
Glycaemic index values for commercially available potatoes in Great Britain
C. Jeya K. Henry
1
*, Helen J. Lightowler
1
, Caroline M. Strik
1
and Michael Storey
2
1
Nutrition and Food Science Group, School of Biological and Molecular Sciences, Oxford Brookes University, Gipsy Lane Campus,
Headington, Oxford OX3 0BP, UK
2
British Potato Council, 4300 Nash Court, John Smith Drive, Oxford Business Park South, Oxford OX4 2RT, UK
(Received 18 February 2005 – Revised 5 July 2005 – Accepted 11 July 2005)
The glycaemic response to eight potato varieties commercially available in Great Britain was compared against a glucose standard in a non-blind, random-
ised, repeated measure, crossover design trial. Seventeen healthy subjects (three males, fouteen females), mean age 32 (
SD 13) years and mean BMI 22·3 (SD
3·6) kg/m
2
, were recruited to the study. Subjects were served portions of eight potato varieties and a standard food (glucose), on separate occasions, each
containing 50 g carbohydrate. Capillary blood glucose was measured from finger-prick samples in fasted subjects (0 min) and at 15, 30, 45, 60, 90 and
120 min after the consumption of each test food. For each potato variety, the glycaemic index (GI) value was calculated geometrically by expressing
the incremental area under the blood glucose curve (IAUC) as a percentage of each subject’s average IAUC for the standard food. The eight potato varieties
exhibited a wide range in GI values from 56 to 94. A trend was seen whereby potatoes with waxy textures produced medium GI values, whilst floury pota-
toes had high GI values. Considering the widespread consumption of potatoes in Great Britain (933–1086 g per person per week), this information could be
used to help lower the overall GI and glycaemic load of the diets of the British population.
Glycaemic index: Potato variety: Great Britain: Glycaemic load
The glycaemic index (GI), first introduced in 1981 (Jenkins et al.
1981), is a classification of the blood glucose-raising potential of
the carbohydrates in foods. It is defined as the incremental area
under the blood glucose curve (IAUC) of a 50 g carbohydrate
portion of a test food expressed as a percentage of the response
to 50 g carbohydrate of a standard (reference) food taken by
the same subject, on a different day (Food and Agriculture
Organization/World Health Organization, 1998).
Carbohydrate foods consumed in isoglucidic amounts produce
different glycaemic responses depending on many factors, such
as particle size, cooking and food processing, other food
components (e.g. fat, protein, dietary fibre) and starch structure
(Bjorck et al. 1994). The principle is that the slower the rate of
carbohydrate absorption, the lower the rise of blood glucose
level and the lower the GI value (Brand et al. 1991). Indeed,
high GI foods are characterised by fast-release carbohydrate and
higher blood glucose levels. A GI value $ 70 is considered
high, a GI value 56–69 inclusive is medium and a GI value
# 55 is low, where glucose ¼ 100 (Brand-Miller et al. 2003).
The GI of foods may have important implications for the
prevention and treatment of the major causes of morbidity and mor-
tality in Western countries, including type 2 diabetes, CHD and
obesity. Today, there is an important body of evidence to support
the therapeutic potential of low-GI diets, not only in diabetes
(Bjorck et al. 1994; Frost et al. 1994; Gilbertson et al. 2001; Augus-
tin et al. 2002) but also in subjects with hyperlipidaemia (Jenkins
et al. 1987a). In addition, low-GI foods have been associated with
prolonged endurance during physical activity (Thomas et al.
1991), improved insulin sensitivity (Frost et al. 1998), reduced
food intake (Holt et al. 1995; Warren et al. 2003) and increased
colonic fermentation (Jenkins et al. 1987b; Wolever et al. 1992).
More recent data support the preventive potential of a low-GI diet
against the development of type 2 diabetes and CVD (Salmeron
et al. 1997a,b; Frost et al. 1999; Meyer et al. 2000).
Potatoes generally have one of the highest GI values of any food,
although some varieties appear to be lower than others. Published GI
values are highly variable (Foster-Powell et al. 2002); however, it
can be difficult to compare values as the variety of potato is rarely
specified. It is necessary to clarify the GI of different varieties of
potatoes as they are a major staple in Great Britain, contributing
approximately 9 % of total carbohydrate intake (National Statistics,
2004). In addition, there is widespread consumption of potatoes.
