United States’ Teen Dating Violence Policies: Summary of Policy
Element Variation
Hannah I. Rochford
1,*
, Corinne Peek-Asa
1
, Anne Abbott
2
, Ann Estin
3
, Karisa Harland
4
1
Injury Prevention Research Center, University of Iowa, Iowa City, Iowa, USA
2
National Resource Center for Family-Centered Practice, Coralville, Iowa, USA
3
College of Law, 290 Boyd Law Building, University of Iowa, Iowa City, Iowa, USA
4
Department of Emergency Medicine, University of Iowa Hospitals and Clinics, 200 Hawkins
Drive, 1008 Roy Carver Pavilion, Iowa City, IA 52242
Abstract
As Teen Dating Violence (TDV) has gained attention as a public health concern across the United
States (US), many efforts to mitigate TDV appear as policies in the 50 states in the form of
for programming in K-12 schools. A keyword search identified 61 state-level school-based TDV
policies. We developed an abstraction form to conduct a content analysis of these policies and
generated descriptive statistics and graphic summaries. Thirty of the policies were original and 31
were additions or revisions of policies enacted by 17 of the 30 states previously. Of a possible
score of 63, the minimum, mean, median, and maximum scores of currently active policies were
3.0, 17.7, 18.3 and 33.8, respectively. Results revealed considerable state-to-state variation in
presence and composition of school-based TDV policies. Opportunity for improving policies was
universal, even among those with most favorably scores.
Keywords
teen dating violence; adolescent dating violence; public health law; K-12 programming
Introduction
Teen dating violence (TDV) is a prevalent and preventable public health challenge. While
this type of harm impacts many societies, and many prevention strategies foreseeably
transcend social, cultural and political contexts, this work offers a summary of the U.S.
policies enacted in an effort to mitigate TDV. The United States Center for Disease Control
and Prevention defines TDV as: “verbal, physical, emotional, psychological, or sexual abuse
in a dating relationship, including stalking and perpetration via electronic media” [1] when
“one or both partners is between thirteen and twenty years of age” [2]. TDV can cause acute
physical injuries and mental health concerns and influence long- term health outcomes,
*
Corresponding author: MPH, Department of Health Management and Policy, College of Public Health, University of Iowa, 145 N.
Riverside Drive, Room N271, Iowa City, 52242-2007, United States. hannah-rochford@uiowa.edu.
Supplemental Material: Supplemental material contains Appendices A, B, and C.
HHS Public Access
Author manuscript
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Published in final edited form as:
J Public Health Policy
. 2022 December ; 43(4): 503–514. doi:10.1057/s41271-022-00365-7.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

including an increased risk for pregnancy, risky sexual behavior, eating disorders, substance
abuse, suicide or suicidal ideation [3], victimization in adult relationships [4], depression,
smoking, and binge drinking [5].
The public health burden of TDV disproportionately falls on teenage girls and teens who
are Lesbian, Gay, and Bisexual [6]. National figures from the US 2015 Youth Risk Behavior
Surveillance System (YRBSS) indicate that among students who dated, the prevalence of
physical TDV victimization was 40% higher among girls than boys (11.7% vs 7.4%), and
sexual TDV rates were 2.6-times higher in girls than boys (14.0% vs 5.4%). State-based
rates of TDV varied widely, with physical TDV highest in Arkansas (15.6%) and lowest
in Massachusetts (6.7%) [7]. Prior research suggests approximately one out of five teens
engage in an abusive relationship, and 10% of reported intentional injuries to adolescent
girls are the result of dating violence by male partners [3].
Efforts to prevent and mitigate the consequences of TDV have largely taken the form of state
policies that attempt to reduce teen dating violence through programming in kindergarten
(K)-12 schools [8, 9]. K-12 schools are a common setting for health-related programming
and supportive services to children and youth, including awareness building and prevention
education around TDV [8]. These programs offer opportune access points for introducing
awareness, prevention, and recognition strategies and opportunities for delivering support
resources to the population at risk for TDV, and to the school staff with whom these teens
engage. Schools are also sites of TDV incidents, and personnel often work with students
who have expressed violent behavior toward someone in or out of school. Recent research,
however, provides reason to suspect many US schools are not adequately prepared to address
TDV for lack of awareness and understanding [4]. In a national survey of high school
guidance counselors, a group often engaged in responding to TDV, 58% had not received
TDV education, 81% were unaware of a school protocol for responding to TDV incidents,
and 90% had not been trained to assist students victimized by TDV [10].
