1
Medicare Managed Care Manual
Chapter 2 - Medicare Advantage Enrollment and Disenrollment
Updated: August 19, 2011
(Revised: November 16, 2011, August 7, 2012, August 30, 2013, August 14, 2014, July 6, 2015,
September 1, 2015, September 14, 2015, December 30, 2015, May 27, 2016, August 25, 2016, June 15,
2017, July 31, 2018 & August 12, 2020)
This guidance update is effective for contract year 2021. All enrollments with an effective date on
or after January 1, 2021, must be processed in accordance with the revised requirements,
including the new model Medicare Advantage (MA)enrollment form for the 2021 plan year
starting October 15, 2020 and model notices, as appropriate. Organizations may, at their option,
implement any new requirement consistent with this guidance prior to the required
implementation date.
It is expected that organizations will assure compliance with all Medicare Advantage
requirements described in this chapter regarding communications made with
beneficiaries/members, including the use of the model notices, and the requirements outlined in
the Medicare Communications and Marketing Guidelines (MCMG).
Organizations are required to provide information to individuals in accessible/alternate formats
(for example, Large Print, Braille), upon request and thereafter, as outlined in Section 504 of the
Rehabilitation Act of 1973 (and subsequent revisions). Such individuals must have an equal
opportunity to participate in enrollment, paying premium bills, and communicating with the plan,
as members who do not request accessible/alternate formats.
Table of Contents
10 - Definitions .......................................................................................................................................9
20 - Eligibility for Enrollment in MA Plans .......................................................................................16
20.1 - Entitlement to Medicare Parts A and B and Eligibility for Part D ...................................17
20.2 - Place of Permanent Residence ............................................................................................17
20.2.1 - Mailing Address .........................................................................................................19
20.2.2 – U.S. Citizenship or Lawful Presence ..............................................................................19
20.3 - Completion of Enrollment Request ....................................................................................19
20.3.1 - Optional Employer/Union Enrollment Request Mechanism ...................................20
20.3.2 - Passive Enrollment by CMS ......................................................................................20
20.3.3 - Group Enrollment for Employer or Union Sponsored Plans ...................................22
20.4 - Agreeing to Abide by MA Organization Rules .................................................................23
20.5 - Grandfathering of Members on January 1, 1999 ...............................................................23
20.6 - Eligibility and the Hospice Benefit ....................................................................................24

2
20.7 - Continuation of Enrollment Option for MA Local Plans ..................................................24
20.8 - Additional Eligibility Requirements for MA Religious Fraternal Benefit (RFB) Plans .25
20.9 - Eligibility Requirements for Medicare Medical Savings Account (MSA) Plans ............25
20.10 - Additional Eligibility Requirements for Enrollment in MA Special Needs Plans ........25
30 - Election Periods and Effective Dates...........................................................................................28
30.1 - Annual Election Period (AEP) ............................................................................................29
30.2 - Initial Coverage Election Period (ICEP) ............................................................................29
30.2.1 - Initial Enrollment Period for Part D (IEP for Part D) ..............................................30
30.3 - Open Enrollment Period for Institutionalized Individuals (OEPI) ...................................31
30.4 - Special Election Period (SEP) ............................................................................................31
30.4.1 - SEPs for Changes in Residence .................................................................................34
30.4.2 - SEPs for Contract Violation ......................................................................................35
30.4.3 - SEPs for Non-renewals or Terminations ..................................................................36
30.4.4 - SEPs for Exceptional Conditions ..............................................................................38
1. SEP EGHP (Employer/Union Group Health Plan) .....................................................38
2. SEP for Individuals Who Disenroll in Connection with a CMS Sanction .................39
3. SEP for Individuals Enrolled in Cost Plans that are Non-renewing their Contracts .39
4. SEP for Individuals in the Program of All-inclusive Care for the Elderly (PACE) ..39
5. SEP for Dual-eligible Individuals and Other LIS-Eligible Individuals......................39
6. SEP for Individuals Who Terminated a Medigap Policy When They Enrolled For
the First Time in an MA Plan, and Who Are Still in a “Trial Period” ...............41
7. SEP for Individuals with ESRD Whose Entitlement Determination Made
Retroactively ..........................................................................................................41
8. SEP for Individuals Whose Medicare Entitlement Determination Made
Retroactively ..........................................................................................................42
9. MA SEPs to Coordinate With Part D Enrollment Periods ..........................................42
10. SEP for Individuals Who Lose Special Needs Status ...............................................43
11. SEP for Individuals Who Belong to a Qualified SPAP or Who Lose SPAP
Eligibility ...............................................................................................................43
12. SEP for Individuals who Gain, Lose, or Have a Change in their Dual or LIS-
Eligible Status ........................................................................................................43
13. SEP for Enrollment Into a Chronic Care SNP and for Individuals Found Ineligible
for a Chronic Care SNP.........................................................................................44
14. SEP for Disenrollment from Part D to Enroll in or Maintain
Other Creditable Coverage ...................................................................................44
15. SEP to Enroll in an MA Plan, PDP or Cost Plan With a Plan Performance Rating
of Five (5) Stars .....................................................................................................44
16. SEP for Non-U.S. Citizens who become Lawfully Present ......................................46
17. SEP for Providing Individuals who Requested Materials in Accessible Formats
Equal Time to Make Enrollment Decisions .........................................................46
18. SEP for Government Entity-Declared Disaster or Other Emergency ......................46

3
19. SEP for Individuals Enrolled in a Plan Placed in Receivership ..............................47
20. SEP for Individuals Enrolled in a Plan That Has Been Identified by CMS as a
Consistent Poor Performer ...................................................................................47
21. SEP for Other Exceptional Circumstances ................................................................47
30.4.5 - SEPs for Beneficiaries Age 65 (SEP65) ...................................................................48
30.4.6 – SEP for Significant Change in Provider Network ...................................................48
30.4.7 – SEP for CMS and State-Initiated Enrollments ........................................................48
30.5 – Medicare Advantage Open Enrollment Period (MA OEP) ..............................................49
30.6 - Effective Date of Coverage .................................................................................................49
30.6.1 - Effective Date of Auto- and Facilitated Enrollments ...............................................51
30.7 - Effective Date of Voluntary Disenrollment .......................................................................52
30.8 - Election Periods and Effective Dates for Medicare MSA Plans ......................................53
30.9 - Closed Plans, Capacity Limits, and Reserved Vacancies .................................................53
30.9.1 - MA Plan Closures ......................................................................................................53
40 - Enrollment Procedures ..................................................................................................................55
40.1 - Format of Enrollment Requests ..........................................................................................56
40.1.1 - Enrollment Request Mechanisms ..............................................................................57
40.1.2 – Electronic Enrollment................................................................................................58
40.1.3 - Enrollment via Telephone ..........................................................................................59
40.1.4 - Default Enrollment Option for Medicaid Managed Care Plan Enrollees who are
Newly Eligible for Medicare Advantage ...................................................................60
40.1.5 - Auto- and Facilitated Enrollment ..............................................................................62
40.1.6 – Additional Enrollment Request Mechanisms for Employer/Union Sponsored
Coverage.......................................................................................................................71
40.1.6.1 - Group Enrollment Mechanism .........................................................................72
40.1.6.2 - Optional Mechanism For MA Group-sponsored plan Enrollment ................73
40.1.7 - Enrollment for Beneficiaries in Qualified State Pharmaceutical Assistance
Programs (SPAPs) .......................................................................................................74
40.1.8 – Re-Assignment of Certain LIS Beneficiaries ..........................................................74
40.1.9 – Simplified (Opt-In) Enrollment Mechanism ............................................................76
40.2 - Processing the Enrollment Request ....................................................................................78
40.2.1 - Who May Complete an Enrollment or Disenrollment Request...............................85
40.2.2 - When the Enrollment Request Is Incomplete ...........................................................86
40.2.3 - MA Organization Denial of Enrollment ...................................................................87
40.2.4 - MA-PD Enrollment When an Individual has Other Qualified Prescription Drug
Coverage through an Employer or Union Retiree Drug Subsidy (RDS) Plan
Sponsor .........................................................................................................................88
40.3 - Transmission of Enrollments to CMS ................................................................................89
40.4 - Information Provided to Member .......................................................................................90
40.4.1 - Prior to the Effective Date of Coverage ....................................................................90
40.4.2 - After the Effective Date of Coverage........................................................................92

4
40.5 - Enrollment Processing During Closed Periods ..................................................................92
40.5.1 - Procedures After Reaching Capacity Limit ..............................................................93
40.5.2 - Procedures After Closing During the OEP and OEPI..............................................94
40.6 - Enrollments Not Legally Valid ...........................................................................................95
40.7 - Enrollment Procedures for Medicare MSA Plans .............................................................96
40.7.1 - Establishing the MSA Banking Account during the Enrollment Process ..............97
50 - Disenrollment Procedures.............................................................................................................98
50.1 - Voluntary Disenrollment by Member ................................................................................98
50.1.1 – Requests Submitted via Internet ...............................................................................99
50.1.2 - Request Signature and Date .......................................................................................99
50.1.3 - Effective Date of Disenrollment............................................................................. 100
50.1.4 - Notice Requirements ............................................................................................... 100
50.1.5 - Optional Employer/Union MA Disenrollment Request Mechanism ................... 101
50.1.6 - Group Disenrollment for Employer/Union Sponsored Plans ............................... 102
50.1.7 - Medigap Guaranteed Issue Notification Requirements for Disenrollments to
Original Medicare during a SEP .............................................................................. 102
50.2 - Required Involuntary Disenrollment ............................................................................... 102
50.2.1 - Members Who Change Residence ......................................................................... 104
50.2.1.1 - General Rule ................................................................................................... 104
50.2.1.2 - Effective Date of Disenrollment ................................................................... 105
50.2.1.3 - Researching and Acting on a Change of Address ........................................ 106
50.2.1.4 - Procedures for Developing Addresses for Members Whose Mail is Returned
as Undeliverable ................................................................................................. 107
50.2.1.5 - Notice Requirements...................................................................................... 108
50.2.2 - Loss of Medicare Part A or Part B ......................................................................... 109
50.2.3 - Death ........................................................................................................................ 110
50.2.4 - Terminations/Nonrenewals ..................................................................................... 110
50.2.5 – Loss of Special Needs Status ................................................................................. 111
50.2.6 – Failure to Pay a Part D-Income Related Monthly Adjustment Amount (Part D-
IRMAA) .................................................................................................................... 112
50.2.7 – Unlawful Presence Status ....................................................................................... 113
50.3 - Optional Involuntary Disenrollments .............................................................................. 114
50.3.1 - Failure to Pay Premiums ......................................................................................... 114
50.3.2 - Disruptive Behavior ................................................................................................ 120
50.3.3 - Fraud and Abuse ...................................................................................................... 123
50.4 - Processing Disenrollments ............................................................................................... 123
50.4.1 - Voluntary Disenrollments ....................................................................................... 123
50.4.2 – When the Disenrollment Request is Incomplete .................................................. 124
50.4.3 - Involuntary Disenrollments .................................................................................... 125
50.5 - Disenrollments Not Legally Valid ................................................................................... 125

5
50.6 - Disenrollment of Grandfathered Members ..................................................................... 126
50.7 - Disenrollment Procedures for Employer/Union Sponsored Coverage Terminations .. 126
50.8 - Disenrollment Procedures for Medicare MSA Plans ..................................................... 128
60 - Post-Enrollment Activities ........................................................................................................ 129
60.1 - Multiple Transactions ....................................................................................................... 129
60.2 - Cancellations ............................................................................................................... 130
60.2.1 - Cancellation of Enrollment ..................................................................................... 130
60.2.2 - Cancellation of Disenrollment ................................................................................ 131
60.2.3 – When A Cancellation Transaction is Rejected by CMS Systems (Transaction
Reply Code (TRC) 284) ........................................................................................... 132
60.2.4 – Cancellation Due to Notification from CMS (TRC 015) ..................................... 132
60.3 - Reinstatements ............................................................................................................ 132
60.3.1 - Reinstatements for Disenrollment Due to Erroneous Death Indicator, or Erroneous
Loss of Medicare Part A or Part B, Erroneous Incarceration Information, or
Erroneous Unlawful Presence Information ............................................................. 133
60.3.2 - Reinstatements Based on Beneficiary Cancellation of New Enrollment ............ 135
60.3.3 - Reinstatements Due to Mistaken Disenrollment Due to Plan Error .................... 135
60.3.4 - Reinstatements Based on a Determination of Good Cause for Failure to Pay Plan
Premiums or Part D-IRMAA Timely ............................................................................ 136
60.3.4.1 - Process for Good Cause Determinations for Nonpayment of Plan
Premiums ............................................................................................................ 138
60.3.4.2 – Process for Good Cause Determinations for Nonpayment of Part D-
IRMAA ............................................................................................................... 140
60.4 - Retroactive Enrollments ................................................................................................... 142
60.5 - Retroactive Disenrollments .............................................................................................. 143
60.6 - Retroactive Transactions for Employer/Union Group Health Plan (EGHP) Members 144
60.6.1 - EGHP Retroactive Enrollments .............................................................................. 144
60.6.2 - EGHP Retroactive Disenrollments......................................................................... 145
60.7 – User Interface (UI) Transactions Reply Codes (TRC) – Communications with
Beneficiaries .................................................................................................................... 145
60.8 - Election of Continuation of Enrollment Option for MA Local Plans ........................... 148
60.9 - Storage of Enrollment and Disenrollment Records ........................................................ 148
Appendices ......................................................................................................................................... 149
Appendix 1: Summary of Notice Requirements........................................................................ 150
Appendix 2: Summary of Data Elements Required for Plan Enrollment Mechanisms and
Completed Enrollment Requests .................................................................................... 156
Appendix 3: Setting the Application Date on CMS Enrollment Transactions ........................ 159
Appendix 4: Examples of Good Cause Determinations ........................................................... 160
EXHIBITS.......................................................................................................................................... 165
Exhibit 1: MODEL INDIVIDUAL ENROLLMENT REQUEST FORM TO ENROLL IN A
MEDICARE ADVANTAGE PLAN (PART C) ................................................................. 166
6
Exhibit 1a: Information to include on or with Enrollment Mechanism – Attestation of Eligibility
for an Enrollment Period....................................................................................................... 169
Exhibit 1b: Model MA MSA Plan Enrollment Request Form (“Election” may also be used) .... 171
Exhibit 1c: Model PFFS Individual Enrollment Request Form (“Election” may also be used) . 175
Exhibit 1d: Model Simplified Enrollment Form.............................................................................. 180
Exhibit 2: Model Employer/Union Group Health Plan Enrollment Request Form (“Election” may
also be used) .......................................................................................................................... 182
Exhibit 3: Model Short Enrollment Request Form (“Election” may also be used) ...................... 186
Exhibit 3a: Model Plan Selection Form for MA-PD - Switch From Plan to Plan Within Parent
Organization .......................................................................................................................... 190
Exhibit 4: Model Notice to Acknowledge Receipt of Completed Enrollment Request............... 195
Exhibit 4a: Model Notice to Acknowledge Receipt of Completed Enrollment Request –
Enrollment in another Plan Within the Same Parent Organization.................................... 198
Exhibit 4b: Model Notice to Acknowledge Receipt of Completed Enrollment Request and to
Confirm Enrollment .............................................................................................................. 201
Exhibit 4d: Model Notice to Acknowledge Receipt of Completed PFFS Enrollment Request and
to Confirm Enrollment in a PFFS Plan ................................................................................ 208
Exhibit 4e: Model Notice to Acknowledge Receipt of Completed Enrollment Request and to
Confirm Enrollment in Another Plan Within the Same Parent Organization ................... 212
Exhibit 5: Model Notice to Request Information ........................................................................... 216
Exhibit 6: Model Notice to Confirm Enrollment (MA-PD) .......................................................... 217
Exhibit 6a: Model Notice to Confirm Enrollment - Plan to Plan Within Parent Organization ... 219
Exhibit 6b: Model Notice for MA-PD Plans for Individuals Identified on CMS Records As
Members of Employer or Union Group Receiving the Retiree Drug Subsidy (RDS)...... 221
Exhibit 6c: Model Notice to Confirm PFFS Enrollment................................................................. 222
Exhibit 6d: Model Notice to Confirm Enrollment (MA-only) ....................................................... 225
Exhibit 7: Model Notice for MA Organization Denial of Enrollment .......................................... 226
Exhibit 8: Model Notice for CMS Rejection of Enrollment .......................................................... 228
Exhibit 9: Model Notice to Send Out Disenrollment Form (MA-PD enrollee) ........................... 230
Exhibit 9a: Model Notice to Send Out Disenrollment Form (MA-only enrollee) ........................ 232
Exhibit 10: Model Disenrollment Form .......................................................................................... 234
Exhibit 10a: Information to include on or with Disenrollment Form – Attestation of Eligibility for
an Election Period ................................................................................................................. 235
Exhibit 11: Model Notice to Acknowledge Receipt of Voluntary Disenrollment Request from
Member .................................................................................................................................. 236
Exhibit 11a: Model Notice to Request Information (Disenrollment) ............................................ 238
Exhibit 12: Model Notice to Confirm Voluntary Disenrollment Following Receipt of Daily
Transaction Reply Report (DTRR) ...................................................................................... 240
Exhibit 12a: Model Notice for MA Organization Denial of Disenrollment ................................. 242
Exhibit 12b: Model Notice for CMS Rejection of Disenrollment................................................. 244
Exhibit 12c: Confirmation of Disenrollment Due to Passive Enrollment into a Medicare-
Medicaid Plan ........................................................................................................................ 245
7
Exhibit 13: Model Notice of Disenrollment Due to Death ............................................................ 246
Exhibit 14: Model Notice of Disenrollment Due to Loss of Medicare Part A and/or Part B ...... 247
Exhibit 15: Model Notice to Offer Beneficiary Services, Pending Correction of Erroneous Death
Status ...................................................................................................................................... 248
Exhibit 16: Model Notice to Offer Beneficiary Services, Pending Correction of Erroneous
Medicare Part A and/or Part B Termination ........................................................................ 249
Exhibit 17: Model Notice to Offer Reinstatement of Beneficiary Services, Pending Correction of
Disenrollment Status Due to Plan Error .............................................................................. 250
Exhibit 18: Model Notice to Close Out Request for Reinstatement ............................................. 251
Exhibit 19: Model Notice on Failure to Pay Plan Premiums - Advance Notification of
Disenrollment or Reduction in Coverage of Optional Supplemental Benefit(s) .............. 252
Exhibit 20: Model Notice on Failure to Pay Plan Premiums - Notification of Involuntary
Disenrollment ........................................................................................................................ 254
Exhibit 21: Model Notice on Failure to Pay Plan Premiums - Confirmation of Involuntary
Disenrollment ........................................................................................................................ 256
Exhibit 21a: Notification of Involuntary Disenrollment by the Centers for Medicare & Medicaid
Services for Failure to Pay the Part D-Income Related Monthly Adjustment Amount.... 258
Exhibit 22: Model Notice on Failure to Pay Optional Supplemental Benefit Premiums - Notice of
Reduction in Coverage of Optional Supplemental Benefit(s) Within the Same Plan
(PBP) ...................................................................................................................................... 260
Exhibit 22a: Model Notice on Favorable Good Cause Determination for Disenrollment Due to
Nonpayment of Part D-IRMAA – Notification of Plan Premium Amount Due for
Reinstatement ........................................................................................................................ 262
Exhibit 22b: Model Notice on Favorable Good Cause Determination for Disenrollment Due to
Nonpayment of Plan Premiums – Notification of Plan Premium Amount Due for
Reinstatement ........................................................................................................................ 264
Exhibit 22c: Model Notice on Unfavorable Good Cause Determination for Disenrollment Due to
Nonpayment of Plan Premiums ............................................................................................ 266
If you have any questions, please call us at <phone number> between <hours and days of
operation>. TTY users should call <TTY number>. ......................................................... 266
Exhibit 22d: Model Notice to Close Out Good Cause Reinstatement Request – Failure to Pay Plan
Premiums within 3 Months of Disenrollment ..................................................................... 267
Exhibit 22e: Model Notice on Favorable Good Cause Determination for Disenrollment Due to
Nonpayment of Plan Premiums (No Plan Premium Amount Due for Reinstatement) .... 269
Referenced in section: 60.3.4.1 ............................................................................................ 269
Exhibit 23: Model Notices for Closing Enrollment........................................................................ 270
Exhibit 24: Model Notice for Medigap Rights Per Special Election Period ................................ 272
Exhibit 25: Acknowledgement of Request to Cancel Enrollment ................................................. 273
Exhibit 25a - Model Acknowledgment of Reinstatement ............................................................... 274
Exhibit 25b: Confirmation of Cancellation of Enrollment Due to Notice from CMS (TRC 015) 275
Exhibit 26: Acknowledgement of Request to Cancel Disenrollment ............................................ 276
Exhibit 27a: MA-PFFS Model Notice to Inform Full-Benefit Dual Eligible Member of Auto-
Enrollment in PDP ................................................................................................................ 280
8
Exhibit 28: MA Model Notice to Inform Member of Facilitated Enrollment into MA-PD plan 282
Exhibit 28a: MA Model Notice to Inform Member of Facilitated Enrollment into PDP ............ 284
Exhibit 29: Acknowledgement of Request to Opt Out of Auto/Facilitated Enrollment ............... 286
Exhibit 30: Model Notice for Enrollment Status Update ................................................................ 287
Exhibit 31: Model Employer/Union Sponsored MA Plan Group Enrollment Mechanism
Notice ..................................................................................................................................... 289
Exhibit 32: Model Notice for Loss of Special Needs Status.......................................................... 291
Exhibit 33: Model Notice for Loss of SNP Status - Notification of Involuntary Disenrollment . 293
Exhibit 34: MA Model Notice to Research Potential Out of Area Status .................................... 295
Exhibit 35: MA Model Notice for Disenrollment Due to Out of Area Status (No Response to
Request for Address Verification) ....................................................................................... 297
Exhibit 36: MA Model Notice for Disenrollment Due to Confirmation of Out of Area Status
(Upon New Address Verification from Member) ............................................................... 299
Exhibit 37: Notification of Involuntary Disenrollment by the Centers for Medicare & Medicaid
Services due to Incarceration................................................................................................ 301
Exhibit 38: Notification of Involuntary Disenrollment by the Centers for Medicare & Medicaid
Services due to Loss of Lawful Presence ............................................................................ 303
9
For Chapter 2, a reference to an “MA plan” includes MA local plans, MA Regional Preferred
Provider Organization (PPO) plans and MA-PD plans (including special needs plans), unless
otherwise specified.
The instructions provided in this chapter apply to MA plans, including MA-PD plans.
Instructions for enrollment (and disenrollment) in a Prescription Drug Plan (PDP) or an 1876
cost plan are provided in a separate guidance.
10 - Definitions
The following definitions relate to topics addressed in this guidance.
Application Date – For paper enrollment forms and other enrollment request mechanisms, the
application date is the date the enrollment request is initially received by the organization as defined
below. Plans must use this date in the appropriate field when submitting enrollment transactions to
CMS. A summary of application dates for CMS enrollment transactions is provided in Appendix 3 of
this guidance.
• For requests sent by mail, the application date is the date the application is received by the
organization (i.e., arrives in the organization’s mailbox or mailroom); the postmark is irrelevant).
• For requests received by fax, the application date is the date the fax is received on the
organization’s fax machine.
• For requests submitted to sales agents, including brokers, the application date is the date the
agent and/or broker receives (accepts) the enrollment request and not the date the organization
receives the enrollment request from the agent and/or broker. For purposes of enrollment,
receipt by the agent or broker employed by or contracting with the organization, is considered
receipt by the plan, thus all CMS required timeframes for enrollment processing begin on this
date.
• For requests accepted by approved telephonic enrollment mechanisms, the application date is the
date of the call. The call must have followed the approved script, included a clear statement that
the individual understands he or she is requesting enrollment, and have been recorded.
• The Medicare.gov Online Enrollment Center (OEC) uses coordinated Universal Time (UTC,
which was formerly known as Greenwich Meant Time and is four hours ahead of Eastern
Daylight Time and five hours ahead of Eastern Standard Time) as the system time to generate the
timestamp of when an enrollment was received. For requests made via the (OEC), the application
date to be used for processing the enrollment request is the time and date that is 11 hours earlier
than the time and date CMS “stamps” on the enrollment request at the time the individual
completed the OEC process. This is true regardless of when an organization ultimately retrieves
or downloads the request.
Example: An individual completes an enrollment request and submits it via the OEC at
9:00 p.m. EST on December 7. The OEC will “stamp” this request as having been
completed on December 8 at 2:00 a.m., which is the UTC equivalent time and date. The
organization will use December 7, 3:00 p.m., as the application date for the purpose of
addressing CMS enrollment policy requirements (e.g. application date, determination of
election period, etc.).

10
• For electronic enrollment requests made using the organization’s system instead of the OEC, the
application date is the date the applicant completes the request through the organization’s
electronic enrollment process. This is true regardless of when an organization ultimately
retrieves or downloads the request.
• For all enrollments into employer group or union sponsored plans using the Special Enrollment
Period for Employer or Union Group Health Plans (SEP EGHP), the application date used on the
transaction submitted to CMS will always be the
first of the month prior to the effective date of
enrollment for all mechanisms at all times. For the purposes of providing notices and meeting
other timeframe requirements provided in this guidance, use the date the organization receives
the request. For example, if a valid group enrollment mechanism file is received by the
organization on January 24
th
for enrollments effective February 1
st
, the receipt date for the
provision of required notices is January 24
th
and the application date submitted on the enrollment
transactions is January 1
st
.
• For auto- or facilitated enrollment, as described in §40.1.5, the application date is the first day of
the month prior to the effective date of the auto/facilitated enrollment. This will ensure that any
subsequent beneficiary-generated enrollment request will supersede the auto- or facilitated
enrollment in CMS systems.
At-risk Beneficiary – A Part D eligible individual who is determined to be at-risk for misuse or abuse
of a frequently abused drug in accordance with the requirements for drug management programs at 42
CFR 423.153(f). Additional guidance about Part D drug management programs is available at
https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovContra/RxUtilization.html
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Authorized Representative/Legal Representative – An individual who is the legal representative or
otherwise legally able to act on behalf of an enrollee, as the law of the State in which the beneficiary
resides may allow, in order to execute an enrollment or disenrollment request; e.g., court appointed
legal guardians, persons having durable power of attorney for health care decisions, or individuals
authorized to make health care decisions under state surrogate consent laws, provided they have the
authority to act for the beneficiary in this capacity (see §40.2.1). Form CMS-1696 may not be used to
appoint an authorized representative for the purposes of enrollment and disenrollment. This form is
solely for use in the claims adjudication or claim appeals process, and does not provide broad legal
authority to make another individual’s healthcare decisions.
Cancellation of Enrollment Request – An action initiated by the beneficiary to cancel an enrollment
request. To be valid, the cancellation request must be received by the organization before the
enrollment effective date. An enrollment request that has been appropriately cancelled is considered
not to have been used and the election remains available for use within the time frame of the
applicable election period.
Completed Election – An enrollment request is considered complete when:
1. The form/request is signed by the beneficiary or legal representative (refer to §40.2.1 for a
discussion of who is considered to be a legal representative), or the enrollment request
mechanism is completed;

11
2. For enrollments, evidence of entitlement to Medicare Part A and enrollment in Medicare Part B
is obtained by the Medicare Advantage organization (see below for definition of “evidence of
Medicare Part A and Part B coverage”);
3. All necessary elements on the form are completed (for enrollments, see Appendix 2
for a list of
elements that must be completed) or when the enrollment request mechanism is completed as
CMS directs, and, when applicable;
4. Certification of a legal representative’s authority to make the enrollment request is obtained by
attestation (refer to §40.2.1).
5. For Special Needs Plans (SNP), verification of SNP eligibility, as described in §20.11. Chronic
condition SNPs (C-SNP) that utilize a CMS-approved pre-enrollment qualification assessment
tool will consider the enrollment request to be complete upon receipt of the completed tool.
If an individual is involuntarily disenrolled for failure to pay premiums, to re-enroll in that plan, or
enroll into another, he or she would need to request enrollment during a valid enrollment period. In
addition, for enrollments into an MA-only (non MA-PD) plan, an MA organization may also choose to
wait for the individual’s payment of the plan premium, including any premiums due the MA
organization for a prior enrollment before considering an enrollment “complete.”
Continuation Area/Continuation of Enrollment Option – A continuation area is an additional
CMS-approved area outside the MA local plan’s service area within which the MA organization
furnishes or arranges for furnishing of services to the MA local plan’s continuation of enrollment
members. MA organizations have the option of establishing continuation areas for MA local plans.
Conversions – For individuals who are enrolled in a health plan offered by the MA organization the
month immediately before the month of their entitlement to Medicare Parts A and B, their enrollment
in an MA plan offered by the same organization is referred to as a “conversion” from non-Medicare
status to MA enrollee status. In order for the individual’s enrollment with the organization as an MA
enrollee to take effect upon becoming eligible for Medicare, conversions must take place during the
individual’s Initial Coverage Election Period (ICEP).
Denial of Enrollment Request – Occurs when an MA organization determines that an individual is
not eligible to make an enrollment request (e.g., the individual is not entitled to Medicare Part A or
enrolled in Part B, the individual is not making the enrollment request during an election period, etc.),
and therefore determines it should not submit the enrollment request transaction to CMS.
Effective Date of Coverage/Enrollment – The date on which an individual’s coverage in an MA plan
begins. The MA organization must determine the effective date of enrollment for all enrollment
requests. Instructions for determining the correct effective date of coverage are provided in §30.6.
Election – Enrollment in, or voluntary disenrollment from, an MA plan or the traditional Medicare
fee-for-service program (“Original Medicare”) constitutes an election. (Disenrollment from Original
Medicare would occur only when an individual enrolls in an MA plan.) The term “election” is used to
describe either an enrollment or voluntary disenrollment. If the term “enrollment” is used alone,
however, then the term is used deliberately, i.e., it is being used to describe only an enrollment, and
12
not a disenrollment. The same applies when the term “disenrollment” is used alone, i.e., the term is
being used to describe only a disenrollment, and not an enrollment.
Election Period – The time(s) during which an eligible individual may request to enroll in or disenroll
from an MA plan. The type of election period determines the effective date of MA coverage as well as
the types of enrollment requests allowed. There are several types of election periods, all of which are
defined under §30.
Enrollment Request Mechanism – A method used by individuals to request to enroll in an MA plan.
Several model individual enrollment forms are provided in the Exhibits at the end of this guidance. An
individual who is a member of an MA plan and who wishes to elect another MA plan, even if it is
offered by the same MA organization, must complete a new election during a valid enrollment
period to enroll in the new MA plan. However, that individual may use a short enrollment form
(refer to Exhibit 3) or a “plan selection” form (refer to Exhibit 3a) to make the election in place of the
comprehensive individual enrollment form, or, may complete the election via an electronic enrollment
mechanism, as described in §40.1.2 of this guidance, or by telephone, as described in §40.1.3 of this
guidance, if the MA organization offers these options. In addition, MA organizations may want to
collaborate with Employer or Union Group Health Plans (EGHPs) to use a single enrollment form (or
other CMS approved method, if available) for EGHP members; a model EGHP enrollment form for
this purpose is provided in Exhibit 2. Beneficiaries or their legal representatives must complete an
enrollment request mechanism (e.g. enrollment form) to enroll in an MA plan.
Beneficiaries are not required to use a specific form to disenroll from an MA plan; however, a model
disenrollment form is provided in Exhibit 10.
Evidence of Entitlement (Medicare Part A and Part B Coverage) – Documentation, materials or
other information that confirms an individual is entitled to coverage under Parts A and B of Medicare.
Evidence of entitlement is a requirement to determine eligibility for enrollment into a MA plan. It
includes the individual’s coverage start dates for Part A and Part B. CMS systems are updated within
two business days of SSA processing a new or changed Part A or Part B entitlement. MA
organizations must verify Medicare entitlement for all enrollment requests using either the Batch
Eligibility Query (BEQ) process or MARx online query (M232 screen). Therefore, the applicant is not
required to provide evidence with the enrollment request.
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Evidence of Permanent Residence – A permanent residence is normally the enrollee’s primary
residence. An MA organization may request additional information such as voter’s registration
records, driver’s license records, tax records, and utility bills to verify the primary residence. Such
records must establish the permanent residence address, and not the mailing address, of the individual.
Full-Benefit Dual Eligible Individual – For purposes of Medicare Prescription Drug benefits (Part
D), is a Medicare beneficiary who is determined eligible by the state for medical assistance for full
benefits under title XIX of the Social Security Act for the month under any eligibility category
covered under the State plan or comprehensive benefits under a demonstration under section 1115 of
the Act, or medical assistance under section 1902(a)(10)(C) of the Act (medically needy) or section
1902(f) of the Act (States that use more restrictive eligibility criteria than are used by the SSI program)
for any month if the individual was eligible for medical assistance in any part of the month.
13
Good Cause – This term refers to the standards established in § 60.3.4 under which an individual may
be reinstated into his/her MA plan when involuntarily disenrolled for failure to pay the plan’s premium
or the Part D-Income Related Monthly Adjustment Amount (Part D-IRMAA) premium amount.
Incarceration – This term refers to the status of an individual who is in the custody of a penal
authority and confined to a correctional facility, such as a jail or prison, or a mental health institution
as a result of a criminal offense. Such individuals reside outside of the service area for the purposes of
MA plan eligibility, even if the correctional facility is located within the plan service area. Individuals
who are confined to Institutions for Mental Disease (IMDs), such as state hospitals, psychiatric
hospitals, or the psychiatric unit of a hospital, as a result of violations of the penal code, are
incarcerated as CMS defines the term for the purpose of MA eligibility. The place of residence for
these confined individuals is therefore excluded from the service area of an MA plan on that basis.
Individuals who are confined to IMDs, such as state hospitals, psychiatric hospitals, or the psychiatric
unit of a hospital, for other reasons (e.g., because of court orders unrelated to penal violations) are not
incarcerated. Normal service area rules apply to these individuals.
Institutionalized Individual – Please refer to 42 CFR 422.2.
Involuntary Disenrollment – Disenrollments made necessary due to the organization’s determination
that the individual is no longer eligible to remain enrolled in a plan, or when an organization otherwise
initiates disenrollment (e.g. failure to pay plan premiums, plan termination). Procedures regarding
involuntary disenrollment are found in §§50.2 and 50.3.
Late Enrollment Penalty (LEP) – An amount added to the MA-PD plan premium of an individual
who did not obtain creditable prescription drug coverage when s/he was first eligible for Part D or who
had a break in creditable prescription drug coverage of at least 63 consecutive days. The LEP is
considered a part of the plan premium.
Lawfully Present Individual – Refer to 8 CFR 1.3 (Lawfully present aliens for purposes of applying
for Social Security benefits) for a definition of an alien who is considered lawfully present in the
United States. An individual who is not lawfully present in the Unites States is not eligible for any
federal public benefit, including payment of Medicare benefits. (8 U.S.C. 1611)
Medicare Advantage Organization (MA organization) - Refer to Chapter 1 (General Provisions)
for a definition of an “MA organization.”
MA Organization Error – An error or delay in enrollment request processing made under the full
control of the MA organization personnel and one that the organization could have avoided.
Medicare Advantage Plan – Refer to Chapter 1 for a definition of “MA plan.” Enrollment requests
are made at the MA plan level, not at the MA organization level.
Other Low Income Subsidy (LIS) Eligible Individuals – For purposes of Medicare Part D benefits,
individuals who are determined eligible for the Part D low-income subsidy (LIS) who are not full-
benefit dual eligible individuals as defined above. This includes individuals deemed eligible for LIS
by virtue of having QMB-only, SLMB-only, QI, SSI-only; as well as those who apply and are
determined eligible for LIS.

14
Out-of-Area Members - Members of an MA plan who live outside the service area and who elected
the MA plan while residing outside the service area (as allowed in §§20.0, 20.3, 50.2.1, and 50.2.4).
Part D-Income Related Monthly Adjustment Amount (Part D-IRMAA) – A premium amount
separate from the Part D plan’s monthly premium for individuals who have incomes over a certain
amount. The Social Security Administration assesses the amount annually based on the enrollee’s
available tax information. The plan does not collect the Part D-IRMAA as part of its premium.
Typically, individuals pay the Part D-IRMAA through their Social Security, Office of Personnel
Management or Railroad Retirement Board (RRB) benefit withholding. Some enrollees are directly
billed for their Part D-IRMAA through invoices sent by CMS or the RRB. All Part D enrollees who
are assessed the Part D-IRMAA are required to pay the IRMAA even if the Part D coverage is
provided through an EGHP.
Plan Performance Rating – A CMS-assigned rating, measured in stars from one to five, which
indicates an organization’s quality and performance based on criteria established by CMS. A star
rating of one star indicates poor performance, while a star rating of five stars indicates exemplary
performance. The Plan Performance Overall Rating (or “overall rating”) is publicly available on
Medicare.gov. CMS assigns the rating in October for the following year based on the organization’s
most recent quality and performance data.
Potential At-risk Beneficiary – A Part D eligible individual who is identified as being potentially at-
risk for misuse or abuse of a frequently abused drug in accordance with the requirements for drug
management programs at 42 CFR 423.153(f). Additional guidance about Part D drug management
programs is available at
www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovContra/RxUtilization.htm
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Receipt of Enrollment Request – MA organizations may receive enrollment requests through various
means, as described in §40.1. The MA organization must date as received all enrollment requests as
soon as they are initially received. This date will be used to determine the election period in which the
request was made, which in turn will determine the effective date of the request. Please refer to the
definition of “Application Date” in this section for specific information regarding the correct date to
report as the application date on enrollment transactions submitted to CMS.
Reinstatement of Election – An action that may be taken by CMS to correct an erroneous
disenrollment from an MA plan. The reinstatement corrects an individual’s records by canceling a
disenrollment to reflect no gap in enrollment in an MA plan. A reinstatement may result in retroactive
disenrollment from another Medicare managed care plan.
Rejection of Enrollment Request – Occurs when CMS has rejected an enrollment request submitted
by the MA organization. The rejection could be due to the MA organization incorrectly submitting the
transactions, to system error, or to an individual’s ineligibility to elect the MA plan.
Special Needs Plan – Medicare Advantage coordinated care plans that serve the special needs of
certain groups of individuals including; institutionalized individuals (as defined by CMS), those
entitled to Medical Assistance under a State Plan under Title XIX and individuals with severe or
disabling chronic conditions, as defined by CMS.

15
System Error – A “system error” is an unintended error or delay in enrollment request processing that
is clearly attributable to a specific Federal government system (e.g., Social Security Administration
(SSA) system, Railroad Retirement Board (RRB) system), and is related to Medicare entitlement
information or other information required to process an enrollment request.
Voluntary Disenrollment – Disenrollment initiated by a member or his/her authorized representative.

16
20 - Eligibility for Enrollment in MA Plans
42 CFR 422.50
(Rev. 1, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
In general, an individual is eligible to elect an MA plan when each of the following requirements is
met:
1. The individual is entitled to Medicare Part A and enrolled in Part B, provided that he or she
will be entitled to receive services under Medicare Part A and Part B as of the effective date of
coverage under the plan (see exceptions described under §20.6);
2. Effective for plan years beginning on or after January 1, 2021, a beneficiary with ESRD can
choose to join a MA plan. (For additional information on SNP eligibility criteria, see Chapter
16-B Special Needs Plans).
3. The individual permanently resides in the service area of the MA plan (see exceptions in §20.3
for persons living outside the service area at the time of the enrollment request);
4. The individual is a U.S. citizen or lawfully present in the United States (see exceptions in
§20.3.2 for persons unlawfully present at the time of the enrollment request);
5. The individual or his/her legal representative completes an enrollment request and includes all
the information required to process the enrollment or meets alternative conditions for
enrollment specified by CMS (refer to Appendix 2 for a list of items required to complete the
enrollment form, and §40.2.1 for who may sign enrollment request forms or complete other
enrollment request mechanisms);
6. The individual is fully informed of and agrees to abide by the rules of the MA organization that
were provided during the enrollment request; and
7. The individual makes a valid enrollment request that is received by the plan during an election
period, as described in §30;
8. For a Special Needs Plan (SNP) additional requirements apply as described in §20.11 of this
guidance.
9. For an MSA plan, additional requirements apply as described in §20.10 of this guidance.
An MA organization may not impose any additional eligibility requirements as a condition of
enrollment other than those established by CMS in this guidance.
An MA organization must not deny enrollment to otherwise eligible individuals covered under an
employee benefit plan. If the individual enrolls in an MA plan and continues to be enrolled in his/her
employer/union or spouse’s group health benefits plan, then coordination of benefits rules apply.
An MA eligible individual may not be enrolled in more than one MA plan at any given time.
Procedures for handling multiple transactions, cancellations, and reinstatements are described in
§§ 60.1, 60.2 and 60.3.
17
Individuals enrolled in an MA plan may not concurrently enroll in a PDP except for individuals
enrolled in a Medicare MSA plan or individuals enrolled in a PFFS plan that does not offer Medicare
prescription drug coverage. An individual enrolled in an MA PFFS plan that does not include a Part D
benefit may enroll in a PDP, even if under the same MA contract the organization offers another PFFS
plan that includes a Part D benefit.
20.1 - Entitlement to Medicare Parts A and B and Eligibility for Part D
To be eligible to elect an MA plan, an individual must be entitled to Medicare Part A and enrolled in
Part B, and must be entitled to Medicare Part A and Part B benefits as of the effective date of coverage
under the plan. Exceptions for Part B-only “grandfathered” members are outlined in §20.6. Part B only
individuals currently enrolled in a plan created under §1833 or §1876 of the Social Security Act (the
Act) are not considered to be “grandfathered” individuals, and must purchase Medicare Part A through
the Social Security Administration to become eligible to enroll in an MA plan.
An MA organization has the option to continue to offer Part A-equivalent coverage to Medicare Part
B-only “grandfathered” members, as described in §20.6. However, an MA organization may not offer
Part A-equivalent coverage to other individuals enrolled only in Medicare Part B (and not entitled to
Part A) in order to make them “eligible” for enrollment in an MA plan. Eligibility requirements are
met based on Part A entitlement through Medicare and not through the purchase of Part A-equivalent
benefits through the MA organization. The MA organization may refer the individual to SSA if the
individual wishes to enroll in Medicare Part A in order to be eligible to enroll in the MA plan.
Eligibility for Part D does not exist:
• When the beneficiary is incarcerated.
• When the beneficiary is not lawfully present in the United States.
• When the beneficiary lives abroad.
• For any month prior to the month of notification of the entitlement determination when the
entitlement determination for Part A and B is made retroactively.
MA-PDs may not enroll an individual who is not eligible for Part D.
20.2 - Place of Permanent Residence
42 CFR 422.2 and 422.50(a)(3)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
An individual is eligible to elect an MA plan if he or she permanently resides in the service area of the
MA plan. A temporary move into the MA plan’s service area does not enable the individual to elect
the MA plan; the MA organization must deny such an enrollment request.
Incarcerated individuals reside outside of the plan service area for the purposes of MA eligibility, even
if the correctional facility, institution or other place of confinement is located within the plan service
area (see §10 for definition of “incarceration”).
18
EXCEPTIONS
• An MA organization may offer a continuation of enrollment option to MA local plan enrollees
when they no longer reside in the service area of a plan and permanently move into the
geographic area designated by the MA organization as a continuation area (refer to §20.8 for
more detail on the requirements for the continuation of enrollment option).
• Conversions: Individuals who are enrolled in a health plan of the MA organization and are
converting to Medicare Parts A and B can elect an MA local plan offered by the same MA
organization during their ICEP even if they reside in the MA organization’s continuation area.
(“Conversion” is defined in §10 and the time frames for the ICEP are covered in §30.2.)
• A member who was enrolled in an MA plan covering the area in which the member
permanently resides at the time the plan was terminated in that area, may remain enrolled in the
MA plan while living outside the plan’s new reduced service area if:
• There is no other MA plan serving the area at that time;
• The MA organization offers this option; and
• The member agrees to receive services through providers in the MA plan’s service area.
• The MA organization has the option to also allow individuals who are converting to Medicare
Parts A and B to elect the MA plan during their ICEP even if they reside outside the service
and continuation area. This option may be offered provided that CMS determines that all
applicable MA access requirements in 42 CFR 422.112 are met for that individual through the
MA plan’s established provider network providing services in the MA plan service area, and
the organization furnishes the same benefits to the individual as to members who reside in the
service area. The organization must apply the policy consistently for all individuals. These
members will be known as “out-of-area” members. This option applies both to individual
members and to employer or union sponsored group plan members of the MA organization.
Individuals who do not meet the above requirements may not elect the MA plan. The MA organization
must deny enrollment to these individuals.
A permanent residence is normally the primary residence of an individual. Proof of permanent
residence is normally established by the address of an individual’s residence, but an MA organization
may request additional information such as voter’s registration records, driver’s license records (where
such records accurately establish current residence), tax records, and utility bills. Such records must
establish the permanent residence address, and not the mailing address, of the individual. If an
individual puts a Post Office Box as his/her place of residence on the enrollment form, the MA
organization must contact the individual to confirm that the individual resides in the service area. If
there is a dispute over where the individual permanently resides, the MA organization should
determine whether, according to the law of the MA organization’s State, the person would be
considered a resident of that State.
In the case of homeless individuals, a Post Office Box, an address of a shelter or clinic, or the address
where the individual receives mail (e.g., social security checks) may be considered the place of
permanent residence.
19
MA organizations have the option to offer “visitor” or “traveler” programs for currently enrolled
individuals who are consecutively out of the area for up to 12 months, provided the plan includes the
full range of services available to other members (refer to §50.2.1 for more detail on the requirements
for the “visitor/traveler” option). Residence in an area designated for a “visitor” or “traveler” program
does not make an individual eligible to enroll in an MA plan, but rather applies to already enrolled
individuals.
20.2.1 - Mailing Address
As described in §20.3, an individual’s eligibility to enroll in an MA plan is in part determined by the
individual’s permanent residence in the service area of that MA plan. Some individuals may have
separate mailing addresses that may or may not be within the geographic plan service area. If an
individual requests that mail be sent to an alternate address, such as that of a relative, MA
organizations should make every effort to accommodate these requests, and should use this alternate
address to provide required notices and other plan mailings, as appropriate. The model MA plan
enrollment application forms provided in this guidance include a mechanism to collect a mailing
address. Use of an alternate address does not eliminate or change the requirement of residency for the
purposes of MA plan eligibility.
20.2.2 – U.S. Citizenship or Lawful Presence
An individual is eligible to elect enrollment in a MA plan if he or she is a U.S. citizen or lawfully
present in the United States. CMS will notify the MA organization if the individual is not eligible to
enroll on this basis at the time of enrollment. The MA organization must deny an enrollment request
from an individual who does not meet this requirement.
EXCEPTION: In the case where CMS systems show that an individual will have lawful
presence status on or before the enrollment effective date, the plan must accept and process the
enrollment request. An MA organization must not deny an enrollment request on the basis that
the applicant is not lawfully present at the time the request is received if CMS systems indicate
that he or she will be lawfully present in the United States as of the enrollment effective date.
If an individual provides evidence of their lawful presence status to the MA organization, the
organization may not consider it when determining eligibility for enrollment. The organization may
not request from an applicant any documentation of U.S. citizenship or alien status. CMS will provide
the official status to the MA organization at the time of enrollment. However, if an individual has
evidence of their lawful presence status and there is a dispute over their status, the MA organization
should refer the individual to the Social Security Administration to have their status reviewed and
adjusted, if necessary.
20.3 - Completion of Enrollment Request
42 CFR 422.50(a)(5)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
The Medicare beneficiary (or their legal representative, as described in § 40.2.1) must complete an
enrollment request in order to enroll in an MA plan, even if switching plans in the same MA
organization. To consider an election complete, the individual must:
• Complete an enrollment request;
20
• Provide required information to the MA organization within the required time frames; and
• Submit the completed request to the MA organization during a valid enrollment period.
This is required for all enrollments, unless otherwise specified by CMS.
Individuals may use any of the enrollment mechanisms offered by the MA organization to make their
enrollment request. See § 40.1 for more information on the types of enrollment mechanisms allowed.
Individuals switching plans in the same MA organization may use a shortened enrollment form
(sample Exhibit 3 or 3a). Individuals new to Medicare who are already a member of the organization’s
non-Medicare coverage (commercial, Medicaid, Marketplace) may use the simplified enrollment
mechanism, if the MA organization chooses to offer it.
An MA organization must deny enrollment to any individual who does not properly complete the
enrollment form or other mechanism within required time frames. Procedures for completing the
enrollment request are provided in §40.2 and Appendix 2. Refer to §10 for a definition of “completed
enrollment request.”
20.3.1 - Optional Employer/Union Enrollment Request Mechanism
Beginning April 1, 2003, MA organizations that offer MA plans to an employer or union may choose
to accept voluntary enrollment requests directly from the employer or union (or its Third Party
Administrator (TPA)) without obtaining a paper MA enrollment request form from each individual.
The enrollment requests reported to the MA organization by the employer/union will reflect the choice
of retiree coverage individuals made using their employer’s or union’s process for selecting a health
plan. This enrollment request mechanism is optional for MA organizations, and may not be required.
Therefore, MA organizations may specify the employers and/or unions, if any, from which they will
accept this enrollment request format and may choose to accept enrollment and/or voluntary
disenrollment requests.
The record of an individual’s choice of health plan submitted by the employer or union effectively
replaces the paper MA enrollment request form(s). All eligibility, processing and notice requirements,
as outlined in this guidance and other references, that pertain to paper enrollment request forms are
applicable to this enrollment request mechanism; however, this process does not require the MA
organization to obtain a signature. Detailed information and instruction is provided in §40.1.2 for
enrollments and §50.1.5 for disenrollments.
Notices of disenrollment, cancellation or termination of coverage not initiated by an enrollee
enrollment request (i.e. involuntary disenrollment) are not included in this mechanism. Guidance for
these situations is available in §50.1.5.
Additional information regarding employer/union sponsored group health plans can be found in
Chapter 9 of this manual.
20.3.2 - Passive Enrollment by CMS
42 CFR 422.60(g)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
21
Passive enrollment is a process where CMS enrolls an individual into another plan under certain
circumstances specified below (note that CMS may also enroll individuals in plans under auto- and
facilitated enrollment per § 40.1.5 and reassignment per § 40.1.8). The beneficiary receives a notice of
this change and has the opportunity to accept or decline it. If the individual takes no action, the
individual has made a choice to accept the enrollment. Passive enrollments are permitted in specific,
limited circumstances associated with:
• Immediate plan terminations,
• Situations in which remaining enrolled in the plan would pose potential harm to members, and
• Situations where CMS determines passive enrollment is necessary to promote integrated care
and continuity of care for full-benefit dual eligible beneficiaries.
CMS will determine when passive enrollment is appropriate under 42 CFR 422.60(g) and will initiate
contact through the MA organization’s CMS account manager. CMS will consult with the state
Medicaid agency and may authorize passive enrollment for full-benefit dual eligible beneficiaries
enrolled in an integrated dual-eligible special needs plan (D-SNP) to continue access in integrated
care, including when:
• The organization’s Medicaid managed care plans non-renew because the state awards these
contracts to another organization, or
• An integrated D-SNP non-renews at the end of the contract year.
CMS will provide specific instructions directly to the affected organizations (both the plan losing the
member and the plan receiving the member) regarding processing the enrollments and specific
information relevant to the situation for inclusion in notices.
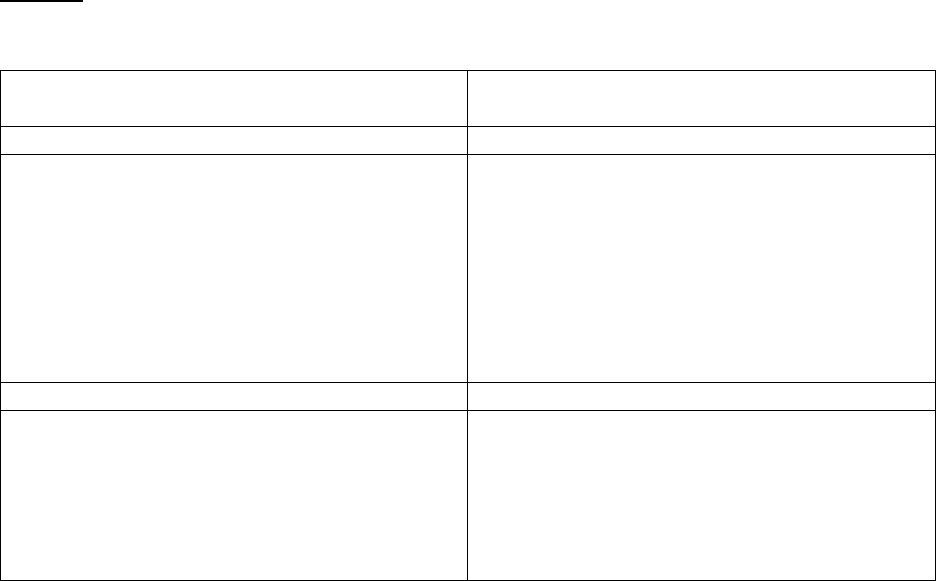
Notices:
Organizations receiving passive enrollments must send required notices. The chart below outlines the
requirements and timing:
Passive enrollment due to immediate plan
termination or potential harm to members
Passive enrollment to continue access to
integrated care
1 notice required
2 notices required
Notice language must:
• describe the costs and benefits of the
plan;
• outline the process for accessing care
in the plan; and
• explain the ability to decline the
enrollment or choose another plan,
how to take that action and by when
Each notice language must:
• describe the costs and benefits of the
plan;
• outline the process for accessing care
in the plan; and
• explain the ability to decline the
enrollment or choose another plan,
how to take that action and by when
Notice language must be approved by CMS
Notice language must be approved by CMS
Notice must be sent:
• prior to the date coverage in the plan
begins; or
• as soon as possible after coverage in
the plan begins, if prior notice isn’t
practical
Notice must be sent:
• at least 60 calendar days prior to the
date coverage in the plan begins; and
• at least 30 calendar days prior to the
date coverage in the plan begins
22
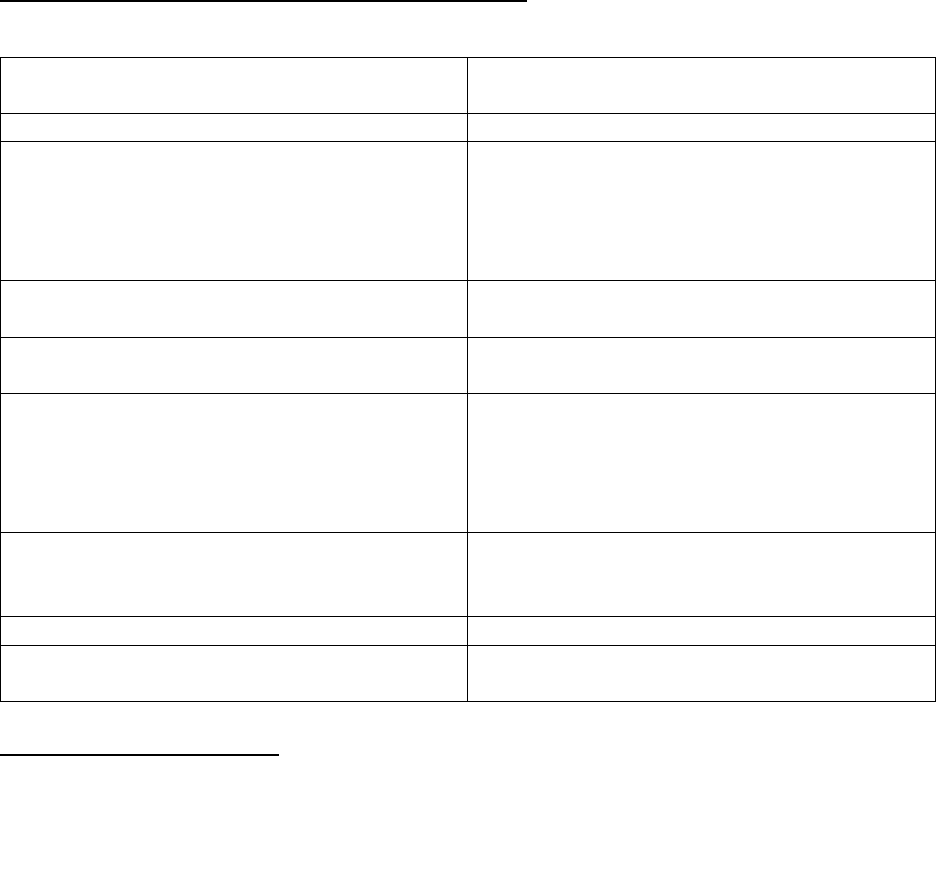
Evaluation of Plans Receiving Passive Enrollments:
For passive enrollment, CMS evaluates the receiving plan as noted in the following chart.
Passive enrollment due to immediate plan
termination or potential harm to members
Passive enrollment to continue access to
integrated care
Key criteria CMS may use:
Requirements (all must be met):
Similar or lower out-of-pocket maximum
Currently operate as a fully integrated dual
eligible SNP (FIDE SNP) or qualify to meet
Medicare-Medicaid integration criteria as D-
SNP that meets a higher standard of
integration (see Chapter 16b)
Similar or lower hospital cost-sharing amount
Substantially similar provider and facility
networks
No additional network restrictions
Substantially similar Medicare and Medicaid
covered benefits
Premium isn’t significantly higher
Have limits on premiums and cost-sharing
that are appropriate for full-benefit dually
eligible beneficiaries (CMS interprets this
standard as having no premium or cost-
sharing ($0) (see Chapter 16b)
Equivalent or higher value Part D benefit and
formulary structure
Have overall MA star rating of at least 3 stars
(Exception: plan is low enrollment contract or
new plan without star ratings)
Similar Part B buy-down feature, if applicable
Not under sanction for new enrollments
Not under sanction for new enrollments
Have capacity (and agree) to accept the
enrollments
Special Enrollment Period:
An SEP is available to all individuals who are passively enrolled in addition to the ability to opt-out of
a passive enrollment. This SEP allows the individual to make an election before the passive enrollment
is effective in the receiving plan or after the coverage in the receiving plan starts. The SEP lasts 3
months beginning from the later of notice of a CMS or State-initiated enrollment action or the
enrollment effective date. See §30.4.7 for more details about this SEP.
NOTE: Individuals in non-renewing or terminating plans also have the ability to use other existing
SEPs outlined in § 30. Dually-eligible individuals may also have the ability to use the duals SEP to
switch plans, provided he or she meets the criteria for that election period (see § 30.4.4 #5). When
more than one SEP is available, the individual may use the SEP that provides him or her with the
greatest flexibility to choose the plan that best meets his or her needs, but use of one SEP does not
negate the availability of other SEPs if the beneficiary chooses to make a subsequent election
(provided that the SEP hasn’t expired and the individual still meets the SEP qualifying conditions).
20.3.3 - Group Enrollment for Employer or Union Sponsored Plans
CMS is providing a process for group enrollment into an employer/union sponsored MA plan. CMS
will allow an employer or union to enroll its retirees using a group enrollment process in which the
beneficiaries participate through advance notification and that provides CMS with any information the
23
employer/union has on other insurance coverage for the purposes of coordination of benefits. MA
organizations must adhere to the guidelines outlined in §40.1.6, as well as all other program
requirements, in developing and implementing this process.
20.4 - Agreeing to Abide by MA Organization Rules
42 CFR 422.50(a)(6)
Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
To be eligible to elect an MA plan, a beneficiary must be fully informed of and agree to abide by the
rules of the MA organization that were provided during the enrollment process (refer to §§ 40.4,
40.4.1, and 40.4.2 regarding what information must be provided to the individual during the
enrollment process). “Fully informed” means that the individual must be provided with the applicable
rules of the MA organization, as described in §40.4.1 of this chapter, as well as in the Medicare
Communications and Marketing Guidelines. The MA organization must deny enrollment to any
individual who does not agree to abide by the rules of the MA organization. Agreement to abide by
the rules of the MA organization in this context is made through the completion of the enrollment
request.
20.5 - Grandfathering of Members on January 1, 1999
An individual who was enrolled on December 31, 1998, in an HMO with a risk contract under §1876
of the Social Security Act was deemed to be enrolled on January 1, 1999, in an MA plan offered by
the same organization if he/she did not choose to disenroll from the organization effective on the latter
date. This deemed enrollment applied even if the enrollee was not entitled to Medicare Part A or did
not live in an MA plan service area or continuation area. The MA organization was not permitted to
disenroll such individuals because they were not entitled to Part A, or did not live in the service or
continuation area. However, if these individuals elect to disenroll from the MA organization, they are
not eligible to enroll in any MA plan until or unless they meet all MA eligibility requirements.
If enrollment in Medicare Part B ends for an individual, the individual may not continue as a member
of the MA plan and must be disenrolled as described in §§50.2.2 and 50.6.
The MA organization must identify all Medicare Part B-only “grandfathered” individuals and inform
them of their status annually. This notification may be included as part of the Evidence of Coverage.
The notice must inform these individuals that if they disenroll from the MA organization, they cannot
elect another MA plan unless they become entitled to Medicare Part A (by enrolling in Medicare Part
A at SSA and by paying the appropriate premium to CMS) and remain enrolled in Medicare Part B.
MA organizations may continue to provide Part A-equivalent benefits to Medicare Part B-only
grandfathered members. In addition, if an MA organization offers Part A-equivalent coverage as a
supplemental benefit in an MA plan, then the MA organization may disenroll a Medicare Part B-only
grandfathered member who fails to pay the organization’s Part A-equivalent premium, just as any
member of the MA organization could be disenrolled for nonpayment of premiums (refer to §50.3.1).
Grandfathered members may enroll in other MA plans in the same MA organization (within the same
State). However, if grandfathered members disenroll from the MA organization (i.e., they switch to
Original Medicare), they will not be eligible to enroll in any MA plan in any MA organization until or
unless they meet all MA eligibility requirements. If the out-of-area grandfathered members disenroll
24
from the MA organization (i.e., they switch to Original Medicare or attempt to enroll in another MA
organization), they will only be able to enroll in other MA organizations if they meet all MA eligibility
requirements, including, but not limited to, that of living in the service area of the MA plan.
20.6 - Eligibility and the Hospice Benefit
An MA organization must not deny enrollment to any individual who has elected the hospice benefit
(except in the case of a Medicare MSA plan; see §20.10 for additional eligibility requirements for
Medicare MSA plans). Until the MA organization acknowledges that it has received the completed
enrollment request and gives a coverage effective date to the individual (refer to Exhibit 4, Exhibit 4a,
and §40), the MA organization must not ask any questions related to the existence of a terminal illness
or election of the hospice benefit. Such questions will be considered impermissible health screening.
The MA organization may not disenroll any member on the basis of the member electing the hospice
benefit either before or after becoming a member of the MA plan.
20.7 - Continuation of Enrollment Option for MA Local Plans
With CMS approval, an MA organization may establish continuation areas, separate and apart from an
MA local plan’s service area. Refer to Chapter 11 (Medicare Advantage Application Procedures and
Contract Requirements) regarding CMS approval of continuation areas. As defined in§10, the CMS-
approved continuation area is an additional area outside an MA local plan’s service area within which
the MA organization furnishes or arranges for furnishing of services to the MA plan’s members.
Members may only choose to continue enrollment with the MA local plan if they have permanently
moved from the service area into the continuation area.
As described in Chapter 11, if an MA organization wants to offer a continuation of enrollment option
under one or more of the MA local plans it offers, then it must obtain CMS’ approval of the
continuation area and the marketing materials that describe the continuation of enrollment option. The
MA organization must also describe the enrollment option(s) in member materials and make the
option available to all members of the MA local plan in question who make a permanent move to the
continuation area. An MA organization may require members to give advance notice of their intent to
use the continuation of enrollment option. If the MA organization has this requirement, then it must
fully describe the required notification process in the CMS-approved marketing materials. In addition,
the MA organization must fully explain any continuation option to all potential members of the MA
local plan, current members of any other health plan of the MA organization members who reside in
the MA local plan service area and/or MA organization continuation area.
If a member who permanently moves from the service area into the continuation area does not choose
the continuation of enrollment option when he/she is eligible for the option, then the individual is no
longer eligible to be a member of the MA local plan, and the MA organization must initiate the
individual’s disenrollment. Procedures for continued enrollment are in §60.8 and procedures
describing disenrollment for permanent change of residence are described in §50.2.1.
25
20.8 - Additional Eligibility Requirements for MA Religious Fraternal Benefit
(RFB) Plans
An MA RFB plan is a plan that an RFB society may offer only to members of the church, or
convention or group of churches with which the society is affiliated. The requirement for membership
can be met by any documentation establishing membership issued by the church, or by using the
church’s records of membership. An individual must also meet all the other requirements to elect an
MA plan.
20.9 - Eligibility Requirements for Medicare Medical Savings Account (MSA)
Plans
There are additional requirements and limitations for individuals who wish to elect a Medicare
Medical Savings Account (MSA) plan. An individual is not eligible to elect a Medicare MSA plan if
any one of the following applies:
• The individual will reside in the United States for fewer than 183 calendar days during the year
in which the enrollment request is effective;
• The individual is enrolled in a Federal Employees Health Benefits program, or is eligible for
health care benefits through the Department of Veterans Affairs or the Department of Defense;
• The individual is dual eligible and is entitled to coverage of Medicare premium and/or cost-
sharing under a Medicaid State plan;
• The individual is receiving hospice benefits under the Medicare benefit prior to completing the
enrollment request; or
• The individual receives health benefits that cover all or part of the annual Medicare MSA
deductible such as through insurance primary to Medicare, supplemental insurance policies not
specifically permitted under 42 CFR 422.104, or retirement health benefits.
20.10 - Additional Eligibility Requirements for Enrollment in MA Special Needs
Plans
MA Special Needs Plans (SNP) must limit enrollment to individuals who meet specified eligibility
requirements in addition to the eligibility requirements in §20 of this chapter. To be eligible for
enrollment in a SNP an individual must meet the eligibility requirements for the specific SNP. Refer to
Chapter 16-B of the Medicare Managed Care Manual for additional information regarding special
needs plan requirements.
Before processing an enrollment into a dual eligible SNP (D-SNP), the SNP must confirm eligibility,
including both MA eligibility and Medicaid eligibility. Acceptable proof of Medicaid eligibility can be
a current Medicaid card, a letter from the state agency that confirms entitlement to Medical Assistance,
or verification through a systems query to a State eligibility data system. The aforementioned
documents or State systems verifications are acceptable proof of Medicaid entitlement for

26
beneficiaries residing in the 50 states and the District of Columbia. Only where a state Medicaid
agency requires a Social Security number to verify Medicaid status may the SNP enrollment request
mechanism include a field for this element. An individual’s current eligibility for the Medicare Part D
Low Income Subsidy (LIS) or any other Medicaid status flag in CMS systems are not acceptable for
initial or ongoing Medicaid eligibility verification for the purposes of determining dual eligible SNP
eligibility. For current enrollees, the SNP must verify continuing eligibility (e.g. full or partial dual
status, as applicable) at least as often as the state Medicaid agency conducts re-determinations of
Medicaid eligibility.
Medicaid subset SNPs may enroll only those dual eligible individuals who meet all applicable MA
eligibility requirements and are eligible to enroll in the organization’s Medicaid managed care plan, as
described in the organization’s State contract.
For enrollments into an institutional SNP (I-SNP), the organization must confirm that the individual
requires an institutional (skilled nursing facility (SNF), nursing facility (NF), SNF/NF, intermediate
care facility for the mentally retarded (ICF/MR) or inpatient psychiatric facility) level-of-care, and that
the need for an institutional level-of-care has lasted 90 days or longer. When an institutional SNP opts
to enroll special needs individuals prior to a 90 day length-of-stay, the needs-assessment (pre-
approved by CMS) must show that the individual’s condition makes it likely that the length-of-stay (or
need for an institutional level-of-care) will be at least 90 days.
For enrollments into a chronic condition SNP (C-SNP), the organization must contact the provider or
provider’s office to confirm that the individual has the qualifying condition. The organization must
obtain this information in one of the following two ways:
1) Contact the provider or provider’s office and obtain verification of the condition prior to
enrollment, or
2) Utilize a CMS-approved pre-enrollment qualification assessment tool prior to enrollment and
obtain verification of the condition from the provider or provider’s office on a post-enrollment
basis.
For either method, verification from the provider can be in the form of a note from a provider or the
provider’s office, or documented telephone contact with the provider or provider’s office confirming
that the individual has the condition. The organization may need to obtain written permission
(separately from the enrollment form) permitting it to contact the beneficiary’s provider’s office to
obtain verification of the condition.
If the organization chooses to use a CMS-approved prequalification assessment tool, it has until the
end of the first month of enrollment to confirm that the enrollee has the qualifying condition necessary
for enrollment into the severe/chronic disabling condition SNP. If it cannot confirm that the enrollee
has the qualifying condition within that time, the organization has the first seven calendar days of the
following month (i.e., the second month of enrollment) in which to send the beneficiary notice of his/
her disenrollment at the end of that month for not having the qualifying condition. Disenrollment is
effective at the end of the second month of enrollment; however, the organization must retain the
member if confirmation of the qualifying condition is obtained at any point during the second month
of enrollment. In the event the organization submits a disenrollment request to CMS prior to
confirming the qualifying condition, a reinstatement request must be submitted to CMS (or its

27
designee). The beneficiary has an SEP that begins with the month of notification and continues
through the two following months to enroll in another MA organization for a prospective effective
date. This SEP allows a beneficiary time to find a new plan while reducing the potential for incurring a
late enrollment penalty.
EXAMPLE: A beneficiary submits a request to enroll in a SNP effective March 1st. The SNP
uses a CMS-approved prequalification assessment tool in February and attempts to confirm the
beneficiary’s special needs status but is unable to do so by March 31st. Between April 1st and
April 7
th
(inclusive), the SNP must send a notice of prospective disenrollment to the beneficiary
indicating April 30th as the disenrollment date. If the beneficiary fails to select a new plan by
April 30th, his/her SEP will continue through June 30
th
. S/he can enroll in a plan effective June
1st or July 1
st
.

