IMMUNIZATION VERIFICATION 1
Immunization Verification at Christian Camps
Katherine Stacey
A Senior Thesis submitted in partial fulfillment
of the requirements for graduation
in the Honors Program
Liberty University
Spring 2021
IMMUNIZATION VERIFICATION 2
Acceptance of Senior Honors Thesis
This Senior Honors Thesis is accepted in partial
fulfillment of the requirements for graduation from the
Honors Program of Liberty University.
______________________________
Jonathan Geukgeuzian, D.Ed.Min.
Thesis Chair
______________________________
P. Adam McClendon, Ph.D.
Committee Member
_____________________________
James H. Nutter, D.A.
Honors Director
______________________________
Date
IMMUNIZATION VERIFICATION 3
Abstract
No standard exists among Christian camps regarding immunization verification for program
participants. The best practice for Christian camps regarding immunization verification is
debated because of religious reasons, camper and staff safety, and state mandates. This research
examines the current practice of Christian Camp and Conference Association (CCCA) affiliated
camps regarding immunization verification. It was conducted by emailing a seven-question
survey to over 700 CCCA camps. Just over 100 camps responded. The study found that roughly
two-thirds of CCCA camps practice no method of immunization verification. In response to this
result, the researchers propose a best practice for Christian camps regarding immunization
verification based on American Association of Pediatrics (AAP) guidelines.
IMMUNIZATION VERIFICATION 4
Immunization Verification at Christian Camps
Introduction
In a typical year, over fourteen million people attend a session of camp in the United
States. The American camping industry is worth over $18 billion, employing well over a million
people at over 14,000 camps.
1
The impact these camps have had and will continue to have
cannot be overstated. Outcomes of camp for youth include “organization, self-identity, emotion
regulation, and to a lesser degree, self-confidence and relationship skills.”
2
The development of
these outcomes can be attributed to strategic programming
designed and implemented by camp
staff. Many aspects of campers’ growth are an inherent result of the camp setting: independence,
appreciation for diversity, community, and teamwork.
3
While these and countless other benefits are inherent to camp, the camp setting is also
intrinsically conducive to the spread of diseases.
4
Youth are removed from their familiar home
setting and placed in an unfamiliar context with tens or hundreds of other campers. Although
interacting with peers strengthens interpersonal qualities, it increases the chances of spreading
disease.
5
Many camp activities involve coming in close contact with other persons and sharing
1
American Camp Association, “ACA Facts and Trends,” ACA Camps, accessed December 18, 2020,
https://www.acacamps.org/press-room/aca-facts-trends.
2
Dan Richmond, Jim Sibthorp, and Cait Wilson, “Understanding the Role of Summer Camps in the
Learning Landscape: An Exploratory Sequential Study,” Journal of Youth Development 14, no. 3 (2019): 24.
http://jyd.pitt.edu/ojs/jyd/article/view/19-14-03-FA-01/872.
3
Dan Richmond, Jim Sibthorp, and Cait Wilson, “Understanding the Role of Summer Camps,” 23.
4
Tsalik, Ephraim L. et al., “Clinical presentation and response to treatment of novel influenza A H1N1 in a
university-based summer camp population,” Journal of Clinical Virology 47 (2010): 286.
5
Laura L. Blaisdell et al., “Preventing and Mitigating SARS-CoV-2 Transmission — Four Overnight
Camps, Maine, June–August 2020,” Morbidity and Mortality Weekly Report 69, no. 35 (2020): 1217.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7470465/.

IMMUNIZATION VERIFICATION 5
equipment. Recognizing the long, full days and short nights associated with camp, some question
the influence of fatigue on illness at camps.
6
Just as many benefits of camp are tied to its nature,
so are many of its risks.
Disease outbreak at camps has many detrimental effects on the participants and the
organization. The most obvious and notable effect is the potential for a lasting injury or death of
campers or staff members because of the disease.
7
Even if the camper or staff member does not
experience serious lasting effects because of the disease, they may spread it to an
immunocompromised or at-risk individual who would experience the adverse effects of the
disease more severely. Additionally, disease outbreaks at camps may lead to a shortened camp
season if the camp must close because of the outbreak.
8
This shortened season results in financial
deficits and a lesser amount of time to impact campers. Sick staff cannot work, so a disease
outbreak may result in being understaffed. Many issues come with a disease outbreak at camp.
Risk management is a key aspect of the operation of any camp. Keeping the balance of an
appropriate perceived risk compared to the lowest possible actual risk is essential to
programming activities that stimulate campers’ growth. One aspect of camp that should both
appear and be safe is the way camps care for the health of their program participants (campers
and staff). Camp directors should take reasonable precautions to protect their program
6
American Camp Association, “The Healthy Camp Study: Impact Report,” ACA Camps, accessed
December 18, 2020, https://www.acacamps.org/downloads/healthy-camp-study-impact-report.
7
Thomas Novotny et al., “Measles Outbreaks in Religious Groups Exempt from Immunization Laws,”
Public Health Reports 103, no. 1 (1988): 49.
8
Hannah Lebovits, “We sent our kids to summer camp. It shut down with a COVID-19 outbreak after just
a few days. This is what school will look like,” Business Insider, August 5, 2020,
https://www.businessinsider.com/covid-broke-out-at-our-kids-camp-this-is-what-school-will-look-like-2020-7.

IMMUNIZATION VERIFICATION 6
participants from disease outbreaks. According to the AAP, one necessary precaution is that all
campers should be fully vaccinated.
9
To ensure this precaution is fulfilled, the researchers
recommend camps verify the status of the immunizations of their campers and staff. Christian
camps, for various reasons, hold opposing positions regarding immunization verification for their
program participants. These reasons will be explored in the following literature review, as well
as a recollection of historic guidelines from the AAP. The following literature review and
discussion of the current practices of CCCA affiliated camps will be based on a recent empirical
study. This thesis will conclude with a discussion of best practices for camps to protect program
participants from the various risks immunization verification presents and those it mitigates.
Literature Review
CCCA camps hold their position on immunization verification for many reasons. Those
that do not verify camper immunizations cite factors such as religious reasons, safety, state
mandates, and camp-specific concerns. Those who verify camper immunizations do so for
camper and staff safety and because of state mandates. Each of these points will be explored
further, with information that should be considered when understanding the survey discussed in
the Results section.
9
Michael J. Ambrose and Edward A. Walton, “Improving Health and Safety at Camp,” American Academy
of Pediatrics 144, no. 1 (2019): 3. https://pediatrics.aappublications.org/content/144/1/e20191355.

IMMUNIZATION VERIFICATION 7
Reasons Camps do not Verify Immunizations
Religious Reasons
Some camps do not verify that their program participants are vaccinated for religious
reasons. One main concern is the fact that some vaccines use aborted babies for research. This
traditionally Catholic concern has been questioned in light of the COVID-19 pandemic.
10
Those
who do not verify immunizations for this religious reason found their opinion on the “illicit
origin of human sources of biological material” and the “the dignity of the person.”
11
The
sanctity of human life, rooted in Genesis 1:27-28, is a key point in the argument against
immunization verification.
A second religious objection to immunization verification is some people see vaccines as
“playing God.” Additionally, negative effects that sometimes accompany immunizations are seen
as retribution for taking part in a sinful practice. According to Gordana Pelčić, et al., “Orthodox
Protestant parents who refuse vaccination on religious grounds. . . claim that vaccination is an act
of interfering with divine providence. Those who actually vaccinated their children consider the
side-effects of vaccination as a God’s sign that they made a wrong decision.”
12
As with many
debated current medical practices, vaccinations are seen by some as an orchestration by man of
what only God should arrange. Some camps recognize their participants will be against
10
Chelsey Cox and Miriam Fauzia, “Fact check: COVID-19 vaccine ‘morally acceptable,’ Vatican says,
but some claims missing context,” USA Today, December 29, 2020,
https://www.usatoday.com/story/news/factcheck/2020/12/29/fact-check-covid-19-vaccines-morally-acceptable-
vatican-says/4014905001/.
11
Gordana Pelčić, et al., “Religious exception for vaccination or religious excuses for avoiding
vaccination,” Croatian Medical Journal 57, no. 5 (2016): 517.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5141457/.
12
Gordana Pelčić, et al., “Religious exception for vaccination.”

