
Departments of Rehabilitation Services and
Orthopaedic Surgery
Post-operative Rehabilitation Protocol
following Arthroscopic Hip Surgery for
Femoroacetabular Impingement
Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
2
Departments of Rehabilitation Services and Orthopaedic Surgery
Post-operative Rehabilitation Protocol following Arthroscopic
Hip Surgery for Femoroacetabular Impingement
Hip preservation surgery has become an increasingly common procedure to address a number of intra-
articular hip disorders including labral tears and femoroacetabular impingement. The number of hip
arthroscopies has increased greatly in the past decade. With this increase in number of surgeries have
come advancements and refinements in surgical techniques and increasingly complex considerations for
rehabilitation needs. Hip arthroscopies with labral repair and FAI correction are typically a successful
procedure with improvements in function (mHHS) and pain (VAS) typically seen in patients at 3, 6, and
12 months.
1
This rehabilitation protocol has been written with consideration of current surgical techniques and
avoidance of post-operative complications. Proper rehabilitation to avoid post-operative adhesions, and
appropriate weight bearing, along with manual therapy to manage post-operative impairments are all
important factors to consider in order to minimize the risk of adverse outcomes. The rationale for aspects
of this protocol is provided in the following paragraphs to increase clinician knowledge and
understanding. Since surgical techniques and procedures can vary for each patient, the clinician should
obtain and read the detailed operative report in order to gain a full understanding of what must be
considered in the post-operative period.
Consideration for tissue quality, bone quality, success of repair, and surgical technique should be assessed
and considered by the clinician. Avoidance of irritation and inflammation in the post-operative phase is
imperative. In the first phase of rehabilitation the focus is to protect the repair and avoid irritation. Gluteal
isometrics have been shown to be helpful in decreasing iliopsoas spasm and preventing anterior hip pain
and are therefore initiated in Phase I of the protocol.
2
One surgical technique that merits special consideration in post-operative rehabilitation is capsular
closure. Capsular closure is performed to restore the normal anatomy and minimize the risk of post-
operative issues with instability. With the capsular repair closure technique, it is necessary to protect and
limit hip external rotation and extension in the early healing phase to protect the integrity of the repair.
2
Capsular integrity has been correlated to improved outcomes after hip arthroscopy with FAI correction.
Additionally, the clinician should consider whether the labrum was repaired or reconstructed. If the labral
tissue is inadequate the surgeon may reconstruct the labrum using an autograft or allograft. This
information can be accessed in the operative note and will impact rehabilitation.
The evidence for manual therapy after hip arthroscopy is developing. It is thought that manual therapy to
the musculature and joints around the hip joint helps to decrease nociceptive input and address
impairments that develop in the pre and post-operative period, thereby decreasing abnormal forces to the
hip joint and improving patient outcome.
3
In order to protect the integrity of the labral repair or
reconstruction, capsular repair, and protect the fluid seal, long axis hip distraction should not be
performed until 8 weeks after labral repair and 12 weeks after labral reconstruction. Joint mobilizations of
grade III-IV should not be performed until 8 weeks postoperatively for the aforementioned reasons.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
3
Intra-articular adhesions have been recognized as a cause of surgical complications and pain. In an
analysis of possible risk factors for adhesions following hip arthroscopy, the following factors were
identified: age under 30, Modified Harris Hip score under 50, no microfracture performed, and
rehabilitation without circumduction.
4
Passive range of motion circumduction is incorporated into
treatment to minimize the development of post-operative adhesions.
Appropriate progression of weightbearing and gait retraining are essential aspects of rehabilitation. With
respect to weightbearing, the patient is initially limited to 20 lb of foot flat weight bearing in the
immediate post-operative phase. This limitation is due to the concern for appropriate healing of the labral
repair or reconstruction, and the capsular repair. Foot flat weight bearing is indicated to avoid achilles
irritation or shortening, irritation or shortening of hip flexors and stressing the labral repair or
reconstruction.
2
Patients should be counseled that they should not self select a non-weightbearing pattern
due to increased compressive forces to the hip joint due to hip flexor overactivity.
5
It is expected that the
gluteus medius will be inhibited post-operatively, therefore special attention should be paid to gait
retraining and proper crutch use to avoid contralateral hip drop when weightbearing on the operative leg
to avoid irritation to hip joint or repair.
5
Patients should be advised to continue with use of assistive
device for 6 weeks following surgery, or until their gait without device is without deviation. Allowing
unassisted gait with deviations will cause intraarticular irritation and overuse of accessory muscles around
the hip, possibly delaying the healing process.
6
Clinicians should have a good understanding of the expected progression and healing timeframes as
outlined in this protocol. If patient is not progressing appropriately, or if there is concern for post-
operative complications, the surgeon should be contacted and notified of the patient’s status.
Progression to the next phase of rehabilitation is based on achieving both Clinical Criteria
as well as Time Frames. Variance from this needs to be reviewed by surgeon.
The intent of this protocol is to provide clinicians with a guideline of the post-operative
rehabilitation for patients following arthroscopic hip surgery for femoroacetabular
impingement. This protocol is not intended to mandate the course of patient care. If there are
concerns regarding the patient’s clinical presentation. Please consult with the referring
physician prior to making adjustments to the protocol.