28
30 - Election Periods and Effective Dates
42 CFR 422.62 & 422.68
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
In order for an MA organization to accept an election, a valid request must be made during an election
period (see §10 for the definition of “election”). It is the responsibility of the organization to determine
the election period of each enrollment or disenrollment request. To make this determination, the
organization may need to contact the individual directly. The plan may incorporate specific statements
regarding eligibility of an election period with the enrollment or disenrollment request (see Exhibit 1a
for optional use with enrollment mechanisms). However, if this information is not provided with the
request, the plan must attempt to contact the individual by phone or other communication mechanism,
and determine within the seven (7) day requirement if s/he is eligible to make an election at that time
(see Exhibits 5 & 11a). Use of Exhibit 5 for the sole purpose of requesting information regarding an
applicant’s eligibility for an election period must include a due date that is no later than seven calendar
days from the date the enrollment request was received.
Enrollment requests the plan is not denying must be submitted to CMS within seven (7) calendar days
of the plan’s receipt of the completed enrollment request. (Section 40.3)
Note: An organization’s determination about an individual’s eligibility for an election period is
separate from a determination regarding whether an enrollment/disenrollment request is complete. See
Section 40.2.2 for information pertaining to incomplete enrollment requests.
There are six types of election periods during which individuals may make enrollment requests. They
are:
• Annual Election Period (AEP);
• Initial Coverage Election Period (ICEP);
• Initial Enrollment Period for Part D (IEP for Part D)
1
• Open Enrollment Period for Institutionalized Individuals (OEPI)
• Special Election Periods (SEP); and
• Medicare Advantage Open Enrollment Period ( MA OEP)
Unless a CMS-approved capacity limit or a CMS-issued enrollment sanction applies, all MA
organizations must accept requests to enroll in their MA plans (with the exception of Medicare MSA
plans) during the AEP, an ICEP, an IEP for Part D (MA-PD plans only), the MA OEP and any SEP
that allows enrollment into the specific plan. (Refer to §30.7 for election periods for Medicare MSA
plans.) When an MA plan is closed due to a capacity limit, the MA plan must remain closed to all
1
For MA, allows enrollment requests for MA-PD plans only.
2
The employer/union establishes criteria for its retirees to
participate in the employer/union sponsored MA plan. These criteria are exclusive of and in addition to the eligibility
criteria for MA enrollment. Eligibility criteria to participate and receive employer/union sponsored benefits may include
spouse/family status, payment to the employer/union of the individual’s part of the premium, or other criteria determined
by the employer/union.
29
prospective enrollees (with the exception of reserved vacancies) until the limit is lifted. Refer to §30.9
and §30.9.1 for more information on OEPI plan closures, capacity limits and reserved vacancies.
30.1 - Annual Election Period (AEP)
During the AEP, MA eligible individuals may enroll in or disenroll from an MA plan. The last
enrollment request made, determined by the application date, will be the enrollment request that takes
effect (refer to §60.1 for information on multiple transactions).
Beginning in 2011, the AEP is from October 15 through December 7 of every year. The AEP is also
referred to as the “Fall Open Enrollment” season and the “Open Enrollment Period for Medicare
Advantage AND Medicare prescription drug coverage” in Medicare beneficiary publications and other
tools. MA organizations may use these descriptions of the AEP in their member materials, as well as
in materials for prospective members.
Note: An employer/union sponsored MA plan may have an “open season” as determined by the
employer. This may or may not correspond with the AEP. Therefore, organizations are not required to
accept enrollment requests into employer/union plans during the AEP (unless the AEP and open
season occur simultaneously); however, organizations must accept valid requests for disenrollment.
30.2 - Initial Coverage Election Period (ICEP)
The ICEP is the period during which an individual newly eligible for MA may make an initial
enrollment request to enroll in an MA plan. This period begins three months immediately before the
individual’s first entitlement to both Medicare Part A and Part B and ends on the later of:
1. The last day of the month preceding entitlement to both Part A and Part B, or;
2. The last day of the individual’s Part B initial enrollment period.
The initial enrollment period for Part B is the seven (7) month period that begins 3 months before the
month an individual meets the eligibility requirements for Part B, and ends 3 months after the month
of eligibility. See 42 CFR 407.14 for additional information.
Once an ICEP enrollment request is made and enrollment takes effect, the ICEP election has been
used.
EXAMPLES
• Mrs. Donovan’s 65
th
birthday is June 20, 2009. She is eligible for Medicare Part A and Part B
beginning June 1, 2009 and has decided to enroll in Part B beginning on June 1. Her ICEP
begins on March 1, 2009 and ends on September 30, 2009.
•
Mrs. Smith’s 65
th
birthday is April 20, 2008. She is eligible for Medicare Part A and Part B
beginning April 1, 2008. Because she is still working and has health insurance provided by her
employer, she has decided not to enroll in Part B during her initial enrollment period for Part B.
Upon retiring, she will have the opportunity to enroll in Part B (through a Part B SEP). She has
30
enrolled in Part B effective May 1, 2009. Her ICEP would be February 1 through April 30,
2009.
Please note that the ICEP for an MA enrollment election will frequently relate to either the
individual’s 65th birthday or the 25th month of disability, but it must always relate to the individual’s
entitlement to both Medicare Part A and Part B. When an individual enrolls in an MA-PD plan, s/he
has used both the ICEP and the IEP for Part D (see §30.2.1).
30.2.1 - Initial Enrollment Period for Part D (IEP for Part D)
The Initial Enrollment Period for Part D (IEP for Part D) is the period during which an individual is
first eligible to enroll in a Part D plan. In general, an individual is eligible to enroll in a Part D plan
when he or she is entitled to Part A OR is enrolled in Part B, AND permanently resides in the service
area of a Part D plan. Ultimately, CMS provides a part D eligibility effective date and maintains it in
CMS systems.
At the beginning of the Medicare prescription drug coverage program, all current Part D eligible
individuals had an IEP for Part D that began on November 15, 2005, and ended on May 15, 2006.
During the IEP for Part D, individuals may make one Part D enrollment choice, including enrollment
in an MA-PD plan.
Generally, individuals will have an IEP for Part D that is the same period as the Initial Enrollment
Period for Medicare Part B. The initial enrollment period for Part B is the seven (7) month period that
begins 3 months before the month an individual meets the eligibility requirements for Part B, and ends
3 months after the month of eligibility. See 42 CFR 407.14 for additional information.
EXAMPLE: Mr. Hackerman’s 65th birthday is March 23, 2010. He is currently working, and
while he signed up for his Medicare Part A benefits, effective March 1, 2010, he declined his
enrollment in Part B, given his working status. He is eligible for Part D since he has Part A and
lives in the service area. Even though he did not enroll in Part B, his Part B IEP is still the 3
months before, the month of, and the 3 months following his 65th birthday – that is, December
2009 – June 2010. Hence, his IEP for Part D is also December 2009 – June 2010.
Individuals not eligible to enroll in a Part D plan at any time during their initial enrollment period for
Medicare Part B have an IEP for Part D that is the 3 months before becoming eligible for Part D, the
month of eligibility, and the three months following eligibility for Part D.
EXAMPLE: Mr. Duke lived in Italy at the time of his 65
th
birthday, which occurred on August
3, 2008. His Part B initial enrollment period began on May 1, 2008, and ended November 30,
2008. He plans to return to the U.S. to reside permanently in June 2010. Since he lived out of
the U.S. and was not eligible to enroll in a Part D plan during his IEP for Part B, his initial
enrollment period for Part D will occur when he meets all the eligibility requirements for Part D,
that is, when he has Part A or B and resides in a Part D plan service area. His IEP for Part D is
March 2010 – September 2010.
Individuals eligible for Medicare prior to age 65 (such as for disability) will have another Initial
Enrollment Period for Part D based upon attaining age 65.
31
The ICEP and the IEP for Part D occur together as one period when a newly Medicare eligible
individual has enrolled in BOTH Part A and B at first eligibility. Should an individual delay
enrollment in Part B to a later time, the ICEP and IEP for Part D become separate with the ICEP
changing to then occur as the 3 months immediately preceding entitlement to BOTH parts A and B.
If a Medicare entitlement determination is made retroactively eligibility for Part D begins with the
month in which the individual received notification of the retroactive entitlement decision. Therefore,
the Part D IEP begins the month the individual receives the notice of the Medicare entitlement
determination and continues for three additional months after the month the notice is provided. The
effective date is generally the first day of the month after the organization receives a completed
enrollment request.
In MA context, the IEP for Part D applies only to MA-PD enrollment requests. Accordingly, when an
applicant has both the ICEP and IEP for Part D available to him/her, the organization must submit the
transaction to CMS as an IEP for Part D election. Refer to Chapter 3 of the Medicare Prescription
Drug Benefit Manual for additional information regarding Part D election periods.
30.3 - Open Enrollment Period for Institutionalized Individuals (OEPI)
The OEPI is continuous for eligible individuals. For purposes of enrollment under the OEPI election
period, an institutionalized individual is defined as an individual who moves into, resides in, or moves
out of an institution, as defined in §10. The OEPI ends two months after the month the individual
moves out of the institution.
Special Note for SNP enrollment: In addition, the OEPI is available for individuals who meet
the definition of “institutionalized” to enroll in or disenroll from an MA SNP for institutionalized
individuals.
An MA eligible institutionalized individual can make an unlimited number of MA enrollment requests
during the OEPI. An MA organization is not required to accept requests to enroll into its plan during
the OEPI, but if it is open for these enrollment requests, it must accept all OEPI requests to enroll into
the plan.
Since the OEPI is continuous for eligible individuals, Original Medicare is also open continuously.
Therefore, MA organizations must accept requests for disenrollment from their MA plans during the
OEPI whether or not the MA plan is open to accept enrollment.
Please note the definition of “institution” here differs from that used in determining when an
institutionalized full-benefit dual eligible qualifies for the low-income subsidy copayment level of
zero.
30.4 - Special Election Period (SEP)
42 CFR 422.62(b)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Special election periods constitute periods outside of the usual IEP, AEP or MA OEP when an
individual may elect a plan or change his or her current plan election. As detailed below, there are
various types of SEPs, including SEPs for dual eligibles, and for individuals whose current plan
32
terminates, who change residence and who meet “exceptional conditions” as CMS may provide,
consistent with §1851(e)(4) of the Act and §422.62(b) of the MA regulations.
Depending on the nature of the particular special election period, an individual may:
• Discontinue an enrollment in an MA plan and enroll in Original Medicare
• Switch from Original Medicare to an MA plan
• Switch from one MA plan to another MA plan
Certain SEPs are limited to an enrollment or disenrollment request. If the individual disenrolls from
(or is disenrolled from) the MA plan and changes to Original Medicare, the individual may
subsequently elect a new MA plan within the SEP time period. Once the individual has elected the
new MA plan, the SEP ends for that individual even if the time frame for the SEP is still in effect. In
other words, the SEP for the individual ends when the individual elects a new MA plan or when
the SEP time frame ends, whichever comes first, unless specified otherwise within an SEP.
Note: An individual’s eligibility for an SEP provides an opportunity to make an election but does not
convey eligibility to enroll in the plan; an individual must also meet all applicable MA eligibility
criteria.
It is generally the responsibility of the organization to determine whether the individual is eligible for
an SEP. The exception to this determination requirement would be enrollment and disenrollment
requests completed or approved by CMS staff. To make this determination, the organization may need
to contact the individual directly. The plan may incorporate specific statements regarding eligibility of
an SEP with the enrollment or disenrollment request (see Exhibit 1a for optional use with enrollment
mechanisms and Exhibit 10a for optional use with disenrollment forms). However, if this information
is not provided with the request, the plan must contact the individual to determine if they are eligible
to make an election at that time. Unless stated otherwise in this guidance, the organization MUST
accept an individual’s verbal or written confirmation regarding the conditions that make him or her
eligible for the SEP. Determination of eligibility for some SEPs requires that the organization obtain
the date on which the individual’s circumstances changed (i.e. change in residence, loss of special
needs status, etc.). Organizations that obtain this information on the enrollment or disenrollment
request are not required to obtain an additional verbal or written confirmation of SEP eligibility.
For enrollment requests obtained during a face-to-face interview or telephone request, the
determination of SEP eligibility can be made at that time. For enrollment requests made using paper,
or via an electronic enrollment mechanism or the Medicare OEC (without accompanying CMS
approval), the organization is not required to contact the applicant to confirm SEP eligibility if the
enrollment request includes the applicant’s attestation of SEP eligibility.
If SEP eligibility is obtained orally (by phone or in person), the organization must document this
contact and retain this information with the enrollment or disenrollment record. If the organization
obtains this confirmation through a written notice, such notice must afford the beneficiary the option
of calling the organization and confirming this information verbally. If the organization is not able to
obtain SEP eligibility information from the applicant, the organization must deny the enrollment or
disenrollment request and provide the individual a denial notice (see Exhibit 7).
The following are examples of questions that might be used to determine eligibility for an SEP:
33
Type of SEP?
Examples of Questions
Change in Residence
Have you recently moved? If so, when? Where did
you move from?
Employer/Union Group Health
Plan (EGHP)
Do you currently have (or are leaving) coverage
offered by an employer or union? Have you recently
lost such coverage?
Disenroll from Part D to Enroll
in Creditable Coverage
Are you a member of TriCare? Do you have or want
to obtain VA benefits?
Full Dual Eligible or Other Low
Income Subsidy
Do you currently have Medicaid coverage? Does
your state pay for your Medicare premiums?
Do you receive SSI cash benefits without Medicaid?
Did you receive a letter from Medicare letting you
know that you automatically qualify for extra help?
How much do you pay for your prescriptions?
Retroactive notice of Medicare
entitlement
Have you recently received a notice telling you that
you have been approved for Medicare for a
“retroactive” date? If so, when did you receive this
notice?
PACE
For enrollment – are you currently enrolled in a
special plan called “PACE”?
CMS/State Assignment
Have you recently received a blue letter (i.e.,
Reassignment notice) from Medicare?
Did your state/plan send you a letter to let you know
they are moving you to a different plan?
Did you recently receive a yellow letter (i.e., Auto-
enrollment notice) from Medicare?
Have you recently received a green letter (i.e.,
Facilitated Enrollment notice) from Medicare?
Change in Dual/LIS Status
Have you recently gained/lost coverage under
Medicaid?
Did you recently receive a grey letter (i.e., Loss of
Deemed Status notice) from Medicare?
Did you recently receive an orange letter (i.e.,
Change in Extra Help Co-Payment notice) from
Medicare?
Did you recently receive a purple letter (i.e., Deemed
Status notice) from Medicare?
Please note that the time frame of an SEP denotes the time frame during which an individual may
make an enrollment or disenrollment request. It does not necessarily correspond to the effective date
of coverage. For example, if an SEP exists for an individual from May - July, then an MA organization
must receive an enrollment request from that individual sometime between May 1 and July 31 in order
to consider the enrollment request an SEP enrollment request. However, the type of SEP will dictate
what the effective date of coverage may be.
34
Individuals who disenroll from an MA plan to Original Medicare during an SEP may be provided
Medigap guaranteed issue rights. These rights are not afforded to those individuals who enroll into an
MA plan during an SEP. MA organizations are required to notify members of these guaranteed issue
rights when members disenroll to Original Medicare during a SEP. See §§50.1.7 and 50.2 for the
additional information regarding these notification requirements
The time frames and effective dates for SEPs are discussed in the following sections. SEPs apply to
local and regional MA plans unless otherwise specifically stated. Corresponding Part D SEPs are
provided in separate PDP Enrollment guidance.
30.4.1 - SEPs for Changes in Residence
An SEP for a change in residence exists for these scenarios:
1) individuals who are no longer eligible to be enrolled in an MA plan due to a change in
permanent residence outside of the MA plan service area;
2) individuals who were not eligible for MA because they were incarcerated and have now
been released, or;
3) individuals who will have new Medicare health or Part D plans available to them as a result
of a permanent move.
The SEP permits enrollment elections only; it begins on either the date of the permanent move or on
the date the individual provides notification of such move. Since individuals who do not permanently
reside in the plan service area are ineligible for the plan and must be disenrolled, a SEP is not needed
to effectuate an involuntary disenrollment for that reason (see §50.2.1). Individuals who move and
have new Medicare health or Part D plans available to them as a result of the move, but continue to
reside in the current plan service area, may use this SEP to enroll in any MA or Part D plan for which
they are eligible in their new place of residence. It is the individual’s responsibility to notify the MA
organization that he/she is permanently moving.
When the individual notifies the organization of a permanent move out of the plan service area, the
SEP begins either the month before the individual’s permanent move, if the individual notifies the
organization in advance, or the month the individual provides the notice of the move, if the individual
has already moved. The SEP continues for two months following the month it begins or the two
months following the month of the move, whichever is later.
If the organization learns from CMS or another source (as described in §50.2.1.3) that the individual
has been out of the service area for over six months and the organization has not been able to confirm
otherwise with the individual, the SEP starts at the beginning of the sixth month and continues through
to the end of the eighth month.
The enrollment effective date is determined by the date the MA organization receives the enrollment
request. The individual may choose an effective date of up to three months after the month in which
the MA organization receives the enrollment request. However, the effective date may not be earlier
than the date the individual moves to the new service area and the MA organization receives the
enrollment request.
35
EXAMPLE 1
A beneficiary is a member of an MA plan in Florida and intends to move to Arizona on June 18.
A SEP exists for this beneficiary from May 1 - August 31.
A. If an MA organization in Arizona receives an enrollment request from the beneficiary in
May, the beneficiary can choose an effective date of July 1, August 1, or September 1.
B. If the MA organization receives the enrollment request from the beneficiary in June (the
month of the move), the beneficiary can choose an effective date of July 1, August 1, or
September 1.
C. If the MA organization receives the enrollment request in July, the beneficiary could choose
an effective date of August 1, September 1, or October 1.
EXAMPLE 2
A beneficiary resides in Florida and is currently in Original Medicare and not enrolled in an MA
plan. The individual intends to move to Maryland on August 3. An SEP exists for this
beneficiary from July 1 through October 31.
At the time the individual makes the enrollment request into an MA plan, the individual must provide
the specific address where the individual will permanently reside upon moving into the service area, so
that the MA organization can determine that the individual meets the residency requirements for
enrollment in the plan.
Disenrollment from Previous MA Plan
Please keep in mind that a member of an MA plan who moves permanently out of the service area
must be involuntarily disenrolled from the plan, unless continuation of enrollment applies. A member
of an MA plan who is out of the service area for more than six months must be involuntarily
disenrolled from the plan.
CMS has established an SEP that allows an individual adequate time to choose a new MA plan, given
the fact that the individual will no longer be enrolled in the original MA plan after the month of the
move or after the sixth month (whichever is appropriate). Unless an individual enrolls in a new MA
plan with an effective date of the month after the move or the beginning of the seventh month (e.g., the
individual moves on June 18 and enrolls in a new plan effective July 1), he/she will be enrolled in
Original Medicare until he/she elects the new MA plan during a valid enrollment period. If the
individual had Part D coverage and lost it due to the involuntary disenrollment, s/he may be subject to
a Part D late enrollment penalty (LEP). See Chapter 4 of the Medicare Prescription Drug Manual for
more information.
30.4.2 - SEPs for Contract Violation
In the event an individual is able to demonstrate to CMS that the MA organization offering the MA
plan of which he/she is a member substantially violated a material provision of its contract under MA
in relation to the individual, or the MA organization (or its agent) materially misrepresented the plan
when marketing the plan, the individual may disenroll from the MA plan and elect Original Medicare
36
or another MA plan. The SEP will begin once CMS determines that a violation has occurred. Its length
will depend on whether the individual immediately elects a new MA plan upon disenrollment from the
original MA plan or whether the individual initially elects Original Medicare before choosing a new
MA plan.
We note that in some case-specific situations, CMS may process a retroactive disenrollment for these
types of disenrollments. If the disenrollment is not retroactive:
• A SEP exists such that an individual may elect another MA plan or Original Medicare during
the last month of enrollment in the MA organization, for an effective date of the month after
the month the new MA organization receives the enrollment request.
EXAMPLE
On January 16, CMS determines, based on a member’s allegations, that the MA organization
substantially violated a material provision of its contract. As a result, the member will be
disenrolled from the MA plan on January 31. A SEP exists for this beneficiary beginning
January 16 and lasting until the end of January. The beneficiary promptly applies for a new
MA plan, and the new MA organization receives the enrollment form on January 28 for a
February 1 effective date.
• If the individual in the above example elected Original Medicare during the last month of
enrollment in the MA organization (either by choosing Original Medicare or by not choosing
an MA plan and therefore defaulting to Original Medicare), the individual will be given an
additional 90 calendar days from the effective date of the disenrollment from the MA
organization to elect another MA plan. During this 90-day period, and until the individual
elects a new MA plan, the individual will be enrolled in Original Medicare. The individual may
choose an effective date into a new MA plan beginning any of the three months after the month
in which the MA organization receives the enrollment request. However, the effective date
may not be earlier than the date the MA organization receives the enrollment request.
EXAMPLE
On January 16, CMS determines, based on a member’s allegations that the MA organization
substantially violated a material provision of its contract. The member decides to return to
Original Medicare. As a result, the member is disenrolled from the MA plan on January 31 and
enrolled in Original Medicare with a February 1 effective date. A 90-day SEP continues to
exist for the beneficiary from February 1 through April 30. In this example, a new MA
organization then receives an enrollment request from the individual on April 15. The
beneficiary can choose an effective date of May 1, June 1, or July 1.
If the disenrollment is retroactive, CMS will provide the beneficiary with the time frame for his/her
SEP to elect another plan on a case-by-case basis. Depending on the circumstances surrounding the
contract violation, CMS may determine a retroactive enrollment into another MA plan is warranted.
30.4.3 - SEPs for Non-renewals or Terminations
In general, SEPs are established to allow members affected by non-renewals or terminations ample
time to elect a new plan. Effective dates during these SEPs are described below. CMS has the
37
discretion to modify this SEP as necessary for any non-renewals or terminations when the
circumstances are unique and warrant a modified SEP.
• Non-renewals - A SEP exists for members of MA plans that will be affected by plan or contract
non-renewals and plan service area reductions that are effective January 1 of the contract year. In
order to provide sufficient time for members to evaluate their options, the SEP begins December
8 and ends on the last day in February of the following year.
Enrollment requests received from December 8 through December 31 will have an effective date
of January 1. Enrollment requests received in January will have an effective date of February 1.
Enrollment requests received in February will have an effective date of March 1.
• MA organization Termination of Contract and Terminations/Contract Modifications by
Mutual Consent - A SEP exists for members of plans who will be affected by a termination of
contract by the MA organization or a modification or termination of the contract by mutual
consent (42 CFR §§422.512 and 422.508(a)(1)). The SEP begins two months before the
proposed termination effective date, and ends one month after the month in which the
termination occurs.
Please note that if an individual does not elect an MA plan before the termination effective date,
he/she will be defaulted to Original Medicare on the effective date of the termination. However,
the SEP will still be in effect for one month after the effective date of the termination should the
individual wish to subsequently elect an MA plan (for a current, not retroactive, effective date).
Beneficiaries affected by these types of terminations may request an effective date of the month
after notice is given, or up to two months after the effective date of the termination. However, the
effective date may not be earlier than the date the new MA organization receives the enrollment
request.
EXAMPLE
If an MA organization contract terminates for cause on April 30, an SEP lasts from March 1
through May 31. In this scenario, a beneficiary could choose an effective date of April 1, May 1,
or June 1; however, the effective date may not be earlier than the date the new MA organization
receives the enrollment request.
• CMS Termination of MA organization Contract - A SEP exists for members of plans that will
be affected by MA organization contract terminations by CMS (42 CFR 422.510). The SEP
begins 1 month before the termination effective date and ends 2 months after the effective date of
the termination.
Please note that if an individual does not elect an MA plan before the termination effective date,
he/she will be defaulted to Original Medicare on the effective date of the termination. However,
the SEP will still be in effect for two months after the effective date of the termination should the
individual wish to subsequently elect an MA plan (for a current, not retroactive, effective date).
Beneficiaries affected by these types of terminations may select an effective date of up to three
months after the month of termination. However, the effective date may not be earlier than the
date the new MA organization receives the enrollment request.
38
EXAMPLE
If CMS terminates an MA organization contract effective June 30, an SEP lasts from June 1
through August 31. In this scenario, a beneficiary could choose an effective date of July 1,
August 1, or September 1; however, the effective date may not be earlier than the date the new
MA organization receives the enrollment request.
• Immediate Terminations By CMS - CMS will establish the SEP during the termination process
for immediate terminations by CMS (42 CFR 422.510(b)(2)), where CMS provides notice of
termination to an MA plan’s members and the termination may be mid-month.
Note: Approved plan consolidations are neither terminations nor non-renewals. Thus individuals
affected by plan consolidations are not eligible for the SEP for non-renewals or terminations. Please
see the annual CMS Call Letter and other CMS end-of-year guidance for more information about
approved plan consolidations.
30.4.4 - SEPs for Exceptional Conditions
42 CFR 422.62(b)(4)
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
CMS has the legal authority to establish SEPs when an individual or group of individuals meets
exceptional conditions specified by CMS, including on a case-by-case basis. The SEPs CMS has
established include:
1. SEP EGHP (Employer/Union Group Health Plan)
42 CFR 422.62(b)(4)
An SEP exists for individuals making MA enrollment requests into or out of employer sponsored MA
plans, for individuals to disenroll from an MA plan to take employer sponsored coverage of any kind,
and for individuals disenrolling from employer sponsored coverage (including COBRA coverage) to
elect an MA plan. The SEP EGHP may be used when the EGHP allows the individual to make
changes in their health coverage choices, such as during the employer’s or union’s “open season,” or
at other times the employer or union allows. This SEP is available to individuals who have (or are
enrolling in) an employer or union sponsored plan and ends 2 months after the month the employer or
union coverage ends.
The individual may choose an effective date of up to three months after the month in which the
individual completed an enrollment or disenrollment request; however, the effective date may not be
earlier than the first of the month following the month in which the request was made. The effective
date also may not be earlier than the first day of the individual’s entitlement to both Medicare Part A
and Part B.
NOTE: If necessary due to the employer’s or union’s delay in forwarding the completed
enrollment request to the MA organization, the MA organization may process the enrollment
request with a retroactive effective date, as outlined in §60.6. Keep in mind that all MA eligible
individuals, including those in EGHPs, may elect MA plans during the AEP and ICEP and during
any other SEP. The SEP EGHP does not eliminate the right of these individuals to make
enrollment requests during these election periods.
39
Refer to §30.6 for additional information for situations in which an individual is determined eligible
for more than one election period, one of which includes the SEP EGHP.
2. SEP for Individuals Who Disenroll in Connection with a CMS Sanction
42 CFR 422.62(b)(5)
On a case by case basis, CMS will establish an SEP for individuals enrolled in an MA plan offered by
an MA organization that has been sanctioned by CMS who elect to disenroll in connection with the
matter that gave rise to that sanction. The start/length of the SEP, as well as the effective date, is
dependent upon the situation. The SEP starts with the imposition of the sanction and ends when the
sanction ends or when the individual makes an election, whichever occurs first.
CMS may require the MA organization to notify current enrollees that if the enrollees believe they are
affected by the matter(s) that gave rise to the sanction, the enrollees are eligible for a SEP to elect
another MA plan or disenroll to original Medicare and enroll in a PDP.
3. SEP for Individuals Enrolled in Cost Plans that are Non-renewing their Contracts
42 CFR 422.62(b)(6)
An SEP will be available to Medicare beneficiaries who are enrolled in an HMO or CMP under a
§1876 cost contract that will no longer be offered in the area in which the beneficiary resides.
Beneficiaries electing to enroll in an MA plan via this SEP must meet MA eligibility requirements.
This SEP begins December 8 of the current contract year and ends on the last day of February of the
following year.
Enrollment requests received from December 8 through December 31 will have an effective date of
January 1. Enrollment requests received in January will have an effective date of February 1.
Enrollment requests received in February will have an effective date of March 1.
4. SEP for Individuals in the Program of All-inclusive Care for the Elderly (PACE)
42 CFR 422.62(b)(7)
Individuals may disenroll from an MA plan at any time in order to enroll in PACE. In addition,
individuals who disenroll from PACE have an SEP to elect an MA plan. The SEP ends 2 months after
the effective date of PACE disenrollment.
5. SEP for Dual-eligible Individuals and Other LIS-Eligible Individuals–
42 CFR 423.38(c)(4)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
There is an SEP for individuals who have Medicare Part A and Part B and receive any type of
assistance from the Title XIX (Medicaid) program. This includes both “full benefit” dual eligible
individuals as well as individuals often referred to as “partial duals” who receive cost sharing
assistance under Medicaid (e.g. QMB-only, SLMB-only, etc.) and individuals who qualify for LIS
(but who do not receive Medicaid benefits).
40
This SEP begins the month the individual becomes dually-eligible and exists as long as he or she
receives Medicaid benefits; however there are limits in how often it can be used. This SEP allows an
individual to enroll in, or disenroll from, an MA plan once per calendar quarter during the first nine
months of the year. This SEP can be used once during each of the following time periods:
• January – March,
• April – June, and
• July – September.
It may not be used in the 4
th
quarter of the year (October – December).
The SEP is considered “used” based on the month in which the individual makes the election (i.e.,
application date of the enrollment request). If the plan receives an election in March (which would be
effective April 1
st
), this counts as “using” the SEP for the 1
st
quarter, not the 2
nd
quarter.
The effective date of an enrollment request made using this SEP is the first of the month following
receipt of an enrollment request.
NOTES:
• As described in § 40.1.5, the effective date for auto-enrollments of full-benefit dual-eligible
individuals may be retroactive.
• Organizations need to check for prior uses of the SEP via the BEQ or MARx UI to determine
eligibility.
• CMS will reject enrollment transactions for individuals who have already used this SEP in the
calendar quarter.
Use of this SEP is separate from, and in addition to, the SEPs outlined in #12 in this section (SEP for
Individuals who Lose or Have a Change in their Dual or LIS-Eligible Status) and § 30.4.7 (SEP for
Individuals Who Have Been Enrolled into a Plan by CMS or the State). If a dual or other-LIS eligible
beneficiary is making an election and is also eligible for another SEP, the organization should use the
other SEP instead of this SEP.
Limitation for “At-Risk” and “Potential At-Risk” Beneficiaries:
Once an individual is identified by the MA-PD organization as a “potential at-risk” or “at-risk”
beneficiary and the plan sponsor has sent written notice to the individual, he or she cannot use this
SEP to change plans while this designation is in place. The notice to the individual explains that this
SEP is no longer available. Additional information on drug management programs is available at
www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/RxUtilization.html
Duration of Limitation – This limitation starts as of the date on the initial notice provided to the
“potential at-risk” beneficiary. The chart below outlines when the limitation ends:
Situation
SEP limitation ends
Plan decides not to identify the “potential at-
risk” beneficiary as an “at-risk” beneficiary
60 days from the date on the initial notice, or the
date the beneficiary receives notice of the plan’s
decision, if earlier.
The “potential at-risk” or “at-risk” beneficiary
identification is subsequently removed by the
The date that the designation is removed by the
plan or upon effectuation of a favorable appeal
41
Situation
SEP limitation ends
plan or through beneficiary’s favorable appeal of
an “at-risk” determination
The plan determines the beneficiary is “at-risk”
12 months from the date the individual is
determined to be “at-risk”
The plan extends the “at-risk” designation
beyond the initial 12 months
24 months from the date the individual is
determined to be “at-risk”
NOTE: This is the maximum consecutive time
the SEP limitation can be imposed for each “at-
risk” limitation a sponsor implements.
The limitation ends based on whichever situation occurs first. If a plan sponsor removes the
individual’s status as an “at-risk” beneficiary or the designation expires, the plan may subsequently
determine that the individual is “potentially at-risk” again, in accordance with the requirements for
drug management programs in 42 CFR 423.153(f)(1). Consequently, the SEP would, once again, not
be available to the individual based on the date the plan sends the new notification. For more
information on “potentially at-risk” or “at-risk” designations, see
www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/RxUtilization.html
.
NOTE: Organizations need to check for this designation via the BEQ or MARx UI to determine
eligibility. The enrollment limitation for a “potential at-risk” or an “at-risk” individual will not apply
to other Part D enrollment periods, including the AEP or other SEPs.
6. SEP for Individuals Who Terminated a Medigap Policy When They Enrolled For the First
Time in an MA Plan, and Who Are Still in a “Trial Period”
42 CFR 422.62(b)(8)
For Medicare beneficiaries who terminated a Medigap policy when they enrolled for the first time in
an MA plan, §1882(s)(3)(B)(v) of the Act provides a guaranteed right to purchase another Medigap
policy if they disenroll from the MA plan while they are still in a “trial period.” In most cases, a trial
period lasts for 12 months after a person enrolls in an MA plan for the first time.
This SEP is for individuals who are eligible for “guaranteed issue” of a Medigap policy under
§1882(s)(3)(B)(v) of the Act upon disenrollment from the MA plan in which they are enrolled. This
SEP allows a qualified individual to make a one-time election to disenroll from their first MA plan to
join Original Medicare at any time of the year. The SEP begins upon enrollment in the MA plan and
ends after 12 months of enrollment or when the beneficiary disenrolls from the MA plan, whichever is
earlier.
7. SEP for Individuals with ESRD Whose Entitlement Determination Made Retroactively
42 CFR 422.62(b)(9)
If a Medicare entitlement determination is made for a retroactive effective date, an individual has not
been provided the opportunity to elect an MA plan during his/her ICEP. Therefore, these individuals
will be allowed to elect an MA plan for a prospective effective date.
This would also be allowed in cases when there is an administrative delay and the entitlement
determination is not made timely. For example, an individual who performs self-dialysis will have
42
his/her entitlement date adjusted to begin at the time of dialysis, rather than the customary 3-month
period AFTER dialysis begins.
The SEP begins the month the individual receives the notice of the retroactive Medicare entitlement
determination and continues for 2 additional calendar months after the month the notice is received.
The enrollment effective date is the first day of the month after the MA plan receives the enrollment
request. This SEP is not available after December 31, 2020.
8. SEP for Individuals Whose Medicare Entitlement Determination Made Retroactively
42 CFR 422.62(b)(10)
If a Medicare entitlement determination is made for a retroactive effective date, an individual has not
been provided the opportunity to elect an MA plan during his/her ICEP. Therefore, these individuals
will be allowed to elect an MA plan for a prospective effective date. This would also be allowed in
cases when there is an administrative delay and the entitlement determination is not made timely by
SSA and/or received by the individual in a timely manner.
The SEP begins the month the individual receives the notice of the retroactive Medicare entitlement
determination and continues for two additional calendar months after the month the notice is received.
The effective date is the first day of the month after the MA plan receives the enrollment request.
9. MA SEPs to Coordinate With Part D Enrollment Periods – Individuals eligible for an
enrollment period under the guidance for Part D enrollment and disenrollment may use that SEP to
make an election into or out of an MA-PD plan (as applicable). Most Part D SEPs are duplicated in the
MA program as described above; however, those that are not described elsewhere are provided here:
A. Involuntary loss of creditable coverage, including a reduction in the level of coverage so that it
is no longer creditable, not including any such loss or reduction due to a failure to pay
premiums. The SEP permits enrollment into an MA-PD and begins when the individual is
advised of the loss of (or reduction in) creditable coverage. The SEP ends two calendar
months after either the loss (or reduction) occurs or the individual received notice, whichever is
later. The effective date of this SEP is the first of the month after the election is made or, at the
beneficiary’s request, may be up to 3 months prospective. (42 CFR 422.62(b)(19))
B. Individuals who are not adequately informed of a loss of creditable coverage, or that they never
had creditable coverage, have an SEP that permits one enrollment in, or disenrollment from, an
MA-PD plan. CMS determines eligibility for this on a case-by-case basis, based on its
determination that an entity offering prescription drug coverage failed to provide accurate and
timely disclosure of the loss of creditable prescription drug coverage or whether the
prescription drug coverage offered is creditable. This SEP begins the month of CMS approval
of this SEP and continues for two additional calendar months following this approval. (42 CFR
422.62(b)(20))
C. Individuals whose enrollment or non-enrollment in a Part D plan is erroneous due to an action,
inaction or error by a Federal Employee. The SEP permits disenrollment and/or enrollment in a
Part D plan on a case-by-case basis. Requests for this SEP must be developed and presented to
the CMS Regional Office serving the MA-PD plan for which the SEP will apply. This SEP
begins the month of CMS approval of this SEP and continues for two additional months
following this approval. (42 CFR 422.62(b)(21))
43
D. An individual eligible for an additional Part D IEP, such as an individual currently entitled to
Medicare due to a disability and who is attaining age 65, has an MA SEP to coordinate with the
additional Part D IEP. The SEP may be used to disenroll from an MA-only or MA-PD plan to
Original Medicare, or to enroll in an MA-only plan (regardless of whether the individual uses
the Part D IEP to enroll in a PDP). The SEP begins and ends concurrently with the
additional Part D IEP. (42 CFR 422.62(b)(22))
For more information about PDP enrollment and disenrollment, please refer to the CMS guidance for
PDPs.
10. SEP for Individuals Who Lose Special Needs Status
42 CFR 422.62(b)(11)
CMS will provide an SEP for individuals enrolled in a SNP who are no longer eligible for the SNP
because they no longer meet the specific special needs status. This SEP begins the month the
individual’s special needs status changes and ends when he or she makes an enrollment request or
three calendar months after the effective date of involuntary disenrollment from the SNP, whichever is
earlier.
11. SEP for Individuals Who Belong to a Qualified SPAP or Who Lose SPAP Eligibility
42 CFR 422.62(b)(12)
Individuals who belong to a qualified State Pharmaceutical Assistance Program (SPAP) are eligible
for an SEP to request enrollment in an MA-PD plan at any time through the end of each calendar year
(i.e. once per year). SPAP members may use this SEP to enroll in a Part D plan outside of existing
enrollment opportunities, allowing them, for example, to join an MA-PD plan upon becoming a
member of an SPAP or to switch to another MA-PD plan. In summary, a beneficiary may use this SEP
to switch from an MA-PD plan to another MA-PD plan, from Original Medicare without a PDP to an
MA-PD plan, from a PDP to another PDP or MA-PD plan or from an MA-only plan (no prescription
drug coverage) to an MA-PD plan. This SEP is available while the individual is enrolled in the SPAP
and, upon loss of eligibility for SPAP benefits, for an additional 2 calendar months after either the
month of the loss of eligibility or notification of the loss, whichever is later.
12. SEP for Individuals who Gain, Lose, or Have a Change in their Dual or LIS-Eligible Status–
42 CFR 423.38(c)(9)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
An SEP is provided for individuals who receive “Extra Help.” It includes those who:
• Become eligible for any type of assistance from the Title XIX program (including “partial
duals” who receive cost sharing assistance under Medicaid) and individuals who qualify for
LIS (but who do not receive Medicaid benefits);
• Lose eligibility for any type of assistance; and
• Have a change in the level of assistance they receive (e.g., stop receiving Medicaid benefits,
but still qualify for LIS, those who have a change in cost sharing, or become eligible for
additional Medicaid benefits [e.g., when an individual newly qualifies as needing nursing
home level of care and thus becomes eligible for certain Medicaid long term supports and
services, or becomes eligible for full Medicaid after having previously been eligible for
Medicaid coverage of Medicare premiums or cost-sharing]).
44
The SEP allows the individual one opportunity to make an election within three months of any of the
changes noted above, or notification of such a change, whichever is later. The effective date for
enrollments under this SEP is the first day of the month following receipt of the enrollment request by
the plan.
NOTE: Use of this SEP does not count towards the once per calendar quarter limitation outlined in
SEP #5 in this section.
13. SEP for Enrollment Into a Chronic Care SNP and for Individuals Found Ineligible for a
Chronic Care SNP
42 CFR 422.62(b)(13)
CMS will provide an SEP for those individuals with severe or disabling chronic conditions to enroll in
a SNP designed to serve individuals with those conditions. This SEP is available while the individual
has the qualifying condition(s); it ends upon enrollment in the chronic care SNP. Once the SEP ends,
that individual may make enrollment changes only during applicable MA election periods. In addition,
individuals enrolled in a Chronic Care SNP who have a severe/disabling chronic condition which is
not a focus of their current SNP are eligible for this SEP. Such individuals have an opportunity to
enroll in a Chronic Care SNP that focuses on this other condition. Eligibility for this SEP ends at the
time the individual enrolls in the new SNP.
Individuals who are found after enrollment not to have the qualifying condition necessary to enroll in a
Chronic Care SNP will have an SEP to enroll in a different MA-PD plan or an MA-only plan with
accompanying Part D coverage. This would normally occur when the required post enrollment
verification with a provider did not confirm the information provided on the pre-enrollment
assessment tool. This SEP begins when the plan notifies the individual of the lack of eligibility and
extends through the end of that month as well as the following two calendar months. The SEP ends
when the individual makes an enrollment election or on the last day of the second of the two calendar
months following notification. Any enrollments made during this election period are for prospective
effective dates.
14. SEP for Disenrollment from Part D to Enroll in or Maintain Other Creditable Coverage
42 CFR 422.62(b)(14)
Individuals may disenroll from an MA-PD plan) to enroll in or maintain other creditable drug
coverage (such as TriCare or VA coverage). The effective date of disenrollment is the first day of the
month following the month a disenrollment request is received by the MA organization. Additionally,
individuals enrolled in an MA-PD plan who have or are enrolling in other creditable coverage may use
this SEP to disenroll from the MA-PD plan by enrolling in an MA-only plan.
15. SEP to Enroll in an MA Plan, PDP or Cost Plan With a Plan Performance Rating of Five (5)
Stars
42 CFR 422.62(b)(15)
An eligible individual may enroll in an MA plan offered by an MA organization with a Star Rating of
5 Stars during the year in which that plan has the 5-star overall performance rating, provided the
enrollee meets the other requirements to enroll in that plan (e.g., living within the service area).
45
Individuals may use the 5-Star SEP to disenroll from a Medicare Advantage plan by enrolling in a 5-
Star cost plan that is open for enrollment.
As overall ratings are assigned for the plan contract year (January through December), possible
enrollment effective dates are the first of the month from January 1 to December 1 during the year for
which the plan has been assigned an overall performance rating of 5 stars. An individual may use this
SEP only one time from December 8 through November 30 of the following year in which the
organization has been granted a 5-star overall rating. The enrollment effective date is the first of the
month following the month in which the plan receives the enrollment request.
EXAMPLE: Plan X has an overall rating of 4.5 stars in 2020 and 5 stars for 2021. An
individual could use this SEP to request enrollment in Plan X beginning December 8, 2020 for
an effective date of January 1, 2021. An individual could not use the SEP to enroll in Plan X for
an effective date on or before December 1, 2020, as the enrollment effective dates available
during that period are prior to the calendar year for which Plan X has been assigned a 5-star
overall rating.
EXAMPLE: Plan Y has an overall rating of 5 stars for 2020 but has lost that 5-star rating for
2021. A beneficiary could use this SEP to request enrollment in Plan Y for the first of the
following month until November 30, 2020, with the last possible effective date available being
December 1, 2020. The beneficiary could not use the SEP to enroll in Plan Y on or after
December 1, 2020, as the enrollment effective dates available during that period are after the
calendar year for which Plan Y has been assigned a 5-star overall rating.
An individual using this SEP can enroll in an MA-only or an MA-PD plan, even if coming from
Original Medicare (with or without concurrent enrollment in a PDP). Individuals enrolled in a plan
with a 5-star overall rating may also switch to a different plan with a 5-star overall rating. An
individual in an MA-only or MA-PD coordinated care plan who switches to a PDP with a 5-star
overall rating will lose MA coverage and will revert to Original Medicare for basic medical coverage.
Regardless of whether the individual has Part D coverage prior to use of this SEP, any individual who
enrolls in a 5-star MA Private Fee-for-Service plan without prescription drug coverage or a 5-star cost
plan is eligible for a coordinating Part D SEP to enroll in a PDP. (See Chapter 3, Section 30.3.8 #8,
letter H, of the Medicare Prescription Drug Benefit Manual for more information.)
Note that use of this SEP does not guarantee Part D coverage. If an individual in either an MA-PD
plan or a PDP chooses to enroll in an MA-only coordinated care plan with a 5-star overall rating, that
individual would lose Part D coverage and must wait for a subsequent enrollment period to obtain Part
D coverage under the normal enrollment rules. Late enrollment penalties might also apply.
Individuals may use the 5-Star SEP to disenroll from an MA plan by enrolling in a 5-Star cost plan
that is open for enrollment.
EXAMPLE: A cost plan has an overall rating of 5 stars for 2020 and is open for enrollment. An
individual enrolled in a MA plan uses this SEP to enroll in the cost plan. The cost plan submits the
enrollment transaction to MARx using the “R” election type code, and the MA plan accepts and
processes the subsequent disenrollment per the Daily Transaction Reply Report (DTRR).
46
16. SEP for Non-U.S. Citizens who become Lawfully Present
42 CFR 422.62(b)(16)
CMS will provide an SEP for non-U.S. citizens who become lawfully present in the United States.
The individual may use this SEP to request enrollment in any MA plan for which he or she is eligible,
including an MA-PD. This SEP begins the month the individual attains lawful presence starts and
ends the earlier of when the individual makes an enrollment request or two (2) full calendar months
after the month it begins.
17. SEP for Providing Individuals who Requested Materials in Accessible Formats Equal Time
to Make Enrollment Decisions
42 CFR 422.62(b)(17)
(Rev. 2, Issued: August , 2020; Effective/Implementation: 01-01-2021)
As outlined in Section 504 of the Rehabilitation Act of 1973 (Section 504), organizations are required
to comply with its requirements, and provide materials in accessible formats to its members. This
generally includes formats such as Braille, Data, and Audio files, or other formats accepted by the
member in place of, or in addition to, the original print material.
A SEP is available to an individual who was adversely affected by having requested, but not received,
required notices or information in an accessible format within the same timeframe that the MA
organization or CMS provided the same information to individuals who did not request an accessible
format. This limited SEP ensures that beneficiaries who have requested information in accessible
formats are not disadvantaged by any additional time necessary to fulfill their request, including
missing an election period deadline.
The SEP begins at the end of the election period during which the beneficiary was seeking to make an
election. The length of the SEP is at least as long as the time it took for the information to be provided
to the individual in an accessible format. Organizations may determine eligibility for this SEP when
the criterion is met, ensuring adequate documentation of the situation, including records indicating the
amount of time taken to provide accessible versions of the requested materials and the amount of time
it takes for the same information to be provided to an individual who does not request an accessible
format. Individuals seeking assistance for this SEP may also contact 1-800-MEDICARE.
18. SEP for Government Entity-Declared Disaster or Other Emergency
42 CFR 422.62(b)(18)
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
A SEP exists for individuals affected by a disaster or other emergency declared by a Federal, state or
local government entity who were unable to, and did not make an election during another valid
election period. This includes both enrollment and disenrollment elections. Individuals are eligible for
this SEP if they:
• Reside, or resided at the start of the SEP eligibility period described in this guidance, in an area
for which a federal, state or local government entity has declared a disaster or other
emergency or they do not reside in an affected area but rely on help making healthcare
decisions from one or more individuals who reside in an affected area; and
• Were eligible for another election period at the time of the SEP eligibility period; and
47
• Did not make an election during that other valid election period due to the disaster or other
emergency.
The SEP starts as of the date the declaration is made, the incident start date or, if different, the start
date identified in the declaration, whichever is earlier. The SEP ends 2 full calendar months following
the end date identified in the declaration or, if different, the date the end of the incident is announced,
whichever is later.
19. SEP for Individuals Enrolled in a Plan Placed in Receivership
42 CFR 422.62(b)(24)
A SEP exists for individuals enrolled in a plan offered by an MA organization that has been placed
into receivership by a state or territorial regulatory authority.
The SEP begins the month the receivership is effective and continues until it is no longer in effect or
until the enrollee makes an election, whichever occurs first. When instructed by CMS, the MA plan
that has been placed under receivership must notify its enrollees, in the form and manner directed by
CMS,
of the enrollees’ eligibility for this SEP and how to use the SEP.
20. SEP for Individuals Enrolled in a Plan That Has Been Identified by CMS as a Consistent Poor
Performer
42 CFR 422.62(b)(25)
A SEP exists for individuals enrolled in a plan that has been identified with the low performing icon in
accordance with 42 CFR 422.166(h)(1)(ii). This SEP exists while the individual is enrolled in the low
performing MA plan.
21. SEP for Other Exceptional Circumstances
422.62(b)(26)
CMS will establish a SEP, on a case by case basis, for individuals whom CMS determines have
experienced exceptional circumstances related to enrollments into or disenrollments from an MA plan
that are not otherwise captured in regulation. Consistent with current practice, CMS will consider
granting an enrollment or disenrollment opportunity in situations such as the following:
• Circumstances beyond the beneficiary’s control that prevented him or her from submitting a
timely request to enroll or disenroll from a plan during a valid election period. This is
inclusive of, but not limited to, a serious medical emergency of the beneficiary or his or her
authorized representative during an entire election period, a change in hospice status, or
mailed enrollment or disenrollment requests returned as undeliverable on or after the last day
of an enrollment period.
• Situations in which a beneficiary provides a verbal or written allegation that his or her
enrollment in a MA or Part D plan was based upon misleading or incorrect information
provided by a plan representative or State Health Insurance Assistance Program (SHIP)
counselor, including situations where a beneficiary states that he or she was enrolled into a
plan without his or her knowledge or consent, and requests cancellation of the enrollment or
disenrollment from the plan.
48
• A SEP may be warranted to ensure beneficiary access to services and where without the
approval of an enrollment exception, there could be adverse health consequences for the
beneficiary. This is inclusive of, but not limited to, maintaining continuity of care for a chronic
condition and preventing an interruption in treatment.
CMS will review supporting details and documentation to determine eligibility for the SEP for
exceptional circumstances. CMS’s review can be in response to an individual beneficiary’s request for
an exception to the current enrollment rules, as well as CMS’ determination that an exception is
warranted for a group of beneficiaries.
The SEP would take effect once CMS makes its determination and the enrollee has been notified. The
effective date for an enrollment or disenrollment election using an approved enrollment exception
would be based on the beneficiary’s circumstances and may be either prospective or retroactive.
30.4.5 - SEPs for Beneficiaries Age 65 (SEP65)
MA eligible individuals who elect an MA plan (other than an MSA plan) during the initial enrollment
period (IEP) for Part B surrounding their 65th birthday have an SEP. This “SEP65” allows the
individual to disenroll from this MA plan and elect the Original Medicare plan any time during the 12-
month period that begins on the effective date of coverage in the MA plan.
The IEP for Part B is established by Medicare and begins 3 months before and ends 3 months after the
month of the individual’s 65th birthday. Individuals entitled to Medicare prior to age 65 are not
eligible for the SEP65.
30.4.6 – SEP for Significant Change in Provider Network
42 CFR 422.62(b)(23)
(Rev. 1, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
CMS will establish a SEP, on a case by case basis, for situations in which CMS determines that
changes to an MA plan’s provider network are significant based on the affect, or potential to affect,
current plan enrollees who are assigned to, are currently receiving care from, or who have received
care within the past 3 months from a provider or facility being terminated from the provider network.
The SEP can be used only once per significant change in provider network. It begins the month
enrollees are notified of eligibility for the SEP and continues for an additional two calendar months
thereafter.
30.4.7 – SEP for CMS and State-Initiated Enrollments
42 CFR 422.60(g)(5) and 423.38(c)(10)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Individuals who are enrolled into a plan by CMS or a State (i.e., through passive enrollment, auto-
enrollment, facilitated enrollment, and reassignment) have an SEP to disenroll from their new plan or
enroll into a different plan. The SEP permits a onetime election within three months of the effective
date of the assignment, or notification of the assignment, whichever is later. It allows the individual to
make an election before the enrollment is effective in the receiving plan or after the coverage in the

49
receiving plan starts. This SEP must be used within three months of the start of coverage in the
receiving plan. In the case where the notice is sent after the coverage in the receiving plan starts, the
SEP ends three months after the date of the notice. This SEP is provided so that an individual may
exercise any mandatory “opt-out” right provided to the enrollee as part of the CMS or State-initiated
enrollment.
The effective date for enrollments under this SEP is the first day of the month following receipt of the
enrollment request by the plan.
Individuals passively enrolled due to a plan’s non-renewal or termination (outlined in § 20.4.2) may
also be eligible for an SEP as outlined in § 30.4.3 of this Chapter.
30.5 – Medicare Advantage Open Enrollment Period (MA OEP)
42 CFR 422.62(a)(3)
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
During the MA OEP, MA plan enrollees may enroll in another MA plan or disenroll from their MA
plan and return to Original Medicare. Individuals may make only one election during the MA OEP.
This chart outlines who can use the MA OEP and when:
Who can use the MA OEP:
MA OEP occurs:
Individuals enrolled in an MA plan
January 1 – March 31
New Medicare beneficiaries who are enrolled in
an MA plan during their ICEP
The month of entitlement to Part A
and Part B – the last day of the 3rd
month of entitlement
Individuals enrolled in an MA plan may add or drop Part D coverage during the MA OEP. Individuals
enrolled in either MA-PD or MA-only plans can switch to:
• MA-PD
• MA-only
• Original Medicare (with or without a stand-alone Part D plan)
The effective date for an MA OEP election is the first of the month following receipt of the enrollment
request.
NOTE: The MA OEP does not provide an opportunity for an individual enrolled in Original Medicare
to join a MA plan. It also does not allow for Part D changes for individuals enrolled in Original
Medicare, including those enrolled in stand-alone Part D plans. The MA OEP is not available for those
enrolled in Medicare Savings Accounts or other Medicare health plan types (such as cost plans or
PACE).
30.6 - Effective Date of Coverage
42 CFR 422.68(c)
(Rev. 2, Issued: August 12, 2021; Effective/Implementation: 01-01-2021)
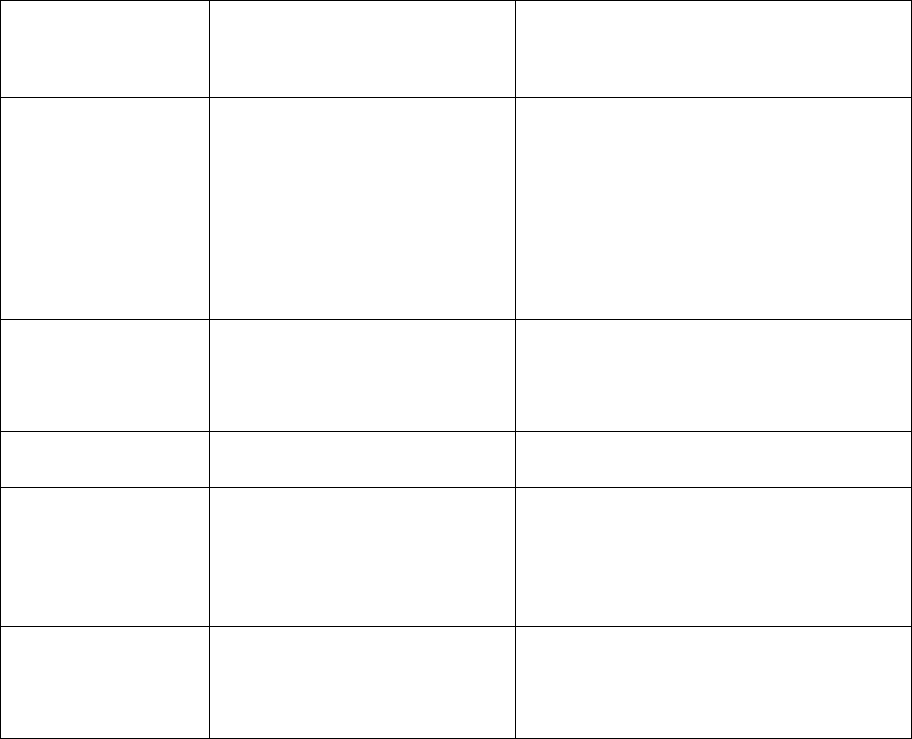
50
With the exception of some SEPs and when election periods overlap, generally beneficiaries may not
request their enrollment effective date. Furthermore, except for EGHP enrollment requests, the
effective date is generally not prior to the receipt of an enrollment request by the MA organization. An
enrollment cannot be effective prior to the date the beneficiary or his/her legal representative
completed the enrollment request. The effective date may not be earlier than the first day of the
individual’s entitlement to both Medicare Part A and Part B. §40.2 includes procedures for handling
situations when a beneficiary chooses an unallowable enrollment effective date.
To determine the proper effective date, the MA organization must determine which election period
applies to each individual before the enrollment may be transmitted to CMS. The election period may
be determined by reviewing information such as the individual’s date of birth, Medicare card, a letter
from SSA, or by the date the enrollment request is received by the MA organization.
Once the election period is identified by the MA organization, the MA organization must determine
the effective date. Refer to §60.8 to determine the effective date for a continuation of enrollment. In
certain circumstances, EGHP enrollments may be retroactive (refer to §60.6 for more information on
EGHP retroactive effective dates).
Effective dates are as follows:
Election Period
Effective Date of
Coverage
Do MA organizations have to
accept enrollment requests in
this election period?
Initial Coverage
Election Period
and Initial
Enrollment Period
for Part D
First day of the month of
entitlement to Medicare Part
A and Part B – or-
The first of the month
following the month the
enrollment request was made
if after entitlement has
occurred.
Yes – unless capacity limit applies
(see §30.9 for capacity limit
information). IEP for Part D is
applicable only to MA-PD enrollment
requests.
Open Enrollment
Period for
Institutionalized
Individuals (OEPI)
First day of the month after
the month the MA
organization receives an
enrollment request
No - the MA organization can choose
to be “open” or “closed” for
enrollments during this period.
Annual Election
Period
January 1 of the following
year
Yes – unless capacity limit applies
Special Election
Period
First day of the month after
the month the MA
organization receives an
enrollment request, unless
otherwise noted.
Yes – unless capacity limit applies
Medicare
Advantage Open
Enrollment Period
(MA OEP)
First day of the month after
the month the MA
organization receives an
enrollment request
No - the MA organization can choose
to be “open” or “closed” for
enrollments during this period.
51
It is possible for an individual to make an enrollment request when s/he is eligible for more than one
election period, resulting in more than one possible effective date. Therefore, if an organization
receives an enrollment request and determines the applicant is eligible for more than one election
period, the organization must allow the individual to choose the enrollment effective date (see
exception in the next paragraph regarding the ICEP). To accomplish this, the organization must
attempt to contact the individual, and must document its attempt(s), to determine the individual’s
preferred effective date. Note: This requirement does not apply to beneficiary requests for enrollment
into an employer/union sponsored plan using the group enrollment mechanism, as these may be
submitted to CMS with the EGHP SEP election type code.
If one of the election periods for which the individual is eligible is the ICEP, the individual may not
choose an effective date any earlier than the month of entitlement to Medicare Part A and Part B.
EXAMPLE
If an individual will be entitled to Medicare Part A and Part B in February his ICEP is November
through May. If an MA organization receives an enrollment request from that individual during
the AEP, the individual may NOT choose a January 1 effective date and must be given a February
1 effective date for the ICEP because January 1st is earlier than the month of entitlement to
Medicare Part A and Part B.
If an individual is eligible for more than one election period but does not indicate a preferred effective
date or the organization is unable to contact the individual, the organization must assign an effective
date using the following ranking of election periods. The election period with the highest rank
generally determines the effective date of enrollment (refer to §30.7 for procedures to determine the
effective date of voluntary disenrollment).
Individuals eligible for the SEP EGHP and one or more other election periods who make an election
via the employer or union election process will be assigned an effective date according to the SEP
EGHP, unless the individual requests a different effective date that is allowed by one of the other
elections periods for which s/he is eligible.
Ranking of Election Periods: (1 = Highest, 5 = Lowest)
1. ICEP/IEP-D
2. MA OEP
3. SEP
4. AEP
5. OEPI
30.6.1 - Effective Date of Auto- and Facilitated Enrollments
The effective dates for auto-enrollment and facilitated enrollment are described in §40.1.5 of this
chapter.
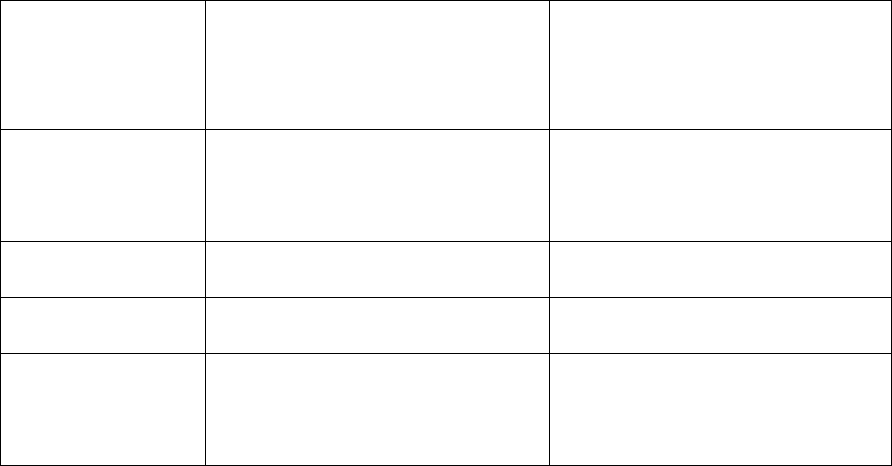
52
30.7 - Effective Date of Voluntary Disenrollment
42 CFR 422.68
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
With the exception of some SEPs and when election periods overlap, generally beneficiaries may not
select their effective date of disenrollment. §50.1 includes procedures for handling situations when a
beneficiary chooses a disenrollment effective date that is not allowable based on the requirements
outlined in this section.
When a member disenrolls through the MA organization or 1-800-MEDICARE, the disenrollment will
return the member to Original Medicare. If a member elects a new MA plan while still a member of a
different plan, he/she will automatically be disenrolled from the old plan and enrolled in the new plan
by CMS systems with no duplication or delay in coverage.
As with enrollments, it is possible for a member to make a disenrollment request when more than one
election period applies. Therefore, in order to determine the proper effective date, the MA organization
must determine which election period applies to each member before the disenrollment may be
transmitted to CMS.
If an MA organization receives a disenrollment request when more than one election period applies,
the MA organization must allow the member to choose the effective date of disenrollment. If the
member does not make a choice of effective date, then the MA organization must give the effective
date that results in the earliest disenrollment.
Effective dates for voluntary disenrollment are as follows (refer to §§50.2 and 50.3 for effective dates
for involuntary disenrollment).
Election
Period
Effective Date of
Disenrollment*
Do MA organizations have
to accept disenrollment
requests in this election
period?
Medicare
Advantage Open
Enrollment Period
First day of the month after the
month the MA organization
receives the disenrollment
request.
Yes
Annual Election
Period
January 1 of the following year. Yes
Special Election
Period
Varies, as outlined in §30.4 Yes
Open Enrollment
Period for
Institutionalized
Individuals
First day of the month after the
month the MA organization
receives the disenrollment
request.
Yes
*NOTE: CMS may allow up to 90 days retroactive payment adjustments for EGHP disenrollments.
Refer to §60.6 for more information.

53
30.8 - Election Periods and Effective Dates for Medicare MSA Plans
42 CFR 422.56, 422.62(d)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Individuals may enroll in Medicare MSA plans (should one be offered in their area) only during the
ICEP or the AEP; they may not enroll in Medicare MSA plans during a SEP (see exception below).
The effective date of coverage is determined by the election period in which an enrollment request is
made. Effective dates are provided in §30.6 of this chapter.
Individuals may disenroll from Medicare MSA plans only during the AEP or an SEP. The effective
date of disenrollment during an SEP depends on the type of SEP. Additionally, MSA enrollees may
not use the MA OEP to disenroll from the MSA.
Exception: To facilitate the offering of employer/union sponsored MSA plans, CMS will permit
individuals to request enrollment into an employer/union sponsored MSA plan using the
Employer Group Health Plan Special Enrollment Period (EGHP SEP).
30.9 - Closed Plans, Capacity Limits, and Reserved Vacancies
42 CFR 422.60(a)(2), 422.60(b) and 422.66(d)(2)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
An MA organization may specify a capacity limit for one or all of the MA plans it offers and reserve
spaces for individual and employer or union group commercial members who are converting from a
commercial product to an MA product at the time the member becomes eligible (i.e., conversion
enrollments). When an MA plan is closed due to a capacity limit, the MA plan must remain closed to
all prospective enrollees (with the exception of reserved vacancies) until space becomes available. All
requests from MA organizations for a capacity limit should be submitted to the CMS Regional Office
account manager.
All MA plans (with the exception of Medicare MSA plans; see §30.8) must accept enrollment requests
made during the AEP, ICEP and SEP unless an approved capacity limit applies. Only with an
approved number of reserved vacancies may an MA organization set aside openings for the enrollment
of conversions (i.e., ICEP enrollment requests).
Unlike the mandatory election periods (AEP, ICEP and SEP), an MA organization has the option to
voluntarily close one or more of its MA plans to OEP and OEPI enrollment requests. If an MA plan is
closed for OEP and OEPI enrollments, then it is closed to all individuals who are making OEP or
OEPI enrollment requests for that plan. All MA plans must accept OEP and OEPI disenrollment
requests, regardless of whether or not it is open for enrollment.
NOTE: For purposes of auto-enrollment and facilitated enrollment, MA organizations must
ensure that the MA-PD plans into which beneficiaries are deemed to have enrolled have the
capacity to accept them. Should a capacity limit be proposed for an MA-PD plan, it must be set
high enough to ensure all beneficiaries may be transitioned.
30.9.1 - MA Plan Closures

54
The decision to be open or closed for OEP and OEPI enrollment requests rests with the MA
organization and does not require CMS approval. However, if an MA organization has an MA plan
that is open for OEP and OEPI enrollment requests, and decides to change this process, it must notify
CMS and the general public 30 calendar days in advance of the new limitations on the open enrollment
process.
If an MA organization has more than one MA plan, those plans may be open or closed to OEP and
OEPI enrollment requests independent of one another, as the MA organization determines. Further,
each MA plan may be open for OEP and OEPI enrollment requests:
1. Only certain months of the year;
2. Some portion of certain months; and/or
3. During the first 25 days (or any part) of each month.
When an MA plan is voluntarily closed for OEP and OEPI enrollments, it is closed to ALL OEP and
OEPI enrollment requests, but it must accept enrollment requests made during the ICEP and SEP as
well as be open for the AEP, unless an approved capacity limit applies and has been reached
(excluding reserved vacancies). CMS may approve a partial service area closure for capacity reasons.
If a plan is closed in a portion of its service area for capacity reasons, that plan may be open for OEP
and OEPI enrollments in the remaining portion of the service area.
When an MA plan is closed due to an approved capacity limit that has been reached, it may continue
to accept ICEP (i.e., conversion) enrollments only if there are reserved vacancies set aside. If there are
no reserved vacancies, or once all of these vacancies have been filled, the MA organization cannot
accept any new enrollees into the MA plan until space becomes available. Refer to §40.5.1 for more
information on enrollment processing after reaching capacity.
Refer to §40.5 of this chapter for additional information on enrollment processing during closed
periods.
If an MA organization has an MA plan that is approved by CMS for a capacity limit, it should estimate
when a capacity limit will be reached and notify CMS and the general public 30 calendar days in
advance of the closing of the open enrollment process. If CMS approves the capacity limit for
immediate closing of enrollment, the MA organization must notify the general public within 15
calendar days of CMS approval that it has closed for enrollment.
Exhibit 23 contains three model notices that MA organizations can use to notify the public when they
are closing for enrollment. NOTE: Public notices must receive CMS approval under the usual
marketing review process.
When an MA organization has a plan that re-opens after being closed to OEP and OEPI enrollment
requests or as a result of a capacity limit, there is no requirement for the MA organization to notify the
general public. However, the MA organization should notify CMS when this occurs.

55
40 - Enrollment Procedures
42 CFR 422.66
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
An MA organization must accept enrollment requests it receives, regardless of whether they are
received in a face-to-face interview, by mail, by facsimile, or through other mechanisms defined by
CMS.
An individual (or his/her legal representative) must complete an enrollment request mechanism to
enroll in an MA plan and submit the enrollment request to the MA plan during a valid enrollment
period. If an individual wishes to elect another MA plan in the same parent organization, he/she must
complete a new enrollment request to enroll in the new MA plan. Enrollment may also be made via
Auto- and Facilitated enrollment processes as described in §40.1.5 of this chapter and via the group
enrollment process for employer or union sponsored plans as described in §40.1.6.
Upon receiving an enrollment request, an MA organization must provide within 10 calendar days, one
of the following:
• Acknowledgement notice (as described in section 40.4.1);
• Request for additional information (as described in 40.2.2); or
• Notice of denial (as described in 40.2.3).
If a plan uses the combined acknowledgment/confirmation notice, the plan may send the notice of
rejection within 7 calendar days of receiving the DTRR indicating a rejection instead of sending the
above items (as described in 40.4.2).
Unless otherwise directed in this guidance, the organization must provide required notices in response
to information received from CMS on the DTRR that contains the earliest notification.
MA organizations may not delay the processing of enrollment requests unless the beneficiary’s
enrollment request is being placed on a waiting list, as allowed under §40.5.
Refer to §40.2.5 for MA-PD enrollments in which an individual has other qualified prescription drug
coverage through an employer or union group.
Special Rule for the Annual Election Period (AEP):
Medicare Advantage (MA) organizations may not solicit submission of paper enrollment forms or
accept telephone or on-line enrollment requests prior to the beginning of the AEP. Brokers and agents
under contract to MA organizations may not accept or solicit submission of paper enrollment forms
prior to the start of the AEP. MA organizations and their brokers and agents also should remind
beneficiaries that they cannot submit enrollment requests prior to the start of the AEP.
Despite these efforts, CMS recognizes that MA organizations may receive unsolicited paper
enrollment forms prior to the start of the AEP, given that marketing activities may begin prior to this
date. To be considered unsolicited, the MA organization must have received the paper AEP
enrollment request directly from the applicant and not through a sales agent or broker. Other
enrollment request mechanisms may not be accepted prior to the actual start of the AEP. Paper AEP
enrollment requests received prior to the start of the AEP for which there is indication of sales agent or
56
broker involvement in the submission of the request (i.e., the name or contact information of a sales
agent or broker) must be investigated by the organization for compliance with the requirements in the
Medicare Communications and Marketing Guidelines. If an MA organization receives unsolicited
paper enrollment forms on or after October 1
st
but prior to the start of the AEP, it must retain and
process them as follows:
• Within 7 calendar days of the receipt of a paper enrollment request, the MA organization must
provide the beneficiary with a written notice that acknowledges receipt of the complete
enrollment request, and indicates that the enrollment will take effect on January 1 of the
following year (refer to Exhibits 4, 4a, 4b and 4c for model notices).
• For AEP enrollment requests received prior to the start of the AEP, the MA organization must
submit all transactions to CMS systems (MARx) on the first day of the AEP with an “application
date” of the same date. For example, unsolicited AEP paper enrollment requests received
October 1 through October 14 must be submitted on October 15
th
with an “application date” of
October 15
th
of the current year in the appropriate data field on the enrollment transaction. If a
beneficiary has submitted more than one AEP paper enrollment request prior to the start of the
AEP, the beneficiary will be enrolled in a plan based on the first application that is processed.
• Once the MA organization receives a MARx DTRR from CMS indicating whether the
individual’s enrollment has been accepted or rejected, it must meet the remainder of the
requirements (e.g., sending a notice of the acceptance or rejection of the enrollment within 10
calendar days following receipt of the DTRR from CMS) provided in §40.4.2.
Note: If organizations receive incomplete unsolicited AEP paper enrollment requests prior to the start
of the AEP, they must follow existing guidance for working with beneficiaries to complete the
applications (refer to §40.2.2).
Again, this policy applies only to the receipt of unsolicited paper enrollment forms prior to the
beginning of the AEP. To help ensure a successful AEP season, it is imperative that organizations
follow these steps and submit valid enrollment transactions promptly as directed.
40.1 - Format of Enrollment Requests
42 CFR 422.60(c)
Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
MA organizations must have, at minimum, a paper enrollment form process available for potential
enrollees to request enrollment in an MA plan.
In addition to the paper enrollment form, MA organizations have the option to accept enrollment
requests through other approved mechanisms as described in §§ 40.1.2, 40.1.3, 40.1.4 and 40.1.5
below.
57
40.1.1 - Enrollment Request Mechanisms
Rev. 1, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
The MA organization must use an enrollment mechanism that complies with CMS’ guidelines in
format and content.
Specific model enrollment forms have been developed for each plan type as follows:
Exhibit 1 - MA coordinated care plans
Exhibit 1b - MSA plans
Exhibit 1c - PFFS plans
Organizations should utilize the model appropriate to the plan type for all enrollment request
mechanisms to ensure all required elements are included. CMS has also developed a model EGHP
enrollment (Exhibit 2) for EGHP members, a model short enrollment form (“short form”) (Exhibit 3)
and a model plan selection form (Exhibit 3a) to allow for enrollment requests into another plan (PBP)
offered by the same parent organization. For determining the appropriate use of the short form or
model plan selection form, CMS defines parent organization as the contract numbers (H#) and legal
entities that are owned and operated by a single organization in a single State. As a result, a short
form or a model plan selection form may be used only for enrollment requests into another plan of the
same type (i.e., HMO to HMO, PPO to PPO, or PFFS to PFFS).
Organizations can utilize model enrollment forms included in Exhibits 1-3a, or choose to develop their
own materials using these models as a guide. Materials are subject to the CMS review and approval of
plan marketing materials.
In addition to the information collected on the request, the enrollment mechanism must include
information indicating that the applicant acknowledges--
• The requirement to keep Part A and B;
• That they will abide by the rules of the MA plan;
• The release of information to Medicare and other plans. Information may be used to track
enrollment and for other purposes, as allowed under federal law;
• That enrollment in the MA plan automatically disenrolls him or her from any other Medicare
health plan and prescription drug plan. Note: The model PFFS and MSA enrollment
mechanisms provide language as appropriate; and
• The right to appeal service and payment denials made by the organization.
Please refer to Appendix 2 for a complete listing of required elements that must be included on
enrollment mechanisms and Exhibits 1 – 3a for complete information on these statements.
The plan premium is not required to be displayed or disclosed on the enrollment mechanism unless it
is part of the plan name. Organizations may include the premium amount on the enrollment
58
mechanism if they choose to do so, but they must do so consistently for all PBPs listed on the
enrollment mechanism.
Special Needs Plans (SNPs) must include elements on the enrollment mechanism that correspond to
the special needs focus of the particular SNP.
Medical Savings Plans (MSA) must include elements on the enrollment form as provided in
Exhibit 1b.
No enrollment form or other enrollment request mechanism may include a question regarding binding
arbitration, whether the individual receives hospice coverage (except MSA plans) or any other health
screening information, with the exception of questions regarding nursing home status (some additional
exceptions apply for SNPs; please refer to §40.2, item “D” of this chapter).
Refer to §60.9 for requirements regarding retention of enrollment request mechanisms.
40.1.2 – Electronic Enrollment
42 CFR 422.60(c)
Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
MA organizations may develop and offer electronic enrollment mechanisms made available via an
electronic device or secure internet website.
The following standards, in addition to all other program requirements, apply to electronic enrollment
mechanisms:
• Submit all materials, web pages, and images (e.g. screen shots) related to the electronic enrollment
process for CMS approval following the established process for the review and approval of
marketing materials and other enrollment request mechanisms.
• Provide individuals with all the information required by Medicare regulations and communication
and marketing guidelines for the MA program.
• At a minimum, comply with CMS’ data security policies.
• Advise each individual at the beginning of the electronic enrollment process that he or she is
completing an actual enrollment request to the MA organization.
• Capture the same data as required on the model enrollment form (see Exhibit 1 and Appendix 2).
o For enrollment requests from one plan to another plan within the same parent organization,
the data required on the model short enrollment form are sufficient, provided the plan can
verify that the individual is currently enrolled in the parent organization at the time the
individual submits the enrollment request.
o Electronic ICEP enrollment requests from individuals enrolled in a non-Medicare plan
under the same organization (or parent organization) and transitioning to the MA plan
without a break in coverage may be based on the simplified opt-in enrollment mechanism
as described in § 40.1.9.
• As part of any electronic enrollment process, obtain an electronic signature from the applicant or
include a clear and distinct step that requires the applicant to activate an “Enroll Now,” or “I
Agree,” type of button or tool. By taking this affirmative step, the individual indicates his or her
intent to enroll. It must also be made clear to the applicant that, by taking this action, he or she
agrees to the release of information as provided on the model enrollment form (see Exhibit 1), and

59
attests to the truthfulness of the data provided. The process must also remind the individual of the
penalty for providing false information. See §40.2 for information about legally binding electronic
signatures.
• The electronic enrollment mechanism must capture an accurate time and date stamp at the time the
applicant executes the electronic signature or activates the step in the previous bullet (i.e. “Enroll
Now or I Agree” button or tool). The organization will use this data to establish the application
date for the enrollment request. This time stamp also marks the start of the seven day
timeframe for processing the enrollment request, as it is at this time that the enrollment
request is considered by CMS to be received by the MA organization.
• If a legal representative is completing this enrollment request, he or she must attest that he or she
has such authority to make the enrollment request and that proof of this authority is available upon
request by the MA organization or CMS.
• Inform the individual of the effects of completing the electronic enrollment, including that the
individual will be enrolled (if approved by CMS), and that he or she will receive notice (of
acceptance or denial) following submission of the enrollment to CMS.
• Include a tracking mechanism (e.g., a confirmation number) to provide the individual with
evidence that the MA organization has received the electronic enrollment request.
• Optionally, may request or collect premium payment or other payment information, such as a bank
account number or credit card numbers.
• Maintain electronic records that are securely stored and readily reproducible for the period
required in §60.9 of this chapter. The MA organization’s record of the enrollment request must
exist in a format that can be easily, accurately and quickly reproduced for later reference by each
individual member and/or CMS. A data extract file alone is not acceptable.
• Plans have the option of obtaining technical and related services from outside entities in support of
the MA organization’s electronic enrollment mechanism, (e.g. licensed software). MA
organizations may use downstream entities, such as a broker or third party website, as a means of
facilitating and capturing the electronic enrollment request. However, organizations retain
complete responsibility for ensuring enrollment policies in this guidance are followed, and for
ensuring the appropriate handling of any sensitive beneficiary information provided as part of the
online enrollment, including those facilitated by downstream entities.
• From the point at which an individual selects the plan of his or her choice on the third-party
website and begins the online enrollment process, CMS holds the organization responsible for the
security and privacy of the information provided by the applicant and for the timely disclosure of
any breaches.
Medicare Online Enrollment Center
In addition to the process described above, CMS offers an online enrollment center (OEC) through the
Medicare.gov
website and the 1-800-MEDICARE Call Center for enrollment into Medicare
Advantage plans (except for MSA) and Medicare prescription drug plans. The date and time
“stamped” by the Medicare OEC will serve as the application date for purposes of determining the
election period and enrollment effective date. MA organizations must promptly retrieve enrollment
requests from the OEC and should check for requests at least daily.
40.1.3 - Enrollment via Telephone
(Rev. 2, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
MA organizations may accept requests for enrollment into their MA plans via an incoming (in-bound)
telephone call to a plan representative or agent. MAOs may also accept enrollment requests during
60
communications initiated by the organization when, during the course of outreach to provide
information about their Medicare plan offerings to individuals with whom they have an existing
business relationship, the individual expresses a desire to enroll in one of the organization’s MA plans.
The following standards apply, in addition to all other applicable program requirements:
• Enrollment requests from individuals with whom the organization does not have an existing
business relationship may be accepted only during an incoming (or in-bound) telephone call
from a beneficiary. This includes inbound calls to an incorrect department or extension
transferred internally.
• For all telephonic enrollment requests, the MA organization must ensure that the telephonic
enrollment request is effectuated entirely by the beneficiary or his or her authorized
representative.
• Individuals must be advised that they are completing an enrollment request.
• Each telephonic enrollment request must be recorded (audio) and include a statement of the
individual’s agreement to be recorded, all required elements necessary to complete the
enrollment (as described in Appendix 2), and a verbal attestation of the intent to enroll. If the
request is made by someone other than the beneficiary, the recording must include the attestation
regarding the individual’s authority under State law to complete the request, in addition to the
required contact information. All telephonic enrollment recordings must be reproducible and
maintained as provided in section §60.9.
• Include a tracking mechanism to provide the individual with evidence that the telephonic
enrollment request was received (e.g. a confirmation number).
• Optionally, organizations may request or collect premium payment or other payment information
needed, such as a bank account number or credit card numbers, to process the form of premium
payment requested by the individual.
• A notice of acknowledgement and other required information must be provided to the individual
as described in §40.4.1.
• Telephonic enrollment requests into a plan offered by the same parent organization may be based
on the model short enrollment form (Exhibit 3) or the model plan selection form (Exhibit 3a)
instead of the comprehensive individual enrollment form.
• Telephonic ICEP enrollment requests from individuals enrolled in a non-Medicare plan under
the same organization (or parent organization) and transitioning from the non-Medicare plan to
the MA plan without a break in coverage may be based on the simplified opt-in enrollment
mechanism as described in § 40.1.9.
The MA organization must ensure that all MA eligibility and enrollment requirements provided in this
chapter are met. Scripts for completing an enrollment request in this manner must be developed by the
MA organization and submitted to CMS for review and approval. The scripts must contain the
required elements for completing an enrollment request as described in Appendix 2, and must receive
CMS approval in accordance with applicable Medicare regulations before use.
40.1.4 - Default Enrollment Option for Medicaid Managed Care Plan Enrollees
who are Newly Eligible for Medicare Advantage
42 CFR 422.66(c) and 422.68(a)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
61
Subject to prior CMS approval, MA organizations may automatically enroll newly eligible Medicare
beneficiaries into a dual eligible MA special needs plan (D-SNP). Default enrollment is permitted
only for individuals who:
• are newly eligible for Medicare Advantage;
• are currently enrolled in a Medicaid managed care plan offered by the MA organization (or by
an entity under the same parent organization as the MA organization); and
• will remain in the Medicaid managed care plan upon their conversion to Medicare.
CMS approval of default enrollment
To qualify for default enrollment, an MA organization must have an affiliated Medicaid managed care
plan. An affiliated Medicaid managed care plan is one that is offered by the MA organization that also
offers the D-SNP (or is offered by an entity under the same parent organization as the MA
organization). The MA organization must be able to demonstrate:
• State approval for the use of a default enrollment process in its contract with the state Medicaid
agency; and
• State agreement to provide the information that is necessary for the MA organization to
identify individuals in their Medicaid managed care plan who are in their MA initial coverage
election period.
NOTE: Data provided by the State must include all information necessary to submit the enrollment
transaction to CMS (i.e., Medicare number, date of birth, etc.).
MA organizations must have a minimum overall quality rating from the most recently issued ratings of
at least 3 stars (or be a low enrollment contract or new MA plan as defined in § 422.252) and must not
have any prohibition on new enrollment imposed by CMS. MA organizations must submit proposals
to their CMS Account Manager via HPMS and receive CMS approval before beginning any default
enrollments under this authority.
Proposals for default enrollment must include a description of the MA organization’s process to
identify individuals eligible for default enrollment, including:
• Those currently enrolled in a Medicaid managed care plan offered by the organization and who
are about to convert to Medicare;
• How the process ensures the organization will identify eligible individuals in time to provide
the required written notice to these individuals no fewer than 60 days prior to the date of their
initial Medicare eligibility (the conversion date); and
• How the process ensures identification of individuals whose upcoming Medicare eligibility is
based on disability as well as age.
Notice to individuals about automatic (default) enrollment
Proposals must include a copy of the required written notice and copies of any written, telephonic or
electronic outreach materials for CMS prior approval, as well as a description of the organization’s
outreach activity for its default enrollment process. The required written notice must include the
following:

