Policy Implementation Challenges and Barriers to Access
Sexual and Reproductive Health Services Faced By People
With Disabilities: An Intersectional Analysis of Policy
Actors’ Perspectives in Post-Conflict Northern Uganda
Muriel Mac-Seing
1,2*
ID
, Emmanuel Ochola
3
ID
, Martin Ogwang
4
ID
, Kate Zinszer
1,2
ID
, Christina Zarowsky
1,2,5
ID
Abstract
Background: Emerging from a 20-year armed conflict, Uganda adopted several laws and policies to protect the rights
of people with disabilities, including their sexual and reproductive health (SRH) rights. However, the SRH rights of
people with disabilities continue to be infringed in Uganda. We explored policy actors’ perceptions of existing pro-
disability legislation and policy implementation, their perceptions of potential barriers experienced by people with
disabilities in accessing and using SRH services in post-conflict Northern Uganda, and their recommendations on
how to redress these inequities.
Methods: Through an intersectionality-informed approach, we conducted and thematically analysed 13 in-depth
semi-structured interviews with macro level policy actors (national policy-makers and international and national
organisations); seven focus groups (FGs) at meso level with 68 health service providers and representatives of disabled
people’s organisations (DPOs); and a two-day participatory workshop on disability-sensitive health service provision
for 34 healthcare providers.
Results: We identified four main themes: (1) legislation and policy implementation was fraught with numerous
technical and financial challenges, coupled with lack of prioritisation of disability issues; (2) people with disabilities
experienced multiple physical, attitudinal, communication, and structural barriers to access and use SRH services; (3)
the conflict was perceived to have persisting impacts on the access to services; and (4) policy actors recommended
concrete solutions to reduce health inequities faced by people with disabilities.
Conclusion: This study provides substantial evidence of the multilayered disadvantages people with disabilities face
when using SRH services and the difficulty of implementing disability-focused policy in Uganda. Informed by an
intersectionality approach, policy actors were able to identify concrete solutions and recommendations beyond the
identification of problems. These recommendations can be acted upon in a practical road map to remove different
types of barriers in the access to SRH services by people with disabilities, irrespective of their geographic location in
Uganda.
Keywords: Intersectionality-Based Policy Analysis, People With Disabilities, Sexual and Reproductive Health, Health
Equity, Policy Implementation, Uganda
Copyright: © 2022 The Author(s); Published by Kerman University of Medical Sciences. This is an open-access
article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/
licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the
original work is properly cited.
Citation:
Mac-Seing M, Ochola E, Ogwang M, Zinszer K, Zarowsky C. Policy implementation challenges and
barriers to access sexual and reproductive health services faced by people with disabilities: an intersectional analysis
of policy actors’ perspectives in post-conflict Northern Uganda.
Int J Health Policy Manag. 2022;11(7):1187–1196.
doi:10.34172/ijhpm.2021.28
*Correspondence to:
Muriel Mac-Seing
Email:
muriel.k.f.mac-seing@umontreal.ca
Article History:
Received: 19 December 2020
Accepted: 28 March 2021
ePublished: 13 April 2021
Original Article
Full list of authors’ affiliations is available at the end of the article.
2022, 11(7), 1187–1196
doi
Background
More than 180 Member States have ratified the United
Nations (UN) Convention on the Rights of Persons with
Disabilities (CRPD), which aims to promote, protect and
ensure the fundamental human rights of people with
disabilities.
1
The CRPD was adopted in 2006 and came
into force in 2008 after two decades of negotiation among
international organisations, activists, disabled people’s
organisations (DPOs), and governments.
2
According to the
CRPD, people with disabilities are people “who have a long
term physical, mental, intellectual or sensory impairments
which in interaction with various barriers may hinder their
full and effective participation in society on an equal basis
with others.”
3
Worldwide, one person in seven is estimated
to live with some form of disability, with 80% of them living
in low and middle resource income countries.
4
In 2019, the
UN report on the realisation of the Sustainable Development
Goals stated that despite improvement in development,
people with disabilities continue to experience exclusion and
face numerous barriers to their full participation.
5
In sub-Saharan Africa, Uganda cited as an exemplary
disability rights promoter,
6,7
was among the first countries
to ratify the CRDP in 2008.
1
One fifth of its population was
estimated to live with some disability.
8
In 1995, Uganda
Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–11961188
Implications for policy makers
• An intersectionality-informed analysis goes beyond describing a problem. It enables policy actors and researchers to examine intersecting social
identities, diverse sources of knowledge, and multilevel factors, and to consciously explore complex policy issues for transformative policy
solutions.
• Pro-disability policy implementation challenges are multiple and people with disabilities still experience physical, attitudinal, communication,
and structural barriers to access and use sexual and reproductive health (SRH) services in post-conflict Northern Uganda.
• Policy actors, including health service providers, disabled people’s organisations (DPOs), national and international organisations, and national
policy-makers, proposed numerous recommendations and solutions which can be applied within the normative space created by the recent
adoption of the 2019 Disability Act.
• The combination of these recommendations contributes to redress situations of social inequity and injustice, and advances Uganda’s progress
towards the Sustainable Development Goals for universal health coverage.
Implications for the public
The fundamental rights of people with disabilities, including their sexual and reproductive health (SRH) rights, continue to be violated despite the
existence of many laws and policies adopted to promote the rights of people with disabilities in Uganda. The study found that multiple forms of
barriers and policy implementation challenges still exist, preventing people with disabilities from accessing and using SRH services. Many actionable
solutions at individual, community and national levels exist and can be implemented to redress historic health inequities and injustice. People with
and without disabilities, health service providers, civil society organisations (CSOs) and policy-makers have a renewed opportunity to contribute to
concretely ‘leave no one behind’, as promoted by the Sustainable Development Goals.
Key Messages
enacted its Constitution, and in 2005 it was amended,
providing a legal space for the promotion of people with
disabilities’ rights. In the following years, several legal
instruments that contain sections or articles related to the
rights of people with disabilities were adopted. Among
these, Uganda approved the Parliamentary Election Statute
in 1996 and the Local Government Act in 1997. These laws,
respectively, make provision for people with disabilities to be
elected to Parliament, and at the district and subcounty levels.
6
In 2003, the National Council for Disability (NCD) Act was
adopted and specified the role of this national body in the
promotion, monitoring, and advocacy of equal opportunities
for Ugandans with disabilities.
9
Three years later, Uganda
further adopted a Disability Act with sections related to
such as accessibility, social services, and health, including
access to reproductive health and user-friendly health facility
materials.
