MICHIGAN
HEAD LICE MANUAL
A comprehensive guide to identify, treat,
manage, and prevent head lice

i | P a g e
The purpose of this manual is to provide schools, local health departments, healthcare facilities, and other
group settings a comprehensive guide to identify, treat, manage, and prevent head lice infestations. This
manual was designed to serve as a universal guide providing information about head lice in a technical
sense, as well as a quick reference. This manual represents an update to the previous “Michigan Head
Lice Manual” published in 2004 and was compiled by members of a workgroup consisting of school
nurses, local public health officials, entomologists, and epidemiologists. Recognizing that head lice can
be a sensitive topic, the group strived to examine the current body of research about head lice and make
recommendations in the best interest of children and others impacted by them.
Thank you to those who assisted in the revision of this manual:
Susan Boley, RN, BS, CSN Marshall Public Schools
Brenda Brennan , MSPH Michigan Department of Community Health
Erik Foster, MS Michigan Department of Community Health
Judith Goldberg, RN, BSN Detroit Country Day School
Ronda Harrison, RN, BSN, NCSN Michigan Association of School Nurses
Jayne Heringhausen, RN, MSN Saginaw County Department of Public Health
Mary Larsen, RN, BSN, CSN Farmington Public Schools
Linda Meeder Michigan Department of Community Health
RN, MS, C-FNP, NCSN Michigan Department of Education
Nancy Polmear-Swendris Ann Arbor Public Schools
RN, MS, CSN
Kimberly Signs, DVM Michigan Department of Community Health
Various peer reviewed resources and references were utilized in the revision of the Michigan Head Lice
Manual. Special thanks to Tracy Miller, MPH, North Dakota Department of Public Health, and all those
involved in the development of “Head Lice: A Lousy Problem” (April 2012).
This publication is available on the Michigan Department of Community Health website at
www.michigan.gov/cdinfo.
This publication was partially supported with funding from the U.S. Centers for Disease Control and
Prevention, Building Epidemiology Laboratory Capacity, Cooperative Agreement Number
U50CI000895.
Revised August 2013

ii | P a g e
Table of Contents
Preface .........................................................................................................................................1
What are Head Lice? .................................................................................................................2
Life Cycle of Head Lice ..............................................................................................................3
Head Lice Myths and Facts .......................................................................................................4
Transmission of Head Lice ........................................................................................................6
Symptoms of Head Lice .............................................................................................................7
Detecting Head Lice ...................................................................................................................8
Inspection/Head-Check ........................................................................................................8
Supplies Needed for a Head Lice Inspection ...........................................................8
Inspection Method ...................................................................................................9
Management and Treatment ...................................................................................................10
Treatment with Pediculicides .............................................................................................10
Important Things to Know About Pediculicides ...................................................11
Treatment Failure ...................................................................................................11
Nit Removal after Treatment with a Pediculicide ..................................................11
Safety and Precautions .......................................................................................................12
Over the Counter (OTC) Pediculicides ..............................................................................13
Prescription Pediculicides ..................................................................................................14
Manual Removal of Lice and Nits .....................................................................................16
Alternative or Natural Methods .........................................................................................17
Other Substances ................................................................................................................18
Table Comparing Various Head Lice Treatments ................................................................18
Cleaning of Personal Items and Environment .......................................................................20
Developing a Head Lice Treatment and Prevention Policy ..................................................21
Michigan Department of Community Health and Michigan Department of Education
Recommended Head Lice Policy ............................................................................................22
Policy Recommendation ....................................................................................................22
Roles and Responsibilities .................................................................................................22
Recommended Procedures .................................................................................................23

iii | P a g e
Appendices
Quick Guide for Managing Head Lice ............................................................................. 25-26
Sample Letters ..........................................................................................................................27
Head Lice Identified on Child – Sample Letter 1 ..............................................................27
Head Lice Identified on Child – Sample Letter 2 ..............................................................28
Parent Education Letter – Sample Letter 1 ........................................................................29
10 Steps to Keep Ahead of Head Lice ....................................................................................30
Head Lice: Fast Facts ......................................................................................................... 31-32
1 | P a g e
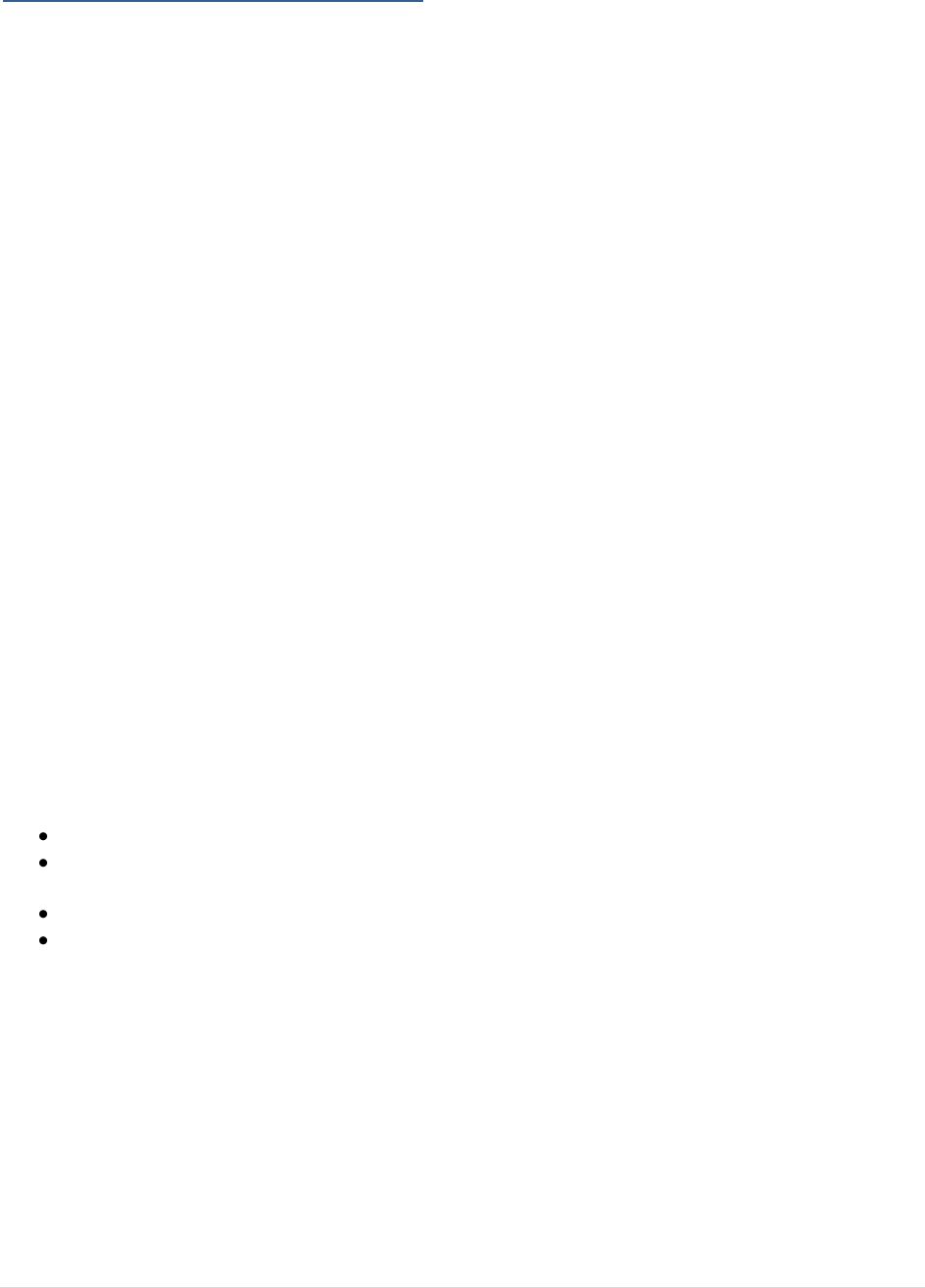
Head lice (Pediculosis humanus capitis) have been
plaguing people for millennia. Once accepted as a
common and unremarkable occurrence in society, head
lice have attained almost “legendary status” for creating
panic among parents of school-aged children in the United
States.
Pediculosis is an infestation of head lice, not an infection.
Infestations of head lice mostly affect children between
the ages of 3-12 years. Head lice infestations are not a
health hazard, and these lice do not spread disease.
1
However, inappropriate treatments can pose real and
significant health hazards to the child and his or her household. The most common symptom of a head
lice infestation is itching due to sensitization to allergens in lice saliva. Many times, there are no
symptoms. Occasionally, scratching leads to chafing and secondary bacterial infection requiring
treatment with an antibiotic.
While the public health impact from head lice is negligible, the social and economic costs can be
substantial. Anxiety over head lice can actually cause much more harm than the infestation itself. A
single case of head lice in a school or day care setting can create fear and anger among the community
that is out of proportion to the actual threat it poses to others. Infested children and their families
frequently suffer social punishment in the form of shame and embarrassment in the community. The
economic impact of head lice in the U.S. is estimated to approach $1 billion dollars annually, including
both direct costs (products and treatments used to kill lice and their eggs) and indirect costs (missed
school and work days, misdiagnosis, misuse of pediculicides and other agents).
2
Ineffective and outdated
“no nit” policies contribute greatly to the social stigma of lice infestations, but have no impact on
preventing additional infestations in the community.
3
(See MDCH and MDE Recommended Head Lice
Policy, page 22)
Utilizing the 2010 recommendations of the American Academy of Pediatrics and many other peer
reviewed scientific resources, this updated manual intends to provide clarification of new
recommendations for the effective treatment and management of head lice.
1
Frankowski BL, Bocchini JA, (2010). Council on School Health and Committee on Infectious Diseases, “Head Lice,” Pediatrics,
126 (2): 392-403.
2
Hansen RC, O-Haver J, (2004). “Economic Considerations Associated with Pediculus humanus capitis Infestation,” Clinical
Pediatrics, 43 (6): 523-527.
3
Mumcuoglu KY, Meinking TA, Brukhart CN, Burkhart CG, (2006). “Head louse infestations: the “no nit” policy and its
consequences,” Int J Dermatol, 45 (8): 891-6.