Violence prevention theoretical frameworks like the socioecological model suggest a need
to implement interventions beyond the individual level [10], and studies of TDV laws
and policies support this. Recent work has affirmed that improving TDV perpetration and
responses to TDV behaviors require effective interventions to facilitate re-shaping social
norms and culture around TDV [11]. Some states have enacted legislative action only
recently, since 1992. The oldest TDV policy that has not been updated since its enactment
in 2002. Thus, our figures display 2002 as the oldest year of enactment for a currently
active policy, although the first state to enact a law did so in 1992, then updated it.) Policies
meant to address public health concerns vary widely in terms of their written quality,
implementation integrity ( the extent to which a policy’s implemented form aligns with what
a policy’s authors intended to occur), and overall capacity to help implementers achieve
the intended impact on health outcomes. A community-based participatory research effort
conducted by Gulliot-Wright et al. [12] on Texas-specific TDV legislation and school-based
curriculum found gaps in uptake of school-based prevention programming. They identified
legislation that addressed individual- and system-level causes for violence as an important
opportunity for prevention. Jackson et al. [13] also examined Texas-specific TDV policies
Rochford et al.
Page 2
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

from an implementation perspective and found most districts had developed basic policies
and were making progress in implementation.
Nationally, Black, Hoefer, & Ricard [14] scored TDV policies using the advocacy group
Break the Cycle’s
A – F grading system. This system focuses on ability youth (those under
age 18) to make use of civil protective orders and modeled their relationship with other
system-level factors (state political and economic conditions) to TDV prevalence. They
found an inverse association between the caliber of a TDV policy and TDV outcomes.
Cascardi, et al. [15] examined TDV policies in the context of policies against ‘bullying’(a
pattern of unwanted, aggressive behaviors involving a perceived power imbalance, and
occurring between youths who are not family members or dating partners) based on the
binary inclusion or exclusion of a purpose statement and discussion of prohibited behaviors
and harmful effects, enumeration of school jurisdiction, discussion of protected groups,
local or district policy development and implementation, designation of a specialist within
schools, reporting or investigation procedures, and sanctions recommended.
To our knowledge, although TDV state policies have been studied and scored, a gold
standard for assessing the elements in state laws does not yet exist. The goal of this
work was to synthesize current approaches to TDV legislation and position future research
efforts to elucidate what drives policy variation, and how TDV policy variation shapes
TDV outcomes. Thus, we systematically abstracted and described states’ TDV law content
and distinguished among those with presence, partial presence, or absence of 34 policy
components.
Methods
Law students identified school-based state TDV policies from keywords searches in
Westlaw
®
. Westlaw Codified Law Index terms for the search are reported elsewhere.
[16] The study period was defined by the enactment dates of all policies identified in
2019: related policies were enacted as early as 1992 and as recently as 2018. The project
leader (KH) organized the legal language by state and by effective periods in MonQcle
(a software system developed by the Temple University Center for Public Health Law
Research to support policy surveillance and scientific legal research projects) in preparation
for component scoring.
School-based TDV Policy Abstraction Form Development
To understand states’ approaches to school-based TDV policy, the authors (HR, CP, AA, AE,
KH) developed and applied an abstraction form to measure TDV policy components based
on our literature search of peer-reviewed health sciences, social sciences, education, and law
publications available as of 2019. As no one has yet established best practices to guide TDV
legislative evaluation, our study team developed a scoring system to identify components
of a comprehensive law and allowed for components to be designated as present, partially
present, or absent. Four sources guided our scoring system for components: US Department
of Education (DOE) recommendations on best practices for anti-bullying laws and policies
[17], policy elements in existing laws [18], S
tart Strong
’s TDV model school policy [19]
and best practices for public health law evaluation [20]. The team (HR, CP, AA, AE, KH)
Rochford et al.
