Journal of Family Strengths Journal of Family Strengths
Volume 11 Issue 1 Article 10
November 2011
Connecting the Dots: Families and Children with Special Needs in Connecting the Dots: Families and Children with Special Needs in
a Rural Community a Rural Community
Saundra Starks
Western Kentucky University
Dana J. Sullivan
Western Kentucky University
Vella Mae Travis
Western Kentucky University
Follow this and additional works at: https://digitalcommons.library.tmc.edu/jfs
Recommended Citation Recommended Citation
Starks, Saundra; Sullivan, Dana J.; and Travis, Vella Mae (2011) "Connecting the Dots: Families and
Children with Special Needs in a Rural Community,"
Journal of Family Strengths
: Vol. 11: Iss. 1, Article 10.
DOI: https://doi.org/10.58464/2168-670X.1015
Available at: https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
The Journal of Family Strengths is brought to you for free
and open access by CHILDREN AT RISK at
DigitalCommons@The Texas Medical Center. It has a "cc
by-nc-nd" Creative Commons license" (Attribution Non-
Commercial No Derivatives) For more information, please
contact [email protected].tmc.edu
Over the past 20 years, there has been a rise in diagnoses of autism
spectrum disorders as well as other developmental disorders and delays
(Autism Speaks, n.d.). While low-birth weight babies are more likely to
survive due to advanced medical care and technology, these babies are
also more likely to have delays and disabilities (Carpenter, 2000). Autism
is the fastest growing developmental disability and has an incidence rate
of 1 in 110 births (formally 1 in 150 until 2009 and 1 in 10,000 in the early
1990’s). For males, the rate is 1 in 70 births, unsurprising since boys are
four times more likely than girls to be diagnosed with the disorder. The
number of children with autism is more than the numbers of children with
AIDS, cancer, and diabetes combined (Autism Speaks, n.d.). According
to the 2010 Kentucky KIDS COUNT Data Book, the number of children in
a south-central Kentucky Area Development District receiving social
security income due to disability in 2000 totaled 1,183, whereas in 2008
when the count was updated, the number jumped to 1,512 (Kentucky
Youth Advocates, 2010).
It takes a village to address these increasing social phenomena of
the rise in numbers of families with special needs children. Whether these
children have autism spectrum disorders, pervasive developmental
disorders, or any myriad number of other limiting physical, psychological,
social, or emotional issues, the habilitative response has to be
collaborative and well integrated. This village must include, but not be
limited to, the families, the professionals in the special needs community,
the students/interns in training, and the agencies and facilities that provide
the services. So what would the creation of such a village look like in a
rural southern community with both a university and a community
committed to having such services? What theories would support and
ground such an initiative? What system of inquiry would be used to
explore the needs and the gaps in services? What results would come
from such an initiative?
The following discussion answers the above questions and
presents not only the theoretical models but also the process of
developing a special needs forum that applied training, support, and
research to issues of families and children with special needs in a rural
community. The exploration of these needs and gaps within the rural
community is critical since rural communities in general are often
considered communities in transition (Ginsberg, 2005) and can lag behind
urban areas in terms of resource development and social service delivery.
The strengths perspective and systems model are integral
components of all social work education and practice (Zastrow, 2002) and
1
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
are critical to service development and delivery. The strengths
perspective provides an orientation that
emphasizes the client’s resources, capabilities, support systems
and motivation to meet challenges and overcome adversity. . . . It
emphasizes the client’s assets that can be used to achieve and
maintain individual and social well-being. (Barker, 2003, p. 420)
In order to connect the dots for services for the special needs community,
the village would need a clear understanding of how all the elements work
together. Systems theories inform us about the interrelatedness and
interconnectedness of people, issues, and elements. Any discussion of,
or planning for, a response to major biopsychosocial issues should
ethically include an understanding of systems theory. Thus begins the
process in a village that includes a small force of individuals connected by
their commitment to address the issues of families with special needs.
Functioning as a Clinical Education Complex (CEC) connected to a
university in rural south-central Kentucky, this village proceeded to move
beyond services as usual. The CEC is comprised of six programs that
provide services in the areas of 1) acquired brain injury, 2) communication
disorders, 3) early childhood education/intervention, 4) family counseling,
5) family resources, and 6) autism support. These programs work
together collaboratively to provide services to individuals, families, and
professionals in this rural community. Research and multidisciplinary
training complement the service delivery and are critical to the mission of
a CEC in an academic setting.
The Family Resource Program (FRP) of the CEC is a
service/resource program staffed with social work faculty, students, and
community volunteers. Comprehensive family needs assessments are
provided to families to evaluate their needs and connect them to services
within the CEC as well as community, state, and national resources.
Support networks are encouraged and fostered through the services of the
FRP. Education and support are also available to families who have a
child newly diagnosed with autism or any other developmental disorders.
Professional staff and interns are available to meet with family members
and significant others to provide information, resource material, screening
services, case management, counseling, and referrals.
As an integral part of a university community, the FRP strives to
proactively empower individuals and caregivers. While building bridges
between individuals and needed services within the community, the FRP
enhances the community’s knowledge and awareness of individual and
family needs. The services at the FRP are offered to individuals and
families referred from other programs within the CEC, from the community
2
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
agencies and programs, and from area schools; they are also available to
anyone seeking resource assistance in the region.
Overall, the FRP’s goals are to provide resource information and
referrals to individuals and families in need of services, to identify
individual strengths and assess individual needs, to assist families in
connecting with needed resources in the community, especially families
who have children with special needs, and to encourage and promote
community partnerships in service delivery.
