
4
th
and 5
th
Year Medicine
Study Notes
Edited by David Tripp
Second Edition
February 2003
Volume 1
Credits and Introduction ...................................................... 1
Patient Management ............................................................ 3
Systems:
Cardiovascular ...................................................... 13
Respiratory ............................................................ 57
Endocrine and Electrolytes ................................... 93
Neuro-sensory ..................................................... 116
Gastro-Intestinal .................................................. 153
Renal and Genitourinary ..................................... 201
Musculo-skeletal ................................................. 229
Haematology and Immunology ........................... 285
Skin ..................................................................... 313
Reproductive and Obstetrics ............................... 337
Index ............................................................................. 388
To Helen, Laura and Esther
My precious wife and daughters
Thanks for your support and patience

4
th
and 5
th
Year Notes
1
Credits and Introduction
This workbook collates all the study material lavished upon us in the 4th and 5th Year
Medicine course taught at the Wellington School of Medicine. It is an attempt to organise
and summarise the zillion and one things that of course you should know.
This second edition also includes further material gained as a Trainee Intern. Thankfully
this added to the practical material without impacting on the bulk! Revising these notes
also gave me a change to remove another round of bloopers.
This document is intended to help you cram for exams. It is not intended as a
clinical reference, and should not be used for making real life decisions. Find
something (much) more reliable. I have endeavoured to be as accurate as
possible, but a patient on the end of a needle deserves better than the ravings of a
6
th
year student.
Sections whose headers are marked with an „*‟ are sections I compiled from books –
these were not taught as discrete topics, but I thought they should be in here.
I am indebted to Matthew Kelly for his review of parts of this document (thanks Matt!)
and the many lecturers who taught us. Where I drew from substantial handouts, these are
referenced.
I have also used the following books:
Oxford Handbook of Clinical Medicine, 4
th
Edition, R A Hope, J M Longmore, S K
McManus and C A Wood-Allum, Oxford University Press, 1998
N J Talley and S O‟Connor, Clinical Examination – a Systematic Guide to Physical
Diagnosis, Third Edition, MacLennan & Petty Pty Ltd, 1998
T J B Maling and C D Burgess, Clinical Pharmacology and Therapeutics, 9
th
Edition,
Wellington School of Medicine, 2000
These are good books – buy them!
Feedback – especially any bloopers – would be most welcome. Email them to me at
Enjoy!
© David Tripp, November 2002
2 4
th
and 5
th
Year Notes
Relationship to Wellington School of Medicine Runs
Run/Module
Where to find the material from that run in this document
Clinical Skills
Material from this run is included in the relevant systems
chapters, mainly Cardiovascular, Respiratory and Renal.
Endocrine is a separate chapter.
Neuro-sensory
All in the Neuro-sensory Chapter
Health Care and the
Elderly
All in the Health Care of the Elderly Chapter, or referenced
from there
Psychological Medicine
All in the Psychological Medicine Chapter
Gut
Mainly in the Gastro-Intestinal Chapter (incorporating the
substantial run handout). IV Fluids and Nutrition are in the
Surgery and Fluid Management Chapter.
Community Medicine/GP
Run
Material from this run is scattered through the relevant
system chapters. Dermatology is in the Skin Chapter,
Consultation Skills is in the Patient Management Chapter,
Grief and Terminal Illness is in Psychological Medicine
Chapter, Screening and the Health System in NZ is in the
Public Health Chapter, Sexual Health in the Reproductive
and Obstetrics Chapter
Anaesthetics and
Emergency
Material is split across the Anaesthetics Chapter and the
Emergency Management Chapter, or referenced from there
Women‟s, Sexual and
Reproductive Health
All in the Obstetrics and Gynaecology Chapter, except for
Urinary Incontinence in the Renal Chapter and Post-natal
depression in the Psychological Medicine Chapter
Public Health
All in the Public Health Chapter
Paediatrics
Mainly in the paediatrics Chapter. Meningitis is in the
Infectious Diseases chapter and some paediatric skin
conditions are in the Skin Chapter. UTIs are covered in the
Renal and Genitourinary Chapter
Musculo-Skeletal
All in the Musculo-skeletal chapter or referenced from there
Medicine
In the Cardiovascular, Respiratory, Renal or Endocrine
Chapter
Pathology
Pathology of specific systems is merged into those system
chapters. Haematology material is the Haematology
Chapter, in the Blood Tests section of Patient Management
Chapter, and Blood Products section of the Surgery and
Fluid Management Chapter. Genetics is in the Genetics
chapter, or referenced from there. Forensic Pathology is
mainly in the Professional Development Chapter.

Patient Management 3
Patient Management
This chapter contains aspects of history taking, examination, investigations and management that don’t
sit neatly in another chapter. It therefore focuses on principles and general exam features, and covers
some bits and pieces. For specific history taking or examination refer to the relevant chapter.
History Taking ................................................... 4
Frameworks for consultation ........................ 4
History Taking .............................................. 4
History Outline ............................................. 4
Examination ....................................................... 5
Purpose of Examination ................................ 5
General ......................................................... 5
Fever ............................................................. 5
Pyrexia/Fever of Unknown Origin
(PYO/FUO) ............................................. 6
Tiredness....................................................... 6
Oedema ......................................................... 7
Hands ............................................................ 7
Head .............................................................. 8
Investigations ..................................................... 9
CT and MRI Imaging ................................... 9
Blood Tests ................................................... 9
Treatment ......................................................... 10
Differential Diagnosis ................................. 10
Formulating a case ...................................... 11
Treatment Checklist .................................... 11
Behavioural Change ................................... 11
Breaking Bad News .................................... 12
4 4
th
and 5
th
Year Notes
History Taking
Frameworks for consultation
4 tasks for consultation:
Management of presenting problems
Modification of help-seeking behaviour (did they come too soon/too late)
Management of continuing problems
Opportunistic health promotion
Objective: integration of:
Doctor‟s agenda: Correct diagnosis, preventative health care
Patient‟s agenda: expectations, feelings, fears, understanding of illness experience
Silverman and Kurtz: - five phases of the consultation:
Initiating the session: introduce yourself, why are you here, how can I help (not how are you)
Gathering information: start with open questions, physical exam
Building the relationship
Explanation and planning: what you‟ll do, what you want the patient to do. Involve patient in
planning. Give them as many choices as possible
Closing the session: any more questions, check understanding, follow up, emergencies, etc
Double Diamond model:
First phase: patient presents problems, doctor hones down
Second phase: diagnosis reached, expansive phase of explanation, management options, then
brought to closure
FIFE: Feelings, Ideas, Function/Dysfunction, Expectations
Remember: listen, reassure
History Taking
Always ask why they‟ve come: and why that is a concern to them (what are they scared of?)
Key skills:
Establishing rapport
Asking questions in a logical order
Observing non-verbal queues
Proper interpretation
Record positive & negative findings. Always amplify positive findings:
Time course
How quickly did it come on (what were you doing then), pattern since then
Site and radiation
Character
Severity
Aggravating or relieving factors
Associated symptoms
Previous occurrences
For each potential cause of a symptom think of:
Detail of the symptom
Other symptoms you would expect if that cause
Ask about risk factors of that cause
See also Talking with Children, page 567 and Talking with Adolescents, page 665
History Outline
History:
Identifying data
Presenting complaint (or complaints) eg Cough with green sputum 2 days, Dizziness 4 weeks
History of presenting complaint
Drug and medication use, including allergies, OTC drugs, herbal/alternative medicines
Past medical and surgical history (including hospital admissions)
Screen for hypertension, heart disease, asthma, diabetes, epilepsy, rheumatic fever, TB, bleeding
tendency, hepatitis B
Family history of illness (if genetic illness draw family tree)
Patient Management 5
Social history: smoking, alcohol, job, living situation, social supports, overseas travel, functional
history in the elderly or disabled
If a child, then obstetric, neonatal, growth and development, immunisations
Review of systems
At end of history always ask „is there anything else you want to tell me‟
Note mental function and communication: dementia/delirium common
Physical Exam:
Vital signs: temperature, respiratory rate, pulse, blood pressure
General observations: distress, pallor, hydration, cyanosis, weight
Relevant systems exams
Formulation and problem list:
List of active problems or clusters of problems (always include smoking if they smoke)
List of inactive problems or clusters of problems
For each problem, list a set of differential diagnoses, investigations to establish which it is,
immediate management, other management strategies
Progress notes:
Changes in symptoms
Changes in physical exam or investigation
Assessment of what this means
Plan for what to do now
Examination
Purpose of Examination
Aims to:
Confirm suspicion
Exclude other causes that mimic it
Measure severity
General
Are the conditions OK to do an exam? Is the light in the room OK, is the patient positioned and
exposed, etc
ALWAYS OBSERVE FIRST: stand back and look.
Distress, comfort, central or peripheral cyanosis, pallor, jaundice, dehydration, SOB, how sick or well
Cachectic = severe loss of weight and muscle wasting. Usually malignancy, but also severe cardiac
disease (due to anorexia from liver congestion and impaired absorption due to intestinal venous
congestion)
Facies: features of the face suggesting diagnoses: eg acromegaly, Cushing‟s, Down‟s, myxoedema,
Parkinson‟s, hair distribution in men and women, etc
Weight, body habitus and posture, including deformities
Include vital signs in general assessment: pulse, blood pressure, temperature, respiratory rate
Fever
See also Fever in Children, page 616
Taking a temperature:
Serial measurements the most useful
Also take pulse – if temp should have heart rate (except in typhoid)
Normal Values
Low
High
Oral
36.6
37.2
In hot weather
+0.5
+0.5
Rectal
+0.2
+0.5
Axillary
-0.5
-0.5
Children. The most common emergency presentation in paediatrics. Most common cause is viral
infection, otitis media, pharyngitis, and tonsillitis. Also consider bladder infection, Rheumatic fever,
Meningitis. Kids spike temperature easily. Febrile convulsions occur between 18 months and 5 years.
At other ages investigate other causes
6 4
th
and 5
th
Year Notes
Types of fever:
Continued: does not remit e.g. typhoid, drug fever
Intermittent: falls to normal each day – pyogenic infections, lymphomas
Relapsing: returns to normal for days then rises again – Malaria, lymphoma, pyogenic
Pyrexia/Fever of Unknown Origin (PYO/FUO)
See also:
Pyrexia of unknown origin if returning from 3
rd
world, page 511
Fever in a Neutropenic Patient, page 301
Formal definition: > 38 C, > 3 weeks, no known cause (ie normal admission tests already done).
However, often used to describe a temperature that that you haven‟t done any tests on yet
Usually an unusual presentation of a common disease
History, exam, investigations, time course, urgency and likely cause depend on setting:
Community acquired (Classic PUO)
Nosocomial PUO (ie hospital acquired)
Immune-deficit or HIV related PUO
Differential:
Neoplasm: lymphoma, leukaemia (check lymph nodes), other (hepatic, renal, other)
Infection:
Bacterial: Tb, abscess (subphrenic, hepatic, pelvic, renal – look for neutrophils),
endocarditis (any dental work?), pericarditis, osteomyelitis, cholangitis, pyelonephritis, PID,
syphilis, cystitis
Viral: EBV, CMV, HBV, HCV, HIV, Varicella-Zoster
Parasitic: malaria, toxoplasmosis
Fungal
Connective Tissue: RA, SLE, Vasculitis (eg polyarteritis nordosa – check for Raynaud‟s
phenomena – abnormal response in fingers to cold)
Miscellaneous: drug fever (especially penicillins, sulphonamides), Rheumatic fever, inflammatory
bowel disease, granulomatous disease (eg Sarcoid), Fictitious/Munchausen‟s (eg injecting
themselves with saliva)
Clues:
Weight loss chronic
Check eyes: iritis in connective tissue disease, jaundice, etc
Check tonsils, glands, ears for infection
History:
Travel (eg malaria, did they have prophylaxis)
Exposure to others
Sexual history
Weight loss
Been to other doctors (had any antibiotics)
Occupational exposure (eg cows)
Exam:
Lymph nodes
Heart murmurs
Skin for rashes
Abdominal exam
Possible investigations:
Blood count
Blood cultures
Urine microscopy & culture
Liver function (eg hepatitis)
Viral serology
Malaria film
Chest X-ray
Tiredness
Differential:
Sleep disturbance: eg anxiety, sleep apnoea, narcolepsy,
Patient Management 7
Depression
Anaemia
Endocrine: hypothyroidism, hypocortisol (Addison‟s), diabetes, hypercalcaemia (due to PTH)
Infection (eg EBV)
Cancer
Drugs: alcohol intoxication, sedative drugs,
Head injury (eg subdural haematoma)
Post ictal states
Hypoglycaemia
Hepatic encephalopathy, Wernicke‟s encephalopathy
Chronic heart failure
Malabsorption (eg coeliac disease)
Pregnancy
See also Sleepiness, page 90
Oedema
Include in exam of appropriate system
Need to retain 3 – 4 litres before pitting begins
Exam:
Where is it? Distribution
Is it pitting
Other signs of inflammation
Mechanisms:
↓colloid osmotic pressure
↑hydrostatic pressure
↓permeability of wall
Localised Cause:
Inflammatory (e.g. infection, allergy - cytokine mediated) pain/heat/redness/swelling
Trauma
Venous occlusion by tumour or lymph nodes
Thrombis (e.g. DVT)
Generalised Cause:
Is it bilateral? Usually worse in the evenings
Heart Failure:
Mechanism: ↑preload ↑venous pressure, ↓renal perfusion ↑renin ↑Na/H20
History: check SOB, orthopnea, PND
Signs/Tests: CXR, ECG, Echo
Liver:
Mechanism: liver failure/malnutrition ↓colloid pressure ↓renal flow ↑retention
History: check alcohol, cholestasis, hepatitis, bleeding, bruising
Signs/Tests: portal hypertension, enlarged liver, jaundice, bloods (Liver Function, INR)
Renal:
Mechanism: nephrotic syndrome ↓colloid pressure (have to loose 3.5 g protein a day to be
nephrotic. NB nephritis is inflammation)
History: check change in urination, nocturia (due to diuresis), diabetes
Signs/tests: ↑BP, urine test, 24 hr urine, dipstick, urea/creatinine
Drugs (eg vasodilators, like calcium channel blockers) can cause ankle oedema
Gastrointestinal: Malabsorption hypoalbuminaemia
Non-pitting lower limb oedema
Lymphoedema (eg malignant invasion of lymphatics, allergy) doesn‟t pit – push for 10 seconds
Hypothyroidism
Hands
Nails:
Takes ~ 6 months for fingernails to grow out
Clubbing:
Respiratory: carcinoma, fibrosis, cystic fibrosis, TB, chronic suppuration (eg bronchiectasis),
idiopathic pulmonary fibrosis, NOT asthma or CORD alone

8 4
th
and 5
th
Year Notes
Cardiovascular: infective endocarditis
Other (uncommon): cirrhosis, IBD, coeliac disease, thyrotoxicosis
Blue: cyanosis, Wilson‟s disease
Red: Polycythaemia (red-blue), carbon monoxide poisoning (cherry red)
Pale nail bed: anaemia
Koilonychia: spoon shaped nails in Fe deficiency
Leuconychia: white nails in hypoalbuminaemia
Mee‟s lines: single white transverse line in renal failure
Splinter haemorrhages: usually trauma (especially manual workers) or infective endocarditis,
rarely vasulitis (eg in rheumatoid arthritis), polyarteritis nodosa, sepsis, blood malignancy or
profound anaemia
Check capillary refill: squeeze nail and see how long it takes to return to red – sign of peripheral
circulation. Normal < 2 sec
Hands:
Palmar erythema: pink spots on pale background – should be bilateral - Chronic liver disease,
pregnancy, rheumatoid arthritis, polycythaemia, thyrotoxicosis, SLE
Skin: subcutaneous bleeding: petechiae small, purpura bigger, ecymosis – biggest. Petechiae
caused by a platelet problem, not due to coagulopathy
Dupuytren‟s Contracture: extend fingers back – shortening of palmar aponneurosis – in alcoholic
liver disease, epilepsy, manual workers and idiopathic
Asterixis: metabolic flap – coarse, non-symmetrical – neural inhibition encephalopathy in renal
failure (urea), respiratory failure (CO2), liver failure (nitrogenous material), hypoglycaemia,
barbiturate poisoning
Raynaud‟s Syndrome: intermittent attacks of ischaemia of fingers or toes due to intense arterial
vasospasm, often precipitated by cold or emotional stimuli
Tendon Xanthomata: lipid deposits in tendons of hands or arms in hyperlipidaemia
Head
Headache
See Headaches, page 139
Eyes
Jaundice: primary liver disease, liver congestion secondary to heart failure
Anaemia: pale conjunctiva – especially anterior border just inside eye lid
Sclera not affected by hypercarotenaemia
Puffiness below eye: early nephritis (before feet oedema), myxoedema of hypothyroidism
Mouth
Mouth: Foetor hepaticus, ulceration, pigmentation, telangiectasia, gingivitis/hypertrophy, glossitis
Ulcers: aphthous, drugs (e.g. gold), trauma, Crohn‟s, infection (HVZ, HS)
Pigmentation: heavy metals (lead, iron), drugs (anti-malarials), Addison's, Melanoma, Kaposi‟s
sarcoma
Snotty nose = coryza
Throat
Bacterial
Viral
High fever
Runny nose
Pus/exudate
Red raw throat
Productive cough (if any)
Persistent dry cough
Whitish-yellow membrane over tonsils - ?EBV
Patches of exudate on mucosa - candida
Differential: Bacterial sore throat, viral URTI, glandular fever, rheumatic fever, quinsy (peri-tonsillar
abscess, can lead to airway obstruction)
See also Acute Pharyngitis, page 63
Lymph Nodes
Occipital Nodes: scalp infections, bad nits, infected cradle cap, rubella
Mastoid and posterior auricular
Patient Management 9
Parotid: mumps
Posterior sternomastoid
Anterior sternomastoid: sore throat
Jugulodigastric
Submandibular and Submental: tooth infection, glandular fever
Superior, deep and lateral cervical (internal jugular) nodes
Supra & sub-clavicular: lung and lung surface infections, Tb, lung metastasis
Enlarged lymph nodes and oral thrush ?AIDS
Investigations
CT and MRI Imaging
CT:
Looks for density bones are white (hyper-dense), air is black
If it is contrast enhanced then vessels will appear whitish
MRI (=Magnetic Resonance Imaging):
Looks for H atoms
Very strong magnet lines up H atoms (effectively little dipoles), radio waves emitted which disturb
net magnetic vector, then measure radio frequency emitted by atoms as they return to aligned state
Describe as hypo or hyper intense – as relates to signal intensity not density
Bones on both are black (no free fluid)
T1 weighting: simple fluid black (eg CSF, urine). Shows exquisite anatomy
T2 weighting: simple fluid turns white. Shows pathology, due to tissue hydration (eg infection,
tumour). T2 shows H2O. Flowing blood is black
Blood Tests
Why test
Before ordering any test always ask yourself why you are ordering it. Labs confirm a diagnosis – don‟t
give it
Diagnosis: to confirm diagnosis/exclude differential diagnosis from history & exam
Prognosis: severity/progression
Monitoring: Measure target of treatment rather than drug level (e.g. INR rather than warfarin)
Screening: Only where test is reliable and you can do something about it
Parameters of a Test
Normal range: either arbitrary (level which leads to risk) or statistical (what most people are)
Reliability:
Accuracy: mean of test results = real result
Precision: variability in results (i.e. want a small standard deviation). Important for serial
monitoring. Only different if 2½ SDs from previous test
Sensitivity: what rate of true positives does it pick up (are all positives found?)
Specificity: False negative rate
For further details on sensitivity, specificity, etc, see Sensitivity and Specificity, page 704
Test Results
Results may be:
Real & require interpretation
Erroneous: will always be some errors – there should be known rates of error for a lab and these
should be within acceptable limits
Artefact: affected by non-disease factors:
Pre-analytical artefacts: mainly at time of collection
Incorrect labelling
Wrong tube/anticoagulant
Haemolysis
Delayed transport
Temperature effects e.g. refrigerating stuffs up electrolytes
Sample incorrectly taken (e.g. through or close to IV lines)
10 4
th
and 5
th
Year Notes
Pre-analytical factors:
Not fasted/wrong time for sample
Medications interfere
Wrong reference range
Urgent Tests
If the result may change the immediate management of a patient or if it plays a major role in on going
assessment of a critically ill patient
Routine ordering/screening not appropriate in A&E
Emergency electrolytes:
Frequently over-ordered
Indications include D/V, seizure of unknown cause, muscle weakness, > 65, known renal/diabetes
disease
Blood gases:
Don‟t need for uncomplicated asthma/MI, or if normal systemic perfusion and no
dyspnoea/hyperventilation
Indicated if: cyanosis, severe dyspnoea, hypotension, vasoconstricted and sweaty, septic shock,
pneumonia, suspected PE, CORD in acute exacerbation
Beware overdoses: people miscalculate/lie about consumption
Timing important: test for paracetamol overdose after 4 hours to judge treatment required.
Changes in liver function take 24 hours
Ethanol levels: check in unconscious patient, for medicolegal reasons, or if intoxicated but
potentially multiple problems
Toxicology Testing:
Serum levels for paracetamol, aspirin, ethanol, methanol, ethylene glycol, lithium,
anticonvulscents, digoxin, iron, theophylline
Urine screen for drugs of abuse
Toxilab screen: long and slow for about 400 therapeutic drugs. Qualitative only
Emergency use of cardiac markers: Beware timing - only after 6 hours unless as baseline. Can‟t
size infarcts on cardiac enzymes
Abdominal pain:
Common to find no specific biochemical change
Baseline Na, K, creatinine if D/V or surgery likely
Amylase, glucose, HCG, LFT, calcium, cardiac enzymes
More rarely: urinary porphobilinogen, blood lead
Acute pancreatitis may not have amylase, and amylase can present in other conditions e.g.
perforated/ischaemic bowel, ruptured ectopic pregnancy, diabetic ketoacidosis, renal failure
Treatment
Differential Diagnosis
Always consider:
Autoimmune
Degenerative
Drugs
Doctors
Hereditary/congenital
Infective
Inflammatory
Idiopathic
Mechanical
Metabolic
Nutritional
Neoplastic
Pregnancy
Psychiatric
Trauma
Vascular
Patient Management 11
Formulating a case
Differential diagnosis
What are the risk factors
Problem list
Complications of problems and risk factors
Prognosis: how does this impact on treatment decisions
Investigations
Treatment + management/monitoring of side effects
Integration: stand back and think – am I missing something
Treatment Checklist
Listen (therapeutic relationship)
Education
Lifestyle (diet, exercise, etc)
Environment/social change
Psychological
Drugs
Surgery
Referral: to specialists, other health providers, support groups
Family involvement
Prevention
Public Health measures
Behavioural Change
Health Education is an attempt to achieve behavioural change
See Parent and Adolescent Education, page 567
Stages of Change Model
Stages of changes (Prochaska and Di Clemente 1982): Discussion must be tailored to the stage they‟re
at:
Pre-contemplation
Contemplation
Determination
Action
Maintenance (and maybe permanent exit)
Relapse (and maybe return to contemplation)
Readiness to Change/Motivational Interviewing
Motivation = the probability that a person will enter into, continue and adhere to a specific change
strategy. It fluctuates. It is a state not a trait. Measure motivation by what they say not what they do
Motivational interviewing: goal is to get from the patient their reasons for concern and their arguments
for change. Especially helpful in precontemplation/contemplative stages
Confrontation tends to evoke resistance. Resistance the chance of change
Approaches at each stage:
Pre-contemplation:
Lack of knowledge or inertia
Rebellion: try to provide choices
Resignation: given up – try to instil hope/explore barriers
Contemplation:
Not equivalent to commitment
Extra information may not make any difference
Work through ambivalence, anticipate barriers, desirability of present behaviour
Dealing with ambivalence:
“Yes, but…” is normal
Helping people resolve ambivalence is key to change
Further education may result in conflict or denial
Try to get the patient unstuck
Poor self-esteem, social context and values may make this difficult
12 4
th
and 5
th
Year Notes
Highlight discrepancy between personal goals and behaviour. Best if they can identify this
discrepancy themselves, rather than feeling pressured
Motivational Strategies (NB importance of empathy – understanding where the patient is at):
A – give Advice
B – remove Barriers
C – provide Choices
D – decrease Desirability: alter balance of perceived costs, barriers and rewards
E – practice Empathy. Accept and understand without agreeing
F – provide Feedback
G – clarify Goals
H – active Helping
Counselling techniques:
Open ended questions
Reflective listening: voice what you think the patient means by what they are saying
Affirm: self esteem and support the patient
Summarise
Brief Interventions in General Practice
Brief but repeated interventions avoid stigmatism, and are more effective than one long session
Direct advice normally provokes resistance
Opening lines:
“What are some good things about…. What are the less good things…”
Ask permission before giving information: “I wonder, would you be interested in knowing more
about ….”. When you‟ve finished: “What do you make of all this?”
“What concerns do you have about …”
Breaking Bad News
Prepare patient for what is to come – give an honest explanation of why you‟re doing investigations
before you do them
Think ahead – invite family members when results come back
If there is no family, take a nurse (who has probably been preparing them anyway)
Ask patient what they understand is happening or what they‟re scared of – gives you a good intro
It is the patient‟s information – let them decide the pace and level of detail
If the patient asks „have I got cancer‟ then they will have been thinking about it and will have a reason
for asking – this is helpful
If the patient asks „What do you think‟ then they‟re likely to be anxious. Need to open up discussion
and give them opportunity to express their fears
Break up the information – „chunk and check‟. Check understanding bit by bit
„Denial‟ can be shock, disbelief, or failure to understand. Denial is a longer-term pattern of behaviour.
Whether denial is bad or not depends on the consequences
Document your discussion and what you‟ve said

Cardiovascular 13
Cardiovascular
See also Heart Disease in Children, page 596
References: Prof Delahunt's Pathology Notes
Physiology and Anatomy ................................. 14
History .............................................................. 15
Differentiating Chest Symptoms ...................... 16
Cough ......................................................... 16
Chest Pain ................................................... 16
Breathlessness ............................................. 17
Cyanosis ..................................................... 18
Physical Exam* ................................................ 18
Peripheral Exam ......................................... 18
Praecordium ................................................ 21
Heart sounds ............................................... 21
Heart Murmurs ........................................... 23
Lungs, Abdomen and Legs ......................... 24
ECG Interpretation* ......................................... 24
Chest X-ray ...................................................... 27
Cardiovascular Risk factors*............................ 30
Vessel Pathology .............................................. 31
Atherosclerosis ........................................... 31
Aortic Aneurysm ........................................ 32
Dissecting Aneurysms ................................ 32
Arteritis ....................................................... 33
Other Vessel Abnormalities ........................ 33
Ischaemic Heart Disease .................................. 33
Hypertension ............................................... 34
Angina Pectoris .......................................... 36
Myocardial Infarction (MI)......................... 36
Arrhythmias...................................................... 40
Atrial Fibrillation ........................................ 40
Sinus Arrhythmia ........................................ 41
Other Abnormal Rhythms........................... 41
Heart Block ................................................. 42
Drugs for Acute, Life Threatening
Arrhythmias .......................................... 42
Emergency cardiac pacing .......................... 43
Valvular Heart Disease ..................................... 43
Aortic Stenosis ............................................ 43
Aortic Regurgitation ................................... 44
Mitral Stenosis ............................................ 45
Mitral Regurgitation (MR) ......................... 45
Tricuspid Regurgitation .............................. 46
Infective Endocarditis ................................. 46
Heart Failure..................................................... 48
Myocarditis ...................................................... 50
Cardiovascular Pharmacology .......................... 51
Cardiomyopathy ............................................... 54
Primary Cardiomyopathy............................ 54
Secondary Cardiomyopathy........................ 54
Neoplasia of the Heart and Blood Vessels ....... 54

14 4
th
and 5
th
Year Notes
Physiology and Anatomy
Physiology
Cardiac Output (CO):
CO = MAP/TPR (ie flow = pressure / resistance)
CO = SV * HR
Normal adult at rest = 5 L/min
Can be measured with Doppler/echo
Mean Arterial Pressure:
MAP = Cardiac Output*TPR
MAP = Diastolic + 1/3(systolic-diastolic)
Stroke volume:
SV = End diastolic volume – end systolic volume
Normal 60 – 80 ml
Ejection fraction = ESV/EDV. Determined by:
Preload (=EDV): dependent on blood volume, venous tone, posture, intrathoracic pressure,
peripheral muscle pump, and atrial contraction (20% of filling). Affects stroke volume through
Starling‟s Law: myocardial fibre length (ie filling) SV until ventricle is over-stretched. Can
be measured for the left ventricle using pulmonary artery/capillary wedge pressure (CAWP) and
for the right using central venous pressure
Force of Contraction (Inotropy): Shifts Starling Curve up and to the left. Increased by
sympathetic stimulation, Ca, thyroxine, angiotensin, drugs, temp, HR. Decreased by
acidosis, hypoxaemia, K, drugs (general anaesthetics, beta blockers)
Afterload = tension in the ventricular wall at the end of systole. Results from ventricular
distension, elasticity of arterial walls and arterial network resistance. Measure with arterial
catheter
Changes given certain shock states:
Cause
CVP
PAWP
BP
HR
Urine Output
Blood Loss
L V Failure
R V Failure
Fluid overload
Peripheral vascular resistance:
Resistance proportional to radius to the power of 4
= (Mean aortic pressure – right atrial pressure)/cardiac output
Cardiac Anatomy
Heart Valves:
Mitral valve (left AV): anterior and posterior leaflets
Tricuspid valve: anterior, posterior and septal cusps
Aortic valve: left, right and posterior cusps
Pulmonary valve: left, right and anterior cusps
Blood supply:
Left main stem (LMS) LAD (anterior wall of LV and anterior 2/3 of septum) and Circumflex
(lateral wall of left ventricle and most of the posterior wall of the LV). Also supplies AV node,
and SA node in 60%
Right coronary artery right atrium, right ventricle (except for left part of anterior wall), right
posterior and inferior walls of LV and posterior 1/3
rd
of septum
Pericardial effusion: normal content of pericardial sac = 50 ml. Effusion can be serous, chylous or
haemorrhagic. Sign of pericarditis but also accompanies MI
Cardiovascular 15
Regional Blood Flow
Organ (mass)
% Of Cardiac Output
O2 consumption
(ml/100g/min)
Regulation of blood flow
Heart – 300 g
5% - 250 ml/min
10
Metabolites (CO2, K, H, lactate,
adenosine); & adrenergics
Kidneys – 300 g
20 % - 1000 ml/min
6
Myogenic autoregulation,
angiotensin, adrenergics, PGs,
juxta-glomerular feedback
Brain – 1500 g
15% - 750 ml/min
3
H+; myogenic mechanisms
Liver – 2500 g
30% - 1500 ml/min
2
MAP, portal blood flow (local
metabolites), adrenergics
Muscle – 35 kg
15% - 750 ml/min
0.2
& adrenergics; local metabolites
(K+)
Skin – 3500 g
10% - 500 ml/min
0.2
adrenergics; kinins
(thermoregulation); axonal reflex;
sympathetic cholinergic
Cerebral Perfusion:
Cerebral blood flow (CBF) = [MAP – ICP (or CVP, whichever is greatest)]/cerebral vascular
resistance
Minimal desirable perfusion pressure is 60 mmHg. This is reduced by arterial pressure, venous
pressure, constriction/spasm of cerebral vessels or intra-cranial pressure (ICP)
Autoregulation keeps CBF at 50 ml/100g/min. Less than 15 changes in electrical activity
Coronary Perfusion:
Perfused during diastole
Coronary perfusion = (Mean diastolic pressure – VEDP)/Coronary Vascular Resistance
So treat poor perfusion with:
High diastolic pressure (eg systemic vasoconstrictor - agonist)
Reducing end diastolic ventricular volume (prevent volume overload)
Decrease coronary vascular resistance (eg coronary vasodilator)
Slow heart rate longer diastolic phase (eg beta blockers)
Preload (nitrates and Ca channel blocker)
O2 therapy and maintain haemoglobin
Renal Perfusion:
Normally autoregulated down to 80 mmHg systolic. When BP , renal blood flow renal
failure and acute tubular necrosis
Treatment:
Colloid/saline BP
Dopamine 2 – 5 mg/kg/min renal vascular resistance
History
Major symptoms:
Chest pain/heaviness/discomfort
SOB (exertional, orthopnoea, PND)
Ankle swelling
Palpitations (due to EDV, or do they mean arrhythmia – usually sudden onset – or tachycardia –
usually gradual onset)
Syncope
Intermittent claudication (pain in legs on exertion due to ischaemia)
Fatigue
Key differentials:
Does it change with breathing? ( ?respiratory cause)
Does it change with movement or localised pressure ( ?musculoskeletal cause)
Past history screen: Rheumatic fever, STDs, recent dental work, thyroid disease, history of heart
disease, drugs
Social history: tobacco (ask „have you ever smoked‟ not „do you smoke‟ just in case they „gave up this
morning‟), alcohol, occupation
Family history: Ischaemic heart disease, valve disease, congenital disease, Marfan‟s
16 4
th
and 5
th
Year Notes
Risk factors of Coronary Artery disease: hyperlipidaemia, smoking, hypertension, family history,
diabetes mellitus, obesity, exercise, male, advanced age
Differentiating Chest Symptoms
Cough
Due to non-specific irritation from pharynx to lungs
Note duration:
Short Respiratory tract infection (especially if fever)
Long asthma, CHF
Long + irritating and dry ?reflux and aspiration
Long + sputum bronchiectasis
Note time of day:
Night asthma, heart failure
After food reflux
Infective respiratory causes:
Yellow/green sputum bronchitis, pneumonia
Dark, fowl smelling sputum anaerobic abscess
Other potential causes:
CORD
Psychogenic
ACE inhibitors
Sputum:
Yellow or green: lobar pneumonia or bronchiectasis
Foul smelling and dark: anaerobic abscess
Pink and frothy: not sputum but pulmonary oedema
Haemoptysis (coughing blood) can be: bronchitis, cancer, bronchiectasis, cystic fibrosis, abscess,
pneumonia, TB, foreign body, Goodpasture‟s syndrome, rupture of a blood vessel after coughing, LV
failure or mitral stenosis. Exclude nasal bleeding and haematemesis
Chest Pain
Very common reason for A & E attendance: but only a few have S-T elevation MI
Very localised pain (i.e. point to it with a finger) unlikely to be ischaemic
History taking:
Often a lot of denial
Key question is time course (acute & on-going, episodic, persistence, etc)
What causes it? If exertion, how far can you walk? Worse going up hill or into a cold wind? How
long does it take to settle? What do you do to relieved it? Is the pain related to breathlessness
Family history: not when did family die but when did it start – if patient young then looking for
early onset in family
Risk factors: smoking, hypertension, diabetes, hyperlipideamia, obesity, homocsytinaemia, age,
sex (women better prior to menopause).
Causes:
Cardiac:
Myocardial ischaemia (narrowing of arteries, acute thrombosis, stenosis ↓perfusion
pressure, angina pectoralis). Gripping, crushing central chest pain. Pain may radiate.
Provoked by exercise, relieved by rest
Myocardial infarction
Pericarditis (if infectious then severe inflammation, if secondary to MI then more mild. ST
elevation on all leads). Pain changes with position/movement, respiration & coughing. Sharp
& severe central chest pain
Aortic Stenosis
Vascular:
Aortic aneurysm: central chest pain radiating to the back. Can mimic MI pain
Pulmonary Embolism (PE): very sudden onset of SOB – may ease gradually (as clot
disperses). Several days later – pleuretic chest pain, may have high fever, haemoptasis
Dissection: brachial pulse in each arm different, very sudden onset of very severe pain (c.f. MI
has unstable angina phase first)
Cardiovascular 17
Right ventricular strain
Pulmonary:
Pleuritis or Pneumonia
Tracheobronchitis
Pneumothorax
Tumour
Emphysema
Gastrointestinal:
Oesophageal reflux
Oesophageal spasm
Mallory-Weiss tear
Peptic disease (injury to oesophagus, ulcers, pancreatitis, bilary)
Biliary disease
Pancreatitis: do amylase to exclude
Musculoskeletal (will be localised – can point to it, will be palpable tenderness, pain on movement
and maybe history of trauma)
Cervical disk disease
Costochondritis
Arthritis of shoulder or spine
Intercostal muscle cramps
Subacromial bursitis
Other:
Breast disorders
Chest wall tumours
Herpes Zoster prior to eruption
Psychogenic causes
Breathlessness
Normal up to 16 breaths per minute. 20 is definitely high
History questions should include:
Ask patient what they mean by breathless
How much exertion does it take to make them breathless (eg distance walked, stairs climbed)
Exclude obesity and lack of fitness
Chest pain: pleuretic is sharp and made worse by coughing and deep inspiration. Usually localised
Occupational triggers: e.g. asbestos, legionella, occupational allergens, hobbies, birds, animals
Onset (slow over years ?fibrosis)
SOB on raising arms (eg reaching into a cupboard) using accessory muscles to breath
Orthopnoea: breathless when lying down
Fever at night: consider TB, pneumonia, mesothelioma
Sleep apnoea: ask about snoring, daytime somnolence, chronic fatigue
Anxiety symptoms
Immune status ( PCP or TB)
Medications for clues to condition and for possible side effects, eg PE from OC pill, cough from
ACE inhibitors, cocaine
SMOKING
Check: cyanosis, can they complete a sentence, peak flow, consciousness level, pulse
Divide into:
Acute: PE, hyperventilation (tingling, strange pains – alkalotic), acute LVF (no oedema c.f. CHF),
pneumothorax, lung collapse due to many causes, pneumonia
Chronic: COPD (asthma, bronchitis, emphysema), interstitial lung disease
Asthma is fluctuating not progressive (i.e. „Do you have good days and bad days‟)
Obstructive: trouble breathing out
Restrictive: trouble breathing in
Think of systems: cardiac, respiratory, blood (anaemia, jaundice), hyperthyroidism, psychogenic,
acidosis etc
Paroxysmal Nocturnal Dyspnoea (PND):
Paroxysmal = sudden recurrence or intensification of symptoms
18 4
th
and 5
th
Year Notes
Heart failure: wakes feeling like they‟re suffocating, get out of bed and open window, may wheeze
(cardiac asthma), may take ½ an hour to settle
Sleep apnoea: wakes feeling like they‟re suffocating, panics, sits up, and settles very quickly. Get
collaborative history
Asthma: wakes up coughing
Cyanosis
Caused by > 50 gm/L of reduced Hb (so if Hb concentration and CORD then easy to be cyanosed
blue bloaters)
< 66% saturation at normal HB (ie late sign)
< 40% saturation in anaemia
Causes:
Cardiac: shunts or congenital heart disease
Non-cardiac: e.g. hypoxia
Physical Exam*
Position patient at 45 degrees
General appearance, including cachectic state, Marfan‟s, Down‟s or Turner‟s Syndromes
Dextrocardia = heart on right hand side (1 in 400??). Need right-sided heart leads
Peripheral Exam
Hands
Check for clubbing (congenital cyanotic heart disease), warmth (perfusion), capillary refill, anaemia
(palmar creases), peripheral cyanosis, splinter haemorrhages
Pulse
Radial pulse: assess rate, rhythm, and delay from radial to femoral pulse (radio-femoral delay)
Brachial or Carotid pulse: Character and volume
Rate:
Sinus Tachycardia:
= Sinus rhythm > 100 bpm. 120 bpm could be physiological, > 140 – 150 bpm more likely to
be an aberrant rhythm
Causes: fever, exercise, emotion, anxiety, pain, pregnancy, anaemia, hypoxia, thyrotoxicosis,
HF, catecholamine excess, constrictive pericarditis, myocarditis, shock, MI, drugs, smoking,
coffee, autonomic neuropathy (eg in DM), PE
Sinus bradycardia:
= Sinus rhythm < 60 bpm
Causes: athlete, during sleep, drugs (-blockers, digoxin, amiodarone), hypothyroidism,
hypothermia, severe jaundice (due to bilirubin in conducting system), 3
rd
degree heart block,
MI, paroxysmal bradycardia (eg vasovagal syncope)
Rhythm:
Regular
Irregular:
Irregularly irregular: usually atrial fibrillation
Regularly irregular: Sinus arrhythmia (rate with respiration and with expiration) or 2
nd
degree heart block (Mobitz type 1)
Quality:
If „thin‟ then volume
Slow rising, low volume aortic stenosis
Radial/femoral delay aortic stricture e.g. coarctation,
Bounding pulse = a pronounced pulse – big difference between systolic and diastolic pressure (i.e.
large pulse pressure). If bounding then always do a collapsing check
Collapsing pulse = bounding pulse + thumping pulse felt over wrist with palm of your hand when
patient‟s arm raised - ?aortic regurgitation (higher column of blood regurgitation)
Pulse deficit = difference between the radial pulse rate and heart rate. If rapid or irregular contraction
then no time for ventricular filling there may not be a corresponding radial pulse beat
Cardiovascular 19
Measuring Blood Pressure
Ways of measuring blood pressure:
Mercury sphygmomanometer: listen for Kortokoff sounds
Oscillotonometer: detects arterial pulsations transmitted by the cuff. Tend to over-read very low
pressures (oscillations diminish in amplitude)
Ultrasound sphygmomanometer: uses Doppler shift
Direct measurement: intra-arterial pressure with transducer
How to measure with a sphygmomanometer:
Patient relaxed/seated for 5 minutes
Arm at heart level
Hold their hand under your right arm, straighten their arm and support under elbow. Use right
thumb to feel brachial pulse as cuff is inflated (so you don‟t over-inflate). Inflate to 30 mmHg
above point where pulsation stops
Don‟t push stethoscope diaphragm too hard (otherwise bruit)
Start of Kortokoff sound 1 = systolic. Disappearance of Kortokoff sound 5 = diastolic
In obese people a normal width cuff will over-estimate blood pressure – must use a large one
Repeat several times, and on several occasions before deciding to treat
Sources of operator error:
Wrong sized cuff
Poor positioning of the patient
Too rapid release of cuff pressure
Use of non-standard diastolic end points
Rounding to 5‟s or 10‟s
Watch for:
Pulsus paradoxus: Normally inspiration systolic and diastolic blood pressure (more negative
intrathoracic pressure pooling in pulmonary vessels filling). Pulsus paradoxus = this
decrease is exaggerated (ie fall of > 10 mmHg). Can occur in constrictive pericarditis, pericardial
effusion or severe asthma
Postural hypotension:
Fall of more than 15 mmHg systolic or 10 mmHg diastolic on standing
Causes: hypovolaemia, drugs (vasodilators, antidepressants, diuretics), Addison‟s disease,
hypopituitarism, autonomic neuropathy
Pulse on standing. For vasovagal syncope pulse
See also Hypertension, page 34
Face
Eyes:
Jaundice from liver congestion secondary to heart failure
Anaemia
Roth‟s spots on retina: areas of retinal infarction and haemorrhage caused by septic emboli in
bacterial endocarditis
Xanthelasma: intracutaneous yellow cholesterol deposits around the eye. Normal variant or
?hyperlipidaemia
Mitral facies: rose cheeks with dilated blue veins and cyanosed tongue. Due to pulmonary
hypertension and cardiac output (eg as in severe mitral stenosis)
Mouth: diseased teeth (cause of infective endocarditis), tongue for central cyanosis, and mucosa for
petechiae
Carotid Arteries
Never palpate both at once occlude blood supply to brain
Information about aorta and left ventricular function
20 4
th
and 5
th
Year Notes
Pulse wave forms:
Type
Causes
Anacrotic: small volume, slow uptake
Aortic stenosis
Bisferiens: anacrotic and collapsing
Aortic stenosis and regurgitation
Collapsing
Aortic regurgitation, hyperdynamic circulation
(eg exercise, fever), patent ductus arteriosus,
atherosclerotic aorta
Small volume
Aortic stenosis, pericardial effusion
Alternans: alternating strong and weak
beats
Left ventricular failure
Jerky
Hypertrophic cardiomyopathy
Jugular Venous Pressure (JVP)
Information about right atrial and right ventricular function
in RVF, volume overload, impaired RV filling, SVC syndrome
Positioning:
Patient should be at 45 degrees
Internal jugular is medial to the superior end of sterno-mastoid then runs behind it as it descends
External is lateral, is easier to see, but is more tortuous and therefore less reliable
Sternal angel is the zero point – pulsations are visible above this point at 45 degrees (centre of the
right atrium is 5 cm lower). Normal is pulsations just above the clavicle (+3 cm)
Differentiating from carotid pulse. The JVP is:
Visible but not palpable
Flickers twice with each cardiac cycle
Usually decreases with respiration
Is obliterated then filled from above following light pressure at the base of the neck
Pressure waves in atria:
a wave: atrial contraction at end of diastole atrial pressure. Coincides with first heart sound
and precedes carotid pulse. Closely followed by …
c point: bulging of AV valves into atria during systole atrial pressure. Not usually visible
x descent: atrial relaxation between S1 and S2
v wave: End of atrial filling during systole – venous inflow into atria with AV valve closed
atrial pressure
y descent: rapid ventricular filling following opening of the AV valve
Height (the easy bit – ha ha!):
If > 3 cm above the zero point then right heart filling pressure is raised
Rises with 10 seconds pressure on the liver (hepatojugular reflex). A rise is normal. If it remains
raised then ventricular failure
Causes of height: Right ventricular failure, tricuspid stenosis or regurgitation, pericardial
effusion or constrictive pericarditis, SVC obstruction (no waves), fluid overload, hyperdynamic
circulation
Should normally fall on inspiration. If it rises then ?constrictive pericarditis. Investigate with echo
Character (the hard part):
Causes of a dominant a wave: tricuspid stenosis (also causes a slow descent), pulmonary stenosis,
pulmonary hypertension
Causes of cannon a waves (wave - right atrium contracts against closed tricuspid valve):
intermittently in complete heart block (two chambers beating independently), retrograde
conduction
Cause of dominant v wave: tricuspid regurgitation (should never miss this, watch for movement of
ear lobe)
x descent: absent in AF, exaggerated in cardiac tamponade, constrictive pericarditis
a
c
x
v
y
Cardiovascular 21
y descent: Sharp: severe tricuspid regurgitation, constrictive pericarditis, slow in tricuspid stenosis,
right atrial myxoma
Praecordium
Inspection of the Praecordium
Scars:
Median sternotomy: any surgery requiring cardiopulmonary bypass
Left lateral Thoracotomy: ?closed mitral valvotomy
Note structural abnormalities: Pectus excavatum (sunken chest = funnel chest) or kyphoscoliosis may
distort position of heart and vessels (ie shifting the apex beat). If severe then pulmonary function
Note presence of pacemaker
Pulsations: apex beat and others (eg over pulmonary artery in severe pulmonary hypertension)
Palpation of the Praecordium
Apex beat:
Count down intercostal spaces (the 2
nd
space is the first one palpable, opposite the sternal angle).
Find most lateral and inferior point at which pulsations are felt
Normal = 5
th
intercostal space, mid-clavicular line
If not palpable then thick chest wall, emphysema, pericardial effusion, shock (or rarely
dextrocardia – inversion of heart and great vessels onto right side)
Pressure overloaded = systolic overloaded: Forceful, sustained, not displaced. Due to
hypertension, aortic stenosis
Volume loaded = diastolic overloaded = hyperkinetic: displaced, unsustained, uncoordinated, large
area. Due to aortic or mitral regurgitation, dilation, LV dysfunction (eg anterior MI)
Double or triple impulse = hypertrophic cardiomyopathy
Parasternal impulse: heal of hand rested just to the left of the sternum. Feel movement with systole in
right ventricular enlargement or severe left atrial enlargement (right ventricle pushed anteriorly)
Tap of pulmonary valve closure (P2) over pulmonary areas in pulmonary hypertension
Thrills = palpable murmurs. Apical thrills felt best with patient rolled onto left side. Pulmonary or
Aortic thrills best felt with patient sitting up, leaning forward and on expiration. A thrill coinciding
with the apex beat is a systolic thrill, otherwise a diastolic thrill
Percussion of the Praecordium
A waste of time!
Heart sounds
Stethoscope head:
Bell: good for low pitched sounds, eg diastolic murmur (mitral stenosis) or 3
rd
heart sound. Don‟t
press too hard otherwise skin becomes a diaphragm
Diaphragm: good for high pitched sounds, eg systolic murmur or 4
th
heart sound
Using stethoscope, ausciltate:
Mitral area (4
th
intercostal space, left mid-clavicular line) with bell and diaphragm
Tricuspid area (5
th
intercostal space, left sternal edge) with diaphragm
Pulmonary area (second intercostal space, left sternal edge) with diaphragm
Aortic area (second intercostal space, right sternal edge) with diaphragm
Heart Sounds:
First heart sound: closure of mitral and tricuspid valves at beginning of systole. Mitral closes
slightly before tricuspid but you won‟t hear the difference
Second heart sounds: closure of aortic and pulmonary valves. Lower pitch. End of systole. Aortic
closes first (higher back pressure on valve) splitting of heart sounds. But pulmonary closure is
not heard over all the praecordium, so splitting best heard over pulmonary area. Inspiration
venous return later closure of pulmonary valve enhanced splitting
Use carotid pulsation to orientate to timing. This occurs during systole, between S1 and S2
22 4
th
and 5
th
Year Notes
Abnormal Heart Sounds
S1
Loud
Mitral or Tricuspid Stenosis limited ventricular filling no easing
of low at end of filling valves snap shut. Also diastolic filling (eg
in tachycardia)
Soft
Prolonged filling (eg 1
st
degree heart block) or failure of leaflets to
close properly (eg mitral regurgitation), delayed LV systolic (eg
LBBB)
Splitting
Most often due to right bundle branch block
S2
Loud
Loud aorta in patients with hypertension and congenital aortic stenosis
( forceful closure). Pulmonary closure loud in pulmonary
hypertension
Soft
Aortic calcification or regurgitation leaflets don‟t close well
Increased Splitting
If abnormal delay in right ventricular emptying, eg right bundle
branch block, pulmonary stenosis, pulmonary hypertension,
ventricular septal defect ( right ventricle filling). Also mitral
regurgitation earlier aortic valve closure
Fixed splitting
Doesn‟t change with respiration atrial septal defect and both atria
have equal volumes
Reversed splitting
P2 occurs before A2, and gap increases on expiration. Due to delayed
left ventricular emptying (left branch bundle block, severe aortic
stenosis, coarctation of the aorta, or large patent ductus arteriosus)
Extra Heart Sounds
Description
Cause
S3
Low-pitched mid-diastolic
sound. Called Gallop Rhythm
?Caused by tightening of mitral or
tricuspid muscle at the end of rapid
ventricular filling. Normal in children and
young people. Pathological when
ventricular compliance, so get S3 even
when filling is not rapid
Left Ventricular S3
Louder at apex than at sternal
edge, and louder on expiration
Normal under 40 years and in pregnancy.
Otherwise, left ventricular failure, also
aortic regurgitation, mitral regurgitation,
ventricular septal defect and patent ductus
Right Ventricular S3
Louder at sternal edge than
apex, and louder with
inspiration
Due to right ventricular failure of
constrictive pericarditis
S4
Late diastolic sound, higher
pitched than S3. Can sound
like a gallop rhythm.
Always abnormal. Due to high-pressure
atrial wave reflected back from a poorly
compliant ventricle. Doesn‟t occur in AF
as it requires atrial contraction
Left Ventricular S4
Often during angina or MI
Left ventricle compliance: aortic
stenosis, acute mitral regurgitation,
systemic hypertension, ischaemic heart
disease, age
Right Ventricular S4
Ventricular compliance: pulmonary
stenosis or pulmonary hypertension
Summation Gallop
If the heart rate > 120 bpm, S3
and S4 may be superimposed,
and therefore more audible
Only implies ventricular stress if S3 or S3
persists when heart rate slows
Miscellaneous Sounds
Opening Snap: High-pitched sound after S2 in mitral stenosis, due to sudden opening of the mitral
valve. Don‟t confuse with widely split S2 (snap is higher pitched)
Cardiovascular 23
Systolic ejection click: early systolic high-pitched sound over aortic or pulmonary areas. Is caused by
pulmonary or aortic congential stenosis and is followed by a systolic ejection murmur
Non-ejection systolic click: high pitched systolic sound over the mitral area. Common. May be
followed by systolic murmur. Due to mitral prolapse and atrial septal defects
Diastolic pericardial knock: may occur if there is a sudden cessation of ventricular filling in constrictive
pericardial disease
Heart Murmurs
Timing of Murmurs
Murmur
Nature
Cause
Pan systolic
Pan-systolic: extend from S1 to S2,
loudness and pitch vary during
systole
Ventricular leakage: Mitral or
tricuspid regurgitation, ventricular
septal defects
Ejection (mid) systolic
Intensity greatest in early to mid-
systole then wanes
Turbulent flow through an orifice:
Aortic or pulmonary stenosis,
hypertrophic cardiomyopathy,
atrial septal defect
Late systolic
Noticeable gap between S1 and
murmur, and continues to S2
Mitral valve prolapse or papillary
muscle dysfunction
Early Diastolic
Begins with S2 and fades
(decrescendo). High pitched.
Regurgitation through a leaky
valve: Aortic or pulmonary
regurgitation.
Mid Diastolic
Begin after S2, may extend to S1.
Lower pitched.
Impaired flow during filling: Mitral
or tricuspid stenosis
Pre Systolic
Just before S1
Atrial systole increases blood flow
across the valve: Mitral or tricuspid
stenosis
Continuous murmurs
Through systole and diastole
Communication where there‟s a
permanent pressure gradient:
Patent ductus, numerous
malformations or fistulas
Combined systolic and
diastolic murmurs
Aortic stenosis and aortic
regurgitation
Pericardial friction rub
Superficial scratching sound at any
time in the cycle. Intermittent.
May varies with respiration and
posture
Pericarditis
Listening for Murmurs
Areas of greatest intensity: Mitral regurgitation is loudest over the apex and radiates into the axilla –
but may be heard over the whole praecordium. Aortic murmurs radiate into the carotid arteries
Benign murmur of pregnancy – ejection systolic. Pan systolic or diastolic murmurs are abnormal
In general, systolic murmurs are easier to hear than diastolic murmurs
Loudness: Doesn‟t always correlate with severity but a change is significant (eg after an MI).
For systolic:
Grade 1/6: very soft. Consultants only!
Grade 2/6: soft. Detected immediately by an experienced operator
Grade 3/6: moderate but no thrill
Grade 4/6: loud, thrill just palpable
Grade 5/6: very loud, thrill easily palpable
Grade 6/6: audible without stethoscope
For diastolic: Usually graded 1 to 4
Pitch: low pitched turbulent flow under pressure (eg mitral stenosis), high pitched high velocity
(eg mitral regurgitation)
24 4
th
and 5
th
Year Notes
Clues can also be obtained from peripheral signs (eg tricuspid regurgitation pulsitile liver, slow
rising pulse aortic stenosis)
Dynamic manoeuvre testing:
Respiration: Right sided murmurs louder on Inspiration (due to venous return), Left sided louder
on Expiration (brings heart closer to the chest wall – especially for aortic regurgitation) – RILE
Valsalva manoeuvre ( preload): Hold nose, close mouth, breathe out hard to pop ears and hold.
Listen over left sternal edge for changes in the systolic murmur of hypertrophic cardiomyopathy,
and over the apex for mitral valve prolapse. Other murmurs will be quieter due to left and right
filling
Squatting or leg raise (preload): venous return and arterial resistance most murmurs are
louder
Handgrip (afterload): aortic stenosis quieter
Lungs, Abdomen and Legs
Percuss and ausciltate lung bases on the back for pulmonary oedema, then check for sacral oedema
Abdomen:
Tender or enlarged liver ?heart failure
Pulsitile liver ?tricuspid regurgitation
Ascites ?heart failure
Splenomegaly ?infective endocarditis
Legs:
Femoral artery pulses: palpate and ausciltate for bruits
Popliteal pulse
Feel leg pulses both sides at once, standing at end of bed (gives you two chances to find them!):
Posterior tibial pulse: posterior to medial malleolus
Dorsalis pedis pulse: just lateral to the extensor hallucis longus tendon (seen when big toe
dorsiflexed)
Palpate the distal shaft of the tibia for oedema – press for 15 seconds. If present, note upper level
Cyanosis and clubbing of the toes, pallor, cool, capillary refill of toes
ECG Interpretation*
Reference: ECG Made Easy, J R Hampton, Churchill Livingston, 1997. Well worth a read
5 mm (one large square) = 0.2 secs 300 squares per minute
Leads
Depolarisation:
R > S: depolarisation spreading toward lead
R < S: depolarisation spreading away from lead
I
AVL (-30 degrees)
aVR (-150 degrees)
II (60 degrees)
aVF (90 degrees)
III (120 degrees)
V1 V2
Right Ventricle
V 3 V4
Septum
V5 V6
Anterior and Lateral
Left Ventricle
Cardiovascular 25
R = S: depolarisation at right angles to lead
Axis
To check axis, look at I, II and III. Normal is between VL and VF
Alternative: cardiac axis is at right angles to lead in which R & S are the same size
Right Deviation: ? hypertrophy of RV or tall and thin.
Left deviation: ?hypertrophy of LV
QRS Complex in V Leads
Shape is determined by:
Septum is depolarised first, and the wave spreads from L to R in the septum:
V1 initially up as depolarisation in the septum (L R) is towards the lead
V6 initially down as depolarisation in the septum is away from lead
Muscle mass: LV dominates so V1 is down and V6 is up.
Bundle Branch Block
Delay in depolarisation of part of the muscle widened QRS. If QRS > 3 small squares (0.12 secs)
slowed conduction bundle block or ventricular ectopic beat.
Right Bundle Branch Block (Can be benign. ?Atrial septal defect): Left depolarises first, then right.
May just be delay to the terminal end of QRS (especially in V5)
Left Bundle Branch Block. Always pathological. RV depolarises, then wave spreads to LV. T wave
inversion in anterior and lateral leads is common (I, VL, V4 – V6). Wide QRS
Left bundle divides into the anterior and posterior fascicles. Failure of the anterior fascicle left
axis deviation (depolarisation is through the posterior fascicle)
If LBBB: ?aortic stenosis, ischaemic disease
To determine side of block: W in V1 and M in V6 is Left (WiLLiam). M in V1 and W in V6 is Right
(MaRRow). LBBB prevents any further interpretation of the ECG
Reporting an ECG
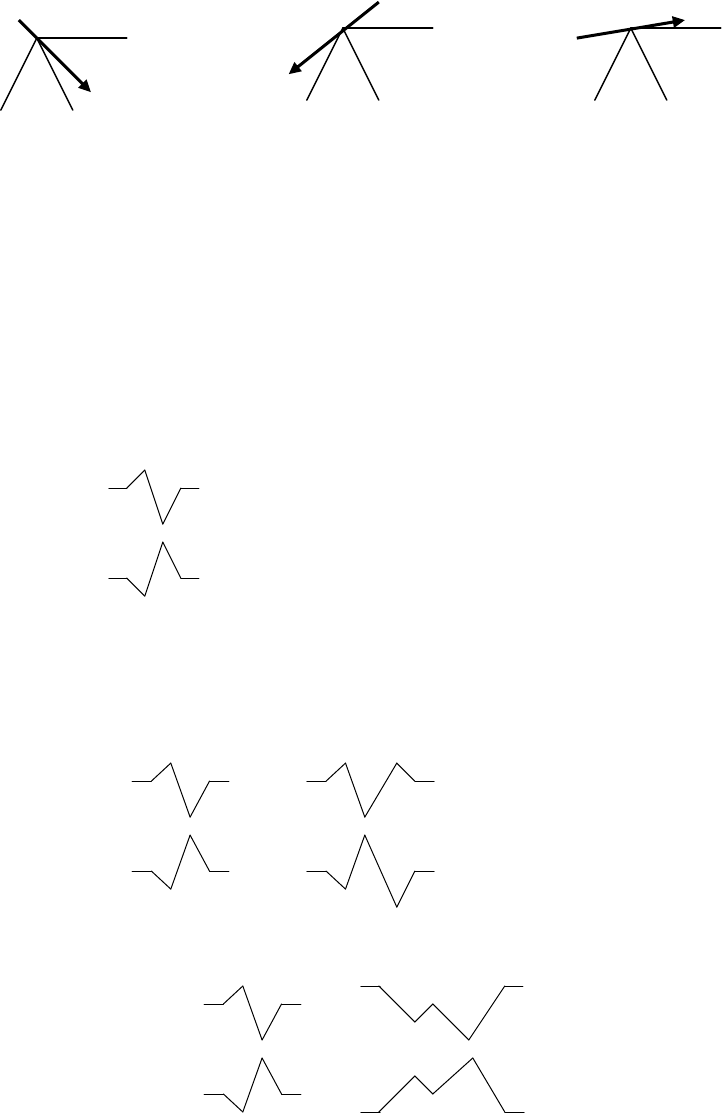
Check rate: bradycardia or tachycardia?
Check rhythm:
I +
II ++
III +
I -
II +/-
III ++
I +
II -
III -
Normal
Right Deviation
Left Deviation
V1
V6
V1
V6
RSR‟ Complex
V1
V6
„M‟ Pattern
26 4
th
and 5
th
Year Notes
See also Arrhythmias, page 39
Regular or irregular
Sinus rhythm = one P wave per QRS complex depolarisation begins in SA node.
Sinus arrhythmia:
Bradycardia: athletes, fainting attacks, hypothermia, myxoedema, drugs
Tachycardia: exercise, fear, pain, shock, thyrotoxicosis
Supraventricular arrhythmia:
= Sinus, atrial or junctional/nodal arrhythmia
QRS is normal width (unless also bundle block)
Escape beats are atrial, nodal or ventricular pacemakers that fire if the SA node fails, as they
have a slower intrinsic rate. Escape beats come late.
Atrial escape: abnormal P wave after SA node fails. Normal QRS
Nodal escape: no P wave (either none or buried in Normal QRS)
[Ventricular escape – not supraventricular: usually in complete heart block. Fast P waves.
Slow wide QRS. Shape of QRS may vary.]
Extrasystole/ectopic beats come early – some part of the heart has depolarised prematurely
Distinguish Ventricular Tachycardia and supraventricular tachycardia with bundle branch block:
Both have wide QRS
But Supraventricular Tachycardia has P waves (check all leads). Compare QRS with normal
QRS – if similar then bundle block.
Wolff-Parkinson-White Syndrome (a type of ventricular pre-excitation): Accessory conducting
bundle, usually to LV short PR and QRS has abnormal slurred upstroke (delta wave)
Treatments:
Atrial Fibrillation: Digoxin
Junctional Tachycardia: Carotid sinus pressure then adenosine
Atrial Flutter: Carotid sinus pressure, adenosine, flecainide, DC conversation
Ventricular Tachycardia: lignocaine, DC conversion
Check Cardiac Axis
Check P wave: shape:
Normal is < 2 * 2 small squares
Right atrial hypertrophy (eg tricuspid stenosis) peaked P
Left atrial hypertrophy (eg mitral stenosis) broad, twin-peaked P, especially in II, III, aVF
Potassium: K P, K P
Check conduction intervals - PR interval:
From beginning of P wave to beginning of QRS = time for AP to spread from SA node to
ventricular muscle.
Normal is 0.12 – 0.2 sec. (3 – 5 small squares)
Description of QRS Complex. Width of QRS complex = time for AP to spread through ventricles:
Normal is <= 0.12 sec. (3 small squares)
Height muscle mass
Right Ventricular Hypertrophy:
V1: R becomes higher (> 25 mm)
V6: S becomes deeper
Also look for:
Right axis deviation
Peaked P (right atrial hypertrophy)
Inverted T in V1 – V3
This picture is similar to a PE (which also has a Q wave in III)
Left Ventricular Hypertrophy:
V1: deep S wave
V6: Tall R wave (> 25 mm)
Inverted T wave in II, VL, V5 and V6
Left axis shift
Q waves:
Negative wave at start of QRS
If > one small square wide and > 2 mm deep patch of non-active muscle in the wall and the
lead is „looking inside‟ the heart, not at the wall old MI. Usually permanent
Anterior/septal infarct Q wave in V2, V3 and V4 (Left anterior descending artery)
Cardiovascular 27
Anterior-lateral infarct Q waves in I, II, VL. V3 – V6 (Left circumflex)
Lateral infarct Q wave in I, V5, V6
Inferior infarct Q wave in II, III and VF ( right coronary artery)
Inferior-lateral Q wave in II, III, aVF, V5, V6
Bundle Branch Block
Description of ST segments:
If raised acute injury – recent MI or pericarditis. Anterior V5, V6. Inferior III and VF
Depression ischaemia not infarction
T wave:
Normally inverted in aVR and V1 (also V2 in young people and V3 in blacks)
If not full thickness infarct T wave inversion but no Q wave (no „window‟ into heart) non-Q
wave infarction
If abnormal QRS abnormal T of no significance (repolarisation also skewed)
Digoxin T wave inversion and sloping depression of the ST segment
Electrolyte imbalances:
K T wave flattening
K tall, wide peaked T waves
QT interval
Ca QT interval
Ca QT interval
Progression following MI:
Elevation of ST
Q waves appear
T becomes inverted – may be permanent
ECG Abnormalities Due to Electrolyte Disturbances
Abnormality
Common Cause
ECG
Emergency Treatment
Potassium
Renal failure
Addison‟s disease
Peaked T
Prolonged PR
Small P
Wide QRS
VT, VF, asystole
Calcium chloride
Bicarbonate
Insulin/Glucose
Beta agonists
Dialysis
Potassium
Diuretics
Hyperaldosteronism
Vomiting
Gastric aspiration
Wide, flat or inverted T
Depressed ST segment
Small QRS
Prolonged PR
Prominent U wave
Large P wave
Potassium
Magnesium
Magnesium
Renal Failure
Bradycardia
AV block
Asystole
Calcium Chloride
Magnesium
Alcoholism
Starvation
Urinary Loss
Diuretics
GI loss
Malabsorption
Long QT
Short QT
Broad T
VF, VT, asystole
Magnesium
Calcium
Hypoparathyroidism
Acute pancreatitis
Renal failure
Long QT
Elevated ST
Peaked or inverted T
AV block
Tachyarrhythmias
Calcium Chloride
Chest X-ray
First check:
Is it the right patient
Is it the right date
Is it the right way round (ie L and R)
Then ask what is their age (and therefore likely pathologies)
28 4
th
and 5
th
Year Notes
How was the film taken:
Normal is PA erect, inspiratory:
PA as all Xray sensitive tissues are on the front (breasts, eyes, gonads, thyroid) – less exposure
Scapula off chest (in an AP then scapula projected onto chest)
Differences in Supine film:
Air collects on front of chest not top (important for pneumothorax)
Fluid distributes over back of pleura not in costophrenic angles
Normally more blood flow in lower zones, but in supine equal vascular markings at top
Better venous return in supine distended great vessels
To tell if it‟s supine where is gastric bubble: fundus = erect, body = supine
Is the film good enough:
Is it rotated: medial ends of clavicle equidistant from spinous process
Is it a good exposure: can you see lung veins in periphery – if you can see the spine clearly then
over exposed
Good inspiration: 5 – 7 anterior ribs on the right (hemidiaphragm is higher – must take a bigger
breath to get it down) or 9 – 11 posterior ribs
Key questions:
Is there any area that is lighter (opacity)
Is there any area that is darker (lucency)
Is there any abnormality of normally seen anatomy
Normally seen anatomy/silhouettes:
Right Upper quadrant (above the right bronchi):
SVC: free edge abutting lung
Right paratracheal strip (lung abutting right side of trachea). If strip wider than 5 mm then
lymph node enlargement
Arch of azygous in tracheal bronchial angle, just above carina. If enlarged think RH failure or
IVC obstruction
Left Upper Quadrant (above the left bronchi):
Arch of aorta (aortic knuckle) and free edge of descending aorta behind heart
Pulmonary trunk
Between them is the aortic pulmonary window: should be concave, if convex then lymph node
enlargement
Right lower quadrant (below right bronchi): Right atrium forming the border of the heart
Left lower quadrant (below left bronchi):
Border of heart = left ventricle + left auricle of atrium (NB its below the bronchi – a bulge
above the bronchi must be something else)
Left hemidiaphragm (lower than the right)
Lateral view:
Spine should get blacker as you go down
Retrosternal and retrocardiac areas should be the same density
Left hemi-diaphragm is the one that the heart sits on
Heart size:
Enlargement: greatest transverse diameter = largest horizontal distance from midline to right
border + largest horizontal distance from midline to left border. If this is > 50% of greatest
internal diameter then the heart is enlarged
Signs of left atrial enlargement:
2
nd
heart border parallel and medial to RH border (atrium bulging around behind the RA)
Density medial to this 2
nd
border
A prominent left atrial appendage
Elevation of the left main bronchus
Right atrial enlargement: bulges into right lung and elevation of right main bronchus
Right ventricle enlargement: Apex tilts upwards. On the lateral film, area of contact between the
heart and the sternum
Left ventricle enlargement: Elongates along its long axis apex shifts down and out. Posterior
bulge on the lateral film
Causes of global heart enlargement:
Sack like dilatation: due to pericardial effusion, cardiomyopathy or multi-valvular disease
Multi-valvular disease
Cardiovascular 29
Upper lobe
Lower lobe
Middle lobe
Horizontal fissure
Oblique fissure
Hypertrophic cardiomyopathy
Pericardial effusion
Progression of pulmonary oedema:
Prominence of upper zone vessels due to redistribution of blood to upper zones
Leakage interstitial changes: peribronchial cuffing, Kerley B lines, effusion
Flooding of the airspaces „Bats wing‟ appearance
With treatment, resolves in the reverse order
Ribs
Posterior of rib connects with midline, anterior doesn‟t as it turns to cartilage which isn‟t calcified
(but maybe in old person)
If 1
st
and 2
nd
ribs fractured, this takes massive force, consider concurrent damage to great vessels
If sternum fractured, consider cardiac contusion – do cardiac enzymes
If 11
th
and 12
th
ribs fractured, consider damage to kidney‟s, liver, spleen
If multiple fractures: flaccid chest Paradoxical Breathing (segment of chest moves in on
inspiration)
Lobes:
Upper: apical, posterior, anterior
Medial: superior, inferior
Lower lobe: Anterior, posterior, lateral, medial, apical
Pathology to look out for:
Pulmonary contusion: Opacity in parenchyma = bleeding. Should clear in 3 – 6 days (cf
consolidation which may take 6 weeks to clear). May resolve leaving clots filling cavities created
from shearing forces
Pneumothorax: must see visceral pleural edge AND no vascular markings lateral to this edge.
Edge alone might be other things
ARDS: soft and fluffy over all the lung parenchyma
Aspiration: won‟t be symmetrical. If it‟s global is it the „bats wing‟ appearance of pulmonary
oedema?
Is it effusion or pneumonia: Pleura is 2 cells thick. If pleural cavity fills up loose sharp edge. If
unsure, take another film lying on side (De Cubitus view) and see if fluid level shifts. If the
opacity is heterogeneous (eg polka-dots) then pneumonia, if homogenous (a smear) then effusion
Miliary pattern: occurs in Tb, fungi, Thyroid cancer, pneumoconiosis, rarely Sarcoid
Cysts cystic bronchiectasis. Especially in Cystic Fibrosis and Staph.
Enlarged hilum can be:
Enlarged vessels
Lymph node enlargement (like bunches of grapes): sarcoid, Tb, lymphoma
Cancer – usually unilateral
Differential if CXR is normal:
Airflow obstruction: asthma, COPD
PE
Pneumothorax (look again…)
Hidden pneumonia: check apices, angles and behind both sides of the heart (can you see the
diaphragm below the heart or the ribs behind the heart?)
Chest X ray checklist:
A – airway – midline
B – bones and soft tissue. Check for gaps in bones ?bony metastases
C – cardiac size and silhouette. Should be < 50% of maximal internal chest width
D – diaphragm – right higher than left, angles sharp, contract with lung sharp
E – equal volume, density symmetrical
F – fine detail (pleura & lung parenchyma)
Is upper darker than lower
30 4
th
and 5
th
Year Notes
Pronounced/wider vessels in upper lobes pulmonary venous congestion
Interstitial/pulmonary oedema fine diffuse shadowing
Kerley B lines oedematous interlobular septa
Fluff extending from hilum (bat‟s wing appearance): alveolar pulmonary oedema
Atelectesis: dense, short, usually peripheral horizontal lines. If large then collapsed lung
Are L & R main bronchus < 75 degrees at carina
If there are dots, are they hollow (if so then likely to be blood vessels end on)
G – gastric bubble
H – hilum – left higher than right, no larger than thumb + Hardware
Don‟t make pathological diagnoses – say an opacity consistent with consolidation
Treat the patient not the x-ray
Cardiovascular Risk factors*
Ref: 1996 National Heart Foundation Clinical Guidelines for the Assessment and Management of
Dyslipidaemia, NZMJ, 1996; 109:224-32
Framework:
Collect information on risk factors
Estimate prognosis
Decide on Treatment based on assessment of benefits and risks:
Assessment of risk
Absolute risk of cardiovascular disease depends on the combination of all risk factors. Treatment
decisions should be based on assessment of total risk – not one factor in isolation (eg raised blood
pressure or cholesterol)
Absolute risk is usually stated as the risk of a cardiovascular event in the next 5 years (Based on the
Framingham Study):
Very high risk: > 20% risk in next 5 years. Includes by definition people with:
Proven cardiovascular disease (past MI, positive treadmill, stroke, claudication, etc)
Familiar hypercholesterolaemia and familial combined hyperlipidaemia
Established diabetic nephropathy (albumin excretion > 300 mg/day)
High risk: 15 – 20% risk in next 5 years
Moderate risk: 10 – 15% risk in next 5 years
Mild risk: < 10% in next 5 years
Over age 70, risk for all individuals is very high, and age effect dominates
Risk factors in the Framingham tables are age, gender, blood pressure, dyslipidaemia, smoking and
diabetes/IGT
Risk factors not included in the tables are: Family history of coronary disease, physical inactivity,
obesity (especially BMI > 27), left ventricular hypertrophy, fibrinogen, lipoprotein (a). The presence
of these should bias treatment decisions towards treatment at any level of risk.
Dyslipidaemia
High levels of LDL („bad‟ cholesterol), low levels of HDL (“good” cholesterol) : normal ratio < 4.5
LDL reflects heredity, diet (both high cholesterol & high saturated fat) and exercise
TAG and HDL may be related to insulin resistance, without total Cholesterol being appreciably
raised
Raised triglyceride levels are closely related to low HDL levels hard to separate their independent
effects on risk
Secondary causes: diabetes mellitus, obesity, alcohol abuse, hypothyroidism, renal disease,
corticosteroids, exogenous sex hormones, pregnancy
Levels should be measured in early adulthood, especially if other risk factors or significant family
history of heart disease
Fasting lipids best measure of TAGs (from which LDL can be inferred – more accurate than total
cholesterol)
Within 24 hours of an MI, and up to 3 months later, total cholesterol and HDL , so measurements
over this period are not reliable
Treatment:
A 10% relative reduction in total cholesterol reduces relative risk by 15 – 20% over 5 years
Cardiovascular 31
Treatment goal: total cholesterol < 5 , HDL > 1, TAG < 2. TC: HDL < 4.5. Realistic goal is 25%
reduction in total cholesterol through diet and drugs
Thresholds for drug treatment following dietary treatment:
For very high risk: treat if TC or TC:HDL > 5.5
For high risk: treat if TC or TC:HDL > 6.5
For moderate risk: treat if TC or TC:HDL > 7.5
For mild risk: treat if TC or TC:HDL > 8.0
Dietary advice: reduce saturated and trans unsaturated fats + exercise
For drugs, see Lipid Lowering Drugs, page 53
Other Specific Risks
Hypertension: Blood pressure > 160/95 has 5 times risk. Vibrational stress damages intima. Pressure
wave tears the intima and this heals by scarring. Large pulse pressure also significant. Atheroma
occurs most commonly at vascular bifurcations. See Hypertension, page 34
Cigarette smoking: 2 times risk. Intimal microulceration (a complication to a plaque) predisposes to
thrombosis. Tobacco oxidises LDL poorly digested form that accumulates in the intima
Diabetes: 2 times risk factor advanced glycosylation end-products (non-enzymatically glycosylated
proteins) bind to endothelium permeable, causes cells to produce fibrous tissue
Vessel Pathology
Arteries
3 layers:
Intima: thin, includes endothelium, underlying thin layer of connective tissue containing
smooth muscle, and elastic interna – elastic fibre layer
Media: thick, smooth muscle and collagen. Large arteries have elastic fibres as well
Adventitia: thin layer containing elastic fibres in loose connective tissue
3 sizes: large (elastic), medium (muscular), small
Veins: thin wall, large lumen, IEL intact only in large vessels, scant media, contain valves
Atherosclerosis
Epidemiology
Causes 50% of all deaths in US – including coronary, cerebral and peripheral vascular disease
A disease of Western civilisation. Absent in certain 3
rd
world ethnic groups
Aetiology
Multifactorial
Endothelial damage permeability, monocyte adhesion and endothelial proliferation intimal
hyperlipidaemia with invasion of foamy macrophages cytokines (IL1 and TNF) and growth factors
(PDGF and FGF) cause inflammatory response and proliferation of smooth muscle with sclerosis;
plaque thickened by organisation of superimposed thrombi
Gross Morphology
Lesions appear in childhood as fatty streaks
Adult plaques: discrete, yellow white random elevations, more prominent around ostia of large
branches
Plaques may have sclerotic firm surfaces or ulcerate exposing soft cholesterol laden material
Severity increases with age
Microscopic Morphology
Plaque: intimal lesion – deposition of cholesterol esters, necrotic debris, smooth muscle and foam cells.
Chronic fibrotic inflammatory response forming a superficial fibrous cap
Complications are ulcers with thrombi, bleeding into plaque, embolisation, calcifications, atrophy of
media aneurysms
Reduplication of internal elastic lamina: shows with Elastin Van Geesen (EVG) stain
Adventitial fibrosis and chronic inflammation
32 4
th
and 5
th
Year Notes
Complications
Calcification rigid pipe pulse pressure distal atherosclerosis. (NB Calcium laid down in two
ways: dystrophic calcification – Ca laid down in necrotic tissue – and metastatic calcification - serum
Ca Ca laid down abnormally
Ulceration: fibrous cap cracks – debris discharged into lumen embolisation/thrombis
Thrombis: can embolise, or occlude artery. Cause of majority of myocardial infarcts and cases of
unstable angina pectoris. If collateral circulation, can recannalise thrombis
Haemorrhage: a weak little new artery in the plaque bursts pushes plaque against opposite wall
Aortic Aneurysm
Aetiology
Severe arteriosclerosis
20% familial incidence defect in connective tissue component (?type III procollagen)
Syphilis and other bacterial infections
Cystic medial necrosis denudation of elastic layer
Trauma
Common in Marfan's syndrome (eg Abraham Lincoln). Long ulnar, femur, weak aorta, and high
arched pallet
Clinical
75% occur in abdominal aorta. Easy to repair cf thoracic and thoraco-abdominal cases
Often asymptomatic incidental finding
Can cause back pain (due to retroperitoneal blood). Differential pancreatitis
44% of symptomatic aneurysms rupture. Distension inevitable rupture (Law of La Place)
Pathogenesis
Arteriosclerosis gradual destruction of media focal weakening of wall distensibility w +
r tension + blood velocity (T Pr/W)
Pressure radius tension radius, etc
Gross Description
Fusiform dilatation of severely atherosclerotic aorta with sharp superior and inferior margins
Typically abdominal aorta, from just below ostia of renal arteries to bifurcation of aorta
Larger aneurysms contain thick old laminated thrombus reducing patent luminal size
Aneurysmal thrombus does not organise due to the paucity of functioning vasa vasorum in fibrotic wall
Microscopic Description
Aneurysm wall: barely identifiable media, fibrotic lesions with focal aggregates of mononuclear cells
Adventitia is fibrotic with chronic inflammation
Complications
Thrombus distal gangrene, calcification, bacterial infection (salmonella, shigella), rupture,
dissection, fistula (eg aorta-vena cava)
Dissecting Aneurysms
Usually involves the aorta
Fatal in 75 – 90% of cases
Causes: atherosclerosis, also hypertension, Marfan‟s syndrome, trauma, inflammation of media
Pathogenesis:
Cystic medial necrosis: mucoid cysts in the media, elastic fragmentation and fibrosis
Commences as a transverse intimal tear, 90% in ascending aorta
Splits the media between the mid and outer 1/3
Proceeds down occluding branches
Outcomes:
Acute perforation sudden death
Subacute progression perforation in several days
Chronic rupture back into the lumen double barrel aorta
Cardiovascular 33
Arteritis
Diverse group of diseases classified by aetiology, vessel size or histologic changes
Infectious arteritis
Wide range of organisms, pyogenic, TB, parasites, viruses, fungi, syphilis
Vessel infected by septic emboli ( lodges and forms mycotic aneurysm) or direct extension from
adjacent abscesses
Histology: oedema, fibrin, dense neutrophilic infiltrate
Outcome: scarring, obliteration of lumen distal infarction
Syphilis: occludes vasa vasorum ischaemic damage to artery, small vessel occlusion obliterative
end arteritis, perivascular lymphocyte and plasma cell cuffing. Famous for causing proximal aortic
aneurysms
Physical/Chemical Agents
Irradiation, trauma, vascular toxins, sulphonamides, penicillin
Arteritis syndromes
See Vasculitis, page 282
Other Vessel Abnormalities
Arteriosclerosis:
= Thickening and loss of elasticity of arterial walls. Seen in chronic hypertension, and to a lesser
degree with ageing
Hyaline arteriosclerosis: blood vessel takes on glassy „hyaline‟ appearance. Reflects mild or
„benign‟ hypertension. Particularly seen in kidneys
Hyperplastic arteriosclerosis: concentric rings of increased connective tissue and smooth muscle
give arteries an onion skin appearance. Signifies acceleration/malignancy of the hypertension
Fibromuscular dysplasia: non-inflammatory thickening of large and medium sized muscular arteries
causing stenosis. Most significant in renal arteries secondary hypertension
Thrombophlebitis: inflammation and secondary thrombosis of veins, usually small veins as part of a
local reaction to bacterial infection
Varicose veins: enlarged, dilated, tortuous blood veins and incompetent venous valves – mainly in legs.
Predisposing factors include older age, female, heredity, posture and obesity. Varicose veins at other
sites include haemorrhoids (rectal), oesophageal varices and varicocoele (scrotum)
Vasculitis: inflammation and necrosis of blood vessels – including arteries, veins and capillaries. May
be due to infection, trauma, radiation, toxins or immune (eg disposition of immune complexes)
Leukocytoclastic vasculitis: a form of hypersensitivity angiitis in the skin presenting as purpura
Ischaemic Heart Disease
Most common cause of death in Western countries
Incidence peaked in NZ in 1968 at 320 deaths /100,000. Now 200/100,000
In NZ, 4,500 acute MI per year, 3,200 CIHD per year (=25% of all deaths)
Risks factors:
Cigarette smoking 5.2 x
Hypertension 3.3 x
Hyperlipidaemia 3.7 x
Diabetes mellitus
Male gender
Family history
Pathogenesis
Myocardial blood flow < metabolic demand of myocardium
Coronary perfusion related to:
Atherosclerosis occluding coronary arteries (fixed coronary stenosis), acute plaque changes
(eg rupture), thrombosis, vasoconstriction
Differential between ostia (aortic diastolic pressure) and coronary sinus (right atrial pressure)
Compression of intramuscular arteries during contraction myocardium perfused in diastole
Decreased coronary blood flow also due to intraventricular pressure & myocardial
contraction, aortic valve stenosis/regurgitation, right atrial pressure
34 4
th
and 5
th
Year Notes
Cross sectional area of major vessels must be reduced by 75% to significantly affect perfusion
Hypertension
See Measuring Blood Pressure, page 19, for measurement
Is a risk factor not a disease
Definition:
No dividing line between normal and high blood pressure. There are arbitrary levels set based on
the risk of complications (the main ones being stroke, MI, heart failure and renal failure)
In determining whether the blood pressure is „bad‟, take into account the systolic and diastolic
pressure, age, sex, other diseases (eg DM, hyperlipidaemia), smoking. Older age is the greatest
risk factor: treat high blood pressure in an older person regardless of other risk factors
WHO definitions:
Category
Systolic
Diastolic
Normal
< 130
< 85
High Normal
130 - 139
85 – 90
Hypertension
Stage 1 (mild)
140 – 159
90 – 99
Stage 2 (moderate)
160 – 179
100 – 109
Stage 3 (severe)
180 – 209
110 – 119
Stage 4 (very severe)
> 210
> 120
Also classified according to retinopathy, see Hypertensive Retinopathy, page 146
Classified as:
Primary/essential (what most people have – but a diagnosis of exclusion): contributing factors
include hereditary, obesity, alcohol intake, salt intake (60% of patients respond to salt intake –
but compliance difficult)
Secondary causes: renal disease (eg renal artery stenosis, diabetic kidney disease, etc), endocrine
(eg cortisol, aldosterone, acromegaly, oral contraceptives), neurogenic (eg psychogenic), sleep
apnoea (major changes in baroreceptor reflexes)
Epidemiology:
Prevalence with age. Older people at greater risk at any given blood pressure compared with
young
Strong risk factor for stroke, congestive heart failure, coronary artery disease and renal failure
Probably 10 – 20% of older adults require treatment (ie have essential hypertension with diastolic
pressure > 95 mmHg)
Treatment reduces related complications. Stroke risk reduces in line with BP, MI risk doesn‟t
reduce as much for a given drop in BP
History:
How accurate is the diagnosis?
Usually symptomless
Possibly related symptoms: palpitation, flushing, headache
Related risk factors: history of renal, cardiac or neurological disease
Asthma, diabetes, gout, renal disease: complications with drug treatment
Occupational
Diet: salt, fat
Smoking and alcohol
Family History
Detection and assessment:
Blood pressure more labile in older adults measure 2 to 3 times (in same arm). Measure
standing and sitting
In primary hypertension usually on standing. In secondary hypertension, usually on standing
Basic workup:
Urine for protein, blood and glucose DM, renal disease
FBC for polycythaemia, renal disease, alcohol
Electrolytes (especially K): exclude odd endocrine causes
ECG: any end organ damage
Additional tests if indicated:
Microscopic analysis of urine (for casts)
Plasma lipids
Blood glucose: need to modify drug treatment

Cardiovascular 35
Serum Ca, PO4, uric acid (gout – associated with hypertension, may also due to drugs)
Echocardiogram or CXR
Special tests for secondary causes if indicated: eg renal imaging, 24 hour urine for
catecholamine metabolites (phaeochromocytoma)
Pathology:
Pathophysiology: poorly understood. Older people have renin, and are more responsive to Na
depletion. „Hardening‟ of arteries systolic pressure. Responsiveness to -mediated vascular
relaxation
Leads to hypertensive heart disease: left ventricular hypertrophy relative myocardial ischaemia.
Aortic valvular disease also LV hypertrophy
Malignant hypertension (accelerated hypertension): hypertension leading to rapidly progressive
vascular compromise. Blood vessels show fibrinoid necrosis or concentric hyperplasia („onion
skin‟ changes)
Non-drug treatment
Remove/substitute drugs: eg NSAIDs, OCP, Prednisone
Always attempt lifestyle changes first:
Stop smoking (little effect on BP, but biggest impact on risk factors)
Weight loss
Alcohol (max 2 drinks per day)
Salt intake (max 70 mmol/day)
exercise
Saturated fats
Drug Treatment
When to treat:
Given it is such a strong risk factor, consider hypertension above systolic 140 mmHg
Always treat > 170 systolic or > 110 diastolic
Hardly ever treat < 140 and < 90 diastolic
In between, controversial. Consider other risks. If over 65 no other risk factors needed (eg
diabetes, etc). Give considerable attention to non-pharmacological approaches for 3 – 6 months.
Long term follow up necessary
Treat 72 older adults for 5 years to prevent 1 death, treat 43 for 5 years to prevent one
cerebrovascular event
Aim of treatment: diastolic < 90
Rules of thumb:
Use low doses of several agents, rather than increasing doses of one drug (especially thiazides)
First line: thiazides (with or without a potassium sparing agent) and/or -blocker (atenolol most
used in trials). If tolerate them both then add them together
ACE inhibitors: not so effective but rated best quality of life
Don‟t take diuretic, ACE inhibitor and NSAIDS together (renal side effects)
Introduce slowly, monitor for symptoms and postural hypotension
Aim for 140/90, and then attempt back titration 3 monthly
Individualise depending on co-morbid conditions:
Condition
Implication
Atrial Fibrillation
Some Ca channel blockers and -blockers may help. Watch
for drug interactions with digoxin
COPD
Avoid -blockers (also in Asthma)
CHF
ACE inhibitors improve the CHF. If diastolic dysfunction is
prominent then -blockers or Ca antagonists
Diabetes Mellitus
ACE inhibitors delay renal failure. Thiazides worsen
diabetic control. -blockers may mask hypoglycaemic
symptoms
Gout
Thiazides may worsen hyperuricaemia
Ischaemic Heart Disease
Consider -blockers
Renal Failure
half life of some drugs (eg atenolol)

36 4
th
and 5
th
Year Notes
Voiding Dysfunction
In men with urine flow, consider -blockers (eg terazosin)
History of IHD, stroke or
DM
Aspirin
See Cardiovascular Pharmacology, page 51
Angina Pectoris
Symptom complex characterised by attacks of chest pain, causing ischaemia but not infarction
Patterns:
Stable angina (typical): pain on exertion, relieved by rest or vasodilators. Subendocardial
ischaemia with ST-segment depression
Variant or Prinzmetal‟s angina: classically occurs at rest. Caused by reversible spasm in normal to
severely atherosclerotic coronary arteries. Can see ST-segment elevation or depression
Unstable angina: variable, prolonged pain, pain at rest or worsening of pain in stable angina. ST-
segment depression – but may be elevated. Most common complication: arrhythmias (especially
VF). Within 3 months 4% will have sudden death and 15% a myocardial infarct
Sudden cardiac death. Usually within an hour of a cardiac event or without symptoms. Usually
high-grade stenosis. Usually associated with arrhythmias, especially ventricular ectopic beats and
subsequent VF
Treatment options for stable angina:
Nitrates: short & long acting
-blockers (myocardial O2 consumption)
Ca antagonists
Aspirin
Unstable angina:
= Acute Coronary Syndrome (ACS) = acute heart problems without ST elevation
Investigations:
ECG. Serial or continuous if high risk
Bloods: Troponin (repeat after 6 hours), FBC, Cr, electrolytes, CK, blood glucose. Want to
test lipids/cholestrol – but false positives following an acute coronary event. Do later.
CXR: cargiomegaly? Pulmonary oedema? Dissection?
Medical therapy:
Aspirin: reduces progression to MI. Neither Warfarin nor Heparin confers little further
benefit. Use heparin if high risk.
-blockers: reduce progression to MI
iv nitroglycerine for symptomatic relief
Maybe calcium channel blockers that reduce the heart rate
Low risk:
Normal ECG and no detectable troponin despite angina frequency or severity
Management: discharge for outpatient assessment
High risk:
If even a minor degree of ST depression or a significant elevation of troponin minor
myocardial damage so now is the time to act
Overlap between High Risk ACS and non-STEMI (non-ST elevation MI)
Management: Admit for coronary angiography and, if positive, early percutaneous coronary
intervention (ie more aggressive treatment than previously)
Long term management:
Obesity, diabetes, smoking, exercise
Referral to a cardiac rehabilitation programme
Statins if serum cholesterol raised
ACE inhibitors if hypertension or diabetes
Myocardial Infarction (MI)
Definition and Classification
Old WHO definition: two out of three of: chest discomfort for > 30 minutes, enzyme rise and typical
pattern of ECG involving the development of Q waves (ie normal ECG does not rule out infarction)
Cardiovascular 37
New definition: Blood levels of sensitive and specific markers are raised in the clinical setting of acute
ischaemia (ie importance of biochemical tests). See Laboratory Diagnosis, page 38
2 classifications:
ST elevation MI verses none (ie STEMI and non-STEMI). Often ST elevation progresses to Q
wave
Q wave verses none (older classification) transmural or not
Epidemiology
Same risk factors as for atherosclerosis
5% occur under age 40, 45% over age 65
Oestrogen protective in women pre-menopause
30% mortality with 20% dying before admission
Symptoms
Crushing chest pain (absent in 15% of cases). But < 25% with chest pain have an MI
Can also present as epigastric, arm, wrist, or jaw discomfort with exertion or at rest
May be associated with dyspnoea, sweating, nausea, vomiting, weakness, dizziness, fainting
Pathogenesis
Irreversible damage in 20 – 40 minutes
Occlusive intracoronary thrombus, overlying ulcerated or stenotic plaque:
Causes 90% of transmural acute MIs.
For blood to clot need: abnormal flow, damage to vessel wall and clotting factors.
Thrombis formation: activated platelets adhere to exposed collagen of damaged endothelium
release thromboxane A2 expanding platelet mass + coagulation
Vasospasm: with or without atherosclerosis. Postulate where no findings at post-mortem (10%) – but
many of these will be thrombi that have lysed
Emboli: from left sided mural thrombosis, vegetative endocarditis
Arteritis: polyarteritis nordosa, Kawasaki disease
Other: dissecting aneurysm occluding coronary ostia, O2 supply (anaemia, CO, cyanide), O2
demand (hyperthyroidism, fever)
Gross Morphology
Transmural infarct: entire thickness of wall from endocardium to epicardium. Usually Anterior wall
(50%) or posterior free wall/septum in 15 – 30%. Q wave
Subendocardial infarct: multifocal necrosis confined to inner 1/3 to ½ of left ventricle wall. More
commonly associated with temporary hypoperfusion (eg shock). No Q wave
Occlusion:
LAD: 40 – 50%
RCA: 30 – 40%
LCA: 15 – 20%
Gross changes over time:
18 – 24 hours
Pallor of myocardium – anaemic, grey brown (cf normal brown-red)
24 – 72 hours
Pallor (yellow/brown) with increasingly defined hyperaemia border
3 – 7 days
Hyperaemic border (darker brick red) with central yellowing,
haemorrhagic areas
10 – 21 days
Maximally yellow and soft with vascular margins (red edge – granulation
tissues moves in)
7 weeks
White fibrosis
Microscopic Appearance
1 – 3 hours
Wavy myocardial fibres
2 – 3 hours
Staining defect with tetrazolium
4 – 12 hours
Coagulative necrosis with loss of cross striations, oedema, haemorrhage,
early neutrophil infiltrate (WBCs with multilobed nuclei), loss of
myocardial striations
38 4
th
and 5
th
Year Notes
18 – 24 hours
Continuing coagulation necrosis, pyknosis (margination) of nuclei
(healthy myocardial nuclei are usually central)
24 – 72 hours
Total loss of nuclei and striations, heavy neutrophilic infiltrate
3 – 7 days
Macrophage and mononuclear infiltration, fibrovascular response begins
(starts at edges), myocardium at its weakest
10 – 21 days
Prominent granulation tissue: fibroblasts and neovascularisation,
macrophages (tissue scavengers – high fat content yellow, high iron
brown), plasma cells
7 weeks
Fibrosis
Laboratory Diagnosis
Troponins:
Increases highly specific for MI injury – but not synonymous with MI or ischaemia, but probably
indicates irreversible injury
Increases above the 99
th
percentile are significant (lower than previously)
Prognosis related to degree of elevation
Rises no faster than CK (ie starts to rise within 3 – 12 hours) and more expensive but substantial
rise after MI (400 fold)
Causes besides MI:
Subendocardial injury from wall stress in left ventricular hypertrophy (eg heart failure)
Right ventricular injury in severe PE
Direct trauma (eg contusion)
Toxic injury by drugs or in septic shock
Myocarditis
Cardioversion
Troponin T
= Cardiac troponin T, cTnT, TnT: only available from Boehringer Mannheim
Normal < 0.03 g/l
Increases in renal failure due to clearance ( false positive)
Troponin I:
Everyone else‟s test. Normal value depends on which assay is used
I remains elevated for 5 – 9 days and T for 2 weeks. Better marker for recent MI than LDH.
Harder to interpret in re-infarct – don‟t know whether it‟s the 1st or 2
nd
infarct
Test on admission to either see if already raised (poor prognosis) or to establish baseline
CK – total: not specific to myocardial injury. Do baseline and use to check for reinfarction (Troponins
not so good for this)
Older tests:
CK – MB fraction:
MM fraction is in both skeletal and myocardial muscle. But 15 – 40% of cardiac CK is MB,
compared with 2% skeletal. BB found in brain, bowel and bladder. The MB fraction is
therefore very specific
MB fraction rises within 2 – 8 hours. Dissipates within 1 – 3 days. So also a good marker of
reinfarction
CK – MB isoforms: Ratio of isoform 2 to isoform 1 > 1.5 early acute MI (changes before
CK- MB elevated). Requires electrophoresis, so labour intensive. False positives with heart
failure
Myoglobin: Oxygen binding protein in skeletal and cardiac muscle. Elevated before CK-MB, but
is not specific to cardiac muscle. Negative myoglobin can help rule out MI
LDH: supplanted by other tests. Rises later (24 – 48 hours) and elevated for 7 – 14 days.
Isoenzyme measurement of LDH 1 and 2 necessary for cardiac specificity
AST and ALT: intermediate timing but rather non-specific
Other Investigations: CXR, echo, ABG, FBC, ?perfusion scan, ?amylase
Management*
Exclude differentials:
Aortic dissection
Pericarditis
PE or other causes of pleuretic chest pain
Cardiovascular 39
Peptic ulcer
Investigations as for Unstable Angina, see page 36
They will be frightened. Reassure. > 90% survival if low risk (< 60, no diabetes, no past history, pulse
< 100)
High flow O2 (unless CO2 retaining)
Morphine 5 – 15 mg iv at < 1 mg/min (+ antiemetic eg metoclopramide 5 – 10 mg iv). Effects:
analgesic, anxiolytic, anti-arrhythmic, venodilatory
Restoring/Maintaining vessel patency:
Aspirin 300 mg (unless contra-indicated)
Thrombolysis:
Indicated if with 12 hours of MI
Best within 60 mins
Contraindications:
General bleeding tendency: warfarin, haemophilia, severe liver disease, thrombocytopenia
Local bleeding risk: Past haemorrhagic stroke or recent surgery, prolonged resuscitation
( rib fractures, contusion, etc), peptic ulcer, GI bleeding, pregnancy, cavitating Tb
Severe hypertension (systolic > 200, diastolic > 120)
Pre-existing thrombis that might embolise (eg endocarditis, aortic aneurysm)
Options:
Streptokinase: restores perfusion in 30%
TPA: restores perfusion in 54%. Expensive. Use tPA if previous reaction to SK, or if SK
has been used between 1 year and 5 days ago
Complications: 1% risk of stroke
Watch this space for platelet receptor blocking drugs (eg IIb/IIIa inhibitors)
Consider for primary angioplasty (acute stenting of an occluded coronary artery) if large anterior
infarct refractory to thrombolysis
Management of preload, afterload and heart rate and rhythm:
Glyceryl trinitrate
ACE inhibitor + -blocker (unless contra-indicated)
Bed rest
Monitor ECG, BP, cardiac enzymes, ABGs
Stop smoking
Early stress/treadmill test
Prognosis
Good prognostic indicators:
No pre-existing hypertension
Normal heart size
No post MI pulmonary oedema
No significant arrhythmias after day 1
No post-MI angina
If good prognosis, discharge on aspirin and -blocker. Add an ACE inhibitor if LVF. Consider a
statin if lipids.
Complications
35% die within one year, 10% per year thereafter. NZ overall hospital mortality 19%
Arrhythmias and conduction defects: eg premature ventricular beats, sinus bradycardia, VT, VF, heart
block
Extension of infarction, re-infarction
Congestive heart failure (pulmonary oedema): everyone who‟s had a significant MI will have some
degree of this
Cardiogenic shock: if more than 40% of the left ventricle is infarcted. 70 – 90% die
Pericarditis: fibrinous adhesions in the pericardium overlying the infarct (Dressler‟s syndrome –
autoimmune adherent pericarditis – occurring 2 – 6 weeks post MI or cardiac surgery. Treatment -
steroids)
Mural thrombosis embolisation
Myocardial rupture tamponade. Maximum incidence day 5 - 7. Can include rupture of
interventricular septum
Papillary muscle rupture or infarct mitral incompetence
40 4
th
and 5
th
Year Notes
Ventricular aneurysm formation: 12 – 20% of cases
Ischaemic cardiomyopathy: severe atherosclerosis involving all major branches inadequate vascular
supply myocyte loss and interstitial fibrosis compliance & dilation compensation by
myocyte hypertrophy slow progressive heart failure and enormous heart size (up to 2 to 3 times
normal)
Time to complications:
1 – 3 days: arrhythmia, CHF, pericarditis
5 – 7 days: rupture
Later: recurrent MI, angina, embolism from mural thrombosis, mitral regurgitation, Dressler‟s
syndrome (Post MI syndrome)
Arrhythmias
For cardiac arrest rhythms (VT, VF, Torsade and asystole) see Cardiac Arrest Rhythms, page 479
Atrial Fibrillation
= a type of supra-ventricular arrhythmia
Mechanism:
Wave of depolarisation circulates in atria at much faster rate than the discharge from the SA node.
Disorders changing the conduction characteristics of the AV node predispose to AF: atrial size,
fibrosis, inflammation, thyrotoxicosis, ischaemia, altered autonomic tone, alcohol use, after bypass
surgery (30%), after valve replacement surgery (50%)
AV node receives irregular impulses at a rate of 250 – 400 per minute. Conducted through the
node at a frequency dependent on the pathway‟s refractory period
Typical ventricular rate is 120 per minute: but this may if sympathetic stimulation (
refractory period) or alternative conducting path to the AV node (eg Wolf-Parkinson-White
syndrome)
Epidemiology: most common cardiac arrhythmia. M > F. 5% of over 70s
Causes:
IHD: especially post MI
Mitral valve disease
Alcohol
Thyroid disease
Idiopathic
Potential implications:
Thrombo-embolism: Especially cerebral (also mesenteric arteries or lower limbs). If no other risk
factors then 1% per year. 5% if one other risk factor (age over 65, BP, heart failure, diabetes,
IHD, previous embolism, RF). If RF and AF then 20% annual rate
Reduced cardiac output: Ventricular filling Cardiac output heart failure or exercise
tolerance. Also high ventricular rate filling CO
Other symptoms: palpitations (25%) and dizziness or syncope (20%)
Diagnosis: should always be confirmed by ECG. Ventricular rhythm in AF can be deceptively regular,
and not all irregular rhythms are AF (eg variable AV block, ventricular or atrial ectopics)
Assessment:
Exclude thyrotoxicosis
Manage contributing MI, respiratory disease or alcohol abuse
Check electrolytes
Assess cardiovascular risk factors: eg glucose, lipids
Echocardiogram to assess atrial size or abnormal ventricles (eg valvular heart disease). These are
harder to cardiovert (also have a higher risk of embolism). Echocardiogram is poor at detecting
thrombis (trans-oesophageal echocardiogram is better)
Management:
Cardioversion: indicated if onset is within 24 – 48 hours and no other risk factors (eg no atrial
enlargement or ventricular abnormality). Involves general anaesthetic and synchronised DC shock
at 100 then 200J. Successful in about 85%. May need anticoagulation for cardioversion (thrombi
may get dislodged if normal rhythm returns).
Chemical cardioversion: flecainide and amiodarone – successful in 60 – 90%. (Digoxin does not
cardiovert)
> 50% revert in one year if no ongoing drug treatment
Cardiovascular 41
Drug treatment: consider digoxin (increases heart block slows ventricle improved pump
action), flecainide (in those without structural heart disease), Amiodarone (extensive toxicity
issues) or Sotalol:
Agent
Action
Adverse effects
Amiodarone
Prolongs action potential, -
blocker activity. Hepatic
metabolism, active metabolites.
T½ of weeks.
Pulmonary fibrosis, thyroid and
hepatic dysfunction (do baseline
bloods), muscle weakness, peripheral
neuropathy, skin discoloration
Digoxin
vagal tone, renal elimination, T½
= 36 hours
Nausea, vomiting and confusion. K
(eg diuretics) toxicity. Diltiazem,
amiodarone and flecainide digoxin
concentration.
Diltiazem
Ca channel blocker. Hepatic
elimination. T½ = 4 hours.
Hypotension, headache, bradycardia,
oedema, heart failure. Digoxin
levels.
Flecainide
Na Channel blocker. Renal and
hepatic metabolism. T½ = 10 – 17
hours
Sudden cardiac death in those with
structural heart disease, CHF or heart
block
Metoprolol
-blocker. Hepatic metabolism.
T½ = 4 hours. High first pass
metabolism
Hypotension, heart block, worsening
of heart failure if larger doses, asthma
Sotalol
-blocker, prolongs action
potential. Renal elimination. T½ =
8 hours
Ventricular arrhythmia, hypotension,
heart block, worsening of heart failure,
asthma
Antithrombotic therapy: Reduces annual risk in those at risk from 5% to 1.5% (60% relative risk
reduction), with 1% having material anti-coagulant side effects. Use warfarin with a goal of an
INR from 2 to 3. Use aspirin if warfarin contra-indicated (only 10 – 15% relative risk reduction)
Atrial flutter: probably due to atrial re-entry. Regular atrial saw tooth pattern with ventricular beat
every 3:1 or 4:1. If unstable hypotension, synchronised counter-shock at 50J (treat as for AF)
Sinus Arrhythmia
Normal sinus rhythm: rate 60 to 100 per minute, P wave upright in leads I, II and AVF
Sinus tachycardia:
discharge of sinus node. Rate is > 100/minute and regular
P wave is upright in leads I, II, AVF. Treat underlying cause
Sinus bradycardia:
Constant and normal PR interval
< 60 bpm: but this is relative. An athlete may normal at 40, and a hypovolaemic patient
bradycardic at 65 bpm
Causes: SA node disease, parasympathetic tone, drug effect
Treat if hypotension or ventricular escape beats present
Treatment: atropine (0.6 mg) unless MI, transthoracic pacing, dopamine or adrenaline
Sick Sinus Syndrome: Common in elderly. Bradycardia +/- arrest, AV block, or SVT alternating with
bradycardia/asystole (Tachy-Brady Syndrome). Pace if symptomatic
Other Abnormal Rhythms
Atrial tachycardia (paroxysmal atrial tachycardia) – SVT (Supraventricular Tachycardia):
Narrow QRS complex (always exclude atrial flutter with 2:1 block)
Often abrupt onset, last for seconds to many hours, then abrupt offset
Rate is usually 160 – 200/min
Therapy: vagal stimulation (carotid massage, one side at a time), adenosine, amiodarone, beta-
blockers or digoxin. If LV failure, chest pain or HR > 220 bpm then synchronised counter-shock
Premature Atrial Complexes (PAC): atrial ectopic beats. Small spike before premature but normal
width QRS
Junctional or Nodal rhythm: regular rhythm. May be no detectable P wave (due to retrograde firing
into atrium) or inverted P-wave with short PR interval. P wave may be buried in QRS complex. Rate
of 40 – 60 bpm. Reduction in atrial filing. Treatment often not indicated
42 4
th
and 5
th
Year Notes
Premature Ventricular Complexes (PVC‟s): bizarre, wide QRS complexes triggered by an ectopic
ventricular focus. Most common post-MI rhythm. Unifocal PVC‟s (each complex looks the same) or
multifocal (each complex looks different from others)
Heart Block
Atrioventricular block/Heart Block: Delay or interruption in conduction between atrium and ventricle
First degree (partial block): PR interval prolonged beyond 0.2 secs (5 small squares). Often seen
in normal people. ?Acute MI or Rheumatic Fever. No urgent action needed.
Second degree AV block (partial block): some impulses are conducted and some not. Heart
disease. Often seen in acute MI:
Mobitz type 1 (Wenckebach): progressive prolongation of PR interval before an impulse is
completely blocked – then sequence starts over. Usually transient and prognosis is good
Mobitz type 2: PR interval does not lengthen but some beats are not conducted. May lead to
bundle branch block ( wide QRS), transvenous pacing may be required
2:1 block (every second beat gets through). Also 3:1 block. May need pacing if ventricular
rate too slow.
Third degree (complete heart block): no conduction – either at AV, bundle of His or bundle branch
level. More often fibrosis than ischaemia:
At level of AV node: junctional escape pacemaker will fire at 40 – 60 bpm with normal QRS.
Prognosis favourable. Due to parasympathetic tone from inferior MI or drug effect
At infranodal level: Implies extensive disease of both bundles. Associated with anterior MI.
Distal escape rhythm, slow rate (<40) plus wide QRS, possibly asystole. Management:
transvenous or transthoracic pacing, dopamine or adrenaline, pacemaker
Drugs for Acute, Life Threatening Arrhythmias
For tachycardias:
Ventricular Tachycardia:
Lignocaine: dose 1 – 1.5 mg/kg by slow iv bolus, followed by infusion of 1 – 4 mg/min.
Reduce dose in heart failure, shock, > 70 years, blockade & hepatic disease. Side effects
include convulsions. Action on sodium channels reduces myocardial excitability, especially in
ischaemic myocardium. Raises threshold for VF, and suppresses VT and ventricular
ectopy. Should be considered in VF after 3 defibrillatory loops. No evidence of usefulness in
converting VF but may prevent return to VF. Reduces blood pressure and slows the heart rate
Bretyllium: anti-adrenergic, although initially causes adrenergic stimulation (for 20 minutes),
raises VF threshold. Use if lignocaine fails
Procainamide: powerful antiarrhythmic and strong negative inotropic agent, but slow to act.
Use where lignocaine has failed to suppress recurrent ventricular tachycardia
Magnesium: prevention and treatment of refractory ventricular arrhythmias
SVTs:
Adenosine: slows sinus rate and AV conduction. Use for SVT due to re-entry. Very short
T½
Verapamil: Ca blocker. Suppresses pacemaker activity in SA and AV nodes. For SVT where
adenosine has failed
Amiodarone: delays repolarisation with less cardiac depression than other antiarrhythmics.
Good for SVT, less so for ventricular arrhythmias. Via central line, long T½
-blockers: useful in treatment of hypertension, supraventricular arrhythmias and recurrent VT
where LV function is not severely impaired. E.g. propranolol (unselective), atenolol (1
selective), metoprolol (relatively selective), labetalol ( & selective, short acting, for acute
hypertensive crises), sotalol (non-selective blocker + antiarrhythmic), esmolol (ultra-short
acting block)
For bradycardias:
Atropine: Competitive anticholinergic at muscarinic nerve endings. Enhances SA discharge and
AV conduction. Use in bradycardia or AV block. Care in MI – may increase pulse extension
of ischaemia
Isoprenaline: agonist - use for significant bradycardia refractory to atropine. Use dopamine or
adrenaline first
Other supra-ventricular arrhythmias:
Digoxin: force of contraction and AV conduction – for heart failure and supraventricular
arrhythmias (particular AF). Avoid in recent MI, heart block, renal impairment, and hypokalaemia
Cardiovascular 43
Dopamine: for treatment complete heart block. A catecholamine. Infuse at 5 – 20 g/kg/min.
Adjust to keep heart rate at 60 beats per minute. renal blood flow ( renal output) through
renal vasodilator and due to CO and perfusion generally
Others:
Inotropes: dopamine and dobutamine – for supporting blood pressure once cardiac output has been
established. Useful in cardiac failure secondary to ischaemia.
Nor-adrenaline: intense vasoconstrictor – use for restoring MAP where vasodilation induced
hypotension
GTN: venous vasodilator - blood pressure and improve artery blood flow. Preload and afterload
reduced
Diuretics: frusemide – also causes venodilation ( preload)
Antihistamines: H1 antagonists (promethazine / Phenergan), H2 antagonists (ranitidine)
Emergency cardiac pacing
Complete heart block most common indication. Also for non-response bradycardias and asystole with
P waves
Transcutaneous/transthoracic pacing: Electrodes over apex and sternum. Sedation + analgesia
required. Temporary measure only
Transvenous pacing: via arm or neck vein into right atrium or ventricle
Valvular Heart Disease
= Stenosis, insufficiency/regurgitation or mixed
Insufficiency may be due to diseased cusp or supporting structures (valve ring, chordae tendinae,
papillary muscles, ventricular wall). Can be acute or chronic
Stenosis: disease of valve cusps, usually always chronic
See Heart Murmurs, page 23 for clinical descriptions
Aortic Stenosis
Compared with regurgitation/incompetence:
Have different effects on the LV (can‟t have severe stenosis and severe regurgitation together):
Stenosis: pressure but no in volume. LV tolerates pressure loads less well than volume loads
stenosis is the worse of the two
Regurgitation: volume but no in pressure. However, some in afterload due to stroke
volume
Causes or aortic stenosis:
Post inflammatory scarring (eg rheumatic fever): 10%
Senile (degenerative) aortic stenosis: commonest, in 8
th
– 9
th
decade
Calcification of deformed valve in 6
th
– 7
th
decade (associated with coarctation check for radio-
femoral delay)
Congenital stenosis
Infective
Symptoms: Occur late
Dyspnoea and chest tightness related to exertion
Exertional syncope: due to inability to increase CO and transient ventricular arrhythmias
Angina pectoris/MI, fibrosis, ventricular arrhythmia and sudden death due to impact on myocardial
O2 supply and demand:
O2 demand due to pressure and LV mass (LV workload concentric hypertrophy)
coronary blood flow due to diastolic aortic pressure coronary vascular resistance and
systole compared with diastole time for perfusion
ischaemia
No pulmonary oedema unless eg mitral problems secondary to LV hypertrophy, etc
Signs:
Sounds:
Harsh systolic ejection murmur (unless in severe LV failure) +/- systolic ejection click and a
short aortic diastolic murmur. Heard in base, apex and carotids
May have paradoxic (reversed) splitting of S2 if severe stenosis or LBBB. 3
rd
and 4
th
sounds
common
Pulse pressure and low blood pressure
44 4
th
and 5
th
Year Notes
Slowing and shuddering of the carotid upstroke
LV hypertrophy on ECG or x-ray and heave on examination. Palpable LV hypertrophy with a
dynamic quality is more related to incompetence – the ventricular impulse reflects stroke volume
more than pressure
LV failure: progression from LV hypertrophy to LV dilation in late stages
AF in 10%
Diagnosis:
Often a discrepancy between symptoms and severity. Pre-symptomatic progression is highly
variable
Usually at least some regurgitation as well
ECG: LV hypertrophy, occasionally left or right BBB
Pressure differential with Doppler estimate valve area
Gross:
Look for commissural fusion (rheumatic)
Heaped up calcified masses in leaflets. Beginning at the base senile, beginning at the edge
abnormal valve
Management:
If mild/moderate (ie < 50 mmHg pressure gradient across the valve) then monitor
Fix/replace valve before LV failure
Complications:
Sudden death
LVF
Conduction defects
Infective endocarditis
Embolisation
Differential:
Can rarely be due to supraventricular or subvalvular lesions, with no problem with the valve
Left ventricular failure
Hypertrophic obstructive cardiomyopathy: pulse is jerky and upstroke rapid. Longer, harsher
murmur best heard at the left sternal edge
Hard to confuse with mitral regurgitation (!!): Pansystolic murmur and rapid upstroke
Coarctation
Aortic Regurgitation
Causes:
Intrinsic valvular disease:
Acute lesions: Rheumatic fever, infective endocarditis (have high index of suspicion),
traumatic rupture, aortic dissection (may also have dissected coronary arteries MI)
Chronic lesions: Congenital lesions, rheumatic heart disease, arteritis, aortic aneurysm,
collagen diseases, ankylosing spondylitis and Reiter‟s Syndrome (may be secondary to
aortitis)
Aortic disease: degenerative aortic dilatation, syphilitic aortitis, Ankylosing Spondylitis,
rheumatoid arthritis, Marfan‟s syndrome
Key features:
LV hypertrophy
Large aorta
Stroke volume
Wide pulse pressure eg 140/50 (systolic due to extra work of the heart, diastolic due to back
flow)
Symptoms:
Acute: dyspnoea – often paroxysmal, orthopnea, pink frothy sputum. Chest pain, sudden death,
etc. If sub-acute, possibly embolisation
Chronic: Symptoms unrelated to severity. Either awareness of force of contraction (palpitations)
or LV disease/failure
Signs:
Pulses: prominent pulsations in the neck (Corrigan‟s Sign), throbbing peripheral pulses, prominent
apex beat over a wide area
Auscultation: high-pitched, blowing diastolic murmur beginning immediately after S2. The more
severe the longer it lasts. Systolic flow murmur
Cardiovascular 45
Pathogenesis:
Acute: LV blood volume left atrial and pulmonary pressure oedema. Pressure inside a
non-compliant pericardium RH pressures. Myocardial flow due to aortic diastolic pressure
and constricted pericardium ischaemia, further dysfunction, etc
Chronic/Gradual: eccentric hypertrophy with low filling pressure. Stroke volume systolic
pressure baroreceptor reflex peripheral vasodilation further widening of the pulse
pressure. Copes with tachycardia better than stenosis: proportion of cycle in diastole
proportion of blood flowing back into the ventricle. However, peripheral resistance (eg cold,
iso-tonic exercise, sympathetic nervous stimulation) pressure load on the heart
Complications:
LV failure + myocardial fibrosis (secondary to hypertrophy, ischaemia, etc) late in the progression
Infective endocarditis
Conduction defects less common
No pulmonary oedema unless LV hypertrophy
Differential diagnosis:
Pulmonary regurgitation + pulmonary hypertension
Other causes of rapid run-off: patent ductus, arterio-venous fistula
Mitral Stenosis
Causes: rheumatic heart disease, infection (less common than aortic) fusion of the leaflets
Symptoms: dyspnoea, PND, haemoptysis, arrhythmia ( palpitations), RH signs if pulmonary
hypertension
Signs:
Loud S1, opening snap after S2 (loudest at apex)
Long, loud diastolic murmur accentuated just before S1 (atrial systole – not if AF). Loudest with
bell at apex and left lateral side
Pulmonary oedema is worse than in other causes (eg mitral regurgitation)
If pulmonary hypertension then low cardiac output failure thin patient, peripheral cyanosis, cool
extremities, small pulse volume. Dilated veins and cyanosis of cheeks = mitral facies
Leads to:
LA enlargement:
pulmonary hypertension (> 7.5 mmHg/L/min) and pulmonary oedema
AF
Bronchitis
Investigations:
ECG: broad P wave, RV hypertrophy (NB – LV enlargement is not typical – key differential with
mitral regurgitation)
X-ray: LA enlargement, RH enlargement
Echo: good at imaging the mitral valve
Differential: Left atrial myxoma (much less common)
Treatment:
Prophylaxis for RF (till 20) and infective endocarditis (eg dental work)
Surgery: valvotomy, balloon valvuloplasty, replacement
Mitral Regurgitation (MR)
Causes:
Abnormalities of leaflets:
Rheumatic heart disease post inflammatory scarring
Infective endocarditis
Degenerative change
Floppy valve syndrome = mitral valve prolapse. Immaterial haemodynamic changes (
normal heart size, etc). Common - ?5-10% of young women. Mid/late systolic murmur +/-
mid/late systolic click. Complications (3% of affected) are infective endocarditis, mitral
regurgitation, and embolism of leaflet thrombi
Congenital
SLE can cause Libman-Sacks endocarditis: sterile immune mediated endocarditis mainly
affecting underside of mitral valve (cf other vegetative endocarditis on top)
Abnormalities of tensor apparatus: Previous MI: e.g. fibrosis or rupture of papillary muscle
46 4
th
and 5
th
Year Notes
Abnormalities of LV cavity or valve ring:
Calcification of mitral ring (especially elderly women)
LV enlargement (whole ventricle expands). Dilatation of the mitral annulus and lateral
displacement of the papillary muscles
Hypertrophic cardiomyopathy (thickening in parts of wall – e.g. enlarged septum disrupts flow
to aortic valve). Anterior displacement of the anterior leaflet
Existing MR – begets MR. Enlargement of LV pulls posterior leaflet away from the mitral orifice
Signs:
Pan-systolic murmur: regurgitation throughout the whole of systole. Loudest at apex. Radiates
over precordium and into axilla. No S1. No opening snap unless concurrent stenosis. Early
diastolic flow murmur
In severe MR, Aortic valve closes prematurely split S2
S3 caused by sudden tensing of papillary muscles, chordae tendinae and valve leaflets
Small volume pulse
Significant difference between acute and chronic presentations:
Pulmonary oedema and RV overload much more significant if acute. In chronic, enlargement of
the LA reduces pulmonary „back flow‟
AF better tolerated than in mitral stenosis
RHF rare unless acute presentation or LVF
Leads to:
Eventually leads to LV and LA hypertrophy (may take decades)
AF common – mostly correlated with age
Infective endocarditis (in 20%)
Systemic embolisation
Pulmonary hypertension (but much later compared with mitral stenosis)
Differential:
Hypertrophic cardiomyopathy: both long systolic murmurs, but MR radiates to the axilla,
hypertrophic cardiomyopathy radiates centrally
VSD
Tricuspid Regurgitation
Commonest cause is right heart failure/enlargement secondary to left ventricular failure. Left atrium is
also likely to be enlarged AF common too
Infective Endocarditis
= Infection of mural endothelium or heart valves. May also include the proximal aorta
See also Rheumatic Fever, page 602
Classification
Now all called infective endocarditis
Acute bacterial endocarditis (ABE):
< 6 weeks duration
Virulent organisms
Normal valves (eg IVDU)
Bulky friable vegetations: may extend to adjoining endocardium and chordae tendinae.
Destructive (directly proportional to virulence of organism). Much more destructive than
Rheumatic Fever. Microscopically vegetations show a suppurative exudate, fibrinous thrombi,
and large bacterial colonies destroying valve substance
Sub-acute bacterial endocarditis (SBE)
> 6 weeks duration
Avirulent organisms: normal flora
Abnormal valves
Evolution slower, gradual valvular dysfunction, flatter vegetations with deeper chronic
inflammatory component including a vascular fibrous tissue healing response
Predisposing Factors
1950s: rheumatic heart disease (most cases) – affect 15 – 35 year olds
1990s: degenerative, rheumatic, congenital (low pressure side of a septal defect gets infected),
prosthetic valves – affects 50 year olds
Cardiovascular 47
Circulatory factors:
Regurgitant blood stream (incompetent valve)
Large pressure gradient across valve (i.e. rarely right heart except IVDU)
Anatomic sites of infection
Nearly always where there‟s a pre-existing abnormality
Usually on the top of the valve
Incompetent mitral and aortic valves: 40% mitral, 40% mitral and aortic valve
Calcific aortic stenosis
Prosthetic heart valves
Congenital septal or valve defects
Also in Intra-venous drug users (IVDU) with normal hearts (Right side commonly affected).
Causal organisms
In theory: any organism (including fungi and chlamydiae)
In practice:
Native valves:
Streptococci: 70%
Staph: 20 – 25%
Miscellaneous (including enteroccoci) 5%
Culture negative 5%
Prosthetic valves:
< 3 months (early PVE): staphylococci > streptococci
> 3 months: staph = streptococci
Streptococcal causes of endocarditis:
Oral Commensals: Viridians Streps – more in younger people, good at sticking, don‟t cause much
infection elsewhere: S. sanguis, s. salivarius, s. mitis, s. milleri, s. mutans
Faecal: called enterococcal
Staphylococcal causes:
S. aureus: coag +ive – 60% mortality (common in intravenous drug user)
S. epidermidis + 20 others: coag –ive – 40% mortality
Miscellaneous causes: Haemophilus, Actinobacillus, Cadriobacterium/Candida Albicans (in
prosthetic valves, mortality 100%), Eikenella, Kingella
Pathogenesis of infection
Abnormal valve
NBTE (non-bacterial thrombotic endocarditis) – little blood clots – we all have them but risk on a
deformed valve
Transient bacteraemia from possibly trivial infection adherence of bacteria
Acute inflammatory reaction – WBCs, fibrin & platelets laid down
Mature vegetation – sheds bacteria
Diagnosis
Always a differential in pyrexia of unknown origin. Malaise, weakness
Existing immunosuppression, neutropenia, diabetes, and alcohol increases risk
Heart murmur, isolated petechiae (eg nail beds, retinal) and splenomegaly significant
Blood culture: 3 times – organism load in blood may be low
Echocardiogram (although may miss flat vegetations)
Complications
Valvular insufficiency or stenosis (aortic stenosis LV hypertrophy coronary artery insufficiency)
Local extension: down septum, into wall of aorta, perforated valve, suppurative pericarditis, ring
abscesses
Embolism: small infarcts (e.g. in kidney cortex) or abscess (each emboli has bacteria in it) eg in lungs
Mycotic aneurysms, focal and diffuse glomerulonephritis
Septicaemia
Antigenaemia: antigen/antibody complexes skin lesions, clogged up kidneys
48 4
th
and 5
th
Year Notes
Treatment
Identify causal organism with antibody sensitive tests (MIC & MBC)
Empiric antibiotic therapy - regimes:
Staphylococcal: Flucloxacillin (or vancomycin) 2g iv 4 hourly for 2 weeks, then 1 g orally 6 hourly
for 4 weeks
Streptococcal: penicillin + gentamycin or amoxycillin + gentamycin iv for 2 weeks, then 4 weeks
oral
Heart Failure
Background
= Pump function is inadequate to maintain body homeostasis Na and H20 retention
Left atrial pressure above 25 mmHg transudate of ECF into alveoli pulmonary oedema
20% have infarcts without knowing it
Strong association with old age. A common diagnosis amongst the most disabled elderly
Symptoms may be non-specific: energy, nausea, poor appetite, poor mobility, confusion, sleep etc
Classification
Classify as:
High output failure: due to O2 requirements and heart can‟t keep up. Happens quicker if pre-
existing heart disease. Eg anaemia, pregnancy, hyperthyroidism, Paget‟s disease. Initial features
of RH failure. Progresses to LH failure
Low output failure: Inadequate output (ejection fraction < 0.35 – 0.40) or only adequate with high
filling pressure:
Excessive preload: eg mitral regurgitation or fluid overload
Pump failure due to heart muscle disease, restricted filling, inadequate heart rate (eg heart
block, post MI)
Chronic excessive afterload (eg aortic stenosis, hypertension)
Can also classify as diastolic dysfunction (eg poor filling due to, for example, tamponade or restrictive
cardiomyopathy) or systolic dysfunction (eg poor contraction due to a large floppy heart)
Left HF pulmonary oedema:
Caused by:
Ischaemic heart disease
Hypertension
Aortic and mitral valve disease (aortic stenosis/rheumatic heart disease)
Myocardial disease
Hypertrophied L ventricle secondary atrial enlargement atrial fibrillation
Leads to:
Renal flow Na retention oedema
Pulmonary hypertension pulmonary oedema and bronchospasm
Symptoms: exertional dyspnoea, orthopneoa, PND, wheeze („cardiac asthma‟), cough + pink froth,
haemoptysis, fatigue
Signs: tachypnoea, tachycardia, end-inspiratory basal crackles, dullness to percussion over lung
bases, S3, cardiomegaly, cyanosis, pleural effusion
Right HF:
Due to:
Left Heart failure pulmonary hypertension RV failure
Cor pulmonale (R ventricle ↑ pressure due to disease of lung or pulmonary vasculature)
Constrictive pericarditis
Leads to:
Symptoms: fatigue, abdominal pain, oedema, anorexia, wasting, weight gain
Signs: enlargement of liver, spleen, kidneys, subcutaneous tissues and brain JVP, pulsitile
liver, hepatomegaly, pitting oedema, ascites
Congestive HF: both sides
Aetiology
Age associated changes:
Reduction in adrenergic responsiveness inotropic response and vasodilation
Cardiovascular 49
Increased arterial stiffness compliance afterload
Alterations in cardiac filling: connective tissue content of myocardium stiffer ventricle
filling more dependent on atrial contraction pressure and size of left atrium predisposes to
AF ( further filling problems)
Failure of reserve capacity of mitochondria
Age associated diseases:
Hypertension risk factor for atherosclerosis, and size and stiffness of left ventricle. By the
time they have heart failure, may no longer have hypertension as they can‟t sustain the cardiac
output necessary to be hypertensive
Coronary artery disease
Also respiratory function and renal function
Precipitating factors unmask the subsequent reduced cardiac reserve, eg arrhythmia, infarction, AF,
infection, thyroid disease, anaemia, PE, COPD hypoxia, DRUGS, etc
Decreased perfusion due to decreased pump action ↓kidney perfusion ↑renin/aldosterone
↑blood volume to try and increase pre-load and push heart up the starling curve (however, they‟re often
into negative marginal gain from increased volume). However, ↑ BP also raises after-load and
increases work of the heart ↑ischaemia
Cardiac dysfunction due to:
Disruption of circulatory system
Disorders of conduction
Lesion preventing valve opening
Pump failure (contraction/dilation) ↓SV and ↑EDV ↓CO
Beriberi = heart failure due to deficiency of Vitamin B1 (Thiamine): bradycardia, premature ventricular
beats, VF, AF, and heart block
Differential
Must be able to prove the heart is the problem
Otherwise consider:
Renal failure (eg nephritic syndrome) oedema
Liver disease or malnutrition albumin oedema
Investigations
Bloods: FBC, Cr, electrolytes, Trop I, U&E, glucose, TFTs, LFTs, Cholesterol, ?ABG
ECG
CXR: although concomitant COPD may obscure changes in heart size and pulmonary vasculature
Echocardiogram:
LV hypertrophy (normal thickness 1 cm), valve regurgitation or stenosis (check rate of flow), areas
of hypokinetic myocardium
Normal velocity of blood through the heart = 1 m/sec. If aortic valve narrowed then faster flow
then > 3 m/sec (same amount of blood through smaller space). Velocity between ventricles and
aorta is proportional the change in pressure
Angiography
Treatment
Principles:
Reverse underlying process (eg thyrotoxicosis)
Halt progression
Help symptoms
Acutely:
Treat cause if any: hyperthyroid, hypertension, anaemia, alcohol, valve lesions
Symptomatic treatment:
Sitting position venous return
O2 therapy (care with CO2 retainers)
Frusemide 40 – 80 mg iv (if not already on it) afterload, vasodilation (preload and ECF
volume). Watch for K+
Morphine 5 – 10 mg iv: (as long as not low BP) a potent vasodilator (↓preload work of heart
and ↓pulmonary capillary pressure), bradycardic and sedative effects
Also consider:
50 4
th
and 5
th
Year Notes
Aminophyline 250 mg over 5 – 10 min (+ive inotrope, mild diuretic, bronchospasm. iv form
of theophylline)
Blood pressure control: Nitrates, Oral ACE inhibitors (preload and afterload, and heart
remodelling)
Arrhythmia control: Digoxin, amiodarone
Inotropes: dopamine, dobutamine
DVT prevention
Not -blocker acutely, but use in chronic management
Intensive treatment:
Mechanical ventilation with positive end-respiratory pressure (CPAP) preload and intra-
alveolar pressure
Aortic balloon pump
Heart transplant
Monitoring: weight, fluid balance, telemetry and U&Es (eg K)
Chronic:
Balancing act, especially in elderly: eg risks of polypharmacy, comorbid disease, what is the goal
of treatment, postural hypotension if over-treated falls, etc
Non-drug treatment:
Stop smoking
Control of blood pressure, DM, alcohol
Exercise within ability to tolerate it (prevent further deterioration and problems of immobility)
Dietary advice: weight, Na and H2O depending on weight (ie educate patient about illness
and to monitor weight daily), low fat, high calorie
Physio: mobilisation and breathing control
Vaccination against influenza and pneumococcus
„Core‟ drugs:
ACE Inhibitors: Drug of first choice in CHF. dyspnoea, exercise tolerance, mortality,
admissions. Even if low blood pressure
Diuretics: for all people with volume overload and CHF. In elderly, effect of loop diuretics
may be delayed through poor absorption, and elimination effect. Accumulation can
deafness. Limited if poor renal perfusion. May exacerbate urinary incontinence. Low dose
spironolactone may be useful (if high dose and ACE inhibitor K and renal function)
Aspirin
Second line drug treatment for systolic dysfunction:
-blockers, used cautiously, are gaining wider use:
If sympathetic drive is causing a relative tachycardia then -blockers will help (will get
worse on -blockers if reliant on sympathetic drive to maintain CO)
Criteria: chronic, stable, LV systolic impairment (ejection fraction < 45%), resting HR >
50 bpm, no contraindications (eg asthma, AV block). Not if very low ejection fraction
Start at low dose, titrate up as out-patient with carvedilol ( + blocker) or metoprolol
Clear instructions to patient of symptoms of deterioration
See Clinical Use of Beta-Blocker Therapy in Patients with Heart Failure, Doughty RN and
Richards AM, NZMJ, 9 Feb 2001
Spironolactone
Other Vasodilators (e.g. nitrates, calcium channel blockers) - work of heart, efficiency of
heart, peripheral redistribution of blood. But problems with postural hypotension (especially
if already volume depleted – check for hyponatraemia)
Inotropic agents if low BP, eg digoxin. Controversial in heart failure, main role is in AF
Limited role for anti-arrhythmic agents
Drug treatment for diastolic dysfunction (ie normal ejection fraction):
Avoid over diuresis
Tolerate AF poorly
Aspirin
-blockers
Statins if cholesterol > 4 mmol/l
Myocarditis
= Inflammation of the myocardium, excluding IHD
Cardiovascular 51
Suppurative myocarditis: focal necrosis, pyogenic abscesses or diffuse spreading infection. Neutrophil
infiltrate
Interstitial myocarditis:
Characteristic of viral myocarditis
Occurs mainly in children and young women
Most have benign, self limiting course
Microscopic appearance: oedema, chronic inflammatory cells
Parenchymatous myocarditis: diffuse, patchy destruction of muscle cells. Associated with diphtheria,
typhoid, some haemolytic streptococci, protozoa and parasitic infections
Miscellaneous: Idiopathic (giant cell, Fiedler‟s). Also autoimmune disease or hypersensitivity to drugs
Cardiovascular Pharmacology
For Anti-coagulation, see Anticoagulant Treatment, page 75
Idiot’s guide
Always push non drug treatment: lifestyle, smoking, etc
Hypertension: Thiazides (not diabetics or gout) + -blockers (not CORD/asthma). Maybe ACE
inhibitors
Angina: -blockers + aspirin + nitrates. Maybe Ca channel blockers (HR), statins, ACE (if
hypertension/diabetes)
Post MI: Aspirin, -blockers, ACE if LVF +/- statin
Heart Failure: ACE + diuretic + aspirin. Maybe -blockers, spironolactone, other vasodilators, statins,
etc
ACE Inhibitors
Block the formation of angiotensin II diuretic, peripheral vascular resistance, and better tissue
remodelling/healing of damaged myocardium. But 30% of hypertensives are non-responders
Eg Captopril, quinapril
Many patients (especially the elderly) don‟t respond on its own. Synergistic effect with diuretic (ie
shifts ACE inhibitor dose-response curve to the left). If it‟s not working, add in a low dose diuretic
Adverse effects:
Metabolic taste, hypotension (especially with first few doses), hyperkalaemia, angioedema,
neutropenia, proteinuria.
Renal function, especially if existing renal impairment (efferent flow glomerular filtration)
Dry cough (due to bradykinins). If cough a problem, then use an angiotensin II receptor
antagonist (eg Losartan)
Rash: may be long time after starting, especially captopril due to sulphur group
Interactions:
Diuretics: hypotension + renal function
NSAIDS: renal failure, hyperkalaemia
Contra-indications:
Bilateral renal artery stenosis
Pregnancy, breast feeding
LV outflow obstruction (eg Aortic Stenosis)
Marked hypotension
Other drugs: K supplements, Li, NSAIDs
Monitor for: Na, K, Cr > 200, rare neutropenia
Diuretics
Common types:
Thiazides eg bendrofluazide. Flat dose response curve so dose only side effects. No effect
from a dose above 2.5 mg. Effect: mainly vasodilation, also inhibit Na/K co-transport in distal
convoluted tubule salt and water loss. VERY cheap. Take 6 – 8 weeks to work
Frusemide: blocks Na/K/Cl transport in Loop of Henle. No role in lowering blood pressure
Interactions:
General: NSAIDs, lithium, digoxin, ACE inhibitors, corticosteroids
Loop: antibiotics
Thiazides: calcium supplements
52 4
th
and 5
th
Year Notes
Adverse drug reactions are dose dependent ( use in low dose):
General: dehydration, electrolytes, lipids, endocrine, skin
Loop: ototoxicity, K, Ca. Frusemide water rush. Difficult if you‟re out and about
compliance
Thiazide:K, Ca, Mg, urate (+/- gout), lipids, progressive glucose rise over years,
thrombocytopenia, impotence in high doses
Spironolactone:
Acts at distal renal tubule as an aldosterone antagonist
Adverse effects: hyperkalaemia, diarrhoea, gynaecomastia
Interactions: ACE inhibitors, digoxin
-blockers
Action (effect takes 2 – 4 weeks):
Renal effect (renin)
Pre-synaptic -receptor blocker
Cardiac output due to rate and strength of myocardial contraction ( O2 consumption).
Acutely TPR (so not if peripheral vascular disease otherwise ischaemia). CO resolves over
time
?Central action
Use in angina, hypertension, heart failure
Classified by:
Lipid vs H2O soluble
-receptor selectivity
-blocking activity (eg labetalol prone to postural hypotension)
Contraindications:
Arrhythmias: bradycardia and AV block
Asthma
Peripheral vascular disease: lead to unopposed 1 stimulation
Diabetes: block the symptoms of hypoglycaemia, potentiate effects of insulin and oral
hypoglycaemics
Overt cardiac failure: negative inotropes – but still OK in heart failure at low dose
Adverse effects (generally dose dependent):
Common: Lethargy, heavy legs (slowed up feeling due to CO), cold extremities, lipids,
headaches, nightmares (in lipid soluble propranolol, not water soluble atenolol)
Less common: GI disturbances and rashes
Rapid withdrawal angina, arrhythmias due to 1 up-regulation
Interactions with:
Verapamil: severe bradycardia
Cimitidine: inhibits metabolism potentiates effect
Consider -blockers for hypertension– but not as first line agents (may exacerbate heart failure). Dilate
peripheral arterioles (modern ones don‟t cause reflex tachycardia), less arterial dilation. Start low to
avoid profound hypotension (especially elderly). Good for lipids
Ca Channel Blockers
Uses: Angina, dysrhythmias, hypertension, NOT heart failure
Hypertension: only in isolated systolic hypertension (eg due to hardened arteries)
Not better than diuretics or -blockers for hypertension, but additive effect
Action: myocardial work, decrease afterload, vasodilate coronary arteries
Verapamil (originally an anti-arrhythmic, derivative of theophylline, less effect on vasodilation but
bradycardia) and Diltiazem: slow conduction at the AV node and cause coronary vasodilation
Nifedipine: vasodilator good for coronary artery spasm, but may also cause reflex tachycardia
so may use with a -blocker
Adverse effects:
All cause headache, flushing, dizziness, hypotension, LV function
Verapamil: constipation
Verapamil and diltiazem: heart block
Nifedipine and verapamil: blood sugar
Cardiovascular 53
Interactions:
plasma digoxin levels
Enzyme inhibitors plasma levels of carbamazepine and cyclosporin
Don‟t use verapamil with -blockers: bradycardia + LVF
Also consider long acting nitrates
Positive Inotropes
Digoxin: only oral inotrope. Slows AV conduction and increases contractility
Use: in AF, slows rate output. But poor for rate control – still HR in response to standing up
Orally takes a week to reach steady state (T½ is 36 – 40 hours)
Shortens QT interval causes digitalis effect on ST interval (not a sign of toxicity)
Low therapeutic index (although wide therapeutic range) toxicity common:
CV: any arrhythmia, arrest, worsening heart failure
GI: anorexia, nausea, vomiting, diarrhoea, abdominal pain
CNS: headache, drowsiness, unsteadiness, blurred/yellow vision, confusion
Worse if:
Electrolyte disturbance: hypokalaemic, hypercalcaemia, alkalosis
Potassium sparing diuretics, steroids, verapamil, amiodarone, spironolactone
Disease: hypothyroidism, hypoxia, renal failure
Old age
Management: stop digoxin, check plasma level and K, treat arrhythmias, antidote (Digibind)
Dopamine (precursor of nor-adrenaline)
In low doses renal vasodilation and improved renal function
In higher doses acts on cardiac 1 receptors inotropic effects
Dobutamine: acts on cardiac 1 receptors inotropic effects
Lipid Lowering Drugs
See Dyslipidaemia, page 30
Lipids:
Cholesterol is most concentrated in LDL
HDL is beneficial
VLDL carries TAGs
Hypercholesterolaemia:
Primary: Hepatic overproduction of VLDL VLDL/LDL/Remnant lipoproteins
Secondary: Obesity, diabetes, hypothyroidism, nephrotic syndrome, alcohol, drugs (oestrogen,
Retinoids, -blockers, thiazides….)
Drug groups:
Action
Effect
HMG Co-A Reductase Inhibitors:
Statins
Simvastatin, Pravastatin,
Atorvastatin
Cholesterol synthesis
LDL 20 – 40%
HDL 5 – 15%
TAG 10 - 20
Fibric-acid derivatives:
Benzafibrate, Gemfibrozil
Lipoprotein lipase activity.
release of FFA from periphery
LDL 10 –15 %
HDL 10 – 15 %
TAG 20 – 50%
Bile Acid Sequestrants:
Cholestyramine, Colestipol
Non-specific binding of bile acids
LDL 15 – 30%
HDL 3 – 5%
TAG: no affect (but can
rise)
Nicotinic acid derivatives:
Acipimox
VLDL. FFA from periphery
LDL 10 – 25
HDL 15 – 35
TAG 20 - 50
Commencement of treatment depends on HDL:cholesterol ratio plus other risk factors
54 4
th
and 5
th
Year Notes
HMG-CoA Reductase Inhibitors (Statins):
Treatment: Requires health benefits approval (it‟s expensive) and is always accompanied by diet
More effect in lowering plasma concentrations of LDL and total cholesterol mortality in
hypercholesterolaemia + angina
SE: rare. GI, headaches, LFTs, myopathy from Ck. Potentiates warfarin
Fibrates: HDL and TAGs
Bile-acid sequestrants: Indicated for children and women of childbearing age. SE: constipation, skin
rashes. Bind fat soluble vitamins and other drugs (eg warfarin, give two hours before or 4 hours after)
Cardiomyopathy
= Primary or idiopathic diseases involving the myocardium. Diagnosed by excluding other more
common causes of heart failure: IHC, hypertension, rheumatic fever, and infectious myocarditis
Primary Cardiomyopathy
Congestive-Dilated Cardiomyopathy
Presents as congestive heart failure at any age
Men twice as common as women
Exclude pre-existing hypertension and alcoholism
Macroscopic appearance: greatly dilated ventricles, heart weighs 500 – 1000g (normal is 300g female,
350 g male)
Microscopic appearance: patchy interstitial fibrosis, interstitial oedema, hypertrophy of remaining
fibres
Complications: arrhythmia, mural thrombus, mitral and tricuspid insufficiency
Prognosis: progressive disease, no cure
Hypertrophic Cardiomyopathy
Disproportionate hypertrophy of the interventricular septum ventricular outflow obstruction
Familial and non-familial forms
Macroscopic appearance: heart weighs 600 – 1300g. Septum thicker than free wall of left ventricle
Microscopic appearance: diffuse hypertrophy of tangled myocytes. Interstitial collagen
Prognosis: poor. 1/3 die from outlet obstruction (can be precipitated by digoxin)
Restrictive Cardiomyopathy
Endocardial fibroelastosis: cartilage-like thickening of the left sided endocardium. Most common < 2
Endomyocardial fibrosis: Only tropical Africa. Fibrosis thickening of chordae tendinae and aortic
valve leaflets
Secondary Cardiomyopathy
Alcohol, cobalt, sarcoid (infiltrative granulomatous), amyloid (accumulation of insoluble pleated
proteins derived from immunoglobulins in elderly patients), metastatic carcinoma, storage diseases (eg
haemochromatosis), ischaemia
Effect of alcohol on the heart:
Binge drinking (also exercise and caffeine) AF a day later lasting for a day
Fibrotic cardiomyopathy
Arrhythmia
Neoplasia of the Heart and Blood Vessels
Haemangioma:
Common congenital vascular lesions usually occurring in the skin
Haemangioendothelioma: endothelial vascular tumour, intermediate between haemangioma and
frankly malignant angiosarcomas
Multiple Haemangiomatous syndromes: angiomatous lesions present in two or more tissues
Kaposi‟s sarcoma: malignant tumour of endothelial cells. Associated with AIDS. Painful purple to
brown lesions
Myxoma: most common primary benign tumour of the heart. Jelly like appearance, typically located
on the atrial side of the mitral valve
Cardiovascular 55
Rhabdomyoma: primary benign striated muscle cell tumour of the myocardium, typically found in
children
56 4
th
and 5
th
Year Notes

Respiratory 57
Respiratory
Physiology ........................................................ 58
Blood Gases ................................................ 58
Lung Function Tests ................................... 58
Respiratory Failure ..................................... 59
Oxygen Therapy ......................................... 60
Respiratory History .......................................... 60
Respiratory Exam ............................................. 60
Upper Respiratory Tract ................................... 62
Nasal & Sinus ............................................. 62
Acute Pharyngitis ....................................... 63
Other URTIs ............................................... 65
Antibiotic Treatment of URTI .................... 65
Larynx ........................................................ 65
Adult Pneumonia .............................................. 67
Classifications ............................................. 67
History ........................................................ 67
Epidemiology ............................................. 67
Types of Infectious Pneumonia .................. 67
Community Acquired Pneumonia .............. 70
Pleural Disease ................................................. 73
Venous Thromboembolism .............................. 74
Deep Vein Thrombosis (DVT) ................... 74
Pulmonary Embolism (PE) ......................... 76
Asthma ............................................................. 77
Chronic Obstructive Pulmonary Disease
(COPD) ....................................................... 80
Chronic Bronchitis ...................................... 81
Emphysema ................................................ 81
Bronchiectasis ............................................. 82
Restrictive/Interstitial Pulmonary Disease ....... 83
Acute Interstitial Lung Disease .................. 83
Chronic Infiltrative (Restrictive) Lung
Disease .................................................. 84
Neoplasia of the Respiratory Tract ................... 86
Cancer of the Nasal Cavity and Paranasal
Sinuses .................................................. 86
Tumours of the Larynx ............................... 86
Lung Cancer ............................................... 87
Sleep Apnoea ................................................... 90
Miscellaneous Lung Diseases .......................... 92

58 4
th
and 5
th
Year Notes
Physiology
For acid-base disturbances, see Acid-Base balance, page 113
Blood Gases
Normal Values:
PaO2: 75 – 100 mmHg, 10 – 13.3 KPa. Dependent on ventilation/perfusion balance (A-a gradient)
and inspired O2 concentration
O2 saturation: 95 – 100%
PaCO2: 36 – 46 mmHg. If high then hypoventilation, if low then hyperventilation. Measured with
a capnograph. pH falls by 0.1 for every rise of 10 CO2
Plasma HCO3 (arterial): 22 – 26 mmol/L
To convert mmHg to kPa divide by 7.5 (multiply by 0.133)
PAO2 is lower than inspired PO2 because:
It becomes saturated with water vapour
It is diluted by expired CO2
O2 is absorbed into the blood
Factors affecting the A-a gradient (normally 5 mmHg at FIO2 of 21%, may be up to 100 at 100%):
Ventilation/Perfusion balance (V/Q): most common cause of a fall. Responds well to O2 therapy
Diffusion
Shunts (pathological or anatomical)
Calculating the A-a gradient:
PIO2 = (PB – PH2O) * FIO2 = (760-47) * 21% = 150 mmHg
PAO2 = PIO2 – PaCO2/R
A-a gradient = PAO2 – PaO2. Normal is 5 – 15
Saturation = % of haemoglobin that is fully bound. Determined by PO2 and shape of dissociation
curve
Oxyhaemoglobin dissociation curve
Shifted right by blood temp, CO2, H+, 2,3BPG
Shifted left by blood temp, CO2, H+, 2,3BPG
O2 available to tissues (Oxygen flux) depends on:
O2 saturation
Hb concentration
Blood flow
Normal flux is 1000 ml/min. If flux falls below 250 then hypoxia
Cyanosis:
Peripheral cyanosis: capillary de-oxy Hb > 50 g/litre. Eg due to being cold and vasoconstricted
Central cyanosis: due to saturation and de-oxy Hb > 50 g/litre eg in mouth and tongue
Lung Function Tests
(S)VC
IC:
TLC
(Slow) Vital Capacity
Inspiratory Capacity
Vt: Tidal Volume
Total Lung Capacity
FRC: Functional
RV: Residual Volume
Residual Capacity
RV: Residual Volume
Definitions:
PEFR = peak expiratory flow rate
FEV1.0 = maximum volume of air that can be exhaled during the first second of a Forced Vital
Capacity (FVC= maximum expired volume = FV). May use SVC if its higher
Normally 80% of FVC
< 75% obstructive lung disease
> 75% restrictive lung disease, eg lung fibrosis, neuro-muscular disease, chronic PEs (
scarring) and heart failure
But this can lead you astray. Eg if bronchodilator FVC by more than FEV, then the ratio
drops
FEV 25-75%: Mean forced expiratory flow from 25 to 75% of vital capacity = Mean Mid-
expiratory Flow (MMEF). Gets rid of peak flow which is very effort dependent more reliable
measure
Respiratory 59
VC = vital capacity:
FVC: forced vital capacity
SVC: slow vital capacity
FIF50%: Forced inspiratory flow at 50% of vital capacity
PIFR: Peak inspiratory flow rate
Patterns:
Obstructive
Restrictive
FEV1
FVC
FEV/FVC
TLC
RV
DLCO
Diffusing Capacity: DL CO: Diffusing capacity of the lung for Carbon Monoxide (needs adjustment for
Hb – eg anaemia, polycythaemia)
Performing Lung Function Tests:
Requires at least 3 manoeuvres, the best two having FEV1.0‟s and FVCs within 5% of each other
Biggest problems with serial reproducibility are obtaining maximum inspiration first, and getting
maximum effort
All are reported at BTPS (body temperature, saturated)
If assessing broncho-dilator responsiveness, should have no inhaler for 2 hours before hand.
Maximum responsiveness usually 20 minutes after dosing
Predicted values are based on age, height and sex. Different racial groups and people with varying
proportions (eg long legs/short torso) may be very poorly approximated by predicted values
Flow-volume Loop gives very valuable information. Eg in emphysema, expiratory flows but
inspiratory flows normal
Patterns of disease:
Obstruction: flow
Restrictive: volume
Other lung function tests:
Asthma provocation: for pilots, divers, police, etc
Cardiopulmonary exercise testing – finds how much of shortness of breath is due to pulmonary
causes and how much to cardiac causes
Respiratory Failure
Ventilatory failure: When bellows function inadequate to excrete CO2 produced (ie above 60 mmHg)
Respiratory Failure: (PaO2 < 60 mmHg)
Type 1: PaCO2 < 50 mmHg VQ mismatch (less O2 absorbed in hypoperfused areas,
hyperperfused can‟t compensate due to the sigmoid shape of the dissociation curve) plus other
causes (e.g. heart failure)
Type 2: PaCO2 > 50 mmHg hypoventilation – both gases are affected reciprocally – only lung
problem can cause this
Respiratory Failure can be due to:
Central respiratory depression:
Drugs: opiates, alcohol, barbiturates
Brain stem: CVA, coning
If A-a gradient normal but patient hypoventilating central depression. If young then ?OD
Sleep Apnoea syndromes
Lung Pump Failure: neuromuscular disease, chest wall, lung disease. E.g. diaphragm dysfunction:
Unilateral paralysis may be asymptomatic
Bilateral paralysis: neurological (e.g. polio, motor neuron, Gillian Barre) or myopathic (e.g.
hypothyroid)
Signs: orthopnea, morning headache (hypercapnea over night), paradoxical breathing (chest
wall and abdomen go in opposite directions when breathing), lung function worse when lying
down
Treatment: treat cause, positive pressure ventilation systems
60 4
th
and 5
th
Year Notes
Oxygen Therapy
Ensure PO2 is on plateau of O2 saturation curve (ie PaO2 > 70 mmHg)
Shunt is resistant to O2 therapy, whereas a diffusion abnormality and V/Q mismatch respond well
Complications:
Reduced respiratory drive in CORD. Consider if PCO2 but pH not as low as you‟d expect.
Don‟t give too much O2 otherwise respiratory drive CO2. Aim for saturation of ~ 90%
Loss of nitrogen splint, etc
Levels of O2 therapy:
21%: Room air
24%: nasal prongs at 1 litre
28%: nasal prongs at 2 litres
32%: nasal prongs at 3 litres
35%: Hudson mask at 6LO2/min
40%: Hudson mask at 8LO2/min. Maximum level obtainable with a mask (inspiratory flow > flow
from wall)
50%: Hudson mask with rebreather bag
Types of ventilation:
CPAP: Continuous positive airways pressure – splints airways open at end of respiration
BiPAP: Positive pressure for inspiration only. Good if CO2 retention – makes it easier to blow off
CO2
IPPV = intermittent positive pressure ventilation: complete control
PEEP = positive end expiratory pressure ventilation: splints collapsed or fluid filled alveoli
Complications of ventilation:
Application of pressure to lungs rupture, thoracic pressure venous return
Artificial airway obstruction, trauma to teeth, pharynx, cilial damage, infection
Ventilation mismanagement inappropriate ventilation, hypoxic gas mixture, equipment
failure
Respiratory History
See Differentiating Chest Symptoms, page 16
Respiratory Exam
For Chest X-ray, see Chest X-ray, page 27
Inspection, Palpation and Percussion *
Inspection:
Count respiratory rate (at rest should be < 14 per minute)
Chronic airways disease barrel (expended chest) can‟t find apex beat
Look for use of accessory muscles. Are intercostals depressed (ie being used a lot)? Look for
paradoxical breathing of the abdomen
Cyanosis (eg tongue)
Ask patient to cough. Listen for wheeze, gurgling, etc
Inspect sputum
Listen for stridor or hoarseness (laryngitis, cancer affecting left recurrent nerve or larynx)
Hands:
Clubbing (and maybe Hypertrophic Pulmonary Osteoarthropathy – „swollen‟ metacarpals and
elsewhere, eg in lung cancers). See Hands, page 7 for causes of clubbing
Staining from cigarettes
Wasting (Pancoast tumour)
Pulse rate: tachycardia
Flapping tremour: late and unreliable sign of severe CO2 retention
The face:
Eyes for Horner‟s syndrome (constricted pupil, partial ptosis)
Tenderness over sinuses sinusitis
Nose: check for polyps (associated with asthma), deviated septum (nasal obstruction), etc
Throat for URTI
Check lymph nodes
Respiratory 61
Trachea:
Check for displacement
Tracheal Tug: trachea moves inferiorly with inspiration, due to over expansion of the lung in
airflow obstruction
Chest:
Inspect:
Shape and symmetry, including funnel chest (= pectus excavatum or sunken sternum),
kyphosis (forward curvature) and scoliosis (lateral bowing)
Scars, signs of radiotherapy
Subcutaneous emphysema – crackling under the skin due to air from pneumothorax
Prominent veins in SVC obstruction
Movement when breathing in and out – better from behind. Look for uni-lateral or bi-lateral
reduction in movement
Palpation:
Check expansion: the affected side dose NOT expand – regardless of pathology
Apex beat: if not found then ?hyper-expanded. Maybe displaced by pathology
(pneumothorax, fibrosis, etc)
Vocal fremitus: Feel with hand while patient says 99, each side font and back
Compress sternum to spine pain if fracture or bone tumour
Percussion:
Ask patient to move elbows forward to move scapula off the lungs
Around lung and also directly on the clavicle
Normal lung is resonant, pneumothorax is hyper-resonant, liver is dull, consolidation is dull,
effusion is stony dull
Chest Sounds
When auscultating, ask patient to breath through mouth – not to take deep breaths
Vesicular breath sounds
(= normal breathing)
Bronchial breathing
Length
Inspiration > expiration (inspiration
requires work, expiration is elastic
recoil – snaps back)
Inspiration =< Expiration (takes
longer for air to get passively
squeezed out through reduced
bronchioles)
Relative Volume
Inspiration louder
Equal (sounds like Darth Vader)
Gap between in and
out
No
Yes
Crackle:
= Crepitations
Coarse or fine (like hair rubbing)
Short, discontinuous, non-musical sounds heard mostly during inspiration
Fine (high pitched) are from distal air-spaces, coarse (low pitched) are proximal air spaces
Produced when there is fluid inside a bronchus with collapse of the distal airways and alveoli
Disease
Early Crackle
Late Crackle
Congestive Heart Failure
Very Common
Common
Obstructive Lung Disease
Present
Absent
Interstitial fibrosis
Absent
Present
Pneumonia
Absent
Present
Wheeze
= Rhonchi, rhonchus, rale
Continuous musical sounds heard mostly during expiration
Produced by airflow through narrowed bronchi
Narrowing may be due to swelling, secretions, spasm, tumour, or a foreign body
Pleural Rub
Grating sound like Velcro ripping or walking on snow on inspiration and expiration
Produced by motion of roughened or thickened pleura
Caused by inflammatory or neoplastic cells or fibrin deposits
62 4
th
and 5
th
Year Notes
Differentiating Consolidation from Pleural Effusion
Consolidation = exudate into alveoli. Signs are:
Expansion: reduced on affected side
Vocal resonance and tactile fremitus (patient says „99‟ and listen with stethoscope/feel with
hand): on affected side
Percussion: dull but not stony dull
Breath Sounds: increased volume and bronchial not vesicular (ie will hear coarse breath
sounds like over the trachea)
Additional Sounds: inspiratory crackles (as pneumonia resolves)
Vocal Resonance: increased
Plural Rub: may be present
Effusion = fluid in pleural space (but not blood – that‟s haemothorax, and not pus – that‟s
empyema). Signs of effusion are:
Displaced trachea if massive effusion
Expansion: reduced on affected side
Percussion: stony dullness over effusion
Breath Sounds: reduced or absent
Vocal Resonance: reduced
The key differences are therefore:
Consolidation
Effusion
Percussion
Dull
Stony Dull
Breath Sounds
Bronchial
Reduced
Vocal Resonance
Increased
Reduced
Common presentations:
Expansion
Percussion
Breath sounds
Vocal
Resonance
Trachea
Consolidation
Dull
, Bronchial,
course crackles
-
Effusion
- or
Stony dull
-
COPD
Hyper-
expanded
Hyper-resonant
Wheeze
-
-
Pneumothorax
- or
Hyper-resonant
Deviated if
tension
PE
-
- (unless
effusion)
-
-
-
Fibrosis
- or dull
Crackles
Depends
LV Failure
Dull
Fine crackles
-
-
Collapse
Dull
Deviated
Other systems *
Check JVP for right heart failure
Listen to P2 of second heart sound, at 2
nd
intercostal space on the left. If louder ?pulmonary
hypertension
Check liver for tumour 2
nd
to lung cancer, and for „ptosis‟ – displaced downwards in emphysema
Pemberton‟s sign: SVC obstruction – hold arms over head facial plethora, inspiratory stridor and
JVP
Feet: check for oedema (pulmonary hypertension) and DVT
Upper Respiratory Tract
See also URTI in Respiratory Tract Infections in Children, page 605
Nasal & Sinus
For Nasal neoplasms, see Cancer of the Nasal Cavity and Paranasal Sinuses, page 86
Warms, cleans and humidifies inspired air. By back of nose air is 98% humidified and 35 C
Anatomy: maxillary, ethmoid, frontal and sphenoid sinuses. Concha and turbinate bones
Respiratory 63
Nasal obstruction
Mechanical:
Defect in cartilage or bone
Septal deviation. Overtime paradoxical obstruction – hypertrophy of turbinate on other side
bilateral obstruction. Treatment: septoplasty
Mucosal:
Blocked nose, mucoid discharge, smell
Vasomotor rhinitis (VMR): there is normally a cycle between one nostril blocked and other
cleared. This cycle upset. Treatment: cauterise turbinates reduce venous congestion
Allergic rhinitis
Polyps: sessile or pedunculated. Usually inflammatory – related to asthma and aspirin sensitivity.
Can be idiopathic or secondary to infective sinusitis
Treatment: topical steroids (allergy, primary polyps, VMR), antihistamines, mast cell
stabilisers
Epistaxis
Kids: from Little‟s area (= Kiesselbach‟s area). Anterior septum. Naso-palatine plexus. Treatment:
cauterise
Adults: From further back – septal or lateral wall. In elderly, mortality from severe epistaxis 1% - from
secondary effects eg stroke (aspirin common cofactor bleeding)
Sinusitis
See also Acute Sinusitis, page 608
Face pain after cold
Maxillary most common presentation, although ethmoid more commonly infected
Causes: Strep pneumoniae, Strep pyogenes, H. influenzae, B. catarrhalis
Treatment: Amoxil
Complications:
Orbital cellulitis via orbital periosteum optic nerve compression compression of ophthalmic
artery retinal blindness. Need to drain pus and iv antibiotics
Sphenoidal and frontal sinusitis can cerebral complications (eg cavernous thrombosis)
Chronic sinusitis: puss, smell, no pain. Can be from dental infection
Allergic Rhinitis
See also Allergy and Hypersensitivity Disorders, page 309
Symptoms: Recurrent or acute
Sneezing, blocked or runny nose, itchy watery or puffy eyes, itchy throat
May also be epistaxis, snoring, mouth breathing
Examination: look at anterior nares for nasal patency, polyps (chronic rhinitis), secretions, oedema
Two types:
Seasonal Allergic Rhinitis = Hay fever. Allergy to birch or grass pollen etc. especially rye grass
Perennial Allergic Rhinitis: allergy to dust mites, cat dander, moulds, etc
Non-drug treatment:
Avoid allergen
Avoid other irritants: perfume, temperature change, other smoke
Drug treatment:
Antihistamines: Some can cause sedation, especially if taken with alcohol
Decongestants: Vasoconstrictors. Can have stimulant effects (including BP). Overuse
rebound congestion
Mast cell stabilisers: Nasal spray. Slow onset
Topical nasal steroids: Slow onset. Can cause mucosal atrophy nose bleeds
Desensitisation: Injections of increasing doses of allergen. Expense and takes time (eg up to two
years)
Acute Pharyngitis
See also Pharyngitis, page 607
Clinical signs: fever, respiratory distress, cervical lymphadenopathy, pharyngeal erythema, pharyngeal
exudates
64 4
th
and 5
th
Year Notes
Causal Organisms
Viral causes (commonest):
Agent
Disease
Symptoms
Rhinovirus,
coronavirus
Common Cold
Common cold. Fever uncommon
except in kids
Influenza (A & B)
„Flu
As for common cold + fever, headache,
generalised myalgia
Parainfluenza virus 1-3
Croup =
Laryngotracheobronchitis
Initial: sore throat, rhinorrhoea, mild
cough
Leading to: severe cough (seals bark),
hoarseness, inspiratory stridor
(subglottic inflammation)
Adenovirus
Pharyngo-conjunctival
fever
Sore throat (often erythema and
exudate – even though virus), fever,
headache, myalgia, conjunctivitis
Herpes Simplex
Mild: indistinguishable from other viral
URTI. Severe: pharyngeal
exudate/erythema, shallow ulcers,
vascular rash on lips
Epstein Barr Virus
Infectious Mononucleosis
– Glandular fever (See
Epstein Barr Virus, page
505)
Usually adolescents/young adults.
Sore throat (erythema/exudate in 50%),
fatigue, malaise, fever, headache,
cervical lymphadenopathy, atypical
mononucleosis on blood film,
splenomegaly
Bacterial Causes:
Agent
Disease
Symptoms
Streptococcus
Pyogenes (Lancefield
Gp A) & Strep Group
C
Pharyngitis/Tonsillitis
Marked variation: Mild:
indistinguishable from viral URTI,
minimal erythema. Severe: Marked
pharyngeal erythema & florid tonsillar
exudate, high fever, cervical
lymphadenopathy, leucocytosis on
blood film. Type M strains
Rheumatic fever.
Mixed anaerobes
Gingivitis/Pharyngitis
Polymicrobial infection, due to poor
dental hygiene, bad breath
Corynebacterium
diphtheriae
Diphtheria
Pharyngeal diphtheria rare. Range
from mild non-specific illness to
severe. Sore throat/fever, pain on
swallowing, headache, vomiting.
Characteristic greyish-green
membranous exudate on pharynx
Neisseria gonorrhoeae
Pharyngitis
Mostly asymptomatic. Mild
pharyngitis. Pain/difficulty swallowing
Fungal causes:
Agent
Disease
Symptoms
Candida Albicans
Thrush
Usually immunocompromised.
Creamy white plaques on
tongue/mucosa. Complication of
asthma steroids and long-term
antibiotics
Respiratory 65
Diagnosis
Throat swabs:
For routine bacterial culture: especially to confirm/exclude Strep Pyogenes
Low sensitivity (?30%) and specificity (?75%)
40 – 50% of people with sore throats have bacteria isolated
Lots of variability: swab-taking technique, delays in transport, etc
Worth it for $18?
Nasopharyngeal washings (kids): Antigen detection by immunoflouresence for RSV, Influenza A & B,
Parainfluenza 1 – 3 and adenovirus
Other URTIs
Infection
Common causative organisms
Acute Otitis Media
Strep pneumoniae, H influenzae, Branhamella catarrhalis.
See Acute Otitis Media, page 605
Acute Sinusitis
Strep pneumoniae, H influenzae
Acute Epiglottitis
H influenzae type B. See Epiglottitis, page 609
Chronic Bronchitis (acute infectious
exacerbations)
Strep pneumoniae, H influenzae, Branhamella catarrhalis
Bronchiolitis
Respiratory Syncytial Virus. See Bronchiolitis, page 610
Antibiotic Treatment of URTI
See also Acute Otitis Media, page 605
Treatment for Strep Pharyngitis (Path lecture):
Oral Penicillin:
On empty stomach (before food)
500 mg (200 for kids) 8 hourly for 10 days (adults)
If compliance in doubt, IM benzathine penicillin G (single dose)
Allergic to Penicillin: Erythromycin 500 mg (200 for kids) 8 hourly for 10 days
Antibiotic treatment (source –„ Just Say No‟, Thomas and Arroll, NZMJ, 14 July 2000):
No benefits in patients with colds
Trivial benefit in patients with acute bronchitis
Trivial benefit in all but a minority of patients with acute exacerbations of COPD
Modest benefit in sinusitis
But, in real life, antibiotics are prescribed for a majority of patients with URTI
Antibiotic treatment (Cochrane review):
Absolute benefits modest
Preventing complications can only be achieved by treating many who will derive no benefit
Symptoms: reduced duration by about half a day, especially at 3 days (although 50% of untreated
had also settled by then)
Non-suppurative complications: Reduces rheumatic fever to less than one third. Possible
protection against acute glomerulonephritis (although rare)
Suppurative complications: Reduces rate of otitis media to a quarter (NNT = 29), acute sinusitis to
about one half and reduced incidence of quinsy
No risk of delaying antibiotic treatment for possible Strep Pyogenes pharyngitis until culture results
received. Late treatment as effective as early treatment
Risks of „over treatment‟ with antibiotics: Penicillin resistance – 2 to 9 times, risk of subsequent
otitis media, pneumonia, bacteraemia or meningitis being caused by resistant S. Pneumoniae. „Cherish
your normal flora and don‟t assault it with antibiotics‟
Delayed/contingent prescription can allow antibiotics without morbidity. Eg antibiotics dispensed
for sore throat dropped from 99% to 31% with wait of 2 days
For Treatment of Otitis Media, see Acute Otitis Media, page 605
Larynx
See also Tumours of the Larynx, page 86
Function: protect airway from saliva and food, voice production
Vocal chords shut during coughing, straining, lifting maximal splinting from thoracic muscles
Anatomy:
Recurrent laryngeal: maintains open vocal chords via abductor muscle. If damaged stridor.
Rest of muscles supplied by superior laryngeal nerve
66 4
th
and 5
th
Year Notes
Pharynx: superior, middle and inferior constrictor muscles attach on the cervical spine at medium
raphae
Paediatric problems:
See also Neonatal Acute Airway Problems, page 595 and Respiratory Illness, page 604
Signs: stridor, feeding difficulties
Failure of canalisation severe (normally dies)
Laryngomalatica: Supra glottic structures floppy collapse on inspiration inspiratory stridor.
Improves with muscle tone/innovation
Subglottic stenosis: congenital or trauma (eg too big a ventilation tube)
Croup:
= Laryngo-tracheo bronchitis.
Inspiratory and expiratory stridor, barking cough
If frequent, may have anatomical narrowing
Usually viral infection. If severe, steroids inflammation
Obstructive sleep apnoea:
Very different to adults: usually due to enlarged adenoids/tonsils – snore loudly
Failure to thrive, behavioural problems, etc
Obstructive apnoea up to age 7 take adenoids out
Epiglottis:
Symptoms: obstruction, sore throat, drooling, toxic/septicaemia
Cause: bacterial infection (eg H. Influenzae)
Medical emergency: can deteriorate quickly. Don‟t examine throat – may cause spasm and
obstruct
Emergency treatment: Geudal airway and ambubag. If unsuccessful get a very experienced
person to intubate. If unsuccessful cricothyroidotomy with 14 gauge needles
Tonsillitis:
Tonsils are not normal lymph nodes: don‟t have capsule or afferent vessels
Bulk of lymphoid tissue is in base of tongue
Decrease in size with age. At 40 half the size as when 15
Foreign bodies:
Can‟t eat or drink.
In kids: 10-cent pieces, inhaled peanuts. Differential: asthma (cough and wheeze). If < 2 years
old, do CXR and look for collapse distal to obstruction
In elderly with dentures: can‟t chew or feel unwell
Must take out: if stuck in gullet, will perforate within 7 days. Can linger for months in lung
Vocal chords:
Papillomas: usually solitary. Very low incidence of malignant change. Laser them (usually
repeatedly)
Nodules: usually bilateral. Keratinised lesions from chords banging together. Treatment: vocal
rest, correct voice abuse
Polyps: usually unilateral. Granulation tissue/inflammatory
Reincher‟s disease: in middle aged female smokers. Degenerative, gelatinous polyps of
surrounding mucosa hoarse voice, obstruction. Cause unknown
Recurrent Laryngeal Palsy:
Usually left nerve: longer. Right only goes round subclavian
40% idiopathic
Exclude: bronchogeneic cancer, mediastinal lymph nodes (eg lung or breast Ca), Ca of larynx,
mononeuropathic infection
Voice disorders (Dysphonia, Aphonia):
Obstruction to vocal chord closure: vocal chord thickening/oedema, nodules, papilloma, ulcers,
polyps
Larynx growths: leukoplakia, hyperkeratosis
Trauma: intubation, external
Paralysis: superior or recurrent laryngeal nerve
Vocal hyperfunction: spastic dysphonia, tension due to voice abuse (singers, teachers)
Presbyphonia: in the elderly
Other: chronic laryngitis mucosal atrophy, Parkinson‟s, Motor neuron disease, following
laryngectomy
Respiratory 67
In all cases refer to speech-language therapy for assessment/management
Adult Pneumonia
= Inflammation and consolidation of the pulmonary parenchyma
Classifications
Community acquired vs. hospital acquired
Typical vs. atypical organisms
Lobar vs. diffuse/non-lobar/bronchopneumonia (although no clinical relevance as it doesn‟t tell you
which bug)
Normal vs. immunocompromised
Severe or not
Includes: bronchopneumonia, lobar pneumonia, interstitial pneumonia, and infectious granulomas
History
Previous pneumonia, asthma, bronchitis
Aspiration risk
Social History: smoking, alcohol, occupational or hobby exposure (birds, dust, healthcare worker, etc)
Infectious: overseas travel, recent arrival
TB History: race, previous history, family history, exposure, living situation, BCG status
History or immuno-suppression: transplant, cancer, high dose steroids, HIV risk (sexual, weight loss,
night sweats)
Epidemiology
10% of hospitalisations
At risk:
Infants and children: more frequent exposure, immature immune system, narrower bronchial tree
Elderly
Altered level of consciousness: post-operative, CVA, fits, drugs/alcohol, diabetic coma:
diminished cough reflex
Smokers
Patients with pulmonary oedema
Immune deficiencies: leukaemia, lymphoma, renal transplant patients, cytotoxic drugs
80% of AIDs patients die of respiratory failure: 60% of these will have a pulmonary infection
Types of Infectious Pneumonia
Bronchopneumonia
Patchy consolidation of the lung. Infection centered on a bronchus or bronchiole, involving
immediately adjacent alveoli. Pleura not usually involved. Can overlap with lobar pneumonia.
Infection is spread through the airways
Macroscopic appearance: patchy consolidation – firm, raised, nodular, red to grey-white. Colour varies
with the amount of necrosis and haemorrhage, and due to stage. May involve one or more lobes
Microscopic appearance:
Bronchocentric lesions
Early: congestion and oedema
Progresses to: neutrophils + proteinaceous (fibrinous) exudate + RBCs fill distal airways and
alveoli.
Resolution: airways clear but may organise into fibrous tufts. Parenchymal destruction depending
on organism
Causative organisms:
Depends on whether community or hospital acquired, depressed pulmonary defences, etc
G +ive cocci (staphs and streps) and G –ive H Influenza, Pseudomonas, E Coli and Klebsiella
S. Aureus and G -ives more common in hospital acquired (eg in ICU) – also more destructive
Pseudomonas aeruginosa: can infect lung haematogenously infection of vascular walls
haemorrhagic pneumonia. Common in burn, immunocompromised and cystic fibrosis patients.
Usually fulminant course
Legionella pneumonia: characteristic morphology is acute fibrino-purulent exudative pneumonia –
neutrophils + macrophages within a fibrinous exudate. Inflammatory response spares alveolar
68 4
th
and 5
th
Year Notes
walls, so no necrosis or haemorrhage. Mild and self-limiting, except in elderly and smokers. 10 –
20% mortality in immunocompromised. Rumoured to have prominent GI symptoms (diarrhoea
and vomiting) – but ?any difference in incidence to other agents. Characteristic in air conditioning
(ie plumbers, office workers, etc) and carriage in potting mix (ie gardeners).
Lobar pneumonia
Involves whole lobe uniformly, often with reactive fibrinous pleuritis
95% of cases are Strep pneumoniae
Pathogenesis: bacteria inhaled profuse fluid exudate (good growth medium) infection spreads
through interalveolar pores throughout lobe
Macroscopic and Microscopic appearance: 4 stages based on macroscopic appearance:
Congestion: 12 – 24 hours, oedema
Red hepatisation: 2 – 3 days. Redness due to congestion and haemorrhage. Fibrinous neutrophilic
exudate, consistency of liver
Grey hepatisation: 3 – 4 days, grey due to WBCs and fibrin, and blood due to compression of
capillaries
Resolution: 2 – 5 days, macrophage phagocytosis and clearance. Pulmonary architecture usually
maintained, or fibrous tufts fill distal airways and alveoli and are then incorporated in the
interstitium interstitial fibrosis
Complications: 20 – 30% get bacteraemia meningitis, endocarditis, arthritis, etc.
Presentation: fever, chills, productive cough with sputum from watery to rusty as the disease advances.
Functional parenchyma SOB and cyanotic. Pleural rub.
Lung Abscesses
Can occur secondary to pneumonia or independently. There are two patterns:
Multiple abscess: haematogenous spread or bronchopneumonia from a virulent organism that
causes necrosis
Solitary abscess: usually due to anaerobic organism – eg following aspiration in alcoholic with
depressed reflexes
Infectious Granulomas
Three possibilities for a granuloma:
Tb: no neutrophil infiltrate in granuloma caseating necrosis
Fungal: causes abscess neutrophils/puss in the middle
Sarcoidosis: non-necrotising (non-infectious)
Mainly Mycobacterial Tuberculosis: can infect any organ but commonly the lung
Immune cells in granulomas:
Histiocyte = epithelioid cell = macrophages („eating phase‟ as opposed to circulating in blood
when its called a monocyte)
Bigger and more cytoplasm than a lymphocyte
If cytoplasm fuses giant cell with multiple nuclei
Tuberculosis
See also Mycobacteria, page 502
Usually Mycobacterium Tuberculosis. In AIDS, may be M. avium-intracellulare. M. bovis causes GI
Tb in 3
rd
world from contaminated milk
Epidemiology:
Affects 33% of world‟s population and causes 3 million deaths a year.
In first world, improved sanitation has reduced incidence – but is climbing again due to AIDS and
antibiotic resistance
NZ: 300 notifications per year: European < Maori < PI < Other
Clinical:
Non-specific fever and weight loss (due to macrophage cytokines), coughing, blood-tinged
sputum. If in GI, can present with obstruction
Takes 6 weeks to 3 months before Tb sensitivity develops (ie Mantoux positive)
Predisposing host factors: malnutrition, alcohol, diabetes, age, immune suppression (diseases or
drugs), background population prevalence
Respiratory 69
Progression:
Primary infection: initial exposure is self-limiting, leading to formation of a solitary granuloma
(Ghon focus), often with granulomas along lymphatic drainage and in hilar lymph nodes (Ghon
Complex). Lesions usually asymptomatic and undergo fibrosis and calcification
Spontaneous recovery: may still have bacilli on board
Progressive primary infection: rare, primary lesion erodes into airways or vasculature airway
spread or miliary spread fulminant bronchopneumonia
Post-primary pulmonary Tb: granulomas coalesce consolidation evident on X-ray cavity
ruptures into a bronchus productive cough, fever, sweating, haemoptasis
Secondary infection: in small percentage of those who had primary infection. Reactivation of
latent mycobacteria. Usually in lung apices (higher O2 tension). Can become progressive. Can
have isolated involvement of the intestine or adrenals ( acute Addison‟s Disease). Cell mediated
immunity or delayed type hypersensitivity contributes to tissue destruction
Diagnosis:
Samples: sputum, bronchial wash, gastric lavage in the morning, bronchoscopy, pleural tap
Culture (6 weeks), ZN stain, PCR (not very sensitive or specific for serious disease)
Treatment:
Combinations always required for a long duration
Drugs:
Isoniazid: best and cheapest. Bacteriocidal. Side effects: rash, peripheral neuropathy,
hepatotoxicity
Rifampicin: Destroys rapidly dividing bacilli quickly ( good for fulminant disease). SE:
enzyme induction, orange secretions, rash, flu like illness, purpura
Pyrazinamide: bacteriocidal, works intra-cellularly (ie bacilli inside macrophages). SE rash,
hepatotoxicity, gout
Ethambutol: SE optic neuritis. In kids too young to monitor visual acuity, use streptomycin
Regime: 2 months of isoniazid + rifampicin + pyrazinamide + 4 months of just isoniazid and
rifampicin
Compliance a major issue ( directly observed therapy. Is cost effective compared to self-
administered therapy. Treatment completion rates up to 90% are possible), also toxicity
May need steroids (in addition to antibiotics) if adrenal suppression, miliary Tb or pleural effusion
Pathology:
Bacterium is ingested by macrophages, but resists lysis due to waxy coat. Multiplies inside
macrophage. Immune response forms granuloma through unknown mechanisms
Macroscopic appearance: lesions in any organ – but mainly in lungs and lymph nodes. Initially
small focus of consolidation < 3cm with central caseation, which cavitates if it communicates with
a bronchiole. Resolution fibrocalcific scarring puckering the pleural surface. Large nodules
have extensive cavitation and necrosis, and are lined with a ragged white material containing
millions of mycobacteria
Microscopic appearance: granulomas composed of epitheliod cells surrounded by fibroblasts and
lymphocytes, containing giant cells and Langhans cells (nuclei around the edge). Central caseous
necrosis. Acid-fast bacilli with ZN stain
Fungal Pneumonias
Second most common cause of infectious granulomas
Often form necrotising granulomas with central cavitation similar to Tb
Uncommon in NZ: but query in returned travellers or immunosuppressed
Causative agents:
Candida: includes yeast and pseudohyphae. Oral commensal multiple scattered lesion in the
lung
Aspergillus: a saprophytic hyaline mould causing bronchopneumonia, possibly with vascular
invasion and dissemination haemorrhage and necrosis. Most common in immunocompromised
– especially acute leukaemia
Mucormycosis (Zygomycosis): 2 infectious types: Rhizopus and Mucor. Tendency to invade
blood vessels and cause haemorrhagic pneumonia
Cryptococcus neoformans: pleomorphic round to oval 4 – 10 micron yeast with thick mucinous
capsule. Found in bird (pigeon) droppings. Most common infection is meningitis. Stains with
Indian Ink stain
Others: histoplasma capsulatum, coccidioides immitis and blastomycosis dermatitidis

70 4
th
and 5
th
Year Notes
Viral pneumonias
Usually acquired through inhalation
Typically result in diffuse interstitial oedema and lypmhocytic cellular infiltrates in the septae. Lungs
tend to be heavy and diffusely firm without focal lesions. If severe microvascular injury
pneumocyte necrosis and leakage of proteinaceous fluid into alveoli hyaline membrane formation
Most due to influenza viruses (elderly), respiratory syncytial virus (kids) and rhinovirus (kids)
Viruses of note:
Cytomegalovirus: Herpes virus causing cytomegaly or enlargement of infected cells. May have
multiple small cytoplasmic inclusions that are purple and PAS-positive. Subclinical infection
unless immunocompromised. Commonest viral pneumonia in immunosuppressed. Focal or
diffuse interstitial pneumonia. CMV primary infects epithelial and endothelial cells
Herpes Simplex Virus types I and II. Have characteristic nuclear inclusions in epithelial cells.
Two patterns of spread: Necrotising Tracheobronchitis mechanism (spread by contiguity through
necrotic mucosa) or Haematogenous dissemination (more random distribution through lung)
Varicella Zoster: Lung involvement similar to H. Simplex
Measles: RNA virus, infection leads to multinucleate giant cells, interstitial pneumonia, and focal
bronchilobar necrosis. Mainly in immunocompromised kids with measles
Adenovirus: DNA virus mainly causing mild upper RTI. Clinical disease in transplant patients (eg
bone marrow). Necrotising bronchitis and bronchiolitis. Smudge cells seen (large cells with dense
mass filling the nucleus)
Influenza: RNA virus seen in older adults
Respiratory Syncytial Virus: RNA virus causing RTI in the young. Causes bronchiolitis,
sometimes necrotising, and less frequently interstitial pneumonia
Mainly Influenza A or B, Adenovirus or RSV
Other pneumonias
Mycoplasma pneumonia: Common cause of URTI. Smallest free-living organism. 15% of all
pneumonias in general population. Benign and self-limiting with few complications. Peak incidence is
5 – 15 years. Causes a bronchiolar lesion with neutrophil rich exudate, and bronchiolar metaplasia
Pneumocystis Carinii Pneumonia: Extracellular protozoan parasite almost exclusively infects the lung.
Selective attachment to type I pneumocytes injury. Usually in AIDs. Microscopic appearance:
interstitial infiltrate of lymphocytes and plasma cells, and foamy intra-alveolar exudate containing the
organism. Stain with silver (GMS). Occurs as cysts, excysted forms and trophozoites. Ground glass
appearance on X-ray
Lipid Pneumonia: Exogenous lipid pneumonia – aspirated mineral oil being taken by the elderly for
constipation segmental opacification (whiting-out) of the lung and granulomatous fibrous reaction.
Endogenous lipid pneumonia occurs distal to an obstruction (eg cancer) due to coalescing lipid droplets
from dead alveolar macrophages
Mixed bacterial flora is normally found in patients with chronic pulmonary infections (eg cystic
fibrosis, bronchiectasis). Principle organisms are Pseudomonas Aeruginosa (commonest),
staphylococcus aureus and Haemophilus influenzae
Community Acquired Pneumonia
Epidemiology
1 per 1,000 admitted annually
Mortality = 10 % (especially old, young, underlying disease)
Pathogens:
Organism
Proportion
Presentation
Bacteria
Strep. Pneumoniae
60 – 70%
Under 5, Over 50
Abrupt
Focal chest signs – usually lobar
Mycoplasma
Pneumoniae
5 – 18%
Kids & young adults, 4 yearly
epidemic
Flu like, minimal respiratory signs
H Influenzae
4 – 5%
Type A: Smokers, CORD, all ages,
no distinguishing signs
Type B in unvaccinated pre-schoolers

Respiratory 71
Legionella
2 – 5%
Classic presentation: 40 – 70 year old
working smoking man
Organ transplants
Fewer respiratory symptoms
>50% have headache or delirium
Often diarrhoea/liver pain
hyponatreamic
Chlamydia (esp. from
farm animals), S
Aureus, G- anaerobes
< 3%
Virus
Influenza
8%
Other
2 – 8%
Unknown organism in 1/3 of cases despite extensive testing. Dual infections occur
GI symptoms in typical and atypical
Clinical clues:
2 – 3 days: pneumococcus, staph aureus
1 – 3 weeks: mycoplasma/legionella
Sputum: foul smelling anaerobic, rust coloured pneumococcal
Season: summer legionella, mycoplasma comes in 4 yearly cycles
Chronic lung disease: H Influenzae, Moraxella catarrhalis (ie lactams)
HIV: PCP
Neutropenia: G –ive, fungal
Alcohol: G –ive, legionella, staph
Aspiration (6 – 10%) risk of anaerobe cavitation. Upper respiratory commensals
Cavitation S Aureus, G- & Tb
Previous viral infection common in bacteria
If immunocompromised:
Pneumocystis carinii (AIDs)
G – ive bacilli: pseudomonas aeruginosa, Klebsiella pneumoniae (neutropenic cancer patients)
Fungi: Candida albicans, Cryptococcus neoformans
Virus: cytomegalovirus
Diagnosis
Suggested by fever + respiratory symptoms (cough, sputum, dyspnoea)
May present with GI symptoms most prominent
Confused with acute bronchitis
Signs: fever in > 80%, Respiratory Rate > 20, crackles on auscultation, consolidation in 30%
Post influenza: 70% (?) S. Aureus infection ( micro abscesses)
Can be secondary to abscess, empyema, lung cancer
Investigation Options
CXR: extent, cavitation, effusion, cardiomegaly. False negatives possible if PCP or during first 24
hours
Blood gases
FBC: White cell count, if > 15,000 * 10E9 bacteria likely cf. virus
Urea/electrolytes/liver severity and underlying disease
Urine: glycosuria
Microbiology:
Sputum (but 1/3 don‟t expectorate and many causative organisms are URT commensals): culture
and pneumococcal antigen test (most sensitive test for strep pneumoniae). If can‟t get sputum
sample, can nebulise with hypo-osmotic saline.
Blood serum for pneumococcal antigen
Blood cultures
Culture plural effusion
Lavage via bronchoscopy may be indicated in immunosuppressed patients and in those suspected of TB
who can‟t produce adequate sputum
72 4
th
and 5
th
Year Notes
Acute and convalescent serum for antibodies to mycoplasma pneumoniae, legionella, chlamydia
pneumoniae (Convalescent = 5 – 6 weeks later, a 4 fold rise in antibody titre or the presence of IgM
specific antibody is evidence of recent infection)
Prognosis
Classified as severe if (21 times risk of mortality)
Age > 65
Respiratory rate > 30 bpm. (key prognostic indicator)
Systolic BP < 90, Diastolic BP < 60 mmHg or low urine output (ie shocked)
Confusion
Serum urea > 7 mmol/L
Comorbid disease: heart failure, diabetes, CORD, cancer, HIV, renal failure, chronic alcohol, etc
Other markers of severe prognosis:
WBC < 4000 or > 30000
PO2 < 60 or inability to get Sats above 90% despite O2 therapy
CXR shows multilobed or pleural effusion
Haematocrit < 30%
Treatment
Community treatment:
Immediate empirical therapy:
Should cover S pneumonia
Erythromycin if legionella/Mycoplasma suspected
Antibiotics: for 5 – 10 days (10 – 14 if Mycoplasma or Chlamydia)
Oral amoxycillin 500mg td
If allergic to penicillin: erythromycin
IV benzyl penicillin 1.2 g qd IV if poor absorption (e.g. vomiting)
If severe: erythromycin 1g qd + 3
rd
generation cephalosporin
Types of antibiotics:
Penicillin: strep pneumoniae. Even if resistant, iv penicillin dose exceeds the MIC, so it‟s still
effective (doesn‟t work though for Meningitis caused by Strep Pneumoniae because CSF
penetration is lower)
Augmentin, Cefaclor, Tetracycline (not kids), cefuroxime (iv): H Influenzae (5% resistant to
amoxycillin), Branhamella Catarrhalis
Flucloxacillin: Staph aureus
Ceftriaxone: penicillin resistant strep pneumoniae, G- bacilli
Erythromycin (ie macrolides): mycoplasma, legionella, chlamydia
Rifampicin + isoniazid + pyrazinamide: Tb
Cotrimoxazole: Pneumocystis carinii
Fluconazole or Amphotericin B: Candida, Cryptococcus
Ganciclovir: CMV
Resistant to Augmentin (ie have -lactamase):
Mycoplasma pneumoniae
Chlamydia pneumoniae
Legionella
Penicillin resistant strep pneumoniae
Hospital treatment:
Only 0.1% of chest infections get to hospital not typical of population as a whole
Hospitalise if high pyrexia, cyanosis, tachycardia, tachypnoea, confusion
Oxygen:
See Oxygen Therapy, page 60
Give sufficient O2 to keep PO2 > 60 mmHg
O2 saturation > 90 % preferable
Transfer to ICU if:
Severe
Blood gases bad: PO2 < 60 on FIO2 > 60%, or PCO2 > 48 (should breath faster PCO2
should fall – if normal or raised person getting tired bad sign)
Shocked
Respiratory 73
CCHL preferred medicines list:
Uncomplicated: Penicillin G 1.2 g iv 4 – 6 hourly or amoxycillin 1g iv 8 hourly. Consider
adding erythromycin 500 mg iv 6 hourly if the patient is > 60, no response to penicillin
antibiotics, or mycoplasma or legionella are suspected (atypicals less likely if leucocytosis)
History of CORD or other disease: Augmentin 1.2 g iv 8 hourly or Ceftriaxone 1.5 g iv 8
hourly. Consider adding erythromycin for above complications
Failure to Respond
Is treatment failing?
Some improvement should be seen in 48 – 72 hours, don‟t change treatment over this time unless
there is a marked deterioration
CXR may worsen initially after therapy started: if mild pneumonia this may be normal. If severe,
this is a poor prognostic indicator
Fever lasts 2 – 4 days, S pneumoniae resolves quickest
Crackles will last beyond 7 days in up to 40%. May take more than a month for CXR to clear
If treatment is failing, consider:
Incorrect diagnosis: PE, pulmonary oedema, Wegerner‟s granulomatosis (ie non-infectious illness)
Antibiotic resistant organism
Resistant infection: mycoplasma, chlamydia, Staph aureus, TB, PCP (immunodeficient)
Complication: empyema (see Pleural Disease, page 73), abscess, PE, drug induced fever
Underlying disease: lung cause, cardiac failure, immunodeficiency
Drug compliance in outpatients
Pleural Disease
Common problems:
Effusion
Empyema
Pleural pain
Pleural disease
Pneumothorax. See Tension Pneumothorax, page 490
Usually presents with pain related to breathing: cough, deep inspiration
Investigations:
CXR: PA, lateral and lateral decubitus (does pleural opacity move with gravity)
Pleurocentesis
Pleural biopsy
US for septa or cysts
CT. MRI rarely superior to CT
Pleural space:
Usually 0.4 mls of fluid
If then either production or clearance (eg Tb or malignancy blocking lymphatics)
Pleural fluids:
Takes 300 – 500 ml before visible on CXR
Transudate:
Pleural membrane not diseased
Due to change in hydrostatic or osmotic pressure due to distant disease
Eg nephrotic syndrome, cirrhosis or CHF
Exudate:
Protein rich (> 30 – 40 g/L)
Due to pleural disease: Parapneumonic effusion, empyema, malignancy, Tb, SLE/RA,
asbestosis, drug induced
Empyema:
= Collection of purulent material (with or without bugs) in any body site: usually refers to
pleural space
Commonly associated with underlying pulmonary parenchymal infection
Low pH differentiates it from effusion, as does growth of organism on culture
Strep pneumoniae and Staph aureus are the main pathogens
Closely related to lung abscess (necrotising pneumonia)
Symptoms: fever, sweats, cough, dyspnoea, weight loss, pleurisy
74 4
th
and 5
th
Year Notes
Signs: stony dullness to percussion, breath sounds, maybe quite localised, fluid in
costophrenic angles on X-ray
Need to drain. Reduced antibiotic penetration, especially if loculated
Usually heals with pleural fibrosis
If blood in a pleural tap then:
Hit an artery
Haemothorax (need to evacuate. NB can bleed 3 litres into one side of the chest profound
shock)
Blood in an effusion (eg Tb/cancer). To differentiate from a haemothorax measure the
haematocrit
Testing pleural fluid:
Total protein
Albumin: If (effusion albumin)/(serum albumin) > 0.5 then transudate
LDH: in exudates
pH < 7.2 empyema
Amylase. Normally none. If present then oesophageal rupture or pancreatitis
Cytology for malignancy
Microscopy and culture: low sensitivity. Organisms causing empyema are hard to culture (eg
anaerobes, Tb, fungi, etc)
Venous Thromboembolism
Deep Vein Thrombosis (DVT)
Risk Factors
Key risk factors:
Age
Obesity
Immobility
Co-morbidity
These can present as:
Post-operatively (immobile + hypercoagulable)
Stasis (long period of immobility)
Pregnancy & immediately post-partum
Thrombophilia
Smokers on the pill. See Combined Oral Contraceptive, page 341, for risk ratios
Obesity, Cancer, Polycythaemia
PMHx or FHx of DVT
Presentation
May be rapidly offset by collateral bypass
Less than 1/3 present with classic syndrome of calf discomfort, distal oedema, venous distension &
pain on forced dorsiflexion of foot
Homen's sign: pull big toe up stretch calf pain. Of little diagnostic value and theoretically could
dislodge a clot
Exclude Baker‟s cyst: herniation from joint space into popliteal space – wouldn‟t cause leg swelling
Approx. 50% are asymptomatic
Investigations
See Possible Investigations, page 77
Treatment
Aims:
Prevent PE
Restore venous patency
Options:
Anticoagulant: See below
IV or subcutaneous heparin for 5 days: aim for APTT 1.5 – 2.5 times normal
Respiratory 75
Oral warfarin for 3 months: 5mg daily then dose adjust to aim for INR 2.0 – 3.0. Can continue
longer – haemorrhages, if they occur, are usually early on
Surgery: really only if limb at risk. Veins often re-occlude
Thrombolytic Treatment: better clearance of occlusion, no change to PE risk, risk of bleed or
intra-cranial haemorrhage little evidence of net benefit
Prophylaxis:
Cost effective if risk high. Base assessment on clinical risk – lab results not good predictor. If low
risk after surgery – early ambulation and stockings may be sufficient
2/3rds decrease in risk with Low molecular weight Heparin (inject daily for duration of risk)
Mechanical: intermittent external compression with inflatable cuffs as effective as drugs in
moderate risk people – but frequently misused
Antiplatelet: aspirin not as effective as anticoagulant but good in the community as LMM Heparin
not funded (ie can be prescribed by GP for a temporarily bed-bound elderly or obese person)
Anticoagulant Treatment
Standard (unfractionated) Heparin:
Potentiates antithrombin III at all sites of coagulation activation (cf Low Molecular weight Heparin
which only acts at Factor 10)
Dosing:
10 fold variability in individual dose response individual titration required
T½ = 100 minutes
Monitor APTT and aim for 1.5 – 2.5. (If goes above 3 then 8 * risk of bleed)
Monitor after 10 hours (4 – 5 half lives)
Emboli doses:
IV dose: Loading 5000 IU, maintenance 1400 IU/j (20 IU/kg/hr)
Subcutaneous: 17,5000 IU 12 hourly, duration of action 9 – 10 hours
T½ in large PE need infusion not bolus
Standard Heparin Prophylaxis:
Medical view (surgeons disagree!): 5% DVTs in general surgical operations, 20% in
orthopaedics
Pre-op Prophylaxis:
Non-fatal PE by 40% and fatal by 65%
Risk of excess bleeding from 3.7% to 6%
Low dose heparin (never warfarin):
5000 IU standard heparin 12 hourly start 2 hourly pre-op
LMW Heparin single dose: more costly and no advantage in most cases
Continue for 2 weeks for patients at high risk (biggest mistake is to stop too soon)
Heparin induced bleeding:
Uncommon for 1
st
2 days, then common for days 3 – 10
Retroperitoneal is a common occult site of bleeding
Thrombocytopenia after 5 days
Antidote: Protamine sulphate + FPP (clotting factors)
Low Molecular Weight Heparin:
Lots of different types, all with different T½s and doses
Longer T½ (can have once daily dosing), better bioavailability, less platelet inactivation, and
potentially less bleeding
Elimination is not dose dependent (heparin approaches this at high dose)
Need to adjust for obesity
Protamine reversal less efficient
Warfarin:
Competitive inhibition of Vitamin K dependent clotting factors (II, VII, IX, X) and inhibits
proteins C and S
Pharmacokinetics:
Very narrow therapeutic index
10 fold variability from dose to plasma concentration, and further 10 fold variability from
plasma concentration to effect
99% albumin bound Vd = intravascular space
T ½ = 25 – 60 hours, biological effect lasts 2 – 5 days
76 4
th
and 5
th
Year Notes
Contraindications:
Teratogenic, but not in breast milk
Risks of bleeding, eg peptic ulcer, haemorrhagic stroke
On NSAIDs ( GI bleed)
Consider:
Can the patient cope with therapy and monitoring (infirm, alcoholic, etc)
Warfarin sensitivity if > 65 years due to liver metabolism
Patient education important – lots of different sized/coloured pills
Dose:
Do pre-test INR
Start low, monitor on day 3
Dose range approx 3 – 9 mg daily (contrary to New Ethicals)
Target range for INR:
Venous thromboembolism: INR of 2 – 3 for 3 months for 1
st
VTE
Non-rheumatic atrial fibrillation:
> 60 with no risk factors: INR 1.5 – 2.7
Risk factors: hypertension, previous VTE, recent heart failure
Don‟t anticoagulate patients < 60 years if no risk factors
MI: 20% in mortality and reinfarction but no advantage of warfarin over aspirin except with
added fibrillation (in which case aim for INR 2 – 3)
Bleeding:
Risk factors: age, haemostatic disorder, malignancy, uraemia, GI ulceration, recent surgery,
haemorrhagic strokes, low protein states (ie clotting factors)
Management:
If INR < 7 withhold doses until INR in normal range (unless severe bleed)
INR > 7 and no prosthetic heart valve: 0.5 mg iv vitamin K (never IM)
If INR > 7 and prosthetic heart valve, don‟t use vitamin K unless evidence of an inter-
cranial haemorrhage
If overt bleeding: stop warfarin, give FFP or Prothrombin complex concentrates
Drug interactions:
Inducers: take 10 days to warfarin concentration, and warfarin toxicity when stopped.
Phenytoin, carbamazepine, phenobarbitone, rifampicin
Inhibitors: immediate effect warfarin toxicity. INR when these are stopped: macrolides,
metronidazole, fluoxetine, quinolones (eg ciprofloxacin), chloramphenicol, cimitidine,
disulphram
If massive PE, consider thrombolysis. Echocardiogram to determine RV function useful in assessing
risks and benefits
Pulmonary Embolism (PE)
Very important to do a risk assessment for everyone in hospital or bed-bound at home: are they low,
medium or high risk. Prevention is better than cure
Presentation
Frequently undiagnosed (71% of PEs are not diagnosed): always have it as a differential to SOB
If episodic SOB unresponsive to treatment ?PE
May not have chest pain. May have fever, but rarely sweating or rigours
Severity:
Small: transient chest pain, cough, SOB. If pre-existing pulmonary disease may get small infarct
with pleuretic chest pain and fever
Multiple small emboli: pleuretic chest pain, haemoptysis, gradually SOB
Medium: Bronchial arteries are enough to maintain viability of healthy lung tissue. Get chest pain
(not always pleuretic), SOB, maybe haemoptysis
Large: Classical – 10 days post op, sudden SOB and collapse while straining on toilet. If fatal, die
within an hour. May mimic MI with comma (acute SOB, severe chest pain, hypotension, temp,
LDH, syncope). Also cyanosis, gallop rhythm, JVP, pleural rub, haemoptysis
Course: Frequent PE pulmonary hypertension dilated pulmonary artery enlarged right heart
(Cor Pulmonale)
Respiratory 77
Possible Investigations
Imaging:
CXR: most are normal
Doppler US for DVT
Ventilation-Perfusion Scan
Pulmonary arteriogram: gold standard but not often done
CT Pulmonary Angiogram: pretty good and getting better
ECG:
Small-medium PE: usually normal except for tachycardia. May be signs of AF or right ventricular
strain
Massive PE: S1Q3T3 pattern: S wave in lead I, Q wave in lead III, inverted T wave in lead III.
Tall peaked T waves in lead II.
Bloods:
ABGs: Aa gradient
FBC - check Hb, WBCs, platelets (eg hypercoagulable)
Clotting times: likely to be normal – these test bleeding disorders, not clotting disorders
D-dimmer test for fibrin degradation products digested clot (cheap and easy):
+ive for cancer, trauma, post surgery, sepsis lots of false positives
Don‟t use as first line test – only in the context of a complete algorithm
Decision analysis:
If > 6% risk of a PE then test
If > 48% risk of a PE then treat
If risk > 6% but < 48% then further testing
Test sequence:
Chest X-ray and D-dimmer: if d-dimmer negative then no DVT/PE. Positive test doesn‟t
change pre-test odds. If Chest X-ray normal then V/Q scan. If abnormal go straight to CT
angiogram
V/Q Scan: if positive then treat. If negative, doesn‟t change pre-test odds
CT angiogram
Treatment
See Anticoagulant Treatment, page 75
If massive (Hypotension and multiple clots): thrombolysis or surgery
If submassive (RV strain or lots of clots): consider thrombolysis
Asthma
Is chronic and obstructive, but not usually categorised with CORD
History
Viral infections likely to trigger asthma
Night time cough and low peak flow can be asthma, ?hay-fever, a cold or bronchitis
Ask about:
Living situation
Occupation
Allergies, any pets?
Seasonal
Cold air
Irritants (eg fumes)
Exercise
Night cough
History of atopy: eczema
Classic symptoms: SOB, wheeze, cough, tightness (like in angina)
Assessment
Always do peak flow. Not the same as FEV1, which is more accurate. FEV1 of 50% of predicted = PF
of 70% predicted
If can‟t get a wheeze on auscultation, then take a big breath and blow out fast to elicit wheeze (=Forced
End Expiratory Wheeze). Also listen to heart to ensure it‟s not a cardiac cause
78 4
th
and 5
th
Year Notes
Can you demonstrate reversible bronchial constriction? If peak flow (or FEV1 if spirometry available)
by 15% (60 – 70 litre/min) following bronchodilator. Do best of 3 peak flows, then repeat 15
minutes (= peak response time) after >= 2 doses of a reliever
There will be significant pathology even if mild: pseudo stratified epithelium gone, thickened basement
membrane, eosinophils, hypertrophy of smooth muscle and glands, mucus
High-risk asthmatic (markers of risk of death):
Hospital admission in last 12 months
Previous life threatening attack
Repeated self-administration of high doses of reliever (eg requesting 2 or more reliever
prescriptions per month)
Precipitating factors in a life-threatening attack:
In kids (80%) and adults (30%): viral URTI. Most commonly rhinoviruses and coronaviruses
(„common cold‟)
Allergen exposure in a sensitised individual
Drug sensitivity, eg aspirin
If severe, then ?other causes: PE, pneumothorax, etc
Classification of severity
How they feel (ie breathlessness) does NOT correlate to severity (as measured by FEV1). Due to
temporal adaptation – if chronically breathless, body turns off perception of breathlessness (cf don‟t
hear trains if living by a railway line). Unless you MEASURE lung function, you CANNOT assess
severity. However, in kids have to rely on symptoms as peak flow unreliable
PEF
Symptoms
Action
Under Control –
stable
> 80% predicted (best
PEF they‟ve ever
had)
Can exercise easily,
symptom-free most days,
Not needing reliever on
most days.
Take preventer every
day – can it be
reduced? Would a
spacer help?
Getting Worse -
unstable
< 80%
Daily symptoms, waking at
night, getting a cold, more
short of breath with
exercise, needing more
reliever
Start or increase dose
of preventer. Use
reliever as required.
Severe
< 60%
More breathless or wheezy,
reliever only lasting 2 – 3
hours. Getting worse
despite more preventer
Start prednisone and
see doctor within 1 or 2
days. Use reliever as
required.
Emergency
< 40%
Hard to speak, feeling faint
or frightened, reliever not
working.
Ambulance/emergency
doctor, sit upright, keep
calm, keep using
reliever.
Key time to measure peak flow is when asthma is getting worse. No one will do it all the time so don‟t
ask them to
Asthma in Young Children
See Asthma in Young Children, page 613
Principles of management
Asthma self-management plans are recommended as essential in the long-term treatment of adult
asthma. Those with formal management plans have half the morbidity of those without them, despite
the same treatment
Also need to establish, avoid and control triggers
Factors associated with asthma deaths:
Long term:
Lack of appreciation of chronic asthma severity and risk
Poor compliance
Discontinuity of medical care
Under utilisation of inhaled steroids
Fatal attack:
Respiratory 79
Delay in seeking medical help
Inability to recognise severity
Over-reliance on bronchodilator
Insufficient systemic steroid use
Lack of written information
If the management plan is too complicated for the patient, modify (eg just the point at which to see the
doctor)
Compliance is critical ownership of treatment by the patient is fundamental – negotiate and educate
Treatment
Status asthmaticus: severe acute asthma that does not respond to treatment. See Asthma, page 485
Most important part is use of inhaled corticosteroid. Patient may favour reliever (it obviously does
something – reinforce that preventer stops it happening to start with)
Inhaled Corticosteroids:
Action: Anti-inflammatory and hyper-reactivity
Effect: lung function, symptoms, admissions (only drug to do this)
If using a -agonist most days then should be on an inhaled steroid
Doses:
200 to 1000 g/day of Beclomethasone Dipropionate (BDP/Becotide) or Budesonide
(BUD/Pulmicort), or
100 to 500 g/day of Fluticasone Propionate (Flexatide - only difference is potency, not
efficacy, ?side effects)
Starting dose: if steroid naïve, better to start low and step up not start high and step down – too
hard to wind it back
Back titration: in stable patients back titration may be attempted. ½ dose as a one off. If cut
too far too fast can rebound within a month. Stopping treatment altogether is likely to cause a
relapse
Doses by severity:
Stable: inhaled steroid bd, agonist prn. If well controlled can take total steroid dose once a
day at night rather than bd better compliance
Unstable: inhaled steroid qid, agonist prn. If still not controlled then oral theophylline at
night or long acting agonist
Severe: systemic steroids, high dose agonist, O2, medical review. Bronchodilators and
inhaled steroids don‟t work so well in severe asthma as the major cause of obstruction is
mucus plugging and the drugs don‟t get through. Steroid dose: start early (takes approx 12
hours to have an effect), 0.4 – 0.6 mg/kg/day = 40 mg for normal adult. In practice: 30 – 40
mg/day until PEF normal, then 20 mg/day for as many days again
Side-effects: Dose dependent redistribution of fat, electrolyte disturbances, hypertension (ie
Cushing‟s features), stunted growth in children
Bronchodilator:
Reliever. Short acting inhaled agonist.
Potent and rapid bronchodilator and a relatively low toxicity. Relaxes airway smooth muscles
(plus other effects, e.g. release of mast cell mediators). Adverse effects: muscle tremour and
tachycardia common. Use as needed – not regularly – then becomes a guide to severity
Salbutamol and terbutaline sulphate common.
Long acting agonists for more severe asthmatics: Salmeterol and Eformoterol (similar effect but
potency). Peak effect 2 – 4 hours, duration 9 – 12 hours.
Theophylline:
May have additive effect with agonist, but risk of side effects (including K).
Narrow TI.
T½ in heart and liver failure, viral infections, elderly, enzyme inhibitors eg: cimitidine,
erythromycin, contraceptives
T½ in smokers, chronic alcohol, phenytoin, carbamazepine, rifampicin, and barbiturates
Given IV (very slowly) as aminophylline (too irritant for IM) for severe attack unresponsive to
nebuliser
Others:
Sodium cromoglicate: non-steroidal preventer – less effective than steroids but fewer side effects.
Single dose good for prevention of exercise induced asthma
80 4
th
and 5
th
Year Notes
Anti-leukotrienes: Leukotrienes vascular permeability, mucus production, mucus transport,
etc. Oral montelukast 15 % in FEV1, use of agonist. Place in therapy still uncertain
Follow-up (eg good liaison with GP) following emergency admission is critical to preventing
recurrence
Inhalers
Advantages: minimum possible dose, highly targeted, patient controls therapy
Inhaled steroids deposition in mouth. If not using spacer, need to rinse, gargle and spit otherwise
risk of thrush and croaky voice. At best, 10% gets to lower airways without spacer
Metered dose inhalers (MDI):
Autohaler: shake, push lever up, suck. Lower level of suck needed than powder inhalers – but still
require good suck to get lower airways deposition. As expensive as powder inhalers. OK from
age 8 upwards
Standard MDI: (cheap, light and rapid delivery of drug, but co-ordination difficult). From age 12
onwards. Instructions for use:
Shake an inhaler between each puff
Remove cap
Hold it upright and pointed backwards
Breath out
Fire during 1
st
25% of long slow inhalation
Hold breath
Breath out after removing inhaler from mouth
Inhalers through a spacer:
As effective as a nebuliser. Increases LRT deposition by 4 times
Eliminate oral deposition of steroids and lung deposition of both preventers and relievers
Breath-a-tech with a facemask up to 6. Remove mask as soon as you can (stops nasal filtering –
try at age 4 - 5). Need smaller spacer as they have a small tidal volume
Volumatic without facemask. Need to be able to mouth breath well (ie try from age 2 – 3
onwards)
Need to inhale within 30 seconds of a puff into the space
One puff at a time
But plastic spacer static charge particles stick. So wash in detergent once a week and do not
rinse bubbles off ( microfilm of detergent)
If using a new space without washing, need to prime it (10 puffs). Don‟t do this in front of patient
Dry Powder Inhalers: oral deposition. Use from age 5 up (good for use at school when they don‟t
want to lug a spacer around but their MDI technique is inadequate). Advantages: light, quick delivery,
don‟t need co-ordination, CFC free. Disadvantages: cost, require high respiratory flow
Accuhaler: 60 doses, easy to use, has dose meter
Disk haler: 6 doses
Turbohaler: easier to use than disk haler. Red mark inside indicates when its empty
Chronic Obstructive Pulmonary Disease (COPD)
= Increase resistance to air flow due to partial or complete obstruction at any level
= Permanent or minimally reversible obstruction of expiratory airflow caused by chronic bronchitis,
emphysema or both
Lung Function results:
FEV1/FVC ratio < 70% with a concave expiratory loop
RV secondary to air trapping
DL CO due to loss of parenchyma
Severity:
Mild: FEV1 > 50% predicted
Moderate: FEV1 35 – 49% predicted
Severe: FEV1 < 35% predicted
Chest Xray:
Emphysema: absent peripheral vessels, hypertranslucency, flattened diaphragm, bullous change
Bronchitis: thickened bronchial walls (especially end on)
Respiratory 81
Abnormalities in gas exchange:
Pink Puffer (Emphysema)
Blue Bloater (Bronchitis)
Presentation
Dyspnoea
Cough, sputum, RHF
CXR
Hyperinflated
markings at bases
ABG
PaO2, PCO2
PO2, PaCO2
Lung Function Tests
TLC, DL CO
Normal TLC and DL CO
Sleep
Moderate desaturation
Marked desaturation
Treatment:
Only smoking cessation and long term oxygen alters the natural course
No evidence that daily bronchodilators are beneficial in asymptomatic patients
20% benefit from oral corticosteroids. Should be used primarily for exacerbations. Inhaled
steroids show no significant benefit
Management of an exacerbation:
Exclude differentials: PE, LVF, pneumothorax, hyperventilation
Is there an infective component: Upper or Lower RTI
Are there complications of COPD:
Cor pulmonale/pulmonary hypertension (look for signs of RH failure)
Polycythaemia secondary to chronic hypoxia
Low body weight/osteoporosis (from steroids and acidosis)
Investigations:
FBC (is Hb or WBC ), U & E, Glucose
ECG
If Sats < 92% then ABG
CXR
Sputum microscopy, culture and sensitivity
Peak flow is asthmatic component
Spirometry when resolved
Echo if cor pulmonale or LVF suspected
Treatment:
O2 with goal of saturation 90 – 92% (beware CO2 narcosis)
Broncho dilation: Combivent
Antibiotics: Usually oral. Augmentin, erythromycin, etc. Commonly H Influenzae or M
Catarrhalis
Steroids: 30 – 40 mg/day, stepping down over around 2 weeks
Chronic Bronchitis
= Persistent cough with sputum for at least 3 months in 2 consecutive years
Follows prolonged exposure of the tracheobronchial trees to non-specific irritants hypersecretion of
mucus and structural changes
Types:
Simple chronic bronchitis: no airway obstruction
Chronic asthmatic bronchitis: intermittent bronchospasm and wheezing
Chronic obstructive bronchitis: heavy smokers with chronic airways obstruction, usually with
emphysema. Sputum will be clear/white, only occasionally will be infected (yellow/green)
[Cf Chronic infective bronchitis with green sputum bronchiectasis]
Pathogenesis:
Chronic irritation (eg inhaled substances such as smoking) and microbiological infections
hyper-secretion of mucus obstructing airways. Hypertrophy of submucosal glands in larger
bronchi and hyperplasia of goblet cells in small airways.
Infection maintains the hyper-secretion and causes acute exacerbations
Macroscopic appearance: hyperaemia, swelling, mucopurulent secretions in the bronchi
Microscopic appearance: increased size of mucous glands. Reid index (ratio of mucous gland layer to
thickness of epithelium to cartilage) greater than 0.4. Chronic inflammation metaplasia to squamous
epithelium and dysplasia. Mucous plugging, inflammation and fibrosis. If severe luminal
obliteration
Emphysema
Enlargement of air-spaces distal to terminal bronchioles and destruction of alveolar walls without
fibrosis
82 4
th
and 5
th
Year Notes
Moderate to severe emphysema is rare in non-smokers
Aetiology:
Cigarettes: usually had a 20-pack year history. Only 15 – 20% of smokers develop obstruction
Alpha-1 antitrypsin deficiency
Dusts: coal, gold mining, textile, cement and steel making
FEV1 best single indicator of prognosis
Pathogenesis: Disruption in balance of elastin synthesis: in elastolytic activity from neutrophil
elastase (smoking neutrophils) and 1-antitrypsin (elastase inhibitor – oxidants in cigarette
smoke inhibit 1-antitrypsin). Neutrophils also release free radicals that inhibit 1-antitrypsin
Types:
Centriacinar (Centrilobular): enlargement of respiratory bronchioles, distal alveoli are spared.
(Small particles deposited here – don‟t make it right to the end). More severe in upper lobes.
Blackened. Bronchi and bronchioles have chronic inflammation. Seen in smokers and coal
workers pneumoconiosis
Panacinar (Panlobular): acinus is uniformly involved from respiratory bronchiole to terminal
alveoli. Seen in 1-antitrypsin deficiency (ZZ or MZ alleles on chromosome 14) and as an
extension of centrilobular emphysema in smokers. Mean age of onset is 45 – 50 years in non-
smokers and 30 – 40 in smokers. Liver disease in 5 – 10 % of adults. Heterozygotes (MZ)
predisposed to emphysema if they smoke. Treatment same as for smoking induced
Paraseptal (distal acinar): proximal acinus is normal, distal part affected. Most prominent sub-
pleurally and next to interlobular septi. Often seen in cases of spontaneous pneumothorax in
young people
Irregular emphysema: acinus irregularly involved. Associated with scarring
Macroscopic appearance: voluminous lungs
Microscopic appearance: large abnormal airspaces, blebs and bullae. Bronchitis and bronchiolitis
Clinical features:
60 years or older
Prolonged history of exertional dyspnoea
Minimal non-productive cough
Usually have lost weight
Use accessory muscles for respiration
Prolonged expiration period (lungs collapse due to elastin)
Pink puffers: respiratory rate maintains O2. Xray: central pulmonary artery size, peripheral
vascular markings
Blue bloaters: PaCO2, PaO2, cyanotic, respiratory centre insensitive to CO2, instead rely on
hypoxic drive to breathe. Dangerous to give O2 ventilatory drive
Medical management:
Bronchodilators and inhaled corticosteroids: only if reversible obstruction
Smoking cessation (nicotine replacement doubles quit rate)
Antibiotics
O2 with care
Exercise/physio
Attention to nutrition
Bronchiectasis
Chronic necrotising infection of bronchi and bronchioles (ie a pneumonia that doesn’t clear)
abnormal airway dilation and destruction of bronchial walls obstruction due to inflammation,
ulceration and distortion
= Chronic infective bronchitis
Pathogenesis:
Obstruction (especially during growth) due to tumour, foreign bodies, mucous impaction (eg in
cystic fibrosis and immotile cilia)
Infection with bronchial wall weakening and atelectesis (eg in necrotising pneumonia). Especially
Tb, pertussis, MAC
Macroscopic appearance: affects lower lobes, especially vertical airways and more distal bronchi.
Airways may be cylindrical, fusiform or saccular
Microscopic appearance: Acute – inflammatory exudate with desquamation and ulceration of the
epithelium. Chronic – peribronchial fibrosis
Respiratory 83
Clinical course: foul, bloody sputum, especially in the morning. (cf Clear sputum in chronic
bronchitis). Repeated „bronchitis‟ with wheezing, haemoptysis, and dyspnoea. Coarse crepitations,
wheezing, and clubbing.
Complications: obstructive ventilatory insufficiency dyspnoea and cyanosis. Rarely cor pulmonale,
metastatic brain abscesses and amyloidosis
Restrictive/Interstitial Pulmonary Disease
= Reduced expansion of the lung parenchyma
British and Americans give them different names
Over 150 different disease processes primarily affecting alveoli epithelium, interstitium and capillary
endothelium, not airways
Leads to expansion of lung parenchyma, total lung capacity, lung compliance
Other causes:
Secondary to drugs (eg amiodarone)
Secondary to radiotherapy
In some connective tissue diseases (eg Ankylosing Spondylitis)
Acute Interstitial Lung Disease
Adult Respiratory Distress Syndrome (ARDS)
= Diffuse Alveolar Damage (DAD)
= Shock Lung
Clinical: rapid onset of life-threatening respiratory insufficiency, cyanosis and hypoxaemia refractory
to O2 therapy
Diagnostic criteria: acute onset, fluid on CXR, capillary wedge pressure < 19 ( not LH failure),
hypoxia
Aetiology – types of injury:
Aspiration: gastric contents or drowning
Inhalation of fumes or toxic aerosols, smoke, chlorine, oxygen toxicity
Circulating toxins: bacterial endotoxins
Other: DIC, high altitude, trauma, radiation therapy, chemotherapy
Pathogenesis:
Results from leakage from capillaries to alveoli spaces: non-cardiogenic pulmonary oedema
Leads to a non-compliant lung: smaller tidal volume, poor gas exchange, risk of lung rupture
when ventilating
Prototypical injury is oxygen toxicity: hyperoxia damage alveolar macrophages (AM) release
O2 radicals injure lung tissue; AM release cytokines attract neutrophils, stimulate
intravascular adherence, and release further O2 radicals. Vicious circle of damage, especially to
septum
Other possible initiating mechanisms (alone or in combination): activation of complement cascade,
neutrophil aggregation, activation of coagulation fibrin deposition, etc
Restrictive Lung Diseases
Affecting chest wall or
pleural space bellows
function. Eg polio and
kyphoscoliosis
Interstitial or infiltrative diseases
DAD/ARDS
Acute
Chronic
Known causes, including:
BOOP
Idiopathic Pulmonary Fibrosis
Pneumoconioses
Hypersensitivity Pneumoconioses
Unknown
causes
Honeycomb lung
84 4
th
and 5
th
Year Notes
Macroscopic appearance: Affects WHOLE lung (if only one lobe affected ?pneumonia). Heavy lungs
due to fluid accumulation (interstitial and later alveolar)
Microscopic appearance:
Early change: interstitial oedema, few cell infiltrates
Acute exudative stage: microvascular injury breakdown of basement membrane leakage of
plasma proteins into alveoli. Sloughing of injured type 1 pneumocytes. Cell debris + exudate
form hyaline membrane. Inflammatory cells in interstitium. No neutrophils in alveoli (key
differential from pneumonia)
Proliferative stage: Type II pneumocytes proliferate to cover alveolar surface. Fibroblasts lay
down collagen in interstitium and alveolar spaces interstitial and intra-alveolar fibrosis
Prognosis: 50% mortality. Surviving patients may have mild to extensive diffuse interstitial pulmonary
fibrosis
Acute Interstitial Pneumonia (AIP)
= Hamman-Rich Disease
Rapidly progressive interstitial pneumonitis that resembles the organising stage of DAD (?may be a
variant)
Affects young adults, presenting with flu-like syndrome and bilateral infiltrates. Most die of
respiratory failure within two months
Chronic Infiltrative (Restrictive) Lung Disease
Common clinical and radiologic features but diverse aetiology and pathology
Clinical features:
Cyanosis due to severe hypoxemia from ventilation-perfusion mismatch
Clubbing of digits
Late in disease: pulmonary hypertension due to destruction of alveolar capillary bed
Interstitial infiltrate and some exudate in small airspaces
Diseases leading to chronic infiltrative lung disease:
Idiopathic chronic interstitial pneumonias: 13%
Environmental lung disease: 25%
Sarcoidosis: 20%
Types of Idiopathic Pulmonary Fibrosis (IPF)
Usual Interstitial Pneumonia (UIP, US):
= Cryptogenic Fibrosing Alveolitis (UK)
Most common type of IPF
Presents with gradual onset of dyspnoea and cough (usually dry)
Non-uniform slowly progressive disease starting in middle age. Die in several years. No known
treatment (don‟t respond to steroids). Airflow and blood flow disrupted
Macroscopic appearance: when advanced lung is small and firm with a honeycomb appearance on
cut section
Microscopic appearance: ranges from normal to fibrotic alveolar walls, with marked variation in
the degree of fibrosis from field to field (cf other IPFs which are uniform). Capillary bed slowly
destroyed pulmonary hypertension and cor pulmonale. Inflammatory cells (lymphocytes +
macrophages + neutrophils) in interstitium and airspaces
Desquamative Interstitial Pneumonia (DIP): more uniform than UIP, with no alternating areas of
scarring and normal lung. Filling of alveolar with alveolar macrophages (not desquamated as originally
thought). Is it an early stage of UIP? However, may respond to steroids and have a better prognosis.
X-ray shows bilateral lower lobe ground glass infiltrates
Lymphocytic Interstitial Pneumonia (LIP)
Granulomatous Interstitial Pneumonia
Bronchiolitis Obliterans Organising Pneumonia (BOOP)
Obliterans airways sealed off
Organising fibrosis
Common response to lung injury from infections, inhaled toxins, drugs, etc
Major finding: plugs of loose fibrous tissue filling bronchioles and alveoli. Variable chronic
inflammatory cell infiltrate is present
Patients improve gradually with steroids (ie different from UIP)
Respiratory 85
Pneumoconioses
= Pulmonary diseases caused by the inhalation of inorganic dust (usually stimulating fibrosis)
Asbestos:
Occupational exposure to asbestos is linked to:
Localised fibrous plaques: dense fibrotic plaques on X-ray – generally asymptomatic
Pleural effusions cough, SOB
Asbestosis: Parenchymal interstitial fibrosis. Progressive SOB on exertion. FVC, FEV but
FEV/FVC, DL CO, restrictive pattern
Bronchogenic carcinoma (5 times risk, 14 times risk if smoker): most common
Mesotheliomas (1000 times risk) but still rare. See Types of Lung Cancer, page 88
Laryngeal and perhaps extrapulmonary neoplasms
When asking about occupational exposure, need to go back a long time. Will present in an older
man. Ask them what they did when they left school and go from there.
Pathogenesis: depends on which type of asbestos. Serpentine crysotile form (curly, flexible) is
more common, less dangerous, cleared more easily from bronchi and more soluble so don‟t persist
in the alveoli. Amphibole type (straight, stiff, brittle) rarer, more dangerous, go deeper, penetrate
epithelial cells and lodge in the interstitium
Coal Workers Pneumoconiosis (CWP):
Two forms:
Simple CWP: accumulation of dust laden macrophages with little pulmonary dysfunction
Complicated CWP: progressive fibrosis induced by macrophages
Macroscopic appearance: Anthracosis, coal nodules progressing to black scars larger than 2 cm in
complicated CWP
Microscopic appearance: Coal laden macrophages, fibrous scarring
Caplan‟s Syndrome: Rheumatoid arthritis with a pneumoconiosis nodular pulmonary lesions
Silicosis:
Exposure to crystalline silicon dioxide: sand blasting, rock mining, foundry work
Silica causes activation and release of inflammatory factors by macrophages
Morphology: discrete pale to black tiny nodules which coalesce into fibrous scars
Hypersensitivity Pneumonia
= Extrinsic Allergic Alveolitis
Sometimes grouped with Pneumoconioses Occupational Lung Disease
Immune resistance to protein antigens acute or chronic attacks on re-exposure
Lots of causes: farmer‟s lung (antigen is thermophilic actinomyces), pigeon breeder HSP, air-
conditioner HSP
Morphology: chronic inflammatory cells in the alveolar septi, septal fibrosis, obliterative bronchiolitis
and non-necrotising granuloma formation (diagnostic on biopsy)
Honey Comb Lung
End stage of many chronic interstitial lung diseases
Morphology: small lungs with nodular pleural surface due to interstitial fibrosis retracting the pleura.
Large air spaces cause honeycomb effect. Destruction of the capillary bed in the lung pulmonary
hypertension, RV hypertrophy, cor pulmonale death
Sarcoidosis
Multisystem disorder, most common in the young and in females
Aetiology: ?antigenic stimulus cell mediated (type 4) immune injury
Pathogenesis: poorly understood. Deficient cell mediated immunity. Eg anergic to the TB skin test.
Stimulated B-cell population with resultant hyperglobulinaemia. ?Antigen T cells inducing B cells.
Monocytes recruited granuloma formation
Macroscopic appearance: Chest X-ray shows bilateral hilar lymphadenopathy and/or diffuse interstitial
disease. Granulomas also found in spleen, liver, bone marrow, skin, eye and salivary glands
Microscopic appearance: non-caseating (non-necrotic) granulomas (unlike TB). Occur in all organs but
most commonly in all parts of the lungs. Tightly clustered epithelioid histiocytes, multiple giant cells,
and a few peripheral lymphocytes
Clinical course: Treat with steroids. 70% recover, 20% have some loss of function, 10% die
86 4
th
and 5
th
Year Notes
Neoplasia of the Respiratory Tract
Cancer of the Nasal Cavity and Paranasal Sinuses
Inflammatory Polyp:
Not a true tumour: overgrowth of stromal tissue – no malignant potential
Common in adults, rare in children
Associated with cystic fibrosis
Sinonasal papilloma:
Benign. Can become malignant. 3% become malignant after removal (poor prognosis). 3% have
malignancy in polyp (prognosis better)
Usually in adult. Presents with nasal obstruction and painless epistaxis
?Associated with HPV 6 & 11
Sinonasal Carcinoma:
Occupational association: wood turners (adenocarcinoma) and nickel mining
Relatively rare (<1% of cancer deaths)
60% 5 year survival, surgical treatment
Squamous cell most common (look for keratin whirls), also adenocarcinoma
Stromal overgrowth = desmoplasia sign of invasive cancer
Nasopharyngeal Carcinoma:
Most common in SE Asia and N Africa, occurs in 15 – 25 and 60 – 69. Presents with epistaxis or
obstructed eustachian
No occupational association
Associated with EBV
Biphasic tumour: Small cells superimposed on squamous cell carcinoma, with lots of lymphocytes
(don‟t confuse with lymphoma)
Aggressive: early lymph node spread
Treatment: radiotherapy +/- surgery
Tumours of the Larynx
Benign non-neoplastic neck lumps:
Inflammatory:
Lymph nodes: anterior cervical for tonsillitis, jugular digastric for tongue
Atypical Tb (especially kids)
Deep Neck abscesses: para-pharyngeal or retro-pharyngeal abscesses (can track down into
mediastinum)
Thyroglossal cysts: cysts in embryological track from tongue to thyroid (usually at level of hyoid)
Branchial cysts: ?embryological. Like enlarged anterior node. Contain lots of cholesterol
Pharyngeal pouch: Mucosa herniates out through triangle between the cricopharyngeus and
thyropharyngeal muscles under pressure from swallowing when upper oesophageal sphincter
doesn‟t relax properly. Catches food, becomes infected. Treatment: surgery
Laryngeal Nodule:
Due to trauma of vocal chords banging together oedema (early) scarring/granulation tissue
(late)
Only on anterior 1/3
rd
of vocal fold
Completely benign
Gravely voice
Laryngeal Papilloma:
Like sinonasal papillomas
Most commonly seen in children
Associated with HPV 6, 11
Tendency to recur: can become unmanageable airway obstruction
Benign squamous overgrowth
Laryngeal Carcinoma:
Presentation:
Presenting early: if affect vocal chords, invade recurrent pharyngeal nerve, front of mouth
Presenting late: supraglottic lesions due to airway obstruction or pain ( deeper), sinus (lots
of space)
Dysphagia rare

Respiratory 87
90% are squamous cell carcinoma (like lung)
Mostly in males, smoking a major risk factor, also alcohol, radiation, family history, tend to be
older (> 50)
Classification, prognosis and treatment depends on site (prognosis also depends on stage):
Glottic: 60%, on chords, maintained in larynx by cartilage. Treatment: radiotherapy unless
spread through cartilage
Supraglottic: 30%, above chords, involves false chord. More aggressive, metastasise to
cervical lymph nodes
Transglottic: < 5%, crosses from one chord to another
Infraglottic < 5%, below chords, more aggressive
Don‟t usually metastasise elsewhere, but lymph node infiltration common
Treatment: radiotherapy ( dry mouth) +/- surgery (superficial, hemilaryngectomy, laryngectomy,
laryngectomy +/- radical neck resection. Chemo has little effect against SCC (most of them). If
laryngectomy then need a tracheostomy ( can‟t cough, infection, humidification, etc)
Lung Cancer
Smoking
1998 Statistics for NZ:
Adults
24%
Male
25%
Female
23%
Maori
44%
Maori Male
40%
Maori Female
47%
Cigarette smoking and lung cancer:
Relative risk is 10 times in regular smoker, 20 times in those smoking > 40 per day
Most important avoidable cause in 20 – 30% of cancers: including Respiratory tract, liver,
stomach, cervix
Tobacco and alcohol have a multiplicative relationship in oral cavity, throat and oesophagus
Fall in lung cancer mortality begins 5 – 9 years after quitting, back to baseline at 14 years
Abnormal cytology and squamous metaplasia in smokers
Passive smoking:
Passive smoking: relative risk is 3 times normal
Relationship to URTI in children
Possibility of younger children being affected e.g. SIDS
Children of smokers more likely to smoke
Active Smoking:
Demonstrates that knowledge/education is insufficient to ensure behaviour or behaviour change
Health promotion principles of acting at all levels (i.e. individual/community/government) to make
healthy behaviour the easy choice
Measurement: Pack-years = (cigarettes per day * years smoked) / 20
Smoking cessation:
Listen first: Why do you smoke? (If it‟s stress – what will you do in the future)
What do you know about risks (don‟t assume they know about risks – maybe information lack or
cognitive dissonance)
Estimate cost for them: what would you do with $2-3,000 per year
Give a positive message: do you want to live longer/better
Need to negotiate with patient: be smart not paternalistic, be realistic, honest
Always put smoking on problem list
Information: Quit Book or Can Quit (from cancer society). Quitline 0800 778 778
Epidemiology of Lung Cancer
Commonest cancer in the world
In New Zealand, leading cause of cancer death in men (23%, bowel 15%, prostate 14%) and third most
common in women. Maori women have the highest death rate from lung cancer of any female
population in the world
Males predominate. Females catching up
88 4
th
and 5
th
Year Notes
60% not resectable at the time of diagnosis
23% of all lung cancers are mixed
Smoking:
> 90% are caused by smoking and are therefore preventable
25% of lung cancer in non-smokers is due to passive smoking
Types according to smoking status:
% Smokers
% Non-smokers
Squamous Cell
98
2
Small Cell
99
1
Large Cell
93
7
Adenocarcinoma
82
18
Bronchioalveolar
70
30
Presentation and Survival:
Smokers
Non-smokers
Distant disease at presentation
> 50%
10%
Endocrine disorders
10 – 25%
5%
5 year survival
5%
17%
Relative incidence changing rapidly:
Squamous cell
Adenocarcinoma (now more common than squamous cell in most countries)
Bronchioalveolar carcinoma
Large cell constant
Presentation
Fatigue 84%
Cough 71%
Dyspnoea 59%
Anorexia 57%
Pain 48%
Haemoptysis 25%
Diagnosis
Cytology necessary for management. Use the least invasive route (eg FNA of a neck node if there is
one)
Sputum cytology
Bronchoscopy:
Can do washings, brushings, biopsy or lavage (to get more distal stuff)
If can‟t produce sputum sample, can nebulise with hypo-osmotic saline to induce sputum
1% of transbronchial biopsy haemorrhage or pneumonia
Fine Needle Aspiration (FNA): good for peripheral tumours
Types of Lung Cancer
Squamous Cell Carcinoma:
Most common form
Males > females, with age
Central tumour: presents late with invasion of lymph nodes
Can block airway distal pneumonia
Pathogenesis: BPDE in smoke binds p53 mutational hot spots mutation. Sequence of changes
from squamous metaplasia to dysplasia to carcinoma in situ to invasive carcinoma
Macroscopic: Arises in major bronchus, grey-white hard granular neoplasm, central cavitation in
large cancers, uninvolved lung shows smoking related pathology (eg emphysema)
Microscopic appearance: pink when stained (due to cytoplasm), keratin whirls and intracellular
bridges (diagnostic), band in central cytoplasm, large irregular nucleus, nuclear pleomorphism,
hyperchromatism (ie darker), coarse chromatin clumping, mitosis, large nucleoli, usually arranged
in sheets
Complications: metastatic disease to lymph nodes, brain, liver and adrenals
Overall five year survival 10%
Respiratory 89
Surgical treatment preferred: but may patients may have insufficient pulmonary reserve
Small Cell Carcinoma:
= „Oat cell‟ carcinoma
Central poor prognosis
Very aggressive
Treatment: chemotherapy +/- radiotherapy – not surgery as will have metastasised
Neuroendocrine origin
Pathogenesis: BPDE in smoke binds p53 mutational hot spots mutation
Macroscopic description: perihilar and surround large bronchi. Grey-white or haemorrhagic. May
be more extensive microscopically
Microscopic appearance: small cells, scant cytoplasm (blue when stained – predominantly nuclei),
ovoid, dense, hyperchromatic so nucleoli not usually seen, mitotically active, pleomorphic nuclei.
Fragile crushed causing blue streaks
Complications: metastatic disease to lymph nodes, brain, liver and adrenals
Two year survival 25%
Treatment: chemotherapy. Surgery useless unless palliative
Large cell carcinoma:
Undifferentiated (the „waste basket‟ category)
Central
White desmoplastic
Microscopic appearance: Can‟t tell cell of origin, contains giant cells, moderate amount of
cytoplasm
Quite aggressive
Adenocarcinoma:
Less common, Male = female
Occurs peripherally not centrally more easily respectable (unless into pleura – poor prognosis)
Less association with smoking
Association with previous scarring (eg Tb)
Microscopic appearance: looks like it‟s trying to form glands, ascini, desmoplastic stroma
Bronchioalveolar carcinoma:
Distinctive variant of adenocarcinoma
Slowly crawls along bronchioles
Good 5 year survival but poor prognosis: drown in mucin
Type of adenocarcinoma
Carcinoid tumour:
Low grade tumour derived from neuroendocrine cells
Occurs younger (mean is 45) than the more frequent bronchogeneic carcinomas
Occur in lung, bowel, other sites
90% Central types: 70% survive 5 years
10% Peripheral types: rarely metastasise
Look like oat cell, but behave very differently. Grows by expansion rather than infiltration
Mesothelioma:
Primary pleural tumours, including benign and malignant (also tumours of the peritoneum, tunica
vaginalis and pericardium)
Benign mesothelioma does not produce pleural effusion and has no relationship to asbestos
Malignant mesotheliomas arise in either visceral or parietal pleura, produce pleural effusion (can
be unilateral) and are related to asbestos. Drain effusion and re-xray (looking for lumpy pleura).
Do cytology on fluid. Invades lung and often other thoracic structures. Presents in 5
th
to 7
th
decade, with lag after exposure of > 20 years. Diagnosis by imaging and biopsy. Poor prognosis.
See Pneumoconioses, page 85.
Adenosquamous carcinoma: rarer tumour with squamous and glandular features. Aggressive, bulky,
peripheral tumour
Pancoast tumour/syndrome: lung cancer (usually squamous) in the apex extending to supraclavicular
nodes and involving 8
th
cervical and 1
st
and 2
nd
thoracic nerves shoulder pain radiating in ulnar
distribution. May also involve cervical sympathetic nerves and cause Horner‟s Syndrome (ipsilateral
enophthalmos – sunken eye, ptosis, miosis and dry skin)
Systemic Effects of Lung Carcinoma
Often the presenting problem:
90 4
th
and 5
th
Year Notes
Type
Effect
Squamous cell carcinoma
Hyperparathyroidism (PTH) ( Ca which may
arrhythmias)
Small Cell Carcinoma
Cushing‟s Syndrome (ACTH)
Carcinoid Syndrome
Hyponatraemia (ADH)
Neuropathy and Psychosis (may be due to neurotransmitter)
All Types
Gynaecomastia (HCG) in many poorly differentiated
cancers
Prognosis
No improvement in last 40 years
5 year survival for all cases 13%
Prognostic factors:
Stage: most important factor
Age < 40 worse (diagnosed late)
Gender: female worse (diagnosed late)
Site
Size > 6 cm worse
Staging:
Critical to prognosis and treatment decisions
Staging systems are regularly refined
TNM system (not usually used for Small Cell as these have usually metastasised by diagnosis):
T: Size and invasion
N: which mediastinal nodes are involved
M: no metastases or metastases present
TNMs are grouped to give stage groups ranging from IA to IV
Treatment
Significant difference between Non-small cell and Small cell:
Non-small Cell:
Resection is the gold standard, but only 20% have resectable disease at diagnosis. Surgical
studies are highly selected and not representative of the general population
Majority will require radiotherapy. Usually palliative, (eg for haemoptysis, pain or dyspnoea)
can also be radical or adjuvant
Chemotherapy: not used much in NZ, standard treatment in the US. Cost a factor in newer
agents. Myriad of dosing regimes, combinations, etc. Can be used prior to
surgery/radiotherapy to control micro-metastases/improve operability, or palliatively.
Cisplatin and Etoposide are the gold standards amongst the older agents
Small Cell:
70 – 80% have metastasised at diagnosis
Very rapid doubling time
No place for surgery
Mainly managed with chemo +/- radiotherapy (makes a dismal outlook a bit better)
Sleep Apnoea
See also:
Treatment of Insomnia, page 534 for Treatment of Insomnia
See also Tiredness, page 6
Sleepiness
Varies according to circadian cycle: two sleep gates each day, 2 – 3 pm and 10 – 11 pm (correlates with
melatoin)
Obstructive sleep apnoea is the most common cause of excessive sleepiness. MVA (driving drowsy
is the same as driving drunk)
Causes of day time sleepiness:
Insufficient sleep (eg sleep restriction)
Obstructive sleep apnoea
Respiratory 91
Central sleep apnoea: absent or diminished ventilatory drive. Variety of causes including
neuromuscular and chest wall deformities
Cheyne-Stokes Respiration: usually with advanced heart failure. Destabilisation of respiratory
control centres
Upper airway resistance syndrome (no actual apnoea)
Periodic limb movements in sleep (PLMS: associated with restless leg syndrome) fragmented
sleep. Also hot legs at night, cramps. Occurs in renal failure and anaemia. Treatment: codeine or
anti-Parkinson drugs
Narcolepsy: Normal sleep at night and frequently going to sleep during the day. (Sleep study
looks at daytime napping more than nighttime). Goes into REM sleep early. Equivalent to 48
hours sleep deprivation, vivid dreams (hypnogogic hallucinations), HLA linkage, affects young,
twice as common as MS. Can also be complicated by cataplexy (sudden loss of muscle tone in
response to emotional stimuli). Treatment: stimulants during the day
Idiopathic hypersomnolence
Drugs: alcohol, sedatives
Psychiatric
Hypothyroid
Anaemia
Normal breathing:
Inspiration: uses Genioglossus and other muscles to dilate trachea, and intercostals and diaphragm
to create negative pleural pressure
Expiration: much more passive
Normal changes during sleep:
Carotid bodies much less sensitive to CO2 and O2
Intercostal & accessory muscle tone
tidal volume ventilation PCO2 by 5 mmHg HR, flushed, warm periphery
Obstructive Sleep Apnoea Syndrome
Pathogenesis: muscle tone + anatomical factors (eg obese) + neural factors (eg stroke) upper
airway narrows apnoea due to collapse arousal impairment overtime of sensitivity to daytime
PCO2
Epidemiology:
Prevalence = 4% of adult population
More common in:
Men and post-menopausal women
Middle age
In kids with facio-cranial syndromes
Short jaw
Alcohol users
Over weight
Symptoms: Loud snoring, apnoea, daytime tiredness, early morning headache
History questions:
When do you go to bed and when do you get up (sleep restriction)
Do you snore, in any posture (the norm with OSAS). Need witness accounts
Do you feel refreshed on waking
Where do you fall asleep (normal places but more often)
Other medical conditions: depression, anaemia, hypothyroidism, etc
Medications and when do you take them: can keep awake at night or make you sleepy during the
day
Consequences:
concentration, memory, accident risk, libido, premature mortality, hypertension, MI, CVA,
precipitate respiratory failure in mild CORD
In kids: less apnoea (if there is apnoea then ?SIDS/epilepsy), more noisy breathing/restlessness,
wake a lot at night, hyperactive during the day, growth delay (GH secretion due to slow wave
sleep)
Diagnosis requires sleep study Polysomnography. Measures muscle movements, airflows, O2 and
CO2, EEG waves, eye movements, ECG etc during sleep
92 4
th
and 5
th
Year Notes
Treatment:
Conservative:
Weight loss (did it start with weight gain?), smoke reduction, sleep posture modification
Nasal CPAP for moderate/severe: air splint prevents airway collapse through whole breath
cycle. Need to titrate pressure
Treat allergic rhinitis
Medication: Sleeping pills make it worse – stop them
Dental devices
Surgery:
Kids – tonsils and adenoids.
Adults:
Mandibular advancement
Gastric bypass weight
Tracheostomy
Uvulopalatopharygnoplasty (UPPP) – but doesn‟t deal with all sites of occlusion and stops
CPAP working
Miscellaneous Lung Diseases
Goodpastures Syndrome (= Antibasement Membrane Antibody Disease – ABMA):
Simultaneous rapidly progressive glomerulonephritis and haemorrhagic pneumonitis
Present with renal failure and haemoptysis
Due to anti-basement membrane antibodies deposited along alveolar walls and in glomeruli (type
II immune reaction)
Usually occurs in young men, treated with steroids and cytotoxic drugs
See also Goodpasture‟s Syndrome, page 214
Alveolar Proteinosis: Peripheral alveoli filled with pink, granular, acellular material. No treatment,
variable course, clears in a few years. Prone to infection so steroids worsen the condition by depressing
the immune system. Bronchial lavage effective in acute episodes
A number of vasculitis affect the lung. Eg Wegner‟s granulomatosis, allergic angiitis and
granulomatosis. Also collagen diseases such as SLE and Rheumatoid arthritis
Pulmonary Hamartoma: benign localised proliferation of normal tissue components (hyaline cartilage
with respiratory epithelium, maybe fibrous tissue, fat, blood vessels). Usually found as incidental
findings on X-ray
Primary Pulmonary Hypertension: rare, usually in young women. Usually secondary to COPD,
congenital or acquired heart disease, etc
Langerhans cell: diagnostic cell seen in eosinophilic granuloma. = histiocytosis X and pulmonary
eosinophilic granuloma. A large histiocyte with one bland folded nucleus, abundant eosinophilic
cytoplasm with indistinct cell borders. Proliferative disorder of histiocytes. X-rays show multiple
nodules scattered through both lungs
Langhans giant cell: (not the same as Langerhans cell) multinucleated giant cell in granulomas, with
nuclei arranged around the periphery of the cell in a horseshoe pattern
Sequestration:
Extralobular: Congenital. Mass of lung tissue not connected to bronchial tree and outside the
visceral pleura
Intralobar sequestration: usually acquired. Within the visceral pleura but not connected to the
bronchial tree
Differential of Solitary lung nodule:
Tumour: benign (bronchial adenoma or pulmonary hamartoma) or malignant
Tb
Sarcoidosis
Other granuloma: eg fungal
Haematoma (ie blood clot, eg in cavity following lung contusion)

Endocrine and Electrolytes 93
Endocrine and Electrolytes
History .............................................................. 94
Diabetes Mellitus ............................................. 94
Thyroid ............................................................. 97
Hyperthyroidism ......................................... 98
Hypothyroidism .......................................... 99
Thyroid Nodules ....................................... 100
Parathyroid ..................................................... 101
Adrenal Cortex ............................................... 102
Cushing‟s Syndrome ................................. 102
Hypoadrenalism ........................................ 103
Hyperaldosteronism .................................. 104
Phaeochromocytoma ................................ 104
Pituitary Gland ............................................... 104
Hypopituitarism ........................................ 105
Pituitary Tumours ..................................... 106
Prolactinaemia .......................................... 106
Acromegaly .............................................. 107
Other Endocrine Problems ............................. 107
Electrolytes ..................................................... 107
Sodium Summary ..................................... 107
Hyponatraemia ......................................... 108
Hypernatraemia ........................................ 110
Diabetes Insipidous................................... 110
Potassium .................................................. 111
Calcium..................................................... 112
Magnesium * ............................................ 113
Chloride .................................................... 113
Acid-Base balance .................................... 113
94 4
th
and 5
th
Year Notes
History
Symptoms widespread and often insidious
Enquire about previous endocrine gland problems, surgery, etc
Major symptoms:
Changes in appetite and weight:
Appetite
Appetite
Weight
Cushing‟s Syndrome, hypoglycaemia,
hypothalamic disease
Hypothyroidism
Weight
Thyrotoxicosis, uncontrolled DM
Adrenal insufficiency (also GI
causes and malignancy)
Bowel:
Diarrhoea hyperthyroidism or adrenal insufficiency
Constipation hypothyroidism or hypercalcaemia
Sweating: hyperthyroidism, phaeochromocytoma, hypoglycaemia, acromegaly (also anxiety and
menopause)
Subcutaneous thinning: either androgens (old men and post-menopausal women) or Cortisol
Amenorrhoea: PRL (by only a little), Cortisol (takes bigger increase), hyperthyroidism
Nocturia: ADH, or Diabetes from insulin, cortisol or GH
Diabetes Mellitus
Diagnosis of diabetes
1999 criteria (ie textbooks out of date):
For Diabetes:
Fasting Blood glucose
2 hours post glucose tolerance test
Diabetes (one or the other)
> 7.0 (was 7.8) mmol/l
> 11.1 mmol/l
Impaired Glucose
Tolerance: IGT
< 7.0
7.8 – 11.1
Impaired Fasting
Glycaemia: IFG
(New category)
6.1 – 6.9
< 7.8
For Gestational Diabetes:
Screening: at 28 weeks, non-fasting glucose load of 50g. If >= 7.8 should have gestational
glucose tolerance test
Gestational Glucose tolerance test: 75 g load when fasting. Fasting level >= 5.5 OR 1 hour
post glucose load of >= 11 OR 2 hour post glucose load of >= 8.5 (some say 9.0)
gestational diabetes.
1 – 3 % of pregnancies have gestational diabetes
Suggested regime for Screening for type 2 diabetes (Screening for type 2 diabetes, NZMJ 26 April
2002)
Test if > 5% of diabetes Europeans over 50 and non-Europeans > 40 years of age
Yearly screening for anyone found to have IGT or IFG
Best to test with morning fasting glucose – although use random test with caution if conditions
approach fasting or post-glucose load conditions
Finger prick testing not accurate enough
HBA1c not recommended for screening: different methods for testing and different normal ranges
IDDM – Type 1 (Juvenile Onset Diabetes)
A chronic, progressive autoimmune process in genetically susceptible people, triggered by
environmental factors
Eventually cannot survive without insulin treatment. Ketoacidosis will develop unless insulin given (if
any endogenous insulin then no ketones)
Incidence up to 20 yrs: 10 – 15/100,000
Prevalence: 0.25 – 3 % (10 – 15% of all diabetics)
Endocrine and Electrolytes 95
Peak age of incidence is 12 – but can present at any age (even after 40). Surges in presentation at 3- 4,
starting school. ?Viral exposure
85 – 90% have no family history, but family history confers risk
Antibodies:
Islet Cell Antibodies: risk of IDDM with level of ICA. Frequency in newly diagnosed IDDM
is 65 – 85%. Frequency in population is < 0.5%
GAD (glutamic acid decarboxylase) antibodies: mildly specific antigenic enzyme released from
islet cells when destroyed. Can test for these in prodromal stage
Insulin autoantibodies
Acute presentation: hyperglycaemia (polyuria when glucose > 10 mmol/l, thirst, polydypsia), tiredness,
weight loss. Also cramps, blurred vision, superficial infections. Ketoacidosis (now rare) also has
nausea, vomiting, and drowsiness
Kids presenting with mild hyperglycaemia: don‟t know if they will become IDDM or are MODY
(Maturity Onset Diabetes Of The Young – ie Type 2). So when start insulin replacement back titrate
(after stabilised) – type 1 may have honeymoon period until no endogenous insulin
Currently being investigated for prevention in high risk individuals (ie have antibodies but not frank
disease):
Cow‟s milk avoidance until 6 months of age
Early oral insulin therapy autoimmune modulation
Nicotinamide (vitamin B) supplementation
Treatment goals: stable blood sugar, prevent/monitor complications, promote normal growth and
development, maintenance of normal weight
Investigations for both Type 1 and Type 2 Diabetes
Glucose testing
HbA1C. Any reduction worthwhile. Target is <= 7.0. Not all willing or able to achieve this
Ketonuria
24 hour urine and measure C-peptide: a by-product of insulin production (have they any endogenous
insulin – as long as replacement insulin hasn‟t islet cell atrophy)
Fundoscopy
Lipids
BP: want diastolic < 85 and systolic < 135 (especially for young or existing microalbuminuria)
Microalbuminuria:
Nephropathy has two phases:
Normal blood pressure, creatinine, and urines but microalbuminuria.
Overt neuropathy: proteinuria, hypertension, creatinine and GRF
Normal level < 20 mg/24 hours. Microalbuminuria = 30 – 300 mg/24 hours. Dipsticks detect >
150 g/l (ie insensitive)
Microalbuminuria hard to test (needs 24 hr urine). So use albumin : creatinine ratio. Normal < 2.8
in men, < 4.5 in females in random test
If abnormal result then patients qualify for statins with cholesterol > 6 (normal threshold > 9)
See Diabetic Nephropathy, page 207
Complications
Microvascular disease:
Due to thickened walls and laying down of advanced end glycosylation products
Eye disease: mainly retinopathy. After 30 years 80% have background retinopathy and 7 – 8% are
blind (see Focal Ischaemic Retinal Disease, page 145). Also Sorbitol cataracts.
Nephropathy
Neuropathy: peripheral and autonomic
Macrovascular disease:
Coronary heart disease. Male diabetics have 2 times risk, females 4 times risk. Very high risk if
other risks present (eg BP, lipids, smoking etc)
Accelerated atherosclerosis (but lesions look the same)
Kidney disease:
See also Diabetic Nephropathy, page 207
Onset of diabetes leads to:
Functional changes: GFR, Reversible albuminuria
Structural changes: GBM thickening, mesangial expansion
96 4
th
and 5
th
Year Notes
After 30 years, 30 – 40% have nephropathy. Unlikely if hasn‟t developed after 30 years (?some
protective factors)
Glomerular damage:
Nodular glomerulosclerosis. Acellular hyaline material (Kimmelstiel-Wilson Lesion): BM
proliferates (ie collagen expansion of mesangial matrix) sclerosed and fibrotic due to
fibroblast infiltration chronic renal failure. Earliest sign is microalbuminuria, due to pores
getting bigger
Diffuse glomerulo-sclerosis: glomerular loop obstruction necrosis (seen in hypertension or
any end-stage renal disease)
Papillary necrosis: least blood supply susceptible to ischaemia
Also pyelonephritis and reflux lead to kidney damage
Immune deficiency: White cells affected when glucose > 14 mmol/l
Neuropathy:
Glycosylation of nerve
Demyelination of nerve due to sorbitol accumulation in Scwhann cells slowed conduction
Peripheral sensory AND motor neuropathy (eg foot deformity, fallen arches)
Autonomic neuropathy leads to bladder problems, impotence, gastroenteropathy
Diabetic foot
Special management in surgery, pregnancy and in intercurrent illness
Management of Diabetic Ketoacidosis or Hyperglycaemia
Diabetic Ketoacidosis:
Signs: nausea, vomiting, thirst, abdominal pain, delirium, coma, acetone fetor, hypotension,
tachycardia, metabolic acidosis (Kussmaul breathing), hyperosmolality
Treatment:
ABC, oxygen
IV crystalloid: may need 4 – 6 L. Will be severely dehydrated due to osmotic diuresis. Use
normal saline, and reduce to hypotonic fluid once rehydrated and glucose < 15 mmol/l or if Na
> 150 mmol/l
Potassium 20 mmol in first 6 hours then 10 mmol/hr according to plasma levels. If plasma K
high then delay adding K until this has normalised
Insulin: actrapid 10 – 20 units. Resistance to insulin may suggest sepsis, insulin antibodies
Monitor acidosis. May need HCO3
Ongoing Management of Diabetes:
Acute symptoms are main reason for seeking treatment. But good control is more than just
keeping out of trouble. Involves significant education
For Impaired Glucose tolerance and Impaired fasting glucose: lifestyle change and monitoring
Diet: Saturated fats, low glycaemic index foods (sugar presented slower to liver, able to convert
more to glycogen). Space out CHO more evenly throughout the day. If normal BMI and NIDDM
try fats and CHO may insulin release (BMI ~ level of insulin resistance)
Warn about effects on blood sugars of another illness (eg „flu) blood sugars. Requires more
regular monitoring. Don‟t just stop taking insulin if not eating.
Insulin:
Use fast acting for glucose peaks following meals, and long acting for basal rate ( suppress
gluconeogenesis overnight, etc)
Conventional regime: twice daily with both fast and long acting
Intensive regime: fast acting before each meal and long acting at night (= 4 jabs a day)
Diabetes Complications Control Trial (1993) examined 1441 volunteers (ie motivated) in two
groups: conventional treatment (insulin once or twice daily) and intensive (3 or 4 times daily).
Intensive therapy reduced risk in all categories, but hypoglycaemia and some weight gain
Biguanides: eg metformin. Insulin sensitivity, gluconeogenesis, won‟t hypoglycaemia.
Nausea, vomiting, B12 malabsorption. Not in hepatic and renal disease or pregnancy. Not in
hypoxic lung disease or cardiac disease
Sulphonylureas: insulin release from -islet cells (must have some left for it to work),
gluconeogenesis and glycogenolysis. Can hypoglycaemia. Nausea, vomiting. Not in hepatic
and renal disease or pregnancy.
Monitoring: HbA1C (normal < 6.5), daily blood sugars (before breakfast)

