Research Article
Volume 6 • Issue 3 100
The Problem of Home Therapy during COVID-19 Pandemic in Italy:
Government Guidelines versus Freedom of Cure?
Serano Fazio¹, Marco Cosentino², Franca Marino², Sergio Pandol
3
, Elisabetta Zanolin
4
, Paolo Bellavite
5
,*
Aliation:
1
Medical School University Federico II, Naples
(retired professor), Italy
2
Center of Research in Medical Pharmacology,
University of Insubria, Varese, Italy
3
High School Master of Oxygen-Ozone Therapy,
University of Pavia, Italy
4
Department of Diagnostics and Public Health,
University of Verona, Italy
5
Medical School University of Verona, Verona
(retired professor), Italy
*Corresponding author:
Paolo Bellavite, Homeopathic Medical School of
Verona, Vicolo dietro Santi Apostoli, 2 – 37121
Verona, Italy.
E-mail: [email protected]
Citation: Serafino Fazio, Marco Cosentino,
Franca Marino, Sergio Pandolfi, Elisabetta
Zanolin, Paolo Bellavite. The Problem of Home
Therapy during COVID-19 Pandemic in Italy:
Government Guidelines versus Freedom of Cure?.
Journal of Pharmacy and Pharmacology Research
6 (2022): 100-114
Received: July 19, 2022
Accepted: July 28, 2022
Published: August 02, 2022
Keywords: COVID-19 treatment; treatment guidelines; COVID-19 lethality;
outpatient care; SARS-CoV-2 epidemiology; paracetamol; healthcare system
Introduction
COVID-19 is a new disease due to the acute severe respiratory syndrome
coronavirus-2 (SARS-CoV-2). After its onset in Wuhan, China, at the
end of 2019, it rapidly spread worldwide leading to the development of a
pandemic. After China, Italy was the rst Western nation to be severely
aected and, during the rst months of 2020, the health system care was
particularly disoriented and unprepared to deal with the surging epidemic.
In this paper we analyze in historical and narrative terms the evolution of the
therapeutic approaches to COVID-19 in Italy and the critical discussions that
arose between doctors and public health professionals working within the
communities and the government and regulatory authorities.
Since the 1990s, the practice of medicine has been completely changed by
the advent of evidence-based medicine (EBM), leading to major changes and
advances in the medical management of patients. The scientic demonstration
Abstract
After starting in late 2019, COVID-19 spread worldwide, and Italy
was one of the rst Western nations to be seriously aected. At that
time, both the virus and the disease were little known and there were no
Evidence-Based Medicine indications for treatment. The Italian Health
Ministry guidelines claimed that, unless oxygen saturation fell to <92%,
no pharmacological treatment was necessary during the rst 72 hours,
other than on a purely symptomatic basis, preferably with paracetamol.
As later conrmed, that delay in therapeutic intervention may have been
responsible for numerous hospital admissions and a very high lethality
(3.5 %). To try to remedy this situation, several volunteer groups were
formed, managing to promptly cure thousands of patients at home with
non-steroidal anti-inammatory drugs and a variety of re-purposed drugs
(principally hydroxychloroquine, ivermectin) and supplements (such as
antioxidants, polyphenols and vitamin D). Although not documented by
any randomized controlled studies, these approaches were nonetheless
based on the best available evidence, were aimed at addressing otherwise
unmet major needs and produced a signicant reduction of hospitalizations,
of symptom duration, and a complete recovery from the disease compared
with late treatment, according to some retrospective observational studies
and the clinical experience of many physicians. A prompt discussion, with
a clear and open exchange between healthcare Institutions and the said
groups of voluntary physicians, could clarify the most eective approaches
to reduce the number of hospitalizations and the lethality of this disease.

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 101
of previously established evidence seeks to prevent errors as far
as possible. It is therefore obvious that faced with established
medical evidence it would be truly inconsistent not to use it.
However, it should also be kept in mind that, at the onset
of the SARS-CoV-2 pandemic, when the virus and ensuing
disease were scarcely known, there were no EBM-based
guidelines for the proper treatment of this disease available,
nor would there be for a long time to come. Furthermore,
the vast majority of doctors who found themselves dealing
with the new pandemic situation had grown up and practiced
professionally in an EBM environment and many of them felt
ill at ease to treat patients with COVID-19 at home, lacking
the support of clear guidelines.
For all these reasons, it would have been absolutely
necessary for the competent international institutions to
step in, such as the World Health Organisation, the major
regulatory bodies, such as the Food and Drug Administration
and the European Medicine Agency, and in the case of Italy,
in particular, the Ministry of Health and the Italian Medicines
Agency (AIFA), to establish that – lacking any available
medical evidence – it was up to the medical judgment of each
doctor to decide the best possible treatment, on a case by
case basis, in agreement with the generally accepted ethical
principles of the medical profession (cf. Article 13 of the
code of ethics of Italian doctors at https://portale.fnomceo.it/
codice-deontologico/) and with the applicable laws (in Italy,
prescription outside authorized indications is regulated by
Law 94 of 1998).
Already at the beginning of 2020, some of us were
expressing an opinion on the subject by saying that “while
waiting for denite EBM-based facts for the treatment of
COVID-19, it would be absolutely unethical to leave patients
at home without treatment, accepting the risk that the disease
could worsen, instead we should be looking to try other, even
o-label, pharmacological treatments with available well-
proven drugs for other conditions, which might prove eective
against COVID-19 as well, based on the pathophysiological
mechanisms of the disease, which were gradually becoming
known and on the well-known actions of these drugs” [1].
Even back then, Indomethacin was already indicated as one
of the drugs that could bring benets in the treatment of
COVID-19, due to both its powerful anti-inammatory action
and, above all, its known antiviral action [2].
In Italy, instead, the Ministry of Health issued
recommendations to treat the disease on a symptomatic basis
alone, using only paracetamol for fever and pain, waiting and
monitoring oxygen saturation by means of a pulse oximeter
and intervening only in the event that the oxygen saturation
level dropped below 92%, when hospitalization would be
inevitable [3]. These guidelines failed to take into account the
fact that the disease has several stages and, in many patients, if
not adequately treated, the stage of respiratory tract infection
is rapidly and unpredictably followed by severe multi-
systemic inammation with involvement of the coagulation
systems and cytokine and bradykinin "storms". Moreover,
a drop in oxygen saturation to below 92% indicates that
signicant damage has by then already occurred to the lungs,
and probably to other organs as well, and that the risk of other
chronic conditions setting in could not be ruled out, even after
recovery from COVID-19, with a subsequent burden on the
national health system.
These ocial recommendations also stated that no
drugs were needed before 72 hours (pages 9 and 10) [3]. In
the presence of a diagnosed infectious disease, however, it
seems unethical to stand by and not initiate pharmacological
treatment to combat the infection and attempt to halt
progression of the disease, particularly in this case where
it has been seen that the subsequent stages of the disease
can be truly dangerous to the point of the possible onset of
complications which then becomes dicult to control. This
delay in home care, as subsequently conrmed, may have
been responsible, particularly in the rst months of the year
2020, for both the high number of hospital admissions, with
overloading of hospitals that were ill-organised to respond to
the rising demand, and the very high lethality rate recorded at
the time (13.7%).
Worldwide, but particularly in Italy, the pandemic has
been tackled almost exclusively through anti-COVID-19
vaccination, even though these vaccines were still only
authorized for emergency use and therefore their safety, in
the short, medium and long term, had not yet been claried
with certainty. Furthermore, it became apparent as the
months went by that not only did the vaccine not prevent
the possibility of being infected with the virus, as a result of
which even vaccinated persons could spread the infection, but
also that the vaccine rapidly reduced its level of protection,
thus requiring boosters, which were also administered with
dierent vaccines from the basal vaccine. Thus, even many
fully vaccinated persons caught the disease, albeit mostly
less severely, although a number of them still required
hospitalization, intensive care, and many even died [4-6].
A discussion of the worrying signals of the pathogenicity of
these newly designed vaccines and of the variable benet /
risk ratio in dierent ages of life is beyond the scope of this
paper.
In the light of these facts, which are becoming more
and more obvious as experiences of physicians around the
world are gathered, it is necessary to ask whether focusing
all resources on the vaccine was a good choice. So why not
also focus on home therapy protocols, even while waiting
for precise EBM-based treatment protocols? In Italy, many
doctors have treated patients at home, also by way of
telemedicine systems, drawing on their knowledge and guided
by science and conscience. The majority of these doctors,
Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 102
the quickest and most important of the various means at our
disposal to understand the mechanisms and eects of the
disease on our bodies. However, the circular of the Italian
Ministry of Health of 1 April 2020, no. 11285 [9] (Page 3),
reads as follows on the subject of autopsy examinations and
diagnostic ndings on deceased COVID-19 patients: “For
the entire period of the emergency phase, no autopsies or
diagnostic ndings should be carried out in con-rmed cases
of COVID-19...”.
While not a blanket ban, this circular led to no or very
few autopsies actually being carried out, precisely during the
period when they would have been crucial to rapidly further
our knowledge of the disease. In fact, it was precisely thanks
to subsequent studies, carried out also using the autopsy
method, that it became clear that one of the factors that
aggravated the disease was endothelitis with the triggering
of pulmonary micro- and macro-thromboses, as well as
multi-district thrombosis [10]. It was precisely for this reason
that a new circular of the Italian Ministry of Health, dated
11/01/2021, no.0000818 [11], corrected the aim by removing
the wording that “advised against” performing autopsies.
Factors such as the signicant impact of COVID-19 on
the elderly population, the decision to manage the disease at
an advanced stage only and exclusively in hospital settings,
and the critical nature of the home treatment approach to
people infected with SARS-CoV-2, may have contributed to
the increase in the number of deaths from COVID-19 in Italy
[12, 13]. The average lethality rate for COVID-19 in Italy
was very high in 2020 (3.5%) and has gradually declined to
0.33% today, with an average gure for the entire pandemic
period of about 1% (Table 1, data from Worldometers
Coronavirus site). Vice versa, in countries such as Portugal,
where the healthcare service responded particularly well, due
to an excellent organisation at local community level, the
average recorded lethality during the pandemic was 0.55%,
i.e., still about 50% lower than in Italy [12], and this cannot
be justied only by the fact that the over-65 segment of the
population in Italy is 21%, while in Portugal it is 18%.).
