
Recommendations and Reports / Vol. 68 / No. 4 December 13, 2019
Use of Anthrax Vaccine in the United States:
Recommendations of the Advisory Committee
on Immunization Practices, 2019
U.S. Department of Health and Human Services
Centers for Disease Control and Prevention
Morbidity and Mortality Weekly Report

Recommendations and Reports
CDC Adoption of ACIP Recommendations for MMWR
Recommendations and Reports, MMWR Policy Notes, and
Immunization Schedules (Child/Adolescent, Adult):
Recommendations for routine use of vaccines in children,
adolescents, and adults are developed by the Advisory
Committee on Immunization Practices (ACIP). ACIP is
chartered as a federal advisory committee to provide expert
external advice and guidance to the Director of CDC on
use of vaccines and related agents for the control of vaccine-
preventable diseases in the civilian population of the United
States. Recommendations for routine use of vaccines in
children and adolescents are harmonized to the greatest
extent possible with recommendations made by the American
Academy of Pediatrics (AAP), the American Academy of Family
Physicians (AAFP), and the American College of Obstetricians
and Gynecologists (ACOG). Recommendations for routine use
of vaccines in adults are harmonized with recommendations
of AAFP, ACOG, and the American College of Physicians
(ACP). ACIP recommendations approved by the CDC
Director become agency guidelines on the date published in the
Morbidity and Mortality Weekly Report (MMWR). Additional
information is available at https://www.cdc.gov/vaccines/acip.
The MMWR series of publications is published by the Center for Surveillance, Epidemiology, and Laboratory Services, Centers for Disease Control and Prevention (CDC),
U.S. Department of Health and Human Services, Atlanta, GA 30329-4027.
Suggested citation: [Author names; first three, then et al., if more than six.] [Title]. MMWR Recomm Rep 2019;68(No. RR-#):[inclusive page numbers].
Centers for Disease Control and Prevention
Robert R. Redfield, MD, Director
Anne Schuchat, MD, Principal Deputy Director
Chesley L. Richards, MD, MPH, Deputy Director for Public Health Science and Surveillance
Rebecca Bunnell, PhD, MEd, Director, Office of Science
Barbara Ellis, PhD, MS, Acting Director, Office of Science Quality, Office of Science
Michael F. Iademarco, MD, MPH, Director, Center for Surveillance, Epidemiology, and Laboratory Services
MMWR Editorial and Production Staff (Serials)
Charlotte K. Kent, PhD, MPH, Editor in Chief
Christine G. Casey, MD, Editor
Mary Dott, MD, MPH, Online Editor
Terisa F. Rutledge, Managing Editor
David C. Johnson, Lead Technical Writer-Editor
Catherine B. Lansdowne, MS, Project Editor
Martha F. Boyd, Lead Visual Information Specialist
Maureen A. Leahy, Julia C. Martinroe,
Stephen R. Spriggs, Tong Yang,
Visual Information Specialists
Quang M. Doan, MBA, Phyllis H. King,
Terraye M. Starr, Moua Yang,
Information Technology Specialists
MMWR Editorial Board
Timothy F. Jones, MD, Chairman
Ileana Arias, PhD
Matthew L. Boulton, MD, MPH
Jay C. Butler, MD
Virginia A. Caine, MD
Katherine Lyon Daniel, PhD
Jonathan E. Fielding, MD, MPH, MBA
David W. Fleming, MD
William E. Halperin, MD, DrPH, MPH
Jewel Mullen, MD, MPH, MPA
Jeff Niederdeppe, PhD
Patricia Quinlisk, MD, MPH
Stephen C. Redd, MD
Patrick L. Remington, MD, MPH
Carlos Roig, MS, MA
William Schaffner, MD
Morgan Bobb Swanson, BS
CONTENTS
Introduction ............................................................................................................1
Methods
....................................................................................................................2
Risk for Exposure to Anthrax
.............................................................................3
Summary of Key Findings...................................................................................3
Recommendations for Prevention of Anthrax Among Persons with
Potential Risk for Exposure: PrEP
................................................................... 7
Recommendations for Prevention of Anthrax Among Persons with
Suspected or Known Exposure: PEP
...........................................................8
Vaccine Adverse Events Reporting and Additional Information
....... 10
Future Directions
................................................................................................ 10
References
............................................................................................................ 11

Recommendations and Reports
MMWR / December 13, 2019 / Vol. 68 / No. 4 1
US Department of Health and Human Services/Centers for Disease Control and Prevention
Use of Anthrax Vaccine in the United States: Recommendations of the
Advisory Committee on Immunization Practices, 2019
William A. Bower, MD
1
; Jarad Schiffer, MS
2
; Robert L. Atmar, MD
3
; Wendy A. Keitel, MD
4
; Arthur M. Friedlander, MD
5
; Lindy Liu, MPH
1
;
Yon Yu, PharmD
6
; David S. Stephens, MD
7
; Conrad P. Quinn, PhD
8
; Katherine Hendricks, MD
1
1
Division of High-Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Diseases, CDC;
2
Division of Bacterial Diseases,
National Center for Immunization and Respiratory Diseases, CDC;
3
Department of Medicine, Baylor College of Medicine, Houston, Texas;
4
Department of
Molecular Virology & Microbiology and Department of Medicine, Baylor College of Medicine, Houston, Texas;
5
U.S. Army Medical Research Institute of Infectious
Diseases, Frederick, Maryland;
6
Division of Preparedness and Emerging Infections, National Center for Emerging and Zoonotic Infectious Diseases, CDC;
7
Department of Medicine, Emory University, Atlanta, Georgia;
8
Office of Laboratory Science, CDC
Summary
This report updates the 2009 recommendations from the CDC Advisory Committee on Immunization Practices (ACIP) regarding
use of anthrax vaccine in the United States (Wright JG, Quinn CP, Shadomy S, Messonnier N. Use of anthrax vaccine in the
United States: recommendations of the Advisory Committee on Immunization Practices [ACIP)], 2009. MMWR Recomm
Rep 2010;59[No. RR-6]). The report 1) summarizes data on estimated efficacy in humans using a correlates of protection model
and safety data published since the last ACIP review, 2) provides updated guidance for use of anthrax vaccine adsorbed (AVA) for
preexposure prophylaxis (PrEP) and in conjunction with antimicrobials for postexposure prophylaxis (PEP), 3) provides updated
guidance regarding PrEP vaccination of emergency and other responders, 4) summarizes the available data on an investigational
anthrax vaccine (AV7909), and 5) discusses the use of anthrax antitoxins for PEP.
Changes from previous guidance in this report include the following: 1) a booster dose of AVA for PrEP can be given every
3 years instead of annually to persons not at high risk for exposure to Bacillus anthracis who have previously received the initial
AVA 3-dose priming and 2-dose booster series and want to maintain protection; 2) during a large-scale emergency response, AVA
for PEP can be administered using an intramuscular route if the subcutaneous route of administration poses significant materiel,
personnel, or clinical challenges that might delay or preclude vaccination; 3) recommendations on dose-sparing AVA PEP regimens
if the anthrax vaccine supply is insufficient to vaccinate all potentially exposed persons; and 4) clarification on the duration of
antimicrobial therapy when used in conjunction with vaccine for PEP.
These updated recommendations can be used by health care providers and guide emergency preparedness officials and planners
who are developing plans to provide anthrax vaccine, including preparations for a wide-area aerosol release of B. anthracis spores.
The recommendations also provide guidance on dose-sparing options, if needed, to extend the supply of vaccine to increase the
number of persons receiving PEP in a mass casualty event.
Introduction
Anthrax is an acute febrile illness caused by infection with
Bacillus anthracis. The mortality rate, even with treatment,
ranges from <2% for cutaneous anthrax (1) to 45% for
inhalation anthrax (2) and 92% for anthrax meningitis (3).
B. anthracis is a zoonotic pathogen that primarily infects sheep,
goats, cattle, and other herbivores. Humans become infected
after exposure to infected animals or contaminated animal
products or, rarely, as a complication from injection drug use
(4). B. anthracis is also a tier 1 select agent and is considered one
of the bioterrorism agents that is most likely to be used because
it is relatively easy to acquire from the natural environment,
mass produce, and disseminate as spores via aerosolization (5).
Anthrax vaccine adsorbed (AVA) (BioThrax) is licensed for
preexposure prophylaxis (PrEP) for adults aged 18–65 years
at high risk for exposure to B. anthracis (6). The dosage
approved by the U.S. Food and Drug Administration (FDA)
is 0.5 mL administered intramuscularly (IM) at 0, 1, and
6 months with boosters at 6 and 12 months after completion
of the primary series and at 12-month intervals thereafter.
AVA also is licensed for postexposure prophylaxis (PEP) in
combination with antimicrobials for adults aged 18–65 years
with suspected or known exposure to aerosolized B. anthracis
spores. The dosage approved by FDA is 0.5 mL administered
subcutaneously (SC) at 0, 2, and 4 weeks. For persons not
included in the FDA-approved indication for PEP, AVA
will be available for PEP use for children, pregnant women,
nursing mothers and older adults (i.e., ≥66 years) under
Corresponding author: William A. Bower, Division of High-
Consequence Pathogens and Pathology, National Center for Emerging
and Zoonotic Infectious Diseases, CDC. Telephone: 404-639-0376;
E-mail: [email protected]v.
Recommendations and Reports
2 MMWR / December 13, 2019 / Vol. 68 / No. 4
US Department of Health and Human Services/Centers for Disease Control and Prevention
appropriate emergency use regulatory provisions. Although
data are lacking on the immune impact of mixing the IM and
SC routes of administration, as might occur when switching
from PrEP to PEP, switching between routes would be
unlikely to adversely impact immunity because both routes
provide adequate immunity.
AV7909 (AVA plus CpG 7909 adjuvant) is a second-
generation anthrax vaccine produced by Emergent BioSolutions
that is in a phase 3 trial (https://clinicaltrials.gov). The
CpG 7909 adjuvant binds to the Toll-like receptor 9 to enhance
the immune response to coadministered antigens (primarily
B. anthracis protective antigen) (7,8). The PEP schedule,
under clinical evaluation for AV7909, is 0.5 mL AVA with
0.25 mg CpG 7909 adjuvant administered IM at 0 and 2 weeks
postexposure, combined with antimicrobials.
