Parental leave policies in graduate medical education: A systematic
review
Laura S. Humphries, Sarah Lyon, Rebecca Garza, Daniel R. Butz, Benjamin Lemelman,
Julie E. Park
*
Section of Plastic and Reconstructive Surgery, Department of Surgery, University of Chicago, Chicago, IL, United States
article info
Article history:
Received 10 February 2017
Received in revised form
1 June 2017
Accepted 20 June 2017
Keywords:
GME
Leave of absence
Maternity leave
Paternity leave
Parental leave
abstract
BACKGROUND: A thorough understanding of attitudes toward and program policies for parenthood in
graduate medical education (GME) is essential for establishing fair and achievable parental leave policies
and fostering a culture of support for trainees during GME.
METHODS: A systematic review of the literature was completed. Non-cohort studies, studies completed
or published outside of the United States, and studies not published in English were excluded. Studies
that addressed the existence of parental leave policies in GME were identified and were the focus of this
study.
RESULTS: Twenty-eight studies addressed the topic of the existence of formal parental leave policies in
GME, which was found to vary across time and ranged between 22 and 90%. Support for such policies
persisted across time.
CONCLUSIONS: Attention to formal leave policies in GME has traditionally been lacking, but may be
increasing. Negative attitudes towards parenthood in GME persist. Active awareness of the challenges
faced by parent-trainees combined with formal parental leave policy implementation is important in
supporting parenthood in GME.
© 2017 Published by Elsevier Inc.
1. Introduction
Parenthood during graduate medical education (GME) has been
a topic of interest since the late 1970s. With increasing percentages
of women in medicine, this subject has resurfaced recently as part
of a broader conversation within government and industry about
gender in the American workplace.
1
Women physicians face
particular challenges because their training programs, which can
span nearly a decade, coincide with traditional childbearing years.
Although these challenges are well known, formal and informal
support for parenthood in GME remains variable and poorly defined.
The Accreditation Council for Graduate Medical Education (ACGME)
does not have a single, defined parental leave policy that all GME
programs must follow.
2
While the ACGME mandates that GME
programs must have leave policies in place, the ACGME does not
provide specific recommendations or guidelines for their
development. Instead, individual GME programs are left to create
their own leave policies that are consistent with applicable laws
(Table 1) and that satisfy the relevant certifying board
requirements.
2
The goal of this study is to provide a systematic review of
parental leave policies in graduate medical education. Specifically,
we aim to identify the number of studies available in the literature
addressing the existence of parental leave policies in GME.
2. Methods
An electronic search of the PubMed, Medline, Scopus, and Psy-
chInfo databases was completed using multiple search terms
(Fig.1), including internship, residency, leave and pregnancy (Table 2).
Search criteria incorporated relevant articles from January 1,1960 to
December 13, 2015. Studies that pertained to family planning or
leave (including pregnancy/childbearing, paternity/maternity/
parental leave, breastfeeding and childcare issues) during GME in
the United States (including studies addressing these issues in res-
idency, fellowship, or across multiple training time periods) were
included in the initial pool of studies reviewed. Non-cohort studies
* Corresponding author. The University of Chicago Medicine and Biological Sci-
ences, 5841 S. Maryland Avenue, MC 6035, Chicago, IL 60637, United States.
Contents lists available at ScienceDirect
The American Journal of Surgery
journal homepage: www.americanjournalofsurgery.com
http://dx.doi.org/10.1016/j.amjsurg.2017.06.023
0002-9610/© 2017 Published by Elsevier Inc.
The American Journal of Surgery 214 (2017) 634e639
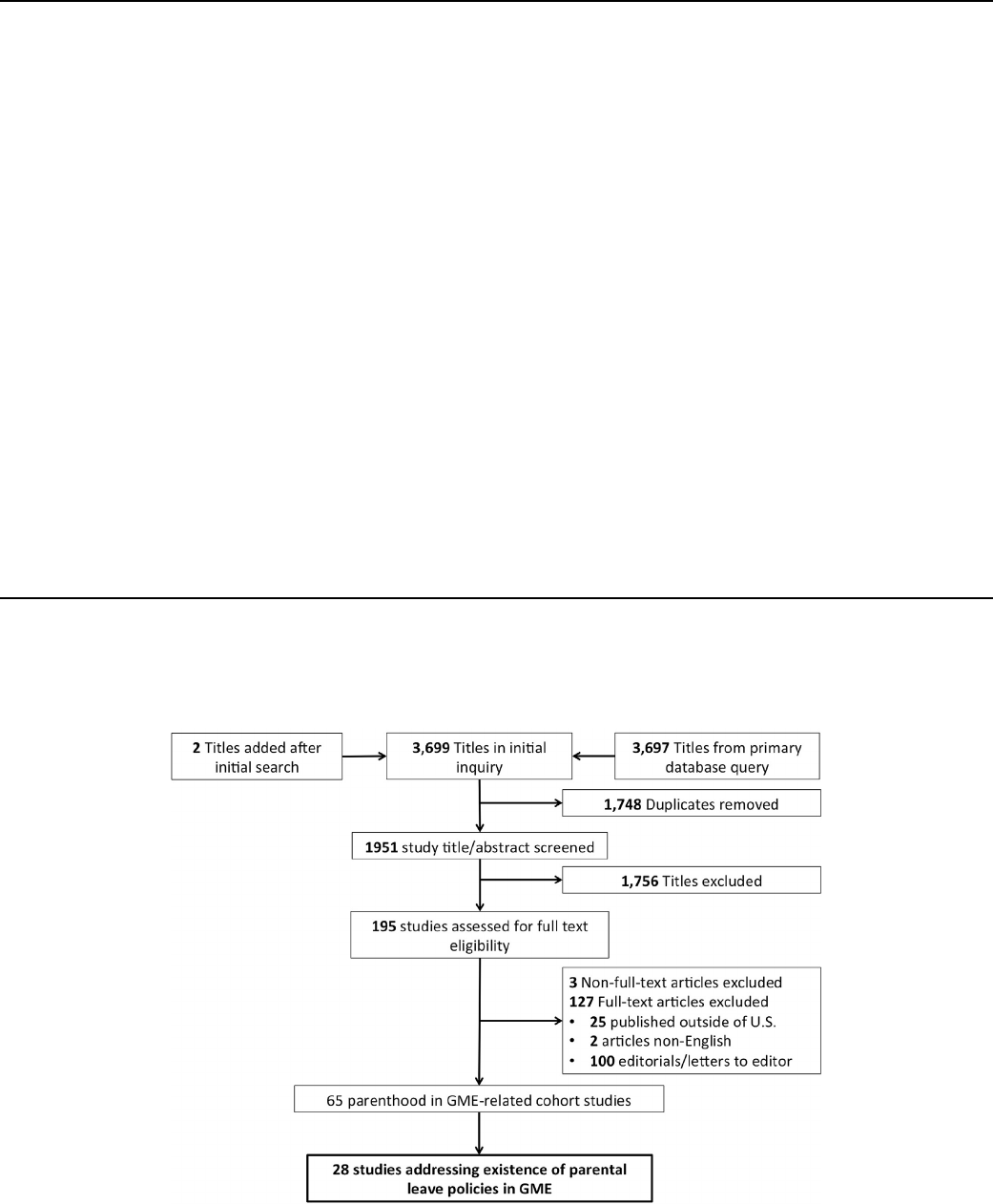
Table 1
Parental leave policies: United States government laws and Graduate Medical Education regulations.
United States Government Laws
Civil Rights Act of 1964, Title VII
3