Endocrine and Electrolytes 97
Examples:
Case
Age
BMI
Fasting Gl
Post-prandial Gl
Ketones
Symptoms
1
50
35
6.5
12
-
-
2
50
35
12
14
-
Nocturia
3
50
25
12
14
-
-
4
50
18
12
14
+
Weight loss
Case 1: Has more insulin than case 2 (insulin resistance is proportional to BMI, but her glucose is
lower more insulin) earlier presentation than case 2. Treatment: diet + metformin (can
diarrhoea secondary to malabsorption). If very overweight, check LFT
Case 2: pancreas starting to fail
Case 3: Weight loss may not do much. Are they CHO deficient (CHO insulin release)? May
start with sulphonylureas. May need insulin sooner
Case 4: Type 1/IDDM. Will be catabolic – need protein. Quick test with sulphonylureas but will
need insulin at earlier stage
Thyroid
Assessment
Clinical
Biochemical
The gland itself: enlarged, smooth, nodules, tender, etc
Specific features: eg autoimmune (exophthalmos) or pituitary disease
Physiology
TRH (hypothalamus) TSH (anterior pituitary) T3 and T4 (thyroxine peripherally converted to
T3)
T3 & T4 stored in thyroid follicles as thyroglobulin
T3 exerts greater negative feedback on the pituitary. Only takes a 10% rise in fT4 to suppress TSH
T3 is considerably more metabolically active (ie potent) than T4
Liver converts T4 T3, as does kidney and muscle
T4 goes down first in hypothyroid. Only measure T3 in hyperthyroid (as it drives symptoms)
Bound in plasma to thyroid binding globulin
Intercurrent illness: fT4 rises (liver stops converting T4 to T3 straight away – want to be catabolic) then
T4 falls to subnormal levels as thyroid production slows. FT3 falls from onset. TSH slowly falls to
subnormal levels with severe illness. (ie similar pattern to hypopituitarism)
Goitre
Normal gland weighs about 30 g
Nodular or diffuse?
Can be hyper, eu, or hypo-thyroid
Check size, shape, consistency, mobility
Check for dysphagia, stridor, laryngeal nerve palsy (especially multinodular)
Thyroid Tests
Free T4 and T3
Plasma T4 (= bound T4 + free T4). False high in pregnancy, oestrogens (TBG). False lows in
NSAID, phenytoin, steroids, TBG deficiency
Plasma TSH: Newer sensitive test means low levels can be measured don‟t do TRH anymore
If low T3 and T4 and normal TSH ?pituitary failure
Thyroid isotope scanning: to look for hot spots or cold spots
Thyroid antibodies: raised in Hashimoto‟s and some Graves
TRH test: Inject to test thyroid. If minimal increase in TSH then: Hyperthyroidism, multinodular
goitre, thyroxine replacement, euthyroid Graves disease, autonomous thyroid nodule
Thyroid imaging
Can use nuclear medicine, ultrasound (little routine use – can guide FNA), CT (not for intra-thyroid
lesions but demonstrates extension and mass effects) or MRI. Only when suspicion of significant
pathology
98 4
th
and 5
th
Year Notes
Before scanning thyroid (with 99MTc pertechnetate), stop Iodine supplements (eg kelp), thyroxine, and
angiography (contrast contains Iodine). Gland must be „hungry‟
Normal uptake is 1 - 3 %. If it takes up too much then hyperthyroid
If diffuse uptake then Grave's. If multinodular then:
Cold nodules: 80% are cysts or regressive nodules. 20% are malignant. FNA
Hot nodules: maybe with decompensation in rest of gland (uptake due to TSH)
Thyroid Eye Disease
Retro-orbital inflammation and lymphocyte infiltration. May optic nerve compression ( colour
desaturation and acuity). Does not parallel degree of toxicosis
At presentation, patient may be euthyroid, hypothyroid or hyperthyroid
Management: Early referral. Check for keratitis with Rose Bengal eye-drops. Lubricant eye drops.
Systemic steroids. Surgical and other treatments
Hyperthyroidism
Symptoms: weight, appetite, frequent stools, tremor, irritability, hot intolerance, sweating,
oligomenorrhoea, infertility
Signs: Tachycardia, AF, warm peripheries, thyroid enlargement or nodules
Additional signs in Grave‟s disease: exophthalmos (bulging eyes), lid lag (lid lags eye when following
your finger descending slowly), vitiligo (growing patches of skin depigmentation due to
melanocytes), Pretibial Myxoedema (due to amyloid)
Tests:
Progression:
TSH is suppressed first, while fT3 and fT4 normal TSH is the most sensitive test.
Suppresses with minor changes in fT4
fT3 rises next mild symptoms
fT4 rises last severe symptoms
Screening: fT4 and TSH
Severity: fT4 and fT3
Thyroid microsomal and thyroglobulin antibodies (only present in 80% of Graves at presentation)
If goitre, ultrasound, thyroid scan
Test visual fields, acuity and eye movements. Referral if positive. Steroids to reduce swelling
Causes:
Grave‟s disease: F:M = 9:1.
Most common when < 50 ( multinodular goitre as you get older)
Probably results from Autoantibodies against TSH receptors. Check for hTSABs (human
Thyroid stimulating antibodies)
May cause normochromic, normocytic anaemia, ESR, calcium, abnormal LFTs
Histology: large hyperchromatic nuclei, retracted thyroglobulin. Follicles same as in follicular
carcinoma but carcinoma shows invasion of blood vessels
Toxic adenoma (= Plummer‟s Disease, Thyroid autonomy): a nodule producing T3 or T4 hot
spot on scan
Subacute Thyroiditis:
= De Quervain‟s Disease. Usually resolves in 3 – 6 months. If rapidly destructive then acute
thyroiditis
= Inflammation of the thyroid secondary to:
Pregnancy: autoimmune. Gland may not be tender
Infection: coxaxyvirus and mumps. Tender gland
Goitre (often painful). Usually self-limiting
If severe, then 3 phases:
Prodromal: may be 4 – 6 weeks longs
Hyperthyroid: Release of preformed T3 and T4. TSH low. If very bad, fT4 will be 100
(normal = 10 – 24). ESR in parallel with T4
Hypothyroid/regenerating: For 2 weeks – 2 months. In proportion to severity of
hyperthyroid phase. T3 and T4 will go very low (?gland exhausted), TSH will remain
depressed for a while longer (ie resembles secondary failure)
Doesn‟t respond to carbimazole as it‟s releasing preformed hormone. Carbimazole stops
formation of hormone. If mild then wait. If severe, then antagonise peripheral effects (eg
propranolol). Steroids work but prolong illness
Endocrine and Electrolytes 99
Histology:
Neutrophils attack cuboidal epithelium (acute inflammation)
Thyroglobulin leaks out granuloma formation
Resolution
Post-partum thyroiditis: hyper or hypo thyroid. Hypothyroid may persist
Other: Toxic Multinodular Goitre, self medication (T4 but T3), follicular carcinoma of thyroid
Treatment:
Drugs: Thyourylenes: Carbimazole (40 mg/day PO for 4 weeks, then reducing every 1 – 2 months,
withdraw after 18 months, 50% relapse) – or try block and replace strategy (ongoing carbimazole
and replacement T4), propylthiouracil. Risk of agranulocytosis with Carbimazole and
propylthiouracil
Toxic multi-nodular goitre and toxic adenoma unlikely to remit following drugs
Partial thyroidectomy: risk to recurrent laryngeal and parathyroids. May be hypo or hyper post
surgery
Radioactive iodine (I131): will ultimately become hypothyroid
Hypothyroidism
= Myxoedema if severe
Signs and symptoms:
Symptoms: Unhappy, no spark, weight, constipation, cold intolerance, menorrhagia (excessive
menstruation, T3 oestrogen breakdown), lethargy, depression, dementia, sleep. Symptoms
insidious and subtle (T3 receptors in nuclei of nearly all cells – govern metabolism, modulation of
other hormones, O2 consumption, regulation of protein synthesis, etc, etc)
Signs: bradycardia, dry skin and hair, goitre
Signs of myxoedema (hydration of subcutaneous tissue): non-pitting oedema (eyelids, hands,
feet), yellowing of skin (myxoedema absorbs carotene. Sclera unaffected), thickened tissues, voice
change (oedema in vocal chords), hirsutism, carpal tunnel syndrome
If severe: slow, slurred speech (swollen tongue, slow thought), intention tremour (cerebellar
effects), muscle weakness and pain, deafness (reverses with treatment), paranoid ideation,
agitation, coarser hair, hair stops growing but no diffuse hair loss, slowly relaxing reflexes
(contraction normal, relaxation slow – not specific to hypothyroidism), plethora (deep red cheeks),
hypotension, ADH release hyponatraemia, normocytic normochromic anaemia, but no
neuropathy (except secondary to, say, carpel tunnel)
Myxoedema coma: presents in coma with history of above symptoms. Exclude: alcoholism,
epilepsy, diabetes mellitus, use of sedative medication, or clear suggestion of a fall predisposing to
a subdural haematoma. With myxoedema may find pleural effusion, ascites, myocardial oedema
( arrhythmias), no focal neuropathies (unless concurrent CVA), possibly hypoglycaemia
Progression of primary hypothyroidism:
Normal TSH is 0.35 – 5.3
Prodromal hypothyroidism:
TSH 4.0 – 10.
fT4 usually still normal. fT3 up marginally (failing gland proportion of T3)
Partial hypothyroidism:
Early symptoms
TSH > 10 – 15
fT3 and fT4 falling, but may still be normal. fT3 falls later than fT4
Severe:
With time develop myxoedema
TSH > 60. fT4 < 6.0
Diagnosis:
Screening and severity: fT4 and TSH
Primary: TSH rises with minor changes in fT4 (before clinical features).
Secondary (rare): Test fT4. TSH remains in normal range but is inappropriately low for the fT4
level
Thyroid antibodies: almost all have positive antibodies at diagnosis
Thyroid scan not indicated
Normochromic macrocytic anaemia
Causes:
Spontaneous (autoimmune)
100 4
th
and 5
th
Year Notes
Hashimoto‟s Thyroiditis: autoimmune disease, lymphocyte and plasma cell infiltration.
Goitre. Usually older women. Often euthyroid + goitre. Invasion of polyclonal lymphocytes.
Have oncocytes (cells with mitochondria)
Spontaneous primary atrophic hypothyroidism. Autoimmune, = Hashimoto‟s without the
goitre, associated with IDDM, Addison‟s and Pernicious anaemia. F:M = 6: 1
Woody Thyroiditis (Riedel‟s Thyroiditis): fibrous replacement of the thyroid
Iatrogenic:
Following thyroidectomy and radio-iodine treatment
Drug induced: eg amiodarone ( hypo or hyper), lithium, iodine in expectorants
Not deep x-ray treatment to face and neck (does lead to nodular goitre),
Juvenile:
Dyshormonogenesis: eg partial deficiency of peroxidase gland hyperplasia restore
deficiency. Expect: mild TSH, goitre and mildly hypothyroid
Agenesis/sublingual thyroid
Di George Syndrome. Absent thymus, hypoplasia of parathyroid blands, lymphopenia
TSH deficiency: isolated, panhypopituitarism, hypothalamic disease
1% of Grave‟s go onto hypothyroidism
Iodine deficiency
High doses of iodine (eg ask about kelp)
Treatment:
Thyroxine. Takes 4 – 5 days to have any impact (ie not useful acutely). Review after 12 weeks.
Adjust dose to keep TSH < 5 mu/L. T½ = 7 days so adjusting dose takes long time
Note: hypothyroid slow drug metabolism
If pre-existing heart disease, introduce very slowly. Consider propranolol
Thyroid Nodules
Are common (occur in 10 – 60% depending on definition) but clinical malignancy is rare (2 –
10/100,000/year)
Evaluation:
Presents with lump in lower neck
Age: young with nodules more likely to be cancer
Gender: Females have more nodules, male‟s nodule more likely to be cancer
Risk factors: radiation, family history, large solitary nodule bigger risk than many small ones
Symptoms:
Systemic: weight and appetite, night sweats
Local: pain, stridor
Tests:
Usually normal thyroid function
Tumour markers: thyroglobulin, calcitonin
Imaging: Not specific: Cold spots – can be cancer but also normal. Hot spots unlikely to be
cancer
US
FNA best
Benign types:
Haemorrhage into a thyroid cyst: painful and instantly palpable
Adenoma: always follicular, encapsulated, universally benign. Usually cold on scan, may be hot
Malignant:
Papillary Thyroid Cancer:
60% of carcinomas
Have papillary (finger like) architecture with fibro vascular core
Metastasises to lymph nodes
May also have calcified bits Psammoma Bodies (also found in meningiomas, serous
cystadenoma of the ovary)
Prognosis: If extra-thyroid lesions then 62% survival @ 15 years
Follicular carcinoma: rarely multifocal, capsular invasion, metastasises via blood vessels. If gross
invasion then 50% survival at 6 years. Hard to differentiate from adenoma on FNA
Anaplastic (undifferentiated carcinoma): highly malignant, old age, poor prognosis
Endocrine and Electrolytes 101
Medullary/C Cell carcinoma: parafollicular cells (serum calcitonin). Usually part of Multiple
Endocrine Neoplasia Syndrome (MEN)
Treatment: near total thyroidectomy. If staging indicates high risk then radioiodine for remnant
ablation
Also lymphoma
Multinodular Goitre:
With time, all thyroids have:
Anatomical heterogeneity: cold/fibrosed regions, hyperplasia, calcification, etc
Functional heterogeneity: various degrees of autonomy
If pronounced, then multinodular goitre:
Can be substantially enlarged with cystic appearance
Growth may haemorrhage tender
Treatment: Cut it out or thyroxine (slows it down)
In addition to a tumour, a single nodule may be:
A hyperplastic nodule (ie physiological)
Multinodular goitre with a prominent nodule
Thyroglossal duct cysts (see Cervical Lumps, page 648)
Parathyroid
Calcium metabolism:
Hyperparathyroidism:
Primary: PTH Ca2+.
Usually detected as incidental finding. If symptoms: pain/fracture, renal stones, constipation,
abdominal pain, depression. Also maybe dehydration, BP, thirst, nocturia, stuff joints,
myopathy
Associations: endocrine neoplasia (eg pancreas, pituitary, phaeochromocytoma and thyroid)
Causes: Single (90%) or multiple adenoma, carcinoma, hyperplasia
Tests: Ca, PO4 (unless renal failure), ALP, PTH raised or normal. CXR for „pepper pot
skull‟ and pelvis
Treatment: surgery
Ca from
osteoclast
activity,
ALP
Parathryoid Gland
Ca
PTH
Kidney
Liver
Gut
Bone
Ca, PO4
PO4 (reabsorption)
7-hydrocholestrol
Sunlight
D3 – also absorbed as fat
soluble vitamin
25,OH D3
Enzyme: 1-hydroxylase
1,25(OH)2D3

102 4
th
and 5
th
Year Notes
PTH related protein (PTHrH): produced by some tumours – causes some of the hypercalcaemia
seen in malignancy
Secondary Hyperparathyroidism: Ca PTH. Causes: Vitamin D and chronic renal failure
(see 210 – complications of chronic renal failure)
Tertiary Hyperparathyroidism: continued secretion of PTH after prolonged secondary hyperPTH
Hypoparathryoidism:
Primary HypoPTH. Eg after neck surgery. Ca and PO4, normal ALP. Associations with
pernicious anaemia, Addison‟s, hypothyroidism, hypogonadism
PseudohypoPTH: Failure of target cell response to PTH. Round face, short metacarpals and
metatarsals
Adrenal Cortex
Produces:
Glucocorticoids: eg Cortisol - affects CHO, protein and lipid metabolism
Mineralocorticoids eg aldosterone
Androgens and oestrogens
Cortisol:
Corticotrophin releasing factor (CRF from the hypothalamus) ACTH (from pituitary)
Cortisol
Postulated that Cortisol inhibits a general or uncontrolled inflammatory response to tissue damage
following insult. Raised in trauma, infection, severe psychiatric disease
ACTH production is inhibited potently by Betamethasone and Dexamethasone, Prednisone has
intermediate potency and hydrocortisone (ie cortisol) has the lowest potency of these agents
Cortisol is excreted as urinary free cortisol
Morning level (2am – 8 am) is twice evening. Severe stress can override diurnal pattern
Summary of best tests:
Cortisol
Cortisol
24 hour urine
Renin
Low dose dexamethasone
Short Synacthen test
Cushing’s Syndrome
= Chronic glucocorticoid excess, either exogenous or endogenous (adrenal or pituitary neoplasm, or
ectopic ACTH secretion)
Signs: Tissue wasting, myopathy, thin skin, purple abdominal striae, easy bruising, osteoporosis, water
retention, supraclavicular fat-pad (“buffalo hump”), predisposition to infection, bad wound healing,
hirsutism, amenorrhoea, hyperglycaemia (30%)
Tests:
Confirm source biochemically before looking radiologically. CT adrenal „incidentalomas‟ are
common does not prove adrenal source of cortisol excess
Screening tests:
24h urinary free cortisol (normal < 280 nmol/24 hr). If positive then high dose dexamethasone
suppression test.
Alternative is low dose dexamethasone suppression test: give 1 mg po at midnight, check
cortisol at 8 am (normal 450 – 700 nmol/L). False positives with depression, obesity and drugs
affecting metabolism of dexamethasone (eg phenytoin, phenobarbitone)
Midnight cortisol nearly as good: but must do as an inpatient (need to wake to do it and be
unstressed) – midnight is low point of diurnal cycle, if high then diurnal cycle depressed
Do high dose dexamethasone test (8mg) to determine type of Cushing‟s or if obese
Causes and treatment:
Exogenous corticosteroid administration: reduce as much as possible. In asthma, use inhaled
steroids
Cushing‟s Disease: (adrenal hyperplasia secondary to pituitary tumour, F > M, peak age 30 – 50).
Some, but not normal, suppression of cortisol with high dose dexamethasone. Treatment: Surgical
removal of pituitary adenoma
Adrenal gland adenoma or carcinoma: No suppression of cortisol with high dose. Undetectable
ACTH. Treatment: surgical removal
Endocrine and Electrolytes 103
Ectopic ACTH production: especially small cell carcinoma of the lung and carcinoid. No
suppression of cortisol with high dose dexamethasone. Plasma ACTH generally >250 ng/L.
Hypokalaemic alkalosis is common. CT relevant areas (lung, pancreas, mediastinum, thyroid)
Can block adrenal cortisol production with ketoconazole
Hypoadrenalism
Addison’s Disease
Primary adrenal failure: Failure of gluco- and mineralo-corticoids – both have similar hypotensive and
electrolyte effects (different mechanisms but additive)
Pure glucocorticoid (eg cortisol) deficiency gives:
Hypotension (postural and resting BP) due to:
Depletion of plasma renin substrate (angiotensinogen): Cortisol is permissive to PRS
production and lowers angiotensin levels and hence vascular tone
Reduced cardiac contractility and stroke volume due to sodium shift from ECF to ICF (with
tendency to hyperkalaemia reciprocal to the Na cell influx)
These lead to secondary effects including renal plasma flow, reduced GFR and mild
elevation in urea
Hyponatraemia results from:
Shift of Na+ from ECF into cells – K shifts out
Very high ADH (vasopressin) levels
Reduced renal free water clearance (in part from ADH excess and from the reduced GFR)
Pure mineralocorticoid (ie aldosterone) deficiency gives:
Reduced Na uptake exchanging for K+ and H+ in renal distal tubule and in other epithelial
surfaces (gut, sweat) hyponatraemia
Secondary effects: hypotension, reduced GFR, clearly raised urea, raised K+
With suspected Addison‟s, need to check for features of:
Mineralocorticoid deficit (few, but relate to salt depletion)
ACTH excess (hyperpigmentation)
A pituitary lesion (space occupying effects)
Hypopituitarism (gonadal, thyroid, prolactin or GH deficiency, PRL excess, ADH/vasopressin)
History of glucocorticoid medication
Symptoms: very non-specific, weakness, abdominal pain, depression, „viral illness‟, anorexia, D&V,
nausea, pigmentation in palmar creases and buccal mucosa (takes ACTH), arthralgia, myalgia,
weight loss, nocturia, confusion, irritability, constipation, dehydration, dizziness (eg due to Na
depletion postural hypotension), hypoglycaemia (reduced gluconeogenesis. Lack of cortisol will
obscure adrenergic effects of hypoglycaemia), diarrhoea, libido, vitiligo (autoimmune mediated
depigmentation of patches of skin). Not constipation or dehydration in pure cortisol deficiency
Addisonian Crisis: tachycardia, fever, shock, coma
Diagnostic tests:
Plasma renin (most sensitive indicator of mineralo-corticoid insufficiency)
Short ACTH stimulation test (Synacthen)
Better than 24 hr urine Cortisol (midnight cortisol test is equivalent to 24 hour urine).
Usually test at 0 and 30 minutes
Use long Synacthen test (0, 4, 6 hours) only when in doubt
If Cortisol doesn‟t rise then do prolonged ACTH stimulation test over 3 days (eg to
differentiate between Addison‟s and prednisone suppression).
Basal (8 – 9 am) plasma ACTH will determine gland or origin (if high then primary, if low then
secondary)
Basal (8 – 9 am) plasma Cortisol little help due to wide normal range
Test for adrenal antibodies and check for signs of Tb (eg calcification on Xray)
Also test for: hyperkalaemia, hyponatraemia, hypoglycaemia, uraemia, mild acidosis, hypercalcaemia
(?from pre-renal failure), normocytic anaemia, abnormal LFTs, eosinophilia, neutropenia
Causes:
80% idiopathic (autoimmune). Associated with Graves, Hashimoto‟s, IDDM, pernicious anaemia
Tb, metastases (insufficiency only after 90% of both adrenals destroyed)
104 4
th
and 5
th
Year Notes
Secondary Hypoadrenalism: Pituitary Failure
Tests for longstanding (ie > 6 – 8 years)
Short Synacthen test: measures adrenal atrophy
Insulin tolerance test: check for ACTH and cortisol release. Little data to judge normal range
not often used clinically
Adrenal atrophy from glucocorticoid therapy
Occasionally short Synacthen test shows a delayed response
Long Synacthen less convenient but more reliable
Steroid Medication
Replacement doses for Cortisol:
Hydrocortisone = 15 mg per day, have to take 3 times a day due to short T½, and to avoid plasma
peaks ( side effects, eg osteoporosis)
Prednisone: 7 mg per day. Longer T½
Adjust by measuring cortisol (ie 24 hour urine cortisol). Replacement therapy does not usually
suppress elevated ACTH
No abrupt changes in dose, increase in intercurrent illness. If vomiting then iv dose
Use Fludrocortisone for aldosterone replacement
Withdrawal:
Withdrawal of long term prednisone needs to be done slowly (ie monthly reductions) due to
atrophy
Signs of CG deficiency imply withdrawal is too fast
Hyperaldosteronism
Excess of aldosterone independent of renin-angiotensin system
Signs: hypertension, hypokalaemia, alkalosis, Na is normal or slightly raised
Causes: >50% due to unilateral adrenocortical adenoma (Conn‟s Syndrome). Other causes include
hyperplasia, carcinoma, genetic defect
Tests: Test K 3 times on salt replete diet (no diuretics, etc for 4 weeks). If < 3.7 mmol, test for
aldosterone or renin. Exclude renal artery stenosis (BP and K+), high renin (eg secondary to
hepatic failure)
Treatment: surgery and/or spironolactone
Phaeochromocytoma
= Benign (usually) unilateral tumour in adrenal medulla producing catecholamines
Signs: episodic hypertension, restlessness, anxiety, sweating, weight loss, tremor, cold feet,
palpitations, extensive heart investigations
Test: HMMA (breakdown products) in urine
Treatment: surgery – careful management of BP before and after surgery
Pituitary Gland
Anterior pituitary releases: ACTH, GH, FSH, LH, TSH, PRL
Posterior pituitary releases: ADH, Oxytocin
Under dominant tonic control (stalk failure hormone failure): LH, FSH, GH, TSH, ACTH
Under dominant inhibitory control (stalk failure ): PRL
Vasopressin (ADH): produced in hypothalamus, released in pituitary. Stalk failure polyuria for a
few weeks until release in median eminence
Imaging the Pituitary
Pituitary fossa is in the superior sphenoid bone, covered superiorly by the diaphragm sellae, with a
central aperture for the infundibulum. The suprasellar cistern includes the infundibulum and the optic
chiasm
Pituitary is usually 6 mm in kids, 8 mm in men and postmenopausal women, 10 mm in women of child
bearing age, 12 mm in pregnancy and postpartum. Gradual involution beyond 50 years old
„Pituitary bright spot‟: posterior pituitary is normally hyperdense. Lost in diabetes insipidous
Normal pituitary fossa has a flat top, or concave (dips down)
Endocrine and Electrolytes 105
Microadenomas: < 10 mm, don‟t normally take up contrast. Are usually hormone secreting (that‟s why
they‟re found)
Macroadenomas: > 10 mm, most are not hormone secreting, found because of space occupying effect
Sellae and suprasellar lesions:
An empty sellae is due to herniation of the suprasellar cistern in to the sellae flattening of gland
(with or without disturbance). Also secondary to hypophysectomy, post-radiation or infarction
Craniopharyngiomas: suprasellar tumours that may extend into the sellae. Kids and young adults.
Cause pituitary insufficiency, visual impairment, hydrocephalus, hypothalamic disturbance
Meningiomas: MRI shows close meningeal attachment and enhancement post-contrast
Optic nerve gliomas: in kids. Extend along optic nerve
Hypopituitarism
Causes: hypophysectomy, pituitary irradiation, adenoma (either functional or non-functional), other
intracranial tumours, Sheehan‟s Syndrome (pituitary necrosis after post-partum haemorrhage), TB
Check symptoms of:
Gonadal and GH ( bone strength): early to fail
Thyroid: intermediate to fail
Adrenal: last to go.
Also look for PRL (need a little for LH peak to happen), vasopressin, space occupying lesions (test
visual fields and for Oculmotor palsy)
ADH/Oxytocin only fail completely if hypothalamic tumour or major suprasellar extension
Symptoms: insidious onset, afternoon tiredness, pallor, anorexia, libido (can be due to many illnesses
to and PRL), impotence, amenorrhoea, no menarche by 16, headache, depression, hypothyroidism,
reduced body hair in males (due to hypogonadism – is also normal in older age – but not front baldness
– that‟s due to androgens), intolerance of intercurrent illness and postural hypotension (hypocortisone),
mild fluid retention (myxoedema and cortisol water retention), mild anaemia, pallor (yellow of
myxoedema, and anaemia), also marked behavioural changes
Signs: breast atrophy, small testes, muscle to fat ratio, hair, thin flaky wrinkled skin, postural
hypotension, visual field defect
Differentials: depression, dementia, subdural bleed (although more acute), slowly progressive tumour
The age of presentation makes a difference:
Prepubertal failure slows growth, delays puberty
Post-pubertal failure reduces gonadal activity
Post-menopausal women: High FSH and LH would be normal. If FSH within normal range then
very sensitive test of early pituitary failure (if menopausal should normally be high)
Craniopharyngiomas are the commonest cause of pituitary failure in children, but can be found at
any age
Types of lesion:
Mostly hypopituitarism comes from non-functioning pituitary adenomas (adenomata)
But also craniopharyngioma, GH or prolactin secreting tumours
Most other causes are rare: pituitary apoplexy (a pituitary haemorrhage, mostly into a pre-existing
tumour) and pituitary infarction (occasionally during delivery)
Sites of tumour extension from the fossa
Suprasellar affects optic nerve
Parasellar affects III, IV and VI nerves
Infrasellar shows xray changes
Tests:
CT/MRI, visual fields, basal T4, TSH and PRL, U&E (hyponatraemia), FBC (normochromic
normocytic anaemia)
Triple stimulation test (unless heart disease or epilepsy): As inpatient with iv access, inject insulin,
TRH and GnRH. Look for GH, Cortisol (due to ACTH), TSH, PRL (due to TRH)
LH and FSH insufficient on their own, without checking testosterone as well (may be due to
testosterone). Also LH & FSH tests are not sensitive enough to distinguish low from low-normal
Cortisol too variable to be a useful check of pituitary
Very high PRL indicates a prolactinoma, which can cause pan-hypopituitarism
An overnight Metyrapone test - give Metyrapone orally at midnight and measure plasma cortisol
and its biosynthetic precursor at 8.30am. Metyrapone blocks the synthesis of cortisol leading to a
build-up of 11-deoxycortisol and reduced negative cortisol feedback a raised ACTH. Cortisol,
106 4
th
and 5
th
Year Notes
ACTH and 11-deoxycortisol all remain low in hypopituitarism or long-standing suppression of the
HP adrenal axis by drugs
Assessing severity:
Gonadal: Males – testosterone, LH and FSH. Females: menstrual history, LH and FSH
Thyroid: fT4 and TSH
Adrenal: Short Synacthen test (false negatives possible) or urine free cortisol (not sensitive)
Growth Hormone: simple sample (after 10 am) or IGF1
Vasopressin: overnight urine concentration (osmolality)
Treatment: Hydrocortisone and thyroxine. Maybe GH. Testosterone in men, Oestrogen for pre-
menopausal women
Pituitary Tumours
Symptoms caused by local pressure, hormone secretion or hypopituitarism
Almost always benign adenomas
Histological classification:
Chromophobe (70%): half produce PRL, some non-secretary, a few produce ACTH or GH
Acidophil (15%): Secrete GH or PRL
Basophil (15%): secrete ACTH
Effects of pressure: headache (felt anywhere over head, local or general), bilateral hemianopia (initially
of superior quadrants), III, IV or VI palsy, CSF rhinorrhoea (erosion through floor of sellae)
Tests: as for hypopituitarism. Water deprivation test if diabetes insipidous is suspected
Treatment: surgery (trans-sphenoidal or transfrontal). Hormone replacement. Bromocriptine for PRL
secreting tumours. Radiotherapy (but side-effects common)
Prolactinaemia
Physiology:
PRL has pulsitile and diurnal pattern: rises dramatically during sleep
Dopamine inhibits prolactin
PRL is raised by:
Oestrogen slightly PRL (ie women higher than men)
TRH slightly PRL (used in pituitary stimulation test)
T5 Dermatome stimulation PRL (but breastfeeding won‟t increase the size of a
prolactinoma)
PRL rises through pregnancy
Drugs: most major tranquillisers (ie antipsychotics), Metoclopramide (Maxolon) therapy for
nausea blocks dopamine PRL. Aldomet (alpha-methylDOPA) is the only hypotensive
agent which increases prolactin (via dopamine depletion)
Can rise due to emotional or physical stress (including stressful venipuncture artefact)
High in chronic renal failure
Hypothyroidism TRH PRL
Sarcoidosis
Post-pill amenorrhoea (if due to other causes usually resolves < 1 year)
PRL level is not effected by Progesterone or nausea
Most common pituitary presentation. Presents early in women (amenorrhoea), late in men
Symptoms:
Women: libido, weight gain, apathy, vaginal dryness (due to hypooestrogen), amenorrhoea (very
sensitive to PRL, infertility due to PRL LH peak, PRL suppresses progesterone),
galactorrhoea (will need to differentiate from breast inflammatory exudate – clear or green). If
infertility, always check the man (cause of 1/3 of problems of infertility)
Men: impotence, libido, reduced facial hair, local pressure effects, galactorrhoea (30%), mildly
testosterone (but asymptomatic). Not gynaecomastia (usually only in testosterone or
oestrogen)
Investigations: basal prolactin between 10.00 – 12.00 h (repeat 2 – 3 times), CT, MRI, assess pituitary
function
Management:
If tumour < 10 mm (unlikely to be seen on Xray): bromocriptine to restore fertility avoids
complications of oestrogen due to PRL (could take pill instead). May postural hypotension.
Commence slowly otherwise nausea. Good prognosis. No known teratogenic effects of
bromocriptine – but still withdrawn on becoming pregnant if possible
Endocrine and Electrolytes 107
Treat macroadenoma with surgery if bromocriptine fails to reduce size of PRL. But if pressure
effects or pregnancy is contemplated then surgery. Monitor PRL
Prolactin deficiency causes failure of lactation but has no other know ill effects. Deficiency is very rare
Acromegaly
Usually presents between 30 – 50 years. Rare (3/million/year)
Symptoms: insidious onset (look at old photos), coarse oily skin, large tongue, bossing of supraorbital
ridge, shoe size and teeth spacing, spade-like hands, carpel tunnel syndrome, progressive heart failure,
goitre
Symptoms due to: periosteal growth (gigantism if the condition starts before closure of the bony
epiphyses), fibrous tissue growth ( skin thickening), organomegaly (eg cardiomegaly,
hepatomegaly, splenomegaly, testicular enlargement), cartilaginous growth (ears, nose,
costochondral junctions), neurological overgrowth ( peripheral neuropathy, exacerbated by the soft
tissue swelling)
Complications: DM, BP, cardiomyopathy, lipids, hypopituitarism
Tests:
GH (highly variable – normally undetectable, spikes 10 times a day, mainly during deep sleep),
IGF-1 (insulin like growth factor) indicates GH secretion over the previous 24 hrs.
Oral glucose tolerance test. If GH doesn‟t fall then acromegaly, anorexia nervosa, poorly
controlled DM, or Cushing‟s.
Tests as for pituitary tumour
Treatment: trans-sphenoidal surgery if young. External irradiation for elderly. Somatostatin
(Octreotide) if patient is not a good operative risk
GH deficiency in children growth retardation. One high GH level excludes deficiency. Take after
sleep or exercise
Other Endocrine Problems
Hirsutism: Male pattern of hair in a female. Common (10%). If normal menstruation then no increased
testosterone production benign. If abnormal menstruation then ?polycystic ovary syndrome with
androgen hypersecretion or late onset congenital adrenal hyperplasia with deficiency of 21-hydroxylase
enzyme
Virilism: Male secondary sex characteristics in a woman. Rare. Amenorrhoea, deep voice, temporal
hair recession, hirsutism. Refer for androgen secreting adrenal and ovarian tumours
Galactorrhoea: may come with thyroid failure (primary or secondary), with a raised prolactin
(prolactinoma, pituitary stalk section and especially drugs) and occasionally with acromegaly
Gynaecomastia. Abnormal amount of breast tissue in males. May occur in normal puberty. Due to an
in the oestrogen : androgen ratio. May result from liver disease (metabolism of oestrogen) or
testicular tumours (oestrogens) or with hyperthyroidism. Commonest causes are drugs: eg
spironolactone, cimitidine, digoxin
Hypogonadism: Due to hypopituitarism, post-orchitis (eg from mumps), chemotherapy, irradiation,
cirrhosis, alcohol (toxic to Leydig cells), various syndromes
Impotence: Common in old age. Psychological causes are common (eg if clear stressor, or if morning
erections still occur). Major causes: diabetes, drugs (diuretics, -blockers, major tranquillisers, alcohol,
antidepressants, cimetidine), hyperthyroidism, hypogonadism, PRL, cirrhosis, cancer
Electrolytes
See also ECG Abnormalities Due to Electrolyte Disturbances, page 27
Arrest due to electrolyte abnormalities is uncommon except for hyperkalaemia.
Sodium Summary
Low sodium:
Dilution: appropriate or inappropriate (SIADH)
Loss: sweat, GI, renal
High sodium:
Retention: central or renal
Water loss
108 4
th
and 5
th
Year Notes
Hyponatraemia
Key Points
Normal value of Na: 135 – 145 mmol/L
Hyponatraemia is not a diagnosis – it is found in diverse conditions. Body Na may be low, normal or
high. Relative water retention is a common factor
Condition and treatment can be hazardous. If correct too fast then pontine demyelination
Treatment must be slow and monitored closely. Treatment can range from water restriction or diuresis
to sodium restriction or normal saline. Need to know underlying cause
Don‟t use hypotonic fluids post-op unless Na is high. Eg dextrose saline – glucose absorbed very
quickly post surgery hypotonic
Symptoms
The big boogie is underlying cerebral oedema. Bigger problem if abrupt onset. Rapid correction can
cause central pontine melanosis
Symptoms don‟t correlate well with [Na]
Early: anorexia, headache, nausea, vomiting, muscle cramps, weakness
Advanced: mutism, dysarthria, impaired response to verbal or painful stimuli, bizarre behaviour,
hallucinations, asterixis, incontinence, respiratory insufficiency, spastic quadriparesis in 90%
Far advanced: (too late to do much) decorticate or decerebrate posturing, bradycardia, hypo or
hypertension, dilated pupils, seizures, respiratory arrest, coma, polyuria (central diabetes insipidous)
Should always be a differential in post-operative coma
Aetiology
Either Na depletion or water gain (usually water gain)
Inappropriate water retention: eg drugs (most common – eg antiepileptics), ADH, kidney or thyroid
problems
May be borderline hyponatraemic before (eg long term use of diuretics)
Normal ADH will if osmolality or blood volume
Operative stress or serious illness syndrome of inappropriate ADH (in most people) water
retention (especially in women, smaller starting fluid volume). NB it‟s not really inappropriate – the
body is making a justifiable physiological response: I‟m stressed so conserve water rather than
throwing it out.
Ageing impairs fluid homeostasis wider swings happen easily
Assessment
History: fluid losses, diuretics, other medications
Clinical findings: pulse, blood pressure, volume assessment, oedema, thirst, skin, input/output
Laboratory:
Creatinine, urea, glucose, HCO3, K, plasma osmolarity, urine Na and Osmolarity
Severe hyponatraemia is < 125 mmol/l: nausea, malaise, headache
< 115 mmol/l: convulsions
Look for:
Low Na and serum osmolality
Urine osmolality higher than expected (>200 and usually > serum osmolality)
Urinary sodium higher than expected (> 30)
Normal pituitary, adrenal, cardiac, and renal function
Clinically useful grouping ( volume assessment critical):
Hyponatraemia with oedema: heart failure + diuretic, cirrhosis, nephrosis (impairment of water
loss via increased ADH +/- Na loss)
Hyponatraemia with dehydration:
Urine [Na] > 20 mmol/l: Diuretics, Addison‟s Disease, Salt losing nephritis
Urine [Na] < 20 mmol/l: Vomiting, Diarrhoea, Skin loss
Usually rehydrate slowly with normal saline
Hyponatraemia with euvolaemia and reduced plasma osmolality:
Urine [Na] > 20 mmol/l: Chronic water overload (eg primary polydypsia, chronic SIADH –
central or malignancy, etc)
Urine [Na] < 20 mmol/l: Acute water overload (eg acute SIADH, oxytocin for induced labour,
etc)
Endocrine and Electrolytes 109
Treat with fluid restriction < 1000 ml/day, and treat underlying cause
Complicating factors:
If plasma osmolarity is high then measure glucose. Hyperglycaemia shift of water out of
muscle cells: Na 1 mmol/L for every 4 mmol/L in glucose
If osmolarity is normal then pseudo-hyponatraemia (eg hyperlipidaemia, hyperprotinaemia). An
artefact: Na has been incorrectly measured in plasma volume rather than plasma water
Syndrome of Inappropriate ADH secretion
= SIADH
See Diabetes Insipidous, page 110
Ectopic ADH Production (relatively rare): malignancies of lung, bronchus, brain, kidney, duodenum,
pancreas
Central production:
Cerebral infections, trauma, tumours, haemorrhage
Lung disease, eg pneumonia
Drugs, eg morphine, carbamazepine (anti-epileptic)
Can be seen in AIDS patients (?combination of above factors)
Common Scenarios
Prolonged vomiting and rehydration with Gastrolyte – only contains 60 mmol/L Na
If dehydrated (eg vomiting) and on diuretic, ADH still conserves water, but Na retention so [Na].
We preserve volume at the expense of osmolarity
Serious post-operative problem. Especially women after elective surgery (eg gynaecology wards).
Hypothesis: surgery ADH (eg due to pain), dextrose also given in belief that it slows catabolism
and promotes healing – but together they lead to [Na]
Sample cases:
Case
1
2
3
4
5
6
7
8
Na
130
126
125
125
125
128
128
128
K
3.7
3.5
3.5
3.5
3.5
6.5
2.1
5.7
Creat
130
56
56
56
700
200
220
HCO3
15
40
3.0
Uos/Sos
0.4
1.6
Sos
285
Alb
16
Heart
Failure
+
diuretic:
too
dried
out
Nephrosis
Water
overload
SIADH
Pseudo
hyponatraemia
or something
osmotically
active (eg
glucose)
Renal
failure
Severe
vomiting
Ketoacidosis
Treatment
Principles:
Raise the sodium at a safe rate
Treat the cause
Basic regimes:
If volume depleted (Renal/GI losses, diuretics, adrenal insufficiency): saline isotonic to the patient
or normal saline. Extra Na will have a small effect but volume ADH excess water
excreted
Normovolaemic or oedematous (SIADH, renal failure, polydypsia, oedema): Water restriction
If severe symptoms or if sodium < 110 then ?hypertonic saline. Na by no more than 12 mmol per
24 hours: keep rate smooth. Key judgement is speed of infusion. No front loading. Animal
studies show correction by > 14/mmol/24 hours lesions in 71% of dogs. If no symptoms –
maybe go slower
Monitor 2 hourly. Manage in high dependency unit. Detect and treat hypoxia
Adverse neurological consequences of rapid correction: myelin breakdown in the pons, patchy
symmetrical lesions elsewhere in the brain. But risk of not treating acute cerebral oedema far exceeds
the small risk of osmotic demyelination
110 4
th
and 5
th
Year Notes
Maybe frusemide to free water excretion
Dehydration or Volume Depletion
Dehydration:
Often used loosely to describe a volume depleted patient
Correctly it refers to intracellular water, following fluid shifts from ICF to ECF
Water is lost (either as pure water or as hypotonic fluid) osmolality and thirst
Treatment is water replacement (dextrose)
Volume depletion:
Losses from the ECF (isotonic sodium) circulating volume
BP, tachycardia, tissue turgor
Treatment is replacement of NaCl
Dehydration and volume depletion can co-exist
Hypernatraemia
Indicates ICF volume contraction
Usually not due to total body sodium – total sodium is low, normal or high. Kidney is good at
excreting excess Na (except if swamped – eg near drowning)
Always means the patient is hyperosmolar
Thirst and ADH protect against hyperosmolality don‟t see hypernatraemia where the thirst
mechanism is normal and there is access to water
Cellular dehydration neurologic symptoms: lethargy, weakness, irritability, seizures, etc. Cerebral
oedema if it is rapidly corrected
Classification:
Water and sodium deficiency with water loss > sodium loss (ie lost hypotonic fluid), eg vomit,
diarrhoea, sweat, osmotic diuresis (urine osmolarity not low), burns
With normal total body sodium (pure water depletion): unable to drink (old, babies, sick, etc),
central or nephrogenic diabetes insipidous (see page 110)
With increased total body sodium: excess iv hypertonic saline, ingestion of sea water,
mineralocorticoid excess (low sodium output) ( expanded ECF)
Treatment:
Chronic: may be asymptomatic even at 170 – 180 mmol/l due to adaptation by brain gradual
correction
If water deficit then:
Stop the water loss: give ADH, prevent osmotic diuresis, etc
SLOWLY give oral water or iv dextrose (Watch for hyperglycaemia, rate ~ 300 ml/hr. Add
sodium if history suggests loss of sodium containing fluid and patient is not polyuric)
Aim for Na reduction of 1 mmol/L/hr and no more than 12 mmol/24 hours
If Na: diuretics and give free water
Oral replacement is best if feasible
Diabetes Insipidous
Symptoms: polyuria, dilute urine despite dehydration, polydypsia
Central Diabetes Insipidous:
Water resorption in kidney due to ADH secretion from posterior pituitary low urine
osmolality (eg 150 mosmol/kg) despite dehydration. > 5/l per day urine requires hypothalamic
damage as well as posterior lobe
Causes of central DI: head injury, tumour, metastasis, sarcoidosis, vascular lesion, inherited, drugs
(eg phenytoin), idiopathic (50%)
Nephrogenic DI:
Reduced response by kidney to ADH
Causes of nephrogenic DI: K, Ca, drugs (lithium), pyelonephritis, congenital, loss of medullary
hypertonicity (eg renal interstitial disease)
Tests:
U&E, Ca, plasma and urine osmolalities
Water deprivation test. Stop drinking then measure urine for 8 hours. If osmolality > 800
mosmol/kg then DI excluded. If diuresis continues, give nasal desmopresson and continue
measuring
Endocrine and Electrolytes 111
Potassium
Normal value of K: 3.5 – 5 mmol/L
Standard western diet contains ~ 70 mmol/day
Shifts from ICF to ECF in response to:
Insulin deficiency
-blockers
Acidosis
Cell necrosis
Excreted in the distal tubule (K and H swapped for Na) under the influence of aldosterone. High
HCO3 excretion also K loss (eg alkalosis)
Investigations:
H+
HCO3-: usually when K and visa-versa except when there is acidosis (eg renal tubular
necrosis, diarrhoea)
Creatinine
Urinary K: > 20 mmol/L renal K loss
Na: in hyperkalaemia, consider renal tubule disorder, mineralocorticoid
Glucose
ECG (if widened QRS complexes give Ca). See ECG Abnormalities Due to Electrolyte
Disturbances, page 27
Key differentials: Diabetic ketoacidosis, renal failure
Summary
Low:
Redistribution: alkalosis, -agonists
Loss: GI, renal, thiazide or loop diuretics
Intake (starvation, surgery)
High:
Redistribution: acidosis
Massive cell lysis
Excretion: DRUGS (eg ACE inhibitors), renal failure, hypoaldosteronism
Hyperkalaemia
Causes:
Usually renal excretion
Shift from ICF (eg acidosis, massive cell lysis)
Low aldosterone: ACE inhibitors (instead use spironolactone), renin (renal disease, NSAIDs,
diabetes), poor adrenal function (eg Addison‟s)
Renal unresponsive to aldosterone: interstitial nephritis, K sparing diuretics
Renal failure: hyperkalaemia once GFR < 25 ml/min
Signs: myocardial depression, peaked T wave, flat P wave, wide QRS, VF, diarrhoea, abdominal pain,
muscle excitability
Treatment:
If severe (> 6.5 mmol/L) consider:
Glucose 50 g + soluble insulin 10 U over 15 mins
IV calcium gluconate – stabilises myocytes but doesn‟t change K
2 agonist (salbutamol)
Dialysis if extreme
If moderate (5.5 – 6.5 mmol/L): Calcium resonium 15 g po (calcium binding resins), renal loss
through diuretics, mineralocorticoids
Hypokalaemia
Causes:
GI losses (ECF volume contraction):
Vomiting, NG suction alkalosis HCO3 in urine and aldosterone renal loss of K
Diarrhoea: K loss and metabolic acidosis
Urinary losses:
Diuretics: thiazides or loop
112 4
th
and 5
th
Year Notes
Alkalosis (also shift to ICF if significant alkalosis)
ECF normal or high: high aldosterone or hypermineralocorticoid (eg Cushing‟s)
K shift into cells: metabolic alkalosis, insulin, -adrenergics
Intake (starvation, surgery)
Symptoms:
Muscle weakness, cramps
GI: constipation, ileus
Polyuria, nocturia
Urine – if volume then diuretics or osmotic diuresis, if not consider aldosterone action
Signs: arrhythmias, PR prolonged, inverted T waves, U waves, VF, GI ileus, muscle weakness,
hypotonicity, digoxin toxicity, alkalosis
Treatment: May have large total body deficit (eg DKA). Replacement KCl up to 40 mmol/hour
Calcium
See also Parathyroid, page 101
Summary
If low Mg, then no in PTH in response to Ca
Low:
Hypothyroidism: abscess/gland destruction, Mg, resistance to PTH (pseudo)
Vit D: renal failure, malnutrition
High:
PTH: primary, secondary or tertiary
Paraneoplastic: PTHrH, bone metastasis
Vitamin D: nutritional, conversion (sarcoid)
Hypercalcaemia*
Signs: “Bones, stones, groans and psychic moans”. Also abdominal pain, vomiting, constipation,
polyuria (Ca potentiates ADH effect), depression, anorexia, weakness, BP, renal stones, cardiac arrest
Most commonly:
Primary hyperPTH in the community
Malignancy in hospital
NB: acidosis H displaces Ca on albumin free Ca
If albumin raised:
Urea raised dehydration
Urea normal cuffed specimen
Albumin normal or low:
Phosphate low or normal (and urea normal): primary or tertiary hyperparathyroidism
Phosphate or normal:
ALP: Bone metastases (most common primaries are breast, kidney, lung, thyroid, prostate,
ovary, colon), sarcoidosis (Vitamin D conversion in the lungs), thyrotoxicosis
Normal ALP: myeloma, vitamin D excess, Ca supplements
Treatment: if Ca > 3.5 mmol/l or severe symptoms:
Rehydrate and correct any hypokalaemia and hypomagnesaemia
Diuretics once rehydrated (frusemide, avoid thiazides)
Bisphosphonates (pamidronate): lower Ca over 2-3 days by inhibiting osteoclasts
Hypocalcaemia
Normal value of Ca: 2.12 – 2.65 mmol/L
40% of calcium is bound to albumin. Adjust Ca for changes in albumin (0.025 per 1g of Albumin).
Take sample uncuffed
Symptoms: Tetany, depression, carpo-pedal spasm (wrist flexion and fingers drawn together),
neuromuscular excitability (eg tapping over parotid causes facial muscles to twitch – Chvostek‟s sign)
Causes of hypocalcaemia:
Mg PTH hypocalcaemia
Thyroid or parathyroid surgery
If PO4 then chronic renal failure (failure of Vitamin D conversion), hypoPTH or
PseudohypoPTH
If PO4 normal or then osteomalacia (ALP), over hydration or pancreatitis

Endocrine and Electrolytes 113
Magnesium *
Stored 65% in bone, 35% in cells
Concentration generally follows Ca and K
Excess:
Usually in renal failure treat renal failure not magnesium
Symptoms: neuromuscular depression BP CNS depression
Deficiency:
Causes: severe diarrhoea, ketoacidosis, alcohol, TPN, with Ca or K (especially diuretics)
Symptoms: tetany (same as Ca, K gives weakness), fits, arrhythmia
Treatment: Mg salts either po or iv
Chloride
Anion Gap = Na + K – (Cl + HCO3)
Usually 8 – 16 milliequivalent/l (measure of charge)
High Anion Gap: Ketoacidosis, lacticacidosis, renal failure, poisoning (salicylate, methanol,
ethanol, ethylene glycol)
Low anion Gap: GI or GI loss of HCO3, therapy for diabetic ketoacidosis, ingestion of HCl or
NH4Cl
Practical use limited – cause of metabolic acidosis obvious from history and observation
Most labs have deleted it from electrolyte profile
Cl normally tracks Na except in metabolic acidosis. Eg severe vomiting: HCl ( hypochloraemic
metabolic alkalosis) and volume depletion ( kidney retains Na generation of HCO3 and K
depletion). Correction of alkalosis requires correction of volume, chloride and K
Acid-Base balance
Physiology
Metabolism produces two acids:
Volatile: carbonic
Non-volatile: eg lactic
Buffer systems:
H+ + HCO3- H2CO3 (H2O + CO2)
Henderson Hasselbach Equation:
PCO2][ * 0.03
[HCO3]
log 6.1(pKa)pH
, or
CO2 of Regulationy Respirator
HCO3 of ProductionKidney
log 6.1(pKa)pH
, or
Normal range for pH is 7.35 – 7.45 (=45 – 35 nmol/L of H+ ion)
Range of pH compatible with life is about 6.8 – 7.8 = H+ concentration of 160 – 16 nmol/l
Lots of other buffering systems
Compensation:
Never complete
Respiratory: pH measured in the medulla. Compensates rapidly
Renal:
Alter bicarbonate reabsorption
Titratable acid excretion: organic buffers in tubules acidifies urine. Excretes 30 – 50% of acid
produced each day
NH4 excretion: formed in tubules, takes days. Excretes 50 – 70% of acid
Respiratory Alkalosis
Hyperventilation
Causes:
Hypoxia
Lung disease: PE, asthma

114 4
th
and 5
th
Year Notes
Anxiety
Fever, sepsis
Salicylate overdose: stimulates respiration, will subsequently develop metabolic acidosis
PaCO2, pH, initial alterations in [HCO3] are minimal, if it persists then kidneys compensate
Compensation:
Acute: HCO3 by 2 for each 10 PCO2
Chronic: HCO3 by a further 3 (ie total of 5) for each 10 PCO2 [renal loss of HCO3]
Respiratory Acidosis
Hypoventilation
Causes:
PCO2 excretion lags production – eg severe asthma (initially asthmatics hyperventilate)
Pulmonary disease, muscular diseases, etc
CNS depression: primary or drugs/toxins
Asphyxia, smoke inhalation
As PCO2 then CO2 + H20 H+ + HCO3-
PaCO2 pH, initial alterations in [HCO3] are minimal, if it persists then kidneys compensate
(HCO3 reabsorption, NH3 formation and excretion):
Acute: HCO3 by 1 for each 10 PCO2
Chronic: HCO3 by a further 2.5 (ie 3.5 of total) for each 10 PCO2
For example:
PCO2
HCO3
pH
Uncompensated
80
24
7.10
Acute
80
28
7.17
Chronic
80
38
7.30
Metabolic acidosis
Net gain of acid
Causes:
Accumulation of acid (anion gap > 18 mmol/L): H+ (ketoacidosis, lactic acidosis, ingestion of
salicylates, methanol), renal failure (failure to excrete H+)
HCO3 (anion gap < 18 mmol): GI tract loss (eg diarrhoea), renal loss (eg carbonic anhydrase),
hypoaldosteronism
Compensation:
Rapid: PCO2 by 1.2 for each 1 in HCO3 (baseline = 24) - rapid
Slow: HCO3 reabsorption and NH4 excretion by the kidneys
Metabolic alkalosis
Net loss of acid
Causes:
Loss of H+:
Vomiting (suspect surreptitious if low Cl)
NG suction
Renal loss (hyperaldosteronism)
Increase in HCO3 reabsorption:
K depletion (Conn‟s, Cushing‟s, drugs, diuretics).
Volume depletion, eg Aldosteronism Na/H exchange
Gain in alkali: eg NaHCO3 administration
Compensation:
PCO2 by 0.6 for each 1 in HCO3. Limited by hypoxia
Final compensation is by renal excretion of HCO3 – requires correction of Cl, K and volume
Endocrine and Electrolytes 115
Summary of compensation rules
Change in HCO3 per 10 CO2
CO2
Acute
Chronic
Acidosis
1
further 2.5 (total 3.5)
Alkalosis
2
further 3 (total 5)
HCO3
Change in PCO2 for each HCO3
Alkalosis
0.6
Acidosis
1.2
Mixed Acid/Base disorders
Suspect if:
Clinical grounds
Compensation rules not obeyed
Normal pH but abnormal PCO2 and HCO3
Examples:
Respiratory + Metabolic Acidosis: Pulmonary oedema + cardiac arrest
Respiratory + Metabolic Alkalosis: Over-ventilation + Nasogastric suction
Respiratory Alkalosis + Metabolic Acidosis: Septic shock or Salicylate OD
Respiratory Acidosis + Metabolic Alkalosis: CORD + Diuretic
Metabolic Acidosis + Metabolic Alkalosis: Renal failure + vomiting
Interpreting Blood Gas Results
Arterial blood taken in 2 ml syringe containing heparin (to stop clotting) and transported on ice
Look at pH: 7.36 to 7.44 is normal
Look at PCO2. If < 36 then hyperventilation. If > 44 then hypoventilation.
Look at HCO3. If < 22 then metabolic acidosis. If > 26 then metabolic alkalosis. But HCO3 depends
on PCO2. So (to work out if its just compensation, or there is a metabolic problem as well as a
respiratory one):
For acute changes (hours): a fall in PaCO2 a normal HCO3 2 less for every 10 mmHg in
PaCO2. A rise in PaCO2 normal HCO3 1 greater for every 10 mm Hg in PaCO2
For chronic changes (days): a rise in PaCO2 results in a normal HCO3 4 greater for every 10
change in PaCO2
Base Excess
Given on all arterial blood gas results
= Concentration of titratable base when titrating blood or plasma with a strong acid or base to a plasma
pH of 7.40 at PCO2 of 40 mmHg at 37C
Intent is to remove the impact of the respiratory component leaving just the metabolic component:
If +ive: metabolic alkalosis deficit of non-carbonic acid
If –ive: metabolic acidosis excess of non-carbonic acid
BUT recognises normal compensation as an extra disturbance. May be useful for an anaesthetist (eg
simple and acute disturbances)

116 4
th
and 5
th
Year Notes
Neuro-sensory
References: Neurology, a 4
th
year Student Teaching Resource by Drs David Abernethy and Stuart
Mossman, Wellington School of Medicine
See also Dementia and Delirium, page 439
Neurology ....................................................... 117
History ....................................................... 117
Physical Exam ........................................... 117
Cognitive Functions .................................. 122
Common Peripheral Nerve Lesions .......... 123
Brain Anatomy .......................................... 123
Intracranial Haemorrhage .......................... 123
Stroke ........................................................ 125
Head Trauma ............................................. 129
Coma and Stupor ....................................... 130
Syncope (Fainting) .................................... 131
Abnormal Speech ...................................... 131
Parkinson‟s Disease .................................. 131
Dystonias ................................................... 132
Demyelinating Disease .............................. 132
Other CNS Degenerative Diseases ............ 133
Epilepsy ..................................................... 133
Brain Tumours .......................................... 136
Spinal Chord Syndromes ........................... 138
Headaches ................................................. 139
Myasthenia Gravis .................................... 140
Other neurological emergencies ................ 140
Other.......................................................... 140
Eyes ................................................................ 140
History ....................................................... 140
Physical Examination ................................ 140
Anatomy .................................................... 141
Loss of Vision ........................................... 141
The Red Eye .............................................. 142
Glaucoma .................................................. 143
Eye Infections............................................ 144
Optic Nerve Lesions .................................. 145
Nerve Lesions Affecting Eye movement .. 145
Retinal Vascular Disease ........................... 145
Focal Ischaemic Retinal Disease ............... 145
Tumours .................................................... 146
Paediatric Ophthalmology ......................... 147
Vestibular ........................................................ 148
Ear ................................................................... 149
External Ear ............................................... 149
Middle Ear ................................................. 149
Ear Testing ................................................ 150
Hearing Loss ............................................. 151
Neuro-sensory 117
Neurology
UMN = Upper Motor Neuron, LMN = Lower Motor Neuron
History
Want to know the answer to two questions:
Where is the lesion (based on history and exam): Eg Weakness:
Upper motor neuron: motor cortex, internal capsule, brain stem or spinal chord
Lower motor neuron: nerve root, brachial/lumbosacral plexus, or peripheral nerve
Neuromuscular junction
Muscle
What is the lesion (based on history – mode of onset and progression)? Is it infarct, haemorrhage,
inflammatory, tumour or degenerative
Differentials:
Inability to walk: Parkinson‟s, spinal chord (demyelination, compression, disease due to B12 or
syphilis), cervical spondylosis, polymyositis, myasthenia gravis, Guillain Barre, hereditary motor
and sensory neuropathy, MS, diabetic neuropathy, motor neuron disease, alcoholic neuropathy
Brief loss of consciousness: Stokes Adams attacks, VT, postural hypotension, hysterical
unconsciousness, vasovagal syncope (fainting), epilepsy, CVA
Coma and Stupor: hypoglycaemia, Wernicke‟s encephalopathy, sedative or narcotic drug overdose,
post anoxic coma, CVA, status epilepticus, meningitis, encephalitis, delirium, coning. See Coma
and Stupor, page 130
Space occupying lesion: bleed, tumour, cyst, abscess, TB granuloma, AVMs, hydrocephalus
Physical Exam
Hard to incorporate with rest of physical exam do it on its own
Tailor the exam to the clinical problem (full exam can take an hour)
Avoid suggestion: rather than „Is this sharp‟ or „do you smell the perfume‟ say „what do you feel/smell‟
Quick list:
Observe: including wasting and fasciliculations
Cranial nerves
Tone
Power
Reflexes
Coordination
Sensation: position, vibration, pin prick, light touch
Mental State Exam
Wanting to test:
Distributed cognitive function:
Attention/concentration
Memory
Word finding
Localised cognitive functions
Speech
Visuo-spatial
If suspicious from history need assessment of the following:
State of consciousness: alert, drowsy, stuporose, comatose (assess with GCS)
Other observations from mental state exam (See Mental State Examination, page 414)
Orientation: date, their name, age, who are their relatives
Remote or long-term memory: phone number, Prime Minister, recent events in the news
Registration and Immediate recall: Memorise 3 objects, recall after 3 minutes. Repeat 4 or 5 digits
in reverse
Others: abstract thinking, serial 7‟s
Can use Mini-mental status test: but not sensitive to subtle impairments
Language
If difficulty following instructions, appears confused, etc
118 4
th
and 5
th
Year Notes
Requires assessment of spoken and written response to both spoken and written questions
Observations: fluency, word finding, grammatical errors, understanding questions
Naming objects: ask about whole object then parts – wrist watch and strap
Repetition: No Ifs ands or buts
Auditory comprehension: Increasingly complex commands, eg Close your eyes, touch your left ear
with your right thumb and stick out your tongue
Writing: write a simple sentence, their name and address
Reading: read aloud
Cranial Nerve Exam
1: Olfactory: Smell. Not if doing general screen. Close eyes. Check each nostril patent then test (eg
scented soap on ward). Poor smell common (smoking, allergies, ageing). Also in Alzheimer‟s,
Parkinson‟s, MS, chemotherapy. Most serious association: frontal lobe tumour, presents with
personality change, self-neglect, dementia
2: Ophthalmic nerve: lesions common and serious. Check if they normally wear glasses. Test:
Acuity: (use pinhole if they‟ve forgotten their glasses). Test each eye separately
Visual fields: confrontational testing: first just hold hands in each visual field and ask what they
see. Then wiggle one finger, then the other, then both, in all visual fields (or count fingers)
Red pinhead test: test for colour sensitivity – more sensitive than acuity (good for vague
hemianopia). Loss of colour = “desaturation”. Blind spot = “scotoma”
Hemianopia:
Pituitary lesion bitemporal hemianopia (nasal retina affected). Bring red pin from affected
field into normal – gain of red colour is convincing. Upper temporal field in one eye is
typically affected first
Parietal lesion visual inattention
3, 4, 6: Seeing double. Complicated to sort out
Look for ptosis
Smooth tracking: Fix on finger, draw H in the air, ask for report of diplopia, watch for one eye
lagging or nystagmus (a few beats in extreme gaze is normal)
Examine pupils at rest, light reflexes and near reflex
Voluntary eye movement:
Look up, down, left, right. Often elderly have trouble looking up anyway
Cover test: look at target, cover one eye, does other eye move? Reverse. Shows which is
fixing eye
If diplopia found, find field where it‟s maximal. Weak eye moves less; good eye overshoots.
Use stick man drawn on tongue depressor
Problems locating target (overshoot and come back) ?cerebellar
5: Trigeminal Nerve
Sensory 5
th
: Test light touch and pinprick in all 3 divisions on both sides (separate pathways in the
brain stem). Test corneal reflex (early sign of lesion) – patient looks up, use cotton wool on cornea
(more sensitive than sclera)
Motor 5
th
: jaw opening in midline (tests pterygoids). Jaw deviates to the side of weakness. Clench
jaw and palpate maesseters. Jaw jerk only if indicated
7: Facial Nerve. Wrinkle forehead and „show your teeth‟ (not smile). Look for lower face weakness.
Upper face (eg screw up eyes) better preserved in UMN, both similarly affected in LMN (eg Bell‟s
palsy – can be due to HSV, onset in days, recovery in weeks/months, rarely parotid tumour). Note
symmetry, fasciculation, and abnormal movements. Don‟t normally test taste
8: whispered voice at arms length, with patient‟s eyes close. Mask opposite ear by rubbing your finger
and thumb together beside it.
9 (glossopharyngeal and vagus nerves): back of mouth, say ahh, uvula up in midline. Check
swallowing. Gag normally not tested – if you do, test both sides. Unilateral absence abnormal,
bilateral absence may be normal.
11 (accessory): shake and shrug shoulders. Observe sternomastoid and trapezius at rest for wasting,
fasciculation, or dystonia. Look sideways, try to return head against resistance. Compare strength of
shoulder shrug on each side. Rarely useful, unless confirming site or suspected lesion. Always test
neck extension if diffuse muscle weakness – if abnormal indicates lesion above C1/C2
12: Hypoglossal nerve. Tongue. Examine at rest then protrude. If fasciculation ?motor neuron
disease. Deviates towards the weak side. Push tongue into check against your finger. Try rapidly
alternating movements of protruded tongue or rapid la-la-la
Neuro-sensory 119
INSERT Cranial Nerve Table
120 4
th
and 5
th
Year Notes
Motor Examination
Observation for congenital maldevelopment, wasting, fasciculation and abnormal movements (tremor,
chorea, myoclonus, dystonia)
Assessment of tone: resistance to passive movement (must be relaxed). Tone due to:
Rigidity (Basal ganglia): uniform resistance to slow passive movement, may be jerky (cogwheel
rigidity). Affects flexors and extensors equally
Spasticity (upper motor neuron). Rapid passive movement maximal tone to start with,
decreases suddenly as muscle is lengthened. Most marked in flexors of arms and extensors in legs.
Due to reflex contraction to muscle stretch
Clonus: maintaining stretch (eg of ankle plantar flexors) further repetitive beating
Power: compare between sides
Test in position where patient has mechanical advantage: you shouldn‟t be able to win then if its
normal
Grade as follows:
0: no contraction
1: a flicker/trace of contraction
2: active movement with gravity eliminated
3: active movement against gravity but not against resistance
4: active movement against gravity and resistance, but reduced power (covers wide range –
can classify as mild, moderate or severe weakness)
5: normal power
Motor exam of the arms:
Observe arms at rest, then outstretched with eyes closed (check for drift – non-specific test). Look
for wasting of 1
st
dorsal interosseus and abductor pollicis brevis
Assess tone at elbow (flexion/extension and supination) and wrist (flexion/extension) with slow
and rapid movements
Arms (start at top and work down)
Shoulder abduction (deltoid, C5, axillary nerve). Arms out like chicken wings – push it down
Elbow flexion (biceps, brachialis, C5-6, musculocutaneous nerve) – pull me in
Elbow extension (triceps, C7, radial). Arm bent up in front - push me out
Wrist extension. (Extensor carpi ulnaris and radialis, C6-7, radial nerve). Extended „cocked‟
wrist – push it down
Finger extension (extensor digitorum, C7). Fingers straight out – push them down just distal to
MP joint
Finger flexion (flexor digitorum, C8). Try to uncurl curled up fingers
Abduction of index finger (ulnar nerve, T1, dorsal interosseus)
Abduction of thumb (median nerve, T1, abductor pollicis). Try and push raised thumb down
into palm. Look for atrophy of thenar eminence
Motor Exam of the legs:
Observation of legs: while standing, walking, lying down. ALWAYS observe posture and gait:
movement of arms, stride length, broadness, smoothness. Stand with eye‟s closed and feet
together (Romberg test). Look for wasting of tibialis anterior and small muscles of feet
Check for tone
Check for clonus. Flex hip and knee to 45 degrees, externally rotate hip, rapidly dorsiflex foot and
hold. Two or three beats of clonus may be normal if symmetrical
Power in Legs (patient lying down):
Hip flexion (ilio-psoas, L1-2, lumbar plexus). Push down on raised straight leg
Hip extension (gluteus maximus, sciatic nerve, L5-S1). Lift ankle of straight leg
Knee Extension (quadriceps, femoral n, L3-4). Bend knee, try to push ankle in
Knee Flexion (hamstrings, sciatic nerve, L5 – S1)
Ankle dorsiflexion (tibialis ant peroneal n, L4 – 5): push on top of foot while toes raised
Ankle plantarflexion (gastrocnemius, sciatic nerve, S1 – 2): push on bottom of foot
Ankle inversion (tibialis ant & Post, peroneal and tibial n, L4 – 5). Patient bends foot in and
try and pull it back
Ankle eversion (peronei, peroneal nerve, L5 – S1): Patient bends foot out and try and pull it
back
Rapid leg tests:
If they can walk on their heals, then no foot drop (L5 or common peroneal)

Neuro-sensory 121
If they can walk on their tiptoes, then no S1 lesion (plantar-flexion)
To test proximal leg function, crouch and stand up
Differentiating Upper and Lower Motor Neuron lesions
Upper
Lower
Tone
(unless acute), Spasticity or
Rigidity (mainly Parkinson‟s)
Wasting
No
Yes
Reflexes
(unless acute)
Reflexes
Key is for them to be relaxed
Arm (Clench teeth if no response):
Biceps (C5/C6)
Triceps (C7)
Supinator (C5/C6)
Can also do finger reflex if suspect C8 lesion: tap your fingers while placed over outstretch fingers
of face up hand. Often normally absent
Leg (if no response, interlock fingers of both hands and pull just before tap)
Patella (hold knees up) (L3/L4)
Ankle (passively dorsiflex ankle) (S1). 3 ways: hand on dorsum of foot and tap hand, directly on
Achilles tendon, or kneel on chair with foot hanging off, tap Achilles tendon (most sensitive)
Grading reflexes:
0: absent
+-: just present
+: normal
++: brisk normal
+++: very brisk
Plantar responses: put patient at ease! Normal response is plantar flexion (down). If upper motor
neuron lesion, big toe up and other toes fan out (Babinski). Not positive if withdrawal response (hip
and knee flexion) due to over response
Superficial Abdominal reflexes: Not tested routinely. Stroke lightly with sharp object in each quadrant
towards midline. Normal reflex is contraction. Tires quickly
Co-ordination
Rapid alternating movements of hand: supinate and pronate hand rapidly (dysdiadokinesia)
Finger-nose-finger test. Not too fast (may mask intention tremour)
Heel-knee-shin test
Heel-toe walking: tests midline cerebellar vermis
Romberg: tests dorsal column sensory loss (ie proprioception). Rare in clinical practice
Important syndromes including ataxia:
Cerebellar haematoma: Sudden onset of progressive headache, vomiting, and inability to stand or
walk. Later progressive drowsiness, lateral gaze palsy from pontine compression. Decompressive
surgery can be lifesaving
Wernicke‟s Encephalopathy: Confusion, ataxia, nystagmus. 6
th
nerve palsy. On recovery: impaired
short-term memory, confabulation. Common with prolonged vomiting, poor nutrition, not
confined to alcohol
Sensory test
Issue is where and why to test. What do you expect to find? Do this last so you have some idea what
to look for. Very easy to suggest to patient
Common scenarios:
Hemisensory loss: stroke, peripheral root and nerve lesion
Glove or stocking: spinal chord lesion or peripheral neuropathy
Get patient to close eyes. Stimulate at irregular intervals so patient can‟t anticipate them. Test from
abnormal to normal. Don‟t try to completely map – just test key boundaries
Key Dermatomes:
Stand on S1
Sit on S3
Groin: L1
122 4
th
and 5
th
Year Notes
Umbilicus: T10
Nipple: T5
T2 meets C4 on line connecting axilla: should be clear difference across this line in any lesion
between T2 and C4
Middle Finger: C7
Position sense: hold big toe by the sides, explain which way is up and down, then test. Has low yield in
practice. Try functional test: can they stand up with eyes closed?
Vibration: 128 Hz fork. On bony prominences (what do you feel?). Move up until its positive. Bunion
medial melleolus tibial tuberosity anterior iliac spine. Test fingers for completeness. First
sensation to go in progressive deterioration
Pinprick: Use large safety pin and discard after use. Toes, fingers, face (no more unless suspicious, eg
reflexes). Is it sharp or blunt? Can alternate sharp and blunt end to see if they can tell the difference.
More reliable than light touch if both damaged
Temperature: Not usually done if pin prick done
Light touch (cotton wool)
Others (not routine):
Two point discrimination
Stereognosis: recognising objects by their feel (coin, key, etc). Normal hand first
Graphaesthesia: write numbers on the hand
Sensory inattention: touch sides separately and together – which is being touched?
Cognitive Functions
Localised Cognitive Functions
Dominant hemisphere:
Speech, reading and writing
Calculation
Praxis (higher motor control of learned movement)
Non-dominant hemisphere:
Neglect: visual, auditory, tactile
Dressing or constructional apraxia
Visuo-perceptual: object recognition (fragmented drawings) and faces (Prosopagnosia)
Prosody: Expressive aspects of speech
Attention/Concentration
Depends on the reticular activating system, thalamus, frontal and medial temporal lobes
Test: orientation in time and place, serial subtractions, spelling WORLD backwards etc
Memory
Implicit: learned responses, reflexes and motor skills
Explicit:
Episodic:
Left hippocampus: verbal, right visuo-spatial, faces, etc
Temporally specific personal experiences
Lost in diffuse brain disease (dementia) and bilateral limbic disease (amnesic syndrome)
Semantic:
Facts, concepts, words, meanings (eg object naming, what do you cut bread with, etc)
In the temporal neocortex (left)
Lost in dementia
Working memory:
Very short term recall: words, numbers, melodies
Under frontal lobe executive control: important for dual task performance
Patients can have damage to just one of working or long term memory (eg Korsakov)
Psychosis patients have normal working memory, but cannot make:
New memories (anteriograde): Word list learning
Retrieve long-term memories: recall public events, autobiographical details
Higher Cognitive Function/Executive Function
Situated in the pre-frontal area (non-motor frontal lobes)

Neuro-sensory 123
Functioning best established from informants and observation
Clinical features of frontal lobe lesions:
Poor planning: can‟t initiate and carry out a sequence of actions to complete a goal, can‟t do two
things at once
Can‟t control impulses: irritable, irascible
Deterioration of personal relationships, social habits and hygiene
Dulling of curiosity and vitality, jocular, puerile
Lack energy
Common Peripheral Nerve Lesions
Patterns of presentations:
Unilateral defined areas of weakness/sensory loss in hand or foot
Peripheral neuropathy
Paraparesis: weakness of both legs. Rare but critical. Usually spinal chord lesion
Muscle disease (rare): initial proximal pattern of weakness – neck flexion, shoulder abduction, hip
flexion
Hemiparesis due to stroke: 1/day in Wellington (this one is not peripheral)
Hand:
Common Lesions:
Ulnar neuropathy: Elbow compression weakness of finger but not thumb abduction.
Thumb adduction weak (paper test). Weakness of long flexors of 4
th
and 5
th
fingers. Wasting
of interossei. Sensory loss on little finger
Median nerve compression in Carpal Tunnel Syndrome: weakness and wasting of abductor
pollicis brevis, with numbness of palmar surface of fingers 1,2,3 and lateral 4. Tingling/pain
which wakes at night
C7 Radiculopathy: pain from neck, shoulder, arm and forearm. Weakness of elbow, wrist
and finger extension
C6 Radiculopathy: Weakens elbow flexion and wrist extension. Sensory loss of dorsolateral
forearm, thumb and index finger
Radial nerve (Saturday night Palsy): Unable to dorsiflex the wrist or extend fingers or thumb.
Less Common Lesions:
Peripheral neuropathy: weakens small muscles of the hand, glove sensory loss
T1 root lesion: Weakness of small hand muscles, sensory loss on medial arm and often
Horner‟s syndrome
Leg:
S1 Radiculopathy: Pain in back, buttock, thigh, leg, and foot, numbness of the lateral border of
the foot. Mild weakness of eversion and dorsiflexion, depressed ankle jerk
L5 Radiculopathy: Pain in back, buttock, thigh, leg, and foot, numbness of medial border of the
foot and big toe, weakness of inversion and dorsiflexion. No reflex change
Common peroneal nerve lesion from compression at the fibula head: Painless, severe
weakness of dorsiflexion and eversion, with normal inversion, and numbness on the lateral foot
and dorsum of the foot. Maybe sudden onset with severe footdrop. Ankle jerk normal. 80% of
nerve palsies causing foot drop recover over 3 – 4 months. Differentiating foot drop:
Common Peroneal Lesion
L5 Lesion
Ankle jerk
OK
May be depressed (normally S1)
Inversion
OK
Weak
Eversion
Weak
Brain Anatomy
Revise it!
Cerebro-spinal Fluid – CSF:
Made in coroid plexus on floor of lateral ventricles and roof of 3
rd
ventricle
Flow: Lateral ventricles foramen of Munro (intraventricular foramen) 3
rd
ventricle
Aqueduct of Sylvia 4
th
Ventricle via 3 foramen to cisternal spaces of subarachnoid space
arachnoid granulations venous sinuses
Intracranial Haemorrhage
Usually due to:
Trauma: typically extra/epi-dural or subdural
124 4
th
and 5
th
Year Notes
Spontaneous (usually due to cerebrovascular disease): brain parenchyma and subarachnoid
Extradural Haemorrhage
Due to head trauma, especially with skull fracture (although not necessary in children)
Lentiform shaped arterial bleed ( high pressure rapid progression)
Skull fracture leads to one of:
Blood from middle meningeal artery forces its way between dura and inner table of skull (normally
intimately related) – rapid, displacing cerebral tissue herniation
Laceration of dural venous sinus slow, delayed findings, less dense, less common
Dura fixed at sutures so doesn‟t go past these (eg will be bounded by coronal and lamdoid sutures)
Dura has two layers: the outer forming the internal periosteum of the calvarium, the inner forming the
septae which compartmentalise the calvarium
Subdural Haemorrhage
Following trauma: 50% also have a brain injury (swelling, contusion, laceration, etc)
Bleed from bridging vein into the space between the arachnoid and dura mater (low pressure slower
progression)
Risk in old people due to relative cerebral atrophy
Traverses right round the inside the calvarium: cresenteric shaped bleed, very flat (may need to look
carefully to distinguish from the skull)
Most common location is over the lateral aspects of the cerebral hemispheres
Poor prognosis due to large size and associated brain injury
Classification:
Acute < 3 days
Subacute 4 – 21 days
Chronic > 21 days (eg minor injury in elderly, hypodense (blood broken down), lots of midline
shift
If not detected, the haematoma undergoes organisation granulation tissue. This can rebleed
Subarachnoid Haemorrhage
Into the space between the dura mater and pia mater – where CSF is
Bleed may be focal, or diffusely spread through subarachnoid space (will flow into sulci and be
bilaterally symmetrical)
Incidence: 15 per 100,000
Signs/symptoms: Sudden severe headache, loss of consciousness, meningism (neck stiffness, vomiting,
photophobia, fever), maybe focal neurological signs, fundi
Spontaneous: ruptured aneurysm (70%), Arteriovenous Malformation (AVM, 10%), hypertensive
bleed, bleed into a tumour, hypocoagulable state
Traumatic: injury to leptomeningeal vessels, rupture of intracerebral vessels, contusion, laceration
Aneurysm:
Mostly situated on the circle of Willis (ie 40% are at the junction of the anterior cerebral artery and
the anterior communicating artery)
Associated with connective tissue disorders (eg Marfan‟s)
Mostly saccular rather than fusiform
Saccular: due to elastic laminar (?congenital) = Berry Aneurysm. No muscle layer and
thickened hyalinised intima
Fusiform: due to atheromatous degeneration
Mycotic: due to septic emboli – usually more peripheral in brain
Dissecting: may extend either from aortic dissection or from internal carotid artery (complication
of angiography)
85% are in the anterior circle of Willis. Posterior communicating artery unilateral 3
rd
nerve
palsy (dilated pupil, ptosis, etc)
Arterio-venous Malformations:
Localised developmental failure shunt from an artery to a vein gradually dilates
distension of veins under arterial pressure
Most in the territory of the middle cerebral artery
Can present with haemorrhage or epilepsy
Investigations: CT, CSF if CT not helpful and no risk of ICP (make sure blood is not from a bloody
tap)
Neuro-sensory 125
Treatment:
Analgesia, rest (maintain normotensive)
Rebleeding: 30% die from 1
st
bleed, 60% from rebleed (25% within 2 wks)
Clip or endovascular obliteration if GCS > 6
Vasospasm: 5 – 15% have stroke due to vasospasm (peak 3 – 10 days post bleed) despite all
treatment. Cause: ?oedema around vessels compression. Prevention with fluids, drugs and
monitoring electrolytes
Complications:
Acute: if intraventricular extension ependymitis obstruction of aqueduct acute obstructive
hydrocephalus. Also cerebral oedema and vasospasm of the affected artery ( infarct)
Delayed: fibroblast proliferation in arachnoid space and at granulations communicating
hydrocephalus
Hypertensive Intracerebral Haemorrhage
Mainly due to rupture of small penetrating vessels secondary to hypertension – which causes:
Hyaline arteriolosclerosis in small arteries and arterioles weakening of vessel
Minute aneurysms
Main sites are: Putamen, thalamus, pons, cerebellum
Haematoma compression brownish discolouration of surrounding tissue
How old is blood on a film
On a CT:
< 24 hours: homogenous high density lesion, well defined margins, prognosis related to size of clot
Then oedema develops, increasing the mass effect, less homogenous
For the first week is hyperdense cf brain tissue (clotting contracting)
2 – 3 weeks isodense
3 – 4 weeks is hypodense cf brain tissue. Breakdown of haemoglobin osmotically active
particles water diffuses in.
On MRI:
T1: fluid is black: hypointense
T2: fluid is white: hyperintense
If contrast enhancement ring enhancement, then either an abscess or metastatic deposit
Stroke
= The acute onset of focal or global neurologic deficit presumably of vascular origin lasting > 24 hours
(WHO). This includes ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage
Aetiology:
Risk in NZ in 65 – 74 is 1:100, in 85+ is 1:30
80% due to atheroma, thrombosis and embolism, especially following heart (recent MI, AF, RF
disease) or vessel pathology
Nearly half the people having a new stroke are already in institutional care or needing help with
daily activities
25% of strokes are in people who have had a previous stroke
Differential to stroke: TIA, Migraine, Trauma, space occupying lesion (sub-dural haematoma, tumour,
abscess), infections, hypoglycaemia, delirium, MS and spinal chord pathology/injury
Isolated signs seldom due to a TIA or stroke: dizziness, unconsciousness
Site of Lesion
Site of lesion:
75% hemisphere
25% posterior circulation
20% lacunar
Pathophysiology: Brain has high and constant need for blood supply
Signs of cerebral involvement:
Dominant hemisphere: language disorder (dysphasia, middle cerebral artery)
Non-dominant hemisphere: disorders of knowing (agnosia) and doing (apraxia), visual or sensory
neglect
Loss of integrated cerebral function (eg cognitive impairment, memory, abstract thought)
Failure of inhibition of lower centres (eg spasticity and urinary incontinence)
126 4
th
and 5
th
Year Notes
Seizure activity: abnormal electrical activity in brain tissue around areas of ischaemia
Hemianopia
Four classes:
Total anterior circulation infarction (TACI. Anterior = Carotid artery anterior and middle
cerebral arteries): language or visuospatial disorder (depending on side) + homonymous
hemianopia + motor deficit in two or more of face, arm or leg
Partial anterior circulation infarction (PACI): 2 of 3 of TACI criteria
Posterior circulation infarction (POCI. Posterior = Basilar artery posterior cerebral artery):
variety of presentations, including ipsilateral cranial nerve palsy with contralateral motor
and/or sensory deficit, isolated cerebellar dysfunction, isolated homonymous visual field
defect
Common lacunar syndromes (small deep white matter infarcts):
Pure motor hemiparesis
Pure sensory abnormality
Ataxic hemiparesis
Sensori-motor stroke
Dysarthria and clumsy hand
Signs of brain stem involvement:
Diplopia, bilateral weakness or numbness, vertigo, ataxia
Brain stem syndromes: *
Syndrome
Structures Affected
Symptoms
Medial Medullary due
to Ant. Spinal or
Vertebral artery
Hypoglossal nerve (12)
Atrophy and paresis of tongue,
deviates to ipsilateral side
Medial lemniscus
Contralateral loss of discriminative
touch and proprioception
Pyramid
Contralateral hemiparesis
Lateral Medullary, due
to Vertebral, PICA,
maybe AICA
Spinal trigeminal n. & tract
Ipsilateral loss of pain/temperature
on face
Spinothalamic tract
Contralateral loss of
pain/temperature on body
N. ambiguous
Loss of gag reflex, dysphagia,
dysarthria, swallowing problems
Inferior cerebellar peduncle
Ipsilateral ataxia
Vestibular n.
Nystagmus, vertigo
Dorsal motor n.
Vomiting
Descending sympathetic
fibres
Ipsilateral Horner‟s syndrome
Basal Pontine
Syndrome, due to
Basilar and pontine
arteries
Abducens
Ipsilateral medial deviation of the
eye
Facial
Ipsilateral paralysis of face
Medial lemniscus
Contralateral loss of discriminative
touch and position sense
Corticospinal tract
Contralateral hemiparesis
Mediobasal
mesencephalic
syndrome due to
aneurysm of posterior
Circle of Willis or
Basilar
Oculmotor
Ipsilateral outward deviation of eye
Edinger-Westphal
Ipsilateral dilated pupil, no light
reflex
Corticospinal tract
Contralateral hemiparesis
Red nucleus
Contralateral cerebellar ataxia
Transient Ischaemic Attacks (TIAs):
30% of untreated TIAs eventually have a stroke, aspirin reduces this by a quarter
Presence of carotid bruit not very sensitive for stenosis (ie can have stenosis without it, may not
have significant stenosis with it)
Surgery for carotid stenosis giving TIAs: beneficial if stenosis > 70%, risk of ipsilateral
stroke. Other studies less variable (NNT if asymptomatic = 17, if symptomatic then 6 – 7)
Angiogram morbidity = 1.5%, surgical morbidity 1.5 – 6.3% (if not vascular trained)
Neuro-sensory 127
Also consider multi-infarct dementia
Management
Investigations:
FBC: exclude polycythaemia and anaemia. Do electrolytes and renal function
ESR: exclude vasculitis
Glucose
ECG/CXR for heart disease, AF
?CT – 5% don‟t have a stroke, also exclude haemorrhage before antithrombotic treatment, and to
assess for carotid surgery (>70% stenosis)
Treatment:
Aspirin small improvement in outcome if not haemorrhagic
Heparin has a negative effect: although beneficial for DVT prophylaxis
Warfarin anticoagulation if mitral stenosis or AF
tPA if within 4 hours and there is visible evidence of infarct covering < 1/3 of MCA territory on
CT
Immediate anti-hypertensive therapy only if hypertensive encephalopathy is suspected (will have
papilloedema)
Assessment of swallowing by a speech-language therapist: 40% of hospitalised stroke patients
have swallowing problems, can aspiration. Gag reflex is not sufficient to indicate normal
swallowing. Nil by mouth until assessed (ie for 12 – 24 hours) unless clearly dehydrated
Watch for cerebral oedema over next 24 hours if large stroke. Restrict fluids, iv mannitol
Early rehabilitation: turning to prevent bed sores, limiting bed rest
Assessment for depression (common following stroke) and urinary incontinence
Prognosis
After 6 months, 1/3 are dead, 1/3 have moderate disability, 1/3 have good recovery
Poor prognosis if haven‟t started to make a good recovery after 2 weeks (acute assessment not reliable)
Risk factors for poor prognosis: prior stroke, persistent incontinence, cognitive/perceptual deficits, poor
previous functional status or social supports, poor sitting balance
Vascular Pathology
Primary intra-cerebral haemorrhage:
Eg Sub-arachnoid haemorrhage or Intra-cerebral haemorrhage related to trauma
Due to high blood pressure or lobar haemorrhage (?due to amyloid deposition in vascular walls)
Ischaemic stroke:
Thrombotic: occlusion – depending on collateral flow
Embolic stroke
Other: vasculitis, cerebral venous thrombosis, carotid artery dissection, etc
Extent of infarction depends on:
Adequacy of collateral flow (via circle of Willis). Little/no collateral flow for the deep penetrating
vessels supplying the thalamus, basal ganglia, and deep white matter
Presence of previous occlusive lesions
Location and rapidity of the occlusive process
Infarcts are of two types:
Haemorrhagic (red) infarcts
Non-haemorrhagic infarcts: pale, bland, anaemic
Thrombotic infarction
Arterial occlusion usually due to in-situ thrombosis over a plaque, or emboli
Most common sites for atherosclerotic involvement are:
Carotid bifurcation
Origin of the middle cerebral artery
Either end of the basilar artery
128 4
th
and 5
th
Year Notes
Pathology
Imaging
< 24 hours
Cytotoxic intracellular oedema
CT: normal. Subtle loss of grey-white matter
interface. Little/no mass effect
MRI more sensitive than CT in first 24 hours.
See cortical thickening and loss of sulci
MRI, T2: signal intensity
MRI, T1: signal intensity
1 – 7 days
Tissue necrosis, maximal
intracellular oedema, blurring of
grey-white interface, tiny
haemorrhagic infarcts
CT: hypodense, homogenous area with sharp
margins. Variable mass defect
MRI, T2: hyperintense
7 – 21 days
(Subacute)
Resolving oedema. Marginal
capillary ingrowth. Progressive
liquifications
CT: Isodense surpigenous bands and nodular
regions develop in the hypodense infarct.
Infarcted white matter does not show density
change. Contrast ring enhancement
MRI: loss of previous hyperintensity.
Chronic
Phagocytic removal of necrotic
tissue. Cystic cavitation (esp in
white matter). Gliosis
(proliferation of fibrillary
astrocytes glial membrane)
CT and MRI. Lesion becomes homogenous.
Approach density of CSF. Gliosis
contraction. Dilation of adjacent ventricle.
Overlying cortex is atrophic, enlarged sulci
and cisterns. Stable by end of 3
rd
month.
Healing in the brain: don‟t want scarring as the remaining tissue doesn‟t need protection (it‟s still
within the skull) and scar contraction would damage surrounding tracts. So instead of scarring,
you get gliosis and cavity formation
Embolic Infarction
Mural thrombosis emboli. Most common sources are plaques within the carotid arteries and cardiac
mural thrombi
Most commonly affects middle cerebral artery
Embolus responsible for ischaemia lyses within 1 – 5 days reperfusion into ischaemic brain (lost the
ability to autoregulate)
This leads to perfusion, especially of grey matter and basal ganglia (lots of capillaries). Oedema
(would be if thrombotic) mass effect. Cortical petechial haemorrhages. If these are extensive
and merge haemorrhagic infarct
CT: previously hypodense become iso/hyper dense
Haemorrhagic Infarcts
Usually secondary to embolic infarct
Result from high reperfusion pressure, or following anticoagulation in thrombotic infarcts (eg heparin)
May develop within 21 days following an embolic infarct
Difference between haemorrhagic infarct and Intracerebral haemorrhage:
Haemorrhagic infarct
Intracerebral Haemorrhage
Inhomogeneous
Homogeneous
Wedge-shaped or rectangular
Round/Oval
Indistinct border
Sharp margins
Predominantly cortical
Predominantly white matter
Haemodynamic Infarcts
~ Border zone infarcts
Vaso-occlusive disease + disturbed autoregulation temporary uncompensated decrease in perfusion
pressure
Affects watersheds between vascular territories (may haemorrhagic infarct), especially between the
middle and anterior cerebral arteries
Can lead to transient ischaemic attacks and infarction
Lacunar Infarcts
Hypertension arteriolar sclerosis of the deep penetrating arteries of the:
Middle cerebral artery basal ganglia and internal capsule
Neuro-sensory 129
Posterior cerebral and basilar communicating arteries mid-brain and thalamus
Arteriolar sclerosis hyaline disrupted lumen small infarct small round lacunae (hole)
Cerebral Venous Occlusion
Confined to certain patients: pregnancy, post-partum, diabetes mellitus
Head Trauma
Types of Injury
Effects of head trauma:
Direct trauma (eg under skill facture)
Cerebral contusion (local or contracoup)
Shearing: diffuse axonal injury petechial haemorrhage in midbrain, corpus callosum and
cerebrum
Cerebral swelling
Intracranial haemorrhage: epidural, subdural, subarachnoid, intracerebral
Concussion: no absolute definition but period of loss of consciousness and anteriograde or
retrograde amnesia
Types of skull fracture:
Simple: linear of vault
Depressed
Compound: open to skin or sinuses
Skull base rhinorrhoea or otorrhoea
Principal injuries from acceleration/deceleration injury:
Contusion: coup and coutracoup
Subdural haematoma from ruptured bridging veins
Diffuse axonal injury (shearing injury). Ranges from concussion (very mild, temporary,
physiological disturbance) to severe
Assessment
ABC
Gross assessment:
Localise injury by looking for lumps, depressed fractures, etc
CSF from nose or ears basal skull fracture
Neuro assessment:
Use level of consciousness: GCS – best response to verbal, motor and eye response. See
Glasgow Coma Scale (GCS), page 481
Also pupillary size and exam, limbs
In diffuse injury the main enemy is ischaemia, which leads to oedema. In localised injury, oedema is
the main enemy – acts like a mass lesion
Presume cervical spine injury until cleared:
Need 3 xray views: anterior, lateral and peg (open mouth to view facet joints of C1 and C2, and
odontoid peg)
Clearance requires clear X-rays AND normal exam. If x-rays clear but tender C spine then CT
Assess other systems
Investigations:
SXR for minor HI (OK now but were knocked out): mainly for medico legal cover!
Cervical spine Xray, even if minor, for occult dens or cervical fracture
CT brain if GCS < 15, neuro signs in limbs, cranial nerve palsy or CSF leak
Criteria for admission, etc:
Discharge if GCS 15, low velocity, no seizures or fractures, adequate supervision at home and
readmission checklist given to patient
Admit if: loss of consciousness/marked post traumatic amnesia or under 5 or over 50
CT indicated if GCS < 15 at 4 hours or < 9 at any time, seizures or focal neurological signs
Neurosurgical referral if compound head injury or GCS < 15
Raised Intracranial Hypertension (ICP)
Other causes of intracranial pressure:
Bleeding
130 4
th
and 5
th
Year Notes
Neoplasm
Brain oedema results from:
Inflammatory lesions
Infarction
Head injury
Neoplasms
Types of brain oedema:
Vasogenic cerebral oedema: permeability of cerebral vessels
Cytotoxic cerebral oedema: rare. Toxic effect intracellular oedema
If severe acts as a space occupying lesions
ICP leads to displacement of CSF and compression of veins, then:
Herniation of the:
Cingulate gyrus under the falx
Parahippocampal gyrus past the free edge of the tentorium cerebelli
Cerebellar tonsils into the foramen magnum (fatal)
And pushing of the midbrain against the tentorium on the opposite side
Treatment of intracranial hypertension:
Aim: Keep ICP low. Principle danger is ICP ischaemia, transtentorial herniation (uncus of
temporal lobe on ipsilateral side) and coning
ABC:
Maintain airway. If breathing OK then lateral position. 100% O2
Intubate if GCS < 9
Aim to keep CPP (Coronary Perfusion Pressure) > 70. CPP = MAP less the greater of ICP or JVP.
Coronary blood flow = CPP / CVR (cerebral vascular resistance)
In general, keep BP normal:
If hypotension then perfusion pressure (bad)
Use colloids to maintain BP at 120 – 160 systolic (don‟t over-hydrate, especially infants)
Diuretic: frusemide 40 mg iv
Tilt head up venous return venous pressure perfusion pressure
O2 requirements by sedation (Propofol or barbiturates eg thiopentone) and cooling
Hyperventilate reduce CO2 to 30 – 35 mmHg cerebral blood flow cerebral blood
volume brain volume ICP (but only for short term otherwise ischaemia)
Cushing's Reflex (bradycardia, hypertension) kicks in when O2 falls below 20 mls/100g/min
Mannitol 0.5 – 1g/kg over 20 mins iv if life threatening – draws fluid from brain, but also a
diuretic, so watch for hypotension
Drain fluid from ventricle if severe
Evacuation of intra-cerebral bleeds
Seizures: Clonazepam 0.25 mg/min up to 1 mg plus loading dose of phenytoin
Nutrition, urine and bowel management
Steroids not effective after head injury
Coma and Stupor
Checking eyes:
Doll‟s Eye: do eyes remain fixed on target when head is turned. Tests inputs from the neck
muscles. Requires linking via medial longitudinal fasiculus of nerves 3, 4, and 6 on both sides
Vestibulo-Ocular reflexes: caloric response. 1 ml of ice water evokes nystagmus beating to the
opposite side in a normal person. If unconscious, see only deviation without corrective nystagmus
In deepening diffuse coma without structural damage, the Dolls eye disappears, then the Caloric
response. If pupils still reactive then no coning
Due to Structural damage
Only if affecting brain areas required to maintain consciousness: usually infarct, bleed or inflammation
Reticular Activating System: periventricular grey matter from mid pons up, including the hypothalamus
and deep grey matter of both hemispheres
Most supra-tentorial lesions produce coma due to oedema compression of deep hemispheric
structures (paramedian diencephalon)
Features of coning:
Transtentorial: progressive drowsiness followed by pupil changes
Neuro-sensory 131
If unilateral cerebral swelling then stretching of ipsilateral 3
rd
nerve parasympathetic
innervation
If diffuse bilateral swelling involving brain stem then impairment of both sympathetic and
parasympathetic mid position, irregular pupils
Posterior fossa coning: headache, stiff neck, BP, pulse
Due to Diffuse depression of brain function
Usually metabolic encephalopathy
Key differential from structural damage: Pupillary reflexes retained
Features: clouded consciousness, difficulty concentrating, altered sleep wake patterns
Two basic types:
Delirium or acute toxic psychosis: agitated, hallucinatory, severely disorientated
Acute confusional state: quieter than delirium
Immediate evaluation: Glucose, thiamine, Na, Ca, Creatinine, pH, PO2, PCO2, lumbar puncture, sepsis
(septicaemia, lung, urinary tract, meningitis)
Later: LFT, Sedatives, Blood and CSF culture, Electrolytes and Mg, Coagulation, EEG (absence status)
Outcome:
Sedative drug poisoning: equivalent to GA and will recover with treatment
Other medical causes: depends on cause, severity and extent. Only 15% make a good recovery if
in coma for more than a few hours
Traumatic: better outlook, related to age, 50% die (many instantly), if ophthalmologic signs of
brain stem dysfunction then 90% die or remain vegetative
Syncope (Fainting)
Temporary loss of consciousness (ie up to a minute or so)
In physically or emotionally stressful situations (eg sight of blood), going out with new partner or boss
Vasodilation from alcohol, warmth or drugs may contribute
Usually standing or sitting
Often groggy and unwell afterwards
Myoclonus common (seizure like movements, vocalisations): only 10% motionless
Due to cerebral blood flow:
Postural Hypotension
Cardiac output: arrhythmia, VT, periods of asystole (Stokes Adam disease)
NOT due to: TIA, hypoglycaemia, alcohol. These take longer to recover
Abnormal Speech
Types:
Dysphonia/dysarthria: problems with the mechanics, not ideas, of speech production (eg nerves
involved in motor control, connective tissue disease, etc). Say „baby hippopotamus‟
Broca‟s (expressive) dysphagia: Non-fluent speech with malformed words. Reading and writing
are impaired but comprehension intact. Patients understand questions. Inferio-lateral frontal
lesion
Wernicke‟s (receptive) dysphasia: Empty fluent speech. Maybe mistaken for psychotic speech.
Reading writing and comprehension are impaired. Posterior Superior temporal lobe lesion.
Cerebellar disease: ataxia of the muscles of speech slurred and irregular speech
Pseudo-bulbar palsy: UMN. Exaggerated jaw jerk, difficultly swallowing, maybe emotional
liability. Due to upper motor neuron lesion above the mid pons due to bilateral CV disease, severe
MS or motor neuron disease
Bulbar palsy: LMN eg facial nerve, Guillian Barre, etc
Assessment:
If speech fluent, grammatical and meaningful or patient can repeat a sentence dysphagia
unlikely
If the patient can comprehend simple instructions with several steps Wernicke‟s unlikely
Parkinson’s Disease
Bradykinesia, tremour (70% of cases) and rigidity (unilateral onset) but no early difficulty with gait
Also lack of arm swing (usually only one side at outset), lack of facial expression, paucity of
movement. 30% become demented (either due to Alzheimer‟s or widespread Lewy bodies). Also
postural hypotension
132 4
th
and 5
th
Year Notes
Gradual progression and prolonged course
Pathology:
Gross: Pallor of substantia nigra
Micro: in melanin-containing dopaminergic neurones with secondary reactive gliosis. Lewy
Bodies may be present in remaining neurones (eosinophilic intracytoplasmic inclusions).
Treatment:
L-Dopa dyskinesias, and on-off effects after 3 – 5 years. The mainstay of treatment. Give
minimum dose to control symptoms, not necessarily signs
Carbidopa: prevents peripheral conversion of L=Dopa
For younger patients, begin with a dopamine agonist (bromocriptine, pergolide)
Selegiline, a MAOB inhibitor delays the time needed for the subsequent introduction of L-Dopa
Anticholinergics: stop ACh induced hyper-reactivity: but dry mouth, urinary retention, blurred
vision
Other causes of Parkinsonism. Parkinson Disease is a disease of exclusion:
Drug induced parkinsonism eg phenothiazines including antiemetics (eg Maxolon)
Multisystem atrophy: also have cerebellar ataxia, eye movement disorder, autonomic dysfunction
and pyramidal signs
Huntington‟s Disease: early presentation may mimic Parkinson‟s, rather than a movement disorder
with chorea, myoclonus and dystonia
Wilson‟s Disease: consider in younger patients. Behaviour disturbance, dystonia, flapping
tremour. Rare but treatable
Diffuse Lewy Body Dementia: Males 2:1. All demented eventually. Most have rigidity,
bradykinesia but tremour uncommon. Usually begins with cognitive impairment. See Dementia,
page 439
Dystonias
Most dystonias are caused by basal ganglia disturbance
Blephrospasm
Causes eyes to close all the time, especially in light, wind, etc
Tx: inject botulinum toxin
Hemifacial spasm
Cervical dystonia: neck turning, head back, etc
Demyelinating Disease
= Selective, primary destruction of myelin
Diseases of CNS and PNS myelin do not affect the other
CNS Demyelinating disease:
Multiple Sclerosis
Acute Disseminated Encephalomyelitis
Progressive Multifocal Leucoencephalopathy (PML)
Toxins
Leucodystrophies
PNS Demyelinating Diseases:
Guillain-Barre Syndrome
Diphtheria
Diabetes Mellitus
IgM Paraproteinaemia
Leucodystrophies
Hypertrophic neuropathies (eg Charcot-Marie Tooth Disease)
Secondary Demyelination:
Infarction
Abscess
Contusion/Compression
Multiple Sclerosis
Chronic autoimmune demyelination of CNS neurons
Epidemiology:
Female to male = 2: 1
Peak age of onset 20 to 40 years
Neuro-sensory 133
Marked racial difference in susceptibility. Caucasian most common. Africans/Asians rare
Genetic risk modified by environmental risks up to age 15 (from studies of immigrants)
Risk 15 times higher if first degree relative with MS. Associated with HLA-DR2 haplotype
Can be sensory or motor
Diagnosis: Two lesions in different places at different times. Lesions normally visible on MRI
One spinal chord lesion may account for diffuse symptoms. As it grows through a spinal chord column
a single lesion may progressively affect other areas
Highly variable course. Relapsing and remitting
Worse after exercise
Pathology:
Autoimmune destruction of oligodendrocytes, ?triggered by a viral infection in a genetically
susceptible host
Multiple plaques distributed throughout the cerebral hemispheres (especially periventricular white
matter), optic fibres, brain stem, cerebellum and spinal chord
Active plaques: are soft yellow or pink and granular. Myelin breakdown foamy macrophages,
T-suppressor cytotoxic cells, T-helper cells, and plasma cell infiltrate. Also reactive astrocytes
Chronic plaques: well defined, sclerotic and grey. Sharply defined areas of demyelination with
compacted astrocytes processes ( gliosis)
Lesions expand by concentric outward growth. Poor correlation between number of plaques and
symptoms
Tx: -interferons
Progressive Multifocal Leukoencephalopathy (PML)
Like MS: multiple discrete foci of myelin destruction with relative preservation of axons
Caused by JC virus (DNA papovavirus common in the community) in immunodeficient patients
Relentlessly progressive
Pathology: multiple lipid laden macrophages, oligodendrocytes with ground-glass nuclei (viral
inclusions)
Other CNS Degenerative Diseases
Amyotrophic Lateral Sclerosis (ALS)
Most common form for progressive Motor Neurone Disease
Affects upper motor neurones (ie layer five of the motor cortex) and lower motor neurones (anterior
horn cells)
1 – 3 per 100,000 per year
5 – 10% autosomal dominant, rest sporadic
Cause unknown
Clinical presentation:
Lower motor neurons: fasciculations, progressive wasting of muscles, bulbar involvement
difficulty chewing etc, weakness of respiratory muscles
Upper motor neurons: spasticity, muscle stiffness, hyperreflexia
Sensory, bowel, bladder, ocular movements and cognitive functions relatively preserved
Median survival 3 years
Pathology:
Neurons shrink and accumulate lipofuscin
No macrophage or inflammatory response
Disappearance of axons in Corticospinal and corticobulbar tracts astrogliosis lateral sclerosis
Epilepsy
See Seizures, page 625 for Epilepsy in Childhood, Benign Febrile Convulsions and Anoxic Seizures
1:200
Onset after age 20 10% chance of tumour
Symptoms:
Abrupt onset, brief duration, rapid recovery, and stereotypical recurrence
Not just fits: focal signs depending on where in the brain it arises
Very long list of differentials to epileptic seizure: See Other Spells, page 136
134 4
th
and 5
th
Year Notes
Is it epileptiform:
Pseudo-seizure (or Non-Epileptic Seizure): either factitious disorder (are deliberately faking) or
conversion disorder (they think it‟s real) (See Somatoform Disorders, page 439)
Hard to differentiate: going blue, frothing at mouth and incontinence can happen in pseudo-seizure.
Epiletics may not have post-ictal phase
Gold standard is EEG: but can‟t do this in A&E. Fall back is checking whether the person is in
any way aware (then it can‟t be generalised) – eg localising to pain (sternal rub, squeeze thumb
nail), drop their hand onto their face
Check history: evidence of brain injury, infection, on anticonvulsant meds
Pseudo seizure more common in women (10:1) and those with a medical connection (eg
doctor/nurse in family, someone with epilepsy)
Epileptic seizures happen more if: tired, ill, fever, stressed, not taking medication (but these are not
classified as „provoked‟ as they wouldn‟t provoke a seizure in a normal person)
Seizure Types
Generalised: bilaterally symmetrical without local onset
Tonic-clonic (Grand mal) seizures: Tonic phase: 10 – 20 secs – extension phase then tremour
begins – repetitive relaxation of tonic contraction. Clonic phase: usually 30 seconds, random
movements, tongue often bitten
Absence (Petit Mal) Seizures: Characteristic type of absence attack. Childhood or adolescent
onset, associated with 3/sec spike and wave on the EEG. Blank stare and unresponsive for 5 – 15
seconds. No post-ictal confusion or sleepiness. May also have automatisms and mild clonic
motion (usually eyelids at 3 Hz). May be induced by hyperventilation. 80% have no further
seizures after 20 years old. Can also have atypical absence seizures. Treat with ethosuximide or
sodium valproate
Atonic: complete, sudden loss of tone – completely collapse, may injure themselves
Tonic: sustained contraction, maybe with fine tremour
Myoclonic: Sudden, very brief jerk but still generalised
Clonic: rhythmic jerking
Infantile spasms:
Sudden bilateral symmetrical jerk, extensor or flexor. Can be subtle, come in clusters
Usually around 3 – 6 months, boys > girls
Grow out of the spasms
Bad prognosis: cerebral palsy, retardation, etc
Medical emergency: try to urgently get them under control
Partial: Begin locally
In simple partial seizures consciousness is preserved.
Complex partial seizures are focal seizures in which consciousness is altered (eg blank
unresponsiveness followed by automatisms, eg lip smacking, other semipurposeful activity) –
usually temporal lobe but may be frontal. Can go on for minutes. Aware it is coming (cf absence
which is sudden)
Partial seizure secondarily generalised: they have an awareness first
Localising it:
Preceding aura: olfactory, visceral, auditory, visual, déjà vu
Dystonic posturing: contraction of agonist and antagonist muscles
Post-ictal Todd‟s Syndrome: if they have one area of weakness after a seizures (ie one hand
weaker than the other) then it started locally
Automatic behaviour usually seen in complex partial seizures: but can be in absence (petit mal)
seizures. Eg Oral or manual automatisms
Seizure location:
Frontal: focal tonic or clonic motor activity, posturing, prominent motor automatisms but no
orofacial or experiential automatisms
Central: focal clonic seizures with preservation of awareness
Temporal: experiential, gustatory or olfactory hallucination. Motion arrest, automatisms
Parietal: exclusively somatosensory manifestations
Posterior: polymodal sensory, visual, auditory or somatosensory hallucinations
Sorting out type of seizure:
When do the seizures occur
Does patient know they‟re going to have a seizure
Neuro-sensory 135
What can the patient recall
Detailed description from observers:
Are they aware – will they respond
Are their automatisms
Is there dystonic posturing
How long did it last
After the seizure: are they confused, can they speak, any post-ictal Todd‟s
Treatment
Diagnosis is clinical. EEG helps with severity, classification, to localise a surgically remediable
abnormality (eg hippocampal sclerosis), and to differentiate pseudo-seizures
Don‟t treat until you‟re sure it‟s epilepsy
Anticonvulsants suppress seizure activity in 80%
Principles of drug treatment:
When to treat: often wait for second seizure – although treatment after the first occurrence, but
no long term change in outcome
Use only one drug
Tailor drug to seizure type
Introduce slowly. Takes about 5 days to stabilise a change in dose
Monitor drug level: for other than phenytoin, this is to check compliance. Beware – plasma level
at which seizure control is obtained is variable
Consider withdrawal of drugs after 2 years without seizure, slowly over 6 months
Mode of action unknown – but may GABA breakdown, as well as modifying flux of Na, K and Ca
ions
Usual drugs:
Idiot‟s guide: carbamazepine for partial seizures and Valproate for generalised
Seizure type
Examples of conventional drugs
Partial Seizures
Simple partial,
Complex partial and
Partial secondarily generalised
Carbamazepine (Tegretol),
Phenytoin, Sodium Valproate
(Epilim), Penobarbitone,
Primidone
Generalised seizures
Absence
Clonazepam (a BZD),
Ethosuximide, Valproate
Myoclonic
Valproate
Tonic-clonic
Carbamazepine, Phenytoin,
Valproate, Penobarbitone,
Primidone
Conventional drugs have hepatic clearance
Side Effects:
General lethargy, concentration, unsteadiness, dizziness
LFTs: but serious hepatotoxicity rare. Especially Valproate
Rarely bone marrow suppression
Pregnancy:
Epilepsy often worsens during pregnancy
Plasma concentration of drugs falls due to pharmokinetic changes and compliance
Teratogenic: 3% risk of malformation on 1 drug (also, epilepsy itself can be teratogenic -
?hypoxia during seizure)
% in breast milk varies by drug
Specific drugs:
Carbamazepine: enzyme inducer
Phenytoin: Dose-dependent kinetics small in dose may in plasma concentration,
SE: ataxia, peripheral neuropathy, gingivitis
Must be seizure free (with or without treatment) for 12 months before you can drive. Obliged to tell
LTSA on diagnosis if the patient won‟t and continues to drive
Status Epilepticus
Repeated seizures without regaining consciousness
No one knows how long is too long: but after 10 minutes risk of damage
136 4
th
and 5
th
Year Notes
If not sure whether it‟s epileptiform then must still treat for status
Treatment:
Protect and maintain airway, insert oral airway
Prevent injury
100% oxygen
Diazepam 10 – 20 mgs iv, not exceeding 2 – 5 mgs per minute. If no iv access give rectally with
10 – 20 ml normal saline. Duration is brief and another anticonvulsant is required. Avoid
repeating diazepam cardiorespiratory collapse. If no response give clonazepam 1 – 4 mg iv
Phenytoin 50 mg/min iv (25 mg/min in cardiovascular disease), usual adult dose 1250 mg in 100
mls saline over no more than 20 minutes. Monitor BP and heart rate
If established, give phenobarbitone
If refractory, then anaesthesia with propofol or thiopentone. Taper after 12 – 24 hours
Other Spells
Commonly misdiagnosed as seizures
Paroxysmal non-epileptic events without altered consciousness: Jitteriness, migraine with focal aura,
hyperventilation, acute paroxysmal vertigo, shuddering attacks, anxiety states (eg panic attack),
psychosis, drug induced dystonias, masturbation, tics, etc
Paroxysmal non-epileptic events with altered consciousness: Day dreaming, breath holding spells,
reflex syncope, TIAs, psychosis, pseudo-seizures, delirium, metabolic disorders, other brain insult
(infection, haemorrhage), ritualistic movements, migraine, arrhythmias, drugs substance abuse
Paroxysmal non-epileptic events related to sleep: benign sleep myoclonus of infancy, head banging,
night terrors, hypnogogic jerks, sleep walking, sleep apnoea
Brain Tumours
Epidemiology
2% of all cancer deaths
20% of paediatric neoplasms (21 per 100,000 at 2 years)
Incidence 8 – 10 per 100,000 per year
Incidence lowest in teens rises to 16 per 100,000 in 70‟s
Histology
Cell types in the brain: neurons, microglia (lymphocytic derived, phagocytic function), oligodenrocyte
(myelination), choroid cells (make CSF), astrocytes (structural support, star shaped, multiply in sites of
injury), ependymal cells (line ventricles), meninges, pituitary, lipophages (histiocytes which
phagocytose lipid rich myelin – non-specific marker of white matter destruction)
Neuropil = intercellular matrix in the CNS – tangled processes of neurones, astrocytes,
oligodendrocytes
Tumour vasogenic oedema
Incidence of neoplasms:
Neuroepithelial (ie intrinsic brain cells) Gliomas: 52%
Astrocytoma: 44%. When severe = Glial Blastoma Multiforme (GBM)
Ependymoma 3%
Oligodendrioglioma: 2%
Medulloblastoma: 3%
Metastatic 15% (eg breast, lung)
Meningioma: 15%
Pituitary: 8%
Vestibular Scwhannoma: 8%
Also retinoblastoma
Different incidence in children:
Normally posterior fossa (as opposed to anterior fossa in adults) and different frequencies of
different types
Most common tumours are pilocytic astrocytoma and medulloblastoma
Astrocytoma
Locally invasive
Neuro-sensory 137
Presentation:
ICP from obstructive hydrocephalus and from space occupying lesion
Focal neurological deficit
Epilepsy: ¾ of high grade astrocytoma present with seizure
Endocrine
By age:
Cerebral hemispheres in middle and old age
Spinal cord in young adults
Cerebellum and pons in childhood
Pathology:
Benign = won‟t recur if removed. However, also need to be accessible to have a good prognosis
Heterogeneous – range from well-differentiated to anaplastic
Characteristic fibrillary background of cytoplasmic processes containing Glial Fibrillary Acidic
Protein (GFAP). Can use immunohistochemistry to stain for these. May congregate to form
Rosenthal fibres
Graded from 1 (low grade, and hard to differentiate from reactive gliosis although these rarely
produce a distinct mass) to 3 (anaplastic) to 4 (glioblastoma multiforme – GBM, mitoses common
compared with low grade, pallisading necrosis differentiates it from grade 3). Low grade have a
tendency to become high grade and are also hard to cure due to their infiltrative nature
Grossly: Infiltrative. Either firm or soft/gelatinous. GBM is heterogeneous with focal
haemorrhage and necrosis
Pilocytic variant of astrocytoma: most common astrocytoma of childhood. Excellent prognosis.
Cystic. Usually in cerebellum
Astrocytomas (grade 3 or 4) are the most common gliomas to arise subsequent to radiotherapy
(usually 5 – 25 years later)
Investigations: CT and MRI. Xray and angiography obsolete
Management:
Dexamethasone: vasogenic oedema ICP
Anticonvulscents seizures
MR spectroscopy biopsy by framed stereotactic or image guidance
Surgery: debulking or macroscopic excision (only if not deep or eloquent areas otherwise too much
damage from surgery – use radiotherapy for these)
Arguments for macroscopic excision. High-grade gliomas weigh 100g at diagnosis = 10E11 cells.
After macroscopic excision will still have 10E10 cells. Effective radiotherapy 10E8 cells.
Chemo/radio therapy only kills cells in division
Prognosis
For GBM: Median survival:
Without surgery, 17 wks
With surgery, radio and chemo, 51 wks
For low grade glioma: 50% 5 year survival if total macro excision
Other Neuroepithelial Tumours
Subendymal giant cell astrocytoma: associated with tuberous sclerosis
Neuronal tumours: not common. Include:
Gangliocytomas
Gangligliomas: better prognosis
Cerebral neuroblastoma: Rare, in children. Resemble peripheral neuroblastomas – „small round
blue-cell tumours‟
Oligodendroglioma:
5 – 15% of gliomas
Radiographically, well demarcated and often show calcification (key differential)
Grossly: gelatinous masses +/- cysts and/or haemorrhage
Ependymoma: usually in fourth ventricle outflow obstruction. Also in intramedullary portions of
the spinal chord. Slow growing and not malignant but poor prognosis. CSF spread is common.
Significant histological features: „true‟ rosette and perivascular pseudo-rosette. Numerous subtypes
Choroid Plexus Papilloma: rare. In ventricles. Usually children. Cauliflower type projections into
ventricular lumen
138 4
th
and 5
th
Year Notes
Pineal Neoplasma: Intrinsic tumours are Pineocytoma and Pineoblastoma. Germ cell tumours are the
most common, including choriocarcinoma, teratoma, etc. Present with mass effects in men aged 20 –
40. Differential: lymphoma or metastatic cancer
Hemangioblastoma: Highly vascularised, cystic tumours, mainly in the cerebellar hemispheres
Craniopharyngioma: Arise from the epithelium of Rathke‟s pouch – part of the embryonic nasopharynx
the forms the anterior lobe of the pituitary. Present due to mass effects in children and adolescents.
Histology: see keratin pearls.
Primitive Neuroectodermal Tumours (PNETS):
Rare tumours in children arising from primitive glial or neuronal precursor cells. Aggressive and
poor prognosis. Usually “small round blue-cell tumour” (differential includes lymphoma)
Medulloblastoma: a distinctive PNET. Occurs exclusively in the cerebellum, mainly in children,
mainly as a midline mass. Cause CSF obstruction and spread via CSF
Scwhannoma: In the cranial vault, nearly all schwannomas are attached to the 8
th
cranial nerve in the
cerebellar pontine angle acoustic neuroma
Lymphoma: Either originated in the CNS or from systemic invasion (usually affect the meninges).
Usually B-cell lymphomas
Pituitary
Pituitary Adenoma: benign neoplasm in anterior lobe of the pituitary
Present with either mass effects (including on the rest of the pituitary) and excess hormone
secretion
At any age or sex, but most common in men aged 20 – 50
Classified on the basis of hormones they secrete by immunocytochemistry. Poor correlation
between acidophils, basophils and chromophobes and the hormones secreted
Carcinomas are rare. Diagnosis requires gross brain invasion or discontinuous spread
Metastatic Brain Tumours
20% have intracranial mets at autopsy
In 15% primary organ not found
Surgery for solitary met if primary site controlled or for symptomatic control or for diagnosis
Most mets are carcinomas. 80% are due to (in decreasing frequency): lung, breast, skin (melanoma),
kidney and GI
Prognosis:
Melanoma & lung solitary: < 30% 1 year survival
Breast solitary: 50%
Undetermined solitary: 50%
Meningioma
20% of primary intracranial neoplasms
Incidence peaks in females aged 40 - 50
Benign in 90 – 95%
Occur anywhere round brain
Well circumscribed mass effects
Histology: meningothelial whorls and psammoma bodies
Tx: surgical excision
Spinal Chord Syndromes
Prognosis depends on time to treatment: speed is important
Trauma:
Transfer to specialist unit within 24 hours unless medically unstable
Catheterise: bladder won‟t work urinary retention
Check underneath them before transferring. An unfelt pen or other object will cause a full
thickness pressure sore during 2 hour transfer 3 months to heal
200 per year in NZ (same as severe HI). Mainly young men long term disability, lots of
ongoing psychological problems
Extradural spinal cord compression (EDSCC)
Usually cancer. Also haemorrhage (epidural haematoma) or epidural abscess
Key questions: where is the lesion, what is the lesion (eg weight loss, past cancer history
cancer)
Neuro-sensory 139
If there is a clear level below which these is sensory abnormality spinal chord
If both legs then spinal chord (usually). Can be parasagital meningioma (very rare)
Are arms normal: if so T2 highest possible level
If there are signs of an upper motor neuron lesion in the legs then it MUST be above the cell
bodies of L3 – S5 in the conus of the spinal chord, which is at T12 vertebral level if UMN
lesion then it is in thoracic spine or above
95% have pain at the site of compression very good indicator. Tap gently down spinal chord
with tendon hammer
Imaging: MRI
If can‟t be completely sure it‟s cancer MUST biopsy (eg chronic infection)
Cancers:
Lymphoma
Female: breast
Male: lung, sometimes prostate
Transverse Myelitis:
Inflammation of spinal chord itself
Same symptoms as EDSCC, but no compressing signs on MRI (usually normal – NO mass lesion)
Usually due to a demyelinating type inflammation – can be due to MS (= 2 demyelinating lesions
in the CNS at different times and different places)
Could also be sarcoidosis granulomas and inflammation (very rare to only occur in spinal
chord)
Corda Equina Syndrome (CES)
Triad: leg weakness, sensory loss, sphincter problems (usually overflow not urgency – ie LMN)
Classic description: „saddle anaesthesia‟ – anaesthesia in sacral dermatomes – eg feels like cotton
wool when sitting on the toilet seat. May be only symptom. Usually bilateral
If due to central disc prolapse can be fixed if treated urgently medical emergency
95% of disc prolapses are at L4/L5 or L5/S1: but most are laterally into nerve root, not central into
cauda equina
Acute Inflammatory Demyelinating Polyradiculopathy (AIDP)
= Guillian-Barre
= Demyelination of multiple peripheral nerves
Symptoms: ascending paralysis. Affects arms, legs and respiratory. Only a portion will get to
ventilatory arrest, but can deteriorate very quickly test FEV1 4 hourly while normal (normal >
4 l), to ICU if < 2 l. (O2 saturation and PO2 won‟t tell you till too late)
Predominantly motor problem: unlikely to be AIDP if lots of sensory symptoms
Signs: LMN and arreflexia (arreflexia is a classic sign)
Tests:
Lumbar puncture: protein but no WBC
Nerve conduction studies: motor conduction < 30 m/sec (normal > 40 – 50 m/sec)
Treatment: IV globulin and plasmaphoresis (plasma exchange). Heparin to prevent PE
Not related to Chronic Inflammatory Demyelinating Polyradiculopathy
Headaches
See also Headaches, page 624 for Headaches in Children
Recent onset of severe headache: the most common cause is idiopathic
Ask about associations/antecedents
Red flags: fever, change in mental status/personality, fits, focal neurological signs, sudden and severe,
affected by postural change, normally headache free, waking at night or in the morning with a headache
Types of headache:
Tension headaches, eg chronic daily headache, gradual onset (chronic), sleep not disturbed, treat
by stress (massage, relaxation). ? Depression. Types: post-coital, ergotamine misuse
Cluster headache: clusters of extreme, recurrent non-throbbing deep pain in and around an eye,
spreading onto the face. Eye typically becomes swollen and watery
Migraine: visual symptoms, unilateral, throbbing, nausea, aura
Facial structure: eg TMJ dysfunction, sinusitis, NOT teeth
Neuralgic: eg idiopathic, trigeminal neuralgia
„True vascular headache‟: associated with TIA/stroke, artery dissection, giant cell arteritis
Associated with ICP: focal lesions, venous thrombosis, meningitis, severe hypertension
140 4
th
and 5
th
Year Notes
Acute: ?meningitis, sinusitis, head injury
Associated with post Lumbar puncture
Treatment: Ongoing unchanged tension or migraine headache: TCAs
Differential of morning headache:
ICP
CO2 (eg sleep apnoea)
Diabetic going hypoglycaemic overnight
Myasthenia Gravis
Antibodies to Ach receptors weakness, fatigues with repetition
Affects eye movement in 15%
Treatment:
Immunosuppressives: Prednisone, azathioprine, cyclosporin
Take out thymus – many have hyperplasia or thymoma
Myasthenia Gravis Crisis:
Triggers: Respiratory infection, change in medication
Respiratory failure due to weakness, can be insidious
Consider ICU admission and ventilation
Other neurological emergencies
Meningococcal meningitis. See Infections of the CNS, page 495.
Encephalitis: fever, stiff neck, strange behaviour, unable to make new memories, seizures. Acyclovir
10 mg/kg 8 hourly (> 20% caused by Herpes Simplex)
Temporal arteritis/Giant Cell Arteritis: See Giant Cell arteritis/Temporal Arteritis, page 282
Other
Trigeminal neuralgia: momentary severe shooting pain in one division of 5
th
nerve due to touching,
chewing or speaking. Responds to Tegretol
Locked-in syndrome: pontine infarction quadriplegia and variable loss of all reflex and horizontal
eye movements. Vertical eye movement or eyelid movement may be the only means of
communication
Cerebellar infarction/haemorrhage: vertigo, headache, and abnormalities of eye movements (eg
saccadic deficits). May lead to life threatening compression/coning of the brainstem
Eyes
History
Common presenting complaints:
Loss of vision: blurred, double, distorted, field loss, glare, colour defect
Disturbance of sensation: pain, itching, photophobia. If sharp pain surface, if throbbing pain
deeper lesion
Changes in appearance: red and/or discharge
Associated symptoms
Past ocular history: trauma, surgery, spectacles
General medical history: diabetes, allergy, medications
Family History: squint, glaucoma, refractive error
Social History: Assess impact on function (eg work, hobbies, support, dependents). Also smoking
incidence of cataract
Physical Examination
Trying to work out where is the problem: refractive, obstruction of light through the transparent tissues
of the eye, or neural problem
Measure Visual Acuity:
One at a time. Wear glasses
Snellen‟s Chart: Distance of chart (normally 6 metres)/Distance they could read. Smaller fraction
is worse
If can‟t see chart at all, then Count Fingers (CF) at X metres
If can‟t count fingers then Perceive Light (PL): flash torch on and off in eyes – can they see it

Neuro-sensory 141
Check with pinhole, if clearer refractive error or corneal scarring, refer to optometrist. If worse
retinal pathology
Also check visual fields, colour, stereo vision
External inspection:
Be systematic: look for changes in shape, size, position, colour, transparency, is it focal or diffuse
Pupil reflexes: Should be simultaneous and equal. Swinging light test: Alternate light from one
eye to the other, swapping it quickly. Both pupils should stay the same. Sensitive and complete
test of neural pathways. If this shows a problem, test for an efferent pupillary defect with the near
reflex test
Internal inspection with ophthalmoscope:
Get patient to look at target a long way away: relaxes accommodation. Dim the light dilation
Dilate pupil with Madriasil (not atropine, T½ too long)
Check for:
Red reflex defects: eg cataract, intra-ocular blood
Reduced transparency (compare two eyes)
Cup and disk:
Disk is 15 degrees nasal to fixation. To examine macula, get patient to look directly at the
light
Check disk for distinct margins and symmetry
Physiology cup is blood vessels in the centre of the nerve – not nerves
Normal cup to disc ratio < 1/3 (but lots of variation). Check it‟s the same in both eyes
Large and/or deep cup sign of glaucoma (vessels „diving into‟ the cup) – especially if eyes
different. Large ratio
Papilloedema: non-inflammatory nerve oedema due optic nerve axon flow obstruction or ICP
red disk swelling towards you, blurred margins of disk but no early visual loss. Venous
obstruction may haemorrhage. If bilateral then ICP
Papillitis: optic nerve head inflammation swollen disk with visual loss. If unilateral then
optic neuritis (colour vision, orbital pain), sarcoidosis, Tb, Syphilis, etc
Pseudopapilloedema: occurs in hypermetropia, disc is smaller than normal and crowded
Fundus pathology: maculopathy, optic neuropathy, retinal detachment
Refractive errors: hard to focus on retina
Arteries: narrow, bright red, windy. Veins: thicker, straight
Amount of melanin in choroid layer variation in pigmentation of retina. Deep green patch =
coronial nevus (benign)
Clinical usefulness depends on good instrument, good technique, knowledge of normal anatomy
and normal variations
Anatomy
Fovea: dip in middle of retina. Only photoreceptors, neural connections heaped up around it
Macula: ill defined area around fovea
Uvea = iris, ciliary body and choroid. Iritis = anterior uveitis
Reflex pathway: retina optic nerve optic chiasm optic tract lateral geniculate nuclei
optic radiation and brain stem Edinger Westphal nucleus 3
rd
nerve
Loss of Vision
Is it bilateral or unilateral?
Sudden: Woke up with it Vascular: Central retinal artery or vein occlusion, ischaemic optic
neuropathy, vitreous haemorrhage, CVA, preretinal haemorrhage
Suddenish: Gradual over a few days: Closed angle glaucoma (hours), infection, inflammation, retinal
detachment, optic neuritis
Gradual: Months to Years: Refractive, cataract, primary open angle glaucoma, age related macular
degeneration, retinopathy (eg diabetes, hypertension)
Chronic visual loss:
Uniocular
Binocular
Cornea & Red Reflex
Keratoconus, cataract, uveitis
Corneal dystrophies, cataract,
uveitis
Visual Fields
Retinal detachment, meningioma
Retinitis pigmentosa, pituitary
lesions
Pupils and IOP
Glaucoma
Glaucoma

142 4
th
and 5
th
Year Notes
Dilate for Fundoscopy
Malignant melanoma, optic
atrophy
Maculopathies, optic atrophy,
papilloedema
Age Related Macular Degeneration
Loss of visual acuity with peripheral vision in tact
Observe stippling and depigmentation of macular
Can be uni or bilateral
Age-related types:
Dry (atrophic) macular degeneration: thinning of macula, gradual. No cure. Atrophy of
photoreceptors, loss of outer nuclear layer
Wet (exudative) macular degeneration: May be due to Choroidal Neovascular Membranes,
unilateral with onset over several weeks. Straight lines appear wavy refer as laser treatment
slows progression
Symptoms: blurred central vision, distortion of straight lines
Eye Trauma
Mechanical: blunt/sharp, superficial/penetrating
Chemical: alkali the worst. Local anaesthetic then irrigate for 30 minutes (less time already irrigated
before presentation). If not toxic nor significantly inflamed, if VA OK and no fluorescein staining then
chloramphenicol eyedrops qid for 5 days
Radiation: UV, thermal, arch flash. Comes on hours after exposure, is very painful. Eye is very red,
multiple fine specks of fluorescein staining. Usually resolves in 24 hours. Treat as an abrasion (pad
both eyes)
Hyphema: blood in anterior chamber. Refer for opinion but don‟t normally treat. Check for corneal
abrasion, traumatic mydriasis, eye movements, blowout fracture of orbital floor, intra-ocular bleed
Penetrating Eye Injuries can be missed by subconjunctival bleed. Always refer if at risk. If metal vs.
metal, always do an xray otherwise blind from Fe toxicity. Also rose thorns. Teardrop shaped cornea
is a PEI until proven otherwise. Refer immediately. Lie down, im antiemetic to prevent vomiting.
Keep nil-by-mouth
Distorted pupil: penetrating injury until proven otherwise nil by mouth, shield eye, antibiotics,
antiemetic, refer
Foreign bodies: remove with 25-gauge needle and topical anaesthetic drops. Steady fixation of eye is
key. Always evert upper key lid to look for further foreign bodies
Corneal abrasions: Very painful and photophobic. Stain with fluorescein. Most heal within 24 hours.
Refer if abrasion large or central, if cornea hazy, VA reduced or eye is very inflamed. Double pad eye
well. Apply chloramphenicol ointment stat and bd for 5 days. Never give anaesthetic drops to take
home – can cause ulceration and blindness
Lid laceration: sow up anything not penetrating, or not involving lid margin or tear drainage (refer
these)
Retinal Detachment
Higher risk in near-sighted (myopic)
Can be caused by blunt trauma
Due to vitreous shrinkage, tears/holes in retina (eg with age), or underlying pathology
Symptoms: sudden changes in vision – watery or shadowy patch, sudden in number of floaters (spots
in vision), loss of visual field (like a descending curtain)
Need rapid treatment: seal tear with laser
Causes:
Exudative detachment: accumulation of fluid under the retina due to leaky vessels, eg tumour,
vascular abnormality
Traction detachment: vitreous becomes organised following trauma or neovascularisation and pulls
on the retina
The Red Eye
Never use steroids in an undiagnosed red eye (can worsen ulcers, etc)
Diagnostic Tree:
Uniocular:
No Pain, vision normal: subconjunctival haemorrhage, episcleritis, pterygium, conjunctivitis
Pain and normal vision: if no corneal staining: Anterior uveitis, scleritis, HZO. If corneal
scarring: HSV, marginal ulcer
Neuro-sensory 143
Pain and vision reduced: If no corneal staining: severe uveitis, angle closure glaucoma,
secondary glaucoma. If corneal staining: HSV, Bacterial keratitis, HZO
Binocular:
No pain, good vision: bacterial, viral or allergic conjunctivitis
Pain, vision good or poor: viral or chlamydial keratoconjunctivitis
Subconjunctival bleed: self limiting unless severely hypertensive or coagulopathy
Conjunctivitis:
Initially unilateral, may bilateral due to cross infection
Feeling of surface grittiness
Causes:
Infective: See Eye Infections, page 144
Allergic: eg eczema, allergy to protein deposits on poorly cleaned soft contacts
Chemical/mechanical
Baby: 1 month with pussy discharge urgent referral (?blocked and infected lacrimal duct)
Never pad a discharging eye
Blepheritis
= Lid inflammation
Eyelash „dandruff‟
Meibomian gland dysfunction: usually staph infection. 30ish glands under they eyelid normally
secrete lipid to cover tear film
Clean with saline or bicarbonate solution
Chalazion: Red nodule in the lid. Due to obstruction and infection of a Meibomian gland.
Microscopically granulomatous inflammation (basically a burst sebaceous gland)
Corneal Ulcer: See HSV infections below.
Keratitis:
Corneal inflammatory disease
Symptoms: deeper, aching pain
Aetiology: infective, contact lens, staph hypersensitivity, exposure keratopathy (eg 7
th
nerve palsy)
Signs: speckled light reflex corneal oedema
Shingles affecting face: refer within 7 – 10 days to check for intra-ocular complications. Pain is due to
trigeminal neuralgia
Iritis:
Frontal headache, photophobia, not watering. Usually unilateral
White cells and fibrous exudate in anterior aqueous. May be white cells at bottom of cornea
Usually autoimmune: Ankylosing Spondylitis, Crohn‟s. Treat with steroids, and dilating drops to
keep iris mobile
Rarely infective (eg Tb)
Episcleritis:
= Localised inflammation of sclera. Treatment: topical NSAIDs
Acute onset, mild pain, young adults, usually sectorial, no corneal signs
Cf Scleritis: pain, VA decreased, tender, sectorial or diffuse, corneal signs
Pterygium:
Conjunctival overgrowth growing over cornea. Age related changes due to sun exposure
Refer if enlarging and vascularised. Differential: squamous cell carcinoma.
Pinguecula: White epibulbar nodule similar to pterygium
Acute Glaucoma: See Primary Closed-angle Glaucoma, page 144
Glaucoma
Usually due to outflow obstruction: damage to the trabecular meshwork overlying the channel of
schlemm resistance to flow steady state intraocular pressure vascular perfusion of the
neural tissue blindness
Classification:
Primary:
Open angle (chronic)
Closed angle (acute)
Secondary: eg iritis, trauma, blood in the eye, etc
144 4
th
and 5
th
Year Notes
Primary Open-angle Glaucoma
Epidemiology:
Leading cause of preventable blindness
Risk factors: age, near-sightedness, African/Asian ancestry, family history, past eye injury, a
history of severe anaemia or shock, steroid medication
Most common sort, gradual impairment of aqueous drainage, insidious loss of sight
2% of over 50 years
1 in 7 risk if primary relative has it
Presentation:
Central field defect – arcurate shape with macular sparing
Cupping of the disk due to ischaemic atrophy of the nerve fibre layer
Bullous keratopathy – oedema of the cornea
Screen with tonometry (measuring intra-ocular pressure), test visual fields.
Is diagnosed by cupping of the optic disk: not by intra-ocular pressure. 17% of people with glaucoma
have „normal‟ IOP.
Pathology:
Resistance to outflow (pathogenesis not clearly understood) aqueous humour intra-
ocular pressure (normal is < 22 mmHg)
Leads to damage to ganglion nerve cell axon (final output) at the optic nerve head. Due to vascular
insufficiency as nerves exit the eye
Affects peripheral bundles preferentially: spares papillo-macular bundle
Treatment: Medication, laser treatment to enlarge the drain (trabeculoplasty)
Primary Closed-angle Glaucoma
Iris is pushed forward and acutely occludes the trabecular meshwork drainage
Rare but vision threatening
Unilateral, acute visual loss, pain, nausea and vomiting, dilated, non-reactive pupil
Precipitating factors: long sited (narrow anterior chamber, narrow iridocorneal angle), and when pupil
dilated for a long time (dim light)
Can be congenital
Once resolved, put hole through iris (iridotomy): no further obstruction possible
Secondary Glaucoma
Secondary open angle glaucoma: Outflow system is obstructed mechanically by debris (ie gunge up
trabecular meshwork). Rare. Eg Haemolytic glaucoma, lens protein glaucoma
Secondary closed angle glaucoma: Can be due to neovascularisation „zipping up‟ the angle, secondary
to ischaemic eyes (eg diabetes, central retinal vein occlusion)
Eye Infections
Viral Infections:
Adenovirus types 8 (epidemic) and 3 and 7 (sporadic). Conjunctivitis with pre-auricular lymph
node hyperplasia. Over about a week get small white spots (WBC accumulations) just below the
surface of the cornea
HSV:
Gives Herpes Simplex Keratitis.
Dendritic ulceration with neovascularisation. Chronic inflammation and scarring. May lead
to small white vesicles around the eye.
Viewed with fluorescein drops under cobalt light (stains where there is no epithelium)
Branching pattern Herpes Simplex Virus. Never give steroids: worse infection
permanent damage
Bacterial: Usually puss. Always bilateral:
Standard bacterial conjunctivitis: treatment chloremphenicol eye drops
Trachoma: Due to Chlamydia. Commonest cause of blindness in the tropics. Less common than
other causes in NZ. Chronic. Suspect if no response to topical antibiotics. Initially the
conjunctival epithelium is infected scarring of the eye lid abrasion of cornea over years
get panus (fibrovascular layer) over the cornea
Gonorrhoea: pre-auricular nodes
Neuro-sensory 145
Optic Nerve Lesions
Optic atrophy: pallor of the optic disk, and damage to the retinal nerve layer, optic nerve or tract
leading to visual acuity or field loss. Due to neuritis, compression, ischaemia, glaucoma
Optic Neuritis: Age 18 – 40, more common in women. Pain on movement of eye, with central fog
patch, colour desaturation. Worsens over hours to days, may lose sight completely, gradually improves
over 4 – 6 weeks. 70% chance of developing MS over 10 years
Anterior Ischaemic Optic Neuropathy: Sudden painless unilateral visual loss in an older person.
Seldom improves. Due to occlusion of the arterioles to the optic nerve head
Compressive Optic neuropathy: insidious loss of central vision in one eye, especially colour. Usually
meningioma of optic nerve
Nerve Lesions Affecting Eye movement
Droopy lid (ptosis) and small pupil (Horner‟s syndrome) – due to lesions in the brain stem, in the apex
of the lung, in the neck or on the carotid artery (eg carotid dissection)
Droopy eye lid and large pupil non reactive to light: 3
rd
nerve palsy – eye turned down and out due to
weakness of MR, SR, IO, and IR
Differential for Ptosis: idiopathic (esp elderly), myasthenia, muscular dystrophies, myotonic dystrophy
Nystagmus: if present in all directions will be central (commonest cause is antiepileptics)
Retinal Vascular Disease
Damage to large vessels in the eye
Occlusion of the central retinal artery:
Due to atheroma, thrombus, embolis, arteritis
Retina is white and totally infracted
Occlusion of the central retinal vein:
Haemorrhagic infarction
Collateral supply means some vision is recoverable
Retina is a mass of red, veins big and tortuous, cotton wool spots
Focal Ischaemic Retinal Disease
Affects little vessels
Features:
Cotton wool spots:
Fluffy and off-white/yellow
Due to micro-infarction superficial area of necrosis and oedema
Axons are disrupted and become distended (cytoid bodies)
Resolve in 6 weeks
Hard exudates:
Discrete, brighter white, often around macula
Plasma leaks from damaged capillaries (secondary to thickened basement membrane) in the
outer plexiform layer (deeper in the retina) and forms proteinaceous lakes
Resolves over several months
Haemorrhage: usually arises from microemboli/thrombi damaging vessels
Flame: a small arteriole bursts into nerve fibre layer and spreads along nerve fibres
Dot: capillary bursts into outer plexiform layer
Blot: into the subretinal space
Roth‟s spots: central white infarct surrounded by haemorrhage
Microaneurysms:
Round or oval dilations of capillaries – look like lots of very little red dots
Central in diabetes, peripheral in central retinal vein occlusion
Due to reduced numbers of pericytes surrounding capillaries
Neovascularisation:
Response of the eye to vascular insufficiency, secondary to angiogenesis factors from
ischaemia: proliferate around the margin of non-perfusion. Detect with fluorescein angiogram
Appears as fine lace work of new vessels. They leak and bleed
Sites:
Iris surface neovascular glaucoma, ectropion uvea
Pupillary membrane Posterior Synichiae
146 4
th
and 5
th
Year Notes
Vitreal Surface haemorrhage, pre-retinal fibrovascular membranes scarring
retinal detachment
Easy to see if over optic disk (normally should only be large vessels)
Differentiating between Hypertensive and diabetic retinopathy:
Hypertensive Retinopathy
Diabetic Retinopathy
Vessel
Arterioles
Capillaries/veins
Site
Superficial nerve fibre layer
Deep (non-proliferative)
Superficial (proliferative)
Pathology
Medial hypertrophy
Pericyte loss
BM thickening
Microaneurysms
New vessel formation
Diabetic Retinopathy
See also Diabetes Mellitus, page 94
1/3 diabetes with > 30 years disease will loose some sight. Diabetics 25 times more likely to go blind
Risk related to duration Type 1 (juvenile onset) more likely to cause damage
Retinal exam essential:
At diagnosis for maturity onset (may have had diabetes for 5 – 10 years)
After 5 years for juvenile onset and annually thereafter
Fluorescein angiography (injected in arm then photograph retina) to test for neovascularisation
Causes: Thickened basement membrane of retinal microcirculation leakage, oedema, nonperfusion
and micro-aneurysms
Macular retinopathy: boggy, leaky macula blurred vision
Non-proliferative retinopathy (= Background Retinopathy): Progression: oedema ( blurred vision)
microaneurysms hard exudates cotton wool spots small haemorrhages venous bleeding
Proliferative retinopathy:
Neovascularisation
Retinal detachment due to shrinkage of subsequent scars
Vitreous haemorrhage (can also be due to vitreous collapse tearing at retina or retinal venous
occlusion – usually due to BP expanded artery compresses adjacent vein)
Treatment:
Regular checks
Blood sugar control
Treatment of vascular disease (eg BP)
Laser treatment (photocoagulation): 2 – 3,000 burns (but NEVER on macula). O2 demand
neovascularisation. Complications: peripheral and night vision, macula oedema
Vitrectomy: if non-resolving vitreous haemorrhage or fibrovascular contraction of vitreous (which
has risk of retraction of retina tear)
Retinal repair: reattach retina
Diabetes can also cause: neovascular glaucoma (blocking flow past lens), more susceptible to damage
from IOP, cataract, extraocular muscle palsy
Hypertensive Retinopathy
Rarely causes visual loss. Requires diastolic BP > 120 for many years
Stages:
Stage 0: no changes
Stage 1: „copper-wiring‟ of arterioles due to thickening of the walls due to medial thickening (very
subjective)
Stage 2: Arteriovenous nipping – thickened arterioles compressing underlying veins
Stage 3: Soft-exudates and/or flame haemorrhages (spread longitudinally along fibres)
Stage 4: Papilloedema plus the above
Bilateral and symmetric. More cotton wool spots (nerve fibre hypoxia)
Retinopathy regresses if hypertension controlled (cf diabetes which doesn‟t)
See also Hypertension, page 34
Tumours
Can occur on the iris, ciliary body, choroids
Neuro-sensory 147
Malignant Melanoma of the Choroid
Presentation: elderly, usually white, visual loss from retinal detachment or incidental
Retinal appearance: light to darkly pigmented ovoid, elevated mass. Many variants
2
nd
most common site of melanoma after the skin
Prognosis depends on cell type (Spindle A, Spindle B, Epithelioid or Mixed) and Stage. Overall 50%
at 15 years
Retinoblastoma
Life threatening
1:20,000 live births. First few years of life
Types:
60% sporadic
40% familial (90% bilateral and/or multifocal)
Presentation: strabismus (squint), „white‟ patches on papillary/red reflex (leukocoria), red eye
Pathogenesis:
Due to variety of mutations in the tumour suppressor gene RB1 at 13q14 – inactivated a protein
which down regulates cell growth
Need both alleles to be mutated to cause cancer. Hereditary neuroblastoma = inherit one defective
gene from parent, with other allele in one cell undergoing spontaneous mutation. If non-
hereditary, need to acquire mutations to both alleles in one cell
Gross appearance: flat, elevated, diffuse, multicentric pale tumour nodules of plaques
Microscopic appearance: small round cells with hyperchromatic nuclei, rosettes are characteristic, areas
of necrosis and calcification
Treatment: remove eye
Complications:
Metastasis eg in CNS. From occurrence in eye to spreading down the optic track is ~ 6 months
Survivors have a 20% chance of developing malignant tumours at 10 years: osteosarcoma or
rhabdomyosarcoma
Prognosis: 90% 5-year survival (less if optic nerve invasion).
Paediatric Ophthalmology
Assessment
Vision: fixation (test independently and together), pictures, symbol matching, E
Alignment: inspection, alternating cover test
Squint inspection:
Corneal reflection when looking at bright light source. Should be in the centre of the pupil on both
sides. Cover good eye and see if corneal reflection shifts over the pupil of the bad eye
Check for equal schlera on either side of iris. Wide bridge of nose may give pseudo squint
Can have squint without amblyopia as long as brain alternates which eye it looks through. If
preference for one eye, then amblyopia
Amblyopia
= “Lazy eye”
Affects 2 to 3 per 100 children. Can only occur in childhood while visual pathway still developing
Usually unilateral: maybe bilateral if bad astigmatism or hypermetropia. If unilateral no effect on
reading/writing. Treat as insurance against problems in good eye
Affects central vision: peripheral vision OK
Three major causes:
Squint: Most common cause: misaligned or crossed eyes. The crossed eye is „turned off‟ to avoid
double vision
Unequal focus (refractive error). One eye is more near/far sighted or astigmatic
Visual obstruction: eg Cataract
Also caused by ocular motor defects
Treatment: force the use of the weak eye by covering the good one (for weeks or months), plus
correcting refractive errors with glasses
Refractive errors
Myopia
148 4
th
and 5
th
Year Notes
Hypermetropia: if equal and severe then squint due to accommodation
Stigmatism
Anisometropia: difference between two eyes (especially if one normal and other long sighted) –
accommodation just makes normal eye go out of focus
Other
Congenital cataract
Can be autosomal dominant
Check for red reflex within 6 weeks
May be uni or bilateral, part of a syndrome or isolated
Congenital epiphora
Watery eye. Common – lacrimal system not fully developed
Spontaneous resolution the norm. Conservative treatment until 12 months. Massage +/-
antibiotics (stagnation of tear drainage)
Perinatal eye infections
Retinoblastoma: See Retinoblastoma, page 147
Retinopathy of prematurity
Very premature babies (low risk if over 30 weeks or 1200 g)
Spectrum from severe to norm
Problem with vascularisation retinal detachment over time
Congenital Glaucoma: rare. One cause of red watery eye
Vestibular
Examination of Eye Movements
Nystagmus:
Peripheral cause: fine, unidirectional, horizontal or rotatory
Beats to the side opposite the lesion, worse when looking to that side
Named for the direction of the fast phase
Is inhibited by fixation (ie will be quicker if you close one eye and try fundoscopy on the other)
Bi-directional or vertical nystagmus is always central in origin
Control of eye movement:
Saccades: voluntary quick refixation eye movement. If hypometric then undershot number of
small saccades to catch up. Hypermetric saccades overshoot reverse saccade
Parietal lobe controls ipsilateral smooth pursuit and contralateral saccades. Impairment over 70
may be normal
Impaired pursuit also due to cerebellar and brainstem lesions
Vestibulo-ocular reflexes:
Eye movements to compensate for head movement: maintain stable picture on retina
Doll‟s eye: eyes stay focused on target when head moves
Benign Paroxysmal Positional Vertigo (BPPV)
Usually posterior semicircular canal. Due to debris in canal (CaCO3 crystals). Usually cause unknown
or aging, but may follow trauma or infection. Fluid movement distorted stimulations to nerve due to
particles different input from 2 vestibular end organs
Posterior canals are in the snow-plough position, and are the lowest. Collect debris from the anterior
and horizontal canal
Leads to discharge to ipsilateral superior oblique and contralateral inferior rectus torsional
nystagmus
Can also be due to horizontal semicircular canal
Symptoms:
Brief attacks of vertigo precipitated by certain head movements (eg getting into or out of bed,
rolling over). Less severe when repeated
May spontaneously remit and relapse
Hallpike manoeuvre: Rotatory or torsional nystagmus beating toward affected ear when tipped
down, after a brief latent period (5 – 10 secs). If immediate then ?central cause. Last about 20
secs and reoccurs again when sitting up. Effect fatigues with retesting (material disperses in
process of testing)
Neuro-sensory 149
Usually resolves over weeks or months
No cochlear symptoms
Treatment:
Drug therapy not helpful
Canalith Repositioning: induce symptoms shifts particles into a chamber not sensitive to
movement
For right ear: sit on edge of bed, turn head 45 degrees to the left, lean all the way down to the right
then quickly through 180 degrees to the left, then back to upright. May be easier with eyes closed.
Repeat after 2 – 3 minutes. Do every three hours
Acute Peripheral Vestibulopathy
= Acute labyrinthitis
Symptoms: acute and continuous vertigo, worse with any movement, lasting several days with nausea
and vomiting, but no auditory or neurological symptoms
Signs: unsteady walking (eg heel-toe). Fine horizontal/rotatory nystagmus beating away from the
lesion. Vestibulo-ocular reflex is absent/impaired on passive head rotation toward the lesion, requiring
voluntary eye movement to regain fixation (catch-up saccade)
Most likely to be horizontal canal affected
Other
Vertigo may follow Head injury. Eg temporal bone fracture tearing 8
th
nerve
Infarct with occlusion of the internal auditory artery affects hearing and balance
Chronic bilateral vestibulopathy imbalance and oscillopsia (sensation of the world moving on head
movement) due to inadequate vestibulo-ocular reflex. Usually due to gentamycin toxicity
Migraine may have vestibular symptoms
MS: vertigo is a classic feature
Ear
External Ear
Congenital Abnormalities: usually unilateral. Common ones:
Preauricular tag: only cosmetic
Preauricular sinus: get infected
Otitis Externa:
Localised: furnuncle or furnuculosis
Very painful, may abscess and discharge
Usually staph aureus
Tx: Oral antibiotics, may need drainage
Diffuse (more common)
Skin infection: viral or bacterial, or underlying dermatitis (more chronic, less pain and
swelling but itchy). If longstanding and treatment resistant, ?fungal (eg aspergillus) – less
painful, but blocked and debris, look for hyphae
Treatment: swab, clean out canal, topical antibiotics (drops with steroids swelling)
Canal trauma from itching, ear cleaning. Resolves spontaneously (unless infected)
Wax: produced by suruminous glands (only in the ear) over cartilaginous part. Slightly acid
antibacterial. Carries debris out
Insect in ear. Drown it and take out at leisure
Exostosis: common benign finding. Overgrowth of bone in internal 1/3 of canal, following exposure to
cold water (surfers, divers). May obstruction
Neoplasms: on pinna: BCC or SCC – require excision
Middle Ear
Middle ear cleft = ear drum + tympanum + eustachian tube
Ear drum:
Should see malleous, top towards the back
May see incus through the drum. If internal jugular very high, may see it at bottom
Main part called pars tensa, pars flaccida at top
150 4
th
and 5
th
Year Notes
Otitis Media
See Acute Otitis Media, page 605
Other Middle Ear Conditions
Cholesteatoma:
Most commonly affects the attic (=epitympanum) and antrum of the mastoid
Pars flaccida gets sucked in, expands, erodes surrounding tissue
May present with:
Chronically discharging, smelly ear, resistant to treatment
Conductive hearing loss: ossicles eroded
Complication: brain or mastoid abscess
Treatment: remove diseased bone
Otosclerosis:
New bone formation fixes the footplate of stapes
Conductive hearing loss but ear looks normal
F > M, familial, in pregnancy, menopause
1:20 – 25,000K, can be bilateral
Treatment: Stapendectomy (put in piston) or hearing aid
Tympanic sclerosis. White plaques on ear drum. No consequence
Barotrauma: from flying/diving. Bleeding and bruising around malleolus. Will settle spontaneously
Haemotympanum: Blood in middle ear. ?Temporal bone fracture. Battle‟s Sign (of temporal
fracture): bruising behind the pinna
Ear Testing
Voice Testing
Tuning fork tests:
Rinne Test: 512 Hz fork beside the ear. If conductive loss then bone conduction is better than air
conduction. If sensorineural, air conduction best
Weber Test: Tuning fork on top of the head. Louder in affected ear if conductive loss, softer in
affected ear if sensory loss
Pure Tone Audiometry:
Can establish severity of hearing impairment and whether sensorineural or conductive
Measures thresholds across a range of frequencies. Threshold = lowest intensity that can be
detected
Usually only test in range of conversational speech (250 Hz to 8 KHz)
Normal hearing is 0 – 20 dB (zero is based on population surveys)
Harder if child aged 3 – 5: need to play games etc
Auditory Brainstem Response (ABR):
Detects evoked potentials in the brainstem in response to sound
Used for neonatal testing (reliable from full term), in older kids where behavioural responses are
unclear and for testing the auditory nerve (eg acoustic neuroma – but MRI is gold standard, CT
with contrast poorer)
Tympanomtery:
Measures compliance of middle ear
Normal is -100 to 100 daPa
Type A: normal (peak compliance over 0 daPa). If peak is low ?scarring or adhesions
Type B: Flat curve (ie not compliant at any pressure).
Low volume type B: wax impaction or middle ear infusion
High volume type B: perforation or grommet
Type C: Peak shifted to the left. Eustachian tube obstruction
Otoacoustic emissions:
Test for cochlear function, eg in neonatal screening
Also for tinnitis: is it cochlear or non-cochlear
Paediatric testing:
0 – 3 months: referred from neonatal high-risk register. Need to correct (eg hearing aid implants) by 9
– 10 months otherwise speech impairment
6 – 12 months: distraction testing – looking for head turning, etc
1 – 2½ years: in a room with speakers
Neuro-sensory 151
Hearing Loss
See Hearing, page 580 for developmental delay resulting form hearing loss
Congenital Sensorineural Deafness
Irreversible
Pathology: problems with nerve or cochlear
Profound hearing loss at birth: 2 per 1,000
Most often detected by parents (ie believe them!)
Aetiology: genetic or acquired, etc:
Idiopathic 60%
Genetic: most are spontaneous mutations rather than family history
Low birth weight
Infection (fairly rare now), eg Rubella, also toxoplasmosis, CMV, syphilis
Maternal drugs: eg aminoglycosides, alcohol
Lots of others, eg hypoxia, high bilirubin
Sudden Onset Sensorineural Hearing Loss
=Uni/bilateral sudden onset within 3 days. May also get dizzy, tinnitis
Could be inflammatory, infective, ototoxicity, acoustic neuroma ( always investigate)
Urgent specialist referral within 24 hours
Spontaneous remission likely, poor prognosis if elderly, diabetic, vascular disease (Cochlear artery is
an end artery – if blocked no collateral flow)
Presbycusis
= Age related hearing loss, especially at higher frequencies
Bilateral, symmetrical. May get recruitment (some sounds sound louder – eg toilet flushing, doing
dishes)
M > F, 24% of 64 – 74 year olds, 40% of over 75s
May have word discrimination: hard to help, volume doesn‟t help
Aetiology: age, noise, hypertension, genetic predisposition
Pathology: degenerative changes, eg of cochlea and also of central procession (this part won‟t respond
to volume)
Clinical: progressive deafness, „social‟ deafness, especially 1 KHz, tinnitis. Often judged worse by
spouse/partner
Exclude: wax impaction, otosclerosis, Paget‟s disease of the middle ear bones, acoustic neuroma
Management:
Screen elderly people (eg questionnaires or audiometry)
Hearing aid: only ¼ who would benefit use one, although there are many barriers to use (including
cost)
Speaking facing the person, clearly, slowly, not too loud, paraphrasing sentences that aren‟t heard
rather than repeating them (also give this advice to spouse and caregivers),
Aids (telephone boosters, lights that flash when the doorbell rings, etc)
Rehabilitative services available through the Hearing Association
Noise Induced Hearing Loss
Commonest cause of hearing loss < 60
Usually industrial noise exposure: factories, builders, firearms, jack hammers
Safe limit: 80 db for not more than 4 hours
Classic damage at 4 & 6 KHz on audiogram. Usually bilateral
Treatment: Prevention, hearing aids not much help
Meniere’s Disease
Diagnostic triad: tinnitus (usually low pitched), deafness, vertigo, (+ feeling of aural fullness)
Clinical: acute onset of triad, disabling vertigo (world spinning, vomiting) for 6 – 12 hours then low
frequency hearing loss
30 – 55 years, M > F
Stages:
Early: occasional attacks
Later: fluctuating low tone deafness
152 4
th
and 5
th
Year Notes
End stage: low tone deafness, imbalance but no vertigo
Pathology: endolymphatic hydrops: distension of endolymphatic space
Aetiology: unknown. ?Production of endolymph
Diagnosis: possibly nystagmus, fluctuating SN loss
Treatment: Supportive, low Na diet (endolymph), thiazides, antivertigo, antiemetic and histamine
medication
Acoustic Neuroma
Progressive loss of hearing in one ear with tinnitus.
Not usually associated with vestibular function – slow enough to compensate (ie CNS adjusts so
world doesn‟t seem on a tilt). But, everyone with acute vertigo should have a pure tone audiogram to
screen for the (rare) possibility of acoustic neuroma
MRI is definitive, CT is unreliable and should not be done
Aural Rehabilitation
When hearing loss cannot be corrected, use hearing aids, listening devices and communication
strategies

Gastro-Intestinal 153
Gastro-Intestinal
References: Dr Kenwright‟s Pathology Notes and Gastro Intestinal Run Handbook
Abdominal Physiology ................................... 154
Abdominal History ......................................... 154
Abdominal Exam ............................................ 154
Abdominal Tests ............................................ 157
Abdominal X-ray ...................................... 157
Other Abdominal Tests ............................. 157
Developmental Abnormalities ........................ 157
Oral Pathology................................................ 157
Oesophagus .................................................... 158
Dysphagia ................................................. 158
Oesophageal Tumours .............................. 158
Achalasia .................................................. 159
Dyspepsia.................................................. 159
Oesophagitis ............................................. 160
Gastro-Oesophageal Reflux Disease
(GORD) .............................................. 160
Hiatus Hernia ............................................ 161
Stomach and Duodenum ................................ 161
Gastritis ..................................................... 161
Acute Ulcers ............................................. 161
Peptic (Gastric & Duodenal) Ulcer ........... 161
Pernicious Anaemia .................................. 163
Gastric Neoplasia ...................................... 163
Ceoliac Disease ......................................... 164
Other Malabsorption Syndromes .............. 165
Small & Large Bowel ..................................... 165
Pathology .................................................. 165
Ischaemic Bowel Disease ......................... 165
Bowel Obstruction .................................... 166
Appendicitis .............................................. 167
Ulcerative Colitis (UC) ............................. 168
Crohn‟s Disease ........................................ 169
Small Bowel Tumours .............................. 171
Colorectal Cancer ..................................... 171
Diverticular disease of the colon .............. 174
Irritable Bowel Syndrome (IBS) ............... 175
Bacterial Overgrowth of Small Intestine .. 176
Pseudomembranous Colitis....................... 176
Diarrhoea – Infectious Agents .................. 176
Constipation .............................................. 177
Other Bowel Diseases ............................... 179
Anorectal problems ........................................ 179
GI Bleeding .................................................... 180
Liver Disease .................................................. 181
Assessment ............................................... 181
Alcoholic Liver Disease ........................... 185
Viral Hepatitis .......................................... 186
Hepatitis A ................................................ 186
Hepatitis B ................................................ 187
Hepatitis C ................................................ 189
Other Viral Hepatitis ................................ 191
Tumours of the Liver ................................ 191
Other Liver Diseases ................................ 192
End Stage Liver Disease ........................... 194
Gallbladder and Bile Ducts ............................ 195
Cholelithiasis ............................................ 195
Cholecystitis ............................................. 195
Tumours .................................................... 197
Pancreas ......................................................... 197
Acute Pancreatitis ..................................... 197
Chronic Pancreatitis .................................. 198
Pancreatic Tumours .................................. 199

154 4
th
and 5
th
Year Notes
Abdominal Physiology
Fluid into GI tract each day:
Drink 2L
Saliva 1L
Bile 1 – 1½L
Stomach Secretion 1 – 2 L
Pancreas 2L
Small Bowel 1L
7 – 9 L per day into top end of small bowel
Output of H2O in faeces = 150 – 200ml in faeces. 7.5 L absorbed in small intestine. 1- 3 L absorbed
in Colon
Normal stool is 70 – 80% water: held by fibre or in bacteria. Stool H2O by 25 ml diarrhoea. By
25 ml constipation
Abdominal History
Abdominal Pain:
Frequency and duration
Site and radiation: pancreas or peptic ulcer may radiate to the back, diaphragm to shoulder and
oesophagus to the neck
Pattern: colicky pain is due to peristaltic movements against obstruction in bowel or ureters.
Biliary pain usually lasts for hours (ie is not colicky)
Aggravating or relieving factors, including food, vomiting, defaecation, flatus, lying still in
peritonitis
Appetite and weight change:
Anorexia and weight loss ?malignancy
Appetite and weight loss ?malabsorption
Nausea and vomiting, ask about vomit (blood, bile, old food outlet obstruction, etc)
Heartburn and acid regurgitation
Dysphagia: differentiate painful swallowing from actual difficulty
Diarrhoea: check frequency and consistency. Can be:
Secretory diarrhoea: large volume
Osmotic diarrhoea: disappears with fasting
Abnormal intestinal motility
Exudative diarrhoea: with blood or mucus
Malabsorption: steatorrhoea
Constipation: Check what they mean. Check drugs, hypothyroidism, diabetes, etc. Is it recent (cancer
can cause obstruction)?
Mucus: ?IBS or rectal ulcer, fistula or villous adenoma
Bleeding:
Haematemesis (vomiting blood)
Melaena (jet black stools)
Haematochezia (bright red rectal bleeding)
Jaundice: also ask about dark urine and pale stools ( obstructive jaundice)
Pruritis: itching skin. Can be caused by cholestatic liver disease
Abdominal swelling. Also check ankles
Lethargy: common in liver disease
Drugs: especially NSAIDS
Social history: alcohol, occupational exposure to hepatitis, travel, sexual and recreational drug history
Abdominal Exam
Trying to filter symptoms for:
Upper vs. lower
Functional (motility) vs. structural (infection etc)
Alarm symptoms
Gastro-Intestinal 155
Periphery
General:
Lie flat and comfortable ( relaxed muscles)
General appearance:
Jaundice
Weight and wasting (weight them)
Skin: pigmentation (eg haemochromatosis)
Mental state: hepatic encephalopathy
Hands for peripheral stigmata of abdominal disease (mainly liver):
Nails: Leuconychia (nail bed opacity in hypoalbuminaemia), clubbing in cirrhosis
Palms: Palmar erythema (reddened palms) in chronic liver disease, anaemia (from GI loss,
malabsorption or chronic disease)
Dupuytren‟s Contracture: thickening of the palmar fascia permanent flexion, especially of the
ring finger. In manual workers, alcohol, and familial
Hepatic flap: extend wrists and separate fingers for 15 seconds
Arms:
Bruising:
Large bruises (ecchymoses) from clotting disorders
Small bruises (petechiae) from alcohol toxicity platelets (also portal hypertension
splenomegaly platelets)
Also muscle wasting, scratch marks, spider naevi (cirrhosis – usually alcohol, due to oestrogen
excess)
Face:
Eyes for jaundice, anaemia, or scleritis/iritis (associated with inflammatory bowel disease)
Bilateral swollen parotids due to fatty infiltration with alcohol
Smell of breath: fetor hepaticus (sweet smell) or alcohol
Ulceration (eg in Crohn‟s) or candida in the mouth
Angular stomatitis: cracks at the corners of the mouth: causes include Vit B 6 and 12, folate and
iron deficiency
Neck and Chest:
JVP
Cervical lymph nodes and especially supraclavicular nodes (always bad)
Gynaecomastia: due to oestrogen to testosterone ratio (alcoholic effect on Leydig cells), or due to
spironolactone (used to treat ascites)
Examine chest:
Gynaecomastia
Spider naevi
Body hair
Abdomen
Regions:
Right & left hypochondrium, epigastrium
Right & left lumbar/mid-lateral region
Right & left iliac fossa, hypogastrium or suprapubic
Why examine:
Enlarged organs
Abnormal masses (e.g. tumour or inflammation – abscess) & fluid (ascites)
Signs of peritoneal irritation (hurts with cough)
Hernia
Inspection:
?Abdomen moves with respiration (look from side on to view asymmetry ?mass)
Scars: what were operations
Hernias - Hernial Orifices: Umbilical, Inguinal, femoral
Visible lumps/organs
Skin lesions/pigmentation (eg Shingles causes strange pains until it erupts)
Distension: Due to Fat, Fluid, Fetus, Flatus, Faeces, Filthy big tumour. Umbilicus is shallow or
everted in ascites or pregnancy
156 4
th
and 5
th
Year Notes
Veins. Test direction of flow. In portal hypertension, flow is away from umbilicus (rare, = Caput
Medusae). In IVC obstruction, flow is upwards
Striae: Ascites, pregnancy, recent weight loss, rarely Cushing‟s Syndrome
Pulsitations: abdominal aorta. Visible in thin people. If fat then ?aneurysm
Palpation:
Relax patient, use warm hands. Bend knees up if necessary to relax muscles
Gently all round: look at face – check for tenderness/peritonism, obvious lumps. Do most painful
quadrant last. If tense, use their hand
Percuss before palpation for organs. Check for shifting dullness
More firmly: looking for organs, masses
What to palpate for:
Liver:
Don‟t usually feel in normal adult, may in child. Normal span in mid-clavicular line is 10 - 12
cm. Don‟t measure on lateral side, right lobe hangs down in some giving appearance of bigger
liver (Riedel‟s lobe)
Describe as hard or soft, tender or non-tender, regular or irregular, pulsitile or non-pulsitile
Spleen: needs to be enlarged 3 or 4 times to palpate. Palpable spleen is ALWAYS bad. Start
palpation inferior to the umbilicus
Kidney: if palpable either tumour or obstructed
Aorta: can nearly palpate in most people – key issue is width
Gallbladder: Murphy‟s sign: lay fingers along costal margin, patient takes a deep breath and it
hurts. Enlarged gallbladder is unlikely to be gallstones as chronic gallstones fibrosis that can‟t
then expand. Instead, ?carcinoma of the head of the pancreas.
Also palpate for bladder, uterus
What to note: Site, size, shape, consistency, tender, pulsitile
Signs of inflammation, infection or haemorrhage:
Tenderness: how severe is pain in response to pressure
Guarding: muscles resist pressure. Can be voluntary or involuntary (latter suggests peritonitis)
Rigidity: muscles tight
Rebound tenderness: push down surreptitiously then remove hand quickly – watch face for pain
(peritonitis)
Percuss for:
Liver
Spleen: unreliable
Kidneys: but overlying bowel makes this problematic
Bladder: supra-pubic dullness indicates upper border of an enlarged bladder or pelvic mass
Shifting dullness in ascites
Ausciltate:
Bowel sounds: just below umbilicus. Are either present or absent (increased or decreased
meaningless)
Over liver, spleen, renal areas for rubs and bruits
Groin: genitalia, lymph nodes, hernial orifices
Rectal:
Observe for tags, haemorrhoids, pylonodal sinuses, blood, faeces colour
Feel for anal tone, masses or strictures in the rectum
Legs: bruising, muscle wasting, oedema (check sacral as well)
Causes of Splenomegaly
Chronic granulocytic leukaemia
Malaria
Lymphoma
Myelofibrosis
Polycythaemia
Gastro-Intestinal 157
Abdominal Tests
Abdominal X-ray
Gas:
Normal in colon and stomach, some in small bowel OK
Define colon: has haustrations – but don‟t cross tinea coli. Only part of bowel with faeces
If they have ulcerative colitis shouldn‟t be bigger than 5cm – otherwise toxic megacolon
Transverse diameter of caecum shouldn‟t be bigger than 9 cm otherwise risk of rupture
Small bowel: circularis goes right round. Max diameter 3 cm. Gas if obstructed, diarrhoea, ileus
or swallowing gas due to pain
Gas under diaphragm = pneumo-peritoneum
Can have gas in bilary tree (esp. after ERCP, or if fistula to bowel), and retroperitoneal from
perforated 2
nd
part of duodenum
Stripes:
Edges of psoas: demarcated against fat
Lateral abdominal wall: flank line is peritoneum. If exudate in the paracolic gutter then distance
from the colon is increased
Renal outline: parallel to upper psoas
Edge of liver
Edge of spleen (not always seen)
Stones:
Any extraoscious calcifications
Bladder, kidney, gallbladder
Bones
Other Abdominal Tests
Endoscopy
Complications: Mallory Weiss tear, perforation (1/2000), aspiration pneumonia (rare)
Ultrasound for Ascites
Need 1 litre of fluid before it can be detected
Rectal biopsy
For ulcerative colitis, microscopic colitis, amyloidosis, cancer
Stool test
Occult blood
Culture (for bacteria): would either be self-limiting or very sick
Ova, parasites & giardia antigen: if high risk, repeat 3 times. Needs to be warm on arrival in lab
Barium Enema
Make sure they got to the caecum (i.e. want to see contrast in the appendix or terminal ileum)
Also need to know that bowel was clean enough for them not to miss anything
Developmental Abnormalities
See Congenital abnormalities, page 639
Oral Pathology
Same pathology in the mouth as with skin, mucosa, nerves, blood vessels, etc. But also specialised
stuff
Teeth and Teeth forming tissue:
Genetic defects
Severe illness eg measles bands on teeth
Tetracycline discolouration
Vomiting, regurgitation (eg bulimia) erosion
Cysts or tumours of teeth forming tissue (eg ameloblastoma)
158 4
th
and 5
th
Year Notes
Gums: loose more teeth through gum disease than caries. Immunosuppressive disease can lead to
abnormal gums (eg leukaemia)
Salivary glands:
Calcification in duct of major gland blockage
Tumours/cysts
Recurrent infections: short/wide ducts retrograde flow infection with oral commensals
Post-radiotherapy to head and neck. Salivary tissue very sensitive dry mouth
Drug induced dry month: made worse by anxiety, smoking, dehydration
Sjogern‟s Disease: autoimmune attack of salivary and lacrimal glands
Dry mouth rapid tooth decay (no buffering from saliva)
Oral Mucosa:
Hyperkeratosis with hyperplasia or atrophy: looks white
Upsets to normal flora. Eg candida overgrowth. Can lead to loss of papilla (atrophic candidiasis),
hyperkeratosis
Ulceration: lots of causes: eg trauma (new dentures, burns), herpes, Aphthous ulcers (if recurrent
then check serum ferritin, hormonal cycle, stress, food allergy [eg benzoic acid in Coca Cola],
heredity)
White lesions (due to thickened keratin layer):
Lichen Planus: white patches surround by red erosions
Lichenoid drug reactions
Malignant and premalignant (eg leukoplakia - white, erythroplakia – red). Eg squamous cell
carcinoma. Related to smoking – 60 – 75% of white lesions go away if they stop
Oesophagus
Dysphagia
=Difficulty swallowing
Define level and whether progressive or intermittent
History: Time course, reflux symptoms, cough, asthma, chest infections, weight loss, pain
Examination:
Lymphadenopathy
Chest signs: consolidation, effusion
Hepatomegaly
Ascites
Raynaud‟s: connective tissue disorders
Investigations:
Barium swallow (video)
CT scan: staging malignancy
Endoscopy: assess mucosa, strictures
Manometry: assess motility
Oesophageal motility causes:
Fluids get through OK, solids the problem
Pharynx: neurological diseases causing failure of high pressure contraction
Cricopharyngeal sphincter: failure due to cricopharyngeal spasm or pharyngeal pouch
Oesophagus: failure of peristaltic wave due to diffuse oesophageal spasm
Cardiac sphincter: failure of opening due to achalasia
Oesophageal obstruction causes:
Fluids also a problem
Extrinsic compression: thyroid, other neck mass, lymph nodes (Ca lung)
Carcinoma of the oesophagus. Often diagnosed at advanced stage. Either squamous or
adenocarcinoma. Diagnosis by endoscopy + biopsy +/- CT. Treatment – surgical reconstruction.
Palliation: radiation + internal stent
Reflux stricture of the lower oesophagus
Oesophageal Tumours
Symptoms & signs:
Dysphagia: when disease advanced
Inability to swallow saliva
Gastro-Intestinal 159
Pain
Weight loss, anaemia, lymphadenopathy, hepatomegaly
Investigations:
Endoscopy: biopsy
Bloods: FBC (anaemia), ALP (metastases. in liver or bone)
CT, MRI: localised tumours
Differential diagnosis:
Benign stricture
Motility disorders, especially achalasia
Extrinsic compression of oesophagus (e.g. bronchial carcinoma)
Treatment:
Adequate nutrition (enteral feeding tube if necessary)
Pain management
Surgery/radiotherapy: usually only palliative
Squamous cell carcinoma:
90 % of oesophageal cancer
Epidemiology: M>F 4:1, B>W, approx 5 per 100,000
Aetiology: dietary (fungal, nitrites, leafy greens), oesophagitis, alcohol, tobacco, genetics
Macroscopic appearance: Site: 50% middle, 30% lower, 20% upper. Early lesion a small grey-
white thickening. Later: fungating tumour, ulceration, infiltration (may present as stricture)
Microscopic appearance:
Sheets of neoplastic squamous cells with intercellular bridges
Keratin whirls well differentiated
Mitoses, necrosis, pleomorphism (as with all malignant tumours)
Invasion of mediastinal structures and lymphatics
Clinical outcome: Insidious ( late presentation). 70% dead at one year
Adenocarcinoma of the oesophagus:
10% of oesophageal carcinomas. Arise in Barrett‟s mucosa
Elderly, mainly males
Macroscopic: mass or nodule
Microscopic: pleomorphism, irregular gland formation
Achalasia
= Failure to relax lower sphincter
Symptoms & signs
Dysphagia: with both solids and liquids
Intermittent chest pain
Regurgitation/reflux
Weight loss
Nocturnal cough (related to regurgitation & aspiration)
Investigations
Chest x-ray: dilated oesophagus
Barium swallow: delayed passage through cardia, oesophageal dilation
Endoscopy: may be normal, may be food in oesophagus ( secondary oesophagitis)
Manometry: impaired relaxation of lower oesophageal sphincter, absent peristalsis
Differential diagnosis
Benign or malignant stricture
Malignancy at cardia
Treatment
Medical: nitrates and calcium antagonists sphincter pressure
Balloon Dilation
Botulinus toxin injection
Cardiomyotomy
Retrosternal pain may continue following treatment. May need H2 antagonist
Dyspepsia
= Upper abdominal discomfort. Includes bloating, fullness, early satiety, nausea, anorexia, heartburn,
regurgitation. Chronic not acute.
160 4
th
and 5
th
Year Notes
Exclude bilary colic, pancreas and heart pain
Functional/idiopathic/essential dyspepsia = all investigations normal but still pain = Up to 60% of
dyspepsia. ?Increased visceral sensitivity, ?delayed gastric emptying, ?H Pylori gastritis
Abdominal pain without significant pathology very common
Ask about weight: if overweight – think reflux, if loosing weight think cancer
Oesophagitis doesn‟t cause anaemia until proved otherwise
Types:
Reflux like heartburn/regurgitation – treat with empiric H2 antagonist
Dysmotility like bloating, nausea, fullness (?delayed gastric emptying) – treat with prokinetics
(e.g. cisapride & domperidone)
Oesophagitis
Caused by:
Reflux oesophagitis
Irritants (eg alcohol, tobacco)
Fungal or viral infection
Systemic blistering diseases (rare)
Radiation (eg for breast cancer) or cytotoxics
Graft vs. host disease (affects whole GI)
Gastro-Oesophageal Reflux Disease (GORD)
Includes reflux oesophagitis
An acid and motility disease
Mechanisms for reflux:
Lowered sphincter pressure/incompetence: Aggravated by large meals, acidic (e.g. citrus), fatty
food, chocolate, smoking, peppermint, caffeine
Abdominal pressure: effects right crus of diaphragm which acts like an external LOS: aggravated
by obesity, straining, pregnancy, bending over
Presentation:
Heart burn
Dyspepsia, nocturnal cough or chest pain
Poor correlation between symptoms and severity
Diagnosis:
Therapeutic trial
If going to investigate, don‟t treat in meantime: otherwise inflammation (if any)
Endoscopy most sensitive and specific: use after failure of therapeutic trail or if alarm symptoms.
Biopsy only to exclude malignancy or Barrett's oesophagus. 50% are normal on endoscopy
Gold standard: 24 hour ambulatory pH monitoring
Lesions graded 1 (mild) to 4 (severe), 5 (metaplasia – Barrett‟s). If Grade >= 3, then indefinite,
significant acid suppression.
Alarm Symptoms:
Dysphagia
Early satiety
Night waking
Abrupt onset
Recurrent hoarseness
Severity
Weight loss
Vomiting blood
Symptoms for the first time > 45 years or soon after any treatment
Differential: Peptic ulcer, gastric or oesophageal cancer, angina/IHD, hiatus hernia
Macroscopic appearance: Oedema, hyperaemia (redness), ulceration, white patches with candida
Microscopic appearance:
Intraepithelial eosinophils
Neutrophils in the epithelium and lamina propria
Regenerative and degenerative features of the epithelium ( thickening)
Ulceration
Gastro-Intestinal 161
Treatment hierarchy:
Try antacids & lifestyle changes first (e.g. tilt bed, no food before bed, avoid problem foods,
weight loss)
Paracetamol for pain not aspirin
High fibre diet: reduces straining reduces reflux due to intra-abdominal pressure (only helps if
straining to start with)
Prokinetics: cisapride, metoclopramide or domperidone
H2 antagonists (OK for mild): healing after 8 – 12 weeks
PPI (more effective in severe): omeprazole, lansoprazole, pantoprazole
Nissen fundiplication (operation): also reduces hiatus hernia at same time
Complications:
Barrett's oesophagus: long-standing reflux Metaplasia: columnar changes above gastro-
oesophageal junction. Predisposes to cancer
Ulceration, stricture (always biopsy strictures as some cancers present like this)
Adenocarcinoma
Hiatus Hernia
Common. May be asymptomatic
Two types: sliding or rolling/para-oesophageal
Symptoms:
Sliding: Reflux, cardiac and pulmonary symptoms (mass in thoracic cavity)
Rolling: cardiac and pulmonary symptoms, dysphagia, hiccough, volvulus
Stomach and Duodenum
Gastritis
Acute gastritis:
Transient, acute, mucosal inflammation
Causes: aspirin, alcohol, chemotherapy, stress, shock, severe systemic infection
Macroscopic appearance: oedema, hyperaemia, superficial erosion
Microscopic appearance: neutrophils, sloughing, haemorrhage in the lamina propria
Chronic gastritis:
Lost velvety appearance, flat (no folds)
Autoimmune type: Associated with antibodies to parietal cells ( achlorhydria) and intrinsic
factor. Pernicious anaemia develops in 10%. Usually affects body of the stomach
Helicobacter pylori infection:
Hypertrophic gastritis: enlargement of rugal folds due to hyperplasia. Several causes. Differential:
lymphoma can also present with enlargement of rugae
Acute Ulcers
Stress ulcers: shock, burns, sepsis
Due to mucosal hypoxia
Usually heal quickly
Appearance: multiple circular ulcers < 1cm. Penetrate submucosa. Occasionally massive bleeding
Peptic (Gastric & Duodenal) Ulcer
Symptoms & Signs
Gastric & duodenal usually indistinguishable clinically
Uncomplicated: can be silent, epigastric pain after food, relived by antacids, and waking at night due to
pain, weight change
Complicated: haematemesis/melaena, vomiting, severe pain pancreatitis or perforation (but 50% of
patients with fatal complications present without ulcer pain), shock, anaemia, peritonitis
Epidemiology
10% of the population have one at some time in their lives
M>F 3:1
Genetic risk (50% twin concordance)
162 4
th
and 5
th
Year Notes
Aetiology
Need mucosal injury
H. Pylori infection. Damages D cells gastrin acid & pepsin metaplasia + helicobacter
damage ulcer
Smoking, alcohol, etc
NSAIDs
If neither H. Pylori infection nor NSAIDs then ulcer very unlikely
Not due to acid (except for Zollinger-Ellison syndrome)
Macroscopic appearance: well demarcated, punched out, with radiating mucosal folds. Most <4 cm
diameter
Microscopic appearance – 4 layers/zones:
Exudative zone: fibrin, debris, neutrophils, etc
Necrotic zone: necrotic debris
Granulation tissue zone
Zone of fibrous tissue
Adjacent: blood vessel thickening, mucosal hyperplasia, chronic inflammation
Helicobacter Pylori
Curved gram negative organisms in gastric mucus
From contaminated water
Prevalence in NZ 30% but declining, 20% in Wellington, lower in Dunedin. Causes 60% of antral
gastritis (other causes include bile reflux)
H. Pylori infection in 70-80% of gastric ulcers, 95% of duodenal
Also associated with gastric adenocarcinoma and gastric MALT lymphoma (i.e. it‟s a carcinogen)
Lives beneath gastric mucus: pH of 5 – 7 (compared with 1 – 2 in stomach lumen)
H. Pylori always gives gastritis, usually in the antrum, but usually asymptomatic. Eradication only of
benefit if ulcer‟s present
Microscopic appearance: chronic atrophic gastritis. Chronic inflammatory infiltrate gland atrophy
over time, intestinal metaplasia of remaining glands
Investigations
Bloods: FBC (anaemia), amylase
Refer for endoscopy if > 45 years or alarm symptoms (See Gastro-Oesophageal Reflux Disease
(GORD), page 160)
At endoscopy check for H Pylori, CLO test from biopsy sample, or histology/culture, and biopsy from
antrum of stomach. 1% of gastric ulcers are cancers – always biopsy – but ulcers don‟t predispose to
cancer
Urease breath test (gold standard): swallow C13 labelled urease and check for expired labelled CO2.
H. Pylori has Urease to turn urea NH2 + CO2
CXR: subdiaphragmatic gas in perforation
Contrast Xray (less accurate than endoscopy)
Differential
Pain: Reflux, gastric ulcer, gastric cancer, gallbladder disease, chronic pancreatitis, IBS
Acute Severe Pain: acute pancreatitis, bilary colic, aortic dissection, MI
Zollinger-Ellison syndrome: uncontrolled gastric acid secretion driven by plasma gastrin released by a
gastrinoma - 50% malignant multiple peptic ulcers
Crohn‟s, Lymphoma, CMV
Treatment
If on NSAIDs: stop them. Normally curative
Antacids
H2 receptor antagonists: good healing over 4 – 8 weeks (ranitidine, cimetidine)
PPIs: for unresponsive ulcers - superior to H2RA for healing and maintenance
Triple therapy for H. Pylori:
75% effective under normal conditions. Reinfection is rare (< 1%)
2 weeks optimal – 7 days pretty good
pH has effect on antibiotic bioavailability: want to pH (e.g. omeprazole)
Bismuth (De-Nol) + tetracycline & metronidazole + ranitidine, or
Gastro-Intestinal 163
Clarithromycin & metronidazole + ranitidine, or
Amoxycillin + metronidazole + omeprazole
Treatment of H. Pylori in non-ulcer dyspepsia has little effect. Only proven benefit of eradication
is in ulcer disease and MALT lymphoma
Always re-scope an ulcer to check healing. You want to be sure it‟s not a cancer missed on histology
(and PPIs will mask symptoms)
Complications
Only time surgery is involved
Haemorrhage: 2.5% of PU per year occult, melaena or haematemesis. 10% mortality
Perforation: 1% of PU per year, usually NSAID users
Penetrating: pancreas, liver, biliary
Obstruction: of pylorus due to chronic scarring/stenosis functional obstruction
Pernicious Anaemia
Symptoms & signs (due to anaemia or B12 deficiency):
SOB/lethargy
Sore tongue (glossitis in 50%)
Parasthesiae and gait disturbance (peripheral neuropathy), loss of proprioception/reflexes
Depression, impaired memory
Mild splenomegaly
Investigations:
Bloods: macrocytic anaemia, leucopenia, hypersegmented neutrophils, bilirubin, serum B12
Schilling Test: < 10% urinary excretion of 58Co labelled B12, corrected when administered with
intrinsic factor
Also serum gastrin measurement and endoscopy for gastritis
Differential:
Dietary (e.g. vegan) or malabsorption (e.g. Crohn‟s) deficiency of B12
Chronic H Pylori gastritis
8% of pernicious anaemias develop gastric cancer
Treatment: iv B12, loading dose then 1 mg every 3 months (watch for folate deficiency initially)
Gastric Neoplasia
Symptoms & Signs
„Ulcer-like dyspepsia‟ lasting more than a few weeks in middle aged or older
Early satiety, fullness small cancer in pylorus, large in body of stomach, extrinsic compression,
or linitis plastica (infiltrates stomach so can‟t distend)
Vomiting, haematemesis/melaena
Weight loss, malaise
Anaemia
Metastases: Knobbly enlarged liver, ascites, pleural effusion, left anterior axillary node
Investigations:
FBC (anaemia), LFT (mets?)
Endoscopy: biopsy and assess obstruction
CT/ultrasound to assess metastases
Differential:
Ulcer or non-ulcer dyspepsia
Reflux oesophagitis
Anaemia of other causes
Depression
Types:
Benign Tumours:
Polyps: hyperplastic/inflammatory – 90%, Neoplastic/adenomatous – 10%
Stromal tumours: leiomyomas, etc
Gastric Carcinoma:
Epidemiology: high in Japan (due to diet screening programme), China, decreasing in
Western world (better water helicobacter and better food preservation oxidised food
which is carcinogenic). 6/100,000. M > F
164 4
th
and 5
th
Year Notes
Aetiology: Diet (pickles, smoked food, green leafy vegetables), genetic, associated with
chronic gastritis and adenomatous polyps, and helicobacter
Evolution: dysplasia carcinoma-in-situ (confined to submucosa) invasive
Macroscopic: Early – thickening, hyperaemia. Go on to 1) ulcerating, fungating masses,
rolled overhanging edge, 2) diffusely infiltrative (linitis plastica – “leather bottle stomach” –
thickened wall and folds), 3) polypoid mass
Microscopic appearance: 1) Intestinal type: malignant glands, 2) Diffuse or gastric type:
cygnet ring cells
Outcome: depends on stage not type. Metastasis to lymph nodes, peritoneum, liver, lungs
Treatment:
Resection
Chemotherapy for palliation only
Symptomatic drug treatment
Ceoliac Disease
= Gluten sensitive enteropathy: sensitive to gliaden protein fraction in gluten (found in BROW: barley,
rye, oats and wheat)
Epidemiology
In Wgtn: prevalence 70 per 100,000, incidence 1.8 per 100,000
Male:female = 1:3
10% familial recurrence
Association with HLA 8
Symptoms
Abdominal pain (related to meals), diarrhoea, steatorrhoea, no fever, sudden onset, early satiety,
vomiting
Symptoms secondary to malabsorption: anaemia (common presentation – Fe absorbed in duodenum),
failure to thrive, weight loss, tetany, osteoporosis (Ca or Mg), Wernicke‟s encephalopathy
Clubbing
Diagnosis
Bloods: ferritin, folate, B12, and Ca
Faecal fat
Contrast Xray
Antigliadin IgG antibodies
Antigliadin IgA antibodies
Endomysial antibodies: high predictive value
Diagnosis: histology + histological improvement on gluten-free diet
Differential
Other causes of diarrhoea: e.g. Lactose intolerance, IBD, IBS
Thyrotoxicosis ( bowel motility)
Ca
Aetiology
Dietary factors + environmental agents + genetic pre-disposition (HLA B8, DR3, Celtic ancestry)
Latent-compensated gluten sensitivity (proximal only, B12 absorbed in terminal ileum)
Unmasking factors (nutrient deficiency, metabolic stress, infections, etc)
Symptomatic
Pathology
Subtotal villous atrophy
Crypt hyperplasia
Leading to abnormal small bowel mucosa and malabsorption. Primarily affects distal duodenum. In
severe cases can extend to terminal ileum
Treatment
Gluten free diet for life: refer to dietician
If severe, prednisone
Gastro-Intestinal 165
Replenish deficiencies: iron, folate, vitamins
Bones: due to Ca malabsorption – do bone scan, Ca supplements. A diary free diet pre-diagnosis may
have improved things as less lactase in coeliac disease
?Family screening: but antibodies only +ive with mucosal damage (doesn‟t detect latent disease). Keep
kids growth charts up to date
Refer patients to Ceoliac Society
Other Malabsorption Syndromes
Lactose Intolerance:
Lactose intolerance very common: especially where diary products are uncommon. Either
congenital (rare), acquired, or secondary to enteritis (i.e. be careful with milk for several weeks
after bad diarrhoea)
Lactose breath test: Give lactose. Broken down by lactase. If lactase then osmotic diarrhoea
rapid transit early & large rise in H2 as lactose is broken down by bacteria. Check with serial
breath H2 measurements
Tropical Sprue: Enterotoxic E coli infection in visitors to the tropics. Affects distal intestine
Whipple's Disease: Tropheryma whippelii (bacteria) infection. Obstruction to lymphatics causes
malabsorption. Treat with erythromycin, otherwise death from systemic spread
Abetalipoproteinaemia: genetic defect, unable to synthesise apoproteins
Small & Large Bowel
Pathology
Differentiating small and large bowel: large bowel has teniae coli, and haustra are not continuous
around inside of lumen
Type of colitis:
Infective
Collagenous
Microscopic
Pseudomembranous
Acute & chronic irradiation
Necrotising enterocoloitis
Ischaemic
Amoebiasis
Crohn‟s and Ulcerative
Gut layers:
Mucosa and muscularis mucosa
Submucosa with lamina propria
Muscularis propria (two layers)
Serosa/adventitia
Melanosis Colis: brown cells at base of crypts - lipofuscin from broken down organelles, correlated
with laxative use, no impact
Ischaemic Bowel Disease
Distribution:
Vascular occlusion: superior mesenteric
Watershed lesions (eg splenic flexure, rectum)
Transmural infarction:
Pathogenesis: arterial thrombosis, embolic occlusion, venous thrombosis or strangulation and
torsion
Macroscopic appearance: Red and intensely congested. Subsequently gangrenous
Microscopic appearance: transmural necrosis, congested with blood, epithelium sloughed off,
inflammation, perforation in 3 – 4 days
Clinical: severe pain, nausea, collapse, 50 – 75% die
Mucosal Infarction:
Pathogenesis: non-occlusive hypoperfusion damaging only the inner layers due to shock, cardiac
failure, etc
166 4
th
and 5
th
Year Notes
Macroscopic appearance: congested in patches or large areas. Mucosa haemorrhagic, oedematous,
ulcerated
Microscopic appearance: Necrosis of mucosa, remainder OK
Clinical: pain, bloody diarrhoea, shock, potentially reversible
Bowel Obstruction
Presentation
High small bowel: mainly vomiting, less distension/pain, no constipation, more rapid onset
Low large bowel: mainly distension/constipation/pain, evolves over days/week („sub-acute‟)
Visceral pain poorly localised to either epigastric, peri-umbilical or subrapubic regions
Classification
Small vs. Large
Complete vs. Incomplete
Open loop vs. closed loop
Open loop: mainly colicky pain – comes in waves. Either top end or bottom end still open
Closed loop:
Isolated loop peristalsis & fluid intramural pressure capillary perfusion &
compromised venous drainage gangrene perforation (rapidly fatal through sepsis and
mass cytokine release)
Symptoms: quick (6 hours start to finish), constant severe pain that started colicky,
temperature & pulse once infarction starts
X-rays & WBCs may be normal
Differential diagnosis pancreatitis (do amylase)
Causes
Intraluminal: e.g.
Choleocystoduodenal fistula gallstone ileus. Gallstone moves from gallbladder to duodenum
via fistula ( air into bilary tree). Also following ERCP
Bezoar: lump of stuff (e.g. hair) intermittently blocking ileocaecal valve
In the bowel wall:
Crohn‟s
Tb
Tumours of small bowel. (Less common) – lymphoma, carcinoid (neuro-endocrine),
adenocarcinoma, melanoma secondaries
Outside wall
Hernia of small bowel, especially indirect inguinal or femoral ( always examine groin)
Adhesion from previous surgery ( look for scars): can take years to present acutely
Small bowel volvulus: malrotation of embryonic mesentery (can also be acquired, e.g. drugs)
easy rotation of mesentery
Intussusception: piece of bowel forced into distal section. Rare, most common in kids (2 months
2 years). Especially around ileocaecal valve
Also in large bowel:
Diverticular stricture and cancer (most common in sigmoid)
Volvulus: of any part of colon (especially sigmoid)
Distal obstruction can also cause ileocaecal valve to shut close loop obstruction. Caecum
ischaemic first as biggest radius (Law of La Place)
Pseudo-obstruction: motility problem (esp. after recent surgery). Check with barium enema,
contrast will go through OK but rectum will be empty
Management
History: bowel movements, previous surgery, weight loss
Exam: dehydration (from vomiting) & distension
Treatment:
Rehydration: crystalloid (i.e. saline) – only want to restore ECF (i.e. not dextrose)
Nasogastric tube: suck out stomach contents vomiting & aspiration
Urinary catheter: monitor fluids
Monitor creatinine: if hypoperfusion kidney failure
Gastro-Intestinal 167
FBC: group & save
Pain relief: 10 mg im morphine or slow infusion. If dose is bad enough to need another then need
surgery
If no scars & no hernias surgery
If scars may settle (if operate more adhesions). Regular review
Appendicitis
= Acute Suppurative Appendicitis
Lifetime incidence = 6%
Most common surgical emergency
Incidence declining (?Hygiene pathogen exposure)
Gut organisms invade appendix wall after lumen obstruction
If suspected then nil by mouth. If no diarrhoea or vomiting then no immediate danger of dehydration
If you diagnose it, or if you don‟t, you‟ll be wrong 50% of the time!
Symptoms & Signs
Very difficult to diagnose – considerable variety in presentation
Fever: 37.5 – 38.5. Typically low grade. Higher if perforated. Swinging fever more typical of an
abscess
Pain:
Initially: central abdominal colic (obstructed appendix and lumen pressure)
Ball-valve relief of obstruction often leads to colicky pain
Once peritoneum inflamed: constant RIF pain.
If perforated: generalised tenderness, maybe distension. If really sick, abdomen may not be hard
However, considerable variation – pain may stay central, may be situated elsewhere in abdomen
Lying on back and lying still, coughing hurts (peritonitis)
Push on left side hurts more on right
Evoking pain: cough or hop on right leg. In a child, look for tenderness and guarding – not
rebound – won‟t let anyone touch them after that.
Systemic signs:
Kids: vague pain, off food (won‟t eat favourite food), diarrhoea, vomiting
Elderly: shocked, confused, no pain
Anorexia, maybe vomiting
Constipation or diarrhoea
Tachycardia (not always)
May be urinary symptoms and signs: especially in children with appendix in the pelvis – e.g. dysuria,
white cells in urine (always do dipstick)
Differential
Appendicitis may co-exist with acute tonsillitis, pneumonia, UTI or even gastro-enteritis
Salpingitis in female, ectopic pregnancy, food poisoning, diverticulitis, cholecystitis, perforated ulcer,
cystitis, Crohn‟s disease, inflammation of Meikels diverticulum (if operate and appendix OK, always
check a metre up the small bowel), radiation of torsion of right testis, strangulated inguinal hernia,
pyelonephritis
Pathology
Pathogenesis: Obstruction of the lumen (faecal, tumour, worms) intraluminal pressure
ischaemia and bacterial invasion inflammation oedema
Macroscopic appearance: congested, dull, fibropurulent exudate on serosa, luminal abscess, gangrene,
rupture
Microscopic appearance: neutrophils in mucosa, submucosa and muscularis propria, necrosis +/-
abscess
Treatment
If not sure, observe: it will get better or worse
Supportive care: IV, NG, restore hydration
Appendicectomy
Metronidazole + cefuroxime (reduce wound infection)
168 4
th
and 5
th
Year Notes
Children
Anatomic variations:
Typical site only 30 – 40% of time
PR: pain on right side retrocaecal appendix (30%). Pain may radiate up right flank. May be no
abdominal tenderness
Pelvic (23%). If in contact with bladder sterile pyuria. If in contact with sigmoid diarrhoea
Course accelerated:
Tiny lumen, inflammation, perforate quickly
Dehydration, tachycardia and shock
Board-like abdomen after resuscitation
Treatment:
Resuscitation first: HG, IV, antibiotics
Operate when: urine output, temperature, pulse rate. Anaesthetics vasodilation and cardiac
depression BP if not well hydrated
Complications
Wound infection
Perforation peritonitis infertility in girls ( lower threshold for surgery in girls)
Abscess
Bowel obstruction (related to perforation adhesions)
Other Disorders of the Appendix
Mucocoele of the appendix: dilation of the appendiceal lumen by mucus duct hyperplasia (either
benign or malignant)
Pseudomyxoma peritonei: „Jelly Belly‟. Mucinous cystadenocarcinoma invading the peritoneum, fills
with tenacious semisolid mucus. Treated with serial resection
Ulcerative Colitis (UC)
= Chronic inflammation of colonic mucosa (only). Unknown aetiology
Epidemiology
More common than Crohn‟s.
1 in 1500 in US. Rare in developing countries
Peak incidence in 25 – 30 year olds
Smoking is protective
Risk in 1
st
degree relatives increases 15-fold
F > M, W > B
Symptoms & Signs
Diarrhoea if disease extends above rectosigmoid junction
Mucus and blood per rectum
Urgency to defaecate
Abdominal pain, tenderness
Relapsing-remitting in 65% patients
If severe attack: fever, tachycardia, hypoalbuminaemia
May have: erythema nodosum, arthropathy, aphthous ulcers in mouth and liver complications
Investigations
Stool culture: exclude infectious
Bloods: ESR and acute phase proteins
Possible deficiencies: Fe, Hb, albumin, electrolyte abnormalities
Sigmoidoscopy: red, raw, granular mucosa
Colonoscopy & biopsy. Spreads from rectum to some point in colon.
Pathology
Macroscopic appearance:
Begins in rectum and extends in continuity to left colon. 40 – 50% limited to rectosigmoid colon.
10% have pan-colitis, may also develop „backwash‟ ileitis.
Gastro-Intestinal 169
Mild: Erythema only. Severe: Mucosal haemorrhages and broad-based ulcerations (not deep
though). Normal appearance during relapses
Pseudopolyps: islands of remaining, regenerating mucosa
Microscopic appearance:
Mucosal inflammation only: mucosal ulcers
Neutrophils, plasma cells, histiocytes in lamina propria
Crypt abscesses (neutrophils in crypt) suggestive of UC rather than Crohn‟s. May extend into
laminar propria to produce ulcers
Chronically, mucosa becomes thin and atrophic
Distortion of crypt architecture, branching
Overtime dysplasia flat carcinomas (cf raised in colorectal cancer)
Differential diagnosis
Microscopic (lymphocytic colitis), Collangenous colitis or Crohn‟s colitis
Irradiation proctitis
Infection, IBS, or Cancer
CMV or herpes simplex in immunosuppressed patients
Complications
Anaemia due to chronic blood loss
Toxic megacolon: diameter of transverse colon > 5.5 cm. Acute dilation of colon due to loss of muscle
tone gas distension vascular occlusion necrosis. May rupture peritonitis. Emergency
Risk of colon carcinoma. Key risk facts:
How long have they had it (main one): 1% at 10 years, 30% at 30 years. Require regular screening
How much bowel is affected: greatest in pancolitis. Minimal with only rectal involvement
How well controlled is the inflammation
Aggressive flat lesions, infiltrates quickly into lymphatics in submucosa
Perforation
Fibromuscular strictures (check to exclude malignancy)
Treatment
Sulphasalazine +/- steroids (or azathioprine). Need regular FBCs
Crohn’s Disease
= Chronic granulomatous inflammation of the gut
Epidemiology
Incidence increasing. Peaks in 2
nd
to 3
rd
decade
1 per 1000 in UK
F > M, W > B
Symptoms & Signs:
Malaise, weight loss (65 – 75%), failure to thrive, malabsorption
Diarrhoea (70 – 90%)
Rectal bleeding (45%)
Pain (50%, from inflammation, infection, obstruction, colicky from intermittent obstruction of terminal
ileum)
Perianal disease (50 – 80%)
Mild fever (30 – 40%)
Anaemia, glossitis (due to malabsorption)
Aphthous ulcers in mouth
Erythema nodosum (painful red nodular lesions on shins), pyoderma gangrenosum (recurring skin
ulcers – 10 cm), clubbing
Asymptomatic periods for weeks-months
Attacks may be precipitated by emotional/physical stress
Risk factors: genetic, smoking, high sugar/low fibre
Aetiology
Type 4 immune reaction: trigger unknown. Cause: ?immune hyper-reactivity
170 4
th
and 5
th
Year Notes
Proposed agents: viruses, disordered immunologic response to ingested antigen
Genetic susceptibility. 10-fold risk in first-degree relatives
Multifactorial abnormal regulation of inflammatory mediators
Investigations
Bloods: check for anaemia (including anaemia of chronic disease), malabsorption, inflammatory
measurements, ESR and acute phase proteins
Deficiencies: folate, iron, B12, etc, electrolyte abnormalities
Culture to exclude infective causes
Sigmoidoscopy/colonoscopy + biopsy
Upper GI endoscopy
Barium contrast of small & large bowel: strictures, fistula, cobblestone appearance, skip lesions etc
Differential
Ileal disease: Tb, Lymphoma
Colonic disease: colitis (ulcerative, ischaemic, radiation, collagenous), infection (salmonella, shigella,
campylobacter), cancer
Malabsorption: lactose intolerance, coeliac disease
Pathology
Location:
75% terminal ileum
50% also involves colon
25% colon only (predominantly right side)
<5% oesophagus, mouth
Macroscopic appearance:
Skip lesions
Transmural inflammation
Thickened, inflexible (resembles rubber hose) with narrow lumen
Thickened, fibrosed mesentery and enlarged regional lymph nodes
Strictures, fistulas, abscesses
Mucosa: varying degrees of erythema and oedema. Cobblestone mucosa
Microscopic appearance:
Submucosal and subserosal inflammation with only secondary mucosal involvement (ie glands
may be straight, unaffected)
Aphthoid ulceration of the mucosa
Lymphocytic infiltrate, fibrosis
Multifocal granulomatous vasculitis
Non-caseating granulomata (only 60%): can have some Langhans/giant cells (horseshoe pattern of
nuclei around periphery of a giant cell), but usually granulomas poorly circumscribed
Treatment
Aim: suppress activity, restore quality of live, prevent complications
Diet: nutritional supplements. Malnutrition a real risk, growth retardation in kids. May need enteral
or TPN feeding for „Bowel Rest‟ antigen load (controversial)
Corticosteriods e.g. prednisone: symptomatic relief
5-aminosalicylic acids e.g. mezalazine
Antibiotics (mainly colonic and perianal disease, antigen load): metronidazole
Steroid sparing immunosuppressives: azathioprine
Cholestyramine: absorbs bile (normally absorbed in the terminal ileum) to stop it getting into the large
bowel, where it causes irritation
Surgery
Monitor: inflammatory markers
Complications
Episcleritis (reddened sclera)
Stricture, obstruction, fistulas (to bowel, bladder, vagina)
Malnutrition
Large & small bowel cancer (5% at 10 years – ie small risk – not screened for)
Gastro-Intestinal 171
Ankylosing Spondylitis
Pyoderma gangrenosum
Iritis
Arthritis
Comparison with Ulcerative Colitis
Crohn‟s
Ulcerative Colitis
Macroscopic
Skip lesions
Transmural inflammation
Thickened wall
Often proximal to large bowel
Cobblestone appearance
Continuous
Mucosa only affected
Large bowel only
Pseudopolyps
Microscopic
Granulomas (only 60%, poorly formed –
pale area with giant cells)
Crypt architecture preserved (like a row
of soldiers)
Muscularis involved
Superficial
No granulomas
Crypt abscesses
Distorted crypt architecture
Ulcers
Complications
Minor cancer risk
Major cancer risk
Fistulas, strictures, fissures
Toxic megacolon
Surgery
Recurs at anastamosis. Surgery for
obstruction and abscess common
Colectomy = „cure‟
Small Bowel Tumours
Benign: Polyps (Peutz-Jeghers), Juvenile Polyps, Adenomas, Stromal tumours
Malignant:
Carcinoid tumours:
Tumours arising from neuroendocrine cells
Mainly midgut. Similar tumours occur in lungs, ovaries, biliary tree
Macroscopic appearance: submucosal elevations, yellow/grey, infiltrative, ulceration, multiple
Microscopic appearance: Uniform cells, oval nucleus, fine chromatin, pink cytoplasm,
neuroendocrine granules
Clinical: malignancy depends on site. Appendix and rectum better, ileal and colonic worse
Carcinoid Syndrome: due to excess serotonin. Occurs with hepatic metastases (liver
efficiently removes 5HT from portal circulation) wheezing, right sided heart failure,
diarrhoea (motility), abdominal pain, oedema, skin lesions
Lymphomas of the GI tract
Affects stomach, ileum, colon, jejunum. Arise in the gut, or spread there from elsewhere
3 types: MALT, Sprue associated, and immunoproliferative small intestinal disease
Macroscopic appearance: plaque-like expansion of the mucosa ulcerating, fungating mass,
can obstruction or perforation
Microscopic appearance: tumour cells diffusely infiltrate the wall, cytologically resemble
follicular lymphoma cells
Clinical outcome: prognosis depends on depth of invasion, size, direct extension
Adenocarcinoma: Uncommon. Resembles those in the colon
Colorectal Cancer
Presentation
Change in shape of stools significant (e.g. pencil shaped)
Rectal bleeding/mucus
Persistent changes in bowel habit
Tenesmus: constant feeling of need to defacate, even after passing stool
Weight loss
Anaemia
Abdominal or rectal mass in late presentation
Hepatomegaly (from secondaries)
172 4
th
and 5
th
Year Notes
By 75 years, 1 in 20 males and 1 in 25 females (Victoria)
Risk Factors
Environmental factors: diet, lifestyle, smoking
Family history
Premalignant lesions
Family History and Colorectal Cancer
Average risk = up to two 1
st
or 2
nd
degree relatives with bowel cancer at 55 or older (as long as on
different sides of family). 98% of population
Moderate risk = either one 1
st
degree relative diagnosed before 55 years, or two 1
st
or 2
nd
degree
relatives on one side of family diagnosed at any age. 1% population. Refer for colonoscopy every 5
years from age 50 or 10 years younger than earliest diagnosis in family
High risk = more than above, including FAP or identified high-risk mutation in near relative. <1% of
population. Suggest genetic testing. Referral to plan appropriate surveillance
Incidence has been declining since 1950‟s (5.8% decrease in men, 12.9% decrease in women)
People may not know family history: can they get death certificates of relatives
Polyps
= Any lesion which protrudes above the level of the surrounding mucosa
Hyperplastic polyps
90% of all polyps, measure < 0.5 cm, mainly in rectosigmoid
Benign, no premalignant potential
“Dew drop” appearance, on top of mucosal fold
Sessile (no stalk), often multiple, very common
Microscopically: elongated crypts, goblet and absorptive cells, excess mucin
Adenomatous polyps
10% of polyps
Neoplasms: precursors of most colonic carcinomas. Normally removed as don‟t know which will
become invasive
Malignancy related to size: <1.5 cm only 1% contains a carcinoma, > 1.5 cm 10% will contain a
carcinoma-in-situ. As long as it‟s confined to the mucosa, there is no metastatic potential. If
submucosal invasion then segmental resection
Macroscopically: stalk (ie pedunculated)
Microscopically: neoplastic glands, hyperchromatic, etc
Tubular adenomas: Most common (75%), usually pedunculated, most common in left colon, M >
F, 50% are solitary, continued colonoscopic follow-up necessary. Head has closely packed
tubules/glands lined by non-differentiated neoplastic columnar cells. Stalk has normal colonic
mucosa
Villous adenomas: Papillary projections, larger, more likely to harbour carcinoma, sessile, 10 –
15% of adenomatous polyps, mainly rectosigmoid
Tubulovillous adenomas: contain 25 – 75% of villous component. May secrete lots of mucous
Juvenile polyps:
Left side of large bowel of kids
Cause rectal bleeding
Grossly look similar to adenomas
Microscopically not neoplastic. Cystically dilated mucous glands, inflammation of lamina propria,
maybe ulceration
Peutz-Jeghers Syndrome: Polyp containing mucin filled cysts and smooth muscle in the lamina propria.
No malignant potential. Maybe pigmentation in the mouth
Polyposis syndromes:
Familial Adenomatous Polyposis (FAP): 0.5% of all colorectal cancers. Autosomal dominant,
antioncogene mutation of APC gene. APC gene: 1 in 10,000 have mutation 100s of
adenomatous polyps appearing in 2
nd
or 3
rd
decade. Will develop carcinoma prophylactic
colectomy. APC gene also mutated in sporadic cancer
Hereditary Non-polyposis Colon Cancer (HNPCC): Aka Lynch Syndrome. 5% of non-FAP
colorectal cancers. Patients often young with multiple tumours. 1 – 5 % of all CR cancer.
Autosomal dominant – defect of DNA mismatch repair genes – MMR gene (mismatch repair) - 1
in 1,000 have mutation
Gastro-Intestinal 173
Gardener‟s Syndrome: colonic polyposis, epidermoid cysts (skin), osteoid osteomas (benign bone
tumours). High risk of carcinoma
Turcot‟s Syndrome: colon polyps + brain tumours
Adenocarcinomas of the Colon
Epidemiology:
In US, 2
nd
only to lung cancer in cancer deaths. Much lower in third world ( environmental
factors)
Peak incidence in 7
th
decade (ie old), except APC and UC
70% in recto-sigmoid colon, rest all the way back to caecum
M:F is 2:1 for rectal, equal for right sided
Aetiology:
Adenomatous polyps (esp villous)
Ulcerative colitis
Familial multiple polyposis
Family History
Environmental factors: High incidence in Europe/North America, low in Asia/Africa. Urban >
rural
Diet: High fat and low fibre (slower transit ?exposure to carcinogens)
Pathogenesis: increasing loss of heterozygosity in genes involved in DNA repair, tumour suppression
and oncogene activation. Either through turnover due to mucosal damage risk of gene match
failure or directly genotoxic mechanism
Presentation:
Left sided: annular encircling napkin ring or apple core constriction. Signs of obstruction.
Poorer prognosis despite earlier detection due to invasion
Right sided: large fungating or sessile masses, necrotic areas, occult bleeding, anaemia, weight loss
May produce mucin, ulceration blood loss
Doubling time of about 2 years
Macroscopic description: Early: may still appear to be a polyp or sessile. Later: obliterate precursor
adenoma
Microscopic appearance: Most are moderately differentiated, irregular glands with pleomorphic cells,
usually lack mucin production. Mucinous carcinomas (10 – 15%) have pools of mucin, cleaves
through tissue aiding spread (worse prognosis)
Variants: Adenosquamous carcinoma, small cell undifferentiated (rare), Ulcerative colitis poorly
differentiated colitis
Other large bowel tumours (Gastro-intestinal stromal tumours: GIST)
Carcinoid tumours: most common in appendix and stomach. See Small Bowel Tumours, page 171
Lymphomas: Non-Hodgkin's. Eg MALT
Mesenchymal tumours (eg leiomyomas): much less common
Diagnosis
Rectal exam
FOBT: sensitivity 50% and low specificity
Sigmoidoscopy picks up 40% (& take biopsy).
Colonoscopy: expensive, miss rate for cancer 2-3%
Double contrast barium enema: cheaper, miss rate for cancer 10 – 15%
Check for dissemination: LFT, Abdominal CT, CXR (25% have metastatic disease at presentation)
Differential
Diverticular disease, Inflammatory Bowel Disease, Irritable Bowel Syndrome, Rectal ulcer
Treatment of Colorectal Cancer
No role for radiotherapy in colon
Adjuvant chemotherapy:
Improves 5 year survival over surgery alone from 50 to 60/65% (but can‟t predict who will benefit)
Quality of life (side effects of cancer are pretty severe, chemo reduces these)
Given after surgery
Six months of 5FU

174 4
th
and 5
th
Year Notes
Currently given to:
Dukes C: All patients (C1 = Muscularis propria + lymph node, C2 = serosa + lymph node)
Dukes B2 (serosa): High risk groups, perforation, invasion of adjacent organs, diploid tumours
Rectal cancer:
No serosa around rectum – cancer infiltrates straight into fat – harder to get clear resection margins
Radiation in rectal cancer good: but impaired function and may irradiate small bowel
fibrosis. Try and predict who needs irradiation and do it pre-operatively
Palliation: hospice + chemotherapy better quality of life than hospice alone
Prognosis of Colorectal Cancer
Invade into serosal fat, metastasise to regional lymph nodes then to liver and lungs. Rarely
intraperitoneal spread
Complications: Obstruction, perforation, haemorrhage, fistulas
Prognosis mainly related to stage (how far it‟s spread), to a lesser extent the grade and location
Pre-operative staging: ultrasound of liver, Xray of lungs
Duke‟s Post-operative staging:
Dukes Stage
5 year survival
Level of Invasion
A
100%
Mucosa
B
60%
Serosal wall but not lymph nodes
C
30%
Lymph nodes
D
5%
Distant Metastasis
Wgtn Hospital uses APC staging (Australasian Pathologists): minor differences to Dukes
5 year survival = cured – unlikely to relapse after that
Follow-up
Colonoscopy (e.g. initially rest of colon for 2
nd
primary, then every 3 years)
Monitor tumour marker CEA (colonic embryonic antigen). Also raised in a variety of other tumours &
benign cancers. Not sensitive for early cancers (4% of Duke‟s A). Neither sensitive nor specific
Diverticular disease of the colon
Aetiology & Epidemiology
Dietary fibre stool weight and colonic transit colonic pressure
50% in > 70 years
Symptoms & Signs:
Most asymptomatic
Uncomplicated disease (Diverticulosis): non-specific tender sigmoid colon, cramping lower abdominal
pain (esp. LIF), altered bowel habit (hard or ribbon like stools, e.g. due to stricture)
Complicated disease (Diverticulitis): constant pain worse with movement, fever, shock, peritonitis,
haemorrhage, guarding, palpable mass, ileus, distension, obstruction (= “Left sided appendicitis”)
PR bleeding not usually concurrent with guarding
Pathology
Diverticulosis: multiple out-pouchings or herniations (= diverticula) of the mucosa through the muscle
wall of the bowel at the point where arteries penetrate the bowel wall
Diverticulitis: inflammation of the diverticulum caused by obstruction of the neck, faecal impaction,
constricted blood supply, infection from luminal flora
Complications:
Abscesses obstruction, bleeding due to erosion of blood vessels
Stricture from scarring
Investigations
Bloods usually normal in uncomplicated disease: do FBC and LFT
Complicated disease: inflammatory/infection markers (eg blood cultures if temp > 38 C)
CT, ultrasound, colonoscopy
Contrast enema one month later (never acutely – risk of perforation) to confirm diverticulum and
exclude cancer
Gastro-Intestinal 175
Differential
Cancer
Inflammatory bowel disease
Drug induced colonic symptoms
Abscess/perforation: pyelonephritis, perforated peptic ulcer, ischaemic colitis
Haemorrhage: polyp, angiodysplasia, GI bleeding
Stricture: radiation damage, ischaemic colitis, endometriosis
Malabsorption: lactose intolerance, coeliac disease
Infection: campylobacter, other infection
Treatment:
Acute management:
Fluids (nil by mouth to rest gut)
For diverticulitis: antibiotics (eg cefuroxime and Metronidazole. If really nasty then Gentamycin,
Amoxycillin and Metronidazole)
Epidural would be good for pain but is contraindicated if risk of sepsis
Usually settles with conservative management. If not, then resect affected colon:
Hartman‟s procedure: Remove affected segment. Bring proximal bowel out to a colonostomy.
Temporarily close off distal segment
Reverse colonostomy 3 months later
Chronic management:
Fibre, fluids, exercise
For constipation: bulking agents, lactulose
For pain relief: anticholinergics (cicyclomine), antispasmodics
Irritable Bowel Syndrome (IBS)
Very common (up to 15 – 20%)
F > M
Symptoms & Signs
Crampy lower abdominal pain relieved by defaecation or flatus, associated with change in stool
frequency/consistency
Diarrhoea (rarely at night) and mucus
Distension, variable abdominal tenderness
Nausea, heartburn, early satiety
Urinary frequency
Exacerbated by anxiety or stress
Age < 50 years
Feeling of incomplete evacuation
But NO blood, weight loss or recent onset
Diagnosis
A diagnosis of exclusion
Continuous or recurrent symptoms for at least 3 months
Abdominal pain relieved by defecation or associated with a change in bowel habit
Irregular pattern 25% of time with 2 or more of:
Change in frequency (> 3 per day or < 3 per week)
Change in form (lumpy/hard/loose)
Change in passage (straining/urgency/feeling of incomplete evacuation)
Mucus
Bloating/distension
Investigations
Exclude other conditions, e.g.:
FBC: anaemia and nutritional deficiency
LFT: exclude bilary colic
Thyroid function: exclude myxoedema ( constipation) or thyrotoxicosis ( diarrhoea)
Colonic imagining for new or different symptoms in > 40 years – exclude cancer/IBD
Faecal fat, breath test, lactose tolerance test
176 4
th
and 5
th
Year Notes
Differential
Diagnosis of exclusion, so the differential is everything else
Cancer, IBD, diverticular/ceoliac disease, infection, diverticular disease, chronic pancreatitis,
bilary/liver disease, peptic ulcer, motility disorder, bacterial overgrowth, laxative abuse, endometriosis,
ovarian malignancy, thyroid disease
Aetiology
Abnormal gut motility
Enhanced visceral sensitivity
Psychological/psychiatric disorder
Food allergy/intolerance
Treatment
Supportive, reassurance, stress reduction,fibre (RDA = 25 – 30 grams, average is 15), fluids (2 litres
per day), exercise
For constipation: bulking agents, lactulose
For pain relief: anticholinergics (cicyclomine), antispasmodics
For confirmed diarrhoea: antimotility drugs (loperamide, codeine phosphate)
If depressed then antidepressants
Bacterial Overgrowth of Small Intestine
=Aerobic G+ bacteria replaced by anaerobic G-, esp. E coli & clostridium difficile (toxin causes
diarrhoea) often in a blind loop of bowel, or in the small bowel which usually has low bacterial load
Symptoms & Signs:
Diarrhoea, abdominal pain, weight loss
Steatorrhoea, anaemia, ataxia/neuropathy (due to B12 deficiency – bacteria eat it all)
Investigations:
Blood: check for anaemia, B12, folate
Schilling test
Stool fat
Barium x-ray for jejunal stricture/diverticulitis, motility
Duodenal aspiration and biopsy
Differential:
Coeliac disease
Chronic pancreatitis
Crohn‟s disease
Infections: campylobacter, Giardia, AIDs enteropathy
Breath tests: H2 after lactulose, etc
Aetiology
Motility disorders
Bacteria: e.g. stomach acid (hypochlorhydria)
Impaired immunity
Treatment:
High protein diet, vitamin supplementation, stop antibiotics
Antibiotics: Metronidazole 400 mg TD, Ciprofloxacin 500 mg BD, or vancomycin
Pseudomembranous Colitis
Acute diarrhoeal illness following broad-spectrum antibiotics
Overgrowth of clostridium difficile
Macroscopic appearance: Puss erupting from glands (like little volcanoes, cauliflowers)
Microscopic appearance: superficial necrosis of epithelium and crypts, mucus/puss over the surface
Diarrhoea – Infectious Agents
= Acute Enterocolitis
Symptoms & Signs:
Dysphagia (e.g. Candida)
Flatulence, colic, distension, diarrhoea (watery, fatty, bloody)
Vomiting, fever
Gastro-Intestinal 177
Investigations
Blood: eosinophilia, HIV
Faecal microscopy, parasitology, culture
H2 breath test
Endoscopy/Colonoscopy +/- biopsy
Pathology: Red, oedematous bowel (all look the same), microscopically non-specific inflammation
Differential
Drug induced diarrhoea: laxatives, magnesium compounds, diuretics
Severe alcohol intake
Diabetic autonomic neuropathy
IBD
Malabsorption: coeliac, lactose intolerance, lymphoma, pancreatitis, bilary/liver disease
Management:
Rehydration
Investigate cause
Monitor complications: anaemia (due to haemorrhage), septicaemia, perforation, appendicitis
Strict food hygiene
Avoid milk secondary hypolactasia
Antibiotic treatment
Infectious agents
Bacterial enteroinvasive:
Campylobacter Jejuni
Poultry
Haemorrhagic colitis
Erythromycin (used to be ciprofloxacin but it‟s been put in chicken feed resistance)
Escheria Coli
Enterotoxic subspecies
Travellers diarrhoea
Salmonella/Shigella: Poultry
Bacterial enterotoxins:
Vibrio Cholerae
Staph Aureus: Food poisoning (eg cream buns)
Clostridium Botulinum
Some subtypes of E Coli
Protozoa
Giardia
Trophozoites reside mainly in duodenum, also small bowel
Cysts in faeces
Small bowel diarrhoea diarrhoea during night (large bowel „sleeps‟)
Entamoeba histolytica: causes amoebic dysentery (colitis)
Cryptosporidium
Common in kids
Is chronic in immunocompromised
No effective antibiotic treatment
Constipation
= Infrequent bowel action (ie > 3 days) or difficult/painful defecation
Affects 3% in young adults 20% in elderly
Physiology:
Muscular movements: segmentation mixes bowel contents. Peristalsis moves it along. Mass
movements occur once or twice a day (usually after a meal)
Faecal mass in rectum internal anal sphincter opens by reflex. External sphincter remains
contracted voluntarily, but will tire quickly leakage
Defaecation requires relaxation of external sphincter, pelvic floor muscles and abdominal straining
Motility affected by sympathetic (segmentation) and parasympathetic ( peristaltic and mass
movement) system, hormones, fibre, acid pH, lactobacilli
Age related changes: mucosal atrophy (mucus), muscular atrophy, etc
178 4
th
and 5
th
Year Notes
Assessment:
History: What do they mean? Frequency, stool consistency, presence of blood/mucus, ease of
evacuation, onset of symptoms, and drug history.
In elderly screen for risk factors: fibre following changed diet or false teeth, can‟t shop or prepare
food, physical activity transit time, dehydration, neurological disease (eg diabetic
neuropathy)
Exam: systemic disease, abdominal exam and perianal sensation
Investigations: Usual, plus blood tests to exclude anaemia, hypothyroidism and electrolyte
abnormality
Management:
Review medication, eg:
Opioids
Anticholinergics (eg antihistamine, antiemetics)
NSAIDS
Serotonin antagonists
Phenothiazines
Tricyclic antidepressants
Bowel retraining. Try during high motility periods – first thing in the morning and after meals.
Exercise to improve abdominal muscles
Adequate fibre and fluid
Laxatives:
Hydrophilic bulk forming agents, eg Normacol, Metamucil. Must also take adequate water.
Not useful in palliative care (patients are too sick to eat it)
Osmotic agents, eg lactulose or sorbitol not broken down in small bowel osmotic
gradient water content. Take 1 to 2 days to act. Safest agent in the long term
Stool softeners and lubricants. Take 1 to 3 days to act. Act as detergents top increase water
penetration and thus softening of the stool. Eg docusate agents, Coloxyl (a detergent effect
breaks up stool, may be hepatotoxic) and lubricants. Oil based lubricants (eg paraffin) can
affect vitamin and drug absorption and be aspirated
Stimulants and irritants peristalsis and net fluid secretion. Eg Senna. Take 6 to 12 hours
to act. Stimulates the myenteric plexuses to produce peristalsis. Avoid irritant laxatives
unless impaction, severe muscle weakness. Long term use of laxatives causes constipation by
damaging the nerve supply of the gut
Locally acting agents eg glycerol suppository at peak motility time. Can have osmotic and
irritant agents
Investigational agents such as cisapride (prokinetic agent)
Rectal Laxatives:
For faecal impaction
On exam will either have a loaded rectum or ballooning of the rectum (dilated distally
impacted further up)
Types:
Glycerine suppositories: soften stool by lubrication and osmosis
Bisacodyl (Dulcolax) suppositories: Causes peristalsis
Sodium Phosphate enemas
Oil Enemas
Fibre
Dietary Fibre: the undigested and unabsorbed polysaccharide (cereal, fruit, vegetable) that remains at
the end of the small bowel. Contains cellulose and non-cellulose polysaccharides, lignin, gums and
waxes
Worth a trial in constipation, IBS (esp. with constipation) and non-ulcer dyspepsia of dysmotility type
Get good 24 hour dietary history
Intake from cereal source is 4 or 5 times greater than fruit or vegetables. It is also less fermented in
large bowel
Ideal level = 30g/24 hours. Usual NZ adult approx. 15 g/24 hours
20 g of fibre in 6 tablespoons of bran, 2 Weetbix or 4 large thick slices of whole meal bread
Suggestions for use:
Increase SLOWLY (i.e. aim for a full bowl of All bran in 2-3 months): otherwise bloating,
distension, gas
Gastro-Intestinal 179
Take fibre every day
Necessary amount is not a weight – but the amount necessary to keep stools soft
Drink lots of water (2 L per day is recommended)
Will increase gas (fibre promotes bacterial growth): take stairs not lift!
Other Bowel Diseases
Collagenous colitis:
Chronic or episodic watery diarrhoea
F > M, 30 + years, autoimmune association
Macroscopic appearance: Looks normal at colonoscopy
Microscopic appearance: subepithelial hypocellular collagen band (prevents H2O absorption)
Anorectal problems
Haemorrhoids:
Dilated veins beneath the submucosa. Bleeding from overlying mucosa
Don‟t cause pain unless prolapsed or thrombosed
Can cause Pruritis ani
Treatment: injection with injected sclerosant (eg almond oil), banding (but infection and bleeding
risk), infra-red coagulation
Rectal Prolapse:
Self-limiting in kids, in elderly due to weakened pelvic floor (childbirth or denervation)
Treatment is surgical, faecal incontinence improved in half
Rectal Cancer:
Majority can be felt on digital examination
Adenocarcinomas
Presentation: bleeding and tenesmus, rarely pain
Treatment: local excision or resection
Fissures:
Vertical tear in anoderm. 90% posteriorly
Acute or chronic
Vicious circle: tight internal anal sphincter tear reflect spasm constipation etc.
History: severe pain and bleeding on defaecation
Associated with high resting anal pressure
Treatment: High fibre diet, lots of H2O, local analgesic cream, GTN paste (relaxes sphincter) (all
conservative), limited internal sphincterotomy
Abscesses and fistulae:
Infection of tiny glands emptying at dentate line.
Infection can burrow into perianal fat or ischiorectal fat
Drainage may result in anal fistula
Pruritis Ani (itchy anus):
Usually worse at night
Causes by anal or dermatological conditions
Anal: haemorrhoids, keyhole deformity, pinworm infection, anal warts and cancers
Dermatological: Bowen‟s disease, Paget‟s disease of anus, eczema
Treatment: avoiding strong steroid creams, avoiding itching, and drying carefully
Anal warts: Condylomata acuminata. Caused by HPV 8 and 11. Usually an STD
Anal Cancer: Uncommon. Spreads to inguinal glands. Can be adenocarcinoma, basaloid carcinoma
(this and next two caused by HPV 16 and 18), squamous carcinoma, muco-epidermoid carcinoma, anal
melanoma.
Perianal suppuration
Angiodysplasia (submucosal proliferation of vessels – associated with age and aortic stenosis)
Anal cancer (rare): related to HPV (as with cervical cancer) anal intraepithelial neoplasia. Risk
factors as for cervical cancer (number of partners, age of first intercourse, etc). Above dentate line –
endodermal origin adenocarcioma. Below dentate line – ectodermal origin squamous or basal
cell carcinoma or melanoma
180 4
th
and 5
th
Year Notes
GI Bleeding
Upper GI Haemorrhage
Symptoms/Signs:
Haematemesis (either fresh or coffee ground appearance): check not coughing it up. Can check
vomit with urine dipstick for blood
Melaena (black/sticky foul smelling stools): stomach denatures haemoglobin black. So no
melaena if bleed beyond proximal small bowel. Exclude iron tablets, bismuth preparations &
Guinness
Rectal bleeding (haematochezia)
Anaemia: tired, pale, breathless, faint (brain struggles to compensate if PO2 <60 mmHg)
Hypovoleamia: carotid bodies sympathetic ↑HR & peripheral vasoconstriction; ↓renal
perfusion ↑renin ↑angiotensin (vasoconstriction) ↑aldosterone (H2O retention); ↑ADH
thirst and H2O retention. If serious hypovoleamia: postural hypotension, cold & clammy,
confused, thirsty, weak pulse & tachycardic, ↓urine output
Check stridor: tumour compressing trachea – expiratory wheeze
History:
Always ask about CV and respiratory history, and when they last ate, in case surgery is needed
Medications: NSAIDs (if so, then steroids further increase risk), anticoagulants
Investigations:
Bloods: anaemia, reticulocytes, group & hold, U &Es, Liver fn (is it varicies?), clotting (either
poor liver function or Warfarin bleeding)
Endoscopy (can do biopsy)
Barium swallow (not so good)
Causes: Tear, varices (check splenomegaly, spider naevi, palmar erythema, risk of death 30%, risk of
rebleed, 30%), oesophagitis (e.g. from reflux or ulcer), Mallory-Weiss tear from repeated vomiting,
gastritis (e.g. alcoholic), ulcer, malignancy (check for masses, lymph gland enlargement,
organomegaly), ulcer (NSAIDs)
Causes of small bowel bleeding (eg if no upper or lower cause found):
Under 25: Meckel‟s diverticulum
30 – 50: Small bowel tumour
Over 50: angiodysplasia
Lower GI Haemorrhage
Symptoms/Signs:
Blood in/with stool. Colour indicates site: if bright red 95% of pathology distal to splenic
flexure (usually anus & rectum)
Pain on passing motions anal fissure (haemorrhoids don‟t cause pain unless prolapsed)
Anaemia
Angina (in elderly with CHF, anaemia angina due to ↓O2 ↑heart work)
Check: Meikels diverticulum – lined with gastric mucosa
Family Hx: colorectal cancer/inflammatory bowel disease
Rectal Exam (Always do abdominal exam as well)
Look first: skin tags Crohn‟s, sentinel tags chronic anal fissure
Digital examination: if acute fissure this will be very painful ( give up)
Rigid sigmoidoscope: in 2/3 can only see rectum
Investigations: rectal exam, sigmoidoscopy, colonoscopy, barium enema, bloods (anaemia,
reticulocytes)
Causes:
Diverticular disease (brisk bleeding with sudden onset)
Inflammation (ulcerative colitis, etc)
Infection (e.g. campylobacter)
Colorectal cancer
Angiodysplasia
Haemorrhoids (blood coats bowel motion with drops after motion passed)
Anal Fissure (pain passing motion)
Anal Cancer
Upper GI bleeding (check with an NG aspirate)
Gastro-Intestinal 181
Treatment of Major GI Haemorrhage
Resuscitate:
Colloid drip (expand vascular volume – not crystalloid – that shifts into interstitial space, 14 or 16
gauge)
If meet any of the criteria for shock then transfer to ICU: postural hypotension > 15 mmHg fall,
tachycardia > 100, systolic BP < 100.
Check thirst/urine output (insert catheter)
Max O2
Bloods: group and hold (don‟t match until sure you need it), ABG, Hb, baseline creatinine before renal
failure, ↑urea – may be due to breakdown of blood in gut, check platelets, INR & APTT for liver
disease, bleeding disorders, warfarin OD)
Find cause:
ANY melaena upper GI down to proximal small bowel
Endoscope for upper:
Don‟t endoscope until resuscitated – but do it early. If they rebleed and surgery is required,
the surgeon will want to know where its from
Endoscope for varices injection sclerotherapy (e.g. ethanolamine oleate), balloon
tamponade
For lower bleeding:
Sigmoidoscope: check no mass
Colonoscopy
If pain ischaemic colitis
If aortic surgery aorticduodenal fistula
If not stopping, either labelled red cell scan (view with gamma camera) or mesenteric
angiogram (contrast via femoral artery into mesenteric arteries) to guide surgery. These only
detect active bleeding
65% will spontaneously stop resuscitate/transfuse and investigate less urgently
Indications for surgery:
Failure of conservative treatment
In shock, rebleed, etc
Consider if > 6 units of blood needed over 24 – 48 hours
Liver Disease
NB: This section combines notes from the Gut run, and from Microbiology and Chemical Pathology
Assessment
Presentation
Found coincidentally when clinically well (e.g. medicals)
Family screening e.g. abnormal irons, HBV
Non-specific illness and found to have abnormal LFT: ?alcohol, medicines, viral, jaundice, liver/bilary
disease
Is it acute, chronic, acute on chronic, or a failing chronic
Aetiology
Acute hepatitis:
Viral: A, B, C, D, others
Toxic:
Drugs
Poisoning (eg alcohol)
Chronic hepatitis:
Viral: B, C, B + D, CMV
Toxic:
Drugs
Chronic Alcohol
Autoimmune
Metabolic:
Alpha-1-antitrypsin
182 4
th
and 5
th
Year Notes
Wilson‟s disease
Haemochromatosis
Fatty liver: Obesity, NIDDM, Drugs, alcohol
History
Surgery: e.g. cholecystectomy
Heart disease: congestive heart failure
Pregnancy
HIV positive, sexual orientation
Contact with hepatitis: family, sexual
Travel: malaria, parasites
Hepatitis infection risk: Tattoos, body piercing, health care worker, transfusion, IVDU
Alcohol acute alcoholic hepatitis
Ethnic group
Medications – ALWAYS ASK ABOUT DRUGS
Family History: e.g. anaemias, Gilbert‟s syndrome, haemochromatosis, gallstones, alcoholism,
autoimmune disease, Wilson‟s disease (copper)
Symptoms: itch, urine and stool colour
Liver Function Tests (LFTs)
Investigations:
Bloods:
Bilirubin
LFT: AST, ALT, ALP, GGT
Total protein, albumin
Tests can be widely variable for the same condition
Other: Coagulation studies, ammonia
Special tests: 1 antitrypsin, feta protein, hepatitis markers, specific autoantibodies, Igs,
caeruloplasmin
Any liver disorder may ferritin (also an acute phase protein)
Also test for other causes of liver disease: HBV, HIV, iron studies (ferritin), immune liver disease
(Anti-nuclear Antibodies – ANA)
Imaging: ultrasound +/- CT, MRCP, ERCP. Ultrasound and CT have high false negatives for
bilary
Percutaneous transhepatic cholangiogram – PCT
Liver biopsy the gold standard
Aim to decide if liver disease is present, is progressing or is severe
Aiming to answer three questions:
1) Is there liver cell death – inflammation and hepatonecrosis? Check:
Bilirubin: in acute hepatitis will be 50:50 direct and indirect
Raised aminotransferases predominate. If AST > ALT think severe cirrhosis, liver malignancy,
alcohol. In normal hepatitis ALT > AST
Common liver causes:
Non-alcoholic steatohepatitis (fatty liver): probably the most common cause of mildly
elevated LFTs, especially if obese, Type 2 diabetes and hyperlipideamia
Acute/chronic viral hepatitis
Genetic haemochromatosis
Autoimmune hepatitis
Less commonly: 1 antitrypsin deficiency and Wilson‟s disease
Causes of abnormal LFTs other than Liver disease:
Diseases of other organs affecting liver, e.g. RA
Medicines, alcohol, tonics, remedies, poisons
Congestive heart failure hepatic congestion
AST: also produced by:
Muscle: If normal ALT and AST then do a CK for muscle breakdown
Blood: Haemolysis