Historical Perspective
In 2010, the Family Resource Program (FRP), in collaboration with the
other five CEC programs, developed a forum to target professionals in the
community as well as parents and caregivers of children with special
needs. The first forum was titled “Special Needs Family Summit” and was
presented to the community in May 2010. This event was modeled after
“The Family Café,” an annual conference for individuals and families with
special needs in Florida. The annual statewide conference of Florida’s
special needs community provides information on resources and services
available to the special needs community, while also involving the families
in the programs, agendas, and entertainment of the conference (The
Family Café, n.d.).
“The Family Café” annual conference’s mission is “to provide
individuals with disabilities and their families with an opportunity for
collaboration, advocacy, friendship, and empowerment by serving as a
facilitator of communication, a space for dialogue, and a source of
information” (The Family Café, n.d.) This conference, reportedly the
largest of its kind in the country, has impacted over 40,000 individuals
through “education, training, and networking,” providing families and
individuals with the opportunity to collaborate with professionals and other
families (The Family Café, n.d.)
The state of Florida has a unique history of responding to the needs
of children with special needs since 1994 (Stoutimore, Williams, Neff, &
Foster, 2008). Several initiatives, which included placing behavioral
analysts in child welfare programs as well as in-home placements for
parent coaching and training, were implemented. Collaboration was a key
element in the success of the programs developed. A training curriculum
of behavioral management skills and tools was utilized for caregivers.
Using the Florida conference or “Family Café” as a model, the FRP
proceeded with the assistance of a committee comprised of other CEC
program directors, interns, parent volunteers, and faculty to develop the
first Summit. Sessions were provided on the following: “Feeding
3
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
Disorders,” “Common Psychiatric Disorders in Children,” “Waiver
Services,” “Applied Behavioral Analysis,” and “Play-based Parenting
Strategies,” along with a psycho-drama and panel presentation on “How to
be an Effective Advocate as a Parent with a Child with Special Needs in
the Public School System.” Area health-care providers and other
professionals were given the opportunity to earn continuing education
credits through this forum.
Like the Florida conference, the Summit provided similar
information and activities, although on a much smaller scale. One
difference in the two forums was the research component. The Special
Needs Family Summit provided an opportune time for data collection
around the issues of resource availability, accessibility, and gaps in
services as well as an assessment of needs directly from the stakeholders
or those most impacted. This very unique Summit was the first of its kind
in the area and was repeated the following year (2011) as the “Special
Needs Summit.”
The 2011 Summit expanded on the original with an increase in
continuing education offerings and opportunities for education and
activities. The Summit concluded with a panel of college-aged students,
all with a diagnosis on the autism spectrum. These students contributed
their personal reflections of opportunities experienced through the service
delivery programs of the CEC, in particular the mentoring and tutoring
offered through the autism program.
The success of both of the Summits will be discussed further in the
results and discussion sections of this article. The results from both not
only provided answers to the research questions but also were consistent
with the current literature on families and children with special needs.
Literature Review
A review of the literature on the issues faced by families of children with
special needs produces several common themes. Parents of children with
special needs tend to 1) experience chronic stress in caring for their child
with special needs, 2) be more prone to feelings of social isolation, 3)
experience financial difficulties in caring for their child, 4) be likely to
experience frustration in trying to locate and access services, and 5)
experience frequent anxiety and worry over their child’s future or life span
issues (Abery, 2006; Aitken et al., 2009; Autism Speaks, n.d.; Barr, 2010;
Benson & Karlof, 2009; Freedman & Boyer, 2000; Sloper, 1999). For the
scope of this article, families are defined in a broad context that includes
biological parents, adoptive parents, grandparents, extended family
members, siblings, and fictive kin. The term “parents” refers to individuals
4
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
in the parenting or caregiving role for the child with special needs. The
terms “parents” and “families” will be used interchangeably due to the
primary relationships between the children and those individuals in the
parenting or caregiving role.
Stress
Several studies indicate the connection between a child’s disability or
health condition with parental stress and mental health issues such as
depression. Parents of children with special needs are more likely to
experience stress than parents of children who are considered to be
typically developing (Abery, 2006; Benson & Karlof, 2009; Sloper, 1999).
Having a child with a disability has a ripple effect on the family across
several domains.
Specifically, studies have shown that parents of children with ASD
(autism spectrum disorders) are at greater risk for mental health issues,
including depression, than parents of children with disabilities other than
autism. According to Benson and Karlof (2009), the symptoms and
behaviors of children with ASD, which are often pervasive and chronic,
may disrupt family roles and activities in multiple ways such as finances,
employment, and social interaction. This in turn may lead to parental
depression and other issues. In their study of parents of children with
ASD, Benson and Karlof (2009) found that having a child with ASD can
lead to considerable “psychological distress” (p. 358), including
comparatively higher levels of depressed mood and anger.
For families who have children with special needs, higher levels of
parental stress could contribute to higher parental divorce rates; however,
it is difficult to draw conclusions due to the existence of contradictory
studies. Differing divorce rates for families who have children with special
needs seem to be related to the type and severity of disability. For
example, in families where a child has autism, divorce rates appear to be
higher. In studies of families with an infant who has a health condition or
health risk, the family is more likely to experience parental divorce and
parental separation, and the family is more likely to have a stay-at-home
mother, in addition to a father with reduced work hours. In these same
families, the mother is more likely to rely on public assistance (Reichman,
Corman, & Noonan, 2008), probably due to the family’s loss of income.
However, one study by the Vanderbilt Kennedy Center found that
the divorce rate is actually lower than the national average for families
who have a child with Down Syndrome (Barr, 2010). Regardless of the
actual divorce rates for families of children with special needs, there is a
general consensus that these families need extra support due to the
5
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
higher levels of stress experienced, especially in families where a child
presents challenging behaviors (Osborne & Reed, 2009), including
sleeping problems (Williams, Sears, & Allard, 2004).