Procedures Performed:
☐
Acetabuloplasty
☐
Labral repair
☐
Labral debridement
☐
Labral reconstruction
☐
Chondroplasty
☐
Microfracture
☐
Fibrin glue repair
☐
Femoroplasty
☐
Capsular repair
☐
Iliopsoas Release
☐
Endoscopic Trochanteric Bursa Excision
☐
Endoscopic Abductor Repair
Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
4
Specific Case Complexity and Limitations:
☐Primary Procedure
☐Revision Procedure
Comments: ___________________________________________________________________
Pace of Protocol:
☐ROUTINE
☐LESS-AGGRESSIVE
Comments: ___________________________________________________________________
Weightbearing
Timeframe
Weightbearing
0-21 days
Partial weightbearing 20 lbs, step to pattern,
foot flat gait
3-6 weeks
Gradually increase weight bearing to WBAT
pain-free
6 weeks-8 weeks
Gradually wean from crutches, decrease to
single crutch, then without device as tolerated
Range of Motion
Hip
Motion
ROM Days 0-
21
ROM Week 3-6
ROM Week 6-12
ROM Week 12+
Flexion
0-90 degrees
Gradually increase
in pain free
manner
Gradually increase in
pain free manner
Gradually increase in
pain free manner
Extension
0 degrees, no
motion beyond
neutral
0-10 degrees
Gradually increase to
fully ROM as
tolerated
If full ROM not
attained, gradually
increase to full ROM
Abduction
0-30 degrees
0-45 degrees
Gradually increase to
full ROM as tolerated
If full ROM not
attained, gradually
increase to full ROM
External
Rotation
0-30 degrees
0-45 degrees
Gradually increase to
full ROM as tolerated
If full ROM not
attained, gradually
increase to full ROM
Internal
Rotation
0-30 degrees
0-45 degrees
Gradually increase to
full ROM as tolerated
Gradually increase to
full ROM as tolerated
Bracing: none

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
5
Phase I – Immediate Post-Surgical Phase (Day 1-28):
Initial Physical Therapy Evaluation to be scheduled 2 weeks after surgery. Patient instructed on initial
exercise program by surgical team.
Goals:
• Minimize pain and inflammation
• Protect integrity of repair
• Avoid post-operative adhesions
• Improve pain-free AROM/PROM within stated parameters
• Attain non-antalgic gait with use of device and appropriate weight bearing
• Address muscle inhibition
• Patient demonstrates independence with initial home exercise program
Precautions/Guidelines:
• No active straight-leg raises throughout rehabilitation period
• Avoid ambulation to fatigue or pain
• No active hip flexion for days 0-21, hip flexion should be self-assisted for functional mobility
• No Gr III-IV hip joint mobilization for 1
st
8 weeks
• No long axis hip distraction for first 8 weeks for labral repair
• No long axis hip distraction for first 12 weeks for labral reconstruction
• At all times pain and pinching in the hip joint should be avoided.
Throughout rehabilitation period every effort should be made to avoid:
o Hip flexor tendinitis
o Synovitis of operative joint
o Trochanteric bursitis
o Lower back pain or sacroiliac pain
Criteria for progression to the next phase:
• Minimal pain with ambulation
• Non-antalgic gait with use of crutches
• Minimal pain at rest
• Patient able to perform exercise program without increase in baseline pain
Patient compliant with weight bearing, home exercise program, and activity precautions

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
6
Treatment Strategies
Patient Education
Activity modification, bed mobility, positioning:
o No crossing of legs
o Avoid sitting for more than 30 minutes for first 2 weeks, vary position frequently
throughout the day. Gradually increase sitting time as tolerated after first 2 weeks.
o Sit with hip angle less than 90 degrees by sitting on a high chair or sit slightly reclined
o Prone lying 15 minutes 2-3 times per day to avoid hip flexor contracture
o Assist operative leg when getting in/out of bed, in/out of car and for all functional
mobility
o Consider obtaining raised toilet seat to avoid hip flexion greater than 90 degrees when
sitting on toilet
Manual Therapy
• Soft tissue mobilization as appropriate for quadriceps, hamstrings, TFL, gluteus medius, iliacus,
psoas, quadratus lumborum, lumbar paraspinals. Avoid suture sites until sutures removed and
incisions healed.
• Joint mobilizations to lumbar spine/sacrum to address lumbosacral dysfunction as indicated
• Gr I-II hip joint mobilizations for pain modulation as appropriate
• Initiate hip circumduction and passive IR as indicated below
PROM Hip Circumduction at 70° Hip Flexion
• Setup: The patient should begin lying on their
back. The provider should hold the patient's leg
just above the knee and under the heel, with the
patient's hip bent at a 70 degree angle.
• Movement: The provider should gently move
the patient's hip in a small clockwise motion,
then counterclockwise direction.
• Tip(s): The provider should only move the
patient's leg in a gentle, pain-free range of
motion.
PROM Hip Internal and External Rotation
• Setup: The patient should be lying on their
back with their legs straight. The provider
should grasp the patient's closest leg with one
hand on the thigh and the other on the shin.
• Movement: The provider should then gently
rotate the patient's leg inward approximately 30
degrees, then back to neutral, then outward
approximately 30 degrees keeping it on the bed
with the knee straight.
• Tip(s): The patient should stay as relaxed as
possible during the exercise.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
7
Gait Training
• Gait training with B axillary crutches maintaining indicated weight bearing
• Stair training with step to pattern, maintaining indicated weight bearing with rail/assistive device
Modalities
• Cryotherapy as needed
• Electrical stimulation for pain management as needed
Therapeutic Exercise:
Note: Dosage of exercises to be prescribed by physical therapist as appropriate.
Recommendations have been made when appropriate. Exercise instructions are written in patient
friendly language.
Supine Ankle Pumps
• Setup: Begin lying on your back with your legs
straight.
• Movement: Slowly pump your ankles by
bending and straightening them.
• Tip(s): Try to keep the rest of your legs relaxed
while you move your ankles.
Supine Quad Set
• Setup: Begin lying on your back on a bed or
flat surface with your legs straight.
• Movement: Tighten the muscles in the thigh of
your surgical leg as you straighten your knee.
Hold, then relax and repeat.
• Tip: Make sure to keep your toes pointing
toward the ceiling during the exercise. Try to
flatten the back of your knee towards the bed.
