
REPORT TO THE
UTAH LEGISLATURE
Report No. 2002-01
A Performance Audit
of
Medical School Admissions
January 2002
Audit Performed by:
Audit Manager Tim Osterstock
Auditor Supervisor James Behunin
Audit Staff Mark Roos
Ivan Djambov
Aaron Eliason

Table of Contents
Page
Digest ................................................. i
Chapter I
Introduction ............................................ 1
Selection of a Medical School Class Is a Difficult Process ......... 2
Utah’s Selection Process Consists of Three Phases .............. 4
Steps Taken to Promote Fairness ..........................7
Audit Scope and Objectives .............................. 8
Chapter II
Rate of Acceptance Higher for Women and Minorities ............. 9
Gender Affects Likelihood of Acceptance ....................9
Minority Applicants Accepted At a Higher Rate .............. 14
Acceptance Rates for Other Variables Show Little Difference .... 17
Chapter III
Diversity Policy Explains the High Rate of Female and
Minority Admissions ..................................21
A Student’s Diversity Is Considered During the Admissions
Process ........................................... 21
Diversity Program Is Not a Population-based Quota System ..... 27
Diversity Policy Conflicts With Policy on Non-discrimination .... 30
Recommendations ....................................37
Chapter IV
Deviations from Admissions Process Have Raised Questions ....... 39

Office of the Utah Legislative Auditor General – 3 –
Table of Contents (Cont.)
Review Committee Decisions Are Not Always Followed ........ 39
Interview Problems Raise Question of Fairness ............... 44
Selection Committee Process Can be Streamlined ............. 49
Recommendations ....................................53
Appendices ............................................ 55
Agency Response ........................................ 75
-i-
Office of the Utah Legislative Auditor General – i –
The School of Medicine
seeks to enroll the
same portion of
minorities and women
found in the state’s
general population.
Women and minorities
are accepted at over
twice the rate of white
males.
Digest of
A Performance Audit of
Medical School Admissions
The University of Utah School of Medicine’s admissions practices have
changed in recent years to, among other things, better enable the school
to mirror the diversity of race and gender found in the general population.
This is a difficult task because relatively few women and minorities apply
to the School of Medicine. In seeking to enroll a class of students that
reflects the same general proportion of minorities and women, the school
has had to increase the rate of acceptance among minorities and women.
As a result, the fairness of the school’s admissions practices have been
questioned.
These questions arise because the school has elevated the importance
of diversity over academics and has conflicting internal policies. The
school’s diversity policy is, however, consistent with the policies of the
university administration and the Board of Regents. The policy on
diversity also fits within a broader strategy of affirmative action that is
promoted by the Association of American Medical Colleges.
The report’s main themes are summarized below.
Rate of Acceptance Higher for Women and Minorities
School of Medicine records show that over the past two years, roughly
one out of every two women who applied to medical school were
accepted while only one of five men were accepted. Similarly, about one
out of every two minority applicants were accepted during the past two
years but only one in five white applicants were accepted.
While gender and minority status appear to effect the rate of
acceptance, there is no significant difference in the rate of acceptance when
the applicant’s undergraduate college, rural/non-rural status or age is
considered. Also, we could not identify any systematic bias against
applicant’s religious background.

-ii-
– ii – A Performance Audit of Medical School Admissions
The high rate of
acceptance among
women and minorities
is explained by the
school’s efforts to
promote diversity.
Diversity Policy Explains the High Rate
of Female and Minority Admissions
The high rate of acceptance of women and minority applicants at the
School of Medicine can be attributed to the school’s effort to promote
diversity without relying on a rigid system of quotas. To gain greater
diversity in its student body, the School of Medicine has elevated the
importance of diversity-related selection criteria and reduced the
importance of academic achievement. The school has adopted lower
academic requirement (GPA and MCAT) for applicants it considers
disadvantaged while maintaining a higher set of standards for non-
disadvantaged applicants.
One obstacle to the school’s application of diversity is the apparent
conflict with the university’s policy on non-discrimination. Reconciliation
of the school’s promotion of racial and gender diversity within the student
body and the school’s often-stated prohibition against considering an
applicant’s gender, race, and religion, should be addressed.
We recommend that the School of Medicine adopt a single set of
academic standards, prohibit admission committee consideration of
applicant demographics, and consider providing under-represented
populations with, as needed, pre-admittance course work.
We recommend the Board of Regents examine the apparent conflicts
regarding its policies of diversity and non-discrimination.
Deviations from Admissions Process
Have Raised Questions
The school’s emphasis on the subjective evaluation of an applicant’s
character and background and its reduced consideration for an applicant’s
academic achievements has made it more difficult to evaluate applicants
consistently. In addition, inconsistencies in the administration of the
admissions process show there is a need to improve admissions procedures
and policies.
Central to the problems facing the admissions process is the
relationship between the school’s Dean of Admissions and the three
committees responsible for the selection of applicants. Although the
members of the admissions committee receive specific instructions from

-iii-
Office of the Utah Legislative Auditor General – iii –
Although 100
volunteers participate
on the admissions
committees, the Dean
of Admissions is often
the person that decides
whether an application
will receive further
consideration.
the school’s Office of Admissions, they are often unable or unwilling to
decide whether an application should continue in the system. This
indecision means that the Dean of Admissions often must decide whether
or not an applicant will receive further consideration. Reliance on the
Dean to ultimately decide so many of the applications appears to defeat
the school’s use of over 100 selection committee members to eliminate
individual bias.
Moreover, it appears that some applications sent to the selection
committee for final consideration may not be those considered to be the
best applicants by other admissions committees. Greater diligence in
policy and procedure control could eliminate a number of the problems
currently encountered.
We recommend the School of Medicine eliminate all courtesy
interviews and better define the relationship of admissions and
diversity.
We recommend interview forms be revised to eliminate confusion
regarding the results of an interview and limit the final evaluation
to either a “yes, forward to selection” or “no, reject applicant”.
We recommend the selection committee follow existing policies and
drop outlying scores and that all rankings be combined in order to
accept the next best scoring applicant.

-1-
Office of the Utah Legislative Auditor General – 1 –
Medical schools
throughout the
country are giving
special consideration
to students who add
diversity.
Chapter I
Introduction
The University of Utah School of Medicine’s (School of Medicine) has
followed a nationwide trend among medical schools to place greater
emphasis on subjective admissions criteria. Medical schools throughout
the United States are placing less emphasis on the objective indicators
such as a student’s MCAT score and GPA and are focusing more on
subjective factors such as a students character, leadership skills, and
compassion. In addition, special consideration is given to students who
can add diversity to a class of students. One result of the use of subjective
selection criteria is that many people who would like to apply to medical
school do not understand the requirements for admission and the relative
importance of objective factors such as the MCAT score and subjective
factors such as service in the community. The emphasis on subjective
criteria has also led some to question the fairness of the admissions
process.
The changes in selection criteria, particularly the heightened value of
diversity, has altered the demographics of students entering the School of
Medicine. Acceptance rates of various under-represented population
groups applying to the school have increased while rates for non-minority
males, who do not add to the school’s diversity, have decreased.
Although there is no evidence that unqualified individuals have been
admitted to medical school, the school’s emphasis on diversity has led to
claims by some applicants that they have not been given an equal
opportunity.
The school’s goal to create a diverse student body is an especially
difficult task in Utah because the state’s school of medicine tends to attract
a rather homogenous pool of applicants. The vast majority of applicants
are white males who tend to have similar backgrounds and experiences.
At the same time, relatively few women and minorities apply to medical
school in Utah. As a result, the school’s effort to enroll a diverse class can
make it difficult for a white male to stand out and be viewed as someone
who can offer something different. On the other hand, the push for
diversity tends to work in favor of female and minority applicants who,
because of their low numbers and varied backgrounds, find it relatively
easy to appear unique.

-2-
– 2 – A Performance Audit of Medical School Admissions
AAMC encourages
schools to place more
weight on an
applicant’s character
and background than
on GPA and MCAT.
An applicant with an
MCAT of 27 (or a 21 if
disadvantaged) is
considered to be as
equally prepared
academically as an
applicant with an
MCAT of 39.
Selection of a Medical School Class
Is a Difficult Process
The University of Utah School of Medicine has the difficult task of
selecting a medical school class of 102 students from 500 to 600 qualified
applicants each year. Like most other medical schools, the School of
Medicine follows an admissions process that is largely prescribed by the
Association of American Medical Colleges (AAMC).
The AAMC processes a basic medical school application form that is
used jointly by medical schools throughout the country. In addition,
AAMC administers the Medical College Admissions Test (MCAT) and
advises the School of Medicine on the best admissions policies and
procedures. Occasionally, AAMC will provide training to the school’s
interviewers. Due to the school’s reliance on the national association, the
admissions procedures used by the School of Medicine are similar to those
used by medical schools in other states.
In recent years there have been two policies promoted by the AAMC
that have gained wide acceptance among the nation’s medical schools.
AAMC has encouraged medical schools to first, place less emphasis on
academic measures (MCAT and GPA) as selection criteria and second, to
adopt policies that promote diversity.
AAMC Discourages the Use of MCAT and GPA as Primary
Selection Criteria. In recent years, AAMC and many of its member
colleges have reconsidered their longstanding use of the applicant’s
academic achievements as the primary criteria for admission to medical
school. Instead, AAMC now encourages schools to place more weight on
an applicant’s character and background than on academics. This change
reflects an interest by many in the profession to select and train physicians
who can communicate effectively and be sensitive to the needs of patients.
It is ironic that the AAMC would discourage the use of the MCAT
and GPA as primary selection criteria because it is the organization that
administers the MCAT exam. In fact, the AAMC’s own research shows
that a student’s MCAT score and GPA correlate with their performance
during the first two years of medical school. Their concern, however is
that the test scores and grades (at least above certain levels) are not good
predictors of how effective a person might be as a physician. Instead, they
place more emphasis on an applicant’s character traits such as “altruism,

-3-
Office of the Utah Legislative Auditor General – 3 –
The medical school
has a goal to create a
student body with the
same proportion of
women and minorities
as the state’s general
population.
fervor for social justice, leadership, commitment to self sacrifice, empathy
for those in pain.”
In keeping with the suggestions of the AAMC’s president, the
University of Utah School of Medicine has adopted a policy of using the
MCAT score and the GPA only as a minimum standard for consideration.
Because academics do not seem to be as important as once thought,
minimum academic requirements for admission have been reduced. As
long as students have a GPA above a 3.2 and an MCAT of 27 (or, if
disadvantaged, a GPA of 2.5 and a MCAT of 21), then they are all
considered to be equally qualified in terms of their ability to handle the
curriculum of medical school. In other words, the applicant with an
MCAT of 27 )or a 21 if disadvantaged) is considered to be as equally
prepared academically as an applicant with an MCAT of 39.
By considering all applicants equal in terms of their academic
preparation, the School of Medicine can use their time to assess attributes
they associate with an effective physician. These other attributes include
leadership skills, communication skills, compassion, maturity,
understanding of the profession, humility and cultural sensitivity.
AAMC’s Push for Greater Diversity Is Followed by Most
Schools. AAMC’s President, Dr. Jordan J. Cohen, is a leading advocate
for expanding diversity within the nation’s medical schools. Speaking for
all medical schools, Dr. Cohen has said that “our mandate is to select and
prepare students for the profession who, in the aggregate, bear a
reasonable resemblance to the racial, ethnic, and, of course, gender
profiles of the people they will serve.” He also said “there is simply no
way we can select an adequately diverse class of medical students today
without taking race and ethnicity explicitly or implicitly into account.”
Like many other member schools, the University of Utah School of
Medicine supports the views of Dr. Cohen and the AAMC. For example,
school officials, with the support of the Board of Regents, have adopted
AAMC’s goal to create a student body that has the same proportion of
women and minorities as found in the state’s general population. In
addition, the School of Medicine offers special services and waives certain
requirements for five minority groups that the AAMC suggests are
“under-represented” in the state’s medical schools. These include

-4-
– 4 – A Performance Audit of Medical School Admissions
The medical school
uses ten cognitive and
non-cognitive selection
criteria.
• Native American
• African American
• Mexican American
• Native Hawaiian
• Mainland Puerto Rican
Specifically, applicants from these minority groups are offered advice and
assistance in their preparation for and application to medical school. In
addition, certain requirements imposed on non-resident applicants are
waived for those who belong to the above listed minority groups. The
following provides an overview of the admissions process used by the
School of Medicine and the changes the school has made in recent years to
promote a fair and objective selection process.
Utah’s Selection Process
Consists of Three Phases
The School of Medicine has declared that it evaluates each applicant
according to ten criteria that it says are used by medical school’s
nationally. The evaluation of applications is performed by three distinct,
independent committees. Each committee is assigned an evaluation
component and works to filter down the number of applications to the
point that a class is selected.
School of Medicine Uses AAMC Criteria
For its Selection Process
The ten cognitive and non-cognitive selection criteria promoted by the
AAMC and adopted by the University of Utah admissions program are
• Undergraduate GPA, overall and science
• MCAT, all sections
• Leadership/management skills
• Physician shadowing
• Exposure to patient care
• Community service
• Research experience
• Letters of recommendation
• Personal statements
• Interviews
-5-
Office of the Utah Legislative Auditor General – 5 –
Once the minimum
academic requirements
are met, an applicant’s
character and
background are the
primary consideration.
Although each application is evaluated against the above criteria, some
factors are given greater weight than others. In addition, the above list
does not include certain other factors that are considered, such as an
applicant’s compassion, motivation for services, and ability to add
diversity to the class of students. Two factors that are given relatively less
weight than other criteria are the GPA and MCAT score. The School of
Medicine uses GPA and MCAT scores only as minimum requirements for
consideration. Once the academic requirements are met, the applicant’s
character and background are the primary consideration.
In some respects, the personal essay, leadership positions, volunteer
service, and letters of recommendation are not really used as selection
criteria. Rather, they are the means used to consider a wide range of
attributes not specifically identified in its list of ten criteria. For example,
the applicant’s list of volunteer service is not used to merely identify the
extent of service rendered. The admissions committee also uses the list of
volunteer service to consider the applicant’s level of empathy, humility,
problem solving skills, exposure to other cultures, leadership skills, ability
to overcome hardships, openness to new/different ideas, and diversity of
experience. Although not specifically mentioned as selection criteria, these
character traits are all given considerable weight during the admissions
process.
Applicant Evaluation Is Divided
Into Three Committees
Operating under the control and guidance of the Dean of Admissions,
the medical school admissions process is carried out by three separate
committees. The three committees are described as follows:
• Review Committee - examines applicant’s basic qualifications and
determines whether the applicant should be interviewed.
• Interview Committee - holds interviews with applicants and
decides which applications should be presented to the Selection
Committee.
• Selection Committee - decides which of all the remaining
applicants should be accepted for admission to the medical school.
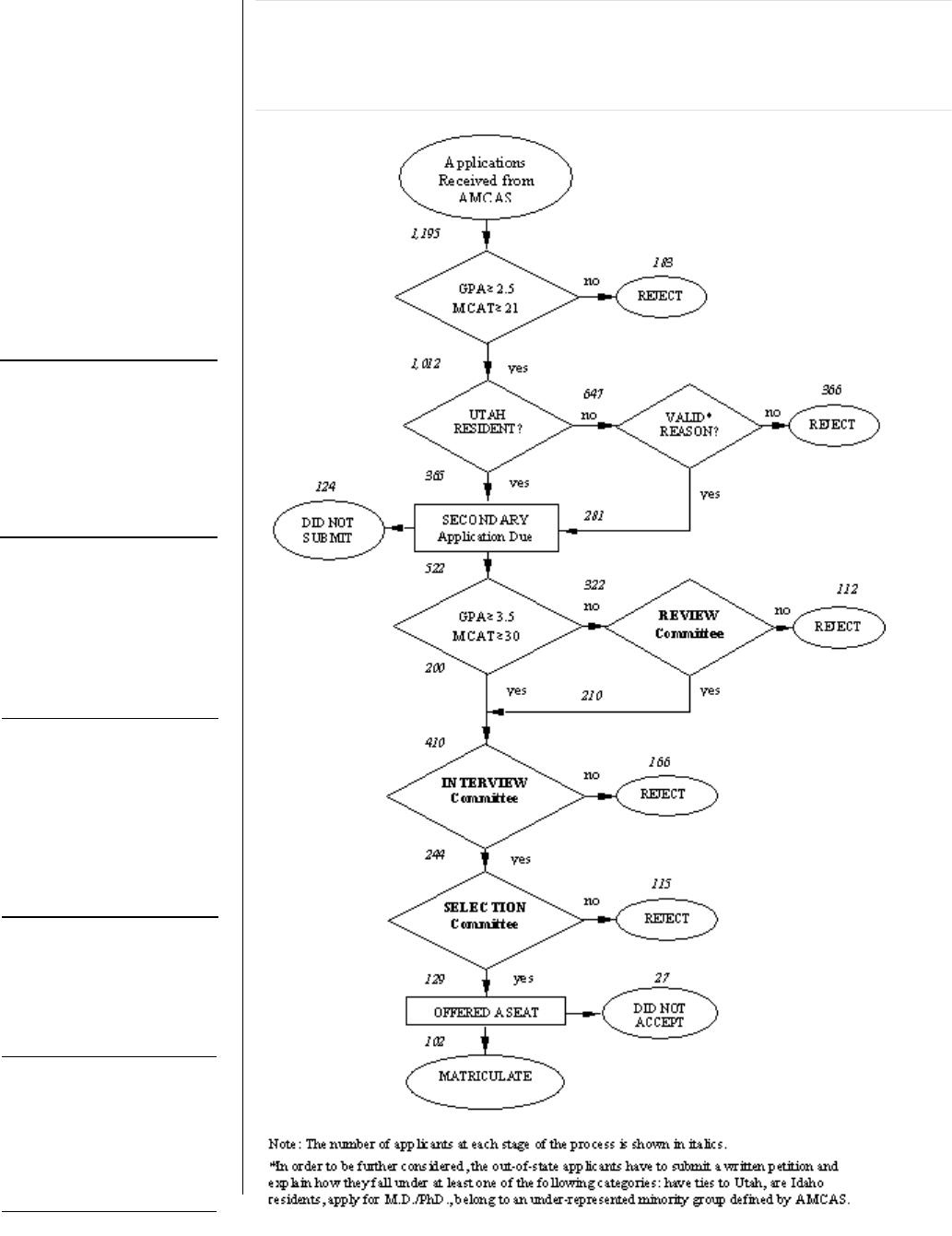
Figure 1 describes the flow of applications through the admissions
process.
-6-
– 6 – A Performance Audit of Medical School Admissions
Interview Comm ittee:
after conducting
interviews and
reviewing application,
committee
recommends
applicants for further
consideration.
Review Committee:
reviews academic
record and
disadvantaged status
to decide if applicant
should receive an
interview.
Selection Committee:
ranks and makes the
final class selection,
based on information
from the review and
interview committees.
Figure 1. The Application Process. During the 2001 recruitment
year, 1,195 individuals asked that their MCAT score be sent to the
University of Utah. Of those, only 522 completed the secondary
application form and 102 were admitted.