Page 3
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

that developed the scoring system was multidisciplinary with broad expertise: a legal expert
on family law pertaining to intimate partner violence, an epidemiologist with experience
in domestic violence research, two injury epidemiologists with experience conducting
violence research and policy evaluations, and a biostatistician with experience conducting
longitudinal, hierarchical modeling analysis.
Select authors (HR, AA, KH)revised our original abstraction form using an iterative process
during a pilot period. Three individuals (HR, AA,KH) with graduate training in public health
and experience working with sexual and intimate partner violence policies piloted use of the
abstraction form with policies from two states that the same select authors (HR, AA, KH)
perceived to present low risk for error in coding (Michigan and Pennsylvania), from two
states perceived to present moderate risk for error in coding (Delaware and Massachusetts),
and from two states perceived to present high risk for error in coding (California and
Connecticut). In coding, the project leader (KH) assessed initial abstraction results of two
authors (HR, AA) for areas of frequent (recurrent in piloted policies) or severe discrepancy
(scores by one party indicating full presence of a component and another party indicating
absence), or both. The authors (HR, CP, AA, AE, KH) clarified intent and criteria for coding
each abstraction item of concern. The authors (HR, CP, AA, AE, KH) retained in the final
version all the originally proposed sections of the instrument. Full abstraction occurred after
the pilot process was complete.
Policy Element Abstraction & Analysis
Abstraction Process—We included 34-items in the abstraction form, organized into 7
sections. The full abstraction form is available in Appendix A. We scored each item in
each Section from 0 – 2 scale where 0 indicated the element was not present, 1 that it was
partially present or encouraged, and, 2 that it was fully present or required. We standardized
the item on the minimum number of years of TDV prevention education for students to a
0-12 scale (of years of schooling) from a 0-13 scale (thus some scores involve decimals).
Two graduate students (HR, AA) with training in public health, public policy, and violence
research (neither of whom participated in the piloting of the instrument) completed formal
abstraction using MonQcle
®
; the project leader (KH) adjudicated discrepancies. During the
abstraction process, we first coded the original policies of the 30 states that had any policy,
then coded any subsequent updates. Each student carried out abstraction independently, prior
to the generation of the Krippendorff’s alpha for inter-rater reliability to correct for change
agreement, handle multiple coders, and measure intercoder agreement for nominal, ordinal,
and interval data. [21] The inter-rater reliability score generated using Krippendorf’s alpha
was 0.88.
Analysis of Abstracted Data—We separated states according to the presence or absence
of school-based TDV policies, and assigned a scored of 0 for those with no laws. We
isolated scores of states with school-based TDV policies to derive their distribution and a
series of descriptive statistics. We generated descriptive statistics for each of the 7 policy
component sections.
Rochford et al.
Page 4
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Several states had more than one score because they updated their school-based policy
between the start and end of the analysis period (1992 – 2018). In these instances, we used
the overall score and Section-specific scores of the current policy. To determine the presence
of a temporal trend we assessed changes in state policy scores, in each state, over time, using
a Pearson correlation test for policy score and year of enactment.
Results
Thirty states had enacted at least one related policy by 2019, scoring between 3 and 33.77
out of a possible 68. Our TDV policy search yielded 61 policies from 30 states. Of these,
30 policies were original, and 31 were additions or revisions enacted by 17 of the 30
states. Table 1 displays states with policies, scores for currently active policies, and the
year the state enacted its latest policy. Twenty-one states enacted no TDV policy between
1992 and 2018. States enacted policies with the lowest scores in 2005, 2015, and 2017, and
with the highest scores in 2011, 2017, and 2018. The highest component score was Ohio’s
at 33.77, and the lowest component score observed was 3, held by both Maryland and
Washington. California, Connecticut, Tennessee, Ohio, and Virginia implemented or revised
TDV policies most recently. Maine Michigan and Washington maintained policies for the
longest duration. The association between the date of enactment and the component score is
not significant (correlation of 0.501). For policies active in 2018 or earlier, the mean year of
enactment was 2012. California had the largest number of policy updates (5 revisions since
1994).