Prohibits employment discrimination based on race, color, religion, sex and national origin.
Pregnancy Discrimination Act (PDA) (1978)
4
Amendment to Title VII of Civil Rights Act of 1964. Prohibits discrimination in employment against women
affected by pregnancy or related conditions.
Americans with Disabilities Act (ADA) (1990)
5
Prohibits discrimination against people with disabilities in employment, public services, public accommodations
and in telecommunications.
Employers must treat women who are temporarily unable to perform their jobs due to medical condition related
to pregnancy or childbirth similar to any other temporarily disabled employee
Family and Medical Leave Act (FMLA) (1993)
6
Entitles eligible employees of covered employers to take unpaid, job-protected leave for speci fied family and
medical reasons.
12 workweeks leave in a 12-month period.
Patient Protection and Affordable Care Act (PPACA)
(2010)
7
Amendment to Section 7 of the Fair Labor Standards Act (FLSA)
Employers required to provide “reasonable break time for an employee to express breast milk for her nursing
child for 1 year after the child's birth each time such employee has need to express the milk.”
Employers required to provide “a place, other than a bathroom, that is shielded from view and free from
intrusion from coworkers and the public, which may be used by an employee to express breast milk”
Graduate Medical Education Regulations
Accreditation Council for Graduate Medical
Education (ACGME)
2
IV.A.3. An applicant invited to interview for a resident/fellow position must be informed in writing or by
electronic means of the terms, conditions and benefits of appointment to the ACGME-accredited program, either
in effect at the time of the interview or that will be in effect at the time of his or her eventual appointment
A) Information that is provided must include: financial support; vacations; parental, sick, and other leaves of
absence; and professional liability, hospitalization, health, disability, and other insurance accessible to residents/
fellows and their eligible dependents.
IV.B.2. The contract/agreement of appointment must directly contain or provide a reference to the following
items:
h) disability insurance for residents/fellows;
i) vacation, parental, sick, and other leave(s) for residents/fellows, compliant with applicable laws
j) timely notice of the effect of leaves on the ability of residents/fellows to satisfy requirements for program
completion
IV.G Vacation and Leaves of Absence
IV.G.I. The sponsoring institution must have a policy for vacation and other leaves of absence, consistent with
applicable laws.
IV. G.2. This policy must ensure that each of its ACGME-accredited programs provides its residents/fellows with
accurate information regarding the impact of extended leave of absence upon the criteria for satisfactory
completion of the program and upon a resident's/fellows' eligibility to participate in examinations by the
relevant certifying board(s).
Fig. 1. Article selection process.
L.S. Humphries et al. / The American Journal of Surgery 214 (2017) 634e639 635
(e.g. editorials, letters to the editor), studies completed or published
outside of the United States and studies not published in English
were excluded. Studies that addressed the existence of parental
leave policies in GME were identified and were the focus of this
study. Two of the investigators independently completed study
selection, and a third investigator resolved discrepancies. Data
extraction was completed by one individual (LSH).
This study adhered to standardized methodological principles of
PRISMA for reporting systematic reviews.
8
Due to the heterogeneity
of the data reporting amongst articles, a qualitative analysis was
performed for each results category. Themes included existence of
formal leave policies, amount of leave time allowed, impact of
parental leave on training and support for parenthood in residency.
3. Results
3.1. Systematic review results
In the first inquiry of the systematic review, 3,699 papers were
identified. After duplicates were removed, 165 articles
9e73
met
initial inclusion criteria. Editorials that otherwise met initial in-
clusion criteria (n ¼ 100) were removed to compile the final list of
65 articles. All were cross-sectional studies: 62 survey, 1 database
58
and 2 interview studies.
