https://doi.org/10.29399/npa.28527
148
RESEARCH ARTICLE
Arch Neuropsychiatry 2024;61:148−153
Evaluation of Sexual Behavior and Sexual Functions of BDSM Practitioners:
A Controlled Study
Ender CESUR
1
, Barış SANCAK
2
1
Psychiatrist, Acıbadem Mehmet Ali Aydınlar University, The School of Medicine, Maslak Hospital, Istanbul, Turkey
2
Psychiatrist, Acıbadem Mehmet Ali Aydınlar University, The School of Medicine, Atakent Hospital, Istanbul, Turkey
148
Correspondence Address: Ender Cesur, Acıbadem Maslak Hospital, Darüşşafaka Büyükdere Caddesi, No:40, 34457, Sarıyer, İstanbul, Turkey • E-mail: [email protected]
Received: 09.07.2023, Accepted: 23.10.2023, Available Online Date: 29.05.2024
©Copyright 2023 by Turkish Association of Neuropsychiatry - Available online at www.noropskiyatriarsivi.com
BDSM is an acronym for “bondage-discipline, dominance-submission,
sadism, masochism” (1). It is difficult to establish a precise definition
of BDSM, but it often includes sexual behavior involving some type of
exchange of power between partners and/or the use of pain for sexual
pleasure, although there are sensations other than pain (1). These
practices are based on the consent of individuals (2).
“Kink”
is an umbrella term to address a wide range of erotic interests,
identities, practices, and relationships (3). Although it is sometimes
thought that “kink” always includes genital contact or orgasm, “kink” can
serve different purposes. In a study conducted with 1580 participants from
the kink community, 126 different forms of erotic stimuli were identified
(4). Historically, BDSM has been associated with paraphilic disorders, as
BDSM was thought to result from psychiatric illnesses, childhood traumas
(5,6) or it does not include sexual behaviors that aim reproduction. DSM-
5 includes diagnoses of sexual sadism disorder and sexual masochism
disorder. The diagnostic criteria of these disorders emphasize that these
practices should contain nonconsenting partners and they must cause
clinically significant distress and loss of functionality (7). Having BDSM
interests alone no longer meets the criteria for a mental disorder or a
paraphilic disorder. It is stated that most BDSM practitioners do not differ
from the general population in terms of depression, anxiety, and phobias
(8). While sadomasochism is no longer considered a disorder in ICD-11,
it has suggested to include some paraphilic disorders, mostly involving a
lack of consent from the partner such as coercive sexual sadism disorder
(1). These updates can be interpreted as a change to avoid stigma and
establish higher tolerance for various sexual fantasies, urges, or behaviors.
INTRODUCTION
Cite this article as: Cesur E, Sancak B. Evaluation of Sexual Behavior and Sexual Functions of BDSM Practitioners: A Controlled Study. Arch Neuropsychiatry 2024;61:148−153.
Introduction: The purpose of this study was to obtain information
about the sexual behaviors, sexual functioning of “bondage-discipline,
dominance-submission, sadism, masochism” (BDSM) practitioners.
Methods: The study group (n=141) consisted of 65 women and 76 men
who defined themselves as BDSM practitioners included in the study
with the snowball technique through websites that are accessible on
online BDSM groups. A control group (n=167) who stated that they
were not BDSM practitioners was also recruited through websites.
Sociodemographic and Sexual Behavior Evaluation Form and Arizona
Sexual Experience Scale (ASEX) were used online to gather data.
Results: No significant difference was found between BDSM practitioners
and controls with regard to ASEX scores. Yet, in women, the mean ASEX
score was lower in BDSM practitioners than in the control group whereas
in men, the mean ASEX score was higher in the BDSM practitioners.
Conclusion: Gender might be an important factor in terms of sexual
functioning in cisgender BDSM practitioners. Awareness on problems of
this sexual minority should be increased.
Keywords: BDSM, masochism, sadism, sexual behavior, sexual
dysfunctions, stigma
ABSTRACT
Although BDSM fantasies and practices are common (9), the stigma
associated with the sexual behavior of BDSM practitioners is still prevalent
among healthcare providers (10). Less than half of kink-oriented patients
receiving healthcare can talk about their sexual activities to healthcare
providers because they are afraid of being stigmatized (11). BDSM
practitioners may seek psychiatric support for both BDSM-related and
different mental problems, but most healthcare professionals are not
familiar with these practices (12). One of the consequences of prejudices
of BDSM practices is that very few studies have focused on sexual
functioning and related distress in this population (11).
In a study comparing groups with and without BDSM practices, it is
reported that, apart from maintaining arousal, there was no significant
Highlights
• BDSM practitioner men and women show difference in
terms of sexual dysfunctions.
• Difficulty in the ability to reach orgasm is significant in
BDSM practicing men.
• The probability of sexual dysfunction was found to be
lower in women practicing BDSM.
• BDSM group thought that they could not talk about their
sexuality comfortably.

