Select Preferred Clinic Location (map and addresses on re
verse side)
Date: _________________________
Patient Name: ________________________________
______ DOB: ________________
Mobile Phone: ______________________ Alt Phone:
__________________________
Email: _____________________________ Insurance: _
_________________________
Member ID: ________________________ Group #: ___
_________________________
Pre-Cert #: _____________________________________________________________
Independence Lee’s Summit Liberty North Olathe Overland Park Pl
aza St. Joseph Wyandotte County
Contact Patient to Schedule DIC to Pre-C
ert
PLEASE FAX COMPLETED FORM TO 913-344-9957 OR
816-444-9957
Referring Provider (Please Print):
*Provider Signature: __________________________
Provider Phone: Provider Fax:
Special Ins
tructions:
Call Report
Send CD with Courier
C
ontrast: Yes No
Hold patient/Call Report A
fter Hours Phone
(If different from above):
Send CD with Patient
Radiologist Discretion
C
reatinine: DIC to obtain (if needed) Results/Date: _______________________________________
Diagnosis/Symptoms: _________________________________________________________________________________
Electronic Signature on file
MR Cervical Spine
MR Thoracic Spine
MR Lumbar Spine
MR Pelvis
MR OTHER
(Please Specify)
MR UPPER Extremity (Please Specify)
MR LOWER Extremity (Please Specify)
CT OTHER (Please Specify)
CT Cervical Spine
CT Thoracic Spine
CT Lumbar Spine
CT Pelvis
CT UPPER Extremity
(Please Specify)
CT LOWER Extremity (Please Specify)
GENERAL RADIOLOGY
Cervical Spine x-ray
2 - 3 views
4 - 5 views
Lumbar Spine x-ray
2 - 3 views
4 view minimum
Complete w/ Flexion & Extension
Thoracic Spine x-ray, 3 views
Chest x-ray, 2 views
RT LT Bilateral
Ribs and PA Chest x-ray
RT LT Bilateral
Shoulder x-ray, 2 views
RT LT Bilateral
Hip x-ray, 2 views
RT LT Bilateral
Pelvis x-ray, 1 view
Bilateral Hips and Pelvis x-ray
Knee x-ray, 2 views
RT LT Bilateral
Ankle x-ray, 3 views
RT LT Bilateral
Foot x-ray, 3 views
RT LT Bilateral
OTHER
(Please Specify)
RT LT Bilateral
RT LT Bilateral
RT LT Bilateral
Form #CL188 Copyright© Diagnostic Imaging Centers, P.A. 2005
Revised: 11-08-19
*MRI CPT CODES LISTED ON REVERSE SIDE
*CT CPT CODES LISTED ON REVERSE SIDE
EXAM SCH
EDULING ORDER FORM
CHIROPRACTIC
Online Scheduling Available!
You are now able to schedule most exams online and on our
mobile
app. Schedule online at www.dic-KC.com, or download our free
mobile app today! Search for "DICImaging" in your App
Store and
look for our logo!
To reach
our
Schedulin
g
Center,
call
913
-344-9989 or 816-444-9989
MRI
MRI Availability & Table Weight Limits:
High Field 3T Wide-Bore MRI/500 lbs. - Overland Park
High Field 1.5T Wide-Bore Oval MRI/550 lbs. - North
High Field 1.5T Wide-Bore MRI/500 lbs. - Olathe
High Field 1.5T MRI/350 lbs. - Independence, Lee's Summit,
Liberty, St. Joseph
High Field 1.5T MRI/300 lbs. - Plaza
High Field 1.2T OPEN MRI/660 lbs. - Overland Park
Open MRI/500 lbs. - Independence, Plaza, Wyandotte County
CT
C
T Scan Table Weight Limits:
Table Limit: 500 lbs. - Liberty, North, Olathe, Overland Park
Table Limit: 450 lbs. - Independence, Lee’s Summit, Plaza
Table Limit: 400 lbs. - St. Joseph, Wyandotte County
PLEASE NOTE:
If you are taking medications on a dail
y basis, please do not withhold medication unless discu
ssed as part of your exam preparation.
