
Suggested citation: European Centre for Disease Prevention and Control. Invasive pneumococcal disease. In: ECDC. Annual
epidemiological report for 2018. Stockholm: ECDC; 2020.
Stockholm, September 2020
© European Centre for Disease Prevention and Control, 2020. Reproduction is authorised, provided the source is acknowledged.
aged
SURVEILLANCE REPORT
Invasive pneumococcal disease
Annual Epidemiological Report for 2018
Key facts
In 2018, 24 663 confirmed cases of invasive pneumococcal disease (IPD) were reported in the EU/EEA.
The crude notification rate was 6.4 cases per 100 000 population, continuing the increasing trend
observed since 2014.
Age-specific rates were highest in adults aged 65 years or older (18.7 confirmed cases per 100 000
population) and in infants under one year (14.4 confirmed cases per 100 000 population), with higher
rates reported in males than females.
The 10 most common serotypes were 8, 3, 19A, 22F, 12F, 9N, 15A, 10A, 23B and 6C (in order of
decreasing frequency), accounting for 70% of typed isolates.
Of all the cases under five years of age, 75% were caused by a serotype not included in any
pneumococcal conjugate vaccine (PCV).
Among cases aged 65 years and over, 73% were caused by serotypes included in the 23-valent
polysaccharide vaccine and 29% were caused by serotypes in the 13-valent PCV.
Methods
This report is based on data for 2018 retrieved from The European Surveillance System (TESSy) on 11 March 2020.
TESSy is a system for the collection, analysis and dissemination of data on communicable diseases. For a detailed
description of methods used to produce this report, refer to the
Methods
chapter [1].
An overview of the national surveillance systems is available online [2].
Additional data on the disease are accessible from ECDC’s online
Surveillance atlas of infectious diseases
[3].
In 2019, 29 Member States reported data on invasive pneumococcal disease (IPD). Twenty-four Member States used
the EU-2008/2012 case definition. One Member State used the EU-2002 case definition and for four Member States,
the case definition was unknown/not specified. The EU-2008/2012 case definition differs from the EU-2002 case
definition by excluding possible and probable cases and including detection of
S. pneumoniae
antigens at a normally
sterile site as the definition of a confirmed case [4].
National IPD surveillance systems were heterogeneous. Of the 29 countries reporting data, 22 countries conducted
surveillance with compulsory reporting and national coverage. Six countries had voluntary sentinel systems. The
Netherlands and Spain had surveillance systems that covered 25% and 80% of the national population respectively.
The population coverage of the Belgian surveillance system was unknown, so notification rates were not calculated.
IPD data from France were reported through two different systems: one relying on reports from physicians (FR-
EPIBAC) and the other based on laboratories (FR-PNEUMO-NRL). Data reported from FR-PNEUMO-NRL were used to
analyse serotype and antimicrobial susceptibility, while data reported from FR-EPIBAC provided epidemiological and
clinical information. Germany had a voluntary laboratory-based surveillance system and did not report data to ECDC
[5]. All countries except Belgium, Bulgaria, Croatia and Poland reported case-based data [2].

Annual epidemiological report for 2018 SURVEILLANCE REPORT
2
Epidemiology
In 2018, 24 663 confirmed cases of IPD were reported by 29 countries. The crude notification rate was 6.2 cases
per 100 000 population (Table 1). The United Kingdom reported the highest number of confirmed cases, followed
by France. The highest notification rates were reported in Denmark, Ireland, Finland, the Netherlands, Norway,
Slovenia and Sweden (Table 1, Figure 1). Many countries in the southern and eastern parts of the EU had low
notification rates.