10
In September 2019, Uganda updated this Act with
a more comprehensive version, referencing the CRPD and
using a similar definition of disability.
11
Emerging from a 20-year armed conflict which most affected
its Northern region, Uganda had to rebuild a weakened health
system. It witnessed high levels of sexual and gender-based
violence and unwanted pregnancies as well as poor access to
safe motherhood
12,13
and reproductive healthcare.
14
Despite
an arsenal of well-intentioned legal tools adopted over several
years to promote and protect the human rights of people with
disabilities, including their sexual and reproductive health
(SRH) rights, people with disabilities continue to have limited
access to routinely accessible SRH services in Uganda. Studies
examining SRH service utilisation reported ongoing physical
and costs barriers,
15,16
attitudinal challenges,
15
and multilayered
discrimination and inequities
17
experienced by people with
disabilities. The 2018 Guttmacher-Lancet Commission also
highlighted that people with disabilities constitute a group
‘with specific disadvantages’ and are ‘subjected to harmful
stereotypes and myths’ which contribute to their heightened
risk of physical and sexual abuse.
18
Intersectionality-Based Policy Analysis (IBPA)
can critically address social inequities and multiple
discriminations experienced by people with disabilities.
19
It provides a flexible framework to enable policy actors,
researchers, and group advocates to examine diverse sources
of knowledge, intersecting multiple social identities and
multilevel factors, and to explore complex policy issues
for transformative policy solutions, beyond describing the
problem.
20
Intersectionality addresses the interrelationships
among multiple social identities, social inequities, power
dynamics, context, and complexity.
21
Principles promoted in
the IBPA are the importance of acknowledging intersecting
social categories, a multilevel analysis, power structures, the
context, the diversity of sources of knowledge, reflexivity, and
social justice and equity.
22
Before critical studies started to
be interested in intersectionality to highlight inequality and
multiple oppressions experienced by marginalised groups,
23-27
Black feminists and lesbians of the Combahee River Collective
were already embracing core concepts of this framework and
approach in their struggle in the 1970s.
28
Intersectionality
was first coined in 1989 by Kimberlé Crenshaw to address the
multiple discriminations faced by African American women
workers who were protected by neither anti-racism nor anti-
sexism legislation.
24,29
The study reported here aimed to understand and document
how policy actors perceive the relationships among legislation
and health policy and the utilisation of SRH services by
people with disabilities in the post-conflict Northern region
of Uganda. We were interested in exploring policy actors’
understanding of existing pro-disability legislation and policy
implementation, their perceptions of possible discriminations
experienced by people with disabilities in accessing and using
SRH services, and their recommendations on how to redress
these inequities. This paper reports the qualitative findings
on the perceptions of policy actors at meso and macro
levels, drawing from a larger body of evidence from a mixed
methods study which also involved women and men with
Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–1196
1189
disabilities (micro level). Perspectives of women and men
with disabilities have been reported previously.
17
Methods
The qualitative study methods are reported in detail elsewhere
and summarised here.
17
From November 2017 to April 2018,
we conducted our study in the districts of Gulu, Amuru, and
Omoro in the Northern region and in Kampala, the capital of
Uganda. To assess the rigour of our qualitative research, we
followed the Consolidated Criteria for Reporting Qualitative
Research.
30
Study Participants
A total of 115 people participated in the study: at the national
level, 13 policy actors took part in in-depth semi-structured
interviews; and at the community level, 68 health service
providers and DPO representatives participated in seven
focus groups (FGs) of the Northern districts of Gulu, Amuru,
and Omoro. Additionally, 34 health service providers and
managers participated in a 2-day participatory workshop
on disability-sensitive health service provision (Table 1).
Participants were purposefully recruited, following a snow-
ball approach in which initially recruited study respondents
recommended other potentially relevant policy actors that
could speak to the research objectives.
31
National policy
actors based in the capital of Kampala were selected based
on different types of organisations they belonged to and who
were knowledgeable of disability and SRH related policy and
programmatic processes in Uganda. Health service providers
were recruited from seven health facilities, with a balance of
gender and public and private-not-for-profit health facilities.
Recruitment of study participants continued until saturation
was reached.
32
Data Collection
We used in-depth semi-structured interviews, FGs,
and a participatory workshop to triangulate findings.
32
These techniques were selected to further increase the
trustworthiness of qualitative research process.
32
For fine-
tuning of data collection tools, we first discussed them among
the research team, and pre-tested each tool in FGs and with
sign language interpreters to improve comprehension. The
IBPA framework informed this research and was adapted in
our interview and FG guidelines, which included two sets of
questions
20
: The first set constituted of descriptive questions
related to the identification of problems related to SRH use
among people with disabilities and information on policy
implementation processes. The second set was composed
of transformative questions related to solutions aimed at
reducing inequities and addressing problems identified.
Individual and group interviews were conducted in English,
and research assistants translated concurrently questions and
answers in Luo, when needed. For the few participants with
hearing impairments, we hired locally qualified Ugandan sign
language interpreters who were fluent in English, Luo and sign
language. Each individual or group interview lasted around
60 minutes and was audio recorded with the permission of
study participants.
Consistent with the transformative component of the
IBPA emphasising the search for solutions, we organised a
2-day participatory workshop on disability-sensitive service
provision, following the numerous requests we received
from interviewed health service providers. The workshop
objective was to discuss the barriers people with disabilities
encountered when seeking SRH services and the solutions
to address concretely these problems. It was organised
for health service providers and managers of seven health
facilities of three districts. On the first day, the preliminary
findings of the study and the existing pro-disability policies
and legislation in Uganda were presented. Two women,
one with a physical impairment and another with a mental
impairment, and two men, one with a hearing impairment
and the second with a vision impairment, were invited as
experts to share their experiences and recommendations on
how to improve accessibility and service delivery. On the
second day, a deaf trainer and a hearing trainer who knew
sign language facilitated a series of hands-on sessions for
participants to learn the basics of Uganda sign language in
relation to health and SRH services. With the permission
of workshop participants, we documented the outcomes of
group discussions and exchanges.
To ensure confidentiality, all citations from study
Table 1. Sample Characteristics
Source Total Women (%) Men(%) Disabled (%)
6
7 5 2 2
68 7 (9)
60 26 1
8 2 6 6
19 (56) 0 (0)
27 16 11 0
7 0
115 12 (10)
Note
Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–11961190
respondents have been depersonalised and are referred to
in this paper by their professional function only. For health
service providers, the FG number is specified.