IMMUNIZATION VERIFICATION 8
vaccinations because of this religious reason, and therefore do not verify that their campers are
immunized.
Safety
The questioned safety of vaccinations is another key reason camps do not verify their
campers’ immunizations. One well-known safety issue is the question of whether autism is
linked to vaccinations. Andrew Wakefield, in a 1999 edition of The Lancet, postulated that
autism is linked to the MMR vaccine.
13
However, this study has been researched further and
found to be grossly inaccurate. Jeffrey Gerber and Paul Offit write that twenty studies conducted
show no correlation between vaccinations and autism. Performed across “several countries by
many different investigators who have employed a multitude of epidemiologic and statistical
methods. . . a level of statistical power sufficient to detect even rare associations” has been found
through these studies. No such correlation exists between autism and vaccines.
14
However,
concerns persist that some vaccines are unsafe because of Wakefield’s study.
15
Additional safety concerns concerning vaccinations may spring from the numerous side
effects that accompany the immunizations recommended in most states. The influenza vaccine is
often accompanied by redness, swelling, pain, tenderness, headaches, nausea, fever, and muscle
13
Andrew J. Wakefield, “MMR vaccination and autism,” The Lancet 354, no. 9182 (1999): 949.
https://www.thelancet.com/journals/lancet/article/PIIS0140673605756968/fulltext.
14
Jeffrey S. Gerber and Paul A. Offit, “Vaccines and Autism: A Tale of Shifting Hypotheses,” Clin Infect
Dis. 48, no. 4 (2009). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2908388/.
15
Jeffrey S. Gerber and Paul A. Offit, “Vaccines and Autism.”
IMMUNIZATION VERIFICATION 9
aches.
16
Common side effects of the diphtheria, tetanus, and whooping cough (DTaP) vaccine are
redness, swelling, pain, tenderness, body aches, fatigue, and fever.
17
The inactivated poliovirus
(IPV) vaccine can cause fainting, shoulder pain from the shot, or allergic reactions.
18
The
measles, mumps, and rubella (MMR) vaccine can cause a sore arm from the shot, fever, a mild
rash, and temporary pain and stiffness in the joints.
19
Side effects of the chickenpox (Varicella)
vaccine are a sore arm from the shot, fever, mild rash, temporary pain, and stiffness in the
joints.
20
The Hepatitis B (Hep B) vaccine is linked to soreness, redness, or swelling in the arm,
headaches, and fever.
21
The Haemophilus Influenza Type B (Hib) vaccine can cause redness,
warmth, or swelling from the shot and a fever.
22
The Pneumococcal Vaccine (PCV) may cause a
reaction where the shot was given, redness, swelling, pain or tenderness, fever, loss of appetite,
fussiness or irritability, feeling tired, headaches, or chills.
23
Although all these side effects are
16
Centers for Disease Control and Prevention, “Flu Vaccine Safety Information,” CDC, Centers for
Disease Control and Prevention, revised September 17, 2019, https://www.cdc.gov/flu/prevent/general.htm.
17
Centers for Disease Control and Prevention, “Whooping Cough Vaccines are Safe but Side Effects Can
Occur,” CDC, last modified June 29, 2017, https://www.cdc.gov/pertussis/pregnant/mom/safety-side-effects.html.
18
Centers for Disease Control and Prevention, “Polio Vaccination: What Everyone Should Know,” CDC,
last modified May 4, 2018, https://www.cdc.gov/vaccines/vpd/polio/public/index.html.
19
Centers for Disease Control and Prevention, “Measles, Mumps, Rubella (MMR) Vaccine,” CDC, last
modified September 9, 2020, https://www.cdc.gov/vaccinesafety/vaccines/mmr-vaccine.html.
20
Centers for Disease Control and Prevention, “Chickenpox (Varicella) Vaccines,” CDC, last modified
September 9, 2020, https://www.cdc.gov/vaccinesafety/vaccines/varicella-vaccine.html.
21
Centers for Disease Control and Prevention, “Hepatitis B Vaccines,” CDC, last modified September 9,
2020, https://www.cdc.gov/vaccinesafety/vaccines/hepatitis-b-vaccine.html.
22
Centers for Disease Control and Prevention, “Haemophilus Influenza Type B (Hib) Vaccines,” CDC, last
modified September 9, 2020, https://www.cdc.gov/vaccinesafety/vaccines/hib-vaccine.html.
23
Centers for Disease Control and Prevention, “Pneumococcal Vaccination: What Everyone Should
Know,” CDC, last modified August 7, 2020, https://www.cdc.gov/vaccines/vpd/pneumo/public/index.html.

IMMUNIZATION VERIFICATION 10
rarely serious, they are enough to make some people question the safety of vaccines. Because of
this safety concern, some camps do not verify that their campers are vaccinated.
A final and more recent concern regarding immunizations is the questioned safety of the
newly developed SARS-CoV-2 vaccine. According to the CDC, “The U.S. Food and Drug
Administration (FDA) has granted Emergency Use Authorizations (EUA) for two COVID-19
vaccines which have been shown to be safe and effective as determined by data from the
manufacturers and findings from large clinical trials.”
24
However, because these vaccines are
currently so new, their long-term effects are unknown. Furthermore, their effects and
effectiveness on children are still in question. As of September 2020, researchers Douglas Opel,
Douglas Diekema, and Lainie Friedman Ross concluded that “we currently know too little about
the performance of any of the candidate COVID-19 vaccines or the epidemiology of SARS-
CoV-2 in children to make any firm judgments about whether a COVID-19 vaccine should be
mandatory in children.”
25
This vaccine is something camps will have to wrestle with as time
progresses and more information is ascertained regarding its safety and effectiveness for
children.
State Mandates
An additional reason some camps do not verify that their campers are vaccinated is that
the state in which they are located already mandates youth be immunized to attend public
24
Centers for Disease Control and Prevention, “Ensuring the Safety of COVID-19 Vaccines in the United
States,” CDC, last modified December 22, 2020, https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety.html.
25
Douglas J. Opel, Douglas S. Diekema, and Lainie Friedman Ross, “Should We Mandate a COVID-19
Vaccine for Children?” Jama Pediatrics (2020). https://jamanetwork.com/journals/jamapediatrics/article-
abstract/2770123.

IMMUNIZATION VERIFICATION 11
schools, without exception. Currently, there are five such states in the US: California, New York,
Maine, West Virginia, and Mississippi.
26
These states require different vaccines but do so
without an exemption for religious or philosophical reasons. California requires students to get
the Hep B, DTaP, IPV, MMR, Varicella, and Hepatitis A (Hep A) vaccines. New York, West
Virginia, and Mississippi all mandate the Hep B, DTaP, IPV, MMR, and Varicella vaccines.
Maine requires its students to get the DTaP, IPV, MMR, and Varicella immunizations.
27
In these
states, exemptions are given neither for religious reasons nor personal beliefs. Hence, some
camps in these states do not see it necessary to verify that their campers have been vaccinated.
Camp Specific Reasons
In addition to information gathered through the seven-question survey, the following
anecdotal items were mentioned by survey responders as reasons they do not verify
immunizations: verification has never been considered, vaccinations are required but not
verified, verification is an additional step for camper registration, and the camp only hosts
groups. For many camps, immunization verification has never been considered. Tradition
dictated policy. Whatever the reason, many camps simply have never considered verifying
camper immunization. Others require their campers to be vaccinated, but do not verify that
campers have received their immunizations. Vaccine verification is a time-consuming and
sometimes complex step that makes camper registration more difficult. Some camps do not
26
National Conference of State Legislatures, “States With Religious and Philosophical Exemptions From
School Immunization Requirements,” NCSL, last modified June 26, 2020,
https://www.ncsl.org/research/health/school-immunization-exemption-state-laws.aspx.
27
ProCon.org, “State-by-State: Vaccinations Required for Public School Kindergarten,” ProCon.org, last
modified August 20, 2020, https://vaccines.procon.org/state-by-state-vaccinations-required-for-public-school-
kindergarten/.