Supine Glute Set
• Setup: Begin lying on your back with your
hands resting comfortably.
• Movement: Tighten your buttock muscles, then
release and repeat.
• Tip(s): Make sure not to arch your low back
during the exercise or hold your breath as you
tighten your muscles.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
8
Transversus Abdominis Activation Hooklying
• Setup: Begin lying on your back with your
knees bent, feet resting on the floor, and your
fingers resting on your stomach just above your
hip bones.
• Movement: Tighten your abdominals, pulling
your navel in toward your spine and up. You
should feel your muscles contract under your
fingers. Hold this position, then relax and
repeat.
• Tip(s): Make sure to keep your back flat against
the floor and do not hold your breath as you
tighten your muscles
Prone Knee Flexion
• Setup: Begin lying face down with your legs
straight.
• Movement: Bend one knee, bringing your foot
as close as possible toward your body. Once a
gentle stretch is felt in the thigh, hold the
position for 10 seconds
• Tip: Make sure to keep your upper body
relaxed during the exercise and do not arch your
back as you bend your knee. This should not
cause pain.
Passive Supine Hip Flexor Stretch
• Setup: Lie flat on your back with one pillow
under your hips.
• Movement: relax all muscles and you will feel
a gentle stretch in the front of your operative
leg. Hold position for 10 minutes 3 x per day
Upright Stationary Bike
• Setup: Seat slightly elevated to minimize
excessive hip flexion
• Movement: Pedal with slow, controlled motion.
No resistance
• Tip(s): Start with 5 minutes, 2 x per day
gradually increase to 20 minutes 2 x per day

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
9
Phase II – Protection Phase (day 21-week 6):
Goals:
Progress weight bearing as appropriate per timeline
Progress ROM as tolerated per protocol
Minimize pain and inflammation
Protect integrity of repair
Avoid post-operative adhesions
Improve pain-free AROM/PROM within stated parameters
Attain non-antalgic gait with use of device and appropriate weight bearing
Address muscle inhibition
Patient demonstrates independence with initial home exercise program
Precautions/Guidelines:
• No active straight-leg raises for 8 weeks
• No active hip flexion for days 0-21, hip flexion should be active assisted for functional mobility
• No Gr III-IV hip joint mobilization for 1
st
6 weeks
• No long axis hip distraction for first 8 weeks for labral repair
• No long axis hip distraction for first 12 weeks for labral reconstruction
• At all times pain and pinching in the hip joint should be avoided.
• Avoid functional activities that cause hip pain
Avoid:
• Hip flexor tendinitis
• Synovitis of operative joint
• Trochanteric bursitis
• Lower back pain or sacroiliac pain
Treatment Strategies:
Gait Training
• Increase to weightbearing as tolerated with B axillary crutches and normalize gait pattern. Avoid
contralateral pelvic drop.
• As tolerated decrease to single crutch and normalize gait pattern.
• Wean from crutches by 6-8 weeks as tolerated.
Manual Therapy
• Soft tissue mobilization as appropriate for quadriceps, hamstrings, TFL, gluteus medius,
iliopsoas, quadratus lumborum, lumbar paraspinals
• Joint mobilizations to lumbar spine/sacrum to address lumbosacral dysfunction as indicated
• Gr I-II hip joint mobilizations as appropriate
• Scar mobilization to portal scars as appropriate
• PROM small range hip circumduction at 70 degrees flexion
• PROM log rolls to internal rotation/external rotation
• PROM all motions within allowed ROM
Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
10
Modalities
• Cryotherapy as needed
• Electrical stimulation for pain management as needed
Therapeutic Exercise
Continue with Phase I exercises as deemed appropriate by treating physical therapist
Phase IIa Exercises, Initiate beginning week 3 as tolerated:
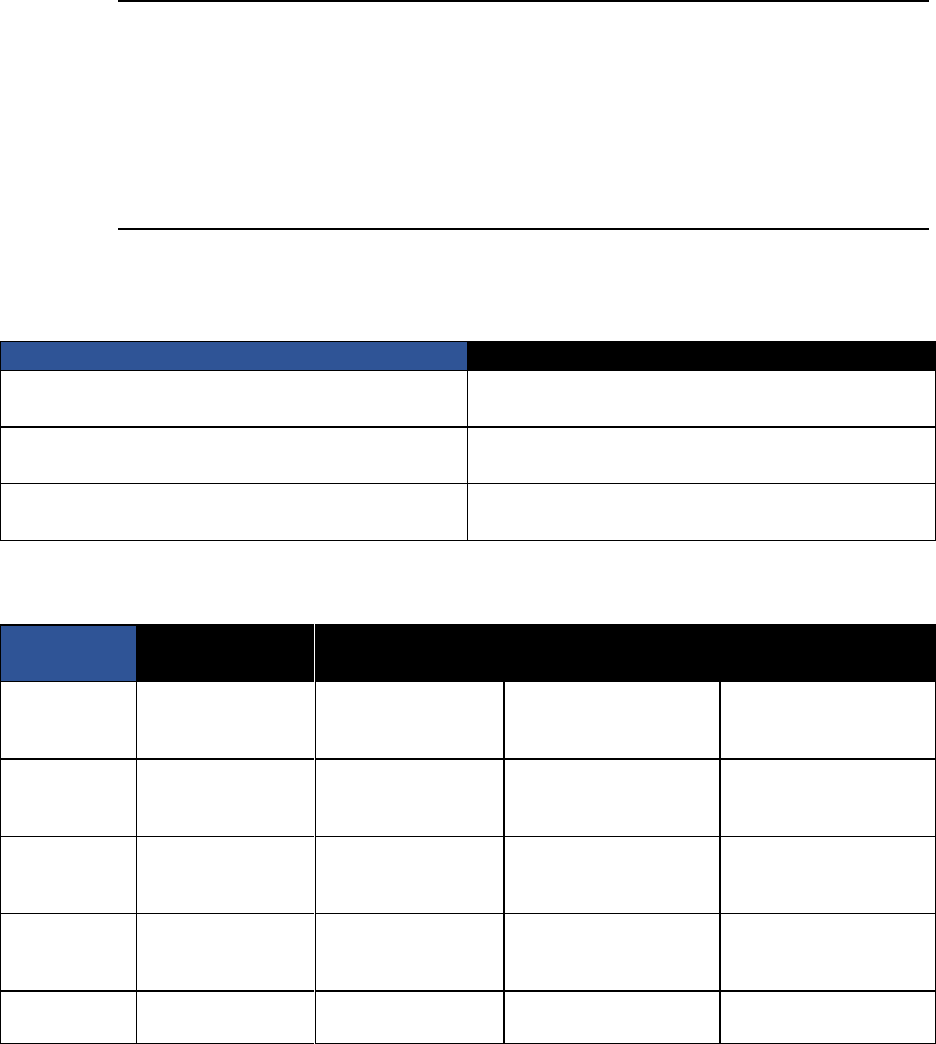
Quadruped Rocking
• Setup: begin on all fours, with your arms
positioned shoulder width apart and your knees
resting on a cushion.