Office of the Utah Legislative Auditor General – 7 –
-7-
Three successive
committees pare down
the number of
applicants based on
selected criteria.
The School of Medicine
has taken steps to
prevent individual
committee members
from having too much
influence.
Figure 1 shows that 1,195 individuals asked that their MCAT scores
be sent to the University of Utah School of Medicine during the 2000-
2001 recruitment year. Of those, 522 completed the application by
submitting secondary forms requested by the University and by paying
their application fee. Of the 522 applicants, 200 were automatically
granted interviews, and the rest were considered by the Review
Committee.
The Review Committee approved interviews for an additional 210
applicants, and 112 were rejected because they did not meet the basic
requirements. The Interview Committee eliminated another 166
applicants and referred 244 applicants to the Selection Committee. Those
244 were each considered by the Selection Committee and given a
ranking or score by each member. The applicants with the highest
average score were sent letters of acceptance. In all, there are 102
positions available in the medical school. However, in order to fill those
positions, 129 applicants were sent letters of acceptance. Of those, 27
decided to attend other institutions.
Steps Taken to Promote Fairness
The selection process is fairly subjective because analyzing the selection
criteria is dependent on the perceptions of each Admissions Committee
member. Recognizing that each committee member has his or her own
unique set of biases and perspectives, the School of Medicine has taken
several steps to ensure that no single member of the admissions committee
has too much influence over the process. The following describes some of
the procedures that have been adopted in recent years:
• Committee members can participate on only one committee. Thus,
any one member cannot promote the cause of one individual applicant
through the entire admissions process. Instead, successful applicants
must receive approval from many committee members.
• No single individual selects the members for the admissions
committee. They are nominated by their organizations: departments
in the School of Medicine, community organizations, local hospitals,
senior medical students, alumni.

-8-
– 8 – A Performance Audit of Medical School Admissions
The school’s database
as well as applicant
admissions files were
used in the audit.
• More than 100 people serve on the admissions committee. Thus,
applications are considered from many different perspectives.
• Applicants have the opportunity to petition for an additional review if
they feel that the review committee has made a mistake or did not take
into consideration the applicant’s most recent accomplishments.
• Applicants who feel the interviewer was biased or asked unfair
questions, may request an additional interview.
• Personal background information regarding an applicant such as the
applicant’s home town, parents’ occupation, the college the applicant
attended, etc., are excluded from the materials presented to the
Selection Committee in order to prevent them from considering issues
that are not relevant.
Audit Scope and Objectives
The audit subcommittee asked that the primary focus of the audit be
the admissions process used by the University of Utah School of Medicine
but granted audit staff some flexibility to pursue other areas if instances of
bias were identified. In keeping with this request, the audit staff focused
mainly on matters relating to the admissions policies and procedures and
whether they were applied in a fair and consistent manner.
First, audit staff obtained a copy of the School of Medicine’s applicant
database and used that information to compile statistical information
describing the rates of admission for the past several years. Next, audit
staff conducted a detailed review of applications submitted for the class
beginning in the fall of 2001. Particular attention was given to the 410
applicants who reached the interview phase of the admissions process.
For each applicant, the written comments prepared by the Review
Committee and the Interview Committee were considered in light of the
school’s admissions policies.
The objective of the audit was to evaluate the fairness of th admissions
policies and procedures used by the School of Medicine.

Office of the Utah Legislative Auditor General – 9 –
-9-
The School of
Medicine accepts
women at a rate that
is two and one-half
times the rate of
acceptance for men.
Chapter II
Rate of Acceptance Higher for
Women and Minorities
There are significant differences in the rates at which men, women and
minorities are accepted to medical school. During the past two years,
roughly one out of every two women who applied to medical school was
accepted while only one of five men was accepted. Similarly, about one
out of every two minority applicants was accepted during the past two
years, but only one in five white applicants was accepted. There does not
appear to be a significant difference in the rate of acceptance when
considering the college where an applicant earned a pre-medical degree, an
applicant’s geographic origin, or age. We also found no evidence of bias
against applicants based on their religious affiliation.
The rate of acceptance among men, women and minorities is a useful
tool because it helps identify whether all applicants have an equal
opportunity to be admitted. According to its Student Information
Handbook, the School of Medicine embraces the concept of “equal
opportunity and non-discrimination.” Because the school says it does not
consider race or gender during the admissions process, one might expect
male, female and minority applicants to be accepted at roughly the same
rate at which they apply.
Gender Affects Likelihood of Acceptance
Men make up the majority of applicants to the University of Utah
School of Medicine and men also make up the majority of those admitted.
Although relatively few women apply, the School of Medicine accepts
women at a rate that is two and one-half times the rate of acceptance for
men. This difference in the rate of acceptance among men and women
sets Utah apart from most other medical schools in the nation. Most
schools have roughly the same number of men and women apply and
typically, with comparable acceptance rates, the schools admit a class of
students that is roughly half women and half men.
-10-
– 10 – A Performance Audit of Medical School Admissions
The number of
women who applied
to medical school
has declined in
recent years.
The University of Utah School of Medicine acknowledges the
difference between their admission rates and those at other schools but
can not explain why their admission rates would be higher for women and
minorities. Some school officials have speculated that the female
applicants are better qualified than the male applicants. Despite this
claim, we found no evidence to support it. In fact, school records show
that men and women applicants are roughly equal in terms of their
academic qualifications.
Female Acceptance Rates Have Increased
As Applications Have Declined
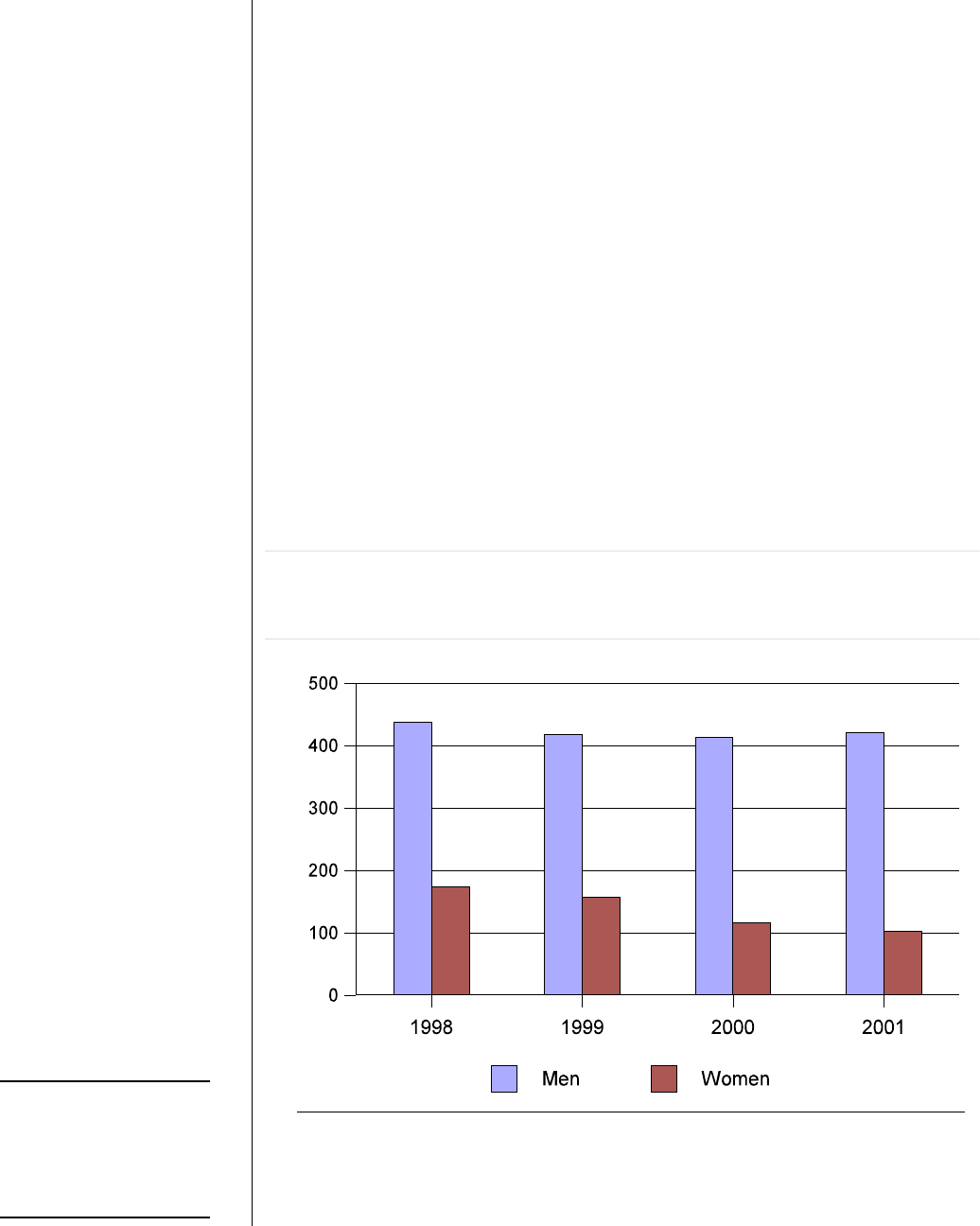
The number of men applying to the School of Medicine, as Figure 2
shows, has changed little during the past four years while the number of
women applicants, already relatively low compared to the number of male
applicants, has declined since 1998.
Figure 2. Number of Men and Women Applicants to the School
of Medicine, 1998 to 2001. The number of female applicants has
decreased by 40 % in recent years.
* See Appendix A for details.
Although Figure 2 shows the relatively low number of women
Office of the Utah Legislative Auditor General – 11 –
-11-
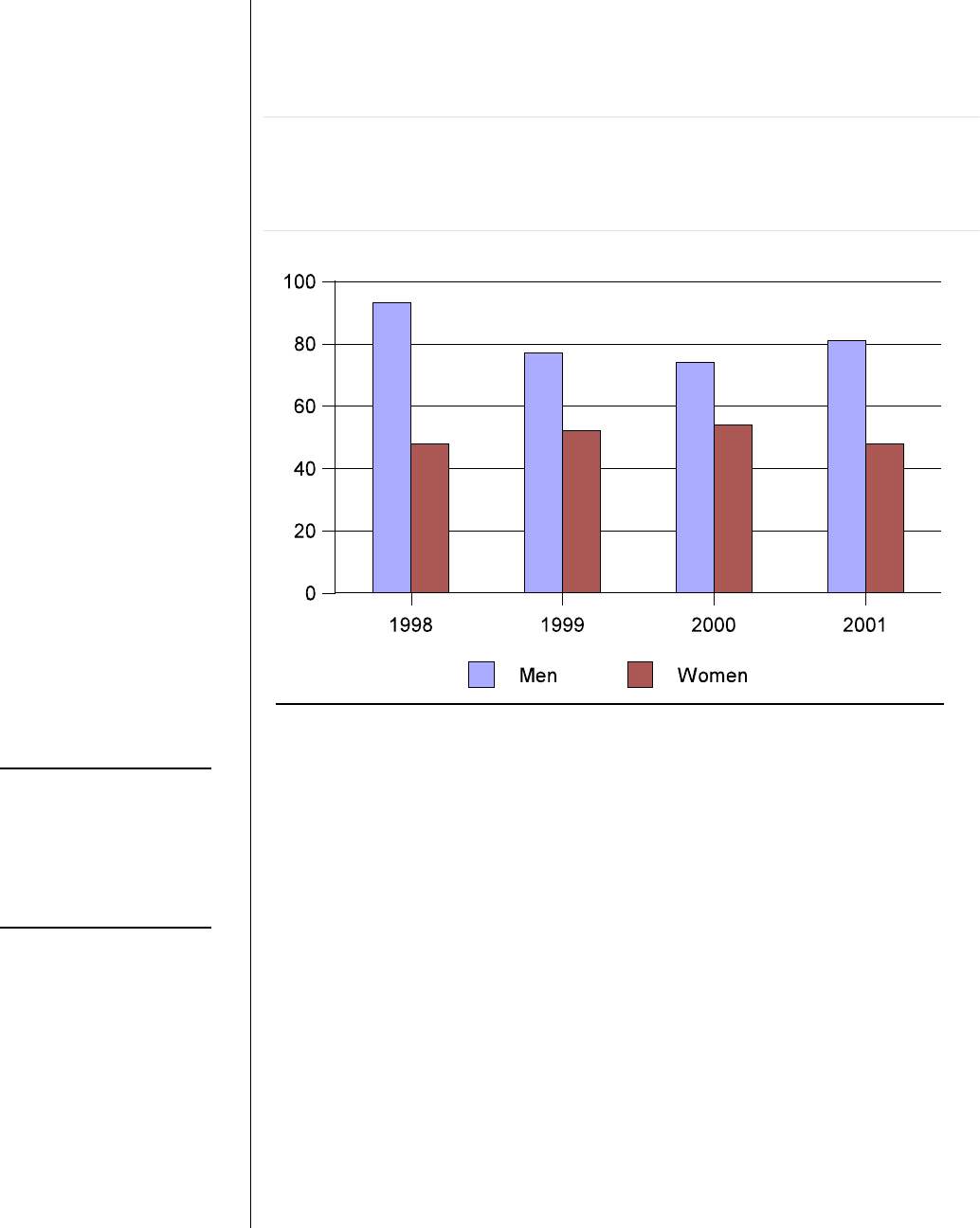
The number of
female applicants
accepted has
remained between
48 and 54 during the
past four years.
applying to medical school has declined in recent years, Figure 3 shows
the number of women accepted to the School of Medicine has remained
steady.
Figure 3. Number of Men and Women Accepted, 1998 to 2001.
The number of men accepted by the school has declined slightly
while the number of women accepted has remained relatively
constant.
* See Appendix A for details.
One effect of the declining number of female applicants, in
combination with a fairly constant number of women accepted, is that
female applicants have a much greater likelihood of being accepted than
they did just a few years ago. This increase in the acceptance rates for
women is described in Figure 4.
-12-
– 12 – A Performance Audit of Medical School Admissions
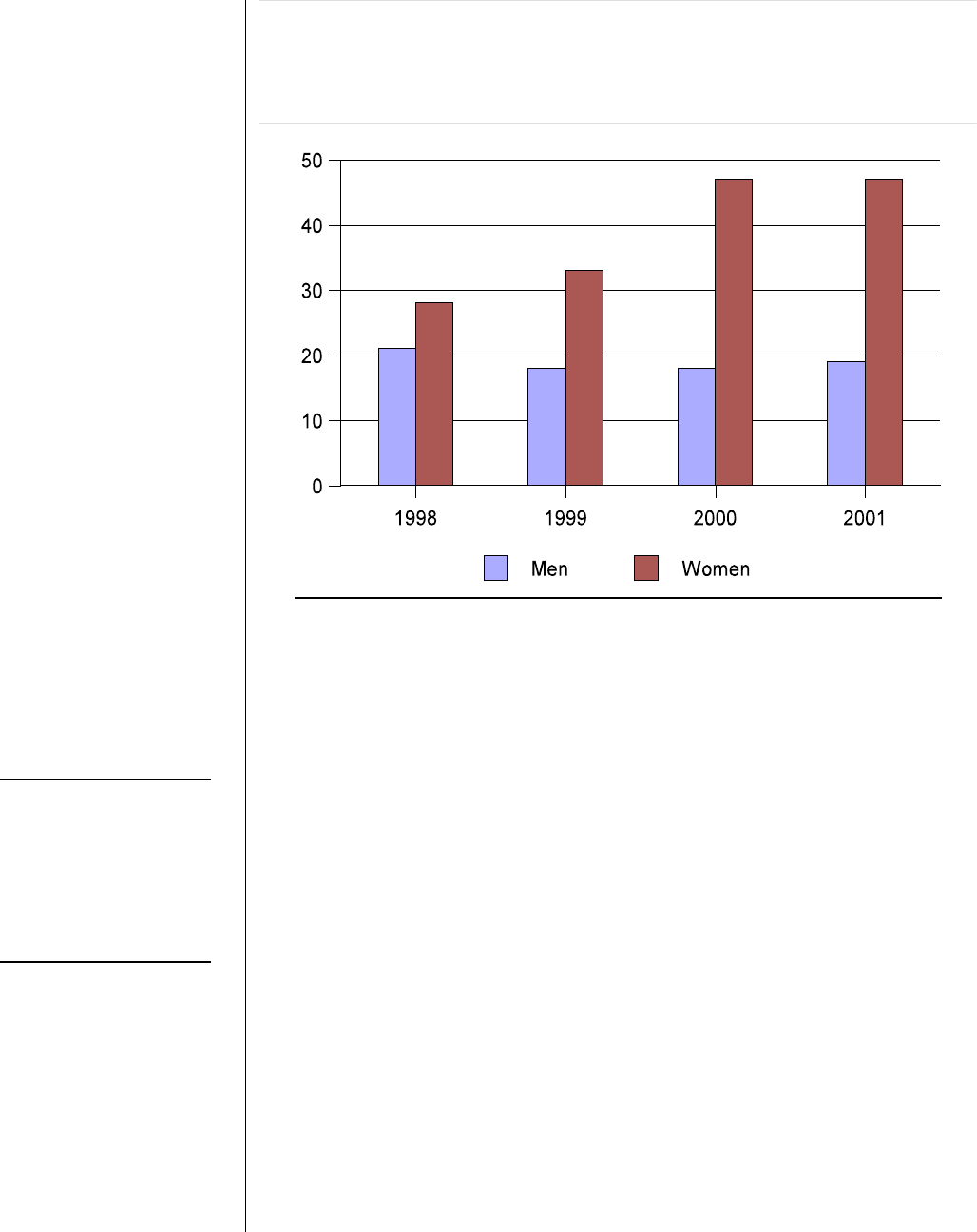
In the last two years,
nearly one out of
every tw o female
applicants was
accepted while only
one in five men was
accepted.
Figure 4. Rate of Acceptance of Female Applicants has
Increased. The percentage of females accepted has increased
significantly during the past four years while the percentage of males
accepted has decreased slightly.
* See Appendix A for details.
Of all those who qualified for medical school in 1998, women had a
slightly higher likelihood of being accepted than men. About 28 percent
of female applicants in 1998 were accepted and 21 percent of men were
accepted. Since that time, the likelihood of a female being accepted has
increased significantly to 47 percent while the percentage of men being
accepted has declined to 19 percent. Thus, nearly one out of every two
female applicants has been accepted to the medical school during the past
two years while only one in five men has been accepted.
Little Evidence to Support School’s Explanation
For the Higher Rate of Females Accepted
School officials offer three possible explanations for females being
accepted at higher rates than males, including
• Better preparation - women who apply are better prepared
candidates than their male counterparts; only the best prepared
women apply for medical school.