Gastro-Intestinal 183
2) Is there cholestasis (=impaired bile flow)? Liver can remove 5 * normal bilirubin from circulation (i.e.
large functional reserve). Cholestasis usually refers to obstruction within the liver. „Obstructive
Jaundice‟ major ducts. Bile salts are 90% reabsorbed in the terminal ileum. They emulsify fats.
Bile also contains cholesterol, phospholipids and bilirubin (reabsorbed urobilinogen urine)
If left or right hepatic duct blocked, other side of liver will be sufficient to keep bilirubin normal
GGT released in inflammation: usually in parallel with ALP in obstruction. If GGT and ALP
then ALP is from the bilary tree
Raised ALP and GGT predominate in cholestatic diseases
Common:
Biliary obstruction: gallstones
Drug hepatotoxicity
Neoplasms (eg head of pancreas)
Less Common:
Primary biliary cirrhosis
Primary sclerosing cholangitis
Sarcoidosis
Autoimmune cholangiopathy
Other causes of ALP:
ALP from bone and cholangiocytes (bilary epithelium). Excreted in urine, but saturated
kinetics serum level
Physiological:
Bone: Growth and fractures. High in puberty
Pregnancy (placental)
Benign with age
Bone disease: Paget‟s, malignancy, renal failure, hyperparathyroidism, Rickets
GI tract can also produce ALP, eg Crohn‟s
Miscellaneous: hyperthyroidism, familial benign, transient of infancy
GGT benignly with age and obesity
3) Is liver function normal? Are detoxification, synthesis, and glucose management working? Has a
large functional reserve. Check:
Bilirubin
Albumin. See below
Prothrombin time (INR): factors 2, 5, 7, 9, 10. Give parental Vitamin K to differentiate between
malabsorption or poor liver function
Tests in cirrhosis
Liver function tests very variable:
Quiescent phase: normal of minor in LFT
Active Phase: in ALT and AST when necrosis is dominant
Causes: idiopathic, alcohol, chronic active hepatitis, primary biliary cirrhosis, haemochromatosis,
Wilson‟s disease, 1 antitrypsin deficiency
Other examples of Liver Function tests:
ALT and AST: viral hepatitis, Paracetamol OD
ALP and bilirubin in a 12 year old with vomiting: Gilbert‟s syndrome (bilirubin when fasting),
ALP normally raised at this age
Bilirubin, ALP, Albumin + neuro signs ?Wilson‟s disease (very rare)
Bilirubin, ALP, Albumin + abnormal electrophoresis ? 1 antitrypsin
Total Protein
Normal Ranges:
Total Protein
60 – 80
Albumin
34 – 46
Globulin Gap
~ 20
Examples:
55 year old man, albumin, normal protein Ig (common in cirrhosis)
14 year old, cholesterol, protein, albumin nephrotic syndrome (relevance of high
cholesterol not understood)
184 4
th
and 5
th
Year Notes
58 year old man with diabetes, protein 94, albumin 56 dehydration (don‟t get albumin > 50
without dehydration)
40year old post-op, protein 26, albumin 11 dilution. Took blood downstream of iv line
46 year old, enlarged nodes, protein 50, albumin 33 globulin gap ?
immunocompromised/lymphoma
60 year old, pneumonia, protein 70, albumin 22 acute phase + maybe Ig
50 year old, recurrent abdominal pain, protein 55, albumin 27 pancreatitis malabsorption
38 year old, SOB, rash, protein 86, albumin 34 sarcoidosis or SLE
Differentials:
Hypoproteinaemia:
Haemodilution: poor iv therapy, drip arm, SIADH, pregnancy
Albumin: synthesis (liver disease, malabsorption, malnutrition), losses (renal, gut, skin),
non-specific (eg illness)
Ig: primary or secondary immunodeficiencies. Only IgG deficiency is enough to show up as
low protein or on electrophoresis
Hyperproteinaemia:
Haemoconcentration: dehydration, haemostasis
Ig:
Monoclonal: myeloma, lymphoma, macroglobulin, MGUS
Polyclonal: liver disease, infection, autoimmune, sarcoidosis
Oligoclonal
Aside: Electrophoresis
Bands: albumin, 1 antitrypsin, haptaglobins (2 band), transferrin, complement, Igs
Two indications:
1 antitrypsin deficiency
Monoclonal antibody band
Monoclonal Gammaglobulinaemia of Uncertain Significance (MGUS)
Benign, but potential for malignant transformation (eg to Myeloma): 5% at 5 years, 25% at 15
years
need to follow up over time
See Aside: Conditions associated with Monoclonal proteins, page 303
Causes of Jaundice
For neonatal jaundice, see Jaundice, page 595
Unconjugated hyperbilirubinaemia
Overproduction: Intravascular or extrahepatic haemolysis
Hepatocellular uptake: drugs, sepsis, starvation
Hepatocellular conjugation: Gilbert‟s syndrome, neonatal jaundice, drugs, diffuse hepatic disease
Conjugated bilirubinaema (cholestatic jaundice)
Impaired hepatocellular secretion: various syndromes, duct stricture, biliary cirrhosis, steroids
Hepatocellular cholestasis – impaired secretion plus liver injury as well: viral infection, drugs,
alcohol
Extrahepatic obstruction: stones, carcinoma, strictures and congenital atresia
Pathology
Normal histology:
Chords of hepatocytes between sinuses running from portal tract to central vein
Zone 3 (perivenular) more sensitive (eg to drugs) than zone 1 (periportal)
Acute Hepatitis:
=Inflammation of the liver: no cause implied
Macroscopic appearance: mildly enlarged, tender liver. Flu like symptoms. Jaundice, itching
Microscopic appearance:
Diffuse liver cell injury with lobular disarray: loss of normal radial array
Focal necrosis of hepatocytes with hepatocyte regeneration (mitotic figures, variation in cell
size)
Portal inflammation: lymphocytes & macrophages. Eosinophils with drugs
Bile stasis: variable (often absent), due to disruption of canaliculi, greenish
NO fibrosis
Gastro-Intestinal 185
Chronic hepatitis:
If longer than 6 months then chronic – otherwise acute (unless chronic signs – e.g. spider naevi)
Chronic active and chronic persistent hepatitis reflect different disease activity but caused by the
same agents
Chronic persistent hepatitis: Benign and self-limiting, following acute hepatitis and lasting several
years. Inflammation limited to portal triad (lymphocytes, macrophages and plasma cells).
Architecture preserved, no fibrosis, no hepatocyte necrosis
Chronic active hepatitis:
Progressive hepatic necrosis and fibrosis, potentially leading to cirrhosis
Clinical course variable. 5 year survival 25 – 50%
Marked portal inflammation extending into lobules
Piecemeal necrosis: „nibbling away‟ at hepatocytes around portal track by lymphocytes
necrosis
Bridging necrosis: creating portal-central or portal-portal tracts
Hepatitis B: ground glass hepatocytes – large, uniform cytoplasm filled with viral protein
Hepatitis C: fatty degeneration, bile duct lesions and lymphoid follicles
Fulminant Hepatitis:
Very rare. Onset to death in 2 – 3 weeks (massive necrosis) to 3 months (submassive failure)
Causes: Viral (60%), drugs/chemicals (30%, eg paracetamol poisoning), numerous other minor
causes
Macroscopic appearance: all/most of liver destroyed. Red, limp, wrinkled capsule. Mushy red
Microscopic appearance: Zonal (2,3) or complete necrosis, liquefaction of hepatocytes, little
inflammation
Management of Acute Hepatitis
Avoid strenuous physical activity while jaundiced, increase slowly afterwards
Best rest only if unwell
No corticosteroids
Perhaps reduce fat, abstinence from alcohol
Care with personal hygiene
Follow liver tests until normal
Progression of Chronic Hepatitis
Acute hepatitis (inflammation/cell death) regeneration resolution or chronic hepatitis, which may
fibrosis (the necessary step for progression to liver failure) disordered architecture cirrhosis
Assessing Liver Biopsy:
Is there inflammation around the portal tract? „Limiting plate‟ surrounds portal tract. Monocytes
migrate through this and cause piecemeal or interface hepatitis. If it extends to another portal tract
then called bridging necrosis
Is there inflammation/necrosis out in the lobule intralobular or focal necrosis
Are there inflammatory cells in the portal tract portal inflammation
How much scar tissue/fibrosis is there?
Knodell index scores each of these to generate a Hepatitis Activity Index (HAI). Score out of 22
Child-Pugh Classification of liver function/failure: sum of scores for encephalopathy, ascites, bilirubin,
albumin, INR, nutrition
Score
5 year survival
Grade A
<= 6
50%
Grade B
7 – 9
20%
Grade C
> 9
Few
Alcoholic Liver Disease
Alcoholic Steatosis (Fatty Liver):
Pathogenesis: synthesis of TAGs + fatty acid oxidation + formation/release of lipoproteins
fat in lymphocytes
Macroscopic appearance: large, pale, liver with soft greasy cut surface
Microscopic appearance: Micro and macro-vesicular types. Intracytoplasmic droplets coalescing
to fill the cell, may rupture (no inflammation before rupture). Perivenular fibrosis
186 4
th
and 5
th
Year Notes
Outcome: Liver function may be normal. If no fibrosis then can be cleared
Fatty liver can also be caused by toxic, metabolic and hypoxic conditions, and occurs in
malnourished kids in the third world
Alcoholic hepatitis:
Acutely following heavy drinking
Often superimposed on fatty change or cirrhosis
Microscopic appearance:
Similar to viral hepatitis
Liver cell necrosis and inflammatory infiltrate
Mallory bodies (alcoholic hyaline): intracytoplasmic collection of cyto-skeletal proteins.
Looks like candy floss
Fibrosis
Alcoholic Cirrhosis:
Causes 60 – 70% of cirrhosis. Most of the rest is viral
Only 10% of alcoholics get cirrhosis
Requires daily alcohol of > 60 gm (1/3 bottle of spirits)
Macroscopic appearance:
Initially large, fatty, micronodular (liver cells regenerating between fibrosis)
Progresses to small, non-fatty, macronodular (>10 mm) liver. Often micro-macro nodular
presentation
Microscopic appearance:
Early: delicate portal-central fibrosis, fatty parenchyma.
Late: enlarged nodules surrounded by broad fibrous bands (with signs of liver failure). Bile
retention within nodules
Immediate causes of death: hepatic coma, GI bleed, infection, hepatocellular carcinoma, head
injury subdural haematoma
Alcohol also pancreatitis (see Pancreas, page 197)
Viral Hepatitis
Causes:
Prime target is the liver: Hep A, B, C, D, E,
May affect liver secondarily: EVB and CMV
Distribution of cause of acute hepatitis (e.g. ALT > 1000) in Auckland: A - 25%, B – 25%, EBV –
25%, C – 5 – 10%, some CMV
Clinical course: variable – from asymptomatic to fulminant/fatal. Common symptoms:
Malaise, weakness, lethargy
Flu like illness: tiredness, fever, myalgia
Anorexia, nausea, vomiting (especially Hep A)
Jaundice (uncommon)
Hep A
Hep B
Hep C
Incubation
2 – 8 weeks (ave 4)
4 – 17 weeks (ave 6)
3 – 20 weeks (ave 7)
Symptoms
20 – 40%
40 – 60%
Mild
Onset
Abrupt
Insidious
Duration
1 – 3 weeks
1 – 4 weeks, sporadic
Icterus (Jaundice)
30 – 35%
30 – 40%
10 %
Route of Infection
Faecal/oral
Parenteral/sexual
Blood
Chronic infection
None
10 – 15%
50 – 80%
Mortality
0.05 – 0.1%
1 – 2%
Diagnosis
IgM anti-HAV
IgG anti-HAV
IgM Anti-HBc,
HBsAg, HBeAg
Exclusion. After 3
months Anti HVC.
HVC RNA PCR
earlier
Vaccination
Havrix: 99% cover
Engerix B: 90 – 95%
cover
None
Hepatitis A
= Infectious hepatitis
25 – 33% of clinical cases of hepatitis
Especially in kids, normally mild
Gastro-Intestinal 187
Transmitted by food (especially raw shell fish) or contaminated water.
Decreasing over time due to hygiene and good vaccine
Viraemia lasts 7 days after onset of jaundice. Don‟t get virus in the blood (or only transiently). It‟s a
gut bug
Symptoms: arthralgia, weight loss, fatigue, low grade fever, loss of appetite, abdominal pain
Diagnosed by IGM Anti HAV & ?exclusion of HBV
Treatment: supportive, dietary restriction, rest, no alcohol. Notifiable disease
Post exposure prophylaxis with ISG for contacts
Vaccination:
Havrix 1440: 99% immunity after 1 month. One dose im. Booster after 6 – 12 months gives
longer-term immunity. Inactivated HAV
Especially for travellers, sewage workers, health and childcare workers
Can‟t distinguish natural immunity from vaccine immunity (IgG Anti-HAV in both)
Hepatitis B
Epidemiology
350 million with chronic infection, >75% of these Asian
30% of chronically infected die prematurely from the disease
In NZ, approx. 50,000 carriers. Chinese 10%, Maori 5.4%, PI 4.4%, European 0.43%
Transmission:
Body fluids (blood, semen), including transfusion & contaminated needles
Mother to baby (vertical transmission): 95% risk of infection – vaccinate at birth and give Anti-
HBs – immune globulin
Organ transplant
Child to child (horizontal transmission). Must get into blood – e.g. grazes, stubbed toes. Very
resilient virus. Children are most likely to have asymptomatic seroconversion
Diagnosis
ALT elevation to 1000-1500 (usually higher than for Hep C)
Viral antigens:
Antigen
Antibody
Surface
HBsAg
Anti-HBs
E (fraction of core)
HBeAg
Anti-HBe
Core
HBcAg (never in blood)
Anti-HBc, IgM Anti-HBc
Acute Viral Hepatitis due to HBV with recovery:
IgG anti-HAV
IgM Anti-HAV
HA Ag in faeces
Onset of jaundice
188 4
th
and 5
th
Year Notes
Diagnosis from bloods:
With HBsAg, HBeAg, and HBV DNA by PCR.
Acute HBV: IgM Anti-HBc
Carrier: HBsAg
Past infection: IgG Anti-HBc
Vaccine immunity: IgG Anti-HBs > 10 IU
Monitoring for carrier state: Test for HBsAg:
Monthly for first 6 months or until negative
If still positive at 6 months then probably carrier: test 6 monthly till 2 years
Annually thereafter
Also test ALT
Carrier infectivity:
HBsAg
HBeAg
Anti-HBe
High
+
+
-
Intermediate
+
-
-
Low
+
-
+
Presence of HBe has a high correlation with the presence of whole hepatitis virons in the
blood
Screening:
Anti-HBc
HBsAg
Anti-HBs
No infection
-
-
-
Vaccinated
-
-
+
Carrier
+
+
-
Past infection: non infectious
+
-
+
Past infection: low infectivity,
silent carrier
+
-
-
Normal virus called „wild type‟. Also pre-core mutant HBV virus – doesn‟t produce E antigen but will
still be HBV-DNA +ive
Progression
Incubation 45 – 180 days
Symptoms:
Incubation: can be up to 6 months or longer
Minority of first episodes are symptomatic
If symptoms occur: malaise, anorexia, nausea, jaundice. Coincide with appearance of Anti-HBc
antibody in serum
Acute HBV infection leads to:
10% chronic infection („carrier‟ is a misnomer) due to ineffective immune response. 90% of
infected newborn infants, 25% in young children, and 2 % adults. 25% of „carriers‟ develop
chronic active hepatitis and cirrhosis, and 50% have hepatocellular carcinoma peaking in the 5
th
decade
65% transient subclinical infection 100% recovery
25% acute hepatitis 99% recover, 1% fulminant hepatitis
HBsAg
HBeAg
Anti-HBcIgG
Anti-HBs
Anti-HBe
Anti-HBcIgM
Active Virus
Elevated ALT
Jaundice
0 – 6 months
1 – 6 years
Gastro-Intestinal 189
Stages of illness:
Immune tolerant stage (mainly babies): no hepatitis even though circulating virus. HBsAg, HbeAg
in blood
Immune activation ALT
If chronic: called chronic lobular hepatitis (CLH) or chronic active hepatitis (CAH). 6% will clear
it per year. Key issue is how much fibrosis has occurred before clearance
First stage of clearance: E antigen seroconvesion. HBeAg and anti-HBe (was there previously
– but used up too rapidly to detect. As HBeAg, residual anti-HBe)
Second stage: S antigen seroconversion
Vaccination
Most effective means of control: vaccination: Engerix B. 85 – 90% efficacy
Yeast derived subunit vaccine.
Number of notifications has dropped from 400 to 100 since introduction in 1988
Suspension of synthetic HBsAg
Doses at 0, 1 and 6 months immune levels of Anti-HBs in 92%.
Check for seroconversion 2 months later
Booster every 2 – 3 years if high risk
Treatment
Lamivudine
Purine nucleoside analogue: inhibits DNA polymerase. Potent inhibitor of HBV replications
As safe as placebo, no interactions, excreted unchanged
Each year of treatment:
17% HBe seroconversion (30% if concurrent interferon)
15% get YMDD mutant ALT and HBV DNA again. But these also seem to seroconvert in
time
Eligibility:
If ALT > 2 * normal
Pre & post liver transplant
HIV and HBV co-infection (plus multi drug therapy for HIV as well)
Risk of Hepatocellular carcinoma – related to length of time as a carrier
Hepatitis C
An enveloped ssRNA virus (used to be called non A non B). 6 geneotypes identified.
Damage is caused by immune response – not virus
Presentation
Incubation to onset of symptoms average 7 weeks (range 3 – 20)
HCV RNA detectable within 1 – 3 weeks of exposure. Rises rapidly to 10E6 – 10E8 per ml
Only 1/3 have symptoms. . Clinical illness (if any) lasts 2- 12 weeks
ALT elevation to 300 – 800
50% go on to chronic infection (ie higher than Hep B)
May present with end stage liver disease (e.g. may present for first time with variceal bleeding)
Hepatocellular carcinoma found in 1/3, test with ultrasound. ?Evidence that interferon for 6 months
risk of HCC
Risk Factors
NZ prevalence: 0.47%
Low infectivity: mainly transmitted by blood
Transfusion
IV drugs (40-60% of cases)
Sexual contact (very low risk)
Maternal transmission to neonate in 5% of maternal infection (ie low risk)
Viral Serology
Acute HCV: Anti-HCV doesn’t appear for 3 months. Can do PCR. Exclude HAV, HBV, EBV, and
CMV
Chronic HCV: Anti-HCV antibody
190 4
th
and 5
th
Year Notes
Indications for HCV test:
Chronic hepatitis (raised ALT over 6 months)
History of Non-A, Non-B hepatitis but at least 3 months after acute infection
At risk groups: IV users, haemophiliacs
Donors: blood and organs
Indications for HCV RNA test. Test if indeterminate Anti-HCV results, diagnosis in neonates and
monitoring of interferon therapy.
80% of chronically infected have persisting viraemia
Tests
LFT: bilirubin, Albumin
FBC: platelets
APTT/INR
Anti HCV antibodies
PCR for HCV RNA
Ultrasound for size (& to guide biopsy)
?Biopsy degree of fibrosis prognosis
Exclude: Hep A, Hep B, Iron studies, ANA
Progression
If self-limiting HCV RNA undetectable and ALT back to normal in 1 – 3 months
Wide spectrum: 1/3 persistently normal ALT. Majority fluctuating ALT ( immune system active and
causing hepatocyte death). ALT height doesn‟t correlate with histological severity. Acute – ALT 10
times normal
Non-hepatic manifestations: arthritis, dry membranes, lichen planus (white plaques in mouth),
glomerulonephritis, cryoglobulinaeamia, porphyria cutanea tarda (PCT – blisters on skin)
Prognosis
Contributing to progression:
Alcohol fibrosis
HBV
Age at infection - younger have longer period of time with infection
Mode of acquisition: transfusion worse (?greater viral load)
Genotype of virus: effects interferon treatment. Type 1 severe disease and poor response to
interferon
Management
Alcohol
Have liver biopsy before commencing drug treatment. Also, intravenous drug users should have drug
free urines (otherwise risk of reinfection)
Need strong motivation/compliance
Hep C Infection
10 % cleared –
no further Rx
+ive anti HCV
Chronic Infection
80% mild
inflammation (no
further severe
problem)
20 % cirrhosis
Alcohol
5% liver failure
2% cancer
Gastro-Intestinal 191
Interferon - best for:
High ALT
Disease < 5 years
Non-cirrhotic
Not genotype 1
Low viral load
No history of depression (interferon can cause this)
Causes flu like symptoms: appetite, fever, myalgia. Largely resolves after 1-2 weeks. Given it
up-regulates the immune system can also cause autoimmune diseases (e.g. thyroid)
On it‟s own only 15% are PCR negative 6 months after completing treatment
Combination interferon/Ribavirin
Ribavirin is teratogenic: contraception needs to be VERY reliable
Purine nucleoside analogue
Stored and transported in red cells. Dose dependent haemolysis monitor HB and reticulocytes
Only useful in addition to interferon
After 3 months, 35% non-responders. 65% complete responders. For geneotypes 2 & 3 most of
these go on to be sustained responders
Transplantation:
Hep C most common indication
Recurrent (usually mild) infection of graft
Survival: 65% at 5 years
Other Viral Hepatitis
Hepatitis D
Defective virus that can only replicate in the presence of HBV infection (requires HBsAg as a viral
coat)
Common in Middle East, Pacific Islands
Clinical:
Acute D on Acute B: in IV drug users. Often severe/fulminating
Chronic D on Chronic B: endemic in many parts of the world. Perinatal transmission
Complications: Chronic hepatitis more common in HBV carriers who are also infected with HDV
HBV vaccination also protects against HDV
Hepatitis E
Faecally transmitted: contaminated food and water
Epidemic in India, China, Russia, parts of Africa
Higher mortality than HAV, up to 20% in pregnant women
Test for IgM-specific antibody
Epstein Barr Virus
1% of infections present as acute viral hepatitis, with significant elevation of ALT (mild ALT in most
cases)
See Epstein Barr Virus, page 505
Cytomegalovirus (CMV)
See Infectious diseases chapter
Tumours of the Liver
Metastases are the most common
Hepatocellular carcinoma
Epidemiology:
80% of all liver primary cancer
Third world: 40% of all cancer, age 20 – 40
Western world: age 60+
192 4
th
and 5
th
Year Notes
Pathogenesis:
Hepatitis B: Commonest where carrier state begins in infancy. Viral DNA integrates into the
genome
Cirrhosis: chronic regenerative activity
Fungal toxins: aflatoxin, mycotoxin
Macroscopic appearance: Either large, unifocal mass, multifocal widely distributed nodules, or
infiltrative cancer. Yellow-white masses, occasionally bile stained
Microscopic appearance:
Well differentiated: Trabeculae and acini of malignant cells, large irregular nuclei, bile pigment,
cytoplasmic inclusions
Anaplastic: giant cell, small cell, spindle cell
Fibrolamellar carcinoma (important variant): Single mass with fibrous bands, well-differentiated
cells. No cirrhotic background. In kids/young adults. Better prognosis
Cholangiocarcinoma
Arises in intrahepatic biliary tree
Associated with parasitic infestation (ie 3
rd
world)
Microscopic appearance: well to poorly differentiated adenocarcinoma. Malignant ductules in a dense
stroma
Clinical: ill defined upper abdo pain, malaise, fatigue, enlarged nodular liver, poor prognosis due to late
presentation
Rarer Cancers
Angiosarcoma: malignant tumour of blood vessels. Haemorrhagic appearance in liver. Associated
with vinyl chloride (ie plastics manufacture) and arsenic
Hepatoblastoma: In infants, can be epithelial or mixed, recapitulates foetal liver
Benign Tumours of the Liver
Bile duct adenoma: “von Myenberg complex”, 1 cm pale nodules composed of small ducts in fibrous
tissue. Incidental finding at surgery
Liver cell adenoma:
Associated with oral contraceptives, pregnancy, anabolic steroids. Rupture can lead to massive
haemorrhage (eg in pregnancy).
Appearance: soft-yellow bile stained well-circumscribed nodules. Sheets and cords of polygonal
cells, lack normal architecture. No features of malignancy (although mildly pleomorphic)
Other: Cavernous haemangioma, biliary cysts, focal nodular hyperplasia
Other Liver Diseases
Toxic: drugs, alcohol
Fatty Liver: obesity, diabetes, drugs, alcohol
Drugs: e.g. flucloxacillin (and other antibiotics) can cause intrahepatic cholestasis
Haemochromatosis
Bronzed diabetes: triad of micronodular cirrhosis, diabetes mellitus, and skin pigmentation (iron
stimulates melanin)
Affects liver, pancreas, heart, gonads. Also causes osteoarthritis and diabetes
Primary/idiopathic/genetic:
Common autosomal recessive, usually males 40 – 60 years. Most common genetic disorder.
Homozygotes: 65 – 100% will have iron overload. Heterozygotes have elevated ferritin but no
disease
Die from hepatocellular carcinoma, cardiac disease, liver failure
Iron accumulates in the cytoplasm of liver cells (lots of black dots), also in pancreas, endocrine
glands, skin, myocardium, joint linings
Macroscopic appearance: micronodular, brown, cirrhotic liver. Atrophy and fibrosis of pancreas.
Enlarged heart. Brown/grey skin
Microscopic appearance: Initially golden brown periportal ferritin deposits in hepatocytes. Later
Kupffer cells become loaded. Non-inflammatory cirrhosis. Pearl stain: stains iron blue
Monitoring:
If transferrin > 45% or serum ferritin > 300 ng/ml then liver biopsy if > 39 years
Hepatic Iron Index = hepatic iron concentration/age. Normal < 1.9 mmol/gm/yr
Gastro-Intestinal 193
If cirrhosis for > 10 years then screen for hepatocellular carcinoma every 6 or 12 months. If
picked up clinically then too late
Screen for -feta Protein (tumour marker), or inject lipiodol into hepatic artery
preferentially taken up by HCC hypodense on CT
Treatment of HCC: resection or liver transplantation. Chemo ineffective
Treatment of haemochromatosis: if regular venesection before organ damage then normal life
expectancy. Regular initial venesection to iron load, then venesection very 3 – 6 months
Secondary:
Ineffective erythropoiesis (eg thalassaemia, liver disease, high iron intake)
Iron first in Kupffer cells, later in hepatocytes
Cirrhosis unusual
Diseases of Intrahepatic Bile Ducts
Ascending Cholangitis
Suppurative inflammation within the bile ducts with bile stasis
Caused by obstruction, treated with drainage
Common organisms are enteric: E Coli, Klebsiella, Enterobacilli
Primary Sclerosing Cholangitis
Autoimmune destruction of intra and extra hepatic bile ducts
In young males, associated with ulcerative colitis and HLA types
Cirrhosis and liver failure within 5 years
Microscopic appearance: onion skin fibrosis around intrahepatic ducts
Primary Biliary Cirrhosis:
Autoimmune destruction of intrahepatic ducts
F:M = 9:1, average age = 50
Antimitochondrial antibodies typical
Focal inflammatory destruction of bile ducts, no primary inflammation in stroma ducts reduced
in number green bile plugs in canaliculi bile infarct and portal-portal fibrosis cholestasis
and cirrhosis
Secondary biliary cirrhosis: scarring following obstruction and ascending cholangitis
Disappearing bile ducts: Autoimmune, Graft vs. Host, Post transplant – all due to lymphocytic
destruction of biliary epithelium
Vascular Disease of the Liver
Post hepatic disease:
Right sided heart failure:
Enlarged, tense, tender liver
Marked centrilobular congestion and haemorrhagic necrosis: „nutmeg liver‟ – lacy pattern with
dark and light areas
Cardiac Sclerosis:
Less common complication of heart failure
A peri-venular fibrosing reaction following long-standing congestion
Rarely causes portal pressure
Hepatic Vein Thrombosis (Budd Chiari Syndrome)
Hepatic congestion from obstruction to blood flow due to occlusion of hepatic veins or IVC
Associated with anything causing hypercoagulability: polycythaemia vera, pregnancy, oral
contraceptives, hepatocellular carcinoma
Appearance: swollen, red liver, congestion, veins containing thrombi
Intrahepatic Disease: Hepatic veno-occlusive disease. Subendothelial sclerosis of veins. Lumen of
central vein occluded + collagen deposition in Space of Disse
Pre-hepatic disease: Portal vein obstruction due to cancer, peritoneal sepsis, pancreatitis, surgery,
cirrhosis
Gilbert’s Syndrome
Normal variant in ?7% of the population
Raised indirect bilirubin due to „defective‟ uptake and conjugation of bilirubin by liver
Exacerbated by low fat/low calorie diet (e.g. when gastroenteritis). Use this to test: fast and see if it
increases. Also worse when ill due to other causes (may present as a red hearing)
Bilirubin rarely > 100 micromol/L
194 4
th
and 5
th
Year Notes
Is totally benign
Neonatal Liver Disease
Extrahepatic Biliary Atresia: destructive inflammation of bile ducts cirrhosis
Neonatal Hepatitis: non-specific idiopathic response to neonatal hepatic insult (eg virus). Giant cell
transformation of hepatocytes, chronic inflammation around portal tracts, focal necrosis and lobular
disarray
Wilson’s Disease
Rare autosomal recessive: accumulation of dietary copper in liver, brain, eye
Leads to non-inflammatory cirrhosis
Can look like alcoholic liver disease due to mallory hyaline and bile plugging
Alpha-1 Antitrypsin Deficiency
Autosomal co-dominant.
Ineffective protease inhibitor enzymes
Genetics:
Only liver disease if < 10% normal function (ie ZZ allele).
Z is bad, M is normal, S is mildly impaired. Only 10% of ZZ get chronic liver disease.
7 – 10% of the population have a variant associated with mild/moderate deficiency
Abnormal alpha-1AT accumulates in cells as cytoplasmic globules cell death fibrosis
Clinical: neonatal hepatitis, can present as macronodular in adult. Suspect in premature emphysema
End Stage Liver Disease
Hepatic Failure
Conjugated jaundice
Fatigue, muscle wasting, brusiability
Platelet count (reliable early indicator of cirrhosis)
Synthesis: notably of albumin
Fluid retention, ascites, spontaneous bacterial peritonitis
Coagulopathy: synthesis of 2, 5, 7, 9, 10
Hyperammonaemia metabolic encephalopathy
Gynaecomastia (steroid hormones not metabolised)
Hepatocellular carcinoma
Hepato-renal Syndrome:
Renal failure in patients with liver failure urea and creatinine
Blood is hyperosmolar but urine sodium is low
Pathogenesis unknown: possibly vasoconstriction
Hepatic Encephalopathy:
Metabolic derangement of the brain: only mild morphologic changes (eg oedema)
Flapping tremour
Grade 1 – altered mood, confusion, 2 – drowsy, disorientation, ataxia, 3 – marked confusion,
sleepy, obey simply commands, 4 - coma
Which lead to liver failure or transplantation
Portal Hypertension
Diagnosed clinically: if cirrhosis, ascites and varices assume portal hypertension. Can confirm with
Doppler ultrasound
Causes:
Post-hepatic: vascular outflow obstruction (Budd Chari Syndrome)
Intrahepatic: cirrhosis
Prehepatic: portal vein occlusions
Consequences:
Ascites: albumin synthesis, portal pressure, hepatic lymph formation and renal retention of
sodium and water
Portosystemic shunts: oesophageal varices, haemorrhoids and abdominal wall
Splenomegaly and portal congestive gastropathy
Gastro-Intestinal 195
Treatment of varices:
Complicated by hypo-coagulopathy secondary to liver failure (do INR and APPT)
Band oesophageal varices lower down: collapses them further up. Varices are asymptomatic until
eroded by acid or increased pressure from vomiting
Emergency therapy for bleeding varices:
Octreotide infusion (somatostatin analogue but longer T½) reduce portal pressure
Balloon tamponade
Resuscitation
Then emergency endoscopy with sclerotherapy (takes several iterations) or banding, or
TIPS/surgery (portal/caval shunt)
Maintenance treatment:
Sucralfate (an Al carbohydrate): 1 gm 1 hr ac QID - surface protective effect to stop ulcers
over sclerosed varices
Beta blocker: propranolol, nadolol CO due to HR
Nutrition
Malnutrition is common in chronic liver disease due to absorption and synthesis
Give fat and CHO to combat hyperglycaemia resulting from insulin resistance
If encephalopathy, then low protein diet, antibiotics to decrease bacterial ammonia production and
lactulose (transit time & metabolised by bacteria H+ which converts NH3 to less absorbable
NH4)
Gallbladder and Bile Ducts
Cholecystitis = inflamed gallbladder (eg due to stone impacted in gallbladder or cystic duct). Acute or
chronic
Cholangitis = bile duct infection: RUQ pain, jaundice & rigors
Choledocholithiasis = gallstones in common bile duct
Cholecystoliathiasis = gallstones in gallbladder (??)
Cholecystectomy = gall bladder out
Cholelithiasis
= Gall stones.
Cholesterol stones:
85% of stones
Incidence: Northern European ancestry, age, female, obesity
Caused by supersaturation of the bile with cholesterol precipitation around bits of junk (eg
epithelium)
Appearance: either pure pale yellow and radiolucent, or mixed grey „gravel‟ – more dangerous as
can squeeze through cystic duct
Pigment stones:
15% of stones
Incidence: Asian, haemolysis, alcoholic cirrhosis, biliary infection, age
Excess unconjugated bilirubin
Appearance: small, jet black and ovoid
Cholecystitis
Biliary Colic
Symptoms:
Gives a colicky pain – waves of intense pain every 10 – 20 minutes with little pain in between.
Patient is restless – can‟t get comfortable in any position (as opposed to cholecystitis below)
May be mild tenderness on examination
Pathogenesis:
Impaction of stone in the cystic duct
No inflammation of the gall bladder (yet)
Investigations:
Plain xray (mainly to exclude other causes of an acute abdomen – eg obstruction, perforation, etc)
Diagnosis by US – looking for a thickened wall on the gall bladder and filling defects in the ducts
196 4
th
and 5
th
Year Notes
CT the best modality for looking for stones
Management:
IV fluids (may not have been drinking, may need to be nil-by-mouth if they go to surgery)
Bloods: FBC, U&Es, LFTs, Amylase, Clotting factors, Group & Hold, ESR/CRP
Urine: UTI/pregnancy
Pain relief + antiemetics
Antibiotics
Antispasmodics (eg Buscopan) for colic
Acute Cholecystitis
Most dangerous common complication of cholelithiasis
Clinical presentation: acute abdomen. Symptoms may be obscured by the predisposing condition
90% caused by impaction of stone in the neck: calculus acute cholecystitis. If no stones then
acalculous cholecystitis (usually vasculitis)
Inflammation due to pressure, chemical irritation, and secondary infection
Macroscopic appearance: enlarged (bigger than chronic), tense, covered by fibrin, contains turbid bile
or puss. Wall is thick and oedematous and the mucosa is red or green-black (gangrenous cholecystitis,
due to blood flow secondary to pressure)
Microscopic appearance: Acute inflammation, congestion, abscess, necrosis
Symptoms:
70% stones are asymptomatic. If symptomatic there is a 30% 5 year risk of complications
requiring surgery
Uncomplicated: severe constant epigastric/RUQ pain, lasting several hours, radiating to back,
maybe nausea/vomiting. It hurts to move or breath so patient lies still. Local peritonitis (very
tender). If impacted then inflammatory component (fever, WBCs)
Complicated:
Fever, abdominal pain, nausea, vomiting: indicating acute cholecystitis
Fever, pain, jaundice: acute cholangitis
Abdominal and back pain, collapse, vomiting, hypotension: acute pancreatitis
Investigations
Murphy‟s sign: Lay 2 fingers on RUQ. Patient inspiration pain. No pain on LUQ
Gallstones often incidental finding on ultrasound or x-ray (if calcified – only 10% radio-opaque)
Ultrasound picks up 98% of gallbladder stones but only 50% of common bile duct stones. More
can be inferred from a dilated duct (> 6 mm)
Serum Amylase: if > 1000 IU/L acute pancreatitis
ALP & bilirubin
WBC count cholecystitis
Antimitochondrial antibody tests exclude primary bilary cirrhosis
Differential
Obstructive Jaundice: pancreatic neoplasm, cholestatic hepatitis
Bilary colic: pancreatitis, oesophagitis, peptic ulcer, IBS
Ascending Cholangitis
Treatment
If acute, nil by mouth, pain relief, IV antibiotics (e.g. cefuroxime)
Usually settle with conservative treatment (wait 2 days and see). Then schedule for elective
cholesectomy 6 week later (once inflammation settled down)
Surgical Options:
Lithotripsy
Laproscopic cholecystectomy
Percutaneous, transhepatic gallbladder canuulation (PTC)
Long term:
No relationship with high-cholesterol diet. Avoid obesity
Drugs: bile acid treatment – dissolve small cholesterol stones
Chronic Cholecystitis
?Aetiology: no infective or inflammatory agents
Macroscopic appearance: normal to enlarged gallbladder with stones and a fibrous thickened wall
Gastro-Intestinal 197
Microscopic appearance: chronic inflammation, fibrosis and muscular hypertrophy. Rokitansky-
Aschoff sinuses: herniations through submucosa. Lipid laden macrophages extend into the lamina
propria
Symptoms: heartburn, belching, intolerance of fatty foods, discomfort. Can be found in people without
gallstones symptoms not specific
Ascending Cholangitis
Signs of Acute Cholecystitis plus sweats and rigours
Infection of the biliary tract
Often accompanies obstruction due to gall stones
Also following ERCP (probe introduces gut bacteria into the ducts which are normally sterile)
Can be rapidly fatal – have low threshold for treatment
Rare differential Mirrizi Syndrome: no stone in the common duct but its compressed by adjacent
inflamed gallbladder
Mucocoele of the Gallbladder
Cystic duct becomes obstructed. Trapped bile is absorbed and gallbladder fills with mucus
Tumours
Benign tumours:
Adenomas and papillomas: project into the lumen. Benign overgrowths of epithelium
Adenomyoma: nodule at the gallbladder tip composed of smooth muscle around benign ductules
Malignant:
Carcinoma of the gallbladder:
Uncommon: 0.5% of cholelithiasis patients
Associated with gallstones and inflammation
Presentation: insidious until late. Abdo pain, jaundice, anorexia, weight loss, nausea. 1% 5-
year survival
Macroscopic appearance: at fundus and neck. Either infiltrating of fungating type. At
discovery usually involve liver, bile ducts and portal nodes
Microscopic appearance: 95% adenocarcinoma (can be poorly differentiated), 5% squamous
cell carcinoma (from squamous metaplasia)
Carcinoma of the bile ducts and ampulla:
Uncommon, associated with chronic inflammation, parasites, ulcerative colitis
Presentation: obstructive jaundice, pale stools, nausea, LFTs. Differentiate from obstruction
due to stones. Poor prognosis
Macroscopic appearance: papillary fungating mass + intraductal nodules + diffuse infiltration
obstruction. Periampullary tumours have better prognosis
Microscopic appearance: adenocarcinoma, occasionally squamous cell
Pancreas
Acute Pancreatitis
= Inflammation in pancreas and peripancreatic tissues (sometimes with haemorrhage and necrosis)
Causes
90% caused by either (grog or gravel):
Gallstones blocking the ampulla (60%)
Alcoholic (more chronic than acute) (30%). Pathogenesis unclear - ?duct obstruction
Also: trauma, ERCP, drugs
Types:
Interstitial or oedematous pancreatitis: mild, self-limiting
Acute haemorrhagic (necrotising) pancreatitis: severe
Pathogenesis
Activation of pancreatic enzymes cellular injury, release of enzymes and cytokines ischaemia.
Secondary bacterial infection possible. May also follow ERCP – catalysts from duodenum activate
pancreatic enzymes while still in the pancreatic duct
Macroscopic appearance:
198 4
th
and 5
th
Year Notes
Variegated: blue-black haemorrhage, yellow-white fat necrosis
Peritoneal „Chicken-Broth Ascites‟: layer of clear fat floating on turbid liquid – lipase has digested
abdominal fat
With resolution: fibrosis, calcification, pseudocysts
Microscopic appearance: If mild, periductal inflammation. Proteolytic destruction of the pancreatic
substance. Necrosis of blood vessels haemorrhage
Presentation
Upper abdominal constant (ie inflammatory) pain + lumbar back pain
Nausea, vomiting
Peritoneal irritation, ileus
Jaundice, especially in gallstone induced
Tachycardia
Signs (due to haemorrhagic fluid in the extra peritoneal space):
Cullen‟s Sign: Discolouration around the umbilicus
Greg-Turner‟s Sign: Discolouration around the flanks
If severe:
Shock: enzymes into blood, acute peritonitis, massive inflammation
Respiratory failure, circulatory failure
Complications: shock, ARDS, acute renal failure, abscess, duodenal obstruction
Investigations
Serum or urine amylase. Height of amylase does not correlate with severity. Other conditions may
cause raised amylase. Lipase
Also possibly glucose, WBCs, creatinine, calcium, faecal elastase
CXR to exclude gastrointestinal perforation (air under diaphragm)
Ultrasound/ERCP, ALT and bilirubin to check for stones
CT to determine extent of inflammation/necrosis. Use contrast – necrotic tissue doesn‟t light up as it‟s
not perfused
Also FNA
Differential
Abdominal catastrophe: perforation, ectopic pregnancy, infarction, ruptured aneurysm, obstruction,
appendicitis
MI
Acute cholecystitis
Progression
Most fully recover in 4 – 6 days with IV fluids, O2, analgesia
If severe, up to 50% mortality. Treat for renal, cardiac and respiratory failure. Surgery for infected
necrosis
Treat cause: e.g. ECRP + sphincterotomy, later cholecystectomy, alcohol abstinence, etc
Supportive treatment: IV fluids, pain relief, inotropic support if BP or renal hypoperfusion despite
fluids
Chronic Pancreatitis
= Replacement of pancreatic tissue by fibrosis, often with calcification, sometimes with duct dilation
and stones
May result in chronic pain, relapsing acute pancreatitis, exocrine or endocrine deficiency
Causes:
Alcohol (60 – 80%) duct obstruction by protein rich secretions
Obstruction (10%)
Idiopathic (10%)
Genetic factors
Hypercalcaemia and Hyperlipidaemia
Congenital anomalies of duct
Following acute pancreatitis of any cause
Gastro-Intestinal 199
Symptoms
Abdominal pain, weight loss, diarrhoea/steatorrhoea, diabetes mellitus (late complication – islet cells
are the last to fail), acute pancreatitis
Investigations
As for acute, plus check chronic differentials (e.g. ulcer, GORD)
Blood glucose, GTT
Pathology
Chronic calcifying pancreatitis:
In alcoholics
Macroscopic appearance: throughout lobules of pancreas, hardened foci of calcification
Microscopic appearance: atrophy of acini, fibrosis, chronic inflammation. Dilated ducts and
atrophic epithelium
Obstructive pancreatitis
Due to cholelithiasis
Affects periductal regions, mainly head of the pancreas
Ductal epithelium better preserved
Treatment:
Exocrine/endocrine replacement
Analgesia
Surgery: duct dilation, resection of diseased portion
Pancreatic Tumours
Symptoms
Weight loss, anorexia, lethargy
Pain
Jaundice (70%)
Pruritis (itching)
Diabetes mellitus
Investigations
FBC: anaemia, sepsis
LFT: to confirm obstructive jaundice
Ultrasound
ERCP or CT
Differential
Obstructive jaundice
Hepatic jaundice
Cachexia: gastric, colorectal or ovarian cancer
Other pancreatic disease
Types
Pseudocysts (don‟t have epithelial lining so not a true cyst – not neoplastic):
Congenital (rare) or acquired
Solitary cyst 5 – 10 cm diameter, contains serous, turbid fluid
Associated with pancreatitis
Benign tumours: rare. Serous cystadenoma (elderly women), solid cystic tumour (young women)
Carcinoma of the pancreas
Epidemiology:
5% of cancer deaths
Usually fatal, 90% die within one year, 5 year survival 1 – 2%
Associated with smoking, fatty diet, chemical carcinogens
M > F, B > W, 60+
Presentation:
Often perineural invasion (travels along nerves) difficult pain
200 4
th
and 5
th
Year Notes
Affecting head: obstructive jaundice
Affecting tail: weight loss, liver metastases
Macroscopic appearance: 60% head (most pancreatic tissue is there). Grey-white tumour with
infiltrative margins. Extends to duodenum, liver, nodes, etc
Microscopic appearance: 90% adenocarcinoma, 10% adenosquamous. Other rare types
Treatment: palliative. Stenting or ERCP for duct compression
If resection possible:
For body/tail: distal pancreatectomy – usually need to remove spleen as well
For head: pancreaticoduodenectomy (Whipple operation)
Other tumours: benign or malignant endocrine tumours (insulinoma, gastrinoma)

Renal 201
Renal and Genitourinary
References: Renal Medicine handout, General Medicine Run, and Prof Delahunt‟s pathology handout
See also Renal Disease in Children, page 632
History ............................................................ 202
Renal Physiology ........................................... 202
Assessment of Renal Function ....................... 202
Presentation of Kidney Disease ...................... 204
Nephritic Syndrome .................................. 204
Nephrotic Syndrome ................................. 204
Acute Renal Failure .................................. 205
Chronic Renal Failure ............................... 207
Complications of Chronic Renal Failure .. 209
Specific Nephrotoxins .............................. 210
Kidney Disease ............................................... 210
Renal Stones (Nephrolithiasis) * .............. 210
Tubulointerstitial Diseases........................ 211
Glomerulonephritis ................................... 212
Hypertension ............................................. 215
Congenital Abnormalities ......................... 216
Hydronephrosis ......................................... 216
Cystic Renal Disease ................................ 216
Renal Tumours ......................................... 216
Renal Replacement Therapy .......................... 217
Ureter ............................................................. 219
Urinary Tract Infections ................................. 219
UTIs in Children ....................................... 221
Bladder ........................................................... 223
Interstitial Cystitis..................................... 223
Bladder Tumours ...................................... 223
Urinary Incontinence ................................ 223
Male Genitourinary ........................................ 224
Prostate ..................................................... 224
Penis ......................................................... 226
Scrotum..................................................... 226
Testes ........................................................ 226
202 4
th
and 5
th
Year Notes
History
Exposure to nephrotoxic medication (i.e. pre-renal or intrinsic renal failure)
Risks of renal-artery atherosclerotic disease
Volume depletion pre-renal
Rash = allergic interstitial nephritis
Bone pain in elderly multiple myeloma acute renal failure
Renal Physiology
Function of kidneys:
Maintenance of fluid and electrolyte balance
Excretion of metabolic wastes
Excretion of acid
Endocrine (calcitriol, erythropoietin)
Allows regulation of a daily intake of:
Water: 1 – 20 litres
Sodium: 5 – 500 mmol
Potassium: 20 – 200 mmol
Protein: 30 – 150 g
Fluid dynamics:
Kidney‟s receive 20 – 25% of cardiac output
GFR maintained by autoregulation but dependent on glomerular pressure and renal blood flow
Normal urination: 1 ml/kg/hr (down to 0.5 ml/kg/hr OK)
Urine output of 1 – 2 litres/day
Hormones:
Intra-renal:
Renin-angiotensin system: Na, hypotension renin angiotensin II
vasoconstriction, aldosterone and thirst
Prostaglandins: vasodilating, control glomerular blood flow, natriuretic and diuretic
Extra-renal:
Aldosterone: stimulated by Angiotensin II and K Na reabsorption
ADH: controlled by both volume and osmotic stimuli water resorption providing
sufficient medullary concentration gradient
Atrial and brain natriuretic proteins (ANP/BNP): volume overload natriuretic and diuretic
For hypo/hypernatraemia, potassium and acid-base balance, see Electrolytes, page 107
Assessment of Renal Function
Urinalysis
Dipstick:
Blood: indicates bleeding in the urinary tract or free haemoglobin or myoglobin
Proteinuria: sensitive to protein – but use 24 hour urine to quantify, or spot check with protein:Cr
ratio in morning urine. Urine protein is normally albumin. Hyaline and granular casts and Bense
Jones Proteins don’t test +ive for protein
Glucose: diabetes, pregnancy, sepsis, tubular damage or low renal threshold
Nitrates UTI
Microscopy:
Blood: should be less than 8 * 10E6 cells per litre
Normal morphology suggests bleeding from the lower urinary tract: calculi, infection,
neoplasia
Dysmorphic cells suggests glomerular bleeding: glomerulonephritis and vasculitis (including
endocarditis). Microhaematuria can be either nephrotic or nephritic. Macro haematuria is
normally nephritic
WBCs indicate infection, less commonly renal tuberculosis, renal stones and papillary necrosis
Eosinophils interstitial nephritis
Casts:

Renal 203
Hyaline casts: just protein, no cellular elements and may be normal (especially concentrated
urine)
Granular casts: Degenerative cellular material – usually tubular cells pathology
Red cell casts: glomerular bleeding usually active GN
White cell casts: pyelonephritis, interstitial nephritis or glomerulonephritis
Glomerular Filtration Rate (GFR)
Marker of renal excretory function
Determined by intra-glomerular pressure, which in turn is determined by the difference in vascular tone
between afferent and efferent arterioles. Maintained by autoregulation except when blood pressure is
very high or very low
Creatinine:
Filtered at the glomerulus and not reabsorbed, but a small amount is excreted from the tubules (ie
GRF less reliable at small urine flows)
Affected by muscle mass, protein intake and age poor indicator of renal function. Serial
measurements helpful
Normal Creatinine < 0.110 mmol/L
Use Cockcroft-Gault formula:
)/(creatinine serum*50
)(85.0*)(tbody weighlean *)age140(
sec)/GFR(mL
Lmicromil
femalekg
Normal is > 1.5 ml/sec (> 90 ml/min)
Use total body weight but recognise it overestimates if obese
Or collect 24 hour urine and compare to plasma concentration with UV/P
Can measure with radionucliotides
Other
Do volume assessment: lying and standing BP, JVP, change in weight, etc
Tubular Function: test concentrating ability with fluid deprivation and ADH administration
Urinary Acidification: give ammonium chloride and then measure urinary pH
Also consider blood tests: Ca, PO4, FBC, complement, autoantibodies, etc
Renal Imaging
Plain X-ray: shows radio-opaque renal stones (90% are) not uric acid stones (eg Gout). Methodology:
Gas:
Renal colic/pancreatitis focal ileus
Emphysematous pyelonephritis gas in kidney
Emphysematous cystitis gas in bladder
Stripes:
Find the psoas muscle and move out parallel to this to find the kidneys
Assess size: length of kidney = length of 3 vertebrae + disc spaces. Up to 2 cm variation in
size between kidney‟s OK
Stones: check down ureters: down psoas, anterior to sacro-iliac junction, around pelvis, into
bladder
Bones: renal osteodystrophy, etc
Intravenous Urogram (Plain film + contrast) = IVU = IVP (Intravenous pyleogram)
Gives anatomical and functional information
Shows renal contours, presence of scarring, reflux nephropathy, obstruction
Depends on renal uptake of the contrast. Little use if significant renal impairment (eg CR > 200)
Interpretation:
Nephrogram phase (1 minute post injection): renal contour, position, equal in intensity?
Pyelogram phase (5 minutes): see major and minor calicies and bladder
Post micturition phase: look for normal voiding
Antegrade and retrograde pyelography: direct injection of contrast into the renal pelvis or the ureter
Micturating Cystourethrogram: Fill bladder with contrast and image following micturition. For
assessment of vesico-ureteric reflux in children
Ultrasound:
For renal size and contour
204 4
th
and 5
th
Year Notes
Shows hydronephrosis – but may not show the site of obstruction. Reasonable view of renal
masses and cysts
Scarring: asymmetric indentation of renal outline. If young ?reflux. If older ?ischaemia
CT: for complex cysts, masses, renal colic and stones.
Modality of choice for stones. 5 mm slices:
Sensitivity
No contrast risk (mortality 1 in 40,000)
Can sort out differentials of colic (eg appendicitis) on CT that you won‟t see on IVP
Stone filling the whole of the renal calicies = staghorn calyx (in recurrent infection and alkaline
urine)
Nuclear medicine studies:
Renogram for assessing function of each kidney, avoids nephrotoxic contrasts. Eg Technetium
labelled DTPA and Mag3. Especially good for renal artery stenosis and obstruction
DMSA: highlights proximal tubules. Good for showing renal scarring, eg reflux nephropathy
Arteriography: Renal artery stenosis
Renal Biopsy
Under local
Indications: acute renal failure, nephrotic syndrome, heavy proteinuria or haematuria
Only if histology will influence management
Major contraindication: bleeding tendency (check FBC and clotting first)
Complications: bleeding and development of a perirenal haematoma (eg in amyloid disease when rigid
arterioles won‟t contract following bleeding)
Risk of serious complications < 1% (fistula, haematoma, infection, surgery, etc)
Presentation of Kidney Disease
This section outlines how kidney diseases present. A variety of kidney diseases present
symptomatically in a variety of different ways. The major underlying diseases are described in the
following section of Kidney Diseases, page 210
Other presentations of kidney disease:
Hypertension: common symptom of chronic renal failure of any cause
See Renal Osteodystrophy in Increased Bone Resorption, page 263
See Urinary Tract Infections, page 219
Nephritic Syndrome
~ Proliferative glomerulonephritis
Presentation:
Urinary sediment: haematuria, granular and cellular casts
Varying degrees of proteinuria
Oliguria fluid retention and oedema
Renal impairment Cr, electrolyte disturbance
Hypertension
Headache
Histology: Large glomeruli (diffuse changes of predominantly mesangial cells), polymorphs and black
deposits on epithelial side of BM, can occasionally lead to crescents (ie lots of cell proliferation
compared with Nephrotic Syndrome rapidly progressive glomerulonephritis)
Possible causes:
Post-infectious GN
Rapidly progressive GN
Mesangio-capillary GN
Maybe IgA GN
Nephrotic Syndrome
~ Non-proliferative glomerulonephritis
Presentation:
Marked proteinuria (may make urine frothy) > 3 g/day
Hypoalbuminaemia oedema: generalised, insidious onset, may be peri-orbital in the morning,
legs in the afternoon. If gross then ascites and pleural effusion
Renal 205
Hypercholesterolaemia
Renal function is preserved. But may retain Na and H20. May plasma volume
If polyuria then tubular and interstitial damage as well
Pathogenesis: common end point of a variety of disease processes that alter the permeability of the
basement membrane
Possible causes (first 3 reasonably common in adults, Membranous is perhaps the most common):
Minimal change GN
Membranous GN
Focal Segmental GN
Maybe IgA and mesangiocapillary
(Also diabetes, amyloidosis (eg multiple myeloma), drugs)
Management:
Minimal change: very responsive to steroids. The rest need something stronger (eg
cyclophosamide) and commonly renal failure over time
Fluid restrict
Monitor and treat BP
Salt restricted, high protein diet
Oral diuretics + K (beware hypovolaemia pre-renal failure)
Complications: loose Antithrombin 3 protein as well as albumin renal vein (and other) thrombosis.
?Prophylactic anticoagulation
Acute Renal Failure
=Abrupt reduction in glomerular filtration rate plasma urea & creatinine and (usually) urine
volume (oliguria < 400 ml/day, auria < 100 ml/day). If urea but only Cr then ?dehydration or
catabolic state
Assess severity using Cockcroft-Gault equation (see page 203). Normal clearance >= ~ 100 ml/min
Due to acute damage to any part of the kidney or renal tract. Usually Acute Tubular Necrosis but
always consider differentials
Pre-renal Acute Renal Failure
= in glomerular perfusion in absence of structural kidney damage
Kidney usually autoregulates – but can‟t cope with extremes
Can‟t interpret results if patient has had recent diuretics
If prolonged ischaemic damage loss of medullary gradient and reabsorbing capacity dilute
urine
Causes:
Volume depletion: Usually GI loss, but also renal loss, burns, haemorrhage
Cardiac failure renal perfusion
Systemic vasodilation: sepsis or antihypertensives
Also:
Reno-vascular disease: renal artery stenosis
Vasoconstriction in kidneys, e.g. due to NSAIDs ( vasodilating PGs), ACE inhibitors (
efferent arteriolar tone intraglomerular pressure)
Intense reabsorption of salt and water leads to:
Low volume of urine, high osmolality (> plasma), but low urine Na (usually < 20 mmol/l)
Urine to plasma ratio of creatinine and urea
Urea is re-absorbed preferentially to creatinine at low urine flows plasma urea to creatinine is
increased
Hyaline casts: aggregations of urine protein if low urine flow
Kidneys try to compensate by:
Vasodilating afferent arterioles (via PGs)
Activation of renin-angiotensin BP and vasoconstricts efferent arterioles
Management:
Rapid fluid resuscitation
Correct underlying disorder (eg inotropes)
Monitor intravascular volume and watch for ATN
206 4
th
and 5
th
Year Notes
Intrinsic Acute Renal Failure
Possible presentations:
Oliguria (rather than auria)
Nephritic syndrome: haematuria, hypertension, oliguria +/- oedema
Proteinuria: excludes pre and post-renal
Hypertension: intrinsic renal disease BP, pre-renal BP
Systemic features of disorders causing intrinsic failure (eg fever, arthralgia, skin rash, vasculitis
etc)
Due to:
Acute Tubular Necrosis (most common cause): See page 211
Acute Interstitial Nephritis: See page 211
RPGN: Urine chemistry midway between pre-renal acute renal failure and acute tubular necrosis -
urine to plasma ratios for osmolality and creatinine, and Na between 20 – 40 mmol/L. See page
212
Nephrotoxins
Other tubular diseases (eg myeloma)
Investigations:
Urinalysis: cells, casts, protein
US: echogenicity
Renal biopsy
Also blood tests to exclude specific causes: ANA, ANCA, Complement, CK, etc
Post-renal Acute Renal Failure
Presentation:
Complete auria: most pre-renal and intra-renal failure is oliguric. But partial obstruction may give
moderate tubular dysfunction osmotic diuresis polyuria
Normal urinalysis: no proteinuria or casts, any blood (eg from stones, cancer) will be normal not
dysmorphic
Specific diseases pre-dispose: eg diabetes and analgesic use papillary necrosis bits fall off
and cause obstruction. See Acute Papillary Necrosis, page 211
Due to obstruction:
Usually in urethra: bladder stones or tumours. Prostate usually chronic
If at ureteric level must be bilateral to lead to severe kidney failure or obstruction on one side and a
poor functioning kidney on the other
Extrinsic obstruction due to eg retroperitoneal fibrosis following radiotherapy, etc
tubular pressure glomerula filtration
Usually obvious from history, confirm with:
Ultrasound of kidneys for hydronephrosis
CT to determine the level of the blockage
IVU only if the kidney is functioning (ie Cr < 200)
Investigations in Acute Renal Failure
Pre-renal
ATN
RPGN
AIN
Urine Osmolality
>500
<350
300-400
300-400
Urine Na
<20
>40
20-40
20-40
Urine/Plasma urea
>10
<10
Intermediate
Intermediate
Urine/Plasma creatinine
>40
<20
Intermediate
Intermediate
Fractional excretion of Na
<1
>3
<1
>1
Urine Sediment
RBC
Occasional
+
+++
Occasional
WBC
Occasional
Occasional
++
+++
Granular casts
Occasional
++
++
+
Epithelial casts
+++
++
RBC casts
+++
WBC casts
Occasional
Fractional excretion of Na =
Cr Urine* Na Plasma
100 *Cr Plasma * Na Urine
Renal 207
Renal biopsy is rarely needed to differentiate causes of renal failure, mainly in RPGN
Management
Treat cause
Resuscitate if hypovolaemia
Monitor for K
Treat pulmonary oedema, ?dialysis
Monitor fluid balance carefully
Avoid nephrotoxic drugs
Chronic Renal Failure
= Reduction in renal function for > 6 months
Causes in NZ in 1997:
Diabetes Mellitus
44% (and growing)
Glomerulonephritis
20%
Hypertension
13%
Polycystic Kidney Disease
6%
Reflux Nephropathy
3%
Analgesic Nephropathy
< 1%
Miscellaneous
7%
Uncertain diagnosis
7%
Miscellaneous causes include: stone disease, interstitial nephritis, amyloidosis, myeloma,
lithium toxicity, obstructive uropathy, renal cell carcinoma, post-partum failure
Symptoms:
Earlier: nausea, anorexia, lethargy, itch, nocturia, impotence
Later: oedema, SOB, chest pain (from pericarditis), vomiting, confusion, fits
See also:
Adult Polycystic Kidney, page 216
Wegner‟s granulomatosis, Microscopic Polyarteritis, and Henoch-Schonlein Purpura, Vasculitis,
page 282
Multiple Myeloma, page 302
Diabetic Nephropathy
See also Diabetes Mellitus, page 94
Epidemiology: Nephropathy in
30 – 50% of type 1 diabetic patients (after ~ 10 – 15 years of disease)
20 – 30% of type 2 diabetic patients – many with overt disease at the time of presentation
In both cases is associated with poor glycaemic control, hypertension and proteinuria
Definitions:
Overt diabetic nephropathy = proteinuria > 500 mg/day in the absence of other renal disease
Microalbuminuria:
Albumin excretion 30 – 300 mg/day (= 20 – 200 g/minute). Concentration is not relevant –
it is the amount excreted per unit time. Albumin is more specific for nephropathy than total
urine protein (normal protein < 150 mg/day – mainly from tubular cells). Normal dipsticks
not sensitive enough at this level. Random early morning urine is dependent on concentration.
Urinary albumin:creatinine ratio is a useful screening test
Marker for endothelial damage elsewhere. Strong association with retinopathy, IHD, etc
Prognosis for a diabetic with microalbuminaemia is worse than for HIV!
Natural History:
Type 1 Diabetes:
Not usually evident until after 10 – 15 years of disease. If none by 25 years then nephropathy
unlikely
Once overt nephropathy starts, progresses to ESRF over 5 – 7 years
Initial hyperfiltration in about 50% of diabetics (GFR by about 25 – 50%). Overtime this
reduces and hypertension ensues
Type 2 Diabetes: Similar progression to ESRF once overt nephropathy
208 4
th
and 5
th
Year Notes
Pathology:
Intra-glomerular pressure, glomerular hypertrophy, ?deposition of advanced glycosylation end
products
Glomeruli:
Glomerulosclerosis: nodular (Kimmelstiel-Wilson) or diffuse
Mesangial broadening with deposition of eosinophilic material
GBM irregularly thickened
Arterioles show evidence of subintimal arteriosclerosis and hyalinisation
Interstitial changes: tubular atrophy and fibrosis
Look for other renal pathology if:
No retinopathy
Active urinary sediment
Rapid onset nephrotic syndrome
Type 2 diabetes
Management:
Glycaemic control. HBA1c < 8.5% delays progression in early phases – not later
Anti-hypertensive treatment: All effective. ACE inhibitors are best at protein and intra-
glomerular pressure. May delay progression even in normotensive patients. Aim to lower blood
pressure by as much as possible without creating hypotensive symptoms. Also calcium antagonists
(diltiazem and Verapamil proteinuria)
Protein Restriction: Limiting intake may reduce progression. High intake intraglomerular
pressure and hyperfiltration
Dialysis: worse prognosis than non-diabetics due to concurrent IHD. Peritoneal dialysis better if
CVS instability
Transplant: best prognosis in the absence of CV disease. Disease can recur in the graft 5 – 10
years later
Other renal complications:
Urinary tract sepsis. Should be treated even if asymptomatic
Risk of pyelonephritis
Papillary necrosis. May macroscopic haematuria or ureteric obstruction
Autonomic neuropathy neurogenic bladder infection/obstruction
Contrast nephropathy: always hydrate aggressively
Systemic Lupus Erythematosus
Renal involvement common:
Clinically apparent in around 50%
Histologic lupus nephritis in 100%
5% present with a renal syndrome
Presentation:
Usually heavy proteinuria, nephritic syndrome or RPGN
Test for SLE antibodies (see Blood tests in Inflammatory Arthritis, page 270)
Most patients have complement
Histology:
Mimics anything!
Most severe: Diffuse proliferative glomerulonephritis with crescents
Common: membranous pattern, tubulo-interstitial damage
Immunoflouresence (IF): extensive deposition of IgG and C3, also C1q, IgA, IgM and fibrin
See also Systemic Lupus Erythematosus, page 278
Reflux Nephropathy
See also UTIs in Children, page 221
Most common cause of end-stage renal failure in children, secondary to vesico-ureteric reflux +
infection in infancy
May not appear till adulthood (ie slowly progressive)
Investigations:
Renal cortical scarring on ultrasound or DMSA scan
IVU may show clubbing of calyces
Biopsy: chronic interstitial disease with secondary focal glomerulosclerosis
Treatment: aggressive blood pressure control
Renal 209
Thrombotic Microangiopathy
Includes Haemolytic Uraemic Syndrome (HUS), Thrombotic Thrombocytopaenic Purpura (TTP) and
HELLP Syndrome of Pregnancy (Haemolysis, elevated liver enzymes and low platelets)
Presentation:
Microangiopathic haemolytic anaemia, low platelets and renal and neurological manifestations
Renal involvement: haematuria and proteinuria, renal failure in 40 – 80%
Investigations: Blood film marked fragmentation of red cells, Comb‟s test –ive
Treatment: 90% response to plasmapheresis with or without corticosteroids
Amyloidosis
A dysproteinaemia that usually presents renally with nephrotic syndrome
Types:
Primary amyloidosis: idiopathic or associated with myeloma. Amyloid protein is part of the Ig
light chain. Poor prognosis
Secondary amyloidosis: deposition of a different form of protein. Associated with chronic
inflammatory or infective conditions (eg Rheumatoid arthritis, Tb, etc)
Particularly affects glomerular capillary walls, seen with Congo Red Stain
Complications of Chronic Renal Failure
Uraemia
= Symptom complex associated with severe, near end-stage renal failure (ie GFR < 20 mls/min)
Leads to:
Accumulation of uraemic toxins
Anaemia
Hyperparathyroidism
Metabolic acidosis
Common symptoms (NB some of these may be due to anaemia alone):
CNS: Fatigue, weakness, malaise, concentration, restless legs, insomnia
GI: anorexia, nausea, vomiting, gastritis
Blood: anaemia, platelet dysfunction ( bleeding)
CVS: hypertension, oedema, pericarditis
Skin: pruritis, pigmentation
Endocrine: hyperlipidaemia, hypogonadism ( infertility and amenorrhoea), impotence
Investigations:
Serum creatinine and urea: markers of uraemia but also affected by malnutrition and muscle mass
Creatinine clearance: overestimates GFR in severe renal failure as some Cr is secreted in the tubule
Albumin: marker of malnutrition and key prognostic factor
Ca, PO4 and PTH: markers of renal osteodystrophy (see Increased Bone Resorption, page 263)
HCO3: degree of metabolic acidosis
Anaemia due to erythropoietin (but exclude other causes, eg Fe or folate)
Management:
Protein restriction (but beware malnutrition)
Alkalis (eg HCO3) to control acidosis
Aggressive blood pressure control
Fluid restriction if pulmonary oedema
K restriction and avoiding K increasing drugs
Dialysis if these measures fail to control symptoms/signs. See Renal Replacement Therapy, page
217
Anaemia
Normocytic, normochromic
Universal in patients with end-stage renal failure (except that it‟s less common in polycystic disease)
Secondary to erythropoietin deficiency, plus also RBC survival
Also Fe and folate due to dialysis
Management:
Blood transfusion: effective but only temporary benefit. Complications: Fe overload, development
of cytotoxic antibodies ( problems for future renal transplant)
210 4
th
and 5
th
Year Notes
Synthetic erythropoietin: Very effective, including well-being, exercise tolerance, LV
hypertrophy, etc. Most are Fe deficient, so need supplementation (maybe iv). Complications:
worsening hypertension
Secondary Hyperparathyroidism
See Parathyroid, page 101
Pathogenesis:
1,25 (OH)2D3 [calcitrol] from kidneys Ca absorption and PTH
Renal failure PO4 excretion serum PO4 PTH
PTH in most patients with GFR < 50 mls/min
Presentation:
Pruritis (?soft tissue deposition of calcium phosphate)
Bone pain due to calcium resorption
Restless legs
Management:
Early replacement of calcitrol (but watch for hypercalcaemia)
Phosphate reduction: dietary intake and calcium carbonate (binding agent in the gut
absorption)
If these don‟t control the PTH without causing Ca, then parathyroidectomy ( hypocalcaemia
and requirement for ongoing calcitrol)
Other complications
Hyperphosphataemia
Vascular disease
Chronic fluid overload LV hypertrophy and BP
Specific Nephrotoxins
Aminoglycosides
Amphotericin
NSAIDs: PGs which vasodilate afferent arteriole vasoconstriction. Compounded risk if already
dehydrated, elderly, etc
ACE inhibitors. Acute renal failure following introduction of ACE ?renal artery stenosis: already
reduced renal flow, ACE dilates efferent arteriole precipitous fall in GFR.
All radio-contrasts: risk in at risk patients by maintaining hydration with a saline drip
Chemotherapy: eg Cisplatin
Rhabdomyolysis (from trauma, status epilepticus, acidosis, etc):
Injury to membrane of skeletal muscle
Ck
Renal failure due to combined effect of nephrotoxic effect of myoglobin, hypovolaemia and
aciduria
Urinalysis is +ive for blood but no RBCs on microscopy. Urine is dark brown
Kidney Disease
Renal Stones (Nephrolithiasis) *
Symptoms:
Loin pain stone in kidney
Colic anywhere from loin to groin (may just be the tip of the penis) stone in ureter
UTI, haematuria, obstruction
Risk factors:
Low urine output ( drink lots)
Hypercalcaemia: hyperparathyroidism, sarcoid, neoplasia, Addison‟s, Cushing‟s, hyperthyroidism,
Li, could be just due to Vitamin D in summer
Hyperoxaluria: high levels of oxalate in chocolate, tea, rhubarb, spinach
Hypocitraturia
Hyperuricosuria
Investigations:
MSU: RBC, UTI, protein, pH (stones like acid urine)
Renal 211
Plain X-ray of kidneys, ureters and bladder
Blood: U&Es, urate, Ca, PO4, HCO3
Management:
Pain relief: NSAIDS (but care with renal flow) or morphine
Fluid intake
Sieve urine to catch the stone for analysis
If obstruction or infection urgent urologist referral
Tubulointerstitial Diseases
Involve tubules and renal interstitium (not glomerulus)
Acute Tubular Necrosis (ATN)
Ischaemic:
Patchy areas of tubular necrosis (proximal convoluted tubules and straight segments of the loop of
Henle) and thinning of epithelial brush border
Loss of basement membrane scarring, loss of architecture permanent loss
Regeneration if not too severe
Toxin-mediated (e.g. aminoglycosides, radio-contrast agents, heavy metals, arsenic, solvents, also from
myoglobinuria from muscle damage):
Necrosis is continuous not patchy
No loss of basement membrane epithelium can regrow down the nephron resolution
Leads to:
Intra-tubular obstruction GFR. Glomeruli and vessels generally normal
Hyaline casts from cellular debris
Reduction in sodium reabsorption & loss of medullary concentration gradient inability to
concentrate urine isoosmolar urine with Na > 20 mmol/L
Management:
Fluid restrict
Correct electrolytes
Nutrition
Avoid nephrotoxins
Dialysis if:
Severe hyperkalaemia
Pulmonary oedema/severe hypertension
Symptomatic uraemia
Progressive uraemia with oliguria
Severe refractory metabolic acidosis
Lasts 1-2 weeks, followed by gradual improvement in serum urea and creatinine, and diuresis (due to
reduced medullary gradient) – monitor to avoid hypokalaemia and hypovolaemia
Prevent preoperatively by maintaining hydration maintained renal blood flow. No clear benefit
from mannitol, dopamine, frusemide, etc
Acute Papillary Necrosis
Diabetes
Also in urinary outflow obstruction pressure in renal pelvis perfusion
Acute Interstitial Nephritis (AIN)
=Intense, often patchy, interstitial inflammatory infiltrate of lymphocytes & monocytes
Presentation:
Similar to RPGN
Also skin rash, fevers, eosinophilia of urine
Glomeruli normal but may be tubular necrosis
GFR due to tubular obstruction and altered intra-renal haemodynamics
Associated with drugs (e.g. penicillins - especially amoxycillin, and cephalosporins) – sometimes with
infections & systemic diseases. Also NSAIDs – but after months of exposure & severe proteinuria
Symptoms: 1 – 2 weeks after exposure (ie delayed hypersensitivity): fever, maculo-papular rash,
eosinophilia, arthralgia, flank pain
Urine has pyuria, mild haematuria and mild proteinuria
Treatment: withdraw drug +/- steroids
212 4
th
and 5
th
Year Notes
Acute Pyelonephritis
Caused by suppurative infection: E coli, Proteus, Klebsiella, Enterobacter
From ascending UTI or haematogenous spread of infection (eg septicaemia)
See Urinary Tract Infections, page 219
Chronic Pyelonephritis
Not a disease, but a description of what happens to the kidney – it becomes dilated and replaced by fat
Causes:
Recurrent infection
Obstructive uropathy
Vesicoureteric reflux (especially in kids with malformed vesicoureteric valves. Present in puberty
with renal failure – subclinical before that)
Kidney stones ( infection)
Glomerulonephritis
See also Presentation of Kidney Disease, page 204
Overview
Variety of conditions inflammatory changes in the glomeruli. If severe enough to cause crescent
formation rapidly progressive glomerulonephritis (see page 215)
Some forms predominantly present in one way, but any form can present in any way. Can present as:
Nephritic Syndrome
Nephrotic Syndrome
Acute Renal Failure secondary to rapidly progressive GN
Chronic Renal Failure
Asymptomatic Haematuria or proteinuria
Hypertension
Either:
Primary: limited to the kidney
Secondary: part of a more widely disseminated immune process
Systemic diseases that may present as GN:
Lupus nephritis: deposits of immune complexes everywhere within the glomerulus
Arteritis: Microscopic polyarteritis
Amyloid: Nephrotic Syndrome or renal failure. Histology with Congo Red Stain
Diabetes
Hypertension
Terminology:
Proliferative: proliferation of endogenous glomeruli cells
Exudative: infiltration by polymorphs
Diffuse: involves all glomeruli
Focal: involves only some glomeruli
Global: involves the whole glomerular tuft
Segmental: involves only part of the glomerular tuft
Diagnosis:
Urine biochemistry: urine sodium > 20 mmol/L (if pre-renal failure then < 20, ie frantically trying
to reabsorb Na)
Urine analysis: Blood morphology and casts, protein (usually mild)
Ultrasound: exclude obstruction, looking for normal or slightly enlarged kidneys, echogenic (dark
on US fluid)
CXR: look for Goodpastures Syndrome, Wegener‟s Granulomatosis
Bloods: ANA (connective tissue disorders), ANCA (Anti-neutrophil cytoplasmic antigen
Wegener‟s Granulomatosis), Anti-dsDNA ( SLE), anti-GBM
Histology. May see:
Glomerula epithelial cells usually have interdigitating foot processes. If they swell, gaps
between them proteinuria
Mesangial cells (supporting framework) are the first to react to injury and the last to return to
normal
Renal 213
Management
Investigations:
Urine microscopy
24 hour urine for protein and Cr
Serum: U&E, FBC, ESR, CRP, albumin, ANAs, etc
Culture: ?blood, throat, ears, skin
CXR, US, IVU
Biopsy
Treatment:
Prompt referral
Keep BP < 145/90
Specific treatment
Monitor renal function
Clinical and lab features
Proteinuria
Haematuria
Asymp-
tomatic
Nephrotic
Macro
Micro
Nephritic
ARF
CRF
Anti-
GBM
C3
Anti-
strep
Anti
IgA
Minimal
Change
++++
+
FSGN
+++
++++
++++
+++
Membranous
+++
+++
+
+++
++
Post-
Infectious
+
+
+
++++
++++
+
+++
+++
RPGN
+
+
++++
+++
+++
++
++
IgA
+++
++
+++
++++
+
+
+
++
Mesangio-
capillary
+
+++
+
++++
+++
++
+++
+
Minimal Change Disease
Presentation:
Usually nephrotic syndrome, with severe oedema, uncommonly have hypertension and 10% have
microscopic haematuria
Commonly after an URTI
Boys > girls
90% of childhood nephrotic syndrome, 20 – 30% of adult nephrotic syndrome
Renal function normal, unless it deteriorates secondary to hypovolaemia
Weak association with Hodgkin‟s Disease
Investigations:
Light Microscopy (LM): glomeruli are normal
Immunoflourescence (IF): Negative
Electron Microscopy (EM): fusion of foot processes
Management:
Kids: natural history unpredictable:
90% of kids respond to 8 weeks of steroids. If they relapse, respond to steroids again (eg
triggered by intercurrent illness). No renal failure but complications of treatment
10% become steroid dependent or resistant use cyclosporin
Steroids less effective in adults, but still reasonable response rate
214 4
th
and 5
th
Year Notes
Focal and Segmental Glomerulosclerosis (FSGS)
Presentation:
Usually nephrotic, can be nephritic
Usually microscopic haematuria
Accounts for 10 – 20% of nephrotic syndrome in adults
Investigations:
LM: segmental sclerosis of the glomerular tufts. May be mesangial matrix, interstitial fibrosis
and tubular atrophy
IF: Weakly positive for IgM and C3 (?artefact)
Management:
Poor prognosis: 50% have a five year renal survival
Some response but frequent relapse to steroids
Membranous Glomerulonephritis
Presentation:
Nephrotic syndrome, also asymptomatic proteinuria
Microscopic haematuria, hypertension, renal impairment
30% of adult nephrotic syndrome, most commonly middle-aged
Usually idiopathic, but 25% of it is secondary to underlying disease, including:
Lung or colon cancer (< 10% or adults presenting with Membranous GN)
Infections: hepatitis B, malaria
SLE
Drugs: penicillamine, gold, high dose captopril
Investigations:
Is autoimmune – but there is no antibody you can measure
LM: thickened, irregular capillary loops, spikes in BM with silver stain
IF: granular deposition of IgG and C3
EM: Subepithelial deposits
Prognosis: variable – 30% progress to end-stage, 30% improve, and the rest retain stable renal function
but with ongoing proteinuria
Treatment: steroids or cytotoxics for the progressive group
Post-Infectious Glomerulonephritis
8 – 14 days following Group A -haemolytic strep infection of throat or skin, also SBE, osteomyelitis,
etc
Cultures usually negative, strep serology may be helpful
Presentation: Usually nephritic, may be rapidly progressing acute renal failure
Biopsy: usually in adults to rule out a crescentic rapidly progressive GN:
LM: mesangial and endothelial cell proliferation + neutrophils. Crescents if severe
IF: Usually +ive for granular IgG and C3 deposition
Treatment: supportive, not immunosuppressive. Treat culture positive family members with penicillin
Prognosis: slow recovery, mild residual impairment in a few
Goodpasture’s Syndrome
GN +/- pulmonary involvement (ranging from pulmonary infiltrate on x-ray to frank haemoptysis)
Pathogenesis: antibodies against an antigen in the glomerular basement membrane and pulmonary
tissue
Biopsy: Crescents + linear immunoflourescence on the basement membrane
Can measure serum anti-GBM antibody
Treatment: immunosuppression (steroids, cyclophosphamide) +/- plasmapheresis
See also Miscellaneous Lung Diseases, page 92
Mesangial IgA disease (Berger’s Disease)
Most common form of GN. Common cause of recurrent haematuria in young men. Usually more
benign
Presentation, either:
Macroscopic haematuria +/- URTI (= Synpharyngetic haematuria)
Asymptomatic microscopic haematuria picked up on dipstick testing
Nephrotic levels of proteinuria are rare
Renal 215
Biopsy:
LM: Mesangial cell proliferation + matrix formation
IF: Mesangial deposits of IgA and C3
Prognosis: only 15 – 20% progress to end-stage renal failure – these are more likely to have
proteinuria, hypertension and impaired renal function at presentation
No effective treatment. Consider immunosuppressive treatment if rapidly progressive
Similar to Henoch-Scholein Purpura – but HSP is more widespread, causing purpura (especially
buttocks and ankles) and abdominal pain (which may GI bleeding)
Mesangiocapillary (Membranoproliferative) GN*
50% present as Nephrotic Syndrome
Biopsy:
LM: cellular expansion of the mesangium. „Twin track‟ BM
EM: Subendothelial deposits or deposits within the BM
Rapidly Progressive Glomerulonephritis
What is it:
A description not a diagnosis
= Acute renal failure secondary to glomerula disease generally with a nephritic presentation.
Any form of GN can present in a rapidly progressive form. Generally caused by immune mediated
diseases
~ Crescentic glomerulonephritis (marker for severe RPGN)
= Cellular proliferation in glomeruli, and crescent formation.
Pathogenesis of crescents: rupture of the basement membrane fibrin leaks into Bowman‟s
space, macrophages recruited, epithelioid cells form a crescent. Leads to scarring and fibrosis of
glomeruli
Presentation:
Nephritic presentation. Nephrotic range proteinuria is rare
GFR but tubular function OK so Na/H20 reabsorbed oedema
Systemic features of immune mediated diseases: myalgia, arthralgia, fever, etc
Investigations:
Urine chemistry midway between pre-renal ARF and ATN
Light Microscope: Extensive proliferation of cells, numerous crescents, generally without
polymorphs
Immunoflouresence:
Granular IgG and C3 immune complex mediated (Post strep, Lupus, etc)
Linear IgG Goodpastures
None pauci-immune
Due to:
Immune complex mediated GN:
Post-infectious GN: e.g. post-streptococcal (rarely crescents, dialysis rarely needed) also
staph. See page 214. Has granular IgG plus neutrophils
Lupus Nephritis, see page 208. Has granular IgG (plus IgA, IgE, etc)
Others, including vasculitis
Anti-glomerular-basement membrane diseases (Goodpasture‟s syndrome): See page 214
Pauci-immune: (ie no evidence of immune deposits, probably cell mediated immune problem):
Wegener‟s Granulomatosis: Causes GN, URTI, LRTI, non-caseating granuloma, cANCA is
highly specific, -ive immunoflourescence, typically older patients. See also Wegener‟s
Granulomatosis, page 283
Microscopic polyarteritis (also joints)
Prognosis dependent on % of crescents
Treatment: immunosuppressive (iv methylprednisolone, cyclophosphamide) +/- dialysis
Hypertension
Histologic changes: intimal fibrosis, hyaline deposition, downstream infarction progressive scarring,
granular surface
Need to aggressively treat hypertension in people with other risk factors for kidney disease (eg
diabetes)
See Hypertension, page 34
216 4
th
and 5
th
Year Notes
Congenital Abnormalities
Aplasia: absence of a kidney
Hypoplasia: usually unilateral, secondary to obstruction of the ureter in utero
Horseshoe Kidney:
1 in 500
Work normally
Disturbed renal flow: ureter has to flow over the kidney recurrent UTI
Hydronephrosis
Dilation of renal pelvis due to:
Obstruction of the pelvo-ureteric junction (often in kids)
Big prostates
Kidney stones
Leads to renal failure due to:
Chronic interstitial nephritis (as do other things): leucocyte invasion.
Atrophy of the collecting ducts and distal tubule (which are relatively hypoxic compared to the
glomerulus). However, if the tubule goes, the glomeruli scleroses loose whole nephron
Cystic Renal Disease
Adult Polycystic Kidney
Autosomal dominant: PKD1 loci on chromosome 16 (worse), PKD2 on chromosome 4 (better)
1 in 500
Pathogenesis:
Whole nephron blows up squashes other nephrons progressive renal failure
Cystic lesions in other organs: liver, pancreas, lung
Presentation:
Present with hypertension around 50 IHD, CVA
Vary in severity and onset
Usually only moderate proteinuria
Kidney‟s can get very large impair respiration
Diagnose with US or CT
Treatment: slow progression through aggressive blood pressure control
Infantile Polycystic Kidney
Autosomal recessive
In mild forms that escape renal failure, is associated with congenital hepatic fibrosis
Cystic Renal Dysplasia
Due to obstruction of urinary outflow tract prior to the union of metanephric blastema and the
ascending ureteral bud
Disordered kidney development. Contains bone, smooth muscle, etc but is not a tumour
Simple Cortical Cyst
Dilation of a single nephron, usually to 5 mm – 1 cm. Most people usually have 3 or 4
Usually asymptomatic
If large and rupture urinary peritonitis
Other
Infection: Tb and hydatids can present as cystic dilation on US
Medullary Sponge Kidney: Rare. Dilated collecting ducts
Renal Tumours
Renal Adenoma/Papillary Adenoma
Most people have one or two
Associated with renal scarring
< 5 mm diameter
Papillary architecture
Renal 217
No clear cells (if there were then malignant)
Other benign renal tumours
Renal Oncocytoma: Have oncocytes: cells with abundant mitochondria (pink and granular) – tired
epithelial cells. Grossly form a stalate scar
Renal fibroma
Aniomyolipoma: composed of fat, smooth muscle and thick blood vessels. Associated with Tuberous
Sclerosis
Renal Cell Carcinoma
75% of renal epithelial tumours in adults
Annual incidence 3/100,000
Risk factors: smoking, obesity, hypertension, unopposed oestrogen
3% familial, Von Hippel-Lindau disease
Clinical features: haematuria, back pain, abdominal mass. Often metastasised before diagnosis
Histology:
Clear Cell Renal Cell Carcinoma – most common
Metastasise up the renal vein to the heart emboli cannon ball metastasis of the lung
Sheets of clear cells
3 p25 deletion diagnostic feature
Papillary RCC: Better prognosis
Chromophobe RCC: Better prognosis, large cells, abundant cytoplasm, small dark nucleus
Sarcomatoid RCC: Highly malignant, highly anaplastic
Transitional Papillary Cell Carcinoma
Present with painless haematuria
Can cause hydronephrosis, flank pain, and renal colic from clots
Peak in 6
th
– 7
th
decade, M > F
Derived from epithelium of renal pelvis
Associated with smoking, analgesic abuse, azo dyes
Often associated with transitional cell carcinoma of the bladder and ureter
Nephroblastoma (Wilms’ Tumour)
Very aggressive, presents with abdominal mass with or without haematuria. Pain and intestinal
obstruction can occur
50% present < 3 years, 90% < 10 years, rare in adults
Derived from metanephric blastema
Dark with scant cytoplasm
Triphasic histology: epithelial cells, stromal cells, blastema
Now around 80% cure
Associated with syndromes:
WAGR: Wilms, aniridia, genital anomalies and mental retardation
Denys Drash Syndrome: Gonadal dysgenesis, nephropathy
Beckwith-Wiedemann syndrome
Other Renal Tumours
Angiomyolipoma: Benign – but grow and haemorrhage. Composed of fat, smooth muscle and dilated
blood vessels
Juxtaglomerular Cell Tumour: Very rare, benign but causes malignant hypertension
Renal Replacement Therapy
For end-stage renal failure, characterised by:
Severe uraemia
Resistant pulmonary oedema
Uraemic pericarditis
Severe hyperkalaemia
Metabolic acidosis
Anaemia
Renal osteodystrophy
218 4
th
and 5
th
Year Notes
Usually required if:
Cr is 500 – 1000 mol/L (depending on patient‟s size)
Urea > 35 mmol/L
GFR < 10 mls/min
Wherever possible, the type of treatment is open to patient preference with the aim of home self-care
Principles of Diffusion in Dialysis
Replaces excretory function of the kidney. Residual kidney function reduces dialysis requirements –
but this usually „dries up‟ over the first few years on dialysis
Blood is exposed to dialysis solution across a semi-permeable membrane movement of low
molecular weight proteins by:
Diffusion
Ultra-filtration and convection due to pressure gradient carrying compounds passively in fluid
Haemodialysis
Indicated for:
Acute dialysis
Weight > 100 kgs
Patient preference
Contra-indicated:
Profound hypotension: dialysis takes half a unit of blood out of the vasculature through the
machine further hypotension
Cardiac failure: intermittent nature of dialysis (every 2
nd
or 3
rd
day) accumulating fluid in
between times then rapid reduction in fluid. If heart function is dependent on pre-load, then a rapid
reduction in circulating fluid frank failure
Inability to establish long term vascular access: a particular problem with diabetics with vascular
disease
Procedure: 3 times a week for 5 to 6 hours, with a dialysis machine, dialysis membrane and dialysate
(buffer/electrolyte solution). Access is via an arteriorvenous fistula at the non-dominant wrist. There
are other options if this fails. Vascular access can thrombose, become infected, lead to high-output
failure, etc
Complications:
Hypotension
Muscle cramps
Bleeding: due to blood loss in dialysis and the anticoagulation necessary to stop clotting in the
machine
Arrhythmias: due to rapid changes in electrolytes
Infections: mainly staph in patients with temporary or tunnelled catheters
CVVHD = continuous veno-venous haemodialysis (used when BP too low for normal dialysis)
Peritoneal Dialysis
Dialysate introduced into the peritoneal cavity, with diffusion across the peritoneal membrane. Less
efficient so requires longer period of dialysis. Good for dialysis while still some kidney function
remaining. Easier to learn and lower cost than haemodialysis
Indicated if:
Severe cardiac disease: maintains more stable fluid levels in the body
Elderly or frail patients
Diabetic patients
Patient preference
Contraindicated if:
Previous extensive abdominal surgery: requires adequate peritoneal membrane
Greater than 100 kgs: not efficient enough
Types:
Continuous ambulatory peritoneal dialysis: 4 to 5 exchanges each day, each of 2 – 3 litres
Automated Peritoneal Dialysis: Machine automatically exchanges through the night (good for kids
and people who work through the day)
Complications:
Inadequate dialysis
Tenckhoff Catheter problems
Renal 219
Infection at the exit site and peritonitis (abdominal pain and cloudy dialysis fluid). Usually staph.
Intra-peritoneal antibiotics. If G –ive then ?intra-abdominal pathology
Hydrothorax
Hyperglycaemia: glucose is used in the fluid to encourage filtration
Malnutrition
Renal Transplantation
Treatment of choice. If successful provides full excretory and hormonal function
95% of patients and 85% of grafts survival at 1 year. Half life of a graft ~ 13 years
Not considered if significant co-morbidities
Types:
Cadaveric transplantation: donor and recipient must be ABO compatible with a negative direct
cross match test (ie no recipient antibodies which might cause acute rejection)
Live Donor Transplants: 25% of transplants. Donors must be investigated to ensure good renal
function. Good results due to well donors and better preparation of recipients
Life-long immunosuppressive therapy is required, using cyclosporin, mycophenolate and prednisone.
Combination therapy allows doses complications
Acute rejection: oliguria, Cr, fever and swollen graft. May only be picked up biochemically. Most
likely within the first 3 months, but can occur at any time. Treated with high dose corticosteroids
Long term complications:
Infections due to immune compromise, including opportunistic infections, eg CMV, EBV, PCP.
Prophylaxis during the first 3 months common
Malignancy: skin squamous cell, lymphoma, cervical and Kaposi‟s Sarcoma – not breast, lung or
colon
Ureter
Congenital abnormalities:
Double/bifid ureters
Megaureter
Hydroureter
Usually present with UTIs
May have abnormalities elsewhere
Ureteritis:
Associated with generalised UTI
May be caused by stones lodging the ureter
Rarely caused by Tb
Transitional Cell Carcinoma:
Transitional between squamous and glandular epithelium. Tumours typically papillary/frond like
Similar histology to renal and bladder TCC
Infiltrates early to retroperitoneum with poor prognosis
Urinary Tract Infections
Investigations
Dipstick: Under-rated
Nitrites (produced by an enzyme in most infectious bacteria which breaks nitrates down to nitrites)
presumptive diagnosis
If no leukocytes, nitrates, protein or blood then no infection. Ie high negative predictive value.
Positive predictive value only about 30 – 40%
Culture should be done (ie not just dipstick) in pregnancy, diabetics, atypical presentations
recurrent attacks and non-response to treatment
Urine Microscopy:
Some RBC and WBCs are normal
Look for casts, crystals, bacteria. Absence of bacteria not significant (treat empirically)
If RBC > WBC then ?stone
Culture:
Bacteruria 10E5 colony forming units (cfu) per ml of urine. However, this was set using
morning samples in young women via catheterisation not much value.
220 4
th
and 5
th
Year Notes
In kids, a much smaller number may be significant, especially if:
In a boy
Obtained by catheter. In a supra-pubic aspirate any growth is important
Most UTIs are caused by a single bug. If multiple organisms then contaminated sample. Bugs can
grow in transit send to lab straight away or refrigerate
Antibiotic sensitivity: if multi-resistant then usually from Asia where antibiotics are freely
available
Haematuria in 50% - but if asymptomatic ?bladder carcinoma
Intravenous pyleogram / urogram (same thing)
Microbiology
GP
Hospital
E Coli
75%
40%
Coag –ive Staph
7%
6%
Proteus
6%
15%
Klebsiella
3%
12%
Enterococcus
3%
15%
Pseudomonas
1%
6%
Hospital acquired are more antibiotic resistant
Pathogenesis: bacterial adherence
Uropathic strains: fimbriae – microbial adhesions. Different types in different bugs, and different
densities of receptors in hosts genetic predisposition
Catheter adhering strains:
Tightly adherent none grown from urine
Thick layer of „biofilm‟ forms in lumen of catheter containing bugs. Antibiotics can‟t
penetrate change catheter
Risk factors: duration of use (but regular changing makes it worse), female sex, absence of
systemic antibiotics, catheter care violations
Prevention: avoid catheterisation, lots of fluid, alternative method for bladder drainage (eg
condom catheter), closed, sterile bladder drainage, appropriate aseptic technique at insertion
Adults
Epidemiology:
More common in women, older people, and long term care
20% in women 65 – 75, 3% of men
Definition: Lots of terms with subtle variations in meaning: UTI, bacteruria, bladder bacteruria,
asymptomatic, etc, etc
Presentation:
Acute symptomatic urinary infection = urgency, frequency and dysuria (pain on urination). NB
urgency and frequency may be unrelated to infection (eg bladder instability)
In elderly may present atypically: delirium, falls, immobility
Cloudy urine, dark urine (volume depletion), and smelly urine are all normal!
Asymptomatic bacteruria = 2 consecutive positive cultures without symptoms attributable to the
urinary tract
Classification:
Uncomplicated: normal urinary tract and normal renal function
Complicated if:
Abnormal urinary tract: eg calculi, reflux, obstruction, paraplegia, catheter, prostatitis, etc
Impaired host defences: immunosuppressed, diabetes, etc
Impaired renal function
Virulent organism (eg Proteus)
Male
Causes of dysuria:
Urinary tract infection +/- vaginitis
Vaginitis (Candida albicans, trichomonas vaginalis, gardnerella vaginalis)
STDs
Other: trauma, urethral syndrome
Treatment:
Oral trimethoprim in uncomplicated infections. E coli resistance will need to change this soon
Renal 221
Oral quinolones are the main second line agents (eg norfloxacine)
Don’t treat asymptomatic positive urine cultures (ie don‟t test unless symptoms) unless diabetic or
pregnant
Single dose therapy is worse than conventional therapy (7 – 10 days). For adult women, single
does therapy has an odds ratio compared to conventional treatment (5 days or more) of 0.7 for
TMP/SMZ (trimethoprim/sulphamethoxazole), and 0.4 for amoxycillin
Short course possibly as effective as conventional (watch this space)
Complications: Ascending infection renal scarring hypertension, etc
Prophylaxis:
Consider if recurrent infections, eg low dose nightly antibiotics for 3 – 6 months, post-coital
antibiotics
Bladder emptying at night and after intercourse
Topical oestrogen cream if post-menopausal
Adequate fluid intake (> 2 litres per day)
Men:
If unknown cause - ?referral to urologist for kidney scan (e.g. stone)
Always do urine culture in addition to antibiotics
Do swab if discharge
Urethral syndrome
No bacteria isolatable
Can be chlamydia (need to do right test)
Can become very sensitive after a number of infections (general inflammation)
Acidic urine will hurt more if inflamed drink lots (dilute urine) and Uracil
More common in older women
UTIs in Children
Epidemiology:
UTI is common:
Males usually have them in their first year, for girls it‟s on going
By age 7, 9% of girls and 2% of boys will have had at least one episode
Caused by E coli in over 80% of cases. Others are associated with complicated UTIs or long term
antibiotic therapy (eg Candida)
Of 1000 kids with UTI:
400 have vesico-ureteric reflux, 100 have renal scars, 10 will develop premature hypertension
(eg in older childhood or pregnancy), end stage renal failure in 1
10 – 20 will have obstruction due to urethral valves, VU or PUJ obstruction
Greatest risk usually kids < 4 and especially in first year of life
Risk Factors for UTI:
Previous infection
Normal anatomy but functional problem: e.g. vesico-urethral reflux (in child, sibling or parent)
Structural abnormality: e.g. urethral stenosis/stricture (more common in boys – congenital, trauma
or inflammation)
Vulvoanitis from poor perineal hygiene
Incomplete or infrequent voiding
In first year of life, uncircumcised male is 10 times that of circumcised
Sexual abuse: only 2% of patients investigated for sexual abuse have UTI as a symptom. UTI
without other indications (lesions, bleeding, bruising) is very unlikely to be sexual abuse
Antibiotics: disrupt normal peri-urethral flora predispose to infection
Constipation a risk factor: ask about this
Indwelling catheter
Risk factors for VUR:
Children with UTI (30 – 40%)
Siblings affected
Antenatal dilation of the urinary tract (8 – 22%)
No evidence that prophylaxis renal scars (controversial)
Always have appendicitis as differential diagnosis: can have white cells in urine with appendicitis
where appendix is in the pelvis (or elsewhere)
222 4
th
and 5
th
Year Notes
Symptoms are highly variable:
0 – 2: Fever/hypothermia (?sepsis), lethargy, poor feeding, diarrhoea, vomiting, abdominal
distension, failure to thrive
2 – 5: fever, rigours, vomiting, diarrhoea, colic, abdominal pain, some dysuria, offensive urine,
haematuria, weak urine stream
5 – 12: fever, rigours, abdominal pain ( upper tract infection), dysuria, frequency, urgency,
incontinence, haematuria
If systemic illness then likelihood of pyelonephritis as well as cystitis. If under one, can have
Pyelonephritis without systemic signs if UTI under age 1 then presume Pyelonephritis
Diagnosis:
Urine bag:
Wash genitalia before application
Test with urine dipstick. If positive, obtain definitive sample with catheter or supra-pubic
aspiration (SPA)
Do not routinely send bag specimens for culture. Boys have 93% false positive
Catheter:
For children who can‟t void on request and where the bladder is in the pelvis (SPA won‟t
work)
Uncomfortable. Discard first few mls
Growth > 10E6/litre suggest infection
Supra-pubic aspirate:
If child too young to obtain an MSU
Gold standard: any growth suggests infection (but beware contamination with skin
commensals)
MSU: discard first few mls
Exam:
Often normal, other than fever
Do blood pressure, search for loin, abdominal and supra-pubic tenderness, inspect spine and
external genitalia, and brief neuro exam of the lower limbs. Check and plot growth
Management:
Admitted for IV antibiotics if:
Neonate or immunocompromised
Shocked
Vomiting frequently (ie oral antibiotics won‟t stay down)
Hospital treatment:
Bloods: FBC, blood cultures, electrolytes and Cr. If toxic, consider LP and glucose
Antibiotics: Amoxycillin 50 mg/kg/6hr (max 2g) (for enterococcus) and gentamicin 2.5
mg/kg/8hr (if older than 1 week and normal renal function) to cover everything else.
Discharge on oral antibiotics to take total treatment to 10 – 14 days. Then prophylaxis until
follow-up
Repeat urines to check it‟s cleared
Follow-up:
US within, say, 12 hours: checking for obstruction and kidney size. Poor sensitivity for
reflux
If < 2 years then MCU (Miturocysto-urethrogram, for reflux risk of scarring) + delayed
DMSA scan (eg after 6 months, look for filling defects renal scarring)
If > 2 years then delayed DMSA
If reflux, then prophylactic antibiotics until out of nappies and 6 months since last UTI
Oral Antibiotic treatment:
Don‟t give antibiotics unless a definitive urine specimen has been obtained
Antibiotics standard treatment:
Cotrimoxazole 200/40mg in 5 ml, 0.5 ml/kg bd 5 days (= trimethoprim +
sulphamethoxazole – less concern about allergy in kids),
Amoxycillin 15 mg/kg tds po (max 500 mg) for 5 days
Augmentin 15 mg/kg tds po (max 500 mg) for 5 days
Prophylaxis in children with recurrent infection is common – but duration, drug and dose all
remain variable. Cotrimoxazole 200/40mg in 5 ml, 0.25 ml/kg po od
Repeat urines at conclusion of antibiotics to check it‟s cleared
Renal 223
Referral to urologist:
Boys: always refer for confirmed UTI, especially if circumcised
Girls: At least repeat urines after first UTI to check cleared. Refer after second UTI
Bladder
Interstitial Cystitis
Usually elderly patients
Urine sterile
If severe then intractable pain with decreasing bladder capacity
Microscopy ulcerative chronic cystitis
?Viral aetiology
Bladder Tumours
Transitional Cell Carcinoma
Classic association with azo dyes (clothing, plastics, batteries) and smoking
Present with painless haematuria (ALWAYS investigate painless haematuria)
Develop as a flat carcinoma-in-situ papillary tumour infiltrates
Management: regular scrapping it out until pathology says its metastatic then cystectomy
Other Bladder Tumours
Squamous cell carcinoma: common in Egypt due to Schistosoma (parasite). Early infiltration
Adenocarcinoma: Rare. Resembles large bowel adenocarcinoma. Derived from urachal remnant
Rhabdomyosarcoma: In childhood. Aggressive but responds to chemo
Urinary Incontinence
Bladder pressure > urethral pressure = flow of urine
8- 34% of community dwelling older people. Women 1.5 to 2 times rate of men
Only 25 – 50% with urinary incontinence seek medical help
Physiology:
Bladder fills at 25 – 125 ml/hr. Low pressure maintained by reflex arc detrussor muscle
inhibition
Conscious sensation to void at 250 – 350 ml, normal capacity 400 – 600 ml
Micturition co-ordinated by pontine micturition centre parasympathetic nerves S2 to S4
relaxation of urethral sphincter muscles + contraction of detrussor until < 30 ml left in bladder.
Inhibition of pontine centre voiding.
Age related changes:
Uninhibited detrusor contractions
Benign prostatic hypertrophy in men urinary outflow obstruction urinary retention
Oestrogen in women urethral sphincter function
Miscellaneous: bladder capacity, residual urine, nocturnal urine production
Impact of age related diseases:
D: Drugs (diuretics, anticholinergic side effects detrusor contraction, sedatives) and Dementia
(executive function)
R: Retention of urine (eg prostate hypertrophy retention bladder pressure sphincter pressure)
I: Immobility (arthritis, etc), inflammation of bladder (asymptomatic bacteruria), impaction of
faeces
P: Polyuria (Diabetes, heart failure)
Established urinary incontinence:
Overactive detrussor: Detrussor Instability. Spontaneous contraction when attempting to inhibit
voiding (eg stroke, prostate disease) frequency, nocturia, urgency, urge incontinence. = Blabber
instability – common. = Urge incontinence. Usually no pathology found
Under-active sphincter: If normal bladder then Genuine Stress Incontinence (GSI). In small
portion of men with prostate surgery, in women more complex (childbirth trauma, oestrogen,
prolapse etc) momentary loss of small volume of urine with intra-abdominal pressure (eg
cough). Occurs in the absence of detrusor activity. Upper urethra slips through the pelvic floor.
224 4
th
and 5
th
Year Notes
Caused by childbirth, surgery, menopause (atrophy of urethral epithelium), masses, prolapse,
pregnancy, etc
Overactive sphincter: anticholinergics, neural damage or prostate problems retention
overflow incontinence
Overflow incontinence: due to over-distended bladder (without detrusor activity)
Reflex Incontinence: involuntary loss due to abnormal spinal reflex activity without the desire to
void
Assessment:
History: Screen all elderly people. „Have you ever lost control/wet yourself „? Impact on function,
proximity to toilets, fluid intake, medications, etc
Exam: neurological, esp. sacral nerve lesions, signs of stroke. Rectal exam (eg sphincter tone,
faecal impaction, prostate - although large prostate size does not correlate to urethral obstruction),
in women cough induced urine leakage, mobility, eyesight, cognition
Investigations: urinalysis to exclude infection, exclude polyuria due to diabetes, urodynamic
investigations (measuring micturition pressure and volume)
Management:
Genuine stress incontinence: pelvic floor exercises, agonists, oestrogen, surgery
Detrusor instability: bladder retraining, bladder relaxants, remove obstruction
Overflow: surgery to remove obstruction, intermittent/permanent catheter
Other: schedule toileting, pads, etc
Male Genitourinary
Prostate
Anatomy
Normally 20 – 30 g. Grossly enlarged can be 500g
Prostate can become infected, hyperplastic or malignant
Used to be described in lobes. Now described in zones:
Anterior zone
Transition and central zone: main site of benign hyperplasia
Peripheral zone: main site of malignancy. Next to rectum – can palpate on PR
PR exam:
Even if normal, don‟t ignore PSA. Cancers can be small or diffuse, or anterior, in an already
large prostate PR isn‟t sensitive
Nodularity can be detected on PR. This is due to desmoplasia (fibrous reaction) – usually to a
slower infiltrating cancer
Prostatitis
Acute:
Gonorrhoea most common cause: pain, discharge, haematuria, tender on PR
May be infarction secondary to hyperplasia compressing blood supply
Granulomatous:
Tb (rare)
Fungal (only immunocompromised)
Leakage of prostatic secretion into interstitium post surgery
Resolving prostates (hard, knobbly prostate, PSA, mistaken for malignancy). Suspect post
surgery, but still need biopsy
Benign Prostatic Nodular Hyperplasia
Not benign if not treated: hydronephros kidney failure death!
Common: 75% of all men over 75 years of age
Testosterone with age oestrogen potentiates effect of Dihydrotestosterone (DHT) on the
prostate prostatic hyperplasia
Morphology: nodular proliferation of ducts, mainly in the central zone
Histology: epithelial nodules, fibrosis, chronic inflammation, focal infarction
Management:
Transurethral prostatic resection (TURP): always retrograde ejaculation + risk of impotence and
incontinence
Renal 225
5 Reductase Inhibitors (blocks Testosterone DHT). Usually preferred. OK if not acute
obstruction
Prostatic Carcinoma
Occurs in 25% of males over 70 years. (More if include indolent central or transition zone tumours)
6% mortality in males
Predominantly adenocarcinoma occurring in the peripheral zone
Key histological features: single cell basal layer in duct epithelium, prominent nucleolus, lots of small
glands
Prognosis related to Grade (using Gleason score: 2 is good, 10 is very bad)
Spreads to pelvic lymph nodes via perineural infiltration
Prostate Specific Antigen:
PSA – a tumour marker. Screening test only. Serum PSA correlates with tumour burden. PSA is
a lytic agent that makes seminal fluid runny. If > 4 then do free to bound ratio, and/or follow/refer
patient
In benign and malignant tumours, or inflammation
Management:
Transurethral resection
Radiotherapy
Radical prostatectomy (selected on basis of tumour bulk and grade (not if very high grade – will
already have metastasised). 50% have complications (impotence, incontinence)
Workup of Obstruction from Enlarged Prostate
Investigations:
Cr: checking renal function
K and Na: checking renal failure
Blood gases for metabolic acidosis
PSA
Ultrasound: look for distended bladder and hydronephrosis
ECG if K: if ECG changes or if K high then may need anti-arrhythmic
Management:
Catheterise: should see K and Cr resolve over a day (depending on remaining renal function)
If high K, then insulin + glucose
Complications of obstruction:
Enlarged bladder: hyperplasia of detrussor muscle fibres, space between trabeculated fibres
Back pressure in ureter hydronephrosis
Filtration Cr
Function of tubular epithelium due to poor perfusion active transport of K
Acidosis
Moral: Must act on a distended bladder to protect the kidney
Prostate Cancer Screening*
Notes prepared for Public Health Test. Does PSA meet the 6 criteria for a good screening test?
Source: Readings on Closed Reserve
Is it an important health issue:
2
nd
leading cause of cancer death in men in the US. In NZ, 800 cases and 400 deaths per year
A disease of the very old. 1% < 55 years, 65% > 75 years. Would reducing incidence lead to
decline in all-causes mortality?
Is there a suitable test: PSA test + digital rectal exam. PSA test is reasonably good at detecting
pathology, and sensitivity is improving (currently ~ 80%)
Is the natural history well understood:
Wide variety of cancers: from the slow growing, indolent sort to very aggressive
Need long enough asymptomatic duration to allow screening at reasonable intervals
Screening likely to detect indolent cancers (length bias)
Incidence of prostate cancer has increased dramatically since opportunistic screening introduced
treating many cancers that would have remained harmless (ie would die WITH cancer but not
BECAUSE of cancer)
226 4
th
and 5
th
Year Notes
Does treatment at the asymptomatic stage confer positive benefits over later treatment:
No firm evidence that radical prostatectomy is better than conservative treatment for asymptomatic
cancers
For Grade I and II cancers, evidence that conservative treatment is at least reasonably effective
Risks of prostatectomy: 30-day mortality of 0.5% + significant levels of ongoing incontinence and
sexual dysfunction
Assuming 4% rate of detection from screening, 1 in 5000 will die, 1 in 81 will be incontinent, and
1 in 36 will have sexual dysfunction as the result of the screening
Conclusion: Screening is good at detection pathology, but don‟t yet know if treatment is beneficial
in net terms
Infrastructure and cost: of lesser relevance until it can be demonstrated that screening is clinically
effective
Penis
For congential malformations and paediatric presentations see Penis, page 636
Epispadias: abnormal opening of urethra on ventral surface
Fractured Penis: Rupture of corpus cavernosum during erection
Condyloma: Genital wart. Usually flat. Associated with HPV.
Erythroplasia of Queyrat (= Bowen‟s disease): non-invasive cancer of the penis. Premalignant
condition. Usually starts in coronal sulcus.
Squamous cell carcinoma: Very rare, risk if not circumcised. Early spread to lymph nodes but
doesn‟t disseminate widely
Scrotum
Steatocystoma: benign sebaceous cysts, hereditary
Fournier‟s gangrene: Ischaemic necrosis. Little collateral flow to the scrotum so occlusion domino
effect. Treatment: debridement
Squamous cell carcinoma
Testes
For Torsion and Hydrocoele, see Testes, page 636
Infection
Epididymo-orchitis:
Bacterial infection: E Coli, Klebsiella, Proteus
In adults also Gonorrhoea
Usually self-limiting antibiotics
Key differential: torsion. If in doubt, emergency referral and Doppler US to assess blood flow
Primary Orchitis:
Mumps, Tb, tertiary syphilis
Rare
Other
Spermatocoele: dilation of a chord of epididymis: common benign small lump on testis. Translucent to
torch
Haematocoele: Haemorrhage into tunica vaginalis or tunica albicinia (rugby injury, bleeding disorder)
Testicular Tumours
Incidence 3.5/100,000
3% bilateral
7% associated with undescended testis
Germ cell tumours:
95% of testicular tumours
Derived from germ cells
Peak in 15 – 34 year olds
Painless swelling of the testis
Seminoma:
40% of testicular tumours
Gross: lobulated pale tumour mass
Renal 227
Micro: Undifferentiated germ cells + lymphocytes. Aggressive. Metastasise to inguinal and
para-aortic nodes
Treatment: Orchidectomy via inguinal region (never via scrotum different lymphatic
drainage. Also never biopsy suspected testicular cancers). Very responsive to radiotherapy
Teratoma:
30% of testicular tumours
All can recapitulate ectodermal, mesodermal and endodermal tissue
Benign teratoma: More common in ovary than testis. 3% chance of malignant change.
Mature tissues (usually skin elements – epidermis, hair follicles, etc)
Malignant teratoma: metastasise to para-aortic lymph nodes (especially neural cells – very
aggressive). Gross appearance – lots of variety. Treatment: chemo +/- radiotherapy. Chemo
stimulates cells to mature still malignant but slower growing excision of affected lymph
nodes
Embryonal carcinoma: poorly differentiated, resembles adenocarcinoma. Highly malignant. May
express tumour marker alpha-fetoprotein
Choriocarcinoma: Placental tissues (resembles hydatiform mole). Expresses HCG positive
for pregnancy test. Contains highly malignant syncytiotrophoblast and cytotrophoblast cells.
Responds well to chemotherapy
Mixed tumours: Teratoma and seminoma
Sex chord/stromal tumours:
Leydig tumours: 90% benign. Small brown mass. Present with overproduction of testosterone:
precocious puberty or gynaecomastia in post-puberty. Can produce androgens, oestrogen or
corticosteroids
Sertoli cell tumours: Rare. 90% benign. Within seminephrous tubules of the testis. Local
infiltration
Lymphoma: Older males, often bilateral, poorly differentiated and poor prognosis
Testicular tumours present relatively young, lymphoma in older men
Differential of Testicular Swelling
Ref: Casebook 17, July 2002, Medical Protection Society
Testicular Torsion
Epididymo-orchitis
Testicular Caner
Pain
Acute, sudden onset.
30% have lower abdo
pain
Usually develops over a
day or so
Usually painless – but
30% have diffuse pain or
„dragging sensation‟
Scrotum
Increasing oedema and
erythema on affected side
Increasing oedema and
erythema on affected
side
Testis enlarged. 15%
have scrotal inflammation
Palpation
Testis enlarged,
exquisitely tender, may
ride high
Epididymis usually
enlarged
Lump detected in body of
the testicle
Age
Usually babies and
pubescent boys. Can
occur in 20s and 30s
Usually in 19 – 40 year
olds
Peak incidence age 25 –
35, but as young as 15
History
May have had previous
short acute episodes.
Sometimes recent trauma
Sexual activity. UTI
History of undescended
testis or family history
Urinary
symptoms
90% have normal
urinalysis
Dysuria, frequency,
urgency, only 10% have
discharge
Few in early stages
GI symptoms
Nausea in 1/3. 30%
complain of abdo pain
Can be nausea/vomiting
Can be caused by mets
Temperature
Usually normal
May have fever
Usually normal
Cremasteric
reflex
Diagnosis confirmed by
absence, not excluded by
presence
Present
Present
228 4
th
and 5
th
Year Notes

Musculo-skeletal 229
Musculo-Skeletal *
See also Paediatric Orthopaedics, page 618
History ............................................................ 230
Exam .............................................................. 230
Radiology ....................................................... 231
Fractures ......................................................... 232
Soft Tissue Injury ........................................... 235
Nerve Injury ................................................... 237
Back and Neck ............................................... 237
History ...................................................... 237
Exam ......................................................... 237
Neck and Radiating Arm Pain .................. 238
Back Pain .................................................. 239
Pelvic Injury ............................................. 242
Upper Limb .................................................... 243
Shoulder .................................................... 243
Upper Arm and Elbow .............................. 245
Forearm and Hand .................................... 247
Lower Limb .................................................... 250
Gait ........................................................... 250
Hip and Femur .......................................... 252
Knee .......................................................... 253
Lower Leg and Foot ................................. 257
Facial Fractures .............................................. 258
Joint and Bone Infections ............................... 259
Metabolic Bone Disease ................................. 261
Orthopaedic Tumours ..................................... 264
Other ......................................................... 265
Secondary Bone Cancer ............................ 266
Arthritis Overview ......................................... 266
Exam ......................................................... 266
Differentials for Arthritis .......................... 266
Radiology ................................................. 267
Osteoarthritis .................................................. 268
Inflammatory Arthritis ................................... 270
Management of Inflammatory Arthritis .... 270
Blood tests in Inflammatory Arthritis ....... 270
Pharmacology ........................................... 271
Rheumatoid Arthritis ................................ 272
Juvenile Rheumatoid Arthritis .................. 273
Spondyloarthropathies (Seronegative
Arthritis).............................................. 274
Crystal Arthropathy .................................. 277
Connective Tissue Diseases ........................... 278
Systemic Lupus Erythematosus ................ 278
Sjogren‟s Syndrome ................................. 279
Progressive Systemic Sclerosis (PSS) ...... 280
Mixed Connective Tissue Disease ............ 281
Polymyositis and Dermatomyositis .......... 281
Polymyalgia Rheumatica .......................... 281
Vasculitis .................................................. 282
Pain Syndromes .............................................. 283
Plastic and Reconstructive Surgery ................ 284
Accident Compensation Corporation (ACC) . 284
230 4
th
and 5
th
Year Notes
History
HPC:
When it started: gradual, injury (nature of injury, did it swell straight away, after a day etc)
Arthralgia: joint pain without swelling
Arthritis: pain and swelling
What‟s happened till now: gradual, fluctuating, etc
Now:
Site, character, radiation, aggravating and relieving factors
Include:
Morning stiffness, and how long it lasts (classically inflammatory arthritis)
Effect of rest and exercise
Sequence of joint involvement
Severity:
Activities of daily living – what can‟t they do that they would normally do, use of aids and
appliances
How far can you walk
Night pain: is it keeping them awake (always consider neoplasia and infection)
What treatment have they tried: NSAIDS, orthotics, physio, etc
Other features if inflammatory arthritis:
Systemic: Raynaud‟s phenomenon, rash, fever, fatigue, weight loss,
Eyes:
Dry eyes and mouth ( ?Sjogren‟s syndrome)
Red, painful eyes ( ?iritis in seronegative arthritis), conjunctivitis in Reiter‟s
GI: diarrhoea (eg inflammatory bowel disease, scleroderma), mucosal ulcers (eg SLE)
Skin: psoriasis, nodules (rheumatoid), ulcers
Genito-urinary: dysuria, genital ulcers ( ?Reiter‟s)
Lungs: eg Pulmonary fibrosis in systemic sclerosis, ankylosing spondylosis
Kidney: eg Gout
Heart: Rheumatic fever,
PMH
Surgery: any operations
Medical: any medical problems, especially diabetes, asthma, heart and lung disease
Also childhood arthritis
Sexually transmitted diseases, especially non-specific urethritis and gonorrhoea
Drugs, side-effects and allergies (including what the allergy does to them)
Family history:
Especially rheumatoid arthritis, gout, primary osteoarthritis, sero-negative spondyloarthropathies
and inflammatory bowel disease. Note age of onset and outcome
Also Developmental Dysplasia of the Hip
Social:
Always ask about occupation: any potential causes or implications of impaired function
Living situation: who else at home, any family living nearby, steps, etc
Systems review: mainly cardiovascular, respiratory and GI. Also urinary stream in a male with a hip
problem (fix the prostate first, otherwise operation urinary retention catheter infection
dynamite to a recent hip replacement)
Exam
General inspection: observe them closely as the walk into the room – pain, gait, getting out of chair
Joints: gait, look, feel, move
Gait
Inspection:
Need to expose the patient (discretely watch them taking of their clothes – eg undoing
buttons), including the joint above and below. Have sheets available to cover the patient.
Ensure adequate lighting
Compare left with right
Look from outside in:
Musculo-skeletal 231
Skin: scars, redness, swelling, hairs, rashes (eg psoriasis)
Soft tissue: swelling
Muscle: wasting chronic disuse, surrounding inflammation or nerve damage
Bone and joint: deformities – usually a sign of destructive arthritis, also subluxation and
dislocation
Other inspection: eg nails
Palpation:
Warmth
Tenderness (watch their face)
Evidence of:
Synovitis: soft and boggy swelling
Effusion: can shift within the joint
Bony swelling (eg osteophyte formation or subchondral bone thickening): hard and
immobile
Move – Range of movement:
Better information from passive rather than active movement
Fixed Flexion Deformity = Limited extension
Fixed Extension Deformity = Limited flexion
Stability: attempt to move the joint in abnormal directions
Joint crepitus: grating sensation or noise from the joint
Measure angles with a goniometer. Anatomical position = 0
To finish:
Special tests
Joint above and below
Distal pulses
Neurology
Xray and/or aspirate
Think: acute, chronic, impact on function, systemic effects
Is it broken?
Can they walk/use it at all? If they can hobble, fracture less likely
Bony tenderness increases likelihood of fracture
Radiology
Check name and date
Check quality and that film covers the pathology you want
Rules of 2
ALWAYS take 2 views at 90%
Include 2 joints: one above and one below:
Especially in paired bones of arm and leg. If there is a fracture with shortening, there will also be
dislocation
Need to assess rotation relative to joint
Sometimes need to Xray 2 times. Eg May not see a scaffoid fracture until 10 – 14 days later (will see it
with a bone scan after ~ 24 hours)
Sometimes need to do opposite side to get a good idea of normal – especially if dealing with a
complicated joint in a child with lots of epiphyseal plates around. Don‟t do it routinely due to
radiation
Describing a fracture
Which bone
Site (where on the bone):
For a femur it can be capital (through the head), subcapital (below the head), transcervical (through
the neck), intertrochanteral, supracondylar, at the junction of the proximal and middle thirds, etc
Diaphysis: mid-portion or shaft of a long bone. Outer cortex and inner medulla
Epiphysis: Ends of long bones
Metaphysis: rapidly growing trabecular bone underlying the growth plate
232 4
th
and 5
th
Year Notes
Type:
Greenstick: only the convex side of the injured cortex is disrupted, transverse fracture. Only in
kids (higher collagen content and less mineralisation). Can also present as:
Bowing of a long bone
Buckle: fracture around the epiphysis if the force was along the axis of the bone
Transverse: force at 90% to bone ie direct blow ( also soft tissue injury). Stable when reduced
Oblique: force at 90% while weight bearing (net vector is oblique). Slips out of reduction
Spiral: rotatory force – twisting. Don‟t need big force
Comminuted (> 2 pieces)
Epiphyseal: described by Salter-Harris Classification: from I to V (most complex). II most
common (break through epiphysis with a small chip of bone)
Intra-articular
Segmental: 2 breaks separated by a section of normal bone. Big force required
Stress: fractured bone trying to heal itself and refracturing, etc. May be visible on X-ray, will be
visible as a hot spot on bone scan
Avulsion: ligament tears off bone
All fractures can also be:
Pathological
Simple or compound (bone communicates with air). If compound then Gustilo Classification from
I (minor) to III (extensive)
Further description of the fracture: LARD
Length: is it shortened or distracted (lengthened, eg soft tissue falling into the gap at the time of
impact)
Angulation: degree and direction. Described as the distal relative to the proximal portion when in
the anatomical position. Medial is varus, lateral is valgus
Rotation
Displacement/Translation: are the two ends aligned? Range from 0 to 100% displaced, and
direction of displacement
Associated symptoms: eg
Compound wound (eg may see air in soft tissue)
Compartment syndromes
Foreign bodies, etc
Types of joint injury:
Sprain: tearing of ligaments
Subluxation: partial loss of congruity of the articular surfaces
Dislocation: complete loss of congruity of the articular surfaces
Fractured dislocation
Fractures
Management of Fracture of the extremities
Immediate assessment:
Straighten any displaced fracture to allow adequate blood flow
Examine for fractures
Examine for dislocations
Compartment syndromes
Look for vascular injuries: Hard to assess for vascular injuries when SBP is less than 90 mm Hg
Look for nerve injuries
Goals of fracture management:
Upper limb: restore function
Lower limb: obtain and maintain alignment restore alignment, angulation, rotation and length
Principles:
Reduce severe deformity as soon as possible if it is causing soft-tissue or neurovascular
compromise
Open fractures antibiotics
Assess for conservative or surgical treatment
Management is a tension between immobilising it long enough to enable union, and short enough
to stop stiffening/arthritis of immobilised joints
Musculo-skeletal 233
Methods:
Immobilise. However, casting muscle atrophy, stiff joints, OA, DVT
Reduction: by manipulation, traction or open reduction
If it involves joint articulations: open reduction and fixation (especially if displaced) so that early
movement can occur, otherwise secondary OA
Internal fixation: plates, nails (Kuntscher) or wires (Kirschner)
External fixation: screws into bone with external bracing
Rules for manipulation to obtain closed reduction:
If you manipulate, then re-xray now
Review early (eg after 1 week). Can‟t re-manipulate after this should that be necessary
Indications for surgery:
Failure to obtain or maintain closed reduction, or where closed reduction has high failure rate (eg
fractured neck of femur)
Intra-articular fracture (especially if > 1mm displacement after reduction). Failure to operate leads
to:
Short term: irritant effect of synovial fluid non-union
Long term: pain, arthritis, instability
Arterial compromise
Open fracture
Pathological fracture
Multiple injuries
Segmental fracture
Risks of surgery:
Soft tissue damage
Wound healing
Anaesthetic risks
But potentially quicker recovery
Healing of Fractures
Stress fractures occur in:
The elderly with osteoporosis
Metabolic bone disease
Very active runners/sports people (eg tennis, squash)
Never in kids
Factors improving remodelling:
Young age
Long bones (for example, cf carpal bones)
Close to growth plate
If angle is in the principle direction of movement (ie posterior or anterior angulation of the radius,
given this is in line with flexion and extension of the wrist)
Factors impairing healing:
Movement
Non-union
Infection
Poor blood supply
Comminuted
Rule of thumb for fracture healing:
Upper limb: 4 – 6 weeks (kids at shorter end, adults at longer end, etc)
Ankle: 6 weeks (close to a joint so want to mobilise early)
Tibia and femur: up to 12 weeks
Other specific times for some fractures
When to mobilise:
Stable fractures should be mobilised soon
Unstable fractures should be stabilised before mobilising
Patient advice:
If the limb distal to a cast ever goes blue, becomes painful or tingles, elevate it for ½ an hour and if
no improvement return immediately (not the next day). Remove cast and assess for improvement.
If no improvement then urgent opinion

234 4
th
and 5
th
Year Notes
When to start mobilising
Complications of Fractures
Joint stiffness: Cartilage requires motion for nutrition. If held in one position risk of cartilage
deterioration
Delayed Union:
Presents as pain + movement at fracture site with stress
Normal union times
Upper Limb
Lower Limb
Callus Visible
2-3 weeks
2-3 weeks
Union
4-6 weeks
8-12 weeks
Consolidation
6-8 weeks
12-16 weeks
If these times prolonged “delayed union” is likely
Causes: Severe soft tissue damage, inadequate blood supply, infection, insufficient splintage,
excessive traction
Clinically: site tender, painful if subjected to stress, x-rays still show visible line
Treatment: needs to be reviewed if no bridging callus by 3 months. Need internal fixation and
bone grafting
Non Union:
Non-union is likely if delayed union is not treated
Presents as non-painful movement at the fracture site
Causes: Too large a gap (bone missing, muscle in way), interposition of periosteum
Clinical: Painless movement at fracture site. Xray shows smooth and sclerosed bone ends or
excessive bone formation
Treatment: Not all cases need treating eg scaphoid, otherwise fixation and bone grafting necessary.
Infection in open fractures:
Osteomyelitis, slow union and increased chance of refracture
Clinical: History of open fracture or operation on closed fracture. Wound inflamed. Systemic signs
of fever
Treatment: All open fractures require prophylactic antibiotics and excision of devitalised tissue. If
acutely infected, surrounding tissues should be opened and drained + antibiotics.
Malunion:
When bone fractures join in an unsatisfactory position i.e. unacceptable angulation, rotation or
shortening
Aetiology:
Failure to reduce a fracture adequately
Failure to hold reduction while healing proceeds
Gradual collapse of comminuted or osteoporotic bone
Signs and symptoms: Usually obvious eg. Unusual bone alignment, x-ray
Treatment:
If detected before union complete angulation may be corrected by wedging of plaster
Forcible manipulation under anaesthetic
Osteotomy if union complete and deformity severe
Compartment Syndrome:
Elevated pressure in an enclosed space (eg muscle compartment) can irreversibly damage the
contents of that space (eg ischaemia)
Major causes: Processes constricting the compartment or increasing the contents of the space:
Compressive bandages
Tight cast
Haemorrhage and oedema after fracture
Closure of fascical defects
Muscles once infarcted are replaced by inelastic fibrous tissue (eg Volkmann‟s Ischaemic
Contracture of the forearm compartment after humeral supracondylar fracture). Most sensitive test
is passive extension of the muscles. Can still have arterial flow through the compartment while
muscles are becoming ischaemic
Signs and symptoms (The 5 p‟s i.e.):
Pain
Paraesthesia
Musculo-skeletal 235
Pallor
Pulselessness
Paralysis
Diagnosis: Pressure > 30 – 40mmHg (using needle manometer etc) and/or MRI
Treatment: Remove bandages, etc, consider decompression with a fasciotomy if pressure high,
with wound left open for 5 days
Avascular Necrosis:
Aetiology
Rare
Focal subchondral infarction collapse of necrotic segment joint deformity arthritis
Common in bones that derive most of their blood supply from the medullary cavity
Mainly femoral head, also knee, scaphoid, head of talus
Gross: infarct is yellow, opaque and chalky with rim of hyperaemic fibrous tissue
Causes:
Trauma (eg subcapital fractured neck of femur)
Secondary to corticosteroid treatment
Nitrogen embolisation in divers ( Bends Caisson disease)
Sickle cell disease
Alcoholism
SLE
Infective endocarditis
Radiation
Diabetes mellitus
Signs and symptoms:
Joint stiffness
Pain in or near joint
Local tenderness
Restricted movement
Other complications of fractures:
Venous thromboembolism: injury patients are at risk due to immobility, leg injury, etc
Skin necrosis
Pressure sores
Fat embolism: typically day 3 – 10. Confusion, sudden SOB, hypoxia. Immediate ICU
management
Charcot‟s Joint = neuropathic joint:
Causes: diabetic neuropathy, tabes dorsalis, cauda equina, leprosy
Gross disorganisation of the joints (even dislocation) following repeated minor trauma recurrent
stress fractures that aren‟t felt due to neuropathy
Soft Tissue Injury
Prevention of Sport Injuries
Proper warm up
Cooling down
Protective equipment
Good technique and sensible training schedules
Ligament Injuries
Sprain: partial tear of ligament or joint capsule but the joint is still stable. Site of tear is tender and
there may be bruising. Symptomatic treatment and protection from stress until healing is complete
Partial Rupture: If rupture is incomplete, treat conservatively (ranging from rest and analgesia to
casting for 6 weeks). Recurrence common
Complete Rupture: Poor healing as scar tissue is not as tough as the ligament. May attempt surgical
repair – but it may not help
Tendon Injuries
Due to sudden, violent contraction
Most common is Achilles Tendon Rupture. See Lower Leg and Foot Injury, page 257
236 4
th
and 5
th
Year Notes
Can also rupture long head of biceps and supraspinatus
Other tendon injuries:
Paratendonitis: Inflammation due to friction of the paratendon (fatty tissue in the fascial
compartment through which a tendon runs). Usually Achilles or wrist tendons. Try good footwear
or rest in a splint. Steroid injection (but not into the tendon itself) may be effective. NB steroid
injections around the Achilles are controversial – may weaken the tendon
Tendonitis: irritation/tearing of fibres due to repeat trauma. Pain worse on contraction. Rest +
NSAIDs
Frost Bite
Formation of ice-crystals in the skin and soft tissues when temperature < -3 ºC
Presentation: tissue is pale, grey, and doughy – or frozen solid. May develop without person knowing
Treatment:
Warm slowly – this will be painful
Blisters may form over several days. May develop blackened shell as blisters burst
Dry, non-adherent, strictly aseptic dressings and prevention of further trauma (tissues are numb)
Recovery takes weeks. Surgery may be required
Contusion
Characterised by direct trauma to a muscle group with subsequent pain and swelling due to bleeding
within the muscle
Management:
Rest, ice, mild compression and elevation to control swelling, bleeding and pain
Intermittent icing for up to 48 hours
Maybe NSAIDS – but may increase the bleeding
Exclude other injuries, including compartment syndrome
Once swelling has settled, aim is to restore function, beginning with gentle isometric muscle
exercises
Lacerations
Torn, ragged wound
Treat for bleeding: expose wound to assess for blood loss, cover, direct pressure, elevate, pad and
bandage
If severe then sutures. However, muscle divided transversely will not hold sutures well enough to stop
muscular contraction pulling the edges apart
Enthesitis
Inflammation at the site of attachment of bone to a tendon, ligament or joint capsule
Elbow: See Tennis and Golfer‟s Elbow, page 246. Treatment: rest and strapping. Steroid injection if
severe
Plantar Fasciitis:
Insertion of the tendon into the calcaneum
Pain on standing and walking
Is isolated, or with sero-negative arthritis
Treatment: heel pads, reduced walking, steroid injection
Chronic Compartment Syndrome
Caused by tissue pressure in a closed fascial space circulation to muscles and nerves
Presentation: pain or deep ache over compartment. Usually after prolonged exercise. Usually bilateral.
May have palpable muscle hernias
Diagnosis: difficult. Elevated pressure within the compartment during/after exercise with slow return
to resting pressure
Treatment: decrease exercise ( muscle bulk) or elective fasciotomy (can affect muscle strength)
„Shin Splints‟: Shin soreness in unfit runner: can be due to a combination of muscle tears, mild anterior
compartment syndrome or stress fracture
Causes of Non-traumatic Limb Pain
Muscle disease: polymyositis, polymyalgia rheumatica, tendon inflammation, compartment syndrome
Bone disease: osteomyelitis, osteomalacia, osteoporosis, tumours
Vascular disease: Arterial or venous (eg DVT)
Musculo-skeletal 237
Neuropathy: nerve entrapment, neuropathy
Nerve Injury
See Common Peripheral Nerve Lesions, page 123 for common peripheral nerve injuries
Types:
Neuropraxia: transient loss due to external pressure
Aconotmesis: loss of function for weeks/months due to more severe compression. No loss of
neuronal continuity
Neurotmesis: nerve division. No recovery without surgical repair
Mechanisms: Division, stretching, crushing, ischaemia alone or in combination
Common sites:
Upper Limb:
Median nerve: hand through window
Ulnar nerve at elbow: fracture or pressure
Radial nerve: cuts around the elbow
Digital nerve: finger cuts
Brachial plexus: Downward pressure at the shoulder damages the upper cord, upward pressure
damages lower cord
Cervical nerve roots: compression of vertebrae
Lower Limb:
Common peroneal nerve: damage at the neck of the fibula
Lumbar nerve roots: prolapsed discs
Sciatic nerve: hip dislocation
Management:
Immediate primary suture: if clean cut
Secondary suture: Clean and debride then suture two weeks later
Cable Grafts: if long area of damage: graft from another nerve
Back and Neck
Spondylosis = degenerative
Spondylitis = inflammatory
History
Onset
Where is it situated
Sudden or gradual
Radiation
Aggravated by movement, coughing or straining
Effect of rest
If musculoskeletal then usually well localised and aggravated by movement
If progressive and unremitting consider osteoporosis (with crush fractures), osteomalacia, or neoplasia
(secondaries, leukaemia or myeloma)
General health, weight loss, fever, sphincter disturbance
Exam
Inspection
Look at belt line: is the pelvis horizontal.
Scoliosis:
If postural (eg do to a short leg) will correct when sitting down.
If pathological will hump to one side when they bend forward
Dominant hand will usually have a lower shoulder (“Which hand do you sign your name with?”)
Check shape, scars, lumps, muscles spasms, etc
Neck
Examination: Look while sitting
Feel. Place forearm against shoulder and fingers on forehead to stop them tensing when you push on
the spine. Feel down cervical spine
238 4
th
and 5
th
Year Notes
Test movement actively. Extension, flexion and lateral flexion normally 45º. Left and right rotation
normally 70º. If you need to measure, then measure from the sternal notch to the chin in each position
If neck pain, check neurology in arms
Thoracolumbar Spine and Sacroiliac Joints
Look for deformity – inspect from both back and sides. Look for scoliosis, eg from trauma,
developmental abnormalities, vertebral body disease (eg rickets, Tb) or muscle abnormalities (eg polio)
Feel each vertebral body for tenderness and palpate for muscle spasm
Gently tap spine with closed fist: severe localised tenderness suggest infection/tumour/trauma do x-
ray
Movement:
Flexion (touch toes), extension, lateral bending (slide hand down side of leg as far as possible
without bending forward)
Rotation: sit on stool (fixes pelvis) and rotate each direction
Schober‟s Test: for lumbar flexion. Make a midline mark at the level of the posterior iliac spine
(about L5). Make another mark 5cm blow and 10 cm above the first mark. Ask the patient to
touch their toes. An increase of < 5cm between the upper and lower marks limitation of flexion
Lasegue‟s Sign for lumbar disk prolapse: passive lifting of straight leg is limited by pain as Sciatic
nerve is stretched root pain
Palpate sacroiliac joints while they lie on their stomach
Special tests:
Heel/toe walking, squatting may reveal weakness
Measure limb girth for wasting
Nerve tension tests: straight leg raising, sciatic stretch, femoral stretch
Always test legs:
Neuro: sciatic pain, sensation, power, reflexes
Pulses
Abdominal: Is this a bleeding AAA? Pancreatitis radiating to the upper back?
Xray Interpretation (ABCS)
Alignment: anterior and posterior lines should be smooth curves
Bones: Assess each vertebrae – trace each round body. Processes and facet joint may be obscured.
Look for osteophytes
Cartilage and joints: discs should be similar and even. Facet joint dislocation only occurs in
association with severe damage to vertebrae
Soft tissue: disruption of shadows
Non-traumatic injuries very rarely have positive findings on plain X-ray
Neck and Radiating Arm Pain
Cervical Spondylosis
Spondylosis is the most common disorder of the cervical spine. Universal in patients over the age of 40
but seldom causes symptoms
Intervertebral discs degenerate and flatten (ie not synovial not OA)
Bony spurs appear at the anterior and posterior margins of the vertebral bodies. Posteriorly, these may
encroach upon the intervertebral foramina, causing pressure on the nerve roots
Clinical features:
Neck pain and stiffness, usually gradual onset and worse on getting up
Pain may radiate widely, to occiput, scapular muscles and down one or both arms
May be paraesthesia, weakness and clumsiness
Weakness of the legs or bladder disturbance suggest cervical cord compression
The appearance is normal. Tenderness occurs in the posterior neck muscles and scapular region,
all movements are limited and painful
Differential Diagnosis:
Thoracic Outlet Syndrome: pain in the ulnar forearms and hand
Carpal Tunnel Syndrome: pain and paraesthesia are worse at night. Nerve conduction is slowed
across the wrist
Rotator cuff lesions: pain is like one of a prolapsed cervical disc, but shoulder movements are
abnormal and there are no neurological signs
Musculo-skeletal 239
Cervical tumours: Symptoms are not intermittent and x-ray may be abnormal
X-ray: Cervical disc spaces are narrowed. Corners of vertebrae have osteophytes. Oblique views may
show encroachment of the intervertebral foramina
Treatment:
Heat and massage are soothing
Neck collar is the most effective treatment during painful attacks
Physiotherapy
Operation is seldom indicated but if necessary then anterior fusion is appropriate
Prolapsed Cervical Disc
May be precipitated by local strain or injury, esp. sudden flexion and rotation
May be a predisposition abnormality of the disc with increased nuclear tension
Prolapsed disc may press on:
Posterior longitudinal ligament, causing pain and stiffness
Nerve roots, causing pain and paraesthesia in one or both arms
Usually occurs above or below the 6
th
cervical vertebra, nerve roots are C6 and C7
Presentation:
Usually acute in onset and more severe than those of neck strain
Pain may be referred into the scapula, shoulder or hand and there may be associated paraesthesia
Differential:
Cervical spine infections, pain is unrelenting and local spasm severe, x-ray show erosion of the
vertebral end-plates
Cervical tumours, neurological signs are progressive and x-rays show bone destruction
X-rays may show slight narrowing of the disc space. Disc itself is best seen on MRI
Treatment:
Rest: in a collar to prevent unguarded movement
Reduce: traction may enlarge the disc space
Remove: if symptoms are severe enough the disc may be removed
Back Pain
Sources of Pain
Local: processes compressing or irritating nerve endings, e.g. fractures or tears. If it does not vary with
change in position then ?spinal tumour or infection
Pain referred to spine: arises from abdominal or pelvic viscera. Often unaffected by position of spine
Pain of spinal origin: Upper lumbar refers to groin or anterior thighs. Lower lumbar refers to buttocks,
posterior thighs or calves/feet
Radicular back pain: sharp and radiates from spine to leg in territory of nerve root. Coughing, sneezing
or voluntary contraction of abdominal muscles often elicits radiating pain. Increase pain in postures
which stretch the nerve root (e.g. sciatic nerve – L5 & S1 - when sitting as it passes posterior to hip, but
not femoral nerve – L2 – L3 as it passes in front of the hip)
Pain associated with muscle spasm: accompanied by abnormal posture, taut para-spinal muscles and
dull pain
Very hard to differentiate lower back pain cheat and call it lumbar spine dysfunction!
Classification
Pathological (5%): infection, inflammation, metabolic bone disease, neoplasm
Referred (5%): Abdominal or pelvic organs
Mechanical (95%):
Muscle/ligament injury
Intervertebral disc injury
Spondylolysis and spondylolisthesis
Age
Children: congenital or developmental disorders, infection, primary tumours (ie don‟t ignore back pain
in children)
Younger adults: disc disease, spondylolisthesis, acute fractures
Older adults: spinal stenosis, metastatic disease, osteopenic compression
240 4
th
and 5
th
Year Notes
Injuries
Hyperflexion wedge fracture around T12 – L 2
Shearing anterior or posterior displacement, intervertebral ligaments torn
Hyperextension: tears longitudinal ligaments, widens anterior disk space
Axial compression: squeezes T4 – L5 disc squeezes out and disrupts longitudinal ligaments
Spondylolysis: defect/fatigue fracture in the pars interarticularis. Most common cause of low back pain
in children and adolescents. Defect in the neck of the „Scottie dog‟ on oblique x-rays
Mechanical Back Pain
No obvious pathology – following trauma or progressive onset. But major cause of people off-work etc
Spinal movement is complex there are many components that could cause pain
Not related to old age: most common in 25 – 60 year olds
Patterns:
Disc Pain
Facet Joint Pain
Nerve Root Pain
Spinal Stenosis
Location of
pain
Worst in back.
May spread to
buttocks or legs
Worst in back.
May spread to
buttocks or legs
Mainly in legs,
may be some in
the back
Worst in the legs:
heaviness/aching
Pattern
Intermittent or
varying intensity
Always
intermittent
Usually constant
Intermittent,
occurs with
activity
Pain worse
with:
Sitting, bending
forward
Bending
backwards,
standing/walking
for long periods
Sitting and
bending, and by
backwards
movement if
acute
Worse with
activity
Pain better
with
Bending
backwards,
walking better
than standing
better than sitting
Bending forward
Lying face down,
or on back with
legs drawn up
Bending forward,
sitting
Exercises
Face down, push
up with hands
arching spine
Lie on back,
knees to chest.
Pelvic tilt (
tilt on walking)
Lie on back on
the floor with
knees over a
chair
Sit ups to
strengthen
abdominals
Lumbar Spondylosis:
Degeneration of joints and of intervertebral discs
Gel of nucleus pulposis shrinks and looses compliance causing circumferential bulging of annulus
fibrosis.
Osteophytes may form
Most common sites are L5/S1 and L4/L5
Facet joint syndrome – secondary osteoarthritis of the facet joints. Pain worse bending backwards
Presentation: midline pain radiating to groin or buttock, worse towards the end of the day,
aggravated by coughing or sneezing. Straight leg raising is normal
Treatment: analgesics, physio, spinal fusion
Acute lumbar disc prolapse:
Nucleus pulposis extrudes into a fissure in the annulus and bulges beneath the posterior
longitudinal ligament:
Pressure on ligament back ache
Pressure on dural envelope of the nerve root pain referred to lower limbs (sciatica)
Compression of nerve root paraesthesia and muscle weakness
Posture: stand forwards and sideways tilt
Sudden onset lasting for hours/days. Local tenderness and loss of spinal mobility
Differential:
Inflammation (eg due to Ankylosing Spondylitis or Tb)
Vertebral tumours constant pain
Nerve tumours cause sciatic but constant pain
X-ray to exclude bone disease. CT/MRI best for localising the lesion
Treatment:
Musculo-skeletal 241
Rest: most resolve spontaneously
Reduction: continuous bed rest and pelvic traction for 2 weeks
Removal: if cauda equina compression, persistent pain after 2 weeks or neurological
deterioration
Rehabilitation: isometric exercises and advice on bending/lifting
Spinal and root canal stenosis:
Due to progressive loss of disc height, OA of facet joints, posterior osteophytes
Rarely neurogenic claudication (nerve root ischaemia) when walking. Due to blood flow to
the cauda equina (whose metabolic needs on walking)
Differential of vascular and neurogenic claudication:
Activity
Vascular Claudication (no foot
pulse)
Neurogenic claudication
Walking
Distal proximal pain, calf pain
Proximal distal pain, thigh
pain, symmetrical, tingling nerve
pain
Uphill walking
Symptoms develop sooner
Symptoms develop later (leaning
forward opens facet joints
blood flow)
Rest
Relief with standing
Relief when sitting or bending
Bicycling
Symptoms develop
Symptoms do not develop
Lying flat
Relief
May exacerbate symptoms
Treatment:
Vascular bypass
Usually have foot pulses. Rest,
Decompressive laminectomy
Spondylolisthesis:
Anterior or posterior displacement of a vertebrae with or without preceding injury (usually L5
slides forward on S1)
Can be congenital (eg defect of articular processes) or acquired (trauma, OA of facet joints,
pathological, fracture of the neural arch, elongation of the pars interarticularis)
Requires bilateral interarticular defect instability
X-ray (AP and lateral) if:
< 20 years or > 50 years
Suspicious pain
Worse at night and in morning (inflammation, infection, tumour)
Neurological signs ( CT/MRI)
Management:
Conservative: lumbosacral support, exercises to build extensor and abdominal muscles
Surgery: Nerve release and spinal fusion
Other non-mechanical back-pain:
Sway Back: pregnancy: altered spinal posture and ligamentous laxity. Conservative treatment
Osteoporotic: painless or agonising localised pain that radiates around ribs and abdomen. Caution
with spine physio: mechanical lever arm forces on vertebrae are very strong easy damage
Psychogenic pain is a contributing factor in some. Look for signs of secondary gain
Localisation of Lumbar Root Nerve Entrapment
Nerve Root
Usual prolapse
Sensory Changes
Reflex Loss
Weakness
L2
L2/L3
Front of thigh
None
Hip flexor and
adductors
L3
L2/L3
Inner thigh & knee
Knee
Knee extension
L4
L4/L5
Inner calf
Knee
Knee extension
L5
L4/L5
Outer calf, upper
inner foot
None
Inversion, dorsiflexion
of toes
S1
L5/S1
Lateral borders/ sole
of foot
Ankle
Plantar flexion
Red Flags
Continuous or progressive pain which doesn‟t change with movement
Fever (e.g. infection)
242 4
th
and 5
th
Year Notes
Bowel/bladder involvement (sacral roots)
Also:
Young (< 20) or old (> 55)
Violent trauma: MVA or fall from a height
Bilateral or alternating sciatica
Weak legs
Weight loss
ESR
On oral steroids
IV Drug use
Pain with movement in all directions
Localised bony tenderness
Past history of neoplasia
CNS deficit at more than one root level or bilateral
If no red flags then investigations not indicated unless symptoms persist beyond 4 – 6 weeks
Yellow Flags
= Barriers to recovery
Problems at home or work
Management of Back Pain
Conservative:
80 – 90% of back pain resolves in 4 – 6 weeks
Firm bed (eg a board underneath)
No slouching, education on how not to stress back
Analgesia ( break cycle of muscle spasm)
No bed rest, early return to work
Warmth, analgesics
Promote self care and responsibility dependence
Stay active. Eg swimming. But may need to modify normal activities. Lift carefully, wear low
healed shoes, chair which helps good posture, pillow between knees at night, walking, cycling,
swimming
Exercises only help with symptoms – don‟t affect recovery time
Physio – but not while acutely sore
Manipulation may help in the first month
Advice on prevention
Check-ups at 1, 4 and 6 weeks (ACC guidelines)
If not improved after 2 weeks, consider X-ray, referral, etc
Other treatment:
Sciatic pain: epidural steroid injection
Surgery: remove disc protrusion, decompression or stabilisation
Pelvic Injury
Serious
Need to check all midline structures: rectum, bladder, urethra, also ureters, iliac vessels
Immediate risk is bleeding. Usually from iliac veins – retroperitoneal
Signs and symptoms of pelvic bleeding:
Shock (blood loss, visceral damage)
Bruising
Abrasions
Ecchymoses into thigh and perineum
Swelling of labia / scrotum, blood at urethral meatus
Abdominal tenderness
Pain
Investigations
X-rays essential: AP, inlet, outlet, oblique views. Always look for pairs of fractures
If anterior fracture then must also do x-rays of sacro-iliac joints and lumbar
Musculo-skeletal 243
Fractures
Structure and stability:
The stability of the pelvic ring depends on both the bony and ligamentous structures
The anterior position of the pelvic ring does not participate in normal weight bearing, nor is it
essential for maintenance of pelvic stability
The posterior arch (sacrum, sacro iliac joint and ilia) all serve as the weight bearing portion of the
pelvis
The posteriosuperior SI ligaments connecting the iliac tuberosities to the sacrum provide most of
the stability to the SI joints
Fractures may be unstable or stable (those that don‟t involve the pelvic ring or have minimal
displacement of the pelvic ring)
Types of fractures:
AP compression injury hinges the pelvis open onto the intact posteriosuperior S.I. ligaments. Not
grossly unstable
Lateral compression. Caused by direct force to iliac crests. May be stable or unstable
Vertical shear. Forces through femur directed perpendicularly to the pelvic ring. Causes disruption
to the S.I. joint / unimpacted fracture through the sacrum or ilium. Hemipelvis is unstable
If >1 fracture then pelvic ring is unstable and up to 25% will have internal injuries.
Treatment
Quick manoeuvre to bleeding: internally rotate femurs and tie a towel around the pelvis and pull
it tight
Most fractures are stable and can be treated conservatively
If unstable will require surgical stabilisation
Upper Limb
Shoulder
Exam
Look:
Compare both sides
Effusions not scene unless significant.
Look at each muscle group
If shoulder dislocated, there will be a convexity or flattening of the deltoid below the acromion
Feel:
For tenderness and swelling
Start at sterno-clavicular joint AC joint and corocoid process gleno-humeral joint spine of
scapula
Feel along groove between acromion process and head of the humerus for ligaments of teres
minor, infraspinatus and supraspinatus
Feel and look in axilla: lymph nodes, check soft tissues for swelling/tenderness
Move:
If active movement is reduced, try passive movement for the remainder of the normal range
Abduction: test with elbow flexed. Test passively from behind. Normal is 90º
Elevation: If done actively, possible to 180º. Thumbs facing forwards, arms straight. Look for
painful arch from 60 – 120º due to insertion of inflamed rotator tendons catching on the acromion.
Is it the same with the arm laterally or medially rotated? Checks for tendon impingement
Adduction to 50º across the front of the chest. Pain in full adduction if AC joint injury
External rotation: with elbow flexed to 90º, can externally rotate to ~ 60º. Good test of
glenohumeral joint (eg for frozen shoulder)
Internal rotation: Test actively: place hand behind back and scratch as high as they can. Compare
with good arm
Extension is possible to 65º
Testing Rotator Cuff:
Pain worst at 90º abduction
Supraspinatus: test abduction against resistance, especially from 0 - 30º (deltoid doesn‟t help
much in that range) with thumbs pointing to the ground (turns the glenoid tubercle forward
greater impingement)
244 4
th
and 5
th
Year Notes
Infraspinatus: externally rotate against resistance
Subscapularis: „Lift-off test‟: Hold hand behind back, with patient pushing out from their
back. Try and push them in (Pectoralis Major inactive in this position)
Teres Minor: hard to test in isolation
Check for stability:
Sulcus test: pull arm down and look for sulcus deep to the deltoid muscle (distracting the
gleno-humeral joint)
Anterior draw test: from the side, hold acromion and corocoid process between your thumb
and index finger, hold proximal humerus between the other thumb and forefinger and try and
push forward and backwards against each other
Apprehension test for dislocating shoulder: posterior pressure during elevation on an abducted
and externally rotated arm
Push-ups against the wall: look for winging of scapula seratus anterior dysfunction
Always examine neck and elbow (joint above and joint below) and distal pulses
X-rays:
Do AP and lateral obliquely – as scapular is oblique and don‟t want spine and other shoulder in the
lateral film
Can do an axillary film: abducted 90% and x-rayed from above
Differentiating:
Intra-articular disease painful limitation of movement in all directions
Tendonitis painful limitation of movement in one plane only
Tendon rupture and neurological lesions painless weakness
Referred pain:
Cervical root lesions (eg due to cervical spine lesions)
Brachial plexus, thoracic outlet syndromes
Referred pain from abdominal visera, diaphragm
Injury
Most frequently affected by non-arthritic conditions involving bursa and surrounding tendons:
tendonitis, bursitis, frozen shoulder
Frozen shoulder:
= Adhesive Capsulitis
Gradual onset of pain, pain at night, then stiffness as pain gradually subsides
May follow minor trauma
Active and passive movement in all directions, following minor trauma. Cause unknown – but
due to a tendonitis/capsulitis adhesion of capsule to the humeral head
Treatment: physio, mobilisation, NSAIDs, corticosteroid injection into subarcromial bursa
Prognosis: resolution may take years
Differential:
Disuse stiffness
Complex Regional Pain Syndrome Type 1
Rotator Cuff:
Humeral head is held in place by the rotator cuff muscles forming part of the joint capsule:
infraspinatus posteriorly, supraspinatus superiorly, teres minor and subscapularis anteriorly
Due to impingement of rotator cuff tendons under the coraco-acromial arch. May be due to
osteophytes or narrowing under the coraco-acromial arch
With age or injury the tendons of these muscles are prone to hyaline degeneration, fibrosis and
calcification friction, swelling and pain. Prone to rupture
Tendonitis of more than one tendon rotator cuff syndrome
Presentation:
Local tenderness over rotator cuff insertion
Supraspinatus tendonitis: the most common: pain on abduction of the arm
Subscapularis tendonitis: pain on internal rotation
Infraspinatus tendonitis: pain on external rotation
May be accompanies by bicepital tendonitis: pain on resisted forearm flexion and supination
and on pressure on the tendon of biceps in the bicepital grove
Treatment:
Conservative:
NSAIDs
Musculo-skeletal 245
Local injection of steroid with local anaesthetic to tendon insertion
Rest shoulder initially, in sling if necessary
Short-wave diathermy, ultrasound therapy to reduce pain
Exercise to lessen the risk of adhesive capsulitis or help restore movement
Surgical:
„Decompress‟ the rotator cuff
Excise the coraco-acromial ligament, anterior acromial process or any obstructive masses
Cuff reconstruction for large tears
Anterior dislocation:
Head of humerus anterior to the glenoid fossa:
Usually sub-glenoid (ie also inferiorly displaced)
Can rarely be subclavicular
Mechanism: arm abducted and externally rotated then hit from behind (eg tackle injury)
Clinical: Very painful. Patient holds arm at elbow to prevent any movement. Palpate under
acromion, is humeral head there?
Consequential injuries
Check axillary nerve (cutaneous sensation from axillary nerve palsy over regimental badge
area [over deltoid on upper arm] and action of teres major – medial rotator and adductor - and
deltoid – adduction)
Hill-Sackes lesion: injury to posterior of head of humerus
Bankart Lesion: injury to the anterior margin of the glenoid fossa
Reduction: Kocher or Hippocratic manoeuvres
Management: immobilisation in a sling for 2 to 3 weeks while structures anterior to gleno-humeral
joint heal (otherwise recurrence), then physio avoiding external rotation
Posterior dislocation:
Mechanism: Direct trauma from the front, electric shocks or Grand mal seizures
Head of humerus lies posterior to glenoid.
Clinical: Pain, deformity, local tenderness
Shoulder Instability: 2 types:
Atraumatic, multidirectional (ie generalised laxity), bilateral, treatment: rehab (Physio)
Traumatic, unidirectional/unilateral, Bankart Lesion (capsule at the front detaches from the
glenoid), Treatment: surgery. Progressively less traumatic force required to dislocate it. External
rotation causes apprehension
Fracture of Clavicle:
Mechanism: fall on outstretched hand
Clinical: arm clasped to chest to prevent movement, subcutaneous lump
Xray: usually middle third
Treatment: support arm in sling until pain subsides (2-3 weeks)
A/C Joint:
Mechanism: usually involves fall in which patient rolls on shoulder
Clinical: Outer end of clavicle prominent, local tenderness present. Confirm subluxation by
supporting elbow and detecting movement of clavicle downwards.
Clavicle is usually attached to the acromion by the ac joint, coroid ligament and trapezoid
ligament. In serious injuries all three of these areas can be damaged
Treatment: Broad arm sling for 4-6 weeks usually sufficient
Infantile Torticolis: Two types
Congenital shortening of sterno-mastoid muscle
Neurological: damage to the spinal accessory nerve from infected lymph nodes in the posterior
triangle
Brachial Plexus injury:
Erb‟s Palsy: C5, C6: paralysis of deltoid, supraspinatus, teres major, biceps Porter‟s tip position
Klumpke‟s Paralysis: C8, T1: arm in adduction, paralysis of small muscles of the hand. May also
be Horner‟s syndrome
Upper Arm and Elbow
Exam
In the elbow, look for:
Joint effusion
246 4
th
and 5
th
Year Notes
Lumps: rheumatoid nodules, gouty tophi, enlarge olecranon bursa
Feel: especially for tenderness over the lateral epicondyle (tennis elbow) or medial epicondyle
(golfer‟s elbow)
Move: Normal range is from 0 – 150. Limitation of extension early synovitis
Radiology of elbow:
If looking for effusion on an x-ray (eg blood in joint following fracture of the head of the radius)
look for protrusion of the Haversian fat pads in the coronoid and olecranon fossa radiolucent
triangles
Avulsion of the medial epicondyle in children: „Little leaguers‟ injury from pitching in baseball
Medial = Trochlear articulates with the ulnar (literally = „pulley‟)
Lateral = Capitalum articulates with the radius
Injury
Fracture of proximal humerus:
Mechanism: Fall on outstretched arm, most common in post menopausal women
Clinical: Appearance of large bruise on upper arm. Signs of axillary nerve or brachial plexus injury
should be sought. Exclude dislocation of the shoulder
Treatment: Sling. Begin mobilising early as pain permits: gentle arm swinging, climbing fingers
up the wall. If > 2 parts fractured, then surgery
Major complication: shoulder stiffness
Humeral shaft fractures:
Most treated conservatively – u-slab, collar and cuff, sling, brace, etc.
Complication: risk of radial nerve injury in spiral grove
Supra-condylar fracture of the humerus:
Eg child falling onto outstretched hand.
Radial pulse may not return for 24 hours
Can lead to Volkmann‟s Ischaemic Contracture due to disruption to the brachial artery. Muscle
necrosis (especially FPL and FDP) flexion deformity at elbow and wrist. Arm is blue, there is
no radial pulse and passive finger extension is painful (the key sign)
Cast in < 90º flexion
Fractured Head of Radius:
Mechanism: fall on outstretched hand forces elbow into valgus. Common in adults
Clinical: Painful rotation of forearm, tender on lateral side of elbow
Treatment: Sling
Fractures of Olecranon:
Mechanism: Direct blow or fall on elbow causes a comminuted fracture. Clean transverse break is
due to traction when patient falls on hand whilst triceps contracted (attaches to olecranon)
Clinical: Graze or bruise over elbow. With a transverse fracture there may be a palpable gap and
they are unable to extend elbow against resistance
Treatment: Undisplaced transverse needs immobilisation in cast at 60 degrees flexion for 2-3
weeks then exercises begun
Pulled Elbow:
Mechanism: Radial head stretching annular ligament and slipping out from under its cover.
Usually kids 2 – 6 years old when parents have pulled on child‟s arm (esp when crossing road)
Clinical: Tenderness over lateral aspect, supination limited
Treatment: Sling, usually results in spontaneous reduction
Tennis Elbow: enthesitis of the common extensor origin on the lateral epicondyle of the humerus
pain on contraction/stretching of the forearm extensors. Management: rest, physio, NSAIDs in the
early stages, steroid injections, surgery later on
Golfer‟s Elbow (or any throwing sport): Enthesitis of the common flexor origin on the medial
epicondyle
Ulnar Nerve Entrapment:
Fracture at elbow or prolonged or recurrent pressure on the ulnar nerve compression of the
nerve in the cubital tunnel
Presentation: wasting of the ulnar innervated muscles (hypothenar eminence and the interossei)
with sensory loss in the little and ulnar side of 4
th
fingers
Treatment: Decompression
NB: Deep motor branch of the ulnar in the hand can be damaged by recurrent pressure from tools
(screw-drivers, handlebars, crutches, etc)
Musculo-skeletal 247
Forearm and Hand
Exam
Naming:
Don‟t number fingers, name them: thumb, index, middle, ring and little
Don‟t describe structures as medial or lateral, use radial and ulnar
Palmar surface of hand = volar
Always examine whole hand and compare with other hand
Inspection:
Work from wrist to finger tips
Fingers: ulnar deviation, palmar subluxation, joint swelling
Nails:
Psoriasis: pitting (small depressions in the nails), oncyholysis (white across distal, lateral or
proximal portion), hyperkeratosis (thickening of the nail), transverse nail ridges („tide marks‟
– signs of previous inflammation)
Splinter haemorrhages in rheumatoid arthritis and SLE
Rheumatoid vasculitis: small, periungual brown spots
Periungual telangiectases in SLE, erythematosus and scleroderma
Palpation and passive movement together: tenderness, swelling, osteophytes, laxity
Function:
Grip strength: squeeze two fingers. Squeeze a partly inflated sphygmomanometer
Key grip: try and pull thumb and forefinger apart
Opposition: try and pull thumb and little finger apart
Functional test: undo a button, write with a pen
Testing nerves:
Want to test intrinsic muscles that have no extrinsic help
Ulnar Nerve (Medial cord, C8, T1)
Abductor of little finger
Adductor pollicis: grip paper between thumb and side of index finger and try and pull it away.
If they bend the thumb, they‟re trying to use flexors to help (ie fail the test)
Lumbriacls: flex MCP and extend IP joints. Ulnar does ring and little finger
Ulnar claw hand: hyperextend the fingers and the ring and little fingers curve forward due to
lack of lumbriacls
Median Nerve (Lateral and Median Cords, C6,7,8,T1):
Opposition of thumb to little finger: requires median eminence. NB opposition of the thumb
requires flexion, abduction and rotation
Abduction of thumb: Abductor pollicis brevis and longus (other two muscles of thenar
eminence can be ulnar)
Anterior Interosseus Nerve Compression: compressed under the fibrous origin of flexor
digitorum weakness of FPL, pronator quadratus and flexor profundus to the index and
middle fingers „Benediction Hand‟ when they try and make a fist.
Radial Nerve (posterior cord, C5,6,7,8):
Check back of first web space (between thumb and index finger). Only sensory area reliably
supplied by radial nerve
Motor distribution:
Upper arm: triceps
Proximal to supinator, this branch innervates ECRL, ECRB, brachioradialis, supinator
Distal to supinator tunnel: EI, ECU, APL, EPL, EPB
Posterior Interosseus nerve compression: passing through supinator muscle. Weakness of
the long finger extensors, short and long thumb extensors but no sensory loss.
Sensory distribution: Terminal part supplies the dorsum of the hand. Posterior Cutaneous
branch supplies a variable area on the back of the arm and forearm
Common sites affected: axilla (eg pressure from crutches), midhumeral fracture, at and below
the elbow (dislocations and Monteggia fractures)
Testing ligaments:
Ligaments: test like knee. Opening to the sides, forward and posterior displacement when fully
flexed and then when not quite fully flexed
Of flexor pollicis longus: hold proximal phalanx of thumb and flex the end
248 4
th
and 5
th
Year Notes
Of flexor digitorum profundus: hold middle phalanx and flex distal phalanx
Of flexor digitorum superficialis: hold other fingers in full extension, hold proximal phalanx of
middle finger, flex finger and distal phalanx should be floppy
Of extensor pollicis longus: can rupture after a Collies fracture can‟t straighten distal thumb
(Mallet Thumb)
Napier‟s ligament: anterior over the 1
st
CMC joint
Injuries
Fractures of Radius and Ulna:
Mechanism: occur commonly in road accidents, direct blow causes transverse at same level.
Twisting may cause spiral or oblique fractures at different levels
Clinical: Fracture usually obvious. Pulse must be felt and hand examined for circulatory or neural
defects.
Treatment: Kids only need cast for 6-8 weeks. Adults often require internal fixation.
Fractures of either the radius or ulna alone, with shortening (ie angulation or displacement) are
associated with dislocation of the other:
Monteggia Fracture:
Fracture to ulna and dislocation of radial head
Mechanism: fall on hand, body twisting at time of impact
Clinical: Ulnar deformity obvious, but dislocation may be masked by swelling. Look for
pain and swelling on lateral side of elbow. Wrist and hand must be examined for signs of
injury to radial nerve
Treatment: Restore length to ulna then reduce. Above elbow cast, arm at 90 degrees
flexion 6 weeks
Galeazzi Fracture:
Fractured radius and subluxation or dislocation of distal radio-ulnar joint
Clinical: more common than Monteggia, important to check for ulnar nerve injury
Treatment: As for Monteggia
Colles' Fracture:
Fracture of the radius within 2.5cm of the wrist with dorsal angulation/displacement. If
displacement occurs the classic dinner fork deformity occurs.
Mechanism: Most common fracture resulting from a fall on the outstretched hand. Sometimes
TFCC (Triangular Fibrocartilage Complex) is torn therefore disrupting the distal R-U joint and
causing ulnar angulation also
Clinical: Pain and tenderness over distal end of radius after a fall. Deformity and radiology
also often definitive
Treatment: If displaced then reduce, plaster cast in ulnar deviation and slight flexion for 5-6
weeks with finger and wrist exercises
Complications: Radial drift or ulna prominence in mal union. Delayed rupture of tendon of
extensor pollicis longus due to roughness at site of injury or decreased blood supply ( Mallet
thumb). Carpal tunnel syndrome also possible
Smith‟s Fracture: Due to fall on the back of hand. Reverse of Colles fracture (ie volar displacement
rather than dorsal)
Barton‟s Fracture: Intra-articular fracture of the distal radius. Unstable
Distal Radio-ulnar joint:
Triangular ligament (TFCC): holds radius in place while it rotates around the ulnar
Test for dislocation: grip around the proximal wrist and squeeze or supinate pain
Scaphoid fractures:
Rare in skeletally immature children
2
nd
in occurrence to radial fracture – usually young adult males
Waist of scaffoid the most common site
Caused by fall on radial side of outstretched hand land on tubercle of the scaffoid with wrist
hyper-extension
Blood supply is distal to proximal pole prone to avascular necrosis or poor healing
If suspected treat as a fracture, immobilise joints above and below (i.e. Collies cast, with thumb
free, up to 10 weeks to healing) – may not see it on first Xray and prone to non-union. Can see on
bone scan after about 1 day. However, over diagnosed.
Musculo-skeletal 249
Carpal dislocations:
Perilunate dislocation: associated with distal radius fracture. Lunate stays attached to radius, all
other carpals pushed dorsally
Trans-scaphoid perilunate dislocation: as for perilunate dislocation, but fracture through the waist
of the scaphoid leaves the proximal fragment in place. Treatment: reduction/surgery
Metacarpal Fractures:
5
th
most common. Treatment: Buddy strapping, or strapping + slab
1
st
metacarpal: Bennett‟s Fracture – through middle of the metacarpal and intra-articular through
the 1
st
CMC joint. Following a fall or blow on a clenched fist or forced abduction of the thumb
(skiers). Ligament of Napier can commonly be injured as well. Unstable as oblique and proximal
fragment is attached to trapezium and distal fragment has strong muscles attached to it that pull it
proximally. Reduce and plaster with thumb held abducted and extended. Transverse fracture is
straightforward: Scaphoid cast
Multiple metacarpal fractures: twisting and crush injuries. Realignment with Kirschner wires or
small bone plate
MCP dislocation. Uncommon. May require open reduction
Finger injuries:
Mallet Finger: can‟t extend DIP: rupture or avulsion of extensor tendon, eg by ball hitting
outstretched finger. If < one month since injury then splint in extension otherwise surgery (but
may not get full flexion back)
Button Hole (Boutonniere) Deformity: can‟t extend PIP joint of finger and hyperextension of DIP:
Rupture/detachment of central slip of extensor tendon with lateral bands slipping down the side of
the finger
Trigger Finger (Stenosing Tenosynovitis): flexor tendon inflames and then jams going through the
A1 annular pulley over the MP joint (under the palmar crease). May find crepitus, swelling,
triggering and tenderness. Common in RA. Treatment: cut the A1 pulley
De Quervain‟s Syndrome. Pain over the styloid process of the radius (dorsal wrist). Finckelstein‟s
sign: pain on forcible adduction and flexion of the thumb into the palm. Stenosing
tenosynovitis/inflamed tendon sheath of extensor pollicis brevis and abductor pollicis longus.
Management: Rest, NSAIDs, cortisone injection, surgery
Skiers/Gamekeeper‟s Thumb: rupture of the ulnar collateral ligament of the MCP joint of the
thumb, caused by forced abduction. If stable then splint. If unstable (can‟t oppose fingers) then
repair (adductor tendon may get in the way and prevent reattachment)
Dislocation of the phalanges: usually always ligament injury as well. Swelling may take up to 2
years to reduce. Reduction can be spontaneous or via longitudinal traction. Buddy strapping +
early mobilisation
Phalangeal fractures: Buddy taping: encourage flexion, deny rotation, allow for swelling (ie not too
tight)
Dupuytren‟s Contracture: Painless fibrosis of the palmar aponneurosis (can also occur on the foot).
Usually familial (associations with alcoholism and manual work over-rated), anti-epileptics. Causes
puckering of the skin over the distal palmar crease and gradual flexion of the fingers (usually starts
with ring finger). Treatment conservative. If they can‟t push their palmer MCP joints into the table
then consider surgical release. Prognosis worse if younger
Ganglia: Painless, jelly filled swelling caused by a partial tear or bulging of a joint capsule. Commonly
in the wrist. May resolve or cause little trouble. Don‟t respond to injection. Surgical excision.
Carpal Tunnel Syndrome
Compression of the median nerve as it passes through the carpal tunnel in the wrist
Epidemiology: Common. Usually women 3 - 50 years
Causes: Due to thickened tendons or synovitis in the carpal tunnel
Rheumatoid arthritis
Hypothyroidism
Acromegaly
Pregnancy (2
nd
ary to oedema)
Obesity
Amyloid
Diabetes Mellitus
Idiopathic
Symptoms: Pain/tingling in the hand and wrist classically in the median nerve distribution (palm and
thumb, index and middle fingers). Wakes at night, shakes hand, can‟t get it comfortable
250 4
th
and 5
th
Year Notes
Signs:
Wasting of thenar eminence, weak thumb abduction and opposition (late signs).
Tinel‟s Test: pain is reproduced by tapping a tendon hammer over the carpel tunnel
Flex both wrists for 30 seconds – may precipitate paraesthesia if carpal tunnel syndrome: Phalen‟s
Test
Investigations: median nerve conduction velocity test
Treatment:
Light splint to hold wrist in slight dorsiflexion, NSAIDs and vitamin B6
Diuretics
Corticosteroid injection
Surgical Decompression
Lower Limb
Gait
Components of Gait
Aim of gait is to keep the body‟s centre of gravity travelling in smooth line energy
Gait consists of a:
Stance phase (60% of the cycle):
Heal strike: Forefoot not yet in contact. Knee in full extension. Quads contract to prevent
buckling of the knee
Foot Flat: Dorsiflexors slowly relax to bring foot to ground, and hip extensors propel body
forward
Mid stand: body directly over ankle
Heel off: Triceps surae contract
Toe off: Hallucis and flexor digitorum longus contract
Swing phase (40% of the cycle):
Acceleration: iliopsoas contracts (flexes hip), passive knee extension, dorsiflexors contract so
foot clears the ground
Mid swing
Deceleration: hamstrings stop hyper-extension of the knee and gluteus maximus slows hip
flexion
Double stance: both feet on ground for 20% of the cycle when walking. When running this %
reduces to 0% (ie swing > 50% of cycle so both feet off the ground at some point)
Abnormalities of Gait
Causes a limp
The main causes of abnormal gait are:
Pain Antalgic gait (non-specific). Pain shortened stance phase on affected leg, shortened
swing of opposite leg
Weakness
Joint abnormality
Usually noticed during stance phase when one leg is bearing the body‟s weight
Swing phase:
Abnormal heel strike due to:
Pain in hind foot (so land on forefoot)
Quad weakness: Knee won‟t extend by itself, so lands flexed and at risk of buckling. Use
hand to push thigh posteriorly (foot and hip fixed so backward pressure on distal thigh stops
the knee collapsing). May also land on mid foot
Foot Slap Gait: during foot flat phase: weakness of dorsiflexors foot slaps to the ground rather
than controlled lowering
Mid-stance:
Back-knee Gait: due to:
Fixed plantar-flexion deformity of the ankle: Can‟t dorsiflex ankle above neutral so
compensate with knee hyper-extension of the knee (slight flexion is normal)
Quad weakness: Use hyperextension of the knee to lock the leg straight, rather than quads
holding the knee in extension
Musculo-skeletal 251
Abductor muscle action: Either weakness (disuse, polio, L5 lesion) or because use puts
pressure across the hip joint pain if hip pathology:
Abductor Lurch or Gluteus Medius Gait: Lateral shift of the trunk over the sore hip in
stance, rather than use abductors
Trendelenburg Gait: Other hip sags excessively due to inability of abductors to keep
pelvis level. Look at hip and shoulder alignment
Extensor Lurch or Gluteus Maximus Gait: Don‟t have enough strength in gluteus maximus to
hold hip in extension risk that the torso collapses forward at the end of stance. Lurch torso
backwards to compensate
Flat Foot or Calcanial Gait: can‟t toe-off, instead lift whole foot off without extending big toe.
Due to:
Pain or Rigidity in the fore foot
Weakness of plantar-flexors
Swing Phase:
Paralysis of foot and ankle dorsiflexors can cause one or more of the following during toe
clearance:
Steppage or Drop Foot Gait: flex knee more in swing phase so the foot clears the floor
Hip-hike Gait: Lift pelvis to help the foot clear the ground. Can also be due to a stiff knee
Circumduction Gait: Swing leg out to the side so the foot clears the ground. Can also be due
to a stiff knee
Abnormal pelvic rotation: Weakness of hip flexors on the swing side acceleration.
Compensate with forward pelvic rotation to „flick‟ the swing leg forward
Hip Fusion: fused hip on the stance side pelvic rotation on the swing side decreased swing
length
Abnormal gaits by causative muscles:
Quads: Abnormal heel strike, back-knee gait
Abductors: Abductor lurch/Gluteus medius or Trendelenburg gait
Gluteus Maximus: Extensor lurch
Plantar flexors: Flat foot/calcanial gait
Dorsiflexors: foot slap, steppage/drop foot, hip-hike or circumduction gait
Iliopsoas: abnormal pelvic rotation
Other:
Broad based gait: impaired balance/co-ordination/vision, drunk
Short leg: have to drop ipsilateral hip in stance phase so the foot can reach the floor
Observing Gait
Walk the patient
Other aspects of gait to observe:
When observing gait, focus on the pelvis first:
Pelvic tilt
Pelvic rotation
Lateral shift of the torso
Width of base: normally 6 – 8 cm
Stride length (distance from where the heel strikes on one side to where the heel strikes again on
that same side)
Step length (distance from where the heel strikes on one side to where the heel strikes on the
opposite side. Normally the same for both sides)
Also observe shoulder movement
Once you‟ve identified the gait, think of causes from top down:
Stroke
Spinal chord lesion
Nerve root
Peripheral nerve
Muscle (either weakness or pathology)
Joint
Bone (eg fracture)
252 4
th
and 5
th
Year Notes
Hip and Femur
Overview
Primary concerns:
Range of motion
Gait
Also need to examine
The lower back and sacro-iliac joints
Vasculature of the leg: pulses, temperature, capillary refill
Peripheral nerves: eg sensory
Problems arising with the hip:
Fracture
Arthritis
Dislocation: trauma, also in congential abnormalities, infection, Cerebral Palsy
Epiphyseal dislocation (typically a chubby 11 year old boy with a slipped femoral epiphysis)
Infection: septic arthritis
History
Impact on daily activities
Walking distance
Climbing stairs
Getting out of low chairs
Location:
Anterior/groin pain: ?hip
Lateral: ?trochanteric bursitis, referred from spine
Posterior: referred from spine, gluteus medius tendonitis
Hip Exam
Inspection
While standing:
Observe gait
Walking: on toes (tests S1), on heels (test L5)
Observe from front and do Trendelenberg‟s test: thumb on each ASIS while they alternate
standing on one leg. Sagging to contra-lateral side is Trendelenburg positive (ie lack sufficient
abductor strength to stabilise pelvis)
Observe from back: wasting of gluteals, posterior surgical scars, etc
Test the joint above (sacro-iliac joints and lumbar spine): Bend over (measure how far they do
down – eg fingers to floor, toes, mid-calf, etc). Extend back
Test the joint below: crouch down to test knees
Palpate sacro-iliac joints and lumbar spine for tenderness
On bed, look especially for:
Scars, hernia, bruising, inflammation
Muscle wasting: gluteals, quads, biceps and adductors
Leg length (check they‟re lying straight and pelvis is straight):
Real leg length discrepancy: Measure ASIS to medial melleolus on each side. If there is a
discrepancy then flex both knees to isolate the discrepancy to above or below the knee
Apparent leg length discrepancy: measure umbilicus to medial melleolus. If discrepancy
but no real leg length discrepancy then postural cause
Palpation:
Groin: lumps: hernias, lymph nodes, femoral artery aneurysm pain is not hip pain
Check for ilio-tibial band pain over the greater trochanter pain is not hip pain
Range of motion: always state start and end: from X to Y degrees (eg adduction from 0 to 30 degrees)
Compare sides
Thomas test for fixed flexion deformity (ie not full extension): Bring up good leg with hand under
the spine. When pelvis starts to flex the bad leg won‟t be able to remain straight if there is fixed
flexion deformity. Quantify by measuring the degrees that the bad leg has risen from lying flat
Test flexion
To test adduction (0 - 20º) and abduction (0 - 50º), stabilise hip by holding hand across both ASIS
or abduction the opposite leg
Musculo-skeletal 253
Internal (0 - 45º) and external rotation (0 - 45º): flex hip and knee and lever hip using lower leg
Don‟t test extension
Finally check:
Leg pulses relevant to operative risks
Joint above: did this while standing
Joint below: check knee
X-ray
Injury
Fracture of Femoral Neck:
Commonest site in elderly, associated with osteoporosis
Types: subcapital, transcervical, basicervical, intertrochanteric
Clinical: History of fall, pain in hip. Patient lies with limb in lateral rotation and leg looks short
Location: key issue is disruption of blood flow to the femoral head. Most blood flow is via the
attachment of the capsule. If disrupted (via a fracture at or above a basicervical fracture)
avascular necrosis
Treatment: Operative mostly. Displaced fractures will not unite without internal fixation.
Richardson‟s screw often used, otherwise hip replacement
Complications include: dementia, pressure sores, pneumonia, urinary infection, not liver failure
Clinical difference between a dislocated femur and a fractured neck of femur: both are shortened.
Neck of femur: leg externally rotated, dislocation: leg internally rotated („in points out and out
point in‟)
Femoral shaft Fracture:
Clinical: Mostly young adults. Shock is severe and with closed fracture fat embolism common.
Leg is rotated externally may be short and deformed. Thigh swollen and bruised. Shock MUST be
treated, ABG should also be done
Risk of fat embolism: do CXR (?pleural effusion, congested pulmonary veins etc)
Treatment: Intramedullary nailing
Comminuted fractures of the femur:
Mechanism: violent trauma (eg motor bike accident)
Traction or external fixation +/- grafting to fill the gaps
Supracondylar fracture of the distal femur:
Mechanism: Forceful flexion/hyperextension in osteoporotic bone
Gastrocnemius then pulls the femur forward
Internally fixate with long blade plate
Condylar fracture of the femur:
Mechanism: Fractures entering the intercondylar notch can divide a condyle from the femur (eg
knee hitting the dash board)
Management:
Undisplaced: aspirate + traction for 4 weeks then cast
Displaced: open reduction and internal fixation
Complications: avascular necrosis, collapse, varus or valgus deformity
Knee
History
About the injury
How did you do it: Direct blow or indirect (eg twisting consider meniscus lesion)
Immediate disability: Inability to walk, knee collapsing (?ACL injury), locking (?meniscus),
catching, clicking. For days or weeks, hamstring spasm protects the painful knee. As pain and
effusion settle, the knee gradually straightens. NB neither cartilage or inner two thirds of menisci
are innervated – pain from these injuries is caused by consequential tension/damage to other
structures
Sounds and sensations: hearing or feeling a pop, snap or tearing
Swelling: If the knee swells straight after an injury ?ACL injury causing bleeding into the joint
or other haemarthrosis (always serious). Soft tissue swelling/effusion takes up to a day
Always ask about knees:
Locking: question carefully to distinguish from pain-induced hamstring spasm
Giving way
254 4
th
and 5
th
Year Notes
Swelling
Function:
Difficulty with stairs (going up or down?)
Trouble getting out of low chairs
Waking with pain at night after having leg bent
Exam
Adequately expose the leg
Walk:
Stiff knee gait
Valgus deviation (deviation away from midline, eg knock knee – Genu valgus)
Varus deviation (deviation towards midline, eg bow leg – Genu varum)
Lateral thrust: Posterolateral insufficiency, knee goes posterolaterally, a result of Medial
Compartment OA.
Squat on their haunches and duck walk:
Stimulates pain in the front then it is an anterior problem (ie patello-femoral joint)
In the popliteal fossa could be a medial meniscal tear.
View from the side: any fixed flexion deformity
Inspect the popliteal fossa (then you don‟t have to get them to roll over on the bed). Look for
Baker‟s cyst – protrusion of the synovium into the popliteal fossa
Look: Get on bed
Swelling
Muscle wasting: measure thigh circumference
Bony deformity
Arthroscopy scars
Get them to push their knee down into the bed to test:
Extension (fixed flexion deformity)
For muscle wasting in vastus medialis
Can measure angles with a goniometer
Feel:
Feel for temperature compared with rest of leg and with other knee
Feel for effusion (Meniscal pathology often produces an effusion)
Stroke/bulge test
Patellar tap
Palpate joint line along tibial plateau (watch their face): Tenderness here may indicate a meniscal
tear, above or below the joint line the meniscus won‟t be causing it.
Palpate medial and lateral collateral ligaments
Palpate tibial tuberosity and infra-patellar ligament
Move:
Actively raise their leg straight as high as they can: checks extensor mechanism – quads, patella
ligament, etc. If damaged traumatically then urgent surgery (the key knee injury where you
wouldn‟t wait for the swelling to go down before operating)
Flex their knee. Bring the other leg up with the knee in flexion to compare. Have one hand on the
patella to feel for crepitus. Measure distance from heel to buttock
Poster Cruciate Ligament:
Feet back down on the bed leaving both their knees in 90
o
flexion.
Look across the two knees for posterior sag, which could indicate a PCL rupture.
Stabilise the tibia (sit on their foot), relax hamstrings and push tibia towards body (Posterior
draw test)
Anterior Cruciate Ligament:
Anterior draw to test the ACL. Compare with the other side. Sit on foot and pull tibia
towards you
Lachman‟s Test: with leg in slight flexion on the bed (eg rolled up towel or your knee
underneath it) push down on distal femur while pulling up on proximal tibia
Pivot Test (hard to elicit unless relaxed or under GA): Flex the knee, put it in valgus, then
extend it. If ACL is ruptures, the knee jumps smartly forward
McMurray‟s Test for meniscal tears (not particularly reliable): Feel and listen for a click as
meniscal tag snaps free
Start with leg in slight flexion
Musculo-skeletal 255
Medial lemniscus: externally rotate the tibia on the femur, apply valgus pressure. Extending
the leg will cause pain/clicking
Lateral lemniscus: internally rotate the tibia on the femur, apply varus pressure. Further
flexing the leg will cause pain/clicking
Collateral Ligaments:
With leg under your arm Valgus stress test and Varus stress test:
With the knee still in 15
o
steady it as you pull the leg into valgus, this tests the medial
collateral ligament and the ACL. Now Push it into Varus, this tests the lateral collateral
ligament
Lay the leg flat and repeat with the knee in full extension: tests all structures – not just the
collateral ligaments. If laxity in full extension, the ACL or PCL damage as well
Patellar-femoral joint:
Ask about pain going up and down stairs
Palpate
Border
Anterior surface: Push it in – „any pain?‟
Tendon and ligament insertions (especially tibial tuberosity)
Posterior surface (by pushing it to one side and then the other)
Solomon‟s test: With leg in full extension, try and lift patella and get fingers underneath. If
can‟t then effusion/synovitis
Site on edge of bed with legs handing over: Look at the direction that the patellar points in. Have
the patient flex and extend at the knee should follow an inverted J course
Grind or Friction Test
Straighten the leg with your hand over the patella
Will cause painful grating if the central portion of the articular cartilage is damaged
Patella apprehension test: Press the patella laterally and hold it slightly subluxed Watch the
person‟s face and ask them to flex their knee If they grimace or show signs of pain then the test
is positive and is diagnostic of recurrent patellar subluxation or dislocation.
Joint Above and Below. Check the Hip (pain is referred to the knee from there)
Check the Ankle and the foot pulses, and distal neurology
Knee Injury
General principles of ligament injury:
Pain + slight joint opening good (strain/partial rupture)
No pain + big joint opening bad (complete rupture)
Always x-ray adequately. Small bony fragments on x-ray soft tissue injury until proven otherwise
In kids, bone and growth plates are weaker than ligaments
Meniscal Tears:
Variety of types: fragments causing locking, tears on internal or external margins, etc
Clinical: Twisting injury, unable to straighten knee, locking (typically bucket handle tears), pain
Investigations: Arthroscopy or MRI
Management: Excise tears or reattach. Aim is to preserve as much of the meniscus as possible
Lateral/Medial Collateral Ligament:
Most common knee ligament injury
Medial is attached to the medial meniscus. Lateral isn‟t less injury. But if it is, consider check
for fibular head fracture and common peroneal nerve damage
Mechanical: Blow to medial/lateral side of knee pushing the joint into varus/valgus
Presentation: Tenderness over ligament (unless complete rupture no pain), pain worse under
varus/valgus stress, effusion
Management: Isolated tears heal well without operating. Immobilisation in leg plaster at 10º
flexion (6 weeks) then mobilise cautiously. May have ongoing instability
Anterior Cruciate Ligament:
Prevents posterior displacement of the femur on the tibia and hyperextension. Is the weaker of the
2 cruciates. Anterior-medial bundle is taut throughout flexion anterior draw test +ive if AMB
affected
75% of haemarthroses
Mechanism: sharp twisting movement or tackle that pushes the tibia forward cf femur
Presentation: may hear a snap, swelling, pain, effusion (very rapid if due to haemarthrosis). If
delayed then knee gives way, can run in a straight line but can‟t turn corners
256 4
th
and 5
th
Year Notes
Often tear medial meniscus ( OA and instability)
X-ray for avulsion fracture of tibial insertion: seen in young patients
Management:
Conservative: aspirate and physio to strengthen hamstrings
Surgical: reconstruction of ligament (repair impossible as ligaments devitalise rapidly after
injury)
Posterior Cruciate Ligament:
Prevents anterior displacement of femur on tibia and hyper-flexion
Mechanism: blow to anterior tibia when knee flexed (eg bicycle vs car) or hyperextension
Presentation: swelling, pain, effusion, posterior sag at 90º flexion
X-ray for an avulsion fracture ( requires surgery)
Most do well with conservative treatment. Can often manage without a PCL. Quads exercises
decrease backwards tibial sag
Patella Fractures:
Comminuted: from blow to flexed knee (eg knee against dashboard). Put patella together (usually
hard) or remove it (patellaectomy)
Stellate: blow to patella that cracks but doesn‟t displace fragments. Aspirate + long leg cast
Transverse: Due to sudden contraction of quads. Internal fixation with tension wire band
Chondromalacia Patellae: young women. Patellar aching after prolonged sitting due to softening or
fibrillation of the patellar articular cartilage. Conservative treatment: vastus medialis strengthening
Disruption of extensor mechanism:
Rupture of Rectus Femoris: sudden violent contraction transverse tear. Feel defect in muscle.
Conservative treatment: ice, elevation, analgesia, mobilisation within limits of comfort. Functional
deficit negligible
Ruptured Quadriceps tendon: sudden violent contraction. Need to reattach
Ruptured patella tendon: Forced flexion injury. Repair if weakness or extensor lag
Dislocation of the Patella:
Sharp twisting motion on flexed knee or blow to side of leg haemarthrosis ( swelling)
and medial tenderness (medial structures torn).
To reduce: gently extend the knee, then gentle traction. Primary concern is distal circulation
reduce at scene of injury if possible
Aspirate and irrigate if necessary, splint for 4 weeks
Physio to strengthen quads (necessary for patella stability)
If recurrent then ?underdevelopment of lateral femoral condyle
Osteochondral Fractures:
In young person, twisting or direct blow can detachment of sliver of bone and cartilage. Most
common with patellar dislocation
Haemarthrosis and fat from cancellous bone causing a fat-fluid line on lateral radiograph
If small then remove, if large then reattach
Chondral separations or flaps: Fragments of articular cartilage. Need arthroscopy or MRI. Flaps are
usually ground away. Separations are removed
Osteochondritis Dissecans:
Blood to subchondral bone (cause unknown) focal necrosis of cartilage and bone loose
fragment
Presentation: pain in young adulthood, worse on walking and hyperextension, M>F, intermittent
swelling, maybe locking
X-ray: small irregularities on medial condyle +/- fragments
Treatment: wait, or surgery if no radiological signs of union
Bursitis: 16 bursae around the knee. Most commonly affected are:
Prepatellar bursa: „housemaid‟s knee
Infrapatellar bursa: „Vicar‟s knee‟ – they kneel more upright
Anserine bursae: on medial side of the head of the tibia, under the ligaments of semi-tendonosis,
gracilus and sartorius
Aspiration distinguishes friction bursitis from infective or inflammatory bursitis
Haemarthrosis of the knee is the most common presenting complaint of a 0% F VIII haemophilia
Management of knee injury
Weight
Exercises to strengthen hamstrings and quads (eg straight leg raise while seated)
Musculo-skeletal 257
Check for flattened arches exercises
Aquajogging
Analgesics (NSAIDs, consider COX2)
If tense haemarthrosis then aspiration will give immediate relief and aid diagnosis (ie send it to the lab:
?blood, infection or gout)
Lower Leg and Foot
Exam
Look: swelling, deformity, muscle wasting. Deformities include:
Hallux valgus: lateral deviation of the MTP joint of the big toe (bunion). Causes: biomechanical,
pointed shoes or wearing heals, flat foot (flattening of the longitudinal arch)
Hammer toe: Extended at the MTP joint, hyperflexed at the PIP joint, extended at the DIP joint (cf
boutonniere deformity of the finger)
Claw toes: fixed flexion deformity: extended at MTP joints, and flexed at PIP and DIP joints. Due
to imbalance of extensors and flexors (eg previous polio)
Crowding of the toes: rheumatoid arthritis
Sausage deformity of the toes: psoriasis, ankylosing spondylitis and Reiter‟s disease
Inspect transverse and longitudinal arch:
Pes Planus: Flat feet. May be valgus and eversion deformity. Normal when a child is learning
to walk. If the arch forms when walking on toes then OK
Pes cavus: Accentuated longitudinal arches: idiopathic, spina bifida or previous polio
weight on head of metatarsals pain.
Calluses over the metatarsal heads on the plantar surface occur with subluxation of these joints
Feel and move:
Swelling around the lateral and medial malleoli (don‟t confuse with pitting oedema)
Hold midfoot and test dorsiflexion (normal ~ 20º) and plantar flexion (~ 50º)
Subtalar joint: test inversion and eversion. Look for tenderness more than range of movement
Midtarsal (midfoot) joints allow rotation when hindfoot fixed
Squeeze MTP joints: tenderness common in early rheumatoid arthritis
Very tender first MTP joint ?gout
IP joints typically affected in sero-negative arthritis
Palpate Achilles tendon for nodules and Achilles tendonitis
Palpate inferior heal for plantar fasciitis (can occur with seronegative-arthropathies)
Lower Leg and Foot Injury
Ankle anatomy:
Lateral malleolus of the fibula is firmly attached to tibia by the anterior and posterior inferior tibio-
fibular ligaments
Talus is held in place by deltoid ligament on medial side and calcaneo-fibular ligament on lateral
side
Commonest ankle injury occurs when the talus is rotated, fracturing one or both malleoli and
rupturing the ligaments
Fracture of the Tibia
Most common site of open fractures
Clinical: Skin may be undamaged or obviously divided. Foot rolled outwards, leg bruised and
swollen. Need to assess circulation and sensation in toes
Treatment:
Closed fractures need to be observed for compartment syndrome and soft tissue damage.
Obtain fracture alignment and start weight bearing early
Open fractures require immediate antibiotics, debridement, then stabilization and rehab
Distal fibial fracture:
Check even, clear joint space around the ankle
Check ankle joint is not subluxed
Check ligaments on the other side (eg Deltoid). If damaged unstable
Classified as A, B, C1 or C2
If stable, cast for symptomatic relief for 6 weeks
Diastasis:
= Dislocation where no true joint exists
258 4
th
and 5
th
Year Notes
Separation of the distal tibia and fibula. Talus goes with the fibula. Leads to incongruity of the
tibial-talus joint
Ruptured deltoid: always exclude proximal fibular fracture (Maisoneuve Fracture)
Dislocation of the ankle: reduce urgently (ie before lengthy transport) otherwise ischaemia of overlying
skin
Achilles Tendon Rupture:
Mechanism: Forced dorsiflexion against resistance (eg jumping, due to a forward lunge in squash)
– an eccentric injury
Presentation:
Lie on stomach with foot over end of the bed. Foot normally slightly plantar-flexed. If
rupture neutral position
Swelling plus defect felt in tendon. Squeezing is positive (Simmond‟s test). Foot doesn‟t
move when calf is squeezed
Management: Hold the ends together until healed – either surgical or conservative.
Conservative: Casting for both: 4 weeks in full flexion below the knee cast then a further 3
weeks with foot half way to neutral. Walking with heeled shoe for a further 8 weeks but not
bare-foot. Physio + ultrasound to reduce swelling. Rerupture rate 20%
Operative:
Makes the tendon heal at the right length, doesn‟t heal any faster
Indicated if: a re-rupture, late presentation (> 48 hours), open wound, or if strong healing
necessary (eg athlete)
Risk: poor skin healing
Nothing vigorous for 6 months post injury
Ruptured plantaris: severe pain, unable to bear weight
March Fractures: in the shaft of the 2
nd
and 3
rd
metatarsals, following excessive walking. X-rays may
be normal. Conservative treatment unless severe, in which case cast
Lisfranc Dislocation of the 1
st
TMT joint – may impair blood supply to the medial foot
Metatarsalgia: caused by:
Freiberg‟s infarction: collapse and reformation of the epiphyses of the 2
nd
and 3
rd
metatarsal heads
Neuroma of the digital nerve
Synovitis
Sesamoid fracture
Injury
Pes cavis
Facial Fractures
Nasal Fracture
Fracture of the nasal cartilages and nasal bone are common and leave a deformity if not correctly
treated
If a nasal fracture is suspected, hold the patient‟s nose gently and move it slightly. Pain or abnormal
movement indicates a fracture
Treatment: Dislocated or displaced fractures of the nasal bones need to be repositioned accurately.
Refer to ENT
Zygoma
Fractured by a direct blow to the face.
If there is bruise over the cheekbone, check zygoma fracture
On inspection and palpation, the zygoma bone should be depressed
If untreated, depression zygoma will cause diplopia and damage to the infraorbital nerve.
Treatment: Fragments need repositioning. May require fixation with wires or external fixation
Orbital Fractures
If direct trauma to the orbit or eye, look for orbital fracture
Diplopia and the abnormal position of the eye should lead to the diagnosis
Treatment: Surgery
Musculo-skeletal 259
Maxilla
Le Fort classification of maxillary fractures:
1: through the maxilla, leaving nose and orbits intact
2: through the maxilla, into the orbit and across the nose leaving the lateral side of the face mobile
3: same as 2 but fracture extends through the lateral wall of the orbit and across the nose
All maxillary fractures are an emergency because the lateral wall of the face may be unstable and can
fall backwards to obstruct the airway.
Treatment: Secure airway. External fixation to the skull
Mandible
Dislocation of the TMJ can follow direct or indirect trauma, or even a wide yawn
Dislocation can usually be reduced easily if the mandible is intact
Can recognise a fracture by tenderness when the mandible is palpated or squeezed gently, and by a
deranged dental occlusion
X – ray if in doubt
Soft tissue swelling round a fractured mandible can obstruct the airway
Treatment: Surgery. May require internal fixation, interdental wiring and dental treatment
Joint and Bone Infections
Septic Arthritis
Presentation: systemic illness with fever, usually one joint (knee most common), swelling, effusion,
warmth, markedly reduced movement of the affected joint, and very painful to move (cf adjacent
osteomyelitis some pain only). Hip and shoulder have less swelling
In neonates, may overlap with acute haematogenous osteomyelitis
Risk factors: diabetes, recurrent steroid injections, systemic steroids, alcoholic liver disease,
immunosuppression
Differential:
Gout and pseudogout
Haemarthrosis
Acute osteomyelitis
Acute traumatic arthritis
Pathogenesis:
From haematogenous spread or extension of osteomyelitis, often following distant infection. Also
following penetrating injury
WBC enzymes rapidly erode articular cartilage surgical emergency: empiric antibiotics and
rapid drainage. Urgent – can destroy a joint in 24 hours. In neonates/kids can damage growth
plate growth disturbance
S. Aureus, also S pneumoniae and S pyogenes. In high-risk groups, M Tb and Candida. Neonates
consider S agalactiae, Haemophilus and N gonorrhoea (did they have bacterial conjunctivitis soon
after birth?). Pseudomonas from foot wound.
Tb arthritis: usually haematogenous spread from lungs to hips (kids), knees (adults) or spine. X-
ray shows marginal erosions and destruction of sub-chondral bone (like Rheumatoid – but different
distribution). Have granulomas (except in AIDS). Histology: Granulomas are pink, cf lymphoid
aggregates in Rheumatoid that are blue
Investigations:
Joint aspiration (arthrocentesis: opaque fluid with WBC > 50,000/ml)
FBC, ESR, CRP, blood cultures, plain Xray, US (for detection effusion)
Xray delays rather than establishes the diagnosis
Management:
Flucloxacillin: for staph aureus, but also covers S pneumonia, S pyogenes, S agalactiae
If neonate:
And unimmunised consider H. Influenzae: cefuroxime or cefotaxime
Consider G –ive: gentamycin
Arthroscopic washout
Initial splinting for pain relief, but then encourage mobility
If there is a joint prosthesis, revision may be necessary
260 4
th
and 5
th
Year Notes
Complications due to delayed diagnosis:
Joint degeneration, joint dislocation
Damage to the growth plate growth arrest
Osteomyelitis
Common in low socio-economic and warmer weather
May follow minor trauma with or without infection elsewhere in body
Acute haematogenous osteomyelitis:
Presentation:
Early: short, febrile illness, bone pain, metaphyseal tenderness (point tenderness)
Late: Swelling/erythema (suggest abscess). Cellulitis. Adjacent joints sore but some
movement still possible
Vascular supply to bone is compromised and infection spreads to surrounding soft tissue
Differential diagnosis:
Septic arthritis
Cellulitis
Trauma (Facture)
Tumour
Aetiology:
Trauma/surgery direct introduction of bacteria
Direct extension from infective site: eg dental infection jaw, diabetic foot bones of foot
Haematogenous seeding:
Commonest site in children is metaphysis of the long bones. Femur and tibia account for
> ½ all cases (especially around knee joint). Epiphyseal growth plate acts as a barrier to
the spread of infection to the joint. May spread through Haversian and Volkmann‟s canal
system to form a subperiosteal abscess (requires drainage)
In adults, haematological spread less common. Tends to affect subperiosteal corticies of
long bones. Also cancellous bone of vertebral bodies, may compression fracture
Eg: sluggish blood flow easy thrombosis following trauma predisposes to infection
(esp staph aureus)
Pathology: Inflammatory response oedema compromise vascular supply necrosis
spread of infection through cortices pus under periosteum shearing of periosteum further
disruption to blood vessels
Causative organisms:
Under one year: staph aureus, strep agalactiae, E coli. May be non-specific illness
Children: staph aureus, strep pyogenes, H influenzae
Adults: staph aureus, staph epidermis and G negatives (E coli, salmonella and pseudomonas
from foot wounds)
M. Tb and Candida in high risk groups
Complications:
Spread of infection septicaemia, joint infection
Fracture, abscess formation
Chronic osteomyelitis in 5 – 20% of cases
Subacute osteomyelitis: Focal rather than systemic response to infection. Xray shows bone
destruction. Differential includes bone tumour and stress fracture
Chronic osteomyelitis:
Usually delayed or inadequate treatment.
Pain, swelling +/- discharging sinuses.
Xray: destruction, with sequestrum (areas if necrotic bone which can‟t be resorbed) harbouring
bacteria and involucrum (formed from periosteum raised over an abscess). Brodie‟s abscess:
abscess surrounded by sclerotic bone due to organisms of low virulence
Treatment: sequestrum must be removed, may require repeated surgery. Poor penetration of
antibiotics
Complications:
Persistently discharging sinus
Chronic ill health
Pathological fractures/deformities
Malignant change SCC
Musculo-skeletal 261
Investigations:
Blood: FBC, ESR, CRP, Blood cultures (+ive in 50%)
Imagining:
Plain films: no changes until day 10
US: subperiosteal abscesses
Bone scan: very sensitive but not specific
MRI: very sensitive but expensive
CT: good for detecting degree of bone destruction
Treatment:
High dose IV antibiotics for at least 2 – 4 days (for children, Flucloxacillin 50 mg/kg/6 hourly,
max 2 g), followed by 3 – 4 weeks of oral therapy
Surgery to decompress and remove necrotic bone if late or failed medical treatment, or
subperiosteal abscess drainage
Specific presentations:
Osteomyelitis of the calcaneum: infection 5 – 10 days after puncture wound. P aeruginosa
Discitis: inflammation of the lumber disc, usually < 8 years
Pelvic osteomyelitis: pain referred to the abdomen, buttock or leg. S aureus. Bone scan diagnostic
Tb Osteomyelitis: rare in developed world. Occurs in 1-3% of patients with pulmonary Tb.
Insidious. After months: pain on movement, fever, night sweats, weight loss. Destructive. If
lumber or thoracic vertebrae may hunchback deformity
Pyogenic infections of the hand
Usually history of trauma
Paronychia: common infection of periungual tissues, usually by Staph Aureus
Felon: deep infection of the pad of the finger. Usually Staph aureus following puncture wound
Cellulitis: Strep Pyogenes infection
Suppurative flexor tenosynovitis:
Infection of flexor tendon sheaths
Presentation: Swollen finger with painful motion. Symmetrical swelling, tenderness, erythema
along tendon sheath. Semi flexed posture and severe pain on passive extension of DIP joint
Signs: crepitus, erythema, vesicle formation, colour, pain, puss
Tests:
Culture of puss, blood culture, FBC
X-ray to rule out foreign body, air in tissue or joint, associated fracture
Treatment: irrigate, leave wound open and dress after swelling has decreased, antibiotics, splint
Atypical infections:
Herpes infections of the thumb and fingers (eg Whitlow‟s lesions)
Fungal infections: more indolent. Sporotrichosis common
Metabolic Bone Disease
Osteoporosis: bone matrix reduced in amount but normally mineralised (ie bone mass due to loss of
both protein matrix and Ca in equal proportions)
Osteomalacia: normal amount of bone matrix but deficient mineralisation (ie Ca)
Both will appear on x-ray as osteopenia (poverty of bone)
Bone Metabolism
Osteoblasts:
Synthesise osteoid: normally this is a thin layer as the time between matrix deposition and
mineralisation is short. If either osteoid or delayed mineralisation thick layer
(hyperosteoidosis), eg:
Bone formation: fracture callus, Paget‟s disease, hyperparathyroidism
Calcium, phosphorous, or vitamin D
Blocked mineralisation due to inhibitory/toxic substances (eg aluminium, iron, fluoride)
Mediate osteoclast activity
Flat when inactive, plump when active. Become buried in cortex (then called osteocytes)
Activity due to physical activity, PTH, growth factors, fluoride. Suppressed by inactivity and
steroid hormones
262 4
th
and 5
th
Year Notes
Osteoclasts:
Regulated by PTH and osteoblasts
Large cells containing 2 – 4 nuclei
Adhere to bone and are seen in depressions referred to as Howship‟s lacunae or resorption bays
scalloped appearance of resorbed bone
Woven bone: immature bone laid down by osteoblasts in a callus (eg healing of a fracture)
Lamellar bone: parallel and organised
Tetracycline:
Give pulses before bone biopsy
Binds to actively mineralising surfaces and fluoresces in UV light under the microscope
Shows the extent of mineralisation and amount of bone formed over a given time
Osteoporosis
Normal bone composition – just less of it. Either primary or secondary
Epidemiology:
Often presents with a hip fracture. 3 per 1000 in men and 6 per 1000 in women over 65 per year.
Number of vertebral fractures and resulting disability unknown
¼ of those > 80 going to hospital with a fracture don‟t return to their previous residential status
Pathogenesis:
Bone is constantly turning over. From the 3
rd
decade, resorption exceeds bone formation – the two
become uncoupled. In women, this accelerates post menopause (oestrogen is protective). Around
menopause will loose 6 – 10% of bone mass, then returns to gradual decline
Trabecular bone (20% of skeleton) turnover 8 times that of cortical bone (80% of skeleton).
Femoral head has lots of trabecular bone good place to measure loss. Use Singh Index of
number of trabecular groups present (6 = good, 1 = bad)
Also thinning and attenuation of the cortices
Fracture risk a combination of density (which we can measure) and structure (which we can‟t)
By the time they present with a fracture, osteoporosis is usually advanced
Severity depends on:
Peak bone mass. Peaks at around age 30. Largely determined by type of inherited vitamin D
receptor. Also calcium intake in teens, etc
Sex: peak bone mass of males > females
Age: men affected later than women
Also physical activity positive (disuse localised osteoporosis), smoking negative, calcium intake
Distribution:
Osteoporotic vertebrae (most common fracture):
Loose secondary trabeculae 1
st
(leaves vertical lines of primary trabeculae) clear glass
appearance
Changes in shape: wedge, biconcave, planar (ie flat)
Anterior of vertebrae reduced
May occur with trivial trauma or lifting
Small fractures don‟t cause immediate pain – comes on after several days. If no scoliosis then
can heal
Fractures affecting proximal femur, proximal humerus, distal radius resulting from falls
Look for insufficiency factors in the sacrum, pubis, and supra acetabular
Differential of osteoporosis:
Male: hypogonadism ( testosterone), excess alcohol
Female: Ca and Vit D post menopause
Scanning for osteoporosis:
Plain x-ray insensitive: don‟t show changes until 30 – 40% of bone mass lost. Radiodensity varies
due to exposure, developing, and patient‟s build
Dual Energy X-ray Absorbiometry = DEXA:
Measures bone density (ie Ca density) by firing X-rays of 2 different wave lengths – one
maximally absorbed, the other absorbed as much as carbon, and subtract the two
Number of standard deviations from the mean (of 30 year old women) more important than
actual density. T < -2.5 standard deviations = Osteoporosis. Osteopenia: -1 < t < -2.5
Management:
Prevention:
Physical exercise ( bone laid down)
Musculo-skeletal 263
Adequate Ca (prevents bone resorption)
Vitamin D if house bound (a small amount of sun is sufficient)
Rocaltrol: 1,25(OH)2D3
HRT: most stop before 5 years – compliance problem. Can start at any age – but if elderly
need to build up gradually
Treatment: alendronate (or Fosamax) osteoclast action turnover gain bone
Osteomalacia
Osteomalacia in adults = Rickets in kids
Present with bone pain, fractures (eg neck of femur) or waddling gait (proximal myopathy)
Aetiology:
Deficiency or abnormal metabolism of vitamin D
Calcium deficiency
Pathology:
Intracortical tunnelling (due to secondary hyperPTH)
Coarsened indistinct trabecular pattern (due to seams of osteoid) frosted glass appearance
Looser‟s zones: the hallmark of osteomalacia: lateral margin of scapula, ribs, pubic rami, proximal
femur, proximal ulna
Micro: in unmineralised bone (up to 40 – 50%) + disorganisation of trabecular architecture
In children: changes around metaphyses of most rapidly growing bones (knee and wrist), with irregular
and broadened epiphyseal growth plates
Investigations:
X-rays: generalised osteopenia + multiple, bilateral, symmetrical partial linear fractures (stress
fractures)
May be ALP, vitamin D
PTH assay not very helpful: normal range is too wide (0.5 – 5) so can mask an increase. Mild
increase osteoclastic activity, but serum Ca normal so remineralising normally osteopenia
and not osteomalacia
Increased Bone Resorption
Hyperparathyroidism:
See also Parathyroid, page 101
Old term: osteitis fibrosa cystica
PTH (either primary of secondary) Ca and PO4
Presentation: kidney stones, peptic ulcer, bone pain, nausea, vomiting, weakness, headaches,
depression (bones, stones, groans). Now rare – usually picked up as an incidental finding of
hypercalcaemia
Affects cortical bone more than cancellous/trabecular bone
Osteoclast and osteoblast activity
May reactive fibrosis tissue (eg following microfractures and secondary haemorrhages) mass
called a „Brown tumour‟
X-ray: generalised osteopenia and tufts on end of distal phalanges
Differential:
Blood sample with dehydration or tourniquet Ca
Malignant disease and/or neoplastic syndrome with PTHrH secretion
Sarcoidosis
Vit D intoxication
Diuretic therapy
Treatment: neck exploration for parathyroid adenoma
Renal Osteodystrophy:
= All skeletal changes resulting from chronic renal disease, including:
Osteoclast resorption (mimicking hyperPTH)
Delayed matrix mineralisation (osteomalacia)
Osteosclerosis
Growth retardation
Osteoporosis
Due to:
PO4 retention Secondary HyperPTH Osteoclast activity
Metabolic acidosis bone resorption

264 4
th
and 5
th
Year Notes
Conversion of 1,25(OH)2D3 in kidneys hypocalcaemia
Aluminium deposition (from antacids, dialysis fluid) at the site of mineralisation
mineralisation
Similar impact to osteomalacia: PTH osteoclastic bone resorption
Investigations:
X-ray and bone densitometry
Bloods: Ca, albumin, phosphate, PTH, ALP, Vitamin D3 levels
Urine Ca usually low and faecal Ca high
Paget’s Disease:
Common in northern Europeans, rare in Blacks/Asians, M = F, usually old
Presentation:
Monostotic, asymptomatic and incidental finding on x-ray (doesn‟t spread)
In a small number, widespread, polystotic lesions with bone pain (worse at night), fracture,
arthritis or development of a sarcoma
Usually axial skeleton (spine, skull, pelvis) and femur
Pathogenesis: ?viral infection (paramyxovirus) of osteoclasts osteoclast activity
osteoblast activity disorganised, woven bone. Normal bone mineralisation. Also genetic and
geographic predisposition
Gross: enlarged bone with thick cortices
Micro: irregular trabeculae with numerous osteoclasts and plump osteoblasts, jigsaw pattern
Prognosis:
Progressive bone deformity and micro fractures, anterior bowing of the femur. Arthritis due to
deformed joints
Osteosarcoma in 5 – 10% of those with severe disease
Investigations:
X-ray: early radiolucency. Late: loss of distinction between cortical and cancellous bone (may
be confused with primary bone tumour)
Bone formation ALP but Ca and PO4 normal. Urinary hydroxyproline
Treatment:
Mild: NSAIDs – indicated if pain
Severe: biphosphonates (alendronate), calcitonin
Complications:
Fractures
Spinal stenosis nerve compression
Osteosarcoma
Enlargement of the skull, femur, clavicle, tibia („Sabre Tibia‟)
Neural deafness due to bone overgrowth
High output heart failure (due to blood flow to bone)
Orthopaedic Tumours
Primary bone tumours are rare.
Myeloma accounts for half of malignant bone neoplasms:
Old, M > F, pathogenic fractures, pepper-pot skull, normocytic anaemia with Rouleaux
Gross: red current jelly lesions
See Multiple Myeloma, page 302
Classification based on histology of tumour cell – cell of origin is unknown/debated. Diagnosis
difficult. Requires clinician, radiologist, pathologist
Classification:
Histiologic Type
Benign
Malignant
Haematopoietic
Myeloma
Lymphoma
Chondrogenic
Osteochondroma
Chondroma
Chondroblastoma
Chondromyxoid fibroma
Chondrosarcoma
Secondary chondrosarcoma
Mesenchymal Chondrosarcoma
Osteogenic
Osteoid osteoma
Osteoblastoma
Osteosarcoma
Parosteal osteosarcoma

Musculo-skeletal 265
Unknown
Giant Cell Tumour
Malignancy in giant cell tumour
Ewing’s sarcoma
Chondrosarcoma
Malignant tumour of cartilage, with no tumour osteoid or bone being formed
Pain becomes severe and persistent, swelling
Typically age 40 – 60 (average 45 years)
Most common in the medullary cavity of the flat bones of the pelvis, large limb bones and ribs. Rare to
involve the extremities
Types:
Conventional: eg diaphysis or metaphysis of long bones. Margins poorly defined. Eroded or
thickened cortex. X-ray: fluffy calcification. Grossly, pearly blue/white colour of cartilage
Secondary to multiple exostosis in chondrodysplasia
Dedifferentiated
Treatment: tend to metastasise late (to lung and other bones) attempt local excision and replacement
with prosthesis
Prognosis: Grade 1 and 2 80 – 90% 5-year survival, Grade 3 (rare) 40% 5-year survival. Local or
distant metastasis may occur up to 20 years later
Osteosarcoma (Osteogenic Sarcoma)
Proliferating malignant spindle-cell stroma producing osteoid
After multiple myeloma, it is the most common primary malignant bone tumour
50 – 60% of cases are near the knee (either distal femur or proximal tibia)
Types:
Conventional osteosarcoma: Most common. Adolescent growth (age 10 – 20). M:F = 2:1, eg
metaphyses of distal femur and proximal tibia. X-ray: geographic destruction, dense of lytic,
raised periosteum. May also appear fibroblastic or predominantly chondroid. Gross:
haemorrhagic. Micro: osteoid formation, malignant spinal cells (often see spindle cells in
mesencymal tumours)
Second, smaller peak in 60 – 70s, secondary to existing disease (eg in < 1% of Paget‟s), previous
irradiation, etc. Microscopically look like a osteosarcoma
Also Telangiectatic osteosarcoma, low-grade osteosarcoma, small cell osteosarcoma (like Ewing‟s
but produces osteoid) and surface osteosarcomas (on the surface of the bone)
Investigations: X-ray, serum ALP (markedly ), and biopsy
Very aggressive: assumed to have metastasised at diagnosis – usually to lung (in preference to lymph
nodes)
Treatment: chemotherapy resection prosthesis post-op adjuvant chemo (high dose
methotrexate)
5 year survival 60%
Other
Benign:
Osteochondroma: most common benign tumour of bone. Growth of an aberrant focus of cartilage
on the surface of the bone (?adherent growth plate). Cartilage-capped lateral bony projection from
the metaphysis, usually long bones. Also know as an exostosis. Can be hereditary ( multiple).
Symptoms due to size, impingement or fracture. X-ray: mushroom like growth from metaphysis.
Regular shape. If irregular then ?malignant
Enchondroma: benign cartilaginous neoplasm usually arising in the medullary cavity of bone.
Most common in age 20 – 50 in small bones of the hand or foot. Usually clearly circumscribed.
Differential is chondrosarcoma – suspect if large bone in an older patient, erosion of the cortex or
suspicious histology
Chondroblastoma: benign chondroid neoplasm at the end of long bones during teens
Osteogenic tumours: produce osteoid:
Osteoid osteomas: Rare. Males in teens. Exquisite pain especially at night relieved by aspirin.
Well-circumscribed lesion of bony trabeculae, with variable mineralisation. < 1.5 cm. X-ray:
radiolucent central zone surrounded by opaque sclerotic bone
Osteoblastoma: Roughly speaking, an osteoid osteoma that is > 1.5 cm
Fibrous dysplasia: developmental defect of bone formation enlargement and distortion of the
bone. Feels firm, fibrous and may be gritty.
266 4
th
and 5
th
Year Notes
Malignant:
Ewing‟s Tumour: Rare. t(11;22)(q24;q12) usual fusion gene is an oncogene. Usually age 5 –
10. Usually shaft of long bones, presenting with localised pain or swelling. Small round blue cell
tumour. ?neural origin. 75% 5-year survival. Can mimic osteomyelitis
Giant Cell Tumour: F > M, age 20 – 40, ends of long bones, lytic lesions, contains multinucleated
giant cells. Usually benign. High local recurrence, rarely metastasises
Fibrosarcoma
Malignant tumour of fibroblasts (ie collagen producing cells)
Occurs in any connective tissue but more common in the extremities and middle aged
Fibrosarcoma of the bone is rare. Swelling, pain, pathological fracture
Synoviosarcoma:
Rare malignant tumour of the synovium, usually sharply circumscribed
Rapid enlargement of the joint with pain. Usually knee, hip or shoulder
May extend along fascial lines and invade bone
Treatment: if small then excise, if high grade: resection + radiotherapy + chemotherapy
Secondary Bone Cancer
Most common bone cancer always ask about previous primaries
Source: breast > prostate > kidney > lung > thyroid
Sites: vertebrae, pelvis, proximal femur, humerus
Spread: usually haematogenous. Occasionally local extension
Usually osteolytic pathological fractures
Presentation:
Pain + history of cancer in 50 – 70 year old
In children < 6 years: from neuroblastoma
Symptoms of hypercalcaemia: anorexia, nausea, weakness, depression, polyuria
Investigations:
Xray: usually osteolytic lesions (if osteoblastic probably carcinoma)
Bone scan, FBC, ALP, Electrophoresis (myeloma)
FNA: determining cell of origin helps guide management
Treatment: usually palliative, control pain, prophylactic fixation, spinal stabilisation, radiotherapy (
pain)
Arthritis Overview
Exam
Screening exam (OHCS, p 666):
Observe from behind: muscle bulk (shoulders, buttocks), straight spine, swellings, deformities
Observe from the side: cervical and lumbar lordosis, thoracic kyphosis
Touch your toes: spine and hip flexion
Observe from in front
Ear to shoulder: lateral cervical flexion, flexion, extension and rotation
Open and close the mouth: TMJ, orofacial pain
Hands behind head: shoulder and sternoclavicular movement, then straight above
Arms straight: elbow extension
Examine hands: nails, pray sign, press dorsum of both hands together
Observe legs: bulk, swelling, deformity
Knee effusion
Observe feet
Observe walking
Differentials for Arthritis
Causes of Monoarthritis
Acute Monoarthritis:
Septic arthritis: either haematogenous (staph or gonococcal) or following penetrating injury
Traumatic
Gout, pseudogout
Musculo-skeletal 267
Haemarthrosis (eg haemophilia)
Sometimes seronegative spondyloarthritis
Chronic monoarthritis:
Chronic infection (eg Tb)
Osteoarthritis
Seronegative spondyloarthritis
Metastasis
Causes of Polyarthritis
Acute polyarthritis
Infection: viral (mumps, rubella, EBV, etc), bacterial
Rheumatic fever
Onset of chronic polyarthritis
Drug allergies
Chronic polyarthritis:
Rheumatoid arthritis
Seronegative spondyloarthritis
Primary osteoarthritis
Gout, pseudogout or hydroxyapatite arthropathy
Connective tissue disease (eg SLE)
Infection (eg Tb)
Differential by Distribution
Inflammatory:
Peripheral, symmetrical, small joint polyarthritis:
RA
Lupus and Connective Tissue Diseases (non-deforming and non-nodular)
Asymmetrical, large joint, oligoarthritis, possibly with spinal disease: Sero-negative
spondyloarthropathies:
Ankylosing Spondylitis
Reactive Arthritis and Reiter‟s Disease
Psoriatic Arthritis
Arthritis of IBD
Acute inflammatory mono or oligo arthritis: septic arthritis or gout
Non-inflammatory:
Osteoarthritis: weight bearing joints or hands
Soft tissue or locomotor pain syndromes
Sacro-ilitis: occurs in Ankylosing Spondylitis, Reiter‟s Syndrome, Crohn‟s Disease, Chronic
Polyarthritis
Causes of Arthritis and Nodules
Rheumatoid arthritis
SLE (rare)
Rheumatic fever (very rare)
Granulomas, eg sarcoid (very rare)
Raynaud’s Syndrome
Episodic digital ischaemia, precipitated by cold or emotion
Fingers ache and go pale blue red/purple (pain most severe in this stage, during reperfusion)
May be:
Idiopathic: Raynaud‟s disease
Associated with underlying cause (Raynaud‟s phenomenon): Scleroderma, SLE, RA,
arteriosclerosis, leukaemia, drugs, etc. Not polyarteritis nordosa
Keep warm, stop smoking, try Ca channel blockers (eg diltiazem)
Radiology
Principles: Looking for:
Morphologic change in an individual joint
The skeletal distribution
268 4
th
and 5
th
Year Notes
Features:
Joint space narrowing, either localised or uniform
Erosions (if at the margin then periarticular erosions)
Osteophytes: bony lip at edge of joint
Subchondral cysts: formed by synovium getting through fissures in the cartilage
Subchondral Sclerosis: micro-fractures in the subchondral bone attempted repair dense white
band
Periarticular osteopenia: cytokine mediated thinning of the surrounding bone (check other joints)
Periarticular soft tissue swelling:
Fusiform: in inflammatory
Asymmetric: in gout
Features of different arthropathies:
Rheumatoid
Primary Osteoarthritis
Gout
Signs
Uniform joint space
narrowing
Erosions
Periarticular
osteopenia
Fusiform soft tissue
swelling
Can get cysts (call
geods in RA)
Localised joint space
narrowing (ie not
whole joint space)
Subchondral cysts
Marginal osteophytes
Subchondral sclerosis
Erosions (often para-
articular or long way
from the joint, may
have cave like
opening with
overhanging margins)
Relative preservation
of joint space and
bone density until late
in the disease
Asymmetric soft
tissue swelling
Distribution
Hand: proximal joints
All large joints
Symmetric
Weight bearing joints:
hip, knee, C5-C6
(fulcrum for flexing
the neck)
Distal Hand: DIP, PIP
and 1
st
carpo-
metacarpal joint
Asymmetric
Any small joints of
hands and feet
Elbows and knees
Asymmetric
Other arthropathies are variations on this:
Secondary osteoarthritis (eg due to previous trauma or infection). Looks like OA but not
standard (eg uniform joint space)
If inflammatory but wrong distribution ?sero-negative
Idiot‟s rule of thumb for hand arthritis:
Rheumatoid: MCP and MTP joints
Psoriasis: PIP joints
Osteoarthritis: DIP
Osteoarthritis
= Loss of articular cartilage in a synovial joint, and associated changes in underlying bone and other
joint tissues
Is degenerative not inflammatory
Very common, although prevalence unknown due to variations in diagnosis
Risk facts:
Age: 75% of over 70 year olds and 90% of 80 year olds
Previous injury
Female and obesity (especially hip and knee) are debated
Non-specific symptoms:
Pain: initially with/after exercise or at the end of the day, later also at rest and related to other
factors. Pain with sleeping on hip at night
Stiffness: not as prominent as in inflammatory arthritis
Swelling: due to synovial fluid (may contain a few mononucleocytes) and bony thickening
Loss of function (common to all arthritis)
Musculo-skeletal 269
Signs: joint instability, crepitus, joint tenderness, derangement, range of movement, effusion,
fixed deformity
Distribution:
Primary osteoarthritis:
Often – but not always - symmetrical
Fingers: DIP and PIP, MCP joint of thumb but not of fingers. Can lead to Heberden‟s Nodes:
marginal osteophytes at the base of the distal phalanx. Bouchard‟s Nodes on proximal IP
joints
Weight bearing joints: Hips, knees
Less Common:
Acromioclavicular joints
Lower cervical and lumbar spine
MTP joints of big toes
Secondary Osteoarthritis (secondary to joint disease or injury – consider especially if it doesn‟t fit
the joint distribution of primary):
Asymmetrical
Trauma (eg intra-articular fracture, dislocation, etc)
Infection
Metabolic: haemophilia, gout (or pseudogout if bigger joints), haemochromatosis
Avascular necrosis: see Complications of Fractures, page 234
Congenital (eg DDH)
Inflammatory (reactive or primary)
Neoplasia (eg prostate femoral head)
Pathology:
Cartilage = collagen proteoglycans + water (70%). Made by chrondrocytes
Elasticity of cartilage mechanical stress causes deformation and stress on underlying bone.
Fissuring and flaking of cartilage. Roughened cartilage surface. Blood vessels invade cartilage.
?Inflammatory cytokines mediate cartilage destruction
Micro: villus fronds in cartilage
Gross: Shiny, subchondral bone (eburnisation), subchondral cysts, osteophytes (extra-articular
overgrowth of bone attempt to weight bearing area)
Investigations:
X-ray
Lab tests usually normal (check for normal ESR, CRP, RF, ANAs, joint aspirate)
Management:
Conservative:
Inform, education
Do nothing, or
Pharmacology (analgesics, NSAIDs): Paracetamol. NSAIDs have little evidence of further
improvement, and cause renal impairment and GI bleeds. Potential for COX-2 inhibitors.
Also glucosamine (from health food shop, 1500 mg/day)
Steroid injection if secondary inflammatory component
Physiotherapy:
Obtain and maintain full range of motion (range of motion loading on a smaller area
of cartilage wears out faster)
Exercise: eg quad exercises for osteoarthritis of the knee
Orthotics and other devices:
Weight loss and devices to reduce weight bearing across affected joints
Raising bed and chairs to reduce strain, walking sticks, handrails, etc
Aspiration of joint fluid
Surgery, especially for knee and hip (determined on functional/pain criteria):
Arthroscopic debridement (buys time)
Osteotomy: take out a wedge of bone above or below the joint – realigns stress through the
joint more even wear
Arthroplasty: a prosthesis (considerable variety). Main indication is pain. Surgery to correct
fixed flexion deformity is less successful. NB don‟t forget DVT prophylaxis
Arthrodesis: joint fusion
270 4
th
and 5
th
Year Notes
Inflammatory Arthritis
Management of Inflammatory Arthritis
The different arthropathies overlap
The issue is less which arthritis it is, but whether there are risk factors for serious disease (of which the
type of arthritis is but one factor). This risk assessment will determine whether treatment is aimed at:
Aggressive treatment: use of immunosuppressives and DMARDs to induce/maintain remission
Symptomatic treatment
Risk factors for any inflammatory disease:
Evidence of active inflammation: eg morning stiffness, function, biochemical markers
Extra-articular involvement: eg lung, vasculitis, etc
Gradual onset (this is worse than sudden onset)
Large joint involvement
Genetic markets: HLA DR1 and DR4, etc
Presence of rheumatoid factor (-ive prognostic factor for erosions in rheumatoid arthritis)
Radiographic abnormalities
Blood tests in Inflammatory Arthritis
Gout and seronegative arthritis are not normally positive for rheumatoid factor and auto-antibodies
Rheumatoid Factor: IgM against Fc portion of IgG. Can be tested with the Rose-Waaler titre. Positive
in:
70-80% of RA
< 40% of SLE
100% of Sjogren‟s
30% of PSS
ANA: Autonuclear Antigens
Screening test of SLE: present in > 95% at titre > 1:200 – but not specific
Present in RA (30%), Sjogren‟s (68%), PSS (64%), and normal (0 – 2%)
Also with age, other autoimmune diseases, drugs, infections
Patterns:
Diffuse ANA suggests dsDNA may be +ive
Speckled ANA suggests ENA may be +ive
Anti-DNA histone: suggests active SLE. Also in 95% of drug SLE
Anti-centromere: suggests systemic sclerosis
dsDNA: 70% of SLE. Specific (ssDNA is not). Titres correspond to clinical activity and risk of
nephritis
ENA: Extractable Nuclear Antigens (not all speckled ANA results are due to ENAs):
Anti-Ro (SSA): Sjogren‟s, SLE (30%)
Anti-La (SSB): Sjogren‟s. Always associated with SSA. Found in only 10% of SLE
Anti-Sm: 30% of SLE. Specific
Anti-RNP: SLE (40%), polymyositis, scleroderma, mixed disorders
Anti Jo-1: polymyositis and dermatomyositis
Anti-phospholipid antibodies (attacks phospholipid on platelets)
Occurs in 50% of SLE. Do Lupus anti-coagulopathy test
3 types:
Lupus anticoagulant: Causes APTT, but causes thrombosis in vivo
Anti-cardiolipin
False positive VRDL test
1 and 2 associated with fetal loss, clotting, thrombocytopenia, valvular heart disease
Antiphospholipid Syndrome: recurrent miscarriages, thrombocytopenia and recurrent arterial or
venous thrombosis
ANCA: Associated with some small vessel vasculitis. Can divide arteritis into ANCA +ive and –ive
(although pANCA may also be found in 20% of polyarteritis nordosa):
Cytoplasmic anti-neutrophil cytoplasmic antibody (cANCA): Specific but not sensitive for
Wegener‟s disease > 90% +ive
Perinuclear anti-neutrophil cytoplasmic antibody (pANCA): Microscopic polyangitis ~ 75%
(vasculitis in kidney and lung) and PAN
ANCA negative small vessel vasculitises include Henoch-Schonlein Purpura
Musculo-skeletal 271
CD4+:CD8+ ratio (normally ~3) in Polymyalgia Rheumatica
Pharmacology
NSAIDS
Action: Many! Inhibit PG synthesis by inhibiting cyclo-oxygenase (converts arachidonic acid to PGG2
and PGH2):
COX-1: present in blood vessels, stomach, kidney (eg might actually help in heart disease – eg
aspirin)
COX-2: induced during inflammation PGs (eg Celecoxib/Celebrix and rofecoxib/Vioxx)
Effects:
Analgesic: Effective against pain where PGs sensitise nociceptors
Anti-inflammatory: Reduce vasodilation, oedema, pain. Effect may not be clinically obvious for 2
– 3 weeks
Antipyretic: acts in hypothalamus
Pharmacokinetics: well absorbed, no first pass metabolism (except aspirin), highly protein bound
Side effects:
Risk in elderly
GI: dyspepsia, mucosal irritation, ulceration (relative risk 5 times, if on warfarin, etc)
Renal: Little effect on renal function in normal people. If chronic renal impairment, CHF, gout, or
longer T½ NSAIDs then Na retention and oedema in 3 – 5%
Skin: rashes, urticaria, photosensitivity and erythema multiform
Other: headache, platelet function bleeding time, blood dyscrasias (aplastic anaemia with
indometacin and phenylbutazone)
Interactions:
Antihypertensive effect of ACE inhibitors
Diuretic action of frusemide and thiazide diuretics
Methotrexate levels
Not if on anti-coagulants GI bleed
Patient instructions: Only take them PRN to avoid risk of bleed – so don‟t take them on good days.
Watch for abdominal pain, black stools. Smoking and alcohol the risk. Don‟t supplement them with
OTC NSAIDs
Commonly used NSAIDs:
Salicylates: Aspirin (not in kids) and Diflunisal
Propionic Acids (better tolerated and more sensitive for COX-2): Ibuprofen, Naproxen
Pyrazoles: Phenylbutazone
Acetic Acids: Indometacin (potent, CNS side effects), sulindac
Paracetamol (no anti-inflammatory or GI effects)
Other Pain relief
Amitriptyline: a TCA which in low dose has pain modifying effects
Tramadol: opiod analgesic with less respiratory depression, constipation and addiction
Immune Suppressive Drugs
For acute inflammatory problem (arthritis, connective tissue, etc)
Prednisone: 60 mg/day starting dose
Methylprednisolone (iv)
Disease Modifying Anti-Rheumatic Drugs (DMARDs)
Aim: to suppress inflammatory activity destructive changes (NSAIDs reduce inflammation but
don‟t act on the pathway that leads to joint destruction)
Indicated for patients at an early stage with high markers of disease activity don‟t wait for RF,
nodules or erosions
Effect:
Suppress inflammatory activity
Reduce the need for NSAIDS and corticosteroids which have greater potential toxicity
First line agents (high efficacy especially in combination, low toxicity):
272 4
th
and 5
th
Year Notes
Sulphasalazine: start low, increase to 2-3g per day. Best tolerated and most often used. Effect
after 3 – 6 months. SE: nausea, rashes, sperm count, hepatitis, oral ulcers, rarely: blood
dyscrasia, Stevens-Johnson, neutropenia, monitor CBC and LFTs
Methotrexate: Takes several months to work. Action: IL-1, IL-10, neutrophil chemotaxis.
SE: nausea, bone marrow suppression, GI ulceration, teratogenic. Inhibits folate metabolism
give folic acid 5 – 10 mg/wkly, rare: irreversible liver toxin. Monitor CBC, LFTs, Cr
Antimalarials: Hydroxychloroquine: weak disease modifying drug, doesn‟t stop periarticular
osteopenia. SE: nausea, rash, headache, tinnitus. Rarely: bone marrow suppression, corneal &
retinal damage. Monitor: Cr and 6 – 12 monthly ophthalmological review. Chloroquine more
toxic.
Others:
Gold: Sodium Aurothiomalate / Myocrisin. Similar efficacy to Sulphasalazine/methotrexate but
more toxic. When it works it works well. Action: accumulates in macrophages. SE: rash
thrombocytopenia, nephrotic syndrome, proteinuria. Not with allopurinol, SLE, breast feeding,
liver/renal disease. Monitor CBC, Cr, Urine dipstick for protein
Cyclosporin A: SE nephrotoxicity
Salazopyrin
Beneficial but don‟t alter progression of radiological changes:
Azathioprine
D-Penicillamine. SE: marrow, proteinuria, taste, oral ulcers, myasthenia, Goodpasture‟s
The future: anticytokine therapy: eg against Tissue Necrosis Factor
Rheumatoid Arthritis
Persistent, symmetrical, deforming, peripheral arthropathy
Epidemiology:
Peak onset: 4
th
decade
Prevalence: 1-3%
Female:male = 3:1
Pathogenesis:
Microbial agent initiates the disease: current suspect is EBV, plus others
Presentation of (unknown) antigen to CD4+ T-helper cells + plasma cells and macrophages
cytokine-mediated synovial neutrophilic exudate + vascularity cartilage-degrading enzymes +
fibrosis + panus formation (inflamed synovium) + osteoclastic activity + ligament and tendon
damage
Painful, unstable, disrupted joint (eg subluxed, deformed, etc)
65 – 80% are HLA DR4 or DR1 +ive, plus further specific DR alleles (eg Q(k/R)RA motif in the
DRB1-HV3 region of the T-cell antigen receptor)
Autoimmunity to type 2 collagen can be demonstrated in most patients with RA
80% have Rheumatoid Factors: autoantibodies (mainly IgM) to the Fc portion of autologous IgG
Implicated mediators are cytokines: TNF, IL-1, IL-6, IL-15, interferon-, growth factors,
proteases, elastases
Presentation:
Common: Swollen, painful, stiff hands and feet, especially in the morning. Progresses to larger
joints
Less common:
Palindromic: relapsing and remitting monoarthritis of different large joints
Persistent monoarthritis (especially the knee)
Systemic illness: weight, pericarditis, pleurisy
Vague limb girdle aches
Sudden-onset widespread arthritis
Greatest damage occurs in first 4 – 5 years
Pattern of involvement:
Usually symmetrical
Most RA involves:
PIP and MCP joints and wrists (DIP spared) in the hands
Tarsal and MTP joints in the foot
Also involves:
Elbows
Shoulders (eg Pencilling – erosion of distal end of the clavicle)
Musculo-skeletal 273
Small joints of upper cervical spine: Atlanto-Axial instability: anterior subluxation of C1 on
C2 with cervical flexion due to erosion of the transverse atlantal ligament threatens spinal
cord
Lumbo-sacral region usually spared
Hips
Knees
Deformities:
Initially sausage-shaped fingers and MCP joint swelling
Ulnar deviation and volar subluxation (partial dislocation) of the fingers
Fingers: Swan Neck and boutonniere (buttonhole)
Z deformity of the thumb: hyperextension of the IP joint and fixed flexion and subluxation of the
MCP joint
Subluxation of the wrist, with prominent radial head
Extra-articular involvement:
Nodules: subcutaneous central zone of fibrinoid necrosis surrounded by pallisading histiocytes and
fibroblasts. May occur in viscera, including heart, lung and GI
Anaemia
Lymphadenopathy
Vasculitis
Carpel Tunnel Syndrome (early manifestation)
Multifocal neuropathies (= Mononeuritis Multiplex): Sequential, multifocal, random involvement
of non-contiguous peripheral nerve trunks (there are other causes besides RA)
Splenomegaly
Eyes: episcleritis, scleritis, keratoconjunctivitis sicca
Pericarditis
Pulmonary fibrosis
Amyloidosis
Not glomerulonephritis
Investigations
X-ray
Bloods: Rheumatoid factor +ive in 75% (See Blood tests in Inflammatory Arthritis, page 270)
Treatment:
Regular exercise
Physiotherapy
Occupational therapy
Household and personal aids (eg wrist splints)
Intralesional steroids
Surgery
Drugs:
NSAIDs (eg ibuprofen): Least likely to cause a bleed. Contraindicated if asthma or peptic
ulcer. To control inflammation/pain
Steroids: To control flare-ups. Can reduce erosions if given in early disease. Need to keep
dose low (ie 7.5 mg/day) – but due to symptomatic improvement patients often want more.
SE: bony density, cataract, fluid retention, peptic ulcers
Disease modifying drugs: See Disease Modifying Anti-Rheumatic Drugs (DMARDs), page
271. All have side effects, monitoring essential. All can cause rash
Juvenile Rheumatoid Arthritis
= Arthritis beginning at or before 16 years of age (usually early childhood)
= Still‟s Disease
Signs: High, swinging, early evening fever, pink maculo-papular rash, arthralgia, arthritis, myalgia,
generalised lymphadenopathy
Number of different types:
Oligoarthritis (persistent): asymmetrical, affecting 4 or fewer joints, especially wrist, knees, ankles.
Usually remission in 4 – 5 years
Oligoarthritis (extended): Oligoarticular onset progressing to > 4 joints
Polyarticular JCA: Usually in teenagers progressing to widespread joint destruction, especially
hands (less so the DIPs)
274 4
th
and 5
th
Year Notes
Extra-articular involvement can include: pericarditis, myocarditis, pulmonary fibrosis,
glomerulonephritis, uveitis and growth retardation
Differences from Adult RA:
Oligoarthritis is more common
Systemic onset is more frequent
Large joints affected more than small joints
Rheumatoid nodules and rheumatoid factor are usually absent
ANAs often positive
Treatment:
Referral to specialist
Low dose NSAIDs/paracetamol (Aspirin: beware of Reyes Syndrome)
Corticosteroids
Prognosis: variable: up to 50% have long term disability
Completely different disease entity to Juvenile Spondyloarthropathies – although clinically may
overlap. Enthesitis common
Spondyloarthropathies (Seronegative Arthritis)
Rheumatoid factor is negative – but exclude seronegative RA
Clinical overlap between the conditions
Acronym: PEAR: Psoriasis, Enteropathic, Ankylosing Spondolytis, Reactive/Reiter‟s
Have in common:
Involvement of spine and sacroiliac joints (= axial arthritis)
Usually asymmetrical large joint mono or oligo-arthritis
Inflammation then calcification of tendon insertions (enthesopathy)
Extra-articular manifestations: uveitis, aortic regurgitation, upper zone pulmonary fibrosis
Familial tendency + HLA-B27 +ive predisposition
If type not clear then classified as „Undifferentiated spondyl-arthropathy‟:
AS
Reiter‟s
Reactive
Psoriatic
Enteropathic
Sex
M > F
M > F
M = F
F > M
F = M
Age of onset
~ 20
Any
Any
Any
Any
Uveitis
++
++
+
+
+
Conjunctivitis
-
+
+
-
-
Peripheral joints
Lower>Upper
Usually lower
Lower>upper
Upper>lower
Lower>upper
Sacroiliitis
Always
Often
Often
Often
Often
HLA-B27
95%
80%
80%
20 – 50%
50%
Onset
Gradual
Sudden
Sudden
Variable
Gradual
Symmetry spinal
+
-
-
-
+
Ankylosing Spondylitis
= Chronic systemic inflammatory disorder of the axial skeleton, affecting SI joints and spine
Ankylosing = fibrous replacement of the joint bony fusion
Epidemiology:
Prevalence: 2 – 5 per 1,000 males. Men have more progressive disease
Men more common and present earlier (6:1 at 16 years, 2:1 at 30 years)
Onset usually between 15 – 40 years
Closely linked to HLA-B27:
5 – 20% risk for positive individual
11 HLA subtypes identified with different disease susceptibilities
Strong ethnic variances in HLA prevalence: present in Caucasians, absent in indigenous
people of South America and Australia, high prevalence in Eskimos….
Clinical presentation:
75% first present with insidious onset of dull back ache, worse at night, improved by exercise
Morning stiffness, backache, sacroiliac pain, loss of spinal movement (spinal ankylosis, distraction
of < 10 cm on flexion with Schober‟s test)
Leading to flattening of lumber spine, thoracic kyphosis, neck hyperextension
Fatigue common
Distribution:
Sacroiliac joints and spine (lumbar to start with, C-spine later):
Bilateral sacro-iliac joint tenderness
Musculo-skeletal 275
Tenderness of the lumbar vertebrae
Loss of thoracic kyphosis and lumbar lordosis
Early restriction in lateral flexion of the spine – test by seeing how far they can slide their
hand down the side of their leg without bending forward. Later loss of movement in all
directions
Hips (30%), also knees and shoulders
Peripheral arthritis infrequent
Other features:
Commonly:
Enthesitis
Iritis/Anterior Uveitis (25 – 30%): unilateral, acute, painful, with photophobia and blurred
vision. To test: shining light in opposite eye causes pain in the affected eye
Costocondriasis + chest pain referred from thoracic vertebrae
Chest wall rigidity VC
Plantar fasciitis
Rare:
Neurological involvement: secondary to spinal fracture (eg C-spine), atlanto-axial subluxation,
cauda equina syndrome
Amyloidosis
Carditis and aortic regurgitation due to fibrosis of the aortic valve (can also affect AV bundle
arrhythmias)
Apical lung fibrosis (rare)
Pathogenesis:
Cross reactivity between Klebsiella pneumoniae antigens and HLA B27
Antibody complexes cause synovitis, enthesopathy (including tendon attachment calcification)
capsular ossification, ankylosis (bony fusion) of the sacroiliac joint, inflammatory arthritis of the
synovial joints in the spin and ossification of spinal ligaments
Diagnosis is clinical: History of inflammatory spine disease + SI tenderness, L-spine mobility, chest
expansion
Differential from RA:
Spine rarely affect in RA
Small peripheral joints rarely affected in AS
In AS there are no subcutaneous nodules and no RF (but there may not be in RA either)
Investigations:
X-rays: „bamboo‟ or „railroad‟ spine, squaring of vertebrae, syndesmophytes, erosions of the
apophyseal joints (between rib tuberosities and spinal processes), eventually bony ankylosis of the
SI joints (also seen in Reiter‟s and Crohn‟s diseases)
Bloods:
FBC (mild normochromic anaemia in 15%)
ESR and CRP
Treatment:
Physiotherapy/Exercise (not rest) to maintain posture and mobility
NSAIDs to relieve pain and stiffness (especially phenylbutazone). If ineffective try sulphasalazine
Local corticosteroids for uveitis, enthesitis, peripheral synovitis
Disease Modifying drugs if severe
Psoriatic Arthritis
Epidemiology: occurs in 5 – 7% of psoriasis patients, age 35 – 45, male = female
Pathology:
Can have a reactive type presentation due to a host of possible infective/inflammatory agents
Primary lesion = synovitis (similar to RA): hypertrophic villi, T-cell infiltration, aggregates of T
cells. But usually only minimal joint impairment. Articular destruction in a subset (25%) with
panus formation, cartilage erosion, etc = Arthritis Mutilans
Clinical presentation:
Usually psoriasis develops first, then arthritis, but 15% go the other way
Usually insidious but can present acutely
Check for nail pitting, transverse ridging, oncyholysis
Extra-articular manifestations are uncommon (except for conjunctivitis and iritis)
276 4
th
and 5
th
Year Notes
Distribution:
Often asymmetric, mainly oligo but can be poly arthritis
Often upper limb
DIP joints in hands and feet especially affected – unique to PA
Sacroiliac joints and spine (20 – 40%) – asymmetric involvement common
Rheumatoid pattern
Inflammation of digital tendon sheaths sausage finger (dactylitis)
Enthesitis: Achilles tendonitis and plantar fasciitis
Diagnosis: Psoriasis (exclude seborrhoeic dermatitis and fungal infections) or psoriatic nail
involvement + sero-negative arthritis. Increased likelihood in B27 +ive
Investigations: X-ray of hands DIP involvement + resorption of the terminal phalanges
Treatment:
NSAIDs for pain – but may worsen skin lesions
Corticosteroid injections for local synovitis
If severe: methotrexate, cyclosporin, sulphasalazine, gold etc
Differentiating from RA:
Presence of skin rash
Asymmetric
DIP and PIP involvement
Can overlap with RA and present as a symmetrical, destructive arthritis. Look for psoriasis and
nail changes
Reiter’s Syndrome
Classic triad: urethritis, conjunctivitis and seronegative arthritis. Recurrence in 50%, attacks can last
several months
Caused by sterile synovitis following chlamydia/NSU/shigella infection
Distribution of arthritis usually lower limb (may be chronic or relapsing):
Sacroiliac joints and spine
Hips
Knees
Ankles and most of the joints of the feet
Other features:
Iritis
Keratoderma blenorrhagica (brown, aseptic abscesses on soles and palms)
Mouth ulcers
Circinate balanitis (painless serpiginous penile rash)
Enthesopathy (plantar fasciitis, Achilles tendonitis)
Not onycholysis (differentiates from psoriasis)
Investigations:
Chlamydia: First of 2 glass urine test shows more debris in the first glass in urethritis (cf
prostatitis where there is more in the 2
nd
)
Anti-chlamydial antibodies
Neutrophils in synovial fluid
X-rays: periosteitis at ligamentous insertions. Rheumatoid like changes if chronic
Pathogenesis: following non-specific urethritis, Chlamydia or Shigella infection in those genetically
pre-disposed (ie HLA B27). Hyperaemic synovial membrane, but no panus or cartilage erosion (except
if progressive). Profuse osteolysis and formation of new periosteal bone
Management: treat causal agent, rest, NSAIDs, steroid injections, recovery may be slow
Other Reactive Arthritis
Infective causes: Yersinia, Chlamydia, Campylobacter, Salmonella, Shigella, Clostridium difficile…
(all have lipopolysaccharide in their outer cell membrane)
Sterile immunological reaction in joints due to cross reactivity of antigens
Usually B27+
Presentation:
Acute asymmetrical polyarthritis (esp of lower limb) 1-2 weeks post infection lasting for 3 – 6
months
Can become chronic with relapsing and remitting course
Enthesitis is common (eg plantar fasciitis or Achilles tendonitis)
Musculo-skeletal 277
Can also get:
Skin lesions resembling psoriasis: Circinate balanitis, keratoderma blenorrhagica and nail
dystrophy
Iritis
Investigations:
Causative agent: Blood culture/serology for antibodies/stool culture
HLA-B27, X-ray, ESR, joint aspiration for sceptic arthritis
Diagnosis is clinical
Management:
Treating persisting infection has little impact on course
NSAIDs/corticosteroids
Sulphasalazine etc if necessary
Also in leukaemia, endocarditis, acne, acromegaly, Wilson‟s disease, sarcoid, sickle cell,
haemochromatosis
Enteropathic Arthropathies
Associations:
Inflammatory bowel disease (15% of Crohn‟s and UC get arthritis)
Also associated with intestinal bypass surgery and Whipple‟s Disease
Asymmetrical lower large joint mono- or oligo arthropathy
No joint destruction
Sacroiliitis or Spondylitis in 5% (70% of these have HLA-B27)
Manage underlying condition:
Sulphasalazine for both bowel disease and arthritis
NSAIDs and steroid injections for monoarthritis
Crystal Arthropathy
Gouty Arthritis
Prevalence: ½ - 1%, male:female = 5:1. Common in Maori and Polynesian populations. Most people
with hyperuricaemia don‟t have gout
Family history common
Types:
Acute Gout:
Severe pain, redness and swelling, may be febrile
Differential of acute gout: septic arthritis or haemarthrosis
Chronic Recurrent Gout:
Urate deposits with inflammatory cells surrounding them (tophi) in avascular areas: pinna,
infra-patella and Achilles tendons, joints, eye, etc chronic tophaceous gout = gouty tophi
Bone erosion and loss of cartilage
Distribution:
Acute gouty arthritis is usually monoarticular
Affects MTP joint of the great toe in 75% of cases
Ankles and knees involved after recurrent attacks
Fingers, wrists and elbows affected late
Pathogenesis:
Uric acid is the last step in the breakdown of purines
Hyperuricaemia (uric acid > 0.41 mmol/L) deposition of monosodium urate crystals (MSU) in
joints (and viscera, especially the kidney) chemotactic to leukocytes and activate complement
accumulation of neutrophils and macrophages erosion, inflammation, secondary OA
May be precipitated by trauma, surgery, starvation, infection and diuretics
Hyperuricaemia results from turnover or excretion
Causes of excretion:
Primary gout
Renal failure hyperuricaemia which rarely gout
Hypertension
Primary hypoparathyroidism
Hypothyroidism
278 4
th
and 5
th
Year Notes
Lactic acid production (eg from ETOH)
Cell turnover (turnover of purines) due to:
Lymphoma, leukaemia, severe psoriasis, haemolysis, muscle necrosis
Disorders of purine synthesis (eg Lesch-Nyhan syndrome)
Hyperuricaemia can also cause renal failure eg cytotoxic treatment
Diagnosis:
Needle shaped, negatively birefringent urate crystals in tissues and synovial fluid (serum urate not
always ) – also neutrophils (+ ingested crystals)
ESR
Check renal function and BP
X-rays: in early stages may only show soft tissue swelling
Treatment:
Acute:
NSAID (eg ibuprofen, Naproxen, indometacin, not aspirin) – but problematic in renal failure
and heart failure ( fluid retention). Also contra-indicated if on anticoagulants ( GI bleed)
Colchicine
Prevention:
Avoid purine-rich foods (offal, oily fish, beer), obesity and excess alcohol (which is why it
used to be called the „disease of kings‟)
No aspirin: salicylates competes with uric acid for excretion serum urate
Long term („interval‟) treatment: Allopurinol:
Xanthine-oxidase inhibitor serum urate
But not during an acute attack – wait three weeks. Mobilises gouty tophi systemic
urate precipitates acute gout. Use with colchicine cover
SE: rash, fever, WCC
Allopurinol can also be used during chemotherapy for leukaemia/lymphoma/myeloma to
prevent gout from purines
Also uricosuric drugs ( excretion): probenecid or sulfinpyrazone
Pseudogout
= Calcium Pyrophosphate Deposition (CPPD)
Onset in 30s
Deposition of chalky white crystalline material – usually calcium pyrophosphate
Chondrocalcinosis: deposition in articular cartilage calcification on x-ray
Predominantly large joints (especially the knees)
Aspirate: positively birefringent rhomboid shaped crystals
In some there are signs of hyperparathyroidism and haemochromatosis
Connective Tissue Diseases
= Collagen vascular diseases
Affect many organ systems, associated with systemic fever and malaise, run a chronic course, respond
to steroids, associated with anaemia of chronic disease and a raised ESR
Systemic Lupus Erythematosus
Non-organ specific autoimmune vasculitis with positive ANAs
Epidemiology:
Peak age of diagnosis: 30 - 40
Female:male = 9:1
Prevalence: 0.2%
Commoner in pregnancy, Afro-Caribbeans, Asians
Genetic predisposition: HLA B8, DR3, DR2
Presentation (OHCM p 672):
Gradual or sudden onset
General: Fever (77%), splenomegaly, lymphadenopathy, extreme fatigue
Musculo-skeletal symptoms (95%): joint/muscle pain, non-erosive small joint polyarthritis, bone
necrosis, rare joint deformity due to capsular laxity
Musculo-skeletal 279
Skin (81%): photosensitive butterfly rash (hyperkeratosis, follicular plugging), scarring alopecia,
Raynaud‟s, purpura, oral ulcers, discoid lupus (3 stage rash: erythema pigmented hyperkeratotic
oedematous papules atrophic depressed lesions), nailfold vasculitis
Renal (<75%): proteinuria, casts, oedema, uraemia, glomerulonephritis. See Systemic Lupus
Erythematosus, page 208 for renal complications
CNS (<18%): Depression, psychosis, fits, cranial nerve lesions, retinal exudates
Pulmonary (<48%): Pleurisy (+/- effusion), fibrosing alveolitis, BOOP
CVS (38%): BP, pericarditis, Libman-Sacks endocarditis
Blood: Normocytic anaemia (75%), Coombs +ive haemolysis, WCC, INR, platelets, ESR,
normal CRP
Mortality is due to renal failure
Pathology: Autoantibodies fibrinoid change fibrosis
Investigations:
FBC
ESR > 20, CRP often low
80% are ANA +ive: High dsDNA ANA almost exclusive to SLE (+ive in 40 – 60%)
40% are RF +ive
30% are anti-Sm positive
Lupus anti-coagulopathy test
Antibodies to Ro (SS-A), La (SS-B) and anti-RNP (ribonuclear protein) help define overlap
syndromes
VDRL false positive in 30%
Organ/skin biopsy
Pain disproportionate to radiological damage on X-ray
Monitoring:
BP
Urinalysis
FBC, U&E, Complement (C3, C4 – better than ESR)
dsDNA ANA titres
Treatment:
Sun block creams
Analgesics/NSAIDs: joint pain, swelling, fever
Hydroxychloroquine for skin and joint pain. For disease not controlled by NSAIDs SE:
retinopathy – check eyes annually
Prednisolone: higher dose for exacerbations, lower dose for chronic disease – mainstay of
treatment
Cyclophosphamide: either daily or monthly pulse (fewer side effects): helps renal function more
than steroids
Azathioprine: steroid sparing. SE: lymphoma
Cyclosporin or methotrexate
Drug Lupus:
Caused by isoniazid, hydralazine, procainamide, chlorpromazine, anticonvulsants
Lung and skin effects greater than renal and CNS
ENA anti-histone more likely to be positive
Remits if drug stopped
Sulfonamindes and the Pill may exacerbate idiopathic SLE
Discoid lupus = skin involvement only. See Discoid Lupus Erythematous (DLE), page 330
Sjogren’s Syndrome
= Dry eyes, dry month and associated with rheumatoid arthritis
Epidemiology: onset 15 – 65 years, more common in women
Types:
Primary (ie no other connective tissue disease)
Secondary: associated with other connective tissue diseases: Rheumatoid (50% of Sjogren‟s have
RA), SLE, Scleroderma, Polymyositis, Primary biliary cirrhosis (ie autoimmune disorders), graft-
verses host disease, AIDs
Presentation:
Gritty, sore eyes: keratoconjunctivitis sicca (lacrimation dry eyes)
280 4
th
and 5
th
Year Notes
Dry mouth: xerostomia (salivation) – can‟t swallow, need sips of water at night, enlarged tender
parotids
Also dry nose, vagina
Tiredness/depression
Arthritis as in SLE
Raynaud‟s
Pulmonary fibrosis, pleurisy
Also peripheral neuropathy, renal involvement, hepatosplenomegaly, pancreatitis, etc
Compared to RA:
ANA is more strongly positive in Sjogren‟s
Arthritis is not destructive
Investigations:
Schirmer test: < 10 mm of filter paper under the lower eye lid is wet after 5 minutes
ESR & CRP. May have normal CRP (can get this in most CTDs, but not RA)
100% have RF
ANA positive in 60 – 70%
Anti-Ro (SSA) and Anti-La (SSB) present in 70% of primary, and 10% of secondary. NB Ro and
La antibodies cross the placenta causing congenital heart block
Pathology:
Connective tissue disease
Lymphocytes and plasma cells infiltrate secretory glands (also skin, lungs and liver) causing
fibrosis
Inflammation and destruction of exocrine glands: especially salvia and tears, with CD4+
lymphocytes
HLA DR3 association
Treatment
Artificial tears and saliva
Hydroxychloroquine and methotrexate
Progressive Systemic Sclerosis (PSS)
Connective tissue disease with inflammation, vasculitis and fibrotic changes in skin and viscera
Epidemiology: female = 3 * male. Any age, but peak is 30 – 50 years
Pathology:
Small vessel damage + oedema collagen laid down fibrosis and contraction
Dilation of other vessels telangiectasia
Presentation:
Raynaud‟s (90%) may precede other signs by years
Then swelling of fingers and hands
Then skin gets tight, waxy and tethered (eg fingers – pointy fingers, forearms, face – no wrinkles,
pointy nose)
Other: telangiectasia, nail bed spots, symmetrical polyarthritis
Types:
Diffuse/Generalised Progressive Systemic Sclerosis: widespread skin involvement with early
visceral involvement kidney (proteinuria, sediment, maybe crisis BP), polyarthritis,
myopathy, lung fibrosis (expansion + gas transfer SOB) and GI fibrosis
CREST Syndrome (probably very different disease entity to Diffuse): Calcinosis (subcutaneous
calcium deposits on hands) + Raynaud‟s phenomenon + disordered oesophageal motility (heart
burn and dysphagia) + sclerodactyly (Scleroderma of the hands) + telangiectasia. Centromeric
ANA
Limited Scleroderma:
Tightening and fibrosis of the skin: proximal skin scleroderma (eg face – can they open their
mouth wide, any wrinkles – if so then no involvement. Limited mouth opening =
microstomia) or any 2 of sclerodactyly (can they make a fist, Prayer sign: can they oppose
palmar MCP joints), digital pitting scars, pulp loss, bibasilar lung fibrosis. Late visceral
involvement
Scleroderma limited to the hands and maybe face („Limited Scleroderma‟) is probably a
presenting symptom of CREST syndrome even if the other features aren‟t present
Morphoea (localised skin sclerosis) rarely, if ever, progresses to PSS
Musculo-skeletal 281
Investigations:
FBC: normocytic anaemia, haemolytic anaemia
ESR
ANA positive in 75%. May have autonuclear autoantibodies in any of these three forms to:
topoisomerase (Scl-70), RNA polymerases and centromeres. Anticentromere (ACA) in Limited
and CREST. AntiScl-70 in diffuse.
RF +ive in 30%
24 hour urine
Hand x-ray. Can get distal phalanges resorption
Barium swallow and CT of lung
Treatment:
No cure
Education, support groups, etc
Raynaud‟s: warmth and vasodilators (Ca blocker)
Oesophageal mobility: omeprazole, cisapride, reflux prevention
Renal & Raynaud‟s: ACE inhibitors
Scleroderma: D-penicillamine (antifibrotic) or immunosuppressants (little efficacy from steroids)
Prognosis: Limited disease has 70% 10-year survival; diffuse has 55% 10-year survival. Death from
lung/renal effects
Mixed Connective Tissue Disease
Features of SLE, PSS and polymyositis
Anti-RNP (ribonuclear protein) +ive without other types of ANA
Polymyositis and Dermatomyositis
Peaks in age 10-14 (mainly dermatomyosis) and 45 – 60 years (mainly polymyositis). Rare
Presentation:
Voluntary muscle inflammation insidious, symmetrical, proximal muscle weakness (shoulders,
hips, trunk, neck – compared to polymyalgia rheumatica which just has stiffness). May atrophy
and contractures
Skin (only Dermatomyositis): Gottron‟s lesions: erythematous plaques or macules over MCP
joints, extensor knees, wrist and elbows. Rash over upper chest, neck, etc
Other symptoms: Fatigue, malaise, weight loss, fever
Causes dysphagia, dysphonia, facial oedema, respiratory weakness
Also Raynaud‟s, lung involvement (interstitial fibrosis), polyarthritis, retinitis, myocardial
involvement, purple rash on cheeks and light exposed areas
Differential Diagnosis:
Infection
Muscular dystrophy
Endocrine: thyroid, PTH, Ca, K
Neurology: motor neurone, Guillian Barre, Myasthenia Gravis
Drugs
Investigations:
ESR, CRP, CK, maybe AST and LD
RF positive in 50%
ANA may be +ive, as well as myositis specific antibodies (eg AntiJo-1 – linked to HLA DR3)
EMG denervation and myopathy (not usually done)
Biopsy: inflammatory muscle infiltrate + fibrosis
Associations:
Other autoimmune rheumatological diseases
Malignancy in 10%
Coxsackie virus, rubella & influenzae
Diagnosis of exclusion
Treatment: rest, steroids, methotrexate, Ig, active graded exercise between attacks
Polymyalgia Rheumatica
Old ladies with morning stiffness in proximal muscles +/- mild polyarthritis, depression, fever,
anorexia, maybe jaw claudication, angina, hypopituitarism, not weakness
282 4
th
and 5
th
Year Notes
May be features related to underlying CTDs (arthritis if superimposed RA, headache in GCA ask
about headaches, visual disturbance etc)
?Syndrome with many underlying causes (eg variety of connective tissue diseases)
Differential:
RA with onset of central joints
Frozen shoulder
Carcinomas: breast, thyroid, prostate
Myeloma
Polymyositis
Bacterial endocarditis
Investigations: ESR, anaemia, no abnormality on X-ray, usually RF and ANA negative, CK not
usually raised, liver involvement ALP
Treatment: dramatic response to low dose steroids (eg 15 mg/day)
Vasculitis
Associations:
Occurs in non-organ specific autoimmune diseases (eg RA, SLE)
Principal feature of other connective tissue diseases that may or may not be autoimmune
Also occurs in conditions not usually included in connective tissue diseases (eg drug reactions)
Types:
Large vessel vasculitis: Giant cell arteritis, Takayasu‟s arteritis
Medium sized vessels: Polyarteritis Nodosa (PAN), Kawasaki‟s disease
Small vessel vasculitis: Wegener‟s Granulomatosis, Microscopic Polyarteritis, Henoch-Schonlein
purpura
Giant Cell arteritis/Temporal Arteritis
Medium and small arteries (especially temporal arteries medical emergency – affects retinal
arteries).
From 50 years, peaking at 75.
Clinical: Initially persistent headache, then superficial pain and tenderness over temporal arteries,
unilateral visual disturbance, arthritic pain, jaw claudication, fever, malaise, ESR (Age and ESR both
over 60 in 3/4 cases)
Immune reaction with internal elastic lamina
Diagnosed by biopsy showing giant cells engulfing the IEL and inflamed media. Biopsy is critical as
treatment should continue for 2 years and therefore want to be sure of diagnosis
Presumptive treatment with steroids. Immediate risk is blindness, but longer-term morbidity is due to
steroid treatment!
Overlaps with Polymyalgia Rheumatica in 25% of cases ( stiff proximal muscles in the morning).
See Polymyalgia Rheumatica, page 281
Polyarterititis nodosa
Affects young adults. M:F = 4:1.
Presents with non-specific symptoms – fever malaise, abdominal pain, renal failure, purpura.
Immune complex mediated arteritis (type 3 hypersensitivity)
40% associated with Hep B
Necrotising vasculitis of medium sized arteries (not arterioles). Involves smaller arteries – kidney,
heart, liver, GI. Often patchy distribution. Macroscopic: small nodules. Microscopic: fibrinoid
necrosis, intimal proliferation, media destruction, inflammation of adventitia, scarring if chronic.
Investigations: FBC, biopsy of affected organ, ECG, ANCA may be +ive
Treatment: steroids/immunosuppressives (azathioprine/cyclophosphamide)
Kawasaki Disease
= Mucocutaneous Lymph Node Syndrome ~ Childhood Polyarteritis Nordosa
Immune mediated injury to vascular endothelium, including coronary artery arteritis
?post viral
Fever in kids (usually < 5) for > 5 days with bilateral, non-purulent conjunctival infection, oral mucosal
changes, cervical lymphadenopathy, changes in the extremities (eg swelling of hands), & generalised
rash
Investigations: Echo for coronary aneurysm, FBC (WBC, platelets), CRP
Musculo-skeletal 283
Differential: Scarlet fever, EBV
Complications: pancarditis, aneurysms or dilatation
Treatment: none, or high dose IgG/steroids
Wegener’s Granulomatosis
Generalised necrotising arteritis of small-medium sized arteries of the respiratory tract and kidney with
non-caseating granuloma formation
Wegner‟s triad: aseptic necrosis of the lower and upper respiratory tract and focal glomerulonephritis
of the kidney
Presentation:
Upper airways disease (chronic rhinitis/epistaxis/sinusitis/mouth ulcers) unresponsive to therapy.
CXR shows spots. May have haemoptysis. Progresses to ulceration of nasal mucosa, perforation
of the septum, heavy nose bleeds, granulomatous invasion of large bronchi bronchial stenosis
Glomerulonephritis. If untreated then slow progression to end stage renal failure
Systemic: fever, night sweats, weight loss, et
Non-deforming arthritis and arthralgia
Progression highly variable
Investigations:
ESR, c-ANCA positive, CXR (nodular masses, cavitation)
Renal biopsy: necrotising glomerulonephritis: may be focal and crescentic. Immunoflouresence is
–ive pauci-immune
Treatment: steroids +/- cyclophosphamide 90% remission but frequent relapse. Continue for a year
then taper off
Microscopic Polyarteritis
Vasculitis of small-medium sized vessels
Multisystem involvement including glomerulonephritis
Kidney involvement: crescentic rapidly progressive GN common, no immune deposits on
immunoflouresence (ie pauci immune)
Biopsy: fibrinoid necrosis and cellular proliferation within capillaries
Frequently positive for p-ANCA
Treatment: similar to Wegener‟s
Henoch-Schonlein Purpura
Leukocytoclastic vasculitis of small vessels with deposition of IgA immune complexes in the skin, gut
and kidney
Usually in young children, associated with URTIs
Palpable purpuric rash over the buttocks and ankles, abdominal pain and arthralgia
Renal involvement: macroscopic or microscopic vasculitis, mesangial proliferative glomerulonephritis,
maybe crescentic, IF +ive for mesangial IgA deposition
Usually self-limiting, otherwise steroids
Others
Hypersensitivity angiitis (Leukocytoclastic vasculitis): Type 3 immune injury. Associated with
medicines, lupus, HBV. Microscopically: neutrophils, fibrinoid necrosis
Takayasu’s arteritis: Aortic thickening with autoimmune granulomas = Pulseless Disease. Rare, in
young females, hypertension, pain of affected artery
Thromboangiitis Obliterans = Buerger‟s disease. Neurovascular bundles – mainly in legs and arms
of young/middle aged smokers – become inflamed and thrombosed
Behcet’s Disease: Systemic vasculitis, commoner in Turkey and Japan, oral and genital ulcers, eye
lesions, arthritis of knee, ankles, wrists and elbows
Pain Syndromes
Chronic/Complex Regional Pain Syndrome (Type 1)
= Reflex Sympathetic Dystrophy
=Algodystrophy
Can develop as a consequence of trauma affecting the limbs with or without obvious nerve lesion
284 4
th
and 5
th
Year Notes
Cause: ?peripheral sympathetic over-activity, pathological interaction of sympathetic and afferent
systems
Presentation:
Pain
Abnormal blood flow (cold or hot) and sweating (including distal to the trauma)
Structural changes eg muscle wasting (over months to years can contractures)
Treatment: difficult: pain relief, rehabilitation, physio, early refer to pain management clinic
Fibromyalgia
Aetiology: unknown
Presentation:
Diffuse musculoskeletal pain (over all 4 quadrants and axial) but normal muscle power
Morning stiffness
Paraesthesia
Tender points over the body
Skin fold tenderness
Sleep disturbance, fatigue and vertigo
ESR usually normal
Associations: Raynaud‟s phenomenon, anxiety/depression, IBS
Diagnosis: based on finding a number of separate, defined tender points
Treatment: analgesics and exercise
Plastic and Reconstructive Surgery
Restoration of function and correction of deformity
Resulting from trauma, neoplasia, etc
Largely about transferring tissue
Techniques:
Direct closure
Graft: gets blood supply from wound site
Flaps: brings blood supply with it (especially over bony prominences, and if further surgery will go
through it again)
Tissue expansion
Always:
Repair in layers
External layers everted (if inverted then retraction depression)
Burns: See Burns, page 486
See Mr Tan‟s very interesting but non-examinable hand-outs
Accident Compensation Corporation (ACC)
Provides economic support for injured people and aims to reduce the physical impact of injury
Is a no fault, compulsory scheme
NZers gave up right to sue in return for specified support
Resources available:
Costs of retrieval from accident scene
Costs of diagnosis and physical rehabilitation
Compensation for loss of earnings (80% of pre-injury income after 1 week off work)
Vocational support: retraining if necessary to return to work
Range of personal support to help make living with an injury more comfortable