62
• Information and materials required under § 422.111 for initial enrollments (e.g., Evidence of
Coverage and Summary of Benefits);
• Information on how to opt-out of (decline) the enrollment prior to the enrollment effective
date, and either enroll in Original Medicare or choose another MA plan. This must include the
opportunity to contact the MA organization either in writing or by telephone to a toll-free
number. The MA organization is prohibited from discouraging declination. The organization
will submit opt-out requests to CMS as enrollment cancellations;
• Information on the differences in premium, benefits, and cost sharing between the individual’s
current Medicaid managed care plan and the D-SNP;
• Information on the process for accessing care under the D-SNP; and
• A general description of alternative Medicare health and drug coverage options available to an
individual in his or her Initial Coverage Election Period.
Default enrollment process
The MA organization will send the enrollment transaction to CMS at the same time that it sends the
written notice (i.e., no fewer than 60 days prior to the conversion date). Default enrollment
transactions must be submitted with
election code type ‘J’ and must always use the first day of an
individual’s ICEP as the application date. The enrollment effective date must always be the date of the
individual’s first entitlement to both Medicare Part A and Part B. Opt-out requests received after
coverage begins are to be processed as disenrollment requests; once enrolled in the MA plan, these
individuals may use the MA OEP to either enroll in Original Medicare or choose another MA plan
(see § 30.4 for more information).
Approval Period
CMS may approve an MAO using the default enrollment for a period of up to five years. Such
approval shall continue after contract consolidations or other CMS-approved changes to the Plan
Benefit Package if the D-SNP continues to be offered by the same parent organization and continues
to meet all qualifying criteria for default enrollment. CMS may suspend or rescind approval prior to
the expiration of this period if CMS determines the MA organization is not in compliance with the
requirements of this section. An MA organization that wants to continue default enrollment after the
expiration of an approval period must re-apply and CMS must approve the request to use default
enrollment before the MA organization begins default enrollments again. MA organizations may not
continue to use default enrollment if they are pending a response from CMS at the time their approval
period expires.
40.1.5 - Auto- and Facilitated Enrollment
42 CFR 423.34
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
CMS requires that MA organizations offering both MA-PD and MA-only plans have a process for
auto- and facilitated enrollment. All LIS eligible individuals who elect an MA plan without Medicare
prescription drug benefits (“MA-only plan”) will be auto- or facilitated enrolled into an MA-PD plan
in the same organization or into a PDP offered by the same organization, unless the individual declines
the enrollment. The MA organization’s auto- and facilitated enrollment processes will occur monthly.
As noted in the preamble to the final regulation for Part D (Federal Register/Vol. 70, No. 18, January
28, 2005), the legal authority for both auto- and facilitated enrollment processes is technically termed
"facilitated" enrollment, since auto-enrollment is limited to PDPs. However, the term "auto-

63
enrollment" is used here to denote the process that applies to full-benefit dual eligible individuals, and
“facilitated enrollment” to others with LIS
.
CMS has safeguards in place to prevent existing MA and cost plan enrollees from being auto- or
facilitated enrolled by CMS into a PDP. However, there may be instances in which a beneficiary’s
request to enroll into an MA plan will not yet be reflected in CMS systems at the point in time when
CMS processes auto- or facilitated PDP enrollments. In these cases, the beneficiary will receive a
notice from CMS informing him/her that s/he has been enrolled into a PDP. However, once the
beneficiary’s request to enroll into the MA plan is processed by CMS, it will prevail over the
previously processed auto- or facilitated PDP enrollment submitted by CMS.
Please note this section does not apply to MA organizations that offer only MA-PD plans, as all their
enrollees already have Part D coverage. Nor does it apply to PFFS plans offered by organizations that
do not offer any MA-PD plans (these beneficiaries are included in the standard CMS auto/facilitated
enrollment process into PDPs), nor to MA organizations in the U.S. territories, including Puerto Rico,
or to employer sponsored MA plans.
Starting January 1, 2010, CMS implemented the Limited Income Newly Eligible Transition (Limited
Income NET) demonstration, which modified its procedures for auto/facilitating enrollment of LIS
beneficiaries into PDPs for those who have retroactive enrollment effective dates. That demonstration
does not impact the auto/facilitated requirements for MA organizations as specified in this section,
except for MA-PFFS plans that autoenroll new full benefit dual eligible enrollees into a PDP owned
by the same organization (see §40.1.5, item B as well as Exhibit 27A).
A. Populations
1. Auto-Enrollment
Full-benefit dual eligibles in MA-only plans will be auto-enrolled by the MA organization into an
MA-PD plan. Full-benefit dual eligible individuals are defined as those eligible for comprehensive
Title XIX Medicaid benefits as well as eligible for Medicare Part D. This includes those who are
eligible for comprehensive Medicaid benefits plus Medicaid payment of Medicare cost-sharing
(sometimes known as QMB-plus or SLMB-plus). Please note that full-benefit dual eligible
individuals do not include those eligible only for Medicaid payment of Medicare cost-sharing (i.e.
QMB-only, SLMB-only, or QI). In Part D, these distinctions are key to distinguishing full-benefit dual
eligibles, who need to be auto-enrolled, from other types of dual eligibles, who need to be facilitated
enrolled.
Full-benefit dual eligible individuals to be auto-enrolled include those who are full-benefit dual
eligible upon initial enrollment into an MA-only plan, as well as existing Medicare enrollees of an
MA-only plan who become newly Medicaid eligible. This includes full-benefit dual eligible MA-only
enrollees who reside in the 50 states or the District of Columbia.
This excludes full-benefit dual eligibles who:
• Live in any of the five U.S. territories;
• Live in another country;

64
• Are individuals for whom an employer or union is claiming the retiree drug subsidy, or are
enrolled in an employer-sponsored MA-only plan, including MA-only “800 series” plans.
• Are incarcerated, as defined in §10;
• Are not lawfully present in the U.S.; or
• Have opted out of auto-enrollment into the Part D benefit.
• [For MA-PFFS only] Are already enrolled in a stand-alone Prescription Drug Plan
2. Facilitated enrollment
Other LIS eligibles are defined as those deemed automatically eligible for LIS because they are QMB-
only, SLMB-only, QI (i.e. only eligible for Medicaid payment of Medicare premiums and/or cost-
sharing); SSI-only (Medicare and Supplemental Security Income [SSI], but no Medicaid); or those
who apply for LIS at the Social Security Administration (SSA) or a State Medicaid Agency and are
determined eligible for LIS. This includes those who apply and are determined eligible for either the
full or partial level of the LIS.
Other LIS eligible individuals to be facilitated enrolled include those who are Other LIS eligible upon
initial enrollment into an MA-only plan, as well as existing Medicare enrollees of an MA-only plan
who become newly Other LIS eligible. This includes Other LIS eligible MA-only enrollees who reside
in the 50 states or the District of Columbia.
This excludes Other LIS eligible individuals who:
• Live in any of the five U.S. territories,
• Live in another country,
• Are individuals for whom the employer or union is claiming the retiree drug subsidy, or are
enrolled in an employer-sponsored MA-only plan, including MA-only “800 series” plans,
• Are incarcerated, as defined in §10;
• Are not lawfully present in the U.S.; or
• Have opted out of facilitated enrollment into the Part D benefit.
• [For MA-PFFS only] Are already enrolled in a stand-alone Prescription Drug Plan
B. Auto/Facilitated Enrollment Process
The procedure for auto/facilitated enrollment is as follows:
1. The MA organization will identify full-benefit dual eligibles to be auto-enrolled, and Other LIS
eligibles to be facilitated enrolled. Please see subsection C for details on how to distinguish the
two populations.
a. Auto/facilitated enrollment specifically excludes individuals in employer-sponsored MA-
only plans, including “800 series” plans, and individuals with Retiree Drug Subsidy
(RDS).
b. For PFFS plans, the organization must exclude individuals who are already enrolled in a
stand-alone PDP. The organization may submit a Batch Eligibility Query (BEQ)
transaction or access the MARx online query (M232 screen) to determine whether
individuals are enrolled in a stand-alone PDP.
65
2. The MA organization will then identify MA-PD plans in the same service area, and in the same
MA organization, with the lowest combined Part C and Part D premium amount. If more than
one MA-PD plan have the same lowest premium amount, auto-enrollment must be random
among the available MA-PD plans. The selection of MA-PD plan is without regard to the Part
C cost-sharing. The only exception to this is when the MA-PD plan is a high-deductible plan,
unless the high-deductible plan is the only MA-PD plan offered in the area. Please note that
the Part D premium is the dollar amount equaling the premium charged to a beneficiary with a
100 percent premium subsidy.
If an MA Special Needs Plan (SNP) meets these criteria, the MA organization must ensure that
the individual meets the eligibility criteria for the SNP (e.g. type of dual eligible, type of
chronic condition, or institutionalized). Please note the “MA full dual file” uses LIS deemed
reason code to identify full duals, meaning they were full dual in at least one month in the past
year; it cannot be used by MA organizations to confirm dual status in the current month. If the
MA SNP does not meet the criteria of lowest combined Part C and D premium (with the Part D
premium equaling the premium charged to a beneficiary with a 100 percent premium subsidy),
the MA organization may not auto-enroll full benefit dual eligibles into it, even if it is a dual
eligible SNP.
Organizations offering both an MA-PD PFFS plan and a stand-alone PDP in the same region
with a basic benefit and a premium at or below the low-income premium subsidy amount for
that region may auto/facilitate enrollment into either the MA-PD PFFS plan or the PDP, but
must apply this policy consistently for all PFFS plans offered by the organization. CMS will
conduct auto/facilitated enrollment of LIS individuals enrolled in MA-only PFFS plans where
the organization does not offer an MA-PD PFFS plan, even if they also offer a stand-alone
PDP.
3. Within 10 calendar days of identifying an individual as needing auto/facilitated enrollment, the
MA organization sends an auto/facilitated enrollment notice to the beneficiary (see Exhibits 27,
27A, 28 and 28a).
4. If the person does not respond or opt-out by the deadline below, submit a Code 61 transaction
(PBP change) for the auto/facilitated enrollment into the MA-PD plan and include the
appropriate effective date within the timelines specified below (see subsection C). The new
MA-PD plan will be notified of the auto/facilitated enrollment via a transaction reply.
• Auto-enrollment – within 10 calendar days of sending notice
• Facilitated enrollment – by last day before effective date of facilitated enrollment

66
C. Effective Date of Auto/Facilitated Enrollments
1. Auto-Enrollment
The effective date of auto-enrollment is retroactive to the first day of the month the individual first
became a full-benefit dual eligible, or January 1, 2006, whichever is later. For individuals who are
full-benefit dual eligible upon enrollment into an MA-only plan, the effective date would be
retroactive to the effective date of enrollment in the MA-only plan. For existing MA-only Medicare
enrollees who subsequently become Medicaid eligible, the effective date is retroactive to the first day
of the month the person became Medicaid eligible. In no case will the effective date of auto-
enrollment precede the date that the individual became an enrollee of the MA organization.
For MA-PFFS plans that elect to auto-enroll a full-benefit dual eligible beneficiary into a PDP offered
by the same organization, the effective date will be prospective, i.e., the first day of the second month
after the enrollee is identified as a new full benefit dual eligible. This is because CMS implemented
the Limited Income NET demonstration in January, 2010, in which a single contractor addresses all
retroactive periods of PDP auto-enrollment. The MA-PFFS may not submit an election on behalf of a
beneficiary into the Limited Income NET demonstration contractor. To ensure the beneficiary is
aware s/he can request retroactive coverage from the demonstration contractor, Exhibit 27a includes
instructions on how to do so.
There is nothing that prohibits a full-benefit dual eligible from initially electing an MA-only plan. To
ensure they understand the consequences of doing so, marketing material and the acknowledgement
letter emphasize that prescription drugs are not covered.
2. Facilitated Enrollment
The effective date of facilitated enrollment for all Other LIS eligible members is the first day of the
second month after the person is identified as qualifying for facilitated enrollment. For example, if the
plan is notified in August 2010 that an existing member of an MA-only plan has become LIS eligible,
the effective date is October 1, 2010.
The MA organization may move up the effective date of a facilitated enrollment by a month if an
Other LIS beneficiary requests this in a timely fashion, i.e. before start of earlier month. The SEP
under §30.4.4 #12 should be used.
Example: The MA organization facilitates enrollment of an Other LIS eligible in May, 2010,
effective July 1, 2010. The beneficiary receives the facilitated enrollment by the last day in May,
and requests the MA organization makes the facilitated enrollment effective June 1. The MA
organization submits an enrollment transaction to do so.
3. Distinguishing Between Full-Benefit Dual Eligible and Other LIS Individuals
MA organizations need to distinguish full benefit dual eligibles from others with LIS for purposes of
setting the effective date. The first step is to identify all LIS eligibles in the MA-only plan. In the
past, CMS did not transmit a data element to plans that could be used to distinguish full-benefit dual
eligibles from other LIS. As a result, CMS sends a monthly “Auto Assignment Full Dual Notification
File” (for file format and technical specifications, please see section 8.1 of the Plan Communications

67
User Guide, on the CMS website at http://www.cms.hhs.gov/mmahelp/. This file identifies full-benefit
dual eligibles.
However, starting December, 2010, the monthly membership report (MMR) will include a new field
(Medicaid dual status code) that will provide the dual status code of the enrollee, if that enrollee has
Medicaid status. The new field will be aligned with the already-existing Field 40 (Current Medicaid
Status). If Field 40 indicates that the enrollee has Medicaid status, Field 85 will provide the dual status
code for that enrollee. Field 40 indicates that an enrollee is Medicaid when that enrollee has a
Medicaid period reported to CMS for either the month prior to payment or two months prior to
payment. Please note that Field 40 and, thus the new field, are not related to payment, but are provided
for purposes of benefits coordination and bidding. The new field will be coded as follows:
The valid values when Field 40 = 1 are:
01 = Eligible is entitled to Medicare- QMB only
02 = Eligible is entitled to Medicare- QMB AND Medicaid coverage
03 = Eligible is entitled to Medicare- SLMB only
04 = Eligible is entitled to Medicare- SLMB AND Medicaid coverage
05 = Eligible is entitled to Medicare- QDWI
06 = Eligible is entitled to Medicare- Qualifying individuals
08 = Eligible is entitled to Medicare- Other Dual Eligibles (Non QMB, SLMB,QDWI or QI) with
Medicaid coverage
09 = Eligible is entitled to Medicare- Other Dual Eligibles but without Medicaid coverage
99=Unknown
The valid value when Field 40 = 0 is:
00 = No Medicaid Status
The valid value when Field 40 is blank is: Blank
Full-benefit dual eligible beneficiaries are represented by dual status codes 02, 04, and 08.
To ensure a sufficient period of transition, CMS will continue to send the Auto Assignment Full Dual
Notification File to identify the subset of the LIS enrollees in the MA-only plan who are full-benefit
dual eligibles. Plans may begin using the MMR instead, but starting August, 2011, plans will be
required to use the MMR as CMS will discontinue transmission of the Auto Assignment Full Dual
Notification File.
To determine the auto-enrollment effective date, identify the LIS copay start date data provided on
other files (i.e., Transaction Reply Report or monthly LIS history report). MA-PFFS plans that elect
to auto/facilitate enroll new LIS beneficiaries into a PDP offered by the same organization do not need
to distinguish between full-benefit dual eligible enrollees and others with LIS because the effective
date will always be prospective.
The remaining LIS eligibles in the MA-only plan qualify for facilitated enrollment, and the effective
date should be set as noted in item 2 above.
D. Notice
68
The MA organization will notify the beneficiary in writing that she/he will be enrolled in the given
MA-PD plan on the specified effective date. The notice must be sent within 10 calendar days of
identifying the individual as qualifying for auto/facilitated enrollment. The notice will inform the
beneficiary that they may choose another Part D plan (either another MA-PD plan or Original
Medicare with a PDP) or opt out of auto/facilitated enrollment into the Part D benefit. If the
beneficiary does not opt out, or choose another Part D plan within the specified deadline, the person’s
silence will be deemed to be an election of the auto/facilitated enrollment and it will take effect on the
effective date. These individuals will also be informed they have a Special Enrollment Period (SEP)
that permits them to change Part D plans, even after the auto/facilitated enrollment takes effect.
1. Auto-Enrollment
Please use the model notice language in Exhibit 27. For MA-PFFS auto-enrolling into a PDP, please
use Exhibit 27a. The deadline for responding is 10 calendar days from when the notice is sent.
2. Facilitated enrollment
Please use the model notice language in Exhibit 28. For MA-PFFS auto-enrolling into a PDP, please
use Exhibit 28a. The deadline for responding is the last day before the facilitated enrollment effective
date.
E. Opt-Out
Full-benefit dual eligible and Other LIS individuals may opt-out, or affirmatively decline, the Part D
benefit. Beneficiaries may opt-out verbally or in writing. For an MA-only plan enrollee, this
primarily means declining auto/facilitated enrollment into an MA-PD plan in the same organization
and maintaining enrollment in the MA-only plan. MA organization may check the common User
Interface to see if the individual has previously opted out; if so, the person should not be
auto/facilitated enrolled. Once a beneficiary has opted out, the MA organization should document this
and not include him/her in future auto/facilitated enrollment processing.
The MA plan should counsel the individual to ensure they understand the implications of their request
to decline, and should confirm this in writing (see Exhibit 29) within 10 calendar days of the
individual’s request to opt-out. If a beneficiary opts out of auto/facilitated enrollment by the deadline
in the auto/facilitated notice, do not submit an enrollment transaction that would move them to an MA-
PD plan. This will have the effect of leaving him/her in the MA-only plan.
If the individual opts-out after the Code 61 transaction has been submitted, the effective date of
returning to the MA-only plan is normally prospective, i.e. first day of the following month. However,
through the 15
th
of the month after the month in which the notice was sent, at a full-dual eligible
beneficiary’s request, the MA organization may restore the person to the MA-only plan retroactive to
the auto-enrollment effective date. This is accomplished by submitting a Code 61 transaction with the
same effective date, and setting the opt-out flag as noted below.
Individuals who want to opt-out of auto/facilitated enrollment into an MA-PD plan must do so with
their MA organization, not through 1-800-MEDICARE. This differs from the procedure for
individuals who want to opt-out of auto/facilitated enrollment into a stand-alone PDP. If a 61
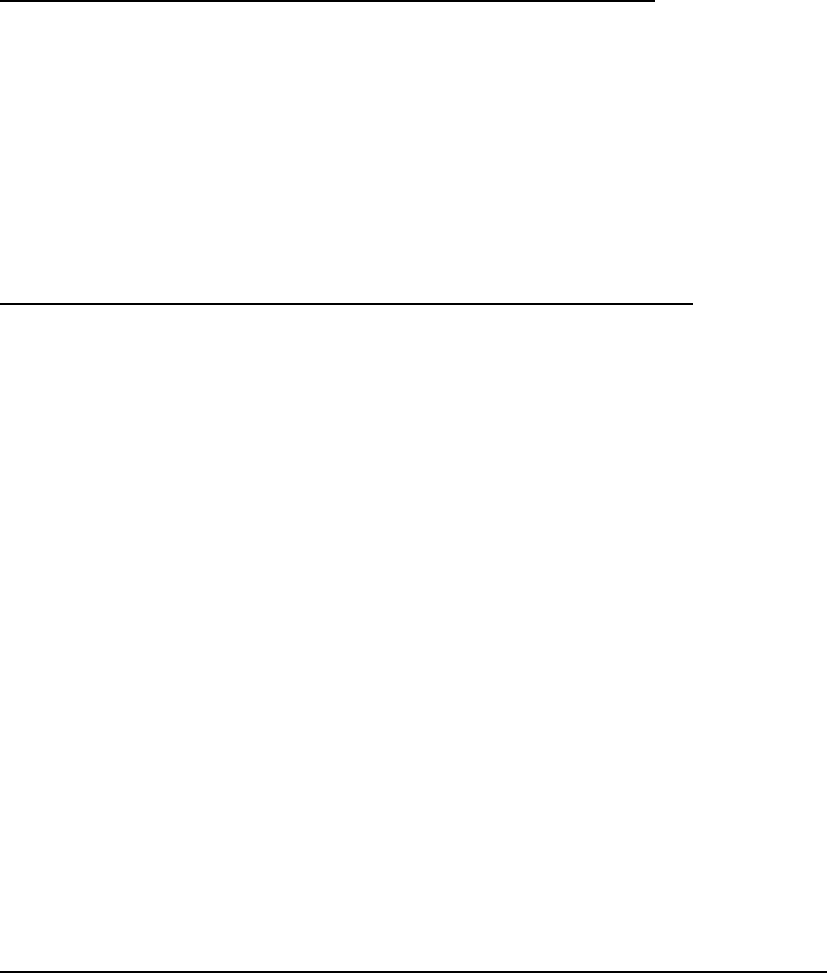
69
transaction has already been submitted to move the person to the MA-PD plan, the MA organization
sends another 61 transaction (to move the person back to the MA-only plan), setting the Part D Opt-
Out Flag (field 38) to Y (opt-out of auto-enrollment) . If it has not, submit just the opt out indicator on
a 79 transaction.
An individual who opts out does not permanently surrender his or her eligibility for, or right to enroll
in, a Part D plan; rather, this step ensures the person is not included in future monthly auto/facilitated
enrollment processes. To obtain Part D benefits, the beneficiary simply makes a voluntary request to
enroll into a plan that offers Part D benefits.
F. Special Procedures for Individuals With Employer Coverage
When the individual’s employer or union-sponsored enrollment, including in “800 series” plans, or
Retirement Drug Subsidy (RDS) status is known, the MA organization shall exclude the individual
from auto/facilitated enrollment. It is possible the MA organization will not be aware an individual has
RDS until they submit a Code 61 transaction to auto/facilitate his/her enrollment. As with all
enrollment transactions for individuals with RDS, MARx will enforce a two-step process, initially
rejecting the transaction. The MA organization must follow normal procedures of confirming with the
beneficiary that she/he wants to be enrolled in the Part D benefit and, if confirmed, resubmit the
transaction with the employer subsidy override.
G. Information Provided to Auto/Facilitated Enrolled Beneficiaries
The MA-PD plan into which the beneficiary has been auto/facilitated enrolled must send a modified
version of the pre- and post-enrollment materials required to be provided to new enrollees. If the
effective date is retroactive into the previous calendar year, only send the current year’s version of the
documents below.
Prior to effective date, the MA-PD plan must send:
• The information required in §40.4.1, and
• A Summary of Benefits (those who are auto/facilitated enrolled still need to make a decision
whether to stay with the plan into which they have been auto/facilitated enrolled or change to
another one that better meets their needs). Providing the Summary of Benefits, which is
considered marketing material normally provided prior to making an enrollment request,
ensures that those auto/facilitated enrolled have a similar scope of information as those who
voluntarily enroll.
After the effective date of coverage:
• The guidance in §40.4.2 applies, including guidance on what to do if the MA-PD plan is not
notified early enough of an auto/facilitated enrollment to meet the timelines in §40.4.1 on
materials required to be provided prior to the effective date.
H. Summary of Differences between Auto- and Facilitated Enrollment Processes
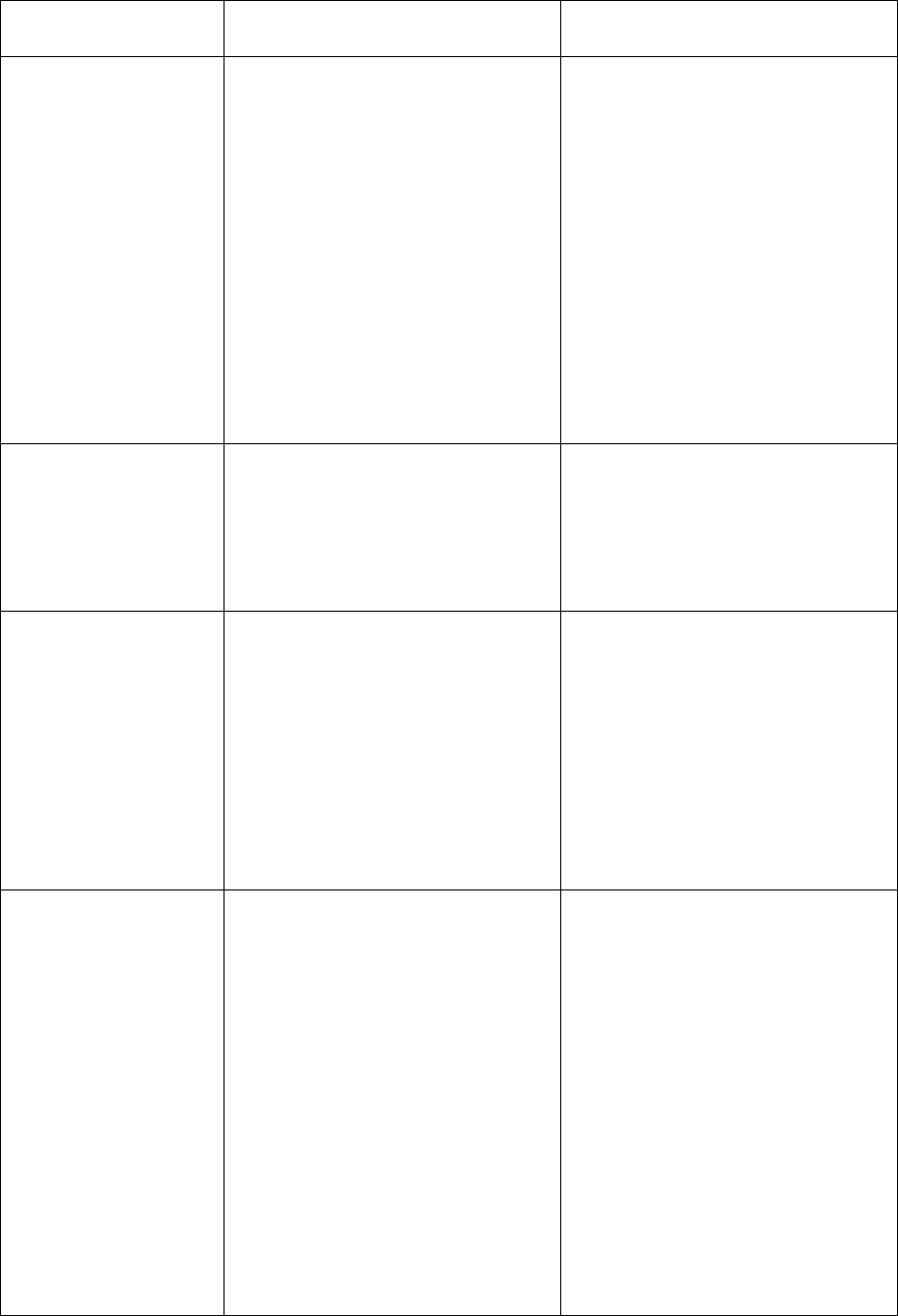
70
Auto-Enrollment of Full Duals
Facilitated Enrollment of
Other LIS
Steps
• Identify full dual eligibles in
MA-only plan who need to
be enrolled into MA-PD plan
• Send notice to beneficiary
within 10 calendar days of
identifying need for person
to be auto-enrolled
• If no answer or person does
not opt out within 10
calendar days, submit 61
transaction to move to MA-
DPD plan
• Identify non-full dual LIS
beneficiaries in MA-only plan
who need to be enrolled into
MA-PD plan
• Send notice to beneficiary
within 10 calendar days of
identifying need for person to
be facilitated enrolled
• If no answer or person does
not opt out by last day before
effective date of facilitated
enrollment, submit 61
transaction to move to MA-PD
plan
Who needs to be
moved
• Full dual who newly enrolls
in MA-only plan
• Beneficiary in MA-only plan
who recently became
Medicaid eligible and is thus
newly full dual
• Non-full dual with LIS who
newly enrolls in MA-only plan
• Beneficiary in MA-only plan
who recently became LIS-
eligible
Who does not need
to be moved
• Those who have already
opted out
• Those with RDS
• Those in “800 series”
employer sponsored plans
• Those in employer sponsored
plans (other than “800
series” plans)
• Those who have already opted
out
• Those with RDS
• Those in “800 series”
employer sponsored group
plans
• Those in employer sponsored
plans (other than “800 series”
plans)
Data to identify
those in MA-only
plan who need to be
moved to MA-PD
plan
Monthly MA full dual file or on
MMR with dual status code 02,
04, or 08
LIS data (DTRR or monthly LIS
history report):
• Premium subsidy = 25%, 50%,
75%
OR
•
Premium subsidy = 100 and
LIS copay = 4 (15%)
OR
• Premium subsidy = 100 and
LIS copay = 1, 2, or 3, and
person is not on MA full dual
file or on MMR with dual
status code 02, 04, or 08
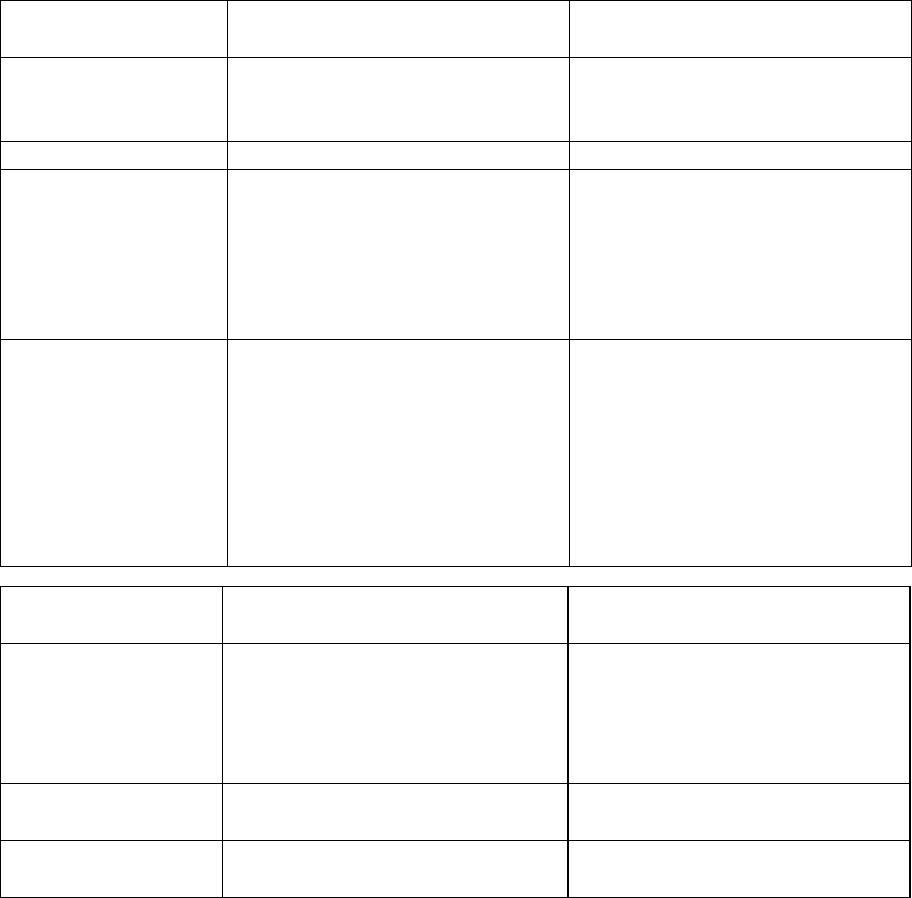
71
Auto-Enrollment of Full Duals
Facilitated Enrollment of
Other LIS
Plan Into Which
Beneficiary Should
be Enrolled
MA-PD plan with the lowest
combined Part C and D premium
MA-PD plan with the lowest
combined Part C and D premium
Notice to send
Exhibit 27 (27a if applicable)
Exhibit 28 (28a if applicable)
Effective date
• First day of month person
qualified for LIS (will be
retroactive)
• Cannot be prior to start of
enrollment in the MA-only
plan
• First day of second month
after person identified as
needing enrollment
• Cannot be prior to start of
enrollment in the MA-only
plan
Opt out
• Document and do not enroll
again in future.
• Confirm with beneficiary (see
Exhibit 29)
• If submitting 61 transaction
to move beneficiary back to
MA-only, set Opt-Out flag to
Y (field 38)
• Document and do not enroll
again in future.
• Confirm with beneficiary (see
Exhibit 29)
• If submitting 61 transaction
to move beneficiary back to
MA-only, set Opt-Out flag to
Y (field 38)
Data on
Transaction
Auto-Enrollment of Full Duals
Facilitated Enrollment of
Other LIS
Application date
First day of month prior to
enrollment effective date OR day
after current application date on
MA-only plan enrollment,
whichever is later.
First day of month prior to
effective date of the enrollment
Election type Code
Z = MA auto-enrollment period*
U = Dual/LIS Special
Enrollment Period
Enrollment Source
Code
E (MA-submitted auto-
enrollment)*
F (MA-submitted facilitated
enrollment)
* Use of the enrollment period of “Z” and enrollment source code of “E” permits these 61 transactions
for retroactive auto-enrollments to bypass normal MARx suspension of processing for retroactive
effective dates (i.e. they will process immediately).
40.1.6 – Additional Enrollment Request Mechanisms for Employer/Union
Sponsored Coverage
MA organizations may choose to accept voluntary enrollment requests directly from the employer or
unions who sponsor MA coverage for its members in any of the enrollment mechanisms described in
this guidance (except auto or facilitated enrollment). In addition, the MA organization may also
accept enrollment requests using either the optional enrollment request mechanism or group
enrollment process described in this section.
It is the MA organization’s responsibility to ensure that all applicable MA enrollment requirements are
met, regardless of the process utilized, as required by CMS. In any case, the enrollment requests
72
provided to the MA organization by the employer or union will reflect the choice of retiree coverage
individuals made using their employer’s or union’s process for selecting a health plan.
For enrollments processed using the SEP EGHP, the application date on the enrollment transaction
submitted to CMS is the first day of the month prior to the effective date of enrollment into the
employer or union group-sponsored plan. For the purposes of providing notices and meeting other
timeframe requirements provided in this guidance, use the date the organization receives the request.
40.1.6.1 - Group Enrollment Mechanism
CMS will allow an MA organization to accept enrollment requests into an employer or union
sponsored MA plan using a group enrollment process in which beneficiaries enroll in an employer or
union sponsored MA plan. Beneficiaries participate in this process through advance notification that
provides each individual with all the information necessary to make an informed choice. Furthermore,
the process must provide CMS with any information the employer/union has on other insurance
coverage for the purposes of coordination of benefits. It is the MA organization’s responsibility to
ensure the group enrollment process meets all applicable MA enrollment requirements. MA
organizations must ensure that any contracts and other arrangements and agreements with employers
and unions intending to use the group enrollment process make these requirements clear.
The group enrollment process must include providing the following information to each beneficiary as
follows:
• Beneficiaries participate in the group enrollment mechanism by receiving an advance notice that
the employer/union intends to enroll them for a prospective coverage effective date in an MA
plan that the employer/union is sponsoring; and
• Clear instruction that the beneficiary may affirmatively opt out of such enrollment; explaining
the process to opt-out; and any consequences to employer or union benefits opting out would
bring; and
• This notice must be provided by the MA organization, or the employer or union acting on its
behalf, not less than 21 calendar days prior to the effective date of the beneficiary’s enrollment in
the employer/union sponsored MA plan; and
• Additionally, the information provided to each beneficiary must include a Summary of Benefits
offered under the employer/union sponsored MA plan, as well as an explanation of how to get
more information about the MA plan, and an explanation on how to contact Medicare for
information on other Medicare health plan options that might be available to the beneficiary; and
• Each individual must also receive in the group enrollment notice materials the information
contained in Exhibit 2 under the heading “Please Read & Sign Below.”
The organization must ensure all of the above requirements are met prior to submission of the
enrollment transactions to CMS. For enrollments processed using the SEP EGHP, the application date
on the enrollment transaction submitted to CMS is the first day of the month prior to the effective date
of the group enrollment. This will ensure that any subsequent beneficiary-generated enrollment request
will supersede the group enrollment in CMS systems.
73
The employer or union must provide in the group enrollment file(s) all the information required for the
MA organization to submit a complete enrollment request transaction to CMS, including permanent
residence information (refer to Appendix 2 of this chapter for a complete list of the required data
elements and any other relevant CMS systems guidance). Records must be maintained as outlined in
§60.9 of this chapter.
40.1.6.2 - Optional Mechanism For MA Group-sponsored plan Enrollment
This enrollment request mechanism is optional for MA organizations and may not be required.
Therefore, MA organizations may specify the employers or unions, if any, from which they will accept
this enrollment request format. It is the MA organization’s responsibility to ensure that the process it
uses, as well as the process used by the employer or union, meets the following requirements:
The MA organization must inform its Regional Office Account Manager of its intent to use this
mechanism and identify the employer group(s) or union(s) for which it will be accepting enrollments
made in this manner.
The enrollment information (i.e., the electronic file) submitted to the MA organization by an employer
or union (or TPA) must accurately reflect the employer’s or union’s record of the election of coverage
made by each individual according to the processes the employer or union has in place, and may be
accepted without a paper MA enrollment request form.
Sales package minimum information requirements are not changed by using this option. These
include, but are not limited to, providing the applicable rules of the MA organization. Each
individual’s enrollment request must clearly denote his/her agreement to abide by the MA organization
rules, certify his/her receipt of required disclosure information and include authorization by the
beneficiary for the disclosure and exchange of necessary information between the U.S. Department of
Health and Human Services (and its designees) and the MA organization. The requirements for all
other information provided to enrollees, both pre- and post-enrollment, are unchanged by this option
and must be satisfied.
The enrollment request transaction must include all the data necessary for the MA organization to
determine each individual’s eligibility to make an enrollment request as described in §20 of this
chapter of the MMCM. Agreements with employer groups or unions should identify required data
elements. A detailed list of these elements is provided in Appendix 2.
This alternate enrollment request mechanism is used in place of paper MA enrollment request forms
and does not require a signature. For purposes of compatibility with existing instructions in this
chapter, the application date of enrollments processed using the SEP EGHP will be the first day of the
month prior to the effective date of enrollment into the employer/union sponsored plan. This will
ensure that any subsequent beneficiary-generated enrollment request will supersede the enrollment
submitted by the employer or union.
Effective date calculation of voluntary enrollment requests and the collection and submission of
enrollment requests to CMS will follow existing procedures.
74
To accept electronic records of employer or union enrollment requests, the MA organization must, at
minimum, comply with the CMS security policies regarding the acceptable method of encryption
utilized to provide for data security, confidentiality and integrity, and authentication and identification
procedures to ensure both the sender and recipient of the data are known to each other and are
authorized to receive and decrypt the information. (See the CMS web site at:
http://www.cms.hhs.gov/informationsecurity for additional information.)
The employer’s or union’s record of the request to enroll must exist in a format that can be easily,
accurately and quickly reproduced for later reference by each individual member, the MA organization
and/or CMS, as necessary, and be maintained (by the employer/union or the MA organization, as they
agree) following the guidelines for MA enrollment request forms (see §60.9). Included in this
requirement is the MA organization’s record of information received from the employer or union.
40.1.7 - Enrollment for Beneficiaries in Qualified State Pharmaceutical Assistance
Programs (SPAPs)
CMS will allow MA organizations to accept enrollment requests in an agreed-upon electronic file
format from qualified SPAPs, provided the SPAP has met the following requirements:
• The SPAP must attest, as required by §40.2.1 of this guidance, that it has the authority under
state law to enroll on behalf of its members.
• The SPAP must coordinate with the MA Organization to provide the required data elements for
the organization to process and submit an enrollment request to CMS.
• The SPAP must provide a notice to its members in advance of submitting the requests that
explains that it is enrolling on their behalf, how the enrollment works with the SPAP and how
individuals can decline such enrollment.
In return, MA organizations that agree to accept mass enrollment requests from SPAPs are required to
process them like any other enrollment and in accordance with notification timeframes. Additionally,
the organization must ensure the SPAP has met the above requirements prior to submission of the
enrollment transaction to CMS. It is important for the MA organization to work with the SPAP in the
event that the organization encounters any problems processing the enrollment request in the format
provided. Because the SPAP is the authorized representative of the beneficiary, the organization is
responsible for following up with the SPAP if the enrollment is incomplete in any way (to obtain
missing information) or if the enrollment is conditionally rejected due to the existence of employer or
union sponsored drug coverage (to confirm that the individual understands the implications of
enrolling in a Part D plan).
Special note for SPAP enrollment requests during the AEP - For enrollment processing purposes,
the application date on the enrollment transaction submitted to CMS for the AEP must be set to
October 15
th
. This will ensure that subsequent beneficiary-generated enrollment requests made during
the AEP will supersede the SPAP enrollment in CMS systems.
40.1.8 – Re-Assignment of Certain LIS Beneficiaries
CMS has the discretion to re-assign LIS beneficiaries, including situations in which their current MA
plan will terminate. CMS will announce its intent to conduct reassignment in the Call Letter. CMS will
75
conduct the reassignment in the fall of each year, and ensure all affected LIS beneficiaries are notified.
Affected MA organizations are not responsible for initiating any disenrollment transactions for
reassigned beneficiaries. Gaining PDP sponsors are only responsible for responding to the CMS
enrollment transaction promptly when they receive it and for providing appropriate beneficiary notices
and materials, as described below.
A. Population to be Re-Assigned
CMS will reassign all current LIS enrollees in terminating MA plans. This includes non-renewing
MA only plans, as well as MA-PD plans and MA PFFS plans. CMS will perform this reassignment
when plan benefit packages are being non-renewed in their entirety, as well as MA plans that will
continue but have service area reductions (SARs). In the case of an MA-only or MA-PD plan with a
SAR, reassignment will only be performed for counties that will no longer be served by the plan in the
following year).
Beneficiaries who have LIS this year and will continue to do so next year will be included in this
reassignment process, regardless of whether the individual was assigned to or voluntarily enrolled in a
plan. The only exception is when an LIS beneficiary in an MA-PFFS plan that does not offer drugs is
concomitantly enrolled in a stand-alone PDP. In these cases the beneficiary will not be reassigned.
Reassignment is not performed for LIS beneficiaries in a non-renewing MA-only or MA-PD plan in
the U.S. Territories, or in an employer-sponsored MA-only or MA-PD plan.
The actual reassignment process is typically run on a single day in mid-October. CMS will only
reassign beneficiaries who meet the above criteria as of the day of the reassignment run. CMS does
not subsequently “sweep” for individuals who may meet the criteria at later points in time.
B. Re-assignment Process
CMS will reassign LIS beneficiaries from a non-renewing MA plan or MA plan with a SAR to a
stand-alone prescription drug plan (PDP). Beneficiaries retain the option to elect another MA plan.
CMS will attempt to reassign beneficiaries to a PDP offered by the same organization that offers the
MA plan in which they are currently enrolled, wherever possible. CMS will identify PDPs that qualify
to receive reassignment and are sponsored by the same parent organization (see §40.1.5 in Chapter 3
of the Medicare Prescription Drug Benefit Manual for details on PDPs to which beneficiaries will be
reassigned as well as for the responsibilities of those “gaining” PDPs). If the organization has more
than one such plan in that region, CMS will randomly reassign beneficiaries among those plans.
If the organization does NOT offer a qualifying PDP, CMS will randomly reassign affected
beneficiaries to PDP sponsors that have at least one qualifying PDP in that region. CMS will follow
the two-step process used under auto/facilitated enrollment (i.e. random distribution first at the sponsor
level, then randomly among qualifying plans within the sponsor).
C. CMS Notification to Beneficiaries
CMS will ensure that all beneficiaries being re-assigned are notified. These notices will be on blue
paper, and will instruct beneficiaries who are being reassigned because of a premium increase to

76
contact their current plan if they wish to remain with the plan for the following year. Per section 1860
D–14 (c) of the Social Security Act, CMS will also provide reassigned beneficiaries with information
on formulary differences between the individual’s former plan and new plan (with respect to the
individual’s drug regimen), and a description of the right to coverage determination, exception,
reconsideration, appeal or grievance.
D. Plan Communication to Affected Beneficiaries
Non-renewing MA plans or MA plans with a SAR are not required to send any beneficiary notices
specific to the reassignment process. Please refer to the Call Letter for details on general notification
requirements related to non-renewals and SARs.
“Gaining” PDPs are responsible for providing enrollment confirmation (See Exhibit 29 of Chapter 3 of
the Prescription Drug Manual) and enrollment materials to beneficiaries within 10 calendar days of
receiving confirmation of reassignment on a DTRR.
40.1.9 – Simplified (Opt-In) Enrollment Mechanism
42 CFR 422.66(d)(5)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
This mechanism permits an MA organization to use data it has from its non-Medicare lines of business
(commercial, Marketplace, Medicaid, etc.) to obtain some of the information it would normally need
to receive from the beneficiary in the enrollment request. The organization is required to obtain any
data necessary from the individual that it doesn’t have from its data sharing.
Use of this mechanism is not required. It is up to the MA organization whether it has the capability
and wants to share data between its Medicare and non-Medicare lines of business.
MA organizations may only offer simplified enrollment to individuals who:
• Are in their ICEP based on their initial enrollment in Medicare;
• Are enrolled in any type of non-Medicare plan under the same organization (or an entity under
the same parent organization as the MA organization); and
• Do not have a break in coverage between the non-Medicare plan and the MA plan.
The MA organization identifies individuals who are enrolled in its non-Medicare coverage, nearing
Medicare eligibility (or recently enrolled), and in their ICEP. It may conduct outreach to these current
members and offer them the opportunity to enroll in their plan. Outreach efforts are considered
marketing, and should clearly articulate the various plan offerings, plan structure, premium, costs,
network, etc.
MA organizations may offer simplified enrollment via paper, telephone or electronically, as outlined
in §§ 40.1, 40.1.1 through 40.1.3. For telephonic or electronic requests, the plan may limit the data to
be collected from the applicant to those items it does not already have.
The MA organization must collect the following data for the simplified enrollment:
• Minimal personal data sufficient for the MA organization to correctly identify the current
member and his or her information within its systems;
77
• Medicare number;
• Name of the MA plan selected for enrollment;
• Statement of a language or alternate format preference (beneficiary response is optional; does
not effect enrollment if not completed);
• Applicant’s acknowledgement of the following items:
o The plan has a contract with the federal government;
o Sales agents/brokers may be compensated if they are helping the individual to enroll;
o Release of information to Medicare and other plans, as necessary. Information may be
used for research and other purposes, as allowed under federal law and regulations;
o Obtaining benefits and services from the plan in order to be covered;
o Maintain enrollment in both Part A and B;
o Information provided in the enrollment request is correct; intentionally falsifying
information will result in disenrollment; and
o Understanding that completion/signature indicates an understanding of the enrollment
application, and that authorized representatives have legal authority to complete the
enrollment request.
• Signature or attestation of intent to enroll and, as applicable, from an authorized representative
acting on the beneficiary’s behalf, contact information; and
• Any other data the MA organization doesn’t already have in its records that is necessary to
meet the requirements in Appendix 2.
Organizations are encouraged, but are not required, to request premium payment method information
in the simplified enrollment request. In the absence of a stated preference, individuals are to be placed
in direct billing status, as outlined in §40.2.M. Additionally, the parameters outlined in
§§ 40.1.1 through 40.1.3 must be met based on the method of the simplified enrollment request
(telephonic, electronic, or paper).
Enrollments requested using this mechanism are the same as any other new ICEP enrollment the plan
receives and should be processed similarly.
Example:
Mr. Smith is turning 65 in June 2018 and is enrolled in commercial coverage with an organization
named Good Insurance. Good Insurance identifies in its records that Mr. Smith’s Medicare Part A and
B Initial Enrollment Period begins March 2018. Based on its data from Mr. Smith’s commercial
enrollment, Good Insurance knows that Mr. Smith lives in the service area of MA plans that Good
Insurance offers.
A representative of Good Insurance calls Mr. Smith in May 2018 and identifies herself as his
commercial health insurance plan. Using the plan’s internal protocols, she confirm his identity on the
call. In this call, she informs Mr. Smith that because he’s soon to be eligible for Medicare, he can
enroll in a plan that Good Insurance offers just for people with Medicare. She provides information on
Good Insurance MA plans available in Mr. Smith’s area and asks if he is interested in enrolling in one
of these or learning more. Mr. Smith expresses his interest in enrolling in Good Insurance’s MA plan
with prescription drugs.
Good Insurance already has Mr. Smith’s personal information via its internal systems and, while on
the call, the representative obtains what is needed for the MA enrollment that Good Insurance doesn’t
already have. The representative uses this information to complete the telephonic enrollment request
in Good Insurance’s internal MA enrollment system. Good Insurance confirms the MA plan Mr. Smith
78
wants to enroll in and asks for his Medicare number. Good Insurance explains the legal requirements
for enrollment, release of information, and confirms Mr. Smith’s understanding and
acknowledgement/approval to process the request. Good Insurance also provides information to Mr.
Smith to process his disenrollment from the commercial coverage to be effective as of May 31, 2018.
Good Insurance processes the telephonic enrollment the same as other received requests and submits
the enrollment transaction to CMS. Mr. Smith’s MA plan coverage will begin on June 1, 2018, when
his Medicare coverage begins.
40.2 - Processing the Enrollment Request
42 CFR 422.60
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
If an individual completes an enrollment request during a face-to-face interview, the MA organization
may ask to see the individual’s Medicare card to verify the spelling of the name, and to confirm the
correct recording of Medicare Number, and entitlement dates for Medicare Part A and Part B. The
individual does not have to show or provide the Medicare card or other evidence when submitting the
request. The other forms of evidence as listed in item “B” are only requested when the enrollment
request doesn’t include the Medicare Number and the plan is unable to locate the individual in CMS
systems. For processing all enrollment requests, the MA organization must verify Medicare
entitlement as described in item “B” below in this section.
Appendix 2 lists all the elements that must be provided in order to consider an enrollment request
“complete.” If the MA organization receives an enrollment request that contains the required
elements, the MA organization must consider the enrollment complete even if the optional data
elements on the enrollment request are not provided. If an MA organization has received CMS
approval for an enrollment request that contains data elements in addition to those included in
Appendix 2, then the enrollment request is considered complete even if those additional elements are
not provided.
If an MA organization receives an enrollment request that does not have all necessary elements
required in order to consider it complete, it must not immediately deny the enrollment. The MA
organization must always check available systems (i.e. BEQ, MARx online query) for information to
complete an enrollment before requiring the beneficiary to provide the missing information. For
example, if a beneficiary failed to fill out the “sex” field on the enrollment request and the MA
organization has access to this information via available systems, the organization must use that source
to complete the application instead of requesting the information from the beneficiary. If the required
but missing information is not available via CMS systems, the enrollment request is considered
incomplete and the MA organization must follow the procedures outlined in §40.2.2 in order to
complete the enrollment request.
For EGHP enrollees, the MA Organization may choose to accept enrollment requests as described in
§40.1.2 or §40.1.6. All required elements as listed in Appendix 2 must be included in the record of the
enrollment request provided by the group for the enrollment request to be considered complete (except
signature). Follow the procedures outlined in §40.2.2 to address incomplete enrollment requests.
For paper, telephone and electronic enrollment requests, all required elements as listed in Appendix 2
must be included. The “Beneficiary Signature and/or Authorized Representative Signature” element
79
for a paper request is satisfied with a pen-and-ink signature, for a telephone request it is satisfied with
a verbal attestation of intent to enroll, and for an electronic request it is satisfied with an electronic
signature or a clear and distinct step that requires the applicant to activate an “Enroll Now,” or “I
Agree,” type of button or tool. Follow the procedures outlined in §40.2.2 to address incomplete
enrollment requests.
Electronic signatures have the same legal effect and validity as pen-and-ink signatures. An MA
organization utilizing electronic signatures in electronic enrollment must, at a minimum, comply with
the CMS security policies. For more information on the requirements for legally binding electronic
signatures, see the Electronic Signatures in Global and National Commerce Act, 15 U.S.C. §7001, and
“Use of Electronic Signatures in Federal Organization Transactions” published by the CIO Council.
The following should also be considered when completing an enrollment:
A. Permanent Residence Information - The MA organization must determine whether or not the
enrollee resides within the MA plan’s service area. If an individual puts a Post Office Box as
his or her place of residence on the enrollment request, the MA organization must consider the
enrollment request incomplete and must contact the individual to determine place of permanent
residence. If the applicant claims permanent residency in two or more states or if there is a
dispute over where the individual permanently resides, the MA organization should consult the
State law in which the MA organization operates and determine whether the enrollee is
considered a resident of the State.
Refer to §10 for a definition of “evidence of permanent residence,” and §20.3 for more
information on determining residence for homeless individuals.
Individuals for whom the Batch Eligibility Query (BEQ) or MARx online query (M232 screen)
reflects an incarcerated status, that beneficiary is considered to reside outside of the service
area and are, therefore, not eligible to enroll.
B. Entitlement Information and Medicare Number –
42 CFR 422.50(a)(1)
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Following the procedures outlined in the CMS Plan Communications User Guide, MA
organizations must verify Medicare entitlement using the Batch Eligibility Query (BEQ)
process or MARx online query (M232 screen) for all enrollment requests, except enrollment
requests from a current enrollee of an MA plan who is requesting enrollment into another MA
plan offered by the same parent organization with no break in coverage (i.e. “switching
plans”).
Individuals are not required to provide evidence of entitlement to Medicare Part A and
enrollment in Part B with the enrollment request. If the systems (BEQ or MARx online query)
indicate that the individual is entitled to Medicare Part A and is enrolled in Part B, no further
documentation of Medicare entitlement is needed from the individual.
80
CMS systems are updated within two business days of SSA processing new or changed Part A
or Part B entitlement for a Medicare beneficiary. The CMS systems are the most up-to-date
data regarding Medicare entitlement for the beneficiary.
The Medicare Number will be assigned at the time CMS first receives entitlement information
for a new beneficiary. In the event that the enrollment request doesn’t include the Medicare
Number and the plan is unable to locate the individual in the BEQ or MARx online query, the
organization should consider the enrollment request incomplete and follow § 40.2.2.
The individual may provide the Medicare Number to the organization verbally or in writing.
Examples of documents the beneficiary may send to the plan which display the Medicare
Number (and entitlement information) include:
• Medicare card;
• Medicare Award notice from SSA (shows Medicare entitlement dates only);
• Benefit Verification notice from SSA (includes Medicare Number and entitlement start
dates);
• Medicare card information from the individual’s MyMedicare.gov account; and
• A notice from CMS regarding change in Medicare Number.
NOTE: If the beneficiary provides any of the notices listed above, the date on the letter should
be no more than two months before the enrollment request was received by the organization. If
there is a discrepancy between the entitlement information in a document and the information
in CMS’ systems, use the data in CMS systems to determine eligibility for enrollment.
For auto- and facilitated enrollments, as described in §40.1.5 of this chapter, entitlement
verification is deemed complete, as the individual is already an MA enrollee.
C. Effective Date of Coverage - The MA organization must determine the effective date of
coverage as described in §30.5 for all enrollment requests. If the individual fills out an
enrollment form in a face-to-face interview, then the MA organization representative may
advise the individual of the proposed effective date, but must also stress to the individual that it
is only a proposed effective date and that the individual will hear directly from the MA
organization to confirm the actual effective date. The MA organization must notify the member
of the effective date of coverage prior to the effective date (refer to §40.4 for more information
and a description of exceptions to this rule).
With the exception of some SEPs and when election periods overlap, beneficiaries may not
choose their effective date (effective dates are described in §30.5). Instead, the MA
organization is responsible for assigning the appropriate effective date based on the election
period. During face-to-face enrollments, the MA organization staff are responsible for ensuring
that a beneficiary does not choose an effective date that is not allowed under the requirements
outlined in §30.5.
If a beneficiary completes an enrollment request with an unallowable effective date, or if the
MA organization allowed the beneficiary to choose an unallowable effective date, the MA
organization must notify the beneficiary in a timely manner and explain that the enrollment
must be processed with a different effective date. The organization should resolve the issue
with the beneficiary as to the correct effective date, and the notification must be documented. If
81
the beneficiary refuses to have the enrollment processed with the correct effective date, the
beneficiary can cancel the enrollment request according to the procedures outlined in §60.2.1.
MA organizations must ensure enrollees have access to plan benefits as of the effective date of
enrollment the MA organization has determined and may not delay provision of plan benefits
in anticipation of the submission to or reply from CMS systems.
For auto- and facilitated enrollments, refer to §40.1.5 of this chapter for more information.
D. Health Related Information - MA organizations may not ask health screening questions
during completion of the enrollment request. MA organizations are only permitted to send
health assessment forms after enrollment. However, MA organizations may ask very limited
health status questions related to a beneficiary’s eligibility to join an MA plan, such as whether
the individual is enrolled in Medicaid, or is currently admitted to a certified
Medicare/Medicaid institution. Queries for this information are included on the model EGHP
form in Exhibit 2. These queries are not considered to be health screening questions. The
responses to these questions must not have an effect on eligibility to enroll in an MA plan.
Exception for certain MA-SNPs - An SNP that is being offered to individuals with certain
medical conditions (i.e. an SNP for chronic and disabling conditions), as permitted by CMS,
will need to establish that the individual has such a condition to determine eligibility for
enrollment in that specific SNP. Refer to §20.11 for more information.
E. Statements of Understanding - As outlined in §20.5, a beneficiary must understand and agree
to abide by the rules of the MA plan in order to be eligible to enroll. If the MA organization
lists such statements in an itemized format, it is at the MA organization’s discretion to decide
whether it will:
• Consider the beneficiary signature on the form (or completion of the enrollment request
process) to signify that the individual has read and understands the statements (as shown
on Exhibits 1, 1b, 2 and 3); or
• Have fields next to the statements and require the applicant’s initials next to each
statement.
The MA organization must apply the policy consistently. If the MA organization requires the
initials and the applicant fails to initial his/her understanding of each item listed on the
enrollment form, the MA organization may contact the applicant to clarify the MA
organization rules in order to complete the enrollment form. The MA organization must
document the contact and annotate the outcome of the contact. If the MA organization is
unable to contact the applicant to ensure their understanding, the enrollment form would be
considered incomplete.
F. Applicant Signature and Date - The individual must sign the enrollment form or complete the
enrollment request mechanism. If the individual is unable to do so, a legal representative must
sign the enrollment form (refer to §40.2.1 for more detail) or complete the enrollment request
mechanism. If a legal representative enrolls an individual, the legal representative must attest
to having the authority under State law to do so, and confirm that a copy of the proof of court-
82
appointed legal guardian, durable power of attorney, or proof of other authorization required by
State law that empowers the individual to effect an enrollment request on behalf of the
applicant is available and can be presented upon request by the MA organization or CMS.
The individual and/or legal representative must indicate his/her relationship to the individual
and date he/she signed the enrollment form or completed the enrollment request; however, if
he/she inadvertently fails to include the date on the enrollment request, then the date the MA
organization receives the enrollment request may serve as the signature date of the form.
If a paper enrollment form is submitted and the signature is not included, the MA organization
may verify with the individual with a phone call and document the contact, rather than return
the paper enrollment form as incomplete. The documentation of this contact will complete the
enrollment request (assuming all other required elements are complete).
Certain enrollment request mechanisms do not include a pen-and-ink, or “wet,” signature. The
signature element listed in Appendix 2 is satisfied by specific procedures provided for the other
enrollment request mechanisms in this chapter; for example, see §40.1.2 for information about
enrollment.
For auto and facilitated enrollment as described in §40.1.5, an enrollee signature is not
required.
G. Other Signatures - If the MA organization representative helps the individual fill out the
enrollment form, then the MA organization representative must clearly indicate his/her name
on the enrollment form. However, the MA organization representative does not have to include
his/her name on the form when:
• He/she pre-fills the individual’s name and mailing address when the individual has
requested that an enrollment form be mailed to him/her,
• He/she fills in the “office use only” block, and/or
• He/she corrects information on the enrollment form after verifying information (see “final
verification of information” below).
The MA organization representative does have to include his/her name on the form if he/she
pre-fills any other information, including the individual’s phone number.
H. Old Enrollment Requests - If the MA organization receives an enrollment request that was
executed more than 30 calendar days prior to the MA organization’s receipt of the request, the
MA organization is encouraged to contact the individual to re-affirm intent to enroll prior to
processing the enrollment and to advise the beneficiary of the upcoming effective date.
I. Determining the Application Date - The MA organization must date all enrollment requests as
soon as they are initially received. Except for enrollment requests submitted via the CMS
Online Enrollment Center, requests made by the group enrollment mechanism and auto or
facilitated enrollments, the date the enrollment request is initially received is equivalent to the
“application date” (refer to §10 for definitions of “receipt of enrollment request,” “completed
83
enrollment request” and “application date”). If the enrollment request is not complete at the
time it is received, then the additional documentation required for the enrollment request to be
complete must be dated as soon as it is received. Appendix 3 describes the appropriate
application date to include in the enrollment transaction submitted to CMS under various
conditions.
J. Final Verification of Information - Some MA organizations verify information before
enrollment information has been transmitted to CMS. In these cases the MA organization may
find that it must make corrections to an individual’s paper enrollment form. The MA
organization should make those corrections, and the individual making those corrections must
place his/her initials and the date next to the corrections. A separate “correction” sheet, signed
and dated by the individual making the correction, may be used by the MA organization (in
place of the initialing procedure described in the prior sentence), and should become a part of
the enrollment file. These types of corrections will not result in the MA organization having to
co-sign the enrollment form.
K. Premiums Owed to the MAO - For individuals enrolling in an MA-only plan, an MA
organization may choose to wait for an enrolling individual’s payment of the MA-only plan
premium before considering the enrollment request complete. An MA organization cannot
consider an enrollment request incomplete if the individual enrolling has indicated that he or
she wants the plan premium withheld from an SSA benefit check.
For enrollment into either an MA-only or MA-PD plan, an MA organization may consider an
enrollment request incomplete if there are premium amounts due to the organization from a
prior enrollment, whether or not premium withhold from an SSA benefit check is selected.
The option chosen by the MA plan to consider the application complete or incomplete must be
applied consistently to all potential enrollees of the plan.
Optional Exception for Dual-Eligible Individuals and Individuals who Qualify for the
Low Income Subsidy
For enrollment requests submitted by dually eligible individuals and individuals who qualify
for the low income subsidy (LIS), an MA organization may consider an enrollment request
complete if there are premium amounts due to the organization from a prior enrollment, even if
the MA organization has a policy to consider such enrollment requests incomplete.
The MA organization has the discretion to implement this exception to dually eligible
individuals and individuals who qualify for LIS within each of its MA plans. If the MA
organization offers this exception in one of its plans, it must apply the policy to all such
individuals who request enrollment in that MA plan.
L. Completed Enrollment Requests - Once the enrollment request is complete, the MA
organization must transmit the enrollment to CMS within the time frames prescribed in §40.3,
and must send the individual the information described in §40.4 within the prescribed time
frames. There are instances when a complete enrollment can turn out to be legally invalid.
These instances are outlined in §40.6.
M. Plan Premium Payment and Premium Withhold Options –
84
42 CFR 422.60(c)(1)
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
MA organizations may include on all enrollment request mechanisms (except the simplified
enrollment mechanism) the option for individuals to: 1) pay plan premiums by being billed
directly by the plan or 2) have the premiums withheld from their SSA benefit check. The plan
may also choose to offer other payment methods, such as automatic deduction from the
individual’s bank or other financial institution or from the individual’s credit card. The
enrollment mechanism can also advise that if the individual does not select a premium
payment option, the default action will be direct bill.
MA-only plans that do not have a premium may omit the “Paying your Plan Premium” section
from their enrollment request mechanism. MA-PD plans that do not have a plan premium may
include, at minimum, the direct bill and SSA withhold options for those individuals subject to
the LEP to select how they will pay this penalty (premium); however, such plans may also
include introductory language to indicate that the premium payment section applies only to
individuals subject to the LEP.
Railroad Retirement Board (RRB) enrollees may also submit requests to have their premiums
withheld from their RRB retirement payments. Organizations may choose to offer this option
on all enrollment mechanisms as well.
MA-PD plans can also include on the enrollment request a statement in the premium payment
section advising those individuals who qualify for extra help that, if the extra help does not
cover the entire plan premium, the individual is responsible for the amount that Medicare does
not cover.
Model language has been provided on Exhibits 1, 1c, 3 and 3a to reflect these options. In
addition, suggested optional language for MA-PD plans without premiums has also been
provided.
N. Additional Information for MA-PD Enrollment Requests – Individuals enrolling in a Part
D plan must disclose any other existing coverage for prescription drugs.
O. U.S. Citizenship or Lawful Presence Information – MA organizations must use the CMS
Batch Eligibility Query (BEQ) (individual or batch submission) or, via online access, the
MARx M232 screen, to verify eligibility on the basis of incarceration status or unlawful
presence status. An exception to this are enrollment requests from a current enrollee of an MA
plan who is requesting enrollment into another MA plan offered by the same parent
organization with no break in coverage (i.e., “switching plans”).
Individuals are not required to provide evidence of U.S. citizenship or lawful presence status
with the enrollment request, nor are MA organizations permitted to request such information or
documentation. The systems (BEQ or MARx online query) will indicate the lawful presence
status of a non-U.S. citizen, including the start and, if applicable, the end date of the unlawful
presence status of the individual.
85
CMS eligibility queries will only reflect data for the existence of an unlawful presence status.
When neither the BEQ nor the MARx online query shows any indication of unlawful presence
in the U.S., the MA organization must treat the lack of information as confirmation of evidence
of U.S. citizenship or lawful presence status.
When either the BEQ or the MARx online query shows an indication of unlawful presence in
the U.S. and the organization receives documentation of lawful presence from the applicant,
the plan cannot use this documentation to establish eligibility. If the MA organization is
provided evidence of lawful presence by the applicant in the form of a document from the
Department of Homeland Security or SSA and neither the BEQ nor the MARx online query
reflects this lawful presence status, the organization should refer the applicant to SSA to
request that SSA update its records.
40.2.1 - Who May Complete an Enrollment or Disenrollment Request
42 CFR 422.60(c)
A Medicare beneficiary is generally the only individual who may execute a valid request for
enrollment in or disenrollment from an MA plan. However, another individual could be the legal
representative or appropriate party to execute an enrollment or disenrollment request as the law of the
State in which the beneficiary resides may allow. CMS will recognize State laws that authorize
persons to make such requests for Medicare beneficiaries. For example, persons authorized under State
law may be court-appointed legal guardians, persons having durable power of attorney for health care
decisions or individuals authorized to make health care decisions under State surrogate consent laws,
provided they have authority to act for the beneficiary in this capacity.
If a Medicare beneficiary is unable to sign an enrollment form or disenrollment request or complete an
enrollment request mechanism due to reasons such as physical limitations or illiteracy, State law
would again govern whether another individual may execute the enrollment request on behalf of the
beneficiary. Usually, a court-appointed guardian is authorized to act on the beneficiary’s behalf. If
there is uncertainty regarding whether another person may sign for a beneficiary, MA organizations
should check State laws regarding the authority of persons to sign for and make health care treatment
decisions for other persons.
Where MA organizations are aware that an individual has a representative payee designated by SSA to
handle the individual’s finances, MA organizations should contact the representative payee to
determine his/her legal relationship to the individual, and to ascertain whether he/she is the appropriate
person, under State law, to execute the enrollment or disenrollment request. Representative payee
status alone is not sufficient to enroll a Medicare beneficiary.
When someone other than the Medicare beneficiary completes an enrollment or disenrollment request,
he or she must:
1) Attest to having the authority under State law to do so;
2) Confirm that proof of authorization, if any, required by State law that empowers the individual
to make an enrollment or disenrollment request on behalf of the individual is available and can
be provided upon request by CMS. MA organizations cannot require such documentation as a
condition of enrollment or disenrollment; and
3) Provide contact information.
86
The MA organization must retain the record of this attestation as part of the record of the enrollment
or disenrollment request. CMS provides a sample attestation as part of the model MA enrollment form
(Exhibit 1).
If anyone has reason to believe that an individual making an election on behalf of a beneficiary may
not be authorized under State law to do so, the organization should contact its CMS account manager
with all applicable documentation regarding State Law and the case in question. The account manager
may request supporting documentation from the individual making the election.
When an authorized representative completes an enrollment request on behalf of a beneficiary, the MA
organization should inquire regarding the preference for the delivery of required notifications and
other plan materials (i.e. sending mail to the beneficiary directly or to the representative, or both) and
make reasonable accommodations to satisfy these wishes.
40.2.2 - When the Enrollment Request Is Incomplete
42 CFR 422.50(a)(5)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
When the enrollment request is incomplete, the MA organization must document all efforts to obtain
additional documentation to complete the enrollment request and have an audit trail to document why
the enrollment request needed additional documentation before it could be considered complete. The
organization must make this determination and, within 10 calendar days of receipt of the enrollment
request, must notify the individual that additional information is needed, unless the required but
missing information can be obtained via CMS systems. This notification is not required for SNP
enrollment requests for which the only missing information is confirmation of the applicant’s special
needs status.
Note: An enrollment request is considered complete even if the only information missing is the
eligibility for the election period. In such circumstances, the plan must contact the individual to assure
they have a valid election period before processing the enrollment. (See Section 30 for more
information regarding eligibility for election periods and Section 40 for enrollment processing
requirements.)
If the request is missing the Medicare Number, see §40.2.B for more information.
If a paper enrollment form is missing a signature, see §40.2 F for more information.
For incomplete ICEP enrollment requests received prior to the month of entitlement to Part A and
enrollment in Part B, additional documentation to make the request complete must be received during
the first three months of the ICEP, or within 21 calendar days of the request for additional information
(whichever is later). For incomplete ICEP enrollment requests received during the month of
entitlement to Part A and enrollment in Part B or later, additional documentation to make the request
complete must be received by the end of the month in which the enrollment request was initially
received, or within 21 calendar days of the request for additional information (whichever is later).
For incomplete AEP enrollment requests, additional documentation to make the request complete must
be received by December 7, or within 21 calendar days of the request for additional information
87
(whichever is later). For all other enrollment periods, additional documentation to make the request
complete must be received by the end of the month in which the enrollment request was initially
received, or within 21 calendar days of the request for additional information (whichever is later).
EXAMPLES:
• Ms. Stears’ 65
th
birthday is April 20, 2011. She is eligible for Medicare Part A and Part B
beginning April 1, 2011 and has decided to enroll in Part B beginning on April 1. Her ICEP
begins on January 1, 2011 and ends on July 31, 2011. She submits an incomplete ICEP
enrollment request on January 15, 2011, and the MAO requests the required but missing
information on January 20, 2011. The enrollment request must be denied if the required
information is not received by March 31, 2011.
• Ms. Mohan’s 65
th
birthday is June 10, 2011. She is eligible for Medicare Part A and Part B
beginning June 1, 2011 and has decided to enroll in Part B beginning on June 1. Her ICEP
begins on March 1, 2011 and ends on September 30, 2011. She submits an incomplete ICEP
enrollment request on July 5, 2011, and the MAO requests the required but missing
information on July 7, 2011. The enrollment request must be denied if the required information
is not received by July 31, 2011.
When the MA organization receives an incomplete enrollment request near the end of either a month
or an enrollment period, the use of the full 21 calendar day period to complete the request may extend
beyond CMS systems plan submission “cut-off” date (these dates are provided in the CMS Plan
Communications User Guide). MA organizations may utilize a code 61 enrollment transaction to
directly submit the request to CMS as provided in the CMS Plan Communications User Guide.
If additional documentation needed to make the enrollment request “complete” is not received within
allowable time frames, the organization must deny the enrollment using the procedures outlined in
§40.2.3.
Requesting Information from the Beneficiary - To obtain information to complete the enrollment
request, the MA organization must contact the individual to request the information within ten
calendar days of receipt of the enrollment request. The organization may contact the beneficiary either
in writing (see Exhibit 5 for a model letter) or orally. If the contact is made orally, the MA
organization must document the contact and retain the documentation in its records. The MA
organization must explain to the individual that s/he has 21 calendar days in which to submit the
additional information or the enrollment will be denied. Since an incomplete enrollment request is an
invalid enrollment (as explained in §40.6), if the additional documentation is not received within
allowable time frames, the MA organization must send a denial of enrollment letter (see Exhibit 7).
If all documentation is received within allowable time frames and the enrollment request is complete,
the MA organization must transmit the enrollment to CMS within the time frames prescribed in §40.3,
and must send the individual the information described in §40.4.
40.2.3 - MA Organization Denial of Enrollment
MA organization denials occur before the organization has transmitted the enrollment to CMS. For
enrollment requests that do not require additional information from the applicant, an MA organization
88
must deny an enrollment within 10 calendar days of receiving the enrollment request based on its own
determination of the ineligibility of the individual to elect the MA plan. For an incomplete enrollment
request that requires information from the applicant and for which the applicant fails to provide the
information within the required time frame, an MA organization must deny the enrollment within 10
calendar days of the expiration of the time frames described in §40.2.2.
Notice Requirement - The organization must send notice of the denial to the individual that includes
an explanation of the reason for denial (refer to Exhibit 7 for a model notice). This notice must be sent
within ten calendar days of either 1) receipt of the enrollment request or 2) expiration of the time
frame for receipt of requested additional information, as described in the following examples:
• An MA organization receives an enrollment request from an individual on November 7 and
determines on that same day that the individual is ineligible due to place of residence. The
organization should send notice of denial within ten calendar days from November 7.
• An MA organization receives an enrollment request from an individual on January 7 and is
unable to determine, through direct contact with the beneficiary or the beneficiary’s authorized
representative, that the beneficiary has a valid enrollment period available. The organization
should send notice of denial within ten calendar days from January 7.
• An MA organization receives an enrollment form on November 7 from an individual, identifies
the enrollment form as incomplete, and notifies the individual of the need for additional
information, on November10. The beneficiary does not submit the information by December (as
required under §40.2.2), which means the organization must deny the enrollment. The
organization should send notice of denial within ten calendar days from December 1.
40.2.4 - MA-PD Enrollment When an Individual has Other Qualified Prescription
Drug Coverage through an Employer or Union Retiree Drug Subsidy (RDS) Plan
Sponsor
CMS systems will compare MA-PD enrollment transactions to information CMS has regarding the
existence of employer or union sponsored qualified prescription drug coverage for which the
beneficiary is also being claimed for the Retiree Drug Subsidy (RDS). If there is a match indicating
that the individual may have such other coverage, the enrollment will be conditionally rejected by
CMS systems as incomplete.
Within 10 calendar days of receipt of the Code 127 conditional rejection, the MA organization must
contact the individual to confirm the individual’s intent to enroll, and that the individual has discussed
and understands the implications of enrollment in a Part D plan on his or her employer or union
coverage. Individuals will have 30 calendar days from the date they are contacted to respond. The
organization must ensure that plan benefits are available to the individual as of the effective date of the
initial enrollment request and must not delay the provision of plan benefits in anticipation of the
applicant’s confirmation of intent to enroll. The organization may contact the individual in writing
(See Exhibit 6b) or by phone and must document this contact and retain it with the record of the
individual’s enrollment request. If the individual indicates that s/he is fully aware of any consequence
to his/her employer or union coverage brought about by enrolling in the Part D Plan, and confirms s/he
still wants to enroll, the MA organization must update the transaction with the appropriate “flag”
(detailed instructions for this activity are included with CMS systems guidance) and re-submit it for