For parents of children with special needs, finding appropriate and
affordable child care can add to family stress (Reichman et al., 2008).
Perhaps because locating affordable and quality child care is difficult,
many parents of children with special needs choose to remain at home to
care for their child or one or both parents reduce their work hours in order
to provide care at home (Reichman et al., 2008). Concern about how their
child would be treated by caregivers outside the family could also
contribute to parents’ decisions to care for their child at home. For some
families, their child’s challenging behaviors result in one parent remaining
at home to care for the child.
Social Isolation
Parents of children with special needs tend to have lower rates of social
participation than parents without a child with a disability (Reichman et al.,
2008), which may contribute to parental depression. In general, parents of
children with special needs are more prone to social isolation than their
peers who do not have children with special needs (Autism Speaks, n.d.;
Abery, 2006). In a preliminary study by the organization Autism Speaks
and the Kennedy Krieger Institute (2011), extremely challenging behaviors
resulted in social isolation for the whole family, due to the family remaining
home in order to stick to routines and avoid challenging behaviors in
public, as well as the public’s response to their child’s behaviors.
Financial Difficulties
Financial issues and work issues are significant stressors for families of
children with special needs (Aitken et al., 2009; Bachman & Comeau,
2010; Kogan et al., 2008; Lindley & Mark, 2010; Porterfield & McBride,
2007). Several factors contribute to special needs families experiencing
financial difficulties; these factors include the cost of treatments and
therapies, cost of child care, loss of income due to parents’ not being able
to work or work full-time, the time needed to receive appropriate therapies
and treatments, and the costs of money and time to transport children to
and from appointments (Parish & Cloud, 2006).
Not having adequate income means that families will not be able to
access or purchase services and resources that their children need.
Families with children who have special needs tend to have lower incomes
compared to other families; this exacerbates the process of obtaining
needed services and treatments (Bachman & Comeau, 2010). Since
6
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
children with special needs are more likely to be living in poverty than
children in general, financial worries greatly contribute to family stress
(Bachman & Comeau, 2010; Porterfield & McBride, 2007). In rural areas
with high poverty rates, higher levels of stress produced by financial
strains may be experienced.
Contributing to financial difficulties is the lack of access to and
affordability of adequate insurance coverage (Bumbalo, Ustinich,
Ramcharran, & Schwalberg, 2005; Freedman & Boyer, 2000). Of those
with insurance, many have found that insurance does not cover needed
interventions such as physical therapy, speech-language services,
occupational therapy, applied behavior analysis, case management, and
parent support (Kennedy Krieger Institute, 2011).
Locating and Accessing Services
In order to make informed decisions about their children’s care, parents
need information about available resources and programs (Freedman &
Boyer, 2000). However, information about their child’s condition or
diagnosis, available services, available financial resources, material
supports, and respite is often missing (Sloper, 1999). In one study by
Davis et al. (2010), families reported that they did not feel supported by
services that they accessed. Another study found that lower-income
families frequently hold negative perceptions about existing community
resources (Silverstein, Lamberto, DePeau, & Grossman, 2008). Without
effective case managers who can connect families with services and
resources across several agencies, the family may be forced to
“piecemeal” services and thus experience higher levels of stress and
frustration (Freedman & Boyer, 2000).
Special needs families often require interventions and services from
multiple agencies, such as health-care, social services, education, federal,
and state agencies; this leads to contact with numerous service providers
(Abery, 2006; Ello & Donovan, 2005; Sloper, 1999). Having several
agencies or programs involved with the family without a “key” or single
point of contact leads to fragmentation of services and lack of coordination
of care (Sloper, 1999). In addition, the families who receive the least
services may be those in greatest need, including single-parent families,
lower-income families, and large families (Sloper, 1999). Families need
help in navigating the complex system of services (Freedman & Boyer,
2000).
In one study, parents often perceived that programs or agencies
involved in their children’s care did not communicate with each other,
duplicated paperwork and procedures, and provided contradictory
7
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
information. Thus, they identified a need for agencies to communicate
and collaborate, as well as the need for a single point of entry for services
(Freedman & Boyer, 2000).
Life Span Issues
A major concern for parents of children with special needs is worry over
what will happen to the children after the parents die. Easter Seals, along
with the Autism Society of America, conducted the Living with Autism
study, in which 1,652 parents of children with autism and 917 parents of
typically developing children were surveyed regarding their daily lives,
relationships, employment, finances, healthcare, independence, and so
forth. This study found that close to 80% of parents with autism reported
that they are extremely concerned or very concerned about their child’s
ability to be independent as an adult, in stark contrast to only 32% of
parents with typically developing children. In comparison to parents of
children who are typically developing, much smaller percentages of
parents felt their child with autism would be able to make life decisions,
befriend others in the community, take part in recreational/leisure
activities, or have a life partner or spouse (Easter Seals, 2008).
Strengths
In spite of the increased demands and increased stress on families of
children with special needs, many families not only cope with the
additional demands and stress but find ways to thrive. In families of
children with developmental disabilities, parents often find ways to cope
with caregiving demands, build strong marriages, and raise children
without disabilities who appear to be well adjusted (Abery, 2006). As
mentioned earlier, in families with a child who has Down Syndrome, the
parental divorce rate was actually lower than the national average (Barr,
2010).
Some positive benefits to the family have been identified in families
with a child who has an intellectual disability. Though having a child with
an intellectual disability is not stress-free, it can be very rewarding and
enriching. Family members may have positive experiences which
contribute to an overall appreciation of life. For siblings of children with an
intellectual disability, several positive outcomes included “increased
empathy, love, sense of social justice, advocacy for those in need,
protection-nurturance, loyalty, implicit understandings and acceptance of
difference” (Dykens, 2005, p. 361).
