Fiscal Policies
for Diet and Prevention of
Noncommunicable
Diseases
Technical Meeting Report
5–6 May 2015, Geneva, Switzerland

Fiscal Policies
for Diet and Prevention of
Noncommunicable
Diseases
Technical Meeting Report
5–6 May 2015, Geneva, Switzerland

4 5
© World Health Organization 2016
All rights reserved. Publications of the World Health Organization are available on
the WHO website (www.who.int) or can be purchased from WHO Press, World Health
Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264;
fax: +41 22 791 4857; email: [email protected]).
Requests for permission to reproduce or translate WHO publications –whether for
sale or for non-commercial distribution–should be addressed to WHO Press through
the WHO website (www.who.int/about/licensing/copyright_form/index.html).
The designations employed and the presentation of the material in this publication
do not imply the expression of any opinion whatsoever on the part of the World
Health Organization concerning the legal status of any country, territory, city or area
or of its authorities, or concerning the delimitation of its frontiers or boundaries.
Dotted and dashed lines on maps represent approximate border lines for which there
may not yet be full agreement.
The mention of specic companies or of certain manufacturers’ products does not
imply that they are endorsed or recommended by the World Health Organization
in preference to others of a similar nature that are not mentioned. Errors and
omissions excepted, the names of proprietary products are distinguished by initial
capitalletters.
All reasonable precautions have been taken by the World Health Organization to
verify the information contained in this publication. However, the published material
is being distributed without warranty of any kind, either expressed or implied.
Theresponsibility for the interpretation and use of the material lies with the reader.
In no event shall the World Health Organization be liable for damages arising
fromitsuse.
Printed by WHO Document Production Services, Geneva, Switzerland.
Layout design: Eddy Hill Design
WHO Library Cataloguing-in-Publication Data
Fiscal policies for diet and prevention of noncommunicable diseases:
technical meeting report, 5-6 May 2015, Geneva, Switzerland.
1.Diet. 2.Food Habits. 3.Chronic Disease. 4.Health Behavior. 5.Taxes.
6.HealthPolicy. 7.Meeting Abstracts. I.World Health Organization.
ISBN 978 92 4 151124 7 (NLM classication: WT 500)

4 5
Contents
Acknowledgements 6
Abbreviations 7
Glossary 8
Executive summary 9
1. Introduction 10
2. Overview of noncommunicable diseases and the role
of scal policies to promote healthy diets 11
3. Rationale and evidence of scal policies 12
Rationale for scal policies on diet 12
Existing evidence on scal policies for diet 13
4. Country experiences and lessons learned 14
5. Implications for design and implementation of scal policies 19
A typology for consideration 19
Fiscal policies and price elasticity 20
Health and substitution eects of scal policies 21
Overcoming barriers to scal policies 21
Nutrient proling 22
Policy development 23
Earmarking of tax revenues 23
6. Conclusions 24
7. Recommendations 26
References 27
Annex 1. List of participants 30
Annex 2. Meeting programme 34
Figures
Figure 1: Pathways for the effect of fiscal policy interventions 12
Figure 2: Summary of main findings of meta-review 13
Figure 3: Types of taxes 19
Figure 4: Different tax base options for beverages 20
Figure 5: Fiscal policy development and implementation framework 23
Contents

6 7
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
Acknowledgements
The meeting report was prepared by Temo Waqanivalu and Leo Nederveen
withsupport from Doris Oppong and Paulina Sosa of the Department of Prevention
ofNoncommunicable Diseases.
Sta in the WHO regional oces and colleagues from the WHO departments
of Prevention of Noncommunicable Diseases, and Nutrition for Health and
Development, participated in the organization of the meeting and provided
valuablecontributions to the meeting report.
WHO also wishes to thank the authors of the background paper provided to the
meeting, in particular Dr Anne Marie Thow and Dr Shauna Downs of the Menzies
Centre for Health Policy, University of Sydney, Australia.
Photos: Front cover: Gutsulyak (background, also back cover, p. 7), Mariyana M (also p. 8, 26),
Xiaorui (also p. 8, 26), Irina Rogova (also p. 8, 25), Billion Photos (also p. 8, 22, 26), Zelenskaya
(also p. 8, 11, 26), 5second Studio (also back cover, p. 9, 11), Claudio Divizia (also p. 9, 11, 25),
Yuttana Samol (alsop.9, 22, 25), Worananphoto (also p. 9, 25). Back cover: Yellow Cat (also
p. 5), Kanchana P (also p. 5), Andrey Popov, Niwat Chaiyawoot, BillionPhotos (also p. 20, 30),
AfricaStudio (also p. 5), Claudio Divizia (alsop.5, 21, 26), Ultimathule (also p. 5, 23), Africa
Studio. Page 33: Martin Good / all Shutterstock.

6 7
Abbreviations
CN Combined nomenclature
DALY Disability-adjusted life year
DKr Danish krone
EU European Union
FINI Food Insecurity and Nutrition Incentives
GAP Global Action Plan on Noncommunicable Diseases
HIP Health Incentive Pilot
ICN2 2nd International Conference on Nutrition
MRA Mauritius Revenue Authority
NCD Noncommunicable disease
OECD Organisation for Economic Co-operation and Development
PAHO Pan American Health Organization
PHPT Public health product tax
SNAP Supplemental Nutrition Assistance Programme
SSB Sugar-sweetened beverage
USA United States of America
VAT Value added tax
WHO World Health Organization
Abbreviations

8 9
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
Glossary
Ad valorem tax:
Method for charging a duty, fee, or tax according to the
value of goods and services, instead of by a xed rate, or
by weight or quantity.
Fiscal policy:
A government’s revenue (taxation) and spending policy.
This report focuses on non-trade related taxes and
subsidies related to food, as non-discriminatory scal
policy approaches.
Noncommunicable diseases:
Noncommunicable diseases (NCDs) – also known
as chronic diseases – are not passed from person
to person. They are of long duration and, generally,
slow progression. The four main types of NCDs are:
cardiovascular diseases (such as heart attacks and
stroke); cancers; chronic respiratory diseases (such as
chronic obstructed pulmonary disease and asthma); and
diabetes.
Non-sugar sweetener:
A food additive (other than a mono- or disaccharide
sugar), which imparts a sweet taste to a food.
Technological purposes for this functional class includes:
sweetener, intense sweetener, bulk sweetener. It should
be noted that products like sugars, honey and other
food ingredients that can be used to sweeten are not
associated with the term “sweetener”.
Nutrient proling:
The science of classifying or ranking foods according
to their nutritional composition for reasons related to
preventing disease and promoting health.
Price elasticity of demand:
The degree to which demand for a good or service varies
with its price.
Regressivity:
The extent to which the burden of a tax is higher for
people on lower incomes, and/or represents a smaller
percentage of a higher income earner.
Specic excise:
A set amount of tax charged on a given amount
ofproduct.
Substitution:
An eect caused by a rise in price that induces a
consumer (whose income has remained the same)
tobuy more of a relatively lower-priced good and less
ofahigher-priced one.
Sugar-sweetened beverages:
Sugar-sweetened beverages (SSBs) are beverages
containing added caloric sweeteners, such as sucrose,
high-fructose corn syrup, or fruit-juice concentrates.
These include, but are not limited to, carbonates, fruit
drinks, sports drinks, energy and vitamin water drinks,
sweetened iced tea, and lemonade.
Value-added tax:
Tax on each stage of production that adds value to
aproduct or process.
Sources: World Health Organization ( www.who.int ); Online Business
Dictionary ( ww w.businessdictionary.com );
Using price policies to promote healthier diets. Copenhagen:
WHORegional Office for Europe; 2015.

8 9
Executive summary
The Global Action Plan for the Prevention and Control of
Noncommunicable Diseases 2013–2020 proposes that
“as appropriate to national context, countries consider
the use of economic tools that are justified by evidence,
and may include taxes and subsidies, to improve access
to healthy dietary choices and create incentives for
behaviours associated with improved health outcomes
and discourage the consumption of less healthy options”.
The Comprehensive Implementation Plan on Maternal,
Infant and Young Child Nutrition 2012 also considers
that “trade measures, taxes and subsidies are an important
means of guaranteeing access and enabling healthy
dietary choices”.
To address the increasing number of requests from
Member States for guidance on how to design scal
policies on diet, WHO convened a technical meeting
of global experts in scal policies on 5–6 May 2015 in
Geneva. The main objectives of the meeting were to
review evidence and existing guidance, discuss country
case studies and provide considerations with regards to
the scope, design and implementation of eective scal
policies on diet. The meeting consisted of presentations
and discussions during plenary and in working groups
on the evidence, country experiences and technical
aspects of policy design and implementation.
It was concluded that there is reasonable and increasing
evidence that appropriately designed taxes on sugar-
sweetened beverages would result in proportional
reductions in consumption, especially if aimed at raising
the retail price by 20% or more. There is similar strong
evidence that subsidies for fresh fruits and vegetables
that reduce prices by 10–30% are eective in increasing
fruit and vegetable consumption. Greater eects on
thenet energy intake and weight may be accomplished
by combining subsidies on fruit and vegetables and
taxation of target foods and beverages. Vulnerable
populations, including low-income consumers, are
most price-responsive and, in terms of health, benet
most from changes in the relative prices of foods
andbeverages.
Consistent with the evidence on tobacco taxes, specic
excise taxes – as opposed to sales or other taxes – based
on a percentage of retail price, are likely to be most
eective. In countries with strong tax administration,
taxes that are calculated based on nutrient content
can have greater impact. A proper situation analysis,
good political advocacy, appropriate objective setting
and evaluation, should be part of the multidisciplinary
development and implementation of such policies.
It is also important in this process to be proactive in
counteracting the industry arguments and eorts to
oppose the development and implementation of tax
measures or attenuate their eects.
There are evidence gaps that could be addressed, with
more countries developing and implementing such scal
policies. Lack of standards or criteria for determining
exactly what to tax is a challenge experienced by
countries and the development of a nutrient prole
model for designing and implementing scal policies
was recommended. In addition, there was a call for
a manual on developing and implementing scal
policiesfor diet.
Executive summary

