
UvA-DARE is a service provided by the library of the University of Amsterdam (http
s
://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Man vs. machine: A meta-analysis on the added value of human support in text-
based internet treatments (“e-therapy”) for mental disorders
Koelen, J.A.; Vonk, Anne; Klein, A.; de Koning, L.; Vonk, P.; de Vet, S.; Wiers, R.
DOI
10.1016/j.cpr.2022.102179
Publication date
2022
Document Version
Final published version
Published in
Clinical Psychology Review
License
CC BY-NC-ND
Link to publication
Citation for published version (APA):
Koelen, J. A., Vonk, A., Klein, A., de Koning, L., Vonk, P., de Vet, S., & Wiers, R. (2022). Man
vs. machine: A meta-analysis on the added value of human support in text-based internet
treatments (“e-therapy”) for mental disorders.
Clinical Psychology Review
,
96
, Article 102179.
https://doi.org/10.1016/j.cpr.2022.102179
General rights
It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s)
and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open
content license (like Creative Commons).
Disclaimer/Complaints regulations
If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please
let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material
inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter
to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You
will be contacted as soon as possible.
Download date:04 Aug 2024
Clinical Psychology Review 96 (2022) 102179
Available online 9 June 2022
0272-7358/© 2022 The Authors. Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-
nc-nd/4.0/).
Review
Man vs. machine: A meta-analysis on the added value of human support in
text-based internet treatments (“e-therapy”) for mental disorders
J.A. Koelen
a
,
*
, A. Vonk
a
, A. Klein
a
, L. de Koning
a
, P. Vonk
b
, S. de Vet
a
, R. Wiers
a
,
c
,
d
a
Developmental Psychology, Department of Psychology, University of Amsterdam, the Netherlands
b
Department of Research, Development and Prevention, Student Health Service, University of Amsterdam, the Netherlands
c
Center for Urban Mental Health, University of Amsterdam, the Netherlands
d
Addiction Development and Psychopathology (ADAPT)-Lab, Department of Psychology, University of Amsterdam, the Netherlands
ARTICLE INFO
Keywords:
Text-based internet treatment
Technological guidance
Human guidance
Optional support
Therapist qualication
Mental disorders
ABSTRACT
Guided internet-based treatment is more efcacious than completely unguided or self-guided internet-based
treatment, yet within the spectrum of guidance, little is known about the added value of human support
compared to more basic forms of guidance. The primary aims of this meta-analysis were: (1) to examine whether
human guidance was more efcacious than technological guidance in text-based internet treatments (“e-ther-
apy”) for mental disorders, and (2) whether more intensive human guidance outperformed basic forms of human
guidance. PsycINFO, PubMed and Web of Science were systematically searched for randomized controlled trials
that directly compared various types and degrees of online guidance. Thirty-one studies, totaling 6215 in-
dividuals, met inclusion criteria. Results showed that human guidance was slightly more efcacious than tech-
nological guidance, both in terms of symptom reduction (g = 0.11; p < .01) and adherence (0.26 < g < 0.29; p's
< 0.01). On the spectrum of human support, results were slightly more favorable for regular guidance compared
to optional guidance, but only in terms of adherence (OR = 1.89, g = 0.35; p < .05). Higher qualication of
online counselors was not associated with efcacy. These ndings extend and rene previous reports on guided
and unguided online treatments.
1. Introduction
An increasing number of studies have shown that internet-based
interventions are efcacious for a variety of mental disorders, such as
anxiety disorders, depression, and problematic alcohol use (Andersson
& Cuijpers, 2009; Domhardt, Geßlein, von Rezori, & Baumeister, 2019;
Hadjistavropoulos, Mehta, Wilhelms, Keough, & Sundstr
¨
om, 2020).
With internet-based treatment, we refer to a specic form of online
intervention that makes use of texts, images, and videos to provide the
client with therapeutic material in an interactive way, often in the shape
of a xed number of sequential modules, consisting of psycho-education,
in-session exercises, and homework assignments. This predominantly
text-based intervention is referred to as “e-therapy” throughout this
manuscript. The effects of e-therapy are similar to those found for face-
to-face therapy, at least when restricted to cognitive-behavior therapy
(CBT; Andersson & Titov, 2014; Carlbring, Andersson, Cuijpers, Riper, &
Hedman-Lagerl
¨
of, 2018; Cuijpers, Donker, Van Straten, Li, & Andersson,
2010). Moreover, some follow-up studies have indicated that the effects
of e-therapy are maintained for as long as ve years after treatment
(Hedman et al., 2011). There is burgeoning evidence that e-therapy,
despite high initial costs, could be a cost-effective treatment, both as
stand-alone treatment, or as an initial treatment option within a
stepped-care model (Salivar, Rothman, Roddy, & Doss, 2020; Weisel,
Zarski, Berger, Krieger, Schaub, et al., 2019).
E-therapy offers many other benets for people with mental health
issues, as they have the potential to overcome barriers to regular mental
health services (Andersson, 2015; Lovell & Richards, 2000). For
example, it may provide people living in remote or underprivileged
areas with the opportunity to gain access to mental health care. Across
the globe, nearly 10% of the world population have to travel for over an
hour to reach the help they might need (Weiss et al., 2020). In addition
to providing more exibility and autonomy, some people may prefer to
receive treatment in the privacy of their homes, likely related to stigma
surrounding mental health problems (Andersson, Titov, Dear, Rozental,
& Carlbring, 2019). Moreover, e-therapy, when implemented on a large
scale, offers great potential for the prevention of mental disorders
* Corresponding author at: Nieuwe Achtergracht 129B, 1018 WT Amsterdam, the Netherlands.
E-mail address: [email protected] (J.A. Koelen).
Contents lists available at ScienceDirect
Clinical Psychology Review
journal homepage: www.elsevier.com/locate/clinpsychrev
https://doi.org/10.1016/j.cpr.2022.102179
Received 3 September 2021; Received in revised form 28 April 2022; Accepted 4 June 2022
Clinical Psychology Review 96 (2022) 102179
2
(Deady et al., 2017). Finally, during the recent COVID-19 pandemic,
online treatment (including remote face-to-face therapy) has offered
many people access to therapy without running the risk of contracting
the virus. In summary, e-therapy increases access to mental health care
across the globe and offers some important advantages that make this a
promising avenue for future mental health care.
1.1. Guidance within e-therapy
In research contexts, many of the e-therapies studied have been
”unguided” (sometimes called “self-guided”), where the client pro-
gresses through the treatment without any assistance. Increasingly,
research is becoming available that better mirrors clinical practice, in
which a therapist or counselor guides the client through the treatment
(Andersson, 2015). Online guidance can be delivered in an asynchro-
nous way, for example with regular individualized or semi-standardized
email feedback, or in a synchronous way, through brief phone or chat
sessions (Riper & Cuijpers, 2016). Videoconferencing is becoming
increasingly popular, but is not the focus of this review, because this
could be considered face-to-face treatment, and is usually sharply
demarcated from modular internet-based treatments, that are the focus
of this review (e.g., Berryhill, Culmer, Williams, Halli-Tierney, Betan-
court, et al., 2019). The focus of this review is on guided e-therapy.
Guidance offers the possibility to tailor the therapy to the in-
dividual's needs, and to intervene better in case of non-adherence, crisis,
or after a sudden increase in symptoms (Andersson & Titov, 2014). Most
meta-analyses suggested that guidance renders e-therapy more efca-
cious (Andersson & Cuijpers, 2009; Johansson & Andersson, 2012;
Richards & Richardson, 2012; Spek et al., 2007; Van 't Hof, Cuijpers, &
Stein, 2009). However, these meta-analyses did not compare guided and
unguided e-therapy directly with each other. Instead, they compared
one group of studies that contrasted guided e-therapy with treatment as
usual (TAU), with another group of studies that contrasted unguided e-
therapy with TAU. The nding that the effect sizes for guided e-therapy
was larger than those for unguided led to the conclusion that guided e-
therapy was more efcacious. However, given that guided and unguided
e-therapies were not offered within the same setting, this conclusion
should be conrmed in analyses with direct comparisons.
Three more recent meta-analyses with head-to-head comparisons
tended to conrm the superiority of guided e-therapy for a range of
mental disorders (Baumeister, Reichler, Munzinger, & Lin, 2014; Dom-
hardt et al., 2019; Karyotaki et al., 2021). For example, in a meta-
analysis of 8 studies into a variety of mental disorders (mostly social
phobia and depression), Baumeister et al. (2014) reported a standard-
ized mean difference of d = 0.27 in favor of the guided e-therapy.
Domhardt et al. (2019), examining the efcacy of e-therapy for anxiety
disorders, found a similar effect size difference of d = 0.39 in favor of
guided e-therapy. However, this result was based on only four included
studies. Karyotaki et al. (2021), in an individual patient data network
meta-analysis including 39 studies on e-therapy for depression, reported
moderate differences (d = 0.6) between guided and unguided treat-
ments, in favor of the guided conditions. These ndings were stronger
for patients with higher depression scores (they beneted more from the
guided treatment). However, the differences disappeared at 6- or 12
months following randomization, although it should be noted that the
latter nding was based on a subgroup of 8 studies only (Karyotaki et al.,
2021). Findings were based on online CBT in patients with depression
only, and treatment duration (i.e., dosage of guidance) was not taken
into account.
A signicant concern is that despite supercial agreement between
these meta-analyses, basic forms of support are sometimes included in
the so-called “unguided” treatment conditions (e.g., Karyotaki et al.,
2021). Newer unguided e-therapies differ in the sense that participants
often do receive automated messages intended to increase adherence
and to reinforce their progression through treatment, which was much
less the case in older forms of e-therapy (Dear, Staples, Terides, Fogliati,
Sheehan, et al., 2016). This could be considered “technological support”,
yet was not taken into account in some of the older meta-analyses and
reviews. Riper et al. (2018), for example, found that human-supported
e-therapies were more efcacious to reduce problem drinking than
“fully automated” ones, yet it was not made explicit what the automated
interventions entailed. To elucidate these issues, in this review we will
make a clear distinction between fully unguided and technologically
guided treatments. As noted, the comparison between guided and fully
unguided e-therapy was the focus of other reviews; our focus lies on the
full spectrum of guidance, consisting of technological guidance at the
one end, and varieties of human guidance at the other end of the
spectrum.
1.2. Varieties of human guidance
Within the spectrum of human guidance, a further distinction can be
made between intensive and more basic human guidance (Domhardt
et al., 2019; Newman et al., 2011; Richards & Richardson, 2012). In the
aforementioned meta-analysis of anxiety disorders, Domhardt et al.
(2019) differentiated between “guided” and “mostly unguided” in-
terventions. Treatment was considered mostly unguided when “tech-
nical support” was offered at the request of the patient. Please note that
technical support (i.e., a human being helping to solve a technical issue)
should be differentiated from “technological” support mentioned
earlier, which is non-human by denition. However, to complicate
matters further, in some studies the “technical” support refers to
scheduled, motivational support, and encouragement from psycholo-
gists (e.g., Dirkse et al., 2020; Johnston et al., 2011); a component
considered a “common factor” of effective therapies (Cuijpers, Reijnd-
ers, & Huibers, 2019; Wampold & Imel, 2015). In other studies, “tech-
nical support” is provided by non-psychologists on a weekly basis to
encourage and motivate participants (e.g., Titov, Andrews, Davies,
Mcintyre, Robinson, et al., 2010). Richards and Richardson (2012), in
their meta-analysis, differentiated between studies that offered therapist
support with those that offered “administrative” support, which appears
similar to some denitions of “technical support”. From these examples,
it becomes clear the type/degree of human support, and the qualica-
tion of the person supporting the treatment are sometimes conated.