2 | P a g e
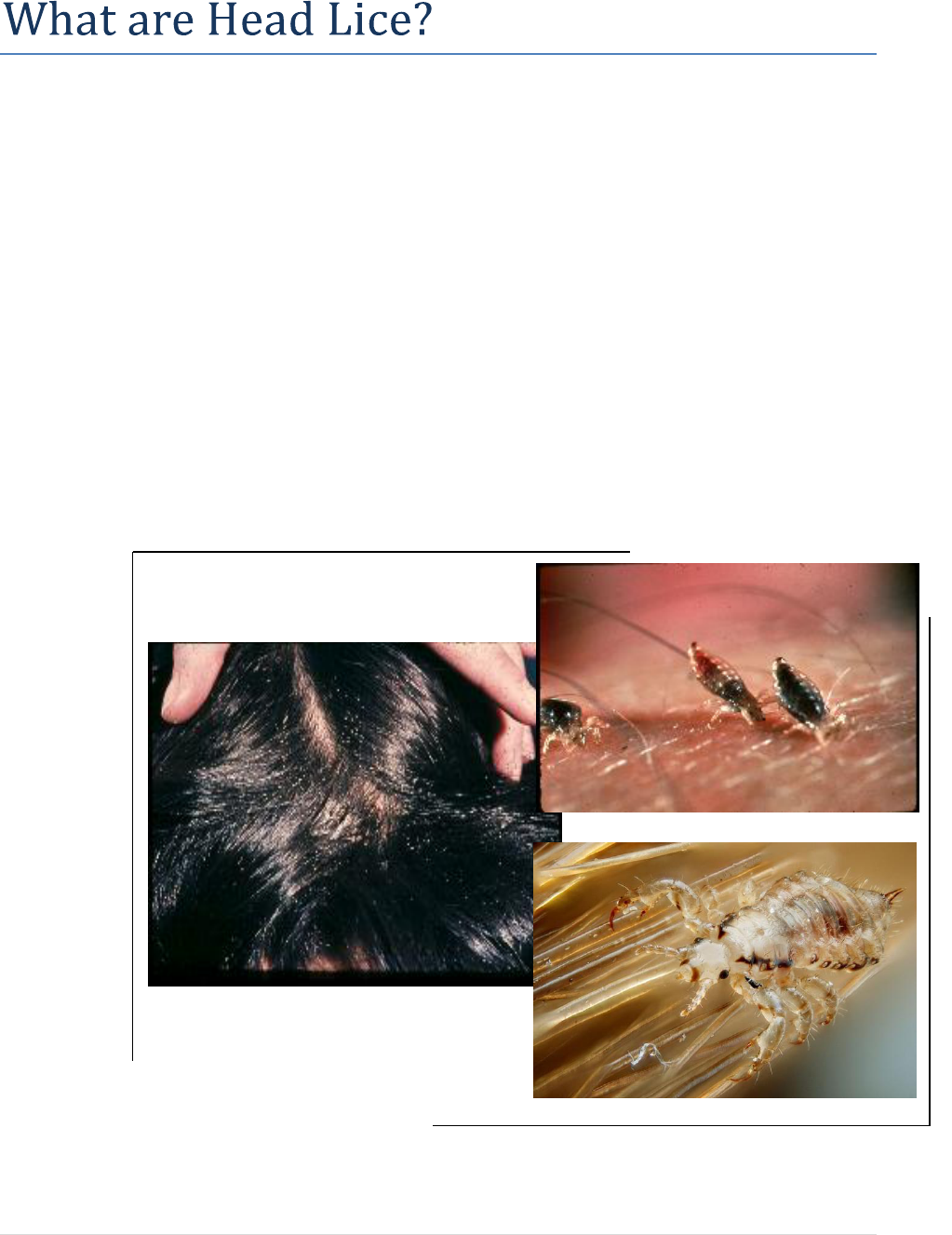
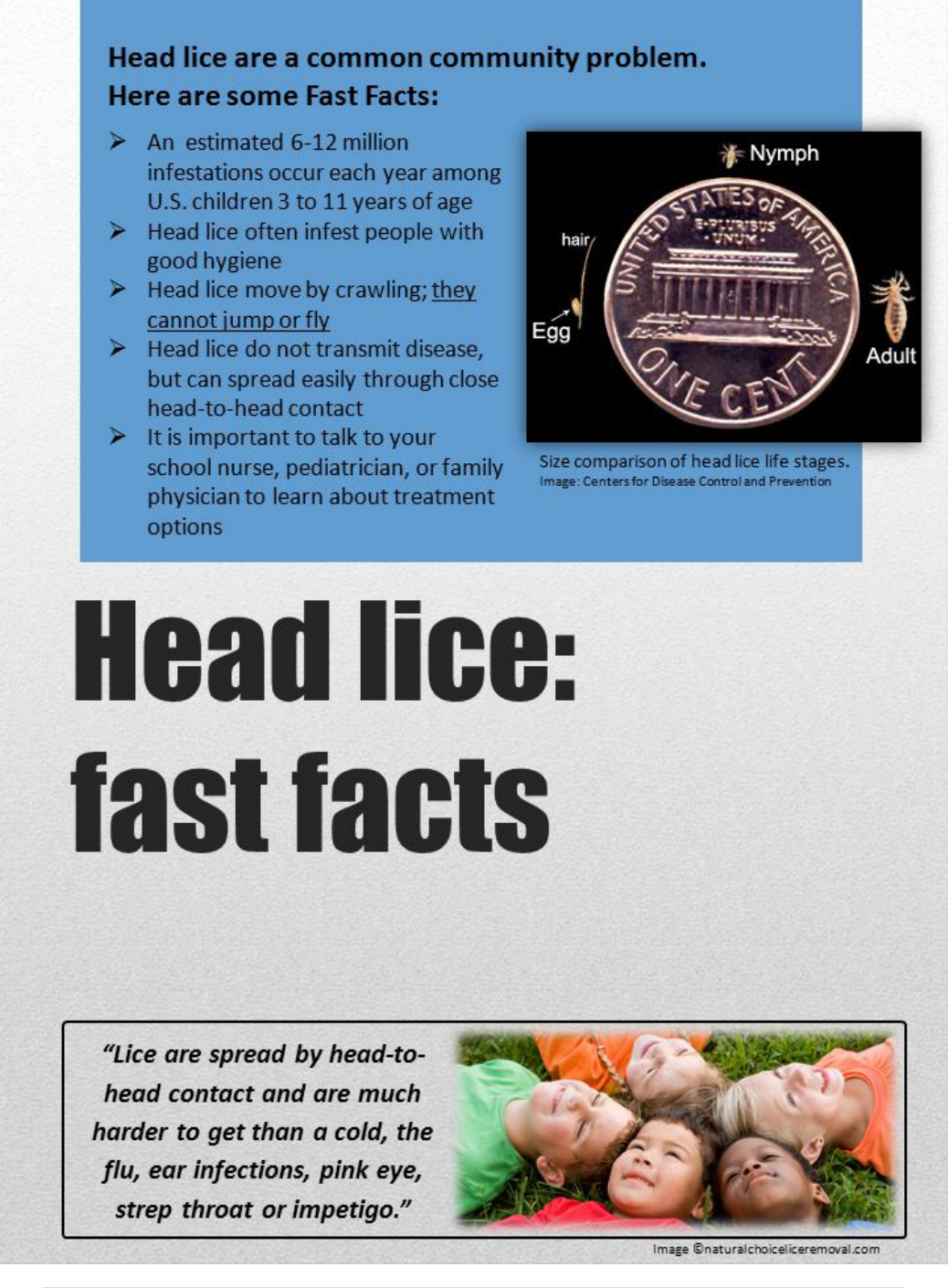
Human head lice (Pediculus humanus capitus) have been associated with humans for thousands of years.
Head lice are minute (about the size of a sesame seed), wingless parasitic insects that must live on a
person to survive. They survive by piercing the skin to feed on blood and are almost exclusively
associated with hair on the neck and scalp (Figure 1).
Lice are flattened dorso-ventrally, or top to bottom, and have six jointed legs with specially adapted claws
for holding on to hair (Figure 2). They can move about readily from hair to hair, but are most adept at
clinging to prevent dislodgement. Head lice tend to adapt their color to their surroundings and may range
in color from red to brown, gray, or black. Red colored head lice have likely recently fed. Because of
their small size, flattened bodies, and color, they may be very difficult to see on someone’s head.
The head louse feeds by using rasping teeth to penetrate scalp skin at the base of a hair or behind the ears.
The louse then inserts its “straw-like” mouthparts into a blood vessel and feeds much like a mosquito.
Over time, this feeding activity can be irritating to the skin and leads to the itching/scratching
characteristic of the infestation. A louse can ingest several blood meals per day.
Figure 1.
Head lice feeding
on a human scalp.
Lice engorge and
enlarge on blood
and will become a
reddish color when
recently fed.
Figure 2.
A close up high-
resolution image of
an adult male head
louse in its natural
environment.
Figure 3.
Head lice eggs (nits)
on a person’s hair.
Dandruff, hair casts,
globules of hair
spray, and scalp
conditions such as
psoriasis or eczema
may easily be
mistaken for nits.
Figure 3
Figure 1
Figure 2

3 | P a g e
Nits/Eggs:
Head lice begin their lives as eggs, or “nits.” The female adult head louse may lay an average of five
eggs per day.
4
Eggs are attached singly to a hair shaft with a “glue” that is resistant to chemical and
mechanical dislodgement (Figure 4). Eggs are normally cemented to the shaft of the hair very close to the
scalp. Nits are oval or teardrop-shaped and may range in color from white, yellow, or tan to gray,
depending upon age and whether or not the egg has hatched or been killed by head lice treatments. It is
thought that eggs attached to hairs greater than one-quarter inch from the scalp have either already
hatched, or will not hatch.
Nymphs:
Eggs spend seven to ten days incubating close to the scalp before hatching to release the first nymphal
stage (Figure 5). Nymphal stage head lice look very much like a miniature adult louse (Figure 6).
The newly hatched nymph will crawl and seek a place to feed immediately. There are three nymphal
stages punctuated by molting (the shedding of exoskeleton or “skin”). The three nymphal stages last
about 8-12 days.
Adults:
The final molt leads to an adult stage (Figure 6) where body growth stops and sexual maturation occurs.
Adult head lice continue to feed on blood every three to six hours. There are separate sexes in head lice,
and females must mate and be
fertilized in order to produce
viable eggs. A mated female can
continue to produce eggs for the
duration of her life, which is about
30 days. She can lay an average of
five eggs daily during this period.