Cesur and Sancak. Sexual Practices of BDSM Practitioners in Turkey
149
Arch Neuropsychiatry 2024;61:148−153
difference between women in both groups in terms of distress in sexual
functioning (13). For men, it is reported that sexual dysfunction is less
common in BDSM practitioners, except for premature orgasm and
anorgasmia (13). Botta et al. stated that very few of the participants
describe distress related to BDSM activities (14).
To the best of our knowledge, there is no study on BDSM in Türkiye.
The scarce of knowledge of BDSM practitioners’ sexual lives, level of
knowledge about sexual and mental health makes it difficult to provide a
qualified health service to this community and contributes to prejudices.
The aim of our research is to obtain information about the sexual lives,
sexual behaviors, and sexual functioning of BDSM practitioners, to
determine whether there is a difference about sexual practices between
them and those who do not practice BDSM, and to provide clinicians with
information about BDSM practitioners’ sexual practices and problems,
if any. Therefore, we aimed to test the hypothesis that cisgender BDSM
practitioners do not differ from the general population in terms of sexual
dysfunctions.
METHODS
A hundred and forty-one people (65 cisgender women, 76 cisgender
men) aged 18 and over who defined themselves as BDSM practitioners
were included in the study with both convenience and snowball
techniques through websites that are accessible on the internet and
BDSM groups in social networks. In order to reach our research sample
in the most accurate way, the most popular Turkish-language websites
and social networks used by BDSM practitioners living in Türkiye were
chosen. The moderators of the selected websites were contacted and
informed about the study. Persons who volunteered to participate were
included in the study. The study was carried out with the Google forms
survey application, which was sent individually to those who agreed to
participate in the research via the internet. Consent was obtained from
the participants who identified themselves as BDSM practitioners, and
the questionnaire was administered completely anonymously to protect
their privacy.
To reach the control group, another form was prepared (which only
excludes BDSM practices) and was placed on two popular national
websites. With the approval of the moderators of these websites, the
control form was advertised. A hundred and sixty-seven volunteer
participants (88 cisgender women, 79 cisgender men) who stated that
they were not BDSM practitioners and filled out the form completely
were determined as the control group.
While 4 trans women, 2 trans men, and 3 nonbinary participants
answered the questions in the study group; the questions in the control
group were answered by 4 trans women, 2 trans men, and 5 nonbinary
people. However, transgender participants’ data could not be included in
the study, since the number of trans participants is quite small to pursue
subgroup analysis.
Data were collected between 01.05.2021 and 31.07.2021.
Measurements
Sociodemographic and Sexual Behavior Evaluation Form
It is a questionnaire prepared by researchers that include questions about
sociodemographic and sexual identity-related features, preferences in
BDSM practices, sexual development histories, medical characteristics,
and sexual health-related knowledge levels. In the form delivered to the
control group, there is no statement about BDSM, except for a question
asking whether they are BDSM practitioners. First, a BDSM definition
was made and participants were asked if they identified as a BDSM
practitioner. Then we questioned the sociodemographic characteristics.
When questioning sexual identity-related features, definitions were
made initially and the participants were asked to mark the option most
suitable for them.
In the second part, the medical history of the participants has been
questioned: whether they had been diagnosed with a physical or
psychiatric illness in the past, whether they have attempted suicide,
whether they have received professional help for a sexual problem in
the past, whether they have been discriminated against during medical/
psychological assistance due to their sexual practices, whether they delay
seeking medical/psychological help because they think they cannot talk
about their sexuality comfortably.
In the last part of the form, their sexual histories, practices, and sexual
health knowledge levels were questioned.
The BDSM group was also asked about their roles in BDSM, their preferred
BDSM practices, sexual intercourse during BDSM sessions, their preferred
activities during BDSM practices, and at what age they first experienced
BDSM.
Arizona Sexual Experience Scale (ASEX)
The scale developed by McGahuey et al. (2000) was prepared in a six-
point Likert type, and has separate forms for men/women (15). The
validity and reliability of the Turkish form of the scale were established,
and the cut-off score of the scale was determined as 11 (16). The increase
in score is directly associated with the severity of the sexual dysfunction.
There are questions that examine sex drive, arousal, physiological arousal
(vaginal lubrication/erection), ability to reach orgasm, and satisfaction
from orgasm.
Statistical Analyses
All the data obtained in the study was analyzed using the IBM
Statistical Package for Social Sciences (SPSS) program version 21.0
package program (IBM Inc., Chicago IL, USA). In the study, categorical
independent variables were shown with frequency and percentage
values; continuous variables with mean and standard deviation values.
Skewness and kurtosis indices, histogram graph, QQ plot graph, and
Kolmogorov-Smirnov normality test were used to determine whether the
variables showed a normal distribution. Descriptive statistics were used
to determine the participants’ characteristics. Regarding the hypotheses,
Chi-square analysis was used to determine history of psychiatric disorder
frequency and the discrimination and help-seeking behavior of BDSM
practitioners compared to the control group. An independent t-test was
used to examine the hypothesis that BDSM practitioners do not differ
from the general population in terms of sexual dysfunctions. In the post
hoc power analysis, we assessed the statistical power of our study. The
analysis revealed a power of 0.961 for comparing ASEX scores between
female BDSM practitioners and the control group. For the comparison of
ASEX scores among male groups, the study exhibited a power of 0.817. P
≤0.05 was considered statistically significant.