IMMUNIZATION VERIFICATION 12
verify camper vaccinations because they want registration to be as easy as possible. Lastly, some
camps do not require their program participants’ vaccinations to be verified because they only
host groups, similar to a convention center or a hotel. They see the verification of vaccinations as
the responsibility of the organizing party, not the host location.
Reasons Camps Verify Immunizations
Just as there are several reasons camps do not verify their campers’ immunizations, there
are many reasons those who do verify immunizations hold this stance. Similar to the opposing
viewpoint, camps verify camper immunizations for camper safety, staff safety, and because of
state mandates.
Camper Safety
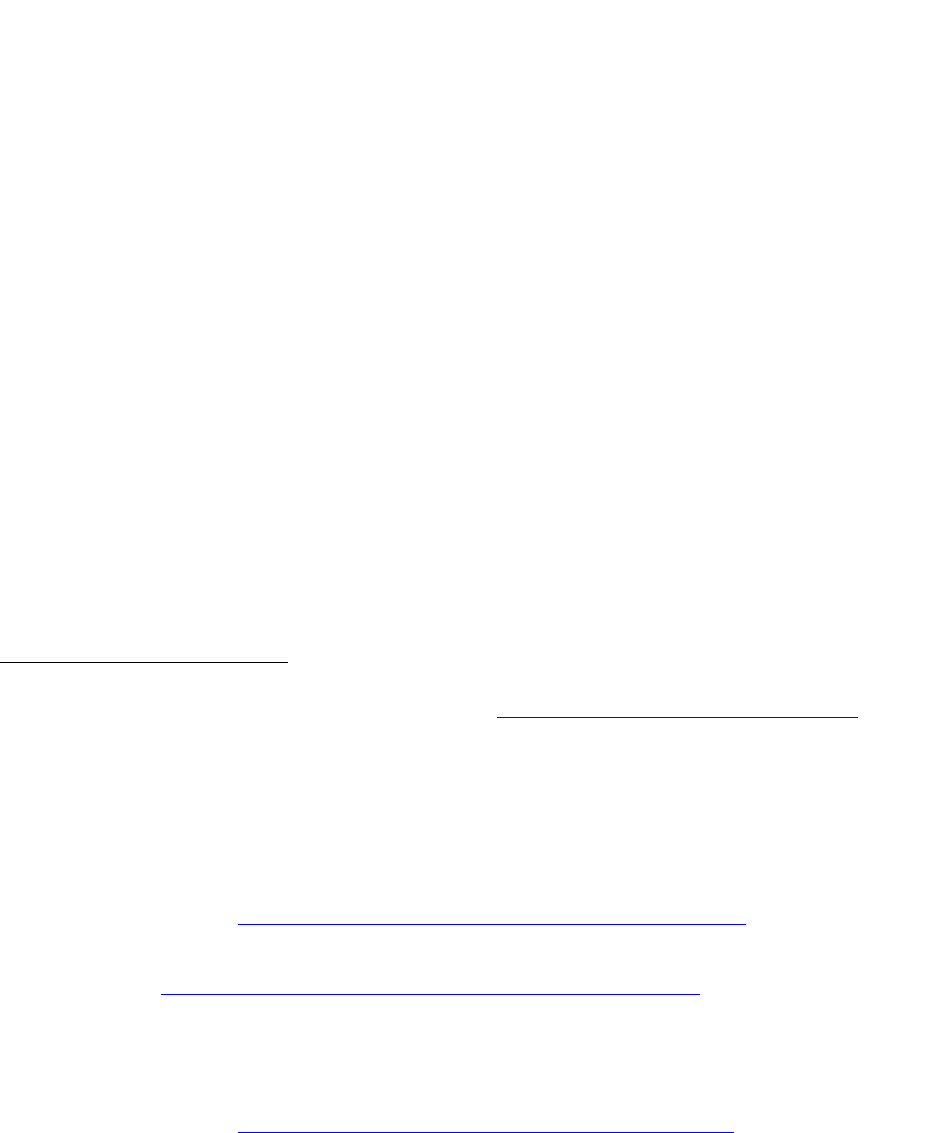
Recommended for All Children. The AAP recommends the Hep B, Rotavirus (RV),
DTaP, Hib, Pneumococcal conjugate (PCV13), Inactivated poliovirus (IPV), Influenza, MMR,
Varicella, and Hep A vaccines and boosters before children reach eighteen months of age. The
Tdap, Human papillomavirus (HPV), and Meningococcal vaccines and boosters are all
recommended for children between the ages of eighteen months and eighteen years, with varying
ages suggested based on the vaccine.
28
This vaccine schedule (Figure 1) is suggested, with minor
alterations for extenuating circumstances or late doses, for all children eighteen or under, except
for those with immunodeficiencies.
29
According to the AAP:
28
American Academy of Pediatrics, “Immunization Schedules for 2020,” AAP, last modified February 3,
2020, https://redbook.solutions.aap.org/selfserve/ssPage.aspx?SelfServeContentId=Immunization_Schedules.
29
American Academy of Pediatrics, “Immunization Schedules.”
IMMUNIZATION VERIFICATION 13
Figure 1. AAP Point-of-Care Solutions, "Immunization Schedules for 2020," AAP (2020):
https://redbook.solutions.aap.org/selfserve/ssPage.aspx?SelfServeContentId=Immunization_Schedules
This schedule is recommended by the Advisory Committee on Immunization Practices
(ACIP) and approved by the Centers for Disease Control and Prevention (CDC),
American Academy of Pediatrics (AAP), American Academy of Family Physicians
(AAFP), American College of Obstetricians and Gynecologists (ACOG), and American
College of Nurse-Midwives (ACNM).
This schedule shows the vaccines recommended for all children for their safety. Because of the
many vaccines recommended by medical experts, many camps believe immunization verification
is beneficial for camper safety and therefore require it.
Recommended for Schools. Additionally, public schools across the United States
require a number of vaccines for the majority of their students. All fifty states and Washington,
DC require their students to get the DTaP, IPV, MMR, and Varicella vaccines. Additionally,
IMMUNIZATION VERIFICATION 14
forty-three states and Washington, DC require their students to get the Hep B vaccine.
Connecticut, North Carolina, and Wyoming require students to get the Hib vaccine. Connecticut
and Washington, DC require students to get the PCV vaccine. Finally, Massachusetts requires
students to get the flu shot.
30
In forty-five states and Washington, DC, religious exemptions to
vaccines are allowed. This exemption “Indicates that there is a provision in the statute that allows
parents to exempt their children from vaccination if it contradicts their sincere religious
beliefs.”
31
Additionally, in fifteen states, philosophical exemptions to vaccines are allowed. This
exemption “Indicates that the statutory language does not restrict the exemption to purely
religious or spiritual beliefs. For example, Maine allows restrictions based on ‘moral,
philosophical or other personal beliefs,’ and Minnesota allows objections based on
conscientiously held beliefs of the parent or guardian.’”
32
Recommended for Camps. The ACA has a number of recommendations for camps
regarding immunization verification. These recommendations emerged in light of the 2015
Measles outbreak and are applicable today. The ACA requires camps within their association to
use a health form which has “A statement from the custodial parent/guardian attesting that all
immunizations required for school are up to date and including the actual date (month/year) of
last tetanus shot. . . .”
33
However, as of 2019, the ACA allowed exemptions for non-vaccinated
30
ProCon.org, “State-by-State.”
31
National Conference of State Legislatures, “States With Religious and Philosophical Exemptions.”
32
National Conference of State Legislatures, “States With Religious and Philosophical Exemptions.”
33
American Camp Association, “Emerging Issues: Immunizations, Measles, and other Communicable
Diseases,” ACA Camps, April 2015, https://www.acacamps.org/resource-library/campline/emerging-issues-
immunizations-measles-other-communicable-diseases.

IMMUNIZATION VERIFICATION 15
campers because of religious and philosophical exemptions or medical reasons. They noted,
however, that camps must recognize the risk that comes with allowing non-vaccinated campers
and weigh these risks accordingly.
34
Here, the AAP differs in its recommendation:
Before starting camp, all campers and staff should be in compliance with the
recommended childhood immunization schedule published annually by the American
Academy of Pediatrics (AAP), the Advisory Committee on Immunization Practices of the
Centers for Disease Control and Prevention (CDC), and the American Academy of
Family Physicians. . . Camp administrators should be aware that individual states might
require other immunizations in addition to those recommended by these organizations.
Immunization requirements for participation at camp provide a safe environment for
those participating.
35
They furthermore note:
Nonmedical exemptions to required immunizations are inappropriate, and these
exemptions should be eliminated by camps. Participation by campers and staff who are
incompletely immunized or unimmunized because of nonmedical exemptions is
inappropriate for individual, public health, and ethical reasons. Camps should support
medical exemptions to specific immunizations as determined for each individual (eg,
those with congenital conditions, with compromised immune systems, or taking specific
medications).
36
A final instance that highlights the importance of immunization verification for camper
safety is a 2005 outbreak of mumps at a New York summer camp. A study was conducted to find
the effectiveness of the vaccination in protecting campers for this instance. This study was
possible because of a “retrospective review of immunization records for 507 attendees who were
34
American Camp Association, “Measles Update for the 2019 Summer Camp Season,” ACA Camps, May
20, 2019, https://www.acacamps.org/news-publications/blogs/camp-connection/measles-update-2019-summer-
camp-season.
35
Michael J. Ambrose and Edward A. Walton, “Improving Health and Safety at Camp,” 3. Emphasis
added.
36
Michael J. Ambrose and Edward A. Walton, “Improving Health and Safety at Camp,” 3.
IMMUNIZATION VERIFICATION 16
eligible for vaccination and had verified immunization history.”
37
This study concluded and
confirmed two doses of the mumps vaccine were needed for the camper to gain optimal
immunity.
38
This outbreak and subsequent study highlight the importance of immunization and
verification for the protection of campers.
Staff Safety. Many camps verify immunizations for the safety of their staff. Both the
ACA and AAP recommend immunization verification for staff safety. The ACA emphasizes the
importance of verifying the vaccinations of international staff, as many countries do not follow
the same rigorous immunization schedule the United States does.
39
As with campers, the ACA
echoes that risks accompany hosting unvaccinated staff.
40
Like previously noted, the AAP also
says, “all. . . staff should be in compliance with the recommended childhood immunization
schedule. . . .”
41
Because it is beneficial for staff safety, some camps verify program participant
vaccination.
State Mandates. One reason some camps verify their campers’ immunizations is that
they are required to by the state in which they are located. For instance, Massachusetts requires
camps within the state to certify their campers’ immunizations through written documentation.
This documentation may include “any form or letter signed and dated by a physician or designee,
37
Joshua K. Schaffzin et al., “Effectiveness of Previous Mumps Vaccination during a Summer Camp
Outbreak,” Pediatrics 120, no 4. (2007): e862.
38
Joshua K. Schaffzin et al., “Effectiveness of Previous Mumps Vaccination,” e867.
39
Marla Coleman, “American Camp Association Immunization Recommendations for International Staff,”
ACA Camps, accessed January 20, 2021, https://www.acacamps.org/resource-library/campline/american-camp-
association-immunization-recommendations-international-staff.
40
American Camp Association, “Measles Update.”
41
Michael J. Ambrose and Edward A. Walton, “Improving Health and Safety at Camp,” 3.

IMMUNIZATION VERIFICATION 17
or. . . a dated report from the Massachusetts Immunization Information System; provided that
either document specifies the month and year of administration and the type/name of the
vaccines(s) administered to the camper or staff person, or alternative evidence of immunity.”
42
Massachusetts does permit religious and medical exemptions from immunizations for camp
program participants. However, in these cases, written documentation of the exemption must be
submitted to the camp and recorded. The Massachusetts requirements for camps notes, “In
situations when one or more cases of a vaccine-preventable or any other communicable disease
are present in a camp, all susceptible children, including those with medical or religious
exemptions, are subject to exclusion. . . .”
43
Although not all campers are required to be
vaccinated, camps in Massachusetts are all required to know the status of their campers’
immunizations and act accordingly. These requirements vary from state to state and are the
reason some camps verify immunizations.
Furthermore, the potential exists that the COVID-19 vaccine may be required to attend
school and play youth sports. Since the camp environment (day camp and overnight) includes
camper interaction in close proximity, they may require COVID-19 immunizations also. If this
vaccine is required to attend camps, then the verification of this vaccine may be required. This
vaccine presents an additional potential state mandate that camps may have to consider regarding
immunization verification.
42
Massachusetts Department of Public Health, Minimum Standards for Recreational Camps for Children
(State Sanitary Code, Chapter IV), 105 CMR 430.000, 12.
43
Massachusetts Department of Public Health, Minimum Standards for Recreational Camps, 12.

IMMUNIZATION VERIFICATION 18
Past Recommendations and Current Practices
Because of the similar bases for these opposing viewpoints, camps may find ascertaining
the best practice for immunization verification difficult. However, an additional important
concept to consider is the recommendations from medical experts for camps regarding
immunization verification practices. The guidelines from the AAP over the past twenty years
offer a range of suggestions for camps that have influenced the ACA’s current practice.
Historic AAP Recommendations
The AAP’s recommended best practice for camps regarding immunizations and their
verification has changed several times over the past twenty years. These practices reflect possible
approaches for CCCA camps toward immunization verification. A discussion of the strengths
and weaknesses of each approach follows the description of the approaches.
2000 Recommendation. In the AAP’s 2000 health guidelines for camps, they
recommend “All camps should be in compliance with immunization schedules recommended by
the AAP and as required by state and local health departments.”
44
Furthermore, they recommend:
Camp personnel should request and keep on file the following information: . . .
Immunizations: full record of series according to the “Recommended Childhood
Immunization Schedule-United States,” which is published every January by the AAP,
the Advisory Committee on Immunization Practices of the Centers for Disease Control
and Prevention, and the American Academy of Family Physicians.
45
44
Committee on School Health, “Health Appraisal Guidelines for Day Camps and Resident Camps,”
Pediatrics 105, no. 3 (2000): 643.
45
Committee on School Health, “Health Appraisal Guidelines,” 644.