• Movement: Slowly rock back and forth,
shifting your weight between your arms and
your legs.
• Tip: Make sure to keep your back straight and
chin tucked during the exercise. Maintain equal
weight distribution between both sides of your
body.
Hip rotations on stool IR/ER
• Setup: Begin in a standing upright position with
the knee of your affected leg resting on a
spinning stool or chair.
• Movement: Slowly turn your thigh inward so
your foot moves out to your side, then turn your
thigh outward so your foot moves in toward
your opposite leg, and repeat.
• Tip(s): Make sure to maintain an upright
posture and keep your balance during the
exercise.
Prone B hip IR
• Setup: Begin lying on your stomach.
• Movement: Bend both knees to a 90 degree
angle, tighten your abdominals, and let both of
your legs fall outward as far as you can. Bring
them back together, then repeat.
• Tip: Make sure to keep your abdominals tight
and do not let your low back arch during the
exercise

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
11
Hook-lying Lumbar Rotation (small range)
• Setup: Begin lying on your back with your
knees bent and feet resting on the floor
• Movement: Keeping your back flat, slowly
rotate your knees slightly toward one side, then
back to the other side.
• Tip: Make sure that your back and shoulders
stay flat on the floor.
Hip ABD/ADD Isometrics Hook-lying
• Setup: Begin lying on your back with your
knees bent, a ball between your knees, and a
belt looped around your knees.
• Movement: Gently press your knees out into
the belt, hold briefly, then squeeze your knees
into the ball, and hold briefly. Continue
alternating these movements.
• Tip: Make sure to continue breathing evenly.
There should be little to no movement during
the exercise.
Hook-lying Gluteal Set
• Setup: Begin lying on your back with your
knees bent and heels on the floor.
• Movement: Tighten your buttock muscles,
digging your heels into the floor, then release
and repeat.
• Tip: Make sure to keep your low back flat on
the floor during the exercise.
Standing Knee Flexion
• Setup: Begin in a standing upright position with
your hands resting on the back of a chair in
front of you for support.
• Movement: Slowly bend your operative knee,
lifting your foot as far as possible.
• Tip: Make sure to maintain your balance, stand
up straight, and do not bend at your waist
during the exercise.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
12
Quadruped Hip Extension Knee Slides for
Operative Leg w/TrA Activation
• Setup: Begin on all fours.
• Movement: Tighten your abdominal muscles,
pulling your navel in and up towards your spine.
Then slide the knee of your operative hip back
approximately 6 inches
• Tip: Your hips should stay level and your lower
leg should stay on the surface
Quadruped ‘Cat and Camel’ Exercise
• Setup: Begin on all fours with your arms
directly under your shoulders and knees bent 90
degrees.
• Movement: Slowly round your back up toward
the ceiling, then let it sag down to the floor
while looking up, and repeat.
• Tip: Make sure to use your entire back for the
motion and keep your movements slow and
controlled. You should not feel any pain in your
hip.
Supine Modified Thomas Stretch (operative leg
straight)
• Setup: Begin lying on your back with your legs
straight.
• Movement: Slowly lift your non-operative leg
and hug your knee toward your chest until you
feel a gentle stretch in the front of your hip of
the leg that is straight.
• Tip: Make sure to keep your abdominals
engaged and your opposite leg flat on the
surface.
Sidelying Piriformis Stretch
• Setup: Patient sidelying operative hip up, bend
knee of operative leg and support on 1-2
pillows.
• Movement: Should feel gentle stretch in gluteal
muscles without any pain or pinching in hip.
Cardiovascular Exercise:
Upright bike up to 20 minutes, 2 x per day with seat slightly elevated to minimize excessive hip
flexion, no resistance.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
13
Phase IIb Exercises, Initiate week 4 as tolerated:
Bilateral Bridging
• Setup: Begin lying on your back with your
knees bent and feet resting flat on the floor.
• Movement: Lift up through your pelvis as you
exhale, inhale and slowly lower back down, and
repeat.
• Tip: Make sure to engage your core, maintain a
neutral spine, and keep your upper back on the
floor during the exercise.
Standing Hip Abduction
• Setup: Begin in a standing upright position
with your hands resting on a counter.
• Movement: Lift your operative leg out to the
side and back on a diagonal, then return to the
starting position and repeat.