Researchers do not appear to agree on what is meant by “technical” or
“administrative” support. In our opinion, more clear denitions of de-
grees of guidance in e-therapy, as well as the distinction between in-
tensity of guidance and qualication of counselors, are needed in order
to analyze and understand their effect.
Therefore, in this meta-analysis, we compared varying degrees of
human support that were restricted to clinical guidance, i.e., support
aimed at the content of the program and not at its usage, using a clearly
dened taxonomy. This spectrum of human guidance includes three
levels: (1) Minimal human guidance, excluding mere assistance for
technical problems. Minimal guidance refers to support on demand, i.e.,
optional support is provided only when the patient asks for it; (2) Reg-
ular (scheduled) guidance in the form of e-mail feedback (asynchronous)
to assignments or questions, or brief support via telephone or chat
(synchronous). Regular guidance followed the established regime of
planned weekly support, and (3) Intensive guidance, i.e., human support
that is offered more frequently (a xed higher frequency of contact, i.e.,
2 or 3 times a week), or more quickly (e.g., within 24 h), than regular
support. We realize that optional support (level 2) could in practice be
more intensive than level 3 type of support (i.e., when there is high
demand for it). Therefore, studies offering optional vs. regular support
were also analyzed separately, to control for the potential confound of
intensity. Studies with a focus on levels of counselor qualication were
compared separately from the matter of intensity, to allow for a com-
parison of high-qualied guidance from low-qualied guidance (Bau-
meister et al., 2014).
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
3
1.3. Denition of technological guidance
All types of guidance share the common aim of guiding the patient
through online treatment modules, and increasing adherence (Ander-
sson, 2015; Riper and Cuijpers, 2016). Technological guidance in our
conceptualization consisted of automated reminders and feedback or
encouragement. “Reminders” imply messages to inform participants
about new material available, additional resources, or the aim to insti-
gate planning exercises. These messages were usually sent at xed in-
tervals, or when participants were unresponsive. “Automated feedback”
or encouragement/reinforcement refers to automatic standardized
(template-based) messages that the participant receives upon session
completion, usually to congratulate with completion of the session and
thus reinforce progress, and/or to provide a summary of the contents.
1.4. Aims of the present study
In sum, e-therapy studies use a wide variety of denitions to refer to
the type and nature of guidance being offered. Yet, most reviews and
meta-analyses used a dichotomization by comparing the coarse cate-
gories of ‘guided’ and ‘unguided’ interventions, which fails to consider
the wide spectrum of guidance and its variations (Farrand & Woodford,
2013). Moreover, previous meta-analyses have rarely made head-to-
head comparisons. These two issues render it difcult to draw denite
conclusions with respect to which type of support is optimal.
The primary aims of this study were to rstly clarify whether human
guidance would increase efcacy compared with technological guidance
only, and secondly whether more intensive human guidance would in-
crease efcacy of e-therapy compared with more basic forms of human
guidance. To address these aims, we created two separate sets of com-
parisons. Our rst set of comparisons was between studies that directly
compared technological and human guidance. Our second set of com-
parisons concentrated solely on varieties within the spectrum of human
guidance, in which we differentiated between three levels of human
guidance, as introduced above. This approach differs from previous
meta-analyses and reviews in three ways: (1) We did not include in-
terventions that were completely self-guided, as well as studies with
technical support only; (2) Compared to ‘regular guidance’ (weekly
human support), we included both less and more intensive forms of
human guidance; (3) We included only studies directly comparing va-
rieties of guidance.
Furthermore, due to the confusion between qualication of the on-
line counselor and so-called “technical” or “administrative support” (e.
g., Dirkse, Hadjistavropoulos, Alberts, Karin, Schneider, et al., 2020;
Richards & Richardson, 2012; Titov, Andrews, Schwencke, Solley, &
Robinson, 2009), we compared studies that examined the impact of
therapist qualication on outcome separately, thus updating previous
reviews (e.g., Baumeister et al., 2014). Finally, a number of moderators
were examined, such as offering a pretreatment interview or actively
reminding participants of their assignments.
2. Methods
2.1. Literature search
An initial, systematic multi-phase search was conducted May 2020 in
three databases (PsycINFO, PubMed and Web of Science) to obtain
studies that reported on the impact of therapist guidance in e-therapy
(see Supplement 1, Appendix A for the search strategy). This search was
updated December 2021. Our meta-analysis focused on e-therapy, and
not on combinations of face-to-face and e-therapy (blended therapy).
Publication year of published articles was not constrained. Within
the domain of randomized controlled trials (in English), we used the
following search terms (see also Appendix A in Supplement 1): web-
based, online, internet*, digital* or computer* together with cognitive
behav* or therap* or treatment, and assistance, support or guidance in
conjunction with various qualications of guidance. To detect recently
completed trials, registered trials in the U.S. National Library of Medi-
cine (https://www.clinicaltrials.gov) were searched. In case (published)
results were to be expected, researchers were contacted to obtain po-
tential results to be included in this meta-analysis. This yielded no
additional studies. Authors were also contacted in case of incomplete or
missing data. This meta-analysis was pre-registered (PROSPERO 2021
CRD42021243964).
2.2. Inclusion and exclusion criteria
Randomized controlled trials were included if they fullled the
following criteria:
(1) adult participants (18+);
(2) a mental disorder according to either relevant classication sys-
tems or a subthreshold disorder, using a validated cut-off
(screener), or both. The disorder or the dimensional equivalent
had to be enlisted in the ofcial handbooks of mental disorders
(DSM-IV or 5, ICD-10 or 11);
(3) the outcome of the intervention was assessed in terms of
depression, anxiety, or both. Thus, sleep disorders, sexual disor-
ders, and somatic symptom disorders were also included, as long
as the focus was on the alleviation of depression and/or anxiety;
(4) publication in English;
(5) examination of variations of therapist guidance in internet
treatment with at least two guided interventions with different
intensities (e.g., regular or optional, high or low frequency) of
guidance. Studies comparing different levels of therapist quali-
cation were also included;
(6) trials had to report (a) symptom (depression/anxiety) severity
levels at posttreatment or (b) adherence to the program as out-
comes (or both). Adherence was operationalized following Don-
kin et al. (2011) as the percentage of participants that completed
the whole treatment, and as the mean number of sessions
completed.
Studies were excluded if they:
(1) contained no e-therapy as dened here (e.g., attentional bias
modication training, psychoeducation only, cognitive or phys-
ical remediation therapy);
(2) combined e-therapy with face-to-face therapy (blended therapy),
either simultaneously or sequentially, or only face-to-face treat-
ment, or face-to-face treatment as a control group;
(3) examined only “self-guided” treatments with no form of guid-
ance. Note that all studies that claimed to examine “self-guided
treatments” were scrutinized for the actual absence of guidance
in any shape or form (technological support), as newer types of
internet therapies often provide automated support in “self-help”
interventions;
(4) static webpages offering psychoeducation only;
(5) comparison of two types of treatment with the same level of
guidance;
(6) inclusion of fully automated programs with virtual therapists or
chatbots, with unlimited access to the program;
(7) test of therapeutic effects of programs using virtual or augmented
reality or games;
(8) inclusion of supportive communication or supportive therapy as a
control (“attention control”) without any guidance of modules (e.
g., e-mails alone);
(9) inclusion of non-moderated internet forums as main ‘interven-
tion’ platform. Forums were allowed when offered in addition to
modules, and if moderated (and not just monitored) by a clinical
psychologist.
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
4
2.3. Selection of studies
The studies were selected in two phases: (1) screening of title and
abstract and (2) inspection of full text. To complement the electronic
search, reference lists of recent meta-analyses and reviews on this topic
(i.e., Baumeister et al., 2014; Domhardt et al., 2019; Karyotaki et al.,
2021) were screened for relevant articles during the rst phase. In
addition, reference lists of the screened full-text papers were inspected
when deemed relevant.
Two researchers (JK and AV) independently assessed the inclusion
and exclusion criteria after an initial calibration. Both authors screened
all retrieved search hits. A conservative approach was taken, so when
the title and abstract did not provide enough information, the article was
inspected full text. In the rst phase, the agreement between the two
raters was 92% (Cohen's kappa = 0.62), which is considered substantial
agreement. For the second phase, the agreement was 74% (Cohen's
kappa = 0.48), which is considered moderate agreement. The main
reason the agreement dropped in the second phase was a lack of clarity
about what constituted guidance, and which control groups were
allowed (e.g., supportive therapy without any modules). These issues
were rened during consensus meetings and yielded the denitions
introduced above. Disagreement was resolved by discussion until
consensus was reached. There was no need to consult a third party to
reach consensus.
2.4. Data extraction
For each study included, the same raters extracted the statistics
necessary for effect size calculation (means, standard deviations, drop
out or adherence rate, sample sizes) for the relevant treatment condi-
tions and the relevant outcome data. The primary outcomes differed per
study and were usually determined by the main disorders under treat-
ment. Psychological symptoms were chosen as outcome, also for studies
in the realm of medical psychology. Effect sizes were calculated for
psychological symptoms and for adherence to treatment (see denition
above). Post-treatment scores were obtained where available within
three months of treatment completion. Because follow-up outcome pe-
riods are likely to vary across studies, and because we were interested in
the immediate impact of guidance, we focused only on post-treatment
outcomes. Self-report measures were included as most studies use self-
report instruments only.
Finally, study characteristics were extracted (or calculated), that
could be used as moderators, including primary diagnosis or complaint,
setting (community/website, primary care, clinic, or hospital), type of
treatment (i.e., CBT or not), number of sessions or modules, and thera-
pist qualication (level of training, and/or role).
2.5. Assessment of study quality
To determine the methodological quality of included studies, they
were rated with the RCT Psychotherapy Quality Rating Scale (RCT-
PQRS; Kocsis et al., 2010). After registration, but before data-extraction,
we decided to use this instrument instead of the Cochrane risk of bias
tool (Higgins & Green, 2011), because the PQRS is better tailored to the
particularities of (psycho)therapy (e.g., that clinician and patient are not
blind to the treatment provided). The RCT-PQRS was specically
developed for RCTs in psychotherapy research and contains 25 items
covering six domains: (a) description of patients; (b) denition and
delivery of treatment; (c) outcome measures; (d) data analysis; (e)
treatment assignment; and (f) overall quality. The last ‘omnibus’ item is
scored on a 7-point scale; other items on a 3-point scale (0–2), yielding a
range of 1–55, with scores ≤9 representing abominable quality, scores
10–14 very poor quality, 15–24 poor quality, 25–33 adequate quality,
34–42 good, 43–50 very good, and ≥ 51 excellent quality.
One independent judge (a Master psychology student) trained by the
rst author coded all studies. To establish interrater reliability, the rst
author rated a random sample of 9 studies. Intraclass correlations (ICC)
coefcients were calculated using SPSS Statistics for MacIntosh, version
24 (IBMCorp., 2018), based on a mean rating (k = 2), absolute-
agreement, 2-way mixed-effects model. The intraclass correlation of
single measures was 0.84, which indicates a good reliability (Koo & Li,
2016).