4
Takano-Lee et al. (2003). In Vivo and In Vitro Rearing of Pediculus humanus capitis (Anoplura: Pediculidae), J. Med. Entomol.,
40 (5): 628-635.
Adult louse
actual Size
Image: Centers for Disease Control/James Gathany
Figure 5
Figure 4
Figure 6
1st
Nymph
2nd
Nymph
3rd
Nymph
Adult
Male
Adult
Female
1 mm
Figure 4.
Head lice eggs, or nits, are attached
singly to hair shafts close to the
scalp. They may be confused with
dandruff or dried particles of hair
spray or gel.
Figure 5.
Head lice eggs will hatch into first
stage nymphs in 7-10 days.
Figure 6.
Head lice progress through three
nymphal stages into the sexually
mature adult stage. All stages of
head lice feed on blood.
4 | P a g e
Definitions
Infestation = having multiple insects present and reproducing, in this case, on a human head
Lice = more than one louse
Louse = small insect that lives on the scalp (singular)
Nits = eggs, dead or alive, of a louse
Parasite = an organism that lives off another, i.e. lice surviving on the blood of humans
Pediculosis = having an infestation of lice
Myth
Fact
It is easy to get lice.
Lice are spread by head-to-head contact and are much harder to
get than a cold, the flu, ear infections, pink eye, strep throat or
impetigo.
Avoiding lice is important, as they are
dirty and spread disease.
Lice do not spread any known disease, nor are they impacted by
hygiene.
Head lice are very sturdy creatures and
can survive many days off a human
head in furniture, linens, or clothing.
Head lice need a blood meal every few hours in addition to the
warmth and humidity of the human scalp to survive. When off
the human body, in optimal conditions, they cannot survive for
more than 24 to 36 hours.
Nits (lice eggs) can fall off a person’s
head, hatch, and cause another person
to get lice.
Nits are glued to the hair shaft by a cement-like substance and
are very hard to remove. When a nymph is hatched, it must
quickly have the warmth and food source of a head to survive.
Cutting a person’s hair will prevent
head lice infestations.
The length of a person’s hair does not prevent head lice
infestations.
You can get head lice from sitting at a
desk next to someone who is infested
with head lice.
Head lice are spread through direct head-to-head contact. The
lice do not hop, jump, or fly, so sitting near someone with head
lice does not increase the risk of getting the lice.
Lice are commonly spread throughout
schools.
Transmissions in schools are rare. It is more common to get
head lice from family members, overnight guests, and
playmates who spend a lot of time together.
Lice are commonly spread through
hats, helmets, or headphones.
Although the spreading of lice through hats, helmets, or
headphones is possible, it is rare. It is more common for
transmission to occur from pillows, hairbrushes, or bedding.
Transmission primarily occurs through head-to-head contact.
5 | P a g e
Myth
Fact
Schools and child-care facilities should
screen all children for head lice, so
everyone can be treated and the spread
of head lice will be prevented.
Having regularly scheduled mass screenings does not reduce
the incidence of head lice.
“No-nit” policies reduce the risk of
head lice in schools and child-care
facilities.
Research shows “no-nit” policies do not decrease the number of
cases of head lice. They do increase the risk of incorrect
diagnosis of head lice, the number of days children are out of
school, and negative social stigma associated with head lice.
They also may hinder academic performance.
You can get lice from your dog or other
pets.
Head lice are specific to humans. You can get human lice only
from other humans. You cannot give your pets lice.
“Lice are spread by head-to-head
contact and are much harder to
get than a cold, the flu, ear
infections, pink eye, strep throat
or impetigo.”
Image ©naturalchoiceliceremoval.com
6 | P a g e
Head lice are transmitted by:
Person-to-person transmission (direct contact) – The majority
of transmissions of head lice occur by direct head-to-head
contact with an infested person. Most of the time this is a
close friend or relative.
Vector transmission (indirect contact) – This type of
transmission may occur through the sharing of bedding, or by
using personal items such as combs, brushes, scarves, hair
ornaments, or hats of an infested person. Although
transmission via indirect contact is possible, it is rare.
Common ways of transmission through head-to-head contact include:
Slumber parties
Shared beds
Sport activities
Reading circles
Without head-to-head contact, these ways of transmission are highly unlikely:
School buses
Hats, helmets, or headphones
Gym mats
Sitting at a desk
Anyone can get head lice, but some people are at greater risk than
others. Those people include:
Children between the ages of 3 and 11 years
Girls are more likely to get head lice than boys, possibly because of their play styles and
sharing of personal items.
5
People with long or short hair can contract head lice. Although all races can get head lice,
studies show that children of African-American descent are less likely to become infested.
5
5
Centers for Disease Control and Prevention, Head Lice Epidemiology: http://www.cdc.gov/parasites/lice/head/epi.html.
Quick Facts
1. Head lice are adept at moving from hair-to-hair because of their specialized “claws.” They cannot
jump, fly, or crawl great distances over hard surfaces.
2. Head lice
cannot survive long away from a human head.
A nymph or adult louse that falls from
its host will perish within a couple days under the most optimal conditions. Louse eggs do not
hatch at normal room temperatures; they require the higher temperatures associated with a human
body.
7 | P a g e
Parents, teachers, and other care givers should be aware of the signs and symptoms of a head lice
infestation because young children may not be able to express their discomfort directly. The following
symptoms should raise the level of suspicion for a head lice infestation:
Itching (“pruritis”): Caused by an allergic reaction to lice bites. When lice feed, they inject a
small amount of saliva into the skin. Over time, the host can develop an immune reaction to the
saliva which results in inflammation and itching. It may take four to six weeks for this reaction to
occur in people infested for the first time. However, itching may not be present in all cases.
Sores on the head: Rarely, scratching can lead to abrasions on the skin, allowing bacteria to enter
and possibly lead to infection. In severe cases, lymph nodes around the head, neck and
underarms can become swollen.
Tickling sensation: Lice movements in the hair may be felt by some infested individuals.
Sleeplessness and irritability: Lice are more active at night, possibly disrupting sleep.
Some people with head lice infestations have no symptoms. A lack of symptoms does not mean a lack of
head lice. See page 8 for how to screen an asymptomatic person for head lice.
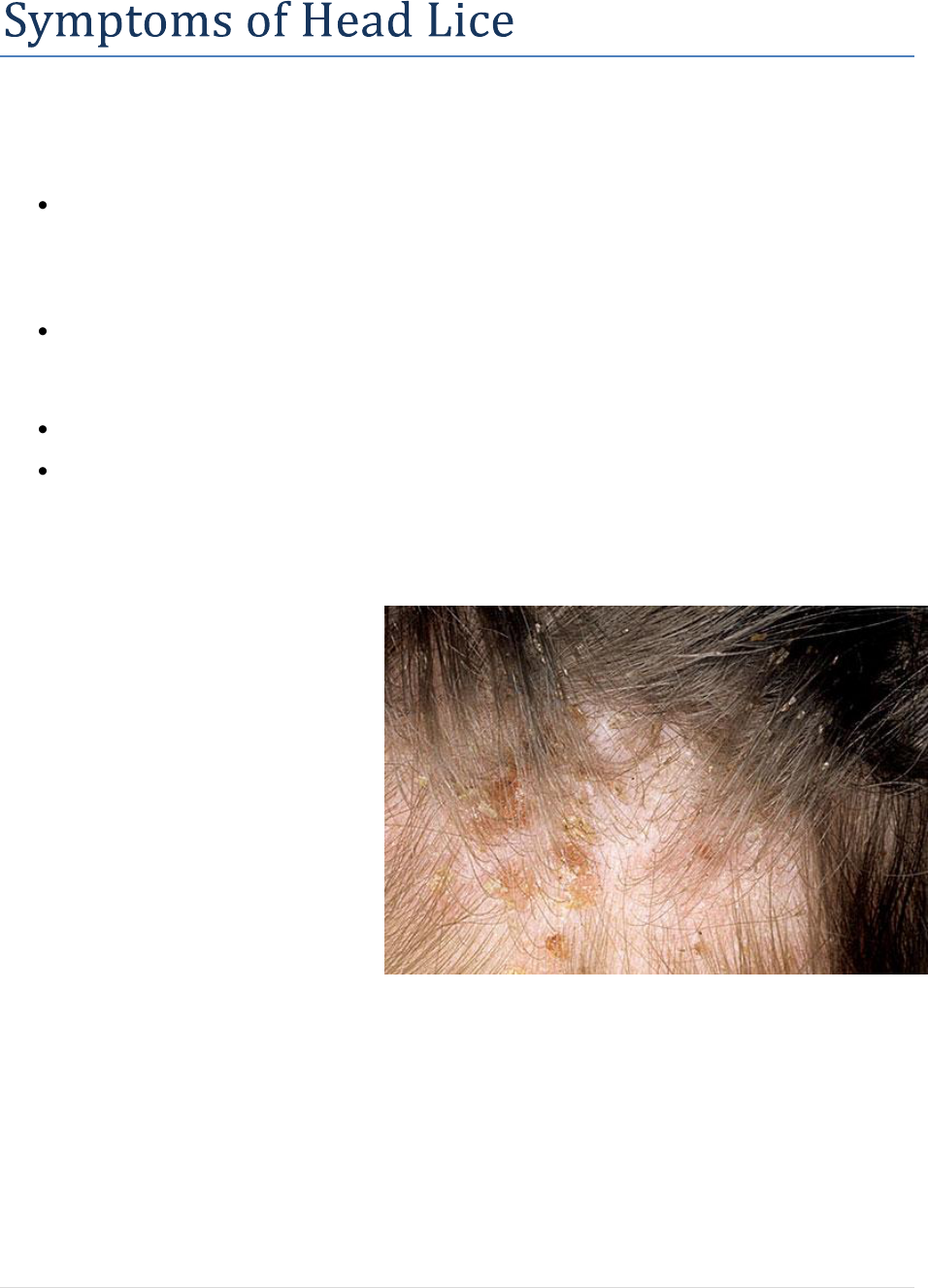
Head lice infestation may sometimes be characterized by the
presence of scabs or scars on the scalp from itching. In the above
photo, nits are also evident on hair shafts.
Image: Dermnet
8 | P a g e
Inspection/Head-Check
Head lice may be brought home after a person has had direct head-to-head contact with someone who has
an active head lice infestation. This is most often a close family contact or friend. Lice may spread
rapidly to others throughout the home because of the close contact of family members. Whenever one
person in the family has been identified to have lice, everyone living in the home should be checked. Any
friends, family members, or other people who have had close head-to-head contact with the infested
person over the previous week should be notified so they can be checked for head lice as well.
