
1 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Attachment 1
District of Columbia Home & Community-Based Waiver Settings Compliance Update-Operations
Submitted to CMS December 21, 2022
Description of how the state’s oversight systems (licensure and certification standards, provider manuals,
person-centered plan monitoring by case managers, etc.) have been modified to embed the regulatory criteria
into ongoing operations;
Excerpt from District of Columbia Statewide Transition Plan (September 30, 2020 Update)
The following excerpts address each oversight area below by Intellectual and Developmental Disability (IDD) and
Elderly and persons with Physical Disabilities (EPD) groups respectively:
1. Policy on compliance with HCBS Settings Rule
2. HCBS service definitions and requirements
3. All regulations governing HCBS
4. Provider requirements
5. Licensing requirements and regulations
6. All relevant policies, procedures, and protocols
7. Provider training requirements
8. Human Care Agreements (IDD only)
Section V: Assessment & Remediation
A. Policy on Compliance with HCBS Settings Rule
1. DDS Policy on Compliance with HCBS Settings Rule (2015-DDS-POL23).
2 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
DDS issued a policy requiring that agency staff and providers participate in efforts to assess and achieve compliance
with the HCBS Settings Rule. This includes the expectation that providers conduct a critical and honest self-
assessment; cooperate fully with the assessment and transition process; and demonstrate on-going efforts, cooperation
and progress towards compliance with the HCBS Settings Rule. The policy was issued by the projected date of April 1,
2015 and posted on the DDS website at: http://dds.dc.gov/publication/hcbs-settings-rule-compliance-policy.
September 2019 Update: No update. The District of Columbia has completed all required policy updates, with final
policies published in September 2018, as discussed above.
September 2018 Update: In M
ay 2018, DDS issued a Home and Community Based Services for People with
Intellectual Disabilities Day Setting Heightened Scrutiny Review Procedure, 2018-DDS-PR-02, and accompanying
Transmittal # 18-2, incorporating the methodology described within this Statewide Transition Plan. Please see
https://dds.dc.gov/publication/heightened-scrutiny-procedure and https://dds.dc.gov/publication/heightened-scrutiny-
transmittal-18-2, respectively.
2. DHCF Policy on Compliance with HCBS Settings Rule
DHCF will issue a transmittal informing all providers of DHCF’s expectations that they will come into compliance
with the HCBS Settings Rule. The transmittal is planned for release during the third quarter of 2017.
September 2019 Update: DCHF adjusted its policy strategy by incorporating the settings requirements in its
monitoring assessment for Assisted Living Facilities. HCBS Settings requirements are reinforced annually with each
ALF during an on-site visit as a part of the annual monitoring process. This strategy has proven effective as evidenced
by 100% compliance in the first quarter of Fiscal Year 2019.

3 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
September 2018 Update: In anticipation of the March 17, 2022 initial deadline for full compliance with the HCBS
Settings rule, DHCF will issue a transmittal as planned in 2018. As policies and procedures are drafted for the waiver,
the settings requirements will also be incorporated.
B. State Level Self-Assessment Process, Results and Remediation
1. HCBS Settings for People with IDD
DDS established an HCBS Settings Rule Advisory Group and held a series of meetings to assess all rules, regulations,
licensing requirements, certifications processes, policies, service definitions, protocols, practices and contracts to
determine which characteristics of HCBS settings are already required and where there are gaps. The review group
identified areas where changes are needed to ensure compliance with the HCBS settings characteristics rule and made
recommendations for remediation.
1. DDS invited representatives of the groups below to participate in the review group and invited and consulted with
others, including the Department of Health (DOH), as needed. DDS posted the meeting dates on its website and
members of the public were welcome to attend and participate. DDS State Office of Disability Administration
(SODA) is responsible for arranging and facilitating the meetings. DDS Information Technology (IT) Unit posts
items, as needed, on the website. Although the state level self-assessment process has been completed, meetings
will continue, as needed, through the remediation process. For example, DDS reconvened the group to provide
input into a draft of proposed Host Home regulations. Planning is underway to conduct a meeting to discuss
challenges and solutions for compliance with the leasing/ written residency agreement sections of the HCBS
Settings Rule.
Although meetings are open, invited members of the review group include:

4 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
a. DDS, including representatives from DDA Service Coordination, DDA Waiver Unit, SODA, a Person-Centered
Thinking Leader, DDS/DDA’s Provider Certification Review team and others, as needed, including
representatives from DDS/DDA Quality Management Division;
b. DHCF;
c. DC Developmental Disabilities Council
d. Project ACTION!, DC’s self-advocacy group;
e. DC Supporting Families Community of Practice;
f. Quality Trust for Individuals with Disabilities;
g. Disability Rights DC/ University Legal Services, DC’s protection and advocacy organization;
h. DC Coalition of Disability Services Providers; and
i. Georgetown University Center for Excellence in Developmental Disabilities.
2. The state level assessment was completed, as projected, by September 1, 2015 and has resulted in DC having a list
of required changes needed to the waiver itself, implementing regulations, and policies, procedures and practices.
The self-assessment included a review and analysis of:
a. All HCBS waiver service definitions and provider requirements (including all residential, day and
vocational services) are attached.
The HCBS waiver is available on-line on the DDS Waiver Amendment Page at:
http://dds.dc.gov/node/1220341
Remediation: The District is planning several additional waiver amendments to support compliance with the HCBS
Settings Rule and seeks public comment on these as described below and welcomes additional ideas. DDS will
ensure appropriate public notice and comment periods for the proposed waiver amendments, including posting of
the entire waiver application with the proposed amendments. DDS will also ensure appropriate due process notice
5 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
to all impacted HCBS IDD waiver beneficiaries. Changes to the waiver will be completed by November 2017, as
part of the waiver renewal, and may vary from what is described below based upon public comment. .
• Provider Qualifications for All HCBS Settings: Modify language in provider qualifications for Supported
Living, Supported Living with Transportation, Host Home, Residential Habilitation, Day Habilitation, and
Employment Readiness to require that any new settings must meet all requirements of the HCBS Settings
Rule. Require that all Supported Living, Supported Living with Transportation, and Host Home settings
fully comply with the HCBS Settings Rule as of the effective date of the waiver renewal.
• Residential Habilitation: Limit the size of all new settings to no more than 4 peopleor less per setting;
those who wish to stay with their housemates are not required to move. After November 1, 2020, settings
that are currently for 5 or 6 people will be targeted for reduction through attrition.
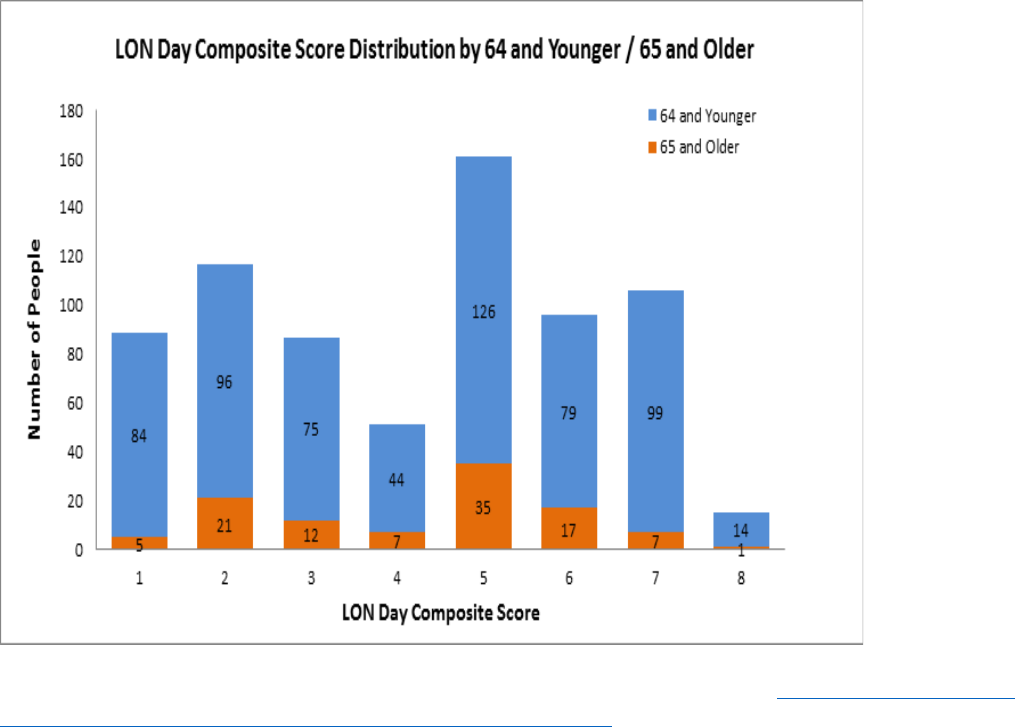
• Day Habilitation: Eligibility Limitations based on Level Of Need (LON):
Service limitations for new individual admissions to Day Habilitation services:
(1) People who are 64 years old and younger and have a Level of Need Day Composite score of 2 or less would
not be eligible to attend Day Habilitation services, unless approved by DDS due to extenuating circumstances or
barriers that are expected to be resolved within six months. Exceptions may only be granted for 6 month
periods and must be accompanied by an Individual Support Plan goal aimed at addressing the barrier to
participation in other day or employment waiver supports. Alternative services, including Employment
Readiness, Small Group Supported Employment, Individualized Day Supports, and Companion services that
are offered during regular day service hours, would be available, in combination, for up to forty hours per
week.
6 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(2) People who are 64 and younger and have a Level of Need Day Composite score of 3 or 4 would not be
eligible to attend Day Habilitation programs, unless they have tried other day and employment options for one
year first unless approved by DDS due to extenuating circumstances or barriers that are expected to be resolved
within six months. Any exceptions must be accompanied by an ISP goal aimed at addressing the barrier to
participation in other day or employment waiver supports. Alternative services including Supported
Employment, Individualized Day Supports, Employment Readiness and Companion would be available in
combination for up to forty hours per week.
(3) In addition to the limitations described above, Day Habilitation services may not be authorized for any
waiver participant for more than 24 hours per week. Wrap around services are available, including Supported
Employment, Individualized Day Supports, Employment Readiness and Companion in combination for up to
forty hours per week. This limitation is not applicable to Small Group Day Habilitation services.
Service limitations for people currently in Day Habilitation services:
(1)Within one year from the waiver effective date, any person with a Level of Need Day Composite score of 1
or 2 would no longer be eligible for Day Habilitation services and services may no longer be
authorized. Instead the person should be offered employment services, either through the waiver, the
Rehabilitation Services Administration, or other community based options, subject to the exception described
below. This would be implemented on a rolling basis over the course of the year, with the new service
limitation discussed and choice of alternative options offered at the person’s next ISP meeting. Exception: For
people with an ISP meeting that is scheduled within 90 days of the first anniversary of the waiver effective date,
DDS may authorize Day Habilitation services for up to 90 days following the ISP meeting to ensure a smooth
transition.
(2) Within one year from the waiver effective date, regular Day Habilitation services may not be authorized for
any waiver participant with a Day Composite Level of Need score above 2 for more than 24 hours per week,
subject to the exceptions described below. Wrap around services are available, including Supported
Employment, Individualized Day Supports, Employment Readiness and Companion in combination for up to
7 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
forty hours per week. Exceptions: This limitation is not applicable to Small Group Day Habilitation
services. Additionally, for people with an ISP meeting that is scheduled within 90 days of the first anniversary
of the waiver effective date, DDS may authorize up to 40 hours of Day Habilitation services per week for up to
90 days following the ISP meeting to ensure a smooth transition.
(3) For any person who is currently receiving Day Habilitation services who will be subject to a reduction in
authorized service hours due to the service limitations listed above, DDS will provide timely and adequate due
process notice of the change in services and the person’s appeal rights.
The chart below indicates the current LON Day Composite Scores amongst people who are attending Day
Habilitation programs.
9 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
• Size Limitations on Day Habilitation and Employment Readiness Settings
a. Current Day Habilitation and Employment Readiness settings that have a daily census under fifty people
in the setting for more than 20% of the day, may only receive authorizations for services for new
participants up to a daily census of fifty people in the setting.
b. Current Day Habilitation settings that have a daily census of fifty people or more in the setting for more
than 20% of the day will not be eligible for authorizations for services for new participants until their
daily census is less than fifty people in the setting. (There are no current Employment Readiness settings
that have a daily census over 50 people in the setting.)
• Employment Readiness: Time Limitation on Services
For people who are not currently enrolled in Employment Readiness services, the service may only be
authorized for up to one year, except that DDS may approve up to a one year extension if there is
documentation that the person is making progress towards competitive integrated employment and would
benefit from extended services.
For people who are currently enrolled in Employment Readiness services, the service may only be reauthorized
for up to one year from the person’s next ISP date, except that DDS may approve up to a one year extension if
there is documentation that the person is making progress towards competitive integrated employment and
would benefit from extended services.
If a person has exhausted Employment Readiness services and: (1) has had at least one year since the end of that
service; (2) expresses an interest in employment; and (3) the support team has identified specific goals around
building employment skills that are reflected in the ISP, then DDS may authorize Employment Readiness
services one time, for up to one year. (Total of up to three years of Employment Readiness services.)

