
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 1 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
UnitedHealthcare
®
Commercial
Medical Policy
Home Health, Skilled, and Custodial Care Services
(for Commercial Only)
Policy Number: MP.022.23
Effective Date: May 1, 2024
Instructions for Use
Table of Contents Page
Application ..................................................................................... 1
Coverage Rationale ....................................................................... 1
Definitions ...................................................................................... 1
Applicable Codes .......................................................................... 2
Description of Services ................................................................. 9
Benefit Considerations .................................................................. 9
U.S. Food and Drug Administration ........................................... 10
References ................................................................................... 10
Policy History/Revision Information ........................................... 10
Instructions for Use ..................................................................... 11
Application
This Medical Policy applies to all UnitedHealthcare Commercial benefit plans.
Coverage Rationale
See Benefit Considerations
Home health and skilled care services are considered medically necessary in certain circumstances. For medical
necessity clinical coverage criteria, refer to the InterQual
®
LOC: Home Care Q & A:
Home Care Services, Adult
Home Care Services, Pediatric
Click here to view the InterQual
®
criteria.
Definitions
The following definitions may not apply to all plans. Refer to the member specific benefit plan document for applicable
definitions.
Place of Residence: Wherever the member makes his/her home. This may include a dwelling, an apartment, a relative's home,
or a facility-based long-term care residence, such as a board and care home, an assisted living facility, a nursing home, and a
continuing care retirement community (National Institute on Aging, 2017a).
Related Commercial Policies
• Home Hemodialysis
•
Private Duty Nursing Services
Community Plan Policy
• Home Health, Skilled, and Custodial Care Services
Medicare Advantage Coverage Summary
• Home Health Services, Home Health Visits, Respite
Care, and Hospice Care
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 2 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
Respite Care: Short-term relief for primary caregivers that can be provided at the member’s Place of Residence, in a healthcare
facility or at an adult day center. The relief period can be arranged for just an afternoon or for several days or weeks (National
Institute on Aging, 2017b).
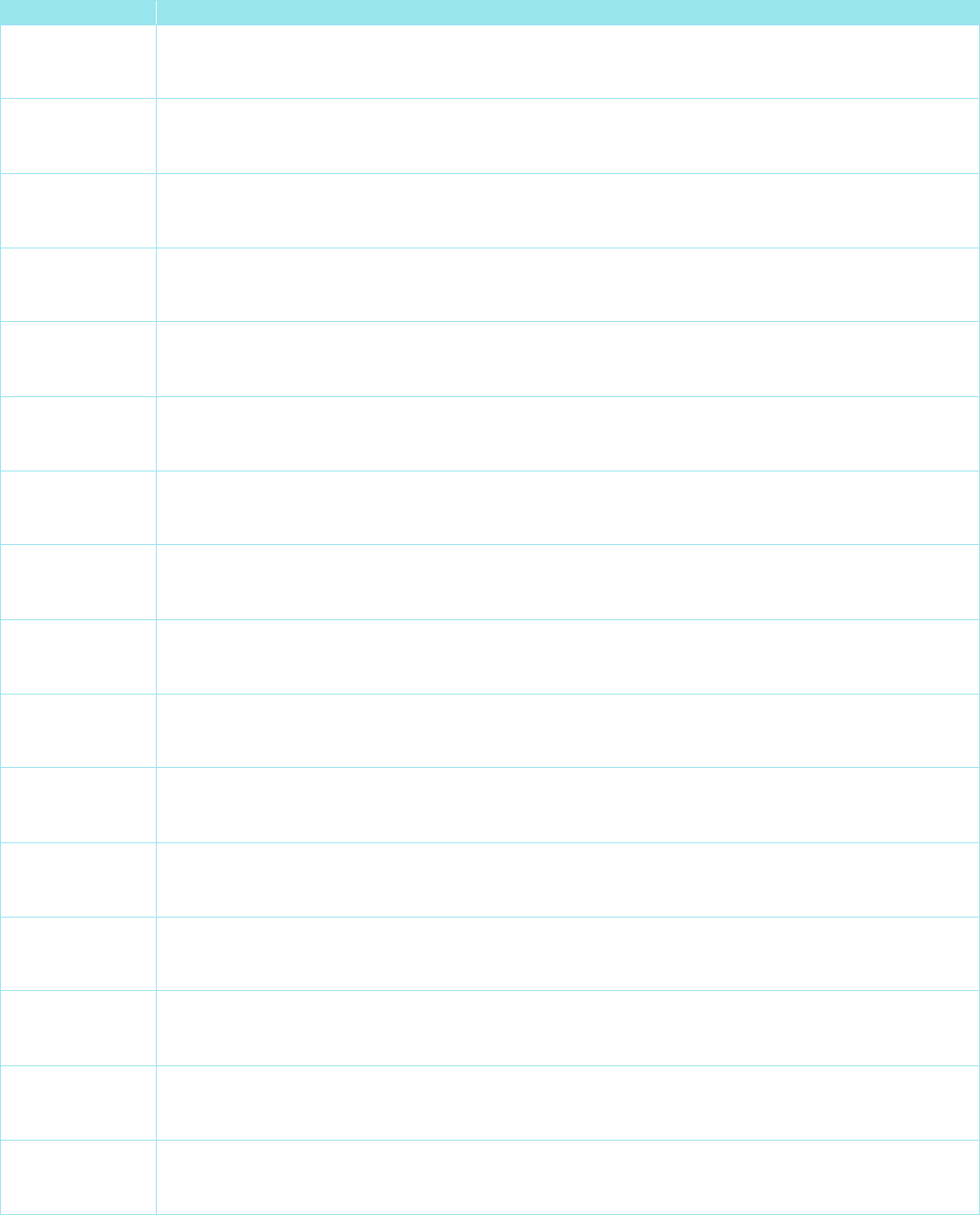
Applicable Codes
The following list(s) of procedure and/or diagnosis codes is provided for reference purposes only and may not be all inclusive.