Since the publication in 2010 of the Advisory Committee on
Immunization Practices (ACIP) recommendations for use of
anthrax vaccine in the United States (9), published studies have
1) addressed the efficacy, immunogenicity, and reactogenicity
of the recommended and alternate dose-sparing schedules of
AVA; 2) estimated AVA efficacy in humans from data on animal
efficacy and human antibody levels by using a correlates of
protection model; and 3) evaluated whether developing chronic
illnesses or having adverse pregnancy outcomes are associated
with previous AVA receipt. In addition, AV7909 phase 1 and 2
clinical trials have demonstrated the potential of AV7909 for
use as the vaccine component of PEP (PEP-Vx) (10–12).
Given these newly available data, CDC asked ACIP to
revise the recommendations for use of anthrax vaccines in
the United States. These revised recommendations address
the IM versus SC administration of AVA for PEP and the use
of reduced-schedule and half-dose AVA during public health
emergencies, shortening the duration of antimicrobials given
in conjunction with PEP-Vx, and extending the AVA PrEP
booster dose interval after the initial priming and booster
series. This report provides recommendations and guidance
regarding the use of AVA for PrEP and PEP and updates the
ACIP anthrax vaccination recommendations published in
2002 and 2010. This report also describes available data for
AV7909 because of its potential for prelicensure emergency
use during a large-scale anthrax public health emergency
if the AVA supply is inadequate. This report can be used
by health care providers to update the current practice for
providing anthrax vaccine for PrEP and PEP and can be used
by emergency preparedness partners to develop emergency
vaccine response plans in preparation for a wide-area
aerosolized release of B. anthracis spores.
Methods
During March 2017–January 2019, the ACIP Anthrax
Vaccines Work Group (AVWG), which comprises professionals
from academic medicine (internal medicine, pediatrics,
obstetrics, and infectious disease specialists), federal and state
public health entities, and medical societies, participated in
monthly telephone conferences facilitated by CDC. During
these meetings, AVWG reviewed relevant scientific evidence
and evaluated the quality of the evidence assessing the
1) immunogenicity and safety of an extended booster dose
interval for PrEP in persons not at high risk for exposure
to B. anthracis but who might have a future high risk for
exposure; 2) benefits and harms of the IM versus SC route
of administration for PEP-Vx; 3) benefits and harms of AVA
dose-sparing schedules (i.e., 2 full doses or 3 half doses) for
PEP-Vx if vaccination demands were to exceed vaccine supply
after a wide-area aerosolized release of B. anthracis spores;
4) immunogenicity and safety of AV7909, based on available
data; and 5) use of anthrax antitoxin for PEP in conjunction
with anthrax vaccine.
A scientific literature search was conducted through a
systematic review for studies involving human subjects or for
animal studies that met criteria for the Animal Rule (13,14)
that reported primary data on important health outcomes
related to AVA or AV7909 published after 2008. The previous
ACIP review summarized the data through 2008 (9). Databases
searched in February 2017 included Medline (OVID), Embase
(OVID), CAB Abstracts (OVID), Global Health (OVID),
CINAHL (Ebsco), Econlit (Ebsco), Cochrane Library, Clinical
Trials.gov, FedRip (Ebsco), the U.S. Department of Defense
(DoD) Technical Information Center, NTIS:NTRL, Scopus,
WHOLIS, and WorldCat. Search terms included anthrax
vaccine, AVA, Biothrax, Nuthrax, AV7909, CpG DNA,
CpG 7909, CpG motifs, CpG oligodeoxynucleotide, Anthim,
Anthrasil, obiltoxaximab, and raxibacumab. In addition, the
work group reviewed unpublished data from the CDC Anthrax
Vaccine Research Program, unpublished data from the vaccine
manufacturer, and results of studies from the Vaccine Analytic
Unit, which is a CDC-led collaboration with DoD and FDA
that assessed potential associations of AVA with development
of chronic conditions (15). The review of vaccine safety also
included adverse events reported to the Vaccine Adverse Event
Reporting System (VAERS) after AVA administration for
January 1, 2009, through June 30, 2017 (16). To qualify as a
candidate for inclusion in the review, a study had to present
immunogenicity or safety data on AVA, AV7909, or infectious
disease vaccines that used CpG 7909 adjuvant. Studies were
excluded if they lacked mention of either AVA or AV7909 for
Recommendations and Reports
MMWR / December 13, 2019 / Vol. 68 / No. 4 3
US Department of Health and Human Services/Centers for Disease Control and Prevention
the prevention of anthrax, lacked primary data, or were outside
the time frame of interest.
Data were abstracted and summarized for immunogenicity
outcomes of interest, including seroconversion, geometric
mean concentration (GMC) of anti-protective antigen
immunoglobulin G (anti-PA IgG, determined by enzyme-
linked immunosorbent assay), geometric mean titer (GMT) of
toxin neutralization activity (TNA), effective dose 50 (ED
50
)
levels, and GMT of TNA neutralization factor 50 (NF
50
)
levels. Data also were abstracted and summarized for safety
outcomes of interest, including injection site adverse events,
systemic adverse events, and serious adverse events. Quality of
evidence was evaluated and presented in tabular format using
the Grading of Recommendations Assessment, Development
and Evaluation (GRADE) approach (17).
Evidence that had been summarized for and reviewed
by AVWG was publicly presented at the ACIP meetings
in June 2017, October 2017, February 2018, June 2018,
October 2018, and February 2019 (18). After a public
comment period, ACIP voting members at the June 2018
and February 2019 meetings unanimously approved the
proposed recommendations.
Risk for Exposure to Anthrax
The risk for exposure to aerosolized B. anthracis spores in
the United States is very low (19). Anthrax is only endemic
in a few sparsely populated areas in the western United States
(20). Certain occupations and other activities place persons at
higher risk for exposure (21). These include laboratory work
that involves bioproduction of large quantities, volumes, or
high concentrations of B. anthracis spores and activities with
a high potential for exposure to aerosolized B. anthracis spores,
such as military deployment to areas designated by DoD as
posing a high risk for anthrax exposure and emergency response
activities after release of B. anthracis spores (9).
The possibility exists of an intentional wide-area aerosolized
release of B. anthracis spores over a densely populated area in the
United States. In 2001, letters containing B. anthracis spores
sent through the U.S. Postal Service led to 22 cases of anthrax,
five of which were fatal (22). In addition, certain countries and
terrorist groups have explored the use of anthrax as a bioweapon
(23–25). An aerosolized release of B. anthracis spores over
densely populated areas could become a mass-casualty incident
(26). However, previously developed, publicly available
clinical recommendations only addressed clinical management
using conventional standards of care (27). To prepare for the
possibility of an anthrax mass-casualty incident, when the
number of patients is likely to exceed the ability of the health
care infrastructure to provide conventional standards of care
and supplies might not meet demand, the U.S. government
has stockpiled equipment and therapeutics (i.e., medical
countermeasures) for anthrax prevention and treatment
and provided recommendations for their use (28). The U.S.
government’s Strategic National Stockpile stores anthrax
vaccine to be used with antimicrobials for PEP of persons with
known or potential exposure to B. anthracis spores, as well
as therapeutics and supplies for anthrax treatment. Animal
models have shown that although 5–30 days of antimicrobials
might be insufficient to prevent anthrax after single exposures
or reexposures to B. anthracis spores, the addition of vaccine
substantially enhances efficacy (29–31). In the event of a
large-scale release of B. anthracis spores, the Strategic National
Stockpile will distribute medical countermeasures to affected
states, and state and local public health agencies will then
dispense antimicrobials to and vaccinate numerous at-risk
persons. Antimicrobials are given long enough (up to 60 days)
to prevent infection until the vaccine can elicit a protective
immune response (29).
Summary of Key Findings
Anthrax Vaccine Adsorbed
Because human efficacy studies of inhalation anthrax are
unethical, the effectiveness of AVA for PEP cannot be directly
assessed in humans. For this situation, FDA allows the use
of the Animal Rule, a set of regulations that allow approval
of products critical for the protection of public health and
national security based on efficacy data only in animals
combined with immunogenicity and safety data in animals
and humans (32). Under the Animal Rule, AVA vaccine-
induced antibody levels were extrapolated from vaccine efficacy
studies conducted in animals to predict vaccine effectiveness
in humans (33). Statistical modeling was used to establish
the relation between survival of AVA-vaccinated animals
challenged with B. anthracis spores and their antibody levels
at the time of infectious challenge. This relation was applied
to postvaccination antibody levels in humans to estimate the
probability of human survival at selected time points (34).
Route of Administration and Immunogenicity of
AVA for PEP
The SC route of administration of AVA is preferred in
adults because SC administration results in higher antibody
concentrations by week 4 than the IM route: males SC,
40.8
µg/mL (95% confidence interval [CI]: 34.0–49.1);
males IM, 26.3
µg/mL (95% CI: 21.9–31.2); females SC,
60.2
µg/mL, (95% CI: 50.1–72.3), females IM, 36.0 µg/ml
Recommendations and Reports
4 MMWR / December 13, 2019 / Vol. 68 / No. 4
US Department of Health and Human Services/Centers for Disease Control and Prevention
(95% CI: 30.0–43.1 (35). Using these antibody concentrations,
survival estimates based on the correlates of protection model
are 3.8% higher for the SC route (92.4%) than the IM route
(88.6%) of administration at week 4 (36). However, by week 9,
the antibody concentrations and predicted survival from the
IM route (95.6%) and SC route (96.1%) are no longer
significantly different (35).
In a wide-area aerosolized release of B. anthracis spores over
a densely populated area, potentially hundreds of thousands of
exposed persons might require PEP-Vx to prevent inhalation
anthrax. In such a situation, rapid and efficient administration
of vaccine to large numbers of persons would be a key
component of the public health emergency response. Health
care providers typically have more experience administering
vaccines by the IM route than the SC route. In addition,
during a conference call with state and local jurisdictions, many
public health officials indicated that they plan to use just-in-
time training for responding vaccinators during a wide-area
aerosolized release of B. anthracis spores. Officials also stated
during this call that training vaccinators to use the IM route
was the easiest (State and local public health preparedness
officials, personal communication, 2018). In addition, a study
comparing the IM and SC route for AVA administration found
significantly less reactogenicity (less injection site warmth,
itching, erythema, induration, swelling, and nodule formation)
with the IM route than with the SC route at 0, 2, and 4 weeks.