21,57
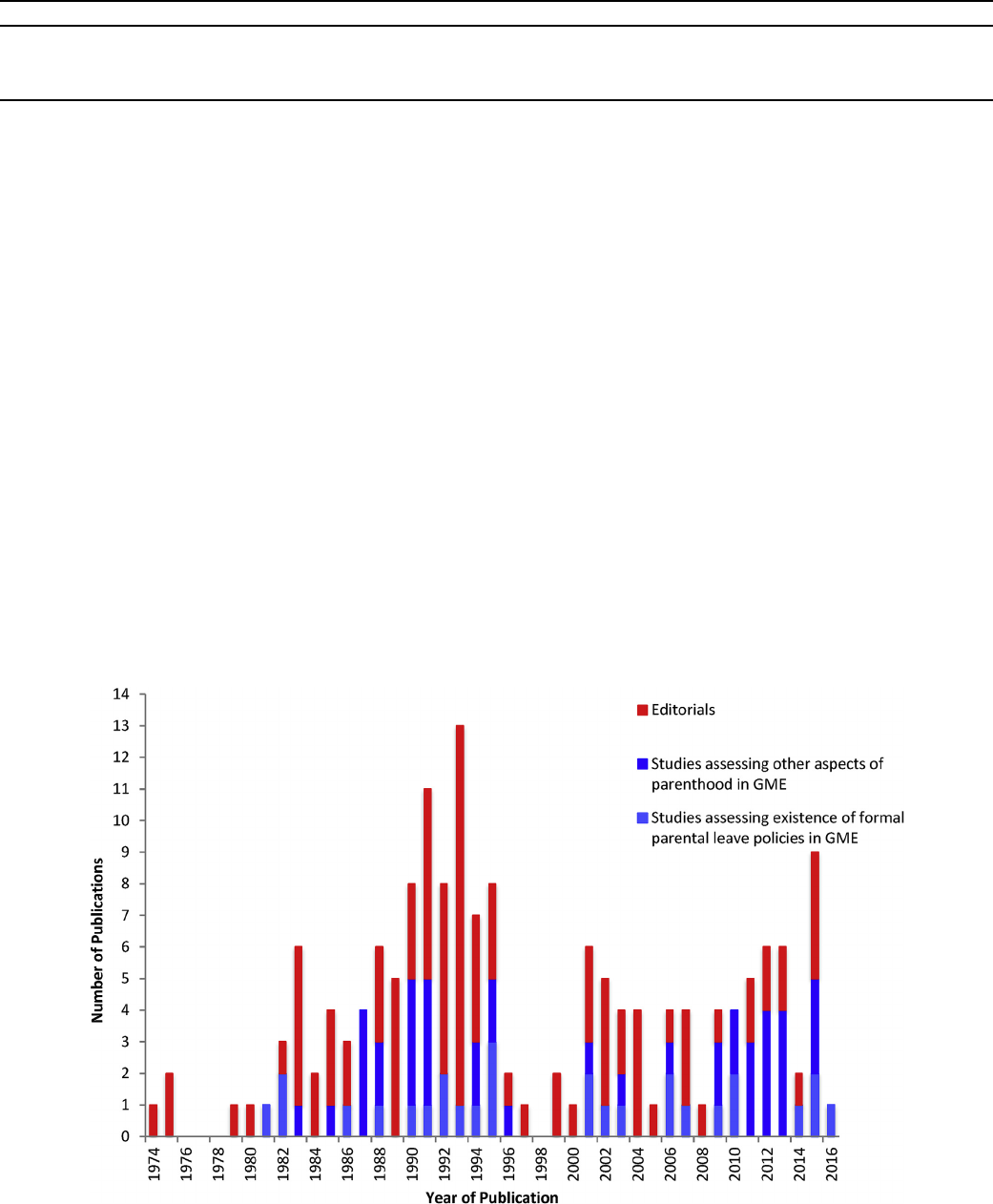
Publications on parenthood in GME
were clustered in two time periods d the late 1980s-early 1990s
and the 2000s (Fig. 2). Of these, 28 articles specifically addressed
the existence of parental leave policies (Fig. 2).
3.2. Subjects
Twenty-one studies focused on parental leave policies during
residency and/or fellowship, and 7 articles focused on this topic
across multiple professional periods. Surveyed individuals varied,
including female residents, male residents, partners of male
residents, fellows, program directors, department chairs, female
faculty, and male faculty. No studies included partners of female
residents. Various medical and surgical specialties were
represented.
3.3. Existence of parental leave policies
Twenty-eight studies addressed the topic of the existence of
formal parental leave policies in graduate medical educa-
tion.
12,1 4e16,18,21,22,24,27e29,33,34,42e45,49,52e54,58e 63,66
Six of the
included 28 studies were from surgical specialties including gen-
eral surgery,
18,44,59
otolaryngology,
21
urology
42
and thoracic
surgery.
49
The existence of formal family leave policies varied across time.
Of the studies published between 1986 and 1992, two studies re-
ported existence of maternity leave policies with 22e66% of sur-
veyed programs having formal policies.
52,60
None in this time
period mentioned paternity leave. Of the studies published be-
tween 1995 and 2016, nine described maternity or family leave
policies.
12,21,22,43e45,54,59
In a 1991 survey of program directors of
Boston-area hospitals, 82% (9/11) of responding hospitals indicated
Table 2
Systematic review search terms used for article search.