Listing of a code in this policy does not imply that the service described by the code is a covered or non-covered health service.
Benefit coverage for health services is determined by the member specific benefit plan document and applicable laws that may
require coverage for a specific service. The inclusion of a code does not imply any right to reimbursement or guarantee claim
payment. Other Policies and Guidelines may apply.
CPT Code
Description
99500 Home visit for prenatal monitoring and assessment to include fetal heart rate, non-stress test, uterine
monitoring, and gestational diabetes monitoring
99501 Home visit for postnatal assessment and follow-up care
99502 Home visit for newborn care and assessment
99503 Home visit for respiratory therapy care (e.g., bronchodilator, oxygen therapy, respiratory assessment,
apnea evaluation)
99504 Home visit for mechanical ventilation care
99505 Home visit for stoma care and maintenance including colostomy and cystostomy
99506 Home visit for intramuscular injections
99507 Home visit for care and maintenance of catheter(s) (e.g., urinary, drainage, and enteral)
99511 Home visit for fecal impaction management and enema administration
99512 Home visit for hemodialysis
99601 Home infusion/specialty drug administration, per visit (up to 2 hours);
99602 Home infusion/specialty drug administration, per visit (up to 2 hours); each additional hour (List
separately in addition to code for primary procedure)
CPT
®
is a registered trademark of the American Medical Association
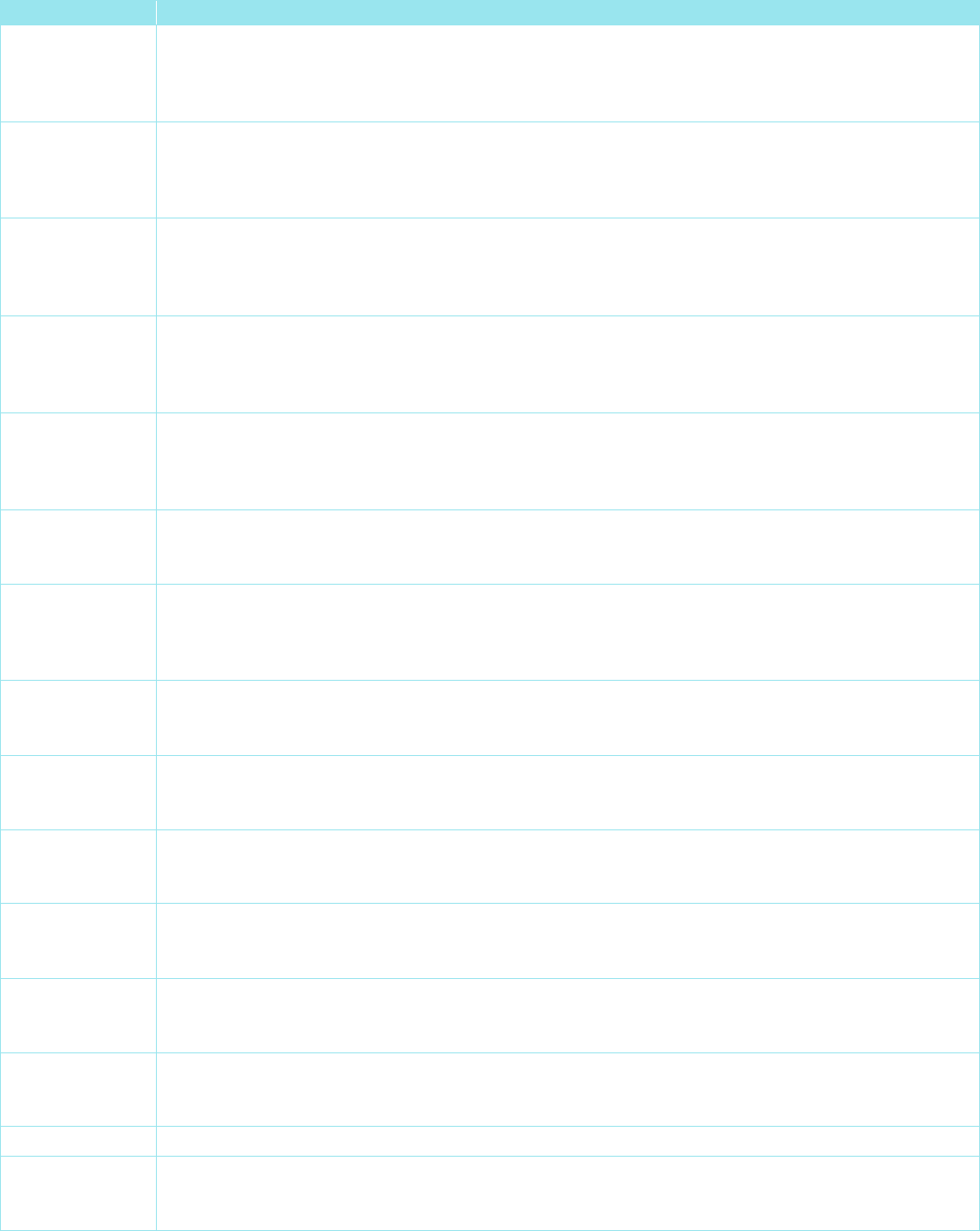
HCPCS Code
Description
G0068 Professional services for the administration of anti-infective, pain management, chelation, pulmonary
hypertension, inotropic, or other intravenous infusion drug or biological (excluding chemotherapy or
other highly complex drug or biological) for each infusion drug administration calendar day in the
individual's home, each 15 minutes
G0069 Professional services for the administration of subcutaneous immunotherapy or other subcutaneous
infusion drug or biological for each infusion drug administration calendar day in the individual's home,
each 15 minutes
G0070 Professional services for the administration of intravenous chemotherapy or other intravenous highly
complex drug or biological infusion for each infusion drug administration calendar day in the individual's
home, each 15 minutes
G0088
Professional services, initial visit, for the administration of anti-infective, pain management, chelation,
pulmonary hypertension, inotropic, or other intravenous infusion drug or biological (excluding
chemotherapy or other highly complex drug or biological) for each infusion drug administration calendar
day in the individual's home, each 15 minutes
G0089 Professional services, initial visit, for the administration of subcutaneous immunotherapy or other
subcutaneous infusion drug or biological for each infusion drug administration calendar day in the
individual's home, each 15 minutes
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 3 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
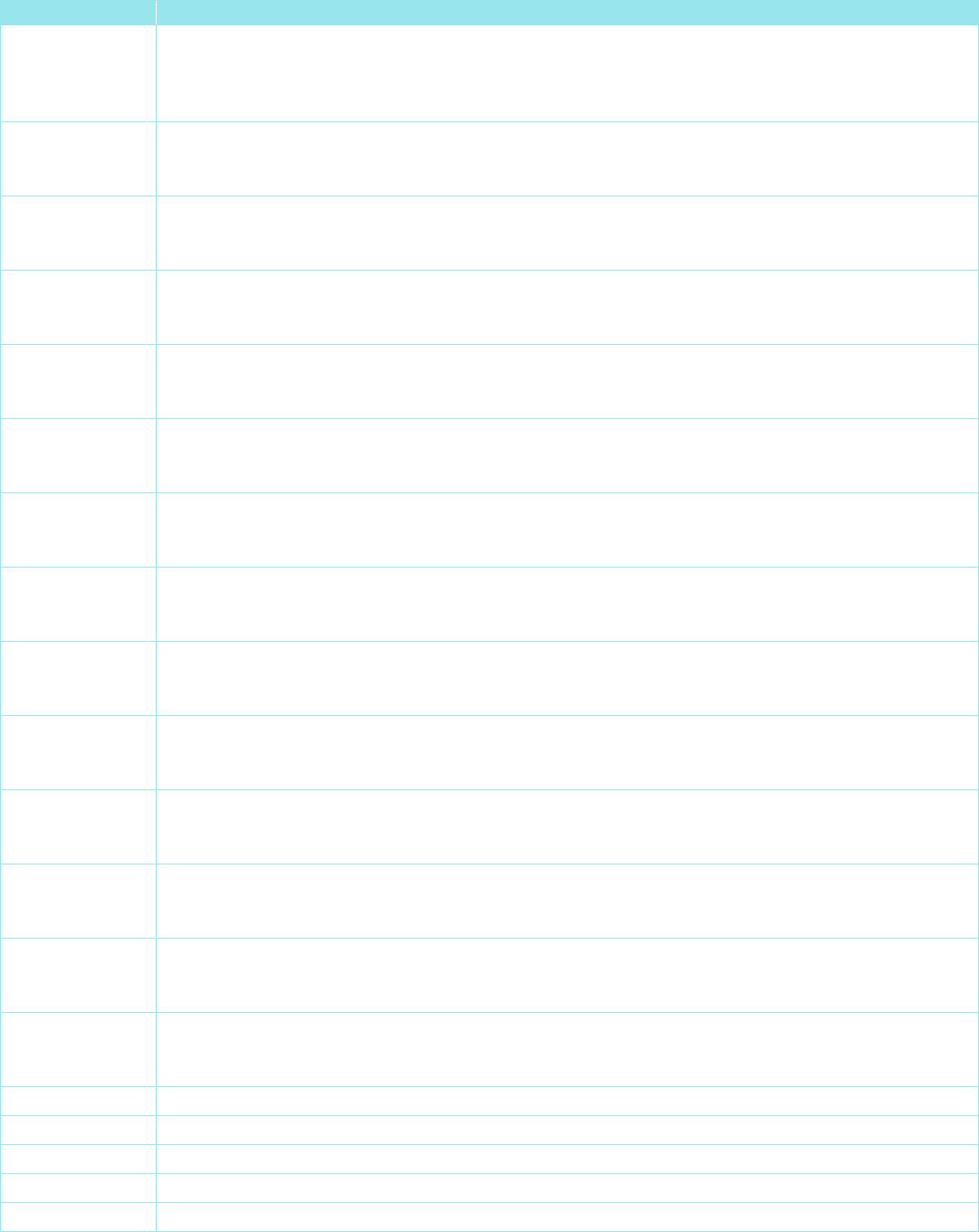
HCPCS Code
Description
G0090 Professional services, initial visit, for the administration of intravenous chemotherapy or other highly
complex infusion drug or biological for each infusion drug administration calendar day in the individual's
home, each 15 minutes
G0153
Services performed by a qualified speech-language pathologist in the home health or hospice setting,
each 15 minutes
G0155 Services of clinical social worker in home health or hospice settings, each 15 minutes
G0156 Services of home health/hospice aide in home health or hospice settings, each 15 minutes
G0157
Services performed by a qualified physical therapist assistant in the home health or hospice setting,
each 15 minutes
G0158 Services performed by a qualified occupational therapist assistant in the home health or hospice setting,
each 15 minutes
G0159
Services performed by a qualified physical therapist, in the home health setting, in the establishment or
delivery of a safe and effective physical therapy maintenance program, each 15 minutes
G0160 Services performed by a qualified occupational therapist, in the home health setting, in the
establishment or delivery of a safe and effective occupational therapy maintenance program, each 15
minutes
G0161 Services performed by a qualified speech-language pathologist, in the home health setting, in the
