REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 1
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
MEDICAL INFORMATION
According to Connecticut State Law, all students born after January 1, 1957, and entering an institution of higher education MUST SHOW proof of having received
immunizations for Measles, Mumps, Rubella (German Measles) and Varicella (Chicken Pox). For your own safety and that of your classmates, you will not be
permitted to register for classes or access your residence hall until the University’s Health Services Oce receives proof of immunity for its records.
•
Necessary Insurance and HIPAA Information: ALL STUDENTS
You must provide a copy of your private insurance company card, including company name, company phone number, and your identification number.
All students are required to have private or university sponsored health insurance.
You must provide a copy of your driver’s license, passport, or other photo identification to be included in your patient chart.
If you are a minor, PLEASE SEE PAGE 8 for additional documents to be completed prior to treatment at the health center.
•
A physical exam within one year prior to start of classes: ALL STUDENTS
Complete Physical Exam Form (To be completed by a medical professional)
University of New Haven Varsity Student Athletes
Please note: According to NCAA guidelines, physicals for varsity student-athletes may not be dated more than six (6) months prior to becoming
eligible for practice or competition. We recommend that varsity student-athletes have a physical dated April 1 or later.
•
Required Immunization: ALL STUDENTS
MMR vaccine (Measles, Mumps, Rubella) — two doses required or blood test to prove immunity (attach results) required. Vaccines given before
the first birthday are not valid. MMRV is also acceptable.
Varicella (Chicken Pox) — two doses required or proof of history of disease, or blood test to prove immunity (attach results) required.
MMRV is also acceptable.
TB Screening- Must be completed by all students — If applicable, a TB skin test result must also be submitted (Part 2 of TB screening form).
Meningitis vaccine (MCV4 Sero Groups A,C,Y and W135) — Only for students living on University-sponsored housing – non commuters and
varsity athletes — Proof of vaccine within five (5) years of enrollment required of all students residing in University-sponsored housing and all
University of New Haven athletes, whether living on or o campus.
If you have received the required vaccines, please submit proof of immunity, i.e., records from school, parents’ records, or copies of lab results of blood
tests (for Rubella, Mumps, Rubeola, and Varicella titers), along with the completed physical form.
If you have not been immunized, we suggest you contact your family physician as soon as possible or have vaccines administered at a local pharmacy if
applicable.
HOW DO I SUBMIT FORMS? What is the Process?
•
All health documents for incoming students must be submitted electronically via the site listed below. Upload your records as soon as possible to
ensure you are cleared to start the semester
•
Login to Medicat (https://ynhh.medicatconnect.com) with your University username and follow the instructions listed there.
•
University of New Haven will eliminate holds on your Banner account after documents are successfully reviewed and completed. All records must
be manually reviewed, and individuals should allow at least two (2) business days from submission for this review to occur. If University sta have
questions or need you to submit additional info, you will be contacted via your University email.
QUESTIONS? Contact the Health Services Oce at 203.932.7079
REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 2
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
HEALTH EXAMINATION REPORT
It is mandatory that all students entering the University of New Haven have a completed Health Examination Report on file, thus enabling the Health Services sta to
render optimum health care when needed.
In the past several years, outbreaks of vaccine-preventable diseases on college campuses throughout the United States have resulted in many lost school days, severe
complications from the diseases, anxieties for students and their parents, and large expenditures of monies to contain these outbreaks. Compliance by each student with the
pre-entrance immunization policy at the University of New Haven protects the student and the general college community.
All students are required to complete the health examination report prior to the beginning of classes in the initial term of enrollment.
Name Last First Middle Initial Student ID #
/ / ( )
Birth Date (MM/DD/YYYY) Age Birth Place Home Phone Cell Phone
Sex Assigned at Birth: Gender Identity: Pronouns: Chosen Name:
Permanent Home Address Street Local O Campus Address or Residence Hall Street
City State Zip City State Zip
If a University of New Haven varsity athlete (or planning to be), name of sport
Parent/Guardian full name#1 Parent/Guardian full name#2
Address Street Address Street
City State Zip City State Zip
Guardian/Spouse Full Name Guardian/Spouse Full Name
IN CASE OF EMERGENCY NOTIFY (Please Print)
Full name Relationship
Address
Work Place Home Phone Cell Phone
IN THE EVENT OF SERIOUS ILLNESS OR INJURY, PARENTS OR GUARDIAN WILL BE NOTIFIED AT THE DISCRETION OF THE PROFESSIONAL STAFF.
Signature(s) Required: I certify that to the best of my knowledge that the information on this form is complete and correct.
