ABSTRACT
February 2001, Vol. 91, No. 2270 American Journal of Public Health
Jac J. L. van der Klink, MD, MSc, Roland W. B. Blonk, PhD,
Aart H. Schene, PhD, MD, and Frank J. H. van Dijk, PhD, MD
Jac J.L. van der Klink, Roland W.B. Blonk, and Frank
J. H. van Dijk are with Coronel Institute, Academic
Medical Center, University of Amsterdam, Amster-
dam, the Netherlands. Jac J. L. van der Klink is also
with the Foundation for Quality in Occupational
Health, Amsterdam, the Netherlands; Roland W.B.
Blonk is also with TNO Work and Employment,
Hoofddorp, the Netherlands. Aart H. Schene is with
the Department of Psychiatry, Academic Medical
Center, University of Amsterdam.
Requests for reprints should be sent to Jac J. L.
van der Klink, MD, MSc, Coronel Institute, Acade-
mic Medical Center, University of Amsterdam, PO
Box 22660, 1100 DD Amsterdam, the Netherlands
(e-mail: [email protected]).
This article was accepted May 12, 2000.
Objectives. This quantitative meta-
analysis sought to determine the effec-
tiveness of occupational stress–reducing
interventions and the populations for which
such interventions are most beneficial.
Methods. Forty-eight experimental
studies (n = 3736) were included in the
analysis. Four intervention types were
distinguished: cognitive–behavioral in-
terventions, relaxation techniques, mul-
timodal programs, and organization-
focused interventions.
Results. A small but significant
overall effect was found. A moderate ef-
fect was found for cognitive–behavioral
interventions and multimodal interven-
tions, and a small effect was found for
relaxation techniques. The effect size for
organization-focused interventions was
nonsignificant. Effects were most pro-
nounced on the following outcome cate-
gories: complaints, psychologic resources
and responses, and perceived quality of
work life.
Conclusions. Stress management
interventions are effective. Cognitive–
behavioral interventions are more effec-
tive than the other intervention types. (Am
J Public Health. 2001;91:270–276)
The efficacy and cost-effectiveness of in-
terventions designed for patients with emo-
tional difficulties is a relevant topic in general
practice.
1
Such considerations also apply in oc-
cupational health care. With the increases in
workloads of the past decades, the number of
employees experiencing psychologic problems
related to occupational stress has increased rap-
idly in Western countries.
2
At the societal level,
costs are considerable in terms of absenteeism,
loss of productivity, and health care consump-
tion. In Britain, it is estimated that 40 million
workdays are lost to the nation’s economy
owing to mental and emotional problems.
3
At
the individual level, there are costs in terms of
high rates of tension, anger, anxiety, depressed
mood, mental fatigue, and sleep disturbances.
These problems, usually referred to in aggre-
gate as distress, are often classified as neuras-
thenia, adjustment disorders, or burnout. Inci-
dence rates in the Netherlands vary from 14 to
50 cases per year per 1000 patients.
4
Interventions designed to reduce occu-
pational stress can be categorized according
to focus, content, method, and duration. In re-
gard to focus, interventions can be categorized
as (1) aiming to increase individual psycho-
logic resources and responses (e.g., coping) or
(2) aiming to change the occupational context.
The first category of intervention is usually
referred to as stress management training.
However, stress management is the common
denominator of an assortment of interventions
ranging from relaxation methods
5
to cognitive–
behavioral interventions
6,7
and client-centered
therapy.
8
The second category refers to inter-
ventions such as organizational development
9,10
and job redesign.
11
We distinguished 4 intervention types ac-
cording to categorizations used in previous re-
views
12–14
: cognitive–behavioral approaches,
relaxation techniques, multimodal interven-
tions, and organization-focused interventions.
Cognitive–behavioral approaches aim at chang-
ing cognitions and subsequently reinforcing
active coping skills.
6,7
Relaxation techniques
focus on physical or mental relaxation as a
method to cope with the consequences of stress.
Multimodal interventions emphasize the ac-
quisition of both passive and active coping
skills. The fourth intervention type involves a
focus on the organization as a whole.
Several reviews have been conducted of
interventions designed to reduce occupational
stress.
2,5,12,14–16
The general finding of these re-
views is that such interventions are effective.
However, the reviews have been qualitative in
nature and thus provide limited information on
which type of intervention is most effective
and for whom. Recently, Bamberg and Busch
conducted the first meta-analysis on occupa-
tional stress–reducing interventions.
17
How-
ever, they included only cognitive–behavioral
interventions in their quantitative analyses.
In the present quantitative review, the fol-
lowing research questions were posed: (1) Are
stress interventions effective, as suggested by
qualitative reviews of the literature? (2) If so,
which type of stress intervention is most effec-
tive, and on which outcome measures? In ad-
dition to these research questions, exploratory
analyses were conducted to determine what
moderator variables (e.g., job characteristics,
preventive/remedial nature of interventions,
length of treatment) were related to the effec-
tiveness of the interventions.
The Benefits of Interventions for
Work-Related Stress

February 2001, Vol. 91, No. 2 American Journal of Public Health 271
Methods
Search and Inclusion Criteria
Two strategies were used to locate appro-
priate studies. First, 4 databases—Medline
(1966–1996), ClinPsych (1980–1996), Cur-
rent Contents (1997), and Nioshtic (1970–
1996)—were used to conduct a computerized
search. Three groups of terms were composed
for this search: (1) terms linked to stress-re-
lated psychologic problems (psychologic stress,
work stress, job stress, neurasthenia, burnout,
minor psychiatric problems, mental fatigue,
minor depression, neurosis, distress, nervous
breakdown, and adjustment disorder), (2) terms
related to the intervention (therapy, treatment,
protocol, program, intervention, primary care,
prevention, and employee assistance program),
and (3) terms related to the population (em-
ployee, occupational, vocational, rehabilita-
tion, work, job, absenteeism, and sickness
leave).
Within each group of terms, searches were
added. Subsequently, these searches were com-
bined. Second, a manual search of relevant re-
views, book chapters, and articles was con-
ducted, with the objective of finding relevant
references missed in the computerized search.
To be included in our database, a study
had to meet several criteria. First, the inter-
vention was required to be specifically designed
to prevent or reduce psychologic complaints
related to occupational stress. Second, in terms
of the target population, participants had to be
recruited from the working population because
of imminent or already-manifested stress-
related psychologic problems not diagnosed
as involving a major psychiatric disorder (e.g.,
depression or posttraumatic stress disorder) or
a stress-related somatic disorder (e.g., hyper-
tension, coronary heart disease). Third, an ex-
perimental or quasi-experimental design in-
volving a no-treatment control group had to
be used. Within the quasi-experimental studies,
we required that the experimental group and
the control group be recruited from identical
populations and have identical baseline values
on dependent variables. In this high-quality
group of primary studies, we applied no rank-
ing for methodological quality aspects because
the consequent choice of a weighting factor in
the quantitative analyses would introduce an
element of subjectivity. Fourth, outcome vari-
ables had to be well defined and of sufficient
reliability. Finally, we required that the study be
published as a journal article in English.
Definitions
The variables used in the meta-analysis
included intervention-related variables, out-
come variables, and population characteristics.
Intervention-related variables were (1) type of
intervention, (2) total number of hours, (3) num-
ber of weeks, and (4) number of sessions. The
latter 3 variables could be considered indexes
of the intensity and extent of the intervention.