establishment or delivery of a safe and effective speech-language pathology maintenance program, each
15 minutes
G0162
Skilled services by a registered nurse (RN) for management and evaluation of the plan of care; each 15
minutes (the patient's underlying condition or complication requires an RN to ensure that essential
nonskilled care achieves its purpose in the home health or hospice setting)
G0299 Direct skilled nursing services of a registered nurse (RN) in the home health or hospice setting, each 15
minutes
G0300
Direct skilled nursing services of a licensed practical nurse (LPN) in the home health or hospice setting,
each 15 minutes
G0320 Home health services furnished using synchronous telemedicine rendered via a real-time two-way audio
and video telecommunications system
G0321
Home health services furnished using synchronous telemedicine rendered via telephone or other real-
time interactive audio-only telecommunications system
G0322 The collection of physiologic data digitally stored and/or transmitted by the patient to the home health
agency (i.e., remote patient monitoring)
G0490
Face-to-face home health nursing visit by a rural health clinic (RHC) or federally qualified health center
(FQHC) in an area with a shortage of home health agencies; (services limited to RN or LPN only)
G0493 Skilled services of a registered nurse (RN) for the observation and assessment of the patient's condition,
each 15 minutes (the change in the patient's condition requires skilled nursing personnel to identify and
evaluate the patient's need for possible modification of treatment in the home health or hospice setting)
G0494 Skilled services of a licensed practical nurse (LPN) for the observation and assessment of the patient's
condition, each 15 minutes (the change in the patient's condition requires skilled nursing personnel to
identify and evaluate the patient's need for possible modification of treatment in the home health or
hospice setting)
G0495
Skilled services of a registered nurse (RN), in the training and/or education of a patient or family
member, in the home health or hospice setting, each 15 minutes
G0496 Skilled services of a licensed practical nurse (LPN), in the training and/or education of a patient or family
member, in the home health or hospice setting, each 15 minutes
G2168
Services performed by a physical therapist assistant in the home health setting in the delivery of a safe
and effective physical therapy maintenance program, each 15 minutes
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 4 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
HCPCS Code
Description
G2169 Services performed by an occupational therapist assistant in the home health setting in the delivery of a
safe and effective occupational therapy maintenance program, each 15 minutes
H1004 Prenatal care, at-risk enhanced service; follow-up home visit
S5035 Home infusion therapy, routine service of infusion device (e.g., pump maintenance)
S5036 Home infusion therapy, repair of infusion device (e.g., pump repair)
S5108 Home care training to home care client, per 15 minutes
S5109 Home care training to home care client, per session
S5110 Home care training, family; per 15 minutes
S5111 Home care training, family; per session
S5115 Home care training, nonfamily; per 15 minutes
S5116 Home care training, nonfamily; per session
S5180 Home health respiratory therapy, initial evaluation
S5181 Home health respiratory therapy, NOS, per diem
S5497 Home infusion therapy, catheter care/maintenance, not otherwise classified; includes administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S5498
Home infusion therapy, catheter care/maintenance, simple (single lumen), includes administrative
services, professional pharmacy services, care coordination and all necessary supplies and equipment,
(drugs and nursing visits coded separately), per diem
S5501 Home infusion therapy, catheter care/maintenance, complex (more than one lumen), includes
administrative services, professional pharmacy services, care coordination, and all necessary supplies
and equipment (drugs and nursing visits coded separately), per diem
S5502 Home infusion therapy, catheter care/maintenance, implanted access device, includes administrative
services, professional pharmacy services, care coordination and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem (Use this code for interim maintenance of vascular
access not currently in use)