In this same study, only two adverse events were more common
among IM AVA recipients than SC AVA recipients: limitation
of arm motion and generalized myalgia (35). Because the
preponderance of injection site adverse events was associated
with the SC route, concern has been raised that using this
route might decrease the likelihood of patients completing the
second and third doses of AVA.
Dose-Sparing Strategies for PEP-Vx
A wide-area aerosolized release of B. anthracis spores over
a densely populated area could potentially require PEP-Vx
of more persons than could be vaccinated with the available
supply of AVA in the Strategic National Stockpile if AVA were
to be administered according to the licensed regimen (0.5 mL
at 0, 2, and 4 weeks) for the PEP-Vx indication. If demand
were to exceed the supply, alternative AVA dose-sparing
regimens might be needed to provide PEP-Vx to all persons
with suspected or known exposure to aerosolized B. anthracis
spores. To address this problem, studies were reviewed that
estimated survival with AVA administered according to the
licensed PEP-Vx schedule (3 full [0.5-ml] doses at 0, 2, and
4 weeks) versus alternate dose-sparing schedules (i.e., 2 full
doses at 0 and 2 weeks, 2 full doses at 0 and 4 weeks, and
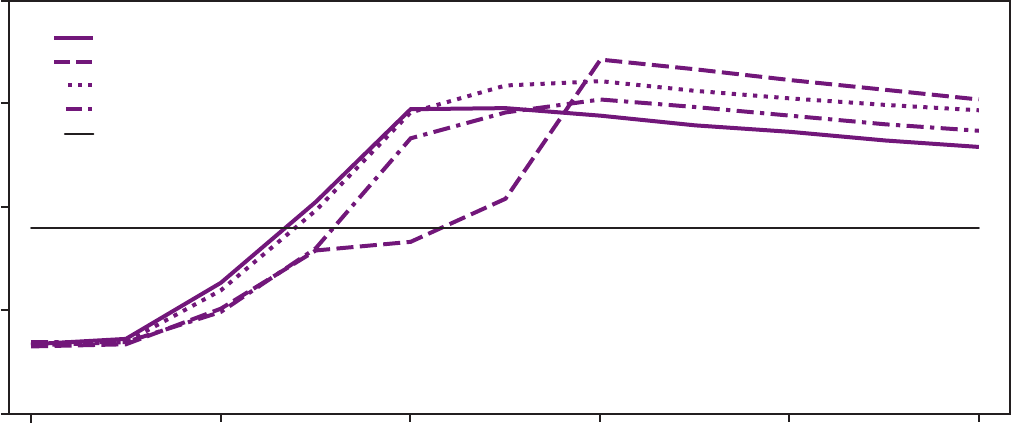
3 half [0.25-ml] doses at 0, 2, and 4 weeks) (Figure). The
three groups who received an AVA dose at week 2 had higher
antibody concentrations at week 4 than the one group who
FIGURE. Group geometric means for anti-protective antigen immunoglobulin G enzyme-linked immunosorbent assay over time after
administration of anthrax vaccine adsorbed*
0.1
1
10
100
1,000
0 2 4 6 8 10
Weeks since rst dose
0, 2 Full dose
0, 4 Full dose
0, 2, 4 Full dose
0, 2, 4 Half dose
PA80
Anti-PA IgG (μg/mL)
Abbreviations: AVA = anthrax vaccine adsorbed; IgG = immunoglobulin G; PA = protective antigen.
* 0, 2 Full dose = 0.5 mL AVA administered at 0 and 2 weeks; 0, 4 Full dose = 0.5 mL AVA administered at 0 and 4 weeks; 0, 2, 4 Full dose = 0.5 mL AVA administered at
0, 2, and 4 weeks; 0, 2, 4 Half dose = 0.25 mL AVA administered at 0, 2, and 4 weeks; PA80 = 80% predicted protection level.

Recommendations and Reports
MMWR / December 13, 2019 / Vol. 68 / No. 4 5
US Department of Health and Human Services/Centers for Disease Control and Prevention
did not. The dose-sparing schedule of 2 full doses administered
4 weeks apart produced the highest antibody concentrations
from week 6 onward after the first dose. The 3 full-dose
regimen produced higher antibody concentrations than when
the vaccine was administered as 3 half doses at all measured
time points after week 1. The peak response was measured
2 weeks after the last dose for the licensed and dose-sparing
PEP-Vx schedules and was estimated to be highly protective
by the correlates of protection model (37). The predicted
survival was estimated to be 97.4% (95% CI: 85.1–100) for the
licensed schedule, 95.8% (95% CI: 92.2–100) for the full dose
administered at 0 and 2 weeks, 98.1% (95% CI: 86.9–100)
for the full dose administered at 0 and 4 weeks, and 96.1%
(95% CI: 83.7–100) for the 3 half doses administered at 0, 2,
and 4 weeks (Table 1). All dosing PEP-Vx schedules maintain
a high level of predicted survival through week 9 (36,38).
Duration of Antimicrobial Administration in
Combination with Vaccine
Since 2000, FDA has approved several oral antimicrobials
(ciprofloxacin in 2000, penicillin G in 2001, doxycycline in
2001, and levofloxacin in 2004) for antimicrobial postexposure
prophylaxis (PEP-Abx) of anthrax. Each PEP-Abx regimen
should be administered for 60 days when not used in
combination with vaccine. However, studies of nonhuman
primates have demonstrated that spores can persist in the
lungs many days after inhalation exposure (up to 100 days
in one animal study) and that anthrax can develop after
discontinuation of PEP-Abx (29,30). Because of the possibility
of delayed infection from persistent spores, recommendations
for PEP require use of AVA in conjunction with antimicrobial
drugs. With this strategy, the antimicrobials protect against
germinating spores until the vaccine can elicit a protective
immune response.
Using the limited data available at the time, in 2015, FDA
licensed a 3-dose regimen of AVA to be given in conjunction
with recommended antimicrobials for PEP for persons
potentially exposed to aerosolized B. anthracis spores (39).
Newer data from a human clinical trial with AVA demonstrate
that, with concurrent receipt of AVA, the duration of
antimicrobial use can be shortened from the recommended
60 days (38). In the trial, persons were given one of four
PEP-Vx regimens: the licensed 3-dose schedule, a dose-sparing
schedule with 2 full doses at 0 and 2 weeks, a dose-sparing
schedule with 2 full doses at 0 and 4 weeks, or a dose-sparing
schedule with 3 half doses at 0, 2, and 4 weeks. Antibody
levels predicted to be protective in humans were extrapolated
from a matched nonhuman primate nonclinical trial in which
48 nonhuman primates were given 2 doses of AVA at 0 and
2 weeks and challenged with a 200 LD
50
dose of B. anthracis
spores at week 4. Protection provided by anti-PA IgG was
modeled using logistic regression of the measured prechallenge
antibody levels at week 4 in nonhuman primates versus survival
of challenge (36). The nonhuman primate prediction curve
was then applied to the human antibody levels to predict
protection in humans (38). The estimated peak protection both
for licensed and dose-sparing AVA PEP-Vx regimens occurred
2 weeks after the last AVA dose was given. All regimens are
estimated to be highly protective; protection is maintained
through day 60, when the antimicrobial component of PEP
is recommended to end (Table 1).
Safety
Since 2008, the vast majority of AVA vaccinations
(approximately 8 million doses administered to approximately
1.9 million persons) have been administered by DoD as PrEP
to its service members. The PrEP route of administration
was SC until FDA approved changing the PrEP route of
administration to IM in December 2008. As defined by the
TABLE 1. Anthrax vaccine adsorbed postexposure prophylaxis schedules and predicted human survival*
Time from rst dose
of PEP-Vx
Predicted human survival by PEP-Vx schedule
Licensed vaccination regimen Alternate dose-sparing schedules
Full dose at 0, 2, and 4 wks Full dose
†
at 0 and 2 wks Full dose at 0 and 4 wks Half dose
§
at 0, 2, and 4 wks
% (95% CI) % (95% CI) % (95% CI) % (95% CI)
Week 4 95.8 (92.2–100) 95.8 (82.6–100) 72.6
¶
(58.2–92.9) 91.1 (78.2–98.7)
Week 6 97.4 (85.1–100) 95.5 (81.7–100) 98.1 (86.9–100) 96.1 (83.7–100)
Week 9 96.4 (83.1–100) 93.3 (78.9–100) 97.0 (84.4–100) 94.2 (80.8–100)
Source: Data from Stark GV, Sivko GS, VanRaden M, et al. Cross-species prediction of human survival probabilities for accelerated anthrax vaccine adsorbed (AVA)
regimens and the potential for vaccine and antibiotic dose sparing. Vaccine 2016;34:6512–7.
Abbreviations: AVA = anthrax vaccine adsorbed; CI=confidence interval; PEP-Vx = AVA postexposure prophylaxis.
* Based on survival data from nonhuman primates that received AVA at weeks 0 and 2 and were challenged with a target dose of 200 LD
50
aerosolized Bacillus anthracis
spores at week 4.
†
0.5 mL of AVA.
§
0.25 mL of AVA.
¶
At 4 weeks before the second dose of vaccine.
Recommendations and Reports
6 MMWR / December 13, 2019 / Vol. 68 / No. 4
US Department of Health and Human Services/Centers for Disease Control and Prevention
U.S. Code of Federal Regulations, an event is classified as
serious if one or more of the following conditions is reported:
death, a life-threatening illness, hospitalization or prolongation
of existing hospitalization, permanent disability, or a congenital
anomaly or birth defect (40).
From January 1, 2009, through
June 30, 2017, a total of 2,439 AVA-related adverse events
were reported to VAERS (16); 329 (13.5%) of these were
considered serious.
During the same period, the 10 most common reported
adverse events were coded as headache (14.7%), injection
site erythema (13.6%), pain (12.6%), fever (11.6%), fatigue
(11.5%), arthralgia (11.2%), erythema (11.2%), injection site
pain (9.9%), injection site swelling (9.8%), and rash (9.4%)
on the basis of coding terms from the Medical Dictionary for
Regulatory Activities. VAERS has numerous strengths, such as
broad national scope and early detection of possible new, rare,
or unusual patterns of adverse events. However, VAERS is a
spontaneous reporting system that has important limitations,
including underreporting, inconsistent data quality and report
completeness, and lack of an unexposed comparison group.
