Universal Screening Panel Report
September 2019
October 30, 2019 1
Introduction
Iowa has been working diligently on the care and nurturance of its most vulnerable citizens for
over 150 years
1
. The goal of providing “safe, healthy, and successful lives with their families
and friends” shows the value and importance of social emotional behavioral health to the
community.
The Iowa Children’s System State Board convened the Universal Screening Panel
2
(herein the
Panel) in the spring of 2019 to provide recommendations based on Board consensus to develop
a universal screening plan for Iowa’s children. The Strategic Plan
3
of the State Board provides
a vision, mission, reason to act, and core value statements as a guide for the Universal
Screening Panel’s work.
It is strongly recommended that implementation of universal screening is approached as a
learning process with opportunities to reflect, improve, and correct in response to lessons
learned as it unfolds. The Panel recommends three broad goals for the implementation of
universal screening in Iowa:
1. Provide public education about the critical need to attend to social and emotional
behavioral health and well-being.
2. Implement universal screening informed by Panel tool and practice guidance,
capitalizing on existing efforts and the natural opportunities to engage families.
3. Provide enhanced family support, targeted training, and funding support and
throughout the state.
Using parameters and guidelines that can be found in the needs assessment section of this
report, the Panel developed the following set of specific recommendations for the
implementation of universal screenings:
Universal screening activities use existing programs of strength, supply strong
communication tools, and activates care coordination functions of the Children’s System;
Leverage the strength of the Iowa EPSDT (Early, Periodic, Screening, Diagnosis, and
Treatment) program, 1
st
Five, Children’s Health Insurance Program
4
, and Department of
Education activities including the use of the MTSS framework for supplying and
broadcasting the message of social emotional behavioral health and well-being;
Public education about universal screening as a proactive strategy for maximizing
healthy social emotional behavioral development and building family and community
strength;
Provide screening in the environments naturally engaging with families: healthcare and
schools, as well as innovative strategies like placing healthcare clinics in or alongside
schools, daycares, early childhood programs;
Provide families, in various contexts, with resource navigators who serve to support,
educate, and accompany families through the identification of need to intervention and
resolution. Examples of resource navigators are found in 1
st
Five
5
and Scott County
6
;
1
https://idph.iowa.gov/Portals/1/Files/LPHS/LBOH%203_history.pdf
2
Membership found in Appendix/Additional Resources
3
https://dhs.iowa.gov/sites/default/files/ChildrensStateBoard_StrategicPlan_Nov2018.pdf?071120191534
4
https://dhs.iowa.gov/hawki
5
http://www.iowapeds.org/home/about-us/programs/1st-five-initiative/
October 30, 2019 2
Provide training for all screeners/practitioners and to use existing stakeholders and
relationships (Systems of Care, AAP Iowa, EPSDT, Family Physicians, 1
st
Five, and the
Department of Education including Areas Education Agencies) to ensure broad capacity,
competence, and networks are developed;
Training includes specific training and support about choosing best screening tools for
the various contexts in which screening will happen;
The State Board endorses the Practice Parameters and Suggested Matrix of Tools
supplied here and institutes a robust periodic review of suggested tools;
A diligent analysis of barriers to universal screening including funding, payment,
personnel, and referral network adequacy. Education and healthcare communities
presently manage extraordinary expectations often with competing demands and limited
time. Removal of impediments and creating efficiencies for these providers is strongly
recommended. Additionally, equity across insurance types (and for the uninsured), in
access to quality care, and of service and provider capacity is a significant concern and
removal of these barriers will be necessary.
Background
Social and emotional behavioral health (SEBH) affects how we think, feel, communicate, act,
and learn. It includes the process by which children and adults acquire and effectively apply the
knowledge attitudes, and skills necessary to understand and manage emotions set and achieve
positive goals, feel and show empathy for others, establish and maintain positive relationships,
and make responsible decisions.
Flexible and competent social and emotional behavioral health is developed through responsive
and nurturing caregiving and relationships. It contributes to resilience, how we relate to others,
respond to stress and emotions, and make choices
7
. Families need essential resources,
support, and attentive care in order to nurture children’s health: mind and body.