10 11
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
The Global Action Plan for the Prevention and
Control of Noncommunicable Diseases 2013–2020
(GAP) (1)provides a roadmap and a menu of policy
options for Member States and other stakeholders
to take coordinated and coherent action to reduce
mortality from noncommunicable diseases (NCDs)
and exposure to risk factors. Under Objective 3 of GAP,
one of the policy options is to “consider economic tools
that are justied by evidence, and may include taxes and
subsidies, that create incentives for behaviours associated
with improved health outcomes, improve the aordability
and encourage consumption of healthier food products and
discourage the consumption of less healthy options”.
Furthermore, the Comprehensive Implementation Plan
on Maternal, Infant and Young Child Nutrition 2012 (2)
states under Action 3: “Trade measures, taxes and subsidies
are an important means of guaranteeing access and
enabling healthy dietary choices. They can be powerful tools
when associated with adequate information for consumers
through nutrition labelling and responsible food marketing,
and with social marketing and promotion of healthy diets
and healthy lifestyles”. In November 2014, during the
Second International Conference on Nutrition (ICN2),
Member States adopted the Rome Declaration (3) and
a Framework for Action (4) which called governments
and partners to “identify opportunities to achieve global
food and nutrition targets, through trade and investment
policies”.
As part of these global mandates to prevent NCDs,
improve nutrition, and address the increasing demand
from Member States for guidance on how to design
scal policies on diet, WHO organized an expert technical
meeting on 5–6 May 2015 in Geneva.
The specic objectives of the meeting were to:
• Review existing evidence of taxes on sugar-sweetened
beverages (SSBs) and other foods and beverages
high in sugar, salt and fat, including the health and
economic impact;
• Present and review evidence from countries with
experience in the taxing of SSBs and other foods and
beverages high in sugar, salt and fat;
• Review and discuss modalities on policy options of
taxes on SSBs and other foods and beverages high in
sugar, salt and fat, including scope, tax rate, tax base
and use of tax revenue.
The expected output of the technical meeting was to
provide considerations based on evidence with regards
to the scope, design and implementation of eective
scal policies on sugar-sweetened beverages and other
foods and beverages high in saturated fats, trans-fatty
acids, free sugars and/or salt. The meeting convened
global experts in public health or health economics
with experience in scal policies for health, particularly
in relation to diet and tobacco. These included country
experts, a politician, academic researchers, and
civil society organization representatives. The WHO
Secretariat consisted of sta from the departments of
Nutrition for Health and Development and of Prevention
of Noncommunicable Diseases.
Dr Oleg Chestnov, Assistant Director-General
Noncommunicable Diseases and Mental Health
welcomed the participants and opened the meeting
by describing it as another milestone in the work on
NCD prevention. Dr Sirpa Sarlio-Lähteenkorva, Senior
Adviser of the Ministry of Social Aairs and Health of
Finland, and Dr Franco Sassi, Senior Health Economist
of the Organisation for Economic Co-operation and
Development (OECD), were elected as co-chairs, and
Professor Jamie Chriqui of the University of Illinois at
Chicago as rapporteur. A full list of participants can be
found in Annex 1.
The meeting consisted of panel presentations and
discussions on the evidence of scal policies, country
experiences and technical aspects of policy design
and implementation. Two working groups discussed
opportunities and challenges for scal policies and
aspects of good scal policy design, particularly with
respect to target foods, type of tax, tax structure, price
elasticity, substitution eects and implications for
revenue generations. This was followed by a plenary
discussion to reach consensus on the conclusions
and recommendations. The meeting programme
canbefound in Annex 2.
1. Introduction

10 11
Noncommunicable diseases, including diabetes
and obesity, are a major challenge for health and
development, particularly in developing countries,
where 85% of premature deaths occur. The 2013 World
Health Assembly endorsed the Global Action Plan on
Noncommunicable Diseases 2013–2020 (1) which
includes a set of actions for Member States, international
partners and the WHO Secretariat to prevent NCDs,
promote healthy diets and physical activity, and to attain
the nine voluntary global NCD targets by 2025. The nine
targets include halting the rise in diabetes and obesity
in adults and adolescents as well as the increase of
childhood overweight and obesity by 2025.
In 2014, 39% of adults worldwide aged 18 years and
older (38% of men and 40% of women) were overweight
(dened as body mass index [BMI] ≥ 25). Between
1980 and 2014, the worldwide prevalence of obesity
nearly doubled, with 11% of men and 15% of women
– i.e.more than half a billion adults – being classied
as obese. In2013, an estimated 42 million children
aged under 5 years (6.3%) were overweight, an increase
from around 5% in 2000 to 6% in 2010 and 6.3% in
2013,with the highest rates of increase being observed
in Africa and Asia. Diabetes was directly responsible
for 1.5million deaths in 2012 and 89 million DALYs.
The global prevalence of diabetes (dened as a fasting
plasma glucose value ≥7.0 mmol/L [126 mg/dl] or being
on medication for raised blood glucose) was estimated
to be 9% in 2014 (5). Excess consumption of calorie-
dense foods containing high levels of saturated fats,
trans-fatty acids, free sugars and/or salt either alone, or in
combination with insucient physical activity, contribute
to obesity and diabetes, as well as other NCDs. National
dietary surveys indicate that foods and beverages high
in free sugars can be a major source of discretionary
calories in the diet, particularly in the case of children,
adolescents and young adults.
Fiscal policies to improve diet – particularly taxation and
subsidies – are key population-based policy interventions
to reduce the consumption of calorie-dense foods and
address obesity and diabetes. They form part of the
menu of policy options of GAP and are being considered
by an increasing number of countries to promote
healthy diets, especially after experiencing progress in
implementing tobacco taxation. There is increasingly
clear evidence that taxes and subsidies inuence
purchasing behaviour, notably when applied to sugar-
sweetened beverages and this contributes signicantly
towards addressing the obesity and diabetes epidemic,
especially when part of comprehensive multisectoral
population-basedinterventions.
2. Overview of noncommunicable
diseases and the role of scal
policies to promote healthy diets
2. Overview of noncommunicable diseases and the role of scal policies to promote healthy diets
12 13
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
There are strong economic and health rationales for
using scal tools: scal interventions play a key role in
correcting for market failure; they can create incentives
to reduce dietary risk factors for NCDs and generate
revenues for the government. Estimates from recent
economic research show that the prices of foods
and beverages eect purchase and consumption
signicantly. Fiscal policy intervention has been
proposed primarily as a mechanism to inuence
consumer behaviour at the point of purchase. By
incentivising consumers to purchase healthier foods (or
disincentivising the purchase of less healthy foods), scal
interventions aim to change consumption of these foods
at the individual and household level, and to thus reduce
diet-related risk factors for NCDs (Figure 1).
Fiscal policy interventions can also work through
changing incentives for the production and manufacture
of healthy, relative to less healthy, foods. As taxes
increase, the purchase price of certain foods increases
and consumers thus reduce their purchases. As a
consequence, industry may produce less of the
food in question. Similarly, a subsidy decreases the
cost for consumers and can lead to increased
consumption, thus triggering increases in
supply to meet the rising demand. Taxes and
subsidies can also incentivise the food industry
to reformulate foods to improve the nutritional
quality of their products.
An additional benet of scal policy interventions,
highlighted in the literature, is revenue generation
and the potential to designate (hypothecate)
these funds for health promoting purposes.
Rationale for scal policies on diet
Source: Fiscal policy options with potential for improving diets for the prevention of
noncommunicable diseases (NCDs) (draft). Geneva: World Health Organization; 2015.
3. Rationale and evidence
ofscalpolicies
As such, the use of scal policies should be considered a key
component of a comprehensive strategy for the promotion
of healthy diet and the prevention and control of NCDs.
The main scal policy interventions that have been proposed
for NCD prevention are: taxes on SSBs, unhealthy nutrients
(saturated/trans fats, salt and sugar) and/or unhealthy foods
(dened through nutrient proling); and subsidies on fruits,
vegetables and/or other healthy foods.
The fundamentals to the eect of scal policies on diet and
the basics of price elasticities include:
a) demand for SSBs is generally elastic, with price elasticities
around -0.9 to -1.3;
b) price elasticity is higher among low-income consumers,
in younger people and people with overweight, which
iscorrelated with income;
c) high consumers of SSBs are also likely to be more
price-responsive.
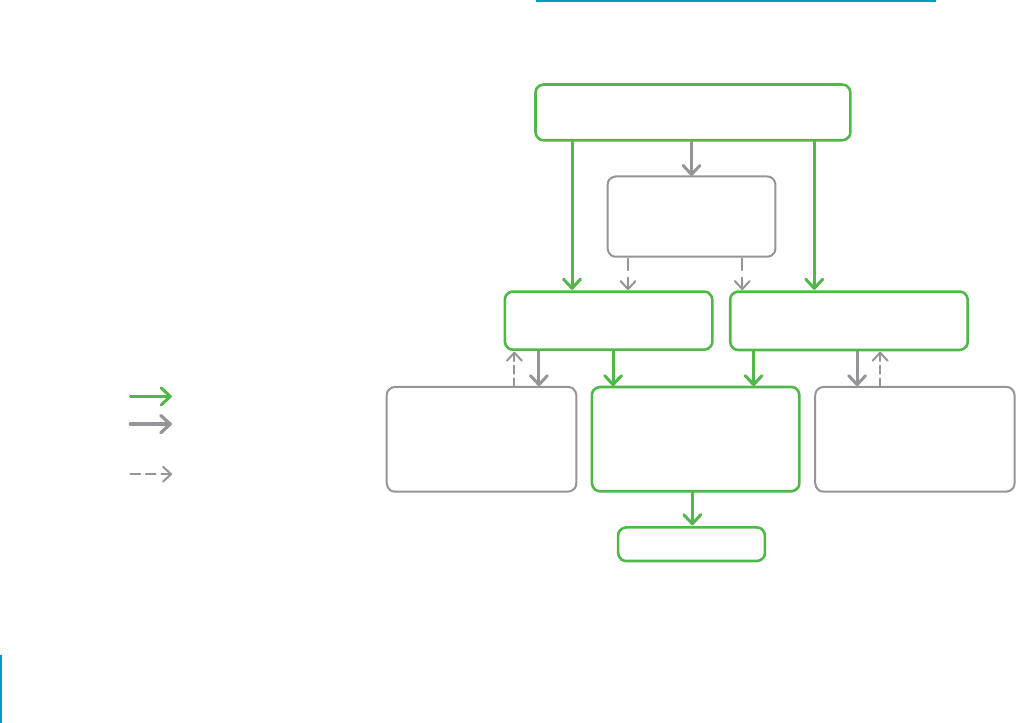
Figure 1: Pathways for the eect of scal policy
interventions
Eect on consumers
Secondary eect
(on industry and revenue)
Possible amplication eect
Tax and/or subsidy – incentives for substitution
with healthier foods and beverages
Increased purchase and
consumption ofhealthy foods
Financial implications
for manufacturers and
producers – incentive for
increased production
Decreased diet-related risk
factors for NCDs (e.g. body
weight; blood pressure;
bloodcholesterol)
Decreased NCD risk
Financial implications for
manufacturers and producers
– incentive for decreased
production andreformulation
Decreased purchase and
consumption of lesshealthyfoods
Revenue generation:
potentialhealth care/
healthpromotion funds
12 13
Growing evidence shows that appropriately designed
scal policies, when implemented with other policy
actions, have considerable potential for promoting
healthier diets. These will improve weight outcomes
and other diet-related risk factors, and will contribute,
ultimately, both to the prevention of NCDs and to the
reduction of the NCD health and economic burden.
A meta-review of 11 recent systematic reviews on the
eectiveness of scal policy interventions for improving
diets and preventing NCDs (6) showed that the evidence
was strongest and most consistent for the eectiveness
of SSB taxes in the range of 20–50% in reducing
consumption, and of fruit and vegetable subsidies in
the range of 10–30% in increasing consumption. While
evidence is mixed on the net eect of fruit and vegetable
subsidies on net caloric intake and weight, overall diet
quality improves thus leading to improvements in health
outcomes. There is also growing evidence for the likely
eectiveness of combinations of taxes and subsidies,
particularly as a mechanism to reduce potential
substitution with unhealthy foods. These combination
interventions can be designed using modelling that
is both eective and revenue neutral. All the reviews
concluded that taxes and subsidies were eective at
changing the consumption and purchasing of target
foods, with the strongest and most consistent eects
seen for SSB taxes and fruit and vegetable subsidies
(Figure 2). The greatest impact was on lower-income,
less-educated younger populations, and populations
atgreater risk of obesity.
Existing evidence on scal policies for diet
Current evidence is based mainly on intervention
studies and modelling. The most accurate and eective
objectives for price policies focus on their upstream
potential to inuence purchasing and consumption
behaviour, rather than on downstream eects, such as
body weight or disease which are also inuenced by
a large number of other factors. One of the evidence
gaps that needs to be lled is research quantifying the
impact of SSB tax on improving weight outcomes and
other diet-related risk factors. In many of the countries
implementing scal policies formal evaluations are
lacking, and when more countries introduce similar
measures, longitudinal research work could be one way
to address this evidence gap. Monitoring and evaluation
eorts are critical in documenting the eectiveness
of the taxes in achieving their objectives in terms of
revenue and its use, impact on purchase patterns,
consumption, and product composition for targeted
products and close substitutes. In addition, monitoring
and evaluation highlight the relevant health outcomes
of tax implementation, while identifying unanticipated
eects - such as a substitution to non-sugar sweeteners.
3. Rationale and evidence ofscalpolicies
Source: Fiscal policy options with potential for improving diets for the prevention of noncommunicable diseases (NCDs) (draft).
Geneva:WorldHealth Organization; 2015.
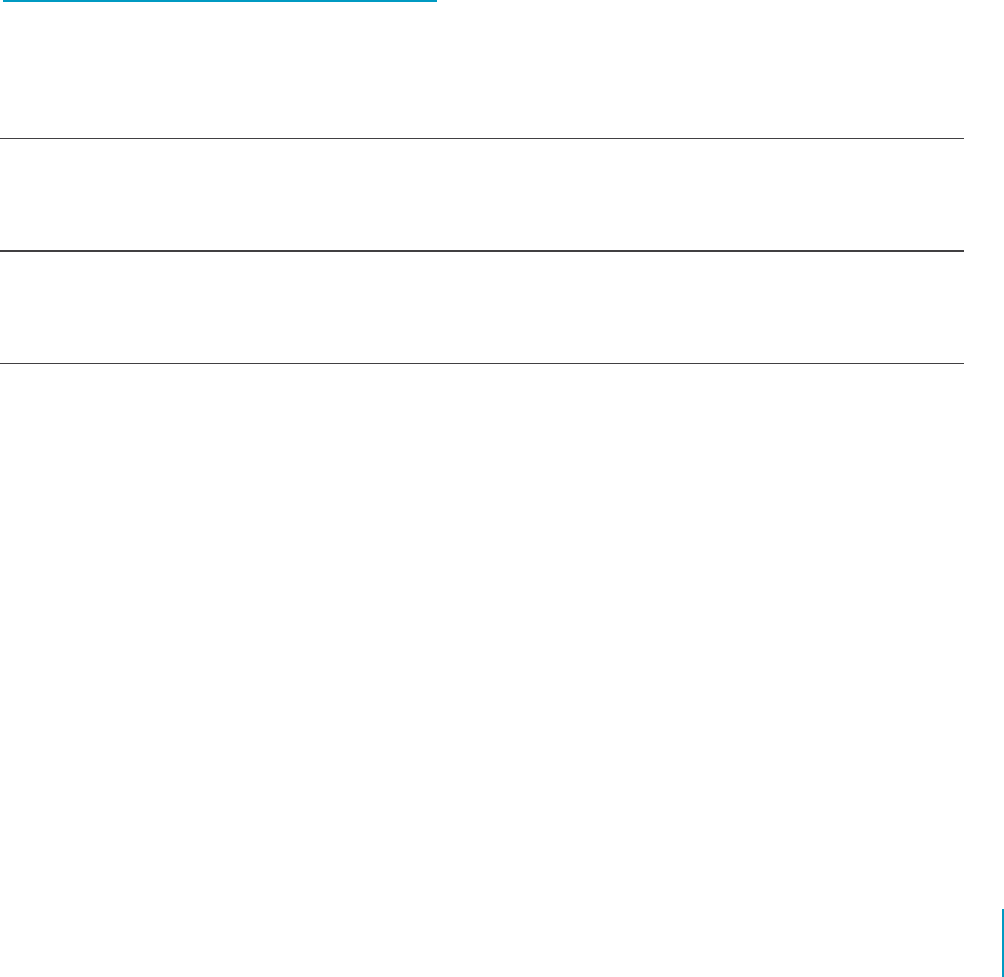
Figure 2: Summary of main ndings of meta-review
of systematic reviews on scal policies on diet
Food/ beverage taxes Nutrient-focused taxes Subsidies
Eect on
consumption
Strongest evidence for SSB taxes – reduce
consumption by same percentage as
taxrate.
Reduce consumption of target but may
increase consumption of non-target
nutritients; may apply to core foods;
better if paired with subsidy.
Subsidies increase healthy food intake.
Strongest evidence for fruit and vegetable
subsidies.
Eects on body
weight/disease
outcomes
Substitution will aect total calorie
intake. Most eective to target sugar-
sweetened beverages. Limited evidence
for disease outcomes.
Disease outcome aected by substitution
– nutrient prole taxes less likely to have
unintented eects than single nutrient-
based taxes.
Subsidies may also increase total calorie
intake and body weight. Very likely to
reduce dietary NCD risk factors.
Dierential
eects
May be most eective for low-income
populations; may have greater eect on
those who consumemost.
May be more likely to have regressive
eects as more likely to apply to
corefoods.
Mixed socioeconomic status eects
for population subsidies, may benet
wealthy. Targeted low-income
subsidieseective.