S5517 Home infusion therapy, all supplies necessary for restoration of catheter patency or declotting
S5518 Home infusion therapy, all supplies necessary for catheter repair
S5520
Home infusion therapy, all supplies (including catheter) necessary for a peripherally inserted central
venous catheter (PICC) line insertion
S5521 Home infusion therapy, all supplies (including catheter) necessary for a midline catheter insertion
S5522 Home infusion therapy, insertion of peripherally inserted central venous catheter (PICC), nursing
services only (no supplies or catheter included)
S5523 Home infusion therapy, insertion of midline venous catheter, nursing services only (no supplies or
catheter included)
S9061 Home administration of aerosolized drug therapy (e.g., Pentamidine); administrative services,
professional pharmacy services, care coordination, all necessary supplies and equipment (drugs and
nursing visits coded separately), per diem
S9097 Home visit for wound care
S9098 Home visit, phototherapy services (e.g., Bili-lite), including equipment rental, nursing services, blood
draw, supplies, and other services, per diem
S9122 Home health aide or certified nurse assistant, providing care in the home; per hour
S9123 Nursing care, in the home; by registered nurse, per hour (use for general nursing care only, not to be
used when CPT codes 99500-99602 can be used)
S9124 Nursing care, in the home; by licensed practical nurse, per hour
S9127 Social work visit, in the home, per diem
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 5 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
HCPCS Code
Description
S9208 Home management of preterm labor, including administrative services, professional pharmacy services,
care coordination, and all necessary supplies or equipment (drugs and nursing visits coded separately),
per diem (do not use this code with any home infusion per diem code)
S9209
Home management of preterm premature rupture of membranes (PPROM), including administrative
services, professional pharmacy services, care coordination, and all necessary supplies or equipment
(drugs and nursing visits coded separately), per diem (do not use this code with any home infusion per
diem code)
S9211 Home management of gestational hypertension, includes administrative services, professional pharmacy
services, care coordination and all necessary supplies and equipment (drugs and nursing visits coded
separately); per diem (do not use this code with any home infusion per diem code)
S9212 Home management of postpartum hypertension, includes administrative services, professional
pharmacy services, care coordination, and all necessary supplies and equipment (drugs and nursing
visits coded separately), per diem (do not use this code with any home infusion per diem code)
S9213
Home management of preeclampsia, includes administrative services, professional pharmacy services,
care coordination, and all necessary supplies and equipment (drugs and nursing services coded
separately); per diem (do not use this code with any home infusion per diem code)
S9214 Home management of gestational diabetes, includes administrative services, professional pharmacy
services, care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately); per diem (do not use this code with any home infusion per diem code)
S9325 Home infusion therapy, pain management infusion; administrative services, professional pharmacy
services, care coordination, and all necessary supplies and equipment, (drugs and nursing visits coded
separately), per diem (do not use this code with S9326, S9327 or S9328)
S9326
Home infusion therapy, continuous (24 hours or more) pain management infusion; administrative
services, professional pharmacy services, care coordination and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9327 Home infusion therapy, intermittent (less than 24 hours) pain management infusion; administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9328 Home infusion therapy, implanted pump pain management infusion; administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and nursing visits coded separately), per diem
S9329
Home infusion therapy, chemotherapy infusion; administrative services, professional pharmacy services,
care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately), per diem (do not use this code with S9330 or S9331)
S9330 Home infusion therapy, continuous (24 hours or more) chemotherapy infusion; administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and nursing visits coded separately), per diem