8
The consequences of inadequate care and insufficient
resources on the brain development of young children
can be dire to individuals and the community. Toxic
stress and adverse childhood experiences
9
, especially
in the early years, impact a person’s overall health,
ability to maintain healthy relationships, make wise
choices, and meaningfully contribute to their
community. Many parts of the community that touch
families – childcare and education, healthcare, housing,
nutrition, and economic support – are essential for
helping families to nurture and support optimal social
emotional behavioral health. Iowa’s Innovation Model
10
and investment in community health is an excellent
6
https://www.scottcountyiowa.com/health/care-kids/developmental-screenings
7
https://www.cdc.gov/hrqol/wellbeing.htm
8
https://www.cdc.gov/ncbddd/childdevelopment/early-brain-development.html
9
https://www.iowaaces360.org/
10
https://dhs.iowa.gov/ime/about/initiatives/newSIMhome/social-determinants-health
A toxic stress response can occur
when a child experiences strong,
frequent, and/or prolonged adversity—
such as physical or emotional abuse,
chronic neglect, caregiver substance
abuse or mental illness, exposure to
violence, and/or the accumulated
burdens of family economic hardship—
without adequate adult support.
https://developingchild.harvard.edu/scien
ce/key-concepts/toxic-stress/
October 30, 2019 3
example of committed leadership and resources in addressing the social determinants of health
(aka unmet social needs).
The Innovation Model describes five unmet social needs:
Economic Stability
Education
Social and Community Context
Health and Health Care
Neighborhood and Built Environment
Unmet social needs should remain a
consideration in system design and
implementation of universal screening. Panel
members cited how identifying an unmet social
need and lacking a viable option for addressing
the need frustrates the opportunity to stabilize a
vulnerable family. The 1st Five
11
program was
highlighted as a powerful engine for connecting
families to resources that can meet material needs
while simultaneously attending to social and
emotional health of all members of the family.
Learning environments are a powerful place to
strengthen social emotional behavioral health. The
Iowa Department of Education has employed the
Multi-Tiered System of Support (MTSS
12
)
framework to help ensure that students are
provided a rich and attentive context in which to
learn and grow. Iowa educational innovators like Scott County Kids
13
use universal screening to
appropriately identify and attend to needs that impact students’ learning and social/emotional
health. The MTSS framework supports accurate knowledge about the needs of individuals,
schools, and communities in support of the sound allocation of resources.
Needs assessment
The Panel initiated its work with an assessment and review of the present practices and
opportunities for universal screening across Iowa and national practices and guidance. At
present, schools, healthcare professionals, and the early childhood community supported by the
Department of Health provide excellent structure to build upon.
The Panel gathered, shared, and reviewed information about the areas of strength in Iowa’s
efforts to attend to children’s social and emotional needs. Innovative and strong efforts include
the work of Scott County Kids
14
, Iowa 1
st
Five
15
, and the medical home model many pediatric
11
http://www.iowapeds.org/home/about-us/programs/1st-five-initiative/
12
https://educateiowa.gov/pk-12/learner-supports/multi-tiered-system-supports-mtss
13
https://scottcountykids.org/
14
https://scottcountykids.org/
15
http://idph.iowa.gov/1stfive
Unmet social needs are the complex,
integrated, and overlapping social structures
and economic systems that are responsible
for most health inequities. These social
structures and economic systems include the
social environment, physical environment,
health services, and structural and societal
factors. Social determinants of health are
shaped by the distribution of money, power,
and resources throughout local communities,
nations, and the world.
https://www.healthypeople.gov/2020/t
opics-objectives/topic/social-
determinants-of-health
October 30, 2019 4
practices employ
16
. Each of these is unique in its attention to sensitive and timely engagement
with families, evidence-based practices of identifying needs and strengths, attention to unmet
social needs, and deliberate coordination of care in the service of attending to needs.
Paramount in successful implementation and efforts at sustaining universal screening is the role
of care coordination and communication between and among families, practitioners, educators,
and service providers. The Panel recommends ensuring universal screening activities use
existing programs of strength, supply strong communication tools, and activates care
coordination functions of the Children’s System.