10 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Exception: At any time that a person loses his or her job, or is employed and is seeking to learn new job skills,
DDS may authorize Employment Readiness services for up to one year.
For any person who is currently receiving Employment Readiness services who will be subject to a reduction in
authorized service hours due to the service limitations listed above, DDS will provide timely and adequate due
process notice of the change in services and the person’s appeal rights, using the process described in the DDS
Person Centered Planning Process and Individual Support Plans policy and procedures, or the successor
documents.
September 2019 Update: No update. As noted in 2018: DC provided all Waiver changes with approval.
September 2018 Update: DC renewed its waiver, effective November 20, 2018. Selected changes include:
• A requirement that all Residential Settings be fully compliant with the HCBS Settings Rule.
• A requirement that all providers of Employment Readiness services become Vocational Rehabilitation
providers
• Size limitations for Residential Habilitation settings
• Time limitations for use of Employment Readiness services
• Limitations on the size of Day Habilitation programs
• Limitations on number of hours a person may be authorized to use Day Habilitation services
• Limitations on who may use Day Habilitation services
• Requirement that Supported Employment and Employment Readiness staff have training that is the
equivalent to ACRE/ CESP training.
b. All regulations governing HCBS
11 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
The regulations are available on the DDS website at: http://dds.dc.gov/page/hcbs-waiver-service-description or
via the DC Regulations website at:
http://www.dcregs.dc.gov/Gateway/ChapterHome.aspx?ChapterNumber=29-19.
Remediation: DDS and DHCF began the publishing the first round of regulation revisions in spring 2015.
However, the regulation implementation date was timed to the effective date of the waiver amendments, which
did not occur until September 2015. Once it became apparent that the waiver would not be approved over the
summer, DDS and DHCF held off on publishing new regulations until we had a better sense of when the waiver
would be approved. Regulatory revisions will continue, on an ongoing basis, as needed, to ensure full
compliance with the HCBS Settings Rule no later than March 17, 2022.
The bulk of the changes made are in the “General Provisions,” which apply to all HCBS Settings. Please see,
online: http://www.dcregs.dc.gov/Gateway/ChapterHome.aspx?ChapterNumber=29-19. First, we
require via
regulation that each waiver provider develop and adhere to policies which ensure that each person receiving
services has the right to the following:
• Be treated with courtesy, dignity, and respect;
• Direct the person-centered planning of his or her supports and services;
• Be free from mental and physical abuse, neglect, and exploitation from staff providing services;
• Be assured that for purposes of record confidentiality, the disclosure of the contents of his or her personal
records is subject to all the provisions of applicable District and federal laws and rules;
• Voice a complaint regarding treatment or care, lack of respect for personal property by staff providing services
without fear of retaliation; and
• Be informed orally and in writing of the following:
o Complaint and referral procedures including how to file an anonymous complaint;
o The telephone number of the DDS customer complaint line;
o How to report an allegation of abuse, neglect and exploitation;
12 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
o For people receiving residential supports, the person’s rights as a tenant, and information about how to
relocate and request new housing.
We also added a new section, below, to the “General Provisions”:
HOME AND COMMUNITY-BASED SETTING REQUIREMENTS
(1) All Supported Living, Supported Living with Transportation, Host Home, Respite Daily, Residential Habilitation,
Day Habilitation, Small Group Day Habilitation, Individualized Day Supports, Supported Employment, Small
Group Supported Employment and Employment Readiness settings must:
(a) Be chosen by the person from HCBS settings options including non-disability settings;
(b) Ensure people’s right to privacy, dignity, and respect, and freedom from coercion and restraint;
(c) Be physically accessible to the person and allow the person access to all common areas;
(d) Support the person’s community integration and inclusion, including relationship-building and
maintenance, support for self-determination and self-advocacy;
(e) Provide opportunities for the person to seek employment and meaningful non-work activities in the
community;
(f) Provide information on individual rights;
(g) Optimize the person’s initiative, autonomy and independence in making life choices including but not
limited to, daily activities, physical environment, and with whom to interact;
13 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(h) Facilitate the person’s choices regarding services and supports, and who provides them;
(i) Create individualized daily schedules for each person receiving supports, that includes activities that align
with the person’s goals, interests and preferences, as reflected in his or her ISP;
(j) Provide opportunities for the person to engage in community life;
(k) Provide opportunities to receive services in the community to the same degree of access as individuals not
receiving Medicaid HCBS;
(l) Control over his or her personal funds and bank accounts; and
(m) Allow visitors at any time.
(2) All Supported Living, Supported Living with Transportation, Host Home, Residential Habilitation, and Respite
Daily, settings must:
a) Be integrated in the community and support access to the greater community;
b) Allow full access to the greater community;
c) Be leased in the names of the people who are being supported. If this is not possible, then the provider
must ensure that each person has a legally enforceable residency agreement or other written agreement
that, at a minimum, provides the same responsibilities and protections from eviction that tenants have
under relevant landlord/tenant law. This applies equally to lease and provider owned properties.
d) Develop and adhere to policies which ensure that each person receiving services has the right to the
following:
14 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(1) Privacy in his or her personal space, including entrances that are lockable by the person (with
staff having keys as needed);
(2) Freedom to furnish and decorate his or her personal space (with the exception of Respite
Daily);
(3) Privacy for telephone calls, texts and/or emails; or any other form of electronic communication,
e.g. FaceTime or Skype; and
(4) Access to food at any time.
(3) All Day Habilitation, Small Group Day Habilitation, Individualized Day Supports, Supported Employment, Small
Group Supported Employment and Employment Readiness settings must develop and adhere to policies which
ensure that each person receiving services has the right to the following:
a) Privacy for personal care, including when using the bathroom;
b) Access to snacks at any time;
c) Privacy for telephone calls, texts and/or emails; or any other form of electronic communication, e.g. FaceTime
or Skype; and
d) Meals at the time and place of a person’s choosing.
Any deviations from the requirements in 1(l) and (m), 2(d) and 3 must be supported by a specific assessed need,
justified in the person’s person-centered Individualized Support Plan, and reviewed and approved as a restriction
by the Provider’s Human Rights Committee (HRC). There must be documentation that the Provider’s HRC
review included discussion of the following elements:
(a) What the person’s specific individualized assessed need is that results in the restriction;
15 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(b) What prior interventions and supports have been attempted, including less intrusive methods;
(c) Whether the proposed restriction is proportionate to the person’s assessed needs;
(d) What the plan is for ongoing data collection to measure the effectiveness of the restriction;
(e) When the HRC or the person’s support team will review the restriction again;
(f) Whether the person, or his or her substitute decision-maker, gives informed consent; and
(g) Whether the HRC has assurance that the proposed restriction or intervention will not cause harm.
Please note that the Provider HRC review is a pre-requisite to the ISP Support Team meeting. The ISP team must
allow review and approve all deviations from the requirements and there must be documentation in the ISP of all
the elements discussed above. DDS is currently piloting a new ISP process that incorporates this review. The
new ISP process will begin for all waiver recipients no later than September 30, 2017 and will be implemented
on a rolling basis throughout as each person has their next scheduled ISP meeting.
All of the above changes have been made through Emergency and Proposed Rulemakings and are in effect.
The public comment period closed on June 13, 2016, without any public comments. A final rulemaking for
“General Provisions” was published on August 12, 2016 (see attached). In addition to the changes described
above, DC updated individual regulations for each of the HCBS Settings, detailed in the Statewide Assessment
Reporting Charts, attached.
DDS recognizes that there is additional regulatory action to take, although much of the HCBS Settings Rule has
already been adopted into DC regulations and requirements. Rather than make all of the changes at once, we
decided to allow some time to give providers an opportunity to build capacity, train staff, and change their
practices. DDS plans to continue to update the General Provisions, and, if needed, the Day Habilitation, and
Employment Readiness regulations, to implement standards that meet the requirements of the HCBS Settings

16 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Rule for all settings. All regulations will be fully updated to ensure HCBS Settings compliance by September
2018, which leaves sufficient time for providers to come to compliance and DDS to move any people who are
in settings we determine will not become compliant with the rule. Additionally, for both day and residential
settings, DDS will continue to analyze the results of the site-by-site assessments and what we learn through
Provider Performance Review to determine whether additional regulatory action is needed to address
compliance with the HCBS Settings Rule.
DC recognizes that changing regulations alone does not always lead to changes on the ground level for people
receiving services. As described throughout this document, DDS is using a variety of quality functions to
measure provider compliance with the HCBS Settings Rule, providing technical assistance, require individual
remediation plans, called Provider Corrective Action Plans, and follow any issues through to remediation. This
includes the changes we have made to our Provider Certification Review process to add questions that test
compliance with all aspects of the HCBS Settings Rule; the new requirements for a Continuing Improvement
Plan for HCBS Settings Compliance in Provider Certification Review through the Provider Performance
Review; the revised Service Coordination Monitoring Tool; the focus on the HCBS Settings Rule at all Provider
Leadership meetings, and more. Simply put, DDS has revised significant portions of our Quality Management
System so that we have the ability to assess provider compliance with the HCBS Settings Rule; provide support
for compliance; and ensure remediation throughout the transition period and ongoing.
September 2019 update: No update. DC completed all regulatory changes for HCBS IDD Waiver providers.
September 2018 update: DC has completed its update of regulatory changes related to compliance for HCBS
IDD waiver providers. Based upon input from the HCBS Settings Advisory Group, DC added information to
the rules that describe examples of what is expected for a setting to be found in compliance. These examples
were taken from the CMS sub-regulatory guidance exploratory questions and recommendations from members
of Project ACTION!, DC’s self-advocacy group.
Emergency and proposed rules were adopted on November 24, 2018, to implement the new waiver. Final rules
were adopted on March 2, 2018. Both sets of rules are available at:

17 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
https://dcregs.dc.gov/Common/DCMR/SectionList.aspx?SectionNumber=29-1938. The full text of the final
rule is as follows:
1938 HOME AND COMMUNITY-BASED SETTING REQUIREMENTS
1938.1 All Supported Living, Supported Living with Transportation, Host Home Without Transportation,
Residential Habilitation, Day Habilitation, Small Group Day Habilitation, Individualized Day Supports,
Companion, Supported Employment, Small Group Supported Employment and Employment Readiness
settings must:
(a) Be chosen by the person from HCBS settings options including non-disability settings. For
residential settings, this includes, but is not limited to, ensuring that:
(1) People select their home and know that they have protections against eviction;
(2) People choose their roommates and know how to request a roommate change; and
(3) People who have a roommate are offered the choice of available residential settings with a
private bedroom, if they have the ability to pay.
(b) Ensure people’s right to privacy, dignity, and respect, and freedom from coercion and restraint.
This includes, but is not limited to, ensuring that:
(1) People are provided personal care assistance in private, as appropriate;
(2) Information is provided to people on how to make an anonymous complaint;
(3) People’s health and other personal information (e.g., mealtime protocols, therapy
schedules) are kept private;
18 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(4) Staff do not talk about people’s private information in front of other people who do not
have a right and/ or need to know; and
(5) Staff address people by their names or preferred nicknames.
(c) Be physically accessible to the person and allow the person access to all common areas. For
residential settings, this includes, but is not limited to, ensuring that:
(1) People have full access to the kitchen, dining area, living room, laundry, and all other
common areas of their home; and
(2) The home is fully accessible to meet the needs of the people living there, including all
common areas and supports as needed, such as grab bars and ramps.
(d) Support the person’s community integration and inclusion, including relationship-building and
maintenance, support for self-determination and self-advocacy;
(e) Provide opportunities for the person to seek employment and meaningful non-work activities in
the community. This is evidenced in part by the following:
(1) People who desire to work are supported to pursue work in the community; and
(2) People engage in meaningful non-work activities in the community.
(f) Provide information on individual rights;
(g) Optimize the person’s initiative, autonomy, and independence in making life choices including,
but not limited to, daily activities, physical environment, and with whom to interact;