• Tip: Make sure to keep your moving leg
straight and do not bend or rotate your trunk
during the exercise. Use the counter to help you
balance as needed
Quadruped Hip Extension for Operative Leg
• Setup: Begin on all fours with your arms under
your shoulders and knees under your hips.
• Movement: Extend your operative leg straight
back so that it is parallel with the ground and
your toes are pointing toward the floor. Hold 2-
3 seconds), then return to the starting position.
• Tip: Make sure to keep your back straight and
maintain a gentle chin tuck during the exercise.
Do not let your trunk rotate while moving your
leg.
Standing Hip Extension to Neutral
• Setup: Begin in a standing with a slightly
flexed trunk in front of a counter or stable
surface for support.
• Movement: Tighten your buttock muscles and
slowly lift your operative leg backward in a
small motion. Return to the starting position
and repeat.
• Tip: Make sure to keep your operative knee
straight and keep your shoulders and hips
facing forward during the exercise. Do not bend
forward at your hips.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
14
Counter Plank
• Setup: Begin standing with your hands resting
on a table.
• Movement: Lean onto the table with both
hands as you keep your elbows straight and
walk your feet backward into a plank position.
Hold this position.
• Tip: Make sure to keep your back straight,
abdominals tight, and maintain a gentle chin
tuck throughout the exercise.
Single Leg Balance
• Setup: Begin in a standing upright position
with your feet together and arms resting at your
sides.
• Movement: Lift one non-operative foot off the
floor, balancing on your operative \leg.
Maintain your balance in this position.
• Tip: Try not to move your arms away from
your body or let your weight shift from side to
side.
Sidelying Clamshell in Neutral
• Setup: Begin lying on your side with your
knees bent at a 90 degree angle behind you.
• Movement: Lift your top knee upward. Hold
briefly, then slowly lower it back down and
repeat.
• Tip: Make sure not to let your hips fall
backward as you lift your leg.
Hip Internal Rotation Prone with Resistance
• Setup: Begin lying on your front with one knee
bent at a 90 degree angle and a resistance band
looped around that ankle, anchored on your
opposite side.
• Movement: Slowly rotate your bent leg
outward against the resistance, then bring it
back to the starting position and repeat.
• Tip: Make sure to keep your hips flat on the
ground during the exercise.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
15
Criteria for progression to the next phase:
• ROM within functional limits
• Ascend/descend 8-inch step with good pelvic control
• Good pelvic control during single-limb stance
• Normalized gait without an assistive device
• No joint inflammation, muscular irritation, or pain
• Good neuromuscular control and optimal muscle firing patterns
Phase III – Intermediate phase (week 6-12):
Goals:
• Performance of exercise program without hip pain
• Normalize hip ROM through appropriate ROM progression as outlined
• Good activation of hip musculature without evidence of muscle inhibition
• Normalized soft tissue of hip and lumbopelvic region
• Normal gait without evidence of gait deviations
Precautions:
• No extreme combined ROM (e.g. flexion/IR, flexion/ER)
• No plyometrics
• No running
• No squatting below 90 degrees
• Avoid painful ROM
• No pivoting on operative leg
• Avoid extreme combined hip ROM
• Avoid symptom provocation during ambulation, ADLs, or therapeutic exercise and avoid post-
activity soreness
• Avoid pinching in operative hip with range of motion exercises