Table 1. Distribution of confirmed invasive pneumococcal disease cases and rates per 100 000
population by country, EU/EEA, 2014–2018
Country
2014
2015
2016
2017
2018
Number
Rate
Number
Rate
Number
Rate
Number
Rate
Confirmed
cases
Rate
ASR
Reported
cases
Austria
322
3.8
422
4.9
439
5.0
545
6.2
611
6.9
6.4
611
Belgium
1 192
-
1 362
-
1 329
-
1 461
-
1 553
-
-
1 553
Bulgaria
21
0.3
31
0.4
35
0.5
34
0.5
24
0.3
0.3
24
Croatia
27
0.6
24
0.6
14
0.3
16
0.4
21
0.5
-
21
Cyprus
14
1.6
9
1.1
5
0.6
20
2.3
17
2.0
2.0
18
Czech
Republic
337
3.2
413
3.9
323
3.1
389
3.7
535
5.0
4.7
535
Denmark
725
12.9
807
14.3
731
12.8
771
13.4
799
13.8
12.7
799
Estonia
12
0.9
24
1.8
30
2.3
45
3.4
43
3.3
3.1
43
Finland
703
12.9
815
14.9
817
14.9
822
14.9
761
13.8
12.5
761
France
3 184
6.6
3 299
6.9
3 800
7.9
3 862
8.0
3 862
7.7
7.2
3 862
Germany
.
.
.
.
.
.
.
.
.
.
.
.
Greece
30
0.3
55
0.5
52
0.5
52
0.5
42
0.4
0.4
42
Hungary
150
1.5
189
1.9
226
2.3
268
2.7
331
3.4
3.1
331
Iceland
24
7.4
25
7.6
19
5.7
27
8.0
30
8.6
9.7
30
Ireland
342
7.4
370
7.9
378
8.0
414
8.7
514
10.6
11.8
514
Italy
957
1.6
1 248
2.1
1 529
2.5
1 705
2.8
1 555
2.6
2.2
1 555
Latvia
51
2.5
87
4.4
65
3.3
75
3.8
76
3.9
3.5
76
Liechtenstein
.
.
.
.
.
.
.
.
.
.
.
.
Lithuania
6
0.2
25
0.9
56
1.9
76
2.7
65
2.3
2.1
65
Luxembourg
1
0.2
0
0.0
0
0.0
1
0.2
1
0.2
0.2
1
Malta
22
5.1
9
2.0
11
2.4
18
3.9
31
6.5
6.2
31
Netherlands
546
13.0
667
15.8
631
14.9
616
14.4
688
16.0
14.8
693
Norway
569
11.1
522
10.1
599
11.5
560
10.6
581
11.0
11.0
581
Poland
705
1.9
979
2.6
967
2.5
1 192
3.1
1 350
3.6
-
1 350
Portugal
-
-
142
1.4
163
1.6
301
2.9
397
3.9
3.5
420
Romania
62
0.3
53
0.3
50
0.3
50
0.3
74
0.4
0.4
74
Slovakia
78
1.4
68
1.3
59
1.1
100
1.8
98
1.8
1.8
98
Slovenia
276
13.4
332
16.1
281
13.6
328
15.9
276
13.4
12.2
276
Spain
1 856
5.0
2 037
5.5
1 825
4.9
2 443
6.6
2 365
6.3
5.9
2 365
Sweden
1 159
12.0
1 314
13.5
1 351
13.7
1 367
13.7
1 408
13.9
12.9
1 408
United
Kingdom
4 157
6.5
5 796
8.9
6 205
9.5
6 333
9.6
6 555
9.9
9.5
6 555
EU/EEA
17 528
4.8
21 124
5.6
21 990
5.8
23 891
6.2
24 663
6.4
6.2
24 692
Source: Country reports.
ASR: age-standardised rate
.: no data reported
-: no notification rate calculated.
Note: The national coverage in France is calculated based on the entire French population. However, the actual surveillance
system only collects data from metropolitan France, thus the coverage of the surveillance system shown here for France is
underestimated.
The number of cases presented from France in Table 1 was collected through the FR-EPIBAC surveillance system.

SURVEILLANCE REPORT Annual epidemiological report for 2018
3
Figure 1. Distribution of confirmed invasive pneumococcal disease cases per 100 000 population by
country, EU/EEA, 2018
Source: Country reports from Austria, Bulgaria, Croatia, Cyprus, the Czech Republic, Denmark, Estonia, Finland, France, Greece,
Hungary, Iceland, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Norway, Poland, Portugal, Romania,
Slovakia, Slovenia, Spain, Sweden and the United Kingdom.
