No 47 Spring 2017
BARGOOSE
Dr Simon P Hughes and Partners
Patient Participation Group
Newsletter No 47 Spring 2017
Contents
Page 2
The late Chris Porter
Dr Hughes 25 years
Page 3 Primary Care
Development Plan
Page 4
Questions to doctors,
and replies, at the
Open Evening
Page 5
Questions and Answers
from the Open Evening
continued
FAST awareness of
strokes
Page 6
Lasting Power of
Attorney
Page 7
Between the two
World Wars by Ivan
Jones
Page 8
The day of the CQC
inspection
THE CARE QUALITY COMMISSION REPORT
T
he CQC report on the Practice inspection at Barton on 17 May 2016
presents a picture of a technically excellent and well equipped
team, devoted to the welfare of the patients, who were treated with
kindness, dignity, compassion and respect. Information on the services
available to patients was available and easily understood.
Appointments with a named doctor and continuing contact with that
doctor were possible. There were emergency appointments available for
those needing same-day help. Older people and those
with long-term conditions had special provision, and a
register of carers, and contact with them, was
developing well. Nursing staff took lead rolls in chronic
disease management and patients at risk of hospital
admission were identified for special care.
T
he leadership and management of the Practice was
highly rated. The partners had demonstrated that
they had the experience, capacity and capability to run
the Practice and deliver high quality care. They
prioritised safe, high quality and compassionate
care. Staff said that the partners were
approachable and always took time to listen to all
members of staff. Staff felt respected, valued and
supported, particularly by the partners. They
were encouraged to take part in discussions about
how to run and develop the practice. Feed back
from patients, the public and staff was
encouraged. The Patient Participation Group
(Bargoose) was part of this. For an account of the
actual inspection day see page 8
Staff were not
mentioned by name in
the report, but clearly
the leadership provided
by Dr Hughes and
colleagues, and the
involvement of all staff,
was seen to be critical
to the success of and
patient satisfaction with
the practice.
Page 2
We have to report the sad news of the
passing on 11
th
December of Chris Porter,
one of our committed and able Bargoose
members.
He was born and spent his early years in
Liverpool, and retained his affection for
the city and Anfield throughout his life. He
served a 5-year apprenticeship in design
and draughtsmanship in Kent and became
a teacher, eventually teaching engineering
drawing and mathematics at Harlington
School.
Chris was a football
and cricket
enthusiast, a
devoted father and
grandfather, a life-
long church member
and supporter of
community projects.
He belonged in this
district, having been
married in Silsoe
church and lived in
Greenfield and
Barton for many years. Pulloxhill church
was packed for the memorial service on 5
th
January.
CHRIS PORTER 1935 - 2016
All 55 GP practices in Bedfordshire are
members of the Clinical Commissioning
Group (CCG). The CCG divides itself into
five areas or ‘localities’. Bedford Locality
covers roughly the same area as Bedford
Borough Council. The other four localities
cover the area of Central Bedfordshire
Council.
● Bedford Locality is a group of 26 GP
Practices covering the towns of Bedford
and Kempston and some north-
Bedfordshire villages.
● Chiltern Vale Locality is a group of 10 GP
practices in the south of Bedfordshire
covering Toddington, Houghton Regis,
Dunstable and the surrounding villages.
● Ivel Vale is a group of 7 GP practices
covering Sandy, Potton, Biggleswade,
Shefford and Stotfold.
● Leighton Buzzard is a group of 3 GP
practices in the south of Bedfordshire.
● West Mid Beds is a group of 6 GP
practices covering a population of
58,790 in Ampthill, Flitwick, Barton le
Clay, and Woburn Sands
The Practice of Dr Simon Hughes and
Partners, Barton le Clay, is part of the
West Mid Beds Locality. This is what it
means.
On 5
th
February
completed 25 years service with the
Practice. We give thanks for all the
help and support he has given us,
patients and staff alike, over those
years, and beg him to continue the
good work for many years to come.
Page 3
PRIMARY CARE DEVELOPMENT IN WEST MID BEDS LOCALITY
P
rimary care, the service provided by doctors, nurses and others at our local
surgeries, is under severe pressure. We have more patients, older patients with
multiple problems needing more attention, a Government demand for complete out of
hours and weekend services, and more administrative duties. Funding for General
Practice has declined by 30% since 2010. Government has promised 5000 additional
General Practitioners within a few years, but there is widespread doubt that this can
be achieved. The work is less attractive to new doctors and recruitment is difficult.