Haematology and Immunology 285
Haematology and Immunology
Haematology Overview .................................. 286
Microscopy of Abnormal Cells ...................... 286
Anaemias ........................................................ 287
Microcytic Anaemia ................................. 287
Macrocytic Anaemia ................................. 288
Pancytopenia ............................................. 289
Hereditary Spherocytosis .......................... 289
Hb abnormalities....................................... 290
Data Interpretation .................................... 290
Porphyria .................................................. 290
Haematology of Systemic Disease ................. 290
Anaemia of Chronic Disease .................... 291
Haemostasis.................................................... 291
Coagulation ............................................... 292
Hypo-Coagulation Diseases...................... 292
Hypercoagulable States ............................ 293
Data Interpretation .................................... 294
Platelets and Platelet disorders ....................... 294
Platelets..................................................... 294
Thrombocytosis ........................................ 294
Thrombocytopenia .................................... 295
Platelet Function Disorders....................... 295
Myeloproliferative Disorders (MPD) ............. 296
Introduction .............................................. 296
Polycythaemia Vera .................................. 297
Essential thrombocythaemia ..................... 298
Myelofibrosis ............................................ 298
Chronic Granulocytic Leukaemia ............. 298
Myelodysplastic syndromes ........................... 299
Leukaemia ...................................................... 300
Chronic Leukaemia................................... 300
Acute Leukaemia ...................................... 300
Fever in a Neutropenic Patient ................. 301
Lymphoproliferative Disorders ...................... 302
Multiple Myeloma .................................... 302
Chronic Lymphocytic Leukaemia ............ 304
Lymphoma ................................................ 305
Hairy Cell Leukaemia ............................... 306
Data Interpretation: Leukaemia &
Lymphoproliferative disorders ............ 306
Immunodeficiency .......................................... 306
Immunology ............................................. 306
Primary Immunodeficiency ...................... 306
Secondary Immunodeficiency (Acquired) 307
Allergy and Hypersensitivity Disorders ......... 309
Hypersensitivity ........................................ 309
Allergy ...................................................... 309
Diagnosis .................................................. 310
Diseases caused by Antibodies ................. 311
286 4
th
and 5
th
Year Notes
Haematology Overview
Cell/System
Disorders
Anaemia
Microcytic: Iron Deficiency, Thalassemia, Chronic Disease (can be
normocytic)
Macrocytic: Alcoholism, B12/folate (Megaloblastic), Newborn. Also liver
disease, marrow disorders, drugs, malaria, idiopathic
Pancytopenia
Aplastic Anaemia
Also alcohol, bone marrow infiltration, megaloblastic anaemia, hypersplenism
Other Red cell
Spherocytosis, Hb abnormalities
Hypocoagulation
Haemophilia A & B, Von Willebrandt's, DIC
Also liver disease, Vit K, Renal failure, iatrogenic (aspirin, heparin)
Hypercoagulation
Primary: Factor V Leiden, Antithrombin 3, Protein C & S
Secondary: Malignancy, pregnancy, stasis, age, myeloproliferative diseases
Thrombocytosis
Reactive: Infection, inflammation, bleeding, malignancy, splenectomy
Primary: Essential thrombocythaemia
Thrombocytopenia
Immune thrombocytopenia, Heparin induced, artefact, dilutional, marrow
production failure, peripheral consumption (drugs, DIC, etc)
Platelet function
disorders
Mainly acquired: aspirin, uraemia, paraproteinaemias
Myeloproliferative
Chronic Myelocytic Leukaemia, Acute Myelocytic Leukaemia, Polycythaemia
Rubra Vera, Essential thrombocythaemia, Myelofibrosis
Myelodysplasia
Lymphoproliferative
Chronic lymphocytic leukaemia, acute lymphocytic leukaemia, multiple
myeloma
Also see Blood Tests, page 9
Also see Blood Products, page 552 (including transfusion)
Microscopy of Abnormal Cells
Red Blood Cells
Oval macrocytes + hypersegmented neutrophils megaloblastic anaemia (B12/folate)
Target cell RBCs (haemoglobin in the middle – non-specific): most commonly seen in patients with
liver disease (eg too much alcohol)
Small pale RBCs, target cells + pencil poikilocytes (elongated RBCs) iron deficiency
Rouleaux: red cells stack like coins, fall fast if high ESR. Stick together due to immunoglobulin or
fibrinogen). Causes: inflammation, myeloma
No lighter patch in middle spherocytes
Spherocytosis: if only some RBCs, then spleen has taken out a bit of membrane => autoimmune
haemolytic anaemia. If all RBCs are spherocytes then hereditary spherocytosis. If spherocytes +
reticulocytes then spherocytic anaemia
Cygnet shape (ring form with blue circumference) inside cell malaria parasite
Tear drop red cells myelofibrosis or polycythaemia
Polychromasia some red cells a bit blue due to stain – still contain some RNA
Reticulocytes: normal is 0.2 – 2%. Look big and blue. Will be high in anaemia (except ?anaemia of
chronic disease)
Howell-Jolly Bodies: Little purple/black dots (like a ball bearing) in RBC = remnant DNA that hasn‟t
been removed by the spleen. Seen in splenectomy patients
Fragmented cell: red cell sliced in circulation (DIC, artificial heart valve)
White Blood Cells
Normal lymphocyte: small, little/no cytoplasm
Neutrophils have multilobed nuclei, >= 6 lobes is hypersegmented (megaloblastic anaemia: B12, folate.
Also drugs, chemotherapy, renal failure)
Plasma cell: eccentric nuclei, clock-face chromatin. If eccentric nucleus (clear area next to nucleus) in
bone marrow multiple myeloma

Haematology and Immunology 287
Neutrophil maturation:
Blast
No granules, fine chromatin
Large
Myelocytes
Large round nucleus
Large
Metamyelocytes
Large bean shaped nucleus
Large
Band
Horse shoe shaped nucleus
Smaller
Neutrophil
Segmented neutrophil, dense
chromatin
Smaller
Normal differentiation: Neutrophils 80%, Lymphocytes 20%
Lymphocyte: Toxic Changes (i.e. „switched on‟): granules, vacuoles, Dohle bodies (blue clumps in
cytoplasm), nuclear clumping. Strong indicator of bacterial infection
If high lymphocytes and lots of „atypical lymphocytes‟ then viral infection: EBV, HIV, CMV
Auer rods in a blast acute myeloblastic leukaemia
Eosinophil: normal is reddish cytoplasmic granules. In toxoplasmosis, allergy (asthma, drugs, etc),
gut parasites
Bone marrow biopsy: normal is about ½ fat, ½ cellular
Leukaemias
Smudge cells CLL. Middle aged, significant lymphadenopathy
WCC, enlarged lymph nodes, splenomegaly, lots of white cells, majority are mature neutrophils
CGL (= CML)
Acute leukaemias: cells not mature
Anaemias
= Hb level below normal for age and sex
Normal Hb levels:
Male 138 – 180 g/l
Female 115 – 165 g/l
Mild is > 100
Moderate is 80 – 100
Severe is < 80
Symptoms
SOB on exertion
Tiredness/fatigue
Lack of concentration
O2 delivery Bring on underlying angina or pain/claudication in legs
Signs: Pale conjunctiva, palmar creases, nail beds: but insensitive test
Microcytic Anaemia
= MCV < 75 fl (normal is 76 – 98)
Causes
Iron deficiency anaemia
Thalassemia
Chronic disease (see Anaemia of Chronic Disease, page 291)
Other Causes: Sideroblastic anaemia, lead poisoning
Iron Protoporphyrin
Haem Globin
Haemoglobin
Iron deficiency,
Chronic inflammation
or malignancy
Sideroblastic anaemia
Thalassemia ( or )
288 4
th
and 5
th
Year Notes
Iron Deficiency Anaemia
See also Iron Deficiency, page 646 for Iron Deficiency Anaemia in Children
Commonest cause of anaemia
15-25% of healthy pre-menopausal women have low ferritin
2 mls of blood = 1 mg of iron. Easy to get anaemia from a small trickle bleed
Average menstrual loss = 60 ml
Iron absorption:
Western diet contains 10 – 15 mg iron
5 – 10 % normally absorbed
20 – 30% absorbed in Fe deficiency and pregnancy
Absorbed in duodenum, proximal jejunum
Iron transport and storage:
Fe carried by Transferrin (MW 80,000): made in liver, T½ 8 – 10 days
Ferritin: Water-soluble protein – MW 465,000. Stores iron in cells. Is proportional to body iron
stores
Clinical features of iron deficiency:
Anaemia
Glossitis: swollen tongue, sore, lost papilla
Koilonychia: spoon shaped nails
Dietary cravings (pica): eating strange stuff – kids eat dirt, pregnant women eat ice
Blue sclera: highly specific
Pharyngeal webs dysphagia
Diagnosis:
Microcytic hypochromic anaemia: use MCV (not MCH – but highly correlated)
On film may see: target cells (haemoglobin in middle – non-specific), pencil poikilocytes,
platelets
Lab findings: serum ferritin (sufficient on it‟s own) – will also see serum Fe (but Serum Iron
useless) and transferrin/ICP (Iron combining protein). Mean cell volume in normal range may
disguise a combination of small Fe deficient cells plus lots of large reticulocytes
Macrocytic Anaemia
= MCV > 96 fl
Causes
New born
B12/folate
Alcoholism (most common cause but usually mild)
Liver disease
Primary marrow disorders
Drugs
Malaria
Idiopathic/others
Megaloblastic Anaemia
Is NOT the same as macrocytic anaemia
Causes:
Folate (comes from veges)
B12 (comes from meat)
Drugs that interfere with B12 metabolism
Leads to defective DNA synthesis and delayed maturation of the nucleus cf. cytoplasm.
Big red cells and hyper-segmented neutrophils (>= 6 segments)
Clinical features:
Anaemia
Infection (neutrophil function)
Jaundice (bilirubin)
Purpura
Malabsorption (gut lining)
Lab features:
Haematology and Immunology 289
MCV > 95 fl
Oval macrocytes
WBC and platelets
Investigations: blood film and B12/folate levels. Serum folate is useless – folate is stored in RBCs
If low B12:
Also have symmetrical peripheral neuropathy
Could be diet: if animal products
Could be malabsorption: pernicious anaemia. Check intrinsic factor antibodies against gastric
parietal cells. Schilling test for absorption
If low folate:
Not eating enough veges (e.g. living on tea and toast)
Exclude malabsorption (e.g. Ceoliac Disease)
Review drugs
Pancytopenia
Stem Cells
Blood stem cells detected by CD34+
Live in bone marrow: biochemical environment there necessary for survival – from fat, fibroblasts,
endothelial & macrophage cells
Pancytopenia
Confirmed RBC, WBC and platelets
Causes:
Production:
Bone marrow infiltration/failure
Megaloblastic anaemia
Miscellaneous (e.g. alcohol)
Aplastic/hypoplastic anaemia
Margination: Hypersplenism
Aplastic Anaemia
Rare
Defect in supportive environment: dysfunctional stem cells, autoimmune damage
Criteria for severe:
Neutrophils < 0.5
Platelets < 20
Reticulocytes < 10 * 10E9
Hypocellular marrow
Causes:
Idiopathic
Drugs/chemicals
Radiation
Viral
Pregnancy
Treatment:
Supportive care
Immunosuppressive treatment
Stem cell transplantation
Hereditary Spherocytosis
Normal RBC has surplus membrane floppy
Spherocytes have less membrane tight
Autosomal dominant
Could take out spleen if symptomatic
290 4
th
and 5
th
Year Notes
Hb abnormalities
= Synthesis of abnormal Hb or rate of synthesis of normal or globin chains
Syndrome
Abnormality
Haemolysis
Crystalline Hbs (S, C, D, E) unstable Hb
Thalassemia
or , due to globin chain synthesis:
Thalassemia major – transfusion dependent, homozygous 0,
Mediterranean, splenomegaly, frontal bossing of forehead, bad teeth
Thalassaemia intermedia
Thalassaemia minor - 0 trait - MCV. 0 trait - MCV, Hb H bodies,
target cells
Familial Polycythaemia
AH1, measure P 50 for O2
Methaemoglobinaemia
Failure of reduction
Data Interpretation
Pregnancy Fe requirements and fibrinogen ( ESR)
If mild microcytic anaemia and normal ferritin it‟s not iron: check either Thalassaemia or anaemia of
chronic disease
Ferritin is an acute phase protein. It will be raised in chronic disease. So if there is chronic
inflammation and a low-normal ferritin, the underlying ferritin is likely to be below normal
Mildly MCV could be because of reticulocytes check haemolysis
Haemolysis tests:
Production: reticulocytes, blood film
Breakdown: Hb and Hatoglobins (binding protein for haem – used up in haemolysis would
fall)
Combes test: is there antibody on the RBC
If Fe in urine (Urine haemosiderin) then intravascular haemolysis (not spleen – which is
extravascular). E.g. aortic value replacement haemodynamic/shear stress from turbulent flow
Porphyria
Disorder of haem synthesis toxic metabolites
Many types, all due to genetic deficiency. Homozygous not viable. Heterozygotes can produce
enough haem, but when the system is challenged toxic metabolites
Symptoms:
Uncommon, but differential in intermittent abdominal pain
Can be intermittent or constant
Can acutely cause psychotic symptoms
Sun sensitivity (accumulation of metabolites in skin)
Neuro-visceral symptoms (pain but no organ pathology)
Rare types can cause sideroblastic anaemia
Investigations:
Urine test for metabolites (porphyrins)
Then specific test for which porphyria
ALA synthase controls the rate limiting step at the beginning of the pathway:
Induced by: BZDs, alcohol, oestrogen and progesterone ( onset at puberty or on starting the
OCP), sulphonamides, tetracycline, theophylline
Inhibited by haem, glucose
Haematology of Systemic Disease
Also see Hypercoagulable States, page 293
E.g. Cancer ESR, Neutrophils, coagulation, anaemia
Erythrocyte Sedimentation Rate (ESR)
Normal varies by age and sex (increases with age)
Rouleaux: red cells stack like coins, fall fast
Due to:
Acute phase reactants: esp. fibrinogen
Gamma globulins
Anaemia
Haematology and Immunology 291
Clinical uses: collaborative test, monitor course of disease
ESR in pregnancy, infection, tumours, connective tissue disorders, multiple myeloma
Leucocytosis
Normal range varies with age (esp. kids)
Neutrophils:
In adults: 2 – 7.5 *10E9
Lobed nucleus, lots of granules in cytoplasm
Made in marrow, transported via blood
Neutrophilia in many states, not just infection, and including stress. Physiological neutrophilia e.g.
exercise margination
Lymphocytosis
In acute infections: pertussis, infectious lymphocytosis, EBV, viral hepatitis
In chronic infections: brucellosis, Tb, Syphilis
In haemopoietic disorders
Toxic Changes (i.e. „switched on‟): granules, vacuoles, Dohle bodies (blue clumps in cytoplasm),
nuclear clumping. Strong indicator of bacterial infection
Anaemia of Chronic Disease
Causes:
Chronic infections e.g. TB, SBE, AIDS
Chronic inflammatory states e.g. RA, ulcerative colitis
Recognise it so patient is not over-investigated
Features:
Mild to moderate anaemia: 70 – 100 g/L (usually 90 – 100)
Normocytic to mild microcytosis
Differential diagnosis
Fe deficiency
Renal impairment
Marrow infiltration
Haemolysis
Iron Studies (highly examinable):
Fe deficiency
Chronic Disease
Serum Iron
Iron Binding Capacity
%Saturation
Marrow Iron
Serum Ferritin
N or
Blood results in chronic disease:
Ferritin
Protein (especially albumin)
Globulins
Pathogenesis
RBC destruction survival
Iron metabolism
Impaired erythropoietin response
Cytokines (TNF-, IL-1, interferons)
Treatment
Won‟t respond to iron, etc
Treat underlying cause
Erythropoietin (but very expensive)
Haemostasis
Necessary factors for haemostasis (stopping bleeding):
Vasoconstriction
Platelets
Coagulation (= fibrin production)
292 4
th
and 5
th
Year Notes
Coagulation
Key reaction: fibrinogen fibrin
Intrinsic pathway:
XII II via IX and VIII
Triggered by damage to endothelium
Measured by Partial thromboplastin Time (PTT) = Activated PTT (APTT). Also called PTTK
Reduced by heparin treatment
Extrinsic Pathway:
VII II
Triggered by chemicals extrinsic to blood stream
Measured by Prothrombin time or INR (International Normalised Ratio): ratio of Patient PT to
Control. Normal < 1.3. INR mainly measures top end of the extrinsic pathway – so INR may not
be affected by heparin even though it affects the common pathway. APPT more sensitive to
common pathway
Reduced by warfarin treatment
Hypo-Coagulation Diseases
Congenital:
Haemophilia A
Haemophilia B
Von Willebrand‟s Disease
Rare factor deficiencies
Acquired:
Liver diseases coagulation factors
DIC
Vitamin K deficiency: needed for factors 2, 7, 9 and 10
Uraemia: renal failure platelets and coagulation function
Massive blood transfusions dilution of clotting factors
Factor inhibitors
Von Willebrand’s Disease
Bleeding time, APTT due to VIII (VW factor is a binding protein for VIII)
Symptoms: Superficial bleeds – mouth, nose, gut, bruising, heavy menstrual bleeding
Autosomal dominant
Comes in mild, moderate and severe forms
Haemophilia
Ratio of 4:1 of A (factor VIII) to B (factor IX)
Prevalence of 13 – 18 per 100,000 males in Wellington (high)
Symptoms: bleeding into soft tissues, joints, dental extraction. Deep bleeds major orthopaedic
implications. NOT superficial or gut
Classification:
Severe: < 1% - joint bleeds, e.g. once a fortnight or month
Moderate: 1 – 4 % - some joint bleeds, main problem with trauma, not spontaneous bleeds
Mild: 5 – 25% - main problem trauma
Lab diagnosis:
INR: normal
APTT: prolonged
Fibrinogen: normal
Platelets: normal
Intrinsic System
Extrinsic system
Fibrinogen (soluble) Fibrin (insoluble)
PT (INR)
APTT
Haematology and Immunology 293
Bleeding time: normal
Factor assay reduced (do VIII first then IX)
Symptoms of a joint bleed:
Strange sensation: not really a pain – treat at this point, they will know despite no signs yet
Swelling
Treatment:
Factor replacement: either prophylactic or on demand
Choice of factor product: blood derived or recombinant
Management of inhibitors
Disseminated Intravascular Coagulation (DIC)
= Laying down fibrin inappropriately within vasculature
Causes:
1. Activation of extrinsic system by thromboplastin (triggers VII). Thromboplastin is a lipoprotein
substance from cell membranes. Due to: massive injury (release of thromboplastin),
septicaemia (damage to endothelium), tumour cells breaking down
2. Activation of intrinsic system: anoxia, acidosis, sepsis, burns
3. Direct activation of II & X: amniotic fluid embolism, pancreatitis ( release of toxic enzymes into
blood)
Outcomes:
Lab screen:
PT (Prothrombin time)
APTT
Fibrinogen
Platelets
Fibrin degradation products
Treatment:
Correct cause
Platelet transfusion
Fresh Frozen plasma
Cryoprecipitate
Hypercoagulable States
Primary Causes:
Factor V Leiden:
Most common primary cause
Point mutation on factor V prevents breakdown levels of Va hypercoagulable
Heterozygous have lifetime risk of 30 – 40% of thrombotic event, Homozygous then 50 – 60%
In thrombotic patients, 20 – 40% have factor V Leiden, mainly in Caucasians
Prothrombin gene mutation
Antithrombin 3 deficiency:
Reduced breakdown of thrombin
Heparin co-factor, 2 globulin
Intravascular activation
of coagulation
Consumption of
coagulation factors
Fibrin deposition in
microvasculature
Secondary fibrinolysis
(Breakdown enzymes)
Bleeding
Ischaemic organ
damage
Microangiopathic
haemolytic anaemia
294 4
th
and 5
th
Year Notes
Autosomal dominant, 1:2-5000 in Caucasian
Found in 2 – 3 % of DVTs
Can also cause mesenteric or brachial thrombosis. These are rare so index of suspicion
Protein C or S deficiency
Homocysteinaemia
Secondary Causes:
Malignancy
Pregnancy and for 6 weeks afterwards: hypercoagulable, stasis, venous compression. If concurrent
primary disorder then prophylaxis with sc heparin (warfarin contra-indicated)
Stasis: immobilisation, surgery, local pressure
Age
Myeloproliferative disorders
Antiphospholipid Syndrome (acquired, aggressive)
Infection
Trauma
Data Interpretation
Serum = plasma that‟s clotted: i.e. no clotting factors
Citrated plasma: citrate chelates calcium – so can‟t act as a co-factor in clotting. Add Ca to reverse
Aspirin for Coronary Heart Disease mimics VWD. (i.e. bleeding time, everything else normal). T½
of platelets = 3 – 4 days. Need to stop aspirin 10 days before surgery. ½ an aspirin enough to increase
bleeding time. 45 minutes to have an effect after oral dose
Heparin APPT
Fractionated Heparin TT (APPT may be normal)
Warfarin INR
Try to determine deficiency (e.g. FVIII or Warfarin 2,7,9,10) or Inhibition (e.g. aspirin, heparin)
Platelets and Platelet disorders
Platelets
No nucleus: contain granular cytoplasm
Normal count: 150 – 400 * 10E9/L
Normal size: 2 – 3 um
From megakaryocyte in bone marrow (from pluripotential stem cell under the influence of
thrombopoietin)
Lifespan 10 days – destroyed mainly in spleen. 20 – 30% of total body platelets are pooled in spleen
Function – form haemostatic plug:
Adherence: via Ia, indirectly via Ib &VWF
Shape change
Release reaction
Aggregation: glycoprotein IIb/IIIa via fibrinogen
Bleeding time: time taken for a standardised skin incision to stop bleeding at venous pressure of 40
mmHg. Normal is 1 – 7 minutes. Depends on platelet numbers, platelet function, vascular factors (e.g.
connective tissue disorders)
Disorders:
Thrombocytosis: too many
Thrombocytopenia: too few
Functional disorders
Thrombocytosis
= > 400 *10E9/l
Causes:
Reactive: infection, inflammation, bleeding, malignancy, splenectomy, Fe deficiency,
haemorrhage. Treat underlying disorder. Not usually necessary to treat platelets, but if so then
aspirin
Myeloproliferative: primary or essential thrombocythaemia – largely diagnosis by exclusion
Increased risk of venous and arterial thromboses
Haematology and Immunology 295
Thrombocytopenia
= <150*10E9/L
Symptoms: bleeding in skin & mucosal surfaces, petechiae (<1 mm), purpura (1-5 mm), ecchymoses
(>5mm), menorrhagia. Bad bleeding (e.g. in stools) usually only becomes significant below platelet
count of 10
Causes:
Artefact (e.g. clot in sample – usually due to using EDTA tube not citrate)
Dilutional thrombocytopenia: splenomegaly, massive blood transfusion
Marrow production failure (low platelet count & reduced/absent megakaryocytes):
Component of pancytopenia
Isolated thrombocytopenia: alcohol, chlorthiazides, rare megakaryocytic hypoplasias
Peripheral consumption (more common – low platelet count, but normal/increased
megakaryocytes):
Immune:
Idiopathic thrombocytopenic purpura
Secondary to drugs (e.g. quinine, heparin), autoimmune disease (SLE), CLL, virus (e.g.
HIV)
Non-immune:
DIC
Haemolytic uraemic syndrome
Immune Thrombocytopenia (ITP)
Autoantibodies or immune complexes bind to platelets and cause premature destruction in spleen –
lifespan reduced to 1 – 2 days
ITP does not cause splenomegaly
Acute IPT:
Immune complex mediated
Majority of childhood ITPs
Often follows viral infection
90% resolve spontaneously within one month
Rarely requires treatment
Chronic ITP:
Autoantibody to platelet glycoprotein
Majority of adult ITP
Usually no preceding illness
10% resolve spontaneously: need to treat, although if platelets at around 30 – 50 may not need
treatment – may dip during a viral illness. Need to review pre-surgery.
Treatment (if any needed):
Steroids (1 mg/kg prednisone per day). 30% don‟t respond
Intravenous immunoglobulins (swamp Fc receptors in spleen so platelets not destroyed –
temporary). 30% don‟t respond
Splenectomy (see Splenectomy, page 307 for risks)
Review if every pregnant: antiplatelet IgG may cross the placenta
Heparin-Induced Thrombocytopenia
1% of patients develop a drug-dependent antiplatelet antibody
3% of these immune complexes bind platelet Fc receptors & induce aggregation
Presentation is thrombocytopenia followed by thrombosis
Can be fatal
Management: stop heparin
Platelet Function Disorders
Congenital: rare
Acquired: common:
Aspirin (inhibits cyclo-oxygenase TXA2 aggregation)
Uraemia (i.e. renal failure)
Cardiac bypass
Myelodysplasia
296 4
th
and 5
th
Year Notes
Acquired abnormality of bone marrow
stem cell
Granulocytic
precursor
Red Cell
precursor
Megakaryocytes
Reactive fibrosis
Clinical
Presentation:
CML
Polycythaemia
Thrombocythaemia
Myelo-fibrosis
AML
70%
10%
20%
10%
Haemopoeitic
stem cell
Abnormal
clone
Failure of proliferation
Proliferation with
differentiation
Proliferation with abnormal
differentiation
Proliferation without
differentiation
Aplastic anaemia
Myeloproliferative
disorders
Myelodisplastic disorders
Acute Leukaemia
DNA
Damage
Paraproteinaemias
Myeloproliferative Disorders (MPD)
Introduction
Myelo = marrow
4 types:
Polycythaemia rubra vera
Essential thrombocythaemia
Myelofibrosis
Chronic granulocytic leukaemia (=chronic myeloid leukaemia)
Primary, clonal proliferation of myeloid (marrow) cells
Arises at pluripotent stem cell level:
Leads to mixed picture as diseases merge
Variation is based on degree and type of proliferation:
Leucoerythroblastosis:
Nucleated RBC and immature neutrophils in blood
Disturbance of blood/marrow barrier (normally stops immature cells getting out)
Causes:
Immature barrier: common in new born
Toxic: septicaemia
Hypoxia: respiratory failure
Marrow function
Mechanical damage: e.g. infiltration of metastatic cancer (breast, lung, prostate go to bones)
Extramedullary haematopoiesis:
Marrow cells outside marrow (e.g. spleen, liver, lymph nodes)
Common in MPD, especially myelofibrosis

Haematology and Immunology 297
Polycythaemia Vera
= Erythrocytosis
Males
Females
Hb
> 17.5 g/dl
>15.5
Red Cells
> 6.0 *10E11/l
> 5.5
PCV (packed cell volume)
>58%
> 48%
Investigation: total red cell volume by 51Cr. Also erythropoietin assay
Classification (given Raised PCV):
RCM (Red cell mass) = Absolute
Normal RCM = apparent
Primary Proliferative Polycythaemia
Clonal stem cell disorder
Predominant age 55 – 60 years
Diagnosis:
RCM > 36 ml/kg (i.e. absolute polycythaemia)
No secondary cause: e.g. O2 saturation > 92% (e.g. CORD)
Effects:
Vascular complications: TIA, cerebral thrombosis, microvascular (e.g. toes), headaches, DVTs
(but usually arterial problems due to viscosity e.g. stroke)
Haemorrhage
Pruritis
Gout
Splenomegaly (also liver)
Lab findings:
Hb & PCV
WBC in 2/3
Serum B12
Low erythropoietin
Platelets 400 – 800 in 50%
Hypercellular marrow: little fat, in megakaryocytes
„Hot‟ looking bone scan: lots of activity
Tear drop red cells
Treatment:
Venesection: take off a unit of blood every 3 or 4 months (if old do it slow)
If platelets as well ( clotting risk) then radioactive P32 (risk of leukaemia 10 years on),
Busulphan & allopurinol ( gout). Also hydroxyurea
Course:
20% progress to myelofibrosis
AML transition
?Splenectomy if massive
Median survival = 8 – 15 years
Secondary Causes of Polycythaemia
Hypoxia: normal erythropoietin. High altitude, lung disease, cyanotic CHD, smoking
Inappropriate erythropoietin: renal tumours, renal ischaemia (ascultate for renal bruits), fibroids,
hepatoma
Miscellaneous: e.g. drugs like androgens for breast cancer
Apparent Polycythaemia
Packed cell volume (=PCV = Haematocrit) but normal RCM (ie RBCs a greater proportion of a unit
of blood, but normal volume of RBCs in the body):
Diuretics
Alcohol
Hypertension
Early primary polycythaemia
High altitude: initially plasma volume then absolute polycythaemia (and O2 curve shifts left)
298 4
th
and 5
th
Year Notes
Essential thrombocythaemia
Clinical presentation:
Any age, usually older
Often asymptomatic
Bleeding OR thrombosis (e.g. digital arteries necrotic toes)
Splenomegaly (2 – 3 cm) in 70%
Lab results:
Platelets, often > 1000 * 10E9
Morphology abnormal, normal plus large platelets
Platelet function studies abnormal
Hb normal or mild anaemia
WBC normal or mild
Bone marrow: many megakaryocytes
Treatment:
Chemotherapy: hydroxyurea
Radioactive phosphorous: P32 – stored in bone so zaps marrow
Interferon
Prognosis: if platelets down then good, if not then bad
Myelofibrosis
Clinical presentation:
Old age
Preceding polycythaemia in 30%
Anaemia
Slow onset, weight loss, night sweats – insidious
Massive hepatosplenomegaly. Large spleen pressure on splenic blood supply infarction
pain
Lab results:
Hb low
WBC high early, low late
Platelets high early, low late
Leucoerythroblastosis
Tear drop red cells
LAP (leucocyte alkaline phosphatase)
Philadelphia chromosome –ive
Fibrosis of bone marrow
Treatment: Mainly supportive: observation, low does chemotherapy, splenectomy (symptomatic effect
only)
Prognosis:
Mean survival 3 – 4 years, may become transfusion dependent
10% develop AML
Chronic Granulocytic Leukaemia
= Chronic Myeloid Leukaemia
Clinical presentation
Any age
Tired, off colour, sweats
Slow onset
Large spleen (also liver)
Lab results:
WBCs (30 – 300). In chronic there will be mature and immature blasts (myelocytes,
promyelocytes and lymphocytes as well. Just a general left shift). In acute there will be immature
only.
Bone marrow has neutrophils
Philadelphia chromosome +ive
Low leukocyte alkaline phosphatase (LAP)
Uric acids
Haematology and Immunology 299
Course:
Chronic phase: median duration 3 – 4 years
Transformation (either to myeloblastic/AML or lymphoblastic) aggressive/acute – end stage
Treatment:
Hydroxyurea: controls proliferation but won‟t stop transformation
Interferon: suppresses marrow, in 15% Philadelphia goes away ( no transformation)
Autotransplant: use patient‟s stem cells
Allotransplant (use sibling): 60% cure, 20% death, 20% remission
MUD (Matched unrelated donor)
„Mini-transplant‟: new stem cell technique with no high dose chemo/radiotherapy. Transplant
mops up weakened immune system without you needing to kill it
New drug: Glevac (STI571) – targets Philadelphia Chromosome:
Acquired genetic defect – 9:22 translocation BCR-ABL oncogene (functional oncogene)
P210-BCR-ABL oncoprotein
Leads to cell proliferation, adhesions and apoptosis without regulation
Myelodysplastic syndromes
Description:
Heterogeneous group of disorders
Clonal abnormality of haemopoietic stem cells
Abnormal, ineffective haematopoiesis
Involves 1 or more lineages
Irreversible quantitative and qualitative defects (ie normal count but bad function)
Tendency to evolve to acute leukaemia
Clinical
Usually elderly
Features of bone marrow failure: tired (anaemia), bleeding, infection, mild splenomegaly in 10 –
20%
Incidental finding on blood film in 20%
4 – 12 per 100,000 per year (definitional problems)
Variants:
Refractory anaemia +/- further features (eg excess blasts)
Chronic myelomonocytic leukaemia
Differential diagnosis:
Megaloblastic anaemia
Acute leukaemia
Heavy metal toxicity (lead, arsenic)
Chronic infection
Immune deficiency (esp HIV)
Anticancer chemo/radio therapy
Myeloproliferative disorders
Bone marrow hypoplasia
Progression:
70 – 80% die of marrow failure
20 – 30% die of progression to leukaemia
Median survival varies with subtype from 6 – 50 months
Treatment:
Response rates to treatment poor
Supportive care
Maybe cytotoxic chemotherapy or stem cell transplants in the few young cases
Growth factors eg erythropoietin
Secondary myelodysplasia:
Incidence
Complication of former treatment: alkylating agents (including cyclophosphamide, widely used as
an immunosuppressive, eg in Rheumatoid arthritis) and topoisomerase II agents
Risk related to cumulative dose and duration of exposure
Peak 5 years post treatment
300 4
th
and 5
th
Year Notes
Poor prognosis
Leukaemia
Leuk: Greek for white
= Cancer dominantly of white cells arising in MARROW. Lymphoma primarily arises in lymph nodes
Summary:
Acute
Chronic
Myeloblastic/Granulocytic
Neutrophil precursors
Sudan black for peroxidase
Auer rod in cell
Mature neutrophils and blasts
Philadelphia +ive
Converts to AML after 3 years
Lymphoblastic
T/B Cell precursors
PAS stain for glycogen
Proliferation of mature B cells
Doesn‟t convert to ALL
Longer mean survival
Chronic Leukaemia
Chronic Myeloblastic Leukaemia (CML): Converts to AML/AGL. See Chronic Granulocytic
Leukaemia, page 298
Chronic Lymphoblastic Leukaemia (CLL): see Chronic Lymphocytic Leukaemia, page 304. Doesn‟t
convert to ALL
Acute Leukaemia
Rapid onset, 100% mortality within 3 months if untreated
Very undifferentiated (anaplastic) cells: blasts, no normal cells in blood
Types:
Acute Myeloblastic Leukaemia (AML). Chance of cure with chemo alone = 20 – 40%. With
transplant = 60%. Has Auer rob in blast
Acute Lymphoblastic Leukaemia (ALL)
Presentation:
Tired due to anaemia, breathless
Bleeding due to platelets, nose bleeds
Bacterial infection
Hepatosplenomegaly, lymph nodes, bone pain (push on sternum)
Investigations:
FBC: Hb, platelets, white count: High, normal or low (sometimes leukaemia cells stay in
marrow)
Bone marrow: > 30% of nucleated cells in the marrow are leukaemic blasts
Classification:
Cytochemistry:
Staining. PAS - +ive stain for glycogen lymphoblastic
Sudan black +ive for peroxidase myeloblastic
Immunology: flow cytometry
Cytogenetics
Treatment
Supportive Care:
Antibiotics, platelet/RBC transfusion
Venous catheter: Hickman catheter
Cytotoxic Treatment:
Complex multi-drug protocols
Remission induction: 1-4 weeks depending on protocol. FBC normal and < 5% blasts in marrow
(that‟s normal). AML – achieved in 70 – 80%. ALL – achieved in 70 – 80% of adults, 95% of
kids
Consolidation: more drugs to mop up residual blasts, including CNS prophylaxis (some drugs
don‟t penetrate CNS well)
But 60 – 80% chance of relapse over next 2 – 4 years
Bone Marrow Transplantation:
= Haematopoietic stem cell transplantation
Haematology and Immunology 301
Kill of leukaemic cells with dose: but limited by marrow toxicity. With marrow transplantation
can push dose higher (limit is organ toxicity) if cancer is responsive
Process: patient and donor preparation, conditioning (chemo & high does radiation), stem cell
infusion, neutropenic phase, post neutropenic phase
Sources of stem cells: Self (autologous), twin (syngenic), HLA matched sibling (allogenic), HLA
partial matched sibling, matched unrelated donor (MUD)
Peritransplant mortality = 20%
Fever in a Neutropenic Patient
Eg in patients undergoing chemotherapy
Indicators of serious infection:
Signs and symptoms of infection will be reduced – can‟t mount an inflammatory response
Temperature:
> 38.5 C
> 38 for 4 hours
Patient fells unwell but no temperature
Neutropenia:
Neutrophils < 0.5 * 10E9/L (less than 0.2 serious concern)
Neutrophils falling
Prolonged neutropenia (> 7 days)
Types of infection (drives focused history)
Respiratory: SOB, cough
Skin infection
Mouth and teeth
Perianal (pain on moving bowels and wiping)
Pain around central line
Less often: bowel & UTI
Focused exam:
Signs of septic shock: Pulse, BP and peripheral circulation
Chest: percussion and auscultation
Mouth: a good look around – abscesses will be sensitive to pain
Skin infections, especially lines
Quick abdominal
Exam perianal area – test for sensitivity to touch. Don‟t do PR (risk of minor trauma
bacteraemia)
Investigations:
FBC
Blood culture (debate about whether to take it from the central line or not)
CXR
Swabs from anything that looks infected, including central line
Maybe CRP: in bacteraemia
Normally don‟t find anything. Over half infections are low grade line infections
If in doubt, treat empirically now. If infected will deteriorate quickly:
Gentamycin + Ticarcillin (synthetic penicillin)
Monotherapy (eg imipenem)
+/- Vancomycin (for staph line sepsis)
Causes of infection:
Frequency
Risk
First Fever
Staph
+++
+
haemolytic strep
+
++
G –ive bacilli
+
+++
Subsequent infections
Staph
+++
+
Fungi
++
+++
Resistant G-ive
+
+++
Subsequent fevers: longer in hospital (hospital acquired infection), longer on antibiotics, etc
302 4
th
and 5
th
Year Notes
If fever persists:
Repeat the above exam and investigations – but unlikely to add anything new
Choices:
Change antibiotics
Consider antifungal: Amphotericin. Watch for nephrotoxicity and the patient feels awful
Obscure fevers:
Central venous line infection
Occult sinusitis (check with CT)
Hepatosplenic candidiasis (check with CT abscess biopsy)
Pulmonary/disseminated aspergillus (doesn‟t respond to amphotericin)
Viral
Drugs
Prevention:
Avoid hospitalisation
Strict hand washing
Avoid invasive procedures (beware interventionist surgeons!)
Care of IV devices
Consider prophylactic antimicrobials
Prophylaxis
Bacteria: selective gut decontamination (origin of many infections is bowel flora): Ciprofloxacin
(fluorinated quinolone). Arguments for and against
Anti-fungal: Fluconazole, Itraconazole (OK for prophylaxis, not so good as amphotericin for
established infection)
Anti-viral: acyclovir (for HSV), ganciclovir (for CMV)
Anti-pneumocystis: co-trimoxazole (but beware marrow suppression) or aerolised pentamidine
Other possible treatments:
Granulocyte-CSF: try to marrow production of neutrophils
Maybe -globulin infusions
Transfuse granulocytes: emerging area
Lymphoproliferative Disorders
Multiple Myeloma
= A neoplastic proliferation of plasma cells, characterised by lytic lesions, bone marrow failure and
homogenous serum and urinary globulin elevations
Epidemiology
10% of haemopoietic malignancies
12 – 16 new cases in Wellington each year
Median age approx. 70 (rare under 40), male > female
Remains incurable
Association with lead, chemicals, agricultural work and FH of autoimmune disorders
Pathogenesis
Monoclonal
Arises in lymphoid follicle and disseminates to bone marrow. Plasma cells not seen in blood until
terminal stage
Stromal cells release IL6 acts on osteoclasts to cause lytic lesions Crush fractures in spine, nerve
compression, diffuse osteoporosis, hypercalcaemia. Treat vertebral fractures with radiotherapy
Presentation
Bone pain, pathological fracture
Anaemia
Amyloidosis in 10 – 15%: macroglossia, cardiomegaly, peripheral neuropathy. Diagnose with
rectal/bone marrow biopsy. Stain with Congo Red
Renal complications:
Presents with heavy proteinuria, also chronic renal failure – due to infiltration
Haematology and Immunology 303
Light chain nephropathy worse prognosis. Casts of free light chains obstruction and are
directly nephrotic
Amyloid deposition nephrotic syndrome
Recurrent bacterial infections
Rarely „Hyper-Viscosity Syndrome‟: due to IgM or IgG retinal haemorrhage
Lab Findings
Normochromic, normocytic anaemia
Platelets in advanced disease
ESR
Serum uric acid
Bone marrow: plasma cells
Monoclonal band on electrophoresis
Light chains (Bense-Jones Proteins) in urine
X-rays: multiple punched-out lytic holes in the bone, no sclerosis
Gross: „currant jelly‟ – soft, red lesion
Micro: resemble plasma cells but variability in cell shape, prominent nucleoli, multinucleation
Differential: chronic osteomyelitis – but will have granulation tissue with at least a sprinkling of other
inflammatory cells
Treatment
General treatment:
Over 65: Melphalan/prednisone
Younger: Vincristine, Adriamycin, Dexamethasone
Emergency treatment:
Hypercalcaemia: pamidronate – coats bone surface to stop osteoclast reabsorption
Anaemia: transfusions
Hyperviscosity: plasmapheresis
Renal failure: dialysis
Prognosis
Median survival 3 years
Some develop AML or MDS
Transplant (auto) extend survival
Allo-transplants may cure a select few
Aside: Causes of Paraproteinaemia
Benign monoclonal gammopathy: level < 30 g/L (low cf. MM), no light chains in urine. Other Ig‟s
normal (cf. suppressed in MM). 15-20% go onto MM but may take 10 – 20 years
Lymphoma or CLL
Multiple myeloma
Waldenstrom‟s Macroglobulinaemia: monoclonal proliferation of B cell lineage (half way between
lymphocytes & plasma cell). Slowly progressive lymphoma. Monoclonal IgM paraprotein. Present
with big glands/liver/spleen – no bone lesions
Aside: Conditions associated with Monoclonal proteins
Associated with uncontrolled proliferation:
Multiple myeloma
Solitary plasmacytoma
Waldenstrom‟s macroglobulinaemia
Lymphoma
Lymphocytic leukaemia
Heavy chain disease
Primary amyloidosis
Associated with controlled proliferation:
MGUS: difficult to distinguish from malignancy, especially in early stages. Tend towards
malignancy if:
Serial M band levels are increasing
Bone lesions
304 4
th
and 5
th
Year Notes
IgG > 30 g/l or IgA > 20 g/l
Serum or urine light chains present
Normal Igs decreased
Marrow plasma cells > 10%
Renal failure
Hypercalcaemia
Anaemia
Chronic infections
Non-lymphoid malignancy
Connective tissue disorders
Transient (virus, drug reaction)
Peripheral neuropathy
Transplants
Chronic Lymphocytic Leukaemia
Monoclonal proliferation of mature B cells (CD 19 & 20+). Being mature, will have surface
expression of immunoglobulins
Epidemiology
Commonest leukaemia: 25%.
Primarily elderly
Male = 2 * Female
Clinical Features
Asymptomatic (40 – 70%)
Insidious, maybe weight loss, fatigue
Symmetrical enlargement of superficial lymph nodes (50%)
Splenomegaly and hepatomegaly
Platelets bruising
Defects in CMI and Ig infections: Herpes Zoster (shingles), fungal, bacterial, viral. Death usually
due to infection
Diagnostic Criteria
Blood lymphocytes > 5 * 10E9/L
Lymphocytes are B cells (CD19, 20 and 24)
Marrow lymphocytosis > 30%
Differential Diagnosis
Reactive lymphocytosis: EBV, CMV, HZV, Toxoplasmosis, Brucellosis, Tb, Viral
Other B cell tumours:
Prolymphocytic anaemia
Hairy cell leukaemia
Splenic lymphoma with villous lymphocytes
Mantle cell lymphoma
Follicular lymphoma
Lab
20% diagnosed on routine blood test
Lymphocytosis: > 5 * 10E9/L, but may be 30 to 300. Small lymphocytes and smudge cells common.
(cytoplasm fragile – breaks easily)
Normal looking lymphocyte: small, little/no cytoplasm
Anaemia in later stages due to marrow replacement and survival. 15% have Combes positive
haemolytic anaemia
Marrow: lymphocytic replacement
10% have haemolytic anaemia
Treatment
Only if nodes painful: Prednisone (1 mg/kg), Chlorambucil, fludarabine. Side effects of prednisone:
weight gain, hyperexia, mood changes (euphoria depression), candidiasis, polyuria (secondary to
glucose intolerance), dyspepsia
Haematology and Immunology 305
Supportive treatment for infections, and radiotherapy for deposits causing pressure symptoms
Little impact on viscosity (its mainly RBCs and blasts that affect that)
Doesn‟t convert to Acute Lymphatic Leukaemia
Median survival from diagnosis: 4 years. But 15% live for 15 years with no treatment
Complications Include
Infections, secondary to hypogammaglobulinaemia, neutropenia, drugs (immunosuppressive)
Cardia dysfunction: secondary to chemo toxicity, etc
DVT: hypercoagulable
Lymphoma
Malignant lymphoma = Clonal proliferation of lymphocytes arising in lymph nodes (or other lymphoid
tissue). Minor exceptions – can get them in spleen, gut, etc
Differentiating lymphoma from leukaemia: was its origin in the bone marrow or lymph nodes?
Clinical features:
Painless lymphadenopathy: non-tender, rubbery
Hepatosplenomegaly
Systemic symptoms: fever, nights sweats, weight loss, tiredness
Involvement of other areas: skin, CNS, GI, salivary glands
If bone involvement (fairly rare) then preference for bones with red marrow, and may present with
bone pain
Diagnosis: excision biopsy (not FNA). Special lab procedures, stains etc. Warn the lab it‟s coming
Classification:
Hodgkin‟s vs non-Hodgkin‟s: histological diagnosis only. No clinical difference. Hodgkin‟s
responds better in general. In general, Hodgkin‟s spreads node to node, non-Hodgkin‟s spreads to
any node in the body
Low (indolent) vs intermediate vs high (aggressive) grade
Staging: Ann Arbor Staging System (Ann Arbor is a place in the USA):
1: one lymph node area only
2: 2 or more lymph node areas on the same side of diaphragm
3: 2 of more lymph node areas on different sides of the diaphragm
4: disease in liver, bone marrow or other extra-nodal sites
Symptom status: A = absence of fevers, sweats, weight loss. B = one of unexplained fever >
38.5 C, weight loss > 10 % in preceding 6 months, drenching night sweats [Unusual to include
symptom status in cancer staging]
Staging investigations: CT of neck, chest and abdomen. Bone marrow. FBC, LFTs, ESR
Compared with leukaemia: if its in your bone marrow its everywhere
Survival:
Hodgkin‟s Disease:
5-year survival (%)
10-year survival (%)
Stage I
90
73
Stage II
87
69
Stage III
71
54
Stage IV
45
< 37
Non-Hodgkin‟s Lymphoma:
5-year survival (%)
Favourable histology
Localised
61 – 90
Widespread
50 – 70
Unfavourable histology
Localised
76 – 100
Widespread
80 - 85
Treatment:
Radiology if localised (main side effect is tiredness)
Chemo if disseminated
Possible bone marrow transplant if chemo fails (permits more toxic dose of chemo)
If treatment fails then gradual progression

306 4
th
and 5
th
Year Notes
Hairy Cell Leukaemia
Indolent B cell neoplasm.
Males to female = 5:1. Median onset age 50
Splenomegaly
Wispy changes to cytoplasm of B cell
Purine analogues 80% remission
Data Interpretation: Leukaemia & Lymphoproliferative disorders
Normal count but atypical lymphocytes viral infection. Check glands/spleen. Test for EBV, CMV,
or HIV. Ensure time to seroconvert
If only a few blasts in blood (e.g. 1%) and some nucleated red cells not acute (blasts not dominant)
but marrow under stress chronic
Immunodeficiency
Immunology
Natural
Specific
Circulating molecules
Complement
Antibodies
Cells
Phagocytes: macrophages,
neutrophils, NK cells
Lymphocytes
Natural immunity:
Integrity of skin & mucosal surfaces
Clearance of surfaces (eg cilia)
Antiseptic chemicals (eg lysozymes in tears)
Specific immunity:
Has memory and specificity
Turns on, then off
Humoral (antibodies): generally extracellular bacteria. First exposure, mainly IgM. Subsequent
exposures, more antibody, and mainly IgG
CMI/T-cells: intracellular
The categories of things that go wrong:
Immune deficiency: can‟t fight an external agent
Auto-immune: inappropriate reaction against an internal antigen
Allergy: inappropriate reaction against an external antigen
Causes of immune deficiency:
Autoimmune Disease
Vitamin/mineral deficiency: B12/Zinc
Genetic patterns: autosomal recessive
Metabolic deficiency e.g. Adenosine deaminase deficiency
Arrest in embryogenesis
Primary Immunodeficiency
Most single gene disorders: range of effects e.g. antibody or complement deficiencies
Clinical features:
Highly suspicious: chronic, recurrent or unusual infections, incomplete response to treatment
Moderately suspicious: skin rash (eczema, candida), diarrhoea, growth failure, recurrent abscesses,
hepatosplenomegaly
Different infections associated with different disorders
Antibodies: sino/pulmonary/gut problems
CMI: multisystem (e.g. CMV), pulmonary (PCP, aspergillus, candida), viruses (e.g. Herpes)
Phagocytic problems: s. aureus
Complement: recurrent neisserial infection
Symptoms depend on where in the lineage the defect is:
Stem cell: eg SCID
Pre-B cell: X Linked Agammaglobulinaemia
Maturation Defect: eg can‟t switch from IgM to IgG
Haematology and Immunology 307
Group 1 – Combined Variable Immunodeficiencies (CVID)
Prevalence 1 in 20 – 50,000
Symptomatic at 15 – 35 years (but long diagnostic delay)
Recurrent pyogenic problems/autoimmune features/respiratory infections
GI infections: giardia, campylobacter, HCV
Normal B cells: but defect in maturation – no plasma cells
Treatment: iv Ig (e.g. Intragam), prophylactic antibiotics
E.g. x-linked SCID (Severe Combined Immunodeficiency), Adenosine deaminase (ADA) deficiency
Group 2 – Antibody deficiencies
Diagnosis of primary antibody deficiencies:
Serum Ig‟s
Quantitative measurement essential (electrophoresis insensitive)
Severe hypogammaglobulinaemia: serum IgG level below 3 g/L in adults
Response to vaccination (important test)
Tetanus and Pneumo-Vax
Do baseline, vaccinate, expect 4 times at 4 weeks
IgG subclass concentrations: interpretation difficult. Based on lymphocyte count. E.g. if
lymphocytes normal then primary, if low lymphocytes then ?SCID
Lymphocyte Subsets:
Absence of B cells in Brutons
CVID: up to 30 % have T cell reductions
CLL - CD5+ B cells
IgA Deficiency (most common genetic deficiency)
Approx 1 in 700
Respiratory & GI infections
Risk of anaphylaxis with blood products due to reaction to exogenous IgA
Don‟t treat with Ig
Runs in families with CVID
Can be associated with:
IgG subclass abnormalities
Impaired responses to vaccination
Group 3 – Immunodeficiency associated with other defects
Group 4 – Complement deficiencies
Opsionisation: attachment of C3 to immune complexes
C3 pyogenic infections due to lysis
Group 5 – defects of phagocytic number or function
E.g. severe congenital neutropenia, chronic granulomatous disease, IFN gamma receptor deficiency
Can test for chemotaxis, adherence and phagocytic function
Management: specific antibodies, G-CSF in neutropenia, etc
Secondary Immunodeficiency (Acquired)
Splenectomy
RR of fatal infection by 200 times: e.g. meningitis, bacteraemia and pneumonia OPSI
(Overwhelming Post Splenectomy Infection)
Biggest problem is encapsulated bacteria plus malaria and salmonella
Treat with vaccination (e.g. for pneumoccal, negligent if you don‟t, always record in notes) +
prophylactic antibiotics
Aggressively investigate any post splenectomy patient with infection
Diabetes
Function of neutrophils & macrophages
Staph skin diseases common
Compounded by ketoacidosis
308 4
th
and 5
th
Year Notes
AIDS
The virus: RNA virus with reverse transcriptase. Has p24 nuclear antigen. Attacks CD4+ T cells.
Transmission: sex (risk in receptive intercourse – male to male most significant, also in other STDs),
blood and maternal transmission ( risk with AZT)
1 % of Europeans lack CXR-5 receptor: if homozygous then resistant
Signs & Symptoms:
Temperature, wasting (chronic ill health)
Rashes: eg shingles, HSV (cold sores), candidiasis, may be drug response (heightened sensitivity
to drug responses)
Lymph nodes
Signs of high risk behaviour: Injection marks, other STD
Mouth: infections, Kaposi‟s Sarcoma (re-purple vascular non-tender tumours – mainly on skin)
Chronic cough common
Hepatosplenomegaly (infections, lymphoma)
Neuropathies: eg due to intracranial lesion (eg lymphoma), peripheral sensory neuropathies
Fundi: cotton wool spots, scars (eg due to toxoplasmosis, CMV)
Early disease:
Seroconversion illness: in 50 – 90% of infected people. May include macular rash
Debate about usefulness of early treatment
Good evidence of value of prophylactic treatment (e.g. following needle stick)
Screening:
3 weeks before positive after infection
Elisa for HIV-1 and HIV-2 antibodies
False positive tests: 4/1000
Confirmatory diagnosis: Western Blot
Can take up to 3 months to get Western Blot Positive
Can give indeterminate, weak positive or strong positive (3 bands)
Course: measure based on viral load and CD4 count
Acute illness: 4 – 8 weeks
Asymptomatic: 2 – 12 years
Symptomatic: 2+ years. AIDS defining illness:
PCP infection (treat with co-trimoxazole): can pneumothorax
Cryptococcus infection: mild headaches: lumbar puncture. Indian ink stain positive
Kaposi‟s sarcoma: can present anywhere
Psychological: HIV related, secondary illness related, or depression
Viral Load:
High T cell turnover: Virus replicates in 1½ days. Infected cell lasts 2.2 days
HIV in sanctuary sites: e.g. brain – hard to treat
Measure through PCR of viral RNA: good indicator of progression. If viral load high, treat now
Immune depletion: Based on CD4+ count:
> 500
200 – 500: Tb, herpes
<200
Subgroups of illness:
Constitutional: fever, diarrhoea, weight loss
Neurological: dementia, neuropathy, cognitive
Opportunistic infections: candida, PCP, toxoplasmosis, CMV, MAC, Tb
Malignancies: Kaposi‟s sarcoma, non-Hodgkin‟s lymphoma
Drug Treatment:
Combination of drugs that inhibit various points of viral replication
Can improve CD4+ count from very low (e.g. 50) to e.g. 500-600
Side-effects: non-specific rashes, „buffalo hump‟ – abnormal fat distribution
Leading cause of death: Respiratory infection
Testing for HIV
Guidelines for HIV pre-test counselling:
What the test for HIV antibodies means: not a test for AIDS
Significance of negative test (Window period)
Haematology and Immunology 309
Significance of positive test: medical implications (prognosis & treatment), social implications
(coping, support, relationships, who needs to know, possible discrimination), notification
requirements (HIV not notifiable, patient can use alias), implications for insurance
Safeguards to preserve confidentiality
Future preventative aspects: safer sex and IVDU
How results are obtained
Any costs
Guidelines for post test counselling:
Explanation of test results
If negative: 3-month window period – especially if recent high risk behaviour. Future prevention
If positive: repeat, confirmatory test organised, arrangement for counselling, support and specialist
assessment
Other Causes of Secondary Immunodeficiency
Malignancy
Drugs e.g. steroids, cyclosporin, cytotoxics
Nutritional Deficiency
Post-viral
Post-transfusion
Alcoholism
Chronic renal disease
Allergy and Hypersensitivity Disorders
Hypersensitivity
A lay term
Stimuli that don‟t cause symptoms amongst general population
Usually reaction of body surfaces (eyes, airways) to environmental factors
Immunological Hypersensitivity Types:
Problem With
Mechanisms
I
Immediate Hypersensitivity
IgE
Allergen reacts with antibody on the
surface of mast cells or basophils
mediator (eg histamine) release
II
Cytotoxic / Antibody
mediated
IgM, IgG
IgG or IgM against antigens on ones own
tissues. Antibody binding complement
activation WBC tissue injury. Eg
Goodpastures Syndrome (Ab against
glomerular basement membrane),
haemolytic disease of the newborn.
III
Immune Complex
Mediated
Antigens + Ig
Antibody complexes are not cleared from
the circulation and fix in capillary beds
WBCs tissue damage. Eg serum
sickness (foreign proteins and drugs – eg
Ceclor [cefaclor] – urticaria (hives, welts) 1
– 7 days later) and some
glomerulonephritis
IV
Delayed Hypersensitivity /
T cell mediated
CD4/8
TcR (T Cell receptor) binds to tissue
antigens clonal expansion and
inflammatory cytokine release. Eg contact
dermatitis, tuberculin sensitivity in Tb.
Autoimmune disease can be any one of types II, III or IV
Hyperreactivity = sensitivity to non-specific stimuli (= irritants), eg cold, perfumes, etc
Allergy
Cross references:
See also Food Allergy, page 647
See also Atopic Eczema, page 319
See also Allergic Rhinitis, page 63
310 4
th
and 5
th
Year Notes
See also Drug Allergy, page 530
= Immunologic reaction to common substances which are harmless to most people
Previous exposure antibodies or specific lymphocytes against these substances
Types:
Atopy:
Predisposition to produce IgE antibodies to common environmental substances (also called
immediate or Type 1 hypersensitivity).
Order of incidence:
Peak in years
Eczema
1 – 2
Food allergy (eg milk, eggs)
2 – 3
Asthma
10
Seasonal Rhinitis (hay fever)
20 +
Adults aged 20 – 44 in New Zealand: Asthma 15%, hay-fever 35%, Maori more symptomatic
Mediators lead to vasodilation, vascular leakage (swelling), smooth muscle spasm (eg
respiratory).
Similar symptoms can occur from non-allergic hypersensitivity => non-atopic
Contact Allergies: direct skin contact with nickel, chrome, rubber. Due to lymphocyte (delayed-
type hypersensitivity, type IV) not IgE antibodies
Allergic Alveolitis lung inflammation. Eg farmer‟s lung, pigeon fancier‟s lung. Due to
lymphocytes and IgG (not IgE)
Risk factors:
Allergy predominates in young adults and children: while non-specific hypersensitivity is more
common later in life
Genetic Factors: One parent doubled risk of child having atopic disease. Both parents 4
times risk
Early childhood factors important in subsequent development of allergic disease:
High house dust mite/cat/pollen exposure in early months risk
Exposure to tobacco smoke in utero/infancy risk
Early life infections risk: ?improved shift from TH2 environment of uterus to non-allergic
TH1 immune responses which dominate in most infections (especially intracellular pathogens)
First born children at greater risk
The workplace is a major source of allergen exposure
Bee sting allergy:
Don‟t have to have atopic history
If anaphylaxis as a child, 1 in 6 chance next time. For adult, 60% chance next time
Carry adrenaline until desensitisation (serial antigen shots 95% effective)
Anaphylaxis: give 0.5 m of 1:1000 adrenaline IM if in community setting (iv in hospital if you can
give slow infusion). IM gives good diffusion, safer, effective and fewer problems with cardiac
vasoconstriction cf bolus
For treatment of Anaphylaxis see Severe Anaphylaxis, page 483
Diagnosis
History: do symptoms occur in particular environments, particular times or seasons, what are dominant
symptoms (eg sneezing/itching more likely to be allergy than chronic nasal blockage)
Skin prick tests
Useful for atopic allergies: especially of the mucous membranes
Use standard panel of allergen extracts (eg grass pollen, house dust mite, cat dander, etc)
Read wheal and flare reaction 10 – 15 minutes later
Safe, accurate and cheap
If they have had an anaphylactic reaction test in a hospital setting. If very highly sensitive
systemic reaction. If anaphylactic reaction, test tryptase (elevated for 1 – 6 hours)
Skin prick tests will be negative in hypersensitivity that is not IgE mediated
Pathophysiology:
Allergen + specific IgE (attached to mast cells) mast cell activation degranulation
histamine and tryptase release + newly generated mediators (arachidonic acid metabolites eg
leukotrienes and PGs) local & systemic effects. Eosinophils may also produce mediators of
inflammation
Haematology and Immunology 311
In the sensitisation process antigen presenting cells (dendritic cells, macrophages) present allergen
fragments (epitopes) to T helper cells using MHC Class II. Mainly Th2 cells involved in inducing
allergic disease IL4, IL5, IL3 IgE production, eosinophil growth and differentiation and mast
cell growth
Lab tests
Tests for IgE antibodies (eg RAST tests) are available for certain allergens. But also rises for parasites
– where in the world were they raised – this could be a cause
Indicate immune sensitisation only. Allergy requires symptoms following exposure
Expensive and less accurate than skin tests, but useful if skin tests not possible, history of anaphylaxis
Challenge tests
Mainly in research setting
Food allergy: can do double blind, placebo-controlled food challenge. In small kids, removing food
allergens from diet will improve severe eczema – but not in adults
Inhalation of cold air, histamine or exercise may be useful in assessing bronchial hyperreactivity in
asthma
Contact Allergy
Affect whole skin and are usually life long
Diagnosed using patch testing on back for 48 hours. Difficult to distinguish between allergic and
irritant reactions
Diseases caused by Antibodies
Antibodies against tissue antigens
Cause disease specific for that cell/tissue
Usually auto-antibodies: but may be a foreign antigen that is immunologically cross-reactive with a
component of self-tissues
Usually IgG or IgM
Antibodies may be specific for cellular structures: eg receptors. May lead to interference in function,
eg myasthenia gravis, Graves disease
Immune complexes formed from a soluble antigen and specific antibody
Formed in the circulation, deposit typically in arteries, glomeruli, synovia
Leads to local leucocyte activation and tissue injury
Antigens can be foreign or self antigens, antibodies are usually IgG or IgM
312 4
th
and 5
th
Year Notes

Skin 313
Skin
References:
Mainly Dr Lisa Judd‟s notes in GP, Paediatrics and Musculo-skeletal
Prof Delahunt‟s Pathology notes
Dr Stanley‟s Paediatric eczema notes
Dermatology Glossary.................................... 314
Diagnosis ........................................................ 314
Skin Infections ............................................... 315
Bacterial infections of skin and soft
tissue ................................................... 315
Fungal Infections/Dermatophytosis .......... 317
Viral Infections ......................................... 318
Other Infections ........................................ 318
Eczema ........................................................... 319
Atopic Eczema .......................................... 319
Seborrhoeic Dermatitis ............................. 321
Contact Dermatitis .................................... 321
Other Eczema Related Conditions ............ 322
Nappy Rash .............................................. 323
Sun Damaged Skin ......................................... 323
Skin Neoplasia ............................................... 324
Naevi and Melanoma ................................ 324
Other Tumours .......................................... 325
Ulcers ............................................................. 327
Inflammatory skin lesions .............................. 328
Acne ............................................................... 330
Other Skin Lesions ......................................... 332
Pharmacology ................................................. 335
Treatments ................................................ 335
314 4
th
and 5
th
Year Notes
Dermatology Glossary
Annular lesion - ring shaped
Erythema: dilation of blood vessels – colour goes away if pressed (blanching)
Macule: an alteration in colour (e.g. macular erythema)
Papule: a small lump, less than 0.5 cm in diameter
Nodule: lump bigger than 0.5 cm
Erythemato-squamous: red and scaly
Plaque: elevated (maybe only very slightly) area of skin > 2 cm. Altered texture
Vesicles and bullae = fluid within or beneath epidermis (blister). Vesicles < 0.5 cm, bullae > 0.5 cm.
Can have both. E.g. vesicular-bullae eruption from a plant allergy
Pustule: accumulation of pus (can be just inflammatory not infectious, e.g. psoriasis)
Cellulitis: inflammation of deep dermis and subcutaneous tissue
Ulcer: loss of dermis and epidermis
Scale: at edge of inflammatory lesion, can be fine, large, dark, silvery (psoriasis)
Scar: fibrous tissue due to healing. Atrophic scar is thin and wrinkled. Hypertrophic scar is elevated
Poikiloderma: cutaneous pigmentation, atrophy and telangiectasia
Comedo – pl. comedones: a plug of keratin and sebum in a dilated pilosebaceous orifice. Closed
comedo = blackhead, open comedo = whitehead
Cyst: any closed cavity with a membranous lining containing fluid
Petechiae – pl., petechiae: a haemorrhagic spot 1 – 2 mm diameter
Purpura: haemorrhagic spot > 2 mm. Pressing down doesn‟t blanch – red cells are extravascular
?vessel damage. If purpura are palpable vasculitis
Ecchymoses: bruises – larger extravasations of blood
Telangiectases: permanently dilated small vessels
Guttate: a profusion of small macules or plaques
Serpinginous: a linear eruption which is S shaped or snake like (e.g. larva migrans – a worm)
Dermatitis: usually means eczema
Structure of skin:
Epidermis:
Stratum corneum
Stratum lucidum
Stratum granulosum
Stratum spinosum
Stratum germanitivum (base of epidermis)
Dermis:
Papillary dermis
Reticular dermis
Subcutaneous tissue
Basic terms: Non-specific reactive changes
Hyperkeratosis: thickening of the stratum corneum. Eg due to trauma (eg the lump where you hold
a pen)
Parakeratosis: Nuclei are seen in the stratum corneum (would normally have died off, eg psoriasis)
Acanthosis: thickening of the epidermis, eg due to irritation
Diagnosis
Where is it:
Psoriasis: likes scalp and extensor elbows/knees
Atopic eczema: likes flexor elbows and knees
Nose & cheeks: lupus, especially if it leaves a pigment behind
Does it itch?
Atopic eczema (if it doesn‟t itch its not eczema)
Chicken pox
Urticaria/allergic reactions
Contact dermatitis
Scabies
Skin 315
Insect bites
Fungal infections
Dermatitis herpetiformis
Pityriasis Rosea
Idiot‟s algorithm:
Skin Infections
Bacterial infections of skin and soft tissue
Impetigo (School Sores)
= Superficial infection involving the epidermis
Most common in children during summer months
Non-bullous impetigo:
= Streptococcal impetigo
Vesicles on erythematous base pustules (highly contagious) yellow-brown scabs (CRUSTY),
associated with regional lymphadenopathy
Ecthyma is deeper version – cut out edge
Commonly result of skin break such as insect bites or chicken pox. Especially if overcrowding and
warmer climates
Goes for limbs and face
Fever uncommon. Check lymph nodes
Caused by Streptococcus Pyogenes with or without co-infection with Staphlococcus Aureus (can
Scalded Skin Syndrome, see page 315)
Commonest cause of post-strep glomerulonephritis
Bullous impetigo:
Due to Staph aureus of phage II (usually type 71)
Usually younger children
Lesions: begin as vesicles – turn into flaccid bullae in response to toxins. Following rupture of the
bullae, a moist red surface remains and varnish like crust appears
Neonatal Impetigo: Staph Aureus. Can spread to deeper tissues, umbilicus, bone and joints. If only
one site, antiseptic bath once a day. If > 1 site then systemic antibiotics
Treatment:
To relieve symptoms, stop new lesions, prevent complications (e.g. cellulitis, acute
glomerulonephritis), and stop spread to others
Flucloxacillin, dicloxacillin, a cephalosporin, erythromycin or clindamycin are all effective
If MRSA: usually susceptible to co-trimoxazole (although not so good against S Pyogenes).
Resistance to fusidic acid is also growing
Resistance is growing to topical agents (e.g. Mupirocin)
Scalded Skin Syndrome
Due to staph aureus toxin (may be distant site)
Skin peels off with little pressure – skin looks abnormal – damage from within
Commonest in infancy
Treatment: flucloxacillin plus burn treatment (including fluid balance)
Itchy?
No
Yes
Fever?
Fever?
Yes
Yes
No
No
Chicken pox
Eczema
Urticaria
(hives)
Tinea
Measles
Rubella
Meningitis
Cellulitis
Moles
Herpes Simplex
Impetigo
Folliculitis
316 4
th
and 5
th
Year Notes
Folliculitis
Pyoderma located within the hair follicle
Usually caused by S aureus
Responds well to topical antibacterial measures
Furuncle
= A „boil‟
A deep inflammatory nodule
In skin areas subject to friction and perspiration and containing hair follicles
Often drain spontaneously, especially with moist heat
If recurrent, then ?nasal carriage of S aureus. Treat with topical intranasal mupirocin or systemic
rifampicin
May progress to a carbuncle: more extensive involving subcutaneous fat. If surrounding cellulitis or if
on face then need iv antibiotics
Cellulitis and Erysipelas
Infection of subcutaneous layer by Strep Pyogenes
Symptoms: inflammation, warmth, erythema, pain, fever
Can sepsis, bullae and small abscesses
Also erythema around anus with puss and blood in stool
May desquamate
Impaired lymphatic drainage predisposes to recurrent cellulitis (e.g. pelvic, joint, breast surgery)
Erysipelas is a distinctive superficial cellulitis, primarily involves dermis. Raised and well demarcated.
Prominent lymphatic involvement. May chills, fever and malaise
Treatment: S Pyogenes still very susceptible to penicillin
Diabetic Foot infections
Due to neuropathy, ischaemia, and infection
Causes: often S aureus, also coagulase negative staphylococci and streptococci
Often nasal carriage of S aureus
Treatment: anti-staphylococcal agents. IV treatment if deep tissues or bone involvement
Deep Tissue Infections
Necrotising Fasciitis: See Streptococcus Pyogenes (Group A, Haemolytic), page 500
Superficial necrotising cellulitis or streptococcal gangrene (rare)
Gas Gangrene (Clostridial myonecrosis): rapidly progressive and life threatening infection of muscle
due to Clostridium Perfringens
Scarlet Fever
See Streptococcus Pyogenes (Group A, Haemolytic), page 500
Lymphadenitis
May require drainage. Distinguish from lymphadenopathy
Usually Staph aureus, also TB
See Cervical Lumps, page 648
Toxic Shock Syndrome
See Streptococcus Pyogenes (Group A, Haemolytic), page 500
Desquamation a week later characteristic
Dog Bites
Clean carefully (may need local anaesthetic)
Treat with broad-spectrum antibiotic. Amoxycillin/clavulanate. NNT = 14. So limit to high risk of
infection only. Consider anaerobe cover (eg metronidazole)
Screen for post-traumatic stress disorder afterwards
Report the dog
Lyme Disease
Tick borne spirochete (Borrelia burgdorferi)
Gives erythema migrans, headache, fever, myalgia, fatigue
Skin 317
Leads later to widespread systemic manifestations
Discovered in Connecticut, USA. No in NZ
Fungal Infections/Dermatophytosis
= Tinea
Fungal infections of animal (zoophilic) origin: These include “ringworm” (which causes a scaling
macule – not a ring – and there is no worm!). Usually in children, for example from cows, dogs, cats or
mice
Clinical Description
Fungal infections usually itch. Have a raised scaling margin that extends outwards
There are several classical presentations:
Tinea Cruris: in the groin. Mainly affects men. Sharp margin. On thighs or buttocks may get
follicular pustules. If feet involvement as well then systemic treatment, otherwise topical
Tinea Capitis: Scalp. Invasion of hair shaft. Causes alopecia. Usually M Canis. Usually children
aged 3 – 7, nearly always cervical occipital lymphadenopathy. Needs systemic treatment (topical
doesn‟t penetrate hair shaft).
Athlete‟s Foot/Tinea pedis: on the feet (usually lateral toe clefts – compared with eczema which in
medial toe clefts). Increased sweating predisposes to fungal infection. It can be spread to the sole
with a powdery scale. To hands by itching, where it presents with a dry, hot rash on one palm,
with well defined lesions with a scaling edge
Tinea Corpus: on the trunk. Presents with an erythema and itching, and a well defined, scaling
edge. May not itch
Tinea manuum: Hand. Almost always a pre-existing foot infection.
Fungal infection of the nail (Onychomycosis): occur mainly in adults, usually in their toenails
(fingernails uncommon, ?psoriasis), and especially following trauma. The nails become thickened,
yellow, and crumble, usually asymmetrically. The changes occur distally, and move back to the
nail fold (compared with psoriasis, which is symmetrical and moves distally from the nail fold)
Tinea Incognito: Fungal infection treated with steroids. Stops inflammation but fungus slowly
spreads follicular pustules etc.
Tinea Versicolor:
Infection due to a commensal yeast Malassezia Furfur (= pityrosporum ovale. Not a fungus). In
young adults, causes hypo- or hyper-pigmented macules with powdery scale, on upper trunk, upper
arms and neck. Slightly itchy
Differential diagnoses:
Vitiligo: but pure white lesion (amelanotic), no scaling
Pityriasis alba: Usually children and on the face. Tinea Versicolor rare in children
Treatment: Imidazole cream, sporanox, selsun shampoo
Diagnosis
Consider in any patient where isolated, itching, dry and scaling lesions occur for no reason (e.g. no
history of eczema). Fungal lesions are usually asymmetric. Clippings or scrapings can be sent for
culture
Pathogenesis
Common: Microsporum Canis (from cats, fluoresce under Wood‟s light), Trichophyton rubrum, and
Trichophyton mentagrophytes
Less common: Trichophyton tonsurans, Epidermophyton floccosum, Trichophyton erinacei
Fungi consist of thread-like hyphae that invade keratin (yeasts do not have hyphae). Vegetative spores
(conidia) develop in culture. When immune response is impaired, superficial infections may invade
deeper tissues
Management
Topical Treatment: imidazole preparations, such as clotrimazole and miconazole. Dusting preparations
are also available. Terbinafine is available as a cream
Systemic Treatment: Diagnosis should be confirmed before commencing treatment. Terbinafine
(250mg, once daily PO) for 2 to 6 weeks for skin infections and 3 months for fingernail infections, 6
months for toe nail infections. (Pregnancy and lactation are relative contraindications). Can take
itraconazole 1 week per month for 3 months (200 mg bd) side effects. Takes 12 – 18 months to
grow a new nail. Given length of treatment, confirm with nail scraping for culture first.
318 4
th
and 5
th
Year Notes
Viral Infections
Molluscum Contagiosum
Viral infection with pox virus
Small solid papules with umbilication in middle. Stay fairly localised
If you squeeze them then virus released (ie infective)
Histology: acanthosis and molluscum bodies
Disappear in under 9 – 12 months. Treat if severe
Verrucae (Warts)
Papova virus: Papillary lesion + polyoma (lots of them) + vacuolation of cells containing the virus
Locations:
Verruca vulgaris
Verruca plana: flat, eg on face
Verruca plantaris: on feet, can be painful
Verruca palmaris: on hands, can be painful
Condyloma accuminatum: Genital. Rarely premalignant
Histology:
Hyperkeratosis/parakeratosis
Acanthosis
Nuclear and cytoplasmic inclusions
Perinuclear vacuolation
Other Viral Illness
See Varicella Zoster504
See Herpes Simplex Virus (HSV), page 503
See Common Paediatric Viruses, page 617
Other Infections
Paronychia
Loss of cuticle (due to eczema, wet work, etc) allows growth of organisms beneath the proximal nail
fold inflammation and nail dystrophy. Acute usually staph, chronic usually candida
Differential:
Onychomycosis
Lupus, psoriasis, chilblains
Treatment: avoid wet work, treat eczema, dying agent, systemic antibiotic if bacterial
Pitted Keratolysis
Small craters in the sole of the foot. Asymptomatic. Foot odour
Variously attributed to Corynebacteria, Dermatophilus, Micrococcus
Treatment: keep feet dry, topical erythromycin, systemic tetracyclines
Pityriasis Rosea
Usually 10 – 35. Starts with herald patch (larger than later lesions). After 5- 15 days general eruption
begins. Oval, dull pink, with marginal scale. Itch varies. On trunk, rarely on face
Was thought to be viral, but erythromycin effective
Fades after 3 – 6 weeks
Differential: eczema, psoriasis, seborrheic dermatitis, tinea versicolor
Candidiasis
Yeast infection
Common in infants – either mouth (esp inside checks) and in nappy area, maybe on hands if sucked.
More common in damp areas. Need to treat Mum‟s nipple as well.
Lesions whitish with satellite lesions characteristic
Also with oral/inhaled steroids or broad spectrum antibiotics
Systemic spread in immuno-compromised is nasty
Treatment: see Antifungals, page 515
Skin 319
Scabies
Irritation from hypersensitivity after 4 weeks of scabies mite burrowing
Papular vesicular lesions
Headlice *
The insect: 2 – 3 mm long, breeds all year round. They live in the scalp and suck blood for food 5 or 6
times a day. They are only transmitted through close head contact. They don‟t come off with
swimming or washing. The eggs are a similar colour to scalp skin. The empty egg shells, known as
nits, are white
Life cycle: female lice lay about 7 – 10 eggs each night, these hatch in 9 days. A louse will live for 40
days
Where to find them: around the hairline at the back of the neck, behind the ears, on the crown
Treat if you find a live insect or an egg within 1 cm of the scalp (hair grows 1 cm a month, so more
than 1 cm from head means they‟re dead)
Use special shampoo from the chemist. Leave on scalp for 5 – 10 minutes. Don‟t use too much water.
Repeat a week later
Don‟t need to wash bedclothes: lice only lay eggs on hair. Instead check kid‟s heads once a week
Prevention: regular hair brushing, don‟t share brushes, keep clothes separate, contact tracing
Eczema
= Dermatitis
Formal definition: pattern of inflammatory response of the skin which can be defined histologically by
the presence of a predominantly lymphohistiocytic infiltrate around the upper dermal blood vessels,
associated with spongiosis (= oedema between keratinocytes) and varying degrees of acanthosis.
Clinical features include itching, redness, weeping, scaling and clustered papulovesicles
Endogenous forms:
Atopic
Seborrheic
Discoid
Juvenile plantar dermatosis
Pompholyx
Pityriasis Alba
Exogenous forms:
Asteatotic
Irritant contact dermatitis
Allergic contact dermatitis
Atopic Eczema
See Allergy and Hypersensitivity Disorders, page 309
Symptoms
Onset usually 2 – 6 months
Acutely:
Itchy
Redness, swelling, usually ill-defined border
Papules, vesicle, extremely large blisters, may look weepy
Exudates and crusting
Scaling
Can be papular
Chronic:
Less vascular and exudative
More scaly, pigmented and thickened
Fissuring
More likely to be lichenified (epidermal thickening with exaggeration of skin markings) and
develop painful fissures
If dark skin: post inflammation change in pigmentation
Pitting of nailed if involved with ridging of nails
320 4
th
and 5
th
Year Notes
In babies:
Common onset in first few weeks
Quite weepy/blistery
Around face (spares eyes and base of nose) and trunk. If extensor distribution think of contact
sensitivity (eg house dust mite)
Can be due to antigens in breast milk
The itch that rashes: itchy skin is scratched and an eruption occurs – don‟t see rash where child
can‟t reach
Children, and older:
Bends of elbows, behind knees
More leathery
Between big toe and 2
nd
toe (compared with tinea between 4 and 5)
Associated with asthma and hay fever
Associated with food allergy – commonly cows milk but this is overstated
Atopic skin has lower threshold to irritation (eg soaps) and is more prone to staph infection
Prognosis: ½ have cleared by 12, few persist after age 30
Increased tendency to: dry skin, urticaria, pityriasis alba, keratosis pilaris, irritant contact dermatitis, etc
Pathogenesis
Genetic predisposition
?Imbalance of Th1 and Th2 cells in the thymus in favour of Th2
?Early childhood infections preferential induction of Th1 type cytokines and prevent atopic
sensitisation. Infections greater risk of atopy
Inversely proportional to the number of older siblings (marker of exposure to infection)
Atopy does not equal allergy:
Level of IgE, which may be elevated, doesn‟t correlate to severity
Up to 50% of children with eczema do not have +ive skin prick tests (especially if mild eczema
and no asthma)
Skin prick tests for histamine release (type 1 reaction) may be positive but the person may have not
reaction when exposed to that allergen
Rast test looks for antigen specific IgE
Type 1: normally asthma, rhinitis, urticaria, not usually eczema
Patch testing (Type 4) may be relevant to childhood eczema
Only 50% with severe eczema develop reactions when challenged with particular foods – most are
delayed reactions
See Allergy and Hypersensitivity Disorders, page 309
Management
Investigations
Patch testing
Is there infection? (Yellow crusts, weepy, failure to respond to treatment) systemic antibiotics
Prevention:
Don‟t itch
Avoid aggravators:
Light cotton clothes, no scratchy woollens
Avoid excess humidity/dryness
Avoid local or systemic aggravators
Care with soaps, perfumes, solvents etc
Baths not shower, not too hot, pat not rub dry
Reduce stress
Control dry skin: Emollients – aqueous cream, white soft paraffin
Medical:
Topical corticosteroids:
Reduce inflammation but doesn‟t treat cause
Use weakest possible – 1% hydrocortisone OK for most
At night use in conjunction with wet dressings (containing emollient)
Not for too long otherwise skin atrophy, striae and rebound afterwards, wrinkling, vascular
markings, also dynamite to viral/bacterial infections. Even worse with systemic steroids
Lotion for scalp, ointment for dry areas (may cause folliculitis), cream
Skin 321
Strength:
Face and flexures: mild only
Scalp, palms and soles: can tolerate very potent steroids (eg betamethasone diproprionate)
Body and limbs: potent for short periods (a week or two), mild to moderate as
maintenance
Systemic steroids for severe eczema, for a short time only
Tar compounds: esp. at night to prevent itching
Antihistamines: stop itching (more in kids and for sedative effect) and urticaria
Antibiotics for infection
For severe eczema: phototherapy, azathioprine, cyclosporin
Seborrhoeic Dermatitis
Scalp, eyebrows and nasal labial folds. Cradle cap in babies whose scalp was clear at birth
Red, greasy scale, sharply circumscribed
In kids = another presentation of atopic. Treat the same. Differential: Infantile psoriasis
In adults = allergy to yeast (Pityrosporum ovale) which arrive with grease gland activation at puberty
Differential:
Psoriasis. But doesn‟t often affect the face
Discoid, and other forms of eczema
Pityriasis rosea (usually on trunk and not on the face)
Fungal infection: annular, scaling isn‟t greasy
Contact Dermatitis
May be irritant or allergic or both. May co-exist with endogenous forms (eg atopic)
Differentiate from endogenous on the basis of history, distribution and maybe allergy testing, not
morphology
Contact Irritant Dermatitis
Irritant: a substance which induces dermatitis in anyone if applied in sufficient concentration for long
enough penetrates skin and produces cellular damage
Individuals vary in their threshold
Heat and or hydration impair barrier function more susceptible
Cumulative effect of different irritants
Irritants include: acids, alkalis, solvents, soaps, detergents, enzymes, abrasives
Diagnosis:
Exposure to irritants for what length of time and frequency
Are sites consistent with exposure
Does it improve after exposure stops
Can contact allergy be excluded (eg have they had it since childhood more likely to be allergy)
Management:
Steroid creams, emollients
Reduce exposure, remove occlusion (ie sweat inside gloves over hydration), other work
Contact Allergic Dermatitis
Type 4 cell mediated immune reaction (see Allergy and Hypersensitivity Disorders, page 309)
Often takes repeated exposure, so no previous symptoms may not be significant (same for type 1
reactions). Eg may have worn rubber gloves for years
Once sensitised, further exposure to even minuscule amounts reaction after a day or two. Takes 24
– 72 hours, compared to type 1 which takes 15 – 20 minutes
Will involve primary sites, and maybe distant sites (eg eyes, genitals)
Photoallergy = need exposure to allergen + UV light to cause rash. Eg sunscreens
Common allergens: nickel (eg pierced ears), rubber additives, plants, chromate in cement, hairdressing
chemicals, perfumes, …
Rubber glove allergy can be:
Type 1 due to rubber
Type 4 due to rubber additives
Contact dermatitis due to sweaty hands - risk of type 1 or 4 reaction (mediated by Langerhans
cells) due to barrier function
322 4
th
and 5
th
Year Notes
Diagnosis:
Exposure to possible allergens
Sites consistent with exposure, goes away when exposure stops. NB some sites resistant (scalp,
soles)
Patch testing
Management:
Steroids, emollients, etc
Avoid exposure
Other Eczema Related Conditions
Discoid Eczema
Descriptive term: round or oval, well circumscribed, red, scaly, +/- vesicular ( weepy)
In kids: often atopic
In Adults: often cause unknown
Differential:
Ringworm: tends to be annular (worse at the edge). May have alopecia or pustules. Take scraping
for culture.
Superficial BCC: doesn‟t usually itch, often a shiny surface, dots of pigment
Psoriasis: silvery scale, not weepy
Juvenile Plantar Dermatosis
Fissured dermatitis of the plantar surface of the forefoot – red, glazed, cracked, symmetrical, toe clefts
normal
In children 3 – 14 years
Usually atopic
Treatment difficult: Urea creams, moisturisers, steroid creams. Has usually resolved by teens.
Pompholyx (dyshidrotic eczema)
Not related to atopic eczema
Vesicles +/- bullae on palms, soles, sides of fingers or toes
Erythema or scaling absent. If present then just a vesicular eczema
Heals with desquamation
Differential: fungal infection
Treatment: ?steroids
Pityriasis Alba
Round/oval, hypopigmented, fine lamellar scaling, from 5 – 20 mm, commonly on face
Usually age 3 – 16
Associated with atopy – but may be independent
No treatment – goes away by itself
Asteatotic Eczema
Related to dry skin
Usually on legs, usually diuretics, excessive washing or hypothyroidism
Superficial fissures create a crazy paving pattern
Treatment: soap substitute, moisturiser +/- topical steroid
Intertrigo
Generic term for inflammatory dermatosis in skin folds (eg submammary or gentiocrural)
May be a form of atopic or seborrheic dermatitis
Can be secondarily infected with candida or staph
Treatment:
Reduce friction, avoid tight clothing
Mild steroid, antibacterial or anti-candida cream
Angular Cheilitis
Affects the fold of skin at the corner of the mouth. Especially in denture wearers
May be a form of intertrigo, can be associated with atopic or seborrheic dermatosis
Skin 323
May be infected with candida or staph, may be folate deficiency, a frequent complication of
Roaccutane treatment
Nappy Rash
Napkin Dermatitis
Irritant contact dermatitis caused by prolonged contact with wet nappies
Spares the flexures
Bacterial conversion of urine to ammonia alkaline irritant
Treatment: frequent changing, carefully washing, protective cream
Differential: Candidiasis
Frequently superimposed on nappy rash
Flexures involved + satellite lesions or superficial pustules on a background of erythema
Treatment: antifungal cream (nystatin)
Sun Damaged Skin
Photo-damage = Dermatoheliosis
Damage results in:
Wrinkling
Pigmented lesions
Sebaceous hyperplasia (?sun damage or age)
Telangiectasia and purpura (thinned epidermis due to basal cells + flattening out of dermo-
epidermal junction shearing forces rupture capillaries bruising
Pseudoscars
Benign and malignant growths
Skin laxity
Diffusely thickened skin with yellowish micropapular appearance (especially temples), etc, etc
Damage relates to life-time dose of UV:
Melanoma risk determined by age 15
After that, sun only affects BCC and SCC risk
Sunscreens
UVA blockers: block in range 320 – 360 nm. Doesn‟t cause sunburn but is implicated in skin cancer as
its harder to filter out
UVB blockers: block UV in the range 290 – 320 nm, the sunburn range, but easily filtered. SPF refers
to ability to block UVB – not UVA need broad spectrum
Types of sunscreen:
Cinnamates: UVB
PABA: UVB (not commonly used – allergies)
Salicylates: UVB
Benzophenones: UVA
Camphor: UVA
Dibenzoylmethane: UVA (good to have in addition to a high SPF)
Can use reflective agents (eg titanium dioxide) in addition to absorbers
Need behaviour change as well as sunscreen
Lesions
Solar Keratosis: See Premalignant Lesions, page 326
Cutaneous Horn: horny outgrowth, arising from a Solar Keratosis, SCC or seborrheic keratosis. Treat
according to underlying lesion
Disseminated Superficial Actinic Porokeratosis: Caucasian. Autosomal dominant. First noticed in 40s.
Up to 1 cm, slightly red/hyperpigmented on lower leg or forearms. Border has 2 parallel rows of scale
Bowen‟s Disease: See Premalignant Lesions, page 326
Chondrodermatitis: On sun damaged ears, may also be due to pressure. Commonly on helix of pinna.
Painful when pressed. Differential SCC (usually large and not as painful) or BCC (pearly, not often on
rim of ear). Treatment: excision including cartilage otherwise recurrence
Lentigo: Brown macules (look like large freckles). Solitary, multiple or generalised. May be part of a
syndrome. In adults they are usually sun induced, on back of hand or back. Can get a solitary dark one
324 4
th
and 5
th
Year Notes
on the lower lip after sunburn. Differential of dark ones: melanoma. May require excision to
differentiate
Idiopathic Guttate hypomelanosis: pale spots in the shape and distribution of largish freckles on sun
damaged skin
Freckle: brown macule. Due to pigment production but anatomically normal. Fades if sun exposure
ceases. Commoner in redheads
Skin Neoplasia
Naevi and Melanoma
Naevi = hamartoma of the skin. With respect to melanocytes, a benign neoplasm
Melanocytic Naevi
Normal skin: epidermal cells, plus melanocytes, Langerhans cells (Antigen Presenting Cells –APC),
prickle cells and merkel cells (sensory receptors)
Benign melanocytic naevi:
Junctional: epidermis only, early active growth to <0.5 cm. Can be non-pigmented. Overgrowth
of melanocytes in nests along the junction of the dermis and epidermis.
Compound: epidermis and dermis, older active growth (moles on palms, soles and genitalia stay
junctional)
Intradermal: stopped growing, loss of tyrosinase small and pale. Don‟t have contact with the
epidermal junction (ie are deep). Don‟t become malignant – must have junctional activity to do
this
Dysplastic melanocytic naevi (Atypical Mole Syndrome):
Uncontrolled proliferation without malignancy (> 100 with at least one Dysplastic more or a mole
> 0.5 cm)
Mostly benign with possibility of malignancy
If have > 100 moles, 100 to 200 times normal risk
Risk of melanoma proportional to the number of moles, plus family history and degree of atypia
Management:
Self checking each month
Annual doctor check (to make sure they‟re self checking)
Most moles that change aren‟t melanoma, but if suspicious need to remove it
Halo naevi: Fairly common, especially in kids. Depigmented symmetrical halo around the mole, but
the mole is normal (cf depigmented melanoma where pigmented lesion is not normal and not central)
Pathogenesis: ?Somatic mutation
Differential:
Melanoma
Dermatofibroma: feels firm
Seborrheic keratosis: altered texture
Melanoma
Host Risk Factors: Skin colour, Naevi, Atypical naevi, DNA repair, Immune status
Environment Risk Factors: UV light (geography, season, time), behaviour. Risk from sun determined
by age 15. After that sunscreen mainly protects against squamous and basal cell carcinomas
Epidemiology:
1 – 3% of childhood cancers
Females 14/100,000, males 9/100,000. Difference is in the distribution on the legs
Spotting them:
A: asymmetry
B: border irregular – e.g. growing a peninsular
C: colour – 3 or more, colour not symmetrical, areas of black, variegated
D: dimension > 0.6 cm (although you can get smaller melanomas, and most larger lesions aren‟t
melanomas
E: elevated dermal penetration (but most are initially flat – superficial spreading melanomas)
Usually asymptomatic: don‟t bleed until late (ie take bleeding seriously) and don‟t usually itch
Watch out for:
Changes: but moles can change for lots of reasons. And patients aren‟t good at detecting changes
(either miss them or think they‟ve changed when they haven‟t)
Skin 325
Bleeding, itching and halo (although can get two tone moles – OK if symmetrical)
Progression:
Radial Growth Phase: initially growth is along the dermo-epidermal junction and within the
epidermis
Vertical Growth Phase: Growth into the dermis malignant cells in contact with lymphatics and
capillaries metastasis
Nodular melanoma: bad news
Acral Letigenous Melanoma: on palms and soles
Differential:
Benign mole
BCC
Seborrheic keratosis: stuck on appearance, monotone and symmetrical, greasy surface, numerous
Angiokeratomas
Dermatofibroma: firm, round, monotone
Any lesion under a nail (usually thumb) is a melanoma or SCC until proven otherwise
Pathology:
Features of malignant cells: irregular, hyperchromatic, large N:C ratio, mitoses (blackberry nuclei),
abnormal number of mitosis
Radical/Superficial/Horizontal growth phase: cells in contact with dermis, don‟t metastasise
Vertical growth: mass of atypical melanocytes infiltrating dermis, lymphocytes, not necessarily
pigmented, metastasises
Will always have junctional activity. If they only exist deeper in the dermis then they‟re not
malignant.
Prognosis:
Breslow tumour thickness (> 0.76 cm bad) or Clarke‟s levels (grade 1- 5, 3 ~ Breslow 0.76, bigger
= worse)
Ulceration > 3 mm (bad)
High mitotic rate (bad)
Regression an indication of metastasis (bad)
Tumour infiltrating lymphocytes (bad)
Treatment: surgical excision
Hutchison‟s Freckle: freckly „in-situ‟ melanoma. Usually on face, tan macule that slowly enlarges and
develops a geographic shape, multicoloured in time. Malignant change of melanocytes along the
epidermis border but no infiltration. Takes years to become invasive. On sun damaged skin. On
elderly watch for a while. Now showing up on younger people – excise before they get too big
Other Naevi
Epidermal Naevi:
Defined according to their predominant cell type
Circumscribed distribution over a part of the body surface, usually dermatomal
Any size, never cross the midline, uncommon on face and head
Sebaceous Naevi: hamartomas of predominantly sebaceous glands. Usually on scalp (lesion is bald).
Raised, velvety surface, present at birth, usually small. Risk of basal-cell carcinoma, but no longer
prophylactically excised
Dermal Melanocytic naevus (Mongolian spot): macular blue-grey pigmentation present at birth, over
sacral area in Mongoloid and some other races. Looks like a large bruise. Rarely persist into
adulthood.
Congenital naevocellular naevus: Small is < 1.5 cm, intermediate = 1.5 – 20 cm, large is > 20 cm. If
over lower sacrum ?spinabifida occulta. May arise or darken in puberty. Large ones have risk of
melanoma
Spitz naevus: appears in early childhood as a firm, round red or reddish brown nodule. May bleed and
crust. Benign. Local excision.
Other Tumours
Benign
Epidermal cyst:
Collection of epidermal cells within the dermis. Either around the base of a hair follicle or from
trauma (eg on a builders hands)
326 4
th
and 5
th
Year Notes
If it becomes infective ulcerates and smells
May be tethered to the epidermis with a central keratin filled punctum
Treatment: surgical excision for cosmetic or nuisance reasons
Seborrhoeic Keratosis ( = Basal cell papilloma)
Incidence with age, sun exposure, familial tendency, often associated with skin tags
Raised, sharply demarcated papule or plaque, shiny, bleeds easily if scrapped. Variable size,
„stuck on‟ appearance with cobblestone or leathery appearance, skin coloured, yellowish or greyish
brown/black
Results from proliferation of squamous basaloid cells which sit on top of and do not invade the
dermis (grow up, compared to BCC which grows down)
Histology: hyperkeratosis, well circumscribed, cystic structures within the epidermis filled with
keratin
Treatment: liquid nitrogen for cosmetic reasons. Fairly harmless
Differential:
Melanoma – but different surface texture
Pigmented solar keratosis: treatment similar so differential not so important
Keratoacanthoma:
Uncommon
On lip, up to 1 cm. Other areas up to 2 cm. Develops quickly (eg 4 weeks – too fast to be an SCC)
then heals with a scar
A „self healing squamous cell carcinoma‟. Inflammatory reaction at the base – body is rejecting it
Dermatofibroma (= sclerosing haemangioma):
Slightly elevated and pink or brown. Firm, button-like dermal lesion. Usually female
Histology: expands into dermis
Not malignant – but recurs if not all cut out
Premalignant Lesions
Actinic keratosis (= Solar Keratosis)
Common: 50% of NZers over 65
In situ proliferation of dysplastic squamous epidermal cells caused by UV light. Often on face,
white
Adherent scale, difficult to pick off. Not well circumscribed. Erythematous base
May spread within the epidermis, stop growing, recede or progress to invasive squamous cell
carcinoma (only 1%)
Histology: large, irregular nuclei, overgrowth of epidermis, hyperkeratosis and parakeratosis
Indicates sun damage has occurred person at risk of SCC, BCC and melanoma
No evidence that removal reduces the incidence of cancer – don‟t need to treat but often do for
cosmetic reasons
Differential:
Bowen‟s Disease: usually larger with a sharper margin
Discoid Lupus: erythema or pigmentation more marked, may have a pitted surface, more
common in Polynesians
Treatment:
Reduce sun exposure
Examine skin regularly for cancer
Remove lesions which are atypical, growing, annoying, unsightly
Liquid nitrogen if few in number
Efudix (5FU) cream: good for treating a large area – goes red and sore, stop cream then
resolution. If you use the cream too long ulcers, etc
Also retinoic acid, laser resurfacing, imiquimod (expensive)
Bowen‟s Disease:
More uncommon – but at least as common as SCC
75% are on the leg
Erythematous, well circumscribed, 1cm or more
Slightly raised plaque with irregular hyperkeratosis. Compared with BCC it‟s not so shiny and has
no pearly rim. May be bright red
May remain stable for a long time. If growing or bleeding or young patient treat. SCC arises in
3%
Differential:
Skin 327
Solar keratosis
BCC: shiny surface, pearly border, few dots of pigment
Psoriasis: silvery scale
Eczema
Treatment:
Excision
Liquid nitrogen – need more aggressive freeze than SK, on leg may ulcerate
Leave and watch
Malignant
Basal cell carcinoma:
Most common malignant tumour
Nodular BCC:
Flat and paler than surrounding skin, pearly or translucent, shiny. May have telangiectases
over the surface
Progresses to „rodent ulcer‟ (ulcer with raised, rolled edges)
Often on bridge of nose where glasses sit
Differential:
Intradermal naevus: Don‟t have the shiny, stretched look of a BCC
SCC: usually in badly damaged skin, and not translucent
Superficial BCC:
Red plaque +/- atrophy +/- dots of pigment. Usually well circumscribed. Raised rim. Less
shiny. Commonest on back, arms, legs, behind ears
Most common form of BCC
Differential:
Eczema: weepy, fissured surface, itchy (BCC isn‟t), atypical sites for a BCC
Psoriasis: silvery scale
Bowen‟s disease: duller surface with more hyperkeratosis
Don‟t metastasis but does invade. Won‟t kill you (at least quickly)
Histology: basophilic (blue) cells, palisaded around the edge
Squamous cell carcinoma:
Skin coloured or purplish nodule/plaque which may ulcerated
On badly sun damaged skin – dorsum of the hand, bald scalp, lower lip (BCC‟s uncommon on
these sites)
Surface may be hyperkeratotic or warty. Margins less well defined than BCC
May have cutaneous horn. Fleshy layer at the base of the horn differentiates it from benign lesions
Commonly misdiagnosed as BCC
If neglected will invade (claw-like infiltration)
4% metastasise
On sun exposed areas, may have cutaneous horns
Histology: hyperkeratosis
Ulcers
Venous Stasis Ulcers
70 – 90% of ulcers on lower extremities are due to venous insufficiency (eg varicose veins)
Below the knee, never on the sole of the foot, usually around the malleoli
Unlike ulcers due to arterial insufficiency, will have good peripheral pulses and no peripheral
neuropathy
Usual isolates: S aureus and/or various G –ive bacilli (including Pseudomonas aeruginosa and other
aerobic G-ive‟s)
Treatment: in absence of extensive surrounding cellulitis or systemic signs, there is no role for systemic
antibiotics
Pressure Ulcers
= Skin necrosis and ulceration as a result of pressure induced ischaemia
Incidence over a 3 week period of bed and chair bound patients is about 8 %
Critical factors in their development:
328 4
th
and 5
th
Year Notes
Pressure: Muscle and subcutaneous tissue are more vulnerable than epidermis. Pressure leads to
venous, arteriolar and lymphatic occlusion. Especially over bony prominences
Shearing: Sliding of adjacent surfaces (eg sacral skin on underlying bone) vulnerability to
pressure induced obstruction
Frictional forces: Eg from being pulled across sheets intra-epidermal blisters
Moisture: eg urinary incontinence, also sweat and faeces. Risk of pressure sores 5 times
Risk factors: age (loss of blood vessels, epidermal atrophy etc) and immobility
Staging:
1: irregular, ill-defined are of soft tissue swelling, induration and heat. Reversible
2: Plus inflammatory and fibroblastic response. Extends through dermis and into subcutaneous fat.
Reversible
3: Plus undermining of edges
4: Plus underlying muscle and bone
Infection. All pressure areas become contaminated. Impairs healing. Can lead to bacteraemia (usually
polymicrobial) with high mortality
Site: most at the sacrum, heel, ischial tuberosities and greater trochanter
Management:
Prevention (responsibility of all involved professionals)
Decreasing pressure: change of positioning, padding, alternating air cell mattresses
Friction: appropriate bed clothes, no particles in bed (eg food)
Moisture: Pads, catheters, reduced sweating
Shearing: avoid shearing positions (eg propped up in bed)
Established sores: Good nutrition, oral vitamin C, ?topical antibiotics (but resistance), saline
dressings + variety of preparations/dressings. If stage 3 or 4 then consider debridement or skin
grafts
Other Ulcers
Ischaemic ulcers:
Large artery disease: usually lateral side of the leg, pulses absent
Small vessel disease (eg vasculitis): palpable purpura
Malignant ulcer: eg basal cell carcinoma (pearly translucent edge), squamous cell carcinoma (hard
everted edge), etc
Neuropathic ulcer: painless penetrating ulcer on the sole of the foot due to peripheral neuropathy (eg
diabetes, leprosy)
Underlying systemic disease: Diabetes, pyoderma gangrenosum, rheumatoid arthritis, lymphoma
Inflammatory skin lesions
Psoriasis
Epidemiology:
Begins at any age
~2% of the population
Chronic characterised by rich red, erythematous silvery scaly plaques. May or may not itch
May be inherited (autosomal dominant with mixed penetrance)
Precipitated or aggravated by:
Cigarette smoking and alcohol consumption
Strep infection
Trauma (Koebner phenomenon)
Hypocalcaemia
Drugs: lithium, beta blockers, Antimalarials, withdrawal of systemic steroids
Stress
Characterised by rapid turnover of epidermis. Normally 28 days, reduced to 4 days parakeratosis
Histology: epidermal squamous cell hyperplasia, neutrophil accumulation
Psoriasis vulgaris:
Elbows, knees, scalp
Histology: parakeratosis, acanthosis, focal thinning, oedema of dermal papillae, micro-abscesses in
the stratum corneum
Pustular psoriasis:
Skin 329
Abscess formation within the epidermal layer widespread sloughing risk of
infection/electrolyte imbalance
Generalised (rare and life-threatening) or localised (most commonly palms and soles)
Nail involvement: pitting, discoloration, subungual hyperkeratosis and onycholysis (especially lateral)
Differential:
Bowen‟s disease: usually over leg
Superficial BCC
Eczema: may show Lichenification or fissures or vesicles
Lichen planus
Fungal: do a scraping
Discoid Lupus: face, leaves scars, has plugs of follicular hyperkeratosis
Seborrheic dermatitis
Treatment:
Mild steroid creams for face and flexures
Stronger steroid creams for short periods on trunk and limbs (but rebound flare up)
Coal tar creams: messy and smells
Dithranol + salicylic acid in white soft paraffin
Scalp: steroid of Betnovate strength to shift scale then a maintenance cream
UVB treatment
PUVA: Psoralen tablets 2 hours prior to UVA treatment twice a week. Effective but may have to
travel
If severe: methotrexate, Acitretin, cyclosporin, etc
Bullous Lesions
Epidermis sloughs off dermis
Intraepidermal: if any of the epidermis is left attached
Burns
Herpes
Pemphigus:
40 – 60 years, very fragile blisters skin, and also on oral and nasal mucosa
Less common than Phemigoid but more serious (40% mortality)
Histology: BM is intact, acantholysis
Pathogenesis: Autoimmune reaction to desmosomes in the epidermis infection etc. IgG
above the basement membrane. Chicken-wire pattern on immunoflouresence within the
epidermis
Types:
Pemphigus vulgaris: suprabasal lesions. More serious of the two. Mucosal and scalp
involvement, more fragile blisters, looks like burn. Generalised bullous phase ~ 5 months
after the onset of oral lesions. Heals without scaring. Patients are ill
Pemphigus foliaceous: acanthosis only in the superficial epidermis. Small flaccid blisters,
rupture leaving erythematous lesion, heals with crusting and scarring. Face, scalp, chest
and back. Oral lesions not common
Treatment: High dose steroids
Subepidermal:
Pemphigoid:
Smaller, localised, sturdy, grape-like blisters, generally rest of skin remains in tact. Ruptured
lesions heal rapidly. No oral involvement
May have only urticarial lesions with no blisters, or just vesicles, or eczema like appearance
Usually self-limiting, chronic relapsing, > 60 years. Can become generalised
Histology: Epidermis lifts in total at the dermo-epidermal junction
Pathogenesis: IgG in the BM, linear stain with immunoflouresence
Differential:
Diagnosis of bullae difficult. Usually need to refer, and histology (prior to treatment)
usually necessary
Pemphigus (flaccid bullae with mucosal involvement)
Eczema (but not itchy)
Russian hog weed et al
330 4
th
and 5
th
Year Notes
Treatment:
Systemic steroids: may need 20 – 40 mg per day. Unsuitable for long term use
problem especially in the elderly
Topical steroids if localised
Tetracycline 1 – 2 g per day, especially in elderly
Other immunosuppressive treatment (eg methotrexate)
Discoid Lupus Erythematous (DLE)
= Mild end of Lupus spectrum and much much more common than SLE. Mild skin rash, normal serum
ANAs and ENAs
Rash usually on the face, usually crosses the nose, sometimes scalp, ears, nose, arms
Erythematous plagues varying from several mm to several cm. Adherent scale (not flaky like eczema)
and pitted surface. Rough feel, doesn‟t itch. May heal with hyperpigmentation or white scar. Scarring
alopecia
Alopecia in scalp lesions which is normally permanent
More common in Polynesians and Maori, F > M
Characteristic histology and direct immunoflouresence (DIF) +ive
Differential:
Eczema (doesn‟t scar, uncommon to get discoid eczema on face, eczema can be weepy)
Solar keratosis or Bowen‟s (but patient usually to young for these)
Treatment:
Topical or intralesional steroids: fairly potent ones but be careful on the face. Systemic if
widespread
Sun protection
Antimalarials (eg hydroxychloroquine. SE: eye problems regular check-ups)
Topical Retinoids – also penetration of topical steroids
See also Systemic Lupus Erythematosus, page 278
Morphoea
Localised cutaneous scleroderma, occurs any age but especially 20 - 40
Thickened dermis with dense collagen, progressive loss of subcutaneous fat
Waxy, ivory coloured skin without hair or sweating
Vary in size from 2 – 15 cm with lilac coloured edge
Any site, especially the trunk
Tend to improve over time (years)
Treatment: intralesional steroid
See Progressive Systemic Sclerosis (PSS), page 280
Vitiligo
Slowly progressive amelanotic macules, initially on sun exposed areas. Usually symmetrical
Affected areas prone to sunburn
?Autoimmune
Associated with family history and other autoimmune disorders (eg alopecia arearta)
In 50% develops before age 20
Differential:
Tinea versicolor (but hypopigmented, not amelanotic, and scaly)
Pityriasis alba (but hypopigmented, not amelanotic, and scaly)
Treatment: usually unsatisfactory
PUVA or narrow band UVB (may need 2 or 3 treatments a week for a year)
Various surgical procedures
Acne
Inflammatory disease occurring in and around the sebaceous glands, generally affecting the face, also
the chest and back. Characterised by papules and pustules, or by cyst and other more specific lesions.
Deeper lesions are associated with scarring: hypertrophic, keloidal or depressed
Differential:
Rosacea
Perioral dermatitis
Skin 331
Acneiform drug eruptions
Pathogenesis
Four factors:
Increased sebum production by the sebaceous glands (normally produced to maintain epidermal
hydration)
Cornification (blockage) of the pilosebaceous duct: abnormal keratinisation and desquamation
of follicular epithelium combine with increased amounts of sebum production to obstruct the duct.
Bacterial proliferation - abnormal colonisation of the follicle duct by Propionibacterium acnes.
But severity not proportional to number of bacteria
Inflammation
If the obstruction is closer to the skin surface it will form open comedo and oxidation of the fatty
material causes discoloration (blackhead). A closed comedo (white head) occurs when the duct is
blocked at a deeper level
Acne is dependent on:
Genetic factors (high concordance in monozygotic twins)
Hormonal factors: androgens sebum production
Environmental factors: aggravated by humidity, some cosmetics and oils (block pilosebaceous
orifice)
Diet rarely implicated
Usually starts in adolescence and resolves by mid 20s (starts earlier in females and is more persistent)
Management
Reassurance: Treat as a physical and psychological disorder. Undermines patient‟s self-confidence,
especially in the adolescents. Myths of poor diet and hygiene make patients feel responsible and/or
guilty - reassured that they are not the cause
General advice:
Avoid humid conditions
Avoid occlusive creams and sunscreens
Only use moisturisers if the skin is dry
Topical agents. For mild to moderate acne:
Comedolytics: most effective option is Tretinion. Normalises desquamation of the follicular
epithelium promoting drainage of pre-existing comedones. This increases penetration of
antimicrobial agents
Antibiotics such as benzoyl peroxide and erythromycin gel reduce bacterial numbers and
inflammation
Oral agents. Are generally used for severe or persistent acne in addition to topical agents:
Antibiotics such as tetracycline, doxycycline, trimethoprim and erythromycin suppress
inflammation by inhibiting neutrophil chemotaxis and production of bacterial lipases and
proteases. For a minimum of six months with an 80-90% improvement expected after this time.
Often recur. SE of Minocycline: vertigo, discolouration of teeth, grey skin pigmentation
Oestrogens. They have a direct effect on sebaceous gland activity. They are combined with
progesterone in an oral contraceptive, which may counteract the effects of the oestrogen
Antiandrogens (in a female only) such as cyproterone acetate and spironolactone act peripherally
to inhibit androgen stimulation of sebaceous glands and hair follicles. They are useful in mature
presenting acne
Isotretinoin (Roaccutane)
A synthetic Vitamin A derivative that inhibits sebaceous gland activity, reduces P. acnes cell
numbers, alters follicular keratinisation and is anti-inflammatory
At adequate doses permanently cures acne in 80% of cases after 4 – 6 months
Highly teratogenic. Women need to be fully informed of the risks, need to have a negative
pregnancy test before starting treatment, and need to be on reliable contraception throughout
course (i.e. belt and braces) and one month after
Causes liver damage and hyperlipidaemia: baseline bloods and then after one month
Causes dry lips and maybe nasal mucosa ( epistaxis), skin and eyes, angular cheilitis
< 10% will get aching muscles, depression, hair loss, headaches
See Retinoids, page 336
332 4
th
and 5
th
Year Notes
Rosacea
Cardinal signs in order of importance:
Erythema
Telangiectasia
Papules
Swelling
Tiny pustules
On cheeks, chin, forehead, nose and neck, sun exposed sites. Flushing may precede other signs
Many theories
May be associated with rhinophyma (bullous swelling of the nose)
Minor ocular involvement in 50%: especially conjunctivitis, may blepheritis, etc
Treatment:
Systemic or topical antibiotics (as per acne)
Retinoids
Metronidazole
Perioral Dermatitis
Mainly young women
Cause a mystery. ?Steroids implicated
Starts in nasolabial fold and spreads to involve the perioral area. Minute papules and pustules on an
erythematous base with some scaling
Treatment: Systemic tetracyclines or erythromycin until rash gone then for another couple of weeks
Other Skin Lesions
Erythema Multiforme
Confusion/overlap between Erythema Multiforme (EM), Stephens Johnson Syndrome (SJS) and Toxic
Epidermal Necrolysis (TEN) [Later two at the severe end of the spectrum]
Varying degrees of mucosal involvement and rash
Typical lesion: target lesion – dull red macule or maculopapule 1 – 2 cm across, erythematous rim with
cyanotic or purpuric centre. May be blistering. Typically affects acral areas (dorsal hands, feet, palms,
soles, forearms, legs). Usually crop over a couple of days and fade after a couple of weeks.
Trunk only in extensive reactions. Also if severe: erosions, haemorrhagic crusting, lesions
uncomfortable (not usually painful). May affect cornea. May get systemic upset (fever, anaemia, etc)
Histology: vacuolar degeneration of lower epidermis
Provoking factors:
HSV – major cause. Rash worst at periphery (+/- oral mucosa). Will get it with subsequent
outbreaks as well. History: Do you get cold sores?
Mycoplasma (<1% of EM)
Drug reactions – more likely if severe outbreak. Not typical targets (eg red blotches), on trunk as
well as acral, may be blistered. Implicated drugs: anticonvulsants, sulphonamides, NSAIDs,
allopurinol. Stops drugs if at all possible. Treat like a burn. Steroids controversial
Idiopathic
Erythema Nodosum
Lesions: 2 –4 cm, erythematous, tender, especially on shins but also on thighs or forearms. A little
raised. Look like purplish bruises
Number from 2 – 50 (usually 5 – 6), erupt over 10 days and subside over 3 – 6 weeks
Regress with bruise like yellow/green colour changes
Systemic signs: fever, generalised aching and malaise
Due to deposition of immune complexes in and around venules in the deep dermis
Causes:
Kids: Streptococcal infection
Sarcoidosis (rare in kids)
TB
Cat scratch disease
Yersinia
Some drugs
Skin 333
Differential:
Nodular vasculitis (tend to ulcerated, don‟t heal with bruise like changes)
Meningococcal or gonococcal septicaemia (smaller lesions, often purpura, ill patient)
Erythema Toxicum Neonatorum
Up to 50% of full term infants (less if preterm), occur up to 4
th
day
Erythematous macules, wheals, papules and pustules – few to several hundred
Face, buttocks, torso, proximal limbs, not palms or soles
Usually resolve in several days
Cause unknown
Differential: HSV
Urticaria
= Hives or welts. Intensely itchy.
Relationship to allergy and atopy:
More likely in atopy
50% related to allergy – type 1 only exposure 15 – 30 minutes prior to onset and last < 24
hours careful history
Allergy likely to be all over, and no further outbreak for weeks/months
Most chronic urticaria is non allergic
Some foods/drugs may cause urticaria without immune involvement (ie histamine release without
IgE involvement)
Common causes:
Idiopathic – common
IgE mediated:
Food: peanuts, strawberries, milk, eggs
Animal dander: horses, cats
Physical: pressure, cold, heat
Complement mediated: hereditary angioedema and blood transfusion reactions
Mast cell releasing agents: opiates, penicillins
Prostacyclin inhibitors: Aspirin, NSAIDs
Infections: cause of 80% of acute childhood urticaria (eg hepatitis)
Serum sickness: type 3 reaction. Drugs, especially penicillin. Fever, raised ESR, starts within 5 –
20 days of exposure and lasts 5 – 28 days. See Allergy, page 309
Papular Urticaria
Hypersensitivity to an insect
Itchy, urticarial weal firm itchy papule
Usually gone in a day to two, may persist for months
Grouped in clusters, and develop crops at irregular intervals
Treatment: try insect repellent
If dark skin, may be post-inflammatory hypopigmentation
Alopecia Areata
Circumscribed areas of hair loss but skin normal.
Presentations:
Often scalp – with a few bald areas 1 – 3 cm
Loss of all scalp hair is alopecia totalis
Loss of hair at all sites is alopecia universalis
Not a diagnosis
Autosomal, autoimmune dominant disorder with variable penetrance
Duration < 1 year in 50 %, relapse common. Kids get it worse
Associated with Atopy, Downs, Hashimoto's Disease, Pernicious Anaemia, Addison‟s Disease, Vitiligo
Treatments include local steroids, topical minoxidil (antihypertensive), etc
Differential diagnosis: all produce circumscribed hair loss, but skin itself is abnormal
Fungal infections
Anything causing scaring (eg skin cancer)
334 4
th
and 5
th
Year Notes
Keratosis Pilaris
Common. More common in atopics
Small whitish plugs of keratin obstruct the follicle mouth. Usually extensor surfaces. Feels like
sandpaper
Variable perifollicular erythema
Facial involvement usually resolves in teens. Elsewhere can persist until middle age
Autosomal dominant with variable penetrance
Differential: Acne (shouldn‟t feel like sandpaper)
Treatment: mild steroids, urea creams, salicylic acid creams, etc
Granuloma Annulare
Ring of smooth, firm, skin coloured or slightly purplish papules from 1 – 5 cm. No scaling (cf ring
worm which is) or blistering ( epidermis fine)
Enlarge centrifugally, with beaded rim gradually flattening until it disappears without trace within 2
years
Dorsal surfaces of feet, hands and fingers are the commonest sites
Lymphohistiocytic granulomata
Mainly children and young adults
Can treat with intra-lesional steroids
Lichen Planus
Occurs in 30 – 60 year olds. Insidious onset, can be explosive, localised or generalised. In 80%
resolves in 18 months
Clinically: flat topped papules, discrete or coalescing. White lines on papules = Wickham's Striae.
Can also get annular, hypertrophic, atrophic or even bullous forms. Should linear lesions characteristic.
Itch variable. Rash resolves with hyperpigmentation. Can be painful on lips or genitals.
Looks like everything else. Differential:
Plane warts
Eczema
Drug reaction: gold, quinine, thiazides, etc
Treatment: Acitretin, steroids, miscellaneous
Tuberous Sclerosis
Disorder of haematoma formation: especially in eye, brain, skin, kidney and heart
Skin lesion:
Angiofibromas: appear from 3 – 10, firm, discrete red/brown telangiectatic papules, 1 – 10 mm,
cheeks and chin
Periungual fibromas: smooth skin coloured excrescences emerging from the nail folds
Shagreen patch: skin coloured plaque in lumbosacral region
Oval white macules (Ash-leaf-macules) seen under Woods light. But also similar lesions common
in normal kids
Classically (but not invariably) seen with epilepsy and mental retardation („zits, fits and nit-twits‟)
Autosomal dominant with variable penetrance, 50% are new mutations
Prevalence ?1/10,000
Neurofibromatosis
Look like intradermal naevi but soft
Type 1: commonest, 1/3000, Autosomal dominant, 30% new mutations
Type 2: 2 or more of:
6 or more café-au-lait macules over 5 mm in pre-pubertal patients
2 or more neurofibromas
Freckling in axillary or inguinal regions
Optic glioma
Others
May lead to short stature, macrocephaly, kyphoscoliosis, intellectual handicap, endocrine problems
(precocious puberty, acromegaly, Addison‟s), neuro tumours (optic nerve glioma, astrocytomas), etc
NF2: characterised by bilateral acoustic neuromas
See Other Congenital Skeletal abnormalities, page 620
Skin 335
Ichthyoses
All genetic
Ichthyosis vulgaris: common, usually mild. Entire skin is scaly. Controlled with moisturises
Rare sorts: Collodion Baby, Bullous and non-bullous ichthyosiform erythroderma, lamellar ichthyosis,
X-linked ichthyosis, Harlequin fetus
Erythroderma
Inflammatory skin disease involving 90% or more of the body surface. Don‟t call it Exfoliative
Dermatitis – meaning is unclear
May have sudden onset over weeks or days. Scaling varies in degrees. Itch varies
Well unwell, feel hot or cold even though temperature normal. Hypoalbuminaemia and oedema
common
Fatal in 20 – 40% due to pneumonia, septicaemia, cardiac failure
Cause:
Eczema: 40%
Psoriasis: 25%
Lymphoma, leukaemia: 15%
Drug reaction: 10%
Unknown: 10% (usually elderly)
History usually helpful, histology usually unhelpful
Management: monitor fluid balance, rest, nutrition (shedding lots of protein), Moisturiser, careful use
of steroids, methotrexate, etc.
Epidermolysis Bullosa
All rare
Variety of inherited forms. An acquired form exists
Can be localised or generalised
Types:
Generalised simple autosomal dominant epidermolysis bullosa
Junctional EB
Autosomal Recessive Dystrophic EB
Autosomal dominant dystrophic EB
Incontinentia Pigmenti
X-linked dominant, usually lethal in males
Presents within first 2 months
Tense bullae on limbs then red nodules or plaques on limbs and trunk
Pigmentation ranges in colour from blue-grey to brown
Pharmacology
Topical treatment systemic side effects
Penetration of drugs into the skin depends on:
Barrier function ( with age and disease)
Nature of the vehicle (greasy better)
Interaction of the drug and vehicle
Hydration
Patient compliance (especially if sticky, smelly or staining)
Types of vehicles:
Liquids: solutions, emulsions (oil in water or water in oil), emulsion, suspension
Semi-solids: ointments (no water), gels, creams, pastes
Greases: oils, waxes, mineral greases (eg vasoline), macrogols
Treatments
Coal tar: in psoriasis, sometimes eczema. Therapeutic agent unknown
Topical Steroids
Double the concentration doesn‟t necessarily double the efficacy
Potency related to receptor binding. Modulates messenger RNA production
336 4
th
and 5
th
Year Notes
Anti-inflammatory effects involve a wide range of mediators
Side effects:
Epidermal thinning
Melanocytic inhibition
Reduction in collagen synthesis and ground substance striae and intradermal haemorrhage
Vascular effects: initial vasoconstriction rebound vaso-dilation oedema, inflammation
Inhibition of pituitary-adrenal axis if excessive use or potent
Grouped into 4 classes according to “potency” – based on vasoconstrictor assays not efficiency
Antifungals
Griseofulvin
Only one till recently
Poorly absorbed orally, carried to skin through sweat
Fungistatic
Rapidly cleared from the skin have to continue till condition cleared
Headaches and nausea common
Only effective against dermatophytes, not yeasts (eg candida)
Lamisil and itraconazole: effective against fungi + yeasts
Itraconazole (= Triazole)
Fungistatic
Absorption dose dependent, take with a fatty meal
Persists in skin for 4 weeks and in nails for up to 6 months after 3 month course
P450 interaction
GI side effects in 7 %
Terbinafine (=allylamine)
Fungicidal
Well absorbed orally
Adverse effects in 10%, no P450 effect
Use:
Cochrane review: no evidence that topical antifungals are of value in fungal toenail infections
Skin infections of the feet: allylamines better than azoles, but much more expensive
Retinoids
Retinol (vitamin A): metabolised by the liver to retinal, then oxidised to retinoic acids. carotine can
also be converted into retinol
A hormone: binds to nuclear receptors
Modifies the expression of a variety of genes involved in cell growth and differentiation
Induces epidermal hyperplasia and desquamation (efficacy without peeling unlikely)
Thins the stratum corneum, dermal capillaries, etc etc, promotes hair growth
Isotretinoin (=Roaccutane, Oratane, 13 cis retinoic acid)
Lipophilic ( take with food)
Teratogenic: contraception till 1 month afterwards
Side effects: dry skin, mucosa, photo-sensitive, aching muscles, headaches
Acitretin (=neotigason)
Inhibits formation of retinoic acid from retinol.
Used in Psoriasis
Teratogenic for 2 – 3 years afterwards, also reduces efficacy of oral contraceptives
Plus dry skin, mucosa, photo-sensitive, aching muscles, headaches

Reproductive and Obstetrics 337
Reproductive and Obstetrics
Gynaecology .................................................. 338
Physiology ................................................ 338
History ...................................................... 338
Exam ......................................................... 340
Contraception ........................................... 340
Suspicion of Abuse or Interpersonal
Violence .............................................. 343
Infertility ................................................... 344
Dyspareunia .............................................. 345
Menstrual Disorders ................................. 345
Polycystic Ovary Syndrome (PCOS) ........ 348
Menopause ................................................ 349
Chronic Pelvic Pain (CPP)........................ 350
Pelvic Mass ............................................... 350
Vulval Lesions .......................................... 350
Cervical Cancer ........................................ 351
Other Cancers ........................................... 354
Obstetrics ....................................................... 355
History and Antenatal Booking ................ 355
Booking Exam and Investigations ............ 357
Minor symptoms of Pregnancy ................. 358
“At Risk” Pregnancies .............................. 358
Multiple Pregnancy................................... 358
Fetal Welfare ............................................ 359
Termination of Pregnancy (TOP) ............. 361
Complications of Early Pregnancy ........... 361
Gestational Diabetes Mellitus (GDM) ...... 363
Hypertension in Pregnancy ....................... 364
Other Complications of Later Pregnancy . 366
Labour ...................................................... 368
Abnormal Labour ..................................... 370
Postnatal assessment ................................. 372
Postpartum Complications ........................ 372
Six Week Check ....................................... 374
Breast ............................................................. 375
Physiology & Anatomy ............................ 375
Breast History ........................................... 375
Breast Exam .............................................. 376
Breast Investigations ................................. 376
Breast in Pregnancy and Breastfeeding .... 376
Breast discharge ........................................ 377
Developmental Problems .......................... 377
Inflammatory Breast Disease .................... 377
Fibrocystic Disease ................................... 378
Generally Benign Breast Tumours ........... 378
Breast Cancer ............................................ 379
Sexual Health ................................................. 382
Sexual History Taking .............................. 382
Exam ......................................................... 383
Sexually Transmitted Diseases (STDs) .... 383
338 4
th
and 5
th
Year Notes
Gynaecology
Physiology
GnRH:
10 amino acids – only lasts seconds requires portal circulation
Pulsitile release
Stimulates release of FSH + LH
Inhibited by progesterone (strongest inhibitor), PRL, inhibin, testosterone, oestrogen, stress
FSH: acts on germ cells
LH: acts on supporting tissue:
Male: Leydig cells testosterone
Female: Thecal cells testosterone acted on by aromatase (produced by granulosa cells)
oestradiol
Oestrogen: three types:
Oestradiol: ovary
Produced by follicles
Mucus
-ive feedback on FSH
Above a threshold LH
Unopposed oestradiol causes endometrial hyperplasia – growth without the maturing effect of
progesterone
Oestriol: placenta
Oestrone: metabolised from androgens (eg testosterone) by adipose tissue
Female fetus has several million eggs, by puberty has 300 – 400 eggs
Follicle at ovulation is 2 cm
Infection control:
Sperm carry bacteria and viruses into uterus. If mucus inhibits sperm infection, which would
otherwise cause inflammation and chances of implantation
Oestrogen Vaginal epithelium thickens during cycle glycogen lactobacilli acidity
other bacteria
Menstrual Cycle:
Inhibin from developing follicle suppresses FSH compared with LH LH surge
Phases for uterus endothelium: menstrual proliferative/follicular secretory/ progestational
Human Chorionic Gonadatrohpin (hCG) from implanted zygote signals corpus luteum to continue
progesterone production.
History
Introduction Data:
Age
Gravidity = total number of pregnancies
Parity = # of deliveries (multiple births = 1 delivery – but definitions vary…). E.g. P1(SB) = one
stillbirth. P1(twins). Eg: G4P2 (+TOP + SAB). SAB = Spontaneous Abortion.
LMP
FSH
LH
Oestrogen
Progesterone
Day 1
Day 28
Pituitary
Hormones
Ovarian
Hormones
Reproductive and Obstetrics 339
+/- Martial status
Presenting complaint: recorded as direct quote from the patient. Give them time to tell you. Stop and
listen!
History of presenting complaint. Include:
Bleeding:
Quantity (eg # of pads per day – but ask why they change – 1 per hour too much), double
protection needed (eg tampon and pad), soaking through, etc
Duration
Quality. Bright red fast flow. Brown slow flow. Clots
Timing: with menses, inter-menstrual, post-coital
Always consider anaemia, look for signs, do FBC if indicated
Pain:
Location (be specific)
Radiation
Circumstances (related to menses, meals, activity, time of day). Want to differentiate from
bowel and bladder pain
Character: sharp, dull, continuous, intermittent, severity
Reliving factors: position, medication
Vaginal Discharge:
Duration
Relationship to menses
Colour, odour, consistency
Associated symptoms: itch, burn, dyspareunia, vulvar irritation
Response to treatment, if any
Urinary symptoms:
Incontinence: stress or urge
Frequency, urgency
Dysuria
Haematuria
Past Gynaecological History:
Age of menarche – probably not a big deal – were you significantly younger or older than friends
Menses: Frequency (normal 21 – 35 days) and duration (normal 3 – 7 days), regularity (some
variation normal). NB:
First day of bleeding = 1
st
day of menstrual cycle. Teenagers will often give their period
length as first day without bleeding to first day of bleeding – check understanding
Ovulation is 12 – 16 days before the start of the next period (determined by timing of the
following period, not the prior period). Fertile for 5 – 7 days before ovulation
If post-menopausal, when did periods stop and are there any symptoms
Past gynaecological problems or procedures
? Sexual history, currently sexually active
Current/past contraception
Past STD‟s, UTIs,
Incontinence
Smear history: last smear date, any abnormal
Past Obstetric History (mainly for obstetric history): See History and Antenatal Booking, page 355
Past Medical and Surgical History (and maybe very brief systems review)
Medications:
Remember vitamins and non-prescription meds – may be bad in pregnancy
Allergies
Family History: Sister or mother with fertility, pregnancy or gynaecological problems
Social History:
Marital/relationship status
Sexual activity, sexual orientation („Are you in a relationship with a man or a woman‟), number of
partners. To avoid embarrassment, just ask straight
Cigarette, alcohol and recreational drug use
Occupation
?Victim of interpersonal violence (but don‟t introduce it in a crisis situation). See Suspicion of
Abuse or Interpersonal Violence, page 343
340 4
th
and 5
th
Year Notes
Gynaecological write-up: [name] is a [age] year old G_P_ LMP (date) who presents complaining of
(PC). Then HPC, including all pertinent (+) and (–) and any relevant past medical, surgical or
gynaecological information.
Exam
Explanation while dressed. Check experiences with past exams
Ensure chaperon if male
Have available: light, additional light source and mirror for the patient
Check bladder is empty
Clear instructions to patient on what clothes to remove and position. Cover with sheet
Position: flat on back on firm surface, unless prolapsed, obese or on a soft bed, in which case left lateral
position (like recovery position) with right knee drawn up
Pulse: indicator of anxiety
BP
General physical exam as indicated
Vaginal Exam:
Bivalve Speculum: warm and check temperature. Introduce at 45 degrees then rotate. Use narrow
speculum for nulliparous, wider speculum for multiparous, and paediatric for child or sometimes
post menopausal. Use Sim‟s Speculum for prolapsed. Warm blade, little (preferably no) lubricant
if doing a smear.
Check size, shape, position and appearance of cervix, view transformation zone and os.
Nulliparous or multiparous cervix
Bimanual:
Check uterus for size, shape, consistency, tenderness and mobility
Check adnexae for abnormal swelling or tenderness
Normal tube and ovaries are not palpable
Explain results when fully dressed
Contraception
Ideal contraceptive is 100% effective, only desirable side-effects, readily reversible, and able to be used
un-supervised
Reference: OHCS + numerous pamphlets
For a younger person wanting to start on the pill:
Discuss the possibility of coercive sex, especially if under 15
Discuss the emotional and physical consequences of sex
Ask about prior contraceptive use
Ask whether they want to become pregnant – establish a context for motherhood in terms of the
next 5 years and their life goals
Find out their thoughts about birth control (many myths: birth defects, fertility)
Inform about all methods
Risk assessment questions:
Current sexual history
Past problems with weight gain
Acne
Headaches/migraines
Dysmenorrhoea/irregular menses
Nausea/abdominal pain
Diabetes
Smoking
Personal or family history of DVT
Hypertension or IHD
Natural Family Planning
No intercourse from 6 days before to 2 days after ovulation – free and no drugs
Monitor fertility by:
Checking cervical mucus – clear and stretchy when fertile
Temperature 0.3 C after ovulation (affected by fevers, drugs, drink)
Success if regular cycles, dedication and self-control
Reproductive and Obstetrics 341
Peak effectiveness is 2% - usually 10 - 20 % (pregnancies per woman years)
Barrier Methods
Low health risk, need high motivation, some STD protection
Condoms, Caps +/- spermicide, female condom (Femidom)
Don‟t use oil-based lubricant or anti-thrush cream with condom
Spermicide gives extra protection
IUCD
Eg Novagard
Very effective (failure rate 1-2 per 1000 woman years)
Inhibit implantation and may impair sperm migration
Need replacing every 3 – 5 years
Best in older, parous women in stable relationships
Contraindications: Pregnancy, high risk for STD, undiagnosed vaginal bleeding, very heavy periods
Complications:
Can be expelled from a nulliparous or distorted (eg fibroids) uterus
Ectopic pregnancy more likely (1 in 2000)
Associated with PID following insertion or STD
If she becomes pregnant then must take the IUCD out (little risk of inducing miscarriage). If it‟s left in
then risk of chorioamnioitis, miscarriage or pre-term labour
Mirena – carries levonorgestrel (a progesterone) risk of implantation and lighter periods (Good for
menorrhagia). Lasts 3 years. 20% experience reversible amenorrhoea. Expensive. Can use with
oestrogen only HRT (no risk of endometrial hyperplasia) and avoid progesterone side effects
Combined Oral Contraceptive
Initial exam should include:
Weight
Blood pressure
Cervical screen if appropriate
= Oestrogen (usually ethinylestradiol) + progestogen:
Oestrogens:
Ethinylestradiol (most common), mestranol (which is converted to estradiol. 50 g mestranol
= 35 g estradiol)
High dose = 50 g estradiol. Low dose is <= 30 g oestrogen. Adverse effects are dose
related give lowest dose that gives good cycle control.
Progestins:
Estranes: norethindrone, ethynosiol acetate, norethindrone acetate (latter two converted to the
former)
Gonanes: norgestimate, levonorgestrel, desogestrel (gonanes have a longer half-life)
About 4 * physiological dose of oestrogen
Triphasic pill: mimic‟s body‟s fluctuation in oestrogen but break through bleeding
Action: G type mucus + GnRH ( no FSH or LH surge). „Puts the ovary to sleep‟
Take for 3 weeks, then pill free for a week withdrawal bleed
Benefits of CoC: 99% effective, reversible, lighter periods, PMS, ovarian and endometrial
carcinoma (but slightly risk of breast cancer), endometriosis
Problems: compliance
Contraindications:
> 35 and smoker (death 8 times more common in smokers – but still as safe as childbirth)
Any disorder predisposing to venous or arterial problems, eg lipids, APC resistance
Many cardiovascular problems (except mild hypertension)
Liver disease
Migraine with aura or for > 72 hours (status migrainosus) or requiring ergotamine. Pill 4 times
risk of ischaemic stroke. Contra-indicated in any woman with migraine if > 1 other risk factor for
stroke (lipids, BP, diabetes, etc)
Pregnancy
Undiagnosed uterine bleeding
Gross obesity or immobility (stop before major surgery)
342 4
th
and 5
th
Year Notes
Special precautions: Family history of DVT, BP or breast cancer; epilepsy, diabetes, illnesses causing
diarrhoea (eg Crohn‟s)
Side-effects: (usually worse when starting the pill), intra-menstrual bleeding, breast tenderness, nausea,
or weight, mood changes, headaches
Risks:
MI. Risk sharply over 40 – 1:2500 for non-smokers, 1:500 for smokers.
Older progesterones: breakthrough bleeding, acne, headache, weight lead to search for new
progesterones (ie 3
rd
generation progesterones like gestodene eg in Mercilon, etc)
Nausea: due to oestrogen. Take with meal or with a snack at bedtime
Blood pressure (rare – but monitor 6 monthly)
DVT Risk (Source: Medsafe flier)
35/100,000 on the pill per year develop a clot, one dies two deaths per year in NZ
Risk increases 3-4 times over population risk on 2
nd
generation, 6 – 8 times on 3
rd
generation.
Increased risk of Diane 35 and Estelle 35 of 4 times over 2
nd
generation.
No risk with PoP
Drugs interfering with the pill: liver enzyme inducers (eg anticonvulsants, rifampicin). Consider higher
dose pill
Monitoring: 6 monthly-BP check. Check weight and breasts etc if > 35. Up to date with smears?
Starting the pill:
On day 1 of cycle, or day of TOP, 3 weeks post-partum or 2 weeks after mobilisation after major
surgery. Contraceptive cover immediate
Breakthrough bleeding is very common – especially in the first 3 months. Can add 20 g estradiol
every 24 hours, 12 hours after the usual pill, for one week.
Missed pill: 12 hours late OK, after that the seven day rule (also if diarrhoea) – take 7 active pills
before unprotected sex (eg if pill free days coming then skip them and go straight onto the next pack)
Stopping:
66% menstruate within 6 weeks, 98% by 6 months
At menopause: Stop at 50 with > 1 years amenorrhoea. CoC masks menopause, so stop at 50 and
use non-hormonal method. Little evidence that it‟s not safe to continue to menopause
Progesterone Only Pill (PoP)
= Mini-pill
Cervical mucus hostile to sperm (G Type mucus) + prevent ovulation in some + tubal motility.
Effectively a barrier method. Woman may still ovulate. Small risk of follicular cyst (one that doesn‟t
pop) pain with full bladder or rectum
Worst side effect: erratic bleeding. Some women have amenorrhoea. Less risk of weight gain, acne,
depression, breast tenderness, headache
Less effective than CoC (0.3 – 4% failure) – age and compliance dependent
OK where CoC contra-indicated and in breast-feeding mums (full breast feeding alone is protective for
3 months). For post-partum contraception see Six Week Check, page 374
Contraindications: History of ectopic pregnancy, breast cancer, liver disease or enzyme inducing drugs
Must be taken same time each day (+/- 3 hours).
Starting on the PoP: Alternative precautions for 7 days
If pill missed then at risk for 2 days. Safe again after 2 days of restarting the pill
Depot progestogen:
Safe, simple and effective (failure rate 0.4 – 1.2 %). Suppress ovulation, G type mucus, motility
and implantation
Eg Depot-provera – deep IM 12 weekly, given during first 5 days of cycle, 5 days post partum if
bottle feeding, 6 weeks if breast feeding.
Contraindications: pregnancy, abnormal undiagnosed vaginal bleeding, acute liver/cardiac disease
Advantages: no oestrogen, PMS, secret, no compliance problems, good with GI disease, Ok with
breast feeding, etc… Particularly good around major surgery, epileptics, after vasectomy and
bowel disease
Problems: irregular bleeding – usually become amenorrhoea, also weight gain and acne. May also
depression and libedo. Median delays of 10 months return to ovulation on stopping (fat soluble
very slow metabolism)
Sterilisation
Reversal is only 50% successful see it as irreversible
Reproductive and Obstetrics 343
Tubal ligation has 1% failure (1:200) – 10 times worse than vasectomy and same as IUCDs
Vasectomy – easier than tubal ligation, but takes up to 3 months before stored sperm used up. Need to
be tested and have 2 sperm-free ejaculates. Has been discussion of risk of prostate cancer – best
evidence says no association.
Emergency Contraception
Ask why: unprotected intercourse, condom broke, etc. If no condom, then check why. If indicated:
„Are you worried about infection?‟ and „Was it OK with you that it all happened the way it did‟
[checking for non-consensual intercourse]
Ask:
How long ago was sex?
LMP
Regular partner ( risk of STD)
Medications
Previously had an ECP – any side effects. Sometimes nausea +/- vomiting with Progesterone only
ECP
Other conditions. Old Oestrogen + Progesterone ECPs required history of DVT and focal
migraine
If sex < 72 hours ago prescribe:
Nordiol 2+2/Antinaus 5mg (12 hours apart, few side effects) or
2/Microval 25+25 (can have while breast feeding, may reduce breast milk for ~ 1 week)
Discuss:
How to take it
Pregnancy test in three weeks
Ongoing contraception, other advice
Emergency IUCD: inserted within 120 hours of unprotected intercourse. Screen for STDs.
Prophylactic cover if suspected
Suspicion of Abuse or Interpersonal Violence
It is common and victims are high users of health services
Epidemiology: 20% of women report sexual abuse before 16, full intercourse reported by 4%. Sexual
abuse of boys is about 1/3 as common as for girls.
Adult women: 25% report sexual abuse, 12% rape
Men: 5% report sexual abuse, 3% rape (?under-reporting)
10 – 16 % of rapes reported to police
Effects:
Acute and long term effects are related to age of victim, extent and duration of abuse, relationship
with abuser and response of others
Acute effects: numbness, shock, disbelief, anxiety
Long-term effects: feelings of helplessness, depression, sleep disturbances, nightmares, flashbacks,
guilt, self-blame, shame. Measurable long-term psychiatric sequalae in 25%
What is patient‟s age:
< 14: all suspected cases should be referred to CYPFS, or if older but abuser still has access to
young people. See also Child Abuse, page 656
14 – 17 don‟t make a decision about what to do on your own need to put caveats on
confidentiality
History questions (but don‟t introduce it in a crisis situation)
Suspect if physical injuries, chronic undiagnosed pelvic pain, heightened anxiety about an
examination, STD‟s without being worried about health risks
They will be reluctant to discuss it
Physical: „have you ever been hit, slapped or shoved by a parent or partner. Ever had bruises or
had to stay in bed…
Sexual: Did anything sexually frightening happen to you as a child or young adult, have you ever
been made to participate in sexual activity that made you feel uncomfortable. Was it your choice,
or were you forced or coerced?
Psychological: Does your partner ever ignore you, call you names, make fun of you, threaten to
leave you, punish the children when he is angry with you, are you fearful of anyone at the
moment?
344 4
th
and 5
th
Year Notes
Most helpful response is: being believed, being supported, not being blamed, being helped not to feel
odd or alone
Rape/Non-Consensual Intercourse
Rape: = sexual contact without consent (including consent under threat) which involves oral, genital or
anal penetration, otherwise unlawful sexual contact
Therapeutic role:
Recognise & treat physical injury
Attention to emotional trauma
Prevention of pregnancy – offer ECP. Legal requirement under the Contraception, Sterilisation
and Abortion Act.
Check for infection (NB incubation of chlamydia is 21 days) and offer prophylaxis (but may
interfere with ECP – do it after)
Referral to support services
If not sure about making a police complaint, bring in crisis counselling team
Victim compensation – inform re ACC entitlement
Forensic role:
When did it happen: If less than 7 days then may be forensic requirements. If very recent then nil-
by-mouth and collect all urine and toilet paper until forensic examination. Ring forensic specialist
(DSAC = Doctors for Sexual Abuse Care)
Keep detailed records at the time of examination
Forensic specialist will do genital exam, blood tests, urine (drug screen), colposcopy (for genital
injury), finger nail scrapings, etc and appear as expert witness
Supportive role:
Communicate empathy: „that sounded really unpleasant for you‟
„You are safe now‟ (don‟t say if not true)
Reinforce „Its not your fault‟ – victims blame themselves
Follow-up at 1 week, 1 month and 3 months (pregnancy, HIV test, Hep B and C, Syphilis)
Infertility
= Inability to establish a pregnancy within a year of unprotected intercourse or > 2 consecutive
miscarriages or still births
Normal fecundability = 25% per month, 85% per year, 90-95% per 2 years
Incidence – approx 10% of couples
Aetiology:
Male factors: 30%
Idiopathic/unexplained: 20%
Ovulatory: 10%
Tubal: 10%
History:
Male: Previous surgery (eg hernia), undescended testes, mumps, etc
Female: surgery, menstrual history, BMI, symptoms of endocrine disorders, nasty polyps, PID,
ectopic pregnancy, nasty appendicitis
Both: general medical and reproductive history, smoking, medications, family history
Exam: include general assessment of endocrine disorders: PRL (Galactorrhoea), thyroid disorders
(goitre, etc), Polycystic ovary ( hirsutism, obese, etc)
Investigations:
Male: semen analysis, sperm antibodies, Plasma FSH (primary or secondary testicular failure),
androgen deficiency, testicular biopsy
Female:
Possible causes: Endometriosis, stress/anorexia/exercise, early menopause, PCO, thyroid,
PRL
Ovulation: if regular menstruation then ovulation likely. Only proof is laproscopic
visualisation – impractical. Can measure temperature, progesterone levels, etc
Test HCG, TSH, PRL, Oestrogen (day 2), progesterone (day 21) for 3 cycles to check for
consistent ovulation
Post-coital test of cervical mucus
Pelvic assessment: US, contrast x rays, etc
Reproductive and Obstetrics 345
Management:
Induce ovulation: risk of multiple pregnancy, also narrow TI. Anovulatory cycles: treat with
Clomifene – stimulates ovulation but risk of multiple pregnancy
IVF (also better for tubal blockage than surgical repair). 1 in 3 have life birth.
Oligospermia: intracytoplasmic sperm injection, donor sperm, artificial insemination
Lots of psychosocial implications of infertility
Workup to point of diagnosis is funded. Criteria based funding for treatment
Also prepare for pregnancy: take folate, do booking bloods, check rubella status and offer vaccination
Dyspareunia
= Pain with sex
Causes:
Superficial pain: vulvitis (eg HSV), introital shrinkage (atrophy, scarring), vaginismus
Vaginal pain: post-menopausal atrophy, medication (eg antihistamines), arousal phase dysfunction
Deep-pain: pelvic disease (endometriosis, adenomyosis), shortened vaginal vault post-
hysterectomy, retroverted uterus
May be cycle of anticipation of pain tense muscles and lack lubrication further pain
Treatment if no aetiology uncovered:
Lubricants
Oestrogen replacement
Position modification
Counselling
Vaginismus: involuntary spasm of the levator ani muscle making penetration difficult. May be related
to prior trauma/abuse. Pain-vaginismus-pain cycle develops. Treatment: behaviour modification,
progressive vaginal dilatation
Menstrual Disorders
Key distinction:
Ovulatory cycles: regular
Anovulatory cycles: irregular
Also consider thyroid and PRL
Amenorrhoea
Primary amenorrhoea: failure to start menstruating. Investigate in a 16 year old or a 14 year old with
no breast development. When did her mum start menstruating? Usually normal. Rarely Turner‟s
syndrome or testicular feminisation
Secondary amenorrhoea: when periods stop for > 6 months, except for pregnancy:
Hypothalamic-pituitary-ovarian causes common. Eg stress, anorexia, breast feeding, weight loss,
PRL, severe disease. Test with a 7-day progesterone challenge. If withdrawal bleed following,
then there is enough oestrogen to produce an endometrium
Ovarian causes are uncommon: Polycystic ovarian syndrome, tumours, premature menopause
Hyperthyroidism oestrogen breakdown
Investigation:
Pregnancy Test
5 day progesterone
challenge:
withdrawal bleed?
Anovulatory:
- PCOD
- Ovarian Failure (PM)
Oestrogen + Progesterone:
Withdrawal bleed?
Uterine problem
hysteroscopy
Measure LH + FSH
Low LH or Low FSH:
?hypothalamic. CT or
MRI. Diagnosis of
exclusion
High LH: PCOD
High FSH: Ovarian failure
-ive
-ive
-ive
+ive
+ive

346 4
th
and 5
th
Year Notes
Oligomenorrhoea: infrequent periods: common in the young and the nearly menopausal. Consider
polycystic ovary syndrome, rapid weight change, PRL, hypothyroidism or primary oligomenorrhoea
Menorrhagia
= Excessive blood loss (technically > 80ml lost/cycle – but hard to measure)
Causes:
?Hypothyroidism: cold intolerance, weight gain, constipation, goitre, etc
Younger: pregnancy, dysfunctional uterine bleeding (diagnosis of exclusion, no pelvic pathology,
associated with anovulatory cycles. If young, may settle)
Older: IUCD, fibroids, endometriosis, adenomyosis, polyps, pelvic infection
Perimenopausal: ?endometrial carcinoma (especially if > 90Kg)
Haematological: low or dysfunctional platelets (not coagulopathy)
Investigation:
HCG: are they pregnant
FBC: anaemic?
Smear if not up-to-date
Menstrual calendar
Abdominal ultrasound
If age > 45, over 90 kg or infertile with heavy bleeding then transvaginal ultrasound and/or
endometrial biopsy (pipelle) to test for endometrial cancer
Hysteroscopy and curettage for histology if irregular bleeding or ultrasound indicating polyps or
fibroids
Treatment if pathology known:
Anti-PGs (eg NSAIDs) as 1
st
line treatment
Progesterone during the follicular phase or CoC
Intra-uterine devices (eg Mirena)
Other drugs: Tranexamic acid, norethisterone, Danazol (bad side effects), etc,
Surgical options: endometrial ablation (problem with recurrence) or hysterectomy
Inter-menstrual bleeding
May follow mid-cycle in oestrogen (ie with ovulation)
Also cervical polyps, ectropion, carcinoma, cervicitis and vaginitis, IUCD, hormonal contraception
(spotting)
If post-coital, then suspicion of more serious pathology (eg cervical cancer)
Appropriate to do an exam and smear – but it is NOT appropriate to reply on the smear result (false
negatives, etc). Should act on clinical suspicion
Dysmenorrhoea
= Painful periods, may be associated with sweating, tachycardia, headache:
Primary
Secondary
Age
< 20
> 20
Onset of pain
With bleeding
Prior to bleeding
Duration
First 1 – 2 days of menses
Through out menses
Intensity
Begins with ovulatory cycles,
remains constant
Begins at any time, progressively
worsens
Aetiology
Probably PG-F2 mediated
Pain without organ pathology
Cervical Stenosis
Endometriosis
Adenomyosis
Pelvic Infection
Fibroid/polyps
Chronic sepsis (eg Chlamydia)
Conditioned behaviour
Treatment:
Reassurance
CoC: at least 3 month trial, combine with NSAIDs if necessary
Progestogens: day 5 – 25
PG inhibitors
Exercise
De-conditioning, eliminate secondary gains
Reproductive and Obstetrics 347
Endometriosis
= Ectopic endometrial tissue, histologically confirmed. Most often on ovaries and uterosacral
ligaments
Chronic and progressive: inflammation and local haemorrhage fibrosis and scarring
Incidence:
10 – 15% of reproductive age. Patients usually in mid 30s – early 40s, nulliparous
Common in infertility and chronic pelvic pain
Aetiology theories:
Retrograde menstruation homologous grafts
Genetics: 7 fold risk if +ive family history. Usually earlier and more severe disease
Symptoms: classic triad = pelvic pain, deep dyspareunia, dysmenorrhoea. Also irregular bleeding,
infertility (scars fallopian tubes)
On exam: tender, retroverted uterus
Confirmation by laproscopy. Red brown nodules on surface of ovaries and pelvic structures, and other
sites (appendix, peritoneal scars, etc). Can develop large cysts, lined by endometrial stroma and glands
and containing changed blood (chocolate cysts).
Treatment:
Conservative (50% recurrence within 5 years): surgical removal (ablation or excision) of affected
tissue and/or hormonal therapy:
Prostaglandin synthetase inhibitors treat pain (NSAIDs)
OCPs – promote inactivity of endometrial tissue
Progesterones – oral or depot
GnRH agonists – short course only due to bone loss
Danazol (testosterone derivative)
Laproscopic resection or ablation of affected peritoneum
Radical: removal of pelvic organs
Fibroids
Benign growths in myometrium (ie underneath the proliferative layer)
Very common, especially in overweight and infertility
Oestrogen enlargement, so grow in pregnancy and shrink after menopause
Aetiology unknown
Symptoms: heavy/irregular bleeding, painful periods, urinary frequency, constipation
Diagnosis: abdominal +/- vaginal ultrasound hysteroscopy
Treatment:
Medical:
GnRHa can shrink fibroids temporarily. Not for > 6 months, menopausal symptoms. Also
Gestrinone and Danazol.
NSAIDs, Progesterone and HRT don‟t shrink fibroids
Surgical: Hysterectomy, hysteroscopic resection if small and submucosal, myomectomy (risk of
uterine rupture in subsequent pregnancy)
Adenomyosis
= Growth of endometrial glands and stroma into the myometrium. Does not undergo cyclic changes
and is not hormone responsive
Symptoms: dysmenorrhoea, menorrhagia, deep dyspareunia
Incidence: age 35 – 50, parous
Exam: globular, enlarged uterus, most tender peri-menses
Treatment: NSAIDs, OCPs, GnRH agonists, Hysterectomy
Premenstrual Syndrome (PMS)
= Recurrence of symptoms, whether emotional or physical, occurring the pre-menstruum but with
complete absence of symptoms in the post-menstruum. Severe symptoms in 5% of women
DSM 4 has „Premenstrual Dysphoric Disorder‟ as a research criteria
Main symptoms:
Depression, irritability, tiredness, headache, bloating, breast tenderness.
Plus 150 others!
Classify as mild, moderate or severe on the basis of interference with daily function
Use of a symptom diary over 2 months is very valuable
348 4
th
and 5
th
Year Notes
Diagnosis:
History
Exam to exclude gynaecological and endocrine disorders
Tests: rule out thyroid, PRL, secondary dysmenorrhoea (eg endometriosis)
Differential:
Psychiatric: depression or anxiety with premenstrual exacerbation
Medical: anaemia, hypothyroidism, cancer, SLE, menopause if > 45, renal causes, polycystic ovary
Management:
Education
Life-style changes: diet, exercise, smoking
Psycho-therapy if psych history, for coping skills, or to manage secondary gains or conditioning
Drugs:
Suppression of ovulation. Eg with CoC – although this can give symptoms (eg depression,
ache, etc)
Fluoxetine 20 mg only when symptoms occurring (30% remission, minimal side effects)
Debated remedies include evening primrose oil, Vitamin B6 (pyridoxine) in low dose
(neuropathy in high dose)
Very high placebo rates
Aetiology:
Multifactorial – includes biological, psychological and societal factors
Biological hypotheses include abnormal response to ovarian hormones, mineralocorticoid effects,
prostaglandins, etc.
Post menopausal Bleeding (PMB)
Bleeding > 1 year after the last period (check it is vaginal bleeding, not urethra or rectal)
Causes:
Vaginitis (often atrophic): fragile trauma, and secretions infection
Foreign bodies (eg pessaries)
Endometrial or cervical polyps, endometrial fibroids (bleed a lot – leiomyoma, adenomyosis,
hyperplasia)
Oestrogen withdrawal (HRT or ovarian tumour)
Carcinoma of the cervix
Endometrial cancer
Distinguish from peri- or post-menopausal on HRT
Investigation: Trans-vaginal US (looks at thickness of endometrium) and trans-abdominal US (finds
other masses)
If bleeding on non-cyclical HRT or intra-cyclical bleeding on cyclical HRT, be a bit more aggressive in
investigation (HRT slight risk of endometrial cancer)
Polycystic Ovary Syndrome (PCOS)
Seek help for: infertility (anovulation), menstrual irregularity and androgen excess
Symptoms: oligomenorrhoea, amenorrhoea, anovulation, infertility, hirsutism, acne, male pattern hair
loss
If rapid viralisation then look for tumour – not PCOS
Associated with:
Obesity
Type 2 diabetes – insulin resistance hyperinsulinaemia
Lipid abnormalities vascular disease (eg 7 times risk of MI)
Pathogenesis:
?Primarily a disorder of LH hypersecretion
Non-cyclical oestrogen (including from adrenal androgens and obesity) leads to:
LH ovarian hyperplasia androgens perpetuates the cycle
FH follicular maturation cyclical oestrogen chronic anovulation
progesterone no menses
Hormonal cycling is disrupted and ovaries enlarged by follicles with have failed to rupture
Investigations:
Serum total testosterone
Sex hormone binding globulin
Reproductive and Obstetrics 349
LH and FSH. Testosterone and LH high.
Fasting HDL, LDL, cholesterol
Glucose tolerance test (if pregnant do at beginning of pregnancy)
Rarely: DHEAS for adrenal androgen tumour + 17-hydroxyprogresterone for congenital adrenal
hyperplasia
Treatment:
Diet and exercise weight peripheral oestrogen
Induce ovulation with Clomifene FSH
Combined pill (Diane 35) to control bleeding and risks of unopposed oestrogen on endometrium
Metformin insulin sensitivity, menstrual disturbance and ovulatory function
Prevention of risks of diabetes and ischaemic heart disease
Established facial hair won‟t go away when hormones corrects (require cosmetic treatment)
Differential: Tumours of the ovary (eg granulosa and thecal cells) chronic anovulation
Menopause
Up to last period and 2 years following
Primary ovarian failure oestrogen feedback FSH
Continue contraception for one year following last period (eg PoP, IUCD, condoms)
Usually age 50 – 51. Cycles start to slow from 47 – 48. Usually follows pattern of her mother.
Factors affecting age:
CoC delays menopause (lots of eggs left over)
Earlier if chronic disease or toxins (eg radiation, chemo, etc)
Signs:
Hot flushes, palpitations
Night sweats
Mood swings/depression
Vaginal atrophy dyspareunia, post-coital bleeding
Urinary frequency/incontinence
Test for high TSH if wanting to exclude thyroid and psychiatric problems
Hormone Replacement Therapy
Replacing normal physiological dose of oestrogen (cf CoC which is much higher)
Contraindications:
History of breast or endometrial cancer (not ovarian or cervical)
Undiagnosed vaginal bleeding
Liver disease (it‟s metabolised in the liver)
Pregnancy or breast-feeding!
Past PE
High cholesterol is NOT a contra-indication – it‟s protective (compared with OC dose of
progesterone which is bad)
Smoking is NOT a contra-indication – it‟s protective
DVT is NOT a contra-indication (whereas OC dose of oestrogen is bad for clots)
Benefits:
Especially good for those with hysterectomy, bilateral oophorectomy, risk of osteoporosis, IHD,
cholesterol, DM, RA
Oestrogen effects: menopause symptoms, osteoporosis, CV disease (LDL, HDL,
vasodilates coronary arteries)
Progesterone effects: risk of endometrial cancer (if they have a uterus) by preventing proliferation
of endometrium by unopposed oestrogen
??Protective against colon cancer and Alzheimer‟s
Side-effects: weight, PMS, cholestasis, vomiting
Risks:
Minimal breast and ovarian cancer risk if taken for less than 5 years
Gallbladder disease
If severe heart disease then slightly risk of CV problems in 1
st
years
350 4
th
and 5
th
Year Notes
Types:
Cyclical: continuous oestrogen, progesterone for any 10 days per cycle (with bleeding 2 – 3 days
after its finished). Good if immediately post-menopausal – cycle them for a while and if no break
through bleeding then continuous HRT after a year
Non-cyclical: Continuous oestrogen and progesterone. No period as oestrogen and progesterone
oppose each other stable endothelium. Don‟t start until after menopause. Ovary may still be
„surging‟ from time to time break through bleeding that you‟ve got to investigate
Chronic Pelvic Pain (CPP)
= Pelvis pain present for 6 months or longer. Can be intermittent (eg related to menses or intercourse)
or continuous
Differential:
Gynaecological: dysmenorrhoea, endometriosis, adenomyosis, pelvic adhesions, PID, uterine
prolapse, vaginitis, pelvic congestion (engorgement of pelvic vasculature – ie varicose veins),
pelvic relaxation (trauma of pregnancy etc)
Non-gynaecologic: UTI, interstitial cystitis, IBS, diverticular disease, musculo-skeletal disorders
Psychosocial: psychosomatic, abuse/rape, drug seeking, attention seeking
Exam:
External genitalia, mono-manual (eg evidence of spasm), bi-manual, recto-vaginal (nodularity over
uterosacral ligaments endometriosis), speculum (eg discharge, cervical erythema)
Musculo-skeletal exam: tenderness over lumbar, lower thoracic muscles, strength
Investigations:
Always: cultures, FBC, urine culture and analysis, US, pap smear
If indicated: pregnancy, GI and GU workup, psych evaluation, laproscopy (if suspicious masses,
other physical findings, acute abdomen, if for reassurance then wait a while first)
Treatment:
Drugs: NSAIDs, PG-inhibitors, ?antibiotics, OCP for at least 3 months
GI: diet changes, stool softeners, bulking agents
Exercise
Pelvic Mass
History: pain, bleeding, urinary and bowel symptoms, constitutional symptoms (weight loss, night
sweats, etc)
Exam: shape, consistency, mobility, etc
Where:
Physiological: full bladder, flatus, faeces, pregnancy, obesity
Congenital: uterine anomaly, pelvic or polycystic kidney
Trauma: rectus abdominis haematoma
Infective: pyosalpinx, pelvic abscess, diverticulitis, TB peritonitis, lymph nodes
Neoplastic: fibroids, tumours of colon, rectum cervix or endometrium, ascites, retroperitoneal
tumour, mesenteric cyst
Hormonal: non-neoplastic cysts
Mechanical: Hydronephrosis
Pregnancy associated: pregnancy in uterine horn or ectopic, trophoblastic disease, corpus luteum of
pregnancy
Investigations:
Pregnancy test
US
Ca125
ESR, FBC
Laproscopy, colonoscopy
Vulval Lesions
Non-neoplastic epithelial disorders:
Lichen Sclerosis:
1/3 of lesions, commonest after menopause
Pruritic, affecting any part of the vulva
Multiple irregular white patches, shiny wrinkled atrophic skin
Risk of SCC
Reproductive and Obstetrics 351
Microscopy: subepithelial homogenous collagen + band of lymphocytes
Autoimmune aetiology treatment with steroids
Squamous Hyperplasia:
Non specific thickening of the epithelium + inflammatory reaction below the BM: acanthosis,
hyperkeratosis
Non specific diagnosis
Other dermatoses: Lichen simplex chronicus, spongiotic dermatitis (contact dermatitis eg perfumed
toilet paper), psoriasis, lichen planus
Vulval Intraepithelial Neoplasia (VIN):
Often multi-focal white-pink-red raised lesions which itch/burn/asymptomatic
Preinvasive dysplastic squamous lesions
Dysplasia is graded VIN1, VIN2, VIN3
Untreated 7/8 progress to SCC (unlike CIN)
Risk factors similar to cervical carcinoma
60% have lesions in other areas
Squamous Cell Carcinoma:
90% of vulval cancer and 5% of gynae cancer
Two types:
Elderly women (70+): 65%, related to Lichen Sclerosis & squamous hyperplasia, well
differentiated – islands of invading cells
Younger women (40+): 35%, related to HPV, Cervical cancer risk factors, poorly
differentiated
Raised white warty mass
Micro: resembles SCC at other sites
Often present late
Prognosis depends on stage. Factors in order of importance are:
Lymph node metastasis
Depth of invasion
Size
See also Non-Sexually Transmitted Genital Skin Lesions, page 386
Cervical Cancer
Reference: Cervical Screening, Information for Health Professionals, National Cervical Screening
Programme, Health Funding Authority, October 1998
Epidemiology
In NZ, about 200 new cases per year, 70 – 80 deaths ( relatively rare compared with other cancers)
One in 97 women can expect to get it before 75
75% of cases and 80% deaths are over 35, but CIN lesions can develop young (ie many woman coming
for colposcopy after abnormal smears are 25 – 30).
Aetiology
Human Papilloma Virus (HPV):
HPV 6, 11: condyloma accuminatum
HPV 16 or 18: Genital dysplasia. Is a necessary but not sufficient condition for cervical cancer
Koilocytes: HPV infected keratinocytes with a perinuclear halo. Episomal viral DNA
Dysplasia: pleomorphic, hyperchromatic mitotically active, high nuclear/cytoplasmic ratio.
Integrated DNA (Kettle fry nuclei)
HPV Carcinogenesis:
Not typical mechanisms
E6 binds to p53 (tumour suppressor and accelerates its degradation)
E7 binds to RB displacing transcription factors usually sequestered by RB
Other risk factors:
Early age at first intercourse
Multiple sexual partners
High risk male partners
Smoking
Herpes
Immunosuppression
352 4
th
and 5
th
Year Notes
Occurs in the transformation zone: junction in the endocervix between squamous cells of the vagina
and columnar cells of the uterus. Completes development at age 18 – 20, shifting into the endocervix.
Previously in the exocervix and more vulnerable to damage/infection significance of age at first
intercourse
Classification
3 grading systems:
Histology
Cytology
Mild dysplasia
CIN1
LSIL
Moderate Dysplasia
CIN2
HSIL
Severe Dysplasia
CIN3
HSIL
Carcinoma-in-situ
CIN3
HSIL
Low grade changes: Low Grade Squamous Intraepithelial Lesion (LSIL) (=CIN1 – Cervical
intraepithelial neoplasia. More likely to be HPV types 6 & 11). Nucleus is slightly enlarged and
irregular. In bottom third of cells on top of base membrane in transformation zone. If found on
screening more regular smears. 50 – 60% return to normal
High Grade Changes: HSIL (covers CIN 2 and 3/CIN – carcinoma-in-situ. More likely to be HPV 16
& 18). Nucleus of every cell is very enlarged and irregular in shape. High nuclear:cytoplasmic ratio.
Affected cells right to surface. If found on screening refer for colposcopy. Treated the same but
CIN3 more likely to progress than CIN2
Invasive cancer: basement membrane has been breached. Can get glandular extension in CIN3 –
metaplasia down glands – but still not invasive as the BM is not breached
Progression
Cervical Dysplasia: grade depends on the proportion of the epithelium occupied by malignant cells
Cervical Carcinoma:
Micro: islands of infiltrating neoplastic squamous cells that may show keratinisation
Outcome: depends on stage
Size and depth of invasion. > 10 mm invasion poorer outcome
Lymph node involvement poor outcome
Stage 1: confined to cervix. 90 – 95% 5 year survival
Stage 3: lymph node positive: 30% 5 year survival
Cervical glandular neoplasia:
Also HPV related, but much less common than cervical squamous carcinoma (which has a higher
rate of replication)
Invasive adenocarcinoma has infiltrating neoplastic glands
Comprises 20% of tumours in a screened population vs 5% in unscreened
Cervical Screening
Pap smears collect exfoliated cells from the cervix
Currently reported on the Bethesda system which divides dysplasia into LGSIL, HGSIL and ASCUS
(Atypical squamous cells of unknown significance – not sure whether they‟re dysplastic or reactive.
Some will be CIN3 so still need follow-up)
Procedure:
Best done mid-cycle (blood and bacteria which are a causes of cytolysis)
Explain first. Ask about LMP, abnormal bleeding, post-coital bleeding, abnormal discharge, if
pregnant, and previous smear history and experiences
Patient Education: discuss feelings about having a smear, emphasise preventative nature, explain
what cervix is, show equipment
Ensure screen/curtain for patient and sheet
Label slides first
Either:
Spatula first, one full turn, and if poor endocervical sample follow with brush (only turn one
turn otherwise bleeding obscures sample) and use a second slide for the brush.
Broom does both well (sample of choice for all age groups) – turn 5 times and wipe both sides
once down slide. Thin prep: cells mixed up and rubbish removed better reading. Can‟t use
wooden spatula.
Reproductive and Obstetrics 353
Putting on slide: wipe spatula once, roll brush (scrubbing it around lyses cells). Fix quickly –
within one second – as drying causes distortion of cells. Fix either in 95% ethyl alcohol for 20 - 30
minutes or cytofix sprayed from 20 – 30 cms.
Data on lab form includes LMP and clinical details.
Biggest cause of sensitivity is poor sampling. Smears can be unsatisfactory if blood,
inflammatory cells or lubricant present. Smears taken 4 – 5 days prior to the next period may show
cytolysis (cellular degeneration due to bacilli)
Relationship between screening results and lesions
From OHCS, p 34:
Papanicolaou class
Histology
1
Normal
0.1% CIN II – III
2
Inflammatory
6% CIN II – III
Mild Atypia
20 – 37% CIN II – III
3
Mild/Moderate dyskaryosis
50 – 75% CIN II – III
4
Severe dyskaryosis
Malignant cells
80 – 90% CIN II – III
5% invasion
5
Invasion suspected
50% invasion
Abnormal glandular cells
?Adenocarcinoma
NZ Protocol:
3 yearly screening should be offered to all women aged 20 – 69 years who have been sexually
active. Can stop if > 5 years with no sex (this bit not in the guideline)
Screening should be yearly for 2 years from 20 (some advocate starting earlier if > 2 years since
commencing regular sex – but as cancer in this age group is very uncommon, it‟s not good
screening practice. If you think cancer is a possibility, you shouldn‟t use a screening test to
diagnose it)
Normal or benign/reactive changes:
Satisfactory
Previously normal
Smear in 3 years
First smear, or more than 5 years since
last smear
Smear in 1 year
Previous abnormal smears
See below
Satisfactory but
limited
Previously normal
Smear in 1 year
First smear, or more than 5 years since
last smear
Smear in 1 year
Abnormal smear in last 5 years
Smear in 6 months
Unsatisfactory smear
Smear in 1 – 3 months
Abnormal:
CIN1 or HPV
Previous normal smear
Smear in 6 months
Previous abnormal smear
Smear in 6 months, if normal then 2
* 1 year, if abnormal then
colposcopy
CIN 2 or 3
Colposcopy
If LSIL or less
Smears at 6 months, 1 year, 1 year, 3
yearly, if abnormal then colposcopy
If HSIL
Smear at 6 months then annual until
70, if abnormal then colposcopy
Effectiveness of Screening
Sensitivity of a single smear is 80% for low and high grade lesions (ie not sufficient for diagnosis, only
for screening)
PPV of HGSIL cytology report: 30 – 40%
NPV of a normal smear is 80% if abnormal appearing cervix (lesion with raised edge, nodular feel,
hard, bleeds when touched) or persistent abnormal bleeding they need a colposcopy not a smear:
DON‟T RELY ON THE SMEAR
Maximum prevention: 91-92 % of squamous cancers with 3 yearly screening. to 92 – 93% with
annual screening. to 87% with 5 yearly screening
354 4
th
and 5
th
Year Notes
Less than 100% because of:
Less than 100% enrolment
False negatives in sampling (eg a lesion is more likely to bleed and compromise the sample)
False negatives in laboratory diagnosis
Interval cancers: minimum time from infection to invasive is ~ 18 months. Normal is ~ 10 to 15
years
Success rate for adequate treatment of pre-cancers is 98 – 100%
Women most likely to get cervical cancer are those not regularly screened
Much less effective at glandular lesions: clinical suspicion should overrule a „normal‟ smear
Other Cancers
Ovarian cancer
Risk factors: nulliparity, infertility, early menarche, family history, no past pill use
Presentation:
75% asymptomatic until advanced
Swelling with palpable mass
Pressure effects (eg on bladder)
Infarction, haemorrhage, peritonism
Ascites
Torsion
Endocrine: virilisation, menstrual irregularity, PMB
Lower incidence than endometrial cancer, but higher death rate due to late presentation
5 Yearly survival ~ 30 – 35% (varies from 80 – 100% for FIGO I to 5 – 10% for FIGO IIIC/IV)
Types:
Epithelium: 70%
Benign (60%): younger – serous cystadenoma, mucinous cystadenoma. If cysts have smooth
internal epithelium likely to be benign
Borderline (20%): mucinous tumour of borderline malignancy. 6% recurrence (but still
treatable) so need long term follow-up
Malignant (20%): serous cystadenocarcinoma
Ovum: 20%
Dermoid cyst (teratoma)
Occur in children and young women, in contrast to epithelial tumours
Commonest is benign, but in young children they are often malignant
Micro: variety of mature cell types: skin, gut, neural tissue, etc
Others: 5%
Stroma: lymphoma, fibroma
Granulosa cell tumour oestrogen amenorrhoea and breakthrough bleeding
Thecal cell tumour androgen infertile, hirsutism, amenorrhoea
Investigations: Ca125, FBC, electrolytes, LFTs, US + CT (for mets or possible primary elsewhere)
Should identify and screen those with high risk – those with genetic tendency (ie BRAC1, BRAC2,
HPNNC). If family history then screen with US plus CA125 – more informative together. NB lead
time bias
Treatment: Surgery for staging +/- debulking, chemo (usually platinum)
Other ovarian cysts:
Present with mass effects of torsion:
Follicular cyst
Corpus luteum cyst
Polycystic ovaries
Endometriosis
Endometrial Neoplasia
Most common gynaecological cancer, but early presentation better prognosis
Endometrial hyperplasia:
Simple hyperplasia: cystic glands with pseudostratified mitotically active cells. No atypia,
minimal risk of carcinoma
Complex hyperplasia: More crowded gland with budding and infolding. With atypia, 5% progress
to carcinoma
Reproductive and Obstetrics 355
Complex hyperplasia with atypia: crowded, folded gland in which the lining cells are pleomorphic
with loss of polarity and increased nuclear cytoplasmic ratio. > 25% progress to carcinoma
Endometrial polyps:
Most are hyperplastic polyps
Often seen with generalised hyperplasia
Due to an area responding to oestrogen but resistant to progesterone
Micro: a polypoid collection of cystic hyperplastic glands in a fibrotic stroma
Endometrial Cancer:
Presentation: irregular PV bleeding, often post menopausal
Risk factors: obesity, nulliparity, diabetes, unopposed oestrogen therapy, pelvic irradiation,
endogenous unopposed oestrogen (functioning ovarian tumour, anovulatory cycles, fat), family
history for breast, ovarian or colon cancer
Peak age 55 - 60
Investigate endometrial thickness with trans-cervical ultrasound:
Reproductive endometrium: 0.5 – 1.5 cm
Menopausal endometrium: < 5 mm. If bleeding, repeat US in 4 – 6 months and look for
change
If menopausal and 5 – 9mm, do endometrial sample. 90% are normal proliferative
endometrium. 5% are atypical (pre-cancerous), 5% are carcinoma
If > 9 mm, straight to D&C to get good endometrial sample (high suspicion of cancer). Not
hysteroscopy (can force malignant cells into the peritoneum)
Macro: fungating mass in the fundus
Micro: adenocarcinoma
Treatment: hysterectomy and oophorectomy + chemo and radiotherapy
Prognosis:
Stage 1: invade wall, 90% 5 year survival
Stage 2: invade cervix, 50% 5 year survival
Stage 3: lymph nodes, 20% 5 year survival
Obstetrics
History and Antenatal Booking
Always assume a woman is pregnant until proven otherwise, always assume a pregnancy is ectopic and
the mother has pre-eclampsia until proven otherwise (these are the common dangerous and treatable
conditions)
Objectives of antenatal care:
Assessment and monitoring of maternal and fetal well-being
Preparing woman and family for childbirth
Preparing woman and family for parenthood
Introduction Data:
Age: NB „Old‟ at 35:
Hypertension/diabetes/DVT more common
Down‟s: Past aged 35 risk of Down Syndrome > risk of amnio (approx 1 in 200)
Gravidity + Parity: Eg: G4P2 (+TOP + SAB). SAB = Spontaneous Abortion.
LMP – date of first day of bleeding in last period. Cycles regular? How long?
+/- Martial status
History of current pregnancy – if yes to any then focused questions
Due date = LMP + 7 days + 9 months (Naegele‟s rule), if 4 weekly cycle. If 6 weekly cycle, add 2
weeks (ovulation set by end of cycle not beginning)
Date it well. Management decisions later in pregnancy depend on dates being accurate. U/S more
accurate early on get accurate dates early on:
1
st
trimester (< 12 weeks) accurate +/- 5 days
2
nd
trimester (12 – 24ish weeks) accurate +/- 10 days
3
rd
trimester (24+ weeks) accurate +/- 2 – 3 weeks
Morning sickness
Contractions/pain
Bleeding
Discharge/leakage (rupture of membranes)
356 4
th
and 5
th
Year Notes
Foetal movements (from 18 – 20 weeks)
Urinary symptoms
Past Obstetric History: For each pregnancy:
When was it
If TOP then:
How many weeks. If 6 – 8 then likely to be choice. If after first trimester maternal or
congenital problem more likely so need to ask the reason for the TOP
Any problems (bleeding, infection, etc)
Antenatal problems/complications: hypertension, diabetes, PTL (Pre-term labour), medical
problems
When did you deliver (how close to your due dates were you)? If pre-term then risk this time.
Was there a reason?
How delivered? If caesarean need to check surgical report for type of incision. If it was low
transverse can trial labour, if vertical then not. Skin incision not reliable indicator.
Weight of baby: big ?diabetes (were they screened for diabetes – they will remember the sugar
load), small ?smoking or growth problem
Post partum bleeding, infection, depression
Breast feed, if so how did it go
How‟s the baby now?
Past Gynaecological History. If indicated. See History, page 338
Actively treat any infection
Any chronic infections (eg Herpes)
Polycystic ovaries, uterine abnormality or surgery risk
Gynaecological cancer: pregnancy hormones may exacerbate the disease
Contraceptive history – talk about restarting after pregnancy
Smear history: last smear date, any abnormal
Past Medical and Surgical History (and maybe very brief systems review):
History of hypertension (any signs of renal disease?), DM, heart disease, asthma, epilepsy, RF,
bleeding tendency, clots, previous STIs, TB, Hep B, gynaecological problems, kidney disease,
clinical depression, autoimmune disease, thyroid
Previous surgery
Medications:
See also Pharmacology of Pregnancy and Breast Feeding, page 528
Remember vitamins and non-prescription meds. Vitamin tablets not recommended in pregnancy
(OHCS, p 95).
On folate (should be from before conception to 13 weeks)
Allergies
Family History:
As for medical history
Clotting problems/DVT
Hereditary anaemias: Thalassemia (Mediteranian), Sickle Cell Anaemia (Africian)
Birth/Congenital defects (including congenital dislocation of hips)
Multiple births
Sister or mother with fertility or pregnancy problems (HT, miscarriages, DM, premature labour)
Social History (key element in determining pregnancy outcome):
Adopted
Marital/relationship status, subject to domestic abuse
Support system
Cigarette, alcohol and recreational drug use
Occupation. Interested in exposures. Also stay away from high impact activity and keep HR <
140 ( placenta perfusion)
Financial well-being
Low socio-economic status pregnancy complications (eg poor nutrition, lack of antenatal care,
etc)
Enquire about anxieties, etc
Offer advice on:
Questions or concerns (especially if first pregnancy or previous miscarriage)
Ante-natal screening
Reproductive and Obstetrics 357
Ante-natal classes
Dental check-up
Smoking and alcohol
Diet, including folate, iron, listeria (nothing from the Deli unless it‟s piping hot, no imported soft
cheeses - unpasturised)
Morning sickness: keep glucose up (ie morning barley sugar)
Rest
Knowledge of social security benefits
Mild exercise
Intercourse OK if there is no vaginal bleeding
Pregnancy write-up: [Name] is a [age] year old G_P_ LMP (date) EDD (estimated date of
delivery)/EDC (estimated date of confinement) at _ weeks by [LMP or US at _ weeks] who presents
for/complaining of etc…. Her prenatal course has been uncomplicated/complicated by…. Should also
include (gestation dependent):
Contractions, abdominal pain
Bleeding
Rupture of membranes – discharge or leakage
Foetal movement – 1
st
baby about 20 weeks, 2
nd
baby maybe as early as 18 weeks
Booking Exam and Investigations
Exam:
Pulse, blood pressure
Weight and height BMI
Signs of thyroid disease
Signs of anaemia
Heart and lungs (eg wheeze, mid systolic murmur common, pan systolic and diastolic abnormal)
Breast exam, including nipples
Abdominal (masses, large liver, etc)
Oedema
Varicose veins
Fundal height
Fetal Heart rate by monitor (if old enough)
Vaginal
Bi-manual – uterus size consistent with dates and no adnexal masses. Uterus becomes an
abdominal organ (rather than pelvic) at 12 weeks
Tests:
Blood:
FBC: check for anaemia
Blood group: check if RH –ive. If so, mark clearly in notes. Give Anti-D following birth or
invasive procedure
RBC Antibodies (eg Anti-D, Anti-ABO, etc)
Serology:
Syphilis (VDRL): treat with course of penicillin IM
Hepatitis B: if +ive, test and immunise partner and close contacts. At birth give Hep B IgG
and Hep B vaccine to baby (repeat at 1 and 6 months)
Rubella: If negative for Rubella and pregnant then NO vaccine (it‟s a live vaccine). Stay
away from kids. If she gets sick, repeat serology 2 – 3 weeks later to see if it was Rubella.
70% fetuses affected in 1
st
trimester, drops to < 5% by 16 weeks.
MSU for protein, bacteria and glucose
High vaginal swab where indicated for chlamydia, gonorrhoea, bacterial vaginosis, candida,
trichomoniasis, etc
If indicated:
Smear if not up-to date
Ultrasound if dates unsure (otherwise offer morphology at 18 weeks)
Tb if high risk (immigrant, family contact, etc)
Sickle cell anaemia if black
-feta protein/triple test if at risk of Down
358 4
th
and 5
th
Year Notes
HIV test if at risk
If > 35 then offer amniocentesis
Subsequent visits: see Assessment of Fetal Growth and Well-Being, page 359
Minor symptoms of Pregnancy
Pregnancy testing: requires a few drops of urine, +ive from first day of missed period until week 20,
false +ives low
Early: amenorrhoea, nausea, vomiting, bladder irritability
Nausea: At 20 weeks, 20% may still vomit. Reassure, small meals and stress
Headaches, palpitations and fainting due to peripheral dilation. Drink lots
Urinary frequency (exclude UTI)
Abdominal pain
Breathlessness
Constipation due to motility. Give fibre and lots of fluid
Reflux oesophagitis
Backache in 3
rd
trimester
Carpal tunnel syndrome (due to fluid retention)
Itchy rashes
Ankle oedema – almost universal. Exclude BP and proteinuria ( pre-eclampsia)
Leg cramps
“At Risk” Pregnancies
Adolescent Pregnancy (usually considered < 16):
Usually no problems with size of pelvis
Psychological and social problems: stability of relationship, financial (no DPB until 16), may
conceal pregnancy or have poor access to care, if very young may involve incest criminal
offence, need support after birth
Obstetric problems:
Inaccurate dates
Compliance issues
Pre-diagnosis exposure to alcohol/drugs
Smoking
Risk for pre-eclampsia (more likely to have less immunological tolerance to partner)
Elderly Primagravid (> 35):
Risk of chromosomal abnormality, twins, pre-eclampsia (more likely to have essential
hypertension, SLE or renal disease), DVT, thyroid disease, gestational diabetes, labour problems
IVF pregnancy risk of prematurity, IUGR
Risk of fibroids (which double in size in pregnancy) malpresentation, outgrow blood supply
( pain) but usually little problem to pregnancy
Grand Multip (>= 5 pregnancies)
Fe deficiency
Precipitate labour: can uterine rupture due to efficiency
Post-partum: relaxes quickly APH
Lie can be very unstable
Multiple Pregnancy
Causes of large uterus for dates (in order of occurrence):
Incorrect date for LMP
Distended bladder
Multiple fetuses
Polyhydramnios
Adnexal mass
Large for gestational age fetus
Fetal macrosomia (in diabetes)
Hydatiform mole
Dizygotic twins:
Baseline risk: 1in 80 pregnancies. 1 in 40 if primary relative a dizygotic twin
Reproductive and Obstetrics 359
Siblings that happen to share the uterus as the same time: separate placentas, amnions, and
chorions
2/3 of twins
7 – 11 per 1000 births
Risk factors: > 35 years, high parity, ethnicity and assisted conception
Monozygotic twins:
Family history has minimal risk for monozygotic
Splitting at two cell stage (< 5 days) gives separate placenta, amnion and chorion
Splitting at inner cell mass (5 – 10 days) gives common placenta and chorionic sac, but separate
amnions (most common – 70%)
Splitting of inner cell mass at later, bilaminar disc stage gives common placenta, amnion and
chorion
Problems:
Cord entanglement: highest risk < 30 wks occlusion and fetal death
Conjoined twins (1% of monozygotes): incomplete splitting of primitive node
Twin reversed arterial perfusion syndrome: one twin develops at the expense of the other
Fetus Papyraceus/Vanishing twin – death and subsequent reabsorption of one fetus
Complications: all complication rates are increased
Maternal:
Pre-eclampsia: 3* risk
APH: 6% (4 – 5% in singleton), PPH: 10% (4 – 6 % in singleton)
Preterm labour: on average 3 weeks early
Mal-presentation: only 40% present cephalic/cephalic
Hypertension
Gestational Diabetes
Miscarriage
Iron and folate deficiency
Acute polyhydramnios
Fetal:
Fetal growth retardation (~500 g less than expected in 25%)
Still births and infant mortality
Congenital malformations, mental retardation and neurological damage
Management:
More regular monitoring: eg hypertension and diabetes
Iron, folate supplementation
Introduction to multiple pregnancy support groups
Hospital delivery: obstetrician, midwife, 2* paediatrician, etc
Aim for vaginal delivery of first twin, syntocinon after delivery of first
Fetal Welfare
Assessment of Fetal Growth and Well-Being
Clinical assessment. Key issue is serial measurement:
Mother:
Blood pressure
Maternal weight
Test urine from 20 weeks for albumin (ie proteinuria) and glucose
Oedema
Check Hb and Rh antibodies (eg at 28 weeks) and do glucose challenge
Baby:
Symphyseal-fundal height (SFH)
Indicator of weeks gestation – roughly 1 cm per week. Drops a bit at term
Measure from top of pubic bone to top of uterus
NB – can just palpate uterus on the abdomen at 12 weeks. At 20 weeks up to umbilicus
Lie and presentation from 32 weeks
Fetal heart: use Doppler (mum can hear it too). Normal is 110/120 to 160 bpm.
Fetal movements (from 19 – 20 weeks in primips, earlier in multips): if no movement then
asleep or sick. Awake foetuses are active
360 4
th
and 5
th
Year Notes
OSCI tips:
First introduce yourself, wash hands, get sheet to cover legs
Explain what you‟re going to do
BP in sitting/semi-reclined position
Look for oedema – especially pre-tibial. Enquire about hands and face
Inspect abdomen for shape, size, scars, striae and linear nigra, symmetry. Is the baby
transverse or longitudinal
Measure fundal height
Find poles to determine lie
Where is the back: Feel laterally (brace hand other side), then walk hands across.
Ask what position it was on last scan and ask where she‟s feeling movements
Pawlicks grip above symphasis then both hands to measure descent. Watch face for pain
20-week morphology scan. Fetal risk 0%. Operator dependent. Assesses:
Fetal number, lie and cardiac activity
Fetal anatomy: CNS, CVS, GIT, GU, musculoskeletal anomalies (eg neural tube)
Gestational age (BPD, head/abdomen circumference ratio, femur length)
Amount of amniotic fluid (poly or oligo-hydramnios)
Placental location (low lying?)
Pelvic pathology: fibroids, cysts, etc
Give reassurance: parental anxiety
Further investigations: Most have high false positives interpret in light of clinical picture
Cardiotocography (CTG - fetal heart rate monitoring). See Cardiotocography (CTG) in Labour,
page 371
Doppler ultrasound of blood flow in umbilical artery (not routine)
Ultrasound scan: fetal size (biparietal diameter, abdominal circumference, femur length), amniotic
fluid estimation, assess fetal breathing (eg in hypoxia)
Biophysical Profile: Only if high risk. Score of fetal heart rate, breathing movements, fetal
movement, fetal tone and amniotic fluid volume. Not often done in NZ
Prenatal diagnosis
Reasons for prenatal diagnosis:
If an abnormality is detected, termination may be considered
Knowledge of an abnormality may give time to adjust/prepare
For Down syndrome see Down Syndrome, page 581
Screening tests (higher false +ive, especially if low risk women) – used to modify existing risks:
Fetal nuchal translucency (= nuchal fold): at 10 - 14 weeks, measure soft tissue thickening on
posterior neck, normal < ~ 3 mm. Thickness (adjusted for maternal and fetal age) associated with
chromosomal abnormalities. Combine with other risk factors (eg age). Fetal risk 0%
Maternal serum screening (triple blood test – now quadruple test): at 15 – 17 weeks, measures
AFP, HCG and free and bound oestriol. Serum levels, maternal age and gestational age are used to
calculate the risk of neural tube defects and chromosomal abnormalities classification as high
risk (eg 1:50 for Down) or low risk (1:2700 for Down). Fetal risk 0%
Diagnostic tests (higher false –ive):
Indications: positive results from screening, previous child affected by a congenital/genetic
disorder or family history, maternal age > 35, maternal condition or medication with possible
effect on baby
All introduce risk of Rh isoimmunisation give anti-D afterwards if RH -ive
Chorionic villous sampling (CVS): from 10 weeks, trans-abdominal or trans-cervical. Karyotyped
in 2 days, gene/enzyme analysis takes longer, 1 – 3% miscarriage. Can‟t detect neural tube
defects. Complicated by maternal contamination or fetal mosaicism (~ 0.5%). If mosaic, skin
cells in fetus closer to the babies karyotype than placental cells
Amniocentesis: from 14 weeks (10 – 13 weeks 5% miscarriage). Culture amniotic cells for 2 –
3 weeks detects chromosomal abnormalities and neural tube defects. Risk 0.5% miscarriage.
Gold standard but late. Difficult if anterior placenta or oligohydramnios
Cordocentesis (Percutaneous umbilical blood sampling): from 18 weeks. Miscarriage rate of 1 –
3%. Rapid karyotyping – good for detection of fetal blood disorders and infection (eg rubella)
Fetal Growth Restriction (FGR)
= Intra-uterine Growth Retardation (IUGR). Don‟t use this term in front of parents!
Reproductive and Obstetrics 361
= Failure to achieve full growth potential. Not quite the same as small for gestational age (< 10
th
percentile)
Causes of SFH: descent, changes in lie, IUGR, oligohydramnios
Common cause of perinatal death (along with prematurity and congenital malformation)
Associated with NIDDM, hypertension, heart and thyroid disease in later life
Asymmetrical:
Chronic placental insufficiency – head preferentially protected
Occurs in maternal illness/smoking, multiple pregnancy, idiopathic
Abdominal circumference cf the head, amniotic fluid
Symmetrical: Everything smaller due to eg congenital malformation, chromosome abnormalities,
infections or toxins
Termination of Pregnancy (TOP)
Crimes Act 1961:
Killing a child: child by definition is not a child until delivered
Killing an unborn child: prison term not exceeding 14 years
Unlawful to unlawfully procure an abortion for a woman
Section 187a: It is not unlawful to procure an abortion for a women if:
Not more than 20 weeks gestation and either:
Continuing the pregnancy „would result in serious danger (not being danger normally
attendant upon childbirth) to the life, or physical or mental health of the woman or girl
That there is a substantial risk that the child, if born, would be so physically or mentally
abnormal as to be seriously handicapped
That the pregnancy is the result of intercourse between a parent and a child, a whole or
half blood brother and sister, grandfather, is the result of sexual intercourse that is an
offence against section 131(1) or the girl or woman is severely subnormal
If the woman is near the beginning or end of child bearing years, or if there is reasonable
grounds to consider the pregnancy was the result of rape, then these factors may be taking
into account (although are not sole grounds for termination)
More than 20 weeks, and the termination is „necessary to save the life of the woman or girl or
to prevent serious permanent injury to her physical or mental health‟
Contraception, Sterilisation and Abortion Act 1977 specifies the process, not the criteria, for getting an
abortion. Abortions must be certified by two certifying consultants. These people to be chosen by the
Abortion supervisory committee, with a view to expeditious access by any woman seeking an abortion.
Supervisory committee also appoints/approves counselling services
Ethics:
Why is killing wrong:
Violates the moral integrity of the entity killed
It has negative consequences
Evidences moral flaws in the killer
Reasons for killing: to end suffering, to protect the innocent, lesser of two evils, to express societal
condemnation
Different views of the moral status of the fetus:
Fetus has the same moral status: absence of a dividing line between a baby and a fetus does
not show lack of difference
Fetus has no moral status: Is seeking an abortion for trivial reasons wrong?
Fetus has some moral status: As the fetus develops, reasons have to be increasingly weighty
Cervical softening before surgical abortion: misoprostol
Medical abortion: use of IU486/mifepristone
Complications of Early Pregnancy
Differential of early pain/bleeding
20% of women bleed in early pregnancy – it is never normal investigate
Obstetric causes: miscarriage, ectopic, trophoblastic disease
Gynaecological causes: period, STI, cervical (eg polyps), vaginitis, endometriosis, ovarian cyst (may be
functional irregular cycles), PID
Non-gynaecological: UTI, GI (eg haemorrhoids)
Exam:
362 4
th
and 5
th
Year Notes
CV, Resp, temp
Abdominal: tenderness/guarding/rebound
Pelvic exam:
Speculum: discharge, bleeding, swabs, os
Bimanual: mass, endometriosis ( fixed, retroverted uterus and utero-sacral nodularity on
PR), cervical motion tenderness ( ?PID)
Investigations:
MSU, FBC
Blood type + Rhesus
Spontaneous abortion/Miscarriage
= Loss of products of conception before the 20
th
week.
10 – 15% of recognised pregnancies. >75% in first trimester and due to fetal causes
Threatened abortion: os is closed and fetus is viable (still has heart beat). Uterus right size for dates.
75% will settle. Associated with preterm delivery
Incomplete abortion: cervix is dilating, more pain, heavier bleeding. Conservative treatment if < 13
weeks. If pain, bleeding or retained tissue on US then suction curettage. Ergometrine (uterine
smooth muscle contractor) for serve bleeding
Complete abortion: Products of conception expelled, bleeding stopped, cervix closed (don‟t confuse
with threatened), uterus small for dates
Septic Abortion: as for incomplete abortion + uterine and adnexal tenderness, purulent loss, pyrexia.
Can lead to severe sepsis
Missed abortion: Fetus dead but not expelled, uterus small for dates, confirmed by 2 US scans 7 days
apart. Usually active management to remove fetus
Causes:
None found – most common
Chromosomal abnormalities
Hormonal imbalance: eg failure of corpus luteum to produce enough progesterone
Maternal illness, abnormalities of the uterus (eg cervical incompetence), immunological factors
Recurrent miscarriage = loss of 3 or more consecutive pregnancies, occurs in < 1%
Ectopic pregnancy
= Any implantation outside the uterine cavity. > 95% in the fallopian tube
0.5 – 1 % of pregnancies. Fatal if untreated. Most common cause of death in 1
st
trimester
Risk factors – anything slowing ovum‟s path to the uterus: salpingitis (eg PID), surgery, previous
ectopic (recurrence in 10 – 20%), endometriosis, IUCD
Presentation:
Abdominal pain or bleeding in any sexually active woman
Usually around 8 weeks amenorrhoea, but may not have missed a period
Can present with acute rupture – sudden severe abdominal pain and shock
Shoulder tip pain due to blood in the peritoneum irritating the diaphragm
Cervical excitation
Diagnosis:
HCG – low for gestational age and rises slower than normal (normal doubling time is 2 days)
?Quantitative HCG: at 1500-2000 should see sac on trans-vaginal US, at 6000 should see sac on
abdominal US
US can visualise in 2% of cases – key finding is empty uterus
Laproscopy is gold standard
Treatment: surgical or methotrexate (folate antagonist)
Trophoblastic disease
Partial Mole
Complete Mole
Choriocarcinoma
Triploid 69 XXX, 69 XXY (ie
fertilised by 2 sperm)
46 XX, (46XY)
46
Normal and dilated villi –
some initially have a fetus
Dilated villi with trophoblast
proliferation
No villi. Atypical
proliferating trophoblast
Little invasive potential
10% invasive,
Choriocarcinoma 5%
Most have metastasised at
diagnosis. 80% survival
Reproductive and Obstetrics 363
Complete or partial hydatiform mole: abnormal placenta without/with a fetus. Placenta replaced by a
mass of grape-like vesicles
Choriocarcinoma: malignant invasion by trophoblastic cells – can arise years after a pregnancy
1 in 2000 pregnancies
Risk factors: early or late maternal age, previous mole, previous multiple pregnancies
Presentation:
Uterus large for dates in 50%
Vaginal bleeding +/- passage of grape-like villus
Early pre-eclampsia
Very high levels of HCG
Ground glass appearance on US and no fetus or absence of fetal movements/heart sounds
Hyperemesis gravidarum*
Rare (1 in 1000). Risk if young and primip
Presents with inability to keep food or drink down, hypovolaemia, polyneuritis (Vit B), liver and renal
failure
Admit to hospital. Rehydrate, exclude UTI, twins, and hydatiform mole
Cardiovascular Problems in Pregnancy
Common clinical findings in pregnancy: pulse volume, JVP pressure waves, heart size (apex beat
displaced by approx 1 cm), loud first heart sound, 3
rd
heart sound, ejection systolic murmur up to grade
3/6 in 90% women, peripheral oedema
Maternal mortality = 1 per 10,000 – most in puerperium (especially mitral problems pulmonary
flow pulmonary oedema, especially during 3
rd
stage of labour due to sudden in blood volume as
uterus contracts).
Risk of heart failure, especially due to Rheumatic fever, congenital disease, Marfan‟s, prosthetic
valves, given reduced functional reserve in pregnancy (ie further stresses an already stressed heart)
Fetal mortality: usually little impact, except mums with cyanotic congenital heart disease
History: breathlessness (although very common in pregnancy), syncope, arrhythmia
ECG: T wave inversion in III, S-T changes and Q waves occur frequently. ECG best for arrhythmias,
not structural problems (use echocardiogram)
Management: avoid exacerbating factors: infection, hypertension, obesity, anaemia, arrhythmias,
smoking etc. Multiple pregnancy further 30% increase in CO which compromises function further
Drug Treatment: digoxin, diuretic therapy, blockers
Labour: care not to fluid overload, monitor BP carefully (don‟t want it either up or down – care with
aorto-caval compression and epidural).
Gestational Diabetes Mellitus (GDM)
= Any degree of glucose intolerance with onset or first recognition during pregnancy
For most it consists of mild glucose intolerance manifest during the 2
nd
or 3
rd
trimester and normalising
following delivery
Affects 4 – 8 % of all pregnancies (Indian women >> than European). Risk factors:
Maternal age > 35 years
Family history of diabetes
Previous macrosomia, unexplained still birth
Obesity
Glycosuria on two or more separate occasions. 20% of women have glucose in their urine not a
reliable indicator
Associated with:
Morbidity for mother – 1.5 times risk of caesarean delivery
Increased risk of type 2 diabetes in the mother (up to 50% over next 10 years). ?Would have got it
anyway. Also hypertension, hyperlipidaemia, etc.
2.5 times morbidity for baby, including:
Large for gestational age, macrosomia (birth weight > 4000 gm – but most macrosomic
babies‟ mothers have normal glucose tolerance)
Risk of inter-uterine fetal death (IUFD)
Possibly neonatal jaundice, polycythaemia, post-natal hypoglycaemia, prematurity – but not
congenital malformations (unless IDDM mother)
But in general risks are low
364 4
th
and 5
th
Year Notes
Is usually asymptomatic (ie no polyuria and thirst). Risk factors have low predictive power
universal screening usual
NZ guidelines:
All women should be tested for glucose intolerance following a 50g glucose load between 24 and
28 weeks, blood sample 1 hour later. Normal < 7.8. If very high risks (eg previous GDM) screen
at 18 weeks as well
If failed screening test then formal test is 75g fasting load with samples at 0,1 and 2 hours. Normal
is <5.5, < 11 and < 8.5 at 0,1 and 2 hours. If any one is abnormal then GDM.
See also Diagnosis of diabetes, page 94
Exam: includes checks of eyes (retinopathy) and hands and legs (neuropathy), urine for protein
Aetiology: human placental lactogen (HPL, increases through pregnancy) insulin resistance
insulin production. May unmask sub-clinical NIDDM.
Management:
Diet and exercise (but don‟t calorie restrict them – ketosis is bad for babies)
Regular monitoring – home glucose monitoring and Hb A1C – normal is less than 6.5, under 8
acceptable. Aiming for pretty tight control
Insulin used if unable to control levels, or evidence of macrosomia. Stop once labour starts –
requirements fall dramatically after delivery
Sulphonylureas and metformin not approved in pregnancy
Frequency of macrosomia but less clear effect on perinatal mortality and rate of caesarean
section
Do GTT 6 weeks after delivery to check for type 1 or 2 diabetes
IDDM:
Need to conceive when Hb A1C < 8. Even if tightly controlled, 4 – 5% risk of congenital
abnormalities (2* general population). Most common are neural tube and heart defects
Check for retinopathy at least twice during pregnancy
Get baseline renal function and ECG/Echo if cardiac problems
Usual insulin injections have shorter action control harder. In early pregnancy, insulin
requirements may reduce. Later they usually increase.
Usually induced before term
Hypertension in Pregnancy
Normal Changes in Blood Pressure
Physiology:
O2 consumption from 300 to 350 ml per minute
CO from 5 to 6.5 - 7 litres per minute due to Stroke volume (10%) and HR (15 bpm)
Peripheral resistance falls (due to hormonal changes)
PCO2 to 31 mm Hg to increase gradient for shifting CO2 from fetus
Blood volume by 40% from early pregnancy to delivery
Ventilation
Glomerular filtration urination
During first and second trimesters, BP (especially diastolic) falls by 10 - 20 mmHg, return to booking
BP by 3
rd
trimester (partly due to hypotension aldosterone)
Venous distensibility + venous pressure predispose to varicose veins
Essential Hypertension
Present before pregnancy and commoner in older multips
If high blood pressure before 20 weeks, probably pre-existing hypertension
Aim to keep BP < 140/90
5 * more likely to develop pre-eclampsia than normotensive women
Watch for „white-coat‟ hypertension
Pre-eclampsia
= Pregnancy-induced hypertension with proteinuria +/- oedema
= Toxaemia
= Pre-eclampsic toxaemia (PET)
= Gestational Hypertension
Reproductive and Obstetrics 365
Signs: > 20 weeks pregnant, oedema, proteinuria, BP (systolic by 20 - 25 or diastolic by 15 over
booking BP)
If < 20 weeks then ?hydatiform mole
Is asymptomatic requires screening
May recur in a subsequent pregnancy
Risk factors:
Primiparity
New partner
Previous or family history of pre-eclampsia or eclampsia
Overweight
< 20 years or > 35 years
Multiple pregnancy (or anything else that placenta size)
Renal disease, essential hypertension, diabetes
IVF
Autoimmune disease (eg SLE, anti-phospholipid syndrome)
Presentations:
In „normal‟ pregnancy (ie low risk) – PET is usually mild and late (eg from 37 weeks)
In „abnormal‟ pregnancy, may begin from as early as 20 weeks and be severe
Pathogenesis: Abnormal vascularisation of the placental decidua by the syncytiotrophoblast during the
secondary invasion (~ 28 weeks). Arterial wall in placenta does not distend enough to allow sufficient
blood flow to placenta in late pregnancy Mother doesn‟t get the right pregnancy triggers from the
placenta mother‟s body doesn‟t completely adapt to being pregnant
Effects:
Mother doesn‟t vasodilate sufficiently BP, plasma volume and peripheral resistance
Generalised oedema eg face
Proteinuria is a late sign renal involvement. Oliguria renal failure
Serious signs ( Urgent admission):
Signs of ICP: headaches, vomiting, hyperreflexia, bilateral clonus
Headache, stomach pain, vomiting, HR (ie mimics viral illness)
Sustained vasoconstriction ischaemia (eg visual changes, brain) and clotting/DIC. Also
effects liver (RUQ pain), kidneys
Placental abruption
Placental ischaemia
Effects on fetus:
Asymmetric growth retardation (brain preferentially preserved)
If untreated symmetric growth retardation (if this occurs on its own then pre-existing fetal
abnormality)
Fetal movements, fetal respiratory effort and amniotic fluid
Assessment:
Baby: CTG and US
Mum:
Most important of the following are platelets and uric acid
FBC:
Either Hb (haemoconcentration secondary to oedema) or Hb (haemolysis secondary to
DIC)
Platelets – adhering to damaged capillary endothelium
Liver function tests: AST/ALT (not ALP – that‟s produced by the placenta). NB exclude
acute fatty liver of pregnancy
Creatinine and Uric Acid: due to renal flow. If bad then 24 hour urine to check for
oliguria/renal failure
Coagulation: fibrinogen due to DIC
Treatment:
Low dose aspirin pregnancy runs closer to term (controversial)
Mild: monitor BP and fetus; rest up (but not bed rest). If problems and > 37/40 then induce
Moderate: (eg BP of 140/90 but stable):
Labetalol (want 2 activity without any activity). Contraindicated in asthma
Methyldopa (causes depression etc but safe for the fetus)
Nifedipine (other Ca blockers cause fetal malformations)

366 4
th
and 5
th
Year Notes
Severe: Hydralazine IV (BP). Aspirin (blocks thromboxane production preferentially make
prostacyclin), antihypertensives, anticonvulsant prophylaxis (Magnesium sulphate). Have to
stabilise before delivery
Delivery is the only cure (although > half of fits occur post partum). Antihypertensives only mask
the disease. Diuretics contra-indicated. May have serious illness with only mild proteinuria (1+).
Usually resolves over 10 days.
Deliver now if platelets, signs of renal failure, unstable BP etc (ie signs of serious disease), or if
at term (>37 weeks)
Eclampsia
1 in 2000 pregnancies
Major cause of maternal and fetal morbidity/mortality
Is unpredictable. BP is not a good marker of disease
Generalised seizures (eclampsia) – treat with Magnesium sulphate (better than diazepam)
Death from stroke (most common), liver, kidney or heart failure
Other Complications of Later Pregnancy
Key complications: preterm labour, pre-eclampsia and small babies
Antepartum haemorrhage (APH)
Any bleeding from the genital tract between 20
th
week and delivery
Differential diagnosis:
Placenta praevia:
Implantation of the placenta in the lower uterine segment near or over the internal os.
Graded 1 to 4 (worst)
Risk factors: prior c-section (uterine scar), grand multiparity (>5), multiple birth, maternal age
>35, tobacco/cocaine use, fibroid uterus (ie anything that causes scarring or reduces places for
embryo to attach)
Placental abruption:
Premature separation of normally implanted placenta from the uterine wall
Risk factors: maternal age, multiparity, maternal shock, poor nutrition, gestational diabetes,
BP, smoking, anything that causes maternal vasoconstriction (trauma, cocaine, etc)
Onset of premature labour
Bleeding from other parts of the genital tract (eg cervical polyps, vaginitis, vulval varicosities)
Fetal: Vasa praevia. Bleeding from an abnormal fetal vessel attached to the membranes over the
internal os. Need ROM for this to occur. Mother will not be shocked
Clinical differences between praevia and abruption:
Placenta praevia
Placental abruption
Shock in proportion to visible blood loss
Shock out of proportion to visible blood loss
(concealed)
Painless
Poorly localised abdominal pain
Bright red bleeding
Dark red bleeding and clots
No contractions, uterus well relaxed
Uterus tense and tender
Fetus easy to palpated with good heart tones
No fetal heart sound detectable
Recurrent
Possible DIC
Assessment:
History: previous bleeds, initiating factors, eg trauma, colitis
ALWAYS ultrasound: exclude placenta praevia (detects 95 – 98% of cases) and major abruption
with placental separation.
NO vaginal exam until praevia excluded
APT test to distinguish fetal from maternal blood
Bloods to monitor hypovolaemic shock, DIC
Fetal well-being, eg CTG
If major blood loss, treat for shock transfuse, give O2
Give steroids
If fetus alive, consider c-section before labour
If fetus dead, induce
Treatment:
If Rhesus negative and no antibodies yet, give Anti-D within 72 hours
Reproductive and Obstetrics 367
Placenta praevia: If substantial, hospitalised till delivery, Caesar at 38 weeks
Placental abruption: Hospitalise. Serious risk of PPH, also acute renal failure, pituitary necrosis,
etc. Monitor retro-placental clot by serial ultrasound
Rhesus haemolytic disease*
Aetiology: if Rhesus –ive mother is „contaminated‟ by blood from a Rhesus +ive baby anti-D IgG
antibodies (isoimmunisation)
Later in the pregnancy, or in a following pregnancy, IgG can cross the placenta causing
Erythroblastosis Fetalis ( stiff oedematous lungs and hydrops – widespread oedema)
Test for anti-D antibodies in all Rhesus –ive mothers at booking and in 2
nd
trimester. If elevated then
monitor carefully
Anti-D immunoglobulin given prophylactically to Rh –ive mothers:
Within 72 hours after incident (eg amnio, threatened miscarriage, spontaneous abortion, any risk of
trans-placental haemorrhage – TPH, etc)
After birth if baby Rh +ive or group not known
This prevents „iso-immunisation‟ – gobbles up antigen before mothers immune system generates
antibodies
Don‟t give anti-D if mother already producing Anti-D
Premature labour
= Labour < 37 weeks
8% of babies, 85% of neonatal deaths
Over-diagnosed – over 80% diagnosed will deliver at term without treatment. Hard to diagnose –
regular uterine contractions are normal, cervical changes in labour can be subtle
Braxton-Hicks contractions are usual from 30 weeks but are not painful
History: Is it true labour: check nature of contractions, urinary frequency (?UTI), backache, spotting or
a change in vaginal discharge (normal in 3
rd
trimester – lots, white, non-smelling).
Risks:
Strongest association is previous preterm birth (4 times risk)
Previous mid-trimester abortions (2 or more) – not 1
st
trimester spontaneous abortions
Aetiology:
Spontaneous: 40%
Multiple pregnancy: 10%, 10 times risk
Maternal or fetal conditions (25%)
Premature, preterm rupture of membranes (PPROM = rupture of membranes before labour
commences and preterm)
APH
> 28 weeks, 80 – 90% survival
> 32 weeks, similar survival as term babies but complications
Management:
Investigations: temperature, BP, pulse, SFH, view cervix for clots etc (do NOT view cervix if risk
of praevia – do US first), ?infection screen, US, MSU, fetal welfare
Consider tocolysis (inhibiting labour):
Inhibit uterine contractions – allows time for steroids to work and for transfer to neonatal unit
agonists – Ritodrine and Salbutamol (risk of pulmonary oedema) prolong labour for ~ 24
hours. Adverse effects: maternal and fetal tachycardia, vasodilation BP.
Contraindications: fetal distress, severe pre-eclampsia, APH, hypotension, tachycardia,
asthma, etc
Oral Nifedipine (Ca channel blocker) is replacing Salbutamol – equal efficacy and side
effects.
If cervix is > 4cm then it should be allowed to progress – shouldn‟t use tocolytics
?Not if PROM (premature rupture of membranes). Can risk of infection
Steroids: dexamethasone and betamethasone (crosses placenta, prednisone doesn‟t) - 2 shots 12
hours apart. Always give first even if close to delivery maturation of lungs if between 24 and
34 weeks (surfactant production fetal distress syndrome) and neonatal better BP control post
delivery
Delivery. If < 26 weeks then vaginal delivery. C-section more likely if multiple pregnancy or
breech. Epidural analgesia preferable to narcotics ( respiratory depression)
368 4
th
and 5
th
Year Notes
Premature Rupture of Membranes*
= Rupture of membranes before labour is established. Normally rupture of membranes follows
establishment of labour
Check: have they really ruptured? Look for pooled liquor in posterior fornix. Do US for liquor volume
and fetal well-being
Management:
Admit and monitor
Swabs for infection (a cause of PROM)
Check for signs of infection: fever, maternal or fetal tachycardia, WBC
After 24 hours (time varies) commence prophylactic antibiotics
Low threshold for induction
Labour
Definition:
Regular contractions (usually 3 in 10 minutes, lasting 40 – 50 seconds)
Cervical change:
More anterior
Effaced: depth of „rim‟ normally 2 cm, 50% effaced = 1 cm
Dilated
Soft (hard = like forehead, normal = like nose, soft = like chin)
+/- Show (mucus plug) or ROM (rupture of membranes)
80% of all pregnancies last 38 - 42 weeks. 10% are preterm. 10% beyond the start of the 43
rd
week
(although biggest cause is inability to reliably date conception)
How does it start:
Uterus: distension, gap junctions in smooth muscle, oxytocin receptors
Cervical ripening: PGE breaks down collagen + effect of Braxton-Hicks contractions
Fetus: ?vasopressin released in response to transient hypoxia, ?other hormones
Examination:
Mother: monitor BP (hypo ?blood loss, hyper ?pre-eclampsia), pulse, temperature (eg
infection if prolonged period post-rupture)
Foetal position: by abdominal inspection and palpation. 2/3rds of babies head first with back on
the left. Descent – what portion of the head is below the pelvis (eg 3/5ths)
Fundal height
Foetal welfare:
CTG for 20 minutes (but incidence of fetal distress in early labour is low. Continuous
monitoring interventions)
Intermittent auscultation every 15 – 30 minutes following a contraction. Approx every 5
minutes in 2
nd
stage.
Fetal position – Definitions:
Lightening:
= Baby dropping. SFH, development of lower segment of the uterus, descent of fetal head
into pelvis
1
st
pregnancy: 2 – 3 weeks before
2
nd
pregnancy: may not be till 2
nd
stage of labour – uterus has lost some of its tone – doesn‟t
push baby down so well
Fetal lie: relation of fetal spine to mother‟s spine. Longitudinal (cephalic or breech), transverse,
oblique (unstable lie)
Fetal presentation: portion of the fetus in the birth canal:
Cephalic (96%): vertex, sinceput, brow, face
Breech (3%): Frank (extended – „foot in mouth‟), Complete (knees and hips flexed),
Incomplete (footling). Only worry after 36 weeks – it can turn fairly easily before then
Transverse or oblique (1%)
Fetal Attitude: “posture” of the fetus, eg extended neck
Fetal Position: Relation of occiput (vertex) to the maternal pelvis. Left or Right, Anterior,
Posterior, or Transverse, eg
LOA = left occiput anterior (face down, 8 o‟clock) – most common position
LOT = left occiput transverse
OA = occiput anterior (6 o‟clock)
Reproductive and Obstetrics 369
Anterior
Coronal
Frontal
Sagittal
Lambdoid
Posterior
LOP = left occiput posterior (face up)
Sutures:
Caput succedaneum: swelling of the fetal scalp immediately over the os
Moulding: Overlapping cranial bones in cephalic presentation. May BPD (biparietal parameter)
by 0.5 – 1.0 cm
Crowning: encirclement of largest diameter of the fetal head by the vulvar ring
Adequate sized pelvis has:
Wide pubic angle (skeleton can fit a fist)
> 10 cm between ischial spines
Can‟t reach sacral prominence (top of sacrum) on vaginal exam
Delivery of the baby:
Engagement: time when BPD passes through the pelvic inlet. Abdominal, 2/5 is palpable. If
engaged, you know the pelvic inlet is big enough
Descent: Extension of fetal body.
Flexion of neck
Internal rotation. Head rotates from 8 o‟clock to 6 o‟clock. Usually descent through pelvis
transverse, then need to rotate face downwards
Extension: once head reaches vulva, occiput in direct contact with symphasis. Ritgen Manoeuvre
– upward pressure on chin through perineum from below, downward pressure on occiput (stop
anterior tear)
External Rotation/Restitution – occiput goes back to original position (transverse) – now realigned
again with shoulder. Check for nuchal cord (around neck), clear nasopharynx
Expulsion: anterior shoulder, followed by posterior shoulder. Clamp and cut cord, with baby
below the level of the placenta if possible or if prem
Episiotomy: NOT routine. In NZ do them medio-lateral at time of Crowning. 1
st
degree =
superficial, 4
th
degree = deep, including rectal sphincter and mucosa
Stages of labour:
Stage 1: Cervical effacement and dilation - Friedman phase – plot on a partogram:
Latent phase (cervical softening). 20 hours in nullip, 14 hours in multip
Active Phase: Acceleration phase and deceleration phase (= transition). Cervix dilates 1.0 –
1.2 cm/hr (Primiparous), 1.5 cm/hour (multiparous) to a maximum of 10cm dilated
Stage 2: begins at 10 cm dilated and ends with delivery of the baby. 2 hours in primip, 45 minutes
– 1 hour in multip.
Stage 3: separation and expulsion of the placenta
Active management of 3
rd
stage
Especially if risk of PPH (big baby/twins/previous PPH/anything that makes the uterus big
eg polyhydramnios). See Postpartum haemorrhage (PPH), page 373
Give 5 – 10 units Syntocinon (IV if risk of PPH, IM otherwise) when shoulder delivers
Can use syntometrin (oxytocin + a little ergometrine – contraindicated if hypotension)
If PPH then IV infusion following bolus (T½ of Syntocinon is 3 – 5 minutes)
Complications of Syntocinon: hyperstimulation ( fetal hypoxia), uterine rupture, water
intoxication (Syntocinon is like ADH), uterine muscle fatigue ( post-delivery uterine
atony risk of PPH)
Signs of placental separation: sudden rush of blood, uterus rises, cord lengthens
OK to wait if no heavy bleeding. Gentle traction on chord with supra-pubic pressure (stops
uterus coming down) or fundal massage and maternal bearing down without traction
Can manually deliver (place hand into uterus and separate) – if no haemorrhage then wait for
anaesthesia
Then inspection, repair, rectal exam
Cord prolapse: Cord comes through cervix before head. C-section usually indicated. In meantime try to
control pressure on cord – don‟t push it back up. Risk if transverse lie
370 4
th
and 5
th
Year Notes
Pain Relief:
Inhalation agent (eg nitrous oxide)
Epidural: complications – hypotension, urinary retention, total spinal block, prolonged expulsive
effort
TENS
Narcotics eg pethidine: action lasts 3 hours and can cause fetal respiratory distress – don‟t give if
delivery expected within 3 hours
See also Obstetric Anaesthesia, page 545
Abnormal Labour
Risks to foetus in distress:
Hypoxia +/- ischaemia
Trauma
Meconium aspiration (meconium = first stool. Abnormal to find it in amniotic fluid).
= Labour does not progress normally. Due to problems with:
Power – eg hypoactive uterine contractions, or hyperactive (eg spasm)
Passage – disproportion between the size of the pelvis and the fetus (eg scarred cervix)
Passenger – abnormal lie, presentation, position or structure of the fetus
Psyche – excessively anxious or sedated mother (but if sedatives can contractions then probably
not true labour), conduction anaesthesia (ie epidural) may weaken lower uterine contractions and
therefore not assist head rotation and flexion
Types:
Protracted labour – takes longer than normal
Arrested labour – progresses normally then stops. During active stage, progress = either further
dilation or further descent
Can happen at any stage
Causes of failure to progress:
Prolonged latent phase
Primary dysfunctional labour: never enters active phase. Associated with primagravids, OP or
deflexed neck, post maturity and unripe cervix
Secondary arrest: enters active phase then stops. More likely than primary dysfunctional labour to
be associated with absolute cephalo-pelvic disproportion
Cervical dystocia: Primary (rare) or secondary (eg following cone biopsy)
Evaluation:
Palpate or monitor uterine contractions
Perform cervical exam (and check history)
Determine lie/position of fetus
Review medication
Treatment:
Hypertonic contractions – pain medication, Syntocinon
Hypotonic contractions – Syntocinon, AROM (artificial rupture of membranes)
Abnormal Presentations:
Breech. More prone to abnormal labour. C-section if < 1000 gm (body comes through at 7 – 8 cm
dilated and head gets stuck = “entrapment of after-coming head) or > 3600 or 4000 gm. C-section
becoming more routine for any breech
Face (rather than occiput first). Occurs with complete extension. Mentum (chin) anterior can be
delivered vaginally. Don‟t use forceps and Syntocinon
Brow. Incomplete flexion (midway between face and vertex). Converts to either face or occiput –
can‟t deliver as brow
Occiput transverse: Head can‟t flex and rotate from transverse to occiput anterior. Gets stuck at
iliac spines. Risk factors include pelvis shape (wide and squashed = platypoid). Rotate manually
or with forceps, or C-section
Occiput posterior (ie face up): 5 – 10 %, prolonged second stage, painful labour (lots of back pain),
bigger tears and episiotomies
Abnormal fetal structure:
Macrosomia
Hydrocephalus
Hydrops Fetalis: total body oedema eg due to heart failure secondary to Rh-isoimmunisation
Meningocoel (a neural tube defect)
Reproductive and Obstetrics 371
Pelvic abnormalities:
Inlet: failure to descend/engage (failure to descend prior to labour in a nullip is a bad sign)
Mid: smaller capacity than inlet, often associated with OT/OP
Outlet: rare in the absence of contracted mid-pelvis
Cardiotocography (CTG) in Labour
= Fetal heart rate monitoring
Look at rate (normal = 110 – 160), variability (> 5 bpm), accelerations (2 of at least 15 bpm in 20
minutes).
Don‟t want: Basal rate < 110 or > 160, variability for longer than 45 – 60 minutes, or spontaneous
decelerations
Early decelerations (ie with a contraction) are probably normal (due to pressure on the head HR -
?Cushings type reflex). Last decelerations (following a contraction) are a sign of fetal hypoxia.
“Shouldering” (brief HR either side of a deceleration) may signal cord compression
Early hypoxia is indicated by a mild tachycardia, reduced variability and consistent late decelerations.
80% sensitivity (ie 1 in 5 unnecessary interventions). A not normal but not abnormal trace has a 20 –
50% sensitivity for hypoxia
A poor CTG is an indicator only. May do scalp sample to confirm (pH < 7.2 or base excess > -12
getting bad deliver now by the safest means). Would act now on a bad trace if not in labour or
prolonged bradycardia < 80
Red hearings:
Check material BP. Hypotensive mother poor trace. Eg following epidural insertion, vena cava
compression (change position)
Hyperstimulation: contractions to long or fast turn down syntocinon
Methods of Induction
Prostaglandins on the cervix
Artificial rupture of membranes
Oxytocin drip
Forceps
To provide traction, rotation or both to the fetal head
Indications: delay in second stage, fetal distress, malposition, poor maternal effort, etc
Types: outlet, mid or low – depends on the station of the fetal head and degree of rotation
Should never be used when fetal head is not at least at 0 station (unengaged) as you don‟t know if the
head will fit through
Requirements: cephalic presentation, known position, contractions present (mum needs to push at same
time), ROM, fully dilated otherwise cervical tear ( bleeding and possible future cervical
incompetence), empty bladder and adequate anaesthesia
Complications:
Maternal: vaginal, cervical or uterine laceration, bleeding, bladder or bowel injury, often
episiotomy
Fetal: bruising, scalp, skull, eye or brain injury
Ventouse/Vacuum
Suction applied over posterior fontanelle
Less space necessary, often leads to spontaneous flexion/rotation, don‟t need to know exact fetal
position, will pop off if too much pressure less risk of trauma to mum or baby
Caesarean section
Types (refers to uterine not skin incision):
Lower segment transverse: risk of uterine rupture in subsequent pregnancy (<1%)
Classical: vertical incision in upper segment of the uterus. 5 – 6 % risk of rupture in subsequent
pregnancy. Bleeding, infection, ileus
Low vertical: vertical incision in the lower segment – treat as classical
Indications for classical: preterm breech, fibroids, anterior placenta praevia, transverse lie with
back down
Risks to mother:
4 – 6 times greater than for vaginal delivery
372 4
th
and 5
th
Year Notes
Anaesthetic risk for mother. Especially aspiration (slow digestion usually something in the
stomach). Give antacid and Maxolon (acidity if aspirates and vomiting). Give 02 to mum
fetal hypoxia. Group and hold. Usually use spinal or epidural anaesthetic (although
vasodilation BP fetal distress)
Infection
Bleed (placenta gets 500mls of blood a minute at term). May hysterectomy.
DVT (pregnant, surgery and immobile) PE (most common cause of maternal death)
Future obstetric complications:
Risk of caesarean section next time. Can normally trial labour and 70% will progress
normally. 1% uterine rupture (pain, hypotensive). Can‟t be induced if previous Caesar –
strong contractions against a closed cervix risk of rupture
Risk of placenta growing in the scar next time. May placenta accreta (abnormal adherence
to uterus which risk of PPH)
Indications:
Placental: praevia, abruption, vasa praevia
Fetal: disease (eg hydrops), malpresentation, distress, cord prolapse
Maternal: eclampsia, severe PET, active HSV, cardiac disease, cervical cancer, prior uterine
surgery, obstruction (eg fibroids, ovarian tumours)
Herpes Simplex Virus: Caesarean indicated if current genital outbreak at delivery. Only approx 1% of
babies infected but approx 50% mortality if infected
Perinatal Asphyxia
Asphyxia: cessation of gas exchange hypoxia and hypercarbia. Can occur in utero, intra-partum or
postnatally.
Fetal Distress: fetus demonstrates one or more clinical indicators of hypoxia (eg early passage of
meconium and HR changes on CTG)
Hypoxic-ischaemic encephalopathy (HIE): clinical manifestation in the neonate of a previous hypoxic-
ischaemic insult. Need for resuscitation (or not) at birth does not necessarily correlate with HIE later
on:
Grade
Features
Mortality
Neurologic Sequalae
in survivors
Mild
Irritability, poor sucking,
hypotonia
0%
0%
Moderate
Convulsions, lethargy, poor
feeding, abnormal tone
5%
21%
Severe
Comatose, seizures, ventilated
75%
100%
Cerebral Palsy: See Cerebral Palsy, page 629
Systemic effects of hypoxia:
Brain: hypoxic ischaemic encephalopathy (all are potentially reversible except for this one)
Kidney: renal failure
CV: hypotension
Liver: coagulopathy
Respiratory: meconium aspiration, pulmonary hypertension
Gut: ischaemia
Postnatal assessment
See Examination of the Newborn, page 587
Postpartum Complications
Maternal mortality used to be mainly due to PPH and puerperal fever, now PE is the biggest cause
Definitions of Perinatal and Maternal Mortality
Perinatal mortality = death of a fetus after 20
th
week or > 500 gm through to the time of delivery +
death in first week
Born dead = late fetal death
Death in first week = early neonatal death
Perinatal mortality rate (PMR) = (LFD + ENND)/1000 live births. In NZ is 6 – 8 per 1,000.
Varies from region to region
Reproductive and Obstetrics 373
Reasons for perinatal death:
Hypoxia (eg placenta separated, maternal hypertension)
Prematurity
Congenital abnormality (eg heart defect, spina bifida)
Trauma (eg difficult birth)
Maternal Death:
Death associated with pregnancy or trophoblastic disease up to 3 months after the event (required
to be reported to Medical Officer of Health)
Causes:
Obstetric causes – 70%. Includes DVT/PE, hypertension, anaesthetic death, haemorrhage
Associated medical deaths (eg asthma, heart disease)
Associated malignancy (eg breast cancer)
Suicide/homicide
Postpartum haemorrhage (PPH)
Primary PPH:
= Loss of > 500 ml < 24 hours after delivery
Limitations: estimating loss is difficult and loss may be concealed
Causes:
Uterine atony (90%). Eg in anything that causes large uterus – twins, polyhydramnios, etc
Genital tract trauma during delivery (7%)
Coagulation defect
Management:
Resuscitate mother. Test bloods for coagulopathy
Rub up a contraction + IV oxytocics
Deliver placenta and inspect for completeness
Inspect genital tract for trauma. Eg vaginal lacerations, ruptured uterus
If bleeding continues uterine atony. IM prostaglandins + other procedures
Secondary PPH:
= Loss of any volume of blood > 24 hours and < 6 weeks post delivery. Usually 1 – 2 weeks after
Cause: retained placenta/clot, often infected
Risk factors: abnormal placentation or accessory lobes on placenta
Diagnosis: Ultrasound +/- signs of infection: fever, tender uterus, offensive lochia (discharge after
delivery)
Management: curettage with US guidance + antibiotics (Broad spectrum + anaerobic cover)
Pharmacology:
Syntocinon: action lasts 20 – 30 minutes, causes hypotension, H2O retention, contraindicated in
CV disease (eg pre-eclampsia). Used for labour induction or augmentation
Ergot alkaloids (eg Ergometrine). For PPH. Causes hypertension and vomiting. Contraindicated
in hypertension.
Prostaglandin F2. IM for PPH. Contraindicated in Asthma, CV disease
Sequalae:
Massive bleed shock and death
Puerperal anaemia and morbidity
Sheehan‟s syndrome: ischaemia of anterior lobe of pituitary pan-pituitary insufficiency
Fear of further pregnancies
Prophylaxis:
Active management of 3
rd
stage
Elective C-section if placenta praevia
50% risk next time, reduces to 20% if active management
If at risk, then have active management of 3
rd
stage labour, have wide bore cannula in place and
specialist backup available
Puerperal Fever
Puerperium
= Time in which reproductive organs return to their pre-pregnant state – usually 6 weeks after
delivery
Uterus involutes from 1 kg to 100 gm. Pelvic organ by ~10 days
Lochia: red for day 1 – 3, yellow next 10 days, white until 6 weeks
374 4
th
and 5
th
Year Notes
Puerperal Pyrexia = temperature of at least 38 C on any 2 of the first 14 days after abortion or delivery,
exclusive of the first 24 hours
Incidence:
After vaginal delivery: 1 – 3 %
After Caesarean: ~10%
Pathogenesis: assume infection until proven otherwise. Can deteriorate quickly – need rapid
assessment
Sources:
Clots, retained placenta, etc can facilitate growth
Generally an ascending infection
Lower genital tract (eg anaerobes).
Bowel: E. Coli and G –ive
Attendants: staph and haemolytic strep
Environment or partner
Severity is related to:
Bacterial factors: virulence, resistance, etc
Host: general health, immune status
Pregnancy related: duration of labour post-ROM, invasive examinations
Causes:
Endometritis (uterine infection):
Most common cause
Fever, uterine tenderness on abdominal palpation, foul-smelling lochia (post-partum vaginal
discharge)
Treat aggressively to avoid abscesses
Can proceed to peritonitis, septicaemia, etc
Mastitis: Usually occurs 2 – 3 weeks postpartum and is associated with cellulites over the affected
area. Staph Aureus is common
UTI: risk from catheterisations, operative vaginal delivery
Thrombophlebitis: 1% of women present with painful tender varicose veins. Look for DVT
symptoms. Risk if obese, high parity, bed-bound, etc. Treat with NSAID
Wound and episiotomy infections
Respiratory tract infection, atelectasis
Investigations: FBC, urine culture, high vaginal swabs
Management:
General: fluids, correct anaemia, pain relief
Antibiotics: start empirical treatment immediately. CCHL protocol is IV Augmentin +
Metronidazole
Six Week Check
Looking for problems that may not have been present at birth (ie don‟t check for imperforate anus,
they‟d be dead by now!)
The main aim of the 6 week check is to:
Detect abnormalities in the baby that may have become clinically detectable since birth
Explain the advantages of immunisation for the baby and offer immunisation
Check the psychological and physical well-being of the mother
Promote breast feeding and healthy attachment
Checks for the baby:
General well-being including sleeping and feeding
Growth: check serial measurements in the Child Development Book
General physical inspection, including fontanelles
Neurological milestones:
Sight (do they follow an object, smile at a face, etc): at risk if premature or birth asphyxia
Hearing (startles with loud noise, etc): at risk if family history, rubella, CMV, toxoplasmosis,
<1500 gm, severe asphyxia
The mother is likely to be aware of the presence of absence of these
Heart: Ausciltate for murmurs, look for pallor, dyspnoea with feeds, failure to thrive (1% affected,
VSD in 30% of these)
Reproductive and Obstetrics 375
Hip dislocation: unstable hips may not present until after birth. 0.4%, girls = 5 * boys. Need to
treat before they begin to walk. Investigate with US and Xray. Treat with Pavlik harness
Genitals: Check boys for undescended testes (cryptorchidism) – 2%, especially if premature,
spontaneous descent unlikely beyond 3 months, surgery at 9 – 12 months. See Undescended testis,
page 636
Checks for the mother:
History:
General well-being
Signs of post-natal depression or adjustment disorder: poor sleep or appetite, feeling „low‟,
anxious or guilty, thoughts of harming herself or the baby. Complete a screening survey such
as the Edinburgh Postnatal Depression Questionnaire. See Postpartum Mood Disorders, page
430
Breastfeeding: Is this going well?
Bowel and urine continence – encourage pelvic floor exercises
Perineum: pain, dyspareunia, etc
Review of pregnancy and child-birth experience
Exam:
Weight: loss of 60% of weight gained during pregnancy
Examine breasts for infection or cracked nipples
Abdominal exam: involution of the uterus – should be at or approach pre-pregnant size
Pelvic exam: healing of laceration or episiotomy, lochia assessed, size and tenderness of
uterus
Cervical smear if not up-to-date
Check of other complications that may have arisen in pregnancy: BP, diabetes, anaemia, UTIs,
etc
Contraceptive advice:
Low levels of sexual interest common
Return of fertility is variable. If not breastfeeding ovulation can occur as soon as 28 days
Complete breast feeding provides 98% protection for the first 6 months (provided they continue to
have amenorrhoea). Normally start contraception at 3 months
POP: Start in early puerperium. Very effective in conjunction with breast-feeding. Start CoC
when feeding frequency has by half, when solid food started or with first bleed (whichever first).
Amount transferred to baby over 2 years = 1 tablet‟s worth
COC: alters quantity and quality of milk. If not breast feeding start on day 21 (thrombosis risk
and won‟t have ovulated yet)
IUCD: Insert 4 - 8 weeks postpartum (higher expulsion rates if inserted after 3
rd
stage, and C-
section scar will have healed by then)
Sterilisation: wait a while – may change their mind
Natural family planning: problematic due to variable effect of lactation on periods
Immunisation is recommended for Diphtheria, Tetanus, Pertussis, Haemophilus Influenza type B,
Hepatitis B and polio vaccine. If the mother is concerned about the baby being unsettled afterwards,
prophylactic oral paracetamol can also be offered.
Breast
Physiology & Anatomy
3 – 4 days before menses, oestrogen and progesterone cell proliferation and water retention
During pregnancy, cell proliferation. Post-partum, prolactin milk production.
At menopause, breast involution due to replacement of glandular tissue by fibrosis and fat. Occurs
with age
Superficial and deep fascia form a sandwich around the breast
Breast is between the 2
nd
and 6
th
intercostals spaces
Breast History
Previous lumps
Pain
Nipple discharge:
Is it blood stained
376 4
th
and 5
th
Year Notes
Is it unilateral or bilateral
Is there an associated lump
Changes related to menstruation
Parous state – breast feed?
Last period
Family History
Breast Exam
7 – 10 days after the beginning of menses
Inspection: while standing, look for dimpling and nipple deformity with patient‟s hands on her hips and
then above her head
Palpation:
Patient supine with hands behind her head
Distinguish glandular tissue from breast fat
Check for loss of pliability as well as for masses
Axilla: checked for enlarged axillary lymph nodes – 1 – 2% of cancers present as axillary lumps
Characteristics of breast cancer: fixed, immobile, single, hard
Breast Investigations
Clinician/surgeon: examination and history
Pathologist: FNA ( cytology) and core biopsy ( histology)
Radiologist: mammography and ultrasound. Clues on mammography:
Calcification:
Benign: very large, well rounded
Malignant: clusters, variable border, cast in a duct
Density
Breast in Pregnancy and Breastfeeding
Changes during pregnancy:
Oestrogen, progesterone, HPL, PRL and HCG acinar cellular hyperplasia in early pregnancy,
hypertrophy in later pregnancy, duct sprouting
By end of pregnancy, breast is composed almost entirely of lobules separated by relatively scant
amount of stroma
Immediately after childbirth:
Progesterone milk production under the influence of PRL
Milk let down: sucking pulsitile oxytocin myoepithelial cells squeezes milk down duct.
Also due to neuroendocrine reflex (eg hearing baby cry). Sensitive to emotional stress
Sucking also stimulates PRL continued milk production
Advantages of breast feeding:
Infant: infant mortality (two fold), bonding, cheap, anti-infective properties (lysozyme, IgA,
lactoferrine, etc), SIDS
Maternal: contraceptive, sucking promotes uterine contractions PPH, pre-menopausal breast
cancer
Sufficient on its own until 4 – 6 months
See also Breast-feeding, page 590
Contra-indications: maternal HBsAg, CMV or HIV +ive, active breast HSV lesions, amiodarone
Breast care:
Sore/cracked nipple prevention:
Poor position, poor hygiene, irritation (clothing, soap)
Treatment: shields, advice on position, break suction with finger
Breast engorgement:
Supply > demand enlarged breast baby can‟t latch on
Management: feed on demand, no other fluids for baby, express, paracetamol
Mastitis:
Cellulitis of interlobular connective tissue (mainly Staph Aureus)
Fever, tiredness, muscle aches and pains
Treatment: antibiotics (flucloxacillin), analgesics, regularly empty breast, massage lumps
towards nipple when feeding
Reproductive and Obstetrics 377
Abscess:
Secondary to mastitis, febrile and toxic, red and tender > 48 hours
Treatment: surgical drainage, antibiotics, antipyretics, analgesics, ?suppress lactation
Inverted or retracted nipples: gently pull out through pregnancy
Breast discharge
Causes:
Causes of galactorrhoea:
Physiological
Drug related (eg dopamine)
Bronchogenic cancer
Prolactinoma
Duct ectasia (periductal mastitis) – most common cause in pre-menopausal women. Discharge
may be serous, greenish or bloody
Carcinoma: usually associated with a palpable mass – cause in 10% over age 55. Cancer unlikely
if discharge is coming from both nipples and/or multiple ducts. Cytologic examination has 50%
sensitivity
Management:
History and exam
Get mammogram, re-examine in 3 and 12 months, and repeat mammogram in 12 months
Sample to discharge to lab
Check serum PRL, especially if a pre-menopausal woman has irregular periods
Pregnancy and discharge:
Epithelial hyperplasia may blood-stained discharge (usually normal)
Galactocoele: a milk filled cyst due to plugged duct
Galactorrhoea:
Physiological: menarche/menopause
Secondary to dopamine: chlorpromazine, haloperidol, metoclopramide, methyldopa
Prolactinoma: bronchogenic cancer or pituitary tumour
Developmental Problems
Inverted nipples are common. If a previously normal nipple inverts cancer until proven otherwise
(although nipple retraction is more likely to be inflammatory than malignant)
Virginal/ Adolescent Hypertrophy: very large breasts developing around puberty. Problem with
stroma. Aetiology unknown
Hypomastia: almost complete failure of breast development. May be unilateral
Accessory nipples (don‟t have lobular tissue underneath)
Inflammatory Breast Disease
Acute Mastitis and breast abscess:
Usually occurs in early lactation
Usually staph aureus (abscess), less often strep (cellulitis)
Fat Necrosis:
A solid mass caused by injury (eg seat belt injury)
Necrotic fat cells surrounded by an inflammatory infiltrate, with later calcification and scarring.
Can mimic carcinoma
Duct ectasia
Uncommon cause of a breast mass. Usually older woman, tender and nipple retraction
Pathogenesis: Dilation of larger ducts with secretions loss of epithelium ulceration blood
or serous discharge infection periductal mastitis (abscess + fibrosis) nipple retraction
Histology: Chronic inflammation and fibrosis around ducts loaded with lipid and macrophage rich
material
Cause unknown. Correlated with smoking
Preductal mastitis: periareolar inflammation, abscess formation, unilateral, single duct, etc
Plasma cell mastitis: Rare cause of a breast mass. Probably the same as duct ectasia but with plasma
cells
A tumour can block lymphatics causing inflammation cancer is always a differential
378 4
th
and 5
th
Year Notes
Fibrocystic Disease
A „catch-all‟ category for gross and micro cysts
Don‟t call it mammary dysplasia
Commonest disease of the breast
Cause obscure – unopposed oestrogen a known factor. Women on combined pill get less fibrocystic
disease
Classification by size:
Gross cysts: very easy to diagnose on US. 40s. Drain with FNA
Micro cysts: usually 30‟s and 40‟s. May have cyclical pain. Resolves after menopause
Galactocoele – milk filled cyst, usually with lactation
5 components (either separately or together):
Cysts:
Dilated ducts containing cloudy serous fluid (sometimes bloody or infected)
All breasts contain microcysts during childbearing years. Abnormal when > ~ 2mm
Histology: epithelium may be flattened, cuboidal, columnar, piled up or show apocrine
metaplasia. Surrounding stroma likely to be fibrous
Fibrosis:
Dense collagenisation distorting/compressing epithelial structures
Most common in upper outer quadrants, patient‟s in 30s
Sclerosing adenosis:
Usually a tender lump in the upper outer quadrant, patient around 40
Benign proliferation of small ductules in a fibrous stroma, but histologically circumscribed
Lining cells proliferate to fill the ducts
Increased risk of cancer with florid (2*) and atypical (4*) hyperplasia
Mimics cancer both clinically and microscopically
Apocrine Metaplasia: Benign metaplastic change to tall cells with eosinophilic cytoplasm
resembling those of secretory glands (eg lactation, sweat, etc)
Duct (and sometimes lobular) epithelial hyperplasia
Generally Benign Breast Tumours
Fibroadenoma
Most common benign breast tumour – no malignant potential
Hypertrophy of a lobule, compressed by stroma ( sharply circumscribed), hard and very mobile – up
to 2 – 3 cm diameter.
Common in 16 – 24 years. Rapid growth for 6 months, 1/3 will regress.
Diagnosis by FNA if < 25 years, surgical enucleation if > 35 years
Histology: fibrous tissue surrounding normal ducts that are often crushed flat. Risk of subsequent
cancer = 2.17
Cytology: cells clump together (cohesive) compared with malignancy which are normally non-cohesive
Giant fibroadenoma: Variant:
Two peaks of incidence: 14 – 18 years and 40 – 50 years
Large: 5 – 10 cm
Typically oriental and black races
Diagnosis: FNA
Treatment: surgical enucleation (no excision margin)
Phyllodes Tumour
Rare but „worrisome‟ mixture of stromal and epithelial cells
30 – 50 years
Shiny skin + vascular markings
Wide spectrum from benign to frankly malignant. Grow rapidly
Diagnosis: FNA + core biopsy. Cleft into the tumour on US is characteristic
Treatment: excision with 1 cm margin
Recur locally
Papilloma
< 1 cm epithelial proliferation in a major duct just below the nipple
Reproductive and Obstetrics 379
Can bloody discharge and/or nipple retraction
1 in 100 is a papillary carcinoma
Breast Cancer
Epidemiology
In NZ, 1600 cases each year, 580 die. Commonest cause of cancer death in women.
10% life time incidence (usually over 70)
Maori rate similar to non-Maori
75% diagnosed with breast cancer are over 50. Uncommon under 40. Mean age of diagnosis is 60 –
65. Younger if genetic risk
If > 70 years, more likely to be indolent and hormone responsive. If < 35 then large and aggressive
Survival:
5-year survival (%)
10-year survival (%)
Stage I
80
65
Stage II
75
55
Stage III
55
40
Stage IV
10
5
Risk Factors
Major risks:
Woman (100 * men)
Age
Previous breast cancer, also previous (or family) history of endometrial, prostate, or ovarian cancer
Biopsy showing an at risk condition e.g. atypical hyperplasia
Genetic predisposition (eg BRAC1 or 2 account for 5% of breast cancers)
Family History:
Most with family history don‟t develop it, most who get it won‟t have a family history
Risk is above population risk for only 1% of female population
4% have a moderate increase in risk if:
A mother, sister or father developed breast cancer before 50, or in both breasts
More than one close relative on the same side of the family who had breast or ovarian
cancer (geneticist said only genetic if 3 or more affected relatives – it is so common have
to have a high incidence in family before suspecting a family loading)
Minor risks:
Oestrogen exposure:
Slight increase for OC and Depo-Provera (only while taking it – and usually young so less of
an issue)
Longer duration between menarche and menopause
First child beyond 35 or no children
Not having lactated slight risk of premenopausal cancer
Obesity
HRT for more than 5 years increases risk by about 30%. Risk disappears within 5 years of
stopping
Radiation, environmental hazards
Not risk factors:
Smoking
Small (now disproven?) relationship with low fat, high fibre diet
Symptoms
Presenting symptoms:
Painless mass: 66%
Painful mass: 11%
Nipple discharge: 9%
Usual presentation is a dominant, painless mass
New lump or thickening
Change in breast shape or size
Puckering or dimpling of the skin
Change in a nipple
380 4
th
and 5
th
Year Notes
Lumpiness in one breast soon after period ends
Pain in the breast that is unusual
Investigations
History and clinical exam
Mammogram:
Not sensitive < age 35
Calcifications: low risk are coarse or rounded, high risk are clustered or branching
Shadows: malignant are less circumscribed
Ultrasound
FNA Cytology
Core or hook wire biopsy
Pathogenesis
Most tumours occur in the epithelial component lining the ducts and lobules. Epithelial hyperplasia (1
– 2 times risk) Atypical hyperplasia – proliferation and atypia of ductal or lobular epithelium. Risk
of subsequent cancer = 4 times.
Tumour cells secrete cytokines fibrosis lump. Easier to detect in an older woman (fat and
intra-lobular fibrosis)
All breast cancers are different. Tumour growth rates vary considerably. On average takes 9 years to
reach 1 cm.
Death is from metastases which can occur at any time
Spreads to lymph nodes via lymphatics and directly to distant sites via blood stream – not via lymph
nodes then to distant sites (although lymph node involved risk of blood spread as well)
Lots of implicated genes. Those in familial breast cancer include:
BRAC1:
Autosomal dominant (but recessive at the level of the cell): if carrier then 65 – 75% risk (ie
high penetrance)
A tumour suppressor gene, expressed in breast, ovary, thymus, testis
Accounts for 40 – 50% of familial breast cancer
BRAC2:
Associated with male breast cancer, not ovarian
10% of inherited breast cancer
Classification of Breast Cancer
Classification:
In-situ
Infiltrative (invasive)
Ductal
Intraductal carcinoma
Infiltrating ductal carcinoma:
No special type (NOS)
Medullary carcinoma
Mucinous carcinoma
Tubular carcinoma
Metaplastic
Lobular
Non-infiltrating (in situ) lobular
carcinoma
Infiltrating lobular carcinoma
Most cancers are intraductal
Plus Paget‟s Disease of the Nipple
Non-infiltrating/in-situ breast cancer: Does not metastasise but recurrence is a problem. Can
become infiltrative and then metastasise
Intraductal carcinoma (20 – 30%):
Comedocarcinoma: solid intraductal proliferation, central necrosis, microcalcifications on
mammogram
Classified by nuclear grade (low, intermediate and high) and the presence or absence of
necrosis.
Can eventually become invasive: removal cure
Paget‟s disease (a type of ductal carcinoma in situ): lesion of the nipple caused by malignant cells
arising from ducts and invading the nipple epithelium. Looks inflamed (early on can look like
eczema). Most often an underlying duct carcinoma.
Lobular carcinoma in situ:
Reproductive and Obstetrics 381
Usually an incidental finding on biopsy affecting terminal ductules
Proliferation of terminal ductules and acini
1% per year risk of invasive carcinoma in same or opposite breast – removal isn‟t necessarily
cure
Invasive/infiltrating breast cancer:
Main risk factor: age
Infiltrative ductal carcinoma (65 – 80%):
No special type: Most common. Grossly stellate or multinodular and very hard.
Histologically compressed ductules in a very desmoplastic stroma
Medullary: Big, bulky and soft, plentiful lymphocytes, better prognosis than other types
Mucinous (colloid, gelatinous) carcinoma: Grossly: gelatinous mass. Histologically: clumps
of cells in lakes of mucin. Better prognosis
Tubular Carcinoma: well-formed glands, best prognosis
Infiltrative lobular carcinoma:
Histological: Indian files around ducts, small cells
Often bilateral
Features of invasive cancers:
Usually dominant mass
Usually painless
In time fixed to deep fascia immobile
Orange peel appearance: blocked lymphatics oedema + suspensory ligaments contract
distorted shape
Also nipple retraction, ulceration of overlying skin
Majority arise in the outer quadrants – particularly the upper, outer quadrant
On mammography:
Infiltrative edge: not well demarcated
Density compared with adipose tissue
Micro-calcifications: small clustered areas of necrosis
Prognosis
Stage: axillary metastases most important, also size. Cancers found on mammography or by self-
examination are smaller better prognosis
Grade
Oestrogen receptor sensitivity: if positive then better – more differentiated and Tamoxifen
regression
Treatment of Breast Cancer
Can‟t cure metastases aim of treatment is local control
Options:
Two options (similar long-term survival):
Removal of the lump + radiation therapy (significant in local recurrence)
Mastectomy (or radical mastectomy) + reconstruction
+/- Radiotherapy (planned to limit dose to the heart, lung or opposite breast
+/- Tamoxifen (anti-oestrogen)
Surgery:
Mastectomy
Breast Conservative
Patient preference
Patient preference
Large tumour or Large tumour/breast ratio
Small tumour or small tumour/breast ratio
Multiple tumours
Single tumour
+ive margins
Focal microcalcification
Previous breast RT
-ive margins
Pregnancy, etc, etc
Most common metastasis is in the bone. Bisphosphonates slow osteolysis
Risk factors for recurrence in breast cancer ( consider adjuvant chemo):
Axillary node status (strongest predictor)
Tumour size (> 1 cm)
Histological tumour type and grade
Adjuvant Chemotherapy:
382 4
th
and 5
th
Year Notes
Approx 25 – 30% risk of recurrence, 15 – 20% risk of death. Improves long term survival in
node positive and node negative disease
4 to 6 courses over 3 – 6 months optimal
2 agents better than one: eg
AC: Adriamycin (an anthracycline) and Cyclophosphamide. „Gold standard‟. Adriamycin
causes vomiting and wasn‟t used so much until 5HT3 antagonists were available
CMF: Cyclophosphamide, Methotrexate and Fluorouracil (another „Gold Standard‟)
Hormone Therapy:
Aim: prevent breast cancer cells from receiving stimulation from oestrogen
Only is oestrogen receptor sensitive
Oestrogen deprivation:
Block oestrogen receptor: eg Tamoxifen – antagonist. Taken for 5 years. Side-effects:
Largely well tolerated
1 in 3 have post menopausal flushes, vaginal dryness/discharge
Initial nausea, weight gain
Rare retinopathy
Agonist in the uterus endometrium risk of endometrial carcinoma (1 in 1000,
usually curable)
PE/DVT (1 – 2 %)
Suppress synthesis: aromatase inhibitors (work in adipose tissue, eg in post menopausal
women), LHRH agonist (pre-menopausal, switches off the ovary)
Destroy ovaries (surgery or RT)
Leads to recurrent, 40% incidence of contralateral breast cancer (although absolute risk low)
Breast Screening
Of proven benefit in reducing mortality in women over 50: benefits under 50 unclear
2 yearly screening after 50 reduces chances of dying from breast cancer by about 1/3. Reduces a one in
42 chance to one in 60
In NZ is free from 50 – 64
Mammograms less reliable in under 50s: denser breast tissue. Higher false positives unnecessary
investigations. Sensitivity for < 50 years is 50% - 60%, for > 50 years is 80+%. 5 – 10 % screened
sent for further investigations. Positive predicative yield is 8.5% (high false positive rate)
Further investigations: ultrasound, FNA, biopsy
Of 1000 screened, 70 to 120 will be positive, 10 to 30 will proceed as far as open biopsy, and 5 to 10
will have cancer
Mammogram less accurate if on HRT
Interval cancers: fast growing cancers appearing between mammograms – never ignore a lump
Application of screening criteria (see Criteria for Screening Programmes, page 690):
It is an important health problem – with a significant incidence. It is preventable
A screening test is available: a two yearly double view double read mammography (double reading
increases cancer detection by 15% compared with single reading and reduces recall rate)
The screening test is available, acceptable (83% a little uncomfortable only), reasonable sensitivity,
but low PPV
Natural history is well understood, and there is a detectable pre-symptomatic stage
Screening leads to interventions that increase the quality of life: relative risk reduction 10 – 30%
for women in the 50 – 65 age group. However, lots of unnecessary interventions, and for a
majority (>70%) whose cancer is diagnosed, the outcome is unchanged (but will live with 2 years
extra knowledge of condition)
Is there an appropriate infrastructure to provide screening and follow-up? There have been pilot
studies
Is it cost effective: Needs at least 70% screening coverage to be cost effective.
Sexual Health
References: Wellington Sexual Health Service, 4
th
and 5
th
year Handout, 2000
Sexual History Taking
Purpose of sexual history is to determine:
Whether or not there has been a risk of exposure to an STI including HIV
Reproductive and Obstetrics 383
If it is an appropriate time to take tests (window period – genital tests are not taken unless at least
14 days has elapsed from unprotected sex, unless symptomatic. For blood tests wait 3 months)
Who else had been at risk and may need testing/treating
Approach:
„Going to ask personal questions – want to be able to offer right tests and care”
Ask why they‟ve come
Use patient‟s language
Don‟t make assumptions about anyone
Lot‟s of reassurance: STD‟s are common, confidentiality, support relationship issues – let them
decide, continue at a later date
Not interested in their orientation but what they do
Questions:
Are you sexually active?
How many partners have you had in the last 6 months – male or female?
Alcohol and drug history
Do you suspect that you may be at risk from HIV or other STD?
Need to ask about sexual abuse – won‟t volunteer it: Ever had sex when you didn‟t want to, ever
been sexually assaulted?
Exam
Female
Inspection: pubic lice, genital warts, ulcers, blisters, scabies
Palpation: inguinal lymph nodes
Vaginal examination with speculum
Bimanual examination of pelvis
Male
Examination of external genitalia
Palpation of inguinal nodes
Palpation of scrotal sac and testes
Sexually Transmitted Diseases (STDs)
Types and incubation:
Chlamydia (7 –21 days) don‟t test till 14 days after contact (unless symptomatic)
Gonorrhoea (range 1 – 14 days, commonly 2 – 5 days)
Trichomonas (3 – 21 days)
Herpes Simplex Virus (2 days onwards – maybe years)
Human Papilloma Virus (2 – 4 months, up to a year, vertical transmission possible)
Human Immunodeficiency Virus (HIV) – (seroconversion illness 2 – 6 weeks after exposure, HIV
antibodies almost always present after 3 months. Mean time to developing AIDS defining illness 9
– 12 years)
Hepatitis B (1 – 6 months)
Syphilis (9 – 90 days)
Non-specific urethritis
Pubic Lice (eggs – 2 weeks to mature, larvae – 1 week to mature)
Scabies (3 – 30 days, 6 weeks for itch to develop)
Hepatitis C and A may be sexually transmitted
Not necessarily sexually transmitted:
Normal anatomical variants
Commensals bacterial vaginosis
Dermatoses
Candidacies (commensals)
Molluscum contagiousum (3 weeks – months)
Urinary tract infections
Prostatitis
Vulval disorders