Search engine Number of articles Search terms
PubMed 1483 ((residency, leave) OR ((residency, pregnancy))
Medline 808 residency, leave OR residency, pregnancy
Scopus 1539 (((internship OR residency) AND leave) OR ((internship OR residency) AND pregnancy))
PsychInfo 135 (residency and leave) OR (residency and pregnancy)
Fig. 2. Published editorials and studies on parenthood in graduate medical education (GME) across time. (Color version of figure available online.)
L.S. Humphries et al. / The American Journal of Surgery 214 (2017) 634e639636
they had a specific written maternity leave policy, and 75% of
programs reported implementation of the policy.
52
Six studies
described having formal paternity leave policies, all after the year
1995.
12,22,28,34,43,45,59
The existence of formal family leave policies varied across spe-
cialty. Surveys of pediatric and radiology residency program di-
rectors indicated high rates of formal maternity leave policies: 90%
and 88%, respectively.
43,45
Within surgery, individual institutions
have demonstrated success with following a set of general guide-
lines for management of maternity in residency.
18,21
Female urol-
ogists reported a 42% formal maternity leave policy at their
institutions,
42
and a recent general surgery study indicated that
67% of programs have a formal maternity leave policy.
59
As to paternity leave, obstetrics-gynecology (OB-GYN) programs
had the highest proportion of such policies at 69%.
22
Forty-eight
percent of surveyed general surgery programs had formal pater-
nity leave policies in 2016, with larger programs more likely to have
these policies (72% of programs with >6 residents vs. 40% of pro-
grams with <6 residents).
59
3.4. Parental leave time and impact on length of training
In the absence of formal parental leave time allotment,
leave time for family purposes was taken from vacation
time,
16,18,29,33,43,53,60
sick leave
29,43,52,53
or disability.
16,52
Two
studies reported that female residents took unpaid leave.
33,53
In a
survey of female residents and partners of male residents, 50% of
female residents were covered by formal maternity leave policies
compared to 70% of working partners of male residents.
33
One
study investigated the impact of parental leave on extending resi-
dency training and the timing of entrance into the specialty board
certification.
58
There were maximum limits of absence from
training for 21 of 26 specialties. The impact of a six-week parental
leave in training could result in no delay in board entry or could
result in delay of up to one year, depending on the rules of different
specialty boards. In this study, most boards did not have specific
policies related to parental leave.
3.5. Parental leave support
High support for the development of standardized policies for
parental leave across specialties was observed, even in the earlier
studies from the 1990s.
12,14,27
Eighty-seven percent of surveyed
residents at a single institution favored maternity/paternity leave in
1994.
27
Seventy-five percent of radiology program directors sup-
ported the development of standardized residency program
guidelines for pregnant residents.
14
Over 50% of pediatric female
residents with children felt that existence of maternity leave,
length of leave and time needed to make up absence were impor-
tant in selecting a residency program, while more than 33% of male
residents felt paternity leave policies were important in choosing a
residency program.
12
A survey study within one general surgery
program demonstrated that resident maternity could be managed
safely and fairly to the satisfaction of both residents and faculty.
18
A few studies, however, found lack of support for parental is-
sues. One study within thoracic surgery indicated that while 76%
(67/88) of surveyed women expressed need for a reproductive
health wellness policy to allow extended time for reproductive
planning, pregnancy and family care issues, only 32% (8/25) of men
expressed this need.
49
4. Discussion
The topic of parenthood in medicine broadly, and in GME spe-
cifically, has been discussed since the late 1970s. Both published and
informal conversations among governing bodies within medical
and surgical specialties have reemerged in recent years, including
among the American College of Surgeons in the last year.
74
This
conversation is timely, as there has been a noticeable shift within
industry (e.g. Google, Facebook,
75
Amazon
76
and Netflix
77
) and the
U.S. military
78
toward more family-friendly employment policies.
Our review shows a number of issues surrounding the topic of
parenthood in GME, specifically in regard to the existence of formal
parental leave policies. The complex nature of these topics and
wide variation between studies preclude performance of quanti-
tative meta-analysis, thus making way for qualitative discussion.
The ACGME does not have a formal parental leave policy that
GME programs must follow. Instead, the ACGME mandates that
GME programs must create leave policies that are consistent with
applicable laws ( Table 1) and that satisfy the relevant certifying
board requirements.
2
As such, there is great variability across
specialties and individual GME programs as to how parental leave is
approached and handled. This inconsistency is reflected in the re-
sults of this study.
The existence of formal parental leave policies varied across
institutions and specialties and has seemed to increase over time.
Maternity leave was the main focus of early studies. The existence
and study of paternity leave and parental leave policies appeared in
more recent years, mostly after 1995. In addition, issues of
parenthood outside of traditional male-female relationships (e.g.
same-sex partnerships, non-married unions), including adoption,
were considered in more recent publications but were still scarce.
In the absence of formal parental leave policies, leave time desig-
nated for other reasons was often used for situations of family leave
(e.g. sick leave, disability, vacation). Female residents were less
likely to be covered by formal maternity leave policies than part-
ners of male residents.
The lack of uniformity in parental leave policy and guidelines
perpetuates the lack of parity for having children during GME
across programs. The attitudes of GME programs toward parent-
hood may range from hostile, to indifferent, to supportive.
Combining a family and medical career is stressful,
37,60,61,65
more so
for females than males.
49,61,71,72
Pregnancy and childbirth altered
trainee choice of GME program, date of completion, career plans
and/or pursuit of additional degrees more often for women than for
men.