Because they were relevant in assessing the
cost-effectiveness and practical applicability
of a program, we used these variables as mod-
erators in the exploratory analyses.
As described earlier, 4 intervention types
were included; 3 involved a focus on individ-
uals and 1 involved a focus on the organiza-
tion. In several reviews, a third focus has been
discerned: the interaction between the indi-
vidual and the organization.
14,18
Thus far, how-
ever, intervention studies conducted with this
focus have been uncontrolled.
19
The outcome variables included were
placed into 5 categories: (1) quality of work
life, including such aspects as job demands,
work pressure, job control, working conditions,
and social support from management and col-
leagues; (2) psychologic resources and re-
sponses, including measures of self-esteem,
mastery, beliefs, and coping skills
20
; (3) phys-
iology, including measures such as tension,
electromyographic activity, (nor)adrenaline,
and cholesterol level; (4) complaints, including
stress or burnout rates or symptoms, somatic
symptoms, and mental health status and symp-
toms (because of their significance in general
health practice, depressive symptoms and anx-
iety symptoms were considered as separate
subcategories); and (5) absenteeism.
A number of population characteristics,
such as sex, age, years of employment, occu-
pational status, and baseline stress level, may
be important moderators of treatment effects
and thus may provide information on which
types of interventions are effective and for
whom. However, for most of these character-
istics, the specific information required was
not available in the studies; the exceptions were
baseline stress level and occupational status.
The predictive influence of these characteris-
tics on treatment effects was investigated in a
number of exploratory analyses.
In line with Newman and Beehr
12
and
with Murphy,
2
2 baseline stress level categories
were distinguished, preventive and remedial.
In the present meta-analysis, a study was con-
sidered preventive if no participant selection
had taken place in regard to stress levels. A
study was considered remedial if participants
were selected by means of a criterion.
As noted by Karasek and Theorell, occu-
pational status may be indicative of level of job
control.
20
On the basis of Karasek and Theo-
rell’s ratings, we categorized study samples as
“high control” or “low control.” Two studies
involving samples with mixed occupations
were classified as low control because most of
the participants in these studies had low-control
jobs
.21,22
Two studies were excluded from these
exploratory analyses because of a lack of suf-
ficient information.
23,24
Statistical Analysis
The Advanced BASIC Meta-Analysis
program
25
was used in conducting statistical
analyses. In this program, several statistics
(e.g., F, t, r, and P) can be entered, and a
product–moment correlation is obtained. These
effect size correlations are transformed to
Fisher z scores. Subsequently, mean Fisher z
scores are calculated and transformed back to
effect size (r) values.
If F or t values were reported, we used
these values; if such values were not reported,
they were computed if the required informa-
tion was available. If this computation was not
possible, P values were used; effects reported
as nonsignificant were rated as P=0.5.
26
A problem in meta-analyses is that stud-
ies with a relatively large number of outcome
measures disproportionately affect the meta-
analytic results. To counteract this problem,
Rosenthal and Rubin
27
proposed a method of
computing a mean effect size in which the in-
tercorrelation of outcome measures is taken
into account.
25(pp45–47)
For all analyses, outcome
variables were combined according to this
method. We used all outcome measures re-
ported in a study in calculating effect sizes.
We report effect sizes in Cohen’s d, which
can be derived directly from r values. Cohen’s d
represents the standardized mean difference
between the intervention group mean and the
control group mean. Thus, a d value of 1 indi-
cates that the intervention group performed 1
standard deviation above the control group on
a particular outcome variable.
Results
Description of Studies
Forty-eight studies
10,21–24,28–67
conducted
between 1977 and 1996 met the inclusion crite-
ria; findings from these studies were published
in 45 different articles. None of the 48 studies
had a curative orientation in the usual sense (i.e.,
target population consisting of people seeking
help). Four studies were considered remedial,
because there was selection in regard to baseline
stress level. Forty-one studies involved employ-