89
enrollment. The effective date of enrollment will be based upon the individual's initial enrollment
request. This effective date may be retroactive in the event that the confirmation step occurs after the
effective date. MA organizations may use the Code 61 enrollment transaction code to submit the
enrollment transaction directly to CMS, as described in the Plan Communication Users Guide
(PCUG).
MA organizations are strongly encouraged to closely monitor their outreach efforts and to follow up
with applicants prior to expiration of the 30 day timeframe. If the individual does not respond in 30
days, or responds and declines the enrollment, the enrollment must be denied. A denial notice must be
provided (see Exhibit 7).
When an employer or union sponsored MA-PD plan is replacing an existing RDS plan offered by that
employer or union group, the MA organization may receive the Code 127 conditional rejection. In
these cases, it is not necessary to contact each individual, as described above. The MA organization
must resubmit the transactions updated with the appropriate flag.
MA organizations should work in close collaboration with employer/union sponsors who are replacing
RDS coverage with Part D coverage to ensure that all individuals are aware of the change and have the
information they need.
40.3 - Transmission of Enrollments to CMS
For all enrollment requests effective January 1, 2008, or later that the organization is not denying per
the requirements in §40.2.3, the MA organization must submit the information necessary for CMS to
add the beneficiary to its records as an enrollee of the MA organization within 7 calendar days of
receipt of the completed enrollment request. CMS system “down” days are included in the calculation
of the 7 calendar days (refer to Appendix C of the Plan Communications User Guide). For the purpose
of assessing compliance with this requirement, CMS will count the enrollment request receipt date as
“day zero” and the following day as “day one.” In the case of enrollment requests that are accepted
after the MA organization is enrolled to capacity, but as a vacancy occurs, the MA organization must
submit the information within 7 calendar days after a vacancy has become available.
All enrollment elections must be processed in chronological order by date of receipt of completed
enrollment elections (refer to §40.5 for procedures when the MA plan is closed for enrollment).
MA organizations are encouraged to submit transactions by the earliest possible MA organization
processing cutoff date (refer to the Plan Communications Users Guide (PCUG)). However, if the
organization misses the cutoff date, it must still submit the transactions within the required 7 calendar
day time frame.
NOTE: The requirement to submit the transaction within 7 calendar days does not affect the
effective date of the individual’s coverage under the plan, i.e., the effective date must be
established according to the procedures outlined in §§30.5 and 30.7
.
More detail on how MA organizations must submit transmissions to CMS are contained in the
Medicare Advantage and Prescription Drug Plans Plan Communications User Guide.
90
40.4 - Information Provided to Member
Much of the enrollment information that an MA organization must provide to the member must be
sent prior to the effective date of coverage. However, some information will be sent after the effective
date of coverage. A member’s coverage begins on the effective date regardless of when the member
receives all the information the plan sends.
As discussed previously (§40), the organization must provide required notices in response to
information received from CMS on the DTRR that provides the earliest notification. Organizations
may choose to send notifications based on the availability of each Batch Completion Summary Status
(BCSS) file if they desire. However, in no case may use of the BCSS for this purpose extend any
timeframe established in this guidance. Organizations choosing to utilize the BCSS for certain
required beneficiary notifications must do so consistently.
The organization may provide the required notices described in §§40.4.1 and 40.4.2 or may utilize a
single (“combination”) notice (see Exhibits 4b and 4e). The combination notice takes the place of
separate acknowledgement and confirmation notices and, as such, requires expedited issuance. To use
the combination notice, the organization must be able to provide this notice within 7 calendar days of
the availability of the DTRR. Additionally, when following this option to use the combination notice,
if the organization is unable to ensure that the beneficiary will receive this combination notice prior to
the enrollment effective date (or within timeframes for incomplete enrollment requests or enrollments
received at the end of the month), the organization still must ensure that the beneficiary has the
information required in §40.4.1 within the timeframes described therein.
If an individual’s enrollment includes a request for SSA or RRB premium withhold and was processed
after the monthly cut-off for payment, the organization must submit the request for premium withhold
separate from the enrollment request. Plans should resubmit the request for premium withhold timely
to assure the individual can have premium withholding at the next possible effective date.
Additionally, the organization must inform the individual that:
• If his/her request for premium withholding is approved, it will start in 1-2 months;
• The effective date for premium withholding will not be retroactive;
• S/he will be responsible for paying the organization directly for all premiums due from the
enrollment effective date until the month in which premium withholding begins; and
• For plans implementing §50.3.1, failure to pay premiums for months in which premium
withholding is not in effect will result in disenrollment from the plan.
40.4.1 - Prior to the Effective Date of Coverage
42 CFR 422.60(e)
(Rev. 2, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Prior to the effective date of coverage, the MA organization must provide the member with all the
necessary information about being a Medicare member of the MA organization, the MA organization
91
rules, and the member’s rights and responsibilities (an exception to this requirement is described in
§40.4.2). The MA organization must also provide the following to the individual:
• For enrollment requests submitted via electronic enrollment or telephonic enrollment
mechanisms (including the simplified enrollment mechanism), evidence that the enrollment
request was received (e.g., a confirmation number). For paper enrollment requests, organizations
are not required to provide evidence of receipt outside of the acknowledgement or combination
notice outlined below. Organizations may choose to provide a confirmation number or other
tracking mechanism indicating receipt of the paper enrollment request. However, organizations
are expected to keep a copy of the paper enrollment form and provide a copy upon request by the
beneficiary.
• A notice acknowledging receipt of the completed enrollment request (refer to Exhibits 4, 4a, and
4c for model letters) and showing the effective date of coverage. This notice must be provided no
later than 10 calendar days after receipt of the completed enrollment request (organizations
choosing to use the combination notice, refer to 40.4 above).
• Proof of health insurance coverage so that he/she may begin using plan services as of the
effective date. This proof must include the 4Rx data necessary to access benefits.
NOTE: This proof of coverage is not the same as the Evidence of Coverage document described
in the Medicare Communications and Marketing Guidelines. The proof of coverage may be in
the form of member ID cards, the enrollment form, and/or a notice to the member (refer to
Exhibits 4, 4a, 4b and 4c, which are model letters with optional language that would allow the
member to use the letter as evidence of health insurance coverage until he/she receives a member
card). As of the effective date of enrollment, plan systems should indicate active membership.
Regardless of whether an enrollment request is made in a face-to-face interview, by fax, by mail, or by
other mechanisms defined by CMS, the MA organization must explain:
• The charges for which the prospective member will be liable, e.g., any premiums (this includes
any Part D late enrollment penalty), coinsurance, fees or other amounts; and any amount that is
attributable to the Medicare deductible and coinsurance, if this information is available at the
time the acknowledgement notice is issued (confirmation notices and combination
acknowledgement/confirmation notices must contain this information).
• The prospective member’s authorization for the disclosure and exchange of necessary
information between the MA organization and CMS.
• The lock-in requirement. The MA organization must also obtain an acknowledgment by the
individual that he/she understands that care will be received through designated providers except
for emergency services and urgently needed care.
• The potential for financial liability if it is found that the individual is not entitled to Medicare
Part A and Part B at the time coverage begins and he/she has used MA plan services after the
effective date.
92
• The effective date of coverage and how to obtain services prior to the receipt of an ID card (if the
MA organization has not yet provided the ID card).
40.4.2 - After the Effective Date of Coverage
42 CFR 422.62(e)
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
The CMS recognizes that in some instances the MA organization will be unable to provide the
materials and required notifications to new enrollees prior to the effective date, as required in §40.4.1.
These cases will generally occur when an enrollment request is received late in a month with an
effective date of the first of the next month. In these cases, the MA organization still must provide the
member all materials described in §40.4.1 no later than 10 calendar days after receipt of the completed
enrollment request. Additionally, the MA organization is also strongly encouraged to call these new
members as soon as possible (such as within 1-3 calendar days) to provide the effective date, the
information necessary to access benefits and to explain the MA organization rules. The member’s
coverage will be active on the effective date regardless of whether or not the member has received all
the information by the effective date.
Acceptance/Rejection of Enrollment
Once the MA organization receives a DTRR from CMS indicating whether the individual’s enrollment
has been accepted or rejected, the MA organization must notify the individual in writing of CMS’
acceptance or rejection of the enrollment within ten calendar days of the DTRR that contains the
earliest notification of the acceptance or rejection (see Exhibits 4d, 6, 6a, 6c, 6d and 8 for model
letters). The enrollment confirmation notice must explain the charges for which the prospective
member will be liable, e.g., any premiums, coinsurance, fees or other amounts; and any amount that is
attributable to the Medicare deductible and coinsurance. For those eligible for the low-income subsidy,
the enrollment confirmation notice must specify the limits applicable to the level of subsidy to which
the person is entitled.
There are exceptions to this notice requirement for certain types of transaction rejections. These
exceptions exist so as not to penalize the individual for a systems issue or delay, such as a plan
transmission or keying error. In this case, the MA organization should not send a rejection notice and
must request a retroactive enrollment from CMS (or its designee) within the timeframes provided in
the Standard Operating Procedures for the CMS Retroactive Processing Contractor. If CMS (or its
designee) is unable to process the retroactive enrollment due to its determination that the individual is
not eligible, the MA organization must notify the individual of the rejection in writing within ten
calendar days after CMS’ (or its designee’s) determination. Retroactive enrollments are covered in
more detail in §60.4.
If an MA organization rejects an enrollment and later receives additional information from the
individual substantiating his/her eligibility, the MA organization must obtain a new enrollment request
from the individual in order to enroll the individual and must process the enrollment with a current
(i.e., not retroactive) effective date. Refer to §60.4 for more information regarding retroactive
enrollments.
40.5 - Enrollment Processing During Closed Periods
42 CFR 422.60(a)(2) and 422.60(b)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
93
As described in §40.3, an MA organization must process elections in order by date of receipt of
completed enrollment election when it is open for enrollment. However, an MA organization may
close an MA plan to OEP and OEPI enrollments or when it reaches a CMS-approved capacity limit.
This section addresses procedures for handling enrollment requests that arrive at the MA organization
when an MA plan is closed for enrollment, either through voluntary closure to OEP and OEPI
enrollments or because a CMS-approved capacity limit has been reached, and for processing those
enrollments when the MA plan re-opens or a vacancy occurs.
If an MA organization believes its MA plan does not have the capacity to accept additional members,
or as the MA plan enrollment grows and the MA organization estimates it may reach capacity during
its next open enrollment period, the MA organization may request a CMS-approved limit on
enrollment.
A capacity limit allows an MA organization to close or limit enrollment for all election periods. Only
with a reserved vacancy may an MA organization set aside vacancies for enrollment of conversions.
40.5.1 - Procedures After Reaching Capacity Limit
42 CFR §§ 422.60(a)(2) and 422.60(b)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
If the number of individuals who elect to enroll in an MA plan exceeds a CMS-approved capacity
limit, then the MA organization may limit enrollment of these individuals, but only if it provides
priority in acceptance.
If an MA organization receives completed enrollment requests between the time it reaches its limit and
the time CMS approves the limit, it may follow one of two options after it receives approval from
CMS to limit enrollment: (1) Deny the enrollment due to the onset of the capacity limit, or (2) Place
the enrollment on a waiting list to be processed as vacancies occur in the priority of acceptance. This
priority requires that the MA organization process enrollments from individuals who elected the MA
plan prior to CMS’ determination that the capacity has been exceeded, in order based on date of
receipt of the completed enrollment request, and in a manner that does not discriminate on the basis of
any factor related to health as described in 42 CFR §422.110.
The MA organization must take the same action for all enrollment requests received. See below for
procedures for following options 1 or 2.
After the enrollments discussed in the above paragraph are acted upon, the MA organization has
similar options for handling any additional enrollment requests received while the plan is closed for
enrollment. The MA organization may follow one of two options: (1) Deny the enrollment due to the
capacity limit, or (2) Place the enrollment on a waiting list to be processed when the plan re-opens for
enrollment. However, to ensure no discrimination is applied to applications processed, all MA
organizations that use option 1 (i.e., deny enrollment) for enrollments discussed in the above
paragraph, must continue to deny all enrollments received while the plan is closed for enrollment, and
may not use option 2. The MA organization must take the same action for all enrollment forms
received. In the case of enrollments received after the plan closes for enrollment, the date the MA plan
re-opens becomes the “receipt date” of enrollment forms received when the plan was closed.
94
EXAMPLE: If the plan was closed in April and re-opens on May 1, then the receipt date of
enrollment requests received in April is May 1. See below for procedures for following options 1
or 2.
If the MA Organization Uses Option 1 - It must notify the individual in writing that it is denying the
enrollment, and should do so within ten calendar days after it receives the enrollment request or after
the MA organization receives approval from CMS to limit enrollment (Exhibit 7). Please note that
CMS encourages MA organizations to use this option if they expect that there will be no enrollment
opportunities for longer than one month. This reduces the likelihood of multiple transactions and/or
mistaken disenrollments that would occur if a potential applicant enrolls in another MA plan while
waiting for the original MA plan to re-open.
If the MA Organization Uses Option 2 - It must notify the individual in writing that he/she has been
placed on a waiting list, and should do so within ten calendar days after the MA organization receives
the enrollment request or after the MA organization receives approval from CMS to limit enrollment.
The notice must also provide an estimated length of time that the individual will be on a waiting list
and instruct the individual that he may cancel his enrollment before a vacancy occurs.
As enrollment spaces become available, if the plan was closed for more than 30 calendar days since
the receipt of the enrollment form, the MA organization must contact (orally or in writing) the
individual to re-affirm the individual’s intent to enroll before processing the enrollment. (The MA
organization may make this contact even if the plan was closed for less than 30 days.) Within ten
calendar days after contacting the individual, the MA organization must send written notice of intent
to not process the enrollment to all individuals who state they are no longer interested in being
enrolled in the MA plan.
For individuals who indicate their continued interest in enrollment, the MA organization must
document the individual’s expressed interest to continue enrollment. This may be done via phone
contact report, notation on the enrollment form, etc.
There may be situations in which the MA organization has closed enrollment in a service area, yet
receives an approval for a capacity limit for a portion of that same service area. Given that MA plans
are either open or closed to OEP and OEPI enrollments for an ENTIRE plan service area, any
vacancies which may open up may only be filled by individuals making AEP, ICEP or SEP enrollment
elections by applying the rules for accepting enrollments when MA plans are closed (see §40.5.2
below). Further, it must take those individuals based upon enrollments received in chronological order.
40.5.2 - Procedures After Closing During the OEP and OEPI
42 CFR §§ 422.60(a)(2) and 422.60(b)
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
As stated in §30, an MA organization must accept all enrollment requests for its MA plans made
during the AEP, ICEP, or SEP. However, an MA organization may not process OEP or OEPI
enrollments for a plan when the plan is closed to OEP and OEPI enrollments.
If an MA plan is closed to OEP and OEPI enrollments and receives new OEP or OEPI enrollment
requests or documentation to complete OEP enrollment requests already received by the MA
95
organization, then the MA organization may do one of the following. The MA organization must take
the same action for all enrollment forms received while the plan is closed:
1. Deny the enrollment;
2. Continue to accept the completed enrollment requests to be placed on a waiting list.
If the MA Organization uses option #1 above - It must notify the individual in writing that it is
denying the enrollment, and should do so within ten calendar days after it receives the enrollment
request (Exhibit 7). Please note that CMS encourages MA organizations to use this option if they
expect that there will be no enrollment opportunities for longer than one month. This reduces the
likelihood of multiple transactions and/or mistaken disenrollments that would occur if a potential
applicant enrolls in another MA plan while waiting for the original MA plan to re-open.
If the MA Organization uses option #2 above - it must notify the individual in writing that he or she
has been placed on a waiting list. The notice must inform the individual that the enrollment request
will not be processed until the plan re-opens for enrollment, must include the date the plan will re-
open, and must inform the individual that he or she may cancel the request for enrollment before the
plan re-opens. All individuals who wish to wait for an opening must be placed on the waiting list.
After the MA plan re-opens, if the plan was closed for more than 30 calendar days since the MA
organization received the enrollment request, it must contact (orally or in writing) the individual to re-
affirm the individual’s intent to enroll before processing the enrollment. (The MA organization may
make this contact even if the plan was closed for less than 30 days.) The MA organization must send
written notice of intent to not process the enrollment to all individuals who state they are no longer
interested in being enrolled in the MA plan, and should do so within ten calendar days after contacting
the individual.
For individuals who indicate their continued interest in enrollment, the MA organization must
document the individual’s expressed interest to continue enrollment. This may be done via phone
contact report, notation on the enrollment form, etc. The date the MA plan re-opened becomes the
“receipt date” of enrollment forms received when the plan was closed.
EXAMPLE: If the plan was closed in February and re-opens on March 1, then the receipt date of
enrollment requests received in February is March 1.
40.6 - Enrollments Not Legally Valid
When an enrollment is not legally valid, a retroactive cancellation of enrollment action may be
necessary (refer to §60.5 for more information on retroactive disenrollments). In addition, a
reinstatement to the plan in which the individual was originally enrolled may be necessary if the
invalid enrollment resulted in an individual’s disenrollment from his/her original plan of choice.
An enrollment that is not complete, as defined in §10, is not legally valid. In addition, an enrollment is
not legally valid if it is later determined that the individual did not meet eligibility requirements at the
time of enrollment. For example, an enrollment is not legally valid if an MA organization determines
at a later date that the individual provided an incorrect permanent address at the time of enrollment and
the actual address is outside the MA plan’s service area. A second example could be an instance
96
where an individual not authorized by State law to make an enrollment request on another’s behalf
attempts to complete an enrollment request.
There are also instances in which an enrollment that appears to be complete can turn out to be legally
invalid. In particular, CMS does not regard an enrollment as actually complete if the member or
his/her legal representative did not intend to enroll in the MA organization. If there is evidence that the
individual did not intend to enroll in the MA organization, the MA organization should submit a
retroactive disenrollment request to CMS. Evidence of lack of intent to enroll by the individual may
include:
• An enrollment request signed by the individual when a legal representative should have signed
for the individual;
• Request by the individual for cancellation of enrollment before the effective date (refer to
§60.2 for procedures for processing cancellations);
• Enrolling in a supplemental insurance program immediately after enrolling in the MA
organization; or
• Receiving non-emergency or non-urgent services out-of-plan immediately after the effective
date of coverage under the plan.
Payment of the premium does not necessarily indicate an informed decision to enroll. For example, the
individual may believe that he/she was purchasing a supplemental health insurance policy, as opposed
to enrolling in an MA organization. In addition, use of an MA plan doctor does not necessarily
indicate an understanding of the lock-in requirement if the doctor also treats non-plan members.
40.7 - Enrollment Procedures for Medicare MSA Plans
MA organizations offering a Medicare MSA plan must follow the procedures outlined in §§40.2, 40.3,
40.4, 40.5.1, and 40.6. MSA plans must have a paper enrollment form available for eligible individuals
to request enrollment. Exhibit 1b is a model MSA plan enrollment form. Organizations may use this
model form as it appears or may customize their enrollment forms based on this model, if they follow
usual Medicare marketing material approval practices and ensure all the required MSA specific
elements are included. Applications for Medicare MSAs must include a question regarding election of
the Medicare hospice benefit.
All information necessary to successfully enroll the individual in the MSA plan must be provided to
consider the enrollment request complete, including the answers to questions 1 – 4 on the model MSA
enrollment form. Additionally, the organization must obtain the necessary banking and account
information before the enrollment can be considered complete. The MA organization must ensure its
materials describing the MSA plan explain the details of having the MSA account and what options
the individual will have regarding the account.
Beneficiaries may enroll into a Medicare MSA plan only through the MA organization offering that
plan. Beneficiaries may enroll directly with the plan by completing an approved paper enrollment
form. Additionally, MSA plans may offer an online enrollment mechanism as defined in §40.1.2
through the organization’s website. MSA plans are not available through the Online Enrollment
Center on the Medicare.gov website.

97
40.7.1 - Establishing the MSA Banking Account during the Enrollment Process
Medicare beneficiaries interested in enrolling in a MSA plan will need to establish an MSA bank
account to accept MSA deposits in accordance with the MSA plan’s procedures. The MA
Organization must have documentation that a beneficiary will open the MSA account before
submitting an enrollment transaction to MARx for that beneficiary. CMS will make the annual deposit
payment to the plan on the same schedule as the monthly capitation payment. Per Section 1853(e)(2)
of the Act, payment of an MSA deposit cannot be made until the beneficiary account has been
established.
Acceptable documentation that an MSA account has been established includes a
written/electronic notice from the bank that the beneficiary has opened an MSA account, or a
written/electronic communication from the beneficiary that the MSA account has been opened, with
the bank routing number and account number reported on the communication. The MSA organization
must retain this documentation. Described below are several procedures that the MSA Organization
could implement to facilitate the establishment of these MSA accounts:
1. The organization provides the beneficiary with specific banking enrollment materials to begin the
process necessary for establishment of the MSA banking account. The specified bank supplies the
beneficiary with the required signature card and items needed for establishing the account. The
beneficiary completes and returns the required documents to the specified bank. The bank
provides the information to the MSA plan to complete the enrollment transaction.
2. For an employer/union sponsored MSA plan, the plan’s designated bank deals directly with the
employer or union allowing the employer or union to facilitate the establishment of an account on
behalf of the Medicare beneficiaries enrolling in the MSA plan.
Finally, these procedures must accommodate the following guidance:
• MSA organizations must educate beneficiaries that the enrollment is not complete until the MSA
account is set up.
• The organization must have documentation that the account has been established prior to
submitting the enrollment transaction to CMS.
• MSA organizations must educate beneficiaries that once the enrollee’s initial deposit has been
received in the MSA account the enrollee may then transfer the funds to his or her own banking
institution.
MARx will not reject an MSA enrollment transaction if CMS records show an open period of
Medicaid or Hospice coverage; however, MARx will provide information about these statuses. MSA
plans should contact the beneficiary to confirm or deny this information.

98
50 - Disenrollment Procedures
42 CFR 422.74
Except as provided for in this section, an MA organization may not, either orally or in writing, or by
any action or inaction, request or encourage any member to disenroll. While an MA organization may
contact members to determine the reason for disenrollment, the MA organization must not discourage
members from disenrolling after they indicate their desire to do so. The MA organization must apply
disenrollment policies in a consistent manner for similar members in similar circumstances.
All notice requirements are summarized in Appendix 1.
NOTE: It is not necessary for an MA plan to send a notice of disenrollment to beneficiaries whose
plan benefit package (PBP) number is changed as part of a CMS-approved plan renewal. The annual
notice of change that the MA organization sends to the beneficiaries as part of the end-of-year
activities serves this function. Instructions and information on the annual notice of change can be
found in§60.7 of Chapter 3 of the Medicare Managed Care Manual.
50.1 - Voluntary Disenrollment by Member
A member may request disenrollment from an MA plan only during one of the election periods
outlined in §§30 and 30.7. The member may disenroll by:
1. Enrolling in another plan (during a valid enrollment period);
2. Giving or faxing a signed written notice to the MA organization, or through his/her employer
or union, where applicable;
3. Submitting a request via the Internet to the MA organization (if the MA organization offers
such an option); or
4. Calling 1-800-MEDICARE.
If a member verbally requests disenrollment from the MA plan, the MA organization must instruct the
member to make the request in one of the ways described above. The MA organization may send a
disenrollment form to the member upon request (see Exhibits 9, 9a, and 10).
The disenrollment request must be dated when it is initially received by the MA organization.
Per §40.2.1, when someone other than the Medicare beneficiary completes a disenrollment request, he
or she must:
1. Attest that he or she has the authority under State law to make the disenrollment request on
behalf of the individual;
2. Attest that proof of this authorization (if any), as required by State law that empowers the
individual to effect a disenrollment request on behalf of the applicant is available upon
request by the MA organization or CMS; and
3. Provide contact information.
99
50.1.1 – Requests Submitted via Internet
The MA organization has the option to allow members to submit disenrollment requests via the
Internet; however, certain conditions must be met. The MA organization must, at a minimum, comply
with the CMS security policies - found at http://www.cms.hhs.gov/informationsecurity/. However, the
MA organization may also include additional security provisions. The CMS policies indicate that with
regard to receiving such disenrollments via the Internet, an acceptable method of encryption must be
utilized to provide for confidentiality and integrity of this data, and that authentication or identification
procedures are employed to assure that both the sender and recipient of the data are known to each
other and are authorized to receive and decrypt such information.
In addition, CMS policies require MA organizations to provide the CMS Office of Information
Services with a pro forma notice of intent to use the Internet for these purposes. The notice is
essentially an attestation that the MA organization is complying with the required encryption,
authentication, and identification requirements. The CMS reserves the right to audit the MA
organization to ascertain whether it is in compliance with the security policy. The effective date of the
request is determined by the election period in which the valid request was received by the MA
organization. The election period is determined by the date the request is received at the site
designated by the MA organization, as described in member materials.
The option of online disenrollment is limited to requests submitted via the MA organization’s website.
Online disenrollment via other means, such as a broker website, as well as disenrollment requests
submitted via email, are not permitted.
50.1.2 - Request Signature and Date
When providing a written request, the individual must sign the disenrollment request. If the individual
is unable to sign, a legal representative must sign the request (refer to §40.2.1 for more detail on who
may complete enrollment and disenrollment requests). If a legal representative signs the request for the
individual, then he or she must attest to having the authority under State law to do so, and confirm that
a copy of the proof of court-appointed legal guardian, durable power of attorney, or proof of other
authorization required by State law that empowers the individual to effect a disenrollment request on
behalf of the applicant is available and can be presented upon request to the MA organization or CMS.
The individual and/or legal representative should write the date he/she signed the disenrollment
request; however, if he/she inadvertently fails to include the date, then the date of receipt that the MA
organization places on the request form will serve as the signature date.
If a written disenrollment request is received and the signature is not included, the MA organization
may verify with the individual or legal representative with a phone call and document the contact,
rather than return the written request as incomplete.
100
50.1.3 - Effective Date of Disenrollment
The election period during which the organization received a valid request to disenroll will determine
the effective date of the disenrollment; refer to §§30.6 and 30.7 for information regarding
disenrollment effective dates.
With the exception of some SEPs and when election periods overlap, beneficiaries may not choose
their effective date. Instead, the MA organization is responsible for assigning the appropriate effective
date based on the election period. During face-to-face disenrollments, or when a beneficiary calls
about a disenrollment, the MA organization staff are responsible for ensuring that a beneficiary does
not choose an effective date that is not allowed under the requirements outlined in §§30.6 and 30.7.
If a beneficiary submits a disenrollment request with an unallowable effective date, or if the MA
organization allowed the beneficiary to choose an unallowable effective date, the MA organization
must call or write the beneficiary to explain that the disenrollment must be processed with a different
effective date. The organization should resolve the issue with the beneficiary as to the correct effective
date, and the call must be documented. If the beneficiary refuses to have the disenrollment processed
with the correct effective date, the beneficiary can cancel the disenrollment request according to the
procedures outlined in §60.2.2.
50.1.4 - Notice Requirements
After the member submits a request, the MA organization must provide the member with a
disenrollment notice within ten (10) calendar days of receipt of the request to disenroll. The
disenrollment notice must include an explanation of the lock-in restrictions for the period during
which the member remains enrolled in the organization, and the effective date of the disenrollment
(see Exhibit 11). The MA organization may also advise the disenrolling member to hold Original
Medicare claims for up to one month so that Medicare computer records can be updated to show that
the person is no longer enrolled in the plan. For these types of disenrollments, i.e., disenrollments in
which the member has disenrolled directly through the MA organization, MA organizations are
encouraged, but not required, to follow up with a confirmation of disenrollment notice after receiving
CMS confirmation of the disenrollment from the DTRR.
Since Medicare beneficiaries have the option of disenrolling through sources other than the MA
organization (such as 1-800-MEDICARE or by enrolling in another Medicare managed care plan or
PDP), the MA organization will not always receive a request for disenrollment directly from the
member and will instead learn of the disenrollment through the CMS DTRR. If the MA organization
learns of the voluntary disenrollment from the CMS DTRR (as opposed to through written request
from the member), the MA organization must send a written confirmation notice of the disenrollment
to the member within ten calendar days of the availability of the DTRR (see Exhibit 12).
Organizations may choose, but are not required, to issue a disenrollment confirmation notice for an
automatic disenrollments resulting from an individual’s enrollment in a PBP within the same MA
contract.
If the MA organization receives a disenrollment request that it must deny, the organization must notify
the enrollee within 10 calendar days of the receipt of the request, and must include the reason for the
denial (see Exhibit 12a).
101
An MA organization may deny a voluntary request for disenrollment only when:
1. The request was made outside of an allowable period as described in §30 of this guidance; or
2. The request was made by someone other than the enrollee and that individual is not the enrollee’s
legal representative (as described in §40.2.1).
3. The request was incomplete and the required information is not provided within the required time
frame (as described in §50.4.2).
50.1.5 - Optional Employer/Union MA Disenrollment Request Mechanism
As described in §20.4.1 of this chapter, beginning April 1, 2003, MA organizations that offer
employer or union group-sponsored MA plans may choose to accept voluntary disenrollment requests
from beneficiaries enrolled in those plans directly from the employer or union (or its TPA) without
obtaining a written disenrollment request from each individual. The disenrollment must be prospective
from the date the request is received by the employer/union group.
• The MA organization must inform its Regional Office Account Manager of its intent to use this
mechanism and identify the employer(s) or union(s) for which it will be accepting
disenrollments made in this manner.
• The disenrollment information (i.e., the electronic file) submitted to the MA organization by
the employer or union (or TPA) must accurately reflect the employer’s or union’s record of the
disenrollment made by each individual according to the processes the employer or union has in
place, and may be accepted without a paper MA disenrollment request form.
• This alternate disenrollment request mechanism is used in place of paper MA disenrollment
request forms and does not require a signature. For purposes of compatibility with existing
instructions in this chapter, the MA organization receipt date will be the date the employer’s or
union’s record of an individual’s disenrollment choice is received by the MA organization. MA
organizations must record these dates.
• Effective date calculation of voluntary disenrollments and the collection and submission of
disenrollments to CMS will follow existing procedures.
• To accept electronic records of employer or union disenrollment requests, the MA organization
must, at minimum, comply with the CMS security policies regarding the acceptable method of
encryption utilized to provide for data security, confidentiality and integrity, and authentication
and identification procedures to ensure both the sender and recipient of the data are known to
each other and are authorized to receive and decrypt the information.
• The employer’s or union’s record of the disenrollment request must exist in a format that can
be easily, accurately and quickly reproduced for later reference by each individual member, the
MA organization and/or CMS as necessary, and be maintained (by the employer/union or the
MA organization, as they agree) for at least 6 years following the effective date of the
individual’s disenrollment from an MA plan. The MA organization must maintain its record of
information received from the employer or union following the guidelines for MA
disenrollment request forms (see §60.9).
102
50.1.6 - Group Disenrollment for Employer/Union Sponsored Plans
CMS is providing a process for group disenrollment from an employer or union sponsored MA plan.
CMS will allow an employer or union to disenroll its retirees from an employer or union sponsored
MA plan using a group disenrollment process.
The group disenrollment process must include notification to each beneficiary as follows:
• All beneficiaries must be notified that the employer or union intends to disenroll them from the
MA plan that the employer or union is offering; and
• This notice must be provided by the MA organization, employer, or union not less than 21
calendar days prior to the effective date of the beneficiary’s disenrollment from the
employer/union sponsored MA plan.
Additionally, the information provided must include an explanation on how to contact Medicare for
information about other MA plan options that might be available to the beneficiaries.
The employer/union must have and provide all the information required for the MA organization to
submit a complete disenrollment request transaction to CMS, as described in this and other CMS MA
systems guidance. Records must be maintained as outlined in §60.9 of this chapter.
50.1.7 - Medigap Guaranteed Issue Notification Requirements for Disenrollments
to Original Medicare during a SEP
MA organizations are required to notify members of their Medigap guaranteed issue rights when
members disenroll from the MA plan and into Original Medicare during a SEP. Model language
discussing these Medigap rights has been provided in Exhibit 11 and Exhibit 12.
There may be cases when a Medigap issuer requires the beneficiary to provide additional
documentation that s/he disenrolled as a result of an SEP and is eligible for such guaranteed issue
rights. A beneficiary may contact the MA organization for assistance in providing such
documentation. The MA organization may provide such a notice to the beneficiary upon request (see
Exhibit 24).
50.2 - Required Involuntary Disenrollment
The MA organization must disenroll a member from an MA plan in the following cases. Refer to
§50.6 for some exceptions to required disenrollment for grandfathered members.
1. A change in residence (includes incarceration – see below) makes the individual ineligible to
remain enrolled in the plan (§50.2.1);
2. The member loses entitlement to either Medicare Part A or Part B (§50.2.2);
3. The SNP enrollee loses special needs status and does not reestablish SNP eligibility prior to the
expiration of the period of deemed continued eligibility (§20.11).
4. The member dies (§50.2.3);
103
5. The MA organization contract is terminated, or the MA organization reduces its service area to
exclude the member. There is an exception to this rule, which is described in §50.2.4;
6. The member fails to pay his or her Part D-IRMAA to the government and CMS notifies the
plan to effectuate the disenrollment (§50.2.6); or
7. The member is not lawfully present in the United States (§50.2.7).
Incarceration – A member who is incarcerated resides outside the plan’s service area, even if the
correctional facility is located within the plan’s service area (see §10 for definition of “incarcerated”).
Notice Requirements - Disenrollment notices must be sent when:
• The individual has a change in residence and is determined to be out of the plan’s service area;
• CMS disenrolls the individual due to incarceration;
• The individual loses SNP status and doesn’t regain eligibility within the period of continued
deemed eligibility;
• The individual loses eligibility for enrollment due to contract termination or service area
reduction by the MA organization; or
• CMS disenrolls the individual for non-payment of Part D-IRMAA.
For disenrollments effectuated by the MA organization, all disenrollment notices must:
1. Advise the member that the MA organization is planning to disenroll the member and why such
action is occurring;
2. Be mailed to the member before submission of the disenrollment transaction to CMS; and
3. Include an explanation of the member’s right to a hearing under the MA organization’s
grievance procedures. (This explanation is not required if the disenrollment is a result of the
MA plan termination or service area or continuation area reduction, since a hearing would not
be appropriate for that type of disenrollment. There are different notice requirements for
terminations and service area reductions, which are provided in separate instructions to MA
organizations.)
For disenrollments effectuated by CMS due to incarceration or nonpayment of Part D-IRMAA, the
disenrollment notice must advise the member that the plan has disenrolled him or her, why such action
is occurring and be mailed within ten (10) calendar days of receiving the disenrollment DTRR from
CMS.
Plans are strongly encouraged, but not required, to send notices for certain CMS-effectuated
disenrollments, including:
• Death (Exhibit 13);
• Loss of entitlement (Exhibit 14); and
• Unlawful presence in the United States (Exhibit 38).
104
For plans that provide disenrollment notices for these situations, the disenrollment notices should
advise the member that the plan has disenrolled him or her and why such action is occurring. Plans are
encouraged to mail these notices within ten (10) calendar days of receiving the disenrollment DTRR
from CMS.
Medigap Guaranteed Issue Notification Requirements for Disenrollments to Original Medicare
during a SEP
MA organizations are required to notify members of their Medigap guaranteed issue rights when
members disenroll to Original Medicare during a SEP. Model language discussing these Medigap
rights has been provided in Exhibit 11 and Exhibit 12.
There may be cases when a Medigap issuer requires the beneficiary to provide additional
documentation that they disenrolled as a result of an SEP and are eligible for such guaranteed issue
rights. A beneficiary may contact you for assistance in providing such documentation. The MA
organization may provide such a notice to the beneficiary upon request (see Exhibit 24).
50.2.1 - Members Who Change Residence
MA organizations may offer (or continue to offer) extended “visitor” or “traveler” programs to
members of coordinated care plans who have been out of the service area for up to 12 months. The
MA organizations that offer such programs do not have to disenroll members in these extended
programs who remain out of the service area for more than 6 months but less than 12 months. As
mentioned at 42 CFR 422.74(d)(4)(iii), MA organizations offering a plan with a visitor/traveler
program must make this option available to all enrollees who are absent for an extended period from
the MA plan’s service area. However, MA organizations may limit this option to enrollees who travel
to certain areas, as defined by the MA organization, and who receive services from qualified
providers. Organizations offering MA-PFFS plans may allow continued enrollment of individuals
absent from the plan service area for up to 12 months, given that PFFS plans provide access to plan
benefits and services from providers located outside the plan service area.
MA organizations offering plans without these programs must disenroll members who have
been out of the service area for more than 6 months.
An SEP, as defined in §30.4.1, applies to individuals who are disenrolled due to a change in residence.
An individual may choose another MA or Part D plan (either a PDP or MA-PD) during this SEP.
50.2.1.1 - General Rule
The MA organization must disenroll a member if:
1. He/she permanently moves out of the service area and his/her new residence is not in a
continuation area;
2. The member’s temporary absence from the service area (or continuation area, for continuation
of enrollment members) exceeds 6 consecutive months;
105
3. The member is enrolled in an MA plan that offers a visitor/traveler program and his/her
temporary absence exceeds 12 consecutive months (or the length of the visitor/traveler
program if less than 12 months);
4. The member is an out-of-area member (as defined in §10), and permanently moves to an area
that is not in the service area or continuation area;
5. He/she permanently moves out of the continuation area of an MA local plan and his/her new
residence is not in the service area or another continuation area of the MA local plan;
6. The member permanently moves out of the service area (or continuation area, for continuation
of enrollment members in MA local plans) and into a continuation area, but chooses not to
continue enrollment in the MA local plan (refer to §60.7 for procedures for choosing the
continuation of enrollment option);
7. The member is an out-of-area member (as defined in §10), who leaves his/her residence for
more than 6 months;
8. The member is incarcerated and, therefore, resides out of area for the duration of the
incarceration.
50.2.1.2 - Effective Date of Disenrollment
Generally disenrollments for reasons 1, 4, 5, 6 and 8 above are effective the first day of the calendar
month after the date the member begins residing outside of the MA plan’s service area (or
continuation area, as appropriate) AND after the member or his or her legal representative notifies the
organization that he or she has moved and no longer resides in the plan service area. In the case of an
individual who provides advance notice of the move, the disenrollment will be the first of the month
following the month in which the individual indicates he or she will be moving.
In the case of incarcerated individuals, CMS will involuntarily disenroll individuals who are
incarcerated based on data CMS receives from SSA. CMS will report the disenrollments to the
organization via the daily DTRR using a specific Transaction Reply Code (TRC). For all such
disenrollments, the effective date of disenrollment will be the first of the month after the incarceration
start date.
MA organizations may receive notification of the individual’s possible incarceration status via another
source. In this situation, the MA organization needs to investigate and, following processes in
§50.2.1.3, determine if the member resides in the plan’s service area and, if appropriate, involuntarily
disenroll the member. If the incarceration information is received from a public entity or other source
with direct access to confirmed incarceration data, such as a penal facility, state Medicaid agency or
other state or federal agency, additional investigation is not necessary. Disenrollment is effective the
first of the month following the organization’s confirmation of a current incarceration. The MA
organization is required to send notification of the disenrollment to the member.
If the member establishes that a permanent move occurred retroactively and requests retroactive
disenrollment (not earlier than the first of the month after the move), the MA organization can submit
this request to CMS (or its designee) for consideration of retroactive action.
106
Disenrollment for reasons 2 and 7 above is effective the first day of the calendar month after 6
months have passed. Disenrollment for reason 3 is effective the 1st day of the 13th month (or the
length of the visitor/traveler program if less than 12 months) after the individual left the service area.
Unless the member elects another Medicare managed care plan during an applicable election period,
any disenrollment processed under these provisions will result in a change to enrollment in Original
Medicare.
50.2.1.3 - Researching and Acting on a Change of Address
Within ten (10) calendar days of receiving a notice of a change of address or an indication of possible
out-of-area residency from the member, the member’s legal representative, a CMS DTRR, or another
source, the MA organization must make an attempt to contact the member to confirm whether the
move is permanent (may use Exhibit 34 if contacting the member in writing). The MA organization
must also document its efforts. The requirement to attempt to contact the member does not apply to a
prospective enrollment for which the organization receives either transaction reply code 011
(Enrollment Accepted) or 100 (PBP Change Accepted as Submitted) accompanied by 016 (Enrollment
Accepted – Out of Area) on the same DTRR, as these represent new enrollments for which the
organization recently confirmed the individual’s permanent residence in the plan service area. MA
organizations may obtain either written or verbal verification of changes in address, as long as the MA
organization applies the policy consistently among all members.
In the case of individuals for which the plan learns of possible incarceration status from a source other
than CMS, the MA organization must confirm the individual’s out of area (i.e., incarcerated) status.
Confirmation may include contacting the individual or other sources to determine confirmation of
incarceration and incarceration start and end dates, if applicable. As described in §50.2.1.2, additional
investigation is not necessary if the incarceration information is received from a public entity or other
source with direct access to confirmed incarceration data. When an organization is notified of a current
member’s past period of incarceration and has confirmed that this member’s period of incarceration
has ended (i.e. individual is no longer incarcerated), the organization must continue the individual’s
enrollment, unless otherwise directed by CMS.
If the MA organization confirms an individual’s current incarceration status but does not obtain the
start date of the current incarceration, the organization must disenroll the individual prospectively for
the first of the month following the date on which the current incarceration was confirmed. If the MA
organization confirms an individual’s current incarceration status as well as the start date of the current
incarceration, the organization must disenroll the individual for the first of the month following the
start date of the incarceration. If that disenrollment effective date is outside the range of effective
dates allowed by MARx (based on the current calendar month), the MA organization must submit the
retroactive disenrollment request to the CMS Retroactive Processing Contractor (see §60.5).
The MA organization must retain documentation from the member or member’s legal representative of
the notice of the change in address, including the determination of whether the member’s out-of-area
status is temporary or permanent.
1. If the MA organization receives notice of a permanent change in address from the member
or the member’s legal representative, and the new address is outside the MA plan’s service
107
area (or continuation area, for continuation of enrollment members), the MA organization must
disenroll the member and provide proper notification (Exhibit 36). The only exception is if the
member has permanently moved into the continuation area and chosen the continuation of
enrollment option (procedures for electing a continuation of enrollment option are outlined in
§60.8).
2. If the MA organization receives notice (or indication) of a potential change in address from a
source other than the member or the member’s legal representative, and the new address
is outside the MA plan’s service area (or continuation area, for continuation of enrollment
members), the MA organization may not assume the move is permanent until it has received
confirmation from the member, the member’s legal representative or, for incarcerated
individuals, public sources (such as a state/federal government entity or other public records).
The MA organization must initiate disenrollment when it verifies a move is permanent or when
the member has been out of the service area (or continuation area, for continuation of
enrollment members) for six months from the date the MA organization learned of the change
in address. The MA organization must notify the member in writing of the disenrollment. If the
member responded and confirmed the permanent move out of the service area, the MA
organization must send the notice (Exhibit 36) within 10 calendar days of the member’s
confirmation that the move is permanent. If the member failed to respond to the request for
address confirmation the MA organization must send the notice (Exhibit 35) in the first ten
days of the sixth month from the date the MA organization learned of the change in address.
MA organizations may consider the six months to have begun on the date given by the
beneficiary as the date that he/she will be leaving the service area. If the beneficiary did not
inform the MA organization of when he/she left the service area, the MA organization can
consider the six months to have begun on the date it received information regarding the
member’s potential change in address (e.g. DTRR, out-of-area claims).
If the member does not respond to the request for verification within the time frame given by
the MA organization, the MA organization cannot assume the move is permanent and may not
disenroll the member until six months have passed. The MA organization may continue its
attempts to verify address information with the member.
3. Temporary absences - If the MA organization determines the change in address is temporary,
the MA organization may not initiate disenrollment until six months have passed from the date
the MA organization received information regarding the member’s absence from the service
area (or from the date the member states that his/her address changed, if that date is earlier).
If the MA organization offers a visitor/traveler program, the MA organization must initiate
disenrollment if it learns that the individual continues to remain out of the service area during
the 12 months (or the length of its visitor/traveler program if less than 12 months).
50.2.1.4 - Procedures for Developing Addresses for Members Whose Mail is Returned as
Undeliverable
If an address is not current, the USPS will return any materials mailed first-class by the organization as
undeliverable.
108
In the event that any member materials are returned as undeliverable, the organization must take the
following steps:
1. If the USPS returns mail with a new forwarding address, forward plan materials to the
beneficiary and advise the plan member to change his or her address with the Social Security
Administration.
2. If the organization receives documented proof of a beneficiary change that is outside of the
plan service area or mail is returned without a forwarding address, follow the procedures
described in §50.2.1.3.
3. If the organization receives claims for services from providers located outside the plan service
area, the organization may choose to follow up with the provider to obtain the member’s
address.
4. If the organization is successful in locating the beneficiary, advise the beneficiary to update
records with the Social Security Administration by:
a. Calling their toll-free number, 1-800-772-1213. TTY users should call 1-800-325-0778
weekdays from 7:00 a.m. to 7:00 p.m. EST;
b. Going to http://www.ssa.gov/changeaddress.html on the SSA website; or
c. Notifying the local SSA field office. A beneficiary can get addresses and directions to
SSA field offices from the Social Security Office Locator which is available on the
Internet at: http://www.socialsecurity.gov/locator/.
An organization is expected to continue to mail materials to the member’s address of record. If the
postal service returns a piece of beneficiary communication to the organization, the plan should
document the return and retain the returned material. It should continue to send future correspondence
to that same address, as a forwarding address may become available at a later date. Additionally, CMS
encourages the MA organization to continue its efforts, as discussed above, to attempt to locate the
beneficiary using any available resources, including CMS systems, to identify new address
information for the beneficiary. If a forwarding address becomes available, an organization can send
materials to that address as in item #1 above.
50.2.1.5 - Notice Requirements
1. MA organization notified of out-of-area permanent move - When the organization receives
notice of a permanent change in address from the member or the member’s legal
representative, it must provide notification of disenrollment to the member. This notice to the
member, as well as the disenrollment transaction to CMS, must be sent within ten (10) calendar
days of the MA organization’s learning of the permanent move.
In the notice, the MA organization is encouraged to inform the member who moves out of the
service area that he or she may have certain Medigap enrollment opportunities available to
them. These opportunities end 63 days after coverage with the MA organization ends. The MA
organization can direct the beneficiary to contact the State Health Insurance Assistance
Program (SHIP) for additional information on Medigap insurance.
109
In the case of incarcerated individuals disenrolled by CMS, we will report the disenrollments to
the organization via the daily DTRR using a specific TRC. An MA organization must send
each affected individual a written notice of the disenrollment within ten (10) calendar days of
receipt of the DTRR indicating disenrollment due to incarceration.
2. Out of area for 6 months - When the member has been out of the service area for 6 months
after the date the MA organization learned of the change in address from a source other than
the member or the member’s legal representative (or the date the member stated that his
address changed, if that date is earlier), the MA organization must provide notification of the
upcoming disenrollment to the member. Organizations are encouraged to follow up with
members and to issue interim notices prior to the expiration of the 6 month period.
The notice of disenrollment must be provided within the first ten calendar days of the sixth
month. The transaction to CMS must be sent within three (3) business days following the
disenrollment effective date.
This notice must also be provided to out-of-area members (as defined in §10) who leave their
residence and that absence exceeds six (6) months.
The CMS strongly encourages that MA organizations send a final confirmation of
disenrollment notice to the member to ensure the individual does not continue to use MA
organization services.
EXAMPLE: MA organization receives a DTRR on January 20 indicating an “out of area”
State and County Code. The 6-month period ends on July 20. The MA organization sends a
notice to the member within ten (10) calendar days of receipt of the DTRR and does not
receive any response from the member indicating this information is incorrect. Therefore,
the MA organization will proceed with the disenrollment, effective August 1. The MA
organization sends a notice to the member during the first ten (10) calendar days of July
notifying him that he will be disenrolled effective August 1. The transaction to CMS must
be sent no later than three (3) business days following July 31.
3. Visitor/Traveler Program Option - When the member has been out of the service area for 12
months (or the length of its visitor/traveler program if less than 12 months), the MA
organization must provide notification of the upcoming disenrollment to the member.
The notice of disenrollment must be provided during the first ten calendar days of the 12
th
month (or the length of its visitor/traveler program). The transaction to CMS must be sent
within 3 business days following the disenrollment effective date.
The CMS strongly encourages that MA organizations send a final confirmation of
disenrollment notice to the member to ensure the individual does not continue to use MA
organization services.
50.2.2 - Loss of Medicare Part A or Part B
With the exception of Medicare Part B-only grandfathered members (as described in §§20.6 and 50.6),
the MA organization cannot retain a member in an MA plan if the member is no longer entitled to both
110
Medicare Part A and Part B benefits. The organization will be notified by CMS that entitlement to
either Medicare Part A or Part B has ended, and CMS will make the disenrollment effective the first
day of the month following the last month of entitlement to either Medicare Part A or Part B benefits
(whichever occurred first).
If a member loses entitlement to Medicare Part A, the MA organization may not allow the member to
remain a member of the plan and receive Medicare Part B-only services. In addition, the MA
organization may not offer Part A-equivalent benefits and charge a premium for such coverage to
members who lose entitlement to Medicare Part A. Likewise, if a member loses entitlement to
Medicare Part B at any time, the MA organization may not allow the member to remain in the MA
plan.
Notice Requirements - CMS strongly suggests that notices be provided when the disenrollment is due
to the loss of entitlement to either Medicare Part A or Part B (see Exhibit 14) so that any erroneous
disenrollments can be corrected as soon as possible. In cases of erroneous disenrollment and
notification, see §60.3.1.
50.2.3 - Death
The CMS will disenroll a member from an MA organization upon his/her death and CMS will notify
the MA organization that the member has died. This disenrollment is effective the first day of the
calendar month following the month of death. Organizations may not submit disenrollment
transactions to CMS in response to the apparent death of a member. If the eligibility query shows a
date of death, the MA organization must submit the enrollment only when the date of death is equal to
or greater than the effective date. In anticipation of official notification from CMS via the DTRR,
organizations may, at their discretion, make note of the reported death in internal plan systems in order
to suppress premium bills and member notices.
Notice Requirements – Following receipt of a CMS notification (via DTRR) of disenrollment due to
death, CMS strongly suggests that a notice be sent to the member or the estate of the member (see
Exhibit 13) so that any erroneous disenrollments can be corrected as soon as possible. In cases of
erroneous disenrollment and notification, see §60.3.1.
50.2.4 - Terminations/Nonrenewals
The MA organization must disenroll a member from an MA plan if the MA organization contract is
terminated or if the MA organization discontinues offering the plan or reduces its service area to
exclude the member.
A member who is disenrolled under these provisions has an SEP, as described in §30.4.3, to elect a
different MA plan or Original Medicare. A member who fails to make an enrollment request during
this SEP is deemed to have elected Original Medicare.
EXCEPTION
MA organizations can offer an option to continue enrollment in an MA local plan in the organization
to members affected by MA plan service area reductions in areas where no other MA plans are
111
available at that time. If the organization chooses to offer this option, it must notify CMS, and must
notify members in the beneficiary non-renewal notification letter.
Members must indicate their desire to take advantage of this option. Members who take this option to
continue enrollment become known as “out-of-area members,” as defined in §10. The organization
may require individuals who choose to continue enrollment in an MA local plan in the organization to
agree to receive the full range of basic benefits (excluding emergency and urgently needed care, renal
dialysis, and post stabilization) exclusively at facilities designated by the MA organization within the
MA local plan service area.
Notice Requirements - The MA organization must give each Medicare member a written notice of
the effective date of the termination or service area or continuation area reduction, and include a
description of alternatives for obtaining benefits under the Medicare program. Required time frames
for these notices are outlined in
42 CFR 422.506 - 422.512.
50.2.5 – Loss of Special Needs Status
A SNP can determine to continue to provide care for an individual that no longer meets the unique
eligibility criteria of the plan (i.e., special needs status), if the individual can reasonably be expected to
again meet the special needs criteria within a period of time not to exceed six (6) months. For
example, a dual eligible individual who loses Medicaid eligibility can be deemed to continue to be
eligible for the plan if that individual would likely regain eligibility within six months. The SNP may
choose any length of time from one month to six months for deeming continued eligibility, as long as
it applies the criteria consistently to all members of the plan and fully informs members of its policy.
CMS expects the plan to take into account the ability to meet the needs of an individual that no longer
meets special needs status if and when applying the period of deemed continued eligibility. If the
member of a SNP does not re-qualify within the plan’s period of deemed continued eligibility, the
SNP should involuntarily disenroll him or her, with proper notice, at the end of this period. The period
of deemed continued eligibility begins the first of the month following the month in which information
regarding the loss is available to the organization and communicated to the enrollee, including cases of
retroactive Medicaid terminations.
For information on premiums, benefits and cost sharing during the period of deemed continued
eligibility, see Chapter 16b of the Medicare Managed Care Manual.
If the SNP is unable to provide continuity of care to a member who loses eligibility, the organization is
expected to involuntarily disenroll the member. For example, when a member of an institutional SNP
leaves the long-term care facility, he or she should be disenrolled from that SNP if the SNP providers
are limited to those within the facility.
Regardless of the date on which the beneficiary loses special needs status, the organization must
provide him/her with a minimum of 30 days advance notice of disenrollment.
Refer to Chapters 1 and 16b of the Medicare Managed Care Manual for additional information on
Special Needs Plans.
Notice Requirements - The SNP is expected to provide each member a written notice regarding the
loss of special needs status within 10 calendar days of learning of the loss of special needs status. This
112
notice should provide the member an opportunity to prove that he or she is still eligible to be in the
plan. In addition, the notice should include information regarding the period of deemed continued
eligibility, including its duration, a complete description of the SEP for which such individuals are
eligible (see §30.4.4, item #10), the consequences of not regaining special needs status within the
period of deemed continued eligibility and the effective disenrollment date (see Exhibit
32). Organizations are encouraged to follow up with members and to issue interim notices prior to the
expiration of the period of deemed continued eligibility.
In the event the individual fails to regain special needs status during the period of deemed continued
eligibility, the SNP is expected to provide the individual a written notice regarding involuntary
disenrollment (see Exhibit 33)
and must submit a disenrollment transaction to CMS. The disenrollment
notice to the individual and the transaction to CMS should be sent within 3 business days following the last
day
of the period of deemed continued eligibility; however, in no case should the disenrollment notice to
the individual be sent after the transaction is submitted to CMS
.
In the event the SNP fails to process disenrollments timely, the organization is expected to take the
following action(s):
a. If the SNP has not provided timely notification to the member of the potential for involuntary
disenrollment due to loss of special needs status (see Exhibit 32), the SNP should provide
this notice to the member and include a proposed disenrollment date that provides the
member the full length of the period of deemed continued eligibility. The SNP may not
shorten the grace period due its delay in issuing the notice.
b. If the SNP has not provided timely notification to the member of the involuntary
disenrollment due to loss of special needs status (see Exhibit 33), the SNP should provide
this notice to the member, revise the disenrollment date accordingly and include an
explanation of the delay and of the revised disenrollment date.
50.2.6 – Failure to Pay a Part D-Income Related Monthly Adjustment Amount
(Part D-IRMAA)
Individuals with Part D-IRMAA must pay this additional premium directly to the government, not to
their plans. CMS has established a 3-month initial grace period before individuals in an MA plan with
Part D coverage (MA-PD) who fail to pay their assessed Part D-IRMAA will be disenrolled from the
MA-PD plan. CMS will report the disenrollments to the organization via the daily DTRR using a
specific Transaction Reply Code (TRC). The effective date of the disenrollment is the first of the
month following the end of the initial grace period.
EXAMPLE: Ms. Jones owes a Part D-IRMAA. CMS bills Ms. Jones her monthly Part D-IRMAA
amount in March, April and May. Ms. Jones does not pay all the Part D-IRMAA amounts owed by the
due date of the May bill. CMS generates a disenrollment and sends the plan a specific TRC via the
daily DTRR. The effective date of the disenrollment will be June 1.
An MA organization must send each affected individual a written notice of the disenrollment within
ten (10) calendar days of receipt of the DTRR indicating disenrollment for non-payment of the Part D-
IRMAA.
113
Notice Requirements - MA organizations are required to notify members of their disenrollment due
to failure to pay Part D-IRMAA (see Exhibit 21a.)
When an individual fails to pay both Part D-IRMAA and the plan premium, and the disenrollment
effective dates are the same, the TRC for the disenrollment action will reflect the first disenrollment
transaction that is processed by MARx. For example, if the plan-generated disenrollment transaction,
resulting from the failure to pay plan premiums, is processed by MARx before CMS initiates a
disenrollment transaction for failure to pay Part D-IRMAA, the TRC will reflect the plan-generated
disenrollment. Thus, plans would issue Exhibit 21 as outlined in Section 50.3 regarding notice
requirements.
Similarly, if the CMS-generated disenrollment transaction for failure to pay Part D-IRMAA is
processed first, plans will receive the TRC reflecting this action. In such cases, CMS will be unable to
process the plan-generated disenrollment transaction (because the individual is already disenrolled);
however, plans may review their own billing records to determine if an individual was slated for
disenrollment for non-payment of plan premiums. If so, and the effective date of the disenrollment
matches the Part D-IRMAA disenrollment effective date, plans have three options for notifying
beneficiaries:
1. Plans may send the notice for failure to pay Part D-IRMAA (Exhibit 21a);
2. Plans may send both the notice for failure to pay Part D-IRMAA (Exhibit 21a) and the
plan notice for failure to pay premiums (Exhibit 21); or
3. Plans may send the plan notice for failure to pay premiums and include information
regarding the Part D-IRMAA disenrollment (Exhibit 21).
Reinstatement for Good Cause – Individuals involuntarily disenrolled from their MA-PD plan for
failure to pay Part D-IRMAA have the opportunity to ask CMS for reinstatement into the plan from
which they were disenrolled. CMS may reinstate enrollment, without interruption of coverage, if the
individual demonstrates good cause and pays in full within three (3) calendar months of the
disenrollment effective date:
• The Part D-IRMAA amounts that caused the disenrollment for nonpayment of Part D-IRMAA,
and
• Any plan premium amounts owed at the time he or she was disenrolled.
For more information on good cause, see §60.3.4.
50.2.7 – Unlawful Presence Status
The MA organization cannot retain a member in a MA plan if the member is not lawfully present in
the United States. The organization may not request from a member any documentation of U.S.
citizenship or alien status, as CMS provides the official status to the MA organization. CMS will
notify the organization (via DTRR) that the individual is not lawfully present, and CMS will make the
disenrollment effective the first day of the month following the notification by CMS.
Notice Requirements – Following the receipt of a CMS notification (via DTRR) of the disenrollment
due to unlawful presence, CMS strongly suggests that a notice be provided within ten (10) calendar
days of receipt of the DTRR (see Exhibit 38) so that the member is aware of the loss of coverage in the
plan and any erroneous disenrollments can be corrected as soon as possible. See §60.3.1 for cases of
possible erroneous disenrollment or notification.
114
50.3 - Optional Involuntary Disenrollments
An MA organization may disenroll a member from an MA plan it offers if:
• Premiums are not paid on a timely basis (§50.3.1);
• The member engages in disruptive behavior (§50.3.2); or
• The member provides fraudulent information on an enrollment request, or if the member
permits abuse of an enrollment card in the MA plan (§50.3.3).
Notice Requirements - In situations where the MA organization disenrolls the member involuntarily
for any of the reasons addressed above, the MA organization must send notice of the upcoming
disenrollment that meets the following requirements:
• Advises the member that the MA organization is planning to disenroll the member and why
such action is occurring;
• Provides the effective date of termination; and
• Includes an explanation of the member’s right to a hearing under the MA organization’s
grievance procedures.
Unless otherwise indicated, all notices must be mailed to the member before submission of the
disenrollment transaction to CMS.
50.3.1 - Failure to Pay Premiums
42 CFR 422.74(d) and Section 504 of the Rehabilitation Act of 1973
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
MA organizations may not disenroll a member who fails to pay MA plan cost sharing under this
provision. However, an MA organization has three options when a member fails to pay the MA plan’s
basic and supplementary premiums. This includes any Part D late enrollment penalty (per Chapter 4 of
the Medicare Prescription Drug Benefit Manual).
For each of its MA plans (i.e. each PBP), the MA organization must take action consistently among all
members of the discrete plan. For example, an MA organization may have different policies among
each of its plans, but it may not have different policies within a plan (other than the optional exception
for dual-eligible individuals and individuals who qualify for the Part D low income subsidy, as
described below).
The MA organization may:
1. Do nothing, (i.e., allow the member to remain enrolled in the same premium plan);
2. Disenroll the member after a grace period and proper notice; or
3. If the member fails to pay the premium for optional supplemental benefits (that is, a package of
benefits that the member is not required to accept), but pays the premium for basic and
mandatory supplemental benefits, reduce the member’s coverage (also known as “downgrade”)
by discontinuing the optional supplemental benefits and retaining the member in the same plan

115
after proper notice. Given these requirements for a downgrade, this option is available only for
MA plans that have optional supplemental benefits offered at a higher premium than the basic
benefit package. Such an action would be considered an addendum to the member’s original
request to enroll in the MA plan, and would not be considered a new enrollment request. Refer
to Chapter 4 (Benefits and Beneficiary Protections) for a definition of “basic benefit,”
“mandatory supplement,” and “optional supplemental benefits.”
If an MA organization chooses to disenroll members for failure to pay premiums, it must apply its
disenrollment policy consistently to all members of a plan including applying a consistent grace period
of no less than two (2) months. Additionally, the organization must promptly effectuate such
disenrollments at the end of the plan’s grace period for payment of premiums.
The MA organization may increase the length of the initial grace period or establish a policy of not
disenrolling members for failure to pay the plan premium during the calendar year. For example, an
MA organization may increase the grace period from 2 months to 6 months to ease the burden for
individuals affected by a natural disaster; however, it must provide this extended grace period to
everyone in the PBP and not only those in the area affected by the natural disaster. An organization
must report any changes to its policy for disenrollment for failure to pay premiums to its CMS account
manager before implementing such changes.
If the MA organization chooses to disenroll the member or reduce coverage, the action may only be
accomplished after the MA organization has made a reasonable effort to collect the premium and
notice has been provided (as described below). If payment has not been received within the grace
period, the individual will be disenrolled (or coverage reduced, as applicable).
Organizations may not disenroll members for failure to pay premiums (or notify them of impending
disenrollment) in cases where the member has requested that premiums be withheld from his/her
Social Security benefit check until the organization receives a reply from CMS indicating that the
member’s request has been rejected. The organization must then notify the member of the premium
owed, provide the appropriate grace period, and comply with other applicable requirements prior to
disenrolling the member.
Organizations may not involuntarily disenroll individuals who are considered to be in premium
withhold status by CMS. Individuals who have requested premium withhold are considered to
remain in premium withhold status until either (1) CMS notifies the organization that the premium-
withhold request has rejected, failed, or been unsuccessful; or (2) the member requests that he/she be
billed directly. Only after one of these actions occurs may a member’s status be changed to “direct
bill.” Once the member is considered to be in “direct bill” status, the organization must notify the
member of the premium owed and provide the appropriate grace period, as described below.
Organizations must always provide members the opportunity to pay premiums owed before initiating
any disenrollment action.
However, even if a member’s premium payment status has been changed to “direct bill,” if the
member can demonstrate that Social Security Administration (SSA) or the Railroad Retirement Board
(RRB) has withheld Part C and/or Part D premiums during the coverage month(s) in question, the
member will be considered to remain in premium withhold status. Such a member cannot be
disenrolled for failure to pay his/her premium(s), whether or not the organization actually receives
these premiums on a timely basis.
116
Example 1 – Incorrect Continuation of Premium Withhold: Individual was enrolled in Plan
A and selected premium withhold. Individual subsequently enrolls in Plan B and does not select
premium withhold. Upon receiving a direct bill from Plan B, the individual provides Plan B with
proof that a premium deduction continues from his SSA benefit check. Since the member
provided Plan B with evidence that a premium amount is currently being deducted from his
check, Plan B cannot initiate the process to disenroll the individual for failure to pay premiums.
Plan B must work with CMS to obtain appropriate premium reimbursement.
Further, an individual will continue to be considered in premium withhold status if an organization is
notified by CMS that the member’s request for premium withholding is not successful as a result of
systems/fund transfer issues between CMS and SSA or RRB, or between CMS and the organization.
CMS recognizes that in some instances organizations have not received premium amounts in their
monthly CMS plan payment for members who have elected SSA or RRB withholding; however,
organizations cannot hold their members responsible for such issues, nor penalize them by attempting
to disenroll them from their plan. Therefore, the organization may not initiate the billing (and
subsequent disenrollment process, if necessary) until a member is in “direct bill” status.
Example 2 – Incorrect Data Due to Systems Miscommunication: An individual requests
premium withhold, and Plan A correctly submits the request to CMS. The transaction request is
submitted successfully by CMS to SSA or RRB and the appropriate premium amount is deducted
from the individual’s SSA or RRB benefit check. However, due to a systems issue between CMS
and SSA or RRB, the premium withhold data is not correctly reflected in CMS systems. Thus,
CMS does not pay the correct premium amount to Plan A. Plan A must work with CMS to obtain
appropriate premium reimbursement and may not initiate the disenrollment process for the
individual for failure to pay premiums while the premium continues to be withheld.
In addition, organizations may not disenroll a member or initiate the disenrollment process if the
organization has been notified that the Part D portion of the premium is being paid by a SPAP, or
other payer, and the organization has not yet coordinated receipt of the premium payments with the
SPAP or other payer (refer to §50.6 of Chapter 14 of the Medicare Prescription Drug Benefit Manual
for additional information regarding coordination of premium payments).
While the MA organization may accept partial payments, it has the right to ask for full payment within
the grace period. If the member does not pay the required amount within the grace period, the effective
date of disenrollment or reduction in coverage is the first day of the month after the period ends.
Unless the member elects another MA plan during an applicable election period, any disenrollment
processed under these provisions will always result in a change of enrollment request to Original
Medicare. The MA organization has the right to take action to collect the unpaid premiums from
the beneficiary at any point during or after this process.
If a member is disenrolled for failure to pay premiums and attempts to re-enroll in the organization,
the MA organization may require the individual to pay any outstanding premiums owed to the MA
organization before considering the enrollment request to be “complete.”
If the individual is involuntarily disenrolled for failure to pay premiums, in order to re-enroll in that
plan, or to enroll in another plan, the individual must request enrollment during a valid period.
Payment of past due premiums after the disenrollment date does not create an opportunity for
117
reinstatement into the plan from which the individual was disenrolled for failure to pay premiums.
Likewise, disenrollment for failure to pay premiums does not, in itself, provide the beneficiary an
opportunity (SEP) to enroll in a different MA plan.
Calculating the Grace Period
An MA organization must provide plan enrollees with a grace period of not less than 2 calendar
months; however, it may provide a grace period that is longer than 2 calendar months, at its discretion
(e.g. organizations may elect to provide a 3-month initial grace period to match the Part D-IRMAA
initial grace period), provided that similarly situated enrollees are treated equally. The grace period
must be a whole number of calendar months and cannot include fractions of months. The grace period
cannot begin until the individual has been notified of (billed for) the actual premium amount due, with
such notice/bill specifying the due date for that amount and providing an opportunity to pay. For new
enrollees of an MA-PD plan, the MA organization must wait until notified by CMS of the actual Part
D premium which the beneficiary is responsible for paying directly before the individual can be
notified of/billed for the amount due; for these individuals, the due date cannot be until after the
organization receives notification from CMS as to the beneficiary’s premium and notifies the
individual of the amount due. The grace period may begin no earlier than the first of the month for
which the premium was unpaid.
NOTE: For individuals who have requested communications in an accessible format, the grace period
cannot begin until the organization provides notification (e.g. the bill) in an accessible format.
MA organizations have the following options in calculating and applying the grace period. The
organization must apply the same option for all members of a plan.
Option 1 - MA organizations may consider the grace period to end not less than 2 calendar
months after the first day of the month for which premium is unpaid.
If the overdue premium and all other premiums that become due during the grace period (in
accordance with the terms of the member’s agreement with the MA organization) are not paid in full
by the end of the grace period, the MA organization may terminate or reduce the member’s coverage.
As mentioned previously, the individual must be notified of/billed for the actual premium amount due
before the premium can be considered “unpaid.” For new enrollees, at a minimum, this cannot occur
until CMS notifies the organization of the total premium due from the individual. Upon CMS
notification, the organization would notify the individual of the amount due, with a prospective due
date.
Under this scenario, MA organizations are encouraged to send subsequent notices as reminders or to
show that additional premiums are due. Subsequent notices, therefore, should determine the
expiration date of the grace period by reference to this date. Notice requirements are summarized in
this section under the heading “notice requirements.”
EXAMPLE A: Plan XYZ has a 2-month grace period for premium payment. Plan member Mr.
Stone’s premium was due on February 1, 2009. He did not pay this premium and on February 7
th
,
the MA organization sent an appropriate notice. Mr. Stone ignores this notice and any subsequent
premium bills. The grace period is the months of February and March. If Mr. Stone does not pay
his plan premium before the end of March, he will be disenrolled as of April 1, 2009.
118
EXAMPLE B: Plan QRS has a 3-month grace period for premium payment. Plan member Mrs.
Monsoon’s premium was due on July 1, 2009. She did not pay this premium and on July 6
th
, the
MA organization sent an appropriate notice. Mrs. Monsoon ignores this notice and subsequent
premium bills. The grace period is the months of July, August and September. If Mrs. Monsoon
does not pay her owed premiums by the end of this period (September 30), she will be disenrolled
effective October 1, 2009.
In short, the MA organization may require that the member pay the overdue premiums in full within
the grace period, as well as all other payments becoming due within that period, in order to avoid
disenrollment (or a reduction in coverage, where applicable). If the MA organization requires the
member to make full payment within the grace period and pay all premiums falling due within that
period; however, the MA organization must state so in its initial delinquency notice to the member.
Option 2 - MA organizations may use a “rollover” approach in applying the grace period.
Under this scenario, the grace period would begin on the first of the month for which the premium is
unpaid, but if the member makes a premium payment within the grace period, the grace period stops
and is revised to reflect the new disenrollment date, depending on the number of months for which
premiums are received. The member would then have a new grace period beginning on the 1
st
day of
the next month for which the premium is due. The subsequent notice also would have to be sent within
15 calendar days, as described below, of the next premium due date. This process continues until the
member’s balance for delinquent premiums is paid in full or until the grace period expires with no
premium payments being made, at which time the MA organization may disenroll the member.
Organizations are not required to issue new notices each time the member submits a partial premium
payment (i.e. less than one month’s premium), since this would not result in a change in the proposed
disenrollment date. However, since payment of at least one month’s past-due premium causes the
disenrollment date to “roll over” (i.e. move forward) commensurate with the number of month’s
premium received, organizations must issue a notice warning of the potential for involuntary
disenrollment (see Exhibit 19) which includes the new disenrollment date whenever payment of at
least one month’s premium is received during the grace period. These subsequent notices are required
to be sent within 15 calendar days of the premium due date that follows receipt of the premium
payment.
EXAMPLE
Plan WXY has decided to offer a 2 month grace period for non-payment of plan premiums and has
chosen the “rollover” approach to calculating the grace period. A member fails to pay his January
premium due January 1. The MA organization sends a notice to the member on January 7
th
stating
that his coverage will be terminated if the outstanding premium is not paid within the grace period.
The notice advises him that his termination date would be March 1. The member then pays the
January premium, but does not pay the February premium. The grace period is recalculated to
begin on the 1
st
of the next month for which the premium is unpaid (February 1). On February 9
th
the MA organization sends a notice to the member reflecting the new grace period and the new
anticipated termination date of April 1
st
. The member pays off his balance in full before the grace
period expires; therefore, the member’s coverage in the MA plan remains intact.