384 4
th
and 5
th
Year Notes
Tests for STD’s
Urethral swab or first pass urine for chlamydia
Anal or throat swab for gonorrhoea if appropriate
Female:
Cervical sample for gonorrhoea, chlamydia (endocervical cells needed)
Cervical smear
High vaginal swab for bacterial vaginosis, candida, trichomonas
Male: Urethral swab for gonorrhoea
Blood tests:
Hepatitis B (Ag and Ab) and C (Ab)
Syphilis: VDRL, TPHA
HIV Ab if appropriate with counselling and consent. Always attend for results
Vaginal Discharge
Cervical secretions in women not on the pill, and which change during the cycle, are part of normal
discharge. Mucus is clear or clear/white. Some inflammatory cells are normal in the latter half of a
cycle
Desquamating vaginal cells with healthy lactobacilli are major part of normal discharge – pH < 4.5
Key history questions:
Colour
Odour
Itch
Differential:
Thrush (Candidiasis): white curds, very itchy, not smelly
Trichomoniasis: grey/green discharge, fishy smell, moderate itch
Bacterial Vaginosis: green, fishy, itchy
Chlamydia: asymptomatic or discharge
Atrophic vaginitis: brown, spotty discharge (from bruising), pain, no itch. Treatment: oestrogen
cream or HRT
Bacterial Vaginosis
Trichomoniasis
Candidiasis
Prominent symptoms
Discharge odour
Discharge, vulval
irritation
Itch
Classical signs
No vulvitis or vaginitis
Vulvitis, vaginitis,
strawberry cervix
Vulvitis, vaginitis –
fissured and sore
Classical discharge
Greyish-white, thin, may be
frothy
Green/yellow, watery,
pools in posterior
fornix, may be frothy
White, flocculent,
thrush plaques
Risk factors
Pregnancy, antibiotics,
steroids, diabetes
Vaginal pH
pH > 4.5 (often 5.0 – 6.0)
pH > 4.5 (often 6.0 –
7.0)
pH < 4.5 (often 3.0)
KOH test
(amine/Whiff test)
Positive
Weakly positive
Negative
Wet mount
preparation
Clue cells present (vaginal
cells covered by anaerobes &
Gardnerella vaginalis).
Replacement of lactobacilli
with small coccobacilli
(Gardnerella) or motile
curved rods (Mobilunus).
Few pus cells
Trichomonads (motile
flagellate), pus cells
Yeast cells
(blastospores)
Gram stained smear
Clue cells: G-ive curved rods.
G variable coccobacilli.
Pus cells: acridine
orange stain

Reproductive and Obstetrics 385
Notes
Also called Gardnerella.
Multiplication of anaerobic
bacteria and gardnerella.
Associated drop in lactobacilli
Risk of prem delivery
Possibly commonest
STI worldwide –
mainly 3
rd
world. A
Protozoa. Doesn‟t
culture well. Can cause
PID, prem delivery.
Exclude gonorrhoea
Most common cause
of discharge
Candida albicans often
normally present.
Poor immunological
control recurrent
candidiasis
Treatment
Anti-anaerobe: oral
metronidazole
Oral: doxycycline
(remember 7 day rule)
Clotrimazole pessary
Neisseria Gonorrhoeae
Description: G –ive diplococci
Symptoms:
Male: 80% symptomatic. Discharge & dysuria (razor blade pain). 30% also have chlamydia
Female: only 20% symptomatic – can have vaginal discharge or pelvic pain. Pick up with
opportunistic/selective screening if under 25, multiple partners, changed partner in last 6 months,
IUCD, etc
Rectal and pharyngeal: often asymptomatic
Diagnosis: gram stain microscopy if symptomatic or contact, or culture on chocolate agar
Advice: no sex until minimum of 3 days since treatment completed
Treatment:
Amoxycillin 3 gm and Probenecid 1 gm stat (not longer standard due to penicillin resistant), or
Ciprofloxacin 500 mgs (a quinolone) stat if penicillin allergy or if resistant. Specialist
endorsement required. If resistant to that then Ceftriaxone (common in Auckland).
Azithromycin will cover gonorrhoea if it is being used to treat concurrent chlamydia
Resistance possible
Contact tracing required. Treat partners
Test for cure at 14 days (legal requirement)
Complications: See Pelvic Inflammatory Disease (PID), page 386
Chlamydia Trachomatis
Description: obligate intracellular bacteria, STIs are types D – K. Highest in 20 – 24 year age group
Symptoms:
Urethritis, unexplained cystitis, mucopurulent cervicitis, pelvic pain, irregular bleeding
80% of females and 50% of males have no symptoms. Suspect and test if sexual contacts have it,
if patients asks for STI tests, patients under 25 with new/multiple partners
Up to 30% associated with concurrent N Gonorrhoea infection
Diagnosis:
Female: swab from affected area, including from endocervix. Rotate 6 – 10 times. Urine test
alone not sufficient. Most common site of single infection is cervix (ie urine is clear)
Male: urine test
New PCR test easier sampling (urine test)
Opportunistic detection has been shown to reduce rates of PID and ectopic pregnancy
Advice:
Abstain until treated – if not use condoms
Contact trace
Treatment:
Without test results: Doxycycline 100mgs bd for 7 days (remember 7 day rule for patients on OC)
Known positive and partners: Azithromycin 1 g stat orally – directly observed treatment
In pregnancy: erythromycin ethylsuccinate 800mg qid for 7 days – must be treated to prevent
amnionitis and premature rupture of membranes
In PID: Doxycycline/erythromycin for 14 days and ornidazole 500 mgs bd for 7 days, plus
consider gonorrhoea in which case penicillin/ciprofloxacin in addition
Test of cure in 3 weeks if non-compliance or re-infection suspected. Urine test is adequate for
males and females
Test high risk patients only for cure
If reinfection, then ?untreated partner
386 4
th
and 5
th
Year Notes
Complications:
Neonatal: conjunctivitis, pneumonitis 2 – 4 weeks later
See Pelvic Inflammatory Disease (PID), page 386
Herpes Simplex Virus (Type 2)
See Herpes Simplex Virus (HSV), page 503
Pelvic Inflammatory Disease (PID)
~ Tubulo-peritoneal Disease
Cause: ascending infection of vagina and cervix to endometrium, fallopian tubes and other structures:
Chlamydia – often chronic
Gonorrhoea – often acute
Can also be anaerobes (e.g. after instrumentation of the uterus or long standing PID)
Symptoms: Acute pain, but 30% asymptomatic, dyspareunia (pain on sex)
Risk factors:
Young age (< 25)
Sexual activity, multiple partners, multiple infections
Postpartum infections
IUCDs in first several weeks after insertion
Decreased rates with condoms, diaphragms, spermicides (bacteria can use sperm as vector), tubal
ligation, OC pill
Diagnosis:
Difficult to make clinically: there are multiple causes of abdominal pain
Cervical motion tenderness (also occurs with ectopic pregnancy)
Purulent cervical/vaginal discharge
Oral temperature > 38 C
Irregular bleeding and break through bleeding on the OC pill
Ultrasound of no help. Test for other STIs. May require laproscopy
Treatment: Antibiotics must cover anaerobes, chlamydia and gonorrhoea. E.g. Doxycycline 100 mg bd
for 10 – 14 days plus an anti-anaerobe such as metronidazole or ornidazole
Sequalae:
Often repeat episodes due to:
Continued at risk behaviour
Partner is not treated
Past infection compromises cilia of the fallopian tubes making another infection more likely
Infertility risk after 1 infection is 11%, but up to 54% after 3 infections
Other sequalae: ectopic pregnancy, adhesions, chronic pelvic pain
Reiter’s Syndrome*
Triad of arthritis (big joints – hot, red swollen, bilateral), urethritis and conjunctivitis
10:1 are males, usually 25 – 35 years
Often (not always) caused by chlamydia (an immunological reaction, HLA B27+ more susceptible)
Treatment: treat residual infection, if any
See Reiter‟s Syndrome, page 276
Genital Warts
Can get anal warts without anal intercourse
External warts usually benign (types 6 & 11 – not oncogenic)
Treatment:
Destructive: Condyline, liquid nitrogen – high recurrence rate
Imiquimod – topical cream, up-regulates immune system, expensive ($150 per month), 19%
recurrence, requires treatment for 8 – 12 weeks
A vaccine is at stage 3 trials
Non-Sexually Transmitted Genital Skin Lesions
Not all skin lesions on the genitals and surrounding areas are due to STDs
Normal anatomical variants:
Pearly penile papules: small papillae around the corona of the penis
Sebaceous cysts of the penis, labia minora and scrotum
Reproductive and Obstetrics 387
Normal papillae in the vaginal vestibule: can be mistaken for warts
Dermatoses:
Contact dermatitis: soaps, deodorants, etc
Psoriasis: especially head and corona of the penis. Red, scaly plaques. Not itchy. Look for it
elsewhere
Reiter‟s Syndrome: urethritis, conjunctivitis, arthritis in addition to skin lesion
Lichen Planus: itchy plaques on the penis
Infections (not necessarily sexually acquired):
Seborrhoeic dermatitis: a fungus, red, sharply defined area covered with honey coloured scales
Candidiasis: red, irritating, itchy rash. Treat with Clotrimazole (Canesten)
Dermatophyte infections (tinea) are common. Characteristic spreading edge, itchy
Folliculitis: small pustule around a hair follicle
Scabies: red, itchy nodules – may not resolve despite treatment. Treat with malathion 0.5%
Erythrasma: scaly, flat, brown, pigmented rash, not itchy. Caused by corynebacterium
Molluscum contagiosum: may be sexually acquired. Small, pearly umbiliated lesions on the thigh
and buttocks
HIV
See AIDS, page 308

Index
-agonist, 79
-blockers, 42, 50, 52
-feta Protein, 193, 469
HCG, 469
5 Reductase Inhibitors, 225
5HT3 Antagonists, 471
A-a Gradient, 58
Abdominal Pain
in Children, 643
Abdominal Radiology, 157
Abductor Lurch, 251
Abetalipoproteinaemia, 165
ABO Blood Incompatibility, 596
Absence Seizures, 134
Absorption of Drugs, 523
Abuse
Child, 656
Management of, 659
Physical, 343
Sexual, 339, 343
Acanthosis, 314
ACC, 284
Accessory Nerve, 118
Accident Compensation
Corporation, 284
Accommodative Esotropia, 632
ACE Inhibitors, 50, 51
Acetylation, 525
Achalasia, 159
Achilles Tendon Rupture, 258
Acid-Base Balance, 113
Acitretin, 336
Acne, 330
Aconotmesis, 237
Acoustic Neuroma, 152
Acrodermatitis Enteropathica,
647
Acromegaly, 107
ACTH, 102, 104
Actinic Keratosis, 326
Activated Charcoal, 488
Activated Partial Thromboplastin
Time, 292
Acute Bacterial Endocarditis, 46
Acute Cholecystitis, 196
Acute Disseminated
Encephalomyelitis, 132
Acute Enterocolitis, 176
Acute Hepatitis, 184
Acute Inflammatory
Demyelinating
Polyradiculopathy, 139
Acute Interstitial Nephritis, 211
Acute Interstitial Pneumonia, 84
Acute Leukaemia, 300
Acute Pancreatitis, 197
Acute Papillary Necrosis, 211
Acute Pharyngitis, 63
Acute Renal Failur
Pre-renal, 205
Acute Renal Failure, 205
Intrinsic, 206
Post-renal, 206
Acute Stress Disorder, 424
Acute Suppurative Appendicitis,
167
Acute Tubular Necrosis, 211
Acyclovir, 515
Addiction, Aetiology of, 446
Addison‟s Disease, 69, 103
Addisonian Crisis, 103
Adenocarcinoma, 89
Colon, 173
Oesophageal, 159
Adenomyosis, 347
Adenosine, 42
Adenosine Deaminase
Deficiency, 307
Adenosquamous carcinoma, 89
Adenovirus, 64, 70
Eye Infection, 144
ADH, 104
ADHD, 572, 659
Adhesive Capsulitis, 244
Adjustment Disorder, 421
Adnexa Oculi, 632
Adolescent Development, 664
Adolescent Health, 664
Adrenal Cortex, 102
Adrenal Hyperplasia, 102
Adrenarche, 667
Adrenogenital Syndrome, 638
Adriamycin, 382
Adult Polycystic Kidney, 216
Adult Respiratory Distress
Syndrome, 83, 482
Adverse Reactions
Drug Reactions, 529
Vaccination, 517
Adverse Selection, 699
Affinity, 528
AFP. See -feta Protein
Afterload, 14
Aganglionic Megacolon, 640
Ageing, 672
Agenesis, 466
Agonists, 527
Agoraphobia, 423
AIDS, 308
Airway Management, 476
Airway Obstruction, 485
Akathisia, 438
Albumin, 183
Alcohol Abuse, 450
Alcohol Regulation, 697
Alcoholic Dementia, 441
Alcoholic Liver Disease, 185
Aldosterone, 102
Alfentanil, 544
Algodystrophy, 283
Alkylating Agents, 299
Allergic Alveolitis, 310
Allergic Dermatitis, 321
Allergic Rhinitis, 63
Allergy, 63, 309, 319, 320, 321,
483, 531, 647
Allocative Efficiency, 698
Allopurinol, 278
Allylamine, 336
Alma Ata Declaration, 562
Alogia, 436
Alopecia Areata, 333
ALP, 183
Alpha-1 Antitrypsin Deficiency,
82, 194
ALT, 182
Alveolar Proteinosis, 92
Alzheimer‟s Dementia, 440
Ambiguous Genitalia, 638
Amblyopia, 147
AMBU Bag, 477
Ameloblastoma, 157
Amenorrhoea, 106, 345
Post Pill, 106
Aminoglycosides, 514, 533
Amiodarone, 41, 42
Amniocentesis, 360
Amoebiasis, 509
Amoxycillin, 513
Amphotericin, 515
Amylase, 10
Amyloidosis, 209, 302, 303
Amyotrophic Lateral Sclerosis,
133
Anaemia, 209, 287
in Children, 646
Neonatal, 589
of Chronic Disease, 291
Anaesthetics, 539
Dose Calculations, 540
Inhalational, 541
Intravenous, 541
Obstetric, 545
Paediatric, 655
Anal Cancer, 179
Anal Fissures, 179
Anal Warts, 179
Anaphylaxis, 483
ANCA, 212, 270
Androgen resistance, 638
Androgens, 102
Anencephaly, 466, 631
Angelman Syndrome, 465
Angina Pectoris, 36
Angiomyolipoma, 217
Angiosarcoma, 192
Angular Cheilitis, 322
Angular Stomatitis, 155
Anhedonia, 436
Aniomyolipoma, 217
Anion Gap, 113
Anisometropia, 148
Ankle, 257
Ankylosing Spondylitis, 171,
274
Anorchia, 636
Anorexia Nervosa, 420, 453
Anoxic Seizures, 628
Antagonists, 527
Antalgic Gait, 250
Antenatal Booking, 355
Antepartum Haemorrhage, 366
Anterior Cruciate Ligament, 254,
255
Anterior Draw Test, 254
Anterior Uveitis, 275
Anti EBNA, 505
Antibasement Membrane
Antibody Disease, 92, 214
Antibiotic Fever, 531
Antibiotic Treatment, 511
Anticipatory Guidance
Neonatal and Infants, 568,
590
Anticonvulsants, 135
Anti-D, 367
Antidepressant Medication, 432
Antidepressants
MAOIs, 434
SSRIs, 433
Tricyclics, 432
Antifungals, 336, 515
Antigliadin Antibodies, 164
Antihistamines, 43
Antiparkinsonian Medication,
438
Antiphospholipid Syndrome,
270, 294
Antipsychotic Medication, 437
Antisocial Behaviour
in Children, 573
Antisocial Personality Disorder,
455
Antithrombin 3, 293
Anuploidy, 464
Anxiety and Depressive
Symptoms, Differentiating,
426
Anxiety Disorders, 420, 422
in Children, 661
Treatment, 424
Aorta, Traumatic Rupture of,
491
Aortic Aneurysm, 32
Aortic Knuckle, 28
Aortic Regurgitation, 22, 44
Aortic Stenosis, 22, 43
Apex Beat, 21
APGAR, 588
APH, 366
Aphthous Ulcers, 158, 168, 169
Aplasia, 466
Aplastic Anaemia, 289
Apnoea, 588
Appendicitis, 167
Appetite, 94
APTT, 292
Arapax, 434
ARDS, 83, 482
Arnold Chiari Malformation, 624
Arrhythmias
Cardiac Arrest, 479
Congential, 601
Drug Treatment, 42
Non-arrest, 40
Artefacts of Blood Tests, 9
Arterial Blood Gases, 58
Interpretation of, 115
Arteriosclerosis, 33
Hylaine, 33
Hyperplastic, 33
Arterio-venous Malformations,
124
Arteritis, 33
Arteritis Syndromes, 282
Arthralgia, 230
Arthritis, 266
Differential in, 266
Inflammatory, 270
Inflammatory, Systemic Signs
of, 230
Osteoarthritis, 268
Radiology, 267
Septic, 259
Seronegative, 274
Arthritis Mutilans, 275
Arthrocentesis, 259
Arthrodesis, 269
Arthroplasty, 269
Asbestosis, 85
Cholangitis, 197
Aschoff Bodies, 603
Ascites, 194
Ultrasound for, 157
Aseptic Meningitis, 499
Asperger‟s Syndrome, 582
Aspergillus, 69
Aspiration, 614
Risk Factors for, 655
Aspirin
Anticoagulant Effects, 294
Assisted Human Reproduction,
722
AST, 182
Asteatotic Eczema, 322
Asterixis, 8
Asthma, 77
Emergency Management, 485
in Children, 78, 613
Astrocytes, 136
Astrocytoma, 136
Asystole, 480
Atherosclerosis, 31
Athlete‟s Foot, 317
ATN, 211
Atonic Neck Reflex, 624
Atopic Dermatitis, 648
Atopic Eczema, 319
Atopy, 310
Atrial Fibrillation, 26, 40
Atrial Flutter, 26, 41
Atrial Septal Defect, 599
Atrial Tachycardia, 41
Atrioventricular Block, 42
Atropine, 42
Atrovent, 614
Attachment, 573
Attachment Disorder, 573
Attention Deficit/Hyperactivity
Disorder, 572, 659
Attribution Theory, 571
Atypical Lymphocytes, 287
Audiometry, 150
Auditory Brainstem Response,
150
Auer Rods, 287
Auerbach‟s Plexus, 640
Augmentin, 513
Autism, 419, 582
Autonomy, 716, 717
Autonuclear Antigens, 270
Autopsy
Child, 569
Autosomal Dominant, 464
Autosomal Recessive, 464
Avascular Necrosis, 235
Avoidant Personality Disorder,
455
Azathioprine, 272
Back Pain, 239
Management, 242
Red Flags, 241
Background Retinopathy, 146
Back-knee Gait, 250
Bacteraemia, 494
Bacterial Overgrowth of Small
Intestine, 176
Bacterial Vaginosis, 384
Bacteroides Fragilis, 502
Bacteruria, 219
Balanced Anaesthesia, 540
Balanitis, 634, 637
Barium Enema, 157
Barlow‟s Test, 619
Barton‟s Fracture, 248
Barts, 551
Basal Cell Carcinoma, 327
Basal Cell Papilloma, 326
Basal Pontine Syndrome, 126
Base Excess, 115
Battle‟s Sign, 150
Beck‟s Triad, 491
Beclometasone Dipropionate, 79
Becotide, 79
Bed Rest, 674
Bed Wetting, 635
Bee Sting Allergy, 310
Behaviour Management
Children, 570
Behavioural Change, 11
Behcet‟s Disease, 283
Benediction Hand, 247
Beneficence, 716
Benign Focal Epilepsy of
Childhood, 626
Benign Paroxysmal Positional
Vertigo, 148
Benign Paroxysmal Vertigo of
Infancy, 625
Benign Prostatic Nodular
Hyperplasia, 224
Bennett‟s Fracture, 249
Bense-Jones Proteins, 303
Benzodiazepines, 425
Bereavement, 458
Berger‟s Disease, 214
Beriberi, 49
Berry Aneurysm, 124
Bezoar, 166
Bias, 683, 703
in Screening, 690
Bile Acid Sequestrants, 53
Bile Duct Adenoma, 192
Bile Ducts, 195
Bile Salts, 183
Biliary Colic, 195
Bilirubin, 595
Binswanger Disease, 441
Bioavailability, 523
Biophysical Profile, 360
Biostatistics, 683
Biotinidase Deficiency, 466
Bipolar Depression, 431
Bivalve Speculum, 340
Bladder, 223
Bladder Infections, 219
Bladder Tumours, 223
Bleeding Time, 294
Blepheritis, 143
Blood Culture, 494
Blood Gases, 58
Interpretation of, 115
Blood Loss, 552
Blood Pressure, 19, See also
Hypertension
Hypotension in Post-op
Patient, 557
Paediatric Normal Values,
565
Blood Products, 552
Blood Tests, 9
Blood Transfusion, 552
Blood Volume, 550, 649
Blue Baby, 596
Blue Bloater, 81
Body Dysmorphic Disorder, 444
Bone Cancer
Secondary, 266
Bone Marrow Transplantation,
300
Bone Pain, 544
BOOP, 84
Borderline Personality Disorder,
455, 456
Bordetella Pertussis, 609
Borrelia Burgdorferi, 316
Bottle Feeding, 591
Bouchard‟s Nodes, 269
Boutonniere Deformity, 249
Bovine Spongiform
Encephalopathy, 441
Bowel Obstruction, 166
Bowen‟s Disease, 226, 323, 326
Boxer‟s Fractures, 621
BPPV, 148
BRAC Gene, 380
Brachial Plexus Injury, 245
Bradford Hill Criteria, 685
Bradycardia
Drug Treatment, 42
Brain Abscess, 498
Brain Death, 713
Brain Tumours, 136
Branchial Cysts, 648
Branhamella Catarrhalis, 502
Braxton-Hicks Contractions, 367
Breast, 375
Breast Cancer, 379
Treatment of, 381
Breast Discharge, 377
Breast Disease
Inflammatory, 377
Breast Feeding, 376, 590
Drugs and, 529
Breast Milk
Nutritional Deficiencies in,
647
Breast Milk Jaundice, 596
Breast Screening, 382
Breathlessness, 17
Palliative management of, 472
Breech, 370
Bretyllium, 42
Brief Psychotic Episode, 435
Brodie‟s Abscess, 260
Bromocriptine, 106
Bronchial Breathing, 61
Bronchiectasis, 82, 615
Bronchioalveolar carcinoma, 89
Bronchiolitis, 610
Bronchiolitis Obliterans
Organising Pneumonia, 84
Bronchitis, 608
Bronchitis, Chronic, 81
Bronchopneumonia, 67
Broncho-Pulmonary Dysplasia,
589
Brutons, 307
Budd Chiari Syndrome, 193
Budesonide, 79
Buerger‟s Disease, 283
Bulbar Palsy, 131
Bulimia Nervosa, 420
Bullying, 662
Bundle Branch Block, 25
Bupivacaine, 545
Burnout, 711
Burns, 486
in Children, 654
Bursitis, 256
Button Hole Deformity, 249
Butyrophenone, 438
BZDs
Prescription, 536
Withdrawal, 534
C Cell Carcinoma, 101
C6 Radiculopathy, 123
C7 Radiculopathy, 123
Ca Channel Blockers, 52
CA125, 469
Cachectia, 5
Caesarean Section, 371
CAGE Questions, 450
Calcanial Gait, 251
Calcification, 32
Calcitrol, 210
Calcium, 27
Calcium Pyrophosphate
Deposition, 278
Campylobacter Jejuni, 177
Cancer, 466
in Children, 648
Cancer Emergencies, 472
Candidiasis, 64, 69, 318, 323,
384
Cannabis, 448, 697
Cannulation, 554
Caplan's syndrome, 85
Caput Medusae, 156
Caput Succedaneum, 369
Carbamazepine, 135
Carbimazole, 99
Carbuncle, 316
Carcinogenesis, 467
Carcinoid Syndrome, 171
Carcinoid Tumour, 89, 171
Carcinoma
Gallbladder, 197
Gastric, 163
Cardiac Arrest
Drug Treatment, 480
Rhythms, 479
Cardiac Asthma, 48
Cardiac Axis, 26
Cardiac Output, 14
Cardiac Pacing, 43
Cardiac Sclerosis, 193
Cardiac Sphincter, 158
Cardiac Tamponade, 491
Cardiogenic Shock, 483
Cardiomyopathy, 54
Cardiopulmonary Resuscitation,
476
Cardiotocography, 360, 371
Cardiovascular Risk factors, 30
Cardioversion, 40, 479
Carotid Pulses, 19
Carpal Tunnel Syndrome, 123,
238, 249
Case-Control Study, 685, 703
Casts
in Urine, 203
Cataract
Congential, 148
Catheterisation, 220
Cavernous Haemangioma, 192
CDC Epidemiology Group, 687
CEA, 469
Cefazolin, 513
Cefipime, 513
Ceftriaxone, 513
Cefuroxime, 513
Cellulitis, 314, 316
Central Pontine Melanosis, 108
Central Retinal Vessels,
Occlusion of, 145
Centre for Adverse Reactions
Monitoring, 530
Ceoliac Disease, 164
Cephalosporins, 513
Cerebellar infarction, 140
Cerebral Palsy, 629
Cerebral Perfusion, 15
Cerebro-spinal Fluid, 123
Cervical Cancer, 351
Staging, 468
Cervical Glandular Neoplasia,
352
Cervical Intraepithelial
Neoplasia, 352
Cervical Lumps, 648
Cervical Screening, 352
Cervical Spondylosis, 238
Chalazion, 143
Charcot‟s Joint, 235
Charcot-Marie Tooth Disease,
132
Chemotherapy, 470
in Breast Cancer, 381
Chest Pain, Differential of, 16
Chest Radiology, 27
Chest Sounds, 61
Cheyne-Stokes Respiration, 91
Chicken Pox, 504
Chicken-Broth Ascites, 198
Child Abuse, 656
Child Development, 574
Child Health
Determinants of, 562
Measures of, 561
Child‟s Body Weight, 550
Child-Pugh Classification, 185
Children, Young Persons and
Their Families Act, 659
Chlamydia
Eye Infection, 144
Trachomatis, 383
Chlamydia Trachomatis, 385
Chloride, 113
Chloroquine, 509
Chlorpromazine, 438
Choanal Atresia, 595
Chocking, 485
Cholangiocarcinoma, 192
Cholangiocytes, 183
Cholangitis, 195
Ascending, 193
Cholecystitis, 195
Cholelithiasis, 195
Choleocystoduodenal Fistula,
166
Cholestasis, 183
Cholesterol, 53
Cholesterol Stones, 195
Cholestyramine, 170
Chondroblastoma, 265
Chondrocalcinosis, 278
Chondrodermatitis, 323
Chondromalacia Patellae, 256
Chondrosarcoma, 265
Chorea, 603
Choriocarcinoma, 227, 363
Chorionic Villous Sampling, 360
Choroid Plexus Papilloma, 137
Chromosome Disorders, 464
Chronic Active Hepatitis, 185
Chronic Bronchitis, 65, 81
Chronic Cholecystitis, 196
Chronic Disease
Effect on Child Development,
582, 669
in Adolescents, 582, 669
Chronic Fatigue Syndrome, 506
Chronic Granulocytic
Leukaemia, 298
Chronic Hepatitis, 185
Chronic Infiltrative (Restrictive)
Lung Disease, 84
Chronic Leukaemia, 300
Chronic Lymphocytic
Leukaemia, 304
Chronic Myeloid Leukaemia,
298
Chronic Obstructive Pulmonary
Disease, 80
Chronic Pancreatitis, 198
Chronic Pelvic Pain, 350
Chronic Persistent Hepatitis, 185
Chronic Renal Failure, 207
Complications of, 209
Chvostek‟s Sign, 112
Chylothorax, 604
Cigarette Smoking, 87
CIN, 352
Ciprofloxacin, 515
Circinate Balanitis, 276
Circumduction Gait, 251
Cisplatin, 90
CJD, 441, 500
CK, 38
CK – MB fraction, 38
Clarithromycin, 514
Classes of Drugs, 536
Clear Cell Renal Cell
Carcinoma, 217
Clearance of Drugs, 522
Cleft Lip, 618
Clinical Practice Guideline, 703
Clinical Trials, 536
Clinodactyly, 581
CLL, 300
Clonidine withdrawal, 534
Clostridium Botulinum, 177
Clostridium Difficile, 176
Clostridium Perfringens, 316,
502
Clozapine, 438
Club Foot, 619
Clubbing, 7
Clue Cells, 384
CML, 300
CMV, 191, 506
Coagulation, 292
Coal Tar, 335
Coal Workers Pneumoconiosis,
85
Coarctation of the Aorta, 600
Cochrane Collaboration, 702
Cockcroft-Gault Formula, 203,
525
Code of Health and Disability
Services Consumer‟s Rights,
712
Cognition, Assessment of, 416
Cognitive Behavioural Therapy,
424, 429, 457
Cognitive Development, 578
Cognitive Functions, 122
Cohort Effect, 673
Cohort Studies, 686
Colchicine, 278
Cold Chain, 517
Cold Sores, 503
Colic, 593
Colitis, 165
Collagenous Colitis, 179
Collateral Ligaments of the
Knee, 255
Colles Fracture, 248
Colloids, 551
Colonic Embryonic Antigen, 174
Colorectal Cancer, 171
Coma, 486
in Children, 651
Myxoedema, 99
Coma and Stupor, 117, 130
Combes Test, 290
Combined Oral Contraceptive,
341
Combined Variable
Immunodeficiencies, 307
Comedo, 314
Common Cold
in Children, 605
Common Peroneal Nerve, 123
Communicable Disease Control,
686
Community Acquired
Pneumonia, 70
Compartment Syndrome, 234
Chronic, 236
Competency
Assessment of, 714
Complement Deficiencies, 307
Complex Regional Pain
Syndrome, 283
Compliance, 528, 535
Compulsion, 718
Compulsory Treatment, 458
Condyloma, 226
Accuminatum, 318
Confidence Interval, 684
Confidentiality, 716
Confounding, 684, 703
Confusion
Differential in an Alcoholic,
451
Differential of, 443
Congenital Adrenal Hyperplasia,
466
Congenital Diaphragmatic
Hernia, 642
Congenital Dislocation of the
Hip, 618
Congenital Heart Disease, 598
Congenital Naevocellular
Naevus, 325
Congestive Heart Failure, 48
Congestive-Dilated
Cardiomyopathy, 54
Congo Red Stain, 209, 212
Coning, 130
Conjunctivitis, 143
Neonatal, 632
Conn‟s Syndrome, 104
Connective Tissue Diseases, 278
Consent, 717
Consolidation, 62
Constipation, 177
in Children, 643
Constitutional Delay, 586
Consultation Frameworks, 4
Contact Allergies, 310
Contact Dermatitis, 321
Contraception, 340
Contraception, Sterilisation and
Abortion Act 1977, 361
Controlled Release
Formulations, 527
Conversion Disorder, 444
Coombs-Gell Types, 531
Co-ordination, 121
COPD, 80
Cord Prolapse, 369
Corda Equina Syndrome, 139
Cordocentesis, 360
Cornerstones of Maori Health,
696
Coroid Plexus, 123
Coronary Heart Disease, 33
Coronary Perfusion, 15
Coronavirus, 64
Coroner, 713
Child Death, 570
Corrigan‟s Sign, 44
Cortisol, 102
Corynebacterium Diphtheriae,
64
Coryza, 8
Cost Effectiveness, 699
Cost Minimisation, 699
Cost Utility, 699
Cost-Benefit, 699
Cotrimoxazole, 515
Cotton wool spots, 145
Cough, Differential of, 16
Counselling
Genetic, 466
Counter-transference, 666
Cows Milk, 591
CPAP, 60
CPR, 476
Adult, 477
Paediatric, 478
CPR Efficacy, 481
Crackles, 61
Cranial Nerves, 118
Examination in Children, 622
Craniopharyngioma, 105, 138
Creatinine, 203
Creatinine Clearance, 525
Crepitations, 61
CREST Syndrome, 280
Creutzfeldt-Jakob Disease, 441,
500
Cri du Chat Syndrome, 464
Cricothyrotomy, 477
Crises, Medical, 711
Critical Medical Incidents, 711
Critically Appraised Topic, 702
Cross-sectional Studies, 685
Croup, 64, 66, 608
Crowning, 369
Crying Baby, 592
Cryoprecipitate, 553
Cryptococcus neoformans, 69
Cryptogenic Fibrosing
Alveolitis, 84
Cryptorchidism, 375, 636
Cryptosporidium, 177, 510
Crystal Arthropathy, 277
Crystalloids, 551
CSF, 123
CTG, 360, 371
Cushing‟s Disease, 102
Cutaneous Horn, 323
CVID, 307
Cyanosis, 18, 58
in the neonate, 597
Cyclophosphamide, 299, 382
Cystic Fibrosis, 466, 614, 615
Cystic Renal Disease, 216
Cystic Renal Dysplasia, 216
Cystitis, 219
Cytochrome P450, 525, 532
Cytoid Bodies, 145
Cytomegalovirus, 70, 191, 506
Cytotoxic Hypersensitivity, 309
Dactylitis, 276
D-dimmer test, 77
De Cubitus View, 29
De Quervain‟s Disease, 98
De Quervain‟s Syndrome, 249
Death
Certification of, 712
Changes following, 713
Diagnosis of, 481, 712
Death Certificate, 713
Declaration of Helsinki, 723
Deep Vein Thrombosis, 74, 557
Defibrillation, 478
Dehiscence, 558
Dehydration, 110
Assessment
in Children, 650
Treatment of, 550
Delayed Hypersensitivity, 309
Delayed Puberty, 668
Delirium, 420, 442
Delusional Disorder, 435
Delusions, 412, 415
Dementia, 420, 439
Demographic Transition, 689
Demyelinating Disease, 132
Dentate Line, 179
Deontological Moral Theories,
716
Dependent Personality Disorder,
455
Depersonalisation, 415
Depot-provera, 342
Depression
in Adults, 426
in Children and Adolescents,
662
Depressive Disorders, 426
Derealisation, 415
Dermal Melanocytic Naevus,
325
Dermatitis, 319
Dermatofibroma, 326
Dermatoheliosis, 323
Dermatology, 313
Glossary, 314
Dermatomyositis, 281
Dermatophyte Infections, 387
Dermatophytosis, 317
Dermis, 314
Dermoid Cysts, 648
Descriptive Studies, 685
Desquamative Interstitial
Pneumonia, 84
Detrussor Instability, 223
Development
Adolescent, 664
Child, 574
Cognitive, 578
Developmental Assessment, 575
Developmental Delay, 579
Hearing, 580
Developmental Dysplasia of the
Hip, 618
Developmental Quotient., 575
DEXA Scan, 262
Dexamethasone Suppression
Test, 102
Dextran, 551
Dextrocardia, 21
Dextrose, 551
Di George Syndrome, 100
Diabetes Insipidous, 109, 110
Diabetes Mellitus, 94
Foot Infections, 316
Gestational, 363
IDDM in Pregnancy, 364
Neonatal Complications, 596
Nephropathy in, 207
Retinopathy, 146
Type 1 (Juvenile Onset). See
Diabetes Mellitus
Diagnostic and Statistical
Manual of Mental Disorders,
419
Dialysis, 218
Diarrhoea, 154
in Children, 643, 644
Infectious Agents, 176
Diastasis, 257
Diastematomyelia, 631
DIC, 293
Dietary Fibre, 178
Differential Diagnosis, 10
Diffuse Alveolar Damage, 83
Diffuse Progressive Systemic
Sclerosis, 280
Diffusing Capacity, 59
Digesic, 470
Digoxin, 27, 41, 42, 53, 533
Dihydrotestosterone, 224
Diltiazem, 41, 52
Diphtheria, 64, 132
Vaccination, 518
Disability, 673
Disability Adjusted Life Years,
683
Disc Prolapse, 240
Discoid Eczema, 322
Discoid Lupus Erythematous,
279, 330
Disease Modifying Anti-
Rheumatic Drugs, 271, 273
Dissecting Aneurysms, 32
Disseminated Intravascular
Coagulation, 293
Disseminated Superficial Actinic
Porokeratosis, 323
Dissociative Disorders, 420
Distribution of Drugs, 524
District Health Boards, 681
Diuretics, 43, 50, 51
Diverticular Disease, 174
Diverticulitis, 174
Diverticulosis, 174
Dizygotic twins, 358
DMARDs, 271, 273
DMSA Scan, 204, 222
DNR Orders, 482
Do Not Resuscitate Orders, 482
Dobutamine, 53
Doctor‟s Health Advisory
Service, 712
Dog Bites, 316
Dohle Bodies, 287
Doll‟s Eye, 130
Domestic Violence, 574
Dopamine, 43, 53, 106
Dorsal Dermal Sinus, 631
Double Effect, Doctrine of, 720
Down Syndrome, 581, 639
Doxycycline, 515
D-Penicillamine, 272
Driving by the Elderly, 676
Droopy Eye Lid, 145
Drop Foot Gait, 251
Drowning, 487
Drug Allergy, 530
Drug and Alcohol Policy, 697
Drug Education, 457
Drug Interactions, 531
Drug Withdrawal Syndromes,
533
Drugs of Abuse, 448
Regulation of, 536
Dry Mouth, 158
DSM IV, 414, 419
Dual Diagnosis, 421, 446
Duct Ectasia, 377
Ductus Arteriosus, Patent, 599
Duke‟s Staging, 174
Duodenal Atresia, 639
Duodenum, 161
Dupuytren‟s Contracture, 8, 249
DVT, 74, 557
With Contraceptives, 342
Dysarthria, 131
Dysdiadokinesia, 121
Dysfunctional Uterine Bleeding,
346
Dyshidrotic Eczema, 322
Dyslipidaemia, 30
Dysmenorrhoea, 346
Dyspareunia, 345
Dyspepsia, 159
Dysphagia, 131, 158
Dysphonia, 66, 131
Dyspnoea
Differential in Children, 604
Dyspraxia, 439
Dysthymic Disorder, 430
Dystonias, 132
Dysuria, 220
E Coli, 67
Ear Testing, 150
Eating Disorders, 420, 453
EC50, 528
Ecchymoses, 314
ECG
Changes in Pregnancy, 363
Interpretation, 24
Echinococcus Granulosa, 510
Echocardiogram, 49
Echolalia, 582
Eclampsia, 366
Economic Evaluations, 699
Ecthyma, 315
Ectopic Beats, 26
Ectopic Pregnancy, 362
Ectopic Thyroid, 648
Ectropion, 675
Eczema, 319
Eczema Herpeticum, 503
Education, 11
Parent and Adolescent, 567
EEG
in Children, 627
Efficacy, 528, 703
Efficiency, 698, 703
Effusion, 73
Eisenmenger‟s Syndrome, 602
Ejection Fraction, 14
Elastin Van Geesen, 31
Elbow Injury, 246
Elder Abuse, 675
Elderly, 671
Electrocution, 487
Electrolyte Abnormalities, 487
Electrolyte Concentrations, 550
Electro-Mechanical Dissociation,
479
Electrophoresis, 184
Elephantitis, 509
Elimination, 522
Embolic Infarction, 128
Embryonal Carcinoma, 227
Emergency Contraception, 343
Emergency Management
in Children, 649
Emotional Abuse, 658
Emphysema, 81
Empyema, 73, 612
Encephalitis, 140, 499
Encephalocele, 631
Enchondroma, 265
Encopresis, 643
Endocardial Fibroelastosis, 54
Endometrial Cancer, 354
Endometrial Thickness, 355
Endometriosis, 347
Endomyocardial Fibrosis, 54
Endomysial Antibodies, 164
Endoscopy, 157
Endotracheal Intubation, 477
Energy Metabolism, 555
Entamoeba Histolytica, 509
Enteral Nutrition, 555
Enteropathic Arthropathies, 277
Enteroviruses, Non-polio, 617
Enthesitis, 236, 275
Enuresis, 635
Environmental Health, 688
Ependymal Cells, 136
Ependymoma, 136, 137
Epicondyle Fractures, 620
Epidemics, 687
Epidemiology, 685
Mental Health, 410
Epidermal Cyst, 325
Epidermal Naevi, 325
Epidermis, 314
Epidermolysis Bullosa, 335
Epididymo-orchitis, 226
Epididymo-Orchitis
in Children, 637
Epidural Anaesthetic
in Labour, 546
Epiglottis, 66
Epiglottitis, 65, 609
Epilepsy, 133
in Children, 626
Epilim, 135
Epiphora, 148
Episcleritis, 143, 170
Epispadias, 226
Epistaxis, 63
EPS, 438
Epstein Barr Virus, 64, 191, 505
Equipoise, 724
Equity, 680, 698
Erb‟s Palsy, 245
Ergometrine, 369, 373
Erysipelas, 316, 500
Erythema, 314
Erythema Infectiosum, 618
Erythema Marginatum, 603
Erythema Multiforme, 332
Erythema Nodosum, 168, 169,
332
Erythema Toxicum Neonatorum,
333
Erythrasma, 387
Erythrocyte Sedimentation Rate,
290
Erythrocytosis, 297
Erythroderma, 335
Erythromycin, 514
Erythroplakia, 158
Erythroplasia of Queyrat, 226
Erythrovirus, 618
Escape Beats, 26
Escharotomy, 486
Escheria Coli, 177
Escherichia Coli, 502
ESR, 290, 687
Essential Thrombocythaemia,
298
Ethics, 715
Ethics Committees, 723, 724
Etoposide, 90
Euthanasia, 719
Evaluation
Diagnostic Tests, 704
History Taking and Clinical
Examination, 704
Prognosis, 707
Therapy, 706
Event Rate, 704
Evidence Based Medicine, 701
Ewing‟s Tumour, 266
Excretion of Drugs, 524
Executive Function, 122
Exfoliative Dermatitis, 335
Exomphalos, 641
Exophthalmos, 98
Exostosis, 149, 266
Extensor Lurch, 251
External Validity, 683
Extractable Nuclear Antigens,
270
Extradural Haemorrhage, 124
Extradural Spinal Cord
Compression, 138
Extrahepatic Biliary Atresia, 194
Extramedullary Haematopoiesis,
296
Extrapyramidal Syndromes, 438
Extrasystole Beats, 26
Extrinsic Allergic Alveolitis, 85
Extrinsic Pathway, 292
Exudate, Pleural, 73
Eye Disorders in Children, 631
Eye Trauma, 142
Facial Nerve, 118
Facilitation, 543
Factor V Leiden, 293
Failure to Thrive, 591, 642
Fainting, 131
Falls in the Elderly, 674
Familial Adenomatous
Polyposis, 172
Families, 568
Farmer‟s Lung, 85
Fast Acetylators, 525
Fatty Streaks, 31
Febrile Convulsion, Benign, 627
Fecundability, 344
Femoral Anteversion, 619
Femoral Epiphysis
Slipped Upper, 621
Femoral Shaft Fractures, 621
Femur, 252
Fentanyl, 544
Ferritin, 290
Fetal Alcohol Syndrome, 624
Fetal Distress, 372
Fetal Growth Restriction, 360
Fetal Position, 368
Fetal Welfare, 359
FEV1, 58
Fever, 5
in Children, 5, 616
in Neutropenic Patient, 6, 301,
470, 472
of Unknown Origin, 6
Fibre, 178
Fibric-acid Derivatives, 53
Fibroadenoma, 378
Fibroids, Uterine, 347
Fibromuscular Dysplasia, 33
Fibromyalgia, 284
Fibrosarcoma, 266
Fictitious Disorder, 454
Fictitious Disorders, 420
FIGO System, 468
Filariasis, 509
Finckelstein‟s Sign, 249
Flagyl, 515
Flail Chest, 491
Flat Foot Gait, 251
Flecainide, 41
Flexatide, 79
Floppy Valve Syndrome, 45
Flow-volume Loop, 59
Flucloxacillin, 513
Fluconazole, 515
Fluid Compartments, 550
Fluid Loss, Assessment, 650
Fluoxetine, 434
Fluticasone Propionate, 79
Focal and Segmental
Glomerulosclerosis, 214
Folate, 630
Follicular Carcinoma, 100
Folliculitis, 316, 387
Food Allergy, 647
Foot Slap Gait, 250
Forceps, 371
Foreign Body, Inhalation of, 614
Foreskin
Retraction of, 637
Formulation, 5
Psychiatric History, 414
Fournier‟s Gangrene, 226
Fovea, 141
Fracture, 232
Complications of, 234
Healing of, 233
of Clavicle, 245
of Femoral Neck, 253
of Femur, 253
of Fibula, 257
of Head of Radius, 246
of Humerus, 246, 620
of Mandible, 259
of Maxilla, 259
of Metacarpal bones, 249
of Nose, 258
of Olecranon, 246
of Orbit, 258
of Patella, 256
of Pelvis, 243
of Phalanges, 249
of Radius and Ulna, 248
of Scaphoid, 248
of Tibia, 257
of Zygoma, 258
Fractured Penis, 226
Fragile X Syndrome, 464, 465
Framingham Study, 30
Freckle, 324
Fresh Frozen Plasma, 553
Frost Bite, 236
Frozen Shoulder, 244
Frusemide, 51
FSH, 104, 338
Fulminant Hepatitis, 185
Functional State, 672
Fungal Infections, 317
Fungal Pneumonias, 69
Furuncle, 316
Futility, 716
GABA, 425
Gait, 250
Galactorrhoea, 107
Causes of, 377
Galactosaemia, 466
Galeazzi Fracture, 248
Gallbladder, 195
Gallop Rhythm, 22
Gallstone Ileus, 166
Gallstones, 196
Gambling, 420, 453
Gamekeeper‟s Thumb, 249
Ganciclovir, 507, 515
Ganglia, 249
Gangligliomas, 137
Gangliocytomas, 137
Gardener‟s Syndrome, 173
Gardnerella Vaginalis, 384
Gas Gangrene, 316
Gastric Neoplasia, 163
Gastritis, 161
Gastroenteritis
in Children, 644
Gastro-Intestinal, 153
Bleeding. See GI Bleeding
Gastro-Oesophageal Reflux
Disease, 160, 162
Gastroschisis, 641
GCS, 129, 481
General Anaesthesia, 540
General Medical Condition,
Psych Disorders due to, 444
Generalised Anxiety Disorder,
423
Generalised Progressive
Systemic Sclerosis, 280
Genetic Testing, 465
Genetics, 463
Genital Herpes, 504
Genital Skin Lesions
Non-sexually Transmitted,
386
Genital Warts, 386
Genitalia, Ambiguous, 638
Gentamicin, 514
Genuine Stress Incontinence,
223
Germ Cell Tumours, 226
Gestational Diabetes Mellitus,
94, 363
Gestational Hypertension, 364
Geudal Airway, 476
GFR, 203
GGT, 183
GH, 104
Ghon complex, 69
GI Bleeding, 180
in Children, 641
Lower, 180
Upper, 180
GI Haemorrhage
Treatment, 181
Giant Cell Arteritis, 140, 282
Giant Cell Tumour, 266
Giardia, 177
Giardiasis, 509
Gilbert‟s Syndrome, 193
Gillick Case, 718
Gingivostomatitis, 503
Gini Co-efficient, 693
Glasgow Coma Scale, 129, 481
Glaucoma, 143
Congenital, 148, 632
Primary Closed-angle, 144
Primary Open-Angle, 144
Secondary, 144
Glevac, 299
Glial Blastoma, 136
Global Environmental Change,
689
Global Warming, 689
Glomerular Filtration Rate, 203
Glomerulonephritis, 212
Glossitis, 288
Glossopharyngeal Nerve, 118
Glucocorticoids, 102
Glucose Tolerance Test, 94
Glue Ear, 606
Gluteus Maximus Gait, 251
Gluteus Medius Gait, 251
Glycaemic Index, 96
GnRH, 338
Gold, 272
Golfer‟s Elbow, 246
Gonadal Stromal Tumours, 227
Gonadarche, 667
Gonorrhoea, 383
Goodpasture‟s Syndrome, 92,
214
GORD, 160, 162
Gottron‟s Lesions, 281
Gouty Arthritis, 277
Grand Mal Seizures, 134
Granuloma Annulare, 334
Granulomas
Differential of, 68
Grave‟s Disease, 98
Gravidity, 338
Grief, 458, 473
Pathological, 459
Griseofulvin, 336
Grommets, 607
Growing Pains, 587
Growth, 585
GTN, 43
Guillian Barre Syndrome, 139,
630
Gustilo Classification, 232
Gut Layers, 165
Guthrie Card, 465
Guttate, 314
Gynaecology, 338
Gynaecomastia, 107, 668
Haemaccel, 551
Haemangioendothelioma, 54
Haemangioma, 54
Haematemesis, 180
Haematochezia, 154, 180
Haematocoele, 226
Haematology, 285
Haematuria
in Children, 633
Haemochromatosis, 192
Haemodialysis, 218
Haemoglobin Abnormalities,
290
Haemolysis Tests, 290
Haemolytic Uraemic Syndrome,
209, 645
Haemophilia, 292
Haemophilus Influenza, 67, 502
Type B, 609
Type B Vaccination, 519
Haemoptysis, 16
Haemorrhagic Disease of the
New Born, 588
Haemorrhagic Infarcts, 128
Haemorrhoids, 179
Haemostasis, 291
Haemothorax, 491
Haemotympanum, 150
Hairy Cell Leukaemia, 306
Half Life, 523
Hallpike Manoeuvre, 148
Hallucinations, 413, 415
Haloperidol, 438
Halothane, 541
Hamartoma, 468
Hamman-Rich Disease, 84
Hand
Infections of, 261
Hand, Foot and Mouth Disease,
617
Handicap, 673
Happy Wheezer, 614
Hard Exudates, 145
Harrison‟s Sulcus, 565
Hashimoto‟s Thyroiditis, 100
Hatoglobins, 290
Haversian Canal, 260
Havrix, 187
Hay Fever, 310
Head Injury
Dementia due to, 441
Effect on child development,
583
Head Size, 624
Headaches, 139
in Children, 624
Headlice, 319
HEADSS Risk Assessment, 666
Health
WHO Definition, 680
Health Act 1956, 687
Health and Disability
Commission, 681
Health and Disability Services
Consumer‟s Rights, Code of,
712
Health Care Delivery, 680
Health Care Expenditure, 680
Health Economics, 698
Health Insurance Markets, 698
Health Policy Agencies, 681
Health Promotion, 691
Health Sponsorship Council, 681
Health Status, 682
Hearing Loss, 151
Heart Block, 42
in Children, 601
Heart Disease
in Children, 13, 596
Heart Failure, 48, 614
in Children, 601
Heart Murmurs, 23
Heart Sounds, 21
Heart Valves, 14
Heat Exhaustion, 488
Heat Stroke, 488
Heberden‟s Nodes, 269
Hegemony, 418
Heimlich Manoeuvre, 485
Helicobacter Pylori, 162
HELLP Syndrome of Pregnancy,
209
Hemangioblastoma, 138
Hemianopia, 118
Henderson Hasselbach Equation,
113
Henoch-Scholein Purpura, 620
Heparin, 75
Heparin-Induced
Thrombocytopenia, 295
Hepatic Encephalopathy, 194
Hepatic Failure, 194
Hepatic Iron Index, 192
Hepatic Vein Thrombosis, 193
Hepatitis
A, 186
A Vaccination, 511
B, 187
B Vaccination, 518
C, 189
Chronic, 185
Classification of, 184
D, 191
E, 191
Hepatitis Activity Index, 185
Hepatoblastoma, 192
Hepatocellular carcinoma, 191
Hepatojugular Reflex, 20
Hepato-renal Syndrome, 194
Herd Immunity, 516
Hereditary Non-polyposis Colon
Cancer, 172
Hereditary Spherocytosis, 289
Hernia
Hiatus, 161
in Children, 641
Herpes 6 and 7, 618
Herpes Simplex Virus, 64, 70,
318, 383, 386, 503, 616
Encephalitis, 499
Eye infection, 144
In Pregnancy, 372
Herpes Viruses, 503
Hetastarch, 551
Hiatus Hernia, 161
Hickman Catheter, 300
Hip, 252
Developmental Dysplasia of
the, 618
Transient Synovitis of the,
621
Hip-hike Gait, 251
Hirschsprung‟s Disease, 640
Hirsutism, 107
History, 117
Abdominal, 154
Abuse, 339, 343
Anxiety Disorders, 412, 415,
422
Back Pain, 237
Breast, 375
Cardiovascular, 15
Endocrine, 94
Gynaecological, 338
History Taking, 4
Knee, 253
Neonatal, 587
Neurology, 117
Obstetric, 339, 355
Ophthalmology, 140
Orthopaedic, 230
Outline of, 4
Paediatric, 563
Psychiatric, 411
Renal, 202
Rheumatological, 230
Sexual, 382
Substance Abuse, 447
Suicide, 416
Histrionic Personality Disorder,
455
HIV, 308, 383
HLA-B27, 274
HMG Co-A Reductase
Inhibitors, 53
Hodgkin‟s Lymphoma, 305, 648
Honey Comb Lung, 85
Hookworm, 509
Hormonal Contraception, 341
Hormone Replacement Therapy,
349
Horner‟s Syndrome, 145
Horseshoe Kidney, 216
Housing, 693
Howell-Jolly Bodies, 286
HPV, 351
Hudson Mask, 60
Human Chorionic
Gonadatrohpin, 338
Human Immunodeficiency
Virus, 383
Human Papilloma Virus, 351,
383
Huntington‟s Disease, 132, 465
Hutchison‟s Freckle, 325
Hyaline Membrane Disease, 589
Hydatid Disease, 510
Hydatiform Mole, 363
Hydraencephaly, 624
Hydralazine, 366
Hydrocele, 636
Hydronephrosis, 216
Hydrops Fetalis, 370, 595, 597
Hydroxychloroquine, 272
Hyperaldosteronism, 104
Hyperalgesia, 543
Hypercalcaemia, 112
Hypercholesterolaemia, 53
Hyperemesis gravidarum, 363
Hyperglycaemia, 96
Hypericum, 434
Hyperkalaemia, 27, 111
Hyperkeratosis, 158, 314
Hyperlipidaemia, 30
Hypernatraemia, 110
Hyperparathyroidism, 101, 263
Secondary to Renal Failure,
210
Hyperproteinaemia, 184
Hypersensitivity, 309
Angiitis, 283
Pneumonia, 85
Types of, 531
Hypertension, 34, 215, See also
Blood Pressure
Definition of, 34
In Pregnancy, 364
Persistent Pulmonary, 600
Portal, 194
Primary Portal, 92
Pulmonary, 598
WHO definitions, 34
Hypertensive Intracerebral
Haemorrhage, 125
Hypertensive Retinopathy, 146
Hyperthermia, 488
Hyperthyroidism, 98
Hypertrophic Cardiomyopathy,
46, 54
Hypertrophic pyloric stenosis,
639
Hyperuricaemia, 277
Hyper-Viscosity Syndrome, 303
Hypnotics, 535
Hypoadrenalism, 103
Hypocalcaemia, 27, 112
Hypochondriasis, 444
Hypo-Coagulation Diseases, 292
Hypogammaglobulinaemia, 307
Hypoglossal Nerve, 118
Hypoglycaemia
of the New Born, 590, 595
Hypogonadism, 107
Hypokalaemia, 27, 111
Hyponatraemia, 108
Hypoparathryoidism, 102
Hypopituitarism, 105
Hypoproteinaemia, 184
Hypospadias, 638
Hypotension
In Post-Op Patient, 557
Hypothermia, 487
Hypothyroidism, 99, 466
Hypovolaemic shock, 483
Hypoxic-ischaemic
Encephalopathy, 372, 589
Iatrogenic Disease, 674
Ichthyoses, 335
IDDM. See Diabetes Mellitus
Idiopathic Pulmonary Fibrosis,
84
IgA Deficiency, 307
IGF-1, 107
IgM Anti-VCA, 505
IgM Paraproteinaemia, 132
Illusions, 415
Imaging
CT, 9
MRI, 9
Immediate Hypersensitivity, 309
Immune Complex Mediated
Glomerulonephritis, 215
Immune Complex Mediated
Hypersensitivity, 309
Immune Deficiency, 614
Immune Thrombocytopenia, 295
Immunisation, 518, See
Vaccination
Immunity, 516
Immunodeficiency, 306
Impaired Fasting Glycaemia, 94
Impaired Glucose Tolerance, 94
Impaired or Incompetent
Colleagues, 721
Impairment, 673
Imperforate anus, 641
Impetigo, 315
Impotence, 107
Imprinting
Genetic, 465
Impulse-Control Disorders, 420,
453
Incidence, 685
Incontinence
Daytime, in Children, 634
Night time, in Children, 635
of Urine, 223
Incontinentia Pigmenti, 335
Induction, 371
Infant Drug Withdrawal
Syndrome, 596
Infantile Polycystic Kidney, 216
Infantile Spasms, 134
Infection Control, 710
Infectious Arteritis, 33
Infectious Diseases, 493
Infective Endocarditis, 46
Infertility, 344
Inflammatory Arthritis, 270
Blood Tests in, 270
Influenza, 64, 70
Vaccination, 519
Informed Consent, 712, 717, 719
Infraspinatus Muscle, 244
Inguinal Hernia
in Children, 641
Inheritance, Patterns of, 464
Inhibin, 338
Injury
in Children, 654
Innovative Treatment, 723
Inotropes, 43, 53
Inotropy, 14
INR, 292
Insomnia, Treatment of, 534
Insulin, 96
Intention-to-treat analysis, 703
Internal Validity, 683
International Normalised Ratio,
292
Interpersonal Violence, Victim
of, 343
Interstitial Cystitis, 223
Interstitial Myocarditis, 51
Interstitial Pulmonary Disease,
83
Intertrigo, 322
Intervention Studies, 686
Intracranial Haemorrhage, 123
Intraductal Carcinoma, 380
Intra-uterine Growth
Retardation, 360
Intravenous Urogram, 203
Intraventricular Haemorrhage,
589
Intrinsic Pathway, 292
Intussusception, 166, 641
Invasive Ductal Carcinoma, 381
Involucrum, 260
IPPV, 60
Ipratropium, 614
Iritis, 143, 171, 275
Iron Deficiency. See Anaemia
in Children, 646
Irritable Bowel Syndrome, 175
Irritant Dermatitis, 321
Ischaemic Bowel Disease, 165
Ischaemic Heart Disease, 33
Isoflurane, 541
Isoniazid, 69
Isoprenaline, 42
Isotretinoin, 331, 336
Itraconazole, 336, 515
IUCD, 341
Emergency, 343
Jakarta Declaration on Health
Promotion, 562
Japanese Encephalitis, 499
Jaundice, 184
Neonatal, 595
Jelly Belly, 168
Joint Swelling
Differential of in children,
620
Jone‟s Criteria, 603
Jugular Venous Pressure, 20
Junctional Rhythm, 41
Justice, 716
Juvenile Onset Diabetes, 94
Juvenile Plantar Dermatosis, 322
Juvenile Polyps, 171
Juvenile Rheumatoid Arthritis,
273
Juxtaglomerular Cell Tumour,
217
JVP, 20
Kaposi‟s Sarcoma, 54, 308
Kappa Statistic, 704
Kawanatanga, 695
Kawasaki Disease, 282
Keratitis, 143
Keratoacanthoma, 326
Keratoconjunctivitis Sicca, 279
Keratoderma Blenorrhagica, 276
Keratosis Pilaris, 334
Kerley B Lines, 29
Kernicterus, 595
Kernig‟s Sign, 495
Ketamine, 542
Ketoacidosis, 96, 487
Kidney Transplantation, 219
Kimmelstiel-Wilson Lesion, 96
Klebsiella, 67
Aerongenes, 502
Pneumoniae, 275
Klinefelter Syndrome, 464
Klumpke‟s Paralysis, 245
Knee, 253
Knee Injury, 255
Koebner, 328
Koilonychia, 8, 288
Koplik‟s Spots, 617
Kupffer Cells, 192
Kuru, 500
Kussmaul Breathing, 650
L5 Radiculopathy, 123
Labetalol, 365
Labour, 368
Abnormal, 370
Analgesic Drugs, 546
Stages of, 369
Labyrinthitis, 149
Lachman‟s Test, 254
Lactobacilli, 338
Lactose, 591
Lactose Intolerance, 165
Langerhans Cells, 92, 324
Langhans Cells, 92, 170
Large Cell Carcinoma, 89
Laryngeal Carcinoma, 86
Laryngeal Nodule, 86
Laryngeal Papilloma, 86
Laryngomalacia, 604
Laryngomalatica, 66
Laryngotracheobronchitis, 608
Larynx, 65
Lasegue‟s Sign, 238
Lateral Decubitus CXR, 73
Lateral Medullary Syndrome,
126
Laxatives, 178
LDH, 38
LDL, 53
Learning Disability, 583
Leather Bottle Stomach, 164
Left Bundle Branch Block, 25
Left Ventricular Hypertrophy, 26
Legg-Calve-Perthes Disease, 621
Legionella Pneumonia, 67
Lentigo, 323
Leucocytosis, 291
Leucodystrophies, 132
Leucoerythroblastosis, 296
Leuconychia, 8, 155
Leukaemia, 300, 649
Leukocoria, 147
Leukocornea, 632
Leukocytoclastic Vasculitis, 33,
283
Leukoplakia, 158
Levels of Evidence, 703
Lewy Bodies, 132
Lewy Body Dementia, 132, 441
Leydig Cells, 338
Leydig tumours, 227
LFTs, 182
LH, 104, 338
Libman-Sacks Endocarditis, 45,
279
Lichen Planus, 158, 334, 387
Lichen Sclerosis, 350
Life Expectancy, 673, 682
Lignocaine, 42, 545
Likelihood Ratio, 705
Limb Length Inequality, 621
Linitis Plastica, 163
Lipid Lowering Drugs, 53
Lipid Pneumonia, 70
Lipids, 53
Lipoma, 631
Lipophages, 136
Lisfranc Dislocation, 258
Lissencephaly, 629
Listeria, 357
Lithium, 431, 533
Liver
Biopsy, 185
Disease, 181
Rupture of, 490
Tumours, 191
Vascular Disease, 193
Liver Cell Adenoma, 192
Liver Function Tests, 182
Loading Dose, 522
Lobar Pneumonia, 68
Lobular Carcinoma In Situ, 380
Local Anaesthesia, 544
Locked-in Syndrome, 140
Loculated Empyema, 612
Long QT Syndrome, 601
Looser‟s Zones, 263
Loss of Consciousness,
Differential of, 117
Lower Motor Neuron Lesions,
121
Lumbar Puncture, 496
Lumbar Root Nerve Entrapment,
241
Lumbar Spondylosis, 240
Lung Abscesses, 68
Lung Cancer, 87
Systemic Effects, 89
Lung Function Tests, 58
Lyme Disease, 316
Lymph Nodes
Neck Anatomy, 8
Lymphadenitis, 316
Lymphadenopathy
in Cancer, 649
Lymphocytic Meningitis, 499
Lymphocytosis, 291
Lymphoma, 227, 305, 649
Lymphoproliferative Disorders,
302
Macrocytic Anaemia, 288
Macrolides, 514
Macrosomia, 363
Macula, 141
Macular Degeneration, 142
Macule, 314
Mad Cow Disease, 441
Magnesium, 27, 42, 113
Magnesium Sulphate, 366
Maintenance Dose, 522
Major Depressive Episode, 427
Major Tranquillisers, 437
Malabsorption Syndromes, 165
Malaria, 508, 688
Malassezia Furfur, 317
Malignant Hyperthermia, 547
Mallet Finger, 249
Mallet Thumb, 248
Malnutrition, 554
Malrotation, 639
MALT, 171
Mammography, 382
Mana, 694
Managed Care, 680
Manic-Depression, 431
MAO - A, 434
MAOIs, 434
Overdose, 435
Maori Cultural Differences, 697
Maori Health, 694
Maori Mental Health, 410
Maori Patient, Treatment of,
410, 428
Maple Syrup Urine Disease, 466
Marcain, 545
March Fractures, 258
Marginal Analysis, 698
Marijuana, 448
Market Failure, 698
Markets, 698
Marmot Study, 694
Mate Maori, 696
Maternal Death, 373
Maternal Serum Screening, 360
Maturity Onset Diabetes Of The
Young, 95
McCallum‟s Patch, 604
McMurray‟s Test, 254
MCU, 222
Mean Arterial Pressure, 14
Measles, 70, 516, 617
Vaccination, 519
Mechanical Back Pain, 240
Meckel‟s Diverticulum, 639
Meconium Aspiration, 370, 596,
605
Meconium Ileus, 615, 640
Medial Medullary Syndrome,
126
Median Nerve, 247
Compression, 123
Medical Council, 712
Medical Error, 712
Medical Misadventure, 712
Medical Mishap, 712
Medical Officer Of Health, 687
Medical Practitioners Act, 711
Medical Referee, 713
Medicine Assessment Advisory
Committee, 530
Medicines Act, 536
Mediobasal Mesencephalic
Syndrome, 126
MedSafe, 536
Medullary Carcinoma, 101
Medulloblastoma, 136, 138
Mee‟s Lines, 8
Mefloquine, 508
Megakaryocyte, 294
Megalencephaly, 624
Megaloblastic Anaemia, 288
Meissner‟s Plexus, 640
Melaena, 180
Melancholic Depression, 428
Melanocytes, 324
Melanoma, 324
of the Choroid, 147
Melanosis Colis, 165
Membranoproliferative
Glomerulonephritis, 215
Membranous
Glomerulonephritis, 214
Memory, 122
Menarche, 667
Meniere‟s Disease, 151
Meningioma, 136, 138
Meningitis, 495
Viral, 499
Meningocele, 631
Meningococcal Disease, 497
Meniscal Tears, 255
Menopause, 349
Menorrhagia, 346
Menses, 339
Menstrual Cycle, 338
Menstrual Disorders, 345
Mental Health
in Children and Adolescents,
659
in New Zealand, 410
Mental Health Act 1992, 458
Mental Health Commission, 681
Mental Illness, Treatment of, 456
Mental State
Cognition, 416
Examamination of, 117
Examination of, 414
Mesangial IgA disease, 214
Mesangiocapillary
Glomerulonephritis, 215
Mesothelioma, 89
Metabolic Acidosis, 114
Metabolic Alkalosis, 114
Metabolic Bone Disease, 261
Metabolism of Drugs, 524
Metastatic Brain Tumours, 138
Metatarsalgia, 258
Methadone Treatment, 449
Methaemoglobinaemia, 290
Methotrexate, 272
Methyldopa, 365
Metoprolol, 41
Metronidazole, 515
Metyrapone Test, 105
MGUS, 184, 303
MI, 36
Michaelis-Menten Kinetics, 523
Miconazole, 515
Microalbuminuria, 95, 207
Microcephaly, 624
Microcytic Anaemia, 287
Microglia, 136
Microsporum Canis, 317
Microstomia, 280
Micturating Cystourethrogram,
203
Midazolam, 542
Migraine, 139
in Children, 624
Miliary Pattern on Xray, 29
Mineralocorticoids, 102
Minimal Change Disease, 213,
633
Minimum Alveolar
Concentration, 541
Miscarriage, 362
Misuse of Substances Act, 536
Mitochondria, 465
Mitral Facies, 19, 45
Mitral Regurgitation, 22, 45
Mitral Stenosis, 22, 45
Mitral Valve Prolapse, 45
Mixed Acid/Base Disorders, 115
Mixed Connective Tissue
Disease, 281
Mobitz, Heart Block, 42
Moclobemide, 434
MODY, 95
Molluscum Contagiosum, 318,
387
Mongolian Spot, 325
Monoclonal Proteins, 303
Mononeuritis Multiplex, 273
Monozygotic Twins, 359
Monteggia Fracture, 248
Mood Disorders, 420, 426
Mood Stabilising Medication,
431
Moral Hazard, 699
Moraxella Catarrhalis, 502
Morbidity, 682
Morning sickness, 357
Morphine, 471, 543
Morphoea, 280, 330
Mortality, 682
Motivational Interviewing, 11
Motor Examination, 120
Motor Neurone Disease, 133
Mucocoele of the Appendix, 168
Mucocoele of the Gallbladder,
197
Mucormycosis, 69
Multinodular Goitre, 101
Multiple Endocrine Neoplasia,
101
Multiple Myeloma, 302
Multiple Pregnancy, 358
Multiple Sclerosis, 132
Mumps, 617
Vaccination, 519
Munchausen‟s By Proxy, 454
Murmurs, 23
Murphy‟s Sign, 196
Murray Valley Encephalitis, 499
Muscle Relaxants, 542
Muscular Dystrophy, 630
Musculo-Skeletal, 229
Myasthenia Gravis, 140
Mycobacteria, 502
Mycoplasma Pneumonia, 70
Myelodysplastic Syndromes, 299
Myelofibrosis, 298
Myelomeningocele, 631
Myeloproliferative Disorders,
296
Myocardial Contusion, 491
Myocardial Infarction, 36
Myocarditis, 50
Myoglobin, 38, 210
Myotonic Dystrophy, 465
Myxoedema, 99
Myxoma, 54
Naegele‟s Rule, 355
Naevi, 324
Napkin Dermatitis, 323
Nappy Rash, 323
Narcissistic Personality
Disorder, 455
Narcolepsy, 91
Nasal Encephalocele, 595
Nasal Obstruction, 63
Nasal Prongs, 60
Nasopharyngeal Carcinoma, 86
National Health Committee, 681
Natural Family Planning, 340
Nausea, Treatment of, 471
Neck, 237
Necrotising Enterocolitis, 590
Necrotising Fasciitis, 316, 501
Need, 680
Needle Stick Injury, 710
Nefazodone, 434
Neglect of Children, 658
Negligence, 712
Neisseria Gonorrhoeae, 64, 385
Neisseria Meningitidia, 497
Neonatal Hepatitis, 194
Neotigason, 336
Neovascularisation
in the Eye, 145
Nephritic Syndrome, 204
Nephroblastoma, 217
Nephrolithiasis, 210
Nephrotic Syndrome, 204
Nephrotoxins, 210
Nerve Injury, 237
Neural Tube Defects, 630
Neuroblastoma, 649
Neurofibromatosis, 334, 620
Neurogenic Claudication, 241
Neuroleptic Malignant
Syndrome, 438
Neuroleptics, 437
Neurology, 117
Paediatric, 621
Neuromuscular Blockade, 542
Neuromuscular Blocking Agents
Depolarising, 542
Non-depolarising, 542
Neuropathic Joint, 235
Neuropathic Pain, 544
Neuropil, 136
Neuropraxia, 237
Neurotmesis, 237
Nifedipine, 52
Nitrous Oxide, 541, 546
Nits, 319
Nociceptors, 543
Nodal Rhythm, 41
Nodular vasculitis, 333
Nodules
in Arthritis, 267
N-of-1 Trials, 703
Noise Induced Hearing Loss,
151
Non-Epileptic Seizure, 134
Non-Hodgkin‟s Lymphoma, 305
Non-maleficence, 716
Non-Polio Enteroviruses, 617
Non-proliferative
glomerulonephritis, 204
Non-Proliferative Retinopathy,
146
Non-Q Wave Infarction, 27
Non-STEMI, 36
Noonan‟s Syndrome, 464
Nor-adrenaline, 43
Norfloxacin, 515
Nosocomial PUO, 6
Notifiable Diseases, 687
NSAIDs, 210, 271
Nuchal Translucency, 360
Number Needed To Treat, 704
Nuremberg Code, 723
Nutrition
Deficiencies in Childhood,
646
in Surgical Patients, 554
in the elderly, 674
Nutritional assessment, 554
Nystagmus, 148
Nystatin, 515
NZ Deprivation Index, 693
NZ Medicines and Medical
Devices Safety Authority, 536
Obsessive Compulsive Disorder,
424
Obsessive Compulsive
Personality Disorder, 455
Obstetric Anaesthesia, 545
Obstetrics, 355
Obstructive Jaundice, 183
Obstructive Sleep Apnoea, 90
Occupational Therapist, 585
Octreotide, 107
Oedema, 7
Oesophageal Atresia, 639
Oesophageal Tumours, 158
Oesophagitis, 160
Oesophagus, 158
Oestradiol, 338
Oestrogen, 338
Olanzapine, 438, 439
Oligodendroglioma, 136, 137
Oligodenrocyte, 136
Oligomenorrhoea, 346
Oncogenesis, 466
Oncology, 466
Onychomycosis, 317
Opening Snap, 22
Ophthalmia Neonatorum, 632
Ophthalmic Nerve, 118
Ophthalmology, 140
Paediatric, 147
Opiod Analgesics, 543
Opportunity Cost, 698
OPSI, 307
Optic Atrophy, 145
Optic Neuritis, 145
Oral Pathology, 157
Oratane, 336
Orbital Cellulitis, 618
Orchitis, 226
Organ Donation, 722
Orthopaedic Tumours, 264
Orthopnoea, 17
Ortolani‟s Test, 619
Oscillopsia, 149
Osteoarthritis, 268
Secondary, 269
Osteoblastoma, 265
Osteoblasts, 261
Osteochondral Fractures, 256
Osteochondritis Dissecans, 256,
621
Osteochondroma, 265
Osteoclasts, 262
Osteoid Osteomas, 265
Osteomalacia, 261, 263
Osteomyelitis, 260
Chronic, 260
Osteopenia, 261
Osteophytes, 268
Osteoporosis, 261, 262
Pain in, 241
Osteosarcoma, 265
Osteotomy, 269
Otitis Externa, 149
Otitis Media, 65
Acute, 605
Chronic with Effusion, 606
Recurrent Acute, 606
Ottawa Charter, 562, 691
Ovarian cancer, 354
Overdose, 488
Overt Diabetic Nephropathy, 207
Ovulation, 339, 345
Oxygen Flux, 58
Oxygen Therapy, 60
Oxyhaemoglobin Dissociation
Curve, 58
P Value, 684
P wave, 26
P53 Gene, 467
Paget‟s Disease of Bone, 264
Paget‟s Disease of the Nipple,
380
Pain
Abdominal, in Children, 643
Bone, 544
Management, 470, 543
Management in Children, 655
Neuropathic, 544
Pharmacology, 543
Physiology, 543
Post-Operative, 544
Syndromes, 283
Pain Disorder, 444
Palliative Care, 473
Palmar Erythema, 8, 155
Panadine, 470
Pancoast Tumour, 89
Pancreas, 197
Pancreatic Tumours, 199
Pancytopenia, 289
Panic Disorder, 423
Papillary Thyroid Cancer, 100
Papillitis, 141
Papilloedema, 141
Papova Virus, 318
Papular Urticaria, 333
Papule, 314
Paracetamol Poisoning, 489
Paradex, 470
Paradoxical Breathing, 29
Parainfluenza Virus, 64
Parakeratosis, 314
Paranoid Personality Disorder,
455
Paraproteinaemia, 303
Parathyroid, 101
Parenchymal Haemorrhage, 589
Parenchymatous Myocarditis, 51
Parenteral Feeding, 556
Parity, 338
Parkinson‟s Disease, 131
Parkinsonism, 132
Paronychia, 318
Paroxetine, 434
Paroxysmal Nocturnal
Dyspnoea, 17
Partial Seizures, 134
Parvovirus, 618
Patella
Dislocation of, 256
Patellar-Femoral Joint, 255
Paternalism, 716
Pauci-immune
Glomerulonephritis, 215
Paul-Bunell, 506
PE, 76
Pectus Excavatum, 21
PEEP, 60
Pelvic Congestion, 350
Pelvic Inflammatory Disease,
385, 386
Pelvic Injury, 242
Pelvic Mass, 350
Pelvic Relaxation, 350
Pemphigoid, 329
Pemphigus, 329
Pencil Poikilocytes, 286
Penicillin G, 513
Penicillins, 513
Penis, 226
Diseases of in boys, 637
Penobarbitone, 135
Pentaspan, 551
Peptic Ulcer, 161
Pericardial Effusion, 14
Periductal Mastitis, 377
Perinatal Asphyxia, 372
Perinatal Mortality, 372
Periodic Limb Movements In
Sleep, 91
Peripheral Vascular Resistance,
14
Peripheral Vestibulopathy, 149
Peritoneal Dialysis, 218
Periventricular Leukomalacia,
589, 629
Pernicious Anaemia, 163
Peroneal Spastic Flat Foot, 619
Personality Disorders, 454
Pertussis, 609
Differential from Asthma, 613
Vaccination, 610
Petechiae, 155, 314
Pethidine, 546
Petit Mal Seizures, 134
Peutz-Jeghers Syndrome, 171,
172
Phaeochromocytoma, 104
Phalen‟s Test, 250
Pharmacodynamics, 527
Pharmacology, 521
Cardiovascular, 51
Pharyngeal Pouch, 158
Pharyngitis, 607
Phenothiazine, 438
Phenylketonuria (PKU), 466
Phenytoin, 135, 533
Philadelphia Chromosome, 299
Phimosis, 637
Phlebitis, 554
Photocoagulation, 146
Phyllodes Tumour, 378
Physical Abuse, 656
Physical Exam
Abdominal, 154
Ankle and Foot, 257
Arthritis, 266
Back, 237
Breast, 376
Cardiovascular, 18
Elbow, 245
Eye Movements, 148
Gentio-urinary, 383
Gynaecological, 340
Hand, 247
Hip, 252
in Adolescents, 667
Knee, 254
Motor, 120
Motor Exam in Children, 623
Musculo-Skeletal, 230
Neonatal, 587
Neurology, 117
Neurology, in Children, 565,
621
Ophthalmology, 140
Paediatric, 564
Respiratory, 60
Shoulder, 243
Physical Hazards of Medicine,
710
Physiotherapist, 585
Pica, 288
Pick‟s Disease, 441
PID, 385, 386
Pierre Robin Sequence, 595
Pigeon Breeder HSP, 85
Pigeon Chest, 565
Pigment Stones, 195
Pinguecula, 143
Pink Puffer, 81
Pinworm, 509
Piperacillin, 513
Pitted Keratolysis, 318
Pituitary Adenoma, 138
Pituitary Gland, 104
Pityriasis Alba, 322
Pityriasis Rosea, 318
Pityrosporum Ovale, 317
Pivot Test, 254
pKa, 524
Placenta Praevia, 366
Placental Abruption, 366
Plasma Cells, 286
Plasmacytoma, 303
Plasmodium
Falciparum, 508
Vivax, 508
Plastic and Reconstructive
Surgery, 284
Platelets, 294
Pleural Disease, 73
Pleural Effusion, 62
on Xray, 29
Pleural Fluids, 73
Pleural Rub, 61
Plummer‟s Disease, 98
PND, 17
Pneumatocele, 604
Pneumatosis Intestinalis, 590,
639
Pneumoconioses, 85
Pneumocystis Carinii, 510
Pneumonia, 70
Pneumonia, 67
in Children, 611
Tb, 612
Treatment, 72
Pneumo-peritoneum, 157
Pneumothorax, 490
on Xray, 29
Pneumovax, 501
Poikiloderma, 314
Poisoning, 486, 488, 533
Polio
Travel Vaccination, 511
Vaccination, 518
Polyarterititis Nodosa, 282
Polycystic Ovary Syndrome, 348
Polycythaemia Vera, 297
Polymyalgia Rheumatica, 281
Polymyositis, 281
Polypharmacy, 531
Polyploidy, 464
Polyps
Colonic, 172
Endometrial, 355
Pompholyx, 322
Population Health, 680
Porphyria, 290
Portal Hypertension, 194
Portal Tract, 184
Portosystemic Shunts, 194
Post Traumatic Stress Disorder,
424
Posterior Cruciate Ligament,
254, 256
Post-Infectious
Glomerulonephritis, 214
Post-Infective Encephalitis, 500
Postmenopausal Bleeding, 348
Postnatal Assessment, 372
Post-Operative Complications,
556
Postpartum
Complications, 372
Depression, 430
Haemorrhage, 369, 373
Mood Disorders, 430
Psychosis, 430
Post-test Probability, 705
Postural Hypotension, 19
Potassium, 27, 111
Potency, 528
Potential Years Of Life Lost, 682
Power, 684
PPPR Act, 713
Prader-Willi Syndrome, 465
Praecordium, 21
Precision, 703
Precocious Puberty, 668
Prednisone
Side Effects of, 304
Pre-eclampsia, 364
Pregnancy
Cardiovascular problems, 363
Drugs in, 528
Early Complications of, 361
General Anaesthetic, 546
Hypertension in, 364
Late Complications of, 366
Minor symptoms of, 358
Multiple, 358
Physiology, 545
Preload, 14
Premature Adrenarche, 667
Premature Atrial Complexes, 41
Premature Labour, 367
Premature Rupture of
Membranes, 368
Premature Thelarche, 667
Premature Ventricular
Complexes, 42
Premenstrual Dysphoric
Disorder, 347
Premenstrual Syndrome, 347
Prenatal diagnosis, 360
Preoperative Assessment, 546
Paediatric, 655
Pre-Orbital Cellulitis, 618
Presbycusis, 151
Presbyopia, 675
Prescriptions, 535
Pressure Overloaded, 21
Pressure Ulcers, 327
Preterm Birth
Complications of, 589
Outcome after, 589
Pre-test Probability, 705
Pretibial Myxoedema, 98
Prevalence, 685
Primary Biliary Cirrhosis, 193
Primary Care, 681
Primary Proliferative
Polycythaemia, 297
Primary Pulmonary
Hypertension, 92
Primary Sclerosing Cholangitis,
193
Primitive Neuroectodermal
Tumours, 138
Prions, 500
PRL, 104
Procainamide, 42
Professional Boundaries, 710
Professional Ethics, 721
Progesterone Only Pill, 342
Prognostic factor, 707
Progressive Multifocal
Leucoencephalopathy, 500
Progressive Systemic Sclerosis,
280, 330
Prolactinaemia, 106
Prolapsed Cervical Disc, 239
Proliferative Glomerulonephritis,
204
Proliferative Retinopathy, 146
Propofol, 541
Propranolol Withdrawal, 534
Proptosis, 649
Prosopagnosia, 122
Prospective Study, 703
Prostate, 224
Prostate Cancer Screening, 225,
691
Prostate Specific Antigen, 225
Prostatic Carcinoma, 225
Prostatitis, 224
Protection of Personal and
Property Rights Act, 458, 676,
713
Protein C & S, 294
Protein, Total, 183
Proteinuria, 202
in Children, 632, 633
Proteus Mirabilis, 502
Prozac, 434
Pruritis Ani, 179
PSA, 225, 469
Psammoma Bodies, 100
Pseudo-bulbar Palsy, 131
Pseudogout, 278
Pseudomembranous Colitis, 176
Pseudomonas Aeruginosa, 67, 70
Pseudomyxoma Peritonei, 168
Pseudopapilloedema, 141
Pseudo-seizure, 134
Psoriasis, 314, 328
Nail Changes in, 247
Psoriatic Arthritis, 275
Psychiatric Disorders, Aetiology,
411
Psychodynamic Psychotherapy,
425
Psychological Medicine, 409
Psychologist, 585
Psychosis, 435
Treatment of, 437
Psychotic Depression, 428
Psychotic Disorders, 420, 435
Pterygium, 143
PTH, 101
PTH Related Protein, 102
Ptosis, 145
PTSD, 424
PTT, 292
Pubarche, 667
Puberty, 667
Delayed, 668
Precocious, 668
Pubic Lice, 383
Public Health, 679
Puerperal Fever, 373
Puerperal Psychosis, 430
Puerperium, 373
Pulmicort, 79
Pulmonary Artery Wedge
Pressure, 14
Pulmonary Atresia, 601
Pulmonary Contusion, 491
Pulmonary Embolism, 76
Pulmonary Hamartoma, 92
Pulmonary Hypertension, 598,
602
Pulmonary Hypertension,
Persistent, 600
Pulmonary Oedema
Emergency Management, 489
Pulmonary Valve Stenosis, 601
Pulse, 18
Bounding, 18
Collapsing, 18
Pulse deficit, 18
Pulseless Disease, 283
Pulseless Electrical Activity, 479
Pulsus Paradoxus, 491
Purchaser-Provider Split, 681
Purpura, 314
Pustule, 314
Pyelonephritis
Acute, 212
Chronic, 212
Pyemia, 494
Pyloric Stenosis, 639
Pyoderma Gangrenosum, 169
Pyrazinamide, 69
Pyrexia
in Children, 616
of Unknown Origin, 6
on Returning from 3rd World,
6, 511
Pyrimethamine, 507
Q waves, 26
QRS Complex, 25, 26
Quinolones, 515
Quinsy, 8
Radial Nerve, 123, 247
Radicular Back Pain, 239
Radiology
Abdominal, 157
Abdominal in Children, 638
Arthritis, 267
Chest, 27
Orthopaedic, 231
Renal, 203
Spine, 238
Thyroid, 97
Radiotherapy, 469
Rape, 344
Rapid Sequence Induction, 540
Rapidly Progressive
Glomerulonephritis, 215
Raynaud‟s Phenomena, 6
Raynaud‟s Syndrome, 8, 267
Reactive Arthritis, 276
Rectal Cancer, 179
Rectal Prolapse, 179
Recurrent Laryngeal Palsy, 66
Red Blood Cells, 286
Red Eye, 142
Refeeding Syndrome, 555
Referred Pain, 543
Reflex Incontinence, 224
Reflex Sympathetic Dystrophy,
283
Reflexes, 121
Reflux
in Children, 642
Reflux Nephropathy, 208
Refusal of Treatment, 719
Regional Blood Flow, 15
Regulation of Drugs of Abuse,
536
Rehabilitation, 676
Rehydration
in Children, 650
Reiter‟s Syndrome, 276, 386,
387
Relative Risk, 704
Renal, 201, 632
Disease in Children, 201, 632
Renal Adenoma, 216
Renal Cell Carcinoma, 217
Renal Failure
Acute, 205
Acute, in Children, 633
Chronic, 207
Chronic, in Children, 634
Renal Oncocytoma, 217
Renal Osteodystrophy, 263
Renal Perfusion, 15
Renal Stones, 210
Renal Transplantation, 219
Renal Tumours, 216
Renin, 103
Renin-Angiotensin System, 202
Renogram, 204
Research Ethics, 723
Residential Care, 672
Residual Volume, 58
Resiliency, 571
Respiratory Acidosis, 114
Respiratory Alkalaemia, 113
Respiratory Distress Syndrome,
589, 597, 605
Respiratory Failure, 59
Respiratory Physiology, 58
Respiratory Syncytial Virus, 70
Respiratory Tract Infections
in Children, 62, 605, 616
Respiratory Tract Neoplasia, 86
Rest Homes, 677
Restless Leg Syndrome, 91
Restrictive Cardiomyopathy, 54
Restrictive Pulmonary Disease,
83
Resuscitation, 476
Cardiopulmonary, 476
Ethics, 481
in Children, 653
Secondary survey, 481
Reticular Activating System, 130
Reticulocytes, 286
Retinal Detachment, 142
Retinoblastoma, 147, 649
Retinoids, 336
Retinopathy
Diabetic, 146
Hypertensive, 146
of Prematurity, 148, 590
Retractile Testis, 636
Reye‟s Syndrome, 500
Rhabdomyolysis, 210
Rhabdomyoma, 55
Rhabdomyosarcoma, 223
Rhesus Haemolytic Disease, 367
Rheumatic Fever, 602
Rheumatoid Arthritis, 272
Juvenile, 273
Rheumatoid Factor, 270, 273
Rhinitis, 63, 310
Rhinophyma, 332
Rhinovirus, 64
Rhonchi, 61
Rib Fracture, 491
Rickets, 263, 647
Riedel‟s Lobe, 156
Riedel‟s Thyroiditis, 100
Rifampicin, 69, 498, 514
Right Bundle Branch Block, 25
Right Ventricular Hypertrophy,
26
Ringworm, 317
Rinne Test, 150
Risk and Resilience, 571
Risk Factor, 707
Risk Ratio, 704
Risperidone, 438, 439
Ritalin, 661
Roaccutane, 331, 336
Rocuronium, 542
Rokitansky-Aschoff Sinuses,
197
Rosacea, 332
Roseola Infantum, 618
Rose-Waaler Titre, 270
Rotator Cuff Syndrome, 244
Roth‟s Spots, 19, 145
Rouleaux, 286
Roundworm, 509
Rubber Glove Allergy, 321
Rubella, 357
Vaccination, 519
S1 Radiculopathy, 123
Saccades, 148
Sacroiliac Joints, 238
Salazopyrin, 272
Salmonella, 177
Salter-Harris Classification, 232
Sarcoidosis, 85
Scabies, 319, 383, 387
Scalded Skin Syndrome, 315
Scarcity, 698
Scarlet Fever, 500, 607
Schilling Test, 163
Schirmer Test, 280
Schizoaffective Disorder, 435
Schizoid Personality Disorder,
455
Schizophrenia, 420, 436
Schizophreniform Disorder, 435
Schizotypal Personality
Disorder, 455
Schober‟s Test, 238
School Sores, 315, 500, 502
SCID, 307
Scleritis, 143
Sclerodactyly, 280
Scleroderma, 280
Sclerosing Haemangioma, 326
Scoliosis, 237, 619
Screening, 689
Screening Programmes, 691
Screening Test, 690
Scrotum, 226
Acute, in Children, 636
Scwhannoma, 138
Scybala, 640
Seasonal Affective Disorder, 428
Sebaceous Glands, 330
Sebaceous Naevi, 325
Seborrhoeic Dermatitis, 321, 387
Seborrhoeic Keratosis, 326
Secondary Biliary Cirrhosis, 193
Secondary Cardiomyopathy, 54
Seizure
in Children, 625
Types of, 134
Self-rated Health Status, 683
Seminoma, 226
Senile Arcus, 675
Sensitivity, 690, 704
Sensorineural Deafness
Congential, 151
Sudden Onset, 151
Separation
Effect on Children, 574
Separation Anxiety Disorder,
661
Sepsis
in Children, 616
Septic Arthritis, 259
Septic Shock, 482
Septicaemia, 494
Sequestration, 92
Sequestrum, 260
Seronegative Arthritis, 274
Serotonin Syndrome, 434
Serous Cystadenoma, 199
Sertoli Cell Tumours, 227
Serum, 294
Serum Amylase, 196
Serum Sickness, 333, 531
Severe Combined
Immunodeficiency, 307
Sexual Abuse, 657
Sexual and Gender Identity
Disorders, 420
Sexually Transmitted Diseases,
383
Sheehan‟s Syndrome, 105
Shigella, 177
Shin Splints, 236
Shingles, 504
in the Eye, 143
Shock, 482
Shock Lung, 83
Short Stature, 586
Shoulder, 243
Dislocation of, 245
Injury, 244
Instability, 245
Shunt
Cardiac, in neonates, 597
SIADH, 109
Sick Sinus Syndrome, 41
Sideroblastic Anaemia, 287
Silicosis, 85
Sim‟s Speculum, 340
Simmond‟s Test, 258
Singh Index, 262
Sinonasal Carcinoma, 86
Sinonasal Papilloma, 86
Sinus Arrhythmia, 26, 41
Sinus Bradycardia, 18, 41
Sinus Tachycardia, 18, 41
Sinusitis, 63, 65
Acute, 608
Six Week Check, 374
Sjogren‟s Syndrome, 158, 279
Skiers Thumb, 249
Skin Ulcers, 327
Slapped Cheek Syndrome, 618
Sleep
Disorders, 420
Hygiene, 534
in Elderly, 534
Management in Children, 593
Sleeping Pills, 534
Training in Children, 594
Treatment of Insomnia, 534
Sleep Apnoea, 17, 90
Children, 66
Sleepiness, Differential of, 90
Slow Acetylators, 525
Small Bowel Atresia, 639
Small Cell Carcinoma, 89
Smegma, 637
Smith‟s Fracture, 248
Smoking, 87
Amongst Maori, 695
Cessation, 87
Smudge Cells, 287
Snellen‟s Chart, 140
Social Gradient, 692
Social Inequalities in Health, 692
Social Phobia, 423
Social Worker, 585
Socio-economic Status, 692
Sodium Aurothiomalate, 272
Sodium Cromoglicate, 79
Sodium Valproate, 135
Soft Tissue Injury, 235
Solar Keratosis, 326
Somatization Disorder, 444
Somatoform Disorders, 420, 444
Somatostatin, 107
Sotalol, 41
Space of Disse, 193
Specific Phobia, 423
Specificity, 704
Speech Language Therapist, 585
Spells, 136
Spermarche, 667
Spermatocoele, 226
Spherocytes, 286, 289
Spherocytosis, 286
Spina Bifida Occulta, 631
Spinal Chord Syndromes, 138
Spinal Cord Compression, 472
Spinal Shock, 490
Spinal Stenosis, 241
Spironolactone, 52
Spitz Naevus, 325
Spleen
Rupture of, 490
Splenectomy, 307
Splenomegaly, 156
Splinter Haemorrhage, 8
Splitting of Heart Sounds, 22
Spondylitis, 237
Spondyloarthropathies, 274
Spondylolisthesis, 241
Spondylolysis, 240
Spondylosis, 237
Spontaneous abortion, 362
Squamous Cell Carcinoma, 88,
327
Oesophagus, 159
of the vulva, 351
Squamous Hyperplasia
of the vulva, 351
Squint, 147
SSPE, 500
SSRIs, 433
St John‟s Wort, 434
ST Segments, 27
St Vitus Dance, 603
Staging of Cancer, 468
Standard Error, 684
Staphlococcus Aureus, 315, 502
Star Chart, 570
Starling‟s Law, 14
Statins, 53
Statistical Power, 703
Status Epilepticus, 135
STDs, 383
Steady State Concentration, 523
Steatocystoma, 226
STEMI, 37
Stenosing Tenosynovitis, 249
Stephens Johnson Syndrome,
332
Steppage Gait, 251
Sterilisation, 342
Sternotomy, 21
Steroid Medication, 104
Steroids, Topical, 335
Stigma, 456
Stomach, 161
Stool test, 157
Strabismus, 632
Strep Pyogenes, 64
Streptococcus
Group A -Haemolytic, 602
Pneumoniae, 501
Pyogenes, 315, 316, 500, 602,
607
Viridians, 47
Stress, 711
Stridor
Differential in Children, 604
Stroke, 125
Stroke Volume, 14
Strongyloides Stercoralis, 510
Sub-acute Bacterial
Endocarditis, 46
Subacute Sclerosing Pan-
encephalitis, 500
Subacute Thyroiditis, 98
Subarachnoid Haemorrhage, 124
Subchondral Cysts, 268
Subchondral Sclerosis, 268
Subconjunctival Haemorrhage,
632
Subdural Haemorrhage, 124
Subglottic Stenosis, 595
Subscapularis Muscle, 244
Substance Abuse
Treatment of, 448
Substance Dependence, 446
Substance Use Disorders, 445
Sudden Infant Death Syndrome,
590, 594
Suicide
Assessment, 413, 415, 416,
663
Management of Risk, 418
Youth, 663
Sulphasalazine, 272
Summation Gallop, 22
Sun Damaged Skin, 323
Sunscreens, 323
Superior Vena Cava Syndrome,
472
Suppurative Myocarditis, 51
Supraspinatus Muscle, 243
Supraventricular Arrhythmia, 26
Supraventricular Tachycardia, 41
in Children, 601
Surfactant, 367, 589
Surrogacy, 722
Suxamethonium, 542
Swan Neck Deformity, 273
Sway Back, 241
Symphyseal-fundal height, 359
Synacthen, 103
Syncope, 131
Syndesmophytes, 275
Syndrome of Inappropriate ADH
Secretion, 109
Synoviosarcoma, 266
Synpharyngetic Haematuria, 214
Syntocinon, 369, 370, 373
Syphilis, 383
Systematic Error, 683
Systematic Review, 703
Systemic Inflammatory
Response Syndrome, 482
Systemic Lupus Erythematosus,
278
Nephropathy in, 208
T Wave, 27
T½, 523
Tachy-Brady Syndrome, 41
Tachycardia, 26
Tactile Fremitus, 62
Taha Hinengaro, 696
Taha Tinana, 696
Taha Wairua, 696
Taha Whanau, 696
Takayasu‟s Arteritis, 283
Talipes Equinovarus, 619
Talking with Adolescents, 665
Talking with Children, 567
Tall Stature, 587
Tamariki Ora, 579
Tamoxifen, 382
Tangi, 696
Tantrums, 572
Tapeworms, 510
Tapu, 694
Tardive Dyskinesia, 438
Target Cells, 286
Tarsal Conditions, 619
Tazocin, 513
Tb, 68
Cutaneous, 648
Meningitis, 498
Mycobacteria, 502
Pneumonia in Children, 612
TB Act 1948, 687
Te Tiriti O Waitangi, 695
Teams, 710
Tear Drop Red Cells, 286
Technical Efficiency, 698
Tegretol, 135
Telangiectases, 314
Teleological Moral Theories,
716
Telomerase, 467
Telomere, 467
Temporal Arteritis, 282
Tenckhoff Catheter, 218
Tendon Injuries, 235
Tenesmus, 171
Tennis Elbow, 246
Tension Headaches, 139
Tension Pneumothorax, 490
Teratoma, 227
Terbinafine, 336, 515
Termination of Pregnancy, 356,
361
Testes, 226
in Children, 636
Testicular Torsion, 637
Testicular Tumours, 226
Undescended, 636
Testicular Feminisation, 638
Testicular Swelling, Differential
of, 227
Testosterone, 224, 338
Tests of Significance, 684
Tetanus
Vaccination, 518
Tethered cord, 631
Tetracyclines, 515
Tetralogy of Fallot, 600
Thalassemia, 290
Thecal Cells, 338
Thelarche, 667
Theophylline, 79, 533
Theory X and Y, 699
Therapeutic Drug Monitoring,
533
Therapeutic Index, 528
Thiamine, 49, 451
Thiazides, 51
Thiopentone, 541
Thoracic Outlet Syndrome, 238
Thoracotomy, 21
Thought Disorder, 412
Thrills, 21
Throat Swabs, 65, 607
Thromboangiitis Obliterans, 283
Thrombocytopenia, 295
Thrombocytosis, 294
Thrombophlebitis, 33
Thrombotic Infarction, 127
Thrombotic Microangiopathy,
209
Thrombotic Thrombocytopaenic
Purpura, 209
Thrush, 64
Thymus
on X-ray, 604
Thyroglossal Cysts, 648
Thyroid, 97
Thyroid Eye Disease, 98
Thyroid Nodules, 100
Thyroid Radiology, 97
TIAs, 126
Tibial Torsion
Internal, 619
Tics
in Children, 628
Tidal Volume, 58
Tinea, 317, 387
Tinea Corpus, 317
Tinea Cruris, 317
Tinel‟s Test, 250
Tino Rangatiratanga, 695
Tipu Ora, 697
Tiredness, Differential
Diagnosis, 6
Tissue Donation, 722
TNM System, 468
Tobacco Control, 697
Tobramycin, 514
Tocolysis, 367
Todd‟s Syndrome, 134
Toddler Behaviour, 571
Tohunga, 696
Tongue Tie, 639
Tonic-Clonic Seizures, 134
Tonsillitis, 66
Tophi, 277
Topical Steroids, 335
TORCH Complex, 500, 506
Torsade de Pointes, 480
Torsion of Appendix Testis, 637
Torticolis, 245
Total Lung Capacity, 58
Total Parenteral Feeding, 556
Total Protein, 183
Toxaemia, 364
Toxic Appearance
in a Child, 566
Toxic Changes, 287
Toxic Epidermal Necrolysis, 332
Toxic Megacolon, 169
Toxic Multinodular Goitre, 99
Toxic Shock Syndrome, 316,
500
Toxoplasmosis, 507, 648
TPN, 556
Trabecular Bone, 262
Tracheomalacia, 604
Transference, 666
Transformation Zone, 352
Transient Ischaemic Attacks, 126
Transient Synovitis of the Hip,
621
Transient Tachypnoea of the
Newborn, 596, 605
Transitional Cell Carcinoma,
219, 223
Transitional Papillary Cell
Carcinoma, 217
Transposition of the Great
Arteries, 601
Transudate, Pleural, 73
Transurethral Prostatic
Resection, 224
Transverse Myelitis, 139, 630
Trauma
Abdominal, 490
Chest, 490
in Children, 652
Travel Medicine, 510
Treaty of Waitangi, 695
Trendelenburg Gait, 251
Tretinion, 331
Triangular Fibrocartilage
Complex, 248
Triazole, 336
Trichomonas, 383
Trichomoniasis, 384
Tricuspid Regurgitation, 46
Tricuspid Stenosis, 22
Tricyclic Antidepressants, 433
Overdose, 433
Trigeminal Nerve, 118
Trigeminal Neuralgia, 140
Trigger Finger, 249
Trimethoprim, 515
Triple Blood Test, 360
Triple Therapy
H. Pylori, 162
Tripsin
Testing for IRT in CF, 615
Trisomy 13, 464
Trisomy 21, 581
Tropheryma Whippelii, 165
Trophoblastic Disease, 362
Tropical Sprue, 165
Troponin I, 38
Troponin T, 38
Truancy, 573
Truncus Arteriosus, 601
Tryptase, 484
TSH, 104
Tubal Ligation, 343
Tuberculosis, 502, See Tb
Tuberous Sclerosis, 334
Tubulointerstitial Diseases, 211
Tumour Markers, 468
Turcot‟s Syndrome, 173
Turner‟s Syndrome, 464
TURP, 224
Tympanomtery, 150
Typhoid, 511
Typhoid Fever
Vaccination, 510
Tyramine, 435
Ulcer
Peptic, 161
Ulcerative Colitis, 168
Ulcers, 327
Ulcers, Mouth, 8
Ulnar Nerve, 247
Ulnar Nerve Entrapment, 246
Ulnar Neuropathy, 123
Ultrasound
Fetal, 360
Umbilical Hernia, 642
Undescended Testis, 636
Uniparental Disomy, 465
United Nations Convention on
the Rights of the Child, 562,
718
Upper Respiratory Tract, 62
Antibiotic Treatment of
Infections, 65
Uraemia, 209
Ureter, 219
Ureteritis, 219
Urethral Syndrome, 221
Urge Incontinence, 223
Urinalysis, 202
Urinary Incontinence, 223
in Children, 634
Urinary Tract Infections, 219
in Children, 221
Urine Dipstick, 202, 219
Urine Haemosiderin, 290
Urine Output, 649
Urobilinogen, 183
Urticaria, 333
Usual Interstitial Pneumonia, 84
Uterine Atony, 373
Uterus
Large for dates, 358
Utilitarianism, 716
UTIs, 219
Uvulopalatopharygnoplasty, 92
Vaccination, 515
At Six Week Check, 375
Travel, 510
Vaccination Schedule, 517
Vaccine Preventable Diseases,
518
Vaccines, 516
Vaginal Discharge, 384
Vaginal Exam, 340
Vaginismus, 345
Vaginitis, 348
Vagus Nerve, 118
Validity, 703
Valsalva manoeuvre, 24
Valuing Human Life, 699
Valvular Heart Disease, 43
Vancomycin, 514
Variant CJD, 441, 500
Varicella Zoster, 504
Varices, Oesophageal, 194
Varicose Veins, 33
Vasa Praevia, 366
Vascular Dementia, 441
Vasculitis, 33, 282
Vasectomy, 343
Vasopressin, 104
Vd, 522
Vector, 688
Venereal Diseases Act, 687
Venous Stasis Ulcers, 327
Venous Thromboembolism, 74
Ventilation, Artificial, 60
Ventilatory Failure, 59
Ventouse, 371
Ventricular Fibrillation, 479
Ventricular Septal Defect, 598
Ventricular Tachycardia, 480
Drug Treatment, 42
Verapamil, 42, 52
Verrucae, 318
Vesicular Breath Sounds, 61
Vestibular, 148
Vestibulo-Ocular Reflexes, 130,
148
Vibrio Cholerae, 177
Viral Hepatitis, 186
Viral Pneumonias, 70
Virilism, 107
Viruses
in Children, 617
Vision, Loss of, 141
Visiting Neurodevelopmental
Therapist, 585
Visual Acuity, 140
Visual Impairment in the
Elderly, 675
Vital Capacity, 58
Vitamin A, 336
Deficiency, 647
Vitamin B1, 49, 451
Vitamin B12 Deficiency, 451
Vitiligo, 98, 103
Vocal Chords, 66
Vocal Resonance, 62
Voice Disorders, 66
Volkmann‟s Ischaemic
Contracture, 234, 246
Volume Depletion, 110
Volume Loaded, 21
Volume of Distribution, 522
Volvulus
Small Bowel, 166
Vomiting
in Children, 644
Von Willebrand‟s Disease, 292
Vulval Intraepithelial Neoplasia,
351
Vulval Lesions, 350
Vulvitis, 345
Waldenstrom‟s
Macroglobulinaemia, 303
Warfarin, 75
Warts, 318
Weber Test, 150
Wegener‟s Granulomatosis, 215,
283
Wenckebach Heart Block, 42
Wernicke‟s Encephalopathy, 121
Wernicke-Korsakov Syndrome,
451
Whakama, 696
Wheeze, 61
Differential in a Child, 614
Whipple‟s Disease, 165
Whistle Blowing, 721
White Blood Cells, 286
Whooping Cough. See Pertussis
Wilms‟ Tumour, 217
Wilson‟s Disease, 132, 194, 440
Windup, 543
Withdrawal
Drug Withdrawal Syndromes,
533
in a Neonate, 596
Wolff-Parkinson-White
Syndrome, 26, 40, 601
Worms, Intestinal, 509
Wrist and Hand Fractures, 620
Wuchereria Bancrofit, 509
X Linked
Agammaglobulinaemia, 306
Xanthelasma, 19
Xanthomata, 8
Xerostomia, 280
X-linked Dominant, 465
X-linked Recessive, 464
Yellow Fever, 689
Travel Vaccination, 510
Yerkes Dobson Curve, 422
Yersinia Enterocolitica, 553
Youth Suicide, 663
Zathachromia, 496
Zn Deficiency, 647

4
th
and 5
th
Year Medicine
Study Notes
Edited by David Tripp
Second Edition
February 2003
Volume 2
Systems:
Psychological Medicine ............................................409
Genetics and Cancer ..................................................463
Treatment:
Emergency Management ...........................................475
Infectious Diseases ....................................................493
Pharmacology ............................................................521
Anaesthetics ...............................................................539
Surgical and Fluid Management ................................549
Other Topics:
Paediatrics ..................................................................559
Health Care of the Elderly .........................................671
Public Health .............................................................679
Evidence Based Medicine .........................................701
Professional Development .........................................709
Ethics .........................................................................712
Crib Cards
Infectious Diseases ....................................................725
Physical Examination and Differentials ....................733
Index ...................................................................................745
To the Creative Genius behind the human body:
Did You have to make it quite so complicated?

Psychological Medicine 409
Psychological Medicine
Mental Health In New Zealand ...................... 410
Epidemiology ............................................ 410
Maori Mental Health................................. 410
Mental Health System ............................... 411
Aetiology of Psychiatric Disorders ................ 411
Psychiatric History ......................................... 411
Summary ................................................... 411
History ...................................................... 412
Mental State Examination ......................... 414
Suicide Assessment and Management ...... 416
Interviewing Aggressive Patients ............. 418
DSM IV Classification* ................................. 419
Diagnostic Axises ..................................... 419
Diagnostic Classes .................................... 419
Using DSM Diagnoses* ........................... 421
Anxiety Disorders .......................................... 422
Introduction .............................................. 422
History Taking in Anxiety Disorders ........ 422
Panic Disorder (with or without
agoraphobia) ....................................... 423
Specific Phobia ......................................... 423
Social Phobia ............................................ 423
Generalised Anxiety Disorder .................. 423
Obsessive Compulsive Disorder ............... 424
Post Traumatic Stress Disorder (PTSD) ... 424
Acute Stress Disorder ............................... 424
Treatment of Anxiety Disorders ............... 424
Differentiating Anxiety and Depressive
Symptoms ........................................... 426
Mood Disorders .............................................. 426
Depressive Disorders ................................ 426
Postpartum Mood Disorders ..................... 430
Dysthymic Disorder .................................. 430
Bipolar Depression (Manic-Depression) .. 431
Antidepressant and Mood Stabilising
Medication .......................................... 432
Psychotic Disorders ........................................ 435
Types of Psychotic Disorder ..................... 435
Schizophrenia ........................................... 436
Treatment of Psychosis ............................. 437
Dementia ........................................................ 439
Dementia Due to Head Trauma ................ 441
Delirium ......................................................... 442
Somatoform Disorders ................................... 444
Somatization ............................................. 444
Disorders due to a General Medical
Condition .................................................. 444
Substance Use Disorders ................................ 445
Diagnostic Criteria .................................... 445
Epidemiology ............................................ 446
Models of Aetiology of Addiction ............ 446
History Taking .......................................... 447
Investigations ............................................ 447
Drugs of Abuse ......................................... 448
Regulation of Addictive Drugs ................. 448
Treatment of Substance Abuse ................. 448
Alcohol Abuse .......................................... 450
Other Disorders .............................................. 453
Eating Disorders ....................................... 453
Impulse Control Disorders ........................ 453
Fictitious Disorder .................................... 454
Personality Disorders ..................................... 454
Diagnosis .................................................. 454
Examples of Personality Disorders ........... 455
Borderline Personality Disorder ............... 456
Treatment of Mental Illness ........................... 456
Care for the Mentally Ill ........................... 456
Stigma ....................................................... 456
Drug Treatment ........................................ 457
Cognitive Behavioural Therapy (CBT) .... 457
Problem Solving Therapy ......................... 457
Compulsory Treatment ............................. 458
Grief and Bereavement ................................... 458
5
th
Year Written Exam Model Answer ........... 460

410 4
th
and 5
th
Year Notes
Mental Health In New Zealand
Epidemiology
Prevalence
Severe mental illness: 3%
Chronic and/or disabling: 5%
Mild and/or transient: 19%
No mental health problems: 73% - includes up to 25% who don‟t meet diagnostic criteria, but face
disability in function. Source: Wilson 1997
NZ Spending:
Mental illness: 8%
All other Illness: 92%
Youth Problems in NZ
17% have had a major depressive episode
10% alcohol dependence
11% social phobias
3% attempted suicide
Disorders commonly presenting in primary care:
Depressed mood
Anxiety
Unexplained physical symptoms
Cognitive disturbance
Substance Abuse
Sleep disturbance
Sexual dysfunction
Weight change or abnormal eating
Psychotic symptoms
International (World Bank) – Disability Life Years Lost
Mental Illness: 17%
All other illness: 83%
Christchurch psychiatric epidemiology study, adults from 18 – 64:
Total Population
Male
Female
Affective Disorders
9.4%
6.3%
12.4
Substance Abuse
9.1%
15.4%
3.0%
Schizophrenia
0.2 (underestimates)
Anxiety
8.4%
5%
12%
Key criteria for all illness is impairment of function
Maori Mental Health
Reference: Trends in Maori Mental Health 1984 - 1993, Ministry of Maori Development
Maori admission rates compared with Pakeha: females similar, Maori males 2 times pakeha
Maori readmission rates have grown faster than non-Maori. Maori males 2 times more likely to be
readmitted
By specific diagnoses:
Maori drug and alcohol first admission rates rising relative to non-Maori
Maori admission rates for schizophrenia are similar to pakeha, readmission rates are higher
Maori more likely to be referred to mental health services by welfare or law agencies than by a doctor
(opposite for Pakeha)
Maori more likely to be compulsorily admitted
Issues:
Maori view of mental health and illness vs. Western psychiatric paradigm
Specifically Maori services
Maori workforce development
Issues in treating a Maori patient:
Uncertain identity and alienation from society distrust of practitioner
Must use interventions that enhance a Maori sense of well-being. Whanau must be basic unit of
service delivery. Therapeutic alliance is with whole family, not just patient
Psychological Medicine 411
Complexity of problems lots of agencies involved in care (eg illness, substance use, poverty)
Mental Health System
Influences over the last 20 years:
Individualised care
Community based delivery: psych hospitals were very expensive and only cared for small
proportion of people with mental illness
Consumer empowerment and patient rights
General management (during 80‟s – non-clinical people involved in management)
Purchaser-provider split
Competition
Public reactivity
Thinking about disability as well as illness
Aetiology of Psychiatric Disorders
Predisposing factors: Determine a person‟s vulnerability to psychological distress. Causes include:
Genetic endowment (eg strong genetic component in psychosis)
Environment in utero minor damage to CNS
Personality: combination of genetic, uterine development, childhood experiences (physical,
psychological, social), adolescence. Particular personalities are prone to certain disorders. Eg
early obsessional traits may obsessive-compulsive disorders
Precipitating Factors: Factors that occur shortly before the onset of the disorders and are likely to have
caused it. Eg:
Physical: hypothyroidism, drugs, drugs of abuse, head injury (either direct disturbance or due to
associated stress)
Psychological: eg loss of self-esteem owing to relationship or financial catastrophe
Social: eg moving house, changing job, family disturbance
Perpetuating factors: Factors that prolong the course of the disorder: eg secondary demoralisation
Psychiatric aspects of physical illness:
Most common psychiatric illnesses in physical illness are mood disorders and acute organic mental
disorders
Occurs in one of three ways:
Psychological distress can precipitate mental illness
Physical distress can cause psychological ill-health (as can the medicines for physical disease)
Physical and psychological disorders may exist simultaneously and independently (especially
in the elderly)
Pain: a common medical symptom. Can cause (eg head, neck, lower back, abdomen, genitalia) or
arise from psychological disturbance (eg facial pain – antidepressant therapy can be effective).
Psychiatric History
Summary
Reasons for referral
Presenting symptoms and duration
History of Current Illness, any medication and compliance with it
Systematic enquiry: anxiety, mood, psychotic symptoms, suicidality, cognitive, neuro-physiological,
alcohol and drug, stressors, medications, impulse-control screen
Past psychiatric history
Medical History
Family History
Personal history
Premorbid personality
Patient‟s attribution of illness
Mental State: appearance and behaviour, speech, mood, affect, thought form, thought content, suicidal
ideation, perceptual phenomena, cognition, intelligence, insight and judgement, rapport
Formulation
Diagnosis and Differential Diagnosis
412 4
th
and 5
th
Year Notes
Management Plan
Suicide Assessment:
Trying to assess nature of suicidal ideation and state of current plans
Predisposing factors: family history of suicide, psych illness, or alcohol & drug, personality,
childhood and developmental difficulties, suicide exposure, other illness, environment (eg living
alone, isolated), age and sex
Precipitating factors (short-term risk factors): major/stressful life event, current mood, thoughts
about the future, mental state (eg psychosis, judgement, impulsivity), alcohol and drug use, current
plans, expectations of outcome, availability and lethality of method
Protective factors: cognitive flexibility, strong social supports, hopefulness, treatment of disorders,
responsibility for children
For screening for psychiatric illness in teenagers see HEADSS Risk Assessment, page 666
History
This will include the patient‟s narrative, and is therefore subject to revision and embellishment
according to the state of mind of the individual and the relationship with the interviewer. The patient
may adjust the history according to the interviewer‟s hypothesis and values. History taking is therefore
collaborative and therapeutic. It is helping to construct the illness story
Identifying Data
Name, date of interview, age, sex, race, country of birth, occupation, date of hospital admission,
marital status
Use as opportunity to put the patient at ease, build rapport
Reasons for and circumstances of referral/admission
Who made the referral, why now, what expectations
List of presenting symptoms and their duration
List each symptom and duration, use patient‟s own words
Is the situation acute or chronic
Suggested questions:
What sort of problems are troubling you/were troubling you when you came to hospital?
What have been the main difficulties
History of Current Illness
Need to know the patient‟s story: patient‟s situation and preceding/precipitating events
Narrative account of development of symptoms
Include medication and compliance
Suggested questions:
When did you last feel well?
What are the worst worries in your life?
Systematic enquiry
Should screen for all these in every patient
Anxiety Symptoms
See History Taking in Anxiety Disorders, page 422
Mood Symptoms
Refers to long-term/sustained emotional state (ie over last week/months) and is subjective
experience of the patient
Prevailing mood at the time: quality (eg depressed, sad, angry, irritable, happy, elated,
suspicious, perplexed, anhedonia), intensity (ask about extremes), reactivity, duration (when
was it last normal)
Persisting or fluctuating: if so what pattern
Aggravating or relieving factors
Associated symptoms
Patient‟s attribution of mood
Psychotic symptoms
= Thought disorder, delusions or hallucinations
Thought disorder = abnormalities in the thinking process – evidenced by disorganised speech,
thinking or behaviour
Delusions
= Fixed, false belief, abnormal/bizarre beliefs held with conviction, are without evidence
and are culturally inconsistent
Fixedness is key, resisting coercion to change, and preoccupying
Psychological Medicine 413
Ask about unusual concerns, preoccupations, thoughts that others find strange
Hallucinations = abnormal perceptual phenomena. Ask about visions, sensations, noises that
are unusual or not shared by other people
Suicidibility or other dangerous behaviour: See Suicide Assessment and Management, page 416
Cognitive functioning: See Cognition, page 416
Neurophysiological changes
Measure severity of primary process
Changed sleep, energy/motivation, concentration, appetite/weight (look for a 5% change over
several weeks), sex
Sleep: initial, middle, terminal phases, how much in total, is it restful
Alcohol or drug use
Present or past
Smoking, alcohol, illicit drugs, sleeping tablets/tranquillisers
Stressors
Medications and Compliance
Impulse-Control Screen: Screen for gambling (comorbidity of gambling with other pscyh
symptoms is common)
Past Psychiatric History
Dates, duration, diagnoses, treatment, response to treatment and outcome
Suggested questions:
Have you had any psychiatric treatment before?
Is the present illness like the previous one?
Medical History: Past serious illnesses, disabilities, current illnesses and medication
Family History
Parents and siblings: age, state of health (mental & physical), occupations, situation, personalities,
relationship to patient. May help to draw up a family tree
Get idea of family atmosphere during childhood: personalities of parents and relationships have
lasting influence on subsequent relationships. How much care did you get from each parent? How
controlling/protective were they?
Ask about grandparents, and parents up brining
Has anyone in the family been treated for nerves, had a breakdown, been admitted to a psych
hospital, committed or attempted suicide, had an A & D problem?
Categorise under:
Structure of family
Description of key people
Description of important relationships
Family roles
Family history of psychiatric illness or alcohol abuse
Personal and Social History
Important events and influences in patient‟s life
Start open ended: Tell me a bit about your childhood and background? What are the important
things you remember?
Birth: difficulties, parents situation at time
Childhood: family situation, illnesses, injury, nervous symptoms (eg enuresis/bedwetting, fears,
phobias, how did they feel going to school, etc). Did you ever have any unpleasant experiences –
did anyone ever harm you, hit you, interfere with you sexually?
School: primary to tertiary. Academic, sporting, relationships with peers and teachers
Employment: types of jobs, reason for leaving, work performance & satisfaction, relationships at
work
Sexual: age at puberty, sexual orientation, sexual experience (current and past), sexual satisfaction,
contraception, sexual abuse, unpleasant or distressing sexual experiences. Introduce when talking
about adolescence. Aim is to establish abnormalities or concerns about sexual functioning or
relationships
Marital: duration of courtship, age at marriage, age, occupation and health of spouse, marital
relationship and problems
Children: pregnancies, ages and names of children, health, personalities, schooling, occupations,
difficulties in relationship with parent
Friendships: long-standing friends and confidences
Current living situation

414 4
th
and 5
th
Year Notes
Difficulties with law
Leisure activities and interests
Religion: upbringing, beliefs and practices, changes in religious belief (important to ask, won‟t
volunteer)
Premorbid personality
Patient‟s opinions and interviewer‟s impressions of premorbid personality
Personality = enduring characteristics, so requires evaluation over time
Patient’s Attribution of Illness
What the patient thinks is the cause of the illness
Possibility include under „insight‟ in mental state exam
Insert Mental State Exam write-up here (See Mental State Examination, page 414)
Formulation
Core of the psychiatric assessment: why did this person become ill in this way at this time?
Opinion about what explains the presentation and what treatment may work
Manner in which patient‟s problems are unique. Not a summary of problems but the crucial
factors, based on a theoretical knowledge of the aetiology of psychiatric illness. The
linkages/connections between different aspects should add something new – all the raw material
should have been presented before
Should cover the 4 Ps: Predisposing factors, precipitating factors, perpetuating factors, protective
factors
Conceptualise by filling in this table:
Predisposing
Precipitating
Perpetuating
Protective
Biological
Psychological
Psychosocial
Suggest outline (one paragraph per bullet):
Describe problem
Why is this patient at risk of a psychiatric illness, using bio-psycho-social framework
Describe triggers to presentation
Describe relevant prognostic factors, positive and negative
Balanced assessment of risks: especially of suicide and violent behaviour
Diagnosis and Differential Diagnosis
Manner in which patient‟s problems are similar to others (cf formulation which emphasises
uniqueness)
Usually presented using DSM-IV or ICD-10. (See DSM IV Classification*, page 418)
In differential diagnosis: concisely state evidence for and against each possible diagnosis in order
of probability – only include evidence that discriminates between diagnoses
Don‟t forget general medical conditions if there is sufficient evidence
Management Plan
Safety: how will the risks identified be contained or minimised. Is the patient consenting or
committed?
Medical: any medical conditions requiring attention
Diagnosis: is it clear? If not, what needs to be done?
Psychiatric Management: can be divided into management of target symptoms and management
aimed at underlying disease. Can be considered under bio-psycho-social headings. Divide into
timeframes – now, the next day or two, longer term
Always mention family in plan: information and support for them, their role in helping the patient,
assistance with the significant stresses the family may face, etc
Experience Interviewing the Patient: difficulties interviewing the patient, reactions/emotions evoked
by patient, how you dealt with these
Mental State Examination
This is NOT an assessment of cognitive function (the mini-mental state is about cognitive function, but
is just part of a description of mental state)
Appearance and Behaviour
General appearance: physique, hair, make-up, tattoos, scars, clothing (self neglect, incongruous
dress, weight loss)
Facial expression: suggestion of depression, anxiety, physical disorder (eg parkinsonian syndrome)
Posture
Psychological Medicine 415
Movements: mood and involuntary movements (tics, dystonia, akathisia, tardive dyskinesia,
parkinsonism), psychomotor agitation (eg how long to answer a question)
Social behaviour: over familiar, disinhibited, withdrawn, preoccupied, co-operative or not, bizarre
behaviour
Speech
Rate – fast/slow, Quantity – a lot/little, Loudness – loud/soft
Spontaneity, Continuity, Articulation, Prosody, Pressure
Mood: Prevailing mood at the time. The patient‟s subjective experience, what they report. Note
fluctuations (eg diurnal variation in depression is common)
Affect
Refers to the objective appearance of emotions observed during the interview: anger, anxiety,
elation, irritability, depressed, etc
Quality, intensity, stability, range
Variations: labile, restricted, blunted, flattened, inappropriate, fluctuating
Appropriateness: congruous with thinking or not
Thought Form
May be best demonstrated by direct quote
Is there a logical connection between ideas or not – from an opening statement through to a goal
Then define type, eg:
Loosened associations
Flight of ideas
Derailment
Thought block (just stops)
Tangential (talks at great length but never gets to the point)
Interpenetration of themes (rapid change to something completely different)
Thought Content
Depersonalisation: feeling detached from oneself, feeling unreal (often with anxiety)
Derealisation: feelings of unreality of the external world
Spectrum: ideas concerns preoccupations overvalued ideas obsessions delusion.
Note different levels of conviction:
Over-valued idea: I think it but accept that others don‟t
Obsessional: I know it‟s not true but I can‟t get it out of my head
Delusional: I think that, and everyone else thinks that, and I don‟t believe them if they say
they don‟t
Obsessional phenomena (see History Taking in Anxiety Disorders, page 422)
Delusions:
Evaluating delusions: Describe unusual statement, experience or event, decide if it is false, is
there any cultural determination, classify it
Passivity phenomena/control:
Thought insertion: reports „alien‟ thoughts
Thought broadcast: thoughts transmitted to other people
Thoughts spoken aloud: feels as if thoughts are audible to others
Thought echo: involuntary repetition of thoughts
Delusional mood
Delusional perception: perception + delusional interpretation
Paranoid delusions: Is anyone trying to harm you?
Referential delusions: have you noticed anything (eg on TV) that refers to you
Grandiose delusions, sexual delusions
Delusions of guilt, hypochondriasis, nihilism
Delusions of misidentification and misrepresentation: refers to the belief that people have been
replaced by impostors
Suicidal and homicidal ideation
See Suicide Assessment and Management, page 416
Perceptual Phenomena
Illusions: misrepresentation of external environment – transformation without perception
Hallucinations:
External perception without any external stimulus. Hearing voices inside your head is not an
hallucination – they should hear them as coming from outside their head
416 4
th
and 5
th
Year Notes
Can be auditory, visual, olfactory, tactile or taste
If auditory, clarify characteristics: sounds or voices, one or more voices, talk to you or to each
other, give commands, do you recognise them, believe them
Cognition
See also Cognitive Functions, page 122
Is defined by how we assess it!
Can test with Mental Status tests, etc
Observe alertness, attention and concentration (serial sevens, spell „world‟ backwards, days or
months backwards), orientation (time, place and person), memory, executive function, localised
functions
Testing memory: short term – recollection at 5 minutes, recent memory – events over past several
days (adapt to patient‟s interests), remote memory – personal events, birth date, sequence of events
[NB – this classification is really an artefact – it doesn‟t correlate with how memory works]
Language: word finding, comprehension, reading, writing
Calculation: needed for getting change, paying bills
Visuospacial: dressing, finding way around, neglect, problem for driving
Visual perception: can‟t recognise what they see
Personality change: usually exaggerates or ameliorates premorbid state: motivation, spontaneity,
persistence, care, social conduct, quality of relationship, aggression
Problem solving ability
Consider in the context of ADLs (Activities of Daily Living) and Instrumental ADLs (eg using
phone)
If confused may need to interview an informant
Patient will usually water down symptoms
Intelligence: Vocabulary, previous and current performance
Insight and Judgement
Awareness of their own mental condition, do they recognise the reasons for their difficulties
Full, partial, limited, grossly impaired
Base around 4 questions:
Are they aware of the phenomena others have observed
If so, do they recognise them as abnormal
If so, do they consider they are caused by mental illness
If so, do they need treatment
Rapport
Sense of empathy, emotional response of interviewer to patient and patient to interviewer
Good, superficial, none
Easy to overestimate: key test is would they do something you asked if they didn‟t want to. Can
you predict future relationship
Suicide Assessment and Management
Always screen all psychiatric patients for suicide
Definitions:
Attempted suicide: self-inflicted harm intended to cause death
Parasuicide: Act intended to communicate distress not intended to cause death
Suicide History
Overview:
Establish and maintain rapport
Evaluate for:
Suicidal thinking
Suicidal intent
Suicidal plans
Future orientation
Relevant mental status: including mood, drugs/alcohol, labile, impulsiveness, insight, etc
Assessment of risk factors
Ideation questions:
Do you see a future for yourself?
Do you think a lot about death?
Have you ever considered harming yourself/wanted to end your life?
Psychological Medicine 417
What specifically have you thought about this? When did you start thinking this way?
Have you talked to anyone about this?
Do you want to die – or do you want others to realise how bad things are for you?
Have you thought of a plan to kill yourself?
Do you have the means?
What has stopped you so far?
Have you thought about the effect your death would have on family and friends?
How do you feel about accepting help?
How does talking about this make you feel?
If can‟t ask the question directly, then „what do you think about suicide‟, „what would you do if it
got that bad‟, „how bad does it get… have you ever felt so bad that you wanted to end your life‟
Have you thought of hurting anyone else
Past Suicide attempt(s):
What did you do?
When did you start thinking about suicide? Why did you think that?
When did you plan to do something? (ie was it impulsive or planned)
When did you start to action the plan? What triggered that (what was the final straw)?
Did you leave a note/say goodbye/wind up your affairs?
What stopped you going through with it?
How did you get to be in hospital?
Are you surprised to be alive? (ie did they genuinely think it was going to kill them)
Has anything changed in the things that made you try?
What did you feel about getting help?
Assessment of Risk
Predisposing Risk Factors:
Present from birth or soon after:
Sex: Female more likely to try, male more likely to succeed
Genetic or congenital factors
Family History of suicide, psychiatric illness or substance abuse
Personality Traits (eg impulsiveness, perfectionism, hopelessness, low self esteem)
Risk Factors developed later in life:
Suicide Exposure
Psychiatric diagnosis: depression, substance abuse (esp. age 40 – 60) and schizophrenia show
strongest correlation
Other illness
Previous suicidal intents: include factors listed above, type and frequency of ideation, etc
Environmental factors: separated, living alone, elderly, isolated, unemployed
High risk situations: eg young males
Protective Factors: decrease risk:
Cognitive flexibility
Strong social supports
Hopefulness
Treatment of disorders
Responsibility for children
Are there other things that would stop them?
Precipitating Factors: short term risk factors:
Humiliating/precipitating life event: job loss, move, separation, death, interpersonal problems
Post partum
Recent discharge from a psychiatric hospital: a high risk time
Current mood: depression increases risk significantly
Thoughts and expectations about the future. Very important to assessing overall risk. Is the future
hopeless? If they have nothing to live for, suicide is easier
Mental State: mood, psychosis ( impaired judgement, voices may tell them to do it, paranoia),
judgement, impulsivity (be aware of effect of alcohol if person is sober when interviewed: when
you drink, how do you feel afterwards)
418 4
th
and 5
th
Year Notes
Current plan: detail, lethality (not how lethal it actually would be, but what did patient think would
happen), fantasies (eg have they thought about other‟s reactions to their death), expectations of
outcome (eg do they want to be found?) Availability of method
High risk if:
Recent well planned attempt. Remains fixed on wish to die or refuses treatment
Patient has had thoughts about suicide and intends to act on them
If the patient is uncooperative and the assessment was incomplete
If the following are present: psych illness, significant stress, history of impulsivity or violence,
family history of suicide
Influence of community standards and norms on suicide*
Individualism: you‟re a failure if you can‟t make it on your own
Copy cat syndrome
Expectations of achievement individuals set high expectations and fail
Community encourages the use of weapons
Community demeans the poor see themselves as unimportant
Community encourages external locus of control can‟t change anything fatalism
Community encourages/condones suicide in certain circumstances:
People with certain conditions alienated, eg psych illness
Minority culture alienated by enforced dominance of the dominant group‟s beliefs and values
(hegemony) alienation
Management of Current Suicide Risk *
For a high risk: emergency assessment (eg CAT team) followed by regular nursing assessment
For lower risk in a GP setting (UK source):
Straight away:
Identify risk on notes in a way that won‟t be missed by you or other members of the team (eg
note or sticker on summary sheet). Won‟t affect life insurance risk if insurance covers a
mortgage or loan, or policy was taken out more than one year before. Suicide risk has no
additional effect on premiums over and above the presence of depression
Don‟t give prescriptions with repeats – get them to come back for each script. Allows better
monitoring and limits the amount of medication they hold at any time
Ensure adequate symptom relief of physical symptoms
Use a counselling approach: empathy, give feedback to clarify the patient‟s problems, provide
advice if appropriate, etc
Further Actions:
Plan the next few days: especially if a weekend, or they have poor social supports. Should be
detailed, and given to the patient on paper to take home. Should include contact with other
people and things the patient enjoys
Ensure family member/responsible friend is available
Encourage use of informal supports: whom can they talk to. If there is nobody, why do they
feel like this?
Use non-statutory Services: Lifeline, Youthline, Samaritans, community organisations,
support groups, sports/hobby groups etc
Offer follow-up: opportunity to reassess patient, and provide further support
Consider referral to specialist care: Community Psychiatric Nurse, social worker, psychiatrist,
psychologist, CATT
Afterwards:
Liase with other professionals
Discuss with another team member to review your risk assessment and management plan
Be aware of your own response: patients like these can cause considerable concern or evoke a
strong emotional response
Interviewing Aggressive Patients
Understanding why they are aggressive is important:
Poor anger control
Inappropriately managed
Overwhelmingly afraid
Most clients are afraid/confused by their own feelings

Psychological Medicine 419
Aggressive patients often try to change the „rules‟ of the relationship between professional and client
by trying to dominate. The interviewer must maintain the boundaries. If „rules‟ are broken (eg threats,
etc) terminate the interview
Interviewing tips:
Is it wise to interview them at all?
Get as much information about their history and current state before you start
Patients home most difficult environment
Ensure you and the client have direct access to a door
Appear confident!
Ensure there are no missiles (tea cups, ash trays)
Don‟t sit eyeball to eyeball. Have the client in a low, soft chair
Have someone else sit in
Remain aware of clients body language
Negotiate breaks with the client – take a walk in the corridor
Responses:
Set limits: “I can‟t help you if you keep shouting”
Demanding patients: “Perhaps I need to know a bit more before I decide to…”
Reflection: “I can see that made you very angry”
Evaluation:
Diagnose psychiatric disorder and assess mental state – especially paranoid states, command
hallucinations, intoxicated, delirium, manic, depressed
History of violence, abuse, neglect
Who are intended victims
Emotional stressors
Quality of self control
External constraints on behaviour
Physical exam: old and new injuries
Sedation: if drug sedation is necessary:
Haloperidol 2.5 – 5 mg PO/IV and Clonazepam 2 mg PO/IM. Effect takes up to 20 – 30 minutes.
Repeat at 30 minute intervals to maximum of 3 doses
If you forcibly restrain or medicate someone, should initiate Mental Health Act (otherwise iT
constitutes common assault)
DSM IV Classification*
Published 1994, replaces Diagnostic and Statistical Manual of Mental Disorders III and III-R
Diagnostic Axises
Axis 1: Clinical Disorders eg major depression, adjustment disorder, schizophrenic disorder. Basis in
medical model
Axis 2: personality disorder or traits and mental retardation. More blurred distinction between person
and pathology
Axis 3: General Medical Conditions (physical disorders and conditions)
Axis 4: Psychosocial and Environmental Problems (eg severity of psychosocial stressors, problems
with primary support group, social environment, educational, occupational, housing, economic, access
to health care system)
Axis 5: global assessment of functioning (eg in the previous year)
Diagnostic Classes
Major Diagnostic Class
Examples of Disorders
Notes
Disorders usually first
diagnosed in infancy, childhood
or adolescence
Mental retardation, learning, Pervasive
Developmental (eg Autistic), Attention
Deficit and Disruptive Behaviour, Tic
420 4
th
and 5
th
Year Notes
Delirium, Dementia and
Amnestic and Other Cognitive
Disorders
Delirium (eg due to GMC, substance
intoxication or withdrawal), Dementia
(eg due to Alzheimer‟s, Vascular,
HIV, Head Trauma, CJD, Parkinson‟s,
Huntington‟s). See Dementia, page
439 and Delirium, page 442
Some with specifiers for
uncomplicated, with delirium, with
delusions, with depressed mood
Mental Disorders due to a
General Medical Condition
(GMC) not elsewhere classified
Catatonic disorder or personality
change due to …
Most of diagnostic classes have a
category „due to a GMC‟ where the
symptoms fit that class – eg Mood
Disorder due to a GMC
Substance Related Disorders
For most substances there are
[Substance] Use and [Substance]
Induced (including psychotic, mood,
anxiety etc)
Specifiers include: with/without
physiological dependence,
full/partial/sustained/early
remission, with onset during
intoxication/withdrawal
Schizophrenia and Other
Psychotic Disorders
Schizophrenia, Schizophreniform,
Schizoaffective, delusional, brief
psychotic
Specifiers for Schizophrenia
include paranoid, disorganized,
catatonic, undifferentiated and
residual types
Mood Disorders
Depressive (Major Depressive
Disorder – single episode and
recurrent – and Dysthymic), Bipolar
(Bipolar I & II, cyclothymic)
Some have specifiers for severity,
psychotic, remission specifiers,
chronic, with
catatonic/melancholic/atypical
features, with post-partum onset,
with seasonal pattern/rapid cycling
Anxiety Disorders
Panic (with/without agoraphobia),
Agoraphobia (without panic), Specific
phobia, social phobia, Obsessive-
Compulsive, Post Traumatic Stress,
Acute Stress, Generalised Anxiety
Somatoform Disorders
Somatization, Undifferentiated
Somatoform, Conversion, Pain,
Hypochondriasis, Body Dysmorphic,
Somatoform
Fictitious Disorders
Factitious Disorder with
predominantly psychological/physical
signs
Patients intentionally produce signs
of medical or mental disorders and
misrepresent their histories and
symptoms. Have compulsive
quality – but behaviours are
purposeful and deliberate
Dissociative Disorders
Dissociative Amnesia, Fugue, Identity
Disorder, Depersonalisation
Patient feels lack of unity in state
of consciousness, confusion
regarding their identity or multiple
identifies
Sexual and Gender Identity
Disorders
Sexual dysfunctions (of desire,
arousal, orgasmic, pain), Paraphillias
(eg paedophilia), Gender identity
Eating Disorders
Anorexia Nervosa (restricting or
binge/purging type), Bulimia Nervosa
(purging type, non-purging type)
Sleep Disorders
Primary Sleep (eg dyssomnias and
parasomnias) and Related to another
mental disorder
Impulse-Control Disorders Not
Elsewhere Specified
Eg Kleptomania, Pyromania,
Pathological Gambling
Psychological Medicine 421
Adjustment Disorder
With depressed mood, anxiety, mixed,
disturbance of conduct/emotions
Where symptoms appear within 3
months of an identifiable stressor.
Should not meet criteria for another
axis I or II disorder, and excludes
bereavement. A short-term
maladaptive reaction to a stressor
(ie impairs social/occupational
function or causes distress).
Personality Disorders
See Personality Disorders, page 454
Other Conditions that may be a
focus of clinical attention
Psychological factors affecting
medical condition (eg mental
disorder/personality traits/maladaptive
health behaviours affecting medical
condition), medication-induced
movement disorders, relational
problems, problems related to abuse or
neglect, Non-compliance,
Malingering, Bereavement
Using DSM Diagnoses*
In DSM IIIR, “Delirium, Dementia and Amnestic and Other Cognitive Disorders”, “Mental Disorders
Due to a General Medical Condition” and “Substance-Related Disorders” were grouped under the
single heading “Organic Mental Syndromes and Disorders”. “Organic mental disorder” is no longer
used as it implies other disorders don‟t have a biological basis
Qualifiers on Diagnostic codes:
Severity and course specifiers: mild, moderate, severe, in partial remission, in full remission, prior
history of (ie have had full recovery)
Principal diagnosis/Reason for visit: if more than one diagnosis, which one was the principle one
leading to admission/contact. Difficult to determine in dual diagnosis (substance related + non-
substance related). Multiple diagnoses can re reported in multiaxial fashion
Provisional: when strong assumption that criteria will be meet, but insufficient evidence currently
available
Not-otherwise specified used when:
Symptoms below clinical threshold or there is an atypical or mixed presentation
Symptom pattern is not included in DSM IV
When there is uncertainty about aetiology: eg whether it is due to a general medical condition, is
substance induced or is primary
There is incomplete or inconsistent information
Frequently used criteria – to exclude or suggest differential diagnoses:
Criteria have never been/are not meet for…
Does not occur exclusively during the course of…
Not due to the direct physiological effects or a substance of a general medical condition – ie these
have had to have been considered and ruled out
Not better accounted for by…
These criteria establish a hierarchy:
Disorders due to a general medical condition or substance-induced disorder pre-empts diagnoses of
primary disorder with the same symptoms (eg Cocaine-induced mood disorder pre-empts Major
Depressive Disorder)
A more pervasive disorder pre-empts diagnosis of a less pervasive disorder with a subset of the
symptoms of the more pervasive disorder (eg Less pervasive disorder will have „Criteria have not
been meet for [the more pervasive disorder])
When there are very difficult diagnostic boundaries, use „not better accounted for‟ to permit use of
clinical judgement
422 4
th
and 5
th
Year Notes
Anxiety Disorders
Introduction
Anxiety is usually normal, useful and protective. We learn to fear normal anxiety. Yerkes Dobson
Curve (1908): moderate levels of anxiety can improve performance, but performance improvement
plateaus and then falls with anxiety. Anxiety becomes debilitating if severe
4 clusters of responses:
Physiological: autonomic nervous system arousal, sleep
Cognitive: perception of danger, threat, loss, hypervigilence
Affective: nervousness, fear, concentration
Behavioural: fight or flight
Anxiety disorders lead to:
Over activation of cognitions about personal danger
Underestimation of ability to cope
Differential Diagnoses:
Exclude anxiety due to substance intoxication or withdrawal, or due to delirium
Physical conditions that cause or exacerbate anxiety (hyperthyroidism, hyperventilation – eg
asthma, phaeochromocytoma, drug withdrawal, etc)
Becomes a disorder when it causes significant distress or interferes with social or occupational
functioning
History Taking in Anxiety Disorders
Introductory Questions:
Are there currently things in your life that are causing distress/worry?
Are there things that have happened in the past that you can‟t stop thinking about?
How is your general health?
Any one else in your family had similar problems?
Most anxiety is part of a mixed anxiety/depression importance of full psychiatric assessment
General Anxiety
Would you describe yourself as a worrier? Do you worry about things that others don‟t worry
about?
Do you sometimes make mountains out of molehills?
Do you every find it hard to make decisions?
Panic
Have you ever felt your heart pounding, felt frightened/afraid – what do you think was the cause?
Ever felt like a disaster was about to happen to you?
Do they occur when other people wouldn‟t feel afraid?
Do you avoid going out?
Phobias/Avoidance:
Is there anything you would avoid if you could? What happens if you are unexpectedly faced with
that object/situation?
Do you have worries/fears that prevent you from doing things you would like – or that others can
do without difficulty?
Are you only worried if others will see you?
Are you worried/anxious in other settings?
Obsessions and Compulsions:
Obsessive thoughts: Any thoughts that keep coming repeatedly into mind, even when you‟re trying
to get rid of them?
Compulsive rituals:
Do you ever have to repeat actions over and over which most people would only do once?
Do you ever find yourself having to do things over and over again to get them just right?
Do you find yourself spending a lot of time doing things like cleaning or checking that
everything is safe?
What happens if you are interrupted when doing these things?
Trauma:
Do you still have recurrent memories of an upsetting event?
Do you have nightmares, have trouble sleeping, or feel jumpy?
Are there things that remind you of the event? Do you avoid these?
Psychological Medicine 423
How has the trauma changed the way you feel about the future, about what you enjoy?
Panic Disorder (with or without agoraphobia)
Panic attack:
= Intense exacerbation of autonomic responses: discrete episode of intense dread, fear or doom
Sudden, abrupt onset
Symptoms include racing heart, trembling, SOB, nausea, fear of dying or losing control, going
crazy. May have limited symptom attacks
Found across anxiety disorders and in non-anxious population
Panic Disorder:
Recurrent and unexpected panic attacks. Situationally-bound panic attacks are characteristic of
social or specific phobias, although situationally-predisposed panic attacks are frequent in Panic
Disorder
Catastrophic misinterpretation of bodily sensations/mental events (eg has palpitations and thinks
they‟re having a heart attack). Normal bodily sensations misinterpreted
High anticipatory anxiety: persistent worry about having additional attacks
Hyper-vigilance for feared sensations
Agoraphobia:
= „Fear of fear‟
Fear of situation where escape may be difficult or embarrassing in the event of a panic attack
Avoid or endure with dread situations associated with panic attacks and feared bodily sensations
Characteristically involve clusters of situations including being outside the home, being in a crowd,
on a bridge, in a car, train or bus
But fear NOT of the situation
Can occur with or without a history of panic disorder
In Panic disorder, the more agoraphobic avoidance there is, the worse the prognosis
Differentiating from Social Phobia: in panic disorder, fear evaluation of what panic causes them to do
(difficulty breathing, dizziness, weakness in limbs). In Social phobia, fear evaluation of what they do
or say regardless of panic (blushing, sweating, trembling)
Specific Phobia
Persistent and irrational fear and avoidance of a specific object or situation
Leads to avoidance or intense anxiety on exposure to feared stimulus
Fear recognised as excessive
Disruptive to functioning (important – who cares about a snake phobia in NZ)
Can also be anxious about fear reaction
Usually related to animals (mice, snakes, spiders), natural environment (earthquakes), blood, injection
or injury; specific situations (eg claustrophobia)
Develop due to:
Direct conditioning through personal experience
Verbal or vicarious transmission (eg develop shark phobia after watching Jaws)
Treatment:
Graded exposure
Cognitive restructuring
Physiological control: relaxation and medication (short-term only)
Social Phobia
Fear of negative evaluation of performance in social situations. Fear they will do or say something
embarrassing or humiliating. Fear visible anxiety symptoms
Probability and cost of negative evaluation is over-estimated
Early onset
Leads to avoidance of social gatherings, public travel, etc
Epidemiology: 6 month prevalence is 2 per 100, more females, onset in teens through to 35 social
isolation
Aetiology: ?conditioned response, genetics
Generalised Anxiety Disorder
Worry about worry: a meta-worry!
424 4
th
and 5
th
Year Notes
Excessive and persistent worry about a number of areas of life including family, health, job, finances,
etc
Worrying dominant source of discomfort: spend half an average day worrying – most recognise they
worry excessively about minor things but can‟t control it
At least six-month duration, chronic fluctuating course
Epidemiology: 2 – 8 % of the population, onset 20 – 40 years, male = female
Symptoms: restlessness, feeling on edge, difficulty concentrating, mind going blank, irritability, muscle
tension, sleep disturbance (esp difficulty getting back to sleep after waking, anticipatory thoughts while
awake)
Co-morbidity/differential: mood disorders, adjustment disorder (clearly identifiable stressor), panic
attacks, socially anxious, low self-esteem, avoidant or dependent personality disorder
Treatment:
Education
Training: relaxation, breathing control, structured problem solving, gradual confrontation of fears
Avoid sedatives: they will love them but will become dependent on them and underlying problems
won‟t be fixed
Specialist referral if symptoms persist for a further 3 months
Obsessive Compulsive Disorder
Upsetting and intrusive obsessional thoughts that are difficult to control (e.g. fear of contamination),
leading to compulsive rituals (although can have rituals in the absence of obvious obsessions)
Common compulsions: cleaning, checking, counting
Treatment:
Hard to treat with CBT and antianxiolytics
Consider antidepressants
Some evidence of effectiveness of low dose respiridone (?may be delusional component)
Post Traumatic Stress Disorder (PTSD)
Long lasting anxiety or memories about a severe traumatic event, including nightmares, flashbacks,
anxiety, avoidance of reminders
Diagnostic criteria:
Actual or threatened severely traumatic event where the response was intense fear, helplessness or
horror
Event is persistently re-experienced: recollections, dreams, distress to cues of an aspect of the
event
Persistent avoidance of stimuli associated with the trauma (triggers) and numbing of general
responsiveness (eg interest in activities, detachment, etc)
Persistent symptoms of increased arousal (eg difficulty sleeping, irritability, concentration,
hypervigilance)
Duration of > 1 month
Causes significant distress or impairment in social/occupational function
Types:
Acute: duration of symptoms < 3 months
Chronic: duration of symptoms > 3 months
Delayed onset: onset > 6 months after stressor
Differential: OCD, Acute stress disorder (resolves within 4 weeks), adjustment disorder, psychotic
disorders, malingering
Acute Stress Disorder
Distinguished from PTSD by duration < 1 month (i.e. short term reaction). Includes avoidance, fear of
being alone, muscle tension, disbelief, problems with sleep, concentration and memory, guilt, self-
doubt
Treatment of Anxiety Disorders
Cognitive Behavioural Therapy (CBT)
Effective for most anxiety disorders
Response more long lived than for drug treatment
Psychological Medicine 425
Includes: breathing retraining, deconditioning, cognitive restructuring, relaxation, graded exposure,
desensitisation
Psychodynamic Psychotherapy
Symptoms result from mental processes outside conscious awareness. Aim is to elucidate these
Identify and alter core conflicts
Drug Treatment
Benzodiazepines: may be useful for the short term or acute treatment of acute stress reactions. Due to
tolerance and dependence, these are not useful for long-term use
Antidepressants:
For severe panic disorder (with or without agoraphobia), TCA‟s (eg imipramine) are the
medication of choice. Suppression of panic attacks may occur after 4 – 6 weeks. Minimum
treatment usually 6 months. Maximum is 18 months. Use alternative therapies if it fails after this
time
For OCD, clomipramine (a TCA) and SSRIs may be a useful adjunct to CBT. Help minimize
compulsions and manage the depression often associated with OCD.
Betablockers: Useful for the treatment of social phobia when performance anxiety is the main problem.
These prevent noticeable symptoms (eg blushing or shaking), which are typically interpreted
catastrophically by individuals. However, these drugs are not useful if the anxiety is more generalized
Benzodiazepines
Mode of action: enhance GABA inhibition throughout the CNS
GABA (gamma-amino-butyric acid) increases membrane Cl- permeability hyperpolarisation
Binding affinity important in governing duration and degree of effect, in addition to elimination and
dosage.
Hypnotics
T½
- Ultra-short acting
Midazolam
1.5 – 2.5
Triazolam
1.5 – 3
- Sleep sustainers
Zopiclone
4 – 6
Loprazolam
6 – 9
Temazepam
6 – 9
- Others
Lormetazepam
9 – 12
Nitrazelam
25 – 35
Flunitrazepam
15 – 35
Anxiolytics
Diazepam
32
Active metabolite T½ is 40 – 200
hours
Chlordiazepoxide
12
Same metabolite as Diazepam
Lorazepam
12
Pronounced withdrawal
Oxazepam
8
Slow absorption
Alprazolam
14
Panic disorders, antidepressant effects
in anxiety states
Clonazepam
Useful anticonvulsant activity
Key pharmacodynamic differences:
Chlordiazepoxide and Diazepam: shorter elimination time than their active metabolites. Doses of
benzos with active metabolites should be reduced in the elderly, especially if renal function
Midazolam: often used as premed for procedures and GA – relaxes and amnesia
Zopiclone (Imovane): differs from BDZs and barbiturates, but has same actions (sedation,
anticonvulsant, anti-aggressive and muscle relaxant). Binds to BDZ binding sites. Peak plasma
conc. in 1 hour, T½ of 4 hours. At higher doses: hangover effect, memory disturbance, rebound
insomnia, interaction with alcohol
Metabolism:
Eg: diazepam temazepam oxazepam
Inactive conjugates excreted
Adverse Effects:
Daytime sedation: with long acting BDZs where slow elimination leads to accumulation of drug
and active metabolites
426 4
th
and 5
th
Year Notes
Daytime agitation/irritability: with ultra short acting BDZs (triazolam, midazolam), especially in
those with anxiety
Psychomotor functional impairment: beware if driving or operating machinery
Amnesia: with short acting BDZs
Physical dependence: All BDZs are addictive
CNS effects of BDZs all exacerbated by alcohol
Broken sleep patterns are particularly common after withdrawal of hypnotics
Discontinuation of long-term use must be gradual (2 – 3 months) never abrupt. Withdrawal similar
to hyperadrenergic state – anxiety, tremor, ataxia, confusion, insomnia, nausea, seizures (especially
with lorazepam). Withdrawal syndrome can be prolonged (ie months). Treating withdrawal:
change to diazepam (greater dose flexibility), reduce dose by 10% every 2 – 4 weeks. Use
counselling and relaxation
Lorazepam as a hypnotic where insomnia is a complication of anxiety – but never just as a hypnotic
See Treatment of Insomnia, page 534
Differentiating Anxiety and Depressive Symptoms
Coexistence of anxiety and depressive symptoms is common:
Depressive symptoms occur secondarily especially in panic disorder, agoraphobia and OCD. If
anxiety disorders go untreated demoralised and progressive restrictions on function
depression
Anxiousness and irritability are seen in the majority of depressed patients, panic attacks may occur
Differentiating:
GAD/Panic disorder don‟t usually have full range of vegetative symptoms
Anxious patients have trouble getting to sleep, depressed wake early
Anxious patients don‟t loose the capacity to enjoy things or be cheered up
Asking which symptoms came first can be helpful
More Common in
anxiety disorders
More common in
depression
Common to both
Bodily
Difficulty falling asleep
Tremor/palpitations
Sweating
Hot/cold flushes
Muscle tension
Nausea
Breathlessness
Early waking,
oversleeping
Diurnal variation
Chronic nagging pain
Agitation or slowed
behaviour
Loss of libido
Sleep disturbance
Appetite change
Non-specific bodily complaints
Fatigue
Restlessness
Headaches
Dry mouth
Feelings
Helplessness
“Stressed out/keyed up”
Apprehension
Sadness, despair
Guilt, hopelessness
Lack of motivation
Lack of pleasure, flatness
Interest in normal
activities, apathy
Irritability
Feelings of doom, anxious
Dependent
Loss of enjoyment
Tearful
Rapid mood swings
Thoughts
Expecting the worst
Catastrophic thinking
Slowed speech, thought
processes, response
times
Suicidal thoughts
Difficulty with concentration
Excessive worry
Indecision
Behaviour
Phobic avoidance of
feared situations
Easily startled
Anxiety reducing rituals
Hyperventilation
Reduced mobility
Downcast expression
Decreased socialising
Daily activities
Dissatisfaction with life
Derealisation
Depersonalisation
Mood Disorders
Depressive Disorders
References: Guidelines for the Treatment and Management of Depression by Primary Healthcare
Professionals, National Health Committee, September 1996
Psychological Medicine 427
Diagnosis of Major Depressive Disorder/Episode (MDE)
Handy pneumonic:
S: Sleep
A: Appetite and weight
D: Dysphoria and anhedonia
F: Fatigue
A: Agitation/retardation
C: Concentration
E: Esteem
S: Suicide
DSM IV criteria:
5 or more of the following present during the same 2-week period and represent a change from
previous functioning. At least one symptom must be depressed mood or loss of interest/pleasure
[NB exclude symptoms clearly related to a general medication condition, delusions or
hallucinations]. Note duration and persistence of each symptom, and compare to normal:
Depressed mood, most of the day, nearly every day (either self report or observed by others)
Markedly diminished interest or pleasure in all, or all most all, activities (exclude grief
reaction)
Significant weight loss/gain or / in appetite (exclude cancer, Tb, hypothyroid)
Insomnia/hypersomnia nearly every day (exclude sleep apnoea)
Psychomotor agitation or retardation (excessive repetitious and pointless motor activity that is
associated with feelings of tension. Needs to be observable, not just felt). Eg have you been
fidgety/restless or felt „stuck in the mud‟ or in slow motion?
Fatigue or loss of energy nearly every day
Feelings of worthlessness or excessive or inappropriate guilt nearly every day. Eg how do you
feel about yourself, have you blamed yourself for things, do you feel guilty?
Diminished ability to think or concentrate, or indecisiveness, nearly every day
Recurrent thoughts of death, suicidal ideation without a plan, an attempt or a plan
Symptoms do not meet criteria for a mixed episode
Symptoms cause significant distress or impairment in social and occupational functioning. Eg
what difficulties have all these symptoms caused?
Exclude depression if symptoms:
Are due to physical illness, medication or street drugs
Occur within 2 months of significant bereavement (except if marked impairment, morbid
preoccupation with worthlessness, suicidal ideation, psychotic symptoms or psychomotor
retardation). Key difference between grief and depression is whether they themselves feel
worthless or not
Also review risk factors:
Prior history of major depressive episode or suicide attempt. Previous episode 50% lifetime
risk of recurrence
Family history of mood disorder or suicide attempts. If no family history then lifetime risk 10 –
20%. If heavy genetic loading this may double the risk (very polygenic)
Chronic or severe physical illness (may demoralisation and hopelessness)
Concurrent substance abuse
Recent stressful life events and lack of social support (stress should not be used to „explain away‟
symptoms, stress may precipitate a major depressive episode)
Childhood trauma, abuse, parental conflict or deficient parental care
Recent childbirth or other family changes (eg divorce, children leaving home)
Responsibilities for caring for others (eg elderly relatives)
Differentials:
Substance abuse
Other psychiatric disorders, eg anxiety, eating and adjustment disorders, personality disorders,
somatization
Dementia in older people (a key differential is memory)
General medical conditions and medication. Drugs affecting mood:
Steroids: on 20 mg 1.3% get depression, on 80mg 20% get depression
Lipid soluble blocker
New drug affecting P450 metabolism and plasma conc. of existing drug
428 4
th
and 5
th
Year Notes
Grief reaction. Depressive symptoms common during periods of grief. Usually begins within 2 –
3 weeks of bereavement and usually resolves without treatment – although supportive
counselling/practical help may be indicated
In children and adolescents, feelings of guilt, emptiness, self-dislike and failure are common – but are
underreported by parents, who may instead report a decline in behaviour or academic performance
Can use questionnaires: e.g. GHQ (General Health Questionnaire) or CES-D – useful either for
screening or in borderline situations – gives something to discuss with patient
Little point in trying to separate exogenous from endogenous depression (often a chicken & egg
situation). It‟s usually multifactorial – regardless of cause may well need a multi-factorial approach to
management
Subgroups
Subgroup
Essential Features
Implications
Psychotic Depression
Hallucinations and/or delusions
More likely to become bipolar than
non-psychotic types (esp under
25s). May be misdiagnosed as
schizophrenia
Melancholic Depression
Loss of pleasure and lower mood
(typically in morning), marked
psychomotor retardation or
agitation, significant weight
changes and inappropriate guilt
Indicative of more severe
depression. More likely in older
patients. Maybe misdiagnosed as
dementia if cognitive impairment
or psychomotor retardation are
prominent
Atypical Depression
Various: overeating, oversleeping,
weight gain, mood still reactive to
events, anxiety symptoms,
heaviness in arms & legs
Common in younger people. May
be misdiagnosed as a personality
disorder.
Postpartum Depression
See page 430
Postpartum Psychosis
See page 430
Seasonal Affective Disorder
Typically onset in autumn and
remits in spring. Summer episodes
may also occur
Recurrent
Epidemiology and Aetiology
Lifetime risk of depression in women is 20%
Female: Male is 2:1, but in younger cohorts an in male depression is bringing the ratio down to 1.6:1.
This is not an artefact of help-seeking behaviour
Rate is increasing
Variety of theories:
Biological (eg neurotransmitter dysfunction)
Freud: unresolved early childhood events resurrected by similar events in later life
Bent (?): Cognitive triad: people feel helpless hopeless worthless. Selective abstraction –
extrapolate from one event to everything. Treatment: Uncover underlying schema. Then
challenge faulty thinking (is it always that bad?), challenge automatic thoughts
Assessment
Cultural issues:
Different cultures have different views on the cause and treatment of depression.
Appreciating the cultural perception of the individual better therapeutic relationship and
effectiveness of intervention.
Consider referral to culturally appropriate service.
Cultural issues may affect the way the interview is conducted. Eg if Maori, establish initial rapport
before asking name and personal information, don‟t make eye contact when discussing sensitive
information, a family member speaking on a patient‟s behalf is not being dominating, etc
Assessment of severity: Use the number of DSM IV criteria met or severity rating scales. Allows
classification into mild, moderate and severe. Can be used to monitor progression of treatment and
relapse
Assess duration: (> 6 months, > 24 months)
Refer to specialist services when:
There is serious risk of suicide (or harm to others, especially younger children)
Psychological Medicine 429
The child is under the age of 13 years
There are psychotic symptoms or bipolar disorder (depressed phase)
The diagnosis is unclear and needs further evaluation
Melancholic features are so severe that they are unable to look after themselves and have
inadequate community support
There are complex problems (eg poor relationship, another psychiatric disorder)
Considering enhancing antidepressants with mood stabilisers (eg lithium)
Failure to respond to recommended treatment within 12 weeks
Treatment of Major Depressive Disorder
Fundamental to treatment is:
Establishing positive therapeutic relationship
Developing shared understanding of problems
Safety: suicide risks common (lifetime risk 25 – 50%). Higher in delusional Major Depressive
Episode. Consider safety of others, especially if psychotic beliefs or Postpartum Depression
Lifestyle changes that have been shown to be effective: stress management, alcohol and drugs, good
sleep patterns, a balanced diet, and physical exercise
Role of family, friends and self help groups important in maintaining a supportive environment
Education (over time):
Depression is an illness not a weakness.
Treatment is effective and recovery is normal.
Recurrence is possible so compliance is important. However, sometimes there is only partial
remission between episodes. Recognition of warning signs and seeking early treatment will reduce
severity
Psychological treatment:
Indicated if:
Person with mild to moderate chooses this as first line
If partial response to drugs at week 6 or 12 and residual symptoms are largely psychological
There are continuing issues/cognitive beliefs that the risk of relapse
Not as sole treatment in severe, psychotic or melancholic depression
Promoting change: behaviour, thoughts, emotion
Different therapies:
Cognitive behavioural therapy (See Cognitive Behavioural Therapy (CBT), page 457)
Problem solving therapy (See Problem Solving Therapy, page 457)
Interpersonal therapy
Hypnotherapy
Psychoanalysis
Transactional analysis
Martial or family therapy
Drug treatment: See Antidepressant and Mood Stabilising Medication, page 431
Electroconvulsive Therapy (ECT):
Relieves symptoms is 80% of all severe depressions (not just those resistant to medication)
Indications:
Psychotic depression
Depressive stupor (severe psychomotor depression)
Severely suicidal
Previous good response to ECT
Risks: little risk of brain injury – risks are those of a general anaesthetic. Most troubling side
effect is memory loss. Anteriograde loss is usually short lived. Some retrograde loss may be
permanent
Response is proportional to length and quality of seizure. Usual course is about 6 cycles. If no
response after 12 cycles then stop
Also need to establish on an antidepressant that they haven‟t failed on
Monitoring treatment in primary care:
Check for treatment response, side effects, and alteration in stressors or supports
If severe, monitor twice weekly by consultation and phone, if mild then weekly
Assess response in week 6
430 4
th
and 5
th
Year Notes
Postpartum Mood Disorders
Frequency
Symptoms
Course
Risks & Treatment
Postpartum
Blues
50 – 80%
Weepiness, anxiety,
irritability, poor
concentration, euphoria
3 – 10 days post
partum
Treatment: support,
reassurance, monitor.
Function not usually
affected
Postpartum
Depression
10 – 15 %
Common symptoms:
anxiety, spontaneous
crying, lack of interest in
baby, guilt, hard making
decisions, panic attacks,
especially insomnia &
fatigue. Mood may
fluctuate. Obsessional
thoughts. Suicidal ideation.
Not before 3
rd
day.
80% onset within
first 6 weeks.
Gradual onset –
may not be
apparent until 4
th
or
5
th
month. Duration
6 – 9 months.
30 – 50% chance of
recurring in next
postpartum period.
May approach 100% if
history of mood
disorder and previous
postpartum depression.
Treat as for MDE.
Puerperal or
Postpartum
Psychosis
(No criteria
in DSM4)
0.1 – 0.2 %
Severe, labile (unstable)
mood. Obsessional
thoughts (eg about baby‟s
health). Suicidal ideation.
Delusions (eg baby
defective), suspicious,
persecuted, confused
Acute onset < 14
days post partum.
Good prognosis.
Duration 2 – 3
months
30 – 50% chance of
recurring in next
postpartum period
Treatment: Ensure
safety. Antidepressant,
Lithium, antipsychotic.
Consider ECT early –
safe and effective.
Screen at post-natal check up (6 weeks) using Edinburgh Postnatal Depression Scale (EPDS), but still
needs careful clinical assessment
Differential: hypothyroidism (more common post-partum), recurrence of previous psychiatric illness,
initial presentation of a psychiatric illness (eg schizophrenia or anxiety disorders – postpartum period
increases risk), adjustment disorder with depressed mood
Possible aetiological factors:
Stress of delivery, difficult pregnancy
Lack of sleep
Hormonal
Isolation, lack of support
Internal conflicts about role as mother: motherhood idealised or devalued, very difficult adjustment
in role, powerless, dependent, alone, may have had unrealistic expectations, etc
May not have wanted to be pregnant, may now feel trapped in unhappy situation (eg relationship)
Cultural factors: cultures vary in support offered (eg by extended family) to new mother, in
pressures to return to work (variable maternity leave policies), differing attitudes to female
children, etc.
Considerable overlap in the risk factors for major depression, post-partum depression, inadequate
parenting and child abuse
Treatment:
Check whether drugs enter breast milk.
Indications for antidepressants similar for those for other mood disorders
If agitated or anxious, more sedating antidepressants are appropriate (eg imipramine) or even small
doses of antipsychotics
Long term effect of postnatal depression on child development: disturbances in mother-infant
relationships (eg attachment), impaired cognitive and emotional development in later infancy, and
risk of longer-term behavioural and social development of the child. These factors compounded by
indices of socio-economic adversity, which are risk factors for these outcomes and for depression. So
good initial diagnosis and treatment important
Dysthymic Disorder
Diagnostic criteria:
Depressed mood for most of the day, for more days than not, for at least 2 years
Other depressive symptoms
But not a major depressive episode, no manic, hypomanic or psychotic features, no substance
abuse or GMC
Psychological Medicine 431
Differential from Major Depressive Disorder:
Difficult as differences in onset, duration, persistence and severity are not easy to retrospectively
evaluate
Major depression often has a more marked contrast from normal. In dysthymic disorder, low
mood is less easily distinguished from person‟s normal function
If major depressive episode on top of existing dysthymic disorder, then may recover more quickly than
normal from the major depression, but are at significantly higher risk of relapse with faster cycles
Treatment: antidepressants for up to three years together with appropriate life skills training and
psychological therapy
Bipolar Depression (Manic-Depression)
Affects 1% of the population (35,000 New Zealanders)
Genetic predisposition:
No family history then risk is 1%
One parent then risk is 20%
Symptoms:
Manic Phase: elation, pleasure, energy, racing thoughts, invincible, grandiose (self esteem),
irritable, aggressive, lack of judgement (eg reckless driving, spending sprees, sexual indiscretion)
Depressive Phase: same symptoms as for major depressive episode
History questions for mania:
How do you feel about yourself?
Do you feel that you are special?
Have you needed less sleep?
How much have you been spending lately
Classifications of Bipolar Depression
Mixed Episode: rapidly alternating mood – at least 1 week in which the criteria are met for a manic
episode and a MDE nearly every day
Bipolar 1: one or more manic or mixed episodes, usually accompanied by MDEs
Bipolar 2: one or more MDEs accompanied by at least one hypomanic episode
Cyclothymia: At least 2 years of numerous periods of hypomanic symptoms and depressive
symptoms that don‟t meet criteria for mania or MDE (cf Dysthymia)
Mood stabilising medication:
Lithium carbonate (requires regular blood tests. Can they get to the lab?)
Carbamazepine (Tegretol)
Sodium Valproate (Epilim)
All have similar efficacy, Lithium most common
Antipsychotic or tranquillising medication often added during early stages to reduce agitation and
hyperactivity
Antidepressant medication can be used during depressive phase (although therapeutic delay a
problem), and withdrawn gradually when it resolves. If used in isolation without a mood stabiliser,
may precipitate a manic phase as the depression lifts
Can be very stressful on relationships for family members
Lithium
Indication: In bipolar, but also recurrent unipolar. Not good for acute mania – takes 2 – 4 weeks, full
response may take 6 months
Pharmacokinetics:
Variable absorption. T½ is 18 hrs in young, 26 hours in elderly. Excreted unchanged. 80%
reabsorbed in proximal tubule
Renal clearance of Li reduced by diuretics, NSAIDs, theophylline, caffeine, dehydration, low
sodium
Clearance related to tubular sodium load. If Na excretion (eg loop and thiazide diuretics) then
Li excretion.
ACE inhibitors Li levels
Monitoring:
Narrow therapeutic range for maintenance treatment: 0.4 – 0.8 mmol/l
Therapeutic drug monitoring for Li is mandatory when: side effects, relapse of symptoms, serious
illness (eg dehydration), dose adjustment
Check thyroid and renal function before starting
432 4
th
and 5
th
Year Notes
Monitoring every three months should include Li levels, electrolytes, thyroid function
Monitor 12 hrs after immediate release, 5 hrs after slow release. Slow release preparations prevent
peaks in plasma conc. ( nausea, headache)
Side Effects:
Minor symptoms such as tremour and nausea do not predict serious toxicity:
Tremor (especially elderly), nausea, loose bowel motions (especially if levels > 0.8 mmol/L)
Polyuria (especially when starting)
Weight gain: approx 4 kg
Pretibial oedema
Metalic taste
Dose dependent adverse effects:
1.5 – 3 mmol/l – ataxia, weakness, drowsiness, thirst, diarrhoea
3 – 5 mmol/l – confusion, spasticity, convulsions, dehydration, coma, death
Dose independent: hypothyroidism (reversible in early stages), nephrogenic diabetes insipidous,
ECG changes & arrhythmias, acne, GI disturbance, weight gain, bone calcium
Long term Li does not change GFR or lead to renal failure
Antidepressant and Mood Stabilising Medication
Indications for antidepressant use:
Generally not indicated for mild disorder until monitoring, lifestyle changes and psychological
therapies have been attempted
Indicated for mild disorder when there is a history of severe episodes or in dysthymic disorder
which is persistent and disabling
For moderate, TCA or SSRIs equally indicated: depending on contraindications and toleration of
side effects:
SSRIs where severe heart disease, significant anticholinergic problems, and where alertness is
important
Amitriptyline and imipramine cause the most postural hypotension and AntiACH effects of
the older TCAs. Good where sleep disturbance is a major symptom
For severe with melancholic features, TCAs at sufficient dose if side effects can be tolerated.
Otherwise SSRIs (caution in pregnancy – risks not fully known)
If psychotic, use antipsychotic or consider ECT
For moderate and severe, continue for at least 9 months. If more than one recent episode, consider
continuing for up to 3 years
During pregnancy: More experience with TCAs (ie more confident effects on fetus will be
minimal)
Maintenance therapy at full therapeutic dose should be considered if high risk of relapse
Li in relapsing bipolar and as possible adjunct in relapsing unipolar depression
Mode of action of antidepressants:
Increase concentration of noradrenergic or serotonin neurotransmitters in the synaptic cleft.
Leads to adaptive changes eg down regulation of post synaptic and 5HT2A receptors (hence
therapeutic delay)
Older agents also had antimuscarinic and antihistaminic activity
Starting and stopping:
Onset of effect can take 1 – 2 weeks, with full effect possibly not for 4 – 8 weeks
Dose-escalation is a trade-off between desire to reach therapeutic plasma levels as soon as possible
while avoiding side-effects
Rapid cessation of any antidepressant can cause a withdrawal syndrome from a few days resolving
in about 4 weeks. Taper off treatment. (?Less risk with SSRIs due to longer T½)
Drug treatment has similar outcomes as psychological or combination treatment (BMJ 2000, 320: 27-
30)
Tricyclic Antidepressants
Examples: Amitriptyline, Imipramine, Doxepin, Nortriptyline (least orthostatic hypotension)
Action: Inhibit reuptake of serotonin, noradrenaline or both
Use:
Clinical response takes 10 – 14 days. Start with low dose and increase gradually.
Relapse common continue for 6 months
Not in acute MI. Care if suicidal (overdose risk), mania, and variety of medical conditions
Psychological Medicine 433
Pharmacokinetics:
Very low Vd dialysing for overdose ineffective
Long T½ once a day dose possible, but may split dose to reduce the dose dependent anti Ach
effects
Well absorbed. Extensive 1
st
pass metabolism to active metabolites.
Individual variability in metabolism difficulty setting dose.
Protein bound and large Vd.
Long T½ (15 – 30 hours), prolonged in elderly. Can be given once daily, but high peak plasma
levels side effects
Side effects of TCAs: Tricyclics
Inhibit reuptake of:
5HT anorexia, nausea, vomiting
NA tremors, tachycardia, erectile and ejaculatory dysfunction, insomnia
DA less significant
Block:
Ach dry mouth, urinary retention, blurred vision, constipation, tachycardia
Alpha 1 postural hypotension (persistent in elderly). Delay in ejaculation and erectile
dysfunction
H1 sedation, weight gain
Other: Possible convulsions, ataxia, manic reactions, respiratory depression, bundle branch block,
delirium. Arrhythmias/arrest in overdose
There are marked differences in side-effect profile between people and between drugs
Withdrawal of TCAs:
GI: nausea, vomiting, abdominal cramps, diarrhoea
General somatic distress: lethargy, flu-like symptoms, headache
Sleep disturbance: insomnia, abnormal dreams including nightmares
Affective symptoms: anxiety, agitation, low mood
Less commonly: movement disorders, mania, hypomania, arrhythmias, tachycardia, ventricular
ectopic beats
TCA Drug interactions:
Alcohol potentiates sedation
Potentiation of antimuscarinic drugs, adrenaline, noradrenaline and pseudoephedrine
Anticholinergics: worsening of dry mouth, tachycardia, constipation, urinary retention, blurred
vision, narrow angle glaucoma
Antihistamines, alcohol, anxiolytics: sedation (especially bad if driving)
Anaesthetics: arrhythmias and hypotension
Diuretics: postural hypotension
Antihypertensives: increased hypotensive effect
MAOIs: CNS excitation (look like they‟re thyrotoxic) and hypo-hypertension
SSRIs: Fluoxetine inhibits TCAD plasma levels/side effects
Tricyclic Overdose:
Gastric lavage up to 18 hours post ingestion, charcoal, support respiration
Symptoms:
Anticholinergic signs: rapid pulse, dilated pupils
Cardiac: hypotension (1 blocking effect), arrhythmia (PR and QRS intervals)
Neurological: CNS, seizures, sedation, extrapyramidal syndromes
Respiratory: depressed CNS
Other: ileus and urinary retention
Sodium bicarbonate if life threatening arrhythmias, lignocaine for ventricular rhythms, magnesium.
Beware use of physostigmine
SSRIs
= Selective Serotonin Re-uptake inhibitors
Action: Initially inhibit 5HT re-uptake. Long term, normalise 5HT1A and 5HT2 receptor density
Pharmacokinetics: Well absorbed. Fluoxetine: active metabolite with T½ of 7 – 10 days. Others, T½
of Use: Therapeutic delay of 3 – 4weeks. Can be given once a day
About 24 hours, inactive metabolites
434 4
th
and 5
th
Year Notes
Examples: Fluoxetine/Prozac, Paroxetine/Arapax, Citalopram (popular in the UK, not subsidised in
NZ)
SSRI Side effects:
Common:
Nausea 23%, headaches, diarrhoea 15%, anxiety (early in treatment, Fluoxetine more
stimulant than Paroxetine), nervousness and insomnia 25%
Sexual dysfunction is common
Weight loss 4%
Less common:
Postural hypotension uncommon, but can be significant
Sweating, constipation, weight loss, EPS (akathisia, dystonias, tardive dyskinesia),
hyponatraemia
Less affinity for aminergic receptors than TCAs
Lack of cardiac toxicity in overdose (significantly less than TCAs) – no effect on QTc
May precipitate serotonin syndrome: fever, tremor, myoclonic jerks, convulsions, diarrhoea, hyper-
reflexia. Can be fatal. NEVER prescribe MAOIs and SSRIs
Care in variety of medical conditions
Withdrawal of SSRIs: Withdraw slowly
GI: nausea, vomiting, diarrhoea, loss of appetites, abdominal pain, abdominal distress
General somatic distress: lethargy, flu-like symptoms
Sleep disturbance: insomnia, abnormal dreams including nightmares and decreased need for sleep
Affective symptoms: irritability, anxiety symptoms, agitation
Problems with balance: dizziness, vertigo, light-headedness, ataxia
Sensory abnormalities: paraesthesia, numbness, blurred vision/diplopia, visual lag
Interactions of SSRIs:
Cytochrome P450 inhibition is a major risk factor: 2D6, 3A4, 2C – depending on drug type (eg
Sertraline, Fluoxetine, Paroxetine
2D6: 10% Caucasians lack it
Inhibited by Fluoxetine, Sertraline and Paroxetine
TCAs plasma levels/effects by 50 – 400%
Haloperidol levels may be increased (Fluoxetine most potent at this)
2C:
Phenytoin (up to 3 fold )
Tolbutamide (hypoglycaemia with Sertraline)
Warfarin ( INRs on sertraline and paroxetine)
Diazepam (sedation with fluoxetine)
3A4: involves many drugs, including triazolam, carbamazepine, erythromycin, terfenadine,
midazolam. Potential for multiple interactions
Nefazodone: An SSRA + 5HT2 antagonist. Not really an SSRI but similar action. Side-effects similar
to TCAs: nausea, dry mouth, dizziness, constipation, blurred vision
St John‟s Wort (Hypericum): inhibits re-uptake of 5HT, noradrenaline and dopamine. In correct dose
is as effective as imipramine and significantly better than placebo. Adverse effects include nausea, but
no antimuscarinic effects. With SSRI can cause mild serotonin syndrome. Mild enzyme inducer
metabolism of warfarin, and others
MAOIs (Monoamine Oxidase Inhibitors)
Action:
Inhibits MAO, which breaks down 5HT and noradrenaline intracellularly. Isoenzymes in gut and
liver (type A) and brain (type B) all inhibited
MAO-A (intestine, placenta): selectively oxidises NA, Ad and 5HT
MAO-B (platelets): oxidises phenylethylamine
Tyramine and Dopamine are substrates for both forms
Types:
Standard MAOIs are irreversible. Eg Tranyl-cypromine, Phenelzine inhibit MAO-A. Selegiline
(deprenyl) irreversibly inhibits MAO-B
Reversible inhibitor of MAO - A (RIMA), eg Moclobemide. Similar efficacy to TCAs and SSRIs.
Given 3 times a day
Use:
MAOIs rare as first line treatment. Use moclobemide instead
Psychological Medicine 435
Therapeutic delay for about a month
Pharmacokinetics:
MAOIs: Well absorbed. Pharmacokinetics of little importance as kinetics depends on irreversible
inhibition
RIMAs: Well absorbed. Wears off quicker than MAOIs. Fairly extensive 1
st
pass metabolism.
50% protein bound. Large Vd. T½ is 2 hours
MAOI side effects. MAO inhibition catecholamine levels:
Postural hypertension, urinary hesitancy, dry mouth, blurred vision
Impotency and anorgasmia 20%
Hepatotoxicity
Carpal tunnel like syndrome
CNS: agitation, anxiety, hypomania, headache, tremour,
Other: weight gain, insomnia.
Contraindicated/caution in variety of medical conditions
Food interaction: tyramine rich foods:
Foods include avocado, aged cheddar, yoghurt, meat, red wine, chocolate, yeast extracts, some
beers, vegemite, pickled herrings, chicken liver.
Tyramine a precursor to dopamine and nor-adrenaline. Normally tyramine metabolised in gut by
MAO.
If inhibited plasma conc. noradrenaline hypertensive crisis, subarachnoid
haemorrhage, etc. Adrenaline breaks down to HMMA, which can be detect in the urine.
RIMAs have 10 times the capacity to metabolise tyramine (ie food much less of an issue)
Drug Interactions:
Sympathonimetics, including indirectly acting sympathonimetics (eg in cough mixtures such as
ephedrine): hypertension
Opiod analgesics: hypo/hypertension
Antihypertensives: loss of effect, exacerbation of hypertension
Anticholinergics: increased effects
SSRIs and pethidine: serotonergic syndrome (fever, sweating, convulsion, confusion)
L-Dopa: dopaminergic crisis
Potentiate oral hypoglycaemics (sulphonylureas)
MAOI Overdose:
Symptoms: CNS hyperactivity, sweating, hyperthermia, tachycardia, hyperventilation, muscle
rigidity +/- dystonic facial and limb movements
Treatment: and blockers, chlorpromazine + supportive management
Psychotic Disorders
Psychosis = distortion or loss of contact with reality (eg delusions, hallucinations, thought disorder)
without change of consciousness (cf Delirium)
See Mental State Examination, page 414, for definitions and history questions relating to psychosis
Diagnostic hierarchy for psychosis:
Organic psychoses: Delirium, dementia, other organic disorders
Functional psychoses: Mania, schizophrenia, depression
Non-psychotic disorders: anxiety disorders, abnormal illness behaviours
Personality disorders
Types of Psychotic Disorder
Brief Psychotic Episode: symptoms have lasted > 1 day but < 1 month, and the patient has returned to
pre-morbid functioning in that time. Uncommon. May develop in response to severe psychosocial
stressor. More common in personality disorders (histrionic, narcissistic, paranoid, schizotypal,
borderline)
Schizoaffective Disorder: manic or depressive syndrome develops concurrently
Delusional Disorder: non-bizarre delusions present for 1 month without any other symptoms of
schizophrenia
Schizophreniform Disorder: duration of > 1 month but < 6 months (may progress to schizophrenia)
Schizophrenia
436 4
th
and 5
th
Year Notes
Schizophrenia
Key features: positive symptoms, negative symptoms, deterioration in functioning over time
It is not a split personality (ie multiple personality disorder)
Epidemiology:
1% (30,000) NZers have or have had schizophrenia
Median age of presentation: males 19, female 24
Symptoms:
Positive symptoms:
Hallucinations: comes from external space. Typically 2
nd
or 3
rd
person auditory hallucinations
Delusions: fixed false beliefs out of cultural context
Thought disorder: „loss of syntax‟, non-linear. Different to confusion or incoherence
Bizarre and/or disorganised behaviour: eg aggressive, disinhibited, violent (often in „self-
defence‟ if paranoid - rare but possible).
Catatonic behaviour: if long term, untreated psychosis then may assume odd positions, waxy
flexibility, totally unresponsive
Negative symptoms:
Deficiency of mental function - Cognitive symptoms: difficulty concentrating, learning, hard
to assemble thoughts. Not a decline in intelligence. Will still remember. Don‟t try to pull the
wool over their eyes
Alogia: poverty of speech or speech content
Affective flattening: including reduced intensity of emotional response
Anhedonia: don‟t care about their lack of interest, cf depression where they want to enjoy
themselves but can‟t
Asociality - uninterested in the company of others, unresponsiveness, withdrawal
Prodrome = gradual change prior to first episode of frank psychosis. Look for:
Concentration, attention drive, motivation
Depression, anxiety
Sleep disturbance
Social withdrawal, suspiciousness
These are common in adolescence: you‟re looking for marked change over previous function
Associated problems:
Suicide in 10 – 15%
Lack of insight ( non-compliant with medication)
Substance abuse: co-morbid problem, ?self medication
Depression in schizophrenia: diagnosed as Depressive Disorder NOS
Neurological symptoms: abnormalities in balance, proprioception, graphesthesia, disorder in
smooth eye pursuit, decreased blinking
EPS (extra-pyramidal side effects) in 20% of drug naïve people suffering from schizophrenia (
it‟s not always due to drugs)
Subtypes:
Paranoid: delusions, hallucinations
Disorganised: disorganised speech, behaviour, flat/inappropriate affect
Catatonic: motor immobility, excessive motor activity, negativism, stereotypies (repeated
monotonous movements), echolalia, echopraxia
Undifferentiated
Residual
Aetiology:
Multi-factorial: don‟t know about relative loadings for predisposing and precipitating factors
Genetic: one parent affected 5% chance, two parents 45% chance, sibling affected 10%
chance
Neurodevelopment: brain injury at birth and perinatal complications (eg low Apgar), born in
winter, ?viral influences. Insults at this age not causal – but some correlation
Social causation: eg Shift and Drift or Breeder theory to try and explain higher incidence in lower
socio-economic groups, Expressed Emotion theory (a lot of critical comment and high expectations
from parents)
Vulnerable personality: schizoid, schizotypal, paranoid
Head injury
Precipitating factors: life events, drug abuse, etc
Psychological Medicine 437
Differential Diagnosis:
Psychiatric disorders: Bipolar (manic phase), Major Depression with Psychotic Features, Brief
psychotic disorder, schizophreniform disorder, schizoaffective disorder, delusional disorder,
depersonalisation disorder
Medical illness: Temporal lobe epilepsy, tumour, trauma, infectious (syphilis, HIV), SLE
Drugs: amphetamines, cocaine, cannabis, PCP (Angel dust), alcohol withdrawal, benzo
withdrawal, barbiturate withdrawal
Assessment:
Establish rapport: this will be the first encounter of a lifetime of encounters with mental health
services. Try to get off to a good start!
Domains for assessment: home, employment/study, activities, drugs, sexuality, suicide
Assess social situation, and family views and functioning
Recovery from psychotic illness:
20% - no further episodes
10 – 15 % die: suicide/early death
60 % ongoing, 20% with serious disability
Treatment of Psychosis
Early intervention improves outcome, reduces disruption/trauma („collateral damage‟), etc. Important
given stage of life (adolescence) and the potential problems for subsequent social and occupational
development etc
Treatment programme involving health professionals, family members, support agencies, and
cultural/community context
Brain‟s ability to process and interpret information is affected think carefully about how information
conveyed is received. Keeps the facts simple, avoid distractions and pressure, ask one question at a
time, give plenty of time to answer
Biological treatment: treat early, immediately if psychotic, key issue with maintenance medication is
compliance
Psychological: supportive, education, self-care skills. Social skills training and community integration
skills overcome withdrawal significant in readmissions
Social: assertive (to combat stigma), community care
Relapse prevention: understanding drugs, warning signs, prognosis, side effects
Antipsychotic Medication
= Neuroleptics or major tranquillisers
May also use lithium, carbamazepine, antidepressants and benzodiazepines for psychosis
Reduced risk of relapse in schizophrenia, but 40% will still relapse within a year
Two effects:
Reduces delusions and hallucinations (may take 1 –2 weeks)
Tranquillising/calming effect (acute agitation, immediate effect)
For first presentation, treat with low dose and use atypicals (side effects compliance). Use
adjunctive long acting benzodiazepine for first few weeks to sedate and agitation
Can be administered orally, IM, IV and some as depot (but not yet for atypicals)
Side effects range over sedation, extra-pyramidal, anti-cholinergic and hypotensive
All relatively effective at reducing positive symptoms, but „atypicals‟ better than „typicals‟ at reducing
negative symptoms (eg motivation, interest, lack of emotional display, restricted speech)
438 4
th
and 5
th
Year Notes
All have hepatic elimination
Class
Drug
Side Effects
T½
Dose equity
EPS
Hypotensive
Sedation
Typicals:
Phenothiazine
Chlorpromazine
+
+++
+++
16 – 30
100 (ie low potency)
Thioridazine
+
+++
+++
26 – 36
100
Trifluoperazine
+++
+
+/-
5
Fluphenazine *
+++
+
+/-
35
3 (ie high potency)
Butyrophenone
Haloperidol *
+++
+
+/-
10 – 22
3
Thioxanthenes
Flupenthixol *
++
+
+/-
35
6
Thiothixene
++
+
+/-
35
4
Atypicals:
Azepine
Clozapine
+/-
+++
+++
9 - 17
60
Olanzapine
+/-
+/-
++
30
3
Benzisoxazoles
Risperidone
+/-
++
+
2.5
2
* = Available as depot
Typicals (ie Older antipsychotics)
Mode of action: block dopamine (D2) receptors. Most also have low affinity for 5HT2 receptors.
Varying amounts of anticholinergic, antihistamine and anti -1 effects
Adverse Effects:
Extrapyramidal Syndromes (EPS):
Acute: Occur early in treatment – usually first two months.
Dystonias (muscle cramps and spasms): treat with benztropine parenterally
Akathisia (restlessness): treat with blocker or benzodiazepine
Parkinsonism (tremor, cog wheel rigidity, bradykinesia, mask like face) – may improve with
time
Anticholinergics only indicated in those whose antipsychotic dose cannot be safely reduced.
(= antiparkinsonian medication, eg antimuscarinic drugs such as Cogentin)
Tardive Dyskinesia:
Late onset dyskinetic syndrome due to antipsychotic drug treatment. Usually months or years
after treatment
Fairly common: 15 – 30%
Slow, repetitive involuntary movements of mouth/face, and maybe limbs and trunk.
Disappear during sleep
Risk factors: old age, organic brain disease, negative symptoms, alcohol abuse
Irreversible in 50%
No established protocol for treatment: try dose reduction, lithium, or change to clozapine
Made worse by dopaminergic agonists and anticholinergics
Other effects:
Sedation
Anticholinergic effects (dry mouth, constipation, blurred vision, urinary hesitancy)
blockade (postural hypotension, tachycardia, delayed ejaculation)
Endocrine effects (PRL, marked weight gain, libido, impotence, amenorrhoea)
Neuroleptic Malignant Syndrome: Rare (0.2 – 1%) with hyperthermia, rigidity, and impaired
consciousness. 20% mortality. Emergency treatment (cooling, fluids, etc)
Interactions:
Potentiate sedation with hypnotics, alcohol, opioid analgesics
Fluoxetine increases risk of EPS
Atypicals
Clozapine:
Mode of action: numerous receptors: D1, D2, D4, 5HT2, blocks -1, H1 and muscarinic receptors
Psychological Medicine 439
Effective in individuals not responsive to classical antipsychotics, effective for positive and
negative symptoms, no extrapyramidal side effects, no impact on sexual or reproductive function.
Side effects:
Sedation, tachycardia, constipation, weight gain, and seizures (3% at highest dose)
Agranulocytosis/blood dyscrasias in 1-2 % by 1 year, most in first 18 weeks regular blood
tests
Potent enzyme inhibitor: significant drug interaction potential
Serotonergic crisis with SSRIs
Hypersensitivity syndrome: PUO, arthritis, rash
Prolongation of QT
Myocarditis
Risperidone:
Mode of action: binds to 5HT2 and D2 receptors, antagonises H and -1 receptors
Similar efficacy as other antipsychotics for positive symptoms. Effective for negative side effects
and also affective symptoms (depression, anxiety).
Some dose related extrapyramidal side effects. PRL at high doses. Also insomnia, agitation,
anxiety, headache
Olanzapine:
Mode of action. Similar to clozapine. Like clozapine has minimal impact on PRL
Similar efficacy to haloperidol, but more impact on negative symptoms
Sedation, headache, dizziness, constipation, dry mouth, weight gain
Dementia
= Chronic, generalised impairment of memory (key feature), intellect, and personality with no
impairment of consciousness (cf delirium)
Acquired
Not a feature of normal ageing
Diagnostic criteria:
Development of multiple cognitive deficits including both:
Memory impairment (either ability to learn or recall), and
One of aphasia (language disturbance), apraxia (impaired motor co-ordination), agnosia
(impaired recognition despite intact sensory function), disturbance in executive
functions/personality/social conduct
Not due to general medication condition, substance use, or delirium
Significant impairment in social or occupational functioning, and a decline on previous function
Epidemiology: 5% of 65 – 80 year olds, 20% of those over 80
Assessment:
General: age, absence of psychiatric history or co-existing physical illness
General account from carer, including memory impairment, behaviour change, mood change,
physical symptoms, disruption of ADLs
Onset: insidious or acute
Stepwise deterioration (suggests vascular), seizures
Fluctuation, including early evening, nocturnal worsening (“sunsetting”)
Family history including Huntington‟s
Clinical Course:
Amnesia:
Early: forget names, appointments, repetitive in conversation, some insight, leaving elements
or taps on
Later: forget faces, recent events
Advanced: forget past, identity, relatives, no insight
Language:
Early: difficulty word finding
Later: articulateness, difficulty following conversation
Advanced: rambling, incoherent
Dyspraxia (difficulty sequencing tasks): Difficulties with dressing, cooking safety issues:
wandering, kitchen/road safety
Other: depression (difficult to distinguish), psychosis, personality & behavioural change
440 4
th
and 5
th
Year Notes
Examination:
General: posture, gait, consciousness level, wandering, restlessness, feeding and dressing
difficulties
Mental Status examination
Neuro: focal signs, involuntary movements, pseudobulbar signs (swallowing, speech production),
primitive reflexes
Investigation:
Cognitive Function: test with mini-mental state: 26 or above = normal, 20 – 26 = mild, 11 – 20 =
moderate, < 10 = severe
FBC (macrocytosis) and LFTs: is it alcohol induced?
Exclude: thyroid, space occupying lesion, B12 deficiency, AIDS, syphilis
CT if focal neurological signs, new or odd psychiatric disorder, or age < 75 with shorter history.
NB include temporal lobe orientated views, as atrophy of medial temporal lobe is one of the
earliest CT findings in Alzheimer‟s disease
Treatment:
Treatment of any cause found. Treatable causes include:
Benign brain tumour, especially subfrontal meningioma
Subdural haematoma
Wilson‟s disease: akinetic rigid syndrome, bulbar palsy
Deficiency: B12, B6, B1
Hypothyroidism
Alcoholic dementia
Infection: HIV, syphilis
Improve functional ability, relieve distressing symptoms (eg secondary incontinence), regular
routines (diaries, reminders), establish enduring power of attorney early on (using PPPR act later
on is more involved), practical assistance (eg meals on wheels, rest home care), support for the
family (involvement in rehabilitations, information, etc)
Drugs:
Cholinesterase inhibitors:
Hold off progression for a year or two? Better motivation, improvement in ADLs
12 weeks before effect can be reliably assessed
Side effects: nausea, diarrhoea, vomiting, muscle cramps, fatigue, anorexia
Eg Rivastigmine (Exalon): titrate up monthly: 1.5 mg bd 3.0 mg bd 4.5 mg bd bd
6.0 mg
Eg Donepezil (Aricept): 5mg od 10 mg od after a month if necessary
Cautions: peptic ulcer disease, arrhythmias
Not currently funded and pretty expensive
Other drugs with possible benefit:
Antioxidants (eg vitamin E)
NSAIDs
Oestrogen
Treatment for vascular dementia: control of blood pressure and aspirin
Aetiology
Alzheimer‟s:
50%. F > M. Course 6 – 8 years ( may die of something else first)
If < 65 then Alzheimer‟s disease, if > 65 then Senile dementia, Alzheimer‟s type
Clinical diagnosis. Diagnosis only certain at autopsy
Presentation:
Marked impairment of memory: anteriograde and retrograde (eg how old are you, are you
married, what are your children‟s names, etc)
Aphasia with word finding defect early on
Visuo-spatial problems: getting lost
Loss of interest: hobbies, dealing with finances, new circumstances, etc
Gross pathology: Atrophy in frontal, parietal, occipital and temporal regions, with secondary
widening of sulci and dilation of ventricles
Micro:
Neurofibrillary tangles: intracytoplasmic bundles of filaments that displace the neuron‟s
nucleus. Contain abnormal form of the protein tau
Psychological Medicine 441
Senile plaques: extracellular intracortical spherical clusters of dilated axons and dendrites
surrounding a spherical deposit of amyloid fibrils (amyloid beta peptide). Motor and sensory
cortex sparing. A few are normal. There are lots in Alzheimer‟s
Amyloid angiopathy
Granulovacuolar degeneration: clear intraneuronal cytoplasmic vacuoles
Pathogenesis:
?Accumulation of amyloid beta protein, with failure to exocytose the protein
Apoe4 allele is a marker for Alzheimer‟s but is not yet recognised as a screening or diagnostic
tool
Vascular:
20%. Previous history of CHD, stroke, high BP, etc. M > F
Caused by discrete infarcts (ie multi-infarct dementia) but also small vessel disease (eg cerebral
arteriolar sclerosis from chronic hypertension)
Presentation: Often impaired attention and frontal features, emotional lability
Multiple subcortical white matter injury Binswanger disease (damage to association fibres)
Defuse Lewy Body Dementia: 20%:
Often associated Parkinsonian features (rigidity, tremor and bradykinesia) – less tremour but
trunkal rigidity
Can have fluctuating attention and visual hallucinations (so like delirium)
Very sensitive to anti-psychotics. A small dose can profound tranquilliser effect
Pick‟s Disease: Much less common, but similarities with Alzheimer‟s. Differences are early onset of
personality, behavioural changes and language impairment. Atrophy of frontal and temporal lobes (ie
clearly localised). Microscopically, surviving neurons show ballooning degeneration (Pick‟s cells) and
Pick‟s bodies (filamentous intracytoplasmic inclusions). No senile plaques or neurofibrillary tangles
Alcoholic Dementia. See Pathological Effects of Alcohol on the Brain, page 451
Rarer causes:
Creutzfeldt-Jakob Disease (CJD)
Fatal, rapidly progressive dementia with psychiatric and behavioural disturbances. Less than 1
per million per year, usually elderly
No helpful lab findings (including CSF)
Aetiology: abnormal neuronal protein coded by the PRNP gene. Prion causes conformational
change from a -helix to a -pleated sheet chain reaction neuronal death
Can be transferred via pituitary extracts, dural grafts, etc
15% of cases familial
No macroscopic changes. Microscopically: spongiform encephalopathy – vacuoles in neurons
and neuropil (ie extracellular) neuronal loss and gliosis (marked astrocytosis)
Variant CJD (vCJD). Affected young adults, progressed more slowly, early behavioural changes.
Spongiform changes plus plaques composed of prion protein. Caught from Bovine Spongiform
Encephalopathy (BSE, Mad Cow Disease). Prions very difficult to inactivate (eg standard
disinfectants, formalin, UV light don‟t work)
Huntington‟s Disease:
Prevalence: 7 per 100,000
Clinical: Choreoathetotic movements and progressive dementia from age 35 – 40. Depression,
erratic behaviour, apathy, problems with speech and swallowing. Death in 15 years on
average
Genetics: Autosomal dominant, short arm of chromosome 4
Gross: diffuse gyral atrophy, marked atrophy of caudate nucleus and putamen, dilation of
ventricles
Micro: loss of neurones in atrophied areas, replaced by fibrillary gliosis
HIV & syphilis
Dementia Due to Head Trauma
= Presence of dementia directly due to head trauma
Severity and type of cognitive or behavioural impairment depends on location and extent of injury
Symptoms include aphasia, attention problems, irritability, anxiety, depression, apathy, aggression,
other personality change
Is usually non-progressive unless repeated head trauma (eg boxer). Progressive decline following
single trauma suggests another problem (eg hydrocephalus or major depressive episode)
442 4
th
and 5
th
Year Notes
Management
Fatigue and stress result from:
Poor concentration, impaired executive function and memory due to injury
Sleep requirements increase, but patients try and do the same amount as before
No knowledge about what to expect (both patients and families)
Fatigue + stress frustration, anxiety and depression. So reduce factors leading to fatigue and stress
Management focuses on:
Education
Proper assessment of cognitive deficits by a psychologist (eg cognitive testing =
neuropsychological testing)
Support from informed family, friends and employers
Regular breaks/sleeps. Take things in small bites and structure day around these
Teach relaxation methods
Compensating for cognitive losses: structured day (ability to plan), lists, diaries
Continual reassurance
Medication:
Use for depression if symptoms do not resolve with counselling and support. SSRIs have least
side effects. TCA if headaches, or sleep is a problem (side effects include daytime sedation
and cognitive function)
Maybe Methylphenidate (Ritalin) - arousal to extend time possible to work
Prognosis
Only 20 – 30% return to full function 1 – 2 years after a mild head injury
Degree of cognitive difficulty in first month NOT a good prognostic indicator
Need to consider PTSD as differential or co-existent diagnosis
Good prognostic indicators: strong social support, early intervention by a specialist HI recovery service
Bad prognostic indicators: persisting cognitive difficulties at 6 – 9 months
Delirium
Global and transient disturbances of consciousness, attention, perception, thinking, memory,
psychomotor behaviour, emotion and sleep-wake cycle
= Acute Confusional State
Epidemiology:
Rare in the community
Common in hospital, especially in elderly, 10 – 25% of > 65 years olds admitted to medical wards
Significant mortality: approx 25% of elderly patient acquiring delirium in hospital die
Will get poor history from the patient. Need informant
Symptoms
Rapid onset (potentially related to new illness/drug). Rarely lasts more than several weeks
Fluctuating consciousness (cf psychiatric illness, which does not present with impaired consciousness)
Marked abnormalities of attention and concentration
Attention unfocused
Thinking: disorganised, delusions, rambling incoherent speech
Memory impairment
Perception: illusions and hallucinations (especially visual)
Psychomotor behaviour: over/under active, purposeless
Mood: labile, agitation, fear, anxiety
Sleep-wake cycle: disrupted or even reversed
Aetiology
Common causes: Often multi-factorial – a little bit of a number of things
Infection: UTI, pneumonia
Drug reactions
Hypoglycaemia
O2 or CO2
Comprehensive list:
Drugs: antiarrhythmics, antibiotics, anti-virals, anti-fungals, -blockers, etc. etc
Psychological Medicine 443
Drugs of abuse
Withdrawal: alcohol, amphetamines, barbiturates, benzos, cocaine
Neurologic: stroke, epilepsy, Parkinson‟s, Huntington‟s, MS, Tumour, normal pressure
hydrocephalus (confusion, incontinence, gait disturbance)
Endocrine: Hyper/hypothyroidism, hyper/hypoPTH, Hyper/hypoadrenocorticolism, diabetes
mellitus, phaeochromocytoma, etc
Metabolic: hyponatraemia, hypokalaemia, hyper/hypocalcaemia, acidosis, hypoxia, uraemia,
porphyria
Vitamin deficiencies: thiamine, folate, B12
Infection: Especially chest and urinary tract, also sepsis, meningitis, encephalitis, AIDS, Hepatitis,
etc
Other: lung/pancreatic cancer, paraneoplastic syndromes, SLE, etc
Differential of acute confusion:
Psych illness: delirium, psychosis, dementia, depression
Drugs, illness, metabolic, trauma, hypoxia, poisoning/overdose, post-ictal, thiamine
Risk factors
Multiple, severe or unstable medical problems
Dementia or cognitive impairment
Polypharmacy
Metabolic disturbances
Advanced age (especially > 80 years)
Infection (especially UTI)
Fractures
Visual impairment
Fever or hypothermia
Psychoactive drug use
Treatment
First, recognise the delirium (it often isn‟t). Careful and repeated assessment. Watch for
confused/disorientated behaviour or inattention, especially at night
Examination:
Mini-mental
Temperature, hydration, ketosis, foetor
Signs of injury, including scalp
Infection screen
Neuro exam
Signs of drug abuse
Investigations:
Bloods: FBC, ESR, U&E, Glucose, Ca, Renal, Liver, Thyroid, Thiamine
Urine, ECG, CXR
Consider: blood alcohol, cardiac enzymes, blood culture, ABG, B12/folate, CT
Treatment of underlying cause: may require history from care giver
Management of delirium:
Supportive:
Reorientation (a smoke and a cup of tea works wonders!)
Reassurance
Attention to noise and light levels (not too much nor too little)
Stimulate during the day: get up and dressed, put on glasses and hearing aid
Continuity of staffing
Family member (or even an orderly) to sit with patient
Familiar objects (eg family photos) in the room
Stimulate during the day: get them dressed, false teeth in, glasses on, hearing aid in
Attention to nutrition and hydration
Target risk factors of cognitive impairment, sleep deprivation, immobility, visual and hearing
impairment
Drugs: only in addition to the above, and usually to treat those caring for the patient!
444 4
th
and 5
th
Year Notes
Haloperidol 0.5 mg bd (iv if possible): low dose (eg 0.5 – 1.5 mg), especially in elderly,
absolute max 2 – 5 mg prn 1 – 2 hourly. Doesn‟t have anticholinergic side effects, but may
cause restlessness. Maori and Pacific Islanders may be more sensitive so lower dose initially
Lorazepam (short acting benzo) 0.5 – 2 mg q 15 – 20 min iv/im/sublingual/po
Somatoform Disorders
= Presence of physical symptoms that suggest a general medical condition but aren‟t explained by that
condition, by substances or medications, or by another mental disorder (eg Panic Disorder)
Must cause significant distress or impairment in social or occupational functioning
Difficult to manage: need to check for physical conditions constant testing reinforces worry. If
find something on tests this validates and reinforces the worry
Processes contributing to symptoms and motivation for symptom production is unconscious. They
don’t know it’s not real.
Cultural, stress, developmental and self-esteem factors may contribute
Disorder
Comment
Somatization Disorder
Polysymptomatic, recurrent and chronic, 5-10% of primary population, often
young female, system review profusely positive, key differentials: physical
disease, depression
Conversion Disorder
Monosymptomatic, mostly acute, high prevalence, often young females, low
education, excellent prognosis unless chronic, key differentials: depression,
schizophrenia, neurological diseases
Hypochondriasis
Disease concern or preoccupation, middle to older age, especially if previous
physical disease, M = F, may be obsessional, course waxes and wanes, key
differentials: depression, physical disease, personality or delusional disorder
Body Dysmorphic
Disorder
Obsessive pre-occupation with feelings of ugliness or concern with body
defect, rarer, adolescence or young adult, key differentials: delusional
disorder, depression, somatization disorder
Pain Disorder
„Simulated‟ pain syndrome incompatible with known physiology or anatomy,
female to male is 2:1, 4
th
or 5
th
decade, very common in pain populations,
key differentials: depression, physical disease, malingering
Somatization
= Somatic symptoms with no cause found (+/- anxiety/depression)
Aim of treatment is to reattribute the symptoms to relate them to psychological problems
Approach to managing in a non-specialise practice setting:
Feeling understood:
Take full history, including pain during a typical day
Watch for emotional clues or links with stressors: “what are you thinking about when it hurts”
Ask about social/family factors
Explore health beliefs: “What do you think is wrong”
Focused exam
Change the agenda:
Feedback results
Acknowledge reality of pain
Reframe complaints: set them in the context of life events. “I‟m struck by the fact that these
pains started shortly after … and that you‟ve been crying a lot… Do you think there might be
a connection”
Making the link:
Make the link to life events clearer to the patient
Use negotiating style: “Do you think that‟s possible… perhaps…”
Projection: “Has anyone else suffered from symptoms like these… Did your mother get
headaches – what caused those”? May be easier to see the connection in others
Disorders due to a General Medical Condition
Psychiatric symptoms occur in a wide range of medical conditions
Neurological:
Degenerative: Parkinson‟s, Huntington‟s, Wilson‟s depression, dementia, psychosis
Epilepsy: 30 – 50 % have psychiatric illness at some stage, can be due to medication
Psychological Medicine 445
Brain tumours: especially frontal lobe or limbic system
Head injury
Demyelinating disorders: eg MS
Infectious:
Herpes simplex encephalitis changed personality, psychosis
Rabies, syphilis, CJD, Kuru (in PNG)
HIV
Autoimmune: Systemic lupus erythmatosus: eventually 50% have psych symptoms
Endocrine:
Hyperthyroid confusion, anxiety, agitated depression, manic, delusions, with weakness and
muscle loss
Hypothyroid if severe then hypomania, depression, hallucinations
Hypercalcaemia (due to PTH disorder) delirium, changed personality, apathy, cognitive
function
Hypocalcaemia (due to PTH disorder) delirium, changed personality, eventually tetany
Hypoadrenocorticism (Addison‟s) apathy, depression
Hyperadrenocorticism (Cushing‟s) agitated depression
Total pituitary failure hypothyroid and hypoadrenocorticism
Metabolic:
Hepatic encephalopathy memory, LOC, changed personality
Uraemia encephalopathy: renal failure memory, orientation, LOC
Hypoglycaemia: agitation/restlessness
Ketoacidosis easy fatigue
Acute intermittent porphyria porphyrins (components of haemoglobin synthesis): acute
colicky abdominal pain, motor polyneuropathy, psychosis, anxiety, insomnia, lability of mood,
depression. Barbiturates absolutely contraindicated. 0.2 – 0.5 % psych patients have undiagnosed
porphyria
Nutritional:
Niacin deficiency
Thiamine deficiency
B12 deficiency neuro degeneration depression, irritability, moodiness
Toxins:
Mercury: depression, irritability, psychosis, tremour, weakness
Lots of others
Cancers Eg carcinoma of the pancreas
Medication:
Mood disturbances from: stimulants, steroids, L-dopa, etc
A previous condition (eg major depressive disorder) can be triggered by medication with the
capacity to cause depressive symptoms
Substance Use Disorders
Diagnostic Criteria
Two types of disorder:
Substance use disorders: abuse and dependence
Substance induced disorders: secondary to substance use (eg withdrawal, psychosis, persisting
dementia or amnestic disorders, etc). Require evidence of substance use and are not related to pre-
existing problems
Abuse vs. dependence:
Abuse implies use is causing job, social, legal or physical problems or impairing function in some
way
Dependence (a step worse) requires signs of withdrawal and tolerance
Used to be a definition for „the addictive personality type‟: but research has shown no consistent
correlation with the proposed criteria
Substance Abuse
A maladaptive pattern of substance use leading to significant impairment or distress, manifested by one
(ie fairly low threshold) or more of the following occurring in the same 12 month period:
446 4
th
and 5
th
Year Notes
Recurrent substance use resulting in a failure to fulfil major role obligations at work, school or
home
Recurrent substance use in which it is physically hazardous (eg driving)
Recurrent substance-related legal problems (eg arrests for disorderly conduct)
Continued use despite it causing or exacerbating persistent or recurrent social or interpersonal
problems
Symptoms have never meet the criteria for substance dependence for this class of substance
Substance Dependence
A maladaptive pattern of substance use leading to significant impairment or distress, manifested by
three or more of the following occurring in the same 12 month period:
Tolerance: either amounts to achieve intoxication or diminished effect with same amount
Withdrawal: either characteristic withdrawal syndrome for that substance, or the same or a closely
related substance is taken to avoid withdrawal symptoms
Substance is taken in larger amounts or over a longer period than was intended
There is a persistent desire or unsuccessful efforts to cut down or control use
A great deal of time is spent obtaining, using or recovering from its effects
Important social, occupational or recreational activities are given up or reduced as a result
Use is continued despite knowing that has caused or exacerbated a physical or psychological
problem
Epidemiology
1986 CHCH Psychiatric Epidemiology Study: Lifetime prevalence rates:
Overall %
Male %
Female %
Substance use disorder
21
34
9
Alcohol abuse/dependence
19
32
6
Drug abuse/dependence
6
7
4
Affective Disorders
15
10
19
Major Depressive Episode
13
9
16
GAD
31
27
35
Any eating disorder
1
0.2
2
Adolescents:
5% of 15 year olds meet criteria for alcohol abuse (Fergusson 1994)
Cannabis dependence 7% at 18 years, 10% at 21 years. Higher in males
Co-morbidity or Dual Diagnosis:
Epidemiologic Catchment Area (ECA) Study 1990 found the lifetime co-morbidity of substance
use disorders by specific diagnoses:
Schizophrenia
47%
Antisocial Personality Disorder
84% (Abuse a diagnostic criteria)
Anxiety Disorders
15%
Panic Disorder
36%
Obsessive Compulsive Disorder
33%
Mood Disorders
32%
Bipolar Disorder
61%
Those with a mental disorder have twice the risk of an alcohol disorder and 4 times the risk of any
other drug disorder
Those with a lifetime alcohol disorder have twice the risk of another mental disorder (37%) and 6
times the risk of another drug disorder (22%)
Those with a lifetime other drug disorder have a 4 times risk of another mental disorder (53%) and
7 times the risk of an alcohol disorder (47%)
Co-morbidity is higher in institutional settings (70- 80%) than in the community
Dual diagnosis is an expectation not an exception
Models of Aetiology of Addiction
Disease model: emphasises the biological and genetic basis of addition. Loss of control is a central
feature
Self-medication hypothesis: use specific pharmacological effects to self medicate for psychological
disturbance and painful affects
Psychological Medicine 447
Biopsychosocial model: Multifactorial causality, interaction of genetic predisposition, biological
factors, and psychological and sociocultural factors
Biological model: impact on mesolimbic reward system – extends from the ventral tegmentum to the
nucleus accumbens, with projections to areas such as the limbic system and the orbitofrontal cortex
Factors influencing behaviour*
Early childhood learning: modelling by parents and significant others
Current environment: reinforcement or punishment for different practices (especially if immediate)
Views/knowledge/beliefs about risk: usually over-rate our health and under-rate the risks
Our resources (usually an excuse)
Physical environment (work/home)
Social influences (friends/media)
History Taking
Attitude of interviewer important: non-judgemental, empathic, detached, normalising behaviour, start
estimates of use at a high level, person can then say „no, not that much‟ – feels less judgemental
Often illegal: won‟t tell unless good rapport
Signs of Substance Abuse
Changed behaviour
Skipping work/school
Drug seeking behaviour
Money problems
Relationship problems
Questions:
Reason for presentation
Which drugs
Ever intravenous
What are the useful effects – why do you continue to use
Quantity and frequency, pattern of use (regular or binge)
Cost per week
Duration of use, age at first use, reason for first use
Heaviest use
Have you or others ever been concerned about your use
Attempts at cutting down and duration of abstinence, what made you start again
Problems associated with use, including relationships, job, legal considerations, etc
Any withdrawal effects
Past treatment and outcome, what was and wasn‟t helpful
Relationship to psychiatric symptoms. Do they drink when they‟re anxious? Have panic attacks
followed drug use, etc
If alcohol, ever been in an accident, had a head injury or fracture
Medical history, psychological history, social situation
Family History: check psych, suicide and A&D history
Corroborative interview
Drug users have high mortality: health consequences, accidents, suicide, high-risk neighbourhoods, etc
Physical examination: yellow fingers/teeth, injection marks, liver, cardiac murmurs, pregnancy/STD,
mental status, signs of intoxification/withdrawal
Investigations
Alcohol abuse: ethanol level, also LFT (GGT) & FBC (macrocytes), nutrition (eg Fe)
Blood tests for drug levels: benzodiazepines & morphine levels
Cannabis: creatinine/cannabis ratio over time
If any intravenous use check for viral serology: Hep B, C, HIV
Urine tests: useful for tracking abstinence, but not reliably effective as a treatment strategy. Can do a
full drug screen (drugs + prescription medications) for $160. Verification of sample source is
important – minimise the risk of substitution (eg giving you someone else‟s urine sample).
448 4
th
and 5
th
Year Notes
Drug
Time after which urine screen will be negative
Amphetamine
1 – 2 days
Cannabis
4 – 28 days
Cocaine
1 – 2 days
Diazepam
2 – 4 days (longer with prolonged use)
Heroin
1 – 2 days
LSD
1 – 3 days
MDMA (ecstasy)
2 – 4 days
Methadone
2 – 4 days
Drugs of Abuse
If therapeutic index is wide, then it‟s good for addiction: good effect but few side effects
IV drugs: opiates, speed, and benzodiazepines. Health risks include infection and non-infectious
sequalae
Marijuana
Ecstasy – amphetamine (party scene)
Fantasy – GHBA
Solvents: younger, failing at school, worried parents, neurological impairment
Tobacco (See Smoking, page 87)
Dependence resulting from various drugs
Drug Class
Physical
Psychological
Tolerance
Alcohol
3
3
2
Sedatives
3
3
2
Benzodiazepines
1
3
1
Opioids
4
4
4
Stimulants
1
3
4
Hallucinogens
-
2
2
Solvents
1
2
3
Nicotine
1
3
3
Cannabis
-
2
1
Cannabis/Marijuana
Psycho active ingredient is 9 tetrahydrocannabinol (9 THC)
Receptor targets in the CNS = CB1, in PNS = CB2
Synthetic cannabinoid drugs used therapeutically for appetite stimulation (eg in cancer),
anticonvulsant/antispastic, analgesic
Effects:
Minimal for occasional use, greater for longer-term heavy use
Respiratory system: hot irritating smoke all the effects of cigarette smoke (inflammation,
mucus, thickened basement membrane, squamous cell metaplasia, destruction of cilia)
CNS: enhanced feelings of well being, disputed dose-dependent effects – reduction in energy,
drive and motivation, psychosis, learning and attention, dependence with associated social and
psychological dysfunction, acute adverse reactions (eg anxiety/panic attacks)
Regulation of Addictive Drugs
See Regulation of Drugs of Abuse, page 536
Treatment of Substance Abuse
Treatment Rationale
Treatment must be for underlying addictive disorder, not just detoxification and withdrawal
Addiction is a chronic not acute illness. Requires long term follow-up and behaviour modification (as
with diabetes and hypertension)
Often unsympathetic response because addiction is perceived as self-afflicted: but there are numerous
involuntary components in the addictive process. Loss of voluntary control turns a drug misuser into
drug addicted. There is a compulsive, often overwhelming, involuntary component
Involves genetic, biological, behavioural and environmental components
Psychological Medicine 449
Success rate for treatment depends on type of drug and variables inherent in the population being
treated (e.g. better for professionals than for poorly educated). Nicotine has the poorest success rate.
Success rates are comparable with other chronic diseases
Treatment is cost-effective
Issues In Treatment
Compliance with treatment. Those who comply with treatment have best prognosis – as with other
chronic diseases
Who should be involved: multidisciplinary approach
Managing the environment: peer pressure, money, job, supports, triggers to former behaviour, family
relationships (can they be helped, education about illness)
The most significant predictor of treatment success is an empathic, hopeful, continuous treatment
relationship
Must also treat any co-morbid diagnosis simultaneously
Types of Treatment
Medication: Antabuse, naltrexone, opioid substitution
Detoxification (inpatient/outpatient)
A&D counselling: motivational interviewing, strategies for change, relapse prevention
Psychotherapy: CBT, psycho-education
Self-help groups
Addressing specific issues: grief, anxiety, childhood sexual abuse, sexual assault, anger, relationship
problems, parenting issues, financial, housing, employment issues, etc
Readiness to Change/Motivational Interviewing
See Behavioural Change, page 11
Services for dependency
Detox: Kenepuru (inpatient)
AA
Narcotics anonymous
Queen Mary – Hamner: uses 12 step process
Odyssey House (Auckland)
Alcohol and drug service
Making the change
Takes a long time
Involves changing lifestyles, supports, habits
GP can assist with motivation for change:
Methadone Treatment
For opiate addiction
Methadone is highly addictive, but is regular, long acting (a dose a day holds for 24 – 46 hours), free
( crime), legal, more effective taken orally than other opiates, no risks from injection
Doesn‟t give a high – just stops „hanging out‟ (withdrawal)
Has to be taken every day
Can cause high mood, drowsiness, pain, small pupils, constipation, histamine release (sweating,
itching, etc), saliva tooth decay, libido – it is a powerful drug
It doesn‟t affect senses, or damage body organs, shouldn‟t affect pregnancy or breast-feeding
Is dangerous in conjunction with tranquillisers and/or alcohol overdose situation (eg vomit and
choke while sedated)
Is taken as part of a planned programme, including counselling, to build a life away from opiate abuse
– can concentrate on sorting out debt, relationships, etc
450 4
th
and 5
th
Year Notes
Alcohol Abuse
Safe Limits and Metabolism
Men and women have different blood alcohol levels given the same dose due to lower Vd in women
Standard Units
One Sitting
Per Week
Male
4, with 2 – 3 alcohol
free days a week
14 – 21 (ie up to 210 g
ethanol)
Female
3, with 2 – 3 alcohol
free days a week
7 – 14 (ie up to 140 g
ethanol)
Standard Unit = 10 g of alcohol. E.g. 1 can normal strength beer, 1 glass (120 ml) table wine, 1 glass
sherry/port, 20 ml spirits (hotel nip)
Effects (if no tolerance):
50 mg: relaxation, emotional liability
100 mg: judgement affected, reactions slow
150 mg: amnestic blackouts (can‟t remember afterwards)
200 mg: ataxia, vomiting, nystagmus, drowsiness
350 mg: coma, respiratory depression, death
Intoxication can be life threatening
Driving:
Legal blood limit = 80 mg/100ml (17.4 mmol/L)
Legal breath limit = 400 g/L breath
Driving skills impaired from 40 – 50 mg/100 ml
Metabolism:
CH3CH2OH CH3- C – H Acetate
10 g per hour, zero order kinetics
= 15 – 20 mg/100 ml blood/hour (3 – 4 mmol/hr) = one standard drink
Twice this rate of clearance with chronic alcohol consumption, less in liver disease
Alcohol changes NAD/NADH ratio alters redox potential widespread effects (eg lipids,
sugars, etc)
Classifying alcohol use
Alcohol Dependence: need to drink every day
Important features:
Tolerance: due to pharmacodynamic and pharmacokinetic (eg enzyme induction) processes
Cross-tolerance, eg alcohol and BZDs
Physical dependence: Withdrawal syndrome on abstinence
Psychological dependence: Emotional need to compulsively take a drug (even if no physical
withdrawal syndrome)
Characterised by: tolerance (CNS adaptation and pharmacokinetic), narrowing of drinking pattern
(stereotyped drinking), amnesic blackouts, withdrawal symptoms, awareness of loss of control,
failed attempts at abstinence, preoccupation with drinking, drinking to relieve withdrawal
symptoms
Look for: compulsive binges with frequency, stereotyped drinking, intake over 60 g ethanol/day,
chronic social and health problems, neurological problems
Use CAGE questions to assess dependency: Have you ever tried to Cut Down, Annoyed by others
telling you to cut down, Guilt, Eye-opener
Hazardous Drinking. Heavy drinking with no “obvious” problem
Characterised by prolonged (eg 5 years or more), regular (eg almost daily, or weekend binges),
excessive consumption with a high risk of physical mental and social implications, but no
dependency features – but maybe some tolerance and occasional amnesic blackouts, may not be
associated with acute intoxication
Look for: episodic heavy social drinking to intoxication, increasing psychosocial problems,
accidents, inflammation of stomach, liver, pancreas
||
O
Alcohol
dehyrogenase
Acetaldehyde
dehyrogenase
Psychological Medicine 451
Problem Drinking: problems related to alcohol without dependency and with or without excessive
regular consumption. May result from isolated acute intoxication or drinking with medical
contraindication – injury, aggression, binge drinking, family, financial, occupational problems
Remember: Drug abusers often abuse multiple drugs (eg alcohol, BZDs, and marijuana)
Assessment
For liver and pancreatic effects see Alcoholic Liver Disease, page 185
Differential of drowsiness/confusion in alcoholic:
Alcohol intoxication
Sedatives
Post-ictal (eg seizures with alcohol withdrawal)
Wernicke‟s encephalopathy
Subdural haematoma: grow slowly, compounded by global atrophy due to alcohol
Hepatic encephalopathy
Alcoholic hypoglycaemia
Assessment of co-existing disease is vital:
Other drug use (BZD, sedatives, opioids also have withdrawal features)
Primary depressive disorder (in addition to alcohol-induced depression which resolves quickly)
Gastro disorders: oesophagitis, pancreatitis, liver disease, small bowel dysmotility
Respiratory: Obstructive sleep apnoea, aspiration pneumonia, TB
Musculoskeletal: chronic proximal myopathy, osteoporosis
Carcinomas: larynx, oesophagus, lung
Neurological: peripheral neuropathy, dementia, cerebellar atrophy, Wernicke-Korsakoff
syndromes, Head injury (subdural haematoma), haemorrhagic stroke
Cardiovascular: arrhythmias, congestive cardiomyopathy, hypertension
Blood and nutritional: macrocytosis, folate and iron deficiency, impaired leucocytes,
hypocalcaemia, hypokalaemia, electrolyte disturbances
Investigations:
Alcohol levels
LFT
FBC (anaemia)
Glucose ( ?hypoglycaemic)
Coagulopathy: INR
Other drugs, eg BZD
Pathological Effects of Alcohol on the Brain
Cerebral atrophy:
Common. Seen in over ¼ of long term alcoholics at post-mortem
Ventricular dilation, widening of the cerebral and cerebellar sulci
No specific cortical changes have been described. No classical changes of multi-infarct dementia
or Alzheimer‟s (see Dementia, page 439)
Wernicke-Korsakov Syndrome:
Due to Vitamin B1 (Thiamine) – Marmite and Cereals are good sources
Thiamine is not stored in the body, signs of deficiency can appear within a month – especially in
beer drinkers (high carbohydrate intake thiamine requirement)
Rare triad of:
VI nerve palsy (vertical/horizontal nystagmus)
Ataxia (vestibular dysfunction)
Confusion
Pathology:
Acute: petechial haemorrhages in the grey matter surrounding the third and fourth ventricles
and aqueduct
Chronic: shrinkage and haemosiderin staining (especially of mamallory bodies)
If prolonged leads to Korsakov‟s amnesic psychosis
Vitamin B12 (cobalamin) deficiency:
Leads to:
Peripheral neuropathy, demyelination and degeneration of the posterior and lateral columns of
the spinal cord
Variety of confusional, amnestic and psychotic alterations
452 4
th
and 5
th
Year Notes
Treatment of alcohol abuse
Drug treatment of alcohol abuse:
Effects of chronic alcohol:
Dopamine activity
Opioid activity ( ?naloxone/naltrexone craving)
Sensitivity to GABA
Serotonin activity
Ie, lots of potential neurotransmitter targets in reward pathways to cravings, etc
Antabuse (disulphram):
Blocks second step of metabolism pathway acetaldehyde flush, vomiting, BP
Takes 12 hours to block enzyme system. Has effect within ½ hour of a drink (one drink is
enough)
Contraindications: heart disease (can‟t cope with BP), makes depression/psychosis worse
Administration needs to be supervised: if taken at own discretion then little impact on
abstinence
Acamprosate (Campral): craving, must be taken 3 times daily (a pain!), start 7 days post detox.
Not in elderly, pregnant, liver or renal disease. No hypnotic, anxiolytic or antidepressant effects
For non-drug treatment, see Treatment of Substance Abuse, page 448
Alcohol Withdrawal
Most common drug withdrawal state. Can be life threatening (unlike opioid withdrawal)
Detoxification is only the first step in treatment
Aetiology of alcohol withdrawal syndrome poorly understood
Features of withdrawal:
A spectrum. Delirium Tremens describes severe withdrawal only
Minor withdrawal (peaks at day 2): restlessness, anxiety, nausea, disordered sleep, headache,
tachycardia, hypertension, tremor
Major withdrawal (peaks at day 5): Agitation, behavioural disorders, confusion, sweating, fever,
paranoia, hyperventilation
Seizures: if they occur, are most likely on day 1 – 3, usually only one, usually grand mal, status
rare
Hallucinations: usually visual (auditory unlikely), on day 2 – 4
Management:
Get pre-detoxification blood alcohol level. Helps with assessment (how tolerant are they?). Avoid
too much sedative if high. Alcohol metabolised at 20 mg/dl/hour (4 mmol/L/hour) – can predict
when it will reach zero
Previous withdrawal severity good indicator of likely current severity. Other indicators of
severity: > 15 standard drinks a day, early morning drinking, hypokalaemia, intercurrent illness
If likely to be severe, or if co-existing medical, psychiatric illness or other addiction, withdrawal
should be medically supervised (ie admit them). Mattress on the floor with constant nursing
attention. If dehydration or constant sweating then iv fluids
Otherwise at home or outpatients if good social support
Routine blood tests: FBC, ESR, U+E, B12/folate, LFT, AST, GGT, PT, BS
Parental thiamine followed by short oral course (25 mg po twice daily)
Treat withdrawal with drugs which have cross-tolerance with alcohol (ie BDZs) once they’re no
longer intoxicated
Use BZDs or chlormethiazole
Give sedatives with extreme caution if measurable blood alcohol levels
Diazepam 10 – 20 mg/4 hourly for moderate withdrawal, 20 mg/2 hourly iv for severe. Resist
protracted sedatives, otherwise addiction. If liver disease then reduce dose
Oral chlormethiazole 1 gm 6 hourly
Additional treatments:
blockers for tremor, hypertension (except if CORD or CV disease).
Haloperidol 1 – 5 mg 6 hourly if hallucinations
Sodium Valproate (Epilim) 600 mg stat po, then 400 mg 8 hourly for 5 days, if history of
seizures – care if liver disease. Likely to occur early in withdrawal, especially if history of
seizures with previous withdrawal
Psychological Medicine 453
Other Disorders
Eating Disorders
History Questions
Do you worry about how much you weigh?
What do you think of your body/weight?
Do you diet?
Do you ever make yourself sick after a meal?
Anorexia Nervosa
Low weight not due to other illness
Persistent refusal to maintain weight (cf depression – don‟t want to eat). Obsession with food, weight
and thinness
90% female, usual onset from 11 – 19 years
Aetiology:
Media message: thin = beautiful
Already painfully aware of body image due to changes in puberty
Stressful life situations
Genetics
Family dynamics
Something they can have control over when they don‟t have control in other areas of their lives
Failure to achieve weight control sense of failure try harder
Signs:
Deliberate self-starvation
Fear of gaining weight
Denial of hunger
Constant exercising
Self perception of being fat
Absent or irregular periods
May purge (vomiting, laxatives)
Complications: starvation, heart, osteomalacia, fertility
Bulimia
Purging a more dominant feature
Don‟t usually loose so much weight
Impulse Control Disorders
Gambling
Reference: General Practitioners Manual on Problem Gambling, Compulsive Gambling Society of NZ
= The addiction you can‟t see. The new mental disorder on the block
Epidemiology:
1 – 3 % of population are pathological gamblers. There are no longer stereotypical groups – young
and women also now affected
Maori 3 times more likely, Pacific Islanders 6 times more likely (heavy socio-economic
confounding)
2/3 of presenting problem gamblers are under 30. Average age is decreasing
90% of the population gamble (Dept Internal Affairs figures). $600 per family per year (cf $200 in
the US)
Gambling has increased by 700% in the last decade. There has been significantly increased access
to all forms of gambling (without social research)
Mode of gambling of people with pathological gambling disorder: 60% non-casino pokies
Diagnosis:
Should screen early on in relationship with GP: later on won‟t tell due to embarrassment
Features: Preoccupation with gambling, needs to gamble more to get the same excitement (ie
tolerance), repeated and unsuccessful efforts to cut back or control, restless or irritable when trying
to cut down (ie withdrawal), gambles as a way of dissociation, after loosing returns to chase their
losses, lies to conceal extent of gambling, has jeopardised or lost a job or relationships, etc
454 4
th
and 5
th
Year Notes
Other features:
Impacts for physical health: can‟t afford to go to doctor, usually heavy smokers, often have
co-morbid anxiety, depression, alcohol or drug disorder (NB – screen for depression in
affected families), high suicidality
Will use their own money then may resort to crime (usually fraud, forgery & theft). Crimes
unsophisticated, effected in haste and often first offence
Theories re aetiology:
Reward deficiency syndrome
General theory of addiction: unresolved/maladaptive issues from the past
Behavioural/environmental conditioning
Social learning (eg permissive culture)
Phases in the course of the illness:
For gambler: winning, losing, desperation, critical, rebuilding, growth
For spouse: denial, stress, exhaustion, critical, rebuilding, growing
Problems with thinking in gamblers:
Irrational style of thinking
Illusions of control (“if I study the horses enough I‟ll win)
Superstitious beliefs (“I feel lucky today”)
Biased evaluations
By the time gambling is pathological, they don‟t care whether they win or lose, just want to do it
Help to offer:
Treat depression
Financial/budget advice: easy way to engage, encourage contemplation
Information (eg about „controlled gambling‟ as an option for „early‟ problem gamblers)
Helpline: 0800 NOGAMBLE
Referral services: outpatients, Compulsive Gambling Society, Odyssey House
Fictitious Disorder
Factitious Disorder by Proxy
= Munchausen‟s By Proxy
Criteria:
Intentional production or feigning of physical or psychological signs or symptoms in another
person under the individual‟s care
Motivation is to assume the sick role by proxy
No external incentives for the behaviour (economic gain, avoiding legal responsibility)
Warning signs: child aged 15 months to 6 years, baffling multisystem symptoms, taken to lots of health
care providers, over attached parent, no symptoms when parent absent, strange poisonings, reported
seizures
Personality Disorders
Diagnosis
Personality disorder =
An enduring pattern of inner experience and behaviour that deviates markedly from the
expectations of the individual‟s culture
Is inflexible and pervasive across a broad range of situations
Has its onset in adolescence or early adulthood, is stable over time and leads to distress
And is manifested in two or more of the following: interpersonal functioning, affectivity
(emotionality), impulse control, cognition (style of thinking)
Key characteristics:
Rigidity: very pervasive rigidity of cognitions and behaviours
Avoidance: don‟t want to look at or experience their thoughts or feelings problem for therapy
(compulsory treatment won‟t change anything)
Long-term interpersonal difficulties
Differentiating from axis 1:
There is substantial comorbidity with axis 1 – but must be distinguished from axis 1 (which is
episodic, different from normal state. Personality disorders ARE the normal state)

Psychological Medicine 455
Need to exclude other possible factors: eg substance abuse, head injury, general medical condition,
mood or psychotic disorder (ie must not occur exclusively in the course of an axis 1 disorder)
Consider axis 2 if: ongoing non-compliance, client unaware of effect of their behaviour on others,
client acknowledges need for change but motivation is questionable, always blame others for their
behaviour
Can‟t diagnose before age 19 (much of the description of the disorders is also descriptive of
adolescence)
Requires longitudinal assessment and collateral information
Must evaluate within a cultural and religious context (DSM 4 is white & American)
Labelling someone with a personality disorder can be difficult, given limited information and possible
reactions often people labelled „traits of disorder X‟
Presentation is often not for the disorder (as it could be, for example, for depression), but for the degree
of impairment due to excessive or little compliance with treatment
Treatment is difficult and long-term: given deeply imbedded nature and genetic predisposition to
personality
Explanation to client:
Behaviours were probably adaptive to survive difficult childhood experiences (at some point
behaviours were helpful – but they‟ve got stuck). Take care to look for an explanation not
someone to blame (people usually do the best they can)
But it is now more functional to use different strategies in different situations
Take care of criticising non-compliance: few are proud of „doing what they‟re told‟ – would you
rather be a sheep or an eagle?
Examples of Personality Disorders
Disorder
Comment
Cluster A: Appear odd or eccentric
Generally distrustful, suspicious, loners. Non-compliant with
treatment as it doesn‟t fit their worldview. See less of them in
GP – don‟t call attention to themselves.
Paranoid
Distrust and suspiciousness such that other‟s motives are
interpreted as malevolent
Schizoid
Detachment from social relationships and restricted range of
emotional responses (eg can‟t express anger, seem
directionless)
Schizotypal
Acute discomfort in close relationships, cognitive or
perceptual distortions, eccentricities of behaviour. Often have
ideas of reference (but not with delusional conviction) eg
preoccupied with paranormal phenomena or have special
powers. Important differential to psychosis. May be
suspicious/paranoid, may seek treatment for associated
depression or anxiety.
Cluster B: Dramatic, emotional, erratic
Call attention to themselves, vocal in asking for help, other
people want them to change but they may see their behaviour
as functional (will bear the cost of dysfunction because they
get what they want)
Antisocial
Disregard for, and violation of, the rights of others (usually
male)
Borderline
Instability in interpersonal relationships, self-image, and
affects, and marked impulsivity (usually female)
Histrionic
Excessive emotionality and attention seeking
Narcissistic
Exaggerated sense of self worth – pattern of grandiosity, need
for admiration, and lack of empathy
Cluster C: Anxious and fearful
May come to attention due to anxiety
Avoidant
Social inhibition, feelings of inadequacy, hypersensitivity to
negative evaluation
Dependent
Submissive and clinging behaviour, related to an excessive
need to be taken care of
Obsessive-
Compulsive
Pattern of preoccupation with orderliness, perfectionism and
control
Disorder Not otherwise specified
Meet criteria for a personality disorder, but are a mixture of
the above or don‟t fit any of the above (eg passive-aggressive)
456 4
th
and 5
th
Year Notes
Borderline Personality Disorder
Incidence: 3 – 5 % (cf 1% for Schizoid)
Criteria include:
Frantic efforts to avoid real or imagined abandonment
Unstable and intense relationships alternating between extremes of idealization and devaluation
Impulsivity in areas that are potentially self-damaging: eg spending, sex, substance abuse, binge
eating
Recurrent suicidal behaviour, parasuicides, threats or self-mutilations
Marked reactivity or mood, difficulty controlling anger
Characterised by:
Schema: I can‟t control myself overdeveloped emotional responsiveness & underdeveloped
self-identity, impulse control
Core belief about self: I‟m defective, helpless, vulnerable, bad
Belief about others: other people will abandon me, can‟t be trusted
Combination of these two leads to extremes of behaviour: need to depend on others but will be
abandoned
Hate being alone: may attend A & E or ring friends late at night for company
Self-harm:
Begins between 10 and 16: often following a major life change
„Toxic self-soothing‟: eases the inner pain – powerful way to feel better. Can either help the
dissociation (turn off emotions) or help them feel real
Communication strategy: there is chaos within family and have never asked for help can‟t ask
for help now. But self-harm is not always a cry for help. For most, self-harm is a private matter
Strategy in the game of life: to manipulate people or drive them away
Always need to screen for concurrent depressive episode: this will need treatment
What helps in situations of self-harm
Non-judgemental acceptance
Teach other ways to self-sooth
Deal with trigger event: what causes the negative feelings
Address underlying issues: but shouldn‟t do trauma counselling without also improving coping
skills
Aetiology:
Genetic loading in temperament: perseverance, impulsivity, affect regulation, stimulation
seeking
Sexual abuse in 75% (but not all severely abused develop the disorder): feeling unsafe,
victimisation, trauma, terror
75% are female (men more likely to react by becoming antisocial – same motivation but take it out
on others rather than themselves – or substance use). Behaviour in collusion with dominant
western values (eg emotionality, dependence)
Other societal factors eg invalidating environments (eg neglect), marginalisation
Most affected people have this cluster of factors, but someone can still get it even if the best of
upbringings ?stronger than normal predisposing temperaments
Treatment of Mental Illness
Care for the Mentally Ill
Illness (especially initially) is very traumatic for individual and family (eg may not cope as normal or
remember anything you say)
Families will often blame themselves or feel guilty
Knowledge/education is key: without it people are powerless
„Recovery‟: issue may not be getting rid of all the symptoms, but getting rid of or managing those
symptoms which are disruptive or distressing
Stigma
Feeling created by stigma is a significant reason for the loss of hope and relapse experience by those
with mental illness
Psychological Medicine 457
Stigma leads to discrimination and sense of shame
Common misconceptions:
People with mental illness are dangerous and violent
People with mental illness never recover: vast majority do recover, some require ongoing treatment
It‟s got nothing to do with me: but mental illness affects people of all ages and backgrounds
Drug Treatment
When using medication:
Don‟t make assumptions about what people want – ask them
What have they used before and what has worked. What‟s worked for family members?
Need to consider side effects: will benefits outweigh costs. Side effects are often significant, and
will be a major cause of problems with compliance. Be ready to change medications if side effects
are intolerable
Need to consider the long term (ie when/how will they come off) as well as the short-term
Make sure alternative/adjunct treatments are considered
Optimal initial dose: the level at which there are maximum therapeutic benefits for minimum side
effects
Maintenance dose: lowest possible dose that provides relief/remission. Will vary from person to
person, and due to psychosocial factors (ie may need to increase it under when under stress)
Regular review is important, until the patient is stabilized on the medication
Drug education:
Understanding the medication‟s purpose is vital to informed consent and to adherence to treatment
Patient needs to know why the medication is needed, what the medication is expected to achieve,
when and how to take it, and possible side effects or restrictions (eg diet), the likely duration of
treatment, how long until an effect should be noticed, whether the medication is addictive, what are
the alternatives
Some medication (eg fat soluble anti-psychotics) clears very slowly from the body, so a patient can
stop taking them without immediate relapse. Patient‟s need to understand that the drugs are
effective only if taken regularly
Cognitive Behavioural Therapy (CBT)
See also Treatment of Major Depressive Disorder, page 429
Was developed as a structured, problem-orientated psychotherapy by Aaron Beck in the 1960s
Focuses on cognitive and behavioural influences on human experience, as well as interpersonal
processes and „unconscious‟ motivation/underlying schema
Draws on my aspects of learning theory and cognitive psychology
Process in depression: early experience formation of dysfunctional assumptions critical incident
assumptions activated negative automatic thoughts behavioural, motivational, affective,
cognitive and somatic symptoms of depression
Cognitive triad in depression: negative view of self, of the world, and of the future
Basic principals of CBT:
The situation itself does not determine how people feel
Emotions and behaviours are influenced by how people perceive events
Information processing biases lead to, or maintain, depressed affect and behaviour
Efficacy of CBT well supported. At least as effective as antidepressants in depressed outpatients
Problem Solving Therapy
For „problems of living‟ causing or contributing to current symptoms
Regaining control mood and less overwhelmed
3 Steps:
Realise symptoms are linked to problems in their life
Define and clarify problems
Solve problems in a structured way
Stages:
Explanation of treatment and it‟s rationale
Recognition of emotional symptoms
Recognition of problems: eg relationships, work, money, housing, legal, alcohol, etc
Acceptance of a link between symptoms and problems
Clarification and definition of problems:
458 4
th
and 5
th
Year Notes
List problems in a concrete form
Break down big problems into more manageable parts
Choose achievable goals given patients resources and obstacles
Patient generates as many solutions as possible
Choose the preferred solution
Implement the preferred solution – set deadlines, etc
Evaluation and encouragement. If unsuccessful consider: low motivation, inappropriate goals,
unsuitable choice of solution, inappropriate implementation
Compulsory Treatment
See also Protection of Personal and Property Rights Act (1988), page 713. Used for people with
diminished competence – especially dementia.
Features of the Mental Health (Compulsory Assessment and Treatment) Act 1992:
Specific legal definition of mental disorder (not a diagnostic definition)
Even if committed, must be treated in the least restrictive environment ( community orders)
Rights of patients are listed: eg to information, to respect for culture, to second opinion, to legal
advice, ability to communicate (phone, letters, visitors, etc)
Can‟t treat without consent (which you must try and get) without a second opinion
Review procedures are specified, including the Mental Health Review Tribunal
Definition of Mental Disorder (Section 2):
An abnormal state of mind characterised by continuous or intermittent delusions, disorders of
mood, volition (energy, drive, will), cognition, or perception, etc
And to such a degree that it poses a serious danger to person or others, or seriously ability to take
care of themselves
Exclusions include (Section 4): if due only to intellectual disability or substance abuse, criminal
behaviour, sexual preferences, political and religious views
Process:
Application must be made by anyone over 18 (section 8)
Medical certificate must be provided by any doctor (who may be the applicant, section 8)
Reviewed by a psychiatrist designated under the Act within 24 hours (section 9)
5 day compulsory assessment period (although can be released, become voluntary, appeal, section
11)
Following reassessment can be held for a further 14 days (section 13)
To extend beyond this require review by family court
Compulsory treatment orders:
Community treatment orders (section 29)
Inpatient orders (section 30)
Duly Authorised Officer = usually an experienced CPN in CATT team – carry out assessments,
start process
Grief and Bereavement
Reference: Material from Mary Potter Hospice, obtained in GP run, and Te Omanga Hospice Material
See also Palliative Care, page 473
Theories of Grief
Freud: work of mourning: detachment from person who has died. Healthy resolution when this is
completed
Kubler-Ross: Stages of terminal illness: denial, anger, bargaining, depression, and acceptance. But it‟s
not sequential, and this only talks of emotions, not physical or behavioural dimensions
Worden: Tasks of mourning:
Accept reality of loss (harder if no body etc)
Experience pain of grief
Adjust to an environment in which the deceased is missing (often very practical – change in roles
etc)
Withdraw emotionally and invest in new relationships (later he revised this to emotionally relocate
the deceased and move on) – put the deceased in another place
Silverman:
There is a continuing bond between deceased and survivor
Psychological Medicine 459
Stages:
Impact: this is not real
Recoil: I‟m going crazy, why am I worse now (can be months later)
Accommodation: what do I carry with me? Being a living memorial – don‟t have to cut off –
can move on and still carry something with them
Stroebe et al: Dual process moving between expression of grief and containment of grief (women
prefer former, men latter)
Characteristics of Grief
Reassure bereaved person that these are normal. If overwhelming, seek help
Emotional: bewildering and intense range or emotions without warning - shock, numbness, relief,
anxiety, anger, blame, guilt, loneliness, helplessness, hopelessness
Physical: hollow stomach, tight chest, breathlessness, weakness, lack of energy, sexual desire, sleep
disturbances, symptoms similar to person who died (this can be pathological)
Cognitive responses: disbelief, confusion, concentration, going crazy, preoccupation
Behaviours: searching, crying, sighing, absent minded, restless, socialising, visiting/avoiding places
that are reminders
Coping with Loss
Losses are a common cause of illness – they often go unrecognised
Conflicting urges lead to a variety of expression of grief – but there is a pattern
Understanding factors that predict problems in bereavement enables these to be anticipated and
prevented
Grief can be avoided or it may be exaggerated and prolonged
Doctors can help to prepare people for the losses that are to come
People may need permission and encouragement to grieve and to stop grieving
Factors Complicating Grief – Risk Factors for Pathological Grief
Dependent family members (children, handicapped, elderly)
Loss of primary care giver/constant companion
Loss of financial provision
Loss of home (feared or actual)
Anxiety about decisions
Unable to share feelings
Family discord
Uncontrolled pain/emotional distress before death
Concurrent life crisis
Prolonged reaction/suicidal thoughts
Lack of community support
Children’s Grief
It is not possible not to communicate to children (ie not telling them is not an option)
Help should start at the time of diagnosis
Talk about what won‟t change as a result of the illness
Maintain things that are important in a child‟s life (e.g. routines)
Talk about practical concerns
Provide extra stability, order, routine and physical affection
They need to know who will take care of them if key people leave or die
Offer reassurance
Children often assume responsibility for what has happened and feel very guilty
Offer clear, simple, truthful information: repeat, repeat, repeat
Don‟t use euphemisms (e.g. asleep – explain death, body stops working)
Signals for attention from a grieving child
Marked change in behaviour: illegal behaviour, persistent aggression (> 6 months), tantrums,
withdrawal, drug abuse
Inability to cope with problems and daily activities
Many complaints of physical aliments
Persistent depressions, panic attacks
460 4
th
and 5
th
Year Notes
Change in school performance
Fearfulness for self, or for loved ones
Helping Families
Listen effectively
Foster communication
Engage siblings
Check social supports
Address symptoms
Provide constant factual data
Help build positive memories
Don‟t take offence
5
th
Year Written Exam Model Answer
These questions normally give a small vignette and then ask the following questions
What is the Diagnosis?
List the factors from the vignette which support your diagnosis
List what other factors you would ask about on further history taking (eg what criteria for your
diagnosis where not mentioned in the vignette)
What risk factors for the diagnosis are there in the vignette or that you would ask about
Is there a significant impairment in social and occupational functioning
Is there a change from previous functioning
What are the possible Differentials?
Always consider including the following
Alcohol and Drug use disorders or withdrawal
Other psychiatric disorders (eg anxiety for depression, etc)
Conversion disorder
Axis 2 disorders (personality disorders)
Medical conditions:
Endocrine: thyroid, cortisol, calcium
Cerebral insult: dementia, stroke, tumour, SLE, AIDS
Medications: -blockers, steroids, etc
What is your recommended management?
Establish a positive therapeutic relationship based on a shared understanding of the problems
Establish an accurate diagnosis:
Take a full history (including past psych history) and mental state exam
Get a corroborative history if necessary
Consider a drug screen if indicated
Do a physical exam and investigations to exclude medical causes
Assess for comorbid psych illness (especially alcohol and drug use)
Establish a formulation:
Why has this person presented in this way at this time
Assess predisposing, precipitating, perpetuating and protective factors across a biopsychosocial
framework, eg genetic factors, coping and relationship skills, stress, risk factors
Consider cultural aspects. Assess their needs and treatment within their cultural context
Assess insight, willingness to change or accept help
Assess severity
Immediate management:
Safety issues: Use of CAT team, Mental Health Act, etc
Do they need admission to stabilise and assess/observe?
Immediate drugs for psychosis: antipsychotic +/- lorazepam
Longer term management:
Multidisciplinary approach
Lifestyle modification: stress management, alcohol and drug, sleep hygiene, exercise
Maintain function and integration with communities of interest
Psychological Medicine 461
Education for patient and their family
Drugs:
Side effects, contraindications, duration
Watch for and treat complications
Psychotherapy:
Modify exacerbating or precipitating behaviours
CBT, coping skills, structured problem solving, relaxation training, breathing retraining,
deconditioning, desensitisation, graded exposure, cognitive restructuring
Psychodynamic psychotherapy: elucidate mental processes outside the person‟s conscious
awareness so as to alter core conflicts
Stop self esteem and manage stigma from having a psychiatric illness
Secure employment, housing
Community support: support groups, psych nurse
On-going review:
Plan for follow-up to reassess illness and monitor treatments
Identify warning signs for a relapse
Plan and prepare for relapses
Set and prioritise goals
462 4
th
and 5
th
Year Notes