Analysis
Informed by the intersectional framework, a thematic
analysis was adopted due to its flexible approach as well as the
opportunity this type of analysis provides us in managing “a
large data set” in a more structured manner.
33
Our thematic
analysis following specific steps which are described in detail
elsewhere,
17
and briefly summarised here. Relevant themes
emerged after a series of iterative activities which included
listening to all recordings, reading a couple of times all
interview transcripts, and writing down analytical memos
along the process. Transcripts were coded through QDA
Miner 5.0.31 (Provalis) following an inductive and deductive
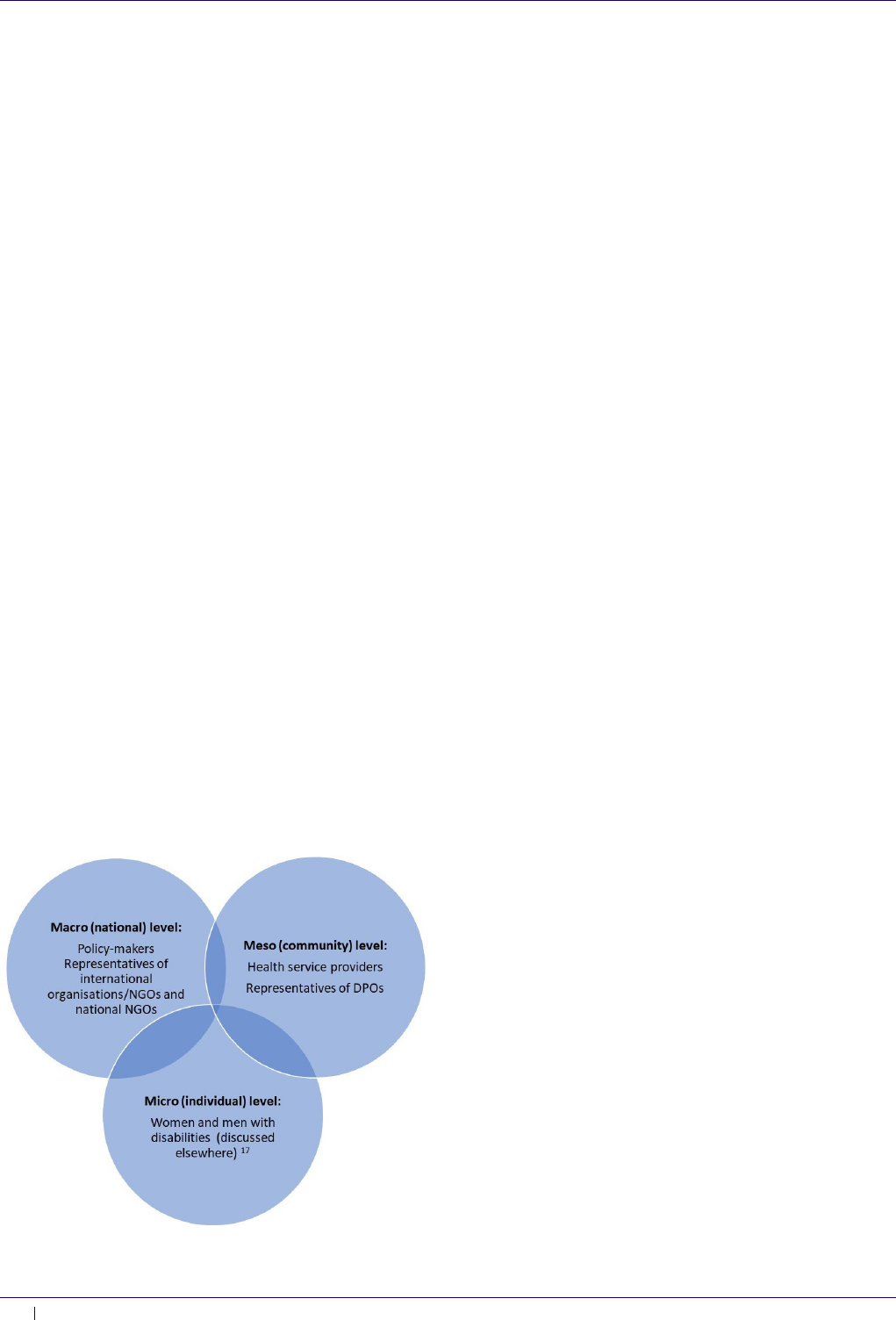
approach. Our analysis was guided by the key principles of the
IBPA framework of intersecting social categories, multilevel
analysis (Figure), power structures, time and space (context),
diverse sources of knowledge, reflexivity, and equity and
social justice.
22
Specifically, when identifying themes, we
were attentive to how policy actors answered descriptive and
transformative questions posed during individual and group
interviews as well as during the workshop.
22
Results
We report here the findings of the perceptions of health service
providers and representatives of DPOs, at meso level, and
those of policy-makers and representatives of international
organisations/non-governmental organisations (NGOs)
and national NGOs, at macro level. They complement the
findings of a larger body of evidence on the perceptions
and recommendations of women and men with different
types of impairments, at micro level, which highlighted the
intersectional discriminations experienced by people with
disabilities when using different types of SRH services.
17
Although we interviewed diverse policy actors at meso and
macro levels, they shared several common narratives around
the relationships between pro-disability legislation and policy
and the use of SRH services by people with disabilities in the
post-conflict Northern region of Uganda.
This study identified four major themes across policy
actors, levels, and districts, as follows: (1) policy and
legislation application challenges; (2) acknowledgment of the
existence of multiple barriers faced by people with disabilities
in accessing and using SRH services; (3) lingering impacts of
the conflict on people with disabilities’ access to services; and
(4) multilevel recommendations to remove barriers.
Policy and Legislation Application Challenges
Policy actors mentioned several challenges related to the
implementation and enforcement of pro-disability policy and
legislation in Uganda. Central to a lack of enforcement is a
widespread lack of awareness and training on disability issues
among policy executors, particularly health professionals,
of existing key policy and laws which focus on the rights of
people with disabilities. To some health service providers, this
implementation gap was illustrated by inaccessible services
and infrastructures.
“It’s unfortunate that most of these things [policies]
stop at Kampala or in offices. They [policy-makers] don’t
come to the ground…. Myself, I have even never seen the
[Disability] Act … This is something that they should also
consider if it must work out very well … because we should
work with references … It was not availed….We also try to
improvise. It is there, though it’s not [up] to standard. But
it is a requirement that we should at least create accessible
[structures] … It’s not very functional because some of our
clients … are still crawling” (Health service provider, FG9,
Omoro).