/ /
Signature of the Student Date (Month/Day/Year)
Entering term: Fall 20 Spring 20
Summer 20 (grad students only)
Degree Program:
Status: Resident
Commuter
Undergraduate
Graduate
Part-time
Full-time
Transfer
Military Veteran
High School Program
REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 3
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
HEALTH CARE PROVIDER (Please print or use stamp)
Print Clinician’s Name Last First Phone Number Fax Number
Address Street City State Zip
Clinician’s Signature and Title
Medication Allergies:
Food Allergies:
Medications (list those currently taking):
Medical Problems:
Past Surgeries:
Health History (to be completed by a clinician)
NAME:
Date of Birth (MM/DD/YYYY):
REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 4
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
Medical Examination: Required within one year prior to admission
TO THE CLINICIAN: Please review the student’s history and complete the Medical Examination Form. The information will be used only as a background
for providing health care and will not be released without student consent.
Examination Date:
Wt. Ht. BP P Vision: Without glasses With Glasses
Right 20/
Left 20/
Status of student’s physical restrictions:
Unrestricted Restricted Full Restriction Partial Restriction
Comment:
Status of student’s health: Excellent Good Poor Comment:
Okay for practice and play of sports: Yes No
Additional Comments:
SYSTEM NORMAL DESCRIBE IF ABNORMAL
Skin
Ears
Nose, throat, teeth, gingival
Neck, thyroid
Chest, breasts
Lungs
Heart (describe murmur, click, etc.)
Abdomen, liver, spleen, kidneys
Hernia
Genitalia
Pelvic (if indicated)
Rectal, Pilonidal
Extremities, back, spine
Lymphatic
Neurological
Psychological
NAME:
Date of Birth (MM/DD/YYYY):
HEALTH CARE PROVIDER (Please print or use stamp)
Print Clinician’s Name Last First Phone Number Fax Number
Address Street City State Zip
Clinician’s Signature and Title
REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 5
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
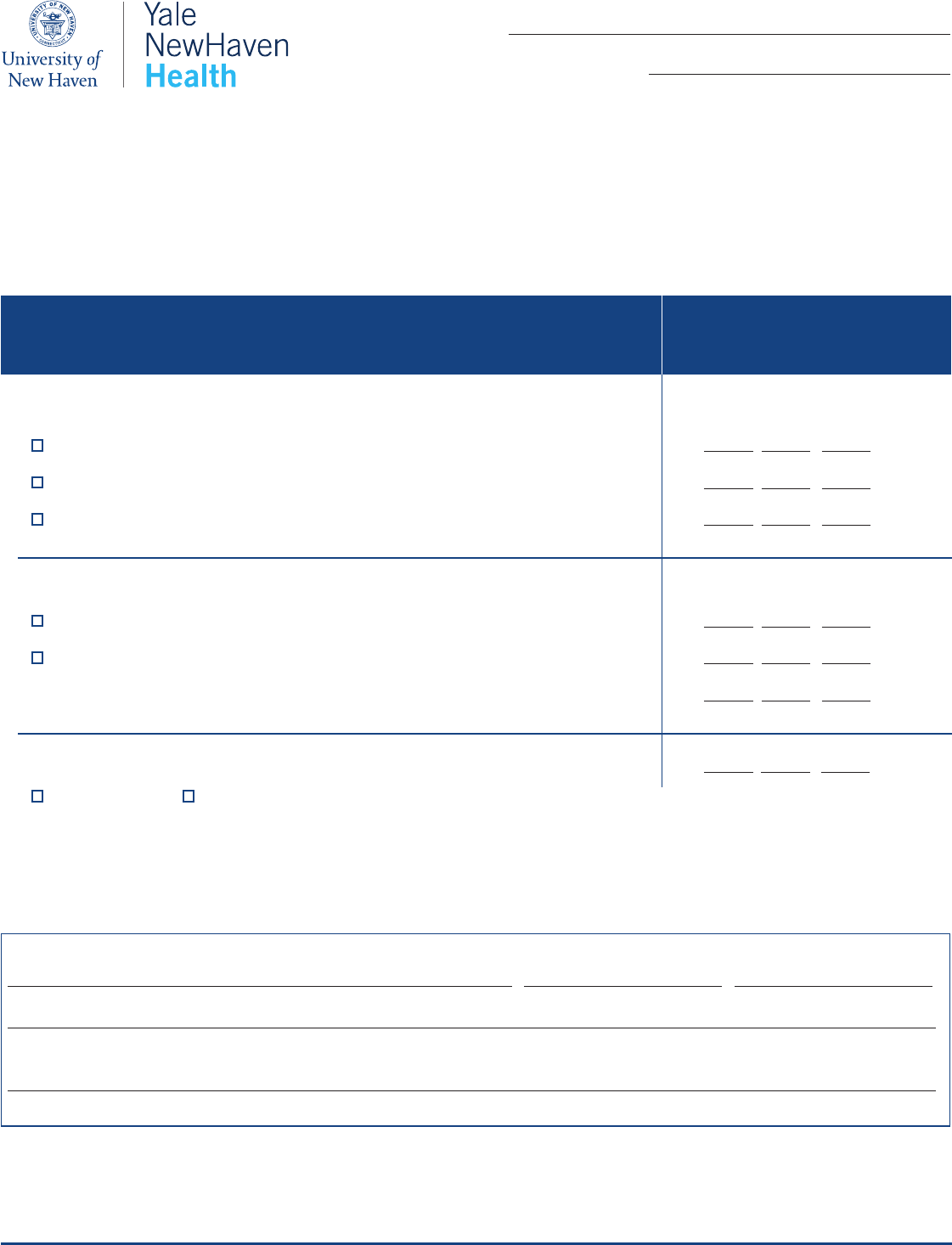
TO BE COMPLETED AND SIGNED BY A HEALTH CARE PROVIDER. (Dates must include month and year.)