119
Notice Requirements - If it is the MA organization’s policy to disenroll the member or to reduce
coverage when a member has not paid premiums, the MA organization must send an appropriate
written notice of non-payment of premium to the member within 15 calendar days of the premium
due date (see Exhibit 19
).
The MA organization may send interim notices after the initial notice.
In addition to the notice requirements outlined in §50.3
, this notice must:
• Alert the member that the premiums are delinquent;
• Provide the member with an explanation of disenrollment procedures advising the member that
failure to pay the premiums within the grace period that began on the 1
st
of the month for which
premium was unpaid will result in termination or reduction of MA coverage, whichever is
appropriate according to the MA organization policy, and the proposed effective date of this
action;
• Explain whether the MA organization requires full payment within the grace period (including
the payment of all premiums falling due during the intervening days, when and as they become
due, according to the terms of the membership agreement) in order to avoid termination of
membership or reduction in benefits; and,
• Explain the implications of a reduction in coverage (e.g., description of lower level of benefits),
if the MA organization policy is to reduce coverage for the nonpayment of optional supplemental
benefit premiums.
If a notice is returned to the organization as undeliverable, the organization should immediately
implement its procedure for researching a potential change of address (see §§50.2.1.3 and 50.2.1.4) as
well. The beneficiary may have moved out of the service area. If the organization confirms the
permanent move such that a disenrollment date earlier than the end of the grace period is required, the
organization must disenroll the beneficiary for the earlier disenrollment date.
If a member does not pay within the grace period, and the MA organization’s policy is to disenroll the
member, the MA organization must notify the member in writing providing the effective date of the
member’s disenrollment (refer to Exhibit 20) and submit a disenrollment transaction to CMS. The
disenrollment notice to the individual and the transaction to CMS must be sent within 3 business days
following the last day of the grace period; however, in no case may the disenrollment notice to the
individual be sent after the transaction is submitted to CMS. In the event the organization submits a
disenrollment request to CMS and later learns that payment was received timely, a reinstatement
request must be submitted to CMS (or its designee). In addition, CMS strongly encourages that MA
organizations send final confirmation of disenrollment to the member after receiving the DTRR (refer
to Exhibit 21 for a model letter).
If a member does not pay within the grace period, and the MA organization policy is to reduce
coverage by eliminating optional supplemental benefits within the current plan, for the nonpayment of
optional supplemental benefit premiums, the MA organization must notify the member in writing no
later than 3 business days after the expiration of the grace period that the MA organization is reducing

120
the coverage and provide the effective date of the change in benefits (refer to Exhibit 22 for a model
letter).
Optional Exception for Dual-Eligible Individuals and Individuals who Qualify for the Low
Income Subsidy
MA organizations offering MA-PD plans have the option to retain dually eligible members and
individuals who qualify for the low income subsidy (LIS) who fail to pay premiums even if the MA
organization has a policy to disenroll members for non-payment of premiums. For MA-only plans,
organizations may retain individuals who are dually eligible for both Medicare and Medicaid (i.e.
individuals who are entitled to Medicare Part A and Part B and receive any type of assistance from the
Title XIX (Medicaid) program).
The MA organization has the discretion to offer this option to dually eligible individuals and
individuals who qualify for LIS within each of its MA plans. If the MA organization offers this option
in one of its plans, it must apply the policy to all such individuals in that MA plan.
The policy to retain individuals is based upon non-payment of premium for the standard benefit
package of the MA plan. If the MA organization chooses this option, any dually eligible individual or
individual who qualifies for LIS who fails to pay premiums for any optional supplemental benefit
offered would be downgraded to the standard benefit package within that MA plan.
CMS requires that organizations provide members advance notice of plan policy changes. An MA
organization will have the discretion as to how it will notify its members of the change, e.g. in an
upcoming newsletter or other member mailing, such as the Annual Notice of Change. CMS
recommends a general statement in such notifications to avoid confusing other members for whom the
policy does not apply.
EXAMPLE: “If you have Medicaid or receive extra help in paying for your Medicare prescription
drugs and are having difficulty paying your plan premiums or cost sharing, please contact us.”
The plan must document this policy internally and have it available for CMS review.
50.3.2 - Disruptive Behavior
42 CFR 422.74(d)(2)
The MA organization may request to disenroll a member if his/her behavior is disruptive to the extent
that his/her continued enrollment in the MA plan substantially impairs the MA organization’s ability
to arrange for or provide services to either that particular member or other members of the plan.
However, the MA organization may disenroll a member for disruptive behavior only after it has met
the requirements of this section and with CMS’ approval. The MA organization may not disenroll a
member because he/she exercises the option to make treatment decisions with which the MA
organization disagrees, including the option of no treatment and/or no diagnostic testing. The MA
organization may not disenroll a member because he/she chooses not to comply with any treatment
regimen developed by the MA organization or any health care professionals associated with the MA
organization.
Before requesting CMS’ approval of disenrollment for disruptive behavior, the MA organization must
make a serious effort to resolve the problems presented by the member. Such efforts must include
121
providing reasonable accommodations, as determined by CMS, for individuals with mental or
cognitive conditions, including mental illness and developmental disabilities. The MA organization
must also inform the individual of his or her right to use the organization’s grievance procedures.
The MA organization must submit documentation of the specific case to CMS for review. This
includes documentation:
• Of the disruptive behavior;
• Of the MA organization’s serious efforts to resolve the problem with the individual;
• Of the MA organization’s effort to provide reasonable accommodations for individuals with
disabilities, if applicable, in accordance with the Americans with Disabilities Act;
• Establishing that the member’s behavior is not related to the use, or lack of use, of medical
services;
• Describing any extenuating circumstances cited under 42 CFR 422.74(d)(2)(iii) and (iv);
• That the MA organization provided the member with appropriate written notice of the
consequences of continued disruptive behavior (see Notice Requirements); and
• That the MA organization then provided written notice of its intent to request involuntary
disenrollment (see Notice Requirements).
The MA organization must submit to its CMS Regional Office account manager:
• The above documentation;
• The thorough explanation of the reason for the request detailing how the individual’s behavior
has impacted the MA organization’s ability to arrange for or provide services to the individual
or other members of the MA plan;
• Member information, including age, diagnosis, mental status, functional status, a description of
his or her social support systems and any other relevant information;
• Statements from providers describing their experiences with the member; and
• Any information provided by the member.
The MA organization may request that CMS consider prohibiting re-enrollment in the MA plan (or
plans) offered by the MA organization in the service area.
The MA organization’s request for involuntary disenrollment for disruptive behavior must be
complete, as described above. The CMS Regional Office will review this documentation and consult
with CMS Central Office (CO), including staff with appropriate clinical or medical expertise, and
decide whether the organization may involuntarily disenroll the member. Such review will include any
122
documentation or information provided either by the organization and the member (information
provided by the member must be forwarded by the organization to the CMS RO). CMS will make the
decision within 20 business days after receipt of all the information required to complete its review.
The CMS will notify the MA organization within 5 (five) business days after making its decision.
The Regional Office will obtain Central Office concurrence before approving an involuntary
disenrollment. The disenrollment is effective the first day of the calendar month after the month in
which the organization gives the member a written notice of the disenrollment, or as provided by
CMS. Any disenrollment processed under these provisions will always result in a change of
enrollment request to Original Medicare.
If the request for involuntary disenrollment for disruptive behavior is approved, CMS may require the
MA organization to provide reasonable accommodations to the individual in such exceptional
circumstances that CMS deems necessary. An example of a reasonable accommodation in this context
is that CMS could require the MA organization to delay the effective date of involuntary disenrollment
to coordinate with an MA enrollment request or Part D enrollment period that would permit the
individual an opportunity to obtain other coverage. If necessary, CMS will establish an SEP on a case-
by-case basis.
Notice Requirements
The disenrollment for disruptive behavior process requires 3 (three) written notices:
1. Advance notice to inform the member that the consequences of continued disruptive behavior will
be disenrollment;
2. Notice of intent to request CMS’ permission to disenroll the member; and
3. A planned action notice advising that CMS has approved the MA organization’s request.
Advance Notice
Prior to forwarding an involuntary disenrollment request to CMS, the MA organization must provide
the member with written notice describing the behavior it has identified as disruptive and how it has
impacted the MA organization’s ability to arrange for or provide services to the member or to other
members of the MA plan. The notice must explain that his/her continued behavior may result in
involuntary disenrollment and that cessation of the undesirable behavior may prevent this action. The
MA organization must include a copy of this notice and the date it was provided to the member in any
information forwarded to CMS. NOTE: If the disruptive behavior ceases after the member receives
notice and then later resumes, the MA organization must begin the process again. This includes
sending another advance notice.
Notice of Intent
If the member’s disruptive behavior continues despite the MA organization’s efforts, then the MA
organization must notify him/her of its intent to request CMS’ permission to disenroll him/her for
disruptive behavior. This notice must also advise the member of his/her right to use the organization’s
grievance procedures and to submit any information or explanation. Refer to Chapter 13, “Grievances,
Organizations Determinations, and Appeals,” for the appropriate procedures for grievances. The MA
123
organization must include a copy of this notice and the date it was provided to the member in any
information forwarded to CMS.
Planned Action Notice
If CMS permits an MA organization to disenroll a member for disruptive behavior, the MA
organization must provide the member with a written notice that, in addition to the notice requirements
outlined in §50.3, a statement that this action was approved by CMS and meets the requirements for
disenrollment due to disruptive behavior described above. The MA organization may only provide the
member with this required notice after CMS notifies the MA organization of its approval of the
request.
The MA organization can only submit the disenrollment transaction to CMS after providing the notice
of disenrollment (Planned Action Notice) to the individual. The disenrollment is effective the first day
of the calendar month after the month in which the MA organization gives the member a written notice
of the disenrollment, or as provided by CMS.
50.3.3 - Fraud and Abuse
42 CFR 422.74(e)(1)
An MA organization may request to cancel the enrollment of a member who knowingly provides, on
the enrollment request form or by another enrollment request mechanism, fraudulent information that
materially affects the determination of an individual’s eligibility to enroll in the plan. The organization
may also request to disenroll a member who intentionally permits others to use his/her enrollment card
to obtain services or supplies from the plan or any authorized plan provider. Such a disenrollment is
effective the first day of the calendar month after the month in which the organization gives the
member the written notice.
When such a cancellation or disenrollment occurs, the organization must immediately notify the CMS
RO so the Office of the Inspector General may initiate an investigation of the alleged fraud and/or
abuse. Any disenrollment processed under these provisions will always result in a change of
enrollment to Original Medicare.
Notice Requirements - The MA organization must give the member a written notice of the
disenrollment that contains the information required at §50.3.
50.4 - Processing Disenrollments
50.4.1 - Voluntary Disenrollments
After receipt of a completed disenrollment request from a member, the MA organization is responsible
for submitting the disenrollment transaction to CMS in a timely, accurate fashion. Such transmissions
must occur within 7 calendar days of receipt of the completed disenrollment request, in order to ensure
the correct effective date.
124
The MA organization must maintain a system for receiving, controlling, and processing voluntary
disenrollments from the MA organization. This system should include:
• Dating each disenrollment request as of the date it is received (regardless of whether the request
is complete at the time it is received by the MA organization) to establish the date of receipt;
• Dating supporting documents for disenrollment requests as of the date they are received;
• Processing disenrollment requests in chronological order by date of receipt of completed
disenrollment requests;
• Transmitting disenrollment information to CMS within 7 calendar days of the receipt of the
completed disenrollment request from the individual or the employer or union (whichever
applies). If the disenrollment information is received through the employer or union, the MA
organization must obtain the member’s written disenrollment request from the employer or
union;
• For disenrollment requests received by the MA organization, notifying the member in writing
within ten calendar days after receiving the member’s written request, to acknowledge receipt of
the completed disenrollment request, and to provide the effective date (see Exhibit 11 for a
model letter). MA organizations are encouraged, but not required, to follow up with a
confirmation of disenrollment letter after receiving CMS confirmation of the disenrollment from
the DTRR;
• For all other voluntary disenrollments (i.e., voluntary disenrollments made by the beneficiary
through 1-800-MEDICARE, by enrolling in another MA plan or PDP or by consenting to
passive enrollment into a Medicare-Medicaid demonstration plan, which the MA organization
would not learn of until receiving the DTRR), notifying the member in writing to confirm the
effective date of disenrollment within ten calendar days of the availability of the TRR (see
Exhibits 12 and 12c for model letters). This notice requirement does not apply to a disenrollment
resulting from a member switching from one benefit package to another within the same
organization (i.e., a PBP change), unless enrollment in the new PBP is the result of passive
enrollment into a Medicare-Medicaid demonstration plan.
50.4.2 – When the Disenrollment Request is Incomplete
When the disenrollment request is incomplete, the MA organization must document all efforts to
obtain additional documentation to complete the disenrollment request and have an audit trail to
document why additional documentation was needed before the request could be considered complete.
The organization must make this determination, and within 10 calendar days of receipt of the
disenrollment request, must notify the individual that additional information is needed.
If a written disenrollment request is submitted and the signature is not included, the MA organization
may verify with the individual with a phone call and document the contact, rather than return the
written request as incomplete.
125
For AEP disenrollment requests, additional documentation to make the request complete must be
received by December 7, or within 21 calendar days of the request for additional information
(whichever is later). For all other enrollment periods, additional documentation to make the request
complete must be received by the end of the month in which the disenrollment request was initially
received, or within 21 calendar days of the request for additional information (whichever is later).
50.4.3 - Involuntary Disenrollments
The MA organization is responsible for submitting involuntary disenrollment transactions to CMS in a
timely, accurate fashion.
The MA organization must maintain a system for controlling and processing involuntary
disenrollments from the MA organization. This includes:
• Maintaining documentation leading to the decision to involuntarily disenroll the member; and
• For all involuntary disenrollments except disenrollments due to death and loss of Medicare Parts
A and/or B, notifying the member in writing of the upcoming involuntary disenrollment,
including providing information on grievances rights.
In addition, CMS strongly encourages MA organizations to send confirmation of involuntary
disenrollment to ensure the member discontinues use of MA organization services after the
disenrollment date.
50.5 - Disenrollments Not Legally Valid
When a disenrollment is not legally valid, a reinstatement action may be necessary (refer to §60.3 for
more information on reinstatements). In addition, the reinstatement may result in a retroactive
disenrollment from another plan. Since optional involuntary disenrollments (as stated in §50.3) are
considered legal and valid disenrollments, individuals would not qualify for reinstatements in these
cases.
A voluntary disenrollment that is not complete, as defined in §10, is not legally valid. In addition,
there are instances in which a disenrollment that appears to be complete can turn out to be legally
invalid. For example, automatic disenrollments due to an erroneous death indicator or an erroneous
loss of Medicare Part A or Part B indicator are not legally valid.
The CMS also does not regard a voluntary disenrollment as actually complete if the member or his/her
legal representative did not intend to disenroll from the MA organization. If there is evidence that the
member did not intend to disenroll from the MA organization, the MA organization should submit a
reinstatement request to CMS (or its designee). Evidence that a member did not intend to disenroll
may include:
• A disenrollment request signed by the member when a legal representative should be signing for
the member; or
• Request by the member for cancellation of disenrollment before the effective date (refer to §60.2
for procedures for processing cancellations).

126
Discontinuation of payment of premiums alone does not necessarily indicate that the member has
made an informed decision to disenroll.
In contrast, CMS believes that a member’s deliberate attempt to disenroll from a plan (e.g. sending a
written request for disenrollment to the MA organization, or calling 1-800-MEDICARE) implies intent
to disenroll. Therefore, unless other factors indicate that this disenrollment is not valid, what appears
to be a deliberate, member-initiated disenrollment should be considered valid.
50.6 - Disenrollment of Grandfathered Members
As discussed in §20.6, any individual who was enrolled in a §1876 risk plan effective December 1,
1998, or earlier, and remained enrolled with the risk plan on December 31, 1998, automatically
continued to be enrolled in the MA organization on January 1, 1999, even if he/she was not entitled to
Medicare Part A or did not live in an MA plan service area or MA organization continuation area.
Disenrollment procedures for grandfathered members are generally the same as those for other
members. The MA organization must disenroll any grandfathered member if:
• The member dies;
• The member loses either Medicare Part A or Part B (or for Part B only members, enrollment in
Medicare Part B ends for the member);
• The member permanently moves into the continuation area, but does not choose to continue
enrollment or moves to an area that is out of the service or continuation area;
• The member permanently moves out of the vicinity, making continued enrollment no longer
reasonable. For example, a move of only a short distance may not affect the member’s ability
to continue to access the plan; therefore, continued enrollment would be reasonable; or,
• The MA organization contract is terminated or the service area or continuation area is reduced
with respect to all MA individuals who live in the area where the individual resides.
NOTE: The member may be offered the option to continue enrollment, as described in
§50.2.4.
50.7 - Disenrollment Procedures for Employer/Union Sponsored Coverage
Terminations
When the contract between an employer or union group and an MA organization is terminated, or the
employer/union determines that a beneficiary is no longer eligible to participate in the employer/union
sponsored MA plan
2
, the MA organization has the option to follow one of two procedures to disenroll
beneficiaries from the current employer/union sponsored MA plan in which the individual is enrolled:
2
The employer/union establishes criteria for its retirees to participate in the employer/union sponsored MA plan. These
criteria are exclusive of and in addition to the eligibility criteria for MA enrollment. Eligibility criteria to participate and
127
For both of the following options, the MA organization must ensure that the employer or union agrees
to the following:
• The employer or union will provide the MA organization with timely notice of contract
termination or the ineligibility of an individual to participate in the employer or union group
sponsored MA plan. Such notice must be prospective, not retroactive.
• The employer or union must provide a prospective notice to its members alerting them of the
termination event and of other insurance options that may be available to them through their
employer or union.
Option 1: Enroll the individual(s) in another MA plan (i.e. individual plan) offered by the same MA
organization unless the beneficiary makes another choice. The individual must be eligible to enroll in
this plan, including residing in the plan’s service area. The individual plan selected for this option
must be the same type of plan. For example, if the employer/union sponsored plan was an MA-PD
coordinated care plan, the individual plan in this option must be an MA-PD coordinated care plan.
• Beneficiaries may elect another MA plan offered by the employer or union, join Original
Medicare or join another MA plan as an individual member instead of electing the individual
MA plan offered by the same MA organization.
• If the beneficiary prefers not to be enrolled in the individual plan, he/she may contact
the MA organization.
• If the beneficiary would prefer enrolling in a different MA plan as an individual
member, he/she must submit an enrollment request to his/her newly chosen MA
organization.
• If the individual takes no other action, he/she will become a member of the individual plan
offered by the same MA organization that offered the employer/union sponsored plan.
• MA Notice requirements - The MA organization (or the employer or union, acting on its
behalf) must provide prospective notice to the beneficiary that his/her plan is changing,
including information about benefits, premiums, and/or copayments, at least 21 calendar days
prior to the effective date of enrollment in the individual plan.
Option 2: Disenroll individual(s) from the employer/union sponsored MA plan to Original Medicare
following prospective notice.
• MA Notice requirements - The MA organization (or the employer or union, acting on its
behalf) must provide prospective notice to the beneficiary that his/her plan enrollment is
ending at least 21 calendar days prior to the effective date of the disenrollment. The notice
must include information about other individual plan options the beneficiary may choose and
how to request enrollment.
receive employer/union sponsored benefits may include spouse/family status, payment to the employer/union of the
individual’s part of the premium, or other criteria determined by the employer/union.

128
• If the employer/union sponsored plan was an MA-PD plan, the individual must be advised that
the disenrollment action means the individual will not have Medicare drug coverage. Notice
must include information about the potential for late-enrollment penalties that may apply in the
future.
The MA organization must outline in its written policies and procedures the option(s) it follows and
must apply the same option for all members of a particular employer/union sponsored plan. It is the
MA organization’s responsibility to ensure that the required elements of the disenrollment procedures
described above are understood by the employer or union and are part of the agreement with each
employer or union, including contract termination notification requirements.
50.8 - Disenrollment Procedures for Medicare MSA Plans
Members of Medicare MSA plans may only disenroll in writing through the MA organization offering
the Medicare MSA plan; they may not disenroll through 1-800-MEDICARE. Election periods and
effective dates for disenrollment from Medicare MSA plans are outlined in §30.7.
MA organizations offering Medicare MSA plans must otherwise follow the disenrollment policies and
procedures outlined in §§50.2 through 50.5.

129
60 - Post-Enrollment Activities
42 CFR 422.60 & 422.66
Post-enrollment activities begin after the MA organization receives the enrollment request from the
individual (e.g., cancellations) and last until a decision is made with respect to an individual’s
enrollment request (e.g., retroactive transactions).
60.1 - Multiple Transactions
Multiple transactions occur when CMS receives more than one enrollment request for the same
individual with the same effective date in the same reporting period. An individual may generally not
be enrolled in more than one MA, cost, HCPP or PDP plan at any given time (however, an individual
may be simultaneously enrolled in a cost plan and a separate PDP plan or in certain MA plan types and
a separate PDP plan).
Generally, the last enrollment request the beneficiary makes during an enrollment period will be
accepted as the plan into which the individual intends to enroll. If an individual elects more than one
plan for the same effective date and with the same application date, the first transaction successfully
processed by CMS will take effect. Because simultaneous enrollment in certain MA plan types and a
separate PDP is permitted, CMS systems will accept both enrollments.
Generally, given the use of the application date to determine the intended enrollment choice,
retroactive enrollments will not be processed for multiple transactions that reject because the
enrollment requests have the same application date.
EXAMPLES
• Two MA organizations receive enrollment forms from one individual. MAO #1 receives a form
on March 4th and MAO #2 receives a form on March 10. Both organizations submit enrollment
transactions, including the applicable effective date and application date. The enrollment in
MAO #2 will be the transaction that is accepted and will be effective on April 1 because the
application date on the enrollment transaction is the later of the 2 submitted. Both plans receive
the appropriate reply on the DTRR.
• Two MA organizations (MAOs) receive enrollment requests from one individual for an April 1
effective date. MAO #1 receives a paper enrollment form with all required information on March
5
th
. The beneficiary completed an enrollment request for MAO #2 by telephone on the same
day, March 5th. Both enrollment requests have the same application date, since they were
received by the MAO on the same date. Both enrollments were submitted to CMS prior to the
April cut-off date. MAO #1 transmitted the enrollment to CMS on March 5th, the day it received
the enrollment request; however, MAO #2 waited until March 8
th
to transmit the enrollment to
CMS. The enrollment for MAO #1 will be the transaction that is effective on April 1, as it was
the first transaction successfully processed by CMS.
In the event a rejection for a multiple transaction is reported to the MA organization, the organization
may contact the individual. If the individual wishes to enroll in a plan offered by the organization that
received the multiple transaction reject, s/he must submit a new enrollment request during a valid
enrollment period.
130
60.2 - Cancellations
Cancellations may be necessary in cases of mistaken enrollment made by an individual and/or
mistaken disenrollment made by a member. Unless otherwise directed by CMS, an individual may
cancel his/her enrollment (or disenrollment) request only by contacting the organization prior to the
effective date of the enrollment (or disenrollment). For enrollments into employer or union sponsored
plans, cancellations received by the employer or union prior to the enrollment effective date are also
acceptable.
If a cancellation occurs after CMS records have changed, retroactive disenrollment and reinstatement
actions may be necessary. Refer to §§60.3 and 60.5.
If a beneficiary verbally requests a cancellation, the MA organization should document the request.
MA organizations have the right to request that a cancellation be in writing. However, they may not
delay processing of a cancellation until the request is made in writing if they have already received a
verbal cancellation request from the beneficiary.
For facilitated enrollment as described in §40.1.5 of this chapter, a beneficiary may cancel the
enrollment and affirmatively decline Part D benefits by telephone. The MA organization may not
require these cancellations in writing.
60.2.1 - Cancellation of Enrollment
An individual’s enrollment request can be cancelled only if the cancellation request is received by the
organization prior to the effective date of the enrollment via phone, in writing or in person, unless
otherwise directed by CMS.
To ensure the cancellation is honored, the MA organization should not transmit the enrollment to
CMS. If, however, the organization had already transmitted the enrollment by the time it receives the
valid request for cancellation, it must submit a cancellation transaction to CMS to cancel the now-void
enrollment transaction. In the event the cancellation transaction fails or the MA organization has other
difficulty, the MA organization must submit the request to cancel the action to the CMS Retroactive
Processing Contractor in order to cancel the enrollment.
When canceling an enrollment transaction, the MA organization must send a letter to the individual
that states that the cancellation is being processed (see Exhibit 25). This notice should be sent within
ten calendar days of receipt of the cancellation request. This notice must inform the member that the
cancellation should result in the individual remaining enrolled in the health plan in which he/she was
originally enrolled, so long as the individual remains eligible to be enrolled in that health plan.
An MA organization may submit a transaction to cancel only those enrollment transactions it
submitted. To cancel an enrollment, the MA organization must submit an enrollment cancellation
transaction (transaction code 80) with an effective date equal to the effective date of the enrollment
being cancelled.
If the member’s request for cancellation occurs after the effective date of the enrollment, the
cancellation generally cannot be processed. (An exception to this is a cancellation requested during the
Outbound Education and Verification (OEV) process.) The organization must inform the beneficiary
131
that he/she is a member of its MA plan. If he/she wants to return to the other MA plan he/she will have
to submit an enrollment request during a valid election period for a prospective enrollment effective
date.
If the member wants to return to Original Medicare instead of returning to his/her previous plan, the
member must be instructed to disenroll from the previous plan as described in §50.1 of this chapter.
The member must be informed that the disenrollment must be made during an election period
(described in §30.5) and will have a current effective date (as prescribed in §30.5), and must be
instructed to continue to use plan services until the disenrollment goes into effect.
Regardless of the plan personnel receiving the request, the plan must document all contact with the
beneficiary associated with the cancellation request.
When an organization receives notification of an individual’s reinstatement, the organization has ten
(10) calendar days to send the individual a notice of reinstatement (Exhibit 25a).
CANCELLATION OF MEDICARE MSA ENROLLMENT REQUEST:
An individual who elects a Medicare MSA plan during an AEP, and who has never before enrolled in
a Medicare MSA plan, may revoke (i.e., “cancel”) that enrollment request, preferably by December 7
(but law allows beneficiaries to do so by December 15) of the year in which s/he requested enrollment
in the Medicare MSA plan. This cancellation will ensure the enrollment request does not go into effect
on January 1. After December 7 and up to December 15, the beneficiary may only return to Original
Medicare and cannot enroll into another MA plan or into a stand-alone PDP.
60.2.2 - Cancellation of Disenrollment
A member’s disenrollment can be canceled only if the request is made prior to the effective date of the
disenrollment, unless otherwise directed by CMS.
To ensure the cancellation is honored, the MA organization should not transmit the disenrollment to
CMS. If, however, the organization had already transmitted the disenrollment by the time it receives
the verbal request for cancellation, it must submit a cancellation of disenrollment transaction,
transaction code 81, to CMS to cancel the now-void disenrollment transaction. In the event the MA
organization has submitted the disenrollment and is unable to submit the transaction code 81, or has
other difficulty, the organization should submit the request to cancel the action to the CMS Retroactive
Processing Contractor in order to cancel the disenrollment.
An MA organization may submit a transaction to cancel only those disenrollment transactions it
submitted. To submit an action to cancel a disenrollment, the MA organization must submit a
transaction code 81 (cancellation of disenrollment), with the effective date equal to the effective date
of the disenrollment being cancelled.
The MA organization must send a letter to the member that states that the cancellation is being
processed and instructs the member to continue using MA plan services (see Exhibit 26). This notice
should be sent within ten calendar days of receipt of the cancellation request.
Within ten (10) calendar days of receipt of confirmation of the individual’s reinstatement, the
organization must send the member written notification of the reinstatement (Exhibit 25a).
132
If the member’s request for cancellation occurs after the effective date of the disenrollment, the
cancellation cannot be processed. In some cases, reinstatement due to a mistaken disenrollment will be
allowed, as outlined in §60.3.2. If a reinstatement will not be allowed, the MA organization should
instruct the member to submit a new enrollment request during a valid election period (described in
§30), and with a current effective date, as prescribed in §30.5.
60.2.3 – When A Cancellation Transaction is Rejected by CMS Systems
(Transaction Reply Code (TRC) 284)
When an MA organization receives a TRC 284 (Cancellation Rejected), while the cancellation
remains valid, it could not be processed automatically in CMS’ systems. The MA organization must
investigate the circumstances behind the rejection. If the rejection was due to incorrect data on the
transaction, the MA organization must correct the data and resubmit it to CMS. If the rejection was
not due to such an error, and the request to cancel is valid, the MA organization must promptly submit
the request to CMS (or its designee) for resolution.
60.2.4 – Cancellation Due to Notification from CMS (TRC 015)
When an MA organization receives a TRC 015 (Enrollment Cancelled), it indicates that an enrollment
must be cancelled. A cancellation may be the result of an action on the part of the beneficiary, CMS or
another plan.
Within ten (10) days of receiving the TRC 015, the plan must send the individual an acknowledgment
notice of the cancellation (Exhibit 25b).
60.3 - Reinstatements
Reinstatements may be necessary if a disenrollment is not legally valid (refer to §50.5 to determine
whether a disenrollment is not legally valid) or if the circumstances justify a reinstatement. The most
common reasons warranting reinstatements are:
1. Disenrollment due to erroneous death indicator;
2. Disenrollment due to erroneous loss of Medicare Part A or Part B indicator;
3. Disenrollment due to erroneous incarceration or unlawful presence information;
4. Reinstatements Based on Beneficiary Cancellation of New Enrollment;
5. Plan error;
6. Demonstration of good cause for failure to pay plan premiums or Part D-IRMAA timely.
When a disenrolled individual contacts the MA organization to state that he or she was disenrolled due
to item 1 (erroneous death indicator), item 2 (erroneous loss of Medicare Part A or Part B indicator) or
item 5 (plan error), and states that he or she wants to remain a member of the MA plan, the MA
133
organization must instruct the member in writing to continue to use MA plan services (refer to
Exhibits 15, 16 and 17). The MA organization must send the notice within ten (10) calendar days of
the individual’s contact with the organization to report the erroneous disenrollment. Accordingly, plan
systems should indicate active membership as of the date the organization instructs the individual to
continue to use plan services.
When a disenrolled individual contacts the MA organization about either item 3 (erroneous
incarceration or unlawful presence information), item 4 (reinstatement based on enrollment
cancellation of new enrollment) or item 6 (good cause), plans should follow the guidance outlined
below pertaining to those unique situations.
A reinstatement is viewed as a correction necessary to “erase” an invalid disenrollment action, and, as
such, does not require an election period. Therefore, reinstatements may be made back to a date when
an MA plan was closed for enrollment. Payment alone of past due premiums after the disenrollment
date does not create an opportunity for reinstatement into the plan from which the individual was
disenrolled for failure to pay premiums.
CMS (or its designee) will review requests for reinstatements on a case-by-case basis.
Within ten (10) calendar days of receipt of DTRR confirmation of the individual’s reinstatement, the
organization must send the member notification of the reinstatement (Exhibit 25a).
60.3.1 - Reinstatements for Disenrollment Due to Erroneous Death Indicator, or
Erroneous Loss of Medicare Part A or Part B, Erroneous Incarceration
Information, or Erroneous Unlawful Presence Information
A member must be reinstated if he or she was disenrolled in error, since the individual continues to be
eligible. This may occur in the following situations:
• Erroneous death indicator;
• Erroneous loss of Part A or Part B;
• Erroneous lawful presence status; or
• Erroneous incarceration information.
As outlined in 42 CFR 422.74(c), MA organizations have the option of sending notification of
disenrollment due to:
• Death;
• Loss of Part A or Part B entitlement; or
• Unlawful presence in the U.S.
134
The CMS strongly suggests that MA organizations send these notices in these three situations, to
ensure any erroneous disenrollments are corrected as soon as possible. Refer to Exhibits 13, 14 and 38
for model letters.
If CMS involuntarily disenrolls an individual due to incarceration, a notice is required because the
individual resides out of the plan’s service area. See §50.2.1.5 for notice requirements for
disenrollment due to incarceration. Refer to Exhibit 37.
Erroneous disenrollments must be corrected and the corresponding reinstatements processed,
regardless of the date on which the individual disputes the erroneous disenrollment or provides
evidence of MA eligibility.
Reinstatements for erroneous death indicator or loss of Part A or Part B entitlement:
Individuals can dispute the disenrollment due to death indicator or loss of Part A or Part B entitlement.
In such cases, the MA organization is expected to acknowledge the individual’s request for
reinstatement and direct him or her to continue to use the MA plan services while the issue is resolved
with the Social Security Administration (SSA). Organizations may request that such individuals
provide evidence of MA eligibility by a particular date; however, should the individual provide
evidence after that date, the error must still be corrected by the MA organization.
To request consideration for reinstatement following disenrollment due to erroneous death indicator,
erroneous loss of Medicare Part A or Part B, the MA organization must submit to CMS (or its
designee) a copy of the letter to the member informing him or her to continue to use MA plan services
until the issue is resolved. The organization must indicate the date the letter was sent. Refer to model
letters in Exhibits 15and 16. Within ten (10) calendar days of receipt of DTRR confirmation of the
individual’s reinstatement, the organization must send the member notification of the reinstatement
(Exhibit 25a).
CMS will attempt to automatically reinstate individuals that were auto-disenrolled by a report of date
of death if there is a subsequent date of death correction that impacts the plan enrollment.
Reinstatements for erroneous incarceration or unlawful presence status information:
Individuals alleging disenrollment due to erroneous incarceration information or erroneous unlawful
presence status must have their complaints reviewed by the MA organization and possibly referred to
SSA. MA organizations are not required to provide coverage to such individuals while the issue is
reviewed by the plan or SSA.
For individuals who contest their disenrollment on these bases, the MA organization should check
CMS’ systems to see if the incarceration or unlawful presence status has been removed (via audit
notification in MARx) and that the person is otherwise eligible to remain enrolled as of the
disenrollment effective date. If the individual is otherwise eligible for enrollment, the reinstatement
request may be sent to the CMS Retroactive Processing Contractor (RPC) instead of referring the
individual to SSA. However, if CMS systems continue to reflect an incarcerated or unlawful presence
status, the plan should refer the beneficiary to SSA so that they may review their records and make
corrections, as appropriate. If the information or status is determined to be erroneous by SSA, CMS’
systems will be updated. The plan may check CMS systems to see if the incarceration or unlawful
presence status has been removed, and, if the person is otherwise eligible to remain enrolled, may send
the reinstatement request to the CMS RPC. The MA organization will receive notification of the
135
individual’s reinstatement from CMS or via the TRR. At that time, services should resume and
coverage should be seamless, as though the individual was never disenrolled. CMS suggests that the
organization send the member notification of the reinstatement (Exhibit 25a) within ten (10) days of
receipt of DTRR confirmation of the individual’s reinstatement.
60.3.2 - Reinstatements Based on Beneficiary Cancellation of New Enrollment
As stated in §50.5, deliberate member-initiated disenrollments imply intent to disenroll. Therefore,
reinstatements generally will not be allowed if the member deliberately initiated a disenrollment. An
exception is made for those members who were automatically disenrolled because they enrolled in
another plan but subsequently cancelled the enrollment in the new plan before the effective date.
In this situation, that is, if an individual has since changed his/her mind and wants to remain enrolled
in the previous plan, the individual must cancel the enrollment into the new plan, as described in
section 60.2.1. When a cancellation of enrollment in a new plan is properly made, the associated
automatic disenrollment from the previous MA plan becomes invalid. Upon successful cancellation of
enrollment in the new plan, CMS systems will attempt to automatically reinstate enrollment in the
previous plan. Because this process is automatic, it is generally not necessary to request reinstatement
via the Regional Office or Retroactive Processing Contractor. Within ten (10) days of receipt of DTRR
confirmation of the individual’s reinstatement, the organization must send the member notification of
the reinstatement (Exhibit 25a).
In cases where the valid cancellation request is not processed timely or CMS systems cannot complete
the request, the new plan must submit a request to the Retroactive Processing Contractor to cancel the
enrollment. This request will require complete documentation, including evidence that the beneficiary
requested cancellation of enrollment in the new plan within required timeframes.
If the previous plan becomes aware of an unsuccessful reinstatement, the previous plan may contact a
CMS Account Manager to investigate the issue with the new plan.
If the disenrolled individual contacts the previous plan requesting to remain a member of that plan, the
MA organization should inform the individual that reinstatement of enrollment is an option only if the
individual successfully cancels enrollment in the “new” plan; accordingly, the organization should
refer the individual to the “new” plan to inquire about his or her options.
60.3.3 - Reinstatements Due to Mistaken Disenrollment Due to Plan Error
A disenrollment that is not the result of either a valid voluntary request or a valid circumstance that
requires involuntary disenrollment is erroneous. When an erroneous disenrollment is the result of plan
error, the plan must reinstate the individuals who were disenrolled.
In the case of an erroneous disenrollment by the organization that is a result of an error the part of the
organization, the organization must restore the enrollment in its records. Additionally, the organization
must cancel the disenrollment action from CMS’s records, if the organization had previously
submitted such a transaction to CMS. Organizations must use the disenrollment cancellation function
to complete this action for effective dates within the parameters that CMS systems allow for such
corrections. For effective dates outside these parameters, the organization must process the request
136
according to the guidance for processing retroactive enrollment and disenrollment requests including
full documentation and explanation as required.
Within ten (10) days of receipt of DTRR confirmation of the individual’s reinstatement, the
organization must send the member notification of the reinstatement (Exhibit 25a).
60.3.4 - Reinstatements Based on a Determination of Good Cause for Failure to
Pay Plan Premiums or Part D-IRMAA Timely
If an individual has been involuntarily disenrolled for failure to pay either plan premiums (under
§50.3.1) or Part D-IRMAA (under §50.2.6), he or she may request reinstatement no later than 60
calendar days following the effective date of disenrollment. Reinstatement for good cause, pursuant to
42 CFR 422.74(d)(1)(v), will occur only when:
1. The individual requests reinstatement within 60 days of disenrollment effective date;
2. The individual has been determined to meet the criteria specified below (i.e., receives a
favorable determination); and
3. (a) Within three (3) months of disenrollment for nonpayment of plan premiums, the
individual pays in full the plan premiums owed at the time he or she was disenrolled or
(b) Within three (3) months of disenrollment for nonpayment of Part D-IRMAA, the
individual pays in full the Part D-IRMAA and any plan premiums owed at the time he or
she was disenrolled.
Criteria for Reinstatement: Reinstatement of enrollment for good cause is provided only in rare
circumstances in which the member or his or her authorized representative (i.e. the individual
responsible for the member’s financial affairs) was unable to make timely payment due to
circumstances over which they had no control and they could not reasonably have been expected to
foresee. Requests for reinstatement must be accompanied by a credible statement (verbal or written)
explaining the unforeseen and uncontrollable circumstances causing the failure to make timely
payment. An individual may make only one reinstatement request for good cause in the 60-day period.
Generally, these circumstances constitute good cause:
• A serious illness, institutionalization and/or hospitalization of the member or his or her
authorized representative (i.e. the individual responsible for the member’s financial affairs),
that lasted for a significant portion of the grace period for plan premium or Part D-IRMAA
payment;
• Prolonged illness that is not chronic in nature, a serious (unexpected) complication to a chronic
condition or rapid deterioration of the health of the member, a spouse, another person living in
the same household, person providing caregiver services to the member, or the member’s
authorized representative (i.e., the individual responsible for the member’s financial affairs)
that occurs during the grace period for the plan premium or Part D-IRMAA payment;
• Recent death of a spouse, immediate family member, person living in the same household or
person providing caregiver services to the member, or the member’s authorized representative
(i.e., the individual responsible for the member’s financial affairs); or
• Home was severely damaged by a fire, natural disaster or other unexpected event, such that the
member or the member’s authorized representative was prevented from making arrangement
for payment during the grace period for plan premium or Part D-IRMAA;
137
• An extreme weather-related, public safety or other unforeseen event declared as a Federal or
state level of emergency prevented premium payment at any point during the plan premium or
Part D-IRMAA grace period. For example, the member’s bank or U.S. Post Office closes for a
significant portion of the grace period; or
• For disenrollments effectuated by CMS for failure to pay Part D-IRMAA, Federal government
error (i.e., CMS, SSA or RRB) caused the payment to be incorrect or late, and the member was
unaware of the error or unable to take action prior to the disenrollment effective date.
There may be situations in addition to those listed above that result in favorable good cause
determinations. If an individual presents a circumstance which is not captured in the listed examples, it
must meet the regulatory standards of being outside of the member’s control or unexpected such that
the member could not have reasonably foreseen its occurrence, and this circumstance must be the
cause for the non-payment of plan premiums or Part D-IRMAA. CMS expects non-listed
circumstances will be rare.
Examples of circumstances that do not constitute good cause include:
• Allegation that bills or warning notices were not received due to unreported change of address,
out of town for vacation, visiting out of town family, etc.;
• Authorized representative did not pay timely on member’s behalf;
• Lack of understanding of the ramifications of not paying plan premiums or Part D-IRMAA;
• Could not afford to pay premiums during the grace period; or
• Need for prescription medicines or other plan services.
For examples of cases for favorable and unfavorable good cause determinations, see Appendix 4.
For the purpose of determining good cause for members with authorized representatives, the criteria
for both favorable and unfavorable determinations apply as though the authorized representative is the
member.
The inability to afford premiums or failure to make timely payment by a member or an authorized
representative alone is not grounds for a favorable good cause determination and reinstatement. In
addition, good cause determinations are not organization determinations related to coverage and,
therefore, are not appealable. (See 42 CFR 422, subpart M.) An individual may not make more than
one reinstatement request for good cause in the same 60-day period following disenrollment, including
instances in which the initial request resulted in an unfavorable determination. However, an individual
has the right to file a grievance against the plan related to the involuntary disenrollment.
An individual who has been disenrolled for failure to pay plan premium, regardless of whether he or
she has also been assessed Part D-IRMAA, remains disenrolled from the plan and does not have
access to plan coverage of services until he or she receives a favorable good cause determination and
the plan receives full payment of the plan premium amounts owed at the time he or she was
disenrolled.
An individual who has been disenrolled by CMS for failure to pay Part D-IRMAA remains disenrolled
from the plan and does not have access to plan coverage of services until the reinstatement occurs and
is reported to the plan on the DTRR or the plan is contacted by the CMS caseworker after he or she
has successfully updated the member’s enrollment record in MARx. Once a reinstatement occurs, the
138
individual’s disenrollment will be cancelled and his or her coverage will be continuous, assuming the
individual continues to be eligible for enrollment in that plan.
60.3.4.1 - Process for Good Cause Determinations for Nonpayment of Plan Premiums
Pursuant to 42 CFR 422.74(d), CMS has assigned the handling of good cause determinations to plans.
When a disenrolled individual initially contacts the MA organization following disenrollment for
failure to pay plan premiums and indicates that he or she “has a good reason for not having paid the
premiums”, the MA organization must:
• Confirm that the request for reinstatement is being made within 60 calendar days of the
disenrollment effective date;
• Inform the individual that reinstatement is a possibility only if it is determined that his or her
failure to make timely payment was due to circumstances over which he or she had no control
and could not reasonably have been expected to foresee;
• Obtain a credible statement from the individual regarding the circumstance that prevented him
or her from making timely payment; and
• Obtain affirmation from the individual indicating his or her willingness and ability to pay all
overdue plan premiums within three (3) months of the disenrollment date in order for
reinstatement to occur.
If all of these preliminary requirements are not met, the individual is not eligible to be considered for
reinstatement for good cause. An individual may not make more than one reinstatement request for
good cause during the same 60-day period. For example, an individual requesting reinstatement
indicates that he had no unusual or unexpected circumstance that caused the nonpayment of premiums
and the plan determines that he does not qualify for his case to be reviewed under good cause. The
plan is expected to clearly communicate that the individual’s request will not be reviewed because the
situation does not meet the criteria (e.g., not unusual or unexpected). The individual remains
disenrolled and may not make another request for good cause during the same 60-day period following
the involuntary disenrollment.
If all of the above criteria are met, the plan will review the request and will make a favorable or
unfavorable good cause determination. CMS expects that plans make such determinations within five
(5) business days of initial receipt of the request, so that the individual has a reasonable amount of
time to make full payment for reinstatement. For requests received by mail, the initial request is
considered received by the plan at the time it arrives in the organization’s mailbox or mailroom. For
requests received by fax, the initial request is considered received by the plan at the time when the fax
is received on the organization’s fax machine. For requests received by telephone, the initial request is
considered received by the plan at the time the organization’s representative receives the incoming
call.
There is no additional time allotted for plans to gather information not collected at the point of initial
contact. Plans would need to collect any additional data they feel is needed to make a determination
and make that determination within five (5) business days of the date on which the individual first
contacts the plan. In such cases where the plan does not have sufficient information to determine if the
member’s circumstances meet the requirements, it should make a good faith effort to collect it within
that timeframe (e.g., making multiple attempts on different days or at different times). However, if
139
attempts are unsuccessful, the plan must use the information provided with the initial request to make
its determination.
If the plan makes a favorable determination and there are amounts owed to the plan for past due
premiums, the plan should notify the individual of this decision within three (3) business days of
making the determination. If the plan offers immediate payment options, such as payment by credit
card via phone, it may provide the notification verbally; however, if the individual does not complete
the payment at that time, the plan should issue a written notice to ensure that the individual has the
information necessary to pay the owed amounts. This notice will specify the amount owed (i.e., the
premiums owed at the time of disenrollment), the date by which payment must be received for
reinstatement (i.e., last day of the third month following the disenrollment effective date), where to
send payment, and/or other payment options such as credit card or direct withdrawal from a bank
account, if offered by the plan. (See Exhibit 22b).
If, at the time the plan makes a favorable determination, there are no amounts owed to the plan for past
due premiums, the plan should notify the individual of this decision either verbally or in writing within
three (3) business days of making the determination. Exhibit 22e is
a model notice for the scenario in
which an individual receives a favorable good cause determination and has already paid the amount
required for reinstatement.
If verbal notification is attempted but unsuccessful, a written notice should
be provided. Verbal notification must be documented by the plan to meet CMS’ retroactive processing
contractor reinstatement submission requirements.
If the plan makes an unfavorable determination, the plan should notify the individual of this decision
by phone or in writing within three (3) business days of making the determination.
If an individual has received a favorable good cause determination, reinstatement in CMS systems
may not occur until and unless all required payments are made within three (3) months of the
disenrollment effective date. If the individual pays all the owed amounts prior to the three-month
deadline, the plan should resume coverage at that time and submit the reinstatement request to the
CMS Retroactive Processing Contractor.
Plans have additional time beyond the deadline (i.e., three (3) months from the disenrollment effective
date) to verify payment by the bank and credit the payment to the member’s account with the plan. To
provide adequate protections for individuals who make timely payment of their owed amounts, plans
have five (5) calendar days beyond the payment deadline to process the payment and submit the
reinstatement request to the CMS Retroactive Processing Contractor..
Reinstatements for good cause are considered complete by CMS when TRC 287 (Enrollment
Reinstated) is sent by CMS to the plan.
Within ten (10) calendar days of receipt of DTRR confirmation of the individual’s reinstatement, the
organization must send the member notification of the reinstatement (Exhibit 25a). In an effort to
prevent members from falling behind in premium payments in the future, plans are encouraged to
educate them on any automated payment mechanisms their plan offers, as well as the availability of
selecting automatic premium withhold through their SSA or RRB benefits.
An individual may not be reinstated in cases where:

140
• the individual pays all plan premiums owed, but does not receive a favorable good cause
determination; or
• the individual receives a favorable good cause determination, but does not pay the plan
premiums owed within three (3) months of the disenrollment effective date.
In both of these cases, the plan may re-enroll the individual for a prospective enrollment effective date
at the individual’s request only if he or she has a valid election period (i.e., AEP, SEP, etc.), following
enrollment procedures outlined in Sections 30 and 40.
Example A: Mr. Smith is disenrolled for failure to pay plan premiums on April 1. Mr. Smith contacts
the plan and makes his request for reinstatement on April 15 and receives a favorable good cause
determination on April 23. The plan notifies Mr. Smith of the amount he owes by June 30 in order to
be reinstated into the plan. Mr. Smith pays the amount due on June 15. Mr. Smith is reinstated into the
plan. (Note: If Mr. Smith did not pay his owed amount by June 30, he would not be reinstated.)
Example B: Mr. Smith is disenrolled by the plan for failure to pay plan premiums on July 1. Mr. Smith
mails in his past due amounts to the plan on July 30. He contacts the plan and makes his request on
August 10, and does not receive a favorable good cause determination. Mr. Smith may not be
reinstated.
Example C: Mr. Smith is disenrolled by the plan for failure to pay plan premiums on November 1. Mr.
Smith mails in his owed amounts to the plan on December 15, but does not contact the plan to request
reinstatement. Thus, Mr. Smith does not have a favorable good cause determination, and he may not
be reinstated.
NOTE: In cases where the involuntary disenrollment for failure to pay plan premiums is the result of
plan error, plans should follow the reinstatement process outlined in Section 60.3.3. Plans should not
refer these individuals to 1-800-MEDICARE, nor should these cases be considered for reinstatement
for good cause.
60.3.4.2 – Process for Good Cause Determinations for Nonpayment of Part D-IRMAA
When a disenrolled individual contacts the MA organization following disenrollment for failure to pay
Part D-IRMAA and indicates that he or she “has a good reason for not paying the Part D-IRMAA,” the
MA organization must advise the individual to contact 1-800-MEDICARE (1-800-633-4227; TTY: 1-
877-486-2048) within 60 calendar days of the disenrollment effective date to make the good cause
reinstatement request. The organization should also inform the individual that in order to be reinstated,
he or she must meet specific good cause standards and must pay all overdue plan premiums and Part
D-IRMAA amounts within three (3) months of the disenrollment date in order for reinstatement to
occur.
Once a request is made with CMS via 1-800-MEDICARE, a Complaint Tracking Module (CTM) case
will be generated for CMS caseworker action. The CMS caseworker will review the request and will
make a favorable or unfavorable good cause determination. If the individual provides any
documentation to the plan regarding the inability to make timely payment of the Part D-IRMAA, the
plan must provide that documentation to CMS (through the CMS account manager) so that it may be
considered in making the determination. If CMS makes an unfavorable determination, CMS will
141
notify the individual of the determination. Notes of the good cause reinstatement request will be
captured in the CTM for CMS and plan viewing.
NOTE: Requests for reinstatement are not considered complaints against the plan; therefore, these
types of CTM cases are excluded from tracking for the purposes of plan ratings.
If CMS makes a favorable determination, a notation will be made in the CTM and the CTM will be
sent to the plan. If there are amounts owed to the plan for past due premiums, the plan should send
notification to the individual within three (3) business days of being informed of the favorable good
cause determination. This notice will specify the amount owed, the date by which payment must be
received for reinstatement (i.e., last day of the third month following effective date of disenrollment),
where to send payment, and other payment options such as credit card or direct withdrawal from a
bank account, if offered by the plan. (See Exhibit 22a).
Plans have additional time beyond the payment deadline (i.e., three months from the disenrollment
effective date) to verify payment by the bank and credit the payment to the individual’s account. To
provide adequate protections for individuals who make timely payment of their owed amounts, plans
have five (5) calendar days beyond the payment deadline to process the payment and notify CMS via
CTM. Even if an individual has received a favorable good cause determination, the actual
reinstatement will not occur until all required payments are made within three (3) months of the
disenrollment effective date.
Within ten (10) calendar days of receipt of DTRR confirmation of the individual’s reinstatement, the
organization must send the member notification of the reinstatement (Exhibit 25a). In an effort to
prevent members from falling behind in premium payments in the future, plans are encouraged to
educate them on any automated payment mechanisms offered by the plan, as well as the availability of
automatic premium withhold from SSA or RRB benefits.
An individual may not be reinstated in cases where:
• the individual pays all Part D-IRMAA amounts and any plan premium amounts owed, but does
not receive a favorable good cause determination; or
• the individual receives a favorable good cause determination, but does not pay the Part D-
IRMAA amounts and/or any plan premiums owed with three (3) months of the disenrollment
effective date.
In both of these cases, the plan may re-enroll the individual for a prospective enrollment effective date
at the individual’s request, but only if he or she has a valid election period (i.e., AEP, SEP, etc.),
following enrollment procedures outlined in Sections 30 and 40.
Example: Mr. Smith is disenrolled by CMS for failure to pay Part D-IRMAA on August 1. He
contacts Medicare and makes his request on September 29 and receives a favorable good cause
determination on October 5. Mr. Smith is also delinquent on his plan premiums. CMS notifies Mr.
Smith that he must pay the Part D-IRMAA amount he owes by October 31. The plan notifies Mr.
Smith that he must also pay the plan premium amount he owes by October 31. Mr. Smith pays his Part
D-IRMAA owed amount on October 25. Mr. Smith pays his plan premium owed amount on
November 5. Because the plan received Mr. Smith’s payment for his owed plan premium amount
after the due date, Mr. Smith may not be reinstated. (Note: If Mr. Smith had paid both his owed Part
142
D-IRMAA and plan premiums by October 31, the plan would have had the additional five (5) days to
process the payment and he would have been reinstated.)
60.4 - Retroactive Enrollments
If an individual has fulfilled all enrollment requirements, but the MA organization or CMS is unable to
process the enrollment for the required effective date (as outlined in §30.5), CMS (or its designee) will
process a retroactive enrollment.
In addition, auto-enrollment for full-benefit dual eligible as described in §40.1.5 may be retroactive to
ensure no coverage gap between the end of Medicaid coverage for Part D drugs and the beginning of
Medicare drug coverage.
In other limited cases, CMS may determine that an individual is eligible for an SEP due to an
extraordinary circumstance beyond his/her control (e.g. a fraudulent enrollment request or misleading
marketing practices) and may also permit a retroactive enrollment in an MA plan as necessary to
prevent a gap in coverage or liability for the late enrollment penalty.
Unlike a reinstatement, which is a correction of records to “erase” an action, a retroactive enrollment
is viewed as an action to enroll a beneficiary into a plan for a new time period. Therefore, retroactive
enrollments may NOT be made back to a date when an MA plan was closed for enrollment.
NOTE: Keep in mind that unless an approved capacity limit applies, all MA plans are open for
ICEP, IEP/D, AEP and SEP enrollment requests; therefore, all MA plans are open for retroactive
enrollments for these types of enrollment requests.
Occasionally, obtaining the information necessary to complete an enrollment request within the
allowable timeframes will extend beyond the CMS systems cut-off date for transaction submission,
thus making the effective date of enrollment “retroactive” to the current payment month. MA
organizations must use the Code 61 enrollment transaction to submit the enrollment transaction
directly to CMS within the Current Calendar Month transaction processing timeframe.
When a valid request for enrollment has not been communicated to CMS successfully within the
required timeframes in this guidance and the Current Calendar Month transaction submission
timeframe, MA organizations are required to submit the appropriate documentation to CMS (or its
designee) for manual review and potential action. The request for a retroactive enrollment should be
made within the timeframes provided in the Standard Operating Procedures for the CMS Retroactive
Processing Contractor. When an individual has fulfilled all enrollment requirements, but the
organization or CMS has been unable to process the enrollment in a timely manner, the following
documentation must be submitted to CMS (or its designee):
• A copy of signed completed enrollment form (the form must have been signed by the
beneficiary (or authorized representative) and received by the organization prior to the
requested effective date of coverage, in order to effectuate the requested effective date of
coverage); or
• A copy of the enrollment request record (the enrollment request record must show that the
enrollment request was made and received by the organization prior to the requested effective
date of coverage).

143
The retroactive enrollment request may be denied if CMS determines that the MA organization did not
notify the member that he/she must use MA plan services during the period covered by the retroactive
enrollment request.
If the request for retroactive enrollment action is due to plan error, the organization must provide a
clear and detailed explanation of the plan error including why the retroactive action is necessary to
correct the error. The explanation must include clear information regarding what the organization has
communicated to the affected beneficiary throughout the period in question. The organization must
also include any relevant information or documentation supporting the requested correction. Such
information could include a copy of the enrollment request form (or clear evidence of the use of
another enrollment mechanism) and evidence of notices sent to the beneficiary related to or caused by
the error.
Special note regarding Regional Office Casework actions
When an MA organization is directed by CMS, such as via an RO caseworker, to submit a retroactive
enrollment or disenrollment request to resolve a complaint, the organization must provide the
following 2 (two) items as documentation to CMS (or its designee):
• A screen print from the Complaint Tracking Module (CTM) or other documentation showing
the CMS RO decision and direction to submit the request to the CMS Retroactive Processing
Contractor, and;
• A copy of the enrollment or disenrollment request, if one is available. Occasionally, due to the
nature of casework, this item may not be available. When that occurs, the organization should
submit a brief statement of explanation for the missing documentation.
60.5 - Retroactive Disenrollments
42 CFR 422.66
If an enrollment was never legally valid (§40.6) or if a valid request for disenrollment was properly
made, but not processed or acted upon (as outlined in the following paragraph), which includes not
only system error, but plan error (see §10 for a definition of “system error” and “plan error”), CMS (or
its designee) may grant a retroactive disenrollment. CMS (or its designee) may also process a
retroactive disenrollment if the reason for the disenrollment is related to a permanent move out of the
plan service area (as outlined in §50.2.1.2), a contract violation (as outlined in 42 CFR 422.62(b)(3))
or other limited exceptional conditions established by CMS (e.g. fraudulent enrollment or misleading
marketing practices).
When a valid request for disenrollment has not been communicated to CMS successfully within the
required timeframes in this guidance and the Current Calendar Month transaction submission
timeframe, MA organizations are required to submit the appropriate documentation to CMS (or its
designee) for manual review and potential action. Retroactive disenrollment requests can be submitted
to CMS (or its designee) by the beneficiary or an MA organization. Requests from an MA
organization must include a copy of the disenrollment request, as well as an explanation as to why the
disenrollment was not processed correctly. MA organizations must submit retroactive disenrollment
requests to CMS (or its designee) within the timeframes provided in the Standard Operating
Procedures for the CMS Retroactive Processing Contractor. If CMS approves a request for retroactive
144
disenrollment, the MA organization must return any premium paid by the member for any month for
which CMS processed a retroactive disenrollment. In addition, CMS will retrieve any capitation
payment for the retroactive period.
A retroactive request must be submitted by the MA organization (or by the member) to CMS (or its
designee) in cases in which the MA organization has not properly processed a required involuntary
disenrollment or acted upon the member’s request for disenrollment as required in §50.4.1 of these
instructions. A disenrollment request would be considered not properly acted upon or processed if the
effective date is a date other than as required in §30.6.
If the request for retroactive disenrollment action is due to the MA organization’s confirmation of an
incarcerated status with a retroactive start date (see § 50.2.1.3), the organization must provide written
confirmation of the incarcerated status, including the start date. Such confirmation could include
documentation of telephonic communications.
If the request for retroactive action is due to plan error, the organization must provide a clear and
detailed explanation of the plan error including why the retroactive action is necessary to correct the
error. The explanation must include clear information regarding what the organization has
communicated to the affected beneficiary throughout the period in question, including evidence that
the beneficiary was notified prospectively of the disenrollment. The organization must also include
any relevant information supporting the requested correction. Such information could include a copy
of the disenrollment request and evidence of notices sent to the beneficiary related to or caused by the
error in question and which demonstrate that the retroactive disenrollment is appropriate under the
circumstances.
60.6 - Retroactive Transactions for Employer/Union Group Health Plan (EGHP)
Members
In some cases an MA organization that has a contract with an EGHP arranges for the employer or
union to process enrollment requests for Medicare-entitled group members who wish to enroll in an
employer or union sponsored MA plan. However, there can be a delay between the time the member
completes the enrollment request through the EGHP and when the enrollment request is received by
the MA organization. Therefore, retroactive transactions for these routine delays may be necessary and
are provided for under this section. Errors made by an EGHP, such as failing to forward a valid
enrollment or disenrollment request within the timeframes described below, must be submitted to
CMS (or its designee) for review. Repeated errors may indicate an ongoing problem and therefore will
be forwarded to the MA organization’s CMS Account Manager for compliance monitoring purposes.
The MA organization’s agreement with the EGHP must include the need to meet the requirements
provided in this chapter that ensure the timely submission of enrollment and disenrollment requests to
reduce the need for retroactivity and to help avoid such errors.
60.6.1 - EGHP Retroactive Enrollments
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
The effective date of EGHP enrollments cannot be earlier than the date the enrollment request was
completed by the beneficiary. The effective date may be retroactive up to, but may not exceed, 90 days
145
from the date the MA organization received the request (which was completed prior to the effective
date) from the employer or union group.
EXAMPLE
In March 2007, the CMS system processing date was March 13, 2007. Enrollment requests processed
by CMS for the March 13, 2007, due date were for the prospective April 1, 2007, payment. For
EGHPs, an effective date of March 1, February 1, or January 1 would reflect 30, 60 and 90 days of
retroactive payment adjustment, respectively. Therefore, if a completed EGHP enrollment request
were to be received by the MA organization on March 5, 2007, the retroactive effective date could be
January 1, February 1, or March 1, as long as the enrollment request was completed prior to the
effective date.
NOTE: Keep in mind that unless a CMS-approved capacity limit has been reached, all MA
plans are open for ICEP, AEP, and SEP enrollment requests. Therefore, all MA plans are open
for retroactive enrollments for these types of enrollment requests.
No retroactive enrollments may be made unless the individual certifies that the MA organization (or
EGHP) provided him/her with the explanation of enrollee rights (including the lock-in requirement) at
the time of enrollment. The MA organization should submit such enrollments using the appropriate
transaction code. Refer to the Medicare Advantage and Prescription Drug Plan Communications User
Guide (PCUG) for more information. The ability to submit limited EGHP retroactive enrollment
transactions is to be used only for the purpose of submitting a retroactive enrollment into an EGHP
made necessary due to the employer’s delay in forwarding the completed enrollment request to the
MA organization.
60.6.2 - EGHP Retroactive Disenrollments
The MA organization must submit a retroactive disenrollment request to CMS (or its designee) if an
EGHP does not provide the MA organization with timely notification of a member’s requested
disenrollment. Up to 90 day’s retroactive payment adjustment is possible in such a case to conform to
the adjustments in payment described under 42 CFR 422.308(f)(2). The EGHP notification is
considered untimely if it does not result in a disenrollment effective date as outlined in §30.6.
The MA organization must submit a disenrollment notice (i.e., documentation) to CMS (or its
designee) demonstrating that the member acted to disenroll in a timely fashion (i.e., prospectively), but
that the EGHP was late in providing the information to the MA organization. Such documentation may
include an enrollment form for a new MA plan signed by the member and given to the EGHP during
an open enrollment season. The documentation may not include a copy of a Medicare supplemental
plan or Medigap plan enrollment form unless the member indicated on that form that he/she has
canceled any other insurance. Such documentation should be sent to CMS (or its designee) as soon as
possible.
60.7 – User Interface (UI) Transactions Reply Codes (TRC) – Communications
with Beneficiaries
Upon receipt of a CMS transaction reply, MA organizations must update their records to accurately
reflect each individual’s enrollment status. Organizations are also required to provide certain notices
146
and information to beneficiaries when enrollment status is confirmed or changes. In the case of UI-
TRC replies, the standard operating procedures for providing these notices and/or information may not
fit some of the unique situations many UI enrollment changes address.
The table below provides guidelines for communicating with beneficiaries when enrollment changes
are reported to MA organizations using the “700 series” TRCs that result from UI enrollment changes.
In all cases, organizations will need to review the situations carefully to determine the necessity and
appropriateness of sending notices. Some UI enrollment change processes will result in multiple 700-
series TRCs being reported. Organizations must determine the final disposition of the beneficiary to
ensure the correct message is provided in any notice sent. In complex situations, CMS encourages
organizations to communicate directly (such as by telephone) with the beneficiary, in addition to any
required notice or materials. When it is necessary to send a notice, organizations must issue the notice
within ten calendar days of receipt of the DTRR.
TRC
Beneficiary Communication Action
701 – New UI Enrollment
Organizations may use existing confirmation notices as provided in
CMS enrollment guidance. If such notice has already been provided
with the same information, it is not necessary to provide it a second
time.
702 – New UI Fill-in
Enrollment
Organizations must use Exhibit 30, “Enrollment Status Update.”
Include the date range covered by the new fill-in period.
703 – UI Enrollment
Cancel
If a cancellation notice applicable to this time period has already been
provided, it is not necessary to provide it a second time. If notice has
not been provided, organizations may use the existing cancellation of
enrollment notice as provided in CMS enrollment guidance. If the
specific situation warrants, organizations may use Exhibit 30 instead,
providing information that clearly indicates that the enrollment period
in question has been cancelled. Include information about the refunding
of plan premiums, if applicable.
704 – UI Enrollment
Cancel - PBP Change
If the UI action is a correction to a plan submission error, the
organization may have already provided the correct plan (PBP)
information; if that’s the case, it is not necessary to send it a second
time. If the beneficiary has not received information about the specific
plan (PBP), the organization must send the materials required in CMS
enrollment guidance that would be provided for any new enrollment.
Organizations must also send Exhibit 30 describing the plan change,
including the effective date. The impact of the change on plan
premiums, cost sharing, and provider networks must be communicated
clearly. It is not necessary to confirm with a notice the associated
“enrollment canceled” TRC that will accompany the enrollment into
the new plan (PBP).
705 – New UI Enrollment
- PBP Change
Follow the guidance provided above for TRC 704.
706 – UI Enrollment
Cancel - Segment change
Plan (PBP) segment changes apply only to MA plans. Provide updated
materials reflecting the new elements of the changed segment, such as
premium and cost sharing increases or decreases.
707- UI New enrollment -
Segment Change
Follow the guidance above for TRC 706.
147
708 – UI End Date
Assigned
This UI action has the same effect as a plan submitted disenrollment
(code 51) transaction. Generally, organizations should follow existing
CMS enrollment guidance for providing notice and confirmation of the
disenrollment. However, since many UI initiated changes are
retroactive, organizations may have already provided notice (with
correct effective dates) and if so, need not provide it a second time.
Additional clarification may be appropriate depending on the specifics
of the case.
709 – UI Earlier Start
Date
An existing enrollment period in the plan has changed to start earlier
than previously recorded. If the organization has already provided
notice reflecting this effective date of enrollment, it is not necessary to
provide it a second time. When the individual has not already received
notice reflecting this effective date, organizations may use existing
confirmation of enrollment notices where there is confidence that such
notice will not cause undue confusion. Alternatively, organizations
may use Exhibit 30, including in it the new effective date and
information about additional premium liability (ensure flexibility in
allowing payment arrangements where necessary). Organizations must
also ensure individuals are fully aware of how to access coverage of
services for the new time period, including their right to appeal.
710 – UI Later Start Date
An existing enrollment period start date has been changed to start on a
later date. Organizations must use Exhibit 30. Organizations must
explain the change in the effective date of coverage, and provide
information on the refunding of any premiums paid. Organizations
must also explain the impact on any paid claims from the time period
affected.
711 – UI Earlier End Date
An enrollment period end date has been changed to occur earlier.
Organizations must use Exhibit 30. Organizations must explain the
change in the effective date of the end of coverage, and provide
information on the refunding of any premiums paid. Organizations
must also explain the impact on any paid claims from the time period
affected.
712 – UI Later End Date
An enrollment period end date has been changed to occur later.
Organizations must use Exhibit 30. Organizations must explain the
change in the effective date of the end of coverage, and provide
information on any premiums the individual may owe for the extended
period. Organizations must also ensure beneficiaries are fully aware of
how to access coverage of services for the new time period.
713 – UI Removed End
Date
An enrollment period that previously had an end date is now open (and
ongoing). Organizations must use Exhibit 25a to explain the change
and that enrollment in the plan is now continuous. Organizations must
provide information on any plan premiums and ensure beneficiaries are
fully aware of how to access coverage of services for the new time
period and going forward.