19 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(h) Facilitate the person’s choices regarding services and supports, and who provides them;
(i) Create individualized daily schedules for each person receiving supports, that includes activities
that align with the person’s goals, interests and preferences, as reflected in his or her ISP, in
accordance with DDS guidance;
(j) Provide opportunities for the person to engage in community life, as evidenced in part by people
being able to shop, attend religious services, schedule appointments, have lunch with friends and
family, etc. in the community, as they choose;
(k) Provide opportunities to receive services in the community to the same degree of access as
individuals not receiving Medicaid HCBS, as evidenced in part by people using community
resources, such as parks, recreational centers, community health clinics, etc.;
(l) Control over his or her personal funds and bank accounts, as evidenced in part by people being
able to access their funds, when they want to, and without advanced notice;
(m) Allow visitors at any time within the limits of the lease or other residency agreement;
(n) Be integrated in the community and support access to the greater community. This is evidenced in
part by the following:
(1) People receive the supports they need to see family and friends and spend time doing
activities of their choosing in the community; and
(2) People are encouraged to learn travel skills so that they can use public transportation.
(o) Allow full access to the greater community.
20 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
1938.2 All Supported Living, Supported Living with Transportation, Host Home Without Transportation, and
Residential Habilitation settings must:
(a) Be leased in the names of the people who are being supported. If this is not possible, then the
provider must ensure that each person has a legally enforceable residency agreement or other
written agreement that, at a minimum, provides the same responsibilities and protections from
eviction that tenants have under the relevant landlord/tenant law for that jurisdiction. This includes
a responsibility to ensure that each person knows their rights regarding housing, as explained by
their lease or written residency agreement, including when they could be required to relocate, and
understand the eviction process and appeals rights. This provision applies equally to leased and
provider owned properties;
(b) Develop and adhere to policies which ensure that each person receiving services has the right to
the following:
(1) Privacy in his or her personal space, including entrances to living spaces that are lockable
by the person (with staff having keys as needed). This is evidenced in part by staff
knocking and receiving permission prior to entering a person’s living space;
(2) Freedom to furnish and decorate his or her personal space, as evidenced in part by people’s
living space reflecting their taste and preferences (e.g., furniture, linens and other
household items reflect people’s choices), within the limits of the lease or other residency
agreement or consistent with the governing Human Care Agreement;
(3) Privacy for telephone calls, texts and/or emails, or any other form of electronic
communication, e.g. FaceTime or Skype, with or without support, based on person’s
preference; and
21 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(4) Access to food at any time, as evidenced in part by:
a. Each person has meals at the time and place of his or her choosing;
b. People can request an alternative meal, if desired; and
c. Snacks are available and accessible at any time unless there is documentation of a
medical condition that requires restrictions.
1938.3 All Day Habilitation, Small Group Day Habilitation, Individualized Day Supports, Supported
Employment, Small Group Supported Employment, Companion and Employment Readiness settings
must develop and adhere to policies which ensure that each person receiving services has the right to the
following:
(a) A secure place to keep their belongings;
(b) Access to snacks at any time;
(c) Privacy for telephone calls, texts and/or emails, or any other form of electronic communication,
e.g. FaceTime or Skype, with or without support, based on the person’s preference; and
(d) Meals at the time and place of a person’s choosing.
1938.4 Any deviations from the requirements in §§ 1938.1(l) and (m), 1938.2(b) and § 1938.3 must be supported
by a specific assessed need, justified and documented in the person’s person-centered Individualized
Support Plan, as well as reviewed and approved as a restriction by the Provider’s Human Rights
Committee (HRC). There must be documentation that the Provider’s HRC review and person-centered
planning meeting included discussion of the following elements:

22 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(a) What the person’s specific individualized assessed need is that results in the restriction;
(b) What prior interventions and supports have been attempted, including less intrusive methods;
(c) Whether the proposed restriction is proportionate to the person’s assessed needs;
(d) What the plan is for ongoing data collection to measure the effectiveness of the restriction;
(e) When the HRC and the person’s support team will review the restriction again;
(f) Whether the person, or his or her substitute decision-maker, gives informed consent; and
(g) Whether the HRC and the person’s support team has assurance that the proposed restriction or
intervention will not cause harm.
September 2019: No update. DC has completed all regulatory changes, with final regulations published in
March 2018, as discussed above.
c. DDS/DDA Provider Certification Review (PCR) process
DDS’s PCR policy, procedure, guidance and tools are available on-line at: http://dds.dc.gov/book/vi-
administrative-dda/provider-certification-review-policy-and-procedures.
Credentials and Training of the PCR staff
The development of the HCBS indicators was completed by the senior managers of the PCR team in partnership
with DDS leadership. The senior managers on the PCR team were responsible for training and ongoing
management of quality measures to insure reliability of the PCR team’s assessment of these indicators. The
senior managers have had years of experience in waiver programs in several states, have received multiple
23 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
trainings in person centered thinking and personal outcome measures from both state agencies and national
leaders in these areas. Specifically, the Senior PCR managers trained the PCR staff members in the
identification of the elements required to be present in order for any one HCBS indicator to be met.
More broadly, the PCR reviewers have been hired to review the provider’s ability to meet all waiver
requirements including HCBS designated indicators for services they offer. They perform these reviews each
week as part of the PCR certification process. All PCR reviews come with at least one year of experience in an
HCBS waiver setting. Many come with case management, quality management, or program management
experience. On hire, each reviewer receives orientation to all indicators including HCBS indicators in the
District’s IDD waiver program. The tools contain written guidance on how to interpret if indicators are met, not
met, or not applicable. A new reviewer is paired with a seasoned reviewer on average for the first three reviews
which involves observing, then conducting a review with the guidance of the season reviewer, then co-
reviewing a person in the sample- in which both reviewers complete an answer sheet, and inter rater reliability
can be established. Senior managers complete an annual inter rater reliability session with each reviewer. All
answer sheets for each review are reviewed by a senior manager before they are approved to determine that
statements accurately fit the designation a reviewer has selected. Only approved answer sheets are submitted to
the database to determine the results. There is often discussion between the senior review manager and the
individual reviewer about how the reviewer arrived at their conclusions, and this assures the Manager that the
reviewer’s thinking is in line with the current guidelines.
Each of the HCBS indicators have a set of sub questions which help the reviewer determine the designation of
the indicator. Sub questions have been selected based on CMS published guidance and the current DDS waiver
rules. All sub questions of an indicator must be satisfied in order for the indicator to be marked as met. This
configuration insures that all reviewers are looking at the same set of criteria, and forms the basis of a “not met”
answer. Here are two examples to illustrate the indicator and the sub questions to that indicator:
Indicator: Does the person have access to use a phone or computer privately, with or without support,
based on the person's preferences?
Subset questions:

24 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Is there a computer or phone available to the person in a private area?
If not, is it due to a restriction based on an assessment?
If there are limitations, is there documentation of the provider HRC review which meets the criteria
outlined in the HCBS Waiver rule, Chapter 19 Section 1938?
Indicator:
Has the provider created a culture in which visitors are accepted and encouraged?
Subset questions:
Does the person express that they can have visitors whenever they want?
Does the family feel they can drop in whenever they want?
Are visitors treated the same as visitors would be in the greater community? If not, is it due to a
restriction based on an assessment?
If there are limitations, is there documentation of the provider HRC review which meets the criteria
outlined in the HCBS Waiver rule, Chapter 19 Section 1938?
Continuing education is ongoing. Each reviewer must attend the District’s Person Centered Thinking Training.
Bi Monthly educational sessions are offered by PCR Senior Managers to reviewers to insure changes to DDS
policy, and Service Rules are understood and implemented. Specific HCBS indicators are selected to be
highlighted in one of these sessions. Included in these sessions are discussions with and among reviewers of
what they are collecting as evidence that indicators are being met to share “best practices” identified by the
staff.
Remediation:
First, to assist providers in completing the Day and Vocational Provider Self-Assessment and the Residential
Provider Self-Assessment the PCR team completed a crosswalk of the self-assessment indicators to the PCR
indicators. This crosswalk was sent out to providers with the self-assessment.
When it was decided by DDS to use the PCR process as a way to collect information and validate the results of
the self-assessment, a closer look was made to the self-assessment indicators and the associated CMS
Recommended Assessment Questions. The PCR team determined that the PCR indicators might be too broad
25 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
and might not be sufficient to successfully demonstrate whether they met the requirements of CMS. At that
time, new indicators were written as part of the PCR tool that better matched the CMS assessment questions.
The PCR tool, as originally designed has a person centered component and an organizational component. The
person centered tools consist of 8 domains:
1. Rights and dignity
2. Safety and Security
3. Health and Wellness
4. Decision Making
5. Community Inclusion
6. Relationships
7. Service Planning and Delivery
8. Satisfaction
Each indicator, within the tool is designated as either QA or QI. QA indicators are based on rules, policies and
procedures and must be met. QI indicators are what would be considered best practice and are not required to be
met. QA indicators have a weighted number assigned to them.
For purposes of completing the self-assessment validation, an addition domain 9 was added, which consisted of
the newly created HCBS indicators. For the purpose of validation, the indicators were designated as QI, no
weight was assigned to them and they do not currently impact a provider’s score. As of July 1, 2016, all but the
indicators having to do with leasing/tenant agreements will become Q/A indicators with weights assigned to
these indicators. At that time, all the HCBS indicators will be placed in the appropriate domains as listed above.
The same process was completed for the organizational indicators. The organizational tool contains 6 outcomes.
They are:
1. The provider has systems to protect individual rights.
2. The provider has a system to respond to emergencies and risk prevention.
26 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
3. The provider ensures that staffs possess the needed skills, competencies and qualifications to support
individuals.
4. The provider has a system to improve Provider certification over time.
5. The provider ensures that each individual has the opportunity to develop and maintain skills in their
home and community.
6. The provider will ensure individuals are safe and receive continuity of services when receiving respite
services.
An additional outcome was added to the organizational tool for HCBS requirements at the organizational level.
Each outcome has individual indicators which must be met and have a weight assigned to them, as in the person
centered tools. The indicators written for the HCBS validation process were given a QI status and assigned to
Outcome 7.
It should be noted, that some of the items being measured in the self-assessment were already things DDS
designated as QA indicators in the PCR such as privacy when completing personal care. In those instances, the
original PCR indicator stayed in its domain and continued to have a weight assigned to it.
Domain 9 and Outcome 7 were added to the relevant tools in the PCR database. They were added to the
following services:
(c) Day Habilitation
(d) Day Habilitation 1:1
(e) Employment Readiness
(f) Supported Living
(g) Supported Living Periodic
(h) Host Home
(i) Residential Habilitation
27 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(j) Organizational tool (for all services)
Once the new indicators were written, research was done to better understand the CMS expectations.
Documents such as the CMS exploratory questions were used. The CQL Toolkit for States prepared by Kerri
Melda and Drew Smith was used to assist in developing exploratory questions. These documents were used to
create guidance for the PCR reviewers. Guidance was suggested as to questions to ask, documents to review
and observations to make. Once the guidance was written, PCR reviewers were trained. They were also given
copies of all documents used to develop the guidance.
On October 1, 2015 the PCR team began completing the validation assessment questions as a part of the PCR
process.
Meetings were held with the database support team to best determine how the information could be entered and
reports generated. The database was set up to run a report by provider with the scores for each HCBS indicator.
The database was also set up to run aggregate scores for all providers by service and for a defined time period.
After conducting reviews for about six (6) weeks, it became clear through meetings with the PCR reviewers
additional guidance was needed for completing the assessments.
Each HCBS indicator was dissected and 2-4 subset questions were written for each indicator. The subset
questions were designed, so that if one of them was marked no, then the indicator had to be marked no.
However, if all of them were marked yes, it did not guarantee the indicator could be marked yes. This is based
on the rationale that the reviewer would be forced to focus on 2-4 things per indicator, but would still have the
flexibility to mark the indicator as “not met” if additional things were discovered during the course of the
review. The subset questions were reviewed by the full PCR team and training was conducted. The subset
questions were then added to the database.
When an indicator is designated as “not met”, the reviewer must write an evidence statement identifying what
they observed, read or heard to support the indicator being not met. The database allows DDS to see the
individual statements.