2.6. Data analysis
2.6.1. Computation of effect sizes
2.6.1.1. Calculations of between-group contrasts. The post-treatment
scores for the two conditions that were being compared were con-
trasted and divided by their pooled standard deviation [M
1
– M
2
/
sd
pooled
]. First, we provided a global estimate for between-group con-
trasts across all studies, generalizing across types of guidance. Second,
subgroups addressing frequency or speed of feedback were analyzed
separately from those that compare regular vs. optional guidance. When
a study included multiple outcomes, the means of z-transformed vari-
ables were used to calculate an average effect size per study. This
approach yields a conservative estimate, because the correlation for the
separate outcomes per study is assumed to be 1 (while in reality it will be
lower) (Borenstein, Hedges, Higgins, & Rothstein, 2009). Some studies
yielded more than one effect size, because they contained more than two
treatment groups. In this case, we considered these pairwise compari-
sons separately. To avoid “double counts” in the shared intervention
group (that served as the comparison), the shared group N was split in
half (Higgins & Green, 2011).
2.6.1.2. Computation of pooled effect sizes across studies. Meta-analyses
were performed using Comprehensive Meta-Analysis (Borenstein, Hed-
ges, Higgins, & Rothstein, 2005). Standardized mean differences with
95% condence intervals (95% CI) were computed for all continuous
outcomes. Hedges' g was used because this corrects for small sample
sizes (Hedges & Olkin, 1985). Effect sizes of 0.20, 0.50 and 0.80 are
considered small, medium, and large (Cohen, 1988). For dichotomous
variables, odds ratios (OR) with 95%CI were computed. Positive effect
sizes imply that higher levels of guidance yielded higher effect sizes.
A random-effects model was used to compute weighted mean effect
sizes, because we expected true population effect sizes to vary across
studies due to differences in sample, methodology and treatment. The
random-effects model results in more conservative results and broader
95%CI than the xed-effects model. With this procedure, effect sizes are
weighted by their inverse variance, thus giving more weight to larger
studies (with smaller sampling error) and increasing the reliability of the
effect estimates. To examine the robustness of the global effects, we
employed the ‘one study removed’ method. Furthermore, effects were
recalculated without outliers. A study was judged an outlier when the
condence interval of the study did not overlap with the pooled effect
size (Harrer, Cuijpers, Furukawa, & Ebert, 2021). Finally, effects were
recalculated for studies with data for the full randomized sample
(intention-to-treat sample, or ITT). ITT samples usually give more con-
servative estimates of relative treatment effects, especially when
dropout is high, as is often the case in internet treatments.
2.6.1.3. Heterogeneity. Heterogeneity of effect sizes within and between
subsamples were calculated using the Q and the I
2
statistic (Higgins &
Thompson, 2002). Signicant p-values for the Q test indicate the pres-
ence of heterogeneity. I
2
represents the percentage of total variance in
effect estimates that is due to systematic heterogeneity between studies
rather than due to chance or sampling error. Low percentages indicate
low heterogeneity and percentages above 75% substantial
heterogeneity.
2.6.1.4. Moderator analysis. For the purpose of moderator analyses,
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
5
studies were divided into subgroups. For each subgroup the pooled
mean effect size was calculated, and differences in effect sizes between
the subgroups (with a minimum of four studies) were examined for
statistical signicance using the Q statistic. For the comparison of sub-
groups, the mixed-effects model was used. This model uses the random-
effects models to estimate the effect size for each subgroup, while the
xed-effects model is used to test the difference between the subgroups
(Borenstein et al., 2009).
The following moderators were examined: (1) studies providing a
pre-treatment interview were analyzed separately and compared to
studies without, because, based on previous ndings (Boettcher, Berger,
& Renneberg, 2012), we hypothesized that a pre-treatment screening or
motivational session would decrease the between-group effect sizes, and
may outweigh the effect of guidance during treatment (Johansson &
Andersson, 2012); (2) we compared studies that offered reminders in
both treatment conditions, to those that did not, as this likely decreases
between-group differences; (3) studies were analyzed separately for
those that treated anxiety disorders, and compared to those that did not,
as internet treatments for anxiety disorders show inconsistent ndings,
and the desired level of guidance is unclear (Farrand & Woodford, 2013;
Spek et al., 2007); (4) studies offering CBT were analyzed separately and
compared to those with another therapeutic orientation; (5) studies
were grouped according to their mode of delivery. We distinguished
between ‘synchronous’ communication mode (chat, telephone), ‘asyn-
chronous’ communication mode (email), and mixed, in line with other
meta-analyses (Baumeister et al., 2014).
2.6.1.5. Publication bias. We tested potential publication bias by means
of the iterative non-parametric trim and ll procedure as implemented
in CMA. This procedure controls for the association between individual
effect sizes and their sample sizes (i.e., sampling error) by inspecting
funnel plots. Publication bias is assumed to be present when the effect
sizes of small studies - with larger sampling variation than large studies -
are represented asymmetrically within and around the funnel (Sterne &
Egger, 2001). The Duval and Tweedie procedure (Duval & Tweedie,
2000) provides a correction of the effect size after publication bias has
been taken into account by trimming away studies suggesting asym-
metry. We used the random-effects model. In addition, we used Egger's
regression intercept (Egger, Smith, Schneider, & Minder, 1997) and
Begg and Mazumdar's (1994) rank correlation test.
3. Results
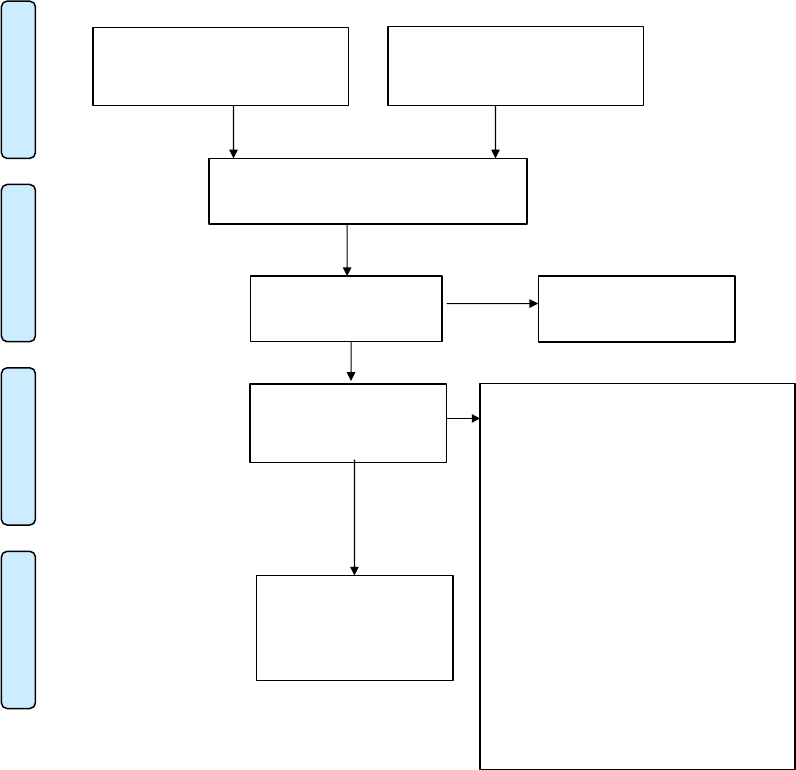
The electronic database search yielded 1629 hits, and 24 additional
records were identied through other sources (online registers, cross-
references, etc.). After removal of duplicates, 1272 articles remained.
Records identified through
database searching
(n = 1462 + 86 + 81)
ScreeningIncluded
Eligibility
Identification
Additional records identified
through other sources
(n =10 + 13 + 1)
Records after duplicates removed
(n=1118+83+71)
Records screened
(n = 1272)
Records exclud ed
(n = 1093)
Full-text articles
assessed for eligibility
(n =179)
Full-text articles excluded, with reasons
(n = 148)
Guidance identical in both groups (n = 39)
No RCT (n = 2)
“Add-on” design (n = 2)
No mental disorder (n = 8)
No relevant outcome measure (n = 2)
Secondary study (n = 1)
Blended or face to face treatment (n = 11)
Follow-up study (n = 6)
Duplicate (n = 3)
Control group or both groups:
- Social network or forum (n = 3)
- No text-based internet treatment (n = 8)
- Not online (n = 9)
- TAU or wait-list (n = 9)
- No guidance (pure self-help) (n = 19)
- Psycho-education (n = 7)
- Both treatment and guidance differ (n = 8)
- No modules (n = 11)
Studies included in
quantitative synthesis
(meta-analysis)
(n = 31)
Fig. 1. Flow diagram of screening process.
Note. An original search (May,2020)and two subsequent searches were conducted (March and December 2021). This is depicted in the diagram by rst mentioning
the results from the original search, and then (with+) the results from the second and third searches. All searches were identical in that they were conducted with the
same search strings, in the same databases, and the by the same author (JK).
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
6
Screening of title and abstract resulted in the exclusion of 1093 articles.
The remaining 179 articles were scrutinized full text. During this phase,
a total of 148 studies were excluded (see Fig. 1 for reasons), leaving 31
studies to be included in the meta-analysis, totaling 6215 participants.
The study selection process is detailed in the PRISMA ow chart (Fig. 1).
3.1. Characteristics of the included studies
Appendix B (Supplement 1) provides a summary of the included
studies and their main characteristics. Two publications turned out to
stem from one original study, albeit with different outcome measures
(Brabyn et al., 2016; Gilbody et al., 2017). Thus, 30 unique studies were
included, with 32 potentially relevant comparisons (two studies had
three relevant treatment conditions). Eleven studies compared various
degrees of human guidance, fourteen studies compared human guidance
with technological guidance. Two studies could not be allocated to our
pre-dened comparisons. Schulz et al. (2016) compared group (forum)
versus individual treatment. Another study (Sundstr
¨
om et al., 2016)
compared different modalities of guidance (choice of xed chat or
email) versus therapist contact through email. Seven studies compared
different levels of therapist qualication. From another study (Pihlaja
et al., 2020) symptom reduction could not be obtained, yet data from
adherence measures was available.
All but ve studies (83.3%) treated anxiety and/or depression.
Thirteen studies (43.3%) addressed panic disorder, ying phobia, social
anxiety disorder, generalized anxiety disorder or severe rumination
(Berger et al., 2011; Campos et al., 2019; Cook et al., 2019; Dear et al.,
2015, 2016; Fogliati et al., 2016; Ivanov et al., 2016; Johnston et al.,
2011; Klein et al., 2009; Oromendia et al., 2016; Robinson et a., 2010;
Schulz et al., 2016; Titov et al., 2009). Eight studies (26.7%) treated
depressive symptoms (Farrer et al., 2011; Gilbody et al., 2017; Mohr
et al., 2013; Montero-Marin et al., 2016; Pihlaja et al., 2020; Titov et al.,
2010; Westerhof et al., 2019; Zagorscak et al., 2018), and four studies
(13.3%) targeted a combination of anxiety and depression (Hadjis-
tavropoulos et al., 2017; Hadjistavropoulos, Peynenburg, Nugent, et al.,
2020; Hadjistavropoulos, Peynenburg, Thiessen, et al., 2020; Kleiboer
et al., 2015). Three other studies focused on other disorders: insomnia
(Lancee et al., 2013), severe symptoms of eating disorders (Aardoom
et al., 2016), and problematic alcohol use (Sundstr
¨
om et al., 2016). The
remaining two studies were conducted in medical settings, and focused
on psychological symptoms in cancer survivors (Dirkse et al., 2020), and
haemodialysis patients (Hudson et al., 2017). The latter two studies used
a threshold to screen for depression and anxiety as part of the inclusion
process.