Unless some action is taken General Practice as we know it will collapse.
The Bedfordshire Clinical Commissioning Group has asked each locality to
produce a 2-year plan to alleviate some of the present problems. Our
West Mid Beds Locality has produced the following proposals, the
development of each section of which has been allocated to one or
more of the surgeries. Overall management of the plan is by Gill
Hiscox, our Practice Manager.
The plan is based on national guidance which emphasises the need
for practices to work together, not to make further demands on
already overstretched GP’s, to accept that evening and weekend
access to primary care is mandatory but not necessarily depending
on GP’s, and to make more extensive use of digital technology. The
main proposals are as follows:
· A Locality website providing information, advice,
eventually on-line consultations and possibly shared phone
lines.
· Further training of administrative staff to enable them to take over more
of the paper work at present overwhelming GP’s.
Urgent home visiting service
· Inclusion of pharmacists in the Practice team for minor illness clinics,
medication reviews for complex patients, care home ward rounds and joint
working with other professionals.
· Improvements in working premises to include joint
Health and Social Care premises in the Ampthill or Flitwick
area to house health and social care staff which could provide
services such as physiotherapy to all patients within the
locality
Gill Hiscox will be the overall manager of the programme, with
each Practice taking the lead on one of the projects under the
direction of their Practice Manager and one of the clinical staff. We will
be kept informed of progress over the next two years.
A PLAN AIMED AT GREATER EFFICIENCY THROUGH COOPERATION AND JOINT
WORKING WITH OTHER LOCAL PRACTICES, CHANGES IN WORKING METHODS
AND THE RELEASE OF MORE DOCTOR AND NURSE TIME FOR DIRECT CONTACT
WITH PATIENTS
Miriam Coffee,
working with the
Locality Group, has
played a leading part
in the preparation of
this plan.
Gill Hiscox
Page 4
Question: Are the Health Checks for the 40-74 year olds useful and
how many of the patients (percentage wise) need treatment for
conditions that they were not aware of?
Dr Sulakshana replied: 664 invitations were issued and 400 were
accepted. 66% were counselled on diet, exercise and lifestyle choices. 2%
were diagnosed with blood pressure, 2% were advised to take statins to
reduce cholesterol, 15% had blood sugar levels higher than ideal and 1%
had diabetes.
Question: What plans have been put in place to combat the
increasing number of patients joining the Practice due to the ever
increasing developments in both areas?
Dr Westgarth replied: The Practice is not restricted by the number of
patients but more by the complexity of their conditions. The income of the
Practice, which has a direct bearing on the services that are provided for
the patients, rises with patient numbers.
Government recently introduced a central audit group to look at practice
patient registers and delete any patients who had not made an
appointment in the last 5 years. These so called ‘phantom patient’ records
were archived in a centre at Warrington. Dr Hughes made the point that
many of our younger and fitter patients did not require any treatment over
very long periods and it may be unreasonable for them to be de-registered.
Question: There was a pilot scheme at the L&D aimed at ensuring that elderly patients
being discharged from the hospital obtained all the relevant services they needed at
home. Was this a success?
Dr Gurram replied: The pilot has finished and was found to be generally
useful, but no funding was available for it to become a permanent feature.
Question: Why hasn’t the path to the entrance to Barton Surgery
been repaired for a long time?
Able bodied people occasionally park close up to the surgery door,
taking spaces that would otherwise be used by others who have
difficulty in walking from the main car-park. Perhaps a sign, or signs,
encouraging able bodied people to park elsewhere, would help.
Gill Hiscox, Practice Manager, replied: We are aware that some areas of tarmac are in
poor condition. Three bodies are responsible for the relative roads and paths – The Parish
Council, the Village Hall, and the Practice. Recently we paid £800 to repair a 6 metre
section of the tarmac, and the Parish Council replaced many paving slabs after three elderly
people suffered falls on them. More tarmac improvements have been scheduled for the near
future. Continued on the opposite page
MORE OF THE QUESTIONS PUT TO THE DOCTORS, AND THE REPLIES,
AT THE OPEN EVENING IN SEPTEMBER

Page 5
A sign or signs about parking near the front door are a problem. It is not
possible to mark the gravel parking spaces, and any signs we install
are quickly vandalised. We plan to tarmac two of the bays and have
them marked with yellow paint for disabled use. It would be helpful if
able bodied patients did not use any of the front spaces and let those
with restricted mobility, but not necessarily having a disabled card, use
them.