Therefore, the data generally cannot be used to assess whether
a vaccine caused an adverse event (16).
Nine studies, including clinical vaccine trials and observational
studies (10,12,35,37,41–45), also assessed serious adverse
events after administration of AVA, AV7909, or both in
human subjects. Serious adverse events were reported in three
studies (12,35,43); however, only in the Anthrax Vaccine
Review Program study (35) were the serious adverse events
considered possibly related to AVA. In this study, 231 adverse
events were identified in recipients of approximately 8,300
doses of AVA. Six serious adverse events, none of which was
fatal, were considered to be possibly related to the vaccine,
including ductal carcinoma of the breast, generalized allergic
reaction, new onset bilateral arthralgia of the metacarpal
joints associated with positive antinuclear antibody (ANA),
bilateral pseudotumor cerebri, supraspinatous tendon tear, and
new onset of generalized seizures associated with aqueductal
stenosis (35).
In studies from the Vaccine Analytic Unit and other groups
published since 2010, no association was found between AVA
receipt and the following chronic health conditions: reduction
in health-related quality of life measures (46), multisystem
illness (47), long-term disabilities (48,49), type 1 diabetes (50),
atrial fibrillation (51), and diffuse connective tissue diseases
(52). In one case-control study, an association was identified
between AVA receipt and new-onset rheumatoid arthritis if a
look-back period of 3 months was used (odds ratio [OR]: 3.93;
95% CI:1.08–14.27). However, no association between AVA
and rheumatoid arthritis was identified if a longer look-back
period of 3 years was used (OR: 1.03; 95% CI:0.48–2.19)
(52), suggesting that AVA exposure might trigger onset of
rheumatoid arthritis in persons who would eventually have
developed rheumatoid arthritis later in life.
Although AVA is not intended for use during pregnancy,
DoD maintains a registry of women inadvertently vaccinated
while pregnant. Studies of adverse outcomes and a cohort study
of birth defects using this registry did not detect any increased
rates of adverse fetal or infant outcomes among women who
received AVA during their first trimester compared with receipt
at other time points or no receipt of AVA (53,54). Finally,
because no safety data are available for AVA use in adolescents, a
presidential ethics commission proposed comparing AVA safety
data for the group aged 18–20 years (the youngest group) and
the group aged 21–29 years. If no significant safety difference
could be found between the two age groups, then evaluations
could proceed in successively younger adolescents. In a study
following these suggested methods, AVA was deemed safe
in adults aged 18–20 years (44); no additional studies have
been conducted in younger age groups. AVWG reviewed the
VAERS reports and the published literature and presented
their findings to the ACIP committee. On the basis of these
data, the committee concluded that no clinically significant
safety concerns have been identified related to receipt of AVA
since 2010 (9).
AV7909
AV7909 is an investigational second-generation anthrax
vaccine that is under development for PEP of inhalation
anthrax in conjunction with appropriate antimicrobials.
AV7909 consists of the licensed AVA combined with a
novel adjuvant, CpG 7909, a synthetic immunostimulatory
oligodeoxynucleotide. CpG 7909 is a Toll-like receptor 9
agonist that has been demonstrated to augment Th1 responses
in humans and enhance innate and adaptive immunity (7,8)
AV7909 is intended to be added to the Strategic National
Stockpile. CDC has submitted a pre–Emergency Use
Authorization (EUA) request to FDA to allow potential
emergency use of AV7909, in conjunction with appropriate
PEP-Abx, for PEP of inhalation anthrax when the supply of
the currently licensed AVA is inadequate. EUA is an authority
given to the FDA commissioner to legally permit the use of
an unapproved medical product or unapproved use of an
approved medical product (55). Under the proposed EUA,
AV7909 would be administered by the IM route as a 2-dose
series 2 weeks apart in conjunction with PEP-Abx for adults
aged 18–65 years. Pregnant or nursing mothers, older adults
(aged ≥66 years), and children (aged <18 years) should receive
AVA until data to adequately support AV7909 use in these
additional populations under EUA become available.
Recommendations and Reports
MMWR / December 13, 2019 / Vol. 68 / No. 4 7
US Department of Health and Human Services/Centers for Disease Control and Prevention
Available data indicate that AV7909 might provide the
following advantages over AVA:
• Two IM doses of AV7909 administered 2 weeks apart
might provide protective immunity 1–2 weeks sooner than
the licensed 3-dose PEP-Vx regimen of AVA.
• Compared with the licensed 3-dose AVA PEP-Vx schedule,
the 2-dose schedule of AV7909 PEP provides an operational
advantage in a large-scale, mass vaccination response.
• Adherence might be better because more persons are likely
to complete the 2-dose AV7909 PEP series than the 3-dose
AVA PEP series.
Immunogenicity
The initial phase 1 clinical trial assessed immunogenicity
of AVA alone and AVA plus CpG 7909 in 69 healthy adults
aged 18–45 years (12). Vaccinations were administered IM on
weeks 0, 2 (±1 day), and 4 (±2 days). The CpG group received
AVA plus 1 mg of CpG 7909. The results showed that the
peak GMT of TNA for the AV7909 group was 8.8-fold higher
than that observed for the AVA-alone group; antibody peaked
at week 6 in both arms. By week 3, GMT in the CpG group
exceeded the peak GMT in the AVA group (reached at week 6).
The TNA results paralleled those observed with anti-PA IgG,
and in both assays the differences between AVA and AV7909
were statistically significant. Analysis of the phase 2 TNA
threshold of protection data for AV7909 revealed that addition
of the CpG 7909 adjuvant to AVA improved the kinetics and
magnitude of the immune response (56). A 2-dose AV7909
regimen with 0.25 mg of CpG 7909 administered IM resulted
in a similar serological response at week 9 compared with a
3-dose AVA regimen administered IM and achieved a peak
response by week 4 versus week 6 for AVA.
Safety
Adverse events were assessed in three clinical trials available
at the time of this review, including a total of 241 subjects who
were administered at least 1 dose of AVA plus CpG 7909 in
varying dose combinations (10,12,45). The most common
adverse events, reported in ≥20% of persons receiving AV7909
across these clinical trials, were injection site reactions (e.g.,
mild to moderate pain, tenderness, and arm motion limitation);
these typically resolved within 48 hours of administration.
Systemic reactogenicity manifested primarily as mild to
moderate fatigue, muscle ache, and headache. No deaths or
serious adverse events assessed as being causally associated have
been reported in AV7909 clinical studies.
In healthy adults aged 18–50 years who received
CpG 7909-adjuvanted experimental vaccines for malaria and
hepatitis B in the 0.25-mg dose that is combined with AVA
in AV7909 (57,58), local and systemic reactions were similar
to those observed in the groups who received malaria and
hepatitis B vaccines without CpG 7909, and the proportion
of subjects who dropped out because of adverse events
did not differ between treatment and control groups (58).
Reasons for discontinuation included rash, positive ANA,
generalized pruritus, urticaria, and fever. These clinical trial
reports suggested that these adverse events might be a result of
activation of proinflammatory innate immune responses at the
injection site. Theoretically, CpG 7909 could trigger the onset
of autoimmune disease, possibly as a result of nonspecific T or B
lymphocyte activation. Some studies reported mild to moderate
increases in anti–double-stranded DNA antibody, rheumatoid
factor, or positive ANA results. However, these increases in
immune markers were typically transient. No adverse events
suggesting autoimmune disease have been reported in the
reviewed published data on CpG 7909-adjuvanted infectious
disease vaccine trials (57–61). No safety data are available for
CpG 7909-adjuvanted vaccines, including AV7909 among
special populations (e.g., children, persons aged >65 years,
and pregnant women).
Recommendations for Prevention of
Anthrax Among Persons with
Potential Risk for Exposure: PrEP
ACIP previously recommended AVA PrEP for prevention of
anthrax in persons at high risk for exposure to B. anthracis (e.g.,
members of the U.S. military deployed to areas designated by
DoD as high risk for exposure, laboratory workers who work
with high concentrations of B. anthracis, and persons such
as farmers, veterinarians, and livestock handlers who might
handle infected animals or contaminated animal products) (9).
In this report, ACIP recommends that a booster dose of AVA
PrEP be given every 3 years to persons who are not at high risk
for exposure to B. anthracis who have previously completed
the 3-dose primary and the initial 2-dose boosters AVA series
and want to maintain protection.
The PrEP schedule for persons at high risk for exposure
to B. anthracis is AVA administered IM as a priming series at
0, 1, and 6 months, with booster doses at 12 and 18 months and
annually thereafter. If the vaccination schedule is interrupted,
the series does not need to be restarted. After the priming series
is completed, persons can work in high-risk areas of exposure
with appropriate personal protective equipment and biosafety
measures. Documentation of seroconversion is not required. If
biosafety or respiratory protection measures are breached and
exposure to aerosolized B. anthracis spores might have occurred,
a 30-day course of PEP-Abx is recommended, regardless of
whether PrEP has been fully or partially completed.
Recommendations and Reports
8 MMWR / December 13, 2019 / Vol. 68 / No. 4
US Department of Health and Human Services/Centers for Disease Control and Prevention
Because of the lack of a quantifiable risk, emergency and
other responders are not recommended to receive routine
PrEP vaccination. However, emergency responders, because
of the requirements of their occupation, might be exposed
to aerosolized B. anthracis spores and thus may opt to receive
the vaccine on a voluntary basis. For persons who are not
currently at high risk for exposure to B. anthracis but who
might be at high risk in the future (e.g., persons involved in
emergency response activities), published data (35) support
a booster dose interval of >1 year. Thus, a booster dose of
AVA can be given every 3 years to persons not at high risk for
exposure to B. anthracis who have previously received the initial
AVA priming and booster series and who want to maintain
protection. After completing the initial 3-dose priming
and booster series, persons who have not received a booster
dose in the last 12 months and need to enter an area where
B. anthracis is suspected to be present in the environment or
be in use should be given an IM booster dose and then either
wait 2 weeks to enter the high-risk area or, if required to enter
immediately, take PEP-Abx for 2 weeks. While in a high-risk
area, a booster dose should be given within 1 year of the last
booster dose.
Persons who are exposed to aerosolized B. anthracis spores
but have not completed the initial priming and booster series
for AVA should receive additional AVA doses and PEP-Abx.
