13
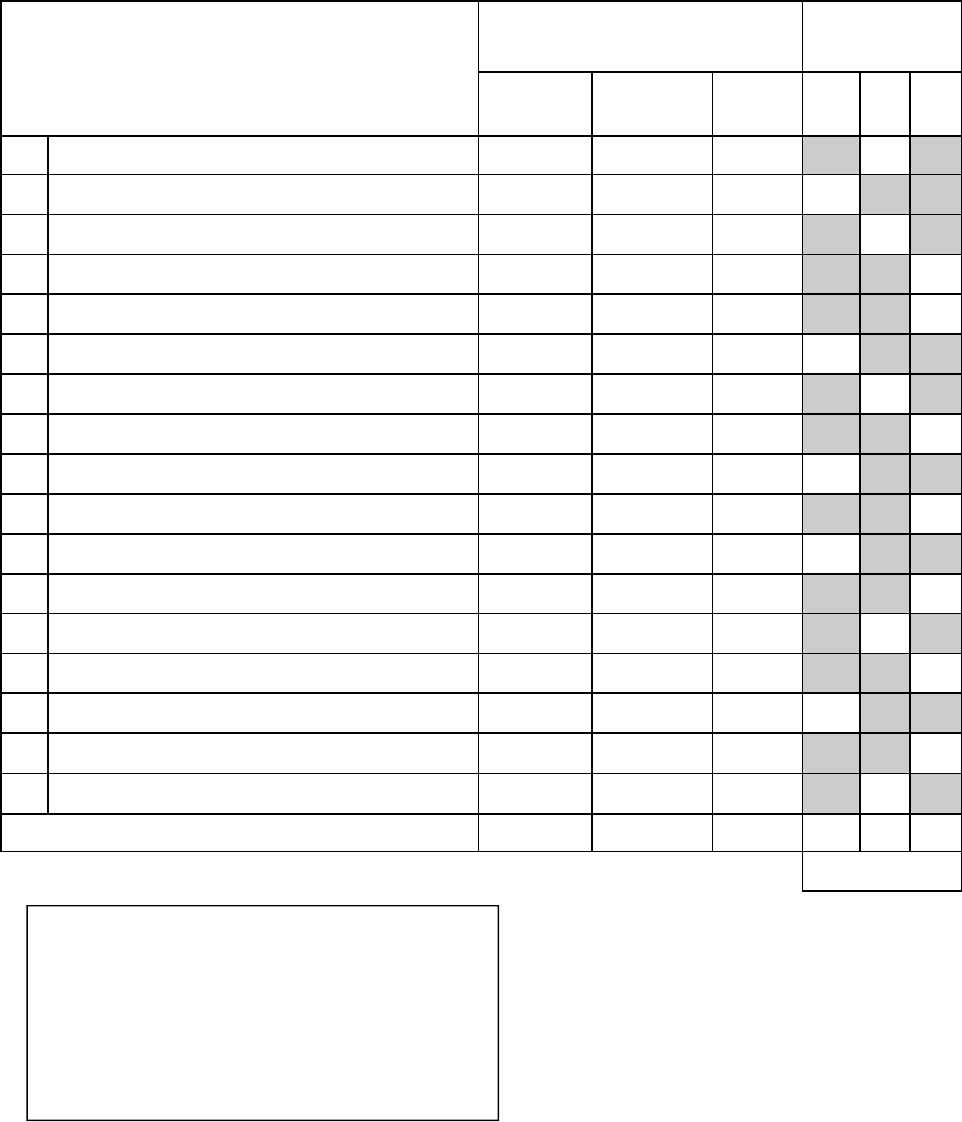
Pediatric Symptom Checklist-17 (PSC-17)
Caregiver Completing this Form: ___________________ Date: _____________________
Name of Child: _______________________
Please mark under the heading that
best fits your child
For Office Use
NEVER
SOME-
TIMES
OFTEN I A E
1.
Fidgety, unable to sit still
2.
Feels sad, unhappy
3.
Daydreams too much
4.
Refuses to share
5.
Does not understand other people’s feelings
6.
Feels hopeless
7.
Has trouble concentrating
8.
Fights with other children
9.
Is down on him or herself
10.
Blames others for his or her troubles
11.
Seems to be having less fun
12.
Does not listen to rules
13.
Acts as if driven by a motor
14.
Teases others
15.
Worries a lot
16.
Takes things that do not belong to him or her
17.
Distracted easily
(scoring totals)
Scoring:
Fill in unshaded box on right with: “Never” = 0,
“Sometimes” = 1, “Often” = 2
Sum the columns.