Table 2 summarizes policy component scores, identifying the state with the lowest and
highest for each. The abstract form version used to score school-based TDV polices is
available in Supplemental Material Appendix C). States’ more recent policies generally had
the highest component score, except for revisions in Maryland and New Jersey. Maryland’s
updated policy lowered the total score from 5 in 2010 to 3 in 2012, reflecting a reduction of
the policy’s Section 5 score from 4 to 2 after that allowing students’ parents to opt them out
of the TDV-related curriculum. New Jersey’s score change over time was the most dramatic,
increasing from 6.0 in 2003 to 20.92 in 2011. New Jersey’s updated policy lowered the total
score from 20.92 in 2011 to 19.85 in 2014, after Section 4 score decreased from 5 to 4 after
removal of the term ‘comprehensive’ (see Supplemental Material Appendix B for full detail
on within-state policy score changes).
All states received the same component score for the types of schools covered, with no
states covering non-public schools (although states do have jurisdiction over educational
content required in all types of schools). Section 2 components most prevalent across
policies included inclusion of: a purpose and prohibition statements, a definition consistent
with the CDC definition of TDV, and specification of policy scope. Fewer policies included
electronic communication (text messaging, social media messaging and posts) components
within their TDV definitions, offered TDV definitions that enumerated groups, or discussed
harms associated with TDV. New Jersey ranked highest in the definition section, (score of
6 of 14). Delaware ranked highest in the district policy section (5 of 6) for having required
districts to adopt policies by a specified date and for having provisions for reviewing district
policies and reports of TDV incidents to the DOE. Some states called for districts to
Rochford et al.
Page 5
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

adopt policies but failed to specify a date or need for policy review and incident reporting
provisions in them. District policy scores in Section 4 were highest for Ohio (11 of 20), then
Delaware (9 of 20). Most leading states had fewer than half of district policy elements of an
ideal policy.
With respect to dating violence education for students, Arkansas led with a score of 9.85 of
14. All states with TDV policies at least encouraged dating violence prevention education
for students, but most did not include the remaining policy components of Section 5.
Maryland, with a score of 2, ranked lowest here. Policies of many states included no dating
violence prevention education for school staff-related (13 of all 30 states with a school-based
TDV policy scored 0 in this section). Alaska, Connecticut, and Louisiana scored highest; 8
of 10, due to including 4 of the 5 major provisions. The final section contained only one
element – availability to victims of school-based alternatives to protective orders or school
transfer options, or both. Except for Pennsylvania and Texas, state TDV policies included
neither of these.
Figure 1 displays a map of scores for 2019 together with the summary statistics for TDV
school policies active as of 2019.
Discussion
This policy content analysis revealed considerable variation in presence and composition
of school-based TDV policies from state-to-state. It also revealed universal opportunity
for policy improvement: even the states with the most comprehensive policies scored
about halfway toward an ideal policy with all components (33.77 / 68.0). Important
opportunities for improvement include: explicitly expanding the scope of school-based
TDV policies to encompass both public and private schools; incorporating broader TDV
training; establishing provisions for in-school protective orders; supporting victims with
protective orders and transfer options; and, eliminating parental ability to opt their student
out of healthy relationship programming. While scores generally improved as states revised
policies over time, no strong relationship appeared between the year of enactment and a
policy score across states.
Acting on these opportunities could advance the health and safety for those at risk because
TDV victims face challenges finding resources to support them outside of school. Judicial
authorities and police hold misconceptions about potential severity of TDV, assuming
damage to be mild and short term [13]. Their views compound barriers TDV survivors
encounter if they seek legal protections available to adult survivors. Thus, state policies
that call for schools to prepare and address TDV are critical to effective prevention and
intervention.
Beyond K-12 educational settings (one dimension of the socioecological model’s societal
and community layer) research has identified other factors that indicate probability of
violence within teen dating partnerships: prosocial beliefs (the view that positive, healthy
interactions will be helpful to an individual, and negative, unhealthy interactions will
be detrimental to an individual), emotional competencies, alcohol consumption patterns,
Rochford et al.