If you have allergies to iodine, other me
dications, or have asthma, please contact our office p
rior to your procedure.
If there is any possibility that you may
be pregnant or are breastfeeding, please let our office k
now at the time of scheduling.
If you have any questions regarding yo
ur procedure, please contact our office and we will be g
lad to help you.
If for any reason
you need to reschedule, please call 913-344-9989 or 816
-444-9989
Form #CL188B Revised: 11-08-19
MRI SPINE:
72141 MRI CERVICAL SPINE without contrast
72156 MRI CERVICAL SPINE
w/o & with
contrast
72146 MRI THORACIC SPINE without contrast
72157 MRI THORACIC SPINE
w/o & with
contrast
72148 MRI LUMBAR SPINE without contrast
72158 MRI LUMBAR SPINE
w/o & with
contrast
MRI OTHER:
72195 MRI PELVIS without contrast
72197 MRI PELVIS
w/o & with
contrast
73218 MRI
UPPER EXTREMITY
without contrast
73220 MRI
UPPER EXTREMITY w/o & with
contrast
73221 MRI
UPPER EXTREMITY JOINT
without contrast
73223 MRI
UPPER EXTREMITY JOINT w/o & with
contrast
73718 MRI
LOWER EXTREMITY
without contrast
73720 MRI
LOWER EXTREMITY
w/o & with
contrast
73721 MRI
LOWER EXTREMITY JOINT
without contrast
73723 MRI
LOWER EXTREMITY JOINT
w/o & with
contras
t
CT SPINE:
72125 CT CERVICAL SPINE wit
hout contrast
72127 CT CERVICAL SPINE
w/o & with
contrast
72128 CT THORACIC SPINE without contrast
72130 CT THORACIC SPINE
w/o & with
contrast
72131 CT LUMBAR SPINE without contrast
72133 CT LUMBAR SPINE
w/o & with
contrast
CT OTHER:
72192 CT PELVIS without contrast
72194 CT PELVIS
w/o & with
contrast
73200 CT
UPPER EXTREMITY
without contrast
73202 CT
UPPER EXTREMITY
w/o & with
contrast
73700 CT
LOWER EXTREMITY
without contrast
73702 CT
LOWER EXTREMITY
w/o & with
contrast
HELPFUL CPT CODES