RESULTS
There was no significant difference between the BDSM practitioners
and the control group in terms of age, gender, and education level. The
comparison of the general characteristics and medical/sexual histories of
the BDSM practitioners and the control group is shown in Table 1.
The mean age of the participants to start BDSM practices is 24.1 (SD=4.12).
In terms of the distribution of participants according to their BDSM
roles, 17.7% (n=25) described themselves as submissive, 21.3% (n=30) as
dominant, 44.7% (n=63) as switch (which can be flexible between dominant
or submissive), and 16.3% (n=23) as other. Regarding the BDSM practices

Cesur and Sancak. Sexual Practices of BDSM Practitioners in Turkey
150
Arch Neuropsychiatry 2024;61:148−153
that are most frequent, it was seen that 42.6% (n=60) of them practice
bondage-discipline, 29.1% (n=41) dominant-submissive, 12.8% (n=18)
sadism, 12.1% (n=17) masochism, and 3.5% (n=5) other practices. When
it was evaluated whether there is vaginal and/or anal penetration during
sexual practices, 12.8% (n=18) of the participants stated that they almost
never had penetration, 60.3% (n=85) of them had penetration sometimes,
and 27% (n=38) of them stated they had penetration frequently.
No significant difference was found between BDSM practitioners and
controls with regard to ASEX scores. In women, the mean ASEX score
was lower in BDSM practitioners than in the control group. In men, the
mean ASEX score was higher in the BDSM practitioners. The comparison
of ASEX item scores for each gender is given in Table 2.
A detailed comparison of the discrimination and sexual characteristics
of both groups is shown in Table 3. To investigate differences in sexual
attitudes among genders, we employed a chi-square test, analyzing both
BDSM practitioners and control groups separately for each gender. Our
analysis yielded no statistically significant differences in sexual attitudes
between the genders.
Table 1. General characteristics of BDSM practitioners and control group
BDSM Practitioners
n (%)
Control Group
n (%)
p
values
Gender
0.249Female 65 (46.1) 88 (52.7)
Male 76 (53.9) 79 (47.3)
Sexual orientation
<0.001
Heterosexual 85 (60.3) 132 (79.0)
Homosexual 38 (27.0) 22 (13.2)
Bisexual 18 (12.8) 13 (7.8)
Marital status
<0.001
Single 122 (86.5) 84 (50.3)
Married/partnered 19 (13.5) 83 (49.7)
Having children
0.166No 123 (87.2) 136 (81.4)
Yes 18 (12.8) 31 (18.6)
Educational level
0.740High school 8 (5.7) 11 (6.6)
University and above 133 (94.3) 156 (93.4)
Working status
0.528
Employed 122 (86.5) 150 (89.8)
Unemployed 10 (7.1) 7 (4.2)
Student 9 (6.4) 10 (6.0)
Information on medical history and sexual life
History of physical illness
0.905
Yes 11 (7.8%) 13 (7.8%)
History of psychiatric disorder
0.411
Yes 29 (20.6%) 29 (17.4%)
Suicide history
0.053
Yes 24 (17.0%) 16 (9.6%)
History of sexual violence
0.019
Yes 72 (51.1%) 63 (37.7%)
M (SD) M (SD)
Age 31.0 (5.17) 31.6 (5.27) 0.101
Age of first sexual intimacy 17.3 (3.37) 16.6 (3.82) 0.088
Age of first sexual intercourse 19.0 (2.86) 20.2 (3.36)
<0.001
p: p value, SD: standard deviation
Cesur and Sancak. Sexual Practices of BDSM Practitioners in Turkey
151
Arch Neuropsychiatry 2024;61:148−153
DISCUSSION
In the female group, the reported rate of sexual dysfunction was lower
in the BDSM group. In the male group, the reported rate of sexual
dysfunction was higher in the BDSM group. While there was no difference
between the BDSM group and the control group in terms of medical
history; BDSM practitioners reported significant difficulties in accessing
healthcare services due to discrimination.
We suggested that BDSM practitioners would not differ from the control
group in terms of sexual dysfunctions. A shift in power dynamics is at
the heart of the BDSM plays (17). When we look at the frequency of
the participants in our study according to their BDSM roles, almost half
of them defined themselves as a “switch”. It is stated that a significant
subgroup of BDSM practitioners switches between dominance and
submission depending on different factors such as mood and partner (18).