Among the Western European countries, Italy recorded
the highest lethality rate: in fact, Spain and Greece had
an average lethality of 0.86%, Belgium 0.76%, Germany
0.53%, France 0.50%, Austria 0.44%, Luxembourg 0.43%,
Switzerland 0.38%, and the Nether-lands 0.27%. Even
seeing that the disease triggered strong organ and systemic
inammation, associated with episodes of micro- and macro-
thrombosis, used NSAIDs in association with antithrombotic
drugs (antiplatelet or low molecular weight heparins), plus
gastric protection.
The poor response and organisation of local community
level healthcare in Italy, in the face of the pandemic, led to the
formation of several groups of volunteers, mainly doctors but
also other healthcare and non-healthcare professionals, who
joined forces in an attempt to remedy the situation that had
been created and help healthcare facilities in the battle against
the pandemic, providing great support to the disoriented
and frightened public. The largest among the many groups set
up at the time were the “Early Home Therapy for COVID-19”
group (https://www.terapiadomiciliarecovid19.org), founded
in March 2020 by a lawyer, Erich Grimaldi, and the
“Ippocrate.org” group (https://ippocrateorg.org/), founded
between May and July 2020 by Mauro Rango.
Both organisations have since treated thousands of
cases of COVID-19 at home, also by remote monitoring,
using personalized treatments with drugs, mainly non-
steroidal anti-inammatory drugs (NSAIDs) but also
vitamins, dietary supplements and repurposed drugs such
as hydroxychloroquine and ivermectin, administered, when
possible, at the onset of the symptoms, in order to prevent
clinical worsening and promote a full recovery. This type
of approach, according to participating physicians, based
on clinical observation, has led to excellent results, as
documented by the clear drop in hospitalizations, the duration
of symptoms and the number of deaths. Preliminary results
with retrospective case histories of these experiences have
already been published by our research groups [7, 8].
Lethality trend in Italy during the pandemic:
Determining factors
When SARS-CoV-2 rst appeared, COVID-19 was a
virtually alien disease, the pathophysiological mechanisms of
which were unknown, and which could even lead to the death
of the infected person. Therefore, all useful measures had to
be taken and implemented to clarify the relevant mechanisms
and to investigate the nature of this disease as quickly as
possible, in order to be able to treat it in the best possible way.
To this end, autopsies of COVID-19 patients are certainly
Italy Portugal
Year 2020 2021 2022* 2020 2021 2022*
No. Cases 2,000,000 4,000,000 10,700,000 420,000 1,412,000 2,412,000
No. Deaths 70,000 62,300 29,500 6,197 12,083 3631
Lethality 3.5 1.55 0.32 1.64 0.85 0.15
* Until 18 of May 2022
Table 1: Lethality during the pandemic in Italy and Portugal compared (from Worldometers Coronavirus site, https://www.worldometers.info/coronavirus/).
Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 103
Sweden, often accused of pandemic mismanagement for
not applying strict restrictions during the various pandemic
waves, recorded a lethality of 0.75%. On the other hand,
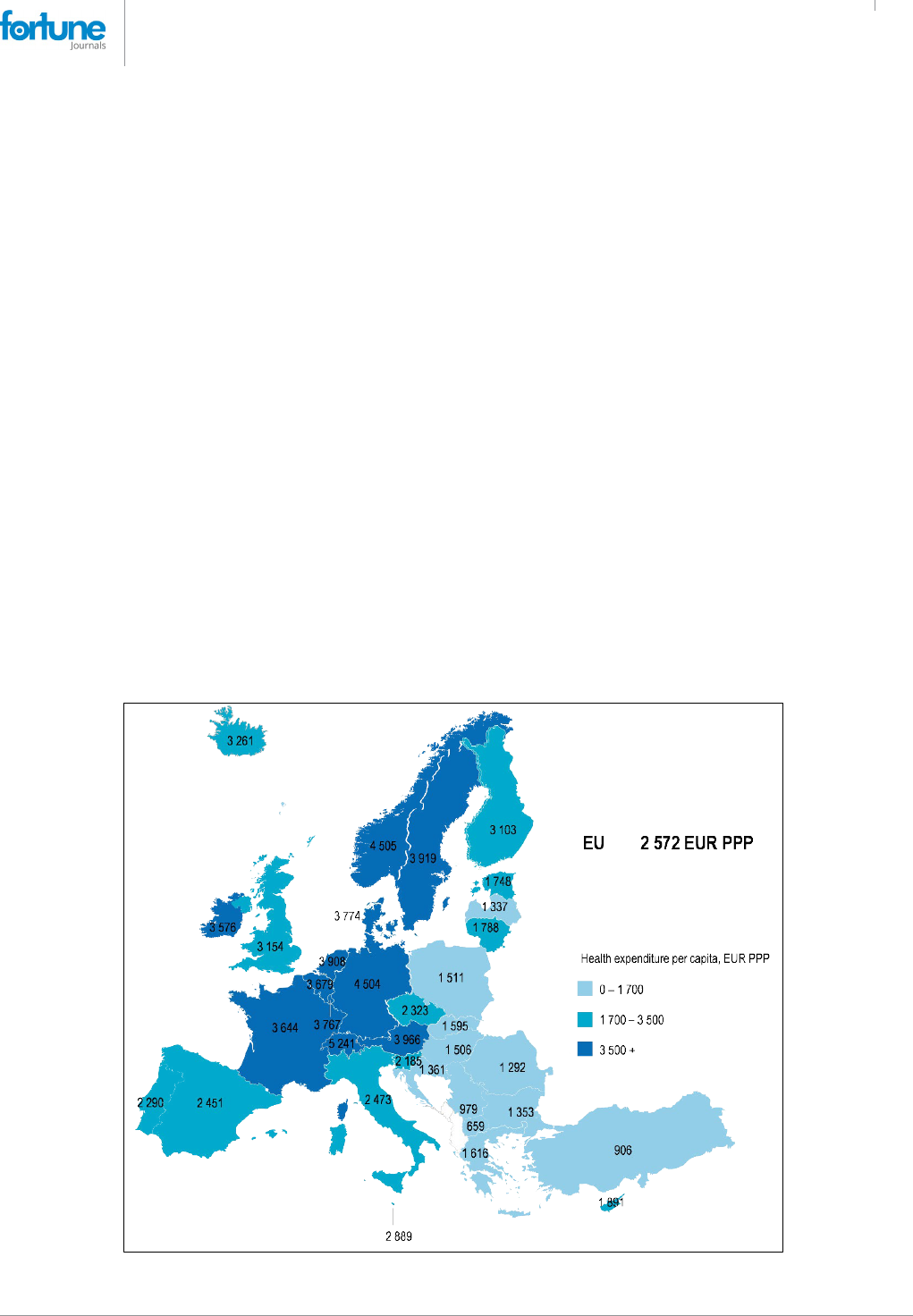
according to the latest OECD iLibrary.org report, Italy is
one of the tail-end countries in terms of per capita health
expenditure, comparable to Greece, Spain and Portugal,
which, however, recorded a much lower average lethality
rate. (From OECD iLibrary.org, Health at a Glance: Europe
2020: State of Health in the EU Cycle) (Figure 1).
There are many likely causes of the important and
progressive reduction in apparent lethality of COVID-19,
from the beginning of the pandemic to the present day,
although the most relevant seem to us to be the following:
NATURAL SELECTION: A relevant factor was the
gradual reduction in the number of frail elderly people, who
died in considerable numbers during the rst months of the
pandemic, with the average age of the sick decreasing and
thus the number of cases destined to unfavorable evolution.
VACCINATION CAMPAIGN: The vaccination campaign,
while failing to reduce the number of infections, probably
conferred some degree of protection from serious illness and
death for COVID-19 in elderly and more frail patients, thereby
reducing lethality. However, in actual fact, the authorization
studies on COVID-19 vaccines have not provided any
evidence of a possible reduction in deaths from COVID-19
[14] since all-cause mortality was not substantially dierent
over a six month period comparing subjects in whom was
administered the BNT162b2 vaccine (15 deaths) with those
who received placebo (14 deaths), and that there were more
cardiovascular and sepsis related deaths in the rst group (12
deaths) that in the second (6 deaths). However, a booster dose
at least 5 months after a second dose of BNT162b2 added
protection also against mortality [15], thus showing that,
perhaps, the protection given by vaccination in the short
term for deaths by COVID-19 may be lost in the long term
as number of all-cause deaths, in the absence of subsequent
booster. It should be noted that the eect of anti-covid-19
vaccines on public health should also be evaluated in the
light of the emerging evidence of the multiple adverse eects
caused by them, which are not always reported.
INCREASED DETECTION OF ASYMPTOMATICS:
Swab testing became mandatory to access the workplace,
public services and all indoor premises, such as restaurants,
cinemas, theatres, etc., initially for those persons who did
not wish to be vaccinated against COVID-19, but which
was then extended also to vaccinated persons after it was
realized that the COVID-19 jab did not provide protection
against the spread of the virus. In order to be able to have a
working and social life, or to travel, it was necessary to either
complete the vaccination program or to have been cured of
COVID-19 within the last 6 months or to have negatively
Figure 1: Per capita health expenditure in Europe, 2019 (From OECD iLibrary.org, Health at a Glance, Europe 2020)

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 104
tested for SARS-CoV-2 every 3 days. Performing these
blanket tests in the population, resulted in the discovery of
many asymptomatic positives. It has been speculated that
the number of asymptomatic positives among the population
with conrmed COVID-19 may be highly variable, but
averages around 40.5% of population [16].
The lethality score
then progressively decreased because so many patients were
asymptomatic, particularly during the wave of the omicron
variant.
