
Range of Joint Motion Evaluation Chart
NAME OF PATIENT CLIENT IDENTIFICATION NUMBER
INSTRUCTIONS: For each affected joint, please indicate the existing limitation of motion by drawing a line(s) on the
figures below, showing the maximum possible range of motion or by notating the chart in degrees. Provide a complete
description of all affected joints in your narrative summary. If range of motion was normal for all joints, please comment in
your narrative summary. If joints which do not appear on this chart are affected, please indicate the degree of limited
motion in your narrative.
1. Back 2. Lateral (flexion)
Right 25
O
Degrees
Right 45
O
Degrees
Right 30
O
Degrees
Right 20
O
Degrees
Right 150
O
Degrees
Extension 25
O
Flexion 90
O
Degrees Degrees
Extension 60
O
Flexion 50
O
Degrees Degrees
Left 80
O
Right 80
O
Degrees Degrees
Left
Knee Flexed Knee Extended
100
O
100
O
Degrees Degrees
Right
Knee Flexed Knee Extended
100
O
100
O
Degrees Degrees
Left 40
O
Right 40
O
Degrees Degrees
Left 25
O
Degrees
Left 45
O
Degrees
Left 30
O
Degrees
Left 20
O
Degrees
Left 150
O
Degrees
3. Neck 4. Neck (lateral bending)
5. Neck (rotation) 6. Hip (backward extension)
7. Hip (flexion) 8. Hip (adduction)
9. Hip (abduction) 10. Knee (flexion)
DSHS 13-585A (REV. 03/2014)
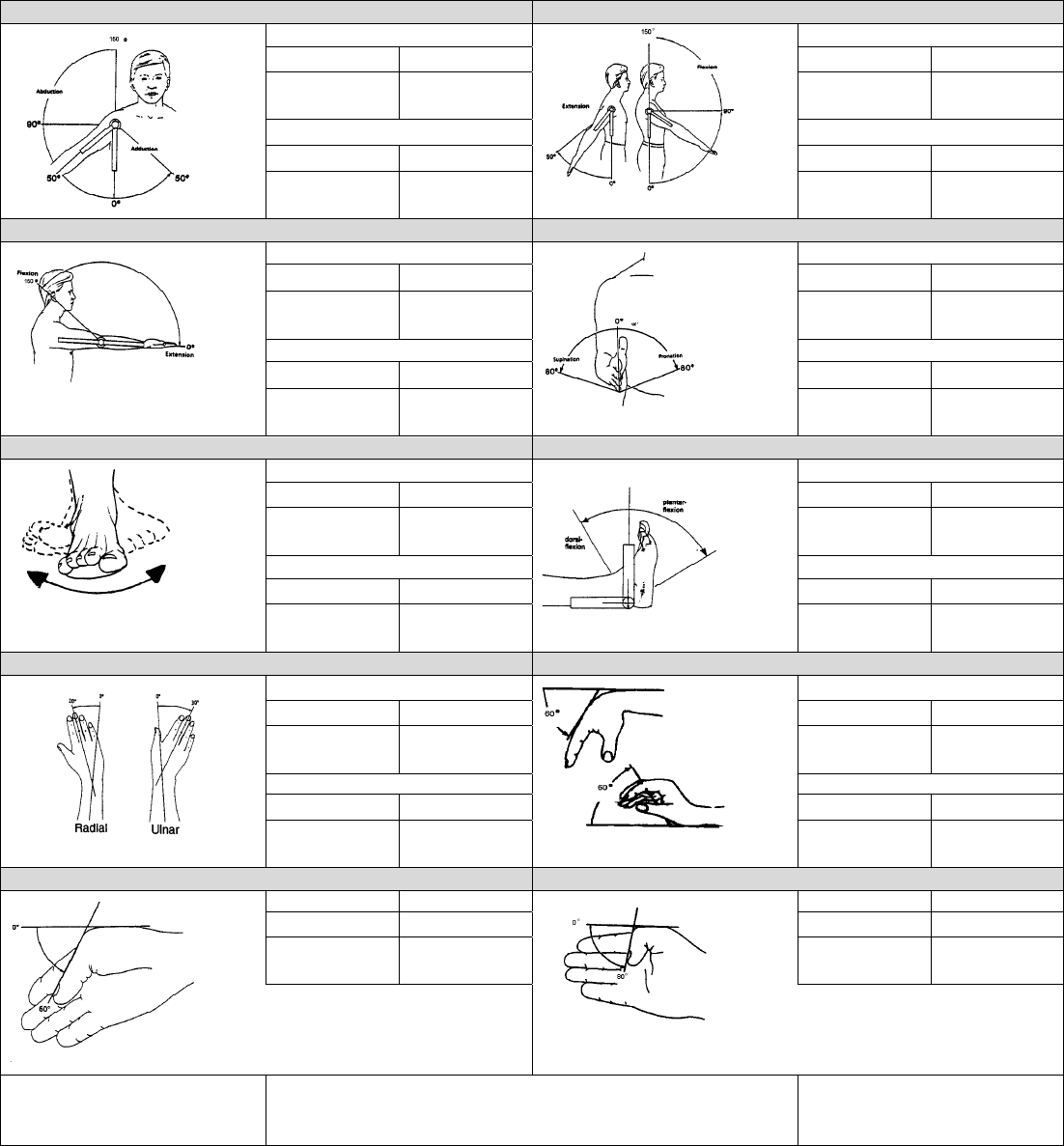
11. Shoulder (Abduction – Adduction) 12. Shoulder (Flexion – Extension)
Left
Left
Abduction 150
O
Adduction 30
O
Extension 50
O
Flexion 150
O
Degrees Degrees Degrees Degrees
Right Right
Abduction 150
O
Adduction 30
O
Extension 50
O
Flexion 150
O
Degrees Degrees Degrees Degrees
13. Elbow 14. Forearm (Pronation – Supination)
Left Left
Extension 0
O
Flexion 150
O
Pronation 80
O
Supination 80
O
Degrees Degrees Degrees Degrees
Right Right
Extension 0
O
Flexion 150
O
Pronation 80
O
Supination 80
O
Degrees Degrees Degrees Degrees
15. Ankle 16. Ankle (Flexion – Extension)
Left Left
Inversion 30
O
Eversion 20
O
Plantar 40
O
Dorsal 20
O
Degrees Degrees Degrees Degrees
Right Right
Inversion 30
O
Eversion 20
O
Plantar 40
O
Dorsal 20
O
Degrees Degrees Degrees Degrees
17. Wrist (radial, ulnar) 18. Wrist
Left Left
Radial 20
O
Ulnar 30
O
Extension 60
O
Flexion 60
O
Degrees Degrees Degrees Degrees
Right Right
Radial 20
O
Ulnar 30
O
Extension 60
O
Flexion 60
O
Degrees Degrees Degrees Degrees
19. Thumb (MP Joint) 20. Thumb (IP Joint)
Left Right Left Right
Flexion 60
O
Flexion 60
O
Flexion 80
O
Flexion 80
O
Degrees Degrees Degrees Degrees
DATE OF EXAMINATION EXAMINING PHYSICIAN’S SIGNATURE DATE OF REPORT
DSHS 13-585A (REV. 03/2014)