PLEASE ATTACH COPIES OF LAB RESULTS IF SUBMITTING TITIERS.
Date of Illness or Dates of Doses
MM/DD/YYYY
IMMUNIZATION RECORD
Immunity is REQUIRED prior to registration.
An ocial printed copy from your physician will be accepted in place of filling out the immunization form.
MMR MEASLES, MUMPS, RUBELLA
Dose 1 – Immunized on or after 12 months of age / /
Dose 2 – Immunized on or after 1/1/1980 (CT State Law) / /
Has report of immune Titer, specify date of Titer (attach copy) / /
VARICELLA CHICKEN POX
History of Disease - from physician oce or Titer proof of immunity (send lab copy) / /
Vaccination: Two doses required / / (Dose #1)
/ / (Dose #2)
MENINGITIS VACCINATION MCV4 SERO GROUPS A, C, Y AND W135 / /
Menactra Other/Document Name
NAME:
Date of Birth (MM/DD/YYYY):
HEALTH CARE PROVIDER (Please print or use stamp)
Print Clinician’s Name Last First Phone Number Fax Number
Address Street City State Zip
Clinician’s Signature and Title
REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 6
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
NAME:
Date of Birth (MM/DD/YYYY):
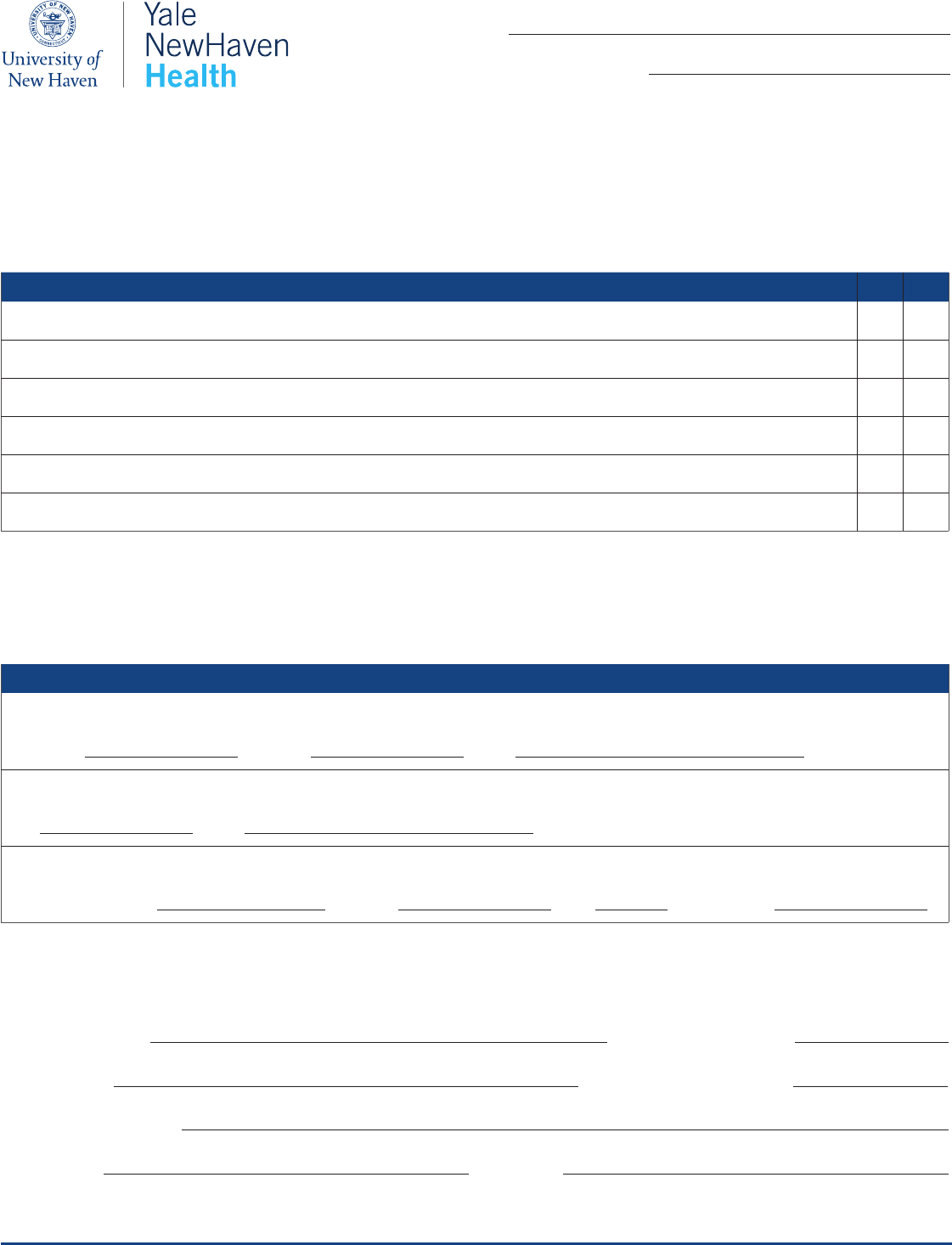
Tuberculosis Screening Questions YES NO
Have you ever had close contact with persons known or suspected to have active TB disease?
Were you born or lived in another country besides the United States, Canada, Australia, New Zealand, or Western/Northern Europe for more than 1 month?
Have you been a resident and/or employee of high-risk congregate settings (e.g., correctional facilities, long-term care facilities, and/or homeless shelters)?