Office of the Utah Legislative Auditor General – 13 –
-13-
School officials say
that only the best
female applicants
apply.
Men and women
applicants had
comparable scores
on the verbal
reasoning section of
the MCAT.
• Better verbal communications - women have better interpersonal
and verbal skills that help them do better in interviews.
• Better writing skills - women commonly write better personal
essays than men.
Little Evidence That Only the Best Females Apply. School officials
have also suggested that, taken as a group, its women applicants are better
prepared than men because only the best prepared women apply. School
officials describe this phenomenon as “self-selection.” There is little
evidence supporting this claim, however.
Although self-selection may occur to some extent, nothing in the
school’s data would suggest that only the best prepared women apply to
medical school. The school’s application data demonstrates that there is
virtually no difference in the level of academic preparation (GPA and
MCAT). Both men and women earned comparable cumulative GPAs,
but the male applicants actually scored slightly higher on the MCAT than
the female applicants. Thus, female applicants appear no better prepared
academically to attend medical school than their male counterparts.
Little Evidence That Women Have Better Verbal and
Interpersonal Skills. School officials also suggest that women have
better interpersonal and verbal skills, and for this reason they perform
better during interviews than their male counterparts. Again, there is little
evidence to support this claim. One objective measure of an applicant’s
verbal skills is the verbal reasoning section of the MCAT exam. We found
that men and women applicants had comparable scores in this category
during the past four years. Similarly, we found little difference between
men and women’s verbal skills as tested by the verbal section of the SAT.
We could not find an objective measure of the interpersonal skills of
applicants. The school’s interviewers give each application a numeric
score for each of ten different selection criteria. In 2001, the interviewers
gave a slightly higher average overall rating to female applicants than they
did to male applicants. However, an interviewer’s evaluation of an
applicant is a subjective matter that tends to be influenced by the
interviewer’s own interests.

-14-
– 14 – A Performance Audit of Medical School Admissions
No difference was
found in the writing
ability of male and
female applicants.
Little Support Found for the Assertion That Women Write
Better Essays. School officials also suggested that women write better
essays. This assertion is also not supported by the facts. We found little
difference in the writing skills of male and female applicants, since male
and female applicants had similar scores on the written portion of the
MCAT exam.
It does appear, however, that while there is no difference in writing
ability, there may be a difference in the subject matter about which male
and female applicants choose to write. As a result, personal essay scores
given by School of Medicine reviewers are slightly higher for women than
for men on average. School officials have observed that women tend to
have more varied backgrounds and activities than their male counterparts,
write better personal statements, and are not as self-centered in their
personal experiences.
Minority Applicants Accepted
At a Higher Rate
In spite of efforts to increase the School of Medicine’s diversity, the
number of minority applications has decreased in the last few years.
However, the number of minorities accepted has remained relatively
steady. The decline in minority applicants, combined with the continued
acceptance of about 20 minority students each year has, in effect, doubled
the likelihood of a minority applicant being accepted.
In 1998, approximately 11 percent of the School of Medicine’s
applicants described themselves as minorities. Over the last four years this
percentage has fallen to about 7 percent. During this same period, the
number of non-minority, or white applicants dropped slightly in the first
year and has since remained relatively constant. Figure 5 shows this
trend.
Office of the Utah Legislative Auditor General – 15 –
-15-
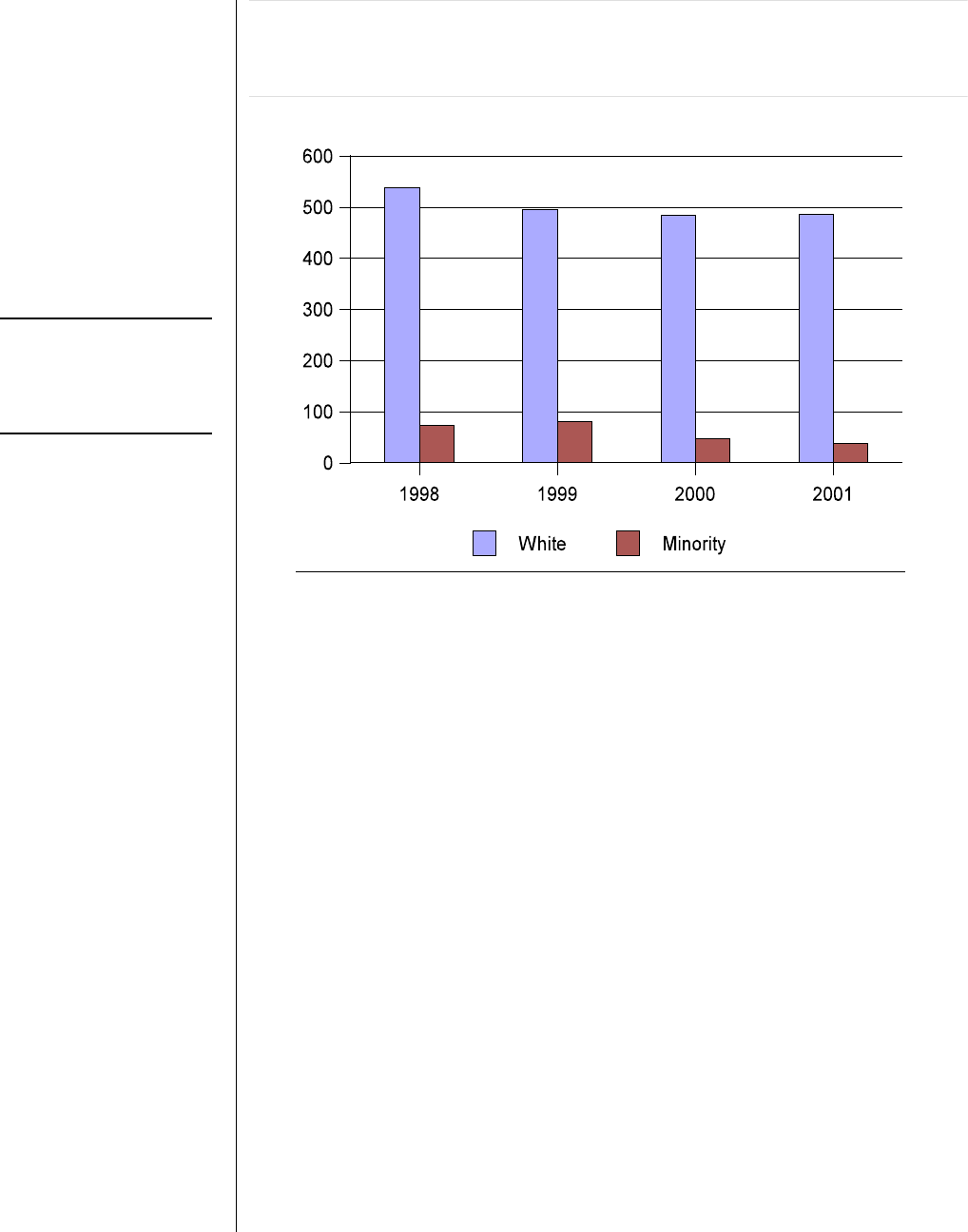
Since 1998, the
number of minority
applicants has
decreased.
Figure 5. Number of Applicants by Minority Status, 1998 to
2001. Since 1999, the number of white applicants has held steady
while the number of minority applicants has decreased.
*See Appendix A for details.
The slight overall decline in the number of applicants to the School of
Medicine reflects a national trend that school officials attribute to the
economy. Reportedly, university enrollment nationwide tends to decline
during an economic expansion. With the recent economic downturn, the
School of Medicine anticipates applications will rebound. The decline in
minority applicants is problematic for the School of Medicine where
minority recruitment has been difficult. When asked why minority
recruitment was declining, school officials could not provide an
explanation.
Although the school has received fewer applications from minorities in
recent years, the number of minority applicants accepted has not changed
significantly. Figure 6 shows this trend.
-16-
– 16 – A Performance Audit of Medical School Admissions
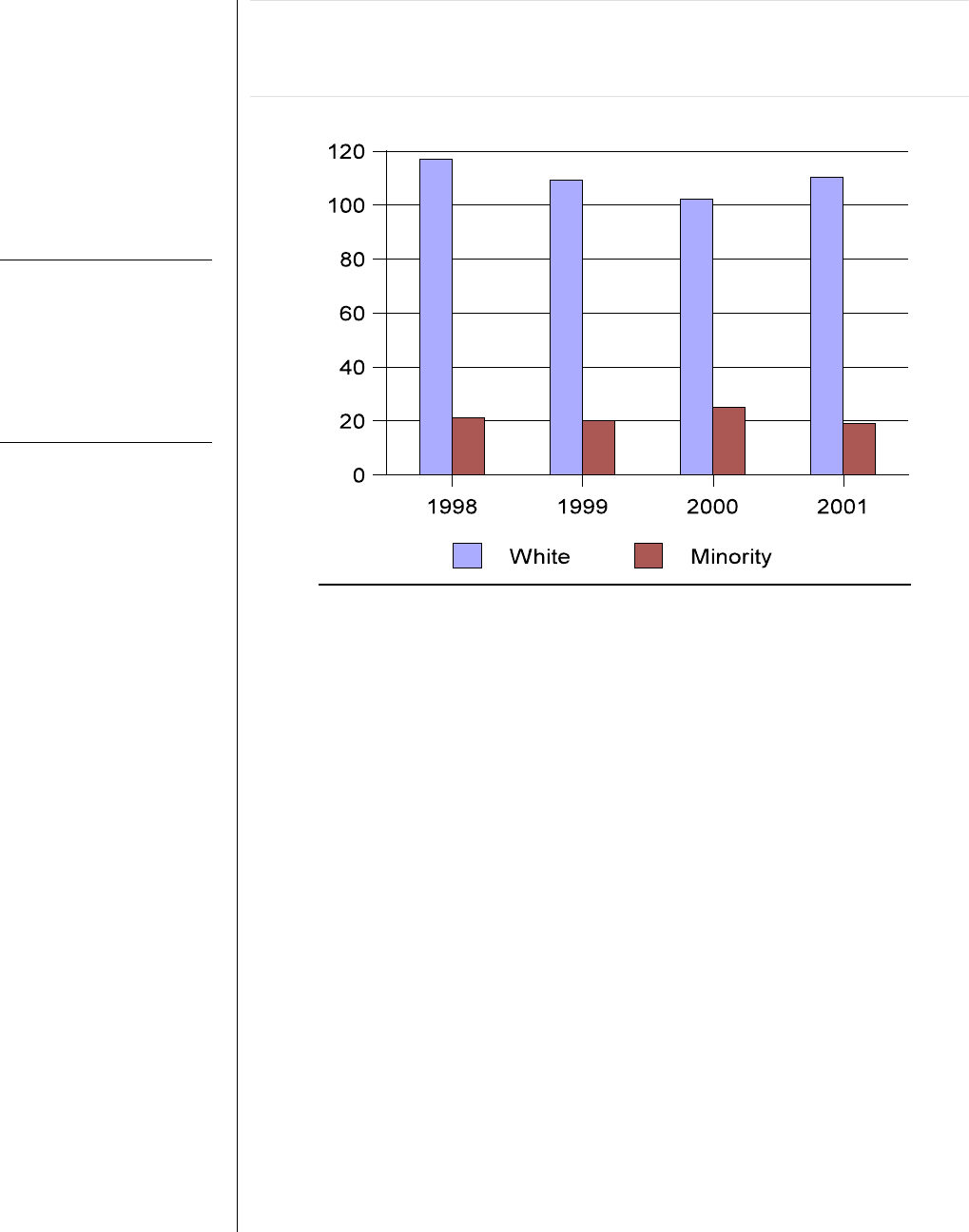
The num ber of both
minority and white
applicants accepted
has remained
relatively constant
over the last few
years.
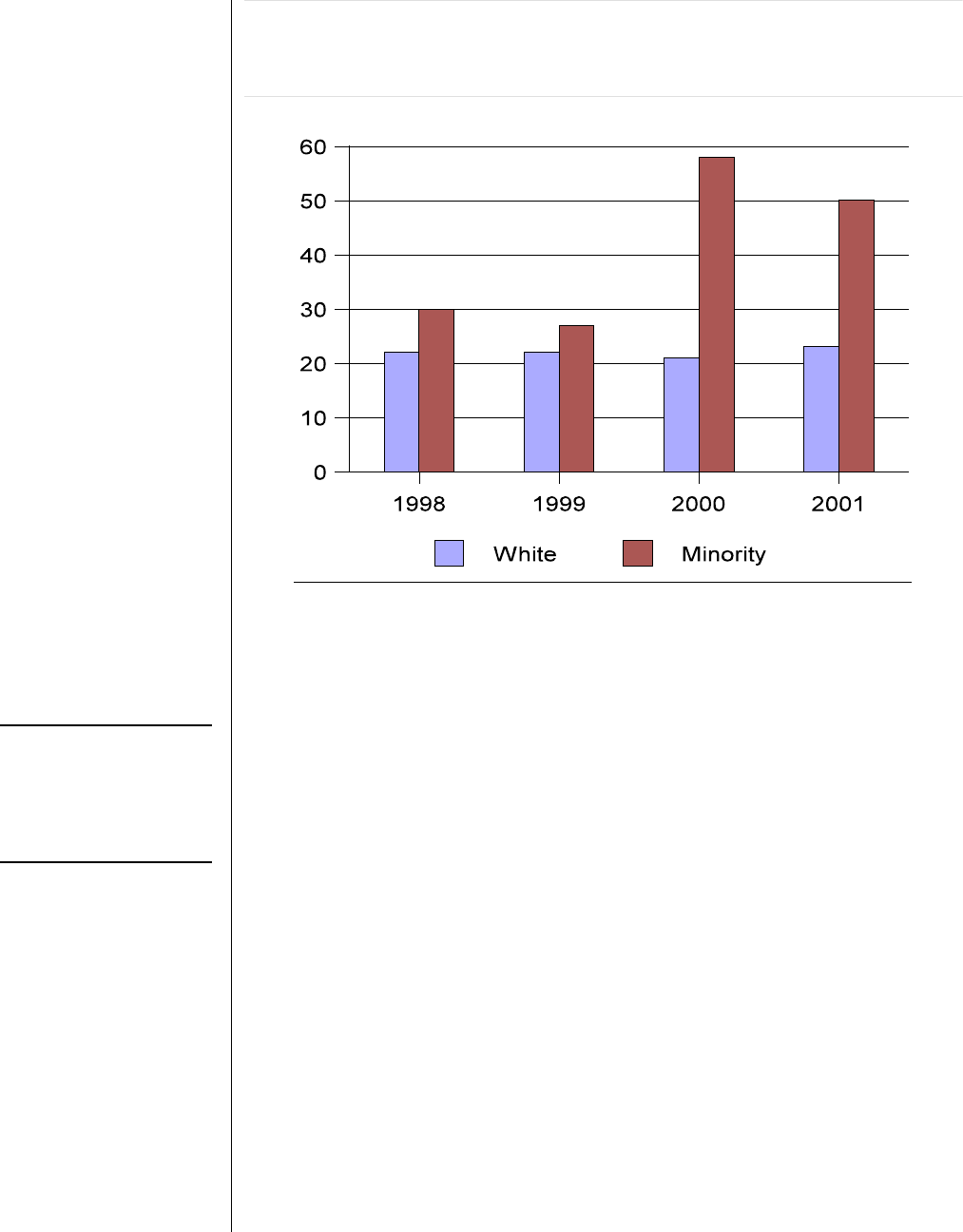
Figure 6. Minority Status of Accepted Applicants, 1998 to 2001.
The number of both minority and white applicants accepted has
remained relatively constant over the last few years.
*See Appendix A for details.
Because the number of minority applicants accepted has remained
constant during a period when fewer minorities have been applying, the
acceptance rate for minority applicants has increased dramatically. Figure
7 shows that in the last two years, minority applicants were much more
likely to be accepted than in the two previous years.
Office of the Utah Legislative Auditor General – 17 –
-17-
The acceptance rate
for minority
applicants has
increased in the last
few years.
Figure 7. Percentage of Applicants Accepted, Minority and
White, 1998 to 2001. The acceptance rate for minority applicants
has increased in the last few years.
*See Appendix A for details.
In years 2000 and 2001, one out of two minority applicants was
accepted by the School of Medicine. Applicants who did not describe
themselves as a minority were accepted at a rate of only one in five. In
previous years (1998 and 1999), minority acceptance rates were much
closer to the rate for non-minority, or white applicants. The rise in
minority acceptance rates appears to reflect the school’s increased
emphasis on diversity. This subject is discussed in some detail in Chapter
III.
Acceptance Rates for Other Variables
Show Little Difference
Although there is strong correlation between an applicant’s race and
gender and their likelihood of being accepted, there is little evidence that
an acceptant’s undergraduate college, age, geographic origin, or religion
affects the likelihood they would be accepted to the School of Medicine.