NEW THERAPEUTIC APPROACHES: A fourth quite
relevant factor was the progressive improvement of the health
response in dealing with the pandemic, with the discovery
of the ecacy of certain drugs (in particular, NSAIDs but
also monoclonal antibodies and appropriate use of steroids
and antivirals) in preventing disease progression and the
realization of the need for early intervention by doctors, even
in the absence of ocial guidelines [7, 8, 17-22].
LESS AGGRESSIVE VARIANTS: Last but not least, one
has to consider the advent of the Omicron variant, which is
highly infectious but with a markedly diminished virulence
compared to the previous variants. This, too, has led to an
exponential increase in cases, but fortunately with fewer
deaths, further contributing to the drop in lethality which,
referring to data from the Worldometers Coronavirus website,
has fallen from 3.5% in 2020 to 1.55% in 2021 and 0.33% in
the first months of 2022 (up to 18 May), settling at an
average lethality of 1% over the entire pandemic period.
Reports from the Ministry of Health and responses
from doctors who acted in the area
During the pandemic a clear dichotomy arose between
local community doctors and emergency room and hospital
doctors, the former coming into contact with the sick at an
early stage of the infection and becoming accustomed to
treating the disease at the onset of the rst symptoms to prevent
it from worsening, while the latter doctors almost exclusively
treating the sick in the later/worse stages (second and third
phases) of the disease, which had to be treated promptly
according to guidelines already available for hospitalized
patients. These are very dierent stages of the disease that
require completely dierent approaches. Furthermore, while
there are still no randomized and controlled trials that have
produced guidelines for the early home treatment of patients
with mild and/or moderate low-risk COVID-19, there are
recommendations for early treatment, based on randomized
controlled trials, for patients at risk of worsening with
monoclonal antibodies [19, 22] and the new antiviral drugs
remdesivir, molnupinavir, ritonavir plus nirmatrelvir [20,
21]. Unfortunately, however, the pandemic has shown us
that even patients with mild and/or moderate COVID-19,
if left untreated, can deteriorate, require hospitalization and
eventually die [23].
Therefore, close cooperation between the various health
care components and institutions would have been necessary
to fully exchange information and collaboration, which could
have resulted in better controlling the pandemic.
Despite urgent and repeated requests, the Minister of
Health never accepted to meet with the representatives of
the doctors who voluntarily treated patients at home at
the first symptoms of the disease, free of charge, thus
building up a great deal of experience on the disease, in
order to discuss the matter. Groups of doctors have called
for changes to be made to the guidelines, even resorting to
the courts, but the Ministry of Health has consistently
opposed these requests. A history of the legislative clashes
between doctors and the Ministry of Health and AIFA can
be found in a Journal of Administrative Law [24] and is
summarized below (see also Table
2).
The guidelines of the Italian Ministry of Health (henceforth
the “Ministry”) echoed those of the Italian Medicines
Agency (AIFA) based on three distinct stages of the disease:
1. An early stage, clinically characterized by the appearance
of general malaise, fever and a dry cough. Cases in
which the host's immune system succeeds in blocking
the infection at this stage (the majority) have an entirely
benign course.
2. The disease may then evolve into a second stage featuring
morpho-functional alterations in the lungs caused by both
the cytopathic eects of the virus and the host's immune
response. This phase is characterized by interstitial
pneumonia, very often bilateral in nature, associated with
respiratory symptoms that are generally limited in the early
phase, but which may subsequently lead to progressive
clinical instability with respiratory insuciency.
3. The second scenario, in a limited number of people,
can evolve towards a clinical picture dominated by the
cytokine storm and consequent hyperinammatory stage,
which leads to local and systemic consequences and
represents a negative prognostic factor producing, in
the lungs, arterial and venous vasculopathy with blood
clots forming in the small vessels and evolution towards
serious and some-times permanent pulmonary lesions
(pulmonary brosis).
This classication was apparently correct and in agreement
with the main scientic reference literature (e.g.: [27, 28]),
but was followed by the very questionable denition of “low-
risk” patient in this way (quoted literally with our translation):
- absence of increased risk factors (e.g., neoplastic
diseases or immunodepression)
- u-like symptoms (e.g., rhinitis, cough without
diculty breathing, myalgia, headache);
- absence of dyspnoea and tachypnoea (documenting
SpO2 > 92% whenever possible);
- fever ≤38 °C or >38 °C since less than 72 hours;
Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 105
- gastro-enteric symptoms (in the absence of dehydration
and/or multiple diarrheal discharges);
- asthenia, ageusia / dysgeusia / anosmia.
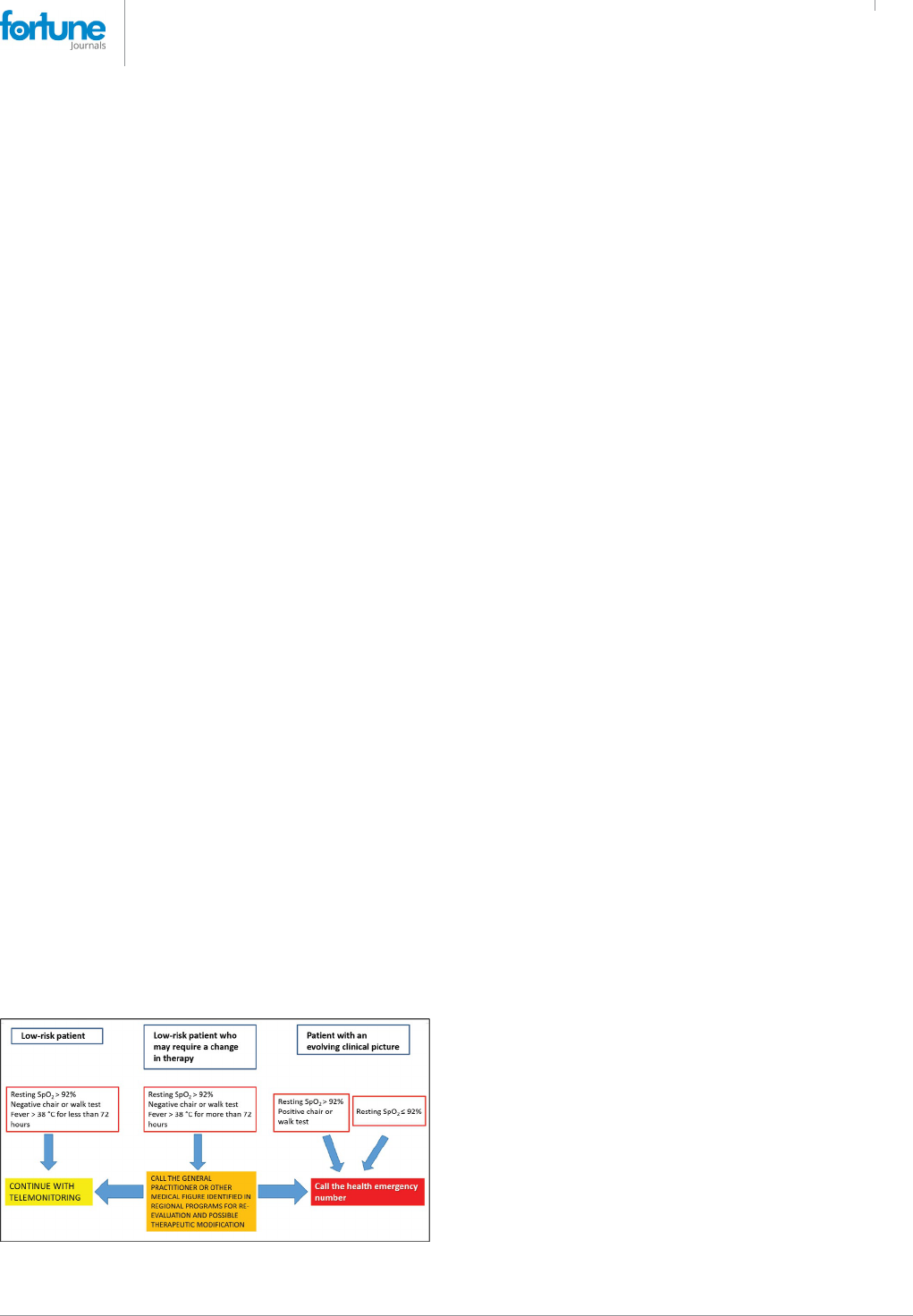
In other words, even patients with overt COVID-19
symptoms were judged to be at low risk and to only require
“remote monitoring”, as a recommendation, according to an
algorithm shown in Figure 2.
The strategy shown here, which is still in force in the
Ministry's guidelines, is highly objectionable, rst and
foremost because it considers patients with overt COVID-19
to be at “low risk” for the rst 72 hours and only recommends
“remote monitoring” for these patients. In fact, for low-risk
patients, the advisable treatment is expressed in these words
(our translation): “Generally speaking, for subjects with
these clinical features, no treatment is recommended except
possible for a symptomatic supportive therapy”. In particular,
in asymptomatic or paucisymptomatic subjects at home, a so
called “watchful waiting”, including periodic measurement
of oxygen saturation levels by means of pulse oximetry,
symptomatic treatment (e.g., paracetamol) and appropriate
hydration and nutrition were recommended, as well as
specic indications for immunocompromised patients [3].
Furthermore, the home treatment guidelines recommended
not to routinely use corticosteroids, not to use heparin, except
in immobilized patients, not to use antibiotics, not to use
hydroxychloroquine, not to administer drugs by aerosol.
Finally, it was stated that “There is no hard, irrefutable
evidence to date (i.e., from controlled clinical studies) of the
ecacy of vitamin supplements and food supplements (e.g.,
vitamins, including vitamin D, lactoferrin, quercetin), the
use of which therefore is not recommended herein”. Such
statements are perplexing, in light of the fact that there is
no hard, irrefutable evidence to date (i.e., from controlled
clinical studies) of the ecacy of paracetamol, which, on the
other hand, is always included in the Ministry guidelines.