S9331 Home infusion therapy, intermittent (less than 24 hours) chemotherapy infusion; administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and nursing visits coded separately), per diem
S9335
Home therapy, hemodialysis; administrative services, professional pharmacy services, care coordination,
and all necessary supplies and equipment (drugs and nursing services coded separately), per diem
S9336 Home infusion therapy, continuous anticoagulant infusion therapy (e.g., Heparin), administrative
services, professional pharmacy services, care coordination and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9338 Home infusion therapy, immunotherapy, administrative services, professional pharmacy services, care
coordination, and all necessary supplies and equipment (drugs and nursing visits coded separately), per
diem
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 6 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
HCPCS Code
Description
S9339 Home therapy; peritoneal dialysis, administrative services, professional pharmacy services, care
coordination and all necessary supplies and equipment (drugs and nursing visits coded separately), per
diem
S9340
Home therapy; enteral nutrition; administrative services, professional pharmacy services, care
coordination, and all necessary supplies and equipment (enteral formula and nursing visits coded
separately), per diem
S9341 Home therapy; enteral nutrition via gravity; administrative services, professional pharmacy services, care
coordination, and all necessary supplies and equipment (enteral formula and nursing visits coded
separately), per diem
S9342 Home therapy; enteral nutrition via pump; administrative services, professional pharmacy services, care
coordination, and all necessary supplies and equipment (enteral formula and nursing visits coded
separately), per diem
S9343
Home therapy; enteral nutrition via bolus; administrative services, professional pharmacy services, care
coordination, and all necessary supplies and equipment (enteral formula and nursing visits coded
separately), per diem
S9345 Home infusion therapy, antihemophilic agent infusion therapy (e.g., factor VIII); administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and nursing visits coded separately), per diem
S9346 Home infusion therapy, alpha-1-proteinase inhibitor (e.g., Prolastin); administrative services, professional
pharmacy services, care coordination, and all necessary supplies and equipment (drugs and nursing
visits coded separately), per diem
S9347
Home infusion therapy, uninterrupted, long-term, controlled rate intravenous or subcutaneous infusion
therapy (e.g., epoprostenol); administrative services, professional pharmacy services, care coordination,
and all necessary supplies and equipment (drugs and nursing visits coded separately), per diem
S9348 Home infusion therapy, sympathomimetic/inotropic agent infusion therapy (e.g., Dobutamine);
administrative services, professional pharmacy services, care coordination, all necessary supplies and
equipment (drugs and nursing visits coded separately), per diem
S9351 Home infusion therapy, continuous or intermittent antiemetic infusion therapy; administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and visits coded separately), per diem
S9353
Home infusion therapy, continuous insulin infusion therapy; administrative services, professional
pharmacy services, care coordination, and all necessary supplies and equipment (drugs and nursing
visits coded separately), per diem
S9355 Home infusion therapy, chelation therapy; administrative services, professional pharmacy services, care
coordination, and all necessary supplies and equipment (drugs and nursing visits coded separately), per
diem
S9357 Home infusion therapy, enzyme replacement intravenous therapy; (e.g., Imiglucerase); administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9359
Home infusion therapy, antitumor necrosis factor intravenous therapy; (e.g., Infliximab); administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9361 Home infusion therapy, diuretic intravenous therapy; administrative services, professional pharmacy
services, care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately), per diem
S9363 Home infusion therapy, antispasmotic therapy; administrative services, professional pharmacy services,
care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately), per diem
