CTA Pulmonary Embolism
CTA Chest (pulmonary angiogram)
Reviewed By: Rachael Edwards, MD; Dan Verdini, MD; Brett Mollard, MD
Last Reviewed: July 2019
Contact: (866) 761-4200, Option 1
In accordance with the ALARA principle, TRA policies and protocols promote the utilization of
radiation dose reduction techniques for all CT examinations. For scanner/protocol combinations
that allow for the use of automated exposure control and/or iterative reconstruction algorithms
while maintaining diagnostic image quality, those techniques can be employed when
appropriate. For examinations that require manual or fixed mA/kV settings as a result of
individual patient or scanner/protocol specific factors, technologists are empowered and
encouraged to adjust mA, kV or other scan parameters based on patient size (including such
variables as height, weight, body mass index and/or lateral width) with the goals of reducing
radiation dose and maintaining diagnostic image quality.
If any patient at a TRA-MINW outpatient facility requires CT re-imaging, obtain radiologist
advice prior to proceeding with the exam.
______________________________________________________________________
The following document is an updated CT protocol for all of the sites at which TRA-MINW is
responsible for the administration, quality, and interpretation of CT examinations.
Include for ALL exams
Scout: Send all scouts for all cases
Reformats: Made from thinnest source acquisition
o
Scroll Display
Axial recons - Cranial to caudal
Coronal recons - Anterior to posterior
Sagittal recons - Right to left
o
Chest reformats should be in separate series from Abdomen/Pelvis reformats, where applicable
kVp
o
100 @ <=140lbs
o
120 @ >140lbs
mAs
o
Prefer: Quality reference mAs for specific exam, scanner and patient size
o
Auto mAs, as necessary
For CTAs: send source data (0.625 mm thick or equivalent) to PACS and TeraRecon
OTHER:
Please call radiologist for OUTPATIENT rule out PE before patient leaves department
o Mark these studies STAT
CTA Pulmonary Embolism
CTA Chest (pulmonary angiogram)
Indication: Evaluate for pulmonary embolism (chest pain, shortness of breath, elevated D-dimer, etc.)
Patient Position: Supine, feet down with arms above head
Scan Range (CC z-axis): Lung apices to L1 (scan cranial to caudal)