In light of our current knowledge, this strategy exposed
patients to the risk of progression and worsening during the
most sensitive period of the disease. In practice, patients at
home were left without any treatment other than paracetamol
as a symptomatic drug. Later on (26 April 2021), partly
due to the continued insistence of physicians working in
the eld and a number of preliminary publications [17, 29,
30], these guidelines were changed by
also introducing
the symptomatic use of NSAIDs, but the above-mentioned
“remote monitoring” strategy continued to apply.
The latest guidelines of the Ministry [26] illustrate the use
of some more recent drugs such as antivirals and monoclonals.
Two dierent approaches are distinguished, based on the
types of patients at low risk or at high risk of complications.
For those at so-called “low risk”, the indications for
monitoring and symptomatic therapies (paracetamol or
NSAIDs) are reiterated. High-risk patients are dened as
those who have one or more of these characteristics: age>
65 years and male, or smoking habit, or chronic diseases
such as neoplasms, immuno-suppressive states, obesity,
cerebrovascular disease, dementia, psychotic disorders,
pathologies neurodegenerative, cardiovascular diseases
(such as arterial hypertension, atrial brillation, heart failure,
cardiomyopathies, coronary artery disease), type I and type
II diabetes mellitus, chronic renal failure, chronic pulmonary
disease (COPD), severe or moderate asthma, cystic
brosis, pulmonary brosis, interstitial diseases, pulmonary
hypertension. Patients with these risk factors are candidates
for early therapy with monoclonal antibodies or with oral or
intravenous antiviral drugs.
Currently in Italy for patients with mild - moderate
Covid-19 who do not require hospitalization, dierent
treatments are available based on the administration
of monoclonal antibodies (combination casirivimab /
imdevibam and the antibody sotrovimab and the combination
bamlanivimab / etesevimab) or antiviral agents (nirmatrelvir
/ ritonavir, remdesevir, molnupiravir). However, ecacy data
on the Omicron variant indicate substantial ineectiveness
of the bamlanivamb / etesevimab and casirivimab /
imdevimab combinations, while sotrovimab appears to
maintain adequate ecacy. The use of lopinavir / ritonavir
or darunavir / ritonavir or cobicistat is not recommended for
either the purpose of preventing or treating the infection. The
randomized clinical trials published to date all conclude that
these pharmacological approaches are ineective.
The selection of the patient to be treated with monoclonal
antibodies or antivirals is entrusted to doctors who have the
opportunity to come into contact with patients suering from
recent onset COVID-19 and with mild-moderate symptoms.
For both types of treatment, the greatest eectiveness is
observed with early administration with respect to the onset
of symptoms, possibly within 72 hours. This position of the
Ministry, which supports a greater ecacy of monoclonals
and antivirals in the rst 72 hours of the disease, could
contrast with the previous statement that in patients with mild
Figure 2: Outline of COVID-19 home treatment according to the Italian
Health Ministry guidelines (see text).
Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 106
disease, no therapies other than symptomatic ones should be
carried out (see also gure 2). In fact, in a progressive disease
such as COVID-19 it is undoubtedly dicult to establish
the evolution of the disease in a short time, especially in the
outpatient context and with telemedicine.
Criticism of the Ministry guidelines by doctors
and patients
Faced with the “therapeutic paralysis” brought about by
the ministerial guidelines, the doctors of the group “Early
Home Therapy for COVID-19” appealed to an administrative
court (TAR) to obtain more therapeutic freedom and the
court decided in their favor, ruling that doctors have (our
translation) “the right/duty, with legal relevance based on
both civil and criminal law, to prescribe the drugs they deem
most appropriate, guided by science and conscience, which
cannot be restricted in the perspective of an expectation,
potentially prejudicial both for the patient and, albeit
for dierent reasons, for the doctors themselves”. The
Regional Administrative Tribunal therefore suspended the
eectiveness of the measure issued by AIFA with immediate
eect and postponed the discussion of the merits to a later
date. However, the disputes between doctors and the
Ministry continued for months (see Table 2) until recently,
without a scientic collaboration agreement that would have
been desirable to solve the problem of the best treatment of
COVID-19.
The doctors operating within the group “Early Home
Therapy for COVID-19” requested, on the basis of their
observational clinical experiences, the possibility of
carrying out randomized and controlled scientic studies, to
denitively conrm the ecacy of their treatments, according
to an EBM approach, with the assistance of the Ministry of
Health and Universities or Research Institutions since their
organisation was ill-equipped to single-handedly perform a
prospective, randomized and controlled scientic study. This
request, to date, has remained unfullled.
Nevertheless, several retrospective observational studies
have been produced showing that treatment with NSAIDs,
administered at the rst symptoms of mild-to-moderate
COVID-19, resulted in a signicant reduction in the number
of hospitalizations, with a clear reduction in healthcare
expenditure. The ecacy of NSAIDs has been proven
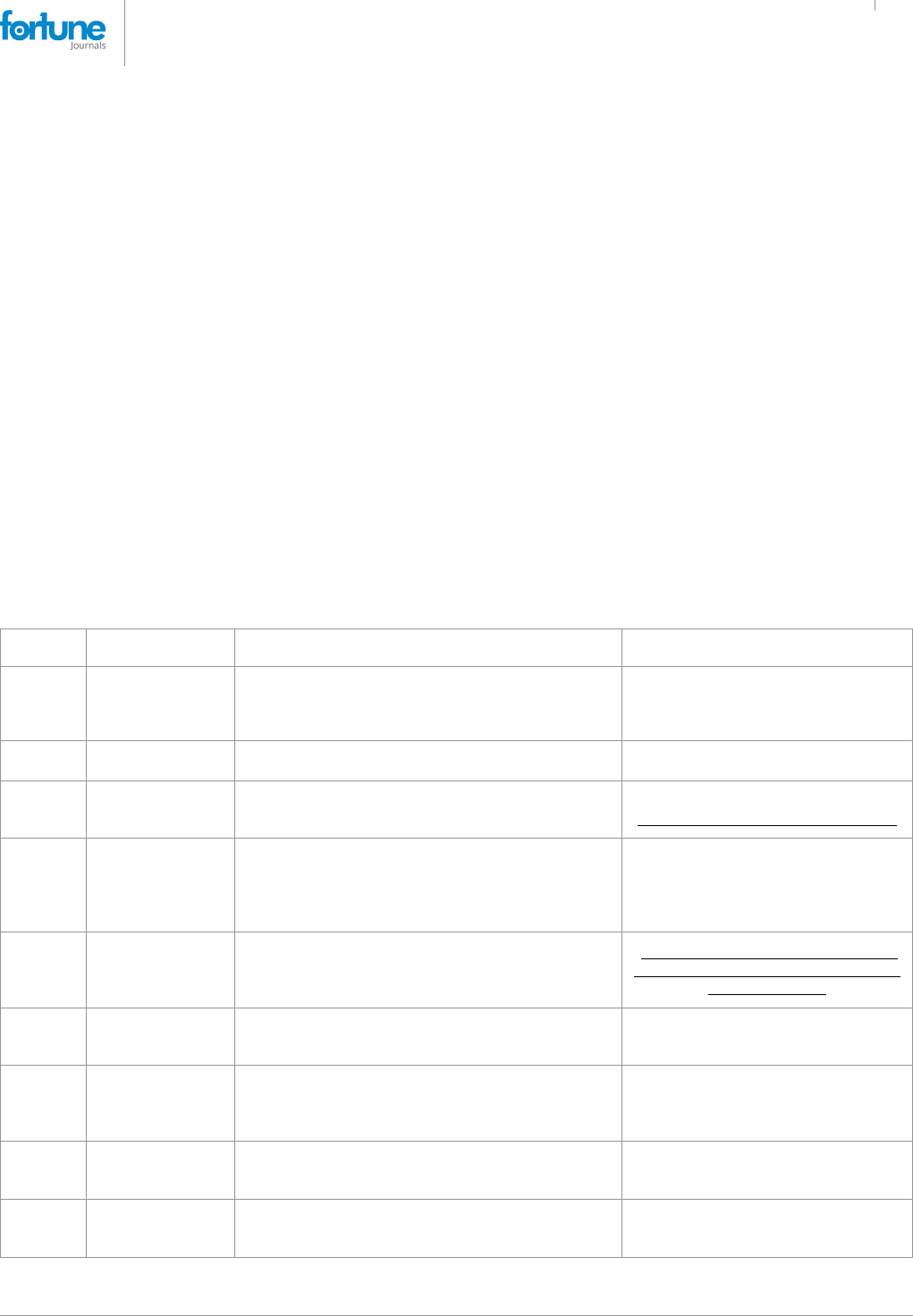
Date Actor Actions concerning home treatment References
22-Jul-20
Italian Medicine
Agency (AIFA)
The use of hydroxychloroquine, alone or in combination
with other drugs, outside of clinical trials, was suspended.
Note of AIFA https://www.aifa.
gov.it/documents/20142/1123276/
idrossiclorochina_22.07.2020.pdf
Accessed 13 June 2022
30-Nov-20
Italian Ministry of
Health
Issued a circular entitled “Home management of patients
with SARS-CoV-2 infection”.
Circular 0024970-30/11/2020-DGPROGS-
DGPROGS-P [3]
10-Dec-20
Italian Council of
State
The note of 22 July 2020 from AIFA, which prohibited
the o-label prescription of hydroxychloroquine, was
suspended
Judgement n. N. 09070/2020 REG.RIC.
allegato7506782.pdf (quotidianosanita.it)
4-Mar-21
Regional
Administrative
Tribunal (TAR) of
Lazio, Rome Branch,
div. III
At the request of a doctors' and patients' association,
the Ministry's circular with guidelines for the home
management of patients was cancelled
TAR Lazio, Div. III quater, precautionary
order no. 1412.
8-Apr-21 Italian Senate
Approved an agenda with a commitment by the
government to update the protocols and guidelines for the
home care of Covid-19 patients, taking into account all the
experiences of professionals working in the eld.