Question: What, in the doctors’ opinions, are the
greatest challenges facing the Practice, and what gives
them the greatest satisfaction or enjoyment in their
work?
The replies: Dr Sulakshana – the love of the job, Dr Westgarth – the love of
the job, the challenges being workload and budgets, Dr Randall – continuity
of care and patient relationships, Dr Hughes – getting a laugh from patients
and helping their situation ( not always able to cure, just help), training
registrars. The main challenge – getting registrars to become practice GP’s rather than do
locum work or going abroad. The job has to be made much more attractive, with pride in it
restored and a good work-life balance.
Dr Randall
Gill Hiscox
QUESTIONS AND ANSWERS CONTINUED
When stroke strikes ACT F.A.S.T.
F. FACE - has it fallen on one side? Can they smile?
A. ARMS - can they raise both arms and keep them there?
S. SPEECH - is it slurred?
T. TIME - to call 999 if you see any single one of these
signs of a stroke
There are other symptoms that may occasionally be due to a stroke:
● Sudden loss of vision or blurred vision
● Sudden weakness or numbness on one side of the body
● Sudden memory loss or confusion
● Sudden dizziness, unsteadiness, or a sudden fall, especially with any of
the other symptoms
( F.A.S.T. is a national campaign aimed at raising awareness of strokes)
Page 6
, formerly known as Enduring Power of Attorney, is a
means of authorising chosen and trusted people, the Attorneys, to act on our
behalf in the event of our being disabled or incapable of managing our own affairs.
There are two types of LPA:
The Attorney can use the LPA for financial decisions while you still have mental
capacity, or you can state that you only want it to come into force if you lose
capacity. If you lose mental capacity and do not have an LPA in place your family
or friends will not be able to make financial decisions on your behalf.
This can only be used when you no longer have mental capacity. It covers all kinds
of health and care decisions. Without this LPA the final decision on health and care
matters rests with the medical advisers.
T
here is no need to be losing mental capacity before making a Lasting Power of
Attorney. It can be done at any early stage and treated like an insurance policy.
You hope you will never need it, but if you do your family will be grateful that you
took the trouble to make dealing with your affairs as simple as possible. Problems
can come on very quickly, and the Power of Attorney needs to be in place.
The role of attorney involves a great deal of power and responsibility so that it is
important that you trust the person or people you choose. This is usually a family
member but could be a spouse or friend, and may be a solicitor. The attorney must
be over 18 and will receive no payment for the time involved unless they are a
professional such as a solicitor. It is usual to have more the one attorney, and it has
to decided whether they will act separately or jointly, or very often separately for
everyday transactions and jointly for property deals. When you choose your
attorneys give them a few days to think about the responsibility before the final
decision.
To apply for a Lasting Power of Attorney you get in touch with the Office of the
Public Guardian who will provide an information pack and the Lasting Power of
Attorney forms online. Contact: https://www.gov.uk/power-of-attorney
You can fill in the forms yourself or it can be done for you. You don’t need a
solicitor or local advice agency, but accepting professional advice can save problems
later on. The LPA must be signed by a certificate provider, any responsible person,
who confirms that you have not been put under any pressure to sign it. Finally, the
LPA must be registered with the Office of the Public Guardian before it can be
used. There is a fee to be paid but this can be reduced or dropped if there are
financial problems. The Public Guardian will provide help and guidance
throughout the process.
We last printed advice on Power of Attorney five years ago. Since that time the
arrangements have been simplified and made more user-friendly.