Therefore, it is conceivable that the power preference in BDSM may not
always be constant over time. When evaluating whether there is vaginal
and/or anal penetration during sexual practices, about a quarter of the
participants stated that there was frequent penetration in our study. Botta
et al. (2019) states that 54.6% of male participants and 63.2% of female
participants often/always prefer penetration during BDSM practices
(14). The exchange of power between partners is sexually arousing for
most practitioners. Even in the general population, it is reported that the
exchange of power between the partners during sexual intercourse and
the behavior of domination/submission are stimulating (19). Therefore,
BDSM practitioners may not always need sexual intercourse to maintain
arousal or orgasm. Considering the ASEX scores in the study, the
probability of sexual dysfunction in both the BDSM and control groups
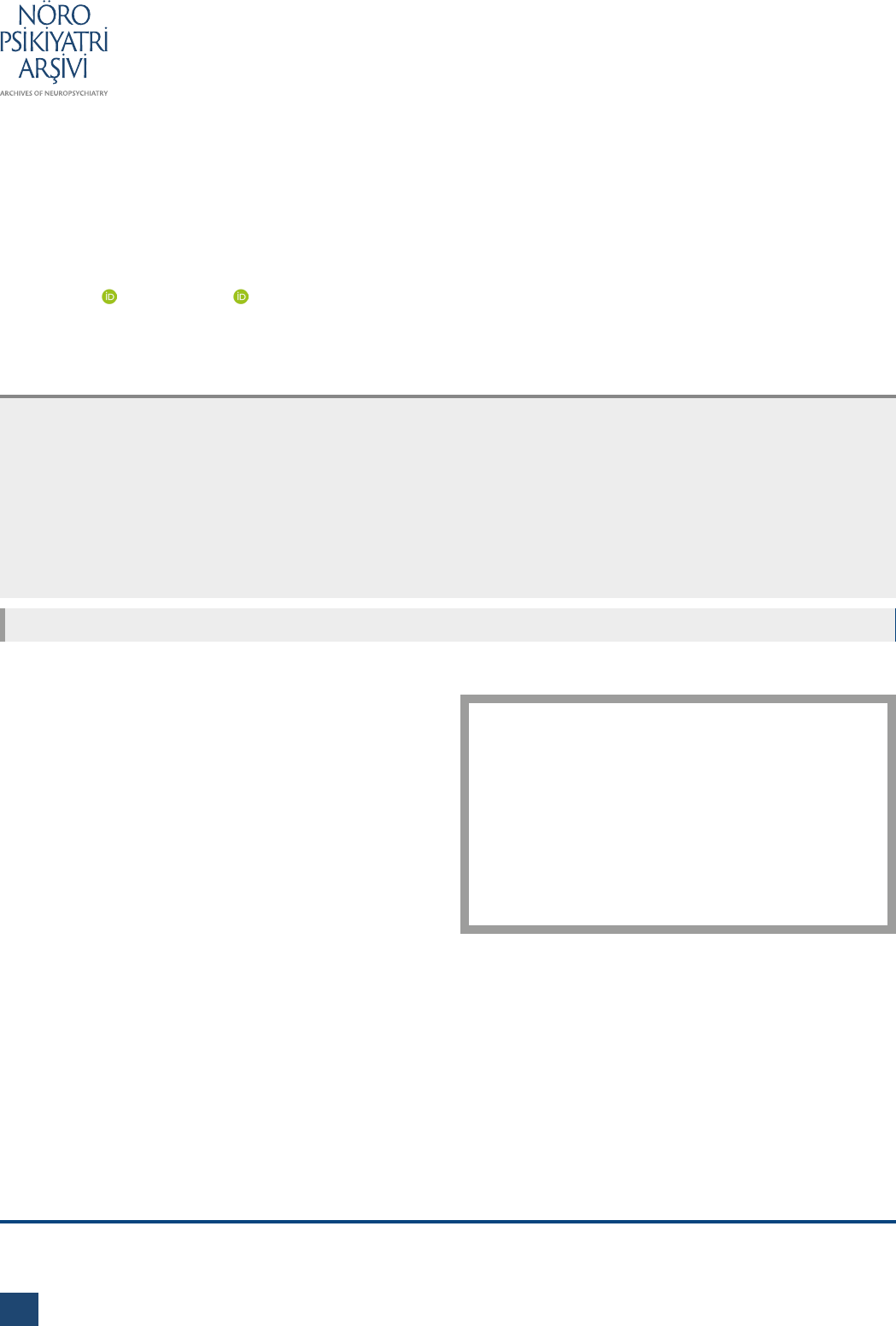
Table 2. Comparison of ASEX item scores for each gender
Female Participants
(n=153)
Male Participants
(n=155)
BDSM
(n=65)
M (SD)
Control
(n=88)
M (SD) p Cohen’s d
BDSM
(n=76)
M (SD)
Control
(n=79)
M (SD) p
Cohen’s
d
Drive 1.83 (0.63) 2.82 (1.23)
<0.001 1
1.99 (0.82) 1.86 (0.76) 0.36 0.16
Arousal 2.26 (1.09) 2.92 (1.17)
<0.001 0.58
2.41 (0.98) 2.11 (0.95) 0.6 0.31
Lubrication/ Erection 3.22 (1.49) 3.67 (1.31)
0.047 0.32
2.30 (1.05) 2.03 (0.95) 0.085 0.26
Orgasm 2.45 (1.12) 2.60 (1.34) 0.45 0.12 3.08 (1.24) 2.46 (1.21)
0.002 0.5
Satisfaction with orgasm 2.62 (0.82) 3.10 (1.01)
0.002 0.52
2.17 (0.93) 1.85 (0.91)
0.03 0.34
Independent samples T-test: values in parentheses indicate standard deviation.