13
The perception of negative impact on one's career may
result in delay in childbearing for many female residents across
specialties.
34
The performance of a pregnant or parent female
resident is likely to be perceived negatively both by the resident
herself
34,35
and her colleagues,
16,26
as well as by the program di-
rector or department chair.
26,60
Perhaps one of the most impactful findings of negative
perception of parenthood in residency was from a 2016 survey of
general surgery program directors.
59
Sixty-one percent of program
directors reported that becoming a parent negatively affected fe-
male trainees' work, including increased burden on fellow resi-
dents (33%), fewer scholarly activities (9%), fewer clinical activities
(8%), less dedication to patient care (6%) and decreased timeliness
(5%).
59
In addition, general surgery program directors were less
likely to report that becoming a parent negatively affects a male
resident's than a female resident's work (34% vs. 61%) and reported
that children decrease female resident well-being more often than
that of male residents (32% vs. 9%). Fifteen percent of general sur-
gery program directors said they would advise against having
children during residency.
This perception of negative impact of parenthood on clinical
performance and academic productivity, especially for women,
persists despite data that indicate the opposite. For example, the
number of clinical cases completed by pregnant OB-GYN residents
has not been shown to be significantly different than peers, and
L.S. Humphries et al. / The American Journal of Surgery 214 (2017) 634e639 637
academic productivity does not seem to differ based on a parent
trainee's gender.
21,40
In a retrospective review of general surgery
residents, factors such as age, sex and incidence of childrearing
during training were not associated with increased risk of attri-
tion.
79
In addition, general surgery residents with children during
training did not have significantly different total case numbers, in-
service scores or written/oral board pass rates than those without
children.
79
In a different study, perceived impact of childbearing on
general surgery resident training had no effect on a resident's de-
cision to have a child during residency for most trainees who had
children in residency.
67
The majority of female surgeons without
children reported that family had no effect on their career, whereas
women with children reported that their family affected their
career a moderate amount. Only 15% of 128 female surgeons with
children felt that having children markedly slowed their career.
32
Furthermore, there remains high career and personal satisfac-
tion among residents and physicians who have children. Career
satisfaction was not significantly different between female physi-
cians with and without children. Ninety-one percent of women
surveyed were “satisfied” or “very satisfied” with their careers.
66
High overall rates of career satisfaction were also reported among
female orthopedic and thoracic surgeons.
32,49
Thus, in the midst of
prevalent negative attitudes toward trainee parents and females in
particular, a culture change toward an environment of support for
trainee parents is imperative to identify means to aid in their
success.
In the face of diverse approaches to parenthood in GME, training
programs have managed to graduate competent physicians and
surgeons, indicating that combining parenthood and residency
training is possible. The environment of support for parenthood in
GME would best be reinforced by formal parental leave policies.
Currently, parental leave policies created by specific GME programs
are often limited by the requirements of their governing specialty
boards.
58
Most specialty boards have a “time spent” requirement
that must be fulfilled in order for graduating residents to be eligible
for their board examinations. For example, the American Board of
Surgery (ABS) requires 48 weeks per year of full-time clinical ac-
tivity over a 5-year residency, allowing an additional 4 weeks of
non-clinical time for “documented medical conditions.” Other ar-
rangements beyond the standard medical leave must be approved
by the ABS. In contrast, the American Board of Plastic Surgery
(ABPS) recently allowed the 48-week/year of clinical training to be
averaged across the 6-year training period to accommodate for
extended leaves of absence; the remaining 4 weeks in the year
could be dedicated to vacation, meeting attendance, medical leave
or other reasons as determined by the institution or program.
80
In
addition, in the final 2 years of training, plastic surgery residents
may have 1 week leave for medical reasons. In contrast, vacation
time allotment is determined by the GME in many institutions as
the residents are considered hospital employees; thus, in these
cases, program directors have less leeway in allocating additional
parental leave time.
The amount of “time spent” engaged in clinical activity in
training may eventually give way to quality of “time spent” with the
introduction of competency-based milestones.
81,82
This transition
in the way trainees are evaluated could impact the actual length of
time required to complete residency, and thus, provide more flex-
ibility for parental leave. Making the process of having children
during training fair for all trainees will require a shift in attitude
toward greater support, and this culture change must be reinforced
with adoption of formal parental leave policies.
5. Conclusion
Although more parental leave policies in training programs have
emerged over time, negative attitudes towards childbearing and
childrearing in training continue to impact residents and fellows.
Issues around paternity leave and adoption have entered the con-
versation only in recent years. Despite persistent challenges,
parenthood in GME seems to have a neutral or positive overall
impact on trainee performance and productivity. A culture shift
toward support and increased awareness of the challenges faced by
parent-trainees, coupled with formal parental leave policies from
medical governing bodies, is needed.
Clinical trial registration
Not applicable.
Funding source
No external funding was secured for this study.
Commercial associations/financial disclosures
None of the authors has a financial interest in any of the prod-
ucts, devices, or drugs mentioned in this manuscript.
References
1. Bass BL, Napolitano LM. Gender and diversity considerations in surgical
training. Surg Clin N. Am. 2004;84(6):1537e1555. http://dx.doi.org/10.1016/
j.suc.2004.06.008.
2. Education ACFGM. ACGME Institutional Requirements. Institutional Organization;
2010. http://www.acgme.org/Portals/0/PDFs/ab_ACGMEPoliciesProcedures.pdf.
3. Civil Rights Act of 1964. Public Law 88-352, 78 Stat. 241. 1964.
4. The Pregnancy Discrimination Act of 1978. Public Law 95-555, 92 Stat. 2076.
1978.