14 15
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
There were important insights from each of the country
presentations: Denmark, Ecuador, Egypt, Finland, France,
Hungary, Mauritius, Mexico, Philippines, Thailand and
the United States of America. Fiscal measures – in
particular food taxation – are being implemented with
promising results; however, the objectives of many
countries focus more on economical benets rather
than on public health. Some of the challenges faced in
implementation include a lack of appropriate capacity
for tax administration, tax set at low levels that prove
inecient in inuencing behavioural choices, and a lack
of monitoring and evaluation of the health impact. It
was established from all presentations that countries
attempting to progress scal policies face considerable
political and industry opposition.
Denmark
Denmark’s tax on saturated fat – implemented on 1
October 2011 and abolished on 1 January 2013 – proved
to be ecient in reducing the intake of saturated fat
as well as in improving other dietary measures and
reducing mortality from NCDs. The tax was paid on
the weight of saturated fat in foods and on saturated
fat used for the production of foods when the content
of saturated fat exceeded 2.3 g/100 g. The excise tax
amounted to DKr 16.00 (€2.15) per kilogram of saturated
fat, plus an additional 25% VAT.
Weaknesses in design, the lack of a coordinated voice
from public health organizations and a lack of public
documentation of the aggregated eects on health and
the overall eects on the economy, gave opponents
of the tax – for example the food industry and trade
organizations – free play to create negative publicity and
to initiate EU jurisdictional actions against it (7–14).
The lessons learned from Denmark are that:
• potential health eects should be estimated before
implementation of a tax, and real health and
consumption eects measured and documented after.
These would include the measuring of potential and
adverse substitution eects;
4. Country experiences
andlessons learned
• health professionals and organizations should be
consulted during the design of the tax to ensure
acoordinated voice;
• total welfare eects on the economy should be analysed
and discussed;
• anti-competitiveness of a tax should be analysed before
implementation to avoid lawsuits; and
• the design of a tax should be clear and logical and based
on clear public health rationale.
Ecuador
In light of the dramatic increases in overweight and
obesity rates across the Ecuadorian population (15), the
government has implemented interventions in the eld of
food regulation. Ecuador is the rst country in Latin America
to implement a trac light front-of-pack food labelling. This
regulation went into eect ocially on 29 August 2014 (16).
The Ecuadorian government made the political decision
to levy a tax on sugar-sweetened beverages and foods
high in fat, sugar and salt (“junk food”). However, the
technical aspect of this proposal faced challenges which
made the tax dicult to implement – the main challenge
being a lack of standard criteria for determining what food
products to tax based on nutrient content. Also, as this was
a public announcement, the national media distorted the
information, stating that certain traditional preparations
consumed in Ecuador would be considered as junk food
because of their high fat content. In order to clarify the
dierence, the energy density criteria (17) were used as
well as denitions developed by the University of Sao Paulo
research group. Nevertheless, application ofthese criteria
was not considered feasible (18).
Egypt
Egypt applies a sales tax on industrial goods with a general
rate of 10%, and specic rates for some goods (excise tax).
The government imposed reduced tax rates, or exemptions,
for specic goods, the purchase of which they considered
essential or desirable. This was put in place without
consideration of the resulting negative health eects
this may have on the consumer, such aswith sugar and
hydrogenated oils.