At the end of the session held on 7 April
2021 https://www.senato.it/3818?seduta_
assemblea=19801
26-Apr-21
Italian Ministry of
Health
Updated the outpatient therapy guidelines with the addition
of symptomatic use of anti-inammatory drugs, while
maintaining the recommendation of paracetamol
Circular 0017948-26/04/2021-DGPRE-
MDS-P [25]
15-Jan-22
Lazio TAR (Rome,
div. III)
At the request of a doctors' and patients' association,
cancelled the new guidelines for the home management
of patients, as contrary to the professional and ethical
standards of doctors
Judgment No. 419/2022
19-Jan-22 Council of State Cancelled the 15 January ruling of the Lazio TAR
Judgement of 9 February 2022, no. 946.
https://www.quotidianosanita.it/governo-e-
parlamento/articolo.php?articolo_id=102213
10-Feb-22
Italian Ministry of
Health
Updated the guidelines by replacing “watchful waiting” with
“monitoring”, while maintaining the recommendation of
symptomatic use of paracetamol or NSAIDs
Circular 0003435-10/02/2022-DGPROGS-
MDS-P [26]
Table 2: Timeline of the key ocial actions concerning home-based care in Italy during the COVID-19 pandemic

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 107
“on the eld” by rigorously designed, though not strictly
randomized, studies [17, 18]. This last paper reported the
results of a cohort study in which patients, at the onset of mild
symptoms of COVID-19, were treated at home on the basis of
a pathophysiological and pharmacological rationale, which
included in particular relatively selective cyclooxygenase-2
inhibitors and, when necessary, corticosteroids,
anticoagulants, oxygen therapy and antibiotics. A cohort
of 108 patients treated at home by their GPs with the
“recommended” treatment, between January 2021 and May
2021, was compared with a cohort of 108 patients of similar
age, gender and comorbidities, combined with other treatment
programs using paracetamol and other drugs (ClinicalTrials.
gov: NCT04854824). The primary outcome was COVID-19-
related hospitalization, which occurred in only one patient
(0.9%) with the “recommended” treatment compared to as
many as 12 patients (11.1%) in the comparison cohort (P
= 0.0136). The proposed algorithm reduced the cumulative
duration of hospital stays by 85% (from 141 to 19 days),
as well as the related costs (from € 60,316 to € 9,058). In
conclusion, the adoption of the proposed outpatient treatment
algorithm during the early and mild phase of COVID-19
reduced the incidence of hospitalization by approximately
10-fold.
An Indian group performed a randomized controlled
trial of indomethacin versus paracetamol, added to standard
background therapy, in which the main outcome was
desaturation to <93% O2 [31]. The results showed that no
patients in the indomethacin group had desaturated, while
as many as 20 patients in the paracetamol group had de-
saturated.
Italian physicians who performed home-based therapies
during the pandemic have already produced two retrospective
studies. The rst [7] chose indomethacin for the early home
treatment of 153 patients with mild-to-moderate COVD-
19 since the beginning of the pandemic, both for its potent
anti-inammatory action and for its documented anti-viral
action against various viruses and, in particular, also in cells
in vitro and in vivo (in dogs) against coronavirus [2] and
more recently also against SARS-CoV-2 [32, 33]. Our multi-
therapeutic treatment is based on a therapeutic rationale
combining various molecules with anti-inammatory,
antiviral and antioxidant properties, such as indomethacin,
hesperidin, quercetin, aspirin in an antiplatelet dosage, and
gastric protection with omeprazole [34]. Intervention within
72 hours resulted in zero hospitalizations with a reduction in
the duration of symptoms and a clear improvement in disease
outcomes, compared to what was observed in a comparison
group of patients who had waited more than 72 hours before
calling the doctor.
Another retrospective observational study, recently
released in preliminary form [8] investigated the
characteristics, management and outcomes in COVID-19
patients treated in Italy by 10 volunteer physicians within the
IppocrateOrg Association, between 1 November 2020 and
31 March 2021. 392 consecutive COVID-19 patients with
various types of comorbidities were treated with vitamins
and supplements (98.7%), aspirin (66.1%), antibiotics (62%),
glucocorticoids (41.8%), hydroxychloroquine (29.6%),
enoxaparin (28.6%), colchicine (8.9%), oxygen therapy
(6.9%), and ivermectin (2.8%). Admission occurred in 5.8%
of the total cases, 390 patients (99.6%) recovered, one patient
(0.2%) was lost at follow-up and one patient (0.2%) died after
hospital admission. It should be noted that the COVID-19
lethality in our cohort was 0.2% (95% condence interval:
0.01-1.4%), whereas the overall COVID-19 lethality in Italy
over the same period was between 3% and 3.8%. The use
of the single drugs and drug combinations described in this
study therefore appears to be eective and safe, as indicated
by the few mild adverse reactions reported.
These results are prompting calls for a study with a
non-inferiority protocol between the dierent therapeutic
schemes and any of the antiviral drugs already authorized in
the early treatment of COVID-19. In the event of a positive
non-inferiority result of our therapeutic scheme against the
chosen antiviral, there would be a truly signicant reduction
in therapeutic expenditure.
Paracetamol: not as safe as was thought?
Paracetamol [N-(4-hydroxyphenyl) acetamide, N-(4-
hydroxyphenyl) ethanamide] is a drug with analgesic and
antipyretic action, widely used in common over-the-counter
preparations for viral colds, or in drugs for the treatment of
acute and chronic pain. It is also among the most widely used
drugs in the home treatment of COVID-19, also because it has
been recommended by the Ministry of Health since the rst
guidelines were issued. However, doubts about the validity
of its use soon emerged [35], based on the fact that it could
interfere with glutathione reserves in the body. In fact, when
administered in high doses, this drug is metabolized with
the formation of N-acetyl-p-benzoquinone imine (NAPQI),
which in turn requires glutathione for hepatic catabolism, to
the point that that the antidote for paracetamol intoxication
is N-acetylcysteine. Glutathione is an indispensable element
of cell metabolism and, in particular, of the defense against
toxic oxygen derivatives (ROS) and thus cellular oxidative
stress [35-38]. Furthermore, NAPQI metabolism in GSH
deciency leads to an accumulation of denatured proteins by
alteration of their sulfhydryl residues.
Oxidative stress has been observed in infection by such
viruses as hepatitis B [39], hepatitis C [40], inuenza [41]
and SARS-CoV-2 [42, 43]. In the latter case, excess ROS
could also lead to an unfavorable evolution in elderly subjects
with low antioxidant capacity [44, 45], possibly because the
intracellular redox environment alters antigen presentation

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 108
[46] and the expression of ACE2 [47, 48]. Indeed, the severity
and mortality risk of SARS-CoV-2 or COVID-19 have been
associated with age [45]. It seems possible that the oxidation
of thiols (-SH residues of proteins) into disuldes (S-S),
under an oxidative stress mechanism, increases the anity of
spike proteins for the ACE2 receptor and thus increases the
severity of COVID-19 [47].
It therefore seems appropriate to reassess the risk-benet
ratio of paracetamol in viral infections [49] particularly in
patients with reduced liver function. Indeed, 37.2 %-76.3 %
of patients with COVID-19 presented abnormal liver function
during COVID-19 [50]. Furthermore, in a retrospective cross-
sectional study conducted in 4 public hospitals in Peru, in
which 1,100 patients admitted with a diagnosis of COVID-19
were enrolled [51], it was found that liver enzymes (AST and
ALT) were altered on admission in more than 60 per cent
of patients. Moreover, patients taking paracetamol featured
a higher risk of liver damage: OR=1.41 (95% CI: 1.01-1.98;
p=0.04). Worsening prognostic factors were dyslipidaemia
and fever; improving prognostic factors were the use of
corticosteroids, enoxaparin and the female gender.
N-acetylcysteine, which supports glutathione and thus
the main antioxidant defense systems [52] has been used
with good results in inuenza syndromes [53] and acute
respiratory distress syndrome (ARDS) [54] and has been
suggested as a potential therapeutic agent for COVID-19 [37,
55-58]. Some positive results have been obtained in critically
ill patients [59, 60], although a randomized study conducted
in Brazil on a patient group treated with an infusion of 21
grams of N-acetylcysteine/day, obtained no therapeutic eect
[61]. Further studies are needed to better evaluate eective
dosages and application at various stages of the disease.
Acetylcysteine was also used to counteract remdesivir-
induced liver failure in two COVID-19 patients [62].
In conclusion, paracetamol, which lacks anti-inammatory
activity and risks depleting the glutathione that is necessary
for antiviral defense purposes, does not appear to be the drug
of choice for the treatment of patients with COVID-19 at an
early stage and may worsen the course of the disease.
Discussion
The problem presented here is part of the continuous debate
between EBM, based on randomized trials and meta-analyses,
and the doctor's freedom of decision, based on observational
studies, personal experience and often intuition, also taking
into account the individual characteristics of each patient.
Furthermore, the experience of Italian doctors engaged on
the front line in the battle against the COVID-19 disease
suggests that the “guidelines” or the “recommendations” of
the public health authorities, governed by political trends, risk
blocking the search for new therapeutic approaches, if they
are intended to be followed in a too rigid and indisputable
way. Paradoxically, the need to formulate guidelines based
on rigorous evidence of ecacy can become an obstacle to
the exploration of new therapies in pandemic emergency
conditions.
However, this apparent contrast is based on a
misconception of EBM. One of the best denitions of EBM is
the following “Evidence based medicine is the conscientious,
explicit, and judicious use of current best evidence in making
decisions about care of individual patients. The practice
of evidence-based medicine means integrating individual
clinical expertise with the best available external clinical
evidence from systematic research” [63]. Therefore, during
a little-known virus pandemic, it would have been more
useful to integrate the scant indications from EBM with the
individual clinical experience that many doctors had gained
by curing promptly at home patients with COVID-19.