Awareness was identified as essential in the pathway to
policy implementation; however, a lack of prioritisation and
budgeting were also identified as detrimental to an effective
response to disability issues from ministry to local levels.
The deficient financial capacity at governmental level was
perceived to be influenced by policy-makers’ worldviews and
their lack of sensitivity towards disability issues.
“I mean the issue of mindset has affected most of our
implementation. If I showed you the percentage for the
[disability] budget … Like the law (…) it should be backed
by resources, financially. If it is a government building, let’s
make sure it’s accessible. That means you need money to
change … Of the Ministry, I think it’s 0.1, is it 1% or something
less than 1%?” (Government policy-maker, Kampala).
Although Uganda has adopted many policies promoting
the rights of people with disabilities, policy actors insisted
on the importance of supervision and monitoring: “There is
no committee in place to supervise the policies that have been
approved, so it is upon the organisation to take it on or not”
(Health service provider, FG4, Gulu). According to policy
actors, the 2006 Disability Act was not substantial enough
to hold the Government imputable to its policy intent:
“People have raised the issue that the Act has so many things
missing … [The Act] doesn’t hold the Government accountable”
(Government policy-maker, Kampala). They further
Figure. Multilevel Analysis of Policy Actors. Abbreviations: DPOs, disabled
people’s organisations; NGOs, non-governmental organisations.

Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–1196
1191
mentioned that the NCD and the civil society organisations
(CSOs) were not fully playing their role of advocacy for and
monitoring of accessible services for people with disabilities:
“It’s the role of disability unions and umbrellas to ensure that they
engage institutions so that they can sign some memorandum
of understanding … help push for disability-friendly services”
(National NGO representative, Kampala).
Acknowledgment of the Existence of Multiple Barriers Faced
by People With Disabilities in Accessing and Using SRH
Services
Irrespective of their background and function, policy actors
at both community and national levels reported similar
barriers regarding the access to and utilisation of SRH services
experienced by people with disabilities. Four types of barriers
were identified: physical, attitudinal, communication, and
structural (related to systems, policies, and norms). According
to respondents, the lack of accessible equipment and
infrastructure, such as toilets, was prevalent and prevented
people with disabilities, especially women, from having optimal
access to maternal and reproductive health services. Health
service providers were frank about the physical accessibility
gaps that they observed in their health facility, prompting
some of them to revisit their service delivery approach.
“Especially in our … maternity ward. You find that it is
very hard to deliver them. Sometimes, we prefer to deliver
them down on the floor. Sometimes, if you have the energy,
you, as the medical person, you have to lift her up on the
bed. She delivers. Again, you lift her down or you use a
trolley to push her … In case of an operation….We don’t
have the equipment for people with [physical] disabilities
like [involving] lower limbs. There is no way you can help
her… [For] most of them, we deliver them on the floor. The
delivery bed is made for normal people … .That is one of
the challenges we’re having” (Health service provider, FG4,
Gulu).
At the attitudinal level, participants reported that for many
health service providers in Uganda, people with disabilities
were perceived to be sexually inactive and incapable of
entertaining sexual activities or having children. This
common perception lead health staff to believe that people
with disabilities did not need to use any SRH services.
This ableist attitude could deny people with disabilities the
possibility of receiving SRH services like anyone else.
“[The] majority of them [health service providers]
do not think disabled people are clients for reproductive
health services … They imagine they might not need these
services … I just asked them a question and I said: ‘If I come
here with a wheelchair, rolling into your health centre, what
will you see?,’ they told me: ‘We see a wheelchair!’ ‘So, you
don’t see the person?!’ … I said ‘It’s just your work to check
whether the baby is lying there [she was pregnant at that
time], and not to look at my disability. It’s the leg that is
disabled … My womb is okay!’” (Government policy-maker
with a disability, Kampala).
According to representatives of DPOs, most of whom were
also people living with different impairments, the negative
and discriminatory attitudes of health service providers were
of concern. Often, these attitudes acted as deterrents among
people with disabilities to seek care for health conditions
that would necessitate medical attention. Moreover, DPO
representatives questioned the professional ethics of health
staff when they were providing SRH services.
“I don’t know whether that is part of their code of conduct,
but most of them are arrogant to clients at the hospital. This
is a big barrier because most of our persons with disabilities
would not want to go to [the] hospital where they are shouted
at. In most cases, our health service providers do not know
how to take care of [people with disabilities]. I think [that is] a
very big barrier in accessing sexual health [and] reproductive
services” (DPO representative, Gulu).
When further probed, most policy actors mentioned
the communication barriers which people with hearing
impairments faced. In Uganda, sign language is officially
recognised. According to the Disability Act, sign language
should be “introduced into the curriculum of medical
personnel.”
10
Interviewed health service providers reported
receiving no training in this regard during their professional
training or continued education opportunities. The inability of
health service providers to communicate health information
or instructions to people with hearing impairments led to
sub-optimal provision of SRH care. These situations could
be detrimental to people with disabilities and frustrating to
health service providers who needed to find alternatives to
understand the needs of people with hearing impairments.
“Last week, we received one [patient who was a] deaf
person. The problem was how to help? Because they use sign
language … but none of us has been trained … I was trying
to handle, doing signs … but I know [figured out] what she
wanted because she came with a paper for HIV test … But
when I wanted to talk to her, she cannot understand … I took
her to the [HIV] counsellor, [but] I don’t know how they
handled it” (Health service provider, FG6, Omoro).
At a structural level, one of the most important barriers
policy actors reported was the lack of disability data collection
and monitoring of service delivery. Although the Ministry of
Health included a specific column on disability (Yes/No) in
the patient registry book made available throughout health
facilities in the country, this information was seldom or
inconsistently collected. Most of health service providers did
not receive any training on how to obtain and use data on
disability nor did analyse the information collected when this
was done.
“We realised that we are not capturing our data well. And
if [it] is captured … we are not reporting … As you report
something, you should be able to analyse, and you put in
practice … At least, there should be a strategy where … even
in the district level, [and at] the facility [level], we should
be able to generate the number of people who are having
disability, so … it can help with planning. We don’t know
how many clients we have who are disabled” (Health service
provider, FG9, Omoro).
During the workshop, participants had the opportunity
to learn directly from people with disabilities who acted as
experts in their SRH care trajectory. The four people with
disabilities explained who they were in their community, what

Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–11961192
happened to them when seeking health services, and how
they were often mistreated by health service providers. They
also described the multiple barriers they faced. While sharing
their stories, they also made sure that health staff recognised
their strengths and resilience, beyond their impairments and
the limitations they were facing due to systemic obstacles,
at environmental, attitudinal, and communication levels.