14 15
To date, the government of Egypt has not adopted taxes
on unhealthy food as a tool to reduce its consumption.
On the contrary, it has imposed low tax rates on some
unhealthy foods, such as sugar, which has tax rates
less than 60 Egyptian pounds per ton. With certain
products, the government has reduced tax rates due to
manufacturers pressure, as, for example, with carbonated
beverages where the excise tax rate was changed from a
two-tiered rate (50% and 60% of the producer price) into
a single sales tax of 25%.
Finland
Finland has a long history of using price policies to
inuence food consumption. Since 1948, free school
meals, paid by tax income, have been oered to all pupils
at elementary schools (19) and university students have
benetted from subsidized meals if nutritional quality
criteria are met (20). Moreover, since 2009, EU school
milk subsidies have not been given to products high in
fat or salt. Since 2011, excise duties have been levied
on sweets, chocolate and non alcoholic beverages (Act
1127/2010). The taxes are primarily levied to generate
revenue for government nance purposes, but potential
health and consumption impacts are acknowledged. The
tax rates were increased in 2012 and 2014.
The current excise tax is €0.95 per kilogram for sweets
and ice cream. For non-alcoholic beverages the tax is
€0.11 per litre; however, beverages containing more than
0.5% sugar pay €0.22 per litre. Products are identied by
CN/Custom tari headings and small-scale production
and exported products are exempted (21).
1
From 2010 to 2013, a Sugar Tax Working Group, set up
by the Ministry of Finance, assessed the suitability and
impact of three tax models: 1) a tax model based on
sugar content; 2) a tax model similar to existing excise
duty on sweets; and 3) a tax model combining the
two. The Working Group found that the combination
model would be optimal in terms of health promotion,
while the excise duty model would be the most
straightforward in terms of practical implementation.
Both the sugar tax and the combination model would
impose a signicant administrative burden on taxpayers
falling within the sphere of the tax (22).
The impact of the tax on purchase, consumption and
health has not been formally evaluated; however
according to unocial reports it has led to decreased
sales and consumption of non alcoholic beverages and
sweets. At the same time, there have been concerns
raised by the industry that a tax targeting such specic
products is unfairly discriminating against particular
manufacturers in the food industry, and therefore
distorting competition.
France
In 2011, France adopted a levy on beverages and liquid
preparations for human consumption that contained
added sugar or other sweeteners. The amount of the
contribution was set at €7.16 per hectolitre, and was
increased to €7.5 per hectolitre in 2015. Since 2013,
thetotal of the contribution is allocated to the National
Social Health Insurance.
According to the Nutrinet
2
study for the General
Directorate of Health of 2013, consumption of sodas
hasdecreased, particularly in young people, low-income
groups and households with adolescents. There is a
need for more detailed impact assessments and eects
on children, dierent socioeconomic groups and on
substitution.
In 2014, the revenue raised by tax was approximately
€300 million. The tax has appeared to have a positive
eect on purchase patterns from a public health
perspective and is generally well accepted by
thepopulation.
Hungary
A public health product tax (PHPT) was introduced in
2011 taxing non-staple food products that carry proven
health risks when consumed. The objectives of the PHPT
were: to encourage healthier eating habits by increasing
the availability of healthy choices; to encourage
reformulation; and to increase revenues for public health.
The PHPT is a specic excise tax on a per unit measure,
based on sugar, salt and methylxantine content in pre-
packaged food products. The tax-related administrative
burden for enterprises is minimal.
The rst impact assessment, conducted one year later,
found that 26–32% of consumers had decreased their
intake of products subject to PHPT. Price increase was
the major driving force, although a high percentage of
consumers (22–38%, depending on food categories)
had reduced their intake due to an increased health
consciousness. Consumers with bad self perceived
health status were, on average, twice as likely to decrease
consumption of foods subject to PHPT compared with
those of good health. Moreover, of the responding
food producers, 40% had carried out reformulation of
their products, 30% had totally removed unfavourable
4. Country experiences andlessons learned
1
On 29 September 2015, a Finnish Financial Parliamentary Committee decided to end the tax on sweets that has been in force since 2011.
www.loc.gov/law/foreign-news/article/finland-tax-on-chocolate-and-sweets-to-be-eliminated-2017
2
https://www.etude-nutrinet-sante.fr/fr/common/login.aspx

16 17
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
components in their products, and 70% had decreased
the quantity of unfavourable components in their
products (23).
In conclusion, PHPT has achieved its public health aims.
The population has reduced its consumption of products
subject to PHPT; food manufacturers have started
reformulation, and the estimated tax revenue has been
almost fully realized.
The second impact assessment of 2014 sought to
determine whether changes in consumption would be
maintained in the long term and how they would be
inuenced by nutritional and socioeconomic status. The
assessment also aimed to obtain information on product
substitution. Initial results showed that consumers of
unhealthy food products responded to the tax by: a)
choosing a cheaper, often healthier product (7–16%
of those surveyed); b) consumed less of the unhealthy
product (5–16%); or c) changed to another brand of the
product (5–11%) or substituted some other food (often
a healthier alternative). Most people (59–73%) who
reduced their consumption after introduction of the tax,
consumed less in 2014 than in previous years, suggesting
that the reduction in unhealthy food consumption has
been sustained.
Mauritius
Mauritius is a sugar producing country. The share
of sugar production in the Mauritian economy
has consequently declined over the years and in
relative terms dwindled to about 3.5% of the gross
domestic product in 2003 (from 25% in the 1970s).
Sugar production nevertheless remains an important
contributor to the country’s economy, with sugar exports
representing approximately 19% of foreign exchange
earnings.
Irrespective of the signicance of sugar to the economy,
in February 2013, the government took the decision
to introduce an excise duty on the sugar content of
“soft drinks”. “Soft drinks” subject to tax in Mauritius
include: any aerated beverage (such as colas); any syrup
for dilution; and any fruit squash, cordial or fruit drink
(including blends and juice with added sugar). The excise
duty excludes bottled water; pure fruit juice, and blends
thereof; pure vegetable juice, and blends thereof; and
dairy milk, and products thereof.
The rate of the excise duty was set at 2 Mauritian cents
per gram of sugar. This was increased to 3 cents per gram
from 1 January 2014.
For imported products, the tax is collected by the
Mauritius Revenue Authority (MRA) (Mauritian customs)
at the time the product is being cleared from customs.
For locally produced products, the tax is collected by
the MRA at the time the product leaves the factory. The
importer, or the local manufacturer, has to produce a
certicate from an accredited laboratory, or the Mauritius
Standard Bureau, indicating the sugar content for
customs clearance. In addition, the MRA also carries out
post-control audit checks on a risk management basis.
The excise duty collected is 330 million Mauritian rupees
(US$9.2 million). Its impact on the sale of soft drinks has
not been assessed.
Mexico
The prevalence of overweight and obesity reached 71%
among adults and 30% in children and adolescents in
Mexico (24, 25). The proportion of adults with diabetes
was estimated at 14% in 2006 (26). In 2012, Mexico had
the highest worldwide consumption of sugar-sweetened
beverages: 160 litres per capita (27). In addition, recent
evidence shows that 71% of the consumption of added
sugars comes from SSBs and 23% from non-basic energy
dense foods (28).
In this context, on January 2014 Mexico implemented
two taxes: 1) a 1 peso per litre excise tax on any
non-alcoholic beverage with added sugar (powder,
concentrates or ready-to-drink), which is paid by the
producer and represents about a 10% increase in price;
and, 2) an 8% ad valorem tax on the purchase price
for a list of non-essential energy-dense foods (snacks,
confectionery products, chocolate and other products
derived from cacao, puddings, ans, ice cream, candies,
peanut butter), that contain 275 calories per 100 grams
or more. This tax is paid by the producer or the retailer.
The SSB tax was proposed by the government to the
congress as a means of reducing the negative eects
of SSB consumption on overweight and obesity, and
the direct and indirect associated costs. Factors that
enabled the approval and implementation of the tax
were: evidence provided by experts on nutrition; high
obesity and diabetes rates; high consumption of SSBs
and non essential high energy dense foods; economics
(price elasticities overall and by income level, potential
substitutes, revenue estimation); the active presence
of the civil society (advocacy, campaigns, mapping
key supporters of the initiative); and interest from
thegovernment.
After implementation of the tax, studies have been
conducted to evaluate the eects on consumer prices
and purchases. Preliminary results show a complete pass
through to consumer prices for SSBs in urban areas, but
incomplete for rural areas and heterogeneous for the

16 17
non essential high-energy dense foods (29). Preliminary
results also show that household purchases have
decreased during 2014 (30).
A study by the Mexican Public Health Institute and
University of North Carolina on the impact of rst year
of introduction of the excise tax on sugar-sweetened
beverages in Mexico concluded that “relative to the
counterfactual in 2014, purchases of taxed beverages
decreased by an average of 6%, and decreased at an
increasing rate up to a 12% decline by December 2014.
All three socioeconomic groups reduced purchases of
taxed beverages, but reductions were higher among the
households of low socioeconomic status, averaging a 9%
decline during 2014, and up to a 17% decrease by December
2014 compared with pre-tax trends” (31, 32).
Philippines
In 2009, the Philippines ranked 11th worldwide in the
consumption of soft drinks (about 1.6 billion litres) which
prompted a lawmaker and health initiatives advocate
in congress to initiate and le a bill imposing an excise
tax on sugar-sweetened beverages to help curb its
consumption and lower the risk of obesity, diabetes
and related illnesses. At the same time, the bill was to
generate tax revenues that would be allocated towards
government health initiatives. These included: providing
medicines and medical assistance for the indigenous
diabetic patients; the promotion of community-
based obesity prevention programmes; diabetes
prevention campaigns and other diet-related health
awareness programmes; funding for research and other
development programmes related to food and nutrition;
providing access to potable water; and establishing
sports facilities in communities and public schools to
promote health and wellness.
The aim of curbing SSBs consumption is supported by
a study (33) that shows that imposing a tax that would
increase the price of SSBs by 20% would reduce overall
consumption by 24%. The ling of the bill in October
2013 sparked negative reactions, not only from the
beverage and sugar industries, but also from some
government agencies and political gures directly
impacted.
Although there is inuence from stakeholders in
deterring the bill within congress, there remains great
optimism that, with the strong support received from
various Philippine and international health organizations
and agencies – including the World Health Organization
– it will be progressed with a positive outcome.
Thailand
Economic growth in Thailand has led to higher incomes
andan increase in consumption of SSBs as Thailand
becomes an emerging market for many ready-to-drink
beverages. Existing taxation is ad valorem and does not
consider the health promotion value. The current tax of
beverages without sugar is US$0.025/440 ml, while the
taxon beverages with sugar is US$0.012/440 ml.
The food system in Thailand includes many dierent food
items, manufacturers and sellers. Tax increases do not always
translate into higher prices. Compared with high-income
countries, Thailand has a smaller proportion of commercial
processed foods and beverages, cheaper retail prices of SSBs
and relatively high prices of fast food. Healthy alternatives
are not always available.
Fiscal policy development and implementation is
dicult due to the many competing policy priorities and
an increasing inuence of international trade treaties
on policies. Human resources for stewardship and
implementation are limited and are coupled with a lack of
verication mechanisms, particularly on food composition
and retail prices. There is also insucient monitoring and
enforcement capacity and limited preparedness of local
governments to administer tax policies.
United States of America: California and Vermont
In the USA, the state of California has been a leader in
establishing public policies to regulate the sale of soda and
other sugar-sweetened beverages. State legislation to ban
the sale of SSBs on school campuses was rst introduced in
1999, and was fully enacted by 2005. Since 2002, California
has considered establishing a tax on SSBs ve times. In 2012,
two cities in California – Richmond and El Monte – voted to
tax SSBs; however, the two-thirds threshold for success was
not achieved. In 2014, two further Californian cities – Berkeley
and San Francisco – similarly voted for an SSB tax. Berkeley
achieved a 75% vote for implementation, well above the 50%
threshold for success and thus became the rst USA city to
pass a tax measure, imposing a 1 cent per ounce tax on SSBs.
In 2014, California was the rst state in the USA to consider
legislation to require warning labels on SSBs.
There was much opposition to these two legislations and two
fundamental lessons emerged from the political campaigns.
The rst was that, using the same well-nanced scare
tactics made famous by the tobacco industry, the beverage
industry, similarly, will do everything it can to prevent tax
implementation; the second is that, as California has shown,
industry can be defeated.
Much of legislative action on SSBs in the USA is at the state
or local (city, county) level. The state of Vermont is another
4. Country experiences andlessons learned