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 7 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
HCPCS Code
Description
S9364 Home infusion therapy, total parenteral nutrition (TPN); administrative services, professional pharmacy
services, care coordination, and all necessary supplies and equipment including standard TPN formula
(lipids, specialty amino acid formulas, drugs other than in standard formula and nursing visits coded
separately), per diem (do not use with home infusion codes S9365-S9368 using daily volume scales)
S9365
Home infusion therapy, total parenteral nutrition (TPN); one liter per day, administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment including
standard TPN formula (lipids, specialty amino acid formulas, drugs other than in standard formula and
nursing visits coded separately), per diem
S9366
Home infusion therapy, total parenteral nutrition (TPN); more than one liter but no more than two liters
per day, administrative services, professional pharmacy services, care coordination, and all necessary
supplies and equipment including standard TPN formula (lipids, specialty amino acid formulas, drugs
other than in standard formula and nursing visits coded separately), per diem
S9367 Home infusion therapy, total parenteral nutrition (TPN); more than two liters but no more than three liters
per day, administrative services, professional pharmacy services, care coordination, and all necessary
supplies and equipment including standard TPN formula (lipids, specialty amino acid formulas, drugs
other than in standard formula and nursing visits coded separately), per diem
S9368 Home infusion therapy, total parenteral nutrition (TPN); more than three liters per day, administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
including standard TPN formula (lipids, specialty amino acid formulas, drugs other than in standard
formula and nursing visits coded separately), per diem
S9370 Home therapy, intermittent antiemetic injection therapy; administrative services, professional pharmacy
services, care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately), per diem
S9372
Home therapy; intermittent anticoagulant injection therapy (e.g., Heparin); administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and nursing visits coded separately), per diem (do not use this code for flushing of infusion devices with
Heparin to maintain patency)
S9373
Home infusion therapy, hydration therapy; administrative services, professional pharmacy services, care
coordination, and all necessary supplies and equipment (drugs and nursing visits coded separately), per
diem (do not use with hydration therapy codes S9374-S9377 using daily volume scales)
S9374 Home infusion therapy, hydration therapy; 1 liter per day, administrative services, professional pharmacy
services, care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately), per diem
S9375 Home infusion therapy, hydration therapy; more than 1 liter but no more than 2 liters per day,
administrative services, professional pharmacy services, care coordination, and all necessary supplies
and equipment (drugs and nursing visits coded separately), per diem
S9376
Home infusion therapy, hydration therapy; more than 2 liters but no more than 3 liters per day,
administrative services, professional pharmacy services, care coordination, and all necessary supplies
and equipment (drugs and nursing visits coded separately), per diem
S9377 Home infusion therapy, hydration therapy; more than 3 liters per day, administrative services,
professional pharmacy services, care coordination, and all necessary supplies (drugs and nursing visits
coded separately), per diem
S9379 Home infusion therapy, infusion therapy, not otherwise classified; administrative services, professional
pharmacy services, care coordination, and all necessary supplies and equipment (drugs and nursing
visits coded separately), per diem
S9474 Enterostomal therapy by a registered nurse certified in enterostomal therapy, per diem
S9490 Home infusion therapy, corticosteroid infusion; administrative services, professional pharmacy services,
care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately), per diem
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 8 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
HCPCS Code
Description
S9494 Home infusion therapy, antibiotic, antiviral, or antifungal therapy; administrative services, professional