Careful inspection of the hair and scalp is necessary to see if a person has head lice.
Supplies needed for a head lice inspection include:
Time – The person who is inspecting for head lice needs to conduct a careful and thorough
search. Times may vary, but this process may take over ten minutes per person.
Strong source of natural light, high intensity lamp, or strong flashlight – Nits reflect
ultraviolet light, so natural light (near a window or outside) are the best. If natural light is not
available, convenient, or sufficient, a lamp (>60-watt bulb) or strong flashlight (LED
recommended) can be used.
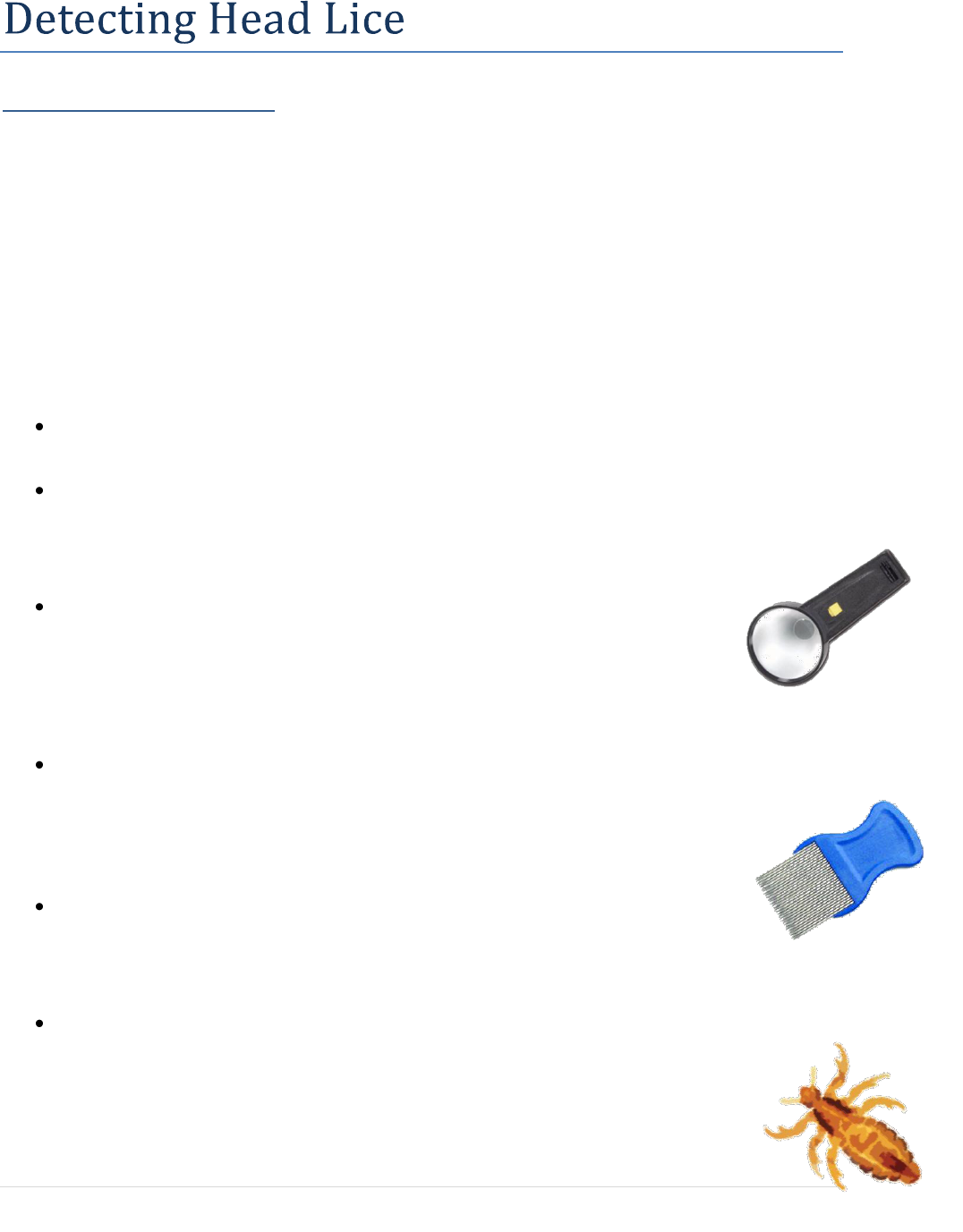
Magnifying glass (with a light source if possible)(optional) – Nits are small and
may be difficult for some people to see. Newly hatched and adult head lice are
also tiny, crawl fast through hair, avoid light, and may be difficult to see in contrast
with certain hair colors. A magnifying glass may assist in focusing on a small area
and detecting movement. It may also be helpful for people with problems focusing at close
distances.
Fine-toothed comb (lice comb) or other disposable hair parting tool (optional) – To examine
the base of the hair nearest the scalp, most examiners will need to use a tool to part and lift the
hair. If more than one person is being inspected, new tools should be used for each
individual. The inspectors should wash hands between checking individuals for general
hygiene.
Disposable gloves (optional) – There is no evidence showing that head lice are
spread through hand contact; however, some organizations or facilities may mandate
barrier precautions for hygienic reasons. If gloves are used, they should be changed between
each inspection.
Transparent tape (optional) – If a head lice infestation is suspected and the person conducting
the inspection is having difficulty identifying the insect, transparent tape may be used to capture
and seal the insect for further identification by someone trained to identify head lice.
9 | P a g e
Inspection Method
Head lice are best identified by inspecting the hair and scalp for live lice or nits (eggs attached to the hair
shaft close to the scalp). The standard for identifying head lice is finding a live louse on the head. Lice
and nits are most often found at the nape of the neck and above and behind the ears.
Carefully part the hair and examine the hair and scalp for nits or crawling lice.
Begin by inspecting the nape of the neck and the area behind the ears. If nothing is seen in these
areas, continue to inspect the rest of the head.
o Most recently laid nits will be opaque, white, shiny, and located on a hair shaft within
one-quarter inch of the scalp. Empty nit cases are more visible and are dull yellow in
color.
o Dandruff, hair casts, globules of hair spray, and scalp conditions such as psoriasis or
eczema may easily be mistaken for nits. To differentiate between nits and other debris,
remember that hair debris is easily detached or loosened from the hair shaft, and nits are
firmly attached to the hair and are not easily removed. Nits are also usually found one-
quarter inch or more from the scalp due to hair growth following the initial attachment.
By the time the hair has grown sufficiently for the egg case to be one-half inch from the
scalp, the egg has either hatched or is non-viable.
o Nits or lice in the eyelashes or eyebrows indicate possible infestation with other species
of lice. Specimens should be submitted to a laboratory for full identification, and the
case referred to a private physician or local health department, as a different form of
treatment will be required.
Questions about identifying lice or nits should be referred to a health care professional familiar with head
lice, such as a school nurse or local health department. Lice may be submitted to a laboratory in a
clean/dry container or on a piece of transparent tape. Pieces of hair with possible nits attached may be
snipped and submitted to a laboratory in the same manner. In Michigan, identification may be obtained
through:
Local or state health department
Michigan State University Extension office
Healthcare provider
STOP
STOP
Mass screenings are NOT recommended! Schools and child-care
facilities should designate an individual or individuals who will be
trained to inspect and assess for head lice on a private and
confidential basis.
10 | P a g e
Head lice infestations have been occurring for thousands of years, and although numerous efforts have
been tried to prevent them from occurring, nothing has proven to be 100 percent successful. However,
when they do occur, head lice infestations can be managed. It is important not to panic and/or to cause
undue stress for those infested and others around them.
If head lice are suspected, it is recommended the individual be inspected by a school nurse, a public
health nurse, or a medical provider.
6
It is recognized that not all families, schools, or child-care facilities
have access to a school nurse, a public health nurse, or medical provider. In those situations, it is
recommended that schools and child-care facilities designate an individual or individuals who will be
trained to inspect and assess for head lice on a private and confidential basis.
Management activities include treating close contacts with head lice, and the elimination of lice and nits
from the living environment and personal items.
Treatment should be considered only if lice or viable eggs are observed. Once a head lice infestation
is determined, there are several treatment options to choose from. Methods include:
1. Treatment with pediculicides (substances used to treat lice)
2. Manual removal
3. Alternative or natural methods
Treatment with Pediculicides
Pediculicides are substances or agents used to kill head lice. There are many medicated products
available for treatment of head lice, and they normally come in the form of shampoos. Most are available
over the counter, but some are by prescription only and may be reimbursable through insurance. All
products must be used strictly in accordance with label directions to ensure effectiveness and
prevent adverse reactions from overuse or misuse. When used properly, their effectiveness has been
reported to be 80-95 percent. Repeat treatment with the pediculicide in 7 to 10 days may be needed if
indicated on the product label. (See Treatment Failure section, page 11)
6
Frankowski BL, Bocchini JA, (2010). Council on School Health and Committee on Infectious Diseases, “Head Lice,” Pediatrics,
126 (2): 392-403.
Image ©suite101.com
11 | P a g e
Important Things to Know About Pediculicides:
Never treat unless there is definite evidence of head lice.
Pediculicides are to be used for the treatment of head lice only when there are active lice or viable
nits present in the hair, or when individuals share the same bed with someone who has live lice or
viable nits (AAP, 2010). They should not be used as routine shampoo or conditioner.
These products do not prevent someone from getting head lice.
No product is 100 percent effective at getting rid of lice and their eggs.
o Head lice infestations will be resolved more quickly by manually removing or combing
nits within one quarter inch of the scalp after treatment. This will prevent eggs not killed
during treatment from hatching. Nits further than one quarter inch from the scalp have
likely hatched or are not viable.
o A second treatment may be required as recommended on the product label.
Non-prescription pediculicidal products generally are effective and safe if used according to the
manufacturers’ directions. To ensure proper treatment, follow all recommendations and
directions on the label. All safety precautions listed on the product label should be observed.
Pediculicidal products are for external use only, and should only be applied to the scalp.
These products are harmful if swallowed or inhaled. If accidental ingestion does occur,
contact poison control at (800) 222-1222.
Treatment Failure
None of the current pediculicides are 100 percent ovicidal (effective at killing nits), and resistance has
been reported with pyrethrins and permethrin
7
products. This is not unusual, as insects can develop
resistance to products over time. Resistance will vary from one community to another.