18 19
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
example of a recent attempt to introduce a state excise tax
on SSBs, proposing a tax doubling the existing penny-per-
ounce (US$1 per almost 3 litres). Given very low SSB prices
in the USA, this translated into a tax burden of, onaverage,
approximately 50%. One of the challenges for economists
is to predict the response of consumers (i.e. price elasticity)
when taxes are very high, and have not been evaluated
based on prior data. Another is to anticipate the tax pass-
through rate (i.e. how much the tax gets passed into the
price). Economic theory predicts a perfect pass-through
(i.e. a 1 cent excise tax increases retail price by 1 cent).
The rst year, data from Berkeley suggested that the tax
pass-through might be initially less than 1 cent, indicating
that prices increase less than the amount of an excise tax
imposed (34).
Cross-price elasticity data are very limited and unstable, with
much variation across studies. Most studies predict a shift
primarily to bottled water and juice, while diet beverages
have a positive cross-price elasticity with SSBs (35). This is
likely the result of the underlying data where promotions
are usually the same for both diet and regular beverages
(e.g. all products of a brand on sale). Shifts to food and the
overall eect on diet should be also considered.
In the USA, the ongoing market trend is for a signicant
reduction in SSB consumption (36), much higher
purchases of bottled water, shifts away from soda towards
water and new healthier (less caloric) beverages (37). Per
capita consumption of SSBs is still very high, which justies
policy action such as taxes. It is likely to have an eect
on SSB consumption per se, since the campaign to pass
a tax (even if unsuccessful) helps to educate consumers,
encourages the industry to reformulate products, and
reduces SSB consumption.
United States of America: Supplemental
Nutrition Assistance Programme
The Supplemental Nutrition Assistance Program (SNAP)
provides food-purchasing assistance for low- and no-
income people living in the USA. The eect of providing
nancial incentives to participants of the SNAP at the
point-of-sale was recently evaluated in a randomized
control trial. Known as the Healthy Incentive Pilot (HIP),
the study showed that a 30% subsidy of targeted fruit
and vegetable purchases increased their consumption,
by SNAP participants, by 26% (38). This would be
predicted by price elasticity data from prior research
(39). There was no eect on total energy intake and no
change in SSB and “junk food” intake. No cost-benet
analysis was done in this evaluation, but it is unlikely that
the intervention would be shown to save money.
There are also incentive programmes, known as “double-
buck programmes”, that provide a match to SNAP benets
for fruit and vegetable purchases at farmers’ markets (40).
These, mostly privately-run, programmes give low-income
consumers “double bucks” (or “health bucks”) coupons that
double the value of food stamps at farmers’ markets and
occasionally grocery stores for buying fruits and vegetables.
The Food Insecurity and Nutrition Incentive (FINI) grant
programme, authorized in the Agricultural Act of 2014, will
provide US$100 million over 5 years to support projects
that increase purchases of fruits and vegetables among
SNAP participants by providing incentives at the point of
purchase (41).
Using price policies to promote healthier diets
inEurope
In 2015, the WHO European Region published a document
on the use of price policies to promote healthy diets (42).
Thedocument provides information on the use of price policies
to promote healthy diets and explores policy developments
from around the WHO European Region. Itexamines the
economic theory underpinning the use of subsidies and
taxation and explores the currently available evidence.
The publication includes several case studies from WHO
European Member States where price policies have been
introduced, including Denmark, Finland, France, Hungary and
the EU School Fruit Scheme.
Specic factors to consider in the design of eective
price policies include possible substitution eects, the tax
mechanism chosen, price pass-through, and impact on
health inequalities. Price policies can also be implemented to
inuence supply-side factors. Comprehensive monitoring and
evaluation, using carefully selected indicators, is essential in
using price policies.
The document concludes that scal policies are an important
tool in tackling unhealthy diets and NCDs and that there is
signicant scope in the future for countries across Europe
to advance their implementation. From the evidence, taxes
on sugar-sweetened beverages and targeted subsidies on
fruit and vegetables emerge as the policy options with the
greatest potential to induce positive changes in consumption;
however there is also demonstrable positive impact with
other approaches. Experience with the implementation of
such policies in the Region has shown that they are feasible
and can inuence consumption and purchasing patterns
as intended, and have a signicant impact on dietary and
health-related behaviour. The revenue raised has, in some
cases, beensuccessfully ring fenced for the health budget.
Continued monitoring and evaluation is considered
important, particularly in terms of establishing baseline data
atthe outsetin order to monitor the eects ofthe policy.
18 19
When designing scal policies on diet, key questions
toconsider are (42–44):
1. What type of tax to apply?
2. What tax structure to implement?
3. What products to tax?
4. What are the implications for revenue generation
anddiet/nutrition-related programming?
Excise tax is tax levied on manufacture, sale, use, or
distribution. It may also include a xed fee or levy on a
purveyor. A special value added tax (VAT) applies to the
production and distribution of goods. It is considered a
consumption tax because the ultimate cost is borne by
the consumer at point of purchase.
A tax can be specic or ad valorem. A specic tax is levied
on the basis of product size or amount. An ad valorem
tax is a percentage of the product value (Figure3).
Consistent with the evidence on tobacco taxes, specic
excise taxes (where a set amount of tax is charged on a
given quantity of the product or specic ingredient) are
likely to be most eective. This is because they reduce
incentives to switch down to cheaper options, in that
they increase the price of all products aected by the tax
in the same way. They also provide more stable revenues,
are not subject to industry price manipulation and are
easier to administer. Inorder to prevent the impact of
specic taxes from being eroded over time, it is essential
that they be adjusted regularly to, at least, keep up with
ination and reduce aordability of the taxed product by
accounting for income growth as well.
In countries with strong tax administration, taxes that
are calculated based on nutrient content (e.g. SSB taxes
based on sugar content) can have the greatest impact,
as they dierentiate between options based on nutrient
content within a product category and can be used to
incentivise consumers to substitute to alternatives while
simultaneously encouraging producers to reformulate
their products. In countries where tax administration is
not as strong, simpler tax systems (e.g. a volume-based
SSB tax) may be more appropriate.
WHO’s tobacco taxation experience
Since 2009, WHO has been working closely with
Member States to improve and increase their excise
taxes on tobacco products and to reduce their
aordability. There are dierent types of indirect taxes
applicable on tobacco products. It is important to
focus on excise taxes (specic, ad valorem and mixed)
as a public health policy rather than other taxes in
order to increase the relative price of the targeted
product eectively and to reduce consumption.
One of the main conclusions derived, and lessons
learned, from tobacco taxation is the importance of
implementing specic excise taxes, or a mixed system,
relying more on the specic excise component.
These taxes lead to higher prices, reduce gaps within
products – therefore reducing risk of substitution –
and are easier to administer. However, specic excise
taxes need to be adjusted to ination – and ideally
to income as well – in order to eectively reduce
aordability and discourage consumption over time.
Additionally, tax policies have to be accompanied by
a system that closely monitors products throughout
the supply chain (track and trace). This will reduce the
chance of products ending in the illicit market.
5. Implications for design and
implementation of scal policies
A typology for consideration
5. Implications for design and implementation of scal policies
Figure 3: Types of taxes
Excise Tax VAT
Specic
+
Ad valorem
+ +
20 21
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
The responsiveness of consumers to price changes (price elasticity) for the food
and beverage products that may be taxed is central in the design of taxes for
health promotion. When consumers can substitute alternative products, their
response to price increases will be greater; but not all substitutions are likely to
be desirable. Carefully designing the tax base (range of products to be taxed)
will help to prevent undesirable substitutions, and possibly steer substitutions
towardshealthyalternatives (Figure 4).
Fiscal policies and price elasticity
In most cases, however, the demand for foods and
beverages is typically inelastic (i.e. consumers are not
very responsive to price changes). This should not be
viewed, per se, as hindering the pursuit of public health
goals. It simply means that the tax rate will have to be
high enough to reduce the consumption of the taxed
products to an extent that will generate meaningful
health eects. A low price elasticity also makes the tax
more likely to be passed on to consumers by suppliers
(i.e. prices will increase at the point of consumption).
Moreover, tax revenues will be larger than in the case
of products with a more elastic demand, providing
greater opportunities for funding other health
promotion activities.
There are areas in which taxation practice is not
entirely in line with theory and some of these
deviations might be desirable from a public health
point of view. For instance, there is a broad consensus
on excise taxes (particularly, specic excises regularly
adjusted for ination) being the scal tool of choice in
the pursuit of public health goals, at least in the area
of food and non-alcoholic beverages.
However, the public health community has also
called for the use of positive scal incentives, for
instance to stimulate the consumption of healthy
foods. This goal could be pursued via the indirect tax
system through rate dierentiation in value added
orsales taxes.
All/most beverages
All sweetened beverages
Only SSBs
Selected SSBs
Figure 4: Dierent tax base options for beverages