Page 6
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

exposure to violent family conflict, parental monitoring and parental discipline practices,
social connectedness in one’s school, and exposure to violent neighborhood settings [22–
24]. Other policies may offer levers to mitigate risk factors / support protective factors for
TDV that are active in societal, community, and relational contexts.
Limitations and next steps
Although we conducted a comprehensive search of state TDV laws that impact schools,
the search process may not have captured every school-based policy relevant to TDV.
We did not examine policies that impact other types of school violence or sexual health
programming, except for that of states which placed their teen dating violence provisions
within sexual health policies. Future research should elucidate additional risk and protective
factors for TDV and model the impact of specific K-12 TDV programming provisions on
TDV outcomes; examine what promotes the uptake of robust K-12 TDV programming and
identify and evaluate strategies beyond school-based interventions for preventing TDV and
mitigating its consequences.
Examining sexual health and wellness education policies at the state and district level may
also shed insight on opportunities for preventing harm in teen dating relationships. Even
so, our detailed data can assist other researchers to explain what factors may be driving the
policy variation and how variation shapes TDV outcomes.
Conclusion
TDV is a preventable harm that compromises population health across societies. The policy
variation measured in this work revealed that all U.S. states have the opportunity to revise
their policies to be more comprehensive. This work also creates a foundation for quasi-
experimental studies to identify which policy components are most protective against TDV
in the U.S.. It similarly offers a foundation for policies of other nations to be abstracted and
analyzed against TDV outcomes of other societies. Related findings can and should inform
policy decisions aiming to reduce TDV within US and international contexts.
Supplementary Material
Refer to Web version on PubMed Central for supplementary material.
Acknowledgements
We acknowledge Maria Doering Critchlow, Paden Hanson, and Erick Orantes for performing the keyword searches
that identified the policies included in this work’s content analysis.
Funding Sources
This work was funded through the CDC/NCIPC-funded University of Iowa Injury Prevention Research Center
(CDC/NCIPC R49CE002108).
About the authors:
Hannah I. Rochford, MPH is a PhD student at the Injury Prevention Research Center, 2190
Westlawn, University of Iowa, Iowa City, Iowa, USA
Rochford et al.
Page 7
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Corinne Peek-Asa, PhD is the Director at the Injury Prevention Research Center, 2190
Westlawn, University of Iowa, Iowa City, Iowa, USA
Anne Abbott, MPP is a PhD Student and Program Director at the National Resource Center
for Family-Centered Practice, University of Iowa, Coralville, Iowa, USA.
Ann Estin, JD, is professor of family law at the College of Law, University of Iowa, Iowa
City, Iowa, USA.
Karisa Harland, PhD, is an assistant professor at the Department of Emergency Medicine,
University of Iowa Hospitals and Clinics, Iowa City, Iowa, USA
References
1. Centers for Disease Control and Prevention. Teen Dating Violence Fact Sheet. 2014. Retrieved from
https://www.cdc.gov/violenceprevention/pdf/tdv-factsheet.pdf Accessed January 6, 2016.
2. Carlson CN. Invisible victims: Holding the educational system liable for teen dating violence at
school. Harv. Women’s LJ. 2003;26:351.
3. Silverman JG, Raj A, Mucci LA, Hathaway JE. Dating violence against adolescent girls and
associated substance use, unhealthy weight control, sexual risk behavior, pregnancy, and suicidality.
jama. 2001 Aug 1;286(5):572–9. [PubMed: 11476659]
4. Levy B, Giggans PO. What parents need to know about dating violence. Seal Press; 1995.
5. Exner-Cortens D, Eckenrode J, Rothman E. Longitudinal associations between teen dating
violence victimization and adverse health outcomes. Pediatrics. 2013 Jan 1;131(1):71–8. [PubMed:
23230075]
6. Centers for Disease Control and Prevention. Youth online: High school YRBS - United States 2019
Results | DASH | CDC. Retrieved from https://nccd.cdc.gov/youthonline/App/Results.aspx?