Age and gender distribution
In 2018, IPD was predominantly reported in the elderly and in infants, with 18.7 confirmed cases per 100 000
population in adults aged 65 years and above, and 14.4 confirmed cases per 100 000 population in infants under
one year (Figure 2). The rates of disease were the lowest in persons aged 5–24 years (0.8 confirmed cases per
100 000 population). The notification rate was higher in males in all age groups. The overall male-to-female ratio
was 1.2:1.

Annual epidemiological report for 2018 SURVEILLANCE REPORT
4
Figure 2. Distribution of confirmed invasive pneumococcal disease cases per 100 000 population, by
age and gender, EU/EEA, 2018
Source: Country reports from Austria, Bulgaria, Croatia, Cyprus, the Czech Republic, Denmark, Estonia, Finland, France, Greece,
Hungary, Iceland, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Norway, Poland, Portugal, Romania,
Slovakia, Slovenia, Spain, Sweden and the United Kingdom.
Seasonality and trend
The seasonal distribution of IPD cases followed a pattern similar to many other respiratory diseases. Case numbers
were lowest during summer, increased rapidly with the onset of autumn, and peaked during the winter months
(Figures 3, 4). There was an increasing trend in reported cases during the period 2014–2017 (Figure 4). The
notification rate increased to 6.2 cases per 100 000 population in 2017, compared to 4.8 in 2014 (Table 1).
Figure 3. Distribution of confirmed invasive pneumococcal disease cases by month, EU/EEA, 2014–2018
Countries included: Austria, Cyprus, Czechia, Denmark, Estonia, Finland, France, Greece, Hungary, Ireland, Iceland, Italy, Latvia,
Lithuania, Malta, the Netherlands, Norway, Poland, Romania, Slovenia, Slovakia, Spain, Sweden and the UK.

SURVEILLANCE REPORT Annual epidemiological report for 2018
5
Figure 4. Distribution of confirmed invasive pneumococcal disease cases by month, EU/EEA, 2018
and 2014–2017
Countries included: Austria, Cyprus, Czechia, Denmark, Estonia, Finland, France, Greece, Hungary, Ireland, Iceland, Italy, Latvia,
Lithuania, Malta, the Netherlands, Norway, Poland, Romania, Slovenia, Slovakia, Spain, Sweden and the UK.
Serotype
Data on serotype were reported from 16 371 sampled cases in EU/EEA countries in 2018. The ten most common
serotypes were 8, 3, 19A, 22F, 12F, 9N, 15A, 10A, 23B, 6C, 11A (in order of decreasing frequency), accounting for
70% of all cases with a known serotype in 2018.
The distribution of these serotypes during the period 2014–2018 is presented in Figure 5 for countries that
reported serotyping data consistently for each year of the reporting period. When comparing distribution in 2018
and 2014, there was a sharp increase in serotypes 8 and 3 during the reporting period (by 184% and 131%
respectively).

Annual epidemiological report for 2018 SURVEILLANCE REPORT
6
Figure 5. Distribution of confirmed serotyped cases of invasive pneumococcal disease: most common
S. pneumoniae
serotypes in 2018
1
Source: Country reports from Austria, the Czech Republic, Denmark, Estonia, Finland, France, Greece, Hungary, Iceland, Ireland,
Italy, Latvia, Lithuania, the Netherlands, Norway, Portugal, Slovakia, Slovenia, Spain, Sweden and the United Kingdom.
˄: covered by PPV23.
†: covered by PCV13 and PPV23
The distribution of serotypes varied according to the age groups affected. The five most common serotypes in each
age group are presented in Table 2. For cases under one year of age, serotypes 8, 10A, 3, 19 A and 24F were
predominant. Serotypes 24F, 3 and 19A were the most common in the 1-4 year age group. Serotype 8 was the most
common for those aged 564 years. Serotype 8 and 3 were the most common serotypes for those over 25 years.
Serotype 19A was among the top five serotypes in all age groups.