IMMUNIZATION VERIFICATION 19
Lastly, this document says camps should ask “whether the child has had chickenpox (varicella)”
and “whether the child has been immunized against chickenpox.”
46
This recommendation is less
stringent than those published later. Camps that follow this model would ask for the program
participant’s immunization history but not require it. Furthermore, the immunization history
submitted would not be verified; therefore, falsification is possible.
2005 Recommendation. In the 2005 health guidelines for camps, the AAP updated their
recommendations to include the following:
Within a period determined by the camp, but before the child’s first day of camp, parents
or guardians should be required to provide camp authorities with a comprehensive health
history. This history should include the child’s significant previous illnesses, surgeries,
injuries, immunizations, and allergies and present state of physical and psychological
health. . . All campers should be in compliance with the recommended childhood
immunization schedule published annually by the AAP, the Advisory Committee on
Immunization Practices of the Centers for Disease Control and Prevention, and the
American Academy of Family Physicians. . . Camps should be aware that individual
states may require other immunizations in addition to those recommended by the AAP.
47
In accordance with this recommendation, camps require parents to submit certain health
information instead of just requesting the information. As in the 2000 recommendation, this
information is not verified.
2011 Recommendation. The AAP once again adapted their recommendations for camps
regarding immunization in this document’s 2011 version. In this edition, the AAP recommends:
Before starting camp, all campers should be in compliance with the recommended
childhood immunization schedule published annually by the American Academy of
Pediatrics (AAP), the Advisory Committee on Immunization Practices of the Centers for
46
Committee on School Health, “Health Appraisal Guidelines,” 643-644.
47
Committee on School Health, “Health Appraisal Guidelines for Day Camps ad Resident Camps,”
Pediatrics 115, no. 6 (2005): 1770-1771.

IMMUNIZATION VERIFICATION 20
Disease Control and Prevention, and the American Academy of Family Physicians. Camp
administrators should be aware that individual states might require other immunizations
in addition to those recommended by the AAP. Polices must also be in place regarding
participation in the camp program by campers who are incompletely immunized or
unimmunized. People who travel internationally as part of a camp program should
consult the Centers for Disease Control and Prevention traveler’s health Web site or visit
a traveler’s clinic for information regarding particular immunization requirements or
health concerns that may be associated with their destination.
48
The most significant addition in this edition of the AAP’s guidelines is the statement on
incompletely vaccinated campers. As it notes, policies must be placed to protect these campers.
As with the 2000 and 2005 guidelines, the 2011 edition does not speak into verification of
program participant immunization status.
2019 Recommendation. The 2019 guidelines for a healthy camp from the AAP give by
far the most strict recommendations for camps. In this document, the most significant change
regarding immunization policy suggestions is nonmedical exemptions to vaccines are deemed
“inappropriate.”
49
While this document does not specify a best practice regarding the verification
of these immunizations, it is clear all campers should be fully vaccinated unless preexisting
medical conditions prevent them from doing so.
Current ACA Practice
As of 2019, the ACA did not require campers to be fully vaccinated. An immunization
history is required, or a waiver for nonvaccinated campers. To protect these campers, the ACA
notes:
48
Council on School Health, “Policy Statement – Creating Healthy Camp Experiences,” Pediatrics 127
(2011): 795.
49
Michael J. Ambrose and Edward A. Walton, “Improving Health and Safety,” 3.