OUT=&SID=HS&QID=&LID=XX&YID=&LID2=&COL=&ROW1=&ROW2=&FR=&FG=&FS
L=&FGL=&PV=&TST=&C1=&C2=&QP=&SYID= . Accessed June 6, 2022
7. Zaza S, Kann L, Barrios LC. Lesbian, gay, and bisexual adolescents: Population estimate and
prevalence of health behaviors. Jama. 2016 Dec 13;316(22):2355–6. [PubMed: 27532437]
8. De La Rue L, Polanin JR, Espelage DL, Pigott TD. A meta-analysis of school-based interventions
aimed to prevent or reduce violence in teen dating relationships. Review of Educational Research.
2017 Feb;87(1):7–34.
9. Break the Cycle. 2010 State Law Report Cards: A National Survey of Teen Dating Violence Laws.
Los Angeles, CA 2010.
10. Khubchandani J, Price JH, Thompson A, Dake JA, Wiblishauser M, Telljohann SK. Adolescent
dating violence: A national assessment of school counselors’ perceptions and practices. Pediatrics.
2012 Aug 1;130(2):202–10. [PubMed: 22778298]
11. Dahlberg LL, Krug EG. Violence: a global public health problem. Ciência & Saúde Coletiva.
2006;11:1163–78.
12. Guillot-Wright S, Lu Y, Torres ED, Macdonald A, Temple JR. Teen Dating Violence Policy: An
Analysis of Teen Dating Violence Prevention Policy and Programming.
13. Jackson RD, Bouffard LA, Fox KA. Putting policy into practice: Examining school districts’
implementation of teen dating violence legislation. Criminal Justice Policy Review. 2014
Jul;25(4):503–24.
14. Hoefer R, Black B, Ricard M. The impact of state policy on teen dating violence prevalence.
Journal of Adolescence. 2015 Oct 1;44:88–96. [PubMed: 26255246]
15. Cascardi M, King CM, Rector D, DelPozzo J. School-based bullying and teen dating
violence prevention laws: overlapping or distinct?. Journal of interpersonal violence. 2018
Nov;33(21):3267–97. [PubMed: 30253722]
Rochford et al.
Page 8
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

16. Harland KK, Vakkalanka JP, Peek-Asa C, Saftlas AF. State-level teen dating violence education
laws and teen dating violence victimisation in the USA: a cross-sectional analysis of 36 states.
Injury prevention. 2021 Jun 1;27(3):257–63.
17. Stuart-Cassel V, Bell A, Springer JF. Analysis of State Bullying Laws and Policies. Office of
Planning, Evaluation and Policy Development, US Department of Education. 2011 Dec.
18. National Conference of State Legislatures. Teen Dating Violence. 2015. Retrieved from http://
www.ncsl.org/research/health/teen-dating-violence.aspx. Accessed December 5, 2015.
19. Schaeffer S, Lee D, Gallopin C, Rosewater A, Vollandt L, Rosenbluth B, Ball B, Miller
K, Alex C. School and District Policies to Increase Student Safety and Improve School
Climate: Promoting Health Relationships and Preventing Teen Dating Violence. Futures Without
Violence. 2012. Retrieved from https://startstrong.futureswithoutviolence.org/wp-content/uploads/
school-and-districtpolicies-and-appendix.pdf Accessed January 6, 2016.
20. Hall MA. Coding case law for public health law evaluation: A methods monograph for the Public
Health Law Research Program (PHLR) Temple University Beasley School of Law. Public Health
Law Research, November. 2011 Nov 26.
21. Kang N, Kara A, Laskey HA, Seaton FB. A SAS MACRO for calculating intercoder agreement in
content analysis. Journal of Advertising. 1993 Jun 1;22(2):17–28.
22. Foshee V, Reyes L, Tharp A, Chang L, Ennett S, Simon T, Latzman N, Suchindran C. Shared
longitudinal predictors of physical peer and dating violence. Journal of Adolescent Health. 2015
Jan 1; 56(1):106–12.