The Panel was charged with and responded to the following parameters for universal screening:
Screenings shall be:
Accessible to all children in Iowa;
Administered at key developmental stages of childhood by qualified individuals after
informed consent is given by the child’s parent or guardian;
Developmentally, age, gender, and culturally appropriate for the child or adolescent
being screened;
Linked to appropriate assessments and services;
Valid and reliable in identifying children and adolescents in need of further
assessment;
Administered at multiple locations including, but not limited to schools, primary care
clinics, and detention centers.
Children and youth in Iowa are commonly screened through schools and healthcare providers.
In the educational setting, panel members evaluated the tools used across early childhood and
through high school and found them to be useful and appropriate. Screening in healthcare
satisfies the objective of EPSDT and is detailed in Iowa’s robust EPSDT program found here:
http://www.iowaepsdt.org/ .
The Panel advocated for the following guidelines for universal screening:
Build on the existing system of already established screenings;
Screening tools are simple, easy to administer checklists or questionnaires used for
identifying biological and environmental factors that put some children at a higher risk for
social emotional behavioral health conditions;
Screening tools are intended to be predictive in nature for assessing strengths and areas
of concern;
Screening tools identify the need for a referral for an appropriate, in-depth assessment
to determine if social emotional behavioral health services are needed;
Periodic screenings are essential for the early detection of social emotional behavioral
health conditions since conditions can present at different stages of development.
Matrix of suggested tools
The matrix of suggested tools and practice parameters are the basis for a universal screening
program in Iowa. The Panel developed a matrix of suggested tools (found in Appendix) having
evaluated each for:
16
https://medicalhomeinfo.aap.org/national-state-initiatives/State-Profiles/Pages/Iowa-State-
Profile.aspx
October 30, 2019 5
a. Appropriateness: the fit of the tool to the screening context, the purpose, and the need of
screening;
b. Technical adequacy: the validity, reliability, and accuracy of the screening tool;
c. Usefulness: the tool generates new and useful information supplemental to existing
information;
d. Feasibility: the ease of implementation and clarity of the referral pathway of the tool;
e. Beneficial properties: the cultural sensitivity and responsiveness and the absence of
harm of the tool.
There is no single tool appropriate for all children or screening situations. All the tools chosen
through expert consensus of the Panel are presently used in Iowa, typically in educational or
healthcare settings. The Panel cautions that the on-going process of suggesting screening
tools should include a rigorous evaluation of psychometric properties, usefulness, cultural
sensitivity, and supporting evidence of effectiveness.
The recommended tools are the best choices to ensure that tools used in Iowa are appropriate
to the child with regard to age, gender, ethnicity, cultural background, sexual orientation,
disability, or any other factor that would influence the developmental appropriateness of the
instrument being administered. The tools are research-informed and evidence-based to ensure
validity and reliability in identifying children and adolescents in need of further assessment.
The Panel recommends the following screening tools:
Modified Checklist for Autism (M-CHAT)
Survey of Wellbeing of Young Children (SWYC)
Patient Health Questionnaire (PHQ)
Ages and Stages Questionnaires (ASQ)
Strengths and Difficulties Questionnaire (SDQ)
Social Academic Emotional Behavior Risk Screener (SAEBERS)
CRAFFT (Car, Relax, Alone, Forget, Friends, Trouble)
Practice Parameters
Practice parameters are outlined by the Panel’s guidance on the following questions:
o When screenings will occur;
o Where screenings will be provided;
o Who will provide screenings; and;
o What will be included in the screenings.
The existing screening practices within Iowa provide a framework and sound rationale for
adopting the EPSDT-approved Bright Futures periodicity schedule (found in Appendix/Additional
Resources). This schedule has been married with the recommended schedule of screenings in
Iowa schools.
WHEN
The Panel recommends including key events in the periodicity schedule detailed here for
healthcare and education. These are the two places that encounter children most frequently
however the Panel encourages inclusion of all available settings (childcare and home visiting,
for example) in universal screening efforts. For both, there is an expectation of on-going
monitoring of development and the periodicity noted here is intended for the use of screening
tools.