In 2018, of all cases in children aged under five years, 7% were caused by a PCV7 serotype (4, 6A, 6B, 9V, 14, 18C,
19F and 23F), 1% by a PCV10/non-PCV7 serotype (1, 5 and 7F), 16% by a PCV13/non-PCV10 serotype (3 and 19A)
and 75% by a serotype not included in any current PCV vaccine. In 2018, among cases aged 5–64 years, 6% were
caused by a PCV7 serotype, 2% by a PCV10/non-PCV7 serotype, 20% by a PCV13/non-PCV10 serotype and 71% by
non-PCV serotypes. Among adults aged 65 years and over, 71% were caused by PPV23 serotypes and 29% were
caused by PCV13 serotypes.
In the under-fives, for countries that reported serotype data consistently each year from 2013–2017, there was a
decrease in the proportion of PCV7 serotypes from 14% to 6%, and in the proportion of PCV10/non-PCV7 serotypes
from 5% to 1% (Figure 6). There was a slight increase in the proportion of PCV13/non-PCV10 serotypes between
2013 and 2017 (13% to 16% respectively) and an increase in non-PCV serotypes from 68% to 75%.
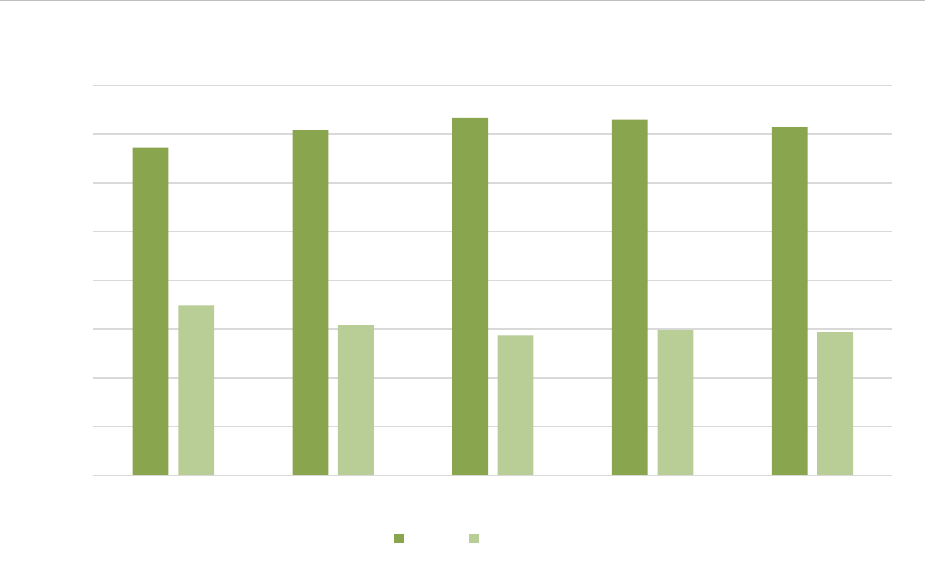
In those aged 65 years and above, in countries that reported serotype data consistently each year during the period
2014–2018, there was a decrease in the proportion of PCV13 serotypes from 35% to 29% (Figure 7). The proportion
caused by PPV23 serotypes fluctuated between 67% and 73%. The proportion caused by PPV23/non-PCV13
serotypes (2, 8, 9N, 10A, 11A, 12F, 15B, 17F, 20, 22F and 33F) increased from 34% in 2013 to 40% in 2018.
1
Different serotypes are covered by different vaccines, as follows:
7-valent pneumococcal conjugate vaccine (PCV7): 4, 6B, 9V, 14, 18C, 19F and 23F
10-valent pneumococcal conjugate vaccine (PCV10): 4, 6B, 9V, 14, 18C, 19F, 23F, 1, 5 and 7F
13-valent pneumococcal conjugate vaccine (PCV13): 4, 6B, 9V, 14, 18C, 19F, 23F, 1, 5, 7F, 3, 6A and 19A.
Although serotype 6A is included in PCV13 and not in PCV7, it is considered to be a PCV7 serotype in the
analysis due to documented cross-protection provided by the serotype 6B antigen in PCV7.
23-valent pneumococcal polysaccharide vaccine (PPV23): 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14,
15B, 17F, 18C, 19A, 19F, 20, 22F, 23F and 33F.