pharmacy services, care coordination, and all necessary supplies and equipment (drugs and nursing
visits coded separately), per diem (do not use this code with home infusion codes for hourly dosing
schedules S9497-S9504)
S9497
Home infusion therapy, antibiotic, antiviral, or antifungal therapy; once every 3 hours; administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9500 Home infusion therapy, antibiotic, antiviral, or antifungal therapy; once every 24 hours; administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9501 Home infusion therapy, antibiotic, antiviral, or antifungal therapy; once every 12 hours; administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9502
Home infusion therapy, antibiotic, antiviral, or antifungal therapy; once every 8 hours, administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9503 Home infusion therapy, antibiotic, antiviral, or antifungal; once every 6 hours; administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and nursing visits coded separately), per diem
S9504 Home infusion therapy, antibiotic, antiviral, or antifungal; once every 4 hours; administrative services,
professional pharmacy services, care coordination, and all necessary supplies and equipment (drugs
and nursing visits coded separately), per diem
S9537
Home therapy; hematopoietic hormone injection therapy (e.g., erythropoietin, G-CSF, GM-CSF);
administrative services, professional pharmacy services, care coordination, and all necessary supplies
and equipment (drugs and nursing visits coded separately), per diem
S9538 Home transfusion of blood product(s); administrative services, professional pharmacy services, care
coordination and all necessary supplies and equipment (blood products, drugs, and nursing visits coded
separately), per diem
S9542 Home injectable therapy, not otherwise classified, including administrative services, professional
pharmacy services, care coordination, and all necessary supplies and equipment (drugs and nursing
visits coded separately), per diem
S9559
Home injectable therapy, interferon, including administrative services, professional pharmacy services,
care coordination, and all necessary supplies and equipment (drugs and nursing visits coded
separately), per diem
S9560 Home injectable therapy; hormonal therapy (e.g., leuprolide, goserelin), including administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9562 Home injectable therapy, palivizumab or other monoclonal antibody for RSV, including administrative
services, professional pharmacy services, care coordination, and all necessary supplies and equipment
(drugs and nursing visits coded separately), per diem
S9590
Home therapy, irrigation therapy (e.g., sterile irrigation of an organ or anatomical cavity); including
administrative services, professional pharmacy services, care coordination, and all necessary supplies
and equipment (drugs and nursing visits coded separately), per diem
T1001 Nursing assessment/evaluation
T1002 RN services, up to 15 minutes
T1003 LPN/LVN services, up to 15 minutes
T1004 Services of a qualified nursing aide, up to 15 minutes
T1005 Respite care services, up to 15 minutes
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 9 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
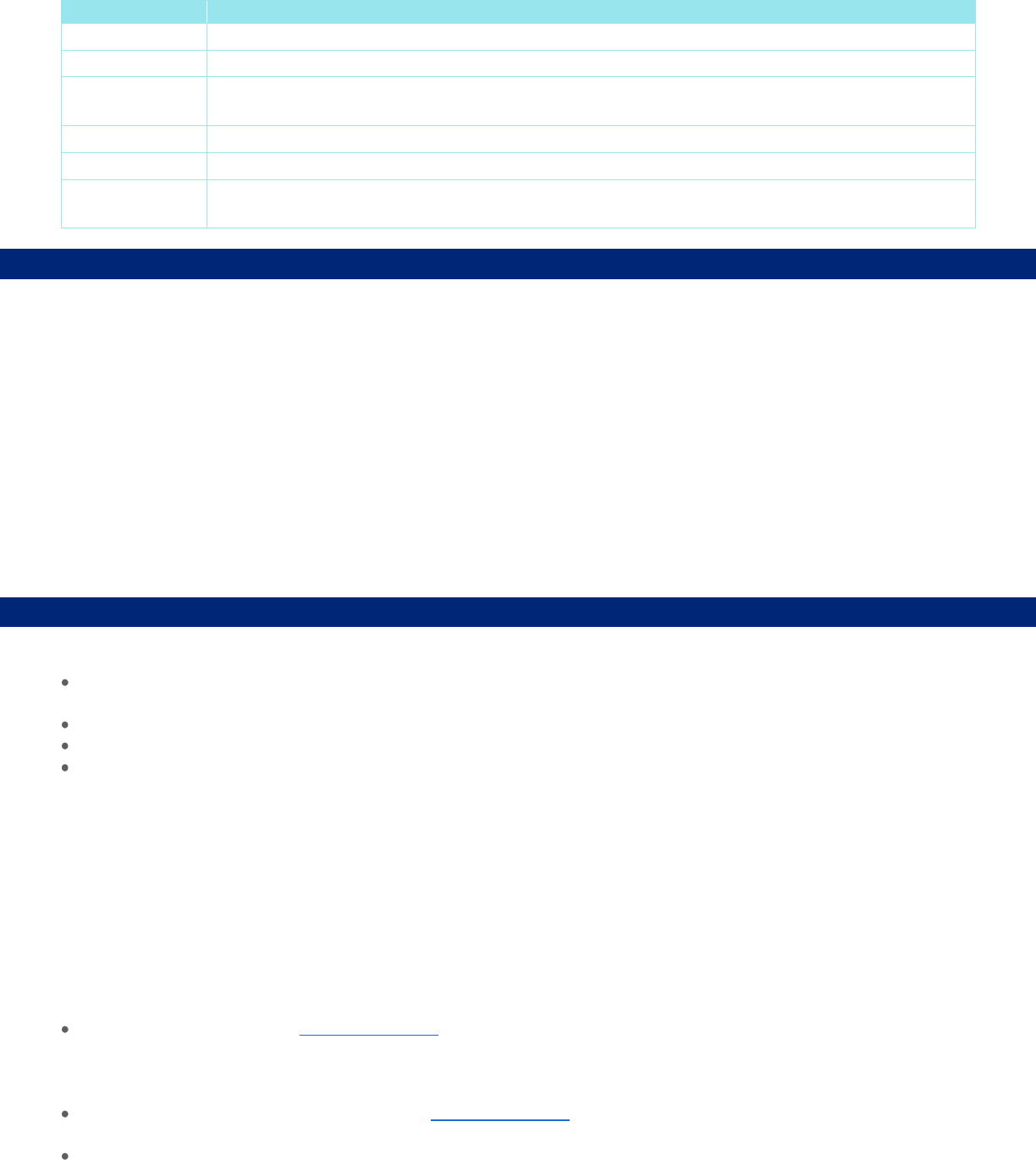
HCPCS Code
Description
T1021 Home health aide or certified nurse assistant, per visit
T1022 Contracted home health agency services, all services provided under contract, per day
T1028
Assessment of home, physical and family environment, to determine suitability to meet patient's medical
needs
T1030 Nursing care, in the home, by registered nurse, per diem
T1031 Nursing care, in the home, by licensed practical nurse, per diem
T1502
Administration of oral, intramuscular and/or subcutaneous medication by health care
agency/professional, per visit
Description of Services
Home health care services are short-term services, prescribed by treating practitioner or specialist (M.D., D.O., P.A. or N.P.)
delivered within a health plan member’s residence and are designed to help a member recover after an illness, injury, hospital
stay, or surgery, or to help manage a chronic condition with the goal of preventing an unplanned hospitalization or prolonging a
current hospitalization. Home health care services are provided intermittently to restore or maintain a member’s maximal level
of function and health in lieu of receiving the services in an outpatient setting or in an acute or sub-acute health care setting.