LASTING POWER OF ATTORNEY - it’s often too late, seldom too early
Page 7
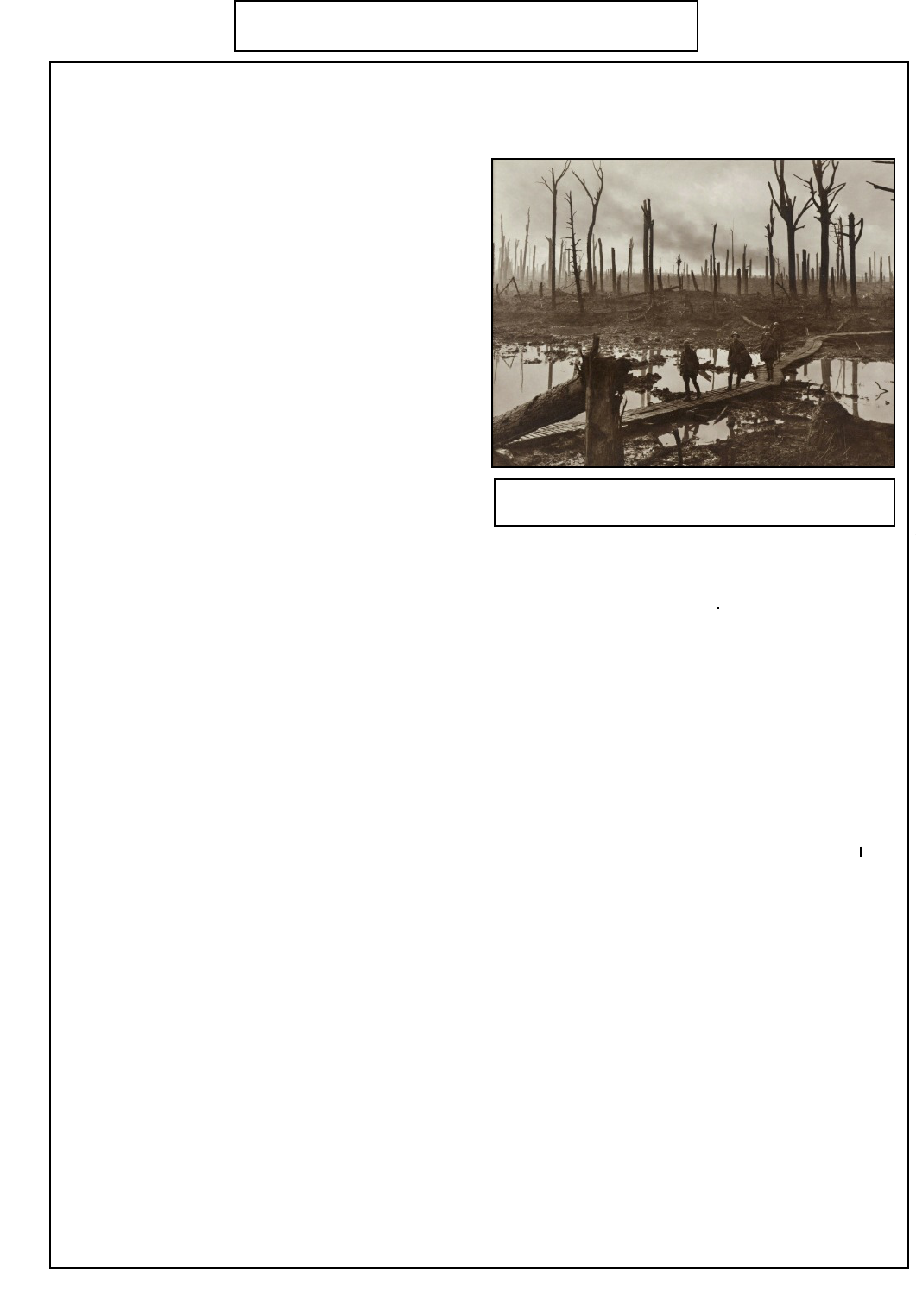
I
n World War II the highest casualty rate was in Bomber Command. In World War I it was
unsurprisingly among the Infantry, and in the infantry the highest casualty rate was among the
officers who went over the top with their men.
They were easily picked out by virtue of their
different uniforms and the fact that they carried
pistols rather than rifles. Officers were almost
exclusively the educated sons of the middle
classes so that although the 'Top Brass' were
usually commanding from cosy headquarters miles
from the front, there was considerable mixing of
the social classes lower down. The officer class
came to have the utmost admiration for the
endurance, stamina and good humour of the
average British 'Tommy' in the face of such
terrible conditions, deprivation and daily
encounters with death. How did men survive such
hardship? The truth was that life in the trenches
was, for many, not much worse than life at home
in squalid slums, dead end jobs, with low pay, poor
diets and few educational opportunities! And yet they were fighting and dying 'for King and
Country' by the hundreds of thousands!
Such was the terrible cost of this war that afterwards there was a frantic search for some good
reasons to explain why it had been fought. One idea that emerged in Britain was that life for ordinary
people had to be made a lot better. It is interesting to note that throughout the 1920's and 30's income
tax never fell below 5/- in the £ (25p.) and few complained. In those times most ordinary people
earned less than £150 per annum which was below the lowest tax level that the tax was levied at, so
income tax was just something for the middle and upper classes to settle twice a year between the
tax office and their accountants! (PAYE for the masses only really got going during World War II
when inflation and vast amounts of overtime for the War effort brought many more in to the tax net.)