148
60.8 - Election of Continuation of Enrollment Option for MA Local Plans
42 CFR 422.54(b)
When a member permanently moves into the MA organization’s continuation area, the member must
make a positive choice to continue enrollment in the MA local plan. The member does not have to
complete and sign a new enrollment form in order for the continuation to occur but must make this
choice in a manner described in the MA organization’s policy and procedure documents.
The MA organization must verify that the member has established permanent residence in the
continuation area. Proof of permanent residence is normally established by the address of the
residence, but the MA organization may request additional information such as voter’s registration
records, driver’s license records, tax records, and utility bills. Such records must establish the
permanent residence address, and not the mailing address, of the individual.
The effective date of a continuation of enrollment change generally is the first day of the month after
the individual moves into the continuation area.
60.9 - Storage of Enrollment and Disenrollment Records
As stated at 42 CFR 422.60(c)(2), MA organizations are required to file and retain enrollment request
forms. MA organizations must retain and have available for evaluation enrollment and disenrollment
records for the current contract period and ten (10) prior years (42 CFR 422.504(e)(4)).
It is appropriate to allow for storage on microfilm, as long as microfilm versions of enrollment forms
and disenrollment requests showing the signature and the date are available to reviewers. Similarly,
other technologies that would allow the reviewer to access signed forms and other enrollment requests
may also be allowed, such as optically scanned forms stored on disk.
Records of MA enrollment and disenrollment requests made by any other enrollment request
mechanism (as described in §40.1) must also be retained as above.
149
Appendices
Summary of
Medicare Advantage Notice and
Data Element Requirements
150
Appendix 1: Summary of Notice Requirements
Referenced in sections: 10, 30, 40, 50, and 60
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
This Exhibit is intended to be a summary of notice requirements. For exact detail on
requirements and time frames, refer to the appropriate sections within this guidance.
Notice Section(s) Required? Timeframe
Model Enrollment Form (Exh. 1)
10, 40.1.1,
40.2, 40.4.1
Yes
3
NA
Information to include on or with
Enrollment Mechanism -- Attestation
of Eligibility for an Enrollment Period
(Exh. 1a)
30.4 No NA
MA MSA Enrollment Form (Exh 1b)
40.1.1
Yes
4
NA
MA PFFS Enrollment Form (Exh 1c)
40.1.1
Yes
5
NA
Simplified Enrollment Form (Exh.
1d)
40.1.9 No NA
EGHP Enrollment Form (Exh. 2)
10, 40.1.1,
40.2, 40.4.1
No NA
Short Enrollment Forms (Exh. 3 and
3a)
10, 40.1.1,
40.2, 40.4.1
No NA
Acknowledgment of Receipt of
Completed Enrollment Request (Exh.
4 and 4a)
40.4.1, 60.4 Yes
6
10 calendar days of
receipt of completed
enrollment request
Combination Acknowledgement and
Confirmation Notice (Exh. 4b)
40.4 Yes
7
7 calendar days of
availability of the DTRR
Acknowledge Receipt of Completed
PFFS Enrollment Request (Exh.4c)
40.4.1, 60.4 Yes
8
10 calendar days of
receipt of completed
enrollment request
Notice to Acknowledge Receipt of
Completed PFFS Enrollment Request
and to Confirm Enrollment in a PFFS
Plan (Exh. 4d)
40.4.1, 60.4 Yes
7 calendar days of
availability of the DTRR
3
Other CMS approved enrollment election mechanisms may take the place of an enrollment form
4
Other CMS approved enrollment election mechanisms may take the place of an enrollment form
5
Other CMS approved enrollment election mechanisms may take the place of an enrollment form
6
Required unless combined acknowledgment/confirmation notice is issued.
7
Required if the MAO has chosen to provide a single notice in response to the DTRR, as described in §40.4.1.
8
Required unless combined acknowledgment/confirmation notice is issued.
151
Notice
Section(s)
Required?
Timeframe
Notice to Acknowledge Receipt of
Completed Enrollment Request and to
Confirm Enrollment in Another Plan
Within the Same Parent Organization
(Exh. 4e)
40.4 Yes
7 calendar days of the
availability of the DTRR
Request for Information (Exh. 5) 30, 40.2.2 No
10 calendar days of
receipt of enrollment
request
Confirmation of Enrollment (Exh.
6,6a, 6d)
40.4.2, 40.6 Yes
9
10 calendar days of
availability of DTRR
Notice to Individuals Identified on
CMS Records As Members of
Employer or Union Group Receiving
Retiree Drug Subsidy (Exh. 6b)
40.2.5 Yes
10 calendar days of
availability of DTRR
Confirm PFFS Enrollment (Exh. 6c) 40.4.2 Yes
10
10 calendar days of
availability of DTRR
MAO Denial of Enrollment (Exh. 7) 40.2.3 Yes
10 calendar days of
receipt of enrollment
request OR expiration of
time frame for requested
additional information
CMS Rejection of Enrollment (Exh.
8)
40.4.2 Yes
10 calendar days of
availability of DTRR
(exception described in
§40.4.2)
Sending Out Disenrollment
Form/Disenrollment Form (Exh. 9,
9a, & 10)
50.1 No NA
Information to include on or with
Disenrollment Form -- Attestation of
Eligibility for an Election Period
(Exh. 10a)
30.4 No NA
Acknowledgment of Receipt of
Voluntary Disenrollment Request
from Member (Exh. 11)
50.1, 50.4.1 Yes
10 calendar days of
receipt of request to
disenroll
Request Information (Disenrollment)
(Exh. 11a)
30, 50.4.2 Yes
10 calendar days of
receipt of disenrollment
request
9
Required unless combined acknowledgment/confirmation notice is issued.
10
Required unless combined acknowledgment/confirmation notice is issued.
152
Notice
Section(s)
Required?
Timeframe
Final Confirmation of Voluntary
Disenrollment Request from Member
(no exhibit)
50.1 No NA
Confirmation of Voluntary
Disenrollment Identified Through
DTRR (Exh. 12)
50.1, 50.4.1.
60.3.2
Yes
10 calendar days of
availability of DTRR
Denial of Disenrollment (Exh. 12a) 50.1.4 Yes
10 calendar days of
receipt of disenrollment
request
Rejection of Disenrollment (Exh.
12b)
50.1
Yes
10 calendar days of
availability of DTRR
Confirmation of Disenrollment Due to
Passive Enrollment into a Medicare-
Medicaid Plan (Exh. 12c)
50.4.1 Yes
10 calendar days of
availability of DTRR
Final Confirmation of Disenrollment
Due to Out of Area > 6 Months (no
exhibit)
50.2.1 No NA
Disenrollment Due to Death (Exh. 13)
50.2.3,
50.4.2, 60.3.1
No NA
Disenrollment Due to Loss of Part A
and/or Part B Coverage (Exh. 14)
50.2.2,
50.4.2, 60.3.1
No NA
Notices on Terminations/Non-
renewals
50.2.4 Yes
Follow requirements in
42 CFR 422.506 -
422.512
Warning of Potential Disenrollment
Due to Disruptive Behavior (no
exhibit)
50.3.2 Yes NA
Disenrollment for Disruptive
Behavior (no exhibit)
50.3.2 Yes
Before the disenrollment
transaction is submitted
to CMS
Disenrollment for Fraud and Abuse
(no exhibit)
50.3.3 Yes
Before the disenrollment
transaction is submitted
to CMS
Offering Beneficiary Services,
Pending Correction of Erroneous
Death Status (Exh. 15)
60.3, 60.3.1 Yes
10 calendar days of initial
contact with member
Offering Beneficiary Services,
Pending Correction of Erroneous Part
A/B Termination (Exh. 16)
60.3, 60.3.1 Yes
10 calendar days of initial
contact with member
Offering Reinstatement of
Beneficiary Services, Pending
60.3, 60.3.1 Yes
10 calendar days of initial
contact with member
153
Notice
Section(s)
Required?
Timeframe
Correction of Disenrollment Status
Due to Plan Error (Exh 17)
Closing Out Request for
Reinstatement (Exh. 18)
60.3.2 Yes
10 calendar days after
information was due to
MA organization
Failure to Pay Plan Premiums -
Advanced Notification of
Disenrollment or Reduction in
Coverage (Exh. 19)
50.3.1 Yes
Within 15 calendar days
of the premium due date
Failure to Pay Plan Premiums -
Notification of Involuntary
Disenrollment (Exh. 20)
50.3.1 Yes
3 business days following
the last day of the grace
period
Failure to Pay Plan Premiums -
Confirmation of Involuntary
Disenrollment (Exh. 21)
50.3.1 No NA
Notification of Involuntary
Disenrollment by the Centers for
Medicare & Medicaid Services for
Failure to Pay the Part D-Income
Related Monthly Adjustment Amount
(Exh. 21a)
50.2.6 Yes
10 calendar days of
notification on the DTRR
Failure to Pay Plan Premiums -
Notice of Reduction in Coverage
(Exh. 22)
50.3.1 Yes
10 calendar days of the
expiration of the grace
period
Notice of Favorable Good Cause
Determination for Disenrollment Due
to Nonpayment of Part D-IRMAA –
Notification of Plan Premium Amount
Due for Reinstatement (Exh. 22a)
60.3.4 No
3 business days following
the notification by CMS
of favorable good cause
determination
Notice on Favorable Good Cause
Determination for Disenrollment Due
to Nonpayment of Plan Premiums –
Notification of Premium Amount Due
for Reinstatement (Exh 22b)
60.3.4 No
3 business days following
favorable good cause
determination
Notice on Unfavorable Good Cause
Determination for Disenrollment Due
to Nonpayment of Plan Premiums
(Exh 22c)
60.3.4 No
3 business days following
unfavorable good cause
determination
Notice to Close Out Good Cause
Reinstatement Request – Failure to
Pay Plan Premiums within 3 Months
of Disenrollment (Exh 22d)
60.3.4 Yes
10 calendar days of the
expiration of the 3 month
period
154
Notice
Section(s)
Required?
Timeframe
Notice on Favorable Good Cause
Determination for Disenrollment Due
to Nonpayment of Plan Premiums
(No Plan Premium Amount Due for
Reinstatement) (Exh 22e)
60.3.4.1 No
3 business days following
favorable good cause
determination
Public Notices For Closing
Enrollment due to Capacity Limit
(Exh. 23)
40.5 Yes
15 days if related to CMS
approved capacity limit
Notice that Enrollment request Placed
on Waiting List (no exhibit)
40.5.1, 40.5.2 Yes
10 calendar days of
receiving enrollment
request or of approval
from CMS to limit
enrollment
Re-affirming Intent to Not Enroll (no
exhibit)
40.5.1, 40.5.2 No
10 days of contacting
member
Intent to Not Process Enrollment (no
exhibit)
40.5.1, 40.5.2 Yes
10 calendar days of
learning beneficiary no
longer wants to enroll
Medigap Rights per Special Election
Period (Exh. 24)
50.2, 50.1 No Upon request.
Request to cancel enrollment (Exh.
25)
60.2.1 Yes
10 calendar days of
request
Confirmation of Reinstatement Per
Notification From CMS (Exh. 25a)
60.2.1,
60.2.2, 60.3,
60.3.1, 60.3.2
Yes
10 calendar days of
DTRR confirming
reinstatement
Confirmation of Cancellation of
Enrollment Due to Notice from CMS
(TRC 015)(Exh. 25b)
60.2.4 Yes
10 calendar days of
DTRR confirming
cancellation
Request to cancel disenrollment (Exh.
26)
60.2.2 Yes
10 calendar days of
request
Inform Member of Auto-Enrollment
(Exh. 27)
40.1.5 Yes
10 calendar days of
identifying individual as
needing auto-enrollment
Inform FBDE Member of Auto-
Enrollment in PDP (Exh. 27a)
40.1.5 Yes
10 calendar days of
identifying individual as
needing auto-enrollment
Inform Member of Facilitated
Enrollment (Exh. 28)
40.1.5 Yes
10 calendar days of
identifying individual as
needing facilitated
enrollment
155
Notice
Section(s)
Required?
Timeframe
Inform Member of Facilitated
Enrollment into PDP (Exh. 28a)
40.1.5 Yes
10 calendar days of
identifying individual as
needing facilitated
enrollment
Request to Decline Part D (Exh. 29) 40.1.5 Yes
10 calendar days of
request
Enrollment Status Update (Exh. 30) 60.7
As
necessary
10 calendar days of
availability of DTRR
Model Employer/Union Group
Enrollment Mechanism Notice (Exh
31)
40.1.6 Yes
21 calendar days prior to
effective date of
enrollment
Loss of SNP Status (Exh 32) 50.2.5 Yes
10 calendar days of loss
of special needs status
Loss of SNP Status - Notification of
Involuntary Disenrollment (Exh 33)
50.2.5 Yes
3 business days of
expiration of period of
deemed continued
eligibility
Research Potential Out of Area Status
(Exh 34)
50.2.1.3 Yes
10 calendar days of
receiving notice of
change of address or
indication of possible out-
of-area residency
Disenrollment Due to Out of Area
Status (No Response to Request for
Address Verification) (Exh 35)
50.2.1.3 Yes
Within first 10 calendar
days of the sixth month.
Disenrollment Due to Confirmation of
Out of Area Status (Upon New
Address Verification from Member)
(Exh 36)
50.2.1.3 Yes
10 calendar days of
receiving confirmation of
out of area status
Exhibit 37: Notification of
Involuntary Disenrollment by the
Centers for Medicare & Medicaid
Services due to Incarceration
50.2 Yes
10 calendar days of
notification on the DTRR
Exhibit 38: Notification of
Involuntary Disenrollment by the
Centers for Medicare & Medicaid
Services due to Loss of Lawful
Presence
50.2.1, 50.2.7 No
10 calendar days of
notification on the DTRR
156
Appendix 2: Summary of Data Elements Required for Plan Enrollment
Mechanisms and Completed Enrollment Requests
Referenced in section(s): 20, 20.4, 40.2, 40.4.1
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
All data elements with a “Yes” in the “Beneficiary response required on request” column are
necessary in order for the enrollment election to be complete. For use of simplified enrollment
mechanism, the plan must be able to obtain, from its internal data sharing, all the required
elements that it does not include on the enrollment request. Elements required on the simplified
enrollment mechanism, regardless of data sharing, are marked with an asterisk (*).
Data Element
CMS
requires
Field on
enrollment
mechanism?
Beneficiary
response
required on
request?
Exhibit # in which data
element appears
1
MA Plan name
11
Yes*
Yes
1, 1b, 1c, 2, 3, 3a
2 Beneficiary name Yes* Yes 1, 1b, 1c, 2, 3, 3a
3
Beneficiary Date of Birth
Yes
Yes
1, 1b, 1c, 2
4
Beneficiary Sex
Yes
Yes
1, 1b, 1c, 2
5 Beneficiary Telephone Number Yes* No 1, 1b, 1c, 2, 3
6
Permanent Residence Address (with
the exception of “County” – see
below)
Yes Yes 1, 1b, 1c, 2, 3
7
County (Optional Field)
No
No
1, 1b, 1c, 2, 3
8 Mailing Address Yes No 1, 1b, 1c, 2, 3
9
Name of person to contact in
emergency, including phone number
and relationship to beneficiary
(Optional Field)
No No 1b, 1c, 2
10 E-mail Address (Optional Field) No No 1, 1b, 1c, 2, 3
11
Beneficiary Medicare number
Yes*
Yes
1, 1b, 1c, 2, 3
12
Additional Medicare information
contained on Medicare card, or copy
of card
12
No No 1b, 1c, 2
13
Plan Premium Payment Option
Yes
13
No
14
1, 1b, 1c, 3, 3a
14 Response to long term care question No No 1, 1b, 1c, 2
11
If enrollment mechanism will be used for multiple plans, all plan names must be listed in a way that permits the
applicant to clearly indicate his/her plan choice.
12
Plans may include the image of the Medicare card in enrollment mechanisms.
13
Zero premium MA-only plans omit this question
14
Response defaults to direct bill if applicant fails to provide information
157
Data Element
CMS
requires
Field on
enrollment
mechanism?
Beneficiary
response
required on
request?
Exhibit # in which data
element appears
15
Response to other insurance COB
information
Yes Yes
15
1, 1b, 1c, 2
16
Option to request materials in
language other than English
(language preference) or in accessible
formats
Yes* No 1, 1b, 1c, 2, 3, 3a
17
Annotation of whether beneficiary is
retiree, including retirement date and
name of retiree (if not the
beneficiary)
No No 2
18
Question of whether spouse or
dependents are covered under the
plan and, if applicable, name of
spouse or dependents
No No 2
19
Question of whether beneficiary is
currently a member of the plan and if
yes, request for plan identification
number
No No 2
20
Name of chosen Primary Care
Physician, clinic or health center
(Optional Field)
No No 1, 1b, 1c, 2, 3
21
Beneficiary signature and/or
Authorized Representative Signature
Yes*
Yes
16
1, 1b, 1c, 2, 3,3a
22
Date of signature
Yes*
No
17
1, 1b, 1c, 2, 3, 3a
23
Authorized representative contact
information
Yes* Yes 1, 1b, 1c, 2,3, 3a
24
Employer or Union Name and Group
Number
Yes Yes 2
25
Question of which MA plan the
beneficiary is currently a member of
and to which MA plan the beneficiary
is changing
Yes Yes 3
15
Refer to CMS COB guidance for additional information
16
For Employer/Union Group MA enrollment elections as described in §40.1.6, and some other CMS approved
enrollment elections, a signature is not required. For paper enrollment forms submitted without a signature,
organization may verify with the applicant by telephone and document the contact instead of returning form.
17
As explained in §40.2, the beneficiary and/or legal representative should write the date s/he signed the
enrollment form; however, if s/he inadvertently fails to include the date on the enrollment form, then the stamped
date of receipt that the MA organization places on the enrollment form may serve as the signature date of the form.
Therefore, the signature date is not a necessary element. For employer group MA elections as described in §40.4.1,
the "signature date" is the date the employer’s process was completed as recorded.
158
Data Element
CMS
requires
Field on
enrollment
mechanism?
Beneficiary
response
required on
request?
Exhibit # in which data
element appears
26
For Special Needs Plans, description
of SNP eligibility criteria
Yes Yes N/A
27
For MSA plans, all additional
elements including proof that MSA
bank account has been established
Yes Yes N/A
28
Information provided under “please
read and sign below”
All elements provided in model
language must be included on
enrollment request mechanisms.
Option -- can be provided as narrative
or listed as statements of
understanding
Yes* Yes 1, 1b, 1c, 2
29
Release of Information
All elements provided in model
language must be included on
enrollment request mechanisms.
Yes* Yes 1, 1b, 1c, 2
30
Notification of receiving plan
materials electronically and ability to
opt out
No No 1, 1b, 1c, 2, 3, 3a
159
Appendix 3: Setting the Application Date on CMS Enrollment Transactions
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
The application date submitted on enrollment transactions plays a key role in CMS system edits
that ensure the beneficiary’s choice of plan is honored. The application date is always a date
prior to the effective date of enrollment. For use of simplified enrollment mechanism, follow the
information based on how the enrollment request is received (e.g., paper, fax, telephone,
electronically.)
Enrollment request
Mechanism
Application Date Special Notes
Paper Enrollment Forms
§40.1.1
The date the paper request is
initially received
Paper requests submitted to or
collected by sales agents or
brokers are received by the MA
organization on the date the
agent or broker receives the form
Enrollment forms received by
Fax
§40.1.1
The date the fax is received on
the MA organization’s Fax
machine
Medicare.gov Online
Enrollment Center (OEC)
§40.1.2
11 hours prior to the time and
date “stamped” by CMS on
the request
Refer to the definition of
Application Date in §10.
MA organization electronic
enrollment process
§40.1.2
The date the enrollee
completes the request via the
electronic enrollment process
The electronic enrollment
process must capture the
application date as the day that
the individual completes the
request as part of the process
itself.
Approved Telephonic
Enrollment
§40.1.3
The date of the call
Default Enrollment Option for
Newly MA Eligible Medicaid
Managed Care Plan Enrollees
§40.1.4
First day of individual’s Initial
Coverage Election Period
(ICEP)
Effective date must always be
the date of the individual’s first
entitlement to both Medicare
Part A and Part B
Other Special Processes for
Application Dates
Application Date
Special Notes
All enrollment requests into
employer or union sponsored
plans using the SEP EGHP,
regardless of mechanism used
1
st
day of the month prior to
the effective date of
enrollment
This applies to all mechanisms
including §§40.1.3 and 40.1.6
Auto and Facilitated
Enrollment
§40.1.5
The 1
st
of the month prior to
the effective date of the
auto/facilitated enrollment
SPAP enrollment requests as
permitted in §40.1.8 made
during the AEP
October 15
th
The effective date of enrollment
is the following January 1
st

160
Appendix 4: Examples of Good Cause Determinations
Referenced in section: 60.3
This listing is to provide examples to assist plans in making favorable and unfavorable
determinations for requests of reinstatement for good cause. For exact detail on the criteria and
requirements for good cause reinstatements, see §60.3.
In all these examples, the individual is disenrolled for nonpayment of plan premiums and makes
a timely request for good cause reinstatement.
Favorable determination examples:
Example A: Ms. Grey was disenrolled on May 31, 2015 following a plan’s two month grace
period. She states that she has a caregiver who is responsible for making her premium payments
to the plan. Ms. Grey attests that her caregiver caught pneumonia, was hospitalized for over 2
months from late March to late May 2015 and wasn’t able to make payments. The plan issues a
favorable good cause determination, since the member’s caregiver was unexpectedly ill and
hospitalized for a significant portion of the plan’s grace period, which prevented the caregiver
from making arrangements for timely payment. The plan’s favorable determination is
appropriate because: 1) The credible statement was provided about a serious illness and the
person paying premiums was hospitalized for a significant portion of the plan’s grace period; 2)
The event (illness and hospitalization) was unexpected and out of the person’s control; and 3) It
is reasonable to conclude that the caregiver could not have paid or made arrangements to pay the
owed premiums within the plan’s grace period as a result of the illness and hospitalization.
Example B: Mr. Lieber was disenrolled on April 30, 2015 following a plan’s two month grace
period. He states that he was in a car accident in mid-February, was hospitalized for one month
and then sent to an assisted living facility for rehabilitation for one month. He indicated that he
wasn’t able to pay his bills during that time and didn’t have any family to assist him. Because
Mr. Lieber’s situation was unexpected and he was hospitalized and institutionalized for a
significant portion of the plan’s grace period, the plan issues a favorable good cause
determination. The plan’s favorable determination is appropriate because: 1) The creditable
statement was provided about a serious illness and that the member was hospitalized and
institutionalized for significant portion of the plan’s grace period ; 2) The event (illness and
hospitalization) was unexpected and out of the person’s control; and 3) It is reasonable to
conclude that Mr. Lieber could not have paid or made arrangements to pay the owed premiums
within the plan’s grace period as a result of the illness.
Example C: Ms. Kim was disenrolled on August 31, 2015 following the plan’s two month grace
period. She states that she was displaced from her apartment due to a building fire in early June,
was unable to access her belongings and as a result, was unable to make timely payment. The
plan issues a favorable determination because Ms. Kim’s home was significantly damaged by an
unexpected and uncontrollable event during the plan’s grace period. The plan’s favorable
determination is appropriate because: 1) The creditable statement was provided about that the
member’s home was severely damaged due to an unexpected event; 2) The event (fire) was
unexpected and out of the person’s control; and 3) It is reasonable that the damage to Ms. Kim’s
home impaired her ability to pay or make arrangements to pay the owed premiums within the
plan’s grace period.
161
Example D: Mr. Jones was disenrolled on June 30, 2015 following a plan’s two month grace
period. His son states that he found out that his father lost his coverage when he recently visited
him. The son states that Mr. Jones was recently diagnosed with dementia and his condition is
quickly worsening, which caused him to not pay his premiums. The son states that because of
his father’s condition, he is taking over financial matters for his father and will pay the
arrearages. The plan issues a favorable determination because Mr. Jones was newly diagnosed
with a serious illness that directly impacts his ability to pay his premiums. The plan’s favorable
determination is appropriate because: 1) The creditable statement was provided about a serious
and prolonged illness with rapid deterioration, that directly impacted the member’s ability to pay
premiums timely; 2) The event (serious illness with rapid deterioration) was unexpected and out
of the person’s control; and 3) It is reasonable to conclude that the onset of dementia caused Mr.
Jones to fail to make the timely payment during the grace period.
Example E: Ms. Brown was disenrolled on July 31, 2015 following the plan’s three month grace
period. She states that for the past four months, her husband was receiving intensive treatment
for cancer and she was taking care of him during this time. During this time, she fell behind in
paying bills due to the care he needed. The plan issues a favorable determination because Ms.
Brown’s husband was seriously ill for a prolonged period time during the plan’s grace period.
The plan’s favorable determination is appropriate because: 1) The credible statement was
provided about a serious and prolonged illness of an immediate family member; 2) The event
(serious and prolonged illness) was unexpected and out of the person’s control; and 3) It is
reasonable to conclude that Ms. Brown’s circumstance in providing caregiver services for her
spouse impacted her ability to pay or make arrangements to pay the owed premiums within the
plan’s grace period.
Example F: Mrs. Duke was disenrolled on August 31, 2015 following the plan’s two month
grace period. She states that her husband had been handling her bills and making payments
timely. However, he passed away in July 2015, leaving her with no caregiver or family member
to take over the responsibility. The plan issues a favorable good cause determination because of
the recent death of Mrs. Duke’s husband, which was unexpected and out of her control. The plan
also offers Mrs. Duke the option to set up electronic payments and premium withholding to help
ensure that she remains current in paying her premiums. The plan’s favorable determination is
appropriate because: 1) The credible statement was provided about the recent death of a spouse;
2) The event (death of spouse) was unexpected and out of the person’s control; and 3) It is
reasonable to conclude that the unexpected death impacted Mrs. Duke’s ability to pay or make
arrangements to pay the owed premiums within the plan’s grace period.
Example G: Mr. Santiago lives in Lucas County, Iowa, and was disenrolled on July 31, 2015
following the plan’s two month grace period. He states that there were severe storms and
significant flooding in his town and the Post Office closed for a week during the grace period
while the flooding receded. The plan checks the FEMA.gov website and verifies that Lucas
County, Iowa, was declared as a federal disaster area. The plan issues a favorable good cause
determination because the declared federal state of emergency occurred during the plan’s grace
period and that emergency impacted Mr. Santiago’s ability to pay his premiums timely. The
plan’s favorable determination is appropriate because: 1) The credible statement provided was an
extreme weather-related event The event (declared state of emergency) was unexpected and out
of the person’s control; 2) The event was unexpected and out of the person’s control; and 3) It is

162
reasonable to conclude that this circumstance impacted Mr. Santiago’s ability to pay or make
arrangements to pay the owed premiums within the plan’s grace period.
Unfavorable determination examples:
Example A: Mr. Smith was disenrolled on June 30, 2015 following the plan’s three month grace
period. He states that he was unable to pay his plan premiums because he was in the hospital for
a week in May for a planned surgical procedure, followed by a two week stay in a rehabilitation
facility. The plan issues an unfavorable good cause determination because Mr. Smith was not
unexpectedly hospitalized or institutionalized for a significant portion of the plan’s grace
period. Even though Mr. Smith was away from his home undergoing medical treatment for three
weeks, he had a reasonable opportunity and ability to resolve the delinquency within the plan’s
grace period. The plan’s unfavorable determination is appropriate because: 1) The credible
statement provided was not one in which hospitalization or institutionalization occurred for a
significant portion of the plan’s grace period; 2) The situation (planned hospital procedure) was
not unexpected, nor did it render the individual without control over timely payment of his
premiums; and 3) It is reasonable to expect that Mr. Smith could have paid or made
arrangements to pay the owed amounts within the plan’s grace period. Mr. Smith may not be
reinstated for good cause.
Example B: Mr. Jones was disenrolled on May 31, 2015 following the plan’s two month grace
period. He states that he was unable to pay his plan premiums because he has End-Stage Renal
Disease (ESRD) and goes to a facility for dialysis three times a week. Mr. Jones states that he
sometimes has difficulty keeping track of his monthly premium billing statements because of his
frequent trips to the dialysis facility. The plan issues an unfavorable good cause determination
because Mr. Jones has a known health issue and his need for routine dialysis is not unexpected in
any way. While he has a chronic illness, he was receiving regular care to treat his condition, and
it is reasonable to expect him, or someone acting on his behalf, to resolve the delinquency at
some point during the plan’s grace period. The plan’s unfavorable determination is appropriate
because: 1) The credible statement provided was not one in which a chronic illness had newly
developed serious complications which inhibited the ability to pay premiums timely; 2) The
situation (chronic condition with no complications) did not render the individual without control
over timely payment of his premiums; and 3) It is reasonable to expect that Mr. Jones could have
paid or made arrangements to pay the owed amounts within the plan’s grace period. Mr. Jones
may not be reinstated for good cause.
Example C: Ms. Ferrera was disenrolled on March 31, 2015 following the plan’s two month
grace period. She states that she and her family were away from home on an extended vacation
and she wasn’t aware that she had been disenrolled until they returned home. Ms. Ferrera states
that she is willing and able to pay the plan premiums that were not paid and added that she needs
her coverage due to her many medications for diabetes. The plan issues an unfavorable good
cause determination because Ms. Ferrera did not have a circumstance that was unexpected or
unforeseen in any way. While she has a chronic illness and requires medicines to treat her
condition, Ms. Ferrera had the ability to make arrangements to have the premiums paid on time
while she was out of town. The plan’s unfavorable determination is appropriate because: 1) The
credible statement provided of being away from home on vacation is listed specifically as the
basis for an unfavorable determination; 2) The situation (planned vacation) was not unexpected
in any way; and 3) It is reasonable to expect that Ms. Ferrera could have paid or made
163
arrangements to pay the owed amounts within the plan’s grace period. Ms. Ferrera may not be
reinstated for good cause.
Example D: Mr. Davis was disenrolled on July 31, 2015 following the plan’s two month grace
period. He states that earlier in the year he moved a short distance from his previous residence
but did not inform the plan of his new address. The plan issues an unfavorable good cause
determination because the plan materials clearly state that it is the enrollee’s responsibility to
inform the plan of a change of address. This is not a case of plan error, since the plan sent the
monthly billing statements and the disenrollment notice to the address most recently provided by
Mr. Davis. (See §60.3.3 for information on reinstatement following disenrollment due to plan
error.) The plan’s unfavorable determination is appropriate because: 1) The credible statement
provided of an unreported change of address is listed specifically as the basis for an unfavorable
determination; 2) The situation (permanent residence change) was not unexpected in any way;
and 3) It is reasonable to expect Mr. Davis to inform the plan of his new address, to avoid any
delay in his receipt of important materials, such as monthly billing statements and notices
regarding his enrollment status. Mr. Davis may not be reinstated for good cause.
Example E: Ms. Adams was disenrolled on April 30, 2015 following the plan’s three month
grace period. She states that the basement in her home and her electricity were affected by recent
flooding and that this prevented her from sending her monthly plan premium payments. Local
road closures and power outages lasted for up to a week for some residents. The plan issues an
unfavorable good cause determination because the local storms and subsequent flooding did not
severely damage Ms. Adams home or prevent her from making the premium payments; further,
there was neither a state nor federal disaster declaration. The plan’s unfavorable determination is
appropriate because: 1) The credible statement provided was not one in which the home was
severely damaged nor was there a federal or state declaration of emergency; and 2) While road
closures and power outages impacted some area residents, it isn’t clear that Ms. Adams was
directly impacted by these events or was impeded from being able to make timely payment; and
3) It is reasonable to expect that Ms. Adams could have paid or made arrangements to pay the
owed amounts within the plan’s grace period. Ms. Adams may not be reinstated for good cause.
Example F: Mrs. Johnson was disenrolled on March 31, 2015 following the plan’s two month
grace period. She states that her husband is responsible for making her premium payments to the
plan. Mrs. Johnson attests that her husband became ill, was hospitalized for two weeks in
February 2015 and was not able to make payments. The plan issues an unfavorable good cause
determination since, although her husband’s illness was unexpected, he was not hospitalized for
a significant portion of the plan’s grace period, which would have caused him to be unable to
make the payment in a timely manner. The plan’s unfavorable determination is appropriate
because: 1) The credible statement provided was not that hospitalization or institutionalization
occurred for a significant portion of the plan’s grace period; and 2) It is reasonable to expect that
Mr. Johnson could have paid or made arrangements to pay the owed amounts for this wife’s
coverage within the plan’s grace period. Mrs. Johnson may not be reinstated for good cause.
Example G: Mr. Patel was disenrolled on September 30, 2015 following the plan’s three month
grace period. He states that his income decreased and he was unable to afford to pay his
premiums. The plan issues an unfavorable good cause determination because there wasn’t an
unexpected or unforeseen circumstance that prevented payment from being made by Mr. Patel in
a timely manner. The plan’s unfavorable determination is appropriate because: 1) The credible
statement provided of personal financial issues is listed specifically as the basis for an
164
unfavorable determination; and 2) It is reasonable to expect that Mr. Patel could have paid or
made arrangements to pay the owed amounts within the plan’s grace period. Mr. Patel may not
be reinstated for good cause.
Example H: Ms. Ulman was disenrolled on June 30, 2015 following the plan’s two month grace
period. She states that she needs to refill her medications and that she paid her owed amounts to
the plan on July 20, 2015, following her disenrollment effective date. The plan issues an
unfavorable good cause determination because Ms. Ulman’s need for medications did not inhibit
her ability to pay her premiums timely. The plan’s unfavorable determination is appropriate
because: 1) The situation (medication needs) was not unexpected or out of the person’s control,
nor did it impede her ability to pay timely; and 2) It is reasonable to expect that Ms. Ulman could
have paid or made arrangements to pay the owed amounts within the plan’s grace period. Ms.
Ulman may not be reinstated for good cause.
Example I: Ms. Taylor was disenrolled on March 31, 2015 following a plan’s three month grace
period. She states that when she enrolled in the plan during the fall open enrollment period, she
selected premium withhold as the method of premium payment. She says that she received a
premium bill from the new plan for January and, in addition, received a delinquency notice in
early January warning of disenrollment at the end of March if she did not pay the premium for
January. She stated that she ignored the bill and the delinquency notice, assuming that her plan
premiums were being withheld from her Social Security benefit check starting with the January
premium. The plan issues an unfavorable good cause determination because the plan explained
in its letter to Ms. Taylor following submission of the enrollment transaction and receipt of the
DTRR that her first month’s plan premium was not withheld, that she was responsible for paying
her premiums until premium withholding started and that she could be involuntarily
disenrolled. The plan concluded that Ms. Taylor had been appropriately advised of her obligation
to pay the bill for the January premium and that this was reiterated by means of the subsequent
premium bills and the delinquency letter the plan sent to her in January. The plan’s unfavorable
determination is appropriate because: 1) The situation (misunderstanding of ramifications of
nonpayment of premiums) was not unexpected in any way; 2) The situation did not impede her
ability to pay timely; and 3) It is reasonable to expect that Ms. Taylor could have paid or made
arrangements to pay the owed amounts within the plan’s grace period. Ms. Taylor may not be
reinstated for good cause.
165
EXHIBITS
Model Medicare Advantage
Enrollment Forms & Notices
This section contains model exhibits for plan issued notices to beneficiaries regarding
enrollment matters. MA organizations may make the following modifications to CMS
model materials and still submit the material to CMS under the ten (10) day review
period: populating variable fields, correcting grammatical errors, changing the font
(within standards described in the CMS marketing guidelines), adding the plan
name/logo, and adding the CMS marketing material identification number.
For more information on CMS marketing and mailing requirements as well as the
instructions for submitting model documents for review, see the CMS Medicare
Communication and Marketing Guidelines.

OMB No. 0938-1378
Expires:7/31/2023
166
Exhibit 1: MODEL INDIVIDUAL ENROLLMENT REQUEST FORM TO ENROLL IN
A MEDICARE ADVANTAGE PLAN (PART C)
Who can use this form?
People with Medicare who want to join a Medicare
Advantage Plan
To join a plan, you must:
• Be a United States citizen or be lawfully
present in the U.S.
• Live in the plan’s service area
Important: To join a Medicare Advantage Plan,
you must also have both:
• Medicare Part A (Hospital Insurance)
• Medicare Part B (Medical Insurance)
When do I use this form?
You can join a plan:
• Between October 15–December 7 each year (for
coverage starting January1)
• Within 3 months of first getting Medicare
• In certain situations where you’re allowed to
join or switch plans
Visit Medicare.gov to learn more about when you
can sign up for a plan.
What do I need to complete this form?
• Your Medicare Number (the number on your
red, white, and blue Medicare card)
• Your permanent address and phone number
Note: You must complete all items in Section 1.
The items in Section 2 are optional — you can’t be
denied coverage because you don’t fill them out.
Reminders:
• If you want to join a plan during fall open
enrollment (October 15–December 7), the plan
must get your completed form by December 7.
• Your plan will send you a bill for the plan’s
premium. You can choose to sign up to have
your premium payments deducted from your
bank account or your monthly Social Security
(or Railroad Retirement Board) benefit.
What happens next?
Send your completed and signed form to:
<Plan Name>
<Plan address>
<Plan address>
<Plan address>
Once they process your request to join, they’ll
contact you.
How do I get help with this form?
Call <Plan Name> at <phone number>. TTY users
can call < phone number >.
Or, call Medicare at 1-800-MEDICARE
(1-800-633-4227). TTY users can call
1-877-486-2048.
En español: Llame a <Plan Name> al <phone
number/TTY> o a Medicare gratis al
1-800-633-4227 y oprima el 2 para asistencia en
español y un representante estará disponible para
asistirle.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
167
Section 1 – All fields on this page are required (unless marked optional)
Select the plan you want to join:
Product ABC – $XX per month Product XYZ – $XX per month
FIRST name: LAST name: [Optional: Middle Initial]:
Birth date: (MM/DD/YYYY)
(__ __/__ __/__ __ __ __)
Sex:
Male Female
Phone number:
( )
Permanent Residence street address (Don’t enter a PO Box):
City:
[Optional: County]:
State:
ZIP Code:
Mailing address, if different from your permanent address (PO Box allowed):
Street address: City: State: ZIP Code:
Your Medicare information:
Medicare Number: _ _ _ _ - _ _ _ - _ _ _ _
Answer these important questions:
[MA-PD / PDPs insert:
Will you have other prescription drug coverage (like VA, TRICARE) in addition to < Plan>? Yes No
Name of other coverage: Member number for this coverage: Group number for this coverage
___________________________ ____________________________ ________________________]
[Special Needs Plans] insert question(s) regarding the required special needs criteria]
IMPORTANT: Read and sign below:
• [MA plans insert: I must keep both Hospital (Part A) and Medical (Part B) to stay in <Plan Name>.]
• By joining this Medicare Advantage Plan, I acknowledge that <Plan Name> will share my information with
Medicare, who may use it to track my enrollment, to make payments, and for other purposes allowed by
Federal law that authorize the collection of this information (see Privacy Act Statement below).
• Your response to this form is voluntary. However, failure to respond may affect enrollment in the plan.
• The information on this enrollment form is correct to the best of my knowledge. I understand that if I
intentionally provide false information on this form, I will be disenrolled from the plan.
• I understand that people with Medicare are generally not covered under Medicare while out of the country,
except for limited coverage near the U.S. border.
• [MA plans insert: I understand that when my <Plan Name> coverage begins, I must get all of my medical
and prescription drug benefits from <Plan Name>. Benefits and services provided by <Plan Name> and
contained in my <Plan Name> “Evidence of Coverage” document (also known as a member contract or
subscriber agreement) will be covered. Neither Medicare nor <Plan Name> will pay for benefits or services
that are not covered.]
• I understand that my signature (or the signature of the person legally authorized to act on my behalf) on this
application means that I have read and understand the contents of this application. If signed by an authorized
representative (as described above), this signature certifies that:
1) This person is authorized under State law to complete this enrollment, and
2) Documentation of this authority is available upon request by Medicare.
Signature:
Today’s date:
If you’re the authorized representative, sign above and fill out these fields:
Name: Address:
Phone number: Relationship to enrollee:
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
168
PRIVACY ACT STATEMENT
The Centers for Medicare & Medicaid Services (CMS) collects information from Medicare plans to track beneficiary enrollment in Medicare Advantage
(MA) Plans, improve care, and for the payment of Medicare benefits. Sections 1851 and 1860D-1 of the Social Security Act and 42 CFR §§ 422.50 and
422.60 authorize the collection of this information. CMS may use, disclose and exchange enrollment data from Medicare beneficiaries as specified in the
System of Records Notice (SORN) “Medicare Advantage Prescription Drug (MARx)”, System No. 09-70-0588. Your response to this form is voluntary.
However, failure to respond may affect enrollment in the plan.
Section 2 – All fields on this page are optional
Answering these questions is your choice. You can’t be denied coverage because you don’t fill them out.
Select one if you want us to send you information in a language other than English.
[ Plans insert the languages required in your service area.]
Select one if you want us to send you information in an accessible format.
Braille Large print Audio CD
Please contact <plan name> at <phone number> if you need information in an accessible format other than
what’s listed above. Our office hours are <insert days and hours of operation>. TTY users can call <TTY
number.>
Do you work? Yes No Does your spouse work? Yes No
List your Primary Care Physician (PCP), clinic, or health center:
I want to get the following materials via email. Select one or more.
[Plans may list those types or categories of materials that are available for electronic delivery]
E-mail address:
Paying your plan premiums
[Plans with premiums insert: You can pay your monthly plan premium [MA-PD plans with premiums insert:
(including any late enrollment penalty that you currently have or may owe)] by mail <insert optional methods:
“Electronic Funds Transfer (EFT)”, “credit card”> each month <insert optional intervals, if applicable, for
example “or quarterly”>. You can also choose to pay your premium by having it automatically taken out of
your Social Security or Railroad Retirement Board (RRB) benefit each month.]
[MA-PD and PDPs with premiums insert: If you have to pay a Part D-Income Related Monthly Adjustment
Amount (Part D-IRMAA), you must pay this extra amount in addition to your plan premium. The amount
is usually taken out of your Social Security benefit, or you may get a bill from Medicare (or the RRB). DON’T
pay [insert appropriate plan and/or organization name] the Part D-IRMAA.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
169
Exhibit 1a: Information to include on or with Enrollment Mechanism –
Attestation of Eligibility for an Enrollment Period
Referenced in section: 30.4
(Rev. 2, Issued: August 25, 2020; Effective/Implementation: 01-01-2021)
Typically, you may enroll in a Medicare Advantage plan only during the annual enrollment
period from October 15 through December 7 of each year. There are exceptions that may
allow you to enroll in a Medicare Advantage plan outside of this period.
Please read the following statements carefully and check the box if the statement applies to you.
By checking any of the following boxes you are certifying that, to the best of your knowledge,
you are eligible for an Enrollment Period. If we later determine that this information is incorrect,
you may be disenrolled.
I am new to Medicare.
I am enrolled in a Medicare Advantage plan and want to make a change during the
Medicare Advantage Open Enrollment Period (MA OEP).
I recently moved outside of the service area for my current plan or I recently moved and
this plan is a new option for me. I moved on (insert date) _______________________.
I recently was released from incarceration. I was released on (insert date)
______________________________________________________.
I recently returned to the United States after living permanently outside of the U.S. I
returned to the U.S. on (insert date) ________________________.
I recently obtained lawful presence status in the United States. I got this status on (insert
date) ______________________________________.
I recently had a change in my Medicaid (newly got Medicaid, had a change in level of
Medicaid assistance, or lost Medicaid) on (insert date) ___________________________.
I recently had a change in my Extra Help paying for Medicare prescription drug coverage
(newly got Extra Help, had a change in the level of Extra Help, or lost Extra Help) on
(insert date) _____________________________________.
I have both Medicare and Medicaid (or my state helps pay for my Medicare premiums) or
I get Extra Help paying for my Medicare prescription drug coverage, but I haven’t had a
change.
I am moving into, live in, or recently moved out of a Long-Term Care Facility (for
example, a nursing home or long term care facility). I moved/will move into/out of the
facility on (insert date) ____________________________________________________.
I recently left a PACE program on (insert date) ___________________________.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
170
I recently involuntarily lost my creditable prescription drug coverage (coverage as good
as Medicare’s). I lost my drug coverage on (insert date) _________________________.
I am leaving employer or union coverage on (insert date) _______________________.
I belong to a pharmacy assistance program provided by my state.
My plan is ending its contract with Medicare, or Medicare is ending its contract with my
plan.
I was enrolled in a plan by Medicare (or my state) and I want to choose a different plan.
My enrollment in that plan started on (insert date) ______________________________.
I was enrolled in a Special Needs Plan (SNP) but I have lost the special needs
qualification required to be in that plan. I was disenrolled from the SNP on (insert date)
_____________________________.
I was affected by an emergency or major disaster (as declared by the Federal Emergency
Management Agency (FEMA) or by a Federal, state or local government entity. One of
the other statements here applied to me, but I was unable to make my enrollment request
because of the disaster.
If none of these statements applies to you or you’re not sure, please contact <plan name> at
<phone number> (TTY users should call <TTY number>) to see if you are eligible to enroll.
We are open <insert days and hours of operation>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
171
Exhibit 1b: Model MA MSA Plan Enrollment Request Form (“Election” may
also be used)
Referenced in §40.1.1
(Rev. 3, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Please contact <plan name> if you need information in another language or format (Braille).
To Enroll in <plan name>, Please Provide the Following Information:
[Required if form used for multiple plans: Please check which plan you want to enroll in:
Product ABC $XX per month Product XYZ $XX per month]
LAST name: FIRST Name: Middle Initial
Mr. Mrs.
Ms.
Birth Date:
(__ __/__ __/__ __ __ __)
(M M / D D / Y Y Y Y)
Sex:
M F
Home Phone Number:
( )
[Optional field:
Alternate Phone
Number: ( )]
Permanent Residence Street Address (P.O. Box is not allowed):
City:
[Optional field: County:]
State:
ZIP Code:
Mailing Address (only if different from your Permanent Residence Address):
Street Address: City: State: ZIP
Code:
[Optional field: Emergency contact: _________________
Phone Number: ________________________ Relationship to You: ____________________ ]
[Optional field: E-mail Address: _____________________ ]
Please Provide Your Medicare Insurance Information
Please take out your red, white and blue Medicare
card to complete this section.
• Fill out this information as it appears on
your Medicare card.
- OR –
• Attach a copy of your Medicare card or
your letter from Social Security or the
Railroad Retirement Board.
Name (as it appears on your Medicare card):
Medicare Number:
Is Entitled to: Effective Date:
HOSPITAL (Part A)
MEDICAL (Part B)
You must have Medicare Part A and Part B to join
a Medicare Advantage plan.
Please read and answer these important questions
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
172
1. To enroll in <MSA plan name>, you may not have other health coverage as described below.
Please answer each of the following questions:
A. Are you enrolled in your State Medicaid program? Yes No
B. Are you receiving Medicare Hospice benefits? Yes No
C. Some individuals may have other health coverage, including other private insurance,
TRICARE, Federal employee health benefits coverage, VA benefits, or other health benefits that
cover all or part of the annual Medicare MSA deductible. If you have any other such coverage, you
aren’t eligible to enroll in <MSA plan name>
Will you have other health coverage in addition to <MSA plan name>? Yes No
If “yes”, please list your other coverage and your identification (ID) number(s) for this coverage so
we can decide if you are eligible to enroll in <MSA plan name>:
Name of other coverage: ID # for this coverage: Group # for this
coverage
_______________________________ __________________________ ________________________
2. Will you reside in the United States for at least 183 days during each year you are enrolled in
<MSA plan>?
Yes No
3. Do you or your spouse work? Yes No
Please check one of the boxes below if you would prefer that we send you information in a
language other than English or an accessible format:
<include list of available languages>
<include list of accessible formats (like Braille, audio tape, or large print>
Please contact <plan name> at <phone number> if you need information in an accessible format or
language other than what is listed above. Our office hours are <insert days and hours of operation>.
TTY users should call <TTY number>.
[
Optional field:
If plan delivers some documents electronically, insert language explaining the types of
documents it sends and how (e.g., information about your enrollment to the email address you provide
to us on this form), as well as how a member can opt to get paper versions of those documents instead
(e.g., a checkbox to opt-out of getting documents electronically).]
Please Read and Sign Below:
By completing this enrollment application, I agree to the following:
<MSA Plan Name> is a Medicare Advantage plan and has a contract with the Federal government. I
will need to keep my Medicare Parts A and B. I can be in only one Medicare Advantage plan at a time
and I understand that my enrollment in this plan will automatically end my enrollment in another
Medicare health plan. It is my responsibility to inform you of any health coverage that I have or may
get in the future. I understand that if I don’t have Medicare prescription drug coverage, or creditable
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
173
prescription drug coverage (as good as Medicare’s), I may have to pay a late enrollment penalty if I
enroll in Medicare prescription drug coverage in the future. Enrollment in this plan is generally for the
entire year. I may leave this plan (“disenroll”) during the Annual Enrollment Period that is October
15
th
through December 7
th
of every year (effective the following January 1
st
) or under certain limited
special circumstances, by sending a request in writing to <MSA plan name>. If I choose a Medicare
MSA plan and haven’t before joined an MSA plan, then change my mind, I may cancel my enrollment
by December 15 of the same year by contacting my plan to cancel my enrollment request. I understand
that my enrollment into an MSA plan isn’t complete until the bank account is established. I understand
that I am enrolling in a plan that doesn’t pay for Medicare covered services until a high deductible is
met, but <plan name> allows me to use funds in my MSA account to pay for health services.
Withdrawals made from the MSA bank account aren’t taxed when used for IRS-qualified medical
expenses. I would owe income tax and up to a 50% penalty for withdrawals used for non-medical
expenses. After the deductible is met the plan pays 100% of Medicare-covered services.
[MSA Demonstration Plans insert: If I am enrolling in a MSA demonstration plan, I may be
responsible for cost sharing for certain preventive services, as described by the plan, before the
deductible is met. After the deductible is met, I may be responsible for cost-sharing until my expenses
for covered services reach the out-of-pocket maximum, after which the MSA demonstration plan pays
100% of Medicare covered services.]
If I have any questions regarding the initial set-up of my MSA bank account or any of the information
in this enrollment form, I should contact the <plan name> at < contact number>.
<MSA plan name> serves a specific service area. If I move out of the area that <MSA Plan Name>
serves, I need to notify the plan so I can disenroll and find a new plan in my new area. Once I am a
member of <MSA plan Name>, I have the right to appeal plan decisions about payment or services if I
disagree. I will read the [insert either Member Handbook or Evidence of Coverage document] from
<MSA plan name> when I get it to know which rules I must follow to get coverage with this Medicare
Advantage plan.
I understand that if I am getting assistance from a sales agent, broker, or other individual employed by
or contracted with <plan name>, he/she may be paid based on my enrollment in<plan name>.
I understand that if I disenroll before the end of the plan year (December 31
st
), <plan name> may debit
my MSA bank account for a prorated share of the current year’s deposit to be returned to Medicare.
The debit amount is based on the number of months left in the year after the disenrollment date. I
understand that, if I die, my estate will be responsible for any money owed to Medicare. My estate
keeps any amount over what is owed to Medicare.
Release of Information: By joining this Medicare health plan, I acknowledge that the Medicare
health plan will release my information to Medicare and other plans as is necessary for treatment,
payment and health care operations. I also acknowledge that <MSA plan name> will release my
information to Medicare, who may release it for research and other purposes which follow all
applicable Federal statutes and regulations. The information on this enrollment form is correct to the
best of my knowledge. I understand that if I intentionally provide false information on this form, I will
be disenrolled from the plan.
I understand that my signature (or the signature of the person authorized to act on my behalf under the
laws of the State where I live) on this application means that I have read and understand the contents of
this application. If signed by an authorized individual (as described above), this signature certifies that
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
174
Office Use Only:
Name of staff member/agent/broker (if assisted in enrollment):___________________________
Plan ID #:_____________________________
Effective Date of Coverage: _______________
ICEP/IEP: __________ AEP: __________ SEP (type): __________ Not Eligible: _______
[optional space for other administrative information needed by plan]
1) this person is authorized under State law to complete this enrollment and 2) documentation of this
authority is available upon request from Medicare.
Signature:
Today’s Date:
If you are the authorized representative, you must sign above and provide the following information:
Name: _________________________________________________
Address: _______________________________________________
Phone Number: (___) ____- _________
Relationship to Enrollee ___________________
Keeping records -- As an authorized representative, it is important that you keep records of when funds
in the MSA account are used, as well as how the funds are used.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
175
Exhibit 1c: Model PFFS Individual Enrollment Request Form (“Election” may
also be used)
Referenced in section(s): 10, 20.4, 40.1, 40.2
(Rev. 3, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Please contact <plan name> if you need information in another language or format (Braille).
To Enroll in <plan>, Please Provide the Following Information:
[Required if form used for multiple plans: Please check which plan you want to enroll in:
Product ABC $XX per month Product XYZ $XX per month]
LAST name: FIRST Name: Middle Initial
Mr. Mrs.
Ms.
Birth Date:
(__ __/__ __/__ __ __ __)
(M M / D D / Y Y Y Y)
Sex:
M F
Home Phone Number:
( )
[Optional field:
Alternate Phone
Number:]
Permanent Residence Street Address (P.O. Box is not allowed):
City:
[Optional field: County:]
State:
ZIP Code:
Mailing Address (only if different from your Permanent Residence Address):
Street Address: City: State: ZIP Code:
[Optional field: Emergency contact: _________________
Phone Number:______________________________ Relationship to You: _________ ]
[Optional field: E-mail Address: __________________ ]
Please Provide Your Medicare Insurance Information
Please take out your red, white and blue Medicare
card to complete this section.
• Fill out this information as it appears on
your Medicare card.
- OR –
• Attach a copy of your Medicare card or
your letter from Social Security or the
Railroad Retirement Board.
Name (as it appears on your Medicare card):
Medicare Number:
Is Entitled to: Effective Date:
HOSPITAL (Part A)
MEDICAL (Part B)
You must have Medicare Part A and Part B to join
a Medicare Advantage plan.
[Zero premium MA-only plans omit this section:
Paying Your Plan Premium
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
176
[Zero premium MA-PD plans insert: If we determine that you owe a late enrollment penalty (or if
you currently have a late enrollment penalty), we need to know how would prefer to pay it. You
can pay by mail <insert optional methods: “Electronic Funds Transfer (EFT)”, “credit card”> each
month <insert optional intervals, if applicable, for example “or quarterly”>. You can also choose to
pay your premium by automatic deduction from your Social Security or Railroad Retirement
Board benefit check each month. If you are assessed a Part D-Income Related Monthly
Adjustment Amount, you will be notified by the Social Security Administration. You will be
responsible for paying this extra amount in addition to your plan premium. You will either have
the amount withheld from your Social Security benefit check or be billed directly by Medicare or
Railroad Retirement Board. DO NOT pay [insert appropriate plan and/or organization name] the
Part D-IRMAA. ]
[MA-only and MA-PD plans with premiums insert: You can pay your monthly plan premium [
MA-
PD plans with premium insert:
(including any late enrollment penalty you have or may owe)] by mail
<insert optional methods: “Electronic Funds Transfer (EFT)”, “credit card”> each month <insert
optional intervals, if applicable, for example “or quarterly”>. You can also choose to pay your
premium by automatic deduction from your Social Security or Railroad Retirement Board
benefit check each month.
[MA-PD plans with premiums insert: If you are assessed a Part D-Income Related Monthly
Adjustment Amount, you will be notified by the Social Security Administration. You will be
responsible for paying this extra amount in addition to your plan premium. You will either have
the amount withheld from your Social Security benefit check or be billed directly by Medicare or
Railroad Retirement Board. DO NOT pay [insert appropriate plan and/or organization name] the
Part D-IRMAA.]
People with limited incomes may qualify for Extra Help to pay for their prescription drug costs. If you
qualify, Medicare could pay for 75% or more of your drug costs including monthly prescription drug
premiums, annual deductibles, and co-insurance. Additionally, those who qualify won’t have a coverage
gap or a late enrollment penalty. Many people qualify for these savings and don’t even know it. For
more information about this Extra Help, contact your local Social Security office, or call Social Security
at 1-800-772-1213. TTY users should call 1-800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp
If you qualify for Extra Help with your Medicare prescription drug coverage costs, Medicare will pay
all or part of your plan premium. If Medicare pays only a portion of this premium, we will bill you for
the amount that Medicare doesn’t cover.
If you don’t select a payment option, you will get a bill each month <optional language in place of “bill
each month”: “coupon book” or “payment book”>.
Please select a premium payment option:
Get a bill <option: “coupon”, “payment” book, etc>
<option to include other billing intervals e.g. bi-monthly, quarterly>
[Optional - Include other payment methods, such as EFT & credit card as follows:
Electronic funds transfer (EFT) from your bank account each month. Please enclose a VOIDED
check or provide the following:
Account holder name: ______________________
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
177
Bank routing number: _ _ _ _ _ _ _ _ _ Bank account number: _ _ _ _ _ _ _ _ _ _ _ _
Account type: Checking Saving
Credit Card. Please provide the following information:
Type of Card: ____________________________
Name of Account holder as it appears on card: _________________________
Account number: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Expiration Date: _ _/_ _ _ _ (MM/YYYY)]
Automatic deduction from your monthly Social Security/Railroad Retirement Board (RRB) benefit
check.
I get monthly benefits from: Social Security RRB
(The Social Security/RRB deduction may take two or more months to begin after Social Security or
RRB approves the deduction. In most cases, if Social Security or RRB accepts your request for
automatic deduction, the first deduction from your Social Security or RRB benefit check will include all
premiums due from your enrollment effective date up to the point withholding begins. If Social
Security or RRB does not approve your request for automatic deduction, we will send you a paper bill
for your monthly premiums.)]
Please read and answer these important questions:
[PFFS-PD plans insert:
1. Some individuals may have other drug coverage, including other private insurance, TRICARE,
Federal employee health benefits coverage, VA benefits, or State pharmaceutical assistance programs.
Will you have other prescription drug coverage in addition to <PFFS plan>? Yes No
If “yes”, please list your other coverage and your identification (ID) number(s) for this coverage:
Name of other coverage: ID # for this coverage: Group # for this
coverage
_______________________________ __________________________ _______________________]
2. Do you or your spouse work? Yes No
[Optional field: Please tell us the name of your Primary Care Physician (PCP):
Doctor’s Name: _____________________________ Phone Number:
___________________________]
[Optional field: Please tell us the name of your preferred hospital, clinic or health center:
Name: _________________________________ City: _____________________ State: ________]
Please check one of the boxes below if you would prefer that we send you information in a
language other than English or in an accessible format:
<include list of available languages>
<include list of accessible formats (like Braille, audio tape, or large print)>
Please contact <plan name> at <phone number> if you need information in an accessible format or
language other than what is listed above. Our office hours are <insert days and hours of operation>.
TTY users should call <TTY number>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
178
[Optional field: If plan delivers some documents electronically, insert language explaining the types of
documents it sends and how (e.g., information about your enrollment to the email address you provide
to us on this form), as well as how a member can opt to get paper versions of those documents instead
(e.g., a checkbox to opt-out of getting documents electronically).]
Please Read and Sign Below
By completing this enrollment application, I agree to the following:
<Plan Name> is a Medicare Private Fee-For-Service plan and has a contract with the Federal
government. I will need to keep my Medicare Parts A and B. I understand that this plan is a Medicare
Advantage Private-Fee-For-Service plan and I can be in only one Medicare health plan at a time. I
understand that my enrollment in this plan will automatically end my enrollment in another Medicare
health plan [PFFS w/PD insert “or Medicare prescription drug plan.”]. It is my responsibility to inform
you of any prescription drug coverage that I have or may get in the future. [PFFS w/o PD only plans
insert: “I understand that since this plan does not offer Medicare prescription drug coverage, I may get
coverage from another Medicare prescription drug plan. If I don’t have Medicare prescription drug
coverage, or creditable prescription drug coverage (as good as Medicare’s), I may have to pay a late
enrollment penalty if I enroll in Medicare prescription drug coverage in the future.”] Enrollment in this
plan is generally for the entire year. Once I enroll, I may leave this plan or make changes only at certain
times of the year if an enrollment period is available (Example: Annual Enrollment Period from October
15 – December 7 of every year), or under certain special circumstances.
Please Read This Important Information
[All PFFS plans insert: <Plan name>, a Medicare Advantage Private Fee-for-Service plan, works
differently than a Medicare supplement plan as well as other Medicare Advantage plans. Your doctor or
hospital isn’t required to agree to accept our plan’s terms and conditions, and may choose not to treat
you, except in emergencies. You should verify that your provider(s) will accept <plan name> before
each visit Providers can find the plan’s terms and conditions on our website at <insert link to PFFS
terms and conditions>.]
[All PFFS plans insert, except for cases in which beneficiary is switching from one PFFS plan to
another PFFS plan offered by the same MAO: Once <plan name> has your enrollment form, you will
get a call from a plan representative. This call is to make sure that you understand how a Private Fee-
for-Service plan works and to confirm your intent to enroll in <plan name>. If <plan name> isn’t able
to reach you by telephone, then you will get a letter by mail that contains similar information.]
[PFFS-PD plans insert: If you currently have health coverage from an employer or union, joining
<PFFS-PD Name> could affect your employer or union health benefits. If you have health coverage
from an employer or union, joining <PFFS-PD Name> may change how your current coverage works.
You or your dependents could lose your other health or drug coverage completely and not get it back if
you join <plan name>. Read the communications your employer or union sends you. If you have
questions, visit their website, or contact the office listed in their communications. If there is no
information on whom to contact, your benefits administrator or the office that answers questions about
your coverage can help.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
179
Office Use Only:
Name of staff member/agent/broker (if assisted in enrollment):___________________________
Plan ID #:_____________________________
Effective Date of Coverage: _______________
ICEP/IEP: ______ AEP: ______ SEP (type): ______ Not Eligible: ______
[optional space for other administrative information needed by plan]
As a Medicare Private Fee-For-Service plan, <plan name> works differently than a Medicare supplement
plan as well as other Medicare Advantage plans. <Plan name> pays instead of Medicare, and I will be
responsible for the amounts that <plan name> doesn’t cover, such as copayments and coinsurances.
Original Medicare won’t pay for my health care while I am enrolled in <plan name>.
Before seeing a provider, I should verify that the provider will accept <plan name>. I understand that
my health care providers have the right to choose whether to accept <plan name>’s payment terms and
conditions every time I see them. I understand that if my provider doesn’t accept <plan name>, I will
need to find another provider that will.
<Plan name> serves a specific service area. If I move out of the area that <plan name> serves, I need to
notify <plan name> so I can disenroll and find a new plan in my new area. Once I am a member of <plan
name>, I have the right to appeal plan decisions about payment or services if I disagree. I will read the
[insert either Member Handbook or Evidence of Coverage document] from <plan name> when I get it to
know which rules I must follow in to get coverage with this Private Fee-For-Service plan. I understand
that people with Medicare aren’t usually covered under Medicare while out of the country except for
limited coverage near the U.S. border.
I understand that if I am getting assistance from a sales agent, broker, or other individual employed by or
contracted with <plan name>, he/she may be paid based on my enrollment in<plan name>.
Release of Information: By joining this Medicare health plan, I acknowledge that the Medicare health
plan will release my information to Medicare and other plans as is necessary for treatment, payment and
health care operations. I also acknowledge that <plan name> will release my information [
PFFS-PD plans
insert:
including my prescription drug event data] to Medicare, who may release it for research and other
purposes which follow all applicable Federal statutes and regulations. The information on this enrollment
form is correct to the best of my knowledge. I understand that if I intentionally provide false information
on this form, I will be disenrolled from the plan.
I understand that my signature (or the signature of the person authorized to act on my behalf under the
laws of the State where I live) on this application means that I have read and understand the contents of
this application. If signed by an authorized individual (as described above), this signature certifies that:
1) this person is authorized under State law to complete this enrollment and 2) documentation of this
authority is available upon request from Medicare.
Signature:
Today’s Date:
If you are the authorized representative, you must sign above and provide the following information:
Name: ________________________
Address: _______________________________________________
Phone Number: (___) ____- ______
Relationship to Enrollee ___________________
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
180
Exhibit 1d: Model Simplified Enrollment Form
Reference: §40.1.9
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
[MA Organizations must collect all required data as outlined in Appendix 2. Additional data
elements must be added for any required data not already available.]
You are requesting enrollment into a Medicare Advantage Plan offered by <name of MA
Organization>. You agree to allow <name of MA Organization> to use your personal
information we have on file from your current enrollment in <our non-Medicare coverage [or
optionally: name non-Medicare plan]> to complete your enrollment request.
Tell Us About Yourself:
LAST Name:
FIRST Name:
Middle Initial:
Your current <non-Medicare
plan name> health plan member
number:
Your Medicare Number:
(Optional)
Part A coverage starts:
Part B coverage starts:
Your Telephone Number (in case we need to reach you):
Tell Us Which Plan You Want to Enroll: [Include plan names and premiums. If using form for
multiple plans, display options for beneficiary to clearly indicate plan choice.]
____ Plan A $XX per month _____ Plan B $XX per month
[If offering a zero premium plan or reduction of the Part B premium, may delete or modify the
references to plan and Medicare premiums:] I understand that this plan may have a different
provider network and that I must pay the monthly plan premium in addition to any Medicare Part
A and Part B premiums I may owe.
[May include options for premium payment. If not offering options for premium payment,
include: You will get a bill from <plan name> for your monthly premium. Contact <plan name>
if you want to pay your premium by <payment options offered by the plan>.]
[Add any other items not available via internal data sharing to collect the remainder of required
information]
Please check one of the boxes if you would prefer that we send you information in a language
other than English or in an accessible format:
____ <include list of available languages>
____ <include list of accessible formats (like Braille, audio tape, or large print)>
Please contact <plan name> at phone <phone number> if you need information in an accessible
format or language other than what is listed above. Our office hours are <insert days and hours of
operation >. TTY users should call <TTY number>.
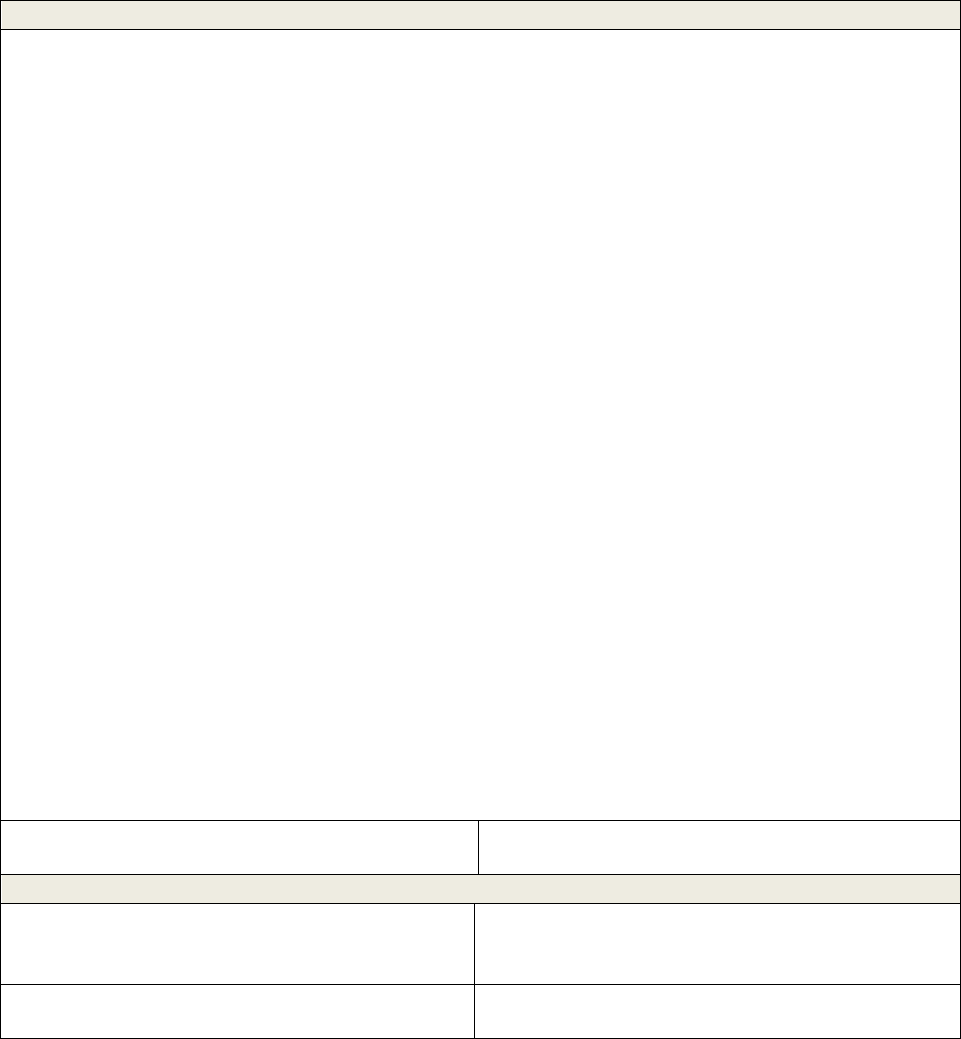
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
181
You are requesting enrollment into a Medicare Advantage Plan offered by <name of MA
Organization>. You agree to allow <name of MA Organization> to use your personal
information we have on file from your current enrollment in <our non-Medicare coverage [or
optionally: name non-Medicare plan]> to complete your enrollment request.
IMPORTANT: Read and Sign Below:
• <Plan name> is a Medicare Advantage prescription drug plan and has a contract with the Federal
government. I must continue to keep both Part A and Part B to stay enrolled in <plan name>.
• I understand that if I am getting assistance from a sales agent, broker, or other individual employed
by or contracted with <plan name>, he/she may be compensated based on my enrollment in <plan
name>.
• Release of Information: By joining this Medicare Advantage Prescription Drug Plan, I
acknowledge that the plan will release my information to Medicare and other plans as is necessary
for treatment, payment and health care operations. I also acknowledge that <plan name> will
release my information, including my prescription drug event data, to Medicare, who may release
it for research and other purposes which follow all applicable Federal statutes and regulations.
• The information on this enrollment form is correct to the best of my knowledge. I understand that
if I intentionally provide false information on this form, I will be disenrolled from the plan. I
understand that people with Medicare are generally not covered under Medicare while out of the
country, except for limited coverage near the U.S. border.
• I understand that when my <plan name> coverage begins, I must get all of my medical and
prescription drug benefits from <plan name>. Benefits and services authorized by <plan name>
and contained in my <plan name> Evidence of Coverage document (also known as a member
contract or subscriber agreement) will be covered. Without authorization, neither Medicare nor
<plan name> will pay for benefits or services.
• I understand that my signature (or the signature of the person legally authorized to act on my
behalf) on this application means that I have read and understand the contents of this application.
If signed by an authorized individual (as described above), this signature certifies that:
1) This person is authorized under State law to complete this enrollment, and
2) Documentation of this authority is available upon request by Medicare.
Signature:
Date:
If you are the authorized representative, you must sign above and provide the following information:
Name:
Address:
Phone Number:
Relationship to Enrollee:
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
182
Exhibit 2: Model Employer/Union Group Health Plan Enrollment Request
Form (“Election” may also be used)
Referenced in section(s): 10, 40.1, 40.2, 50.1
(Rev. 3, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Please contact <plan name> if you need information in another language or format (Braille).
To Enroll in <plan name>, Please Provide the following Information:
Employer or Union Name: Group #:
[Required if form used for multiple plans: Please check which plan you want to enroll in:
Product ABC $XX per month Product XYZ $XX per month]
LAST name: FIRST Name: Middle Initial
Mr. Mrs.
Ms.
Birth Date:
(__ __/__ __/__ __ __ __)
(M M / D D / Y Y Y Y)
Sex:
M F
Home Phone Number:
( )
[Optional field:
Alternate Phone
Number:]
Permanent Residence Street Address (P.O. Box is not allowed):
City:
[Optional field: County:]
State:
ZIP Code:
Mailing Address (only if different from your Permanent Residence Address):
Street Address: City: State: ZIP Code:
[Optional field: E-mail Address: _______________________ ]
Please Provide Your Medicare Insurance Information
Please take out your red, white and blue Medicare
card to complete this section.
• Fill out this information as it appears on
your Medicare card.
- OR –
• Attach a copy of your Medicare card or
your letter from Social Security or the
Railroad Retirement Board.
Name (as it appears on your Medicare card):
Medicare Number:
Is Entitled to: Effective Date:
HOSPITAL (Part A)
MEDICAL (Part B)
You must have Medicare Part A and Part B to join
a Medicare Advantage plan.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
183
Please read and answer these important questions
1. Are you the retiree? Yes No
If yes, retirement date (month/date/year): _________________
If no, name of retiree: ________________________________
2. Are you covering a spouse or dependents under this employer or union plan? Yes No
If yes, name of spouse: ________________________________
Name(s) of dependent(s): _________________________________
3. Do you or your spouse work? Yes No
4. Some individuals may have other drug coverage, including other private insurance, Worker’s
Compensation, VA benefits or State pharmaceutical assistance programs.
Will you have other prescription drug coverage in addition to <plan name>? Yes No
If “yes”, please list your other coverage and your identification (ID) number(s) for this coverage:
Name of other coverage: ID # for Coverage:
_______________________________ __________________________
5. Are you a resident in a long-term care facility, such as a nursing home? Yes No
If “yes” please provide the following information:
Name of Institution: ____________
Address & Phone Number of Institution (number and street):__________________
[Optional field: Please Choose a Primary Care Physician (PCP), clinic or health center: ]
Please check one of the boxes below if you would prefer that we send you information in a
language other than English or in an accessible format:
<include list of available languages>
<include list of accessible formats (like Braille, audio tape, or large print)>
Please contact <plan name> at <phone number> if you need information in an accessible format or
language other than what is listed above. Our office hours are <insert days and hours of operation>.
TTY users should call <TTY number>.
[Optional field: If plan delivers some documents electronically, insert language explaining the types of
documents it sends and how (e.g., information about your enrollment to the email address you provide to
us on this form), as well as how a member can opt to get paper versions of those documents instead (e.g.,
a checkbox to opt-out of getting documents electronically).]
Please Read and Sign Below
By completing this enrollment application, I agree to the following:
<Plan Name> is a Medicare Advantage plan and has a contract with the Federal government. I will need
to keep my Medicare Parts A and B. I can only be in one Medicare Advantage plan at a time and I
understand that my enrollment in this plan will automatically end my enrollment in another Medicare
health plan. It is my responsibility to inform you of any prescription drug coverage that I have or may

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
184
get in the future. [MA-only plans insert: I understand that if I don’t have Medicare prescription drug
coverage, or creditable prescription drug coverage (as good as Medicare’s), I may have to pay a late
enrollment penalty if I enroll in Medicare prescription drug coverage in the future.] Enrollment in this
plan is generally for the entire year. Once I enroll, I may leave this plan or make changes only at certain
times of the year if an enrollment period is available (Example: Annual Enrollment Period from October
15 – December 7), or under certain special circumstances.
<Plan Name> serves a specific service area. If I move out of the area that <Plan Name> serves, I need to
notify the plan so I can disenroll and find a new plan in my new area. Once I am a member of <Plan
Name>, I have the right to appeal plan decisions about payment or services if I disagree. I will read the
[insert either Member Handbook or Evidence of Coverage document] from <plan name> when I get it to
know which rules I must follow to get coverage with this Medicare Advantage plan. I understand that
people with Medicare aren’t usually covered under Medicare while out of the country except for limited
coverage near the U.S. border.
[
MA PFFS do not include the following paragraph: I understand that beginning on the date <plan name>
coverage begins, I must get all of my health care from <plan name>, except for emergency or urgently
needed services or out-of-area dialysis services. Services authorized by <plan name> and other services
contained in my <plan name> Evidence of Coverage document (also known as a member contract or
subscriber agreement) will be covered. Without authorization, NEITHER MEDICARE NOR <Plan
Name> WILL PAY FOR THE SERVICES.]
I understand that if I am getting assistance from a sales agent, broker, or other individual employed by or
contracted with <plan name>, he/she may be paid based on my enrollment in<plan name>.
Release of Information: By joining this Medicare health plan, I acknowledge that the Medicare health
plan will release my information to Medicare and other plans as is necessary for treatment, payment and
health care operations. I also acknowledge that <plan name> will release my information [
MA-PD plans
insert:
including my prescription drug event data] to Medicare, who may release it for research and other
purposes which follow all applicable Federal statutes and regulations. The information on this enrollment
form is correct to the best of my knowledge. I understand that if I intentionally provide false information
on this form, I will be disenrolled from the plan.
I understand that my signature (or the signature of the person authorized to act on my behalf under the
laws of the State where I live) on this application means that I have read and understand the contents of
this application. If signed by an authorized individual (as described above), this signature certifies that: 1)
this person is authorized under State law to complete this enrollment and 2) documentation of this
authority is available upon request from Medicare.
Signature:
Today’s Date:
If you are the authorized representative, you must sign above and provide the following information:
Name: ________________________
Address: _______________________________________________
Phone Number: (___) ____- _____
Relationship to Enrollee ___________________
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
185
Office Use Only:
Name of staff member/agent/broker (if assisted in enrollment):___________________________
Plan ID #:_____________________________
Effective Date of Coverage: _______________
ICEP/IEP: ______ AEP: ______ SEP (type): _____ Not Eligible: ______
[optional space for other administrative information needed by plan]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
186
Exhibit 3: Model Short Enrollment Request Form (“Election” may also be
used)
(Rev. 2, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
This form may be used in place of the model individual enrollment form when a member of a
MA plan is enrolling into another MA plan offered by the same parent organization. This form
is not applicable to MSA.
Referenced in section(s): 10, 20.4, 40, 40.1
Name of Plan You are Enrolling In: ______________________________
Name:
Medicare Number: ________________
(Note: may use “member number” instead of “Medicare Number”)
Home Phone Number:
Permanent Street Address (P.O. Box is not allowed)
City:
[Optional field: County:]
State:
ZIP Code:
Mailing Address (only if different from your Permanent Street Address):
Street Address: City: State: ZIP Code:
Please fill out the following:
I am currently a member of the plan in <MAO name> with a monthly
premium of $ .
I would like to change to the plan in <MAO name>. I understand that
this plan has different health benefits and a monthly premium of $ .
[Optional Field: Name of chosen Primary Care Physician (PCP), clinic or health center: ]
Please check one of the boxes below if you would prefer us to send you information in a language
other than English or in an accessible format:
<include list of available languages>
<include list of accessible formats (like Braille, audio tape, or large print)>
Please contact <plan name> at <phone number> if you need information in an accessible format or
language other than what is listed above. Our office hours are <insert days and hours of operation>. TTY
users should call <TTY number>.
[Optional field: If plan delivers some documents electronically, insert language explaining the types of
documents it sends and how (e.g., information about your enrollment to the email address you provide to
us on this form), as well as how a member can opt to get paper versions of those documents instead (e.g.,
a checkbox to opt-out of getting documents electronically).]
[Zero premium MA-only plans omit this section]
Your Plan Premium