0
2
4
6
8
10
12
14
16
18
20
8^ 3^ 19A^ 22F^ 12F^ 9N^ 15A 10A^ 23B 6C
2014 2015 2016 2017 2018

SURVEILLANCE REPORT Annual epidemiological report for 2018
7
Table 2. Proportion of the five most frequent serotypes of
S. pneumoniae
from confirmed cases of
invasive pneumococcal disease, by age group, 2018
Age group (years)
<1
1–4
5–14
15–24
25–44
45–64
≥65
Five most common
serotypes by age
group (% of all
cases per age
group)
8 (11.0%)
24F
(12.2%)
8 (10%)
8 (32.5%)
8 (28%)
8 (21.5%)
3 (14.7%)
10A (8.4%)
3 (9.2%)
19A (8.3%)
12F (10%)
3 (11.3)
3 (14.6%)
8 (14.0%)
3 (7.6%)
19A (8.4%)
12F (7.5%)
19A (8.7%)
12F (9.5%)
19A (7.2%)
19A (7.6%)
19A (7.0%
12F (7.3%)
23B (7.1%)
3 (7.3%)
19A (7.6%)
12F (7.1%)
22F (7.4%)
24F (6.5%)
23B (7.3%)
3 (5%)
33F (4.7%)
9N (4.5%)
22F (6.4%)
9N (5.4%)
Source: Country reports from Austria, the Czech Republic, Denmark, Estonia, Finland, France, Greece, Hungary, Iceland, Ireland,
Italy, Latvia, Lithuania, the Netherlands, Norway, Portugal, Slovakia, Slovenia, Spain, Sweden and the United Kingdom.
* Number of cases for which information on serotype and age was available : <1 year: n=368; 1–4 years: n=606; 5–14 years:
n= 240; 15–24 years: n=231; 25–44 years: n=1 632; 45–64 years: n=3 481; ≥65 years: n=8 864.
Figure 6. Confirmed cases of invasive pneumococcal disease aged <5 years: serotype distribution by
PCV type and year, 2014–2018
Source: Country reports from Austria, the Czech Republic, Denmark, Estonia, Finland, France, Greece, Hungary, Iceland, Ireland,
Italy, Latvia, Lithuania, the Netherlands, Norway, Portugal, Slovakia, Slovenia, Spain, Sweden and the United Kingdom.
*: Although serotype 6A is included in PCV13 and not in PCV7, for the purposes of this analysis it is considered a PCV7 serotype
due to documented cross-protection provided by the serotype 6B antigen in PCV7.
PCV7 serotypes: 4, 6A, 6B, 9V, 14, 18C, 19F and 23F
PCV10non7 serotypes: 1, 5 and 7F
PCV13non10 serotypes: 3 and 19A
Non-PCV serotypes: all remaining serotypes.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2014 2015 2016 2017 2018
Percentage (%)
PCV10/non-PCV7 PCV7 PCV13/non-PCV10 non-PCV
Annual epidemiological report for 2018 SURVEILLANCE REPORT
8
Figure 7. Confirmed cases of invasive pneumococcal disease aged ≥65 years: serotype distribution by
pneumococcal vaccine type and year, 2013–2017
Source: Country reports from Austria, the Czech Republic, Denmark, Estonia, Finland, France, Greece, Hungary, Iceland, Ireland,
Italy, Latvia, Lithuania, the Netherlands, Norway, Portugal, Slovakia, Slovenia, Spain, Sweden and the United Kingdom.
*: PCV13 serotypes: 1, 3, 5, 4, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, 23F; PPV23 serotypes: 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A,
12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F, 33F.
Antimicrobial susceptibility
Antimicrobial susceptibility data were based on the reporting of Sensitive, Intermediate and Resistant (SIR) and
Minimum Inhibitory Concentration (MIC) data. MIC data were converted to SIR data based on EUCAST
breakpoints. Ten countries reported antimicrobial susceptibility data in 2018. Penicillin susceptibility data were
reported for 5 001 of all IPD cases. Of these, 82% (n=4 081) were reported as sensitive, 16% (n=825) as
intermediate and 2% (n=95) as resistant. Erythromycin susceptibility data were reported for 5 003 of all IPD cases.
