sunset advisory Commission
staff report with Commission deCisions
State Board of Dental Examiners
2016–2017
85th LegisLature

sunset advisory Commission
Representave Larry Gonzales Senator Van Taylor
Chair Vice Chair
Representave Cindy Burke Senator Juan “Chuy” Hinojosa
Representave Dan Flynn Senator Robert Nichols
Representave Richard Peña Raymond Senator Charles Schwertner
Representave Senfronia Thompson Senator Kirk Watson
William Meadows LTC (Ret.) Allen B. West
Ken Levine
Director
Cover Photo: The iron perimeter fence was installed in the 1890s, a few years after the completion of the Texas State
Capitol. The fence surrounds approximately 22 acres of the Capitol Grounds but only on the east, west, and south sides
due to the addition of the Capitol Extension to the north in the early 1990s. Photo Credit: Janet Wood
State Board of dental examinerS
SunSet Staff report with CommiSSion deCiSionS
2016–2017
85th legiSlature

How to Read SunSet RepoRtS
Each Sunset report is issued three times, at each of the three key phases of the Sunset process, to compile
all recommendations and action into one, up-to-date document. Only the most recent version is posted
to the website. (e version in bold is the version you are reading.)
1. SunSet Staff evaluation PhaSe
Sunset sta performs extensive research and analysis to evaluate the need for, performance of,
and improvements to the agency under review.
F V: The Sunset Staff Report identifies problem areas and makes specific
recommendations for positive change, either to the laws governing an agency or in the form of
management directives to agency leadership.
2. SunSet CommiSSion Deliberation PhaSe
e Sunset Commission conducts a public hearing to take testimony on the sta report and the
agency overall. Later, the Commission meets again to vote on which changes to recommend to
the full Legislature.
Second VerSion: e Sunset Sta Report with Commission Decisions, issued after the
decision meeting, documents the Sunset Commission’s decisions on the original sta
recommendations and any new issues raised during the hearing, forming the basis of the
Sunset bills.
3. legiSlative aCtion PhaSe
e full Legislature considers bills containing the Sunset Commission’s recommendations on
each agency and makes nal determinations.
T V: e Sunset Sta Report with Final Results, published after the end of the
legislative session, documents the ultimate outcome of the Sunset process for each agency,
including the actions taken by the legislature on each Sunset recommendation and any new
provisions added to the Sunset bill.

taBle of ContentS
page
SunSet CommiSSion deCiSionS
State Board of Dental Examiners ............................................................................. A1
Adopted Language .................................................................................................... A7
Summary of SunSet Staff reCommendationS
.................................................................................................................................. 1
agenCy at a glanCe
.................................................................................................................................. 7
iSSueS/reCommendationS
1 e Unusually Large Dental Board Inappropriately Focuses on Issues
Unrelated to Its Public Safety Mission ..................................................................... 11
2 State Regulation of Dental Assistants Is Unnecessary to Ensure Public
Protection and Is an Inecient Use of Resources ..................................................... 19
3 e Board Lacks Key Enforcement Tools to Ensure Dentists Are Prepared
to Respond to Increasing Anesthesia Concerns ....................................................... 27
4 Key Elements of the State Board of Dental Examiners’ Licensing and
Regulatory Functions Do Not Conform to Common Licensing Standards ............ 33
5 A Continuing Need Exists for the State Board of Dental Examiners ..................... 39
appendiCeS
Appendix A — Historically Underutilized Businesses Statistics .............................. 45
Appendix B — Equal Employment Opportunity Statistics ...................................... 49
Appendix C — State Board of Dental Examiners Comprehensive
Enforcement Data ........................................................................... 51
Appendix D — Sta Review Activities .................................................................... 53

SunSet CommiSSion deCiSionS

a1
State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
Sunset Advisory Commission January 2017
SunSet CommiSSion deCiSionS
Summary
e following material summarizes the Sunset Commission’s decisions on the sta recommendations
for the State Board of Dental Examiners, as well as modications and new issues raised during the
public hearing.
For a relatively small agency, the dental board has been bueted by more than its share of problems
due to high turnover among its leadership ranks. At 15 members, the dental board itself is oversized
compared to its shrinking duties, leading to board involvement in operational matters well beyond its
proper role and the agency’s needs. Dentist board members have pursued high prole rule packages
that appear more motivated by business interests than demonstrated concern for public safety; all the
while other emerging problems like regulating the administration of anesthesia went largely unaddressed.
In light of high-prole media cases exposing gaps in the board’s regulation of dental anesthesia, the
commission’s recommendations aim to strengthen anesthesia regulation through clear enforcement tools,
improved training and education requirements for permit holders, and broader avenues for stakeholder
input. ese recommendations are consistent with the ndings of a blue ribbon panel commissioned
by Sunset to assess the dental anesthesia problems. Other changes would address deciencies in the
agency’s regulation of dental assistants and update licensing and enforcement processes that have not
kept up with best practices. e Sunset Commission recommends continuing the agency for 12 years.
iSSue 1
The Unusually Large Dental Board Inappropriately Focuses on Issues Unrelated
to Its Public Safety Mission.
Recommendation 1.1, Modied — In lieu of the sta recommendation, sweep the board and reduce
the size of the board from 15 to 11 members, including six dentists, three hygienists, and two public
members. To allow for staggering of terms, the recommendation would provide that all current board
member terms expire on September 1, 2017, with the governor making initial appointments as specied
below. Current members would be eligible for re-appointment if so determined by the governor to
maintain needed expertise. Board members serving on August 31, 2017 would continue to serve until
a majority of new appointments are made.
•
Two dentists and one dental hygienist to initial terms expiring February 1, 2019.
•
Two dentists, one dental hygienist, and one public member to initial terms expiring February 1, 2021.
•
Two dentists, one dental hygienist, and one public member to initial terms expiring February 1, 2023.
Recommendation 1.2, Adopted — Allow the board’s statutory advisory groups to expire and direct
the board to establish clearer processes for stakeholder input in rule.
Recommendation 1.3, Modied — Clarify the use and role of board members at informal settlement
conferences and strike language in the Dental Practice Act regarding informal settlement conferences

State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
a2
January 2017 Sunset Advisory Commission
(Texas Occupations Code, sections 263.007, 263.0075, and 263.0076) and replace with more detailed
language on structure and conduct of informal proceedings. (See Adopted Language, page A7)
•
Dental review committee. Create a state Dental Review Committee consisting of nine governor-
appointed members, including six dentists and three dental hygienists, to serve at informal settlement
conferences on a rotating basis.
iSSue 2
State Regulation of Dental Assistants Is Unnecessary to Ensure Public Protection
and Is an Inefficient Use of Resources.
Recommendation 2.1, Modied — In lieu of the sta recommendation, combine the board’s four dental
assistant certicate programs into one registration for dental assistants. (See Adopted Language, page A9)
iSSue 3
The Board Lacks Key Enforcement Tools to Ensure Dentists Are Prepared to
Respond to Increasing Anesthesia Concerns.
Recommendation 3.1, Modied — Authorize the board to conduct inspections of dentists administering
parenteral anesthesia in oce settings. Provide four levels of anesthesia permits and require the board
to establish minimum standards, education, and training for dentists administering anesthesia. Allow
additional limitations on anesthesia administration for high-risk or pediatric patients. (See Adopted
Language, page A10)
•
Blue ribbon panel. As a management action, Sunset directed the board to quickly establish
an independent 5- to 10-member blue ribbon panel that reviewed de-identied data, including
condential investigative information, related to dental anesthesia deaths and mishaps over the last
ve years, as well as evaluate emergency protocols. e Committee made recommendations to the
Legislature and the Sunset Commission at its January 11, 2017 meeting.
Recommendation 3.2, Modied — As a statutory instead of a management recommendation, direct
the board to revise rules to ensure dentists with one or more anesthesia permits maintain related written
emergency management plans. Also provide that level 2–4 sedation/anesthesia permit holders’ emergency
plans must include current Advanced Cardiac Life Support (ACLS) rescue protocols and advanced
airway management techniques. For level 2–4 sedation/anesthesia permit holders treating pediatric
patients emergency management plans must include current Pediatric Advanced Cardiac Life Support
(PALS) rescue protocols and advanced airway management techniques.
iSSue 4
Key Elements of the State Board of Dental Examiners’ Licensing and Regulatory
Functions Do Not Conform to Common Licensing Standards.
Recommendation 4.1, Adopted — Require the board to monitor licensees for adverse licensure actions.

a3
State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
Sunset Advisory Commission January 2017
Recommendation 4.2, Adopted — Authorize the board to deny applications to renew a license if an
applicant is not compliant with a board order.
Recommendation 4.3, Adopted — Authorize the board to require evaluations of licensees suspected of
being impaired and require condentiality for information relating to the evaluation and participation
in treatment programs.
Recommendation 4.4, Adopted — Remove unnecessary qualications required of applicants for
licensure or registration.
Recommendation 4.5, Adopted — Direct the board to make data on the board’s enforcement activity
information publicly available on its website. (Management action – nonstatutory)
Recommendation 4.6, Adopted — Direct the board to stagger registration and certicate renewals.
(Management action – nonstatutory)
iSSue 5
A Continuing Need Exists for the State Board of Dental Examiners.
Recommendation 5.1, Adopted — Continue the State Board of Dental Examiners for 12 years.
Recommendation 5.2, Modied — Update the standard Sunset across-the-board provision regarding
conicts of interest and apply the newly updated Sunset across-the-board recommendation on board
member training.
adopted new iSSueS
Dental Anesthesia
Advisory committee. Create a standing advisory committee on dental anesthesia to advise the board
on the development and revision of rules related to dental sedation and anesthesia:
•
Require the board chair to appoint nine members to include, but not be limited to: dentists, dentist
anesthesiologists, oral and maxillofacial surgeons, pediatric dentists and physician anesthesiologists.
e board chair may not appoint an active dental board member to the advisory committee.
•
Require the board to provide the committee with a board attorney who will act as counsel to the
committee members. e board attorney shall be present during committee meetings and the
committee’s deliberations to advise the committee on legal issues.
•
Require the committee to report their recommendations and other ndings to the dental board
on an annual basis, or more frequently as necessary to provide input on rulemaking and make this
information available on the board’s website.
Data reporting. Direct the board to track and quarterly report anesthesia-related data and to make
publicly available on its website aggregate enforcement data by scal year and type of license. (Management
action – nonstatutory; see Adopted Language, page A10)

State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
a4
January 2017 Sunset Advisory Commission
Emergency preparedness. Require the board to develop rules establishing minimum emergency
preparedness standards necessary prior to administering sedation /anesthesia including requirements
related to
•
having an adequate, unexpired supply of necessary drugs and anesthetic agents;
•
having an onsite automated external debrillator (AED) immediately available;
•
periodic equipment inspections in a manner and on a schedule determined by the board; and
•
maintenance and retention of an equipment readiness log that shall be made available to the board
upon request and to board sta during inspections.
Portability permits. Provide for the following statutory changes to portability requirements:
•
Dene “portability” as the ability of a permit holder to provide permitted anesthesia services in a
location other than a facility or satellite facility, consistent with the denition in rule.
•
Require the board to establish in rule requirements and methods for a dental sedation and anesthesia
permit holder to obtain a portability permit.
•
Require the board to establish advanced didactic and clinical training requirements necessary for a
portability permit, with consideration for additional requirements for those using their portability
permit to treat pediatric and/or high-risk patients.
Prescription Monitoring Program
Dentist requirements. Beginning September 1, 2018, require dentists to search the Prescription
Monitoring Program and review a patient’s prescription history before prescribing opioids, benzodiazepines,
barbiturates, or carisoprodol. A dentist who does not check the program before prescribing these drugs
would be subject to disciplinary action by the dental board.
Dental board requirements. Require the dental board to query the Prescription Monitoring Program
on a periodic basis for potentially harmful prescribing patterns among its licensees. e dental board
would work with the pharmacy board to establish potentially harmful prescribing patterns that the
dental board should monitor by querying the database for dentists who meet those prescribing patterns.
Based on the information obtained from the Prescription Monitoring Program, the dental board would
be authorized to open a complaint for possible non-therapeutic prescribing.
Fiscal Implication Summary
Overall, the Sunset Commission’s recommendations would result in a positive scal impact to the General
Revenue Fund of approximately $47,900 annually from reducing the size of the board and enhancing
licensing and enforcement eorts.
e recommendation to decrease the number of board members by four would result in a small annual
savings of about $8,300 to the General Revenue Fund resulting from decreased travel costs. Requiring
nine members to attend informal settlement conferences on a rotating basis would cost approximately
$5,400 per year in travel costs, assuming each member attended informal settlement conferences two
times per year.

a5
State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
Sunset Advisory Commission January 2017
e recommendation to authorize the board to inspect dental oces administering anesthesia would not
have a signicant scal impact to the state, though actual implementation would have costs associated
with extra sta, travel, and equipment. ese costs could be mitigated by an adjustment to existing
anesthesia permitting fees.
e recommendation to query the National Practitioner Data Bank would require a $3 increase in
licensing fees to cover the board’s cost and would result in a small revenue gain of approximately $45,000
annually. is gain would result from applicants paying the fee who ultimately do not meet the standards
for licensure and thus do not require of queries the data bank.

State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
a6
January 2017 Sunset Advisory Commission
a7
State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
Sunset Advisory Commission January 2017
adopted language
Recommendation 1.3
Modication Language
Include the following as statutory changes.
Informal Proceedings
•
e board by rule shall adopt procedures governing informal disposition of a contested case. Rules
must require that
(1) not later than the 180th day after the date the board’s ocial investigation of the complaint
is commenced, the board shall determine a future date on which to hold an informal settlement
conference to consider disposition of the complaint or allegation, unless good cause is shown by the
board for scheduling the informal settlement conference after that date;
(2) the board give notice to the licensee of the time and place of the meeting not later than the 45th
day before the date the informal settlement conference is held;
(3) the complainant and the licensee be provided an opportunity to be heard;
(4) the board’s legal counsel or a representative of the attorney general be present to advise the
board or the board’s sta; and
(5) a member of the board’s sta be at the meeting to present to the Informal Settlement Conference
Panel the facts the sta reasonably believes it could prove by competent evidence or qualied
witnesses at a hearing.
•
An aected licensee is entitled to reply to the sta ’s presentation and present the facts the licensee
reasonably believes the licensee could prove by competent evidence or qualied witnesses at a hearing.
•
After ample time is given for the presentations, the Informal Settlement Conference Panel shall
recommend that the investigation be closed or shall make a recommendation regarding the disposition
of the case, unless applicable concerning contested cases requires a hearing.
•
If the license holder has previously been the subject of disciplinary action by the board, the board
shall schedule the informal settlement conference as soon as practicable but not later than the 180th
day after the date the board’s ocial investigation of the complaint is commenced.
•
Notice must be accompanied by a written statement of the nature of the allegations and the
information the board intends to use at the meeting. If the board does not provide the statement
or information at that time, the license holder may use that failure as grounds for rescheduling the
informal meeting. If the complaint includes an allegation that the license holder has violated the
standard of care, the notice must include a copy of the report by the expert dentist reviewer. e
licensee must provide to the board the licensee’s rebuttal at least 15 business days before the date of
the meeting in order for the information to be considered at the meeting.
•
e board by rule shall dene circumstances constituting good cause for not meeting the 180-day
deadline, including an expert dentist reviewer’s delinquency in reviewing and submitting a report
to the board.

State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
a8
January 2017 Sunset Advisory Commission
•
e board by rule shall dene circumstances constituting good cause to grant a licensee’s request for
a continuance of the informal settlement conference.
•
Information presented by the board or board sta in an informal settlement conference is condential.
•
On request by a licensee under review, the board shall make a recording of the informal settlement
conference proceeding. e recording is a part of the investigative le and may not be released to a
third party unless authorized. e board may charge the licensee a fee to cover the cost of recording
the proceeding. e board shall provide a copy of the recording to the licensee on the licensee’s request.
Board Representation in Informal Proceedings
•
Dene the informal settlement conference panel to include members of the Board and the Dental
Review Committee.
•
In an informal settlement conference, at least two Informal Settlement Conference Panel members
shall be appointed to determine whether an informal disposition is appropriate. At least one of the
panelists must be a dentist.
•
Pursuant to Board rules, one panelist must be physically present at the ISC, but one panelist may
appear by video conference.
•
An informal settlement conference may be conducted by one panelist if the aected licensee waives
the requirement that at least two panelists conduct the informal proceeding. If the licensee waives
that requirement, the panelist may be either a dentist, dental hygienist, or a member who represents
the public.
•
Only one panel member is required in an informal settlement conference proceeding conducted by
the board to show compliance with an order or remedial plan of the board.
Roles and Responsibilities of Participants in Informal Proceedings
•
An informal settlement conference panel member that serves as a panelist at an informal settlement
conference shall make recommendations for the disposition of a complaint or allegation. e member
may request the assistance of a board employee at any time.
•
Board employees shall present a summary of the allegations against the aected licensee and of the
facts pertaining to the allegation that the employees reasonably believe may be proven by competent
evidence at a formal hearing.
•
A board attorney shall act as counsel to the panel members and shall be present during the informal
settlement conference and the panel’s deliberations to advise the panel on legal issues that arise
during the proceeding. e attorney may ask questions of participants in the informal settlement
conference to clarify any statement made by the participant. e attorney shall provide to the panel a
historical perspective on comparable cases that have appeared before the board, keep the proceedings
focused on the case being discussed, and ensure that the board’s employees and the aected licensee
have an opportunity to present information related to the case. During the panel’s deliberations,
the attorney may be present only to advise the panel on legal issues and to provide information on
comparable cases that have appeared before the board.
•
e panel and board employees shall provide an opportunity for the aected licensee and the
licensee’s authorized representative to reply to the board employees’ presentation and to present

a9
State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
Sunset Advisory Commission January 2017
oral and written statements and facts that the licensee and representative reasonably believe could
be proven by competent evidence at a formal hearing.
•
An employee of the board who participated in the presentation of the allegation or information
gathered in the investigation of the complaint, the aected licensee, the licensee’s authorized
representative, the complainant, the witnesses, and members of the public may not be present during
the deliberations of the panel. Only the members of the panel and the board attorney serving as
counsel to the panel may be present during the deliberations.
•
e panel shall recommend the dismissal of the complaint or allegations or, if the panel determines
that the aected licensee has violated a statute or board rule, and that violation supports action by
the board, the panel may recommend board action and terms for an informal settlement of the case.
•
e panel’s recommendations must be made in writing and presented to the aected licensee and the
licensee’s authorized representative. e licensee may accept the proposed settlement within the time
established by the panel at the informal meeting. If the licensee rejects the proposed settlement or
does not act within the required time, the board may proceed with the ling of a formal complaint
with the State Oce of Administrative Hearings.
Recommendation 2.1
Modication Language
In lieu of the sta recommendation, remove the separate certication provisions for dental assistants
from law and require one registration for dental assistants who provide the following dental support
services to a licensed dentist: dental x-rays, pit and ssure sealants, coronal polishing, and nitrous oxide
monitoring. A dental assistant would not be authorized to perform any of the four services above without
rst obtaining registration from the board.
Services provided by a registered dental assistant would be performed under the direct supervision of
a licensed dentist, but not to be construed to authorize a dental assistant to practice dentistry or dental
hygiene. Dentists remain responsible for acts delegated to the registered dental assistant. ese changes
would not aect the board’s authority to determine which acts a licensed dentist may delegate to non-
registered dental assistants. is recommendation would establish registration requirements for dental
assistants, as follows:
•
A person may not practice as a dental assistant to perform the four dental support services listed
above after September 1, 2018 unless the person has registered with the board and received a
certicate of registration.
•
e board, by rule, shall establish minimum education requirements for registration as a dental
assistant. Requirements must include a high school diploma or equivalent; and a course of instruction
and examination to demonstrate competency in the following dental support services: dental x-rays,
pit and ssure sealants, coronal polishing, and nitrous oxide monitoring; and training in basic life
support, infection control, jurisprudence, and any other requirements the board determines necessary.
•
e board could consider approving courses of instruction and examinations provided by outside
entities such as the Dental Assisting National Board to qualify for this registration.
•
Dental assistant registrations shall be renewed biennially on a staggered basis, as established by the
board.

State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
a10
January 2017 Sunset Advisory Commission
•
e board shall establish continuing education requirements as a condition of renewing registration
as a registered dental assistant.
•
e board shall establish standards for taking disciplinary action against a registered dental assistant.
•
e board shall establish fees for initial registration and renewals to cover the cost of regulation.
Recommendation 3.1
Modication Language
Include the following as statutory changes.
•
Denitions. Dene “pediatric” as patients ages 0–12. Dene “high-risk patient” as patients with
an American Society of Anesthesiologists (ASA) rating of level 3 or 4 or older than 75.
•
Permitting. Require an annual permit for each of the four dierent levels of anesthesia, dened
based on the depth of the intended procedure to alter the patient’s mental status and the method
of drug delivery.
– Level 1: Minimal Sedation
– Level 2: Moderate Sedation (Enteral)
– Level 3: Moderate Sedation (Parenteral)
– Level 4: Deep Sedation or General Anesthesia
Require the board to develop rules establishing minimum standards for training, education, and other
standards for dierent permit levels. For level 2–4 permit holders, education/training requirements
must include training on pre-procedural patient evaluation including the evaluation of the patient’s
airway and physical status as currently dened by the ASA, ongoing monitoring of sedation and
anesthesia, and management of emergencies.
Require level 2–4 permit holders to provide proof of additional training for the treatment of pediatric
and/or high risk patients including advanced didactic and clinical training requirements. Dentists
would not be allowed to treat pediatric and/or high-risk patients without proof of specialized education.
Allow the board to establish additional limitations on the administration of anesthesia on pediatric
and/or high risk patients.
•
Inspections. Allow the board to conduct pre-permit, random, and compliance inspections. Require
the board to determine an appropriate risk-based inspection schedule for on-site inspections of dental
oces of dentists with a level 2, 3 or 4 permit. Allow the board to stagger inspections as long as all
relevant oces are inspected at least once every 5 years. Allow the board to determine education
and training requirements for inspectors. Require the board to maintain records of inspections.
Data Reporting New Issue
Adopted Language
Direct the board to track and report the following data. All information related to an investigation is
condential, except that the agency shall provide the following information on a quarterly basis to the

a11
State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
Sunset Advisory Commission January 2017
board and the standing advisory committee on dental anesthesia, and to legislative oces upon request:
de-identied, case specic data reecting information about jurisdictional, led complaints resolved
during the reporting period related to anesthesia/sedation including the following.
1. Source of initial complaint: public, other agency, self-report of death, self-report of hospitalization,
or initiated by the board
2. Information about licensee:
a. Whether respondent is Medicaid provider
b. Respondent’s highest sedation/anesthesia permit level
c. Whether respondent holds portability privileges
d. Respondent’s self-reported practice area
3. Information about patient:
a. Patient ASA rating (identied in respondent’s dental records and/or determined by dental review
panel)
b. Patient age: 12 and under, between 13 and 18, between 19 and 75, and over 75
c. Location of treatment investigated by the agency: dental oce, hospital, ASC, oce of other
practitioner
d. Level of sedation/anesthesia administered: local, nitrous, level I, level II, level III, level IV
(determined by dental review panel)
e. Sedation/anesthesia administrator: respondent, other dentist, doctor of medicine, certied
registered nurse anesthetist (determined by dental review panel)
f. Whether treatment investigated by the agency was paid by Medicaid
4. Information about investigation:
a. Allegation categories identied in preliminary investigation
b. Disposition of ocial investigation — dismissed by enforcement, dismissed by legal — no
violation, dismissed by board vote, closed by administrative citation/remedial plan/disciplinary
action
c. If disposition is public action (administrative citation, remedial plan, or disciplinary action), the
violations identied in the public action resolving the ocial investigation
e board must make publicly available on their website aggregate data by scal year and type of license
about the following areas:
1. Number of licensees at the end of the scal year
2. Total number of complaints against licensees originating in that scal year
3. For all resolved complaints in that scal year, break down the resolution by each type of action taken
(nonjurisdictional, dismissed, warning, probation, suspension, revocation, etc.)