Treatment Strategies:
Gait Training:
• Normalize gait without device.
• If patient has pain with ambulation continue to use 1 crutch and wean as tolerated.
Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
16
Manual Therapy:
• Soft tissue mobilization as appropriate for quadriceps, hamstrings, TFL, gluteus medius,
piriformis, quadratus lumborum, lumbar paraspinals
• Joint mobilizations to lumbar spine/sacrum to address lumbosacral dysfunction as indicated
• Gr III-IV hip joint mobilization as needed to address joint hypomobility
• Long axis hip distraction if needed beginning at 8 weeks for labral repair
• No long axis hip distraction for first 12 weeks for labral reconstruction
• PROM small range hip circumduction at 70 degrees flexion
• PROM log rolls to external and internal rotation
• PROM all motions within allowed ROM
Modalities
• Cryotherapy as needed
• Electrical stimulation for pain management as needed
Therapeutic Exercise:
Continue with Phase I and II exercises as deemed appropriate by therapist
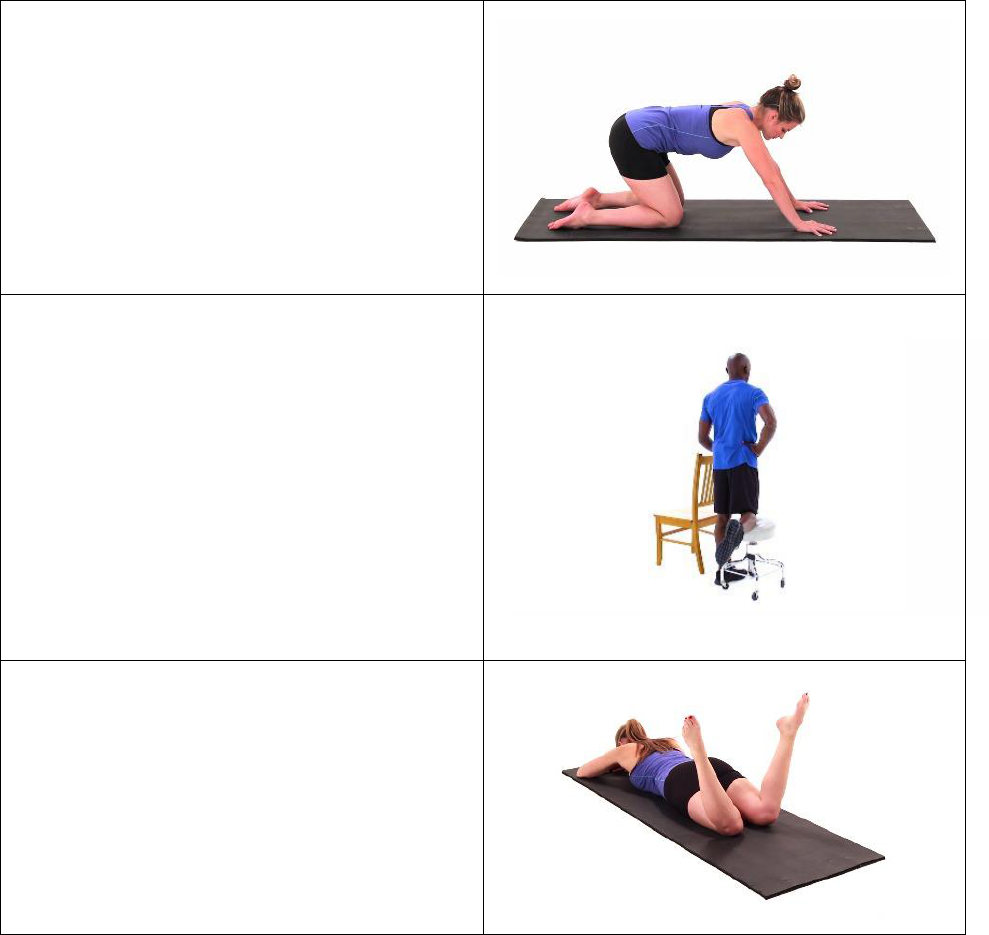
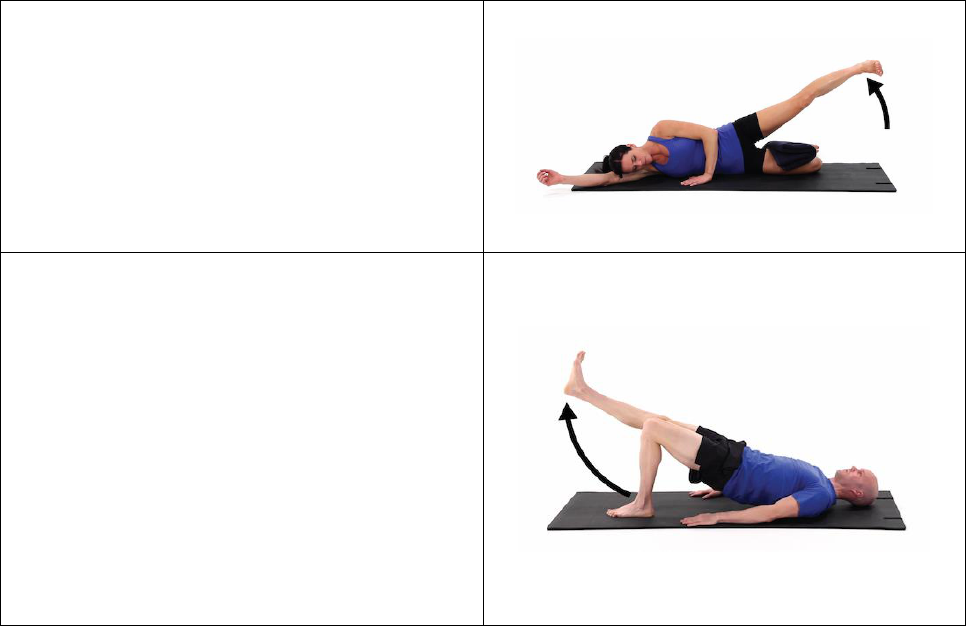
Sidelying Hip Abduction
• Setup: Begin lying on your non-operative side
with your bottom knee bent and your operative
knee lstraight.
• Movement: Raise your operative leg toward the
ceiling , keeping your knee straight.
• Tip: Make sure that your hips do not roll
forward or backward during the exercise.
Bridge with Alternating Leg Extension
Setup
• Setup: Begin lying on your back with your
arms resting at your sides, your knees bent, and
your feet flat on the ground.
• Movement: Tighten your abdominals and
slowly lift your hips off the floor into a bridge
position. Keeping your trunk stiff, straighten
your operative knee and hold.
• Tip: Make sure to maintain your balance during
the exercise and do not let your hips fall
towards the ground.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
17
Side Plank- modified (knees/forearm)
• Setup: Begin lying on yourwith your knees
bent, propped up on your forearm. Your elbow
should be directly under your shoulder.
• Movement: Engage your abdominal muscles
and raise your hips up into a side plank position,
keeping your knees on the ground. Hold this
position, then return to the starting position and
repeat on opposite side
• Tip: Make sure to keep your core engaged
during the exercise. Do not hold your breath or
let your hips roll forward, backward, or drop
towards the floor.
Modified Plank (knees/forearms)
• Setup: Begin lying on your stomach with your
elbows on the ground.
• Movement: Press yourself up into a plank
position, keeping your knees on the ground.
Return to the starting position and repeat.
• Tip: Make sure to keep your back straight in the
plank and look straight down between your
hands during the exercise.
Quadruped Alternating Leg Extension (progress
to opposite arm/leg as tolerated)
• Setup: Begin on all fours with your arms under
your shoulders and knees under your hips.
• Movement: Extend your operative leg straight
back so that it is parallel with the ground and
your toes are pointing toward the floor. Hold
briefly, then return to the starting position and
repeat with the opposite leg.
• Tip: Make sure to keep your back straight and
maintain a gentle chin tuck during the exercise.
Do not let your trunk rotate while moving your
leg
Partial Range Squats (gradually increase to 90
degree squats)
• Setup: Begin in a standing upright position,
with your feet slightly wider than shoulder
width apart.
• Movement: Bend your knees and hips into a
mini squat position, then straighten your legs
and repeat.