When faced with a persistent case of head lice, consider several possible explanations, including:
Misdiagnosis (no active infestation or misidentification)
Noncompliance (not following treatment protocol or directions per manufacturer’s label)
Re-infestation (lice re-acquired after treatment)
Failure to treat all affected family members or close contacts at the same time
Resistance of lice to the pediculicide
Many cases of suspected resistance represent either misdiagnosis of old nits as active cases or a re-
infestation. Individuals who are chronically infested and have been treated multiple times with pyrethroid
shampoos are more likely to have resistant cases.
Although Permethrin 5% lotion has been tried for suspected resistant cases, it is unlikely that an increased
concentration or prolonged application time would be effective in cases of true resistance to Permethrin
1%. Studies have shown that resistance to permethrin is not dose-dependent.
7
Nit Removal after Treatment with a Pediculicide
Because none of the pediculicides are 100 percent ovicidal, manual removal of nits after treatment may be
done to reduce worries of another lice infestation or for cosmetic reasons.
7
Durand et al. (2012). Insecticide resistance in head lice: clinical, parasitological and genetic aspects. Clin Microbiol Infect.,
(4):338-344.
12 | P a g e
Pediculicides are substances that kill live lice and can be dangerous if misused or overused.
Do not use pediculicide products if the following conditions are present. In these instances, consult
a school nurse or other healthcare professional for safe alternative treatments:
Known sensitivity to any component of a product (read package insert thoroughly).
A child younger than the age recommended on the product label. For very young infants and
children, lice and nits may need to be removed manually using a lice comb. (see page 15 for nit
removal instructions)
The person has an infestation of the eyebrows or eyelashes. Many lice medications cannot be
used near the eyes. This can also be indicative of a pubic or body louse infestation.
The following people should consult their healthcare provider before treating themselves or
another person for head lice using a pediculicide:
Pregnant women and nursing mothers.
Individuals with cancer.
Individuals with asthma or other breathing difficulties (some pediculicidal products can cause
breathing difficulties or asthmatic episodes in some individuals).
Individuals who are allergic or sensitive to ragweed or chrysanthemums may have allergic
reactions to some of the pediculicides.
Always read the medication/product label before applying
medication to the head. If there are questions about
contraindications or product safety, contact your
healthcare provider.
13 | P a g e
The following pages will describe active ingredients, brief
instructions, and precautions for over-the-counter
pediculicides, prescription pediculicides, manual removal of
lice, alternative or natural methods, other substances, and
oral treatments for head lice.
Over the Counter (OTC) Pediculicides
Permethrin (1%) - Nix
Manufactured as a synthetic pyrethroid, permethrin 1% is currently the recommended treatment
of choice by the American Academy of Pediatrics (AAP) for head lice in newly diagnosed cases.
It is indicated in treatment of head lice for those individuals aged two months and older.
Permethrin has low toxicity and does not cause allergic reactions in individuals with plant
allergies.
The product is a cream rinse applied to hair that is first shampooed with a non-conditioning
shampoo and then towel dried. It is left on for 10 minutes and then rinsed off. It leaves a residue
on the hair that is designed to kill nymphs emerging from the 20-30 percent of eggs not killed
with the application. In order not to remove the residue, the hair should be rinsed with plain
water after application in a sink rather than the bathtub to limit exposure and with cool rather than
hot water to minimize chemical absorption through the scalp.
It is suggested that the application be repeated if live lice are seen 7 to 10 days later. Many
experts recommend routine re-treatment (preferably on day 9).
Pyrethrins plus piperonyl butoxide - RID, A-200, R & C, Pronto, Clear Lice System
Manufactured from natural extracts from the chrysanthemum, pyrethrins plus piperonyl butoxide
has low toxicity for people, but is neurotoxic to lice.
It is indicated in treatment of head lice for those individuals aged two years and older.
Pyrethrins should be avoided in persons allergic to chrysanthemums or who suffer from asthma.
The labels warn against possible allergic reaction in patients who are sensitive to ragweed, but
modern extraction techniques minimize the chance of product contamination, and reports of true
allergic reactions are rare.
These products are mostly shampoos that are applied to dry hair and left on for 10 minutes before
rinsing. All topical pediculicides should be rinsed from the hair over a sink rather than in the
shower or bathtub to limit exposure. Rinsing should be done with cool rather than hot water to
minimize chemical absorption through the scalp.
None of these natural pyrethrins are totally ovicidal (have the ability to kill a louse through the
egg before hatching), as newly laid eggs do not have a nervous system for several days; 20-30
percent of the eggs may remain viable after treatment.
A second treatment is necessary 7 to 10 days after first treatment to kill newly emerged nymphs
hatched from eggs that survived the first treatment.
14 | P a g e
Prescription Pediculicides
Malathion (0.5%) - Ovide
The organophosphate (cholinesterase inhibitor) 0.5% malathion was reintroduced to the U.S.
market as a head lice treatment in 1999.
It is indicated in treatment of head lice for those individuals aged six years and older.
Available as a lotion that is applied to the hair, left to air dry, then washed off after 8 to 12 hours
(although some studies suggest effectiveness when left on for as short a time as 20 minutes).
Malathion has high ovicidal activity and a single application is adequate for most individuals, but
the product should be reapplied if live lice are still seen in 7 to 9 days.
A concern about this product is its high alcohol content (78% isopropyl alcohol), making it
potentially flammable. Users should be instructed not to use hair dryers, curling irons or flat irons
while the hair is wet, and not to smoke near a person receiving treatment.
There is a risk of severe respiratory depression if accidentally ingested, although no such cases
have been reported.
Benzyl alcohol lotion (5%) - Ulesfia
Approved in 2009, this product kills head lice by asphyxiation.
It is indicated in treatment of head lice for those individuals aged six months and older.
The product is to be applied topically to the scalp for 10 minutes and repeated in 7 days
(retreating in 9 days is optimal).
The most common adverse effects include pruritis, erythema, pyoderma, and ocular irritation.
Benzyl alcohol is not ovicidal (have the ability to kill a louse through the egg before hatching).
Ivermectin lotion (0.5%) – Sklice
Applied as a topical lotion, this product affects the nerve cells of lice, causing paralysis and death.
It is indicated in treatment of head lice for those individuals aged six months and older.
Applied to dry hair in an amount sufficient (up to one tube) to thoroughly coat the hair and scalp
for 10 minutes and then rinsed with plain water.
Ivermectin is both pediculicidal and partially ovicidal.
o Sklice may be a one-time treatment – retreatment may not be necessary. In a study, 73.8
percent of individuals who received one treatment remained lice free after 15 days.
Common side effects include eye redness or irritation, dandruff, dry skin, or burning sensation of
the skin.

15 | P a g e
Spinosad suspension (0.9%) – Natroba
Topical suspension with active ingredient of spinosad which causes neuronal excitement leading
to paralysis and death of lice.
It is indicated in treatment of head lice for those individuals aged four years and older.
Product is applied to dry hair and scalp. Once washed off, a fine-toothed comb may be used to
remove treated lice and nits from the hair and scalp.
Use product in one or two treatments that are one week apart. If live lice are seen one week (7
days) after first use, re-treat.
Contains benzyl alcohol. Common side effects include eye and scalp redness and irritation.
Topical Reactions to Pediculicide Treatment
Itching or mild burning of the scalp caused by inflammation of the skin in response to topical therapeutic
agents can persist for many days after lice are killed and are not a reason for re-treatment. Topical
corticosteroids (i.e., hydrocortisone creams) and oral antihistamines (i.e., Benadryl®) may be beneficial
for relief of these symptoms. Please consult with the child’s physician/pharmacist before starting any
topical therapies.
Image © Melanie Martinez
16 | P a g e
Manual Removal of Lice and Nits
Manually removing lice and nits may be effective at
quickly resolving a head lice infestation. Pediculicide
treatment may not be 100 percent ovicidal. For this
reason, removing viable eggs may prevent the need for
a second treatment. Whether using a pediculicide or
manual removal as a stand-alone treatment, the more
lice and nits that are combed from the hair, the faster
the infestation will be resolved.
To manually remove lice after pediculicide treatment or as a stand-alone treatment:
1. Work in an area with good visibility and light, such as from a lamp or natural sunlight through a
window.
2. Make sure a standard comb moves through the hair without difficulty before attempting to use a
fine-toothed lice comb. Combing may be easier if the person’s hair is slightly wet.
3. Part the hair into sections and hold sections in place with rubber bands or hair clips.
4. Sit behind the person and use a bright light (and magnification if available) to inspect and comb
through the hair, one small section at a time. Remove nits using the comb, fingernails, or by
cutting the strands of hair.
5. Clean the louse comb frequently to remove any caught lice or eggs using soapy water or paper
towel. It may require several hours each night for several nights to successfully remove all nits
and lice. An entertaining video may help keep children occupied during this exercise.
6. Combing may be repeated daily until no lice are seen. Continue monitoring for two to three
weeks.
Many types of fine-toothed combs may be included within packages of pediculicides, or they may be
purchased from most drug stores or internet retailers. The effectiveness depends on their composition
(metal or plastic) and construction (length and spacing) of the comb teeth, the texture of the hair to be
combed, combing technique, and the time and care expended in the effort.
Electronic combs may be useful for detection (if vision is limited), since they
emit a sound when a live louse is present.
17 | P a g e
Alternative or Natural Methods
Several products are marketed as alternative or natural methods of treatment. A number of shampoos and
rinses contain herbs, oils, or enzymes believed to aid in lice removal. The majority of alternative or
natural products are suffocants or enzymes.
Natural or herbal products are not required to meet FDA efficacy and safety standards. These products do
not have licenses for the treatment of head lice, and in some cases, have little or no data to support their
effectiveness. Although natural products are often perceived as being intrinsically safe, the State of
Michigan cannot recommend these treatments without further evidence of their effectiveness.
Please contact your local health department or family physician to make sure there are no potential health
consequences of alternative or natural methods.
Suffocants – petroleum jelly, mayonnaise, plant-based oils, or Cetaphil
Suffocants can obstruct the respiration of adult lice as well as suffocate lice eggs by blocking
efficient air exchange.
For all products except Cetaphil, the product is massaged on the entire surface of the hair and
scalp, covered with a shower cap, and left on for at least eight hours (see safety precautions page
19). The suffocant can then be used as a lubricant to aid in nit removal by combing.
Cetaphil is massaged on the entire surface of the hair and scalp, the excess product is combed out,
hair is dried with a hair dryer, and the hair is washed eight hours or more later.