According to the decision by the Council of State of
9/02/2022 No. 00411/2022 REG.RIC, the ministerial circular
“does not ban or restrict the use of drugs but merely lays down
recommendations and guidelines for the various treatments,
based on the best available evidence in the literature,
depending on the occurrence of specic conditions”. The
decision then stated that the circular “advises against” – but
does not explicitly prohibit – the use of certain drugs in the
home treatment of Covid-19. Individual doctors are free
to exercise their professional judgment, under their own
responsibility, when prescribing the drugs, they deem most
appropriate in each specic case in relation to the individual
patient, on the basis of the scientic evidence collected.
This “open” perspective is certainly acceptable, although
the decision then goes on to state that “Doctors cannot
prescribe a drug based simply on intuition or improvisation
experimented on the individual patients, but on scientic
evidence and therefore on rigorous studies and precise
clinical trials, now numerous at the international level even
in the ght against the Sars-Cov-2 virus, after two years since
the beginning of the pandemic.”
Therefore, the general question remains open as to the
level of “evidence” required in the face of a new and complex
disease, which aects patients with several comorbidities,
and goes through several stages. The adoption of politically-
driven guidelines, especially in the medical sphere, has
already given rise in the past to extensive discussions on their
legal nature and classication within the framework of legal
sources. On the one hand, their inherent nature as guidelines
would prevent them from being considered in regulatory
terms, given that they are indicative and do not claim to be
exhaustive; on the other hand, some have argued that the
wide use of these instruments give them a “binding force” in
an emergency [24].
These issues ended up inuencing the operations of
physicians working in contact with patients in emergency

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 109
conditions, and awareness of this problem has led various
groups of
physicians to call for greater attention to be paid to
their experiences, even in the absence of denite indications
from EBM. Particular mention should be made of a technical
document prepared by a group of experts and submitted to the
attention of Italian political forces in the spring of 2021 [64].
This paper clearly illustrated the situation in which doctors
found themselves working at that time.
The doctors claimed that “Since no study has so far been
proposed, conducted or published on the home therapy of
patients with COVID-19, a doctor faced with a new and
complex condition such as the one in question – taking
into account the available scientic evidence, biological
plausibility and the patient's specic situation – may adopt
the therapeutic approaches that he or she deems necessary
guided by science and conscience”. Furthermore, “doctors
should be given the possibility of proposing on- and o-
label drugs to patients, as well as useful indications for the
prevention and treatment of diseases that can complicate
the course of COVID-19, also by way of general evidence-
based nutritional education and specic advice on nutrition
(also to ensure a proper intake of vitamins and
flavonoids, without ruling out the use of supplements write
where necessary)”. Among the drugs that may prove
useful, according to the doctor's judgement in individual
cases for the prompt home management of patients with
COVID-19, are NSAIDS and, in particular, indomethacin,
that in addition to the anti-inflammatory and anti-
bradykinin actions, also demonstrated a clear antiviral
action in vitro and in vivo against SARS-CoV-2 [2, 7, 31,
32, 34, 65]. While a recent meta-analysis, performed by
analyzing 40 studies, showed that the use of NSAIDs did
not reduce mortality outcomes among people with
COVID-19, it has also shown that NSAIDs can be
used safely among patients positive to SARS-CoV-2
[66]. Moreover, it should be noted that the latter
analysis assessed the effectiveness of ibuprofen, aspirin
and COX-2 inhibitors, it did not mention studies with
indomethacin. The conclusions express the hope that the
therapeutic experience built up in the home set-ting, about
with regard to some of the indicated drugs and their
combinations, or even others that might prove useful in
the treatment of COVID-19 patients over time, would be
the subject of highly valid studies that could evaluate them
and allow appropriate recommendations for their use.
As a result of the cited work [64], the political forces
decided to commit the government (a) to modifying the
guidelines, which were considered too restrictive, and (b)
to setting up a ministerial monitoring committee made up
of representatives of all the professions involved in local
community health care. Other proposed measures included
implementing interventions from the diagnosis stage
capable of involving all health care, social service and
family support personnel to ensure that the various
experiences and clinical
data collected by the regional health systems owed into a
national protocol for the home management of Covid-19
patients, and, last but not least, to support this protocol
with a plan to increase the supply of telemedicine devices
suited to ensuring adequate and constant monitoring of the
patients' clinical condition [64]. Unfortunately, to this day,
the guidelines have remained basically unchanged (the
only dierence being the addition of NSAIDs, alongside
paracetamol, among the symptomatic drugs) and none of
these objectives proposed to the government by the political
forces has been implemented.
From the point of view of the ocial regulations,
the situation is entirely uid and no precise denition
of physicians’ rights and duties, as well as the extent of
“therapeutic freedom” possible in conditions of uncertainty,
has yet been agreed on. The Council of State's ruling on the
AIFA Guidelines for the Home Management of Patients
Infected with Covid-19 and the Ministry of Health's circular
“Home Management of Patients Infected with SARS-CoV-2”,
updated on 26 April 2021, contain mere recommendations
and not binding requirements and are, in legal terms, merely
guidelines for general practitioners, as benchmarks for current
experiences in therapeutic methods at an international level.
Evidence of a pathological link between metabolic
diseases and severe forms of COVID-19 stimulates critical
reection and new considerations. Precisely because
COVID-19 is a disease that most severely aects people
with poor health, diabetes, hypertension and metabolic
syndrome, correct supplementation with dietary factors may
be the key to preventing and countering the complications
of COVID-19. It is highly plausible that a set of natural
agents can inhibit the cytokine storm and hypercoagulability
that characterize a severe COVID-19 infection: vitamin D3,
omega-3 polyunsaturated fatty acids, other nutraceuticals that
can activate anti-inammatory and antioxidant pathways such
as hesperidin, quercetin, rutin, vitamin C, zinc, melatonin,
lactoferrin and glutathione [34, 67-71]. Despite the absence
of meta-analyses, there is much preliminary evidence, even
in double blind, that quercetin can have positive eects on
the evolution of the disease, possibly also in association with
antivirals [72-76].
Each patient should be evaluated for his/her individual
susceptibility and for this reason the evidence deriving from
controlled clinical trials (which involve administration in
homogeneous groups and under standardized conditions)
are important but do not exhaust the possibilities of medical
intervention. From this point of view, it can be understood that
the guidelines cannot yet systematically "recommend" these
innovative approaches, but equally it would be reductive and
counterproductive if they were to ban them. Rigorous studies
will be fundamental to validate preventive and therapeutic
protocols that could combine supplements, vitamins and

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 110
antioxidants with chemical drugs in aid protocols to mitigate
disease progression following SARS-CoV-2 infection.
Conclusions and Perspectives
The Italian approach to the pandemic by the public health
institutions has revealed signicant shortcomings and has
proved to be partly mistaken, based on the contents of this
paper, with the most prominent mistakes, in our opinion,
being: the decision to tackle the pandemic only through the
development of vaccines based on novel and experimental
technology, with insucient information as to the duration
of their ecacy and their medium and long-term safety;
the issuing of guidelines that discouraged doctors from
adopting early home treatment therapy guided by science
and conscience, using the drugs considered most appropriate
for each patient; the decision to strongly recommend
“watchful waiting” and symptomatic drugs alone, especially
paracetamol, going so far as to sanction doctors who did not
comply with the ocial recommendations; the refusal to
enter into any form of dialogue with doctors who promptly
treated thousands and thousands of patients at home,
enormously reducing the number of hospitalizations. This
inecient management of the pandemic can be viewed as one
of the factors whereby Italy is among the countries with most
hospitalizations and deaths due to COVID-19.
Looking ahead, it is necessary to adopt a much more open
and exible approach, starting systematic and comparative
studies between the dierent protocols that emerged from the
experience of doctors who work at the patient's bedside or
through telemedicine in the early stages of the disease. Since
vaccine prevention and early treatment are not alternatives,
it would be necessary, in the near future, for resources to be
allocated to systematic and patient research of the various
therapeutic approaches that have shown promising results,
without focusing only on antiviral drugs in the belief that
they can constitute a “silver bullet” capable of curing the
disease in all instances. Relying only on “big pharma”, which
is engaged in researching next-generation antivirals, could
prove yet another serious mistake in the face of a disease as
complex as COVID-19.
Author Contribution:
Conceptualization, S.F., M.C., P.B.; methodology, F.M.,
E.Z.; validation, S.P., E.Z.; investigation, S.F., M.C., P.B.,
F.M.; writing—original draft preparation, S.F.; writing—
review and editing, P.B.; All authors have read and agreed to
the published version of the manuscript.
Funding:
This research received no external funding.
Potential Conicts of interest:
P.B. has a consultancy agreement with Vanda s.r.l.
(Frascati, Rome). The other authors have no competing
interests to declare.
References
1. Scotto Di Vetta M, Morrone M, Fazio S. COVID-19:
O-label therapies based on mechanism of action while
waiting for evidence-based medicine recommendations.
World J Meta-Anal 8 (2020): 173-177.
2. Amici C, Di CA, Ciucci A, Chiappa L, Castilletti C,
Martella V, et al. Indomethacin has a potent antiviral
activity against SARS coronavirus. Antivir Ther 11
(2006): 1021-1030.
3. Rezza GU, Urbani A. Circolare recante “Gestione
domiciliare dei pazienti con infezione da SARS-CoV-2”.
Direzioni Generali della Programmazione Sanitaria e
della Prevenzione Sanitaria, ed., Ministero della Salute,
Roma (2020).
4. Fabiani M, Puopolo M, Morciano C, Spuri M, Spila
Alegiani S, Filia A, et al. Eectiveness of mRNA vaccines
and waning of protection against SARS-CoV-2 infection
and severe covid-19 during predominant circulation of
the delta variant in Italy: retrospective cohort study. BMJ
376 (2022): e069052.
5. Nyberg T, Ferguson NM, Nash SG, Webster HH,
Flaxman S, Andrews N, et al. Comparative analysis of
the risks of hospitalisation and death associated with
SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2)
variants in England: a cohort study. Lancet 399 (2022):
1303-1312.