State Board of Dental Examiners Staff Report with Commission Decisions
Sunset Commission Decisions
a12
January 2017 Sunset Advisory Commission
4. For all resolved complaints in that scal year, break down the resolution by the nature of the complaint
allegation (standard of care, impairment, dishonorable conduct, continuing education violation, etc.)
5. Number of cases open longer than one year
6. Average administrative penalty assessed
7. Number of cases referred to informal settlement conferences
8. Number of cases resolved in informal settlement conferences
9. Number of cases referred to the State Oce of Administrative Hearings (default + non-default)
10. Number of contested cases heard at the State Oce of Administrative Hearings
11. Number of cases that went on to district court
12. Average number of days to resolve a complaint from complaint received to investigation completed
13. Average number of days to resolve a complaint from complaint received to nal order issued
14. Average number of days to issue a license
15. Number of cases involving mortality and morbidity
16. Total number of anesthesia complaints against licensees originating in that scal year by permit level
17. For all resolved anesthesia complaints in that scal year, break down the resolution by each type of
action taken (dismissed, warning, probation, suspension, revocation, etc.) by permit level
18. For all resolved anesthesia complaints in that scal year, break down the resolution by type of
complication that violated the standard of care by permit level.

Summary of SunSet
Staff reCommendationS
1
State Board of Dental Examiners Staff Report with Commission Decisions
Summary of Sunset Staff Recommendations
Sunset Advisory Commission January 2017
Turnover among the agency’s
leadership ranks has had
a significant effect on the
agency and governing board.
Summary
For a relatively small agency, the State Board of Dental Examiners has had
more than its share of problems over the years. e agency infamously was
abolished through its 1993 Sunset review amid a legislative skirmish not of
its own making. After its re-creation in 1995, the agency was placed under
another Sunset review out of its regular order in 2003 because of concerns
about serious enforcement deciencies. In its last ve years, the agency has
been bueted by high turnover among its leadership ranks, going through four
executive directors and general counsels in that time.
While the older events do not necessarily explain the current situation at the
agency, they do provide an important historical context. Of greater signicance is
the more recent history of employee turnover and the eect it
has had on the agency and the governing board. e revolving
door of executive directors and general counsels means that
senior sta must constantly play catch-up to gain a complete
understanding of the basic elements of the job. e agency
loses institutional knowledge for how and why policies and
procedures were developed, lessons learned, and what works
and what does not. Most important, however, the agency
loses the vision to see emerging problems and the leadership to help address
strategic agency needs, qualities that take time to develop. With experience in
the job and time to see things through, senior sta can work more eectively
with the board to ensure that the agency has the resources — both sta and
systems — and the tools and statutory authority to do its job well. Finally,
sound agency leadership gives condence to the Legislature that the resources
and tools will be used appropriately to protect the public.
In such an environment of high turnover at the top of the organization, the
board itself would understandably emerge to ll the void and take on a larger
role in running the agency. Further, because board members typically have
longer tenure than the agency’s senior sta, they would understandably play a
larger role in calling the shots for the agency. However, at such a disadvantage
to the board, sta is far less likely to take initiative and far more likely to defer
to the board on matters even when the board may need to hear sta ’s more
objective voice.
e issue of board involvement in agency operations is not new to the dental
board. Sunset sta raised the issue in the last review of 2002, noting that the
board no longer developed and administered its own dental examination and
thus had less need for its then-18 members to do its job. Sunset sta ’s initial
recommendation to reduce the board size to 11 members was changed to the
current 15 members through the legislative process.

Sate Board of Dental Examiners Staff Report with Commission Decisions
Summary of Sunset Staff Recommendations
2
January 2017 Sunset Advisory Commission
In the current review, this situation of an oversized board has only continued. e board has even less to
do because of legislation from 2013 eliminating its role in reviewing standard of care complaints, though
dentist board members still nd ways to get involved in such cases. Dentist board members have also
pursued high prole rule packages that appear more motivated by business interests than demonstrated
concern for public safety; all the while other emerging problems like regulating the administration of
anesthesia went largely unaddressed.
is Sunset review occurs at an opportune time for the board. Positive signs are emerging from the
current eorts of the agency’s senior sta, implementing the Legislature’s 2013 operational changes and
other initiatives such as new approaches for engaging stakeholders. While these changes have occurred
with the blessing of the board, the same dynamic that has governed the agency in recent years is still
in place. At the time of this review, the executive director has only been in that position seven months;
the general counsel, less than two years; and the dental director, less than two and a half years. Key
departures could still threaten the progress made.
Structural changes to reduce the size of the board are needed to focus it on its public protection mission
and help ensure the ongoing eectiveness of the agency. Other changes would better focus stakeholder
processes for dental hygienists and dental laboratories; address deciencies in the agency’s regulation
of dentists’ administration of anesthesia; deregulate dental assistants by eliminating the unworkable
patchwork of certicate programs that provides little public protection; and update licensing and
enforcement processes that have not kept up with best practices. Sunset sta recommends continuing
the agency for 12 years.
e following material summarizes all of the Sunset sta ndings and recommendations on the State
Board of Dental Examiners.
Issues and Recommendations
Issue 1
The Unusually Large Dental Board Inappropriately Focuses on Issues Unrelated
to Its Public Safety Mission.
A shift in responsibility for technical complaint reviews to a panel of contracted experts in 2013
signicantly decreased the workload for dentist board members. With less to do, the board, at the behest
of dentist members, pursued signicant rule changes more related to business practices than demonstrated
public safety problems and despite widespread concern by stakeholders and other interests and a lack
of broad consensus. Dentist members also continue their involvement in case resolution, ultimately
undermining those eorts. Better aligning the number of dentist board members with the amount of
technical expertise needed by the agency will help focus the board squarely on issues of public protection
and make better use of sta resources.
In addition, board processes for stakeholder input hold promise for improved involvement, eliminating
the need for two statutorily created advisory committees, the Dental Hygiene Advisory Committee and
the Dental Laboratory Certication Council. Removing advisory committees from statute will allow the
board more exibility to convene more diverse groups of stakeholders for input on an as needed basis.

3
State Board of Dental Examiners Staff Report with Commission Decisions
Summary of Sunset Staff Recommendations
Sunset Advisory Commission January 2017
Key Recommendations
•
Reduce the size of the board from 15 to nine members and adjust its composition to consist of four
dentists, two dental hygienists, and three public members.
•
Allow the board’s statutory advisory groups to expire and direct the board to establish clearer processes
for stakeholder input in rule.
Issue 2
State Regulation of Dental Assistants Is Unnecessary to Ensure Public Protection
and Is an Inefficient Use of Resources.
e board’s regulation of dental assistants has expanded over the past 25 years to consist of four separate
certicate programs for commonly delegated tasks, though assistants can legally perform some work
without holding any certicate. In scal year 2015 the board issued 50,469 dental assistant certicates,
more than all other board issued credentials combined.
State regulation of dental assistants is not needed to protect public safety. Dental assistants can only
work under the delegated authority of the dentist, who remains responsible for patient care and safety.
Because they can only perform reversible tasks, they have very low volume of meaningful complaint and
enforcement activity, little, if any, of which relates to standard of care. In addition, gaps in regulatory
requirements undermine the very promise of public safety the regulations were supposed to provide. e
regulatory program wastes licensing and legal resources and diverts board and sta focus from higher-
risk agency responsibilities. Ultimately, addressing deciencies to x these regulations is not an option
without dramatically expanding the scope of their practice, because the risk to the public relating to the
current practice is so low. National credentialing and private market forces can provide any training or
oversight of dental assistants desired by employers or the public. Removing regulatory responsibility
for dental assistants from the board will allow the agency to focus on licensees that pose a higher risk
to patients and the public.
Key Recommendation
•
Discontinue the board’s dental assistant certicate programs.
Issue 3
The Board Lacks Key Enforcement Tools to Ensure Dentists Are Prepared to
Respond to Increasing Anesthesia Concerns.
Dentists administer anesthesia for a variety of dental procedures. In recent years, the board has seen an
increase in related complaints involving serious patient harm and sometimes death. e board lacks the
authority and resources to routinely inspect the oces of dentists providing some anesthesia services
and does not require written emergency action plans for any dentist administering anesthesia to help
ensure thoughtful planning and readiness for the unexpected. Dentists in other states and Texas doctors
administering anesthesia in oces are subject to related routine inspections, and oce-based Texas
physicians providing anesthesia must maintain written emergency action plans. Allowing the board to
conduct inspections of dentists administering anesthesia in oce settings and requiring related written
emergency management plans of dentists providing anesthesia will incentivize dentists to be prepared
for anesthesia-related complications and train support sta accordingly.

Sate Board of Dental Examiners Staff Report with Commission Decisions
Summary of Sunset Staff Recommendations
4
January 2017 Sunset Advisory Commission
Key Recommendations
•
Authorize the board to conduct inspections for dentists administering parenteral anesthesia in oce
settings.
•
Direct the board to revise rules to ensure dentists with one or more anesthesia permit and maintain
related written emergency management plans.
Issue 4
Key Elements of the State Board of Dental Examiners’ Licensing and Regulatory
Functions Do Not Conform to Common Licensing Standards.
In reviewing the board’s regulatory authority, Sunset sta found that certain licensing and enforcement
processes do not match model standards or common practices observed through Sunset sta ’s experience
reviewing regulatory agencies. Specically, the board does not do enough to ensure licensees are free
from disciplinary action in other states or have complied with past board orders before renewing their
licenses. e board is also unable to require evaluations for licenses suspected of impairment due to
substance abuse or mental illness, and cannot protect the condentiality of licensees participating in
assistance programs.
Key Recommendations
•
Require the board to monitor licensees for adverse licensure actions in other states.
•
Authorize the board to deny applications to renew a license if an applicant is noncompliant with
a board order.
•
Authorize the board to require evaluations of licensees suspected of being impaired and require
condentiality for information relating to the evaluation and participation in treatment programs.
•
Direct the board to make data on the board’s enforcement activity information publically available
on its website.
Issue 5
A Continuing Need Exists for the State Board of Dental Examiners.
Regulating the practice of dentistry and supporting functions continues to support the state’s interest in
protecting the public. Alternative organizational structures, including the transfer of regulatory programs
to other agencies, oer no substantiated benet at this time. Continuing the board in its current form
will provide an independent agency responsible for ensuring quality, safe dental care.
Key Recommendation
•
Continue the State Board of Dental Examiners for 12 years.
5
State Board of Dental Examiners Staff Report with Commission Decisions
Summary of Sunset Staff Recommendations
Sunset Advisory Commission January 2017
Fiscal Implication Summary
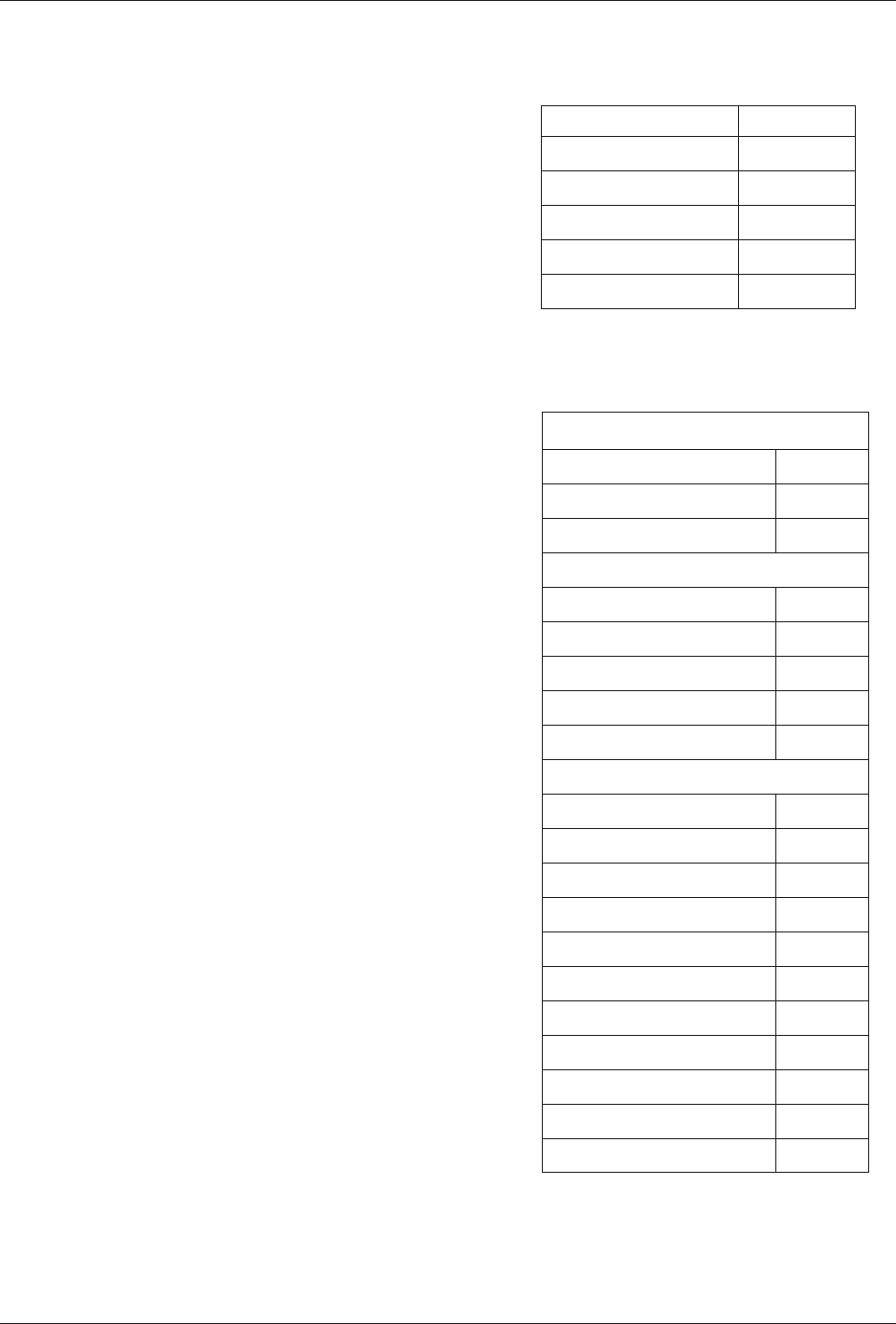
Overall, recommendations in this report would result in a negative scal impact to the General
Revenue Fund of approximately $1,402,000 over the next ve years. e impact comes from ending
the occupational licensing programs for dental assistants, reducing the size of the board, and enhancing
licensing and enforcement eorts.
Issue 1 — Decreasing the number of board members by six would result in a small annual savings of
about $13,000 to the General Revenue Fund resulting from decreased travel costs.
Issue 2 — e recommendation to deregulate dental assistants would have a negative impact to the
General Revenue Fund of about $1.46 million per year resulting from the loss of fee revenue collected
from dental assistants in excess of the cost of regulation.
Issue 3 — Providing the authority for the board to inspect dental oces administering anesthesia
would not have a signicant scal impact to the state, though actual implementation would have costs
associated with extra sta, travel, and equipment. ese costs could be mitigated by an adjustment to
existing anesthesia permitting fees.
Issue 4 — ese recommendations would result in a small revenue gain of approximately $45,000
annually, associated with the $3 increase in licensing fees to cover the board’s cost to query the National
Practitioner Data Bank. is gain would result from applicants paying the fee who ultimately do not
meet the standards for licensure and thus do not require of queries the data bank.
State Board of Dental Examiners
Fiscal Loss to the General
Change in the
Number of FTEs
Year Revenue Fund From FY 2017
2018 $1,402,000 -3
2019 $1,402,000 -3
2020 $1,402,000 -3
2021 $1,402,000 -3
2022 $1,402,000 -3

Sate Board of Dental Examiners Staff Report with Commission Decisions
Summary of Sunset Staff Recommendations
6
January 2017 Sunset Advisory Commission