IMMUNIZATION VERIFICATION 21
If someone not protected through immunization comes in contact with an infected person,
many public health departments have initiated mandatory 21 day quarantine. Each public
health department may handle this differently. For example, where the quarantine occurs
(camp or elsewhere), who is quarantined including potential distinctions between people
who have a medically documented reason for not being immunized (e.g. immune-
compromised) versus those whose parents chose not to immunize, etc.
50
To protect these unvaccinated students, the ACA provides forms with appropriate language that
camps may employ. They also suggest camps “consult with legal counsel regarding the
applicability of the school immunization laws to their business.”
51
The ACA’s suggestion for the
content of this form is included in Appendix A.
Literature Review Conclusion
Stemming from the motivations discussed in this literature review and the potential
merits of both sides, these researchers conducted a study to find what percent of camps in the
CCCA practice immunization verification. Because of the safety benefits for program
participants immunization verification provides both campers and staff, the researchers
hypothesized the majority of CCCA affiliated camps would verify immunizations. This study
and its findings are discussed in the following sections.
Method
Subjects
The camps surveyed in this study were members of the CCCA that operated year-round.
They had to host over five-hundred program participants, including campers and staff,
throughout the year. The individual who responded to the survey on behalf of the camp had to
50
American Camp Association, “Measles Update.”
51
American Camp Association, “Emerging Issues.”
IMMUNIZATION VERIFICATION 22
work full-time and be over eighteen years of age. This individual needed to have access to the
camp’s current policy regarding immunization verification if such a policy existed. This study
was not researching human subjects, so Institutional Review Board (IRB) approval was not
needed (Appendix B).
Apparatus
To collect the desired information from these participants, the researchers used a seven-
question survey. The questions were multiple choice with no open-ended options to protect the
anonymity of the organization. The first question was a screening question, preventing
participants who did not meet the criteria or had not read the consent form from taking the
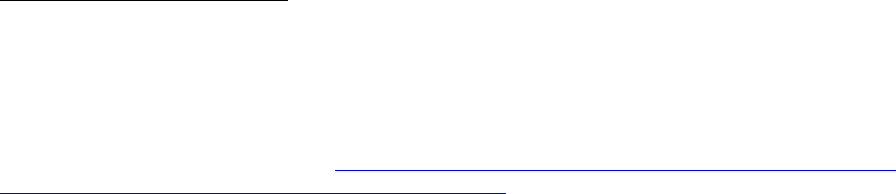
survey. The second question asked, based on Figure 2, in which region the camp is located. The
options given for the participants to select included: West, Midwest, South, Northeast, and Does
not apply (for international camps). The researchers asked this question to determine if there is a
significant difference in policy and practice based on the camp’s location. The third question on
the survey asked, “Over the past five years, how many participants has your camp averaged
annually?” The possible answers were 500-4,999; 5,000-9,999; and 10,000+. The researchers
asked this question to determine if there is a significant difference in policy and practice based
on the camp’s size. The fourth question on the survey asked if the camp represented required
campers to provide proof of immunization. The two options for answers were “yes” and “no.”
This question was used to determine the current practice of the camp. The fifth question on the
survey asked for which vaccinations the camp requires proof of immunization. The options listed
were the vaccines required by many and all public schools in the United States – DTaP, IPV,
Measles and Rubella (MR), Varicella, Mumps, Hep B, Hep A, Flu, Hib, Meningitis,
IMMUNIZATION VERIFICATION 23
Figure 2. Office of Inspector General, “Child Care Providers: Compliance with State Health and Safety Requirements,” U.S.
Department of Health & Human Services, accessed February 8, 2021: https://oig.hhs.gov/oas/child-care/
Pneumococcal Vaccinations – and “Unknown.” The researchers asked this question to determine
the current practice of the camp. Four vaccines – DTaP, IPV, Measles and Rubella, and Varicella
– were marked with an asterisk (*) to indicate they are required by schools in all fifty states and
Washington, DC. Participants could select as many options as desired. The next question asked
how long the camp required proof of vaccination. The options included “Less than 1 year,” “1-5
years,” “6-10 years,” and “Unknown.” The researchers asked this question to determine how
long the camp has practiced its current policy. Lastly, the survey asked why the camp holds its
current position on immunization verification. The options were “Camper safety,” “Staff safety,”
“Religious reasons,” “We have never considered it,” and “Unknown.” The participant could
select as many answers as desired. The researchers asked this question to determine the reasons
behind the camp’s current practice.
IMMUNIZATION VERIFICATION 24
Procedures
The survey was distributed via email to 778 CCCA affiliated camps. To gather the email
addresses used, the researchers used the CCCA’s list of camps, went to each camp’s website, and
found the camp’s email address within their website. When this process took place, there were
842 CCCA affiliated camps. Sixty-four camps did not have publicly accessible emails or did not
have up-to-date email information listed on their websites. Of the 778 camps the survey was sent
to, 106 responded. Of these respondents, four selected “Disagree” on the screening question and
were not able to complete the rest of the survey.
Results
Introduction
The results of the survey gave a fascinating range of answers. Of the 102 camps
surveyed, thirty-one (30.4%) verified camper immunizations. Seventy-one camps (69.6%) did
not verify camper immunizations. Of the camps 101 camps that answered the question of
location, eighteen (17.8%) were located in the West region, thirty-seven (36.6%) in the Midwest
region, twenty-nine (28.7%) in the South, and seventeen (16.8%) in the Northeast region. No
camps surveyed for this research were from outside the United States. Of the ninety-nine camps
that answered the question of size, sixty-eight (68.7%) hosted between 500-4,999 program
participants annually. Fifteen camps (15.2%) hosted from 5,000-9,999 program participants per
year, and sixteen (16.2%) hosted over 10,000 program participants annually.
Of the thirty-one camps that verified immunizations, four (12.9%) have held their policy
for 1-5 years. Two camps (6.5%) have verified immunizations for 6-10 years, sixteen camps
IMMUNIZATION VERIFICATION 25
(51.6%) have for more than ten years, and nine (29%) did not know how long they have verified
immunizations. All the camps surveyed were asked why they held their position on
immunization verification. Thirty-nine camps (39.6%) answered “Camper safety,” twenty-six
(25.7%) answered “Staff safety,” and six (5.9%) selected “Religious reasons.” Thirty-four
(33.7%) camps said they have never considered immunization verification. Thirty camps
(29.7%) did not know why they held their current position on immunization verification.
Twenty-six of the thirty-one camps which verify immunizations (83.9%) require proof of
the DTaP vaccine. Nineteen camps (61.3%) require proof of the IPV vaccine. Twenty-one
(67.7%) require verification of vaccination against MR. Eighteen camps (58.1%) require
verification of the Varicella (Chicken Pox) vaccine. Eleven camps (35.5%) verify that campers
are vaccinated against Mumps; eight (25.8%) verify the Hep B vaccination; five (16.1%) verify
the Hep A vaccine; two (6.5%) verify the Flu vaccination; four (12.9%) verify the Hib vaccine;
eight (25.8%) verify the Meningitis vaccine; and five (16.1%) verify the Pneumococcal
Vaccinations. Four camps (12.9%) selected “Unknown.”
Based on Size of Camp
Overall
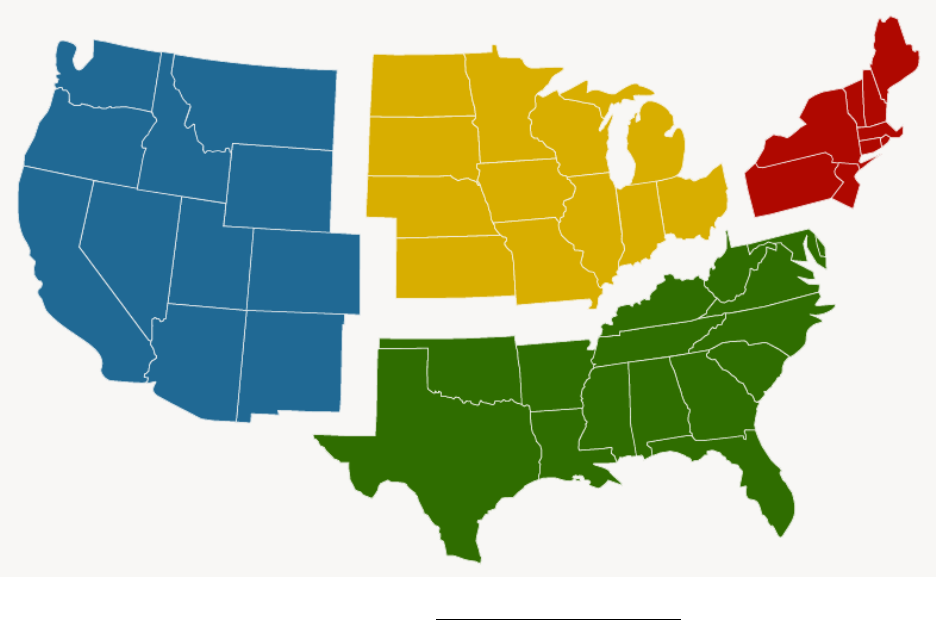
The immunization verification practice of the camps varied significantly based on camp
size. For camps with 9,999 or fewer annual participants, approximately one-third verified
immunizations (twenty-one out of sixty-eight camps with 500-4,999 participants and five out of
fifteen camps with 5,000-9,999 participants). However, for camps with 10,000 or more annual
program participants, less than a quarter verified immunizations. This ratio is illustrated in
Figure 3.
IMMUNIZATION VERIFICATION 26
Figure 3. Immunization Verification by Camp Size. Unless otherwise noted, subsequent figures are the researchers’ originals.
Immunizations Verified
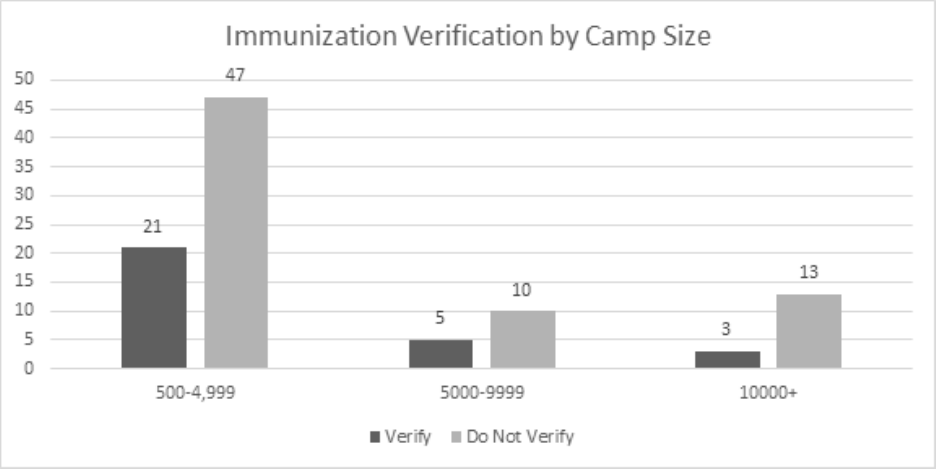
The immunizations verified varied based on the size of the camp. Camps in all size
ranges verified the DTaP, IPV, MR, Varicella, Mumps, and Hep B vaccines. However, no camps
in the medium-size category (5,000-9,999 annual program participants) verified the Hep A, Flu,
Hib, Meningitis, or PCV immunizations. Both large and small camps verified these vaccines but
in mixed proportions. Figure 4 illustrates the percentage of camps, based on size, that verifies
specific vaccines.
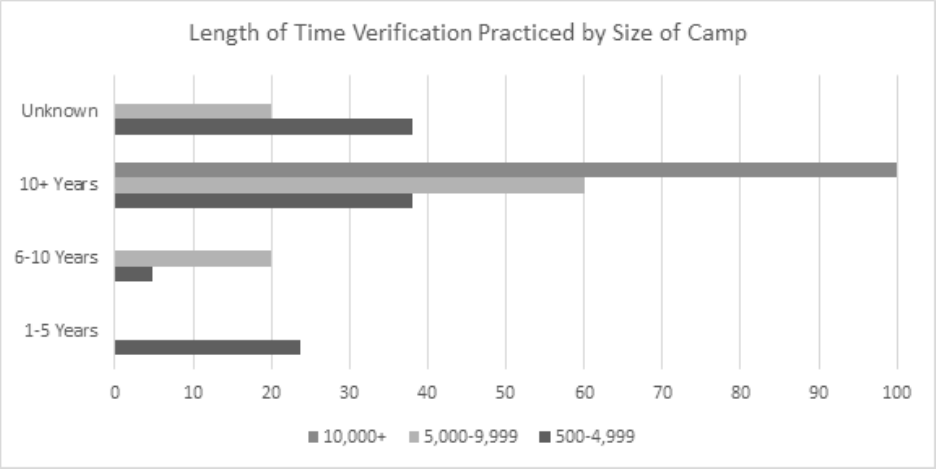
Length of Time
The length of time camps has verified immunizations also varies based on the size of the
camp. All the camps that hosted over 10,000 people annually, which verify immunizations, have
done so for over ten years. Sixty percent of medium-size camps have verified for over ten years;
IMMUNIZATION VERIFICATION 27
Figure 4: Vaccines Verified by Camp Size.
twenty percent for 6-10 years; twenty percent did not know how long they have verified
immunizations. For small camps, 38% had verified for 6-10 years. Five percent have verified for
6-10 years; twenty-four percent have verified for 1-5 years, and 38% did not know how long
they have verified immunizations. This data is represented in Figure 5.
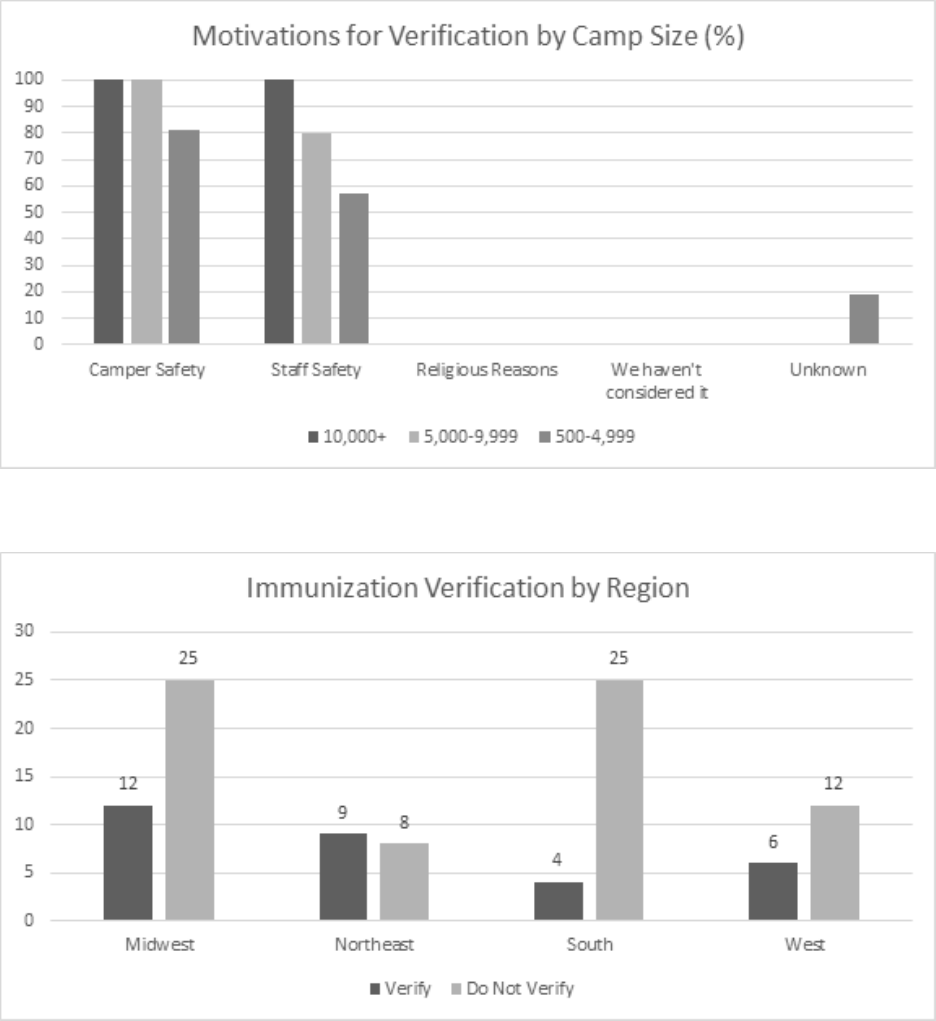
Motivations for Verification
The reasons camps do verify immunizations are similar regardless of the size of the
camp. All large and medium camps which check vaccinations verify program participant
immunizations for camper safety, as do 80% of small camps. Staff safety was also a significant
motivation for these camps: 100% of large camps verify immunizations for staff safety, 80% of
medium camps do, and just under 60% of small camps do. No camp indicated they verified
IMMUNIZATION VERIFICATION 28
Figure 5. Length of Time Verification Practiced by Size of Camp.
program participants’ vaccinations for religious reasons. Just under 20% of small camps did not
know why they verified immunizations. These statistics are illustrated in Figure 6.
Based on the Location of Camp
Overall
The practices of camps regarding immunization verification varied based on the location
of the camp. In the Midwest, twelve out of thirty-seven camps verified immunizations. The
Northeast was the only region in which more camps verified than did not: nine did, eight did not.
In the South, only four of twenty-nine camps verified immunizations. Finally, in the West, six
out of eighteen camps verified program participant immunizations. These ratios are illustrated in
Figure 7.
IMMUNIZATION VERIFICATION 29
Figure 6. Motivations for Verification by Camp Size.
Figure 7. Immunization Verification by Region.
IMMUNIZATION VERIFICATION 30
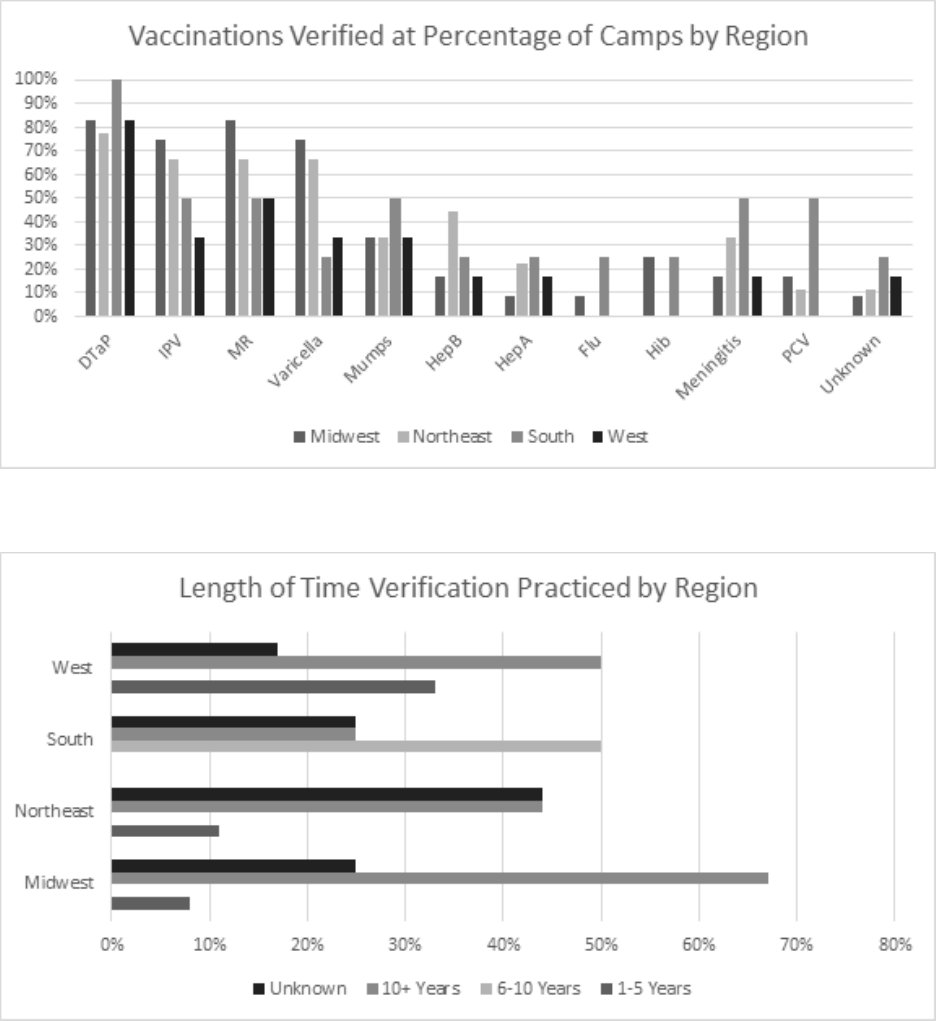
Immunizations Verified
The vaccines verified by region were relatively similar. Camps in all regions verified the
DTaP, IPV, MR, Varicella, Mumps, Hep B, Hep A, and Meningitis vaccines. Only camps in the
Midwest and South verified the Flu and Hib immunizations. PCV is verified in the Midwest,
Northeast, and South. Camps in all four regions selected “Unknown.” The percentage of camps
that verified each immunization varied by region. These percentages are shown in Figure 8.
Length of Time
The length of time camps in the four regions have verified immunizations varies
significantly. The highest percentage of camps in the Midwest have verified for more than ten
years, respectively followed by the West, Northeast, and finally the South. Only camps in the
South – 50% of those which verified immunizations – have done so for 6-10 years. The greatest
percentage of camps in the West have verified for 1-5 years, followed by the Northeast and
Midwest. No camps in the South have verified immunizations in this time range. Across these
four regions, many camps did not know how long they have verified immunizations: 44% of
camps in the Northeast, 25% of camps in the South and Midwest, and 17% in the West. This data
is illustrated in Figure 9.
IMMUNIZATION VERIFICATION 31
Figure 8. Vaccinations Verified at Percentage of Camps by Region.
Figure 9. Length of Time Verification Practiced by Region.
IMMUNIZATION VERIFICATION 32
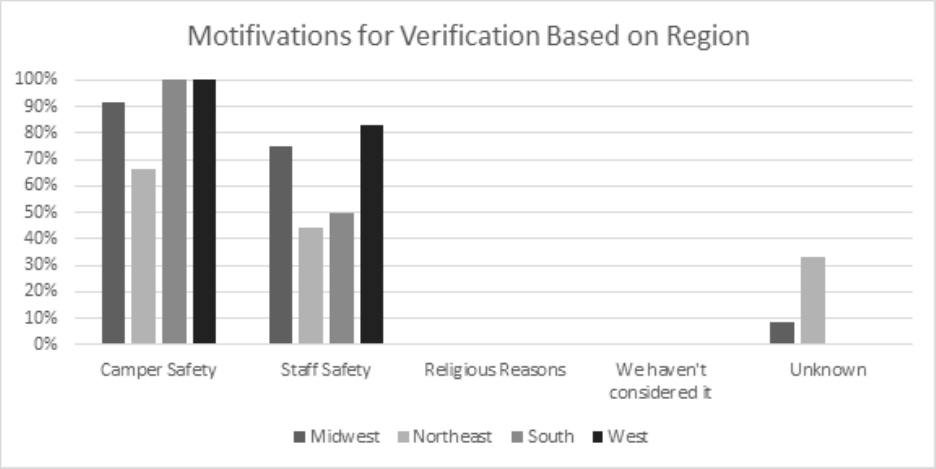
Motivations for Verification
Regardless of the location of the camp, their motivations for verification were similar. In
the West and South, 100% of camps said they verified immunizations for camper safety. Just
over 90% of camps in the Midwest said camper safety was their motivation for immunization
verification, as did 67% of camps in the Northeast. Staff safety was also a key motivation for
immunization verification across all regions. In the West, over 83% of camps said they verified
immunizations for staff safety. In the Midwest, 75% of camps said staff safety was one of their
motivations for immunization verification. In the Northeast, 50% of camps cited staff safety as a
key motivation for immunization verification, as did 44% of camps in the Northeast. 33% of
camps in the Northeast chose “Unknown” on this question, as did 8% of camps in the Midwest.
These ratios are demonstrated in Figure 10.
Discussion
Based on the recommendations of medical experts, the researchers have determined a
best practice which they suggest for camps. This best practice is that which mitigates the most
actual risk and allows the most campers to attend camp safely. This practice would be a form of
immunization verification that prioritizes the health of program participants and the operational
necessities of the camp. Contrary to the results anticipated by the researchers based on these
health guidelines, the majority of CCCA affiliated camps do not verify immunizations in any
way.
IMMUNIZATION VERIFICATION 33
Figure 10. Motivations for Verification Based on Region.
The researchers believe every child is valuable and deserves a camp experience. They
want to see as many children at camp as possible. However, they recognize it is the camps’
responsibility to the public to handle the safety of campers and staff. Camps are responsible for
outbreaks that occur through their programming, such as those mentioned in the above literature
review. Furthermore, a disease outbreak at camp can be operationally disastrous. Sick staff
cannot work. The camp may become understaffed and unable to operate adequately. Because of
the liability of a disease outbreak and the detrimental effect one has on camp operations, the
researchers suggest CCCA camps verify program participants’ immunizations without
exemption.