28 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
The indicators are cross walked with the CMS assessment questions and starting in January 1.2016, each of the
HCBS indicators have a CMS assessment designation making it possible for the database to be able to generate
reports linking these together. Also with the subset questions now in the database, there will be the ability to
report what caused the indicator to not be met due to how the subset questions were answered. This will assist
the District in identifying causes for the not met indicators and make amelioration more accurate and timely.
For reviews beginning October 1, 2015, providers were sent an email at the time of the PCR announcement
explaining the role PCR would have in supporting DDS to validate the results of the HCBS rule. They were sent
the tools that would be used as part of the process.
To assist DDS in meeting required timelines, additional reviews of the day providers are being conducted
outside of the usual PCR calendar. Providers were contacted by phone and sent the tools that would be used.
The tools were also uploaded to the DDS website. Information about the process was shared at the day provider
meeting in November 2015, and again at the February 2016 meeting as well as at the Provider Leadership
meeting in January 2016 and the February 2016 DDA Town Hall Meeting.
September 2019 Update: Additional designations of HCBS indicators have been added and currently the
following services are measured and reported:
• Day Habilitation
• Day Habilitation 1:1
• Day Habilitation Small Group
• Employee Readiness
• IDS and IDS Small Group
• Supported Employment Job Placement and Small Group
• Supported Employment Job Training and Support and Small Group
• Supported Employment Long Term Follow Along and Small Group
• Companion Services and Small Group

29 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
• Supported Living ( Regular and periodic)
• Host Home
• Residential Habilitation
• Organizational Tool ( for all services)
All service designations (individual as well as group) of the services of Individualized Day supports,
Companion Services and Employment Services have been added to the services that are assessed by the PCR
and the PCR tools of these services have been revised to include a review of all HCBS Settings Requirements
for these services.
September 2018 Update: HCBS indicators are measured and reported for the following services:
• Day Habilitation
• Day Habilitation 1:1
• Day Habilitation Small Group
• Employment Readiness
• IDS Small Group
• Supported Employment Job Placement Small Group
• Supported Employment Job Training and Support Small Group
• Companion Services Small Group
• Supported Living (regular and periodic)
• Host Home
• Residential Habilitation
• Organizational Tool (for all services)
As of July 2018, all HCBS indicators became Q/A indicators, are assigned a weight, and are assigned to one of
the organizational outcomes.
30 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
DDS has updated the PCR guide and tools to include the requirement that providers must score 100% on all
HCBS designated indicators in the PCR tools in order to receive an Excellent rating. Prior to this requirement a
provider could receive an excellent rating if they scored 90-100% on indicators. This new criteria recognizes the
importance of meeting the CMS HCBS setting requirements, and DDS’s commitment to insuring providers are
providing people with services per these requirements. When a provider does not meet the requirement of
100%, the will not be able to achieve an Excellent rating, regardless of their score, and are required to remediate
the problem area through a corrective action process that is followed by DDS to resolution.
September 2019 Update: DC completed all needed changes to Provider Certification Review in April 2018.
DC conducted a 100% review of all day settings, as well as a sample of all residential settings, by provider
using the 2018 updated PCR tool.
d. DOH licensing requirements and regulations.
These rules govern Residential Habilitation facilities and are in addition to the waiver rules. They are available
on-line at: http://www.dcregs.dc.gov/Gateway/ChapterHome.aspx?ChapterNumber=22-B35.
Remediation: These regulations, in addition to the waiver regulations, govern Residential Habilitation services.
They were reviewed by the HCBS Settings group, which made recommendations for remediation to DDS in
areas where the rule is either silent or in conflict with the HCBS Settings Rule. DDS has shared those
recommendations with the Mayor's Inter-Agency Task Force on Coordination and Management of the Supports
and Services Delivery System for Persons with Intellectual and Developmental Disabilities. The Task Force is
charged with overseeing and coordinating those steps deemed necessary and appropriate with respect to
improving the District government's supports and services delivery system for persons with intellectual and
developmental disabilities. Membership includes the DDS Deputy Director for DDA, who is the Task Force
Chairperson; the Senior Deputy Director, DHCF; and the Senior Deputy Director, DOH /Health Regulation and
31 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Licensing Administration. The Task Force was established by Mayoral Order, available on-line at:
http://www.dcregs.dc.gov/Gateway/NoticeHome.aspx?NoticeID=388211.
The Task Force is working on revising the Residential Habilitation regulations to comply with the HCBS
Settings Rule, and revised regulations are expected to be published by September 2018.
September 2019 Update: The District of Columbia’s Residential Habilitation providers have made great
strides in meeting compliance with the HCBS Settings Rule, with 100% of all habilitation settings (32 of 32
settings) in full compliance after remediation. This is based upon data from service coordination monitoring of
100% of people residing in residential habilitation settings.
September 2018 Update: DC has
updated its HCBS IDD waiver, implementing regulations, and the Provider
Certification tools, to require compliance with the HCBS Settings for all residential habilitation settings. With
the change to the regulations and certification tools, changes to the licensing regulations are no longer required.
That is because in order to provide residential habilitation services, the provider must meet both certification
and licensing requirements. Therefore, the HCBS Settings Rule requirements need not be contained in both sets
of regulations. As evidence of the effectiveness of these changes, DC notes that Residential Habilitation
providers have made great strides in meeting compliance with the HCBS Settings Rule, with 79% of all
residential habilitation settings (27 of 34 settings) in full compliance, based upon data from service coordination
monitoring of 100% of people living in residential habilitation settings. By comparison, at this time last year
(prior to the changes in the waiver and implementing regulations), only 2 residential habilitation settings were
found to be fully compliant with the HCBS Settings Rule.
e. All relevant DDS/DDA policies, procedures, and protocols, including Quality Management practices
and tools.
These items are available on-line at: http://dds.dc.gov/page/policies-and-procedures-dda.
32 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Remediation: Based on the assessment, DDS has begun to revise policy and procedures and this will continue,
on an ongoing basis, as needed, to ensure full compliance with the HCBS Settings Rule no later than March 17,
2022. DC has established specific timelines and milestones for additional revisions needed to achieve
compliance with the HCBS Settings Rule. In instances where a change in rule or policy requires a public
comment period, time lines have been adjusted accordingly to accommodate time needed to process and
respond to public input and incorporate such comments into document revisions. The Statewide Assessment
Reporting Charts, attached, detail the results of the systemic analysis of policies and procedures and projected
timelines for completion of all revisions by September 2018.
Of note, DDS has made changes to its Provider Performance Review (PPR) policy and procedure (2015-DDS-
QMD-POL001), available on-line at: http://dds.dc.gov/book/iv-quality-management/provider-performance-
review-policy-and-procedure. As part of the FY2016 PPR process, starting in November 2015, the HCBS
Setting Standards are discussed, the provider’s Transition Plan is reviewed, and each provider has a
“Continuous Improvement Plan” (CIP) area of improvement related to ensuring that their agencies policies,
procedures, and protocols reflect the utilization of Person First Language, Person Centered Thinking outcomes,
and compliance with HCBS Settings Standards across all service models. As part of the quarterly CIP follow up
contacts the assigned Quality Resource (QRS) staff will review the provider’s progress towards meeting each of
their agency’s areas of improvement, including benchmarks outlined in their transition plan developed to come
into compliance with the HCBS Settings Rule.
HCBS performance related goals have been added to all CIP’s since FY 16.
PPR will request updated Provider Transition Plans as part of the PPR provider profile starting in
FY17. Additionally, HCBS compliance is monitored through PCR and through the updated Service
Coordination Monitoring Tool (SCMT), the results of which will be added to the PPR process in FY 2017.
September 2019 Update: DDS incorporated the results of service coordination monitoring of HCBS indicators
and PCR into the PPR. HCBS Settings Rule requirements are incorporated into the various PPR domains:

33 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
• Health and Wellness
• Rights and Dignity
• Service Planning and Delivery
• Safety and Security
• Relationships
• Community
• Choice and Decision-making
• Fiscal and Organizational Accountability
PPR results in a provider quality improvement plan to address performance measures falling below established
benchmarks as well as quality improvement strategies in support of advancing best practice. Quality
improvement plans for HCBS waiver providers also include a system for maintaining full compliance with the
requirements of the federal HCBS Settings Rule.
DDS staff are responsible for creating and following an annual schedule of review for each residential, day and
vocational provider. Staff track the effectiveness of their assigned providers’ quality improvement plans on a
quarterly basis through review of performance measures as well as the providers’ progress updates.
No further changes to PPR process is needed. DDS has made all required changes to the PPR.
September Update 2018: PPR has worked with providers to add HCBS performance goals to all CIPs.
However, DDS experienced challenges with adding the results of service coordination monitoring and PCR to
the annual PPR review; it was more difficult to automate than we projected from an IT perspective. Once we
ran into the complications with IT, instead we did a pilot whereby we were able to incorporate findings from the
HCBS Settings assessments into PPR. A redacted example is available upon request from CMS. Based upon

34 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
this pilot, we are training the Quality Resource Specialists on this new method as an interim step, while we
continue to work with our IT department on an automated solution. QRS training will be completed by October
2018.
We expect to fully incorporate the results of service coordination monitoring of HCBS indicators and PCR into
the PPR no later than March 1, 2019. We will roll this out through the PPR year, as providers have their annual
PPR meetings.
Note that although there have been delays in fully transforming our PPR process, DDS remains confident in the
ability of our quality management system, as a whole, to find and remediate issues related to HCBS Settings
Rule compliance on both an individual and systems level. Any negative finding on an HCBS indicator from
service coordination monitoring results in an issue, which is assigned to both a provider and a staff member at
DDS, who follows the issue through to remediation. The same is true for any negative finding from a PCR
issue, whether it is related to an individual or organizational level indicator. Finally, PPR requires providers to
create and follow a CIP that includes addressing any challenges the provider is experiencing with reaching
compliance with the Settings Rule.
f. Provider training requirements.
DDA’s Provider Staff training policy is available on-line at: http://dds.dc.gov/node/735312. In addition to the
HCBS Settings Advisory Group, DDS engaged with stakeholders through our Training Curriculum Committee
to review and revise training requirements. DDS Human Capital Administration led this effort.
Remediation: DDS has made changes to training for all levels of provider employees.
35 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
• Training for Direct Support Professionals: DDS has revised its Phase One training modules for all provider
Direct Support Professionals (DSP) to emphasize person-centered thinking, the importance of self-direction,
and key requirements of the HCBS Settings Rule, such as respect, dignity and privacy, the role of the DSP
in supporting community integration and helping people build relationships, and Employment First.
• Training for Provider Executives, Qualified Intellectual and Developmental Disabilities Professionals, and
Managers: All providers are required to attend training on Person-Centered Thinking and Supporting
Community Integration through Discovery. (see, DDA Provider Staff Training Policy at
http://dds.dc.gov/node/735312).
Finally, DDS has changed the format of its Provider Leadership and Day/ Employment Leadership meetings
to make them more of a forum for training, discussion, information sharing and problem solving. The
HCBS Settings Rule is discussed at each of these monthly meetings. The Day and Employment providers
meeting has become a Community of Practice, aimed at supporting compliance with the HCBS Settings
Rule.
The HCBS related rules are discussed at every meeting with the provider. We will ensure that it is included
on the agenda.
September 2019 Update: DDS has delayed the implementation of the ACRE/CESP requirement for one
year and we are working with providers on developing the ACRE training.
September 2018 Update: DC added the following training requirements for DDA providers of
Employment Readiness, Supported Employment and Small Group Supported Employment services: All
Employment Support Professionals shall complete a professional development course which:

36 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
1. Meets the requirements for an ACRE Basic Employment Certificate (“BEC”); or
2. Meets the requirements for an ACRE Professional Employment Services Certificate; or
3. Meets the requirements for CESP Certification; or
4. Is comparable to ACRE BEC or CESP training. Specifically, the competency-based course must include
40 hours of competency based training in the following:
a. Application of Core Values and Principles to Practice or Federal Policy and Historical Perspective
(four hours required);
b. Individualized Assessment and Employment/ Career Planning or Customer Profile and Employment
Selection; (six hours required);
c. Community Research and Job Development or Organizational Marketing and Job Development (five
hours required);
d. Workplace and Related Supports or Job-Site Training (ten hours required); and
e. Other trainings such as Specific Disabilities, Long Term Support, Funding, Benefits Counseling,
etc.(ten hours required).
As described above, DDS offered a train-the-trainer course and certified 27 new trainers to help providers
meet these new expectations.
g. Human Care Agreements
A sample Human Care Agreement is attached for review.
Remediation: Based on the systemic assessment, in 2015 DDS made the following changes to the District’s
Master Human Care Agreements (HCA) for Residential Supports to support compliance with the HCBS
Settings Rule, applicable to provider owned or operated HCBS Settings for Supported Living, Supported Living
with Transportation, Residential Habilitation and Host Homes services. (Please note that the District’s HCA’s
are funded solely with local funds and do not use any Medicaid funding.)
37 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
DDS updated the language in the Master HCA for Fiscal Year 2017 to require the following:
•
The Provider’s settings must support people’s full access to the greater community.
• Leases shall be in the names of the people who are being supported. If this is not possible, then the Provider
must ensure that each person has a legally enforceable residency agreement or other written agreement that,
at a minimum, provides the same responsibilities and protections from eviction that tenants have under
relevant landlord/tenant law. This applies equally to leased and provider owned properties.
• Each person receiving support, must have access to a telephone or other communication device, as
appropriate, to use for personal communication in private at any time the person is at home, unless there is a
restriction is based on the person’s assessed need and that is justified in his or her person centered plan.
• All residences must offer the person privacy in his or her room (subject to the person having a roommate).
• The entrance to person’s room must be lockable by the person, with only the person, his or her roommate, if
applicable, and appropriate staff having a key. Any exception shall be based on the person’s assessed need
and justified in his or her person centered plan.
• People may choose any provider of services if new room and board funding is not concurrently requested.
• Clothing and furniture reflect the person’s preferences.
• People receiving supports must have the freedom to furnish and decorate their room, subject to the lease or
other residency agreement.
• People receiving supports must have access to food at any time in their home, unless there is a restriction is
based on the person’s assessed need and that is justified in his or her person centered plan.
38 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
• People receiving supports shall have the right to visitors of his or her choosing at any time, in their
residence. Any exception shall be based on the person’s assessed need and justified in his or her person
centered plan.
• The homes must be physically accessible for the person and meet his or her support needs. Any
obstructions that limit a person’s mobility in the home must have environmental adaptations to ameliorate
the obstruction.
• Adds a definition – “HCBS Settings Rule: refers to Home and Community-Based Setting Requirements for
Community First Choice and Home and Community-Based Services (HCBS) Waivers, 79 Fed. Reg. 2948,
3030-31 (Jan. 16, 2014) (to be codified at 42 C.F.R. § 441.301I(4)).”
• Requires the provider to have a detailed Provider Transition Plan, including benchmarks and milestones
that describes how all settings in which waiver services are provided will fully comply with the federal
HCBS Settings Rule by March 17, 2022.
Requires that all new settings must be fully compliant with all requirements of the HCBS Settings Rule at the
time they are established
The HCA also requires that the provider follow all of the governing waiver regulations and DDS policies and
procedures.
DDS staff and providers were trained on the new HCA Agreement on January 31, 2017, with a second training
scheduled for February 21, 2017.
Also, please see the Statewide Assessment Reporting Charts, attached for a summary of the results of the
systemic analysis of DDA’s Master HCA for Residential Supports.

39 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
September 2018 Update: No additional changes were required to the HCA. DC continues to use the HCA with
the requirements detailed above.
2. HCBS Settings for People who have Physical Disabilities
1. DHCF invited representatives of the groups below to participate in the review group and invited and
consulted with others, including the Department of Health (DOH) and Department of Behavioral
Health (DBH), as needed. DHCF posted the meeting dates on its website and members of the public
were welcome to attend and participate. Although the state level self-assessment process has been
completed, meetings will continue, as needed, through the remediation process.
Although meetings are open, invited members of the review group included:
a) DHCF;
b) DOH;
c) DBH;
d) DDS;
e) DC Office of Disability Rights;
f) ADAPT/Direct Action;
g) DC Long Term Care Coalition;
h) DC Long Term Care Ombudsman;
i) DC Health Care Association;
j) DC Home Health Provider Association;
k) DC Center for Independent Living.

40 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
2. The state level assessment was completed by June 30, 2016 and has resulted in DC having a list of
required changes needed to the waiver itself, implementing regulations, and policies, procedures and
practices. The self-assessment included a review and analysis of:
a. All HCBS waiver service definitions and provider requirements (including assisted living and adult day
health services). The HCBS waiver is available on-line at:
http://dhcf.dc.gov/sites/default/files/dc/sites/dhcf/publication/attachments/Home%20and%20Community%20Base
d%20Services%20Waiver%20for%20Persons%20who%20are%20Elderly%20and%20Individuals%20with%20Ph
ysical%20Disabilities%20%28EPD%29%20Notice%20of%20Emergency%20and%20Proposed%20Rulemaking.p
df
Remediation: DHCF submitted a Waiver Amendment to CMS on July 20
th
, 2015 and it was approved on
October 23
rd
, 2015. The changes were as follows: The Waiver Amendment adds new services, amends
existing service descriptions and reimbursement methodologies, adds new provider types and qualification
standards and includes requirements to conform with the new Home and Community-Based Services (HCBS)
requirements under 42 CFR 441.301 of the federal rulemakings by proposing new conflict-free requirements
for case management and person-centered planning to comply with these regulations. It also includes a CMS
required HCBS settings Transition Plan to explain how the District’s assisted living facilities enrolled under the
Waiver will comply with the setting requirements under 42 CFR 441.301.
• Provider Qualifications for All HCBS Settings:
Modify language in provider qualifications for Assisted Living Facilities and Adult Day Health to
require that any new settings must meet all requirements of the HCBS Settings Rule.
b. All regulations governing HCBS. The regulations are available on the DHCF website at:
41 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
EPD Waiver:
http://dhcf.dc.gov/sites/default/files/dc/sites/dhcf/publication/attachments/Home%20and%20Community
%20Based%20Services%20Waiver%20for%20Persons%20who%20are%20Elderly%20and%20Individ
uals%20with%20Physical%20Disabilities%20%28EPD%29%20Notice%20of%20Emergency%20and%
20Proposed%20Rulemaking.pdf#page=5&zoom=auto,-150,613.
Non-Medicaid Mental Health Community Residence Factilities:
http://www.dcregs.dc.gov/Gateway/ChapterHome.aspx?ChapterNumber=22-B38
EPD & Non-Medicaid Assisted Living Facilities Licensed under the Department of Health:
https://doh.dc.gov/sites/default/files/dc/sites/doh/publication/attachments/AssistedLivingLaw.PDF
See the attached Statewide Assessments charts for a detailed analysis of DHCF, DOH, and DBH
regulations relative to compliance with the federal HCBS Settings rule.
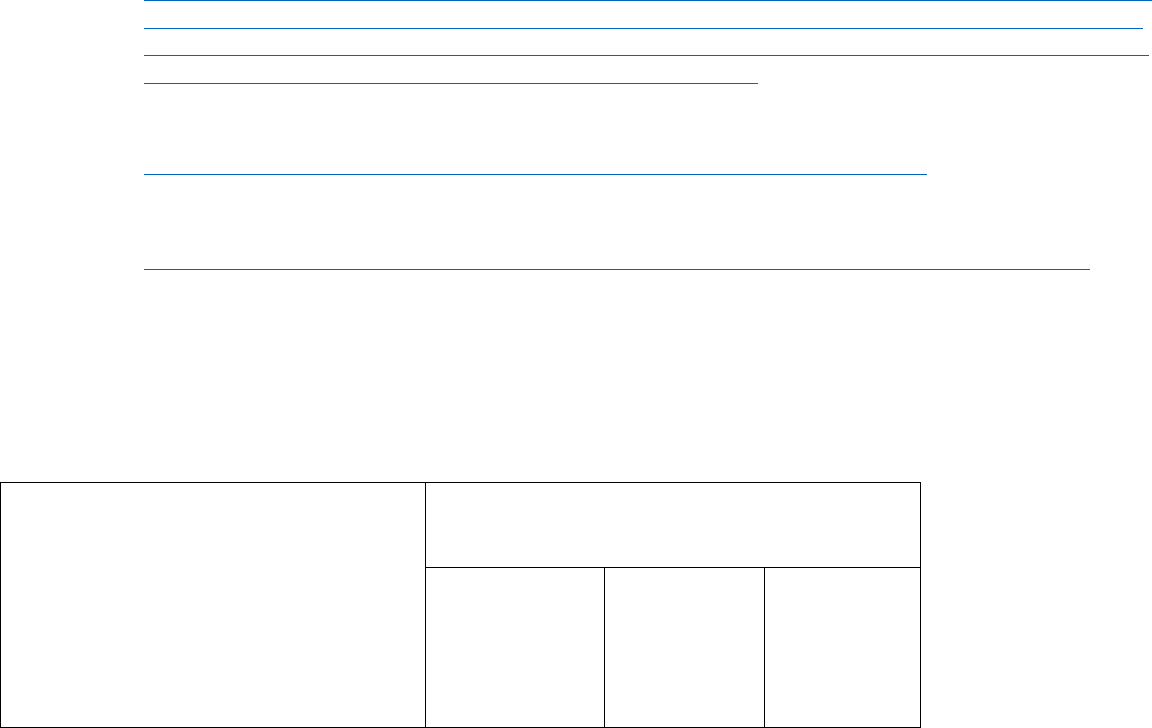
A high level summary of DHCF’s legal analysis is set forth in the table below. Legal Analysis of HCBS Settings
Regulations compared to DC Regulations
CMS HCBS Setting Requirements
Do DC Regulations Meet Federal HCBS
Standards?
Assisted Living
Facilities-EPD
Assisted
Living
Residence-
Mental
Health
Community
Residence
Facilities-
42 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
DOH-Non-
Medicaid
Non-
Medicaid
The setting is integrated in and supports
full access to the greater community
Yes
Yes
No
Is selected by the individual from among
setting options
Yes
Yes
Yes
Ensures individual rights of privacy,
dignity and respect, and freedom from
coercion and restraint
Yes
Yes
No
Optimizes autonomy and independence
in making life choices
No
Yes
No
Facilitates choice regarding services and
who provides them
No
No
No
The individual has a lease or other legally
enforceable agreement providing similar
Protections
Yes
Yes
Yes
The individual controls his/her own
schedule including access to food at any
time
No
No
No
43 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
The individual has privacy in their unit
including lockable doors, choice of
roommates and freedom to furnish or
decorate the unit
No
No
No
The individual can have visitors at any
time
No
No
No
The setting is physically accessible
Yes
Yes
Yes
Remediation: Re
gulatory revisions will continue, on an ongoing basis, as needed, to ensure full
compliance with the HCBS Settings Rule no later than March 17, 2022. An analysis, remediation and
timeline consistent with the crosswalk referenced in Section II. is attached for each setting type listed
above.
1. The District made significant changes to the proposed EPD Waiver Regulations to ensure compliance
with CMS’ settings requirements. These include the following:
Consistent with federal requirements, all EPD waiver service settings that are not an individual’s natural home, including
an assisting living facility and an adult day health program must meet the Home and Community-Based Setting
Requirements pursuant to 42 CFR 441.301(c) (4):
(a) Be chosen by the person receiving EPD Waiver services;
(b) Ensure people’s right to privacy, dignity, and respect, and freedom from coercion and restraint;
(c) Be physically accessible to the person and allow the person access to all common areas;
(d) Support the person’s community integration and inclusion, including relationship-building and
maintenance, support for self-determination and self-advocacy, and opportunities for employment
and meaningful non-work activities in the community;
44 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
(e) Provide information on individual rights; and
(f) Allow visitors at any time, with any exception based on the person’s assessed need to be justified
in his or her person-centered plan.
Additionally, the following requirements were added for all residential EPD settings that are not the individual’s natural
home must:
(a) Be integrated in the community and support access to the greater community;
(b) Provide opportunities for the person to engage in community life;
(c) Allow full access to the greater community;
(d) Be leased in the names of the people who are being supported. If this is not possible, then the
provider must ensure that each person has a legally enforceable residency agreement or other
written agreement that, at a minimum, provides the same responsibilities and protections from
eviction that tenants have under relevant landlord/tenant law. This applies equally to leased and
provider owned properties;
(e) Develop and adhere to policies which ensure that each person receiving services has the right to
the following:
(1) Privacy in his or her personal space, including entrances that are lockable by the person (with
staff having keys as needed);
(2) Freedom to furnish and decorate his or her personal space (with the exception of Respite
Daily);
(3) Control over his or her personal funds and bank accounts;
(4) Privacy for telephone calls, texts and/or emails; and
(5) Access to food at any time.
Because it is not specifically addressed in the rule, the District, in sub-regulatory guidance will stipulate that
the setting must provide individuals who are sharing units a choice of roommates.
2. DHCF is in discussions with the Department of Behavioral Health regarding revising regulations for
community residence facilities for mentally ill persons to comply with the Rule.