Several factors have been identified as contributing to families’
success in raising a child with a disability, including the meanings that
8
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
family members attribute to their situational demands and capacity to meet
those demands, the resources used by or available to the family, and the
coping behaviors used by family members to balance demands and
resources (Abery, 2006). Programs such as those examined in this study
aid families in navigating the needed services and resources as they strive
to maintain and promote the well-being of their children and entire family.
Resource Centers for Families with Special Needs
Across the United States, there are several resource centers serving
families of children with special needs. The Southwest Autism Research
& Resource Center (SARRC), located in Phoenix, Arizona, carries out its
mission to “advance research and provide a lifetime of support for
individuals with autism and their families” (Southwest Autism Research &
Resource Center, n.d.). SARRC provides services and support to children
and families with autism, while conducting research and providing
trainings for and presentations to family members and professionals in the
special needs community (Southwest Autism Research & Resource
Center, n.d.).
Another center that serves professionals in the autism community
as well as families of children with autism is the University of Louisville
Autism Center at Kosair Charities, located in Louisville, Kentucky. The
center combines different departments in the university to provide
evaluations, treatment, and interventions for children while providing
training and information to parents, caregivers, and professionals. The
goal is to provide children, caregivers, and professionals a single place
where they can obtain information, treatment, and referrals (University of
Louisville, n.d.).
In Austin, Texas, the Johnson Center for Child and Health
Development provides diagnostic services, health-care services,
behavioral therapy, educational assessments, community outreach, and
education while also conducting research. This center’s mission is “to
advance the understanding of childhood development through clinical
care, research, and education” (Johnson Center for Child and Health
Development, n.d.). Formerly called the Thoughtful House, the Johnson
Center serves individuals, families, and professionals within the
developmental disorders community (Johnson Center for Child and Health
Development, n.d.).
Located at Vanderbilt University in Nashville, Tennessee, the
Vanderbilt Kennedy Center offers several programs for children, parents,
and professionals within the special needs community. The center
provides information, treatment, interventions, and support for families
9
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
who have a member with developmental disabilities. Within the Vanderbilt
Kennedy Center is the Family Outreach Center, which serves as the point
of entry for families needing services and resources offered at Vanderbilt
University and services offered within the community (Vanderbilt Kennedy
Center, n.d.). All of these centers, including the Clinical Education
Complex (CEC), share similar core values and missions in serving
individuals, families, caregivers, and professionals within the special
needs community while also conducting research to further the knowledge
of evidence-based practices within multiple disciplines. These
multidisciplinary centers provide services, training, and research within the
village of the special needs community.
Method
Consistent with the village approach, inductive methods of research
produce the most effective and user-friendly methods of inquiry.
Grounded theory can be used to capture the multiple dimensions of
phenomena. According to Denzin and Lincoln (2000), grounded theory is
currently the most widely used interpretive paradigm in the social
sciences. The inductive nature of this partially qualitative research
method provides a systematic set of procedures to develop a theory about
a phenomenon that is grounded in data and the experiences of the
participants (Tillman, 2002). Data collection, analysis, and theory
construction are regarded as reciprocally related. This interweaving is a
way to increase insights and clarify the parameters of emerging theory to
ensure that the analysis is based on the data and not on presumptions
(Padgett, 2008; Wilson, 2008). Subsequently, the emergent theory here is
specifically focused on capturing themes related to the needs of families
and children with special needs as well as the professionals who develop
and provide services to them.
This study evaluated the community Summits held over two years
by the CEC to determine if the training was useful and helpful and if it
contributed to the knowledge and skills of the conference participants.
Given the needs of children with special needs and their families, the
researchers also wanted to explore whether participants thought that the
resources were adequate in the area and to get more of a sense of
training and service needs. The training evaluation instrument selected
for this study has been utilized in several studies involving child welfare
and mental health professionals (Antle, Barbee, & van Zyl, 2008; Sullivan,
Antle, van Zyl, & Faul, 2009); it has been found to be a good measure of
training utility and, in the Antle et al. study, appeared to be a factor in
retention of knowledge gained in training. The instrument contained
10
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
questions measured on a 5-point Likert scale. The instrument asked
participants to rate areas such as the training atmosphere, the methods
utilized in the training, the confidence they felt to practice in the topic area,
the usefulness of the material, the amount of material covered, and overall
satisfaction with training. In addition, some needs assessment questions
were asked to determine what supports and services were needed by
families with children with special needs and the professionals who serve
those families. In this study, the researchers wanted to know if the
participants thought the available resources were adequate and wanted to
explore themes around the needs of this targeted population, in order to
consider possible interventions and begin to develop theory around gaps
in services, unmet needs and a continuum of care for these children and
families. Some demographic questions were included to capture
information such as educational level, role of the participant (parent,
professional, student, etc.), age, ethnicity, and length of time involved in
the special needs community.
This study used a convenience sample of training attendees at the
Summit. There was a consent preamble inviting the participants to
complete the survey. They were informed that completing the survey and
participating in the study were voluntary and that they could discontinue
participation in the study at any time. The consent preamble indicated that
their completion of the survey communicates their consent to voluntary
participation in the study. The consent preamble and survey were
included in the participant’s training packet.
Results
Over the two years the Summit was held, 38 participants responded to the
invitation to complete the survey, 20 the first year and 18 the second year.
There were 128 total Summit participants over the two years, which made
this a response rate of 29.6%. Of the participants, 92% were female.