ees with jobs categorized as high in job control.
Five studies evaluated an organization-
focused intervention, 18 evaluated a cognitive–
behavioral intervention, 17 evaluated a relax-
ation technique, and 8 evaluated a multimodal
approach. In all studies, several outcome analy-
ses were conducted. The result was 99
intervention–outcome combinations.
February 2001, Vol. 91, No. 2272 American Journal of Public Health
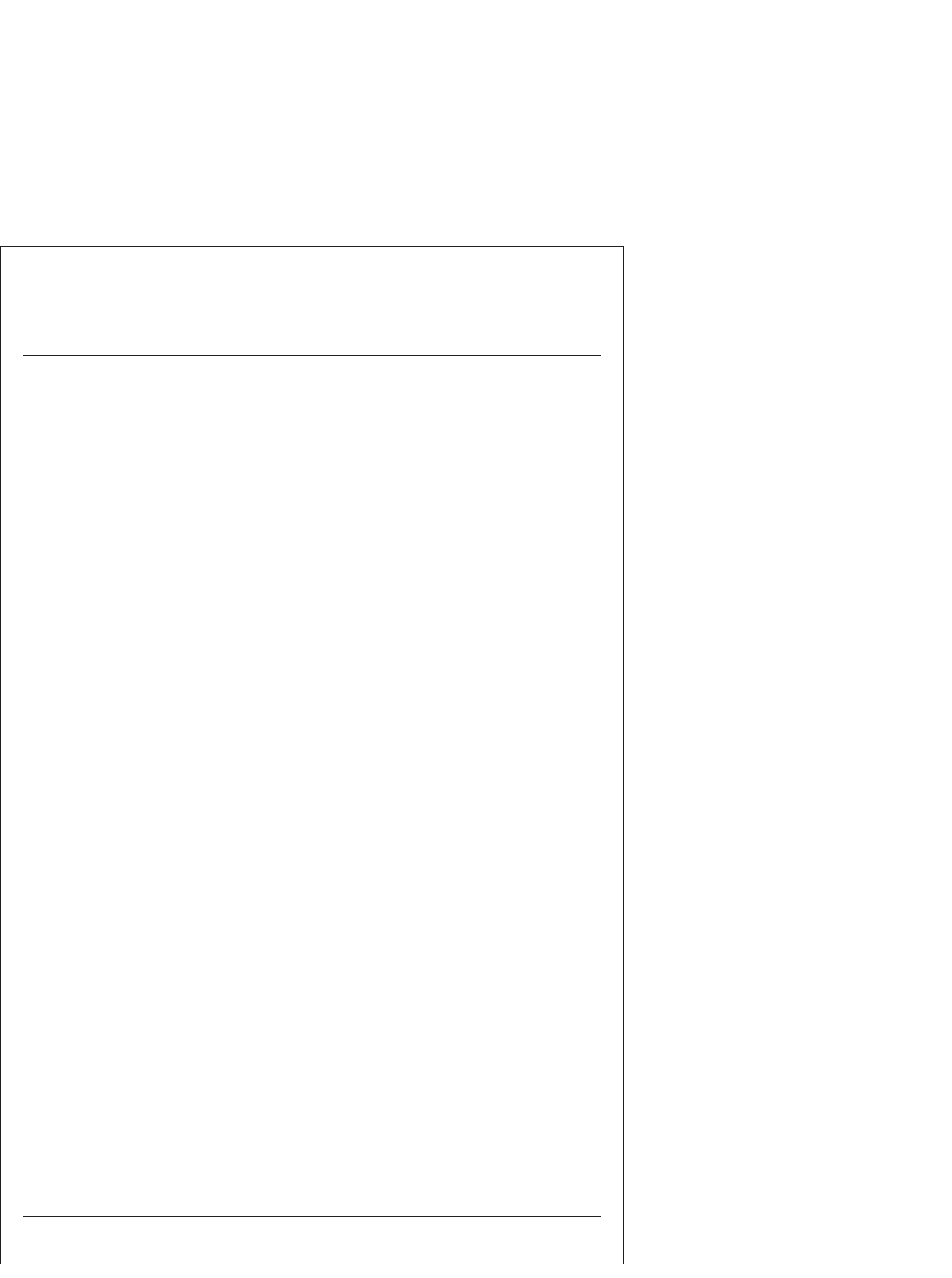
TABLE 1—Effect Sizes per Study Expressed in Cohen’s d and 95% Confidence
Intervals: Meta-Analysis of Occupational Stress-Reducing
Interventions, 1977–1996
Category d 95% Confidence Interval
Organizational
Heaney et al. (1995) 0.06 –0.11, 0.23
Jackson (1983) 0.12 –0.43, 0.67
Jones et al. (1988) 0.5* 0.01, 0.99
Landsbergis & Vivona-Vaughan (1995, 1) –0.2 –0.86, 0.46
Landsbergis & Vivona-Vaughan (1995, 2) –0.04 –0.7, 0.62
Cognitive–behavioral
Bruning & Frew (1986) 0.1 –0.6, 0.8
Cecil & Forman (1990) 0.58 –0.08, 1.24
Curtis (1992) 1.98* 1.32, 2.64
Fava et al. (1991) 1.09* 0.4, 1.78
Forman (1981) 1.62* 0.49, 2.75
Freedy & Hobfoll (1994) 0.26 –0.17, 0.69
Gray-Toft (1980) 0.8 –0.23, 1.83
Grønningsæter et al. (1992) 0.0 –0.55, 0.55
Higgins (1986) 0.39 –0.28, 1.16
Keyes & Dean (1988) 0.87* 0.48, 1.3
Kushnir & Malkinson (1993) 0.41 –0.29, 1.11
Kushnir et al. (1994) 1.43* 0.91, 1.95
Lee & Swanson Crockett (1994) 0.8* 0.26, 1.34
Long (1988) 0.26 –0.22, 0.74
McCue & Sachs (1991) 0.41 –0.12, 0.94
Sharp & Forman (1985) 0.98* 0.42, 1.54
von Baeyer & Krause (1983) 2.2* 0.82, 3.58
West et al. (1984) 0.28 –0.35, 0.91
Relaxation
Aderman & Tecklenburg (1983) 0.72* 0.04, 1.4
Alexander et al. (1993) 0.54* 0.0, 1.08
Arnetz (1996) 0.04 –0.4, 0.48
Bruning & Frew (1986) 0.35 –0.36, 1.06
Carrington et al. (1980) 0.47* 0.07, 0.87
Fiedler et al. (1989) 0.35 –0.17, 0.87
Higgins (1986) 0.3 –0.36, 0.96
Murphy (1983) 0.32 –0.48, 1.12
Murphy (1984) 0.1 –0.74, 0.94
Peters et al. (1977; 2 studies) 0.3 –0.12, 0.72
Toivanen et al. (1993, 1a) 0.28 –0.29, 0.85
Toivanen et al. (1993, 2) 0.45 –0.12, 1.02
Toivanen et al. (1993, 1b) 0.32 –0.25, 0.89
Tsai & Swanson Crockett (1993) 0.43* 0.09, 0.77
Tunnecliff et al. (1986) 0.0 –1.05, 1.05
Vaughn et al. (1989) 1.71* 0.63, 2.79
Vines (1994) 0.0 –0.5, 0.5
Multimodal
Bertoch et al. (1989) 1.15* 0.35, 1.95
Friedman et al. (1983) 0.7* 0.24, 1.16
Ganster et al. (1982) 0.28 –0.23, 0.75
Johanson (1991) 0.82* 0.35, 1.29
Larsson et al. (1990) 0.24 –0.19, 0.67
McNulty et al. (1984) 0.45 –0.15, 1.05
Norvell et al. (1987) 0.26 –0.88, 1.4
Pruitt (1992) 0.37 –0.13, 0.87
*P < .05.
Twenty of the studies involved a follow-
up assessment. In most cases, follow-up was ei-
ther uncontrolled or reported in a way that al-
lowed no retrieval of statistical metrics.
Therefore, only the first postintervention as-
sessment was included in the meta-analysis.
The mean interval between preintervention and
postintervention assessment was 9 weeks for
interventions that focused on individuals (SD=
6 weeks). This deviation was merely due to dif-
ferences in intervention duration. Differences
in interval between intervention types were not
significant. The interval for organization-
focused programs was considerably longer (38
weeks) owing to longer program durations and
longer postintervention assessment intervals.
Pretest-to-posttest dropout rates varied from
0% to 40%. The mean dropout rate for pro-
grams that focused on individuals was 11%;
differences between intervention types were
nonsignificant. Organization-focused programs
had a mean dropout rate of 26%.
Effect Sizes
Effect sizes were calculated as described in
the Methods section.A combined analysis of ef-
fect sizes yielded a significant effect size across
all studies (d= 0.34, 95% confidence interval
[CI]=0.27, 0.41).According to Cohen’s criteria
68
(small effect: d<0.5; medium effect: 0.5<d<0.8;
large effect: d>0.8), however, this effect size was
small. Examination of the data indicated that 17
studies yielded a significant overall effect size,
all in the expected (positive) direction. Of these
17 studies, 2 (both focusing on relaxation tech-
niques) revealed a small effect, 4 (1 organization
focused, 2 relaxation, and 1 multimodal) revealed
a medium effect, and 11 (8 cognitive–behavioral,
1 relaxation, and 2 multimodal) revealed a large
effect. In the 31 remaining studies, overall effects
were nonsignificant; effect sizes for these stud-
ies were small and negative (d≤ –0.2; 1 study),
nonrelevant (–0.2<d≤0.2; 9 studies), small (0.2<
d≤0.5; 19 studies), and medium (0.5<d≤0.8; 2
studies). It should be noted that these 31 studies
yielded many specific outcomes that were sig-
nificant. Table 1 shows effect sizes and confi-
dence intervals for the 48 studies.