45 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Beginning in July through October 2015, DHCF had meetings with the DBH to revise the Mental Health
Community Residence Facility regulations. These regulations provide for the health, safety, and welfare of
individuals with mental illness residing in mental health community residence facilities (MHCRFs). The
revisions ensure that our Waiver beneficiaries reside in settings that are compliant with the HCBS rules, but also
help us to ensure that any Medicaid beneficiary that attends non-residential services such as Adult Day Health
must reside only in settings (Mental Health CRFs , and other CRFs) that also meet all of the requirements of the
federal rules. The regulations are currently posted as second & proposed rulemaking, and incorporate the
settings requirements as outlined in the attached table that accompanies the systemic assessment.
September 2019 Update: On June 28, 2019, DOH posted its third notice of Emergency and Proposed
Rulemaking for Assisted Living Residences. It is available in its entirety at:
https://dchealth.dc.gov/sites/default/files/dc/sites/doh/publication/attachments/ALR%20Regulations%203178_0
01%5B7709%5D.pdf. As noted in last year’s update, the rule incorporates the HCBS settings requirements.
The EPD Waiver regulation remains as amended above, and comports with the HCBS Settings rule.
September 2018 Update: During the year, DOH drafted an Emergency and Proposed Rule for Assisted Living
Residences, amendments to Chapter 101, ASSISTED LIVING RESIDENCES, of Title 22-B, PUBLIC
HEALTH AND MEDICINE, as a supplement to the legislation referenced above. DHCF and DOH agreed to
language that addresses all Medicaid requirements, including the HCBS settings rule, as follows:
“10100.04 An ALR that participates in the Medicaid Home Community-Based Services Waiver
program for the Elderly and Persons with Physical Disabilities, as approved by the Council of the
District of Columbia and the Centers for Medicare and Medicaid Services, shall maintain compliance
with Chapter 42 (Home and Community-Based Services Waiver for Persons Who Are Elderly and
Individuals with Physical Disabilities) of Title 29 of the District of Columbia Municipal Regulations
(“DCMR”).”
46 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
The emergency and proposed rule is available in its entirety at:
https://www.dcregs.dc.gov/Common/DCMR/SectionList.aspx?SectionNumber=22-B10100
c. DHCF Provider Requirements. DHCF’s provider policies, procedures, guidance and tools are
available on-line at: https://www.dc-
medicaid.com/dcwebportal/documentInformation/getDocument/14944 and www.dc-medicaid.com
Remediation:
As mentioned above, DHCF’s Long Term Care Administration (LTCA) revised its EPD Waiver provider
requirements and the application process in order to ensure organizations providing EPD services to DC
residents are supporting and facilitating greater individualized community exploration and integration.
In addition to reengineering the internal mechanism for processing provider applications, the LTCA adopted a
Long Term Care Provider Review Checklist that applicants must use when submitting their application
materials. The Checklist will include HCBS Setting requirements and will be posted on DHCF's provider site
(www.dc-medicaid.com) in FY2017 As this checklist is being refined, a section will be added that reflects the
HCBS settings rule, where applicants, when appropriate, must attest to complying with the rules and submit
their policies and procedures, as appropriate. DHCF will use CMS’ “Exploratory Questions to Assist States in
Assessment of Residential Settings” to amend the checklist. Only applicants with approved policies and
procedures will be referred to DHCF’s Division of Public and Private Provider Services for enrollment as EPD
waiver and 1915(i) providers. As mentioned earlier, provider readiness and enrollment processes for the
District’s new 1915(i) providers included on-site review of compliance with the HCBS Settings requirements.
Additionally, DHCF developed an addendum to the conflict-free assessment tool with the HCBS Setting rule
requirements for prospective 1915(i) applicants. Data collection began in FY15.
47 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
September 2019 Update: As noted in earlier sections, the LTCA universal monitoring tool incorporates the
HCBS settings requirements. Assisted Living Facilities (ALFs) are assessed annually for compliance with
requirements along with other elements of the tool.
d. DOH licensing requirements and regulations. These rules govern Assisted Living facilities and are in
addition to the waiver rules. They are available on-line at:
http://doh.dc.gov/service/health-care-facilities
and https://doh.dc.gov/sites/default/files/dc/sites/doh/publication/attachments/AssistedLivingLaw.PDF .
Remediation: DHCF is working with DOH/HRLA’s Intermediate Care Facilities Division (ICFD) which
licenses group homes for persons with intellectual, developmental and physical disabilities residing in the
District of Columbia. The ICFD also licenses Home Care Agencies, Community Residence Facilities, and
Assisted Living Residences to ensure their compliance with local licensure requirements. In this role, HRLA
staff inspects licensed health care facilities and providers who participate in the Medicare and Medicaid
programs, responds to consumer and self-reported facility incidents and/or complaints, and conducts
investigations. When necessary, HRLA takes enforcement actions to compel facilities and providers to come
into compliance with District and Federal law. DHCF and DDS are working with HRLA to revise the
regulations for community residential facilities which incorporate both licensed small group homes known as
community residence facilities and assisted living residences. The revisions specific to the community residence
facility regulations will be promulgated with a formal opportunity for public comment. Final publication is
anticipated in FY 2017. In FY 2018, DOH will draft regulations relative to Assisted Living Residences that
support compliance with the HCBS settings rule.
As a result of the revised regulations which are under development in FY17, DOH will account for the added
requirements relative to HCBS settings during its monitoring process of ALRs and CRFs. At present, providers
must have their DOH license renewed annually (within 90 days of license expiration). The renewal requires
that a surveyor or team of surveyors (depending on the type/size of provider) make an unannounced site visit
which includes three stages. First, the surveyors will observe staff interaction with individuals receiving HCBS

48 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
services, assess whether the environment is in compliance with the regulations, and interview staff and clients.
Then, the surveyors begin record verification, with includes reviewing medication administration, employment
records, and policies and procedures. From this information, the surveyors make a compliance decision to
determine if there are any deficient practices, which will be shared with the provide during the site visit exit
interview. A written report detailing results of the site visit and the observed deficiencies is shared with the
provider within ten days of the exit interview, and the provider then has ten days to respond with a corrective
action plan. Upon receipt and approval of the plan, DOH may conduct an unannounced follow up site visit to
ensure that the corrective action plan is being adhered to. This monitoring process will account for compliance
with the HCBS settings rule and associated policies and procedures of the provider/licensee. Please note that
DHCF will work with DOH to train staff on the new HCBS settings rules within three (3) months of the rules
being promulgated.
Per DHCF's original submission to CMS, we committed to co-host at least 3 trainings for providers upon
publication of the revised existing DOH standards and completion of the revised EPD Waiver provider
requirements. As mentioned, DOH is still in the process of finalizing regulations, and the EPD waiver rules are
due for publication in summer 2016. DHCF coordinated monthly meetings with case managers to provide
training and technical assistance on LTCA-related issues, including the forthcoming EPD waiver rules. Formal
training will be scheduled upon the actual publication. We anticipate these trainings will begin in the Summer
of 2017 and will be publicized via the DHCF website and provider listserv.
September 2019 Update: On June 28, 2019, DOH posted its third notice of Emergency and Proposed
Rulemaking for Assisted Living Residences. It is available in its entirety at:
https://dchealth.dc.gov/sites/default/files/dc/sites/doh/publication/attachments/ALR%20Regulations%203178_0
01%5B7709%5D.pdf. As noted in last year’s update, the rule incorporates the HCBS settings requirements.
September 2018 Update: During the year, DOH drafted an Emergency and Proposed Rule for Assisted Living
Residences, amendments to Chapter 101, ASSISTED LIVING RESIDENCES, of Title 22-B, PUBLIC
HEALTH AND MEDICINE, as a supplement to the legislation referenced above. DHCF and DOH agreed to
language that addresses all Medicaid requirements, including the HCBS settings rule, as follows:
49 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
“10100.04 An ALR that participates in the Medicaid Home Community-Based Services Waiver
program for the Elderly and Persons with Physical Disabilities, as approved by the Council of the
District of Columbia and the Centers for Medicare and Medicaid Services, shall maintain compliance
with Chapter 42 (Home and Community-Based Services Waiver for Persons Who Are Elderly and
Individuals with Physical Disabilities) of Title 29 of the District of Columbia Municipal Regulations
(“DCMR”).”
The emergency and proposed rule is available in its entirety at:
https://www.dcregs.dc.gov/Common/DCMR/SectionList.aspx?SectionNumber=22-B10100
e. All relevant DHCF policies, procedures, and protocols. While final policies and procedures for the
EPD Waiver are anticipated in the fourth quarter of 2017, the Person-Centered Individualized Service
Plan Guide is currently available l on-line at:
http://dhcf.dc.gov/sites/default/files/dc/sites/dhcf/publication/attachments/PCP%20Template_04-12-
2016_Savable.pdf
Remediation: DHCF’s EPD Monitoring Team has amended its comprehensive monitoring tool for all EPD
waiver services to reflect the HCBS settings requirements. The EPD Monitoring Team also uses the
aforementioned Readiness Checklist for renewals of assisted living providers’ status as EPD Waiver providers.
Beyond DHCF’s efforts to monitor enrolled Medicaid providers for compliance with the HCBS settings
requirements, the LTCA also administers an individual face-to-face, conflict-free assessment to establish the
level of need for beneficiaries who receive long term care services and supports, as mentioned above. Using
’MS' Exploratory Questions to Assist States in Assessment of Residential Settings, DHCF developed an
50 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
Addendum to the LTC conflict-free assessment tool. Nurses conducting the assessment tool were trained on
this new Addendum on April 15, 2015 and have been using this tool to conduct individual assessments of
settings when an EPD waiver beneficiary does not live in their natural home.
1
As mentioned under Training and Capacity Building, the 2
nd
Proposed Rulemaking was published March 18,
2016
(http://dhcf.dc.gov/sites/default/files/dc/sites/dhcf/publication/attachments/Long%20Term%20Care%20Service
s%20and%20Supports%20Assessment%20Process%20Notice%20of%20Second%20Proposed%20Rulemaking.
pdf).
On April 15
th
, DHCF participated in training for all EPD Waiver Providers to ensure that they understood the
setting options. The training materials communicated the various setting requirements including a person’s right
to privacy, dignity, and respect, and the other principles incorporated in the HCBS final rule.
EPD assisted-living service providers deemed noncompliant with the HCBS settings rule will be notified of
areas of deficiency and given 30 days to submit a corrective action plan to DHCF. DHCF will utilize this
corrective action plan as a component of ongoing monitoring processes. If the provider continues to be non-
compliant, DHCF will evaluate the appropriateness of various sanctions as established by DHCF’s amended
rules. In the event that people must be transitioned from one provider to another because the provider setting
does not comply with the HCBS Settings Rule, DHCF will coordinate transitions and ensure continuity of
services in accordance with DHCF’s Transition policy and procedure. Enforcement of compliance rules was
launched in April 2016 subsequent to implementation of monitoring efforts that incorporate HCBS Settings
requirements.
1
The District’s process for conducting individualized settings assessments for EPD Waiver enrollees was reviewed and given approval by
Ralph Lollar before submission of the Statewide Transition Plan in 2015.
51 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
In addition, policies and procedures for EPD Waiver case managers are inclusive of the settings requirements.
The Person-Centered Individualized Service Plan Guide and tool specifically requests that case managers assess
if an individual’s residence was chosen by the person, and is integrated in and supports full access to the greater
community. It further defines access as “access to opportunities to seek employment and work in competitive
integrated settings, engage in community life, control personal resources, and receive services in the community
to the same degree of access as individuals not receiving Medicaid HCBS.” This language is consistent with the
HCBS settings requirements. EPD Case Management, Assisted Living, and Adult Day Health policies and
procedures under development and expected in the fourth quarter of 2017 will incorporate the settings
requirements, as well.
September 2019 Update: No new update.
September 2018 Update: As noted previously, in 2017-2018, the LTCA Oversight and Monitoring Division
collaborated with the Quality Division and EPD Waiver Unit to update its monitoring tool for all EPD
monitoring activities. Through this process, settings for Assisted Living and Community Residence Facilities
monitoring tool was incorporated in the universal tool. The settings requirements were also included in the
person-centered planning template embedded in the District’s new case management system, DC Care Connect,
launched in July 2018.
f. Provider training requirements. DHCF’s provider training policy is available on-line at: www.dc-
medicaid.com and http://doh.dc.gov/service/health-care-facilities.
Remediation: Upon publication of the revised existing DOH standards and completion of the revised EPD
Waiver provider requirements, DHCF will work with DOH and DCOA’s ADRC to co-host no less than three
trainings for providers on both the DOH standards and the new EPD provider requirements. DHCF and the
ADRC will also co-host training for stakeholders on the DOH standards and the new EPD provider
requirements. We anticipate these trainings will begin in the FY18 and will be publicized via the DHCF
website and provider listserv.