-18-
– 18 – A Performance Audit of Medical School Admissions
Those who attended
out-of-state schools
had a greater
likelihood of being
accepted than those
applying from in-
state schools.
For most of the groups tested, we found only modest differences in the
rates of acceptance. Most differences could be explained as random
variations. Some differences can also be explained by the fact that
applicants from some universities and age groups have a higher
proportion of white males. As a result, the slightly lower rates of
acceptance among some groups are best explained by the higher rate of
acceptance among female and minority applicants and not because of any
bias directed towards certain universities, age groups or applicants from a
rural background.
The use of admission rates is supplemented by regression analysis—a
statistical technique that identifies the correlation between various factors
and an applicant’s likelihood of gaining admission. The regression shows
little correlation between a person’s undergraduate institution, age, or
geographic origin and medical school acceptance. The regression does
show that applicant race and gender have the strongest influence on
acceptance (see Appendix B.)
Religious affiliation is not a part of the data collected for each
applicant, so it is impossible to determine whether the rate of admission
was higher or lower depending on the applicant’s religious affiliation.
However, it appears that any perceptions of bias against applicants from
certain religious affiliations are probably due to the lower rate of
acceptance among white males.
Acceptance Rates Are Similar
For Utah’s Undergraduate Colleges
There is also little evidence of bias towards the applicants because of
the undergraduate institution they attended. Although some significant
differences occurred from one year to the next in the number of students
accepted from different universities, these are likely explained as random
events. See Appendix A for the acceptance rates of individual institutions.
The one group who did appear to have an advantage in the admissions
process are the students from Utah who received their undergraduate
training at an out-of-state institution. Utahns attending out-of-state
schools were accepted by the School of Medicine at a rate of 35%. In
contrast, Utahns who attended in-state schools, such as University of
Utah, Brigham Young University, or Utah State University, were
accepted at an average rate of 24%.

Office of the Utah Legislative Auditor General – 19 –
-19-
As a group,
applicants aged 21-
23 were accepted at
a rate of one in four,
whereas only one in
five applicants aged
24-26 was accepted.
The fact that Utahns schooled out-of-state have a greater likelihood of
acceptance reflects the School of Medicine’s emphasis on diversity.
Applicants who attended out-of-state institutions were more likely to be
women and ethnic minorities. Due to their having lived out of state,
these applicants had a college experience that was different from most of
those applying from in-state schools.
In contrast, a higher portion of the applicants from in-state schools
were white males who tended to have similar experiences and
backgrounds. As a result, differences in the higher rate of acceptance for
Utah resident applicants from out-of-state schools does not necessarily
represent bias against certain institutions but the school’s desire to enroll a
diverse student body.
Age and Rural Acceptance Rate
Variations Appear Reasonable
There was some difference observed in acceptance rates for applicants
of different ages, but little difference was observed between applicants
from rural communities and those with no rural background. However,
there are reasonable explanations for the slight differences in acceptance
rates.
Most School of Medicine applicants are between 21 and 26 years old
with 24 being the average age. As a group, applicants aged 21-23 were
accepted at a rate of one in four, whereas only one in five applicants aged
24-26 was accepted. There are two possible explanations for these
differences.
First, the School of Medicine’s published criteria says that they want
applicants who are currently actively engaged in their education to show
they are academically-minded and a “life-long learner.” Second, the lower
rate for the older age group may be due, in part, to the higher percentage
of white males within that group. Eighty-six percent of the 24-to-26
year-old age group were white males and sixty percent of the 21-to-23 age
group were white males. As a result, the older group of applicants does
not offer as much racial and gender diversity as the younger applicants.
Over the four-year period (1998-2001), applicants from rural areas

-20-
– 20 – A Performance Audit of Medical School Admissions
An applicant’s
religious affiliation
is often known, but
there is little
evidence that it
affects the likelihood
of acceptance.
have been accepted at about the same rate as applicants from non-rural
areas. Applicants from rural communities make up a relatively small
portion of the total applicant pool—accounting for 13% of all applicants
and 12% of those accepted. The slight variations in the acceptance rates
among applicants from rural and non-rural communities is most likely a
random event.
Little Evidence That Religious Affiliation
Affects the Likelihood of Acceptance
We could not identify the rate of acceptance based on the religious
affiliation of applicants. Religious affiliation is not part of the data
collected by the AAMC or in the secondary forms that the School of
Medicine asks each applicant to fill out.
Applicant religious affiliation is often identified in the application if
they offered church-related volunteer service or served in a leadership
position within a religious organization. For example, if an applicant
provided religious missionary service, it would be listed among the
applicant’s “post-secondary experiences” on the AAMC form. For an
applicant not to include a major, time-consuming activity such as a
mission would be a glaring omission in the application for which the
school would request an accounting.
Although there were a few applicants who told us they felt their
interviewer was biased against their religious affiliation, such instances
were rare and certainly not the typical experience of most applicants. It
appears that any perception of bias against applicants from a certain
religious affiliation is probably due to the lower rate of acceptance among
white males.

Office of the Utah Legislative Auditor General – 21 –
-21-
Diversity,
considered in terms
of race or gender, is
an attribute
considered during
the admissions
process.
Chapter III
Diversity Policy Explains the High Rate of
Female and Minority Admissions
The high rate of acceptance of women and minority applicants at the
School of Medicine can be attributed primarily to the school’s effort to
promote diversity among its student body. Achieving a diverse student
body is a difficult task for the School of Medicine because the majority of
its applicants are white males. In order to achieve greater diversity, the
School of Medicine has set a goal to enroll roughly the same portion of
men, women and minorities as exist in Utah’s general population.
Although the School of Medicine does not rely on a system of quotas
to achieve its diversity goals, the school’s mission statement says that it is
guided by the “imperatives of affirmative action.” In keeping with its goal
for greater diversity, the school has taken several steps to encourage the
enrollment of greater numbers of women and minorities. The
consideration of diversity during the admissions process may, however,
conflict with the university’s policy on non-discrimination. It is unclear
how the school can follow a policy that promotes racial and gender
diversity and, at the same time, comply with a policy that prohibits the
consideration of an applicant’s gender, race, or religion as part of the
admissions process.
A Student’s Diversity Is Considered
During the Admissions Process
The School of Medicine’s selection criteria includes many factors such
as an applicant’s leadership experience, volunteer service, motivation for
becoming a physician, and familiarity with the profession. The
admissions committee also considers the extent to which a student might
add diversity to the student body. While there are many ways that a
medical school applicant might be viewed as someone who can add
diversity, an applicant’s race and gender are the attributes most often used
to identify their diversity. In fact, most of the School of Medicine’s
programs and policies for creating greater diversity are aimed at providing
more opportunities to women and minorities on campus.

-22-
– 22 – A Performance Audit of Medical School Admissions
The university’s
administration and
the Board of
Regents support
racial and ethnic
diversity.
The school wants
its student body to
mirror the
demographics of the
state’s population.
The School of Medicine’s policy on diversity is based on the following
beliefs:
(1) In order to better serve the public, the school needs to graduate
a class of physicians that has the same percentage of women and
minorities that exists in the community at large.
(2) The school can enhance the richness of the educational
experience by admitting a diverse student body with a broad range
of backgrounds and perspectives.
(3) Cultural and economic barriers prevent minorities from
performing well on standardized tests. For this reason, a different
set of MCAT and GPA standards should be applied to those who
have a disadvantaged background.
These principles are accepted by the Association of American Medical
Colleges and by medical schools throughout the country. The University
of Utah’s administration and the Board of Regents have also expressed
support for diversity.
Improved Medical Access Is the
Primary Goal of Diversity
One justification given for the School of Medicine’s diversity policy is
that women and minorities would have better access to health care
services if there were more female and minority physicians. Enrolling a
diverse student body is also considered an important way to help all
medical students become more sensitive to the needs of patients from
different ethnic communities.
Medical Students That Mirror the General Population May
Improve Access to Health Care. One goal of the School of Medicine is
to admit the same percentage of women and minorities that exist in the
general population. This goal is clearly stated in the school’s Statement on
Student Diversity:
The University of Utah seeks to recruit a student body that reflects
the diversity of the population as a whole. We feel that students
with different cultural and economic backgrounds as well as varied
life experiences add a valuable perspective to student life and

Office of the Utah Legislative Auditor General – 23 –
-23-
School officials
believe that diversity
helps medical
students appreciate
other cultures.
broaden the educational experience of all students. Therefore, the
School of Medicine seeks to foster the aspirations of women to
pursue careers in medicine, and is also committed to recruiting,
admitting and graduating qualified candidates from those minority
groups specifically recognized by the federal government as under-
represented in the health care professions: African-American,
American Indian, Mainland Puerto Rican, Mexican-American and
Native Hawaiians.
To support the above diversity statement, the School of Medicine cites
research suggesting that minority physicians are more likely to practice in
their own ethnic communities. School officials also contend that
minorities prefer to be cared for by physicians from their own ethnic
background. Because many of the state’s ethnic communities tend to have
poor access to health care, the school believes one solution is to admit
more applicants from those communities. As a result, the school’s
diversity policy is also viewed as a means of providing women and
minorities with better access to health care.
While relatively little research exists surrounding the above argument,
one study by the Commonwealth Fund found race is not one of the
primary criteria when minority patients select a doctor. The study showed
minority patients ranked a doctor’s “nationality/race/ethnicity” 12
th
out of
13 factors when selecting a physician. Respondents ranked the ability to
make an appointment quickly, their physician’s location, the doctor’s
reputation in the community and their professional credentials as the most
important factors in selecting a physician. Only two percent of the
African Americans and Hispanics and four percent of Asians surveyed
indicated problems with racial and ethnic differences between themselves
and their physician.
Due to the advent of managed health care plans, another researcher
suggests that patients tend to place more value on the amount of time
their doctors spend with them than their doctor’s race or ethnicity. In
these programs, patients tend to be cared for by a different doctor with
each visit. For these patients it is less likely that they will be able to
establish ties with a doctor of the same racial or ethnic heritage.
Diversity Can Enhance the Educational Experience of All
Students. School officials also believe that diversity helps improve the
-24-
– 24 – A Performance Audit of Medical School Admissions
education of all students. One representative of the School of Medicine
explained this sentiment as follows:
Discovering significant aspects of other cultures is valuable for all
physicians because they are called upon to care for patients of many
races and ethnic origins. This kind of cultural perspective can be
taught in a formal setting, but a more valuable way to experience it
is to get to know individuals of other races and cultures on an
informal basis. Only by having a diverse student body is this type
of experience possible.
The medical school believes that the best way to foster cultural
sensitivity is through the interaction of peers from different cultural
backgrounds.
Minorities Are Disadvantaged by Traditional
Measures of Academic Performance
That minority applicants have, in aggregate, lower MCAT scores and
lower total GPAs is not disputed. What is disputed is the relative value of
these measures for applicants who experienced certain hardships during
their high school and college years. Figure 8 shows how white and
minority applicants compare on MCAT scores and total GPA.
Figure 8. Comparison of Total MCAT and Overall GPA for
Minority and White Applicants to the U of U Medical School.
White applicants scored higher on the MCAT and had a higher GPA
than minority applicants during the last four years.
Average MCAT Average GPA
Year Minority White Minority White
1998 26.2 29.3 3.28 3.57
1999 26.4 29.5 3.32 3.60
2000 28.7 30.1 3.49 3.62
2001 28.8 30.3 3.51 3.63
Although many minority applicants have outstanding academic
records, school officials believe that, as a group, minorities have

Office of the Utah Legislative Auditor General – 25 –
-25-
School officials
believe some
allowance must be
made for the lower
test scores of
disadvantaged
applicants.
experienced social, economic and educational disadvantages that account
for their lower achievement on standardized tests. As a result, the School
of Medicine adopted a lower set of academic standards for
“disadvantaged” applicants, which includes many minority applicants.
They give two reasons for the lower set of academic standards:
(1) Many minorities’ disadvantaged backgrounds affect their
performance on standardized tests, and
(2) There is little correlation between level of academic preparation
and effectiveness as a physician.
For these reasons, disadvantaged applicants can gain entry to medical
school with an MCAT score as low as 21 and a GPA as low as 2.5 while
their non-disadvantaged classmates must have at least an MCAT of 27 and
a GPA of 3.2.
Many Minorities Come from Disadvantaged Backgrounds. The
school recognizes that minorities from disadvantaged backgrounds may
find it difficult to perform well in school. As an example, applicants who
use English as a second language can have difficulty performing on
standardized tests such as the MCAT. As a result, a minority student’s
abilities may not be accurately measured by the traditional measures of
academic achievement. This view is reflected in one of the comments by
an Associate Dean at the School of Medicine who said
Many under-represented minority students come from
disadvantaged educational and economic backgrounds that can
affect their performance on standard measures of academic
achievement. Many must work to support themselves during high
school and college, resulting in limited time for concentration on
academics. In addition, literature published on standardized
testing has indicated that minority groups often score lower on this
type of assessment and this can mask their true academic potential.
For these reasons, the predictors of success in medical school are
somewhat different for minority students.
So, instead of placing so much emphasis on academics, the school
emphasizes other factors in the selection process such as “motivation,

-26-
– 26 – A Performance Audit of Medical School Admissions
MCAT and GPA do
not predict
effectiveness as a
physician.
Once applicants are
approved by the
Review Committee,
they are considered
equally qualified in
terms of their
academic
preparation.
dedication and emotional stability.”
High Academic Scores Do Not Predict Effectiveness as a
Physician. The School of Medicine discounts the importance of MCAT
scores and GPA as indicators of a student’s ability to be an effective
physician. School officials acknowledge that MCAT and GPA scores are
good predictors of how well a student will perform during the first two
academically-focused years of medical school but cite little correlation in
later years.
School officials base their views regarding MCAT and GPA on the
statements of Dr. Jordan J. Cohen, President of the AAMC, whose
writings are included in the training manual for the members of its three
admissions committees. First, Dr. Cohen challenges the traditional view
that “students who have an easier time with tests in medical school make
better doctors.” He then states
Certainly we want our doctors to be smart and to have passed all of
their courses; no one, whether from a minority or majority
background, graduates from medical school who has not done so.
Just as no one practices medicine who has not passed all the
licensing examinations. But good doctoring requires a lot more
than passing requisite exams. And there is no reason to believe
that those other attributes we are looking for in our future doctors
—compassion, dedication, truthfulness, caring—correlate with
scores on multiple-choice exams.
Dr. Cohen then suggests that schools give less emphasis to GPA and
MCAT scores and place more attention on the applicant’s character. In
fact, most recently, Dr. Cohen proposed that medical schools abandon the
consideration of an applicant’s GPA and MCAT scores altogether.
In addition, school officials also believe that an applicant’s MCAT
score and GPA are not good predictors of how successful they might be as
a physician. For this reason, the School of Medicine places less weight on
an applicant’s academic record. Once students have passed the Review
Committee’s screening of their academic records, all applicants are
considered equally qualified in terms of their academic preparation for
medical school. From that point on, the Interview Committee and
Selection Committee only consider an applicant’s non-academic abilities
such as leadership, interpersonal communication skills, compassion,
curiosity and social awareness.