PSC17 Internalizing score is sum of column I
PSC17 Attention score is sum of column A
PSC17 Externalizing score is sum of column E
PSC-17 Total Score is sum of I, A, and E columns
PSC-17 may be freely reproduced.
Created by W Gardner and K Kelleher (1999), and based on PSC by M Jellinek et al. (1988)
Formatted by R Hilt, inspired by Columbus Children’s Research Institute formatting of PSC-17
Suggested Screen Cutoff:
PSC-17 - I ≥ 5
PSC-17 - A ≥ 7
PSC-17 - E ≥7
Total Score ≥ 15
Higher Scores can indicate an increased
likelihood of a behavioral health disorder
being present.
14
The PSC-17 can help primary care providers assess the likelihood of finding any mental
health disorder in their patient. The brief and easy to score PSC-17 has fairly good mental
health screening characteristics, even when compared with much longer instruments like the
CBCL (Child Behavior Checklist by T. Achenbach).
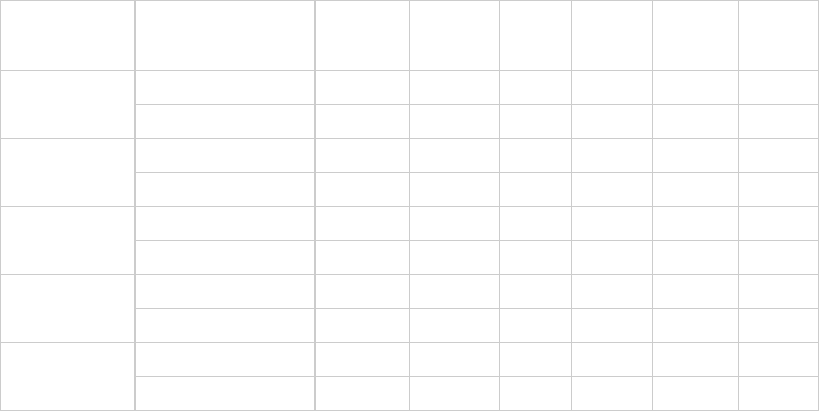
A 2007 study in primary care offices compared use of the PSC-17 to simultaneous use of the
CBCL in 269 children aged 8-15, showing reasonably good performance of its three
subscales compared to similar subscales on the CBCL. The gold standard here was a K-
SADS diagnosis, which is a standardized psychiatric interview diagnosis. These comparison
statistics are summarized below, with positive and negative predictive values shown based
on different presumed prevalence (5 or 15%) of the disorders. Providers should notice that
despite its good performance relative to longer such measures, it is not a foolproof diagnostic
aide. For instance the sensitivity for this scale only ranges from 31% to 73% depending on
the disorder in this study:
W Gardner, A Lucas, DJ Kolko, JV Campo “Comparison of the PSC-17 and Alternative Mental Health Screens in
an At-Risk Primary Care Sample” JAACAP 46:5, May 2007, 611-618
PSC-17 Internalizing score positive if ≥ 5
PSC-17 Externalizing score positive if ≥ 7
PSC-17 Attention score positive if ≥7
PSC-17 Total score positive if ≥15
“Attention” diagnoses can include: ADHD, ADD
“Internalizing” diagnoses can include: Any anxiety or mood disorder
“Externalizing” diagnoses can include: Conduct disorder, Oppositional Defiant Disorder,
adjustment disorder with disturbed conduct or mixed disturbed mood and conduct
PSC-17 Scoring
K-SADS Screen
Sensitiv-
ity
Specific-
ity
PPV
5%
PPV
15%
NPV 5%
NPV
15%
ADHD
PSC-17 Attention
0.58 0.91 0.25 0.53 0.98 0.92
CBCL Attention 0.68 0.90 0.26 0.55 0.98 0.94
Anxiety
PSC-17 Internalizing 0.52 0.74 0.10 0.26 0.97 0.90
CBCL Internalizing 0.42 0.88 0.13 0.38 0.97 0.90
Depression
PSC-17 Internalizing 0.73 0.74 0.13 0.33 0.98 0.94
CBCL Internalizing 0.58 0.87 0.19 0.44 0.98 0.92
Externalizing
PSC-17 Externalizing 0.62 0.89 0.23 0.50 0.98 0.93
CBCL Externalizing 0.46 0.95 0.33 0.62 0.97 0.91
PSC-17 Total 0.42 0.86 0.14 0.35 0.97 0.89
CBCL Total
0.31 0.96 0.29 0.58 0.96 0.89
Any Diagnosis