agenCy at a glanCe
april 2016
7
State Board of Dental Examiners Staff Report with Commission Decisions
Agency at a Glance
Sunset Advisory Commission January 2017
agenCy at a glanCe
e State Board of Dental Examiners (the board) seeks to safeguard public health and safety by regulating
dental care in Texas, a responsibility the board has had since its creation in 1897. To meet its mission
of ensuring high quality and safe dental care, the board
•
licenses dentists and dental hygienists and registers dental assistants, laboratories, and mobile dental
facilities;
•
enforces the Dental Practice Act and board rules by investigating complaints against licensees and
registrants and taking disciplinary action against violators;
•
monitors compliance of disciplined licensees and registrants; and
•
provides a peer assistance program for licensees and registrants who are impaired.
Key Facts
•
State Board of Dental Examiners. e board consists of 15 members: eight dentists, two dental
hygienists, and ve public members. All members are appointed by the governor, with the advice
and consent of the Senate, for no more than two six-year terms. e presiding ocer is chosen by
the governor and must be a dentist; the board annually elects a member to act as secretary. Two
statutorily created advisory committees assist the board. e Dental Hygiene Advisory Committee
is composed of three dental hygienists and two public members appointed by the governor, as well
as one dentist appointed by the board, but not a member of the board. e Dental Laboratory
Certication Council consists of three certied dental technicians appointed by the board.
•
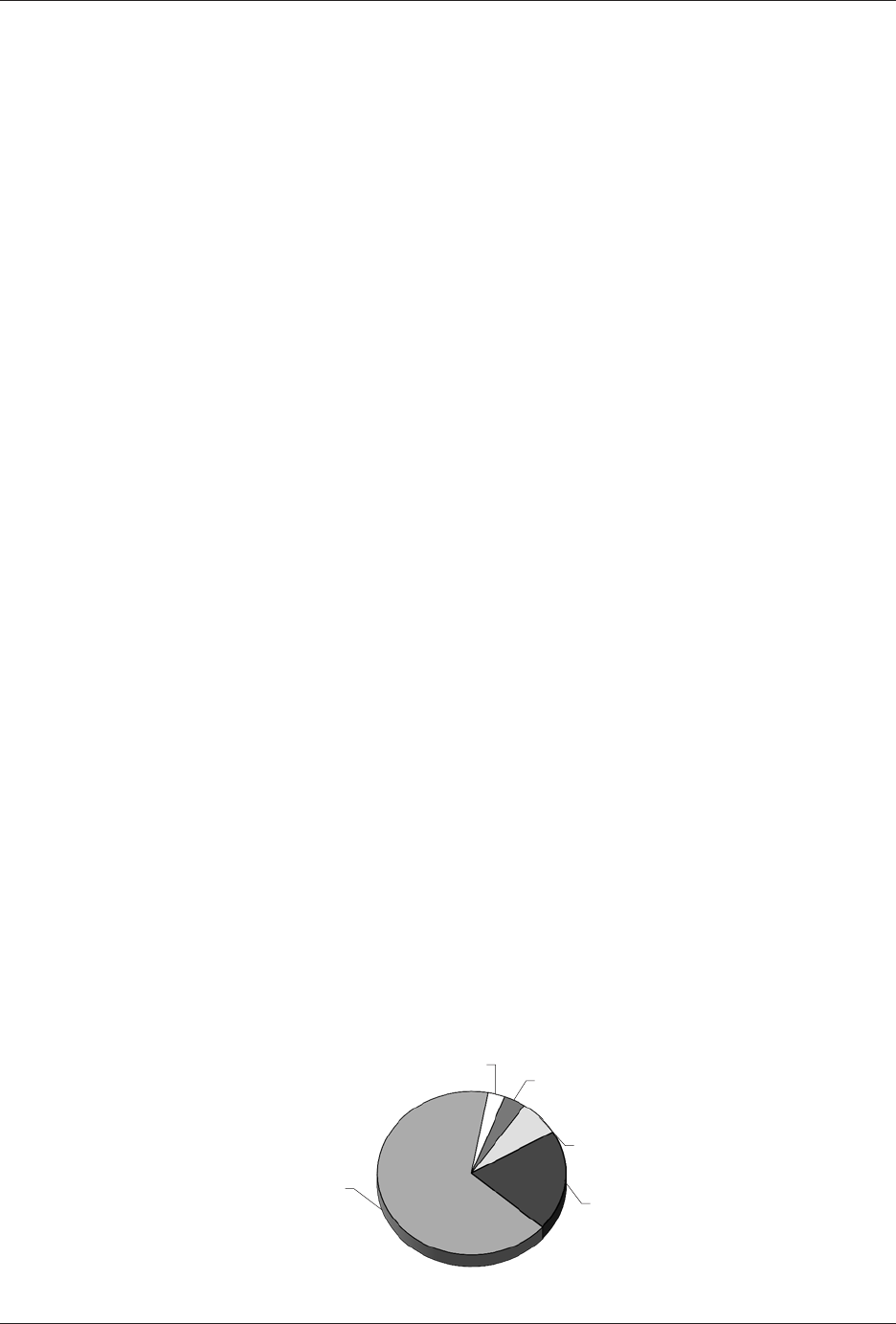
Funding. In scal year 2015, the board operated on a total budget of $4,203,605 with 93 percent of
its funding coming from the General Revenue Fund and the remainder from appropriated receipts.
Revenue generated through fees paid by dentists, dental hygienists, dental assistants, and other entities
regulated by the board is deposited in the General Revenue Fund and more than covers the board’s
operating costs. e pie chart, State Board of Dental Examiners Expenditures by Program, shows the
board’s expenditures in each major program area. Investigating and resolving complaints accounts
for almost two-thirds of total board expenditures.
Peer Assistance Program
$124,250 (3%)
Indirect Administration
$156,882 (4%)
Texas.gov
$300,054 (7%)
Licensure & Registration
$835,900 (20%)
Complaint Resolution
$2,786,519 (66%)
Total: $4,203,605
State Board of Dental Examiners Expenditures by Program
FY 2015
State Board of Dental Examiners Staff Report with Commission Decisions
Agency at a Glance
8
January 2017 Sunset Advisory Commission
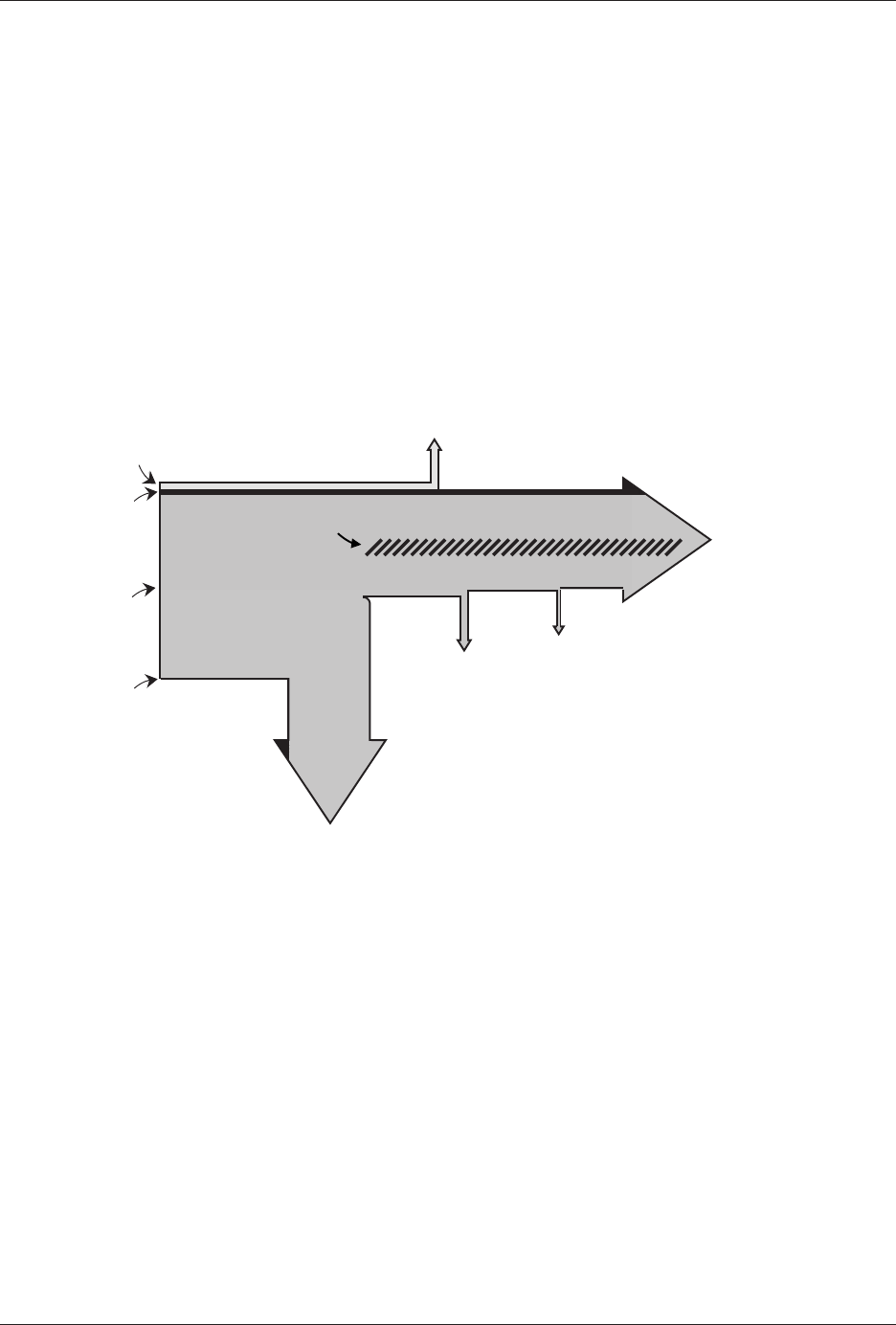
Historically, the board has generated revenue through various fees and charges far in excess of
what is needed to cover agency expenditures. In scal year 2015, the board generated revenue of
$11,814,143, including more than $3 million from the professional fee paid by dentists directly to the
General Revenue Fund and the Foundation School Fund. Although the Legislature discontinued
this professional fee in 2015, the board is still expected to bring in almost $3.8 million more from
its operating fees in scal year 2016 than budgeted to run the agency and pay for employee benets,
as shown in the chart, Flow of State Board of Dental Examiners Agency Revenue and Expenditures. A
description of the board’s use of historically underutilized businesses in purchasing goods and services
for scal years 2013–2015 is included in Appendix A, Historically Underutilized Businesses Statistics.
Texas.gov Fees
$250,000
Texas.gov
$250,000
Agency Costs
$4,586,954
Appropriated
Receipts
$258,500
Agency Fees
and Charges
$8,388,285
Professional Fees
$67,600
Health Professions
Council
$247,019
Peer Assistance
$124,250
General Revenue
$3,756,162
Total: $8,964,385
Employee Benets
$817,093
Flow of State Board of Dental Examiners Agency Revenue and Expenditures
FY 2016 (Budgeted)
•
Stang. e board had 58 authorized positions at the end of scal year 2015 and actually employed
55 individuals. Most employees work in the central oce in Austin, with 16 investigators and
inspectors working in eld oces throughout the state. Additionally, the board is a member of
the Health Professions Council, which provides supplemental information technology stang for
the board and other health professional licensing agencies. A comparison of the board’s workforce
composition to the percentage of minorities in the statewide civilian workforce for the past three
scal years is included in Appendix B, Equal Employment Opportunity Statistics.
•
Licensing and Registration. e board processes initial applications, renewals, and reinstatements
for three regulated dental occupations and two facility types. e table on the following page, Licenses
or Registrations by Type, shows credentials issued by type by the board in scal year 2015. Since
1994, the board has outsourced responsibility for administering licensing examinations for dentists
and dental hygienists to the Western Regional Examining Board. In addition to these licenses and
registrations, the board issues permits for dentists using anesthesia. In calendar year 2016, the board
9
State Board of Dental Examiners Staff Report with Commission Decisions
Agency at a Glance
Sunset Advisory Commission January 2017
will begin monitoring professional involvement with
dental service organizations through a cooperative
agreement with the secretary of state.
•
Complaints, Investigations, and Enforcement.
The board is responsible for receiving and
investigating complaints against licensees. e board
resolves complaints by dismissing those in which no
violation is found or proven, or when a violation is
found, by issuing a recommendation for education
or practice changes, imposing a remedial plan as
a non-disciplinary action, or ordering disciplinary
action. e table, Board Enforcement Data, details
the number of complaints received, subject
of complaints, and disposition of complaints
resolved in scal year 2015. In the same year, the
board averaged 447 days to resolve a total of 943
complaints.
•
Compliance. Sta monitors licensees’ compliance
with disciplinary actions and remedial plans to
ensure that the terms and conditions of board
orders are actually met. e board has two sta
responsible for ensuring compliance of 354 total
open cases at the end of the scal year 2015.
•
Peer Assistance. The agency contracts for
peer assistance services for licensees who may
be impaired by substance abuse or dependence
or mental illness. Through this program,
dentists, dental hygienists, and dental assistants
are evaluated to determine if they are safe to
practice, and if not, may be subject to treatment
and monitoring before being allowed to practice.
Eighty-nine practitioners participated in the peer
assistance program in scal year 2015.
Licenses or Registrations by Type
FY 2015
Dentist 17,540
Dental hygienist 13,740
Dental assistant
50,469
1
Dental laboratory 847
Mobile dental facility 62
Total 82,658
Board Enforcement Data
FY 2015
Complaints Received*
From the public 1,127
Initiated by sta 109
Total 1,236
Subject of Complaints Received*
Dentist 1,137
Dental hygienist 21
Dental assistant 41
Regulated facility 5
Unregulated entity 32
Disposition of Complaints Resolved*
Dismissed 710
Remedial plan 46
Warning or reprimand 128
Administrative penalty 5
Probation 23
Suspension 4
Voluntary surrender 8
Revocation 3
Cease-and-desist order 6
Other 10
Total complaints resolved
943
* Does not include enforcement actions
initiated after criminal history reviews or for
non-jurisdictional cases.

State Board of Dental Examiners Staff Report with Commission Decisions
Agency at a Glance
10
January 2017 Sunset Advisory Commission
1
is number represents the total number of dental assistant registrations issued in scal year 2015 for four separate certicate
programs and does not reect the total number of unique dental assistants registered with the board.

iSSueS
11
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
Sunset Advisory Commission January 2017
iSSue 1
The Unusually Large Dental Board Inappropriately Focuses on Issues
Unrelated to Its Public Safety Mission.
Background
e structure of the State Board of Dental Examiners governing body was last changed following the
2002 Sunset review of the agency, when the number of board members decreased from 18 to 15. e
board now consists of eight dentists, two dental hygienists, and ve public members.
Four standing committees support the board: the Executive, Licensing, Enforcement, and Quality
Control committees. e presiding ocer appoints ad hoc committees to work on special projects or
potential rulemaking eorts. Eight ad hoc committees have been created since 2013 to focus on issues
such as advertising, strategic planning, and ownership of dental practice. Every ad hoc committee
created in recent years has consisted entirely of board members, with mostly dentist board members
participating. Rules allow the board to appoint committees of various stakeholders to advise the board
about contemplated rulemaking.
1
e rst work group in recent history with stakeholder members was
established in February 2016 to examine anesthesia permitting and related inspections.
Two statutorily created advisory groups also
work with the board: the Dental Hygiene
Advisory Committee and the Dental Laboratory
Certication Council. e committee advises
the board, reviews and comments on proposed
rules, and may recommend rules related to the
practice of dental hygiene. e council reviews
applications for laboratory registration and may
also recommend rules related to laboratories to
the board. e Board Advisory Group Composition
textbox lists the membership of each group.
2
Findings
A decline in board duties requiring dental expertise has left
dentist members of the board with less to do.
e board’s oversized number of dentist members is a holdover from when
members had a much larger role in daily agency operations and is no longer
necessary to conduct agency business. In 2013, the Legislature reassigned
standard of care complaint review from the board’s dentist members to a
panel of expert dentists and dental hygienists designated by the board.
3
is
process removes dentist board members from serving as both investigator
and judge in enforcement matters, a position which would aect their ability
to render impartial decisions. ese expert reviewers also represent a much
broader range of dental specialty than is possible on the board. e continuous
availability on a contract basis of the 130 expert reviewers enables a much faster
Board Advisory Group Composition
Dental Hygiene Advisory Committee
•
ree dental hygienists appointed by the Governor
•
Two public members appointed by the Governor
•
One dentist member appointed by the board
Dental Laboratory Certication Council
•
ree members who must be dental technicians or
owners, managers, or employees of a registered dental
laboratory, appointed by the board
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
12
January 2017 Sunset Advisory Commission
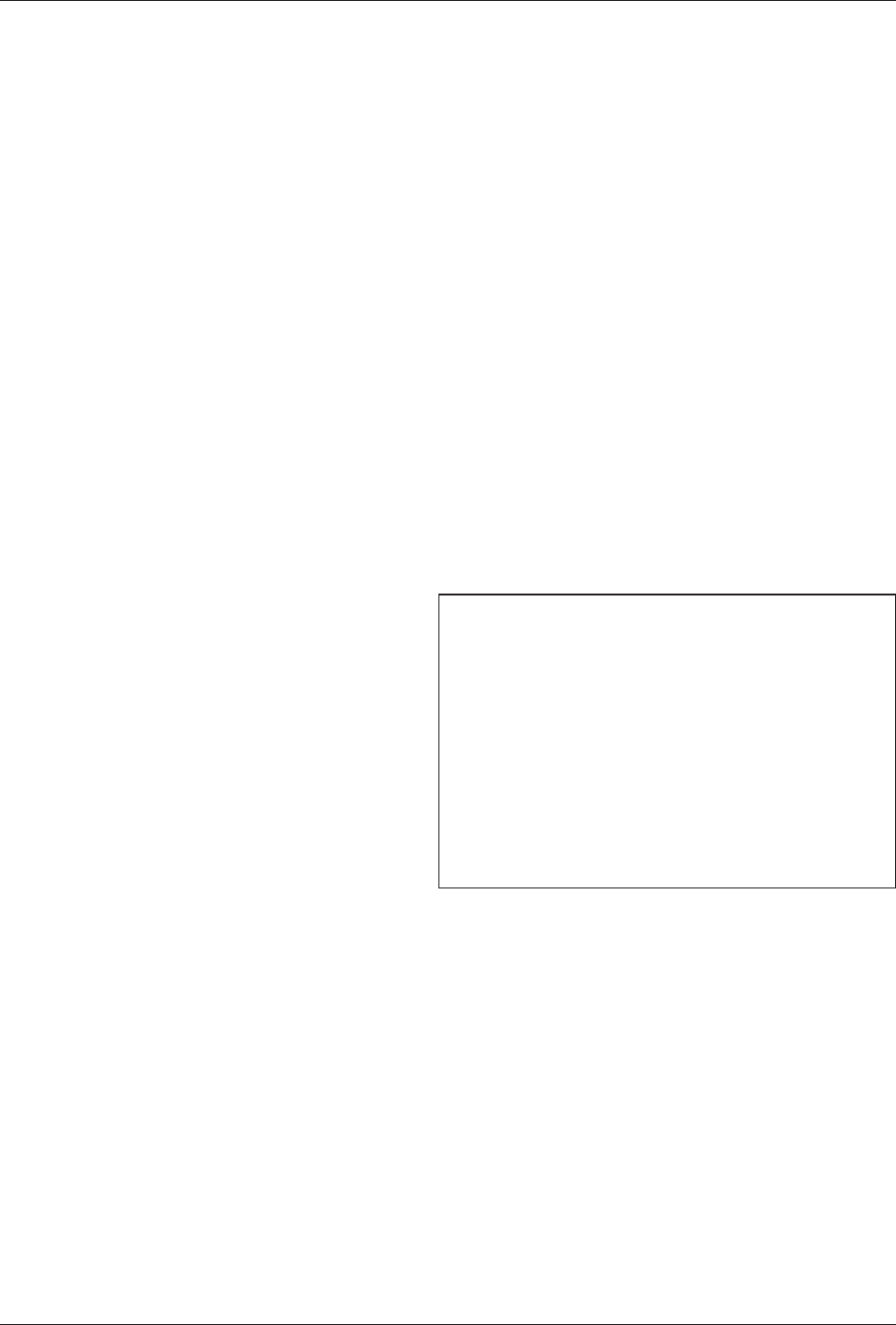
turnaround of reviews for the growing
number of incoming standard of care
complaints shown in the accompanying
chart. e use of panels has relieved
dentist board members of hundreds of
hours of work each year, sped up the
investigative process, and helped the
board make progress on its persistent
backlog of enforcement cases.
With fewer requirements to consume their time, dentist
board members have focused on matters that do not have a
demonstrated public safety impetus, undermining the agency’s
processes and wasting its resources.
•
Ill-fated rule packages. At the behest of dentist members, the board
has shown a propensity to push business-oriented matters without clear
evidence of patient harm. Two recent rulemaking eorts show the board’s
disregard for stakeholder concerns, legislative and legal interests, and the
lack of broad support and consensus.
One set of such proposed rules, regarding dental oce ownership
arrangements, purported to address patient care relating to non-dentist
owners of dental oces, although the board lacks data to suggest that
practice models or ownership arrangements are associated with a higher
incidence of complaints alleging compromised patient safety or demonstrated
harm. Yet, the board’s related ad hoc committee repeatedly promoted rule
revisions addressing the perceived issue in both 2014
and 2015. e board persisted in this matter even in
the face of pointed criticism from the Federal Trade
Commission, opposition from numerous stakeholders,
and requests by six members of the Legislature to
defer to the Legislature on the issue. Federal attention
to state agency rulemaking is unusual; the textbox,
Federal Trade Commission Comments, highlights some
of its comments on the proposed rules.
4
e rules
were ultimately withdrawn, but not before the eort
consumed ve board meetings, six ad hoc committee
meetings, and countless hours of sta support between
May 2014 and May 2015.
e other notable rulemaking eort regarding specialty advertising has a
considerably longer history. e rules reect the board’s long reliance on
a national association for advertising specialty designations. Although
the rules were not challenged for several decades, the regulatory climate
shifted. In 2011, the board began another review of its advertising rules,
an eort spanning numerous board and ad hoc committee meetings.
Ultimately, the board re-adopted rules restricting the advertising of dental
Federal Trade Commission Comments
“Proposed regulations to limit commercial relationships
between dentists and non-licensed entities should
be carefully examined to determine if they are based
on credible and well-founded safety, quality, or other
legitimate justications.”
“e proposed rules appear unnecessary to address any
concerns about the independent judgment of dental
professionals… we urge the Board to consider the
potential anticompetitive eects of the proposed rules,
including higher prices and reduced access to dental
services... and to reject both proposed [rules].”
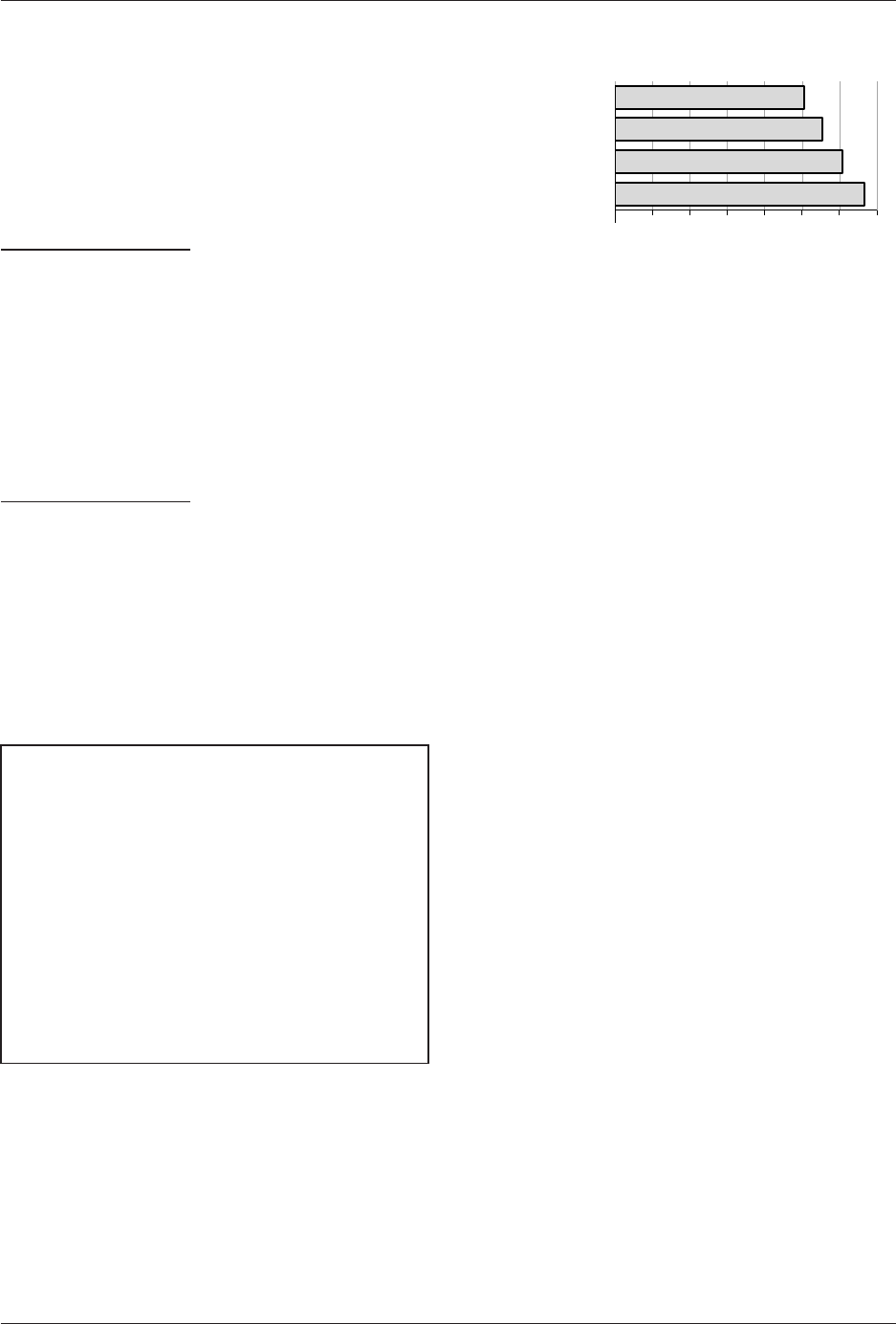
499
455
416
379
0 75 150 225 300 375 450 525
Standard of Care Complaints
FYs 2012–2015
2012
2013
2014
2015
Number of Complaints
The board
has shown a
propensity to
push business–
oriented matters
without clear
evidence of
patient harm.
13
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
Sunset Advisory Commission January 2017
specialties in 2012 and 2013 without clear evidence of patient harm from
an alternative approach to regulating advertising and despite unfavorable
trends in litigation on the subject.
5
e board was sued over the rules
and recently lost, drawing the rebuke of a U.S. District Court in January
2016. As evidenced by the textbox, Specialty Advertising Court Decision,
Federal District Court Judge Sam Sparks’ opinion questioned the board’s
motivation for re-adopting the rules.
6
Despite numerous opportunities to
address the issues raised in the lawsuit and in the court’s ruling, as suggested
by agency sta and stakeholders, the board continues to pursue its own
course, with little apparent concern for the legal liability and potential
nancial impacts its actions could bring on the agency.
Specialty Advertising Court Decision
“Defendants have produced no evidence of actual deception associated with
advertising as specialists in non-ADA [American Dental Association]-recognized
elds, there is no evidence to suggest any of the Plaintis’ elds are illegitimate or
unrecognized, and there has been no accusation any of the Plaintis’ organizations
are shams.”
“Defendants do not oer any competent evidence to substantiate these fears
and admit they did not review any studies, surveys or other evidence regarding
the impact of specialty advertisements before promulgating the Rule. Instead,
Defendants appeal to their own professional judgment and “vast experience dealing
with customers of dental services.” e State Dental Board’s collective common
sense is not a substitute for the “tangible evidence” required…”
“e right to advertise as a specialist in Texas is undoubtedly a nancial boon to
dentists in the state. While ostensibly promulgated to protect consumers from
misleading speech, it appears from the dearth of evidence [the Rule’s] true purpose
is to protect the entrenched economic interests of organizations and dentists in
ADA [American Dental Association]-recognized specialty areas.”
The board missed
opportunities to
address issues
more clearly
related to patient
harm, such
as anesthesia-
related
complaints.
Regulatory boards clearly have exibility to pursue matters they reasonably
believe are within their mission to protect the public, and they should be
given some forgiveness when they miss the mark. However, while this
board was pursuing these two dead-end rule packages — and still has
another regarding sleep apnea being challenged in court — it missed
numerous signs that it was on the wrong road. More importantly, while
these matters were occupying the board’s time, it missed opportunities to
address issues much more clearly related to patient harm, such as a rise
in anesthesia-related complaints. As discussed in Issue 3, board guidance
for strengthening agency oversight of dental anesthesia had been largely
lacking until the board established a work group in February 2016, at the
suggestion of the board’s new executive director, after a spate of media
attention elevated the concern.
e board’s recent misadventures in rulemaking highlight another concern
about obtaining public and stakeholder input on dicult, contentious
issues. e board follows the Administrative Procedure Act and properly
posts rule changes in the Texas Register, but without doing more to include
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
14
January 2017 Sunset Advisory Commission
stakeholders earlier in the rulemaking process, the board gave an appearance
that it had already determined its course of action and was not concerned
with the eect of its policies and regulations on stakeholders. In February
2015, agency sta put a process in place for stakeholders to provide input
on proposed rules earlier, in their formative stages, where they can raise
potential problem areas or identify blind spots that can result without such
a broad perspective. is new process oers promise, but must continue
to focus the board’s rulemaking eorts and ensure that they best serve its
public safety mission.
•
Eect on case resolution. Involvement in the case resolution processes
reects the diculty dentist board members have had accepting the
board’s diminished role. rough the board’s Quality Control Committee,
these members revisit standard of care complaint cases recommended for
dismissal by expert panel reviewers. While the review of dismissed cases is
within the board’s purview, having a standing committee expressly created
to review the work of its appointed experts slows down the resolution of
enforcement cases for little practical result, as detailed in the textbox, Quality
Control Committee Case Review. Of the 10 cases returned to the expert
panel from the Quality Control Committee, only three have resulted in
additional action — requiring nondisciplinary remedial plans. Ultimately,
the committee reects the dentist members’ antipathy for its own dental
review panel, whose members the dentist board members pointedly refuse
to call expert reviewers, despite the designation in law.
7
Quality Control Committee Case Review
September 2014–February 2016
•
290 – Number of cases reviewed
•
7-8 – Weeks, on average, cases wait for committee review
•
10 – Cases returned to expert review panel for additional examination
•
6.7 – Months, on average, added to case resolution for re-reviewed cases
•
2 – Cases dismissed following committee initiated re-review
•
3 – Cases closed by remedial plan following committee initiated re-review
•
5 – Cases pending action following committee initiated re-review
Reviewing work
of appointed
experts slows
case resolution
for little practical
result.
rough informal settlement conferences, board members and agency sta
seek to resolve complaints without going to contested case hearings at the
State Oce of Administrative Hearings. Most settlement conferences
are attended by dentist members to clarify technical issues and questions.
However some dentist board members question the ndings of their own
expert review panel that was designed to provide specic expertise regarding
the specialty of the dentist subject to the complaint. Such freelancing
has the eect of revisiting the facts of the case and revising the agency’s
position, which is not the role of board members at the conferences. It
can also result in less consistent and potentially unfair outcomes for those
15
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
Sunset Advisory Commission January 2017
accused, ultimately undermining the settlement process. Some dentist
board members involve themselves more than others; for example, of six
informal conferences not settled from September 2014 to January 2016, ve
had the same dentist presiding. e regulatory process should work more
consistently and predictably to ensure the fairness and overall eectiveness
of enforcement activities.
•
Sta turnover. Signicant turnover in the executive director and general
counsel positions has left stakeholders and sta without a consistent
vision for agency operations. From 2011 to 2015, the board employed
four separate executive directors and general counsels. Increased funding
for the executive director position in the 84th Legislative Session should
help promote stability for the position. However, board behavior has an
undeniable impact on agency sta in terms of morale and motivation to
do the dicult work of regulating dentistry. Ultimately, the board must
foster an environment to maintain the consistency in leadership and legal
support necessary to focus the board and the agency squarely on clear
issues of public safety and protection.
Recent events highlight the heightened expectations on
occupational licensing boards to adhere to a higher standard of
behavior to protect the public.
•
A recent U.S. Supreme Court ruling put a spotlight on state occupational
licensing board behavior that may be considered anticompetitive.
8
e
impact of the ruling has been to focus attention on board actions that do
not have clear public safety implications, especially actions by active market
participants who may be motivated to act in their self interest. Board
members must clearly show their decisions focus on the agency’s mission
to protect the public.
•
In the 84th Legislative Session, in the heat of the board’s maneuvering
on the dental oce ownership issue, a bill was introduced to single out
the dental board as needing training on the scope and limitations of its
rulemaking authority and establishing a code of conduct.
9
While the bill
was not pursued, the perceived need for such a directed measure indicates
an awareness that existing board training has not resonated with current
board members. e inappropriate actions of dentist board members begs
for a refocusing eort directed toward issues of clear public protection
supported by board licensing and enforcement data.
Statutorily created advisory groups are no longer necessary to
conduct board business and receive input.
•
e Texas Sunset Act states that advisory committees are abolished on
the date set for abolition of an agency unless the committee is expressly
continued by law. e Act also directs the Sunset Commission and sta to
make recommendations on the future of agency advisory committees using
Board behavior
has an impact
on staff morale
and motivation.
Recent court
rulings have
focused attention
on board actions
that do not have
public safety
implications.