Office of the Utah Legislative Auditor General – 27 –
-27-
Preference may be
given to students
that offer diversity to
their class.
The School of
Medicine’s system
does not reserve
slots for minority or
female applicants.
The medical school has accepted disadvantaged students with MCAT
scores as low as 7 on each of the three parts of the MCAT and some with
GPAs less than 3.0. According to the school’s policy, however, these
lower scoring students were considered to be as equally qualified as
students with MCAT’s of 13s and 14s on each section of the test and
GPA’s of 4.0.
Diversity Program Is Not a
Population-based Quota System
The School of Medicine states that it does not use quotas to achieve its
diversity goals nor, in addressing its goals, does it admit unqualified
female and minority students. The school’s position is that, among
equally qualified applicants, preference can be given to female and
minority students that will offer diversity to their class. In this sense, the
School of Medicine is achieving the objectives of affirmative action
without resorting to the questionable admissions practices of past
affirmative action programs.
School of Medicine Supports the Principles of Affirmative Action.
The mission statement of the School of Medicine says that the school is
“guided by the imperatives of affirmative action.” For some, the term
affirmative action is reminiscent of race-based quotas and other policies
that mandated the hiring of a certain of under-represented groups whether
or not they are qualified. Many such policies have been overturned by the
courts.
Several outside observers (including the pre-med advisors from two
other universities in the state) told us that they believe a certain portion of
each freshman class is reserved for females and minorities. This, they say,
is supported by the enrollment figures from the past several years. Since
1998, roughly te same number of female and minorities have been
accepted even though the number of female and minority applicants has
declined.
The School of Medicine does not use an affirmative action quota
system. While the school does have a goal to enroll the same percentage
of women and minorities as in the general population, there are no slots

-28-
– 28 – A Performance Audit of Medical School Admissions
The school
measures diversity
in terms of the
number of women
and minorities that
have been enrolled.
The Office of
Diversity and
Community
Outreach provides
advice, services and
encouragement to
minority applicants.
reserved for minorities or women. Further, the school reports that all
students go through the same admissions process and are subjected to the
same admissions criteria—except for the lower standards applied to
disadvantaged students. The school does allocate a certain number of
positions based on state residency. The School of Medicine reserves 75 of
the 102 positions in each class for residents of Utah. Eight positions are
contracted to residents of Idaho, and the remaining 19 are available to
non-residents.
Medical School and University Administration Both Promote
Diversity. Although the University of Utah does not use quotas to
achieve its affirmative action goals, the school does what it can to
encourage the enrollment of minorities and women. There is an
expectation that the School of Medicine will try to enroll the same
proportion of women and minorities as exist in the general population.
Members of the three admissions committees clearly understand this goal
and that they should give preference to applicants who would add
diversity to the student body.
Although diversity means different things to different people, the term
is most often used to describe the need for an increase in minority and
female students. In fact, the school measures its progress toward its
diversity goals in terms of the number of women and minorities that have
been enrolled each year.
The university administration also encourages diversity through a
published Statement on Affirmative Action and through an annual
diversity award. In its Statement on Affirmative Action the University
states that “affirmative action continues to be needed as a vehicle for
achieving equal opportunity and a diverse population of students... .”
Furthermore, the University Diversity Award is handed out annually to
“programs and persons that have made important contributions to
diversity at the University, especially regarding inclusion of women and
minorities and related issues in the life of the University.” The award was
given to the School of Medicine in recognition of its success of increasing
the involvement of women and minorities within its programs.
Much of the effort to recruit women and minority students is carried
out by the medical school’s Office of Diversity and Community Outreach.
The office is charged with the task of “recruiting, admitting and
graduating qualified candidates from those minority groups” recognized
by AAMC as under-represented. One approach used to attract more

Office of the Utah Legislative Auditor General – 29 –
-29-
Some admissions
committee members
give higher ratings
to applicants they
consider diverse.
women and minorities to the health care profession is the Office’s
recruitment efforts. Occasionally, representatives from the Office of
Diversity and Community Outreach will visit local high schools and
colleges to encourage students to consider a profession in health care.
The Office of Diversity and Community Outreach also helps
minorities through the admissions process. The office contacts minorities
who have applied to the medical school and provides them with services
and advice concerning the application process. For example, they may
offer advice regarding how to write a personal essay or conduct mock
interviews with the applicant. Once an offer of acceptance is made, the
office will encourage minority students to enroll at the University of Utah.
Individual Admissions Committee Members Respond Differently
to the Diversity Policy. We found that members of the admissions
committee responds differently to the school’s goal for greater diversity.
Some members consider diversity specifically in terms of an applicant’s
race and gender. These members give higher ratings to minority and
female applicants because they believe the applicant’s race and gender will
help add to the diversity of the student body.
Other committee members told us that they would never consider
using race or gender as a criteria for selection, but they do look for
applicants with a background and experience that sets them apart from
others. For example, the dean points out that an applicant would be
considered adding diversity with an undergraduate degree in accounting
because the applicant would have a unique background and offer a
different perspective.
Many White Male Applicants Have Such Similar Backgrounds
That They Offer Little in Terms of Diversity. The need for greater
diversity is used to explain why women and minorities are accepted at
higher rates than white men. Women and minorities tend to have more
varied backgrounds and experiences than the typical white male applicant
from Utah. According to school officials, many male applicants from the
Wasatch Front tend to have very similar experiences during their years
leading up to medical school.
Most have attended BYU or the University of Utah, had similar pre-
med degrees, similar volunteer service, and sought out similar experiences

-30-
– 30 – A Performance Audit of Medical School Admissions
Many white male
applicants have
such similar
backgrounds that
they have difficulty
standing out.
to prepare them for medical school. On the other hand, most female and
minority applicants were less likely to pursue a traditional path to medical
school. As a result, the search for applicants with a unique set of
experiences and backgrounds tends to work against many of the white
male applicants and favor women and minorities.
Several Selection Committee members told us most of the applicants
sent to this committee appear quite similar to one another. Our review of
applications and discussions with committee members and school officials
showed this similarity also. So many applicants are highly qualified and
have such similar backgrounds that it is difficult to set them apart. As a
result, we are told, those who have unique experiences and backgrounds
tend to stand out and have a greater likelihood of being accepted. It is
interesting to note that the Selection Committee is not given the
applicants’ MCAT scores and GPAs—two factors that might help them
distinguish applicants who otherwise appear similarly qualified.
We also found through our own observations and discussions with
school officials that serving a mission for their church, while a positive
attribute, does not set applicants apart because so many have had that
same experience. Conversely, school officials told us that serving a
religious mission is a unique attribute for medical schools in other states.
This uniqueness may be one of the reasons why applicants from Utah tend
to have such great success gaining admittance to medical schools in other
states.
Diversity Policy Conflicts
With Policy on Non-discrimination
The goal of creating a diverse student body appears to conflict with
some other school policies. The very factors that make students diverse,
such as their ethnicity, gender, or geographic origin, are specifically
mentioned in the school’s non-discrimination policy as factors that
admissions committee members may not consider. Moreover, the
school’s decision to have lower admission standards for disadvantaged
students also contradicts the goal of the Board of Regents to increase the
academic requirements for admission to the University of Utah.
Office of the Utah Legislative Auditor General – 31 –
-31-
Diversity policy
appears to
contradict policy of
non-discrimination.
Some Attributes Considered as Signs of a Person’s Diversity
Are Listed in the School’s Non-discrimination Policy
It appears that the school’s diversity policy contradicts its policy on
non-discrimination. Although the school’s non-discrimination policies
prohibit the school from considering race, gender, geographic background
and other demographic attributes, the school’s diversity policy encourages
the admissions committee to consider such factors.
Policy on Non-discrimination Prohibits School from Considering
Race, Gender, and Other Attributes. The training manual provided to
each admissions committee member describes the following policy of non-
discrimination:
Factors such as social class, parents’ education and occupation, type
of education establishment attended, geographic location (rural vs
urban), race, ethnicity, gender religion, age, color... should not be
a part of any admissions decision.
Furthermore, representatives from the School of Medicine specifically
mentioned this policy when they met before the Legislative Audit
Subcommittee at its August 2001 meeting:
Being a state institution, we are not allowed to look at race,
gender, religion, geographic location, age, all of those other things
that we can’t look at. So, they are not part of our [selection]
process. They’re not part of our database.
The above statements seem to contradict the school’s policy to
promote the admission of females and minorities. In fact, race, gender,
religion, geographic location and age are all considered during the
admissions process. References to each of these personal attributes are
contained in the written comments made by admissions committee
members regarding applicants. In addition, race, gender, geography and
age are all part of the database of information kept for each student.
Committee Members Do Consider Race, Gender and Other
Demographic Attributes. We reviewed the written comments made by
both the Review Committee and the Interview Committee for each of
410 individuals who applied for the Fall 2001 class and who reached the
interview phase of the admissions process. Most committee members
-32-
– 32 – A Performance Audit of Medical School Admissions
Frequent reference
is made to an
applicant’s race.
Need for rural
physicians is often
cited by committee
members as a
reason to select an
applicant.
focus primarily on the established selection criteria they have been asked
to consider. These include such character traits as the applicant’s
leadership skills, community service, and awareness of the profession.
We did, however, identify 69 applications (or 16 percent) in which
references were made to race, gender, religion or other factors prohibited
by the school’s non-discrimination policy; but, which were listed among
the reasons to accept or reject the applicant. The following describes
some of the references found in applicants’ files regarding these factors
written by members of the Review Committee and Interview Committee:
• A person’s racial or ethnic background is often described favorably as
an indicator of an applicant’s diversity. There were 39 minority
applicants for the class beginning in the fall of 2001. Of those, there
were 30 applications in which one or more of the admissions
committee members made a reference to the applicants’ race as a
reason to consider the person for admission. Often an applicant’s
ethnic background was listed among the applicant’s “strengths” or
under the heading “unique qualities” about an applicant. In addition,
the person’s minority status was sometimes mentioned in the written
summary comments describing why the applicant offered diversity.
• Although the training manual specifically asks that “geographic
location (rural vs. urban)” not be considered, some committee
members are concerned that the school needs to admit more
physicians willing to serve in rural areas. We found 14 instances in
which the applicant was considered favorably because he or she came
from a rural area and expressed an interest in one day practicing
medicine in a rural community.
• Seven applications made reference to the applicant’s gender. Some
were used to describe a reason why the person should be admitted.
For example, one review committee member said that even though an
applicant’s MCAT score was low that the applicant should be
interviewed because the school needed more female students. In other
cases, interviewers made reference to the fact that applicants were
white and male and therefore did not stand out as someone who
would offer anything unique to the school. One interviewer even
admitted in her interview comments that she was biased against an
applicant because he represented what she disliked about white males
in Utah.
• Eight applications made reference to the applicant’s religious activity.

Office of the Utah Legislative Auditor General – 33 –
-33-
An applicant’s ability
to add diversity can
overcome deficits
that normally result
in rejection.
Sometimes the applicant’s unique religious background was listed as a
strength because the person’s religious affiliation would add diversity
to the class. In several instances the committee member discounted
the applicant’s volunteer service or leadership experience because, they
said, it was limited to “church-related” activities.
• There were several references suggesting a committee member was
concerned about the applicant’s age (that he had been out of school
for many years), social status (the applicant was “privileged” or “upper
crust”), or other personal attributes that seemed to have little to do
with qualifications for medical school.
Inasmuch as the committee members are prohibited from considering
race, gender, geography and religion, etc. during the admissions process,
we question how these attributes can also be used as indicators of an
applicant’s diversity. School officials acknowledge that some committee
members make inappropriate statements that are either biased or refer to
such personal attributes as gender and race. However, they also report
that the inappropriate comments are eliminated from copies of the written
interview reports before they are presented to the Selection Committee.
Our concern is that the inappropriate comments may suggest a bias
that is built into the overall rating of an applicant. Even if the gender and
race-based comments are not shown, the overall rating that is presented to
the Selection Committee may be affected by the interviewers’
consideration of race, gender and other personal attributes. In addition,
some applications may not have even been sent to the Selection
Committee because of the inappropriate consideration of gender, race and
other factors prohibited by the school’s non-discrimination policy.
Diversity Can Take Precedence over Other Concerns
The school’s effort to increase diversity is demonstrated by the many
cases we found in which an applicant’s ability to add diversity overcame
the applicant’s deficits. A number of applicants were accepted even
though their applications had problems that would normally result in
rejection. The type of problems that often results in rejection include
• a personal essay that is self-centered, rather than reflective
• out-of-state residency with no ties to Utah
• not currently enrolled in classes

-34-
– 34 – A Performance Audit of Medical School Admissions
Using different
standards for the
disadvantaged
means not everyone
will be judged
against the same
selection criteria.
• low academic scores
• little research experience
• an “arrogant” attitude
• lack of concern for less privileged individuals
• grades that worsen rather than improve over time
• grammatical errors in the personal essay.
For most applicants, any one of the above application problems can
result in a rejection of an otherwise excellent application. For example,
Selection Committee members are very sensitive to any hint of arrogance
on the part of an applicant. If the applicant writes a personal statement
that suggests the applicant is self centered, or insensitive to the needs of
the underprivileged, or overly confident in his or her abilities, the
admissions committee usually concludes that the applicant lacks the
humility and compassion sought in a medical student. However several
applicants who had these same problems with their application were
accepted because they offered diversity.
Lower Academic Standards for Disadvantaged
Inconsistent with Other Policies
The use of lower academic standards for disadvantaged applicants is
inconsistent with the school’s stated policy that all applicants will be
judged against the same criteria. The policy is also inconsistent with the
Board of Regents’ goal of raising admission standards for the University
of Utah.
Different Standards Applied to Disadvantaged Students. As
mentioned previously, the school applies a set of academic standards for
disadvantaged applicants that are lower than those applied to others. The
logic behind this policy is confusing. The policy states,
Students from a disadvantaged background need MCAT scores in
each category of 7 or greater and a GPA of 2.5 or better at the
University of Utah to pass our curriculum. Students from a non-
disadvantaged background need a 9 or better in each category of
the MCAT and 3.2 or better on the GPA to pass in our
curriculum.

Office of the Utah Legislative Auditor General – 35 –
-35-
School policies state
that most people
need a 3.2 GPA to do
well in medical
school, but a
disadvantaged
person only needs a
2.5.
Applicants may be classified as “disadvantaged” if they meet any one of
the following criteria:
• Household annual gross income consistently less than $20,000 for
a family of four,
• Attended a public high school in which less than 50 percent of the
graduates go on to college,
• Raised by a single parent with a low income or primarily by
someone who is not the natural parent,
• Working at least 30 hours a week or more while going to school,
• English is not the primary language of the household in which they
are being raised,
• Neither parent graduating from college nor attending college,
• Growing up in a medically underserved area,
• Growing up with social disadvantages.
However, the school provides little guidance on how committee members
should apply each of these criteria. For the most part, it is up to
committee members to decide on their own whether the applicant truly is
disadvantaged.
Not All Applicants Are Evaluated on the Same Basis. We question
whether the school’s policy toward disadvantaged students is consistent
with the school’s commitment that “all applicants will be evaluated on the
same basis.” The above policy requires that admissions committee
members consider an applicant’s economic, social and ethnic background
when deciding whether an applicant should receive further consideration.
At the same time, however, the school has made a commitment not to
consider some of these same social factors when evaluating applicants.
Policy on Disadvantaged Status Is Confusing. It is also confusing
why the policy states that most people need at least a 3.2 GPA to pass the
medical school’s curriculum but that disadvantaged people need only a
“2.5 GPA... to pass our curriculum.” What this policy suggests is that a
person with a 3.1 GPA would have difficulty with the curriculum, but a
person who has a 2.6 and is disadvantaged would be able to complete the
curriculum.
Disadvantaged Policy Is Inconsistent with Goals Set by the Board
of Regents. The use of a lower standard for disadvantaged applicants is

-36-
– 36 – A Performance Audit of Medical School Admissions
Several states
prohibit their
universities from
considering
diversity in the
admissions process.
also inconsistent with the commitment by the Board of Regents to raise
the admissions standards. As its “flagship institution,” the Board of
Regents recognizes the University of Utah is a major teaching and
research university whose reputation the Board would like to enhance. In
its Master Plan 2000, the Board identified several steps that it will take to
“enhance the University of Utah’s mission by capitalizing on its research
and medical reputation and assuring it is competitive with peer
institutions on an international basis.” Among its other goals, the board
indicated it will “support increased admissions standards” at the
university.
Other Medical Schools Do Not Have Separate Standards for
Disadvantaged Applicants. We surveyed a number of medical schools in
seven western states for information on their admissions standards for
disadvantaged applicants. Each of the seven schools reported that they do
not have separate standards for advantaged and disadvantaged applicants;
all applicants are judged by the same selection criteria.
National Reaction to Diversity Programs Is Polarized
The national debate over diversity policies has resulted in a variety of
reactions. Some states have rejected the policies as a furtherance of
affirmative action. Others see diversity as a positive step and have
initiated programs to elevate minority applicants’ academics prior to
admittance.
Several Other States Do Not Allow Diversity Issues to Be
Considered as Part of the Medical School Admissions. Although
many universities follow the diversity policy promoted by the AAMC, a
few states are concerned with what they believe are unfair policies that
recognize race and gender rather than ability. This resistance is most
notable in states that have had public referendums in opposition to
affirmative action-based programs. For example, California voters passed
proposition 209 which prohibits all affirmative action programs within
state government and public universities. The implementation of the new
law has resulted in a conflict between that state’s Legislature and the
state’s schools of higher education. The Legislature wants the law carried
out and some of the state’s universities continue to promote the
enrollment of minority applicants.
Texas and Washington have also passed similar public referendums
against the use of diversity policies by institutions of higher education.
The Governor of Florida is asking the Florida State Legislature to

Office of the Utah Legislative Auditor General – 37 –
-37-
Some states provide
disadvantaged
minority students
with special pre-
medical training.
consider his “One Florida” plan, abolishing affirmative action in university
admissions and state contracting.
Diversity Can Exist Without Lowering Admission Standards. An
alternative to lowering admission standards for disadvantaged applicants
would be to use some of the techniques of New Mexico and Hawaii that
increases participation among minority applicants. These states focus
their efforts on providing special instruction to disadvantaged minorities
who wish to pursue a career in medicine. For example, the University of
New Mexico offers a special curriculum to applicants from under-
represented populations whose academic training is below that normally
expected from medical students. Students who successfully complete the
additional one-year curriculum are automatically enrolled as first year
medical students the following year.
Similarly, Hawaii has a special post-baccalaureate program which helps
individuals from socially, educationally and economically disadvantaged
backgrounds. These students are enrolled in the program with the
understanding that upon completion of medical school they will serve in
under-served communities within the State of Hawaii and the Pacific
islands. Students are first enrolled in a one year program to help develop
their science skills as well as their communication skills. As with New
Mexico, upon completion of the program, the students are automatically
enrolled as first year medical students. Both New Mexico and Hawaii
program’s are limited and very selective of candidates.
Recommendations
1. We recommend that the School of Medicine adopt a single
minimum MCAT and GPA threshold for all admissions.
2. We recommend that the School of Medicine prohibit the
admissions committee from considering the applicant’s race,
gender, religion, geographic background, etc. If review forms or
interview comments show that such factors have been considered,
they should be considered invalid.
3. We recommend that the School of Medicine consider providing
under-represented populations with special pre-admittance course
work to help them meet the academic standards required of all

-38-
– 38 – A Performance Audit of Medical School Admissions
students.
4. We recommend the Legislature direct the Board of Regents to
examine the apparent conflict between its policies regarding
diversity and those regarding non-discrimination and report their
findings to the Legislature.