20 21
Health and substitution
effectsof scal policies
The overall health eects of food and beverage taxes
depend on the price elasticities of demand, which
are composed of the income and substitution eects.
The size of the substitution eect depends on the
extent to which there are available substitutes, for
example from SSBs to water, milk, unsweetened 100%
fruit juice and beverages with non caloric sweeteners.
Close substitutes give rise to a large substitution
eect. The income eect depends on the extent
to which consumers are able, or willing, to change
behaviour. Lack of behavioural change might imply
that consumers feel burdened by the tax and have less
money to buy either unhealthy or healthy foods.
It is important to consider the tax base since the overall
health eects of the tax depends on the availability
of substitutes for dierent types of consumers.
Consumers might substitute to a healthier type of
product, to another type of unhealthy product, to a
cheaper brand or store. Correct design of the tax and
correct choice of the tax base could minimize any
potential adverse unexpected health eects of food
and beverage taxes (45–48).
Vulnerable populations, including low-income
consumers, young people, and those most at risk
of obesity, are most responsive to changes in the
relative prices of foods and beverages. Well-designed
taxes targeting non-core foods with close, healthier
(untaxed) substitutes may result in greater behaviour
change and would minimize tax regressivity.
There is potential for taxes to be further supported
by complementary subsidies targeted to low-
incomepopulations.
Overcoming barriers
toscalpolicies
Countries experience great challenges in policy
implementation from the undue pressure of the food
and beverage industries. Oppositional arguments
against taxes are usually either false or greatly overstated.
Common myths relate to the impact on jobs, businesses,
those on a low income, and tax avoidance. As has been
conrmed by recent studies in California and Illinois in
the USA, SSB taxes are likely to lead to a net increase
in jobs, in spite of a small decrease in jobs in the
beverage sector (49). This occurs because consumers
redirect their purchases towards untaxed products thus
stimulating growth in other non-beverage sectors. A
study conducted in the USA between 1997 and 2009
found that, contrary to predictions from the tobacco
industry, there was an increase, rather than a decrease,
in the number of convenience stores. This was due to
consumers shifting to buying other products and thus
creating more demand for those products.
Low-income populations have the largest health benet
from taxes, because their pre-tax SSB consumption
is high and post-tax reductions in consumption are
relatively large. The benets for these populations are
even higher if tax revenues are used for targeted obesity
prevention and health promotion programmes and if
targeted subsidies for healthier options exist. There is
likely to be little tax avoidance and evasion in response
to an SSB tax. The strength of governance and presence
of informal distribution networks have a greater eect
than tax and price levels in driving tax avoidance and
evasion.
The role of civil society and health professionals is critical,
not only to counteract undue pressure from food and
beverage companies, but also to monitor scal policies
and ensure their appropriate implementation.
Regarding opposition to taxes, fundamental lessons
are to be learned from the experience of countries
implementing SSB taxes. Firstly, the beverage industry
will do everything it can to avoid taxes, using the same
well-nanced – and well recognized – scare tactics
used by the tobacco industry. In 2014, for example,
the beverage industry spent more than US$10 million
ghting SSB tax measures in Berkeley and San Francisco,
outspending proponents by 18:1, with 99% of funds
provided by corporate interests outside of California.
Tactics ranged from buying television and radio
advertisements, paying for advertising billboards, lawn
signs and advertising space in subway stations (including
5. Implications for design and implementation of scal policies
22 23
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
the oor space) as well as paying members of the
community to go from house to house canvassing
support. Claims were made that the tax was unfair to
poorer people; that it would harm small businesses;
and that revenues would not be spent as promised.
It was also stated that the government should not
interfere with the personal choices of consumers.
A further lesson learned is that, regardless of pressure
and nance from industry, any opposition to taxation
can be overcome with a well-planned campaign
involving a broad coalition of supporters (from
community leaders and health-oriented organizations
to grassroots people and organizations), the ability to
respond to the beverage industry’s propaganda, and
sucient resources. The objective would be to inform
populations of the truth of potential harm caused by
the products. The experiences from countries such as
the USA (in particular the city of Berkeley in California)
and Mexico prove how policies can be progressed
even amidst greatindustryopposition.
As countries around the world enact these policies,
an ever-greater movement to support other countries
to do the same will be created. As with the tobacco
industry, the beverage industry is concerned that
rates of SSB consumption are dropping. However, as
an increasing number of taxes, warning labels, and
other policies are enacted around the world, this
drop may continue and, as a result, diets will become
morehealthy.
Nutrient proling
Health-related taxes applied to foods and beverages
must dene the foods to which the tax applies, and
this often requires some form of nutritional criteria
underpinning the tax. Lack of such criteria or standards
for determining exactly what to tax is a challenge
experienced by many countries. The development of a
nutrient prole model is, therefore, considered important
in identifying the categories of foods subject to the tax
and the nutrient thresholds that apply, thus providing a
tool for countries to implement scal policies.
Nutrient proling is the science of classifying or ranking
foods according to their nutritional composition for
reasons related to preventing disease and promoting
health. Nutrient proling can be used for various
applications, including the marketing of foods to
children; health and nutrition claims; product labelling
logos or symbols; information and education; provision
of food to public institutions; and the use of economic
tools to orient food consumption.
The initial request for WHO to initiate nutrient proling
came in 2007 when the rst technical meeting was
held to review the existing evidence on the eects
of marketing of food and non-alcoholic beverages
to children. The ad hoc development of models by
dierent stakeholders was leading to inconsistencies
andconfusion for target audiences and consumers.
In 2010, WHO prepared guiding principles and a
framework manual for the development and adoption
of nutrient prole models. The main lesson learned from
pre-testing the manual was that it is easier to adapt an
existing model than to develop an entirely new model.
WHO will review and update the manual after country
eld-testing.
Regional nutrient proling models for regulating the
marketing of foods and non-alcoholic beverages to
children have already been developed in the WHO
European and American Regions, and are in the process
of being developed in the Eastern Mediterranean
Region, and the South-East Asia and Western Pacic
Regions. WHO aims to prepare a global nutrient prole
model for: the marketing of food to children; school
food procurement; scal policies; and product labelling
(i.e.front-of-pack labelling).

22 23
Policy development
The importance of a good policy development process
needs to be reinforced when developing scal policies
(Figure 5). An assessment, using all existing relevant
information, should inform appropriate objective-setting
and advocacy and use key policy champions and the
broad coalition of partners for both political buy-in and
for countering industry challenges. Nutrient proling – or
similar tools – need to be developed to dene products
to be taxed as a key part of the multidisciplinary drafting
of the policy. In implementation, tax structure and
administrative issues should be considered as well as
the monitoring of purchases and consumption, while
planning for evaluation and consideration for earmarking
of tax for health is further discussed. Evaluation of the
impact of the policy on purchasing, consumption,
revenues, and, ultimately, health outcomes (e.g. obesity)
is needed, so some consideration for longitudinal
design should be given. Policy coherence is needed to
ensure maximum impact of scal policies on diet. The
requirement of warning labels on taxed products – as
an education strategy and to limit the marketing of
taxed products particularly for children – were discussed
asexamples.
Earmarking of tax revenues
The earmarking of tax revenues is used in many
countries, including in connection with taxes for health
promotion. Earmarking may be aimed at strengthening
health promotion actions, for example by funding
education campaigns or healthy food subsidies, or at
limiting the regressive impact of taxation (when the
impact is indeed regressive). In all cases, earmarking will
improve the transparency of the taxation process and
use of revenues, which will increase the acceptability of
the tax by politicians and the general public. Whenthe
objective of the tax policy is health, rather than solely
economics, it may be easier to discuss earmarking
forhealth in that context.
5. Implications for design and implementation of scal policies
Evidence-gathering
(nance, health,
industry)
Tax environment –
learn from Tobacco
Policy Rationale
Policy Objective
(health and
economic)
Policy coherence
(marketing
restriction etc.)
Public awareness,
education and
support
Tools to dene
products to include
Options of tax
measure
Industry challenges
Key policy
champions
Tax infrastructure
Administrative issues
Enforcement
Purchasing/
consumption
Consider earmarking
of tax for health
Planning evaluation
Systems to support -
monitoring revenue
andconsumption
- longitudinal evaluation of
the impact on purchasing,
consumption, revenues,
health outcomes
(e.g.obesity)
1. Assessment
Figure 5: Fiscal policy development and implementation framework
2. Design
3. Implementation
4. Evaluation

24 25
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
At the end of the meeting the following conclusions were made:
• Growing evidence shows that appropriately designed
scal policies, when implemented with other policy
actions, have considerable potential for promoting
healthier diets. They will also improve weight
outcomes and other diet-related risk factors, and will
ultimately contribute to the prevention and reduction
of the health and economic burden of NCDs. The
use of scal policies should therefore be considered
a key component of a comprehensive strategy for
prevention and control of NCDs.
• The evidence for meaningful health eects is
strongest for taxes on sugar-sweetened beverages,
with suggestions that SSB prices would need to be
raised by 20%, or more. Such taxes lead to more than
proportional reductions in SSB consumption and net
reductions in caloric intake, and thus contribute to
improving nutrition and reducing overweight, obesity
and NCDs.
• Similarly strong evidence shows that subsidies for
fresh fruits and vegetables, that reduce prices by
10–30%, are eective in increasing fruit and vegetable
consumption. While evidence is mixed on the net
eect of fruit and vegetable subsidies on net caloric
intake and weight, overall diet quality improves, with
a resulting improvement in health outcomes. Greater
eects on the net energy intake and weight may be
accomplished by combining subsidies on fruit and
vegetables and taxation of target foods.
• Taxation of other target foods and beverages,
particularly those high in saturated fats, trans fatty
acids, free sugars and/or salt appears promising,
withexisting evidence clearly showing that
increases in the prices of target options reduces
their consumption. Evidence will emerge from
countries that have recently implemented such taxes
showing the impact on health and other outcomes –
forexample NCDmortality.
• Vulnerable populations, including low-income
consumers, young people, and those at most risk of
obesity, are most responsive to changes in the relative
prices of foods and beverages. It is benecial to target
non-core foods and foods for which good healthier
alternatives are available.
• Consistent with the evidence on tobacco taxes,
specic excise taxes (where a set amount of tax is
charged on a given quantity of the product or specic
ingredient), as opposed to sales or other taxes based
on a percentage of retail price, are likely to be most
eective. This is because they reduce incentives to
switch down to cheaper options, in that they increase
the price of all products aected by the tax in the
same way. In order to prevent the impact of specic
taxes from being eroded over time, it is essential that
they be regularly adjusted to keep in line with ination
and to reduce aordability of the taxed product by
accounting for income growth as well.
• In countries with strong tax administration, taxes that
are calculated based on nutrient content (e.g. SSB
taxes based on sugar content) can have the greatest
impact, as they dierentiate between options based
on nutrient content within a product category and
can be used to incentivise consumers to substitute
to alternatives while simultaneously encouraging
producers to reformulate their products. In countries
where tax administration is not as strong, simpler tax
systems (e.g. a volume-based SSB tax) may be more
appropriate.
• Earmarking of tax revenues may be challenging in
some countries, but dedicating some, or all, of the
revenues generated by these taxes for eorts to
improve the health care system, encourage healthier
diets through health promotion and nutrition
education campaigns, increase physical activity, as
well as to build capacity for eective tax administrative
processes (i.e. for monitoring and enforcement)
may increase public support and facilitate the
implementation of earmarking of the revenues.
6. Conclusions

24 25
• Many countries implementing scal policies lack
formal evaluations leading to a shortage of data
on the impact. Monitoring and evaluation eorts
are critical in documenting the eectiveness of the
taxes in achieving their objectives, both in terms of
revenue and its use; impact on purchase patterns;
consumption; and product composition for targeted
products and close substitutes, in addition to relevant
health outcomes, while identifying any unanticipated
eects (e.g. substitution to non-sugar sweeteners).
• Lack of standards or criteria for determining exactly
what to tax is a challenge experienced by the
countries. Development of a nutrient prole model is,
therefore, considered an important action in providing
a tool for countries to implement scal policies. For
countries for which there is a broad knowledge base
on nutrient contents of products this might be used
to include/exclude products from taxation.
• Countries experience great challenges of
implementation from undue pressure from the food
and beverage industries. The role of civil society
and health professionals, not only to counteract
this pressure, but also to monitor and ensure the
appropriate implementation of scal policies is critical.
• Policy coherence is needed to ensure maximum
impact. Requiring warning labels on taxed products
as an education strategy and limiting the marketing
of taxed products, particularly for children, were
discussed as examples.
• The importance of a good policy development
process needs to be reinforced when developing
scalpolicies.
• A proper situation analysis using all existing
relevant information should inform appropriate
objective-setting and the multidisciplinary
drafting of a policy and implementation plan that
includes advocacy for political buy-in, monitoring
and evaluation.
• It is also important in this process to be proactive
in counteracting the industry arguments
and eorts to oppose the development and
implementation of tax measures or attenuate
their eects. A public awareness or education
programme to inform the public about the
positive health consequences, address any
potential negative eects of the tax and keep a
positive public opinion is useful, as it has been
shown to have some eects even if, ultimately,
thetax policy is not passed.
6. Conclusions
26 27
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
It is recommended that:
7. Recommendations
• the report of the meeting be disseminated for use by countries
asinformation to assist in the development and implementation
ofscal policies as appropriate;
• the current evidence gap – including the impact of SSB tax on
improving weight and health outcomes, and ultimately the
prevention of NCDs – be addressed through research and evaluation
in countries;
• a nutrient-proling tool be developed for use by countries for
theimplementation of scal policies;
• an implementation manual be developed to provide further
guidance to countries on the development and implementation
ofscal policies for diet.