**Remember, please isocenter the exam using the lateral scout **
Prep: No solids (liquids OK) for 3 hours prior to examination
Note: Okay to continue examination if prep is incomplete or not done
Oral Contrast: None
IV Contrast Dose, Flush, Rate and Delay:
Dose & Rate: (modify volume if using something other than Isovue 370; 20-gauge or larger IV, at
least 4 inches above wrist or pressure injectable line)
o < 200 lbs 80 mL Isovue 370, 4cc/sec
o > 200 lbs 100 mL Isovue 370, 5cc/sec
Flush: 50 mL saline
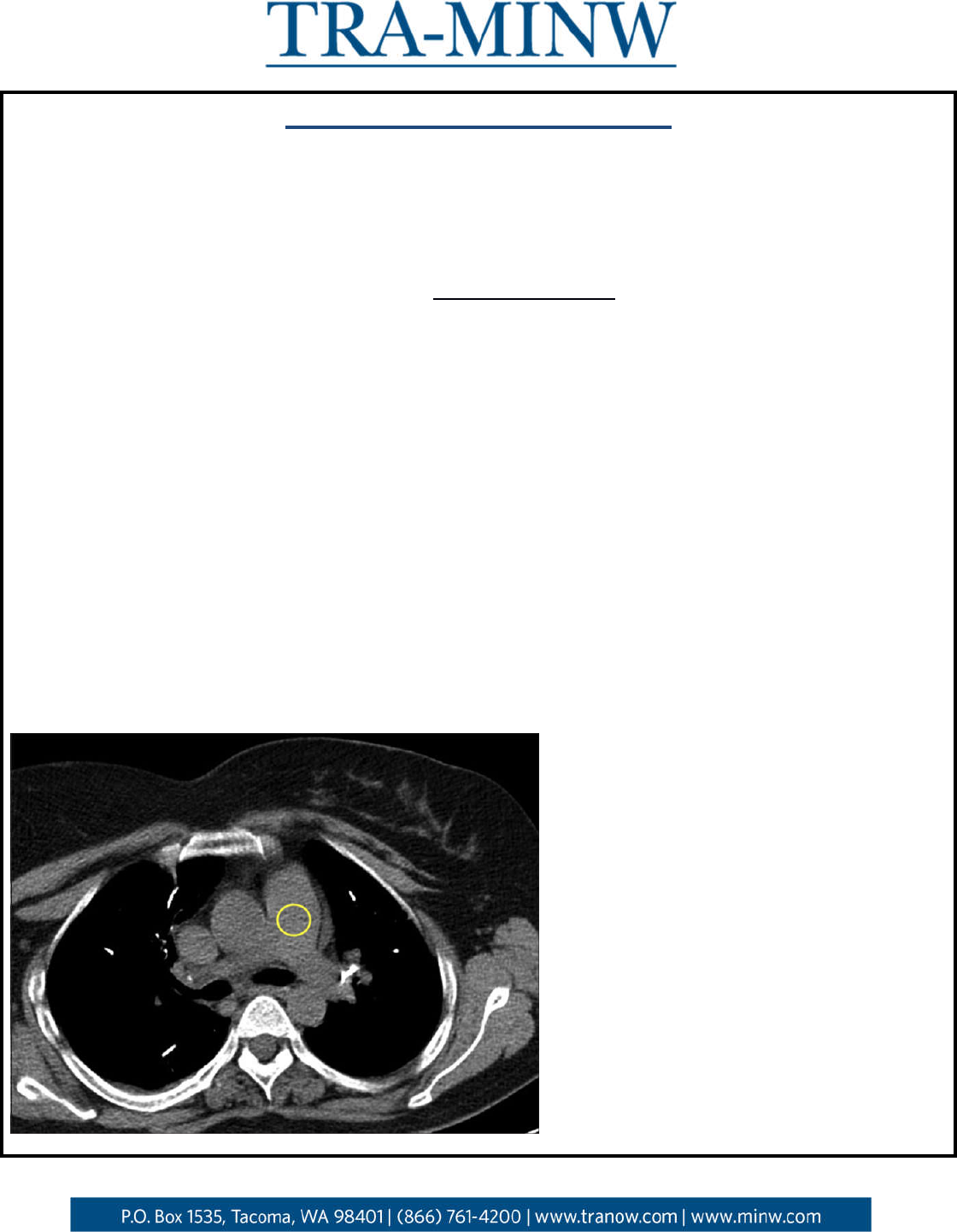
Delay: Bolus trigger in Main Pulmonary Artery (threshold 100HU)
Acquisitions: 1 (post-contrast) scan cranial to caudal
o Pulmonary arterial phase chest - BOLUS TRACK with HU trigger of 100 ROI placed in main
pulmonary artery + 5 second delay
Only if bolus tracking is not available, use fixed scan delay:
16 slice: 15 sec
64 slice: 20 sec
o NOTE: If acquisition is questionable, call radiologist to determine need to re-bolus/re-
scan
o Single breath, full inspiration preferred; mid-expiration should be considered ONLY if
inspiratory images are non-diagnostic
Expiratory imaging significantly limits evaluation of the lung parenchyma
Mid-expiration instructions: “Take a deep breath in, let half of the air out, stop
breathing”
Series + Reformats:
1. Pulmonary arterial phase chest
a. Axial 2-2.5 mm ST kernel
b. Axial 1.2-1.5 mm lung kernel
c. Axial 10 x 2 mm MIP ST kernel
d. Coronal 2 mm ST kernel
e. Sagittal 2 mm ST kernel
f. Oblique 10 x 2 MIP RIGHT Pulmonary Artery ST kernel
– angulation of obliques should be
optimized for each patient’s anatomy to best demonstrate pulmonary arteries
g. Oblique 10 x 2 MIP LEFT Pulmonary Artery ST kernel
– angulation of obliques should be optimized
for each patient’s anatomy to best demonstrate pulmonary arteries
h. Axial 1.25 x 1 mm ST kernel (SuperD where doable)
***Machine specific protocols are included below for reference
Machine specific recons (axial ranges given above for machine variability):
*Soft tissue (ST) Kernel, machine-specific thickness (axial):
GE = 2.5 mm
Siemens = 2 mm
Toshiba = 2 mm
*Lung Kernel, machine-specific thickness (axial):
GE = 1.25 mm
Siemens = 1.2 mm (or 1.5 mm on older generation)
Toshiba = 1 mm
Source: http://pubs.rsna.org/doi/pdf/10.1148/radiol.10090908
General Comments
NOTE:
Use of IV contrast is preferred for most indications aside from: pulmonary nodule follow-up, HRCT, lung