23. Foshee V, McNaughton Reyes H, Chen M, Ennett S, Basile K, DeGue S, Vivolo-Kantor A,
Moracco K, Bowling J. Shared risk factors for the perpetration of physical dating violence,
bullying, and sexual harassment among adolescents exposed to domestic violence. Journal of
youth and adolescence. 2016 Apr;45(4):672–86. [PubMed: 26746242]
24. Flaspohler P, Elfstrom J, Vanderzee K, Sink H, Birchmeier Z. Stand by me: The effects of peer and
teacher support in mitigating the impact of bullying on quality of life. Psychology in the Schools.
2009 Aug;46(7):636–49.
Rochford et al. Page 9
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Key messages:
•
Teen dating violence (TDV) is a prevalent and preventable public health
challenge across societies.
•
Policies enacted by U.S. states to prevent and respond to TDV often make use
of K-12 programming, and vary widely in terms of their presence and written
caliber.
•
All TDV policies active in U.S. states as of 2019 have the opportunity to
improve their comprehensiveness, with the most robust policy (enacted in
Ohio in 2018) scoring only 33.77 out of a possible 68.
Rochford et al. Page 10
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
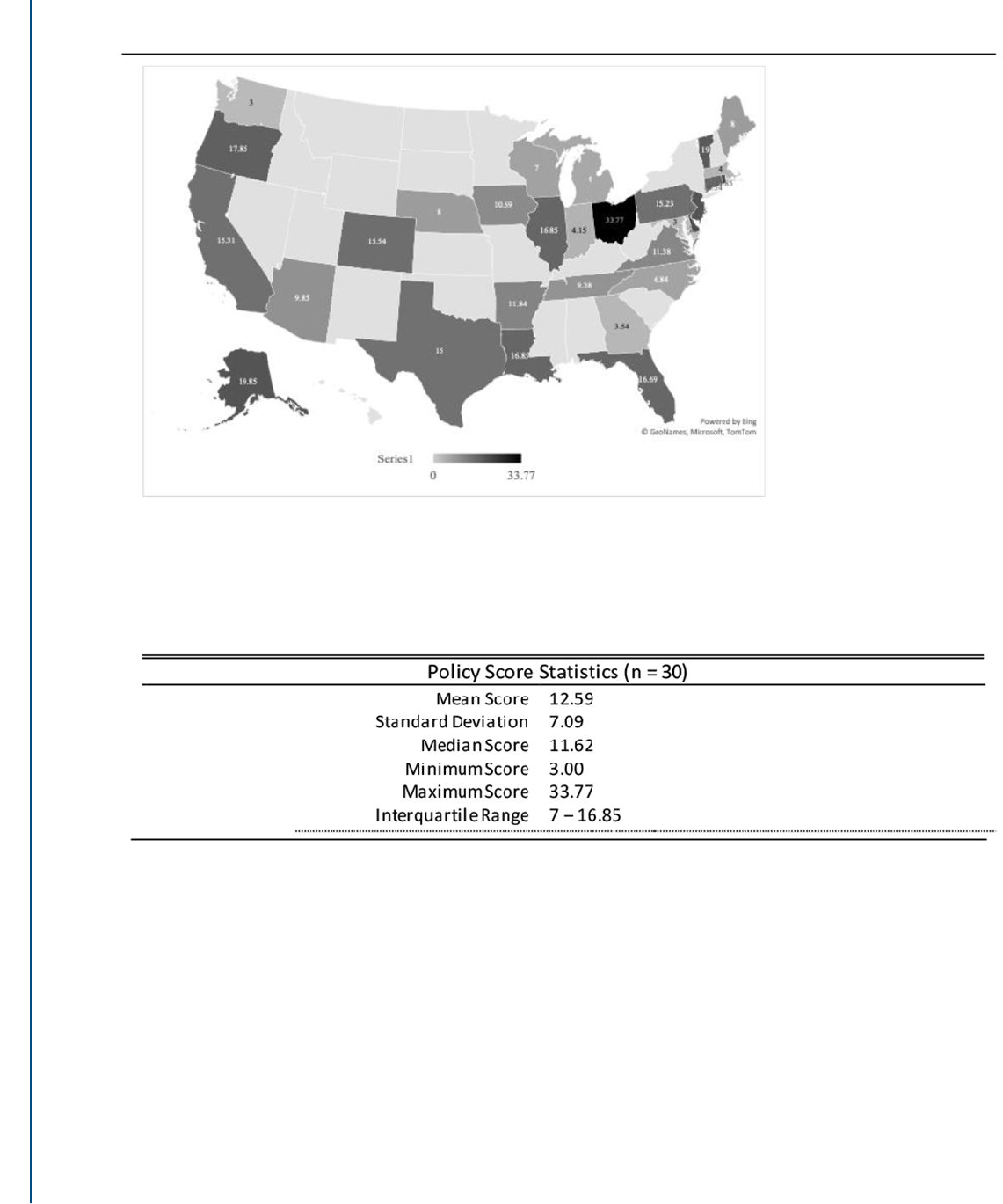
Figure 1.