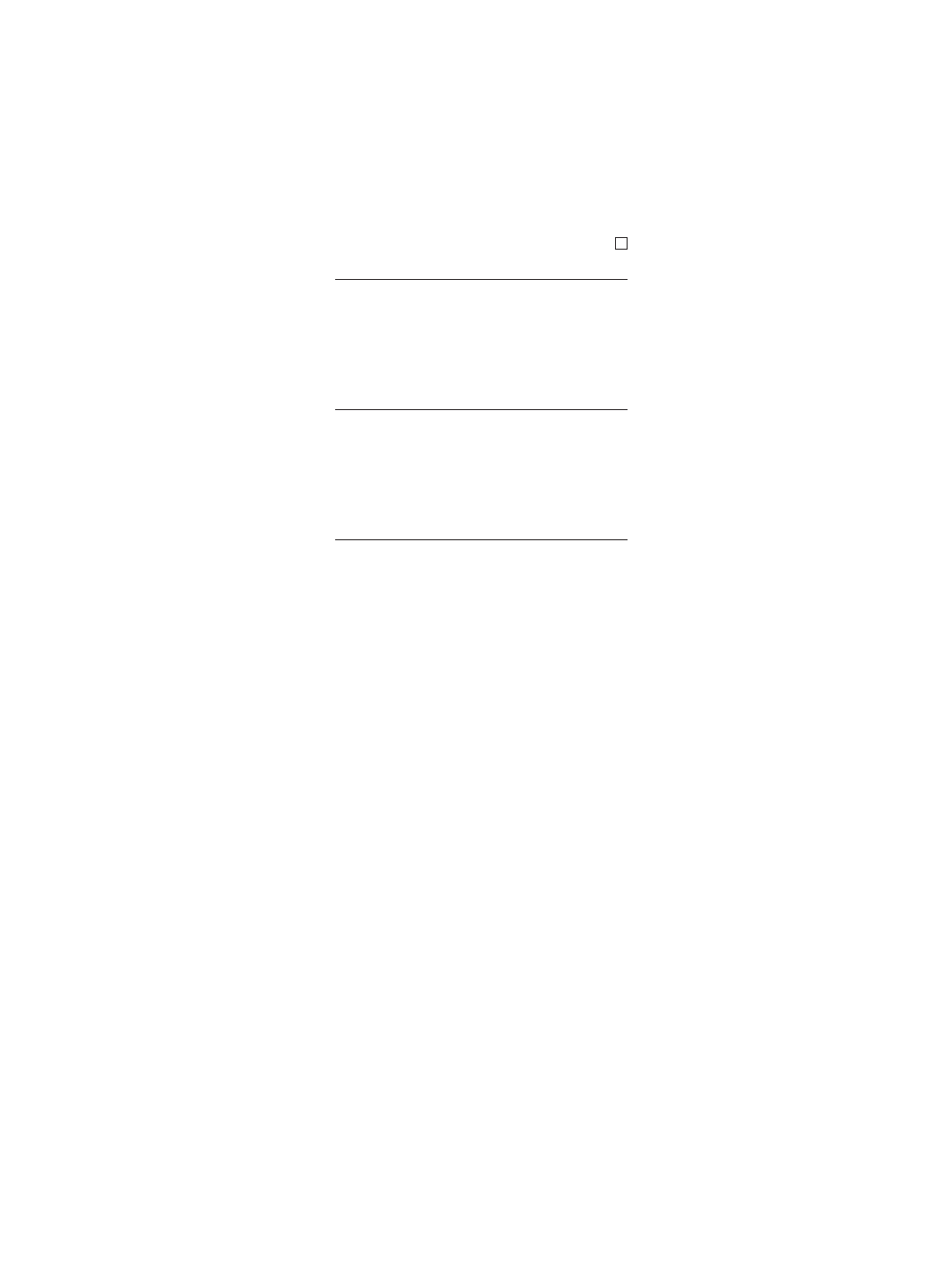
Type of Intervention
Effect sizes were calculated for the 4 dif-
ferent types of interventions. These effect sizes
are shown in Table 2.
The combination of the effect sizes for
interventions that focused on individuals
yielded a significant Cohen’s d of 0.44 (95%
CI=0.36, 0.52; heterogeneous effect). The ef-
fect size difference between interventions fo-
cusing on individuals (combined as well as
separate) and those focusing on the organiza-
tion was significant (P < .05). Furthermore,
cognitive–behavioral interventions were sig-
nificantly more effective than relaxation tech-
niques (P< .005); the difference in effect be-
tween cognitive–behavioral and multimodal
interventions was marginally significant (P=
.06). There were no significant effect size dif-
ferences between relaxation and multimodal
interventions. Cognitive–behavioral interven-
tions yielded heterogeneous effects, indicating
divergent levels of effectiveness among these
studies.
Outcome Variables
Effect sizes were calculated for the 5 out-
come categories across intervention types. As
noted earlier, organization-focused interven-
tions were less effective than interventions fo-
cusing on individuals. Outcome studies on or-
ganizational interventions usually involve
February 2001, Vol. 91, No. 2 American Journal of Public Health 273
TABLE 2—Cohen’s d and Confidence Intervals for the 4 Intervention
Categories: Meta-Analysis of Occupational Stress–Reducing
Interventions, 1977–1996
No. of No. of 95% Confidence
Category Studies Participants d Interval
Organizational 5 1463 0.08 –0.03, 0.19
Cognitive–behavioral 18 858 0.68* 0.54, 0.82
Relaxation 17 982 0.35* 0.22, 0.48
Multimodal 8 470 0.51* 0.33, 0.69
*P < .05.
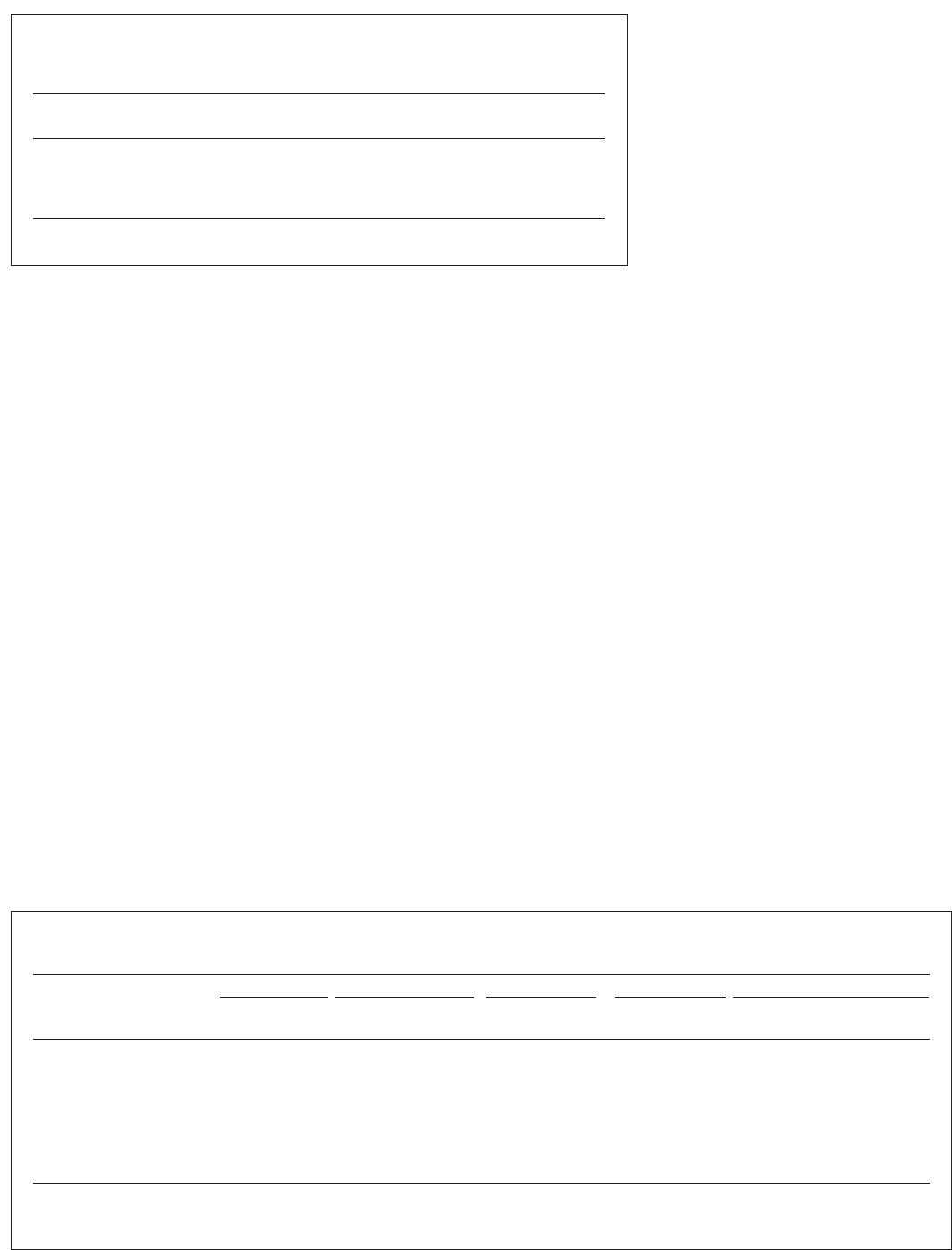
TABLE 3—Effect Sizes, by Intervention, Expressed in Cohen’s d and Weighted for Sample Size: Meta-Analysis of
Occupational Stress-Reducing Interventions, 1977–1996
Organizational Cognitive–Behavioral Relaxation Multimodal Individual Focus (Summation)
No. of No. of No. of No. of No. of No. of
Outcome d Studies d Studies d Studies d Studies d Studies Participants
Quality of work 0.05 4 0.48*** 7 0.29** 8 0.59** 2
a
0.41*** 17 708
Psychologic responses
and resources 0.14** 1 0.65*** 10
a
0.26* 5 0.22 1 0.48*** 16
a
915
Physiology . . . 0 0.11 2 0.31*** 10 0.36* 3 0.30*** 15 808
Complaints 0.05 4 0.52*** 14
a
0.31*** 14 0.48*** 6 0.42*** 34
a
1923
Anxiety symptoms ... 0 0.70*** 7 0.25* 7 0.50*** 4 0.54*** 18 871
Depressive symptoms 0 1 0.23 2 0.11 2 0.59*** 2 0.33** 6 392
Absenteeism 0 1 –0.18 1 –0.09 2 . . . 0 –0.12 3 121
a
Heterogeneous effect.