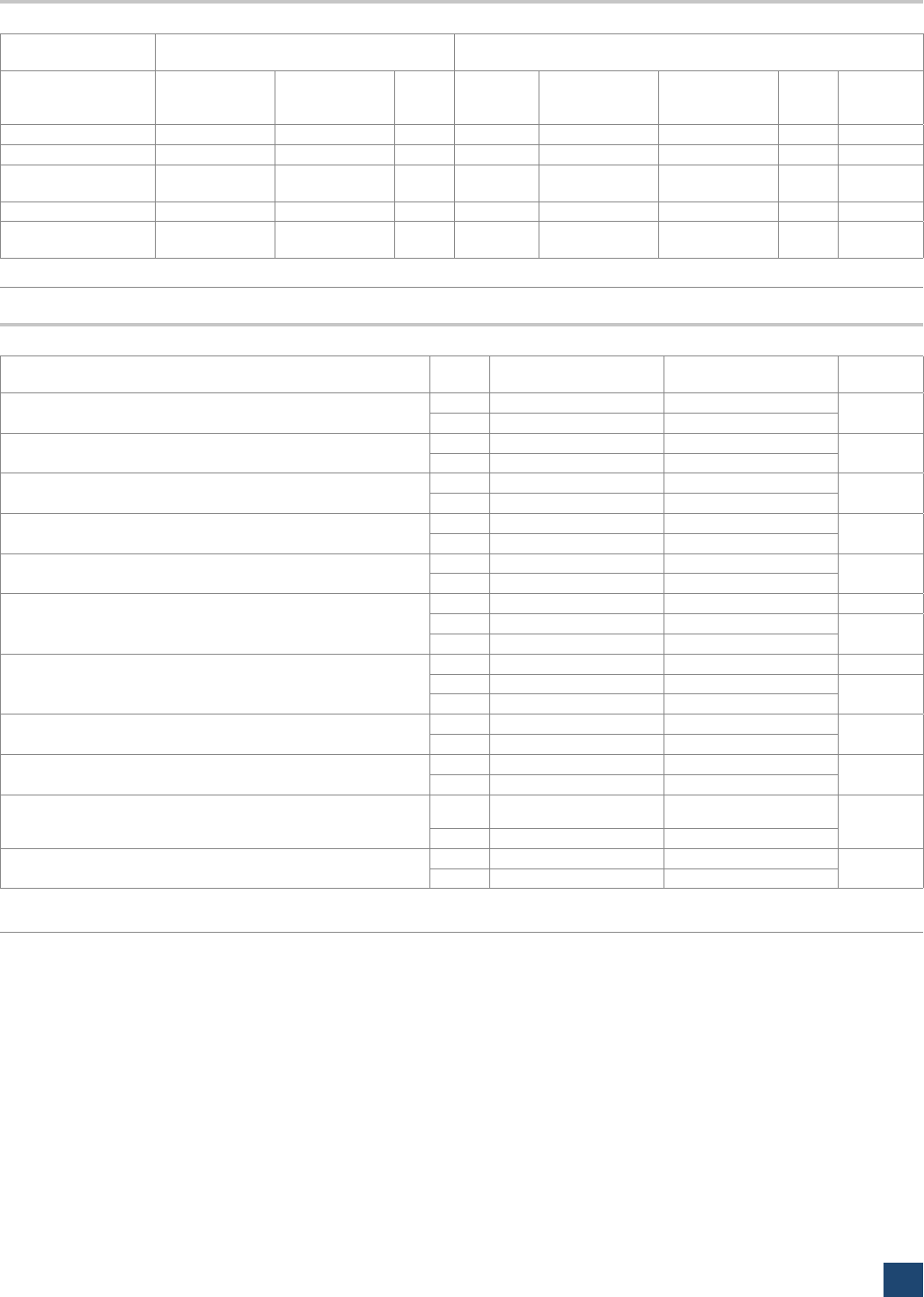
Table 3. Questions about sexual attitudes
BDSM
n (%)
Control
n (%) p
Can you comfortably talk about your sexual desires and expectations
with your partner (s)?
N 18 (12.8) 40 (24)
0.018
Y 123 (87.2) 127 (76)
Do you take into account whether the people you have sex with
consent to your wishes/actions during the intercourse?
N 6 (4.3) 6 (3.6)
0.73
Y 135 (95.7) 161 (96.4)
Have you received any structured education about sexual health and
sexuality in the past?
N 112 (79.4) 125 (74.9)
0.409
Y 29 (20.6) 42 (25.1)
Do you think you know enough about HIV and other sexually
transmitted infections and prevention methods?
N 31 (22.0) 32 (19.2)
0.307
Y 110 (78.0) 135 (80.8)
Do you use an effective protection method (condom, etc.) for sexually
transmitted infections during your sexual relations?
N 34 (24.1) 46 (27.5)
0.234
Y 107 (75.9) 121 (72.5)
Do you use an effective protection method during your sexual
relations?