According to workshop participants, this workshop helped
them to be more reflexive and enabled them to better
understand the situations of people with disabilities.
“I want to apologise. We have been working on people with
different disabilities, but we didn’t know what you people
were going through. I want you to forgive me and us, the
health workers … I would like to tell you that we shall see
that we change the quality of care because disability can
come to anyone, any time. So, I want you not to think that
you are different from us. We shall make a change, I promise”
(Workshop participant, health manager, Gulu).
Lingering Impacts of the Conflict on People With Disabilities’
Access to Services
For many respondents, the impacts of the conflict were
still vivid despite the end of the conflict through a signed
agreement between the Government and the Lord’s Resistance
Army rebels in 2006.
34
According to them, the armed
conflict contributed to “the breakdown of the formal system”
(International NGO representative, Kampala), and generated
widespread disabilities and trauma for Northern Ugandans.
It affected family structure, with persisting sequelae to date.
Others mentioned the high level of gender-based violence
which occurred during the conflict. Many young women and
girls became “child mothers,” after being raped “in the bush,” a
term referencing the period in rebel captivity (Health service
provider, FG3, Amuru). These situations were compounded
by limited access to SRH services: “Access to all health services
or reproductive health services for people with disabilities is
[was] not easily accessible. And it’s worst in Northern Uganda.
This is [was] due to war” (National NGO representative,
Kampala).
Policy actors believed that the impacts of the conflict
were “worse for people with disabilities” (International NGO
representative, Kampala), especially “women with disabilities
in the North [who] are still recovering from war” (Government
policy-maker, Kampala). In the context of insecurity due
to armed conflict, families, in some instances, had to save
their own lives amid the fighting, leaving their relatives with
disabilities behind: “So, if you’re disabled and you have all these
sorts of needs, and the family has to decide between running
away to safety and helping you to access a service?” (National
NGO representative, Kampala). Paradoxically, while the
conflict created different forms of hardship for people with
and without disabilities, camps that were erected to cater
for internally displaced Northern Ugandan populations also
became a source of support considered as “[one stop] shop
centre[s]” (Health service provider, FG9, Omoro) where all
services such as food, education, and healthcare were provided
for free, for all. However, as the conflict ceased, many NGOs
stopped providing their humanitarian services, and people,
including many with disabilities, had to fend for themselves
and survive without any support.
“But after that [the conflict], people were dispersed…
They are now coming from different places. [This situation
has] created distance from points of service delivery. If a
crippled person has to move for more than 10 km to seek for
healthcare, that has become very hard. I would say that this
is negative to them because it is not very easy for them now
to access services, as it used to [be in the camps]” (Health
service provider, FG9, Omoro).
Based on the accounts of a few policy actors, a life spent
in camps not only provided immediate benefits such as
accessible and free services but also generated long-term
social negative consequences. According to them, people lost
their social compass and became dependent upon external
sources to receive services. This situation might have created
other social consequences given the lack of accessible services
of proximity, including healthcare.
“The post-war effect in Northern Uganda has been there.
[There] is still [a] dependency syndrome. We had so many
NGOs which were supporting the household activities. Most
NGOs have gone away, so people have [feel] the effects now.
People resorted to drinking…. We have child-headed families
because of … loss of parents … loss of dear ones” (Heath
service provider, FG3, Amuru).
Multilevel Recommendations to Remove Barriers
At both community and national levels, policy actors
described in detail the multiple barriers people with
disabilities encountered when using health and SRH services.
On the other hand, policy actors also identified specific
recommendations to redress these barriers and better promote
the rights of people with disabilities as enshrined in adopted
policies and laws. Policy actors were reflective about their
shortcomings, but they also went beyond listing problems.
They felt the urgency to instill measures in their institution
and capitalise on the strengths of people with disabilities to
induce change.
“My recommendation goes to the Quality Assurance team
[of the hospital] … Concerning people with disabilities,
much has not yet been done. So, I would advise that we
get a committee that looks at the welfare of persons with
disabilities, to see that this kind of training should be
continuous. And disabled who are doing good things like
these ones [people with disabilities invited in the workshop as
experts] should be used as role models to the other disabled
persons” (Workshop participant, health service provider,
Gulu).
Given the intersectoral and multilayered nature of
barriers to access SRH services and policy and legislation
implementation challenges identified, policy actors
acknowledged that solutions did not lie at a single location, nor
could they be addressed by only one actor. Rather, respondents
recommended solutions targeting specific policy actors. At
the micro level, people with disabilities and their families
were named, highlighting the importance of empowerment
and the exercise of the basic rights of people with disabilities.
At the meso level, both health service providers and local
Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–1196
1193
CSOs were mentioned as playing a crucial role in concretely
removing barriers and in defending the rights of people
with disabilities they served. Respondents argued that at the
macro level, the Government and elected bodies held a prime
position of being held accountable and responsible for putting
in place actionable measures such as devoting financial
and technical resources to mainstream disability in service
delivery, including SRH services. The NCD was pinpointed as
pivotal in monitoring the Government’s policy and legislation
focusing on the promotion and protection of disability rights.
National and international CSOs identified the need for
more research and disability data collection and analysis for
improved planning of services for people with disabilities.
Table 2 summarises the main recommendations made by
policy actors at community and national levels during the
interviews, FGs, and participatory workshop, targeting the
three levels of actors at micro, meso, and macro levels.
Discussion
This paper emphasises the plurality of voices, the exploration of
both problems and solutions, and the triangulation of methods.
An important finding of this study is the convergence of views
collected from policy actors at community and national levels,
who identified multiple policy implementation challenges
and barriers to SRH service use experienced by disabled
users. From the study findings, we highlight learnings which
emerged from our approach of using both an intersectional
analysis and a participatory workshop to validate and
enrich study findings. Study respondents referred to the
principles of intersectionality related to knowledge, power,
multilevel analysis, and the importance of context, equity, and
reflexivity. Specifically, we address the following three points
of discussion: (1) how diverse sources of knowledge and the
reflexivity of policy actors can lead to new insight about their
privileges and the discrimination and barriers faced by people
with disabilities; (2) the importance of the post-conflict
context in understanding policy implementation challenges
and the experiences of barriers to access among people with
disabilities; and (3) the capacity of policy actors to propose
transformative solutions to redress health inequities faced by
people with disabilities.