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
187
[Zero premium MA-PD plans insert: If we determine that you owe a late enrollment penalty (or if you
currently have a late enrollment penalty), we need to know how you would prefer to pay it. You can
pay by mail <insert optional methods: “Electronic Funds Transfer (EFT)”, “credit card”> each
month <insert optional intervals, if applicable, for example “or quarterly”>. You can also pay your
premium by automatic deduction from your Social Security or Railroad Retirement Board (RRB)
benefit check each month. If you are assessed a Part D-Income Related Monthly Adjustment
Amount, you will be notified by the Social Security Administration. You will be responsible for
paying this extra amount in addition to your plan premium. You will either have the amount
withheld from your Social Security benefit check or be billed directly by Medicare or the RRB. Do
NOT pay [insert appropriate plan and/or organization name] the Part D-IRMAA.]
[MA-only and MA-PD plans with premiums insert: You can pay your monthly plan premium [
MA-PD
plans with premium insert:
(including any late enrollment penalty you have or may owe)] by mail
<insert optional methods: “Electronic Funds Transfer (EFT)”, “credit card”> each month <insert
optional intervals, if applicable, for example “or quarterly”>. You can also choose to pay your
premium by automatic deduction from your Social Security or Railroad Retirement Board Check
each month.
[MA-PD plans with premiums also insert: If you are assessed a Part D-Income Related Monthly
Adjustment Amount, you will be notified by the Social Security Administration. You will be
responsible for paying this extra amount in addition to your plan premium. You will either have the
amount withheld from your Social Security benefit check or be billed directly by Medicare or the
Railroad Retirement Board. Do NOT pay [insert appropriate plan and/or organization name] the
Part D-IRMAA.
People with limited incomes may qualify for Extra Help to pay for their prescription drug costs. If you
qualify, Medicare could pay for 75% or more of your drug costs including monthly prescription drug
premiums, annual deductibles, and co-insurance. Additionally, those who qualify won’t have a coverage
gap or a late enrollment penalty. Many people qualify for these savings and don’t even know it. For
more information about this Extra Help, contact your local Social Security office, or call Social Security
at 1-800-772-1213. TTY users should call 1-800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.
If you qualify for Extra Help with your Medicare prescription drug coverage costs, Medicare will pay all
or part of your plan premium for this benefit. If Medicare pays only a portion of this premium, we will
bill you for the amount that Medicare doesn’t cover.
If you don’t select a payment option, you will get a bill each month <optional language in place of “bill
each month”: “coupon book” or “payment book”>.
Please select a premium payment option:
Get a bill <option: Include other optional methods, such as EFT & credit card>
Automatic deduction from your monthly Social Security or RRB benefit check.
I get monthly benefits from: Social Security RRB
(The Social Security deduction may take two or more months to begin after Social Security or RRB
approves the deduction. In most cases, if Social Security or RRB accepts your request for automatic
deduction, the first deduction from your Social Security or RRB benefit check will include all premiums
due from your enrollment effective date up to the point withholding begins. If Social Security or RRB
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
188
does not approve your request for automatic deduction, we will send you a paper bill for your monthly
premiums.)]
Please Read and Sign Below:
<Plan> is a plan that has a contract with the Federal government.
I understand that if I am getting assistance from a sales agent, broker, or other individual employed by or
contracted with <plan name>, he/she may be paid based on my enrollment in<plan name>.
Release of Information: By joining this Medicare health plan, I acknowledge that the Medicare health
plan will release my information to Medicare and other plans as is necessary for treatment, payment and
health care operations. I also acknowledge that <plan name> will release my information [
MA-PD plans
insert:
including my prescription drug event data] to Medicare, who may release it for research and other
purposes which follow all applicable Federal statutes and regulations. The information on this enrollment
form is correct to the best of my knowledge. I understand that if I intentionally provide false information
on this form, I will be disenrolled from the plan. I understand that people with Medicare aren’t covered
under Medicare while out of the country except for limited coverage near the U.S. border.
[
MA PFFS do not include the following paragraph: I understand that beginning on the date [name of plan]
coverage begins, I must get all of my health care from <plan name>, except for emergency or urgently
needed services or out-of-area dialysis services. Services authorized by <plan name> and other services
contained in my <plan name> Evidence of Coverage document (also known as a member contract or
subscriber agreement) will be covered. Without authorization, NEITHER MEDICARE NOR <Plan
Name> WILL PAY FOR THE SERVICES.
I understand that my signature (or the signature of the person authorized to act on my behalf under the
laws of the State where I live) on this application means that I have read and understand the contents of
this application. If signed by an authorized individual (as described above), this signature certifies that: 1)
Please Read This Important Information
[Insert if enrolling in a PFFS plan: <Plan name>, a Medicare Advantage Private Fee-for-Service plan,
works differently than a Medicare supplement plan and other Medicare Advantage plans. Your doctor or
hospital isn’t required to accept the plan’s terms and conditions, and may choose not to treat you, except
in emergencies. If your doctor or hospital does not agree to accept our payment terms and conditions,
they may choose not to provide health care services to you, except in emergencies. You should verify
that your provider(s) will accept <Plan name> before each visit. Providers can find the plan’s terms and
conditions on our website at <insert link to PFFS terms and conditions>.]
[Insert if enrolling in a PFFS plan, except for cases in which the member is switching from one PFFS
plan to another PFFS plan offered by the same parent organization: Once <plan name> has your
enrollment form, a plan representative will call you. This call is to make sure that you understand how a
Private Fee-for-Service plan works and to confirm your intent to enroll in <plan name>. If <plan name>
isn’t able to reach you by telephone, then you will get a letter by mail that contains similar information.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
189
Office Use Only:
Name of staff member/agent/broker (if assisted in enrollment):___________________________
Plan ID #:_____________________________
Effective Date of Coverage: _______________
ICEP/IEP: ______ AEP: ______ SEP (type): ______ Not Eligible: ______
[optional space for other administrative information needed by plan]
this person is authorized under State law to complete this enrollment and 2) documentation of this
authority is available upon request from Medicare.
Signature:
Today’s Date:
If you are the authorized representative, you must sign above and provide the following information:
Name : ________________________
Address: _______________________________________________
Phone Number: (___) ____- _____
Relationship to Enrollee ___________________
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
190
Exhibit 3a: Model Plan Selection Form for MA-PD - Switch From Plan to
Plan Within Parent Organization
This form is not applicable to MSA.
Referenced in section(s): 10, 40, 40.1, 40.2
(Rev. 2, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <plan name> Member:
<Introduction - In the introduction of cover letter, MA organization may include language
regarding plan choices, description of plans, differences, etc.>. [Insert to describe PFFS plans:
<Plan name>, a Medicare Advantage Private Fee-for-Service plan, works differently than a
Medicare supplement plan. Your doctor or hospital is not required to agree to accept the plan’s
terms and conditions, and thus may choose not to treat you, with the exception of
emergencies. If your doctor or hospital does not agree to accept our payment terms and
conditions, they may choose not to provide health care services to you, except in
emergencies. Providers can find the plan’s terms and conditions on our website at <insert link to
PFFS terms and conditions>.]
To make a change in the Medicare Advantage plan you have with <name of MA organization>,
fill out the enclosed plan selection form to make your choice. Check off the plan you want, and
sign the form. Then mail the completed form back to us <optional: in the postage-paid
envelope> by <date>.
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug coverage.
[Plans have the option to omit this language for non-ICEP enrollments: If you join our plan
when you first enroll in Medicare, you can switch to another plan or get Original Medicare (and
join a stand-alone Medicare Prescription Drug Plan). If you’re not happy with your choice in our
plan, you can make a change during the first 3 months you have Medicare.]
If you select another plan and we receive your completed selection form by <date>, your new
benefit plan will begin in <month/year>. Your monthly plan premium will be <premium
amount> and you may continue to see any <current plan name> primary care doctors and
specialists.
Complete the attached form only if you wish to change plans.
To help you with your decision, we have also included <year> <Summary of Benefits or benefit
overview> for the available options.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
191
If you have any questions, please call <plan name> at <phone number - if plan is planning to
have informational meetings - include information about time/place of meetings >. TTY users
should call <TTY number>. We are open <insert days/hours of operation and, if different, TTY
hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
192
Plan Selection Form
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Date:
Member Name:
Member Number:
I want to transfer from my current plan to the plan I have selected below. I understand that if
this form is received by the end of any month, my new plan will generally be effective the 1st of
the following month.
Please check the appropriate box below <list all available plans>:
____ <Name of Plan>
<monthly premium amount>
<brief description of benefit - include items such as: visit copays, emergency room,
durable medical equipment, inpatient care, annual out of pocket maximum on
coinsurance services, etc.>
____ <Name of Plan>
<monthly premium amount>
<brief description of benefit - include items such as: visit copays, emergency room,
durable medical equipment, inpatient care, annual out of pocket maximum on
coinsurance services, etc.>
[Insert to describe PFFS plans: <Plan name>, a Medicare Advantage Private Fee-for-Service
plan, works differently than a Medicare supplement plan. Your doctor or hospital is not required
to agree to accept the plan’s terms and conditions, and thus may choose not to treat you, with the
exception of emergencies. If your doctor or hospital does not agree to accept our payment terms
and conditions, they may choose not to provide health care services to you, except in
emergencies. Providers can find the plan’s terms and conditions on our website at <insert link to
PFFS terms and conditions>.]
[Zero premium MA-only plans omit this section:
Your Plan Premium
[Zero premium MA-PD plans insert: If we determine that you owe a late enrollment penalty
(or if you currently have a late enrollment penalty), we need to know how would prefer to
pay it. You can pay by mail <insert optional methods: “Electronic Funds Transfer (EFT)”,
“credit card”> each month <insert optional intervals, if applicable, for example “or
quarterly”>. You can also choose to pay your premium by automatic deduction from your
Social Security or Railroad Retirement Board Check each month.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
193
[MA-only and MA-PD plans with premiums insert: You can pay your monthly plan premium
[MA-PD plans with premium insert: (including any late enrollment penalty you have or may
owe)] by mail <insert optional methods: “Electronic Funds Transfer (EFT)”, “credit card”>
each month <insert optional intervals, if applicable, for example “or quarterly”>. You can
also choose to pay your premium by automatic deduction from your Social Security or
Railroad Retirement Board Check each month.
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If eligible, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify will not be subject to the coverage gap or a late enrollment penalty. Many people are
eligible for these savings and don’t even know it. For more information about this Extra Help,
contact your local Social Security office or call 1-800-MEDICARE (1-800-633-4227), 24 hours
per day, 7 days per week. TTY/TDD users should call 1-877-486-2048.
If you qualify for Extra Help with your Medicare prescription drug coverage costs, Medicare will
pay all or part of your plan premium for this benefit. If Medicare pays only a portion of this
premium, we will bill you for the amount that Medicare does not cover.
If you don’t select a payment option, you will receive a bill each month <optional language in
place of “bill each month”: “coupon book” or “payment book”>.
Please select a premium payment option:
Receive a bill <option: Include other optional methods, such as EFT & credit card>
Automatic deduction from your monthly Social Security or RRB benefit check.
I get monthly benefits from: Social Security RRB
(The Social Security or RRB deduction may take two or more months to begin after Social
Security or RRB approves the deduction. In most cases, if Social Security or RRB accepts your
request for automatic deduction, the first deduction from your Social Security or RRB benefit
check will include all premiums due from your enrollment effective date up to the point
withholding begins. If Social Security or RRB does not approve your request for automatic
deduction, we will send you a paper bill for your monthly premiums.)]
Please check one of the boxes below if you would prefer us to send you information in a
language other than English or in an accessible format:
<include list of available languages>
<include list of accessible formats (e.g. Braille, audio tape, or large print)>
Please contact <plan name> at <phone number> (TTY users should call TTY number> if you
need information in an accessible format or language other than what is listed above. Our office
hours are <insert days and hours of operation>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
194
[Optional: If plan delivers some documents electronically, insert language explaining the types
of documents it sends and how (e.g., information about your enrollment to the email address you
provide to us on this form), as well as how a member can opt to get paper versions of those
documents instead (e.g., a checkbox to opt-out of getting documents electronically).]
Signature:
Today’s Date:
If you are the authorized representative, you must sign above and provide the following
information:
Name: __________________________________
Address: _________________________________
Phone Number: (___) ____- _________________
Relationship to Enrollee ____________________
Please mail this form to:
<Insert mailing address>
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
195
Exhibit 4: Model Notice to Acknowledge Receipt of Completed Enrollment
Request
Referenced in section(s): 40.4.1, 60.4
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
<Member # >
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Thank you for enrolling in <Plan name>. Beginning <effective date>, you must see your <plan
name> doctor(s) for your health care. This means that starting <effective date>, all of your health
care, except emergency or urgently needed care, or out-of-area dialysis services, must be given
or arranged by a <plan name> doctor(s). You will need to pay your plan co-payments and co-
insurance at the time you get health care services as described in your member materials.
[
Optional language: This letter is proof of insurance that you should show at your doctor
appointments until you get your member card from us.] [Optional language for MA-PD: This
letter is also proof of your prescription drug coverage. You should show this letter at the
pharmacy until you get your member card from us.]
[
MA PPO plans use the following paragraph in place of 1
st
paragraph above: Thank you for enrolling
in <Plan name>. Beginning <effective date>, you must get your health care as provided in your
<insert either ‘Member handbook’ or ‘Evidence of Coverage’>. You will need to pay your plan
co-payments and co-insurance at the time you get health care services, as described in your
member materials. [
Optional language: This letter is proof of insurance that you should show
during your doctor appointments until you get your member card from us.]
What should I do now?
Medicare must review all enrollments. We will send your enrollment to Medicare, and they will
do a final review. When Medicare finishes its review, we will send you a letter to confirm your
enrollment with <plan name>. But, you shouldn’t wait to get this letter before you begin using
<plan name> doctors on <effective date>. Also, don’t cancel any Medigap/Medicare Select or
supplemental insurance that you have until we send you the confirmation letter.
[
MA-PD plans with a premium include the following: If you qualify for Extra Help with your
Medicare prescription drug coverage costs, Medicare may cover all or some portion of your plan
premium.]
[
Plans with a premium include the following:
How do I pay my premium?
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
196
Your enrollment form included the options for paying your plan premium. If you did not choose
one of these options when you enrolled, we will bill you directly. If you chose to have your
monthly premium automatically deducted from your Social Security/Railroad Retirement Board
benefit check, we may have to send you a bill for your first month or two of enrollment if the
deduction doesn’t start right away. Generally, you must stay with the option you choose for the
rest of the year. If you have any questions about how to pay your plan premium, please contact
us at <plan telephone number>. TTY users should call <TTY number>.] [MAOs that disenroll
for non-payment of plan premiums include the following sentence: Members who fail to pay the
monthly plan premium may be disenrolled from <plan name>.]
What do I need to know about getting health care services?
You must have Medicare Part A (Hospital Insurance) and Part B (Medical Insurance) to be a
member of <Plan>. If you don’t have Medicare Parts A and B, we will bill you for any health
care you receive from us, and neither Medicare nor <plan name> will pay for those services.
[
MA PPO plans do not use the following paragraph: Please remember that, except for emergency or
out-of-area urgent care, or out-of-area dialysis services, if you get health care services from a
non-<plan name> doctor without prior authorization, you will have to pay for these services
yourself.]
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
[Plans have the option to omit this language for non-ICEP enrollments: If you join our plan
when you first enroll in Medicare, you can switch to another plan or get Original Medicare (and
join a stand-alone Medicare Prescription Drug Plan). If you’re not happy with your choice in our
plan, you can make a change during the first 3 months you have Medicare.]
[MA-PD plans with a premium include the following two paragraphs:
[Dual-eligible SNPs may omit the following paragraph]
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If eligible, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify will not be subject to the coverage gap or a late enrollment penalty. Many people are
eligible for these savings and don’t even know it. For more information about this Extra Help,
contact your local Social Security office or call Social Security at 1-800-772-1213. TTY users
should call 1-800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
197
[Optional: What else do I need to know about my coverage?
If applicable, insert information instructing member in simple terms on how to select a primary
care provider/site (PCP); how to obtain Medicare Advantage Plan services, e.g., provide the
name, phone number, and location of the PCP, include the membership identification card when
possible, explain unique POS and/or PPO procedures (when applicable), explain which services
do not need PCP approval (when applicable), etc.]
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <days/hours of operation and, if different, TTY hours of
operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
198
Exhibit 4a: Model Notice to Acknowledge Receipt of Completed Enrollment
Request – Enrollment in another Plan Within the Same Parent Organization
Referenced in section(s): 40.4.1, 60.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Member # >
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Thank you for your request to change your enrollment from <old Plan name> to <new Plan
name>. Starting <effective date>, you must see your <new Plan name> doctor(s) for your health
care. This means that starting <effective date>, all of your health care, except emergency or
urgently needed care, or out-of-area dialysis services, must be given or arranged by a <new
plan name> doctor(s). You will need to pay your plan copayments at the time you get health care
services. [
Optional: This letter is proof of health insurance that you should show during your
doctor appointments.] [Optional language for MA-PD: This letter is also proof of your
prescription drug coverage. You should show this letter at the pharmacy until you get your
member card from us.]
[
MA PPO plans use the following paragraph in place of 1
st
paragraph above: Thank you for your
request to change your enrollment from <old plan name> to <new plan name>. Beginning
<effective date>, you must get your health care as provided in your <insert either ‘Member
handbook’ or ‘Evidence of Coverage’>. You will need to pay your plan co-payments and co-
insurance at the time you get health care services, as provided in your member materials.
<Optional: This letter is proof of insurance that you should show during your doctor
appointments until you get your member card from us.>] [Optional language for MA-PD: This
letter is also proof of your prescription drug coverage. You should show this letter at the
pharmacy until you get your member card from us.]
What should I do now?
Medicare must review all enrollments. We will send your enrollment to Medicare, and they will
do a final review. When Medicare finishes its review, we will send you a letter to confirm your
enrollment with <new plan name>. But, you shouldn’t wait to get this letter before you begin
using <new plan name> doctors on <effective date>.
[
MA PPO plans do not use the following sentence: Please remember that, except for emergency or
out-of-area urgent care, or out-of-area dialysis services, if you get health care services from a
non-<new plan name> doctor without prior authorization, you will have to pay for these services
yourself.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
199
[Zero premium plans do not include the following:
How do I pay my premium?
Your enrollment form included the options for paying your plan premium. If you did not choose
one of these options when you enrolled, we will bill you directly. If you chose to have your
monthly premium automatically deducted from your Social Security or Railroad Retirement
Board check, we may have to send you a bill for your first month or two of enrollment if the
deduction doesn’t start right away. Generally, you must stay with the option you choose for the
rest of the year. If you have any questions about how to pay your plan premium, please contact
us at <plan telephone number>. TTY users should call <TTY number>.][MAOs that disenroll
for non-payment of plan premium include the following sentence: “Members who fail to pay the
monthly plan premium may be disenrolled from <plan name>”.]
[MA-PD plans with a premium include the following: If you qualify for Extra Help with your
Medicare prescription drug coverage costs, Medicare may cover all or some portion of your plan
premium.]
[MA-PD plans with a premium include the following paragraph:]
[Dual-eligible SNPs may omit the following paragraph]
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If eligible, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify will not be subject to the coverage gap or a late enrollment penalty. Many people are
eligible for these savings and don’t even know it. For more information about this Extra Help,
contact your local Social Security office or call 1-800-MEDICARE (1-800-633-4227), 24 hours
per day, 7 days per week. TTY/TDD users should call 1-877-486-2048.
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
[Plans have the option to omit this language for non-ICEP enrollments: If you join our plan
when you first enroll in Medicare, you can switch to another plan or get Original Medicare (and
join a stand-alone Medicare Prescription Drug Plan). If you’re not happy with your choice in our
plan, you can make a change during the first 3 months you have Medicare.]
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days/hours of operation and, if different, TTY hours of
operation>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
200
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
201
Exhibit 4b: Model Notice to Acknowledge Receipt of Completed Enrollment
Request and to Confirm Enrollment
Referenced in section: 40.4, 60.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Member # >
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Thank you for enrolling in <plan name>. Medicare has approved your enrollment in <plan
name> beginning <effective date>.
How will this plan work?
Beginning <effective date>, you must see your <plan name> doctor(s) for your health care. This
means that starting <effective date>, all of your health care, except emergency or urgently
needed care, or out-of-area dialysis services, must be given or arranged by a <plan name>
doctor(s). You will need to pay your plan co-payments and co-insurance at the time you get
health care services, as provided in your member materials. Please remember that, except for
emergency or out-of-area urgent care, or out-of-area dialysis services, if you get health care
services from a non-<plan name> doctor without prior authorization, you will have to pay
for these services yourself.
[
MA PPO plans use the following paragraph in place of paragraph above: Thank you for enrolling in
<plan name>. Medicare has approved your enrollment in <plan name> beginning <effective
date>. Beginning <effective date>, you must get your health care as provided in your <insert
either ‘Member handbook’ or ‘Evidence of Coverage’>. You will need to pay your plan co-
payments and co-insurance at the time you get health care services, as provided in your member
materials.]
[Optional: This letter is proof of insurance that you should show during your doctor
appointments until you get your member card from us.] [Optional language for MA-PD: This
letter is also proof of your prescription drug coverage. You should show this letter at the
pharmacy until you get your member card from us.]
[
MA-PD plans insert the following two paragraphs if no low-income subsidy:
What are my costs on this plan?
The monthly premium for your plan is <insert premium>.
Can I get help paying my premiums and other out-of-pocket costs?

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
202
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you think you qualify for Extra Help with your prescription drug costs, but you don’t have or
can’t find proof, please contact <plan name>.]
[
MA-PD plans add the following paragraph if low-income subsidy applicable:
What are my costs since I qualify for Extra Help?
Because you qualify for extra help with your prescription drug costs, you will pay no more than:
- A monthly premium of <insert premium less amount of premium assistance for which
the individual is eligible>,
- <insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
- <insert appropriate LIS copay amount> copayment when you fill a prescription covered
by <plan name>.
If you believe this is incorrect and you have proof that the Extra Help amounts should be
different, please contact <plan name>.]
Will I pay a late enrollment penalty as part of my premium?
[
MA-PD plans insert the following for new members with an existing LEP: Your premium continues to
reflect a late enrollment penalty amount that was based on information sent by your previous
plan. Your plan should have told you about this penalty. If you have questions about the late
enrollment penalty, call <plan name> at the phone number provided at the end of this
letter. You can also get information by visiting www.medicare.gov
or by calling 1-800-
MEDICARE (1-800-633-4227), 24 hours a day/7 days a week. TTY users should call 1-877-
486-2048.]
[
MA-PD plans, if previous paragraph not applicable, insert the following for all other new members:
The late enrollment penalty is an amount added to your monthly Medicare drug plan (Part D)
premium for as long as you have Medicare prescription drug coverage. This penalty is required
by law and is designed to encourage people to enroll in a Medicare drug plan when they are first
eligible or keep other prescription drug coverage that meets Medicare’s minimum standards.
You may owe a late enrollment penalty if you didn’t join a Medicare drug plan when you were
first eligible for Medicare Part A and/or Part B, and:
• You didn’t have other prescription drug coverage that met Medicare’s minimum
standards; OR
• You had a break in coverage of at least 63 days.

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
203
If we determine that you owe a late enrollment penalty, we will notify you of your new monthly
premium amount.]
[
Zero premium plans do not include the following:
How do I pay my premium?
Your enrollment form included the options for paying your plan premium. If you did not choose
one of these options when you enrolled, we will bill you directly. If you chose to have your
monthly plan premium automatically deducted from your Social Security or Railroad Retirement
Board check, we may have to send you a bill for your first month or two of enrollment if the
deduction doesn’t start right away. Generally, you must stay with the option you choose for the
rest of the year. If you have any questions about how to pay your plan premium, please contact
us at <plan telephone number>. TTY users should call <TTY number>.][MAOs that disenroll
for nonpayment of premium include the following sentence: “Members who fail to pay the
monthly plan premium may be disenrolled from <plan name>”.]
[
MA-PD plans with a premium include the following: If you qualify for Extra Help with your
Medicare prescription drug coverage costs, Medicare may cover all or some portion of your plan
premium.] [
Zero premium plans do not include the following: We will bill you for the portion of
your monthly premium that you owe.]
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
[Plans have the option to omit this language for non-ICEP enrollments: If you join our plan
when you first enroll in Medicare, you can switch to another plan or get Original Medicare (and
join a stand-alone Medicare Prescription Drug Plan). If you’re not happy with your choice in our
plan, you can make a change during the first 3 months you have Medicare.] [If applicable, please
insert information instructing member in simple terms on how to select a primary care
provider/site (PCP); how to obtain Medicare Advantage Plan services, e.g., provide the name,
phone number, and location of the PCP, include the membership identification card when
possible, explain unique POS and/or PPO procedures (when applicable), explain which services
do not need PCP approval (when applicable), etc.]
What if I have a Medigap (Medicare Supplement Insurance) policy?
Now that we have confirmed your enrollment, you may cancel any Medigap or supplemental
insurance that you have. Please note that if this is the first time that you are a member of a
Medicare Advantage or Medicare Cost plan, you may have a trial period during which you have
certain rights to leave (disenroll from) <plan name> and buy a Medigap policy. Please contact
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
204
1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a week for further
information. TTY users should call 1-877-486-2048.
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days/hours of operation and, if different, TTY hours of
operation>. Please be sure to keep a copy of this letter for your records.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
205
Exhibit 4c: Model Notice to Acknowledge Receipt of Completed
PFFS Enrollment Request
Referenced in section(s): 40.4.1, 60.4
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
<Member # >
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Thank you for enrolling in <Plan name>. Beginning <effective date>, you will begin to get your
healthcare from <plan name>. You must show your <Plan name> ID card to your doctor or
hospital before you receive healthcare. You may no longer use your red, white and blue
Medicare card to receive healthcare, because Original Medicare won’t pay for your
healthcare while you are enrolled in this plan. You should keep your Medicare card in a safe
place.
How will this plan work?
<Plan name>, a Medicare Advantage Private Fee-for-Service plan, works differently than a
Medicare supplement plan. <Plan name> allows you to go to any Medicare-approved doctor or
hospital that is willing to give you care and accept our plan’s terms of payment. You should
contact your doctor or hospital to ask whether they will accept our plan’s payment terms. Your
doctor or hospital isn’t required to agree to accept the plan’s terms and conditions, and may
choose not to treat you, except in emergencies. You should verify that your provider(s) will
accept <Plan name> before each visit. Providers can find the plan’s terms and conditions on our
website at <insert link to PFFS terms and conditions>.
If any doctor or hospital provides health care services to you after learning about our plan’s
payment terms, they must bill us for services, and aren’t allowed to send the entire bill to you. If
a doctor or hospital does provide services to you, then they are considered to have accepted our
plan’s terms. You will need to pay your plan co-payments and co-insurance at the time you get
health care services, as described in your member materials.
If your doctor or hospital doesn’t accept our plan’s payment terms, they shouldn’t provide
services to you except in emergencies. You may contact us at the phone number provided at the
end of this letter for help locating another provider in your area. [Optional language: You can
also visit the <plan/organization name> website at <plan website address>.]
[Include if plan uses a network of contracted providers: <Plan name> has direct contracts with
some providers who have already agreed to accept our terms and conditions of
payment. [Describe what category or categories of providers the plan has under direct contract
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
206
and how members can get the list of contracted providers.] You can still get care from other
providers who do not contract with <plan name> as long as those providers agree to accept our
terms and conditions of payment. [Indicate if the plan has established higher cost sharing
requirements for members who obtain covered services from non-contracted providers.]]
[Optional: This letter is proof of insurance that you should show during your doctor
appointments until you get your member card from us. Optional language for MA-PD: This
letter is also proof of your prescription drug coverage. You should show this letter at the
pharmacy until you get your member card from us.]
What should I do now?
Medicare must review all enrollments. We will send your enrollment to Medicare, and they will
do a final review. When Medicare finishes its review, we will send you a letter to confirm your
enrollment with <plan name>. But you shouldn’t wait to get that letter before you begin seeing
your <plan name> doctors on <effective date>. Also, don’t cancel any Medigap/Medicare Select
or supplemental insurance that you have until we send you the confirmation letter.
[
Zero premium plans do not include the following:
How do I pay my premium?
Your enrollment form included the options for paying your plan premium. If you did not choose
one of these options when you enrolled, we will bill you directly. If you chose to have your
monthly plan premium automatically deducted from your Social Security or Railroad Retirement
Board check, we may have to send you a bill for your first month or two of enrollment if the
deduction doesn’t start right away. Generally, you must stay with the option you choose for the
rest of the year. If you have any questions about how to pay your plan premium, please contact
us at <plan telephone number>. TTY users should call <TTY number>.][MAOs that disenroll
for non-payment of plan premiums include the following sentence: “Members who fail to pay the
monthly plan premium may be disenrolled from <plan name>”.]
[
MA-PD plans with a premium include the following: If you qualify for Extra Help with your
Medicare prescription drug coverage costs, Medicare may cover all or some portion of your plan
premium.] [
Zero premium plans do not include the following: We will bill you for the portion of
your monthly premium that you owe.]
What do I need to know about getting health care services?
You must have Medicare Part A (Hospital Insurance) and Part B (Medical Insurance) to be a
member of <Plan>. If you don’t have Medicare Parts A and B, we will bill you for any health
care you receive from us, and neither Medicare nor <plan name> will pay for those services.
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
207
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
[
MA-PD plans with a premium include the following two paragraphs:
What are my costs?
[
MA-PD insert the following if no low-income subsidy: The monthly premium for your plan is
<insert premium>. <Explain the charges for which the member will be liable, e.g., coinsurance,
fees or other amounts, and any amount that is attributable to the Medicare deductible and
coinsurance.>
[Dual-eligible SNPs may omit the following paragraph]
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.]
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days/hours of operation and, if different, TTY hours of
operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
208
Exhibit 4d: Model Notice to Acknowledge Receipt of Completed PFFS
Enrollment Request and to Confirm Enrollment in a PFFS Plan
Referenced in section: 40.4, 60.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Member #>
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Thank you for enrolling in <plan name>. Medicare has approved your enrollment in <plan
name> beginning <effective date>.
How will this plan work?
<Plan name>, a Medicare Advantage Private Fee-for-Service plan, works differently than a
Medicare supplement plan. <Plan name> allows you to go to any Medicare-approved doctor or
hospital that is willing to give you care and accept our plan’s terms of payment. You should
contact your doctor or hospital to ask whether they will accept our plan’s payment terms. Your
doctor or hospital isn’t required to agree to accept the plan’s terms and conditions, and may
choose not to treat you, except in emergencies. You should verify that your provider(s) will
accept <Plan name> before each visit. Providers can find the plan’s terms and conditions on our
website at <insert link to PFFS terms and conditions>.
If any doctor or hospital provides health care services to you after learning about our plan’s
payment terms, they must bill us for services, and aren’t allowed to send the entire bill to you. If
a doctor or hospital does provide services to you, then they are considered to have accepted our
plan’s terms. You will need to pay your plan co-payments and co-insurance at the time you get
health care services, as described in your member materials.
If your doctor or hospital doesn’t accept our plan’s payment terms, they shouldn’t provide
services to you except in emergencies. You may contact us at the phone number provided at the
end of this letter for help locating another provider in your area.
[Include if plan uses a network of contracted providers: <Plan name> has direct contracts with
some providers who have already agreed to accept our terms and conditions of
payment. [Describe what category or categories of providers the plan has under direct contract
and how members can get the list of contracted providers.] You can still get care from other
providers who do not contract with <plan name> as long as those providers agree to accept our
terms and conditions of payment. [Indicate if the plan has established higher cost sharing
requirements for members who obtain covered services from non-contracted providers.]]

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
209
[Optional: This letter is proof of insurance that you should show during your doctor
appointments until you get your member card from us. Optional language for MA-PD: This
letter is also proof of your prescription drug coverage. You should show this letter at the
pharmacy until you get your member card from us.]
[
MA-PD plans insert the following two paragraphs if no low-income subsidy:
What are my costs on this plan?
The monthly premium for your plan is <insert premium>.
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you think you qualify for Extra Help with your prescription drug costs, but you don’t have or
can’t find proof, please contact <plan name>.]
[
MA-PD, if low-income subsidy applicable:
What are my costs since I qualify for Extra Help?
Because you qualify for extra help with your prescription drug costs, you will pay no more than:
• A monthly premium of <insert premium less amount of premium assistance for which
the individual is eligible>,
• <insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
• <insert appropriate LIS copay amount> copayment when you fill a prescription
covered by <plan name>.
If you believe this is incorrect and you have proof that that the Extra Help amounts should be
different, please contact <plan name>.]
Will I pay a late enrollment penalty as part of my premium?
[
MA-PD plans insert the following for new members with an existing LEP: Your premium continues to
reflect a late enrollment penalty amount that was based on information sent by your previous
plan. Your plan should have told you about this penalty. If you have questions about the late
enrollment penalty, call <plan name> at the phone number provided at the end of this
letter. You can also get information by visiting www.medicare.gov
or by calling 1-800-
MEDICARE (1-800-633-4227), 24 hours a day/7 days a week. TTY users should call 1-877-
486-2048.]
[
MA-PD plans, if previous paragraph not applicable, insert the following for all other new members:

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
210
The late enrollment penalty is an amount added to your monthly Medicare drug plan (Part D)
premium for as long as you have Medicare prescription drug coverage. This penalty is required
by law and is designed to encourage people to enroll in a Medicare drug plan when they are first
eligible or keep other prescription drug coverage that meets Medicare’s minimum standards.
You may owe a late enrollment penalty if you didn’t join a Medicare drug plan when you were
first eligible for Medicare Part A and/or Part B, and:
• You didn’t have other prescription drug coverage that met Medicare’s minimum
standards; OR
• You had a break in coverage of at least 63 days.
If we determine that you owe a late enrollment penalty, we will notify you of your new monthly
premium amount.]
[
Zero premium plans do not include the following:
How do I pay my premium?
Your enrollment form included the options for paying your plan premium. If you did not choose
one of these options when you enrolled, we will bill you directly. If you chose to have your
monthly plan premium automatically deducted from your Social Security or Railroad Retirement
Board check, we may have to send you a bill for your first month or two of enrollment if the
deduction doesn’t start right away. Generally, you must stay with the option you choose for the
rest of the year. If you have any questions about how to pay your plan premium, please contact
us at <plan telephone number>. TTY users should call <TTY number>.][MAOs that disenroll
for non-payment of plan premiums include the following sentence: Members who fail to pay the
monthly plan premium may be disenrolled from <plan name>”.]
[
MA-PD plans with a premium include the following: If you qualify for Extra Help with your
Medicare prescription drug coverage costs, Medicare may cover all or some portion of your plan
premium.] [
Zero premium plans do not include the following: We will bill you for the portion of
your monthly plan premium that you owe.]
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
[Plans have the option to omit this language for non-ICEP enrollments: If you join our plan
when you first enroll in Medicare, you can switch to another plan or get Original Medicare (and
join a stand-alone Medicare Prescription Drug Plan). If you’re not happy with your choice in our
plan, you can make a change during the first 3 months you have Medicare.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
211
[If applicable, please insert information instructing member in simple terms how to select a
primary care provider/site (PCP); how to obtain Medicare Advantage Plan services, e.g.,
provide the name, phone number, and location of the PCP, include the membership identification
card when possible, explain unique POS and/or PPO procedures (when applicable), explain
which services do not need PCP approval (when applicable), etc.]
What if I have a Medigap (Medicare Supplement Insurance) policy?
Now that we have confirmed your enrollment, you may cancel any Medigap or supplemental
insurance that you have. Please note that if this is the first time that you are a member of a
Medicare Advantage or Medicare Cost plan, you may have a trial period during which you have
certain rights to leave (disenroll from) <plan name> and buy a Medigap policy. Please contact 1-
800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a week for further
information. TTY users should call 1-877-486-2048.
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days/hours of operation and, if different, TTY hours of
operation>. Please be sure to keep a copy of this letter for your records.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
212
Exhibit 4e: Model Notice to Acknowledge Receipt of Completed Enrollment
Request and to Confirm Enrollment in Another Plan Within the Same Parent
Organization
Referenced in section: 40.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Member # >
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Thank you for your request to change your enrollment from <old plan name> to <new plan
name>. Medicare has approved your enrollment in <new plan name> beginning <effective date>.
How will this plan work?
Beginning <effective date>, you must see your <new plan name> doctor(s) for your health care.
This means that starting <effective date>, all of your health care, except emergency or urgently
needed care, or out-of-area dialysis services, must be given or arranged by a <new plan name>
doctor(s). You will need to pay your plan co-payments and co-insurance at the time you get
health care services, as provided in your member materials. Please remember that, except for
emergency or out-of-area urgent care, or out-of-area dialysis services, if you get health care
services from a non-<plan name> doctor without prior authorization, you will have to pay
for these services yourself.
[
MA PPO plans use the following paragraph in place of paragraphs above: Thank you for your
request to change your enrollment from <old plan name> to <new plan name>. Medicare has
approved your enrollment in <new plan name> beginning <effective date>. Beginning <effective
date>, you must get your health care as provided in your <insert either ‘Member handbook’ or
‘Evidence of Coverage’>. You will need to pay your plan co-payments and co-insurance at the
time you get health care services, as provided in your member materials.]
[Optional: This letter is proof of insurance that you should show during your doctor
appointments until you get your member card from us.] [Optional language for MA-PD: This
letter is also proof of your prescription drug coverage. You should show this letter at the
pharmacy until you get your member card from us.]
[
MA-PD plans insert the following two paragraphs if no low-income subsidy:
What are my costs on this plan?
The monthly premium for your plan is <insert premium>.

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
213
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you think you qualify for Extra Help with your prescription drug costs, but you don’t have or
can’t find proof, please contact <plan name>.]
[
MA-PD plans add the following paragraph if low-income subsidy applicable:
What are my costs since I qualify for Extra Help?
Because you qualify for Extra Help with your prescription drug costs, you will pay no more than:
• A monthly premium of <insert premium less amount of premium assistance for which
the individual is eligible>,
• <insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
• <insert appropriate LIS copay amount> copayment when you fill a prescription
covered by <plan name>.
If you believe this is incorrect and you have proof that the Extra Help amounts should be
different, please contact <plan name>.]
Will I pay a late enrollment penalty as part of my premium?
[
MA-PD plans insert the following for new members with an existing LEP: Your premium continues to
reflect a late enrollment penalty amount that was based on information we had from your
previous enrollment in <old plan name>. If you have questions about the late enrollment penalty,
call <plan name> at the phone number provided at the end of this letter. You can also get
information by visiting www.medicare.gov
or by calling 1-800-MEDICARE (1-800-633-4227),
24 hours a day/7 days a week. TTY users should call 1-877-486-2048.]
[
MA-PD plans insert the following for new members who don’t have an existing LEP:
The late enrollment penalty is an amount added to your monthly Medicare drug plan (Part D)
premium for as long as you have Medicare prescription drug coverage. This penalty is required
by law and is designed to encourage people to enroll in a Medicare drug plan when they are first
eligible or keep other prescription drug coverage that meets Medicare’s minimum standards.
You may owe a late enrollment penalty if you didn’t join a Medicare drug plan when you were
first eligible for Medicare Part A and/or Part B, and:
• You didn’t have other prescription drug coverage that met Medicare’s minimum
standards; OR
• You had a break in coverage of at least 63 days.

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
214
As you did not previously have a late enrollment penalty with us, you will not have a late
enrollment penalty with this enrollment change.]
[
Zero premium plans do not include the following:
How do I pay my premium?
Your enrollment form included the options for paying your plan premium. If you did not choose
one of these options when you enrolled, we will bill you directly. If you chose to have your
monthly plan premium automatically deducted from your Social Security or Railroad Retirement
Board check, we may have to send you a bill for your first month or two of enrollment if the
deduction doesn’t start right away. Generally, you must stay with the option you choose for the
rest of the year. If you have any questions about how to pay your plan premium, please contact
us at <plan telephone number>. TTY users should call <TTY number>.][MAOs that disenroll
for nonpayment of premium include the following sentence: “Members who fail to pay the
monthly plan premium may be disenrolled from <plan name>”.]
[
MA-PD plans with a premium include the following: If you qualify for Extra Help with your
Medicare prescription drug coverage costs, Medicare may cover all or some portion of your plan
premium.] [
Zero premium plans do not include the following: We will bill you for the portion of
your monthly premium that you owe.]
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
[Plans have the option to omit this language for non-ICEP enrollments: If you join our plan
when you first enroll in Medicare, you can switch to another plan or get Original Medicare (and
join a stand-alone Medicare Prescription Drug Plan). If you’re not happy with your choice in our
plan, you can make a change during the first 3 months you have Medicare.]
[If applicable, please insert information instructing member in simple terms on how to select a
primary care provider/site (PCP); how to obtain Medicare Advantage Plan services, e.g.,
provide the name, phone number, and location of the PCP, include the membership identification
card when possible, explain unique POS and/or PPO procedures (when applicable), explain
which services do not need PCP approval (when applicable), etc.]
What if I have a Medigap (Medicare Supplement Insurance) policy?
Now that we have confirmed your enrollment, you may cancel any Medigap or supplemental
insurance that you have. Please note that if this is the first time that you are a member of a
Medicare Advantage or Medicare Cost plan, you may have a trial period during which you have
certain rights to leave (disenroll from) <plan name> and buy a Medigap policy. Please contact
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
215
1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a week for further
information. TTY users should call 1-877-486-2048.
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days/hours of operation and, if different, TTY hours of
operation>. Please be sure to keep a copy of this letter for your records.
Thank you.

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
216
Exhibit 5: Model Notice to Request Information
Referenced in section(s): 30, 40.2.2
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Member>:
Thank you for applying with <plan name>. We need additional information from you. Please
see the checked items below.
We cannot process your application until we get the following things from you:
Proof of Medicare coverage. Please provide us your Medicare Number. Your
Medicare Number is printed on your Medicare card. You can also get your
number by:
• Logging into your MySocialSecurity.gov or MyMedicare.gov accounts;
• Calling Medicare at 1-800-MEDICARE (1-800-633-4227; TTY: 1-800-486-
2048); or
• Calling Social Security at 1-800-772-1213 (TTY: 1-800-325-0778).
______ During certain times of the year, Medicare doesn’t let you enroll unless you meet
certain special exceptions, such as if you qualify for extra help with your
prescription drug costs. Please call us at the number below to help us determine
if you’re able to enroll at this time.
Other: ______________________________________________
You will need to send this information to <plan name and address> by <date>. You can contact
us by phone with this information by calling the phone number below. Or, you may also fax it to
us at <fax number> or send it to us at <address>. If we don’t get this information by <date>, we
will have to deny your request to enroll in our plan.
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
217
Exhibit 6: Model Notice to Confirm Enrollment (MA-PD)
Referenced in section(s): 40.40.2, 40.6
<Member # >
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Please be sure to keep a copy of this letter for your records. Medicare has approved your
enrollment in <plan name> beginning <effective date>.
[I
f no low-income subsidy:
What are my costs in this plan?
The monthly premium for your plan is: <premium amount>.
People with limited incomes may qualify for extra help to pay for their prescription drug costs. If
you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this extra help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp.
If you think you qualify for extra help with your prescription drug costs, but you don’t have or
can’t find proof, please contact <plan name> at the phone number provided at the end of this
letter.]
[I
f low-income subsidy applicable:
What are my costs since I qualify for extra help?
Because you qualify for extra help with your prescription drug costs, you will pay no more than:
• A monthly premium of <insert premium less amount of premium assistance for which
the individual is eligible>,
• <insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
• <insert appropriate LIS copay amount> copayment when you fill a prescription
covered by <plan name>.
If you believe this is incorrect and you have proof that the extra help amounts should be
different, please contact <plan name> at the phone number provided at the end of this letter.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
218
Will I pay a late enrollment penalty as part of my premium?
[Insert the following for new members with an existing LEP:
Your premium continues to reflect a late enrollment penalty amount that was based on
information sent by your previous plan. Your plan should have told you about this penalty. If
you have questions about the late enrollment penalty, call <plan name> at the phone number
provided at the end of this letter. You can also get information by visiting www.medicare.gov or
by calling 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a week. TTY
users should call 1-877-486-2048.] If we determine that your penalty needs to be adjusted, we
will notify you of your new monthly premium.
[If previous paragraph not applicable, insert the following for all other new members: If we
determine that you owe a late enrollment penalty, we will notify you of your new monthly
premium amount.]
[Explain the charges for which the prospective member will be liable, e.g., coinsurance, fees or
other amounts, and any amount that is attributable to the Medicare deductible and coinsurance]
What if I have a Medigap (Medicare Supplement Insurance) policy or other supplemental
insurance?
Now that we have confirmed your enrollment, you may cancel any Medigap policy or
supplemental insurance that you have. Please note that if this is the first time that you are a
member of a Medicare Advantage or Medicare Cost plan, you may have certain rights to leave
(disenroll from) <plan name> and buy a Medigap policy. Please contact 1-800-MEDICARE (1-
800-633-4227) anytime, 24 hours a day, 7 days a week for further information about Medigap
policies. TTY users should call 1-877-486-2048.
Please call <plan name> at <phone number> if you have any questions. TTY users should call
<TTY number>. We are open <days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
219
Exhibit 6a: Model Notice to Confirm Enrollment - Plan to Plan Within
Parent Organization
Referenced in section(s): 40.40.2, 40.6
Dear <Name of Member>:
Please keep a copy of this letter for your records. Medicare has approved your enrollment in
<plan name> beginning <effective date>.
[
MA-PD, if no low-income subsidy:
What are my costs in this plan?
The monthly premium for your plan is <premium amount>.
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for extra help to pay for their prescription drug costs. If
you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this extra help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp.
If you think you qualify for extra help with your prescription drug costs, but you don’t have or
can’t find proof, please call <plan name> at the phone number provided at the end of this letter.]
[
MA-PD, if low-income subsidy applicable:
What are my costs since I qualify for extra help?
Because you qualify for extra help with your prescription drug costs, you will pay no more than:
• A monthly premium of <insert premium less amount of premium assistance for which
the individual is eligible>,
• <insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
• <insert appropriate LIS copay amount> copayment when you fill a prescription
covered by <plan name>.
If you believe this is incorrect and you have proof that that the extra help amounts should be
different, please contact <plan name> at the phone number provided at the end of this letter.]
Will I pay a late enrollment penalty as part of my premium?
[
MA-PD plans insert the following for members with an existing LEP: Your premium continues to
reflect a late enrollment penalty. If you have questions about the late enrollment penalty, call
<plan name> at the phone number provided at the end of this letter. You can also get
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
220
information by visiting www.medicare.gov or by calling 1-800-MEDICARE (1-800-633-4227)
anytime, 24 hours a day, 7 days a week. TTY users should call 1-877-486-2048.]
[
MA-PD plans, if previous paragraph not applicable, insert the following for all other new
members: The late enrollment penalty is an amount added to your monthly Medicare drug plan
(Part D) premium for as long as you have Medicare prescription drug coverage. This penalty is
required by law and is designed to encourage people to enroll in a Medicare drug plan when they
are first eligible or keep other prescription drug coverage that meets Medicare’s minimum
standards. You may owe a late enrollment penalty if you didn’t join a Medicare drug plan when
you were first eligible for Medicare Part A and/or Part B, and:
• You didn’t have other prescription drug coverage that met Medicare’s minimum
standards; OR
• You had a break in coverage of at least 63 days.
If we determine that you owe a late enrollment penalty, we will notify you of your new monthly
premium amount.]
[Explain the charges for which the prospective member will be liable, e.g., coinsurance, fees or
other amounts, and any amount that is attributable to the Medicare deductible and coinsurance]
Please call <plan name> at <phone number> if you have any questions. TTY users should call
<TTY number>. We are open <days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
221
Exhibit 6b: Model Notice for MA-PD Plans for Individuals Identified on
CMS Records As Members of Employer or Union Group Receiving the
Retiree Drug Subsidy (RDS)
Referenced in section(s): 40
Dear <Name of Member>:
Thank you for applying with <Plan Name>. To finalize your enrollment, we would like you to
confirm that you want to be enrolled in <plan name>.
Medicare has informed us you belong to an employer group or union health plan whose drug
coverage is as good as Medicare prescription drug plan coverage.
It is important that you consider your decision to enroll in our plan carefully, since enrollment in
<plan name> could affect your employer or union health benefits. You could lose your
employer or union health coverage. If you haven’t already done so, please contact your benefits
administrator to discuss your decision to enroll in a Medicare prescription drug plan.
[PFFS plans insert: <Plan Name>, a Medicare Advantage Private Fee-for-Service plan, works
differently than a Medicare supplement plan and other Medicare Advantage plans. Your doctor
or hospital is not required to agree to accept the plan’s terms and conditions, and thus may
choose not to treat you, with the exception of emergencies. If your doctor or hospital does not
agree to accept our payment terms and conditions, they may choose not to provide health care
services to you, except in emergencies. Providers can find the plan’s terms and conditions on
our website at <insert link to PFFS terms and conditions>.]
If you have already discussed this decision with your benefits administrator and have decided
that you would still like to be a member of <plan name>, please call <plan name> at the phone
number provided below. Your enrollment won’t be complete until you call and confirm
this information. Your effective date will be <effective date>.
We must hear from you to enroll you in our plan. If we don’t hear from you within 30 days from
the date of this notice, we won’t process your enrollment. If you decide not to enroll in <plan
name> you will be responsible for any services you have already received from <plan name>.
To confirm your enrollment or if you have any questions, please feel free to contact <plan name>
at <phone number>. We are open <insert days/hours of operation and, if different, TTY hours of
operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
222
Exhibit 6c: Model Notice to Confirm PFFS Enrollment
Referenced in section: 40.4.2
<Member # >
<RxID>
<RxGroup>
<RxBin>
<RxPCN>
Dear <Name of Member>:
Thank you for enrolling in <Plan name>. Medicare has approved your enrollment in <plan
name> beginning <effective date>. You must show your <Plan name> ID card to your doctor or
hospital before you get healthcare. Don’t use your red, white, and blue Medicare card to receive
healthcare, because Original Medicare won’t pay for your healthcare while you are enrolled
in this plan. You should keep your Medicare card in a safe place. [Optional: This letter is proof
of insurance that you should show during your doctor appointments until you get your member
card from us.] [Optional language for MA-PD: This letter is also proof of your prescription drug
coverage. You should show this letter at the pharmacy until you get your member card from us.]
How does this plan work?
<Plan name>, a Medicare Advantage Private Fee-for-Service plan, works differently than a
Medicare supplement plan and other Medicare Advantage plans. As we told you before, <Plan
name> allows you to go to any Medicare-approved doctor or hospital that is willing to give you
care and accept our plan’s terms of payment. You should contact your doctor or hospital to ask
whether they will accept our plan’s payment terms. Your doctor or hospital isn’t required to
agree to accept the plan’s terms and conditions, and may choose not to treat you, except in
emergencies. You should verify that your provider(s) will accept <plan name> before each
visit. Providers can find the plan’s terms and conditions on our website at <insert link to PFFS
terms and conditions>.
If any doctor or hospital provides health care services to you after learning about our plan’s
payment terms, they must bill us for services, and aren’t allowed to send the entire bill to you. If
a doctor or hospital does provide services to you, then they are considered to have accepted our
plan’s terms. You will need to pay your plan co-payments and co-insurance at the time you get
health care services, as described in your member materials.
If your doctor or hospital doesn’t accept our plan’s payment terms, they shouldn’t provide
services to you except for emergencies. You may contact us at the number at the end of this
letter for help locating another provider in your area.
[Include if plan uses a network of contracted providers: <Plan name> has direct contracts with
some providers who have already agreed to accept our terms and conditions of
payment. [Describe what category or categories of providers the plan has under direct contract
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
223
and how members can get the list of contracted providers.] You can still get care from other
providers who do not contract with <plan name> as long as those providers agree to accept our
terms and conditions of payment. [Indicate if the plan has established higher cost sharing
requirements for members who obtain covered services from non-contracted providers.]
[
MA-PD, if no low-income subsidy:
What are my costs in this plan?
The monthly premium for your plan is <premium amount>. [Explain the charges for which the
prospective member will be liable, e.g., coinsurance, fees or other amounts, and any amount that
is attributable to the Medicare deductible and coinsurance]
[
MA-PD, if no low-income subsidy:
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for extra help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this extra help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp.
If you think you qualify for extra help with your prescription drug costs, but you don’t have or
can’t find proof, please contact <plan name> at the phone number provided at the end of this
letter.]
[
MA-PD, if low-income subsidy applicable:
What are my costs since I qualify for extra help?
Because you qualify for extra help with your prescription drug costs, you will pay no more than:
A monthly premium of <insert premium less amount of premium assistance for which
the individual is eligible>,
<insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
<insert appropriate LIS copay amount> copayment when you fill a prescription
covered by <plan name>.
If you believe this is incorrect and you have proof that that the extra help amounts should be
different, please contact <plan name> at the phone number provided at the end of this letter.]
Will I pay a late enrollment penalty as part of my premium?
[
MA-PD plans insert the following for new members with an existing LEP: Your premium continues
to reflect a late enrollment penalty amount that was based on information sent by your previous
plan. Your plan should have told you about this penalty. If you have questions about the late
enrollment penalty, call <plan name> at the phone number provided at the end of this
letter. TTY users should call <toll-free TTY number>. You can also get information by visiting
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
224
www.medicare.gov or by calling 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day,
7 days a week. TTY users should call 1-877-486-2048.]
[
MA-PD plans, if previous paragraph not applicable, insert the following for all other new members: The
late enrollment penalty is an amount added to your monthly Medicare drug plan (Part D)
premium for as long as you have Medicare prescription drug coverage. This penalty is required
by law and is designed to encourage people to enroll in a Medicare drug plan when they are first
eligible or keep other prescription drug coverage that meets Medicare’s minimum standards.
You may owe a late enrollment penalty if you didn’t join a Medicare drug plan when you were
first eligible for Medicare Part A and/or Part B, and:
• You didn’t have other prescription drug coverage that met Medicare’s minimum
standards; OR
• You had a break in coverage of at least 63 days.
If we determine that you owe a late enrollment penalty, we will notify you of your new monthly
premium amount.]
What if I have a Medigap (Medicare Supplement Insurance) policy or other supplemental
insurance?
Now that we have confirmed your enrollment, you may cancel any Medigap or supplemental
insurance that you have. Please note that if this is the first time that you are a member of a
Medicare Advantage or Medicare Cost plan, you may have certain rights to leave (disenroll
from) <plan name> and buy a Medigap policy. Please contact 1-800-MEDICARE (1-800-633-
4227) anytime, 24 hours a day, 7 days a week for further information about Medigap policies.
TTY users should call 1-877-486-2048.
If you have any questions, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days/hours of operation and, if different, TTY hours of
operation>. Please be sure to keep a copy of this letter for your records.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
225
Exhibit 6d: Model Notice to Confirm Enrollment (MA-only)
Referenced in section(s): 40.4.2
<Member # >
Dear <Name of Member>:
Thank you for enrolling in <plan name>. Medicare has approved your enrollment in <plan
name> beginning <effective date>. Please be sure to keep a copy of this letter for your records.
What are my costs in this plan?
[MA-only plans with a premium insert the following:
The monthly premium for your plan is: <premium amount>.]
[Explain the charges for which the prospective member will be liable, e.g., coinsurance, fees or
other amounts, and any amount that is attributable to the Medicare deductible and coinsurance]
What if I have a Medigap (Medicare Supplement Insurance) policy or other supplemental
insurance?
Now that we have confirmed your enrollment, you may cancel any Medigap policy or
supplemental insurance that you have. Please note that if this is the first time that you are a
member of a Medicare Advantage or Medicare Cost plan, you may have certain rights to leave
(disenroll from) <plan name> and buy a Medigap policy. Please contact 1-800-MEDICARE (1-
800-633-4227) anytime, 24 hours a day, 7 days a week for further information about Medigap
policies. TTY users should call 1-877-486-2048.
Please call <plan name> at <phone number> if you have any questions. TTY users should call
<TTY number>. We are open <days and hours of operation>.
Thank you.

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
226
Exhibit 7: Model Notice for MA Organization Denial of Enrollment
Referenced in section(s): 40.2.3
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Dear <Name of Beneficiary>:
Thank you for applying with <MA Plan>. We cannot accept your request for enrollment in <MA
Plan> because:
1. You don’t have Medicare Part A.
2. You don’t have Medicare Part B.
3. You are unlawfully present in the United States.
4. ______ You are incarcerated and currently reside outside our service area.
5. ______ Your permanent residence is outside our service or continuation area.
6. ______ You attempted to enroll outside of an enrollment period or don’t qualify
for an enrollment period at this time.
7. ______ We didn’t get the information we requested from you within the
timeframe listed in our request.
8. ______ The request was made by someone other than the beneficiary and that
individual isn’t the beneficiary’s authorized representative.
[9. MA-PD plans only: You are not eligible to enroll in prescription drug
coverage at this time.]
[10.______
MA-PD plans only: You have drug coverage from your employer or union
and you told us you don’t want to join <MA plan>.]
[11. ______
Special needs plans only: You are not eligible for this Special Needs Plan
because you don’t <insert special needs criteria>.]
If <plan name> paid for any of your health care services, then we will bill you for the amount
paid.
[Insert if item 3 or 4 is selected: Medicare doesn’t pay for your hospital or medical bills if you’re
not lawfully present in the U.S. or if you’re incarcerated.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
227
[Insert if item 6, 7, 8, or 9 is selected: You can change health plans only at certain times during
the year. From October 15 - December 7, you can join, switch or drop a Medicare health or drug
plan for the following year. In addition, from January 1 - March 31, anyone enrolled in a
Medicare Advantage Plan (except an MSA plan) can switch plans or return to Original Medicare
(and join a stand-alone Medicare Prescription Drug Plan). Generally, you can’t make changes at
other times except in certain situations, such as if you move out of your plan’s service area, want
to join a plan in your area with a 5-star rating, or qualify for (or lose) Extra Help paying for
prescription drug costs.]
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you believe any of the checked items are wrong, or if you have any questions, please call
<plan name> at <phone number>. TTY users should call <TTY number>. We are open <insert
days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
228
Exhibit 8: Model Notice for CMS Rejection of Enrollment
Referenced in section(s): 40.4.2
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Dear <Name of Beneficiary>:
[If sending in place of combined acknowledgement/confirmation notice, insert the following
sentence: Thank you for your request to enroll in <plan name>.] Medicare has denied your
enrollment in <MA Plan> due to the reason(s) checked below:
1. You don’t have Medicare Part A
2. You don’t have Medicare Part B
3. You are unlawfully present in the United States.
4. You are incarcerated and currently reside out of our service area.
5. You attempted to enroll outside of an enrollment period or you
don’t qualify for an enrollment period at this time.
6. You requested to enroll in a different plan for the same effective
date, which canceled your application with <plan name>.
If <plan name> paid for any of your health care services, then we will bill you for the amount
paid.
[Insert if item 3 or 5 is selected: Medicare doesn’t pay for your hospital or medical bills if you’re
not lawfully present in the U.S. or if you’re incarcerated.]
[Insert if item 6 is checked: You can change health plans only at certain times during the year.
From October 15 - December 7, you can join, switch or drop a Medicare health or drug plan for
the following year. In addition, from January 1 - March 31, anyone enrolled in a Medicare
Advantage Plan (except an MSA plan) can switch plans or return to Original Medicare (and join
a stand-alone Medicare Prescription Drug Plan). Generally, you can’t make changes at other
times except in certain situations, such as if you move out of your plan’s service area, want to
join a plan in your area with a 5-star rating, or qualify for (or lose) Extra Help paying for
prescription drug costs.]
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
229
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you believe any of the checked items are wrong, or if you have any questions, please call
<plan name> at <phone number>. TTY users should call <TTY number>. We are open <insert
days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
230
Exhibit 9: Model Notice to Send Out Disenrollment Form (MA-PD enrollee)
Referenced in section(s): 50.1
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Member>:
Attached is the disenrollment form you requested. Please read the important instructions in this
letter regarding requesting disenrollment from <plan name>.
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
What is Extra Help?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
When should I fill out the disenrollment request form?
• You should fill out the attached form if you want to change to Original Medicare only
and do not want Medicare prescription drug coverage.
• You shouldn’t fill out the attached form if you are planning to enroll, or have enrolled, in
another Medicare Advantage plan or other Medicare health plan. Enrolling in another
Medicare plan will automatically disenroll you from our plan.
• You shouldn’t fill out the attached form if you are enrolling in a Medicare prescription
drug plan. Enrolling in a Medicare prescription drug plan will automatically disenroll you
from <plan name> to Original Medicare.
Until your disenrollment date, you must keep using <plan name> doctors. To avoid any
unexpected expenses, you may want to contact us to make sure you’ve been disenrolled before
you seek medical services outside of <plan name>‘s network.
How do I submit the disenrollment request?
If you want Original Medicare, as described above, you may fill out the attached form, sign it,
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
231
and send it back to us in the enclosed envelope. You can also fax the form with a readable
signature and date to us at <fax number>. You can call 1-800-MEDICARE (1-800-633-4227)
for information about Medicare plans available in your area. TTY users should call 1-877-486-
2048, 24 hours a day/7days a week.
What are my Medigap rights?
If you will be changing to Original Medicare, you might have a special temporary right to buy a
Medigap policy, also known as Medicare supplemental insurance, even if you have health
problems. For example, if you are age 65 or older and you enrolled in Medicare Part B within
the past 6 months or if you move out of the service area, you may have this special right.
Federal law requires the protections described above. Your State may have laws that provide
more Medigap protections. If you have questions about Medigap or Medigap rights in your
State, you should contact your State Health Insurance Program <insert name of SHIP> at <SHIP
phone number>. You can also call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a
day, 7 days a week for more information about trial periods. TTY users should call 1-877-486-
2048.
If you need any help, please call us at <phone number>. TTY users should call <TTY number>.
We are open <insert days and hours of operation>.
Thank you.
Attachment
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
232
Exhibit 9a: Model Notice to Send Out Disenrollment Form (MA-only enrollee)
Referenced in section(s): 50.1
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Member>:
Attached is the disenrollment form you requested. Please read the important instructions in this
letter regarding requesting disenrollment from <plan name>.
When can I make changes to my coverage?
You can change health plans only at certain times during the year. From October 15 - December
7, you can join, switch or drop a Medicare health or drug plan for the following year. In
addition, from January 1 - March 31, anyone enrolled in a Medicare Advantage Plan (except an
MSA plan) can switch plans or return to Original Medicare (and join a stand-alone Medicare
Prescription Drug Plan). Generally, you can’t make changes at other times except in certain
situations, such as if you move out of your plan’s service area, want to join a plan in your area
with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription drug costs.
[Dual eligible Special Needs Plans may omit this paragraph: What is Extra Help?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.]
When should I fill out the disenrollment request form?
You should fill out the attached form if you want to change to Original Medicare only and don’t
want Medicare prescription drug coverage.
You shouldn’t fill out the attached form if you are planning to enroll, or have enrolled, in
another Medicare Advantage or other Medicare Health Plan. Enrolling in another Medicare plan
will automatically disenroll you from <plan name>.
[MA-only coordinated care plans insert: You shouldn’t fill out the attached form if you are
enrolling in a Medicare prescription drug plan. Enrolling in a Medicare prescription drug plan
will automatically disenroll you from <plan name> to Original Medicare.]
[MSA plans insert: Please note that if you disenroll before the end of the year, you (or your
estate) will have to pay <MA organization> for a portion of the MSA deposit made by the MSA
Plan at the time you enrolled. The amount you owe is based on the number of months left in the
year after your disenrollment date.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
233
Until your disenrollment date, you must keep using <plan name> doctors. To avoid any
unexpected expenses, you may want to contact us to make sure you’ve been disenrolled before
you seek medical services outside of <plan name>’s network.
How do I submit the disenrollment request?
If you want Original Medicare, as described above, you may fill out the attached form, sign it,
and send it back to us in the enclosed envelope. You can also fax the form with a readable
signature and date to us at <fax number>. You can call 1-800-MEDICARE (1-800-633-4227)
anytime, 24 hours a day, 7 days a week for information about Medicare plans available in your
area. TTY users should call 1-877-486-2048.
What are my Medigap rights?
If you will be changing to Original Medicare, you might have a special temporary right to buy a
Medigap policy, also known as Medicare supplement insurance, even if you have health
problems. For example, if you are age 65 or older and you enrolled in Medicare Part B within
the past 6 months or if you move out of the service area, you may have this special right.
Federal law requires the protections described above. Your State may have laws that provide
more Medigap protections. If you have questions about Medigap or Medigap rights in your
State, you should contact your State Health Insurance Program <insert name of SHIP> at <SHIP
phone number>. Call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a
week for more information. TTY users should call 1-877-486-2048.
If you need any help, please call <plan name> at <phone number>. TTY users should call
<TTY number>. We are open <insert days and hours of operation>.
Thank you.
Attachment
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
234
Exhibit 10: Model Disenrollment Form
Referenced in section: 10
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
If you request disenrollment, you must continue to get all medical care from <plan name> until
the effective date of disenrollment. Contact us to verify your disenrollment before you seek
medical services outside of <plan name>’s network. We will notify you of your effective date
after we get this form from you.
Last name: First Name: Middle Initial
Mr. Mrs. Miss. Ms.
Medicare Number: (Note: may use “Member Number” instead of “Medicare Number”)
Birth Date:
Sex:
M F
Home Phone Number:
( )
Please carefully read and complete the following information before signing and dating this
disenrollment form:
If I have enrolled in another Medicare Advantage or Medicare Prescription Drug Plan, I
understand Medicare will cancel my current membership in <MA plan name> on the effective
date of that new enrollment. I understand that I might not be able to enroll in another plan at this
time. I also understand that if I am disenrolling from my Medicare prescription drug coverage
and want Medicare prescription drug coverage in the future, I may have to pay a higher premium
for this coverage.
Your Signature*: ______________________________ Date: _____________
*Or the signature of the person authorized to act on your behalf under the laws of the State where
you live. If signed by an authorized individual (as described above), this signature certifies that:
1) this person is authorized under State law to complete this disenrollment and 2) documentation
of this authority is available upon request by <plan name> or by Medicare.
If you are the authorized representative, you must provide the following information:
Name : ________________________
Address: _______________________________________________
Phone Number: (___) ____- _____
Relationship to Enrollee ___________________
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
235
Exhibit 10a: Information to include on or with Disenrollment Form –
Attestation of Eligibility for an Election Period
Referenced in section: 30.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Typically, you may disenroll from a Medicare Advantage plan only during the annual
enrollment period from October 15 through December 7 of each year or during the
Medicare Advantage Open Enrollment Period from January 1 through March 31 of each
year. There are exceptions that may allow you to disenroll from a Medicare Advantage plan
outside of this period.
Please read the following statements carefully and check the box if the statement applies to you.
By checking any of the following boxes you are certifying that, to the best of your knowledge,
you are eligible for an Election Period.
I recently had a change in my Medicaid (newly got Medicaid, had a change in level of
Medicaid assistance, or lost Medicaid) on (insert date) ________________________.
I recently had a change in my Extra Help paying for Medicare prescription drug coverage
(newly got Extra Help, had a change in the level of Extra Help, or lost Extra Help) on
(insert date) ___________________________.
I have both Medicare and Medicaid (or my state helps pay for my Medicare premiums) or
I get Extra Help paying for Medicare prescription drug coverage, but I haven’t had a
change.
I am moving into, live in, or recently moved out of a Long-Term Care Facility (for
example, a nursing home or long term care facility). I moved/will move into/out of the
facility on (insert date) ___________________________________________.
I am joining a PACE program on (insert date) _________________________.
I am joining employer or union coverage on (insert date) ________________.
I was enrolled in a plan by Medicare (or my state) and I want to choose a different plan.
My enrollment in that plan started on (insert date) ______________________________.
If none of these statements applies to you or you’re not sure, please contact <plan name> at
<phone number> (TTY users should call <TTY number>) to see if you are eligible to
disenroll. We are open <insert days and hours of operation>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
236
Exhibit 11: Model Notice to Acknowledge Receipt of Voluntary Disenrollment
Request from Member
Referenced in section(s): 50.1, 50.1.4, 50.4.1
Dear <Name of Beneficiary>:
We received your request to disenroll from <plan name>. You will be disenrolled starting
<effective date.> Beginning <effective date>, <plan name> won’t cover any health care you get.
Beginning <effective date>, you can see any doctor through Original Medicare, unless you have
enrolled in another Medicare Advantage plan.
[
MA-PD plans insert: When coverage from <plan name> ends, your <plan name> prescription
drug coverage ends too. If you don’t take any action, you will be covered by Original
Medicare beginning <effective date>. To have new health care coverage and prescription drug
coverage on <effective date> or to buy a Medigap policy while you still have a guaranteed right
to buy one, you need to take action. For example, if you are returning to Original Medicare and
want Medicare prescription drug coverage, you must join a Medicare prescription drug plan. If
you don’t enroll in a Medicare prescription drug plan on your own and you have both Medicare
and Medicaid, Medicare will enroll you in a Medicare prescription drug plan, unless you tell the
plan you don’t want to join. If you don’t enroll in another Medicare Advantage plan with
prescription drug coverage or Medicare prescription drug plan, or if you don’t get creditable
coverage as good as Medicare prescription drug coverage, you may have to pay a late enrollment
penalty if you enroll in Medicare prescription drug coverage in the future.]
[
MA-only plans insert: Disenrolling from <plan name> doesn’t affect any prescription drug
coverage you may have. To have new health care coverage on <effective date> or to buy a
Medigap policy while you still have a guaranteed right to buy one, you need to take action. If
you don’t take any action, you will be covered by Original Medicare beginning <effective
date>.]
[MSA plans insert the following: Please note that if you disenroll before the end of the year, you
(or your estate) will have to pay <MA organization> for a portion of the MSA deposit made by
the MSA Plan at the time you enrolled. The amount you owe is based on the number of months
left in the year after your disenrollment date.]
Please be patient. It will take a few weeks for us to process your disenrollment and update
Medicare’s records. If your doctors need to send Medicare claims, you may want to tell them that
you just disenrolled from <plan name> and there may be a short delay in updating your records.
Information About Medigap Rights
If you will be changing to Original Medicare you might have a special temporary right to buy a
Medigap policy, also known as Medicare supplement insurance, even if you have health
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
237
problems. For example, if you are age 65 or older and you enrolled in Medicare Part B within
the past 6 months or if you move out of the service area, you may have this special right.
Federal law requires the protections described above. Your State may have laws that provide
more Medigap protections. If you have questions about Medigap or Medigap rights in your
State, you should contact your State Health Insurance Program <insert name of SHIP> at <SHIP
phone number>. You can also call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a
day, 7 days a week for more information. TTY users should call 1-877-486-2048.
If you need any help, please call us at <phone number>. TTY users should call <TTY number>.
We are open <insert days and hours of operation>.
[Dual eligible Special Needs Plans may omit this paragraph: Did you know that people with
limited incomes may qualify for extra help to pay for their prescription drug costs? If you
qualify, Medicare could pay for 75% or more of your drug costs including monthly prescription
drug premiums, annual deductibles, and co-insurance. Additionally, those who qualify won’t
have a coverage gap or a late enrollment penalty. Many people qualify for these savings and
don’t even know it. For more information about this extra help, contact your local Social
Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-325-
0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp.]
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
238
Exhibit 11a: Model Notice to Request Information (Disenrollment)
Referenced in section(s): 30, 50.4.2
Dear <Name of Member>:
We received your request to disenroll from <plan name>. However, it is missing information
that will help us to determine if we can accept your request. We cannot process your
disenrollment without this information.
Please review the checked item(s) below and contact us immediately.
Medicare requires that you sign your written disenrollment request. The request
we received from you didn’t include a signature. Please call us at the number
below to confirm that you want to disenroll from <plan name>.
During certain times of the year, Medicare doesn’t let you disenroll unless you
meet certain special exceptions, such as if you qualify for extra help with your
prescription drug costs. Please call us at the number below to help us determine if
you’re able to disenroll at this time.
______ The request we received was from someone other than you and that individual
isn’t listed as your authorized representative. Please call us at the number below
so that we may confirm your request to disenroll.
Other: ______________________________________________
If you have any questions about the information in this letter or would like to provide us with
information to help us process your disenrollment request, you may contact us by telephone or
mail:
<plan name>
<mailing address>
<toll free number and days/hours of operation)
<TTY toll-free number>
You may also fax us information at <fax number>.
If we don’t get this information, we will have to deny your request to disenroll from our plan.
Instead of sending a disenrollment request to <plan name> you can call 1-800-MEDICARE (1-
800-633-4227) anytime, 24 hours a day, 7 days a week to disenroll by telephone. TTY users
should call 1-877-486-2048. If you’re receiving coverage through your employer, you should
contact your employer instead of calling 1-800-MEDICARE to find out how this affects your
retiree benefits.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
239
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
240
Exhibit 12: Model Notice to Confirm Voluntary Disenrollment Following
Receipt of Daily Transaction Reply Report (DTRR)
Referenced in section(s): 50.1, 50.4.1, 60.3.2
Dear <Name of Beneficiary>:
Medicare has confirmed your disenrollment from <MA Plan>. Beginning <effective date,>
<plan name> won’t cover your health care. If your doctor needs to send Medicare claims, you
may want to tell them that there may be a short delay in updating your records since you recently
disenrolled from <plan name>.
[MA-PD plans insert the following: If your <plan name> premium is being deducted from your
Social Security or Railroad Retirement Board benefit, please allow up to 3 months for Social
Security or the Railroad Retirement Board to process a refund. If you have not received a refund
within 3 months of this letter, you should contact 1-800-MEDICARE.]
[MSA plans insert the following: Please note that if you disenroll before the end of the year, you
(or your estate) will have to pay <MA organization> for a portion of the MSA deposit made by
the MSA Plan at the time you enrolled. The amount you owe is based on the number of months
left in the year after your disenrollment date.]
INFORMATION ABOUT MEDIGAP RIGHTS
If you will be changing to Original Medicare you might have a special temporary right to buy a
Medigap policy, also known as Medicare supplement insurance, even if you have health
problems. For example, if you are age 65 or older and you enrolled in Medicare Part B within
the past 6 months or if you move out of the service area, you may have this special right.
Federal law requires the protections described above. Your State may have laws that provide
more Medigap protections. If you have questions about Medigap or Medigap rights in your
State, you should contact your State Health Insurance Program <insert name of SHIP> at <SHIP
phone number>. You can also call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a
day, 7 days a week for more information. TTY users should call 1-877-486-2048.
If you think you didn’t disenroll from <plan name>, and you want to keep being a member of
<plan name>, please call us right away at <phone number> so we can make sure you stay a
member of <plan name>. Medicare gives you only 30 days from the date of this letter to contact
us. TTY users should call <TTY number>. We are open <insert days and hours of operation>.
[Dual eligible Special Needs Plans may omit this paragraph: Did you know that people with
limited incomes may qualify for extra help to pay for their prescription drug costs? If you
qualify, Medicare could pay for 75% or more of your drug costs including monthly prescription
drug premiums, annual deductibles, and co-insurance. Additionally, those who qualify won’t
have a coverage gap or a late enrollment penalty. Many people qualify for these savings and
don’t even know it. For more information about this extra help, contact your local Social
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
241
Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-325-
0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp.]
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
242
Exhibit 12a: Model Notice for MA Organization Denial of Disenrollment
Referenced in section: 50.1.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Beneficiary>:
We recently got your request to disenroll from <plan name>. We cannot accept your request for
disenrollment because:
1. _____ You have attempted to make a change outside of an enrollment period or you
don’t qualify for an enrollment period at this time.
2. _____ You have already made a change to how you get Medicare (see discussion on
limits to changes below).
3. _____ We didn’t get the information we requested from you within the timeframe listed
in our request.
4. _____ The request was made by someone other than the enrollee and that individual isn’t
the enrollee’s authorized representative.
When can I make changes to my coverage?
There are limits to when and how often you can change the way you get Medicare.
• From October 15 through December 7, anyone with Medicare can switch plans or
return to Original Medicare. This includes adding or dropping Medicare prescription drug
coverage for the following year.
• From January 1 through March 31, anyone enrolled in a Medicare Advantage Plan
(except an MSA plan) can switch plans or return to Original Medicare (and join a stand-
alone Medicare Prescription Drug Plan).
Generally, you can’t make changes at other times except in certain situations, such as if you
move out of your plan’s service area, want to join a plan in your area with a 5-star rating, or
qualify for (or lose) Extra Help paying for prescription drug costs.
[Dual-eligible SNPs may omit the following paragraph:]
What is extra help?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
243
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you believe any of the items we checked are wrong, or if you have any questions, please call
us at <phone number>. TTY users should call <TTY number>. We are open <insert days and
hours of operation>.
Thank you.