The number of vaccine doses and duration of PEP-Abx will
vary in a manner commensurate with the number of previously
received doses (Table 2).
Recommendations for Prevention of
Anthrax Among Persons with
Suspected or Known Exposure: PEP
ACIP recommends AVA for use in adults aged 18–65 years
to be given in conjunction with a course of antimicrobials
(Table 3) to prevent infection after suspected or known
exposure to aerosolized B. anthracis spores. Antimicrobial
duration details are provided (Table 4). The vaccine is given
at a dose of 0.5 mL SC at 0, 2, and 4 weeks postexposure,
unless the emergency response requires a change to the IM
route or use of dose-sparing regimens. If the PEP-Vx schedule
is interrupted, the series does not need to be restarted. Instead,
subsequent doses should be administered as soon as possible,
and the series should be finished.
Route of Administration
ACIP recommends the SC route of administration
rather than the IM route for PEP because higher antibody
concentrations are achieved by 4 weeks after AVA vaccination.
However, during a large-scale emergency response, AVA for
PEP can be administered using an IM route if the SC route
of administration poses significant materiel, personnel, or
clinical challenges that might delay or preclude vaccination. In
addition, persons who experienced adverse events from AVA
that was administered SC may elect to receive subsequent
vaccine doses IM after consultation with a health care provider.
Doses of AVA inadvertently administered by the IM route
rather than the SC route do not need to be repeated by the
SC route.
Dose-Sparing PEP Regimens
ACIP recommends use of dose-sparing PEP regimens if the
anthrax vaccine supply is insufficient to vaccinate all potentially
exposed persons. The 2 full-dose strategy will expand the
existing vaccine supply by 50%, and the 3 half-dose strategy
will expand the supply by 100%. Immediately after a wide-area
aerosolized release of B. anthracis spores, the preferred dose-
sparing PEP regimen might not be apparent until the size of
the event is determined. All dose-sparing PEP-Vx regimens
are estimated to provide high levels of protection 2 weeks after
the last dose (Table 5). Existing data indicated that 2 doses
administered 2 weeks apart or 4 weeks apart are effective;
therefore, the 2-dose schedule should be ≥2 weeks apart and
≤4 weeks apart, recognizing that full protection is not achieved
until 2 weeks after the second dose (37).
Antimicrobial Duration in Conjunction
with FDA-Licensed or Dose-Sparing PEP
Regimens of AVA
ACIP recommends that in immunocompetent adults (e.g.,
healthy, nonpregnant adults aged 18–65 years), PEP-Abx
both for the licensed and dose-sparing PEP-Vx regimens can
be discontinued 42 days after initiation of vaccine if AVA is
administered on schedule for both the licensed and dose-
sparing PEP-Vx regimens (Table 4). If the AVA series cannot
be completed, then antimicrobial therapy should continue
for 60 days. However, the second dose of AVA is critical for
producing high antibody concentrations. To account for
delays in initial vaccination that might occur because of the
emergency situation, antimicrobial administration should be
initiated as soon as possible and continued for 42 days after
the first dose or 2 weeks after the last dose of the vaccine series,
whichever comes last. No data on humans are available to
suggest that PEP-Abx should be given for >60 days, which is
the recommended duration for PEP-Abx when given without
Recommendations and Reports
MMWR / December 13, 2019 / Vol. 68 / No. 4 9
US Department of Health and Human Services/Centers for Disease Control and Prevention
TABLE 2. Transition from preexposure prophylaxis* schedule to postexposure prophylaxis schedule for persons who have not completed a
priming and initial booster series
†
and must immediately enter an area that poses a high risk
§
for Bacillus anthracis exposure
Previous
PrEP doses Interval since last dose
PEP
PEP-Vx PEP-Abx
¶
0 — Dose 1 (week 0) Administer until 42 days after first dose of AVA or 14 days after last dose, whichever
occurs later.
Dose 2 (week 2)
Dose 3 (week 4)
1 — Dose 2 (week 0) Administer until 28 days after second dose of AVA or 14 days after the last dose,
whichever occurs later.
Dose 3 (week 2)
2 — Dose 3 (week 0) Administer until 14 days after last dose.
3, 4 >6 mos Booster dose Administer until 14 days after booster dose.
3, 4 ≤6 mos No booster No antimicrobials needed
Abbreviations: AVA = anthrax vaccine adsorbed; PEP = postexposure prophylaxis; PEP-Abx = antimicrobial PEP; PEP-Vx = AVA PEP; PrEP = preexposure prophylaxis.
* No data are available on the effect on the immune response for starting PrEP by the intramuscular route and switching to the subcutaneous route to join the PEP
schedule; however, no evidence suggests that the immune response would be adversely affected by mixing the routes of administration.
†
Priming doses at 0, 1, and 6 mos, with booster doses at 12 and 18 mos.
§
The licensed booster schedule for high-risk exposure applies while in the high-risk area.
¶
If the AVA series cannot be completed, then antimicrobial therapy should continue for 60 days.
TABLE 3. Oral antimicrobial dosages for use in adults in conjunction
with anthrax vaccine adsorbed for postexposure prophylaxis
Strain Drug and dosage*
For all strains, regardless of
penicillin susceptibility or if
susceptibility is unknown
Ciprofloxacin,
†
500 mg every 12 hrs
Doxycycline,
†
100 mg every 12 hrs
Levofloxacin, 750 mg every 24 hrs
Moxifloxacin,
§
400 mg every 24 hrs
Clindamycin,
§
600 mg every 8 hrs
Alternatives for penicillin-
susceptible strains
Amoxicillin,
§
1,000 mg every 8 hrs
Penicillin VK,
§
500 mg every 6 hrs
Abbreviations: FDA = Food and Drug Administration; PEP-Abx = antimicrobial
postexposure prophylaxis.
* Any one of these drug regimens.
†
First-line drugs; alternative drugs are listed in order of preference for PEP-Abx
for patients who cannot take first-line treatment or if first-line PEP-Abx is
unavailable.
§
Not FDA approved for PEP-Abx of inhalation anthrax.
TABLE 4. Antimicrobial duration when used in conjunction with Food
and Drug Administration–licensed or dose-sparing postexposure
prophylaxis regimens of anthrax vaccine adsorbed*
Population with suspected or
known exposure
Duration of antimicrobial
regimen
Immunocompetent adults aged 18–65 yrs 42 days when initiated
concurrently with first dose of
AVA or for 14 days after last
AVA dose, whichever is later
(not to exceed 60 days)
Adults aged 18–65 yrs with
immunocompromising conditions
(e.g., cancer or HIV infection) or receiving
immunosuppressive therapy (e.g.,
high-dose corticosteroids for >2 wks
or radiation therapy)
†
60 days
All older adults (>65 yrs) 60 days
All pregnant women and nursing mothers 60 days
All children (≤17 yrs) 60 days
Abbreviation: AVA = anthrax vaccine adsorbed.
* If the AVA series cannot be completed, then antimicrobial therapy should
continue for 60 days.
†
Source: Löbermann M, Boršo D, Hilgendorf I, Fritzsche C, Zettl UK, Reisinger
EC. Immunization in the adult immunocompromised host. Autoimmun Rev
2012;11:212–8.
TABLE 5. Postexposure prophylaxis with anthrax vaccine adsorbed
dose-sparing regimens
Dose Route of administration Dosing schedule
0.5 mL (full dose) SC or IM* 2 doses: 0 and 2–4 wks
0.25 mL (half dose) SC or IM* 3 doses: 0, 2, and 4 wks
Abbreviations: IM = intramuscular; SC = subcutaneous.
* Can be administered IM if the SC route of administration poses significant materiel,
personnel, or clinical challenges that might delay or preclude vaccination.
vaccine. Thus, PEP-Abx should not be given for >60 days,
regardless of the timing of last vaccine dose.
The shortening of PEP-Abx duration from 60 days to 42 days,
or 2 weeks after the last dose of vaccine, applies to healthy
adults aged 18–65 years. Persons with immunocompromising
conditions that might interfere with their ability to develop an
adequate immune response or populations for whom data on
immune response to AVA are lacking (e.g., children, pregnant
women, and adults aged ≥65 years) should continue to receive
PEP-Abx for 60 days concurrently with AVA.
Potential Emergency Use of AV7909
Because of supply concerns and the investigational status
of AV7909, AVA should be prioritized over AV7909 for
PEP-Vx of potential exposure to aerosolized B. anthracis
spores. However, the limited amount of phase 2 safety and
immunogenicity data indicate that AV7909 appears to be
safe and effective. The benefits of an effective vaccine that
can prevent anthrax outweigh the known potential risks for
adverse events in persons potentially exposed to aerosolized
B. anthracis spores. Therefore, if supplies of AVA are exhausted
or unavailable, AV7909 is an option for PEP of persons exposed
to aerosolized B. anthracis spores under an EUA granted by
FDA. As with AVA, antimicrobials (Tables 3 and 4) should
be taken in conjunction with AV7909. Additional AV7909
Recommendations and Reports
10 MMWR / December 13, 2019 / Vol. 68 / No. 4
US Department of Health and Human Services/Centers for Disease Control and Prevention
data on safety, immunogenicity, and biocompatibility with
antimicrobials will be reviewed by ACIP as they become
available, and recommendations on potential preferential use
will be updated as needed.
No data are available on the immunogenicity or safety of
AV7909 for children or other special populations. However,
a phase 2 clinical trial is being conducted to assess the safety
and immunogenicity of AVA and AV7909 in adults aged
>65 years compared with adults aged 18–50 years (62). In
the absence of such data, AVWG considered it reasonable to
anticipate that risks and benefits of PEP-Vx for children or
special populations would be similar to those for the general
adult population. Therefore, if AVA is not available, emergency
use of AV7909 under an appropriate regulatory mechanism
should be considered for all populations with known or
potential exposure to aerosolized B. anthracis spores. Should
an anthrax exposure event occur that necessitates AV7909 use
while it remains under development and is not yet licensed,
ACIP will convene an emergency meeting to review available
data for specific recommendations on AV7909 emergency use.
No studies have been conducted on the interchangeability
of AVA and AV7909. When feasible, doses of the same vaccine
type should be used to complete a series. However, vaccination
should not be deferred because the previously used vaccine
type is unavailable. When a vaccine series uses a combination
of AVA and AV7909, 3 total doses of anthrax vaccine should
be administered and used in conjunction with appropriate
antimicrobials (Tables 3 and 5).