2019 TDV Policy Score Heat Map by State
Rochford et al. Page 11
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Rochford et al. Page 12
Table 1.
States with currently active TDV school policies and their scores at a scored year
30 States With TDV School Policies
*
Score Scored Year
Maryland 3.00 2017
Washington 3.00 2005
Georgia 3.54 2015
Massachusetts 4.00 2010
Indiana 4.15 2010
Michigan 6.00 2004
North Carolina 6.84 2009
Wisconsin 7.00 2012
Nebraska 8.00 2009
Maine 8.00 2002
Tennessee 9.38 2018
Arizona 9.85 2010
Iowa 10.69 2007
Virginia 11.38 2018
Arkansas 11.84 2015
Texas 15.00 2015
Pennsylvania 15.23 2011
California 15.31 2018
Colorado 15.54 2016
Connecticut 16.54 2018
Florida 16.69 2014
Louisiana 16.85 2014
Illinois 16.85 2013
Oregon 17.85 2016
Vermont 19.00 2011
New Jersey 19.85 2014
Alaska 19.85 2017
Rhode Island 21.85 2011
Delaware 22.00 2017
Ohio 33.77 2018
*
Note: The 21 States without TDV school policies as of 2019 are Alabama, Hawaii, Idaho, Kansas, Kentucky, Minnesota, Mississippi, Missouri,
Montana, New Hampshire, New Mexico, New York, North Dakota, Oklahoma, South Carolina, South Dakota, Utah, Virginia, West Virginia,
Wyoming.
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Rochford et al. Page 13
Table 2.
TDV School Policy Score Elements for States with a Policy
Policy Abstraction Form Elements
Range of
Possible
Scores
Mean
(Standard
Deviation)
State(s) with the
Highest Scoring
Policy
State(s) with the Lowest Scoring
Policy
Section 1
-- Types of schools Covered
(1 2-point item)
0-2 0.93 (0.25)
All other states
scored 1.
VA & WA (0)
Section 2
– Definitions
(6 2-point items)
0-14 1.43 (1.74) NJ (6)
AR, GA, IN, IA, ME, MD, MA, MI,
NE, NC, TN, VT, VA, WA (0)
Section 3
– District Policy
(3 2-point items)
0-6 0.6 (1.19) DE (5)
AZ, AR, CA, CO, GA, IN, IA, LA,
ME, ME, MA, MI, NE, NC, PA,
TN, VT, VA, WA, WI (0)
Section 4
– District Policy Components
(10 2-point items)
0-20 1.7 (2.64) OH (11)
CT, GA, IA, LA, ME, MD, MA, MI,
NE, NC, VT, VA, WA, WI (1)
Section 5
– Dating Violence Prevention
Education for Students
(7 2-point items; items 5c and 5d required
standardization to fit a 2-point scale)
0-14 6.23 (2.24) AR (9.85) MD (2)
Section 6
– Dating Violence Prevention
Education for School Staff
(5 2-point items)
0-10 2.23 (2.78) AK, CT, LA (8)
AZ, AR, GA, IN, IA, MD, MA, MI,
NE, NJ, NC, WA, WI (0)
Section 7
– Protections and Legal Rights
(1 2-point item)
0-2 0.06 (0.25) PA, TX (1) All other states scored 0.
Total Scores 0-68 12.59 (7.09) OH (33.77) MD, WA (3)
J Public Health Policy
. Author manuscript; available in PMC 2023 February 07.