*P < .05; **P < .01; ***P < .001.
significantly larger sample sizes than studies on
individual interventions. As a consequence, ef-
fect sizes for outcome categories may be dis-
proportionately affected by the small effect
sizes found within organization-focused inter-
ventions. Therefore, we analyzed separately
the effect sizes for outcome variables across
all intervention types and across interventions
focusing on individuals only. Across all inter-
vention types, the effect sizes found for the
outcome categories quality of work, psycho-
logic responses and resources, physiology, com-
plaints, and absenteeism were 0.17, 0.28, 0.30,
0.27, and –0.03, respectively. The correspon-
ding effect sizes for interventions focusing on
individuals were 0.41, 0.48, 0.30, 0.42, and
–0.12. With the exception of absenteeism, all
effect sizes were significant at P< .05.
Interactions Between Intervention Types
and Outcome Variables
Table 3 presents results by outcome cat-
egory and intervention type. The overall picture
that emerges from Table 3 is that interventions
involving a cognitive–behavioral approach ap-
pear to be the preferred means of reducing em-
ployees’stress-related complaints. However, it
should be noted that the results were hetero-
geneous for 2 outcome categories, indicating
divergent effects. With regard to psychophys-
iologic outcomes, interventions in which re-
laxation was part of the program appeared to
be most effective. The effect of organization-
focused interventions was small and non-
significant, except for the psychologic re-
sponses and resources category.
Psychophysiologic measures were used
as outcomes only in studies evaluating inter-
ventions that focused on individuals. Relax-
ation techniques and multimodal interventions
appeared to be effective in reducing psy-
chophysiologic stress measures. Absenteeism
was measured in 4 studies; neither the cogni-
tive approach nor relaxation training appeared
to be successful in regard to this outcome vari-
able. Noteworthy is that 1 study included med-
ical malpractice as an outcome variable. The
results of this study, in which an organization-
focused intervention was conducted in hospi-
tals, indicated a significant postintervention
decrease in medical practice failures (d=0.50,
P< .05).
46
Exploratory Analyses
An examination of intervention-related
characteristics (number of weeks, number of
contact hours, number of sessions) across the
4 intervention types revealed no significant
predictive influence of these characteristics on
the overall effect size. Separate analyses for
the intervention types revealed that for
cognitive–behavioral interventions, there was
an inverse correlation between number of ses-
sions and effect size (r=–0.27, P< .05). This
indicates that shorter programs were more ef-
fective. Furthermore, organization-focused pro-
grams were significantly longer than cognitive–
behavioral programs (16.4 vs 6.8 weeks; P<
.05, 2-tailed).
The differential effects of preventive vs re-
medial programs and high vs low job control
both appeared to be marginally significant (P<
.10). Larger effect sizes were found for remedial
programs (n =4, d= 0.59, P<.10) than for pre-
ventive programs (n = 44, d = 0.32, P< .001).
Stress-reducing interventions revealed the largest
effect sizes among employees with high-control
jobs. This latter finding can, however, be attrib-
uted to the fact that all but 1 cognitive–behavioral
intervention and all multimodal interventions
concerned employees with such jobs.
Only relaxation techniques were used with
employees in both types of jobs (low or high in
job control); effect sizes were not significantly
different. For high-control employees, cognitive–
behavioral interventions (n=17, d=0.69, P<.001)
were significantly more effective (P<.001) than
relaxation techniques (n =9, d=0.30, P<.001);
the difference in effect between cognitive–
behavioral and multimodal interventions (n=8,
d=0.51, P<.001) was also significant (P<.05).
The difference between relaxation and multi-
modal interventions was marginally significant
(P<.10). The single cognitive–behavioral study
involving a population with jobs classified as low
in job control did not yield a significant result.
48
Discussion
In the present study, we quantitatively
evaluated the effects of interventions designed

February 2001, Vol. 91, No. 2274 American Journal of Public Health
to reduce occupational stress. Forty-eight stud-
ies met our inclusion criteria of an appropri-
ate design and reliable measures. This is a rel-
atively large number of studies with
methodological rigor, considering the lack of
such studies in the early days of stress inter-
vention research.
5,12
However, despite the con-
siderable increase in methodologically sound
studies in this field, there is a relative lack of
studies with clinically referred employees. Fur-
thermore, the few methodologically rigorous
studies that have been conducted with patients
have not included no-treatment control groups
but have compared 2 treatment types (e.g., Firth
and Shapiro
69
); as a result, these studies could
not be included in our meta-analysis.
Most studies were conducted with vol-
unteer samples rather than clinically referred
samples. Research with clinically referred sam-
ples in settings where treatment is ordinarily
provided is needed to test the generalizability
of the results found in this meta-analysis. Pre-
liminary support was found in the present meta-
analysis: interventions conducted with em-
ployees at high levels of baseline stress
appeared to be at least as effective as inter-
ventions conducted with employees at low lev-
els of baseline stress. However, only 4 studies
involved participant selection in regard to high
baseline stress levels. Furthermore, develop-
ment of treatments that meet the needs of clin-
ically referred employees may generate new
hypotheses and procedures that address clini-
cal exigencies more fully and effectively.
In concordance with earlier qualitative re-
views, the present meta-analysis provides reli-
able evidence that employees benefit from
stress-reducing interventions. Although small
according to Cohen’s criteria,
68
a significant
effect size was found across 48 studies repre-
senting 3736 participants.