Office of the Utah Legislative Auditor General – 39 –
-39-
Often the Dean of
Admissions, rather
than the committee,
decides whether an
applicant is to
receive an interview.
Chapter IV
Deviations from Admissions Process
Have Raised Questions
In recent years the School of Medicine has altered the way it processes
medical school applicants. As stated in Chapter I, greater emphasis is
placed on the subjective evaluation of an applicant’s character and
background and less emphasis is placed on the applicant’s academic
record. However, the school has had difficulty ensuring that the new
selection criteria is fair and consistently applied. To this end the school
needs to reevaluate some of its policies and improve its controls over
admissions procedures.
Central to the problems facing the admissions process is the
relationship between the school’s Dean of Admissions and the three
committees responsible for the selection of applicants. Although the
members of the Review, Interview and Selection Committees all receive
directions from the school’s administration, their decisions are often
inconclusive or overridden by the Dean of Admissions. One result of the
committee’s indecision is that one person—the Dean of Admissions—
must often be the one to decide whether or not an applicant will receive
further consideration.
Inasmuch as the School of Medicine has made many changes to the
admissions process to prevent any one committee member from having
too much influence, it is surprising that the Dean of Admissions has been
given responsibility for deciding individually on many applications.
Another concern is that the responsibilities of the Dean of the Office of
Admissions may conflict with her other role as Dean of the Office of
Diversity and Community Outreach. We question whether the dean can
serve as an impartial manager of the admissions process while also being
responsible for recruiting more minorities and women.
Review Committee Decisions
Are Not Always Followed
The Review Committee is responsible for deciding whether an

-40-
– 40 – A Performance Audit of Medical School Admissions
applicant is academically prepared and fully committed to the highly
demanding field of medicine. This group of 17 faculty and physicians
from the Health Sciences Center and the community make the initial
screening. During the 2001 recruitment year, the Review Committee
considered 322 applications classifying each application as either accepted
or rejected for further consideration or as inconclusive and needed more
review.
The Review Committee’s decisions were given to the Dean of
Admissions where a number of the decisions were overridden. A number
of applications initially rejected by the Review Committee were, either
due to a decision by the Dean of Admissions or due to staff errors,
interviewed anyway. In the case of inconclusive applications, the Dean of
Admissions, rather than the committee, decided which of the applicants
would be granted interviews and which would be rejected.
Review Committee Considers Applications
With Low GPAs and MCAT Scores
The applicants with GPAs higher than 3.5 and scores on the MCAT of
at least 30 are automatically invited for interviews. For the application
year 2001, 200 applications fit that category. The other 210 applications
required a review by the Review Committee because they had GPAs
below 3.5 or an MCAT below 30. In most instances, each application is
reviewed by two committee members. The Review Committee examines
the applicant’s college transcripts, MCAT scores and disadvantaged status,
and then decides whether the person is adequately prepared to handle the
curriculum of medical school. It is the only stage of the process where an
applicant’s academic achievements are considered.
The Review Committee also evaluates applicants’ letters of
recommendation, personal statements, volunteer service, and exposure to
medicine. At the end of the evaluation, each reviewer prepares a written
description of the strengths and weaknesses of the applicant and states
whether the applicant should be interviewed or not (See Appendix C).
Figure 9 shows the flow of applications for the review stage of the
admissions process.
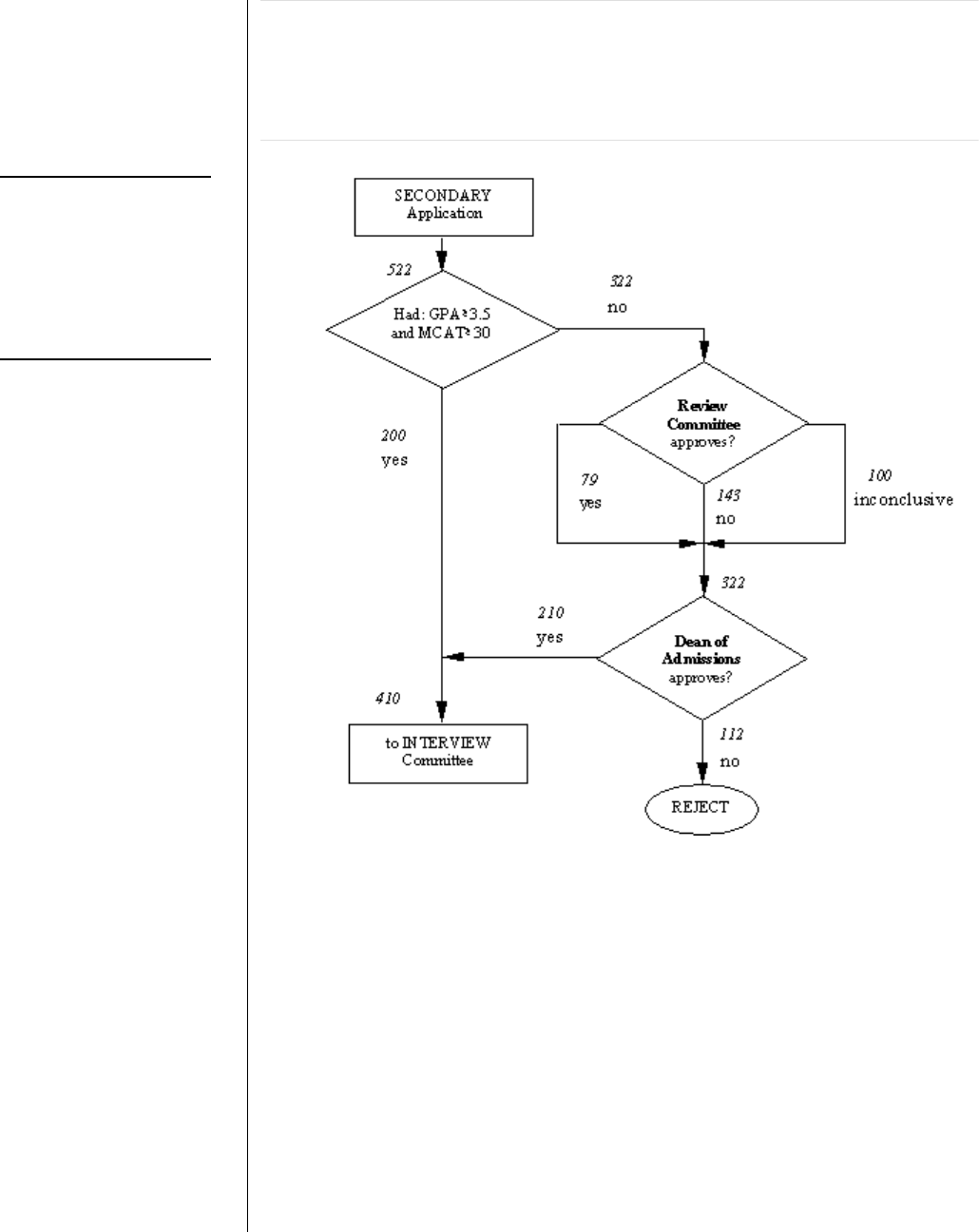
Office of the Utah Legislative Auditor General – 41 –
-41-
Last year 31
applications were
sent to the Interview
Committee even
though they had
been rejected by the
Review Committee.
Figure 9. The Review Committee Selects the Applicants for the
Interviews. The Review Committee is the only committee allowed
to consider applicants’ academics and disadvantaged status. The
reviewers also consider applicants’ exposure to medicine, volunteer
experiences, letters of recommendation, and personal statements.
Some Applicants Rejected by the Review Committee
Were Still Interviewed
During the 2001 recruitment year, 31 applications were sent to the
Interview Committee that the Review Committee had determined should
not have received further consideration. When asked to explain why these
applicant were interviewed even though the Review Committee
recommended against it, the Dean of Admissions provided the following
reasons:
• Sixteen applicants were granted “courtesy” interviews. They were

-42-
– 42 – A Performance Audit of Medical School Admissions
Many applications
considered by the
Review Committee
result in a mixed or
inconclusive
decision. These
applications are
decided by the dean.
interviewed because they are a relative of a physician on campus or
some other prominent individual who might be offended if the school
did not appear to give serious consideration to the applicant. The
dean told us that those given “courtesy” interviews are not allowed to
proceed to the Selection Committee regardless of the outcome.
• Four applicants were scheduled for interviews by administrative
mistake. Although rejected by the Review Committee, an oversight
by admissions office staff led to their being scheduled for an interview.
Before the dean recognized the mistake, several of these were
submitted to the Selection Committee and two were accepted and are
now enrolled in medical school.
• Eleven applications were sent on after the Dean of Admissions
overruled the Review Committee’s recommendations. In most of
these cases, the dean decided that the Review Committee members
had not given sufficient consideration to the applicant’s disadvantaged
background. For example, the committee did not give sufficient
weight to the applicant’s rural background or may not have mitigated
low academics with the applicant’s ethnic heritage.
• In one case, the two reviewers identified seven distinct problems with
an application, any one of which could result in a rejection. Even
though a letter of rejection was sent, the school decided to reconsider
the application and another round of reviews was conducted. The
third reviewer concluded that the applicant should not be interviewed.
However, the fourth reviewer gave a favorable recommendation. In
spite of three negative reviews, the dean made a decision, based on the
applicant’s disadvantaged status, to forward the application to the
Interview Committee. The applicant did well in the interviews and
was eventually approved for admission by the Selection Committee.
Applicants with Mixed Reviews Should Have Received Another
Round of Reviews. We also found that reviewers are often unwilling to
make a clear decision regarding whether an applicant should be
interviewed or not. For the 2001 recruitment year, almost one third of
the decisions made by the Review Committee were either mixed or
inconclusive. In other words, both reviewers said “maybe,” or one of the
reviewers felt that the applicant should be interviewed and the other felt
that he/she should be rejected.
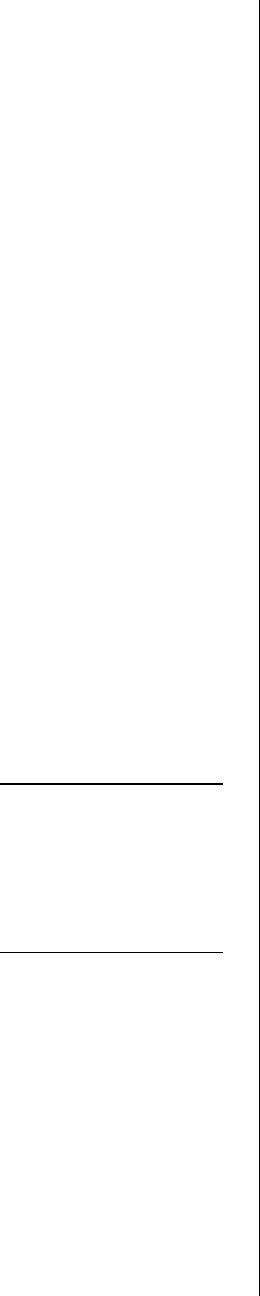
Office of the Utah Legislative Auditor General – 43 –
-43-
It is a concern that
the Dean of
Admissions is also
the Dean of Diversity
and Community
Outreach.
It is a generally accepted practice, though not formalized in policy,
that when two reviews result in a mixed decision, a second round of
reviews is conducted. As a result, it is not uncommon for an application
to receive a third or fourth review. However, many applications with
inconclusive decisions by the Review Committee were never submitted
for another round of reviews. Instead, the Dean of Admissions decided
whether or not to forward the application without additional reviews. Of
the 210 applications that were sent to the review committee and approved
for interviews, 100 received a mixed decision from the review committee
and were decided by the Dean of Admissions without additional reviews.
Role of Dean in the Decision-making Process
Needs Clarification
One reason the dean said she needs to decide whether applicants
should be interviewed is that many Review Committee members are
reluctant to make the decision. This reluctance may be, in part, due to the
subjective nature of the selection criteria and, in part, to the form utilized
by the committee. Review Committee instructions are not concise or
straight forward and the review form allows reviewers to conclude that
“maybe” the applicant should be interviewed.
One concern we have with the dean’s role of deciding whether many
applications will be granted interviews is that the entire purpose of
creating a Review Committee was to help the school reduce bias in the
admissions process. Having so many different people involved in the
selection process is supposed to prevent a single person from having too
much influence. With the dean making many of the decisions for them, it
seems to defeat the purpose of having a Review Committee.
A further concern is that the Dean of Admissions has the additional
role of being the Dean of Diversity and Community Outreach. As the
Dean of Admissions, she is responsible to ensure that each application is
considered in a fair and impartial manner without regard to gender, race,
religion, geographic background. As the Dean of the Office of Diversity
and Community Outreach, she has the responsibility of “recruiting,
admitting and graduating qualified candidates from... minority groups...
as well as disadvantaged students and women applying to medical school.”
It is unclear whether the responsibilities of the Dean of Admissions
conflict with the responsibilities of the Office of Diversity and

-44-
– 44 – A Performance Audit of Medical School Admissions
Community Outreach. However, having the same person fill both roles,
at least, presents the opportunity that the admissions office could give
preference to students being assisted by the Office of Diversity and
Community Outreach.
Interview Problems
Raise Question of Fairness
Several concerns have also been raised about the operation of the
Interview Committee. First, many interviewers are confused about how
to correctly fill out the written interview form. Second, many interviews
do not result in a clear decision whether or not the applicant should be
given further consideration. As a result, the Dean of Admissions must
often make a decision regarding whether to send the application to the
Selection Committee. Finally, a few interviewers appear biased or have
asked inappropriate questions.
Once an application is submitted to the Interview Committee, an
applicant’s MCAT and GPA scores are no longer considered. It is
assumed that all applicants are equally qualified in terms of their academic
preparation for medical school. For this reason, the Interview
Committee, consisting of 66 faculty, staff and fourth year medical
students, focuses on the more subjective selection criteria.
Normally, each applicant is interviewed individually by two and
sometimes three of the members of the interview committee. The
objective of the interview is to evaluate each applicant’s interpersonal skills
and character. Each interviewer also considers the letters of
recommendation, personal statement, and other information included in
the application. During the 2001 recruitment year, 166 applications were
eliminated after the interview process (or about 40 percent of the
remaining applications) and approximately 240 applications were sent on
to the Selection Committee. Figure 10 shows the number of applicants
involved in the interview process.
Office of the Utah Legislative Auditor General – 45 –
-45-
Interview Committee
considers an
applicant’s
character,
background and
interpersonal skills.
Figure 10. The Interview Committee Recommends Which
Applicants Are to Be Presented to the Selection Committee.
Applicants are evaluated based on the interview, their letters of
recommendation, personal essays, exposure to medicine, volunteer
service, and ability to handle issues.
It is the responsibility of the Interview Committee to decide whether
an applicant is to be presented to the Selection Committee. The high
number of applications forwarded to them by the Review Committee and
a desire to give each applicant equal consideration mean the committee’s
66 members will conduct well over 800 interviews.
Time constraints do not permit the committee to conduct as many
interviews as are needed to give each applicant a fair and impartial review.
In order to make the process fair and impartial, the Admissions Office

-46-
– 46 – A Performance Audit of Medical School Admissions
Interviewers are not
consistent in how
they rate applicants.
told us that applicants will typically not be rejected unless both
interviewers conclude that the applicant should not be considered for
admission. In addition, if the applicant feels that the interviewer has asked
inappropriate questions or has shown bias, the applicant can ask the
Admissions Office for another interview with a different interviewer and
the results of the first, questioned interview will be discarded.
Unfortunately, there is often insufficient time to provide all applicants
with a third interview if the first round of interviews resulted in a mixed
or inconclusive decision.
The use of a three-page evaluation form to summarize interviewer
comments is another way that the school has tried to make the interview
process as fair and impartial as possible. The form requires each
interviewer to evaluate and score an applicant according to eight criteria
(see Appendix C for a blank copy of the interview form). Interviewers are
asked to consider a number of different factors. First, the interviewer
considers the applicant’s response to questions asked during the interview.
Then, the interviewer considers the applicant’s written personal statement
and his or her letters of recommendation.
Interviewers use the forms to describe the strengths and weaknesses of
the applicant and to summarize their overall impressions of the applicant.
Interviewers are also asked to give an overall ranking of the applicant on a
five-point scale and to check “yes,” “no,” or “maybe” to the following
questions: “Should this applicant be discussed?” “Should this applicant
be an alternate?” “Should this applicant be accepted?”
The Evaluation Form Causes Confusion. We reviewed each of the
committee member’s written comments for all 410 applicants interviewed
during the 2001 recruitment year. We found that each interviewer has a
unique way of completing the forms. There did not appear to be a great
deal of continuity in the ratings that were given to applicants nor was it
clear that the interviewers understood what they needed to communicate
about the interviews. The greatest confusion comes from the last three
questions on the evaluation form.
For example, in response to the question: “Should this applicant be an
alternate,” one interviewer wrote “I really don’t understand this question.”
In many cases we found that interviewers gave contradictory statements
indicating an applicant should be discussed by the Selection Committee
but not admitted. Others said the applicant should be an alternate but not
discussed by the Selection Committee.
Office of the Utah Legislative Auditor General – 47 –
-47-
Often two interviewers
disagreed on whether
an applicant should be
considered by the
Selection Committee.
The diversity of an
applicant plays a
major role, as
women and
minorities benefit at
a higher rate than
one would expect.
The form also asks interviewers to give an overall ranking to each
applicant on a five-point scale. Some interviewers give glowing comments
about an applicant but only give an average rating by checking the 3
rd
(or
middle) option for “Ranking Among Basic Qualities and/or
Achievements.” Others are somewhat critical of applicants but still give
the applicant the higher rating of “Ranking With some Outstanding
Qualities and/or Achievements.” Still, others rarely give any negative
comments about an applicant and almost always give the highest rating
possible. The result is that it is very difficult to conclude from the
interview forms what the interviewer is recommending.
Many Interviews Result in a Mixed Decision. Just as with the
Review Committee, the Interview Committee often produces a mixed
decision. Often the two interviewers disagree on whether an applicant
should be considered by the Selection Committee. More frequently, the
interviewers provide many positive comments but are not clearly in
support of recommending that the applicant be considered for admission.
It is the general understanding of those involved in the admissions
process that mixed or inconclusive interviews will result in an additional,
tie-breaking interview. In practice, however, most inconclusive interview
cases are determined by the Dean of Admissions. The dean reviews
interviewers’ written comments and decides whether the applicant should
be considered further or be rejected. In making this decision, it appears
that diversity of the applicant plays a major role, as women and minorities
benefit at a higher rate than one would expect. Figure 11 describes the
gender and ethnic status for the applicants for whom the Dean of
Admissions made the final decision.
Figure 11. Applicants with Inconclusive Interview Results that
Were Decided by the Dean. Of those applications decided by the
Dean of Admissions, the women and minority applicants were more
likely to be recommended to the Selection Committee than their
white male counterparts.
Female or Minority Applicants White Male Applicants
Sent To Selection
Committee Rejected
Sent To Selection
Committee Rejected
71% 29% 37% 63%