N/A 27 (19.1) 19 (11.4)
N 23 (16.3) 32 (19.2)
0.118
Y 91 (64.5) 116 (69.5)
If you come into contact with blood during sexual intercourse, do you
think you take adequate precautions to protect yourself?
N/A 72 (51.1) 126 (75.4)
N 52 (36.9) 16 (9.6)
<0.001
Y 17 (12.1) 25 (15.0)
Do you masturbate regularly?
N 18 (12.8) 55 (32.9)
<0.001
Y 123 (87.2) 112 (67.1)
Have you sought professional help for a sexual problem in the past?
N 107 (75.9) 136 (81.4)
0.189
Y 34 (24.1) 31 (18.6)
Have you been discriminated against due to your sexual practices
and sexuality during any medical/psychological assistance you have
received in the past?
N 64 (45.4) 153 (91.6)
<0.001
Y 77 (54.6) 14 (8.4)
Have you delayed seeking medical/psychological help because you
thought you could not talk about your sexuality comfortably?
N 53 (37.6) 141 (84.4)
<0.001
Y 88 (62.4) 26 (15.6)
Chi-square test.
N/A: Not applicable (Does not meet the condition of the question.); N: No; p: p value; Y: Yes.

Cesur and Sancak. Sexual Practices of BDSM Practitioners in Turkey
152
Arch Neuropsychiatry 2024;61:148−153
was higher in the female sample, while the ASEX scores were higher in
the control group than in the BDSM practitioner women. It is observed
that there are difficulties in sex drive, arousal, and vaginal lubrication
functions in women in the control group. It is reported that during BDSM
practices, women may have less anxiety about their bodies and sexual
performance, express themselves more easily and freely, and may have
less difficulty in maintaining arousal (13). This may explain the lower
scores of sexual dysfunctions in BDSM practitioner women in our study.
In the male participants group, the probability of sexual dysfunction was
higher in the BDSM practitioner group. In the BDSM group, difficulty
in the ability to reach orgasm and satisfaction from orgasm functions is
significant. To understand whether a sexual problem can be considered
as sexual dysfunction in the BDSM group participating in our study, it is
necessary to first understand whether it causes distress in participants.
In the study of Pascoal et al. (2015), although premature orgasm and
anorgasmia were equally disturbing individual sexual problems in both
BDSM and non-BDSM male groups, no significant difference was found
between the two groups (13). BDSM activities can be based on various
plays in which intercourse or orgasm are not in the foreground (13,19).
Early orgasm may cause more problems in the BDSM group than in the
control group, as it may interrupt the scene in the BDSM group due to
the difficulties experienced by men in the refractory period in arousal
after orgasm. Therefore, premature ejaculation in men participating in
our study may not be desired in BDSM practices, so ejaculation may take
a long time, and the orgasm experienced before the planned moment
may cause dissatisfaction because it interrupts the activity. Further studies
are needed to understand the reasons for the described difficulty in
ejaculation in BDSM practitioner men.
According to the reports of the online participants, no difference was
found between the groups in terms of physical and psychiatric illness and
past suicide attempts in this study. The belief that psychiatric disorders
are more common in BDSM practitioners has been disproved by studies
showing that their psychological functioning and attachment styles were
not different from the general population (8). The results of our study
supports the opinion that being a BDSM practitioner does not increase
the susceptibility to psychiatric disorders. In our study, participants were
asked about their psychiatric background and no scale and interview
were applied to detect any psychopathology. This is an important
weakness of our study. Studies including more detailed psychiatric
interviews are needed to discover the frequency of psychopathology in
BDSM practitioners.
In our study, the reported rate of sexual violence in the past was higher
in the BDSM group than in the control group. Although studies suggest
that there is no relationship between trauma and BDSM behavior (20,21);
7.9% of the males reported sexual abuse compared to 1–3% in the general
population in a study investigating the history of childhood abuse in
BDSM practitioners; and in women, it was found to be 22.7% and 6–8%,
respectively (22). The rates of discrimination against sexual minorities are
high (23). Discrimination against BDSM practitioners due to their non-
normative sexual practices can be similarly high. Larger-scale studies are
needed to elucidate the relationship between trauma and BDSM.
According to our results, more than half of the BDSM practitioners
reported that they were discriminated due to their sexual practices and
sexuality during a medical/psychological assistance they received in the
past. Moreover, most of the BDSM group stated that they postponed
seeking medical/psychological help because they thought that they could
not talk about their sexuality comfortably. Waldura et al. (2016) state that
less than half of kink-oriented patients receiving healthcare can talk about
their sexual activities with healthcare providers because they are afraid of
being stigmatized (11). Increased stigma by healthcare providers leads
to non-disclosure of kink involvement and delay in seeking care (24). If
healthcare professionals gain sufficient knowledge about the practices of
BDSM practitioners, it may improve the discrimination experienced by
patients with BDSM practitioners in accessing healthcare.