Current figures show that average potato consumption (fresh and
processed) in Great Britain ranges between 933–1086 g per
person per week (National Statistics, 2004).
Previous research has shown no difference in GI values
between three varieties of potato (Sebago, Pontiac and Desiree;
Soh & Brand-Miller, 1999). However, it was demonstrated that
young or ‘new’ potatoes have a lower GI than more mature pota-
toes, which may be attributed to differences in starch structure. If
a low-GI potato variety can be identified, it could be used to lower
the overall GI and glycaemic load of the Western diet and thus
decrease the risk of type 2 diabetes, CHD and obesity (Soh et al.
1999). There are limited data on the GI values of different var-
ieties of commercially available potatoes within Great Britain.
The aim of the current work is to investigate the glycaemic
Abbreviations: GI, glycaemic index; IAUC, incremental area under the blood glucose curve.
British Journal of Nutrition (2005), 94, 917–921 DOI: 10.1079/BJN20051571
q The Authors 2005
https://doi.org/10.1079/BJN20051571 Published online by Cambridge University Press

response of eight varieties of potato commercially available in
Great Britain.
Methods
Subjects
Seventeen healthy subjects (three male, fourteen female) were
recruited through posters distributed throughout Oxford Brookes
University in addition to announcements in lectures and through
personal networks. Subjects were staff and students (undergraduate
and postgraduate) from Oxford Brookes University and were
moderately active, non-smoking men and women. Exclusion
criteria were as follows: age , 18 or . 55 years; BMI $ 30 kg/m
2
;
fasting blood glucose value . 6·1 mmol/l. Mean age was 32 (
SD 13)
years and mean BMI was 22·3 (
SD 3·6) kg/m
2
. Ethical approval for
the study was obtained from the University Research Ethics Commit-
tee at Oxford Brookes University. Subjects were given full details of
the study protocol and the opportunity to ask questions. All subjects
gave written informed consent prior to participation.
Study protocol
The protocol used was adapted from that described by Wolever
et al. (1991) and is in line with procedures recommended by
the Food and Agriculture Organization/World Health Organiz-
ation (1998). To determine the GI of a food, tests should be
repeated in six or more subjects, thus in the present study, for
each test food, ten of the seventeen subjects recruited to the
study were randomly selected. On the day prior to a test, subjects
were asked to restrict their intake of alcohol and caffeine-contain-
ing drinks and to restrict their participation in intense physical
activity (e.g. long periods at the gym, excessive swimming, run-
ning, aerobics). Subjects were also told not to eat or drink after
21.00 hours the night before a test, although water was allowed,
in moderation.
Test foods
Eight potato varieties were tested: Maris Peer; Maris Piper;
Desiree; Estima; Charlotte; Marfona; Nicola; King Edward.
These varieties, all sourced from the British Potato Council,
represent a diverse range of commercial varieties commonly
consumed as fresh, rather than processed, potatoes in the UK.
The eight varieties were compared with a standard food (glucose)
and were tested in equivalent carbohydrate amounts (50 g). The
total solid and carbohydrate content of each potato variety was
obtained from published values (Storey & Davies, 1992; NIAB,
2004). In accordance with Food and Agriculture Organization/
World Health Organization (1998) recommendations, subjects
tested each potato variety once and the standard food three times
in random order on separate days, with at least a 1 d gap between
measurements to minimise carryover effects. Subjects were studied
in the morning after a 12 h overnight fast. To avoid starch retrogra-
dation, potatoes were freshly prepared and cooked each morning.
Potatoes were peeled, cut into quarters and then boiled in 1·5
litres unsalted water for 15 min until tender. Subjects consumed
the standard food/test product at a comfortable pace, within
15 min. The test products and the standard food were served with
200 ml water. A further 200 ml water was given during the sub-
sequent 2 h. Subjects were encouraged to keep physical activity to
a minimum during the testing.
Blood glucose measurements
A qualified technician performed blood glucose measurements.