6. Nordstrom P, Ballin M, Nordstrom A. Risk of SARS-
CoV-2 reinfection and COVID-19 hospitalisation
in individuals with natural and hybrid immunity: a
retrospective, total population cohort study in Sweden.
Lancet Infect Dis 22 (2022): 781-790.
7. Fazio S, Bellavite P, Zanolin E, McCullough PA,
Pandol S, Auso F. Retrospective Study of Outcomes
and Hospitalization Rates of Patients in Italy with a
Conrmed Diagnosis of Early COVID-19 and Treated
at Home Within 3 Days or After 3 Days of Symptom
Onset with Prescribed and Non-Prescribed Treatments
Between November 2020 and August 2021. Med Sci
Monit 27 (2021): e935379.
8. Cosentino M, Vernocchi V, Martini S, Marino F,
Allasino B, Balzola M, et al. Early outpatient treatment
of COVID-19: a retrospective analysis of 392 cases in
Italy MedXriv (2022): https://www.medrxiv.org/conten
t/10.1101/2022.04.04.22273356v1.
9. D'Amario CR, Rossi P. Indicazioni emergenziali
connesse ad epidemia COVID-19 riguardanti il settore
funebre, cimiteriale e di cremazione. Direzione Generale

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 111
della Prevenzione Sanitaria ed., Ministero della Salute,
Roma (2020).
10. Wichmann D, Sperhake JP, Lutgehetmann M, Steurer
S, Edler C, Heinemann A, et al. Autopsy Findings and
Venous Thromboembolism in Patients With COVID-19:
A Prospective Cohort Study. Ann Intern Med 173 (2020):
268-277.
11. Rezza G. Indicazioni emergenziali connesse ad epidemia
SARS-CoV-2 riguardanti il settore funebre, cimiteriali e
della cremazione - Versione 11 gennaio 2021. Direzione
generale della prevenzione sanitaria ed., Ministero della
Salute, Roma (2021).
12. Pandol S, Valdenassi L, Bjorklund G, Chirumbolo S,
Lysiuk R, Lenchyk L, et al. COVID-19 Medical and
Pharmacological Management in the European Countries
Compared to Italy: An Overview. Int J Environ Res
Public Health 19 (2022): 19(7):4262.
13. Pandol S, Chirumbolo S, Ricevuti G, Valdenassi L,
Bjorklund G, Lysiuk R, et al. Home pharmacological
therapy in early COVID-19 to prevent hospitalization
and reduce mortality: Time for a suitable proposal. Basic
Clin Pharmacol Toxicol 130 (2022): 225-239.
14. Thomas SJ, Moreira ED Jr, Kitchin N, Absalon J,
Gurtman A, Lockhart S, et al. Safety and Ecacy of the
BNT162b2 mRNA Covid-19 Vaccine through 6 Months.
N Engl J Med 385 (2021): 1761-1773.
15. Rohban T. BNT162b2 Vaccine Booster and Covid-19
Mortality. N Engl J Med 386 (2022): 1000.
16. Ma Q, Liu J, Liu Q, Kang L, Liu R, Jing W, et al.
Global Percentage of Asymptomatic SARS-CoV-2
Infections Among the Tested Population and Individuals
With Conrmed COVID-19 Diagnosis: A Systematic
Review and Meta-analysis. JAMA Netw Open 4 (2021):
e2137257.
17. Suter F, Consolaro E, Pedroni S, Moroni C, Pasto E,
Paganini MV, et al. A simple, home-therapy algorithm
to prevent hospitalisation for COVID-19 patients: A
retrospective observational matched-cohort study.
EClinicalMedicine 37 (2021): 100941.
18. Consolaro E, Suter F, Rubis N, Pedroni S, Moroni C,
Pasto E, et al. A Home-Treatment Algorithm Based on
Anti-inammatory Drugs to Prevent Hospitalization
of Patients With Early COVID-19: A Matched-Cohort
Study (COVER 2). Front Med (Lausanne) 9 (2022):
785785.
19. Lin WT, Hung SH, Lai CC, Wang CY, Chen CH. The
impact of neutralizing monoclonal antibodies on the
outcomes of COVID-19 outpatients: A systematic review
and meta-analysis of randomized controlled trials. J Med
Virol (2022): 94(5):2222-2229.
20. Vegivinti CTR, Evanson KW, Lyons H, Akosman I,
Barrett A, Hardy N, et al. Ecacy of antiviral therapies
for COVID-19: a systematic review of randomized
controlled trials. BMC Infect Dis 22 (2022): 107.
21. Okoli GN, Rabbani R, Al-Juboori A, Copstein L, Askin
N, Abou-Setta AM. Antiviral drugs for coronavirus
disease 2019 (COVID-19): a systematic review with
network meta-analysis. Expert Rev Anti Infect Ther 20
(2022): 267-278.
22. Kow CS, Ramachandram DS, Hasan SS. The use of
neutralizing monoclonal antibodies and risk of hospital
admission and mortality in patients with COVID-19:
a systematic review and meta-analysis of randomized
trials. Immunopharmacol Immunotoxicol 44 (2022): 28-34.
23. Berlin DA, Gulick RM, Martinez FJ. Severe Covid-19. N
Engl J Med 383 (2020): 2451-2460.
24. Marconi, F. Gestire la pandemia: linee guida e
assistenza domiciliare al vaglio della giurisprudenza
amministrativa. Il Diritto Amministrativo - Rivista
Giuridica anno XIV, Luglio (2022). https://www.
ildirittoamministrativo.it/Gestire-la-pandemia-linee-
guida-e-assistenza-domiciliare-al-vaglio-della-
giurisprudenza-amministrativa-Marconi/stu846.
25. Rezza, GU A. Circolare recante "Gestione domiciliare dei
pazienti con infezione da SARS-CoV-2" aggiornata al 26
aprile 2021. Direzioni Generali della Programmazione
Sanitaria e della Prevenzione Sanitaria, ed., Ministero
della Salute Roma (2021).
26. Rezza GU, Urbani A. Circolare recante “Gestione
domiciliare dei pazienti con infezione da SARS-CoV-2”
aggiornamento del 10 febbraio 2022. Direzioni Generali
della Programmazione Sanitaria e della Prevenzione
Sanitaria, ed., Ministero della Salute, Roma (2022).
27. Cordon-Cardo C, Pujadas E, Wajnberg A, Sebra R, Patel
G, Firpo-Betancourt, A, et al. COVID-19: Staging of a
New Disease. Cancer Cell 38 (2020): 594-597.
28. Turk C, Turk S, Malkan UY, Haznedaroglu IC. Three
critical clinicobiological phases of the human SARS-
associated coronavirus infections. Eur Rev Med
Pharmacol Sci 24 (2020): 8606-8620.
29. Alexander PE, Armstrong R, Fareed G, Lotus J, Oskoui R,
Prodromos C, et al. Early multidrug treatment of SARS-
CoV-2 infection (COVID-19) and reduced mortality
among nursing home (or outpatient/ambulatory)
residents. Med Hypotheses 153 (2021): 110622.
30. McCullough PA, Alexander PE, Armstrong R, Arvinte C,

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 112
Bain AF, Bartlett RP, et al. Multifaceted highly targeted
sequential multidrug treatment of early ambulatory
high-risk SARS-CoV-2 infection (COVID-19). Rev
Cardiovasc Med 21 (2020): 517-530.
31. Ravichandran R, Mohan SK, Sukumaran SK Kamaraj D,
Daivasuga SS, Ravi S, et al. An open label randomized
clinical trial of Indomethacin for mild and moderate
hospitalised Covid-19 patients. Sci Rep 12 (2022): 6413.
32. Shekhar N, Kaur H, Sarma P, Prakash A, Medhi
B. Indomethacin: an exploratory study of antiviral
mechanism and host-pathogen interaction in COVID-19.
Expert Rev Anti Infect Ther (2022): 20(3):383-390.
33. Desantis J, Mercorelli B, Celegato M, Croci F, Bazzacco
A, Baroni M et al. Indomethacin-based PROTACs as
pan-coronavirus antiviral agents. Eur J Med Chem 226
(2021): 113814.
34. Fazio S, Auso F, Bellavite P. A Review of the
Potential Roles of Antioxidant and Anti-Inammatory
Pharmacological Approaches for the Management of
Mild-to-Moderate Symptomatic COVID-19. Med Sci
Monit 28 (2022): e936292.
35. Sestili P, Fimognari C. Paracetamol-Induced Glutathione
Consumption: Is There a Link With Severe COVID-19
Illness? Front Pharmacol 11 (2020): 579944.
36. Rushworth GF, Megson IL. Existing and potential
therapeutic uses for N-acetylcysteine: the need for
conversion to intracellular glutathione for antioxidant
benets. Pharmacol Ther 141 (2014): 150-159.
37. De Flora S, Balansky R, La MS. Rationale for the use of
N-acetylcysteine in both prevention and adjuvant therapy
of COVID-19. FASEB J 34 (2020): 13185-13193.
38. Bellavite P. Reappraisal of Dietary Phytochemicals
for Coronavirus Infection: Focus on Hesperidin and
Quercetin in Antioxidants (Waisundara, VY, ed) (2021)
473-487. DOI: 10.5772/intechopen.95529.
39. Zhang X, Wu X, Hu Q, Wu J, Wang G, Hong Z, et al.
Mitochondrial DNA in liver inammation and oxidative
stress. Life Sci 236 (2019): 116464.
40. Bhargava A, Raghuram GV, Pathak N, Varshney S,
Jatawa SK, Jain D, et al. Occult hepatitis C virus elicits
mitochondrial oxidative stress in lymphocytes and
triggers PI3-kinase-mediated DNA damage response.
Free Radic Biol Med 51 (2011): 1806-1814.
41. Kido H, Indalao IL, Kim H, Kimoto T, Sakai S, Takahashi
E. Energy metabolic disorder is a major risk factor in
severe inuenza virus infection: Proposals for new
therapeutic options based on animal model experiments.
Respir Investig 54 (2016): 312-319.