State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
16
January 2017 Sunset Advisory Commission
the same criteria to evaluate both committees and their host agencies.
10
e Dental Hygiene Advisory Committee and the Dental Laboratory
Certication Council do not eciently support the board and could be
removed from statute without a negative eect on licensees or the public.
•
e board’s advisory groups have outlived their necessity and are no longer
necessary as separate statutorily created entities for eective input to the
board. e Dental Hygiene Advisory Committee has met just four times
in three years and has not prompted any original rulemaking activity in
that time. e Dental Lab Certication Council also seldom meets —
typically just once annually as required by law. e board and specially
convened stakeholder groups can provide any necessary expertise instead.
•
Advisory groups duplicate existing board and sta activity and could be
eliminated from statute without negatively aecting regulatory productivity.
Dental hygienist board members already oer professional expertise to the
full board more eciently than the committee simply by attending board
meetings. Meanwhile, the council’s review of the laboratory registration
applications is also redundant; council members’ expertise is unnecessary
to determine whether an application is complete and meets registration
criteria and the process duplicates the work of agency licensing sta.
Should heightened input regarding the regulation of either dental hygiene
or dental laboratories be required, the board has the authority to convene
working groups including broader interests than are currently represented
by the committee and council.
11
The board has more members than many other Texas health
occupational licensing boards.
Similar Texas health occupational licensing boards function with fewer members,
some while regulating more licensees. e Texas Board of Chiropractic
Examiners has a nine member board; the Texas State Board of Pharmacy has
an 11 member board; and the Texas Board of Nursing has a 13 member board.
Recommendations
Change in Statute
1.1 Reduce the size of the board from 15 to nine members and adjust its composition
to consist of four dentists, two dental hygienists, and three public members.
is recommendation would decrease the size of the State Board of Dental Examiners by six members.
Four dentist members and two dental hygienists on the board would provide necessary professional
expertise in collaboration with the agency’s dental director. e remaining three members would represent
the general public. No workload or special experience needs exist that require a 15-member board. A
nine-member board is large enough to provide professional insight regarding policy and represent the
board in settlement conferences while more appropriately matching dentist representation and overall
board size with workload.
The board can
convene working
groups with
broader interests
than represented
by the committee
and council.

17
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
Sunset Advisory Commission January 2017
Because the board is not structured to represent all areas of dental specialty, it has already had to seek
outside expertise for helping carry out is regulatory responsibilities, as seen in its expert review panels
that review dental standard of care complaints and through its stakeholder process when addressing
other specic issues. With the reduction in dentist members the board would continue its use of expert
panels and stakeholder groups as resources to gain needed insights beyond its experience or knowledge
when addressing specic issues.
To allow for staggering of terms, the recommendation would provide that all current board member
terms expire on September 1, 2017, with the governor making initial appointments as specied below.
Current members would be eligible for re-appointment if so determined by the governor to maintain
needed expertise. To maintain a functioning board and conduct necessary business, board members
serving on August 31, 2017, would continue to serve until a majority of new appointments are made.
•
One dentist, one dental hygienist, and one public member to initial terms expiring February 1, 2019.
•
One dentist, one dental hygienist, and one public member to initial terms expiring February 1, 2021.
•
Two dentists and one public member to initial terms expiring February 1, 2023.
1.2 Allow the board’s statutory advisory groups to expire and direct the board to
establish clearer processes for stakeholder input in rule.
In accordance with the Sunset Act, this recommendation would allow the work of statutorily created
advisory groups to occur more eectively and eciently through existing board members and informal
advisory groups. Allowing the Dental Hygiene Advisory Council and the Dental Laboratory Certication
Council to expire would give the board more exibility to convene working groups to receive input on
related topics on an as needed basis instead of forcing unnecessary annual meetings to meet statutory
requirements. Dental hygienists will retain the opportunity to comment on proposed rules concerning
the practice of dental hygiene through the two dental hygienist members on the board or an ad hoc
advisory group if needed. Application review and approval for dental laboratories would continue by
licensing sta.
As a management action, this recommendation would direct the board to improve and clarify its use
of ad hoc committees and working groups. e board should revise its rules to include a variety of
representation in ad hoc committee and working group membership, including public and dental
hygienist board members, professional associations, interest groups, and other non-industry stakeholders
as appropriate. Stakeholder input should be proactively sought in the development of board rules and
policies. e board should ensure ad hoc committees and working groups are established and working
to meet clearly dened objectives relevant to the board’s mission to protect the public.
1.3 Clarify the use and role of board members at informal settlement conferences.
is recommendation would specify in statute that board members present at informal settlement
conferences are only to make recommendations for the disposition of a complaint or allegation and not
to revisit the ndings of expert reviewers. is recommendation would also direct the board to revise
rules to require all board members, on a rotating basis, to attend informal settlement conferences to
accommodate the workload. Settlement conferences typically occur only a day or so each month. e
board’s dental director and sta hygienists could provide technical dental and dental hygiene expertise
as needed for informal settlement conferences attended by a public or dental hygienist board member.

State Board of Dental Examiners Staff Report with Commission Decisions
Issue 1
18
January 2017 Sunset Advisory Commission
is recommendation would support the work of the legislatively designed expert review panel, make
better use of informal settlement conferences as a complaint resolution tool, and provide a fairer process
to licensees in the enforcement process.
Fiscal Implication
While these recommendations would result in a small savings of $12,800 due to an estimated decrease
in board member travel expenses, the purpose of the recommendations is to enhance eciency, reduce
unnecessary bureaucracy, and improve stakeholder input.
1
22 T.A.C. Section 107.60(e).
2
All citations to Texas statutes are as they appear on http://www.statutes.legis.state.tx.us/. Sections 262.051, 266.051, and 266.052,
Texas Occupations Code.
3
Chapter 709 (H.B. 3201), Acts of the 83rd Texas Legislature, Regular Session, 2013.
4
Letter from Federal Trade Commission Oce of Policy Planning, Bureau of Competition, Bureau of Economics to Simone Salloum,
Assistant General Counsel, State Board of Dental Examiners, October 6, 2014.
5
See Ardt v. Ill. Dept. of Prof 'l Regulation, 607 N.E.2d 1226 (Ill. 1992); Bingham v. Hamilton, 100 F. Supp. 2d 1233 (E.D. Cal. 2000);
Borgner v. Brooks, 284 F.3d 1204 (11th Cir. 2002), cert. denied, 537 U.S. 1080 (2002); Douglas v. State, 921 S.W.2d 180 (Tenn. 1996); Parker v. Ky.
Bd. of Dentistry, 818 F.2d 504 (6th Cir. 1987); Parmley v. Mo. Dental Bd., 719 S.W.2d 745 (Mo. 1986) (en banc); Simm v. La. State Bd. of Dentistry,
No. 01-CV-2608-R (E.D. La. 2002), a 'd, No. 02-30304 (5th Cir. 2003), available at http://www.ca5.uscourts.gov/opinions/unpub/02/02-
30304.0.wpd.pdf.
6
Am. Acad. of Implant Dentistry v. Parker, et al., 2016 U.S. Dist. LEXIS 6956 (W.D. Tex. 2016).
7
Section 255.065, Texas Occupations Code.
8
N.C State Bd. of Dental Exam’rs v. Fed.Trade Comm’n, 135 S. Ct. 1101, 191 L. Ed. 2d 35 (2015).
9
S.B. 357, 84th Texas Legislature, Regular Session, 2015.
10
Sections 325.011, 325.012, and 325.013, Texas Government Code.
11
22 T.A.C. Section 107.60(e).
19
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
Sunset Advisory Commission January 2017
iSSue 2
State Regulation of Dental Assistants Is Unnecessary to Ensure Public
Protection and Is an Inefficient Use of Resources.
Background
Dental assistants perform a variety of functions in dental oces, from oce management to assisting
dentists in oral surgeries. Since 1991, statute has authorized dentists to delegate tasks to dental assistants
as long as the supervising dentist believes the individual can properly and safely perform the procedure
and the actions do not violate other provisions in law.
1
e State Board of Dental Examiners maintains
four separate certicate programs, outlined in the table, Dental Assistant Certicates, regulating specic
duties commonly delegated to dental assistants.
2
e X-Ray, Pit and Fissure Sealant, and Coronal
Polishing Certicates are established in statute; the Nitrous Oxide Monitoring Certicate was created
by board rule.
3
Unregistered dental assistants may still assist in dental procedures by only performing
duties that do not require a certicate.
Dental Assistant Certicates
Certicate Requirements Renewal
Total Active
Certicates FY 2015*
X-Ray
•
Basic life support training
•
Board approved course and exam
•
Jurisprudence test
Annual 34,610
Pit and Fissure
Sealant
•
Basic life support training
•
Board approved course
•
Jurisprudence test
•
Two years’ experience as a dental assistant
Annual 2,353
Coronal
Polishing
•
Basic life support training
•
Board approved course
•
Jurisprudence test
•
Two years’ experience as a dental assistant
None 2,959
Nitrous Oxide
Monitoring
•
Basic life support training
•
Board approved course and exam
•
Jurisprudence test
None 10,547
* Reects number of certicates, not individual certicate holders.
e Sunset Act contains rigorous requirements for evaluating licensing and regulatory functions of
state agencies. As summarized in the textbox on the following page, Sunset Questions for Occupational
Licensing, statutory criteria guide Sunset reviews in determining if an occupation presents a clear threat
to public health, safety, or welfare, and whether ongoing regulation can be justied.
4
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
20
January 2017 Sunset Advisory Commission
Sunset Questions for Occupational Licensing
•
Does the occupational licensing program serve a meaningful public interest?
•
Does the program provide the least restrictive form of regulation needed to protect
the public interest?
•
Could the program’s regulatory objective be achieved through market forces, private
certication and accreditation programs, or enforcement of other law?
•
Are the skill and training requirements for a license consistent with a public
interest, or do they impede applicants, particularly those with moderate or low
incomes, from entering the occupation?
•
What is the impact of the regulation on competition, consumer choice, and the
cost of service?
Complaints
involving patient
care and safety
attach to the
dentist, not the
dental assistant.
Dental assistants
have no direct
role in the
administration
of anesthesia.
Findings
State regulation of dental assistants does not improve public
safety.
•
Dentists are ultimately responsible for patient care and safety. Dentists
are responsible for the quality of all dental care their patients receive. As
detailed in the textbox, Statutory Responsibility, statute is clear that dentists
are accountable for the consequences of all delegated tasks, including those
performed by dental assistants and regardless of the assistant’s registration
status with the board.
5
Complaints involving patient care and safety and
resulting enforcement actions attach to the responsible dentist and not
the dental assistant. Accordingly, the
Statutory Responsibility
regulation of dental assistants by the
state does not oer additional avenues
“A delegating dentist is responsible
of recourse to patients who receive
for a dental act performed by the
person to whom the dentist delegates
substandard care. e dentist has the
the act.”
responsibility to ensure the proper
performance of delegated acts.
•
Dental assistants are limited to performing low risk tasks. e opportunity
for dental assistants to cause serious patient harm is minimal, because all
procedures performed by dental assistants must be reversible or capable
of correction.
6
For example, dental assistants have no direct role in the
administration of anesthesia. State law also prohibits dental assistants
from cutting hard or soft tissue, a stipulation signicantly limiting the
opportunity for in-mouth work by dental assistants.
7
ese limitations
reect the functional relationship between the dental practitioners; dental
assistants perform tasks complementary to dentists’ technical work and at
their direction, but cannot act independently and are therefore unlikely
to injure patients.
•
Regulation produces little meaningful enforcement activity. e board
receives very few complaints against dental assistants, suggesting a lower
risk of harm compared to other related regulatory programs. Not one of
21
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
Sunset Advisory Commission January 2017
the 26 complaints against dental assistants made by the public in scal year
2015 alleged standard of care violations, and most involved professional
conduct or unlicensed practice violations. Additional information about
the board’s complaint and enforcement activity concerning dental assistants
is available in Appendix C, State Board of Dental Examiners Comprehensive
Enforcement Data. e low volume of complaints and regulatory activity
concerning dental assistants’ patient care reects the minimal level of public
risk associated with the vocation.
•
Regulatory gaps undermine the promise of public safety. Exceptions to
the initial requirements for dental assistant certicates challenge assurances
of the education, training, and other competency standards for dental
assistants. By law, dental assistants can take x-rays for up to one year
without registering with the board.
8
e one-year exemption is tied to
the employer, so dental assistants, a highly mobile population, may remain
unregistered indenitely simply by changing employers annually. is
loophole signicantly undermines the registration requirement for dental
assistants, because the board has no way to know when a dental assistant
began employment or began taking x-rays, nor, for that matter, would
patients. As a result, the process largely relies on the honor system between
the dentist and dental assistant to inform the board.
In addition, continuing education provisions do not ensure the ongoing
competency of dental assistants. While continuing education requirements
are clearer for those with the X-Ray and Pit and Fissure Sealant certicates,
which are renewed annually, dental assistants do not have to submit
documentation of continuing education courses to renew certicates, and
the board does not audit compliance. As above, this process ultimately
relies on the honor system for dental assistants to obtain the ongoing
training needed to stay current with the latest developments in the eld.
Continuing education could be better enforced by the employing dentist
without state regulation.
Dental assistant certicates are an unwieldy patchwork of
regulation and waste limited board resources.
•
Dental assistant certicate programs divert licensing resources. Board
resources supporting the dental assistant certicate programs would be of
better use supporting higher risk professional licenses. As illustrated by the
chart on the following page, Credentials Issued, the board issued more dental
assistant certicates in scal year 2015 than all other types of credentials
combined. Managing the application materials for the four distinct dental
assistant certicate programs requires the equivalent of three sta positions
because of separate application processes and dierent requirements. In
contrast, the same number of employees is able to support the processing
of licensing materials for dentists and dental hygienists, professions with
more complex training and education requirements and a greater potential
to cause patient harm.
Dental assistants
can take x-rays
for up to one
year without
registering with
the board.
Staff support for
dental assistant
certificate
programs would
be better used
on higher risk
licenses.
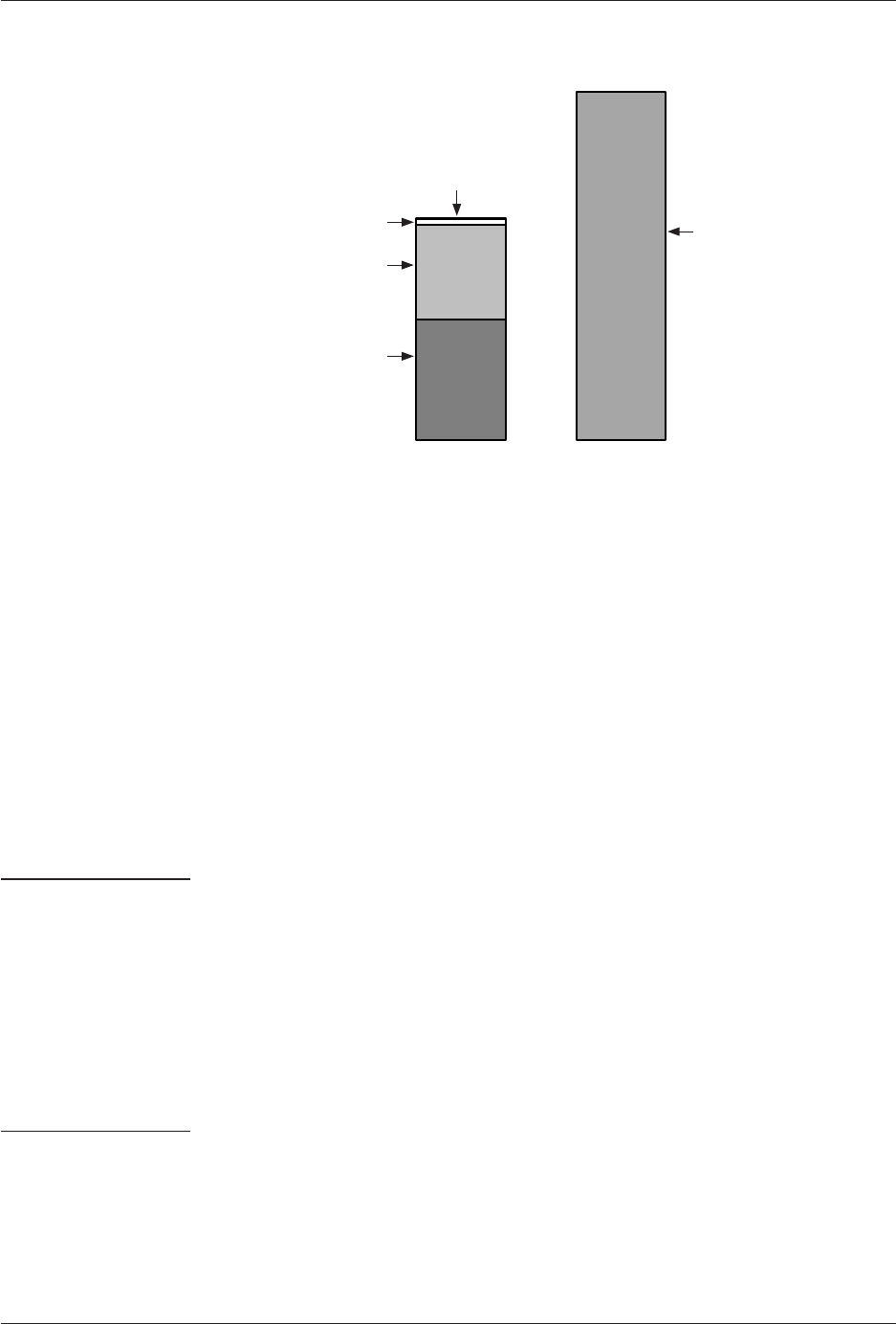
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
22
January 2017 Sunset Advisory Commission
Having a single
certificate for
dental assistants
would not
address the
issue that the
regulation is
unnecessary.
Total: 82,658
Credentials Issued – FY 2015
Mobile/Portable Dental
Facility Permits – 62
Dental Laboratory Permits – 847
Dental Hygienist Licenses
13,740
Dental Licenses
17,540
Dental Assistant Certicates
50,469
•
Board action on dental assistant certicates wastes limited legal resources.
Board action based on applicants’ criminal history needlessly diverts limited
legal resources away from higher priority enforcement responsibilities.
Dental assistants are not subject to background checks before licensure.
However, self-disclosure of criminal convictions on certicate applications
prompts legal review, investigation, and often the issuance of a consent
order with a certicate. e majority of reported criminal history involves
misdemeanors unrelated to the duties or responsibilities of dental assistants
and often occurred years before submitting an application. e impact of
this process on legal sta is out of proportion to the risk; sta attorneys
reviewed about 600 dental assistant applications and prepared 139 associated
consent orders in scal year 2015, requiring signicant legal sta time.
Issuing consent orders in response to dated criminal histories of dental
assistant applicants is an especially ineective use of resources compared
to the legal division’s responsibility to prosecute complex enforcement
cases against dentists and its ongoing eorts to work through a backlog
of complaints.
Addressing the deciencies in the state’s approach to certifying
dental assistants would not enhance public protection.
•
Strengthening the regulation of dental assistants is not justied.
State regulation of dental assistants through a simplied or more robust
regulatory program would not improve patient care and would extend already
unnecessary regulatory oversight. Streamlining the existing registration
processes onto one application or consolidating the certicates into a single
license would not address the fundamental issue that the state’s regulation
of dental assistants is unnecessary to protect the public. Further, to do
so would erect an even higher barrier to the profession for a group that
may be overwhelmed by the expense of required training and coursework,
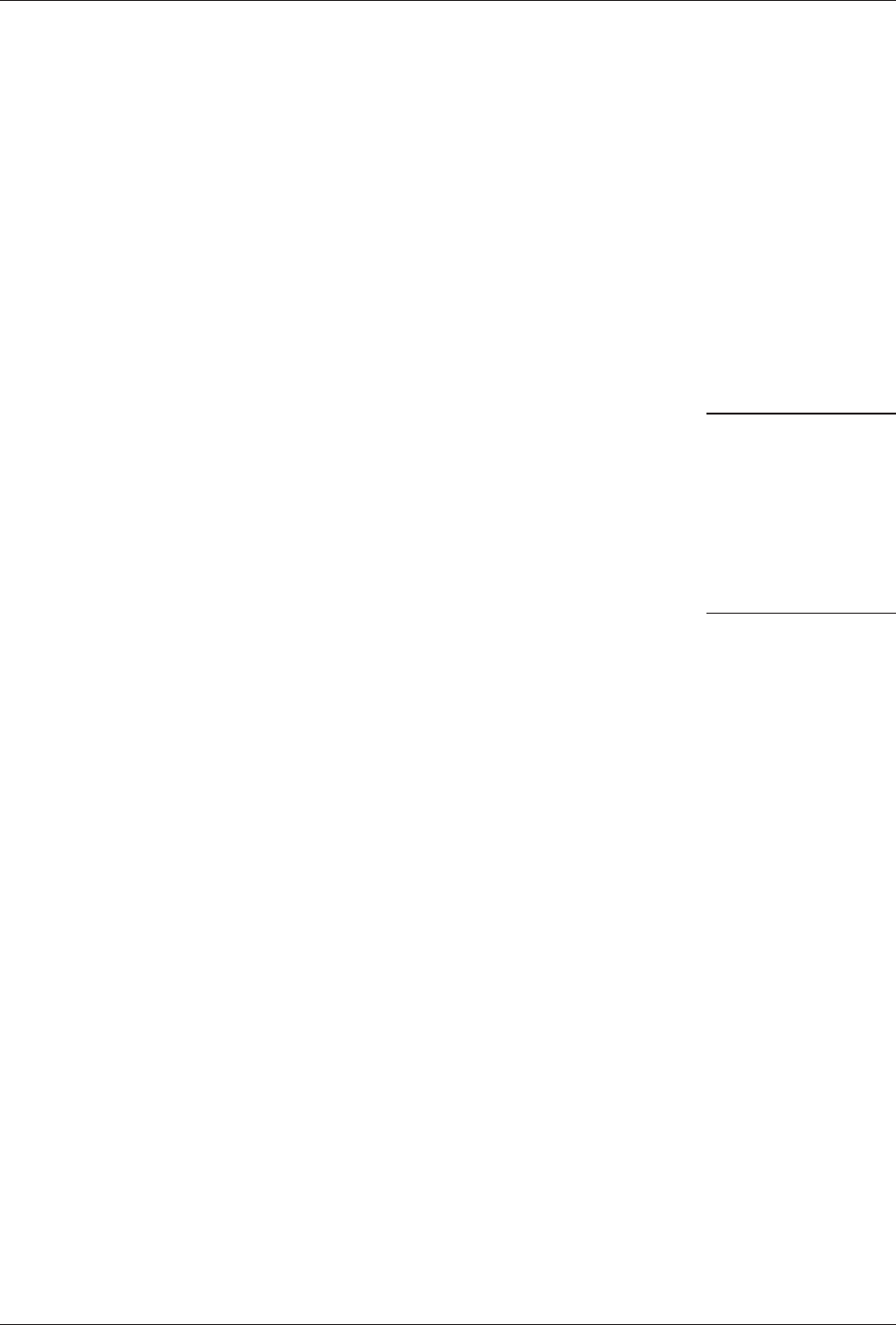
23
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
Sunset Advisory Commission January 2017
agency fees, and continuing education requirements. Establishing a more
comprehensive regulatory system is not needed for someone who can only
perform reversible tasks delegated by a highly trained, and ultimately
accountable, dentist.
•
Other states do not provide a clear model for regulating dental assistants.
Six states license dental assistants, 26 states use registration or certicate
systems to credential dental assistants in some way, and 18 states do not
regulate dental assistants at all.
9
National credentialing and private market forces can provide
desired oversight of dental assistants.
Existing credentialing programs and private market forces already oer
consumers and employing dentists standards and oversight for dental assistants’
training and practice, rendering the state’s certication programs redundant.
e American Dental Association recognizes the Dental Assistant National
Board (DANB) as the national certication board for dental assistants.
10
Credentials from DANB are recognized in 46 states, including 32 states that
require or recognize its certications for certain dental assisting privileges.
Certication through DANB requires education, examinations, and continuing
education, as well as the disclosure of felony criminal history and disciplinary
actions by occupational licensing boards. Dental assistants are disciplined by
DANB for unprofessional, dishonest, or fraudulent behavior.
Using national certication standards would increase market accessibility for
dental assistants looking to relocate to Texas, which already accepts DANB
certication as meeting the education requirements for the X-Ray, Pit and
Fissure Sealant, and Coronal Polishing Certicates. Motivated by statutory
responsibility for all patient care and market forces, dentists are encouraged
to employ only well trained and competent dental assistants, and can rely on
certication through the private DANB as a means to evaluate potential sta
without state interference.
Recommendation
Change in Statute
2.1 Discontinue the board’s dental assistant certicate programs.
is recommendation would eliminate three dental assistant regulatory programs from statute: the X-Ray,
Pit and Fissure Sealant, and Coronal Polishing certicates. As a management action, this recommendation
would also direct the board to discontinue the Nitrous Oxide Monitoring certicate in rule. Removing
the X-Ray Certicate from statute would require clarication of the Medical Radiologic Technologist
Certication Act to ensure the ability of dental assistants to continue to perform x-rays under the
authority of the dentist without having to register with the board.
11
Under this recommendation, the
board’s regulatory functions related to dental assistants would cease on the eective date of the provision
in the resulting Sunset bill.
Statute and
market forces
motivate dentists
to employ well
trained dental
assistants.