26 27
1. Global action plan for the prevention and control
of noncommunicable diseases 2013–2020. Geneva:
World Health Organization; 2013 (http://apps.who.
int/iris/bitstream/10665/94384/1/9789241506236_
eng.pdf, accessed 26 March 2016).
2. Comprehensive implementation plan on maternal,
infant and young child nutrition. Geneva: World
Health Organization; 2014 (http://apps.who.int/iris/
bitstream/10665/113048/1/WHO_NMH_NHD_14.1_
eng.pdf, accessed 26 March 2016).
3. Second International Conference on Nutrition (ICN2)
Rome, 19–21 November 2014, Conference Outcome
Document: Rome Declaration on Nutrition. Rome:
Food and Agricultural Organization of the United
Nations and World Health Organization; 2014 (www.
fao.org/3/a-ml542e.pdf, accessed 26 March 2016).
4. Second International Conference on Nutrition (ICN2)
Rome, 19–21 November 2014, Conference Outcome
Document: Framework for Action. Rome: Food and
Agricultural Organization of the United Nations and
World Health Organization; 2014 (www.fao.org/3/a-
mm215e.pdf, accessed 26 March 2016).
5. Global status report on noncommunicable
diseases 2014, Geneva: World Health
Organization; 2014 (http://apps.who.int/iris/
bitstream/10665/148114/1/9789241564854_eng.pdf,
accessed 26 March 2016).
6. Fiscal policy options with potential for improving
diets for the prevention of noncommunicable
diseases (NCDs) (draft). Geneva: World Health
Organization; 2015.
7. Smed et al. The eects of the Danish saturated fat
tax on food and nutrient intake and modelled health
outcomes: An econometric and comparative risk
assessment evaluation. Forthcoming in European
Journal of Clinical Nutrition, 2016.
8. Smed S. Financial penalties on foods – the fat tax in
Denmark. Nutrition Bulletin. 2012; vol 37, no 2. pp.
142–147.
9. Smed S, Robertson A. Are taxes on fatty foods having
their desired eects on health? BMJ editorial, BMJ.
2012; 16:345;e6885. doi: 10.1136/bmj.e6885.
References
10. Holm AL, Laursen MB, Koch M, Jensen JD,
Diderichsen F. The health benets of selective
taxation as an economic instrument in relation
to ischaemic heart disease and nutrition-related
cancers, Public Health Nutr, 2013; 16(12):2124–31.
doi: 10.1017/S1368980013000153.
11. Vallgårda S, Holm L, Jensen JD. The Danish tax on
saturated fat: why it did not survive. Eur J of Clin Nutr.
2015; 69:223–6. doi: 10.1038/ejcn.2014.224
12. Jensen JD, Smed S. The Danish tax on saturated
fat – short run eects on consumption, substitution
patterns and consumer prices of fats. Food Policy.
2013; 42:18–31. doi: 10.1016/j.foodpol.2013.06.004.
13. Jensen JD, Smed S, Aarup L, Nielsen E. The Danish
tax on saturated fat – demand eects for meat and
dairy products. Paper prepared for presentation
at the EAAE 2014 Congress “Agri-Food and Rural
Innovations for Healthier Societies”, 26–29 August
2014, Ljubljana, Slovenia.
14. Bødker M, Pisinger C, Toft U, Jørgensen T. The rise
and fall of the world’s rst fat tax. Health Policy. 2015;
119(6):737–42. doi: 10.1016/j.healthpol.2015.03.003.
15. Freire WB, Silva-Jaramillo KM, Ramírez-Luzuriaga
MJ, Belmont P, Waters WF. The double burden of
undernutrition and excess body weight in Ecuador.
Am J Clin Nutr. 2014; 100(Suppl):1636S–43S (http://
ajcn.nutrition.org/content/100/6/1636S.full.pdf+html,
accessed 29 March 2016).
16. Registro Ocial. Órgano del Gobierno del Ecuador.
Reglamento Sanitario Sustitutivo de Etiquetado de
Alimentos Procesados para el Consumo Humano,
2014 (in Spanish only) (www.controlsanitario.gob.
ec/wp-content/uploads/downloads/2014/09/R-
Sustitutivo-de-Etiquetado-AM5103-1.pdf, accessed
26 March 2016).
17. World Cancer Research Fund and the American
Institute for Cancer Research. Chapter 12: Public
health goals and personal recommendations. In:
Food, nutrition, physical activity, and the prevention
of cancer: a global perspective. Washington (DC):
AICR; 2007.
References

28 29
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
18. Moubarac J-C, Parra DC, Cannon G, Monteiro
CA. Food classication systems based on food
processing: signicance and implications for policies
and actions: a systematic literature review and
assessment. Curr Obes Rep. 2014; 3(2):256–72. doi:
10.1007/s13679-014-0092-0.
19. Sarlio-Lähteenkorva S, Manninen M. School meals
and nutrition education in Finland. Nutrition Bulletin
2010; 35(2):172–174.
20. Suositus korkeakouluruokailun periaatteiksi.
[Recommendations for college eating principles] Kela
and the National Nutrition Council, Helsinki, 2011 (in
Finnish only) (www.ravitsemusneuvottelukunta./
les/attachments//vrn/korkeakouluruokasuositus.
pdf, accessed 26 March 2016).
21. Using price policies to promote healthier diets.
Copenhagen: WHO Regional Oce for Europe;
2015 (www.euro.who.int/__data/assets/pdf_
le/0008/273662/Using-price-policies-to-promote-
healthier-diets.pdf, accessed 26 March 2016).
22. Sokeriverotyöryhmän loppuraportti [Sugar tax
working group nal report. Ministry of Finance
Publications, 2013 (in Finnish only with English
abstract) (http://vm./documents/10623/1236817/So
keriveroty%C3%B6ryhm%C3%A4+loppuraportti/8eb
df05f-710a-4878-aeb5-9d814f6e63c9).
23. A népegészségügyi termékadó hatásvizsgálata
[The public health impact assessment of taxes on
products]. Budapest: Hungarian National Institute for
Health and Development; 2013 (in Hungarian only)
(www.oe.hu/NETA_hatasvizsgalat.pdf, accessed 29
March 2016).
24. Encuesta Nacional de Salud y Nutrición 2012. Estado
de nutrición, anemia, seguridad alimentaria en la
población Mexicana. Instituto Nacional de Salud
Pública, Mexico, 2012 (http://ensanut.insp.mx/
doctos/ENSANUT2012_Nutricion.pdf, accessed 29
March 2016).
25. Barquera S, Campos-Nonato I, Hernádez-Barrera L,
Pedroza-Tobías A, Rivera-Dommarco JA. Prevalence
of obesity in Mexican adults. Salud Publica Mex. 2013;
55:Suppl 2:S151–60 (in Spanish only).
26. Villalpando S, de la Cruz V, Rojas R, Shamah-Levy T,
Avila MA, Gaona B, et al. Prevalence and distribution
of type 2 diabetes mellitus in Mexican adult
population: a probabilistic survey. Salud Publica Mex.
2010; 52 Suppl 1:S19–26.
27. Valadez B. Desplaza México a EU en consumos de
refrescos de cola, 2012. Milenio. January 2013 (web
document in Spanish only) (www.milenio.com/cdb/
doc/noticias2011/4d61be05ee00877e942fca43bc3ac4
6e, accessed 29 March 2016).
28. Sánchez-Pimienta T, Batis C, Lutter CK, Rivera
Dommarco JA. Main sources of total and added sugars
intake in the Mexican population. 16 Congreso de
Investigación en Salud Pública; Instituto Nacional de
Salud Pública, Cuernavaca, Mexico, 2015.
29. Colchero M, Salgado J, Unar M, Molina M, Ng SW, Rivera
Dommarco JA. Preliminary results of the eect of the
taxes implemented in Mexico in 2014 on prices. 16
Congreso de Investigación en Salud Pública; National
Institute of Public Health, Cuernavaca. 2015.
30. Colchero M, Ng SW, Barry P, Rivera Dommarco JA.
Preliminary results of changes in Mexican Household´s
beverage purchases after the SSB excise tax. 16
Congreso de Investigación en Salud Pública; National
Institute of Public Health, Cuernavaca. 2015.
31. Colchero MA, Popkin BM, Rivera JA, Ng SW. Beverage
purchases from stores in Mexico under the excise
tax on sugar sweetened beverages: observational
study. BMJ. 2016 Jan 6;352:h6704 (www.bmj.com/
content/352/bmj.h6704, accessed 3 February 2016)
32. Taxes on sugar-sweetened beverages as a public
health strategy: the experience of Mexico. Pan
American Health Organization. Mexico Representative
Oce, Mexico, D.F., 2015 (http://iris.paho.org/xmlui/
bitstream/handle/123456789/18391/9789275118719_
eng.pdf?sequence=1&isAllowed=y, accessed 26 March
2016).
33. Powel LM, Chriqui JF, Khan T, Wada R, Chaloupka FJ.
Assessing the potential eectiveness of food and
beverage taxes and subsidies for improving public
health: a systematic review of prices, demand and
body weight outcomes. Obes Rev. 2013; 14(2):110–28.
34. Falbe J, Rojas N, Grummon AH, Madsen KA. Higher
retail prices of sugar-sweetened beverages 3 months
after implementation of an excise tax in Berkeley,
California. Am J Public Health. 2015; 105(11):2194–201.
35. Smith Travis A, Biing-Hwan Lin, Jonq-Ying Lee. Taxing
caloric sweetened beverages: potential eects on
beverage consumption, calorie intake, and obesity.
Economic Research Report number 100, United
States Department of Agriculture, Economic Research
Service, July 2010 (www.ers.usda.gov/media/138598/
err100_1_.pdf, accessed 26 March 2016).