52 of 52
DC HCBS Waiver Settings-Regulatory Compliance Update-Operations 12-21-22
September 2019 Update: No new update.
September 2018 Update: Once the DOH emergency and proposed regulation for ALRs is published, DHCF will
work with the Health Regulation and Licensing Administration to establish trainings specifically for the
Medicaid-enrolled providers, given the general provision in the rule that Medicaid providers must abide by rules
set forth for the District’s EPD Waiver.
1 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
Attachment 2
District of Columbia Home & Community-Based Waiver Settings Compliance
Update-Assessment
Submitted to CMS December 21, 2022
Description of how the state assesses providers for initial compliance and conducts
ongoing monitoring for continued compliance
Excerpt from District of Columbia Statewide Transition Plan (September 30, 2020
Update)
Section VI: Achieving Compliance, Sustaining Ongoing Compliance, and
Amendments to the DC HCBS Waivers Transition Plan
Activities related to the Statewide Transition Plan are done in partnership with sister
District agencies, as appropriate, in particular the Department of Disability Services
(DDS), the Department of Health (DOH), the Department of Behavioral Health (DBH),
the Deputy Mayor of Health and Human Services (DMHHS), and the Office on Aging
(DCOA). The DMHHS oversees the interagency activities, receives and reviews
updated work plans, and convenes interagency meetings, as needed, to check-in with
each agency, discuss progress and any challenges, and to ensure each agency is capably
handling their components of the Statewide Transition Plan.
This STP will be submitted to CMS by September 30, 2017, after public comments,
and will be updated by September 30, 2018, or upon request by CMS.
September 2019 Update: DC has reached full compliance with the HCBS Settings
Rule. This is the final update to the Statewide Transition Plan. In future years,
compliance will be demonstrated through performance measures in both the IDD and
EPD waivers, and upon request by CMS.
September 2018 Update: DC is on target to reach full compliance with the HCBS
Settings Rule by March 2019. DC will provide a final set of updated data by September
30, 2019, or upon request by CMS.

2 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
DC HCBS IDD Waiver
A. As a result of the assessments, DDS has begun issuing revisions to policies
and procedures as needed, continuing on an ongoing basis, as needed, to
ensure full compliance by March 17, 2022. All revised policies will be
distributed to agency staff and providers, posted on the DDS website at
http://dds.dc.gov/page/policies-and-procedures-dda, and will be discussed at
meetings with provider leadership. All policy and procedure updates will be
completed by September 2018.
September 2019: No update at this time.
September 2018 Update: The following is a short description of policy and
procedure changes, particular where the changes we have (or have not made)
varied from previous projections. Additionally, please see the attached updated
Statewide Assessment-I/DD Policies & Procedures chart.
Human Rights and Most Integrated Day: DDS initially thought that we
would amend these policies to include the miscellaneous requirements from
the HCBS Settings Rule and CMS Exploratory Guidance – for example, the
requirement for providers to have an anonymous complaint system, or right to
visitors at any time. Instead, at the request of the DDS HCBS Settings
Advisory Group, we added this level of detail to the District’s revised HCBS
Setting Regulations, as discussed above. This makes sense because our Most
Integrated Day and Human Rights policies apply across DDA settings,
including ICFs and individual homes, while the necessary changes apply only
to HCBS Settings.
Provider HRC Procedure and Behavior Support Policy: DDS initially
planned to update the Provider HRC procedure to require providers to review
all person-centered modifications and potentially to change the definition in
the behavior support policy of the term “restriction” to clarify that BSPs are
not required for these person-centered modifications. Instead, we did this by
revised regulations, revised Individual Support Plans (ISP) Policy and
Procedure and a new Provider HRC Meeting Minutes template.
Additionally, we published a new Person Centered Modifications Procedure
to provide clarity in three processes for both DDS and DDA providers. The
procedure ensures clarity about which HCBS Settings Rule requirements
modifications are permissible, the requirement for Provider HRC and support
3 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
team reviews, and the requirement to have these reviews reflected in Person
Centered Plans.
Personal Funds Policy: Language was added to the updated HCBS
regulations and revised Personal Funds Policy to require that people receiving
HCBS services in a setting have control over his or her personal funds and bank
accounts.
Contribution to Costs: DDS made this change through updated regulations,
requiring that people who have a roommate are offered the choice of available
residential settings with a private bedroom, if they have the ability to pay.
DDS asks about this regularly through Service Coordination monitoring. We
currently have 490 people in our system who live with a roommate and are
not married or otherwise engaged in a romantic relationship. None of them
have expressed a desire to move or change their roommates, and if any person
was interested in having their own bedroom, DDS would call a person-
centered planning meeting to begin the process of transitioning the person to a
Supported Living setting.
Individualized Daily Schedules: DC now requires through updated
regulations and a new Individualized Daily Schedules Policy that providers
create individualized daily schedules for each person receiving supports. They
must include activities aligning with the person’s goals, interests and
preferences, as reflected in his or her ISP, in accordance with DDS guidance.
Lockable Spaces: DDS now requires through updated regulations and a new
Lockable Space Policy that providers ensure people have entrances to living
spaces which are lockable by the person (with staff having keys as needed), as
well as a secure place to keep their belongings at day programs.
Heightened Scrutiny Procedure: Discussed above in Section V.
B. As results of the assessments, DDS and DHCF have begun promulgate revised
regulations for the HCBS waiver, on an on-going basis, continuing on an
ongoing basis, as needed, to ensure full compliance by March 17, 2022. All
regulations are posted on the DDS website and online at the DC Register,
http://www.dcregs.dc.gov/Gateway/ChapterHome.aspx?ChapterNumber=29-
41 . All remaining regulatory updates will be completed by September 2018.
4 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
September 2019: DDS achieved full compliance and will continue to
review and update as needed to ensure that we maintain compliance.
September 2018 Update: As discussed above, all regulatory changes have
been completed by March 2, 2018.
C. For providers needing assistance to come into compliance, the state has
facilitated a Day and Employment Community of Practice, comprised of both
non-compliant and compliant providers who can talk through provider-
specific issues and problem-solve how to achieve compliance together. DDS
also provides one-to-one technical assistance, as well as uses the monthly
Provider Leadership meeting, so that there is support for all providers.
September 2019 Update: As discussed above, the DDS Day and
Employment Community of Practice continues to meet, and DDS continues
to use the monthly Provider Leadership meeting to conduct training, as
needed, on the HCBS Settings Rule.
September 2018 Update: As discussed above, the Day and Employment
Community of Practice continues to meet monthly, and DDS continues to use
the monthly Provider Leadership meeting to conduct training on the HCBS
Settings Rule.
D. As compliance with the HCBS Settings Rule is achieved, strategies to assure
on-going compliance include:
1. Incorporating the assessment by the person into ongoing service
coordination monitoring activities.
Update: The design and staff training has been completed. IT will
complete their work by March 2017. Service Coordinators will complete
the 100% site-by-site assessment by the end of July 2017.
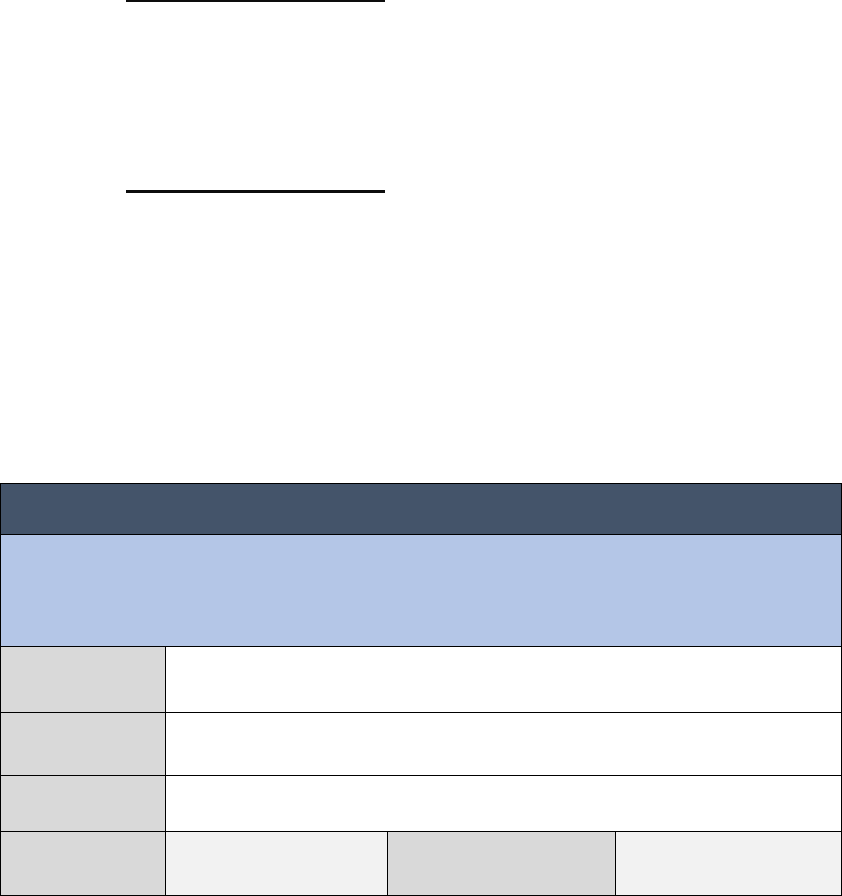
5 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
September 2019 Update: Service Coordinators completed the 100% site-
by-site assessment in July 2018 and immediately began a new round,
which was completed in July 2019. That data was used to update this
Plan. Service Coordinators have now started another monitoring cycle,
which will be completed in July 2020.
September 2018 Update: Service Coordinators completed the 100% site-
by-site assessment in July 2017 and immediately began a new round,
which was completed in July 2018. That data was used to update this
Plan. Service Coordinators have now started another monitoring cycle,
which will be completed in July 2019. Results will be included in the
September 2019 update to this Statewide Transition Plan.
Results will be included in the following HCBS IDD waiver performance
measure: Assurance No. 5 -- Administrative Authority.
Sub Assurance No. 1 (Performance Measure 3 of 3):
The Medicaid Agency retains ultimate administrative authority and responsibility for
the operation of the waiver program by exercising oversight of the performance of
waiver functions by other state and local/regional non-state agencies (if
appropriate) and contracted entities.
Performance
Measure 3/3:
Percentage of settings that meet HCBS settings requirements.
Numerator/
Denominator:
Number of settings that meet the HCBS settings
requirements/Number of settings reviewed
Discovery
Method:
DDS will conduct a 100% review quarterly. DHCF will aggregate
and analyze data quarterly.
Responsible
Party:
DDS Compliance:
Annual
Measure
DDS will submit compliance findings for this sub-assurance annually to DHCF in the
4
th
quarter of the Waiver Year. DHCF will share this information with CMS through
annual evidentiary reporting.
6 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
2. Quality assurance methodologies incorporate monitoring performance
measures that ensure compliance with the HCBS Settings Rule.
Update: The requirements have been incorporated into Provider
Performance Review via a plan of correction for use by providers to
come into compliance with the HCBS Settings Rule. As of October 1,
2016, PPR will incorporate site-by-site data into the PPR process for
more detailed and specific support for compliance by setting.
As of March 2017 any findings of non-compliance through Service
Coordination monitoring generates a provider Issue, which is followed
by assigned DDS staff through to remediation.
Additionally, the DDS Quality Improvement Committee regularly
reviews compliance data. Sample QIC Agendas and meeting minutes
are available upon request.
September 2019 Update: As described above, PPR now fully
incorporates HCBS Settings data.
September 2018 Update: As described above, PPR will more fully
incorporate HCBS Settings data into their reviews by March 1, 2019.
3. Provider certification and licensing requirements will incorporate
requirements that reflect compliance with the HCBS Settings Rule.
Update: New indicators have been added to the PCR process and
these are used with all providers subject to the HCBS Settings Rule.
As of July 1, 2016 any findings of non-compliance require a Plan of
Correction.
September 2018 Update: As of July 2018, all HCBS Settings Rule
requirements have a weighted indicator in PCR with findings of non-
compliance requiring a Plan of Correction.
7 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
September 2019: No update. As indicated above, as of July 2018, all
HCBS Settings Rule requirements have a weighted indicator in PCR
with findings of non-compliance requiring a Plan of Correction.
4. Continued review of NCI data and external monitoring data to support its
ongoing compliance monitoring efforts.
Update: This was completed and continues to be updated as NCI data
is released. Data is shared with the public on the DDS website and
with the DDS Quality Improvement Committee (QIC). Updated NCI
data was reviewed most recently by the QIC on July 5, 2016. QIC
meeting minutes are posted on-line at:
http://dds.dc.gov/publication/quality-improvement-committee-qic.
September 2018 Update: DDS continues to update its analysis of NCI
data annually and share it on the DDS website and with the QIC.
September 2019: No update. As described above, DDS continues to
update its analysis of NCI data annually and share it on the DDS
website and with the QIC.
E. DDS’s Deputy Director for DDA is responsible for monitoring and ensuring
DDS’s compliance with this Transition Plan. DDS has created a work plan to
track each item in this transition plan and ensure timely completion. This is
reviewed with responsible staff, on an ongoing and periodic basis, as needed to
ensure full compliance with the HCBS Settings Rule no later than March 17,
2022. Please see the work plan for the initial Statewide Transition Plan which
indicates that DDS has met almost all timelines and milestones from the initial
Statewide Transition Plan, with the exception being completion of the site-by-
site assessment of residential settings, as discussed above. This is available
on-line at: http://dds.dc.gov/publication/transition-work-plan-website-version-
2-9-2016. An updated version of the work plan that incorporates all
benchmarks and milestones related to the HCBS IDD waiver in this Updated
Statewide Transition Plan will be created by DDS Performance Management
8 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
Unit, to continue to track progress. This will be completed by November 30,
2016 and posted on-line by DDS IT by December 31, 2016.
September 2019 Update: The DDS Deputy Director for QAPMA is
responsible for reporting to DHCF on the waiver performance measure
regarding HCBS Settings compliance, discussed above. The DDS Performance
Management Unit tracks, trends and analyzes on-going provider compliance
with the Statewide Transition Plan. The DDS State Office of Policy, Planning
and Innovation is responsible for ensuring that all policies, procedures,
regulations, and proposed waiver documents comply with the requirements of
the HCBS Settings Rule.
September 2018 Update: DDS Performance Management, in coordination
with the State Office of Policy, Planning and Innovation, tracks on-going
progress with the Statewide Transition Plan.
September 2017 Update: DC does have an updated and detailed work plan
for HCBS IDD waiver compliance, which we will include as an attachment to
the STP. Although DC created this within the timelines listed in the STP, and
is using it to track progress, we did not publish it online. This is because we
have viewed this as an interim document. We understand that DC would soon
be receiving a Milestone Reporting Template from CMS and we planned to
use that to report both to CMS and the public on our progress. Once received,
DC will decide which tool works best for the public. DC will publish updates
on an annual basis on our website.
DC HCBS EPD Waiver
A. DHCF will begin issuing revisions to policies and procedures as needed,
continuing on an ongoing basis, as needed, to ensure full compliance by March
17, 2022. All revised policies will be distributed to agency staff and providers,
posted on the DHCF website at http://dhcf.dc.gov/page/dhcf-medicaid-
regulations and will be discussed at monthly meetings with providers .