State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
24
January 2017 Sunset Advisory Commission
is recommendation would not interfere with the existing ability of dental assistants to perform delegated,
reversible tasks under a licensed dentist’s supervision, nor would it alleviate the responsibility of dentists
to ensure dental assistants have the proper training, such as that provided by private organizations. As
a management action, the board would be directed to clarify the tasks dentists may delegate to dental
assistants in rule. Implementation of this recommendation is intended to allow the board to focus on
the higher risk regulatory programs for dentists and dental hygienists and redirect enforcement resources
to complaints concerning licensees responsible for patient harm.
Fiscal Implication
Because of the eect of licensing fee revenue on the General Appropriations Act, deregulation of
occupations in Texas generally has a negative impact on the General Revenue Fund. is recommendation
would have a negative impact to the General Revenue Fund of $1.46 million per year. Licensing and
administrative fee collections for the dental assistant certicate programs totaled about $1,568,000 in
scal year 2015. is recommendation would eliminate three full-time positions at the board associated
with administering the certicate programs, which would save about $108,000 in salary and benet
expenditures, for a net estimated revenue loss to the state of $1,460,000 annually. Given the continued
backlog of complaints, the board could request the positions and resources associated with the dental
assistant certicate programs to support regulation and enforcement of higher risk licensee groups and
continue working through a backlog of cases.
State Board of Dental Examiners
Fiscal
Year
Loss to the General
Revenue Fund
Change in the
Number of FTEs
From FY 2017
2018 $1,460,000 -3
2019 $1,460,000 -3
2020 $1,460,000 -3
2021 $1,460,000 -3
2022 $1,460,000 -3

25
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
Sunset Advisory Commission January 2017
1
All citations to Texas statutes are as they appear on http://www.statutes.legis.state.tx.us/. Section 258.002(a), Texas Occupations Code.
2
Section 4.04, Chapter 1470 (H.B. 3507), Acts of the 77th Texas Legislature, Regular Session, 2001; Section 25, Chapter 17 (S.B. 263),
Acts of the 78th Texas Legislature, Regular Session, 2003; Section 6, Chapter 476 (S.B. 455), Acts of the 81st Texas Legislature, Regular Session
2009; 22 T.A.C. Section 114.4; (Tex. State Bd. of Dental Exam’rs, Extension of Duties of Auxiliary Personnel--Dental Assistants) adopted 32
Tex. Reg. 627 (2007) (proposed December 1, 2006).
3
Sections 265.004–.006, Texas Occupations Code; 22 T.A.C. 114.4.
4
Section 325.0115(b), Texas Government Code.
5
Sections 258.002(a) and 258.003, Texas Occupations Code.
6
Section 265.0001(2)(C), Texas Occupations Code; 22 T.A.C. Section 114.1.
7
Section 258.001(3)(B), Texas Occupations Code.
8
Section 265.005(l), Texas Occupations Code; 22 T.A.C. Section 114.11.
9
American Association of Dental Boards, e Composite, 26th ed. (Chicago: American Association of Dental Boards, 2015), 83–84 and
90–92.
10
“About DANB,” Dental Assistant National Board, Inc., last modied December 6, 2015, https://www.danb.org/en/About-DANB.
aspx.
11
Sections 601.152 –.153 and 601.252, Texas Occupations Code. e State Board of Dental Examiners would need to be exempt
from Section 601.252(c), Texas Occupations Code, to fully discontinue the X-Ray Certicate program. Additionally, Section 601.153(2), Texas
Occupations Code, would need to be deleted or modied to permit delegation to supervised, but unregistered, dental assistants.