A fasting blood sample was taken at 0 min and the standard
food/test product was consumed immediately after this. Further
blood samples were taken at 15, 30, 45, 60, 90 and 120 min
after starting to eat.
y = 0·9912x + 0·3143
R
2
0·9562
Fig. 1. Pearson regression and Bland –Altman analyses of blood glucose measurements between the Ascensia Contour (ASC) and HemoCue 201 þ analyser
(HEM). For details of procedures, see this page.
Table 1. Incremental area under the blood glucose
curves (IAUC) and glycaemic index (GI) values for
each potato variety (Mean values with their standard
errors)
IAUC GI value
Potato variety Mean
SEM Mean SEM
Maris Peer 182 33 94 16
Maris Piper 167 17 85 4
Desiree 133 18 77 17
Estima 143 13 66 5
Charlotte 134 30 66 5
Marfona 93 21 56 3
King Edward 166 10 75 10
Nicola 130 10 59 7
For details of procedures, see this page.
C. J. K. Henry et al.918
https://doi.org/10.1079/BJN20051571 Published online by Cambridge University Press
Blood was obtained by finger-prick using the Glucolet 2 multi-
patient lancing system (Bayer HealthCare, Newbury, Berks.).
Recent reports suggest that capillary blood sampling is preferred
for reliable GI testing (Food and Agriculture Organization/World
Health Organization, 1998; Wolever, 2003). Prior to a finger-
prick, subjects were encouraged to warm their hand to increase
blood flow. Fingers were not squeezed to extract blood from the fin-
gertip as this may dilute with plasma. Blood glucose was measured
using Ascensia Contour
w
automatic blood glucose meters (Bayer
HealthCare). The blood glucose meters were calibrated daily
using control solutions from the manufacturer and were also
regularly calibrated against a clinical dry chemistry analyser
(Reflotron
w
Plus; Roche, Lewes, Sussex) and the HemoCue
Glucose 201 þ analyser (HemoCue
w
Ltd, Angelholm, Sweden).
Figure 1 shows the Pearson regression and Bland –Altman ana-
lyses (Bland & Altman, 1986) for a random selection of 106
blood samples simultaneously measured using the Ascensia Con-
tour
w
and the HemoCue Glucose 201 þ analyser. There was a
very strong correlation (r 0·978, P# 0·001) and good agreement
(mean difference 2 0.3 mmol; 95 % CI 2 0·3, 2 0·2; limits of
agreement 2 0·75, 0·21) between blood glucose measurements
using the automatic analyser and the HemoCue analyser.
Calculation of glycaemic index
The IAUC, ignoring the area beneath the baseline, was calculated
geometrically for each food (Food and Agriculture Organization/
World Health Organization, 1998). The mean, standard deviation
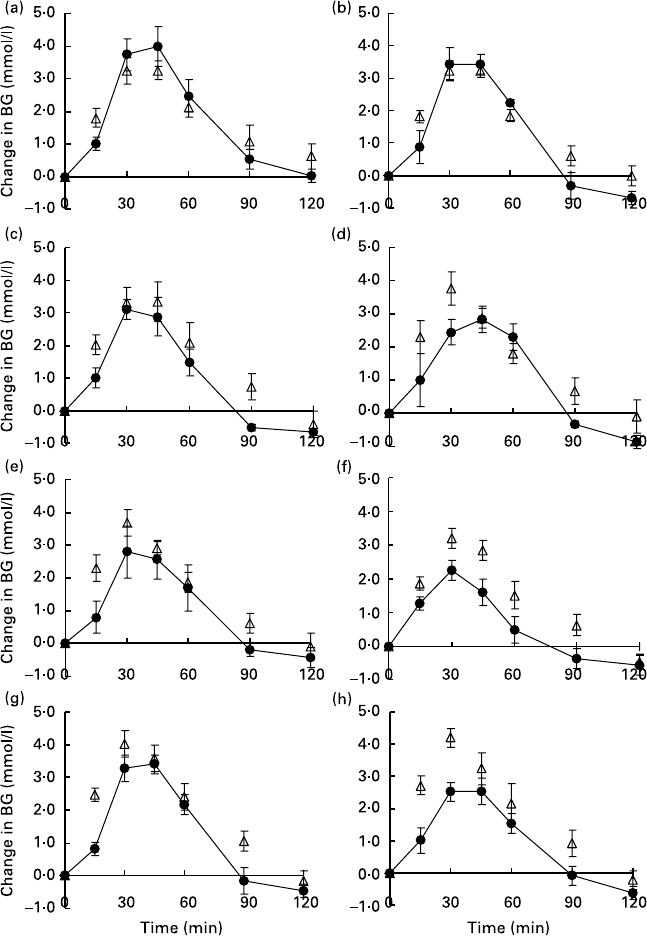
Fig. 2. Incremental area under the blood glucose curves (IAUC) for eight potato varieties ((X), (a) Maris Peer, (b) Maris Piper, (c) Desiree, (d) Estima, (e) Char-
lotte, (f) Marfona, (g) King Edward, (h) Nicola). D, Glucose. For details of procedures, see p. 918. Values are the mean change in blood glucose (BG) with their
standard errors represented by vertical bars (n 10).