-48-
– 48 – A Performance Audit of Medical School Admissions
Diversity is clearly
an issue and either
elevates or reduces
an applicant’s
likelihood of being
accepted.
Figure 11 describes the outcome of those interviews that resulted in a
mixed or unclear conclusions from the Interview Committee. Because the
Interview Committee did not give a clear recommendation whether or not
to send the application to the Selection Committee, the Dean of
Admissions had to make that decision. The data show that among the
female and minority applicants, with a mixed or unclear recommendation
from the Interview Committee, the dean decided to send 71 percent to
the Selection Committee. Among the white male applicants, the dean
chose to send only 36 percent to the Selection Committee. This action
may be best explained by the value that the school places on gender and
ethnic diversity.
We also found 30 applicants who, according to their interviewers,
should have been presented to the Selection Committee but were not. In
these cases the Dean rejected these applicants even though both of their
interviewers recommended they be presented to the Selection Committee.
In that group, 28 of the 30 applicants were white males.
A review of the interview results demonstrates that diversity is clearly
an issue and either elevates or reduces an applicant’s likelihood of
acceptance. The results of the Dean’s decisions raise questions as to how
much influence one individual should have on selecting a medical school
class. The School of Medicine has acknowledged that the Dean should
not be required to decide whether an application should proceed to the
Selection Committee or not. School officials report that in the future a
separate committee will review applications that receive mixed results
from the Review or Interview Committees.
Interviewers with Demonstrated Bias Should Be Removed. As we
reviewed the written comments made by interviews, we noticed that some
interviewers wrote biased comments. Some applicants also told us they
felt they were asked inappropriate questions. The school is aware of these
situations and tries to respond appropriately.
The following describes some of the bias shown by interviewers and
the inappropriate questions they have asked:
• We identified one interviewer who on more than one occasion
made biased comments towards white male applicants in her
written interview evaluations.
• One interviewer, according to the Dean of Admissions,

Office of the Utah Legislative Auditor General – 49 –
-49-
demonstrated bias towards female applicants in that he was much
more demanding and critical of female applicants than he was of male
applicants.
• An interviewer asked each applicant a series of trivia questions such
as “How many periods are in a hockey game?” or “Who shot
Robert Kennedy?” Applicants told us they felt such questions
were unfair because they were asked in an intimidating way and
had little to do with the applicant’s qualifications for medical
school.
• An interviewer quoted religious scriptures in interviews and
discusses them with the applicant.
The Dean of Admissions recognizes that some interviewers have acted
inappropriately and said that she advises them not to ask inappropriate
questions. Moreover, the training manual for interviewers cautions
interviewers to avoid “inappropriate, uncomfortable or possibly
discriminating questions” and requires that questions have a “relation to
the education of the student.”
Unfortunately, the Dean of Admissions appears to either be reluctant
or is unable to remove interviewers who ask inappropriate questions. She
reports that she regularly counsels interviewers when she learns that
inappropriate questions have been asked. In addition, the Dean has
responded by giving fewer assignments to interviewers who have asked
inappropriate questions and may reassign them to other committees
during the next recruitment year. In our opinion, however, if a
committee member is not following the schools’ admissions procedures
and does not improve after having been asked to do so, the interviewer
should be immediately removed from the Interview Committee.
Selection Committee Process
Can be Streamlined
During our discussions with several committee members, we were
impressed by their commitment to this time-consuming process and to
making a fair decision regarding each application. Although we are
confident in the ability of this group to make fair and appropriate
decisions, we question whether some applications should have been sent
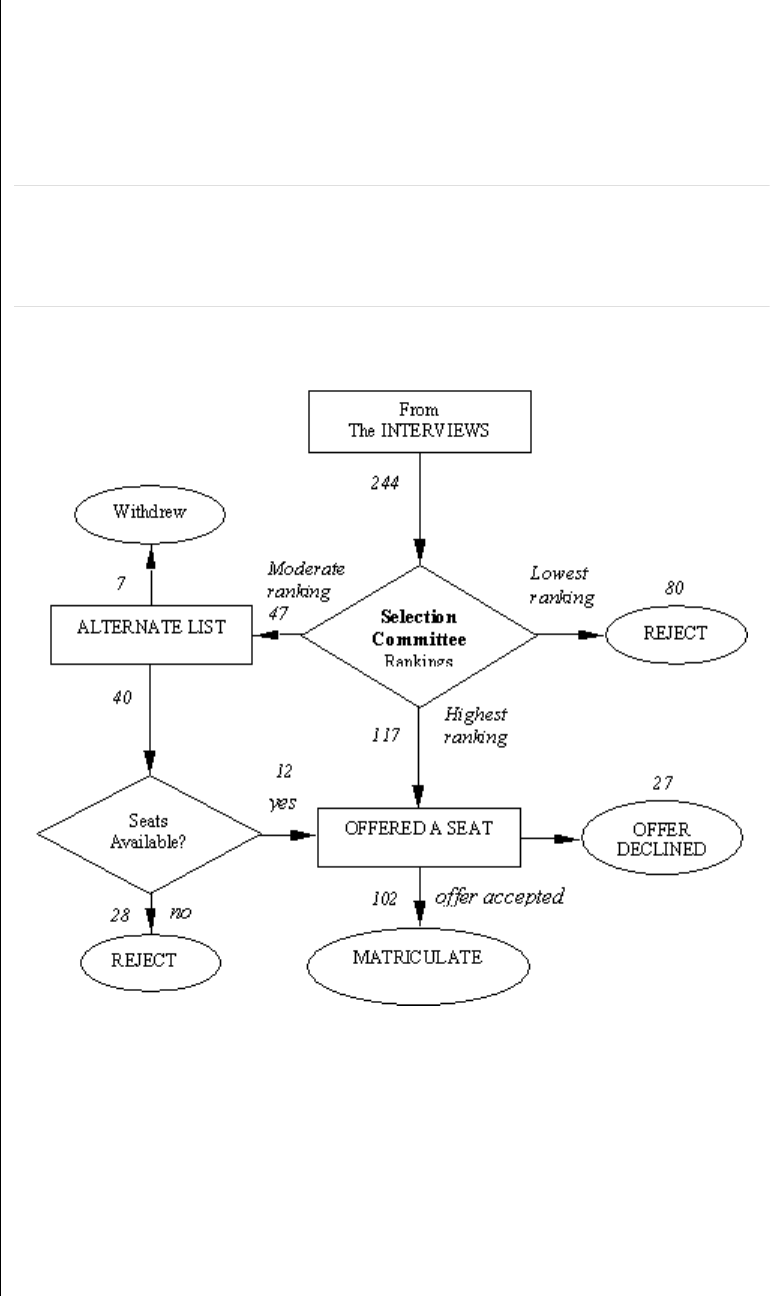
-50-
– 50 – A Performance Audit of Medical School Admissions
to the Selection Committee at all. In addition, we are concerned that the
Selection Committee does not receive all of the information it needs to
make an informed decision. Finally, we are concerned about the way the
admissions office uses the Selection Committee’s scores.
Figure 12. Selection Committee Makes a Final Ranking of the
Applicants. The committee members meet together, discuss and
individually rank each application based on the interview scores and
comments, letters of recommendation, personal essays, etc.
Selection Committee Has Responsibility of Deciding Which
Applicants Will Be Accepted. The members of the Selection Committee
have the difficult task of deciding which of all the applications presented
will be sent letters of acceptance. Because the Selection Committee only
has a limited amount of time to consider roughly 250 applications, it is
important that the committee receive only the top candidates. Figure 12
shows the flow of applicants for this stage of the admissions process.
The Selection Committee has 26 members who meet for about three
hours once a week for about six months. They represent different
departments within the Health Sciences Center and include professors,
Office of the Utah Legislative Auditor General – 51 –
-51-
The dean approved
“courtesy” reviews
even though it was
unlikely the
applicant would be
accepted.
instructors, and fourth year medical students. Several members also
represent the medical community at large. During each meeting they
evaluate from 12 to 15 applications. The strengths and weaknesses of
each application are briefly discussed and then each member is asked to
individually rank the application on a scale of zero to five. The scores are
averaged, and the applicants with the highest scores are sent a letter of
acceptance. Some applicants are placed on an list of alternates and the rest
are sent letters of rejection.
Some Applications Should Not Have Been Presented to the
Selection Committee. During the recruitment for the class entering in
the Fall of 2001, about 60 applications were presented to the Selection
Committee that either did not pass the Review Committee, did not pass
the Interview Committee, or had inconclusive results from the Interview
Committee. Although the dean recognized that these applications had
some serious flaws, she sent about 30 of them to the Selection Committee
as tests to determine whether the Selection Committee would identify the
same flaws in the application that she observed. The dean reports that the
Selection Committee concluded as she did that there were problems with
each of these “test” applications.
Additional applications were sent to the Selection Committee even
though they were not recommended favorably by the Interview
Committee. The dean said she submitted these applications as a courtesy
to the applicant or because other supporters of the applicant wanted the
application to receive consideration by the Selection Committee.
The above cases are a concern for two reasons: First, three
applications apparently failed earlier stages of the review process that were
submitted to the Selection Committee in error and were accepted.
Second, due to time constraints, it is critical to limit the applications
considered by the Selection Committee to those that have been approved
by prior committees. As previously mentioned, during the 2001
recruitment year there were 30 applications that received favorable
recommendations from the Interview Committee yet were not sent to the
Selection Committee because, according to the dean, there was not
sufficient time to consider all of the well-qualified applicants.
Selection Committee Could Benefit by Having Applicants’
Academic Scores. The Selection Committee currently does not receive
any academic information on the presented candidates before them. The

-52-
– 52 – A Performance Audit of Medical School Admissions
The committee is
not given grades
and MCAT scores,
only limited
subjective
information from the
application and
interview forms.
The school admitted
lower ranked out-of-
state applicants over
higher ranked Utah
applicants.
committee is given limited information from the application form and the
interview form. The assumption is made that all applicants have been
approved by the Review Committee and are therefore equally qualified in
terms of their academic preparation for medical school.
During our review of the application files we observed significant
differences in the academic qualifications of the applications that were
eventually sent to the Selection Committee. For the 2000-2001
recruitment year, applicant MCAT scores ranged from 20 to 39, and
GPAs ranged from below 2.8 to 4.0. We find it difficult to understand
why the Selection Committee is required to base its decisions on the
subtle problems they find in the comments made by interviewers,
applicants’ personal statements and the letters of recommendation, while
at the same time the committee is not allowed to consider the obvious
differences in applicants’ academic records.
Dropping Selection Committee Low Scores Has Not Been
Implemented. Occasionally, a Selection Committee member will give a
very low rating to an applicant who fails to impress him or her. This low
rating can have a tremendous effect on an applicant’s average score. For
those on the verge of being accepted or rejected, the extremely low vote
can be the deciding factor.
Because there is a possibility that a single low vote could make the
difference between an applicant being accepted or rejected, the School of
Medicine adopted the policy of dropping any score that is two standard
deviations below the average score. Unfortunately, the policy has not
been implemented.
Selection Scoring and Acceptance Policies Need Review. The
School of Medicine’s current practice is to admit 8 residents from Idaho,
75 Utah residents, and give another 19 positions to out-of-state residents.
Because the admissions office compares the selection committee scores
and awards positions from Idaho, Utah and other states separately, some
applicants from one group may be rejected even though they had higher
scores from the selection committee than applicants who were accepted
from one of the other groups.
For example, one year the Admissions Office admitted its usual 75
Utah applicants and 8 applicants from Idaho. They awarded the
remaining positions to out-of-state applicants. However, the last two out-
of-state applicants to be awarded positions had lower scores from the

Office of the Utah Legislative Auditor General – 53 –
-53-
selection committee than about two dozen applicants from Utah and
Idaho who were not admitted.
In a similar situation, while selecting applicants from the alternate list,
several lower-ranked applicants from one Utah school were selected over
higher-ranked applicants from another Utah institution. At the end of
each admissions process usually a few positions become available when
some applicants who have been previously accepted decide to attend
another medical school. The School of Medicine typically tries to offer
these remaining positions to students who have not been accepted at any
other medical school. Moreover, the school does not necessarily offer the
remaining positions to applicants in the order of their ranking by the
Selection Committee.
During the admissions process for the class admitted in the fall of
2001, five applicants from one school were passed over, and the three
remaining positions were offered to applicants from another school. The
School of Medicine felt this deviation from the rankings was necessary
because the school needed to admit additional students from the one
institution in order to compensate for a mistake made by the school’s pre-
med advisor. Apparently, inappropriate information had been given to
the Selection Committee by the school’s premedical advisory committee
that put students from that school at a slight disadvantage during the
Selection Committee’s deliberations.
Recommendations
1. We recommend that the School of Medicine discontinue offering
courtesy interviews.
2. We recommend that the School of Medicine establish a policy
regarding how to resolve reviews that result in a mixed conclusion.
Specifically, the school should consider having such applications
decided by a third, tie-breaking review rather than by the Dean of
Admissions.
3. We recommend that the School of Medicine review its
administrative structure and determine what the appropriate
relationship should be between the Office of Admissions and the
Office of Diversity and Community Outreach.

-54-
– 54 – A Performance Audit of Medical School Admissions
4. We recommend Review Committee instructions establish
simplified evaluation criteria and eliminate the “maybe” option on
the evaluation form. Only “yes, send to interview” or “no, reject
applicant” conclusions should be available.
5. We recommend that the School of Medicine explore methods of
reducing applications forwarded by the Review and Interview
Committees.
6. We recommend the School of Medicine consider revising its
interview forms to eliminate applicant score confusion either by
assigning a weight and score for each criterium to develop an
overall score or by elimination of all numeric scoring of applicants.
7. We recommend the School of Medicine’s interview form limit final
evaluation options to either a “yes, forward to selection” or “no,
reject applicant”.
8. We recommend that the Selection Committee only be presented
the applicants with positive interview outcomes.
9. We recommend the School of Medicine implement its policy to
drop scores by the Selection Committee members that fall below
two standard deviations from the average score.
10. We recommend that after Utah and Idaho commitments are
made, Selection Committee rankings be combined for all
applicants so the next best scoring applicant is taken regardless of
state affiliation.

Office of the Utah Legislative Auditor General – 55 –
-55-
Appendices

-56-
– 56 – A Performance Audit of Medical School Admissions
This Page Left Blank Intentionally