When asked about their ethnic origin, 76% identified themselves as
Caucasian, 18% African American, 3% Hispanic/Latino and 3% selected
the option “other.” The participants had varying levels of education, with
the majority of participants having a Master’s degree (n = 17) or Master of
Social Work degree (n = 7), 10 having Bachelor’s degrees (2 were in
social work), 1 each having a high school diploma and associate’s degree,
and 2 holding doctoral degrees.
The participants were asked their role within the special needs
community. Thirty-two percent said they worked in an agency serving
children with special needs and their families, 26% worked in a university
setting, 16% were in some sort of private practice, 8% worked for public
11
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
school systems, and 3% were volunteers (number does not equal 100
because some chose “none of the above”). The participants represented
different roles when attending the conference. Most respondents (73%)
were attending as professionals that serve special needs children, 11%
were parents of special needs children, and 16% were students. In terms
of their length of involvement working with the special needs community,
over half the sample had been involved for more than 6 years (51%), only
5% had less than a year’s involvement, while 32% had been involved 1 to
3 years and 11% between 4 and 6 years. Those who work in the field had
been employed an average of 4 years (Mean = 48, SD = 42.3, Range = 8
– 156 months [one outlier of 39 years removed from analysis]).
Overall, the participants reported a high level of satisfaction with the
training. When asked about the importance of the training, on a 5-point
Likert scale, the mean was 4.38 (SD = .83), with 89% indicating they
agreed or strongly agreed about the importance of the training. Their
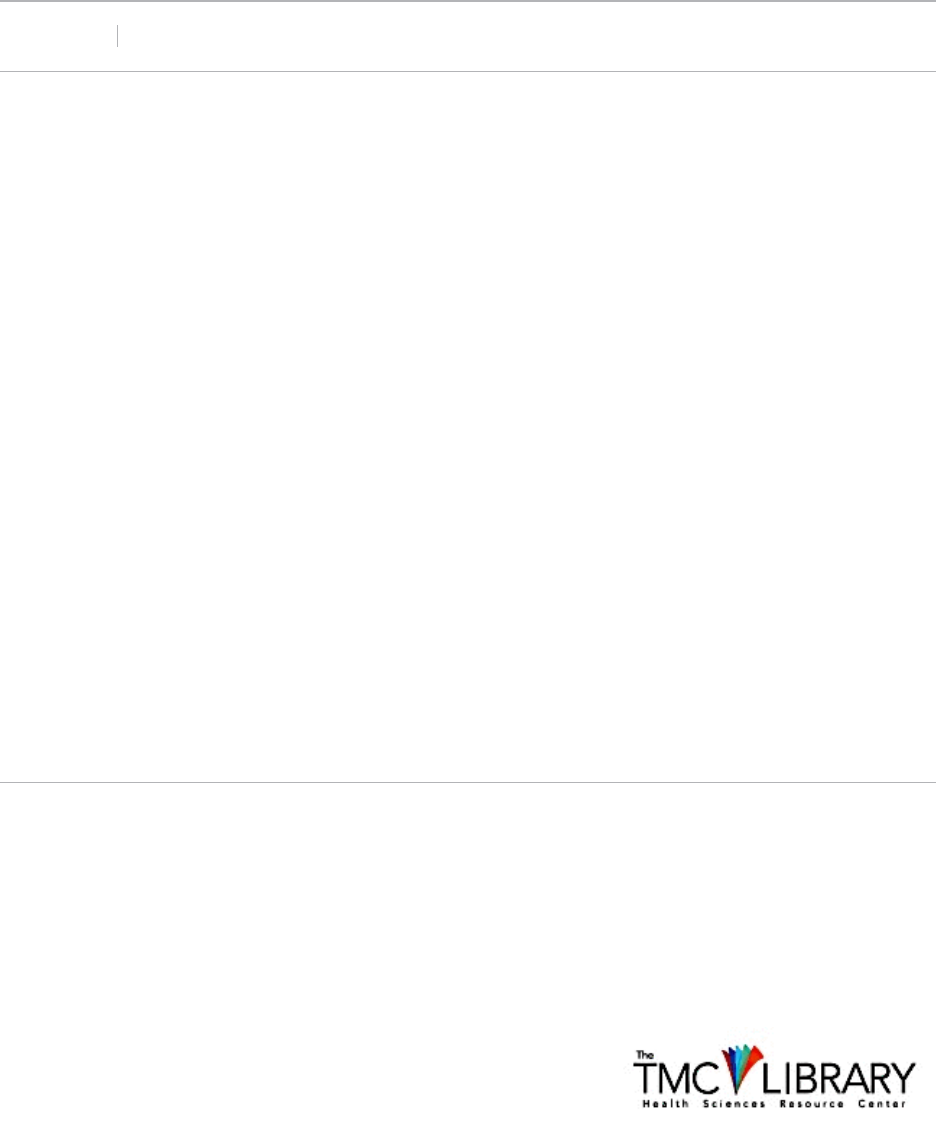
ratings of the helpfulness and practicality of the various training methods
(role play, handouts, and lecture) were very high, ranging from 87% to
97% when combining the “agree” and “strongly agree” responses. See
Figure 1 for a graph of these results. Nearly all respondents (97%)
indicated that the method of training delivery was effective.
The training was seen as useful by 97% of the respondents, and
86.5% said their knowledge had increased as a result of participating in
the Summit. More than half of the sample (62%) indicated the training had
increased their skill in this area, and 65% indicated an increase in their
confidence to practice in this area. A large majority (89%) indicated their
likelihood to apply the knowledge gained from the training, with scores
ranging from 2-5 on a 5-point Likert scale, with a mean score of 4.35 (SD
= .89). See Figure 2 for a summary of these items.