October 30, 2019 6
Primary and Pediatric care:
o Developmental screening (note this includes screening for Autism): 9, 18, 30, and 36
months;
o Yearly developmental monitoring until age 21;
o Annual screening of substance use and depression screening beginning (minimally)
age 12.
Educational setting: Minimally an annual screening with attention to the following
vulnerable times in a child’s life:
o School entry: Kindergarten or 1
st
grade
o 4
th
grade
o 6
th
grade
o 9
th
grade
WHERE
The Matrix of tools includes information about where screenings typically occur. Multiple
opportunities for screening, i.e.: healthcare, school, early childhood setting, ensure that families
and youth engage comfortably and frequently in optimizing social and emotional health, a
breadth of practitioners are involved in collaborative monitoring of social emotional behavioral
health with families, and that screening occurs with more vulnerable families who are often not
as routinely interacting with professionals.
Essential to the implementation of sustainable universal screening practices is the link to follow
up care. Healthcare, ideally as a health home that coordinates care and communication for
families, is the place where most children will be encountered. Healthcare providers will make
appropriate follow up recommendations for care for area(s) of concern identified from any
screening practice employed
17
.
WHO
Screenings should be provided by professionals and paraprofessionals appropriately supported
and trained in screenings and the referral network. Appropriate training is determined by the
screening setting and tool. Efficient and accessible communication tools across settings (for
example school and physician), and clear referral pathways for areas of concern ensure
adequate support of screeners. Screeners should have clear parameters for obtaining consent,
engaging families in the process of screening and discussing area for growth where found, and
be appropriately aware of and connected to pathways to care for addressing concerns.
The Panel encourages the broad use of paraprofessionals in early childhood settings
particularly where their utility and expertise are proven (in Head Start and home visiting
programs for example.)
The Panel also strongly encourages engagement with the primary care community of providers
who see most children and youth in healthcare settings and influence families’ engagement with
supportive services and interventions when these are needed. The development and spread of
health homes throughout Iowa would serve to strengthen the universal screening network.
17
This practice is also best for the 12,000 estimated home-schooled children in Iowa.
October 30, 2019 7
Equally, the role of the Area Education Agencies
18
in early access to screening and care are an
asset to this effort.
WHAT WILL BE INCLUDED
The Matrix reflects the Panel’s recommendation that screenings be appropriate for the age,
developmental needs, and culture of the child and family. Screenings should gather information
about a child’s developmental status, social emotional behavioral strengths and needs, unmet
social needs, and cultural context to supply information about area for growth when identified.
Areas of specific attention like substance use, domestic violence, and depression in the family
are also recommended.
Conclusion
The Panel’s recommendations aim to light the pathways to health for Iowa families. The Panel
is grateful for the opportunity to provide valuable guidance in promoting social emotional
behavioral health early and wisely in Iowa. Promoting the social emotional behavioral health of
children through universal screening as recommended here capitalizes on the existing strengths
of the health, education, and healthcare communities. The care and nurturing of social and
emotional health of Iowa children strengthens schools, families, and communities.
18
http://www.iowaaea.org/

October 30, 2019 8
Definitions and terms
Adverse Childhood Experiences (ACEs): The original study evaluated 10 types of adverse
childhood experiences:
Abuse: physical, sexual, psychological
Neglect: emotional, physical
Household dysfunction: substance abuse, divorce, mental illness, battered
mother, and criminal behavior
The ACE Study revealed that adverse childhood experiences are common. Nearly two-thirds of
participants reported at least one ACE and more than one in five reported three or more ACEs.
The study also linked childhood trauma to a range of health and social outcomes including:
Alcoholism
Chronic obstructive pulmonary disease
Depression
Illicit drug use
Ischemic heart disease
Liver disease
Smoking
Adolescent pregnancy
Sexually transmitted diseases
Intimate partner violence
Health-related quality of life
In addition, as the number of ACEs increase, so does the level of risk for each of these health
issues in a strong and graded fashion
EPSDT (Early, Periodic, Screening, Diagnosis and Treatment): A program for children who are
enrolled in Medicaid. The focus of this program is to assure that eligible children ages birth
through 20 years receive preventive health care services, including oral health care. In Iowa, the
EPSDT program is called Care for Kids. EPSDT Care for Kids services are free to children
enrolled in Medicaid. Care for Kids: http://www.iowaepsdt.org/.