5. Americans with Disabilities Act of 1990. Public Law 101-336, 104 Stat. 327. 1990.
6. Family and Medical Leave Act of 1993. Public Law 103-3, 107 Stat. 6. 1993.
7. Patient Protection and Affordable Care Act. Public Law 111-148, 124 Stat. 119.
2010.
8. Moher D, Liberati A, Tetzlaff J, Altman DG, Grouppara TP. Preferred reporting items
for systematic reviews and meta-analyses: the PRISMA statement. JClinEpidemiol.
2009;62(10):1006e1012. http://dx.doi.org/10.1016/j.jclinepi.2009.06.005.
9. Abbett SK, Hevelone ND, Breen EM, et al. Interest in and perceived barriers to
flexible-track residencies in general surgery: a national survey of residents and
program directors. JSURG. 2011;68(5):365e371. http://dx.doi.org/10.1016/
j.jsurg.2011.04.007.
10. Balk SJ, Christoffel KK, Bijur PE. Pediatricians' attitudes concerning motherhood
during residency. Am J Dis Child. 1990;144(7):770e777.
11. Bergman AS, Adler R. Support services for pediatric trainees. A survey of
training program directors. Am J Dis Child. 1991;145(9):1002e1005.
12. Berkowitz CD, Frintner MP, Cull WL. Pediatric resident perceptions of family-
friendly benefits. Acad Pediatr. 2010;10(5):360e366. http://dx.doi.org/
10.1016/j.acap.2010.06.013.
13. Blair JE, Mayer AP, Caubet SL, Norby SM, O'Connor MI, Hayes SN. Pregnancy and
parental leave during graduate medical education. Acad Med. November
2015;1. http://dx.doi.org/10.1097/ACM.0000000000001006.
14. Blake ME, Oates ME, Applegate K, Kuligowska E. Proposed program guidelines
for pregnant radiology residents. Acad Radiol. 2006;13(3):391e401. http://
dx.doi.org/10.1016/j.acra.2005.10.007.
15.
Bongiovi ME, Freedman J. Maternity leave experiences of resident physicians.
J Am Med Womens Assoc. 1993;48(6), 185e188e193.
16. Braun DL, Susman VL. Pregnancy during psychiatry residency : a study of at-
titudes. Acad Psychiatry. 1992;16(4):178 e 185. http://dx.doi.org/10.1007/
BF03341390.
17. Brogdon BG, Herbert DE. Pregnancy in radiology residents. Investig Radiol.
1991;26(1):102e103.
18. Carty SE, Colson YL, Garvey LS, et al. Maternity policy and practice during
surgery residency: how we do it. Surgery. 2002;132(4):682e688. http://
dx.doi.org/10.1067/msy.2002.127685.
19. Chen MM, Yeo HL, Roman SA, Bell Jr RH, Sosa JA. Life events during surgical
residency have different effects on women and men over time. Surgery.
2013;154(2):162e170. http://dx.doi.org/10.1016/j.surg.2013.03.014.
20. Cochran A, Belder WE, Crandall M, Brasel K, Hauschild T, Neumayer L. Barriers to
advancement in academic surgery: views of senior residents and early career fac-
ulty. AJS. 2013;206(5):661e666. http://dx.doi.org/10.1016/j.amjsurg.2013.07.003.
21. Cole S, Arnold M, Sanderson A, Cupp C. Pregnancy during otolaryngology
residency: experience and recommendations. Am Surg. 2009;75(5):411e415.
22. Davis JL, Baillie S, Hodgson CS, Vontver L, Platt LD. Maternity leave: existing
policies in obstetrics and gynecology residency programs. Obstet Gynecol.
L.S. Humphries et al. / The American Journal of Surgery 214 (2017) 634e639638
2001;98(6):1093e1098.
23. Dixit A, Feldman-Winter L, Szucs KA. Frustrated,”“depressed,” and “devas-
tated” pediatric trainees: US academic medical centers fail to provide adequate
workplace breastfeeding support. J Hum Lactation. 2015;31(2):240e248. http://
dx.doi.org/10.1177/0890334414568119.
24. Dixit A, Feldman-Winter L, Szucs KA. Parental leave policies and pediatric
trainees in the United States. J Hum Lactation. 2015;31(3):434e439. http://
dx.doi.org/10.1177/0890334415585309.
25. Eskenazi L, Weston J. The pregnant plastic surgical resident: results of a survey
of women plastic surgeons and plastic surgery residency directors. Plast
Reconstr Surg. 1995;95(2):330e335.
26. Franco K, Evans CL, Best AP, Zrull JP, Pizza GA. Conflicts associated with phy-
sicians' pregnancies. Am J Psychiatry . 1983;140(7):902e904. http://dx.doi.org/
10.1176/ajp.140.7.902.
27. Franco K, Tamburrino M, Campbell N, Evans C, Jurs S. Conflict with physician
pregnancy revisited. Acad Psychiatry. 1994;18(3):146e153. http://dx.doi.org/
10.1007/BF03341869.
28. Gabbe SG, Morgan MA, Power ML, Schulkin J, Williams SB. Duty hours and
pregnancy outcome among residents in obstetrics and gynecology. Obstet
Gynecol. 2003;102(5 Pt 1):948e951.
29. Gjerdingen DK, Chaloner KM, Vanderscoff JA. Family practice residents' ma-
ternity leave experiences and benefits. Fam Med. 1995;27(8):512e518.