12
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
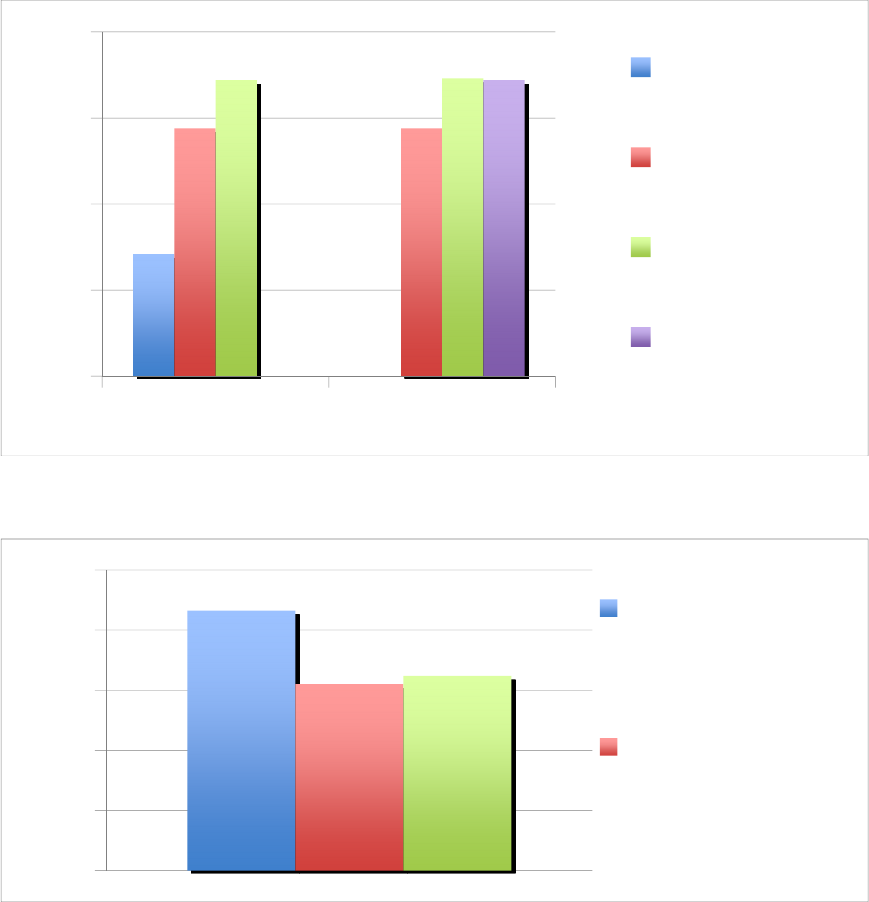
Figure 1. Helpfulness and practicality of training methods (combining
“agree” and “strongly agree”).
Figure 2. Impact of training on practice.
The majority of the participants (89.2%) indicated that they agreed
or strongly agreed regarding the importance of the training, and the
majority (86.5%) indicated their knowledge on the topic had increased
after attending the training. Nearly two-thirds (64%) indicated the amount
of material covered was the right amount while 21.4% indicated they
would have liked more material to be covered during the event. When
asked if they felt more equipped to be an advocate for special needs
80
85
90
95
100
Helpful Practical
Role Playing
Handouts
Lecturing
Training
Overall
0
20
40
60
80
100
Increase
Knowledge
Increase Skill,
Confidence in
Practice
13
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
children after attending the training, 88% indicated they did. Almost all of
the participants (94%) indicated they felt more informed about children
with special needs after attending the Summit. Several themes emerged
regarding how participants felt more equipped to be advocates for children
with special needs. Participants mentioned areas such as feeling better
equipped for families when children have feeding concerns, feeling more
comfortable working with this population, gaining a better understanding of
autism spectrum disorders and related interventions/treatment, and
gaining knowledge to pass on to others to raise awareness about how to
best assist children and families.
Slightly over half (56.3%) indicated that the resources for special
needs children and their families are adequate within the community.
Some of the needed resources listed were as follows: help for learning
resources when new to the area; awareness in the general population to
the needs of children with ASD; more resources for feeding issues;
decreased waiting lists; greater social interaction and assistance with
activities of daily living; more play groups and support groups; financial
resources; transportation to services; more in-home services; and respite
care.
The preferred format for receiving information about working with
special needs children was training events (n = 34), followed by individual
work with staff (n = 12), then electronic sources (n = 8) and newsletters (n
= 6). See Figure 3 for a summary. The training topics most requested by
participants for future events were as follows: strategies for low-
functioning autism, physical disabilities, feeding, sensory issues, speech
behavior, auditory processing/hearing impairment, and in-depth
information on therapy and intervention techniques.
14
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
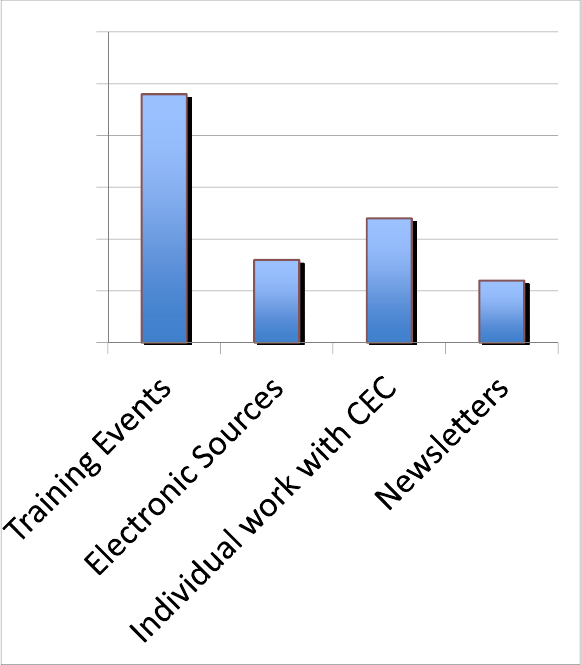
Figure 3. Preferred format for receiving information about working with
special needs children
Discussion
The participants in this study had several years of work experience with
children with special needs and had been involved in the special needs
community for some time. They had varying levels of education, and
more than half had been involved with the special needs community for
more than 6 years. Professionals, parents, and students were all
represented and came together to gain more information about children
with special needs. Those who had worked in the field had been working
there an average of 4 years, indicating that the sample had some
experience already with this population and began the training with some
familiarity of the issues related to this population.