First, through an intersectionality-informed analysis,
we were able to analyse the different voices of different
groups of policy actors. The study methodology capitalised
on their distinctive social positions to shed light on their
understanding of the relationships among legislation, policy
and its implementation, and the use of SRH services by people
with disabilities. Their views corroborated the perceptions
of people with disabilities reported previously.
17
People
with disabilities experienced multiple physical, attitudinal,
Table 2. Main Areas of Recommendations Proposed for and by Policy Actors to Improve the Access to and Utilisation of SRH Services by People With Disabilities
Levels Recommendations
At micro level
“Awareness-raising is needed at all
levels from family, health staff to policy-makers”
“Using people with disabilities
themselves, train them. Use them to target their membership, that would be key”
At meso level
“The
delivery beds... When I went to the Midwifery Day in Fort Portal, Karamoja district, they came with a bed that I have
never seen… those are the beds [for] the use for people with disabilities… They [policy-makers] could come to the
hospital, [and] find out if there are people who are interested in learning sign language… We wait for these things to be
integrated into our curriculums”
“… to create a network of people working in the
area of disability so that we can have a unified voice to address the issues, not only health issues but other social issues
that affect people with disabilities”
At macro level
“The Government needs to [have a] committee in action on the
implementation of the existing laws. The Government must ensure that the accessibility must be universal… to all…
They should widen their scope of consultations when they are coming up with their policies and guidelines… so that you
can be in position to intersect, and also ensure that the needs of all the categories of people, whom you have consulted,
are taken care of”
“One priority is to mainstream disability at all levels of MCH
[maternal and child health] and SRH, in all levels, but don’t separate people with disabilities. It should be integrated,
data collected, and with a budget!”
[There are] too many small disability organisations, and poorly coordinated. The
NCD is not strong because too small…. Competition disadvantages, this decreases their bargaining power… If they are
together at the same time, they have more power to ask for change. So, they need to be strong and give a united voice
from all categories of people with disabilities for advocacy and lobbying”
“The role of research… is to make sure you collect the
appropriate and relevant data [which can] inform the service institutions so that they create the demand of services for
[people with] disabilities”

Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–11961194
communication, and structural barriers. In particular, the
sister study to this paper identified inequitable access to
SRH services in health facilities and numerous intersectional
discriminations related to gender, disability, and experience
of violence.
17
These barriers faced by people with disabilities
have been discussed in the literature regarding Uganda,
15,16,35
other sub-Saharan African countries,
36-39
and globally.
40
Furthermore, the interviewed policy actors were reflexive
about their privilege, and the effects of oppression created by
their inconsideration of the needs of people with disabilities.
They recognised the effects that these internalised biases had
on the experiences of access to and use of SRH services by
users with disabilities.
41,42
According to the IBPA principles,
acknowledging the diverse sources of knowledge and
highlighting the reflexivity of policy actors enable them
to reflect upon the power and privilege they own.
42
This
realisation is a further step toward health equity and acts as a
catalyst toward social justice.
42
Second, the post-conflict context in Northern Uganda
was considered in our analysis. Our findings showed that
time spent in the camps during and after the armed conflict
and the post-conflict period has heavily affected Ugandans.
The post-conflict continues to disadvantage people with
disabilities in the Northern region, up to the current day.
In an intersectionality approach, time and space (context)
are key components in analysis.
42,43
Literature has reported
that the armed conflict in Uganda has caused limited access
to and poor quality of maternal and reproductive health
services,
14
while sexual and gender-based violence aggravated
the physical and psychological health of women.
12
According
to a systematic review on the long-term effects of armed
conflicts, such as in Uganda, findings reported two types of
effects, direct and indirect. Direct long-term effects included
the experience of violence of all forms, disability, illnesses,
injuries, and torture. The indirect long-term effects were
characterised by limited access to healthcare and education as
well as social marginalisation.
44
Specifically, a study conducted
among people with disabilities in the Gulu region reported
the negative effect the conflict had on the psychological and
emotional health of people with disabilities who shared their
traumatic experiences and difficult coping strategies.
45
These
findings also reported difficulties in accessing healthcare
services, including rehabilitation, such as assistive devices,
and mental health services.
45
Literature further mentioned
that people with disabilities, especially women, faced
discrimination and lacked access to health facilities upon
return home, coupled with economic challenges.
46
Third, policy actors identified recommendations
to the numerous barriers to SRH service utilisation
experienced by people with disabilities, disability-focused
policy implementation challenges, and multipronged
recommendations addressed to policy actors at micro, meso,
and macro levels. In an intersectionality-informed analysis,
exploring alternatives and solutions is as important as
identifying problems which need to be addressed.
20
Reflecting
upon and consciously proposing solutions is integral to a
transformative process and contributes to eventually reaching
equity and social justice. For example, the recommendation
made by policy actors to allocate more budget on disability
issues and to reinforce the position of the NCD found an
echo in the revised 2019 Disability Act.
11
Whereas the 2006
Disability Act did not include the scope of the NCD, the 2019
iteration of the Act specified its roles and funds, in addition
to making the provision for representatives of the Council to
work at the district level to enhance the presentation of people
with disabilities in the community. Through the participatory
workshop, health service providers and managers discovered
the strengths of people with disabilities and that they could
be experts in helping them devise health services to be more
accessible and act as role models for others. While policy
actors used to consider people with disabilities as weak and
not capable, Intersectionality enabled them to acknowledge
the multiple social categories a person/group may have,
recognising that they may be simultaneously privileged in one
context and be disadvantaged in another one.
42
Limitations
Given the richness of information elicited from different
groups of policy actors, we were not able to report them all in
a single manuscript. Comprehensive description and analyses
from people with disabilities at individual level have been
reported elsewhere,
17
and the perceptions of policy actors
at meso and macro levels are reported separately here. The
contrasting of convergent or divergent views of policy actors
will subsequently be discussed more in detail. We also did not
include the views of policy actors located in other Northern
districts which have been affected by the armed conflict. This
inclusion may have expanded the depth of data collected
and the richness of description to analyse. With more time
and resources, this expansion would be possible. Given the
convergence of problems and recommendations reported
by study respondents, social desirability could have been a
bias. However, respondents were clear about the observed
multiple barriers faced by people with disabilities and the
policy implementation challenges. They demonstrated the
readiness to address these issues, collectively. Finally, to
reduce the limitations of translation when it was used, we
elaborated a glossary of research and SRH terms in English
and Luo for consistency. Both research assistants were present
during all interviews to support one another for translation
when needed. At the end of each day of interviews, the
research team met and debriefed about the interview process,
including translation, for improvement purposes.