Have you been a volunteer or health-care worker who served clients who are at increased risk for active TB disease?
Are you currently on or plan to be on any type of immunosuppressive medication?
Have you ever had a positive TB skin test or blood test in the past?
Tuberculosis Test Requirements
TB Skin Test (Mantoux Skin Test)
Date Planted:
/ /
Date Read:
/ /
Result: mm of induration
TB Blood Test (QuantiFERON TB Gold)
Date:
/ /
Result: (Please attach copy of results)
Chest X-Ray results if skin test or blood test is positive (please attach copies of results)
TB Treatment: Medication:
Start Date:
/ /
Dose: Completion Date:
/ /
Please complete all information below:
Patient/Student Name: Date of Birth (MM/DD/YYYY):
/ /
Provider’s Name: Assessment Date (MM/DD/YYYY):
/ /
Provider’s Signature/ Stamp
Phone Number: FAX Number:
If you answered YES to any of the above questions, a TB test will need to be performed within 12 months of enrollment at the University of New Haven.
University of New Haven Tuberculosis (TB) Screening Questionnaire
REQUIRED FOR ALL STUDENTS
Part 1: To be completed by the student. Please answer the following questions:
Part 2: To be completed by the health care provider.
REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 7
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
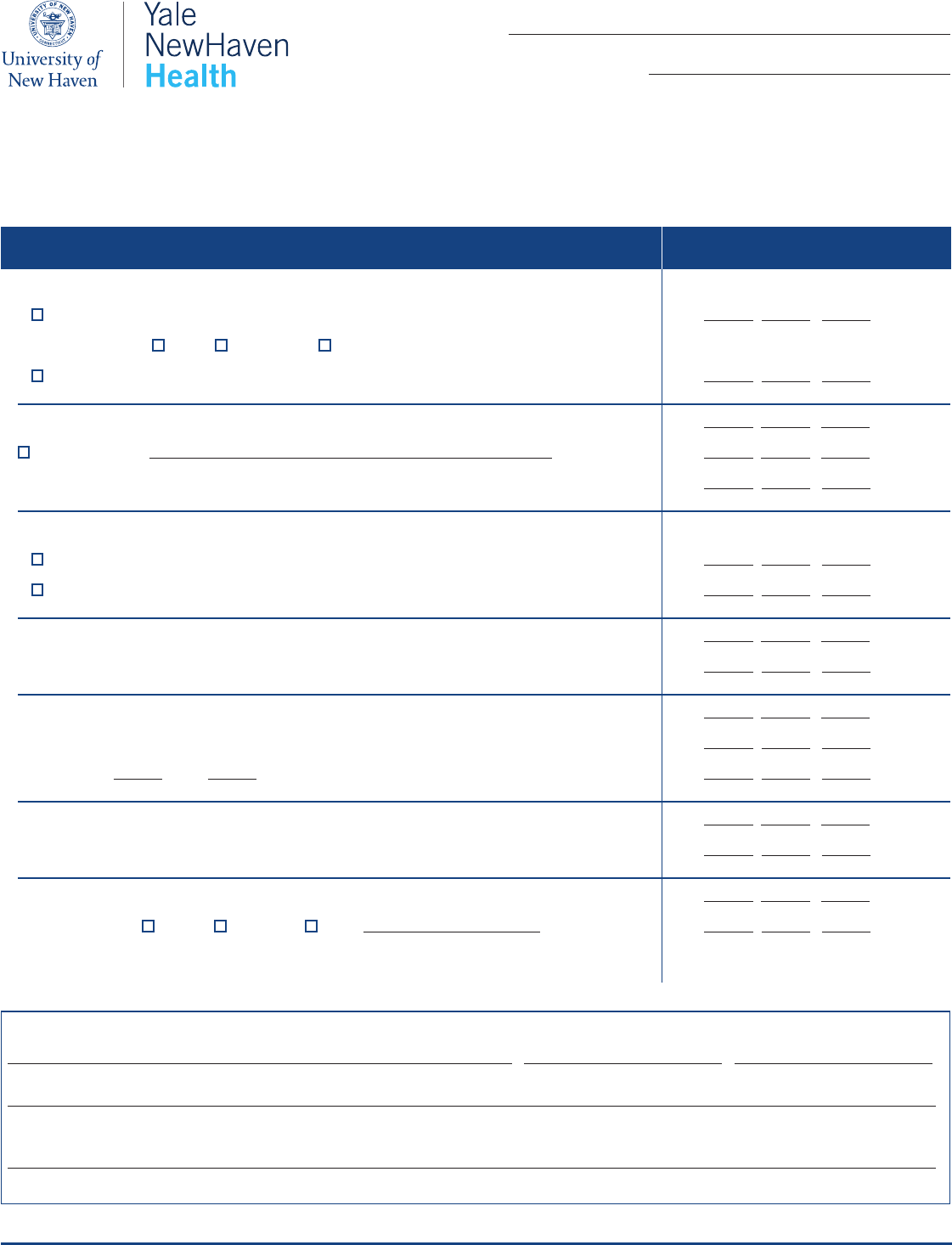
Date of Illness or Dates of Doses
MM/DD/YYYY
Recommended Vaccines
Proof of immunity is not required prior to registration
POLIO
Completed primary series of Polio immunizations / /
Type of vaccine: Oral Inactivated E-IPV
Last Booster Date / /