8
Diligent shampooing is usually necessary for at least the next 7 to 10 days to remove the residue.
To date, little scientifically published information is available on the effectiveness of these
methods.
Enzymes – LiceLogic, Lice B Gone, Lice R Gone
Treatment products containing “enzymes” claim to dissolve or soften the glue that attaches the nit
to the hair shaft, thereby providing easier removal of lice and nits when combing. To date, only
anecdotal information is available on their effectiveness.
Desiccation (Heat Treatment) – LouseBuster, hair dryers, etc.
The LouseBuster is a custom-built machine that uses one 30-minute
application of hot air in an attempt to desiccate active lice and their eggs.
One study has shown that subjects had nearly 100 percent mortality of eggs
and 80 percent mortality of hatched lice.
The LouseBuster is expensive and requires training in its use. Some businesses offer convenient
heat treatments for a fee (normally not covered by insurance).
A home hair dryer should not be used in the same way. Studies have also shown that using home
hair dryers, commercial (salon) dryers, and drying bonnets are not as effective as the steady and
diffused heat offered by professional products.
8
Pearlman, DL (2004). A simple treatment for head lice: Dry-on, suffocation-based pediculicide, Pediatrics, 114 (3): 275-279.
18 | P a g e
Other Substances
Flammable or toxic substances, such as gasoline or kerosene, should never be used. Products intended
for animal use (e.g., flea collars or topical insecticides) should not be used to treat head lice in humans.
Oral Treatments (Used Off-label for Lice)
A promising oral treatment method, oral Ivermectin (Stromectol), is an anti-parasitic agent similar to a
macrolide antibiotic but without antimicrobial activity. Other agents used off-label are currently being
researched, however, the Federal Drug Administration (FDA) has not approved any oral drugs for the
treatment of head lice infestations.
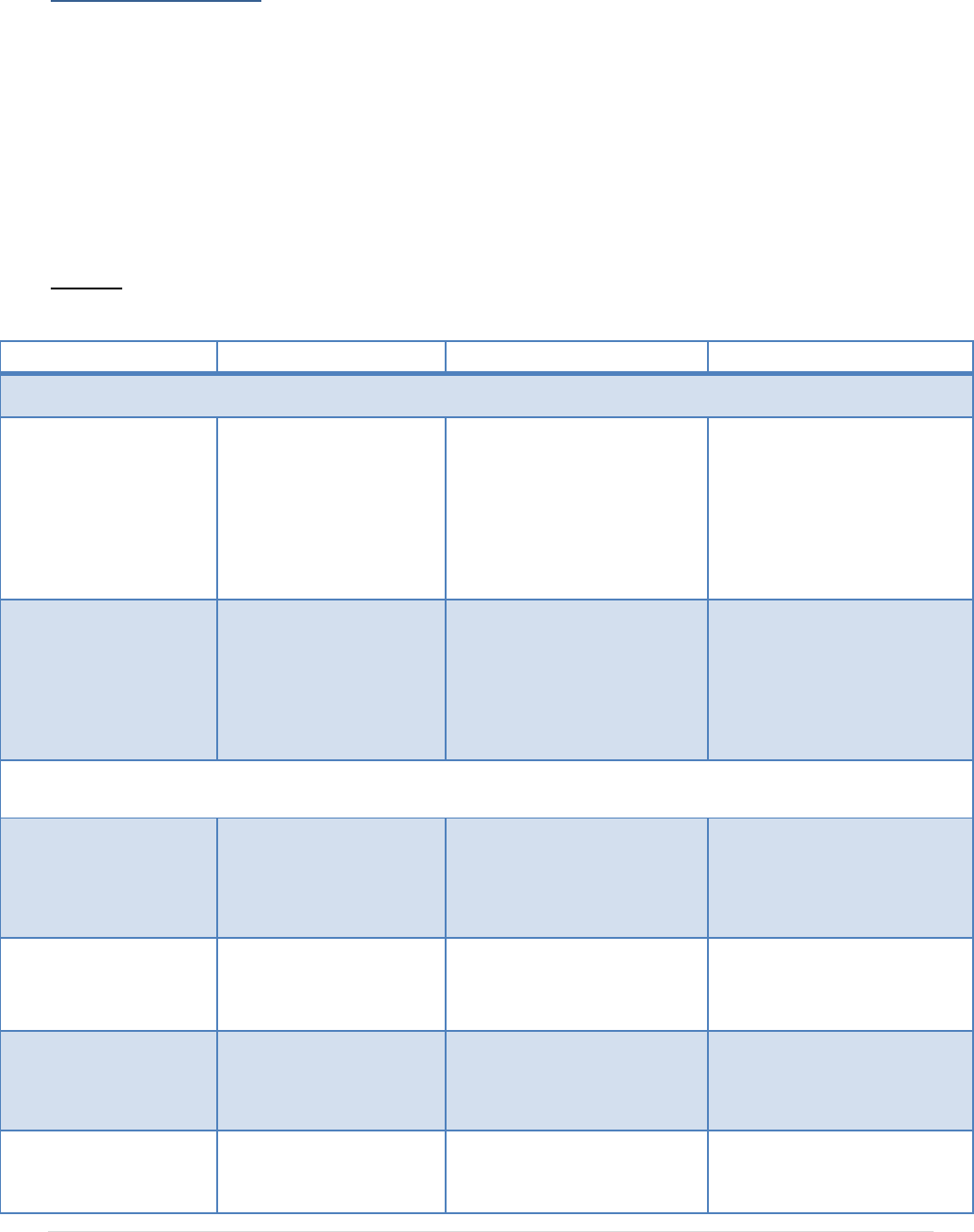
Table 1. Comparison of various head lice treatments including over-the-counter, prescription, and
alternatives.
Treatment
Active Ingredient
Advantages
Disadvantages
Over-the-Counter
Nix
Permethrin lotion 1%
Most studied and least toxic to
humans. Generally effective
and safe if used according to
the manufacturer's directions.
Does not cause allergic
reactions in individuals with
plant allergies. For use in
children over 2 months of age.
Non-ovicidal; adverse effects
include pruritis, erythema, and
edema.
Repeat treatments are often
required or recommended by
the manufacturer.
A-200, Pronto, R&C,
Rid, Triple X
Piperonyl butoxide (4%)
Pyrethrum extract
(equivalent to 0.33%
pyrethrins)
Generally effective and safe if
used according to the
manufacturer's directions. For
use in children over 2 years of
age.
Non-ovicidal; avoid in people
who are allergic to ragweed or
chrysanthemums.
Repeat treatments are often
required or recommended by
the manufacturer.
Prescription
Ovide
Malathion lotion (0.5%)
Single application is adequate
for most patients; partially-
ovicidal. Malathion is
approved for use in children
over 6 years of age.
Due to isopropyl alcohol
content, Ovide is potentially
flammable; use caution. May
cause skin irritation or stinging
sensation.
Ulesfia lotion
Benzyl alcohol lotion (5%)
Not neurotoxic and kills head
lice by asphyxiation. For use in
children over 6 months of age.
Non-ovicidal; contains benzyl
alcohol which may cause eye
and scalp redness and irritation.
Sklice
Ivermectin lotion (0.5%)
May be both pediculocidal and
ovicidal. Approved for use in
children over 6 months of age.
Side effects may include eye
redness or irritation, dandruff,
dry skin, or burning sensation
of the skin.
Natroba
Spinosad lotion (0.9%)
For use in children over 4 years
of age.
Non-ovicidal; contains benzyl
alcohol which may cause eye
and scalp redness and irritation.
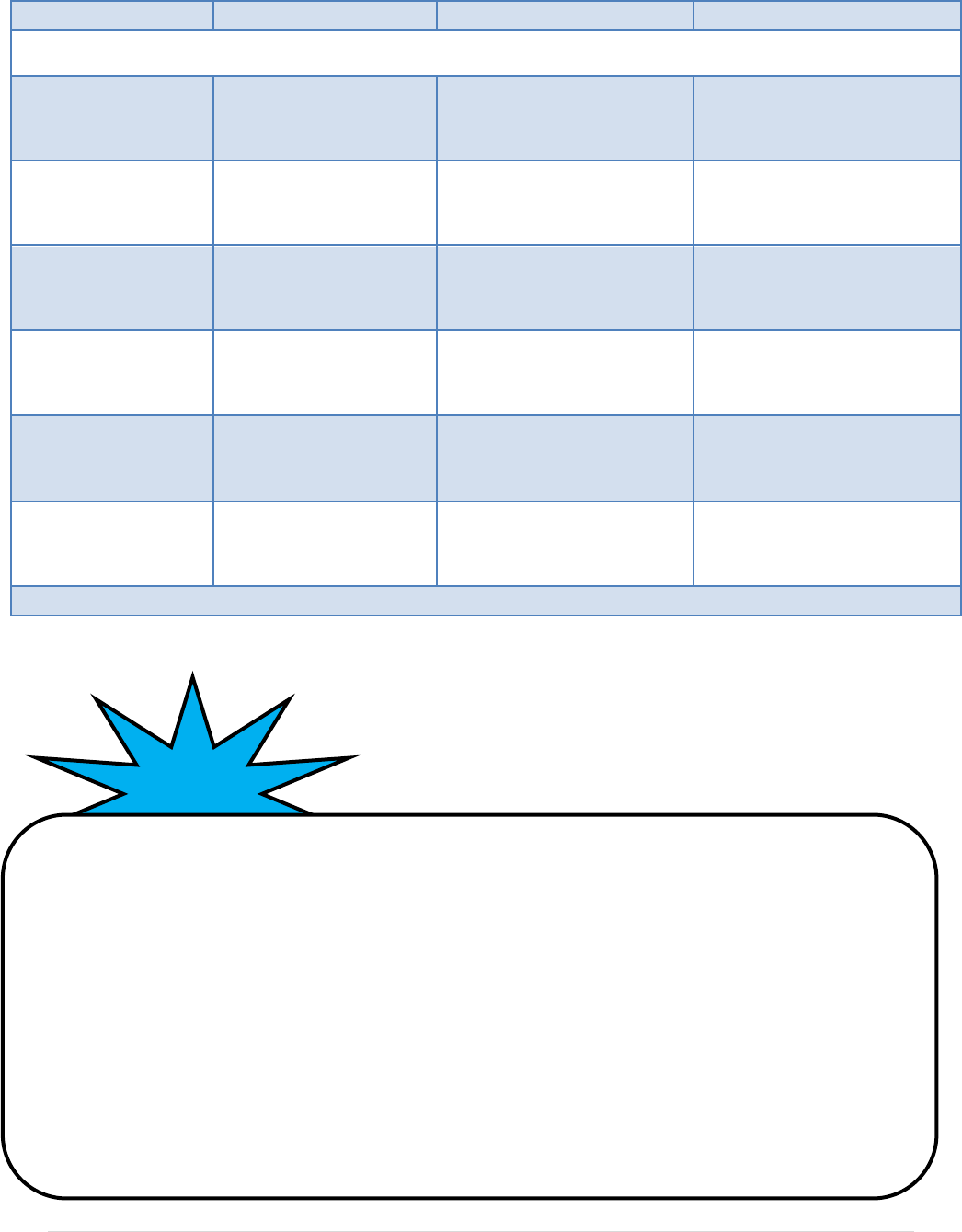
19 | P a g e
Treatment
Active Ingredient
Advantages
Disadvantages
Alternative or Natural
Petroleum jelly
(Vaseline)
Viscous material which
potentially asphyxiates
head lice.