All but 4 studies (86.7%) offered CBT; the median number of mod-
ules was 6 (range: 5–18). One study offered Acceptance and Commit-
ment Therapy (Ivanova et al., 2016), one problem-solving therapy
(Kleiboer et al., 2015), and one study provided life-review therapy
(Westerhof et al., 2019). For one study, the type of therapy was unclear
(Aardoom et al., 2016). More than half of the studies (k = 17; 56.7%)
were conducted in the community: they recruited through websites or
newspapers. Other studies made use of a combination of the community,
websites, and mental health care settings (k = 5; 16.7%). Three studies
(10.0%) were conducted in hospital settings (Hudson et al., 2017; Mohr
et al., 2013; Pihlaja et al., 2020), and one made use of specialized mental
health care facilities (Farrer et al., 2011). The remainder of the studies
(13.3%) were conducted in primary care (Gilbody et al., 2017; Montero-
Marín et al., 2016), university (Cook et al., 2019), and one made use of
the information from the archives of insurance companies (Zagorscak
et al., 2018). Studies were conducted in Australia, Canada, Finland,
Germany, the Netherlands, the United Kingdom, Spain, Sweden,
Switzerland, and the United States.
Most studies used an ITT analysis format and imputed data from
missing cases. However, upon closer inspection, several studies only
analyzed the data of participants who started treatment. For the purpose
of simplicity, this type of analysis is regarded as “modied ITT” analysis.
For studies that reported data from completers only, authors were e-
mailed. Several authors were able to provide us with the estimated av-
erages for the entire sample. For the adherence rates, all 28 studies with
relevant comparisons had adherence data on at least one of the two
outcomes. For approximately one quarter of studies with missing data on
one of the outcomes, data could still be obtained for the other outcome.
3.2. Methodological quality of the included studies
Results from the quality ratings are reported in Appendix C (Sup-
plement 1). Half of the studies were rated as good, 6 studies (20.0%)
were rated as very good, and 9 studies (30.0%) were rated as adequate in
terms of methodological quality.
3.3. Comparison 1: human vs. technological guidance
Before conducting these analyses, we checked for the degree of so-
phistication in the technological support conditions, because in theory,
automated support could be very sophisticated and tailor-made and
potentially more frequently available for patients. Upon closer inspec-
tion, we found one study with a high degree of sophistication, using a
feedback algorithm based on 4 dimensions of symptom severity (Aar-
doom et al., 2016). The other studies used xed templates for their
feedback. In light of this, we also analyzed the subset of studies related
to the comparison of human versus technological guidance separately
without the advanced feedback study.
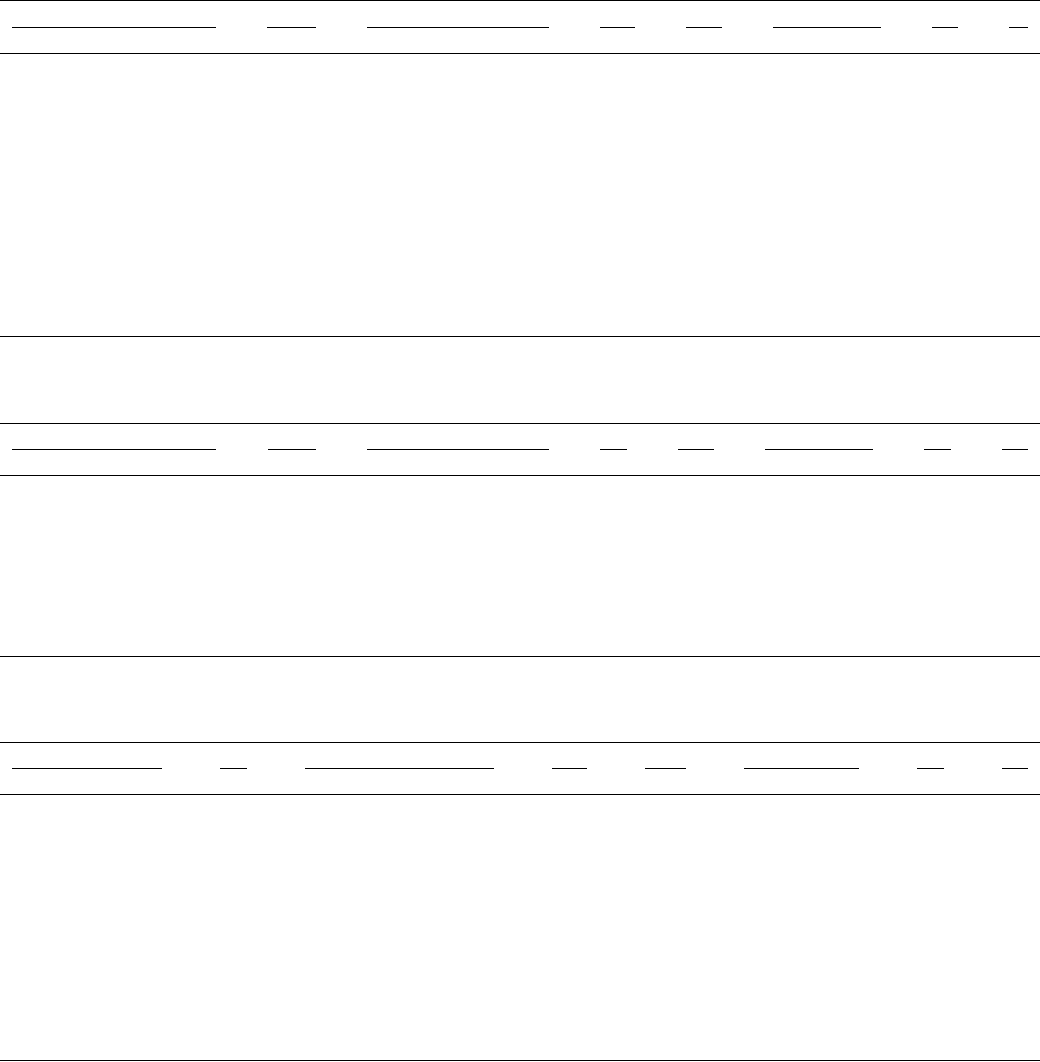
Fourteen studies were available regarding this comparison for the
outcome of symptoms. The pooled effect size was g = 0.11 (95% CI: 0.03,
0.19; p < .01) indicating that human guidance was slightly, yet signif-
icantly, more efcacious than automated guidance (see Table 1). Het-
erogeneity was absent and non-signicant (I
2
= 0%; Q (13) = 7.48; p =
.88). Using the one-study removed method yielded effect sizes in the
range of g = 0.09–0.12. Analyses including only modied ITT-data (k =
6) yielded similar outcomes (Table 1). Re-analyzing the data without the
study with advanced technological guidance yielded similar ndings (g
= 0.12; 95% CI: 0.04, 0.20; p < .01). In three studies (Hudson et al.,
2017; Ivanova et al., 2016; Montero-Marin et al., 2016), the frequency of
human support deviated from the standard frequency of once per week.
We also analyzed the subset without these studies, which yielded similar
results: g = 0.11; 95% CI: 0.03, 0.19; p < .01).
For the outcome of mean number of sessions completed, 9 studies
provided the required data (Table 2). This analysis yielded a pooled
effect size of g = 0.26 (95% CI: 0.13, 0.40; p < .01), indicating that
individuals receiving human support completed more sessions on
average. Heterogeneity was moderate and signicant (I
2
= 52.1%; Q (8)
= 16.71; p < .05). There were no outliers. Using the one-study removed
method, we observed effect sizes between 0.18 and 0.29 (all p's < 0.01).
Excluding the studies with divergent frequencies of human support
(Ivanova et al., 2016; Montero-Marin et al., 2016), yielded a similar
outcome: g = 0.25; 95% CI: 0.09, 0.40; p < .01).
In terms of adherence rates, those receiving human guidance were
more likely to complete treatment (OR = 1.69; 95%CI: 1.30, 2.19; p <
.01). Heterogeneity was moderate but non-signicant (Table 3). Using
the one-study removed method, we found odds ratios between 1.52 and
1.77 (all p's < 0.01). Removing one outlier (Lancee et al., 2013) yielded
a somewhat lower but still signicant odds ratio of 1.52 (95%CI: 1.27,
1.83; p < .01). The outcome was similar without studies with varying
frequencies of human support (Hudson et al., 2017: Ivanova et al., 2016;
Montero-Marin et al., 2016): OR = 1.72; 95% CI: 1.26, 2.35; p < .01.
We performed moderator analyses only for outcomes with sufcient
studies (symptom outcomes). For the moderators “pre-treatment inter-
view”, “anxiety disorder”, and “mode of delivery”, non-signicant dif-
ferences between the designated subgroups were found. For the
moderators “reminders in both groups”, and “CBT vs. other treatment”
not enough studies were available in each subgroup to allow for
meaningful comparisons. Most studies were CBT-based and most offered
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
7
reminders in both groups.