MENINGITIS/SERO GROUP B VACCINE / / (Dose #1)
Note vaccine name: / / (Dose #2)
/ / (Dose #3)
TETANUSDIPHTHERIA
Completed primary series of immunizations / /
Td or Tdap booster recommended within the last 10 years / /
HEPATITIS A 2 DOSES / / (Dose #1)
/ / (Dose #2)
HEPATITIS B 3 DOSES / / (Dose #1)
Hepatitis B surface antibody (quantitative titer) result _______ / / (Dose #2)
Date: Month: / Year: / / (Dose #3)
GARDASIL VACCINE HPV VACCINE / / (Dose #1)
/ / (Dose #2)
COVID VACCINE STRONGLY RECOMMENDED / / (Dose #1)
Type of vaccine: Pfizer Moderna Other: / / (Dose #2)
NAME:
Date of Birth (MM/DD/YYYY):
HEALTH CARE PROVIDER (Please print or use stamp)
Print Clinician’s Name Last First Phone Number Fax Number
Address Street City State Zip
Clinician’s Signature and Title

REV. 8/23 | Produced by the Oce of Marketing & Communications
PAGE 8
HEALTH SERVICES OFFICE
•
300 Boston Post Road
•
West Haven, CT 06516
•
OFFICE: 203.932.7079
•
FAX: 203.937.4099
•
newhaven.edu
If you are less than 18 years of age, you parent or guardian will need to complete two additional forms before treatment can occur at the Yale New Haven
Health Nicholson Student Health Center.
The documents can be obtained on the health services website at newhaven.edu/healthservices under “Health Services Requirements and Forms.”
Please ensure the following are included with your parent or guardian’s signature:
1.
Patient Financial Responsibility Notice
2.
Notice of Privacy Practices
QUESTIONS? Contact the Health Services Oce at 203.932.7079
Additional Information for Minors ONLY (under 18 years of age):