In the context of BDSM, participants ideally interact voluntarily with
predetermined consent based on a mutual understanding of what
activities will take place (2). Therefore, BDSM communities care about
the rules regarding the boundaries of safe and consensual BDSM (25). In
our study, BDSM practitioners reported talking about their sexual desires
and expectations more comfortably with their partners, while there
was no significant difference between the two groups about getting the
consent of their partners during intercourse, taking precautions regarding
sexually transmitted infections and contraception.
All of the BDSM practitioners participating in the research are at least high
school graduates and most of them are working. The number of single
people in the BDSM group is higher than it is in the control group. It is
stated that 17.6% of the participants who practice BDSM describe their
relationships as non-monogamy, 21% as dating, and 15.1% as polyamory
(21). The high number of single people in the BDSM group may be due
to the fact that they do not prefer monogamous relationships. The age
of first sexual intercourse was lower in BDSM practitioners. This result
is consistent with research showing that BDSM practitioners experience
more sexuality throughout their lives and have sex at an earlier age (26).
Although there was no difference between the groups in terms of age,
gender, and education, when considered in terms of sexual orientation, it
was seen that the rate of those who stated that they were homosexual or
bisexual among BDSM practitioners was higher than the control group. In
a large-scale study conducted in Australia by Richters et al. (2008), BDSM
practices were found to be more common among homosexuals and
bisexuals (20). In an online study, it was stated that almost half of those
who stated that they were masochists were bisexual or homosexual (17).
The struggle against the stigma that claims that queer sexuality is wrong
can be cited as a factor in the easier acceptance and spread of BDSM
practices within the queer community (27).
This study has some limitations. Participants were gathered through the
internet using forums and social media accounts. We can guess that the
high education levels in the study is a function of the online surveys,
since people with higher education will be more likely to respond to
online surveys. Accessing and effectively using internet is more common
in people with higher education. Since internet use and access to these
areas are easier for socioeconomically advantaged individuals (13), it may
be possible for this group to reach the study. Since the data is collected
online, there may be problems with the reliability of the participants and
the answers. This may affect the reliability of the study results. To minimize
this problem, we did not put the BDSM form on a general website and
carefully shared it on a limited platform with BDSM practitioners. Also,
we kindly asked the participants to share this form only with their BDSM
practitioner friends. Because the study is an online survey, rates of attrition
is not known exactly. In the advertisement of the form prepared for the
control group, it was stated that the study was about sexual practices,
and sexual dysfunction was not mentioned. However, it may still have
caused a slight increase in the participation of individuals with sexual
dysfunction. Since this is the first study conducted on the BDSM group
in Türkiye, using an anonymous online questionnaire has helped us
reach a difficult-to-reach group more widely. Although the participants
were not asked for their identity information, some participants may
have wanted to refrain from participating in the study due to security
concerns. BDSM was defined in the informed consent form and it was
stated that those who defined themselves as BDSM practitioners should
fill out the study form, but the difficulties in determining the boundaries
of BDSM may have been confusing for the participants. While only

Cesur and Sancak. Sexual Practices of BDSM Practitioners in Turkey
153
Arch Neuropsychiatry 2024;61:148−153
cisgender participants were included in the study, trans and nonbinary
participants were not included. The fact that there were people with
different orientations among the cisgender participants may also have
affected the difference in terms of the discrimination they were exposed
to. Also, it is known that BDSM practices are not only about sexuality and
can be applied by people in the asexual-spectrum. Further studies with
participants from all gender identities are needed.
In conclusion, in our study, no difference was found in the history of
psychiatric illness reported by BDSM practitioners when compared to the
general population. Men and women BDSM practitioners show different
characteristics in terms of sexual dysfunctions. Since the perception of
sexuality is thought to differ culturally, it would be helpful to conduct
similar researches in different societies. The discrimination reported by
the BDSM practitioners negatively affects their help-seeking behavior
and also makes it difficult to conduct research on this group. Therefore,
it is important to raise awareness of this issue, both in medical settings
and in the public.
Ethics Committee Approval: Ethics Committee Approval: Ethics committee approval
was obtained for the study by Acıbadem Mehmet Ali Aydınlar University Medical
Research Evaluation Committee (Date: 21.04.2021, no: 2021/08).
Informed Consent: All patients signed informed consent for data collection during the
visits.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept- EC, BS; Design- EC, BS; Supervision- EC, BS;
Resource- EC, BS; Materials-EC, BS ; Data Collection and/or Processing- ; Analysis and/
or Interpretation-EC, BS ; Literature Search- EC, BS; Writing- EC; Critical Reviews- EC, BS.
Conflict of Interest: The authors declared that there is no conflict of interest.
Financial Disclosure: None.
REFERENCES
1. Brown A, Barker ED, Rahman QA. Systematic scoping review of the
prevalence, etiological, psychological, and interpersonal factors associated
with BDSM. J Sex Res. 2020;57(6):781–811. [Crossref]
2. Dunkley CR, Brotto LA. The role of consent in the context of BDSM. Sex
Abuse. 2020;32(6):657–678. [Crossref]
3. Sprott RA, Vivid J, Vilkin E, Swallow L, Lev EM, Orejudos J, et al. A queer
boundary: how sex and BDSM interact for people who identify as kinky.