• Tip: Make sure to keep your back straight and
do not let your knees bend forward past your
toes.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
18
Prone Hip Extension
Setup
• Setup: Begin lying on your stomach with your
forehead resting on a towel roll. Position a
pillow under your lower abdomen and hips.
• Movement: Slowly lift your operative leg,
hold, then return to the starting position and
repeat with opposite leg
• Tip: Make sure to keep your leg straight and
focus on engaging your buttock muscles during
the exercise. Do not let your back arch or your
hips rotate side to side.
Single Leg Forward Weight Shifts (progressing
to Romanian dead lift)
• Setup: Begin in a standing position balancing
on your operative leg with your hands resting
on your waist.
• Movement: Lean forward by bending at your
hips and knee.
• Tip: Make sure to keep your back straight and
chin tucked
Lateral Band Walk
• Setup: Begin standing upright with a resistance
band looped around your thighs, just above your
knees. Bend your knees slightly so you are in a
mini squat position.
• Movement: Slowly step sideways, maintaining
tension in the band.
• Tip: Make sure to keep your feet pointing
straight forward and do not let your knees
collapse inward during the exercise.
Backwards Monster Walk With Band
• Setup: Begin in a standing upright position with
a resistance band looped around your ankles.
• Movement: Slightly bend your knees into a
mini squat position. Step diagonally backward
with one foot, then slowly bring your feet
together. Repeat in the opposite direction.
• Tip: Make sure to keep your chest upright and
do not bend your knees forward past your toes.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
19
Banded Hip Clamshell
• Setup: Begin by lying on your non-operative
side with your knees bent 90 degrees, hips and
shoulders stacked, and a resistance loop secured
around your legs.
• Movement: Raise your operative knee away
from the bottom one, then slowly return to the
starting position.
• Tip: Make sure not to roll your hips forward or
backward during the exercise.
Single Leg Balance with Clock Taps
• Setup: Begin in a standing upright position.
Imagine you are standing in the middle of a
clock.
• Movement: Bend your legs slightly, then reach
forward with non-operative(?) foot toward 12
o'clock, then bring it back to the starting
position and reach toward 3 or 9 o'clock.
Continue, reaching toward 6 o'clock, and repeat.
• Tip: Make sure to keep your hips level as you
reach with your leg, and do not let your
standing knee collapse inward
Single Leg Balance with Hip ABD and Band
Resistance
• Setup: Begin in a standing upright position,
holding onto a chair for support, with a
resistance loop around your ankles.
• Movement: Lift your operative leg off the
ground and pulse leg a small mount straight out
to your side. Continue this motion this motion
without letting your foot touch the ground.
• Tip: Make sure to keep your abdominals tight
and hips level during the exercise.
Single Leg Balance with Hip Ext and Band
Resistance
• Setup: Begin in a standing upright position,
holding onto a chair for support, with a
resistance loop around your ankles.
• Movement: Lift your operative leg off the
ground and move it straight backward a small
motion. Continue this pulsing the leg without
letting your foot touch the ground.
• Tip(s): Make sure to keep your abdominals
tight and hips level during the exercise.

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
20
Paloff Press
• Setup: Begin in a standing upright position
holding a resistance band in both hands that is
anchored at your side.
• Movement: Press your arms straight forward.
Hold briefly, then bring your arms back in and
repeat. Repeat for opposite side.
• Tip(s): Do not allow trunk to rotate
Standing IT Band Stretch
• Setup: Begin in a standing upright position with
one leg crossed over the other.
• Movement: Move the hip of your operative leg
to be stretched out to the side and reach your
arm overhead to the opposite side. Repeat on
opposite side.
• Tip: Make sure to avoid twisting or rotating
your body during the exercise.
Lower extremity stretching as indicated by patient impairments.
Cardiovascular Exercise:
• Upright stationary bicycle: gradually increase time and resistance as tolerated
• Elliptical training: pedaling forward and backward if pain-free, gradually increase time and
resistance as tolerated
• Swimming: initiate flutter kick as tolerated, avoid frog kicking
Criteria for progression to the next phase:
• ROM within normal limits pain-free
• Alternate Ascend/Descend 8-inch step with good pelvic control no UE support
• Good pelvic control during single-limb stance and dynamic balance
• Normalized gait pain-free without an assistive device
• No Pain at rest, ADL/IADL nor walking
• Strength of operative hip 75% of contralateral hip
• No joint inflammation, muscular irritation, or pain
• Good neuromuscular control and optimal muscle firing patterns
Phase IV – Advanced strengthening phase (week 12-16):
Goals:
• Independent home exercise program
• Optimize ROM
• >=4/5 LE strength, >=4/5 trunk strength
• Improved dynamic balance
• Pain-free ADL
• Pain-free hip flexion with ADLs and functional mobility

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
21
Precautions:
• No extreme combined ROM (e.g. flexion/IR, flexion/ER)
• No plyometrics
• No running
• No squatting below 90 degrees
• Avoid painful ROM
• Avoid extreme combined hip ROM
• No symptom provocation during ambulation, ADLs, or therapeutic exercise
• Avoid pinching in operative hip with range of motion exercises
Treatment Strategies:
Manual Therapy:
• Soft tissue mobilization as appropriate for quadriceps, hamstrings, TFL, gluteus medius,
piriformis, quadratus lumborum, lumbar paraspinals
• Joint mobilizations to lumbar spine/sacrum to address lumbosacral dysfunction as
indicated
• Gr III-IV hip joint mobilization as needed to address joint hypomobility
• Long axis hip distraction if needed beginning at 8 weeks for labral repair
• Long axis hip distraction if needed beginning at 12 week for labral reconstruction
Modalities
• Cryotherapy as needed
• Electrical stimulation for pain management as needed

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
22
Therapeutic Exercise:
Progressive LE and core exercises-
progress exercises from prior phases by
increasing challenge and resistance
Advanced balance exercises as
appropriate for sport or desired recreation
Sport specific plyometrics and agility
exercises as appropriate
Progress core strengthening as deemed
appropriate by therapist
Cardiovascular Exercise:
• Upright stationary bicycle: gradually increase time and resistance as tolerated
• Elliptical training: pedaling forward and backward if pain-free, gradually increase time and
resistance as tolerated
• Swimming: initiate flutter kick as tolerated, avoid frog kicking
Criteria for progression to the next phase:
• Y Balance Test Limb symmetry index 80% of uninvolved side
• Strength of operative hip 90% of uninvolved side
• Perform progressed exercise program without pain
• No joint inflammation, muscular irritation, or pain

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
23
Phase V – Return to activity phase (week 16+):
Please note: Individuals who do not engage in higher level activities may not need to progress to
advanced and sport specific activities.