Office of the Utah Legislative Auditor General – 75 –
-75-
Agency Response

RESPONSE OF
THE UNIVERSITY OF UTAH
SCHOOL OF MEDICINE
INTRODUCTION
The University of Utah School of Medicine (the “School”) appreciates the Auditor
General’s efforts to evaluate the School’s admissions process. The report of the Auditor
General (the “Audit Report”) has identified several areas where the School’s admissions
process can be improved and has offered valuable recommendations to the School. The
School has and will take those recommendations very seriously. In fact, the School has
already implemented changes to its admissions process that address many of the issues
raised in the report. In response to the Audit Report, the School will be implementing
additional changes that should satisfy all recommendations made by the Auditor General.
This audit presents a great opportunity for the Auditor General and the School of
Medicine to educate the Legislature, and all Utah citizens, concerning medical school
admissions processes. Serious misperceptions have developed concerning the School of
Medicine’s process. The audit should go a long way to dispel many of those
misperceptions. Particularly significant in this regard are the Auditor General’s findings
that 1) the School of Medicine has not enrolled applicants who are not qualified for
medical school; 2) the School of Medicine admissions process does not show bias for or
against factors that include religious affiliation, undergraduate college, age or
geographical origin; and, 3) the School of Medicine does not use an affirmative action
quota system.
The School of Medicine has two goals for this Response to the Audit Report. First, the
School wishes to highlight from the Audit Report several important points made by the
Auditor General. Second, the School of Medicine wishes to outline for the Legislature
its plan to implement all recommendations from the Audit Report.
IMPORTANT FINDINGS FROM THE AUDIT REPORT
The Audit Report made some very critical findings that should be noted by the
Legislature. Those findings are as follows:
I. Selecting Each Year’s Medical Class Is An Exceedingly Difficult Task for
the School of Medicine.
In his report, the Auditor General recognizes that the “University of Utah School of
Medicine has the difficult task of selecting a medical school class of 102 students from
500 to 600 qualified applicants each year.” (Audit Report, p. 2). The report recognizes
that the average GPA for all applicants exceeds a 3.5 and the average MCAT score for all
applicants is a 28.8 or better. (Audit Report, p. 24). Coupled with the high academic
achievement of the applicant pool is the fact that most applicants who apply to the School
have followed similar paths to medical school and are hard to distinguish. As the Auditor
General notes, “[s]o many applicants are highly qualified and have such similar
backgrounds that it is difficult to set them apart.” (Audit Report, p. 30).
II. “There is No Evidence That Unqualified Individuals Have Been Admitted to
Medical School.”
This audit has apparently grown out of the perception by some who have not been
selected for admission to the School of Medicine “that they have not been given an equal
opportunity.” (Audit Report, p. 1). Perhaps the most important finding in the Audit
Report is the Auditor General’s conclusion that “there is no evidence that unqualified
individuals have been admitted to medical school.” (Audit Report, p. 1). In fact, there is
strong evidence that the School does an outstanding job of selecting applicants. The
School of Medicine excels among medical schools in terms of graduation rates, passage
of board exams and placement in residency programs for its students. This holds true for
medical students regardless of their age, gender, race, undergraduate academic
achievement, or other distinguishing characteristic. The Audit Report makes no findings
to the contrary.
III. The School of Medicine’s Admissions Process Does Not Show Bias Based
Upon An Applicant’s Religion, Undergraduate College, Age, or Geographical
Origin.
Another important conclusion reached by the Auditor General is that “there does not
appear to be any significant difference in the rate of acceptance when considering the
college where an applicant earned a pre-medical degree, an applicant’s geographic origin,
or age.” (Audit Report, p. 9). The Auditor General also “found no evidence of bias
against applicants based on their religious affiliation.” (Audit Report, p. 9). Also see
findings at pages 17-20 of the Audit Report.
IV. The School of Medicine Does Not Have a Quota System For Women and
Minorities.
Another very important finding by the Auditor General is that the School of Medicine
“does not use an affirmative action quota system” and does not accept women, minorities
or any other groups of candidates in order to fill quotas. (Audit Report, pp. 27-28).
V. The School of Medicine Has Implemented a Selection Process, Recommended
by the Association of American Medical Colleges (“AAMC”), and Used By
Most Medical Schools Throughout the Country.
Important for the Legislature to understand is that the School of Medicine’s admissions
process is not unique. Ad the Audit Report notes, the School’s admissions process is
very similar to the selection process advocated by the AAMC and “used by medical
schools in other states.” (Audit Report, pp. 2).
2
VI. Like Other Medical Schools, the School of Medicine Analyzes Various
Cognitive and Non-Cognitive Factors In Order to Select Applicants Who Will
Be the Best Medical Students and the Best Practicing Physicians.
As the Auditor General notes in his report, the School of Medicine’s admissions process
evaluates both the cognitive and non-cognitive characteristics of its applicants in order to
identify from the entire pool of highly qualified applicants those individuals who will
make the best medical students, and ultimately the best physicians. (Audit Report, pp. 2-
5). Factors considered by the School in the selection process include:
• Undergraduate GPA scores including overall, science, and all other;
• MCAT scores;
• Evidence of leadership and management skills;
• Physician shadowing experience;
• Exposure to patient care;
• Community service;
• Research experience.
(Audit Report, p. 4). As noted in the Audit Report, the School does not place undue
emphasis on an individual’s raw undergraduate GPA’s, or upon a candidate’s MCAT
scores. (Audit Report, pp. 4-5). Substantial research has shown that this raw data,
though a useful benchmark for determining cognitive ability, does not serve as a good
predictor of medical school success (particularly in the clinical years) or of success as a
physician. (See Bibliography attached hereto as Exhibit A). Moreover, research shows
that other criteria besides MCAT and GPA are better predictors of a candidate’s ultimate
success. (See Bibliography, Exhibit A).
VII. The School of Medicine Has Attempted Through Its Admission Process to
Promote Fairness.
As noted by the Auditor General, the School of Medicine has taken steps to promote
fairness in its admission process. (Audit Report, p. 7). “Recognizing that each
committee member has his or her own unique set of biases and perspectives, the School
of Medicine has taken several steps to ensure that no single member of the admissions
committee has too much influence over the process.” (Audit Report, p. 7). These steps
include implementation of a multi-level review process where committee members only
serve at one level; selection of committee members by various departments, community
organizations, hospitals, senior medical students and alumni, rather than by a single
individual; inclusion of over 100 people on admissions committees to accomplish a wide
range of views and perspectives; opportunities for further review of candidates who feel
that a mistake has been made or feel unfairly treated; and, exclusion of certain potentially
prejudicial information from files before they are presented to the Selection Committee.
(Audit Report, pp. 7-8).
The Auditor General was also “impressed by [the committee members’] commitment to
this time-consuming process and to making a fair decision regarding each application.”
(Audit Report, p. 49). Moreover, the Auditor General expressed his confidence “in the
3
ability of the group to make fair and appropriate decisions . . . .” (Audit Report, p. 49-
50).
VIII. The School of Medicine, Along With the University of Utah, the Utah State
Board of Regents, the AAMC, and Medical Schools Throughout the Country,
Promotes Diversity as a Positive Value for Medical Classes.
The School of Medicine promotes diversity as a positive value for its medical classes.
(Audit Report, p. 21). This value is shared by the Utah Board of Regents and promoted
for the entire system of higher education. (Audit Report, p. 22). Moreover, this value is
shared by the AAMC and by nearly every medical school throughout the country. (Audit
Report, p. 22).
While the Audit Report focused on diversity in the narrow sense of race and gender, the
School of Medicine values diversity in the broad sense of the word. As recognized by the
Auditor General, the School of Medicine values diversity for at least two reasons. (Audit
Report, p. 22). First, because medical schools train physicians who will serve many
different kinds of people, a diverse student body will be better able to meet the needs of a
diverse population. (Audit Report, p. 22). Second, though related, a diverse medical
class will expose medical students to a broad range of backgrounds, views and ideas
helping them to appreciate diversity in the people they will ultimately serve and enriching
the entire educational experience. (Audit Report, p. 22). Scholarly research and common
sense support these two concepts. (See Bibliography, Exhibit A).
IX. A Diversity of Experience Also Works to the Benefit of Applicants Who Must
Distinguish Themselves From the Large Pool of Highly Qualified Candidates
Seeking Admission.
As noted throughout the Audit Report, the task of selecting 102 students out of 500 to
600 highly qualified applicants who generally have very similar backgrounds is
immensely difficult. Those applicants who have something unique to offer, in whatever
form, distinguish themselves from the general pool and increase their chances of
selection during the admission process. This diversity comes in many different forms.
The Auditor General has provided a few examples. Utah applicants may distinguish
themselves from other Utah applicants by seeking an out-of-state undergraduate
education. (Audit Report, p. 19). Applicants may distinguish themselves by obtaining a
non-traditional pre-med degree or by pursing other non-traditional paths to medical
school. (Audit Report, pp. 29-30). Anything that applicants can do to distinguish
themselves from their fellow applicants in terms of their background and life experience
will obviously help to set them apart in the minds of people who must make very difficult
selection decisions.
4
X. The Audit Report Identifies Several Factors that May Account for the Higher
Rate of Acceptance for Women at the School of Medicine.
The Auditor General acknowledges that men and women applicants to the School of
Medicine “are roughly equal in terms of their academic qualifications.” (Audit Report, p.
10). Therefore, other factors besides academic achievement certainly play a role in the
selection process. The Audit Report provides insight into what these factors might be.
One factor may be that women tend to receive higher ratings for interpersonal skills than
their male counterparts. (Audit Report, p. 13). Another factor may be that female
applicants tend to select a different subject matter from male applicants for their personal
essays and tend to receive higher scores on those essays. (Audit Report, p. 14). Another
factor may be that more women than men tend to receive their undergraduate educations
from out-of-state institutions. (Audit Report, p. 19). Another factor may be that
“[w]omen . . . tend to have more varied backgrounds and experiences than typical white
male applicants from Utah.” (Audit Report, p. 29). Another factor may be that female
applicants “were less likely to pursue a traditional path to medical school.” (Audit
Report, pp. 29-30). There are undoubtedly other factors, not considered by the auditors,
that set some female applicants apart from their male counterparts. Whatever those
factors may be, there is no reason to assume that women are selected at a higher rate than
men simply because of their gender.
One important point not referenced in the Audit Report is that only 3 of the 126 medical
schools throughout the country admit a lower percentage of female applicants than the
School of Medicine. One factor that may account for this unfortunate statistic is that
most other medical schools have a higher percentage of female applicants than the School
of Medicine.
XI. The Audit Report Identifies Several Factors that May Account for the Higher
Rate of Acceptance for Minorities at the School of Medicine.
Although the Audit Report notes some distinction between the average academic scores
received by minorities and those in the majority, the report shows that this distinction is
relatively minor. In 2001, the average minority GPA was 3.51, as compared to a majority
GPA of 3.63, a difference of only .12. In 2001, the average minority MCAT score was a
28.8 as compared to a majority MCAT score of 30.3, a difference of only 1.4. (Audit
Report, p. 24). Moreover, research shows that MCAT scores and GPA for minorities are
continuing to increase over time. (See Bibliography, Exhibit A). Though raw academic
scores standing alone might favor certain majority applicants over other non-minority
applicants, other equally relevant factors might weigh in the opposite direction. The
Auditor General has noted a few such factors. Minorities, unlike their majority
counterparts, tend to receive their undergraduate educations from out-of-state institutions.
(Audit Report, p. 19). Minorities also “tend to have more varied backgrounds and
experiences than typical [majority] applicants from Utah.” (Audit Report, p. 29). Also,
minority applicants “were less likely to pursue a traditional path to medical school.”
(Audit Report, pp. 29-30). These are a few factors considered by the auditors that could
distinguish a minority candidate from the applicant pool. Others undoubtedly exist.
5
THE UNIVERSITY’S PLAN TO IMPLEMENT ALL RECOMMENDATIONS
FROM THE AUDIT REPORT
As stated in the introduction to this response, the School of Medicine has or will
implement all recommendations from the Audit Report. Those recommendations, and
the University’s actions in response, are as follows:
Recommendations at Page 37 of the Audit Report:
1. Implementation of a Single MCAT and GPA Standard
: The School currently
applies a single standard for all candidates. However, the information contained
in the current admissions manual is confusing and it will be clarified.
2. Inappropriate Comments by Review and Interview Committee Members
: The
School agrees that such comments have no place in the admissions process. The
School commits to revising its training materials and seminars to better educate
committee members on this issue. The School has removed, and will continue to
remove, inappropriate comments from the record when they occur. All applicants
will be encouraged to report inappropriate comments from interviewers.
Interviews containing inappropriate comments will be discarded and new
interviews arranged. Finally, the School will do a better job of excluding
individuals from the admissions process who make inappropriate comments.
3. Preapplication Course for Underrepresented Minorities
: The School has one such
course that takes place in the summer. The School currently does not have
sufficient funding to support a more comprehensive program. However, the
School has recently applied for a federal grant that, if awarded, would supply the
necessary funding for this program.
4. Board of Regents Policies
: The School is comfortable distinguishing policies for
recruitment from the admissions process, but has no objection to the review
suggested.
Recommendations at Pages 53-54 of the Audit Report:
1. Courtesy Interviews
: The practice of courtesy interviews was terminated this
recruiting year.
2. Process for Resolution of Conflicting Recommendations from Reviewers and
Interviewers: In response to this recommendation (as well as recommendations #
5 and # 8 below), the School has established a new executive admissions
committee that will synthesize the recommendations from the review and
interview committees, identify those applicants who should and should not be
presented to the selection committee, and identify those applicants who have
6
conflicting information requiring additional interviews or review. Hereafter, no
single person will ever make decisions concerning applicants. This change in the
admissions process will optimize the number of applicants who progress to the
Selection Committee.
3. Simultaneous Supervision of the Admissions Office and the Office of Diversity
and Community Outreach. The administrative supervision of these offices has
been separated. The Associate Dean for Admissions will no longer be responsible
for the office of Diversity and Community Outreach.
4. Revise Committee Instructions
: The School is currently reviewing and revising
all training materials, forms, admissions materials and web sites. The School’s
goal is to simplify and clarify the process in order to eliminate confusion and
accurately communicate the admissions process to committee members and
prospective applicants. This action will also address the issue of confusion noted
in recommendations # 6 and #7 below.
5. Reduction of the Number of Applicants Going to the Selection Committee
: The
School will accomplish this recommendation by implementation of the process
outlined in the responses to recommendations #2 above and ## 6-8 below.
6. Revise Interview Forms
: The School is in the process of simplifying the
interview form, adding explicit criteria and examples for evaluation. The revised
form will not seek any numerical ranking of candidates but simply ask the
interviewer to describe how well the candidates meet each selection criterion.
The executive admissions committee will consider the information provided by
the interviewers and determine which candidates should proceed to the selection
committee.
7. Limiting Recommendations to “yes” or “no”
: The interview committee will no
longer make the decision as to which candidates proceed to the selection
committee. This decision will be made by the executive admissions committee as
described in the responses to recommendations # 2 and # 6 above.
8. Presentation of Applicants with Positive Interview Outcomes to the Selection
Committee: Only candidates who sufficiently satisfy all selection criteria, as
determined by the executive admissions committee, will proceed to the selection
committee (See responses to recommendations # 2 and # 6 above).
9. Drop Outlier Scores of the Selection Committee
: The School implemented this
procedure for the current admissions cycle.
10. Combining Resident and Non-Residents Admission Pools for Alternates
: The
School has combined the pools for Utah residents and non-residents for the
current admissions cycle. Contractual arrangements with the State of Idaho make
the inclusion of Idaho applicants in this same process impossible.
7

CONCLUSION
The University thanks the Legislature and the Auditor General for this informative and
constructive audit. The University looks forward to next year’s follow-up by the Auditor
General and is confident he will find a much improved admissions process.
8
RESEARCH BIBLIOGRAPHY
• Substantial research exists to support the prevailing view that MCAT scores and
GPA are not good predictors of success for medical students (particularly in
clinical years) or ultimately for physicians.
o Joan Y. Reede, MD, MPH, MS, Predictors of Success in Medicine
, 362
Clinical Orthopedics and Related Research 72, (1999) (GPA and MCAT
have little correlation to success in clinical clerkships, residencies or in
physician practice)
o J.A. Collier, Using a Standard Patient Examination to Establish the
Predictive Value of the MCAT and Undergraduate GPA as Admission
Criteria, 64 Acad. Med. 482 (1989) (MCAT and GPA have weak
correlation to clinical performance).
o H.G. Gough, Some Predictive Implications of Pre Medical Scientific
Competence and Preferences, 53 J. Med. Ed. 291 (1978) (MCAT and
GPA have no predictive value of success in the clinical years)
o R.M. Rippey, A Study of University of Connecticut’s Criteria for
Admissions Into Medical School, 15 Med. Ed. 231 (1981) (MCAT and
GPA have no predictive value of success in the clinical years)
o M.D. Smith, Better Admissions Criteria
, 73 Acad. Med. 1054 (1998)
(differences in MCAT scores do not correlate with significant differences
in academic achievement in medical school)
o J.W. Keck, Efficacy of Cognitive/Non Cognitive Measures in Predicting
Resident-Physician Performance, 54 J. Med. Ed. 759 (1979) (minimal
correlation between standardized tests and grades with clinical success in
residency)
o P.H. Richardson, Grade Predictions for School Leaving Examinations-Do
They Predict Anything?, 32 Med. Ed. 294 (1998) (British research reaches
same conclusion).
• Research demonstrates that other factors besides raw academic information are
better predictors of success in the medical field. Those factors include, breadth of
knowledge, interpersonal skills, problem solving, caring and moral motivation,
motivation to study, interview ratings, prior health care experience, personality,
character, integrity, evidence of leadership, work habits, attitudes, orientation
toward service and altruism.
o W.C. McGaghie, Qualitative Variables in Medical School Admissions
, 65
Acad. Med. 45 (1990) (these cognitive and non-cognitive factors are
critical in medical school admissions decisions)
o D.A. Latif, Moral Reasoning: Should It Serve as a Criterion for Student
and Resident Selection in Pharmacy, 65 Am. J. Pharmaceutical Ed. 119
(2000) (integrity, problem solving, professionalism and caring are better
predictors of decision making ability)
o K.E. Meredith, Subjective and Objective Admissions Factors as Predictors
of Clinical Clerkship Performance, 57 J. Med. Ed. 743 (1982); clinical
1
clerkship success is best predicted by maturity, interpersonal skills,
motivation, judgment and individual achievement)
o C.T. Webb, The Impact of Non-Academic Variables on Performance At
Two Medical Schools, 89 J. Nat. Med. Assoc. 173 (1997) (in study
relating to female medical students, interview ratings, prior health care
experience and personality were better indicators of clinical success than
MCAT and GPA)
o J. Johnson, Medical School Admissions Committee Members’ Evaluations
of and Impressions From Recommendation Letters, 73 Acad. Med. s41
(1998) (exposure to medicine, applicant references and other factors are
critical for accurate analyses by admissions committees)
o William E. Sedalack, Ph.D and Dario O. Prieto, M.Ed., Predicting
Minority Students’ Success in Medical School, 60 Acad. Med. 161 (1990)
(Non-Cognitive factors are better predictors of minority students’ success
in medical school).
• Research suggests that diversity within medical school classes leads to a better
educational experience and more effective medical care for a diverse population.
o J.E. Rolfe, Time for a Review of Admissions to Medical School
, 346
Lancet 1329 (1995) (stressing the importance of a diversity in the
educational experience for effective medical practices)
o R.L. Fishbach, Behind Every Problem Lies an Opportunity: Meeting the
Challenge of Diversity in Medical School, Focus (July 1997) (analyzing
importance of diversity in the education experience for medical practice
and research).
• Research shows that physicians who share unique characteristics with a segment
of the population often serve that population and are preferred as physicians by
the population.
o S.A. Mangus, Medical Schools, Affirmative Action, and the Neglected
Role of Social Class, 90 Am. J. Public Health 1197 (2000) (interpersonal
skills and socioeconomic strata predict a better patient-physician
relationship, particularly in underserved groups).
o M. Komaromy, The Role of Black and Hispanic Physicians in Providing
Health Care for Underserved Populations, 334 N. Eng. J. Med. 1305
(1996) (minorities are more likely to serve minority populations than their
white counterparts).
• Studies have led some researches to recommend that MCAT and GPA scores not
be considered by the interviewers of medical school applicants. D.L. Shaw,
Influence of Medical School Applicants’ Demographic and Cognitive
Characteristics on Interviewers’ Ratings and Noncognitive Traits, 70 Acad. Med.
532 (1995).
2