Sexualities. 2020;24(5-6):708–732. [Crossref]
4. Rehor JE. Sensual, erotic, and sexual behaviors of women from the “kink”
community. Arch Sex Behav. 2015;44(4):825–836. [Crossref]
5. De Neef N, Coppens V, Huys W, Morrens M. Bondage-discipline, dominance-
submission and sadomasochism (BDSM) from an integrative biopsychosocial
perspective: A systematic review. Sex Med. 2019;7(2):129–144. [Crossref]
6. Ten Brink S, Coppens V, Huys W, Morrens M. The Psychology of kink: A survey
into relationships of trauma and attachment style with BDSM interests. Sex
Res Soc Policy. 2021;18:1–12. [Crossref]
7. American Psychiatric Association. Diagnostic and statistical manual of
mental disorders (5th ed.); 2013. [Crossref]
8. Wismeijer AJ, Van Assen MLM. Psychological characteristics of BDSM
practitioners. J Sex Med. 2013;10(8):1943–1952. [Crossref]
9. Lehmiller JJ. Tell me what you want: the Science of sexual desire and how it
can help you improve your sex life. Da Capo Lifelong Books; 2018.
10. Moser C. Paraphilias and the ICD-11: Progress but still logically inconsistent.
Arch Sex Behav. 2018;47:825–826. [Crossref]
11. Waldura JF, Arora I, Randall AM, Farala JP, Sprott RA. Fifty shades of stigma:
exploring the health care experiences of kink-oriented patients. J Sex Med.
2016;13(12):1918–1929. [Crossref]
12. Dunkley CR, Brotto LA. Clinical considerations in treating BDSM practitioners:
a review. J Sex Marital Ther. 2018;44(7):701–712. [Crossref]
13. Pascoal PM, Cardoso D, Henriques R. Sexual satisfaction and distress in
sexual functioning in a sample of the BDSM community: a comparison study
between BDSM and non-BDSM contexts. J Sex Med. 2015;12(4):1052–1061.
[Crossref]
14. Botta D, Nimbi FM, Tripodi F, Silvaggi M, Simonelli C. Are role and gender
related to sexual function and satisfaction in men and women practicing
BDSM? J Sex Med. 2019;16(3):463–473. [Crossref]
15. McGahuey CA, Gelenberg AJ, Laukes CA, Moreno FA, Delgado PL, McKnight
KM, et al. The Arizona Sexual Experience Scale (ASEX): reliability and validity.
J Sex Marital Ther. 2000;26(1):25–40. [Crossref]
16. Soykan A. The reliability and validity of Arizona sexual experiences
scale in Turkish ESRD patients undergoing hemodialysis. Int J Impot Res.
2004;16:531–534. [Crossref]
17 Cross PA, Matheson K. Understanding sadomasochism: an empirical
examination of four perspectives. J Homosex. 2006;50:133–166. [Crossref]
18. Labrecque F, Potz A, Larouche É, Joyal CC. What is so appealing about being
spanked, flogged, dominated, or restrained? Answers from practitioners of
sexual masochism/submission. J Sex Res. 2021;58(4):409–423. [Crossref]
19. Apostolou M, Khalil M. Aggressive and humiliating sexual play: occurrence
rates and discordance between the sexes. Arc Sex Behav. 2018;48:1–14.
[Crossref]
20. Richters J, de Visser RO, Rissel CE, Grulich AE, Smith AMA. Demographic
and psychosocial features of participants in bondage and discipline,
“sadomasochism” or dominance and submission (BDSM): data from a
national survey. J Sex Med. 2008;5:1660–1668. [Crossref]
21. Connolly PH. Psychological functioning of bondage/domination/sado-
masochism (BDSM) practitioners. J Psychol Human Sex. 2006;18:79–120.
[Crossref]
22. Nordling N, Sandnabba NK, Santtila P, Allison L. Differences and similarities
between gay and straight individuals involved in the sadomasochistic
subculture. J Homosex. 2006;50:41–57. [Crossref]
23. Ince Yenilmez M. LGBTQIs in Turkey: the Challenges and resilience of this
marginalized group. Sex Res Soc Policy. 2020;18:440–449. [Crossref]
24. Sprott RA, Randall A, Smith K, Woo L. Rates of injury and healthcare
utilization for kink-identified patients. J Sex Med. 2021;18:1721–1734.
[Crossref]
25. Holt K. Blacklisted: boundaries, violations, and retaliatory behavior in the
BDSM community. Deviant Behav. 2016;37:917–930. [Crossref]
26. Coppens V, Ten Brink S, Huys W, Fransen E, Morrens M. Survey on BDSM-
related Activities: BDSM experience correlates with age of first exposure,
interest profile, and role identity. J Sex Res. 2020;57(1):129–136. [Crossref]
27. Cross PA, Matheson K. Understanding sadomasochism: an empirical
examination of four perspectives. J Homosex. 2006;50:133–166. [Crossref]
28. Burn SM. Heterosexuals’ use of “fag” and “queer” to deride one another:
a contributor to heterosexism and stigma. J Homosex 2020;40(2):1-11.
[Crossref]