9 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
B. As a result of the systemic assessment, DHCF revised regulations for the
HCBS waiver to ensure full compliance. All regulations are posted on the
DHCF website and online at the DC Register,
http://www.dcregs.dc.gov/Default.aspx. The regulation is compliant with the
HCBS settings rule.
C. The District submitted an update to the Statewide Transition Plan upon
completion of the full systemic assessment and review of the site-based
residential assessments.
D. For providers needing assistance to come into compliance, DHCF will provide
one-to-one technical assistance.
E. As compliance with the HCBS Settings Rule is achieved, strategies to assure
on-going compliance include:
1. Incorporating the assessment by the person into ongoing service
coordination monitoring activities.
Update: Ongoing, incorporated in the universal monitoring tool.
2. EPD Waiver Monitoring methodologies incorporate monitoring
performance measures that ensure compliance with the HCBS Settings
Rule.
Update: Ongoing. The requirements have been incorporated into
EPD Waiver monitoring activities.
2. Provider certification and licensing requirements will incorporate
requirements that reflect compliance with the HCBS Settings Rule.
3. A Long Term Care Provider Review Checklist has been added to the
provider certification process, and this is used with all new providers
subject to the HCBS Settings Rule.
10 of 10
DC HCBS Waiver Settings-Regulatory Compliance Update-Assessment 12-21-22
F. DHCF’s Long Term Care Administration is responsible for monitoring and
ensuring DHCF’s compliance with this Transition Plan. DHCF has created a
work plan to track each item in this transition plan and ensure timely
completion. This is reviewed with responsible staff, on an ongoing and
periodic basis, as needed to ensure full compliance with the HCBS Settings
Rule no later than March 17, 2022. A new version of the work plan will be
created by DHCF and DDS, to continue to track progress. This will be
developed by the DDS Performance Management Unit and DHCF staff by
May 2017 and will be posted on the DDS website on the Waiver Amendment
Information page by DDS IT, and on the DHCF website by the Office of the
Chief Technology Officer by June 2017.
September 2019 Update: DHCF demonstrated compliance with the HCBS
Settings rule during the year. All EPD waiver providers in the Statewide
Transition Plan are 100% compliant.
September 2018 Update: LTCA’s Oversight and Monitoring Division, in
collaboration with the EPD Waiver Unit, will continue to track progress toward
compliance with the HCBS settings requirements.
September 2017 Update: A workplan for the HCBS EPD Waiver with an
overview of major tasks is attached. As noted for the HCBS IDD Waiver
workplan above, we understand that DC would soon be receiving a Milestone
Reporting Template from CMS and we plan to use that to report both to CMS
and the public on our progress. Once received, DC will decide which tool
works best for the public. DC will publish updates on an annual basis on our
website.

DC HCBS Waiver Settings-Regulatory Compliance Update-Grievance 12-21-22
1 of 3
Attachment 3
District of Columbia Home & Community-Based Waiver Settings Compliance
Update-Grievance
Submitted to CMS December 21, 2022
Description of a beneficiary’s recourse to notify the state of provider non-
compliance (grievance process, notification of case manager, etc.) and how the
state will address beneficiary feedback.
Intellectual and Developmental Disabilities HCBS Waiver
Excerpt from District of Columbia Statewide Transition Plan (September 30, 2020
Update)
pp. 116-117. First, we require via regulation that each waiver provider develop and
adhere to policies which ensure that each person receiving services has the right to the
following:
• Be treated with courtesy, dignity, and respect;
• Direct the person-centered planning of his or her supports and services;
• Be free from mental and physical abuse, neglect, and exploitation from staff
providing services;
• Be assured that for purposes of record confidentiality, the disclosure of the
contents of his or her personal records is subject to all the provisions of
applicable District and federal laws and rules;
• Voice a complaint regarding treatment or care, lack of respect for personal
property by staff providing services without fear of retaliation; and
• Be informed orally and in writing of the following:
o Complaint and referral procedures including how to file an anonymous
complaint;
o The telephone number of the DDS customer complaint line;
o How to report an allegation of abuse, neglect and exploitation;
o For people receiving residential supports, the person’s rights as a tenant,
and information about how to relocate and request new housing.
p. 217. The new DDA Complaints policy (2016-DDA-POL01) includes an option for
anonymous complaints. Please see: https://dds.dc.gov/page/dda-formal-complaint-
system (Updated December 2022).
DC HCBS Waiver Settings-Regulatory Compliance Update-Grievance 12-21-22
2 of 3
Elderly and persons with Physical Disabilities HCBS Waiver
Excerpt from the District of Columbia Application for 1915(c) HCBS Waiver:
DC.0334.R05.00 - Feb 01, 2022 (EPD)
Appendix F-3 State Grievance/Complaint System
DHCF's Long Term Care Operations Division within LTCA is responsible for the
operation of the grievance/complaint system. Additionally, the District of Columbia
Office of Health Care Ombudsman and Bill of Rights (OHCOBR), an independent
office located within DHCF, operates a separate complaint resolution system, through
which waiver participants may also make complaints. LTCA and OHCOBR coordinate
on the resolution of all types of complaints, including those related to this waiver, and
to facilitate the development of program improvements to address underlying
systemic issues that may have led to complaints.
a) Participants may make all types of complaints or grievances to DHCF pertaining to
the provision of waiver services.
(b) The timelines for resolving complaints are as follows. All complaints that indicate
that a participant's health and/or welfare are at immediate risk are addressed within 24
hours or next business day of the receipt of the complaint. Complaints pertaining to
Medicaid eligibility determination and denial or reduction of service are addressed
within seven (7) business days; all other complaints are addressed within ten business
days and resolved within thirty (30) days of the receipt of the complaint. If the
complaint remains unresolved after the third week, it is elevated to LTCA management
for further intervention. If after thirty (30) days the complaint remains unresolved, it is
elevated to the LTCA Director for intervention. Complainants are also informed upon
the initiation of the complaint of the right to a fair hearing and how to obtain one.
(c) When a participant, or advocate authorized by the participant, contacts the LTCA,
the complaint is documented and logged into a cloud-based, electronic complaints
management system and assigned to one of several staff persons in the LTCA for
investigation and resolution. These staff investigate and use a variety of processes and
mechanisms to resolve the complaint, depending upon the nature of the complaint.
These processes and mechanisms include, but are not limited to: interviewing the
participant, participant representative, service provider, and others with knowledge of
the problem to obtain a clear understanding of the problem; reviewing the participant's
service records and provider documentation; and reviewing billing records. Once the
problem is well understood, staff can take a number of actions as appropriate

DC HCBS Waiver Settings-Regulatory Compliance Update-Grievance 12-21-22
3 of 3
including: directing the provider to develop and implement a corrective action plan (to
be approved by LTCA staff); assisting the participant to choose another provider and
transfer to that provider; referring the situation to Adult Protective Services or other
intergovernmental resources; referring the situation to the DHCF Division of Program
Integrity when instances of provider fraud or abuse are suspected; and referring
complainants to the fair hearing process when certain complaints are not resolvable to
the complainant's satisfaction or involve issues pertaining to eligibility for
or denial of services.
In addition to the LTCA complaints receipt and resolution process, the Office of Health
Care Ombudsman and Bill of Rights (OHCOBR) manages its own complaints process.
The OHCOBR is comprised of two legislative requirements, the Ombudsmans
Program (D.C. Code § 7-2071.01 et seq.), and the Grievance Procedures for Health
Benefit Plans (D.C. Code § 44-301.01 et seq). In February, 2008, the D.C. Medical
Assistance Administration of the D.C. Department of Health (DOH) became a
separate, cabinet-level agency, DHCF, for the administration of the Medicaid program
(D.C. Code § 7-771.01 et seq.) and obtained jurisdiction over matters pertaining to both
requirements. These laws, regulations, and policies pertaining to complaints and
grievances are available to CMS upon request.
December 2022 Update: DHCF LTCA complaint contacts are listed on the Contact
Information page of the LTCA section of the DHCF Website
(https://dhcf.dc.gov/page/contact-information-0).