The acronym EPSDT stands for:
Early
o Children should receive quality health care beginning at birth and continuing
throughout childhood and adolescence including the identification, diagnosis and
treatment of medical conditions as early as possible.
Periodic
o Children should receive well child check-ups at regular intervals throughout
childhood according to standards set by the American Academy of Pediatrics.
Health care may be provided between regularly scheduled check-ups.
Screening
o Children should be screened for health and developmental problems. Services
shall include health history, developmental assessment, physical exam,
immunizations, lab tests, health education, dental exam, and vision and hearing
screenings.
Diagnosis
o Children should receive further evaluation of health or developmental problems
identified during check-ups that may require treatment.
October 30, 2019 9
Treatment
o Children should receive treatment for health or developmental problems
identified during check-ups.
Following the Iowa EPDST Care for Kids Periodicity Schedule, screenings provide the
opportunity to identify concerns through comprehensive assessment of the child and family; and
develop a care plan that is responsive to the family’s strengths, needs and choices.
Screening: The use of a standardized tool to identify risk and determine the need for further
evaluation. Screening includes:
Determining whether your child has any health concerns
Offering ways to keep your child from developing health concerns
Providing support for your child’s overall health and well-being
Talking through health information and offering advice
https://brightfutures.aap.org/Bright%20Futures%20Documents/BF_Family_Tipsheet.pdf:
Surveillance (AKA monitoring): A longitudinal, continuous process based on clinical judgement
that includes eliciting and attending to concerns, maintaining a history of findings, making
observations, and identifying risk and protective factors.
https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Screening/Pages/Definitions-of-
Key-Terms.aspx
Toxic Stress: Prolonged exposure to adverse experiences that activate the stress response
system, potentially disrupting a child’s development and increasing the risk of poor health