Conclusion
This study reveals the multilayered perceptions of policy actors
at meso and macro levels of the relationships among pro-
disability policy and legislation and the use of SRH services
by people with disabilities in three post-conflict Northern
districts of Uganda. The study findings intersect with and
complement the perceptions and recommendations provided
by people with disabilities at micro level. An intersectionality-
informed analysis emphasised the importance of going beyond
the identification of problems by concomitantly searching for
solutions. With the recent adoption of the revised Disability
Act in 2019, Uganda has renewed its commitment to remove

Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–1196
1195
barriers structurally and better protect the rights of people
with disabilities. This creates a normative space for actions
such as those recommended by the participants in our study.
Concrete recommendations included empowering people
with disabilities, families, and their organisations through
awareness-creation and capacity-building, at micro level. At
meso level, policy actors recommended training of health
service providers on disability-sensitive services such as sign
language, improving physical, attitudinal, and communication
accessibility in health facilities, and collecting and analysing
data on disability more systematically. At macro level, more
accountability of policy-makers, active monitoring, and
enforcing of policy implementation with disability budgeting
were identified. The proposed solutions targeting three
levels of policy actors, vertically, and various types of groups,
horizontally, are within the reach and capacity of Government
policy-makers, CSOs’ managers, health decision-makers,
DPO leaders, and people with disabilities. As suggested by
the UN report on the Sustainable Development Goals for
people with disabilities,
5
the recommendations can constitute
the foundation for a hands-on road map to health equity
by removing multiple barriers to access to and use of SRH
services by people with disabilities, irrespective of their
geographic location in Uganda.
Acknowledgements
We thank the study research assistants, Bryan Eryong and
Emma Ajok, and all study participants and stakeholders.
We are grateful to the St-Mary’s Hospital Lacor for its
collaboration during fieldwork.
Ethical issues
This study received ethics approval from the Centre de recherche du Centre
hospitalier de l’Université de Montréal (CR-CHUM) (17.127-CÉR, 1 August
2017); the Research Ethics Committee in Sciences and Health of the Université
de Montréal (CERCES-20-074-D, 13 May 2020), following a change of research
affiliation in Canada; the Lacor Hospital Institutional and Research Ethics
Committee (LHIREC - 019/07/2017); and the Uganda National Council for
Science and Technology (SS-4451, 14 November 2017).
Competing interests
Authors declare that they have no competing interests.
Authors’ contributions
MMS conceptualised the manuscript and collected and analysed the data. All
authors contributed to, reviewed, read, and approved the final manuscript.
Funding
The authors thank the MoCHeLaSS (Mother Child health Lacor-South Sudan)/
IDRC/IMCHA Project for its support. The MoCHeLaSS Project was carried out
with the aid of a grant from the Innovating for Maternal and Child Health in Africa
initiative- a partnership of Global Affairs Canada (GAC), the Canadian Institutes
of Health Research (CIHR) and Canada’s International Development Research
Centre (IDRC). MMS received a doctoral training scholarship from the Fonds
de Recherche du Québec – Santé [0000256736] and a doctoral award from
the International Development Research Centre: [Grant Number 108544-010].
The funding sources had no role in the study design, data collection, analysis,
and interpretation, or writing and preparation of the manuscript, or decision to
publish.
Authors’ affiliations
1
Social and Preventive Medicine Department, School of Public Health,
Université de Montréal, Montreal, QC, Canada.
2
Centre de recherche en
santé publique (CReSP), Université de Montréal et CIUSSS du Centre-Sud-
de-l’Île-de-Montréal, Montreal, QC, Canada.
3
Public Health Department, St-
Mary’s Hospital, Lacor, Uganda.
4
Institutional Direction Department, St-Mary’s
Hospital, Lacor, Uganda.
5
School of Public Health, University of Western Cape,
Bellville, South Africa.
References
1. UN. Convention on the Rights of Persons with Disabilities. https://
treaties.un.org/Pages/ViewDetails.aspx?src=TREATY&mtdsg_no=IV-
15&chapter=4&clang=_en. Accessed July 11, 2020. Published 2020.
2. Kanter AS. The promise and challenge of the United Nations Convention
on the Rights of Persons with Disabilities. Syracuse Journal of International
Law and Commerce. 2006;34:287-321.
3. United Nations. Convention on the Rights of Persons with Disabilities
(CRPD). United Nations; 2006. https://www.un.org/development/
desa/disabilities/convention-on-the-rights-of-persons-with-disabilities/
convention-on-the-rights-of-persons-with-disabilities-2.html. Accessed
July 13, 2020.
4. World Health Organization (WHO), The World Bank. World Report on
Disability. Malta: WHO; 2011.
5. United Nations Department of Economic and Social Affairs (DESA).
Disability and Development Report: Realizing the Sustainable
Development Goals By, for and with Persons with Disabilities 2018. New
York: DESA; 2019.
6. Millward H, Ojwang VP, Carter JA, Hartley S. International guidelines and
the inclusion of disabled people. The Ugandan story. Disabil Soc. 2005;
20(2):153-167. doi:10.1080/09687590500059101
7. Lang R, Murangira A. Disability Scoping Study: Commissioned by DFID
Uganda. Kampala, Uganda: Department for Internal Development; 2009.
8. Uganda Bureau of Statistics (UBOS), ICF. Uganda Demographic Health
Survey 2016. Kampala, Uganda: UBOS, ICF; 2018.
9. Yokoyama A. A comparative analysis of institutional capacities for
implementing disability policies in East African countries: functions of
National Councils for Disability. Disability, CBR & Inclusive Development.
2012;23(2):22-40. doi:10.5463/dcid.v23i2.106
10. Republic of Uganda. Persons with Disabilities Act. Republic of Uganda;
2006.
11. The Republic of Uganda Parliament. The Persons with Disabilities Act,
20192019:46.
12. Liebling-Kalifani H, Ojiambo-Ochieng R, Marshall A, Were-Oguttu J,
Musisi S, Kinyanda E. Violence against women in Northern Uganda:
the neglected health consequences of war. J Int Womens Stud.
2008;9(3):174-192.