So there was a general feeling among the better off in Britain that taxation at 4 or 5 times the level of
the pre-war, Edwardian period had to be accepted to improve the lives of ordinary people who had
sacrificed so much. (The contrast with today's thinking is surely most marked!)
Sadly, of course, the effects of successive governments attempts to raise living standards in the
1920's and 30's were largely masked by the massive world-wide Economic Depression that set in in
1924 as World Trade completely failed to recover from the massive disruption caused by 4 years of
global war. There was massive unemployment (twice as high in Germany as in the UK.)
Unemployment levels varied from area to area. In Merthyr Tydfil at the height of the Depression in
the early 1930's the level was 70%! The birth rate plummeted to it's lowest level ever in this country
in 1932. However, the school leaving age was raised to 14, National Insurance was extended to
cover many more jobs and some Health improvements were made. But perhaps the biggest strides
were in Housing, following on from Lloyd George's 1918 slogan about ' building homes fit for
Heroes'. All Local Authorities were required to purchase land and commence a programme of
building houses to rent which ordinary people could afford. The age of the ‘Council House’ had
arrived to house a third of the population.
The second part of this article by Ivan Jones will appear in the next Newsletter
The terrible conditions on the Somme battlefield,
1916. The junior officer is second in the file.
THE YEARS BETWEEN THE TWO WORLD WARS
Dr Simon P Hughes
and Partners,
The Surgery,
Hexton Road,
Barton le Clay
Beds MK45 4TA
Telephone 01582 528700
BARGOOSE
Health Centre,
Gooseberry Hill,
Luton, Beds LU3 2LB
Telephone: 01582 528721
PRACTICE WEBSITE
www.bartongroupsurgeries.
co.uk
Page 8
EUROPEAN HEALTH
INSURANCE CARD
(EHIC)
A valid European Health
Insurance Card (EHIC)
gives the card holder the
right to access state-
provided healthcare on a
temporary basis as it would
be to a resident of that
country in the European
Economic Area (EEA) This
covers treatment necessary
before the card holder
returns home and includes
treatment for pre-existing
medical conditions.
This is not an alternative to
travel insurance which is
still vital for those
travelling within Europe.
The card is provided free of
charge. Initial contact:
www.ehic.org.uk
T
he Practice were given two weeks’ notice of a CQC (Care
Quality Commission) Inspection to take place on the 17 May
2016. One inspector and three ‘specialists’ arrived just after 8.00
a.m. Prior to the visit we had had to send a forest of paperwork to
the CQC including protocols, surveys, staffing information, reports,
statistics etc.
The ‘specialists’ were a GP, a Pharmacist and an Administrator
who had knowledge of Practice Management. The day was
planned for the GP to spend the morning with Dr Hughes and the
afternoon with Dr Westgarth. The Lead Inspector would be with
Liz, our Lead Nurse and the Pharmacist with Naomi, Dispensary
Manager whilst the Administrator spent the day with me, the
Practice Manager.
During the course of the day the Lead Inspector also interviewed a
number of staff including Kate, Reception Manager and our Chair
of the Patient Group and his wife Bill and Christine Holes.
The inspection covers 5 areas :
Safe
Caring and Responsive
Well Led
Effective
Utilities
Each area has to be evidenced with numerous systems,
procedures and safety certificates. The Administrator sat in my
office surrounded with almost every piece of paper I have! Some
areas covered were checking staff files for references, contracts,
training certificates etc; electric safety checks; complaints
processes; significant event records and so on and so on!
Even though we consider that we are a good Practice, actually
being inspected is an extremely stressful experience for the whole
Practice.
The day ended at 5.00 pm with a meeting of all Partners,
Departmental Heads and myself with the CQC Inspectors feeding
back on their findings. They were very generous with their
comments and were obviously very impressed with us which was a
huge relief.
The final report was received on the 1
st
December (six months
after the inspection) and can be read on the website
www.bartongroupsurgeries.co.uk
Gill Hiscox, Practice Manager
THE CARE QUALITY COMMISSION IS THE INDEPENDENT
REGULATOR OF HEALTH AND SOCIAL CARE IN ENGLAND