30. Grunebaum A, Minkoff H, Blake D. Pregnancy among obstetricians: a com-
parison of births before, during, and after residency. Am J Obstet. Gynecol.
1987;157(1):79e83.
31. Halperin TJ, Werler MM, Mulliken JB. Gender differences in the professional
and private lives of plastic surgeons. Ann Plast Surg. 2010;64(6):775e779.
http://dx.doi.org/10.1097/SAP.0b013e3181b02292.
32. Hamilton AR, Tyson MD, Braga JA, Lerner LB. Childbearing and pregnancy
characteristics of female orthopaedic surgeons. J Bone Jt Surg Am
. 2012;94(11):
1e9. http://dx.doi.org/10.2106/JBJS.K.00707.
33. Harris DL, Osborn LM, Schuman KL, Reading JC, Prather MB, Politzer RM. Im-
plications of pregnancy for residents and their training programs. J Am Med
Womens Assoc. 1990;45(4), 127 e8e131.
34. Holliday EB, Ahmed AA, Jagsi R, et al. Pregnancy and parenthood in radiation
oncology, views and experiences survey (PROVES): results of a blinded pro-
spective trainee parenting and career development assessment. Radiat Oncol
Biol. 2015;92(3):516e524. http://dx.doi.org/10.1016/j.ijrobp.2015.02.024.
35. Hutchinson AM, Anderson NS, Gochnour GL, Stewart C. Pregnancy and child-
birth during family medicine residency training. Fam Med. 2011;43(3):
160e165.
36. Kacmar JE, Taylor JS, Nothnagle M, Stumpff J. Breastfeeding practices of resi-
dent physicians in Rhode Island. Med Health R I. 2006;89(7):230e231.
37. Klebanoff MA, Shiono PH, Rhoads GG. Outcomes of pregnancy in a national
sample of resident physicians. N Engl J Med. 1990;323(15):1040e1045. http://
dx.doi.org/10.1056/NEJM199010113231506.
38. Klebanoff MA, Shiono PH, Rhoads GG. Spontaneous and induced abortion
among resident physicians. JAMA. 1991;265(21):2821e 2825.
39. Klevan JL, Weiss JC, Dabrow SM. Pregnancy during pediatric residency. Atti-
tudes and complications. Am J Dis Child. 1990;144(7):767e769.
40. Lashbrook DL, Frazier LM, Horbelt DV, Stembridge TW, Rall MJ. Pregnancy
during obstetrics and gynecology residency: effect on surgical experience. Am J
Obstet. Gynecol. 2003;189(3):662e665. http://dx.doi.org/10.1067/S0002-
9378(03)00877-9.
41. Lerner LB, Stolzmann KL, Gulla VD. Birth trends and pregnancy complications
among women urologists. J Am Coll Surg . 2009;208(2):293e297. http://
dx.doi.org/10.1016/j.jamcollsurg.2008.10.012.
42. Lerner LB, Baltrushes RJ, Stolzmann KL, Garshick E. Outcomes/epidemiology/
socio economics satisfaction of women urologists with maternity leave and
childbirth timing. JURO. 2010;183(1):282e286. http://dx.doi.org/10.1016/
j.juro.2009.08.113.
43. Manaster BJ, Hulen R. Pregnancy and maternity policies in radiology resi-
dencies: the 1993 survey of the American Association for Women Radiologists.
Acad Radiol
. 1995;2(9):804e806.
44. Mayer KL, Ho HS, Goodnight JE. Childbearing and child care in surgery. Arch
Surg. 2001;136(6):649e655.
45. McPhillips HA, Burke AE, Sheppard K, Pallant A, Stapleton FB, Stanton B. To-
ward creating family-friendly work environments in pediatrics: baseline data
from pediatric department chairs and pediatric program directors. PEDIATRICS.
2007;119(3):e596ee602. http://dx.doi.org/10.1542/peds.2006-2397.
46. Miller NH, Miller DJ, Chism M. Breastfeeding practices among resident physi-
cians. PEDIATRICS. 1996;98(3 Pt 1):434e437.
47. Orth TA, Drachman D, Habak P. Breastfeeding in obstetrics residency: exploring
maternal and colleague resident perspectives. Breastfeed Med. 2013;8(4):
394e400. http://dx.doi.org/10.1089/bfm.2012.0153.
48. Osborn LM, Harris DL, Reading JC, Prather MB. Outcome of pregnancies expe-
rienced during residency. J Fam Pract. 1990;31(6):618e622.
49. Pham DT, Stephens EH, Antonoff MB, et al. Birth trends and factors affecting
childbearing among thoracic surgeons. Ann Thorac Surg. 2014;98(3):890e895.
http://dx.doi.org/10.1016/j.athoracsur.2014.05.041.
50. Phelan ST. Pregnancy during residency: I. The decision “to be or not to be”.
Obstet Gynecol. 1988;72(3 Pt 1):425e431.
51. Phelan ST. Pregnancy during residency: II. Obstetric complications. Obstet
Gynecol. 1988;72(3 Pt 1):431e436.
52. Phelan EA. A survey of maternity leave policies in Boston area hospitals. JAm
Med Womens Assoc. 1991;46(2):55e58.
53. Phelan ST. Sources of stress and support for the pregnant resident. Acad Med.
1992;67(6):408e410.
54. Philibert I, Bickel J. Maternity and parental leave policies at COTH hospitals: an
update. Council of Teaching Hospitals. Acad Med. 1995;70(11):1056e1058.
55. Pincus S. Women in academic dermatology. Results of survey from the pro-
fessors of dermatology.