Genetics and Cancer 463
Genetics and Cancer
Epidemiology of Genetic Disorders ......... 464
DNA ......................................................... 464
Chromosome Disorders ............................ 464
Patterns of inheritance: ............................. 464
Non-Mendelian Genetics .......................... 465
Genetic Testing ......................................... 465
Other ......................................................... 466
Genetic Counselling ....................................... 466
Cancer ............................................................ 466
Epidemiology ........................................... 466
Oncogenesis .............................................. 466
Anatomic Pathology and Neoplasia .......... 467
Staging of Cancer ..................................... 468
Cancer Treatment ..................................... 469
Symptom Management in Cancer ............ 470
Cancer emergencies .................................. 472
Palliative Care .......................................... 473
464 4
th
and 5
th
Year Notes
Epidemiology of Genetic Disorders
9,000 known genetic diseases
5% have genetic diseases before 25
60% during lifetime (includes diabetes, heart disease, cancer)
DNA
There is frequent mutation in rapidly dividing cells: but repair mechanisms „mop up‟
If there is a sustained mutation in:
Essential gene lethal
Non-coding gene no effect
Non-essential gene human variability/disease
Chromosome Disorders
Polyploidy: duplication of whole sets of chromosomes (eg triploidy: n = 69). Non-survivable fetal
wastage
Anuploidy:
One missing or additional chromosome
Trisomy 21: 47XY + 21. See Down Syndrome, page 581
Trisomy 13: next most common, trisomy
Turner‟s Syndrome: 45, XO
Puffy feet, poor toe nails, redundant skin behind head/neck, kidney and cardiac malformation
Later: short, infertile, normal mental ability (unless 2
nd
X ring chromosome mental
disability)
The 10% that survive to term are the good end of the spectrum
Differential: Noonan‟s Syndrome – similar symptoms but karyotype is normal
Klinefelter Syndrome: 47, XXY
1/3 present in childhood with learning difficulty
1/3 present in adolescent: failure of puberty due to no testosterone (ie hypogonadism)
1/3 present in adulthood due to infertility
Chromosome abnormalities:
Deletions, insertions, etc. Will be different in each child variable presentation. Eg deletion in
5p: Cri du Chat syndrome, cat like cry
Fragile X Syndrome: commonest cause of mental disability in males. 1:1,000
In testing for mosaics, may need to test skin, not blood, as abnormal cells don‟t reproduce so well so
get weeded out in tissues (eg blood) with high turnover
Patterns of inheritance:
Autosomal Dominant
=Single gene abnormalities expressed in heterozygotes
M = F, 50% risk of passing it to kids
1 abnormal gene causes disease
Eg Huntington Disease, Marfan Syndrome, Achondroplasia (disturbance of epiphyseal
chrondroblastic bone formation)
But:
Variable expression, variable age of onset
Non-penetrance happens
Gonadal mosaicism (esp if old paternal age) somatic genes normal, mutation in gonads
Autosomal Recessive:
= Only symptomatic when both alleles at a locus on homologous chromosomes are defective
Must have mutations in both genes both parent‟s carriers
Shows up early (no normal genes)
Eg cystic fibrosis, phenylketonuria
X-linked Recessive:
Only affects males
Impact early (no normal gene)
Females are carriers (random X inactivation should mean that 50% of cells are abnormal. But
they‟re usually in the minority. Still may have some traits)
Genetics and Cancer 465
Eg haemophilia, Duchenne muscular dystrophy (wasting muscle disease – most dystrophies are X
linked)
X-linked Dominant: eg Fragile X
Multifactorial:
Common diseases
Genetic predisposition plus environmental influence
Eg Cleft lip/palate
Others: mitochondrial, tumour predisposition
Non-Mendelian Genetics
Genetic Imprinting
= Differential expression of genetic material depending on whether it has been inherited from male or
female parent
Parent of origin of mutation matters for many genes
Affected genes are usually highly conserved (ie the same genes appear in mice and humans –
conserved through evolution)
Myotonic dystrophy:
Autosomal dominant
Progressive weakness from 3
rd
decade
Unstable triplet repeat on 19 (upper limit of normal is 50 repeats)
Most unstable when its from mum (ie parental imprinting)
As number of repeats increases goes from normal premutation carrier affected
Fragile X Syndrome:
Abnormal if triplet repeat > 200
Only expands when passed from mother to son, not to daughter
Huntington‟s:
Unstable triplet repeat syndrome
If father passes it on then greater risk of number of repeats
See Dementia, page 439
Uniparental Disomy (UPD)
= Presence of a cell line containing 2 chromosomes both inherited from only one parent
Has been demonstrated in cystic fibrosis, haemophilia (ie got both mutated genes from the one parent)
Prader-Willi Syndrome:
Floppy baby, low birth weight, retarded, appetite obesity, short statue
Caused by deletion on father‟s Chr 15, or have both normal Chr 15 from mum (ie no 15 from dad)
Angelman Syndrome caused by maternal deletion of the same chromosome low birth weight,
unusual cry, stiff legged gait, tremour and seizures
Mitochondrial Disorder
Mitochondria:
Generate ATP for energy using the respiratory chain
Contain their own DNA: circular double stranded DNA
All come from mother
Have higher mutation rate
Heteroplasmic: up to 200 mitochondria per cell, up to 20 different DNAs per cell
Usually involves all tissues, very variable expression
Difficult to test for and hard to treat
Genetic Testing
Types of test:
Screening tests: done on normal population to identify those at risk (not diagnostic)
Diagnostic tests to confirm the presence of disease
Guthrie Card – for screening all neonates:
Second test needed in about 1 in 100 babies (usually due to poor sample)
466 4
th
and 5
th
Year Notes
Disease
Treatment
Risk
Biotinidase Deficiency
Take vitamin H (biotin)
1:50,000
Congenital Adrenal Hyperplasia
Steroids
1:20,000
Cystic Fibrosis
1:3,000
Galactosaemia
Diet
1:120,000
Hypothyroidism
Thyroid replacement
1:4,500
Maple Syrup Urine Disease
Diet
1:250,000
Phenylketonuria (PKU)
Diet
1:15,000
Indications for neonatal genetic testing: Physical, growth or developmental disorders:
Still birth
Multiple congenital abnormalities
Small for age
Facial dysmorphia
Significant mental retardation
Post-natal growth retardation
Microcephaly
Other
Agenesis: complete absence of an organ
Aplasia: absence of an organ with the persistence of an undeveloped rudiment
Anencephaly: congenital absence of cranial vault – with cerebral hemispheres completely missing
Genetic Counselling
Aim: provide information for an individual/couple to make informed choices about their reproductive
options, and to assist them in coming to terms with the options they face
Requires:
Diagnostic precision
Estimation of risk: either Mendelian or multifactorial (eg cardiac abnormalities, neural tube
defects, etc)
The likely burden of care for a child with the disorder: variability, life expectancy, quality of life,
treatment
Alternatives: childless life style, adoption, intrauterine diagnosis, donor sperm, donor ova
Cancer
See also Childhood Cancer, page 648
Epidemiology
In NZ:
Over 16,000 new cases diagnosed per annum, 7000 deaths
Commonest cancers (incidence):
Male: prostate, large bowel, lung (incidence ~ mortality)
Females: breast, large bowel, melanoma
Commonest cause of death:
Male: lung, large bowel, prostate
Female: breast, lung, large bowel
Prognosis of cancer is determined by:
Tumour related factors: accurate diagnosis, stage, grade, risk factors (eg biochemical markers),
cytogenetics
Patient related factors: age, sex, co-morbidities
Oncogenesis
Cancer causing agents:
„Natural‟ – eg fungus and plant toxins. Eg aflatoxin from fungus contaminating peanuts in Africa
liver cancer
Man-made: enormous diversity. Mainly the metabolites/intermediates in the body that are
carcinogenic. Very often organ specific. Most precarcinogens detoxified to non-carcinogenic
metabolites.
Genetics and Cancer 467
Cancer = uncontrolled cell proliferation due genetic change
The more uncontrolled the proliferation, the more mutations – in final stages anuploidy, translocations,
etc will be very common
Oncogenes: cells related to normal cell proliferation and differentiation. If one allele is mutated then
uncontrolled proliferation ( autosomal dominant)
Tumour suppressor genes: regulatory genes that inhibit cell proliferation. Need to loose both alleles to
have an effect ( autosomal recessive)
Carcinogenesis:
Multifactorial – needs multiple DNA mutations
P53 Gene:
Regulates cell cycle
Inactivated in over ½ human tumours
Activated by hypoxia, DNA damage, viruses
If there is minor cell damage small amount of P53 arrest cell cycle and repair
If major damage P53 apoptosis
Activated P53 binds to DNA activating other genes
Normal P53 can be inactivated by mutating co-factors
Philadelphia Chromosome:
Arises from balanced translocation t(9, 22)(q34,q11)
Brings C-ABL gene beside BCR gene. C-ABL is an oncogene, and is now regulated by BCR
normal regulation has failed
Causative in CML, also seen in other tumours. See Chronic Granulocytic Leukaemia, page
298
Telomere
Non-coding cap to genome
During replication, an enzyme binds and prevents replication telomere shortens with each
replication
Telomerase can produce telomere – usually only in germ cells. But also active in cancer cells
unlimited potential to divide
Research aim: find drug to inhibit telomerase give cancer cells a limited number of
divisions
Tumour starts with single clone, quickly becomes heterogeneous. Only a few descendants will be
able to metastasise
Growing tumour needs blood supply – secrets angiogenic factors. Research aim: find ways of
inhibiting this process. An advantage would be that this would kill all tumour cells, whereas
chemotherapy is selective, leaving resistant cells to grow
Anatomic Pathology and Neoplasia
Describing a histologic section – always include:
Architecture (eg gland formation, infiltration – eg sheet like, chords)
Cytologic atypia: hyperchromatic, nuclear pleomorphism, mitotically active
Tissue reaction (fibrosis, inflammation, etc)
Macroscopic signs of invasion:
Variegated
Poorly circumscribed, not encapsulated, irregular border
Crab like
Areas of haemorrhage
Microscopic signs of malignancy:
Nuclear pleomorphism
Hyperchromatic nuclei
Invasion
Poorly differentiated (anaplastic)
Mitoses
Tumor prognosis:
Stage (how much infiltration, metastasis)
Grade (what type, how well differentiated)
Resection margin
Brisk inflammatory response is good
468 4
th
and 5
th
Year Notes
Hamartoma = overgrowth of tissue native to that site (NOT clonal proliferation/neoplasm)
Headings for answering pathology exam essay questions:
Incidence
Aetiology
Pathogenesis
Macroscopic description
Microscopic description
Natural History
Outcome
Complications
Special types
Staging of Cancer
= Determining the extent of cancer
Why stage:
Affects prognosis
Affects treatment
Allows comparison of results between centres (eg audit)
Staging Systems:
TNM system:
Nomenclature:
T: Size and invasion eg 1 = small, 4 = large
N: which nodes are involved
M: no metastases or metastases present
Variations applied to many cancers (eg NSC lung cancer, breast, etc)
Guides treatment: eg T1N0M0 ?wide local excision, T3N1M0 may start with chemo/RT
TNMs are grouped to give stage groups ranging from IA to IV
FIGO System: Gynae malignancies, eg cervix:
Stage I: confined to cervix
Stage II: Not involving the pelvic wall or lower 1/3 of vagina
Stage III: extends to pelvic side wall
Treatment:
I & IIa: surgery or radiotherapy
IIb & III: radiotherapy
Ann Arbor classification or lymphoma (see Lymphoma, page 305)
Dukes Classification for bowel cancer, see Prognosis of Colorectal Cancer, page 174
How to stage:
History: symptoms suggestive of local extension or distant metastases
Exam: nodal involvement, metastatic involvement (bone tenderness, hepatomegaly)
Bloods: FBC (blood loss, marrow involvement), LFT, ALP and albumin (liver involvement),
tumour markers
Imaging:
CXR, mammography
CT Scanning – to determine primary disease, nodal involvement
MRI: especially CNS and spinal chord tumours
Nuclear medicine: bone scan
US: good for differentiating cystic from solid, especially in the abdomen
Contract studies (barium swallow, enema): largely surpassed by endoscopy
Special investigations:
Bone marrow: lymphomas, small cell lung
FNA: either US or CT guided
Laproscopy: node sampling
Endoscopy
Surgery: role in staging tumours largely over taken
Tumour markers:
Generally only reliable for monitoring treatment in cancer demonstrated to produce a tumour
marker. Generally poor for screening
Genetics and Cancer 469
HCG: germ cell tumours. Used for diagnosis and monitoring treatment
AFP: produced during liver regeneration: hepatocellular cancer, testicular embryonic cancers, yolk
sac tumours
CEA: produced by epithelial elements (colon, ovary, pancreas). Usually in advanced disease so no
use for screening. Also in gastritis and UC
CA125: ovarian cancer (good response marker). Also in endometriosis, hepatitis
PSA: levels correlate well with disease extent. > 10 80% chance of cancer
Cancer Treatment
Treatment objectives:
Cure
Prolong life expectancy
Relieve symptoms
Treatment modalities:
Chemotherapy
Radiotherapy
Symptomatic/Supportive
For Treatment of:
Colorectal cancer, Treatment of Colorectal Cancer, page 173
Breast cancer, see Treatment of Breast Cancer, page 381
Radiotherapy
Superficial X-ray: for skin cancers
Cobalt: no longer used in the west. Max 1.2 MV
Linear accelerators:
6 MV to 18 MV
Skin sparring
Produces electrons and photons. Biological effect of photons is to create free radicals
Does lots of damage to the cell – but only damage which affects reproductive integrity is DNA
damage
Most DNA damage is repaired within 6 – 8 hours, but if lots of damage then non-repair
More damage is done to cells in G2 (ie in mitosis) as DNA is super coiled
Effective use requires:
Good planning: how to maximise dose to the lesion while minimising dose to unaffected tissue
Immobilising the patient
Use of multiple fractions (ie lots of small doses) spares normal tissue as this has time to repair, but
tumour tissue doesn‟t repair so well
Uses:
Aim is curative in head and neck, skin, cervix
Anal (with chemo), rectal (with surgery)
Adjunct in lung, stomach cancer
Toxicity:
Acute: builds up during treatment and settles within ~ 6 weeks
Affects rapidly dividing cells and secretory function
Skin: erythema, desquamation
Mouth: mucositis and dryness
Gut: diarrhoea, colic, ileus
Bladder: cystitis
Marrow (only if widespread dosing): leukopaenia, thrombocytopenia
Late: Months to years
Due to healing with fibrosis or aging of tissues
Affects slowly or non-dividing cells and causes permanent damage
Skin: Telangiectasis, fibrosis
Mouth: Dryness (parotid function), caries, osteoradionecrosis
Gut: stricture, fistula
Bladder: contracture, haematuria
Nerves: myelitis, necrosis, neuropathy
470 4
th
and 5
th
Year Notes
Chemotherapy
Systemic treatment with single or multiple agents
Damages DNA/RNA protein synthesis cell death/apoptosis. Not tumour specific
Predictable side effect depending on the schedule. Side effect management has improved greatly
Can be oral, sc, im, iv, continuous iv
Adjuvant Treatment = after local therapy has removed cancer but where there is a statistical chance of
relapse (eg due to micro metastases)
Uses:
Can be curative in: lymphoma (esp Hodgkin‟s), leukaemia (including ALL), sarcomas of
childhood, Germ cell tumours (Testicular teratoma, Seminoma), etc
Adjuvant in breast, large bowel and ovarian cancer
Prolongation of life: Ovarian, lung (small cell lung cancer is sensitive to chemotherapy), bowel,
breast
Relief of symptoms: shortness of breath, pain/discomfort, local disease
Not in melanoma, renal cell carcinoma
Side effects:
General:
Feeling terrible till 2 – 3 days later
Nausea: 5HT3 antagonists to help
Lethargy, anorexia
Affect on fast growing tissues:
Mucous membranes: mouth ulcers, diarrhoea
Hair loss: not inevitable (depends on regime) but always temporary
Bone marrow: myelosuppression, anaemia, neutropenia, thrombocytopenia
Irritant effects: haematuria, sore eyes
Neutropenia: typically 1 –3 weeks following. See Fever in a Neutropenic Patient, page 301
Fertility (especially in men) but no risk of future fetal abnormality (unless pregnant at the time).
NOT a reliable contraceptive
Other treatment options
Hormones
Immunotherapy
Symptom Management in Cancer
See also Constipation, page 177
Pain Management in Cancer
See also Pain Management, page 543
Principles of symptom control:
Evaluation: identify each problem/pain and make sure it‟s managed
Explanation
Individualised treatment
Monitoring progress
Attention to detail
Anticipate problems
Common problems:
Physical symptoms: pain, anorexia, nausea, insomnia etc
Compounded by anger, losses, fear, financial insecurity, anxiety, isolation, bewildered by
treatment. Always consider emotional, intellectual and spiritual components
Causes of pain:
Destructive/obstructive effects of the cancer
Debility: pressure sores, constipation
Due to treatment
WHO analgesic ladder:
Step 1: mild pain. Paracetamol, aspirin, NSAIDs
Step 2: moderate pain. Codeine, Tramadol (not subsidised, plus combination drugs:
Paradex (Digesic): dextropropoxyphene plus paracetamol
Panadine: codeine plus paracetamol
Genetics and Cancer 471
Step 3: severe pain:
Morphine:
Actions: analgesia, respiratory depression, drowsiness, vomiting, miosis, convulsions,
euphoria or Dysphoria, smooth muscle stimulation ( GI muscle spasm, bilary and renal
tract spasm)
Rapid acting oral: morphine elixir (10 mg 4 hourly) or Sevredol tablet (10 or 20 mg):
maximum effect after 2 hours
Longer acting: MST (duration 8 – 12 hours) or Kapanol (24 hour slow release)
PR: rapid acting suppositories or MST
Parenterally: IM (onset in 10 – 15 minutes, lasts 4 hours), SC, IV
Bioavailability: half parenteral dose over oral
Anticipate constipation
Signs of morphine overdose: RR < 12, if RR < 8 then Naloxone
Methadone (difficult titrating the dose)
Fentanyl: less constipation than morphine, but not subsidised, transdermal fentanyl patches
lasting 72 hours are well suited to patients with stable pain and low to medium opiod
requirements
Adjuvants at any stage: TCAs, anticonvulsants, steroids, muscle relaxants, antiarrhythmics
Anticipate pain and give regular analgesia, plus PRN medication for acute-on-chronic pain
(„breakthrough‟ pain)
Enhance coping skills:
Listen and acknowledge the symptoms
Explanation, information
Shared decision making
Calm supportive environment
Complementary therapies: relaxation, art therapy, music, OT diversional therapy
Spiritual support, counselling
Treat anxiety, depression
Support the family
Management of Nausea
Identify the right pathway and treat it specifically:
“Drugs of choice”:
H1 antagonist: cyclizine
D2 antagonist: Haloperidol
Prokinetic: Oral domperidone, iv metoclopramide (also has anti-D2 effect)
Chemical cause (stimulation of chemoreceptor trigger zone by uraemia, opioid induced,
hypercalcaemia, toxins): stimulates dopamine receptors. Haloperidol is a dopamine antagonist, as is
chlorpromazine, metoclopramide and cisapride
Mechanical cause (squashed stomach, delayed emptying, regurgitation): Metoclopramide and
domperidone prokinetic action
Emetogenic chemotherapy: stimulates release of serotonin in the gut: 5HT3 antagonists are used
(ondansetron, granisetron, tropisetron)
Vestibular and ICP: use antihistamines eg cyclizine
Non-drug therapy: prophylactic treatment of constipation, keep away from sight or small of food;
small, frequent, attractive meals, relaxation therapy, acupressure
Medullary
Vomiting Centre
Intracranial
pressure
Cortex
Chemo Receptor
Trigger Zone
Vestibular
apparatus
GI Tract
H1
H1
H1 &
Muscarinic
Dopamine
& 5HT3
472 4
th
and 5
th
Year Notes
Management of Breathlessness
Due to effusion, anaemia, mass or irritant effect, anxiety, fatigue. Compounded by fear of fighting to
breath. Can also be PE (but don‟t anticoagulate them – it‟s better to die from a clot than a bleed)
Low dose morphine irritant respiratory reflexes
Anxiolytics for panic (eg lorazepam for intermittent breathlessness, diazepam for chronic)
Steroids for anti-inflammatory effect
Nebulised saline: shift sticky secretions, humidify dry airways
Oxygen if symptomatic hypoxia – but commits the patient to the equipment
Advice from physio, especially re controlling expiration
Fan on face, open window
Management of Cachexia
= Marked weight loss and muscle wasting, especially in advanced GI and lung cancers
Due to metabolic rate and food intake, plus abnormal metabolism and cytokine production
May also see altered taste sensation, loose dentures causing difficulty eating, oedema due to hypo-
albuminaemia, pressure sores over bony prominences, etc
Body changes may generate feelings of fear, isolation or difficulty with relationships
Management:
Dietary supplements and NG feeding are unlikely to achieve anything. Patients should eat and
drink as they wish
Corticosteroids in a reducing protocol may help (as well as reducing tumour oedema)
Relining dentures
General support: education, new clothes, aides to maintain independence
Cancer Emergencies
See also Fever in a Neutropenic Patient, page 301
Spinal Cord Compression:
Irreversible damage occurs quickly. Even if poor prognosis from cancer mobility makes a key
difference to quality of life and to ease of nursing at home, etc
Symptoms: pain (often dermatomal at the level of the lesion), weakness, autonomic dysfunction,
sensory loss
95% is extramedullary compression. Thoracic > lumbosacral > cervical
Primary tumours: lung, breast, prostate, lymphoma (very radiation sensitive), myeloma, kidney
Differential: infective or mechanical
Contraindications to Radiotherapy: previous RT (already irradiated to spinal tolerance), radio-
resistant tumour (eg myeloma), no tissue diagnosis (ie don‟t know what you‟re treating)
Contraindications to surgery: widespread systemic disease, multiple levels, vertebral body
collapse, known radio-sensitive tumour
CXR usually done but MRI is investigation of choice
Cauda Equina syndrome
Superior Vena Cava Syndrome:
Compression causing thoracic and neck vein distension, facial and arm (maybe unilateral) oedema
Causes: CNS symptoms (Headache, visual disturbance, dizziness, blackout, altered conscious
state), venous thrombosis
Usually due to lung cancer, also lymphoma and metastases. Benign causes include goitre, fibrosis,
sarcoidosis, syphilis, etc
Investigations: examination, CXR, CT (rather than MRI), biopsy (maybe US guided)
Treatment:
Anticoagulant + thrombolysis if established clot (eg neck veins not compressible)
Endovascular stent if recurrent
Chemotherapy: small cell lung cancer (80% response), Hodgkin‟s Lymphoma or Non-
Hodgkin‟s lymphoma
Radiotherapy: any other malignant cause (80% response)
Hypercalcaemia: stones, groans and moans, also thirst. Tx: Rehydrate + Bisphosphonates
Pathological fracture: orthopaedic referral to stabilise
Haemorrhage: tumours bleed easily, erosion into an artery
Obstruction:
Trachea stridor. Mainly extrinsic compression. Options: RT, steroids (oedema), tracheostomy
Genetics and Cancer 473
Bronchus: dyspnoea
Oesophagus: Dysphagia. Usually progressive not an emergency. Lodged bolus can present
acutely
Bowel
Ureter
Palliative Care
See also Grief and Bereavement, page 458
Palliative Care: care of patients with active, progressive, far advanced disease and a limited prognosis
and for whom the focus of care is the quality of life
Regards death as a normal process
Integrates physical, emotional, social, cultural and spiritual aspects of care
Offers support to help families and care givers
Provide relief from pain and other distressing symptoms
Neither hastens nor postpones death
474 4
th
and 5
th
Year Notes

Emergency Management 475
Emergency Management
References: A New Zealand Guide to Resuscitation Practice, Wellington School of Medicine, New
Zealand Resuscitation Council.
Resuscitation .................................................. 476
Cardiopulmonary Resuscitation (CPR) .... 476
Cardiac Arrest Rhythms ........................... 479
Drugs in Cardiac Arrest ............................ 480
Care Following Arrest .............................. 480
Secondary survey ...................................... 481
Glasgow Coma Scale (GCS) .................... 481
Diagnosis of Death ................................... 481
Resuscitation Ethics .................................. 481
Shock .............................................................. 482
Clinical Signs ............................................ 482
Septic Shock ............................................. 482
Cardiogenic Shock .................................... 483
Hypovolaemic shock ................................ 483
Severe Anaphylaxis .................................. 483
Special Resuscitation Situations and
Common Emergencies .............................. 485
Airway Obstruction .................................. 485
Alcohol Withdrawal ................................. 485
Asthma ...................................................... 485
Burns ........................................................ 486
Coma ........................................................ 486
Convulsions/Status Epilepticus ................ 487
Diabetic Ketoacidosis ............................... 487
Electrolyte Abnormalities ......................... 487
Electrocution ............................................. 487
Head Injury ............................................... 487
Hypertensive Crisis................................... 487
Near Drowning ......................................... 487
Hypothermia ............................................. 487
Hyperthermia ............................................ 488
Poisoning and Overdose ........................... 488
Pulmonary Oedema .................................. 489
Renal failure ............................................. 490
Spinal Shock ............................................. 490
Trauma to Abdomen ................................. 490
Trauma to Chest........................................ 490

476 4
th
and 5
th
Year Notes
Resuscitation
Objective: keep oxygenated blood flowing to the brain – otherwise cell death in 2 – 4 minutes
Basic life support = no special equipment
Advanced life support = basic support + equipment + drugs
Early defibrillation is vital: increasingly non-doctors are being trained to use it outside hospital setting
Cardiopulmonary Resuscitation (CPR)
Summary
Ensure safety
Check responsiveness
Send for help
Open Airway
Check breathing/circulation: no longer than 20 seconds
Precordial thump (if arrest within last 90 secs)
Go for help
2 Effective Breaths – up to 5 attempts
Chest compression/ventilation: adult 2 breaths per 15 compressions at 100 bpm, neonates 1 breath per 5
compressions 100 bpm
ASAP: attach monitor Defibrillator and assess rhythm
VF or VT or AED „shock advised‟:
Defibrillate: 200, 200, 360J (3 * 360J thereafter)
Adrenaline every 3 minutes
I minute CPR
Not VF or VT or No Shock Advised
Adrenaline
3 minutes CPR
Reassess rhythm or circulation
Adjunct Priorities:
Advanced Adjuncts:
Check:
Consider and Correct:
Defibrillation
Advanced airway/
ventilation adjuncts
Oxygen
IV access
Endotracheal Intubation
Laryngeal Mask airway
Adrenaline: 1mg/3
minutes
VF/VT: Defibrillation,
Lignocaine 1mg/kg after
3 loops
Asystole: atropine 3 mg
Consider: pacemaker,
buffers
Defibrillator/ECG:
source, settings and
electrodes
Endotracheal/IV
placement
Hypoxia (give O2)
Hypovolaemia (give colloids,
saline)
Hyper/hypokalaemia (give Ca/K)
Hyper/hypoglycaemia (give insulin
& K/glucose)
Hyper/hypothermia (cool/warm)
Tension Pneumothorax (chest
drain)
Tamponade (pericardiocentesis)
Toxicity
Thromboembolus
A – Approach, Assess, Airway
Ensure own safety, summon help
Assess for responsiveness (gently shake, shout, be careful of other injuries). An arrest may present as a
short grand mal seizure
Cervical spin injury should be suspected, and assumed in unconscious patient esp. trauma. However,
airway management takes precedence
Urgent airway support may be indicated by: respiratory distress, hypoventilation, absent response to
pain or stimuli, major skull, face or neck trauma, chest injuries, high spinal cord injury
Open airway: CNS depression will diminish muscle tone in upper airway tongue and epiglottis will
obstruct airway further hypoxia (faster in kids due to higher metabolic rate)
Tilt head back, chin lift, jaw thrust
Airway Management Techniques
Oropharyngeal airway insertion:
To maintain airway or prevent biting
Use Geudal airway. Male size 4, female size 3
Emergency Management 477
If they tolerate oropharyngeal airway without gagging or coughing no protective reflexes and
need to be endotracheally intubated as soon as practical to protect from aspiration
Laryngeal mask insertion:
For failed endotracheal intubation where Positive Pressure Ventilation indicated
Doesn‟t protect from aspiration
Male size 4, female size 3
Endotracheal intubation:
For control of airway, ventilation, protection from aspiration and prevention of gastric distension
(e.g. in bag mask ventilation)
Sizes: Adult male size 9, female size 8, child (age in years)/4 + 4
If conscious and struggling may require sedative (e.g. thiopentone) and relaxant (suxamethonium)
Always check chest movements and CO2 return to check you haven‟t got it in the oesophagus
Watch for pressure necrosis of tracheal mucosa from too large a tube or inflation
Never attach O2 directly to tube ( over inflation) – always via a ventilation/bag mask system
Bag mask ventilation (AMBU Bag)
Always check chest rising: watch for leaks around mask, check patent airway
Too much pressure gastric distension and aspiration into unprotected trachea
Cricothyrotomy:
Use to gain access to airway where other methods have failed
Clean skin with antiseptic solution
Find cricothyroid membrane, between thyroid cartilage and cricoid ring immediately below it
Make horizontal incision through membrane. Insert handle of scalpel into incision and rotate 90
degrees
Insert largest possible endotracheal tube and attach to ambu bag. Ventilate with O2
Alternatively, use size 14 cannula, at angle of 45 degrees pointing down towards lungs. Attach
cannula to syringe and syringe to ambu-bag
B – Breathing
Ear over mouth and nose and look for chest to rise and fall. Slow gasping respirations may persist after
arrest but these are ineffectual
Assess whether trachea central, breath sounds bilateral, and check for crepitus ( ?pneumothorax)
Exclude life threatening chest injuries: tension or open pneumothorax, flail segment
C – Circulation
Check carotid pulse.
Look for signs of circulation: movement, colour, etc
Action Plan
If breathing and circulation but unconscious recovery position, and maintain airway
If not breathing but there is circulation ventilate with 10 expired air ventilations over a minute and
reassess
If chest moving but there is no flow of air then obstruction head tilt, chin lift, jaw thrust forward
If breathing absent or deteriorating and no or unsure of circulation then presume arrest
Commence CPR/defibrillation, but consider (if you can):
Use O2 if at all possible – they will be hypoxic. Cylinders are black with white shoulder. Connect
to ventilation bag at 4 atm. or to mask if breathing spontaneously (minimum 4 – 5 L per minute).
NEVER connect directly to endotracheal tube (would barotrauma)
Gaining iv access e.g. antecubital vein. Give saline flush after each access and hold limb up
(circulation will be sluggish). Nothing more distal on arm, and don‟t use femoral (unless needed
for fluid replacement in trauma). If can‟t get access, use carotid (subclavian interferes with CPR),
or down endotracheal tube (2 to 2.5 times iv dose) with 10 ml saline
Adult CPR
If defibrillator available, consider immediate use
If no defibrillator and arrest has occurred within 90 – 120 seconds then single precordial thump – may
convert ventricular arrhythmias in small number of cases, should never break bones, never in presence
of palpable pulse (as may cause VF if delivered on T wave – commotio cordis)
Get help: it is most likely a VF (and other things have a poor prognosis) and you need to defibrillate
Continue with cycles of:
478 4
th
and 5
th
Year Notes
2 expired air ventilations (mouth to mouth or nose, normal not big breath otherwise inflate stomach
gastric reflux, allow time for expiration). Theoretical risk of infection take precautions
15 chest compressions:
Raise legs venous return
Press over junction of middle and lower thirds of sternum
Use only heel of hand with thumb side lower
Lock elbows, push straight down, move from hips not shoulders. Get on bed if you‟re too low
Consider putting board under patient or place on floor – soft mattress will impair compression
Depress 4-5cm or one third of chest thickness: it is depth not force that is important, equal
compression and relaxation times, not too jerky. Start gentle to determine correct pressure.
Rib fractures impede filling, cause pneumothorax, lacerations of liver and spleen, and fat
emboli
Rate of 100 per minute for adults and children.
Can achieve systolic pressure of 60 – 80 mmHg, but low diastolic pressure so brain perfusion
maintained but heart perfusion poor. Adrenaline improves diastolic pressure
If two operator, still use 2:15 breaths per compressions. If patient not intubated pause 1 sec for
ventilation. No pause necessary if intubated
After 3 minutes, stop for 10 secs to assess circulation. Continue with assessments every 3 minutes
until defibrillator arrives
Administer adrenaline 1 mg iv with every 3 minute loop
Paediatric CPR
Respiratory distress/failure much more common cause of cardiac arrest than cardiac problems.
Hypoxia and global ischaemia therefore often precede arrest (in adults it follows arrest), which results
in asystole – not VF. Also caused by hypovolaemia, poisoning, drowning, etc
Ventilation therefore more important than defibrillation. Kids have a higher metabolic rate and O2
reserves consumed quicker
Survival associated with duration of arrest (after 5 minutes it plummets), not more than one dose of
adrenaline, and presence of VF
Procedure:
Ensure your and patient‟s safety
Assess responsiveness. Don‟t shake a baby. If unresponsive, shout for help
Open airway: head tilt (not too much extension) and chin lift. Jaw thrust instead if cervical trauma.
Check for obstruction
Assess breathing. If chest moves but no breath, recheck airway
Ventilate: 5 attempted breaths 1 – 1.5 seconds. In babies and infants, give through nose or nose
and mouth. Slow breaths at low pressure better than fast/high pressure (gastric distension).
Ventilate just sufficiently to make chest rise and fall
For no more than 10 secs, check circulation. Infants: brachial, femoral, axillary arteries or apex
beat. If over 8, carotid best
If no circulation or less than 60 bpm, external chest compression. Over junction of middle and
lower 3
rd
of sternum.
In neonates, use two fingers to depth of 1 – 1.5 cm. Rate of 100 bpm, ratio of compressions to
ventilations is 5:1
Kids over 5, heel of one hand, depth approx. 2 – 3 cm
Larger kids, two handed compression, depth of 3 – 4 cm, rate of 80 – 100 bpm, and ratio of
15: 2
After one minute alert emergency services
Resume CPR: reassess circulation after 3 minutes. Give adrenaline. If iv access time consuming,
then 18 gauge perpendicular into anterior surface of tibia, 1 – 3 cm below tibial tuberosity. Failing
this, give 10 times iv dose down endotracheal tube. Repeat cycle and adrenaline
When defibrillator arrives, assess rhythm. Use paediatric paddles if < 10 kg. ONLY if rhythm is
VF or VT deliver 3 shocks at 2, 2, then 4 joules per Kg. Perform CPR for one minute, reassess
rhythm. Every 2
nd
loop give adrenaline
Ventilation: Harder in kids – use two people to do bag-mask. Beware of barotrauma
If hypovolaemia 20 ml/kg saline or Ringers
Defibrillation
Produces a simultaneous depolarisation of myocardial fibres allows coherent rhythm
Emergency Management 479
Ideally within 90 seconds, preferably within 8 minutes. DON‟T delay defibrillation to allow period of
CPR
Apply ECG monitor
Switch on defibrillator (do this in transit)
Check its NOT in synchronised (cardioversion) mode
One paddle (doesn‟t matter which) to right of upper sternum below the clavicle
Other paddle just to the left of the normal apex beat
Use a conducting aid (either electrode gel or pads), wipe up any gel that may short circuit between the
pads
First, use paddles to assess rhythm (check settings on defibrillator). Classify as:
Ventricular fibrillation or ventricular tachycardia (wide QRS complex):
Charge defibrillator to 200J (for kids 2J/kg). This is low, but will charge quicker and do less
damage to myocardium
„Stand clear‟: make sure you‟re not touching patient or bed
Recharge defibrillator
Observe ECG
If VT or VF persists, deliver a second 200J shock, then 360J
If VT/VF persists, 1 minute of CPR (attach ECG leads during this, insert artificial airway, iv access
etc)
Repeat sequence, but with 360, 360, 360 then 1 minute CPR
Adrenaline, 1 mg, with every 2
nd
loop (i.e. every 3 minutes)
If following a shock an organised rhythm appears which could be associated with cardiac output,
check circulation. If absent then 3 minutes of CPR
If following a shock, the rhythm changes from VF/VT to asystole, perform 1 minute CPR and
assess with NO adrenaline. „Stunned myocardium‟ may take 20 – 30 secs to start again
Another rhythm. If asystole or electromechanical dissociation (if normal complex) then continue CPR
in 3 minute loops, 1mg adrenaline per loop. Prognosis poor but consider:
If asystole, is there an electrical fault, low gain on ECG. If in doubt deliver 3 defibrillating shocks
If asystole with P waves (ventricular standstill) consider emergency transcutaneous electrical
pacing
Atropine, 3 mg iv, provides complete vagal blockade, as profound bradycardia may result from
intense vagal over activity
Treatment of precipitating condition
Cardioversion
Is timed via ECG to occur on the R wave – must avoid the T wave (otherwise can VF)
Is used for:
Ventricular tachycardia where pulse is present,
Supraventricular dysrhythmias (SVT, atrial fibrillation, atrial flutter)
Won‟t fire unless it can detect the QRS. So if trying to defibrillate and it‟s not working – check
defibrillator is not set to cardioversion
Cardiac Arrest Rhythms
See also Arrhythmias, page 40
Due either to:
Disordered electrical activity (arrhythmia) such as following an MI, or
Impaired mechanical performance: Pulseless Electrical Activity (PEA) or Electro-Mechanical
Dissociation (EMD) – primary (damaged myocardium, e.g. ischaemia) or secondary (e.g.
hypovolaemia, pneumothorax, anaphylaxis afterload, pulmonary embolus). EMD has worst
prognosis. ECG may be normal but patient is still arresting
Ventricular Fibrillation (VF)
Most non-traumatic arrests are ventricular fibrillation. Only effective treatment is defibrillation
No organised depolarisation doesn‟t contract as a unit. But still contracting still using O2
Coarse VF: irregular, large amplitude ECG waves onset recent. Responds well to defibrillation (if
given within 5 – 8 minutes). CPR not sufficient to maintain the coronary artery perfusion necessary to
offset O2 consumption rapid ischaemia. Precordial thump MAY revert VF
Fine VF: progressively lower amplitude VF until indistinguishable from asystole. 5-10% decrease in
likelihood of successful defibrillation per minute
480 4
th
and 5
th
Year Notes
Treatment:
Defibrillation
CPR and adrenaline help maintain diastolic BP and thus cardiac perfusion
If failing, consider sodium bicarbonate and lignocaine (antiarrhythmic)
Discontinue after 30 minutes
Ventricular Tachycardia
Fast (100 – 220/minute) and wide QRS complexes (> 0.12 sec)
Causes: ischaemia, K or Mg disturbances, PE, etc
Can be confused with supraventricular tachycardia with bundle branch block
Dangerous precursor of VF
Treatment:
If stable (i.e. still sufficient cardiac output pulse):
Oxygen
Lignocaine (1 mg/kg) stat plus 0.5 mg/kg every 8 minutes up to 3 mg/kg
If this fails then cardioversion
If little cardiac output/no pulse: same as for VF
If pulse but unstable:
Sedation
Cardioversion: starting at 50J, then 100 then 200 then 300. If recognisable regular rhythm
then synchronised
If recurrent, give lignocaine, then procainamide 20 mg/min up to 1000 mg then bretyllium 5 –
10 mg/kg and magnesium
Torsade de Pointes
ECG like VT – but QRS amplitude changes due to rotating electrical axis
May be self-limiting for periods of 5 – 10 secs
May be due to anti-arrhythmics prolonging the QT interval (if so, stop them)
Treat by correcting electrolyte abnormalities and by increasing basic heart rate (i.e. over-pacing)
Magnesium sulphate 1-2gms given over 1 – 2 minutes may reverse drug induced torsade
Defibrillate for sustained episodes or use over-drive pacing
Asystole
Complete absence of ventricular electrical activity
Usually end result of major disturbance/myocardial damage
Usually a wandering straight line (if completely flat check ECG)
Invariably fatal after 15 minutes
Atropine + CPR may bring back rhythm
Drugs in Cardiac Arrest
No drug has been shown to consistently improve patient survival after cardiac arrest. CPR,
defibrillation and airway control are therefore most important
Adrenaline: peripheral vasoconstriction raises afterload, aids cardiac perfusion in diastole during CPR.
Short duration of action give 1 mg every 3 minutes. For kids, 10 g/kg, subsequent doses 100
g/kg. Effect wears off as local mediator dilator effects predominate in distal arteries
Sodium bicarbonate: but major acidosis is usually respiratory, in which case bicarbonate CO2 so
will make this worse. Consider after prolonged hypoxia. Also in severe ketoacidosis. Don‟t give via
endotracheal tube
Lignocaine, 1 mg/kg: for ventricular ectopy and stable ventricular tachycardia. No clear evidence of
value in VF. Shock energy required for successful defibrillation. Makes VF less likely – but harder
to get out of
Calcium: if massive blood transfusion will be calcium depleted
Care Following Arrest
Transfer to ICU or CCU
May need short period of elective ventilation
Monitor cardiac rhythms, urine output, cerebral oedema, acid-base balance
Prognosis of neurological function often clear from 24 hours after arrest
Emergency Management 481
Secondary survey
Check BP, respiratory rate, temperature
Check for palpable pulse, capillary return to compressed fingernail bed, and neck veins
Work systematically from head, to chest, abdomen, pelvis.
Check limbs and vertebrae for fractures
External haemorrhage: pressure bandages, splints for fractures, if Military Anti-Shock Trousers
(MAST) used for pelvic/femoral fracture, should only be very temporary and let down slowly (to avoid
hypotension)
Non-obvious injuries to exclude (as they may be life threatening): aortic dissection, pulmonary
contusion, spinal injury, penetrating wounds (esp to back), and intra-abdominal bleeding (e.g. if
persisting shock)
Complications can occur insidiously: hypothermia, acidosis, sepsis, coagulopathies, shock
Need 2 iv access sites with 14 gauge: arms, femoral, jugular, saphenous, subclavian vein, or cutdown to
medial basilic or long saphenous vein (1 cm anterior to medial melleolus). Intraosseous in infants
Fluid replacement: warmed crystalloid (watch for cerebral oedema) or colloid, blood where indicated.
Monitor pulse, BP, skin colour, capillary refill and urine output
Check for neurological disability
Very common, esp in road trauma
Check: Alert, responding to vocal stimuli, pain, or unresponsive
Moving limbs doesn‟t exclude spinal injury
Check pupils
Glasgow Coma Scale (GCS)
Eye opening: E4 spontaneous, E3 to speech, E2 to pain, E1 nil
Verbal response: V5 orientated, V4 confused conversation, V3 inappropriate words, V2
incomprehensible sounds, V1 nil
Best motor response: Obeys M6, localises M5, Withdraws M4, Abnormal flexion M3, Extension M2,
M1 Nil
8 or less = severe head injury
There is also a trauma score, includes GCS, respiratory rate, respiratory expansion, systolic BP and
capillary refill
Diagnosis of Death
Must be made by a doctor
Must have all of: no respiration, no BP, no HR, no pupillary reflex, no response to pain
Resuscitation Ethics
CPR Efficacy
Wide variation in outcome depending on clinical circumstances. Discharge rate is 15%. Biased by
large number of „futile‟ resuscitations.
Outcome
Comment
Elective cardiac surgery
100%
Heart deliberately stopped
Out of hospital arrest, immediate CPR,
ambulance < 2 min
80%
Early defibrillation key predictor of
survival. Survival by 10% per minute.
Arrest under anaesthesia
20%
Would already have had severe
physiological assault prior to arrest
Out of hospital arrest, no CPR, ambulance
> 6 min
< 6%
Malignancy, severe chronic disease,
chronic renal failure, pneumonia, trauma
< 5%
Poor outcomes (e.g. brain damage, organ failure) are inversely correlated with chances of survival.
Age per se is not an independent predictor of survival after CPR – but is correlated with illness
CPR and Consent
Family members are not able to give consent (either for treatment or withdrawal treatment) under
common law in NZ, although H&DC Code has provision for taking into account “the views of other
suitable persons who are interested in the welfare of the consumer…”
482 4
th
and 5
th
Year Notes
Doctor must make a „substituted professional judgement‟: immediate decision on available information
(usually not much) of what is in the patient‟s best interests
Ethically wrong to undertake resuscitation in patients in whom it is possible to predict a very low rate
of intact survival
Futile treatment diverts resources from other people. It is the principle of justice not the principle of
autonomy that creates a right to treatment
Doctor‟s should not make decisions based on their assessment of the patient‟s quality of life. Only the
patient can make this assessment. However, this information is not usually available in acute setting.
Revise further resuscitation/treatment decisions when this becomes available (i.e. the decision to
resuscitate or not is not static)
There is no ethical difference (may be other differences) between withholding and withdrawing
treatment. Can revise decision to resuscitate as the probability of poor outcome grows or other
information (e.g. patient‟s wishes) comes to light
DNR Orders
= Do not resuscitate, DNAR = Do not attempt resuscitation
Reasons for DNR orders:
Refusal by a competent and informed patient
Poor quality of life after CPR (patient‟s, not doctor‟s view)
Futility: a clinical decision – so should the patient be involved or not?
DNR orders should be discussed where:
Requested by a competent patient
Considered on grounds of poor quality of life
Circumstances where it is not necessary to discuss DNR orders:
Patient is incompetent
Competent patient but grounds of quantitative futility
Where discussion of CPR would be detrimental to patient‟s well being
Where patient indicates they do not wish to discuss CPR
Role of family/friends: get their input, but doctor makes the decision regarding CPR unless the patient
has a welfare guardian or has an advance directive
Other points:
A DNR doesn‟t mean other treatment is withdrawn
DNRs must be clearly documented in notes, including discussion of decision making process
DNRs should be reviewed regularly and may be withdrawn if warranted by change in clinical
circumstances
Shock
Clinical Signs
CNS: agitation, anxiety, confusion, changed consciousness, convulsions, focal signs, pupillary
dilatation
Respiratory - RR, respiration effort, cyanosis, SOB, cough
CVS - HR, BP, pulse pressure, capillary return, pallor, sweaty, cool extremities, arrhythmias.
Systolic BP < 90 and HR > 100. Treatment should aim to keep BP above 80 mm Hg
Renal - urine output (< 30 ml/hour or < 0.5 ml/kg/hr)
Cutaneous: flush, angioedema (selling of face/mouth)
GI: abdominal cramps, diarrhoea, vomiting, urinary/faecal incontinence
See Adult Respiratory Distress Syndrome (ARDS), page 83
Septic Shock
Systemic Inflammatory Response Syndrome (SIRS) is the presence of 2 or more of:
Temp >= 38 C or < 35
HR + 90 bpm
RR >= 20/min or PaCO2 <= 32 mmHg
WBC > 12,000 cells/ml
Septic shock evolves from SIRS when BP <= 90 mmHg despite adequate fluid but need e.g. an
inotrope to raise BP
Hyperdynamic circulation: may present early on with warm peripheries because of mediator-induced
vasodilation – confusing as they‟re not cold and clammy
Emergency Management 483
Infection: 70% due to G –ive: endotoxin release inflammatory mediators SIRS changed
haemodynamics
Management:
O2 + ventilation
Circulatory support
Nutrition
Treat infection
Mortality = 30 – 40 %
Cardiogenic Shock
Causes
MI or ischaemia: need to lose 40 – 50% of functional ventricular mass
Trauma
Cardiomyopathy/myocarditis
Dysrhythmia
Valvular/septal defects
Post cardiac surgery: stunned myocardium
Drugs
Contractile mass CO shut down hypoxia, LVEDP pulmonary oedema (more acute
than heart failure)
Management
Maximising coronary perfusion: afterload, maintain CO (inotropes), vessel patency (drugs,
stents, etc), intra-aortic balloon pump
Treat other factors: dysrhythmias, hypertension
Support organ failure
Hypovolaemic shock
Causes:
Blood loss (usually trauma)
GI (vomiting, diarrhoea)
Renal (diuretics)
Surface (burns)
Maldistribution (e.g. sepsis, anaphylaxis)
Estimated losses from fractures:
Femur: 1000 – 1500 mls
Pelvis: 1500 – 2500 mls (usually venous)
Tibia and fibula: 750 – 1200 mls
Humerus: 500 – 750 mls
Also chest, abdomen, retroperitoneum, scalp
Management: ABC, O2, iv fluids, minimise losses
Initial bolus for paediatric shock is 20 ml/kg
Severe Anaphylaxis
= Severe allergic reaction
See also Allergy and Hypersensitivity Disorders, page 309
Problems:
Acute CV collapse: hypotension, myocardial ischaemia, arrhythmias
Lower airway: Bronchospasm respiratory difficulty. Respiratory problems account for 70% of
fatalities. Asthmatics at higher risk.
Upper airway: Laryngeal oedema (ie angioedema)
Also skin problems (urticaria, erythema, itch), nausea, vomiting, diarrhoea, anxiety, etc
Pathogenesis:
Type 1 allergic reactions mediated by IgE antibodies
Previously sensitised IgE antibodies against allergen mast cell activation massive
mediator release (histamine, leukotrienes, prostaglandins, kinins)
Histamine leads to:
Smooth muscle contraction bronchospasm
Vasodilation & permeability (can loose 1½ L of blood volume straight away)
484 4
th
and 5
th
Year Notes
HR and arrhythmias
Noradrenaline
Itch & oedema
Anaphylactoid reaction: activation of mast cells and release of mediators without IgE involvement.
Only relevant to investigating cause – not to treatment
Examples of allergens:
Drugs: 50% of fatalities. Includes penicillin, muscle relaxants (can be sensitised by exposure to
similar drugs), aspirin, contrast media, blood products, streptokinase, preservatives (e.g. in
adrenaline)
Foods: 25% of fatalities. Peanuts, milk, eggs, fish
Insect bites: 25% of fatalities
Also latex, semen, blood products, physical stimuli (eg exercise, cold, heat)
Presentation
Anaesthetics: If IV – then as fast as 1 minute, but normally 5 – 10 minutes. Food up to 30 minutes
1 in 2,500 surgical patients in Wellington. Death rate 4 – 6 %
Treatment
Stop administration of antigen. Call 777
Adrenaline:
If no current venous access then 0.5 ml 1:1000 IM. 0.01 mg/kg for kids
If venous access: 0.3 – 0.5 mls iv of 1:1,000 slowly, repeat until BP > 100. Start low (eg 10 g)
and titrate up
Can be nebulised for laryngeal oedema
If on TCAs then sensitivity to adrenaline
agonist vasoconstriction – but not too much otherwise cardiac vasoconstriction
agonist bronchodilator
Force of heart contraction
Mediator release
T½ is short: common error is to give too little too infrequently
Also:
Metaraminol ( agonist) to stop arrhythmias
?Steroids: prevent late symptoms
Promethazine 25 mg slow iv or im (H1 antagonist) + H2 antagonist (e.g. ranitidine), or
Antihistamines: Phenergan 25 mg iv slowly for itch
If bronchospasm alone:
Salbutamol: 5 – 20 g/min
Hydrocortisone 200 mg iv
Aminophylline 5 mg/kg over 30 minutes
Elevate legs venous return
O2 10 l/min by mask: intubate if necessary
Wide bore cannula 1 – 2 l iv colloid rapidly
If anaesthetic reaction, always investigate so next anaesthetic is safe. Should have skin tests, etc.
Cross reactivity between muscle relaxants is not uncommon
Differential Diagnosis
Measure serum tryptase (longer T½ than histamine) to confirm anaphylaxis
Anaesthetic overdose: Tryptase raised in anaphylaxis, normal in overdose
Respiratory: Pulmonary oedema/embolism, asthma, foreign body
Heart: Pericardial tamponade, MI, arrhythmia, vasovagal faint
Venous air embolism
Septic shock
Pneumothorax
Transfusion reaction
Hypoglycaemia, CVA, epilepsy
Prevention
Avoid treatment with -blockers – makes treatment of anaphylaxis difficult
Carry and use adrenaline (eg Epi-pen)
Emergency Management 485
Medic alert bracelet
Call an ambulance, don‟t „wait and see‟
Special Resuscitation Situations and Common Emergencies
Airway Obstruction
Always consider in rapid cessation of breathing and unconsciousness. Also consider fainting, stroke,
MI, epilepsy and drug overdose
In adults especially related to meat, dentures and alcohol. Will grip throat not chest
Adult obstruction
Partial obstruction distressed and coughing. If conscious and adequate air encourage coughing
and spitting – nothing else
Ask if they are choking: if can‟t talk, breath or cough then:
Remove obvious obstruction from mouth (only if unconscious – may bite). Grasp tongue and
mandible between thumb and fingers and lift up. Hook with other hand
Back slapping: lean well forward onto one hand, 5 sharp slaps between shoulder blades with heel
of other hand. If lying down, roll face down onto your thigh
Abdominal thrusts (Heimlich manoeuvre): fists over midline above naval, always below xiphoid
process and ribs. Upwards thrust. May vomit. If on ground, lie on back and sit astride their thighs.
If pregnant or obese, use chest thrusts
If obstruction is not relieved: check mouth, 5 back slaps, 5 abdominal thrusts, repeat
Paediatric Obstruction
Suspect in any airway distress with coughing, gagging, or stridor with rapid onset. May also be caused
by infections (e.g. croup or epiglottitis). If infective cause then medical emergency
Only intervene if child‟s attempts to clear the obstruction are clearly ineffective and there is inadequate
respiration
For infants (<1 year) and children, 5 back blows with the child‟s head below the level of the chest if
possible
Then 5 chest thrusts to sternum in supine position: sharp, vigorous and rate of 20 bpm
Check mouth: grasp tongue and jaw and lift. Don‟t put finger into mouth unless foreign body is clearly
visible
Reassess airway. If not breathing, attempt to ventilate
Repeat back slaps, chest thrusts, attempted ventilation. In children, alternate abdominal and chest
thrusts
Alcohol Withdrawal
See Alcohol Withdrawal, page 452
Asthma
Arrest due to: bronchospasm ( asphyxia), tension pneumothorax (often bilateral), agonists
arrhythmias
Arrest Prevention:
Maximal O2
Nebulised salbutamol (beware overdose tachycardia and VF/VT) or iv 5 g/min up to 20 g if
necessary
IV hydrocortisone
Adrenaline
IV sodium bicarbonate (acidosis prevents action of sympathonimetics)
Intubation and IPPV: sedate with ketamine or benzodiazepines, paralyse with suxamethonium
During arrest:
Consider assisted exhalation (bilateral manual squeeze over lower chest at end of inspiration)
Plus normal routine
See also Asthma, page 77
486 4
th
and 5
th
Year Notes
Burns
Caused by: thermal, electricity, chemical, mechanical, radiation
History:
Timing – start fluid maintenance calculations from time of injury not time of presentation
Circumstances – eg any risk of inhalational injury
Tetanus immunisation
Classification:
Assessing depth:
1
st
degree burns: Erythema (like bad sunburn)
2
nd
degree: Blistering
3
rd
degree: skin goes like leather
Now classified as:
Partial thickness burns (either 1
st
or 2
nd
degree): superficial heal in 2 – 3 weeks, deep need
grafting
Full thickness burn
Body area covered: Rule of nines to estimate surface area burnt: head 9%, arms 9% each, thorax
18%, abdomen 18%, legs 18% each
Admit if:
Major burn (>15% of adult, > 10% of child)
Special areas (hands, face, over joints, etc)
Circumferential – Require escharotomy to release pressure
Other medical conditions, etc
Respiratory complications:
Upper airway burns: watch for oedema and obstruction. Prophylactic intubation if severe
Lower respiratory tract burns: Suspect if closed space fire, smoke inhalation or upper RT burns.
Treatment: humidified O2, PEEP, pulmonary toilet and physiotherapy. Avoid steroids
Inhalational injury a big killer – eg chemicals from burning materials ARDS 24 hours later
Watch for:
Hypovolaemia. See Replacement fluids, page 550 for fluid resuscitation
Good nutrition critical: calorie and protein requirements. Use NG tube
For minor burns:
Analgesia
Wash gently
Dress with paraffin gauze and padding
Tetanus jab
Review in 3 – 4 days
Coma
Immediate actions:
Establish unresponsiveness
Act as though cervical spine injury
Check ABC
If arrested CPR
Consider ventilation/intubation
100% O2
IV access. Take blood for glucose, U&E, drug levels
Access depth of coma: GCS
Expose and examine patient
Look for localising neurological signs, intracranial pressure
Bladder catheterisation
Further diagnostic options:
Chest, skull and cervical spin X ray
CT scan
Gastric lavage after protection of airway by intubation
Consider:
Drugs/toxic (See also Poisoning and Overdose, page 488):
Alcohol: thiamine 100 mg iv
Opiod overdose: naloxone 0.4 mg iv
Emergency Management 487
Benzodiazepine overdose: flumazenil
Also CO, fumes, antidepressants
Metabolic: renal failure, endocrine (eg hypoglycaemia – Dextrose 25g iv), renal/hepatic
encephalopathy, porphyria
Miscellaneous: hypoxia, post epileptic fit
Extracranial: hypoxia (due to arrest, asphyxia), hypo/hyperthermia, electrocution
Convulsions/Status Epilepticus
See Status Epilepticus, page 135
Diabetic Ketoacidosis
See Management of Diabetic Ketoacidosis or Hyperglycaemia, page 96
Electrolyte Abnormalities
See Electrolytes, page 107. Includes Hyperkalaemia and Hypokalaemia
Electrocution
Depending on shock, reasonable chance of survival from arrest
Ensure your safety, start ventilation and compression ASAP
Watch for airway if face, mouth or neck burns swelling
Rapid iv fluids if hypovolaemic shock or tissue destruction
Head Injury
See Head Trauma, page 129
Hypertensive Crisis
Signs: headache, vomiting, visual changes, convulsion, coma, angina, pulmonary oedema, CVA,
eclampsia
Treatment: sublingual captopril. Labetalol, etc
Caution: vasodilators may increase ICP. May need iv fluids with vasodilators. Don‟t lower blood
pressure too low too fast – cerebral autoregulation may be been reset to a higher blood pressure
Near Drowning
Effective immediate resuscitation critical. Use standard CPR procedure
Remove foreign bodies from airways, don‟t attempt to drain fluid
Suspect spinal injury if diving or in surf
Early tracheal intubation may be indicated. 100% O2
Recovery may occur even after long immersion times, especially in cold water
In hospital, cerebral oedema may require hyperventilation and diuretics
Remember, alcohol or epilepsy may be involved
Avoid steroids, consider antibiotics
Hypothermia
Signs: hypotension, bradycardia, J wave on ECG, SV arrhythmias, VF at 28 C, metabolic acidosis, loss
of consciousness at 28 – 30 C, shivering replaced by rigidity at 33 C, pupils dilated
Lengthens tolerance of arrest: don‟t discontinue till they‟ve been warmed
Arrest prevention:
Prevent further heat loss
Transport avoiding rough movement, which can precipitate VF
If core temperature < 34 C, can rewarm with oesophageal rewarming tubes, peritoneal lavage
(warmed saline or gas). Warm trunk not peripheries. Reduce movement (risk of VF). Rewarm
slowly – 0.5 degrees/hour (unless fit and sudden hypothermia)
During arrest:
Take 30 – 45 secs to confirm cessation of ventilation and pulselessness
Don‟t assume death until resuscitation has failed in an adequately rewarmed patient
If < 30 C give maximum of 3 shocks until core temperature increases
Reduced responsiveness to defibrillation and drugs. Impaired drug metabolism watch for
toxicity
Monitor fluids during rewarming
488 4
th
and 5
th
Year Notes
Hyperthermia
Heat Exhaustion: hypovolaemic shock due to fluid loss through sweating. Cool, restore volume,
position supine with legs raised
Heat stroke: failure of heat regulation through failure to sweat. Hot, flushed and dry. If temperature >
40 degrees neurological disturbances. Rapid cooling, cool iv fluids
Reduces tolerance time for arrest
Cooling can be external or internal
Watch electrolytes and fluid replacement following arrest
Watch for tendency to cerebral oedema and multi-organ failure
Poisoning and Overdose
Cause of significant proportion of arrests in 18 – 35 year olds
Duration of arrest and dose of toxin determinants of survival
Do general management
Manifestations of poisoning:
Exaggerated therapeutic response (eg sedation with BZD)
Pharmacological effects (eg respiratory depression, convulsions)
Accidental: children, single poison
Intentional: adult, often multiple, taken in conjunction with alcohol
Management:
History:
Find out the drug if you can (has someone brought in the packet?): but only a few will change
management (paracetamol, salicylates, lithium, paraquat, quinine, phenobarbitone, iron salts)
Very unreliable – especially the number of tablets taken
Supportive treatment:
A,B,C: Respiratory depression is the most common cause of death.
Maintain airway, check blood gases. Check for hypotension (raise legs except in heart
failure, volume expanders). Monitor electrolytes
Maintain safety: close supervision, no access to drugs on ward, etc
Intensive support treatment: IV fluids, ?NG tube, maintain vital functions, nursing care (eg
suction, pressure sores, limb movement thrombosis)
Treat complications: hypothermia, hyperthermia (salicylates and stimulants – sponge down, use
fan), seizures (iv diazepam), arrhythmias (leave bradycardia, tachycardia – correct acidosis, try
amiodarone), hypoglycaemia (salicylates, oral hypoglycaemics)
Plus treatment specific to poison
Mental health assessment
Investigations:
Blood levels: sometimes useful (eg Li, aspirin, theophylline, carbamazepine). Waste of time for
TCAs
Urine Screen: Rarely changes management, no quantitative information, really only for criminal
cases (eg after MVA)
Corrosives:
Never induce vomiting
Drink copious fluids
Soak eyes, skin, mucous membranes
Petroleum: beware of inhalation, cup of milk
Eliminating poisons. If sure it‟s not petroleum products, caustics, corrosives or acids, then options may
include:
Activated charcoal
Better than emesis
Charcoal powder, mixed with H2O: needs to be within 60 minutes. Give SINGLE 50 g dose in
an adult (1 g/kg)
Reduces GI absorption of paracetamol, aspirin, phenytoin, digoxin, TCAs, theophylline,
carbamazepine.
Don‟t use for volatile hydrocarbons or corrosives or an unprotected airway
Good for unionised drugs. Does not bind with acids, alkalis, alcohols, lithium.
Generally safe but constipation, aspiration may be problems (protect airway)
Emergency Management 489
Multiple doses only for drugs undergoing enterohepatic circulation or diffusing into the gut
drugs with a small Vd, low clearance, low protein binding and long T½. Eg Theophylline,
carbamazepine, quinine, phenobarbitone. NOT Paracetamol.
PH adjusted diuresis:
Alkaline diuresis: aspirin, phenobarbitone
Acid diuresis: amphetamine, methadone. Doubtful use and dangerous
Dialysis: Haemodialysis. Only useful if low Vd, small molecule and low protein binding (eg
lithium, theophylline, salicylates, alcohol and barbiturates)
Whole bowel irrigation: „Go Lightly‟ – Xray prep
Questionable effectiveness:
Emesis: Not effective? Ipecac – never if airway reflexes not intact. Causes emesis in 90%
within 15 – 30 minutes
Gastric lavage: large bore catheter through mouth. 1ml/kg of body temperature water,
recover, repeat. Little evidence of benefit and risk of aspiration. Contraindicated if acid,
alkali, or petroleum
Common poisons
Paracetamol
Walk in, conscious
RUQ pain
Conjugation pathway easily saturated. Of the remainder, 15% is metabolised to a metabolite that
combines with glutathione. If glutathione is depleted, metabolite causes hepatic damage
Toxic dose 140 mg/kg (textbook), 200 mg/kg (Starship), lower if chronic alcoholism, enzyme
inducing drugs or fasting
Measure plasma concentration. Treat if > 200 g/ml, 100 if liver disease, anorexia, etc. Threshold
declines for each hour after ingestion
Absorbed quickly so gastric lavage or activated charcoal only effective within 45 minutes
N-acetylcysteine (NAC) best antidote – saturates alternative pathway so all the paracetamol is
metabolised through the main pathway. Normal dose is 10 - 15 mg/kg per 4 hours acutely, per 6
hours at home
Monitor AST/ALT, PT (INR)
TCAs: see Tricyclic Antidepressants, page 432
MAOIs: see MAOIs (Monoamine Oxidase Inhibitors), page 434
Opioids:
Marked sedation, pinpoint pupils, respiration (differential: stroke)
Naloxone (but short T½ will lapse back)
Stimulants (cocaine type drugs): BP, tachycardia, arrhythmia, dilated pupils [sympathetic effects],
seizures
Barbiturates flumazenil (can cause seizures – so not if SSRIs/TCAs/antihistamines as well – which
also cause seizures)
Dibenzazepine antidepressants: Rapidly absorbed, high Vd, protein bound. Look for myocardial
toxicity, hypotension, hyperreflexia, convulsions. Treatment supportive + naso-gastric tube and
charcoal (up to 24 hours later). Monitor ECG, iv propranolol and NaHCO3
Benzodiazepines: Diazepam, temazepam Post –OD “cerebellar syndrome” (dizziness, confusion,
ataxia, nystagmus, bullous lesions). Supportive treatment
Anticonvulscents: carbamazepine
Bronchodilators: theophylline
Cocaine benzodiazepines
Carbon Monoxide 100% oxygen, treat cerebral oedema. Presentation: pink, headache, vomiting,
tachycardia, seizures, arrest
Cyanide 100% O2 + cobalt edetate
Methanol and ethylene glycol poisoning correct acidosis, ethanol
Chelating agents for arsenic, copper, lead, iron, cyanide
Aspirin: risk is pH balance
Pulmonary Oedema
Sit patient up and give O2
Medication:
IV frusemide: 40 – 80 mg if not on any already
490 4
th
and 5
th
Year Notes
IV morphine: 5 – 10 mg – calming effect, respiratory rate, venodilator preload
Sublingual nitroglycerine
If BP > 100 mmHg then captopril 6.25 mg
Occasionally CPAP or IPPV
Pulmonary oedema resulting from near drowning and ARDS does not respond to morphine & diuretics
– may require ventilation
Renal failure
Causes: potassium, acidosis, uraemia, volume overload, toxic accumulation of drugs
During arrest: give calcium chloride (to antagonise hyperkalaemia) + sodium bicarbonate
Spinal Shock
Due to a shutdown of cord function (e.g. following trauma): may last several days
IV fluids to maintain blood pressure: but don‟t overdo it. BP of 80/50 may be normal in spinal injury
High dose methylprednisolone may be beneficial within 8 hours of spinal injury
NG tube, urinary catheter (monitor output)
Monitor ventilation, temperature, avoid pressure areas
Trauma to Abdomen
Injuries may be blunt or penetrating
Do a diagnostic peritoneal lavage (DPL) to look for bleeding
A surgeon must evaluate all penetrating injuries of the abdomen.
Intra abdominal visceral damage must be strongly suspected following blunt trauma to the abdomen.
Multiple injuries are common and signs and symptoms guide diagnosis. Note that distracting injuries
(eg fractures) may mask abdominal symptoms.
Indications for surgery
Unstable patient
Injury penetrates peritoneum
Significant pancreatic injury on CT
Significant splenic injury in an older patient
Arterial injury
Specific Injuries
Ruptured spleen (intraperitoneal haemorrhage)
Signs and symptoms: May be pain free, may have signs of blood loss
Treatment: Splenectomy if elderly otherwise try to preserve it
Ruptured liver: Treatment: Laparotomy and suturing individual vessels/ packing etc.
Ruptured gut: Presence of gas under diaphragm on x-ray, or history of penetrating wound needs
laparotomy and repair/resection of affected bowel
Trauma to Chest
Tension Pneumothorax
Signs:
Apex beat lost
Blocks IVC venous return JVP
Vocal fremitus
Hyper-resonance
Displaced trachea (maybe)
US may help with diagnosis
On X-ray must have both of no peripheral vascular markings and a visceral pleural line
Types:
Primary/spontaneous: apical sub-pleural blebs are common and occasionally rupture. Especially
tall, thin, young males. Can occur at rest. Recurrence 20%
Secondary: in any lung disease
Treatment:
Insert 14g iv cannula into midaxillary line at level of nipple (any lower and may get diaphragm)
Hissing of air is diagnostic
Emergency Management 491
Remove needle and leave cannula in place. Attach tubing and put other end under water
PP ventilation will help reinflate the lung
Insertion where there wasn‟t a pneumothorax will cause one!
Open Pneumothorax
Sucking wound can‟t create –ive intrathoracic pressure
Occlusive dressing and positive pressure
Massive Haemothorax
1500 ml in thorax or > 200 ml per hour
Mainly penetrating wounds of pulmonary vessels (e.g. intercostals). If great vessels affected usually
don‟t survive
Significant amount of blood needs surgical removal thoracotomy
Flail Chest
Needs lots of force – so suspect pulmonary contusion as well
Independent segment of chest wall paradoxical movement. Requires two breaks
Treat with IPPV for at least a week
Cardiac Tamponade
Commonly results from penetrating injury
Commonly confused with a pneumothorax – think pneumo-thorax first – more common
Signs:
Impaired diastolic filing stroke volume. Initially tachycardia and vasoconstriction maintain
cardiac output and BP. Eventually hypotension and shock
Cardinal signs: Beck‟s triad – hypotension, venous pressure (JVP), small quiet heart
Pulsus paradoxus: > 10 mmHg in systolic BP with normal inspiration
Treatment:
?Emergency pericardiocentesis (either via xyphisternum or into apical area). Surgery essential
Colloid fluid infusion filling pressure and stroke volume
Pulmonary Contusion
Leads to non-compliance: V/Q mismatch, shunting PO2
Ventilate
Myocardial Contusion
Suspect if fractured sternum (requires big force)
There will be a current of injury on ECF and cardiac enzymes
Causes arrhythmias and CO
Treatment: 24 hours observation under ECG – can be arrhythmias
Rib Fracture
Commonest injury: pain impairs ventilation
Complications: atelectasis, pneumonia, contusion, pneumothorax, secondary pleural effusion 2 – 3
weeks later
Treatment: pain relief
Traumatic Rupture of Aorta
Results from rapid deceleration, usually at ligamentum arteriosum
Immediately fatal in 90% of cases. 50% further mortality per 24 hours thereafter untreated
Diagnosis suspected on CXR: widened mediastinum, 1
st
& 2
nd
rib fracture, obliteration of aortic knob,
deviation of trachea. Definitive diagnosis by aortogram
Treatment: repair
Complications: paraplegia due to blood flow to spine
492 4
th
and 5
th
Year Notes

Infectious Diseases 493
Infectious Diseases
References: Predominantly drawn from Dr M Humble‟s Microbiology notes
For notifiable diseases, see Communicable Disease Control, page 686
For infectious diseases of the skin, see Skin Infections, page 315
For infectious diseases in children, see Infectious Diseases, page 616
For respiratory infections, see Acute Pharyngitis, page 63 and Adult Pneumonia, page 67
For urinary tract infections, see Urinary Tract Infections, page 219
For gastro-intestinal infections, see Diarrhoea – Infectious Agents, page 176 and Viral Hepatitis, page
186
Blood Culture ................................................. 494
Infections of the CNS ..................................... 495
Bacterial Meningitis ................................. 495
Brain Abscess ........................................... 498
Viral CNS Infections ................................ 499
Bacterial Disease ............................................ 500
Streptococcus ............................................ 500
Staphlococcus ........................................... 502
Haemophilus Influenzae ........................... 502
Branhamella Catarrhalis ........................... 502
Other G-ives ............................................. 502
Anaerobes ................................................. 502
Mycobacteria ............................................ 502
Herpes Viruses ............................................... 503
Herpes Simplex Virus (HSV) ................... 503
Varicella Zoster ........................................ 504
Epstein Barr Virus .................................... 505
Chronic Fatigue Syndrome ....................... 506
Cytomegalovirus (CMV) .......................... 506
Parasitology .................................................... 507
Toxoplasmosis .......................................... 507
Malaria ...................................................... 508
Other ......................................................... 509
Travel Medicine ............................................. 510
Antibiotic Treatment ...................................... 511
Summary................................................... 511
Antibacterials ............................................ 513
Antifungals ............................................... 515
Antivirals .................................................. 515
Vaccination .................................................... 515
494 4
th
and 5
th
Year Notes
Blood Culture
When to take them:
It takes 30 – 60 minutes for temperature to rise after introduction of bugs into the blood, but
endothelial cells of the vascular system (spleen, kuppfler cells, etc) phagocytose cells in minutes
So when the temperature spikes, bugs may well be gone. So do random cultures in the hope of
getting a hit
Definitions:
Bacteraemia: no host response. Happens all the time (eg after cleaning teeth)
Septicaemia: sustained bacteria in the blood stream – on going delivery of bugs into the blood
stream from a replicating focus (don‟t multiply in blood). Leads to host response and disseminated
loci of infection
Pyemia (older term): Spread of organisms via infected thrombi
Infections associated with bacteraemia:
Community acquired pneumonia (treat strep pneumonia with penicillin, except in children where >
30% resistance so use cephalosporin)
Meningitis with petechial rash (treat meningitidis with penicillin)
Osteomyelitis (treat S Aureus with flucloxacillin or vancomycin if MRSA)
Leukaemia with infected Hickman line (Coag –ive staph, eg epidermidis, treat with vancomycin)
Pyelonephritis (treat E coli with Gentamycin)
Cellulitis (treat Strep pyogenes with Penicillin)
Perforated appendicitis (treat B Fragilis with Metronidazole)
Infective endocarditis (treat viridians Strep, eg S sanguis, with penicillin + maybe gentamycin)
Epiglotitis (treat HIB with cephalosporin)
Premature baby with respiratory distress syndrome (treat Lancefield group B strep with penicillin)
Procedure for blood culture:
Ensure everything sterile – contamination makes interpretation very difficult
5 – 10 mls of blood in two bottles, one general purpose and the other anaerobic
For kids, use single 3 ml paediatric bottle
Choose vein (usually ante-cubital fossa)
Swab with betadine and wait 3 – 4 minutes to dry
Draw blood and inject into bottles
If already on antibiotics, notify lab
Indications for blood cultures:
Infection of any degree of severity – especially if firm clinical diagnosis not possible
Absence of fever doesn‟t rule out infection, so is not a contra-indication (eg confusion, feeling off)
Specific indications:
Acute generalised infection: fever, rigors, sweating, shock
Febrile illness + congenital or acquired heart disease where infective endocarditis suspected
Diseases with a bacteraemic phase (pneumonia, meningitis, acute pyelonephritis, etc)
Shock (especially post-operative following abdominal surgery)
Intercurrent illness in patients with compromised immunity
Usually unnecessary to do more than 2 sets at the time bacteraemia is suspected, 20 minutes apart.
If infective endocarditis, take 3 sets over 24 hours
Bugs isolated in Wgtn Hospital:
Four most common G+ive: Staph aureus, Staph coag –ive (from lines), strep pneumonia,
enterococcus faecalis
Four most common G-ive: E. Coli, Klebsiella, Other Coliforms, Pseudomonas aeruginosa
Most common is staph epidermidis (ie staph coag –ive): It‟s a common contaminant, but also the
most common pathogen in catheter related infections, neonates and neutropenic patients.
Resistance to Flucloxacillin use of vancomycin (expensive, side effects, etc)
Infectious Diseases 495
Infections of the CNS
Bacterial Meningitis
Signs and Symptoms
Rapid onset of:
Meningism: Headaches, photophobia, stiff neck. Kernig‟s sign: Pain on straightening knee with
hip flexed
ICP: Headache, irritable, drowsy, vomiting, fits, pulse, BP, LOC, pin-point pupils,
papilloedema (late sign), tense fontanelle
Septicaemia: fever, arthritis, DIC, BP, pulse, tachycardia, rash (ultimately 80% will have a
purpuric rash, 10 – 15% will have a maculo-papular or urticarial rash, 5 – 10% will have no rash)
In different age groups:
Infants/toddlers: fever, lethargy, poor feeding, vomiting, toxic (drowsy, pallor), rash. Only 30 –
50% have signs of meningism absence doesn‟t exclude. Bulging anterior fontanelle – but if
vomiting may be normal or reduced
Children > 3: fever, headache, vomiting, photophobia, stiff neck, confusion (may be combative),
non-blanching rash (initially blotchy macular rash that rapidly becomes petechial or purpuric)
Adolescents: may present as acute mania or appearance of drug induced psychosis
Pathogenesis
Organisms:
Neonates: E. Coli, -haemolytic streptococci Group B (eg streptococcus agalactiae – normal
vaginal flora), rarely listeria
Children < 14 years: H. Influenza (if < 4 and not immunised), Neisseria Meningitidia Type B,
Strep Pneumoniae, Tb
Adults: Neisseria Meningitidia Type B, Strep Pneumoniae, maybe staph aureus or Cryptococcus
neoformans
Elderly, Immunocompromised: Pneumococcal, Listeria, Tb, G –ive, Cryptococcus Neoformans
Pathogenesis:
Pathology: inflammation of pia mater and arachnoid
Most common are N Meningitidis and S pneumoniae
Nasopharynxbloodsubarachnoid space (via choroid plexus): N meningitides, HIB, S.
pneumoniae
Middle earbloodsubarachnoid space: S Pneumoniae, HIB
Congential abnormalities (eg spina bifida): coliform bacilli, pseudomonas, Strep agalactiae
Trauma: Skull fracture + CSF leak, CNS surgery, shunts: Staph aureus
Depressed immunity: listeria monocytogenes, cryptococcus neoformans
Neonatal meningitis from vaginal flora (especially with prematurity, prolonged ROM, delayed 2
nd
stage): Strep agalactiae, coliforms (E coli), listeria monocytogenes
If recurrent:
Consider immunosuppression (eg hypogammaglobulinaemia or complement deficiency)
Look for lumbosacral defects, especially if enteric bacteria or S aureus
Investigations
Do blood culture before presumptive treatment if possible, but NOTHING should delay presumptive
treatment. Tell lab about antibiotics
Must do:
Blood cultures
CSF via lumbar puncture unless contraindicated (see below)
Urine: supra-pubic aspiration or catheter
If antibiotics have already been administered:
Needle aspirate purpuric lesions for gram stain and culture
Throat swab
Bloods:
Blood Glucose sample – may be hypoglycaemic [ABC = Airway, breathing, circulation. DEFG =
Don‟t Ever Forget Glucose]
FBC, electrolytes, clotting time, ABGs

496 4
th
and 5
th
Year Notes
Lumbar puncture:
Contraindicated if:
Signs of ICP (all meningitis will have ICP) causing cerebral herniation (eg very LOC,
very bad headache, focal signs including abnormal papillary reflexes, tonic seizures,
decerebrate or decorticate posturing, irregular respirations, bradycardia, papilloedema). If in
doubt then CT
Severe cardiovascular compromise with DIC/coagulopathy (eg fulminant sepsis)
Infection over the injection site
Tests of CSF: Gram stain, Tb, cytology, virology, glucose, protein, India ink (Cryptococcus),
culture (if clear then ?virus), antigen testing (especially if partially treated)
May be normal, repeat if symptoms persist
Typical CSF (lots of variation):
Pyogenic
Tb/Fungal
Viral („aseptic‟)
Normal
Main cell seen
Polymorphs
Mononuclear
Mononuclear
< 5 * 10E6 WBC/ml
(< 20 in neonates)
Glucose
- or
2.5 – 5.0 mmol/l
Protein
Mildly or
< 0.4 g/l
Bugs seen
Yes
No
No
NB: early viral meningitis may have predominantly polymorphs
RBCs: None. If there are then either traumatic (more in 1
st
of 3 tubes) or bleed (new if red,
yellow if old – zathachromia)
Appearance on Gram stain:
N Meningitidis: G –ive diplococci
H influenzae: Pleomorphic G –ive bacilli
S pneumoniae & S agalactiae: G +ive diplococci
Listeria: G +ive bacilli
TB: Acid fast bacilli very scant – take at least 5 mls of CSF
Cryptococcus neoformans: Indian ink stain shows capsules
Imaging: To identify subdural collections, abscess, hydrocephalus, thrombosis and infarction. Only if
LP contraindicated and suspected mass lesion or persistent or focal neuro signs
Management
See When is a child really sick?, page 565
Management (based on protocol for a child):
Standard infection control precautions plus surgical mask when examining throat, intubating etc
ICU if:
Coma
Circulatory collapse
Persistent, recurrent seizures
SIADH with cerebral oedema or seizures
Shock or ICP is what kills
Maintain perfusion:
Colloid bolus (20 – 40 ml/kg 4% albumen iv), then colloid + glucose
Inotrope eg dobutamine (10 g/kg/min)
Watch for ADH secretion hyponatraemia and cerebral oedema if too much fluid given
Check Na 6 – 12 hourly. If Na < 135 mmol/l then iv rate. If Na > 145 then rate
Respiratory support:
O2
Early elective intubation if persistent shock (but may exacerbate hypotension due to
vasodilation and sympathetic drive)
Immediate intubation if ICP, hypoxia and/or respiratory failure, pulmonary oedema or
hypotension (uncompensated shock)
Correct abnormalities: anaemia, hypoglycaemia, coagulopathy (FFP), acidosis (NaHCO3),
hypokalaemia
Seizures: anticonvulsants
Watch for ICP:
Conscious state, focal neuro signs, abnormal pupils, hypertension and relative bradycardia.
Infectious Diseases 497
Treatment: ICU, PCO2, diuretics (Mannitol, frusemide), head up, deep sedation, inotropes.
But priority is to correct the shock (CBF = MAP – ICP)
Weight and measure head daily in an infant
Isolate patient, ensure analgesia
Dexamethasone treatment controversial (most benefit in HIB). Not routinely used. Reduces fever
and gives misleading impression of clinical improvement
Antibiotic regimes:
Empiric antibiotic treatment:
Neonate – 3 mths: Amoxycillin 50 mg/kg (for listeria) + Ceftriaxone 50 mg/kg (E coli and
Strep). 2 weeks for G +ive, 3 weeks for G –ive.
Older child:
Cefotaxime 50 mg/kg/6hr, max 2 g, iv for 7 – 10 days or
Ceftriaxone 50 mg/kg/12hr, max 2 g, iv for 7 – 10 days or
Penicillin G 50 mg/kg/4hr iv for 7 – 10 days
If strep pneumonia suspected: Vancomycin 15 mg/kg/6hr, max 500 mg, iv +
cefotaxime/ceftriaxone – synergistic, necessary due to resistance to 3
rd
generation
cephalosporins
If still failing consider adding Rifampicin
Specific Treatment according to culture and susceptibility results:
N Meningitidis, S agalactiae: Penicillin (Cefotaxime if allergic to penicillin) for 5-7 days. For
meningococcaemia only can use penicillin or cefotaxime
S pneumonia:
Penicillin susceptible: penicillin (but 20% are resistant) for 7 – 10 days
Penicillin resistant, 3
rd
generation susceptible: Cefotaxime
Penicillin and 3
rd
generation resistant: Cefotaxime + Vancomycin
H Influenza: Cefotaxime, Ceftriaxone
L Monocytogenes: amoxycillin
Staph Aureus: Flucloxacillin
M Tuberculosis: Rifampicin, Isoniazid, Pyrazinamide, Ethambutol
Coliforms: 3
rd
generation Cephalosporin (ie Cefotaxime, Ceftazidime)
Pseudomonas: Ceftazidime
Cryptococcus Neoformans: fluconazole or amphotericin B
NB: Erythromycin and gentamycin don‟t have good CSF penetration
If not responding, or non-susceptible strain of pneumococci or receiving dexamethasone than
repeat LP after 24 – 48 hours
Complications:
Seizures:
First suspicion should be hyponatraemia (also hypoglycaemia):
SIADH (Na < 130 and urine Na > 20) exacerbates cerebral oedema
Prevent by restricting fluids to 50% of maintenance
Treatment: severe fluid restriction (10 ml/kg/day), in an emergency consider hypertonic
saline, Mannitol or frusemide
Hypoventilation can further ICP hypoxia, hypercapnea, acidosis
Anticonvulsants can also exacerbate these metabolic changes
Management options: diazepam, clonazepam, phenobarbitone, dextrose to control
hypoglycaemia, intubation and ventilation
Major disability in 15%: Deafness, brain damage, peripheral necrosis, etc. All cases should have
audiologist check within 6 – 8 weeks of discharge
Death in 5%, 10 –15% pneumococcal meningitis, 20% in fulminant meningococcaemia
Meningococcal Disease
Cause: Neisseria Meningitidia
Epidemiology:
10-year epidemic started in 1990 with about 50 reported cases. Since then 3696 cases and 163
deaths. Current case fatality rate is 3 – 5 %
Leading infectious cause of death in children
500 reported cases in 2000. NZ rate is 13.3 per 100,000. UK rate is 4 per 100,000
Regional variation: East Cape and Central North Island the highest
Rates per 100,000 < 1 year olds:
498 4
th
and 5
th
Year Notes
Pacific Island: 570
Maori: 230
European: 80
Healthy people can be carriers
Transfer via respiratory secretions
Kids and teenagers more susceptible than adults
Not a cause of Otitis media
Pathogenesis: endotoxins (lipopolysaccharides in the cell wall) activate complement and release of
PAF causing endothelial injury immune activation and vascular permeability
Notifiable to public health (as is HIB)
Prophylaxis to stop nasal carriage of the bug – not to cure incubating illness. Nasal carriage higher in
adults than children
Rifampicin: 4 doses, 600 mg bd for adults, 10 mg/kg bd for kids (very high dose). Broad spectrum
antibiotic
Offer to index case (if only treated with penicillin), all intimate, household and day-care contacts
during last 10 days
Contraindications: pregnancy (use single dose ceftriaxone), liver disease.
Side effects: nausea, vomiting, diarrhoea (GI effects), turns urine/tears/sweat orange/red (will stain
contacts)
Interactions: asthma, blood clotting and oral contraceptives (continue pill, use barrier method until
7 days after antibiotics finished)
TB Meningitis
Rare
Most common < 5 years
Slow onset: malaise and fever progressing to drowsiness, neck stiffness and seizures over 2 weeks
Mantoux testing may be normal, and CXR normal in ½ of cases
Investigations:
Gastric lavage, urine and CSF for Acid fast stain and culture
CT
Treatment: isoniazid, rifampicin, pyrazinamide
Notifiable disease
Brain Abscess
Aetiology:
Chronic otitis media, sinusitis or dental sepsis
Trauma: foreign body, skull fracture, CNS surgery
Haematogenous spread (may be multiple abscess) from congenital heart disease (with R-L shunt),
bronchiectasis, abdominal abscess, endocarditis, etc
Bacteria:
Temporal lobe (from chronic otitis media):
Anaerobes: Bacteroides fragilis
Aerobes: Proteus mirabilis + HIB and E faecalis
Frontal lobe (from chronic sinusitis)
Anaerobes: Bacteroides melaninogenicus
Aerobes: Strep milleri
Traumatic: Staph aureus
Haematogenous spread: Staph aureus, Viridians Strep, Bacteroides fragilis, etc
Treatment:
Surgery
Antibiotics:
Anaerobes: Metronidazole
Aerobes:
Strep: Amoxycillin
Coliforms: Cefotaxime
Staph aureus: Flucloxacillin
Infectious Diseases 499
Viral CNS Infections
Viral Encephalitis
Herpes Simplex:
Clinical: usually short history, fever, headache, confusion, ataxia, focal convulsions coma (if
clouding of consciousness consider encephalitis in addition to meningitis)
CSF: raised leucocyte count, predominantly mononuclear
Diagnosis: PCR test of CSF for Herpes Simplex antigen
Treatment: Acyclovir 10 mg/kg iv 8 hourly for 10 days. Low threshold for treatment
HIV:
Most AIDS patients have a subacute encephalitis caused by direct brain infection
Symptoms: mood changes, depression, lethargy, confusion, dementia
Other viruses: Mosquito born (Murray Valley Encephalitis, Japanese Encephalitis), Rabies virus
Management:
Full blood screen: Cr, electrolytes, glucose, LFT, ABG, urine drug & metabolic screen, blood and
urine cultures, ammonia, cortisol, coagulation screen, ECG
Serology and viral cultures
LP if not contraindicated – may be normal in up to 50% of cases
Consider empiric acyclovir + cefotaxime – at least until HSV is excluded
CT (MRI better still) for focal lesions
Consider differential:
Head injury
Toxic or metabolic encephalopathy
Hypoxic insult
Supportive treatment:
Fluid restriction
Control of seizures
Cardio-respiratory support
Maintenance of nutrition
Viral Meningitis
Causes:
Most due to non-polio enteroviruses:
Faecal oral little kids at risk
ECHO viruses, Polio, Coxsackie A & B
Mumps
Presentation: fever, headache, malaise, photophobia, abdominal pain and vomiting. Neck stiffness in
older children. Maybe a macular or even petechial rash
Differential diagnosis of lymphocytic (aseptic) meningitis
Viral meningitis (eg ECHO, Mumps, Coxsackie)
Viral Encephalitis (eg Herpes Simplex, CMV, Varicella Zoster)
TB meningitis
Fungal meningitis (eg Cryptococcus neoformans)
Neurosyphilis
Acute Leptospirosis
Cerebral toxoplasmosis
Neoplasm
Cerebral sarcoid
Lab tests:
CSF Culture: Enteroviruses, mumps, fungi, TB
Throat culture and Faeces for enteroviruses
CSF Antigen tests: PCR for Herpes Simplex, CMV, VZV, TB, Toxoplasmosis
Serology: antibodies to Treponema pallidum, Leptospira, Toxoplasma gondii
Admit if:
Diagnosis in doubt
Antibiotics are being considered
IV Rehydration is needed
Ensure good analgesia
500 4
th
and 5
th
Year Notes
Post-Infective Encephalitis
Immune hypersensitivity reaction to host cells containing viral antigens
Late onset – 7 – 10 days after acute illness
Viruses involved: Morbilli (Measles), Mumps, Rubella, Varicella-Zoster
Other
Spongiform encephalopathies:
Caused by Prions (Proteinaceous infectious particles)
Histology: vacuolation of brain tissue, deposition of amyloid plaques
Eg: Kuru (in PNG), Creutzfeldt-Jakob Disease (CJD), Variant CJD
Symptoms: Insidious onset of ataxia, dysarthria and dysphagia. Progressive dementia
See Dementia, page 439
Slow virus infections:
SSPE (Subacute sclerosing pan-encephalitis): Measles like virus affecting children and adolescents
PML (Progressive Multifocal Leucoencephalopathy): Affects adults from 40 – 70, Polyoma virus
implicated.
Neonatal Encephalitis:
TORCH Complex: Toxoplasmosis, Rubella, CMV, Herpes Simplex
Usually accompanied by disseminated disease
Reye‟s Syndrome: post-infectious encephalopathy with associated acute liver failure. Most common
antecedent infection is Influenza virus
Bacterial Disease
Streptococcus
Streptococcus Pyogenes (Group A,
Haemolytic)
NB: Lancefield Groups only apply to Haemolytic Streps
Causes:
Commonly: acute pharyngitis, cellulitis, impetigo (also caused by group C)
Uncommonly: necrotising fasciitis (haemolytic strep gangrene), strep toxic shock syndrome,
scarlet fever, erysipelas (= contagious skin infection with strep pyogenes), acute otitis media
Rarely: pneumonia, infective endocarditis
Has remained sensitive to penicillin
Identical strep can lead to a variety of infections:
Sore throat
Impetigo/Cellulitis. See Impetigo (School Sores), page 315
Toxic Shock Syndrome
Myositis
Necrotising Fasciitis
Infection via throat (mainly) or via skin (impetigo/wound infection):
Suppurative: tissue invasion
Non-suppurative (after 2 – 8 weeks):
Rheumatic Fever (See Rheumatic Fever, page 602)
Glomerulonephritis
Super antigens: pyogenic exotoxins – ability to avoid classical antigen processing by APCs
Scarlet Fever:
Direct response to Streptococcal toxins (cf virus rash which is autoimmune and therefore delayed)
Presentation: fever, exudative pharyngitis, scarlatina rash (fine punctate rash with perioral sparing),
desquamation
Skin feels like sandpaper then desquamates. May get purpura in flexures
Tongue affected – white then strawberry red
Streptococcus Toxic Shock Syndrome:
First described in children. Now associated with Tampon use
Early (1 – 7 days): vague, viral like illness: fever, chills, myalgia, diarrhoea
Later: abrupt onset of pain (not necessarily associated with findings), redness, hypotension, renal
failure, ARDS, coagulopathy. May lead to necrotising fasciitis. Also skin diffusely erythematous
like sunburn, conjunctivitis
Infectious Diseases 501
Desquamation a week later characteristic
Age group: 2- 50 year olds, no predisposing or underlying disease
Bacteriology:
Blood culture +ive in 60%
Swab or aspirate in 95%
M protein types 1 & 3: impedes phagocytosis by leucocytes, expressed on cell wall
Lab tests: Haematuria, Cr, albumin and Ca, serum CK for deep tissue infections
Treatment: Ceftriaxone
Necrotising fasciitis:
Diffuse swelling and mild erythema, followed by bullae filled with clear fluid. Spreads along
facial planes
Infection of subcutaneous tissue progressive destruction of fascia and fat but may spare the skin
itself.
25 cases per year in NZ
Requires aggressive surgical debridement
Causative bacteria:
Group A strep most common
Staph Aureus
C. Perfringens
C. Sceptica
Predisposing factors:
Diabetes
Peripheral vascular disease
Chicken pox
Minor trauma/surgical procedures
Use of NSAIDs masks inflammation and delays diagnosis
Streptococcus Lancefield Group B
Haemolytic Streps
Eg Strep agalactiae: differential in neonatal meningitis. Normal vaginal commensal
Streptococcus Pneumoniae
Is haemolytic but not classified as a Viridians
Causes:
Commonly: acute otitis media, acute sinusitis, febrile convulsion in infants, community acquired
pneumonia, infectious exacerbations of chronic bronchitis, meningitis (nasty type)
Uncommonly: peritonitis (2
nd
ary to chronic hepatic/renal disease of to infected IUCD)
Rarely: infective endocarditis
Antibiotic sensitivity:
Parenteral:
Penicillin resistance in 1% blood isolates in adults and 11% in kids Strep pneumonia
penicillin resistance is not an issue in adults but is in kids
Ceftriaxone
Vancomycin (for penicillin resistant strains and MRSA)
Oral: amoxycillin, erythromycin, cefaclor, tetracycline (not kids or pregnant)
Vaccination:
Pneumovax
Polysaccharide-based subunit vaccine containing 23 serotypes covering 90% of strains causing
invasive pneumococcal disease
Contains T-cell independent antigens non-immunogenic if < 2 years (and poor response for
some serogroups up to age 6). Predominant IgM response without induction of memory. 5 yearly
boosters recommended
Recommended for:
> 65 years
> 2 with asplenia, immunocompromised (including nephrotic syndrome) and chronic illness
Conjugate vaccines generating IgG response being worked on….
Viridians Streptococci (plus also Enterococcus faecalis)
Causes UTI, abdominal wound sepsis, infective endocarditis (uncommon)
502 4
th
and 5
th
Year Notes
Staphlococcus
Staphlococcus Aureus
Sources of bacteraemia:
Skin sepsis
Wound infection (esp hospital acquired)
Pneumonia (esp hospital acquired)
Osteomyelitis
Septic arthritis
Lines: Subclavian, IV drips (esp CVP)
Infective endocarditis
See also Impetigo (School Sores), page 315
Staphlococcus coagulase negative (eg epidermidis)
Sources of bacteraemia: IV lines – Hickman, CVP lines, premature neonates with IV lines
Haemophilus Influenzae
Uncapsulated type (not type B which is capsulated)
Causes:
Commonly: acute otitis media, acute sinusitis, acute infectious exacerbation of chronic bronchitis
Uncommonly: community acquired pneumonia (more CORD patients)
Rarely: meningitis
Antibiotic sensitivity:
5% of isolates produce penicillinase resistant to amoxycillin
Augmentin
Cefaclor
Tetracycline (not kids or pregnant)
Cefuroxime (iv)
Is not sensitive to erythromycin
Moraxella Catarrhalis
Previously know as Branhamella Catarrhalis
Commonly causes: acute otitis media, acute sinusitis, acute infectious exacerbation of chronic
bronchitis (same as Haemophilus Influenzae)
Antibiotic sensitivity: 70% produce penicillinase, so use augmentin, cefaclor, tetracycline or
cefuroxime (iv)
Other G-ives
Escherichia coli, klebsiella aerongenes, proteus mirabilis, other Coliform bacilli
Cause: UTI, Pyelonephritis, abdominal wound sepsis, peritonitis, biliary tract infection (gallstones) or
obstruction
Anaerobes
Bacteroides fragilis, Clostridium perfringens, anaerobic streptococci
Cause: Abdominal wound sepsis, peritonitis, pelvic sepsis, septic abortion, puerperal sepsis
Mycobacteria
See Tuberculosis, page 68
Classification:
Tuberculosis complex: M. Tuberculosis and M. Bovis
Other mycobacteria: M. Avium-Intracellulare (MAC), M. Kansasii, M Marinum
Leprosy: M. Leprae
Resulting Diseases:
Tuberculosis Complex
Immunocompetent: In descending frequency: lung, lymph nodes, kidney, genital tract, CNS
Immunodeficient: Lung in > 70%, but extra pulmonary involvement > 70% in blood (25 –
40%), lymph nodes, faeces, CNS due to cell mediated immunity
MAC:
Infectious Diseases 503
Immunocompetent: Kids – cervical lymphadenitis, adults: chronic destructive lung disease
(uncommon)
Immunodeficient: Infection common. Initial colonisation of GI tract, then spread to blood,
lymph nodes, liver, spleen, less lung involvement but invariably fatal
Most strains of MAC are resistant to standard anti-mycobacterial drugs
Drug treatment:
Standard drugs: Rifampicin, Isoniazid, pyrazinamide, ethambutol. Normally first 3, except if from
Pacific Islands where use all 4 due to isoniazid resistance. Rifampicin is the best, if resistant to
this then poor prognosis
Most strains of M Bovis are resistant to pyrazinamide
Many strains of M Tb from AIDS patients in the US (especially NY) are resistant to Rifampicin
and Isoniazid
Other anti-mycobacterial drugs: ciprofloxacin, clarithromycin, amikacin, rifabutin, clofazimine
Vaccination: BCG:
Live vaccine
Indicated for high risk infants: household has individuals from endemic areas of with past or
current Tb
Neonatal BCG is 60 – 90% protective for extra-pulmonary Tb and 65% for pulmonary Tb.
Protection lasts 10 – 15 years
Adverse effects: local abscess in 1%. Treated conservatively. Some require excision
Herpes Viruses
All Herpes viruses exhibit latency
Herpes Simplex Virus (HSV)
Manifestations: systemic (fever, sore throat), gingivostomatitis (ulcers with yellow slough – cold
sores), meningitis (uncommon, self-limiting), encephalitis (fever, fits, headache, dysphagia,
hemiparesis – do PCR on CSF sample – refer urgently)
Incubation: 2 – 25 days. Chronic infection is due to the virus remaining in the sensory nerve ganglia.
Infectious period indeterminate contact isolation
Symptoms:
Blisters which become shallow painful ulcers, often preceded by itching or tingling
First episode may be accompanied by flu like illness, tender inguinal nodes and dysuria
Recurrences can be brought on by stress, fatigue, depression, immunosuppression and concurrent
illness. Recurrences usually less severe and become less frequent
Diagnosis: clinical suspicion. Swab the base of an unroofed ulcer and refrigerate in viral medium. This
will be painful. Culture negative doesn‟t exclude HSV as timing and collection technique important.
Serology possible, but not routinely used
Pathogenesis. There are two antigenic types of Herpes Simplex Virus:
Type 1 is associated with lesions on the face and fingers, and sometimes genital lesions. Treat
with zovirax (topical cream). Prevalence: 70% of population
Type 2 is associated almost entirely with genital infections, and affects the genitalia, vagina, and
cervix and may predispose to cervical dysplasia. 10% of oral lesions caused by type 2.
Prevalence: 10 – 15% of population (depends on population – more in high risk)
Type 1 Herpes Simplex Virus
Infection of fingers or thumb leads to a whitlow (vesicles coalesce)
Can infect eczematous skin eczema herpeticum
Children:
HSV1 the most common type in children.
Primary infection in childhood leads to gingivostomatitis – may lead to dehydration as child won‟t
drink. May need NG tube
Dribbling can perioral spread
Auto-inoculation can conjunctivitis, genital lesions, skin infection with eczema (eczema
herpeticum) can be severe
If neonate or immunocompromised can be life-threatening
Treatment: Oral analgesics (eg lignocaine) and Paracetamol. Acyclovir
504 4
th
and 5
th
Year Notes
Genital Herpes (type 2)
Description:
Painful, recurrent condition.
Male – anus or penis – small grouped vesicles and papules + pain, fever, dysuria. Dysuria may be
severe enough to cause urinary retention
20% may have it, but 20% are asymptomatic and 60% mild or unrecognised
40% caused by type 1, 60% by type 2
Transmission: spread through skin-to-skin contact, usually when skin is broken or lesions present, but
asymptomatic viral shedding a possible route of transmission. Neonatal transmission is rare (1 in
10,000 live births), but carries risk of ophthalmic infection caesarean section indicated if active
blisters at delivery
Prevention of genital herpes: Condoms with new partner (although doesn‟t eliminate risk). Avoid sex
during an outbreak
Can have extra genital lesions on thighs and buttocks. Can radiculoneuropathy urinary
retention/constipation
Treatment of Genital Herpes (type 1 or 2):
Acute: Acyclovir 200 mg 5 times daily for 5 days. Topical creams not effective. Symptomatic
treatment: salt bathing, local anaesthetic creams, oral analgesia, oral fluids. Counselling and
follow-up important – written information for patients and partners, Herpes Helpline (0508 11 12
13)
Suppressive Therapy: Where frequent outbreaks or psychological morbidity. Acyclovir 400 mg
BD for up to a year. Can reduce viral shedding by up to 95%
Can be devastating. Refer to counselling at Sexual Health Service
Complications:
Risk of AIDS transfer
Erythema Multiforme
Neonatal Herpes: 1 % transmission but 50% mortality
In pregnancy:
If first primary episode: miscarriage, prem labour
If recurrent, tiny risk for baby
If lesions at delivery then Caesarean
Varicella Zoster
Primary infection: Chicken Pox.
Macules papules vesicles crusts
Incubation 10 – 21 days (usually 14 – 16)
Infectious for 1 – 2 days before rash appears until it crusts over
Highly infectious, in hospital requires strict respiratory/contact isolation
Complications:
Commonly becomes super-infected (eg with scratching) with Staph aureus (or S Pyogenes)
which leads to scarring
If immunocompromised overwhelming infection, pneumonitis, hepatitis, encephalitis (treat
with Ig and acyclovir)
Post-natal infection can be overwhelming
Immune response can encephalopathy with cerebellar ataxia
Can lead to severe exacerbation of eczema
Then remains dormant in dorsal root ganglia
Treatment: Supportive, antipruritic lotion if itchy, cut fingernails short
Prevention: Live attenuated virus, or im Ig within 96 hours of exposure if at risk and susceptible
(immunocompromised, pregnant, newborn, prem babies)
Tests: culture – swab transported in viral medium
Vaccination:
Live attenuated vaccine recently licensed for both children and adults
Not recommended for general use, but role in protecting non-immune adults (more severe illness)
Contra-indicated if immuno-suppressed or pregnant
Shingles:
Reactivation of infection: affects 20% at some time. Elderly and immunocompromised are high
risk

Infectious Diseases 505
Symptoms: Dermatomal pain, then fever malaise for several days, then macule-papules + vesicles,
especially in thoracic or ophthalmic division of trigeminal dermatomes. If sacral, then urinary
retention may occur. Thoracic (50%), cervical (20%), trigeminal (15%)
Complications:
If shingles around eye (especially end of nose), then are likely to have a dendritic ulcer on
cornea. Stain with Fluorescein and shine on blue light, corneal abrasions will shine green.
Don‟t give steroid blindness. Urgent referral to an ophthalmologist. See Eye Infections,
page 144
Post-hepatic neuralgia – especially in the elderly and trigeminal
Recurrence rare and suggests HIV (or Dermatomal Herpes Simplex)
Treatment if needed: acyclovir as early as possible, 800mg 5 times a day for 5 days. Pain relief –
analgesic or low-dose amitriptyline. Maybe prednisolone to reduce post-herpetic neuralgia.
Report visual loss immediately
Epstein Barr Virus
DNA virus
One of Herpes Group
Spread by respiratory secretions (e.g. sneeze, kiss)
Pre-schoolers an important reservoir: usually just a non-specific URT infection. In later life (e.g.
adolescent) get it more acutely plus hepatitis. 1 – 5% present as hepatitis
Associated with Burkett‟s lymphoma & nasopharyngeal carcinoma
Clinical
Highly variable course. Often asymptomatic if < 5 years
Sore throat (often exudative)
Fever
Lymph nodes up
Tender liver (liver involvement appetite and feeling unwell), maybe big spleen
Rash in 10%
Doesn‟t resolve (especially after antibiotics)
Will be tired for weeks/months
Incubation 30 – 50 days
Association with symptoms:
Sore Throat
Lymphadenopathy
Atypical Mononucleosis
EBV
+++
+++
+++
CMV
-
+
+++
HIV
++
++
++
Toxoplasmosis
+
+++
++
Viral Hepatitis
-
+
++
Investigations
Throat swab
FBC: may be atypical mononuclear lymphocytes
EBV serology
Treatment
Symptomatic
Don’t give penicillin if risk of EBV: leads to rash that can be interpreted as penicillin allergy. (E.g.
amoxycillin, rash in 80 – 90%)
Infectious for months. No isolation required
Steroids if upper airway obstruction in kids
Antibodies to EBV
IgM Anti-VCA (Virus capsid antigen) and IgG Anti-VCA
Usually appear in blood 7 days after symptoms develop in acute primary EBV infection
IgM: usually persists for 2 – 4 months
IgG: usually persists for life
Anti EBNA (Epstein-Barr nuclear antigen): Appears 2 months after primary infection and persists for
life

506 4
th
and 5
th
Year Notes
Profiles:
IgM VCA
IgG VCA
EBNA
No infection
-
-
-
Acute Primary
+
+
-
Past Infection
-
+
+
(ie EBNA +ive rules out acute
infection)
Paul-Bunell now largely obsolete. Negative in 10 – 15 % of cases
Associated diseases
Burkett‟s lymphoma
Nasopharyngeal carcinoma
Hodgkin‟s disease (EBV in 40 – 60% of cases)
Chronic EBV may occur but is very uncommon (recurrent sore throat, cervical lymphadenopathy)
Chronic Fatigue Syndrome
Unknown cause: but key differential to EBV
Diagnosis
Severe chronic fatigue over 6 months or longer, with other known medical conditions excluded, and
4 of the following during 6 consecutive months:
Short term memory or concentration
Sore throat
Tender lymph nodes
Muscle pain
Multi joint pain: without swelling or redness
Headaches of new type/pattern
Unrefreshing sleep
Post-exertional malaise lasting > 24 hours
Differential Diagnosis
Depression
Psycho-social stressors
Cytomegalovirus (CMV)
Transmission:
Blood: transfusions, intra-uterine, perinatal, needle sharing
Cervical secretions and semen
Saliva (eg close contact with kids)
Urine (eg infants to adults)
Organ donation (transplantation)
Immunocompetent:
Kids:
Common in preschoolers, usually asymptomatic. May give URTI
Prolonged excretion in saliva and urine common
Adults:
Usually asymptomatic, if not then usually self-limiting
May be fever (up to 2 weeks, ie a differential of PUO)
Sore throat, cervical lymphadenopathy uncommon
Atypical mononucleosis on blood film
Differential: EBV, HIV, toxoplasmosis
Pregnancy:
Congenital infection (ie crosses placenta) in 20 – 40%
> 90% show no signs at birth, but watch for long term neurological sequalae (eg sensori-
neural deafness, retardation)
Severe cases: respiratory distress, jaundice, microcephaly, etc
Part of TORCH complex: Toxoplasmosis, Rubella, CMV, HSV
Perinatal infection (eg during vaginal delivery):
Full term: usually mild

Infectious Diseases 507
Pre-term: may be severe
Immunodeficient:
AIDS: one of the most common infections CMV retinitis (common), CMV encephalitis (rare),
CMV colitis (rare)
Transplant: greatest risk if they‟re CMV negative and CMV positive organ interstitial
pneumonia and hepatitis (in liver transplant)
Transfusion: blood is not routinely screened for CMV antibody. Should give CMV –ive blood to prem
babies (<1500 g) and seronegative transplant recipients with seronegative transplants
Lab diagnosis:
Serology:
IgG
IgM
No infection
-
-
Past infection
+
-
Acute primary or reactivated
infection
+
+
Cell culture – slow (>7 days). Culture lung biopsy or peripheral blood leucocytes
PCR for CMV DNA on peripheral leucocytes, amniotic fluid, CSF (very specific, less sensitive,
very expensive)
Treatment:
Ganciclovir: bone marrow toxicity
Foscarnet (nephrotoxic)
Ganciclovir prophylaxis used for –ive patients with +ive organs
Parasitology
Toxoplasmosis
A protozoa/parasite
Main source: cysts in meat. Also kitten faeces (eg cyst in garden – pregnant gardeners should wear
gloves)
Presentation:
Immunocompetent:
Lymphadenopathy (eg unilateral)
Maybe: fever, myalgia, acute pharyngitis, hepatosplenomegaly, atypical mononucleosis
Usually self-limiting – may take months to settle
If persistent/recurrent lymphadenopathy ?Need for treatment
Immunodeficient:
Acquired or reactivated
AIDS most common: CNS involvement (solitary space occupying lesion, encephalitis), also
myocarditis, hepatitis
Less common in transplants and encephalitis
Ocular toxoplasmosis: most cases in adolescents and adults reactivation infection. Blurred
vision, photophobia, multiple retinal lesions
Congential Toxoplasmosis:
29% fetal infection if mother has primary CMV infection
Highest risk in 3
rd
trimester (1
st
trimester may miscarry)
Complications: spontaneous abortion, premature, still birth
Surviving neonates: bilateral choroido-retinitis. In severe cases, TORCH type symptoms
Lab diagnosis:
PCR test for toxoplasmosis: amniotic fluid, CSF (AIDS patients)
Lymph node biopsy characteristic histology
Serology:
IgM antibody after 5 – 14 days, peaks at 2 – 4 weeks, traces for up to a year
IgG: high levels for up to 6 months, declines slowly over years
Avidity test: can differentiate between acute phase „immature‟ IgG and „mature‟ IgG
Treatment:
Pyrimethamine (Gold standard, but gives bone marrow suppression + give folate) + sulphadiazine
(not available in NZ)
Pyrimethamine + clindamycin (gives C. difficile diarrhoea)
508 4
th
and 5
th
Year Notes
Spiramycin (only one safe in pregnancy)
Malaria
Transmitted by mosquito and very rarely transfusion
See also Malaria, page 688
Clinical
Irregular fever – peaks on release of parasite from infected RBCs. May only be mild if person has
immunity (ie previous exposure). Various strains have various periodicities
Chills
Headache
Malaise
Vomiting (20%)
Diarrhoea (<5%)
ie similar to Typhoid
History
Travelled to a malaria country
What conditions did you stay in, rural/urban, etc
Was chemoprophylaxis taken, how was compliance
Diagnosed overseas
When did you return to NZ (Plasmodium Falciparum usually in 1 month, P Vivax up to a year)
Length of illness
Diagnosis
Blood film for plasmodium protozoa: a thick film is necessary as well as the standard thin film if
parasites are scant (eg if have some immunity)
Pointless if patient is afebrile
If initially negative, repeat 12 hourly for 48 hours
Critical that you find out which plasmodium species is present, eg:
Plasmodium Falciparum: common in Africa, can cause cerebral malaria (fatal)
Plasmodium Vivax: more common in Asia/Oceania
Features of poor prognosis:
CNS signs: disturbed consciousness, repeated convulsions
Respiratory distress
Haemorrhage, shock
Biochemical markers: Cr, HCO3, bilirubin, glucose
High parasitic load
Prevention
Assessment of risk:
Malaria geography: transmission rates vary by country (eg high in Sub-Sahara, PNG, Solomon
Islands)
Likely extent of contact with mosquitoes (eg standard of accommodation)
Anti-mosquito measures: long sleeves & trousers, insect repellent/sprays, nets
Chemoprophylaxis:
Start 1 week beforehand and continue till 4 weeks after leaving
Mefloquine (effective against chloroquine resistant P Falciparum).
250 mg weekly
Side effects: nausea, diarrhoea, dizziness – usually self-limiting.
At higher doses (eg for treatment) convulsions and sinus bradycardia
Contraindications: drugs altering cardiac conduction, psychiatric disease, epilepsy, pregnant,
kids < 5kg, or where fine CNS co-ordination required (eg airline pilots)
Doxycycline, 100 mg daily
After food otherwise gastritis
In rural areas of SE Asia, where mefloquine-resistant strains of P falciparum are reported
Contraindicated in pregnancy women and children
Chloroquine + proguanil: Only one safe for first trimester. Low efficacy against drug resistant
falciparum
Infectious Diseases 509
Chloroquine weekly – countries without chloroquine-resistant P falciparum (Central America north
of Panama)
Treatment
P Vivax, P Ovale, P Malariae:
Acute treatment: 3 days of Chloroquine
For radical cure in P Vivax or P Ovale:
Primaquine for 2 weeks (screen for G6PD deficiency first)
Eradicates exo-erythrocytic liver cycle. If you don‟t, they will relapse
Relapse common (20%) – maybe several months later. If so, repeat 3 days of Chloroquine
followed by 2 weeks of higher dose of Primaquine
P Falciparum:
Quinine sulphate + Doxycycline for 7 days
No persisting cycle so relapse not a problem
Cerebral malaria: iv quinine: loading dose then maintenance infusion
Drug resistance:
Chloroquine-resistant strains of plasmodium falciparum are widespread
Chloroquine-resistant strains of P Vivax reported in Indonesia and PNG
Other
Amoebiasis (Entamoeba histolytica)
Diagnosis:
Intestinal amoebiasis: stool sample * 3, 48 hours apart, in PVA fixative
Cysts: frequently present asymptomatically (carrier state)
Extra-intestinal amoebiasis (eg amoebic abscess of the liver) maybe months later. Serum antibody
test
Treatment:
Intestinal amoebiasis: metronidazole then diloxanide furoate
Extra-intestinal: metronidazole (surgical drainage may be necessary)
Asymptomatic: Diloxanide furoate
Giardiasis
Diagnosis:
Stool examination for Giardia Lamblia cysts, 3 samples 48 hours apart
Duodenal aspirate and direct examination for trophozoites
Treatment:
Tinidazole 2g stat or Metronidazole 400 mg 8 hourly for 7 days
Test for cure with repeat stool sample. Relapse not uncommon
Filariasis
Commonest is Wuchereria bancrofit imported from Samoa
Elephantitis
Diagnosis: Blood sample
Treatment:
Ivermectin
Most cases are asymptomatic or low grade pyrexia and don‟t require treatment
If severe, surgical relief of major lymphatic obstruction may be necessary
Intestinal Worms
Hookworm:
Ancylostoma duodenale, necator americanus
Diagnosis: stool sample * 3
Roundworm:
Ascaris Lumbricoides
Diagnosis: worms passed in faeces, or stool samples * 3 and examine for Ova
Pinworm:
Enterobius vermicularis
Diagnosis: sellotape swabs of anus
510 4
th
and 5
th
Year Notes
Whipworm:
Trichuris trichura
Diagnosis: stools * 3
Treatment: medendazole 100mg BD for 3 days for Hookworm, Roundworm, Pinworm (treat whole
family) and whipworm (only if severe)
Strongyloides Stercoralis:
Diagnosis: Stools * 3
Treatment: Thiabendazole
Tapeworms:
Taenia saginata, beef tapeworm
Diagnosis: Stools * 3, examine for worm segments
Treatment: niclosamide
Hydatid Disease
Aetiology: Echinococcus granulosa (a flatworm). Infected from ova excreted in dog faeces. Dogs
infected from eating raw sheep offal (ie liver) containing hydatid cysts
Clinical: Often acquired in childhood, present in older age with solitary cysts (liver, lung, brain)
Treatment: surgical drainage + aldendazole as adjunct
Diagnosis: Serology: haemaglutination test + complement fixation test
Cryptosporidium
Common protozoan parasite
Profuse watery diarrhoea for 48 hours. Very common cause of diarrhoea.
Severe and persisting cases in AIDS
Diagnosis: Stool microscopy with ZN stain for acid fast cysts
Treatment: Paromomycin (an oral, non-absorbable aminoglycoside) has some efficacy
Pneumocystis Carinii
Protozoan parasite probably part of normal respiratory flora
Causes interstitial pneumonitis in immuno-compromised patients (transplant, leukaemia, AIDS)
Diagnosis: Bronchial lavage or open lung biopsy
Treatment: Cotrimoxazole (alternatively pentamidine). Relapse in 25%
See also Other pneumonias, page 70
Travel Medicine
Travel History:
Where are you going
How are you getting there
How long there
What will you be doing
Where are you staying
Have you been there before
Examples:
3 week package to Hong Kong, Singapore, Bangkok: Hep A and Tetanus up to date. Typhoid is
overkill
4 month Overland through from Thailand to Turkey (Vivax Malaria): Malaria, Hep A, Tetanus
3 month TI in Tanzania: Hep A, Typhoid, Yellow fever (not Asia)
3 year diplomatic posting in PNG: Malaria prophylaxis if going rural but not continuously
Vaccination
Malaria chemoprophylaxis: unnecessary if in a malarious country for < 7 days. Risk in main resort
areas of Asia is low
Typhoid:
Injectable: salmonella typhi antigen, 70% protection for 3 years
Oral vaccine: attenuated live strain, doses at 0, 3 and 5 days gives protection for one year. Useful
at short notice
Yellow Fever:
Attenuated live strain ( not if immunocompromised)
Infectious Diseases 511
For travel to equatorial Africa and South America
Protection for 10 years
Requires special certificate, stamp, etc only done in designated centres
Polio:
OPV: Oral: 2 drops po (tiny risk of giving it to adults if no previous vaccine use IPV)
IPV: Inactivated polio vaccine: 0.5 mls sc
Booster every 10 years
Tetanus/Diphtheria Toxoid: booster every 10 years. 0.5 mls im into deltoid muscle
Meningococcal Vaccine: For types A, C, W, Y – not B. sc injection gives 3 years protection. Indicated
for travel to countries where epidemics occur – Nepal, West Africa, Brazil
Hepatitis A: Formalin inactivated HAV. IM injection gives protection for one year. Booster dose 6 –
12 months later gives long-term protection. If over 50, check immune status – may be immune and
therefore won‟t need it (its expensive)
Japanese Encephalitis Vaccine: Widespread through SE Asia. Rare for travellers to get it – but high
mortality. Side effects from vaccine
Rabies: Only for people intending to work longer term in rural/agricultural areas of Asia
Pyrexia of unknown origin if returning from 3
rd
world
Diagnose on blood film/culture:
Malaria
Dengue
Typhoid: usually constipated, used to die of peritonitis, bradycardia, high spiking fever, takes days
for temperature to go down
Ross River
Syphilis
Filariasis (eg Samoa)
Other imported infections from Pacific:
Leprosy (mycobacterium leprae)
Yaws (Treponema pertenue)
Eosinophilic Meningitis
Antibiotic Treatment
Summary
G +ive
Cocci
Strep pneumonia
Oral: Amoxycillin. IV: Penicillin G
Allergy: Erythromycin. Resistant (eg kids): Ceftriaxone
Resistant and Meningitis: Cefotaxime + Vancomycin (act
synergistically)
Resistant and Endocarditis: Vancomycin
Strep faecalis
Trimethoprim
Strep agalactiae
Penicillin. [ haemolytic. Normal vaginal flora]
Strep pyogenes
Penicillin. Erythromycin if allergic. Also sensitive to flucloxacillin
Strep sanguis
Penicillin [ haemolytic]
Staph aureus
Flucloxacillin. Allergy: Ceftriaxone. MRSA (resistant to
penicillins and cephalosporins): Vancomycin
Staph epidermidis
Flucloxacillin. Resistant: Vancomycin
Bacilli
Listeria monocytogenes
Amoxycillin. Elderly/immunocompromised: ciprofloxacin
(quinolone – not in kids)
Clostridium difficile
Metronidazole
Enterococcus faecalis
Amoxycillin
G –ive
Bacilli
E Coli
Trimethoprim. Cotrimoxazole (trimethoprim +
sulphmethoxazole), Norfloxacin (Quinolone). 48% resistant to
amoxycillin. Augmentin resistance growing.
Meningitis: Cefotaxime (good CSF penetration). Consider
gentamycin or cotrimoxazole
Campylobacter Jejuni
Erythromycin
512 4
th
and 5
th
Year Notes
H Influenzae
Cefaclor, Augmentin, Tetracycline
5% resistant to penicillin, not sensitive to erythromycin
Legionella
Erythromycin. Add rifampicin if severe
Pseudomonas Aeruginosa
Ciprofloxacin. Maybe Tobramycin or piperacillin
Meningitis: Ceftazidine
Gardnerella Vaginalis
Metronidazole. Metronidazole is otherwise inactive against
aerobes
Bordetella Pertussis
Erythromycin
Branhamella Catarrhalis
Augmentin, cefaclor, tetracycline, cefuroxime
70% penicillinase
Anaerobes
Bacteroides Fragilis
Metronidazole. Not penicillin or cephalosporins
Helicobacter Pylori
Clarithromycin + metronidazole + omeprazole (7 days)
Cocci
Neisseria Meningitidis
Penicillin. Cefotaxime if allergic.
Prophylaxis: Rifampicin, ceftriaxone if pregnant
Neisseria Gonorrhoea
Stat: Amoxycillin + Probenecid
Ciprofloxacin or tetracycline if penicillin allergy or resistant.
Azithromycin if concurrent chlamydia or pregnant
Not G-ive
Chlamydia Pneumoniae
Chlamydia Trachomatis
Erythromycin
STD: Doxycycline, azithromycin, pregnancy: Erythromycin
PID: Erythromycin + ornidazole
NB: Obligate intracellular parasite. Cellular wall similar to G-ive
but not actually a G-ive bacteria
Others
Mycoplasma
Erythromycin. 2
nd
line: Tetracyclines (eg doxycycline) except
pregnant/kids
TB
Rifampicin + isoniazid + pyrazinamide (also ethambutol if
isoniazid resistant). Prophylaxis: rifampicin
MAC
Clarithromycin
Treponema pallidum
= Syphilis. Penicillin G. Resistant: Tetracyclines (eg doxycycline)
Yeasts
Aspergillus
Amphotericin B. Itraconazole prophylaxis
Cryptococcus neoformans
Fluconazole (good CSF penetration), Amphotericin B
Virus
HSV
Acyclovir
CMV
Ganciclovir
Toxoplasmosis
Pyrimethamine + clindamycin. Pregnant: Spiramycin
Protozoa
Cryptosporidium
Nothing effective. Maybe Paromomycin (oral, non-absorbed
aminoglycoside)
Giardiasis
Tinidazole stat or metronidazole 7 days
Trichomonas
Doxycycline, Metronidazole
Pneumocystis Carinii
Pneumonia
Cotrimoxazole
Malaria Prophylaxis
Mefloquine weekly: good for chloroquine resistant falciparum. Not
epilepsy, pregnant, babies
Doxycycline daily: Esp Mefloquine resistant falciparum. Not kids
or pregnant
Chloroquine + Proguanil: if pregnant
Chloroquine weekly: if no chloroquine resistant falciparum
Plasmodium Falciparum
Quinine sulphate + doxycycline
Plasmodium Vivax
Chloroquine 3 days then primaquine 2 weeks
Amoebiasis
Metronidazole + diloxanide furoate
Worms
Filariasis
Ivermectin
Intestinal worms
Hookworm, roundworm, pinworm: Medendazole
Strongyloides Stercoralis: Thiabendazole
Tapeworms: Niclosamide
Infectious Diseases 513
Antibacterials
Penicillins
Use for
Notes
Penicillin G (iv/im)
(Oral form: Pen V)
Streptococci
Not Enterococcus faecalis, resistance in kids to
strep pneumoniae
Staphylococci
But 80% produce penicillinase
N Gonorrhoeae
Some produce penicillinase
N Meningitidis
T Pallidum
Leptospira
Syphilis
Anaerobes
Peptostreptococci, Clostridia, Fusobacteria,
Bacteroides (not B fragilis), Actinomyces
Amoxycillin
As above plus:
Enterococcus faecalis
Listeria monocytogenes
Haemophilus influenzae
6 % produce penicillinase
Some E coli
48% resistant
Most Proteus mirabilis
20% produce penicillinase
Augmentin
Clavulanic acid inhibits penicillinase. Principle
use is infectious exacerbations of chronic
bronchitis
Haemophilus influenzae
Increasing E coli resistance
Branhamella Catarrhalis
Flucloxacillin
Staph Aureus
Penicillinase producers. MRSA resistant to
Flucloxacillin and cephalosporins
Piperacillin
Pseudomonas aeruginosa
Systemic infection only
Tazocin
Neutropenic cancer
patients
= Piperacillin + Tazobactam (a beta-lactamase
inhibitor)
Cephalosporins
Gen
Examples
Use for
1
Cefazolin
Cephalothin (IV)
Cephradine (IV & oral)
Cephalexin (oral)
Better for G+, poor for G-
Gram +ives: Streptococci (not E faecalis), Staphylococci,
Anaerobes (Not B Fragilis)
Gram –ives: Some coliforms: E coli (20% resistant), Klebsiella
Inactive against: H Influenzae, Pseudomonas, Enterococcus
faecalis
2
Cefuroxime (IV+oral)
Cefamandole (IV+IM)
Cefaclor (Oral)
G +ive: as for 1st generation
G -ive: Better against coliforms
Active against H influenzae
Inactive against: Pseudomonas, E Faecalis, B Fragilis
3
Ceftriaxone
Cefotaxime
Ceftazidime
Cefpodoxime (oral)
Good activity against most coliforms
Activity against G+ < 2
nd
generation
No activity against Bacteroides or Enterococcus
Ceftazidime good against pseudomonas aeruginosa
Ceftriaxone has long T½, can be given once daily
Good CSF penetration first choice for meningitis caused by
coliforms or HIB
4
Cefipime
Cefpirome
Highly stable against -lactamases
Good against most aerobic G –ives (coliforms and pseudomonas)
Good against G +ive, incl staph aureus (similar to 1st generation)
but not Enterococcus
Cefotetan
Broad spectrum cephamycin
Good against Bacteroides and Coliforms (not pseudomonas)
Indications: antibiotic prophylaxis for colonic and gynaecological
surgery

514 4
th
and 5
th
Year Notes
Aztreonam
Active against G –ive bacteria only: including coliforms and to a
lesser extent Pseudomonas
Indication: less toxic than aminoglycosides for G-ive infection
Imipenem
Meropenem
A cabapenem (not cephalosporins)
Inhibit nearly all G+ and G-
Restricted as its so good
Indication: Empiric therapy in neutropenic cancer patients
Macrolides
Effective against:
Staph aureus (up to 10% resistance in community strains)
Streptococci (not E faecalis)
Anaerobes (only moderately effective against B fragilis)
Mycoplasma pneumoniae
Chlamydia pneumoniae
Chlamydia trachomatis (but tetracycline is the drug of choice)
Campylobacter jejuni
Ineffective against:
H influenzae
No CSF penetration
Indications:
Treatment of susceptible bacteria if penicillin allergy
Atypical pneumonia (eg Mycoplasma, Chlamydia or Legionella)
Campylobacter
Chlamydia infection in pregnant women
Erythromycin
New analogues:
Roxithromycin (Rulide)
Clarithromycin (Klaricid): Treatment of MAC, especially in AIDS patients
Azithromycin (Zithromax): Single dose treatment for STD‟s caused by Chlamydia trachomatis or
N. gonorrhoeae (especially in pregnancy)
Vancomycin
G+ive wonder drug – active against G+ive only
Indications:
Systemic infections caused by MRSA or MRSE (Epidermidis), or infected Hickman lines in cancer
patients
Infective Endocarditis due to Strep or Staph with penicillin allergy
Clostridium difficile colitis (by mouth). First line is metronidazole
Otto and nephrotoxic
Teicolpanin: similar drug, active against some Vancomycin Resistant Enterococci (VRE)
Rifampicin
Always used in combination (except meningitis prophylaxis)
Active against M. Tb, Staph aureus, Legionella
Indications:
TB (in combination)
Severe Staph aureus infections (eg infective endocarditis) in combination
Severe legionella pneumonia (in combination with erythromycin)
Prophylaxis against N meningitides or HIB
Aminoglycosides
Active against all coliform bacilli (eg E Coli), pseudomonas, staphylococci
Inactive against: streptococci, anaerobes
Indications: G- sepsis, perforated appendix
Drugs:
Gentamicin
Tobramycin: more active against pseudomonas
Amikacin: reserved for Gentamycin resistant bugs
Infectious Diseases 515
Spectinomycin: N gonorrhoeae (penicillinase producers)
Otto and nephrotoxic
Cotrimoxazole
= Trimethoprim + Sulphamethoxazole
Broad spectrum: Staph, Strep, many coliforms (not Pseudomonas), HIB, Pneumocystis, Brucella
Indications: Acute infectious exacerbations of chronic bronchitis, PCP in AIDS
Trimethoprim on its own is the standard treatment against community acquired UTI (E Coli,
Klebsiella, Proteus, Strep faecalis)
Quinolones
Broad spectrum oral antibiotic
Active against: most coliforms, pseudomonas aeruginosa (main use), Staphs (including MRSE and
MRSA), N gonorrhoeae, HIB, Branhamella catarrhalis (good), Salmonella, Shigella, Yersinia,
Campylobacter
Poor activity against Anaerobes, streptococci
Can damage growth cartilage not licensed for children
Indications:
Norfloxacin: resistant UTIs
Ciprofloxacin: Mainly pseudomonas
Tetracyclines
Eg doxycycline (once a day on full stomach), very common in treatment of STIs
Active against Staphs, Streps, Coliforms, HIB
Other indications:
Syphilis and Gonorrhoea if penicillin allergy
Mycoplasma pneumoniae
Contraindications: young children, pregnancy, renal failure (except doxycycline)
Metronidazole
= Flagyl
Active against all anaerobes (eg B fragilis)
Inactive against aerobes (excl Gardnerella vaginalis, causing bacterial vaginosis, where it is drug of
choice)
Active against Protozoa: Trichomonas vaginalis, Giardia lamblia
Other
Fucidin: active against Staph Aureus, must be used in conjunction with, eg Flucloxacillin. Use in
bone/joint infections
Chloramphenicol: for infections caused by Burkholderia cepacia
Antifungals
Nystatin (topical): vaginal or oral candida
Miconazole (topical): Candida and dermatophytes (except scalp or nails)
Terbinafine (oral) Dermatophyte infections of scalp or nails (has superseded Griseofulvin)
Itraconazole (oral): Dermatophyte infections of scalp or nails, prophylaxis in Candida and Aspergillus
in immunocompromised
Fluconazole (Oral/IV): active against yeasts (candida, cryptococcus). Good CSF penetration (eg
Cryptococcal meningitis)
Amphotericin B (IV): Very good but side effects, including nephrotoxicity
See also Antifungals, page 336
Antivirals
Acyclovir: active against HSV and VZV (less active)
Ganciclovir: CMV in immunocompromised patients. Bone marrow suppression neutropenia
Vaccination
Reference: Public Health Module Notes
516 4
th
and 5
th
Year Notes
Vaccination Principles
Jenner first vaccinated using cowpox against smallpox in 1796
Characteristics of immunity:
Specificity: response to specific antigen
Priming
Memory: brisk secondary response
Results of vaccine:
Most stimulate serum antibodies (IgG, IgM)
Some stimulate IgA (eg polio, rubella)
A few promote cell mediated reaction (eg BCG)
Types of vaccine:
Live attenuated vaccine (eg OPV, MMR, VZ, BCG): full and long lasting immunity after a single
dose (except OPV which requires 3 doses)
Inactivated vaccines:
First dose gives a predominantly IgM response. Further doses raise IgG level (depending on
potency of the vaccine, maturity of the immune system and time interval)
Inactivated whole bacteria or viral vaccines: IPV, Hep A, Whole cell pertussis (being
replaced).
Modified toxins (toxoids) eg Diphtheria, Tetanus antibody response to toxin not infective
agent
Sub-unit vaccines: eg Hep B, HIB, Pneumococcus, Influenza – the main focus of modern
vaccines – conjugated vaccines with fewer side effects and easy to grow from genetically
engineered yeasts etc.
Also passive immunity available from injectable IgG. Immediate protection lasting from weeks to
months
Population protection:
Immunisation is delivered to individuals and provides individual protection and benefit
Also provides population protection (herd immunity):
Some level of immunisation protects unimmunised people who would otherwise have caught
it don‟t need to immunise those for whom its contraindicated (eg too young or sick)
Virulence coverage necessary to get herd immunity
„Free riders‟ – because they perceive costs (needles, hassle, side effects) to be greater than
perceived benefits weakens herd immunity
Efficacy and effectiveness:
Efficacy: Does intervention provide a specific outcome (eg an IgG response) under ideal lab
circumstances
Effectiveness: Does it work under normal clinical circumstances
Apparent paradox: as coverage , so does the proportion of cases that have been vaccinated (but
lower absolute numbers of disease), due to vaccination failure. Can create the illusion that the
vaccine is ineffective
Vaccine failure:
Primary vaccine failure: inadequate physiological response to the vaccine (eg freezing or
overheating of the vaccine, or poor host response)
Secondary vaccine failure: waning immunity
Degrees of protection:
Generally provides 80 – 95% protection (BCG 50%, Influenza 70%)
May protect against severe disease rather than infection (eg Diphtheria)
Vaccination coverage:
= Proportion of a population who have completed a specific course of immunisation
In Northern Region in 1996, 63% by 2 years but only 45% for Maori and 53% for Pacific islanders
With measles: coverage time between epidemics as need a pool of 130 – 150,000 measles
susceptible children to sustain an epidemic. Each epidemic 50,000 kids contract measles and
therefore immune in future. 10,000 unprotected kids added to the pool each year.
Policy measures: revise schedule to reduce the number of visits, immunisation certificates on
enrolment at school/early childhood centre.
Surveillance: Generally poor systems
Disease surveillance: notifications, discharge and mortality database, outbreak investigations,
disease modelling
Infectious Diseases 517
Coverage surveillance: registers and periodic surveys
Adverse event surveillance
Cold-chain monitoring
Vaccination Practice
Practical vaccination standards:
Ensure correct storage and transport: maintain the „cold chain‟ at 2 – 8 C. Eg have dedicated
fridge and check its minimum and maximum temperature daily
Check vaccines due for each patient: either age groups (neonates, children, adolescents, adults,
elderly) or specific exposure situations (occupational, travel, post-exposure)
Discuss and obtain informed consent: Written consent only required for children if care giver not
present
Check contra-indications
Administer vaccine
Manage adverse reactions:
Observe for 20 minutes afterwards
Local or systemic reactions (fever, rash, joint pains): symptoms of immune activation. Offer
Paracetamol. Especially whole cell pertussis. MMR may be followed about 7 – 10 days later
by a 2 – 3 day fever and rash (but the vaccine is not infectious)
Anaphylaxis: Distinguish from fainting (which is common). Treatment: ABC, Adrenaline
1:1000 IM injection, 0.01 ml/kg, O2
Report to centre for Adverse Reaction Monitoring if serious (includes persistent screaming > 3
hours and > 5 cm swelling at injection site), but also convulsions, meningitis within 30 days
Manage records: practice notes, HBL claim record and immunisation certificate for parents
Anti-immunisation views:
Risks outweigh benefits: some diseases now rare and specific vaccines have serious side effects
Alternative health views: disease part of growing up (so was death!) and natural infection develops
immune system
Plus a variety of beliefs/values that will be hard to shift
Main reasons for non-immunisation is „passive rejecters‟ – don‟t get around to it
Contraindications:
Acute illness or fever > 38 C: defer vaccine. Otherwise will blame the illness on the vaccine!
Living with an immune suppressed person: use IPV rather than OPV
Reaction to previous dose: encephalopathy with 7 days of DTP vaccines or immediate severe
allergic reaction. If true anaphylaxis seek specialist advice
Immune suppression: don‟t give live vaccine. Likely to have reduced response to inactivated
vaccines
Pregnancy: theoretical risk from live virus vaccines
If in doubt, refer to a paediatrician
False contraindications:
Mild illness, URTI, fever < 38.5 C
Asthma, hay fever, eczema
Prematurity and low birth weight in an otherwise healthy child – these especially need vaccination
Previous clinical history of illness: no harm done from vaccinating and many clinically diagnosed
cases of an illness are in fact something else
On antibiotics, inhaled or low dose steroids
Stable neurological conditions (cerebral palsy, Down)
Currently Vaccine Schedule
Current Vaccination Schedule from February 2002:
Covers Hep B, Diphtheria (child dose = D, adult dose = d – smaller), Tetanus, acellular Pertussis,
Polio (now all intravenous = IPV, not oral), Hib, Measles, Mumps, Rubella
518 4
th
and 5
th
Year Notes
DTaP-
IPV
Hib-
Hep B
Hep B
only
IPV
MMR
DTaP-
Hib
Td
Influenza
6 weeks
3 months
5 months
15 months
4 years
5 years
11 years
If not
had 4
doses
45 years
65 years
For unimmunised adults:
Give jabs over same timeframe
Don‟t need HIB, don‟t give paediatric dose of diphtheria (too big) and more inclined to use
IPV
Additional vaccination in specific age groups:
Neonates:
Babies of HBsAg +ive mothers: Hepatitis B immune globulin (HBIG) and vaccine at birth,
vaccine at 6 weeks, 3 months and 5 months. Also offer vaccination to household and sexual
contacts.
BCG if possible Tb exposure
Women of child bearing age who are susceptible to Rubella should be offered MMR
Adults: Td (after injury and at 45 and 65 – used to be 10 yearly) + annual influenza
Elderly: annual influenza + pneumococcal (5 yearly)
Specific exposure situations:
Splenectomy: Pneumococcal vaccine
Occupational: Health care workers (eg Hep B) or HAV to food workers
Travel: See Travel Medicine, page 510
Future Developments:
Inclusion of Varicella Zoster and pneumococcal for children
Research into Group B meningococcal (currently 10 year epidemic, 250 cases per year), Rotavirus
and RSV, non-infectious diseases including cancer
Vaccine Preventable Diseases
Measles and Pertussis are the main ones still happening that we shouldn‟t have
Hepatitis B: See Hepatitis B, page 187
Diphtheria:
Corynebacterium diphtheriae respiratory and cutaneous infection (grey membrane on throat).
Exotoxin causes cardiac toxicity and ascending paralysis. Spread by nasal droplets
1 imported case in last 20 years. Till 1945 killed 100 babies a year. High is USSR in 90s.
Vaccine: inactivated diphtheria toxoid, boosters every 10 years. > 80% efficacy
Tetanus:
Clostridium tetani from soil and animal faeces muscular rigidity due to neurone specific toxin,
10% mortality
3 notifications per year (old ladies in the garden). Common in environment no herd immunity
Vaccine: Inactivated toxoid, boosters every 10 years, 100% efficacy
Pertussis: See Pertussis, page 609
Polio:
Enterovirus spread by faeces and saliva
Presentation:
Usually asymptomatic or mild (fever, headache, nausea, vomiting
Only 1% of infected get severe clinical disease: severe muscle pain, neck and back stiffness
flaccid paralysis
Last wild virus infection in 1962. Occasional imported and vaccine associated cases
Vaccine:
Infectious Diseases 519
Live oral polio (OPV) > 90% protection after 3 doses. < 1% of recipients develop diarrhoea,
headache or muscle pains. 1 in 2.5 million recipients or close contacts develop paralysis
(more common in immunosuppressed) = Vaccine Associated Polio Paralysis (VAPP)
Inactivated polio vaccine (IPV) for immunocompromised (will be used more widely when it
can be combined with other jabs)
Haemophilus influenzae type B (HIB): See Epiglottitis, page 609
Measles: See Measles, page 617
Mumps: See Mumps, page 617
Rubella:
Togavirus spread by nasal droplets
Presentation:
Incubation 2 – 3 weeks
Fever, headache, mild conjunctivitis, erythematous maculo-papular rash, lymphadenopathy
(especially posterior triangle), arthritis, arthralgia
50% develop the rash and lymphadenopathy
50% of adolescents and adults have arthralgia or even frank arthritis
1 in 5,000 have encephalitis
Complications:
Congenital rubella syndrome: 90% of embryos of mothers infected in 1
st
trimester will abort or
have major abnormalities (severely retarded, seizures, deafness, cardiac defects). Frequent
problems after birth
Rate of congenital rubella is 5 times the US rate
~ 60 notifications per annum (1600 in 1995)
Vaccine:
98 % protective
To protect the unborn child only – relies on herd immunity. Need to vaccinate guys as well
otherwise they will maintain a population reservoir which women with vaccine failure will
catch
5% of adolescents and adults have arthralgia and 1% have non-infectious rash
Contra-indicated in pregnancy and immunosuppressed
Influenza:
Virus types A (H3N2 and H1N1) and B
Causes Fever, rigors, headache, myalgia, protraction. Estimated 400 deaths per annum.
Vaccine: inactivated subunit vaccine for new strains (resulting from „antigenic drift‟). 60 –90%
effective. Contraindicated if egg allergy
Pandemics result from „antigenic shift‟
Tb: BCG: See Mycobacteria, page 502
Pneumococcal Disease: See Streptococcus Pneumoniae, page 501
Varicella Zoster: See Infectious Diseases, page 504
520 4
th
and 5
th
Year Notes

Pharmacology 521
Pharmacology
Generally, specific drugs are covered in the relevant systems chapter
Specific topics elsewhere:
Antibiotics in infectious diseases, see Antibiotic Treatment, page 511
Anticoagulant Treatment, page 75
Antidepressant and Mood Stabilising Medication, page 432
Pharmacokinetics ........................................... 522
Variability of Drug Response ................... 522
Volume of Distribution (Vd) .................... 522
Clearance (Cl) ........................................... 522
Half Life (T½) .......................................... 523
Steady State Concentration ....................... 523
Bioavailability (F)..................................... 523
Absorption ................................................ 523
Distribution ............................................... 524
Metabolism ............................................... 524
Excretion of Drugs.................................... 524
Inter-individual Differences...................... 525
Controlled Release Formulations ............. 527
Pharmacodynamics ........................................ 527
Pharmacology of Pregnancy and Breast
Feeding ..................................................... 528
Adverse Drug Reactions (ADR) ..................... 529
Drug Allergy ............................................. 530
Drug Interactions ...................................... 531
Therapeutic Drug Monitoring (TDM) ...... 533
Poisoning and Drug Overdose .................. 533
Drug withdrawal syndromes ..................... 533
Sleep ............................................................... 534
Treatment of Insomnia .............................. 534
Compliance Issues .......................................... 535
Prescribing ..................................................... 535
Regulation of Medicines and Drugs ............... 536
Clinical Trials ........................................... 536
MedSafe .................................................... 536
522 4
th
and 5
th
Year Notes
Pharmacokinetics
Deals with time course of the drug in the body:
Absorption: rate and amount absorbed
Distribution: amount in the body/volume of distribution
Elimination = Clearance: rate of metabolic and renal elimination
Drug concentration usually plotted as plasma concentration verses time
Variability of Drug Response
Disease, patient and doctor specific factors leading to the prescribing decision
Absorption: formulation, GI motility, polypharmacy (eg Grapefruit juice)
Distribution (ie Vd)
Plasma protein binding (generally not important unless highly bound and low Vd)
Metabolism: age, genetic factors, enzyme induction and inhibition, first pass metabolism, dose-
dependent metabolism, active or toxic drug metabolites, bilary excretion, renal elimination
Tissue Sensitivity
Volume of Distribution (Vd)
Volume of distribution = volume into which the drug appears to be uniformly distributed with a
concentration equal to that of plasma
Relates the amount of drug in the total body relative to that in the plasma. Explains where drug goes –
not what it does. In one compartment model:
Vd = dose/plasma concentration L/kg, or
Amount in body = Vd * conc
Vd = Cl/Ke
Examples:
Gentamycin has an apparent Vd of extracellular H2O
Digoxin has a Vd much larger than physical volume of body
Warfarin has a much smaller Vd than expected
Use Vd to calculate loading dose: LD = Vd * target conc
Vd can be altered in cardiac, liver and renal disease and in obesity
For obese patients, use total body weight for lipid soluble drugs and ideal weight for water-soluble
Clearance (Cl)
= Elimination
Clearance of drug corresponds to the volume of plasma that appears to be cleared of its drug in unit
time e.g. mls/min, l/hr.
Represents the size of the plug hole, rate of elimination (= rate of clearance) is the flow through the
plug hole
Depends on rate at which drug is transported to the organ of elimination and the efficiency of the
eliminating organ in removing the drug
Clearance = rate of elimination/drug concentration (as long as not saturable elimination, eg phyentoin,
alcohol)
Clearance can be:
Concentration dependent/ Capacity limited: saturable metabolic pathway (eg phenytoin)
Flow-dependent: organ elimination rate = concentration * flow * extraction ratio (fraction cleared
on each pass through the organ). Eg will be eliminated on 1
st
pass elimination dependent on
blood flow. If Heart failure vasoconstriction to maintain blood flow liver flow
elimination (eg lignocaine, propranolol). Total body clearance can‟t exceed cardiac output (5
l/min)
Clearance and Volume of Distribution are independent of each other, but T½ is dependent on both
Maintenance Dose = clearance * desired concentration
Compartments:
One or multi compartment models
Ka = absorption into compartment
Ke = elimination from compartment
Pharmacology 523
Linear kinetics
First order kinetics: rate of transport or elimination proportional to drug concentration in the
compartment
Zero order kinetics: elimination has maximum value rate is non-linear and it‟s a capacity limited
process. Eg alcohol is metabolised at 10 ml/hr. Beyond this the enzyme metabolism is swamped. So
if dose rate is greater than clearance rate, then a small increase in dose rate leads to a dramatic increase
in plasma concentration (ie accumulation)
Michaelis-Menten kinetics
For a drug that undergoes zero-order elimination, when the concentration is low enough, elimination no
longer occurs at its maximum rate (V max) but at a rate dependent on but not proportional to the
plasma concentration. As the concentration reaches ½ the maximum rate (km), first order elimination
occurs
So, elimination will increase with increasing dose, but not proportional to the dose
Zero-order kinetics will be approached risk of accumulation
Issue for any drug having zero-order kinetics within its therapeutic range
E.g. salicylic acid (especially in overdose), phenytoin, alcohol
Half Life (T½)
Time for drug concentration to decline by half influences dosing interval
Is dependent on clearance and volume of distribution:
Vd = T½ * clearance / 0.693
Rate at which drug leaves the body is dependent on Cl & Vd. In one compartment model:
Ke = Cl/Vd
= Measure of how the whole body handles the drug – how quickly it gets out
But it doesn‟t work in practice…
For slowly excreted drugs, 5 * T½ and it will be eliminated for practical purposes
But for anaesthetic drugs that you want to switch on and off quickly the therapeutic window is
often in the redistribution phase – not the elimination phase. Need a more complex model where
the drug redistributes to (then from) slow and fast compartments, as well as being excreted from
blood context sensitive half-life. If drug is over infused, it builds up in other compartments and
then takes a long time to wash out. So give a reducing amount over the duration of infusion as
other compartments get saturated and stop „sucking it out‟ of blood
Steady State Concentration
Amount of drug absorbed = amount eliminated
Takes 5 half lives to reach 97% of steady state, if each new dose given at half life spacings
The shorter the T½, the sooner the Css will be reached (steady state concentration)
The shorter the T½, the greater the plasma concentration will fluctuate between doses
If T½ is prolonged, dose should be reduced or dosage interval increased
Css = (F * D) / (Cl * T) where F = bioavailability, D = dose, Cl = clearance and T = dosage interval
As Cl = (Vd * 0.693) / T½, then
Css = (F * D * T½ ) / (0.693 * Vd * T)
Bioavailability (F)
= Fraction of drug that reaches the systemic circulation
F = AUC (Area under curve) after an oral dose/AUC after IV dose
Low F caused by poor absorption, or extensive metabolism in the gut wall or liver
Absorption
3 routes
Passive diffusion:
Most important
Net transfer depends on concentration gradient and lipid:water partition co-efficient
Lipid soluble drugs absorbed more quickly
Non-ionised drugs absorbed quicker (more lipid soluble)
Absorbed along whole GI tract: basis for slow release preparations

524 4
th
and 5
th
Year Notes
Active transport: highly specific – usually for transporting naturally occurring substances (e.g.
amino acids)
Filtration through pores: absorbed via paracellular route in small intestine. E.g. frusemide,
atenolol, digoxin
Factors affecting oral absorption:
Formulation: affects solubility and bioavailability. Presence of other drugs (e.g. Fe, Ca)
Gastric emptying: emptying absorption rate
Food: may slow gastric emptying, alter ionisation, decrease first pass metabolism. Affects
different drugs differently
Alternative sites of absorption:
Plasma concentration rises quickest for iv > im > sc (absorption similar to im but blood supply)
Intramuscular injection: affected by lipid solubility and blood flow
Rectal absorption: avoids GI irritation, good in vomiting, doesn‟t avoid 1
st
pass metabolism
Pulmonary absorption: small particle size
Absorption from mouth: nitrates/buprenorphine
Absorption from nose: desmopressin & other peptides
Percutaneous: zero order absorption – for nicotine, nitrates, scopolamine
Distribution
Drug can be bound or unbound in both plasma and tissues
Drugs bind to albumin (acidic drugs), 1 acid glycoprotein (basic drugs), tissue proteins
Lipid solubility:
Penetrate lipid membranes easily (e.g. placenta, blood/brain barrier)
Rapidly distributed, dissolves in fat plasma levels fall quickly, and large volume of distribution
Is non-polar or unionised
Water soluble:
Excreted by kidneys (some also metabolised by liver)
Redistributes in water, smaller volume of distribution
Ionisation of acid or base:
Depends on pH and pKa (the pH at which 50% of drug is ionised)
As pH (becomes more alkaline) an acid becomes more ionised, and a base less ionised
Only unionised drug will diffuse across lipid membrane
Metabolism
Water soluble: excreted unchanged through the kidney
Lipid soluble: Can‟t be excreted by kidneys (reabsorbed straight away) so conjugated or metabolised
water soluble excretion
Metabolism:
May result in activation of a pro-drug, active metabolites or inactive metabolites
Phase 1: oxidation, reduction, hydrolysis
Phase 2: conjugation, eg methylation, acetylation, glutamine, etc
Occurs in mainly in the liver, also in the lung, kidney, blood, small intestine, gut bacteria
1
st
pass metabolism: high > 70%, e.g. lignocaine, GTN (no use taking them orally)
Examples of drug metabolic reactions:
Reaction
Substrates
Cytochrome P450 (oxidation)
Many drugs, carcinogens
Oxidation of alcohols/aldehydes
Ethanol
Oxidation of purines
Azathioprine
Oxidation by MAO
Tyramine, catecholamines
Hydrolysis
Suxamethonium
Acetylation
Dapsone
Glucuronidation
Phenols, morphine
Factors affecting metabolism: genetics, ethnicity, age, gender, pregnancy, liver disease, time of day,
environment, diet, malnutrition, alcohol, other drugs
Excretion of Drugs
Excretion:
Major routes renal, hepatobilary, pulmonary
Minor routes: saliva, breast milk, tears

Pharmacology 525
Renal:
Few are excreted unchanged. Lipid soluble undergo tubular reabsorption
Only unbound particles excreted if highly bound then slower excretion
Some are secreted by active tubular secretion e.g. penicillin, digoxin
Urine pH: alkaline urine weak acid excretion (eg salicylates) and visa versa
Bilary:
Polar drugs likely to be excreted in bile, e.g. rifampicin, ampicillin
Some drugs undergo entero-hepatic circulation, e.g. oestrogens
Inter-individual Differences
There are large inter-individual differences in the capacity to metabolise drugs, due to:
Genetic factors
Characteristics can be autosomal dominant, autosomal recessive, sex-linked, etc
Either polygenic or monogenic (present either as polymorphisms – more than 1% - or as rare
phenotypes - <1 %)
Cytochrome P450: a group of enzymes located on the endoplasmic reticulum. Divided into families
and sub-families
3 polymorphisms have been well defined:
Acetylation: enzyme: n-acetyl-transferase 2. Leads to slow and fast acetylators. 90% of Japanese
are fast acetylators (autosomal dominant) compared with 55 – 60% of Europeans who are slow
acetylators. Affects eg isoniazid and caffeine
Oxidation: poor metabolisers are deficient in enzyme CYP2D6, affects 4 hydroxylation pathway.
Covers lots of drugs – TCAs, antipsychotics (e.g. haloperidol), blockers (e.g. metoprolol). Risk
of accumulation. Rest of population are extensive metabolisers
Oxidation (CYP2C19): affects diazepam, omeprazole, others
Disease
Absorption in disease:
Can affect gastric emptying rate: affects rate not extent
Absorption rate in migraine, acute MI, labour, malabsorption syndromes (variable effect)
Low cardiac output IM absorption
Distribution:
For drugs with low Vd and high binding (only), changes in protein binding: e.g. albumin in
hepatic disease, nephrotic syndrome, 1AGP in RA, Crohn‟s. Amount of free drug is the same.
But normally total plasma concentration measured (and this will be reduced) danger of
overdose
Cardiac disease altered distribution (eg due to reduced gut flow poor absorption, renal and
hepatic perfusion clearance)
Obesity increased Vd for lipophilic drugs
Metabolism:
Most biotransformation occurs in liver. For some drugs, extraction depends on blood flow (where
extraction ratio tends to 1)
Liver disease capacity of metabolising enzymes (eg warfarin, phenytoin) and possibly
shunting of blood around liver (affects drugs with high first pass metabolism)
Thyroid diseases or metabolism
Diabetes mellitus fatty liver change in metabolism
Low clearance with high (>90%) degree of protein binding – generally clearance
Low clearance, low binding (e.g. paracetamol) – variable but can be clearance
Excretion:
For many drugs, reduction in clearance half-life
Adjust dose using creatinine clearance formula: Cockcroft Gault Formula (a prediction which
saves doing a 24 hr urine):
Cr.Cl ml/sec = (140 – age) * wt(kg)
50,000 * serum Cr (mmol/L)
Normal is 1.5 mls/sec. For mls/min, replace 50,000 by 815
For females, multiply by 0.85

526 4
th
and 5
th
Year Notes
Important for eg digoxin and aminoglycosides which are excreted unchanged. If elderly
excretion plasma concentration
Dose rate for a drug excreted 100% by the kidney (e.g. antibiotics) is:
DR = (Cr.Cl / 1.5) * normal DR
This dose requires adjustment when not all the drug is excreted unchanged.
DR = (1 – fu) + fu * Cr.Cl / 1.5 * DR
Fu = fraction excreted unchanged
Liver disease: arbitrary rule:
Dose by 50% for high clearance drugs (high 1
st
pass metabolism)
Dose by 25% for low clearance drugs (enzyme capacity only)
Dosing in CV disease:
Vd (vasoconstriction)
Renal flow excretion
Mesenteric blood flow absorption of frusemide
Age
Epidemiology:
Elderly > 75 years
More likely to have multiple drugs (median per person over 65 is 3), 90% have one drug
2 * incidence of adverse reactions (20 – 25%). in proportion to number of drugs
30% of elderly admissions due to drug problems
Absorption: little difference compared with young, except if other drugs interfere (eg transit time)
Distribution:
Lean body weight. Vd of fat soluble drugs (eg diazepam), possible problems with accumulation
May be adipose compared with lean body tissue. Eg smaller loading dose of drugs with low Vd
(eg digoxin and cimetidine)
Protein binding: Albumin declines with age significant change only in tightly bound drugs (ie
small Vd, eg phenytoin) or zero order elimination (eg warfarin)
Metabolism: Hepatic clearance:
Liver has significant residual capacity so not much decline with age, especially given lean
body weight
But significant (50%) reduction in liver blood flow, so significant reduction in metabolism of
1
st
pass metabolism (eg propranolol) or capacity limited metabolism (phenytoin or
theophylline). Problem if narrow TI
Hepatic blood flow and hepatic mass
First pass clearance: eg major tranquillisers, TCAs, antiarrhythmics
Excretion:
Decline in renal function. GRF by 50% (although wider spread of function inter-individual
variability). Problems with digoxin, lithium and gentamycin
Renal clearance (see creatinine clearance above). However, variability in serum creatinine (eg
proportional to lean body mass) less reliable estimate of renal function
Delayed action of renal acting drugs (eg diuretics)
Tolerate renal side effects less well (eg NSAIDs)
Need to adjust dose of: digoxin, cimitidine, ACE inhibitors, NSAID, Diazepam, aminoglycosides.
Dose adjustment factor =
1)1(
1
FkF
F = fraction of drug normally excreted unchanged
Kf = relative renal function of a patient =
clearanceCr normal
]formulaGault &Cockcroft [use clearanceCr derivedor actual
Principles of geriatric prescribing:
Full drug history
Reasonable therapeutic objective (ie forget management of long term risk factors if they‟re 95)
Pharmacology 527
Individual dose titration – beware „usual‟ doses
Lowest possible dose
Simplest possible regime
Regular review of drug therapy
Children
Clearance: functional maturity reached from 6 months to 1 year
Vd: have more body water and less fat dose for H2O soluble and for lipid soluble
Guidelines:
If < 6 months: consult a paediatrician
6 months to 1 year: use a nomogram for surface area. Estimates Dose = [wt (kg) ^ 2/1.7 m ^2] *
adult dose
Other Factors
Sex: Women clear BZDs faster, NSAIDs slower
Pregnancy: more rapid clearance of oxidised drugs due to liver flow. See Pharmacology of
Pregnancy and Breast Feeding, page 528
Obesity: Use ideal body weight if actual > 30% above ideal for drugs with low Vd
Environment
Diet: eg smoking, grapefruit juice, malnutrition, alcohol
Controlled Release Formulations
Aim is to prolong short acting drugs, to reduce daily dose frequency
Also a drug company ploy: introduce slow release formulation to extent patent
Good points:
Increased compliance
Side effects (but probably also decreased therapeutic effects)
But:
Often more variability in plasma fluctuation. Eg Slower absorption + variations in 1
st
pass
metabolism wider variation in clinical effect
Effect of variation in gastric emptying reduced
Adhesive patches cause skin reaction in 30%
Fixed dose: harder to titrate
Cost
Pharmacodynamics
=Study of drug/receptor interactions. Dimensions of time, concentration and effect (ie response
intensity)
Types of „receptors‟ for drugs: enzymes, ion channels, receptors, carrier molecules. Most common
targets are transmembrane receptors linked to G proteins
Receptor interactions:
Agonists:
Bind and produce a full effect
Partial agonists: bind and produce sub-maximal effect (ie lower dose-response curve)
Inverse agonists: bind and have opposite effect to that of agonists
Non-competitive agonists cannot be displaced
Competitive agonists reversibly interact, can be reversed by an antagonist.
Antagonists: bind and produce no effect.
Competitive: maximal response is still possible with an in dose of endogenous agonist (ie
dose response curve shifts right). Eg adrenaline can over-ride -blockers
Non-competitive: don‟t allow a maximal response regardless (ie lower-dose response curve).
Progressively lowers maximal response of agonist
Agonist antagonist: has an agonist effect at one subtype of receptor and an antagonist effect at
another
Specificity = effect produced by interaction with a single receptor
Ka = concentration required to occupy 50% of receptor sites at equilibrium
Up-regulation/down-regulation: a very common response to an antagonist/agonist. Watch for
rebound when it stops
528 4
th
and 5
th
Year Notes
Dose response curves:
Relationship between plasma concentration and drug‟s effect
Efficacy: maximal ceiling of effect, regardless of dose. Effectiveness of drug once bound to a
receptor
Potency: quantity required for maximal effect
Affinity: if a drug has lower affinity, it can still produce a maximal effect but will require a larger
dose (ie pushes dose response curve to the right). Higher affinity higher potency.
Individuals vary considerably in the efficacy, slope (difference between small and maximal effect)
and potency of drugs. Eg with age have receptors. So dependent on age, disease, environment,
etc
Concentration vs. response:
EC50 = drug concentration at 50% of maximal effect (describes affinity of the drug for the
receptor)
Therapeutic index is the ratio of the Adverse Effect EC50 to the Therapeutic Effect EC 50
Rise in response intensity is normally less than proportional to drug concentration. It reaches a
point where further increases in concentration have no further effect (but may prolong effect – but
to double time may need 10 fold in concentration). Need to balance against adverse effects
Usually presented as Response vs log drug concentration – this linearises the central part of the
curve
Combining with another drug with a synergistic effect changes the dose response – often allows
dose (eg ACE + diuretic)
Dosing:
„Usual dose‟: set at maximum profit for minimum toxicity. Always half New Ethicals starting
dose!
Objective in chronic disease management: use the lowest possible daily dose of the appropriate
drug. Building up slowly, but this is usually impractical in general practice (requires lots of visits
until therapeutic effect satisfactory, so back titration used)
Loading dose dependent on volume of distribution
Infusion rate dependent on clearance
Constant infusion gradually rising Cp. Bolus instantly high Cp, then declining. Both
stable Cp
Factors in Failure to respond:
Poor compliance: difficult dosage regimes, poor technique (eg inhalers), difficult to swallow, etc.
Frequency critical. Increasing frequency more forgotten. But if T½ < 24 hours, will get better
overall control (avoiding peaks and troughs in Cp) with > once a day
Incorrect drug formulation
Altered drug handling due to disease state (eg impaired absorption of oral frusemide due to
mucosal oedema)
Drug tolerance or bacterial resistance
Disease state too severe (eg thiazide diuretic in heart failure)
Toxicity may prevent attainment of the therapeutic dose
Changes with Age
Blunted homeostatic reserve:
Risk of postural hypotension with antihypertensives, neuroleptics, TCAs
Drugs have greater effect on postural control (eg sedatives)
Changes in neurotransmitters risk of drug induced confusion
Receptor changes. Eg response to agonists and antagonists
Pharmacology of Pregnancy and Breast Feeding
Pregnancy
Risks are often unknown – although usually small
Rule of thumb: DON‟T use drugs in pregnancy
Most drug induced abnormalities are subtle don‟t make link with drug
Effects of harmful drugs:
Gametes sterility
Blastocyst death
Pharmacology 529
Embryo death or major abnormality (heart, limbs, brain, eye form during embryogenesis
Fetus Functional abnormality
Factors affecting dysmorphogenesis:
Critical dose
Timing of dose during development
Fetal susceptibility
Fetal environment (eg already at risk due to diabetes, smoking etc)
Placental drug transfer: all drugs get across but in widely varying amounts. Lipid drugs with polar
metabolites are bad news (drug crosses in, but metabolites can‟t get out, eg diazepam)
Testing safety:
Validity of drug models
RCTs assess efficacy not safety
Can only pick them up with post-market monitoring and careful evaluation in clinical practice
Effects of pregnancy on drug handling:
30 – 50% delay in gastric emptying
Minimal effect on absorption
Albumin reduced by 25% by 15 weeks
Plasma volume increases by 50%
Total body water by 8 litres
50% in renal blood flow
Fetal renal excretion:
Fetal kidney‟s are functionally immature (Ccr = 2 – 4 mls at term – very small)
Renal blood flow only 5% of cardiac output (25% in adult)
Renal elimination not an important route of drug metabolism (baby swallows it again anyway)
Hepatic metabolism:
Shunt 30 – 70% of umbilical blood flow (ductus venosus)
Oxygenation of the Left lobe (umbilical vein) > than right lobe (portal vein)
Slower metabolic rate than adult but extensive CYP450 metabolism
Breast Feeding
Transfer affected by:
PKa: Base transfers more as pH of milk is lower than blood
Lipid solubility
Molecular weight (eg high molecular weight heparin doesn‟t cross)
Avoid:
Excess alcohol
Anticoagulants except heparin
Anti-thyroid drugs
Antibiotics: chloramphenicol, tetracyclines (affect teeth and growth plates), sulphonamides and
quinolones
-blockers: atenolol, sotalol bradycardia. Other antihypertensives OK
Diazepam
Lithium
Combined OCPs
Anti-metabolic agents
Ergot derivatives (eg anti-migraine medication)
?Diuretics
?SSRIs
Phenytoin
NSAIDs – effect breast milk production
Adverse Drug Reactions (ADR)
WHO definition: any response to a drug which is undesirable and unintended, and which occurs at
doses used in man, for prophylaxis, diagnosis or therapy, excluding therapeutic failure
Responsibility of prescriber is to observe, record and report adverse drug effects and interactions
Includes:
Side effects
Intolerance (side effects occurring at levels normally well tolerated)

530 4
th
and 5
th
Year Notes
Anaphylaxis
Interactions with other drugs (e.g. pharmacokinetic reaction due to enzyme induction)
Classification: includes mistakes (knowledge based errors) and lapses (skill based error)
Grading them:
Serious: results in death, hospitalisation or persistent disability
Severity: intensity of reaction not seriousness of reaction (ie a severe skin reaction may not be
serious)
Incidence:
True incidence unknown
Estimated 3 – 5 % of all hospitalisations due to an ADR
Estimated 3 in 1000 hospital deaths due to a drug reaction
Common in elderly
Monitoring:
Medicine Assessment Advisory Committee reviews new drugs prior to licensing
Can be licensed for monitored use through the Intensified Medicines Monitoring Programme
(IMMP). Requires reporting of ALL new clinical events in a patient
Voluntary reporting to the Centre for Adverse Reactions Monitoring in Dunedin (reporting rate
estimated < 15%)
Danger/Warning Notification System with NHI number. Records potentially life-threatening
reactions
Difficulties in recognising ADRs:
May mimic a common symptom (eg headache)
May be so bizarre that a common drug escapes suspicion
May be a long delay (eg hepatoxic reactions)
The ADR may be confused with the disease (eg antibiotic fever in meningitis)
Recognising an ADR: suspicion, how often does this occur without the drug (ie reference rate of the
disorder), temporal sequence, what happens when drug is discontinued and/or rechallenged
Frequency of effect:
Clinical trials are poor indicators of ADRs. Not sufficient numbers to find rare effects, so post
market surveillance important
Eg:
GI bleed
Agranulocytosis
Reference Rate
1:100
1:100,000
Rate with NSAID
5:100
5:100,000
Rate Ratio
5
5
Attributable Fraction
80%
80%
Determinants of ADRs:
The drug itself: rate, route, formulation, dose
The patient:
Age: young (immature conjugating enzymes) and elderly (clearance)
Gender: more common in women. ?Effect of sex hormones, ?less gastric acid, compounding
effect of health seeking behaviour
Disease: diseases of heart, kidneys, liver all affect drug kinetics and dynamics. Eg, AIDs
risk of ADR with co-trimoxazole
Previous history: Previous reaction risk
Genetic and ethnic factors, eg altered rates of metabolism
Extrinsic factors:
Alcohol consumption, tobacco, pollutants
Multiple drug therapy: 1 – 5 drugs 3.3% risk, 6+ drugs 19.8% risks
Mechanisms of ADRs:
Type A – predictable.
Exaggerated primary therapeutic effects. Risk is increased with dose or clearance. Rarely
serious. Eg anticoagulants bleeding, hypotension with antihypertensives
Primary drug effects that are not therapeutic. Eg blockers bronchospasm
Type B - unpredictable. Dose independent, low incidence, serious. Eg anaphylaxis to penicillins,
carcinogenicity, dental discolouration from tetracyclines
Drug Allergy
= Specifically altered potential reactivity to a drug or breakdown product of a drug
Pharmacology 531
Recognition of an allergic drug reaction:
Always a delay in allergic reaction following initial exposure
Once established, a reaction can be precipitated by minute amounts of the drug
There is recurrence on re-exposure
The reaction doesn‟t resemble the pharmacological activity of the drug
Symptoms suggest an allergic response
Four main mechanisms for inducing an immunotoxic reaction:
Drug may be an immunogenic protein
Drug or metabolite may form a hapten by combining with endogenous proteins
Drug/metabolite may cause a reaction between a modified self-antigen and an antibody
Drug/metabolite may cause the synthesis of auto-antibodies, but its continued presence is not
required for binding between the antibody and the antigen
Four types of reaction (Coombs-Gell types): (See Allergy and Hypersensitivity Disorders, page 309)
Type 1 (immediate) hypersensitivity: Drug or drug conjugate binds a specific IgE on the surface
of basophils and mast cells degranulation mediator release bronchospasm, urticaria,
anaphylaxis
Type 2 (cytotoxic) hypersensitivity: IgG or IgM + drug-protein conjugate complement release
complement activation haemolysis or neutropenia or thrombocytopenia (depends on which
cell surface reaction takes place). Eg quinine
Type 3 (immune complex) hypersensitivity: (actually rare) protein complexes + Igs insoluble
matrices complement activation localised vascular damage with Serum Sickness/Antibiotic
Fever (fever, joint pain, lymphadenopathy, neutropenia, glomerulonephritis). Eg Presents 1 – 3
weeks after penicillin/cephalosporin/sulphonamide treatment.
Type 4: (delayed) hypersensitivity (cell mediated): drug-protein complex + target cell
recognised by T-lymphocyte direct cytotoxicity/macrophage activation. Eg contact dermatitis
due to chlorpromazine
Symptoms:
Localised: urticaria (weals, always itch), bronchospasm, angioedema
Generalised: hypotension, bronchospasm, urticaria, laryngeal oedema
Examples:
Haemolytic anaemia: eg levodopa, captopril (ACE inhibitor), penicillins
SLE: eg phenytoin, gold, procainamide (antiarrhythmic)
Glomerulonephritis: eg gold, drugs with sulphydril group
Aplastic anaemia: eg phenytoin
Factors influencing occurrence of allergic reactions
Duration and the number of courses or treatment
Any route (although anaphylaxis more common with iv)
IV anaphylaxis occurs with the same frequency in the general population and atopic individuals.
Anaphylaxis by other routes more common in atopic individuals
More common in adults than children (?less exposure to drug antigens)
Previous history of any allergic reactions and co-existing disease states
Drug Interactions
= Effects of one drug are increased or decreased by another
Lots of interactions: the key is their significance
Often caused by Polypharmacy:
= “Irrational concurrent use of several different drugs”
Common in:
Multiple medical problems
Long term care
“Standing orders”, sedatives, laxatives, antidiarrhoeals, cough medicine
Guide to potential drug interactions:
How commonly are interacting drugs used together?
Does one of the drugs have a low TI? Eg probenecid reduces penicillin clearance, but who cares.
Erythromycin reduces theophylline clearance – critical
Has a potential interaction been validated in in-vivo studies?
Are there case reports of adverse effects?
Is there a reasonable mechanism for the interaction?
532 4
th
and 5
th
Year Notes
Risk factors for drug interactions:
Low volume of distribution (Vd) plasma concentration (esp if protein bound)
Narrow TI (toxicity with small changes)
Capacity limited hepatic clearance (cf blood flow limited), eg phenytoin
Extensive Metabolisers (EM): those genetically predisposed to rapid metabolism. Add in an
enzyme inhibitor more dramatic change
High protein binding ( plasma concentration if protein binding disrupted)
Acidic drugs: readily displace basic drugs
Active renal tubular excretion (other drugs can compete for excretion pathways clearance)
IV administration (risk of mixing drugs that shouldn‟t be mixed)
Pharmacokinetic mechanisms:
Drug Inactivation: Eg Cholestyramine (ion binding resin) binds oral anticoagulants
Altered absorption: Metoclopramide (gastric emptying) + digoxin (takes long time to breakdown
in stomach) absorption. Metoclopramide + paracetamol faster absorption
Protein binding: Adverse reactions do not occur purely because of displacement from protein
binding sites: Eg phenytoin + hypoalbuminaemia binding clearance total
concentration free fraction but free concentration remains the same
Drug excretion: Probenecid + Penicillin – competition for limited capacity of active tubular
excretion. Diuretics Lithium clearance
Drug metabolism: Metabolic reactions are unpredictable and highly variable.
Multiple Cytochrome P450 enzyme phenotypes, each with it‟s own selectivity for inhibitors
(immediate effect) or inducers (takes weeks, requires transcription, etc). Eg sulphinpyrazone:
inhibits tolbutamide, warfarin, and phenytoin. Induces theophylline and verapamil
CYP450: Mixed function oxidase system. Genetic polymorphism results in:
Extensive metabolisers (EM). Inhibition reactions will convert these to PMs
Poor metabolisers (PM). Inhibition reactions won‟t affect these
Ultra-rapid metabolisers (eg CYP2D6). Marked differences in genetic polymorphism (eg
CYP2D6 – 7 % Caucasian, 1% Asian)
Inhibition of CYP450 risk of type A reaction to another drug metabolised by the same
enzyme
CYP3A4 is the most abundant P450 enzyme (metabolises over half of all drugs):
Induced by carbamazepine, rifampicin, dexamethasone
Inhibited by grapefruit juice, azole antifungals, erythromycin
Enzyme inducers: chronic ethanol, anticonvulsants, rifampicin, isoniazid (Tb antibiotic)
Enzyme inhibitors: acute ethanol, ANTIBIOTICS: macrolides (eg erythromycin),
metronidazole, sulphonamides, quinolones (eg ciprofloxacin), azole antifungals, cimitidine,
MAOIs, SSRIs, amiodarone, verapamil, omeprazole, grapefruit juice (inhibits CYP3A4)
Eg non-sedating anti-histamines (eg terfenadine / Teldane). Concentration dependent
inhibition of K influx prolongs action potential QT interval torsade du pois
sudden death (very rare). However, Cp due to CYP450 inhibitors (eg erythromycin,
cimitidine) risk of sudden death
Pharmacodynamic mechanisms:
= Additive or opposing effects at the same or different receptors
Majority of drug effects
Examples:
Combinations of agonists or antagonists at the same receptors: eg Anxiolytics (lorazepam) +
hypnotic (triazolam) BDZ adverse effects
Combinations of agonists and antagonists: eg phenothiazine + L-Dope = antagonism of anti-
parkinsonian effect
Combinations of agonists or antagonists at different receptors: eg ethanol + benzodiazepines
sedation
Pharmaceutic mechanisms: the interaction occurs prior to systemic availability
Common examples:
Ethanol/drug interactions:
CNS depressants: alcoholics need more to sedate but stay under longer
Anticonvulsants: unpredictable
Metronidazole gives a disulfiram reaction (Antabuse)
Warfarin: acute ethanol inhibits metabolism, chronic ethanol induces metabolism
Pharmacology 533
Antihypertensives have decreased effect
Oral contraceptives:
23% of OC failures associated with antibiotics
Mid cycle breakthrough bleeding may indicate important antibiotic effect (oestrogen level)
Should have alternative contraception for the antibiotic course and 7 days afterwards with no
pill free period. No action required for stat antibiotic doses or POPs
Other interactions: antacids, H2 antagonists, NSAIDs, cough and cold remedies
(pseudoephedrine)
Therapeutic Drug Monitoring (TDM)
Used to titrate the „usual dose‟ to an individual
Monitoring Cp (plasma concentration) assumes no receptor tolerance, accurate determination of the
biological effect and accurate determination of the plasma level
Indications for TDM:
Availability of an accurate, precise, specific and inexpensive test
Long term drug therapy where clinical definition of efficacy is difficult (ie won‟t know if it‟s
working by observing the patient)
Dose related adverse effects for which there are few clinical warning signs/symptoms
Substantial inter- and intra-individual variability in pharmacokinetics
Multiple drug interactions
Drugs with a narrow therapeutic index: phenytoin, digoxin, theophylline, lithium, gentamicin
Suspected non-compliance
Unexpected lack of response or signs of toxicity
But TDM should not replace clinical judgement
Therapeutic index: top and bottom are blurred margins/probabilities
Blood sampling for TDM:
Often done badly
When absorption and distribution phases are complete
Steady state plasma conc. (5 half lives after started)
Sample just prior to next dose when dosing 2 * T½. Sample 3 – 5 hours post dose for slow release
formulations
Examples:
Phenytoin: Has dose dependent kinetics. Dose changes should not exceed 20% of total daily dose.
Metabolised by CYP450 with many interactions. CNS toxicity correlates well with blood
concentrations (nystagmus, ataxia, atypical convulsions). Therapeutic concentrations controversial
(based on studies in severe epileptics). Reduce in hypoalbuminaemia (Same dose binding
available free conc.) Frequent error: sample in trough of plasma concentration – then appears
to be below TI
Lithium: narrow TI for maintenance – 0.4 – 0.8 mmol/L. Minor symptoms (eg tremour, nausea)
don‟t predict serious toxicity. Renal clearance by diuretics, theophylline, caffeine, dehydration,
low sodium diet. TDM mandatory when side effect, relapse, serious illness, dose adjustment. 3
monthly monitoring for Li levels, electrolytes, thyroid fn
Theophylline (bronchodilator): Dose related toxicity: seizures, arrhythmias. Elimination reduced
with erythromycin, ciprofloxacin, cimetidine, smoking cessation, hypothyroidism (all P450)
Digoxin: variable bioavailability (eg with cholesterol binding agents, antacids) and large
variability of clearance (with NSAIDs, spironolactone, verapamil, amiodarone). Effect in
hypokalaemia, hypothyroidism, elderly. Effect in hyperthyroidism and `pregnancy. Sample 8 –
12 hours post dose (long distribution phase).
Aminoglycosides: Dose predictions performed by pharmacy
Poisoning and Drug Overdose
See Poisoning and Overdose, page 488
Drug withdrawal syndromes
Alcohol: tremor, sweats, tachycardia, BP, seizures, visual hallucinations, delirium
Opioids: anxiety, lacrimation, fever, runny nose, muscle aches, nausea, vomiting, diarrhoea, dilated
pupils, tachycardia. Give naloxone for overdose (give test dose first, in case its not opiates).
Pentazocine and Buprenorphine also used
534 4
th
and 5
th
Year Notes
BZD Withdrawal:
Anxiety, insomnia, depersonalisation, perceptual disorders, tremor, maybe seizures and confusion
Usually short acting (long acting less likely to give withdrawal affects)
Eg Triazolam: rebound wakefulness (can last 4 – 7 days). Also behavioural disinhibition, amnesia,
confusion, etc
If severe then weight loss, autonomic dysfunction, BP, temp, tachycardia, psychosis, seizures.
Have to restart drug and withdraw slowly
Propranolol withdrawal:
All blockers can do it: but more common with short acting (eg propranolol and metoprolol).
Less common with long acting (atenolol) or slow release
On withdrawal, sympathetic activity overshoots due to receptor up-regulation while on drug
Palpitations, sweating, apprehension, arrhythmias, etc. Peak is 3 – 5 days following withdrawal,
especially with physical activity
Clonidine withdrawal:
Antihypertensive. Pre-synaptic 2 agonists inhibits nor-adrenaline release
Withdrawal in 10% sudden rise in BP 24 – 72 hours later, plus other sympathetic effects
Similar effect in methyldopa (antihypertensive used in pregnancy)
Diuretics: eg frusemide, thiazides. Na retention over 4 – 5 days. Returns to normal
TCAs, phenothiazines, butyrophenones: headache, nausea, vomiting, confusion in elderly. Sleep
disturbance
Sleep
Changes in elderly sleep patterns:
Sleep latency unchanged (= ability to get off to sleep)
Stage 1 and 2 sleep (light sleep) – effects early morning
Deep sleep and REM sleep
Wakefulness
For elderly, less sleep is a normal physiological process – they‟re sleeping the amount they need.
Problem is often anxiety about and during wakefulness
Treatment of Insomnia
A distressing complaint – not an illness
Normal aging increases wakefulness during last 4 hours of sleep (reassure patient insomnia is „normal‟)
Non-drug management:
First check for: anxiety, depression, comfort, incontinence (eg diuretics), dementia, and treat these
Obtain careful sleep history, note factors improving/worsening sleep
Good explanation
Good Sleep Habits (Sleep Hygiene):
Reduce light, noise and extremes of temperature
Ensure physical security
Avoid caffeine, nicotine and alcohol before bedtime
No heavy meal for 2 hours beforehand, but have a light snack if hungry
Regular exercise last in the afternoon/early evening, but nothing vigorous for 3 hours
beforehand
Allow one hour of quiet activity before bedtime (reading, TV, music)
Develop a bedtime ritual, cleaning teeth, reading, etc
Don‟t go too early (ie before you feel sleepy)
Don‟t stay in bed if you are awake. If not asleep within 15 – 20 minutes (estimate – don‟t use
a clock), get up, go elsewhere and do something mundane until you feel sleepy again
Get up at the same time in the morning: don‟t sleep in in weekends or after late nights. This
helps train your body clock
Don‟t nap during the day
Don‟t worry if you can‟t get to sleep at night: worry will delay sleep even more
Drug management:
30% over 65 take sleeping pills
Not for persistent insomnia (common in personality disorders, depression, sleep apnoea, pain,
gastro-oesophageal reflux – treat primary cause).
Pharmacology 535
Hypnotics should only be prescribed for symptomatic temporary insomnia (no more than 2 – 3
weeks) and should only be part of an overall management strategy
If used, for defined period, perhaps intermittently, and should sustain sleep
Not:
Short acting (eg midazolam) get them off to sleep – but don‟t sustain sleep. Don‟t have any
impact on early morning wakefulness. So will wake, and take another – then hangover in the
morning, falls, etc
Long acting (triazolam/Halcyon) - which leads to daytime anxiety
Use intermediate-acting hypnotics (eg zoplicone and temazepam)
Risk of addiction
Shift workers should avoid them
Compliance Issues
Compliance = extent to which person‟s behaviour coincides with medical advice
Few people take their medication as prescribed
Non-compliance is multi-factorial:
Rapport with doctor
Not knowing how to take medication
Not understanding the importance of the drugs
Taking many drugs
Anticipation or experience of side-effects
Forgetfulness
Impaired physical function or other disability
Community and family support
Strategies for improving compliance:
Education about disease and treatments (spoken instructions are quickly forgotten)
Simplifying drug regimes (fewer drugs and fewer doses)
Involving carers
Education about common side effects which may subside
Use of drug diaries, calendars, medication charts
Use of ordinary bottle tops (not childproof) for elderly people
Large print labels
Dosage forms (eg small pill size, pleasant taste)
Compliance aids such as pill trays and blister packs
Return or destruction of old drugs
Prescribing
Definition of a medicine:
Medicines Act 1981 and Medicines Regulations 1984
“Administered to one or more human beings for a therapeutic purpose”:
Treating or preventing disease
Altering the shape, size, structure or weight of the human body
Cleaning, soaking or lubricating contact lenses
Registered medicines:
Registered medicines are gazetted and approved by the Ministry of Health
Unregistered medicines can be used under section 29 – requires special consent process
Unregistered indication
Classification of medicines:
Prescription medicines
Pharmacist only medicines (formerly restricted medicines)
Pharmacy medicines (formerly pharmacy only medicines)
General sales medicines
Controlled drug
Legal requirements for all prescription types:
Legibly and indelibly printed
Signed personally by the prescriber and dated
Contain the address of the prescriber
536 4
th
and 5
th
Year Notes
Contain the surname, initials and address of the patient
If under 13, the child‟s date of birth
Indicate the name and where appropriate the strength of the medicine
Indicate the total quantity to be dispensed on each occasion
Indicate the dose and frequency for medicines intended for internal use
There are special script pads and requirements for controlled drugs (see the Preferred Medicines List)
Regulation of Medicines and Drugs
Medicines Act 1981: prescription medicines can only be supplied or possessed on the prescription of a
doctor and dispensed in a pharmacy. Maximum amount = 3 months supply (6 months for oral
contraceptive)
Regulation of Drugs of Abuse
See also Drugs of Abuse, page 448
Misuse of Substances Act 1975 defines and regulates controlled drugs - prohibits non-therapeutic use.
Mainly Opiates, Ritalin, dexamphetamine and BZDs
Prescriptions for opiates and stimulant-controlled drugs must be on a special triplicate form in the
Doctors own writing. BZDs don‟t require triplicate form
Prescribed for maximum of one month, dispensed in 10 day lots
It is illegal to supply a controlled drug for the treatment of maintenance of dependency (except for
Gazetted drug clinics)
Need good notes to avoid legal recourse (e.g. no automatic repeats)
Many injected drugs have been prescribed „legally‟ by doctors and diverted to illicit use (eg sold to
dealers)
Monitoring of prescription narcotics and abuse prone medicines is carried out by Medicines Control
Advisors, reporting to the Medical Officer of Health
They can issue a Restriction Notice – which prevents the supply of controlled or specified drugs to a
named person – it is then an offence for this person to try and obtain this drugs, and a doctor to
prescribe it for them
Classes of drugs
Responsibilities of the prescriber:
To avoid creating dependence
To see that the patient doesn‟t increase the dose, inducing dependence
To avoid unwittingly supplying the black market
Misuse of Substances Act:
Grades drugs according to harmfulness when misused. Specifies recording, reporting and form
filling requirements. Enforced by Customs, Police (where criminal acts) and by Medical Officer of
Health in the Ministry of Health
Class A: Possession, prescribing, sale are prohibited – street drugs. Use is an offence (e.g. heroin).
Large penalties
Class B: Can only be used for pain. Can only be prescribed for dependency by a gazetted person.
Includes morphine, methadone
Class C: Controlled drugs which are less hazardous (eg codeine, BDZs, etc)
Clinical Trials
Preclinical trials: testing toxicity and potential therapeutic benefit
Phase 1: Human pharmacology
Phase 2: On patients – focus is safety: dose level and frequency, unwanted effects, treatment duration
Phase 3: On more patients – designed to test efficacy not safety
Medicines licensed for use
Phase 4: Adverse reaction monitoring – rare effects only show up with widespread general use big
responsibility on prescribers to report ADR
MedSafe
= NZ Medicines and Medical Devices Safety Authority. Part of the Ministry of Health.
www.medsafe.govt.nz - has data sheets for all drugs
Medicine = any substance … supplied wholly or principally to treat a human for a therapeutic purpose
… treating or preventing a disease
Pharmacology 537
Medsafe regulates:
From production to distribution
Access to medicines (eg prescription, restricted, pharmacy only, general sales
Need to regulate to protect public health and to avoid counterfeit or inferior quality medicines
538 4
th
and 5
th
Year Notes

Anaesthetics 539
Anaesthetics
References: Anaesthesia, Resuscitation and Emergency Management, Wellington School of Medicine,
2000
See also Paediatric Anaesthetics, page 655
General Anaesthesia ....................................... 540
Anaesthetic Agents ......................................... 540
Pain Management ........................................... 543
Local Anaesthesia .......................................... 544
Obstetric Anaesthesia ..................................... 545
Preoperative Assessment ................................ 546
540 4
th
and 5
th
Year Notes
General Anaesthesia
Anaesthesia = absence of all sensation
The reversible induction of:
Hypnosis
Autonomic reflex suppression
Muscle relaxation
One drug doing all (e.g. inhalational anaesthetic such as isoflurane) would require sufficiently high
doses to cause major side effects (e.g. respiratory depression, prolonged recovery)
Balanced anaesthesia: one drug for each component minimal homeostatic depression and quick
recovery:
Hypnotic: e.g. thiopentone or halothane
Opiod: abolish autonomic response to painful stimuli
Muscle Relaxant
Stages:
1 – confusion
2 – exaggerated reflexes, severe confusion
3 – Light, surgical and deep anaesthesia
4 – medullary paralysis
With increasing depth there is:
Loss of reflexes causing cough and swallowing aspiration
Muscle tone airway obstruction
Progressive depression of ventilation
At deep level, medullary paralysis with apnoea and cardiovascular collapse
Major problem is awareness if anaesthetic too light: anaesthetist won‟t know due to paralysis.
Principal signs are stress responses: tachycardia, hypertension, mydriasis (large pupils), sweating,
pallor. Additional hypnotic will remove consciousness of pain, additional opiod will suppress CNS
reception of pain
Monitoring:
ECG: heart rate, rhythm and ischaemia
Blood pressure: depressed by excessive depth, extensive local (e.g. spinal blocks), or blood loss,
elevated by awareness, inadequate pain blockade or hypercarbia
End tidal CO2: if then inadequate ventilation, if then excessive ventilation
Pulse oximeter: O2 saturation
Temperature: anaesthetic agents vasodilation loss of temperature, also cold iv fluids
Muscle relaxation: neuromuscular block monitor
Rapid Sequence Induction/Intubation: Intubation of someone not properly prepared for surgery (eg not
fasted so risk of gastric aspiration/regurgitation). Drugs to paralyse (e.g. Suxamethonium – fast acting)
and sedate (e.g. propofol). Press down on cricoid cartilage until intubated to stop aspiration (closes of
oesophagus) – but not if actively vomiting (otherwise gastric or oesophageal rupture)
Anaesthetic Agents
Dose Calculations of Anaesthetic Drugs
Concentrations. Four most common methods of specifying concentration are:
Mg/ml: weight of drug per volume of dilutent
% - number of grams of drug per 100ml. E.g. 50% = 50 grams per 100 ml or 500 mg/ml. 1% = 10
mg/ml. Multiplying by 10 gives mg/ml. Often used for lignocaine (Xylocaine)
1:1000 is the same as 0.1% (1 mg/ml). Used for adrenaline and isoprenaline
mmol/l: used for electrolytes
Infusions:
Use for drugs with very short T½ where fluctuations in dose of drug are dangerous
Common for adrenaline, dopamine, dobutamine & lignocaine
E.g. post arrest infusion of lignocaine at 2 mg/min with 2% xylocaine. This is 20 mg/ml, so want
0.1 ml per minute. Using a burette system can deliver 6 drops a minute (60 drops = 1 ml) or dilute
10 fold and run at 60 drops per minute (easier)
Anaesthetics 541
Inhalational Anaesthetics
Gases = compounds in the gaseous state at a temperature above their critical temperature.
Vapours = compounds in gaseous phase but can be returned to liquid by in pressure. Ambient
temperature must be below the critical temperature for the compound
The partial pressure in the brain necessary to achieve anaesthesia will depend on its potency
Poorly soluble gases will have higher partial pressure at a given concentration and will have a fast
onset.
Lipid soluble drugs are more potent
So more soluble drugs have slower uptake in blood and require lower partial pressure to achieve their
effect
Factors affecting uptake:
Inspired partial pressure
Alveolar ventilation
Circulation
Properties of the anaesthetic agent (e.g. blood solubility)
Nitrous Oxide (N2O):
Pleasant, non-irritating, non-flammable (but supports combustion)
Stored in blue cylinders
Poorly soluble in tissues rapid uptake and elimination
Good analgesic but low potency
Always given with at least 30% O2 to avoid hypoxia
Expands in enclosed air spaces: so avoided for middle ear operations and where air embolism may
occur
Give 100% O2 at end of N2O anaesthesia to avoid diffusion hypoxia – N2O rapidly leaves
pulmonary capillaries alveolar O2 concentration
Halothane:
High potency (Minimum Alveolar Concentration, MAC = 0.7% - level that produces immobility in
50% of people, NO2 is 105% not so good)
No irritation and moderately rapid induction and recovery
Poor relaxant and analgesic properties
Requires accurate vaporisers
High concentrations produce profound respiratory and cardiac depression
Rare complication is hepatic necrosis
Isoflurane:
Similar to halothane, but more irritant so difficult to use for induction
More potent vasodilator hypotension and tachycardia
Also sevoflurane: not so irritant, quicker onset, but more expensive. Use in kids if can‟t cannulate
Intravenous Anaesthetics
Can be given as bolus for induction or infusion for maintenance
All have similar characteristics:
All are lipid soluble
Unionised fraction crosses the blood brain barrier
Loss of consciousness usually occurs in one arm to brain circulation time (approx. 30 secs)
Rapidly redistributed to tissues with high blood flow so rapid fall in peak plasma concentration
Thiopentone:
Barbiturate derivative containing sulphur ( yellow)
Highly alkaline in solution thrombophlebitis
Blood level results from distribution (seconds), redistribution (e.g. from muscle to fat –
minutes/hours) and metabolism (15%/hour by liver)
CNS depression - cerebral O2 consumption, potent anticonvulsant
Respiratory depression: especially initially – may be apnoeic for short period
Circulatory effects - cardiac outputs, vasomotor depression peripheral vasodilation BP
Poor analgesia and prolonged hangover
Dose: 4 mg/kg – less for elderly, more for robust male
Complications: acute intermittent porphyria and IgE mediated hypersensitivity
Propofol:
White, oil in water emulsions, 20 ml ampoules, 1% solution = 10 mg/ml
542 4
th
and 5
th
Year Notes
Structurally different to barbiturates
Highly lipid soluble: so rapid onset – and short duration due to rapid distribution, metabolism (T ½
= 35 – 50 minutes) and delayed return from poorly perfused tissues (e.g. fat)
Smooth induction, rapid recovery
Poor analgesic
Apnoea for about 30 seconds common
More BP but less nausea/vomiting than thiopentone
Induction dose: 2 mg/kg in young and 1.5 mg in elderly
Midazolam:
H2O soluble benzodiazepine
Muscle relaxant, amnesic, anxiolytic, anticonvulsant
Rapid onset and rapid elimination (T½ = 2 hours) cf. other benzodiazepines
Unlike other iv anaesthetics can be reversed, with flumazenil
Used for minor procedures, ICU sedation
Slower, more variable induction cf. thiopentone. Small dose may deep anaesthesia
Dose for sedation: 1 – 5 mg titrated
Dose of induction: 10 – 15 mg (highly variable)
Ketamine:
Related to angel dust
Dissociative anaesthesia
BP and respiration well supported, bronchodilator
Dose for induction: IV 1 – 2 mg/kg, IM 5 – 12 mg/kg
Smaller doses potent analgesia
A sympathetic stimulant, can have bad dreams
Neuromuscular Blockade
Muscle relaxants are used to:
Facilitate intubation and artificial ventilation
To facilitate abdominal access during abdominal surgery
To allow lighter levels of anaesthetic to be used rapid recovery and less cardiovascular
depression
Block neuromuscular transmission from motor nerve to voluntary muscle (ACh transmission across
synaptic cleft, broken down by cholinesterase)
Non-depolarising blocking agents:
Competitive antagonists of the nicotinic cholinergic motor end plate receptors. E.g. rocuronium,
pancuronium, atracurium, vecuronium
Degree of block determined by train of four stimuli. Each successive twitch is a lower amplitude –
trails off. No interference with twitch response until 75 – 80% receptors blocked. 90 – 95% block
required for surgery
Reversed by anticholinesterase drugs: neostigmine (onset in 2 minutes, lasts 20 minutes),
pyridostigmine, edrophonium. Inhibit acetylcholinesterase ACh, but also effects muscarinic
sites in parasympathetic nervous system. Side effects include salivation, bronchospasm, gut
motility and bradycardia. These effects blocked by atropine – which blocks the parasympathetic
system
Analgesia ended with anticholinesterase (commonly neostigmine 2.5 mg) and atropine 1.2 mg
Depolarising Neuromuscular Blocking Agents:
Faster onset and shorter duration (4 – 6 mins) than non-depolarising. Used for short procedures
(quick intubation), supplemented with non-depolarising for long procedures or given by constant
infusion
Suxamethonium: reacts with ACh receptors to produce depolarisation ( fasciculation), but
because it is not so rapidly eliminated as ACh, depolarisation persists inexcitability of
membrane around endplate. Repolarisation happens when suxamethonium is hydrolysed by
pseudocholinesterase (unless atypical genetic variant prolonged effect). If overdose or poor
elimination drug-receptor complex forms, unavailable for ACh dual or phase II block. No
antagonist to suxamethonium except fresh frozen plasma (contains pseudocholinesterase)
Train of four different to competitive antagonists: each twitch the same height (although reduced
over normal)
Has other muscarinic side effects due to similarity to ACh: BP, intra-ocular pressure,
bronchial secretions, heart rate, post operative muscle pain
Anaesthetics 543
Suxamethonium is contraindicated in major burns, neurological injuries, hyperkalaemia,
myasthenia and myotonic diseases, pseudocholinesterase and history of malignant hyperthermia
Pain Management
See also Symptom Management in Cancer, page 470
Pain Physiology
Pain is vital to survival, but also an important source of human suffering
Subjective response to:
Damage to body tissues stimulation of somatic and visceral nociceptors (nociceptive pain)
Altered function of brain or nerve pathways: neuropathic pain
No detectable damage psychological, social or environmental factors – idiopathic pain
(diagnosis must include a psychological assessment)
Three types of pain:
Acute pain: injury, surgery, acute illness
Cancer pain
Chronic non-cancer pain
Nociceptive pain:
Nociceptors are free nerve endings stimulated by chemicals (e.g. H+), pressure or hot/cold
Sensitivity to noxious stimuli by prostaglandins (long chain fatty acids derived from arachidonic
acid), e.g. PGE2 and PGF2
Conducted by
Fast, myelinated A fibres sharp pain
Slow, poorly myelinated C fibres dull persistent pain
Terminate in thalamus. Fast fibres then to sensory area of cortex pain localisation. Slow fibres
synapse with reticular formation general arousal and limbic system (autonomic responses
and emotion)
Facilitation:
Processes that pain sensation
Primary hyperalgesia: sensation heightened in discrete area due to histamine and serotonin
sensitising adjacent nociceptors
Windup: hyperalgesia beyond areas actually damaged – due to recruitment of other receptors,
mediated by NMDA
Cortical factors: facilitate pain in anxiety, stress, absence of other sensory input (e.g. at night)
Long term changes in pain pathways pain disorders persisting after tissue damage has resolved
Inhibition:
Descending fibres activate encephalinergic neurones within dorsal horn
Release encephalins which inhibit passage of pain impulses, derived from endorphins (in turn
derived from -lipoprotein). Can be antagonised by naloxone
Gate theory: large fibres send inhibitory collaterals to presynaptic C fibres
Referred Pain: visceral pain felt in somatic structures.
Adverse effects of pain:
Psychological effects - adaptive behaviour may become dysfunctional stress, dependency,
isolation, sleep deprivation, psychiatric illness
Neurohumoral reflexes - sympathetic activity, CVS system stimulated, metabolism becomes
catabolic (which can inhibit healing), changes in immune system
Cardiorespiratory effects: e.g. decreased ventilation, secretion clearance hypoxia (especially
given cardiac O2 requirements), infection
Musculoskeletal spasm
Gastro and urinary function - secretions, sphincter tone, motility stasis, urinary retention
Pain Pharmacology
Opiod analgesics:
Main drugs used in severe pain
Act on Mu, kappa and delta receptors in substantia gelatinosa and solitary nuclei in spinal cord,
thalamus, periaqueductal grey matter and amygdaloid
Different opioids have different affinities for different receptor subtypes different effects. E.g.
Morphine agonises all receptors giving strong analgesia, respiratory depression (both mediated
544 4
th
and 5
th
Year Notes
through M receptor) and dependence. Pentazocine is a weak M-receptor antagonist and strong k-
receptor agonist and produces weaker analgesia, low dependence and little respiratory depression
Uses of opioids:
Relief of pain
To supplement regional and general anaesthesia
As primary anaesthetic agents
Premedication to allay anxiety and sedate
Specific indications e.g. pulmonary oedema
Alfentanil, fentanyl and remifentanil are opioids used intra-operatively because they are rapid and
short acting
Side effects: respiratory depression (if dose greater than that necessary for analgesia), addiction
(not a problem in severe or post-operative pain), sedation, nausea and vomiting, constipation,
cough suppression, histamine release
Post-Operative pain relief:
Why:
Humanitarian reasons
Prevent stress and cardiac and endocrine responses
Improve ventilation (especially after abdominal surgery)
Hasten mobility complications (e.g. DVT)
Reasons for poor pain relief: lack of understanding/recognition, poor knowledge of drugs and
doses, fear of overdose or addiction, logistic difficulties (e.g. access to controlled drugs),
willingness to complain about pain, lack of time, problems with side effects, variation in plasma
levels necessary to produce analgesia, wide variations in pharmacokinetics
Factors affecting response:
Lean body mass
Age: neonates sensitive, elderly have slower distribution and metabolism
Liver disease slower metabolism, renal disease slower elimination
Problems in shock: smaller blood volume, but poorer diffusion. Give little and often and
titrate to effect
PaCO2 plasma concentration
Drug interactions (e.g. phenytoin pethidine clearance)
Personality type
Alternatives to IM opiates:
Continuous iv infusion: morphine 10 – 20 mg loading dose over 45 – 60 minutes followed by
2 – 3 mg/hour
PCA
Extradural or regional block
NSAIDs as adjuncts
TENS: transcutaneous electrical nerve stimulation, acupuncture and hypnosis
Chronic Non-cancer Pain relief:
Opioids: orally (morphine tablets, methadone, codeine), epidural, subcutaneous
NSAIDs
Chemical or surgical ablation of nerves: e.g. chemical coeliac plexus block for pancreas pain
Psychological/emotional support
Neuropathic pain (e.g. nerve compression, post herpetic neuralgia, etc):
Burning, stabbing, shooting pain
Treatment:
Amitriptyline: 10- 50 mg nocte, increases descending inhibitory pathways, effect in 48 hours
Anticonvulsants (Carbamazepine, Gabapentin)
Sympathetic blockade
Steroids to reduce inflammation of nerves or adjacent tumour
Plus TENS, psychotherapy, rehabilitation, opioids
Bone Pain:
NSAIDs
If bony metastases: bisphosphonates
Local Anaesthesia
Reversible inhibition of conduction in peripheral nerve fibres and nerve endings
Anaesthetics 545
If local and general GA used, then local can take the place of an opiod in balanced anaesthetic
Methods of local anaesthetic:
Surface or topical anaesthesia
Infiltration anaesthesia
Conduction anaesthesia or regional nerve block
Intravenous regional anaesthesia (into limb with a tourniquet)
Central neural blockade (e.g. spinal or epidural)
Local Anaesthetic Agents
Reversible inhibition of conduction in nerve fibres and endings
Classification:
Esters of benzoic acid: cocaine, tetracaine
Esters of para-aminobenzoic acid: chloroprocaine, procaine
Amides: e.g. lignocaine and bupivacaine (Marcain)
Bind to internal opening of Na channel, preventing threshold and progression of action potential
Pharmacokinetics depends on:
Mass movement of drug around and away from nerve
Diffusion into axon: best if unionised (i.e. weak base)
Absorption is determined by route of administration, site of administration (e.g. vascularity), and
presence of vasoconstrictors (some anaesthetics themselves have vaso-constricting/dilating
properties)
Metabolism: esters hydrolysed by plasma cholinesterase, amides by liver
Adverse effects:
CNS: first cause excitation due to suppression of inhibitory neurons
CVS: negative inotropy, depression of conduction, reduction in automaticity ( sinus bradycardia)
Vasoconstriction – decrease rate of absorption, bleeding. Never use adrenaline in digital
extremities ischaemia
Allergy: extremely rare
Fainting
Treatment of overdose of local anaesthetic:
O2
Diazepam/thiopentone for convulsions
Other resuscitation: airway, ventilation, elevate legs, IV fluids, atropine for bradycardia
Clinical uses:
Topical anaesthesia: slow. Good for cannulating kids but takes an hour
Infiltration: e.g. around suturing. Don‟t inject through wound edge of unsterile wound
Nerve block: large area of analgesia, fewer injections, smaller doses
Extradural: between dura mater and periosteum of vertebral canal. Also blocks autonomic efferent
nerves vasodilation hypotension. If it goes into subarachnoid space total spinal:
respiratory paralysis, hypotension – treat with IPPV O2, IV fluids and vasopressors
Spinal/subarachnoid anaesthesia: direct into CSF. More potent, more pronounced motor block
Intravenous regional anaesthesia: tourniquet inflated to 100mmHg above systolic blood pressure
Obstetric Anaesthesia
Physiology of Pregnancy
Respiratory:
Raised diaphragm functional residual volume
O2 demand: due to maternal metabolism and foetal demands
Respiration respiratory alkalosis (PCO2 approx. 32) with metabolic compensation
Becomes apnoeic more quickly
Cardiovascular:
Blood volume, Hb by not so much physiological anaemia
Blood pressure: if normal pregnancy then small in systolic, in diastolic due to vasodilation
Minimum Alveolar Concentration (MAC) lowers in pregnancy
Volume of CSF reduces dose of spinal by 2/3
GI: lower oesophageal sphincter less effective regurgitation
546 4
th
and 5
th
Year Notes
General Anaesthetic in Pregnancy
More difficult getting endotracheal tube in: throat is smaller, usually done at night in emergency, etc
Mendelssohn‟s syndrome: acid aspiration in surgery when pregnancy bigger A-a gradient compared
with non-pregnant. Give H2 blockers to stomach acid
Awareness: inhaled and induction agents cross placenta – so often more cautious dosing. But muscle
relaxants don‟t cross placenta. Usual dosing. But can‟t tell if they‟re aware
So trend from GA to epidural in pregnancy
If doing GA: use rapid sequence induction. Use anaesthetic agent, muscle relaxant and cricoid pressure
to occlude oesophagus until tube in
Pathology in Pregnancy
Pre-eclampsia: BP, proteinuria, oedema
Eclampsia: circulating blood volume, swollen tissues, fits, death
Placenta praevia: placenta over os big bleed
Abruption: placenta separates from uterus big bleed
Amniotic fluid embolism equivalent of PE and DIC
Aorta-caval occlusion/compression. faint when they lie down. Uterus compresses IVC venous
return HR and vasoconstriction perfusion pressure to uterus. Lie on left side, push uterus to
left if doing CPR
Analgesic Drugs In Labour
Mechanism of pain:
Ischaemic pain during contractions is due to O2
Contraction against resistance colicky pain (like gallbladder)
Mechanical: pelvis and perineum
Epidural:
Very effective
Good in eclampsia and where high suspicion of intervention
Complications:
? Rate of subsequent intervention
Hypotension
Paralysis, infection, haematoma, wrong drug
If into subarachnoid total spinal overdose
If into vein cardiotoxic drugs, CNS damage
If CNS drains out, positional headache
Can‟t have epidural if:
Patient refusal
Hypovolaemic due to haemorrhage
On anticoagulants, in case puncture epidural vein haematoma
Septic: could transfer bug from blood to CSF
Inhalational – N2O/Nitrous Oxide: variable satisfaction, analgesia and dissociative, 50% vomit, 2 min
to peak effect, no further effect once breathed out
Opiates (e.g. Pethidine): variable satisfaction, dissociative, safe (midwives can use it), can
respiratory depression in neonate
Psychoprophylaxis: very effective. If frightened and don‟t know what‟s going to happen, hurts more
Preoperative Assessment
Aim is to investigate and optimise treatment for pre-existing medical conditions before surgery –
especially respiratory and CVS
ASA status = American Society of Anaesthetics: 1 = normal, 5 = expected to die, appended E =
emergency
Cardiovascular conditions requiring assessment:
Hypertension: 1/3 develop intraoperative hypotension, and ¼ develop post-operative hypertension.
Predisposes to MI, stroke and renal failure. Resting diastolic pressure over 100 mmHg should
delay elective surgery until better controlled. Continue previous antihypertensive therapy up to
and following surgery to prevent rebound hypertension (esp beta blockers)
Coronary vascular disease: IHD 10-fold increase of risk of perioperative myocardial infarction.
Delay elective GA until 3 (preferably 6) months after an MI
Anaesthetics 547
Cardiac failure: contra-indication to all but most necessary surgical procedures
Arrhythmias: resulting complications more related to underlying pathology rather than rhythm. If
cardiac efficiency already reduced, GA can lead to cardiac output (e.g. atrial fibrillation with
rapid ventricular response)
Valvular and congenital heart disease. E.g. aortic stenosis may require anticoagulant therapy
(although this increases haemorrhage risk so stop during operation) and prophylactic antibiotics
Respiratory conditions requiring assessment:
Ventilation, gas exchange, cough and mucociliary clearance impaired by GA and into post
operative period
Major risks: sputum retention, lung collapse, infection, ventilatory failure
Preoperative management aims to:
Eradicate infection
Reduce excess sputum production
Treat reversible obstructive disease
Treat co-existing right heart failure
Optimise ventilatory muscle function
Elective surgery should be cancelled if acute infections up to 5 weeks beforehand. (e.g. viral
infections mucociliary clearance)
PEFR (Peak expiratory flow rate), FEV1 and VC (Vital capacity) are useful preoperative measures
Endocrine:
Diabetics are at risk from:
Poor perioperative control: e.g. during pre-operative fasting, stress response, etc. Poor control
poor wound healing, infection, etc
Co-existing cerebral, coronary or renal vascular disease or autonomic neuropathy
Hyperthyroid patients at risk of CVS collapse
Liver Disease: hepatic function commonly deteriorates post operatively. Infection risk to staff from
hepatitis
Alcoholism: complications include withdrawal, nutritional abnormalities, existing cardiac and liver
disease
Anaemia: increases risk of hypotension and hypoxia
Drugs: Corticosteroids suppress cortisol, so patients will require supplementation with hydrocortisone
at induction and by infusion following
Guidelines
GP and RMO should:
Determine what medical conditions are present
Quantify any impairment and improve as much as possible
Make sure appropriate investigations are back in sufficient time before surgery
Advise patient of risks and benefits and obtain consent
Conditions of note:
Cardiac: MI in previous 6 months, evidence of left or congestive heart failure, unstable or
increasing angina, diastolic blood pressure > 110 mmHg, digitalis toxicity, uncontrolled AF
Respiratory: respiratory infections, exacerbation of CORD/Asthma
Hepatitis
Recent stroke
Thyroid or adrenal dysfunction
Poor control of diabetes
Major nutritional disorders
Are the following present:
Family history of anaesthetic problems
Previous anaesthetic problems
Malignant hyperthermia (hypermetabolic response to gases or suxamethonium due to Ca leakage
from cytoplasmic reticulum), suxamethonium apnoea, porphyria (thiopentone precipitates a crisis)
Abnormal hepatic or renal function
Muscle disease
Previous jaundice following anaesthesia
Allergy to anaesthetic or related drugs
Disorders of blood or coagulation
548 4
th
and 5
th
Year Notes
On MAOIs or cholinesterase inhibitors
Also investigate Hb, U+E, CXR, ECG and Respiratory function if indicated

Surgical and Fluid Management 549
Surgical and Fluid Management
Normal Values ............................................... 550
Replacement fluids ......................................... 550
Blood Products ............................................... 552
IV Cannulation ............................................... 554
Nutrition in Surgical Patients ......................... 554
Post-Operative Care ....................................... 556
Post-Operative Complications ........................ 556
550 4
th
and 5
th
Year Notes
Normal Values
Blood volumes
Infant 80-85 ml/kg
Young child 80 ml/kg
Adult 70 ml/kg
Child’s body weight
Under 9 years: kg = 2*age + 9
9 and over: kg = 3*age
Electrolyte concentrations
Extracellular
Intracellular
Sodium
140
12
Potassium
4
155
Magnesium
1
28
Chloride
100
10
Bicarbonate
28
10
Phosphate
1
105
Fluid Compartments and Control
Fluid Compartments in 70 Kg person:
Extracellular: 14 L
Intravascular: 3.5 L
Interstitial: 10.5 L
Intracellular: 28 L
Female: 55% water, male 60 % water
Control through ECF osmolarity:
Thirst
ADH: controls H2O excretion
Renal Na excretion: renin-angiotensin-aldosterone system
Replacement fluids
Signs of extracellular fluid depletion
Symptoms: oliguria (min 0.5 ml/kg/hr), thirst, tachycardia, dry tongue, weakness, confusion
Signs: weight change, tissue turgor, postural hypotension, cool peripheries, dry axilla and mucous
membranes, JVP
Common in surgical patients due to: vomiting, ileus, stomal losses, etc. Not always naso-gastric losses.
Frusemide is a flogging offence! It‟s due to intravascular hypovolaemia
Investigations:
Bloods: Hb, Urea/Creatinine, Na/K
Urine Na
Maybe ABG for acid/base balance
Replace deficit quickly over 30 minutes – 1 ½ hours, not by increasing hourly rate
Give boluses of 200-250 mls N/saline, Hartmanns or plasma expander
Take care in older patients/CHD: don‟t tolerate large Na loads ( pulmonary oedema)
If on IPPV, this pushes up intra-thoracic pressure to 10 – 15 cm H2O (0 – 5 cm H2O is normal), so
when using central venous pressure need to adjust for this before determining whether hypovolaemic
Depletion in children
Can be rapid and profound. Described as:
Mild: loss of 4 – 5 % body mass. History of diarrhoea/vomiting but few signs
Moderate: loss of 6 – 9 % body mass. Sunken eyes & fontanelle. Urine output < 0.5 mls/kg/hour
Severe: 10% loss of body mass. Very ill. Hypotension and rapid weak pulse
See Management of Mild-Moderate Dehydration, page 650, for fluid management in children

Surgical and Fluid Management 551
Types of Replacement Fluids
Crystalloids: isotonic, short intravascular T½ . For replacement of extra-cellular loss. To replace blood
give 3 times blood loss
0.9 % saline: 154 mmol/L NaCl (isotonic)
Hartmanns and Lactated Ringers: electrolyte mixture similar to plasma
Excessive replacement of plasma losses acutely with saline may hyperchloraemic acidosis
Dextrose containing solutions: not for replacing blood loss (hypertonic). For treatment of water loss or
when sodium restrictions are present:
Barts: 4% dextrose/0.18% saline – 30 mmol/L NaCl + 168 Kcal/L
5% dextrose: 200 Kcal/L (calories and water only)
Synthetic Colloids: isotonic, long intravascular T½, for blood volume replacement. More readily
available than blood and no infection risk, don‟t require cross matching. Give 1:1 ratio with blood lost.
If > 1 L required, consider albumin and/or blood. Kidneys take time to excrete, so watch for fluid
overload, especially in renal impairment and kids
Haemaccel: polygeline (degraded gelatine) plus electrolytes (145 mmol/L NaCl + 5.1 mmol/L K +
6.25 mmol./L Ca). T½ = 4 hours, hypersensitivity rare
Dextran 40, 70: dextran with molecular weight 40K (T½ = 2 – 4 hours) or 70K (T½ = 6 hours),
hypersensitivity reactions, impairs coagulation and cross match
Hetastarch (Hespan), Pentaspan: starch solution, MR = 70K, T½ = 17 hours, hypersensitivity rare
Blood products: reserved for > 20% blood loss or continuing bleeding or Hb acutely < 70 g/L
If fluids not hypo-osmotic compared with blood, then red cell would swell haemolysis
Warm fluids, especially if refrigerated. Haemaccel and crystalloids can be microwaved
Child Requirements
Maintenance fluid: 4% dextrose + 0.18% saline + 20 mmol KCl/L at:
Per hour
Per day
First 10 kg
4 mls/kg
100 mls/kg
Second 10 kgs
2 mls/kg
50 mls/kg
All subsequent kgs
1 ml/kg
25 mls/kg
Losses (e.g. nasogastric tube, fever, diarrhoea) replaced with an equal volume of 0.45% NaCl + 20
mmol KCl/L. Give as boluses of 20 ml/kg over 15 – 30 mins. Losses decrease with renal failure
See Management of Mild-Moderate Dehydration, page 650
Adult requirements
Adult daily requirements:
2.5 - 3 litres of fluid
100 mmol Na (60 mmol/day in elderly)
60 mmol of K+ (max of 10 mmol per hour)
Can be given as:
2.5 – 3 litres of dextrose/saline (=0.18% saline + 4% dextrose) per day with 20 mmol/L KCl in
each bag, or
2 litres of 5% dextrose and 500 mls of saline
Run in at 50 – 100 mls per hour (NB, smaller daily requirements for a small person)
If concerned about heart failure/pulmonary oedema than monitor saturation
Intraoperative fluid replacement:
Oral intake withheld before surgery
In major surgery, half the estimated 24 hour maintenance requirement should be given initially
(600 – 1000 ml saline), followed by maintenance requirements plus loses
K is usually excluded for first few post-operative days: due to liberation from cells
Excess use of low Na fluids post-operatively may cause hyponatraemia given ADH
Abdominal losses
GIT has huge internal economy of fluid secretion & absorption
Losses through surgical intervention (stoma, leaking viscous, etc) replaced with iv solution of similar
composition
552 4
th
and 5
th
Year Notes
mls Per day
Saliva 1500
Gastric 1500
Pancreatic 700
Bilary 500
Jejunostomy 2-3000
Ileostomy 500
Colostomy 300
Diarrhoea 0.5 – 15,000 (Normal ileum delivers 1200 – 1500 per day)
See also Abdominal Physiology, page 154
Diarrhoea and Vomiting
Leads to dehydration, hyponatraemia, hypokalaemia, hypochloraemia
Replace ½ calculated losses in first 24 hours with saline plus potassium. Maximum rate of
potassium replacement is 20 mmol/hr
Burns
Burns rapid loss secondary organ damage (e.g. renal)
Give 2-4 mls/kg * %burned area of Hartmanns: half over first 8 hours, rest over next 16, in addition to
maintenance requirements. Consider blood transfusion
See Burns, page 486
Monitoring adequacy of Fluid Replacement
Monitor pulse, BP, respiratory rate and urine output (i.e. put in catheter):
Per hour
Infants in Nappies
2 mls/kg
Kids & adults
1 mls/kg
Elderly
0.5 - 1 ml/kg
Na to K ratio in urine should be > 1. If < 1 then body frantically reabsorbing Na not in balance
Postoperative Hyponatraemia
See Hyponatraemia, page 107
Blood Products
Blood loss
Blood Loss
Clinical signs
Treatment
10% loss (500 ml)
HR, BP normal
Crystalloids, 10 – 20 ml/kg
20% loss (750 – 1500 ml)
HR, moderate hypotension
Colloid +/- red cells, 20 ml/kg
20 – 50% loss (1 – 2.5 L)
Severe hypotension, shock
Colloid and red cells 30 ml/kg
> 50% loss
?irreversible shock
Red cells + coag factors (FFP)
and platelets
Giving blood isn‟t based on how much they‟ve lost, but on Hb measurement and pre-existing
cardiac/respiratory disease. A normal person could survive an Hb of 50 if volume was adequate (below
this CO falls dramatically). But a sick, old person can‟t use CO to compensate, so CO starts to drop
below 100
Blood Component Therapy
Modern transfusion therapy is blood component therapy
Blood components are used to:
Correct intravascular volume (usually non-human products e.g. crystalloids)
Correct O2 transport deficiency
Correct bleeding disorders
Blood components available:
Red cells: one unit is the red cells from one unit of donated blood (450 ml). Hb increases by 10
g/L per unit transfused. Red cell transfusions – transfuse at 1 unit per 2 – 4 hours (if
Surgical and Fluid Management 553
cardiovascularly healthy then 2 hours, if older then 4 hours as you don‟t‟ want to go too fast
otherwise volume overload)
Platelet concentrates: Prophylactic platelet transfusions – 10 g/L pretty good maintenance level in
leukaemia.
Fresh frozen plasma: 250 ml will provide approx 8% of an adult‟s circulating clotting factors
Cryoprecipitate: source of fibrinogen for DIC
VIII & IX concentrates
To separate these: centrifuge – take off plasma first, then platelets, then RBCs
Decision sequence:
What factor is deficient?
Is the deficiency physiologically significant (hard to decide. Not the same as below the normal
range, as normal range includes functional reserve)
What is the appropriate blood product
What is the correct dose to transfuse
Has the transfusion worked?
When blood is required:
Type O immediately, type specific in 10 – 20 minutes and full X match in an hour
If massive transfusion (> 50% loss) use reconstituted red cells and colloid and consult
haematologist re fresh frozen plasma (FFP), platelets and coagulation factors
Tests for coagulation during large transfusions should include:
Full blood count: baseline Hb and platelet counts before transfusion, and repeated throughout
APPT: intrinsic pathway
PT/INR: extrinsic pathway
Thrombin time: fibrinogen availability
Fibrin degradation products: for DIC
Risks:
Most common reaction to transfusion: febrile ½ an hour later:
Due to leukocytes contaminating red cells. If necessary, insert leucocyte filter on line (@$50)
leucocyte poor red cells
Febrile reaction more common if multiple blood transfusions or multiple children (more
antigenically primed)
ABO incompatibility (eg due to incorrect labelling):
Hypotensive, rash, tachycardia
Symptoms of major intravascular haemolysis: nausea, vomiting, low back pain (renal reaction
to free haemoglobin), feeling very unwell
If allergic to plasma proteins washed red cells
For immunocompromised: use irradiated red cells to stop leucocytes grafting into host & then
attacking host
Infection risks (depend on prevalence in population):
Bacteria:
Yersinia Enterocolitica: is cryophilic (likes cold) and blood is a great culture medium.
Comes from transient bacteraemia in infected donor.
Other bacteria: Brucella abortus, salmonella, M. Leprae
Viruses: HBV, HCV, HIV, HTLV-1, CMV, EBV
Parasites: Malaria, Toxoplasma gondii, Trypanosome cruzi
Specific risks:
HIV infection via transfusion: 1 in 1 – 2 million
CJD: no documented case worldwide (although has been done in animals)
HBV: 1 in 200,000
HBC: 1 in 80,000
Complications of massive blood transfusion:
Over transfusion Fluid overload and pulmonary oedema
Coagulation defects: dilutional thrombocytopaenia, factors V, VII & X, DIC
Hypothermia (blood products are stored at 4 C)
Hyperkalaemia: K moves out of red cells in storage
Acidaemia: stored blood becomes acidotic with age
Hypocalcaemia & citrate toxicity cardiac depression and alkalosis
Hypomagnesaemia
554 4
th
and 5
th
Year Notes
Transfusion haemosiderosis (ie iron overload) if on chronic transfusions (eg thalassaemia)
Management of major reaction (either anaphylaxis/haemolysis or sepsis)
If worried during the transfusion, stop it
Call blood bank for advice
Send back blood + samples from the patient
Check for errors
Strategies to stop transmission of infection:
Donor screening – very effective
Blood screening:
But tests not 100% accurate & window periods
Move from serologic tests to PCR for viral antigens
IV Cannulation
Superficial veins of the arm: metacarpal, dorsal venous arch, cephalic (radial – thumb side), basilic
(ulnar), median antebrachial, antecubital
Parts of a cannula: bevel, stylet, catheter, hub of catheter, flash back chamber, air vent
Cannulation procedure: blood return, level off, advance catheter, release tourniquet, pressure upstream
remove stylet
Haematoma by angle of insertion, force
Keeping it going: if infusion stopped, blood can track back through cannula and clot. Intermittent
flushing with saline helps
If hemiplegia, or mastectomy, insert in good arm
Infiltration/tissuing is leakage into surrounding tissues. Will be pale, cold, boggy, painful. If red and
warm then infection
Phlebitis = inflammation of the vein. Caused by
Infection
Chemical irritation (eg antibiotics, especially erythromycin)
Mechanical
Consequences of infection: inflammation of skin, cellulites or bacteraemia
Minimising infection: hand washing, sterile equipment, site care and regular inspection
Always record in notes: date and time of insertion, what gauge, what vein
Replace every 72 hours, unless inserted in emergency in which case replace in 6 – 8 hours
Consent: check armband, explain reasons for iv therapy, duration, what‟s being infused, possible
complications. Obtain verbal consent
Choice of gauge: age, flow required, what‟s being infused.
Gauge
Colour
Uses
24
Yellow
Neonates, extremely small veins
22
Blue
Infants, elderly, fragile veins, small lengths
20
Pink
Most commonly used
18
Green
For viscous fluids (eg blood)
16
Grey
For large quantities of IV fluid. Painful at insertion.
14
Orange
As for 16
Nutrition in Surgical Patients
Consequences of malnutrition
Perioperative mortality (e.g. in 30 days post surgery)
Healing
Respiratory infection
Immune function
Wound infection
Nutritional assessment
Observe: thin?, how strong is finger grip
History: intake over preceding days compared to normal
Anthropomorphic measurement (BMI, girth to hip ratio, skinfold thickness, compare actual to
standardised 24 hour urine creatinine excretion.)
Lab measurements (albumin, transferrin – only for gross malnutrition)
Surgical and Fluid Management 555
Physiological assessment (PEFR, FEV1, hand grip)
Energy Metabolism
Adult needs 25 – 30 kcal/kg/day
Typical diet gives: CHO – 40 – 60% (4 kcal/g)
Fat: 20 – 45% (9 kcal/g)
Protein: 10 – 20 % (4 kcal/g)
Excess CHO stored as fat, otherwise broken down to glucose
Short & medium chain FFA are directly absorbed into the portal vein: so if gut is malabsorbing, give
them this – rapid and easy to absorb
During starvation, FFA saturate Kreb‟s cycle ketones and acids
Protein Metabolism
No body storage. Used, converted to energy or excreted
Maintained by protein intake of 0.8 – 1.0 g/kg/day
Nitrogen balance nitrogen in equal nitrogen out
Protein is 16% N2
Energy metabolism in Starvation
Immediate use: liver and muscle glycogen
Early starvation: Gluconeogenesis from AA, glycerol and lactate. Leads to catabolism. Only supports
CNS and RBCs
After few days: metabolism, FFA used by heart, kidneys and muscles
Prolonged starvation: brain uses ketones. Protein catabolism as fat stores used up
Nutritional Requirements
Basal Energy Requirement (BEE) for otherwise well and sedentary ( when challenged by illness):
Men = 66 + (13.7 * kg) + (5 * height in cm) – (6.8 * years)
Women = 655 + (9.6 * kg) + (1.8 * height in cm) – (4.7 * age)
Nutritional Support
Protein/Calorie Requirements
Well nourished patients without sepsis or injury: H2O and electrolytes OK for 5 days
Non-depleted post-operative patients: 1.2 - 1.5 * BEE + 0.8 – 1.0 g protein/kg/day to prevent
catabolism
Malnourished patients without sepsis or injury: Cautious repletion – avoid refeeding syndrome due to
depletion of co-factors marked in PO4 and Mg – monitor
Nutritionally depleted patients: 1.5 – 1.8 g protein/kg/day + 1.5 * BEE
Patients with sepsis or injury: Well nourished can manage without feeding for a few days.
Malnourished need feeding
Enteral Nutrition
Adult energy requirements: 40 Kcal/kg/day (approx. 2,500 Kcal per day)
Requirement in sepsis, burns, trauma by 50 – 100 %
Protein requirement: 1.5g/kg/day (approx. 105 g protein or 14g N2 per day)
Enteral much safer and less expensive compared with parenteral
Delivered by: NG tube, nasoduodenal tube (risk of aspiration), PEG, jejunostomy
Problems: aspiration, tube blockage, diarrhoea due to intolerance/inadequate digestion
Feed by pump, starting slowly, at 30 – 45 degrees. Stop at night if they can tolerate increased flow
during day
Tradeoffs:
When sick, motility and emptying. Need to be minimal volume but still flow through tube
Don‟t include lactose as lactase when sick. Lactose would diarrhoea
Osmolar load diarrhoea. So need Mr
3 types:
Intact nutrient formulas: Blenderised feedings (don‟t flow well), lactose-free feedings (via tube),
and nutrient-dense feedings (flavoured for oral use)
Pre-digested Nutrients (elemental diets): taste fowl, use NG tube
Feeding modules: concentrated sources of one nutrient (e.g. protein, CHO or fat)
556 4
th
and 5
th
Year Notes
Parenteral Feeding
For nutritional support when GI tract can‟t be used
Via central line: Total Parenteral Feeding (TPN) has very high osmolality. X-ray after insertion to
check no pneumothorax and line is outside pericardium (above anterior third rib) to avoid cardiac
tamponade following catheter erosion
Complete nutrition: electrolytes, glucose, amino acids, fat emulsion, vitamins, etc. Fat a good way of
giving calories without glucose (which could diabetes)
Other major risk: sepsis. Test for coagulase +ive staphylococci. Colony count should be 5 times
higher in central line sample than in peripheral blood
Metabolic problems common, e.g. hyper or hypo glycaemia, acidosis, etc. Alter constitution of TNP
Post-Operative Care
Eg following a laparotomy
Know and watch for complications
Analgesia:
Epidural: watch for low blood pressure
PCA/PRN narcotic (but watch for constipation from morphine/codeine)
Wound care:
Check not too much blood from drain
Rough times to leave a drain in for:
Laproscopic cholecystectomy/vascular surgery: 1 day
Rectal surgery: 3 –4 days
Mastectomy: 4 – 7 days (can go home with it in)
T-tube for biliary surgery: if latex then 10 – 14 days, if silicon then 3 – 4 weeks
Anti-coagulant (eg Clexane)
Fluid balance: if elderly alternate normal saline and dextrose bags (+KCl)
NG tube:
If no aspirate after 24 hours then take it out
If aspirate is green, leave it in
Prophylactic antibiotics: for uncomplicated laparotomy usually one dose intraoperatively
Consider rehabilitation, support at home, work re-entry
Plan follow-up
Post-Operative Complications
Infection
Usually takes 3 – 5 days
Wound infection:
Redness, induration
Either:
Abscess: red, hard mass needs drainage
Cellulitis: red, hot, painful antibiotics
Abdominal infection:
Often 5 – 7 days before apparent: pain, ileus, sweats, rigours
Investigations (to look for abscess): Maybe US. CT better
Treatment:
Small abscess: if deep and < 3 cm try antibiotics
Large abscess: if > 4 cm then drain either surgically or under radiological guidance. Depends
on depth, if its loculated or presence of overlying bowel
Peripheral line
Central line: may look innocent – but consider if no other locus found. Can leave a central line in for 4
– 6 weeks if you look after it
Chest infection:
Usually results from atelectasis following poor ventilation (especially immediately following
extubation, especially if pain)
Look for saturation and fever (especially if it occurs the night following surgery) – this is initially
due to inflammation – so it presents quicker than the above infections
Surgical and Fluid Management 557
Management:
Effective analgesia
Chest physio: deep breaths and cough each hour
Overall management:
Check wound, chest, iv sites, abdomen, UTI. Check for signs of meningism, endocarditis, DVT
Do FBC, culture. Consider MSU, CXR, abdo US
Decreased Blood Pressure
Lie flat and give O2
Check pulse and other vitals
Consider:
Hypovolaemia: check fluid chart, replace losses
Haemorrhage: review wounds
Cardiogenic: any heart history?
Sepsis
Anaphylaxis
Nausea/Vomiting
Causes: Mechanical obstruction, paralytic ileus, emetic drugs (opiates, digoxin, anaesthetics), systemic
or GI illness
Consider AXR, NGT, antiemetic (metoclopramide or cyclizine)
Deep Vein Thrombosis
If it‟s a long operation, a clot may start to form then and propagate inflammation mild fever
If immobile or in pain, then may form post-operatively
High probability of a DVT if:
Calf circumference > 3 cm than the other
Malignancy
Immobile
Local tenderness
Family history
Test using Doppler US (for flow)
See also Deep Vein Thrombosis (DVT), page 74
Confused Patient
Ie Delirium. See also Delirium, page 442
Causes (especially if already borderline):
Infection
Hypoxia
Metabolic: glucose, K
CVA or MI
Drugs:
Too little: eg withdrawal of sleeping pills, insufficient analgesia
Too much: eg morphine respiration, pinpoint pupils. Treat with naloxone (but short T½
so may need to repeat)
Delirium tremens (alcohol withdrawal)
Urinary retention
No cause found
Management: Quiet, gently lit area, familiar faces. Consider midazolam or haloperidol
Decreased Urine Output
= < 30 ml/hour
Causes:
Hypovolaemia: HR, BP, peripherally shut down
Urinary retention: ?palpable bladder
Catheter blockage (especially if sudden drop off)
Renal failure due to hypotension, nephrotoxic drugs, transfusion
Management: If not overloaded then treat with fluids: normal saline unless significant blood loss.
Don‟t use dextrose – won‟t stay in the blood for long
558 4
th
and 5
th
Year Notes
Dehiscence
= Wound breakdown (eg of a gut anastamosis). Usually after 5 – 7 days due to ischaemic tension,
infection, etc
Symptoms: severe pain, bowel sounds
Investigation: CT with gastrographin contrast

Paediatrics 559
Paediatrics
Paediatric topics elsewhere:
Skin conditions, including infections, eczema and other lesions, see Skin, page 313
Consent and Children, see Consent, page 717
Other cross references are included in the relevant section
Epidemiology and Health Systems ................. 561
Epidemiology ............................................ 561
Health Systems ......................................... 562
International Agreements .......................... 562
History and Examination ................................ 563
Difference Between Adult and Child
History Taking .................................... 563
History Outline ......................................... 563
Examination .............................................. 564
When is a child really sick? ...................... 565
Dealing with Children and Families ............... 567
Talking with Children ............................... 567
Parent and Adolescent Education ............. 567
Families .................................................... 568
Preparing a child for surgery .................... 569
The Dying Child ....................................... 569
Autopsy of a Child .................................... 569
Behavioural Issues .................................... 570
Growth and Development .............................. 574
Child Development ................................... 574
Causes of Developmental Delay ............... 580
Effect of Chronic Disease on
Development ....................................... 582
Learning Disability ................................... 583
Child Development Team ......................... 585
Growth ...................................................... 585
Neonatal and Infants ....................................... 587
Examination of the Newborn .................... 587
Outcome after Preterm Birth..................... 589
Neonatal and Infant Anticipatory
Guidance (Parent Education) .............. 590
Breast-feeding ........................................... 590
Failure to Thrive (FTT) ............................ 591
The Crying Baby ...................................... 592
Sleep Management.................................... 593
Sudden Infant Death Syndrome (SIDS) .... 594
Neonatal Acute Airway Problems ............ 595
Hypoglycaemia of the New Born ............. 595
Jaundice .................................................... 595
Other Neonatal problems .......................... 596
Heart Disease in Children ............................... 596
The Blue Baby .......................................... 596
Congenital Heart Disease ......................... 598
Complications of Congenital Heart
Disease ................................................ 601
Rheumatic Fever ....................................... 602
Respiratory Illness .......................................... 604
Symptoms ................................................. 604
Chest Radiology ....................................... 604
Respiratory Tract Infections in Children .. 605
Asthma in Young Children ....................... 613
Differential of Wheezing in a Child.......... 614
Cystic Fibrosis (CF) .................................. 615
Infectious Diseases ......................................... 616
Fever in Children ...................................... 616
Potentially Serious Infections ................... 616
Common Paediatric Viruses ..................... 617
Orbital and Pre-Orbital Cellulitis .............. 618
Paediatric Orthopaedics .................................. 618
Congenital Abnormalities ......................... 618
Bone and Joint Injury and Infection ......... 620
Paediatric Neurology ...................................... 621
Neurological Exam in Children ................ 621
Head Size * ............................................... 624
Headaches ................................................. 624
Seizures..................................................... 625
Tics ........................................................... 628
Cerebral Palsy ........................................... 629
Muscular Dystrophy ................................. 630
Acute Weakness in Childhood .................. 630
Neural Tube Defects ................................. 630
Eye disorders in Children ......................... 631
Renal Disease in Children .............................. 632
Proteinuria ................................................ 632
Haematuria ............................................... 633
Acute Renal Failure .................................. 633
Chronic Renal Failure ............................... 634
Genito-Urinary ............................................... 634
Urinary Incontinence ................................ 634
Testes ........................................................ 636
Acute Scrotum .......................................... 636
Penis ......................................................... 637
Ambiguous Genitalia * ............................. 638
Gastro-Intestinal ............................................. 638
Abdominal Radiology ............................... 638
Congenital abnormalities .......................... 639
Acquired Causes of Obstruction ............... 641
GI Bleeding .............................................. 641
Hernias ...................................................... 641
Common Childhood Presenting Chronic
Symptoms ........................................... 642
Gastroenteritis ........................................... 644
Nutritional Deficiencies in Childhood ...... 646
Food Allergy ............................................. 647
Cervical Lumps ........................................ 648
Childhood Cancer ........................................... 648
Emergency Management ................................ 649
Assessing Fluid State ................................ 649
Paediatric Coma ........................................ 651
Paediatric Trauma ..................................... 652
Paediatric Anaesthetics ............................. 655
560 4
th
and 5
th
Year Notes
Child Abuse .................................................... 656
Mental Health ................................................. 659
Attention Deficit/Hyperactivity Disorder
(ADHD) ............................................... 659
Anxiety Disorders ..................................... 661
Depression ................................................. 662
Youth Suicide ............................................ 663
Other Mental Health Issues ....................... 663
Adolescent Health ........................................... 664
Adolescent Development .......................... 664
Talking with Adolescents .......................... 665
HEADSS Risk Assessment ....................... 666
Physical Exam ........................................... 667
Puberty ...................................................... 667
Chronic illness and disability in
Adolescents .......................................... 669
Paediatrics 561
Epidemiology and Health Systems
Epidemiology
Measures of Child Health
Measures of death/disease:
Mortality
Disease specific mortality/morbidity (eg SIDS)
Hospital Discharges
Disparities: ethic, gender, age, location, etc
Measure of health interventions:
Immunisation coverage
Well child checks
Measures of health or its determinants or impacts:
Breast feeding at 3 months, 6 months
Participation: early childhood education, school, sport, etc
BMI: marker of appropriate nutrition
Self-report (eg questionnaires)
NZ Statistics
Numbers of children:
23% of NZers are aged 0 - 14
Maori and PI children are about double adult proportions as percentage of total population – 1/3 of
Maori and PI people are under 15, compared with 19% of Europeans
Until 2050, fall in the number of children, and fast fall in their proportion of the total population
(from 23 16%) future conflict over resources: “principle of first call” – essential needs of
children should be given high priority in the allocation or resources
Socio-economic status:
Children with no parent participating in the labour force (1996): European 13%, Maori 42%, PI
37%, Asian 30%
Proportion of children in one-parent families (1996): European 15%, Maori 43%, PI 27%, Asian
12%. Increased over all groups from 1986 to 1996
Maori and Pacific Islanders also more likely to not have a car, share a household, less likely to
leave school with a qualification
Mortality:
Under 5 mortality currently around 500 per annum
Age specific rates: 7/1000 live births for 0 – 1 years, 0.4/1000 for children 1 – 4 years, 0.2/1000
after this
All child mortality rates in NZ have declined by 1/3 over the last 15 years, but this is slow in
comparison with other countries. Our OECD ranking for under 5 mortality has fallen from 6
th
to
15
th
. If we had had the same fall as Sweden 194 children would not have died.
Major causes of death:
< 1 year: SIDS (29%), Congential abnormalities (28%), Perinatal conditions (27% -
prematurity, neonatal infection, hypoxia, etc)
1 – 4 years: Injury and poisoning (46%), Congenital abnormalities (18%), Cancer (11%).
Maori injury and poisoning rate 3.5 time Non-Maori
SIDS rate has fallen from 4/1000 in 1989 to 1.5/1000 (UK is 0.6/1000). Rate 4 times higher in
Maori than non-Maori. Low income 3 times higher income (independent of ethnicity) – due to risk
factors of maternal smoking, teen pregnancy, single parenthood, etc
Morbidity:
Under 1‟s most likely to be admitted: NICU, respiratory GI and infectious
Ethnicity patterns same as for mortality: Maori rates range from 1.7 – 4.6 times higher
Conclusions:
Despite improvements, New Zealand hasn‟t made the gains that other countries have
Ethnic and socio-economic disparities are growing
Improvements in curative medicine are unlikely to have an impact on this inequality
562 4
th
and 5
th
Year Notes
Health Systems
Determinants of child health:
Biology: genetic, development in utero
Socio-economic:
Housing
Income
Education (especially maternal – key issue in 3
rd
world)
Environment:
Social
Physical
Health Behaviours
Health Services
Impact of determinants:
Perinatal complications and family adversity have an independent impact on cognitive ability
Social adversity is a bigger factor in mild mental retardation than biological factors
Variations in family social background is a:
Weak determinant of specific problems
Pervasive determinant on generalised vulnerability to a wide range of problems
Large differences in absolute income have little or no effect on mortality. Small increases in
income equality have a large effect
Improving health equality through health services:
Population based measures:
Resource allocation
Intersectorial collaboration
Community development
Data collection on deprivation
Salaried GP services for deprived areas
Individual health services:
Site and mode of provision of services
Communication with consumers
Targeting of preventative services
International Agreements
Alma Ata Declaration on Primary health Care:
Declaration to protect and promote the health of all people
„Health for all by the year 2000‟ through quality primary care
Defined primary care and gave principles for health services
Ottawa Charter on Health Promotion: [See Health Promotion, page 691]
Building health public policy
Creating healthy environments
Strengthening community action – power and control to communities to identify and solve their
problems
Helping people to develop their own skills
Reorientating the health system: balance between preventative and curative services
Jakarta Declaration on Health Promotion in the 21
st
Century:
Comprehensive approaches (using all 5 Ottawa charter principles) are the most effective
Settings offer practical opportunities for the implementation of comprehensive strategies
Participation by the community is essential
Health learning fosters participation
United Nations Convention on the Rights of the Child:
Principles and standards by which governments, organisations and families can be measured
Ratified by NZ in 1993
Rights:
Article 18.2: “render appropriate assistance to parents and legal guardians in the performance
of their child-rearing responsibilities
Article 23: Rights of mentally or physically disabled children: “full and decent life…. Dignity
… self-reliance …. Active participation in the community”
Paediatrics 563
Article 24: Right of all children to “the highest attainable standard of health and to facilities
for the treatment of illness and rehabilitation of health”
Most recent assessment of NZ raised concerns about:
Fragmented approach to the rights of the child
Insufficient data collection on the effects on children of economic reform
“Extensive delegation of support services to children and their families” – but quality remains
the responsibility of the state
NZ Child Health Strategy 1999 had 6 future directions:
A greater focus on promotion, prevention and early intervention
Better co-ordination
Development of a national child health information strategy
Child health workforce development
Improve child health research and evaluation
Leadership in child health
History and Examination
Difference Between Adult and Child History Taking
Kids may not be able to tell you, teens may not want to
Concerned with nutrition: what normal and current feeding practices are, micro-nutrients
Growth: weight, height and head circumference
Developmental perspective:
Gross motor: rolling, sitting, crawling, walking, running, stairs, sports
Fine motor: hand skills, co-ordination (assessed through play art writing)
Vision
Speech/language and hearing
Social development: bonding parents vs strangers peers
Immunisation: „Are your immunisations up to date‟ – usually meaningless. Need to be more specific
Family history:
Congenital abnormalities
Genetic factors
Parental age and experience
Impact of chronic illness on family
Social history:
Abuse and neglect
Living circumstances – overcrowding, smoke exposure
Education settings, eg day care
Peer support for kids (eg in adolescence)
Adolescence: HEADSS Assessment (see page 666)
History Outline
General data: name, DOB, Ethnicity, where they live
Presenting Complaint
History of presenting complaint:
Chronological and including symptoms across all systems
Treatments so far
Contact history
Family history of the complaint
Paediatric Past Medical History:
Antenatal
Birth/perinatal: Gestation, delivery, weight, APGARS, any special care, complications
Feeding (breast, formula, solids) – detailed if relevant (eg which formula, how much, which solids,
how much)
Weight – growth history, where relevant growth and puberty in family members
Immunisations
Milestones – including relevant milestones for the child now: Cover Gross and Fine motor,
receptive and expressive language, social, play and self care skills. See Development Chart:
normal development from 0-60 months, page 576
564 4
th
and 5
th
Year Notes
Past medical history
Social/school
Medications
Allergies
Family History: ages and health of parents and grandparents. Ages, names and health of siblings
Social History:
Parent‟s occupations
Who cares for the child
Schooling/childcare, performance at school
Behaviour at home/school
Sleeping arrangements and home circumstances
Financial circumstances
Alcohol, smoking
Pets
Problems/stresses at home
Systems enquiry (OHCS, p 173):
Neonate
Toddler
Older Child
Cardiorespiratory
Tachypnoea, grunts,
wheeze, cyanosis
Cough, exertional
dyspnoea
Cough, wheeze,
sputum, chest pain
Gastrointestinal
D&V, jaundice, stool
frequency
D&V, stool frequency
D&V, abdominal pain,
stool frequency
Genitourinary
Wet nappies (how
often?)
Wet nappies (how
often?)
Haematuria, dysuria,
sexual development
Neuromuscular
Fits, odd attacks, jitters,
feeding ability
Fits, drowsiness,
hyperactive, vision,
hearing, gait
Headaches, fits, odd
sensations, drowsiness,
academic ability,
vision, hearing, co-
ordination
ENT and teeth
Noisy breathing
Ear discharge, teeth
eruption
Earache/discharge, sore
throat
General questions: fatigue, lumps, itch, fevers, bleeding tendency, family interaction
Examination
Principles:
Leave nasty things till last
Observe
Get on floor and use games
Wait until child familiar with environment but start before bored
Don‟t touch child until rapport established
Use your own toys – they‟re novel
Get parents to undress them (or do anything else that is nasty)
Get them to draw pictures while taking the history
They‟re likely to be scared (depending on previous experience). Build rapport, play games, talk with
child not through parent. Don‟t wear stethoscope around neck
Show them what you want rather than telling them
Blood pressure:
Is important – always do it
Getting them calm is hard – usually anxious artefacts common
Cuff: Bladder should nearly encircle the arm. Width is 2/3 length from should to elbow
Chest exam:
Percussion more sensitive than auscultation (won‟t show anything in the absence of respiratory
signs/symptoms)
Percussion will tell you about hyperinflation, fluid, mediastinal shift
Ausciltate heart early in the exam – but not first
Abdominal exam: Get child to suck in and push out tummy to check for tenderness – then you won‟t
have to hurt them yourself.
Differences in a baby:
More liver in the abdomen (2 finger breaths is normal). Don‟t press too hard – moves with
respiration