13. Roberts B, Odong VN, Browne J, Ocaka KF, Geissler W, Sondorp E. An
exploration of social determinants of health amongst internally displaced
persons in northern Uganda. Confl Health. 2009;3:10. doi:10.1186/1752-
1505-3-10
14. Chi PC, Bulage P, Urdal H, Sundby J. Perceptions of the effects of armed
conflict on maternal and reproductive health services and outcomes in
Burundi and Northern Uganda: a qualitative study. BMC Int Health Hum
Rights. 2015;15:7. doi:10.1186/s12914-015-0045-z
15. Ahumuza SE, Matovu JK, Ddamulira JB, Muhanguzi FK. Challenges
in accessing sexual and reproductive health services by people with
physical disabilities in Kampala, Uganda. Reprod Health. 2014;11:59.
doi:10.1186/1742-4755-11-59
16. Apolot RR, Ekirapa E, Waldman L, et al. Maternal and newborn health
needs for women with walking disabilities; “the twists and turns”: a case
study in Kibuku District Uganda. Int J Equity Health. 2019;18(1):43.
doi:10.1186/s12939-019-0947-9
17. Mac-Seing M, Zinszer K, Eryong B, Ajok E, Ferlatte O, Zarowsky C. The
intersectional jeopardy of disability, gender and sexual and reproductive
health: experiences and recommendations of women and men with
disabilities in Northern Uganda. Sex Reprod Health Matters. 2020;
28(2):1772654. doi:10.1080/26410397.2020.1772654
18. Starrs AM, Ezeh AC, Barker G, et al. Accelerate progress-sexual and
reproductive health and rights for all: report of the Guttmacher-Lancet
Commission. Lancet. 2018;391(10140):2642-2692. doi:10.1016/s0140-
6736(18)30293-9
19. Frohmader C, Ortoleva S. The Sexual and Reproductive Rights of
Women and Girls with Disabilities. Paper presented at: ICPD International
Conference on Population and Development Beyond; 2014.
20. Hankivsky O, Grace D, Hunting G, et al. An intersectionality-based policy
analysis framework: critical reflections on a methodology for advancing
equity. Int J Equity Health. 2014;13:119. doi:10.1186/s12939-014-0119-x

Mac-Seing et al
International Journal of Health Policy and Management, 2022, 11(7), 1187–11961196
21. Collins PH, Bilge S. Intersectionality. Cambridge, UK: Polity; 2016.
22. Hankivsky O. An Intersectionality-Based Policy Analysis Framework.
Vancouver, BC: Institute for Intersectionality Research and Policy, Simon
Fraser University; 2012.
23. Mitchell D Jr. Intersectionality & Higher Education. New York, NY: Peter
Lang; 2014.
24. Carbado DW, Crenshaw KW, Mays VM, Tomlinson B. Intersectionality:
mapping the movements of a theory. Du Bois Rev. 2013;10(2):303-312.
doi:10.1017/s1742058x13000349
25. Cho S, Crenshaw KW, McCall L. Toward a field of intersectionality
studies: theory, applications, and praxis. Signs. 2013;38(4):785-810.
doi:10.1086/669608
26. Chun JJ, Lipsitz G, Shin Y. Intersectionality as a social movement
strategy: Asian immigrant women advocates. Signs. 2013;38(4):917-940.
doi:10.1086/669575
27. Erevelles N, Minear A. Unspeakable offenses: untangling race and
disability in discourses of intersectionality. J Lit Cult Disabil Stud. 2010;
4(2):127-145. doi:10.3828/jlcds.2010.11
28. Combahee River Collective. The Combahee River Collective Statement.
Combahee River Collective; 1977.
29. Crenshaw K. Demarginalizing the intersection of race and sex: a black
feminist critique of antidiscrimination doctrine, feminist theory and
antiracist politics. Univ Chic Leg Forum. 1989;140(1):139-167.
30. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative
research (COREQ): a 32-item checklist for interviews and focus groups.
Int J Qual Health Care. 2007;19(6):349-357. doi:10.1093/intqhc/mzm042
31. Marshall MN. Sampling for qualitative research. Fam Pract. 1996;
13(6):522-525. doi:10.1093/fampra/13.6.522
32. Marshall C, Rossman GB. Designing Qualitative Research. SAGE
Publications; 2016.
33. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis:
striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;
16(1):1609406917733847. doi:10.1177/1609406917733847
34. Advisory Consortium on Conflict Sensitivity (ACCS). Northern Uganda
Conflict Analysis. ACCS; 2013.
35. Nampewo Z. Young women with disabilities and access to HIV/AIDS
interventions in Uganda. Reprod Health Matters. 2017;25(50):121-127.
doi:10.1080/09688080.2017.1333895
36. Casebolt MT. Barriers to reproductive health services for women with
disability in low- and middle-income countries: a review of the literature.
Sex Reprod Healthc. 2020;24:100485. doi:10.1016/j.srhc.2020.100485
37. Mac-Seing M, Zarowsky C. Une méta-synthèse sur le genre, le handicap
et la santé reproductive en Afrique subsaharienne. Sante Publique.
2017;29(6):909-919. doi:10.3917/spub.176.0909
38. Trani JF, Browne J, Kett M, et al. Access to health care, reproductive
health and disability: a large scale survey in Sierra Leone. Soc Sci Med.
2011;73(10):1477-1489. doi:10.1016/j.socscimed.2011.08.040
39. Hanass-Hancock J. Disability and HIV/AIDS - a systematic review of
literature on Africa. J Int AIDS Soc. 2009;12:34. doi:10.1186/1758-2652-
12-34
40. Groce N. HIV/AIDS and Disability: Capturing Hidden Voices: Global
Survey on HIV/AIDS and Disability. New Haven: Global Health Division,
Yale School of Public Health, Yale University; 2004.
41. Nixon SA. The coin model of privilege and critical allyship: implications for
health. BMC Public Health. 2019;19(1):1637. doi:10.1186/s12889-019-
7884-9
42. Hankivsky O. Intersectionality 101. http://vawforum-cwr.ca/sites/default/
files/attachments/intersectionallity_101.pdf. Accessed October 4, 2020.
Published 2014.
43. Hulko W. The time- and context-contingent nature of intersectionality and
interlocking oppressions. Affilia. 2009;24(1):44-55.
44. Kadir A, Shenoda S, Goldhagen J. Effects of armed conflict on child health
and development: a systematic review. PLoS One. 2019;14(1):e0210071.
doi:10.1371/journal.pone.0210071
45. Mulumba M, Nantaba J, Brolan CE, Ruano AL, Brooker K, Hammonds
R. Perceptions and experiences of access to public healthcare by
people with disabilities and older people in Uganda. Int J Equity Health.
2014;13:76. doi:10.1186/s12939-014-0076-4
46. Hollander T, Gill B. Every day the war continues in my body: examining
the marked body in postconflict Northern Uganda. Int J Transit Justice.
2014;8(2):217-234. doi:10.1093/ijtj/iju007