State Board of Dental Examiners Staff Report with Commission Decisions
Issue 2
26
January 2017 Sunset Advisory Commission
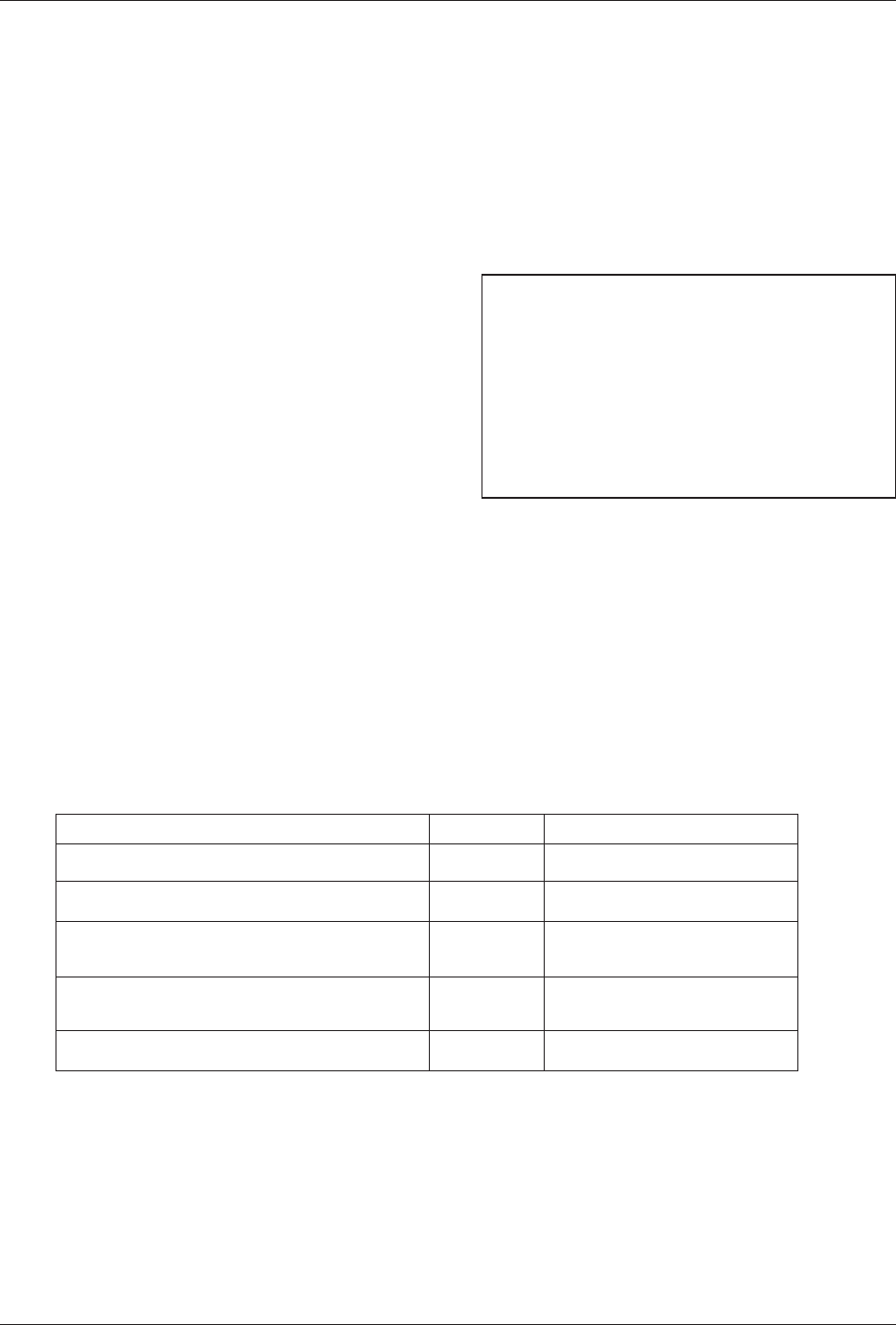
27
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 3
Sunset Advisory Commission January 2017
iSSue 3
The Board Lacks Key Enforcement Tools to Ensure Dentists Are
Prepared to Respond to Increasing Anesthesia Concerns.
Background
Dentists administer varying levels of anesthesia to
perform procedures ranging from routine preventive
care to invasive corrective treatment. Patients typically
receive anesthesia in dental oce, ambulatory surgical
center, or hospital settings using two techniques
described in the textbox, Methods of Anesthesia
Administration. e State Board of Dental Examiners
has issued separate permits allowing dentists to
administer anesthesia since 2001.
1
e board’s anesthesia permitting structure, depicted in the table, Dental Anesthesia Permits, is tiered
based on the intended level of consciousness, method of administration, and amount of practitioner
training. Dentists must hold a separate permit for each type of anesthesia administration they want to
perform, so the numbers include duplicate permit holders. With nitrous oxide permits most numerous,
69 percent of Texas dentists hold at least one anesthesia permit. Level III and IV permit holders can
apply separately for portability permits, allowing provision of anesthesia services in locations other
than a dentist’s primary oce.
2
Dentists with portability permits often administer anesthesia for other
dentists who do not have the same credentials. Nearly 700 Texas dentists held one or more portability
permits in scal year 2015.
Methods of Anesthesia Administration
•
Enteral anesthetic is absorbed through the
intestines, nose, mouth or skin; delivery is typically
through pills and liquids.
•
Parenteral anesthetic is absorbed through
intravenous or intramuscular injection; delivery is
typically through intravenous therapy or localized
injections.
Dental Anesthesia Permits – Fiscal Year 2016
Type Number* Application/Renewal Fees
Nitrous Oxide/Oxygen inhalation sedation 12,086 $32 / $10
Level I: Minimal sedation 7,357 $60 / $10
Level II: Moderate sedation limited
to enteral routes of administration
3,075 $60 / $10
Level III: Moderate sedation which includes
parenteral routes of administration
1,668 $60 / $10
Level IV: Deep sedation or general anesthesia 558 $60 / $10
* Counts reect individual permits issued, not individual permit holders.
Parenteral administration of anesthesia was once the only way to achieve deep sedation in patients,
but advances in pharmacology now allow deep sedation using enteral anesthesia delivery. As a result,
method of administration of anesthesia is less indicative of patient level of consciousness than it once
was. Because individuals respond dierently to anesthesia, the board requires all permit holders to have
certain equipment to rescue patients experiencing adverse reactions or patients who enter a deeper state
of sedation than intended.
3
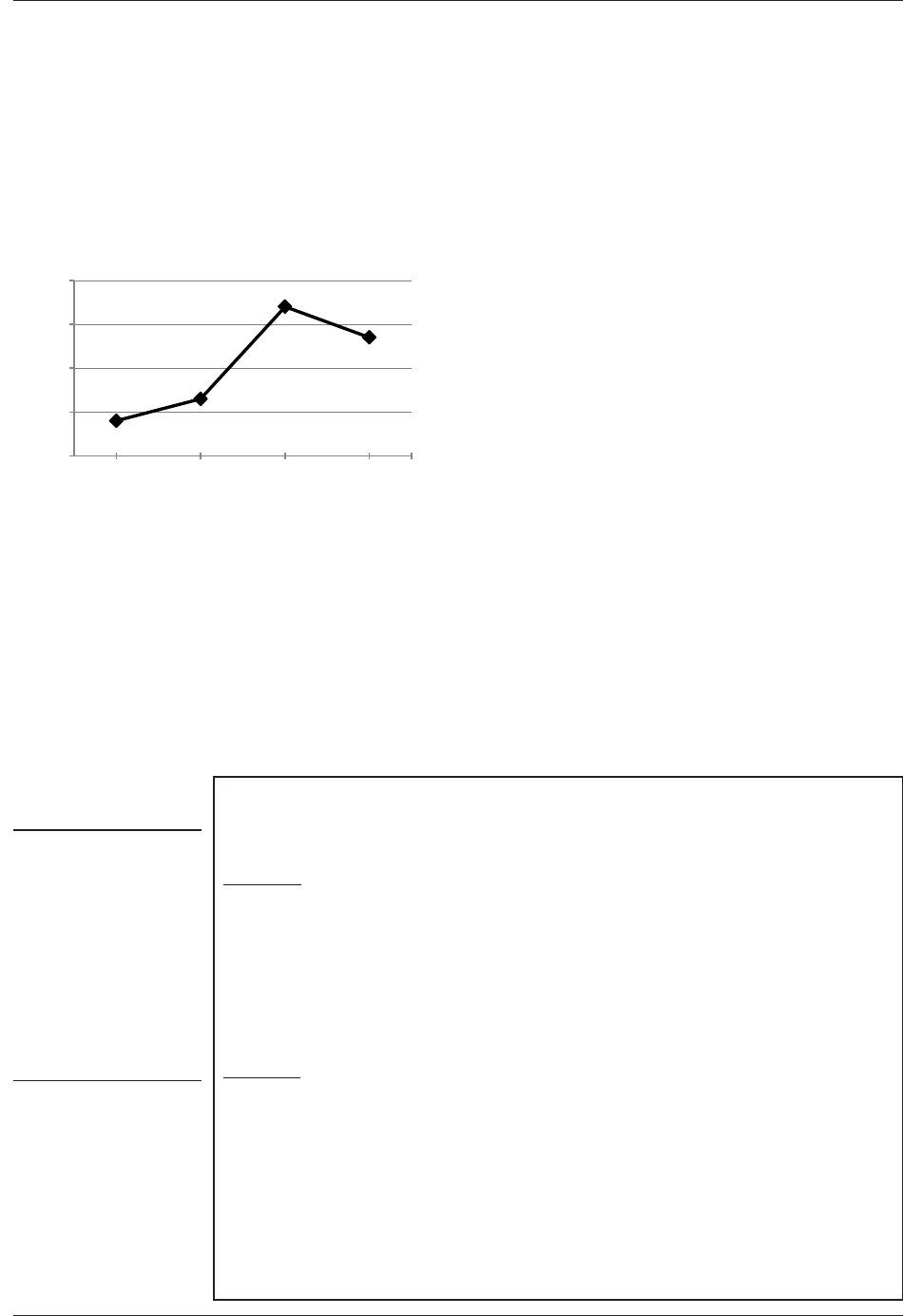
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 3
28
January 2017 Sunset Advisory Commission
Findings
Anesthesia can be high risk to patients, and related complaints
to the board have increased.
As highlighted by recent media coverage, complications from dental procedures
using anesthesia have caused serious harm to Texas patients, including death.
4
To provide a more complete picture of this situation,
a manual examination of standard of care complaints
received by the board from scal year 2011 to mid-
scal year 2016 was performed for this review. Even
without the assurance that the resulting data set is
comprehensive, the number of complaints involving
anesthesia has increased in recent years, as illustrated by
the chart, Anesthesia-Related Complaints. In addition,
the 17 complaints received midway through scal year
2016 were on pace to equal the previous high number
of anesthesia-related complaints in 2014.
Anesthesia can cause serious harm even if correctly administered and supervised.
Of the 100 anesthesia-related complaints compiled in the review, 41 involve a
patient death during or shortly after a dental procedure involving anesthesia.
Board reviewers ultimately determined that most of these deaths were unrelated
to the supervising dentist’s performance, but at least 13 of the 41 death cases
were found to include violations of the dental standard of care, including
inappropriate preparation for or response to anesthesia-related emergencies.
e textbox, Selected Texas Anesthesia-Related Complaint Cases, oers details
of specic harm to patients from recent complaint cases involving dental
procedures using anesthesia.
0
10
20
30
40
2012 2013 2014 2015
Anesthesia-Related Complaints
FYs 2012–2015
8
13
34
27
Number of Complaints
Selected Texas Anesthesia-Related Complaint Cases
e State Board of Dental Examiners investigated and found:
Case One: A child suered severe, irreversible brain damage following moderate enteral
sedation in a dentist’s oce. e treating dentist sedated the patient using oral medications
and nitrous oxide to remove decayed teeth. e child began experiencing seizures after
administration of the anesthesia, but the dentist did not contact emergency medical services
for hours. Instead, the dentist attempted to manage the seizures using oral medications
while the child’s oxygen saturation dropped and was not supplemented. As of the release
of this report, the dentist's license was temporarily suspended. Additional enforcement
action is expected from the board.
Case Two: An adult patient died after receiving deep parenteral sedation for a root canal
procedure. e dentist administering the anesthesia was using a portability permit to
provide services in another dentist’s oce. When the patient stopped breathing during the
procedure, an assistant had to run to the dentist’s car to retrieve resuscitation equipment. e
nal cause of death was determined to be heart disease, which complicated the eect of the
anesthesia on the body. But the board still found that the dentist administering anesthesia
violated the standard of care by failing to recognize the patient’s deteriorating situation,
have rescue equipment at hand, and immediately call emergency medical services. As a
result, the board suspended the dentist's anesthesia permits until the dentist met a number
of requirements including 320 hours of continuing education and an oce inspection.
Anesthesia-
related
complaints
received midway
through fiscal
year 2016 were
on pace to equal
the previous high.
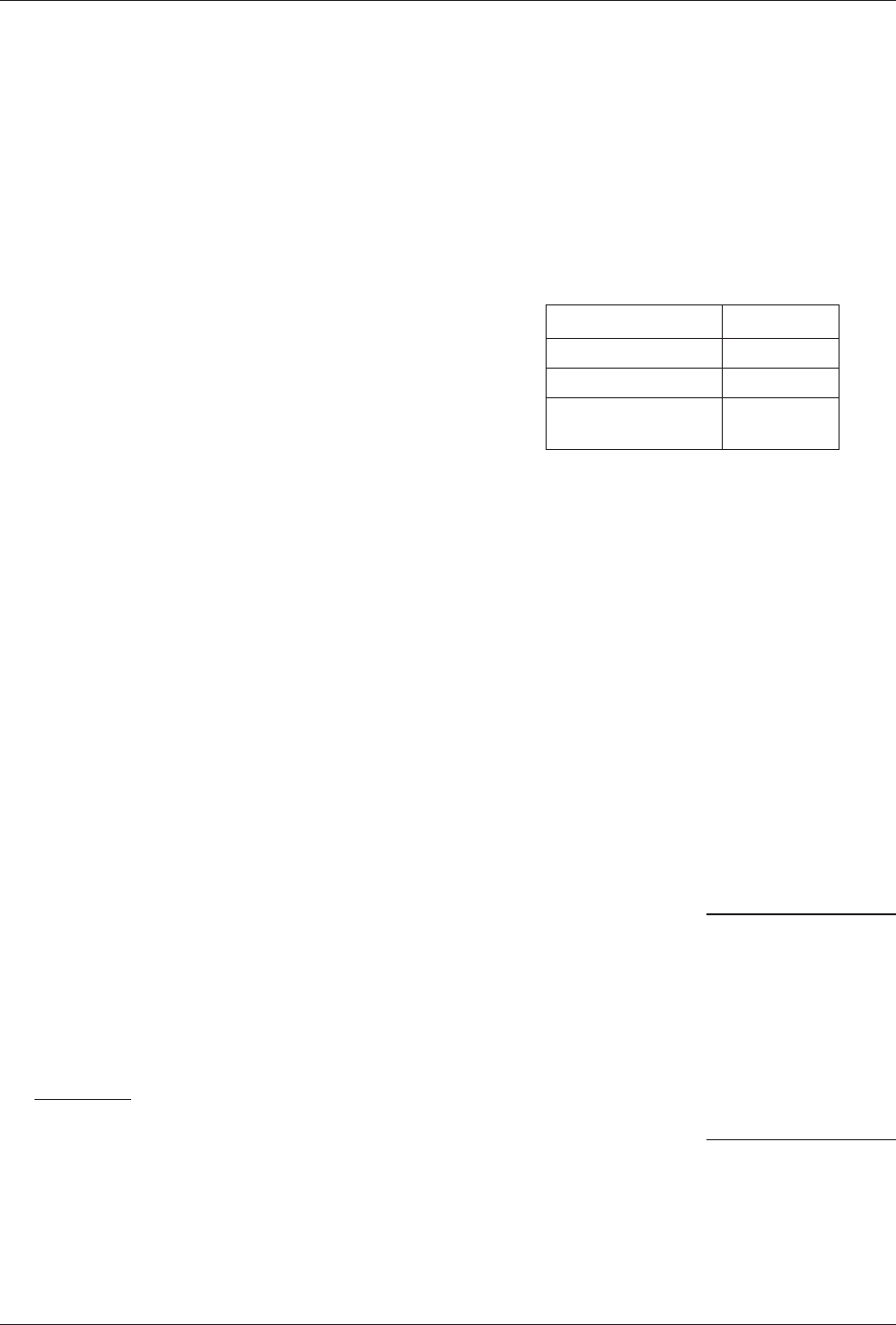
29
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 3
Sunset Advisory Commission January 2017
Gaps in regulatory authority and a lack of leadership have left
the board unprepared to address anesthesia-related problems.
•
Limited inspection authority. Data from the review of more than ve
years of complaints related to anesthesia indicates parenteral delivery of
anesthesia is involved in nearly two-thirds of such complaints, as shown in
the accompanying chart. However, the board only has statutory authority
to perform inspections of dental oces, equipment, and
documents related to enteral anesthesia administration.
e invasive nature and demonstrated risk of parenteral
delivery, combined with a higher number of associated
complaints to the board, suggests a greater need for
similar inspection authority related to parenteral delivery
as it already has for enteral administration of anesthesia.
Without inspection authority, the board is left to react to
problems after they have occurred through its complaint
process and cannot prevent problems and possible
tragedies before they occur by ensuring dentists are ready
to respond to an emergency should the need arise.
•
Lack of board leadership on anesthesia issues. Although it has had
authority since 2001 to routinely inspect the oces of dentists administering
enteral anesthesia, the board has never had or sought the nancial resources
to do so. Until very recently, the board has not even tracked anesthesia-
related complaints to fully understand the extent of related issues. is
inaction may relate to many factors that have aected the board in recent
years, including signicant turnover in key sta positions and the board’s
interest in other projects, as described in Issue 1 of this report. After media
attention to dental anesthesia and at the suggestion of the new executive
director at the February 2016 board meeting, the board appointed a
work group to consider potential inspection criteria, revisions to permit
applications, and other eorts intended to improve the board’s oversight
of anesthesia administration. More of this kind of preventive action is
needed to better ensure the safe delivery of anesthesia in the dental context.
•
Inconsistent regulation of dental anesthesia administration due to
practice location. Dentists providing anesthesia services in oce settings
are not subject to the same preventive and oversight measures as their
hospital — and ambulatory surgical center–based peers, even though the
board has regulatory authority over dentists practicing in both settings.
Inspections. e Department of State Health Services or private accrediting
bodies routinely inspect all hospitals and ambulatory surgical centers in the
state to ensure safety and anesthesia emergency preparedness. As a result,
the workspace of dentists administering anesthesia in those settings is subject
to greater oversight through checks for equipment and written protocols
to help ensure readiness to address anesthesia emergency situations in a
way that does not exist for dentists administering anesthesia in a typical
oce setting.
Anesthesia-Related Complaints
by Method of Administration
FYs 2012–2016 Year to Date*
Method Complaints
Parenteral 63
Enteral 25
Unknown or under
investigation
12
* Reects anesthesia-related complaints
received in only one-half of scal year
2016.
Without
inspection
authority, the
board cannot
ensure readiness
to respond to
emergencies.
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 3
30
January 2017 Sunset Advisory Commission
Emergency Action Plans. Dentists administering anesthesia in oce
settings are required to maintain the equipment, drugs, and training
necessary to respond appropriately to an anesthesia-related emergency.
However, the board has not required dentists practicing in oces to pull
all of these eorts together in a written, actionable plan as is required in
more sophisticated medical facilities or required of physicians administering
moderate anesthesia in oce settings. e distinction is important and
without a basis, considering the equal inherent risk of anesthesia delivery to
patients regardless of treatment location and the danger from mishandling
anesthesia-related complications in oce settings as described in the tragic
cases earlier in this report. Written procedures alone will not save a patient
in distress. But, the exercise of developing and writing out a plan forces
practitioners to consider the role of every oce member when reacting to
anesthesia-related emergencies and identify gaps in preparedness. Plans also
oer references for support sta that can be used for training, an activity
conducive to timely and appropriate reactions should the unexpected occur.
•
Risk-based regulation. Another way of noting the risk associated with
the administration of anesthesia in an oce setting is that 69 of 100 recent
anesthesia-related complaints resulted from procedures performed in such
settings, as noted in the table, Anesthesia-Related Complaints by Location of
Treatment and Method of Administration. By comparison, 20 complaints
emerged from procedures performed in ambulatory surgical centers and
hospitals in the same period. With the noted increase in anesthesia-related
complaints, and the understanding that more of those complaints come
from procedures performed in oces than in other settings, the board has
Anesthesia-Related Complaints by Location
of Treatment and Method of Administration
FYs 2012–2016 Year to Date*
Location of
Treatment Method of Administration
69 Oce
43 Parenteral
20 Enteral
6 Unknown or under investigation
7 Ambulatory
surgical center
7 Parenteral
0 Enteral
0 Unknown or under investigation
13 Hospital
11 Parenteral
1 Enteral
1 Unknown or under investigation
11 Unknown or
under investigation
2 Parenteral
4 Enteral
5 Unknown or under investigation
* Reects anesthesia-related complaints received in only one-half
of scal year 2016.
Plans force
practitioners
to consider the
role of every
office member
in an anesthesia-
related
emergency.
31
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 3
Sunset Advisory Commission January 2017
the opportunity to direct additional attention to these practice settings
and not wait for additional complaints involving serious patient harm to
address current regulatory shortcomings.
Dentists in other states and Texas doctors administering
anesthesia in ofces are subject to related routine inspections.
•
Most other states require oce inspections for dentists delivering
parenteral anesthesia. e inability of the board to routinely inspect the
oces of dentists practicing parenteral anesthesia administration methods
puts Texans at more risk than patients in most other states. irty-
nine states require and three states allow oce inspections for dentists
administering parenteral or general anesthesia, indicating the majority of
states have determined the privilege to administer parenteral anesthesia
should be accompanied by an additional level of oversight beyond the
licensing review of credentials.
5
•
e Texas Medical Board inspects physicians’ facilities providing oce-
based anesthesia services. Since 2001, the medical board has had authority
to perform inspections related to the provision of anesthesia in outpatient
settings, regardless of method of administration.
6
With funding from the
Legislature in 2013, the medical board conducted 239 oce anesthesia
provider inspections in scal year 2014, but had to suspend its inspections
later that year to resolve implementation challenges. e medical board
has since revised related rules and expects to resume inspections again in
scal year 2016.
Recommendations
Change in Statute
3.1 Authorize the board to conduct inspections of dentists administering parenteral
anesthesia in ofce settings.
is recommendation would eliminate the term and related denition of “enteral” in existing statute
to clearly authorize the board to conduct routine, non-complaint based inspections of oce sites
and documents of the practices of dentists providing all methods of anesthesia administration. e
recommendation would not extend existing board inspection authority to licensed hospitals, licensed
ambulatory surgical centers, and other facilities or the dentists performing anesthesia procedures exclusively
in those settings, because these facilities are already subject to inspections through the Department of
State Health Services or other accrediting bodies.
7
However, the board would retain all existing authority
over dentists in those settings. As a management action, the board should adopt rules to support a
risk-based inspection schedule, detailing the framework and procedures for inspections of the oces
and documents of licensed Texas dentists holding any level of anesthesia permit.
Most states see
the need for
extra oversight
of dentists
administering
parenteral
anesthesia.
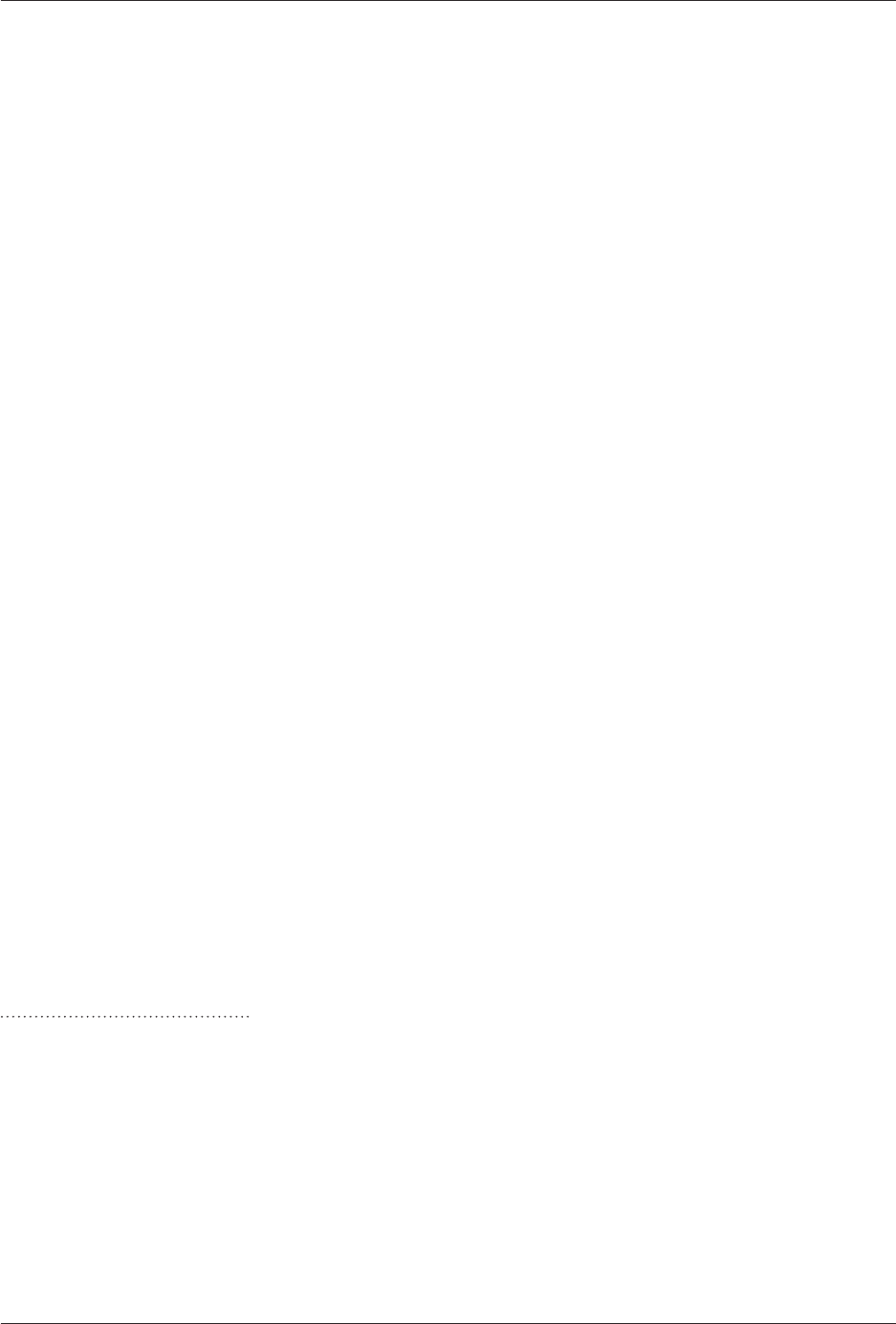
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 3
32
January 2017 Sunset Advisory Commission
Management Action
3.2 Direct the board to revise rules to ensure dentists with one or more anesthesia
permits maintain related written emergency management plans.
is recommendation would direct the board to adopt rules requiring dentists with one or more anesthesia
permit to maintain and annually update written policies and procedures incorporating existing equipment,
drug, and training requirements for responding to emergency situations involving anesthesia. Similar
written procedures are already a part of inspections of licensed hospitals, licensed ambulatory surgical
centers, and other facilities conducted by other entities. Requiring written emergency action plans will
encourage dentists administering anesthesia in all settings to develop actionable, coordinated responses
to adverse reactions or other complications and oer a basis for meaningful related sta training.
Fiscal Implication
Providing the authority for the board to inspect the oces and documents of dentists administering
anesthesia parenterally would not have a signicant scal impact to the state. Implementation of
inspections would have a cost, which could be mitigated by an adjustment to existing anesthesia permitting
fees, listed in the table Dental Anesthesia Permits, on page 27. e board estimates three full-time sta
positions would be necessary to coordinate and support inspections as well as an unidentied amount of
funding for the inspections themselves and related equipment. Depending on whether the inspections
were performed by board sta or contracted reviewers, the board could need additional sta positions.
By comparison, the Texas Medical Board has a $210 biennial fee for physicians oering Level II or
higher oce-based anesthesia services. As registered oce-based anesthesia providers, 2,527 physicians
are technically subject to inspections by the medical board in scal year 2016, though the Board inspects
providers on a four-year cycle.
1
All citations to Texas statutes are as they appear on http://www.statutes.legis.state.tx.us/. Section 258.155, Texas Occupations Code.
2
22 T.A.C. Section 110.7.
3
22 T.A.C. Section192(c) and (i); 22 T.A.C. Section 110.3(c)(7); 22 T.A.C. Section 110.4(c)(7); 22 T.A.C. Section 110.5(c)(7); 22
T.A.C. Section 110.6(c)(8).
4
Brooks Egerton, “Deadly Dentistry” Dallas Morning News, December 9, 2015; Larson, Jace, Deaths at the Dentist, (Houston, TX:
KPRC Channel 2), February 11, 2016.
5
American Association of Dental Boards, e Composite, 26th Ed., (Chicago: American Association of Dental Boards, 2015), 64–65.
6
Section 162.106(a), Texas Occupations Code.
7
Section 162.103, Texas Occupations Code.