Skilled care services are medically necessary services provided in the member’s Place of Residence by licensed health care
professionals and may include services such as medical or psychological evaluation, wound care, medication teaching, pain
management, disease education and management, physical therapy, speech therapy, or occupational therapy.
Custodial care services are non-medical services that provide assistance with personal care such as activities of daily living,
housekeeping, cooking, laundry, or supervision of self-administered medication that can reasonably and safely be provided by
non-licensed caregivers.
Benefit Considerations
The services being requested must also meet all of the following criteria:
A written treatment plan must be submitted with the request for specific services and supplies. Periodic review of the
written treatment plan may be required for continued skilled care needs and progress toward goals; and
Be ordered and directed by a treating practitioner or specialist (M.D., D.O., P.A. or N.P.); and
The care must be delivered or supervised by a licensed professional in order to obtain a specified medical outcome; and
Services are:
o Not custodial care in nature; and
o Not provided for the comfort and convenience of the member or the member’s family; and
o Provided in the home in lieu of skilled care in another setting (including but not limited to a nursing facility, acute
inpatient rehabilitation, or a hospital); and
o Clinically appropriate and not more costly than an alternative health service; and
o Intermittent and part time (typically provided for less than 4 hours per day)
Note: Intermittent care exceptions may be made in certain circumstances when the need for more care is finite and
predictable.
Additional Information
Skilled care in the member’s Place of Residence. Skilled care includes:
o Skilled nursing
o Skilled rehabilitation (physical therapy, occupational therapy, and speech therapy)
o Skilled teaching
For Skilled care to be covered in the member’s Place of Residence, the care provided must require clinical training in order
to be delivered safely and effectively
Eligible physical, occupational, and speech therapy:
Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 10 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
o Received in the home from a home health agency is covered under the home health care benefit
o Received in the home from an independent physical, occupational or speech therapist (a therapist that is not affiliated
with a home health agency) is covered under the rehabilitation services - outpatient therapy benefit
Medical supplies and medications that are used in conjunction with a home health care visit are covered as part of that
visit. Examples include but are not limited to:
o Catheters
o Irrigation devices
o Surgical dressing
o Syringes
Refer to the member’s specific plan document for any applicable visit limitations.
Coverage Limitations and Exclusions
Covered pharmaceuticals, drugs, and durable medical equipment provided in connection with home health services may be
subject to separate benefit categories. Reference the durable medical equipment and the pharmaceutical products benefit
sections of the member specific benefit plan document. Home health care benefits do not include:
Custodial care
Domiciliary care
Private duty nursing
Respite care
Rest cures
Homemaker services such as home meal delivery services (e.g., Meals-on-Wheels) or transportation services (e.g., Dial-a-
Ride)
Independent nurse hired directly by the family/member
Services provided by personal care attendants, family members, or caregivers who are not properly licensed and qualified
by law
Home health services beyond benefit limits (e.g., number of visits)
UnitedHealthcare will determine if benefits are available by reviewing both the skilled nature of the service and the need for
Physician-directed medical management. A service will not be determined to be "skilled" simply because there is not an
available caregiver.
U.S. Food and Drug Administration (FDA)
This section is to be used for informational purposes only. FDA approval alone is not a basis for coverage.
Home health care, including skilled care are services rendered by licensed health care professionals and, therefore, not subject
to regulation by the FDA.
References
National Institute on Aging. Residential Facilities, Assisted Living, and Nursing Homes. U.S. Department of Health & Human
Services; May 01, 2017a.
National Institute on Aging. What Is Respite Care? U.S. Department of Health & Human Services; May 01, 2017b.
UnitedHealthcare Insurance Company Generic Certificate of Coverage 2018.
Policy History/Revision Information
Date
Summary of Changes
05/01/2024
Routine review; no change to coverage guidelines
Archived previous policy version MP.022.22

Home Health, Skilled, and Custodial Care Services (for Commercial Only)
Page 11 of 11
UnitedHealthcare Commercial Medical Policy
Effective 05/01/2024
Proprietary Information of UnitedHealthcare. Copyright 2024 United HealthCare Services, Inc.
Instructions for Use
This Medical Policy provides assistance in interpreting UnitedHealthcare standard benefit plans. When deciding coverage, the
member specific benefit plan document must be referenced as the terms of the member specific benefit plan may differ from
the standard plan. In the event of a conflict, the member specific benefit plan document governs. Before using this policy,
please check the member specific benefit plan document and any applicable federal or state mandates. UnitedHealthcare
reserves the right to modify its Policies and Guidelines as necessary. This Medical Policy is provided for informational
purposes. It does not constitute medical advice.
This Medical Policy may also be applied to Medicare Advantage plans in certain instances. In the absence of a Medicare
National Coverage Determination (NCD), Local Coverage Determination (LCD), or other Medicare coverage guidance, CMS
allows a Medicare Advantage Organization (MAO) to create its own coverage determinations, using objective evidence-based
rationale relying on authoritative evidence (Medicare IOM Pub. No. 100-16, Ch. 4, §90.5).
UnitedHealthcare may also use tools developed by third parties, such as the InterQual
®
criteria, to assist us in administering
health benefits. UnitedHealthcare Medical Policies are intended to be used in connection with the independent professional
medical judgment of a qualified health care provider and do not constitute the practice of medicine or medical advice.