Of these, 82% (n=4 090) were reported as sensitive, 0.6% (n=29) as intermediate and 18% (n=883) as resistant.
Cephalosporin susceptibility data were reported for 4 112 of all IPD cases. Of these, 93% (n=3 815) were reported
as sensitive, 6% (n=262) as intermediate and 1% (n=31) as resistant.
Clinical presentation
Clinical presentation was known for 8 423 (34%) of all cases. Of these, septicaemia was reported in 2 964 cases
(35%), bacteraemic pneumonia in 3 611 (43%), meningitis in 1 627 (19%), meningitis and septicaemia in 56 (1%)
and a further 165 (2%) had other clinical presentations.
The most common clinical presentation in <1 year and 5–14-year-olds was meningitis; in 1–4 year olds
septicaemia and bacteraemic pneumonia were equally frequent and among those aged 15 years and over,
bacteraemic pneumonia was the most common clinical presentation.
Outcome
Among 10 486 cases with known outcome (42%) in 2018, 1 609 (15%) died. The case fatality rate increased with
age: 4% in children <15 years of age, 6% in 15–44-year-olds, 11% in 45–64-year-olds and 21% in those aged 65
years and above.
0
10
20
30
40
50
60
70
80
2014 2015 2016 2017 2018
Percentage (%)
PPV23 PCV13

SURVEILLANCE REPORT Annual epidemiological report for 2018
9
Discussion
The crude notification rate of 6.4 cases per 100 000 population of confirmed IPD in 2018 is slightly higher than in
previous years. The elderly and infants continue to be the most affected age groups. Notification rates varied by
country, ranging from 0.2 to 16.0 cases per 100 000 population. The variation may be due to differences in
healthcare systems, vaccination programmes, case ascertainment and reporting, as well as implementation of
enhanced surveillance systems in a number of countries in recent years [6].
A number of studies have demonstrated the impact of PCVs in reducing the incidence of IPD. They have also provided
evidence of increases in non-vaccine serotypes as a result of introducing PCV10 and PCV13 [7–9]. Moreover, the
vaccination of infants and young children has resulted in indirect protection of older adults by reducing
nasopharyngeal carriage and transmission of the bacterium in children, contributing to a decrease in morbidity and
mortality in older age groups [7,10]. PCV7 was first licensed in 2001 for use in infants and young children and EU/EEA
Member States began introducing the vaccine into routine childhood immunisation schedules in 2006. In 2009, the
higher-valency PCV10 and PCV13 vaccines were licensed and have progressively replaced PCV7.
To date, 29 Member States have introduced conjugate vaccines to their routine national childhood immunisation
programmes (all except Estonia and Malta) [11]. The vaccination is mandatory in six countries (Bulgaria, France,
Croatia, Hungary, Poland and Slovakia). In TESSy, the proportion of IPD cases caused by PCV serotypes has
decreased over time to the extent that 75% of cases among children <5 years of age and 71% in adults 65 years
or above were caused by non-PCV serotypes in 2018. Serotype replacement has gradually reduced the impact of
PCV as the rates of carriage and disease caused by non-vaccine serotypes have increased [12].
In 2018, among infants and children aged 1–4 years, the most common serotypes included 8, 10A, 3, 19A and
24F. Those serotypes are not included in any of the currently licensed PCVs, with the exception of 19A. A better
understanding of the epidemiology of serotype 19A in relation to vaccination strategies is necessary. While
vaccination with PCV13 confers longer and better protection against serotype 19A, it may vary, depending on the
vaccination scheme - 2+1 or 3+1. Longer enhanced surveillance projects are required to better understand factors
associated with fluctuation of serotype 19A.
Twenty-one Member States offer PPV23 and/or PCV13 for persons aged 50 years and over and/or for risk groups
in certain age groups [11]. Among the elderly, the majority of IPD cases continue to be caused by PPV23
serotypes, with less than a third of all cases caused by PCV13 serotypes. In 2011, PCV13 was approved for use in
adults aged 50 years and over. Studies have shown that PCV13 vaccination for the elderly can induce an immune
response against vaccine serotypes that is as good as or better than PPV23 [13]. The vaccine is safe and effective
in preventing non-IPD and IPD caused by vaccine serotypes [13]. However, decreases in PCV13 serotypes and
increases in non-PCV13 serotypes in the elderly as an indirect effect of routine childhood vaccination reduce the
potential additional benefit of PCV13 vaccination in the elderly [14]. Further monitoring of IPD serotype trends in
the elderly and post-marketing effectiveness and impact studies in adults are warranted.