“Non-chemical;” perceived as a
natural option.
Effectiveness unknown; very
difficult to remove from hair.
Mayonnaise
Viscous material which
potentially asphyxiates
head lice.
“Non-chemical;” perceived as a
natural option.
Effectiveness unknown; difficult
to remove from hair.
Oil (vegetable, olive,
mineral)
Viscous material which
potentially asphyxiates
head lice.
“Non-chemical;” perceived as a
natural option.
Effectiveness unknown; difficult
to remove from hair.
Cetaphil
Viscous material which
potentially asphyxiates
head lice.
“Non-chemical;” perceived as a
natural option.
Not approved by the FDA for
use as a pediculicide.
Desiccation (Heat)
Controlled, heated air
causes desiccation in head
lice and eggs.
“Non-chemical;”perceived as a
natural option. Ovicidal; one-
time treatment usually
effective.
Expensive equipment; individual
providing treatment must be
trained and competent.
Enzyme Products
“Non-chemical;” perceived as a
natural option.
Effectiveness unknown.
Note: The use of brand names in this document is for identification purposes only, not for product endorsement.
Safety
Precautions
NEVER USE:
Treatment should never consist of toxic and/or flammable household products such as kerosene,
gasoline, paint thinner, turpentine, or any other household cleaners. Pesticides intended for use
on insects or bugs other than head lice, or pesticides intended for use on animals, should never
be used on humans. Every year children are seriously injured as a result of these types
of products.
CAUTION:
Use caution when putting small children to bed wearing a shower cap. Shower caps may be a
suffocation risk.

20 | P a g e
Head lice are spread most commonly by direct head-to-head (hair-to-hair) contact. However, much less
frequently they are spread by sharing clothing or belongings. The risk of getting infested by a louse that
has fallen onto a carpet or furniture is very small. Head lice survive less than 1-2 days if they fall off a
person and cannot feed; nits cannot hatch and usually die within a week if they are not kept near body
temperature.
9
Items that have been in contact with the head of the person with infestation in the 24-48
hours before treatment should be considered for cleaning.
Check everyone in the household at the same time
Check everyone in the household at the same time, prior to cleaning the environment. This includes
grandparents, younger and older siblings, and parents. Statistics have suggested that 60 percent of
people with head lice don’t know they have them and have no symptoms. They may be
unintentionally infecting others and continuing the cycle.
Launder any personal items that could be infested with head lice
Personal items to be laundered include clothing, bedding, towels, cloth toys, etc. Items should be
washed for at least 10 minutes in hot water and/or dried on high heat for at least 30 minutes. For items
that cannot be washed, seal in a plastic bag and store for 14 days at room temperature or 24 hours in
below freezing temperatures.
Vacuum
Items that should be vacuumed include bare mattresses, carpets, floors, stuffed animals, coat collars,
hats, couches, chairs, and car upholstery. There is no need to discard the vacuum bag after cleaning,
except for aesthetic purposes. Head lice cannot survive without a blood meal.
Inspect hairbrushes, combs, hair ties, and barrettes
For washable accessories, wash and dry (on high heat) for at least 30 minutes. Soak combs, brushes
and barrettes in water hotter than 130ºF. If items cannot be exposed to high heat, soak them in Lysol®
or rubbing alcohol for one hour.
9
Centers for Disease Control and Prevention, Parasites – Lice – Head Lice – Prevention and Control, www.cdc.gov (2013).
Safety
Precautions
DO NOT
spray or “fog” a home with insecticides or pediculicides
. They are not necessary to control head
lice and may be harmful if used in a poorly ventilated area. The CDC, the AAP, and the Michigan Department
of Community Health strongly discourage the use of these spray products for the control of head lice.
21 | P a g e
Michigan’s Department of Community Health, Department of Education, and the Michigan Association
of School Nurses provide a recommended head lice policy for use in Michigan schools. These policy
recommendations are similar to those supported by the American Academy of Pediatrics and the National
Association of School Nurses.
It is recommended that schools and child-care settings develop a written policy addressing how
infestations, or suspected infestations of head lice will be managed in the school/child-care setting. Points
to consider and address within a policy include:
Maintaining confidentiality of the children.
Parent/guardian notification – when, how, and who?
Exclusion protocol.
Communication process for parents and staff regarding education about head lice and local
policy.
Protocol for responding to treatment refusals and failures.
If or when referrals will be made to other agencies.
Written policies and procedures regarding specific responsibilities and recommendations will facilitate
efficient and consistent implementation by all schools and child-care centers. These help to ensure all
children are treated in a fair and equal manner.
Seek input from your local health department, school nurses, clinics/healthcare providers, child-care
health consultants, child-care providers, and school personnel in the development of a head lice
management policy.
22 | P a g e
The Michigan Department of Community Health (MDCH) and the Michigan Department of Education
(MDE) jointly support the following statements for the management of head lice infestations within
school communities. Currently, there is no scientific evidence demonstrating that enforced exclusion
policies are effective at reducing head lice transmission.
10
Although the lice policy is ultimately up to the
school administration, school officials are urged to consider these recommendations.
Policy Recommendation
At this time, MDCH and MDE recommend a policy that focuses on the exclusion of active infestations
only. Active infestations can be defined as the presence of live lice or nits found within one quarter inch
of the scalp. Nits that are found beyond one quarter inch of the scalp have more than likely hatched, or
are no longer viable.
Any student with live lice (or nits within one quarter inch of the scalp) may remain
in school until the end of the school day (see recommended procedures, page 23).
Immediate treatment at home is advised. The student will be readmitted to school
after treatment and examination. If, upon examination, the school-designated
personnel find no live lice on the child, the child may reenter the school.
Any student with nits (farther than one quarter inch from scalp) should be allowed
in school.
Parents should remove nits daily and treat if live lice are observed.
Roles and Responsibilities
Parent’s Role
Parents have the ultimate responsibility for their children. This includes:
Becoming educated about head lice.
Performing regular checks on all individuals in the home.
Treating a child with head lice as soon as possible and committing to following through until
there are no longer signs of an infestation.
Teaching children how to minimize the chance of getting head lice by avoiding head-to-head
contact, not sharing hats, combs, brushes, and hair accessories, and by containing long hair in
braids or pony tails.
10
Frankowski BL, Bocchini JA (2010). Council on School Health and Committee on Infectious Diseases, “Head Lice,” Pediatrics,
126 (2): 392-403.
23 | P a g e
School’s Role
Develop and adhere to school district’s policies and procedures (see “Considerations in
Developing a Head Lice Treatment and Prevention Policy” on page 21).
Periodically disseminate current educational materials on head lice to parents:
o It is recommended to send a general factsheet letter at the beginning and mid-point of the
school year, or as necessary.
o When a significant increase in head lice cases is detected, consider providing a general
factsheet or parent education letter.
Utilize a school nurse or designee to train other school staff to evaluate cases of head lice.
Mass screenings are not recommended. Schools and child-care facilities should designate an
individual or individuals who will be trained to inspect and assess for head lice on a private and
confidential basis.
State and/or Local Public Health Agency’s Role
Provide technical support and knowledge to schools.
Disseminate the most current information on head lice recommendations and control measures.
Recommended Procedures
Student identified during school hours to have an active case of head lice:
1. Student may return to class but restricted from activities involving close head-to-head contact or
sharing personal items with other children. Immediate removal of the child is unnecessary—if
the child has lice, they probably have been infested for weeks and prompt removal of the child
could lead to embarrassment and ridicule. The child can be sent home at the end of the day and
should be allowed to ride the bus.
2. Notify parent/guardian directly. Offer emotional support to the parent/guardian as this is a
difficult situation for all involved.
3. Send home a copy of the “Quick Guide for Managing Head Lice” (see pages 25-26). Schools
may also consider sending the optional parent documentation of treatment form (see page 28).
Student with suspected case of head lice returns to school:
1. Parent must accompany their child to the school office with confirmation of treatment.
2. Designated school personnel will re-examine the student’s hair:
Student will be re-admitted to school if no live lice are found.
If live lice are found and not removed, the student may not be re-admitted to class.
o Review with parent the manual lice removal techniques (caution: if chemical
treatments were used, they should not be used again for another 7-10 days).
o Suggest parent call their pediatrician for further assistance.
o May also contact local health department or school nurse for assistance.
24 | P a g e
Any student with no live lice, but nits farther than one quarter inch from the scalp should
return to class.
If nits are found within one quarter inch of the scalp, educate the parents about the need for
removal of those potentially viable eggs and return the child to class. School personnel re-
check for lice and nits the next school-day to verify removal of potentially viable nits.
3. Periodic checks of the student’s hair by designated school personnel should be done over the next
few weeks to assure successful treatment. **Remember, confidentiality is important.
4. Request parent to continue daily lice checks and nit removal for the next two to three weeks.
5. Retreat as necessary according to product label.
Recurrent or Chronic Cases (Continued active infestation after appropriate treatment has
started, persistent infestation after six consecutive weeks, or three separate cases within one school
year.)
Multidisciplinary group consisting of parent, teachers, administrators, social workers, school
nurse, and other appropriate individuals to determine the best approach to resolving the issue and
improve school attendance.
25 | P a g e
Quick Guide for Managing Head Lice
Management and treatment of head lice
includes:
1. Careful inspection and screening of the hair and
scalp to identify lice and/or nits correctly.