Glycaemic index and potatoes 919
https://doi.org/10.1079/BJN20051571 Published online by Cambridge University Press
and CV of the IAUC of each subject’s repeated standard food
were calculated. The IAUC for each test product eaten by each
subject was expressed as a percentage of the mean IAUC for
the standard food eaten by the same subject. The GI of each
potato variety was taken as the mean for the whole group.
Statistical analysis
Statistical analysis was performed using the Statistical Product
and Service Solutions software version 11.0.1 (SPSS, Chicago,
IL, USA). To examine the correlation and agreement between
the automatic analyser and the HemoCue Glucose 201 þ analy-
ser, Pearson’s correlation coefficient and the method of Bland &
Altman (1986) were used. Levels of inter- and intra-individual
variation of the three standard (glucose) tests were assessed by
determining the CV. One-way ANOVA was used to compare
IAUC values and GI values between the eight potato varieties.
Kendall’s rank correlation coefficient (Kendall’s t) was used to
assess the relationship between GI value and potato texture
rating. Statistical significance was set at P, 0·05.
Results
The mean CV of glycaemic responses to the three standard tests
for the seventeen subjects was 23 %. The inter-individual
variation in glycaemic response to the standard test for the seven-
teen subjects was 30 % CV. These values are consistent with
previously reported data (Wolever, 1990).
Mean IAUC and GI values for each test product are presented in
Table 1 and Fig. 2. There was no significant difference in IAUC
between the different potato varieties (P¼ 0 ·188). The potatoes
exhibited a large variation in GI values ranging from 56 (Marfona)
to 94 (Maris Piper), although the differences in GI were not
statistically significant (P¼ 0·330).
For practical measures, GI values are often grouped into cat-
egories as producing either a low, medium or high glycaemic
response. The cut-off values are as follows: low # 55; medium
56–69 inclusive; high $ 70 (Brand-Miller et al. 2003). The GI
ratings for the tested potato varieties are given in Table 2 along-
side characteristics of the potato varieties. There was a strong
positive correlation (Kendall’s t-b 0·656; P¼ 0·034) between the
GI value and texture rating. In general, potatoes with floury
textures (low in moisture, low in sugar with high starch) were
in the high-GI category, whilst those with firm to waxy textures
(high in moisture, low starch) were in the medium-GI category.
Generally, the earlier crop varieties of potato (second early) and
the salad potatoes tend to have waxy textures while the main
crop varieties tend to have floury textures.
Discussion
The GI values reported here are comparable to those given for
boiled potatoes in the recent international GI tables
(Foster-Powell et al. 2002). A GI value range of 56 – 101 has
been reported for boiled potatoes, where the type of potato has
been specified, and a GI range 23–76 for unspecified potato
type (Foster-Powell et al. 2002). More recently, Fernandes et al.
(2005) reported a GI value of 89 for boiled red potatoes. Small
differences of , 10 –15 units are within the error associated
with the measurement of GI (Wolever et al. 1991; Foster-
Powell et al. 2002). Discrepancies may be due in part to cooking
methods used, which may change the structure of the starch
(Englyst & Cummings, 1987). In particular, it has been reported
that precooking and reheating potatoes before consumption will
elicit a lower glycaemic response compared with potatoes con-
sumed immediately after cooking (Fernandes et al. 2005).