33
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 4
Sunset Advisory Commission January 2017
iSSue 4
Key Elements of the State Board of Dental Examiners’ Licensing
and Regulatory Functions Do Not Conform to Common Licensing
Standards.
Background
e mission of the State Board of Dental Examiners is to protect the public’s health and safety by
ensuring dental professionals are qualied, competent, and adhere to established professional standards.
To accomplish its mission, the board licenses dentists and dental hygienists, registers dental assistants
and facilities, and enforces the Dental Practice Act by investigating complaints and taking disciplinary
action when necessary.
e Sunset Advisory Commission has a long history evaluating licensing agencies, as the increase of
occupational regulation served as an impetus behind the creation of the commission in 1977. Since
then, the commission has completed more than 100 licensing agency reviews, documenting standards
to guide reviews of licensing agencies. While these standards provide a guide for evaluations, they are
not intended for blanket application. Sunset sta continues to rene and develop standards, reecting
additional experience and dierent or changing needs, circumstances, or practices in licensing agencies.
e following material highlights areas where the board’s statute and rules dier from model standards
and common practices by comparable agencies, and describes the potential benets of conforming to
standard practices.
Findings
Nonstandard licensing and enforcement practices detract from
the board’s ability to protect the public.
•
Underutilization of national disciplinary data bank. Licensing agencies
should consult enforcement information compiled by national or federal
data banks to monitor disciplinary actions against practitioners licensed
or seeking licensure in Texas who are also licensed in other states. Federal
law requires each state dental board to report disciplinary actions to the
National Practitioner Data Bank.
1
e data bank provides agencies the
information necessary to decide if licensees disciplined in other states
should be allowed to practice in Texas or if enforcement action is warranted
based on violations that reect a practitioner’s inability to safely perform
their job. e intent is to ensure a licensee’s mobility cannot be used to
evade discipline.
Currently, all applicants for initial licensure must request a self-query from
the data bank and provide the results to the board, but these reports only
provide a snapshot of applicants’ disciplinary history and are not updated
to reect subsequent activity. Additionally, applicants for renewal must
only self-disclose disciplinary actions and do not submit data bank reports
to the board as conrmation. e cost of receiving continuous feedback
The intent of
the data bank
is to ensure a
licensee’s mobility
cannot be used to
evade discipline.
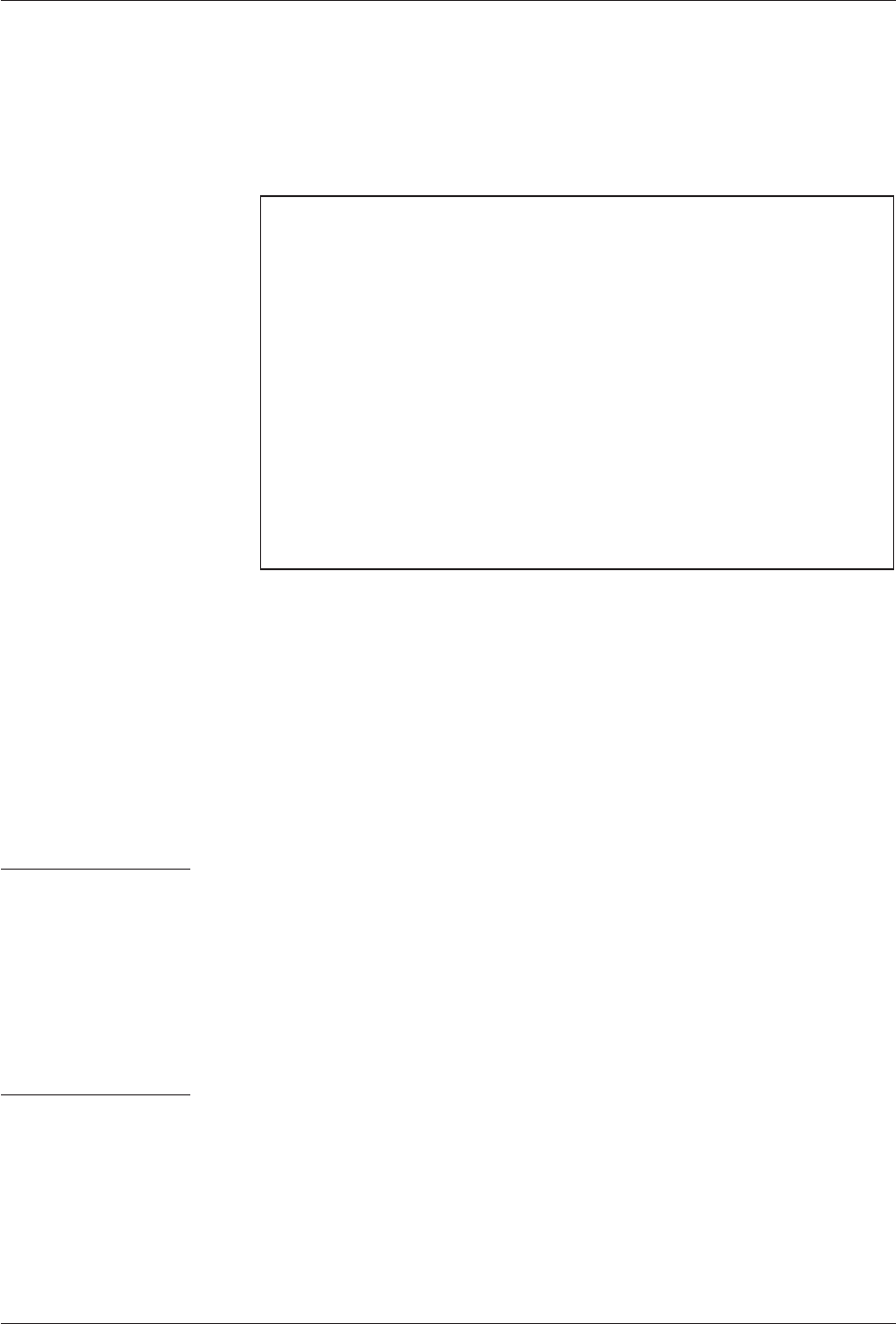
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 4
34
January 2017 Sunset Advisory Commission
from the data bank typically prevents agencies like the board from being
able to obtain up-to-date disciplinary history about licensees. However,
reliance on self-disclosure allows too many gaps for potentially dangerous
licensees to skip through, as demonstrated in the textbox Failure of Current
Self-Disclosure Requirements.
Failure of Current Self-Disclosure Requirements
•
In February 2014, a dentist licensed in Texas and Nevada was disciplined by
the Nevada State Board of Dental Examiners after two patients died following
the dentist’s administration of anesthesia during treatment.
•
In October 2014, the dentist failed to self-disclose the Nevada disciplinary
actions on his Texas renewal application.
•
e dentist was able to treat patients in Texas until November 2015, when
the board discovered the omission and issued a temporary suspension based
on the action taken by Nevada and for having fraudulently obtained a Texas
dental license.
•
Between the renewal in 2014 and license suspension in 2015, a patient was
hospitalized following the dentist’s mismanagement of an anesthesia-related
emergency in Texas.
The board has
no authority
to require the
evaluation of
potentially
impaired
licensees.
•
No statutory authority to deny renewal applications for noncompliance.
e authority to deny renewal applications for failure to comply with
previous board orders bolsters agencies’ enforcement eorts and ensures
that disciplined licensees have fullled their responsibilities and show a
commitment to safe practice. Without authority to deny renewals for
noncompliance, the board must instead open another enforcement case.
Having to pursue a new case in these instances requires additional resources
and time, allowing noncompliant licensees to continue to work and possibly
putting the public at risk.
•
Insucient authority to require evaluations for allegedly impaired
licensees. Most agencies that regulate practitioners with access to controlled
substances have the authority to require licensees suspected of being impaired
due to substance abuse or a physical or mental health condition to submit
to a peer assistance evaluation to determine if they pose a risk to patient
safety.
2
To balance that authority with practitioners’ legitimate concerns
for privacy, these agencies protect the condentiality of information relating
to evaluations and participation in treatment programs.
3
Condentiality
also provides an incentive for licensees to participate in peer assistance
programs. ese agencies allow disclosure in enforcement proceedings
or as otherwise necessary to protect the public, but participants’ medical
information remains private.
4
Unlike other health licensing agencies, the board has no authority to require
the evaluation of licensees to see if a suspected impairment aects their
ability to safely practice. Without the results of an evaluation, the board
35
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 4
Sunset Advisory Commission January 2017
typically lacks evidence to prove that the person’s addiction or condition
aects the person’s ability to practice safely. e inability to practice safely
is already specied as grounds for discipline under the Dental Practice
Act.
5
e act also does not protect the condentiality of information
related to participation in peer assistance programs, potentially deterring
licensees from cooperating with board eorts to get them into treatment,
and ultimately aecting the board’s ability to protect the public.
Nonstandard board procedures could affect the agency's
efciency and accountability in regulating the dental industry.
•
Subjective qualications for licensure and registration. Qualications for
licensure or registration should not overburden applicants or unreasonably
restrict entry into practice. Statute requires applicants for licensure or
registration to be of “good moral character,” which in practice requires boards
to review applicants’ criminal history.
6
Chapter 53 of the Occupations Code
governs licensing agencies’ use of criminal history information, requiring
generally that a crime directly relate to the duties of the licensed occupation
with additional stipulations related to the nature and timing of the crime.
7
While the board generally adheres to the requirements of Chapter 53, its
disciplinary matrix species that it will consider certain crimes unrelated
to dentistry regardless of mitigating factors or rehabilitative eorts.
8
e
statutory requirement for licensees to be of “good moral character” and the
board’s guidance for applying disciplinary action are overbroad and vague,
and can unfairly aect entry into the eld.
•
Insucient reporting of enforcement data. Licensing boards should
maintain adequate information about enforcement activity, including
detailed statistics about complaints received and cases resolved each
year, to improve awareness of trends and areas for improvement. is
information should be readily accessible to policymakers, sta, and the
public in reports to provide greater awareness of an agency’s activities and
maintain accountability for performance. e board receives regulatory data
at each quarterly meeting, but reports are fragmented and limit a complete
analysis of the overall enforcement eort to show agency performance and
identify possible problem areas in the industry. None of this information
is currently included on the board’s website.
•
Inconsistent renewal procedures. Staggering the renewal of credentials
balances sta workload and ensures timely processing. e board renews
most licenses, registrations, and permits on a staggered basis, but renews
dental facility permits on January rst annually.
9
e inux of renewals
for dental laboratories, mobile dental facilities, and portable dental units
can overwhelm agency operations during an already busy month.
Confidentiality
provides an
incentive for
licensees to
participate in
peer assistance
programs.
Enforcement
data should be
readily accessible
to policymakers,
staff, and
the public.

State Board of Dental Examiners Staff Report with Commission Decisions
Issue 4
36
January 2017 Sunset Advisory Commission
Recommendations
Change in Statute
4.1 Require the board to monitor licensees for adverse licensure actions.
is recommendation would require the board to verify, on an ongoing basis, that licensees are not
subject to disciplinary actions taken by other states that warrant similar action in Texas. Under this
recommendation, the board should request continuous query reports from the National Practitioner
Data Bank for each applicant for initial licensure and each renewal applicant to ensure the board receives
accurate, timely notice of actions taken by other states or agencies. is recommendation would require
an increase in licensing fees of $3 per licensee to cover the board’s cost of querying the data bank.
is access to disciplinary information would allow the board to better protect the public by ensuring
licensees in Texas are not subject to disciplinary orders in other states that aect their ability to safely
care for patients.
4.2 Authorize the board to deny applications to renew a license if an applicant is not
compliant with a board order.
Under this recommendation, the board would have the discretion to determine whether noncompliant
applicants can safely perform their job or if their renewal application should be denied. Authority to deny
renewals would help the board better protect consumers from potentially unsafe practitioners, provide
greater incentive for licensees to comply with board orders, and standardize the board’s procedures with
other health occupational licensing agencies’ practices.
10
4.3 Authorize the board to require evaluations of licensees suspected of being impaired
and require condentiality for information relating to the evaluation and participation
in treatment programs.
Under this recommendation, the board would be authorized to order a licensee to submit to an evaluation
by the peer assistance program based on probable cause that the practitioner is impaired due to substance
abuse or a physical or mental health condition. Authority to require an evaluation should be limited
to proving or disproving whether grounds for disciplinary action exists under the existing provisions
of the Dental Practice Act. is recommendation would also require that any information related to
participation in a peer assistance program, including the results of an evaluation, be condential.
e board would only be authorized to disclose this condential information in enforcement and other
proceedings aecting the persons’ license because of the threat to public safety. e board would also
be able to disclose that the license of a person ordered to participate in a peer assistance program is
suspended, revoked, or otherwise limited by referring to the statutory grounds for disciplinary action,
without disclosing the specic impairment or condition that resulted in the board’s action. For example,
the board would be permitted to disclose the suspension of a license based on probable cause that the
licensee is physically or mentally incapable of practicing dentistry safely, but would not disclose the
specic condition or impairment that gives the board probable cause for the suspension.
11
Ultimately,
this recommendation would provide the same tools and license protection as currently available to
comparable licensing agencies to protect the public while also protecting the condentiality of licensees.

37
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 4
Sunset Advisory Commission January 2017
4.4 Remove unnecessary qualications required of applicants for licensure or
registration.
is recommendation would remove the requirement that dental practitioners have “good moral character.”
As a management action, the board would instead be directed to review applicants’ criminal histories in
accordance with the requirements and boundaries of Chapter 53 of the Occupations Code to determine
eligibility for licensure or registration. is recommendation would ensure that qualications for licensure
or registration relate more closely to the duties of dental practitioners and do not unreasonably restrict
entry into practice.
Management Action
4.5 Direct the board to make data on the board’s enforcement activity information
publicly available on its website.
is recommendation would direct the board to synthesize and publish investigative and disciplinary
information, providing policymakers, board members, sta, and stakeholders a more complete picture
of the board’s enforcement eorts. is information would reect compiled data from the board’s
enforcement program, presented in a clear, organized manner. At a minimum, the board should report
•
the number of complaints received in a scal year, distinguishing those received from the public
from those initiated by the agency, for each type of license, certicate, or registration, further broken
out by type of allegation;
•
the outcome of cases resolved in a scal year for each type of credential, describing the type and
number of disciplinary actions taken for each category of violation committed, and the number of
cases dismissed and the basis for dismissal;
•
the average time to resolve cases, as well as the range; and
•
the number and age of all cases open at the end of each scal year.
Compiling and posting this information on the board’s website would help the board and policymakers
judge the performance of the agency and improve transparency to the public. A summary of the board’s
limited enforcement data available for scal year 2015 is provided in Appendix C, State Board of Dental
Examiners Comprehensive Enforcement Data, to demonstrate some of the information that should be
publicly available. e information contained in the summary does not show, and the board is unable
to currently provide, the level of detail imagined by this recommendation and outlined above.
4.6 Direct the board to stagger registration and certicate renewals.
Under this recommendation, the board would be directed to use a staggered renewal system for dental
laboratories, mobile dental facilities, and portable dental units. Staggering renewals is a more ecient
use of limited resources and creates consistency in board operations. is recommendation would take
advantage of existing authority to stagger renewals to alleviate unnecessary burdens on sta responsible
for processing applications.
12
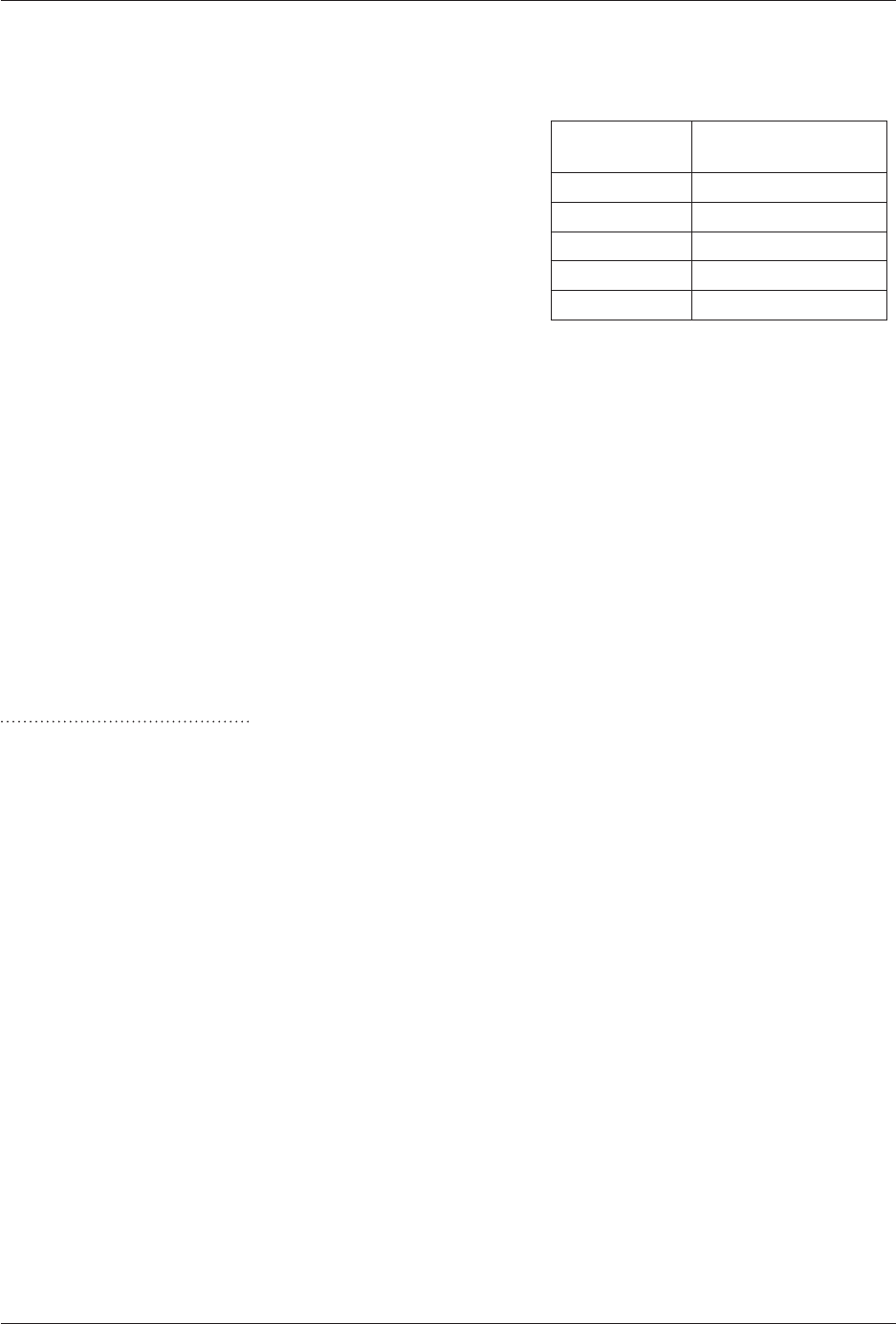
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 4
38
January 2017 Sunset Advisory Commission
Fiscal Implication
ese recommendations would have a small gain to the
General Revenue Fund of about $45,000 annually. e
board’s cost to query the National Practitioner Data Bank
under Recommendation 4.1 would require increasing
licensing fees by $3 for every applicant, reecting the cost of
receiving continuous query services. is fee would generate
excess revenue because more individuals apply for licensure
annually than meet the standards for licensure and do not
require queries of the data bank. e board would be able
to implement the remaining recommendations with current
resources.
State Board of Dental Examiners
Fiscal Year
Gain to the General
Revenue Fund
2018 $45,000
2019 $45,000
2020 $45,000
2021 $45,000
2022 $45,000
1
Health Care Quality Improvement Act of 1986 (42 U.S.C. Section 11101 et seq.).
2
All citations to Texas statutes are as they appear on http://www.statutes.legis.state.tx.us/. Section 164.056, Texas Occupations Code
(Texas Medical Board); Section 301.4521(b), Texas Occupations Code (Texas Board of Nursing); and Section 565.052, Texas Occupations Code
(Texas Board of Pharmacy). See also Section 467.006, Texas Health and Safety Code (general authority); Section 801.401(e), Texas Occupations
Code (Texas State Board of Veterinary Medical Examiners); and Section 202.253(a)(15) and (b)–(c), Texas Occupations Code (Texas State Board
of Podiatric Medical Examiners).
3
Section 167.010, Texas Occupations Code (Texas Medical Board); Section 301.4521(j), Texas Occupations Code (Texas Board of
Nursing); and Section 564.002, Texas Occupations Code (Texas Board of Pharmacy); See also Section 467.007, Texas Health and Safety Code
(general condentiality).
4
Ibid.
5
Section 263.002(a)(7) and (11), Texas Occupations Code.
6
Sections 256.002(a)(2) and 256.053(a)(2), Texas Occupations Code.
7
Chapter 53, Texas Occupations Code.
8
22 TAC Section 101.8; State Board of Dental Examiners, Disciplinary Matrix, accessed February 9, 2016, pp. 8-10, http://www.tsbde.
texas.gov/documents/laws-rules/2015_0603%20Disciplinary%20Matrix.pdf.
9
Sections 257.001(a) and 266.102(b), Texas Occupations Code.
10
Section 155.003(e), Texas Occupations Code (Texas Medical Board); Section 301.452(b)(1), Texas Occupations Code (Texas Board of
Nursing); and Section 565.001(a)(17), Texas Occupations Code (Texas Board of Pharmacy).
11
Section 263.002(a)(11), Texas Occupations Code; see also Section 263.002(a)(3) and (7), Texas Occupations Code.
12
Sections 257.001(a) and 266.102(b), Texas Occupations Code.