In the present study, 4 different types of
stress-reducing interventions were distin-
guished. Three types were considered as fo-
cusing on individuals, and 1 was considered as
focusing on the organization. The analyses
clearly demonstrated that the former were more
effective than the latter. We conclude that an in-
tervention that focuses on individual employees
is the first choice in the case of employees with
stress-related complaints. The rather surpris-
ing lack of a significant effect for organizational
interventions is elaborated on subsequently.
A comparison between interventions that
focused on individuals revealed that cognitive–
behavioral approaches are more effective than
relaxation techniques and tend to be more ef-
fective than multimodal programs. The effect
size found for the cognitive–behavioral inter-
ventions was comparable to those reported in
2 recent meta-analyses on the effectiveness of
such interventions
17
and the effectiveness of
stress inoculation training, a specific form of
cognitive–behavioral intervention.
70
This sup-
ports the robustness of the present finding.
The effectiveness of cognitive–behavioral
interventions has also been shown in compar-
ative treatment outcome studies conducted in
psychotherapeutic settings (e.g., Firth and
Shapiro
69
). This may indicate that interventions
conducted by general practitioners or occupa-
tional physicians or referred by them to psy-
chologists or psychotherapists should be
cognitive–behavioral in nature. However, a het-
erogeneous effect was found for cognitive–
behavioral interventions, which implies that
some interventions were very effective and oth-
ers were not. Future research should be directed
at predictors of treatment effects. Furthermore,
a cautionary note is necessary here because
differential effects in regard to outcome vari-
ables were found for the different interventions
that focused on individuals.
With respect to outcome variables,
cognitive–behavioral interventions appeared to
be effective in improving perceived quality of
work life, enhancing psychologic resources and
responses, and reducing complaints. Multimodal
programs showed similar effects; however, they
appeared to be ineffective in increasing psycho-
logic resources and responses. In terms of psy-
chophysiologic outcomes, relaxation techniques
(whether pure or embedded in a multimodal pro-
gram) appeared to be effective. However, the ef-
fectiveness of cognitive–behavioral programs in
the area of psychophysiologic outcomes was ex-
amined only in 2 studies that yielded no posi-
tive outcomes. The finding that different inter-
ventions resulted in different levels of
effectiveness for specific outcomes indicates that
choice of intervention for a particular individ-
ual or group may be determined by the outcome
sought.
In contrast to the consensus among re-
searchers on the content of interventions, there
was considerable diversity in the outcome vari-
ables used.As a result, some of our outcome cat-
egories were broadly defined.As noted earlier, the
robustness of our findings was supported by com-
parisons with findings from 2 more restricted
meta-analyses, and the pattern of results was con-
firmed as well when we narrowed our outcomes
(to anxiety and depression symptoms). In 18 stud-
ies, anxiety was an outcome variable. In 8 stud-
ies, the State-Trait Anxiety Inventory was used.
There were no differences in effect sizes or sig-
nificance levels between analysis with this in-
strument and those using other anxiety measures.
Regarding cognitive–behavioral inter-
ventions, we found an inverse relation between
number of sessions and effect size. Effect size
plotted against number of sessions showed no
optimum number. The mean number of ses-
sions for the 9 cognitive–behavioral interven-
tion studies with large effect sizes was 6.8; the
mean number of sessions for all cognitive–
behavioral interventions was 7.6. The inverse
relationship found cannot be attributed to a
planned relationship between number of ses-
sions and severity of symptoms. All programs
had a fixed number of sessions, and, because
there were only 2 cognitive–behavioral stud-
ies involving participant selection on baseline
values (both with 8 sessions), there was no
planned relationship at the program level. This
result is in accordance with the finding of Bar-
kum and Shapiro
71
concerning the effective-
ness of brief therapeutic interventions.
Another interesting issue is that of the
marginally significant effect of occupational
status on treatment outcome. Occupational sta-
tus may be indicative of level of job control.
13
Stress-reducing interventions appeared to be
effective for populations at high levels of job
control, in contrast to populations at low lev-
els. Although caution should be exercised here
because level of job control is inferred from
occupational status, and job control can ap-
parently vary extensively within a particular
type of occupational status, elaboration of this
effect may generate new hypotheses.
The difference between employees with
high job control and those with low job control
may be attributed to the fact that all cognitive–
behavioral and multimodal interventions in-
volved the former group. Because cognitive–
behavioral interventions produced the largest
effects, the effect found for occupational status
may be confounded. However, the relatively
large effect size found for cognitive–behavioral
interventions with employees with high job
control may also be explained by the fact that
employees profit most when they are provided
with individual coping skills in a job that allows
them to exercise those skills. If so, these inter-
ventions may be less effective for employees
working in a constrained environment. Unfor-
tunately, this hypothesis could not be tested,
because only 1 study was conducted in which
the effect of a cognitive–behavioral intervention
was investigated with employees with low job
control.
The idea that, in addition to the pattern of
symptoms, the type of work patients do is in-
dicative of the type of intervention that should
be used is in line with the recommendations of
Kahn and Byosiere
72
and, more recently, Kom-
pier et al.
73
In stress reduction programs, the
type of intervention used should be based on
systematic identification of stress risk factors
and risk groups. Without such a systematic risk
assessment, there will be no optimal fit between
intervention and individual, which may result in
the absence of an effect. However, this hypoth-
esis needs to be addressed in future research.
Surprisingly, no effect was found for
organization-focused interventions. This lack
of effect is remarkable in that successes have
been reported in (uncontrolled) evaluations of
February 2001, Vol. 91, No. 2 American Journal of Public Health 275
organization-focused interventions.
73
A num-
ber of factors may explain this lack of effect.
First, with the exception of absenteeism,
all outcomes were assessed at an individual
level. The primary outcomes of organizational
interventions involve aspects of the workplace.
Thus, individual-level outcomes with this kind
of intervention depend on an intermediate ef-
fect. Therefore, it may take time to produce
measurable effects at the individual level.
Second, organization-focused interven-
tions lack an individually tailored focus. Many
organization-focused programs aim at en-
hancing job control. However, individual per-
ception and coping skills are necessary if one
is to use this extra control and make it prof-
itable. Support for this hypothesis may be found
in the Jones et al.
46
study. Of the organization-
focused interventions included in our sample,
only that study incorporated training in per-
ception and coping skills at an individual level.
Contrary to the other organizational studies,
that study yielded a significant effect. Although
such research on the effectiveness of combined
interventions was recommended years ago by
Murphy,
16
this area clearly remains an issue
for future research.
The preceding considerations are in op-
position to the broadly shared vision that there
is a hierarchy of interventions in which pri-
mary prevention should prevail over interven-
tions that focus on individuals in efforts to re-
duce work-related stress.
5,12,50,74
In jobs that
already involve a high degree of decision lati-
tude, cognitive–behavioral interventions seem
to be most effective. These interventions, in
such an environment, can influence individual
variations in perception and use of coping
skills. In jobs with a low degree of decision
latitude, organization-focused interventions
aimed at increasing control potentials should
prevail, accompanied by cognitive–behavioral
interventions. If this strategy is not possible,
interventions that focus on enhancing passive
coping (relaxation techniques) have a moder-
ate but proven effect.
The present study aimed at investigating
the evidence concerning the effectiveness of
stress-reducing interventions. As noted earlier,
support was found for the benefits of such pro-
grams. However, a number of intriguing issues
remain to be addressed in future research.