cancer screening, and in patients with a contraindication to iodinated contrast (see below).
Contrast Relative Contraindications
Severe contrast allergy: anaphylaxis, laryngospasm, severe bronchospasm
- If there is history of severe contrast allergy to IV contrast, avoid administration of oral
contrast
Acute kidney injury (AKI): Creatinine increase of greater than 30% over baseline
- Reference hospital protocol (creatinine cut-off may vary)
Chronic kidney disease (CKD) stage 4 or 5 (eGFR < 30 mL/min per 1.73 m
2
) NOT on dialysis
- Reference hospital protocol
Contrast Allergy Protocol
Per hospital protocol
Discuss with radiologist as necessary
Hydration Protocol
For eGFR 30-45 mL/min per 1.73 m
2
: Follow approved hydration protocol
IV Contrast (where indicated)
o Isovue 370 is the default intravenous contrast agent
o See specific protocols for contrast volume and injection rate
If Isovue 370 is unavailable:
o Osmolality 350-370 (i.e., Omnipaque 250): Use same volume as Isovue 370
o Osmolality 380-320 (i.e., Isovue 300, Visipaque): Use indicated volume + 25 mL (not to
exceed 125 mL total contrast)
Oral Contrast
Dilutions to be performed per site/hospital policy (unless otherwise listed)
Volumes to be given per site/hospital policy (unless otherwise listed)
TRA-MINW document is available for reference if necessary (see website)
Brief Summary
Chest only
Chest W, Chest WO
CTPE
HRCT
Low Dose Screening/Nodule
o None

Pelvis only
Pelvis W, Pelvis WO
o Water, full instructions as indicated
Routine, excluding chest only and pelvis only
Abd W, Abd WO
Abd/Pel W, Abd/Pel WO
Chest/Abd W, Chest/Abd WO
Chest/Abd/Pel W, Chest/Abd/Pel WO
Neck/Chest/Abd/Pel W, Neck/Chest Abd Pel WO
CTPE + Abd/Pel W
o TRA-MINW offices: Dilute Isovue-370
o Hospital sites:
ED: Water, if possible
Inpatient: prefer Dilute Isovue 370
Gastrografin OK if Isovue unavailable
Avoid Barium (Readi-Cat)
FHS/MHS Outpatient: Gastrografin and/or Barium (Readi-Cat)
Multiphase abdomen/pelvis
Liver, pancreas
o Water, full instructions as indicated
Renal, adrenal
o None
CTA abdomen/pelvis
Mesenteric ischemia, acute GI bleed, endograft
o Water, full instructions as indicated
Enterography
o Breeza, full instructions as indicated
Esophogram
o Dilute Isovue 370, full instructions as indicated
Cystogram, Urogram
o None
Venogram
o Water, full instructions as indicated