39
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 5
Sunset Advisory Commission January 2017
Improper practice
of dentistry can
result in a range
of physical harm
to patients.
iSSue 5
A Continuing Need Exists for the State Board of Dental Examiners.
Background
Dentistry, as dened by Texas statute includes a range of activities from the diagnosis, treatment or
removal of stains and decay from human teeth to surgical and other treatment for disease, pain, injury
or physical condition of human teeth, gums, or jaws. Dental hygiene, a supporting function of dentistry,
generally includes removal of tarter or calculus build up and polishing of human teeth, along with other
functions and tasks delegated by licensed dentists. Dental assistants can perform a number of supporting
acts under the delegation and direct or general supervision of a dentist. Dental laboratories generally
make, repair, and t dental appliances such as dentures.
Dental care is one of the longest-standing Texas state regulations, dating back to the creation of the
State Board of Dental Examiners in 1897. Sixty years later, the legislature provided for the licensure
and regulation of dental hygienists. Dental laboratories were added to the board’s regulatory activity
in 1973, and four dental assistant certicate programs were established in statue and rule beginning in
1995. Since 1994, the Western Regional Examination Board has administered licensing examinations
for dentists and dental hygienists seeking licensure in Texas, allowing the agency to focus on licensing
and enforcement functions.
e board seeks to protect public health and safety by issuing licenses and registrations; investigating
and resolving complaints relating to the practice of dentistry or supporting functions; and generally
enforcing the Dental Practice Act. In scal year 2015, the board licensed 17,540 dentists and 13,740
dental hygienists; issued 50,469 dental assistant certicates; and registered 909 facilities.
Findings
The state has a continuing need for regulating the practice of
dentistry and supporting functions.
A primary role of the state is to protect the public from harm. For certain
professions and occupations, the state seeks to provide this protection through
regulation designed to ensure qualied practice and eective enforcement when
practice standards are not met.
•
Potential for harm. For dentistry, the risk to the public is clear. Dental
activities can aect the major life functions of eating and speaking, as
well as overall health and appearance. Improper practice of dentistry can
result in a range of physical harm to patients, from the unnecessary loss
of teeth to infection, pain, and even death. Dentistry may involve the
use of anesthesia in dental procedures, and this access to drugs heightens
the risk to the public. Dentistry also generally involves treatments and
diagnoses well beyond a patients’ ability to judge need or address on their
own. Adverse results can be profound not just to one’s health and safety,
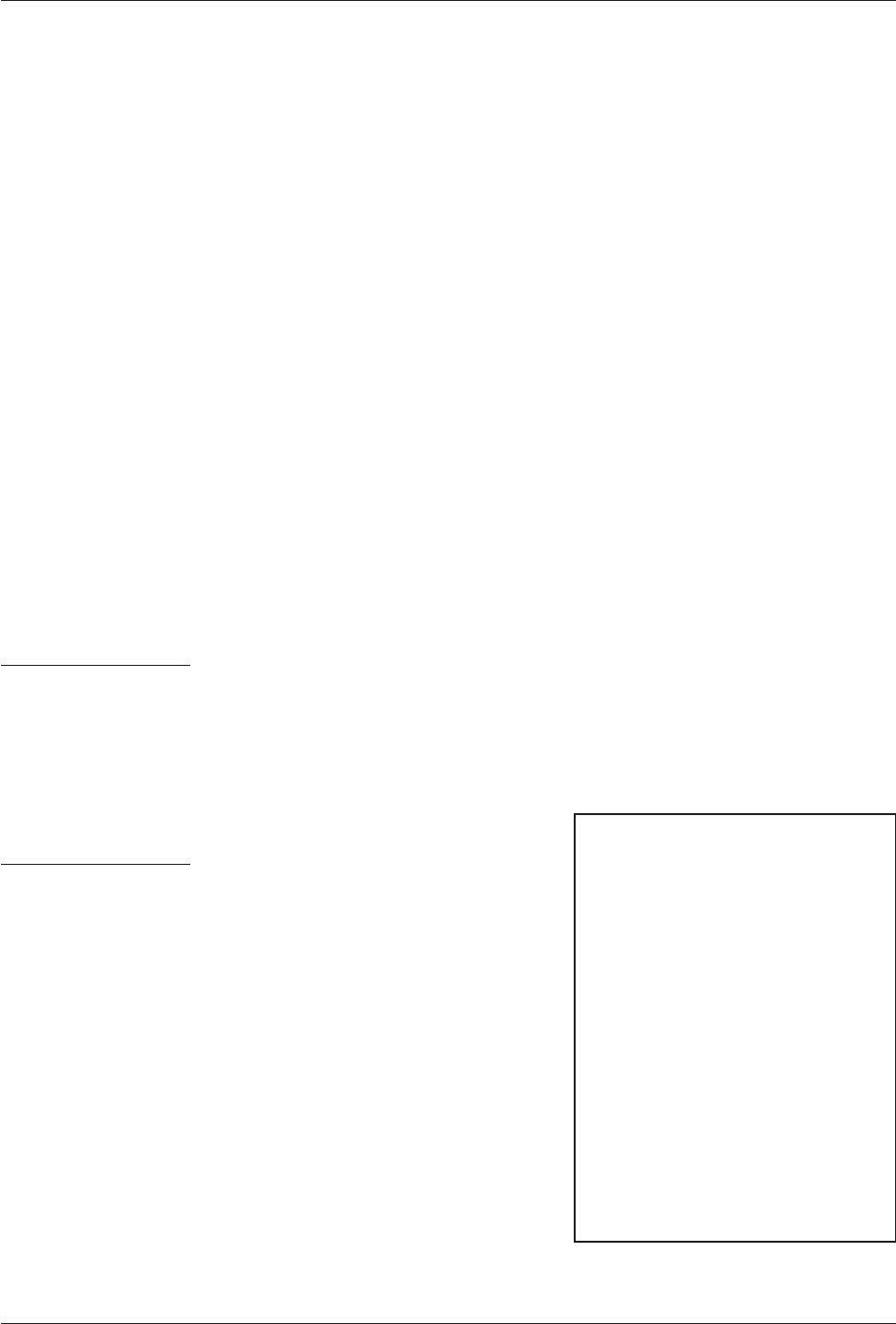
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 5
40
January 2017 Sunset Advisory Commission
but also to one’s nancial well-being for the cost of unnecessary treatment
or to x poorly performed treatment.
•
Qualied practice. State regulation seeks to mitigate the risk to the public
by ensuring dental practitioners are qualied to provide dental services
and by taking enforcement action to ensure compliance with requirements
for safe practice. Requiring practitioners to meet education, training,
and other qualications and to demonstrate competence by passing an
examination is an important way for the state to assure the public that
licensed practitioners can safely perform dentistry. Regulation also promotes
established standards of care and compliance with regulations by providing
a mechanism to investigate and, as necessary, discipline and even remove
practitioners who fail to meet them.
No substantial benet would result for transferring the board’s
functions to another agency at this time.
•
Independent agency structure. For over a century, the state has regulated
dentistry through an independent regulatory agency. is structure reects
the common approach for many health licensing agencies in Texas, especially
larger agencies responsible for overseeing complex medical activities that
pose a signicant and direct risk to public health and safety, such as the
medical, pharmacy, and nursing boards.
is independent structure provides focused regulatory attention on
dentistry. Overseen by a board composed of dental professionals and public
members, the agency receives technical expertise from practitioners in
developing rules and regulations reecting the complex needs of dentistry
and enforcing requirements on those who violate equally complex practice
standards.
As an independent agency, the
board is collocated with other
health regulatory agencies. is
location enables the agency to
easily access best practices and
learn from shared experiences of
neighboring agencies. e board
also achieves administrative
efficiencies among similar
regulatory programs through
the Health Professions Council.
e textbox, Health Professions
Council Functions, lists the
services provided through this
collaboration.
Health Professions
Council Functions
•
Maintenance and security for a
shared licensing database
•
Web-based programming and design
to support the board’s website
•
Operation of a toll-free complaint
hotline
•
Risk management services
•
Mail center operations and courier
services
•
Assistance with job posting and
advertising
•
Board member training
An independent
structure
provides focused
regulatory
attention on
dentistry.
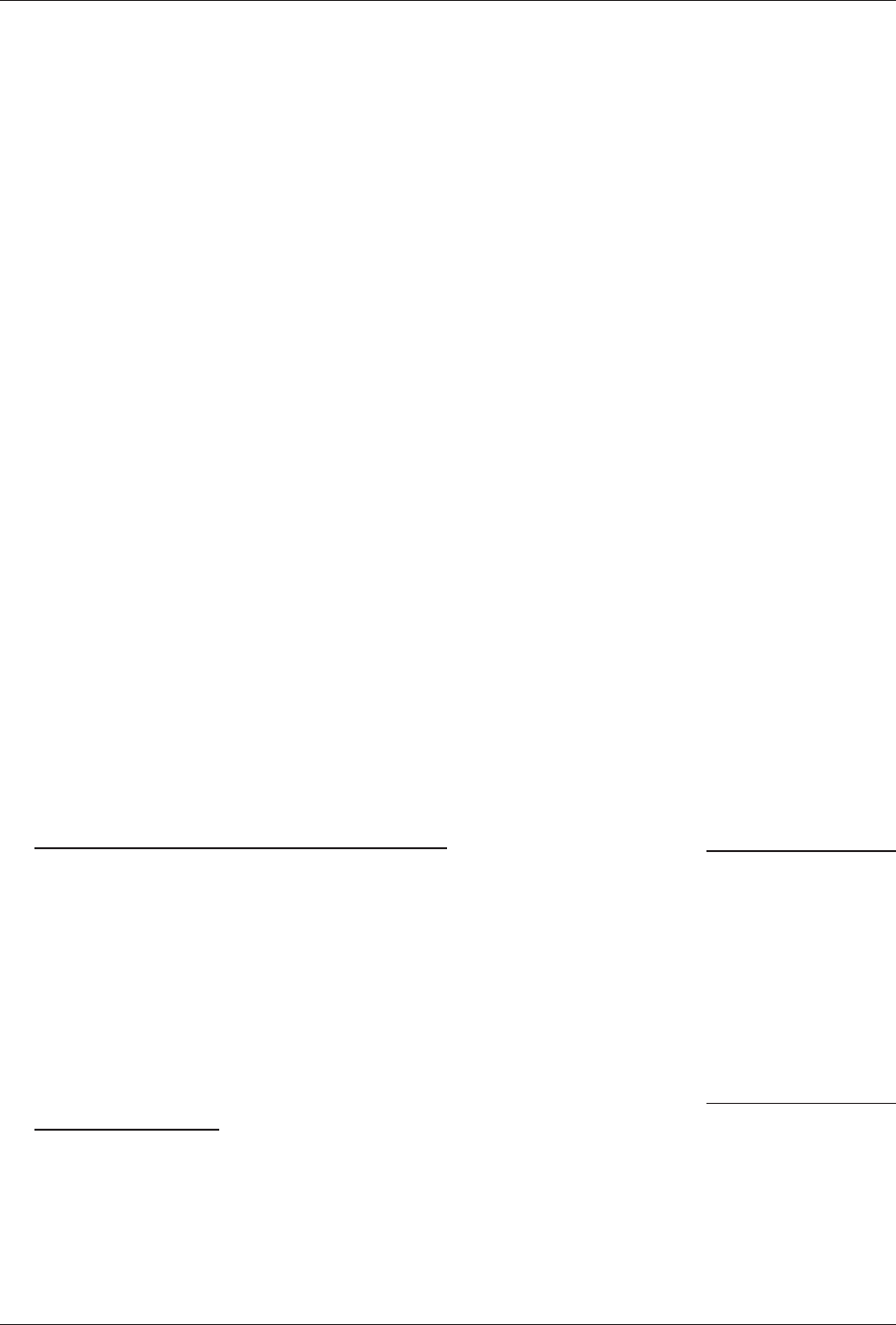
41
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 5
Sunset Advisory Commission January 2017
•
Umbrella agency structure. An alternative approach to having an
independent agency is the consolidation of needed regulatory programs
under an umbrella structure. e state has long regulated various trades under
the umbrella of the Texas Department of Licensing and Regulation (TDLR).
However, the only comparable eort for health regulatory programs at the
Department of State Health Services (DSHS) was ineective and largely
dismantled last session, with numerous programs moved to TDLR or the
Texas Medical Board, while others were deregulated. e rationale for
this change was to focus DSHS on its important public health mission by
freeing it from its health occupations licensing responsibility.
While this same rationale for moving programs from DSHS does not
apply for independent agencies that already focus on licensing, an umbrella
structure can still oer advantages in terms of objective, professional
regulation. By specializing sta along functional lines, umbrella agencies can
provide improved long-term eciency over smaller, single-shot agencies. In
addition, larger umbrella agencies can provide more avenues for developing
and retaining sta, helping to insulate them against the institutional
loss and disruption that can result from the departure of just a few key
personnel in smaller agencies. Umbrella agencies can also provide a more
objective regulatory approach, because their broad responsibilities typically
require oversight boards comprising public members that rely on advisory
committees of practitioners for expertise about the regulated eld. is
separation helps promote the broader public interest, minimizing the
potential for the regulated community to promote its own interest when
it controls these oversight boards.
e review considered structural alternatives presumed to provide these
benets, but found pitfalls that call into question whether such a change
justies the upheaval it would cause.
Texas Department of Licensing and Regulation. As noted above, through
the 2015 Sunset review of DSHS, the Legislature transferred 13 health-
related regulatory programs to TDLR over the next three years. While this
experience has introduced TDLR to the regulation of health professions,
none of the programs transferred require the kind of technical expertise
needed to regulate dentistry, especially from an enforcement standpoint.
In addition, the large expansion of authority may well have brought TDLR
to the limits of its ability — or at least its current capacity to take on a
larger, more complex regulatory program with the level of risk associated
with dentistry.
Texas Medical Board. While the Texas Medical Board is not a traditional
umbrella agency, it regulates a number of health-related programs including
four received through the Sunset review of DSHS. e medical board does
not t the traditional umbrella model because it regulates medical providers
under a physician-oriented board instead of a structure that accounts for
broader regulatory authority. Aside from the regulated medical practices
being signicantly dierent from the practice of dentistry, the oversight
Structural
alternatives have
pitfalls calling
into question
whether such
change justifies
the upheaval
caused.
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 5
42
January 2017 Sunset Advisory Commission
structure would require signicant adjustment to accommodate other
healthcare professionals such as dentists.
Most states regulate dentistry through independent or semi-
autonomous boards.
Texas’ use of an independent board exercising all licensing and disciplinary
powers to regulate dentistry with the outsourcing of certain administrative
functions is an approach similar to most other states. Twenty seven states,
including Texas, use independent dental boards to regulate the industry. An
additional 18 states have a semi-autonomous regulatory structure for dentistry,
wherein boards generally exercise key powers relating to licensing, discipline,
and rulemaking, and a central agency provides most administrative services
and makes some decisions.
1
The Dental Practice Act does not reect standard language
typically applied across the board during Sunset reviews.
e Sunset Commission has developed a set of standard recommendations
that it applies to all state agencies reviewed reecting “good government”
standards designed to ensure open, responsive and eective government. One
such standard in the board’s statutes relates to possible conicts of interest.
e board’s statute restricts certain individuals from serving on the board or as
a high-level agency employee if they or their spouse is closely aliated with a
nonprot Texas trade association.
2
By focusing on nonprot trade associations,
the existing language opens the possibility for a person with a conict because
of an aliation with a for-prot association to serve in such an inuential
capacity. e standard Sunset provision would prevent such a conict.
Recommendations
Change in Statute
5.1 Continue the State Board of Dental Examiners for 12 years.
is recommendation would continue the board until 2029 as an independent agency responsible for
ensuring quality, safe dental care.
5.2 Update the standard Sunset across-the-board provision regarding conicts of
interest.
is recommendation would delete nonprot from the denition of “Texas trade association” in the State
Board of Dental Examiners enabling statute to ensure that a person with a potential conict because of
an aliation with any Texas trade association in the eld of health care cannot serve on the board or as
a high-level agency employee. is recommendation would ensure that both nonprot and for-prot
trade associations are treated equally under statutory conict of interest provisions and better ensure
that agency decisions are made solely in the public interest.
Twenty-seven
states, including
Texas, use
independent
regulatory boards
to regulate
dentistry.

43
State Board of Dental Examiners Staff Report with Commission Decisions
Issue 5
Sunset Advisory Commission January 2017
Fiscal Implication
Based on scal year 2016 appropriations and employee benets, continuing the State Board of Dental
Examiners would require approximately $5.2 million in annual costs associated with the agency. ese
costs are entirely paid for by the licensing and registration fees the agency collects. e state would also
continue to receive approximately $3.8 million collected annually by the board in excess of the agency’s
costs.
1
American Association of Dental Boards, e Composite (Chicago: American Association of Dental Boards, 2015), 1–3.
2
All citations to Texas statutes are as they appear on http://www.statutes.legis.state.tx.us/. Section 252.003, Texas Occupations Code.

State Board of Dental Examiners Staff Report with Commission Decisions
Issue 5
44
January 2017 Sunset Advisory Commission

appendiCeS
45
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix A
Sunset Advisory Commission January 2017
appendix a
Historically Underutilized Businesses Statistics
2013 to 2015
e Legislature has encouraged state agencies to increase their use of historically underutilized businesses
(HUBs) to promote full and equal opportunities for all businesses in state procurement. e Legislature
also requires the Sunset Commission to consider agencies’ compliance with laws and rules regarding
HUB use in its reviews.
1
e following material shows trend information for the State Board of Dental Examiners’ use of HUBs
in purchasing goods and services. e agency maintains this information under guidelines in statute.
2
In the charts, the dashed lines represent the goal for HUB purchasing in each category, as established
by the comptroller’s oce. e diamond lines represent the percentage of agency spending with HUBs
in each purchasing category from 2013 to 2015. Finally, the number in parentheses under each year
shows the total amount spent in each purchasing category.
e board complied with HUB program requirements, but had diculty meeting several statewide
purchasing goals in building construction and other services.
Building Construction
0
20
40
60
80
100
2013 2014 2015
Percent
($0) ($14,179) ($5,306)
Goal
Agency
e board failed to meet the statewide goal for the small amount spent on building construction.
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix A
46
January 2017 Sunset Advisory Commission
Appendix A
Professional Services
0
20
40
60
80
100
2013 2014 2015
Percent
($4,169) ($125) ($0)
Agency
Goal
e board met the state goal for the professional services category in scal year 2013, but had little or
no spending in the same category in scal years 2014 and 2015.
Other Services
0
20
40
60
80
100
2013 2014 2015
Percent
($108,040) ($170,449) ($296,416)
Agency
Goal
e board has not met the state goal in each of the last three scal years in this category, comprising a
large sole-source contract for the peer assistance program and payments for its dental review panelists,
where HUB availability is limited.
47
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix A
Sunset Advisory Commission January 2017
Appendix A
Commodities
0
20
40
60
80
100
2013 2014 2015
Percent
($97,562) ($40,783) ($207,174)
Agency
Goal
e agency has far exceeded the state purchasing goal for commodities in the last three scal years.
1
All citations to Texas statutes are as they appear on http://www.statutes.legis.state.tx.us/. Section 325.011(9)(B), Texas Government Code.
2
Chapter 2161, Texas Government Code.

State Board of Dental Examiners Staff Report with Commission Decisions
Appendix A
48
January 2017 Sunset Advisory Commission
49
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix B
Sunset Advisory Commission January 2017
appendix B
Equal Employment Opportunity Statistics
2013 to 2015
In accordance with the requirements of the Sunset Act, the following material shows trend information
for the employment of minorities and females in all applicable categories by the State Board of Dental
Examiners.
1
e agency maintains and reports this information under guidelines established by the
Texas Workforce Commission.
2
In the charts, the dashed lines represent the percentages of the statewide
civilian workforce for African-Americans, Hispanics, and females in each job category.
3
ese percentages
provide a yardstick for measuring agencies’ performance in employing persons in each of these groups.
e diamond lines represent the agency’s actual employment percentages in each job category from 2013
to 2015. e board met or exceeded several statewide civilian workforce percentages in the last three
scal years, but fell short on its employment of African-Americans in the categories of administration,
professional, and technical, and Hispanics in the professional, technical, and administrative support
categories. e board also failed to meet state employment goals for females in the professional category.
Administration
0
20
40
60
80
100
2013 2014 2015
Percent
Hispanic
0
20
40
60
80
100
2013 2014 2015
Percent
African-American
0
20
40
60
80
100
2013 2014 2015
Percent
Female
Workforce
Agency
Positions: 2 4 5 2 4 5 2 4 5
Agency
Agency
Workforce
Workforce
e board has generally met or exceeded the statewide civilian workforce percentages of Hispanics and
females for the small number of employees in this category, but not African-Americans.
Professional
0
20
40
60
80
100
2013 2014 2015
Percent
Female
0
20
40
60
80
100
2013 2014 2015
Percent
Hispanic
0
20
40
60
80
100
2013 2014 2015
Percent
African-American
Positions: 19 25.5 27 19 25.5 27 19 25.5 27
Workforce
Workforce
Agency
Workforce
Agency
Agency
e board has not met the statewide civilian workforce percentage of African-Americans, Hispanics,
and females in the last three scal years.
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix B
50
January 2017 Sunset Advisory Commission
Appendix B
Technical
0
20
40
60
80
100
2013 2014 2015
Percent
Female
0
20
40
60
80
100
2013 2014 2015
Percent
Hispanic
0
20
40
60
80
100
2013 2014 2015
Percent
African-American
Agency
Agency
Positions: 0 0 1 0 0 1 0 0 1
Agency
Workforce
Workforce
Workforce
e board has only had one employee in this job category, exceeding the civilian workforce percentage
of females in scal year 2015.
Administrative Support
0
20
40
60
80
100
2013 2014 2015
Percent
African-American
0
20
40
60
80
100
2013 2014 2015
Percent
Female
0
20
40
60
80
100
2013 2014 2015
Percent
Hispanic
Agency
Workforce
Workforce
Agency
Positions: 13.5 31 24.6 13.5 31 24.6 13.5 31 24.6
Agency
Workforce
e board exceeded the statewide civilian workforce percentages of African-Americans and females in
each of the three years, but not Hispanics.
1
All citations to Texas statutes are as they appear on http://www.statutes.legis.state.tx.us/. Section 325.011(9)(A), Texas Government Code.
2
Section 21.501, Texas Labor Code.
3
Based on the most recent statewide civilian workforce percentages published by the Texas Workforce Commission.
51
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix C
Sunset Advisory Commission January 2017
appendix C
State Board of Dental Examiners
Comprehensive Enforcement Data – FY 2015
e following information presents a summary of the board’s enforcement activities for scal year 2015.
e State Board of Dental Examiners currently does not maintain detailed statistics and data about
enforcement activities for use by policymakers, sta, and the public. e following information was
hand-counted and organized by Sunset sta into this summary report, and does not provide the level
of detail that would be required under Recommendation 4.5.
Complaints Received by Source
Dentist
Dental
Hygienist
Dental
Assistant
Registered
Facility
Unregistered
Entity Total*
Public 1,051 13 26 5 32 1,127
Agency 86 8 15 0 0 109
Allegations by License Type
Standard of Care Violations 573 8 0 1 13 595
Unlicensed Practice 100 3 7 0 16 126
Professional Conduct 304 8 18 2 13 345
Patient Morbidity or
Mortality
135 0 0 1 0 136
Impairment, Narcotics, or
Drug Diversion
37 0 5 0 0 42
Sanitation 58 1 1 0 5 65
Advertisement Violations 77 0 0 0 3 80
Other/Unreported 145 4 12 2 0 163
* Complaints received by the agency may contain more than one allegation.
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix C
52
January 2017 Sunset Advisory Commission
Appendix C
State Board of Dental Examiners
Comprehensive Enforcement Data – FY 2015
Case Resolutions by License Type
Dentist
Dental
Hygienist
Dental
Assistant
Registered
Facility
Unregistered
Entity
Total*
Remedial Plan 46 0 0 0 0 46
Warning or Reprimand 120 2 3 3 0 128
Administrative Penalty 4 1 0 0 0 5
Probation 14 1 8 0 0 23
Suspension 4 0 0 0 0 4
Voluntary surrender 7 1 0 0 0 8
Revocation 1 0 2 0 0 3
Cease-and-desist order 0 0 0 0 6 6
Other 6 0 4 0 0 10
Total Disciplinary Actions 202 5 17 3 6 233
Total Dismissed ** ** ** ** ** 710
Total Resolved ** ** ** ** ** 943
* Complaints received by the agency may contain more than one allegation.
** is information is not available.
Cases Open – FY 15
Days to
Cases Dismissed by Reason
By Year of Origination
Cases Resolution
Referred to another agency 4
Referred to local law
enforcement
2
Dismissed – no violation found 379
Dismissed by legal 262
Dismissed through informal
settlement
15
Dismissed – insucient
evidence
1
Dismissed with
recommendations/conditionally
18
Dismissed – board vote 29
Total Dismissed 710
2012 2013 2014 2015
Under
Investigation
0 50 195 566
In Legal 20 49 183 50
At State Oce
of Administrative
Hearings
0 2 0 28
Total Open 20 101 378 644
Average 448
Minimum **
Maximum **
** is information is
not available.

53
State Board of Dental Examiners Staff Report with Commission Decisions
Appendix D
Sunset Advisory Commission January 2017
appendix d
Staff Review Activities
During the review of the State Board of Dental Examiners, Sunset sta engaged in the following activities
that are standard to all Sunset reviews. Sunset sta worked extensively with agency personnel; attended
board meetings; met with legislative sta; conducted interviews and solicited written comments from
interest groups, stakeholders, and the public; reviewed agency documents and reports, state statutes,
previous legislation, and literature; researched the organization and functions of similar agencies in other
states; and performed background and comparative research.
In addition, Sunset sta also performed the following activities unique to this agency:
•
Reviewed agency enforcement case les
•
Attended stakeholder meetings concerning contemplated rulemaking topics
•
Surveyed state and national interest groups, individual licensees and registrants, dental schools,
dental support providers, and other stakeholders
•
Attended emergency temporary suspension hearings held by the board and subsequent probable
cause and merits hearings conducted by the State Oce of Administrative Hearings
•
Observed informal settlement conferences of agency enforcement actions
•
Attended a meeting of the Dental Laboratory Certication Council and the Dental Review Panel
Ad Hoc Committee
•
Spoke with sta of the State Oce of Administrative Hearings, State Auditor’s Oce, governor’s
appointments oce, Oce of Inspector General, Texas Medical Board, Health Professions Council,
and Legislative Budget Board

State Board of Dental Examiners Staff Report with Commission Decisions
Appendix D
54
January 2017 Sunset Advisory Commission
Location
Robert E. Johnson Bldg., 6th Floor
1501 North Congress Avenue
Austin, TX 78701
Website
www.sunset.texas.gov
Mail
PO Box 13066
Austin, TX 78711
Email
Phone
(512) 463-1300
Sunset Advisory Commission
Sunset Staff Review of the
State Board of Dental Examiners
Report Prepared By
Anne Allensworth, Project Manager
Julie Davis
Dawn Roberson
Joe Walraven, Project Supervisor
Ken Levine
Director