28 29
36. Kit BK, Fakhouri T, Park S, Nielsen SJ, Ogden CL.
Trends in sugar-sweetened beverage consumption
among youth and adults in the United States:
1999–2010. Am J Clin Nutr. 2013; 98:180–188
(http://ajcn.nutrition.org/content/98/1/180.full.pdf,
accessed29March 2016).
37. Beverage Digest Fact Book 2015. Statistical Yearbook
of Non-Alcoholic Beverages. 20th edition.
38. United States Department of Agriculture, Food and
Nutrition Service, Oce of Research and Analysis.
Healthy Incentives Pilot (HIP) Final Report. Alexandria,
VA; July 2013 (www.fns.usda.gov/sites/default/les/
HIP-Final.pdf, accessed 3 April 2016).
39. Andreyeva T, Long MW, Brownell KD. The impact of
food prices on consumption: a systematic review
of research on the price elasticity of demand for
food. Am J Public Health, 2010; 100(2):216–22. doi:
10.2105/AJPH.2008.151415.
40. Wholesome Wave. Our Initiatives. December 15, 2014
(https://www.wholesomewave.org/our-initiatives,
accessed 26 March 2016).
41. Food Insecurity Nutrition Incentive (FINI) Grant
Program. National Institute of Food and Agriculture,
United States Department of Agriculture. 2014/2015
(http://nifa.usda.gov/sites/default/les/rfa/1415_FINI.
pdf, accessed 7 April 2016).
42. Chriqui JF, Chaloupka FJ, Powell LM, EidsonSS.
Atypology of beverage taxation: multiple
approaches for obesity prevention and obesity
prevention-related revenue generation. J Public
Health Policy, 2013; 34:403–423 (www.palgrave-
journals.com/jphp/journal/v34/n3/full/jphp201317a.
html, accessed 27March 2016).
43. Thow AM, Heywood P, Leeder S, Burns L. The global
context for public health nutrition taxation. Public
Health Nutr. 2011; 14(1):176–186. doi: 10.1017/
S1368980010002053.
44. WHO technical manual on tobacco tax
administration. Geneva: World Health
Organization; 2010 (http://whqlibdoc.who.int/
publications/2010/9789241563994_eng.pdf,
accessed 26 March 2016)
45. Smed S, Jensen JD, Denver S. Socio-economic
characteristics and the eect of taxation as a health
policy instrument Food Policy. Food Policy. 2007;
32(5¬–6):624–639. doi: 10.1016/j.foodpol.2007.03.002.
46. Jensen JD, Smed S. Cost-eective design
ofeconomic instruments in nutrition policy.
IntJBehavNutr Phys Act. 2007; 4:10.
doi: 10.1186/1479-5868-4-10.
47. Economic nutrition policy tools – useful in the
challenge to combat obesity and poor nutrition?
Danish Academy of Technical Sciences, 2007
( www.atv.dk/uploads/1227087410economicnutrition.
pdf ).
48. Adam SA, Smed S. The eects of dierent types of
taxes on soft drink consumption. FOI working paper
2012/9. Institute of Food and Resource Economics,
University of Copenhagen, 2012/9 (http://okonomi.
foi.dk/workingpapers/WPpdf/WP2012/WP_2012_9_
taxes_on_softdrink_revised.pdf,
accessed 26March2016).
49. Powell LM, Wada R, Persky JJ, Chaloupka FJ.
Employment impact of sugar-sweetened beverage
taxes. American Journal of Public Health, 2014;
104(4):672–677 (http://ajph.aphapublications.
org/doi/pdf/10.2105/AJPH.2013.301630,
accessed26March 2016).
References

30 31
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
Dr Tatiana Andreyeva
Associate Professor, Department of Agricultural
andResource Economics
Director of Economic Initiatives
Rudd Center for Food Policy and Obesity
University of Connecticut
1 Constitution Plaza 608
Hartford, CT 06103
USA
Professor Frank J. Chaloupka
Director
Institute for Health Research and Policy
University of Illinois at Chicago
453 Westside Research Oce Bldg
1747 West Roosevelt Road
Chicago, IL 60608
USA
Dr Michel Chauliac
Chef de projet Nutrition
Bureau Alimentation et Nutrition
France
Professor Jamie F. Chriqui
Division of Health Policy and Administration
Institute for Health Research and Policy
University of Illinois at Chicago (MC 275)
University of Illinois at Chicago
453 Westside Research Oce Bldg
1747 West Roosevelt Road
Chicago, IL 60608
USA
Dr Arantxa Colchero
Economist
National Institute of Public Health
Universidad No. 655 Colonia Santa María Ahuacatitlán
Cerrada Los Pinos y Caminera C.P. 62100
Cuernavaca, Morelos
Mexico
Annex 1. List of participants
Dr Anil Deelchand
Acting Director Health Services
Ministry of Health and Quality of Life
Emmanuel Anquetil Building, 5th Floor
Port Louis
Mauritius
Dr Harold Goldstein
Executive Director
California Center for Public Health Advocacy
1947 Galileo Court, Suite 101
Post Oce Box 2309
Davis, California 95617
USA
Dr Michael F. Jacobson
Executive Director
Center for Science in the Public Interest
1220 L St. N.W.
Suite 300
Washington, D.C. 20005
USA
Ms María José Ramírez Luzuriaga
Chief
Nutrition and Food Security
National Ministry of Public Health
Av. República del Salvador 36–64 y Suecia
Quito
Ecuador
Mr Mohamed Madbouly
Ministry of Finance
Nasr City, Al Manteqah Al Oula
Cairo
Egypt

30 31
Dr Éva Martos
Deputy Director
National Institute for Food and Nutrition Science
Directorate General of the National Institute of
Pharmacyand Nutrition
Albert Flórián str. 3/a Budapest 1097
Hungary
Dr Sirpa Sarlio-Lähteenkorva
Senior Adviser
Ministry of Social Aairs and Health
Meritullinkatu 8
00170 Helsinki
Finland
Dr Franco Sassi
Senior Health Economist
Health Division
Directorate for Employment, Labour, and Social Aairs
Health Committee
Organisation for Economic Co-operation and
Development (OECD)
2 Rue André Pascal
75016 Paris
France
Associate professor Sinne Smed
Economist
Department of Food and Resource Economics
University of Copenhagen
Rolighedsvej 23,
1958 Frederiksberg
Denmark
Honourable Estrellita B. Suansing
Representative, Nueva Ecija, 1st District
House of Representatives, Philippines
HOR Complex, Constitution Hills 1126
Quezon City
Philippines
Professor Thaksaphon Thamarangsi
Director, Health Promotion Policy Research Center(HPR)
Manager, Thai NCD Network
Deputy Director and senior researcher
International Health Policy Program (IHPP)
Ministry of Public Health
Tiwanon Rd. Nonthaburi 11000
Thailand
Dr Anne Marie Thow
Menzies Centre for Health Policy
University of Sydney
Victor Coppleson Building D02
NSW 2006 Sydney
Australia
Dr Chonlathan Visaruthvong
Director
The Thai Excise Department
1488 Nakornchaisri Rd
Dusit, Bangkok 10300
Thailand
Annex 1. List of participants

32 33
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
WHO Headquarters:
Dr Tim Armstrong
Coordinator
Surveillance and Population-based Prevention
Department of Prevention of Noncommunicable
Diseases
Dr Douglas Bettcher
Director
Department of Prevention of Noncommunicable
Diseases
Dr Francesco Branca
Director
Department of Nutrition for Health and Development
Dr Oleg Chestnov
Assistant Director-General
Noncommunicable Diseases and Mental Health
Mr Mark Goodchild
Technical Ocer
Tobacco Control Economics Unit
Department of Prevention of Noncommunicable
Diseases
Dr Benn McGrady
Technical Ocer (Legal) National Capacity
Department of Prevention of Noncommunicable
Diseases
Dr Jason Montez
Technical Ocer
Nutrition Policy and Scientic Advice
Department of Nutrition for Health and Development
Mr Leo Nederveen
Technical Ocer
Surveillance and Population-based Prevention
Department of Prevention of Noncommunicable
Diseases
Dr Chizuru Nishida
Coordinator
Nutrition Policy and Scientic Advice Department
ofNutrition for Health and Development
Ms Anne Marie Perucic
Health Economist
Tobacco Control Economics Unit
Department of Prevention of Noncommunicable
Diseases
Dr Vinayak Prasad
Project Manager
Department of Prevention of Noncommunicable
Diseases
Dr Temo Waqanivalu
Programme Ocer
Surveillance and Population-based Prevention
Department of Prevention of Noncommunicable
Diseases
WHO Regional Oce:
Mr Jo Jewell
Technical Ocer
Nutrition, Physical Activity and Obesity
Division of Noncommunicable Diseases and Life-course
WHO Regional Oce for Europe
World Health Organization Secretariat

32 33
Annex 1. List of participants
34 35
Fiscal Policies for Diet and Prevention of NoncommunicableDiseases
Annex 2. Meeting programme
Tuesday, 5 May 2015
08:30–09:00 Registration
09:00–09:30 Opening
• Welcome Remarks
Assistant Director-General, Noncommunicable Diseases and Mental Health
• Election of Chairperson and Rapporteur
• Introduction of participants
• Adoption of agenda and programme
• Administrative arrangements
09:30–10:30 • Noncommunicable diseases overview, and role of scal measures
Dr Temo Waqanivalu
• Review of existing systematic reviews of scal policy interventions to improve diets
Dr Anne Marie Thow
• Existing evidence and guidance on scal policies
Dr Frank Chaloupka
10:30–11:00 Coee Break
11:00–11:30 Tobacco taxation experience
Mr Mark Goodchild, Ms Anne Marie Perucic
11:30–11:45 Using price policies to promote healthier diets in the WHO European Region
Mr Jo Jewell
11:45–13:00 • Countries’ experiences in scal policies
• Objective of tax
• Denition/scope of tax
• Tax structure (tax rate, tax base)
• Development, implementation and administration
• Impacts
• Mexico – Dr Arantxa Colchero
• Egypt – Mr Mohamed Madbouly
• Finland – Dr Sirpa Sarlio-Lähteenkorva
• France – Dr Michel Chauliac
13:00–14:00 Lunch Break
14:00–14:30 Countries’ experiences in scal policies (cont’d)
• Hungary – Dr Eva Martos
• Mauritius – Dr Anil Deelchand
14:30–15:30 Countries’ challenges in implementing scal policies
• Denmark – Associate professor Sinne Smed
• Philippines – Ms Estrellita B. Suansing
• Thailand – Professor Thaksaphon Thamarangsi
• United States of America – DrHarold Goldstein
• Ecuador – Ms María José Ramírez
15:30–16:00 Coee Break
16:00–17:00 Discussion
18:00 Reception
34 35
Wednesday, 6 May 2015
09:00–09:15 Summary of Day 1
09:15–10:45 Evidence of scal policies
• Retail prices: industry structure and scal policies
• Own price elasticities: nal retail prices, use and consumption
• Own price elasticities: socioeconomic groups and target populations (e.g. youth)
• Cross price elasticities: implications for the tax base (e.g. which products to tax
ornot to tax)
Dr Tatiana Andreyeva
Professor Michael Jacobson
Associate professor Sinne Smed
• Discussion
10:45–11:15 Coee Break
11:15–12:45 Policy implications of scal policies
• What type of taxation: excise or special VAT (sales taxes) rates?
• What tax structure: specic or ad valorem?
• Impact of tax rates and tax systems on nal retail prices.
• Fiscal policies and revenue generation potential.
• Nutrient proling to identify target foods and benchmarks
Professor Jamie Chriqui
Dr Franco Sassi
Dr Chonlathan Visaruthvong
Dr Chizuru Nishida
12:45–13:45 Lunch Break
13:45–15:30 Two working groups: identication of gaps, considerations and directions to take
foreach of the following questions:
1. What are the economic and health justications for scal policies?
2. What could be the best approach for a good scal policy design?
15:30–16:00 Coee Break
16:00–17:00 Report back by groups, and discussion
17:00–17:30 Closing remarks and next steps
Annex 2. Meeting programme

ISBN 978 92 4 151124 7