Paediatrics 565
Pelvic organs higher (eg bladder)
Pulses: Radial/ Brachial – take both sides. Must palpate femoral pulse. If feet aren‟t white don‟t
take peripheral pulses
Teenage girls: examine chest underneath clothes
Normal Values
Age
Breathing
Pulse
Systolic BP
< 1 yr
30 – 40
110 – 160
70 – 90
2 – 5 yr
20 – 30
95 – 140
80 – 100
5 – 12 yr
15 – 20
80 – 120
90 – 110
> 12 yr
12 - 16
60 - 100
100 - 120
Stethoscope around your neck adds 10!
Haemoglobin: at birth: 170, day 5: 200, 12 weeks: 120 (lower limit of normal is 90 – 100)
Examination outline
Height, Weight and Head Circumference (and plot them)
General:
Sick or well
Dysmorphic features
Obvious distress
Temperature
Colour/rashes/anaemia/cyanosis/jaundice
Lymph nodes: Check anterior and posterior cervical chains, subhyoid, sub-occipital, sub-
mandibular, sub-lingual, axillary, inguinal and epitrochlear
Hydration/perfusion
Cardiovascular:
Pulses: radial, femoral, synchrony, sinus arrhythmia (normal in all children)
Blood pressure (NB use correct cuff size)
JVP: often hard to see
Peripheral oedema (Periorbital in babies)
Liver enlargement right ventricular failure
Feel the cardiac impulse: Apex may be more lateral in children. Thrills
Auscultation
Respiratory:
Ears, throat, nose, sinuses
Clubbing
Chest deformity
Respiratory rate, effort and accessory muscle use, grunting, ability to talk in sentences
Intercostal, sub-sternal and supraclavicular indrawing, hyperinflation, Harrison‟s sulcus (lower ribs
pulled in chronic airways disease), pigeon chest ( chronic in AP diameter), tracheal tug,
nasal flaring
Auscultation, including cardiac dullness ( hyperinflation). Tracheal position rarely of value
Abdominal:
Inspection, movements, scars, hernia
Liver, spleen and kidneys
Bladder
Masses
Tenderness
External genitalia
Examine anus (PR rarely required)
Neurological:
Developmental assessment: See Child Development, page 574
Neurological Exam: See Neurological Exam in Children, page 621
Joints
Skin
When is a child really sick?
Factors which are not on their own discriminating between mild and severe:
Temperature: spikes easily
566 4
th
and 5
th
Year Notes
Pulse: variable, eg if crying
Blood pressure: hard to measure, and if shocked is still maintained till very late. As soon as they
have any hypotension they‟re the same as an adult with no recordable BP
Factors from history which discriminate:
Intake:
Refusal to feed more severe
Refusal to take solids but still taking liquids not so bad
Losses:
Vomiting:
Frequency and amount: if vomiting their whole feed then bad (vs a small spill)
Colour: Bile is bad. Yellow (from gallbladder), green (after bile has been in the stomach)
or orange. Due to obstruction or sympathetic discharge, eg due to pain (not
necessarily abdominal – could be a torted testicle)
Decreased urine output (wet nappies < 4 per day)
Diarrhoeal losses
Dysuria and pale extremities may be the only warning signs before they crash
Factors which discriminate on exam:
Floppiness: tone
Perfusion: pale, mottled or blue, cold. Capillary refill > 2 secs. (ie Peripheral vasoconstriction)
Fitting
Cyanosis
Tachycardia
Respiratory rate: quality as important as rate
Rash if petechial/purpuric (?meningococcal septicaemia)
pH
Weight (dehydration)
Toxic Appearance =
Decreased level of arousal
Circulatory compromise: pallor, tachycardia, cool + mottled limbs, hypotension
Respiratory impairment:
Tachypnoea, grunting respirations, recession, cyanosis
Due to O2 requirements + trying to blow of CO2 from acidosis + pulmonary oedema from
capillary leak
Shock =
Clinical diagnosis of failure of the circulatory system to deliver sufficient O2
Look for compensatory mechanisms which try to maintain perfusion of vital organs (HR,
peripheral vasoconstriction)
Causes of shock:
Capillary leak cardiac output
Changed vascular tone
Impaired myocardial function
Progression: Toxic Septic Shock
Specific signs:
Meningism: bulging fontanel, rash, stiff neck
Pneumonia: chest sounds (not very sensitive)
Distended abdomen and guarding: obstruction, appendicitis
Lumps in the inguinal region (seen or felt): hernia obstruction acidotic
Blood in faeces: Intussusception
Basic investigations:
Bloods: FBC, electrolytes, culture, ABG, (cross match)
X-rays: chest, abdomen if distended
Urine culture (bladder stab)
Maybe lumbar puncture
Neonates
Check list for a neonate (clinical acumen less reliable):
Fever: consider full sepsis evaluation for any child > 38 C
Feeding: if intake < 50% normal
Paediatrics 567
Urine output: < 4 wet nappies in 24 hours
Peripheral circulation: pallor of recent onset, mottling, cold periphery, slow capillary return
Responsiveness: poor response to stimulation and a weak cry
Activity: movement, sleepiness
Breathing difficulty: signs of distress, cyanosis, RR > 60
Apnoea: pause in respiration > 20 secs. Central (eg premature) or obstructive (eg URTI) or mixed
Vomiting: treat any vomiting in neonate seriously. Look for bile staining
Cyanosis
Seizures
Severe jaundice: risk of bilirubin encephalopathy
Dealing with Children and Families
Talking with Children
Do:
Engage them
Explain who you are and why you are seeing them
Use language and concepts that are age appropriate
Reassure if seeing separate from parents
Outline confidentiality issues with older children or adolescents
Don‟t threaten:
The child‟s sense of loyalty to their family
Their defences against unbearable emotional pain
Interviewing preschoolers (3 – 5 years):
Get down to their level, use simple language
Take things at their pace
Can use play, drawings and stories
Ask about everyday world
Watch verbal and non-verbal communication
See with parent
School age children (6 - 11 years):
Can be structured
Ask about feelings (sadness, anger, etc) as well as daily life
Ask about family, school, friends, problems, worries
Wishes, hopes for the future
Very abstract, open-ended questions can be confusing
For adolescents see Talking with Adolescents, page 665
Parent and Adolescent Education
Aim is to change behaviour. Changing behaviour requires:
Knowledge: necessary but not sufficient
Skills: to manage the change
Motivation: Involves striving towards a goal, not just „trying‟. The goal must be:
Important to the person – „I want this‟. Make it attractive. May need their goals to come
before yours.
Achievable – „I can do this‟. Believe in them
Not too unpleasant. „I don‟t mind doing this‟. Make it easy
Good counselling technique:
Open-ended questions: “tell me about….”
Active listening: “Hmm, I see…”
Reflection: reflect facts and emotions
Summarising: “Let me see if I‟ve got this straight….”
Don’t ask leading questions: eg “You don‟t do that, do you?”
Take a history using open-ended questions, reflecting, summarising:
Help parent or adolescent clarify exactly what it is they want to know
Knowledge: what do you understand about…? Where did you find that out? How convinced are
you?
Attitudes/fears: are you worried about anything in particular?
568 4
th
and 5
th
Year Notes
Practices: What have you actually done so far?
Barriers: What‟s stopping you from doing this?
Then:
Validate/reinforce knowledge they already have: “That‟s terrific – you already understand a
lot….”
Education to correct incorrect beliefs/address fears
Encourage them to find their own solutions: “So, what do you think you could do?”
Reinforce safe practices and responses
See also Neonatal and Infant Anticipatory Guidance (Parent Education), page 590
Families
Ref: notes from Lorraine Christie, Clinical Psychologist
Unuhia te rito o te harakeke
Kei whea te komako?
E hua whakatairantitia
Rere ki uta, rere ki tai
Mau e ki mai He aka te mea nui o te ao?
Maki e ki atu, He tangata, he tangata
If you pluck the young shoot of the flax bush, where will you find the bellbird?
It will be fluttering about flying to the beach and sea!
What is the greatest thing in the world? I tell you, it is people, it is people
The task of childhood is development:
Social relationships
Emotional maturity
Sound set of values and beliefs
Sound thinking patterns
Knowledge
Of body and skills
Self esteem and self respect laid down in the first 7 years are influenced by: Gender, race, culture,
sexuality, temperament, ordinal position, IQ, physical characteristics, creativity, did you arrive in the
family at an okay time
Families are systems with:
Structure
Various roles
Authority
Channels of communication
Five characteristics of healthy families:
The marital relationship is the strongest relationship and the greatest focus of power
Communication is open and honest and permits spontaneous interruption
Warmth and caring predominates over anger and hostility
There are known problem solving techniques which can be instigated quickly
Movement towards independence for all members of the family
The family life cycle: constant reorganisation and change
Two form a couple:
Take on husband/wife/partner roles
Substantial reorganisation of boundaries: family, friends, togetherness vs autonomy
Work through differences
Structuring a relationship: complimentary vs symmetrical
First baby:
Parenting roles
Ensure spouse relationship remains the strongest
Reorganised boundaries to allow for grandparents, friends, interests
Preschoolers:
Protect spouse relationship: contact, support, being together
Parent/child subsystem: affection, encouragement of appropriate autonomy, boundaries for
child, individuating siblings from each other
Paediatrics 569
Continued reorganising of boundaries: grandparents, outside world, work
School age children:
Integrating school and family systems
Allowing age appropriate autonomy
Children less egocentric, more sensitive to other‟s needs, develop sense of fairness and gender
awareness
Adolescence:
Issues of proximity and distance
Extending boundaries to allow independence
Continual renegotiation – autonomy vs control
Sibling individuation from each other
Young Adult: between families
Differentiating self from family of origin
Leaving home, career development
Intimate peer relationships, courtship
Parents: at height of careers, retirement looming
Grandparents: needy, mobility, loss of sight, death
Parents take on grandparent roles
Preparing a child for surgery
Talk to the child about what is going to happen and why. Read books about hospital
Reassure your child that you will be there too
Answer your child‟ questions
Use simple terms that the child can understand
Take a favourite toy. It can have bandages too
Be honest without scaring: „It will hurt for a bit – but we‟ll try and make it better”
Tell the child he/she will be going home with you when it‟s finished
Don‟t be surprised if the child gets angry with you: this is normal
The Dying Child
Anticipated: preterm infants, congenital abnormalities, metabolic disease, etc
Unanticipated: often older, trauma, SIDS
Issues:
Relief of child‟s pain pain management, including neonates
Clear and simple information: check their understanding, explain prognosis, explain disease
process, avoid information overload or jargon, respect silence
Decisions about when to withdraw treatment
Before death: time and space, preparation of child
After death: viewing the body, coroner, funeral options, surviving siblings, other families,
availability of health care team
See also Children‟s Grief, page 459
Autopsy of a Child
Family concerns:
What is an autopsy – like a major operation
Will my child be cut – yes
When will it be done – soon
How long will it take – max 3 hours
What will my baby look like afterwards – won‟t see chest incision if dressed. Vertical cut down
back of head
Can I take my baby home afterwards – yes
Autopsy may provide:
A cause of death – but may take time
Identify unacceptable iatrogenic lesions
Quality control for a neonatal unit
Assist medical knowledge
Information that may help other babies
570 4
th
and 5
th
Year Notes
Common reasons for refusal:
Concerns about disfigurement and further suffering
Lack of information
Objections from family members
Religious beliefs
Interference with funeral arrangements
Must refer to the coroner:
Where death certificates cannot be signed
Thought to be related to an invasive procedure
?Birth asphyxia
Deaths thought to be related to an instrumental delivery
Behavioural Issues
Behaviour doesn‟t exist outside an environmental context
Behaviour Management
History Taking:
Antecedent: what sets him off?
Behaviour: describe exactly what he does?
Consequence: What do you do about this?
Principles:
Remove (time out). Somewhere safe and boring, and where you don‟t mind the child disliking (ie
not the toilet if toilet training or bedroom if sleep training). Leave a minute for every year of age.
Be specific about what they‟re going in for. At the end, remind of the behaviour you want, and
then forget the incident.
Anticipate/avoid situations where conflict is likely
Ignore minor things, particularly tantrums
Distract
Example (set a good one)
Reward acceptable/wanted behaviour
Reward Systems:
Star chart if young, more sophisticated and discrete if older
Agreed between parents and child. Child has to own it (can they help make it?)
Planned: don‟t have to make a decision when the time comes
Anticipated: known about in advance – When you this, then you will have …
Consistently applied: no matter where he is or who he is with
Immediate: not at the end of the week or when dad gets home from work
Strong reward component
Meaningful to child:
Young child: cuddles, praise and attention
8+ years: if you … you can choose what we have for desert/which video, etc (choice is
powerful)
10+: money
Referral options:
Special Education Service (SES): Resource teacher for learning and behaviour (RTLB) or
Behaviour Support Team through SES
Child psychiatry service (CAFS) if severe psychiatric symptoms (anxiety, depression, OCD,
PTSD, sexually abused, ADD), persistent family dysfunction or resistant to simple management
strategies
Paediatrician if medical issues
CYFS if abuse
Paediatrics 571
Risk and Resilience
Good
Bad
Internal (child factors)
Resiliency: High self esteem,
happy temperament, high IQ,
problem-solving skills, coping
strategies, humour
Vulnerability: poor social
skills, low IQ and self esteem,
hopelessness
External (factors in the
environment)
Protective: caring and supportive
adult, reasonable structure and
limits, being believed in
Risks: Family discord, hostility,
lack of warmth and
understanding, lack of friends
Attribution theory: Are their successes and failures due to an internal locus of control („I passed the
test cause I did the work‟ high self-esteem) or an external locus of control („It doesn‟t matter if I
study or not, it won‟t make any difference‟ low self esteem)
Individual traits the build resiliency:
Insight: recognition of ones‟ distressed condition with subsequent action to overcome barriers
Independence: gaining emotional distance and autonomy amid chaos
Initiative: achievements that foster self confidence and constructive activity
Relationship building: Protective and nurturing connections with at least one supportive adult
Creativity: facilities healing and positive activity in a difficult environment
Humour: focuses on hope not harsh realities
Morality: commitment to fairness and compassion
Family traits that build resiliency:
Commitment: loyalty, determination to work things out, sacrifice for mutual benefit
Cohesion: togetherness, respect for the individual, interdependence
Adaptability: flexible, stress coping skills
Communication: listening and speaking skills
Spirituality: shared purpose and values
Connectedness: Support within and beyond family, attitude of service
Effective resource management: Competent use of money, time, etc
Coherence: Optimism and self reliance
Intervention strategies:
Provide opportunity for and encourage contributions
Enhance decision making skills feeling of control
Encourage and give positive feedback
Develop self discipline: involve child in setting the rules and consequences
Toddler Behaviour
Approach:
History, including:
Antecedents, behaviours and consequences
Social context
Collaborative history if necessary
Psychiatric history from mother (is the child the problem?)
PMH: ABFWIMPS
Exam: especially developmental
Education
Most difficult behaviour does not indicate a serious disturbance. Indicators of serious disturbance
include:
Deliberate self harm or messing
Wandering off
Running away
Age inappropriate sexual behaviour
Developmental sequence of everyday habits:
Feeding
Sleeping
Eating
Toilet
572 4
th
and 5
th
Year Notes
Going to bed and getting up
Dressing and undressing
Washing and cleaning teeth
Aim is to achieve regular habits and routines:
To start with need to insist on regular routine and time schedule. Once achieved can be more
flexible
Failure to achieve routine: daily hassle and distress
Regular routines security of child, argument with parents
Factors which behaviour problems:
Routine and regularity
Clear limit setting
Unconditional love and affection
High level of supervision
Consistent care and protection
Age appropriate disciplines and rewards
Tantrums:
Want their way. Purpose of tantrum is to get their way. Giving in reinforces the behaviour
Must be consistent. If you say no, will have to stick with it choose your battles
Options for managing a tantrum (see Behaviour Management, page 570)
Ignore it: eg leave the room
Time out
Distract
Avoid problem areas (eg supermarkets)
Things will get worse before they get better. Once they realise the boundaries are consistent they
will stop testing them
Sleep Management: Sleep Management, page 593
Other points:
Check parent‟s are not expecting too much of the child (eg 3 year old boy not wetting at night)
Keep no for important things
All parents make mistakes
Problems at School
For ADHD see Attention Deficit/Hyperactivity Disorder (ADHD), page 659
Symptoms:
Normal IQ, no disabilities, but fail to develop academic potential
Difficulty with peer relationships, loners, act out, difficult behaviour
Develop associated problems: psycho-somatic, self-esteem
Usually multifactorial:
Constitutional factors: May have subtle defects in:
Receptive or expressive language
Auditory sequencing: can‟t remember verbal sequence (eg instructions). Can have a pervasive
effect on schooling
Visual sequencing: difficulty reading/spelling
Motor problems (eg clumsy)
Attention (may be secondary to the above)
Health, hearing, vision, etc
Environment: cultural, socio-economic status, family disruption, nutrition, etc
School related factors:
School factors associated with antisocial behaviour: poor morale, high turnover, inconsistent
standards, undervaluing children‟s work, bullying
Kids spend 15,000 hours at school – so can have a big impact (just as family does)
Assessment:
History: parents
Information from teachers
Physical and neuro exam
Sensory exam: vision and hearing
Neuro-developmental, educational and psychological assessment
For School refusal, see Separation Anxiety Disorder, page 661

Paediatrics 573
Management of Truancy:
Educational programme appropriate for the child‟s needs
Monitoring child through the day
Assist with the learning process
Child in Trouble with the Authorities
History:
Interview child and caregiver separately
Presenting complaint
History of presenting complaint:
Describe behaviour: Antecedents, Behaviours, Consequences
Social Context in which behaviour occurs: Relationships within family, school, and peers.
Physical or sexual abuse
Collaborative history: parents, teachers, sports coaches – this is important
Psychiatric history: look for depression, anxiety, attentional problems
Formal assessment of learning if academic problems
Exam: especially dysmorphisms, stature, neurocutaneous lesions, observations of reading, writing and
relationship with parents, vision and hearing
Development of antisocial behaviour:
Possible differentials:
Attachment disorder
Developmental delay
Behaviour conduct disorder
Psychiatric illness: Depression, ADHD, PTSD (may appear to be daydreaming)
School refusal/Truancy
Neglect or other abuse
Domestic violence
Management plan:
Keep in him school if at all possible: prognosis plummets if expelled or regularly truant
Ensure a thorough developmental assessment
Referral for psych assessment and counselling
Management: accentuate the positive, minimise the negative
Referral to other services
Attachment Disorder
See also Anxiety Disorders, page 661
Attachment:
Starts in utero and is an ongoing process
Securely attached infants:
Are able to seek and obtain comfort from familiar caretakers
Are willing to explore and master their environment
Insecurely attached infants (eg due to long separation from parents and multiple carer-givers in
hospital) appear:
Anxious: clingy without obvious stress
Avoidant: angry, distrustful of parents, won‟t be comforted after brief separations
Indiscriminately affectionate: won‟t show preference for parents
Concepts:
Separation: the process by which a child develops an identity separate from their parents.
Promoted by secure attachment. At risk when the parents perceive the child is „vulnerable‟
Autonomy: Development of independence ( social competence)
Poor parental
discipline and
violence
Child conduct
problems
Rejection by
normal peers
Academic
failure
Commitment
to deviant
peer group
Delinquency
and crime
574 4
th
and 5
th
Year Notes
Mastery: increasing sense of competence over the physical environment
Together autonomy and mastery lead to an internal locus of control. Struggles for autonomy and
mastery produce normal tantrums
Types of Attachment Disorder:
Disinhibited type: will go to anyone. No stranger awareness and constant, insatiable need for
attention. Likely to be due to neglect. Also see it in chronic hospitalisation
Withdrawn: frozen watchfulness, fearful. Likely to be due to abuse
Test by observing child when parent leaves (separation), when a stranger comes in, and when parent
returns (reunion)
Domestic Violence
Has significant health consequences: injury, psychiatric, chronic pain, drug and alcohol abuse
Is common (some studies report up to 20% of women being hit in the last year), but often missed by
doctors
Domestic violence starts with a cycle of increasing control and disempowerment. Violence is used to
reinforce this
Screening questions:
„I have seen many people who come to see me with problems like yours. In my experience, many
of these women are being hurt in some way by their partner. Is that happening to you?‟
„A lot of tension and violence can be due to relationships within the family – often with a partner.
Is your partner being violent toward you?‟
Management:
Ensure mum and the children are safe. If not, refer to police/CYFS
Refer to Women‟s refuge – be aware of the local services available
Educate: eg the cycle or violence, it won‟t stop without help
Avoid victim blaming („it‟s not your fault‟)
Take careful notes (explain to the women why you are going this)
Display information in your waiting room – signals a willingness to discuss it
When Parents Separate
Responses to parent‟s separation – all signs of distress:
Withdrawn
Clingy
Regression
Difficult behaviour
Helping the child:
Accept the separation – then the child will too
Make sure the child knows you love them
Avoid conflict in front of the child
Allow them to express their feelings
Rely on other adults not the child for support
Tell the kids they‟re not to blame
Things to avoid:
Don‟t abuse their loyalty and trust
Don‟t use them as messengers
Don‟t use them to spy on other parent
Don‟t continue to be angry at partner in front of them
Don‟t let outings/gifts take the place of normal parenting
Don‟t force kids to take sides
Don‟t force a clash of loyalties
Growth and Development
Child Development
Represents the interaction of heredity and the environment:
Heredity: potential of the child
Environment: extent to which potential is achieved. Requires:
Physical needs: warmth, clothing, shelter, food, health, activity with rest
Paediatrics 575
Psychological needs: security, personal identity, self-respect, independence, opportunity to
learn, play, affection and care
Areas of child development:
Gross motor
Find motor
Language (expressive, receptive, non-verbal)
Social (interaction, play, self-care)
Cognitive: all of the above
Requirements for development (need all of them):
Hardware (neurons, muscles, etc)
Motivation (often driven by frustration – a child can‟t do what it wants to)
Nurturing environment
Types of assessment:
Developmental screening: point in time snapshot
Developmental surveillance: following over time
A formal assessment will yield a Developmental Quotient. < 100 delay. 100 advanced.
Developmental assessment
Indirect assessment of the acquisition of life skills
Establish rapport: use names a lot, „thanks for coming‟, etc more valid assessment
History:
Current development and time course of development
Order of questions should be:
When asking about milestones, start with things he is likely to be able to do and work up. Get
better rapport than starting at the upper limit and working down
Hearing: What things can he hear?
Have you been concerned about his hearing?
What makes you confident of that?
Vision: What small things does he see?
Have you been concerned?
What makes you confident of that?
Gross motor: roll, sit, crawl, pull to stand, walk, run, scoot, pedal (progression: head trunk
limbs)
Fine motor: pincer, feeding self, spoon, drawing, blocks
Expressive language: coo, babble, words with meaning, combinations (most common area of
delay – usually focal not global)
Receptive language: Responds to familiar voice, to own name, one or two step instruction,
knows name, gender, address, prepositions, pronouns
Social: smile responsively, laugh, stranger aware, play with peers, name friend
Self care: manage cup, spoon, undress, toilet, dress, laces
Get history of influences on development:
Miscarriages, still births
Pregnancy: toxins, alcohol, infections
Birth: APGAR (usually means brain was vulnerable before birth), gestation, birthweight
Neonatal congential abnormalities, feeding, jaundice, infections
Early milestones (smiling, sitting, walking, first words)
Illness (eg CF, heart/renal disease, epilepsy)
Hearing (speech delay), vision ( good verbal, poor motor)
Nutrition, constipation (especially if mobility problems)
Current development, especially social, self-care
Behaviour problems (sleep, tantrums)
Family stress
Family history, especially of development
History from other sources (eg kindy teacher)
Review previous rate of development: may get slowing before loss
Past Medical History: ABFWIMPS
Observation: Look systematically across each of the 6 areas. Use toys as tools.
Examination:
576 4
th
and 5
th
Year Notes
On lap first (stranger shyness from 8 months)
Dysmorphism: eyes, head shape, body proportions
Height, weight, head circumference – plot them
Vision (do first, affects motor): following, hundreds and thousands
Localise to noise (do before language): if concerned then formal testing
For each of gross motor, fine motor, expressive and receptive language, social and self care on the
table below:
Ask open-ended questions to establish the floor (eg I notice he‟s walking, what other clever
things is he doing)
Then use closed questions to establish a ceiling (eg can he walk backwards, throw over arm)
Then summarise: So he can ….. but is not yet …. Have I got that right?… Therefore he is at
age X for that domain
Summary: age for each domain is X, Y, X. Therefore, overall, he‟s developmentally around age
[Average for X, Y, Z]
Other:
Skin pigmentation (eg tuberous sclerosis – seen under Woods lamp)
Ears, eyes, heart, abdomen, puberty
Neurologic exam
Relationship with parents
Plan: for areas of weakness
If significant delay then early intervention
If some delay then anticipatory guidance – „what could you do to help‟ – use Knowledge,
attitudes/fears, practices, barriers framework
Always pitch safety advice at the level of gross motor skills
Development Chart: normal development from 0-60 months
Ref: Dr Russell Wills
Red flags:
Not smiling by 2 months
No eye contact by 3 months
Not reaching for objects by 5 months
Not sitting unaided by 9 months
Not walking unaided by 18 months
Not using words by 18 months
No 2 – 3 word sentences by 30/12 months
Paediatrics 577
Gross Motor
Fine motor-adaptive
Expressive language
Receptive Language
Personal-Social/Play
Self Care
6 wk
Clear face prone
Follow 180 horizontal
Follow O vertically
Cry, coo
Quiets to voice
Smiles spontaneously
3
m
Up on elbows. No head
lag on pulling up
Grasp
Retain 1 block
Reciprocal vocalisation, laugh
Turn head to voice
Localise bell/keys (horiz)
Reciprocal smiles
6
m
Up on hands
Sit supported
Take 2 blocks
Transfer hand to hand
Consonants
Mono-syllabic babble
Localise bell/keys (vert)
Lifts arms for pick up
9 m
Sit stable
Pull to stand
Crawl
Object permanence: Take 3
blocks 1 at a time and hold onto
them
Bang, index point
Vocalise to communicate
Poly-syllabic babble
Jargon
Understands no, ta
Localise bell/keys (diag)
Peekaboo
Cooperate with
dressing
12
m
Move around furniture
Good pincer
Few words with meaning
Shake head for no
Copy bye bye
Push toy car
Clap hands
Independent with
cup
15 m
Walk independent
Stack 2 blocks
Mark paper with pencil, fist grip
Several words
Understands object names
Wave bye bye on request
Understands pointing
Push large wheeled toy
Casting prom.
Remove item
Indep with spoon
18 m
Walk backward
Kick
Throw over arm
Stack 3 blocks
Vigorous straight scribble
3 shape board
Prom. jargon, two wants
Many common objects
Family names, own name
Few body parts
Hands familiar named object on request
Symbolic play single step
21 mo: likes books
Play alone
Remove hat, shoes,
socks
2 yrs
Run
Throw ball in bin
Seat self at table
Imitate vertical line, then
horizontal; dagger grip for pen
Stack 6, train 3
3 shape board rotated
Combinations; Echolalia; Songs/rhymes
30 mo: Questions: what, who?
3-5 word comb; I, we, you
Verbs: eat, kick, gone
Prepositions: on, in
2 step commands: shut door
Object uses
Several body parts; 30 mo: fetch
Imitative play single step
28 mo: ringaringarosy
30 mo: imit sequence
Indicate wet/dirty
nappies
Dress some
3 yrs
Walking:
tandem, heels, toes
Jump feet together
Pedal; Up stairs adult
Stack 9, 3 stairs/bridge
Imitate circle, cross, tripod grip
42 mo. Count bricks
Echolalia resolved
Full name
Plurals
Prepositions: under, up, down
Mime complex gestures
42 mo: fetch several items
Imagine play seq
Gender
Name friend
Share, turns
T-shirt
Shoes and socks
4 yrs
Hop 3 steps/ Jump off 2
Catch big ball
Down stairs like adult
5 brick gate
4 part man, ladder, square.
Cut with scissors; Higher, longer
Intelligible to strangers
Tenses
Constant Qs: where, why…
Prepositions: between
Opposites: big/little
What would you do if?; Comparisons
Gives age
Co-op play, hide n seek, snap
Dressups, pretend
Undress indep.
5 yrs
Run up stairs
Gallop
Bounce and catch
6 part man, triangle, pencil grip
6 brick stair, castle
Count 15 bricks
Grammatical sentences – conj. & except.
Ask meanings of words
What things are made of: wood, metal
Enjoy jokes, riddles
Knows address
Names best friend
Dress indep.
578 4
th
and 5
th
Year Notes
Older kids:
Gross motor: bike (can ride without trainer wheels at 5), sport (running, kicking), clumsiness
Fine motor: computer, play station
Cognitive: don‟t ask if does OK at school – everyone does OK these days! Instead, does he do age
appropriate work, need extra tuition, etc
Cognitive Development
Overall process:
Autonomy: dependent on parents peers independent
Abstract thinking (what if?): concrete mature
Future consequences of present actions
Gratification: immediate delayed
Satisfaction with body image
Black and white comfort with shades of grey
Infancy (birth – 2 years): Developmental issues:
Later develop goal directed activity
Learn to distinguish between self and surroundings
Develop object permanence
Need secure attachment relationship with parents
Separation, individuation in toddler years
At 2: trial and error problem solving, planned and purposeful play but limited content, egocentric,
parallel play
Preoperational (3 – 5 years):
Egocentric world view (I made it happen, so it‟s my fault)
Use of magical thinking, difficulty distinguishing real from symbolic (if I wish it, it will come true)
Trial and error problem solving only
One aspect of a problem at a time
Cannot order a series of events
Cause and effect thinking: I did X, then Y happened, therefore X Y
Imaginative play
Gradually move from parallel play to interactive play with peers
Separation and autonomy
At 5: symbolic thought (imagination), classify by colour/shape, curiosity, magical thinking, social
values, rules internalised but fixed, turn-taking, cooperative plan, other‟s perspective, increasing
independence
Concrete Operational (6 - 10 years):
Black and white thinking, right and wrong
Capable of simple logic and problem solving
Can order things in a chronological sequence
May have difficulties with multiple perspectives
Peer relationships increasingly important
Sharing games, competition
Analogy, metaphor, figures of speech being
Able to concentrate for longer, delay gratification, predict personal and social consequences of
actions, plan ahead
Formal Operations (10 – 13 years):
Better memory, concentration, forward planning
Social skills refined
Still concrete and literal (black/white, good/bad, right/wrong)
Limited abstraction: eg what if I didn‟t do this? (Contrary-to-fact abstraction)
Dramatic changes to body constant comparisons and normal anxieties
Need to conform with peer norms
Difficult to take others perspective‟s
Difficult to understand complexity
Difficult to apply rules to own situation
Lack future orientation/forward thinking
Clear consequences
Middle Adolescence (14 – 16 years):
Paediatrics 579
Developing abstract and complex thought
Beginning to see other‟s perspectives, starting to cope with shades of grey
Increased self consciousness
Easily swayed – not certain of own view
Still difficult to integrate conflicting ideas
Narcissistic (feels good/what I want therefore its right impulsiveness)
Less need to conform to peer norms, try alternative beliefs and philosophies
Need limits to be secure, limit testing
Late adolescence
Adult memory and concentration
Mature abstractions, problem-solving, self reflection and long range planning
Weigh up multiple information
See multiple meanings, complex relationships, different points of view, tolerant of shades of grey
Able to think hypothetically and plan for possible events
Remains more difficult to use new abilities in challenging situations
Autonomous: able to leave home and return for counsel, rely on own opinion
Developmental Delay
Constant slow development leads to widening gap
Investigations: hearing, vision, chromosomes, DNA screen (eg Fragile X, Angelman, Prader-Willi),
thyroid, metabolic, mucopolysaccharide screen, CK (Duchenne‟s), brain imaging, EEG
Type of Diagnosis:
Functional Diagnosis:
Mobility, communication, learning, self-care, socialising, etc
What does the child need to achieve age-appropriate function
Pattern diagnosis:
Autism: see Autism, page 582
Cerebral palsy: see page 629
Other syndromes
Biological diagnoses: DNA disorders, brain injury
IQ scores:
< 20 profound intellectual disability
20 – 35 severe
35 – 50 moderate
50 – 70 mild
70 – 85 borderline
Definite or highly probable cause in majority < 50. Cause in about half < 70
Management:
Objectives:
Maximising function
Preventing and treating secondary problems
Supporting carers
Referral: paediatrician, geneticist, psychologist (eg cognitive testing), SLT (speech, swallowing,
play), physiotherapist (gross motor problems), OT (fine motor, self care, aids and equipment),
early intervention groups, VNDT (Visiting Neurodevelopmental therapist), support groups
Medical assessment of a diagnosed, disabled child
Always consider new illnesses
Look for syndrome specific health problems
Feeding difficulties, nutrition
Constipation
Medication
Carer Stress
Access to services and allowances
Tamariki Ora (Well Child) National Schedule
Covers:
Health education and promotion
Health protection and clinical assessment
580 4
th
and 5
th
Year Notes
Family/whanau care and support
Health education/promotion topics to cover at appropriate stages
Prevention:
Types:
Primary: shifting the whole population curve improves the overall standard
Secondary: identifying risk factors early or targeted intervention
Tertiary: minimising impact of established disease
Benefits of prevention: adult sequalae: injury, child abuse, delinquency and arrest rates
PPV of parental concerns about delay is about 80 –90%. Must act or refer on parental concern
Causes of Developmental Delay
Causes of abnormal development:
Environmental
Genetic (eg chromosomal, metabolic)
Disability (vision, hearing, motor)
Brain injury (hypoxia, trauma, toxins, infection, prenatal & post-natal)
Illness, nutrition
Unknown
Hearing
See Hearing Loss in Hearing Loss, page 151
1 in 500 has significant permanent hearing loss receptive and/or expressive language delay
All infants babble, even hearing impaired
Suspect deafness when:
Parental concern
At risk babies (should be routinely screened):
Family history
Inter-uterine infection: rubella, CMV
Defects of ENT: cleft palate, external ear
Low birth weight
Neonatal distress
Poor response to sound
Not using words by 15 months
General developmental delay
Poor speech, comprehension and hearing failure
Following brain trauma, infection, neurotoxic drugs
Recurrent or persistent ear infections
Normal development: See Development Chart: normal development from 0-60 months, page 576
History:
Can he hear – how do you know?
Previous development: first word, use of consonants, etc. Check Well Child Book
Ear infections
Antenatal: rubella, prematurity, jaundice, drugs
Family history of hearing problems, developmental delay, neuro problems
Exam:
Dysmorphic features: cleft palate, external ear, skin, heart murmurs, liver enlargement, normal
genitalia
Basic neuro exam, gait, symmetry of movement (including face), eye movement
Investigations:
Tympanogram
Don‟t do distraction testing – hard unless you‟re well trained. Send straight for audiology
Others depending on clinical findings: eg if regression then EEG, brain scan, check stressors,
chromosome problems, CK for Duchenne‟s
Differential of language delay:
End of normal range
Deafness
Isolated language delay (usually expressive more delayed than receptive – but not necessarily)
General delay or mild intellectual handicap formal cognitive testing

Paediatrics 581
Autism
Epilepsy: absence seizures – especially if fluctuates or regressive
Possibly poor environment with little stimulation – but would also expect socialisation and self
care
Congenital problems: cleft palate, macroglossia (eg Down‟s)
Rare isolated CNS or motor problems
Management: Speech language therapist, early intervention service, multidisciplinary team if problems
over other domains. GP to support and co-ordinate, anticipate problems – especially at transitions (eg
school, moving) and checking for comorbidity (eg behavioural problems, self esteem)
Prognosis: Good if early intervention – but maybe problems with higher language function (eg essay
writing)
Down Syndrome
Trisomy 21: 47XY + 21
Accounts for 95% of presentations of Down Syndrome. Usually (80%) non-disjunction at first
meiotic division
5% have different karyotypes:
Mosaic Down: 3 %
Robertsonian translocation t14:21: 4.8%
Epidemiology:
Overall incidence is 1 in 700
At least 20% still born
Incidence increases with maternal age: at 16/40 gestation, 1 in 300 at 35 years, 1 in 22 at 45 years
Accounts for 25% of children with IQ < 50
¼ of all chromosomal abnormalities. Chromosomal anomalies represent 15% of congenital
anomalies
Risk:
Maternal age at birth
Down in live births
25 - 29
1:1100
30
1: 900
35
1:350
37
1:200
40
1:100
43
1:50
45 and over
1:25
Neonatal Screening:
Only 30% of children with Down are born to women over 35. Widespread screening of those > 35
will have only minor increase in detection rate
Screening with the triple test will increase detection, but at the expense of significantly higher rates
of invasive testing as there is a high false positive given the low incidence in younger women
See Prenatal diagnosis, page 360
Neonatal signs:
Hypotonia
Moro reflex
Joint hyper-extensibility
Excess skin at the back of the neck
Flat facial profile
Misshapen low set ears
Protruding tongue
Blunt inner eye angle
Single palmer crease in 50%
Clinodactyly (incurving) of little fingers in 50%
Big „saddle‟ gap between big and 2
nd
toe
Complications:
IQ generally from 45 – 55
Congenital heart malformations in ~50%: VSD, ASD, patent ductus
Susceptible to respiratory infections
Duodenal atresia
Also cataracts (2%), epilepsy (10%), hypothyroidism (3%), acute leukaemia (1%)
582 4
th
and 5
th
Year Notes
Development:
Most will walk and develop simple language
Puberty is often delayed and incomplete
Average adult height is 150 cm
Pre-senile dementia (similar to Alzheimer‟s disease) supervenes after age 40
8% live past 40 years
Autism
Onset before age 3 of:
Ability to form social relationships: slow to smile, don‟t enjoy being cuddled, indifferent eye
contact
Use of both verbal and non-verbal communication: slow onset, echolalia, no use of gesture, poor
pragmatics (eg turn taking and eye contact in conversation). If it was isolated language delay you
would expect compensation in other areas (eg social) but here that‟s affected as well
Restrictive and repetitive behavioural repertoire – dislike change
May start from birth, or regress after normal development
Other behavioural problems: outbursts, sleep problems, distractibility, poor toileting
Rare: 2 – 4/10,000. Boys = 3 * girls
75% show some degree of general intellectual impairment
Asperger‟s Syndrome:
Symptoms overlap with autism
Social interaction and behavioural problems similar to autism but not associated with significant
language or intellectual delay
Effect of Chronic Disease on Development
See also Chronic illness and disability in Adolescents, page 669
10 – 15 % of children have some chronic health condition. 1 – 2% are severe enough to interfere with
their ability to take part in normal activities
Chronic illness can effect development by:
Direct effect: eg deafness language delay
Effect of treatment: eg neuro-radiation
Indirect effect: reduced energy in cystic fibrosis
Social environment: sense of differentness withdrawal or bullying
Transaction: impact on parents (eg maternal depression) affects child‟s adaptation
May lead to failure to develop independence (self control) and competence (control over their
environment), leading to self-doubt or indecision.
Issues to consider:
Burden of care: don‟t give them more helpful ideas if they‟re already over-stretched!
Unpredictable future: Clear idea for the parent and child of what the future might hold
Social/school: Watch for „vulnerable child syndrome‟, bullying, and access issues.
Cost: check relevant benefits received
Respite care: do parents need a break? Deal with feelings of guilt and indispensability
Activities of daily living: the daily routine will be revealing
Multiple professions: check these are co-ordinated and organised around the family‟s needs
Psychological: consider impaired attachment, depression, stress, family dysfunction
Also ensure:
Information for child and parents
Access to services
Access to consumer groups
Equipment and transport needs
Environmental modification
Vocational training for an adolescent
Infants
Effect on parents of congenital malformation:
Shock, disbelief, upset, problem solving processes slowed
Adaptation over time
Grief reaction similar to death of a child (must mourn the loss of a „normal‟ child) – but parent
must also attach to the living child
Paediatrics 583
Management:
Support good bond-enhancing practices before and immediately after birth:
Normal preparation for birth (learn about routines, processes, options, etc)
Time to establish rapport with paediatrician and visit NICU
Long periods together in first few days and breast-feed if possible. Is any separation really
necessary?
Avoid criticism – a very sensitive time
Watch for signs poor attachment. See Attachment Disorder, page 573
For the toddler:
Watch for „vulnerable child syndrome‟: continued parental concern after child has recovered
adverse affects on child. Problem is parents‟ expectations, not attachment. More
complicated when some ongoing vigilance is required
Support appropriate attitudes and plans
Mobilise family support
Remain optimistic
If in hospital, use separations to reinforce that parents will return. Limited number and
consistency in nursing staff
Pre-schooler
Social and emotional development may be limited through lack of opportunity to achieve goals in play
and by limited peer interactions
Management:
Refer for early intervention, especially low socio-economic and disabled children
Promote normal development: separation, appropriate discipline
In hospital: encourage rooming in, maximum contact with families
Warn parents to anticipate behavioural problems especially if hospitalisation is prolonged or
frequent
Head injured child
Initial crisis: grieving put on hold, waiting to see if things improve, child still looks the same, swinging
between hope, despair and disbelief
Restructuring:
Reassign tasks in the family
Move out of crisis reorganisation into long term reorganisation
Inclusion of outside help into family
Appropriate time for husband/wife/other children
Time for self
Grieving:
Allow for grief and acknowledge the loss
Avoid dichotomy of one person (eg mother) taking hope position and others despair
Promote openness. Devastation of silence
Denial can also be a coping mechanism
Develop an acceptance of a new identity through the crisis:
Seeing how the child is different
Finding positives in this new identity and helping the family value these
Achieve a sense of movement through the crisis. Mark positives and achievements of the family
Encouraging compliance:
For the highly compliant: teaching, directions
For the non-compliant (those who respond „yes – but….‟): general indirect messages,
metaphor/story telling
Subsequent learning disabilities: may have problems with learning from then on – but may not show up
till those skills are needed (eg trouble reading when they start school)
Learning Disability
History:
Start with things he is likely to be able to do and work up
Questions over traditional domains for learning:
Reading: „what is she reading now‟, „can she read three letter words‟
Spelling
584 4
th
and 5
th
Year Notes
Numeracy
Writing
Drawing, art, craft
Social skills
Strengths
Collaborative history:
Previous assessments, IQ tests
Talk to the teacher
Comorbidity screen:
Is the norm in developmental paediatrics
Can be:
Primary: eg biological morbidity such as learning and co-ordination difficulties, ADHD
and clumsiness
Secondary: eg acquired psychological and behavioural problems such as loss of self-
esteem, non-compliance, etc
Differential:
Behaviour: aggression, attention seeking, school refusal
Mood, anxiety, attention
Relationship with peers, teasing, bullying
Family issues – get good social history
If adolescent then HEADDSS assessment (See page 666)
School factors: teacher skills, interest/ability to manage the child‟s needs, available skills
Parental insight: are they helping or hindering
Use questionnaires: eg Child Behaviour Checklist (screen for anxiety, depression, etc) or Connor‟s
(specific for ADHD) to provide diagnostic information and provide a pre-treatment baseline
Exam:
Screen for gross and fine motor delay
Refer for vision and hearing tests
Possible differentials:
Hearing and vision
Medical: hypothyroid
Intellectual disability
Specific learning disabilities
Head Injury
Psycho-social: Abuse, stress, etc
Psychological: depression, anxiety, ADHD
Principles for management:
Review and follow-up (eg 3 monthly), especially at times of transition (eg changing schools)
Multidisciplinary approach: OT, Physiotherapist, SLT, VNDT, Educational Psychologist
Excellent communication between professionals
Helping parents to create realistic goals
Dealing with normal parent grief
Strategies for management:
Demystify: Explain strengths and weaknesses to the child, parents and teacher. Removes guilt,
pejorative labels (eg lazy), gives optimism
Bypass strategies: adjust rate, volume, complexity, format or use devices to make the task easier
Remediation of skills: focus on study skills, organisation, use strengths to remediate weaknesses
Developmental therapies: Eg speech therapy, gross and fine motor, etc. More effective when skill
deficits reflect lack of opportunity, and when instituted earlier
Modify the curriculum: Eg drop subjects they‟re not succeeding in
Strengthen strengths: sport, art, mechanics, etc
Individual/family counselling: especially with behaviour management, family dysfunction
Advocacy
Medication
Longitudinal case management
Check whether parents get the child disability allowance. Can get a needs assessment done for respite
care, home help, etc
Paediatrics 585
Child Development Team
For children with:
An identified disability
Developmental delay
At risk of developmental delay/difficulties
Involves multi-disciplinary assessment and intervention
Social Worker:
Conducts individual, marital and family social assessments
Liases with other community services (CYFS, WINZ, etc) and facilitates brokerage of services
Provides emotional support
Teaching parenting skills
Advocacy
Psychologist:
Assessment: neuropsychological, development, behaviour/emotion, family function
Intervention: For individual, skills for parents, family relationships
Physiotherapist:
Functional assessment of gross motor skills: delay, abnormal muscle tone, loss of range of
movement, gait abnormalities, mobility, co-ordination
Therapy (including hydrotherapy) and home/school exercise programmes
Assessing for standing frames, walking aides and wheelchairs (with OT)
Occupational therapist:
Assessment of fine-motor skills (use of hands):
Tool manipulation: grasp and grip, bilateral hand use, release, eye-hand co-ordination (eg
stacking)
Pre-writing: lines, circles, picture of a person
Handwriting: grip, control, sizing, closure, hand dominance, speed
Cutting with scissors: accuracy and co-ordination
Assessment of self-care skills:
Undress/dress, buttons, zips, shoelaces, etc
Feed themselves
Sit unsupported in the bath
Toileting, including sitting on toilet, pulling pants down, wiping
Clean teeth, brush hair, wipe face
Assess for equipment to help with the above
Speech language therapist: assesses and assists with:
Receptive language: understanding
Expressive language: including gesture and facial expression
Phonology: sound system
Pragmatics: social rules – sharing, turn taking, eye contact (biggest problem in autism)
Feeding: transition from tube to oral feeding, behavioural feeding issues
Voice: vocal nodules due to abuse (eg screaming)
Fluency: stammering
Visiting Neurodevelopmental Therapist:
Home based assessment
Family support
Liaison with other health professionals and community agencies
Assessment for equipment
Developmental paediatrician:
Developmental assessments/examination for suspected delay
Investigates cause
Review of developmental progress
Growth
Growth velocity = change in height over time. Declines till about 4, levels out, spike at puberty then
zero
Factors influencing growth:
Genetic potential
Psychosocial factors (eg psychosocial dwarfism)
586 4
th
and 5
th
Year Notes
Nutrition (including in utero): adequate calories, balance of nutrition
Diseases in major systems: uses energy (eg respiratory effort) and nutritional effects (eg GI)
Hormones and Growth factors
Measurement:
Method: Use stadiometer, fixed to wall, feet together, knees straight, lift mastoid processes
Accuracy and reliability:
SD of a single measurement ~ 0.25 cm. In a 5 year old this can cause a range in growth
velocity from 10
th
to 50
th
centile
Taller in morning than at night
Minimising error: Same measurer, calibrate regularly, careful measurement, don‟t look at last
measurement, measure at beginning and at end of exam
Short Stature
Definition:
> 2 standard deviations below the mean = below 5
th
centile
Reduced growth velocity
Exclude failure to thrive
Growth pattern is more important than height
Normal variants:
Familial (genetic) short stature
Constitutional delay of growth and development. Presents mid to late childhood
Familial (genetic) short stature
Constitutional Delay
Height
< -2 SDs
< -2 SDs
Bone age (hand xray)
= Chronological
< Chronological. Delayed
through childhood, accentuated
when peers reach puberty
Puberty
Normal
Delayed
Growth velocity
Normal
Normal
Final height
Short
Normal/Tall (keep growing for
longer)
Parents
Short
Normal
Family History
Positive (for short stature)
Positive (for constitutional)
Pathological causes:
Systems: eg subclinical GI or renal disease (reflux, coeliac, malabsorption, CF, etc)
Psychosocial
Genes:
Turner syndrome: webbed neck, wide nipples, wide carrying angle
Skeletal dysplasia: eg achondroplasia
Syndromes
Hormones: Thyroid or GH deficiency, glucocorticoid excess
Drugs: Steroids
Assessment:
History:
Height: measured accurately and over time
Mid-parental height: assessment of genetic potential (adjusted so both parents are same sex as
child. Male = female + 13 cm or average their centiles)
Family history: eg constitutional delay
Systems
Psychosocial
Development
Examination:
Growth parameters
Dysmorphic features ?syndrome
Proportions: limbs vs trunk, eg arm span vs height, or upper segment (head to pubic bone) vs
lower segment (pubic bone to floor)
Blood pressure (?renal disease)
Fundi and visual fields (?pituitary tumour)
General
Investigations:
Paediatrics 587
Bone age: accurate to about 3 months
Specific depending on history/exam, eg renal creatinine, coeliac antibodies
Karyotype in girls
Treatment:
Treat cause
Growth hormone:
Effective in GH deficiency and Turner‟s syndrome
May help in chronic renal failure, intrauterine growth retardation and severe idiopathic short
stature
Androgens: consider in constitutional delay – won‟t influence final height but get there faster.
Tall Stature
Arbitrary definition
Associated stigma (females more often seek help)
Causes:
Familial/genetic
Over-nutrition
Syndromes (eg XXY, Marfan‟s, Homocystinuria)
Precocious puberty (tall early, but stop growing eventually short)
Growth hormone excess is extremely rare
Growing Pains *
Occurs frequently: 15% of children with peak age of 11
Diagnosis of exclusion – no organic pathology usually found. ?Child more vulnerable to pain and
stress-induced exacerbations
Occurs at least monthly for a three-month period. Between times the child is well
Differential:
Orthopaedic disorders
Collagen vascular disease
Infection
Neoplastic disorders
Management:
Reassure, even if you can‟t find a cause
Symptom diary (also check for psycho-social stressors)
Symptomatic relief
Neonatal and Infants
Neonatal is < 4 weeks
Examination of the Newborn
History
Maternal history:
General health and well-being: past medical history and social history (partner, planned pregnancy,
etc)
Pregnancy: mediations, alcohol and other drugs, complications, infectious illness (toxoplasmosis,
rubella, etc), EDD, scan findings, parental blood groups
Family history: perinatal deaths, paediatric deaths, congenital problems (especially congenital
dislocated hip)
Delivery history: length of labour, infection, resuscitation, APGAR, any concerns
Post-natal history: feeding, colour changes (blue, jaundice), behaviour, stools, urine
Have you any concerns about your baby?
Examination
Initial assessment immediately after birth to check adaptation to extra-uterine life (eg APGAR) and to
look for major congenital anomalies, especially:
Dysmorphic features
Choanal atresia
Major limb defects
588 4
th
and 5
th
Year Notes
Spina bifida
Anal atresia
Genital abnormalities
Birth trauma: bruising, cephalhaematoma
Examine on Resuscitare. Check all equipment carefully first.
APGAR assessment – at one minute, then 5 minutes then every 5 minutes till a score of 10:
Heart rate: 2 for > 100, 1 for < 100, 0 for not present
Colour: 2 for pink, 1 for blue, 0 for pale
Respiration: 2 for regular or strong cry, 1 gasping intermittently (may be bad sign – secondary
hypoxia), 0 for none. May slow due to maternal drugs (eg pethidine)
Tone: 2 for active movement, 1 for limb flexion
Response to stimuli: On suction, 2 for coughs well, 1 depressed
Apnoea:
Primary Apnoea: pulse < 60 and cyanosis. Give O2 and wait a minute
Secondary Apnoea: pulse < 60, pallor and floppiness: suction, ventilate, intubate
General inspection:
Dysmorphisms: eyes, ears, mouth, cry
Colour: central, peripheral
Respiratory effort: grunting, indrawing, flaring nostrils
Posture and movements:
Normal: hips abducted, partially flexed, knees flexed, arms adducted, flexed at elbow, hands
closed (not tightly), fingers over thumb
Abnormal: hypotonia, irritability
Skin: colour, rashes
Systemic examination:
Head:
Skull: fontanelles, sutures, birth trauma
Eyes: red reflex, opacities, conjunctivitis
Nose: patency
Mouth: palate and suck
Ears: hearing, tags
Neck: upper airway
Chest: shape, deformities, respiratory distress, cardiac auscultation, peripheral pulses, respiratory
auscultation
Abdomen: cord, 3 vessels (2 arteries and a vein), shape, liver, spleen, kidneys, bladder, genitalia,
urine stream, anus, passage of meconium, femoral pulses,
Limbs and other bones: upper limbs, digits, palmar creases, clinodactyly, grasp, lower limbs,
digits, hips, talipes (club foot), spine
Neurological status: cry, jittery, spastic, grasping, activity, irritability, symmetry of movement,
tone, neonatal reflexes
Neonatal reflexes: stepping, walking, Moro, grasp, rooting
Also:
Growth: weight, length, OFC plot
Offer vitamin K IM as prophylaxis against Haemorrhagic disease of the new born
Cord blood for blood typing and Rhesus -ive, and also measure Cord pH (from artery) – measure
of hypoxia
If baby has patches of yellow sitting in meconium for a while stain
If uncertainty about gestational age then formal assessment
Re-examine at end of the first week of life, especially for signs of congenital heart disease. Takes
~ 48 hours for ductus to close
Other observations:
Micturition: usually soon after birth, infrequent for first 24 hours
Bowel: 99.9% passed meconium by 48 hours/ Otherwise ? Cystic Fibrosis, Hirshprungs
Jaundice: 40% develop it, but transient, resolves by day 5
Vomiting: a little is common. Green is bad (= bile)
Temperature: rectal best. Same range as adults when dressed appropriately
Weight: 1
st
3 – 5 days may loose 5 – 10% of birth weight. Should regain it in 7 – 10 days
In first week:
Paediatrics 589
Immunisations: if mother HBsAg +ive then Hep b Vaccine and HBIG
Guthrie card. See Genetic Testing, page 465
Outcome after Preterm Birth
At 27 weeks, 90% survive to discharge
Definitions:
Prematurity: < 37 = weeks Preterm, < 33 = weeks Very preterm
Birth weight (?relevance to Pacific Island Babies – usually heavier):
< 2.5 Kg: LBW
< 1.5 Kg: VLBW
< 1.0 Kg: Extremely low birth weight
Factors affecting prognosis:
Prenatal: Socio-economic, maternal smoking, infertility
Antenatal: multiple birth, IURG, maternal illness, smoking, steroids before delivery
Birth: time of transfer, method of delivery, APGAR, resuscitation
Postnatal:
Size of NICU, surfactant, breast feeding
Hypoxic-Ischaemic Encephalopathy (HIE): O2 delivery to brain becomes oedematous
over next 24 – 48 hours
Assessment of outcome: lots of problems with cohort studies: which population, admission, length of
follow-up, what‟s measured, etc
Issues for mothers of NICU babies:
How they perceive health workers
Postnatal Depression
Visiting family commitments
Breast feeding: often expressing
Complications of Preterm Birth
Anaemia:
Miss out on the „iron loading‟ that happens through 3
rd
trimester
Haemorrhage: feto-maternal, twin to twin, placental, cephalhaematoma, etc
Haemolysis: Rhesus disease, ABO incompatibility, spherocytosis, G6PD deficiency
Infection: CMV, rubella, septicaemia, UTI
Bleeding disorder: haemorrhagic disease of the new born
Respiratory Distress Syndrome:
=Hyaline Membrane Disease
Inversely proportional to gestational age and birth weight, also diabetic mothers, asphyxia, cold
stress, etc
Surfactant deficiency alveolar collapse haemorrhage/protein leaking hyaline membrane
Signs: indrawing and expiratory grunt
CXR: ground glass appearance with air bronchogram. See Chest Radiology, page 604
Broncho-Pulmonary Dysplasia (BPD):
Follows ventilation for respiratory distress and O2 toxicity
Histology: necrotising bronchiolitis and alveolar fibrosis
Mortality 40%
Long term: airways obstruction, airways hyper-reactivity and hyper-inflation
CXR: patchy collapse and fibrosis with areas of cystic change and over-distension
Intraventricular Haemorrhage (IVH): small haemorrhages into the germinal layer lining the lateral
ventricles with hypoxia. May hydrocephalus. Most have no serious long term sequalae
Parenchymal Haemorrhage:
Into brain, not IVH
Incidence 1 – 2 % of preterms
Most are unilateral
Outcome depends on site
Varies from nil to severe hemiplegia
Periventricular Leukomalacia:
Incidence 4% of preterms
?Associated with maternal infection
590 4
th
and 5
th
Year Notes
Frontal, usually watershed lesion
Cysts long term spastic diplegia (legs worse than arm)
Retinopathy of Prematurity: Abnormal vascularisation of retina following exposure to high O2
concentrations. Screen all babies < 31 weeks or 1500 g
Necrotising Enterocolitis:
During first 3 weeks (up to 3 months in VLBW infants). Rare in term babies
Aetiology uncertain:
Hypoxic damage to bowel wall (?umbilical catheterisation, apnoeic spells, septicaemia)
Colonisation with certain bacteria: Clostridium perfringnes, E Coli, S Epidermidis, Rotavirus
Necrotic segment of intestine with Pneumatosis Intestinalis („string of pearls‟ sign on X-ray
plus portal gas seen in liver) perforation, sepsis, etc
Presentation: sepsis, bloody stools, bile stained vomiting
Pathogenesis:
Necrotising inflammation of the small and large intestine
Mucosal oedema necrosis gangrene, perforation, peritonitis
Sequalae: malabsorption, strictures, short bowel syndrome
Skin easily irritated (eg alcohol, tape, drips) long term scars
Also:
Jaundice more common
Hypoglycaemia more common
Failure of closure of patent ductus (give anti-PGs, eg endomethacin)
Problems associated with Intrauterine Growth Retardation:
Immediate:
Hypoglycaemia (see Hypoglycaemia of the New Born, page 595)
Polycythaemia (eg due to placental insufficiency) heart failure (due to viscosity),
pulmonary hypertension, NEC. Treat with exchange transfusion (eg or saline) Hb
Hypocalcaemia (test ALP)
Jaundice
Plus others (eg Cerebral Palsy)
Neonatal and Infant Anticipatory Guidance (Parent Education)
See Parent and Adolescent Education, page 567
Consider the topics for discussion about a neonate:
Vision and hearing: Can your baby hear and see (how do you know?)
SIDS prevention: sleep on back, smoke exposure, breast feeding, nothing over head when
sleeping (see Sudden Infant Death Syndrome (SIDS), page 594)
Immunisation: the schedule, genuine and non-genuine contra-indications, common myths, benefits
and risks (see Vaccination Practice, page 517)
Maternal mental health: screening and assessing for post-natal depression (See Postpartum Mood
Disorders, page 430)
6 week screening: dysmorphic features, cleft lip and palate, growth, eyes, heart, hips (see Six
Week Check, page 374)
Contraceptive advice
Smoke cessation
Always ask why has the mother really presented
When neonatal and/or later, consider the following:
Recognition of illness, emergency contacts
Feeding: breast feeding and maternal nutrition, introducing solids, nutrition
CPR
Parenting skills: eg management strategies for sleep and toddler behaviour, toileting, eating
Injury prevention: seat belts, fire safety, falls, hot water, sun exposure, poisoning, safe child care,
pools, playgrounds, road
When to expect which developmental milestones. Reassure for parents. Also early identification
early intervention
Developmental needs of kids: play, language, nutrition, social etc
Breast-feeding
See also Pharmacology of Pregnancy and Breast Feeding, page 528
Paediatrics 591
See also Breast in Pregnancy and Breastfeeding, page 376
Advantages:
Prevention of disease: passive immunity against gastro-enteritis and otitis media due to better
Eustachian tube drainage
Bonding
PPH
SIDS
Cheap and convenient (available, portable, sterile – cf bottle feeding, especially in 3
rd
world)
Contents vary with circumstances (fore milk has water content)
No constipation
Less spilling, less irritating than bottle feeding
Supply matches demand
Smells nicer at both ends. No constipation with breast milk
?Higher IQ
Males can‟t do it!
Disadvantages:
Discomfort establishing
Limits mum
Limited iron and phosphate, Vit D and C if preterm (cf bottle feeding which can be fortified)
Can‟t easily measure intake
Leaking
Maternal drugs are included (eg lithium)
Breast milk jaundice
Establishing breast feeding:
Babies don‟t feed much for 1
st
48 hours
Breast milk comes in around day 3 (especially 1
st
baby) baby‟s hungry on day 3
Can hurt – usually uncomfortable
Growth is best way of proving adequacy
Very hard to overfeed compared with bottle feeding (sucking is a reflex will keep bottle feeding
even if they don‟t want the feed)
Ongoing issues:
If feeding too regularly then baby will be getting CHO rich foremilk but not fat rich hind milk
hungry
Attachment to the breast is key: Is the baby nipple feeding or breast-feeding. If nipple then
repeated trauma pain, cracked nipples, etc
Mastitis or blocked duct express lots (try it in the bath)
Establishing bottle feeding:
Day 1: average intake 60 ml/kg (= 40 calories/kg)
by 15 ml/kg/day until average of 150 ml/kg/day
If too much then stools, vomiting, misery
Alternatives to cows milk: goat (but no folate), soya, hydrolysed (if allergic to everything else)
Allergy: eczema reaction mainly to casein proteins, but can also be allergic to whey protein
Can be intolerant (ie non allergic reaction) to:
Lactose (galactose + glucose): lactase osmotic diarrhoea + fermentation by bacteria
gas frothy acid stools acid burns round perianal skin. More common as
secondary intolerance (eg following Rotavirus). Breast milk has lactose too.
Fructose (eg fruits)
Sorbitol (artificial sweeteners)
Failure to Thrive (FTT)
= Failure to gain weight normally (< 3
rd
percentile, or falling serial measurements) [cf Stunted growth
= failure to gain height]
If also failure of linear growth long standing problem (weight always falls first, then length, then
head circumference falls last)
History:
What goes in (diet):
What and how much (and does it actually go in, or is it just offered?). Milk, other drinks,
meat, fruit and vegetables, cereals and breads, lollies
592 4
th
and 5
th
Year Notes
Assess parents knowledge base
Feeding difficulties: appetite, behavioural, structural, swallowing
What comes out (poos) – especially steatorrhoea. People usually overestimate vomit
Chronic illness: cardiac, renal, neurological
PMH: ABFWIMPS
Development
Social history: especially PND, other psych stresses, violence, drugs and alcohol
Examination:
End of bed: fat, thin, energy, pallor, well/sick, dysmorphisms
Muscle and fat stores – look for scraggy buttocks
Signs of abuse and injury
Signs of chronic disease:
Cyanosis due to heart: L R shunt and heart failure or cyanotic lesion (R L shunt)
Respiratory: clubbing, nasal polyps (CF, asthma)
Gut: coeliac (not if breast feed) – distended abdomen and thin legs
Renal: blood pressure
Assess suck, chew, swallow
Rickets (vitamin D), anaemia (Fe), Bruising (vitamin K), dermatitis & neuropathy (Vitamin
B) (all late signs)
Differential:
Parent‟s expectations: In the 2
nd
year of life: appetite, rate of growth, activity are all normal.
Parents may need reassurance
Non-organic failure to thrive:
Inadequate parenting/poor nutrition the most common cause (will feed and gain weight well
while in hospital).
Usually complex situation: eg young mum, unwanted pregnancy, obstetric problems, poor
bonding, bottle feed, maternal depression, etc.
Is the milk being made up properly, any strange stuff (eg tea, Milo, etc)
To cheek for attachment: observe mum chatting to baby while they dress – is she talking to the
baby
Organic causes:
Intake secondary to:
Underfeeding (eg engorged breasts poor latching on, inverted nipples)
Congenital abnormalities (eg cleft palate)
Dyspnoea (eg chronic heart failure, CF, chronic URTIs)
Neurological lesions (eg pseudobulbar palsy)
Behavioural factors (eg alert, restless)
Abnormal losses:
Vomiting: need to be severe and persistent to FTT. Eg pyloric stenosis, chronic UTIs,
renal disorders
Stools: diarrhoea, steatorrhoea
Urine: eg diabetes, renal failure, diabetes insipidous, adrenal insufficiency
Failure of utilisation:
Chronic infection (eg Tb, UTIs, immune disorders)
Metabolic disorders (eg phenylketonurea)
Endocrine disorders (eg hypothyroidism)
Constitutional and genetic abnormalities: Short stature, Down‟s, Turner‟s, Achondroplasia
Increased requirements: Chronic lung disease, heart disease, etc
Macrosomic babies (ie mum diabetic) will loose excess weight after birth looks like failure
to thrive
Management:
If non-organic failure to thrive, then educate regarding a baby‟s dietary needs. See Parent and
Adolescent Education, page 567
Investigations: rarely necessary. Maybe Fe for anaemia
The Crying Baby
A multifactorial problem
Normal crying:
Paediatrics 593
Babies cry their most at 6 weeks – just when the honeymoon period is over and all the supports
have gone back to work/gone home
Range for ½ to 7 hours per day
It‟s their only means of communications
May be hungry, overfeed, tired, pain, bored, hot, cold, inadequate burping, switching breasts too
soon ( low fat feeds), solids before 3 months.
Note especially babies cry when they‟re tired – common mistake is to stimulate and sooth them
when they need to sleep
Not due to parental stress. Crying leads to stress not the other way round. Harder for older women
and professional who worked up to delivery to cope with ( sense of isolation post delivery)
Colic: definitions vary from crying lots to “well thriving baby who develops muscle spasms, flushing
face, pulls up legs, screams. On and off every few minutes for several hours, loud tummy rumbles,
relieved by flatus or passage of stool”
Theories:
Gut immaturity disordered intestinal motility GI pain
CNS immaturity immature, disorganised response to stimuli response to most things is
to cry
Very unlikely to be lactose intolerance (rare before 3 months) or maternal cows milk
consumption
History:
Clarify what the parent wants to know – address their issues
HPC: How often, when, associated behaviours, timing, pattern
Vomiting and bowel patterns
Feeding and sleep patterns
PMH: ABFWIMPS
Maternal social history: attitude to baby, supports, PND, drugs and alcohol
Exam and investigations:
Check growth
Exclude physical causes:
Acute: otitis media, intestinal cramping/diarrhoea, corneal abrasion, incarcerated hernia
Chronic: gastro-oesophageal reflux
Nutritional intolerances from mother‟s diet (rare)
Issues:
Baby‟s safety: Is mum is at breaking point?
Feeding problems: sore nipples, nipple infection (eg thrush)
Maternal mental state: depression, lacking support, sleep deprived, anxious
Maternal nutrition: is she eating well?
Management:
Acknowledge strain
Reassurance: “I have looked carefully for physical causes and there are none that I can see”.
“Baby is growing well so is getting the food they need”
Things to try: rocking, pram, vacuum cleaner, ride in car, dummy, massage, warm bath
Feeding: not too often, burp well, having enough?, no solids till 4 – 6 months, maternal diet
(caffeine, cabbage, onions, experiment with what causes baby to cry)
Optimistic outlook: from 6 weeks to 3 – 4 months amount of crying normally reduces significantly
Active advice: plan what mum can do to make it easier
Referral to Plunket nurse or Plunket Karatane centre and/or lactation consultant
Sleep Management
Principles:
Sleep is a learned process – you train your baby to do it
After 6 months a night feed becomes a reward for waking up trained night waker
Parents also need time for themselves
For babies:
Night feeds: quick, quiet, dim light
Leave the baby to cry for a while
Wrap them well, then not woken by their own reflexes (eg startle reflex when lightly asleep)
Toddlers:
594 4
th
and 5
th
Year Notes
Evening routine: won‟t harm toddler if you‟re firm with bedtime routines. No energetic games
beforehand
Approach to Sleep Training:
Agree with partner/family what you are going to do
Plan in advance (eg start on a long weekend). Warn neighbours
Tell the child how it is going to be and why
Quiet bedtime routine every night
Put in bed, say good night, walk out
If they come out, return them to bed with no reinforcement or eye contact
If they cry, wait 5 minutes, then 7 minutes, then 9 minutes, etc. When going in, no
reinforcement
Stick with it. May get worse before it gets better. Should see improvement by 5
th
night
Sudden Infant Death Syndrome (SIDS)
Defn: death < 1 year, and still unexplained after autopsy, review of clinical history and examination of
the death scene (in practice none of these is usually done well)
Epidemiology:
1990: approx 4.5 per 1000 live births
2000: approx 1 per 1000 live births (about 70 per year). Pakeha lower, Maori about 4 per 1000
Epidemiological risk factors:
Age (3 – 5 months)
Maternal smoking – now greatest modifiable risk factor given sleeping on back well established
Prone sleeping position
?Bed sharing
Seasonal (winter worse)
Previously well
Race (eg higher in indigenous minorities)
Male
Low birth weight
Low maternal age
Low Socio-economic status
Theories:
Re-breathing of expired gases (eg prone or bed sharing)
Hyperthermia
Co-sleeping (bed sharing)
Differential diagnosis:
Child abuse (eg shaking injury, suffocation)
Metabolic disease
Cardiac disease (congenital or acquired)
Overwhelming sepsis
Accidental asphyxia (eg in bed) – requires good death scene exam and history
SIDS follow-up:
Explanation of death
Explanation of grieving process
Follow up with next child
Screen for risk factors
Role of monitoring (no evidence of effectiveness but reassuring for parents)
Prevention:
Supine sleep position
No smoking
Own cot
Avoid bed sharing or sofa if tired or smoker or alcohol intake or pillows
Dress for room temperature (ie don‟t let them get too hot, no hat in bed)
Make up bed so they can‟t slip under the covers (ie short-sheet the bed)
Complications of prone position: Plagiocephaly (flat spot on skull). Prevent by varying position of the
head when lying
Paediatrics 595
Neonatal Acute Airway Problems
Choanal Atresia: failure of formation of nasal passages. Baby goes blue until someone opens the
mouth. Can‟t pass NG tube. Can be unilateral
Congenital masses: nasal encephalocele and nasal dermoid. Care with nasal intubation. Beware the
midline lesion
Pierre Robin Sequence: short jaw, cleft palate and tongue falls back and obstructs. Nurse prone.
Associated with oligohydramnios
Subglottic Stenosis: due to intubation trauma in a preterm baby
Hypoglycaemia of the New Born
Not a big deal, but needs to be recognised and managed
Causes (either big babies or small babies):
Hyperinsulin: Child of poorly controlled diabetic mother. Maternal glucose fetal glucose
fetal insulin (important growth factor in utero) fatter and larger baby, haemoglobin
Small babies: Double whammy: lack of substrate and requirements (eg cold quicker)
If septic or otherwise sick (may also go hyperglycaemic due to cortisol and adrenaline)
Symptoms:
Usually none. Can be asymptomatic at < 1 mmol/litre of glucose [would cause convulsion in
adult]
May be jittery (but most common cause is difficult delivery)
Convulsions or floppy (post-ictal) – late sign
Prevention:
Identify at risk babies and monitor blood glucose
Feeding is usually required (normal babies can go 48 hours without a feed)
May need IV glucose
Prevent hypothermia. If they‟re small and get cold they will become hypoglycaemic
Jaundice
Key question is why, not by how much (although this is important too)
Two types of bilirubin:
Unconjugated:
If unconjugated kernicterus: cerebral palsy, deafness, IQ
Can die acutely (seizures, bilirubin encephalopathy)
If survive: deaf, athetoid cerebral palsy (snake like movements – the harder they try to move
the harder it becomes), normally intelligent
Conjugated: water soluble, conjugated in liver by glucuronyl transferase
Early onset (in 1
st
24 hours):
Always pathological
Causes:
Haemolysis of any cause (eg Rhesus, ABO blood incompatibility, spherocytosis, G6PD
deficiency etc)
Sepsis: respiratory distress + jaundice (not common)
Exam:
Maybe hydrops fetalis, large liver, large spleen (site of haemopoesis in newborn)
Sepsis: especially breathing (indrawing and difficulty) – if in doubt then culture and stat
antibiotics
Prevention:
Expect ABO if they‟ve had it before
Check for Rhesus disease
Jaundice in 1
st
week:
Emphasis on extent of the jaundice (as well as consideration of the cause)
Treatment:
Phototherapy (visible light at the blue end of the spectrum – not UV)
Exchange transfusion
Persistent jaundice:
If it doesn‟t got away by 10 – 14 days then revisit
Causes:
Conjugated bilirubin (go green) – needs treatment
596 4
th
and 5
th
Year Notes
Liver obstruction abnormalities (eg biliary atresia, secondary to liver damage from
infection, toxins, etc)
Hepatitis/liver inflammation
Unconjugated (yellow) – needs treatment if high. Eg Breast milk jaundice – progesterone in
breast milk delays maturation
Diseases picked up on Guthrie card causing jaundice:
Hypothyroidism
Galactosaemia
Cystic Fibrosis
Aside: ABO Blood Incompatibility
Maternal antibodies from mother with type O blood attack fetal blood cells if type A, B, or AB.
Not isoimmunisation – it‟s an existing immune response. Doesn‟t get worse with subsequent
pregnancies
Transfusion:
Want to transfuse type O RBCs – aren‟t antigenic to anyone
Want to transfuse type AB plasma – won‟t contain antibodies to either type A or B blood
Other Neonatal problems
Infant Drug Withdrawal Syndrome *
For first 2 weeks after delivery if mother is abusing heroin, methadone, other narcotics:
Jitteriness
Sneezing
Yawning
Poor Feeding
Vomiting
Diarrhoea
Weight loss
Seizures
Child of Diabetic Mother *
Maternal complications: polyhydramnios, preterm labour, still birth near term
Fetal: malformations, macrosomic, growth retarded
After birth: hypoglycaemia, hypocalcaemia, respiratory distress (surfactant doesn‟t till later in
gestation) , polycythaemic (venous haematocrit > 0.65, looks plethoric. May require exchange
transfusion to remove RBCs)
Transient Tachypnoea of the Newborn *
Occurs in both term and prem babies
?Delayed absorption of amniotic fluid from lungs
Risk factors: C-section, perinatal asphyxia, excessive analgesia, hypothermia
Presentation: subcostal recession, grunting, and cyanosis all seen but not prominent
CXR: inflated lung fields, perihilar opacities, vascular markings
Treatment: O2 for several days, respiratory failure uncommon. Penicillin if ?congenital pneumonia
Meconium Aspiration *
Hypoxia during labour gasp aspirate meconium (+/- vernix, meconium, blood)
Patchy lung collapse and over inflation (ball valve effect)
Complications: pneumothorax and pneumomediastinum ( angel wing appearance on CXR due to air
under the thymus)
Treatment: suction via ET tube
Heart Disease in Children
The Blue Baby
Neonatal adaptation:
With first breath:
Alveolar oxygen tension increases
Pulmonary bed dilates
Paediatrics 597
Ductus arteriosus starts to constrict
Cord clamp:
In LV and LA pressure
Functional closure of foramen ovale
Ductus: closes at 24 – 48 hours. A murmur may be normal. Can open or close it with drugs
(NSAIDS close, prostaglandins open)
Replacement of HbF with HbA from 24 weeks (90%) to birth (70%) to 6 months (trace)
Clinical Signs of Heart Disease
Clinical warning signs:
Early murmurs in a clinically well baby
New-born who becomes hypoxic
Classifying:
Cyanotic Heart Disease
Acyanotic Heart Disease
Respiratory Disease
Cyanosis
Severe
Variable
Variable
Tachypnoea
Mild
Variable
Variable
Respiratory Effort
Not major
Variable
Variable
Heart Murmur
+/-
+/-
None
When
First 1 – 7 days
First 1 – 4 weeks (effect
of failure – takes longer)
Often at birth
Causes of Cyanosis
Respiratory Causes:
Hypoventilation: Central apnoea from drugs, apnoea of prematurity, sepsis, metabolic (eg
hypoglycaemia), seizures
Mechanical interference with lung function: airway obstruction, abdominal distension,
pneumothorax, thoracic and sternal deformities, etc
V-Q mismatch with lung disease:
Infection (Gp B Strep, G – ive): pneumonia on X-ray hard to distinguish from wet-lung of
early respiratory distress. Have high index of suspicion, low threshold for antibiotics
Respiratory Distress Syndrome: X-ray appearance: Ground glass + air bronchogram
surfactant. If maternal diabetes, are deficient in surfactant until later in gestation
Aspiration: meconium, milk, blood
Pulmonary oedema, hydrops fetalis ( in heart failure before delivery. Used to be due to
Rhesus negative disease prior to Anti-D treatment, now numerous other causes)
Lung haemorrhage: complication in premature
Primary lung disease
Cardiac causes of cyanosis:
R to L shunt: Cyanotic heart disease or pulmonary hypertension
L to R shunt and Heart failure
Differentiating Heart and Lung Disease:
History and exam:
When did it start
Relationship of cyanosis to birth. If heart, pink to start with then go blue as ductus closes
(blood gets to lungs via reverse flow through ductus if right heart not functioning well)
Check respiration:
If apnoea heart. If heart problems, won‟t work so hard at breathing
Respiratory distress and effort airway or lung problem
By investigations:
CXR (heart size, lung fields)
ABG/O2 saturation monitoring. If lung disease, may have CO2
Hyperoxia test: put in 100% O2 – if heart disease then won‟t change PO2 as gas transfer is not
the problem
Echocardiography
Also consider sepsis and anaemia
598 4
th
and 5
th
Year Notes
Congenital Heart Disease
Summary
Congenital
Acyanotic: Ventricular septal defect (VSD), Atrial septal defect (ASD), Atrioventricular Septal
Defect (AVSD) and Patent ductus (PDA)
Cyanotic:
Decreased Pulmonary Flow ( dark lungs on X-ray):
Critical pulmonary atresia/stenosis, critical aortic stenosis (if not critical the acyanotic)
Tricuspid atresia
Fallot‟s Tetralogy (commonest congenital cyanotic problem, presents about 3 months of
age, no murmur)
Increased pulmonary flow:
Transposition of the great arteries (TGA): Fine till birth, goes blue as ductus closes
Total anomalous pulmonary venous drainage (TAPVD): very rare
Other: Coarctation
Acquired: Rheumatic fever
Arrhythmia: Long QT, SVT, Pre-excitation, VT
If chronic leads to developmental delay and clubbing
Associated with:
Chromosome disorders: Trisomy 21 (40% have cardiac lesion – mainly AVSD), 18, 13 and
Turners (coarctation)
Numerous syndromes
Aetiology
Genetic causes:
6 – 8/1000 live, full term births (higher in premature and still born). Second most common
congenital malformation after the brain
Chromosomal eg Down Syndrome
Single gene eg Marfan‟s (prolapsing mitral valve)
Environmental:
Infection (eg Rubella)
Maternal (eg Diabetes)
Substance abuse (eg alcohol)
Drugs (eg phenytoin, thalidamide)
Usually leads to an abnormality in tissue migration
Incidence (Pathology not Paediatrics’ numbers!)
Acyanotic (L-R Shunt)
Ventricular Septal Defect
25 – 30%
Atrial Septal Defect
12 – 20%
Patent Ductus
10 – 15%
Cyanotic (R-L Shunt)
Tetralogy of Fallot
8 – 15%
Transposition of Great Vessels
8 – 10%
No Shunt
Coarctation of the Aorta
5 – 7 %
Pulmonary Stenosis
5 – 7%
Aortic Stenosis
4 – 5 %
Ventricular Septal Defect
Epidemiology: 12/10,000
Types are muscular, perimembranous and outlet (affects aortic valve)
90% involve membranous septum which grows down to meet muscular wall
Clinical:
Wide range: from asymptomatic through life to fulminant heart failure in infancy
Signs:
Pansystolic murmur (often with thrill)
Features of heart failure
Features of pulmonary hypertension if large: JVP, sternal heave (RH work), loud P2
Investigations:
ECG: LV hypertrophy (due to volume loading)
Paediatrics 599
CXR: heart size, vascular markings in lungs
Echo: size and location of defect
Management: Treat only if large: surgical repair
Prognosis dependent on size of defect:
Small defects often close over spontaneously. Remaining ones at risk of infective endocarditis.
Prophylaxis if dental work.
Large defects Eisenmenger‟s syndrome (see below, pulmonary hypertension, shunt reversal and
cyanosis)
Atrial Septal Defect (ASD)
Epidemiology: 6 – 8/10,000 live full term births. F:M = 2:1. Higher in stillborn and premature births
Aetiology unknown in > 90% of cases
Pathogenesis:
Septum primum closes foramen primum at week 5. Failure to form completely results in a low
ASD adjoining AV valve
Septum secundum closes over foramen secundum at week 4 – flap forms a one-way value. If it
fails to reach far enough leads to fossa ovalis ASDs. Common in trisomy 21
Defects in primitive sinus venosus lead to ASD near vena cava ostia
Clinical:
A L R shunt increases pulmonary flow but if < 1 cm may be asymptomatic through life
Larger defects arrhythmias and/or murmur in 3
rd
decade. Evaluate for corrective surgery to
prevent pulmonary hypertension, heart failure or arrhythmia
Chronic pulmonary flow 2 – 4 times normal pulmonary hypertension with R L shunt and
heart failure in less then 10% of cases
Signs:
May have evidence of RH overload: JVP, sternal heave, loud P2
Ejection systolic murmur in pulmonary region (flow murmur due to flow, not due to defect).
This is not specific – many children have it, especially when ill P2 important in
differentiating benign from ASD
Fixed splitting of S2
Investigations:
ECG: RV hypertrophy and Right axis deviation (due to RV volume loading)
CXR: heart size, prominent pulmonary artery with vascular markings
Echo to confirm diagnosis
Management: Surgical or percutaneous closure by age 5 (unless small and spontaneous closure)
Patent Ductus Arteriosus
Aetiology: Occurs as an isolated lesion or in combination with other abnormalities (eg Tetralogy of
Fallot). Association with Rubella. 90% isolated defects. Incidence 1 in 2000
Pathogenesis:
Connects aorta to left pulmonary artery (acts as R L shunt in foetus).
Oxygenation at birth PGs (lungs metabolise them) muscular contraction functional
closure at 2 days, anatomic closure at 2 – 3 months. Forms ligamentum arteriosum.
If hypoxia at birth then it can remain patent. A patent ductus allows up to 75% of LV output to
flow from the aorta to the pulmonary artery (ie becomes a L R shunt)
If persistent then pulmonary hypertension becomes a R L shunt (Eisenmenger‟s
Syndrome – see below), deoxygenated blood flows more to legs than arms clubbing in toes not
fingers
In term infants: Delayed closure due to PaO2: pulmonary disease (eg meconium aspiration),
pulmonary hypertension, high altitude
In preterm:
Incidence with birth weight
Sensitivity to PaO2 and sensitivity to PGE2
Haemodynamic effect of hypoperfusion and hypotension: associated with intraventricular
haemorrhage and necrotising enterocolitis
Clinical:
Murmur at left sternal edge, 2
nd
or 3
rd
intercostal space: systolic only. Silent if high pulmonary
artery pressures (can be heard in first few hours in many infants)
Active precordium with bounding pulses and pulse pressure (collapsing pulse)
600 4
th
and 5
th
Year Notes
Hepatomegaly
LV failure: apnoea, bradycardia
LV hypertrophy, RV hypertrophy secondary to pulmonary hypertension if persistent
Investigations:
ECG usually normal. LV and/or RV hypertrophy if large and persistent
CXR: cardiomegaly and pulmonary plethora
Echo: diagnostic
Management:
Requires closing:
NSAIDs (anti-PG) promote closure
Surgical or device closure
Small risk of endocarditis if closed
Persistent Pulmonary Hypertension
Failure of pulmonary capillary bed to dilate sufficiently after birth
Return to fetal circulation (ie RL shunt): pulmonary flow
Causes:
Aspiration, eg meconium
Hypoxia: asphyxia
Infection: Group B strep
Hyaline membrane disease
Lung hypoplasia
Coarctation of the Aorta
Preductal or infantile form:
Narrowing of the arch of the aorta between the left subclavian artery and ductus arteriosus.
Association with patent ductus and ASD (?due to low flow in this area after birth) and with
bicuspid aortic valves. Associated with Turner‟s Syndrome. Severe consequences: LH failure,
cyanosis in lower half of body
Variety of presentations:
Heart failure in infancy (LV hypertrophy due to pumping against an load)
Hypertension in child/young adult
Asymptomatic murmur
Exam:
Femoral pulses, radio-femoral delay
Upper limb hypertension
Systolic murmur heard anteriorly and posteriorly (in back). Continuous murmur if severe
Investigations:
ECG shows evidence of LV hypertrophy
CXR:
Rib notching due to collaterals (> 5 years of age)
Abnormal aortic arch contour: look for faint post stenotic dilatation below cardiac knuckle
Echo: shows lesion – harder to see descending aorta
Cardiac catheter: assess haemodynamics
Treatment: surgery, balloon angioplasty and ongoing management (hypertension, risk of
dissection, etc)
Post ductal or adult form: Less severe narrowing with possible post-stenotic aneurysm due to
turbulence. Ductus is closed. May be asymptomatic. Possible LV hypertrophy. Left intercostal artery
provides collateral flow. (NB Proximal aneurysms occur in Syphilis, Coarctation and Marfan‟s)
Left and right pulses may be different (left bounding)
Tetralogy of Fallot
Malformation during closure of the interventricular septum leads to:
Transposition/over-riding aorta
High VSD
Pulmonary valve stenosis/atresia
Right ventricular hypertrophy (giving a boot shaped heart – diagnose on X-ray)
Survival requires a patent ductus
Paediatrics 601
Clinical: RH failure, commonly endocarditis with subsequent brain abscess. Present several months
after birth with episodic blueness. Death likely at puberty if not corrected
Transposition of the Great Arteries (TGA)
Aortic and pulmonary arteries transposed 2 separate circuits
Requires a patent ductus +/- VSD
OK until birth. Go blue as ductus closes
Pulmonary Valve Stenosis
Similar effect to pulmonary atresia
Right heart development. Blood has always got to LA via foramen ovale, rather than through
lungs
Other
Truncus arteriosus: congenital malformation in which the pulmonary artery and aorta have failed to
separate from their common precursor truncus
Arrhythmias in Children
Relatively uncommon in paediatric population
Often not associated with other heart disease (cf adults, associated with structural disease)
Clinical
Asymptomatic or palpitations
If prolonged may growth retardation, heart failure, arrest, etc
Classification:
Bradycardias:
AV Block:
1
st
and 2
nd
degree: normal variant
3
rd
degree: Associated with AVSD, post-surgical, Rheumatic fever, myocarditis, maternal
mumps, etc. Acute treatment: Isoprenaline/Atropine HR. Long term: pacemaker.
Sinus node dysfunction
Tachycardias:
Supra-ventricular tachycardia (SVT): due to re-entrant pathway associated with A-V node.
Generally paroxysmal. Regular rhythm. Normal QRS duration. 1:1 A-V conduction.
Management: Terminate tachycardia: vagal manoeuvres (ice on face, valsalva – breathing
against closed glottis, carotid massage), IV adenosine (A-V node blocker), -blockers,
DC cardioversion. Prevent recurrences with -blockers or ablation of re-entry pathway
Ventricular Tachycardias: rare in children. Cardiovert.
Pre-excitation Syndromes: Wolfe-Parkinson White. Accessory pathway from atria to ventricle
short PR interval, wide QRS and delta wave. Risk of cardiac arrest and sudden death. Treatment:
ablation
Long QT syndrome: due to congenital (K+ channel abnormality) or acquired (drugs,
hypocalcaemia). Susceptible to arrest, torsades and bradycardias. Consider in unexplained
syncope or convulsions. Treatment: cardiovert if arrhythmia, -blockers or pacemaker to prevent
Complications of Congenital Heart Disease
Heart disease with failure
Definition: inability of myocardium to meet metabolic needs of the body
Causes:
Congential Heart disease:
Lesions with left to right shunt: Large VSD ( blood to pump overloaded heart), AV
canal defect, Patent ductus
Left outflow obstruction: Hypoplastic left heart, Coarctation of the aorta, aortic stenosis
Arrhythmia: usually SVT
Cardiomyopathy: Usually ischaemic, due to birth asphyxia
Incidence by age:
Infants: congential heart lesions, rarely arrhythmias (eg SVT)
> 1 year: cardiomyopathy, right heart disease, dysrhythmias
602 4
th
and 5
th
Year Notes
Symptoms of heart failure: respiratory effort, sweating, poor feeding (no energy to suck), failure to
thrive (hypermetabolic state and poor feeding due to breathlessness)
Signs of heart failure: Tachycardia (160 in infants), tachypnoea (intercostal indrawing, wheeze),
gallop rhythm, hepatomegaly
Features not found in children:
JVP
Peripheral oedema
Crepitations in lung fields
Key differential to acute onset is sepsis
Treatment:
Rest
Diuretics
Digoxin
O2
Adequate calories: fortified feeds
Treatment of underlying cause (arrhythmias, infections, anaemia, etc)
Eisenmenger’s Syndrome (Pulmonary Hypertension)
Sequalae of large L R shunt with untreated VSD, PDA or ASD. Rare – as there usually corrected
Usually present in 3
rd
to 4
th
decade
Pulmonary flow oversupply of blood pulmonary capillary hypertrophy resistance
pulmonary hypertension :
Reversal of shunt (R L) development of cyanosis
RH hypertrophy and failure
Also abnormal flow mural thrombosis endocarditis (as in most congenital defects)
Clinical:
Signs of pulmonary hypertension: RV heave, loud P2, hepatomegaly
Little or no murmur
Cyanosis, clubbing
Prognosis:
Arrhythmias and sudden cardiac death
Hb due to cyanosis (polycythaemia) viscosity clotting problems
Risk of systemic emboli (lungs don‟t act as a filter for emboli)
Haemoptysis due to pulmonary infarct/haemorrhage
Treatment: Supportive or heart-lung transplant
Rheumatic Fever
Incidence:
Incidence has declined over last 50 years, from death rate of about 20/100,000 to 6/100,000
1 per 1000 people in NZ (highest rate in western world).
Annual incidence in NZ per 100,000: European 0.1 – 0.3, Maori 6.1 – 11.3 (ie 50 – 100 times),
Pacific Island 13.3 – 24.3 (ie 100-200 times). Pockets in Porirua, South Auckland
Acute attacks occur mainly between 5 – 15 years of age. Peak 10 – 11 years.
Aetiology:
Incidence following strep throat is 0.3 % (sore throat for 1 week) to 3% (sore throat for 3 weeks)
?Some at risk due to longer carriage of strep antibody response
Pathogenesis: Group A -haemolytic streptococci infection (eg Streptococcus Pyogenes) cross
reactive antibodies – substances in myocardium similar to strep antigens to significant inflammatory
reaction in cardiac muscle acute rheumatic fever 1 – 5 weeks following infection (average 19 day
latent period).
Clinical features:
Carditis:
Endo +/- myo +/- peri
Usually mild in first attack
New left sided diastolic murmur: mitral and/or aortic regurgitation
Tachycardia
PR prolongation (may be buried in T wave)
Cardiomegaly: due to valve dysfunction ( dilation) or myocarditis
Paediatrics 603
Arthritis:
Migratory polyarthritis – as one joint starts to recover another flares
Usually large joints. Can be red and swollen
Dramatic response to aspirin
Never permanent joint damage
Chorea (St Vitus Dance):
Sudden or gradual onset. Acute onset chorea in a child only occurs in RF
Usually generalised, although can be focal
Deterioration at school, eg writing
Stops during sleep
Increased by anxiety/stress
Rare symptom. Always resolves, after 2 – 3 weeks
Erythema Marginatum:
= Red rash around edge, centre normalises as it expands
Evanescent (comes and goes quickly)
Not itchy, blanches with pressure, mainly on trunk and proximal limbs
Subcutaneous nodules: small, painless, over bony prominences, RARE
Investigations:
Throat swab: +ive for strep in 15%
ESR usually > 100 (not if chorea or CHF)
CXR: looking for cardiomegaly
ECG: prolonged PR in 14%
Echocardiogram
Streptococcal titres
Diagnosis:
Acute Phase: Jone‟s criteria: evidence of strep throat (serum titres) plus 2 major or 1
major/2minor:
Major criteria: carditis, migratory polyarthritis of major joints (75%), erythema marginatum
(non pruritic, non painful), subcutaneous nodules, and chorea (later)
Minor criteria: fever, arthralgia, acute phase proteins, c-reactive protein, ESR, PR interval
Also watch out for murmurs, arrhythmias (from focal fibrosis)
Very difficult to diagnose. Always consider as differential in pyrexia of unknown origin
Chronic Phase: recurring attacks magnify cardiac injury. Mitral and/or aortic stenosis progresses
to congestive heart failure. Recurrent attacks make it worse ?long term prophylaxis
Treatment:
Eradicate streptococcus
Aspirin: 75 mg/kg/day (inflammation)
Bed rest if cardiomegaly or CHF, others should avoid rigorous exercise
Steroids for acute treatment – but doesn‟t affect long term prognosis
Diazepam for chorea
Course:
Acute phase lasts 6 – 8 weeks, monitored by ESR
Dental check
Ongoing management:
Will get it again if they get another strep infection, and more severe
Penicillin prophylaxis: 4 weekly IM benzathine penicillin until 18 if no cardiac damage (for
life if damaged).
Regular dental care. Prophylaxis for deep dental work (erythromycin or clindomycin – won‟t
have any penicillin sensitive organisms on board)
Valves can recover
Macroscopic appearance:
Acute (exudative and proliferative) phase: Pancarditis grossly visible in valves and pericardium.
Valve leaflets have evenly spaced small 1 – 2 mm sterile/inflammatory (not infective) „verrucae‟ –
small vegetations resulting from deposition of fibrin along edges of value. Verrucae resolve but
Aschoff bodies (areas of necrosis surrounded by macrophages) organise and fibrose. Mitral valve
always involved. Pericardium show non-specific serofibrinous (bread and butter) pericarditis
similar to uraemia or acute MI
604 4
th
and 5
th
Year Notes
Chronic (healed) phase: Heals with organised fibrosis deformed valves (50% mitral, 50% mitral
and aortic) and/or shortening/thickening/fusion of chordae tendinae. Subendocardial fibrosis
fibrous plaque (McCallum‟s patch). Characteristic “fish mouth” stenosis atrial hypertrophy and
LV atrophy. Aortic stenosis LV hypertrophy. May lead to murmurs or arrhythmias
Microscopic appearance:
Exudative phase: fibrinoid necrosis with neutrophils, lymphocytes, plasma cells and macrophages
Proliferative phase: Aschoff body in the myocardium is pathognomonic. Consists of central
fibrinoid exudate/necrosis with aggregates of large mononuclear or multinuclear cells (Aschoff
giant cells), fibroblasts, plasma cells, lymphocytes and oedema. Aschoff bodies may also be seen
in perivascular spaces, joint capsules, tendons, subcutaneous tissues
Susceptible to later valvular infection
Treatment: Possible surgical replacement of deformed valves
Respiratory Illness
See Allergic Rhinitis, page 63
Symptoms
Differential of dyspnoea
Heart failure
Cerebral hypoxia
Metabolic acidosis
Respiratory Causes
Differential of Stridor:
Retropharyngeal abscess: lymph nodes in midline behind pharynx, usually under 4 years, mainly
strep, maybe staph aureus. Acute toxicity, hyper-extended, quiet stridor, CT diagnostic
Croup
Epiglottitis
Foreign Body
Angio-oedema
Peritonsillar abscess
Laryngomalacia: noisy breathing due to floppy larynx from birth, especially inspiratory, crying or
exertion
Tracheomalacia: soft tracheal cartilages: Brassy cough (honking). May get severe obstruction
Adenoid and tonsillar hypertrophy: reaches peak at 8 – 10 years, but relatively largest at 5 – 6.
Snoring and obstructive sleep apnoea. Acutely enlarged stridor (eg in EBV – treat with
steroids)
Chest Radiology
Initially:
Name, date, and view
Orientation: L & R
Check exposure: lung fields and intervertebral discs
Centering: check rib length on each side for rotation (clavicles unreliable)
Lung field size:
5 – 7 anterior ribs to the midline of the Right diaphragm
7 – 9 posterior ribs to the spine
If too many, then hyperinflated: asthma, CF
If too few, then inspiratory film: hard to interpret
Middle right lobe is against RH border – consolidation there will obscure border. No other
consolidation will
Staph pneumonia pneumatocele (air filled cysts). Generally resolve
Pneumo-mediastinum „angel wing‟ appearance as air lifts up thymus
Chylothorax: lymph surrounding lung in the newborn ?thoracic duct dysfunction
Trachea: in an infant is floppy, so in an expiratory film can have a kink
Lateral CXR:
Vertebrae should get blacker as go down
Retrosternal clear space: in infant whiter due to thymus
Thymus on AP CXR:
Paediatrics 605
Lots of variation – can look like large heart
Thymic notch: lower right or left edge as it abuts the heart
Thymic wave sign: contour down the side of the thymus
Thymic sail sign: sail-like shape sticking into the lung fields
Respiratory Distress Syndrome:
= Alveolar collapse (not bronchi)
Xray: diffuse opacity, air bronchograms and small lung volume
Severity assessed by blurring of heart borders and diaphragm
Group B Strep infections in full term babies can look a bit like it
Transient Tachypnoea of the Newborn:
Xray: Retained lung fluid, lung volumes normal to large, and pleural effusions
Mild recover
Meconium Aspiration:
Xray: Diffuse, coarse lung field opacity (fluffy), hyperinflated (airway pathology not air space
pathology plugging and ball/valve effect)
Can get pneumothorax, pleural effusions due to the work of breathing
Mainly in term babies – they have the grunt to suck it down. Also, pre-term babies less likely to
pass meconium when stressed
Respiratory Tract Infections in Children
Reference: Mainly from Prof Grimwood‟s extensive infectious diseases handout
Epidemiology:
Common: During the first 3 years of life, a child may have up to 6 episodes of otitis media, 2
episodes of gastro-enteritis and 6 respiratory infections per year. 10 – 15% have 12 colds per year.
Other risk factors:
Breast feeding is protective
Passive smoking
Exposure to infection: older siblings, day care, etc
Socio-economic status (multifactorial)
95% of respiratory infections involve the upper respiratory tract and 90% are viral
But antibiotics prescribed in 70% of cases. Leads to:
Unnecessary adverse effects: rashes, diarrhoea, thrush, plus more serious ADRs
Cost
Antibiotic resistance major increases in cost. Especially S pneumoniae and S. aureus
Reduce unnecessary prescribing by developing guidelines, practitioner education, public
relations and OTC antibiotic sales (eg mupirocin)
Pathogenesis: 60% due to rhinoviruses and coronaviruses, then RSV, parainfluenza viruses, influenza
and adenovirus
Common cold
Starts with nasal congestion, throat irritation sneezing, watery nasal discharge
Low grade fever, malaise, cough, headache
After 1 – 3 days nasal discharge becomes thicker and mucopurulent. This is part of the natural history
of URTI and does not indicate a bacterial super-infection
Generally improved by day 10, although cough (in 30%) and nasal discharge (in 40%) may persist for
> 2 weeks
Numerous RCTs have consistently failed to show that antibiotics alter the course of the common cold
Acute Otitis Media
= Infection of the middle ear cleft
Presentation:
Eardrum opaque (not semitransparent), red, normal landmarks lost, bulging. But if kid is
screaming, ear will be red regardless
Otalgia, otorrhoea, hearing loss
Systemic signs: fever, irritability
If it ruptures, child will be instantly better (but parents will panic!). Acutely ruptured eardrum will
heal in 24 hours
Pathogens:
S pneumoniae (30 – 50%)
606 4
th
and 5
th
Year Notes
Non-typeable strains of H influenzae (20 – 30%)
M Catarrhalis (10 – 20%)
Viral (10 – 20%) especially RSV
Mixed bacterial/viral infections account for 50% of antibiotic failures
Treatment:
Without treatment, 70 –90% of infections resolve spontaneously
Those least likely to respond are:
Aged < 2 years
Those with constitutional disturbance (eg > 39 C)
Where S pneumoniae is the pathogen
Antibiotics:
Should be directed against S pneumoniae: it is the most common pathogen, the least likely to
resolve spontaneously, and the most commonly associated with mastoiditis. Amoxycillin for 7 –
10 days (?5 days just as good) is the treatment of choice, even when there are non-susceptible S
pneumoniae isolates. Good penetration of middle ear. Erythromycin/cotrimoxazole if allergic.
Main reason for antibiotics is to prevent rare complications
For the 90 – 95% of otitis media that responds to antibiotics, 90% are due to spontaneous
resolution
If < 2 years, constitutional disturbance and persistent symptoms > 48 hours:
Amoxycillin 15 – 30 mg/kg TID for 10 days (ie high dose).
If no improvement after 48 – 72 hours try Augmentin (cover H influenzae and Moraxella)
Main aim is to reduce the very small chance of suppurative complications
Treatment for Acute Otitis Media in children (NZ Guideline for Acute Otitis Media):
Main benefit from antibiotics is less pain on the 2
nd
or 3
rd
day in 1 in 17 kids, and failure to
spread to other side in 1 in 17. No effect on pain on first day, prevention of recurrence or
build up of middle ear fluid
Side effects of skin rash, vomiting or diarrhoea are as common as benefits
Recommendation: use Paracetamol, return to doctor if symptoms persist beyond 48 hours, and
have ears checked in a month for persisting fluid (common in first several weeks) – this occurs
in about 1 in 10
Oral cephalosporins and 2
nd
generation macrolides don‟t penetrate the middle ear and/or have poor
activity against S pneumoniae
Complications:
Mastoiditis in 0.1%. Incidence is not increased by delayed treatment
Little evidence to suggest that untreated otitis media causes mastoiditis
Very rare: petrositis, labyrinthitis, facial palsy, subdural/epidural/brain abscess
Recurrent Acute Otitis Media
Risk factors for recurrent acute otitis media: childcare centres, passive smoking, family history, reflux
Management:
Ensure correct diagnosis
Reassure: spontaneous improvement in many after age 2 – 3 years and during summer
Limit passive smoking, discourage pacifier use
Encourage breast feeding in infancy
Antibiotic prophylaxis generally ineffective
Avoid unproven therapies: antihistamines, decongestants, chiropractic, homeopathy and
naturopathy
Refer to paediatrician/ENT surgeon if febrile seizures, antibiotic intolerance, hearing loss/speech
problems, underlying facio-cranial abnormalities
In the future, conjugate pneumococcal vaccines are likely to play an important role
Chronic Otitis Media with Effusion
= Presence of sterile or infected fluid in middle ear
Chronic OME (=Glue Ear) if > 3 months. If it hasn‟t cleared by then, less likely to clear
spontaneously.
Common up to age 5 or 6
Symptoms:
Incidental finding in asymptomatic child
Paediatrics 607
Hearing loss and its effects: speech delay, slurred speech, failing at school, irritable, poor balance,
falling over. But delayed language and cognitive problems related more to genetic and SES than
previous otitis media
Pathogenesis: eustachian tube dysfunction (not just blockage)
Sequalae of otitis media: Middle ear effusion:
In 70% after 2 weeks
In 50% after 1 month
In 20% at 2 months
In 5 – 10% after 3 months
Associated with mild hearing loss.
Treatment:
Effusion common after an ear infection. Watch and wait
If bubbles behind ear drum then it‟s resolving itself
Drugs: antibiotics and decongestants not very effective
If persisting > 3 – 6 months:
Test hearing
Limit passive smoke exposure
Treat underlying allergic rhinitis/adenoidal enlargement with intra-nasal steroids
Refer after 3 – 6 months if hearing loss and:
Failure to respond to antibiotics
Recurrent acute otitis media
Persistent otalgia
Retraction pockets
Expressive/receptive language delay
Underlying cranio-facial abnormalities (eg Down syndrome)
ENTs say grommets are the treatment of choice: Aerate middle air ( CO2 squamous
metaplasia goblet cells effusion). Extrude over 18 months – 2 years. Take out if still there
5 yrs later. May take out adenoids at same time eustachian tube function (Paediatricians say
adenoidectomy is treatment of choice).
Precautions with grommets:
Plug ears when washing hair and bathing
Can swim in clean fresh water but no diving below the surface
Chronic Suppurative Otitis Media – with hole in drum. Treatment: get rid of infection then surgical
repair
Pharyngitis
See Acute Pharyngitis, page 63
Almost 100% given broad-spectrum antibiotics. Inappropriate in 90% of cases
Pathogens:
Viruses: Adenovirus, also rhinovirus, coronaviruses, RSV, Parainfluenza virus, influenza,
enteroviruses, EBV
Bacteria: S Pyogenes (GABHS = Group A Beta-Haemolytic Strep) in about 20 – 30% of cases,
predominantly in those over 4 years
Differentiating (at best 70% predictive accuracy):
Exudative tonsillitis: Adenovirus, GABHS, EBV
> 4 years, enlarged tender anterior cervical lymph nodes and diffusely inflamed pharyngeal
structures (+ exudates) suggests S Pyogenes
Diffuse, sandpaper-like red rash, accentuated in skin creases (Pastia lines) suggest Scarlet Fever.
See Streptococcus Pyogenes (Group A, Haemolytic), page 500
Nasal discharge, cough, hoarseness, conjunctivitis or diarrhoea +/- fever +/- tonsillar exudates
suggests virus
Throat swabs: usually identify organism, but 10 – 50% are carriers
Treatment:
Aim: Prevent acute rheumatic fever, suppurative complications (peri- or para tonsillar abscess) and
hasten recovery
But
Only benzathine penicillin has been shown to reduce RF – and this was in military personnel
No convincing data which shows antibiotics reduce the risk of rare suppurative complications
608 4
th
and 5
th
Year Notes
Antibiotics reduce symptoms by 8 hours only
Reinforces the notion that antibiotics are effective and increases the likelihood of their future
use for trivial illnesses
If high risk for RF (eg Maori, PI, > 4 years of age) take swabs or treat empirically. However,
prescribing penicillin for sore throat hasn‟t altered the rates of RF, and many children with RF
haven‟t consulted their doctor
S Pyogenes: penicillin, 500 – 1000 mg BID for 10 days (Allergy: erythromycin)
Acute Sinusitis
Uncommon. Bacterial sinusitis complicates 0.5 – 5% of viral upper respiratory tract infections
With most colds, nasal discharge and obstruction are improving after 2 weeks. Children with acute
sinusitis will not be improving
A minority present with high and persistent fever, periorbital swelling, facial and dental pain
Imaging:
Plain x-rays don‟t differentiate well between common cold and sinusitis
CT more useful. Air-fluid levels, opacification, mucosal thickening > 4 mm
Maxillary and ethmoid sinuses present at birth (although small). Frontal and sphenoid sinuses begin at
4 – 6 years of age
Pathogens: S pneumoniae (30 – 70%), H influenzae (20%), M Catarrhalis (20%), virus alone (10%)
Treatment:
High spontaneous cure (60% by 10 days vs 85% with amoxycillin)
Treat for S Pneumoniae in children with persisting symptoms which are not improving
Amoxycillin 15 – 30 mg/kg TID for 5 days. Higher limit if < 2 years, attend child-care, or have
received antibiotics in the last month in areas with > 10% penicillin resistance
Consider Augmentin, co-trimoxazole, cefuroxime or ceftriaxone if no improvement after 48 – 72
hours
Bronchitis
Inflammation in bronchial mucosa productive cough
Most cases are from viruses (eg RSV)
Numerous studies have not found any evidence to support antibiotic treatment (but they‟re usually
prescribed….)
Production, colour or culture or sputum does NOT predict aetiology
Consider treatment if:
Prolonged cough in older child: ?M pneumoniae erythromycin
Pertussis and cough < 4 weeks: erythromycin (or co-trimoxazole) reduces infectivity
Cystic fibrosis/other chronic lung disease: tailored antibiotics
Prolonged cough (> 8 – 12 weeks and not from URTI): investigate for asthma, Tb, pertussis, CF,
foreign body, Subacute-sinusitis, psychogenic cough
Croup
= Laryngotracheobronchitis
Pathogens: Usually viral: Parainfluenza 1 and 2 are the most common. Measles and influenza are the
most severe. Don‟t give antibiotics
Presentation:
Child < 5 years
Coryza and fever over 1 – 2 days
Then characteristic harsh “barking” cough, hoarseness +/- signs of upper airway obstruction
(stridor, respiratory distress), inspiratory stridor
Worse at night, and peak on 2
nd
or 3
rd
night. Varies hour to hour (ie don‟t send them home just
yet…)
Lasts 3 – 4 days then changes to sound productive. May last for another 2 weeks
Differential:
Epiglottitis: Absent/minimal cough, low-pitched expiratory snore
Bacterial tracheitis: toxic appearing, older child, high fever, brassy cough, stridor, tender trachea
Laryngeal foreign body: sudden onset, unable to vocalise
Angioneurotic oedema: associated signs usually present
Retropharyngeal abscess: High fever, dysphagia, hyperextension of neck
Assessment:
Paediatrics 609
Severe if restless, anxious, pallor, lethargy, tachycardia, tachypnoea, indrawing, cyanosis or
breath sounds
Loudness of stridor is not a reliable guide to severity of obstruction
Risk of obstruction if: pre-existing upper airway narrowing (eg sub-glottic stenosis) or Down
Syndrome
Management:
Avoid distressing the child, settle them on parent‟s lap
Blood tests, pulse oximetry, O2 masks and nebulisers rarely needed
Mild:
Not distressed, no stridor at rest
No treatment, management at home, return if signs of obstruction, lots of comfort
Paracetamol
Moderate:
Frequent barking cough, distressed, persistent inspiratory stridor, tracheal tug or sternal
retraction at rest, but no signs of hypoxia
Observe or admit
Steroids (Dexamethasone or betamethasone 0.6 mg/kg orally or im, prednisolone 1 mg/kg)
orally. May be repeated 12 – 24 hours later (but consider alternative diagnoses first)
Disturb child as little as possible
Severe:
Signs of obstruction, hypoxia (restless, irritable, anxious, cyanosis), breath sounds
?ICU admission
Nebulise adrenaline + Steroids (Prednisolone 1 mg/kg/day)
Monitor closely
Epiglottitis
Caused by Haemophilus Influenza Type B
Incidence ~ 20 cases pa (dropped from 160 in 1992 prior to vaccination)
Presentation:
Incubation for 2 – 4 days
Acute, febrile illness, toxic looking child
Snore, mouth always open, drooling, prefers to sit upright. Soft inspiratory stridor, louder
expiratory stridor
No cough (cf croup)
Management:
Blood cultures
Intubate first, then give iv antibiotics (if given first, pain panic respiratory arrest)
Cefotaxime 25 – 50 mg/kg/8hr iv (max 2g) due to penicillin resistance
Amoxycillin 50 mg/kg/4 hr iv (max 2g) if penicillin sensitive
Other illnesses caused by H Influenzae type B:
Meningitis: 5% mortality, 10% with sequalae (retardation, seizures, hearing loss, etc), 20 – 30%
have functional disabilities (eg learning difficulties)
Also pneumonia, empyaema, septic arthritis, periorbital or facial cellulitis
Vaccination:
Prior to immunisation was the most common cause of life threatening bacterial infection < 5 years
of age.
Herd immunity now works well
Subunit vaccine is 95% effective. Few side effects (< 5% with local reactions)
Notifiable disease
Pertussis
Bordetella Pertussis = Whooping Cough
Epidemiology:
Highly contagious. Regular epidemics every 3 – 5 years in NZ
Incidence: up to 5000 cases a year (only a small proportion notified)
In first year of life 80% are hospitalised and 0.2% die
Presentation:
Phases:
Incubation 2 – 3 weeks
610 4
th
and 5
th
Year Notes
Coryzal phase: ~ 1 week
Paroxysmal phase:
Develops into paroxysmal bouts: unprovoked cough followed by inspiratory gasp
(whoop), apnoea, vomiting.
Thick tenacious sputum can‟t clear coughing spasm. Whoop may be absent in
infant. If severe may need suction
In between paroxysms looks well, is afebrile and has no chest signs
Median length: 6 weeks. Can be up to 12 weeks
Infectious for 2 – 3 weeks of paroxysmal phase
Persistent cough for 3 – 4 months (convalescent phase – bacteria cleared)
Treatment: if < 4 weeks duration: erythromycin. Doesn‟t impact illness after paroxysmal phase is
established, but will infectivity
Admit if under 6 months and/or cyanosis or apnoea in paroxysms
Complications:
Anoxic seizures in 1 – 3%
Encephalopathy in 0.1 – 0.3% retardation, spasticity and seizure disorders. Rate of severe
neurological complications of immunisation negligible compared with the risk of encephalitis from
whooping cough
Vaccine:
Whole cell vaccine effective in 60 – 90%, has higher efficacy for more severe outcomes, local
reactions or fever in 50%. 1 in 1 million are associated with an encephalopathy (? No causal
relationship established)
Acellular pertussis has higher efficacy and is better tolerated (< 10 – 15% adverse reactions) – now
being introduced
Bronchiolitis
Epidemiology
Classically RSV
Highly infectious acute viral respiratory illness in kids 2 weeks to 12 months of airways < 1 mm
diameter
Epidemics every winter with RSV, also parainfluenza, influenza and adenoviruses
Major cause of URTI in kids: up to 50% of 1 year olds have had RSV infection
Seasonal in winter/spring
Presentation:
Short incubation: 3 – 4 days
Contacts: older siblings will have had nothing more than a snotty nose
Difficulty with expiration (cf Croup – inspiratory)
Typical pattern: Starts as URTI - 1 day of runny nose, 1 day of cough, then wheeze.
Illness/breathlessness worst on 4
th
day of wheeze (6
th
or 7
th
day of illness)
Low-grade fever, non-toxic, cough, wheezy, difficulty feeding, hyperinflated chest, diffuse fine
inspiratory crackles and expiratory wheeze
If more severe then irritability, pallor, pulse > 160/min, respiratory rate 50 – 70/min, expiratory
grunt (not stridor), head nodding, more marked retractions
Respiratory failure in 1 – 2%: pallor, sweating, drowsiness, respiratory effort, breath sounds,
apnoea. Cyanosis is a late sign
Feeding a good indicator of respiratory distress (and one which parents can monitor at home)
Recurrence common (?hypoplastic airways and smoke exposure)
Usual recovery is 7 – 10 days
Can get repeat viral illness – in which history suggests fluctuation – getting better, then got worse
again, etc
Distribution of LRTI from RSV:
Bronchiolitis: 40 – 90%
Pneumonia: 5 – 40%
Tracheobronchitis: 10 – 30%
Risk factors for severe presentation:
< 6 weeks old
Older siblings
Maternal smoking
Preterm delivery
Paediatrics 611
Underlying conditions: congenital heart disease, chronic lung disease of infancy, congenital
abnormalities, immunodeficiency
Differential:
Recurrent bronchiolitis, history of eczema, strong family history of atopy ?asthma. Trial of
nebulised salbutamol.
Persistent cough, failure to thrive cardiac disease, cystic fibrosis, structural lung disease,
aspiration, immunodeficiency
Investigations:
Nasopharyngeal aspirate for culture and viral immunoflouresence
Bloods for culture and serology
Imaging: CXR shows hyperinflation, peribronchial thickening, often patchy areas of consolidation
and collapse. Hyperinflation and wheeze differentiate it from pneumonia
Treatment:
Not bronchodilators, steroids, ribavirin or antibiotics
Symptomatic treatment: O2, rehydration, minimal handling
Can go home if they‟re feeding OK and don‟t need O2
Admit if respiratory distress, difficulty feeding, or adverse social circumstances. If sending home
early in the illness, arrange for review within 24 hours
Put on NG feeds: not hungry distress
If respiratory rate > 70/min and feeding poorly then IV or NG fluid at 50 – 75% of maintenance
requirements (risk of SIADH)
If oximetry < 92% then O2
If severe, monitor blood gases, consider CPAP or ventilation (especially chronic respiratory/heart
disease)
Maybe wheezy for 2 weeks and a cough for 4 weeks
Pneumonia
Epidemiology: Peak incidence in first 2 years, and in Maori and PI children
Presentation:
Initial prodromal coryzal symptoms for a few days
Fever, cough, tachypnoea, signs of consolidation
Young children may present with predominantly systemic features: fever, lethargy, vomiting,
abdominal pain
Older children may have headache, pleuretic chest pain, irritating cough, maybe abdo pain if lower
lobe or even signs of meningism if upper lobe
Severe if:
Toxic: lethargy or arousal, circulatory compromise, abnormal respiration (eg apnoea,
cyanosis)
Respiratory distress: pallor, restless, agitated, nasal flaring, grunting, head nodding, chest wall
recession, paradoxical abdominal movement, difficulty feeding
Signs on exam:
In infants: may be few signs, usually limited to a few focal crackles
Older children: chest wall movement, breath sounds, fine crackles, later dull to percussion and
bronchial breath sounds
Pathogens:
Viruses are the most common cause in infants and young children:
RSV and Parainfluenza 3 most common
Suggested by: infant or young child, coryzal prodrome, mild or moderate constitutional
disturbance, hyperinflation and diffuse inspiratory crackles, patchy consolidation on CXR
Rarely, infections with influenza A, adenovirus 3, 7 or 21 can be severe leading to death or
severe lung damage
Bacterial:
S pneumoniae most common bacteria
S aureus uncommon but severe, H influenzae uncommon
M pneumoniae common in school age children, insidious onset including anorexia, headache,
scattered fine inspiratory crackles, bilateral
S pyogenes: typically follows Varicella, influenza A or measles, protracted course and often
empyema
612 4
th
and 5
th
Year Notes
Chlamydia: in 1
st
2 months. Vertical transmission + eye infection in first 5 – 7 days. See Eye
disorders in Children, page 631
Investigations:
Imaging: CXR to:
Confirm diagnosis
Detect complications: pleural effusion, pyopneumothorax, lung abscess
Exclude other causes: congential lung lesions, lung abscesses
Blood cultures before antibiotics
Nasopharyngeal aspirate for RSV detection
Serology for M pneumoniae or RSV
Aspiration of pleural fluid (assists diagnosis, and is therapeutic – antibiotics won‟t penetrate a large
effusion)
Treatment:
Penicillin G is the treatment of choice for uncomplicated bacterial pneumonia (unless allergy).
Despite 20% of S pneumonia‟s showing reduced sensitivity, concentrations in the serum and lung
tissue exceed the MIC by several fold. More treatment failures are associated with erythromycin
and co-trimoxazole
Admit if any of:
< 2 years
Signs of toxicity, hypoxia, respiratory distress
Extensive consolidation or an effusion
Clinical or x-ray signs of Tb
Adverse social circumstances, no transport or no access to phone
If sent home, then review within 12 – 24 hours
For uncomplicated bacterial pneumonia: Penicillin G 25 – 30 mg/kg/6hr iv (max 2.4g)
If not afebrile within 24 hours on penicillin G, then review microbiology results, repeat CXR,
consider other causes and treatments. Treatment failure: consider Viral, Mycoplasma, S aureus,
resistant H influenzae
Supportive therapy: minimal handling, careful fluid management (max 50% of maintenance fluids
if IV), O2
Management of pleural effusion. Before antibiotics do diagnostic aspiration and urgent gram stain.
Discuss with paediatric surgeon:
Thin clear fluid: aspirate as much as possible
Thin purulent fluid: intercostal drain
Thick purulent fluid: loculates so drain won‟t work thoracotomy (consider flucloxacillin +/-
Cefotaxime)
Infected effusion = Empyema = pus in pleural cavity
Fibrous septae will form around empyema = loculated empyema
Tb Pneumonia
Rarely presents as acute pneumonia
Consider if:
Known exposure to Tb
Child or family born in an endemic area
> 4 week history of cough, especially if fever, sweats and weigh loss
Refractory pneumonia
Suggestive CXR
Nurse in respiratory isolation:
Virtually all child cases are primary and non-infectious with a small burden of disease
But adolescents, those with extensive or cavitating disease, or infected visiting family are
infectious
Investigations:
FBC, ESR, electrolytes, CR and LFT
Mantoux test
Specimen collection: sputum if available. Early morning gastric aspirates better than lavage. Also
consider urines, pleural biopsy and LP
Empiric treatment: isoniazid, rifampicin, pyrazinamide
Notify to Medical Officer of Health

Paediatrics 613
Asthma in Young Children
See also Asthma, page 77, especially for Medication and Spacer Use
3
rd
most common reason for admission (after Bronchiolitis and URTI/Otitis media).
Much much less common in < 1 years (NB bronchiolitis causes wheezing in young). Peak in 2 – 4
years
Peak flow very unreliable under age 7 (and most bad asthmatics diagnosed from 2 – 5) have to rely
on history
History:
Symptoms: waking at night with cough/wheeze, after exercise, how often are attacks, had time off
school/kindy as a result, how long does preventer last
Environmental factors: smokers, pets, damp, obvious triggers
Current treatment: medicines, do the family understand the difference between reliever and
preventer, assess technique and compliance, is spacer accepted by child and is it washed
2 patterns on history:
Episodic (intermittent): viral URTI cough and wheeze. No interval symptoms
Persistent (with exacerbations): interval symptoms (with exercise, at night), exacerbations with
viral infection, interferes with everyday life
Symptoms in a toddler:
Cough, often worse at night
May vomit with cough (NB exclude pertussis: cough choke vomit OK for an hour. In
asthma, cough again straight away)
Usually wheezy with URT infection
Diagnosis difficult in an infant unless recurrent, strong immediate family history or evidence of
atopy
Physical findings in a toddler:
Often normal chest exam
If severe chronic symptoms:
Hyperinflated chest ( AP diameter)
Harrison‟s sulcus: dip in chest wall where diaphragm attaches
Eczema
Reduced growth (if severe)
Stethoscope can be confusing
Diagnosis:
Cough is very common in kids (8 – 10 per year). But more during the day than at night. Won‟t
slow them down when running
Is it asthma, bronchitis, bronchiolitis?
Trial of therapy (preventative as well as relievers) and review
Criteria for admission:
Pulse rate > 1.5 * normal
Respiratory rate > 70 minute
Chest movements
Restlessness/apathy/CNS depression or cyanosis/pallor [signs of exhaustion]
Severity assessment:
Mild
Moderate
Severe
Critical
Mental State
Normal
Normal
Agitated
Confused/drowsy
Accessory Muscle use
Nil
Minor
Mod/marked
Maximal/exhaustion
Treatment:
Avoid triggers: passive smoking, pets, house dust mite (dehumidifiers don‟t work), pollens, cold,
exercise, damp houses, certain foods (overstated)
Infrequent episodic asthma:
Consider no therapy, avoid triggers
If distressed with attacks: use bronchodilators + spacer only. Start during URTI phase. No
preventative
Frequent Episodic Asthma (only get it with a cold):
Intervals between attacks < 6 weeks
Bronchodilator as needed with URTIs
Prophylaxis:
614 4
th
and 5
th
Year Notes
Sodium cromoglycate (Vicrom + spacer). ?Evidence of poor efficacy
Nedocromil (Tilade + spacer)
Inhaled steroids: if it makes no difference then stop
Persistent Asthma
Male: female = 4:1
Preventative. If mild try Vicrom or Tilade. Moderate or severe use inhaled steroids (takes 2 –
3 months for maximal effect). Titrate back once controlled
Bronchodilators as required
Poor control: consider dose, check inhaler device and technique, poor compliance,
environmental triggers
Other treatment options:
Long-acting -agonists: salmeterol (Serevent), eformoterol (Foradil, Oxis)
Theophylline (Nuelin, Theodur): 3
rd
line, gut ache poor compliance
If severe: alternate day oral prednisone treatment – reduced side effects (short and fat), and
reasonable asthma control
Protocol for an acute attack:
Salbutamol dose: up to 5 years: 6 puffs via space. Over age 5: 12 puffs via space
For severe add ipratropium (Atrovent)
For moderate and severe, give doses at 0, 20, 40 and 60 minutes and review at 75 minutes
Oral Steroid for all except minor attacks: 1 mg/Kg/day relapse
Differential of Wheezing in a Child
Common:
Asthma
„Happy wheezer‟:
Diagnosis of exclusion
Usually < 12 months
Chronic daytime wheeze and no cough
Child undistressed and not impact (ie feeding OK, not waking)
Less wheeze when asleep
Requires no therapy
?Collapsible airways
Can become an „unhappy‟ wheezer when they get a cold, in which case treat as for
bronchiolitis
Bronchiolitis: See 610
Uncommon:
Inhalation: If convincing episode of inhaling a foreign body (stridor, went blue, etc) should be
bronchoscoped – even if they you think they brought it all back up. Signs: unilateral wheeze or
stridor. May present months or years later with haemoptysis. CXR – will have hyperinflation or
collapse on side of inhaled object
Cystic Fibrosis: [see Cystic Fibrosis (CF), page 615]
If breast feed can still thrive for a month or two
Respiratory symptoms often present with wheeze not cough
Heart Failure:
Sweat when feeding + poor feeding/cyanosis
Wheezy – sounds like bronchiolitis
Look for enlarged liver (but beware, bronchiolitis hyperinflation liver lower)
Aspiration:
If due to neurological problems, will cough and splutter when swallowing
Long vague history with unclear start
Gives acute onset of wheeze – eg OK when you put them to bed, but sudden coughing and
wheezing later
If lying on back, most likely to aspirate into right upper lobe, but in practice they are wheezy
everywhere
Hard to prove. Diagnosis of exclusion. Can do reflux probe to show they reflux often
Immune deficiency:
Rare. Only consider if lots of serious illnesses
Paediatrics 615
Cilia dyskinesia: usually starts with ears (middle ear has respiratory epithelium with cilia),
then lungs and sinuses. Associated with dextrocardia
Hypogammaglobulinaema
Can confuse wheezing with soft stridor: eg laryngomalacia. Inspiratory sound
Rare congenital causes: cysts, tumours, lobar emphysema, tracheomalacia/bronchomalacia (not
properly formed floppy)
Smoking contributes to all the above:
Prenatally, maternally smoking airway size
Post-natal inflammation/irritation
Cystic Fibrosis (CF)
Autosomal recessive. 1 in 25 are carriers
Disease of epithelial lined organs:
Lungs: mucus plugging chronic inflammation necrosis, adjacent pneumonia, bronchiectasis.
Leads to chronic infection, emphysema and pseudomonas colonisation. Eventually Cor
Pulmonale
Pancreas: fibrosis around ducts, dilated ducts, islets cells relatively preserved. pancreatic
insufficiency
Gut meconium ileus, biliary cirrhosis, recurrent RLQ pain
Bile ducts obstructed
Middle ear
Vas deferens infertility
Presentation:
Newborn screening (80% will turn out to be carriers, not diseased). Guthrie card for Immuno
Reactive Tripsin (IRT). Tripsin leaks into blood from pancreas if pancreatic duct blocked.
Sensitivity high (~95%) but not at all specific. If positive then gene screen
Neonates: Meconium ileus:
> 90% with meconium ileus will have CF obstruction at birth. Occurs in 15% of those with
CF
Presentation: bilious vomiting, palpable bowel loops, distension if perforated
CXR: distended bowel loops with thickened walls
May also have associated volvulus, small bowel atresia, perforation, neonatal meconium
peritonitis secondary to perforation
Treatment: enema + IV fluids or surgery
Failure to thrive
Sibling with CF
Pathogenesis:
Abnormality of cAMP dependent chloride transport due to mutation of the CFTR protein. Less
water gets out thicker mucus obstruction and ciliary clearance
In 70% of the mutations, the protein is not glycosylated normally not transported to site
Testing:
Guthrie screening
Sweat test (lack of Cl channel can‟t reabsorb NaCl from isotonic secretions salty sweat)
Gene screen DF508/U on chromosome 7.
Advantages of early diagnosis: lung function, nutrition, less traumatic diagnostic process
Post-natal management:
Good nutrition: enzyme replacement, high calories, fat soluble vitamin supplements
Antibiotics for URTI
Grommets at 2 years
Multidisciplinary approach
Possible monitoring tests:
CXR, lung function tests, sputum culture (esp pseudomonas lung infection – key prognostic
indication)
FBC, electrolytes, total protein, albumin, Vit A, D, E, blood glucose
Faecal elastase (testing pancreatic insufficiency)
Complications include bronchiectasis (CF is commonest cause): bronchi dilated and filled with
purulent secretions. Like CF requires regular physio
616 4
th
and 5
th
Year Notes
Infectious Diseases
See also:
Respiratory Tract Infections in Children, page 605
Gastroenteritis, page 644
Epstein Barr Virus, page 505
Herpes Simplex Virus (HSV), page 503
Varicella Zoster, page 504
Streptococcus, page 500
Bacterial Meningitis, page 495
Polio and Rubella in Vaccine Preventable Diseases, page 518
Fever in Children
Most fevers caused by respiratory tract viral infection, are self-limiting, and require only symptomatic
treatment.
Kids have 6 – 8 viral infections each year they are common
Role of doctor:
Identify source of infection
Counsel caregivers and child
Manage the illness
Identify and refer those with potentially serious illness
If no focus found:
Consider UTI, occult pneumococcal bacteraemia, meningitis
Consider non-infectious causes: rheumatic fever, poisoning, drug fever, more rarely leukaemia and
other autoimmune diseases (eg Kawasaki‟s Disease)
On exam, pay attention to:
General appearance: activity, perfusion, colour
Vital signs: pulse, respiration, blood pressure
Exclude: fontanelle, neck stiffness, respiratory distress, abnormal chest signs, ears, throat,
lymphadenopathy, hepatosplenomegaly, abdominal distension, bone or joint
tenderness/swelling, skin rashes
At greater risk: neonates, immunocompromised, congenital abnormalities, toxic appearance,
epidemiological risk (eg Maori)
WBC are unreliable for detection serious infection
Review within 24 hours and parent education
Advice for parents:
Light clothing
Small, frequent drinks of water or fruit juice diluted 1:4, 5 – 7 mls/kg/hr
Paracetamol, 15 mg/kg/6 hourly, max of 90 mg/kg/day for 2 days
Return to doctor if refusing drink, pale or floppy, difficulty breathing, headache/neck
stiffness/photophobia, doesn‟t improve in 48 hours
Clues for predicting serious illness (even over the phone):
Responsiveness and activity
Feeding
Urine output
Breathing
Colour
Potentially Serious Infections
See When is a child really sick?, page 565
Sepsis: leads to systemic inflammatory response syndrome (SIRS). Also get it in major trauma,
pancreatitis, etc. Mass release of cytokines. (Cf bacteraemia: bugs in blood but no major systemic
reaction)
Sepsis + focus (pneumonia, kidneys, joints/bones):
Neonate: Gp B Strep (S agalactiae), E Coli, S aureus
Infant/older child: S Pneumoniae, N Meningitidis, S aureus (complication of skin infections), S
pyogenes, [HIB]
Meningitis: infection of CSF via choroid plexus
See Bacterial Meningitis, page 495
Paediatrics 617
Neonate: Group B Strep, E Coli, Listeria
Common Paediatric Viruses
Reference: Prof Grimwood‟s Paediatric Infectious Diseases Handout (all 94 pages of it!)
Measles
Highly contagious paramyxovirus spread by coughing and nasal droplets
Epidemiology:
Overall mortality 0.5%
Risk of infection 100% if not immunised
Epidemics occur every 7 years
Incidence up to 3000 notifications in epidemic years. Lab confirmations drop in epidemics as high
incidence high PPV of clinical diagnosis. Very few cases in non-epidemic years will actually
be measles
Presentation:
Incubation 10 – 14 days
Fever, ALWAYS a cough (“measles bronchiolitis), coryza, conjunctivitis for 2 –3 days
Then red maculo-papular rash beginning on face and spreading to rest of body. White spots on
cheery-red buccal mucosa for 24 hours before rash (Koplik‟s Spots) – pathognomonic
Treatment: Supportive, antibiotics for 2
nd
ary infection
Complications:
Otitis media (10%)
Pneumonia (1 – 5%)
Encephalitis (0.1%): 15% die and 25% left severely disabled. 1 in 100,000 develop the fatal grey
matter degenerative disorder Subacute Sclerosing Panencephalitis (SSPE)
Vaccine:
Live attenuated virus. Now MMR2 given at 4 years to time between epidemics and address 2 –
5% chance of primary vaccine failure in first dose
Mild fever, malaise or rash develops in about 1% 7 – 10 days after vaccination
1 in 1 million develop encephalitis (1,000 fold less likely than if infected with wild virus)
Contraindicated during pregnancy and in immunocompromised hosts
Mumps
Contagious paramyxovirus spread by saliva and droplets
~ 80 notified cases per annum. Used to be 3 – 4 year epidemics, now longer
Presentation:
Incubation 2 – 3 weeks
70% develop fever and swelling and tenderness of salivary glands
15% have aseptic meningitis
0.2% develop encephalitis
20% of post-pubertal males have painful orchitis
Case fatality is 0.02% - usually from encephalitis
Infective 1 week before and after parotid swelling starts
Vaccine: Live attenuated virus (contraindicated during pregnancy and immunosuppression). Efficacy
95%. Only introduced because it can piggy back other vaccinations
Non-Polio Enteroviruses
Include Coxsackie A and B, echoviruses and enteroviruses
Cause: non-specific febrile illnesses, pharyngitis, gastroenteritis, viral meningitis, encephalitis,
pericarditis, myocarditis, hepatitis, haemorrhagic conjunctivitis, etc
Viral exanthem: macular rashes, maculo-papular, vesicular and petechial rashes
Hand, Foot and Mouth Disease: Coxsackie A16. Mild illness, low-grade fever and sore throat.
Scattered vesicular lesions in the mouth with similar lesions surrounded by erythematous areolae on the
hands and feet.
Incubation for 3 – 6 days, infectious for at least 1 week after onset of symptoms
Diagnosis: culture (including from faeces – if isolates persist for several weeks may be unrelated to
illness), possible PCR for blood and CSF. Serology difficult
618 4
th
and 5
th
Year Notes
Human Herpes 6 and 7 (Roseola Infantum)
Acute febrile illness of young children for several days with occipital adenopathy, then reduced fever
and appearance of a fine red maculo-papular rash over the trunk and arms for 1 – 2 days (confused with
antibiotic rash)
70% of 2 year olds are sero-positive. Serology and PCR problematic due to latent infection
Incubation 5 – 15 days
Rare complications: encephalitis or benign intracranial hypertension
Erythrovirus (Parvovirus) B19
= Erythema Infectiosum or Slapped Cheek Syndrome
Mild illness, fever in 30%, bright red rash on cheeks for 2 – 3 days
A few days later, a maculo-papular, then lace-like rash may appear on arms, then trunk, buttocks and
thighs. May recur over following weeks after hot baths
Incubation 4 – 14 days
Infectious period is before the rash appears
Complications: Adolescents and adults may also have polyarthralgia/arthritis, aplastic crisis if
chronically anaemic (eg immunocompromised)
Orbital and Pre-Orbital Cellulitis
Want to determine if its:
Orbital cellulitis:
Eg spread from anterior ethmoid sinus
Proptosis (eye pushed forward) and/or ophthalmoplegia (limitation of movement) and/or
visual acuity
Surgical emergency: discuss with ENT, ophthalmologists, radiologist re imaging (CT not
MRI)
Bugs: S Aureus, also S pneumoniae, S pyogenes, HIB
Cefotaxime and flucloxacillin
Complications: intracerebral extension (lumbar puncture contra-indicated until this is ruled
out)
Periorbital cellulitis: in superficial facia around the eye but not into the orbit. Fever and local
tenderness
Investigations: FBC, blood cultures
S pyogenes and S aureus especially if contiguous skin lesion, S pneumonia, HIB if not fully
immunised (can check urine for antigens). If HIB then ?HIB meningitis and Rifampicin
prophylaxis for patient and family
Treatment:
If < 5 and not fully immunised: cefuroxime or Cefotaxime (50 mg/kg/6hr, max 2 g)
If > 5 or <5 and fully immunised: flucloxacillin (50 mg/kg/6 hr, max 2 g)
If no response after 24 – 48 hours, treat as for orbital cellulitis or underlying sinus disease
Local allergic reaction: eg just erythema without tenderness or temperature
Paediatric Orthopaedics
Congenital Abnormalities
Cleft Lip and Palate
Failure of fusion of maxillary and premaxillary processes during week 5. With cleft lip, the lesion runs
from the lip to the nostril, can be bilateral
Incidence: 0.8 – 1.7 per 1000
Cause: genes, drugs (benzodiazepine, antiepileptics), rubella
Treatment:
Feeding with special teats
Surgery: repair lip at 3 months old, palate at 1 year old
Prognosis: Unilateral or incomplete good results. Bilateral lesions some residual deformity
Complications: otitis media, aspiration pneumonia, speech problems (refer to SLT)
Developmental Dysplasia of the Hip
Encompasses Congenital Dislocation of the Hip
Paediatrics 619
Occurs after birth. Coves a spectrum from instability through subluxation to dislocation
Commoner on the left. 25% bilateral
Incidence: 1 in 1000
Risk factors: extended breech, females, positive family history, first child, post-maturity,
oligohydramnios
Clinical: From 12 months shortening of the limb, external rotation and asymmetrical skin creases.
Delayed walking, Trendelenburg gait and OA in early 30s
Diagnosis:
Ortolani‟s Test: Flex hips to 90º then abduct them click as femoral head slips back into the
acetabulum
Barlow‟s test: Test for instability. Fix the pelvis with one hand and try and press the head and
neck of the femur backwards out of the acetabulum
Investigations. Neonatal ultrasound. > 4 months then xray
Treatment: achieve and maintain a stable reduction. Neonate Pavlik harness. Later: open reduction
Prognosis:
The earlier the treatment the better the outcome. Otherwise degenerative changes in the femoral
head (eg anteversion), acetabulum, capsule, altered alignment
Poor prognosis: boy, late detection, Ortolani‟s negative (ie doesn‟t reduce easily)
Clicking: a common finding and rarely associated with CCH
Club Foot
Congenital Talipes Equinovarus
Small foot at birth, plantar flexed (equinus), heal in varus, forefoot displaced towards midline, fore
foot inverted and lateral border convex, ankle is fixed, calf is wasted
Incidence: 1 in 1000. Twice as common in boys. 50% bilateral. Associated with other
abnormalities (eg myelomeningocele)
Aetiology: multifactorial inheritance
Treatment: early diagnosis, stretching and strapping then serial casting from 10 days. Surgery at
12 weeks if not right yet to release tight tissues (eg tendons) on inner side of foot. Raised outside
of shoe when walking. Follow-up: prone to relapse
Calcaneo-Valgus Foot: Dorsiflexed and heal in valgus
Tarsal Conditions
= Peroneal Spastic Flat Foot (old term)
An abnormal union between one or other of the bones of the hind foot
Autosomal dominant failure of segmentation or maturation of the mesenchyme
Incidence 1%
Diagnosis: flat foot as child with increasing stiffness of the hind foot. Progressive onset of pain in
adolescence
Diagnosis: lateral and oblique x-rays. MRI
Treatment: 6 weeks casting, rigid orthosis, resection of the bar if found early, otherwise fusion
Internal Tibial Torsion
Internal bowing of the tibia caused by inter-uterine positioning
Exclude other problems of hip, knee and foot
Usually self corrects by age 5
Femoral Anteversion
Angle between femoral shaft and neck – normal is 15 degrees
Exam: intoed gait and excess internal rotation of the hip. Egg-beater running style
Treatment: Trend to correct up to 5 years of age. Avoid sitting with legs in internal rotation.
Osteotomy if deformity is severe and does not correct
Scoliosis
Lateral spine curvature
Types:
Non-structural or postural curves, eg due to limb length inequality (curve disappears on bending
forward)
620 4
th
and 5
th
Year Notes
Structural curves: has lateral deviation and rotation of the vertebra. When child bends forward
there is a hump to one side and curve is still present/exaggerated eg congential, neuromuscular,
miscellaneous
Idiopathic types often present during adolescent growth phase
Causes pain, deformity and impaired lung function
Usually progressive. Follow carefully or active management (casts or surgery)
Other Congenital Skeletal abnormalities
Neurofibromatosis:
Commonest single gene disorders – autosomal dominant
NF1, 1:3,500
NF2, 1:50,000
Neurofibromatoma, Café au lait, scoliosis, skeletal overgrowth, tibial bowing, thinning, fracture
See Neurofibromatosis, page 334
Osteochondritis juvenilis (osteochondrosis): bony centres in children/adolescents become temporarily
softened deformity due to pressure harden again in 2 – 3 years in deformed shape
Skeletal dysplasia: achondroplasia, osteogenesis imperfecta, plus numerous others
Soft tissue disorders: Marfan‟s, plus numerous others
Chromosomal disorders: Trisomy 21, 13, 18
Metabolic: Numerous, including Wilson‟s, haemophilia
Neuromuscular: Charcot Mari Tooth, Duchenne, Cerebral palsy
Spinal dysraphism
Bone and Joint Injury and Infection
See Joint and Bone Infections, page 259, for Infection
Differential of joint swelling:
Acute rheumatic fever
Septic arthritis
Reactive arthritis
Henoch-Scholein Purpura
Juvenile chronic arthritis
Sero-negative arthritis
Rickets and vitamin deficiencies: A, folate, B12, C
Transient synovitis
Trauma
Haemophilia
Osteomyelitis
Supracondylar Humeral Fracture
Most common fracture above the elbow, typically extension injury by fall on outstretched hand
Type 1: undisplaced. Type 2: displaced but some cortical contact. Type 3: Completely displaced
Complications: nerve palsy (usually resolves after 6 - 8 weeks), vascular injury (esp brachial artery),
compartment syndrome
Treatment: closed reduction and percutaneous pin fixation. Non-displaced fractures without collapse of
the medial or lateral columns can be treated by immobilisation. Open reduction if unsatisfactory closed
reduction, open fracture or if vascular compromise
Medial Epicondyle Fractures
Often accompanied by dislocation. Bony fragment may be trapped in the joint preventing reduction
Usually treated non-surgically
Fractures of the Forearm
75% are fractures of the distal radial metaphases. Loss of reduction in 1/3 of cases
Wrist and Hand Fractures
Radius and ulnar fractures account for 45% of childhood fractures
Scaphoid fractures account for only 0.45% of paediatric upper extremity fractures
75% of finger injuries are stable and can be treated with simple immobilisation (often little finger)
Paediatrics 621
In toddlers and young children, most common pattern of injury is a crush injury of the finger, leading to
distal phalangeal fracture, nail bed laceration and/or distal tip amputation
In teenagers, diaphyseal level phalangeal fractures are common, with malrotation most apparent with
digital flexion
In teenagers, fractures of the metacarpal neck are common (“Boxer‟s Fractures”)
Fingertip trauma may lead to complete or incomplete amputation. Various treatment approaches. For
more proximal amputations, replantation is now standard over 1 year. Best prognosis with sharp
injuries (more common in adolescents, crush more common when younger)
See also Forearm and Hand, page 247
Transient Synovitis of the Hip
Transient synovitis is common and self-limiting, often following URTI.
Hip or knee pain, limp, decreased motion but normal xray
Main differential: septic joint. If in doubt, aspirate
Slipped Upper Femoral Epiphysis
Most common disorder of the hip in early adolescence, especially overweight and boys
90% are chronic and stable (can bear weight) with limp for several months
Pain on abduction, flexion, internal rotation
Often pain refers to the knee
Treatment: Percutaneous fixation
Femoral Shaft Fractures
Common, generally solid healing
Various treatment options including spica casting and traction
Subsequent limb overgrowth is common but not predictable
Limb Length Inequality
Various causes: check for soft-tissue hypertrophy, vascular anomalies, etc etc
Often idiopathic. If mild (< 1.5 cm) then monitor with serial exam and x-rays
Treatment depends on severity – involves surgical, gait, etc
Other
Legg-Calve-Perthes Disease: Poorly understood. Typically affects boys 4 to 8 years. Osteochondritis
and osteonecrosis of the femoral epiphysis. Softens bone then gradually reforms in a deformed shape.
?Due to interference with venous drainage of the femoral head. May present as an incidental finding.
Treatment controversial. Younger the patient the better the prognosis. Usually benign. Maintain
motion
Knee injury:
Osteochondral fractures of the knee: associated with patellar dislocations
Osteochondritis Dissecans: Fragmentation or separation of a portion of the articular surface of the
knee. Symptoms include vague pain, clicking, popping or effusion. Initial treatment is
immobilisation
See also Knee Injury, page 255
Physeal fractures of the distal tibia
Paediatric Neurology
Neurological Exam in Children
General (ALWAYS do these)
Are they well or unwell (esp toxic)
Growth:
Weight, height, and head circumference
Head exam:
Anterior and posterior fontanels (while upright). Anterior closes ~ 18 months, posterior ~ 4
months
Sutures, shape of head,
Check for shunts (subcutaneous tubes behind the ears),
622 4
th
and 5
th
Year Notes
Auscultation over closed eyes and temporal are for bruit
Dysmorphic features
Neurocutaneous stigmata: marks on skin, port-wine stains, Care-au-lait spots, use Woods lamp to look
for depigmented lesions if fair skinned
Higher cortical function
Ask questions appropriate to child‟s age
State
Attention: serial sevens, repeat numbers
Memory:
Dependent on attention, processing and storing, ability to access and ability to communicate
Immediate (repeat numbers), recent (3 items at 5 minutes but not visual things), remote (old
teachers name)
Object permanence
Visual: geometric reconstruction
Reading and spelling
Speech: dysphasia and dysarthria
Draw a man
Following instructions
Behaviour
Right left discrimination (crossed)
Name objects – visual agnosia
Construction of complex geometric figure
Cortical sensation
Abstract thought
Looking for:
Frontal lobe disturbances: personality changes, irritability, lethargy, sphincter incontinence,
primitive reflexes such as rooting, grasp re-emerge
Temporal lobe disturbances: altered ability to read, write and understand speech, memory
dysfunction
Parietal lobe dysfunction: sensory perception abnormalities, 2 point discrimination, graphesthesia,
stereognosis, apraxia
Cranial Nerves
1: Olfactory: don‟t often test unless abnormalities in the same area. Rarely impaired. Check each
nostril separately. Use chocolate, mint or vanilla essence.
2: Optic
Visual Acuity:
Babies: fix and follow, optokinetic nystagmus, blink reflex (50% of 5 months, 100% by 1
year)
Toddlers: offer toys of different sizes. Look in books for smaller and smaller things
Visual Fields:
Screen first: objects in the periphery – make sure they can‟t follow your arm to your hand
If suspicious: test with wiggly finger („look at my nose and grab the finger that wiggles‟)
Optic disc:
Very important
Use low light and small aperture
Get mum or dad to make funny faces behind you
Stay still and wait for optic disk to come into view
Look for venous pulsations – take pulse to get rhythm. If still can‟t see them, push lightly on
orbit – if veins collapse then OK. If no pulsations then ? ICP.
Pupils
III, IV and VI: Oculomotor, Trochlear and Abducens
Ptosis: nerve II and sympathetic. One eye doesn‟t open as much as the other
III: down and out
IV: Up and out
VI: in
Sun-setting: paralysis of upward gaze = pressure on quadregeminal plate
Get them to follow an object past the limit of head turning – don‟t hold head
Paediatrics 623
Hold them to your stomach and spin around with their head out. Nystagmus is normal
Dolls eye
V: Trigeminal
Motor: temporalis – bulk, power, clenching, chewing. Get them to bite on a wooden spatula while
you pull it away
Sensation: test from out of sight with feather
Reflexes: jaw and cornea (only if unconscious or other signs point to a problem)
VII: Facial
Taste: anterior 2/3: very hard in children
Lacrimation and salivary glands
Motor:
Tickle nose with tissue (try and get them to wrinkle face up)
Close eyes/mouth open: look for asymmetry of facial creases
Watch when crying – emotional movements less affected than voluntary ones (helps localised
to UMN/LMN)
VIII: Vestibulochoclear
Ask parents
Testing: whisper words (ice-cream, Wiggles) – rub fingers next to other ear ( white noise)
Spinning
IX and X:
Symmetry of uvula and palate movement
Swallowing
Gag: only if really necessary
Taste on posterior tongue: too hard
Voice: nasal „b‟, „d‟ and „k‟, hoarse
XI: Accessory shrug shoulders, turn heads with resistance
XII: Hypoglossus: stick out your tongue at me – bulk, fasciculation, power. Poke tongue through
cheek and feel it
Motor
Observe:
Abnormal movements: ticks, seizures, chorea, etc
Bulk
Scars
Contractures
Symmetry (eg small thumb nail on one side – contra-lateral parietal lesion)
Posture: eg frog leg posture in hypotonia, fisting
Tone:
Must be relaxed. Lie on back and shake arms and legs to a song
Range of movements: passive and active
Power:
Functional: Observe, including:
Gait: walking forward and backward, running, hopping, tandem gait (eg heal-to-toe), on
tiptoes, on heals, on insides and outsides of feet (Fog test). Look for dystonic posturing of
hands while they do this.
Proximal weakness: up steps, Gower‟s sign, wheelbarrows, play ball, push-ups. Gower‟s: lie
on back – tell them to get up as quick as they can when you say „go‟. Muscular dystrophy will
roll onto front then climb up legs.
Handedness
Formal strength testing (grade 5 down to 0): Pull a toy, push me away, crazy glue (pretend to stick
their finger to their nose and then try and pull it away), resistance, squeeze fingers
Pronator sign
Remember:
Proximal weakness: myopathy
Distal weakness: neuropathy (except myotonic dystrophy)
Reflexes
Must be relaxed, be patient
Hit your hand, not the child
624 4
th
and 5
th
Year Notes
Test ankle jerk on the sole
Swing with gravity, don‟t bash
Use distraction (look over there…) and reinforcement: clenched teeth (chewing sticky lolly)
Check for clonus
Primitive reflexes (go at various ages): Moro, ATNR (atonic neck reflex) – turn head suddenly
extend arm on that side, Babinski
Sensation
Difficult
Test from out of range
Test with a broken spatula: show them sharp and dull and then always use sharp
Touch, pain, vibration, proprioception
Cerebellar
Gait: Walk along a line on the floor – should be able to do it well by 6
Rhomberg
Finger nose: reach for toys (make sure they stretch)
Foot tapping
Rapid alternating movement
Hands outstretched with eyes closed, look for drift
Head Size *
Microcephaly
Head circumference below the 3
rd
centile with abnormally slow head growth
Incidence: 1/1000, recurrence in siblings 1/50
Causes:
Familiar: not associated with developmental delay
Autosomal recessive condition, associated with severe learning delay
Congenital infection: Rubella, CMV, Toxoplasmosis, Varicella Zoster, Listeria, Syphilis
Brain insult: eg perinatal hypoxia, neonatal meningitis. Likely to be accompanied by cerebral
palsy, seizures, visual impairment, etc
Fetal Alcohol Syndrome
Large Head
Megalencephaly = oversized brain
Hydrocephalus: dilated cerebrum:
CSF volume associated with ventricular dilatation and intraventricular pressure
Due to:
Aqueduct obstruction: injury, infection or genes
Arnold Chiari Malformation (downward displacement and elongation of hind brain, with
herniation into the cervical canal)
Acquired causes: meningeal adhesions, mass lesions, etc
Chronic Subdural Haematomas
Hydraencephaly: no cerebrum
Benign familial anatomic megalencephaly or macrocephaly
Metabolic Megalencephaly: late manifestation of many cerebral degenerative disorders (eg lysosomal
storage diseases)
Neurofibromatosis
Cerebral Tumour
Headaches
History:
Pain characteristics: how bad, do they vary from one to the next, throbbing (migraine)/tight
(tension)
Auras: visual, unilateral slowly spreading tingling/numbness/weakness
Photo & phonophobic
Look pale/unwell ?migraine
Late afternoon ? hypoglycaemic
Paediatrics 625
Suspect ICP if vomit in the morning (without much nausea), increasing severity, or wake in the
morning or at night with a headache
Stress: relationship to headaches to school and holidays
Relieving factors: Sleep, medication
Associated with migraines:
Motion sickness – patient and family
„Ice-cream‟ headaches – like shooting pain into head when biting an ice-block
Benign Paroxysmal Vertigo of Infancy (not the same as adult BPPV): 2 – 3 minute episodes of
unsteadiness, queasiness, nystagmus
Cyclical vomiting
Abdominal migraine
Past Medical History: head injury. To assess severity ask: did he loose consciousness, did he go
to hospital and stay overnight, have any stitches or need imagining
Family history:
What kinds of headaches do the rest of the family get (don‟t talk about migraine – different
meanings to different people)? There is a family history in 80% of migraine sufferers
Serious neurological disorders, strokes
Exam:
General: Well/unwell, growth (if big head then measure parents), dysmorphic features, skin
(stigmata)
BLOOD PRESSURE
ICP: venous pulsations in retinal veins, papilloedema, visual acuity, 3
rd
and 4
th
nerve palsy
Focal neurological signs: especially cerebellar (common site of lesion in kids 2 – 10)
Cranial bruit to check for AVM: common finding. Interested in asymmetry, or if it can be
eliminated by compressing the ipsilateral carotid artery
Check sinuses, teeth, TMJ
Differential:
Is it acute or chronic, recurrent or progressive, etc
Migraine: normally throbbing. when stressed. Most common cause in children
Tension headache: Rare before adolescence. Presentation: constant daily bilateral headaches
without well defined onset and ending, less impairment of function. Stress (ie doesn‟t differentiate
from migraine. But children usually somatise rather than tense up). More common in older girls
ICP
Drugs: eg daily use of analgesics
Management:
Reassure: most parents seek help to check its not serious
Education: Migraines are familial, due to ischaemia and vasodilation (which stretches pain fibres
in blood vessels)
Symptom diary: check for food association (fairly rare)
Avoid triggers
?Psychologist referral:
Stress, get to the bottom of stress problems, relaxation, coping
It will be life long – learning skills to cope better than life long medication
Medication:
Paracetamol: need a big dose and right at the start to make a difference (otherwise gastric
motility and fail to stop spread)
Propranolol: tested in RCT, but not if asthmatic
Ergotamine: contraindicated if complex migraine (focal neurological signs)
Migraine Definition:
Recurrent paroxysmal headaches with pain free intervals with normal health, plus two of:
Unilateral pain, nausea, visual or other aura, family history in parents or siblings
Seizures
See also Epilepsy, page 133
Classification:
Either partial or generalised
And one of:
626 4
th
and 5
th
Year Notes
Acute symptomatic: any person in that situation would seize eg hypoglycaemia, heatstroke,
meningitis, hyponatraemia. Seizure will stop when cause goes away (unless scarring – when it
becomes a „remote symptomatic‟ seizure)
Single
Benign Febrile Convulsion
Epilepsy: Repeated unprovoked seizures
If Epilepsy then:
Localised: Idiopathic, symptomatic or cryptogenic
Generalised: Idiopathic, symptomatic or cryptogenic
Unclassified
Seizures:
A symptom – not a diagnosis or a disease
Hyper-synchronous excessive discharge of CNS neurons associated with a clinical sign
Diagnostic process:
Is it a seizure or not
What type of seizures – is it generalised or localised, etc
Is it a single seizure, acute symptomatic, afebrile or epilepsy
If epilepsy, what syndrome is it (this step is critical to treatment and prognosis, but often ignored in
practice)
Brain tumours cause 1 – 2 % of all seizures in children, and 4 – 6% of partial seizures
Neuro-imaging:
Indicated for:
Neurological deficit/asymmetry
Neurocutaneous syndrome
Developmental regression
Partial seizures
Infantile spasms or myoclonic seizures in 1
st
year of life
Persisting unclassifiable seizures
Not indicated for:
Idiopathic generalised epilepsy
Benign childhood epilepsy with centrotemporal spikes (Rolandic)
Simple Febrile Seizures
CT:
Initial scanning technique for exclusion of tumour
Show calcification
Available and easier to perform
MRI:
Preferred imagining technique
Sensitive to migrational abnormalities or very small lesions
PET/SPECT scan: localise lesion on the basis of metabolism. Only if considering epilepsy surgery
Epilepsy in Childhood
Incidence: 0.5 – 1 %
Lifetime prevalence of a seizure is 5%
Aetiology:
Idiopathic: normal kids, no structural abnormality, often family history, EEG normal, generally
benign and good prognosis. Cause is assumed to be genetic – usually a channelopathy
Symptomatic: An underlying cause is known, and there are usually other signs of a problem
Cryptogenic: There are other problems besides seizures, eg retardation, focal signs, etc, but can‟t
find a cause
Symptomatic and Cryptogenic: abnormal children, abnormal background on EEG, prognosis not so
good and often seizures difficult to control
Benign focal (Rolandic) Epilepsy of Childhood:
= Benign Childhood Epilepsy with Centrotemporal Spikes
Commonest focal seizures in children
Onset 3 – 10 years
80% focal, especially mouth and face. 50% only have fits in sleep
EEG diagnostic. Prognosis excellent
Paediatrics 627
Childhood absence epilepsy:
Onset 4 – 10 years – often confused with daydreaming
Almost all outgrow the absence seizures, but 30% will have GTCS in adolescence
Usually easily treated
EEG:
Need to do when sleep deprived and not on medication
2 – 4 % of normal children have an abnormal EEG
55% of epileptic children have an abnormal EEG
Looking at frequency, morphology, location, reactivity, symmetry, dysrhythmia, etc
Paroxysmal events:
Noises
Benign variants: associated with age and state
Epileptiform: inter-ictal and ictal
Psychosocial aspects: More important than drugs. Peoples attitudes will do far more damage than a
few seizures
Education
Counselling
Normalising
Seizure precautions: when driving, swimming, bathing, scuba diving, etc
Pharmacology:
Aim:
Seizure free with no side effects
Start low and go slow
Never stop abruptly
Start after 2 or more seizures
Stop after 2 years seizure free
Common drugs:
Carbamazepine
Valproic acid
Less common:
Clobazam
Ethosuximide
Phenytoin
Phenobarbitone
Rarer:
Vigabatrin
Lamotigine
Status Epilepticus:
Continuous or intermittent fitting > 30 mins
ABCDEFG – does airway need protecting
Give effective anticonvulsant – 2 doses of rectal diazepam, if it continues consider paraldehyde,
phenytoin, general anaesthesia
Benign Febrile Convulsion
Types of seizure occurring with fever:
Benign febrile convulsion
Epilepsy: eg first epileptic seizure unmasked by fever
Acute symptomatic seizure: meningitis, etc
Benign Febrile Convulsions:
Frequency: 2 – 5% of all children
Age: 6 months – 5 years
Temperature: usually > 38.5 C
Boys: Girls = 1.4:1
Family history common (polygenic inheritance)
Unrelated to prenatal and perinatal brain damage
Have seizures with fever only
Treatment:
Stop seizure: rectal diazepam (0.5 mg/kg) at home or in ambulance
628 4
th
and 5
th
Year Notes
Find the cause of the fever: seizure won‟t hurt them but meningitis might!
DON‟T use anticonvulsants – decrease recurrences but potentially significant side effects to
treat something that is benign
Prevention: Avoid over heating. Paracetamol/ibuprofen or tepid sponging don‟t risk of seizure
Types:
Simple (75%): generalised, brief (< 15 minutes), does not recur in 24 hours
Complex (25%): Focal and/or prolonged and/or recurrence within 24 hours
Recurrence: 30% will have a recurrence, 70% of these within the next year
Risk of subsequent epilepsy:
Increased risk if neurologically abnormal prior, family history of epilepsy or first seizure is
complex
Otherwise very slight increase in risk only
Neurological sequalae:
No impact on behaviour, growth, IQ
Prolonged febrile seizures associated with hippocampal sclerosis (temporal lobe).
Controversial. (eg which direction is causation)
Parental education:
Seizure does not cause brain damage (if less than 30 – 45 minutes)
30% chance of another seizure
Next time: stay clam, clear airway, recovery position when stopped (low tone), time the seizure
Call ambulance at 5 minutes:
Most seizures stop by 5 minutes – so those that haven‟t are more likely to go on for longer
Want to be at hospital and have it stopped by 45 minutes
Anoxic Seizures
White breath-holding attacks:
Vaso-vagal events due to stimulus: eg anger, pain, vomiting, etc. [Big sympathetic drive
parasympathetic overcompensation????]
Occur in children from 2 – 10
Reflex bradycardia or brief asystole or peripheral vasodilation
Symptoms: pallor, ocular revulsion, don‟t breath, extensor posture, a few symmetrical clonic
movements, spontaneous resolution and then fine
Blue breath-holding attacks:
1 – 5 years
Follow a stimulus, eg crying
Get worked up, don‟t breath in, run out of breath and don‟t breath in (actually stop breathing)
Cyanosis with retained heart rate
May lose consciousness and have some clonic movements
Blow on face to start breathing
Both white and blue breath holders are often iron deficient do dietary history and Hb test
Don‟t treat them. Ensure parent isn‟t being manipulated by breath-holding by child
Tics
Brief, sudden involuntary stereotyped purposeless movement involving the muscles of the face,
extremities and trunk
Worsens with anxiety
May be able to be controlled for a short while
Go away in sleep
If florid, look like repeated myoclonic seizures
Chronic Motor Tics:
Goes on for more than a year
Life long tendency
Chronic Multiple Tics:
= Gilles de la Tourette Syndrome
Onset usually 2 – 15 years
Boys > girls
Tendency for life
Multiple motor and vocal tics which wax and wane
Paediatrics 629
Wide spectrum from minor severe
Cerebral Palsy
= A persistent disorder of posture or movement caused by a non-progressive, non-hereditary lesion of
the immature brain, acquired either in utero or later at a time of rapid development of the CNS (up to
several years after birth)
May be accompanied by other impairments, eg retardation, vision defects or epilepsy
Though lesion is static, the clinical features may develop for several years as brain function matures
(may give appearance of being progressive – clinical signs have to wait until that part of the brain
„kicks in‟)
Incidence:
Stable at about 2/1000.
80/1000 for very preterm babies
Stages of brain development:
Up to 20 weeks major brain malformations:
Lissencephaly (brain without cortex)
Microgyria: lots of little indentations
Migration defects: islands of grey matter in the middle of white matter
26 – 32 weeks: neurons climb glial fibrils: intense growth – prone to ischaemia. If born then,
prone to germinal matrix bleeds. But ischaemia more important Periventricular Leukomalacia
(PVL)
Myelination starts at about 30 weeks, but most is after birth. Damage only becomes obvious as
myelination complete (conscious control of arm at 4 – 5 months, leg at 9 months)
Causes:
Anything that damages neurons: ischaemia, hypoglycaemia, infection, trauma, toxins
Only 10-30% attributed to “intrapartum asphyxia”. Normal PO2 in utero is 15 – 25 mmHg well
adjusted to hypoxia
For many it‟s due to an unknown earlier adverse event
Significant proportion preterm (43%)
Intrauterine Growth Retardation risk by 5 times
Exam findings:
Hyperactive reflexes
Abnormal movements of chorea, athetosis, dystonia
Abnormal absence or persistence of infantile reflexes
Differential:
Metabolic disorder
CNS degenerative diseases
Cerebellar dysgenesis or spinocerebella degeneration
Classification
Hemiplegia:
0.79/1000
Congential:
Spastic paralysis of arm and leg on same side. Arm usually weaker than the leg. Distal parts
worse than proximal. Growth of affected parts reduced
Face not involved
Epilepsy common – correlates with degree of mental retardation (but IQ often normal)
Mechanism: vascular (ie stroke in utero). If preterm, usually periventricular rather than
cortical and leg weaker than arm
Acquired:
Following infection, trauma, CVA, status epilepticus, etc
Most in first 3 years of life
Flaccid with facial involvement, spastic later
Diplegia:
0.9/1000
Spastic:
Problem in preterm 28 – 32 weeks
Follow bilateral periventricular injury, especially with hydrocephalus complicating, or injury
to basal ganglia or parasagital cortex
630 4
th
and 5
th
Year Notes
Stiff lower limbs (may be floppy as neonates): flexion of hips and knees, scissoring (internal
rotation and adduction), weak trunk and eventual contractures. May dislocate hips
Upper limbs variably affected (if worse then more global)
Hyperreflexia and spasticity with variable wasting
Epilepsy uncommon, intellect may be retained (69%). Head growth mirrors intellect
Quadriplegia:
Global cerebral insult: massive haemorrhage, shock, obstructed umbilical chord
Upper limbs often worse than lower, generalised spasticity and wasting.
Severe mental retardation, cranial nerve palsies, aspiration, etc
Athetoid:
Extrapyramidal injury, especially perinatal insults (including kernicterus – unconjugated
hyperbilirubinaemia)
Appears after 5 months: involuntary movements and posturing, poor trunk control, hypotonia or
normal, normal reflexes
Impaired speech, drooling, facial grimacing, often deaf (especially high tone)
IQ often normal but difficulties communicating. Epilepsy in 25%
Ataxic:
Cerebellar symptoms predominate
Cerebellum abnormal on imagining
Presents at 1 – 2 years, but floppy and docile from the start
Ataxia, intention tremor, late walking, high tone deafness, normal IQ in 50%
Can be familial disease
Management:
Team approach: physio, OT, orthopaedic surgeon, etc
Prevent contractures and encourage normal developmental stages
Treat epilepsy
Rule out deafness, check special senses
Encourage communication
Prevent malnutrition
Encourage mobility and upright posture (frees up hands for „learning‟ activities)
Support for child and family
Manage constipation, incontinence
Muscular Dystrophy
Not common. Most common is Duchenne: 1 in 3,500
X linked recessive, females usually asymptomatic. 1/3 new mutations
Caused by failure to make dystrophin (in muscle cell membrane)
Present with muscle weakness that is slowly progressive. Gower‟s sign: proximal weakness climb
up their legs with hands to stand up
Often mild intellectual handicap (IQ 85)
Wheel chair bound by 12. Respiratory function and scoliosis terminal bronchopneumonia
Diagnosis: genetic tests, CK markedly elevated, myogenic pattern on EMG
Treatment: supportive only
Acute Weakness in Childhood
Consider:
Guillian Barre (LP shows elevated protein but normal cells), post-infectious (eg mycoplasma),
often sensory involvement, treat with Ig
Transverse Myelitis: post-infectious, distinct spinal level, responds to steroids
Neural Tube Defects
A neural tube defect – failure of closure of the neural tube (4 weeks gestation – often already happened
by the time a woman knows she‟s pregnant)
At lower ends leads to spina bifida and at upper end anencephaly or encephalocele
Rate varies on population. High in Irish, Welsh, Scottish (3%) and those from poor backgrounds (poor
nutrition, folate, etc)
Multifactorial causes:
Genetic
Paediatrics 631
Environmental (eg diet)
Drug associations (eg antiepileptics)
Any midline lesion of the skin overlying the CNS from the nose to the sacrum may indicate a lesion
below the skin (same embryological origin) – eg hair, pigmentation, etc
Types
Myelomeningocele:
Most common: 90% of spina bifida, failure of caudal closure of neural tube failure of closure of
skin and absence/leaking of the dura/meninges.
Lumbar sacral (25%), lumbar or thoracolumbar (50%) or thoracic/cervical (11%).
Spinal cord opened out flat. Variable neuro deficit below lesion. Possible tethering
Leads to:
Paraplegia: paralysis of knee and hip extensors with retained flexion. Talipes (club foot) –
equinovarus is commonest
Variable loss of sensation
Autonomic problems: faecal incontinence, dribbling urinary incontinence on lifting baby or
spastic urethral sphincter ( urinary retention), spastic bladder ( reflux, hydronephros)
Open lesion risk of ascending infection
Hydrocephalus: very common (Arnold-Chiari malformation). Dislocation of cerebella tonsils
and medulla into cervical canal, aqueduct stenosis (?primary lesion or tethering). Signs of
hydrocephalus and ICP: bulging fontanelles, rapid head growth, poor feeding, separation of
sutures, „sun-setting eyes‟ (looking down), drowsiness, venous congestion of skull. If acute:
vomiting, bradycardia, hypertension
Management:
Interdisciplinary team
Close back to prevent infection
Drain hydrocephalus (ventriculoperitoneal shunt)
Bladder and bowel management
Review motor and sensory function, prevent contractures and aid mobility
Etc
Spina Bifida Occulta: Range from failure of formation of dorsal spine (cord intact) to abnormal cord
contents
Diastematomyelia: bone or cartilage spur into the cord progressive loss of spinothalamic function
(pain and temperature) with growth (slices as spine elongates). Not common. Leads to regression of
acquired skills.
Lipoma: fatty mass pressure effects
Tethered cord: complication of many types. Cord fixed lower down and gets stretched as spinal
column grows loss of power, sensation and autonomic function (ie sphincter function, weakness in
toes and forefoot, saddle anaesthesia)
Dorsal Dermal Sinus: Epithelium lined tube from skin (lumbar/sacral) to dura or into spinal canal.
Risk of meningitis (coliform) and tethered cord
Meningocele:
Rarer. Swollen lesion on back, full of CSF, brilliant translumination. Little neurological deficit,
risk of tethering
Cranial meningocele: occurs on skull and contains CSF
Encephalocele: occurs on skull and contains brain. Prognosis more guarded
Anencephaly: Failure of cephalic closure of neural tube absence of cranium. Frequent
polyhydramnios. Most live births die within 24 hours. Also occurs in other syndromes ( always do
karyotype)
Prevention
Folic acid levels in pregnant women only half the recommended
Recurrence after one affected child is 3 – 5% (?inborn error of folate metabolism)
Low dose folate prophylaxis highly effective – but 50% pregnancies unplanned
Adequate dietary intake hard (5 portions of broccoli a day!)
Can detect with antenatal ultrasound or maternal or amniotic fluid alpha-fetoprotein
Eye disorders in Children
See also The Red Eye, page 142
632 4
th
and 5
th
Year Notes
Routine eye checks for infants:
Fixing and following: ophthalmology referral if not doing this by 4 months
Pupillary red reflexes: view from about 50 cm. Leukocornea (white pupil) ?retinoblastoma.
Other irregularities ?congenital cataract
Ocular alignment: symmetrical corneal light reflex (don‟t have to be exactly central). Strabismus
(misalignment of visual axis) amblyopia. May be intermittent. Test with cover test.
Accommodative Esotropia = convergent strabismus related to accommodation
Eye movements: if not following then test vestibulo-ocular reflexes using dolls eye
Adnexa Oculi: Eyelids. Check for Congenital Naso-Lacrimal Duct Obstruction (tears, puss or
mucus discharged by pushing on lacrimal duct) due to incomplete canalisation. Most resolve by
age 1 ( usually managed conservatively by twice daily lacrimal sac massage)
Globes and cornea: of equal size
Serious disorders in the neonate ( urgent referral):
Congenital Glaucoma: photophobia, corneal haze/opacity, corneal enlargement or asymmetry
Ophthalmia Neonatorum: conjunctivitis with infection and inflammation of the conjunctiva in first
month of life. Urgent microbiology and iv antibiotics for chlamydia and/or N Gonorrhoeae
Red Eye in Children
Conjunctivitis:
Common in newborns – may be serious
Bacterial: rapid onset, usually spills from one eye to the other. Puss.
Neonatal often Neisseria gonorrhoea (prevented with silver nitrate drops in new born if
high risk). Can lead to perforation of orbit. If systemic spread then septic arthritis.
Treatment: B Penicillin 25 mg/kg/12hr iv + 3 hourly 0.5% chloramphenicol drops for 7
days
3 – 5 days post delivery: Chlamydia. Can progress to rhinitis and pneumonitis. Diagnosis
requires special chlamydia swab. Treatment: Erythromycin 10mg/kg/6hr po for 21 days
to eliminate lung organisms + 1% tetracycline drops
Acute causes often Staph aureus, S pneumoniae, H influenzae or S pyogenes. Treatment:
drops up to hourly (eg chloramphenicol)
Chronic: usually toxins or immune (eg Kawasaki, Erythema Multiforme, Reiter‟s
Syndrome)
Viral: acute onset, often bilateral, minimal pain, thin watery discharge, photophobia.
Adenovirus, Herpes Simplex, measles, etc. Generally clears spontaneously. If Herpes
suspected (eg eyelid vesicles), start 4 hourly acyclovir and immediate referral
Allergic: history of atopy and itchy eyes. If mild then use astringent, topical anti-histamine or
cromoglycate
Subconjunctival haemorrhage: common after blunt trauma (eg birth), coughing (eg whooping
cough) and vomiting.
Corneal abrasions: trauma or infection (esp HSV)
Iritis/Uveitis: uncommon in children. May have no pain but strabismus or visual loss. Cornea red
near iris (unlike conjunctivitis). Look for white cells in anterior chamber.
Renal Disease in Children
See also Renal and Genitourinary, page 201
Proteinuria
Definition: > 150 mg protein/day (same cut off as adults)
Normally protein is lost from tubular cells. Pathological if:
Filtered protein from glomerulus
Loss from tubular cells
Categories:
Gross proteinuria: > 1 gm/day ( nephrotic syndrome if severe)
Acute low grade
Chronic low grade
Diagnosis:
Dipstick: measures concentration of protein, so if urine is concentrated protein concentration
as well
24 hour urine: problem if not continent
Paediatrics 633
Nephrotic syndrome:
= Proteinuria + oedema + albumin in blood (hypoproteinaemia)
Oedema is due to colloid osmotic pressure aldosterone Na H2O retention this
leaks out as well
Caused by leaky glomeruli
Causes
Minimal Change Disease:
See also Minimal Change Disease, page 213
= No change under light microscope
Passing up to 8 – 10 gm per day gross oedema
3 rare complications:
Hypoperfusion: classically the gut abdominal pain
Loose Ig‟s as well risk of bacterial infection (eg pneumococcal)
Thrombosis (eg renal vein)
Usually grow out of it (eg over 6 months, although may persist until an adult). Unpleasant but not
usually life-threatening
Treatment: steroids but side-effects
10 – 20% have other causes which may chronic renal failure
Acute low-grade proteinuria:
No long term significance
Can be:
Exercise induced in some teenagers/adults
Urinary tract infection
Postural proteinuria (when standing up)
Have to demonstrate that it‟s gone (ie that its not chronic)
Persistent/chronic low grade proteinuria
Always have some. Exclude exercise and postural
Significant finding: risk of renal disease, eg in adult
Haematuria
Definition: > 5 RBC in high powered microscope field
Categories:
Gross/Macroscopic:
UTI (most common cause by far)
Trauma: visceral damage easier in kids
Post-streptococcal glomerulonephritis
Stones
Wilm‟s tumour
Bleeding disorder (eg haemophilia)
Red food colourings (eg beetroot)
IgA nephropathy: IgA deposits on glomeruli
Acute microscopic:
Infection
Plus above list (which are more likely to be microscopic than macroscopic, and may be
intermittent/chronic)
Acute Renal Failure
= Acute renal „success‟. If kidney didn‟t shut down after ATN, would continue filtering at 1-2 l/hr with
no reabsorption very rapid dehydration
Causes:
Ischaemia
Obstruction (eg congenital malformation)
Sepsis: toxins killing tubular cells + hypoperfusion
Drugs: at glomeruli or tubular cells
Complications:
Fluid overload: fluid restrict to insensible losses (breath, stools, skin = 400 mls/m2 of body
surface) plus urine and vomit
634 4
th
and 5
th
Year Notes
Hyperkalaemia:
No symptoms, so have to monitor
Treatment: salbutamol or insulin + glucose shifts K into ICF
Calcium resonium: chelates K
Encourage anabolism with calories cell creation
Frusemide if any urine output
CaCl or Ca Gluconate: prevents arrhythmia
Dialysis
Uraemia: vomiting, encephalopathy dialysis
Hypertension: due either to aldosterone release or fluid overload
Chronic Renal Failure
Incidence: 1 – 2 kids per million per year
Disaster for families very demanding treatment
Causes:
Obstruction/congenital
Dysplasia (never developed normally)
Severe reflux
Glomerulonephritis
Problems:
Nutrition (need calories ?NG tube)
Linear growth: due to nutrition, PO4 secondary hyperparathyroidism, vitamin D
Anaemia: due to erythropoietin
Na/H2O/K balance (may loose or retain too much)
Hypertension: angiotensin, overload, drugs
Ca balance
Development (always tired)
Treatment: peritoneal dialysis
Genito-Urinary
Urinary Incontinence
See UTIs in Children, page 221
Daytime incontinence
History:
Previously continent?
Frequency, volume, urgency, pain, colour, continuous dribble (are nappies never dry - nearly
always pathological)?
Infection history:
Associated symptoms
Past infections, kidney complications
Constipation ( urinary retention due to pressure infection). Need to fix bowels first
Family History
Exam:
Palpable/distended bladder
Kidneys: palpable, tender?
Boy: examine penis carefully: balanitis (inflamed foreskin), constricted urethra
Girl: effusion of the perineum, can labia be parted
Signs of occult spina bifida (eg skin or vascular lesions over sacrum)
Are legs neurologically normal
Blood pressure: whenever risk of kidney disease
Screen for infection
Not PR
Investigations:
Urine microscopy
Paediatric US referral
Further tests:
Paediatrics 635
Bladder volume scanning
Paediatric MCU
Cystoscopy
Urodynamics
If repeat infection:
?Genitourinary malformation: do US or MCU to check for reflux
Infection leads to temporary scarring, which predisposes to infection. Break the cycle with
prophylactic antibiotics
Bed Wetting/Enuresis
Very common: 12% at age 6, 4% at age 14
History:
Just at night time, or day as well (pathology more likely – must fix this first)
Is it primary or secondary:
Primary: have never been dry, most common, usually no associated pathology. No daytime
problems. Pass large volume without waking. Ask about proportion of dry nights, getting
worse or better?
Secondary: were dry, now wets (regression) pathology common. Detailed history of when
it began, pattern since then ( or ), symptoms of infection (dysuria, frequency), diabetes
(weight loss, thirst), physical abuse. Can be induced by stress (eg starting boarding school,
family disruption)
How much wetting: big patch, small patch. How often in the night (if several times then will take
longer to come right)
Urinary symptoms: polyuria, dysuria, frequency
?Constipation or soiling need to fix this first
Family history (if one parent wet the bed, 40% of children will wet, if both parents then 80%).
This is key information – normalises it for parents and child anxiety
Parents management style: punitive (unhelpful but common) or supportive (ignore wet pants,
praise for waking to pass urine, not common but more helpful)
Previous treatment experiences
Expectations of parents and child
General developmental screen, including faecal continence, bladder training
Social history: how much extra support will the child or parent need to manage the treatment
Exam:
End of bed: note weight loss, hydration
Growth
Lumbosacral area (midline defects ?spina bifida), perianal sensation and neurological exam of
legs
Abdominal palpation: kidneys, distended bladder, constipation
External genitalia
Blood pressure
Investigations:
If primary then tests usually reveal nothing
MSU: blood, protein, glucose, casts, bacteria, urine analysis
May be: blood sugar (diabetes) and electrolytes (renal failure)
Treatment:
Reassurance: a nuisance, but normal and curable. Not silly or on purpose. Primary enuresis is
NOT a psychological problem, a personality disorder or ADD, but one of delayed maturation.
However, stress will make a tendency to bedwetting worse
Parental intolerance will worsen it and self-esteem
Avoid covert rewards (eg getting into parent‟s bed when their bed is wet)
No night nappy, leave lights on in toilet, normal fluids before bed
Convenient hygienic care of bed (eg waterproof under-blanket)
Keep a diary (good for any symptom):
Day, time of bed, hourly check till parents go to bed, size of wet patch
Helps keep accurate record and has therapeutic value (gives feedback, is something to do, etc)
Don‟t treat until age 6 or 7 – but do treat then otherwise psychological sequalae as they head into
teens
Four options:
636 4
th
and 5
th
Year Notes
Encouragement (rewards). See Behaviour Management, page 570
Systematic Waking: wake half an hour before normal wetting time, and shift toileting time
closer to bedtime/morning by half an hour a week
Pad Alarms: Good ones best. Not funded. Parents need to be instructed on how to get
maximum value from them. Explain and demonstrate to child. Hard work for parents as they
must get up (take turns, may need extra support if solo parent). Must wake child properly (eg
cold flannel on face). Relapse immediate resumption of pad and alarm. Relapse reduced
by over-training (once consistently dry, push fluids at bedtime, will recommence wetting but
overcome it quickly)
Bladder training exercises
Which options:
Wets once or twice a week: Rewards for 4 weeks then pad and bell
Wets at the same time each night: systematic awakening
Wets many times through the night with small patches: bladder retraining and alarm
Wetting more than twice a week at unpredictable times: bell and pad
If not improvement after two lots of 4 weeks then ?anatomical problem
Not medication: Nasal ADH/vasopressin (specialist only) treats symptoms but doesn‟t change
behaviour. Maybe useful for short term protection (eg school camps, etc)
Testes
Undescended testis
= Cryptorchidism
Descent complete in 96% at birth, in 99% at 3 months
Premature will have rate of undescended testis (5% at 1 year)
Two types:
Arrest of descent: at internal or external ring, or at scrotal neck
Ectopic: outside of the line of descent
May present with a hernia
Surgical correction at about 12 months
Sequalae of non-descent:
20 times risk of malignancy
?Impact on fertility (due to ?higher temperature impairs spermatogenesis)
If don‟t bring them down they may end up over the pubic ramus very uncomfortable sex!
No testis
If bilateral undescended testis and hypospadias ambiguous genitalia urgent referral
Torsion in utero no testis
No testis = anorchia. Maybe no kidney on that side check
Retractile Testis
Normally in scrotum but retracts upwards during examination
Testis normal size
Follow-up 2 yearly
Surgery unnecessary. Will drop into scrotum at puberty
Hydrocele
Fluid collection between the layers of the tunica vaginalis secondary to trauma, infection or idiopathic.
Implies a patent process vaginalis
May be bigger in the evening than in the morning
Transluminates well, is non-tender and non-reducible
Herniotomy if not resolved by age 2. 50% disappear in first year. Remove tunica vaginalis removes
potential space
Predisposes to hernia
Acute Scrotum
Must examine the genitalia of every boy who presents with acute lower abdominal pain (may not
localise to testis)
In descending order of frequency, causes of an acute scrotum are:
Paediatrics 637
Torsion of the appendix testis
Testicular torsion
Idiopathic scrotal oedema. Symmetric swelling, no testicular tenderness. May include penis,
inguinal and perineal regions. Exclude torsion
Rarely, epididymo-orchiditis
Management of torsion:
High probability: short duration and negative urinalysis surgery
Low probability: longer duration and positive urinalysis ?Doppler US for blood flow
Torsion of Appendix Testis
Most commonly caused by Hydatid of Morgagni (Mullerian duct remnant) at top of testis
Peak incidence at 10 – 12 years. Oestrogen stimulates enlargement of the remnants predisposes to
torsion
Symptoms range from minimal inflammation to florid, swollen hemi-scrotum indistinguishable from
testicular torsion
Urgent surgical referral
Testicular Torsion
Testes are covered by tunica vaginalis – has parietal and visceral surface (like lungs in pleura)
Testis rotates on its chord within parietal tunica vaginalis
Once torsion has occurred in one, more likely in another
< 6 hours will probably not cause infarct
Two peaks for incidence:
Neonatal: Testis usually dead by diagnosis. May not operate (will atrophy). May „pex‟
contralateral side to prevent torsion
Age 13 – 15: History and presentation variable. Surgical emergency. If testis viable, untwist and
fix. Fix contra-lateral side
Need to remove a torted testis, otherwise he will develop autoantibodies for spermatozoa infertility
of other testis
Epididymo-Orchitis
Very rare in children. Two peaks
Newborn, with underlying urinary tract anomaly. Do US and MCU. MSU to rule out infection
In 13+ due to reflux up the vas infection/inflammation
Mumps orchitis does not occur in pre-pubertal boys
Penis
Smegma
Yellowish coloured secretion-desquamation which occurs normally and keeps the foreskin separate
from the glans
May appear like a dermoid cyst underneath the skin
Is normal, and will eventually extrude spontaneously
Retraction of the foreskin
By age 4 most boys foreskins will be able to be retracted
May have intermittent pain during separation of the adhesions and the foreskin may be red or swollen
for a day or two
Phimosis
Irretractable, scarred foreskin. May balloon on urination
If mild, application of Betnovate ointment to the tight portion of the foreskin (retract loose bit to access
it) is effective
If ongoing problems circumcision
Paraphimosis: foreskin stuck behind glans swollen. Always put foreskin back after catheterisation
Balanitis
Infection of the foreskin, may remain distal or involve whole penile shaft
Can be secondary to phimosis
Treat with topical bactrim or oral antibiotics
638 4
th
and 5
th
Year Notes
Hypospadias
Combination of dorsal hood, proximal urethral opening and chordee (central penile tilt)
Presentation varies from mild to severe peno-scrotal type with ambiguous genitalia (check for testis)
Correct at 9 – 12 months
UTIs
Infertility as the opening moves closer to the base of the penis
Ambiguous Genitalia *
Relative complexity of male differentiation vulnerable to wide variety of incomplete
masculinisation
History and exam:
Exposure to progesterone, testosterone, phenytoin, aminoglutethamide
Previous neonatal deaths
Phallic size, position of urethral orifice, fused labia, descended gonads
Don‟t rely on appearances whenever babies have:
Bilateral cryptorchidism, even if there is a phallus
Unilateral cryptorchidism with hypospadias
Peno-scrotal or perineoscrotal hypospadius
Causes:
Androgen resistance (extreme form: testicular feminisation)
Early in boys development, sertoli cells release anti-mullerian peptide stops formation of
the fallopian tubes, uterus and the upper 1/3 of the vagina
Testosterone and dihydrotestosterone from Leydig cells responsible for the rest of male
genitalia. If a problem in this pathway Girl with short vagina.
Present in puberty with primary amenorrhoea
Adrenogenital Syndrome:
Incidence: 1 in 14,000
Congenital adrenal hyperplasia: masculinsed females
Androgenic hormones because of 21-hydroxylase, 11-hydroxylase or 3-B-hydroxysteroid
dehydrogenase
Can‟t produce cortisol adrenal hyperplasia overproduction of cortisol precursors
androgens
Presentation: vomiting, dehydration and ambiguous genitalia. Hyponatraemia (with
paradoxically high urine Na) and hyperkalaemia is common may present with circulatory
collapse in early life or hyponatraemic seizures (misdiagnosed as febrile convulsions)
Boys may present with precious puberty or have ambiguous genitalia (reduced androgens in
17-hydroxylase deficiency)
Gastro-Intestinal
See Appendicitis, page 167
Abdominal Radiology
Should always be gas in the:
Stomach. If not, then ask why. ?Oesophageal atresia without fistula to the bronchus. ?To sick to
swallow
Rectum
RLQ (Caecum)
Gas bubbles. If only:
1: pyloric stenosis. Do US to confirm (not barium meal)
2: Duodenal atresia – “double bubble trouble”. Associated with Down‟s. Ante-natally:
polyhydramnios (can‟t swallow)
3: Jejunal atresia
Lots of bubbles but no normal caecal gas: Ileal atresia (Colonic atresia very rare)
Other signs:
Gas on both sides of bowel wall wall stands out as opaque line Rigler‟s sign
Malrotation: wandering small bowel below duodenum with barium meal. If corkscrew then
?malrotation with volvulus
Paediatrics 639
Pneumatosis Intestinalis: gas bubbles in intestinal wall („string of pearls‟): if also in portal venous
system (eg bubbles in liver) then necrotising enterocolitis
Congenital abnormalities
Tongue Tie
Short lingual fraenulum
Rarely interferes with eating or speech
Generally requires no treatment
Oesophageal Atresia
Happens early in embryonic life:
Lots else happening then too – look for associations as well
Cardia, Renal, Anus, Vertebral, Oesophagus, Trachea: CRAVET
Symptoms: dribbles all the time
Usually distal oesophagus attached to trachea (fistula) air in stomach
Urgent neonatal repair
Pyloric Stenosis
= Hypertrophic pyloric stenosis
4:1 boys to girls. Males 1/200 – 1/400
Family history: in 15% of siblings or previous generation
Pathophysiology: circular muscle hypertrophy progressive narrowing of pyloric stenosis
Presentation: 3 – 6 weeks, initial spilling progressive dysfunction several days of non-bilious
high volume projectile vomiting with or between feeds. Dryish nappies (from dehydration)
Exam: peristaltic waves of exaggerated gastric peristalsis + palpable lump in RUQ (= pyloric tumour)
when hips flexed and relaxed (eg immediately after a feed)
Differential:
Gastro-oesophageal reflux – but baby well and growing
Exclude infection: UTI, meningitis, gastroenteritis, chest infection
Investigations: usually clinical diagnosis. Check electrolytes and blood gases for hypochloraemic
hypokalaemic alkalosis
Treatment:
Rehydration: IV saline + KCL + glucose
Surgery: pyloromyotomy
Duodenal Atresia
Present in first 24 hours with green vomiting after feed
Xray shows double-bubble sign: gas in stomach
Associations: 1/3
rd
have Down syndrome, 10% of Downs have duodenal atresia
Small Bowel Atresia
Due to loss of blood supply to that part of the gut in utero. Infarcts and heals (as opposed to after birth
when bacteria gangrene)
Bowel distal to the obstruction may be malformed
Malrotation
In 80% of cases, diagnosed in first month of life. Usually presents after 2 –3 days with bilious
vomiting
Exclude: strangulated hernias, bowel obstruction secondary to adhesions, intussusception and sepsis
Investigations: barium meal duodenal jejunal junction hasn‟t ascended to level of pylorus and is not
to the left of the midline
Pathogenesis: Dates from time when the midgut is in the umbilical chord. Failure of fusion (sygosis) of
the small bowel mesentery to the posterior abdominal wall narrow “universal mesentery” with the
superior mesenteric artery supplying the whole mid-gut torsion leads to mid-gut ischaemia
Surgical emergency
Meckel’s Diverticulum
Most frequent congenital abnormality of the gut (2% of autopsied adults). Due to persistence of
omphalomesenteric duct
640 4
th
and 5
th
Year Notes
Illness of 2‟s: incidence 2%, 2 feet from ileocaecal valve, symptomatic from 2 years onwards
Wide mouthed diverticulum (approx 5 cm), on antimesenteric border of the ileum, usually within 100
cm of ileocaecal valve. 30% of the time ectopic tissue is opposite the diverticular
50% have normal ileal mucosa, rest have duodenal, pancreatic, colonic or gastric (not subject to
feedback ulcers) mucosa
Symptoms:
40% of GI bleeds
Maroon not melaena
Intermittent
HB but no shock
30% present with intussusception or band, 20% with diverticulitis like appendicitis, 5% with
umbilical mass
Meckel‟s diverticulitis: blocked, inflamed enlarged burst
Rarely symptomatic after age 5, but may
Haemorrhage, before age 10, due to peptic ulceration of surrounding ileal mucosa,
Inflammation, may mimic acute appendicitis
Obstruction in kids/teenagers: intussusception into lumen of bowel, or twist on fibrous remnant of
the omphalomesenteric duct extending from bowel to abdominal wall (remnant of the yoke sac)
Diagnosis and treatment:
Pertechnetate scan: looking for hot spot
Diagnostic Laproscopy
Treatment with laparotomy and end to end anastamosis
Meconium Ileus
Tenacious meconium won‟t shift, gets colonised and gas
Cystic fibrosis. See page 615
Hirschsprung’s Disease (Aganglionic Megacolon)
= Aganglionic Megacolon
1
st
described by Hirshsprung in 1886
Incidence: 1 in 3 – 5,000 live births. Boys four times girls. Familial tendency
Aetiology: ?arrest in migration of ganglion cells from neural crest down GI tract
Pathology:
Absent GI ganglion cells (co-ordinate motility of bowel – Meissner‟s and Auerbach‟s plexuses).
Always includes internal anal sphincter and spreads proximally a variable length:
50% to recto-sigmoid junction, through to
10% including total colon
Affected colon can‟t relax greatly dilated proximal segment
Macroscopic: affected segment may look normal, proximal segment damaged mucosa, possible
perforation, thickened wall
Microscopic: absence of normal ganglion cells (visible with acetyl cholinesterase stain) and
hypertrophy of nerve fibres (non-specific – can occur with other conditions)
Clinical presentation:
Age of presentation unrelated to length of affected segment. Eg someone with their total colon
affected can present after years
3 groups of kids:
Neonate: acute lower GI obstruction, abdominal distension, bilious vomiting, maybe fulminant
diarrhoea, maybe perforation. Clue: no gas in rectum on x-ray
Infancy: constipation, abdominal distension, possibly precipitated by change in bacterial flora
on introducing other foods after exclusive breast-feeding (may massive diarrhoea)
Older: severe constipation, chronic abdominal distension, scybala (hard mass of faecal matter),
failure to thrive, never soil pants
Diagnosis:
Barium enema: narrow rectum, enlarged proximally. Usually rectum lumen twice the diameter of
the colon. Don‟t do an enema if risk of perforation (barium in the peritoneumserious peritonitis)
Rectal manometry: inflate balloon in rectum, distal rectum and internal anal sphincter should
normally relax, this won‟t
Rectal biopsy: But finding ganglion cells is hard even in a normal specimen. Histochemistry – test
for Ach (preganglionic nerve cells looking for ganglion cells)
Paediatrics 641
Treatment: Two stage surgery:
Stage 1: Disobstruct: ostomy in lowest portion of bowel with ganglia
Stage 2: Later, bring ganglionated bowel to anus
Imperforate anus
In girls, often attaches into the posterior wall of the vagina
Adequacy of the levator sling depends on how high the lesion is. If low, only a superficial problem. If
high (growth arrested above levator sling), then reconstruction is more difficult
Look for other developmental abnormality: eg GU, vertebral, etc
Other
Gastroschisis: paraumbilical defect with evisceration (extrusion of viscera) of abdominal contents.
Incidence 1.6/10,000. No covering. Usually only bowel hanging out. Usually no other defect.
Corrective surgery has good outcome. Delivery in tertiary centre
Exomphalos: Herniation of abdominal contents (may include liver) into the base of the umbilical chord.
Covered with peritoneum. Incidence 4.3/10,000. Other abnormalities often present
Acquired Causes of Obstruction
In addition to congential causes above (malrotation volvulus, atresia, etc):
Hernias
Adhesions (always ask about previous surgery)
Intussusception
Volvulus
Intussusception
Peak incidence 3 months – 2 years
Usually ileocolic
Causes:
95% idiopathic
5% mechanical: intestinal polyp, Meckel‟s diverticulum, lymphosarcoma (> 6 years old)
Symptoms:
Often URTI 10 days before ( adenovirus in Payer‟s patch)
Initial: severe abdominal colic every 15 – 30 minutes, very well in between
Later: red-current jelly stools, prostration, pallor (shock)
Exam: sausage shaped mass clinical diagnosis
Treatment:
Hydrostatic reduction: blow air or barium up anus at 50% diastolic pressure. Not if small bowel
obstruction or peritonitis (barium in peritoneum is nasty)
Surgery
GI Bleeding
Causes:
Serious, life threatening bleeding rare: varices, stress ulcer, etc
Serious disease more common (the bleeding itself is not life-threatening):
Necrotising Enterocolitis (NEC)
Intussusception
Inflammatory bowel disease
Familial polyposis
Other differentials: Meckel‟s Diverticulum, A-V malformation, Anal fissure
History:
Is it really blood? Is baby vomiting mum‟s blood (swallowed in delivery or cracked nipple), is it a
UTI not rectal?
Do they have clotting problem? (Did they get vitamin K?)
How much, how fast
Hernias
Inguinal Hernia
4:1 male to female. 1% of boys
642 4
th
and 5
th
Year Notes
Virtually all indirect. A widely patent proximal process vaginalis allows bowel (and ovary in girls) to
enter the inguinal canal
Presentation: intermittent swelling overlying the external inguinal ring that has been noticed by a parent
50% right, 25% left, 25% bilateral
Do not resolve spontaneously
If < 1 more likely to present with strangulation
Incarcerated (bowel loop stuck through):
Peak incidence in first year – main cause of obstruction. High index of suspicion in any child with
abdominal distress
If neglected will strangulate – testes will die first due to venous return
Management: Should be repaired ASAP.
98% of acute or strangulated hernias can be reduced by taxis: manipulating it back in. Then fix
electively (ie within a week)
If signs of ischaemic gut or peritonitis surgery
Complications:
Girls: fallopian tube and ovaries may be within the hernia. May tort. Care with surgery. Can
completely close the internal ring.
Boys: damage to vas or testicular atrophy if surgery while acute
Umbilical hernia
Rarely cause problems, even if large
Repair at age 3 if haven‟t resolved by then
Congenital Diaphragmatic Hernia
1:5,000 live births. 1:2,000 total births ( lots of still births)
Diaphragm should close just before mid gut comes back from umbilicus. In this case, returning gut
enters chest. Compromises ipsilateral lung development (more common on left) mediastinal shift
and lung hypoplasia
Symptoms:
Early respiratory distress/cyanosis
Scaphoid abdomen
Bowel sounds in chest
Dextrocardia (diaphragmatic hernia most common cause)
Treatment: don‟t bag the child bagging also blows up stomach and guts compromises lung
expansion further. Ventilate. Surgery
Complications: pulmonary hypertension in severe cases
Overall survival of 40 – 60%
Common Childhood Presenting Chronic Symptoms
My Child Won’t Eat
Key issue: do they have normal growth:
Normal growth:
1
st
year: go from 3.5 9 or 10 Kg
2
nd
year: from 9 or 10 kg to 12.5 or 13 kg. Ie Growth slows markedly
Normal intake for first year:
100 cal/kg/day
150 mls fluid/kg/day
Breast milk has 67 cal/100 mls 100 mls breast milk at 150 mls/kg gives 100 cal/kg
If normal growth – what are parent‟s perceptions of amount the child does and should eat. If
perceptions not right then stress, unhelpful dynamics around food (especially for strong willed
child) parents give them lots of milk so they at least get something iron deficient
If not normal growth consider disease, congenital syndromes, are they being offered enough (eg
maternal depression/anorexia). See Failure to Thrive (FTT), page 591
Reflux
Symptoms: poor growth, vomiting, cry (especially after food), cough
But:
All babies have some reflux
Paediatrics 643
All babies cry – parents may not realise how much is normal! Average baby peaks at 4 hours per
day at 6 weeks, then declines. Is an association between crying and maternal depression
Can measure pH via NG tube over 24 hours, or scope them (only in Auckland). But most babies with
presentation of reflux don‟t have oesophagitis.
If neuromuscular problems (eg Cerebral Palsy) then more likely to have problems with severe reflux
oesophagitis
Treatment:
Antacids, ranitidine, omeprazole
Crying decreases from 6 weeks – is this a treatment effect or normal development
Ensure good support: wider family, Plunket, etc
See The Crying Baby, page 591 for Colic
Abdominal Pain
„Functional‟ pain (no organic cause) is „benign‟:
Parents didn‟t know until child said
Distractible from it
Central pain (point to umbilicus)
No sleep disturbance
No associated symptoms
Intermittent
Organic causes mimicking functional pain:
Constipation (parents may not be aware that child has problem with constipation)
Abdominal migraine: migraine in 3 – 8 year old often presents as abdominal pain. Intermittent,
goes pale, last an hour or two, not distractible. As they get older may develop into normal
migraine. Check family history
Always examine genitalia in a boy with acute abdominal pain
Other causes: appendicitis, intussusception, UTI, testicular torsion, volvulus secondary to malrotation,
Meckel‟s diverticulitis, renal colic, pyelonephritis, acute glomerulonephritis, drug ingestion, reflux
oesophagitis
Other causes are rare without associated symptoms (eg coeliac, Crohn‟s)
Diarrhoea
Is growth normal
Yes no significant malabsorption:
Low grade infection, eg Giardia, Cryptosporidium
Diet, eg too much juice overload sucrose absorption osmotic diarrhoea
„Toddlers diarrhoea‟: 18 – 24 months, sloppy poos 3 – 4 times a day. ?Variation of normal.
Gets less messy/tiresome when toilet trained
No:
Chronic infection: giardia, Cryptosporidium, parasites/worms
Immunosuppressed: any infection (eg Rotavirus, campylobacter etc) may become chronic
Coeliac: bloating, miserable, diarrhoea, signs of malabsorption
IBD: uncommon < 10 years. Abdominal pain, diarrhoea, blood in stool
Constipation ?overflow diarrhoea
Encopresis/Constipation
See also Constipation, page 177
Definitions vary: mainly long term constipation/soiling pants, but may also include inappropriate
toileting behaviour (eg going on the lounge floor!)
Constipation is common
The main issue is that hardness of the stool, not the frequency
History:
Need information from both parent and child. Parent is unlikely to know about an older child‟s
toileting habits. Perhaps ask child while you‟re doing the exam – that way parents are off to one
side. “I‟m going to ask you some really silly questions about your poos…”
Soiling (HPC): duration, frequency, severity, ever been continent
Associated constipation, withholding, absence of warning (likely), pain (eg fissure), associated
wetting
Toileting behaviour: avoidance, motions in toilet rare
644 4
th
and 5
th
Year Notes
Associated behaviours: hiding soiled underpants (common), scared of toilets at school, more
serious conduct disorder (rare)
Parent‟s management style: what‟s been tried, punitive (unhelpful but common), supportive
(ignore soiled pants, praise for toileting, not common but more helpful)
General developmental milestones
Exam:
Inspection of perineum: situation of anus, dilated anus
Inspection of lumbo-sacral area
Neurological exam of the legs: (spina bifida), test ankle jerk (S1-2, anal reflex is S2-5)
Abdominal palpation: for palpable faeces
PR usually not necessary
Differentials:
Fissure: usually secondary to constipation vicious cycle
Drugs: morphine, codeine, leukaemia drugs
Hypothyroidism (NB: associated with Downs)
Rare causes: Spina bifida occulta, Hirschsprung‟s (ask about delayed passage of meconium), anal
stenosis (often anal opening is more anterior)
Pathogenesis:
Vicious cycle: chronic dilation of rectum, sigmoid and descending colon sensation of fullness
go less often faeces dry out more hard don‟t completely evacuate distension
strength overflow diarrhoea (with no awareness)
Constipation is common post-gastroenteritis or after surgery
Can more rarely be due to food allergy
Management:
Explain normal anatomy and function of the rectum. Use a diaphragm.
Explain process: withholding stool dilated rectum loss of normal sensation no warning its
coming he‟s not being naughty and will take a while to come right (ie stick with treatment)
Test transit time by eating a pile of whole kernel corn and seeing how long it takes to come out the
other end. The ideal is < 24 hours
Structured toileting programme: diary and reward system for sitting (take a book if they‟re bored)
not for clean pants. Toilet for 10 minutes after each meal. Use timer
Fibre and adequate fluids to keep stools soft
Treatment of severe constipation:
Use enemas to completely empty bowel – get visiting paediatric nurse to do it – easier on
Mum and Dad
Laxatives every day to empty bowel (eg lactulose, magnesium sulphate) + regular toileting.
Coloxyl drops (a stimulant) may colic in kids. Lubricants (eg paraffin oil) are good but not
very palatable
Continue for weeks/months until rectum normal size again
Frequent visits for support of parents and encouragement of child
Gastroenteritis
Differential of acute vomiting/diarrhoea
Enteric infection:
Virus: rotavirus (45% of acute gastro), also enteric adenovirus, caliciviruses, astroviruses
Bacteria: Campylobacter, Salmonella (more common spring/summer), also Yersinia,
enterohaemorrhagic E coli, shigella
Protozoa: giardia, cryptosporidia, also microsporidia, amoeba
Food poisoning: (had anything different to eat from the rest of the family?) Staphylococcus
enterotoxin, bacillus cereus, Campylobacter, salmonella, E coli, Norwalk virus
Systemic infection: if sicker than history suggests then UTI, Pneumonia, otitis media, meningitis,
sepsis (including meningococcaemia)
Surgical conditions: Appendicitis, intussusception, bowel obstruction, Hirschsprung‟s enterocolitis,
pyloric stenosis, incarcerated inguinal hernia, testicular torsion
Other disorders:
Diabetic ketoacidosis
Antibiotic associated diarrhoea
Paediatrics 645
Haemolytic uraemic syndrome (renal failure, haemolytic anaemia and thrombocytopenia, eg due to
E Coli verocytotoxin, also drugs, SLE, etc)
Poisoning
Warning Signs
Seek urgent advice if any of:
Vomiting bile or blood
Severe abdominal pain
Toxic appearance (ie more than just gastro): lethargy, poor perfusion, hypo/hyper ventilation,
cyanosis
Abdominal signs: distension, tenderness, guarding, mass, hepatomegaly
Failure to thrive
Neonate
Diagnostic Clues
Sudden onset of fever, vomiting and watery diarrhoea: viral gastroenteritis
Cramping abdominal pain and frequent bloody, mucousy stools: bacterial gastroenteritis. If an infant
and severe pain or pallor, consider intussusception
Colicky pain, RIF pain, bile stained vomiting and distension surgical case
Season: Rotavirus during winter epidemics, giardia and cryptosporidia during the spring and
campylobacter in the summer
History
Vomiting: bile, blood, coffee grounds, volume, frequency, total duration
Diarrhoea: nature, colour, consistency, blood, mucus, frequency, volume, total duration
Amount and type of recent food and fluid intake
Urinary output
Other symptoms:
Fever
Abdominal, groin or scrotal pain
Urinary symptoms
Respiratory symptoms
Recent illness
Other:
Antibiotics and other drugs
Infectious contacts
Possible contaminated food ingestion, including shellfish
Overseas travel in the last 2 months
Immunisation
Other medical conditions, GI, diabetes, heart or renal
Management
Principles:
Dehydration is the most important complication. In infants it can appear in several hours
See Assessing fluid loss, page 650 for assessment of dehydration and rehydration
Investigations:
Stool microbiology: Only if:
Blood in the stool
Recent overseas travel
Suspected epidemic or food poisoning
Child in an institution
Chronic diarrhoea (> 3 weeks)
Biochemistry: Na, K, Cr +/- glucose +/- ABG if severe, < 3 months, or on IV therapy
Other: urines, blood, and CSF culture, CXR, AXR, LFT etc if indicated
Management:
Ambulatory if diagnosis not in doubt, family able to cope, have transport, no dehydration and good
fluid intake
646 4
th
and 5
th
Year Notes
Admission if: diagnosis in doubt, < 3 months, high risk, dehydration, failure to improve, pre-
existing condition (get sicker quicker: eg Ileostomy, short gut, cyanotic heart disease, renal failure,
diabetes, etc)
IV Rehydration if: shocked, severely dehydrated, failed trial of oral therapy
Treatment principles:
For a non-dehydrated child:
Small, frequent sips of Gastrolyte (doesn‟t fix diarrhoea) – not for bloody dysentery
(dehydration not the biggest concern). 5 – 7 ml/kg/hr
½ strength formula feeds
Fruit juice diluted 1:4
Maintain nutrition: Get back to solids within 6 – 12 hours if possible: banana, apple, rice, potato,
noodles, toast and vegemite
Breast-feeding is continued
Do not use anti-emetics nor anti-diarrhoeal agents
For a dehydrated child, see page 650
Lactose Intolerance
Small bowel injury temporary lactose intolerance
Most common in bottle feed babies < 6 months. Uncommon in breast-feed babies.
Clues are consistent fluid stools, or their restarting with reintroduction of milk feeds, excess flatus,
perianal excoriation
Testing: Collect 5 drops of stool from a plastic lined nappy, mix with 10 drops of water and add a
Clinitest tablet. Colour reaction of > ¾% indicates sugar is present
Change to a lactose free formula for 3 – 4 weeks, then introduce the old feed over 2 – 3 days
Nutritional Deficiencies in Childhood
Iron Deficiency
See Iron Deficiency Anaemia, page 288
Commonest deficiency in NZ and worldwide
Marker of poor diet generally
Associated with:
Inadequate iron intake:
Homogenised cows milk
Late introduction of iron-rich foods
Prolonged sole breast feeding (> 6 months)
Intrauterine growth retardation and placental insufficiency (especially rapid catch up growth)
Excess losses: chronic gut losses (eg infestation, food intolerance) and skin loss in severe ectopic
eczema
Sources of iron:
Poor sources:
Spinach: poorly absorbed
Cows milk: poor source and may lead to gut bleeding
Breast milk: only sufficient to 4 – 6 months, but absorption once food is introduced
Good sources:
Meat: haem iron well absorbed. Especially dark red meat (eg liver)
Pulses: lentils, peas, baked beans and soya beans (not green beans), but gas
Dark fish, shell fish and spices
Breast milk and vitamin C absorption, Cows milk and tea absorption (NB some Polynesians call
tea milo – so ask what sort of tea)
Anaemia:
At birth, Hb = 170, several weeks later = 105
Clinical effects: tired, lethargic, irritability, slow cell mediated immunity, pica (eat anything)
which may lead poisoning (small RBCs and anaemia)
Diagnosis:
Look for pale earlobes
Blood tests, iron studies etc. MCV < 71 in child over 3 months
Ferritin low (but high if infection – test CRP as well and ignore ferritin if raised)
Paediatrics 647
Serum iron – altered in presence of infection. Zinc Protoporphyrin is a new, sensitive test (Zn
substituted for Fe in haem).
Reticulocyte count useful test of response to treatment. Should respond within a week
Treatment:
Find and fix cause: if diet then dietician.
Ferrous gluconate elixir: 50 mg/kg/day (= 6mg/kg/day elemental iron) in 2 – 3 doses with fruit
juice until MCV normal
Rickets
See Parathyroid, page 101
Usually a lack of Vitamin D. With fear of sunburn, it is likely to increase
At risk:
Pigmented people with low dietary vitamin D intake and low sunlight exposure. Breast milk is not
a very rich source of vitamin D
Preterm infants with low Vitamin D intake
Fat malabsorption
Other rarer causes: anticonvulsant therapy, chronic renal disease, Ca or phosphate deficiency
Diagnosis:
Clinical: broad wrists, tender joints, avoidance of weight bearing, bowed legs if weight bearing,
bent pelvis ( obstructed labour later in life), Rickety Rosary (swelling of costochondral
junctions)
Lab: ALP, PO4, Ca usually normal
Xray: Widened metaphysis and splaying of softened bones, generalised osteopenia
Treatment:
1- cholecalciferol: 0.05 – 0.1 mcg/kg/day until ALP normal
Surgery to bones not usually necessary, even when very bent
Other deficiencies
Breast Milk is short of:
Vitamin K (fat soluble). Deficiency haemorrhagic disease of the new born in first few
weeks/months
Vitamin B12: if mother is vegan CNS symptoms (fits, abnormal movements, mental
retardation) + macrocytic anaemia
Chronic malabsorption or prolonged TPN Zn deficiency Acrodermatitis Enteropathica (rash,
especially around buttocks) and immunodeficiency
Vitamin A deficiency: from fat malabsorption or intake night blindness and risk of
complications from eg measles
Folic Acid: Deficiency during pregnancy risk of neural tube defects
Food Allergy
See also Allergy and Hypersensitivity Disorders, page 309
Commonest in first years of life (gut less good at keeping allergens out)
5 – 6% of children cf 1 – 2 % of adults
Commonest allergens: milk, eggs, peanuts, soy, wheat
Mechanisms include:
IgE mediated – rapid onset, due to mast cell activation and histamine release
Delayed hyper-sensitivity
Scenarios:
Urticaria/angio-oedema:
Rapid onset after contact with oral mucosa
Chronic urticaria rarely due to foods (except ?food colourings)
Confirmed by skin testing
IgE mediated
Risk of future anaphylaxis (systemic reaction distant from contact point).
Risk factors for fatal outcome: Asthma, peanut/nut allergy
Treatment: Adrenaline 0.01 ml/kg of 1:1000 im (10 mcg/kg) [relatively safe im, compared
with iv, which risks tachycardia and arrhythmia so would only want to do it in cardiogenic
shock]
648 4
th
and 5
th
Year Notes
Atopic dermatitis: takes days to weeks following food exposure. Strong association between
severe asthma and food allergy (60%)
GI symptoms may be at any point in the gut: oesophagus (reflux), stomach (vomiting), small bowel
(colic, diarrhoea, malabsorption) to large bowel (diarrhoea, gas, bloody stools, mucus,
constipation)
Respiratory symptoms: much less common with foods. Oral allergy syndrome: pollen allergic
individuals may get oral tingling/swelling after eating some fruits/vegetables
Cervical Lumps
99% of general neck lumps are lymph nodes:
Large nodes can take up to 6 – 8 weeks to go down
Three types:
Reactive hyperplasia: due to infection, not painful
Acute lymphadenitis:
Acutely tender, erythematous mass with accompanying fever, usually settle with
rest/analgesia
Results from URTI, cellulitis or other skin infections
Cervical lymphadenitis: S aureus or S pyogenes
Management: antibiotics and/or drainage
Lymph node abscess: lymphadenitis may progress to abscess. Doughy feeling. Overlying
skin erythematous. If raised, red and soft ? Staph abscess flucloxacillin (always on an
empty stomach). Augmentin for Strep abscess. Otherwise excise and drain under GA
Rare causes of lymph node enlargement: Consider if subacute, minimal tenderness, fixed or
overlying skin changes consider:
Cat-scratch disease
Toxoplasmosis
Cutaneous Tb (collar stud abscess, bruised looking, no systemic symptoms, non-tender,
tethered to skin, 6 mths to 5 years): excision, Mantoux and chest x-ray
Hodgkin‟s Lymphoma: Child > 5, rapid enlargement, rubbery spherical lymph non-tender
nodes, night sweats, fever, weight loss, lymphadenopathy elsewhere, splenomegaly
Lateral Neck Lumps: branchial cysts and branchial sinuses
Midline Neck Swellings:
Thyroglossal Cysts:
80% of midline cervical lumps
Peaks in pre-school child and young adulthood
Swelling near the hyoid that moves with swallowing or when pokes tongue out
May trans-illuminate
Early referral: get it out before it becomes infected
Treatment: surgery (Sistrunk procedure) and excision of the tract
Submental nodes: Usually superficial and anterior. Check mouth for primary infection (eg ulcer)
Dermoid Cysts: Common at the corner of the eyebrow (external angular dermoid). In the cervical
region they are subcutaneous and mobile, and appear yellowish. Require excision
Ectopic Thyroid: Rare. May be only thyroid tissue. Tend to become hypothyroid
Childhood Cancer
Cancer: 10% of childhood deaths, most common cause of death after accidents have high index of
suspicion
Distribution:
% of cancers
ALL
23
CNS
21
Neuroblastoma ( chemo)
7
Non-Hodgkin‟s Lymphoma
6
Wilm‟s (Kidney)
6
Hodgkin‟s Lymphoma
5
AML
4
Melanoma
2
Signs and Symptoms:
Paediatrics 649
Often non specific
Adult symptoms rare, eg epistaxis, dysphagia, non healing lesion, rectal bleeding, change in bowel
habit
Para-neoplastic syndromes are rare
Headaches warranting investigation. Headaches are common, but watch out for:
Recurrent morning headaches
One that awakens the child
Intense and incapacitating
Headaches that change in quality, frequency and pattern (eg getting more frequent)
Focal signs or ataxia
MRI more sensitive than CT
Lymphadenopathy:
Common finding in cervical, axillary and inguinal chains. Usually < 1 cm
Most enlarged nodes are due to infection
Suspicious if found in mediastinum, posterior auricular, epitrochlear and supraclavicular
Bone and Joint Pain:
Early symptoms rarely include pain – except in bone (bone cancer and malignancy)
Usually no pathognomic signs on Xray need biopsy
Pancytopaenia:
Common finding in ALL and AML
Need neutrophil count specifically. Lymphocytes may mask neutrophils.
From 6 months to puberty, anaemia is 110 g/L. 50% of leukaemia presents with Hb < 75 g/L
Involvement of two or more lines bone marrow evaluation
Leukocytosis: Common in AML and ALL. But count may get up to 50,000 with septicaemia and
some viruses, also in Down syndrome and post-natal
Presenting signs of cancer:
Recurrent bone pain, paleness, weight loss: leukaemia
Morning headache with vomiting: brain tumour (usually a migraine)
Lump in neck not responsive to antibiotics: Lymphoma
White dot in new born eye: Retinoblastoma
Proptosis (bulging eye): Leukaemia, neuroblastoma
Swollen face and neck: lymphoma, leukaemia (compression of veins)
Abdominal mass: Wilm‟s, neuroblastoma, liver & spleen enlargement in leukaemia
Cough, stridor, haemoptasis, Horner‟s: Mediastinal tumour
Diagnosis: tumour markers (only in neuroblastoma: catecholamine), imaging, bone scan, biopsy
Emergency Management
Assessing Fluid State
Assessing Vital Signs
Rate is always subservient to quality:
Thready pulse: eg palpable at neck and groin only
Respiration: more important that rate are grunting, flaring, subcostal retraction, use of accessory
muscles (in neonate bobbing of head)
Blood volume:
Neonate
90 ml/kg
Child
80 ml/kg
Adult
70 ml/kg
In a trauma situation, guess the weight: (age + 4) * 2
Urine output:
In nappies: 2 ml/kg/hr
Toilet trained: 1 ml/kg/hr
Normal fluid requirements in absence of sweating:
Per hour
Per Day
First 10 kg
4 ml/kg
100 ml/kg
2
nd
10 kg
2 ml/kg
50 ml/kg
Each 10kg thereafter
1 ml/kg
25 ml/kg
650 4
th
and 5
th
Year Notes
Nutrition: to maintain weight need 75 calories/kg/day
Heat loss:
70 kg person: surface to mass ratio is 0.02
2 kg person: surface to mass ratio is 0.08
Rate of heat loss is proportional to (body temp – room temp) to the power of 4. Best way to
maintain body heat is therefore to heat the room.
Assessing fluid loss
Only reliable indicator is pulse. BP doesn‟t drop till severe dehydration (compared with adult where
BP declines proportionately with losses)
No physical signs until > 3% loss
Most signs of dehydration are those of shock
Change in body weight is the most accurate estimate of fluid loss – but is rarely available
Dehydration in obese children is often under-estimated
Mild
Moderate
Severe
Loss: total body weight
3 – 5%
6 – 9%
> 10%
Mental state
Thirsty, alert
Thirsty, lethargic
Drowsy, hypotonic
Skin turgor
Mucus membranes
Dry
Very dry
Parched
Skin colour
Pale
Grey
Mottled
Urine
Oliguria
Oliguria
Marked oliguria
Blood pressure
Normal
+/- Normal
< 70 systolic
Peripheral temperature
Cool
Cool
Cold & clammy
Pulse
+/-
& thready
Assessing turgor: pinched edge of skin goes down slowly. Do centrally on abdomen, chest, thighs
Also when severe: rapid, sighing respirations (Kussmaul breathing)
Poor predictors of dehydration: Sunken eyes or anterior fontanelle, dry mucous membranes, absence of
sweat or tears
Management of Non-Dehydrated Child
If no or infrequent vomiting that is not interfering with fluid intake then 5 – 7 ml/kg/hour of:
Breast milk
½ strength formula
Fruit juice 1 part in 4 with water
After 6 – 12 hours introduce: bananas, rice, potato, parsnips, pumpkin, dry biscuits/toast with vegemite
Management of Mild-Moderate Dehydration
Admit or observe in a short stay facility for several hours
Don‟t use homemade solutions – use Gastrolyte
Orally, of by NG tube if necessary:
Replace calculated losses over 6 hours (don‟t worry about maintenance requirements). Hourly
observations and reassess and reweigh after 6 hours
Give the remainder of the daily fluid maintenance over the next 18 hours
Resume breast feeding as soon as rehydration is complete or sooner if this takes longer than 6-hours
If after 4 – 6 hours the child remains dehydrated, then IV
Management of Severe Rehydration
WEIGH THE CHILD to assess progress
3 stages:
Initial bolus if necessary. 10 - 20 ml/kg of Ringers Lactate or normal saline over 10 – 15 minutes,
reassess and repeat if necessary
Replacement + maintenance
Maintenance only
Rehydration of isotonic dehydration:
Replacement: Normal saline (or Ringer‟s Lactate or Hartmanns – more physiological)
Maintenance: 1/5
th
normal saline + 5% Dextrose + 20 mmol/l KCl [Barts] (gives a bit much Cl but
the kidneys can sort that)
Paediatrics 651
If initially shocked, do not add KCl until urine is passed. If they have ATN following shock (
renal failure) don‟t want to overload K
Timing:
Infuse replacement fluid over 24 hours with the first 24 hours of maintenance using ongoing
replacement: ½ normal saline + 2.5% dextrose + 10 mmol KCL (in 500 ml)
Monitor electrolytes before, and during, up to 6 hourly
Once they are able to tolerate oral fluids, treat as for mild/moderate dehydration
Theme and variations:
Diarrhoea:
Lost Na, HCO3, Cl and K from GI mucosal cells – replace slowly
Resuscitation with bolus of crystalloids, eg Ringer‟s lactate, normal saline
Maintenance with: ½ normal saline + 2.5% dextrose + 20 mmol/L KCL
If persistent acidosis due to HCO3 loss or lactic acidosis then add in HCO3
Rehydration of hypernatraemic dehydration (eg serum Na > 150):
Often the result of administering hyper-osmolar fluids (eg sports drinks) with vomiting and
diarrhoea greater water loss due to water sucked into GI from circulation then
vomited/passed
Will be more dehydrated than they appear due to fluid shifts from ICF ECF
If shocked give 10 ml/kg boluses of normal saline until circulation restored
Calculate deficit
Calculate ongoing requirements over 48 hours
Give both over 48 hours – serum sodium should not fall faster than 0.5 mmol/hr
If oral rehydration, replacement is over 24 hours
Diabetic ketoacidosis:
If give insulin too fast, serum glucose will drop quickly rapid change in ECF osmolality
cerebral oedema
If giving hypotonic solution then cerebral oedema – go slow
Rehydration of hyponatraemic dehydration (serum Na < 130):
Resulting from gut or renal losses, or excessive hypotonic fluid administration
Appear more dehydrated than they are as fluid shifts into the ICF. Can cerebral oedema,
seizures, etc
Never give 1/5
th
normal saline (except to keep vein open). Do serial Na measurements
If asymptomatic: As for rehydration of isotonic dehydration, over 24 hours. Fluid restrict to
50% of maintenance
If symptomatic (seizures, coma) or if severe (Na < 120) then give 5 – 10 ml/kg or 3%
hypertonic saline IV over 60 – 120 minutes in addition to the calculated fluid requirements
Notes:
Be careful about measuring volume: never hang a bag straight into a child
If lung or brain disease (eg meningitis), SIADH is common may need to fluid restrict (eg to
50% maintenance fluids). Check serum Na regularly
In a term baby, born water logged (ECF > ICF). Can pass 500 ml urine per day (7 ml/kg/hour).
Handles water well but not used to passing a NaCl load
Enemas for constipation can dehydration
Paediatric Coma
Assessment: Coma scales – main function is to assess progress
AVPU scales
Glasgow scale (but designed for adults)
Child Coma scale
General observation:
Alert states:
Fully alert (what this mean depends on age of child)
Confused
Delirium: agitated and confused
Reduced alertness:
Lethargic: fails to maintain wakefulness without stimulation
Obtunded: drifts into sleep unless constantly woken
Stuporose: unconscious but withdraws to painful stimuli
652 4
th
and 5
th
Year Notes
Comatose: fails to respond. May be decorticate or decerebrate. At risk of airway failing
Differential in children:
Hypoxic: respiratory or circulatory failure
Epileptic seizures
Trauma: intracranial haemorrhage, brain swelling
Infections: meningitis, encephalitis
Poisons
Metabolic: Renal, hepatic failure, Reye‟s syndrome, hypoglycaemia, diabetes, hypothermia,
hypercapnea
Vascular lesions: bleeding, AV malformations, arterial or venous thrombosis
Hypertension
Diagnosis:
Must be bilateral cortex or brainstem involvement
Is it focal, multifocal or diffuse
Is it getting better or worse
Metabolic disturbances (including hypoxia and seizures) account for 90% of unconscious children
Supratentorial mass lesions compressing the brain stem: 3
rd
nerve palsy and dilated pupil on same
side – NOT 6
th
nerve palsy
Subtentorial lesions affecting the brain stem directly: slow pulse, high BP, irregular breathing
Management:
Stabilise vital functions: ABC then DEFG
Complete history: esp trauma, poisoning, previous diseases – diabetes, epilepsy
Exam: vital signs and progression, trauma, neck stiffness, CNS function, and:
Verbal responsiveness
Ocular responses: eye opening, papillary responses and spontaneous eye movement, ocular
reflexes (eg Dolls eye)
Respiratory patterns: Cheyne Stokes (rate slows down, stops, restarts), irregular, apnoeas,
stridor
Motor system: Motor responses, reflexes, tone, posture
Investigations:
Blood: gases, electrolytes, glucose, FBC, LFT, ammonia, calcium, lactate, clotting factors
Urine: poisons, sugar, organic acids, ketones
Chest Xray, consider skeletal survey
ECG
CT Scan
LP only when safe: risk factors – prolonged fits, focal neuro signs, purpuric rash, CGS < 13,
dilated pupils, reduced Dolls Eye, abnormal posture, signs of herniation, coagulation disorder,
papilloedema, hypertension
Paediatric Trauma
Most common cause of death < 14 years (way out in front)
Under 1 year: cause of death – congenital abnormalities > infection > trauma
Trauma: poisoning > suffocation > MVA
What makes kids different:
Large, poorly supported head. Always land head first
Thin skin evaporative skin losses and burn at a lower temperature
Surface area: mass ration rate of heat loss
Relatively large, poorly attached spleen
Renal function, conserves water, secretes sodium
Greenstick fractures
Child abuse: differential diagnosis in all cases of trauma (do history and physical findings
correlate)
Dealing with children:
Never lie – say if it‟s going to hurt
Kid that is injured will almost always have been injured doing something they were told not to do
– child will consider you part of the punishment
Parents will get mad at you because they feel guilty. Wear it – this is not the time to deal with it
Child will regress
Paediatrics 653
See When is a child really sick?, page 565
Resuscitation
Summary:
A. and cervical spine
B.C.
Exsanguinating haemorrhage (if it‟s not bleeding, ignore it)
Get help early
Airway and cervical spine immobilisation: Look/listen/feel
Airway opening: Jaw thrust
Suction of foreign material under direct vision
Airway devices:
Oropharyngeal/nasopharyngeal airways, ET tube, surgical airways.
Oropharyngeal: Right size: should reach from midline of lips to angle of the jaw. Use tongue
depressor to help insert oropharyngeal (cf adult)
Breathing:
Monitor:
Work of breathing: rate, noises, recession, accessory use, grunting
Effectiveness of breathing: breath sounds, chest expansion, SpO2
If inadequate commence assisted ventilation
Indications for intubation:
Inadequate O2 via bag mask
Inability to protect airway (eg do they have gag reflex, muscle tone in jaw, etc)
Prolonged ventilation required, or control required (eg in transport)
Flail chest
Inhalational burn injury
Intubating
If using sedating drugs, must be confident you can completely manage ventilation, do surgical
airway if necessary, etc
Pre-oxygenate if possible with high flow O2
Need: working, correctly sized laryngoscope, suction, bag valve mask, syringe
Take collar off to intubate
Tube size = (age/4) + 4 (or size of kids little finger)
Must secure tube or it will slide out
Ausciltate the chest to check air entry and check end-tidal CO2
Identify and treat life-threatening problems:
Tension pneumothorax: sounds on affected side, trachea shifts to good side needle
decompression in 2
nd
intercostal space, midclavicular line, then chest drain. Little harm if they
don‟t have a pneumothorax.
Open pneumothorax: 3 sided sealed dressing then chest drain
Massive haemothorax: chest drain and cardiothoracic consult
Flail chest: intubate and ventilate. Rare in kids as ribs too spongy – but can get very severe
injury without breaking ribs
Cardiac tamponade: Urgent cardiothoracic consult
Circulation:
Assess: heart rate, pulse volume, central capillary refill < 2 secs (eg over sternum after 5 secs
pressure), skin temperature
Identify and treat life threatening problems:
Shock
Stop uncontrolled haemorrhage
Stabilise pelvis
Initial management of shock:
O2
Large IV line placement. If can‟t then inter-osseous needle. 1 cm medial and distal to tibial
tuberosity. Have to squeeze in fluid
Crystalloid 20 mls/kg bolus. Reassess and repeat if needed. After that, warmed blood. After
transfusion of > ½ blood volume then FPP.
If still unstable consider blood and urgent surgical opinion
654 4
th
and 5
th
Year Notes
Keep them warm
Disability (ie simplified coma scale):
A: Alert
V: Responds to voice
P: Response to pain
U: unresponsive
Pupils and posture (decorticate/decerebrate)
Exposure:
Uncover to inspect for injuries
Keep warm and minimise embarrassment
Glucose: all severely injured children at risk of hypoglycaemia: check during primary survey
Assessment:
Monitors: Pulse/BP/RR/SpO2/Temperature + EtCO2 if intubated
History taking: parents/ambulance crew/child, past medical history, medications, allergies, last
meal
Blood tests: baseline FBC and U&Es, cross matching, glucose
X-rays: Trauma series – AP chest, AP pelvis, lateral C-spine. NB Soft bones are less likely to
break despite strong force chance of internal organ damage in absence of breaks than in an
adult (eg ribs)
Urinary catheterisation/naso-gastric tube placement
Analgesia: morphine, 0.1 – 0.2 mg/kg IV (not IM)
NG tube to empty stomach: kids graze all day so stomach never empty. Also, swallow lots of gas
when in pain tube lets air out risk of aspiration due to pressure in stomach and less pressure
on thorax
Then secondary survey: head to toe inspection
Traumatic Injury
Head injury almost never causes shock
Frequency of visceral injury: spleen > liver > kidney
Splenectomy. The younger the child the greater the risk of fatal post-splenectomy sepsis (adults have
greater previous antigenic exposure so less susceptible). Leave it in if vital signs stable
Kidney trauma: most common injury is contusion mild haematuria
Bladder: easily ruptured
Closed head injury:
Full neuro exam
Level of consciousness: Awake, responds to Voice, to Pain, or is Unresponsive
Localising signs: can be very subtle, watch for changes
Pupils
Can rupture middle-meningeal artery without fracturing skull
Pain management: early – consider regional blocks (eg femoral nerve block in fractured femur)
Car crash
Without seat belt, risk of death is 10 times. All children being held in the front seat die
Assessment of severity:
Speed of crash
Was seatbelt on
Was child thrown from car
Was any other child killed
Burns
> 50 % of burn admissions are children
Full thickness burns don‟t hurt (nerves are dead)
Partial thickness burns blister and heal
Rule of 9‟s doesn‟t work – needs age adjustment
Fluid resuscitation: Ringer‟s 4ml/kg/% of burn (half in 1
st
8 hours) + maintenance (ie pour it in till they
urinate)
Paediatrics 655
Paediatric Anaesthetics
Pre-operative assessment of child with a URTI
Peri-operative risk variably increased
Postpone high risk:
Neonates and infants
Existing upper airway/respiratory pathology (eg CF) - reserve – easy to tip over the edge
Systemic symptoms
Lower respiratory tract involvement
Surgical impact on respiratory function (eg upper abdo surgery)
Complications usually manageable
Pre-operative assessment of child with a murmur
Innocent murmurs often detected by anaesthetists
Murmurs in up to 95%, but pathology in only 0.5%. May need referral for investigation
3 Common innocent murmurs:
Early systolic from ventricular outflow tracts (either pulmonary or aortic)
Continuous murmur from SVC
Grade 1 – 2
Bad murmurs mimicking benign ones:
Severe hypertrophic obstructive cardiomyopathy
Critical aortic stenosis
These develop after birth – so may not have been picked up in post natal checks
Postpone and refer if suspicious, esp if < 1 year
ECG recommended if echo unavailable (can fax to a paediatric cardiologist for interpretation)
SBE prophylaxis may be indicated
Risk Factors for Aspiration
High risk for aspiration: Treat as full stomach
Full stomach
Regurgitation
Impaired protective reflexes
Airway obstruction (big negative pressure in thorax in order to suck air in past obstruction – but
this also sucks contents out of stomach)
Hazards of fasting:
Discomfort
Hypovolaemia. Guidelines are:
Clear fluids till 2 hours before
Breast milk till 4 hours before
Food till 6 hours before (no chewing gum)
Hypoglycaemia: only an issue for neonates
Assessment for Sedation
Need to risk assess any child before any sort of sedation – its all too easy for something to go wrong (or
more usually, for lots of little things to mount up)
Always need to be confident you could ventilate, intubate and get IV access quickly if necessary
Pain Management in Children
Myths:
Neonates don‟t experience pain
Neonates have no memory of pain (they retract from a needle the 2
nd
time)
Pain is not harmful (it leads to stress response healing, etc. ? Impact on the development of
pain pathways)
It is dangerous to treat pain
Management principles:
Mild to moderate pain relief is achieved through oral or rectal doses
Children hate needles, especially repeated IM injections
Using loading doses and regular maintenance doses to achieve therapeutic effect
Don‟t overdose with paracetamol (may hepatotoxicity). Limit duration
656 4
th
and 5
th
Year Notes
Child-friendly environment and parental involvement important
Available drugs:
Paracetamol (oral better than rectal). Only use aspiring where specially indicated (eg Rheumatic
fever)
NSAIDs: Diclofenac, Ibuprofen, Naproxen
Codeine Phosphate (metabolised to morphine): constipation, plus dose related opiod side-effects –
sedation, respiratory depression, nausea and vomiting
Morphine for serious pain (eg burns and fractures)
Pethidine less used in kids - toxicity (including seizures)
Tramadol – not often used but less respiratory depression
Nitrous Oxide (always administered with O2). OK for brief analgesia (eg fracture immobilisation).
Ensure resuscitation equipment available. Month pieces preferred to masks
Child Abuse
Central elements in maltreatment
Parent‟s strong negative and irrational engagement with the child, featuring a distorted perception of
the child
Parent‟s lack of ability to engage positively with the child
Child is continually left in a state of worry or anxiety
General History
History of injuries – how, who, when, where. Note details of different caregivers, change over times,
etc. Clarify custody arrangements well
Developmental history
PMH, especially previous injuries (do you need notes from hospital, other GPs etc)
Social history: supports, domestic violence, other stresses, previous CYFS referral
What are parent‟s expectations of toddler behaviour, etc
Physical Abuse
Non-accidental injury to a child or young person
Includes: bruises, cuts, fractures, head injuries, injuries to internal organs, suffocation, poisoning, burns
Risk factors:
Hard to parent child: eg handicapped or behaviourally difficult
Poor parenting skills/experience
Unrealistic expectations of the child
Poor mental health of the parents
Reduced social support
Alcohol or substance abuse
Domestic violence
History of child abuse in the abuser
Triggering event precipitating loss of control by the perpetrator
Be suspicious when:
No history is given for the injury
The history changes
History is partial
Unbelievable explanation
Unreasonable delay in seeking help
Previous similar episodes
Parents affect or behaviour is abnormal
Questions to include in history taking:
When, where and how did the injury occur
What was the child doing at the time
Who saw it
What is the child‟s developmental level
Is a scene examination necessary
Patterns of injury suggesting non-accidental injury:
Paediatrics 657
Fractures: multiple sites or different ages, rib fractures, any fracture in a child < 2: consult
radiologist. Look for missing teeth
Head injuries: any child < 1, unexplained coma, retinal haemorrhages (from shaking). Usually
closed head injury rather than a fracture
Bruises: on face or back, non-mobile baby, fingertip pattern bruises, other pattern bruises (strap,
belt), yellowing older than 18 hours. If suspicious, referral immediately to a paediatrician (who
can arrange for evidential photos to be taken). Tell mum you need to refer so they can be checked
for other injuries
Burns: Child will withdraw hand or foot before a burn is full thickness, pattern burns (eg held in
hot bath, cigarette burns), burns on back
Examination:
Normal general assessment: growth, consciousness, play and behaviour, language
Carefully full survey: looking for bruises, tenderness, acute abdomen (eg splenic rupture), genital
bleeding (leave full genital exam for an expert)
Developmental assessment
Systems Review – any other possible cause for the injuries
Document everything carefully, use a body chart and measure lesions, ask for explanation of each
injury
Investigations:
FBC and coagulation
Referral for specific investigations: X-ray, ophthalmologist, ENT surgeon, CT
Consider urine toxicology
Differential to physical abuse:
Bruising: Mongolian spots, coagulopathies, coin rubbing
Cigarette burns: bites or vesicles
Hot fluid burns may be non-intentional
Fractures: osteogenesis imperfecta, spiral fractures of the tibia in toddlers
Sexual Abuse
Any act resulting in sexual exploitation of a child – whether consensual or not, including:
Non-contact abuse: exhibitionism, suggestive behaviours, exposure to pornography
Contact abuse: fondling, masturbation, oral sex, object or penis penetration
Risk factors:
Family dysfunction
Female sex
Pre-adolescence
Previous victimisation: don‟t think they‟re worth it – won‟t say no
Non-biological parent
Developmental delay: don‟t understand, scarred to say no
Alleged perpetrators are all ages. If < 10 years, are they acting out abuse to them. 60% are family
members
History taking:
Evidential interview is the job of the police and CYPFS – usually videoed
If child discloses to a doctor, record questions and answers carefully. Don‟t ask leading questions.
Qualify notes with “the above history was taken in order to direct the exam and does not
necessarily constitute a full or detailed history”. If not acute, leave questions for police
Presentation:
Behavioural indicators: non-specific so don‟t over interpret. They‟re the same for anything that‟s
upset them, eg parents separating: sleep disturbance, change in appetite, regression, running away,
fear (specific or generalise), anger, concentration, sexualised behaviour
Adolescence: self-harm, suicidal ideation, alcohol/drug abuse, eating disorders, unprotected
consensual sex, promiscuity, school failure, loss of peer group
Vaginal discharge in a pre-pubertal child is common:
Non-specific eg irritant/allergic
Infection: Gp A strep, shigella, Candida (uncommon once out of nappies)
Foreign bodies
Polyps
Systemic illness eg measles, chickenpox
Vulvar skin disease
658 4
th
and 5
th
Year Notes
Vaginal bleeding: accidental straddle injury, vaginitis, foreign body, precocious puberty
Normal sexual development:
0 – 2: genital exploration, masturbation (boys > girls), learning names
3: talk about sexual differences, genital interest increases, masturbation common
4: Play doctors and nurses, mothers and fathers, games involving undressing, exhibitionist
activities, demand privacy for themselves, interested in others bodies
5 – 6 years: familiar with and has less interest in sexual differences, likely to be more modest
Sexualised behaviour:
Masturbation is normal, but inappropriate if older and still public
Sexual play: if > 5 shouldn‟t be touching other genitals
Physical findings in abuse:
> 50 % of disclosures will have no physical findings
Urgent forensic exam only if incident < 72 hours ago
Perpetrator usually doesn‟t want to hurt the victim, otherwise won‟t have continued access
physical injuries less common
Investigations:
Pre-pubertal: don‟t screen for STD‟s unless symptomatic. HIV testing in time if high risk
Adolescents: screen for STDs and ?pregnancy test
Prognosis: 25% have no adverse psychological sequalae. The more invasive the abuse, the more severe
the effects long term
Neglect
= Act or omission that results in impaired physical functioning or development, or injury. Includes
physical neglect, neglectful supervision, medical neglect, abandonment, refusal to assume parental
responsibility
Risk factors:
Poor attachment
Parental psychiatric illness
Maternal depression
Isolated unsupported parent
Poverty
Presentation:
Often associated with physical and emotional abuse
In an infant: failure to thrive, frequent attendance at A&E, severe nappy rash, unexplained
bruising, cold injury, developmental delay, attachment disorder
Pre-schoolers: short stature, unkempt and dirty, delayed language, very disorganised play (eg
aggressive and impulsive, indiscriminate friendliness)
School children: short stature, poor hygiene (including teeth), unkempt, learning difficulties, self
esteem, disordered/few relationships, unusually patterns of defecation or urination
Emotional Abuse
= Act or omission that impairs the psychological, social, intellectual or emotional development of a
child or young person. Includes: Rejection, isolation, oppression, deprivation of affection,
inappropriate criticism, threats or humiliation, exposure to violence, involvement in illegal or anti-
social activities, negative impact of substance abuse or mental/emotional condition of parent or
caregiver
Risk factors:
Poor attachment
Parental psychiatric illness
Maternal depression
Isolated unsupported parent
Parental alcohol and/or drug addiction
Domestic violence
Presentation:
Socio-emotional indicators: can‟t enjoy themselves, refuses to defend self, cheats, steals, bizarre or
extreme behaviours, failure to accept responsibility for behaviour, low self-esteem, withdrawal,
defiance, compulsivity, seeks love and acceptance outside the home, apathy
Cognitive indicators: learning problems, short attention span, hypervigilance, hyperactivity,
developmental delay, lack of curiosity
Paediatrics 659
Physical indicators: Failure to thrive, accident prone, self destructive behaviour, eating disorders,
GI and bowel problems, poor posture, sleep disorders, energy
Differential: Munchausen‟s by proxy
Management of Abuse
Paramount principle: The interests, safety and well being of the child should be the paramount concern
(Section 6, Children, Young Persons and Their Families Act)
Doctor‟s role is medical management, not the assessment of child abuse
If child abuse is suspected:
Trust your instincts
Look for signs of abuse
Document the facts
Recognise and treat medical sequalae
Prevent pregnancy
Provide ongoing support, and watch for and help behavioural sequalae
Contact CYPFS immediately and discuss your concerns. You cannot be guaranteed anonymity,
but when reporting to CYPFS or the police you are protected from court action if acting in good
faith
Mother/other person can also contact CYPS [good approach if you consider this is really a custody
issue. Alternatively advise the mother to get a lawyer]
There is no legal requirement to contact CYPFS or to give a CYPFS social worker information if
they contact you. There is likely to be an ethical obligation, and referral guidelines will exist and
should be followed.
Investigation and management is multi-disciplinary: should involve paediatrician, social worker, police,
psychologist
If a child discloses abuse:
Listen to the child but do not interview them
Well being of the child comes before the interests of any other person
Write down what the child says
Reassure them they‟ve done the right thing
Tell them that they will get help – but don‟t make promises. Say it‟s got to stop but that you‟ll
need to tell someone else who will help
Tell your manager/supervisor as soon as possible
Look after yourself: discuss the matter with someone you trust
If nothing seems to be happening, contact CYPFS again
Complete an ACC M45 form and forward to the Sensitive Claims Unit at ACC
Care for mother: may be domestic violence, depression, addiction, etc
Care for perpetrator: talk with intake social worker about help for them (eg violence prevention
programmes)
Mental Health
Attention Deficit/Hyperactivity Disorder (ADHD)
Background:
Estimates range from 2 – 5%
Boys > girls
60% take some symptoms into adulthood (eg restless, disorganised, poor attention, impulse
control)
Was first described 100 years ago – only recently received appropriate recognition
Could be better described as „behaviour inhibition disorder‟
Is strongly genetic and is biological
Diagnosis:
Behaviour:
Inattention: easily distracted, doesn‟t finish tasks, works best with supervision, poor short-term
memory. “How does he get on with daily tasks like dressing/eating breakfast/doing
homework” “Do you ever have to stand over him to make sure he finishes”
Impulsiveness: acts without thinking, short fuse, aggressive, little self-control. “How often
does he get into trouble for not thinking before he does something”
660 4
th
and 5
th
Year Notes
Overactivity: restless, fidgets. “How easy is it for him to sit still”
Insatiability: rarely satisfied, interrogates, over-intrudes in others space
Also poor co-ordination, disorganisation, fluctuation, and specific learning disabilities
Older child: low self esteem, mood swings, aggression, underachievement
Inappropriate for age and development
Pervasive across at least 2 settings
Onset < 7 years
Impairs social and academic functioning
Hard to diagnose pre-school – tantrums and attention common. Issue is whether they mature on
transition to school. Gap widens as they get older. A 6 year old should be able to complete tasks,
concentrate, etc
Usually normal to high IQ
Diagnostic boundary is disputed – this falls on a continuum (like everything else!)
Differential:
Learning disability not coping at school, frustrated acting out
Gifted child whose bored
Psychosocial stress: disruption at home, abuse
Anxiety
Psychiatric disorders (mood, anxiety or personality)
Problems with parenting – no boundaries or inconsistent boundaries
Associated factors:
Lower socio-economic status: poverty, poor housing, unemployment, illness, family breakdown
Childhood depression/anxiety concentration
Auditory/visual perceptual difficulties inattention, loose interest
Reading problems: visual sequencing, letter-word orientation appears inattentive
Assessment:
Onset of behaviours
Situation specific or pervasive
Other learning difficulties
Context: parents management style, life events, teacher, etc
Use parent questionnaire
What are child‟s strengths – basis of self esteem
Get information from school: general behaviour, problems in specific situations (transitions
between lessons, unstructured time eg playground, changes to routines eg outings, academic
problems
Thorough developmental history (ABFWIMPS), especially:
Head injury
Perinatal problems
Attachment problems in first 2 years (eg PND, stresses, violence, drugs)
Exam: dysmorphic features, tics (more common in ADHD and also side effect of ADHD
medication), observation during interview
Classifications:
Primary: early onset, feeding/sleeping problems from early on, overactive/unmanageable toddler,
parents exhausted
Secondary:
Psychosocial causes: family disruption, demands of school, etc
Specific learning disability (stress once school starts)
Mixed: an adolescent presenting with all of the above, plus self-esteem
Management:
Multidisciplinary assessment
Behaviour strategies:
Clear, firm, consistent guidelines
Check understanding of instructions
Anticipate problems and have planned responses ready parental stress and consistency
Avoid triggers (eg crowds)
Predictable routines (eg at bedtime)
Managed use of time out, withdrawal of privileges
Encouragement: see Behaviour Management, page 570
Paediatrics 661
At school:
Structured approach – plan day
Sit near teacher, between quieter kids
Brief, clear instructions
Supervision during transition times (coming in from breaks, etc)
At home:
Force leads to confrontation, resentment, broken relationships
Behavioural techniques work poorly – it‟s a biological problem
Ignore all but the important misbehaviours. Have a few clear rules, with clear
consequences, if broken act without argument. Don‟t debate or escalate
Esteem: Encourage. Find something they are good at. Swimming, bike riding, cooking, judo
and computers may be better than team sports. Encourage friendships – take a friend on
outings
Diet: < 10% sensitive to synthetic food colouring
Many dodgy therapies: avoid unless proven
Stimulant medication:
Concentrate for longer (stimulates inhibition) complete tasks less disruptive and
self-esteem
First: education for child and parents.
“Have you heard about medication – what?”
Address myths: they‟re addictive, they sedate the child, child at risk of substance abuse
later in life
Side effects: sleep disturbance, appetite suppression (small effect, if marked growth
suppression), moodiness, rebound, tics
First line options are Methylphenidate (Ritalin) or Dexamphetamine. Both require specialist
endorsement. Introduce slowly. Short T½ need to fine tune dose times. Eg give before
school Ok at school but difficult by the time they get home. Not in evening otherwise
sleep. Review – should have noticeable improvement, if not re-evaluate
Referral if:
Diagnosis/differential in doubt
Assistance with management of challenging behaviour
Assessment of role of family relationships in perpetuating the problems
Anxiety Disorders
See also Anxiety Disorders, page 422
Fears are normal during childhood and adolescence:
Age 1 – 2: fear of separation from parents
Young child: scared of the dark, animals, storms, monsters
Age 7 – 8: begin to worry about their performance
Adolescents: concern about being disliked, rejected, or criticised by their peers
Fears generally reflect developmental stage
Anxiety disorder:
Fears become intense or pervasive and substantially impair functioning
Can follow chronic, fluctuating course
Not easy to recognise as young people often know that their fears are groundless and feel ashamed
of what they think is a flaw in their character
Anxiety disorders: Separation anxiety disorder, social phobia, generalised anxiety disorder, obsessive
compulsive disorder, post-traumatic stress disorder
Separation Anxiety Disorder
Child very anxious away from home or from their parents
May present with:
Refusal to attend school – but school‟s not the problem, the separation is
Feeling physically ill in the morning. Monday‟s the worst day
Reluctance to sleep at friends places, school camps, etc
Worried that harm will befall their parents while they‟re away
Difficulty coping with parents going out
Difficulty going off to sleep, or needing company of a parent while they do
History should include:
662 4
th
and 5
th
Year Notes
School: problems, bullying, fears, etc
Home: stressors, conflicts
Maternal depression, anxiety, adjustment disorder, etc
Parents may have some insight – but usually underestimate the severity of the maternal-child
dependence and are very defensive
Diagnosis: irrational fear of harm to parents or that they will be abandoned by them
Differential for school non-attendance:
Truancy, conduct disorder: doesn‟t go to school – but doesn‟t stay at home either
Anxiety-based refusal
Major depression: lacks motivation
Other reasons: at home to help with work, etc
Epidemiology: F > M. Peaks in early adolescence
Course:
May be triggered by a worrying or traumatic incident. May be family history of anxiety problems
Eventually become isolated from friends and get behind at school. Feel embarrassed and different.
Self esteem. All makes returning to school more difficult
Prognosis depends on the young person, family strengths and severity
Increased risk of agoraphobia in adulthood
Management:
Support for parents and child
Quick return to school before problem becomes entrenched, even if only for a small portion of the
day
Education for child and parent. Facing the fear is initially distressing but reduces the anxiety,
avoidance increases it
Parents need to be consistent in their commitment to return the child to school
Involve school teachers (eg meet at gate, etc). Problem is actual separation – once settled into the
day problem is likely to reduce
Severe or chronic referral. Support for parents if they‟re having difficulties. SES Behaviour
Support Teams or Resource Teachers for Learning and Behaviour (RTLBs) for child.
No place for medication unless underlying conditions
Bullying
= An act of aggression/harassment by a child/youth
Starts mid-primary, peaks 3
rd
form, nearly gone by 7
th
form
Typical bullying behaviour: boys hit, girls tease and exclude
Teachers generally under-estimate bullying
Characteristics of someone who is bullied:
Something different: high achiever, less physically attractive, etc
Vulnerable: more anxious, cry easily, don‟t fight back
Problem compounded for the bullied in that no one wants to be friends with a person who is bullied
isolation. Standing up to a bully is pretty sophisticated behaviour in early teens – not
developmentally consistent with wanting to identify with the peer group
Long term outcomes worse for the bully than for the bullied
Depression
See also Mood Disorders, page 426
Mood disorders are prevalent and serious disorders in children and adolescents. Leads to difficulties at
school and in social relationships
1 year prevalence estimated as high as 10%
Same diagnostic criteria as for adult – but diagnosis harder. More likely to present with separation
anxiety, phobias, somatic complaints and behaviour issues. More likely to talk of profound boredom
and feeling unloved and lonely than appetite and sleep change
Most do recover, but recurrence is more common than in adults
Clinical approach:
See the teen on their own
Observe: energy, anxiety, anger, shame, variability in affect
Listen: the teen is more likely to talk if they feel they are being heard
Consider differentials: Depression, drug abuse, eating disorder, psychosis (actual or prodrome),
medical
Paediatrics 663
Suicide assessment
Aetiological factors to consider:
Family context
Cultural context: are they comfortable about who they are in a cultural sense
Peer group: Have they friends, how do they support him/her?
School: bullying, what‟s hard at school, current stressors
Life events: losses, abuse
Psychological: negative ways of thinking, learned helplessness
Treatment involves the child, parents and school. Aim is to shorten the episode. Treatment can
include:
Education
Counselling: for milder depression, no remediable family factors, recent life events, if they want it
Family therapy
A range of individual therapy types – usually through referral
Medication: less evidence of effectiveness in adolescents. Consider discussion with a psychiatrist.
Usually SSRIs
Referral when:
Significant suicide risk
Possible psychosis
Abuse
Severe family discord
Failure to improve
Youth Suicide
See also Suicide Assessment and Management, page 416
Epidemiology:
Second only to MVA as cause of death – but still uncommon.
3 fold rise in last 30 years.
Females attempt, males succeed
Second highest rate for 15-24, Finland higher
Postulated factors contributing to increase:
Depression and substance abuse
Unemployment
Isolation and alienation
Key issue: identifying those at risk
Risk factors:
Male gender
Psychiatric illness: depression (most common association), alcohol or substance abuse, personality
disorder, psychosis
Previous suicide attempts
Available means: firearms, toxic medications
Social adversity: recent interpersonal loss, homelessness, school failure or drop-out, family or
relationship problems, unemployment
Recent exposure to suicide
Most common presentations are over-dose, self-poisoning and lacerations
Management:
Treat underlying psychiatric disorder (not TCAs – too lethal in overdose. Use SSRIs)
Reduce ongoing stress: counselling to reduce interpersonal conflict
Promote social supports
Liase with specialist health services
Other Mental Health Issues
Eating disorders: See Eating Disorders, page 453
Substance Abuse:
Drug and alcohol use prevalent
Often comorbidity

664 4
th
and 5
th
Year Notes
Sexual maturation: sexual behaviours, orientation, attitudes to sex and relationships, awareness of
socially defined roles. Knowledge about pregnancy and STIs doesn‟t automatically translate into
behaviours
Risk taking behaviour:
Adolescence is a time of experimentation, pushing boundaries
Contributing factors: ignorance, impulsiveness, cognitive immaturity (sense of omnipotence and
poor comprehension of long term consequences), peer groups, drugs and alcohol
Adolescent Health
Definition of Adolescence
Developmental period between childhood and adulthood
Age of majority in NZ = 20 years
WHO definitions:
Adolescents: 10 – 19
Youth: 15 – 24
10 – 24: Young people
Demographics
Young people are the only age group whose health status has not improved in the last 40 years
Current issues:
Accidents and injuries
Mental health issues
Health risk behaviours: smoking, alcohol, drugs, sex
Chronic illness: eg obesity, asthma, diabetes, etc
Access to health services for adolescents fragmented – fall between child and adult services
Adolescent Development
Summary:
An age of transition
Experimentation and change: inherent risk taking
Behaviours reflect maturational tasks
May use maladaptive behaviours to achieve developmental goals (eg smoking to gain peer
acceptance). Need to change them to adaptive behaviours
Also see Cognitive Development, page 578
Physiological:
Puberty: highly variable – generally from 9 – 14 years. Can take 2 – 5 years to complete
Gain 25 cm in height, 50% of ideal adult body weight
Stages of adolescence:
Early: coming to terms with body/biological changes
Middle: establishing self among peers as a worthwhile individual
Late: vocational/education direction and one-to-one intimate relationships
Developmental issues
Abstract reasoning
Preoccupied with their own thinking
Peer group membership and conformity important
Consolidation of self image and identity
Psychosocial:
Who am I and where do I fit in
Identity: self, culture, ethnicity, sexuality
Autonomy vs relatedness/connectedness
Goals and future direction
Developmental tasks of adolescence:
Tasks
Early: 10 – 13 years
Mid: 14 – 16 years
Late: 17 – 21 years
Psychological tasks
Independence
Separates from parents:
questions, tests
Separation creates
anxieties, ambivalence as
retreats to family
Comfortable away
form home, able to
return for counsel

Paediatrics 665
without shame
Body image
Adjust to dramatic
changes in body
Constant comparisons
Try on images to find real
self (incl. Sexual
identify), attempts to
improve image
Satisfied with realistic
body image
Sexual drives
Marked sexual
curiosity, masturbation
Sexual experimentation,
narcissistic sexual
relationships
Beginnings of intimacy
and caring
Social Tasks
Relationships
Boys „gangs‟, girls
„best friends‟. Crushes
on adults
Other sex friendships,
dating, try on other
philosophies and beliefs
Individual relationships
more important than
group, intensity of
relationships
Career plans
Vague, unrealistic
Efforts but influenced
by „escape‟ from home,
glamorousness of career
Hard decisions
occupational identity.
Delayed by higher
education
Cognition
Concrete, literal,
limited abstraction
Formal operations; use
abstractions (what if…),
introspection, less literal
Mature abstractions,
problem-solving &
self-reflection
Moral Growth:
values
Need to follow rules of
peer group or family
Narcissistic: feels good or
is what I want right
impulsiveness
Idealism, rigid
standards of right and
wrong, intolerance
Talking with Adolescents
Keys to effective intervention:
A positive relationship
Thorough assessment
Inclusive of family and young person
Plans made with the young person and family
Building a trusting relationship: introductions
Friendly, confident welcome but still professional
Introduce yourself directly to the teen, „And is this your mum?‟
Clear introductions: yourself, your role, what you‟ll be doing and why
Clear boundaries: explain that you see young people alone and with family and why:
„You‟re on your way to being an adult. Want to support that process. But your parents also
still have a role‟
Allows them both to say things they might not in front of the other
Outline confidentiality:
„I want to talk about confidentiality. Do you know what that means?…. Want to keep your
information private‟
„There are 3 things I can‟t keep a secret: if someone‟s harming you, if you‟re harming
yourself or if you‟re harming someone else. I need to do something about it – but will tell you
what I‟m doing‟
„Will talk to my colleagues for review – to check I‟m doing the best I can‟
Consider what you put in notes (they get around). Use standardised abbreviations.
If adolescent doesn‟t want you to tell parents (and you think it‟s in adolescents best interests for
them to know):
Why doesn‟t teen want parents to know („You seem worried about your parents knowing this.
Can you tell me about that?‟)
Attempt to persuade the teen to tell her parents
Offer to tell them yourself
Keys to building the relationship:
Be keen to get to know this young person now
Accepting atmosphere
Respect
Non-threatening explanations
Give adolescent some control – encourage normal independence
666 4
th
and 5
th
Year Notes
Reveal hidden agendas
Give them time to talk – hold off asking questions
Make plans with the young person and family
If they don‟t want to talk, probably anxious/frightened. “It seems you‟re pretty angry about being
here. Did someone make you come?”
Communication:
Use language that is understood (no medical or adult jargon). Check understanding
Listen
Move from less sensitive to more sensitive topics
Move from third person approach to the personal
Set clear boundaries: It is appropriate to identify what is and is not acceptable behaviour (eg creating
risk of harm to themselves or others). Middle adolescents still require the security of clear boundaries.
However, try not to be judgemental
Beware:
Transference: person projects their feelings about someone else (eg parents) onto you
Counter-transference: You transfer feelings appropriate to someone else (eg your own kids) onto
the adolescent (eg act as though you were their parent)
Objectivity: understand the most likely reason they won‟t talk is that they‟re frightened
HEADSS Risk Assessment
Gives an overview of this individuals risk and resiliency
If you don‟t ask they won‟t tell you
Do ask, even if you think you know the answer
Home:
Where do you live and whom do you live with?
Who do you get on with, who would you talk to if you had a problem?
What‟s good about home? What‟s not so good?
Who makes the rules and what happens if they‟re broken?
Is there ever any violence at home?
Education/Employment:
What do you enjoy most about school?
What subjects do you like?
How are you getting on at school?
Do you get into any trouble?
How do you get on with your teachers/friends
Activities:
What do you do after school/in the weekends?
What do your mates do? (Get an idea of peer relationships)
What did you do last weekend that you enjoyed?
Drugs:
„I check with all young people – not picking on you. Remember it‟s confidential. You don‟t have
to answer if you don‟t want to‟
Lot‟s of people your age smoke/take drugs/drink. Is it like that at your school?
What do you think about that?
What have your friends tried? What about you?
If no, make it positive „that‟s fantastic - how come you don‟t and lots of others do?
Sexuality:
Most young people have become interested in sex at your age. Have you had sex education at
school? What was it about – body changes, infection, preventing pregnancy, relationships?
Do you talk with anyone in your family about sex
Have you had a sexual relationship with anyone?
Do you have sexual feelings to boys or girls? Ever had sexual experiences with someone your own
sex? If this is confusing or frightening for them then need to talk further.
Want to help you stay healthy…ask about safe sex
If not active – encourage them. But also check they can get condoms, etc: „if you ever were to,
where would you go for information or contraceptives (tie them down to specifics)
Suicide risk and Depression:
„Everyone has good days and bad days. Do you ever have really good days? Really bad days?‟
Paediatrics 667
„Often adolescents see me because they‟ve been feeling down. How have you been?‟
„Have you been happy with the way things are going? How would you rate yourself over the last
couple of weeks if 1 was foul and 10 was brilliant?‟
„Do you ever feel like you want to end it all?‟
„Do you have a plan to hurt/kill yourself?‟
„How do you plan to?‟
Determining the degree of risk:
Well adjusted
Vulnerable
Experimenter
Troubled
Out of control
See Youth Suicide, page 663
Physical Exam
Use chaperones
Be thorough but assure privacy and modesty (work around clothing)
Talk and explain (especially about growing bodies)
Pubertal ratings: Get them to self report genital development off an Adelaide chart – don‟t examine
yourself unless specific problem
Puberty
Physiology:
Pre-puberty: Inhibition of GnRH pulse generator by higher centres
Puberty: increasing frequency and amplitude of pulsitile GnRH secretion, initially at night, with
FSH ( follicles or Sertoli cells) and LH ( hormone production) secretion in response
Also involvement of adrenal glands androgens secondary sex characteristics (eg pubic hair
but not testicular size)
Terminology:
Gonadarche: onset of gonadal function
Thelarche: onset of breast development
Adrenarche /Pubarche: Onset of development of sexual (pubic/axillary) hair
Menarche: Onset of menstruation
Spermarche: Onset of production spermatozoa
Clinical signs:
Measured in Tanner stages (1 = no development, 5 = adult)
Girls: breast development first (ovaries enlarge first but can‟t see them)
Boys: Testicular enlargement (use orchidometer)
Pubic hair development initially related to adrenal androgens and may be discordant with other
changes
What‟s normal:
Girls: traditionally < 8 years or > 13 years abnormal. But number of girls have breast
development at 7. Menarche relatively unchanged at 12 (ie earlier onset, but endpoint relatively
unchanged). Getting earlier by 3-4 months per decade (but psycho-social development unchanged)
Boys: < 9 or > 14 abnormal. No strong evidence of it getting younger
Normal variants
Mini-puberty in neonatal period
Usually neonate – but up to 4 months
Due to hormones in utero and underdeveloped CNS inhibitory mechanisms
Breast development +/- milk (Witches milk - completely normal)
Withdrawal uterine bleeding (following endometrial development in utero)
Estrogenic effects on genitalia
Premature Thelarche
Isolated early breast development
Tanner 2 or 3 maximum
No advancement in bone age
Follow-up to ensure it is isolated not progressive (ie that it‟s a normal variant)
Premature Adrenarche:
668 4
th
and 5
th
Year Notes
Isolated early pubic hair development +/- acne +/ BO
Caused by adrenal androgens
No advancement in bone age and normal menarche/spermarche
Need follow-up (eg to exclude adrenal tumour)
?Association with future hyperandrogenism (eg Polycystic Ovary Syndrome)
Gynaecomastia:
Breast development up to stage 3 during male puberty (75% of males)
Usually in early puberty – resolves in about 2 years
Reassurance, occasionally surgery
Pathological:
In rare instances: Klinefelter‟s syndrome, gonadal failure
Outside of puberty (eg oestrogen producing tumour)
Key sign indicating normal: normal bone age/no growth spurt
Precocious Puberty
Definition arbitrary
Consequences:
Short stature
Psychosocial (out of sync with peers)
Clinical signs: Old bone age and growth spurt (in addition to eg breast development)
Gonadotrophin Dependent:
= Central/complete. Hypothalamic or pituitary cause and balanced development
Girls:
Normal progression through puberty (ie variant of normal?)
Rapid progression suggests pathology
Boys:
Normal progression of puberty
Less common than girls, more likely to be pathology
Causes:
Idiopathic (95% in girls)
Hypothalamic hamartoma: developmental anomaly
Tumours (eg of hypothalamus or pituitary)
Other CNS conditions (eg hydrocephalus, spina bifida)
Gonadotrophin Independent:
= Peripheral/Incomplete. Peripheral cause and not all characteristics of normal puberty
Girls: rapid progression or viralisation
Boys: Testes remain small, rapid progression
Causes:
Hormone ingestion
Congenital Adrenal Hyperplasia (ie adrenal androgens)
Tumours: adrenal, gonadal or hCG secreting
Autonomous hormone production (rare)
Investigations:
Bone age from hand x-ray
Measure hormones
GnRH stimulation test
Imaging
Treatment:
GnRH agonist for central precocious puberty via depot. If GnRH is not pulsitile it switches off
FSH and LH
Girls: progesterone delays menarche
Delayed Puberty
Hypogonadotropic: Hypothalamic/pituitary causes:
Constitutional delay (check for bone age)
Exercise/nutrition (eg anorexia)
Generalised pituitary failure (eg post surgery/radiotherapy for CNS tumour)
Rare isolated deficiencies
Paediatrics 669
Hypergonadotrophic: Gonadal failure
Chromosomal: eg XO, XXY
Infections (eg mumps, especially during puberty)
Autoimmune
Surgery, radiotherapy, chemotherapy
Galactosaemia
Other:
Structural (eg normal puberty but no menarche)
Intersex disorders: chromosomal sex <> phenotypic sex
Pubertal arrest: always pathological (eg pituitary tumour)
Investigation and treatment:
Gonadotrophins +/- GnRH stimulation test
Hormone replacement
Fertility issues (eg with gonadal failure)
Chronic illness and disability in Adolescents
See also Effect of Chronic Disease on Development, page 582
Between 1- 20 % of young people have a chronic or disabling condition
US prevalence:
Asthma: 50/1,000
Mental retardation: 25/1,000
Epilepsy: 4.1/1,000
Diabetes mellitus: 4.1/1,000
Down syndrome: 1.1/1,000
Cystic fibrosis: 0.2/1,000
Survival rates are improving
Developmental impacts:
Primary: effects of the disease
Secondary: effects of delayed development
Tertiary: effects of treatment
Similar risk taking behaviours to healthy adolescents
Impacts on development:
Most don‟t have major problems, and consider their illness less severe than doctors do
Process of separation from parents may be slowed if dependent on parents for care or limited
opportunities to socialise with peers
Learning disorders embarrassment, failure, frustration, self worth, performance anxiety,
learned helplessness
Slowed sexual development or physical deformity problems with sexual identity
Normal developmental issues such as struggle for independence, concrete thinking, narcissism
(what feels good is right) and sense of omnipotence (future is a long way off) non-compliance
with treatment
Mental health in those with chronic illness:
Highly variable
Vulnerable periods: early years, transitions, severe illness
Important variables: onset, disruption to early attachments, premorbid function, family stress,
mental health of parents, experience of failure or victimisation, repeat hospitalisation, life
expectancy
Resilience:
Focus on the young person not just the disability/illness
Focus on building strengths, achieving successes
Competence in self-care/management of illness/disability
Access to age appropriate coping strategies
Opportunities for responsibility/required helpfulness
Family relationships
Peer relationships
School attendance
670 4
th
and 5
th
Year Notes