Among these issues are the evaluation of oc-
cupational stress interventions with patients
treated by occupational physicians or general
practitioners and the development and con-
trolled evaluation of interventions involving a
combined individual and organizational focus.
Research on predictors of treatment effects
(e.g., job control) will be important in terms
of enhancing effects and processes of change.
Insight into the conditions under which an in-
tervention is most effective may enhance the
development of more effective intervention
strategies. We also recommend that a controlled
follow-up of at least 12 weeks be part of the
design of intervention studies.
Finally, we noted considerable diversity
in the outcome variables used, apparently rooted
in conceptual ambiguity about the core dimen-
sions of stress outcomes. Research on the core
dimensions of stress outcomes, which will lead
to more consensus about outcomes and instru-
ments used, is indispensable for the further de-
velopment and evaluation of interventions.
Contributors
All of the authors participated in planning the study,
in interpreting the analysis outcomes, and in writing
the paper. J. J. L. van der Klink and R.W.B. Blonk con-
ducted the analyses.
Acknowledgments
This study was supported in part by grants from the
Occupational Health Service of Royal PTT Neder-
land (KPN) and the Netherlands Organisation of Sci-
entific Research (NWO).
References
1. Friedli K, King MB, Lloyd M, Horner J. Ran-
domised controlled assessment of non-directive
psychotherapy versus routine general-practi-
tioner care. Lancet. 1997;350:1662–1665.
2. Murphy LR. Stress management in working set-
tings: a critical review of the health effects. Am
J Health Promotion. 1996;11:112–135.
3. Cartwright S, Cooper CL. Managing Workplace
Stress. London, England: Sage Publications;
1997.
4. Terluin B. Nervous Breakdown Substantiated:
A Study of the General Practitioner’s Diagno-
sis of Surmenage [in Dutch] [thesis]. Zeist, the
Netherlands: Kerckebosch; 1994.
5. Murphy LR. Occupational stress management:
a review and appraisal. J Occup Psychol. 1984;
57:1–15.
6. Roskies E. Stress Management for the Healthy
Type A: Theory and Practice. New York, NY:
Guilford Press; 1987.
7. Meichenbaum DH, Cameron R. Stress inocula-
tion training. In: Meichenbaum DH, Jarenko
ME, eds. Stress Reduction and Prevention. New
York, NY: Plenum Press; 1983:115–154.
8. Cooper CL, Sadri G. The impact of stress coun-
seling at work. In: Crandall R, Perrewé PL, eds.
Occupational Stress: A Handbook. Washington,
DC: Taylor & Francis; 1995:273–282.
9. Golembiewski RT, Hilles R, Daly R. Some ef-
fects of multiple OD interventions on burnout
and work site features. J Appl Behav Sci. 1987;
23:295–313.
10. Heaney CA, Price RH, Rafferty J. Increasing
coping resources at work: a field experiment to
increase social support, improve work team
functioning, and enhance employee mental
health. J Organ Behav. 1995;16:335–352.
11. Schurman SJ, Israel BA. Redesigning work sys-
tems to reduce stress: a participatory action re-
search approach to creating change. In: Murphy
LR, Hurrell JJ Jr, Sauter SL, Keita GP, eds. Job
Stress Interventions. Washington, DC: Ameri-
can Psychological Association; 1995:235–261.
12. Newman JE, Beehr TA. Personal and organiza-
tional strategies for handling job stress: a review
of research and opinion. Personnel Psychol.
1979;32:1–43.
13. DeFrank RS, Cooper CL. Worksite stress man-
agement interventions: their effectiveness and
conceptualisation. J Manage Psychol. 1987;2:
4–10.
14. Ivancevich JM, Matteson MT, Freedman SM,
Phillips JS. Worksite stress management inter-
ventions. Am Psychol. 1990;45:252–261.
15. McLeroy KR, Green LW, Mullen KD, Foshee V.
Assessing the effects of health promotion in
worksites. Health Educ Q. 1984;11:379–401.
16. Murphy LR. Workplace interventions for stress
reduction and prevention. In: Cooper CL, Payne
R, eds. Causes, Coping, and Consequences of
Stress at Work. Chichester, England: John Wiley
& Sons Inc; 1988:301–339.
17. Bamberg E, Busch C. Employee health im-
provement by stress management training: a
meta-analysis of (quasi-)experimental studies
[in German]. Z Arbeits Organisationspsychol.
1996;40:127–137.
18. van der Hek H, Plomp HN. Occupational stress
management programs: a practical overview of
published effect studies. Occup Med. 1997;47:
133–141.
19. Pearlin LI, Schooler C. The structure of coping.
J Health Soc Behav. 1978;19:2–21.
20. Karasek RA, Theorell T. Healthy Work: Stress,
Productivity, and the Reconstruction of Work-
ing Life. New York, NY: Basic Books; 1990.
21. Aderman M, Tecklenburg K. Effect of relax-
ation training on personal adjustment and per-
ceptions of organizational climate. J Psychol.
1983;115:185–191.
22. Carrington P, Collings GH Jr, Benson H, et al.
The use of meditation-relaxation techniques for
the management of stress in a working popula-
tion. J Occup Med. 1980;22:221–231.
23. Vaughn M, Cheatwood S, Sirles AT, Brown KC.
The effect of progressive muscle relaxation on
stress among clerical workers. Am Assoc Occup
Health Nurs J. 1989;37:302–306.
24. Vines SW. Effects on employees’ psychological
distress and health seeking behaviors. Am Assoc
Occup Health Nurs J. 1994;42:206–213.
25. Mullen B. Advanced Basic Meta-Analysis.
Hillsdale, NJ: Lawrence Erlbaum Associates;
1989.
26. Mullen B, Rosenthal R. BASIC Meta-Analysis:
Procedures and Programs. Hillsdale, NJ: Law-
rence Erlbaum Associates; 1985.
27. Rosenthal R, Rubin DB. Meta-analytic proce-
dures for combining studies with multiple ef-
fect sizes. Psychol Bull. 1986;99:400–406.
28. Alexander CN, Swanson GC, Rainforth MV,
Carlisle TW, Todd CC, Oates RM Jr. Effects of
the transcendental meditation program on stress
reduction, health, and employee development:
a prospective study in two occupational settings.
Anxiety Stress Coping. 1993;6:245–262.
29. Arnetz BB. Techno-stress: a prospective psy-
chophysiological study of the impact of a con-
trolled stress-reduction program in advanced
telecommunication systems design work. J
Occup Environ Med. 1996;38:53–65.
30. von Baeyer C, Krause L. Effectiveness of stress

February 2001, Vol. 91, No. 2276 American Journal of Public Health
management training for nurses working in a
burn treatment unit. Int J Psychol Med. 1983;
13:113–125.
31. Bertoch MR, Nielsen EC, Curley JR, Borg WR.
Reducing teacher stress. J Exp Educ. 1989;57:
117–128.
32. Bruning NS, Frew DR. Can stress intervention
strategies improve self-esteem, manifest anxi-
ety, and job satisfaction? A longitudinal field
experiment. J Health Hum Resources Adm.
1986;9:110–124.
33. Cecil MA, Forman SG. Effects of stress inocu-
lation training and co-worker support groups on
teachers’ stress. J Sch Psychol. 1990;28:
105–118.