The SpiDnet project
From August 2012 to January 2020, in order to obtain further insight into the epidemiology of IPD, ECDC provided
funding for SpIDnet (
Streptococcus pneumoniae
invasive disease network). This project aimed to establish active
enhanced surveillance of IPD in the EU/EEA in order to monitor changes in the epidemiology of IPD, estimate the
effectiveness of PCV vaccines and evaluate the impact of PCV vaccination programmes. The project had 13 study
sites in 10 Member States and covered around 20% of the total EU/EEA population. The project complemented
routine surveillance performed at the European level by actively collecting additional data using a common
protocol. A recent publication showed that during the PCV10/13 period, the incidence of IPD caused by any
serotype in children under five years decreased by 47%, compared to the PCV7 period (i.e. before the introduction
of PCV10/13) [15]. The decrease was even more substantial (55%) when the period after the introduction of
PCV10/13 was compared to the period before the introduction of PCV7. This decline demonstrates the positive
overall effect of PCV programmes on IPD incidence in children. However, the incidence of IPD caused by non-
PCV13 serotypes in children below the age of five increased by 62% against the average incidence when PCV7 was
used, and by 115% compared to the period before PCV7 was used. Another recent publication from the SpIDnet
project showed a 9% decline in IPD cases in adults aged ≥65 years five years following the introduction of
PCV10/13 vaccination in children [14]. On the other hand, during the period 2014–2015 an overall increase in IPD
cases among older adults was observed at 12 out of 13 project sites. The decreases observed in IPD cases caused
by PCV vaccine types (77% due to PCV7 serotypes, 73% due to PCV10/non-PCV7 serotypes and 38% due to
PCV13/non-7 serotypes) were in fact countered by a large increase (63%) in IPD cases due to non-PCV13 vaccine
types. These results suggest the occurrence of serotype replacement, probably due to the use of PCV [16].

Annual epidemiological report for 2018 SURVEILLANCE REPORT
10
Public health implications
PCVs have provided significant protection against IPD as a result of the vaccine serotypes, with effects extending
to all age groups through the introduction of herd immunity. At the same time, limited serotype coverage of the
vaccines has resulted in serotype replacement. It is therefore essential to continue monitoring circulating serotypes
in order to evaluate current vaccination programmes and inform development of new vaccines. The decision to
introduce a vaccine to a routine national immunisation programme depends on context-specific factors in each
country such as disease burden, serotype distribution and cost-effectiveness. Further monitoring of antimicrobial
resistance is also needed to guide vaccination strategies and antibiotic treatment. It would also be of great value to
improve the completeness of serotyping and antimicrobial susceptibility data in TESSy. ECDC is working towards
molecular surveillance of IPD using whole-genome sequencing, which will probably give further information on the
effects of vaccination on clonal expansion and capsular switching, and also inform vaccination strategies.

SURVEILLANCE REPORT Annual epidemiological report for 2018
11
References
1. European Centre for Disease Prevention and Control. Introduction to the Annual Epidemiological Report. In:
ECDC. Annual epidemiological report for 2017 [Internet]. Stockholm: ECDC; 2017 [cited 31 January 2019].
Available from: http://ecdc.europa.eu/annual-epidemiological-reports/methods
2. European Centre for Disease Prevention and Control. Surveillance systems overview [Internet,
downloadable spreadsheet]. Stockholm: ECDC; 2018 [cited 31 January 2019]. Available from:
http://ecdc.europa.eu/publications-data/surveillance-systems-overview-2017
3. European Centre for Disease Prevention and Control. Surveillance atlas of infectious diseases [Internet].
Stockholm: ECDC; 2017 [cited 31 January 2019]. Available from:
http://atlas.ecdc.europa.eu/public/index.aspx?Dataset=27&HealthTopic=40
4. European Centre for Disease Prevention and Control. EU case definitions [Internet]. Stockholm: ECDC; 2018
[cited 15 May 2018]. Available from: http://ecdc.europa.eu/en/aboutus/what-we-
do/surveillance/Pages/case_definitions.aspx
5. van der Linden M, Falkenhorst G, Perniciaro S, Imohl M. Effects of Infant Pneumococcal Conjugate
Vaccination on Serotype Distribution in Invasive Pneumococcal Disease among Children and Adults in
Germany. PLoS One. 2015 Jul 1;10(7):e0131494.