Arch Dermatol. 1994;130(9):1131e1135.
56. Riggins C, Rosenman MB, Szucs KA. Breastfeeding experiences among physi-
cians. Breastfeed Med. 2012;7(3):151e154. http://dx.doi.org/10.1089/
bfm.2011.0045.
57. Rodgers C, Kunkel ES, Field HL. Impact of pregnancy during training on a
psychiatric resident cohort. J Am Med Womens Assoc. 1994;49(2):49e52.
58. Rose SH, Burkle CM, Elliott BA, Koenig LF. The impact of parental leave on
extending training and entering the board certification examination process: a
specialty-based comparison. Mayo Clin Proc. 2006;81(11):1449e1453. http://
dx.doi.org/10.4065/81.11.1449.
59. Sandler BJ, Tackett JJ, Longo WE, Yoo PS. Pregnancy and parenthood among
surgery residents: results of the first nationwide survey of general surgery
residency program directors. J Am Coll Surg. January 2016:1e7. http://
dx.doi.org/10.1016/j.jamcollsurg.2015.12.004.
60. Sayres M, Wyshak G, Denterlein G, Apfel R, Shore E, Federman D. Pregnancy
during residency. N Engl J Med. 1986;314(7):418e423. http://dx.doi.org/
10.1056/NEJM198602133140705.
61. Shapiro J. Children during residency: it“s easier if you”re a man. J Am Med
Womens Assoc. 1981;36(7):227e231.
62. Shapiro J. Pregnancy during residency: attitudes and policies. J Am Med
Womens Assoc. 1982;37(4), 96e7e101e3.
63. Shapiro J. Attitudes of physician faculty members and residents toward the
pregnant medical resident. J Med Educ. 1982;57(6):483e486.
64. Shaw PM, Vouyouka A, Reed A. Time for radiation safety program guidelines
for pregnant trainees and vascular surgeons. YMVA. 2012;55(3):862e868.
http://dx.doi.org/10.1016/j.jvs.2011.11.045. e862.
65. Sheth S, Freedman MT, Arak G. Policies and attitudes toward the pregnant
radiology resident. Investig Radiol. 1985;20(4):413e
415.
66. Sinal S, Weavil P, Camp MG. Survey of women physicians on issues relating to
pregnancy during a medical career. J Med Educ. 1988;63(7):531e538.
67. Smith C, Galante JM, Pierce JL, Scherer LA. The surgical residency baby boom:
changing patterns of childbearing during residency over a 30-year span.
J Graduate Med Educ. 2013;5(4):625e629. http://dx.doi.org/10.4300/JGME-D-
12-00334.1.
68. Tucker JB, Margo KL. Profile of women family practice residents. Fam Med.
1987;19(4):269e271.
69. Turner PL, Lumpkins K, Gabre J, Lin MJ, Liu X, Terrin M. Pregnancy among
women surgeons. Arch Surg. 2012;147(5). http://dx.doi.org/10.1001/
archsurg.2011.1693.
70. Verheyden CN, McGrath MH, Simpson P, Havens L. Social problems in plastic
surgery residents. Plast Reconstr Surg. 2015;135(4):772ee778e. http://
dx.doi.org/10.1097/PRS.0000000000001098.
71. Willett LL, Wellons MF, Hartig JR, et al. Do women residents delay childbearing
due to perceived career threats? Acad Med. 2010;85(4):640e646. http://
dx.doi.org/10.1097/ACM.0b013e3181d2cb5b.
72. Wilson MD, Carpenter RO, Radius SM, Oski FA. Attitudes and factors affecting
the decisions of men and women pediatrics residents toward having children
during their residencies. Acad Med. 1991;66(12):770e772.
73. Windsor AM, Julian TM. Sexuality, reproduction, and contraception among
residents in obstetrics and gynecology. Obstet Gynecol. 1995;85(5 Pt 1):
787e792.
74. Statement on the importance of parental leave. Bull Am Coll Surg. 2016;101(4):
35e36.
75. Cohen D. Facebook Offers All Employees 4 Months' Parental Leave. Published.
AdWeek; December 1, 2015. http://www.adweek.com/digital/four-months-
parental-leave/. Accessed 8 February 2017.
76. Tepper T. Amazon's parental leave: the new free Soda? Money. Published
http://time.com/money/4098026/amazon-paid-parental-leave-benefits/;
November 3, 2015. Accessed 8 February 2017.
77. Tepper T. The pros and cons of Netflix's new parental leave plan. http://time.
com/money/3985632/netflix-unlimited-parental-leave/; August 2015.
78. Ferdinando L. Carter Announces 12 Weeks Paid Military Maternity Leave, Other
Benefits. U.S. Department of Defense. Published; January 28, 2016. https://www.
defense.gov/News/Article/Article/645958/carter-announces-12-weeks-paid-
military-maternity-leave-other-benefits. Accessed 8 February 2017.
79. Brown EG, Galante JM, Keller BA, Braxton J, Farmer DL. Pregnancy-related
attrition in general surgery. JAMA Surg. 2014;149(9):893. http://dx.doi.org/
10.1001/jamasurg.2014.1227.
80. The American Board of Plastic Surgery, Inc. May 2016:1e 92.
81. Bluth M. The General Surgery Milestone Project. July 2015:1e19.
82. McGrath MH. The plastic surgery milestone project. J Graduate Med Educ.
2014;6(1s1):222e224. http://dx.doi.org/10.4300/JGME-06-01s1-25.
L.S. Humphries et al. / The American Journal of Surgery 214 (2017) 634e639 639