IMMUNIZATION VERIFICATION 34
CCCA camps are religious organizations. The philosophical concerns of these camps and
their clients should be respected. Sadly, religious exemptions to vaccines are frequently abused.
52
Even with legitimate religious exemptions, the dangers of disease outbreaks persist. Some
campers may not attend camps that follow this practice and require unexempted immunization
verification. However, camps should consider it because it increases the safety of the program
participants within their care. Not every camp will follow this practice. Opportunities will still
exist for those who do not want to verify their immunizations to have a camp experience.
Recognizing the AAP recommends all campers be vaccinated without exception,
53
camps
should consider implementing strategies that allow program participants to verify immunizations
as painlessly as possible. There are many ways in which this practice may be executed. Some of
these methods include forms with attached doctors’ notes, verification from schools, or through
local immunization registries.
54
These methods are further discussed in Appendix C. Camps are
encouraged to consult this appendix and adapt a method for implementation.
Conclusion
Camps hold various positions regarding immunization verification for program
participants. Their motivations for and against this practice include religious reasons, camper and
staff safety, state mandates, and camp-specific motivations. The majority of CCCA affiliated
52
Dorit Rubenstien Reiss, “Thou Shalt Not Take the Name of the Lord Thy God in Vain: Use and Abuse of
Religious Exemptions from School Immunization Requirements,” Symposium: Children's Health, Mental Health,
and the Law 65 (2014): 1570.
53
Michael J. Ambrose and Edward A. Walton, “Improving Health and Safety,” pg. 3.
54
Center for Disease Control and Prevention, “Finding and Updating Vaccine Records,” CDC, last
modified February 25, 2020. https://www.cdc.gov/vaccines/parents/records/find-records.html.
IMMUNIZATION VERIFICATION 35
camps do not verify their campers’ immunizations. However, a best practice for these camps
should be considered for implementation. This practice protects the program participants and
allows camps to maximize Gospel impact by remaining open. CCCA camps should consider
verifying all camper and staff immunizations without exemption.
IMMUNIZATION VERIFICATION 36
Bibliography
Ambrose, Michael J. and Edward A. Walton. “Improving Health and Safety at Camp.” American
Academy of Pediatrics 144, no. 1 (2019): 1-10.
https://pediatrics.aappublications.org/content/144/1/e20191355.
AAP Point-of-Care Solutions, "Immunization Schedules for 2020," AAP (2020):
https://redbook.solutions.aap.org/selfserve/ssPage.aspx?SelfServeContentId=Immunizati
on_Schedules
American Academy of Pediatrics. “Immunization Schedules for 2020.” AAP. American of
Academy of Pediatrics. Last modified February 3, 2020.
https://redbook.solutions.aap.org/selfserve/ssPage.aspx?SelfServeContentId=Immunizati
on_Schedules.
American Camp Association. “ACA Facts and Trends.” ACA Camps. American Camp
Association. Accessed December 18, 2020. https://www.acacamps.org/press-room/aca-
facts-trends.
———. “Emerging Issues: Immunizations, Measles, and other Communicable Diseases.” ACA.
American Camp Association. Published April 2015. https://www.acacamps.org/resource-
library/campline/emerging-issues-immunizations-measles-other-communicable-diseases.
———. “Camper Health History Form 1.” ACA Camps. American Camp Association. Last
modified January 2014.
https://www.acacamps.org/sites/default/files/resource_library/forms/Camper-Health-
History-Form.pdf
———. “Measles Update for the 2019 Summer Camp Season.” ACA. American Camp
Association. Published May 20, 2019. https://www.acacamps.org/news-
publications/blogs/camp-connection/measles-update-2019-summer-camp-season.
———. “Standards-At-A-Glance.” ACA Camps. American Camp Association. Last modified
December 2019.
https://www.acacamps.org/sites/default/files/page_documents/accreditation/Standards-at-
a-glance-2019-updated-Nov19.pdf. Emphasis ours.
———. “The Healthy Camp Study: Impact Report.” ACA Camps. American Camp Association.
Accessed December 18, 2020. https://www.acacamps.org/downloads/healthy-camp-
study-impact-report.
Centers for Disease Control and Prevention. “Chickenpox (Varicella) Vaccines.” CDC. Last
modified September 9, 2020. https://www.cdc.gov/vaccinesafety/vaccines/varicella-
vaccine.html.
———. “Contacts for IIS Immunization Records.” CDC. Last modified June 7, 2019.
https://www.cdc.gov/vaccines/programs/iis/contacts-locate-records.html#state.
———. “Ensuring the Safety of COVID-19 Vaccines in the United States.” CDC. Last modified
December 22, 2020. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety.html.
IMMUNIZATION VERIFICATION 37
———. “Finding and Updating Vaccine Records.” CDC. Last modified February 25, 2020.
https://www.cdc.gov/vaccines/parents/records/find-records.html.
———. “Flu Vaccine Safety Information.” CDC. Last modified September 17, 2019.
https://www.cdc.gov/flu/prevent/general.htm.
———. “Haemophilus Influenza Type B (Hib) Vaccines.” CDC. Last modified September 9,
2020. https://www.cdc.gov/vaccinesafety/vaccines/hib-vaccine.html.
———. “Hepatitis B Vaccines.” CDC. Last modified September 9, 2020.
https://www.cdc.gov/vaccinesafety/vaccines/varicella-vaccine.html.
———. “Measles, Mumps, Rubella (MMR) Vaccine.” CDC. Last modified September 9, 2020.
https://www.cdc.gov/vaccines/vpd/polio/public/index.html.
———. “Pneumococcal Vaccination: What Everyone Should Know.” CDC. Last modified
August 7, 2020. https://www.cdc.gov/vaccines/vpd/pneumo/public/index.html.
———. “Polio Vaccination: What Everyone Should Know.” CDC. Last modified May 4, 2018.
https://www.cdc.gov/vaccines/vpd/polio/public/index.html.
———. “Whooping Cough Vaccines are Safe but Side Effects Can Occur.” CDC. Last modified
June 29, 2017. https://www.cdc.gov/pertussis/pregnant/mom/safety-side-effects.html.
Coleman, Marla. “American Camp Association Immunization Recommendations for
International Staff.” ACA. American Camp Association. Accessed January 20, 2021.
https://www.acacamps.org/resource-library/campline/american-camp-association-
immunization-recommendations-international-staff.
Committee on School Health. “Health Appraisal Guidelines for Day Camps and Resident
Camps.” Pediatrics 105, no. 3 (2000): 643-644.
———. “Health Appraisal Guidelines for Day Camps ad Resident Camps.” Pediatrics 115, no. 6
(2005): 1770-1773.
Cox, Chelsey and Miriam Fauzia. “Fact check: COVID-19 vaccine ‘morally acceptable,’ Vatican
says, but some claims missing context.” USA Today. USA Today. Published December
29, 2020. https://www.usatoday.com/story/news/factcheck/2020/12/29/fact-check-covid-
19-vaccines-morally-acceptable-vatican-says/4014905001/.
Council on School Health. “Policy Statement – Creating Healthy Camp Experiences.” Pediatrics
127 (2011): 794-799.
Blaisdell, Laura L., Wendy Cohn, Jeff R. Pavell, Dana S. Rubin, and Jeffrey E. Vergales.
“Preventing and Mitigating SARS-CoV-2 Transmission — Four Overnight Camps,
Maine, June–August 2020.” Morbidity and Mortality Weekly Report 69, no. 35 (2020):
1216-1220. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7470465/.
Gerber, Jeffrey S. and Paul A. Offit. “Vaccines and Autism: A Tale of Shifting Hypotheses.”
Clin Infect Dis. 48, no. 4 (2009): 456-461.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2908388/.
IMMUNIZATION VERIFICATION 38
Lebovits, Hannah. “We sent our kids to summer camp. It shut down with a COVID-19 outbreak
after just a few days. This is what school will look like.” Business Insider.
businessinsider.com. Published August 5, 2020. https://www.businessinsider.com/covid-
broke-out-at-our-kids-camp-this-is-what-school-will-look-like-2020-7.
Massachusetts Department of Public Health. Minimum Standards for Recreational Camps for
Children (State Sanitary Code, Chapter IV). 105 CMR 430.000. 1-33.
National Conference of State Legislatures. “States With Religious and Philosophical Exemptions
From School Immunization Requirements.” NCSL. National Conference of State
Legislatures. Last modified June 26, 2020. https://www.ncsl.org/research/health/school-
immunization-exemption-state-laws.aspx.
Novotny, Thomas, Charles Jennings, Mary Doran, C. Ralph March, Richard S. Hopkins, Steven
G.F. Wassilak, and Lauri E. Markowitz. “Measles Outbreaks in Religious Groups
Exempt from Immunization Laws.” Public Health Reports 103, no. 1 (1988): 49-54.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1477942/.
Office of Inspector General, “Child Care Providers: Compliance with State Health and Safety
Requirements,” U.S. Department of Health & Human Services, accessed February 8,
2021: https://oig.hhs.gov/oas/child-care/
Opel, Douglas J., Douglas S. Diekema, and Lainie Friedman Ross. “Should We Mandate a
COVID-19 Vaccine for Children?” Jama Pediatrics (2020).
https://jamanetwork.com/journals/jamapediatrics/article-abstract/2770123.
Pelčić, Gordana, Silvana Karačić, Galina L. Mikirtichan, Olga I. Kubar, Frank J. Leavitt,
Michael Cheng-tek Tai, Naoki Morishita et al. “Religious exception for vaccination or
religious excuses for avoiding vaccination.” Croatian Medical Journal 57, no. 5 (2016):
516-521. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5141457/.
ProCon.org. “State-by-State: Vaccinations Required for Public School Kindergarten.”
ProCon.org. ProCon. Last modified August 20, 2020. https://vaccines.procon.org/state-
by-state-vaccinations-required-for-public-school-kindergarten/.
Richmond, Dan, Jim Sibthorp, and Cait Wilson. “Understanding the Role of Summer Camps in
the Learning Landscape: An Exploratory Sequential Study.” Journal of Youth
Development 14, no. 3 (2019): 9-30. http://digitalcommons.liberty.edu/eleu/vol2/iss1/5/.
Rubenstien Reiss, Dorit. “Thou Shalt Not Take the Name of the Lord Thy God in Vain: Use and
Abuse of Religious Exemptions from School Immunization Requirements.” Symposium:
Children's Health, Mental Health, and the Law 65 (2014): 1551-1601.
Schaffzin, Joshua K., Lynn Pollock, Cynthia Schulte, Kyle Henry, Gustavo Dayan, Debra Blog,
and Perry Smith. “Effectiveness of Previous Mumps Vaccination during a Summer Camp
Outbreak.” Pediatrics 120, no 4. (2007): e862-e868. www.pediatrics.org/cgi/doi/10.1542/
peds.2006-3451
IMMUNIZATION VERIFICATION 39
Tsalik, Ephraim L., Edward F. Hendershot, Devdutta G. Sangvai, Hannah M. Cunningham,
Coleen K. Cunningham, Maria G. Lopez-Marti, William K. Purdy, Christopher W.
Woods, L. Brett Caram. “Clinical presentation and response to treatment of novel
influenza A H1N1 in a university-based summer camp population.” Journal of Clinical
Virology 47. (2010): 286-288.
Wakefield, Andrew J. “MMR vaccination and autism.” The Lancet 354, no. 9182 (1999): 949-
950. https://www.thelancet.com/journals/lancet/article/PIIS0140673605756968/fulltext.
IMMUNIZATION VERIFICATION 40
Appendix A
ACA’s Mandatory Accreditation Standard
The ACA addresses immunization in their accreditation standard, in the portion on health
and wellness. They require the following for accreditation:
ACA’s mandatory accreditation standard HW-5 addresses the issue of immunization:
HW 5.1: Does the camp require each camper to submit a current, signed health history
that includes all of the following information in relation to the activities in which the
camper may participate?
A. Description of any camp activities from which the camper should be exempted for
health reasons;
B. Record of past medical treatment, if any;
C. Record of allergies and/or dietary restrictions;
D. A statement from the custodial parent/guardian attesting that all immunizations
required for school are up to date and including the actual date (month/year) of last
tetanus shot;
E. Record of current medications, both prescribed and over-the-counter; and
F. Description of any current physical, mental, or psychological conditional requiring
medication, treatment, or special restrictions or considerations while at camp?
Furthermore, the “Contextual Education” for HW-5 further explains that:
“If camps have minors who do not have immunizations, for religious or other reasons, a
“record” can be a signed refusal or a signed waiver form.”
Camps should consult with legal counsel regarding the applicability of the school
immunization laws to their business. Camps that include un-vaccinated individuals
should require a signed exemption form. The form might include language such as:
“Because our camp program has a potential for communicable diseases, we recommend
that program participants are appropriately immunized for, at minimum, the following
diseases: tetanus, mumps, measles, rubella, polio, pertussis (whooping cough), and
diphtheria. This being said, we recognize that some individuals may not be fully
immunized for reasons that are biophysical (e.g., the individual is allergic to a serum