Antitoxin Use for PEP
Three licensed anthrax antitoxins are available from the
Strategic National Stockpile: anthrax immune globulin
intravenous (AIGIV) (63), obiltoxaximab (Anthim) (64), and
raxibacumab (ABthrax) (65). AIGIV is a polyclonal antibody,
whereas obiltoxaximab and raxibacumab are both monoclonal
antibodies. All work by binding to protective antigen, which
blocks movement of toxins into cells and therefore the effects
of toxins within the cells. All three antitoxins are indicated
in all adults and children for the treatment of inhalation
anthrax due to B. anthracis, in combination with appropriate
antimicrobial drugs.
Obiltoxaximab and raxibacumab also have an indication
for PEP of inhalation anthrax due to B. anthracis when
alternative therapies are not available or are not appropriate.
In these situations, obiltoxaximab or raxibacumab may be
considered to help prevent inhalation anthrax. The predicted
effectiveness of both antitoxins for this indication is based
solely on efficacy studies conducted in animal models of
inhalation anthrax (66,67).
Data indicate that raxibacumab can be coadministered
with AVA for PEP without affecting vaccine immunogenicity
(68). No data are available to assess whether obiltoxaximab
coadministered with AVA impairs vaccine immunogenicity.
AIGIV does not have a PEP indication because coadministration
of AIGIV and AVA in a rabbit model has been shown to
significantly reduce the development of an immune response
to AVA (68).
Vaccine Adverse Events Reporting
and Additional Information
Surveillance for serious adverse events is important for
all antimicrobials, biologics, and vaccines. All clinically
significant adverse events after receipt of antimicrobials or
anthrax antitoxin for PEP or treatment of anthrax should be
reported to the MedWatch Program (https://www.fda.gov/
safety/medwatch-fda-safety-information-and-adverse-event-
reporting-program or 888-463-6332). All clinically significant
adverse events after receipt of either AVA or AV7909 should be
reported to VAERS (https://vaers.hhs.gov or 800–822–7967).
Additional information about anthrax and anthrax vaccines is
available at https://www.cdc.gov/anthrax.
Future Directions
Research priorities for future studies on anthrax vaccines
should include assessment of immunogenicity and safety in
special populations, such as children, older adults, and pregnant
and nursing mothers; additional evaluations of the dose-sparing
schedules; evaluation of the interchangeability of AVA and
AV7909; determination of the optimal booster schedule to
provide long-term protection after receiving the PEP vaccine
schedule; testing of the stability of AVA and AV7909 outside
the cold chain; assessment of whether coadministration of
obiltoxaximab with AVA impairs vaccine immunogenicity;
and the optimal duration of antimicrobial use in postexposure
settings. Studies are planned to evaluate the effect of longer
intervals between PrEP boosters on vaccine responses. On
approval of AV7909 as a licensed vaccine, the additional data
leading to the licensure of AV7909 will be reviewed by ACIP,
and recommendations will be updated as needed.
Recommendations and Reports
MMWR / December 13, 2019 / Vol. 68 / No. 4 11
US Department of Health and Human Services/Centers for Disease Control and Prevention
Acknowledgments
Marissa Persons, Modupe Osinubi, Division of High-Consequence
Pathogens and Pathology, National Center for Emerging and Zoonotic
Infectious Diseases, CDC; Amanda Cohn, Jessica MacNeil, Office
of the Director, National Center for Immunization and Respiratory
Diseases, CDC. Advisory Committee on Immunization Practices
(ACIP) member roster for March 2017–January 2019 is available at
https://www.cdc.gov/vaccines/acip/committee/members.html.
Conflicts of Interest
All authors have completed and submitted the International Com-
mittee of Medical Journal Editors form for disclosure of potential
conicts of interest. No potential conicts of interest were disclosed.
References
1. Davies JC. A major epidemic of anthrax in Zimbabwe. The
experience at the Beatrice Road Infectious Diseases Hospital, Harare.
Cent Afr J Med 1985;31:176–80.
2. Holty JE, Bravata DM, Liu H, Olshen RA, McDonald KM, Owens
DK. Systematic review: a century of inhalational anthrax cases from
1900 to 2005. Ann Intern Med 2006;144:270–80. https://doi.
org/10.7326/0003-4819-144-4-200602210-00009
3. Katharios-Lanwermeyer S, Holty JE, Person M, et al. Identifying
meningitis during an anthrax mass casualty incident: systematic review
of systemic anthrax since 1880. Clin Infect Dis 2016;62:1537–45.
https://doi.org/10.1093/cid/ciw184
4. Booth MG, Hood J, Brooks TJ, Hart A; Health Protection Scotland
Anthrax Clinical Network. Anthrax infection in drug users. Lancet
2010;375:1345–6. https://doi.org/10.1016/S0140-6736(10)60573-9
5. US Department of Agriculture; CDC. Federal Select Agent Program:
select agents and toxins FAQS. Washington, DC: US Department of
Agriculture; Atlanta, GA: CDC. https://www.selectagents.gov/faq-
general.html
6. US Food and Drug Administration. Full prescribing information:
BioThrax (Anthrax Vaccine Adsorbed). Silver Spring, MD: US Food
and Drug Administration. https://www.fda.gov/media/71954/download
7. Klinman DM, Xie H, Little SF, Currie D, Ivins BE. CpG oligonucleotides
improve the protective immune response induced by the anthrax
vaccination of rhesus macaques. Vaccine 2004;22:2881–6. https://doi.
org/10.1016/j.vaccine.2003.12.020
8. Krieg AM. Therapeutic potential of Toll-like receptor 9 activation. Nat
Rev Drug Discov 2006;5:471–84. https://doi.org/10.1038/nrd2059
9. Wright JG, Quinn CP, Shadomy S, Messonnier N. Use of anthrax vaccine
in the United States: recommendations of the Advisory Committee on
Immunization Practices (ACIP), 2009. MMWR Recomm Rep
2010;59(No. RR-6).
10. Hopkins RJ, Daczkowski NF, Kaptur PE, et al. Randomized, double-
blind, placebo-controlled, safety and immunogenicity study of
4 formulations of anthrax vaccine adsorbed plus CPG 7909 (AV7909)
in healthy adult volunteers. Vaccine 2013;31:3051–8. https://doi.
org/10.1016/j.vaccine.2013.04.063
11. Minang JT, Inglefield JR, Harris AM, et al. Enhanced early innate and
T cell-mediated responses in subjects immunized with anthrax vaccine
adsorbed plus CPG 7909 (AV7909). Vaccine 2014;32:6847–54. https://
doi.org/10.1016/j.vaccine.2014.01.096
12. Rynkiewicz D, Rathkopf M, Sim I, et al. Marked enhancement of the
immune response to BioThrax® (anthrax vaccine adsorbed) by the TLR9
agonist CPG 7909 in healthy volunteers. Vaccine 2011;29:6313–20.
https://doi.org/10.1016/j.vaccine.2011.05.047
13. Burns DL. Licensure of vaccines using the Animal Rule. Curr Opin
Virol 2012;2:353–6. https://doi.org/10.1016/j.coviro.2012.01.004
14. US Food and Drug Administration. Product development under the
Animal Rule. Silver Spring, MD: US Food and Drug Administration.
https://www.fda.gov/media/88625/download
15. Payne DC, Franzke LH, Stehr-Green PA, Schwartz B, McNeil MM.
Development of the Vaccine Analytic Unit’s research agenda for
investigating potential adverse events associated with anthrax vaccine
adsorbed. Pharmacoepidemiol Drug Saf 2007;16:46–54. https://doi.
org/10.1002/pds.1213
16. Shimabukuro TT, Nguyen M, Martin D, DeStefano F. Safety monitoring
in the Vaccine Adverse Event Reporting System (VAERS). Vaccine
2015;33:4398–405. https://doi.org/10.1016/j.vaccine.2015.07.035
17. CDC. GRADE (Grading of Recommendations, Assessment, Development
and Evaluation). Atlanta, GA: US Department of Health and Human
Services, CDC. https://www.cdc.gov/vaccines/acip/recs/grade
18. CDC. ACIP meeting information. Atlanta, GA: US Department of
Health and Human Services, CDC. https://www.cdc.gov/vaccines/acip/
meetings/index.html
19. Bales ME, Dannenberg AL, Brachman PS, Kaufmann AF, Klatsky PC,
Ashford DA. Epidemiologic response to anthrax outbreaks: field
investigations, 1950–2001. Emerg Infect Dis 2002;8:1163–74. https://
doi.org/10.3201/eid0810.020223
20. Blackburn JK, McNyset KM, Curtis A, Hugh-Jones ME. Modeling the
geographic distribution of Bacillus anthracis, the causative agent of
anthrax disease, for the contiguous United States using predictive
ecological [corrected] niche modeling. Am J Trop Med Hyg
2007;77:1103–10. https://doi.org/10.4269/ajtmh.2007.77.1103
21 Anthrax in humans. In: World Health Organization. Anthrax in humans
and animals. 4th ed. Geneva, Switzerland; World Health Organization;
2008:36–52. https://www.who.int/csr/resources/publications/anthrax_
webs.pdf
22. Jernigan DB, Raghunathan PL, Bell BP, et al; National Anthrax
Epidemiologic Investigation Team. Investigation of bioterrorism-related
anthrax, United States, 2001: epidemiologic findings. Emerg Infect Dis
2002;8:1019–28. https://doi.org/10.3201/eid0810.020353
23. Christopher GW, Cieslak TJ, Pavlin JA, Eitzen EM. Biological warfare:
a historical perspective. JAMA 1997;278:412–7.
24. Cole LA. The specter of biological weapons. Sci Am 1996;275:60–5.
25. Zilinskas RA. Iraq’s biological weapons: the past as future? JAMA
1997;278:418–24.
26. World Health Organization. Health aspects of chemical and biological
weapons, report of a WHO group of consultants. Geneva, Switzerland;
World Health Organization; 1970.
27. Hendricks KA, Wright ME, Shadomy SV, et al; Workgroup on Anthrax
Clinical Guidelines. Centers for Disease Control and Prevention expert
panel meetings on prevention and treatment of anthrax in adults. Emerg
Infect Dis 2014;20. https://doi.org/10.3201/eid2002.130687
28. Bowere WA, Hendricks K, Pillai S, Guarnizo J, Meaney Delman D.
Clinical framework and medical countermeasure use during an anthrax
mass-casualty incident: CDC recommendations. MMWR Recomm Rep
2015;64(No. RR-4).