outcomes into adulthood.
https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Screening/Pages/Definitions-of-
Key-Terms.aspx
Unmet Social Needs (AKA social determinants of health): The social determinants of health
(SDH) are the conditions in which people are born, grow, work, live, and age, and the wider set
of forces and systems shaping the conditions of daily life. These forces and systems include
economic policies and systems, development agendas, social norms, social policies and
political systems (https://www.who.int/social_determinants/en/). SDH include the opportunity to
work, access quality childcare, healthcare, and education, have safe housing, and access to
food and nutrition.
October 30, 2019 10
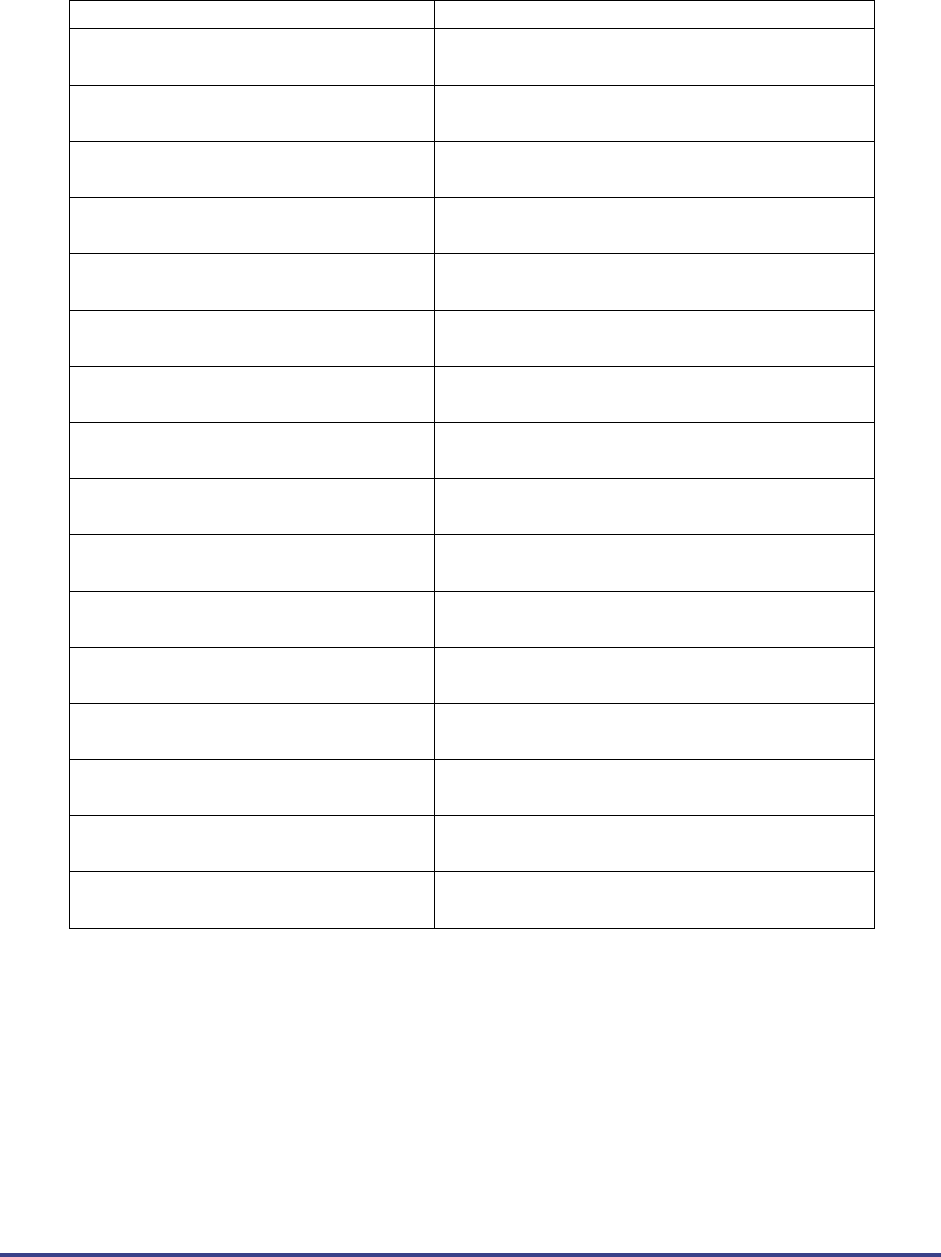
APPENDIX
Working Matrix
BLUE:
SCHOOLS
GREEN:
HEALTHCARE
Tier 1 or 2
Tool
ACCESSIBILITY
ADMINISTRATION
DETAILS
AGES
CULTURAL
SENSITIVITY
1
M-CHAT: (screening tool for autism in toddlers)
Free online; instant score
https://m-chat.org/
Quick online
administration by any
caregiver
16 to 30
months
Translations underway:
https://mchatscreen.co
m/m-chat/translations/
1
SWYC: Survey of Well Being of Young
children: The SWYC covers 3 domains of functioning
(Behavior and Emotion, Family Risk Factors, and
Development), and it is composed of 6 questionnaires:
Preschool Pediatric Symptom Checklist, Baby Pediatric
Symptom Checklist, Family Questions, Parents
Observation of Social Interaction, Developmental
Milestones, and Parent’s Concerns. It is comprehensive,
including cognitive, language, motor, and social-emotional
development as well as family risk factors (parental
depression, conflict, or substance abuse, and hunger).
Free: SWYC was created in order
to provide a screening instrument
that is free of cost and easily
accessed by parents,
pediatricians, preschool teachers,
nurses, and other professionals
involved in child care and
education
10 minutes or less
https://www.floatinghospital.or
g/-/media/Brochures/Floating-
Hospital/SWYC/SWYC-
Manual-v101-Web-Format-
33016.ashx?la=en&hash=E0C
2802F003ED312E9D5268374
C540A112151FB3
1 to 66
months
Spanish, Khmer,
Burmese, Nepali,
Portuguese, Haitian-
Creole, Arabic, Somali
and Vietnamese.