3.4. Comparison 2: degrees of human guidance
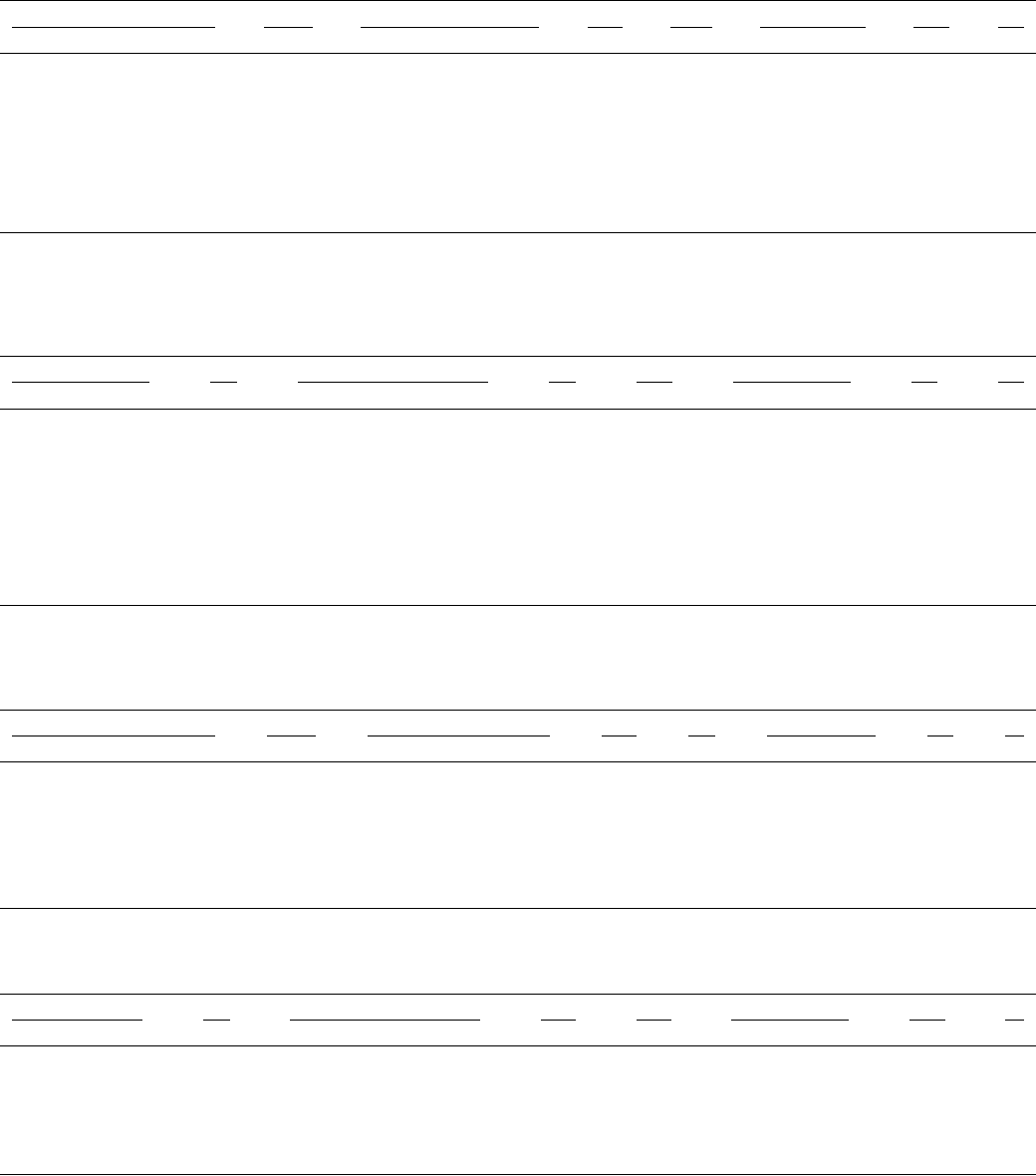
Next, we compared studies with varying degrees of human guidance
on the three outcomes. In terms of symptoms, we calculated the pooled
effect size for ten studies (Table 4). These studies consisted of those
comparing regular vs. optional guidance (Berger et al., 2011; Farrer
et al., 2011; Gilbody et al., 2017; Hadjistavropoulos et al., 2017; Klei-
boer et al., 2015; Oromendia et al., 2016), and those that compared a
(xed) higher frequency (i.e., 2 or 3 times a week) or speed (i.e., within
one business day) of contact with a standard frequency (Aardoom et al.,
2016; Hadjistavropoulos et al., 2020a, 2020b; Klein et al., 2009). The
pooled effect size was non-signicant at g = 0.05 (95% CI: − 0.04, 0.15;
p = .27), indicating that higher levels of human guidance were not more
efcacious than lower levels of human guidance in terms of symptom
reduction. Heterogeneity was low and non-signicant (I
2
= 9.0%; Q (9)
= 9.89; p = .36). Analyzing this subset again with one outlier (k = 9)
removed or ITT data only (k = 8) yielded similar results.
In terms of mean number of sessions completed, 7 studies were
Table 1
Results for human guidance vs. technological guidance – symptoms.
95% Condence interval Heterogeneity
Study name Hedges'g Lower limit Upper limit Z p Q df p I
2
Aardoom2016 (1) 0.00 − 0.30 0.29 − 0.02 0.99
Campos2019 0.12 − 0.56 0.80 0.35 0.73
Cook2019 − 0.12 − 0.48 0.24 − 0.66 0.51
Dear2015 0.02 − 0.29 0.34 0.15 0.88
Dear2016 0.08 − 0.30 0.46 0.42 0.67
Dirkse2020 0.15 − 0.28 0.58 0.67 0.50
Fogliati2016 0.02 − 0.50 0.54 0.08 0.93
Hudson2017 0.07 − 0.79 0.93 0.16 0.87
Ivanova2016 0.29 − 0.10 0.68 1.45 0.15
Kleiboer2015(2) 0.12 − 0.15 0.38 0.84 0.40
Lancee2013 0.32 0.08 0.57 2.62 0.01
Mohr2013 − 0.02 − 0.48 0.45 − 0.06 0.95
Montero-Marin2016 − 0.05 − 0.40 0.31 − 0.26 0.80
Zagorscak2018 0.13 0.01 0.24 2.07 0.04
Weighed mean g (random effects) 0.11 0.03 0.19 2.79 <0.01 7.48 13 0.88 0%
ITT only (k = 6) 0.14 0.05 0.23 3.12 <0.01
Table 2
Results for human guidance vs. technological guidance – session average completed.
95% Condence interval Heterogeneity
Study name Hedges'g Lower limit Upper limit Z p Q df p I
2
Campos2019 0.03 − 0.54 0.59 0.09 0.93
Dear2015 0.26 0.04 0.47 2.36 0.02
Dear2016 0.08 − 0.18 0.34 0.59 0.56
Dirkse2020 0.49 0.07 0.92 2.27 0.02
Fogliati2016 0.07 − 0.26 0.39 0.40 0.70
Ivanova2016 0.48 0.08 0.88 2.36 0.02
Lancee2013 0.61 0.36 0.86 4.85 <0.01
Montero-Marin2016 0.22 − 0.14 0.58 1.21 0.23
Zagorscak2018 0.15 0.03 0.27 2.46 0.01
Weighed mean g (random effects) 0.26 0.13 0.40 3.79 <0.01 16.71 8 0.03 52%
Table 3
Results for human guidance vs. technological guidance – rate of patients completing all sessions.
95% Condence interval Heterogeneity
Study name OR Lower limit Upper limit Z p Q df p I
2
Campos2019 0.81 0.17 3.78 − 0.27 0.79
Cook2019 1.82 0.92 3.62 1.72 0.09
Dear2016 1.20 0.67 2.14 0.61 0.54
Dear2015 1.42 0.91 2.23 1.54 0.12
Dirkse2020 3.12 0.74 13.20 1.54 0.12
Fogliati2016 1.05 0.52 2.11 0.13 0.90
Hudson2017 0.39 0.02 7.64 − 0.62 0.54
Ivanova2016 1.60 0.70 3.66 1.12 0.26
Kleiboer2015(2) 1.75 0.84 3.63 1.49 0.14
Lancee2013 4.40 2.60 7.44 5.52 < 0.01
Montero-Marin2016 1.62 0.77 3.44 1.26 0.21
Zagorscak2018 1.66 1.24 2.23 3.40 0.01
Weighed mean OR 1.69 1.30 2.19 3.97 <0.01 18.95 11 0.06 42%
ITT only (k = 5) 1.97 1.31 2.95 3.26 <0.01
Outliers removed (k = 11) 1.52 1.27 1.83 4.49 <0.01
Note. Study names in italics represent outliers.
J.A. Koelen et al.

Clinical Psychology Review 96 (2022) 102179
8
compared (Table 5). This yielded a pooled effect of g = 0.30 (95%CI:
0.07, 0.53; p < .05), which indicates that more intensive human guid-
ance was more efcacious than lower levels of support in terms of
adherence. Heterogeneity was high and signicant (I
2
= 75.1%; Q (6) =
24.13; p < .001). Using the one-study removed method, we observed
effect sizes between g = 0.20 and g = 0.37 (all p's < 0.05). Repeating
these analyses with ITT data only (k = 6) yielded similar results.
Excluding one outlier (Oromendia et al., 2016) led to a somewhat lower
effect size: g = 0.20 (95%CI: 0.02, 0.37; p < .05), and reduced the
heterogeneity to a moderate level (I
2
= 56.7%; Q (5) = 11.54; p < .05).
The results for adherence rates (Table 6) were similar. Nine studies were
analyzed together, which resulted in an OR = 1.57 (95%CI: 1.09, 2.25; p
< .01). This suggests that individuals with higher levels of human
guidance were more likely to complete treatment. Heterogeneity was
moderate and signicant (I
2
= 54.2%; Q (8) = 17.46; p < .05). Using the
one-study removed method, we observed odds ratios between OR = 1.28
and 1.75 (all p's < 0.05).
As noted, to control for potential confound of intensity, we re-
analyzed degrees of human guidance without studies that compared
intensive guidance with regular guidance, so that only those comparing
optional vs. regular guidance remained (k = 4–6). This analysis (for
symptoms) yielded a somewhat higher, yet non-signicant Hedges' g of
0.12 (95%CI: − 0.06, 0.30; p = .18) for standard guidance compared to
optional guidance (k = 6). Heterogeneity was low and non-signicant
(I
2
= 35.6%; Q (5) = 7.77; p = .170). For number of completed ses-
sions, comparing regular guidance with optional guidance (k = 4)
yielded a signicant effect: g = 0.46 (95%CI: 0.02, 0.91; p < .05). Yet,
again heterogeneity was high (I
2
= 73.9%; Q (3) = 11.51; p < .001), so
this estimate was not reliable. In terms of adherence rates (k = 5), we
observed an OR = 1.89 (95%CI: 1.07, 3.34; p < .05), indicating that
regular guidance was more efcacious than optional guidance.
For the remaining set of studies (k = 4) comparing higher frequency/
speed with regular frequency/speed, the effect was non-signicant: OR
= 1.24 (95%CI: 0.83, 1.85; p = .29). Heterogeneity was low to moderate
and non-signicant (I
2
= 40.3%; Q (3) = 5.03; p = .170). For reduction
of symptoms (k = 4), the effect was also non-signicant (g = 0.01 (95%
CI: − 0.11, 0.12; p = .93). Heterogeneity was low and non-signicant (I
2
= 0.0%; Q (3) = 0.52; p = .914). Not enough studies were available with
mean number of completed sessions to make this comparison.
Moderator analyses were performed only for sufciently large sub-
groups (viz. symptoms). For the moderators “anxiety disorder” and
“mode of delivery”, non-signicant differences between the designated
subgroups were found. The result for “reminders in both conditions” was
marginally signicant (Q (1) = 3.00; p = .08), showing an effect of g =
0.00 (k = 6) for those studies offering reminders in both groups, and g =
0.24 (k = 4) for those that did not. For the moderators “pre-treatment
interview” and “CBT vs. other treatment” not enough studies were
available in each subgroup to allow for meaningful comparisons. Most
studies offered CBT and a pre-treatment interview.
3.5. Comparison 3: qualication of online counselors
Seven studies were found comparing different qualications of on-
line coaches/technicians and psychologist, or community-based vs.
specialized psychologists): two studies from Hadjistavropoulos et al.
(Hadjistavropoulos, Peynenburg, Nugent, et al., 2020; Hadjistavropou-
los, Peynenburg, Thiessen, et al., 2020), Johnston et al. (2011), Rob-
inson et al. (2010), Titov et al. (2009, 2010), and Westerhof et al.
(2019). The pooled effect size was g = 0.04 (95% CI: − 0.06, 0.14; p =
.45), indicating that qualication was not associated with efcacy
(Table 7). Heterogeneity was absent and non-signicant (I
2
= 0%; Q (6)
= 5.79; p = .45). For adherence rates (Table 8), the weighed mean OR
was 1.02 (95% CI: 0.27, 3.91; p = .97). Heterogeneity was absent and
non-signicant (I
2
= 0%; Q (5) = 0.09; p > .99). Not enough studies
were available that provided the average number of sessions completed
for this analysis.