Health Care of the Elderly 671
Health Care of the Elderly
References: Medicine in the Older Adult, Dr Mark Weatherall, Wellington School of Medicine
History ............................................................ 672
Ageing ............................................................ 672
Concepts ................................................... 673
Disability .................................................. 673
Age Related Problems .................................... 673
Iatrogenic Disease..................................... 674
Nutrition ................................................... 674
Falls .......................................................... 674
Visual Impairment .................................... 675
Elder Abuse .............................................. 675
Driving ...................................................... 676
Services for the Elderly .................................. 676
Rehabilitation ........................................... 676
Rest Home and Hospital Care ................... 677
672 4
th
and 5
th
Year Notes
History
History should include:
Function of the person before their illness
Current function of the person
Their aims and aspirations:
Where do they anticipate living on discharge from hospital
What functional level must they achieve for this to happen
Has the availability, ability and opinions of carers and family been taken into account
Are there special social or cultural considerations
Are the goals of the person and the family reasonable within a realistic timeframe
Has there been sufficient consultation
What is the physical layout of the home, access to and within it
Screen for disorders
Assessment of Functional State
Include the following in the social history
Basic activities of daily living:
Mobility: can they move in bed, get in and out of bed, in and out of a chair, on and off a toilet,
ability to get around the house, to get outside, to get to the shops or visit friends. Can steps and
stairs be managed
Urinary & Faecal Continence: is there a problem, how is it managed
Bathing, shaving, teeth, dressing: how much assistance in needed, can they reach all body parts
Feeding: how much assistance is needed (eg cutting up food)
Advanced activities:
Handling of finances
Shopping
Use of public transport
Preparation of a hot drink
Screen for Disorders
Cognitive impairment: delirium, dementia, focal cognitive impairments (dysphasia, non-dominant
hemisphere problems). May need to use an assessment instrument (eg mini-mental state) and/or
interview others
Visual and hearing impairment
Postural hypotension
Malnutrition
Faecal impaction
Pressure areas
Iatrogenic disease, including adverse drug reactions
Weakness secondary to immobility
Untreated or under-treated pain
Residential Care History
Reasons for living in a residential care facility, how long have they lived there
Past health problems and current concerns
Current medical treatment
Current functional state
Social network (family and other visitors), and interests and activities
General physical examination
Screen for common impairments
Formulate a problem list, and management strategies (including preventative) that may be appropriate
Ageing
= Net effect of age related of age related changes likelihood of dying
Age related changes affect all body systems: cardiac, respiratory, CNS, musculoskeletal, vision,
hearing, skin, immune and renal

Health Care of the Elderly 673
Demographics:
In absolute number of 60, and > 60s as a proportion of total population
Number > 65
% of total population
1976
275,000
8.9%
1996
423,000
11.7%
2016
659,000
15.5%
Life expectancy at birth for NZ females is 79.5 years and for males 74.3 years (3
rd
to lowest in
OECD)
Concepts
Cohort Effect: Each current age group (eg adults now aged 80 – 90) have experienced a distinctive
history, leading to the following cohort effects:
Disease and disability with roots in environmental exposure varies from cohort to cohort (eg
tobacco use, diet, peak bone mass)
Cross sectional studies should consider cohort effect (eg medical care available to 80 year olds
when they were 30, compared with 30 year olds now). A difference may not be due solely to aging
Cultural and social differences between cohorts: eg response to health professionals, access to
services, gender and spiritual issues
Diversity of physiology and function increases with age: stereotypes are unhelpful, need individual
assessment
Multiple pathology: Not a single disease process presenting acutely, but a person presenting with
disease(s) and/or disabilities. Need a model of care and assessment that considers individual disease
processes, individual experience, the social context, and interactions between and within these
dimensions
Failure to present (professionals need to initiate strategies to overcome):
Self stereotyping: I‟m just old, there‟s nothing they can do, etc
Cognitive impairment and depression
Disability: eg mobility
Atypical presentation: Strange or unusual presentations are more common compared with younger
people, due to multiple diseases, reduced homeostatic capability, etc. Can be non-specific (not coping,
immobile, etc)
Threshold effect: Change in functional status can occur in the absence of a clear precipitant due to
build up of subclinical dysfunction and loss of physiologic reserve
Disordered homeostasis and the cascade effect: Age related effects ability to maintain homeostasis
in the presence of a threat (eg medication). Disordered homeostasis in one system can trigger
dysfunction in another
Caring for carers is important in maintaining people in the environment of their choice
Disability
Disability is understood by (WHO definition):
Pathology: abnormal structure or function of an organ or system. Eg osteoarthritis
Impairment: Loss or abnormality of psychological, anatomical or physiological function. In
decreasing order of prevalence in the elderly these are (in a CHCH study): visual impairment,
hypertension, symptomatic spinal osteoporosis, hearing impairment, stroke/TIA, osteoarthritis of
the hip or knee, urinary incontinence, dementia, postural hypotension
Disability: Any restriction or lack of ability to perform a task or activity. Eg for elderly women in
Mosgiel: housekeeping, shopping, bathing, mobility
Handicap: disadvantage for a particular individual resulting from impairment or disability that
limits fulfilment of a role normal for someone of that age, culture, gender, etc. Eg reading a
newspaper, shopping, etc
However, some things don‟t fit well into this model (eg psychiatric illness). WHO currently
revising. Will also include impact of environment (eg not being able to drive is not always a
disability – eg if you live in the 3
rd
world)
Interventions should address all levels, and acknowledge the interaction between each level
Reported disability has a clear age associated increase
Age Related Problems
For Osteoporosis and Osteoarthritis, see Metabolic Bone Disease, page 261
674 4
th
and 5
th
Year Notes
For Postural Hypotension see Measuring Blood Pressure, page 19
For Congestive Heart Failure see Heart Failure, page 48
For Hypertension see Hypertension, page 34
For Alcohol Withdrawal see Alcohol Withdrawal, page 452
For Delirium and Dementia, see Dementia, page 439
For Urinary Incontinence, see Urinary Incontinence, page 223
For Constipation see Constipation, page 177
For Pressure Ulcers see Pressure Ulcers, page 327
For Pharmacology and Age see Age, page 526
For Stroke see Stroke, page 125
For Hearing Impairment see Presbycusis, page 151
For Insomnia, see Sleep, page 534
Iatrogenic Disease
Hospitalisation is dangerous to older people, especially leading to: drug toxicity, injury and mental
deterioration
There is often a decline in functional status following discharge, unrelated to disease process
Elderly have susceptibility to variety of stressors
Bed rest (eg in hospital, especially if on drips, monitors etc) generally leads to outcomes, due to:
Muscle strength and aerobic activity
Volume depletion therapy (also results from bed rest) + age related vasomotor instability
postural hypotension
Supine position worsens V/Q mismatch
Bone demineralisation
Urinary incontinence due to high beds or distance from toilet
Pressure sores
Sensory deprivation (eg boring rooms, not wearing glasses or hearing aids)
Nutrition (altered dietary habits, unappetising food, social component to eating)
All lead to a cascade of interaction
Most deterioration happens in first two days in hospital. Examples of prevention include:
Low bed without rails
Carpeting
Minimisation of tethers
Encouragement and assistance
Orientate with clocks, calendars, dressing, undressing, communal dining
Sensory stimulation: proper lighting, decoration, glasses, hearing aids, available recreation
Nutrition
Can be measured through body weight (eg BMI), body composition, or direct measurement of micro-
nutrients
Under-nutrition in the elderly can be due to:
Age related in gastro-intestinal function predisposes to poor nutrition (eg teeth, pancreatic
secretion, etc)
Life-style factors: inability to shop, prepare and cook food, living alone, alcohol abuse, poverty
Diseases: eg stroke, arthritis, dementia make eating harder
Anorexic effect of illness and drugs
Management:
Multidisciplinary: dietician to advise on what and how much to eat. Occupational therapist to
advise on food preparation. Meals on wheels. Social worker in involve family and ensure
adequate finance
Medication review
Nutritional supplements: eg add milk powder to food, eat high-density foods, take supplements
Falls
In elderly, refers to a fall during an activity that is usually safe
25 – 35% of those over 65 fall each year. Occurrence with age
< 5% of falls cause a fracture (40% of these to proximal femur). Soft tissue injury in 40%
Staying upright (a homeostatic function) requires:
Health Care of the Elderly 675
Safe environment
Information on body position: visual, vestibular, mechanoreceptors, proprioception, central
processing
Motor systems: cortex, brainstem, cerebellar, spinal chord, muscles
Stable base: joints, limbs, feet
Intact judgement
Causes of falls:
„Threshold model‟ in which a number of factors combine to risk
Sedative use, cognitive impairment, abnormalities of balance and gait, polypharmacy, history of
stroke, hypotension
Fall over things that are safe to others changing the person more important than changing the
environment. But check for rugs, clutter, cords. In hospital, care with ability to transfer, agitation
and frequent toileting
Associated diseases:
Nervous system: stroke, Parkinson‟s, dementia, seizure, peripheral neuropathy, visual acuity
Musculoskeletal: proximal muscle weakness, arthritis of lower extremity
Cardiac: aortic stenosis, arrhythmia, postural hypotension
Iatrogenic: sedatives, psychotropic medication, alcohol
Assessment:
Previous history of falls
When, where, what was experienced, associated environmental factors
History of vertigo, dizziness, imbalance, blackouts, medication
Examination: postural changes in BP, vision and hearing
Observation: stand up without using hands, observe gait, stop smoothly, turn around, stand with
eyes closed, stand on one leg, reach up, bend over, heal toe walking, can they speed up, nudge
them, sit down without hands
Management:
Active management of injuries: watch for occult pelvic fractures, hypothermia. Care with soft
tissue wounds – can easily go on to ulcers
Acute precipitating illness that requires treating: eg stroke, MI
Identification of risk factors
Rehabilitation: active mobilisation after a fall. Interventions targeted at identified risk factors,
including medical review of medication, physiotherapy for transfer skills and exercise program
Avoid giving psychotropic medication to people at risk; it WILL make them fall over
Visual Impairment
Major causes of visual acuity in adults are (See also Loss of Vision, page 141):
Cataract: due to bulk of the lens and discolouration. Age, diabetes, and UV light are the main
risk factors. Treatment by extraction and implantation improves visual acuity in about 90% but a
smaller proportion benefit in terms of activities of daily living
Age related macular degeneration: Variety of causes. More serious ones include choroidal neo-
vascularisation detachment and scarring
Glaucoma
Diabetic neuropathy
Senile arcus: ring of lipid and calcium salts in a ring at the junction of the cornea and sclera. Very
common in elderly. Not a sign of hyperlipidaemia (as it is in the young)
Ectropion: low lid falls away and tears don‟t drain into lacrimal sac
Lens becomes thicker and less flexible (Presbyopia) can‟t accommodate, need reading glasses
Elder Abuse
= When a person aged over 65 experiences harmful physical, psychological, sexual, material or social
effects caused by the behaviour of another person with whom they have a relationship implying trust
(Age Concern definition)
Elder abuse can be:
Physical: physical pain, injury, force, under/over medication
Psychological: causing emotional anguish or fear, including intimidation, humiliation, harassment,
threats, removal of decision making powers
Sexual
Financial: improper use of funds or other resources
676 4
th
and 5
th
Year Notes
Can be:
Active neglect: conscious deprivation by a carer of basic necessities
Passive neglect: refusal/failure of a carer to provide the basis necessities due to inadequate
knowledge, infirmity, or dispute over the value of services
Prevalence: Significant under-reporting due to cognitive impairment, fear, life long pattern of abuse,
access to someone to complain to, stigma associated with domestic violence. ?About 5% of elderly
people subject to abuse, usually by a spouse, child or relative
Risk factors for abuse:
Dependence by the older person for all or part of their care
Cognitive impairment, especially disruptive or aggressive behaviour
Substance abuse or mental illness of the abuser
Shared living arrangements
External stress
Social isolation
History of violence
Screening for elder abuse:
Will not be volunteered: need to ask the right questions
Watch for injuries or health or emotional problems with vague or inconsistent explanations
Observe interactions, especially in own environment
Question older person away from carer:
Do you feel safe at home?
Are you afraid of anyone at home?
Have you ever been hit or pushed?
Question carer in empathetic not confrontational way: Caring for X must be difficult… How do
you cope…. Have you ever lost control?
Careful physical examination and documentation of findings
Management:
Age Concern have people trained in the assessment of abuse, plus case workers and advisory
groups
Use ATR social workers
If person accepts intervention, then initiate a safety plan
If person declines intervention (but has the capacity to do so) then educate and review
If person declines but doesn‟t have the capacity to make this judgement, then family court can
decide on welfare guardianship through the Protection of Personal and Property Rights Act (PPPR
Act)
Driving
50% of 76 – 80 year olds still have a licence, 27% of those over 80. Half still drive regularly
Driving depends on cognitive function, motor function and sensori-perceptual function
Elderly are only 14% of those killed in crashes, but have a higher death to injury ratio
Older drivers more likely to be at fault in accidents involving intersections, merging and manoeuvring
In elderly people with Alzheimer‟s, crash rates approach those of 15 – 25 year old males
Age associated changes affecting driving include: vision, psychomotor function, strength and dexterity,
cognitive function (especially attention to multiple stimuli and finding ones way, in dementia)
Medical assessment a legal requirement at 75, then 80 and every two years thereafter (including vision
check). Cognitive screening should be included due to the profound effect on driving, the insidious
nature of cognitive impairment, good social facades by patients, and frequent lack of insight.
Psychoactive drugs (especially BDZs) psychomotor function
Practical test performed by the Ministry of Transport is required at 80 and every two years thereafter
Services for the Elderly
Rehabilitation
Can classify approaches to rehabilitation by patterns of disability:
Localised injury or isolated disability: involvement of one discipline may be appropriate
Expectation of return to premorbid function: but more than one discipline necessary (eg fractures)
Where optimal recovery depends on well integrated team approach (eg amputation, stroke)
Health Care of the Elderly 677
Progressive deteriorating conditions where the aim is to maintain optimum ability, with regular
review of goals, and emphasis on emotional, social and environmental factors rather than specific
rehabilitation techniques (eg Parkinson‟s)
Can classify rehabilitation by types of people:
Impaired physical function, but not obviously ill disability management
Chronic illness without manifest disability education and anticipatory care
Those with a combination of illness and disability
Can classify rehabilitation by approaches:
Medical: specific control of disease and impairment
Prevention: Of secondary disability (eg pressure areas, constipation)
Restoration: Using physiotherapy, occupational therapy and nursing interventions to function
Adaptation: Equipment, modification of living environment, and family adjustment
Also need to assess the strengths and abilities of the individual and carers
Goal Setting:
Central task in management of disability
Needs accurate assessment of pre-morbid and current function (eg using formal assessment tools).
Is often unrealistic to aim for future function better than pre-morbid function
Goals must be meaningful and appropriate to the problems and circumstances
Goals should be agreed by negotiation with older person, the carer and the rehab team
Goals should include: who, will do what, under what circumstances, and to what degree of success
Barriers to Rehabilitation:
Unidentified medical problems: don‟t want to over or under-medicate. Check for malnutrition,
anaemia, fluid and electrolyte abnormalities
Cognitive impairment: If they can‟t concentrate or remember, their involvement is compromised.
Always screen for impairment
Depression: Unwell and disabled people have a high prevalence of usually treatable depression.
Diagnosis can be complicated due to overlapping symptoms (eg fatigue, apathy, psychomotor
retardation and sleep disturbance)
Communication problems: Screen for poor eyesight and hearing
Low expectations and ageism: decline is not always as inevitable or severe as thought. Patients,
carers and professionals can all have misconceptions and unrealistically low expectations
Right to dependency: some old people may not participate because they feel they should be looked
after
Common rehabilitation interventions: physiotherapy (especially musculo-skeletal problems and
mobility), occupational therapy (therapy to function in tasks, impairment), doctors (diagnosis,
prescribing, prognosis, co-ordination), nursing (implementing therapies, assessing disease, function and
well being), speech language therapy (including swallowing), dieticians, appliances, adaptations, daily
living aids, advice, education, counselling, encouragement, listening
Whether inpatient or outpatient setting is assessed on the basis of: level of dependency (especially night
care), degree of complexity of disability, speed of response needed, housing and domestic
circumstances, availability of in or outpatient services
Rest Home and Hospital Care
6% of the population over 65 live in institutions (about 25,000), 24.5% of those over 85
Rest homes are licensed by the Ministry of Health and payments are made by the Ministry of Health
Access to funding by an individual is dependent on a needs assessment done by an HHS or other
assessment unit and an asset test done under contract from the Ministry of Health by WINZ
Maximum weekly fee paid is $636: average rest home fees are around $550 per week and hospital fees
around $1100
If receiving the subsidy, you loose super and get and allowance of $27 per week
Needs assessment assigns a Support Need Level (SNL) from 1, little help needed, to 5, 2 person help
needed – levels 1 and 2 general aren‟t funded to be in rest homes
Comorbidity common in rest homes, plus evidence of mental illness (in addition to stroke and
dementia)
Other health issues include vitamin D supplementation, immunisation (including of staff), and loss of
continuity of care on shifting into a rest home
Also broader issues are maintenance of privacy, whether sexual needs can be met, encouragement of
health promotion activities such as exercise, appropriate recreation, monitoring dietary intake,
provision of alcohol and attitudes to smoking
678 4
th
and 5
th
Year Notes

Public Health 679
Public Health
Introduction .................................................... 680
Health Care Delivery ...................................... 680
Measures of Health Status .............................. 682
Biostatistics .................................................... 683
Epidemiology * .............................................. 685
Communicable Disease Control ..................... 686
Environmental Health .................................... 688
Classification ............................................ 688
Inter-relationship of Host and
Environment ........................................ 688
Consequences of Global Environmental
Changes ............................................... 689
Screening ........................................................ 689
Health Promotion ........................................... 691
Social Inequalities in Health .......................... 692
Maori Health .................................................. 694
Who is Maori* .......................................... 694
Epidemiology ........................................... 694
The Treaty of Waitangi (Te Tiriti O
Waitangi) ............................................ 695
Cornerstones of Maori Health .................. 696
Death and Dying * .................................... 696
Maori services .......................................... 697
Maori Cultural Differences ....................... 697
Drug and alcohol policy ................................. 697
Health Economics .......................................... 698
680 4
th
and 5
th
Year Notes
Introduction
WHO Definition of Health: A state of complete physical, mental and social well being, not just the
absence of disease or infirmity
Public Health:
= The art and science of preventing disease, prolonging life and promoting health through the
organised efforts of society
= Population health, not the public health system
Roles of Public Health:
Traditional role: communicable disease control, environmental and occupational health
Information: disease and health surveillance
Policy: Policy, legislation, goals, priority setting
Health Services: planning, evaluation, needs assessment
Health promotion/disease prevention: promotion, screening, immunisation
Steps in public health:
Public health intelligence (monitoring/analysis)
Developing policy
Delivering services
Equity and access:
Need = capacity to benefit (but from whose perspective?)
Vertical verses horizontal equity (but equity of what – outcomes, access, opportunity)
Dimensions of affordability, accessibility, availability, acceptability, accommodation
Health Care Delivery
Issues in Service delivery *
Key international trends:
Changing demographics: esp elderly
Communicable non-communicable diseases
Concern with economy given rising costs
Who should pay: public vs private
Issues in service delivery:
Institutional arrangements:
Output funding
Priority setting
Funder/provider splits
Managed care
„Cultural‟ issues:
Competition vs cooperation
Control vs community voice
Management vs technology
Influences on NZ history:
19
th
century legacy:
Parochialism (isolation self-government)
Adhocracy (new problem new organisation)
Egalitarian myth: services by right
System in NZ
References: Introduction to the New Zealand Health System, Peter Crampton and Anne Viccars,
Departments of Public Health and General Practice, Wellington School of Medicine
Factors facing health systems in developed countries:
Ageing populations
Medical technology
Rising expectations
Treaty of Waitangi
Health Care expenditure in New Zealand:
1998 total: around $8 billion. Vote health was $5.6 billion in 97/98.
Public Health 681
7.6% of GDP (compared with Australia 8.3% and UK 6.7%)
Public 77%, private 23%.
18% of total government expenditure.
Proportion of people covered by health insurance has declined since 1994/95
Health Legislation:
Health and Disability Services Act 1993 (now repealed)
Health Act 1956: main piece of public health legislation
Health Policy Agencies:
Ministry of Health
Other central agencies: Te Puni Kokiri, Treasury, State Services Commission
Other advisory bodies:
National Advisory Committee on Health and Disability (National Health Committee)
Mental Health Commission: established in 1986 following Mason Inquiry
Health and Disability Commission: established in 1994 – responsible for the Code of Health
and Disability Consumers‟ Rights
Health Sponsorship Council: Established under smoke-free environments Act 1990 to sponsor
activities previously sponsored by tobacco companies
Purchasers: Used to be the HFA, including Pharmac and Health Benefits Limited
Purchaser-Provider Split:
Potential benefits were:
Efficiency: due to competition
Equity: reflect need not historical provision
Accountability clearer
Cost containment due to capped budgets
Consumer sovereignty
Better information
Improvements in primary care: IPAs and Maori services
Problems:
Short term market lead decision making
CHE debt/missed business plans
Transaction costs bad contracting relationships 3
rd
party intervention
Asset specificity: providers locked in little real competition
Fragmentation of services
Loss of co-operation
Primary Care:
Numbers:
2,800 GPs (about 2,500 FTEs)
1,600 practice nurses
1800 – 2000 practising midwives
Funding:
GP income derived from: Subsidies (depending on patient age and CSC/HUHC), patient fees,
ACC
Primary Care Expenditure: 59% pharmaceuticals, GMS 15%, labs 13%, maternity benefit 8%
Themes: managed care, budget holding, integrated care
Latest reforms:
Ministry of Health and HFA merged
21 District Health Boards created (roughly around old Hospital and Health services): have a
purchasing and a provision function
Maternity providers funded by MoH
DHBs fund NGOs, GPs, Private providers, public health providers
ACC continues direct purchasing from primary and secondary providers
Key changes:
No purchaser-provider split
Community control
Budget tension between primary and secondary services forced down from central agencies to
DHBs
21 Boards too many: diseconomies of scale

682 4
th
and 5
th
Year Notes
Measures of Health Status
No single or ideal way of measuring a person‟s or a population‟s health status wide range of tools
Purposes of measuring health status:
Diagnostic: to discriminate between people with different health states
Prognostic: to predict future events
Evaluative: eg before and after a health intervention
Measuring health status of individuals and populations:
Dimension of Health
Measures in Individuals
Measures in Populations
Mortality
Age at death
Life expectancy
Disability
Existence of a disability
Prevalence of a disability
Self-rated Health
Self-rated health
Average self-rating
Mortality
Definitions:
Crude Mortality Rate: number of deaths per year for an entire population
Specific Mortality Rate: Number of deaths occurring within a subgroup of the population. Eg age,
sex, or cause specific
Age adjusted mortality rate: adjusts with reference to a standard population to allow comparisons
between populations with different age distributions
Premature mortality: death occurring before the average life expectancy within a given population
Advantages:
Death is easy to diagnose
Is recorded, and doctors are legally bound to state the cause
Disadvantages:
Cause not always accurately described
Reduces health status to being alive or not. Ignores the continuum of suffering and unhappiness
Life Expectancy
= The expectation for life at birth for a population born in a specific year
Calculation:
Period life expectancies: average life-time of a hypothetical group born in a specific year, assumes
age and sex specific death rates won‟t change
Cohort life expectancy: follow through a real cohort until all are dead
Making comparisons, eg between Australia and NZ:
Migration between the two countries
Ethnic groups (Maori, Pacific Islanders, Aborigines)
Socio-economic differences
Potential years of life lost (PYLLs): potential years of life lost for a specific cause. Difference between
age of death and the life expectancy at that age
Changes over time have largely been due to social and economic changes (particularly public and
personal hygiene). Contribution from health services is much less important
Morbidity
= Incidence or prevalence of a condition or disease in a population over a set period of time
Measurement:
„Objective‟ measures:
Biochemical markers (eg blood glucose)
Physiological markers (eg blood pressure)
Pathological markers (eg tumour size)
Functional measures:
See also Disability, page 673
Impairment: reduction in physical or mental capacity – usually due to an organ/system. May
be able to be corrected (eg reading glasses)
Disability: restriction in a person‟s ability to perform a certain task (eg walking)
Handicap: If disability limits ability to perform a normal role – depends on social context
Many measures assess degree to which people can undertake activities of daily living
Sources of morbidity data: cancer registers, notifications (infectious diseases, workplace accidents),
hospital discharges, GP registers
Public Health 683
Advantages: examines range of diseases beyond those that cause death
Disadvantages:
Diagnosis can be ambiguous
Variation in recognition or reporting of disease
Self-reported or Self-rated Health Status
More subjective
Overlaps with health-related quality of life, encompassing physical health, psychological well-being,
emotional well-being and social functioning
For assessing Maori health need to incorporate relations with extended family and spirituality
(obviously non-Maori are not spiritual and don‟t care about family!!)
Composite Measures of Health Status
Independent Life Expectancy: average number of years living without disability. Equals life
expectancy + prevalence of dependency. Ignores reversibility of some disabilities and transition from
good to poor health
Measures of the burden of disease:
Takes into account fatal and non-fatal outcomes
Disability Adjusted Life Years:
Estimate of years of healthy life lost
Similar to QALYs but standardised for use between populations and they also use age weights
(lower weights in childhood and elderly)
Used to assess the burden associated with certain diseases or with particular risk factors (eg
smoking)
In NZ, CV disease accounts for 24% of DALYS lost, followed by cancers and mental
disorders
Criticisms:
Limited use to policy makers because they focus on health loss rather than potential gains
Don‟t take into account disability associated simply with old age
Requires extensive epidemiological data
Biostatistics
Choosing study subjects:
Group
Specified by
Criteria
Target population
Clinical and demographic
characteristics
Well suited to the research
question
Accessible population
Temporal and geographic
characteristics
Representative of the target
population and easy to study
Intended sample
Sampling procedure
Representative of the
accessible population and easy
to do
Actual sample
Availability, and obtaining
informed consent and required
information
May or may not be still
representative of accessible
population
Populations may be people, institutions, records or events
Sampling frame is a complete list of individuals in the accessible population
A sampling procedure is used to select a representative intended sample from the sample frame
Avoiding systematic errors:
Trying to use sample mean to estimate the population mean
Statistic = parameter + bias + confounding bias + chance
Statistic: summary measure in a sample
Parameter: underlying value in the target population
Bias or Confounding internal validity
External validity is whether the study can be applied to the population I‟m interested in – is it
similar enough to the study population?
Bias:
Bias = systematic deviation between the statistic and the parameter, due to defect in the design,
conduct or interpretation
Occurs predominantly in design and data collection
684 4
th
and 5
th
Year Notes
Selection bias: systematic error due to those who were selected and those who were not, so sample
not representative of the defined population
Information bias: a flaw in measurement exposures or outcomes that results in a differential quality
of information between sub-groups/individuals.
Misclassification bias: Subjects erroneously categorised. If a random bias then association
in results and odds ratio moves towards 1
Interviewer bias: systematic difference in soliciting, recording and interpreting of responses (
by training the interviewers – always check this has been done)
Recall bias: should be < 2 weeks for health events. Diet recall ~ 24 hours. If not random (eg
case-control studies) then biased (eg if cases taken from records then there is variability in
what was asked and recorded, verses uniform questionnaire for controls)
Response bias: systematic error due to differences between those who volunteer and those who do
not (eg bias from drop-outs and non-responders)
See EBM Glossary, page 703, for further examples of bias
Confounding bias:
A measure of the effect of an exposure on the risk of an outcome is distorted by an association
of the exposure with other factors that influence the outcome
Standard ones: age, gender, ethnicity, socio-economic status, obesity, smoking, alcohol
As long as you collect data about the confounding factor, you can do something about it
Can control for confounding using matching, logistic regression or stratifying data
Chance effect:
Standard error:
sizesample
deviationstandard
errorstandard
Quantifies the precision with which the sample mean estimates the population mean
Says NOTHING about variability in the data
Confidence interval:
Turns standard error into something we can interpret: sample mean +/- 1.96 * standard error
95% sure the underlying value lies in the range
Width is dependent on:
Variation in observed data
The sample size (larger sample narrower confidence interval more precise estimate)
Degree of confidence we want
Accuracy depends on presence or absence of bias
Tests of significance:
Tests of significance are a tool for statistical inference
Test compatibility of a set of data with the null-hypothesis: assume there is no difference
between the means – what is the probability we would observe a difference as big by chance
P value: the probability of getting a value at least as extreme as the observed statistic.
Threshold usually 0.05
Most common test statistics are chi-squared and t-statistic (compares two means). Both
depend on degrees of freedom
Power: = probability that the study will find a statistically significant difference if a true difference
of a given size exists
Data:
Qualitative: not numeric (eg hair colour)
Quantitative: can be continuous or discrete
Measurement scales can be nominal (categorical and unordered), ordinal (categorical and ordered)
or interval (continuous)
Data description:
Categorical and discrete date: bar graphs, frequency distributions
Continuous data: histograms, frequency polygons
Central tendency: Mean or median (best measure of central tendency if skewed distribution)
Spread/variability: Standard deviation, percentiles or inter-quartile range
Correlation co-efficiency – degree of clustering around a straight line
If two variables are categorical and unordered then use relative risks and odds ratios
Public Health 685
Epidemiology *
Includes 2
nd
and 3
rd
year PDS notes
= Study of distribution and determinants of health and disease in populations
For Definitions of Risk and Odds Ratios, see Risks and Odds, page 703
Bradford Hill Criteria for causation:
Time sequence: did the factor come before the disease – only necessary factor
Strength: large relative risks are seldom artefacts
Consistency: has an association been found elsewhere, using different methods?
Specificity
Dose-response relationship: does the risk with the level of exposure to the factor
Biological plausibility: is a causal risk consistent with current knowledge
Experiment: can an intervention study validate the result
Summary of study types: (increasing power as you go down)
Descriptive (ecological) studies
Analytical (observational) studies:
Cross-sectional studies
Case-control studies
Cohort studies
Intervention (experimental) studies
Descriptive studies
Personal characteristics (age, sex, occupation, social class, etc), place and time
Measures of occurrence ( descriptive):
Prevalence: Number with disease/Relevant population at a designated time
Incidence: Rate of development of a disease in a group over a period of time = number of new
cases during a specific period/total at risk population
Need to compare for specific groups, or standardise for compositional differences in populations
Long duration illness prevalence, short duration prevalence
Incidence and prevalence are similar for short illnesses (eg diarrhoea) but not for long illnesses (eg
TB)
Useful for:
Understanding occurrence
Suggesting hypothesis – but correlation doesn‟t prove cause
Often called ecological studies
Don‟t have unaffected people in the series so no information about relative risks
Cross-sectional studies
Examine relationship between disease and other variables (eg risk factors) in a defined population at
one time
If prevalence not high enough, use sentinel populations (ie those with greater risk)
Normally considering prevalence, not incidence also called Prevalence Studies
Limitation: time sequence of cause and effect cannot be determined
Case-control studies
Factors amongst patients with a disease compared with the frequency among a control group without
the disease
Looking backwards to the exposure (ie the outcome has already happened) also called retrospective
studies
Advantages:
Can be done quickly (compared with cohort study)
Are therefore cost effective
Can do it with diseases with low prevalence (cohort study better for more prevalent diseases)
Defined endpoint
Disadvantages:
Retrospective, so can introduce bias
Selection criteria create difficulty
Biases: non-volunteer bias, recall bias, etc
Causation not proven – just an association

686 4
th
and 5
th
Year Notes
Can only get information on one outcome
Selection of cases:
Representative of those presenting over a defined period
Select according to diagnostic criteria. If these cast the net widely, then will include people with
unrelated disease odds ratio moves towards 1 (if random effect)
Selection of controls:
Representative of the population from which cases drawn but without the outcome
Aim is to establish expected exposure in case group
Want to compare exposures between the cases and the population at large. If, for example, you
match on age, you won‟t be able to conclude anything about age as a risk factor, so choose controls
so you get an unbiased example of risk factors in the population. Matching does reduce the effect
of confounding – but there are other ways to deal with that when doing the number crunching
Identical methods must be used to collect information from both
Can‟t estimate relative risk in a case-control study:
Outcome (eg Disease)
Exposure
Yes (Cases)
No (Controls)
Yes
A
B
No
C
D
Odds Ratio = (A/C)/(B/D)
Relative Risk
= [ A/(A+B) ] / [ C/(C+D)]
= Risk of disease among exposed/risk of disease if not exposed)
In a case-control study, the ratio between the cases and the controls is fixed by the study
design, not the prevalence in the population. The relative risk is therefore meaningless. That
is, you can‟t estimate the risk of the disease in the population in those not exposed to the risk
factor
But if the condition is rare and there is no bias in controls, then the odds ratio approximates the
relative risk ratio well
See also Risks and Odds, page 703
Cohort Studies
Groups observed over time: forward looking from exposure, waiting for outcome also called
Prospective or Follow-up Studies
Either compare within the cohort, or select a comparison cohort
Advantages:
Bias over a case-control study
Can examine more than one outcome
People who don‟t take part don‟t bias the outcome, just its generalisability
Disadvantages:
Large numbers are required information collected has to be simpler risk of confounding
Need to follow people over time expensive and takes a long time
Not good for rare diseases
Strengths: People who don‟t take part don‟t bias the result – just affect its representativeness (ie
external validity) less susceptible to bias
Intervention or Experimental Studies
Test whether removing suspected aetiological factors reduces frequency of disease
Evaluate preventative measures and treatments ( clinical and community trials)
Best test of cause and effect
Often not ethical nor logistical to do a RCT
Blind assessment information bias
Communicable Disease Control
See Vaccination, page 515
Reasons for notification:
High morbidity and mortality (in epidemiology terms, ie deaths per 100,000 of well population).
Intervention available
Other:
Public Health 687
High public interest. Eg CJD – is both rare and untreatable
Historical. Eg decompression sickness
Notifiable Diseases:
Under Health Act 1956
Section A: infectious diseases notifiable to a medical officer of Health and Local Authority
[involve water or food transmission]: acute gastro-enteritis (where common source or person
in high risk occupation), cholera, giardiasis, legionellosis, primary amoebic
meningoencephalitis, shigellosis, yersiniosis, campylobacteriosis, cryptosporidiosis, Hepatitis
A, Listeriosis, salmonellosis, typhoid and paratyphoid fever
Section B: infectious diseases notifiable to Medical Officer of Health: AIDS, CJD, HIB,
Hepatitis C, Hydatid disease, Leptospirosis, measles, Neisseria meningitidis, plague, rabies,
rickettsial diseases, tetanus, yellow fever, anthrax, brucellosis, diphtheria, Hepatitis B,
Leprosy, malaria, mumps, pertussis, poliomyelitis, rheumatic fever, rubella
Notifiable non-infectious diseases: cysticercosis, taeniasis, trichinosis, decompression
sickness, lead poisoning, poisoning from contamination of the environment
All forms of TB (under TB Act 1948)
Venereal Diseases Act (1986?): covers gonorrhoea and syphilis, and contract tracing
Classification of notifiable diseases:
Vaccine preventable diseases
Blood borne and sexually transmitted diseases
Food and water borne diseases
Vector borne eg Malaria
Zoonoses (ie animal stage) eg Brucellosis, Hydatids, Rabies
Other Infectious diseases: eg CJD, Hepatitis, Leprosy, TB
Non-infectious diseases: Decompression illness, Lead poisoning, environmental
contamination
Process of notification:
Is a legal requirement, although compliance is poor with common things like campylobacter. Only
a small proportion contact doctor, only a few of these tested, only a few of these reported, etc
When to notify:
If serious on suspicion (eg meningitis)
If not serious (eg gastroenteritis) then on confirmation
Possible interventions:
Food borne – isolate source and close it down
If AIDS and spread by blood products screen blood
If AIDS and confined to a locality education campaign
Surveillance system:
Report to medical officer of health
Clinical labs also report to medical officer of health (if a special case then refer sample to the CDC
Reference Lab – ESR).
These all report to the CDC Epidemiology Group (also at Porirua), produce the Public Health
Report
In turn report to the Ministry of Health and MAF, so they can form surveillance and disease
control policy (eg vaccination and screening policy, promotion, etc)
Other surveillance systems: coroner, Births, Deaths and Marriage, OSH, Cancer Registry
Epidemics:
An outbreak or epidemic is relative, is „more than you would expect‟
An outbreak investigation involves analysis of the time over which illnesses have occurred, the
places and the characteristics of the people affected
Patterns of epidemic:
Point source out-break (eg food poisoning) – short duration
Multiple source out-break: eg measles, index case spreads to multiple cases – long duration
with fluctuating incidence
Want to find:
Agent
Vector
Source
Can affect rate without known the agent. Eg cholera was controlled through clean water in
London before the bug was discovered

688 4
th
and 5
th
Year Notes
Host
Pathogen
Vector
Environmental Health
Classification
= Effect of environment on health at a population level (want to stop people being sick…)
Classify by route of exposure to agent of harm: Classify water, air and soil by physical, chemical and
microbial (prion, virus, bacteria, protozoa, etc):
Water:
Physical
Drought
Drowning: in NZ have the hazard and lots of exposure (outdoor pursuits, fishing,
swimming pools)
Microbial:
Virus: HAV, rotavirus
Bacterial: shigella, campylobacter
Protozoa: amoeboea, Cryptosporidium, Giardia
Chemical: arsenic poisoning in Bangladesh
Air:
Physical:
Suffocation: plastic bags, volcanic gases, faulty gas appliances
High winds
Noise
Microbial: Tb, legionaries
Chemical: pesticides, asbestos, work place
Soil/Food:
Physical: landslide, earthquake, desertification
Microbial: tetanus
Chemical: heavy metals, selenium deficiency
Other: Sun (UVB cancer), radiation
Occupational health and psycho-social health often separated off from environmental health
Need multi-disciplinary teams to solve problems (eg housing: doctors, engineers, sociologists,
economists)
Inter-relationship of Host and Environment
Malaria
Background:
Lifecycle: plasmodia in human blood mosquito sucks blood migrate into mosquito saliva
glands passed on in next bite
Host factors:
Sickle cell anaemia contagious
Immunocompromised: kids, malnourished, concurrent infection, maybe AIDS
Pathogen factors: which strain
Vector attributes: right species of mosquito
Interventions:
Vector – Host relationship: Interrupt exposure eg nets, repellent, clothing
Host: general health, nutrition
Host – Pathogen relationship: chemoprophylaxis
Pathogen: Air-conditioning temp plasmodium
Pathogen – Vector relationship: Remove infected hosts (ie cure them)
Vector: source reduction (spray, water traps)
Effect of the environment:
Vector: if warm and wet breed faster
Host: if hot take clothes off and open windows
Public Health 689
Pathogen: plasmodium replicated faster if warmer
See also Malaria, page 508
Yellow Fever*
Swotted for Public Health Test Question. Source: Harrison‟s and CDC Website
Haemorrhagic fever with prominent hepatic necrosis
Incidence declining since the turn of the century. Outbreaks mainly now only in West Africa. South
America also at risk
Urban Yellow Fever:
Spread by Aedes Aegytpi mosquito
Human – mosquito – human cycle. Mosquitoes pass it to their offspring via ovary infection
Deposit eggs in any container with water in or around homes (so can still get it if low rainfall or
dry season) women and children more at risk if they‟re around home a lot
Sylvatic Yellow Fever:
Mosquitoes infected from viraemic monkeys (monkey‟s don‟t get ill so are a continuing reservoir)
Infects humans in or living around forests men who do the hunting more at risk
Prevention (in addition to Malaria factors above):
Put bed nets over infected people – stops onward transmission of infected people. They are
viraemic for 3 – 6 days, following a 3 – 6 day incubation period.
Treatment is supportive only. There is no chemoprophylaxis
Vaccination:
Safe, lasts for 10 years
Only vaccinate child < 12 months and pregnant women if high risk
Epidemics occur if poor maintenance of vaccination and lack of plans for detection and response to
epidemics
Consequences of Global Environmental Changes
Population:
Main driver of global changes
Carrying capacity of the world around 10 – 15 billion, currently 6 billion
Compounded by unequal distribution of resources: 20% have 80% of the resources
Technological change will only affect the 20% with resources little impact on carrying capacity
Demographic transition: As countries shift from „3
rd
world‟ to „1
st
world‟ their pattern of disease
shifts from infectious diseases with high infant mortality to degenerative diseases The 80% will
have resource requirements following this transition
Global warming (due to ozone depletion, CO2, etc)
Vector born disease
Thermal expansion of oceans (melting ice caps comes later) + more frequent storms flood low
lying areas
Resource depletion:
Wood, fossil fuels, food
Sources resources used by people sinks. If transfer is too fast, sources and sinks can‟t keep
up
Deforestation/desertification as a result of resource use and climate change
War:
Due to competition for resources
Leads to all extremes of environmental health (death in combat, poor health, refugees, socio-
economic effects)
Trans-boundary population shifts (eg refugees)
Screening
Definitions
Screening:
The presumptive identification of unrecognised/preclinical disease or defects by the application of
tests, examinations or other processes that can be applied rapidly (and cheaply)
Sorts people into high and low risk groups for further diagnosis of high risk.
Is NOT diagnostic on its own
690 4
th
and 5
th
Year Notes
Mass/population Screening: systematic screening of populations
Opportunistic screening: Non-systematic, when the opportunity arises
Selective Screening: systematic screening of high risk groups
Screening test: a test performed without a clinical indication
Objectives of screening:
Mortality/morbidity from disease on the individual
Limit the impact of disease on a community
Identify compensatable disability (eg poor eyesight in kids)
Criteria for Screening Programmes
Is the disease an important health problem (incidence, impact, preventability)
Is a suitable screening test available:
Acceptable, simple,
High sensitivity, as specific as possible
PPV: probability that a person with a positive test does have the disease, depends on sensitivity,
specificity AND prevalence
NPV: probability that a person with a negative test does not have the disease
Yield (proportion of cases of the disease accurately identified by a screening test),
Repeatability (depends on variation in method, subject variation, observer variation)
Is the natural history of the disease well understood:
A recognisable latent or early symptomatic stage
The length of the asymptomatic stage determines screening frequency. Is this long enough to
make the screening interval reasonable?
Does screening lead to interventions that improve quality of life:
Does early intervention offer benefits over later intervention
Accepted treatment, proven effectiveness. Ideally want an RCT that demonstrate screening verses
no screening improves mortality/morbidity
Is there an appropriate infrastructure available to provide screening and follow-up services:
Are there pilot studies demonstrating how it should work?
Is there local and national support?
Are the services accessible (in terms of geographic, cultural barriers, cost), does the system have
sufficient capacity, and is there appropriate quality control processes in place
Is the screening programme cost effective?
Screening Test
Eg PSA for prostate cancer, intra-ocular pressure for glaucoma, etc
For a screening test, you want a test that maximises sensitivity: maximise true positives (minimises
false negatives), so that you identify all diseased cases. The downside is an increasing rate of false
positives who have unnecessary further investigation
A highly specific test would maximise true negatives (ie minimise positives, so would not further test
anyone unnecessarily), but at the cost of increasing false negatives – who are the people you actually
want to detect
See also Evaluation of Diagnostic Tests, page 704
Biases
Lead-time bias: interval from detection to point where diagnosis would have been made without
screening. Depends on length of pre-clinical phase, frequency of testing, and the test sensitivity
Length bias: Cases with a disease with a longer natural history are more likely to be detected by a
screening programme. But these cases also have a better prognosis. Thus screening leads to a better
prognosis, regardless of whether screening itself confers any benefits
Increasing result of
screening test
Well
Diseased
Maximum
sensitivity
Maximum
specificity
Public Health 691
Selection bias: selection, referral or volunteer bias results in a selected subset of the population being
screened
Screening Programmes in NZ
National screening programmes:
Neonates: inborn errors of metabolism – Guthrie Card (See Genetic Testing, page 465)
Cervical Cancer (See Cervical Cancer, page 351)
Vision/hearing testing at school entry (erratic)
Mammography (see Breast Screening, page 382)
Controversial and not currently recommended population screening programmes:
Prostate (PSA)
Colorectal cancer
Otitis media with effusion
Current screening pilots: Hepatitis B
Opportunistic screening
Antenatal screening
Blood pressure
Cholesterol
Blood glucose
HIV
Osteoporosis
Glaucoma, etc
Deciding to implement a screening programme:
The decision to implement a population based screening programme is complex, must be justified
on the basis of standard WHO criteria and supported by research evidence
The rules to do with population health are NOT those of an individual clinician (ie just because
you would screen an asymptomatic man for prostrate cancer is not a reason to implement a
national programme)
Potential to do harm at a population level is considerable („first do no harm‟)
We are „imposing‟ something – need sound evidence
Ethical Considerations
Costs and benefits:
Costs should include adequate support, counselling, etc. Benefits should include quality of life
(but subjective)
Many harms are personal – false alarm, false reassurance. Difficult to account for
Justice:
Distribution: benefits accrue to a few and are large; harms fall on many and are minor. Is this fair?
Inconvenience borne by many to benefit the few – but this also benefits the group (social welfare
function)
Collective gains depend on high levels of individual participation
Autonomy:
Motivation: altruism only effective if participants well informed/educated
Imposition: Opt-out strategies – trade-off between recruitment level and maximal choice
Results: safeguards on third party disclosure
Opportunistic screening:
Cost and benefit usually borne by the same individual
Offered responsively rather than proactively
Appropriate treatment or other follow-up available
For Prostate Screening, see Prostate Cancer Screening*, page 225. Prepared for Public Health test.
Health Promotion
= Health promotion is the “process of enabling people to increase control over, and to improve, their
health” (Ottawa Charter)
Ottawa Charter had 5 strategies:
Build healthy public policy
Create supportive environments

692 4
th
and 5
th
Year Notes
Strengthen community action
Develop personal skills
Reorient health services
The Treaty Understanding of Hauora in Aotearoa NZ (TUHANZ) is a framework adapting this to NZ
(issued by the NZ Health Promotion Forum):
Goal for Article 1 (kawanatanga/Governance): achieve meaningful Maori involvement in all
aspects of health promotion
Goal for Article 2 (Tino rangatiratanga/Maori control and self-determination): actively support the
advancement of Maori health aspirations
Goal for Article 3 (Oritenga/Equity): Prioritise health promotion action that improves Maori health
outcomes
Progress has been made on: Heart disease, SIDS, Road traffic accidents, cervical cancer
Issues of concern: Maori to non-Maori gap, melanoma, youth suicide, obesity, STDs
Compared to other OECD countries, NZ has high mortality from ischaemic heart disease, respiratory
diseases, breast and bowel cancers, MVA, suicide
Role of health care sector:
See patients as part of a community, not just as individuals
Integrate with programmes delivered by others
Move to a focus on the determinants of health (including socio-economic status – income and
housing – culture, health care system, in addition to genetics, etc)
Strategies in the health care sector:
Care and support
Screening: eg alcohol in pregnancy, cervical, six week check, opportunistic screening for diabetes,
breast screening
Immunisation: childhood and influenza
Health education: eg antenatal education including sun protection, diabetes, HIV, nutrition,
exercise, smoking
Helping to build healthy public policy
Creating healthy institutions (eg Healthy Hospitals – integrating health promotion into their work)
Barriers:
Insufficient time with patients
Perceived or real cost disincentives
Uncertainty among providers about the evidence
Social Inequalities in Health
Deprived social and economic conditions strongly associated with poor health
There is a social gradient in health – it exists in all countries but the slope varies
Targets for intervention:
Socio-economic status: issues around distribution
Intermediary factors: housing, targeted support
Health issues: access. Most countries target their intervention here
Link from Health to SES: disability support
Poor health deprivation through stigma and earning potential
Deprivation poor health through the following:
Structural features of society, economy and environment
Health related behaviours, disposable income and psychosocial coherence
Individual health
Community health
Public Health 693
Effect of Deprivation on Health
Poor access to health care:
Culturally foreign
Financial barriers: GP services, transport, class and language differences between doctor and
patient
Income:
Key SES lever. Can have a rapid effect on:
Effects of a drop in absolute income
Rise in income inequality divisive effect on society alienation of „work poor
households‟:
Measured by the Gini Co-efficient for household equivalent disposable income
Has for NZ since 1988 from 0.26 to 0.33 (biggest change in the OECD)
Is followed with a small lag by indicators such as youth suicide, youth unemployment, etc
Formation of social capital. People in „survival‟ mode don‟t have energy to contribute to
community
Policy levers: monitoring income inequality, change tax rates and social wage, alter WINZ rules
about supplements
Single parent families, women, Maori and Pacific Islanders are over-represented in the poor
Education: Increases human capital. Students from poor households are more likely to underachieve,
have lower participation rates in tertiary education.
Occupation and labour force participation:
Translates human capital into income. Also indicator of social class
Higher injury rates in low SES jobs (forestry, construction)
Unemployment: stress, social isolation, lack of purpose self esteem
Housing:
Impacts of rent, neighbourhood, number of bedrooms, quality of construction and maintenance (eg
insulation, ventilation).
Issue for the poor, and also for former institutionalised psychiatric patients
Damp housing respiratory illness, overcrowding infectious diseases, mental distress
Feelings of hopelessness and being devalued less cohesive society violence, exploitation, drug
use
Ethnicity:
Interacts with SES
Sensitive policy area
NZDep (NZ Deprivation Index) is a composite measure of deprivation
Individual health risks:
Adequate food in sufficient quantities („food security‟)
Physical exercise: affected by range or sports facilities, clubs, etc
Alcohol/tobacco consumption: affected by taxes, restrictions on distribution
Early pregnancy
Also indicators such as obesity, high blood pressure, high cholesterol, diet, exercise
Health behaviours/At-risk behaviour (eg lifestyle factors)
Health damaging behaviours more common in low SES
Knowledge alone insufficient to change behaviour (eg smoking may be a coping strategy)
Relate these factors to health status using measures of mortality, morbidity (including measurement of
self-rated health status, suffer from specific diseases or measure role limitation), health risks, health
service utilisation
NZ approach:
Monitor social and economic determinants of health
No systematic cross country comparisons
Slow policy development and implementation
Lacks cross party and public support
Emphasis on health providers not determinants
Conclusions:
Socio-economic determinants of health are multi-causal
Issues around policy making under conditions of uncertainty
Policies should be monitored against goals
694 4
th
and 5
th
Year Notes
Maori Health
Includes 2
nd
and 3
rd
year PDS notes on Maori Health
Who is Maori*
3 concepts:
Biological: amount of blood
Descent: descended from a Maori but not worried about %age of blood
Cultural identification: group to which individual feels most closely aligned
Ethnic Classification in the Census:
Prior to 1974: based on > 50% Maori blood
Till 1986: Based on descent
1986 census: What is your ethnic origin (ie self-identification)
1991 census: What ethnic group do you belong to
All leads to differences in the way trend data are presented (ie adjustments made to the
denominator)
World-view:
Io (supreme being)
Te korekore (the nothingness at the beginning)
3 realms which interpenetrate each other:
Realm of ultimate reality: Io, Rangi (sky father), Papa-tua-nuke (earth mother), Tipuna (Gods,
spirits, ancestors), mana and tapu
Realm of the human
Realm of the dead
Mana:
Enduring, indestructible power of the Gods
Mana atua: sacred power of the Gods
Mana tupuna: power or authority handed down through chiefly lineage
Mana whenua: power associated with possession of lands
Mana tangata: power acquired through developing skills
Tapu:
Sacred, set apart, forbidden, restricted
Everything created by gods has Tapu (people, land, river, forests)
People become tapu by their desire to stay under the influence and protective powers of the gods
There is good tapu and bad tapu (the devil has tapu too!)
Compares with noa (free from tapu, common)
Epidemiology
Life expectancy has improved compared to Pakeha since 1950, has levelled off, and is now about 10
years less than Pakeha
Maori have worse health statistics but fewer hospitalisations (ie use services less)
Wide disparities across all indicators of Education, health, income, housing, employment and criminal
justices
Maori concentrated in lowest 3 deciles of deprivation index – 25% in lowest
When controlling for deprivation, Maori life expectancy is still worse, and gets even worse in the
lowest decile Maori are not just sick because they‟re poor. Possible explanations:
Not Maori behaviour – common to ethnic minorities around the world
Not genetic – why would Maori and black Americans have the same predispositions given the
degree of genetic separation
Social and economic determinants of health:
Michael Marmot: epidemiology of British civil service – position in hierarchy better predictor of
life expectancy than smoking, hypertension, etc
Postulate: Don‟t have more problems but have fewer choices chronic stress from poor control
over life (can only worry, can‟t do anything else) elevated hormone response (eg
Corticosteroids) lipids, obesity, insulin resistance, CHD, etc. Effectively aging quicker.
Stress levels impact on the degree of impact of lifestyle factors on your health
Urban shift:
In 1945, 25% of Maori lived in urban areas. In 1980, 80% lived in urban areas
Public Health 695
Due to development of manufacturing industries and centralisation of agricultural production (eg
freezing works) fewer jobs in traditional tribal areas
Reasons for smoking
Part of history: tobacco given as gifts at Waitangi, Goldie images of smokers, etc
Advertising: eg Howard Morrison (role model) advertising lighters
It has become culturalised: carved pipes, woven pouches for lighters reinforce link between smoking
and Maori
Responses:
Smoke free hui
Aim at young („Why start‟) – counter image that its cool to smoke
Smoke free areas
Enforce bans on underage sales
Needs whanau, local, national integration
The Treaty of Waitangi (Te Tiriti O Waitangi)
Pre-treaty history:
Increasing availability of guns and overcrowding in the north inter-tribal wars
Introduced diseases high mortality
1831: Chiefs wrote to the king to ask for protection. Busby sent as NZ resident in 1832
1835: Northern tribes declaration of independence
1839: Hobson sent by colonial office to do a new deal
At the time of the treaty:
Maori significantly outnumbered non-Maori
Settlers wanted land
Maori needed British government to control sailors, whalers and convicts who came here
Maori needed national identity to trade inter-nationally (eg ships needed a flag)
Maori and non-Maori had a mutual need for each other
The Treaty:
1. Kawanatanga (Governance) vs Sovereignty in English – no Maori would have given this up
2. Tino Rangatiratanga (Chieftainship, Control, Autonomy) vs Possession in English
2a: Queen promised protection, and exercise of their chieftainship over lands, villages and
treasures
2b: Queen had exclusive right to buy land (and sell it on at a profit to finance the colony)
3. Oritenga: Equity
Application of Treaty to health:
Implicit in treaty were concepts of equity, partnership, economic and cultural security
Concepts of health firmly based in Maori culture, which under the treaty are recognised and
protected
Kawanatanga (Governance): Government has responsibilities to govern and should take reasonable
steps to improve health. Crown has obligations as well as power. Applies to all citizens
Tino Rangatiratanga (Chieftainship, Control, Autonomy). Applies to Maori. Right to establish
and provide services (but its not just a right, it is also effective)
Oritenga: Equity. Maori have poorer health and poorer access, so neither equality of opportunity
nor outcome
Post Treaty:
Treaty was basically sound – but the Crown didn‟t stick to it:
Others brought land directly
Crown brought land unfairly or confiscated it
Maori discriminated against in social policy, entitlement to vote, treatment of returned
servicemen, etc
1841: unused land deemed Crown land
1844: law enabling Maori to be educated in English. Speaking Maori in school punishable offence
till relatively recently
1852: right to vote given to individual land owners – Maori excluded as land held collectively
1863: law allowing confiscation of the land of rebels
1867: Maori individual ownership of land threat of majority in some electorates set up 4
Maori sets so Maori remain a minority
696 4
th
and 5
th
Year Notes
Rapid loss of land (from 26.8 m hectares to 3 m hectares by 1900), Pakeha, concern among
Maori about loss of clout Kingitanga movement
Land wars in Taranaki and Waikato: complex and changing politics, many tribes at one point or
another were allied with the British against Maori enemy tribes
Impact on Health
Socio-economic: low incomes, poorer housing, higher unemployment, less education
Lifestyle: diet smoking, alcohol, drug use
Cultural factors: alienation, loss of wairua and cultural identity, urban drift fragmentation of whanau
Due to:
Failure to give same rights and privileges
Failure to protect treasures
See also Maori Mental Health, page 410
Cornerstones of Maori Health
Cornerstones
Attempt to get away from purely bio-medical model of health
Taha hinengaro: mind and emotions
Includes cultural identity: Te whanau (family), te whenua (land) and te reo (language)
Mana important to maintenance of mental health
Whakama: encompasses shyness, embarrassment, shame. Confused with depression, guilt,
subordination
Taha wairua: spiritual health
Life force: reflects where you come from, guides your future
Taha tinana: physical health
Tapu: complex: places/objects (eg tiki)/body parts (head & genitals)
Don‟t mix food and heads, 2 ends of GI tract should never meet
Taha whanau: family.
Belonging, identity, security
Whakapapa: whanau hapu iwi
Fragmented by urbanisation
Check family and social history (eg family effected by mental illness, family health impacts on
personal health eg abuse, etc)
Eg – application to type 2 diabetes:
Taha hinengaro: Need understanding to manage disease and prevent disability, needs coping
strategies
Taha wairua: colonisation and cultural dislocation cultural identity and recovery: need a passion
to live, to know their place in the world more likely to beat the illness
Taha tinana: Medical response, treatment of complications
Taha whanau: Family breakdown contributes to poor lifestyle and support. Need support of family
in making lifestyle changes
Other factors *
Tino rangatiratanga: control of own destiny
Economic security
Self esteem, pride and confidence
Measures of Maori health: value of resources in Maori ownership, drop in crime rate, use of te reo
Tohunga: traditional Maori healer (common in Maori communities)
Mate Maori: illness due to wrong doing refer to kaumatua
Death and Dying *
For family and friends, seeing the patient while alive is important, bring koha, say karakia
Following death:
Everything is tapu – those at the bedside are responsible for ensuring customs carried out
Avoid post-mortem: sanctity involved, impedes release of spirit (spirit lingers 3 – 8 days)
Dead person never left unattended
Tangi:
2 – 5 days after death
Public Health 697
Farewell speeches and lamenting
Conflict over where to bury the deceased: te tupapaku may be taken to a number of marae as a
compromise
Encourage wairua to depart
After burial: hakari – sacred feast – turning point
Maori services
Tipu Ora: in Rotorua, building on traditional role of „Kuia‟ (“nanny”) – Maori, non-smoking, young
grandmothers. Pragmatic focus (ie get them to smoke outside rather than insisting on smoking
cessation). Has reduced SIDS
Maori Cultural Differences
Contributing factors to cultural dislocation:
Perceived value of self
Social position
Cultural dislocation shattered spirituality Taha wairua
Ignore cultural values and they‟ll ignore you
Responses:
Don‟t blame – beating up on beaten up people doesn‟t change anything
Give them resources: e.g. to population group (cf. AIDS control)
Use cornerstones on consultation check list
Are we contributing to peoples stress or reducing it?
Drug and alcohol policy
See also Regulation of Medicines and Drugs, page 535
See also Cannabis/Marijuana, page 448
Drug epidemiology:
Deaths attributed to drug use:
79% Tobacco
19% Alcohol
1 %Other drugs
Male deaths twice female deaths
Social costs (including lost production, mortality, health costs, benefits from consumption etc)
reveal alcohol is more „expensive‟ than tobacco (Tangible and intangible costs of alcohol = 6% of
GDP, tobacco = 4.9%). Alcohol takes people from production and has greater secondary costs (on
family, accidents, etc, and effects production from earlier in life)
Prevention Paradox: To get greatest gain from prevention need to target the mean, not the tail (although
they drink the most), as most people, and therefore the biggest cost, relates to people around the mean.
(Eg cholesterol, alcohol, etc)
Historical influences:
Colonial society: more men than women (miners, whalers, etc)
Brewing industry and pubs a large employer of labour
Brewing industry characterised by wealthy and influential families
Other communities had other drugs (Chinese – opium, Italians – wine, which were subject to
different regulations)
Women settlers in later 19
th
century saw alcohol as a problem strong temperance
movement push for regulation in early 20
th
century
Interests/stakeholders in drug policy today:
Politicians: libertarian vs conservative
Legal drug companies: tobacco/alcohol (invest $$ into „education‟ to control the climate of what is
„cool‟)
Illicit drug dealers: large gang involvement
School sector: teachers/principals
Medical profession (also issues around medicinal use, eg of cannabis)
Lobby groups: ASH, DARE, Drug foundation, Life Education Trust
Police: $30 mill per year for cannabis control, 12,000 arrests for cannabis offences, 6000
prosecutions, only 500 get diversion
Maori: 2 views: its dangerous so should be illegal vs it is criminalizing young Maori
698 4
th
and 5
th
Year Notes
Cannabis: have had a debate without good information
Health Economics
= The study of how individuals and societies, experiencing virtually limitless wants, choose to allocate
scare resources to best satisfy their wants
Scarcity:
Resources (main factors of production – natural resources, capital, labour) are scare
Goods and services produced from them are scarce
Can‟t have as much as we would want if they are free
Will always be medical interventions that cannot be funded
Choice: Because of scarcity, we must make choices
Opportunity cost:
The loss of the next best opportunity we could have chosen (ie if we use time/money on one thing,
it‟s not available for something else)
When doing an evaluation: deduct GST (it‟s a transfer), use real price (eg not subsidised cost of a
drug), include indirect costs (eg patient travel)
Can be calculated from different perspectives: eg provider, funder, society
Marginal analysis:
= Incremental benefit (ie marginal benefit) from incremental cost (ie marginal cost)
Decisions are usually about whether to expand or contract – not stop or start
Marginal cost is NOT the same as average cost
Efficiency:
= Maximising benefits from certain cost of inputs
Not the same as cost-cutting: if you cut costs and output falls then haven‟t improved efficiency
Effectiveness: are patients better off (eg have better health) with intervention than without
Technical efficiency: providing effective services at least cost – doing things right
Allocative efficiency: concentrating resources on effective services that offer the biggest payoff in
terms of health – doing the right things
Inefficiency is unethical (if budget is constrained)
Equity:
= Fairness: usually of distribution or payment
Equal access for equal need (what is need – ill health or capacity to benefit)
Equal resources for equal need (same amount of money for equal needs – basis of the DHB
funding formula)
Equal outcomes: allocate resources to achieve same health status of different populations
Markets:
Means of allocating scarce resources
Result from the interaction of demand and supply, mediated by price
Consumers can signal demands, maximise their „well-being‟ or utility, producers can shift
resources accordingly
If there is perfect competition, theoretically you get allocative efficiency
For this to work, requires:
Perfect information (eg about quality, costs, etc)
No externalities (someone else bears a cost or benefit)
Goods and services must be rival in consumption (ie if I buy it no one else can have it) and
excludable (you can‟t have it if you can‟t pay)
Freedom of entry and exit
Perfect competition – no monopolies
No supplier-induced demand
Equity is not an issue (ie no merit goods – goods that society believes should be more widely
available than would occur through markets alone)
Market failure in health care:
Externalities eg immunisation
Monopolies eg secondary services, labour markets
Asymmetric information eg health professionals
Supplier induced demand (especially if fee-for-service)
Highly inelastic demand
Health Insurance Markets
Public Health 699
Uncertainty about future health needs + high costs demand for insurance
Moral Hazard: will now consume more health care than they otherwise would as someone else
is paying (can control with co-payments)
Adverse selection: patients who know they will need it are more likely to purchase it. Insurers
won‟t know so premiums won‟t reflect risk
Want to getting advantages of market efficiency and overcoming market failure ?government
failure, purchaser provider splits, quasi markets (health care plans)
International Comparisons: Health Expenditure per capita and GDP. NZ is on the line
Economic Evaluations :
= Comparative analysis of alternative courses of action in terms of their costs and consequences
Informs choices about the allocation of scarce resources
Needed to determine efficacy (in lab conditions), effectiveness (more good than harm in practice)
Can be prospective or retrospective
Types of evaluation:
Cost minimisation: compare inputs, assume outputs are equal
Cost benefit: compares different outcomes (eg flu jabs and hypertension screening). Convert
to common unit ($) to compare – but can human life be valued?
Cost effectiveness: relates cost to a clinical measure (eg blood pressure, morbidity, life years
gained). Has superseded cost-benefit analysis due to problems allocating monetary values to
all outputs
Cost utility: cost per QALY gained. Can compared across a whole range of interventions –
but methodological problems. Example: Impact on QALYs of dialysis verses kidney
transplant.
Common approaches to valuing human life:
Human capital: future earnings (but elderly have none)
Implied valuations: value implicit in past policies
Insurance values: but this is paid to survivors
Willingness to pay to reduce low probability of death: survey or observe (eg how much do people
spend on safety)
Theory X and Y: Summarising different approaches to health care in health economics
Theory X
Theory Y
View of Health
Health and disease occur randomly
Health determined by lifestyle
choices
Medical Care
Special. Market Failure
Same as other goods and services
Practice of Medicine
A Science
An art
Economics
Financial rewards reduce the
quality of caring
Financial rewards generate high
quality care
Policy
Regulation needed to mitigate
economic forces. Tax the health,
subsidise the sick. Discourage new
medical technologies
Reduce regulation, encourage
market forces. Tax the sick, not
the healthy. Encourage new
technologies
700 4
th
and 5
th
Year Notes

Evidence Based Medicine 701
Evidence Based Medicine
Reference: 4
th
Year Evidence Based Medicine Notes
Introduction .................................................... 702
Risks and Odds ............................................... 703
Evaluation of History Taking and Clinical
Examination .............................................. 704
Evaluation of Diagnostic Tests....................... 704
Evaluation of Therapy .................................... 706
Evaluation of Prognosis ................................. 707
702 4
th
and 5
th
Year Notes
Introduction
What is Evidence Based Medicine
= „The conscientious, explicit and judicious use of current best evidence in making decisions about the
care of individual patients. This practice means integrating individual clinical experience with the best
available external clinical evidence from systematic research‟
Why is it necessary:
Wide variation in clinical practice
To minimise clinical error
High use of treatments not proven to do more good than harm
Can be extended from medicine to health care
Need to understand new types of evidence: randomised controlled trials (started in 1948), meta-analysis
and systematic reviews
EBM approach is better than traditional continuing medical education (which is largely ineffective).
Clinical knowledge and performance deteriorates over time
Application of evidence:
Generalisability: do trials apply to a whole population
Applying probabilities from a population to an individual
Multiple treatments: trials only test one at a time
Acceptability
Also need to consider economic impact given limited resources
Developing a CAT (Critically Appraised Topic)
Title: Answer to the clinical question that initiated the search
Clinical Scenario: brief summary of the context in which the question arose
The clinical bottom line: a description of the clinical action to be taken as a result of the critical
appraisal
Well Built Question: good for defining pre-test probability and narrowing search strategy
The Patient or problem being addressed in what setting (e.g. In otherwise healthy, non-smoking
adults presenting to a GP with a common cold…)
The intervention being considered (…does a 5 day course of XX ….)
The comparison intervention (where relevant) (…compared with a placebo…)
The clinical outcome of interest (…improve symptomatic control and/or reduce the duration of an
existing common cold)
Search The Evidence: list search terms
Description of study methodology
Table summarising key results
Quantitative take home messages
Notes on validity issues: bias, levels of evidence, research design and methodology, harmful effects of
intervention, etc
References to the articles used in the critical appraisal
Cochrane Collaboration
Aims:
Evidence based
Easily accessed
Clinically useful
Quality controlled
Periodically updates
Prepares, maintains and disseminates systematic reviews.
Systematic reviews are a structured process:
Well formed question
Comprehensive data search (including non-English, unpublished)
Unbiased selection and abstraction process
Critical appraisal of data
Synthesis of data
Width of diamond on Cochrane logo = confidence interval of meta-analysis

Evidence Based Medicine 703
Levels of Evidence
1 – RCT or reviews of them
2 – Cohort studies or reviews of them
3 – Case control studies
4 – Case series or poor quality cohort or case-control studies
5 – Expert Opinion
EBM Glossary
Bias: systematic deviation of study results from true results due to the study design.
Interviewer bias: systematic error due to interviewer‟s gathering of selective data.
Lead time bias: if patients not enrolled at similar point in their illness, differences in outcome may
only reflect differences in duration in illness.
Recall bias: systematic error due to differences in accuracy or completeness of recall. Referral
filter bias – process of referral from primary to secondary proportion of severe cases
unfavourable outcomes.
Selection bias: a bias in study design rather than chance when study and control groups differ in
ways that may affect the outcome
Publication Bias: results from studies with positive results are more likely to be published
Study types:
Case-Control Study: retrospective comparison of exposures of persons with disease and without
disease
Prospective Study: cohorts who have not yet had the outcome event are monitored for the
occurrence of the event
Systematic Review: study in which trials on a topic have been systematically identified, appraised
and summarised according to predetermined criteria. May or may not include a meta-analysis
combining the results of the trials
Clinical Practice Guideline: systematically developed statement to assist decision-making in specific
clinical circumstances
Study Design:
Decision Analysis: application of explicit, quantitative methods to analyse decisions under
conditions of uncertainty
Intention to treat analysis: analyses individuals according to the group to which they were
randomised, even if they didn‟t receive the treatment, rather than confining to those who
completed treatment (treatment may have intolerable side-effects). Better measure of
effectiveness.
N-of-1 trials: blinded patient and doctor undergoes pairs of treatment periods with experimental
and placebo treatment with outcomes monitored
Study Analysis:
Confounding: a variable associated with the factor under investigation. Unless it is possible to
adjust for the confounding variables, their effects cannot be distinguished from those of the factors
being studied
Efficacy: benefit of an intervention under ideal conditions
Efficiency: benefit of intervention, including efficacy and acceptance (e.g. compliance, side effects
– does it do more harm than good)
Precision: the range in which the best estimates of a true value approximate the true value
Statistical power: statistical chance of a study being able to detect a difference if one actually exists
Strength of inference: likelihood that an observed difference represents a real difference, rather
than due to chance. Is weakened by bias and small sample sizes
Validity: results are unbiased and give trust estimate of the measured effect. Extent to which a
variable or intervention measures or accomplishes what it is supposed to. Does it measure what it
claims to measure – described by specificity and sensitivity, etc
Risks and Odds
Outcome
Exposure
Yes
No
Yes
A
B
No
C
D
704 4
th
and 5
th
Year Notes
Event Rate: proportion of patients in a group in whom an event is observed. Applied to Controls and
Experimental groups CER and EER
Relative Risk = (A/(A+B))/(C/(C+D)) = EER/CER
Absolute Risk Reduction (ARR) = C/(C+D) – A/(A+B) = CER - EER
Relative Risk Reduction: percent reduction in events in the treat group event rate compared to the
control group = (CER – EER)/CER * 100 = (C/(C+D) – A/(A+B))/(C/(C+D))
Risk Ratio = EER/CER Odds: ratio of events to non-events
Odds ratio: odds of an experimental patient suffering an adverse event relative to a control patient =
(A/C)/(B/D)
Number needed to treat (NNT): number of patients needing treatment to achieve one favourable
outcome = 1 /ARR – always rounded up to the nearest whole number and accompanied by the 95% CI
Number needed to harm (NNH): number of patients who need to be treated to achieve one adverse
outcome = 1/Absolute Risk Increase (ARI = EER - CER)
RRR and OR do not say anything about absolute risk. An RR of 30% can mean a risk reduction from
60% to 20%, or from 3% to 1%. The ARR and NNT varies dramatically
Time frame: all measures (RR, RRR, ARR, OR) must be qualified by giving them a time frame (e.g.
the length of the period of the study)
Evaluation of History Taking and Clinical Examination
Using an article about history taking or clinical examination
See Using an article about a diagnostic test, page 706
Kappa Statistics
A measure of agreement after chance is removed from consideration
= Actual agreement beyond chance / potential agreement beyond chance:
E.g.. If observed agreement = 78% of cases, and agreement on the basis of chance is 51%, then Kappa
= (78 – 51)/(100 – 51) = 0.55
Kappa Statistic
Degree of Agreement
-1
Perfect disagreement
0
Chance agreement
0 – 0.4
Poor agreement
0.4 – 0.6
Moderate
0.6 – 0.8
Substantial
0.8 – 1.0
Almost perfect
Hard to compare between studies – a different case-mix would yield a different k
A weighted k can be used to measure agreement in ordinal data
For larger samples (> 100) sampling distribution is normal, so it is possible to calculate a standard
error, confidence intervals and P values
Other non-parametric tests (e.g. chi-squared, correlation coefficient) are measures of association not
agreement
Evaluation of Diagnostic Tests
Sensitivity and Specificity
Sensitivity: proportion of people with disease who have a positive test (i.e. true positive). How good is
the test at picking up people who have the condition? SnNout = when a test has a high sensitivity, a
negative result rules out the diagnosis
Specificity: the proportion of people free of a disease who have a negative test (i.e. false positive).
How good is this test at correctly excluding people without the condition? SpPin = When a test is
highly specific, a positive test rules in the diagnosis
Necessary Sensitivity and Specificity depend on setting. E.g. if screening for a disease occurring 1 in
10,000 in a population of 100,000 then a test with sensitivity of 99% and specificity of 99% will find
9.9 true positives and 999.9 false positives. But if the disease occurs 1 in 100 then you‟ll find 9990
true positives and 998 false positives – far better strike rate
Evidence Based Medicine 705
Pre-test Probability
= P (D+) = probability of target disorder before a diagnostic test result is known. Depends on patient
(history and risk factors), setting (e.g. GP, A&E, etc) and signs/symptoms
Is useful for:
Deciding whether to test at all (testing threshold)
Selecting diagnostic tests
Interpreting tests
Choosing whether to start treatment without further tests (treatment threshold) of while awaiting
further tests
Based on epidemiology (e.g. prevalence) or clinical experience
Likelihood Ratio
Positive Likelihood Ratio = the likelihood that a positive test result would be expected in a patient with
the target disorder compared to the likelihood that the same result would be expected in a patient
without the target disorder
Negative Likelihood Ratio = same but for negative result
Less likely than sensitivity and specificity to change with the prevalence of a disorder
Can be calculated for several levels of the symptom or test
Can be used to calculate post-test odds if pre-test odds and LR known
Impact of LR:
< 0.1 or > 10: large changes in disease likelihood (i.e. large change to pre-test probability)
0.2 – 0.5 or 2 – 5: small changes in disease likelihood
1: no change at all
Post-test Probability
= Proportion of patients with a positive test result who have the target disorder
Positive Predictive Value (+PV): proportion of people with a positive test who have disease. If the
person tests positive, what is the probability that s/he has the disease? Determined by sensitivity and
specificity, AND by the prevalence of the condition
Predictive value of test depends on sensitivity and specificity AND on prevalence. E.g., for a test with
99% sensitivity:
Prevalence
Positive Predictive Value
1
19
2
33
5
56
10
73
20
86
So significance of test may vary between, say, hospital and GP
Formulas
Diseased
Normal
Test
+ive
a
b
-ive
c
d
Sensitivity = a/(a+c)
Specificity = d/(b+d)
LR + = sensitivity /(1-specificity)
LR - = (1-sensitivity)/specificity
Positive Predictive Value = a/(a+b)
Negative Predictive Value = d/(c+d)
Prevalence = (a+c)/(a+b+c+d)
Pre-test odds = prevalence /(1-prevalance)
Post-test odds = pre-test odds * LR
Post-test probability = post-test odds/(post-test odds+1)
Accuracy = (a+d)/(a+b+c+d) = what proportion of results have given the correct result
706 4
th
and 5
th
Year Notes
Study design for researching a test
Spectrum composition: what population was it tested on. Sensitivity and specificity may vary between
populations with significant disease and the general population
Are pertinent subgroups assessed separately? Condition for test use must be narrowly defined to avoid
heterogeneity
Avoidance of work-up bias: if there is bias in who is referred for the gold standard. All subjects given
a test should receive either the gold standard test or be verified by follow-up
Avoidance of Review Bias: is there objectivity in interpretation of results (e.g. blinding)
Precision: are confidence intervals quoted?
Should report all positive, negative and indeterminate results and say whether indeterminate ones
where included in accuracy calculations
Test reproducibility: is this tested in tests requiring interpretation
Using an article about a diagnostic test
Is the evidence about the accuracy of a diagnostic test valid?
Was there an independent, blind comparison with a reference standard?
Did the patient sample include an appropriate spectrum of patients to whom the diagnostic test will
be applied in clinical practice
Did the results of the test being evaluated influence the decision to perform the reference standard?
Were the methods for performing the test described in sufficient detail to permit replication?
Does the evidence show the test can accurately distinguish between those who do and don‟t have the
disorder? Are the likelihood ratios for the test results presented or data necessary for their calculation
provided?
Can I apply this test to a specific patient?
Will the reproducibility of the test and its interpretation be available, affordable, accurate and
precise in my setting? Is interpretation of the test tested on people with my skill level?
Can I generate a sensible estimate of the patient‟s pre-test probability?
Are the results applicable to my patient? (e.g. do they have the same disease severity)
Will the results change my management?
Will the patients be better off as a result of the test? An accurate test is very valuable if the target
disorder is dangerous if undiagnosed, has acceptable risks and effective treatment exists
Bayesian Theory
Combining information from history, exam and investigations to determine overall likelihood
Puts test results in context
Use as part of decision analysis to determine the level at which the probability of disease is sufficiently
low to withhold treatment or further tests, or sufficiently high to start treatment. In between, do further
tests to raise or lower probability
Balance between: severity of illness, efficiency, complications of test and treatment, and properties of
the test
Evaluation of Therapy
Assessment of an article about Therapy
Are the results of the study valid?
Was the assignment of patients to treatments randomised?
Was follow-up complete? (Non-follow-ups may have died, etc bias)
Were patients analysed in the groups to which they were randomised?
Were patients and researchers „blind‟ to the treatment
Were the groups similar at the start of the trial
Other than the intervention, were the groups treated equally?
What were the results?
How large was the treatment effect? RR, RRR, ARR
How precise was the estimate of the treatment effect? Point estimate & Confidence intervals.
What is the P value?
Will the results help me in caring for my patients?
Can the results be applied to my patient care?
Evidence Based Medicine 707
Were all clinically important outcomes considered: were the outcomes relevant for the patient? Or
was only a benefit to intermediate outcomes considered?
Do treatment benefits out-weight harms and costs? ARR and NNT/NNH
Evaluation of Prognosis
Glossary
Prognosis: the possible outcomes of a disease or condition and the likelihood that each one will occur.
How to estimate your patient‟s likely clinical course over time, or anticipate likely complications of the
disorder
Prognostic factor: characteristics associated strongly enough with a condition‟s outcome to predict
accurately the development of these outcomes. E.g. demographic (e.g. age), disease specific (e.g.
tumour stage), or co-morbidity (e.g. other conditions present)
Prognostic results are the number of events occurring over time, expressed in absolute terms (e.g. 5
year survival rate), relative terms, or survival curves
Risk factor: patient characteristics associated with an increased probability of developing a disease in
the first place. Neither prognostic or risk factors imply a cause and effect relationship
Using an article about prognosis
Are the results of the study valid?
Was there a representative and well-defined sample of patients at a similar point in the course of
the disease? (ideally at its onset). Is the disease clearly defined (what are the inclusion/exclusion
criteria)? Is the sample representative of the whole spectrum of disease? Sources of bias: e.g.
selection bias (referrer bias) or lead-time bias
Was follow-up sufficiently long and complete (what were the potential characteristics of those lost
to follow-up?
Were objective and unbiased outcome criteria used? Were the investigators blind?
Was there adjustment for important prognostic factors? Were subgroups with different prognoses
stratified?
What are the results?
How large is the likelihood of the outcome event(s) in a specified period of time
How precise are the estimates of likelihood? Precision best expressed in confidence intervals
Will the results help me in caring for my patients?
Were study patients similar to my own?
Will the results lead directly to selecting or avoiding therapy?
Are the results useful for reassuring or counselling patients?
708 4
th
and 5
th
Year Notes

Professional Development 709
Professional Development
Professional Boundaries ........................... 710
Recognising and Respecting Differences . 710
Working in Teams .................................... 710
Physical Hazards of Medicine .................. 710
Medical Crises .......................................... 711
The Doctor‟s Health ................................. 711
Code of Health and Disability Services
Consumer‟s Rights .............................. 712
Medical Error and Misadventure .............. 712
Medical Council ....................................... 712
Certification of Death ............................... 712
Coroner ..................................................... 713
Protection of Personal and Property
Rights Act (1988) ................................ 713
710 4
th
and 5
th
Year Notes
Professional Boundaries
Defines proper/improper behaviour in a professional relationship
Types of boundaries:
Physical
Emotional: strengthened by right to say yes/no, respect, weakened by ridicule, belittling,
judgementalism
Sexual: serve to protect most sensitive part of us
Differences from personal boundaries: Paid for, time limited, power more imbalanced, greater
responsibility for maintaining relationship, requires knowledge and training
Sources of power:
Personal power: size, gender, age, strength, skills, intellect, charisma, money, weapons
Position power: role, job, money, legal status
Recognising and Respecting Differences
Sometimes differences obvious, sometimes subtle
Can lead to misunderstanding, poor compliance
Avoiding recognition of differences is a way of preventing challenge to our world view
Working in Teams
7 components of teams that need to be functioning for the team to work:
Raison d‟etre: clear idea of what the team is therefore
Rules: each person needs to know them
Roles: same person often adopts the same role in different teams
Relationships
Rituals: joining and farewell rituals, birthdays, etc
Rewards
Results: do you achieve your raison d‟etre
Developmental cycle:
Forming:
Becoming acquainted: polite, impersonal, hierarchical
Trial and error: pairing, turf guarding, role conflict, ambiguity (still working as individuals)
Storming:
Collective indecision: covert anger, decision by default, poor morale, no
accountability/leadership
Crisis: open anger, recognition of conflict, leadership assumed
Maintenance: commitment to team work
Performing: management of conflict, sharing information, tolerance or ambiguity/difference,
flexibility, breaking down of inter-professional rivalries
Power in groups:
Always ask „who holds the power‟
Positional (assigned from outside the group), assigned, knowledge, personal, factional
Group processes:
Problem solving
Decision making: who, when, how, what
Conflict management:
Competing: It‟s win/loose and I‟m going to win
Accommodating: I don‟t mind loosing
Avoiding
Compromising
Collaborating
Physical Hazards of Medicine
Hospital hazards:
Biological (infection control):
Blood and body fluid exposure (e.g. risk of seroconversion following needle stick HBV 30%,
HCV 3%, HIV 0.3%)
Tb (high prevalence high index of suspicion, wear face mask in high risk situations, ensure
contact tracing)
Professional Development 711
Meningitis (spread via respiratory secretions, need close contact, wear mask)
MRSA (spread via direct contact, could be almost totally managed by hand-washing).
Manage via vaccination, possible prophylaxis
First aid after exposure (needle stick, splash, spill, bite): rinse affected area under running
warm water for at least 3 minutes, squeeze a puncture wound gently, paint with povidone-
iodine or isopropyl alcohol
Chemical (drugs, latex, hand washing hand dermatitis: usually irritant dermatitis not allergic
dermatitis dose dependent)
Ergonomics (patient handling, keyboards)
Physical (lasers, radiation, heat, noise)
Stressors (shift work, overload – usually insidious)
Behaviour:
Knowledge doesn‟t change behaviour
Consider own and patient safety
Hazard vs. risk vs. perceived risk
Medical Crises
Need to:
Understand and manage our reactions to critical medical incidents
Learn methods of debriefing
Maintain confidentiality when managing reactions to unusual events
A crisis can be:
Death of a patient: especially if similar age or if relationship has developed
Patient complaints, medico-legal action
Blaming yourself for bad outcomes
Responses can be depression, anger, physical illness, use of alcohol or self medicated drugs, isolation,
suicide
Coping strategies:
Accept that it is normal to be stressed by stressful events
Develop an active interest in details of the crisis (eg read up)
Be open about your feelings, don‟t say you‟re fine
Actively pursue social support, leisure pursuits
If medico-legal action, keep close contact with your lawyer and as much contact with the patient as
the patient desires
Watch out for avoidance behaviours (dropping out, sick days) or intrusive re-experiencing (eg
nightmares) –usually indicates need for help
Talk to counsellor, GP, colleagues, mentor – not to family or non-medical friends
The Doctor’s Health
Stress = Marked discrepancy between perceived demands and perceived ability to respond
Burnout = set of symptoms leading to a debilitating psychological condition usually associated with:
Chronic stress
Emotional exhaustion
Depersonalisation
Reduced personal accomplishment
Development of negative and callous attitudes about the people one works with
Negative self worth
Result of a prolonged period of trying to cope with demanding stressors
Medical Practitioners Act: Must notify the Medical Council if you consider a colleague‟s health is
affecting his or her competence
Doctor is unfit to practice if: unable to make safe judgements, demonstrate reasonable skill, behaves
inappropriately, risks infecting patients, etc
Medicine has many stresses: business demands, patient expectations, difficult patients, mistakes,
rosters tiredness, litigation, time for family
On population estimates, there should be 200 – 300 medical practitioners who are alcoholic – only
about 50 are being treated
There are many barriers to seeking help: admitting to illness, financial consequences, not wanting to be
seen as inadequate, isolation
712 4
th
and 5
th
Year Notes
Prevention is key: good health habits (especially in hard times), avoid self-treatment – have your own
GP, formal and informal peer support, develop interests outside medicine, seek help early
Resources to help:
Doctor‟s Health Advisory Service (DHAS): partly funded by the medical council
In Sickness and In Health: a handbook for medical practitioners
Code of Health and Disability Services Consumer’s Rights
Right 1: Right to be treated with respect (incl. privacy respected and right to services that respect their
needs/culture/religion)
Right 2: Right to freedom from discrimination, coercion, harassment and exploitation
Right 3: Right to dignity and independence
Right 4: Right to services of an appropriate standard (incl. co-operation among providers)
Right 5: Right to effective communication (incl. right environment and interpreter if necessary)
Right 6: Right to be fully informed
Right 7: Right to make an informed choice and give informed consent
Right 8: Right to support (ie to have support people present if at all possible)
Right 9: Rights in respect of teaching or research – all other rights extend to when patient is
participating in research or teaching
Right 10: Right to complain
Provider compliance:
A provider is not in breach of this code if they have taken reasonable actions in the circumstances
to comply with duties in the code
The onus is on the provider to prove that it took reasonable actions
Relevant circumstances includes consumer‟s clinical situation and the provider‟s resource
constraints
Medical Error and Misadventure
Medical mishap = treatment was properly given but suffered a rare side-effect (<1% occurrence) and
was severe (ACC definition is in hospital for at least 14 days, in capacitated for 28 or died)
Medical error = Person treating you did not provide treatment of a reasonable standard.
Medical misadventure = mishap + error
Negligence:
Do you owe a duty of care
Did you fail in that duty (according to standard of a reasonable practitioner)
In failing, did the person suffer as a consequence
Court decides whether error is negligence
Types of censure:
From Health and Disability Commissioner (mediate, refer to professional body, referral to their
director of proceedings)
From Medical Council (censure, practice restrictions, struck off, fines)
Criminal charges – eg Manslaughter – only if „major departure‟ from accepted practice (1997
Crimes Act amendment)
Medical Council
Protects public by determining competence of and registering doctors
To be registered must have: acceptable degree, competent in English, no convictions with a possible
prison term > 3 months, be mentally and physically fit and not subject to disciplinary proceedings
Types of registration include: probationary, general, vocational
Council can review or monitor competence or „fitness to practice‟
Also has disciplinary process
Council consists of 4 doctors elected by doctors, 4 people appointed by the Minister, 1 Ministry of
Health and 1 Med School Dean.
Certification of Death
Confirm identity of patient
Signs of death:
No circulation: no carotid pulse or heart sounds over 1 – 3 minutes
Absent respiration: no movement or fogging of a mirror
Unreactive pupils

Professional Development 713
„Railroading' of retinal blood vessels – rows of RBCs settling out
Absence of pattern on EEC or ECG
Signs of brain death (ie on respirator)
Fixed dilated pupils
No corneal reflex
No tracheal reflex (ie tug on ET tube)
No eye movements on putting cold water in ear
No Cranial nerve response to pain (eg supra-orbital pressure)
No respiratory response to hypercapnea
Problems when deeply unconscious: near drowning, hypothermia, epilepsy, drugs (eg barbiturate
poisoning)
Suspicious injuries on a dead person: bruise, abrasion, laceration, incised wounds (suicide look for
tentative cuts, assault look for defence injuries), stab wounds (go deeper than the length of the blade,
always check), pattern wounds
Person certifying death should have no conflict of interest
Death Certificate:
If you‟ve attended a patient must issue a certificate or report to the coroner, if you are „available‟
Are now able to sign for eg GP partner if you‟ve reviewed notes and seen body
Different form for infants over 20 weeks gestation or > 400 gm and < 28 days old. Can be filled in
by midwife
Other forms:
Need an additional form before cremation, which is then cleared by the Medical Referee
Certificate of Life Extinct: police form to say the person is dead – eg if being referred to the
Coroner. Does not include cause of death. Always take your own careful notes
Changes following death:
Rigidity – „rigor mortis‟. Linking of actin and myacin fibres following ATP depletion. Lasts from
6 – 8 hours after death to about 36 hours.
Lividity – bloods seeps downwards – red congestion on downside of body
Temperature – indicator of time elapsed since death. Depends on temperature at death, BMI,
clothing, etc
Decomposition
Rough guide to time of death:
Warm
Flaccid
< 3 hours
Warm
Stiff
3 – 8 hours
Cold
Stiff
8 – 36 hours
Cold
Flaccid
> 36 hours
Homicide:
= Killing another, either directly or indirectly, or by accelerating death
Murder = intent to kill or cause serious injury or to facilitate another crime
Infanticide = death of child under 10 by a mother who has given birth or lactating
Can be hard to distinguish murder from suicide or accident in MVA, fire, drowning, or cot death
Coroner
Has the status of a district court judge
To initiate a coroners case, report the death to the police (who act as the coroner‟s investigating agents)
Must refer a death to the coroner if:
No known cause, suicide, unnatural or violent
No certificate issued
Died undergoing medical, surgical or dental procedure
Detained under A&D Act, committed or in prison
Child in CYPS or foster care
Coroner can order an autopsy and/or hold an inquest
Other court settings: District or High court
Expert witness can give an opinion, ordinary witness can only recount facts
Don‟t take sides, be fair, stick to what you know, use notes taken on the occasion (with the
permission of the judge)
Protection of Personal and Property Rights Act (1988)
= PPPR Act
714 4
th
and 5
th
Year Notes
Designed originally with intellectual handicap in mind. In acute or geriatric care, used mainly in cases
of dementia
Two underlying principles:
A person is competent until proven otherwise. Acts asserts right to autonomy, to refuse treatment
and to manage their own affairs
Any order imposed shall be the least restrictive alternative. Encourages self-reliance,
normalisation and community integration
The judge has three decisions to make:
Determine jurisdiction
Determine whether an order needs to be made
Determine the type of order:
Enduring power of attorney (normally Powers of Attorney expire if the person becomes
incompetent)
Welfare Guardian order (wholly lost capacity)
Property Manager order (wholly or partially lost capacity)
Personal order (wholly or partially lost capacity)
5 questions to assessing competency:
Does the person appreciate their situation
Can they understand the options that address their situation
Are they aware of the pros and cons of their choice
DO they express their choice clearly
Is their choice influenced by a distorted mind
6 stages in an application:
Consider clinical strategies
Assess competency
Complete application forms and a medical report
File application at family court
Family court appoints counsel
Pre-hearing conference, may lead to a full hearing

Ethics 715
Ethics
Ethical Principles ...................................... 716
Morality and Standpoints .......................... 716
Two Classes of Moral Theory .................. 716
Confidentiality .......................................... 716
Consent ..................................................... 717
Compulsion............................................... 718
Refusal of Treatment ................................ 719
End of life issues....................................... 719
Ethical Issues in Dealing with Impaired
or Incompetent Colleagues.................. 721
Professional Ethics ................................... 721
Tissue Donation ........................................ 722
Assisted Human Reproduction ................. 722
Innovative Treatment ................................ 723
Research Ethics ........................................ 723
716 4
th
and 5
th
Year Notes
Ethical Principles
Beneficence: acting in a way that benefits the patient
Paternalism: Substituting the doctor‟s judgement for that of the patient. The patient‟s autonomy is
over-ridden. If the patient is not autonomous there is no paternalism. Can be justified or unjustified
Non-maleficence: minimising harm. Harms should be outweighed by benefits
Justice: fairness – all members of society share in its benefits and burdens
Autonomy: ability to make one‟s own decisions. Exercising autonomy requires intellectual and
emotional competence and the opportunity for action
Dignity: preserving self respect, treating as a means not an end
Truthfulness: central or absolute?
Futility: endeavours that are doomed to failure. Depends on what the goal is
Morality and Standpoints
Standpoints: law, religious belief, social conventions, morality – all give standpoints from which can
define right and wrong – and they may disagree
The scope of morality:
Self-imposed from within (cf. law – imposed form without)
Prescriptive: guides my action
Has universal character (moral principles don‟t always apply to everyone – but demand
consistency in judgements)
But these things don‟t demarcate morality from other standpoints
Bernard Gert: morality is a public system applying to all rational persons governing behaviour which
affects others and which has the minimisation of evil as its end. I.e. it is an „invention‟ for improving
the human condition
4 competing concepts of ethics:
General principles impinging on human well-being
Principles providing a practical antidote to certain types of behaviour (e.g. those which exhibit
limited sympathies) which impact on human well-being
Principles guiding the behaviour of a particular professional group (which makes a distinctive
contribution to he human good)
Principles focusing on a particular dimension of human well being
Two Classes of Moral Theory
Deontological: right/wrong due an essential feature of the behaviour – intrinsic
Excludes relevance of consequences
How do you work out what duties are – have to explain it in terms of intrinsic qualities
Kant is a prominent theorist: the principle (e.g. value of human life) embodied in an action makes
an action a duty. End never justifies the means
Teleological: right/wrong depending on whether it‟s a means to a good or a bad end – instrumental
Largest group is consequentialists of which utilitarianism is the most popular flavour
Utilitarianism: judge consequences by the greatest good for the greatest number
Must know consequences before you can judge it right or wrong
Is it limited to human happiness (what about animals)
Both theories say liberty is important – but for different reasons
Confidentiality
Hippocratic Oath: “Whatsoever things I see or hear concerning the life of men, in my attendance on the
sick or even apart there from, which ought not to be noticed abroad, I will keep silence thereon,
counting such things to be as sacred secrets”
NZMA code of ethics:
Protects patients secrets even after death
Maintain confidence unless patient consents or required by law
Benefits:
Access to information for the patient‟s benefit
Autonomy: patient control over information about them, respect for patient‟s choice
Dignity
Consequences: positive reinforcement of trust
Ethics 717
Legal requirements:
Health Information Privacy Code
Rule 10 (1): information obtained for one purpose cannot use that information for any other
purpose
Rule 11(1): An agency must not disclose information unless…
Code of Health and Disability Service Consumer‟s Rights: Every consumer has the right to have
his or her privacy respected
Legal exceptions:
With patient‟s consent
Within the team of doctors caring for the patient. Not disclosed to students unless anonymised
Statutory e.g. Notifiable diseases, Land Transport Safety Authority (Driver‟s licence)
Disclosure in the public interest: Health Information Privacy Code allows disclose to prevent a
„serious and imminent threat‟
Common Law: e.g. Tarasoff v Regents of the University of California case, Duncan v Medical
Practitioners‟ Disciplinary Committee
Special cases:
Children: does the child have the understanding and maturity to form a relationship of confidence
Incompetent adults: duty of confidentiality remains. The Health Information Privacy Code allows
a representative of the patient to authorise disclosure
The dead: Patient‟s representative must authorise disclosure of information.
Collection of health information discusses (Privacy code?):
Purpose e.g. necessary for a lawful purpose
Source: usually individual concerned
Collection: reasonable steps to ensure individuals aware of purposes, recipients and rights of
access & correction
Manner: e.g. overly intrusive
Storage and security
Rights of access
Right for correction
Reasonable steps to ensure accuracy
Retention: not kept longer than required
Use limited to purpose for which it was collected
Limits on disclosure – breaching confidentiality:
Necessary to prevent/lessen serious and imminent threat to life/safety
Disclosure will lessen or prevent risk
Minimal information released compatible with preventing harm
Patient must be identified to reduce this risk
There is no better alternative
Recipient of the information can do something about it
Consent
Function: to uphold and enhance the patient‟s autonomy – the right to think and act without coercion
Code of HDS right 7: to make an informed choice and give informed consent except where any
enactment of common law provides otherwise… (The code treats adults and children the same)
Consent is a process of communication, openly gives information, honestly answers questions, in a
setting and manner that the patient can understand
Autonomy:
Requires the ability to form beliefs, make decisions, form preferences, form practical intent
Problems when these are completely or incompletely lacking, fluctuating, manifestly irrational
= A set of practical skills through which we make and act on decisions which accord with our own
values
We should respect autonomy as this gives superior outcomes and because of underlying
assumption that individual is best judge of his/her own good
Requirements for consent:
Competence (ie autonomy)
Provision of information
Information is understood
Voluntary. Patient has control over the decision – ie lack of negative consequences, accustomed to
obeying authority figures, feeling threatening by someone
718 4
th
and 5
th
Year Notes
Individual must be able to understand that:
They have a choice (no coercion)
Why they are being offered treatment
What is involved
Probably benefits, risks, side effects, failure rates
Alternatives
When you can‟t get consent:
Children lack legal capability to consent until 16. If patient under 16 doesn‟t want parents to know
can‟t tell them.
If the are mentally or physically incapacitated
Can NOT use implied consent if the patient is incompetent – need consent of guardian, etc. But
must treat in an emergency
Presumption of competence: assumed competent until demonstrated otherwise (including children)
Varies with complexity of condition and treatment
Ask the patient! Do they understand why treatment is needed, what is involved, benefits, risks and
alternatives
Children:
Issue is not whether to get consent – but how
Inconsistency about when they are autonomous:
Guardianship Act: 16
Common Law (Gillick case 1985) and H&D code: Capacity to make decision
Exceptions to age limits and parental consent
Emergencies
Blood transfusion when life saving (if under 20 years)
Compulsory treatment (eg Mental health Act, Tb)
Blood alcohol
Abortion and contraception (CSA Act 1977): at any age, and no requirement to inform parents
Child Abuse examination (CYFS Act 1989)
When Guardianship invested in the Court or DG of Social Welfare
Good practice to involve the parents wherever possible
Consent and the UN Convention on the Rights of the Child
The best interests of the child are paramount (article 3)
Have the right to express their views and have them taken into account (article 12)
Privacy and Confidentiality (article 16)
Accessibility of information (article 17)
Conflict over consent:
Maori issues: greater expression of autonomy collectively, and collective responsibility for
Tamariki. Involve whanau
If a child says no – it‟s usually because they are frightened. Take a child‟s views seriously.
Reduce fear by ensuring understanding. But best interests may be in conflict with their wishes
If parents say no, consider reasonable alternatives and legal (last option). CYPS Act, sections
14 & 67 – child in need of protection. Guardianship Act 1968 may place child under
guardianship of the court
Allow time to work it through, plan ahead
Avoid rushing important decisions
Give information, check it is understood, opportunity to ask questions
Enlist supports, Maori/PI staff, translator, etc
Consent in Research:
Dates from Nuremberg trials Declaration of Helsinki
Underlying principle: Concern for patient must be greater than the concern for science
Patient has same right to informed consent as with treatment
Compulsion
Reasons for over-riding autonomy:
Autonomy is lacking: individual is no longer the best judge of his/her own good
Public well-being takes priority: autonomy present but over-ridden – well-being of others takes
priority
Ethics 719
Paternalism: autonomy present (perhaps diminished) – prioritising the doctor‟s view of the
patient‟s good over that of the patient
Current legislation:
TB Act 1948: compulsory treatment
Health Act 1956: compulsory treatment of some infectious diseases
Alcohol and Drug Act 1966
Guardianship Act 1968: Dr can apply to make a child a ward of the court
CYPF Act 1989: some services parents can‟t refuse for their kids
Criminal Investigations Act 1995 and Land Transport Act 1998: compulsory taking of DNA/blood
alcohol samples
Mental Health Act (Compulsory Assessment & Treatment Act) 1992 (See Compulsory Treatment,
page 458)
Refusal of Treatment
Refusing Consent:
Adults may refuse medical treatment even if it results in the person‟s injury or death (Section 11,
Bill of Rights)
A pregnant woman may refuse treatment even if that jeopardises the life of her unborn baby
Not clear whether a competent child (under 20) can refuse treatment
Parents may refuse on behalf of children, except where refusal endangers the life of the child.
Parent‟s right to practice religion etc does not extend to placing their child‟s health at risk
Issues to consider:
Competence: are they „autonomous‟. Normal presumption is that they are, unless clear evidence to
the contrary. Is the condition affecting their judgment? You can only have „justified paternalism‟
where the person is autonomous. You are not being paternalistic where patient in incompetent.
The higher the level of risk, the greater need for evidence of competence (not just competence per
se, but evidence of competence)
Informed consent: requires a competent person to voluntarily make a decision, who understands all
the relevant information, including the doctor‟s recommendation.
Prognosis: if advanced terminal illness then this is different to where recovery is likely
Is the patient absent from coercion
Irreversibility of a decision not to intervene vs. reversibility of decision to intervene. Given this
asymmetry, strong bias to intervention.
Weighing families wishes against patients
Loss of liberty and prolongation of misery if you intervene
When is paternalism justified:
If intervention will probably prevent significant harm
Where benefits outweigh risks
Where the least autonomy restricting option that ensures the benefit is adopted
Refusal of treatment on grounds of religious belief:
They still want treatment
Danger in accepting refusal to accept treatment at face value
Ensure understanding („Why do you think this? Do you realise you are going to die without it?‟)
Ensure authenticity of beliefs (do they say they JW to avoid blood products they think are
contaminated)
Identify acceptable treatment options
Consequences of treating without consent:
Battery/assault
Breach of the patient‟s rights under the Bill of Rights/Code
Negligence
Disciplinary action
End of life issues
Euthanasia
Euthanasia:
= Killing someone where, because of his or her distressing physical or mental state, this is thought
to be in the person‟s own best interests
Voluntary euthanasia: killing a competent person, when that person requests it
720 4
th
and 5
th
Year Notes
Non-voluntary euthanasia: assumed to be in the person‟s best interests – but they are not competent
(eg babies, unconscious, mental incapacity)
Involuntary euthanasia: against the person‟s will
Arguments for euthanasia:
Autonomy and the right to die
Gives the person the choice to avoid pain and distress, loss of dignity, etc
Arguments against:
Hazards of voluntary euthanasia in practice: fluctuating views, pressure from family
Life belongs to God
Intrinsic value of life
Legal position is clear: doing anything to bring about death is murder, regardless of motive
Doctor Assisted Suicide
If doctor gives the patient the means (eg leaves pills by the bed) then they have committed the offence
of aiding and abetting suicide, punishable by up to 14 years imprisonment under s 179 of the Crimes
Act
Different from euthanasia as:
Doctor may not approve, but may respect the patient‟s choice
Clearer that the patient is making their own decision without coercion
Reasons why doctors should be involved:
For:
They understand the medical condition (ie know the prognosis)
They are not an interested party (unlike families)
They know the best way of helping
Against:
They have a duty to preserve life
It might undermine confidence in the medical profession
Doctrine Of Double Effect
It is wrong to perform a bad act even if there are good consequences
It may be possible to do a good act, even if there may be bad consequences (eg giving pain relief
knowing that it may hasten death)
If the consequence is virtually certain, then it is considered „intended‟ even if it wasn‟t the primary
reason
Acts and Omissions
Legally there is a distinction between doctors not doing something (ie failing to provide treatment) and
doing something (ie giving a lethal injection). However, if the person has a legal obligation to act (eg a
doctor), failing to do so may be culpable
Doctors have a duty to provide the necessities of life to those under their care. Failing to do so is an
offence under s151 of the Crimes Act. Considering medical treatment is not indicated, or that it is not
in the patient‟s best interests, is a lawful excuse
Ethically, omission is generally less bad than acts of commission
Withdrawal of life-sustaining treatment
Is the patient competent – if so, the decision is the patient‟s. They have the right to refuse medical
treatment under the bill of rights
Incompetent patients:
Any advance directive?
Anyone authorised to make the decision on the patient‟s behalf (a guardian under the PPPR act or a
formally appointed attorney). Patient‟s next of kin are not entitled to consent on a patient‟s behalf
Decisions about whether treatment serves no therapeutic purpose are a medical decision (although
see section 7(4) of code or rights re informed consent). There is no duty to continue with life-
sustaining treatment where there is no prospect of recovery or any quality of life
Should discuss with family
Discuss with colleagues (safety in numbers)
Cause of death will be the underlying cause, not the withdrawal of treatment
Withdrawal will be treated as an omission, not an act. Courts have ruled there is no difference between
turning the ventilator off and not turning it on to start with
Ethics 721
Rules of thumb:
Intention is always to act in the patient‟s best interests
Err on the side of caution. Always get a second opinion. If in doubt, seek a court judgement
Advance Directives
Every competent patient has the right to refuse treatment, even if this leads to his or her death. This
includes the right to leave clear instructions in case they may be incompetent in the future an
advance directive. Recognised in the Bill of Rights
A directive is valid if:
The patient was competent at the time is was made
They were free from undue influence
They were sufficiently informed
They intend their directive to apply to circumstances which subsequently arise
These conditions should be tested at the point where a directive is applied
Ethical Issues in Dealing with Impaired or Incompetent Colleagues
Summary:
Collective responsibility as important as individual
Maintenance of public trust vital
Better team work and error reporting will help
Self regulation: use it or loose it
Issues:
Trust of patients in doctors: patients in vulnerable position
Beneficence
Legal requirement to report impaired or incompetent doctor
Collective responsibility: to patient population as a whole
Uncertainty: may explain but not excuse failure to act
Professional etiquette (often disguised as „clinical freedom‟) – not wanting to interfere in other‟s
livelihoods
Loyalty to the group: key to cooperation but should be overridden by maleficence
Pattern of error not a single mistake is indicative of incompetence
Criteria for whistle-blowing:
Evidence of severe harm
Good chance of reducing harm
All other avenues explored
Ethical institutions
Encourage reporting of error (ie about safety not culpability)
Mechanisms for self/peer assessment
Internal complaints mechanisms (with protection)
Guard against malicious complaints
Culture within a group:
Less competent influencing each other
Professional isolation (big risk factor for incompetence)
Hard to pin down doctors because:
Lack of benchmarking (little medical practice has been validated)
Clinical freedom
„Half of all doctors are below average‟
The learning curve: period of necessary and acute incompetence
Informed consent: what is it reasonable for patients to know about their doctors (eg individual success
rates) vs. doctors right to privacy
Professional Ethics
Characteristics of a profession: an important service, monopoly, self regulating, extensive training with
intellectual component, autonomy in work
Professional ethics:
Ethics and values in roles and conduct of professionals
Aspirational and regulatory component
Ethics should reflect common social values: freedom, protection, equality, privacy, etc
722 4
th
and 5
th
Year Notes
Obligations to patients:
Previously paternalism
Then contractual model (but didn‟t acknowledge power imbalance)
Fiduciary model – built on trust – Doctor makes a recommendation, patient has informed consent
Values:
Honesty – eg conflict of interest
Competence
Diligence – give sufficient time and effort to the patient
Loyalty and objectivity
Fairness
Discretion
Professionals as employees: issues around obligation to obey vs autonomy, whistle blowing,
strikes
Economic issues: fee splitting (eg taking a cut out of a referral), accepting gifts, limits on advertising
Professional self-regulation: admitting, setting and applying norms
Tissue Donation
Problems of supply:
Fair distribution (resource allocation)
Dead bodies:
When are they dead (brain death criteria, PVS, anencephalic infants)
Who gives consent, family distress vs need for a quick decision
Should there be a presumption of donation (with right of opt out) – small constraint on
freedom outweighed by significant benefit?
Live bodies:
Increased supply
Operative and consequent risks for donor
Consent (especially if donor is a child or non-competent adult)
Donor/recipient relationship as source of pressure
Buying and selling:
Increase supply
Objections: Consent (free and informed?), exploitation, degradation, misinformation
Fetal tissue:
Increases supply
Fewer rejection problems
Sourced from abortion
„Surplus‟ embryos
Animal Tissue
Regulation:
Health Act 1956 controls donation and prohibits profit making
Human Tissue Act 1964 regulates organ removal after death – mixed opting in/opting out
arrangement
Living Donors: common law – unlawful to remove a body part if not therapeutic for the donor
[Blood is covered by the Health Act)
Assisted Human Reproduction
3 types:
Couples using their own genetic material
Techniques using other people‟s genetic material
Techniques using another women‟s womb (surrogacy)
Current issues:
Surrogacy – non-commercial IVF
Posthumous use of sperm (creation of fatherless families)
Should women have access to IVF if they already have children (eg following tube reversal) – is
there a fair innings?
Intergenerational gamete donation (assisted incest!)
Pre-implantation genetic diagnosis (PGD)
To what extent should families be free to make their own choices
Ethics 723
The significance of life
Does PGD devalue affected individuals
What is the meaning of disability
Who will have access to these diagnostic techniques
Ethical issues:
Human dignity, the value of life and what it is to be human
Autonomy
Procreative liberty vs the role of the state (reflecting the welfare of society)
Informed consent – eg pressure on surrogate mums
Beneficence:
Who benefits
What are the best interested of the child not yet conceived. They should be an end in
themselves, not a means to someone else‟s end
Non-maleficence (do no harm)
Commodification of children
Incrementalism – the „slippery slope‟
Unknown/possible harms – Intra-cytoplasmic sperm injection has become common without
any long term trials looking for any effects on kids
Justice
Fair access to AHR procedures
Prioritisation of need and benefit
Infertility vs social reasons (eg post vasectomy, freezing eggs till after you‟ve had a career,
etc)
Innovative Treatment
Ethics committees must review research and innovative treatments
The difference:
Research is for the benefit of society and future patients
Treatment is for the benefit of the patient
Innovative practice sites between these
Defn: Innovative treatment is those procedures which are new to a particular provider setting in NZ, or
which are being used for a new purpose (Has often been harmful, at a minimum it introduces greater or
new risk of harm)
3 issues:
Proving they are safe and effective. Issues here vary – if it is an established technique overseas the
issue is whether the NZ practitioners are and will remain competent. If it‟s entirely new, is it safe?
Etc. Proving safety is difficult in surgical procedures – the surgeon is gaining skill, case
comparison is complicated, random allocation may be unethical. Safety should be established
early on. Effectiveness should be assessed in a way that gives good statistical evidence
Gaining informed consent to non-standard treatment
Defining what constitutes an innovative procedure
Research Ethics
Codes:
Nuremberg code:
Informed consent of subjects, and liberty to withdraw
Benefits to society (can‟t be got by other means)
Avoid unnecessary suffering and injury
Degree of risk not greater than potential benefit of problem to be solved
Only conducted by scientifically qualified persons
Declaration of Helsinki: 1964, revised 1975. Main difference: required to be supervised by
medically qualified person
Experiments on people that won‟t benefit current patients
If study not sound then won‟t answer questions risk not worth it and waste of resources
Informed consent by participants
Ensure study remains ethical in progress „stop‟ criteria and monitoring of interim results
„Therapeutic Research‟ a misnomer (although used in Declaration of Helsinki). In research, if the
patient happens to benefit that‟s coincidental. Research subject gives up normal expectation of
tailored treatment.
724 4
th
and 5
th
Year Notes
Placebos:
„Equipoise‟: randomisation only ethical if there is justifiable uncertainty of merit between
intervention and control – but reasonable possibility that the new treatment is better than placebo
Must be significant knowledge to be gained from a placebo trial
Implications of randomisation
Severs normal connection between patient and individually tailored treatment
Must be able to break the code if things don‟t go as expected
Investigator requirements:
Competence
Moral Character? Hard to specify or enforce
Conflicts of interest:
Intrinsic: interested in gaining knowledge verses care for the patient
Extrinsic: funding, reputation
Clinical equipoise
Balancing harms and benefits:
Principle of non-maleficence
Healthy problems: only very small risk acceptable. Problem of financial inducements (attract
people to take too much risk?)
Extrapolation from healthy volunteers not always possible
Equitable subject selection:
Respect for people (informed consent)
Principle of justice (equal sharing of benefits and burdens)
Vulnerable groups: reduced capacity to protect their own interests: eg incompetent, dying, minority
groups, 3
rd
world countries (but nothing in ethical codes to preclude their use – justification
becomes harder as degree of risk and degree of vulnerability increases)
Therapeutic orphans:
= Drugs not licensed for some groups, eg:
Children: difficulties of doing research on children. So package says “not recommended”
informed consent issues for the doctor and patient
Women: pregnancy and lactation, financial implications of teratogen testing
Problems with informed consent:
People often don‟t easily understand things like randomisation
People often reticent to ask questions
Role of Ethics Committees:
No statutory requirement for ethical review – but defacto requirement
Composition: Lay chairperson, 50% lay membership (following Cartwright)
Should journals publish research that hasn‟t undergone ethical review:
For: if its sound, would deprive society of valuable information and would require the study to
be repeated
Against: journal editors should be ethical gatekeepers
Problems with Prof Greens cervical cancer experiment:
Poor study design but still approved
Consent not gained from patients
Study not monitored properly (should have been stopped due to evidence of harm)
Concerns of other doctors not acted on properly
Questions it raises:
To whom should the doctor be accountable: their own conscience, patients or colleagues
Women were vulnerable, being examined by men asymmetry of power exaggerated

725
Cram Cards
726 4
th
and 5
th
Year Notes
Causes of Acute Sinusitis
Strep pneumoniae
H influenzae
[Also B catarrhalis and Strep pyogenes]
Causes of Acute Infectious exacerbations
of Chronic Bronchitis
Strep Pneumoniae
H Influenzae
Branhamella Catarrhalis
Causes of Otitis Media
Strep Pneumoniae
H Influenzae
Branhamella Catarrhalis
Urinary Tract Infections
Usually E. Coli.
Treatment:
1
st
line: Oral Trimethoprim (effective
against community acquired E Coli,
Klebsiella, Proteus, Strep faecalis)
2
nd
line: Oral Quinolones (eg
Norfloxacin)
Single dose therapy less effective
Causes of Acute Pharyngitis
Viral (commonest): Rhinovirus, coronavirus,
Influenza A & B, Parainfluenza 1 – 3,
Adenovirus, Herpes Simplex, EBV
Bacterial: Strep Pyogenes (Gp A), Strep
Group C, Mixed anaerobes (gingivitis – poor
dental hygiene), Corynebacterium diphtheria,
Neisseria gonorrhoeae
Fungal: Candida Albicans
Adenovirus
Sore throat (erythema + maybe exudate
even though a virus), fever, headache,
myalgia, conjunctivitis
Aspergillus
A saprophytic hyaline mould – lives on
dead organic matter
Haemorrhagic pneumonia in
immunocompromised (incl. acute
leukaemia)
Treatment: Amphotericin B.
Itraconazole for prophylaxis
Bacteroides Fragilis
G –ive anaerobic bacilli. Dominant gut
microbe
Causes: abdominal wound sepsis,
peritonitis, pelvic sepsis, septic abortion,
puerperal sepsis, any abscess incl. brain
abscess from otitis media or haematogenous
spread
Treatment: Metronidazole (not penicillin)
Bordetella Pertussis
Causes whooping cough
Cough followed by inspiratory gasp
(whoop), apnoea, vomiting
Can encephalitis. 50% of < 6
months get admitted
Incidence: up to 5000 cases a year
Treatment: Erythromycin
Candida Albicans
Yeast causing white plaques
Infection in immunocompromised, steroid use
or long term antibiotics
Treatment:
Topical: Nystatin
Oral: Terbinafine for scalp or nails
STD: Clotrimazole pessary
Severe: Fluconazole (good CSF penetration) or
Amphotericin B (good but nasty side effects)
Campylobacter Jejuni
G –ive rod
Treatment: Erythromycin (used to be
ciprofloxacin [a quinolone] but it‟s
been put in chicken feed
resistance)
Chlamydia Trachomatis
Obligate Intracellular bacteria
Rarer cause of pneumonia (farm animals). Tx:
erythromycin (has penicillinase)
STD (types D – K):
Incubation 7 – 21 days. Need Endocervical sample
Doxycycline 7 days or Azithromycin stat. Pregnancy:
Erythromycin (to avoid PROM). PID: Doxycycline/
erythromycin + ornidazole (antianaerobe like
metronidazole)
Reiter‟s syndrome (autoimmune): arthritis + urethritis +
conjunctivitis
Clostridium
G +ive anaerobe, spore forming
C Perfringens: Abdo wound sepsis, peritonitis, pelvic
sepsis, puerperal sepsis, gas gangrene (clostridial
myonecrosis), food poisoning (Enterotoxic)
C Tetani
C Botulinum
C Difficile: Pseudomembranous colitis following
antibiotics, anaerobe. Tx: Metronidazole (2
nd
line
Vancomycin)
Cytomegalovirus (CMV)
Transmission: saliva, blood, organ donation
Immunocompetent:
Kids: asymptomatic
Adults: self-limiting – maybe fever for 2 weeks
Pregnancy: Congenital infection in 20 – 40%.
Occasional long term sequalae (deafness, retardation,
respiratory distress)
AIDS: retinitis common, rarely encephalitis & colitis
Organ transplant: Interstitial pneumonia, hepatitis
Tx: Ganciclovir
Coliforms (= G –ive bacteria)
Incl. E. Coli + Klebsiella + Proteus mirabilis
Cause UTIs, Pyelonephritis, abdo wound
sepsis, peritonitis, biliary tract infection
Tx:
Meningitis & brain abscess: 3
rd
gen
Cephalosporin – good CSF penetration
(Cefotaxime, Ceftazidime). Consider also
Gentamicin & Cotrimoxazole
Corynebacterium Diphtheriae
G+ive bacilli
Causes diphtheria
Rare now (1 NZ case in last 20 years)
Sore throat, fever, pain on swallowing,
headache, vomiting, grey/green exudate
on pharynx
Toxin cardiac & neuro toxicity
Cryptococcus Neoformans
Yeast with mucinous capsule
Indian ink stain +ive
Causes encephalitis in AIDS,
Pneumonia & aseptic (=lymphocytic)
meningitis in immunocompromised
Tx: Fluconazole or Amphotericin B
Cryptosporidium
Common protozoan parasite
Profuse watery diarrhoea
Diagnosis: stool microscopy (ZN stain
for acid fast cysts)
No effective antibiotic treatment (can
try Paromomycin – oral, nonabsorbable
aminoglycoside)
E Coli
G –ive rods. A coliform. Grows on Maconkey
agar
Most are harmless bowel commensals but can
peritonitis (burst appendix), cystitis, neonatal
meningitis
Tx:
48% resistant to amoxycillin. Augmentin
resistance growing
Gentamycin or Trimethoprim
Epstein Barr Virus
Respiratory spread, usually young adults
Sore throat (erythema/exudate in 50%), fatigue,
malaise, fever, headache, posterior cervical
lymphadenopathy, splenomegaly, hepatitis, atypical
mononucleosis
Don‟t give penicillin rash mistaken for allergy
Diagnosis:
After 7 days Anti-EBV IgM (lasts 2-4 months) and
IgG (lasts for life)
After 2 months EBNA (lasts for life)
Enterococcus Faecalis
Aerobe
Causes UTI, abdominal wound sepsis
Tx: Amoxycillin (not penicillin G)

Otitis Media
Acute Infectious Exacerbations
of Chronic Bronchitis
Acute Sinusitis
Adenovirus
Acute Pharyngitis
Bladder Infections (UTIs)
Bordetella Pertussis
Bacteroides Fragilis
Aspergillus
Chlamydia Trachomatis
Campylobacter Jejuni
Candida Albicans
Coliforms
CMV
Clostridium
Cryptosporidium
Cryptococcus Neoformans
Corynebacterium Diphtheriae
Enterococcus Faecalis
EBV
E Coli
Gardnerella Vaginalis
Causes Bacterial Vaginosis
Symptoms: greyish-white, smelly
discharge
Clue cells on Gram stain
Crowds out Lactobacilli
Tx: Anti-anaerobe: Metronidazole (oral
and/or pessaries)
Haemophilus Influenzae
G –ive bacilli
Type A: Causes acute otitis media, sinusitis, infections,
exacerbation of chronic bronchitis, pneumonia in
chronic lung disease, rarely meningitis (3
rd
gen
Cephalosporin – CSF pen)
Tx: 6% resistant to penicillins, not sensitive to
erythromycin cefaclor, cefuroxime (iv), ceftriaxone,
augmentin, tetracycline (not kids/pregnant)
Type B: causes epiglottitis in kids
Herpes Simplex 1 & 2
Incubation 2 – 25 days
Type 1: face, use zovirax cream. Also STI.
Type 2: STI. Prevalence 20%. Tx Acyclovir
Encephalitis: confusion, convulsions. PCR
test of CSF. Give acyclovir on suspicion
Pharyngitis: Mild like other URTI. Severe
exudate/erythema, shallow ulcers, vascular
rash on lips
Helicobacter Pylori
G –ive rod, curved/spiral shaped
Urease breath test: swallow C13 labelled Urease,
expire C13 labelled CO2
Investigations: CLO test, biopsy, micro, serology
Prevalence 30% but declining
Causes gastritis (usually asymptomatic)
In 70-80% of gastric ulcers, 95% of duodenal ulcers
Triple therapy: eg clarithromycin + metronidazole +
omeprazole ( pH antibiotic bioavailability)
Influenza A & B
Causes flu: common cold + fever,
headache, generalised myalgia; most
common cause of viral pneumonia
400 deaths per annum
Vaccinate each year for new strains due
to antigenic drift
Listeria Monocytogenes
G +ive bacilli
Tx: amoxycillin
Neonatal meningitis
Elderly/immunocompromised: Tx
ciprofloxacin (a quinolone – not in
kids)
Legionella
Pneumonia: fibro-purulent exudate in
40 – 70 year old smoker. Slow onset,
headache, delirium, ?more GI effects
Tx: erythromycin (has penicillinase) +
rifampicin if severe
Mycoplasma
Common cause of URTI
Pneumonia: benign, self-limiting, age 5 – 15
Tx:
Erythromycin
2nd line: Tetracyclines (eg doxycycline)
except pregnant/kids
Resistant to Augmentin
Measles
Interstitial pneumonia in
immunocompromised kids
Moraxella Catarrhalis
(=Branhamella Catarrhalis)
Causes: acute otitis media, acute
sinusitis, acute infectious exacerbation
of chronic bronchitis, pneumonia in
chronic lung disease
Tx: 70% has penicillinase
augmentin, cefaclor, tetracycline,
cefuroxime
Neisseria Gonorrhoea
G-ive diplococci, bean shaped, hard to culture
(chocolate agar), survives intracellularly
STD incubation: 1 – 14 days
Male: discharge and dysuria. Female: only 20%
symptomatic PID
Tx:
Stat: Amoxycillin + Probenecid
Ciprofloxacin (quinolone) or tetracycline (eg
doxycycline) if penicillin allergy or resistant
Azithromycin if concurrent chlamydia or pregnant
Neisseria Meningitidis
G –ive diplococci (bean shaped).
Liberated endotoxin
Kids & adults meningitis, not otitis
media
Notifiable disease
Tx: Penicillin, Cefotaxime if allergic
Prophylaxis: Rifampicin (broad
spectrum), ceftriaxone if pregnant
Parainfluenza virus (1-3)
Causes Croup
(laryngotracheobronchitis)
Initial: sore throat, rhinorrhoea, mild
cough
Leads to: sever cough (seals bark),
hoarseness, inspiratory stridor
(subglottic inflammation)
Pneumocystis Carinii Pneumonia
Extracellular protozoan parasite
Exclusively infects the lung, mainly in
AIDS (also transplant, leukaemia)
Tx: Cotrimoxazole (=trimethoprim
+sulphamethoxazole)
Relapse common
Pseudomonas aeruginosa
G -ive rod. Low virulence but antibiotic
resistance. Grows in anything
Common in burns, immunocompromised and CF
Causes haemorrhagic pneumonia
Tx:
Increasing resistance. Always to sensitivities
Meningitis: Ceftazidine
Ciprofloxacin (Quinolone) – its main use
Tobramycin (Aminoglycoside) or piperacillin
Respiratory Syncytial Virus
Major cause of URTI, esp winter/spring
Starts as URTI (cough, fever, sore
throat) LRTI (mainly bronchiolitis)
with dyspnoea, tachypnoea
Tx: If severe then Ribavirin aerosol
Rhino Virus and Coronavirus
Common cold
Fever uncommon except in kids
Staph Epidermidis
G +ive, Coagulase –ive
Causes infected Hickman line, IV lines
(esp neonates)
Less virulent than Staph Aureus
Tx: Flucloxacillin (one EMPTY
stomach). If resistant then Vancomycin
Staph Aureus
G +ive, Coagulase +ive (fibrinogen fibrin)
Causes: mastitis, diabetic foot infections, furnuncles
(if recurrent then ?nasal carriage rifampicin),
infected lines, hospital acquired pneumonia, abscess,
endocarditis, food poisoning (esp in cream),
osteomyelitis
Tx: Flucloxacillin. Allergy: Ceftriaxone. MRSA
(resistant to flucloxacillin and cephalosporins):
Vancomycin (also quinolones)
Strep Pneumoniae
G+ive diplococci, haemolytic
Causes: acute otitis media, sinusitis, community
acquired pneumonia, infectious exacerbation of chronic
bronchitis, meningitis
Oral: amoxycillin. IV: Penicillin G (1% adults
resistant, 10% kids). Allergy: erythromycin (not for
meningitis, poor CSF penetration)
Penicillin resistant: Ceftriaxone (3
rd
gen) or
Vancomycin. Resistant and Meningitis: Cefotaxime.
Resistant and Endocarditis: Vancomycin
Syphilis
Caused by Treponema pallidum
Lumen of small arteries due to intima
Primary: chancre – painless hard macule at site of sexual
contact. Secondary: 4 – 8 wks later, fever, malaise,
lymphadenopathy, rash, alopecia
Tertiary: latent for 2 – 20 yrs, gummas (granulomas),
ascending aortic aneurysm, aortic regurgitation, cranial nerve
palsies, dementia
Diagnosis; serology (VDRL test). Tx: Penicillin G (im). If
resistant then tetracyclines (eg doxycycline)

Herpes Simplex 1 & 2
H
Haemophilus Influenzae
Gardnerella Vaginalis
Listeria Monocytogenes
Influenza A & B
Helicobacter Pylori
Measles
Mycoplasma
Legionella
Neisseria Meningitida
Neisseria Gonorrhoea
Moraxella Catarrhalis
Pseudomonas aeruginosa
Pneumocystis Carinii
Pneumonia
Parainfluenza Virus 1 - 3
Staph Epidermidis
Rhino Virus and Coronavirus
Respiratory Syncytial Virus
Syphilis
Strep Pneumoniae
Staph Aureus
Haemolytic Strep Group B
Haemolytic = clear on blood agar
Eg Strep agalactiae (vaginal flora).
[NB Strep pyogenes in haemolytic
Lancefield Group A]
Causes: meningitis, respiratory distress
syndrome
Tx: Penicillin
Strep Pyogenes
haemolytic, Lancefield Group A. G +ive singly
or in chains
Common cause of cellulitis, pharyngitis, impetigo
Can Rheumatic fever & glomerulonephritis
Tx: Penicillin (little resistance)
Erythromycin if allergic
Not amoxycillin unless Pyogenes is proven – if
virus rash which is mistaken for allergy
Viridians Strep
= haemolytic (green on blood agar).
G +ive
Eg Strep Sanguis
Causes: UTI, wound sepsis
Infective endocarditis: Tx: penicillin or
amoxycillin +/- gentamycin (for G –ive
cover)
TB
Mycobacterium Tuberculosis
Waxy coat resists lysis after phagocytosis
granulomas. Infects anything (lung, lymph nodes,
brain, gut)
Acid fast bacilli – use ZN stain
Tx: Rifampicin + isoniazid + pyrazinamide (also
ethambutol)
In AIDS, consider M avium intracellulare. Resistant
to Tb drugs. Consider Clarithromycin
Trichomonas
Causes Trichomoniasis
Watery green/yellow fishy smelling
vaginal discharge
Protozoa
Common 3
rd
world STD
Tx: Doxycycline, metronidazole
Varicella Zoster
Chicken pox.
Latent in dorsal root ganglia shingles
Culture possible if transported in viral
medium
Tx for shingles:
Acyclovir as early as possible
Analgesic or low-dose amitriptyline for pain
Toxoplasmosis
Protozoa/parasite. In meat cysts (and kitten faeces)
Causes: lymphadenopathy (eg unilateral), maybe fever,
myalgia, acute pharyngitis, hepato-splenomegaly,
atypical mononucleosis, takes while to settle. AIDS:
CNS involvement, retinal lesions
Congenital: Prem, still birth, choroido-retinitis, (worse
in 3
rd
trimester)
Lab: PCR of amniotic fluid, CSF. Serology: IgM peaks
at 2-4 weeks, traces for up to a year
Tx: Pyrimethamine+clindamycin, Pregnant: Spiramycin
Malaria
Irregular fever, headache, malaise, vomiting (like
typhoid). Lab: Blood film when febrile.
Chemoprophylaxis
Mefloquine weekly: good against chloroquine resistant
Falciparum. Not if epilepsy, pregnant, babies
Doxycycline daily: Esp in SE Asia (mefloquine-
resistant Falciparum). Not kids or pregnant
Chloroquine + Proguanil: Only one safe if pregnant
Chloroquine weekly (if no chloroquine-resistant
falciparum eg Central America)
Plasmodium Falciparum
No reinfection, cerebral malaria, Africa
Quinine sulphate + Doxycycline 7 days
Cerebral malaria: IV quinine
Plasmodium Vivax
Asia/Oceania, exo-erythrocytic liver
cycle
3 days of Chloroquine
Radical cure (P Vivax or P Ovale):
Primaquine 2 weeks (test for G6PD
deficiency first)
Relapse common 3 days chloroquine
then higher dose of primaquine
Giardiasis
Explosive, watery diarrhoea
Stool exam, 3 samples, 48 hours apart
trophozoites
Tx: Tinidazole stat or Metronidazole 7
days
Relapse not uncommon
Amoebiasis
Lab – look for cysts.
May be extra-intestinal (eg abscess)
antibody test
Metronidazole + diloxanide furoate
Filariasis
Eg Wuchereria Bancroft
Elephantitis. May need Surgery to
relieve blocked lymphatics
Tx: Ivermectin
Intestinal Worms
Hookworm, roundworm, pinworm:
Medendazole (treat whole family)
Strongyloides Stercoralis:
Thiabendazole
Tapeworms: Niclosamide
Travel Medicine
Malaria: prophylaxis if > 7 days. Risk in resort areas
low
Hep A: Usually given
Typhoid: injectable or oral vaccine
Yellow fever: equatorial Africa & South America
Polio, tetanus and diphtheria
Meningococcal (Types A,C,W,Y): Nepal, West Africa,
Brazil
Japanese Encephalitis: SE Asia. Rare for travellers to
get it
Cephalosporins
1: Cefazolin: Better for G+ (not E faecalis) and
anaerobes (not B Fragilis)
2: Cefuroxime: Better against Coliforms. Active
against H influenzae
3: Ceftriaxone, Cefotaxime: Good against most
coliforms. Not Bacteroides or Enterococcus. Good
CSF penetration.
4: Cefipime: Good for -lactamases, coliforms &
pseudomonas
Macrolides
Good against streps, mycoplasma, chlamydia or
legionella pneumoniae, Campylobacter
Not H influenzae
No CSF penetration
Chlamydia trachomatis in pregnancy
Erythromycin, Roxithromycin (Rulide),
Clarithromycin (for MAC), Azithromycin (Stat, for
Chlamydia or Gonorrhoea STDs in pregnancy)
Vancomycin
Only active against G+
Systemic MRSA/MRSE infection
Staph or Strep Endocarditis with
penicillin allergy
C Difficile colitis (oral) – use
Metronidazole first
Otto and nephrotoxic
Rifampicin
Always in combination (except
meningitis and HIB prophylaxis)
Tb, Severe staph or legionella infection
Aminoglycosides
Active against all coliforms,
pseudomonas
Inactive against strep, anaerobes
For G- sepsis, perforated appendix
Otto and nephro toxic
Cotrimoxazole
= Trimethoprim + sulphamethoxazole
Broad spectrum
For acute infectious exacerbations of
chronic bronchitis, PCP
Trimethoprim only for community
acquired UTI (so those with sulphur
allergy can use)

Viridians Strep
Strep Pyogenes
Haemolytic Strep Group B
Varicella Zoster
Trichomonas
Tb
Plasmodium Falciparum
Malaria
Toxoplasmosis
Amoebiasis
Giardiasis
Plasmodium Vivax
Travel Medicine
Intestinal Worms
Filariasis
Vancomycin
Macrolides
Cephalosporins
Cotrimoxazole
Aminoglycosides
Rifampicin
Quinolones
Broad spectrum (except anaerobes and
streps)
Not in kids (damages growth cartilage)
Norfloxacin: resistant UTIs
Ciprofloxacin: Pseudomonas
Tetracyclines
Eg Doxycycline
Active against staph, streps, coliforms, HIB
Used in STDs
Syphilis and Gonorrhoea if penicillin
allergy
Mycoplasma pneumoniae
Not in pregnancy or kids < 12 (stains teeth
and deposits in bone)
Metronidazole
Active against all anaerobes (eg B
fragilis)
Inactive against aerobes (except
Gardnerella Vaginalis – drug of choice)
Active against protozoa: eg Giardia
Antifungals
Nystatin (topical): vaginal/oral candida
Miconazole (topical): Candida and dermatophytes
(except scalp and nails)
Terbinafine (oral): dermatophytes of scalp and nails
Fluconazole (oral/iv): Yeasts (candida,
cryptococcus). Good CSF penetration
Itraconazole (oral): Dermatophytes of scalp & nails,
candida/aspergillus prophylaxis in AIDS
Amphotericin B (iv): very good but nephrotoxicity
Metronidazole
Tetracyclines
Quinolones
Antifungals
Back Exam
Walk: gait, walk on toes (S1), walk on heels (L5, ie
neuro signs)
Look:
Is belt line horizontal
Skin: Scars, pigmentation
Shape & Posture: if scoliosis then bend over
Palpate:
Spinous processes (support forehead for neck) for
tenderness or a step
Sacroiliac joint
Move:
Neck: flexion, extension, rotation, lateral flexion
Back:
Flexion: Schober‟s test
Extension
Lateral Flexion
Rotation (sitting on a chair)
Special tests:
Check neurology in arms and legs if neck or
lumbar pain (Sciatic pain – Lasegue‟s test, power,
tone, reflexes, sensation, co-ordination)
Do abdominal exam if lumbar pain (eg AAA)
Hip Exam
Standing:
Gait
On toes (S1), on heels (L5) (checking neurology)
Bend over – how can they reach (examine back)
Crouch down (test knees and extensor mechanism)
Observe: gluteus bulk, posterior scars
Trendelenburg test and sacroiliac joint
Look:
Skin: scars, redness
Soft tissue: swelling
Muscle: wasting – quads, abductors, adductors
Bony deformity
Apparent and real leg length
Feel:
Groin: hernias, lymph nodes
Greater trochanter tenderness ilio-tibial band
pain
Move (compare sides):
Thomas test: fixed flexion deformity
Flexion (comparing sides)
Adduction and abduction with pelvis fixed
Internal and external rotation (comparing sides)
Exam knee and lower back (did this while standing)
Check pulses
Check leg neurology
Knee Exam
While standing:
Observe:
Varus/valgus or fixed flexion deformity
Scars, symmetry, swelling
Popliteal fossa: Baker‟s cyst
Gait
Squat down and duck walk
Observe on the bed:
Swelling, muscle wasting, scars, deformity
Actively push knee into bed (muscle bulk, fixed
flexion deformity)
Straight leg raise: tests extensor mechanism
Palpate:
Warmth each side
Effusion: stroke test, patellar tap
Joint line (meniscal tears), collateral ligaments,
ischial tuberosity and patellar ligament. Baker‟s
cyst, popliteal pulse
Move: Flex both knees
Ligaments: (sit on foot, compare sides)
PCL: posterior sag and posterior draw test
ACL: anterior draw test, Lachman‟s, Pivot-shift
Collaterals: Varus and valgus stress test
McMurray‟s for meniscal tears
Patellar-femoral joint: Solomon‟s test. Feet over side:
pointing straight ahead, raise leg (crepitus?),
apprehension test
Hip, distal pulses and neurology
Shoulder Exam
Look (comparing both sides):
Skin: redness, scars
Shape (in front and behind): asymmetry, wasting,
dislocation, swelling, sub-acromial sulcus
Feel:
Temperature
Around bones from clavicle to scapular
Tendons under acromion
In axilla: tenderness, lymph nodes
Move:
Abduction to 180º and adduction across chest
Flexion and extension
External rotation (forearms at 90º)
Internal rotation (scratch up back)
Rotator Cuff:
Supraspinatus: abduction from 0 - 30º against
resistance with thumbs to the ground
Infraspinatus: externally rotate against resistance
Subscapularis: Lift-off test (try and push it away)
Stability:
Sulcus test: pull arm down and look for sulcus
Anterior draw test
Apprehension test
Push-ups against the wall
Examine neck and elbow
Distal pulses and neurology
Respiratory Exam (Chest Only)
Introduce yourself, wash hands, light, position patient
Observe:
General: Cyanosis, pallor, cachexia, distress, LOC
Chest:
Respiratory distress, dyspnoea, rhythm
Listen for cough, wheeze, hoarseness, stridor
Scars
Shape: scoliosis, kyphosis, pigeon
Movement: accessory muscles, indrawing,
paradoxical breathing of abdomen, expansion
COUNT RESPIRATORY RATE
Palpate:
Neck:
Nodes – especially supraclavicular
Trachea – central, inspiratory tug
Chest expansion
Push sternum to spine (broken ribs)
Tactile fremitus: 99 (on front and back)
Percussion: Stony dull, dull, or hyper-resonant
Ausciltate:
Breath Sounds (front and back):
Air entry each side
Vesicular or bronchial
Wheeze, crackles, rubs
Forced expiration
Vocal resonance
Peak Flow
CVS Exam (Precordium Only)
Introduce yourself, wash hands, light, patient at 45º
Observe:
General: cyanosis, pallor, cachexia, distress, LOC,
Marfan‟s, Down‟s etc, oedema
Chest: Scars, deformity, pacemakers, pulsations
(look from side as well)
JVP
Palpation:
Apex beat (and count down ribs – 2
nd
IC space at
sternal angle): sustained, hyperkinetic, etc
Parasternal heaves (RV activity), Aortic and
pulmonary thrills
Auscultation (ALWAYS time from carotid pulse):
Diaphragm and bell at mitral, tricuspid, pulmonary
and aortic areas
Axilla with diaphragm (mitral regurg if systolic)
Carotid arteries (bruit, aortic murmur)
To refine murmurs:
Left lateral position: Mitral stenosis (bell)
Leaning forward, full expiration, parasternal with
diaphragm: Aortic regurg, hypertrophic
cardiomyopathy
Tricuspid murmurs: check JVP and pulsitile liver
Pulmonary oedema: Percuss and ausciltate posterior
lung bases. Check sacral oedema
Abdomen Exam (Abdomen only)
Introduce yourself, wash hands, light, patient at 0º
Inspection:
General: jaundice, pallor, pigmentation,
weight/wasting, gynaecomastia, spider naevi, body
hair, bruising
Abdomen:
Scars
Distension
Veins
Striae
Hernias, visible masses
Pulsations (aorta, liver)
Palpation (warm hands, watch face):
Light palpation
Deep palpation: test for rebound
Percuss then palpate liver (span, firm, nodular,
tender, pulsitile). Test for movement on inspiration
Percuss then palpate spleen
Ballot kidneys
Percuss for shifting dullness of ascites
Bladder
Ausciltate:
Bowel sounds
Renal bruit
Testicular, PR and inguinal hernias (cough)
Neurology Limb Exam
Observe:
General: alertness, speech
Posture
Wasting, fasciculations, abnormal movements
(tics, tremour, chorea, athetosis)
Power: compare sides, 0 – 5
Tone: of all movements: hypo or hyper tonic (rigidity,
spasticity), ankle clonus
Reflexes:
Arm: triceps, biceps, supinator
Leg: patellar, ankle, Plantar
Sensory:
Light touch
Position sense
Vibration
Pinprick
Temperature (same pathway as pinprick)
Coordination:
Arms: rapid-alternating movements, finger-nose
test, drift, flap
Legs: heel-shin test, Romberg, heel-toe walking
Function:
Legs: Gait, walk on heels (L5), toes (S1), crouch
Hands: identify objects with eyes closed
Examination of Cranial Nerves
2: Ophthalmic nerve: acuity, visual fields, fundoscopy
3, 4 and 6: Oculmotor, Trochlear, and Abducens:
Pupils: ptosis, corneal light reflex, swinging light
test (turn off light), accommodation reflex, squint
Eye movement: draw H, watch for lag or
nystagmus, ask about diplopia
5: Trigeminal:
Light touch and pin prink in all 3 divisions
Corneal reflex
Motor:
Wasting of muscles of mastication
Jaw opens in the midline
Clench jaw, palpate maesseters
7: Facial:
Wrinkle forehead
Show your teeth
Puff up cheeks
8: Vestibulochoclear:
Rinne: conductive deafness if mastoid louder
Weber: hear loudest in good ear if sensori-neural
deafness
9 & 10: glossopharyngeal and Vagus:
Uvula in midline (say „ah‟)
Swallowing and speech (ask about hoarseness)
11: Accessory: Shrug shoulders, turn head against
resistance
12:Hypoglossal: wasting, fasciculation, protrudes in
midline, „la la la‟ quickly, push against inside of cheek
Examination of Leg Vasculature
Inspection:
Colour
Presence of hairs
Varicose veins (while standing)
Dilated superficial veins ( DVT)
Ulcers
Swelling
Wasting – compare muscle bulk on each side
Clubbing of the toes
Oedema
Palpation:
Compare size, tenderness and warmth of calves
Oedema
Temperature of feet
Capillary return
Sensation
Veins: hard thromboses. Tender
thrombophlebitis
Peripheral pulses:
Femoral: Palpate and ausciltate for bruits
Palpate popliteal, posterior tibial, dorsalis pedis
Buerger‟s test:
Elevate leg to 45 º. Pallor is rapid if poor arterial
supply
Then hand over bed. Cyanosis rapid if poor
arterial supply
Bed side test: ABI (Ankle Brachial Index): ultrasound
comparison of blood flow in the arm and leg
Abnormal Menstruation
Basic Menstrual History:
LMP
Normal cycle length, days of bleeding, regularity
How heavy is bleeding (number of pads, clots, etc)
Associated pain
Other bleeding: between periods, post-coital
Age at menarche
Age at menopause, post menopausal symptoms and
any bleeding
Contraception
Amenorrhoea:
Primary: Never menstruated. Rare. Turner‟s,
Testicular feminisation, etc
Secondary:
Pregnancy related: pregnant or breast feeding
PoP, Depot
Stress: Anorexia, athlete, disease (weight)
Prolactinoma pituitary function, visual
fields, headaches
Ovarian causes (PCO, tumours): virilisation,
weight
Premature menopause
Hyperthyroidism
Menorrhagia:
Young: abnormal menstrual bleeding
Older: IUCD, fibroids, endometriosis, polyps,
cancer
Infection (any pain, fevers, discharge)
Hypothyroidism cold intolerance, weight gain
Abnormal platelets
Intermenstrual: mid-cycle in oestrogen + above factors
Gynaecological History
Introductory data:
Age
Gravidity (pregnancies) + Parity (Deliveries)
LMP
HPC: including details of bleeding, pain, discharge and
urinary symptoms
Past Gynae History:
Age at menarche
Menstrual history
Past gynae problems/procedures/abdo surgery
Sexual history
Current/past contraception
Past STDs
Incontinence
Smear history
Past Obstetric history
PMH
Medications
FHx: mother or sisters with gynae/obstetric problems
Social Hx: Relationship status, sexual activity, alcohol
& smoking, occupation, any inter-personal violence or
abuse
Obstetric History
Introductory data:
Age
Gravidity (pregnancies) + Parity (Deliveries)
LMP
Current pregnancy:
Due date (check accuracy)
Contractions/pain
Bleeding
Discharge
Fetal movements
Past Obstetric History:
When was it
Antenatal problems (eg BP, diabetes, etc)
Delivered: pre-term, post-term?
Delivery: vaginal, C-section
Weight of baby
Post partum: any bleeding, infection, depression
Baby: any problems – how are they now
Feeding: breast or bottle
Past Gynae history:
Previous problems: infection, surgery, etc
Contraceptive history
Smear history
PMH: hypertension, DM, heart disease, asthma, DVTs,
infections (esp STIs, Hep B, Tb), depression, endocrine
Medication: especially folate
FHx: DVTs, birth defects, multiple births, pregnancy
problems
Social: relationship, smoking & alcohol, occupation
Pelvic Pain
Pain with sex = dyspareunia
Superficial: eg HSV, atrophy, vaginismus
Deep: pelvic disease (eg endometriosis, PID), post-
hysterectomy
Period pain = dysmenorrhoea:
Primary: Young, first 2 days of menses, no organ
pathology, started at menarche and not getting
worse
Secondary: Older, prior to and through out
bleeding, pelvic disease/infection, PMS
For > 6 months = Chronic pelvic pain
Intermittent (with sex/menses, etc) or continuous
Gynae: dysmenorrhoea, endometriosis,
adenomyosis, PID, prolapse, post-delivery trauma,
etc
Non-gynae: UTI, IBS, diverticular, musculo-
skeletal
Sexual History
Number & duration of relationships
Previous similar symptoms
UTI questions: frequency, discharge, abdo pain,
testicular pain, joint pain
Screen for high risk behaviour:
Alcohol and drug use
Unprotected sex
Multiple partners
Anal/oral sex
Psych History
Identifying data: name, age, occupation
HPC (including when did you last feel well, what‟s
your worst worry)
Systematic enquiry:
Anxiety + phobias
Mood
Psychotic
Suicidality
Cognitive
Neurophysiological: sleep, appetite, weight
Alcohol and drug
Impulse-control screen
Medications
Past psych history
PMH
Family: anyone had psych illness, had a breakdown,
attempted suicide, had an A&D problem
Social: including personal history, past difficulties
(abuse, legal, relationships, etc)
Mental state: appearance and behaviour, speech, mood,
affect, thought form, thought content, suicidal ideation,
perceptual phenomena, cognition, intelligence, insight
and judgement, rapport
Suicide Assessment
History:
Ideation:
Do you think a lot about death
Do you want to die – or want others to know
how bad it is
Do you have the means
What‟s stopped you so far
How do you feel about accepting help
Past attempts:
What did you do
Why did you do it
What was the final straw
Did you leave a note
What stop you going through with it
Risk assessment:
Predisposing factors: Family history, psych illness,
alcohol and drug problem, suicide exposure, other
illness, age and sex, living alone
Precipitating factors: Stressful events, current
mood, thoughts about the future, mental state,
current plans, availability of method
Protective factors: cognitive flexibility, social
supports, hopefulness, treatment of disorders,
responsibility for children
Shortness of Breath
Very sudden:
MI: palpitations, pain, anxious, risk factors
(hypertension, diabetes, lipids, smoking, previous
MI, stroke or claudication, FHx)
PE: Palpitations, Leg swelling, immobility,
surgery, pregnancy, past or family history
Pneumothorax
Over a few hours:
Asthma: night cough, wheeze, previous history.
Test peak flow
Pneumonia: fevers, sweats, cough, sputum, blood,
pain with coughing
Gradual:
Heart failure: oedema, tired, orthopneoa, PND,
history or risk factors for IHD
Anaemia
Carcinoma
Others:
Metabolic acidosis (eg Diabetic ketoacidosis)
Psychiatric – eg anxiety
Remember to ask about medications and smoking
Investigations:
Examine the patient, including BP, pulse & JVP
Peak flow
Bloods: FBC, Electrolytes, cardiac enzymes
ABGs
Sputum/blood cultures
CXR, ECG
Treatment: include O
2
Key Differentials
Sleepiness/Fatigue:
Sleep disturbance/restriction (?anxiety)
Sleep apnoea
Depression
Hypothyroidism
Heart failure
Anaemia
Acute or chronic disease (eg EBV)
Drugs: -blockers, anti-histamines, sedatives,
alcohol
Passing out:
Arrhythmia
Epilepsy (any aura, witness report, post-ictal state,
past head injury)
CVA
Postural hypotension
Vasovagal faint
Hypoglycaemia
Fall
ECG Interpretation
Rate (brady or tachycardia). 300/no of big squares
Rhythm: Relationship of P waves to QRS sinus
arrhythmia, supraventricular arrhythmia, escape beats
Cardiac Axis: Normal if I and II positive
Left deviation = I+, II and III –
Right deviation = I-, II +/-, III +
Description of P wave:
Peaked P: RA hypertrophy
Twin peaked P: LA hypertrophy
Large P K, small P K
Conduction intervals: Start of P to start of QRS = 3 –5
small squares (0.12 – 0.2 secs)
Description of QRS:
Normal <= 3 small squares. > BBB or ventricular
Q waves (or 25% of QRS). Anterior: V2, V3.
Lateral: I, II, VL, V3-6. Inferior: III and VF
Bundle Branch: Marrow and William in V1/V6
RV Hypertrophy: R in V1/2 + S in V5/6
LV Hypertrophy: S in V1/2 + R in V5/6
ST Segment:
Raised: infarction. Anterior V5, V6. Inferior III,
VF
Depressed: ischaemia
T wave: Normally inverted in VR and V1. Abnormal
if –ive in I, II, V4-6. If not full thickness infarct T
wave inversion but no Q wave. Digoxin: T wave
inversion, slopping of ST. K flat, K wide,
peaked
QT interval
Paediatric Differentials
Quick screen for severity of illness: responsiveness,
feeding, urine, colour, breathing
Fever in a child without clear focus:
Infection: UTI, bacteraemia, meningitis
Rheumatic Fever
Poisoning
Leukaemia
Drug Fever
Gastroenteritis in a child:
Infection: Rotavirus, campylobacter, protozoa
Systemic: UTI, Pneumonia, otitis media
Surgical: appendicitis, intussusception, obstruction
(eg hernia), pyloric stenosis, torsion, secondary to
adhesions
Other: diabetic ketoacidosis, antibiotic diarrhoea,
poisoning
PR Bleeding: necrotising enterocolitis, intussusception,
IBD (unlikely), familial polyps
Abdo pain is likely to be benign if: didn‟t know about it
till the child said, they‟re distractible from it, it is
central, no sleep disturbance, no symptoms, intermittent
Coma: hypoxic, epileptic, trauma, infection, poison,
renal failure, hypo/hyperglycaemia, hyper/hypo-
thermia, hypertension

Index
-agonist, 79
-blockers, 42, 50, 52
-feta Protein, 193, 469
HCG, 469
5 Reductase Inhibitors, 225
5HT3 Antagonists, 471
A-a Gradient, 58
Abdominal Pain
in Children, 643
Abdominal Radiology, 157
Abductor Lurch, 251
Abetalipoproteinaemia, 165
ABO Blood Incompatibility, 596
Absence Seizures, 134
Absorption of Drugs, 523
Abuse
Child, 656
Management of, 659
Physical, 343
Sexual, 339, 343
Acanthosis, 314
ACC, 284
Accessory Nerve, 118
Accident Compensation
Corporation, 284
Accommodative Esotropia, 632
ACE Inhibitors, 50, 51
Acetylation, 525
Achalasia, 159
Achilles Tendon Rupture, 258
Acid-Base Balance, 113
Acitretin, 336
Acne, 330
Aconotmesis, 237
Acoustic Neuroma, 152
Acrodermatitis Enteropathica,
647
Acromegaly, 107
ACTH, 102, 104
Actinic Keratosis, 326
Activated Charcoal, 488
Activated Partial Thromboplastin
Time, 292
Acute Bacterial Endocarditis, 46
Acute Cholecystitis, 196
Acute Disseminated
Encephalomyelitis, 132
Acute Enterocolitis, 176
Acute Hepatitis, 184
Acute Inflammatory
Demyelinating
Polyradiculopathy, 139
Acute Interstitial Nephritis, 211
Acute Interstitial Pneumonia, 84
Acute Leukaemia, 300
Acute Pancreatitis, 197
Acute Papillary Necrosis, 211
Acute Pharyngitis, 63
Acute Renal Failur
Pre-renal, 205
Acute Renal Failure, 205
Intrinsic, 206
Post-renal, 206
Acute Stress Disorder, 424
Acute Suppurative Appendicitis,
167
Acute Tubular Necrosis, 211
Acyclovir, 515
Addiction, Aetiology of, 446
Addison‟s Disease, 69, 103
Addisonian Crisis, 103
Adenocarcinoma, 89
Colon, 173
Oesophageal, 159
Adenomyosis, 347
Adenosine, 42
Adenosine Deaminase
Deficiency, 307
Adenosquamous carcinoma, 89
Adenovirus, 64, 70
Eye Infection, 144
ADH, 104
ADHD, 572, 659
Adhesive Capsulitis, 244
Adjustment Disorder, 421
Adnexa Oculi, 632
Adolescent Development, 664
Adolescent Health, 664
Adrenal Cortex, 102
Adrenal Hyperplasia, 102
Adrenarche, 667
Adrenogenital Syndrome, 638
Adriamycin, 382
Adult Polycystic Kidney, 216
Adult Respiratory Distress
Syndrome, 83, 482
Adverse Reactions
Drug Reactions, 529
Vaccination, 517
Adverse Selection, 699
Affinity, 528
AFP. See -feta Protein
Afterload, 14
Aganglionic Megacolon, 640
Ageing, 672
Agenesis, 466
Agonists, 527
Agoraphobia, 423
AIDS, 308
Airway Management, 476
Airway Obstruction, 485
Akathisia, 438
Albumin, 183
Alcohol Abuse, 450
Alcohol Regulation, 697
Alcoholic Dementia, 441
Alcoholic Liver Disease, 185
Aldosterone, 102
Alfentanil, 544
Algodystrophy, 283
Alkylating Agents, 299
Allergic Alveolitis, 310
Allergic Dermatitis, 321
Allergic Rhinitis, 63
Allergy, 63, 309, 319, 320, 321,
483, 531, 647
Allocative Efficiency, 698
Allopurinol, 278
Allylamine, 336
Alma Ata Declaration, 562
Alogia, 436
Alopecia Areata, 333
ALP, 183
Alpha-1 Antitrypsin Deficiency,
82, 194
ALT, 182
Alveolar Proteinosis, 92
Alzheimer‟s Dementia, 440
Ambiguous Genitalia, 638
Amblyopia, 147
AMBU Bag, 477
Ameloblastoma, 157
Amenorrhoea, 106, 345
Post Pill, 106
Aminoglycosides, 514, 533
Amiodarone, 41, 42
Amniocentesis, 360
Amoebiasis, 509
Amoxycillin, 513
Amphotericin, 515
Amylase, 10
Amyloidosis, 209, 302, 303
Amyotrophic Lateral Sclerosis,
133
Anaemia, 209, 287
in Children, 646
Neonatal, 589
of Chronic Disease, 291
Anaesthetics, 539
Dose Calculations, 540
Inhalational, 541
Intravenous, 541
Obstetric, 545
Paediatric, 655
Anal Cancer, 179
Anal Fissures, 179
Anal Warts, 179
Anaphylaxis, 483
ANCA, 212, 270
Androgen resistance, 638
Androgens, 102
Anencephaly, 466, 631
Angelman Syndrome, 465
Angina Pectoris, 36
Angiomyolipoma, 217
Angiosarcoma, 192
Angular Cheilitis, 322
Angular Stomatitis, 155
Anhedonia, 436
Aniomyolipoma, 217
Anion Gap, 113
Anisometropia, 148
Ankle, 257
Ankylosing Spondylitis, 171,
274
Anorchia, 636
Anorexia Nervosa, 420, 453
Anoxic Seizures, 628
Antagonists, 527
Antalgic Gait, 250
Antenatal Booking, 355
Antepartum Haemorrhage, 366
Anterior Cruciate Ligament, 254,
255
Anterior Draw Test, 254
Anterior Uveitis, 275
Anti EBNA, 505
Antibasement Membrane
Antibody Disease, 92, 214
Antibiotic Fever, 531
Antibiotic Treatment, 511
Anticipatory Guidance
Neonatal and Infants, 568,
590
Anticonvulsants, 135
Anti-D, 367
Antidepressant Medication, 432
Antidepressants
MAOIs, 434
SSRIs, 433
Tricyclics, 432
Antifungals, 336, 515
Antigliadin Antibodies, 164
Antihistamines, 43
Antiparkinsonian Medication,
438
Antiphospholipid Syndrome,
270, 294
Antipsychotic Medication, 437
Antisocial Behaviour
in Children, 573
Antisocial Personality Disorder,
455
Antithrombin 3, 293
Anuploidy, 464
Anxiety and Depressive
Symptoms, Differentiating,
426
Anxiety Disorders, 420, 422
in Children, 661
Treatment, 424
Aorta, Traumatic Rupture of,
491
Aortic Aneurysm, 32
Aortic Knuckle, 28
Aortic Regurgitation, 22, 44
Aortic Stenosis, 22, 43
Apex Beat, 21
APGAR, 588
APH, 366
Aphthous Ulcers, 158, 168, 169
Aplasia, 466
Aplastic Anaemia, 289
Apnoea, 588
Appendicitis, 167
Appetite, 94
APTT, 292
Arapax, 434
ARDS, 83, 482
Arnold Chiari Malformation, 624
Arrhythmias
Cardiac Arrest, 479
Congential, 601
Drug Treatment, 42
Non-arrest, 40
Artefacts of Blood Tests, 9
Arterial Blood Gases, 58
Interpretation of, 115
Arteriosclerosis, 33
Hylaine, 33
Hyperplastic, 33
Arterio-venous Malformations,
124
Arteritis, 33
Arteritis Syndromes, 282
Arthralgia, 230
Arthritis, 266
Differential in, 266
Inflammatory, 270
Inflammatory, Systemic Signs
of, 230
Osteoarthritis, 268
Radiology, 267
Septic, 259
Seronegative, 274
Arthritis Mutilans, 275
Arthrocentesis, 259
Arthrodesis, 269
Arthroplasty, 269
Asbestosis, 85
Cholangitis, 197
Aschoff Bodies, 603
Ascites, 194
Ultrasound for, 157
Aseptic Meningitis, 499
Asperger‟s Syndrome, 582
Aspergillus, 69
Aspiration, 614
Risk Factors for, 655
Aspirin
Anticoagulant Effects, 294
Assisted Human Reproduction,
722
AST, 182
Asteatotic Eczema, 322
Asterixis, 8
Asthma, 77
Emergency Management, 485
in Children, 78, 613
Astrocytes, 136
Astrocytoma, 136
Asystole, 480
Atherosclerosis, 31
Athlete‟s Foot, 317
ATN, 211
Atonic Neck Reflex, 624
Atopic Dermatitis, 648
Atopic Eczema, 319
Atopy, 310
Atrial Fibrillation, 26, 40
Atrial Flutter, 26, 41
Atrial Septal Defect, 599
Atrial Tachycardia, 41
Atrioventricular Block, 42
Atropine, 42
Atrovent, 614
Attachment, 573
Attachment Disorder, 573
Attention Deficit/Hyperactivity
Disorder, 572, 659
Attribution Theory, 571
Atypical Lymphocytes, 287
Audiometry, 150
Auditory Brainstem Response,
150
Auer Rods, 287
Auerbach‟s Plexus, 640
Augmentin, 513
Autism, 419, 582
Autonomy, 716, 717
Autonuclear Antigens, 270
Autopsy
Child, 569
Autosomal Dominant, 464
Autosomal Recessive, 464
Avascular Necrosis, 235
Avoidant Personality Disorder,
455
Azathioprine, 272
Back Pain, 239
Management, 242
Red Flags, 241
Background Retinopathy, 146
Back-knee Gait, 250
Bacteraemia, 494
Bacterial Overgrowth of Small
Intestine, 176
Bacterial Vaginosis, 384
Bacteroides Fragilis, 502
Bacteruria, 219
Balanced Anaesthesia, 540
Balanitis, 634, 637
Barium Enema, 157
Barlow‟s Test, 619
Barton‟s Fracture, 248
Barts, 551
Basal Cell Carcinoma, 327
Basal Cell Papilloma, 326
Basal Pontine Syndrome, 126
Base Excess, 115
Battle‟s Sign, 150
Beck‟s Triad, 491
Beclometasone Dipropionate, 79
Becotide, 79
Bed Rest, 674
Bed Wetting, 635
Bee Sting Allergy, 310
Behaviour Management
Children, 570
Behavioural Change, 11
Behcet‟s Disease, 283
Benediction Hand, 247
Beneficence, 716
Benign Focal Epilepsy of
Childhood, 626
Benign Paroxysmal Positional
Vertigo, 148
Benign Paroxysmal Vertigo of
Infancy, 625
Benign Prostatic Nodular
Hyperplasia, 224
Bennett‟s Fracture, 249
Bense-Jones Proteins, 303
Benzodiazepines, 425
Bereavement, 458
Berger‟s Disease, 214
Beriberi, 49
Berry Aneurysm, 124
Bezoar, 166
Bias, 683, 703
in Screening, 690
Bile Acid Sequestrants, 53
Bile Duct Adenoma, 192
Bile Ducts, 195
Bile Salts, 183
Biliary Colic, 195
Bilirubin, 595
Binswanger Disease, 441
Bioavailability, 523
Biophysical Profile, 360
Biostatistics, 683
Biotinidase Deficiency, 466
Bipolar Depression, 431
Bivalve Speculum, 340
Bladder, 223
Bladder Infections, 219
Bladder Tumours, 223
Bleeding Time, 294
Blepheritis, 143
Blood Culture, 494
Blood Gases, 58
Interpretation of, 115
Blood Loss, 552
Blood Pressure, 19, See also
Hypertension
Hypotension in Post-op
Patient, 557
Paediatric Normal Values,
565
Blood Products, 552
Blood Tests, 9
Blood Transfusion, 552
Blood Volume, 550, 649
Blue Baby, 596
Blue Bloater, 81
Body Dysmorphic Disorder, 444
Bone Cancer
Secondary, 266
Bone Marrow Transplantation,
300
Bone Pain, 544
BOOP, 84
Borderline Personality Disorder,
455, 456
Bordetella Pertussis, 609
Borrelia Burgdorferi, 316
Bottle Feeding, 591
Bouchard‟s Nodes, 269
Boutonniere Deformity, 249
Bovine Spongiform
Encephalopathy, 441
Bowel Obstruction, 166
Bowen‟s Disease, 226, 323, 326
Boxer‟s Fractures, 621
BPPV, 148
BRAC Gene, 380
Brachial Plexus Injury, 245
Bradford Hill Criteria, 685
Bradycardia
Drug Treatment, 42
Brain Abscess, 498
Brain Death, 713
Brain Tumours, 136
Branchial Cysts, 648
Branhamella Catarrhalis, 502
Braxton-Hicks Contractions, 367
Breast, 375
Breast Cancer, 379
Treatment of, 381
Breast Discharge, 377
Breast Disease
Inflammatory, 377
Breast Feeding, 376, 590
Drugs and, 529
Breast Milk
Nutritional Deficiencies in,
647
Breast Milk Jaundice, 596
Breast Screening, 382
Breathlessness, 17
Palliative management of, 472
Breech, 370
Bretyllium, 42
Brief Psychotic Episode, 435
Brodie‟s Abscess, 260
Bromocriptine, 106
Bronchial Breathing, 61
Bronchiectasis, 82, 615
Bronchioalveolar carcinoma, 89
Bronchiolitis, 610
Bronchiolitis Obliterans
Organising Pneumonia, 84
Bronchitis, 608
Bronchitis, Chronic, 81
Bronchopneumonia, 67
Broncho-Pulmonary Dysplasia,
589
Brutons, 307
Budd Chiari Syndrome, 193
Budesonide, 79
Buerger‟s Disease, 283
Bulbar Palsy, 131
Bulimia Nervosa, 420
Bullying, 662
Bundle Branch Block, 25
Bupivacaine, 545
Burnout, 711
Burns, 486
in Children, 654
Bursitis, 256
Button Hole Deformity, 249
Butyrophenone, 438
BZDs
Prescription, 536
Withdrawal, 534
C Cell Carcinoma, 101
C6 Radiculopathy, 123
C7 Radiculopathy, 123
Ca Channel Blockers, 52
CA125, 469
Cachectia, 5
Caesarean Section, 371
CAGE Questions, 450
Calcanial Gait, 251
Calcification, 32
Calcitrol, 210
Calcium, 27
Calcium Pyrophosphate
Deposition, 278
Campylobacter Jejuni, 177
Cancer, 466
in Children, 648
Cancer Emergencies, 472
Candidiasis, 64, 69, 318, 323,
384
Cannabis, 448, 697
Cannulation, 554
Caplan's syndrome, 85
Caput Medusae, 156
Caput Succedaneum, 369
Carbamazepine, 135
Carbimazole, 99
Carbuncle, 316
Carcinogenesis, 467
Carcinoid Syndrome, 171
Carcinoid Tumour, 89, 171
Carcinoma
Gallbladder, 197
Gastric, 163
Cardiac Arrest
Drug Treatment, 480
Rhythms, 479
Cardiac Asthma, 48
Cardiac Axis, 26
Cardiac Output, 14
Cardiac Pacing, 43
Cardiac Sclerosis, 193
Cardiac Sphincter, 158
Cardiac Tamponade, 491
Cardiogenic Shock, 483
Cardiomyopathy, 54
Cardiopulmonary Resuscitation,
476
Cardiotocography, 360, 371
Cardiovascular Risk factors, 30
Cardioversion, 40, 479
Carotid Pulses, 19
Carpal Tunnel Syndrome, 123,
238, 249
Case-Control Study, 685, 703
Casts
in Urine, 203
Cataract
Congential, 148
Catheterisation, 220
Cavernous Haemangioma, 192
CDC Epidemiology Group, 687
CEA, 469
Cefazolin, 513
Cefipime, 513
Ceftriaxone, 513
Cefuroxime, 513
Cellulitis, 314, 316
Central Pontine Melanosis, 108
Central Retinal Vessels,
Occlusion of, 145
Centre for Adverse Reactions
Monitoring, 530
Ceoliac Disease, 164
Cephalosporins, 513
Cerebellar infarction, 140
Cerebral Palsy, 629
Cerebral Perfusion, 15
Cerebro-spinal Fluid, 123
Cervical Cancer, 351
Staging, 468
Cervical Glandular Neoplasia,
352
Cervical Intraepithelial
Neoplasia, 352
Cervical Lumps, 648
Cervical Screening, 352
Cervical Spondylosis, 238
Chalazion, 143
Charcot‟s Joint, 235
Charcot-Marie Tooth Disease,
132
Chemotherapy, 470
in Breast Cancer, 381
Chest Pain, Differential of, 16
Chest Radiology, 27
Chest Sounds, 61
Cheyne-Stokes Respiration, 91
Chicken Pox, 504
Chicken-Broth Ascites, 198
Child Abuse, 656
Child Development, 574
Child Health
Determinants of, 562
Measures of, 561
Child‟s Body Weight, 550
Child-Pugh Classification, 185
Children, Young Persons and
Their Families Act, 659
Chlamydia
Eye Infection, 144
Trachomatis, 383
Chlamydia Trachomatis, 385
Chloride, 113
Chloroquine, 509
Chlorpromazine, 438
Choanal Atresia, 595
Chocking, 485
Cholangiocarcinoma, 192
Cholangiocytes, 183
Cholangitis, 195
Ascending, 193
Cholecystitis, 195
Cholelithiasis, 195
Choleocystoduodenal Fistula,
166
Cholestasis, 183
Cholesterol, 53
Cholesterol Stones, 195
Cholestyramine, 170
Chondroblastoma, 265
Chondrocalcinosis, 278
Chondrodermatitis, 323
Chondromalacia Patellae, 256
Chondrosarcoma, 265
Chorea, 603
Choriocarcinoma, 227, 363
Chorionic Villous Sampling, 360
Choroid Plexus Papilloma, 137
Chromosome Disorders, 464
Chronic Active Hepatitis, 185
Chronic Bronchitis, 65, 81
Chronic Cholecystitis, 196
Chronic Disease
Effect on Child Development,
582, 669
in Adolescents, 582, 669
Chronic Fatigue Syndrome, 506
Chronic Granulocytic
Leukaemia, 298
Chronic Hepatitis, 185
Chronic Infiltrative (Restrictive)
Lung Disease, 84
Chronic Leukaemia, 300
Chronic Lymphocytic
Leukaemia, 304
Chronic Myeloid Leukaemia,
298
Chronic Obstructive Pulmonary
Disease, 80
Chronic Pancreatitis, 198
Chronic Pelvic Pain, 350
Chronic Persistent Hepatitis, 185
Chronic Renal Failure, 207
Complications of, 209
Chvostek‟s Sign, 112
Chylothorax, 604
Cigarette Smoking, 87
CIN, 352
Ciprofloxacin, 515
Circinate Balanitis, 276
Circumduction Gait, 251
Cisplatin, 90
CJD, 441, 500
CK, 38
CK – MB fraction, 38
Clarithromycin, 514
Classes of Drugs, 536
Clear Cell Renal Cell
Carcinoma, 217
Clearance of Drugs, 522
Cleft Lip, 618
Clinical Practice Guideline, 703
Clinical Trials, 536
Clinodactyly, 581
CLL, 300
Clonidine withdrawal, 534
Clostridium Botulinum, 177
Clostridium Difficile, 176
Clostridium Perfringens, 316,
502
Clozapine, 438
Club Foot, 619
Clubbing, 7
Clue Cells, 384
CML, 300
CMV, 191, 506
Coagulation, 292
Coal Tar, 335
Coal Workers Pneumoconiosis,
85
Coarctation of the Aorta, 600
Cochrane Collaboration, 702
Cockcroft-Gault Formula, 203,
525
Code of Health and Disability
Services Consumer‟s Rights,
712
Cognition, Assessment of, 416
Cognitive Behavioural Therapy,
424, 429, 457
Cognitive Development, 578
Cognitive Functions, 122
Cohort Effect, 673
Cohort Studies, 686
Colchicine, 278
Cold Chain, 517
Cold Sores, 503
Colic, 593
Colitis, 165
Collagenous Colitis, 179
Collateral Ligaments of the
Knee, 255
Colles Fracture, 248
Colloids, 551
Colonic Embryonic Antigen, 174
Colorectal Cancer, 171
Coma, 486
in Children, 651
Myxoedema, 99
Coma and Stupor, 117, 130
Combes Test, 290
Combined Oral Contraceptive,
341
Combined Variable
Immunodeficiencies, 307
Comedo, 314
Common Cold
in Children, 605
Common Peroneal Nerve, 123
Communicable Disease Control,
686
Community Acquired
Pneumonia, 70
Compartment Syndrome, 234
Chronic, 236
Competency
Assessment of, 714
Complement Deficiencies, 307
Complex Regional Pain
Syndrome, 283
Compliance, 528, 535
Compulsion, 718
Compulsory Treatment, 458
Condyloma, 226
Accuminatum, 318
Confidence Interval, 684
Confidentiality, 716
Confounding, 684, 703
Confusion
Differential in an Alcoholic,
451
Differential of, 443
Congenital Adrenal Hyperplasia,
466
Congenital Diaphragmatic
Hernia, 642
Congenital Dislocation of the
Hip, 618
Congenital Heart Disease, 598
Congenital Naevocellular
Naevus, 325
Congestive Heart Failure, 48
Congestive-Dilated
Cardiomyopathy, 54
Congo Red Stain, 209, 212
Coning, 130
Conjunctivitis, 143
Neonatal, 632
Conn‟s Syndrome, 104
Connective Tissue Diseases, 278
Consent, 717
Consolidation, 62
Constipation, 177
in Children, 643
Constitutional Delay, 586
Consultation Frameworks, 4
Contact Allergies, 310
Contact Dermatitis, 321
Contraception, 340
Contraception, Sterilisation and
Abortion Act 1977, 361
Controlled Release
Formulations, 527
Conversion Disorder, 444
Coombs-Gell Types, 531
Co-ordination, 121
COPD, 80
Cord Prolapse, 369
Corda Equina Syndrome, 139
Cordocentesis, 360
Cornerstones of Maori Health,
696
Coroid Plexus, 123
Coronary Heart Disease, 33
Coronary Perfusion, 15
Coronavirus, 64
Coroner, 713
Child Death, 570
Corrigan‟s Sign, 44
Cortisol, 102
Corynebacterium Diphtheriae,
64
Coryza, 8
Cost Effectiveness, 699
Cost Minimisation, 699
Cost Utility, 699
Cost-Benefit, 699
Cotrimoxazole, 515
Cotton wool spots, 145
Cough, Differential of, 16
Counselling
Genetic, 466
Counter-transference, 666
Cows Milk, 591
CPAP, 60
CPR, 476
Adult, 477
Paediatric, 478
CPR Efficacy, 481
Crackles, 61
Cranial Nerves, 118
Examination in Children, 622
Craniopharyngioma, 105, 138
Creatinine, 203
Creatinine Clearance, 525
Crepitations, 61
CREST Syndrome, 280
Creutzfeldt-Jakob Disease, 441,
500
Cri du Chat Syndrome, 464
Cricothyrotomy, 477
Crises, Medical, 711
Critical Medical Incidents, 711
Critically Appraised Topic, 702
Cross-sectional Studies, 685
Croup, 64, 66, 608
Crowning, 369
Crying Baby, 592
Cryoprecipitate, 553
Cryptococcus neoformans, 69
Cryptogenic Fibrosing
Alveolitis, 84
Cryptorchidism, 375, 636
Cryptosporidium, 177, 510
Crystal Arthropathy, 277
Crystalloids, 551
CSF, 123
CTG, 360, 371
Cushing‟s Disease, 102
Cutaneous Horn, 323
CVID, 307
Cyanosis, 18, 58
in the neonate, 597
Cyclophosphamide, 299, 382
Cystic Fibrosis, 466, 614, 615
Cystic Renal Disease, 216
Cystic Renal Dysplasia, 216
Cystitis, 219
Cytochrome P450, 525, 532
Cytoid Bodies, 145
Cytomegalovirus, 70, 191, 506
Cytotoxic Hypersensitivity, 309
Dactylitis, 276
D-dimmer test, 77
De Cubitus View, 29
De Quervain‟s Disease, 98
De Quervain‟s Syndrome, 249
Death
Certification of, 712
Changes following, 713
Diagnosis of, 481, 712
Death Certificate, 713
Declaration of Helsinki, 723
Deep Vein Thrombosis, 74, 557
Defibrillation, 478
Dehiscence, 558
Dehydration, 110
Assessment
in Children, 650
Treatment of, 550
Delayed Hypersensitivity, 309
Delayed Puberty, 668
Delirium, 420, 442
Delusional Disorder, 435
Delusions, 412, 415
Dementia, 420, 439
Demographic Transition, 689
Demyelinating Disease, 132
Dentate Line, 179
Deontological Moral Theories,
716
Dependent Personality Disorder,
455
Depersonalisation, 415
Depot-provera, 342
Depression
in Adults, 426
in Children and Adolescents,
662
Depressive Disorders, 426
Derealisation, 415
Dermal Melanocytic Naevus,
325
Dermatitis, 319
Dermatofibroma, 326
Dermatoheliosis, 323
Dermatology, 313
Glossary, 314
Dermatomyositis, 281
Dermatophyte Infections, 387
Dermatophytosis, 317
Dermis, 314
Dermoid Cysts, 648
Descriptive Studies, 685
Desquamative Interstitial
Pneumonia, 84
Detrussor Instability, 223
Development
Adolescent, 664
Child, 574
Cognitive, 578
Developmental Assessment, 575
Developmental Delay, 579
Hearing, 580
Developmental Dysplasia of the
Hip, 618
Developmental Quotient., 575
DEXA Scan, 262
Dexamethasone Suppression
Test, 102
Dextran, 551
Dextrocardia, 21
Dextrose, 551
Di George Syndrome, 100
Diabetes Insipidous, 109, 110
Diabetes Mellitus, 94
Foot Infections, 316
Gestational, 363
IDDM in Pregnancy, 364
Neonatal Complications, 596
Nephropathy in, 207
Retinopathy, 146
Type 1 (Juvenile Onset). See
Diabetes Mellitus
Diagnostic and Statistical
Manual of Mental Disorders,
419
Dialysis, 218
Diarrhoea, 154
in Children, 643, 644
Infectious Agents, 176
Diastasis, 257
Diastematomyelia, 631
DIC, 293
Dietary Fibre, 178
Differential Diagnosis, 10
Diffuse Alveolar Damage, 83
Diffuse Progressive Systemic
Sclerosis, 280
Diffusing Capacity, 59
Digesic, 470
Digoxin, 27, 41, 42, 53, 533
Dihydrotestosterone, 224
Diltiazem, 41, 52
Diphtheria, 64, 132
Vaccination, 518
Disability, 673
Disability Adjusted Life Years,
683
Disc Prolapse, 240
Discoid Eczema, 322
Discoid Lupus Erythematous,
279, 330
Disease Modifying Anti-
Rheumatic Drugs, 271, 273
Dissecting Aneurysms, 32
Disseminated Intravascular
Coagulation, 293
Disseminated Superficial Actinic
Porokeratosis, 323
Dissociative Disorders, 420
Distribution of Drugs, 524
District Health Boards, 681
Diuretics, 43, 50, 51
Diverticular Disease, 174
Diverticulitis, 174
Diverticulosis, 174
Dizygotic twins, 358
DMARDs, 271, 273
DMSA Scan, 204, 222
DNR Orders, 482
Do Not Resuscitate Orders, 482
Dobutamine, 53
Doctor‟s Health Advisory
Service, 712
Dog Bites, 316
Dohle Bodies, 287
Doll‟s Eye, 130
Domestic Violence, 574
Dopamine, 43, 53, 106
Dorsal Dermal Sinus, 631
Double Effect, Doctrine of, 720
Down Syndrome, 581, 639
Doxycycline, 515
D-Penicillamine, 272
Driving by the Elderly, 676
Droopy Eye Lid, 145
Drop Foot Gait, 251
Drowning, 487
Drug Allergy, 530
Drug and Alcohol Policy, 697
Drug Education, 457
Drug Interactions, 531
Drug Withdrawal Syndromes,
533
Drugs of Abuse, 448
Regulation of, 536
Dry Mouth, 158
DSM IV, 414, 419
Dual Diagnosis, 421, 446
Duct Ectasia, 377
Ductus Arteriosus, Patent, 599
Duke‟s Staging, 174
Duodenal Atresia, 639
Duodenum, 161
Dupuytren‟s Contracture, 8, 249
DVT, 74, 557
With Contraceptives, 342
Dysarthria, 131
Dysdiadokinesia, 121
Dysfunctional Uterine Bleeding,
346
Dyshidrotic Eczema, 322
Dyslipidaemia, 30
Dysmenorrhoea, 346
Dyspareunia, 345
Dyspepsia, 159
Dysphagia, 131, 158
Dysphonia, 66, 131
Dyspnoea
Differential in Children, 604
Dyspraxia, 439
Dysthymic Disorder, 430
Dystonias, 132
Dysuria, 220
E Coli, 67
Ear Testing, 150
Eating Disorders, 420, 453
EC50, 528
Ecchymoses, 314
ECG
Changes in Pregnancy, 363
Interpretation, 24
Echinococcus Granulosa, 510
Echocardiogram, 49
Echolalia, 582
Eclampsia, 366
Economic Evaluations, 699
Ecthyma, 315
Ectopic Beats, 26
Ectopic Pregnancy, 362
Ectopic Thyroid, 648
Ectropion, 675
Eczema, 319
Eczema Herpeticum, 503
Education, 11
Parent and Adolescent, 567
EEG
in Children, 627
Efficacy, 528, 703
Efficiency, 698, 703
Effusion, 73
Eisenmenger‟s Syndrome, 602
Ejection Fraction, 14
Elastin Van Geesen, 31
Elbow Injury, 246
Elder Abuse, 675
Elderly, 671
Electrocution, 487
Electrolyte Abnormalities, 487
Electrolyte Concentrations, 550
Electro-Mechanical Dissociation,
479
Electrophoresis, 184
Elephantitis, 509
Elimination, 522
Embolic Infarction, 128
Embryonal Carcinoma, 227
Emergency Contraception, 343
Emergency Management
in Children, 649
Emotional Abuse, 658
Emphysema, 81
Empyema, 73, 612
Encephalitis, 140, 499
Encephalocele, 631
Enchondroma, 265
Encopresis, 643
Endocardial Fibroelastosis, 54
Endometrial Cancer, 354
Endometrial Thickness, 355
Endometriosis, 347
Endomyocardial Fibrosis, 54
Endomysial Antibodies, 164
Endoscopy, 157
Endotracheal Intubation, 477
Energy Metabolism, 555
Entamoeba Histolytica, 509
Enteral Nutrition, 555
Enteropathic Arthropathies, 277
Enteroviruses, Non-polio, 617
Enthesitis, 236, 275
Enuresis, 635
Environmental Health, 688
Ependymal Cells, 136
Ependymoma, 136, 137
Epicondyle Fractures, 620
Epidemics, 687
Epidemiology, 685
Mental Health, 410
Epidermal Cyst, 325
Epidermal Naevi, 325
Epidermis, 314
Epidermolysis Bullosa, 335
Epididymo-orchitis, 226
Epididymo-Orchitis
in Children, 637
Epidural Anaesthetic
in Labour, 546
Epiglottis, 66
Epiglottitis, 65, 609
Epilepsy, 133
in Children, 626
Epilim, 135
Epiphora, 148
Episcleritis, 143, 170
Epispadias, 226
Epistaxis, 63
EPS, 438
Epstein Barr Virus, 64, 191, 505
Equipoise, 724
Equity, 680, 698
Erb‟s Palsy, 245
Ergometrine, 369, 373
Erysipelas, 316, 500
Erythema, 314
Erythema Infectiosum, 618
Erythema Marginatum, 603
Erythema Multiforme, 332
Erythema Nodosum, 168, 169,
332
Erythema Toxicum Neonatorum,
333
Erythrasma, 387
Erythrocyte Sedimentation Rate,
290
Erythrocytosis, 297
Erythroderma, 335
Erythromycin, 514
Erythroplakia, 158
Erythroplasia of Queyrat, 226
Erythrovirus, 618
Escape Beats, 26
Escharotomy, 486
Escheria Coli, 177
Escherichia Coli, 502
ESR, 290, 687
Essential Thrombocythaemia,
298
Ethics, 715
Ethics Committees, 723, 724
Etoposide, 90
Euthanasia, 719
Evaluation
Diagnostic Tests, 704
History Taking and Clinical
Examination, 704
Prognosis, 707
Therapy, 706
Event Rate, 704
Evidence Based Medicine, 701
Ewing‟s Tumour, 266
Excretion of Drugs, 524
Executive Function, 122
Exfoliative Dermatitis, 335
Exomphalos, 641
Exophthalmos, 98
Exostosis, 149, 266
Extensor Lurch, 251
External Validity, 683
Extractable Nuclear Antigens,
270
Extradural Haemorrhage, 124
Extradural Spinal Cord
Compression, 138
Extrahepatic Biliary Atresia, 194
Extramedullary Haematopoiesis,
296
Extrapyramidal Syndromes, 438
Extrasystole Beats, 26
Extrinsic Allergic Alveolitis, 85
Extrinsic Pathway, 292
Exudate, Pleural, 73
Eye Disorders in Children, 631
Eye Trauma, 142
Facial Nerve, 118
Facilitation, 543
Factor V Leiden, 293
Failure to Thrive, 591, 642
Fainting, 131
Falls in the Elderly, 674
Familial Adenomatous
Polyposis, 172
Families, 568
Farmer‟s Lung, 85
Fast Acetylators, 525
Fatty Streaks, 31
Febrile Convulsion, Benign, 627
Fecundability, 344
Femoral Anteversion, 619
Femoral Epiphysis
Slipped Upper, 621
Femoral Shaft Fractures, 621
Femur, 252
Fentanyl, 544
Ferritin, 290
Fetal Alcohol Syndrome, 624
Fetal Distress, 372
Fetal Growth Restriction, 360
Fetal Position, 368
Fetal Welfare, 359
FEV1, 58
Fever, 5
in Children, 5, 616
in Neutropenic Patient, 6, 301,
470, 472
of Unknown Origin, 6
Fibre, 178
Fibric-acid Derivatives, 53
Fibroadenoma, 378
Fibroids, Uterine, 347
Fibromuscular Dysplasia, 33
Fibromyalgia, 284
Fibrosarcoma, 266
Fictitious Disorder, 454
Fictitious Disorders, 420
FIGO System, 468
Filariasis, 509
Finckelstein‟s Sign, 249
Flagyl, 515
Flail Chest, 491
Flat Foot Gait, 251
Flecainide, 41
Flexatide, 79
Floppy Valve Syndrome, 45
Flow-volume Loop, 59
Flucloxacillin, 513
Fluconazole, 515
Fluid Compartments, 550
Fluid Loss, Assessment, 650
Fluoxetine, 434
Fluticasone Propionate, 79
Focal and Segmental
Glomerulosclerosis, 214
Folate, 630
Follicular Carcinoma, 100
Folliculitis, 316, 387
Food Allergy, 647
Foot Slap Gait, 250
Forceps, 371
Foreign Body, Inhalation of, 614
Foreskin
Retraction of, 637
Formulation, 5
Psychiatric History, 414
Fournier‟s Gangrene, 226
Fovea, 141
Fracture, 232
Complications of, 234
Healing of, 233
of Clavicle, 245
of Femoral Neck, 253
of Femur, 253
of Fibula, 257
of Head of Radius, 246
of Humerus, 246, 620
of Mandible, 259
of Maxilla, 259
of Metacarpal bones, 249
of Nose, 258
of Olecranon, 246
of Orbit, 258
of Patella, 256
of Pelvis, 243
of Phalanges, 249
of Radius and Ulna, 248
of Scaphoid, 248
of Tibia, 257
of Zygoma, 258
Fractured Penis, 226
Fragile X Syndrome, 464, 465
Framingham Study, 30
Freckle, 324
Fresh Frozen Plasma, 553
Frost Bite, 236
Frozen Shoulder, 244
Frusemide, 51
FSH, 104, 338
Fulminant Hepatitis, 185
Functional State, 672
Fungal Infections, 317
Fungal Pneumonias, 69
Furuncle, 316
Futility, 716
GABA, 425
Gait, 250
Galactorrhoea, 107
Causes of, 377
Galactosaemia, 466
Galeazzi Fracture, 248
Gallbladder, 195
Gallop Rhythm, 22
Gallstone Ileus, 166
Gallstones, 196
Gambling, 420, 453
Gamekeeper‟s Thumb, 249
Ganciclovir, 507, 515
Ganglia, 249
Gangligliomas, 137
Gangliocytomas, 137
Gardener‟s Syndrome, 173
Gardnerella Vaginalis, 384
Gas Gangrene, 316
Gastric Neoplasia, 163
Gastritis, 161
Gastroenteritis
in Children, 644
Gastro-Intestinal, 153
Bleeding. See GI Bleeding
Gastro-Oesophageal Reflux
Disease, 160, 162
Gastroschisis, 641
GCS, 129, 481
General Anaesthesia, 540
General Medical Condition,
Psych Disorders due to, 444
Generalised Anxiety Disorder,
423
Generalised Progressive
Systemic Sclerosis, 280
Genetic Testing, 465
Genetics, 463
Genital Herpes, 504
Genital Skin Lesions
Non-sexually Transmitted,
386
Genital Warts, 386
Genitalia, Ambiguous, 638
Gentamicin, 514
Genuine Stress Incontinence,
223
Germ Cell Tumours, 226
Gestational Diabetes Mellitus,
94, 363
Gestational Hypertension, 364
Geudal Airway, 476
GFR, 203
GGT, 183
GH, 104
Ghon complex, 69
GI Bleeding, 180
in Children, 641
Lower, 180
Upper, 180
GI Haemorrhage
Treatment, 181
Giant Cell Arteritis, 140, 282
Giant Cell Tumour, 266
Giardia, 177
Giardiasis, 509
Gilbert‟s Syndrome, 193
Gillick Case, 718
Gingivostomatitis, 503
Gini Co-efficient, 693
Glasgow Coma Scale, 129, 481
Glaucoma, 143
Congenital, 148, 632
Primary Closed-angle, 144
Primary Open-Angle, 144
Secondary, 144
Glevac, 299
Glial Blastoma, 136
Global Environmental Change,
689
Global Warming, 689
Glomerular Filtration Rate, 203
Glomerulonephritis, 212
Glossitis, 288
Glossopharyngeal Nerve, 118
Glucocorticoids, 102
Glucose Tolerance Test, 94
Glue Ear, 606
Gluteus Maximus Gait, 251
Gluteus Medius Gait, 251
Glycaemic Index, 96
GnRH, 338
Gold, 272
Golfer‟s Elbow, 246
Gonadal Stromal Tumours, 227
Gonadarche, 667
Gonorrhoea, 383
Goodpasture‟s Syndrome, 92,
214
GORD, 160, 162
Gottron‟s Lesions, 281
Gouty Arthritis, 277
Grand Mal Seizures, 134
Granuloma Annulare, 334
Granulomas
Differential of, 68
Grave‟s Disease, 98
Gravidity, 338
Grief, 458, 473
Pathological, 459
Griseofulvin, 336
Grommets, 607
Growing Pains, 587
Growth, 585
GTN, 43
Guillian Barre Syndrome, 139,
630
Gustilo Classification, 232
Gut Layers, 165
Guthrie Card, 465
Guttate, 314
Gynaecology, 338
Gynaecomastia, 107, 668
Haemaccel, 551
Haemangioendothelioma, 54
Haemangioma, 54
Haematemesis, 180
Haematochezia, 154, 180
Haematocoele, 226
Haematology, 285
Haematuria
in Children, 633
Haemochromatosis, 192
Haemodialysis, 218
Haemoglobin Abnormalities,
290
Haemolysis Tests, 290
Haemolytic Uraemic Syndrome,
209, 645
Haemophilia, 292
Haemophilus Influenza, 67, 502
Type B, 609
Type B Vaccination, 519
Haemoptysis, 16
Haemorrhagic Disease of the
New Born, 588
Haemorrhagic Infarcts, 128
Haemorrhoids, 179
Haemostasis, 291
Haemothorax, 491
Haemotympanum, 150
Hairy Cell Leukaemia, 306
Half Life, 523
Hallpike Manoeuvre, 148
Hallucinations, 413, 415
Haloperidol, 438
Halothane, 541
Hamartoma, 468
Hamman-Rich Disease, 84
Hand
Infections of, 261
Hand, Foot and Mouth Disease,
617
Handicap, 673
Happy Wheezer, 614
Hard Exudates, 145
Harrison‟s Sulcus, 565
Hashimoto‟s Thyroiditis, 100
Hatoglobins, 290
Haversian Canal, 260
Havrix, 187
Hay Fever, 310
Head Injury
Dementia due to, 441
Effect on child development,
583
Head Size, 624
Headaches, 139
in Children, 624
Headlice, 319
HEADSS Risk Assessment, 666
Health
WHO Definition, 680
Health Act 1956, 687
Health and Disability
Commission, 681
Health and Disability Services
Consumer‟s Rights, Code of,
712
Health Care Delivery, 680
Health Care Expenditure, 680
Health Economics, 698
Health Insurance Markets, 698
Health Policy Agencies, 681
Health Promotion, 691
Health Sponsorship Council, 681
Health Status, 682
Hearing Loss, 151
Heart Block, 42
in Children, 601
Heart Disease
in Children, 13, 596
Heart Failure, 48, 614
in Children, 601
Heart Murmurs, 23
Heart Sounds, 21
Heart Valves, 14
Heat Exhaustion, 488
Heat Stroke, 488
Heberden‟s Nodes, 269
Hegemony, 418
Heimlich Manoeuvre, 485
Helicobacter Pylori, 162
HELLP Syndrome of Pregnancy,
209
Hemangioblastoma, 138
Hemianopia, 118
Henderson Hasselbach Equation,
113
Henoch-Scholein Purpura, 620
Heparin, 75
Heparin-Induced
Thrombocytopenia, 295
Hepatic Encephalopathy, 194
Hepatic Failure, 194
Hepatic Iron Index, 192
Hepatic Vein Thrombosis, 193
Hepatitis
A, 186
A Vaccination, 511
B, 187
B Vaccination, 518
C, 189
Chronic, 185
Classification of, 184
D, 191
E, 191
Hepatitis Activity Index, 185
Hepatoblastoma, 192
Hepatocellular carcinoma, 191
Hepatojugular Reflex, 20
Hepato-renal Syndrome, 194
Herd Immunity, 516
Hereditary Non-polyposis Colon
Cancer, 172
Hereditary Spherocytosis, 289
Hernia
Hiatus, 161
in Children, 641
Herpes 6 and 7, 618
Herpes Simplex Virus, 64, 70,
318, 383, 386, 503, 616
Encephalitis, 499
Eye infection, 144
In Pregnancy, 372
Herpes Viruses, 503
Hetastarch, 551
Hiatus Hernia, 161
Hickman Catheter, 300
Hip, 252
Developmental Dysplasia of
the, 618
Transient Synovitis of the,
621
Hip-hike Gait, 251
Hirschsprung‟s Disease, 640
Hirsutism, 107
History, 117
Abdominal, 154
Abuse, 339, 343
Anxiety Disorders, 412, 415,
422
Back Pain, 237
Breast, 375
Cardiovascular, 15
Endocrine, 94
Gynaecological, 338
History Taking, 4
Knee, 253
Neonatal, 587
Neurology, 117
Obstetric, 339, 355
Ophthalmology, 140
Orthopaedic, 230
Outline of, 4
Paediatric, 563
Psychiatric, 411
Renal, 202
Rheumatological, 230
Sexual, 382
Substance Abuse, 447
Suicide, 416
Histrionic Personality Disorder,
455
HIV, 308, 383
HLA-B27, 274
HMG Co-A Reductase
Inhibitors, 53
Hodgkin‟s Lymphoma, 305, 648
Honey Comb Lung, 85
Hookworm, 509
Hormonal Contraception, 341
Hormone Replacement Therapy,
349
Horner‟s Syndrome, 145
Horseshoe Kidney, 216
Housing, 693
Howell-Jolly Bodies, 286
HPV, 351
Hudson Mask, 60
Human Chorionic
Gonadatrohpin, 338
Human Immunodeficiency
Virus, 383
Human Papilloma Virus, 351,
383
Huntington‟s Disease, 132, 465
Hutchison‟s Freckle, 325
Hyaline Membrane Disease, 589
Hydatid Disease, 510
Hydatiform Mole, 363
Hydraencephaly, 624
Hydralazine, 366
Hydrocele, 636
Hydronephrosis, 216
Hydrops Fetalis, 370, 595, 597
Hydroxychloroquine, 272
Hyperaldosteronism, 104
Hyperalgesia, 543
Hypercalcaemia, 112
Hypercholesterolaemia, 53
Hyperemesis gravidarum, 363
Hyperglycaemia, 96
Hypericum, 434
Hyperkalaemia, 27, 111
Hyperkeratosis, 158, 314
Hyperlipidaemia, 30
Hypernatraemia, 110
Hyperparathyroidism, 101, 263
Secondary to Renal Failure,
210
Hyperproteinaemia, 184
Hypersensitivity, 309
Angiitis, 283
Pneumonia, 85
Types of, 531
Hypertension, 34, 215, See also
Blood Pressure
Definition of, 34
In Pregnancy, 364
Persistent Pulmonary, 600
Portal, 194
Primary Portal, 92
Pulmonary, 598
WHO definitions, 34
Hypertensive Intracerebral
Haemorrhage, 125
Hypertensive Retinopathy, 146
Hyperthermia, 488
Hyperthyroidism, 98
Hypertrophic Cardiomyopathy,
46, 54
Hypertrophic pyloric stenosis,
639
Hyperuricaemia, 277
Hyper-Viscosity Syndrome, 303
Hypnotics, 535
Hypoadrenalism, 103
Hypocalcaemia, 27, 112
Hypochondriasis, 444
Hypo-Coagulation Diseases, 292
Hypogammaglobulinaemia, 307
Hypoglossal Nerve, 118
Hypoglycaemia
of the New Born, 590, 595
Hypogonadism, 107
Hypokalaemia, 27, 111
Hyponatraemia, 108
Hypoparathryoidism, 102
Hypopituitarism, 105
Hypoproteinaemia, 184
Hypospadias, 638
Hypotension
In Post-Op Patient, 557
Hypothermia, 487
Hypothyroidism, 99, 466
Hypovolaemic shock, 483
Hypoxic-ischaemic
Encephalopathy, 372, 589
Iatrogenic Disease, 674
Ichthyoses, 335
IDDM. See Diabetes Mellitus
Idiopathic Pulmonary Fibrosis,
84
IgA Deficiency, 307
IGF-1, 107
IgM Anti-VCA, 505
IgM Paraproteinaemia, 132
Illusions, 415
Imaging
CT, 9
MRI, 9
Immediate Hypersensitivity, 309
Immune Complex Mediated
Glomerulonephritis, 215
Immune Complex Mediated
Hypersensitivity, 309
Immune Deficiency, 614
Immune Thrombocytopenia, 295
Immunisation, 518, See
Vaccination
Immunity, 516
Immunodeficiency, 306
Impaired Fasting Glycaemia, 94
Impaired Glucose Tolerance, 94
Impaired or Incompetent
Colleagues, 721
Impairment, 673
Imperforate anus, 641
Impetigo, 315
Impotence, 107
Imprinting
Genetic, 465
Impulse-Control Disorders, 420,
453
Incidence, 685
Incontinence
Daytime, in Children, 634
Night time, in Children, 635
of Urine, 223
Incontinentia Pigmenti, 335
Induction, 371
Infant Drug Withdrawal
Syndrome, 596
Infantile Polycystic Kidney, 216
Infantile Spasms, 134
Infection Control, 710
Infectious Arteritis, 33
Infectious Diseases, 493
Infective Endocarditis, 46
Infertility, 344
Inflammatory Arthritis, 270
Blood Tests in, 270
Influenza, 64, 70
Vaccination, 519
Informed Consent, 712, 717, 719
Infraspinatus Muscle, 244
Inguinal Hernia
in Children, 641
Inheritance, Patterns of, 464
Inhibin, 338
Injury
in Children, 654
Innovative Treatment, 723
Inotropes, 43, 53
Inotropy, 14
INR, 292
Insomnia, Treatment of, 534
Insulin, 96
Intention-to-treat analysis, 703
Internal Validity, 683
International Normalised Ratio,
292
Interpersonal Violence, Victim
of, 343
Interstitial Cystitis, 223
Interstitial Myocarditis, 51
Interstitial Pulmonary Disease,
83
Intertrigo, 322
Intervention Studies, 686
Intracranial Haemorrhage, 123
Intraductal Carcinoma, 380
Intra-uterine Growth
Retardation, 360
Intravenous Urogram, 203
Intraventricular Haemorrhage,
589
Intrinsic Pathway, 292
Intussusception, 166, 641
Invasive Ductal Carcinoma, 381
Involucrum, 260
IPPV, 60
Ipratropium, 614
Iritis, 143, 171, 275
Iron Deficiency. See Anaemia
in Children, 646
Irritable Bowel Syndrome, 175
Irritant Dermatitis, 321
Ischaemic Bowel Disease, 165
Ischaemic Heart Disease, 33
Isoflurane, 541
Isoniazid, 69
Isoprenaline, 42
Isotretinoin, 331, 336
Itraconazole, 336, 515
IUCD, 341
Emergency, 343
Jakarta Declaration on Health
Promotion, 562
Japanese Encephalitis, 499
Jaundice, 184
Neonatal, 595
Jelly Belly, 168
Joint Swelling
Differential of in children,
620
Jone‟s Criteria, 603
Jugular Venous Pressure, 20
Junctional Rhythm, 41
Justice, 716
Juvenile Onset Diabetes, 94
Juvenile Plantar Dermatosis, 322
Juvenile Polyps, 171
Juvenile Rheumatoid Arthritis,
273
Juxtaglomerular Cell Tumour,
217
JVP, 20
Kaposi‟s Sarcoma, 54, 308
Kappa Statistic, 704
Kawanatanga, 695
Kawasaki Disease, 282
Keratitis, 143
Keratoacanthoma, 326
Keratoconjunctivitis Sicca, 279
Keratoderma Blenorrhagica, 276
Keratosis Pilaris, 334
Kerley B Lines, 29
Kernicterus, 595
Kernig‟s Sign, 495
Ketamine, 542
Ketoacidosis, 96, 487
Kidney Transplantation, 219
Kimmelstiel-Wilson Lesion, 96
Klebsiella, 67
Aerongenes, 502
Pneumoniae, 275
Klinefelter Syndrome, 464
Klumpke‟s Paralysis, 245
Knee, 253
Knee Injury, 255
Koebner, 328
Koilonychia, 8, 288
Koplik‟s Spots, 617
Kupffer Cells, 192
Kuru, 500
Kussmaul Breathing, 650
L5 Radiculopathy, 123
Labetalol, 365
Labour, 368
Abnormal, 370
Analgesic Drugs, 546
Stages of, 369
Labyrinthitis, 149
Lachman‟s Test, 254
Lactobacilli, 338
Lactose, 591
Lactose Intolerance, 165
Langerhans Cells, 92, 324
Langhans Cells, 92, 170
Large Cell Carcinoma, 89
Laryngeal Carcinoma, 86
Laryngeal Nodule, 86
Laryngeal Papilloma, 86
Laryngomalacia, 604
Laryngomalatica, 66
Laryngotracheobronchitis, 608
Larynx, 65
Lasegue‟s Sign, 238
Lateral Decubitus CXR, 73
Lateral Medullary Syndrome,
126
Laxatives, 178
LDH, 38
LDL, 53
Learning Disability, 583
Leather Bottle Stomach, 164
Left Bundle Branch Block, 25
Left Ventricular Hypertrophy, 26
Legg-Calve-Perthes Disease, 621
Legionella Pneumonia, 67
Lentigo, 323
Leucocytosis, 291
Leucodystrophies, 132
Leucoerythroblastosis, 296
Leuconychia, 8, 155
Leukaemia, 300, 649
Leukocoria, 147
Leukocornea, 632
Leukocytoclastic Vasculitis, 33,
283
Leukoplakia, 158
Levels of Evidence, 703
Lewy Bodies, 132
Lewy Body Dementia, 132, 441
Leydig Cells, 338
Leydig tumours, 227
LFTs, 182
LH, 104, 338
Libman-Sacks Endocarditis, 45,
279
Lichen Planus, 158, 334, 387
Lichen Sclerosis, 350
Life Expectancy, 673, 682
Lignocaine, 42, 545
Likelihood Ratio, 705
Limb Length Inequality, 621
Linitis Plastica, 163
Lipid Lowering Drugs, 53
Lipid Pneumonia, 70
Lipids, 53
Lipoma, 631
Lipophages, 136
Lisfranc Dislocation, 258
Lissencephaly, 629
Listeria, 357
Lithium, 431, 533
Liver
Biopsy, 185
Disease, 181
Rupture of, 490
Tumours, 191
Vascular Disease, 193
Liver Cell Adenoma, 192
Liver Function Tests, 182
Loading Dose, 522
Lobar Pneumonia, 68
Lobular Carcinoma In Situ, 380
Local Anaesthesia, 544
Locked-in Syndrome, 140
Loculated Empyema, 612
Long QT Syndrome, 601
Looser‟s Zones, 263
Loss of Consciousness,
Differential of, 117
Lower Motor Neuron Lesions,
121
Lumbar Puncture, 496
Lumbar Root Nerve Entrapment,
241
Lumbar Spondylosis, 240
Lung Abscesses, 68
Lung Cancer, 87
Systemic Effects, 89
Lung Function Tests, 58
Lyme Disease, 316
Lymph Nodes
Neck Anatomy, 8
Lymphadenitis, 316
Lymphadenopathy
in Cancer, 649
Lymphocytic Meningitis, 499
Lymphocytosis, 291
Lymphoma, 227, 305, 649
Lymphoproliferative Disorders,
302
Macrocytic Anaemia, 288
Macrolides, 514
Macrosomia, 363
Macula, 141
Macular Degeneration, 142
Macule, 314
Mad Cow Disease, 441
Magnesium, 27, 42, 113
Magnesium Sulphate, 366
Maintenance Dose, 522
Major Depressive Episode, 427
Major Tranquillisers, 437
Malabsorption Syndromes, 165
Malaria, 508, 688
Malassezia Furfur, 317
Malignant Hyperthermia, 547
Mallet Finger, 249
Mallet Thumb, 248
Malnutrition, 554
Malrotation, 639
MALT, 171
Mammography, 382
Mana, 694
Managed Care, 680
Manic-Depression, 431
MAO - A, 434
MAOIs, 434
Overdose, 435
Maori Cultural Differences, 697
Maori Health, 694
Maori Mental Health, 410
Maori Patient, Treatment of,
410, 428
Maple Syrup Urine Disease, 466
Marcain, 545
March Fractures, 258
Marginal Analysis, 698
Marijuana, 448
Market Failure, 698
Markets, 698
Marmot Study, 694
Mate Maori, 696
Maternal Death, 373
Maternal Serum Screening, 360
Maturity Onset Diabetes Of The
Young, 95
McCallum‟s Patch, 604
McMurray‟s Test, 254
MCU, 222
Mean Arterial Pressure, 14
Measles, 70, 516, 617
Vaccination, 519
Mechanical Back Pain, 240
Meckel‟s Diverticulum, 639
Meconium Aspiration, 370, 596,
605
Meconium Ileus, 615, 640
Medial Medullary Syndrome,
126
Median Nerve, 247
Compression, 123
Medical Council, 712
Medical Error, 712
Medical Misadventure, 712
Medical Mishap, 712
Medical Officer Of Health, 687
Medical Practitioners Act, 711
Medical Referee, 713
Medicine Assessment Advisory
Committee, 530
Medicines Act, 536
Mediobasal Mesencephalic
Syndrome, 126
MedSafe, 536
Medullary Carcinoma, 101
Medulloblastoma, 136, 138
Mee‟s Lines, 8
Mefloquine, 508
Megakaryocyte, 294
Megalencephaly, 624
Megaloblastic Anaemia, 288
Meissner‟s Plexus, 640
Melaena, 180
Melancholic Depression, 428
Melanocytes, 324
Melanoma, 324
of the Choroid, 147
Melanosis Colis, 165
Membranoproliferative
Glomerulonephritis, 215
Membranous
Glomerulonephritis, 214
Memory, 122
Menarche, 667
Meniere‟s Disease, 151
Meningioma, 136, 138
Meningitis, 495
Viral, 499
Meningocele, 631
Meningococcal Disease, 497
Meniscal Tears, 255
Menopause, 349
Menorrhagia, 346
Menses, 339
Menstrual Cycle, 338
Menstrual Disorders, 345
Mental Health
in Children and Adolescents,
659
in New Zealand, 410
Mental Health Act 1992, 458
Mental Health Commission, 681
Mental Illness, Treatment of, 456
Mental State
Cognition, 416
Examamination of, 117
Examination of, 414
Mesangial IgA disease, 214
Mesangiocapillary
Glomerulonephritis, 215
Mesothelioma, 89
Metabolic Acidosis, 114
Metabolic Alkalosis, 114
Metabolic Bone Disease, 261
Metabolism of Drugs, 524
Metastatic Brain Tumours, 138
Metatarsalgia, 258
Methadone Treatment, 449
Methaemoglobinaemia, 290
Methotrexate, 272
Methyldopa, 365
Metoprolol, 41
Metronidazole, 515
Metyrapone Test, 105
MGUS, 184, 303
MI, 36
Michaelis-Menten Kinetics, 523
Miconazole, 515
Microalbuminuria, 95, 207
Microcephaly, 624
Microcytic Anaemia, 287
Microglia, 136
Microsporum Canis, 317
Microstomia, 280
Micturating Cystourethrogram,
203
Midazolam, 542
Migraine, 139
in Children, 624
Miliary Pattern on Xray, 29
Mineralocorticoids, 102
Minimal Change Disease, 213,
633
Minimum Alveolar
Concentration, 541
Miscarriage, 362
Misuse of Substances Act, 536
Mitochondria, 465
Mitral Facies, 19, 45
Mitral Regurgitation, 22, 45
Mitral Stenosis, 22, 45
Mitral Valve Prolapse, 45
Mixed Acid/Base Disorders, 115
Mixed Connective Tissue
Disease, 281
Mobitz, Heart Block, 42
Moclobemide, 434
MODY, 95
Molluscum Contagiosum, 318,
387
Mongolian Spot, 325
Monoclonal Proteins, 303
Mononeuritis Multiplex, 273
Monozygotic Twins, 359
Monteggia Fracture, 248
Mood Disorders, 420, 426
Mood Stabilising Medication,
431
Moral Hazard, 699
Moraxella Catarrhalis, 502
Morbidity, 682
Morning sickness, 357
Morphine, 471, 543
Morphoea, 280, 330
Mortality, 682
Motivational Interviewing, 11
Motor Examination, 120
Motor Neurone Disease, 133
Mucocoele of the Appendix, 168
Mucocoele of the Gallbladder,
197
Mucormycosis, 69
Multinodular Goitre, 101
Multiple Endocrine Neoplasia,
101
Multiple Myeloma, 302
Multiple Pregnancy, 358
Multiple Sclerosis, 132
Mumps, 617
Vaccination, 519
Munchausen‟s By Proxy, 454
Murmurs, 23
Murphy‟s Sign, 196
Murray Valley Encephalitis, 499
Muscle Relaxants, 542
Muscular Dystrophy, 630
Musculo-Skeletal, 229
Myasthenia Gravis, 140
Mycobacteria, 502
Mycoplasma Pneumonia, 70
Myelodysplastic Syndromes, 299
Myelofibrosis, 298
Myelomeningocele, 631
Myeloproliferative Disorders,
296
Myocardial Contusion, 491
Myocardial Infarction, 36
Myocarditis, 50
Myoglobin, 38, 210
Myotonic Dystrophy, 465
Myxoedema, 99
Myxoma, 54
Naegele‟s Rule, 355
Naevi, 324
Napkin Dermatitis, 323
Nappy Rash, 323
Narcissistic Personality
Disorder, 455
Narcolepsy, 91
Nasal Encephalocele, 595
Nasal Obstruction, 63
Nasal Prongs, 60
Nasopharyngeal Carcinoma, 86
National Health Committee, 681
Natural Family Planning, 340
Nausea, Treatment of, 471
Neck, 237
Necrotising Enterocolitis, 590
Necrotising Fasciitis, 316, 501
Need, 680
Needle Stick Injury, 710
Nefazodone, 434
Neglect of Children, 658
Negligence, 712
Neisseria Gonorrhoeae, 64, 385
Neisseria Meningitidia, 497
Neonatal Hepatitis, 194
Neotigason, 336
Neovascularisation
in the Eye, 145
Nephritic Syndrome, 204
Nephroblastoma, 217
Nephrolithiasis, 210
Nephrotic Syndrome, 204
Nephrotoxins, 210
Nerve Injury, 237
Neural Tube Defects, 630
Neuroblastoma, 649
Neurofibromatosis, 334, 620
Neurogenic Claudication, 241
Neuroleptic Malignant
Syndrome, 438
Neuroleptics, 437
Neurology, 117
Paediatric, 621
Neuromuscular Blockade, 542
Neuromuscular Blocking Agents
Depolarising, 542
Non-depolarising, 542
Neuropathic Joint, 235
Neuropathic Pain, 544
Neuropil, 136
Neuropraxia, 237
Neurotmesis, 237
Nifedipine, 52
Nitrous Oxide, 541, 546
Nits, 319
Nociceptors, 543
Nodal Rhythm, 41
Nodular vasculitis, 333
Nodules
in Arthritis, 267
N-of-1 Trials, 703
Noise Induced Hearing Loss,
151
Non-Epileptic Seizure, 134
Non-Hodgkin‟s Lymphoma, 305
Non-maleficence, 716
Non-Polio Enteroviruses, 617
Non-proliferative
glomerulonephritis, 204
Non-Proliferative Retinopathy,
146
Non-Q Wave Infarction, 27
Non-STEMI, 36
Noonan‟s Syndrome, 464
Nor-adrenaline, 43
Norfloxacin, 515
Nosocomial PUO, 6
Notifiable Diseases, 687
NSAIDs, 210, 271
Nuchal Translucency, 360
Number Needed To Treat, 704
Nuremberg Code, 723
Nutrition
Deficiencies in Childhood,
646
in Surgical Patients, 554
in the elderly, 674
Nutritional assessment, 554
Nystagmus, 148
Nystatin, 515
NZ Deprivation Index, 693
NZ Medicines and Medical
Devices Safety Authority, 536
Obsessive Compulsive Disorder,
424
Obsessive Compulsive
Personality Disorder, 455
Obstetric Anaesthesia, 545
Obstetrics, 355
Obstructive Jaundice, 183
Obstructive Sleep Apnoea, 90
Occupational Therapist, 585
Octreotide, 107
Oedema, 7
Oesophageal Atresia, 639
Oesophageal Tumours, 158
Oesophagitis, 160
Oesophagus, 158
Oestradiol, 338
Oestrogen, 338
Olanzapine, 438, 439
Oligodendroglioma, 136, 137
Oligodenrocyte, 136
Oligomenorrhoea, 346
Oncogenesis, 466
Oncology, 466
Onychomycosis, 317
Opening Snap, 22
Ophthalmia Neonatorum, 632
Ophthalmic Nerve, 118
Ophthalmology, 140
Paediatric, 147
Opiod Analgesics, 543
Opportunity Cost, 698
OPSI, 307
Optic Atrophy, 145
Optic Neuritis, 145
Oral Pathology, 157
Oratane, 336
Orbital Cellulitis, 618
Orchitis, 226
Organ Donation, 722
Orthopaedic Tumours, 264
Orthopnoea, 17
Ortolani‟s Test, 619
Oscillopsia, 149
Osteoarthritis, 268
Secondary, 269
Osteoblastoma, 265
Osteoblasts, 261
Osteochondral Fractures, 256
Osteochondritis Dissecans, 256,
621
Osteochondroma, 265
Osteoclasts, 262
Osteoid Osteomas, 265
Osteomalacia, 261, 263
Osteomyelitis, 260
Chronic, 260
Osteopenia, 261
Osteophytes, 268
Osteoporosis, 261, 262
Pain in, 241
Osteosarcoma, 265
Osteotomy, 269
Otitis Externa, 149
Otitis Media, 65
Acute, 605
Chronic with Effusion, 606
Recurrent Acute, 606
Ottawa Charter, 562, 691
Ovarian cancer, 354
Overdose, 488
Overt Diabetic Nephropathy, 207
Ovulation, 339, 345
Oxygen Flux, 58
Oxygen Therapy, 60
Oxyhaemoglobin Dissociation
Curve, 58
P Value, 684
P wave, 26
P53 Gene, 467
Paget‟s Disease of Bone, 264
Paget‟s Disease of the Nipple,
380
Pain
Abdominal, in Children, 643
Bone, 544
Management, 470, 543
Management in Children, 655
Neuropathic, 544
Pharmacology, 543
Physiology, 543
Post-Operative, 544
Syndromes, 283
Pain Disorder, 444
Palliative Care, 473
Palmar Erythema, 8, 155
Panadine, 470
Pancoast Tumour, 89
Pancreas, 197
Pancreatic Tumours, 199
Pancytopenia, 289
Panic Disorder, 423
Papillary Thyroid Cancer, 100
Papillitis, 141
Papilloedema, 141
Papova Virus, 318
Papular Urticaria, 333
Papule, 314
Paracetamol Poisoning, 489
Paradex, 470
Paradoxical Breathing, 29
Parainfluenza Virus, 64
Parakeratosis, 314
Paranoid Personality Disorder,
455
Paraproteinaemia, 303
Parathyroid, 101
Parenchymal Haemorrhage, 589
Parenchymatous Myocarditis, 51
Parenteral Feeding, 556
Parity, 338
Parkinson‟s Disease, 131
Parkinsonism, 132
Paronychia, 318
Paroxetine, 434
Paroxysmal Nocturnal
Dyspnoea, 17
Partial Seizures, 134
Parvovirus, 618
Patella
Dislocation of, 256
Patellar-Femoral Joint, 255
Paternalism, 716
Pauci-immune
Glomerulonephritis, 215
Paul-Bunell, 506
PE, 76
Pectus Excavatum, 21
PEEP, 60
Pelvic Congestion, 350
Pelvic Inflammatory Disease,
385, 386
Pelvic Injury, 242
Pelvic Mass, 350
Pelvic Relaxation, 350
Pemphigoid, 329
Pemphigus, 329
Pencil Poikilocytes, 286
Penicillin G, 513
Penicillins, 513
Penis, 226
Diseases of in boys, 637
Penobarbitone, 135
Pentaspan, 551
Peptic Ulcer, 161
Pericardial Effusion, 14
Periductal Mastitis, 377
Perinatal Asphyxia, 372
Perinatal Mortality, 372
Periodic Limb Movements In
Sleep, 91
Peripheral Vascular Resistance,
14
Peripheral Vestibulopathy, 149
Peritoneal Dialysis, 218
Periventricular Leukomalacia,
589, 629
Pernicious Anaemia, 163
Peroneal Spastic Flat Foot, 619
Personality Disorders, 454
Pertussis, 609
Differential from Asthma, 613
Vaccination, 610
Petechiae, 155, 314
Pethidine, 546
Petit Mal Seizures, 134
Peutz-Jeghers Syndrome, 171,
172
Phaeochromocytoma, 104
Phalen‟s Test, 250
Pharmacodynamics, 527
Pharmacology, 521
Cardiovascular, 51
Pharyngeal Pouch, 158
Pharyngitis, 607
Phenothiazine, 438
Phenylketonuria (PKU), 466
Phenytoin, 135, 533
Philadelphia Chromosome, 299
Phimosis, 637
Phlebitis, 554
Photocoagulation, 146
Phyllodes Tumour, 378
Physical Abuse, 656
Physical Exam
Abdominal, 154
Ankle and Foot, 257
Arthritis, 266
Back, 237
Breast, 376
Cardiovascular, 18
Elbow, 245
Eye Movements, 148
Gentio-urinary, 383
Gynaecological, 340
Hand, 247
Hip, 252
in Adolescents, 667
Knee, 254
Motor, 120
Motor Exam in Children, 623
Musculo-Skeletal, 230
Neonatal, 587
Neurology, 117
Neurology, in Children, 565,
621
Ophthalmology, 140
Paediatric, 564
Respiratory, 60
Shoulder, 243
Physical Hazards of Medicine,
710
Physiotherapist, 585
Pica, 288
Pick‟s Disease, 441
PID, 385, 386
Pierre Robin Sequence, 595
Pigeon Breeder HSP, 85
Pigeon Chest, 565
Pigment Stones, 195
Pinguecula, 143
Pink Puffer, 81
Pinworm, 509
Piperacillin, 513
Pitted Keratolysis, 318
Pituitary Adenoma, 138
Pituitary Gland, 104
Pityriasis Alba, 322
Pityriasis Rosea, 318
Pityrosporum Ovale, 317
Pivot Test, 254
pKa, 524
Placenta Praevia, 366
Placental Abruption, 366
Plasma Cells, 286
Plasmacytoma, 303
Plasmodium
Falciparum, 508
Vivax, 508
Plastic and Reconstructive
Surgery, 284
Platelets, 294
Pleural Disease, 73
Pleural Effusion, 62
on Xray, 29
Pleural Fluids, 73
Pleural Rub, 61
Plummer‟s Disease, 98
PND, 17
Pneumatocele, 604
Pneumatosis Intestinalis, 590,
639
Pneumoconioses, 85
Pneumocystis Carinii, 510
Pneumonia, 70
Pneumonia, 67
in Children, 611
Tb, 612
Treatment, 72
Pneumo-peritoneum, 157
Pneumothorax, 490
on Xray, 29
Pneumovax, 501
Poikiloderma, 314
Poisoning, 486, 488, 533
Polio
Travel Vaccination, 511
Vaccination, 518
Polyarterititis Nodosa, 282
Polycystic Ovary Syndrome, 348
Polycythaemia Vera, 297
Polymyalgia Rheumatica, 281
Polymyositis, 281
Polypharmacy, 531
Polyploidy, 464
Polyps
Colonic, 172
Endometrial, 355
Pompholyx, 322
Population Health, 680
Porphyria, 290
Portal Hypertension, 194
Portal Tract, 184
Portosystemic Shunts, 194
Post Traumatic Stress Disorder,
424
Posterior Cruciate Ligament,
254, 256
Post-Infectious
Glomerulonephritis, 214
Post-Infective Encephalitis, 500
Postmenopausal Bleeding, 348
Postnatal Assessment, 372
Post-Operative Complications,
556
Postpartum
Complications, 372
Depression, 430
Haemorrhage, 369, 373
Mood Disorders, 430
Psychosis, 430
Post-test Probability, 705
Postural Hypotension, 19
Potassium, 27, 111
Potency, 528
Potential Years Of Life Lost, 682
Power, 684
PPPR Act, 713
Prader-Willi Syndrome, 465
Praecordium, 21
Precision, 703
Precocious Puberty, 668
Prednisone
Side Effects of, 304
Pre-eclampsia, 364
Pregnancy
Cardiovascular problems, 363
Drugs in, 528
Early Complications of, 361
General Anaesthetic, 546
Hypertension in, 364
Late Complications of, 366
Minor symptoms of, 358
Multiple, 358
Physiology, 545
Preload, 14
Premature Adrenarche, 667
Premature Atrial Complexes, 41
Premature Labour, 367
Premature Rupture of
Membranes, 368
Premature Thelarche, 667
Premature Ventricular
Complexes, 42
Premenstrual Dysphoric
Disorder, 347
Premenstrual Syndrome, 347
Prenatal diagnosis, 360
Preoperative Assessment, 546
Paediatric, 655
Pre-Orbital Cellulitis, 618
Presbycusis, 151
Presbyopia, 675
Prescriptions, 535
Pressure Overloaded, 21
Pressure Ulcers, 327
Preterm Birth
Complications of, 589
Outcome after, 589
Pre-test Probability, 705
Pretibial Myxoedema, 98
Prevalence, 685
Primary Biliary Cirrhosis, 193
Primary Care, 681
Primary Proliferative
Polycythaemia, 297
Primary Pulmonary
Hypertension, 92
Primary Sclerosing Cholangitis,
193
Primitive Neuroectodermal
Tumours, 138
Prions, 500
PRL, 104
Procainamide, 42
Professional Boundaries, 710
Professional Ethics, 721
Progesterone Only Pill, 342
Prognostic factor, 707
Progressive Multifocal
Leucoencephalopathy, 500
Progressive Systemic Sclerosis,
280, 330
Prolactinaemia, 106
Prolapsed Cervical Disc, 239
Proliferative Glomerulonephritis,
204
Proliferative Retinopathy, 146
Propofol, 541
Propranolol Withdrawal, 534
Proptosis, 649
Prosopagnosia, 122
Prospective Study, 703
Prostate, 224
Prostate Cancer Screening, 225,
691
Prostate Specific Antigen, 225
Prostatic Carcinoma, 225
Prostatitis, 224
Protection of Personal and
Property Rights Act, 458, 676,
713
Protein C & S, 294
Protein, Total, 183
Proteinuria, 202
in Children, 632, 633
Proteus Mirabilis, 502
Prozac, 434
Pruritis Ani, 179
PSA, 225, 469
Psammoma Bodies, 100
Pseudo-bulbar Palsy, 131
Pseudogout, 278
Pseudomembranous Colitis, 176
Pseudomonas Aeruginosa, 67, 70
Pseudomyxoma Peritonei, 168
Pseudopapilloedema, 141
Pseudo-seizure, 134
Psoriasis, 314, 328
Nail Changes in, 247
Psoriatic Arthritis, 275
Psychiatric Disorders, Aetiology,
411
Psychodynamic Psychotherapy,
425
Psychological Medicine, 409
Psychologist, 585
Psychosis, 435
Treatment of, 437
Psychotic Depression, 428
Psychotic Disorders, 420, 435
Pterygium, 143
PTH, 101
PTH Related Protein, 102
Ptosis, 145
PTSD, 424
PTT, 292
Pubarche, 667
Puberty, 667
Delayed, 668
Precocious, 668
Pubic Lice, 383
Public Health, 679
Puerperal Fever, 373
Puerperal Psychosis, 430
Puerperium, 373
Pulmicort, 79
Pulmonary Artery Wedge
Pressure, 14
Pulmonary Atresia, 601
Pulmonary Contusion, 491
Pulmonary Embolism, 76
Pulmonary Hamartoma, 92
Pulmonary Hypertension, 598,
602
Pulmonary Hypertension,
Persistent, 600
Pulmonary Oedema
Emergency Management, 489
Pulmonary Valve Stenosis, 601
Pulse, 18
Bounding, 18
Collapsing, 18
Pulse deficit, 18
Pulseless Disease, 283
Pulseless Electrical Activity, 479
Pulsus Paradoxus, 491
Purchaser-Provider Split, 681
Purpura, 314
Pustule, 314
Pyelonephritis
Acute, 212
Chronic, 212
Pyemia, 494
Pyloric Stenosis, 639
Pyoderma Gangrenosum, 169
Pyrazinamide, 69
Pyrexia
in Children, 616
of Unknown Origin, 6
on Returning from 3rd World,
6, 511
Pyrimethamine, 507
Q waves, 26
QRS Complex, 25, 26
Quinolones, 515
Quinsy, 8
Radial Nerve, 123, 247
Radicular Back Pain, 239
Radiology
Abdominal, 157
Abdominal in Children, 638
Arthritis, 267
Chest, 27
Orthopaedic, 231
Renal, 203
Spine, 238
Thyroid, 97
Radiotherapy, 469
Rape, 344
Rapid Sequence Induction, 540
Rapidly Progressive
Glomerulonephritis, 215
Raynaud‟s Phenomena, 6
Raynaud‟s Syndrome, 8, 267
Reactive Arthritis, 276
Rectal Cancer, 179
Rectal Prolapse, 179
Recurrent Laryngeal Palsy, 66
Red Blood Cells, 286
Red Eye, 142
Refeeding Syndrome, 555
Referred Pain, 543
Reflex Incontinence, 224
Reflex Sympathetic Dystrophy,
283
Reflexes, 121
Reflux
in Children, 642
Reflux Nephropathy, 208
Refusal of Treatment, 719
Regional Blood Flow, 15
Regulation of Drugs of Abuse,
536
Rehabilitation, 676
Rehydration
in Children, 650
Reiter‟s Syndrome, 276, 386,
387
Relative Risk, 704
Renal, 201, 632
Disease in Children, 201, 632
Renal Adenoma, 216
Renal Cell Carcinoma, 217
Renal Failure
Acute, 205
Acute, in Children, 633
Chronic, 207
Chronic, in Children, 634
Renal Oncocytoma, 217
Renal Osteodystrophy, 263
Renal Perfusion, 15
Renal Stones, 210
Renal Transplantation, 219
Renal Tumours, 216
Renin, 103
Renin-Angiotensin System, 202
Renogram, 204
Research Ethics, 723
Residential Care, 672
Residual Volume, 58
Resiliency, 571
Respiratory Acidosis, 114
Respiratory Alkalaemia, 113
Respiratory Distress Syndrome,
589, 597, 605
Respiratory Failure, 59
Respiratory Physiology, 58
Respiratory Syncytial Virus, 70
Respiratory Tract Infections
in Children, 62, 605, 616
Respiratory Tract Neoplasia, 86
Rest Homes, 677
Restless Leg Syndrome, 91
Restrictive Cardiomyopathy, 54
Restrictive Pulmonary Disease,
83
Resuscitation, 476
Cardiopulmonary, 476
Ethics, 481
in Children, 653
Secondary survey, 481
Reticular Activating System, 130
Reticulocytes, 286
Retinal Detachment, 142
Retinoblastoma, 147, 649
Retinoids, 336
Retinopathy
Diabetic, 146
Hypertensive, 146
of Prematurity, 148, 590
Retractile Testis, 636
Reye‟s Syndrome, 500
Rhabdomyolysis, 210
Rhabdomyoma, 55
Rhabdomyosarcoma, 223
Rhesus Haemolytic Disease, 367
Rheumatic Fever, 602
Rheumatoid Arthritis, 272
Juvenile, 273
Rheumatoid Factor, 270, 273
Rhinitis, 63, 310
Rhinophyma, 332
Rhinovirus, 64
Rhonchi, 61
Rib Fracture, 491
Rickets, 263, 647
Riedel‟s Lobe, 156
Riedel‟s Thyroiditis, 100
Rifampicin, 69, 498, 514
Right Bundle Branch Block, 25
Right Ventricular Hypertrophy,
26
Ringworm, 317
Rinne Test, 150
Risk and Resilience, 571
Risk Factor, 707
Risk Ratio, 704
Risperidone, 438, 439
Ritalin, 661
Roaccutane, 331, 336
Rocuronium, 542
Rokitansky-Aschoff Sinuses,
197
Rosacea, 332
Roseola Infantum, 618
Rose-Waaler Titre, 270
Rotator Cuff Syndrome, 244
Roth‟s Spots, 19, 145
Rouleaux, 286
Roundworm, 509
Rubber Glove Allergy, 321
Rubella, 357
Vaccination, 519
S1 Radiculopathy, 123
Saccades, 148
Sacroiliac Joints, 238
Salazopyrin, 272
Salmonella, 177
Salter-Harris Classification, 232
Sarcoidosis, 85
Scabies, 319, 383, 387
Scalded Skin Syndrome, 315
Scarcity, 698
Scarlet Fever, 500, 607
Schilling Test, 163
Schirmer Test, 280
Schizoaffective Disorder, 435
Schizoid Personality Disorder,
455
Schizophrenia, 420, 436
Schizophreniform Disorder, 435
Schizotypal Personality
Disorder, 455
Schober‟s Test, 238
School Sores, 315, 500, 502
SCID, 307
Scleritis, 143
Sclerodactyly, 280
Scleroderma, 280
Sclerosing Haemangioma, 326
Scoliosis, 237, 619
Screening, 689
Screening Programmes, 691
Screening Test, 690
Scrotum, 226
Acute, in Children, 636
Scwhannoma, 138
Scybala, 640
Seasonal Affective Disorder, 428
Sebaceous Glands, 330
Sebaceous Naevi, 325
Seborrhoeic Dermatitis, 321, 387
Seborrhoeic Keratosis, 326
Secondary Biliary Cirrhosis, 193
Secondary Cardiomyopathy, 54
Seizure
in Children, 625
Types of, 134
Self-rated Health Status, 683
Seminoma, 226
Senile Arcus, 675
Sensitivity, 690, 704
Sensorineural Deafness
Congential, 151
Sudden Onset, 151
Separation
Effect on Children, 574
Separation Anxiety Disorder,
661
Sepsis
in Children, 616
Septic Arthritis, 259
Septic Shock, 482
Septicaemia, 494
Sequestration, 92
Sequestrum, 260
Seronegative Arthritis, 274
Serotonin Syndrome, 434
Serous Cystadenoma, 199
Sertoli Cell Tumours, 227
Serum, 294
Serum Amylase, 196
Serum Sickness, 333, 531
Severe Combined
Immunodeficiency, 307
Sexual Abuse, 657
Sexual and Gender Identity
Disorders, 420
Sexually Transmitted Diseases,
383
Sheehan‟s Syndrome, 105
Shigella, 177
Shin Splints, 236
Shingles, 504
in the Eye, 143
Shock, 482
Shock Lung, 83
Short Stature, 586
Shoulder, 243
Dislocation of, 245
Injury, 244
Instability, 245
Shunt
Cardiac, in neonates, 597
SIADH, 109
Sick Sinus Syndrome, 41
Sideroblastic Anaemia, 287
Silicosis, 85
Sim‟s Speculum, 340
Simmond‟s Test, 258
Singh Index, 262
Sinonasal Carcinoma, 86
Sinonasal Papilloma, 86
Sinus Arrhythmia, 26, 41
Sinus Bradycardia, 18, 41
Sinus Tachycardia, 18, 41
Sinusitis, 63, 65
Acute, 608
Six Week Check, 374
Sjogren‟s Syndrome, 158, 279
Skiers Thumb, 249
Skin Ulcers, 327
Slapped Cheek Syndrome, 618
Sleep
Disorders, 420
Hygiene, 534
in Elderly, 534
Management in Children, 593
Sleeping Pills, 534
Training in Children, 594
Treatment of Insomnia, 534
Sleep Apnoea, 17, 90
Children, 66
Sleepiness, Differential of, 90
Slow Acetylators, 525
Small Bowel Atresia, 639
Small Cell Carcinoma, 89
Smegma, 637
Smith‟s Fracture, 248
Smoking, 87
Amongst Maori, 695
Cessation, 87
Smudge Cells, 287
Snellen‟s Chart, 140
Social Gradient, 692
Social Inequalities in Health, 692
Social Phobia, 423
Social Worker, 585
Socio-economic Status, 692
Sodium Aurothiomalate, 272
Sodium Cromoglicate, 79
Sodium Valproate, 135
Soft Tissue Injury, 235
Solar Keratosis, 326
Somatization Disorder, 444
Somatoform Disorders, 420, 444
Somatostatin, 107
Sotalol, 41
Space of Disse, 193
Specific Phobia, 423
Specificity, 704
Speech Language Therapist, 585
Spells, 136
Spermarche, 667
Spermatocoele, 226
Spherocytes, 286, 289
Spherocytosis, 286
Spina Bifida Occulta, 631
Spinal Chord Syndromes, 138
Spinal Cord Compression, 472
Spinal Shock, 490
Spinal Stenosis, 241
Spironolactone, 52
Spitz Naevus, 325
Spleen
Rupture of, 490
Splenectomy, 307
Splenomegaly, 156
Splinter Haemorrhage, 8
Splitting of Heart Sounds, 22
Spondylitis, 237
Spondyloarthropathies, 274
Spondylolisthesis, 241
Spondylolysis, 240
Spondylosis, 237
Spontaneous abortion, 362
Squamous Cell Carcinoma, 88,
327
Oesophagus, 159
of the vulva, 351
Squamous Hyperplasia
of the vulva, 351
Squint, 147
SSPE, 500
SSRIs, 433
St John‟s Wort, 434
ST Segments, 27
St Vitus Dance, 603
Staging of Cancer, 468
Standard Error, 684
Staphlococcus Aureus, 315, 502
Star Chart, 570
Starling‟s Law, 14
Statins, 53
Statistical Power, 703
Status Epilepticus, 135
STDs, 383
Steady State Concentration, 523
Steatocystoma, 226
STEMI, 37
Stenosing Tenosynovitis, 249
Stephens Johnson Syndrome,
332
Steppage Gait, 251
Sterilisation, 342
Sternotomy, 21
Steroid Medication, 104
Steroids, Topical, 335
Stigma, 456
Stomach, 161
Stool test, 157
Strabismus, 632
Strep Pyogenes, 64
Streptococcus
Group A -Haemolytic, 602
Pneumoniae, 501
Pyogenes, 315, 316, 500, 602,
607
Viridians, 47
Stress, 711
Stridor
Differential in Children, 604
Stroke, 125
Stroke Volume, 14
Strongyloides Stercoralis, 510
Sub-acute Bacterial
Endocarditis, 46
Subacute Sclerosing Pan-
encephalitis, 500
Subacute Thyroiditis, 98
Subarachnoid Haemorrhage, 124
Subchondral Cysts, 268
Subchondral Sclerosis, 268
Subconjunctival Haemorrhage,
632
Subdural Haemorrhage, 124
Subglottic Stenosis, 595
Subscapularis Muscle, 244
Substance Abuse
Treatment of, 448
Substance Dependence, 446
Substance Use Disorders, 445
Sudden Infant Death Syndrome,
590, 594
Suicide
Assessment, 413, 415, 416,
663
Management of Risk, 418
Youth, 663
Sulphasalazine, 272
Summation Gallop, 22
Sun Damaged Skin, 323
Sunscreens, 323
Superior Vena Cava Syndrome,
472
Suppurative Myocarditis, 51
Supraspinatus Muscle, 243
Supraventricular Arrhythmia, 26
Supraventricular Tachycardia, 41
in Children, 601
Surfactant, 367, 589
Surrogacy, 722
Suxamethonium, 542
Swan Neck Deformity, 273
Sway Back, 241
Symphyseal-fundal height, 359
Synacthen, 103
Syncope, 131
Syndesmophytes, 275
Syndrome of Inappropriate ADH
Secretion, 109
Synoviosarcoma, 266
Synpharyngetic Haematuria, 214
Syntocinon, 369, 370, 373
Syphilis, 383
Systematic Error, 683
Systematic Review, 703
Systemic Inflammatory
Response Syndrome, 482
Systemic Lupus Erythematosus,
278
Nephropathy in, 208
T Wave, 27
T½, 523
Tachy-Brady Syndrome, 41
Tachycardia, 26
Tactile Fremitus, 62
Taha Hinengaro, 696
Taha Tinana, 696
Taha Wairua, 696
Taha Whanau, 696
Takayasu‟s Arteritis, 283
Talipes Equinovarus, 619
Talking with Adolescents, 665
Talking with Children, 567
Tall Stature, 587
Tamariki Ora, 579
Tamoxifen, 382
Tangi, 696
Tantrums, 572
Tapeworms, 510
Tapu, 694
Tardive Dyskinesia, 438
Target Cells, 286
Tarsal Conditions, 619
Tazocin, 513
Tb, 68
Cutaneous, 648
Meningitis, 498
Mycobacteria, 502
Pneumonia in Children, 612
TB Act 1948, 687
Te Tiriti O Waitangi, 695
Teams, 710
Tear Drop Red Cells, 286
Technical Efficiency, 698
Tegretol, 135
Telangiectases, 314
Teleological Moral Theories,
716
Telomerase, 467
Telomere, 467
Temporal Arteritis, 282
Tenckhoff Catheter, 218
Tendon Injuries, 235
Tenesmus, 171
Tennis Elbow, 246
Tension Headaches, 139
Tension Pneumothorax, 490
Teratoma, 227
Terbinafine, 336, 515
Termination of Pregnancy, 356,
361
Testes, 226
in Children, 636
Testicular Torsion, 637
Testicular Tumours, 226
Undescended, 636
Testicular Feminisation, 638
Testicular Swelling, Differential
of, 227
Testosterone, 224, 338
Tests of Significance, 684
Tetanus
Vaccination, 518
Tethered cord, 631
Tetracyclines, 515
Tetralogy of Fallot, 600
Thalassemia, 290
Thecal Cells, 338
Thelarche, 667
Theophylline, 79, 533
Theory X and Y, 699
Therapeutic Drug Monitoring,
533
Therapeutic Index, 528
Thiamine, 49, 451
Thiazides, 51
Thiopentone, 541
Thoracic Outlet Syndrome, 238
Thoracotomy, 21
Thought Disorder, 412
Thrills, 21
Throat Swabs, 65, 607
Thromboangiitis Obliterans, 283
Thrombocytopenia, 295
Thrombocytosis, 294
Thrombophlebitis, 33
Thrombotic Infarction, 127
Thrombotic Microangiopathy,
209
Thrombotic Thrombocytopaenic
Purpura, 209
Thrush, 64
Thymus
on X-ray, 604
Thyroglossal Cysts, 648
Thyroid, 97
Thyroid Eye Disease, 98
Thyroid Nodules, 100
Thyroid Radiology, 97
TIAs, 126
Tibial Torsion
Internal, 619
Tics
in Children, 628
Tidal Volume, 58
Tinea, 317, 387
Tinea Corpus, 317
Tinea Cruris, 317
Tinel‟s Test, 250
Tino Rangatiratanga, 695
Tipu Ora, 697
Tiredness, Differential
Diagnosis, 6
Tissue Donation, 722
TNM System, 468
Tobacco Control, 697
Tobramycin, 514
Tocolysis, 367
Todd‟s Syndrome, 134
Toddler Behaviour, 571
Tohunga, 696
Tongue Tie, 639
Tonic-Clonic Seizures, 134
Tonsillitis, 66
Tophi, 277
Topical Steroids, 335
TORCH Complex, 500, 506
Torsade de Pointes, 480
Torsion of Appendix Testis, 637
Torticolis, 245
Total Lung Capacity, 58
Total Parenteral Feeding, 556
Total Protein, 183
Toxaemia, 364
Toxic Appearance
in a Child, 566
Toxic Changes, 287
Toxic Epidermal Necrolysis, 332
Toxic Megacolon, 169
Toxic Multinodular Goitre, 99
Toxic Shock Syndrome, 316,
500
Toxoplasmosis, 507, 648
TPN, 556
Trabecular Bone, 262
Tracheomalacia, 604
Transference, 666
Transformation Zone, 352
Transient Ischaemic Attacks, 126
Transient Synovitis of the Hip,
621
Transient Tachypnoea of the
Newborn, 596, 605
Transitional Cell Carcinoma,
219, 223
Transitional Papillary Cell
Carcinoma, 217
Transposition of the Great
Arteries, 601
Transudate, Pleural, 73
Transurethral Prostatic
Resection, 224
Transverse Myelitis, 139, 630
Trauma
Abdominal, 490
Chest, 490
in Children, 652
Travel Medicine, 510
Treaty of Waitangi, 695
Trendelenburg Gait, 251
Tretinion, 331
Triangular Fibrocartilage
Complex, 248
Triazole, 336
Trichomonas, 383
Trichomoniasis, 384
Tricuspid Regurgitation, 46
Tricuspid Stenosis, 22
Tricyclic Antidepressants, 433
Overdose, 433
Trigeminal Nerve, 118
Trigeminal Neuralgia, 140
Trigger Finger, 249
Trimethoprim, 515
Triple Blood Test, 360
Triple Therapy
H. Pylori, 162
Tripsin
Testing for IRT in CF, 615
Trisomy 13, 464
Trisomy 21, 581
Tropheryma Whippelii, 165
Trophoblastic Disease, 362
Tropical Sprue, 165
Troponin I, 38
Troponin T, 38
Truancy, 573
Truncus Arteriosus, 601
Tryptase, 484
TSH, 104
Tubal Ligation, 343
Tuberculosis, 502, See Tb
Tuberous Sclerosis, 334
Tubulointerstitial Diseases, 211
Tumour Markers, 468
Turcot‟s Syndrome, 173
Turner‟s Syndrome, 464
TURP, 224
Tympanomtery, 150
Typhoid, 511
Typhoid Fever
Vaccination, 510
Tyramine, 435
Ulcer
Peptic, 161
Ulcerative Colitis, 168
Ulcers, 327
Ulcers, Mouth, 8
Ulnar Nerve, 247
Ulnar Nerve Entrapment, 246
Ulnar Neuropathy, 123
Ultrasound
Fetal, 360
Umbilical Hernia, 642
Undescended Testis, 636
Uniparental Disomy, 465
United Nations Convention on
the Rights of the Child, 562,
718
Upper Respiratory Tract, 62
Antibiotic Treatment of
Infections, 65
Uraemia, 209
Ureter, 219
Ureteritis, 219
Urethral Syndrome, 221
Urge Incontinence, 223
Urinalysis, 202
Urinary Incontinence, 223
in Children, 634
Urinary Tract Infections, 219
in Children, 221
Urine Dipstick, 202, 219
Urine Haemosiderin, 290
Urine Output, 649
Urobilinogen, 183
Urticaria, 333
Usual Interstitial Pneumonia, 84
Uterine Atony, 373
Uterus
Large for dates, 358
Utilitarianism, 716
UTIs, 219
Uvulopalatopharygnoplasty, 92
Vaccination, 515
At Six Week Check, 375
Travel, 510
Vaccination Schedule, 517
Vaccine Preventable Diseases,
518
Vaccines, 516
Vaginal Discharge, 384
Vaginal Exam, 340
Vaginismus, 345
Vaginitis, 348
Vagus Nerve, 118
Validity, 703
Valsalva manoeuvre, 24
Valuing Human Life, 699
Valvular Heart Disease, 43
Vancomycin, 514
Variant CJD, 441, 500
Varicella Zoster, 504
Varices, Oesophageal, 194
Varicose Veins, 33
Vasa Praevia, 366
Vascular Dementia, 441
Vasculitis, 33, 282
Vasectomy, 343
Vasopressin, 104
Vd, 522
Vector, 688
Venereal Diseases Act, 687
Venous Stasis Ulcers, 327
Venous Thromboembolism, 74
Ventilation, Artificial, 60
Ventilatory Failure, 59
Ventouse, 371
Ventricular Fibrillation, 479
Ventricular Septal Defect, 598
Ventricular Tachycardia, 480
Drug Treatment, 42
Verapamil, 42, 52
Verrucae, 318
Vesicular Breath Sounds, 61
Vestibular, 148
Vestibulo-Ocular Reflexes, 130,
148
Vibrio Cholerae, 177
Viral Hepatitis, 186
Viral Pneumonias, 70
Virilism, 107
Viruses
in Children, 617
Vision, Loss of, 141
Visiting Neurodevelopmental
Therapist, 585
Visual Acuity, 140
Visual Impairment in the
Elderly, 675
Vital Capacity, 58
Vitamin A, 336
Deficiency, 647
Vitamin B1, 49, 451
Vitamin B12 Deficiency, 451
Vitiligo, 98, 103
Vocal Chords, 66
Vocal Resonance, 62
Voice Disorders, 66
Volkmann‟s Ischaemic
Contracture, 234, 246
Volume Depletion, 110
Volume Loaded, 21
Volume of Distribution, 522
Volvulus
Small Bowel, 166
Vomiting
in Children, 644
Von Willebrand‟s Disease, 292
Vulval Intraepithelial Neoplasia,
351
Vulval Lesions, 350
Vulvitis, 345
Waldenstrom‟s
Macroglobulinaemia, 303
Warfarin, 75
Warts, 318
Weber Test, 150
Wegener‟s Granulomatosis, 215,
283
Wenckebach Heart Block, 42
Wernicke‟s Encephalopathy, 121
Wernicke-Korsakov Syndrome,
451
Whakama, 696
Wheeze, 61
Differential in a Child, 614
Whipple‟s Disease, 165
Whistle Blowing, 721
White Blood Cells, 286
Whooping Cough. See Pertussis
Wilms‟ Tumour, 217
Wilson‟s Disease, 132, 194, 440
Windup, 543
Withdrawal
Drug Withdrawal Syndromes,
533
in a Neonate, 596
Wolff-Parkinson-White
Syndrome, 26, 40, 601
Worms, Intestinal, 509
Wrist and Hand Fractures, 620
Wuchereria Bancrofit, 509
X Linked
Agammaglobulinaemia, 306
Xanthelasma, 19
Xanthomata, 8
Xerostomia, 280
X-linked Dominant, 465
X-linked Recessive, 464
Yellow Fever, 689
Travel Vaccination, 510
Yerkes Dobson Curve, 422
Yersinia Enterocolitica, 553
Youth Suicide, 663
Zathachromia, 496
Zn Deficiency, 647