1
Patient Health Questionnaire (PHQ): The
PHQ, a self-administered version of the PRIME-MD,
contains the mood (PHQ-9), anxiety, alcohol, eating, and
somatoform modules as covered in the original PRIME-
MD. The GAD-7 was subsequently developed as a brief
scale for anxiety. The PHQ-9, a tool specific to depression,
simply scores each of the 9 DSM-IV criteria based on the
mood module from the original PRIME-MD. The GAD-7
scores 7 common anxiety symptoms.
Free
https://www.phqscreeners.com/se
lect-screenere:
Seems most useful for
parents
0-13
years
1
ASQ: General psychosocial screening Sensitivity: 63%
to 94% for emotional symptoms, Specificity: 88% to 98%
conduct problems, hyperactivity/inattention, peer
relationship problems, and pro-social behavior (not
included in score); a separate scale assesses impact of
symptoms on global functioning.
About .50c per screen
Parents, caregivers,
teachers, clinicians10 min;
25 items; self-
administered for 11-17
1 month
to 5.5
years
40 languages
2
ASQ-SE2 & 3: “highly reliable, parent-completed tool
with a deep, exclusive focus on children’s social and
emotional development, it’s easier than ever to screen
important areas of social-emotional competence, pinpoint
behaviors of concern, and identify any need for further
assessment or ongoing monitoring.”
10–15 minutes to
complete, 1-3 minutes to
score;
https://agesandstages.com/free-
resources/articles/using-asq-3-and-
asqse-2-together/
1-72
months
40 languages
1
SDQ: 1) Emotional symptoms; 2) conduct problems; 3)
hyperactivity &/or inattention; 4) peer relationship
problems; 5) prosocial behavior.
Used in research and clinically worldwide
$.25/screen
Additional information:
https://www.cebc4cw.org/assessment-
tool/strengths-and-difficulties-
questionnaire/
https://depts.washington.edu/dbpeds/S
creening%20Tools/Strengths_and_Diffi
culties_Questionnaire.pdf
https://www.nctsn.org/measures/strengt
hs-and-difficulties-questionnaire-child-
report
Self-screener; Parent,
teacher, clinician, youth
3-16
years
Abundant languages
available
1
SAEBRS: The SAEBRS is a brief tool supported by
research for use in universal screening for behavioral and
emotional risk. The measure falls within a broad class of
highly efficient tools, suitable for teacher use in evaluating
and rating all students on common behavioral criteria
(Severson, Walker, Hope-Doolittle, Kratochwill, &
Gresham, 2007). The SAEBRS is designed for use in the
K-12 setting
$7 a student
1-3 minutes;
Online portal
5-18
years
Multiple languages
2
CRAFFT: (screening tool for substance-related risks)
Free -
https://www.integration.samhsa.g
ov/clinical-
practice/sbirt/CRAFFT_Screening
_interview.pdf;
https://www.integration.samhsa.g
ov/clinical-
practice/sbirt/adolescent_screeni
ng,_brieft_intervention_and_referr
al_to_treatment_for_alcohol.pdf
6 questions; designed for
primary care
ages 14-
20
Spanish, Portuguese,
Hebrew, French,
Czech, Khmer,
Russian, Vietnamese,
Haitian Creole,
Laotian, Chinese, and
Japanese
October 30, 2019 11
APPENDIX
Membership
Member
Agency
Dr. Joyce Vista Wayne
Chair/ Mercy Hospital
Ben Barry
Carlisle School District
Brad Niebling
Department of Education
Dana Miller
Central Rivers AEA
Dr. Amanda Boeke
YSS
Dr. Amy Shriver
Blank Children’s Hospital
Dr. Marguerite Oetting
University of Iowa Hospital and Clinics
Dr. Stephen R. Mandler
Orchard Place
Kay Augustine
Department of Education
Kelly Betsworth
ChildServe
Marcus Johnson-Miller
Department of Public Health
Melanie Cleveringa
Sioux Center School District
Nicole Mann
Scott County Kids
Rick Shults
Department of Human Services
Sally Oudekerk
Department of Human Services
Shanell Wagler
Early Childhood Iowa
Grant funds provided by Mid-Iowa Health Foundation were used to support the Panel
and their work.