Overall, the participants rated the training as useful, important, and
practical. The qualitative comments indicated that the participants liked
the speakers, that the training was interesting and helpful, and that a great
0
5
10
15
20
25
30
15
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
deal of good information was covered. Needed resources and future
training topics were identified. Many of these topics are in line with the
literature, which indicates these families need assistance in areas such as
accessing services (Freedman & Boyer, 2000). The majority of
participants indicated they felt better equipped after the training to be
advocates for children with special needs. They were highly satisfied with
the training and indicated an increase in knowledge, skills, and confidence
to practice in this area. Even though many in this sample indicated that
there are adequate resources for children with special needs, the small
sample size limits the generalizability of these findings. Future studies
should continue to explore the needs of children with special needs and
their families as well as to examine outcomes from programs such as the
CEC, programs which are designed to help meet these multiple needs.
Conclusion
The rise in prevalence of children with special needs presents challenges
for families and communities. A child’s disability affects several areas of
family life, and parental well-being impacts the child’s well-being.
Therefore, it is imperative to address the whole family’s needs and not just
the needs of the individual with a disability. Particularly in rural areas, as
more and more children are diagnosed with autism spectrum disorders
and other developmental disabilities, families often struggle to locate
information, support, and referrals for various therapies, services, and
resources.
A review of the literature identifies several issues faced by parents
of children with special needs such as chronic stress, social isolation,
financial issues, difficulty locating and accessing services, and life span
issues. In order to meet the needs of families with special needs, a
holistic approach is critical (Freedman & Boyer, 2000). This holistic
approach was supported by the results of the research conducted in this
study. Linking families with needed resources and giving parents options
to make choices and decisions about the services their children receive
empowers them, and all family members benefit.
The Special Needs Summit was developed by a Clinical Education
Complex (CEC) to provide education, support, and training for families,
professionals, paraprofessionals, and students within the special needs
community. The Summit provided the following for its participants, who
were parents, caregivers, professionals, paraprofessionals, and students:
workshops on relevant topics, continuing education credit, informational
booths, panel of college students with autism spectrum disorders, a talent
show featuring children with special needs, and family festival activities.
16
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
This forum allowed an opportunity for research, and data were
collected through the use of an evaluation training instrument.
Participants were able to provide feedback through the use of a survey
that requested information about the following: 1) relevance of the
training, 2) future needs for training, 3) needs for development of
additional resources, and 4) the best vehicle for service delivery.
Based on data from participants, the majority agreed the training
was important and rated highly the helpfulness and practicality of the
training methods. As a result of the Summit, participants reported their
knowledge and skill in a particular area had increased. Participants
indicated they felt more equipped to advocate for children with special
needs, and almost all felt more informed about children with special needs
after attending the Summit. Some of the gaps in services or needed
resources which were identified included: help in locating and accessing
services when new to the area, community awareness of children with
autism spectrum disorders, financial resources, transportation, and respite
care; this list corresponds to the needs of parents found in the literature.
The feedback from participants in this study will also contribute to the
existing literature on diversity as it relates to families of children with
special needs.
More studies are needed to further explore the challenges of
members within the special needs community, particularly families. More
detailed feedback regarding specific needs would be helpful in developing
future Summits and parent training and support events. Forming a
coalition of service providers dedicated to serving families with special
needs could make service provision more effective and responsive to
families. In order to connect the dots for these families, it will take a
village approach. This village should be multidisciplinary, inclusive of
parents, siblings, formal and informal caregivers, and the professional and
academic communities.
17
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
References
Abery, B. H. (2006). Family adjustment and adaptation with children with
Down Syndrome. Focus on Exceptional Children, 38(6), 1-18.
Aitken, M. E., McCarthy, M. L., Slomine, B. S., Ding, R., Durbin, D. R.,
Jaffe, K. M. . . . & Mackenzie, E. J. (2009). Family burden after
traumatic brain injury in children. Pediatrics, 123(1), 199-206.
Antle, B. A., Barbee, A. P., & van Zyl, M. (2008). A comprehensive model
for child welfare training evaluation. Children and Youth Services
Review, 30(9), 1063-1080.
Autism Speaks Incorporated. (n.d.). What is autism? Retrieved from
http://www.autismspeaks.org/what-autism
Bachman, S. S., & Comeau, M. (2010). A call to action for social work:
Minimizing financial hardship for families of children with special
health care needs. Health & Social Work, 35(3), 233-238.
Barker, R. L. (Ed.). (2003). The social work dictionary (5th ed.).
Washington, DC: NASW Press.
Barr, K. N. (2010, February). When parents of children with special needs
divorce. Exceptional Parent Magazine, 4-7.
Benson, P. R., & Karlof, K. L. (2009) Anger, stress proliferation, and
depressed mood among parents of children with ASD: A
longitudinal replication. Journal of Autism and Developmental
Disorders, 39, 350-362.
Bumbalo, J., Ustinich, L., Ramcharran, D., & Schwalberg, R. (2005).
Economic impact on families caring for children with special health
care needs in New Hampshire: The effect of socioeconomic and
health-related factors. Maternal and Child Health Journal, 9(2
Suppl.), S3-S11.