3.6. Publication bias
We inspected for the presence of publication bias in two sets of
studies: those for human vs. technological guidance (k = 14) and those
than compared degrees of human guidance (k = 10). Regarding the rst
set of studies reporting symptom outcomes, no signs of publication bias
were present when inspecting the funnel plot for missing studies on the
left. Using Duval and Tweedie's trim and ll procedure, no studies
needed to be trimmed (random effects model). Likewise, Begg and
Mazumdar's rank correlation test was non-signicant (
τ
= − 0.08; p [one-
tailed] = 0.35), as was the case for Egger's regression intercept (inter-
cept = − 0.40; p [one-tailed] = 0.18). For the subset of studies
addressing degrees of human support (reporting symptoms), there was
also no indication of publication bias. According to Duval and Tweedie's
trim and ll procedure, no studies needed to be trimmed. Begg and
Mazumdar's rank correlation test was non-signicant (
τ
= 0.24; p [one-
tailed] = 0.16), as well as Egger's regression intercept (intercept = 0.86;
p [one-tailed] = 0.17).
4. Discussion
This meta-analysis addressed the role of guidance in text-based
internet treatments (“e-therapy”) using a more ne-grained taxonomy
of guidance than previous meta-analyses, and a broader range of mental
complaints, while including only studies with direct comparisons be-
tween different types of guidance. Whilst previous meta-analyses usu-
ally focused on a categorical distinction of guidance versus self-help, we
Table 4
Results for degrees of human guidance – symptoms.
95% Condence interval Heterogeneity
Study name Hedges'g Lower limit Upper limit Z p Q df p I
2
Aardoom2016 (2) − 0.08 − 0.37 0.21 − 0.53 0.60
Berger2011* 0.04 − 0.49 0.57 0.15 0.88
Farrer2011* 0.01 − 0.42 0.44 0.05 0.96
Gilbody2017* 0.24 0.00 0.49 1.95 0.05
Hadjistavropoulos2017* − 0.09 − 0.39 0.21 − 0.60 0.55
Hadjistavropoulos2020a − 0.01 − 0.19 0.18 − 0.07 0.95
Hadjistavropoulos2020b 0.03 − 0.13 0.19 0.39 0.69
Kleiboer2015(1)* 0.07 − 0.20 0.34 0.50 0.61
Klein2009 0.08 − 0.45 0.62 0.31 0.76
Oromendia2016* 0.74 0.16 1.32 2.50 0.01
Weighed mean g (random effects) 0.05 ¡0.04 0.15 1.10 0.27 9.89 9 0.36 9%
ITT only (k = 8) 0.02 − 0.07 0.12 0.44 0.66
Outliers removed (k = 9) 0.04 − 0.05 0.12 0.78 0.43
Note. Studies with * compare regular with optional support.
Study names in italics represent outliers.
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
9
made two main comparisons: (1) human guidance vs. technological
guidance and (2) degrees of intensity of human guidance. In addition,
we compared studies with counselors of varying qualications.
Our ndings indicated that technological guidance was less efca-
cious compared to human guidance, which was found consistently
across outcomes. For the purpose of our discussion, it is important to
note that in most studies (11/14 = 79%), technological support was
compared to regular (i.e., weekly) human support. Effects for symptoms
and adherence were comparable. Yet, it is difcult to compare the two
effect sizes directly, as they may differ in terms of their sensitivity to
change. These effects also stem from slightly different subsets of studies,
depending on availability of outcomes. In the studies included in this
Table 5
Results for degrees of human guidance – session average completed.
95% Condence interval Heterogeneity
Study name Hedges'g Lower limit Upper limit Z p Q df p I
2
Berger2011* − 0.10 − 0.65 0.44 − 0.37 0.71
Farrer2011* 0.26 − 0.17 0.69 1.20 0.23
Hadjistavropoulos2017* 0.51 0.21 0.81 3.30 < 0.01
Hadjistavropoulos2020 0.05 − 0.11 0.21 0.64 0.53
Hadjistavropoulos2020b 0.07 − 0.09 0.23 0.83 0.41
Oromendia2016* 1.26 0.65 1.87 4.04 < 0.01
Pihlaja2020 0.48 0.08 0.87 2.36 0.02
Weighed mean g (random effects) 0.30 0.07 0.53 2.56 <0.05 24.13 6 <0.01 75%
ITT only (k = 6) 0.27 0.03 0.52 2.16 <0.05
Outliers removed (k = 6) 0.20 0.02 0.37 2.21 <0.05
Note. Studies with * compare regular with optional support.
Study names in italics represent outliers.
Table 6
Results for degrees of human guidance – rate of patients completing all sessions.
95% Condence interval Heterogeneity
Study name OR Lower limit Upper limit Z p Q df p I
2
Farrer2011* 1.15 0.36 3.68 0.24 0.81
Gilbody2017* 2.07 1.03 4.19 2.03 0.04
Hadjistavropoulos2017* 3.59 1.80 7.17 3.62 <0.01
Hadjistavropoulos2020a 1.02 0.69 1.53 0.11 0.91
Hadjistavropoulos2020b 1.12 0.78 1.62 0.61 0.54
Kleiboer2015(1)* 1.10 0.62 1.95 0.31 0.75
Klein2009 1.40 0.42 4.72 0.54 0.59
Oromendia2016* 7.98 0.39 163.33 1.35 0.18
Pihlaja2020 4.95 1.30 18.81 2.35 0.02
Weighed mean OR 1.57 1.09 2.25 2.44 <0.05 17.46 8 0.03 54%
ITT only (k = 7) 1.54 1.00 2.38 1.96 <0.05
Note. Studies with * compare regular with optional support.
Table 7
Results for qualication of therapists – symptoms.
95% Condence interval Heterogeneity
Study name Hedges'g Lower limit Upper limit Z p Q df p I
2
Hadjistavropoulos2020a 0.11 − 0.08 0.30 1.15 0.25
Hadjistavropoulos2020b 0.01 − 0.15 0.17 0.10 0.92
Johnston2011 − 0.34 − 0.76 0.07 − 1.62 0.11
Robinson2010 0.10 − 0.29 0.50 0.51 0.61
Titov2010 0.09 − 0.33 0.50 0.40 0.69
Titov2009 0.03 − 0.40 0.46 0.12 0.90
Westerhof2019 0.54 − 0.21 1.28 1.41 0.16
Weighed mean g (random effects) 0.04 ¡0.06 0.14 0.76 0.45 5.79 6 0.45 0%
Table 8
Results for Qualication of therapists – rate of patients completing all sessions.
95% Condence interval Heterogeneity
Study name OR Lower limit Upper limit Z p Q df p I
2
Hadjistavropoulos2020 0.99 0.04 26.71 − 0.01 >0.99
Johnston2011 0.96 0.04 24.21 − 0.03 0.98
Robinson2010 0.98 0.04 23.81 − 0.01 >0.99
Titov2009 1.10 0.05 25.76 0.06 0.95
Titov2010 0.78 0.03 19.74 − 0.15 0.88
Westerhof2019 1.58 0.04 60.47 0.25 0.81
Weighed mean OR 1.02 0.27 3.91 0.04 0.97 0.09 5 >0.99 0%
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
10
review, technological support referred to basic support in the form of
regular reminders in case of non-response, or motivating messages in
case of response. According to our denition of technological support,
this did not include continuous support with highly sophisticated tech-
niques based on articial intelligence (AI), such as chatbots (e.g.,
Bendig, Erb, Schulze-Thuesing, & Baumeister, 2019). Although tech-
nological advances are moving fast, the studies included in this review
made use of basic, template-xed messaging. These ndings resonate
with other meta-analytic ndings (e.g., Riper et al., 2018), although this
is the rst meta-analysis based only on direct comparisons between
technological and human support.
Results for varying degrees of human support were less consistent.
Only for one of the outcome measures (adherence rates), results were
signicant and could be reliably estimated. This nding indicated that
more intensive human support is more likely to reduce drop out than less
intensive support. Furthermore, these effects turned out to be driven
only by the subsets of studies comparing regular versus optional support.
Although subgroups were small, these ndings complement those of a
recent meta-analysis focused on people with anxiety disorders, which
included only two studies for this particular comparison (Domhardt
et al., 2019). In practice optional guidance could be more intensive than
regular guidance, this was not the case in the included studies. Some of
the included studies in this comparison explicitly mentioned how often
patients had initiated contact (Berger, Caspar, Richardson, Kneubühler,
Sutter, et al., 2011, Hadjistavropoulos, Schneider, Edmonds, Karin,
Nugentet, al., 2017, Kleiboer, Donker, Seekles, van Straten, Riper, et al.,
2015; Oromendia, Orrego, Bonillo, & Molinuevo, 2016). In all of these
studies, patients in the condition with support on demand ended up
receiving less support than those with xed (weekly) contact. To give a
few examples: In one of the largest studies in this domain (Kleiboer et al.,
2015), only 19% of those in the “support on request” condition asked for
advice. Likewise, in the study by Berger et al. (2011), over half of the
participants in the “Step-up condition” did not ask for additional sup-
port. In another study, patients in the “Optional support” condition
logged in fewer times, spent fewer days enrolled in the program, and
sent fewer and briefer emails to their therapists (Hadjistavropoulos
et al., 2017). In conclusion, due to the small groups of studies, the
nding that regular support yields better outcomes than optional sup-
port should be regarded as preliminary, and limited to adherence, and
should be replicated with more primary studies.
In the current meta-analysis, we found an average attrition rate of
48% (range: 7–94%) for human guidance, and 51% (range: 26–86%) for
technological guidance, which shows that the attrition is generally high
in internet treatments, even with guidance. Compared to face-to-face
CBT, for example, the dropout is approximately twice as high (24%;
Linardon, Fitzsimmons-Craft, Brennan, Barillaro, & Wiley, 2019). It is
essential that therapists make an effort to increase adherence, and this
meta-analysis indicates that offering human guidance aimed at thera-
peutic content slightly increases adherence, which in turn could increase
efcacy. Future studies should aim to clarify whether staying in treat-
ment indeed leads to better outcomes (mediation effect), which regular
forms of therapy seem to indicate, or that patients drop out at the high-
point of their optimal curve (Reich & Berman, 2020).
Because of the conation between type of support and level of
therapist qualication in previous studies (Dirkse et al., 2020; Johnston
et al., 2011), obscuring clear conclusions, we analyzed studies
comparing clinical to (mostly) non-clinical support separately under the
heading of “qualication”. We found that online counselors with higher
levels of education/training were not more efcacious. This is in line
with other meta-analyses, including partially overlapping studies
(Baumeister et al., 2014; Domhardt et al., 2019), lending some support
to the conclusion that online counselors with higher levels of training or
education are not more efcacious. Yet, at the same time, in several
studies included in these analyses, the more qualied counselor offered
more support and/or moderated an online forum designed to assist a
group of patients, instead of providing individual guidance (Robinson
et al., 2010; Titov et al., 2009, 2010). These results should therefore be
considered inconclusive, and future studies should strive to systemati-
cally disentangle qualication and intensity or format (group/individ-
ual) of treatment. This could also answer the question whether online
group formats are more effective than individual formats.