29. Henderson DW, Peacock S, Belton FC. Observations on the prophylaxis
of experimental pulmonary anthrax in the monkey. J Hyg (Lond)
1956;54:28–36. https://doi.org/10.1017/S0022172400044272
30. Friedlander AM, Welkos SL, Pitt ML, et al. Postexposure prophylaxis
against experimental inhalation anthrax. J Infect Dis 1993;167:1239–42.
https://doi.org/10.1093/infdis/167.5.1239
31. Vietri NJ, Purcell BK, Lawler JV, et al. Short-course postexposure
antibiotic prophylaxis combined with vaccination protects against
experimental inhalational anthrax. Proc Natl Acad Sci U S A
2006;103:7813–6. https://doi.org/10.1073/pnas.0602748103
Recommendations and Reports
12 MMWR / December 13, 2019 / Vol. 68 / No. 4
US Department of Health and Human Services/Centers for Disease Control and Prevention
32. US Food and Drug Administration. Pathway to licensure for protective
antigen-based anthrax vaccines for a post-exposure prophylaxis
indication using the Animal Rule: briefing document for the Vaccines
and Related Biological Products Advisory Committee Meeting. Silver
Spring, MD: US Food and Drug Administration; November 16,
2010. http://wayback.archive-it.org/7993/20170113080506/http:/
www.fda.gov/downloads/AdvisoryCommittees/
CommitteesMeetingMaterials/BloodVaccinesandOtherBiologics/
accinesandRelatedBiologicalProductsAdvisoryCommittee/
UCM232400.pdf
33. Fay MP, Follmann DA, Lynn F, et al. Anthrax vaccine-induced antibodies
provide cross-species prediction of survival to aerosol challenge. Sci Transl
Med 2012;4:151ra126. https://doi.org/10.1126/scitranslmed.3004073
34. Schiffer JM, Chen L, Dalton S, Niemuth NA, Sabourin CL, Quinn CP.
Bridging non-human primate correlates of protection to reassess the
anthrax vaccine adsorbed booster schedule in humans. Vaccine
2015;33:3709–16. https://doi.org/10.1016/j.vaccine.2015.05.091
35. Wright JG, Plikaytis BD, Rose CE, et al. Effect of reduced dose schedules
and intramuscular injection of anthrax vaccine adsorbed on
immunological response and safety profile: a randomized trial. Vaccine
2014;32:1019–28. https://doi.org/10.1016/j.vaccine.2013.10.039
36. Sivko GS, Stark GV, Tordoff KP, et al. Evaluation of early immune
response-survival relationship in cynomolgus macaques after anthrax
vaccine adsorbed vaccination and Bacillus anthracis spore challenge. Vaccine
2016;34:6518–28. https://doi.org/10.1016/j.vaccine.2016.04.048
37. Bernstein DI, Jackson L, Patel SM, et al. Immunogenicity and safety of
four different dosing regimens of anthrax vaccine adsorbed for post-
exposure prophylaxis for anthrax in adults. Vaccine 2014;32:6284–93.
https://doi.org/10.1016/j.vaccine.2014.08.076
38. Stark GV, Sivko GS, VanRaden M, et al. Cross-species prediction of
human survival probabilities for accelerated anthrax vaccine adsorbed
(AVA) regimens and the potential for vaccine and antibiotic dose sparing.
Vaccine 2016;34:6512–7. https://doi.org/10.1016/j.vaccine.2016.06.041
39. US Food and Drug Administration. Summary basis for regulatory
action—BioThrax (Anthrax Vaccine Adsorbed). Silver Spring, MD:
US Food and Drug Administration; 2015.
40. US Food and Drug Administration. 21 CFR Sec. 310.305 Records and
reports concerning adverse drug experiences on marketed prescription
drugs for human use without approved new drug applications. Federal
Register 2018;5. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/
cfcfr/CFRSearch.cfm?fr=310.305
41. Zhang Y, Martin SW, Rose CE Jr, et al. Evaluation of body mass index,
pre-vaccination serum progesterone levels and anti-anthrax protective
antigen immunoglobulin G on injection site adverse events following
anthrax vaccination in women. Pharmacoepidemiol Drug Saf
2008;17:1060–7. https://doi.org/10.1002/pds.1657
42. Ionin B, Hopkins RJ, Pleune B, et al. Evaluation of immunogenicity
and efficacy of anthrax vaccine adsorbed for postexposure prophylaxis.
Clin Vaccine Immunol 2013;20:1016–26. https://doi.org/10.1128/
CVI.00099-13
43. Hopkins RJ, Howard C, Hunter-Stitt E, et al. Phase 3 trial evaluating
the immunogenicity and safety of a three-dose BioThrax® regimen for
post-exposure prophylaxis in healthy adults. Vaccine 2014;32:2217–24.
https://doi.org/10.1016/j.vaccine.2014.01.073
44. King JC Jr, Gao Y, Quinn CP, Dreier TM, Vianney C, Espeland EM.
Evaluation of anthrax vaccine safety in 18 to 20 year olds: a first step
towards age de-escalation studies in adolescents. Vaccine 2015;33:2470–6.
https://doi.org/10.1016/j.vaccine.2015.03.071
45. Hopkins RJ, Kalsi G, Montalvo-Lugo VM, et al. Randomized, double-
blind, active-controlled study evaluating the safety and immunogenicity
of three vaccination schedules and two dose levels of AV7909 vaccine
for anthrax post-exposure prophylaxis in healthy adults. Vaccine
2016;34:2096–105. https://doi.org/10.1016/j.vaccine.2016.03.006
46. Stewart B, Rose CE, Tokars JI, et al. Health-related quality of life in the
CDC anthrax vaccine adsorbed human clinical trial. Vaccine
2012;30:5875–9. https://doi.org/10.1016/j.vaccine.2012.06.076
47. Phillips CJ, Matyas GR, Hansen CJ, Alving CR, Smith TC, Ryan MA.
Antibodies to squalene in U.S. Navy Persian Gulf War veterans with
chronic multisymptom illness. Vaccine 2009;27:3921–6. https://doi.
org/10.1016/j.vaccine.2009.03.091
48. Sulsky SI, Luippold R, Garman P, et al. Disability among U.S. Army
veterans vaccinated against anthrax. Vaccine 2012;30:6150–6. https://
doi.org/10.1016/j.vaccine.2012.07.067
49. Sulsky SI, Luippold RS, Garman P, Hughes H, Amoroso PJ. Risk of
disability for U.S. Army personnel vaccinated against anthrax, 1998–2005.
Vaccine 2011;29:6035–41. https://doi.org/10.1016/j.vaccine.2011.06.028
50. Duderstadt SK, Rose CE Jr, Real TM, et al. Vaccination and risk of
type 1 diabetes mellitus in active component U.S. military, 2002–2008.
Vaccine 2012;30:813–9. https://doi.org/10.1016/j.vaccine.2011.10.087
51. McNeil MM, Duderstadt SK, Sabatier JF, Ma GG, Duffy J. Vaccination
and risk of lone atrial fibrillation in the active component United States
military. Hum Vaccin Immunother 2019;15:669–76. https://doi.
org/10.1080/21645515.2018.1549453
52. Bardenheier BH, Duffy J, Duderstadt SK, et al. Anthrax vaccine and
the risk of rheumatoid arthritis and systemic lupus erythematosus in the
U.S. military: a case-control study. Mil Med 2016;181:1348–56. https://
doi.org/10.7205/MILMED-D-15-00485
53. Conlin AM, Bukowinski AT, Gumbs GR; Department of Defense Birth
and Infant Health Registry Team. Analysis of pregnancy and infant
health outcomes among women in the National Smallpox Vaccine in
Pregnancy Registry who received anthrax vaccine adsorbed. Vaccine
2015;33:4387–90. https://doi.org/10.1016/j.vaccine.2015.05.054
54. Conlin AMS, Sevick CJ, Gumbs GR, Khodr ZG, Bukowinski AT. Safety
of inadvertent anthrax vaccination during pregnancy: an analysis of birth
defects in the U.S. military population, 2003–2010. Vaccine
2017;35:4414–20. https://doi.org/10.1016/j.vaccine.2017.06.032
55. US Food and Drug Administration. Emergency use authorization of medical
products and related authorities. Silver Spring, MD: US Food and Drug
Administration; 2017. https://www.fda.gov/media/97321/download
56. National Institutes of Health. A phase 2 safety and immunogenicity
study for an anthrax vaccine using 3 schedules and two dose levels.
Washington, DC: National Institutes of Health; 2015. https://
clinicaltrials.gov/ct2/show/results/NCT01770743?view=results
57. Cooper CL, Davis HL, Morris ML, et al. CPG 7909, an
immunostimulatory TLR9 agonist oligodeoxynucleotide, as adjuvant
to Engerix-B HBV vaccine in healthy adults: a double-blind phase I/II
study. J Clin Immunol 2004;24:693–701. https://doi.org/10.1007/
s10875-004-6244-3
58. Ellis RD, Martin LB, Shaffer D, et al. Phase 1 trial of the Plasmodium
falciparum blood stage vaccine MSP1(42)-C1/Alhydrogel with and
without CPG 7909 in malaria naïve adults. PLoS One 2010;5:e8787.
https://doi.org/10.1371/journal.pone.0008787
59. Cooper CL, Davis HL, Morris ML, et al. Safety and immunogenicity of
CPG 7909 injection as an adjuvant to Fluarix influenza vaccine. Vaccine
2004;22:3136–43. https://doi.org/10.1016/j.vaccine.2004.01.058
60. Cooper CL, Davis HL, Angel JB, et al. CPG 7909 adjuvant improves
hepatitis B virus vaccine seroprotection in antiretroviral-treated HIV-
infected adults. AIDS 2005;19:1473–9. https://doi.org/10.1097/01.
aids.0000183514.37513.d2
61. Mullen GE, Ellis RD, Miura K, et al. Phase 1 trial of AMA1-C1/
Alhydrogel plus CPG 7909: an asexual blood-stage vaccine for
Plasmodium falciparum malaria. PLoS One 2008;3:e2940. https://doi.