The lower GI rating of firm/waxy potato varieties agrees with
previous findings (Soh & Brand-Miller, 1999). However Maris
Peer, which was originally bred as a low-DM potato for use by
the canning industry, is the one variety in the trial that appears
to differ markedly in its GI rating (high) relative to its commercial
usage as an early potato and as such may warrant further study.
Changes in the nature of the starch, predominantly an increase
in the amount of amylopectin (Soh & Brand-Miller, 1999), may
be partly responsible for the difference in glycaemic response
seen with floury, more mature potatoes. Amylopectin has a
branched structure that makes it more readily digestible than
linear chain starch leading to a higher glycaemic response
(Van Amelsvoort & Westrate, 1992).
In conclusion, these results provide a comparison of the glycae-
mic responses of several commercially available varieties of
potato. Considering the widespread consumption of potatoes in
Great Britain (933–1086 g per person per week), it is useful to
have information regarding the glycaemic response of common
varieties. The identification of potato varieties with lower glycae-
mic responses may help lower the GI of the British diet and
potentially have benefit in the management and prevention of
some chronic diseases.
Acknowledgements
This study was supported by the British Potato Council Project
R256.
References
Augustin LS, Franceschi S, Jenkins DJA, Kendall CWC & La Vecchia C
(2002) Glycemic index in chronic disease: a review. Eur J Clin Nutr
56, 1049 – 1071.
Bjorck I, Granfeldt Y, Liljeberg H, Tovar J & Asp NG (1994) Food prop-
erties affecting the digestion and absorption of carbohydrates. Am J
Clin Nutr 59, S699–S705.
Bland JM & Altman DG (1986) Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet I, 307–310.
Brand JC, Colagiuri S, Crossman S, Allen A, Roberts DCK & Truswell
AS (1991) Low-glycemic index foods improve long-term glycemic
control in NIDDM. Diabetes Care 14, 95 – 101.
Table 2. Glycaemic index (GI) classification and characteristics of each
potato variety
Potato variety GI classification Crop type Texture†
Texture
rating*
Maris Peer High Second early Firm 5
Maris Piper High Main crop Floury 5
Desiree High Main crop Firm 5
Estima Medium Second early Firm, moist 4
Charlotte Medium Salad Firm, waxy 4
Marfona Medium Second early Waxy 3
King Edward High Main crop Floury 6
Nicola Medium Salad Firm 4
* Information obtained from the British Potato Council website www.potato.org.uk. Texture
ratings are measured on a scale from 1 to 9 (1 being most waxy and 9 being the most
floury).
For details of procedures, see p. 918.
C. J. K. Henry et al.920
https://doi.org/10.1079/BJN20051571 Published online by Cambridge University Press
Brand-Miller J, Foster-Powell K & Colagiuri S (2003) The New Glucose
Revolution. New York: Marlowe and Company.
Englyst HN & Cummings JH (1987) Digestion of polysaccharides of
potato in the small intestine of man. Am J Clin Nutr 45, 423–431.
Food and Agriculture Organization/World Health Organization (1998)
Carbohydrates in Human Nutrition. Report of a Joint FAO/WHO
Expert Consultation. Rome: FAO.
Fernandes G, Velangi A & Wolever TMS (2005) Glycemic index of potatoes
commonly consumed in North America. J Am Diet Assoc 105, 557–562.
Foster-Powell K, Holt SHA & Brand-Miller JC (2002) International table
of glycemic index and glycaemic load values: 2002. Am J Clin Nutr 76,
5–56.
Frost G, Leeds AA, Dore CJ, Madeiros S, Brading S & Dornhorst A
(1999) Glycaemic index as a determinant of serum HDL-cholesterol
concentration. Lancet 353, 1045 – 1048.
Frost G, Leeds A, Trew G, Margara R & Dornhorst A (1998) Insulin sen-
sitivity in women at risk of coronary heart disease and the effect of a
low glycemic diet. Metabolism 47, 1245–1251.