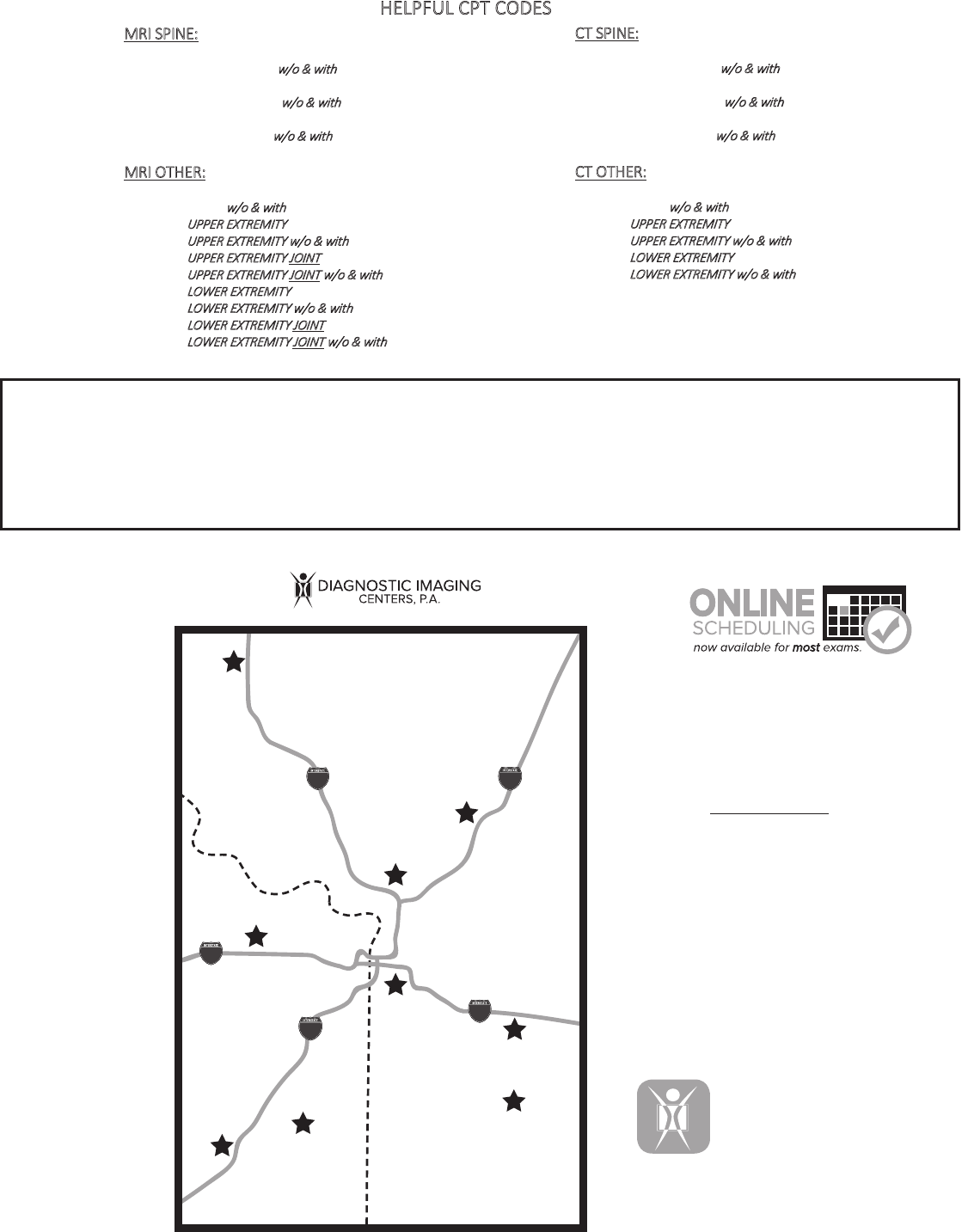
Life takes you places,
and we’re never far.
Find our clinic
nearest you!
LOCATIONS
From CTs to MRIs, to
mammograms and
more, learn about
our exams here.
WE OFFER
EXAMS
Paperwork made
simple -save time
and fill it out ahead
of your visit!
FORMS
Schedule your exam
online. Pick the location,
date, and time!
*available for MOST exams
AND ON THE GO.
THE METRO
O
nline Scheduling Available!
You are
now able to schedule most exams
onl
ine, and on our mobile app.
V
isit www.dic-KC.com
Se
lect Appointment
An
swer a few Appointment Questions
Ch
oose Time & Location
D
ONE!
You wi
ll need to have an order from your doctor.
*Your annual
screening mammogram DOES NOT
require an order.
70
70
35
35
Saint Joseph
Liberty
29
KC North
Independence
Plaza
Lee’s Summit
Overland
Olathe
Park
Wyandotte
29
70
70
35
35
KANSAS
MISSOURI
Download our free mobile
app today! Search for
"DICImaging" in your App
Store and look for our logo!
INDEPENDENCE
4911 S Arrowhead Dr #100
Independence, MO 64055
LEE’S SUMMIT
301 NE Mulberry St #100
Lee’s Summit, MO 64086
PLAZA
4801 Main St #200
Kansas City, MO 64112
KC NORTH
303 NE Englewood Rd
Kansas City, MO 64118
LIBERTY
9151 NE 81st Ter #250
Kansas City, MO 64158
ST. JOSEPH
3937 Sherman Av
St. Joseph, MO 64506
e
OLATHE
13795 S Mur-Len Rd #100
Olathe, KS 66062
OVERLAND PARK
6650 W 110th St #100
Overland Park, KS 66211
WYANDOTTE COUNTY
9201 Parallel Pkw
Kansas City, KS 66112
y
MOBILE 3D
MAMMOGRAPHY
PLEASE NOTE:
If you are taking medications on a dail
y basis, please do not withhold medication unless discu
ssed as part of your exam preparation.
If you have allergies to iodine, other me
dications, or have asthma, please contact our office p
rior to your procedure.