6. Navarro Torné A, Dias JG, Quinten C, Hruba F, Busana MC, Lopalco PL, et al. European enhanced
surveillance of invasive pneumococcal disease in 2010: data from 26 European countries in the
post-heptavalent conjugate vaccine era. Vaccine. 2014 Jun 17;32(29):3644-50.
7. Flasche S, Van Hoek AJ, Sheasby E, Waight P, Andrews N, Sheppard C, et al. Effect of Pneumococcal
Conjugate Vaccination on Serotype-Specific Carriage and Invasive Disease in England: A Cross-Sectional
Study. PLoS Med. 2011 Apr;8(4):e1001017.
8. D'Ancona F, Caporali MG, Del Manso M, Giambi C, Camilli R, D'Ambrosio F, et al. Invasive pneumococcal
disease in children and adults in seven Italian regions after the introduction of the conjugate vaccine,
2008–2014. Epidemiol Prev. 2015 Jul-Aug;39(4 Suppl 1):134-8.
9. Waight PA, Andrews NJ, Ladhani SN, Sheppard CL, Slack MP, Miller E. Effect of the 13-valent pneumococcal
conjugate vaccine on invasive pneumococcal disease in England and Wales 4 years after its introduction: an
observational cohort study. Lancet Infect Dis. 2015 May;15(5):535-43.
10. Tocheva AS, Jefferies JM, Rubery H, Bennett J, Afimeke G, Garland J, et al. Declining serotype coverage of
new pneumococcal conjugate vaccines relating to the carriage of
Streptococcus pneumoniae
in young
children. Vaccine. 2011 Jun 10;29(26):4400-4.
11. European Centre for Disease Prevention and Control. Vaccination Scheduler – Vaccine schedules in all
countries of the European Union [Internet]. Stockholm: ECDC; 2019 [cited 22 March 2019]. Available from:
http://vaccine-schedule.ecdc.europa.eu
12. Lynch JP 3rd, Zhanel GG.
Streptococcus pneumoniae
: epidemiology and risk factors, evolution of
antimicrobial resistance, and impact of vaccines. Curr Opin Pulm Med. 2010 May;16(3):217-25.
13. Tomczyk S, Bennett NM, Stoecker C, Gierke R, Moore MR, Whitney CG, et al. Use of 13-Valent
Pneumococcal Conjugate Vaccine and 23-Valent Pneumococcal Polysaccharide Vaccine Among Adults Aged
≥65 Years: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb
Mortal Wkly Rep. 2014 Sep 19;63(37):822-5.
14. Hanquet G, Krizova P, Valentiner-Branth P, Ladhani SN, Nuorti JP, Lepoutre A, et al. Effect of childhood
pneumococcal conjugate vaccination on invasive disease in older adults of 10 European countries:
implications for adult vaccination. Thorax. 2019 May;74(5):473-482.
15. Savulescu C, Krizova P, Lepoutre A, Mereckiene J, Vestrheim DF, Ciruela P, et al. Effect of high-valency
pneumococcal conjugate vaccines on invasive pneumococcal disease in children in SpIDnet countries: an
observational multicentre study. Lancet Respir Med. 2017 Aug;5(8):648-656.
16. Feikin DR, Kagucia EW, Loo JD, Link-Gelles R, Puhan MA, Cherian T, et al. Serotype-Specific Changes in
Invasive Pneumococcal Disease after Pneumococcal Conjugate Vaccine Introduction: A Pooled Analysis of
Multiple Surveillance Sites. PLoS Med. 2013;10(9):e1001517.