Frost G, Wilding J & Beecham J (1994) Dietary advice based on the gly-
caemic index improves dietary profile and metabolic control in Type 2
diabetic patients. Diabet Med 11, 397–401.
Gilbertson HR, Brand-Miller JC, Thorburn AW, Evans S, Chondros P &
Werther GA (2001) The effect of flexible low glycemic index dietary
advice versus measured carbohydrate exchange diets on glycemic con-
trol in children with type 1 diabetes. Diabetes Care 24, 1137–1143.
Holt SHA, Miller JCB, Petocz P & Farmakalidis E (1995) A satiety index
of common foods. Eur J Clin Nutr 49, 675–690.
Jenkins DJA, Wolever TMS, Collier GR, Ocana A, Rao AV, Buckley G,
Lam Y, Mayer A & Thompson LU (1987b) Metabolic effects of a low
glycemic index diet. Am J Clin Nutr 46, 968–975.
Jenkins DJA, Wolever TMS, Kalmusky J, et al. (1987a) Low-glycemic
index diet in hyperlipidemia: use of traditional starchy foods. Am J
Clin Nutr 46, 66–71.
Jenkins DJA, Wolever TMS, Taylor RH, Barker H, Fielden H, Baldwin
JM, Bowling AC, Newman HC, Jenkins AL & Goff DV (1981)
Glycemic index of foods: a physiological basis for carbohydrate
exchange. Am J Clin Nutr 34, 362–366.
Meyer KA, Kushi LH, Jacobs DR, Slavin J, Sellers TA & Folsom AR
(2000) Carbohydrates, dietary fiber, and incident type 2 diabetes in
older women. Am J Clin Nutr 71, 921–930.
National Statistics (2004) Family Food. A Report on the 2002–03 Expen-
diture and Food Survey. London: TSO.
NIAB (2004) Pocket Guide to Varieties of Potato. Cambridge: NIAB.
Salmeron J, Ascherio A, Rimm EB, Colditz GA, Spiegelman D, Jenkins
DJ, Stampfer MJ, Wing AL & Willett WC (1997a) Dietary fiber, gly-
cemic load, and risk of NIDDM in men. Diabetes Care 20, 545–550.
Salmeron J, Manson JE, Stampfer MJ, Colditz GA, Wing AL & Willett
WC (1997b) Dietary fiber, glycemic load, and risk of non-insulin-
dependent diabetes mellitus in women. JAMA 277, 472– 477.
Soh NL & Brand-Miller J (1999) The glycaemic index of potatoes: the
effect of variety, cooking method and maturity. Eur J Clin Nutr 53,
249– 254.
Storey RMJ & Davies HV (1992) Tuber quality. In The Potato Crop. The
Scientific Basis for Improvement, pp. 507 – 569 [PM Harris, editor].
London: Chapman and Hall.
Thomas DE, Brotherhood JR & Brand JC (1991) Carbohydrate feeding
before exercise: effect of glycemic index. Int J Sports Med 12,
180– 186.
Van Amelsvoort JM & Westrate JA (1992) Amylose–amylopectin ratio in
a meal affects postprandial variables in males volunteers. Am J Clin
Nutr 55, 712–718.
Warren JM, Henry CJK & Simonite P (2003) Low glycemic index break-
fasts and reduced food intake in preadolescent children. Pediatrics 112,
e414– e419.
Wolever TMS (1990) The glycemic index. World Rev Nutr Diet 62,
120– 185.
Wolever TMS (2003) Carbohydrate and the regulation of blood glucose
and metabolism. Nutr Rev 61, S40– S48.
Wolever TMS, Jenkins DJA, Jenkins AL & Josse RG (1991) The glyce-
mic index: methodology and clinical implications. Am J Clin Nutr
54, 846 – 854.
Wolever TMS, Jenkins DJA, Vuksan V, Jenkins AL, Buckley GC, Wong
GS & Josse RG (1992) Beneficial effect of a low glycemic index diet in
Type 2 diabetes. Diabet Med 9, 451 – 458.
Glycaemic index and potatoes 921
https://doi.org/10.1079/BJN20051571 Published online by Cambridge University Press