4.1. Limitations
Some limitations need to be considered when interpreting the re-
sults. First, it should be kept in mind that for some of the included
studies, the main aim was not to reduce mental distress, although this
was our primary outcome measure. Some studies did not target
depression or anxiety primarily, but addressed, for example, sleep dif-
culties or issues with eating instead. Effects for depression/anxiety for
these studies may have been underestimated as a result but should have
affected both tested treatment conditions in equal ways. Second, this
paper focused on the immediate impact of subtleties of guidance and no
conclusions can be drawn with respect to follow-up effects. Although
there is burgeoning evidence that the effects of guidance may be long-
lasting (Lancee et al., 2013; Oromendia et al., 2016; Ruwaard et al.,
2009; Vernmark et al., 2010), more systematic support is needed. Third,
our conclusions seem to apply mostly to the effects of online CBT, as
these dominated the included studies. Furthermore, we tested for a
differential impact of guidance on CBT versus other approaches, but
other approaches were available to a limited extent, hampering sound
conclusions. Fourth, not all authors were able to share data for adher-
ence, which resulted in lower power for these meta-analyses. Moreover,
although we did our best to obtain ITT samples, comparisons contained
different degrees of completer and ITT samples, which could have
resulted in inaccurate estimates. Fifth, we tested for the impact of
therapist qualication on outcome, yet the variance in qualication was
limited. Some of the studies compared two types of trained (specialized
and community) psychologists, other studies compared one clinical
psychologist to a person with no training, introducing a lot of “person-
variance”. We think that this needs further study, before any rm con-
clusions can be drawn. We did not consider cost-effectiveness in this
study. Although we detected a small to moderate difference between
regular vs. optional support, it remains to be considered whether the
minor increases in efcacy outweigh the additional costs of more
intensive human support. Please note that in case of regular support,
support was scheduled at once a week, yet it was contingent upon par-
ticipants completing their assignments. We could not systematically
determine the actual frequency of support they received. Seventh,
although we did our best to establish the degree of sophistication of the
technological support in the studies included, we are not familiar with
all programs used. Eighth, included publications were limited to the
English language. On a related note, the included studies represent
ndings from Western, educated, industrialized, rich and democratic
(WEIRD) countries. In the future, the questions raised in this meta-
analysis should be extended to internet treatments in low and middle
income countries, which were shown to be efcacious as well (Fu,
Burger, Arjadi, & Bockting, 2020). Ninth, our ratings of methodological
quality were based mostly on ratings by a junior psychologist, which
could have limited their validity. Tenth, our moderator analyses were
based on small subgroups, which likely resulted in low power to detect
differences. These analyses should therefore be considered explorative.
Eleventh, we excluded blended therapies from this meta-analysis,
including those with videoconferencing. As a result of this, the gener-
alizability of our ndings to clinical practice may be reduced, as in
clinical practice internet-based treatments are often provided in tandem
with face-to-face services (e.g., Kooistra, Ruwaard, Wiersma, van
Oppen, van der Vaart, et al., 2016; Wentzel, Van der, Bohlmeijer, & Van
Gemert-Pijnen, 2016). Furthermore, most studies recruited in the com-
munity, which limits the generalizability of ndings for clinical patients.
Finally, we were not able to establish the impact of “technical support”.
We did not include this in our spectrum of guidance, because this type of
J.A. Koelen et al.

Clinical Psychology Review 96 (2022) 102179
11
support is non-clinical. Most studies seem to offer this to participants,
yet it was not systematically reported. Another type of support called
“safety monitoring”, was offered in some studies, and this is most
pertinent to patients with depression and suicidal problems. It is possible
that these types of support were offered “behind the scenes” in some
studies, which could have obscured the impact of guidance that we tried
to establish. In other words, participants in the minimal human support
conditions may in some cases have received more support than we could
reasonably determine.
Yet, despite these limitations, we believe our meta-analysis deepened
and extended the knowledge concerning the impact of various levels and
types of guidance on treatment outcomes for e-therapies, by introducing
and employing a more nuanced and “clean” taxonomy of types of
guidance. Most results can be considered robust and apply to a broad
range of mental health difculties. Moreover, most of the included
studies had good to very good methodological quality.
4.2. Research implications
Some directions for future research should be considered. First, since
we could not reach any denite conclusions concerning the qualication
of online therapists, this should be more extensively studied. This could
be done by including a sufcient number of highly qualied, experi-
enced clinical psychologists or therapists, in comparison to, for instance,
psychology students. Second, more systematic research is needed into
the additional benet of regular versus optional support. In this respect,
it is important to be clear about any additional support that participants
receive (e.g., safety monitoring, or technical support) to enable sound
conclusions. Moreover, more detailed information is required concern-
ing the degree of sophistication of the computer programs used,
particularly with respect to (automated) reminders and motivating
messages sent to the users. Taking these factors into account would
allow to address additional, still more nuanced aspects of guidance, both
human and non-human. Moving forward, it is likely that applications of
e-therapy will become more sophisticated, and the impact of more
interactive “conversational agents” should be incorporated into these
examinations.
5. Conclusions
This meta-analysis indicates human support has superior effects over
(simple) technological guidance alone. Findings regarding adherence
further suggest that regular human guidance should be preferred over
optional human guidance, but this nding did not generalize to clinical
outcomes. These ndings extend and rene previous reports addressing
the coarse distinction between “guided” and “unguided” internet treat-
ments. Future research should aim to clarify the added value of more
qualied therapists, the degree to which regular over optional support is
preferred, other questions related to mediation/moderation of efcacy,
and the impact of more advanced use of AI-driven conversational agents.
Role of funding sources
This study was funded from internal resources from the University of
Amsterdam.
Contributors
Jurrijn Koelen: Conceptualization, Methodology, Formal Analysis,
Investigation, Resources, Writing – Original Draft, Visualization, Su-
pervision, Project administration Anne Vonk: Conceptualization,
Methodology, Investigation Anke Klein: Writing - Review & Editing
Lisa de Koning: Writing - Review & Editing Peter Vonk: Conceptuali-
zation, Writing - Review & Editing, Funding acquisition Sabine de Vet:
Investigation, Formal Analysis Reinout Wiers: Conceptualization,
Writing - Review & Editing, Funding acquisition
Declaration of Competing Interest
None.
Supplementary data
Supplementary data to this article can be found online at https://doi.
org/10.1016/j.cpr.2022.102179.
References
1
Andersson, G. (2015). The internet and CBT: a clinical guide. Taylor & Francis.
Andersson, G., & Cuijpers, P. (2009). Internet-based and other computerized
psychological treatments for adult depression: a meta-analysis. Cognitive Behaviour
Therapy, 38(4), 196–205. https://doi.org/10.1080/16506070903318960
Andersson, G., & Titov, N. (2014). Advantages and limitations of internet-based
interventions for common mental disorders. World Psychiatry, 13(1), 4–11. https://
doi.org/10.1002/wps.20083
Andersson, G., Titov, N., Dear, B. F., Rozental, A., & Carlbring, P. (2019). Internet-
delivered psychological treatments: from innovation to implementation. World
Psychiatry, 18(1), 20–28. https://doi.org/10.1002/wps.20610
Baumeister, H., Reichler, L., Munzinger, M., & Lin, J. (2014). The impact of guidance on
internet-based mental health interventions - a systematic review. Internet
Interventions, 1(4), 205–215. https://doi.org/10.1016/j.invent.2014.08.003
Begg, C. B., & Mazumdar, M.. Operating characteristics of a rank correlation test for
publication bias Author ( s ): Colin B. Begg and Madhuchhanda Mazumdar Published
by : International Biometric Society Stable. URL http://www.jstor.org/stable/
2533446.
Bendig, E., Erb, B., Schulze-Thuesing, L., & Baumeister, H. (2019). Next Generation:
Chatbots in Clinical Psychology and Psychotherapy to Foster Mental Health—A
Scoping Review. Verhaltenstherapie, 29(4), 266–280. https://doi.org/10.1159/
000499492
Berger, T., Caspar, F., Richardson, R., Kneubühler, B., Sutter, D., & Andersson, G. (2011).
Internet-based treatment of social phobia: A randomized controlled trial comparing
unguided with two types of guided self-help. Behaviour Research and Therapy, 49(3),
158–169. https://doi.org/10.1016/j.brat.2010.12.007
Berryhill, M. B., Culmer, N., Williams, N., Halli-Tierney, A., Betancourt, A., Roberts, H.,
& King, M. (2019). Videoconferencing Psychotherapy and Depression: A Systematic
Review. Telemedicine and E-Health, 25(6), 435–446. https://doi.org/10.1089/
tmj.2018.0058
Boettcher, J., Berger, T., & Renneberg, B. (2012). Does a pre-treatment diagnostic
interview affect the outcome of internet-based self-help for social anxiety disorder?
A randomized controlled trial. Behavioural and Cognitive Psychotherapy, 40(5),
513–528. https://doi.org/10.1017/S1352465812000501
Borenstein, M., Hedges, L., Higgins, J., & Rothstein, H. (2005). Comprehensive meta-
analysis (2.0). Biostat.
Borenstein, M., Hedges, L. V., Higgins, J. P., & Rothstein, H. R. (2009). Introduction to
meta-analysis. United Kingdom: Wiley-Blackwell Publishing Ltd.
Carlbring, P., Andersson, G., Cuijpers, P., Riper, H., & Hedman-Lagerl
¨
of, E. (2018).
Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and
somatic disorders: an updated systematic review and meta-analysis. Cognitive
Behaviour Therapy, 47(1), 1–18. https://doi.org/10.1080/16506073.2017.1401115
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. L. Erlbaum
Associates. http://books.google.nl/books?id=Tl0N2lRAO9oC.
Cuijpers, P., Donker, T., Van Straten, A., Li, J., & Andersson, G. (2010). Is guided self-
help as effective as face-to-face psychotherapy for depression and anxiety disorders?
A systematic review and meta-analysis of comparative outcome studies. Psychological
Medicine, 40(12), 1943–1957. https://doi.org/10.1017/S0033291710000772
Cuijpers, P., Reijnders, M., & Huibers, M. J. H. (2019). The role of common factors in
psychotherapy outcomes. Annual Review of Clinical Psychology, 15(1). https://doi.
org/10.1146/annurev-clinpsy-050718-095424
Deady, M., Choi, I., Calvo, R. A., Glozier, N., Christensen, H., & Harvey, S. B. (2017).
eHealth interventions for the prevention of depression and anxiety in the general
population: a systematic review and meta-analysis. BMC Psychiatry, 17(1), 1–14.
https://doi.org/10.1186/s12888-017-1473-1
Dear, B. F., Staples, L. G., Terides, M. D., Fogliati, V. J., Sheehan, J., Johnston, L., …
Titov, N. (2016). Transdiagnostic versus disorder-specic and clinician-guided
versus self-guided internet-delivered treatment for Social Anxiety Disorder and
comorbid disorders: A randomized controlled trial. Journal of Anxiety Disorders, 42,
30–44. https://doi.org/10.1016/j.janxdis.2016.05.004
Dirkse, D., Hadjistavropoulos, H. D., Alberts, N. A., Karin, E., Schneider, L. H., Titov, N.,
& Dear, B. F. (2020). Making Internet-delivered cognitive behaviour therapy scalable
for cancer survivors: A randomized non-inferiority trial of self-guided and
technician-guided therapy. Journal of Cancer Survivorship, 14(2), 211–225. https://
doi.org/10.1007/s11764-019-00810-9
Domhardt, M., Geßlein, H., von Rezori, R. E., & Baumeister, H. (2019). Internet- and
mobile-based interventions for anxiety disorders: a meta-analytic review of
intervention components. Depression and Anxiety, 36(3), 213–224. https://doi.org/
10.1002/da.22860
1
See Supplement 2 for the references included in the meta-analysis.