34. Curtis KA. Altering beliefs about the impor-
tance of strategy: an attributional intervention. J
Appl Soc Psychol. 1992;22:953–972.
35. Fava M, Littman A, Halperin P, et al. Psycho-
logical and behavioral benefits of a stress/type A
behavior reduction program for healthy middle-
aged army officers. Psychosomatics. 1991;32:
337–342.
36. Fiedler N, Vivona-Vaughan E, Gochfeld M.
Evaluation of a work site relaxation training pro-
gram using ambulatory blood pressure moni-
toring. J Occup Med. 1989;31:595–602.
37. Forman SG. Stress-management training: eval-
uation of effects on school psychological serv-
ices. J Sch Psychol. 1981;19:233–241.
38. Freedy JR, Hobfoll SE. Stress inoculation for
reduction of burnout: a conservation of resources
approach. Anxiety Stress Coping. 1994;6:
311–325.
39. Friedman GH, Lehrer BE, Stevens JP. The ef-
fectiveness of self-directed and lecture/discus-
sion stress management approaches and the
locus of control of teachers. Am Educ Res J.
1983;20:563–580.
40. Ganster DC, Mayes BT, Sime WE, Tharp GD.
Managing organizational stress: a field experi-
ment. J Appl Psychol. 1982;67:533–542.
41. Gray-Toft P. Effectiveness of a counseling sup-
port program for hospice nurses. J Counseling
Psychol. 1980;27:346–354.
42. Grønningsæter H, Hytten K, Skauli G, Chris-
tensen CC, Ursin H. Improved health and cop-
ing by physical exercise or cognitive behavioral
stress management training in a work environ-
ment. Psychol Health. 1992;7:147–163.
43. Higgins NC. Occupational stress and working
women: the effectiveness of two stress reduc-
tion programs. J Vocational Behav. 1986;29:
66–78.
44. Jackson SE. Participation in decision making as
a strategy for reducing job-related strain. J Appl
Psychol. 1983;68:3–19.
45. Johanson N. Effectiveness of a stress manage-
ment program in reducing anxiety and depres-
sion in nursing students. J Am Coll Health. 1991;
40:125–129.
46. Jones JW, Barge BN, Steffy BD, Fay LM,
Kunz LK, Wuebker LJ. Stress and medical
malpractice: organizational risk assessment
and intervention. J Appl Psychol. 1988;73:
727–735.
47. Keyes JB, Dean SF. Stress inoculation training
for direct contact staff working with mentally
retarded persons. Behav Residential Treatment.
1988;3:315–323.
48. Kushnir T, Malkinson R. A rational-emotive
group intervention for preventing and coping
with stress among safety officers. J Rational
Emotive Cognitive Behav Ther. 1993;11:
195–206.
49. Kushnir T, Malkinson R, Ribak J. Teaching stress
management skills to occupational and envi-
ronmental health physicians and practitioners.
J Occup Med. 1994;36:1335–1340.
50. Landsbergis PA, Vivona-Vaughan E. Evaluation
of an occupational stress intervention in a pub-
lic agency. J Organ Behav. 1995;16:29–48.
51. Larsson G, Setterlind S, Starrin B. Routiniza-
tion of stress control programs in organizations:
a study of Swedish teachers. Health Promotion
Int. 1990;5:269–278.
52. Lee S, Swanson Crockett M. Effect of as-
sertiveness training on levels of stress and as-
sertiveness experienced by nurses in Taiwan,
Republic of China. Issues Ment Health Nurs.
1994;15:419–432.
53. Long BC. Stress management for school per-
sonnel: stress-inoculation training and exercise.
Psychol Schools. 1988;25:314–324.
54. McCue JD, Sachs CL. A stress management
workshop improves residents’coping skills. Arch
Intern Med. 1991;151:2273–2277.
55. McNulty S, Jefferys D, Singer G, Singer L. Use
of hormone analysis in the assessment of the
efficacy of stress management training in po-
lice recruits. J Police Soc Adm. 1984;12:
130–132.
56. Murphy LR. A comparison of relaxation meth-
ods for reducing stress in nursing personnel.
Hum Factors. 1983;25:431–440.
57. Murphy LR. Stress management in highway
maintenance workers. J Occup Med. 1984;26:
436–442.
58. Norvell N, Belles D, Brody S, Freund A. Work-
site stress management for medical care per-
sonnel: results from a pilot program. J Special-
ists Group Work. 1987;12:118–126.
59. Peters RK, Benson H, Porter D. Daily relaxation
response breaks in a working population, I: ef-
fects on self-reported measures of health, per-
formance, and well-being. Am J Public Health.
1977;67:946–953.
60. Peters RK, Benson H, Peters JM. Daily relax-
ation response breaks in a working population,
II: effects on blood pressure. Am J Public Health.
1977;67:954–959.
61. Pruitt RH. Effectiveness and cost efficacy of in-
terventions in health promotion. J Adv Nurs.
1992;17:926–932.
62. Sharp JJ, Forman SG. A comparison of two ap-
proaches to anxiety management for teachers.
Behav Ther. 1985;16:370–383.
63. Toivanen H, Länsimies E, Jokela V, Hänninen
O. Impact of regular relaxation training on the
cardiac autonomic nervous system of hospital
cleaners and bank employees. Scand J Work En-
viron Health. 1993;19:319–325.
64. Toivanen H, Helin P, Hänninen O. Impact of reg-
ular relaxation training and psychosocial work-
ing factors on neck-shoulder tension and ab-
senteeism in hospital cleaners. J Occup Environ
Med. 1993;35:1123–1130.
65. Tsai S, Swanson Crockett M. Effects of relax-
ation training, combining imagery, and medita-
tion on the stress level of Chinese nurses work-
ing in modern hospitals in Taiwan. Issues Ment
Health Nurs. 1993;14:51–66.
66. Tunnecliff MR, Leach DJ, Tunnecliff LP. Rela-
tive efficacy of using behavioral consulting as
an approach to teacher stress management. J Sch
Psychol. 1986;24:123–131.
67. West DJ, Horan JJ, Games PA. Component
analysis of occupational stress inoculation ap-
plied to registered nurses in an acute care hos-
pital setting. J Counseling Psychol. 1984;31:
209–218.
68. Cohen J. Statistical Power Analysis for the Be-
havioral Sciences. New York, NY: Academic
Press Inc; 1988.
69. Firth J, Shapiro DA. An evaluation of psycho-
therapy for job-related distress. J Occup Psy-
chol. 1986;59:111–119.
70. Saunders T, Driskell JE, Hall Johnston J, Salas
E. The effect of stress inoculation training on
anxiety and performance. J Occup Psychol.
1997;70:170–186.
71. Barkum M, Shapiro DA. Brief psychotherapy
interventions for job-related distress: a pilot
study of prescriptive and exploratory therapy.
Counseling Psychol Q. 1990;2:133–147.
72. Kahn RL, Byosiere P. Stress in organizations.
In: Dunette MD, Hough LM, eds. Handbook of
Industrial and Organizational Psychology. 2nd
ed. Vol 3. Palo Alto, Calif: Consulting Psychol-
ogists Press; 1992:571–650.
73. Kompier MAJ, Geurts SAE, Gründemann
RWM, Vink P, Smulders PGW. Cases in stress
prevention: the success of a participative and
stepwise approach. Stress Med. 1998;14:
155–168.
74. Baker DB. The study of stress at work. Annu
Rev Public Health. 1995;6:367–381.