2. Use of a pediculicidal (head lice) product if live lice
or viable nits are found.
3. Cleaning of personal items and the environment.
4. Repeat treatment with the pediculicidal product
following the label instructions. If the label does not
provide a guide for a second treatment, repeat
treatment nine days following the initial treatment.
1. Careful inspection of the hair and scalp
to identify lice and/or nits correctly.
Lice are tiny insects (about the size of sesame seeds)
ranging in color from red to brown, yellow, tan, gray,
white, or black. They attach their eggs (nits) to the
hair shaft near the scalp with a glue-like substance.
The nits are small, about the size of a knot of thread,
and can be white, tan, pale gray, or yellow in color.
Nits can be hard to see, so it is important to take your
time and separate the hair into thin sections. The nits
are most commonly found at the nape of the neck
and behind the ears, but can be anywhere, so check
the entire head.
A person is infested with head lice if live lice or nits on
the hair shaft closer than one quarter inch from the
scalp are found.
All individuals living with an infested person, as well
as those who have head-to-head contact with the
person, should be screened for lice.
2. Use of a pediculicidal (head lice)
product if live lice or viable nits are
found.
When someone is infested with head lice, he or she
should be treated with a medicated hair product that
will kill the lice (a pediculicide). Pediculicides are not
meant to be used for prevention.
There are many lice treatment products available,
which can be found at area drug stores or grocery
stores. Most non-prescription pediculicidal products
contain permethrin 1% or pyrethrin (such as Nix or
RID
11
). Permethrin 1% is recommended as the first
choice of treatment. Once you have selected a
product, it is very important that you follow the label
directions on the product EXACTLY to treat those who
are infested.
Treat only those people with live lice or nits less than
one quarter inch from the scalp. The American
Academy of Pediatrics recommends treating anyone
who shares the same bed with those who are
infested.
Prescription pediculicides are also available. For
further information on pediculicidal products, contact
your local public health department, healthcare
provider, clinic, or pharmacy.
Before using the product, review all safety
statements on the label. Do not use the product if
any of the precautions apply to you or the person
being treated. Consult with a healthcare provider for
further instructions. Using a head lice treatment
product will not prevent you from getting head lice.
11
Use of a brand name does not endorse the specific product. A
similar product may work as well as those mentioned.

26 | P a g e
Quick Guide for Managing Head Lice (continued)
3. Cleaning of personal items and the
environment.
No special cleansers, sprays, or chemicals are needed
for cleaning your home.
Soak hair care tools in hot water (130ºF) for at least
10 minutes. Heat may damage some plastic combs
and brushes. Place these items in a sealed bag for two
weeks.
To kill lice and nits, machine-wash all washable
clothing and bed linens that have been used by the
infested person(s) during the two days before
treatment. Use the hot water cycle during the
washing process. Dry laundry using high heat for 30
minutes.
Washing clothes to remove lice and nits is only
necessary on the day of treatment and does not need
to be repeated daily.
Another option is to place the item in a hot dryer for
30 minutes, if the recommended care label approves
use of dryers.
Articles that cannot be machine washed, or placed in
a hot dryer can be vacuumed, dry cleaned, or stored
in a sealed plastic bag for two weeks.
Floors, carpets, upholstered furniture, pillows, and
mattresses should be vacuumed to pick up any hairs
that may have living lice or nits attached to them.
4. Repeat treatment with the
pediculicidal product following the label
instructions. If the label does not provide
a guide for a second treatment, repeat
treatment nine days following the initial
treatment if live lice or nits within one
quarter inch of the scalp are found.
The use of lice sprays for the
house can be dangerous and is
not recommended.

27 | P a g e
Head Lice Identified on Child - Sample Letter 1
Date:
Dear Parent/Guardian
You are receiving this letter because head lice or recently laid nits (eggs) have been found on your child’s
head. Don’t panic! Head lice are not considered a health risk because they do not spread disease or
illness. Head lice among school children are a common frustration; however, the spread of head lice can
be controlled and prevented.
To help prevent the spread of head lice, it is important to treat your child today after school. Use a lice
shampoo or other method to kill live lice, such as manual removal with a lice comb. Always follow the
package directions when using a lice product. To remove nits after a treatment is done, use a lice comb,
combing small sections of wet hair at a time. Once a treatment has been done, your child may return to
school, but check in at the school office so designated personnel can re-examine your child’s hair in a
private location.
Remember to check everyone in the household and treat anyone that has live head lice. If you think you
see nits within one quarter inch of the scalp, but no live lice, continue to check daily. Check for live lice
for two to three weeks following any treatment. A second treatment may need to be done in seven to ten
days to kill any lice that may have hatched after the first treatment.
Head lice are spread by head-to-head contact. Head lice do not jump or fly. Off the human head, lice
cannot move with speed or direction. They feed off blood in the scalp and survive only on a human head.
Lice do not survive much longer than one to two days off a human head. This makes it difficult for them
to be transmitted environmentally. Adult female lice lay their eggs (nits) close to the scalp so the new
louse can eat as soon as it hatches (otherwise it dies quickly). Nits are attached with a glue-like
substance, making them very difficult to remove. Combing the hair when wet with a lice comb is a good
way to find evidence of lice and remove nits.
Remind your children not to have close head-to-head contact with others. Girls with long hair can wear it
braided or in a ponytail to help avoid hair-to-hair contact. Please see attached instructions on treating head
lice.
If you have any questions, contact your school nurse, the office, your primary care provider, or the public
health department.
Yours truly,
28 | P a g e
Head Lice Identified on Child - Sample Letter 2
Date:___________________________
Dear Parent/Guardian of:___________________________________________
It is suspected that head lice or recently laid nits (eggs) have been found on your child’s head. Head lice
have nothing to do with the cleanliness of a house or parenting skills. Head lice are spread by head-to-
head contact. Rarely, sharing hats, combs, and other hair accessories may also spread head lice.
It is important to treat your child before he/she returns to school. Please begin treatment as soon as
possible and then send your child back to school so that they do not miss learning opportunities in the
classroom. Also, remember to check everyone in the household and treat anyone that has live head lice
and/or nits within one quarter inch of the scalp. Continuous checking may be required for two to three
weeks to avoid re-infestation.
(See attached Health Department Treatment Recommendations)
Following initial treatment, please complete the bottom portion of this letter and return with your child to
the school office. Your child’s hair will be re-examined by designated school personnel prior to returning
to class.
Sincerely,
Student Name:_______________________________________ Room #:________________________
Has been treated for head lice with (Product/treatment/action taken):
___________________________________________________________________________________
___________________________________________________________________________________
On (Date):_____________________________.
Parent/Guardian Signature:______________________________________ Date:__________________
29 | P a g e
Parent Education Letter – Sample
Start of school year or when deemed necessary
Date
Dear Parents/Guardians,
We are sending this letter to all parents to increase head lice awareness so that you may take steps at
home to help prevent your child from becoming infested with head lice. Any time children come together,
particularly at the start of the school year or following any social grouping like Girl/Cub Scouts,
Brownies, Little League, dance groups, or sleepovers, detected head lice cases commonly increase.
Recent studies show that head lice are seldom spread in the school setting.
Direct, physical, head-to-head contact is the usual method of transmission. Lice do not jump or fly. They
survive only for a short time away from the human head and have difficulty crawling or clinging to
smooth surfaces. Check your child’s head weekly for lice and/or nits (eggs). Mature lice, which are
no bigger than a sesame seed, avoid light and are hard to see. Lice eggs or “nits” are usually found close
to the scalp – usually within one quarter inch. They appear as tiny whitish ovals that are “glued” to the
hair shaft. They cannot easily be flicked away as dandruff can. Head lice do not transmit disease and are
not a serious medical condition. They cannot survive on your pets.
If you find head lice on your child, please notify the school and treat him/her with lice shampoo following
package instructions. A second treatment may be required in seven to ten days. Continue to examine the
child and all family members for three weeks and treat only if live lice or if nits are found one quarter
inch or less from the scalp.
Check Regularly – Treat Quickly
Help Keep Head Lice Off Your Child
Check your child’s head weekly for signs of head lice.
Teach your child not to share or trade personal items such as hats, combs, brushes, headbands,
and barrettes.
Contain long hair in braids or ponytails, especially in younger children.
Teach children to avoid head-to-head contact.
For more information regarding head lice or its treatment, please feel free to contact the school office or
your local health department. Thank you for your help and support.
Sincerely,
** You may want to include information about head lice with this letter, such as “Facts and Myths.”

30 | P a g e
1) Watch for signs of head lice, such as frequent head scratching, flaky or irritated scalp,
scabs, or the presence of nits. Anyone can get lice, mainly from direct head-to-head
contact or possibly by sharing hats, brushes, beds, pillows, towels, etc.
2) Check all household members and close contacts for lice and nits (lice eggs) at least once
a week.
3) Be sure not to confuse nits with hair debris (i.e., dandruff, hair spray droplets, or hair
casts). Nits are yellowish-white, oval-shaped, and are attached at an angle to the side of
the hair shaft.
4) Consult a pharmacist, physician, or school nurse before applying pesticides or other lice
treatments. If anyone to be treated is pregnant or nursing, has allergies, asthma, or has
nits in the eyebrows or lashes, contact your physician. Never use a pesticide or lice
treatment on or near the eyes.
5) Consider all of your treatment options. Remember, lice-killing products are pesticides
and must be used with caution. If you choose alternative methods, they may not have
been studied thoroughly enough to determine long-term outcomes. The most effective
and safe alternative is manual removal by combing.
6) Remove all nits. Separate hair sections and remove nits with a lice comb, baby safe
scissors, or your fingernails.
7) For lice treatment, follow package directions carefully. Use the products over the sink,
not in the tub!
8) Wash bedding and all recently worn clothing in hot water and dry in high heat for at
least 30 minutes. Combs and brushes should be soaked in hot water (not boiling) for 10
minutes.
9) Avoid lice sprays! Vacuuming is the safest and best way to remove lice or fallen hairs
with attached nits from furniture, rugs, stuffed animals, and car seats.
10) Notify your child’s school, camp, child-care provider, play partners, and neighborhood
parents. Check for lice on a regular basis.
10 Steps to Keep Ahead of Head Lice
31 | P a g e
32 | P a g e
33 | P a g e
For more information, contact:
Communicable Disease Division
Michigan Department of Community Health
201 Townsend Street, 5
th
Floor
Lansing, MI 48913
517-335-8165