J.A. Koelen et al.
Clinical Psychology Review 96 (2022) 102179
12
Donkin, L., Christensen, H., Naismith, S. L., Neal, B., Hickie, I. B., & Glozier, N. (2011).
A systematic review of the impact of adherence on the effectiveness of e-therapies.
Journal of Medical Internet Research, 13(3), 1–12. https://doi.org/10.2196/jmir.1772
Duval, S., & Tweedie, R. (2000). A nonparametric “Trim and Fill” method of accounting
for publication bias in meta-analysis. Journal of the American Statistical Association,
95(449), 89–98. https://doi.org/10.1080/01621459.2000.10473905
Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis
detected by a simple, graphical test. British Medical Journal, 315, 629–634.
Farrand, P., & Woodford, J. (2013). Impact of support on the effectiveness of written
cognitive behavioural self-help: a systematic review and meta-analysis of
randomised controlled trials. Clinical Psychology Review, 33(1), 182–195. https://doi.
org/10.1016/j.cpr.2012.11.001
Fu, Z., Burger, H., Arjadi, R., & Bockting, C. L. H. (2020). Effectiveness of digital
psychological interventions for mental health problems in low-income and middle-
income countries: a systematic review and meta-analysis. The Lancet Psychiatry, 7
(10), 851–864. https://doi.org/10.1016/S2215-0366(20)30256-X
Hadjistavropoulos, H. D., Mehta, S., Wilhelms, A., Keough, M. T., & Sundstr
¨
om, C.
(2020). A systematic review of internet-delivered cognitive behavior therapy for
alcohol misuse: study characteristics, program content and outcomes. Cognitive
Behaviour Therapy, 49(4), 327–346. https://doi.org/10.1080/
16506073.2019.1663258
Hadjistavropoulos, H. D., Schneider, L. H., Edmonds, M., Karin, E., Nugent, M. N.,
Dirkse, D., … Titov, N. (2017). Randomized controlled trial of internet-delivered
cognitive behaviour therapy comparing standard weekly versus optional weekly
therapist support. Journal of Anxiety Disorders, 52, 15–24. https://doi.org/10.1016/j.
janxdis.2017.09.006
Harrer, M., Cuijpers, P., Furukawa, T. A., & Ebert, D. D. (2021). Doing meta-analysis with
R. A Hands-on guide. Chapmann & Hall/CRC Press.
Hedges, L. V., & Olkin, I. (1985). Statistical methods for meta-analysis. Academic Press.
Hedman, E., Furmark, T., Carlbring, P., Lj
´
otsson, B., Rück, C., Lindefors, N., &
Andersson, G. (2011). A 5-year follow-up of internet-based cognitive behavior
therapy for social anxiety disorder. Journal of Medical Internet Research, 13(2).
https://doi.org/10.2196/jmir.1776
Higgins, J. P., & Green, S. (2011). Cochrane handbook for systematic reviews of interventions
(p. Version 5.1.0 (updated March 2011)). The Cochrane Collaboration.
Higgins, J. P. T., & Thompson, S. G. (2002). Quantifying heterogeneity in a meta-
analysis. Statistics in Medicine, 21(11), 1539–1558. https://doi.org/10.1002/
sim.1186
Johansson, R., & Andersson, G. (2012). Internet-based psychological treatments for
depression. Expert Review of Neurotherapeutics, 12(7), 861–870. https://doi.org/
10.1586/ern.12.63
Johnston, L., Titov, N., Andrews, G., Spence, J., & Dear, B. F. (2011). A RCT of a
Transdiagnostic Internet-Delivered Treatment for Three Anxiety Disorders:
Examination of Support Roles and Disorder-Specic Outcomes. PLOS ONE, 6(11),
Article e28079. https://doi.org/10.1371/journal.pone.0028079
Karyotaki, E., Efthimiou, O., Miguel, C., Bermpohl, F. M. G., Furukawa, T. A.,
Cuijpers, P., … Forsell, Y. (2021). Internet-based cognitive behavioral therapy for
depression: A systematic review and individual patient data network Meta-analysis.
JAMA Psychiatry, 78(4), 361–371. https://doi.org/10.1001/
jamapsychiatry.2020.4364
Kleiboer, A., Donker, T., Seekles, W., van Straten, A., Riper, H., & Cuijpers, P. (2015).
A randomized controlled trial on the role of support in Internet-based problem
solving therapy for depression and anxiety. Behaviour Research and Therapy, 72,
63–71. https://doi.org/10.1016/j.brat.2015.06.013
Kocsis, J. H., Gerber, A. J., Milrod, B., Roose, S. P., Barber, J., Thase, M. E., … Leon, A. C.
(2010). A new scale for assessing the quality of randomized clinical trials of
psychotherapy. Comprehensive Psychiatry, 51(3), 319–324. https://doi.org/10.1016/
j.comppsych.2009.07.001
Koo, T. K., & Li, M. Y. (2016). A guideline of selecting and reporting Intraclass
correlation coefcients for reliability research. Journal of Chiropractic Medicine, 15
(2), 155–163. https://doi.org/10.1016/j.jcm.2016.02.012
Kooistra, L. C., Ruwaard, J., Wiersma, J. E., van Oppen, P., van der Vaart, R., van
Gemert-Pijnen, … Riper, H. (2016). Development and initial evaluation of blended
cognitive behavioural treatment for major depression in routine specialized mental
health care. Internet Interventions, 4, 61–71. https://doi.org/10.1016/j.
invent.2016.01.003
Linardon, J., Fitzsimmons-Craft, E. E., Brennan, L., Barillaro, M., & Wiley, D. E. (2019).
Dropout from interpersonal psychotherapy for mental health disorders: a systematic
review and meta-analysis. Psychotherapy Research : Journal of the Society for
Psychotherapy Research, 29(7), 870–881. https://doi.org/10.1080/
10503307.2018.1497215
Lovell, K., & Richards, D. (2000). Multiple access points and levels of entry (maple):
ensuring choice, accessibility and equity for cbt services. Behavioural and Cognitive
Psychotherapy, 28(4), 379–391. https://doi.org/10.1017/s1352465800004070
Oromendia, P., Orrego, J., Bonillo, A., & Molinuevo, B. (2016). Internet-based self-help
treatment for panic disorder: A randomized controlled trial comparing mandatory
versus optional complementary psychological support. Cognitive Behaviour Therapy,
45(4), 270–286. https://doi.org/10.1080/16506073.2016.1163615
Reich, C. M., & Berman, J. S. (2020). Are psychotherapies with more dropouts less
effective? Psychotherapy Research, 30(1), 23–40. https://doi.org/10.1080/
10503307.2018.1534018
Richards, D., & Richardson, T. (2012). Computer-based psychological treatments for
depression: a systematic review and meta-analysis. Clinical Psychology Review, 32(4),
329–342. https://doi.org/10.1016/j.cpr.2012.02.004
Riper, H., & Cuijpers, P. (2016). Telepsychology and e-health. In J. C. Norcross, &
D. Freedheim (Eds.), vol 3. APA handbook of clinical psychology: Applications and
methods (pp. 451–463). American Psychological Association.
Riper, H., Hoogendoorn, A., Cuijpers, P., Karyotaki, E., Boumparis, N., Mira, A., …
Smit, J. H. (2018). Effectiveness and treatment moderators of internet interventions
for adult problem drinking: An individual patient data meta-analysis of 19
randomised controlled trials. PLoS Medicine, 15(12), 1–26. https://doi.org/10.1371/
journal.pmed.1002714
Ruwaard, J., Schrieken, B., Schrijver, M., Broeksteeg, J., Dekker, J., Vermeulen, H., &
Lange, A. (2009). Standardized web-based cognitive behavioural therapy of mild to
moderate depression: a randomized controlled trial with a long-term follow-up.
Cognitive Behaviour Therapy, 38(4), 206–221. https://doi.org/10.1080/
16506070802408086
Salivar, E. J. G., Rothman, K., Roddy, M. K., & Doss, B. D. (2020). Relative Cost
Effectiveness of In-Person and Internet Interventions for Relationship Distress.
Family Process, 59(1), 66–80.doi. https://doi.org/10.1111/famp.12414
Spek, V., Cuijpers, P., NykIí
ˇ
cek, I., Riper, H., Keyzer, J., & Pop, V. (2007). Internet-based
cognitive behaviour therapy for symptoms of depression and anxiety: a meta-
analysis. Psychological Medicine, 37(3), 319–328. https://doi.org/10.1017/
S0033291706008944
Sterne, J. A. C., & Egger, M. (2001). Funnel plots for detecting bias in meta-analysis:
guidelines on choice of axis. Journal of Clinical Epidemiology, 54, 1046–1055.
Titov, N., Andrews, G., Schwencke, G., Solley, K., Johnston, L., & Robinson, E. (2009).
An RCT Comparing Effect of Two Types of Support on Severity of Symptoms for
People Completing Internet-Based Cognitive Behaviour Therapy for Social Phobia.
Australian & New Zealand Journal of Psychiatry, 43(10), 920–926.
Titov, N., Andrews, G., Davies, M., Mcintyre, K., Robinson, E., & Solley, K. (2010).
Internet treatment for depression: A randomized controlled trial comparing clinician
vs. Technician assistance. PLoS ONE, 5(6), 1–9. https://doi.org/10.1371/journal.
pone.0010939
Van’t Hof, E., Cuijpers, P., & Stein, D. J. (2009). Self-help and internet-guided
interventions in depression and anxiety disorders: a systematic review of meta-
analyses. CNS Spectrums, 14(2 Suppl 3), 34–40. https://doi.org/10.1017/
s1092852900027279
Vernmark, K., Lenndin, J., Bj
¨
arehed, J., Carlsson, M., Karlsson, J.,
¨
Oberg, J.,
Carlbring, P., Eriksson, T., & Andersson, G. (2010). Internet administered guided
self-help versus individualized e-mail therapy: a randomized trial of two versions of
CBT for major depression. Behaviour Research and Therapy, 48(5), 368–376. https://
doi.org/10.1016/j.brat.2010.01.005
Wampold, B. E., & Imel, Z. E. (2015). The great psychotherapy debate (2nd ed.). Routledge.
Weisel, K. K., Zarski, A. C., Berger, T., Krieger, T., Schaub, M. P., Moser, C. T., …
Ebert, D. D. (2019). Efcacy and cost-effectiveness of guided and unguided internet-
and mobile-based indicated transdiagnostic prevention of depression and anxiety
(ICare Prevent): A three-armed randomized controlled trial in four European
countries. Internet Interventions, 16, 52–64. https://doi.org/10.1016/j.
invent.2018.04.002
Weiss, D. J., Nelson, A., Vargas-Ruiz, C. A., Gligori
´
c, K., Bavadekar, S., Gabrilovich, E., …
Gething, P. W. (2020). Global maps of travel time to healthcare facilities. Nature
Medicine, 26(12), 1835–1838. https://doi.org/10.1038/s41591-020-1059-1
Wentzel, J., Van der Vaart, R., Bohlmeijer, E. T., & Van Gemert-Pijnen, J. E. W. C. (2016).
Mixing online and face-to-face therapy: How to benet from blended care in mental
health care. JMIR Mental Health, 3(1), 1–7. https://doi.org/10.2196/mental.4534
J.A. Koelen et al.