Goals:
• Progress to sport specific training without pain
• Progress to jogging pain free when cleared by surgeon
• Independent home exercise program
• Optimize ROM
• 5/5 LE strength, >=4/5 trunk strength
• Normal Muscle Length of B LE
• Good, dynamic unilateral balance of operative extremity
• Pain-free with all activities
Precautions:
• Avoid pain in hip joint with functional activities or exercises
• If post-exercise joint pain or limping occurs, activity level should be decreased
• Avoid joint inflammation
• Focus on quality of movement and exercise
Treatment Strategies:
Manual Therapy:
• Soft tissue mobilization as appropriate for quadriceps, hamstrings, TFL, gluteus medius,
piriformis, quadratus lumborum, lumbar paraspinals
• Joint mobilizations to lumbar spine/sacrum to address lumbosacral dysfunction as
indicated
• Gr III-IV hip joint mobilization as needed to address joint hypomobility
• Long axis hip distraction as needed for labral repair or reconstruction
Modalities
• Cryotherapy as needed
• Electrical stimulation for pain management as needed
Therapeutic Exercises:
Progress strength, proprioception, dynamic balance, agility, and power to address sport specific
demands. Sport specific retraining as tolerated.
Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
24
Cardiovascular Exercise:
• Upright stationary bicycle: gradually increase time and resistance as tolerated
• Elliptical training: pedaling forward and backward if pain-free, gradually increase time
and resistance as tolerated
• Swimming: gradually progress time and swimming strokes at tolerated
• Jogging: initiate at 16-18 weeks as indicated by referring surgeon and patient status
Outcome Measures:
• Hip Outcome Score (HOS) has been validated in the hip arthroscopy population and is an
appropriate outcome measure. (Enseki)
• If unavailable Lower Extremity Functional Scale (LEFS) may be used.
Criteria for discharge from skilled therapy:
• Cross over triple hop for distance 90% of uninvolved side
• Y Balance Test Limb symmetry index 80% of uninvolved side
• Patient able to jog 30 minutes
• Patient able to perform sport specific drills without pain
• Good neuromuscular control and optimal muscle firing patterns

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
25
This protocol has been written utilizing the available literature, clinical experience of physical
therapists, and surgeon experience and preference. The Department of Rehabilitation Services at
Brigham & Women’s Hospital has accepted this protocol as our standard protocol for the
management of patients following arthroscopic hip surgery for femoroacetabular impingement.
If you have any questions regarding this protocol, please contact:
Dawn Rogers-Hyde, PT, OCS
or
Clare Safran-Norton, PT, PhD, OCS
If you have any concerns regarding your patient, please contact:
Richard M. Wilk, MD, FAAOS
Chief, Hip Preservation Service
Sports Medicine, Shoulder & Knee Surgery
Brigham and Women’s Hospital
Clinical Instructor
Harvard Medical School
Office: 617-732-5352 | Mobile: 781-504-9191
brighamandwomens.org
Authors: Reviewers:
Dawn Rogers-Hyde, PT, OCS Richard M. Wilk, MD, FAAOS
Clare Safran-Norton, PT, PhD, OCS Madhuri Kale, PT, OCS

Arthroscopic Hip Surgery for Femoroacetabular Impingement
Copyright © 2020 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
26
References
1. Dippmann, C., Thorborg, K., Kraemer, O., Winge, S., Palm, H., & Hölmich, P. (2014). Hip
arthroscopy with labral repair for femoroacetabular impingement: short-term outcomes. Knee Surgery,
Sports Traumatology, Arthroscopy, 22(4), 744-749.
2. Kuhns, B. D., Weber, A. E., Batko, B., Nho, S. J., & Stegemann, C. (2017). A four-phase physical
therapy regimen for returning athletes to sport following hip arthroscopy for femoroacetabular
impingement with routine capsular closure. International journal of sports physical therapy, 12(4), 683.
3. Heerey, J., Risberg, M. A., Magnus, J., Moksnes, H., Ødegaard, T., Crossley, K., & Kemp, J. L.
(2018). Impairment-based rehabilitation following hip arthroscopy: postoperative protocol for the HIP
ARThroscopy International Randomized Controlled Trial. journal of orthopaedic & sports physical
therapy, 48(4), 336-342.
4. Willimon, S. C., Briggs, K. K., & Philippon, M. J. (2014). Intra-articular adhesions following hip
arthroscopy: a risk factor analysis. Knee Surgery, Sports Traumatology, Arthroscopy, 22(4), 822-825.
5. Enseki, K. R., & Kohlrieser, D. (2014). Rehabilitation following hip arthroscopy: an evolving
process. International journal of sports physical therapy, 9(6), 765.
6. Enseki, K. R., Martin, R., & Kelly, B. T. (2010). Rehabilitation after arthroscopic decompression for
femoroacetabular impingement. Clinics in sports medicine, 29(2), 247-255.