If there is any possibility that you may
be pregnant or are breastfeeding, please let our office k
now at the time of scheduling.
If you have any questions regarding yo
ur procedure, please contact our office and we will be g
lad to help you.
If for any reason
you need to reschedule, please call 913-344-9989 or 816
-444-9989
Form #CL188B Revised: 11-08-19
MRI SPINE:
72141 MRI CERVICAL SPINE without contrast
72156 MRI CERVICAL SPINE
w/o & with
contrast
72146 MRI THORACIC SPINE without contrast
72157 MRI THORACIC SPINE
w/o & with
contrast
72148 MRI LUMBAR SPINE without contrast
72158 MRI LUMBAR SPINE
w/o & with
contrast
MRI OTHER:
72195 MRI PELVIS without contrast
72197 MRI PELVIS
w/o & with
contrast
73218 MRI
UPPER EXTREMITY
without contrast
73220 MRI
UPPER EXTREMITY w/o & with
contrast
73221 MRI
UPPER EXTREMITY JOINT
without contrast
73223 MRI
UPPER EXTREMITY JOINT w/o & with
contrast
73718 MRI
LOWER EXTREMITY
without contrast
73720 MRI
LOWER EXTREMITY
w/o & with
contrast
73721 MRI
LOWER EXTREMITY JOINT
without contrast
73723 MRI
LOWER EXTREMITY JOINT
w/o & with
contras
t
CT SPINE:
72125 CT CERVICAL SPINE wit
hout contrast
72127 CT CERVICAL SPINE
w/o & with
contrast
72128 CT THORACIC SPINE without contrast
72130 CT THORACIC SPINE
w/o & with
contrast
72131 CT LUMBAR SPINE without contrast
72133 CT LUMBAR SPINE
w/o & with
contrast
CT OTHER:
72192 CT PELVIS without contrast
72194 CT PELVIS
w/o & with
contrast
73200 CT
UPPER EXTREMITY
without contrast
73202 CT
UPPER EXTREMITY
w/o & with
contrast
73700 CT
LOWER EXTREMITY
without contrast
73702 CT
LOWER EXTREMITY
w/o & with
contrast
HELPFUL CPT CODES
Life takes you places,
and we’re never far.
Find our clinic
nearest you!
LOCATIONS
From CTs to MRIs, to
mammograms and
more, learn about
our exams here.
WE OFFER
EXAMS
Paperwork made
simple -save time
and fill it out ahead
of your visit!
FORMS
Schedule your exam
online. Pick the location,
date, and time!
*available for MOST exams
AND ON THE GO.
THE METRO
O
nline Scheduling Available!
You are
now able to schedule most exams
onl
ine, and on our mobile app.
V
isit www.dic-KC.com
Se
lect Appointment
An
swer a few Appointment Questions
Ch
oose Time & Location
D
ONE!
You wi
ll need to have an order from your doctor.
*Your annual
screening mammogram DOES NOT require an orde
r.
70
70
35
35
Saint Joseph
Liberty
29
KC North
Independence
Plaza
Lee’s Summit
Overland
Olathe
Park
Wyandotte
29
70
70
35
35
KANSAS
MISSOURI
Download our free mobile
app today! Search for
"DICImaging" in your App
Store and look for our logo!
INDEPENDENCE
4911 S Arrowhead Dr #100
Independence, MO 64055
LEE’S SUMMIT
301 NE Mulberry St #100
Lee’s Summit, MO 64086
PLAZA
4801 Main St #200
Kansas City, MO 64112
KC NORTH
303 NE Englewood Rd
Kansas City, MO 64118
LIBERTY
9151 NE 81st Ter #250
Kansas City, MO 64158
ST. JOSEPH
3937 Sherman Av
St. Joseph, MO 64506
e
OLATHE
13795 S Mur-Len Rd #100
Olathe, KS 66062
OVERLAND PARK
6650 W 110th St #100
Overland Park, KS 66211
WYANDOTTE COUNTY
9201 Parallel Pkw
Kansas City, KS 66112
y
MOBILE 3D
MAMMOGRAPHY