IMMUNIZATION VERIFICATION 41
component) or of personal choice (e.g., faith belief). This form is intended to capture
information about individuals who are not fully immunized.”
55
55
American Camp Association, “Emerging Issues.”
IMMUNIZATION VERIFICATION 42
Appendix B
IRB Communication
The IRB sent the following email describing their approval for this research:
June 11, 2020
Katherine Stacey
Philip McClendon, Keith Oglesby, Jonathan Geukgeuzian
Re: IRB Application - IRB-FY19-20-376 Extent of Immunization Requirement and
Verification at Camps
Dear Katherine Stacey, Philip McClendon, Keith Oglesby, Jonathan Geukgeuzian:
The Liberty University Institutional Review Board (IRB) has reviewed your application
in accordance with the Office for Human Research Protections (OHRP) and Food and
Drug Administration (FDA) regulations and finds your study does not classify as human
subjects research. This means you may begin your research with the data safeguarding
methods mentioned in your IRB application.
Decision: No Human Subjects Research
Explanation: Your study does not classify as human subjects research because it will not
involve the collection of identifiable, private information.
Please note that this decision only applies to your current research application, and any
modifications to your protocol must be reported to the Liberty University IRB for
verification of continued non-human subjects research status. You may report these
changes by completing a modification submission through your Cayuse IRB account.
If you have any questions about this determination or need assistance in determining
whether possible modifications to your protocol would change your application's status,
please email us at [email protected].
Sincerely,
G. Michele Baker, MA, CIP
Administrative Chair of Institutional Research
Research Ethics Office
56
56
G. Michele Baker, e-mail message to researcher, June 11, 2020.