42. Saleh J, Peyssonnaux C, Singh KK, Edeas M.
Mitochondria and microbiota dysfunction in COVID-19
pathogenesis. Mitochondrion 54 (2020): 1-7.
43. Suhail S, Zajac J, Fossum C, Lowater H, McCracken C,
Severson N, et al. Role of Oxidative Stress on SARS-
CoV (SARS) and SARS-CoV-2 (COVID-19) Infection:
A Review. Protein J (2020): 39(6):644-656.
44. Keles ES. Mild SARS-CoV-2 infections in children
might be based on evolutionary biology and linked with
host reactive oxidative stress and antioxidant capabilities.
New Microbes New Infect 36 (2020): 100723.
45. Delgado-Roche L, Mesta F. Oxidative Stress as
Key Player in Severe Acute Respiratory Syndrome
Coronavirus (SARS-CoV) Infection. Arch Med Res 51
(2020): 384-387.
46. Trujillo JA, Croft NP, Dudek NL, Channappanavar
R, Theodossis A, Webb AI, et al. The cellular redox
environment alters antigen presentation. J Biol Chem
289 (2014): 27979-27991.
47. Hati S, Bhattacharyya S. Impact of Thiol-Disulde
Balance on the Binding of Covid-19 Spike Protein with
Angiotensin-Converting Enzyme 2 Receptor. ACS
Omega 5 (2020): 16292-16298.
48. Dalan R, Bornstein SR, El-Armouche A, Rodionov RN,
Markov A, Wielockx B, et al. The ACE-2 in COVID-19:
Foe or Friend? Horm Metab Res 52 (2020): 257-263.
49. Roberts E, Delgado Nunes V, Buckner S, Latchem
S, Constanti M, Miller P, et al. Paracetamol: not as
safe as we thought? A systematic literature review of
observational studies. Ann Rheum Dis 75 (2016): 552-9.
50. Yadav DK, Singh A, Zhang Q, Bai X, Zhang W, Yadav
RK, et al. Involvement of liver in COVID-19: systematic
review and meta-analysis. Gut 70 (2021): 807-809.
51. Marin-Duenas I, Vega J, Carrillo-Ng H, Veramendi-
Schult I, Zavaleta-Alva R, Vasquez-Elera L, et al.
Alteration in liver function tests among patients
hospitalized for COVID-19: a multicentric study in Peru.
Rev Gastroenterol Peru 41 (2021): 86-93.
52. Santus P, Corsico A, Solidoro P, Braido F, Di MF,
Scichilone N. Oxidative stress and respiratory
system: pharmacological and clinical reappraisal of
N-acetylcysteine. COPD 11 (2014): 705-717.
53. De FS, Grassi C, Carati L. Attenuation of inuenza-like
symptomatology and improvement of cell-mediated
immunity with long-term N-acetylcysteine treatment.
Eur Respir J 10 (1997): 1535-1541.
54. Soltan-Shari MS, Mojtahedzadeh M, Naja A, Reza
KM, Reza RM, Moradi M, et al. Improvement by

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 113
N-acetylcysteine of acute respiratory distress syndrome
through increasing intracellular glutathione, and
extracellular thiol molecules and anti-oxidant power:
evidence for underlying toxicological mechanisms. Hum
Exp Toxicol 26 (2007): 697-703.
55. Poe FL, Corn J. N-Acetylcysteine: A potential therapeutic
agent for SARS-CoV-2. Med Hypotheses 143 (2020):
109862.
56. Andreou A, Trantza S, Filippou D, Sipsas N, Tsiodras
S. COVID-19: The Potential Role of Copper and
N-acetylcysteine (NAC) in a Combination of Candidate
Antiviral Treatments Against SARS-CoV-2. In Vivo 34
(2020): 1567-1588.
57. Zhou N, Yang X, Huang A, Chen Z. The potential
mechanism of N-acetylcysteine in treating COVID-19.
Curr Pharm Biotechnol (2020).
58. Luo P, Liu Y, Liu D, Li J. Perspectives for the use of
N-acetylcysteine as a candidate drug to treat COVID-19.
Mini Rev Med Chem (2020) 10.2174/138955752066620
1027160833 [doi].
59. Ibrahim H, Perl A, Smith D, Lewis T, Kon Z, Goldenberg
R, et al. Therapeutic blockade of inammation in severe
COVID-19 infection with intravenous N-acetylcysteine.
Clin Immunol 219 (2020): 108544.
60. Shi Z, Puyo, CA. N-Acetylcysteine to Combat
COVID-19: An Evidence Review. Ther Clin Risk Manag
16 (2020): 1047-1055.
61. de Alencar JCG, Moreira CL, Müller, AD, Chaves
CE, Fukuhara MA, da Silva EA, et al. Double-
blind, randomized, placebo-controlled trial with
N-acetylcysteine for treatment of severe acute respiratory
syndrome caused by COVID-19. Clin Infect Dis (2020):
5910353.
62. Carothers C, Birrer K, Vo M. Acetylcysteine for
the Treatment of Suspected Remdesivir-Associated
Acute Liver Failure in COVID-19: A Case Series.
Pharmacotherapy 40 (2020): 1166-1171.
63. Sackett DL, Rosenberg WM, Gray JA, Haynes RB,
Richardson WS. Evidence based medicine: what it is and
what it isn't. BMJ 312 (1996): 71-2.
64. Allegri PMM A, Gulisano P, Burigana F, Ortolani
R, Donzelli A, Valsecchi M, et al. La gestione dei
pazienti COVID-19 in ambito domiciliare. Indirizzi
operativi proposti dal gruppo di lavoro promosso da
Luca Coletto, Capo Dipartimento Sanità Lega-Salvini
premier in Documento depositato al Senato (Bagnai,
LCaA, ed), Atti parlamentari Roma (2021). https://www.
sanitainformazione.it/wp-content/uploads/2021/04/
Terapia-domicliare-Covid.pdf.
65. Ravichandran R PP, Vijayaragavan S, Kalavakollu
RT, Gaidhane S, Kumar RK. Ecacy and safety of
indomethacin in COVID-19 patients. MedRxiv (2020).
https://www.medrxiv.org/content/10.1101/2020.12.14.2
0245266v1
66. Zhou Q, Zhao S, Gan L, Wang Z, Peng S, Li Q, et al. Use
of non-steroidal anti-inammatory drugs and adverse
outcomes during the COVID-19 pandemic: A systematic
review and meta-analysis. EClinicalMedicine 46 (2022):
101373.
67. Bellavite P, Donzelli A. Hesperidin and SARS-CoV-2:
New Light on the Healthy Function of Citrus Fruits.
Antioxidants (Basel) 9 (2020). 10.3390/antiox9080742
[doi].
68. Ricordi C, Pacici F, Lanzoni G, Palamara AT, Garaci
E, Della-Morte D. Dietary and Protective Factors to Halt
or Mitigate Progression of Autoimmunity, COVID-19
and Its Associated Metabolic Diseases. Int J Mol Sci 22
(2021).
69. Rizzuti, B; Grande, F; Conforti, F; Jimenez-Alesanco,
A; Ceballos-Laita, L; Ortega-Alarcon, D, et al. Rutin
Is a Low Micromolar Inhibitor of SARS-CoV-2 Main
Protease 3CLpro: Implications for Drug Design of
Quercetin Analogs. Biomedicines 9 (2021).
70. Colunga Biancatelli RML, Berrill M, Catravas JD,
Marik PE. Quercetin and Vitamin C: An Experimental,
Synergistic Therapy for the Prevention and Treatment
of SARS-CoV-2 Related Disease (COVID-19). Front
Immunol 11 (2020): 1451.
71. El-Missiry MA, El-Missiry ZM, Othman AI. Melatonin
is a potential adjuvant to improve clinical outcomes in
individuals with obesity and diabetes with coexistence of
Covid-19. Eur J Pharmacol 882 (2020): 173329.
72. Rondanelli M, Perna S, Gasparri C, Petrangolini G,
Allegrini P, Cavioni A, et al. Promising Eects of 3-Month
Period of Quercetin Phytosome((R)) Supplementation
in the Prevention of Symptomatic COVID-19 Disease
in Healthcare Workers: A Pilot Study. Life (Basel) 12
(2022).
73. Pawar A, Russo M, Rani I, Goswami K, Russo GL, Pal A.
A critical evaluation of risk to reward ratio of quercetin
supplementation for COVID-19 and associated comorbid
conditions. Phytother Res (2022): 36(6):2394-2415.
74. Shohan M, Nashibi R, Mahmoudian-Sani MR,
Abolnezhadian F, Ghafourian M, Alavi SM, et al. The
therapeutic ecacy of quercetin in combination with
antiviral drugs in hospitalized COVID-19 patients: A
randomized controlled trial. Eur J Pharmacol 914 (2022):
174615.

Serano Fazio et al., J Pharm Pharmacol Res 2022
DOI:10.26502/fjppr.055
Citation: Serano Fazio, Marco Cosentino, Franca Marino, Sergio Pandol, Elisabetta Zanolin, Paolo Bellavite. The Problem of Home Therapy during
COVID-19 Pandemic in Italy: Government Guidelines versus Freedom of Cure?. Journal of Pharmacy and Pharmacology Research 6 (2022):
100-114.
Volume 6 • Issue 3 114
75. Di Pierro F, Iqtadar S, Khan A, Ullah Mumtaz S, Masud
Chaudhry M, Bertuccioli A, et al. Potential Clinical
Benets of Quercetin in the Early Stage of COVID-19:
Results of a Second, Pilot, Randomized, Controlled and
Open-Label Clinical Trial. Int J Gen Med 14 (2021):
2807-2816.
76. Di Pierro F, Derosa G, Maoli P, Bertuccioli A,
Togni S, Riva A, et al. Possible Therapeutic Eects of
Adjuvant Quercetin Supplementation Against Early-
Stage COVID-19 Infection: A Prospective, Randomized,
Controlled, and Open-Label Study. Int J Gen Med 14
(2021): 2359-2366.