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
244
Exhibit 12b: Model Notice for CMS Rejection of Disenrollment
Referenced in section: 50.1
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Beneficiary>:
Medicare has denied your disenrollment from <plan name> due to the reason(s) checked below:
1. You have attempted to make a change outside of an enrollment period or
you don’t qualify for an enrollment period at this time.
2. You have already made a change to how you get Medicare (see discussion
on limits to changes below.)
When can I make changes to my coverage?
There are limits to when and how often you can change the way you get Medicare.
• From October 15 through December 7, anyone with Medicare can switch plans or
return to Original Medicare. This includes adding or dropping Medicare prescription
drug coverage for the following year.
• From January 1 through March 31, anyone enrolled in a Medicare Advantage Plan
(except an MSA plan) can switch plans or return to Original Medicare (and join a stand-
alone Medicare Prescription Drug Plan).
Generally, you can’t make changes at other times except in certain situations, such as if you
move out of your plan’s service area, want to join a plan in your area with a 5-star rating, or
qualify for (or lose) Extra Help paying for prescription drug costs.
[Dual-eligible SNPs may omit the following paragraph:]
What is extra help?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you believe any of the items we checked are wrong, or if you have any questions, please call
<plan name> at <phone number>. TTY users should call <TTY number>. We are open <insert
days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
245
Exhibit 12c: Confirmation of Disenrollment Due to Passive Enrollment into a
Medicare-Medicaid Plan
Referenced in section: 50.4.1
IMPORTANT INFORMATION ABOUT YOUR UPCOMING DISENROLLMENT
FROM YOUR MEDICARE ADVANTAGE PLAN
<Date>
Dear <Name of Member>:
Your state has enrolled you into a new plan that will provide all of your Medicare and Medicaid
benefits, including prescription drugs. You should have already gotten a letter from your state
telling you about the new plan.
This letter confirms your disenrollment from <MA plan name>. You will continue to get your
Medicare benefits from <MA plan name> until <disenrollment effective date>. Beginning <day
following disenrollment effective date>, your new plan will cover your health care.
You will be automatically enrolled in your new plan starting <day following disenrollment
effective date>, so you don’t have to do anything if you want to be a member of this new plan. In
a few weeks, you should get a letter from your new plan confirming your enrollment. There will
be no gap in your Medicare and Medicaid coverage [MA-PD plans insert the following:
including your prescription drug coverage].
The letter from your new plan will tell you how to contact them. You can call your new plan
with questions about your new coverage or to see if you can still see your current doctors in your
new plan. You can also ask for lists of network primary care providers, covered drugs and
pharmacies.
If you have questions about your disenrollment from <MA plan name>, please call us at <phone
number> (TTY users should call <TTY number>). We are open <days and hours of operation>.
If you do not wish to be automatically enrolled in a new plan, call your state or call Medicare at
1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. Call 1-877-486-2048 if
you use a TTY. You can also call 1-800-MEDICARE if you have questions about Medicare or
need help with your Medicare options.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
246
Exhibit 13: Model Notice of Disenrollment Due to Death
Referenced in section(s): 50.2.3, 50.4.2, 60.3.1
To the Estate of <Member Name>:
Medicare told us of the death of <Member’s Name>. Please accept our condolences.
<Member’s name>’s coverage in <plan name> [ended; will end] as of <effective date>. If plan
premiums were paid for any month after <effective date>, we will issue a refund to the Estate
within 30 days of this letter.
[MA-PD plans insert the following: If the <plan name> premium is being deducted from
<Member Name>’s Social Security or Railroad Retirement Board benefit, please allow up to 3
months for Social Security or the Railroad Retirement Board to process a refund. If the estate
has not received a refund within 3 months of this letter, a representative of the estate should
contact 1-800-MEDICARE anytime, 24 hours a day, 7 days a week. TTY users should call 1-
877-486-2048.]
[MSA plans insert the following: Please note that the Estate has to pay <MA organization> for a
portion of the MSA deposit made by the MSA Plan at the time of enrollment. The amount owed
is based on the number of whole months left in the year after the date of death.]
If this information is wrong, please call us at <phone number>. TTY users should call <TTY
number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
247
Exhibit 14: Model Notice of Disenrollment Due to Loss of Medicare Part A
and/or Part B
Referenced in section(s): 50.2.2, 50.4.2, 60.3.1
Dear <Name of Member>:
Medicare has told us that you [will] no longer have Medicare Part <insert A and/or B, as
appropriate>. You need to have coverage under both Medicare Part A and Part B to remain
enrolled in a Medicare Advantage plan. Therefore, your membership in <plan name> [ended;
will end] on <date>. If this information is wrong, and you want to stay a member of our plan,
please contact us. Also, if you haven’t already done so, please contact your local Social Security
office to have their records corrected.
[
MA-PD plans insert: When coverage from <plan name> [ends; ended] on <date>, your Medicare
prescription drug coverage [will end; ended] too. If you still have either Medicare Part A or
Medicare Part B you are eligible for Medicare prescription drug coverage. To get Medicare
prescription drug coverage, you must enroll in a Medicare prescription drug plan such as a
Medicare Advantage Plan with prescription drug coverage or a Medicare Prescription Drug
Plan. If you are eligible to join a Medicare prescription drug plan but don’t join, and you don’t
have other drug coverage that is at least as good as Medicare’s, you may have to pay a late
enrollment penalty if you join later. This means you pay a higher premium for as long as you
have Medicare prescription drug coverage. Remember, Medicare limits how and when you can
make changes to your coverage. Call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a
day, 7 days a week. TTY users should call 1-877-486-2048.]
If you have any questions, please call us at <phone number>. TTY users should call <TTY
number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
248
Exhibit 15: Model Notice to Offer Beneficiary Services, Pending Correction
of Erroneous Death Status
Referenced in section(s): 60.3, 60.3.1
Dear< Name of Member>:
Medicare records incorrectly show you as deceased.
If you haven’t already done so, please go to your local Social Security Office and ask them to
correct your records. Please send us written proof at <address> after you do this. When we get
this proof, we will share it with Medicare.
In the meantime, you should keep using your <plan name> primary care physician for your
health care. [Note: If PCP not applicable, omit this sentence. MA plans may insert “physicians”
or “doctors” or “providers” instead of “primary care physician,” if that is more appropriate.] If
you have any questions or need help, please call us at < phone number>. TTY users should call
<TTY number>. We are open <insert days and hours of operation>.
Thank you for your continued membership in <plan name>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
249
Exhibit 16: Model Notice to Offer Beneficiary Services, Pending Correction
of Erroneous Medicare Part A and/or Part B Termination
Referenced in section(s): 60.3, 60.3.1
Dear < Name of Member>:
On <date of request> you told us that your enrollment in Medicare was ended in error and that
you want to stay a member of <plan name>.
[Organizations that are able to verify current Medicare entitlement may omit the following:
To do this, please complete the following three steps no later than <insert date: 60 days from date
of disenrollment notice>:
1. Contact Social Security at 1-800-772-1213 between 7AM to 7PM, Monday to Friday,
to have them fix their records TTY users should call 1-800-325-0778.
2. Ask Social Security to give you a letter that says they have fixed your records.
3. Send the letter from Social Security to us at: <address of MA Plan> in the enclosed
postage-paid envelope. You may also fax this information to us at <fax number>.
When we get this letter, we will tell the Medicare to correct its records.]
[Organizations that are able to verify current Medicare entitlement insert: Social Security
corrected the error. We will tell Medicare to correct its records.]
In the meantime, you should keep using your <plan name> primary care physician for your
health care. [Note: If PCP not applicable, omit this sentence. MA plans may insert “physicians”
or “doctors” or “providers” instead of “primary care physician,” if that is more appropriate.]
[Organizations that are able to verify current Medicare entitlement omit the following:
If we find out that you don’t have Medicare Part <insert “A” and/or “B” as appropriate>, or if we
don’t get proof that you have Medicare by <insert date: 60 days from date of disenrollment
notice>, you will have to pay for any service you got after <disenrollment date>.]
If you have any questions or need help, please call us at <phone number>. TTY users should call
<TTY number>. We are open <insert days and hours of operation>.
Thank you for your continued membership in <plan name>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
250
Exhibit 17: Model Notice to Offer Reinstatement of Beneficiary Services,
Pending Correction of Disenrollment Status Due to Plan Error
Referenced in section(s): 60.3, 60.3.3
Dear <Name of Member>:
Thank you for letting us know that you want to remain a member of <plan/sponsor name> after
we mistakenly [select one based on the circumstance: disenrolled you from/cancelled your
enrollment in] our plan. [Insert brief summary of the plan error that caused the disenrollment.]
We apologize for the inconvenience. We have changed our records to show that you are still a
member of <plan/sponsor name>. You should keep seeing your <plan name> [insert appropriate
term: <primary care physician, physicians, doctors, providers, pharmacies, etc.] for your health
care.
If you have any questions or need help, please call us at <phone number>. TTY users should call
<TTY number>. We are open <insert days and hours of operation>.
Thank you for your continued membership in <plan name>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
251
Exhibit 18: Model Notice to Close Out Request for Reinstatement
Referenced in section(s): 60.3.2
Dear <Name of Beneficiary>:
We cannot process your request to be in <plan name> again because we haven’t gotten the
information we requested. As discussed in our letter of <date of letter> you must send us this
information by <date placed on notice in Exhibit 16> to remain a member of our plan.
You were no longer a member of our plan as of <effective date>. If <plan name> paid for any
services after this disenrollment date, we will have to bill you for those services.
If you have any questions, please call <phone number>. TTY users should call <TTY number>.
We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
252
Exhibit 19: Model Notice on Failure to Pay Plan Premiums - Advance
Notification of Disenrollment or Reduction in Coverage of Optional
Supplemental Benefit(s)
Referenced in section: 50.3.1
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Member>:
Our records show that we haven’t gotten payment for your plan premium as of <premium due
date>.
[MA organizations who will disenroll all members (and not use the downgrade option) use the
following sentences: If we don’t get payment by <date grace period expires>, we will have to
disenroll you from <plan name>, effective <disenrollment date>. After <disenrollment date> you
will be covered by Original Medicare instead of <plan name>.]
[Note: As required in section 50.3.1, the MA organization must state whether full payment of
premiums is due to prevent disenrollment.]
[MA organizations who will reduce the member’s coverage (also known as “downgrade”) by
discontinuing the optional supplemental benefit(s) use the following sentences: If we don’t get
payment by <date grace period expires>, we will make some changes to your membership in
<plan name> that will reduce the amount of health care coverage you have in <plan name>. This
means that <describe lower level of benefits, e.g., routine dental care will not be covered>
beginning <date>.]
[Note: As required in section 50.3.1, the MA organization must state whether full payment of
premiums is due to prevent the downgrade.]
[Insert if applicable in state where member resides: If you get medical assistance (Medicaid)
from your State (including paying your premiums, deductibles, or coinsurance), you should
check with your State Medicaid Agency to find out if they have been paying for, or have stopped
paying for, your plan premium. If you are no longer eligible for assistance from Medicaid, you
may have a special temporary right to buy a Medigap policy if you voluntarily disenroll from our
plan. If you have questions about Medigap policies, you should contact your State Health
Insurance Program, <name of SHIP>, at <SHIP phone number(s)> to get more information.]
If you wish to disenroll from <plan name> and change to Original Medicare now, you should do
one of these two things:
1. Send us a written request at <MA Plan address>.
2. Call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a week. TTY
users should call 1-877-486-2048.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
253
Remember, there are limits to when and how often you can change the way you get Medicare:
• From October 15 through December 7, anyone with Medicare can switch plans or
return to Original Medicare. This includes adding or dropping Medicare prescription drug
coverage for the following year.
• From January 1 through March 31, anyone enrolled in a Medicare Advantage Plan
(except an MSA plan) can switch plans or return to Original Medicare (and join a stand-
alone Medicare Prescription Drug Plan).
Generally, you can’t make changes at other times except in certain situations, such as if you
move out of your plan’s service area, want to join a plan in your area with a 5-star rating, or
qualify for (or lose) Extra Help paying for prescription drug costs.
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you paid the premium recently and you think we have made a mistake, or if you have any
questions, please call us at <phone number> between <hours and days of operation>. TTY users
should call <TTY number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
254
Exhibit 20: Model Notice on Failure to Pay Plan Premiums - Notification of
Involuntary Disenrollment
Referenced in section(s): 50.3.1
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Member>:
On <date> we sent you a letter that said your plan premium was overdue. The letter said that if
we didn’t get payment from you, we would disenroll you from <plan name>. Since we didn’t get
that payment, we asked Medicare to disenroll you from <plan name> beginning <effective date>.
You will be covered by Original Medicare beginning <effective date>.
[
MA PFFS do not include this paragraph: Please note that until <disenrollment effective date>,
you must keep using <plan name> doctors except for emergency or urgently needed care or out-
of-area dialysis services. After that date, you can see any doctor through Original Medicare,
unless you join a Medicare Advantage plan or another Medicare health plan.]
What if I think there’s been a mistake?
If you think that we have made a mistake, please call us at <phone number>. You also have the
right to ask us to reconsider your disenrollment through the grievance procedure written in your
<insert “Member Handbook” or “Evidence of Coverage,” as appropriate>.
I had an emergency that kept me from sending my payment. What can I do?
You can ask us to review this decision if you had an emergency or unexpected situation that kept
you from paying your premiums on time. If we approve your request, you will have to pay all
owed premium amounts within three (3) months of your disenrollment in order to get your
coverage back. To ask us to review this decision, please call us at <phone number> between
<hours and days of operation>. TTY users should call <TTY number>. You must make your
request no later than <insert the date that is 60 calendar days after the disenrollment effective
date>.
When can I make changes to how I get my Medicare coverage?
Medicare limits when you can make changes to your coverage. From October 15 through
December 7 each year, you can enroll in a new Medicare Prescription Drug Plan or Medicare
health plan for the following year. You may not enroll in a new plan during other times of the
year unless you meet certain special exceptions, such as you move out of the plan’s service area,
want to join a plan in your area with a 5-star rating, or you qualify for (or lose) Extra Help with
your prescription drug costs.
[
MA-PD plans insert: Please remember, if you don’t have other creditable coverage (prescription
drug coverage expected to pay on average as much as Medicare), you may have to pay a Part D
late enrollment penalty if you enroll in Medicare prescription drug coverage in the future.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
255
[Dual-eligible SNPs may omit the following paragraph:]
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a Part D late enrollment penalty. Many people qualify for
these savings and don’t even know it. For more information about this Extra Help, contact your
local Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-
800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.
For more information:
If you have any questions or if you have recently sent us a payment, please call us at <phone
number> between <hours and days of operation>. TTY users should call <TTY number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
256
Exhibit 21: Model Notice on Failure to Pay Plan Premiums - Confirmation of
Involuntary Disenrollment
Referenced in section(s): 50.3.1
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Beneficiary>:
Medicare has confirmed your disenrollment from <plan name> because you didn’t pay your plan
premium. Your disenrollment begins <effective date>. You are now enrolled in Original
Medicare.
What if I think there’s been a mistake?
If you think that we have made a mistake, please call us at <phone number>. You also have the
right to ask us to reconsider your disenrollment through the grievance procedure written in your
<insert “Member Handbook” or “Evidence of Coverage,” as appropriate>.
I had an emergency that kept me from sending my payment. What can I do?
You can ask us to review this decision if you had an emergency or unexpected situation that kept
you from paying your premiums on time. If we approve your request, you will have to pay all
owed premium amounts within three (3) months of your disenrollment in order to get your
coverage back. To ask us to review this decision, please call us at <phone number> between
<hours and days of operation>. TTY users should call <TTY number>. You must make your
request no later than <insert the date that is 60 calendar days after the disenrollment effective
date>.
When can I make changes to how I get my Medicare coverage?
Medicare limits when you can make changes to your coverage. From October 15 through
December 7 each year, you can enroll in a new Medicare Prescription Drug Plan or Medicare
health plan for the following year. You may not enroll in a new plan during other times of the
year unless you meet certain special exceptions, such as you move out of the plan’s service area,
want to join a plan in your area with a 5-star rating, or you qualify for (or lose) Extra Help with
your prescription drug costs.
[MA-PD plans insert: Please remember, if you don’t have other creditable coverage
(prescription drug coverage that is expected to pay on average as much as Medicare), you may
have to pay a Part D late enrollment penalty if you enroll in Medicare prescription drug coverage
in the future.]
[Dual-eligible SNPs may omit the following paragraph:]
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a Part D late enrollment penalty. Many people qualify for
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
257
these savings and don’t even know it. For more information about this Extra Help, contact your
local Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-
800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.
For more information:
If you have any questions, or need help, please call <plan name> at <phone number> between
<hours and days of operation>. TTY users should call <TTY number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
258
Exhibit 21a: Notification of Involuntary Disenrollment by the Centers for
Medicare & Medicaid Services for Failure to Pay the Part D-Income Related
Monthly Adjustment Amount
Referenced in section: 50.2.6
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Important – You have been disenrolled from your Medicare Advantage
Prescription Drug Plan
<Date>
Dear <Beneficiary Name>:
Medicare has disenrolled you from <MA-PD plan name> because you didn’t pay the extra
amount (called the Part D-Income Related Monthly Adjustment Amount or Part D-IRMAA). As
of <effective date>, you will no longer have coverage through <MA-PD plan name>. Your
Medicare prescription drug coverage will also end on the same date. Since the disenrollment has
already processed, you can’t pay the owed amounts now to keep your Part D coverage.
Before you were disenrolled, Medicare (or the Railroad Retirement Board) sent you notices that
showed the amount that you owed and provided information on how to pay this amount. If your
plan premium was paid for any month after <disenrollment effective date>, you’ll get a refund
from us within 30 days of this letter.
The decision to disenroll you was made by Medicare, not by <plan name>.
What if I think there’s been a mistake?
If you paid the Part D-IRMAA or think that there has been a mistake, please call Medicare at 1-
800-MEDICARE (1-800-633-4227).
I had an emergency that kept me from sending my Part D-IRMAA payment. What can I
do?
You can ask Medicare to review this decision if you had an emergency or unexpected situation
that kept you from paying your premiums on time. If Medicare approves your request, you will
have to pay all Part DIRMAA and plan premium amounts owed within three (3) months of your
disenrollment in order to get your coverage back. Call Medicare at 1-800-MEDICARE (1-800-
633-4227) to make a request as soon as possible, but no later than <insert the date that is 60
calendar days after the disenrollment effective date>. TTY users should call 1-877-486-2048.
Please remember, if you don’t request reinstatement within 60 days and pay all owed amounts
within 3 months, you will not get your coverage back and will have to wait for another
opportunity to enroll. If you don’t have other creditable coverage (prescription drug coverage
that is expected to pay on average as much as Medicare), you may have to pay a Part D late
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
259
enrollment penalty in addition to the monthly Part D-IRMAA and plan premium, if you enroll in
Medicare prescription drug coverage in the future.
When can I get Part D coverage?
Medicare limits when you can make changes to your coverage. From October 15 through
December 7 of each year, you can enroll in a new Medicare Prescription Drug Plan or Medicare
health plan for the following year. You may not enroll in a new plan during other times of the
year unless you meet certain special exceptions, such as you move out of the plan’s service area,
want to join a plan in your area with a 5-star rating, or you qualify for (or lose) Extra Help with
your prescription drug costs.
Who can I call to get more information?
You can call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a week if
you have questions about your disenrollment because you didn’t pay the Part D-IRMAA. TTY
users should call 1-877-486-2048. You can also call < plan name> at <phone number> if you
have questions about your plan’s premium. TTY users should call <TTY number>. We are open
<days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
260
Exhibit 22: Model Notice on Failure to Pay Optional Supplemental Benefit
Premiums - Notice of Reduction in Coverage of Optional Supplemental
Benefit(s) Within the Same Plan (PBP)
Referenced in section(s): 50.3.1
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Dear <Name of Member>:
We recently sent you a letter dated <date> that said your plan premium was overdue. The letter
said that if we didn’t get payment from you, we would have to make some changes in your
membership in <plan name>. Our records show that we did not get payment from you as of
<date>. Therefore, we have reduced your coverage in <plan name>, beginning <effective date>.
<Explain in simple terms lower level of benefits, e.g., routine dental care won’t be covered>
You have the right to ask us to reconsider this change through the grievance procedure written in
your <insert “Member Handbook” or “Evidence of Coverage”, as appropriate>.
Remember, there are limits to when and how often you can change the way you get Medicare:
• From October 15 through December 7, anyone with Medicare can switch plans or return
to Original Medicare. This includes adding or dropping Medicare prescription drug
coverage for the following year.
• From January 1 through March 31, anyone enrolled in a Medicare Advantage Plan
(except an MSA plan) can switch plans or return to Original Medicare (and join a stand-
alone Medicare Prescription Drug Plan).
Generally, you can’t make changes at other times except in certain situations, such as if you
move out of your plan’s service area, want to join a plan in your area with a 5-star rating, or
qualify for (or lose) Extra Help paying for prescription drug costs.
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you think we have made a mistake, or if you have any questions, please call us at <phone
number> between <hours and days of operation>. TTY users should call <TTY number>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
261
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
262
Exhibit 22a: Model Notice on Favorable Good Cause Determination for
Disenrollment Due to Nonpayment of Part D-IRMAA – Notification of Plan
Premium Amount Due for Reinstatement
Referenced in section: 60.3.4
(Rev. 2, Issued: August 12, 2020; Effective/Implementation: 01-01-2021)
Dear <Name of Member>:
Medicare has notified us that you received a favorable decision on your request for reinstatement
into <plan name>. Our records show that we haven’t gotten payment for your plan premium as
of <premium due date>. In order for your coverage to be reinstated, we must receive payment in
the amount of <enter amount owed> no later than <date 3 months from the effective date of
disenrollment>.
This amount is due in addition to the amounts you owe <Medicare or RRB> for your Part D-
IRMAA. You do not pay us your owed Part D-IRMAA amounts. <Medicare or RRB> will send
you a letter regarding the amount you owe and how you can pay. You must pay <Medicare or
RRB> this amount by <date 3 months from the effective date of disenrollment> to be reinstated.
[MA organizations that include a payment coupon with the letter, insert the following sentences:
You can mail your payment to us using the enclosed coupon. Be sure to make full payment of
your owed amount and include your member number on the check.]
[MA organizations that do not include a payment coupon with the letter, insert the following
sentences: You can mail your payment to us at the following address: <billing address>. Be sure
to make full payment of your owed amount and include your name and [insert one: member
number/billing number/ID number] on the check.]
If we don’t get payment by <date 3 months from the effective date of disenrollment>, you will
remain disenrolled from <plan name>. You will be covered by Original Medicare instead of
<plan name>.
When can I make changes to how I get my Medicare coverage?
Medicare limits when you can make changes to your coverage. From October 15 through
December 7 each year, you can enroll in a new Medicare Prescription Drug Plan or Medicare
health plan for the following year. You may not enroll in a new plan during other times of the
year unless you meet certain special exceptions, such as you move out of the plan’s service area,
want to join a plan in your area with a 5-star rating, or you qualify for (or lose) Extra Help with
your prescription drug costs.
[MA-PD plans insert: Please remember, if you don’t have other creditable coverage
(prescription drug coverage that is expected to pay on average as much as Medicare), you may
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
263
have to pay a Part D late enrollment penalty if you enroll in Medicare prescription drug coverage
in the future.]
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a Part D late enrollment penalty. Many people qualify for
these savings and don’t even know it. For more information about this Extra Help, contact your
local Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-
800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.
For more information:
If you have any questions regarding the plan premium amount you owe and how you can pay,
please call <plan name> at <toll-free number> <days and hours of operation>. TTY users should
call <toll-free TTY number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
264
Exhibit 22b: Model Notice on Favorable Good Cause Determination for
Disenrollment Due to Nonpayment of Plan Premiums – Notification of Plan
Premium Amount Due for Reinstatement
Referenced in section: 60.3.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Beneficiary Name>:
We reviewed your request to get your coverage back, and your request has been approved. Our
records show that we haven’t gotten payment for your plan premium as of <premium due date>.
In order for your coverage to be reinstated, we must receive payment in the amount of <enter
amount owed> no later than <date 3 months from the effective date of disenrollment>.
[MA organizations that include a payment coupon with the letter, insert the following sentences:
You can mail your payment to us using the enclosed coupon. Be sure to make full payment of
your owed amount and include your member number on the check.]
[MA organizations that do not include a payment coupon with the letter, insert the following
sentences: You can mail your payment to us at the following address: <billing address>. Be sure
to make full payment of your owed amount and include your name and [insert one: member
number/billing number/ID number] on the check.]
If we don’t get payment by <date 3 months from the effective date of disenrollment>, you will
remain disenrolled from <plan name>. You will be covered by Original Medicare instead of
<plan name>.
When can I make changes to how I get my Medicare coverage?
Medicare limits when you can make changes to your coverage. From October 15 through
December 7 each year, you can enroll in a new Medicare Prescription Drug Plan or Medicare
health plan for the following year. You may not enroll in a new plan during other times of the
year unless you meet certain special exceptions, such as you move out of the plan’s service area,
want to join a plan in your area with a 5-star rating, or you qualify for (or lose) Extra Help with
your prescription drug costs.
[MA-PD plans insert: Please remember, if you don’t have other creditable coverage (prescription
drug coverage that is expected to pay on average as much as Medicare), you may have to pay a
Part D late enrollment penalty if you enroll in Medicare prescription drug coverage in the future.]
[Dual-eligible SNPs may omit the following paragraph:
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a Part D late enrollment penalty. Many people qualify for
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
265
these savings and don’t even know it. For more information about this Extra Help, contact your
local Social Security office, or call Social Security at 1-800-772-1213.
TTY users should call 1-800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.]
For more information:
If you have any questions regarding the plan premium amount you owe and how you can pay,
please call us at <phone number> between <hours and days of operation>. TTY users should
call <TTY number>.
For questions about making changes to the way you get Medicare, call 1‐ 800‐MEDICARE (1‐
800‐633‐4227). TTY users should call 1‐877‐486‐2048.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
266
Exhibit 22c: Model Notice on Unfavorable Good Cause Determination for
Disenrollment Due to Nonpayment of Plan Premiums
Referenced in section: 60.3.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Beneficiary Name>:
We reviewed your request to get your coverage back, and your request has been denied. This is
because [Insert one of the following: your request doesn’t meet the criteria for reinstatement OR
[Insert if unable to make a decision based on the original request and unable to reach
beneficiary: we were not able to reach you to get the information needed to see if your
circumstances meet the criteria for reinstatement.] This means you’ll remain disenrolled from
your plan. This decision is final and can’t be appealed.
You are still responsible for paying the plan premiums you owed at the time you were
disenrolled.
When can I make changes to how I get my Medicare coverage?
Medicare limits when you can make changes to your coverage. From October 15 through
December 7 each year, you can enroll in a new Medicare Prescription Drug Plan or Medicare
health plan for the following year. You may not enroll in a new plan during other times of the
year unless you meet certain special exceptions, such as you move out of the plan’s service area,
want to join a plan in your area with a 5-star rating, or you qualify for (or lose) Extra Help with
your prescription drug costs.
[MA-PD plans insert: Please remember, if you don’t have other creditable coverage (prescription
drug coverage that is expected to pay on average as much as Medicare), you may have to pay a
Part D late enrollment penalty if you enroll in Medicare prescription drug coverage in the future.]
[Dual-eligible SNPs may omit the following paragraph:
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a Part D late enrollment penalty. Many people qualify for
these savings and don’t even know it. For more information about this Extra Help, contact your
local Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-
800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.]
For more information:
If you have any questions, please call us at <phone number> between <hours and days of
operation>. TTY users should call <TTY number>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
267
For questions about making changes to the way you get Medicare, call 1‐800‐MEDICARE (1‐
800‐633‐4227). TTY users should call 1‐877‐486‐2048.
Thank you.
Exhibit 22d: Model Notice to Close Out Good Cause Reinstatement Request –
Failure to Pay Plan Premiums within 3 Months of Disenrollment
Referenced in section: 60.3.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Date>
<Beneficiary full name>
<Address>
<City, State Zip>
Dear <Beneficiary Name>:
We recently sent you a letter letting you know that we gave you a favorable decision on your
request to get your coverage back.
The letter told you that in order to be reinstated into <plan name>, you had to pay all plan
premiums you owe by <insert date 3 months after disenrollment effective date>. The amount
owed was <$ insert total premium amount owed>. The letter also told you that if we didn’t get
full payment by the deadline, you would stay disenrolled [insert if Part D coverage included in
plan: and you would not have Medicare prescription drug coverage].
Your Payment Wasn’t Received on Time
Because you didn’t pay the full amount you owe by the deadline, you will stay disenrolled
from your Medicare plan. This decision is final and can’t be appealed.
You are still responsible for paying the plan premiums you owed at the time you were
disenrolled.
When can I make changes to how I get my Medicare coverage?
Medicare limits when you can make changes to your coverage. From October 15 through
December 7 each year, you can enroll in a new Medicare Prescription Drug Plan or Medicare
health plan for the following year. You may not enroll in a new plan during other times of the
year unless you meet certain special exceptions, such as you move out of the plan’s service area,
want to join a plan in your area with a 5-star rating, or you qualify for (or lose) Extra Help with
your prescription drug costs.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
268
[MA-PD plans insert: Please remember, if you don’t have other creditable coverage (prescription
drug coverage that is expected to pay on average as much as Medicare), you may have to pay a
Part D late enrollment penalty if you enroll in Medicare prescription drug coverage in the future.]
[Dual-eligible SNPs may omit the following paragraph:
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a Part D late enrollment penalty. Many people qualify for
these savings and don’t even know it. For more information about this Extra Help, contact your
local Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-
800-325-0778. You can also apply for Extra Help online at
www.socialsecurity.gov/prescriptionhelp.]
For more information:
If you think we have made a mistake, or if you have any questions, please call us at <phone
number> between <hours and days of operation>. TTY users should call <TTY number>.
For questions about making changes to the way you get Medicare, call 1‐800‐MEDICARE (1‐
800‐633‐4227). TTY users should call 1‐877‐486‐2048.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
269
Exhibit 22e: Model Notice on Favorable Good Cause Determination for
Disenrollment Due to Nonpayment of Plan Premiums (No Plan Premium
Amount Due for Reinstatement)
Referenced in section: 60.3.4.1
<Member # >
[Insert RxID, RxGroup, RxBin and RxPCN if individual is being reinstated into Part D coverage]
Dear <Beneficiary Name>:
We reviewed your request to get your coverage back, and your request has been approved. Our
records show that we received the plan premium you needed to pay in order for your coverage to
be reinstated.
We have updated our records to show that you are enrolled in <plan name> with no break in
coverage. We will ask Medicare to correct its records to show the same.
You should keep using your <plan name> primary care physician for your health care. (If PCP
not applicable, terms such as “physicians” or “doctors” or “providers” may be used instead of
“primary care physician.”)
If you have any questions about your plan premium and how you can pay, please call us at
<phone number> between <hours and days of operation>. TTY users should call <TTY
number>.
Thank you for your continued membership in <plan name>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
270
Exhibit 23: Model Notices for Closing Enrollment
Referenced in section(s): 30.8.1
Model A: Closing Enrollment for Partial Month(s)
<MA organization> PUBLIC NOTICE
As of <date> <MA organization> will no longer offer continuous open enrollment under its
Medicare Advantage contract with Medicare for <plan name> in <service area>.
Instead, <MA organization> will offer open enrollment for all eligible individuals from the
<insert date> to the <insert date> of each month.
<MA organization> will continue to accept enrollments into <plan name> during an entire month
from people who meet certain special exceptions, such as if someone moves out of the plan’s
service area or qualifies for extra help with prescription drug costs.
Also, <MA organization> will continue to accept enrollments into <plan name> from all eligible
individuals from October 15 through December 7.
Current members of <plan name> aren’t affected by this change. For information regarding this
notice, call <MA organization> at <phone number> between <hours and days of operation>.
TTY users should call<TTY number>.
Thank you.
Model B: Closing Enrollment for Whole Month(s)
<MA organization> PUBLIC NOTICE
As of <date> <MA organization> will no longer offer open enrollment under its Medicare
Advantage contract with Medicare for <plan name> in <service area>.
However, <MA organization> will continue to accept enrollments into <plan name> from
eligible individuals who are in a Special Election Period or an Initial Coverage Election Period.
Also, <MA organization> will continue to accept enrollments into <plan name> from all eligible
individuals during the Annual Election Period from October 15 through December 7.
Current members of <plan name> aren’t affected by this change. For information regarding this
notice, call <MA organization> at <phone number> between <hours and days of operation>.
TTY users should call <TTY number>. Thank you.
Model C: Closing Enrollment for Capacity Reasons
<MA organization> PUBLIC NOTICE
As of <date>, <MA organization> will no longer accept enrollment under its Medicare
Advantage contract with Medicare for <plan name> in <insert service area>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
271
<MA organization> is limiting enrollment in <plan name> so plan members have greater access
to providers and services.
Current members of <plan name> aren’t affected by this change. Also, individuals who are
enrolled in other <MA organization> plans may still be able to enroll in <plan name> when they
become eligible for Medicare.
For information regarding this notice, call <MA organization> at <phone number> between
<hours and days of operation>. TTY users should call <TTY number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
272
Exhibit 24: Model Notice for Medigap Rights Per Special Election Period
Referenced in section(s): 50.1 and 50.2
Dear <Name of Beneficiary>:
This is to confirm that you disenrolled from <plan name> effective <date> and returned to
Original Medicare because of the special circumstances indicated below:
______ You permanently moved.
______ You get help from the Medicaid program.
______ You wanted to use certain Medigap protections while in your trial period.
______ Other circumstances defined as eligible for a Special Election Period.
Please save this letter as proof of your Medigap rights.
[Information about Medigap rights
Since you will be changing to Original Medicare, you might have a special temporary right to
buy a Medigap (Medicare supplement insurance) policy, even if you have health problems. For
example, if you are age 65 or older, and you enrolled in Medicare Part B within the past 6
months or if you move out of the service area, you may have this special right.
Federal law requires the protections described above. Your State may have laws that provide
more Medigap protections. If you have questions about Medigap or Medigap rights in your
State, you should contact your State Health Insurance Program <insert name of SHIP> at <SHIP
phone number>. You can also call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a
day, 7 days a week for more information. TTY users should call 1-877-486-2048.]
If you have any questions, please call us at <phone number>. TTY users should call <TTY
number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
273
Exhibit 25: Acknowledgement of Request to Cancel Enrollment
Referenced in section(s): 60.2.1
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <name of applicant>:
As requested, we have cancelled your request to enroll with <plan name>.
Please be patient. It may take up to 45 days for Medicare to update your records. If you are in
Original Medicare, you may want to tell your doctors that if they need to submit Medicare
claims, there may be a short delay in updating your records.
Important: If you were enrolled in another Medicare Advantage plan or Medicare
prescription drug plan before enrolling with <plan name>, you should be automatically
enrolled back into that plan.
If you don’t receive an enrollment acknowledgement letter from your previous plan within
two (2) weeks of receiving this letter, please contact them to confirm your enrollment. They
may request a copy of this letter for their records.
Please remember that if you don’t have or get Medicare prescription drug coverage or other
creditable prescription drug coverage, you may have to pay a late enrollment penalty if you
enroll in Medicare prescription drug coverage in the future.
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you have any questions, please contact <plan name> at <number>. TTY users should call
<TTY number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
274
Exhibit 25a - Model Acknowledgment of Reinstatement
Dear <member name>:
Please be sure to keep a copy of this letter for your records.
Medicare has enrolled you back in <plan name> with no break in coverage as of <effective
date>.
[If PCP not applicable, omit following sentence. Terms such as “physicians” or “doctors” or
“providers” may be used instead of “primary care physician”: You should keep using your
<plan name> primary care physician for your health care.]
[Insert one of the following sentences depending on plan policy: We will be sending you a new
membership card and other important documents for <plan name>. or You can continue using
the <plan name> membership card that you currently have. or If you no longer have your
membership card, contact us at the number below to get a new card.]
[Insert information regarding plan premiums required to maintain enrollment, or use the following
language: The monthly premium for <plan name> is <monthly premium amount>. You must pay
this premium amount each month to remain enrolled in our plan. For more information regarding our
disenrollment policy for non-payment of plan premiums, please see our policy written in your <insert
“Member Handbook” or “Evidence of Coverage”, as appropriate>.]
Please call <plan name> at <phone number> if you have any questions. TTY users should call
<TTY number>. We are open <days and hours of operation>.
Thank you for your continued membership in <plan name>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
275
Exhibit 25b: Confirmation of Cancellation of Enrollment Due to Notice from
CMS (TRC 015)
Referenced in section(s): 60.2.4
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Date>
Dear <name of applicant>:
Medicare has told us that you have canceled your enrollment in <plan name> effective <insert
date of enrollment that was canceled>. If this information is wrong, and you want to stay a
member of our plan, please contact us.
Please remember that if you don’t have or get Medicare prescription drug coverage or other
creditable prescription drug coverage, you may have to pay a late enrollment penalty if you
enroll in Medicare prescription drug coverage in the future.
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
If you have any questions, please contact <plan name> at <number>. TTY users should call
<TTY number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
276
Exhibit 26: Acknowledgement of Request to Cancel Disenrollment
Referenced in section(s): 60.2.2
Dear <name of member>:
As requested, we have cancelled your disenrollment with <plan name>. [
If PCP not applicable,
omit following sentence. Terms such as “physicians” or “doctors” or “providers” may be used instead of
“primary care physician”:
You should keep using your <plan name> primary care physician for
your health care.] Thank you for your continued membership in <plan name>.
IMPORTANT: If you have also enrolled in another Medicare Advantage plan or Medicare Cost
plan or Medicare Prescription Drug Plan, you may appear on their records as being enrolled. If you
want to stay enrolled in <plan name>, you will need to notify the other Medicare plan that you are
canceling enrollment in their plan before that enrollment takes effect. They may request you write
them a letter for their records.
If you have any questions, please contact <plan name> at <phone number>. TTY users should
call <TTY number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
277
Exhibit 27: MA Model Notice to Inform Full-Benefit Dual Eligible Member
of Auto-Enrollment in MA-PD Plan
Referenced in section: 40.1.5
[Member #]
[RxID]
[RxGroup]
[RxBin]
[RxPCN]
Dear <insert member name>
Our records show that you have Medicare and Medicaid. [
Insert for those with retroactive effective
dates:
To make sure that you don’t lose a day of your drug coverage,] [Insert for those with
prospective effective dates:
To make sure you have prescription drug coverage,] Medicare has
asked us to enroll you in our <MA-PD plan name> that includes Medicare prescription drug
coverage, beginning <effective date>, unless you tell us you don’t want to join our plan.
Starting <effective date>, all of your health care, except emergency or urgently needed care, or
out-of-area dialysis services, must be given or arranged by a <plan name> doctor(s). You will
need to pay our copayments when you get health care. [Optional: This letter is proof of
insurance that you should show during your doctor appointments.] [Optional: This letter is also
proof of your prescription drug coverage. You should show this letter at the pharmacy until you
get your member card from us.]
What are my costs in this plan?
With this Medicare prescription drug coverage, you will pay no more than:
• $0 for your yearly prescription drug plan deductible,
• <insert appropriate LIS copay amount> copayments when you fill a prescription
covered by the plan.
If you believe this is incorrect and you have proof that the extra help amounts should be
different, please contact <plan name> at the phone number provided at the end of this letter.
[Include cost of premium less low-income premium subsidy amount, brief description of benefit,
emergency room, durable medical equipment, inpatient care, annual out of pocket maximum on
coinsurance services, etc. if changes. If no changes, simply state that there will be no changes.]
What do I need to know about getting health care services?
[
MA PPO and PFFS plans do not use the following paragraph: Please remember that, except for
emergency or out-of-area urgent care, or out-of-area dialysis services, if you get health care from
a non-<new plan name> doctor without prior authorization, you will have to pay for the health
care yourself.]
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
278
[MA PPO plans use the following paragraph: Beginning <effective date>, you will get your health
care as provided in your <insert either “Member handbook” or “Evidence of Coverage’’>. You
will need to pay your plan co-payments and co-insurance at the time you get health care services,
as provided in your member materials.]
[
MA PFFS plans use the following paragraph: Beginning <effective date>, you will begin to
receive your healthcare from <new plan name>, which allows you to go to any Medicare-
approved doctor or hospital that is willing to give you care and accept our plan’s terms of
payment. <new plan name>, a Medicare Advantage Private Fee-for-Service plan, works
differently than a Medicare supplement plan as well as other Medicare Advantage plans. Your
doctor or hospital doesn’t have to agree to accept the plan’s terms and conditions, and may
choose not to treat you, except in emergencies. You should verify that your provider(s) will
accept <Plan name> before each visit. Providers can find the plan’s terms and conditions on our
website at <insert link to PFFS terms and conditions>.]
What if Medicaid used to pay for my prescription drugs?
Remember, Medicaid will not pay for most prescription drugs. Federal law will not let Medicaid
continue the drug coverage you currently get. Some state Medicaid programs may cover a few
prescriptions that won’t be covered under Medicare prescription drug coverage. This coverage
alone won’t be at least as good as Medicare prescription drug coverage. To continue to have
prescription drug coverage, you must be enrolled in a Medicare prescription drug plan, like <new
plan name>.
What if I have other prescription drug coverage?
If you now have drug coverage through an employer or union plan, joining a Medicare drug plan
may NOT be right for you. You or your dependents could lose your other health or drug
coverage completely and not get it back if you join <plan name>. Read all the materials you
get from your insurer or plan provider to learn how joining a Medicare drug plan may affect you
or your family current coverage. You may not need to join a Medicare drug plan. Examples of
other types of prescription drug coverage include coverage from an employer or union,
TRICARE, the Department of Veterans Affairs, or a Medigap (Medicare Supplement Insurance)
policy.
What if I want to join another plan?
You aren’t required to be in our Medicare prescription drug plan and can stay in <name of MA-
only plan>. You can also decide to join a different Medicare prescription drug plan. Call 1-800-
MEDICARE anytime, 24 hours a day, 7 days a week for help in learning how. TTY users should
call 1-877-486-2048.
What if I don’t want Medicare prescription drug coverage?
If you don’t want Medicare prescription drug coverage at all, call <plan name> at <phone
number> within 10 days of the date on this letter. TTY users should call <TTY number>. We
are open <insert days/hours of operation and, if different, TTY hours of operation>. You will
need to tell us you don’t want Medicare prescription drug coverage.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
279
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
280
Exhibit 27a: MA-PFFS Model Notice to Inform Full-Benefit Dual Eligible
Member of Auto-Enrollment in PDP
Referenced in section: 40.1.5
[Member #]
[RxID]
[RxGroup]
[RxBin]
[RxPCN]
Dear <insert member name>
Our records show that you have Medicare and Medicaid. To make sure you have prescription
drug coverage. Medicare has asked us to enroll you in our <PDP name> that provides Medicare
prescription drug coverage, beginning <effective date>, unless you tell us you don’t want to join
our plan.
How does this plan work?
Starting <effective date>, all of your health care will continue to be covered under your <current
MA-only plan name> and your prescription drug coverage will be provided through our <PDP
name>. Your medical benefits and member copayments under <current MA-only plan> won’t
change. [Optional: You will be sent a membership card along with more detailed information
about your prescription drug coverage in the next several days. Until you get your prescription
drug card, you can use this letter to buy your prescriptions.]
With the addition of this Medicare prescription drug coverage, you will pay no more than:
• $0 for your yearly prescription drug plan deductible,
• <insert appropriate LIS copay amount> copayments when you fill a prescription
covered by the plan.
If you believe this is incorrect and you have proof that the extra help amounts should be
different, please contact <plan name> at the phone number provided at the end of this letter.
There will be no changes to your premium, medical benefits or member copayments under the
<current MA-only plan name>.
What if Medicaid used to pay for my prescription drugs?
Remember, Medicaid won’t pay for most prescription drugs. Federal law will not let Medicaid
continue the drug coverage you currently get. Some state Medicaid programs may cover a few
prescriptions that won’t be covered under Medicare prescription drug coverage. This coverage
alone won’t be at least as good as Medicare prescription drug coverage. To continue to have
prescription drug coverage, you must be enrolled in a Medicare prescription drug plan, like
<PDP name>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
281
What if I have other prescription drug coverage?
If you now have or are eligible for other types of prescription drug coverage, you may not need
to join a Medicare drug plan. You or your dependents could lose your other health or drug
coverage completely and not get it back if you join <plan name>. Read all the materials you
get from your insurer or plan provider to learn how joining a Medicare drug plan may affect you
or your family’s current coverage. Examples of other types of prescription drug coverage include
coverage from an employer or union, TRICARE, the Department of Veterans Affairs, or a
Medigap (Medicare Supplement Insurance) policy. Please call your insurer or benefits
administrator if you have any questions.
What if I paid for drugs before my new coverage starts?
If you filled any covered prescriptions before <effective date>, you might be able to get back
part of what the prescriptions cost if you were eligible for Medicare and Medicaid but not
enrolled in a Medicare drug plan. Call Medicare’s Limited Income NET program at 1-800-783-
1307. TTY users should call 711. You can also visit www.humana.com/pharmacists.
What if I want to join another plan, or I don’t want Medicare prescription drug coverage?
You aren’t required to be in our Medicare drug plan and can stay in <name of MA-only plan>.
You can also decide to join a different Medicare drug plan. Call 1-800-MEDICARE anytime, 24
hours a day, 7 days a week for help in learning how. TTY users should call 1-877-486-2048.
If you don’t want Medicare prescription drug coverage at all, call <plan name> at <phone
number> within 10 days of the date on this letter. TTY users should call <TTY number>. We are
open <insert days/hours of operation and, if different, TTY hours of operation>. You will need
to tell us you don’t want Medicare prescription drug coverage.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
282
Exhibit 28: MA Model Notice to Inform Member of Facilitated Enrollment
into MA-PD plan
Referenced in section: 40.1.5
[Member #]
[RxID]
[RxGroup]
[RxBin]
[RxPCN]
Dear <insert member name>
Our records show that you qualify for extra help with your prescription drug costs. Medicare has
asked us to enroll you in our <MA-PD plan name> that offers Medicare prescription drug
coverage beginning <effective date>, unless you tell us you don’t want to join our plan.
[
MA PPO and PFFS plans do not use the following paragraph: Starting <effective date>, all of your
health care, except emergency or urgently needed care, or out-of-area dialysis services, must be
given or arranged by a <MA-PD plan name> doctor(s). You will need to pay our copayments
when you get health care.]
[Optional: This letter is proof of insurance that you should show during your doctor’s
appointments until you get your member card from us.] [Optional: This letter is also proof of
your prescription drug coverage. You should show this letter at the pharmacy until you get your
member card from us.]
What are my costs in this plan?
With Medicare prescription drug coverage, you will pay no more than:
• <insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
• <insert appropriate LIS copay amount> copayments when you fill a prescription
covered by our plan.
[Include cost of premium less amount of premium assistance for which the member is eligible,
brief description of benefit, emergency room, durable medical equipment, inpatient care, annual
out of pocket maximum on coinsurance services, etc. if changes. If no changes, simply state that
there will be no changes.]
If you believe this is incorrect and you have proof that the extra help amounts should be
different, please contact <plan name> at the phone number provided at the end of this letter.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
283
What do I need to know about getting health care services?
[
MA PPO and PFFS plans do not use the following paragraph: Please remember that, except for
emergency or out-of-area urgent care, or out-of-area dialysis services, if you get health care from
a non-<MA-PD plan name> doctor without prior authorization, you will have to pay for the
health care yourself.]
[
MA PPO plans use the following paragraph: Beginning <effective date>, you will get your health
care as provided in your <insert either “Member handbook” or ‘Evidence of Coverage’>. You
will need to pay your plan co-payments and co-insurance at the time you get health care services,
as provided in your member materials.]
[
MA PFFS plans use the following paragraph: Beginning <effective date>, you will begin to
receive your healthcare from <new plan name>, which allows you to go to any Medicare-
approved doctor or hospital that is willing to give you care and accept our plan’s terms of
payment. <MA-PFFS plan name>, a Medicare Advantage Private Fee-for-Service Plan, works
differently than Original Medicare. Your doctor or hospital isn’t required to agree to accept the
plan’s terms and conditions, and may choose not to treat you, except in emergencies. You should
verify that your provider(s) will accept <Plan name> before each visit. Providers can find the
plan’s terms and conditions on our website at <insert link to PFFS terms and conditions>.
What if I have other prescription drug coverage?
If you now have or are eligible for other types of prescription drug coverage, you may not need
to join a Medicare drug plan. You or your dependents could lose your other health or drug
coverage completely and not get it back if you join <plan name>. Read all the materials you
get from your insurer or plan provider to learn how joining a Medicare drug plan may affect you
or your family’s current coverage. Examples of other types of prescription drug coverage include
coverage from an employer or union, TRICARE, the Department of Veterans Affairs, or a
Medigap (Medicare Supplement Insurance) policy. Please call your insurer or benefits
administrator if you have any questions.
What if I want to join another plan, or I don’t want Medicare prescription drug coverage?
You aren’t required to be in our Medicare drug plan and can stay in <name of MA-only plan>.
You can also decide to join a different Medicare drug plan. Call 1-800-MEDICARE anytime, 24
hours a day, 7 days a week for help in learning how. TTY users should call 1-877-486-2048.
If you don’t want Medicare prescription drug coverage at all, call <plan name> at <phone
number> before <effective date>. TTY users should call <TTY number>. We are open <insert
days/hours of operation and, if different, TTY hours of operation>. You will need to tell us you
don’t want Medicare prescription drug coverage.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
284
Exhibit 28a: MA Model Notice to Inform Member of Facilitated Enrollment
into PDP
Referenced in section: 40.1.5
[Member #]
[RxID]
[RxGroup]
[RxBin]
[RxPCN]
Dear <insert member name>
Our records show that you qualify for extra help with your prescription drug costs . To make
sure you have prescription drug coverage, Medicare has asked us to enroll you in our <name of
PDP> that provides Medicare prescription drug coverage, beginning <effective date>, unless you
tell us you don’t want to join our plan.
Starting <effective date>, all of your health care, will continue to be covered under your <current
MA-only plan name>, and your pharmacy coverage will be provided through our <PDP name>.
Your medical benefits and member copayments under <current MA-only plan name> won’t
change. [Optional: You will be sent a pharmacy card along with more detailed information
about your pharmacy coverage in the next several days. Until you receive your pharmacy card,
you can use this letter to purchase your prescriptions. This letter includes the information needed
to obtain your prescriptions.]
With the addition of this Medicare prescription drug coverage, you will pay no more than:
• <insert appropriate LIS deductible amount> for your yearly prescription drug plan
deductible,
• <insert appropriate LIS copay amount> copayments when you fill a prescription
covered by our plan.
If you believe this is incorrect and you have proof that the extra help amounts should be
different, please contact <plan name> at the phone number provided at the end of this letter.
There will be no changes to your premium, medical benefits or member copayments under
<current MA-only plan name>.
What if I have other prescription drug coverage?
If you now have or are eligible for other types of prescription drug coverage, you may not need
to join a Medicare drug plan. You or your dependents could lose your other health or drug
coverage completely and not get it back if you join <plan name>. Read all the materials you
get from your insurer or plan provider to learn how joining a Medicare drug plan may affect you
or your family’s current coverage. Examples of other types of prescription drug coverage include
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
285
coverage from an employer or union, TRICARE, the Department of Veterans Affairs, or a
Medigap (Medicare Supplement Insurance) policy. Please call your insurer or benefits
administrator if you have any questions.
What if I paid for drugs before my new coverage starts?
If you filled any covered prescriptions before <effective date>, you might be able to get back
part of what the prescriptions cost if you were eligible for Medicare and Medicaid but not
enrolled in a Medicare drug plan. Call Medicare’s Limited Income NET program at 1-800-783-
1307. TTY users should call 711. You can also visit www.humana.com/pharmacists.
What if I want to join another plan, or I don’t want Medicare prescription drug coverage?
You aren’t required to be in our Medicare drug plan and can stay in <name of MA-only plan>.
You can also decide to join a different Medicare drug plan. Call 1-800-MEDICARE anytime, 24
hours a day, 7 days a week for help in learning how. TTY users should call 1-877-486-2048.
If you don’t want Medicare prescription drug coverage at all, call <plan name> at <phone
number> before <effective date>. TTY users should call <TTY number>. We are open <insert
days/hours of operation and, if different, TTY hours of operation>. You will need to tell us you
don’t want Medicare prescription drug coverage.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
286
Exhibit 29: Acknowledgement of Request to Opt Out of Auto/Facilitated
Enrollment
Referenced in section(s): 40.1.5
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <name of member>:
As requested, we have processed your request to decline (opt out of) Medicare prescription drug
coverage. You will continue to be a member of <plan name> that doesn’t offer Medicare
prescription drug coverage.
If you have Medicaid drug coverage, it won’t pay for your prescription drugs.
Remember, even if you don’t use a lot of prescription drugs now, you still should consider
joining a Medicare prescription drug plan. As we age, most people need prescription drugs to
stay healthy.
From October 15 through December 7, you can join, switch or drop a Medicare health or drug
plan for the following year. You can join, switch or leave a plan at other times while you qualify
for (or lose) Extra Help paying for prescription drug costs.
If you change your mind and would like to join, you can call <plan name> at <phone number>.
TTY users should call <TTY number>. We are open <insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
287
Exhibit 30: Model Notice for Enrollment Status Update
(For use with Transaction Reply Codes (TRC) from User Interface (UI) changes)
Referenced in section: 60.7
[Member #]
Dear <Name of Member>:
Your enrollment in <Name of Plan> has been updated.
[Insert one or more of the following, including sufficient detail to describe the specific
enrollment change:
• You have been enrolled in <name of plan>. Your coverage will start on <insert start date>
and will end on <insert end date>. [Insert information about premiums, if applicable, and
how to access coverage, etc.].
• Your enrollment in <name of plan/old PBP> has been changed to <name of plan/new
PBP>. Your coverage in <name of plan/new PBP> will start on <date>. [Insert
information on premium differences (if any), cost sharing information, and other
details the individual will need to ensure past and future coverage is clear]
• Your enrollment in <Name of Plan> has been changed to start on an earlier date. Your
coverage will start <date>. [Include information about premiums, coverage, and how to get
refunded for prescriptions purchased in the period of retroactive coverage.]
• Your enrollment in <Name of Plan> has been changed to start on a later date. Your
coverage with <Name of Plan> will start on < date>. [Insert information about
refunding premium, where applicable, and impact to paid claims]
• Your enrollment in <Name of Plan> [ended, will end] on < date>. This means you [don’t,
won’t] have coverage from <Name of Plan> after <date>. [Insert appropriate descriptive
information, such as premium owed if the date has moved forward, or premium refunds if the
date has moved back, and impact on paid claims or how to submit claims, as applicable]
• Your enrollment in <Name of Plan> has been cancelled. This means that you don’t
have coverage from <Name of Plan>. [Insert information about refund of premium, if
applicable, and impact to any paid claims]
[Insert other pertinent and appropriate information regarding the enrollment status
update and the resulting impact to the beneficiary as necessary]
[Insert if enrolling in a PFFS plan: <Name of Plan>, a Medicare Advantage Private Fee-for-
Service plan, works differently than a Medicare supplement plan. Your doctor or hospital isn’t
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
288
required to agree to accept the plan’s terms and conditions, and may choose not to treat you,
except in emergencies. You should verify that your provider(s) will accept <Plan name> before
each visit. Providers can find the plan’s terms and conditions on our website at <insert link to
PFFS terms and conditions>.]
[Dual-eligible SNPs may omit the following paragraph:]
People with limited incomes may qualify for extra help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this extra help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp.
Call <toll-free number> <days and hours of operation> to get more information. TTY users
should call <toll-free TTY number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
289
Exhibit 31: Model Employer/Union Sponsored MA Plan Group Enrollment
Mechanism Notice
Dear <name>
<Name of Employer/Union> is enrolling you in <plan name > as your retiree health benefit plan
beginning <effective date>, unless you tell us by <insert date no less than 21 days from date of
notice> that you don’t want to join our plan. <Plan name> is a Medicare Advantage plan. This
enrollment will automatically cancel your enrollment in a different Medicare Advantage plan or
a Medicare Prescription Drug (Part D) plan. Please call us if you think you might be enrolled in a
different Medicare Advantage plan or a Medicare Prescription Drug plan.
What do I need to know as a member of <plan name>?
This mailing includes important information about this plan and the coverage it offers, including
a summary of benefits document. Please review this information carefully. If you want to be
enrolled in this Medicare health plan, you don’t have to do anything, and your enrollment will
automatically begin on <effective date>.
Once you are a member of <Plan Name>, you have the right to appeal plan decisions about
payment or services if you disagree. Read the [insert either Member Handbook or Evidence of
Coverage document] from <plan name> when you get it to know which rules you must follow to
get coverage with this Medicare Advantage Plan. Enrollment in this plan is generally for the
entire year.
[
MA PFFS do not include the following paragraph: Beginning on the date <plan name> coverage
begins, you must get all of your health care from <plan name>, with the exception of emergency
or urgently needed services or out-of-area dialysis services. Services authorized by <plan name>
and other services contained in my <plan name> Evidence of Coverage document (also known
as a member contract or subscriber agreement) will be covered. Without authorization,
NEITHER MEDICARE NOR <Plan Name> WILL PAY FOR SERVICES.]
You will need to keep Medicare Parts A and B as <Plan Name> is a Medicare Advantage Plan.
You can be in only one Medicare Advantage Plan at a time. It is your responsibility to inform
<Plan Name> of any prescription drug coverage that you have or may get in the future.
By joining this Medicare health plan, you acknowledge that the Medicare health plan will release
your information to Medicare and other plans as is necessary for treatment, payment and health
care operations. You also acknowledge that <plan name> will release your information [
MA-PD
plans insert:
including your prescription drug purchase history] to Medicare, who may release it
for research and other purposes which follow all applicable Federal statutes and regulations.
What happens if I don’t join <plan name>?
You aren’t required to be enrolled in this plan. <insert information about other group sponsored
plan options, if there are any>. You can also decide to join a different Medicare plan. Call 1-
800-MEDICARE for help in learning how. However, if you decide not to be enrolled <insert
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
290
consequences for opting out of group plan, like that you cannot return, or that other benefits are
impacted>. To request not to be enrolled by this process <insert clear instruction for opting out
including telephone numbers and times of operation where those numbers will be answered>.
What if I want to leave <Plan Name>?
You may leave this plan only at certain times of the year, or under certain special circumstances,
by sending a request to <Plan Name>.
<Plan Name> serves a specific service area. If you move out of the area that <Plan Name>
serves, you need to notify the plan so you can disenroll and find a new plan in your new area.
[
MA-only plans insert the following, unless the employer/union provides other creditable coverage:
Remember that if you leave this plan and don’t have creditable prescription drug coverage (as
good as Medicare’s prescription drug coverage), you may have to pay a late enrollment penalty if
you enroll in Medicare prescription drug coverage in the future.]
Thank you.
Attachment
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
291
Exhibit 32: Model Notice for Loss of Special Needs Status
Referenced in section: 50.2.5
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Member>:
<Insert plan or organization name> must disenroll a member from <Insert plan name> if a
member doesn’t <describe special needs status> and doesn’t reestablish <describe required
special needs status> prior to the expiration <insert length of period of deemed continued
eligibility >.
Why am I receiving this notice?
Our records indicate that you no longer <describe special needs status that individual has lost>.
To be a member of <plan name>, you must <describe required special needs status>.
How long will I continue to receive coverage?
<Plan name> will continue to cover your Medicare benefits until <insert end date for period of
deemed continued eligibility>. You have <insert length of period of deemed continued
eligibility> to re-qualify for our plan.
When will coverage end?
If, at the end of <insert length of period of deemed continued eligibility>, you haven’t <describe
special needs criteria that must be met> and you haven’t enrolled in a different plan, we will
disenroll you and you will be covered by Original Medicare beginning <insert end date for
period of deemed continued eligibility>.
What do I do if my coverage ends?
When coverage from <plan name> ends, your Medicare prescription drug coverage ends too. To
have new health care coverage and prescription drug coverage after <date> or to buy a Medigap
policy while you still have a guaranteed right to buy one, you need to take action. For example, if
you are returning to Original Medicare coverage, to get Medicare prescription drug coverage you
must join a Medicare prescription drug plan. Please remember, if you disenroll from <plan
name> and don’t have or get other creditable prescription drug coverage (as good as Medicare
prescription drug coverage), you may have to pay a late enrollment penalty if you enroll in
Medicare prescription drug coverage in the future.
When can I join another plan?
Because you are no longer eligible for our plan, Medicare will give you a special one-time
opportunity to change to a different Medicare Advantage Plan or Medicare Prescription Drug
Plan. This opportunity begins now and ends when you enroll in a different plan or on <insert
date three months after the expiration of the period of deemed continued eligibility>, whichever
is earlier. If you don’t take any action, <plan name> will continue to cover your Medicare
benefits until <insert end date for period of deemed continued eligibility>.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
292
Once you use the special one-time opportunity to change plans, there are limits to when and how
often you can change the way you get Medicare:
• From October 15 through December 7, anyone with Medicare can switch plans or return
to Original Medicare. This includes adding or dropping Medicare prescription drug
coverage for the following year.
• From January 1 through March 31, anyone enrolled in a Medicare Advantage Plan
(except an MSA plan) can switch plans or return to Original Medicare (and join a stand-
alone Medicare Prescription Drug Plan).
Generally, you can’t make changes at other times except in certain situations, such as if you
move out of your plan’s service area, want to join a plan in your area with a 5-star rating, or
qualify for (or lose) Extra Help paying for prescription drug costs.
[Dual-eligible SNPs may omit the following paragraph:]
What is extra help?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
What if I don’t agree with this decision or if I have questions?
If this information is wrong and you continue to be eligible for <plan name> or if you believe
you have already re-qualified for our plan and you want to stay a member of our plan, please
contact us immediately at <phone number>. TTY users should call <TTY number>. We are open
<insert days and hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
293
Exhibit 33: Model Notice for Loss of SNP Status - Notification of Involuntary
Disenrollment
Referenced in section(s): 50.2.5
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
Dear <Name of Member>:
On <date> we sent you a letter that said you no longer <describe special needs status that
individual has lost>. The letter said that if you didn’t <describe special needs criteria that must
be met>, we would disenroll you and you would be covered by Original Medicare beginning
<insert end date for period of deemed continued eligibility>.
Why am I receiving this notice?
According to our records, you remain ineligible for <plan name>. Therefore, we asked Medicare to
disenroll you from <plan name> beginning <date>.
What if I don’t agree with this decision?
You have the right to ask us to reconsider this decision through the grievance process described
in your [insert “Member Handbook” or “Evidence of Coverage”, as appropriate].
What happens next?
Due to your disenrollment from <plan name>, you will be covered by Original Medicare,
beginning <effective date> unless you take action.
When can I join another plan?
As described in our earlier letter, you have a special one-time opportunity to enroll in a different
Medicare Advantage Plan or Medicare Prescription Drug Plan. This opportunity will end when
you enroll in a different plan or on <insert date three months after the expiration of the period of
deemed continued eligibility>, whichever is earlier.
Once you use the special one-time opportunity to change plans, there are limits to when and how
often you can change the way you get Medicare:
• From October 15 through December 7, anyone with Medicare can switch plans or return
to Original Medicare. This includes adding or dropping Medicare prescription drug
coverage for the following year.
• From January 1 through March 31, anyone enrolled in a Medicare Advantage Plan
(except an MSA plan) can switch plans or return to Original Medicare (and join a stand-
alone Medicare Prescription Drug Plan).
Generally, you can’t make changes at other times except in certain situations, such as if you
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
294
move out of your plan’s service area, want to join a plan in your area with a 5-star rating, or
qualify for (or lose) Extra Help paying for prescription drug costs.
[Dual-eligible SNPs may omit the following two paragraphs:]
What is extra help?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
Why is it important to find new drug coverage?
Please remember, if you don’t enroll in another Medicare Advantage Plan with prescription drug
coverage or a Medicare Prescription Drug Plan or other creditable prescription drug coverage,
you may have to pay a late enrollment penalty if you enroll in Medicare prescription drug
coverage in the future.
Information About Medigap Rights
You might have a special temporary right to buy a Medigap policy, also known as Medicare
supplement insurance, even if you have health problems. For example, if you are age 65 or older
and you enrolled in Medicare Part B within the past 6 months or if you move out of the service
area, you may have this special right.
Federal law requires the protections described above. Your State may have laws that provide
more Medigap protections. If you have questions about Medigap or Medigap rights in your
State, you should contact your State Health Insurance Program <insert name of SHIP> at <SHIP
phone number>. You can also call 1-800-MEDICARE (1-800-633-4227) 24 hours a day, 7 days
a week for more information. TTY users should call 1-877-486-2048.
If you have any questions, please call us at <phone number> between <hours and days of
operation>. TTY users should call <TTY number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
295
Exhibit 34: MA Model Notice to Research Potential Out of Area Status
Referenced in section: 50.2.1.3
<Date>
<Member ID>
Dear <member name>:
We have recently received information that your address may have changed and that you may
not live in the service area of <plan name>. If you don’t contact us to verify your address,
you will be disenrolled from <plan name> effective <disenrollment effective date>.
It is important that you contact us to verify your permanent address. You may use this form and
return it to us in the enclosed envelope or you may call our <Customer Service, Member
Services> department at <phone number> <days and hours of operation>. TTY users should call
<TTY number>.
Please note that your permanent address must be inside our service area in order for you to be a
member of <plan name>. You may request that we send mail to you at another address outside
of our service area. You may also temporarily reside for up to [insert either “six” or the length
of the plan’s visitor traveler program (if any)] months outside our service area and remain a
member of <plan name>. But if you permanently move outside our service area or if you
temporarily live outside our service area for more than six months in a row, we must disenroll
you from <plan name>. You will have an opportunity to enroll in a plan that serves the area
where you now live.
Your Permanent Address
Please tell us the permanent address where you live. Do not use a post office box.
Street: _____________________________________________________________
City, State, ZIP: _____________________________________________________
County: ___________________________________________________________
Current Phone Number:_____________________________ __________________
Your Temporary Address
If you are currently living somewhere other than your permanent address, please provide the
address. Do not use a post office box. (You may skip this section if you are living at your
permanent address.)
Street:________________________________________________________________
City, State, ZIP:________________________________________________________
County:_______________________________________________________________
Current Phone Number:___________________________________________________
When did you begin living at this address?___________________________________

<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
296
When do you expect to return to your permanent address?_______________________
Your Mailing Address
If the address that you want us to use to send information to you is different than your permanent
address, please provide it below. (You may skip this section if your mailing address is the same
as your permanent address that you provided.)
Street or P.O. Box: ______________________________________________________
City, State, ZIP: _________________________________________________________
County: ________________________________________________________________
If you have moved and have not notified Social Security of your new address, you may call them
at 1-800-772-1213 (TTY: 1-800-325-0778) Monday-Friday, 7am to 7pm.
If you have any questions or need help, please call us at <customer service phone number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
297
Exhibit 35: MA Model Notice for Disenrollment Due to Out of Area Status
(No Response to Request for Address Verification)
Referenced in section: 50.2.1.3
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Date>
<Member ID>
Dear <member name>:
On <date of notice requesting address verification> we asked you to contact us so that we could
determine whether you had moved out of the [Optional: Parent Organization Name] <plan
name> service area. As we explained in our earlier letter, in order to be a member of our plan,
you must live in the <plan name> service area, although you may be out of the service area
temporarily for up to [insert either “six” or the length of the plan’s visitor traveler program (if
any)] consecutive months.
Our records show that you have not responded to our earlier letter. Therefore, you will be
disenrolled from <plan name> effective <disenrollment effective date>.
Beginning <effective date>, <plan name> won’t cover any health care you get. Beginning
<effective date>, you can see any doctor through Original Medicare, unless you have enrolled in
another Medicare Advantage plan.
[MA-PD plans add the following: When your coverage from <plan name> ends, your Medicare
prescription drug coverage ends too. Beginning <effective date>, <plan name> also won’t cover
any prescriptions you get. You won’t have any prescription drug coverage beginning <effective
date> unless you have enrolled in another prescription drug plan.]
What if I disagree with this decision?
You have the right to ask us to reconsider this decision. You can ask us to reconsider by filing a
grievance with us. Look in your <EOC document name> for information about how to file a
grievance.
Can I enroll in a new plan?
You may have up to two months to join a new Medicare Advantage Plan or a Medicare
prescription drug plan that serves the area where you now live. You may call 1-800-
MEDICARE (1-800-633-4227) for information about plans that may serve your area.
What if I don’t enroll in a new plan right now?
If you don’t enroll in a Medicare Advantage Plan during this special two-month period, you may
have to wait to enroll in a new plan. You can join or change health plans only at certain times
during the year. From October 15 – December 7, you can join, switch or drop a Medicare health
or drug plan for the following year. Generally you can’t make changes at other times except in
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
298
certain situations, such as you want to join a plan in your area with a 5-star rating, or you qualify
for (or lose) Extra Help paying for prescription drug costs.
[MA-PD plans insert: What happens if I don’t enroll in another Medicare Prescription
Drug Plan?
Please remember, if you don’t enroll in another Medicare Prescription Drug Plan (or a Medicare
Advantage Plan with prescription drug coverage) or you don’t have or obtain other coverage that
is at least as good as Medicare drug coverage (also referred to as “creditable coverage”), you
may have to pay a late enrollment penalty if you enroll in Medicare prescription drug coverage in
the future.]
What if my premium was being deducted from my Social Security benefit check?
If your plan premium is being deducted from your Social Security benefit, please allow up to 3
months for us to process a refund. If you haven’t received a refund from Social Security within
3 months of this letter, you should contact 1-800-MEDICARE anytime, 24 hours a day, 7 days a
week. TTY users should call 1-877-486-2048.
[Dual-eligible SNPs may omit the following paragraph:]
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
What should I do if I’ve moved?
If you have moved and haven’t notified Social Security of your new address, you may call them
at 1-800-772-1213 (TTY: 1-800-325-0778) Monday-Friday, 7am to 7pm.
What should I do if I have more questions?
If you have any questions or need help, please call our <Customer Service, Member Services>
department at <phone number> <days and hours of operation>. TTY users should call <TTY
number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
299
Exhibit 36: MA Model Notice for Disenrollment Due to Confirmation of Out
of Area Status (Upon New Address Verification from Member)
Referenced in section: 50.2.1.3
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Date>
<Member ID>
Dear <member name>:
Thank you for informing us of your recent change of permanent address. Your permanent
address is now outside the <plan name> service area. In order to be a member of our plan, you
must live in the <plan name> service area, although you may be out of the service area
temporarily for up to [insert either “six” or the length of the plan’s visitor traveler program (if
any)] consecutive months. Therefore, you will be disenrolled from <plan name> effective
<disenrollment effective date>.
Beginning <effective date>, <plan name> won’t cover any health care you receive. Beginning
<effective date>, you can see any doctor through Original Medicare, unless you have enrolled in
another Medicare Advantage plan.
[MA-PD plans add the following: When your coverage from <plan name> ends, your Medicare
prescription drug coverage ends too. Beginning <effective date>, <plan name> also won’t cover
any prescriptions you get. To have new prescription drug coverage after <date>, you need to
join a new Medicare Advantage plan with prescription drug coverage or join a Medicare
prescription drug plan.]
What if I disagree with this decision?
You have the right to ask us to reconsider this decision. You can ask us to reconsider by filing a
grievance with us. Look in your <EOC document name> for information about how to file a
grievance.
Can I enroll in a new plan?
You may have up to two months to join a new Medicare Advantage Plan or Medicare
prescription drug plan that serves the area where you now live. You may call 1-800-
MEDICARE (1-800-633-4227) for information about plans that may serve your area.
What if I don’t enroll in a new plan right now?
If you don’t enroll in a Medicare Advantage Plan during this special two-month period, you may
have to wait to enroll in a new plan. You can join or change health plans only at certain times
during the year. From October 15 – December 7, you can join, switch or drop a Medicare health
or drug plan for the following year. Generally you can’t make changes at other times except in
certain situations, such as you want to join a plan in your area with a 5-star rating, or you qualify
for (or lose) Extra Help paying for prescription drug costs.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
300
[MA-PD plans insert: What happens if I don’t enroll in another Medicare Prescription
Drug Plan?
Please remember, if you don’t enroll in another Medicare Prescription Drug Plan (or a Medicare
Advantage Plan with prescription drug coverage) or you don’t have or obtain other coverage that
is at least as good as Medicare drug coverage (also referred to as “creditable coverage”), you
may have to pay a late enrollment penalty if you enroll in Medicare prescription drug coverage in
the future.]
What if my premium was being deducted from my Social Security benefit check?
If your plan premium is being deducted from your Social Security benefit, please allow up to 3
months for us to process a refund. If you haven’t received a refund from Social Security within
3 months of this letter, you should contact 1-800-MEDICARE.
[Dual-eligible SNPs may omit the following paragraph:]
Can I get help paying my premiums and other out-of-pocket costs?
People with limited incomes may qualify for Extra Help to pay for their prescription drug
costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly
prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who
qualify won’t have a coverage gap or a late enrollment penalty. Many people qualify for these
savings and don’t even know it. For more information about this Extra Help, contact your local
Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-
325-0778. You can also apply for Extra Help online at www.socialsecurity.gov/prescriptionhelp.
What should I do if I’ve moved?
If you have moved and haven’t notified Social Security of your new address, you may call them
at 1-800-772-1213 (TTY: 1-800-325-0778) Monday-Friday, 7am to 7pm.
What should I do if I have more questions?
If you have any questions or need help, please call our <Customer Service, Member Services>
department at <phone number> <days and hours of operation>. TTY users should call <TTY
number>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
301
Exhibit 37: Notification of Involuntary Disenrollment by the Centers for
Medicare & Medicaid Services due to Incarceration
Referenced in section: 50.2
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Date>
Dear <Beneficiary Name>:
Medicare has disenrolled you from <plan name> because its records show that you are
incarcerated. As of <effective date>, you no longer have coverage through <plan name>. [MA-
PD plans insert: Your Medicare prescription drug coverage ended on the same date.] You will
have Original Medicare; however, Medicare generally doesn’t pay for your hospital or medical
bills if you’re incarcerated.
If your plan premium was paid for any month after <disenrollment effective date>, you’ll get a
refund from us within 30 days of this letter.
The decision to disenroll you was made by Medicare, based on information from SSA, not by
<plan name>.
What if I think there’s been a mistake?
If you aren’t incarcerated or think that there has been a mistake, please call us at <phone
number>. TTY users should call <TTY number>. We are open <days and hours of operation>.
What happens to my Medicare and Part D coverage?
While you are incarcerated, you are not eligible to enroll in a Medicare health or Part D plan.
However, once you are released and report it to SSA, you will have a special opportunity to join
a Medicare health or Part D plan. This opportunity begins the month you are released and lasts
for two additional months. If you don’t enroll at that time, you can enroll in a new Medicare
health plan or Medicare prescription drug plan from October 15 through December 7 of each
year for coverage to start the following year. Generally, you can’t make changes at other times
except in certain situations, such as if you move out of your plan’s service area, want to join a
plan in your area with a 5-star rating, or qualify for (or lose) Extra Help paying for prescription
drug costs.
Please remember, if you go without other drug coverage that is at least as good as Medicare drug
coverage (also referred to as “creditable coverage”) for 63 days or more after your release, you
may have to pay a lifetime Part D late enrollment penalty in addition to any plan premium, if you
enroll in Medicare prescription drug coverage in the future.
Who can I call to get more information?
You can call Social Security at 1-800-772-1213, if you have questions about your incarcerated
status. TTY users should call 1-800-325-0778. If you have questions about your Medicare
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
302
coverage, you can call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day, 7 days a
week. TTY users should call 1-877-486-2048. You can also call < plan name> at <phone
number> if you have questions. TTY users should call <TTY number>. We are open <days and
hours of operation>.
Thank you.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
303
Exhibit 38: Notification of Involuntary Disenrollment by the Centers for
Medicare & Medicaid Services due to Loss of Lawful Presence
Referenced in section: 50.2.1, 50.2.7
(Rev. 1, Issued: July 31, 2018; Effective/Implementation: 01-01-2019)
<Date>
Dear <member name>:
Medicare has disenrolled you from <plan name> because the Social Security Administration
(SSA) reported that you are not lawfully present in the United States. As of <effective date>,
you no longer have coverage through <plan name>. [MA-PD insert: Your Medicare prescription
drug coverage ends on this date.] You will have Original Medicare; however, Medicare doesn’t
pay for your hospital or medical bills if you’re not lawfully present in the U. S.
If your plan premium was paid for any month after <disenrollment effective date>, you’ll get a
refund from us within 30 days of this letter.
The decision to disenroll you was made by Medicare, based on information from SSA, not by
<plan name>.
What if I think there’s been a mistake?
If you aren’t unlawfully present in the U.S. or think that there has been a mistake, please call us
at <phone number>. TTY users should call <TTY number>. We are open <days and hours of
operation>.
What happens to my Medicare and Part D coverage?
While you are unlawfully present in the United States, you are not eligible to receive any
coverage in the Medicare program. This includes coverage through Original Medicare, a
Medicare health plan or Medicare prescription drug coverage.
If you become lawfully present in the U.S. in the future and report it to SSA, you will have a
special opportunity to join a Medicare health or Part D plan. This opportunity begins the month
you regain lawful presence status and lasts for two additional months. If you don’t enroll at that
time, you can enroll in a new Medicare health plan or Medicare prescription drug plan from
October 15 through December 7 of each year for coverage to start the following year. You
may not enroll in a new plan during other times of the year unless you meet certain special
exceptions, such as you move out of the plan’s service area, want to join a plan in your area with
a 5-star rating, or you qualify for (or lose) Extra Help with your prescription drug costs.
<Contract#, alpha-numeric identifier, “CMS Approved/File & Use” [date] (as applicable)>
304
Please remember, if you go without other drug coverage that is at least as good as Medicare drug
coverage (also referred to as “creditable coverage”) for 63 days or more after you become
lawfully present in the U.S., you may have to pay a lifetime Part D late enrollment penalty in
addition to any plan premium, if you enroll in Medicare prescription drug coverage in the future.
Who can I call to get more information?
You can call Social Security at 1-800-772-1213, if you have questions about your lawful
presence status. TTY users should call 1-800-325-0778. If you have questions about your
Medicare coverage, you can call 1-800-MEDICARE (1-800-633-4227) anytime, 24 hours a day,
7 days a week. TTY users should call 1-877-486-2048. You can also call < plan name> at
<phone number> if you have questions. TTY users should call <TTY number>. We are open
<days and hours of operation>.
Thank you.