IMMUNIZATION VERIFICATION 43
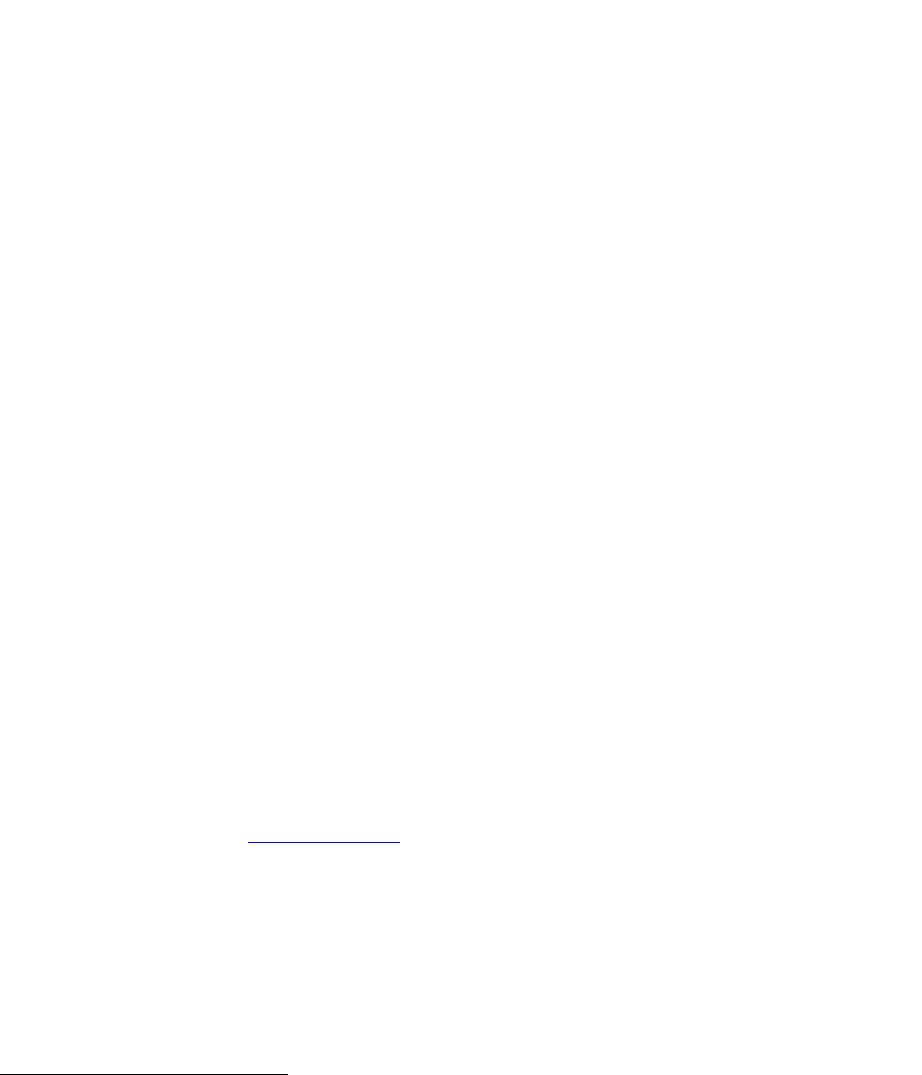
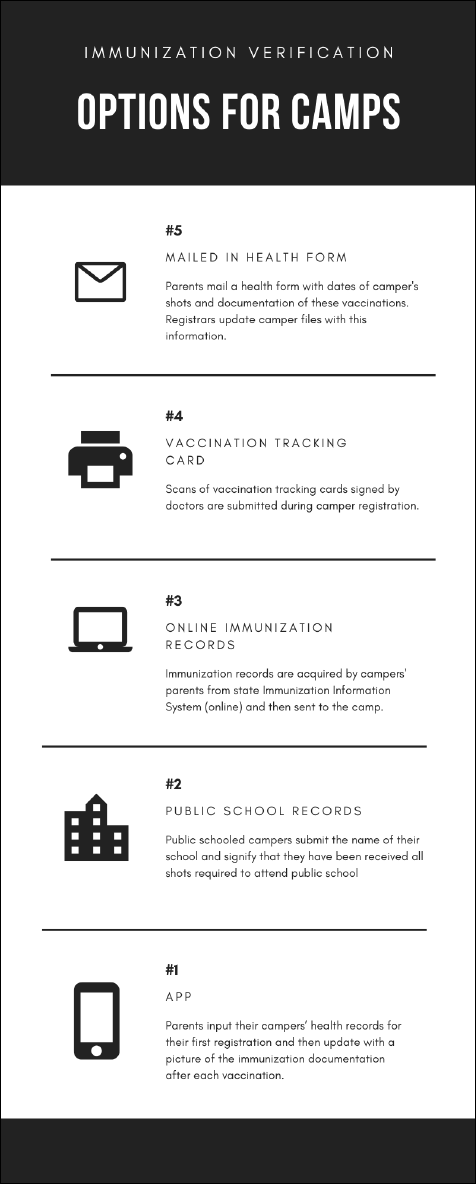
Appendix C
Methods of Immunization Verification
Methods for immunization verification are listed in Figure 11. Support for these methods
can be found in the footnotes below.
57
,
58
,
59
57
American Camp Association, “Camper Health History Form 1,” ACA Camps, American Camp
Association, last modified January 2014.
https://www.acacamps.org/sites/default/files/resource_library/forms/Camper-Health-History-Form.pdf
58
Center for Disease Control and Prevention, “Finding and Updating Vaccine Records.”
59
Centers for Disease Control and Prevention, “Contacts for IIS Immunization Records,” CDC, last
modified June 7, 2019. https://www.cdc.gov/vaccines/programs/iis/contacts-locate-records.html#state.
IMMUNIZATION VERIFICATION 44
Figure 11: Methods for Immunization Verification Infographic