Carpenter, B. (2000). Sustaining the family: Meeting the needs of families
of children with disabilities. British Journal of Special Education,
27(3), 135-144.
Davis, E., Shelly, A., Waters, E., Boyd, R., Cook, K., Casey, E., . . .
Reddihough, D. (2010). The impact of caring for a child with
cerebral palsy: Quality of life for mothers and fathers. Child: Care,
Health, and Development, 36(1), 63-73.
Denzin, N. K., & Lincoln, Y. S. (2000). Handbook of qualitative research.
Thousand Oaks, CA: Sage Publications.
Dykens, E. M. (2005). Happiness, well-being, and character strengths:
Outcomes for families and siblings of persons with mental
retardation. Mental Retardation, 43(5), 360-364.
Easter Seals. (2008). Living with autism study. Retrieved from
18
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
http://www.easterseals.com/site/PageServer?pagename=ntlc8_livin
g_with_autism_study_home
Ello, L. M., & Donovan, S. J. (2005). Assessment of the relationship
between parenting stress and a child’s ability to functionally
communicate. Research on Social Work Practice, 15(6), 531-544.
Freedman, R. I., & Boyer, N. C. (2000). The power to choose: Supports for
families caring for individuals with developmental disabilities. Health
& Social Work, 25(1), 59-68.
Ginsberg, L. H. (Ed.). (2005). Social work in rural communities (4th ed.).
Alexandria, VA: Council on Social Work Education.
Johnson Center for Child and Health Development. (n.d., para. 1).
What is the Johnson Center for Child Health and
Development?.Retrieved from http://www.johnson-
center.org/index.php/site/FAQ
Kennedy Krieger Institute. (2011). Interactive autism network research
report: Family stress—part 1. Retrieved from
http://www.autismspeaks.org/news/news-item/ian-research-report-
family-stress-%E2%80%94-part-1
Kentucky Youth Advocates. (2010). Kentucky KIDS COUNT county data
book. Jeffersonville, KY: Kentucky Youth Advocates.
Kogan, M. D., Strickland, B. B., Blumberg, S. J., Singh, G. K., Perrin, J.
M., & van Dyck, P. C. (2008). A national profile of the health care
experiences and family impact of autism spectrum disorder among
children in the United States, 2005-2006. Pediatrics, 122(6), e1149-
e1158.
Lindley, L. C., & Mark, B. A. (2010). Children with special health care
needs: Impact of health care expenditures on family financial
burden. Journal of Child and Family Studies, 19, 79-89.
Osborne, L. A., & Reed, P. (2009). The relationship between parenting
stress and behavior problems of children with autistic spectrum
disorders. Exceptional Children, 76(1), 54-73.
Padgett, D. K. (2008). Qualitative methods in social work research (2nd
ed.). Thousand Oaks, CA: Sage Publications.
Parish, S. L., & Cloud, J. M. (2006). Financial well-being of young children
with disabilities and their families. Social Work, 51(3), 223-232.
Porterfield, S. L., & McBride, T. D. (2007). The effect of poverty and
caregiver education on perceived need and access to health
services among children with special health care needs. American
Journal of Public Health, 97(2), 323-329.
19
Starks et al.: Connecting the Dots
Published by DigitalCommons@TMC, 2011
Reichman, N. E., Corman, H., & Noonan, K. (2008). Impact of child
disability on the family. Maternal and Child Health Journal, 12, 679-
683.
Silverstein, M., Lamberto, J., DePeau, K., & Grossman, D. C. (2008). “You
get what you get”: Unexpected findings about low-income parents’
negative experiences with community resources. Pediatrics, 122(6),
e1141-e1148.
Sloper, P. (1999). Models of service support for parents of disabled
children: What do we know? What do we need to know? Child:
Care, Health, and Development, 25(2), 85-99.
Southwest Autism Research & Resource Center. (n.d.) About SARRC.
Retrieved from
http://www.autismcenter.org/about_sarrc.aspx
Stoutimore, M. R., Williams, C. E., Neff, B., & Foster, M. (2008). The
Florida child welfare behavior analysis services program. Research
on Social Work Practice, 18(5), 367-376.
Sullivan, D. J., Antle, B. F., van Zyl, M. A., & Faul, A. C. (2009).
Implementing evidence-based practice into public mental health
settings: Evaluation of the Kentucky Medication Algorithm Program.
Best Practices in Mental Health, 5(2), 112-128.
The Family Café. (n.d., para 1). The Family Café: About Us. Retrieved
from
http://familycafe.net/index.php?option=com_content&view=section&
id=3&Itemid=90
Tillman, L. C. (2002). Culturally sensitive research approaches: An
African-American perspective. Educational Researcher, 31(9), 3-
12.
University of Louisville Autism Center at Kosair Charities. (n.d.) Our
mission statement. Retrieved from http://louisville.edu/autism/
Vanderbilt Kennedy Center (n.d.) The Family Outreach Center. Retrieved
from
http://kc.vanderbilt.edu/site/services/disabilityservices/default.aspx
Williams, P. G., Sears, L. L., & Allard, A. (2004). Sleep problems in
children with autism. Journal of Sleep Research, 13, 265-268.
Wilson, S. (2008). Research is ceremony: Indigenous research methods.
Winnipeg, Canada: Fernwood Publishing.
Zastrow, C. (2002). The practice of social work (7th ed.). Pacific Grove,
CA: Brookes/Cole Publishers.
20
Journal of Family Strengths, Vol. 11 [2011], Iss. 1, Art. 10
https://digitalcommons.library.tmc.edu/jfs/vol11/iss1/10
DOI: 10.58464/2168-670X.1015