org/10.1371/journal.pone.0002940
62. US National Library of Medicine. BARDA Securing Anthrax Immunity
For the Elderly (B-SAFE) study. Bethesda, MD: US National Library
of Medicine. https://clinicaltrials.gov/ct2/show/NCT03518125?cond=
AV7909&draw=1&rank=3
Recommendations and Reports
MMWR / December 13, 2019 / Vol. 68 / No. 4 13
US Department of Health and Human Services/Centers for Disease Control and Prevention
63. Anthim. Package insert. Pine Brook, NJ: Elusys Therapeutics; 2016. https://
www.accessdata.fda.gov/drugsatfda_docs/label/2016/125509lbl.pdf
64. Raxibacumab. Package insert. Rockville, MD: GlaxoSmithKline;
2012. https://www.accessdata.fda.gov/drugsatfda_docs/
label/2012/125349s000lbl.pdf
65. Anthrasil. Package insert. Manitoba, Canada: Emergent BioSolutions;
2015. https://www.fda.gov/media/91577/download
66. Migone TS, Subramanian GM, Zhong J, et al. Raxibacumab for the
treatment of inhalational anthrax. N Engl J Med 2009;361:135–44.
https://doi.org/10.1056/NEJMoa0810603
67. Yamamoto BJ, Shadiack AM, Carpenter S, et al. Obiltoxaximab prevents
disseminated Bacillus anthracis infection and improves survival during
pre- and postexposure prophylaxis in animal models of inhalational
anthrax. Antimicrob Agents Chemother 2016;60:5796–805. https://
doi.org/10.1128/AAC.01102-16
68. Malkevich NV, Basu S, Rudge TL Jr, et al. Effect of anthrax immune
globulin on response to BioThrax (anthrax vaccine adsorbed) in New
Zealand white rabbits. Antimicrob Agents Chemother 2013;57:5693–6.
https://doi.org/10.1128/AAC.00460-13
Recommendations and Reports
14 MMWR / December 13, 2019 / Vol. 68 / No. 4
US Department of Health and Human Services/Centers for Disease Control and Prevention
Advisory Committee on Immunization Practices
Membership as of February 27, 2019
Chair: José R. Romero, MD, University of Arkansas for Medical Sciences and Arkansas Children’s Hospital, Little Rock, Arkansas.
Executive Secretary: Amanda Cohn, MD, National Center for Immunization and Respiratory Diseases, CDC, Atlanta, Georgia.
Members: Robert L. Atmar, MD, Baylor College of Medicine, Houston, Texas; Kevin A. Ault, MD, University of Kansas Medical Center, Kansas City, Kansas;
Henry Bernstein, DO, Zucker School of Medicine at Hofstra/Northwell Cohen Childrens’ Medical Center, New Hyde Park, New York; Echezona Ezeanolue,
MD, University of Nevada, Las Vegas, Nevada; Sharon E. Frey, MD, Saint Louis University Medical School, Saint Louis, Missouri; Stefan Gravenstein, MD,
Providence Veterans Administration Hospital, Providence, Rhode Island; Paul Hunter, MD, City of Milwaukee Health Department, Milwaukee, Wisconsin;
Grace M. Lee, MD, Lucile Packard Children’s Hospital, Stanford University School of Medicine, Stanford, California; Veronica V. McNally, JD, Fanny
Strong Foundation, West Bloomfield, Michigan; Kelly Moore, MD, Vanderbilt University School of Medicine, Nashville, Tennessee; José R. Romero, MD,
University of Arkansas for Medical Sciences and Arkansas Children’s Hospital, Little Rock, Arkansas; David Stephens, MD, Emory University School of
Medicine, Atlanta, Georgia; Peter Szilagyi, MD, University of California, Los Angeles (UCLA), Los Angeles, California; Helen Keipp Talbot, MD, Vanderbilt
University, Nashville, Tennessee; Emmanuel Walter, Jr., MD, Duke University School of Medicine, Durham, North Carolina.
Ex Officio Members: Mary Beth Hance, Centers for Medicare and Medicaid Services; Eric Deussing, MD, Department of Defense; Jane A. Kim, MD,
Department of Veterans Affairs; Doran Fink, MD, Food and Drug Administration; Narayan Nair, MD, Health Resources and Services Administration; Thomas
Weiser, MD, Indian Health Service; Tammy Beckham, National Vaccine Program Office; John Beigel, MD, National Institutes of Health.
Liaison Representatives: American Academy of Family Physicians, Pamela G. Rockwell, DO, Ann Arbor, Michigan; American Academy of Pediatrics, Yvonne
Maldonado, MD, Stanford, California; American Academy of Pediatrics, David Kimberlin, MD, Birmingham, Alabama; American Academy of Physician
Assistants, Marie-Michèle Léger, MPH, Alexandria, Virginia; American College Health Association, Susan Even, MD, Columbia, Missouri; American
College of Nurse Midwives, Carol E. Hayes, MN, Atlanta, Georgia; American College of Nurse Midwives, Pamela M. Meharry, PhD; American College of
Obstetricians and Gynecologists, Linda O’Neal Eckert, MD, Seattle, Washington; American College of Physicians, Jason M. Goldman, MD, Boca Raton,
Florida; American Geriatrics Society, Kenneth Schmader, MD, Durham, North Carolina; America’s Health Insurance Plans, Mark J. Netoskie, MD, Houston,
Texas; American Immunization Registry Association, Rebecca Coyle, MSEd, Washington DC; American Medical Association, Sandra Adamson Fryhofer,
MD, Atlanta, Georgia; American Nurses Association, Charles Rittle, MPH, Pittsburgh, Pennsylvania; American Osteopathic Association, Stanley Grogg, DO,
Tulsa, Oklahoma; American Pharmacists Association, Stephan L. Foster, PharmD, Memphis, Tennessee; Association of Immunization Managers, Christine
Finley, MPH, Burlington, Vermont; Association for Prevention Teaching and Research, Paul W. McKinney, MD, Louisville, Kentucky; Association of State
and Territorial Health Officials, Nathaniel Smith, MD, Little Rock, Arkansas; Biotechnology Industry Organization, Phyllis A. Arthur, MBA, Washington,
DC; Council of State and Territorial Epidemiologists, Christine Hahn, MD, Boise, Idaho; Canadian National Advisory Committee on Immunization,
Caroline Quach, MD, Montreal, Québec, Canada; Infectious Diseases Society of America, Carol J. Baker, MD, Houston, Texas; National Association of
County and City Health Officials, Matthew Zahn, MD, Santa Ana, California; National Association of County and City Health Officials, Jeffrey Duchin,
MD, Seattle, Washington; National Association of Pediatric Nurse Practitioners, Patricia A. Stinchfield, MS, St. Paul, Minnesota; National Foundation for
Infectious Diseases, William Schaffner, MD, Nashville, Tennessee; Mexico National Immunization Council and Child Health Program, Luis Duran, MD,
Mexico; National Medical Association, Patricia Whitley-Williams, MD, New Brunswick, New Jersey; Pediatric Infectious Diseases Society, Sean O’Leary,
MD, Colorado; Pediatric Infectious Diseases Society, Mark H. Sawyer, MD, San Diego, California; Pharmaceutical Research and Manufacturers of America,
David R. Johnson, MD, Swiftwater, Pennsylvania; Society for Adolescent Health and Medicine, Amy B. Middleman, MD, Oklahoma City, Oklahoma; Society
for Healthcare Epidemiology of America, David Weber, MD, Chapel Hill, North Carolina.
ACIP Anthrax Vaccine Work Group
ACIP Members: David S. Stephens, MD, Chair, Emory University School of Medicine, Atlanta, Georgia; Robert L. Atmar, MD, Baylor College of Medicine,
Houston, Texas; Sharon E. Frey, MD, St. Louis University Medical School, St. Louis, Missouri.
Ex Officio Members: Eric Espeland, PhD, Biomedical Advanced Research and Development Authority, Washington, DC; Chia-Wei Tsai, PhD,
Biomedical Advanced Research and Development Authority, Washington, DC; Amanda Zarrabian, MS, Biomedical Advanced Research and Development
Authority, Washington, DC; Eric Deussing, MD, Department of Defense, Atlanta, Georgia; Alexandra Worobec, MD, Food and Drug Administration,
Washington, DC; Julianne Clifford, PhD, Food and Drug Administration, Washington, DC; Judy Hewitt, PhD, National Institutes of Health, Bethesda,
Maryland; Kim Taylor, PhD, National Institutes of Health, Bethesda, Maryland.
Liaison Representatives: American College of Obstetricians and Gynecologists, Richard Beigi, MD, Pittsburgh, Pennsylvania; Infectious Diseases Society of
America, Kathleen Neuzil, MD, Baltimore, Maryland; American Academy of Pediatrics, James D. Campbell, MD, Golden, Colorado; National Association
of County and City Health Officials, Matthew Zahn, MD, Orange, California.
Invited Consultants: Wendy Keitel, MD, Baylor College of Medicine, Houston, Texas; Arthur Friedlander, MD, United States Army Medical Research
Institute of Infectious Diseases, Fort Detrick, Maryland; Phillip Pittman, MD, United States Army Medical Research Institute of Infectious Diseases, Fort
Detrick, Maryland; Andy Pavia, MD, University of Utah, Salt Lake City, Utah; Stacy Hall, MSN, Louisiana Office of Public Health, New Orleans, Louisiana.
CDC Contributors: Kate Hendricks, MD, CDC, Atlanta, Georgia; Jarad Schiffer, MS, CDC, Atlanta, Georgia; Conrad Quinn, PhD, CDC, Atlanta,
Georgia; Charles Rose, PhD, CDC, Atlanta, Georgia; Michael M. McNeil, MD, CDC, Atlanta, Georgia; Jennifer Wright, DVM, CDC, Atlanta, Georgia;
Yon Yu, PharmD, CDC, Atlanta, Georgia; Marie de Perio, MD, CDC, Cincinnati, Ohio.
Work Group Secretariat: William Bower, MD, CDC, Atlanta, Georgia.

ISSN: 0149-2195 (Print)
The Morbidity and Mortality Weekly Report (MMWR) Series is prepared by the Centers for Disease Control and Prevention (CDC) and is available free
of charge in electronic format. To receive an electronic copy each week, visit MMWR at https://www.cdc.gov/mmwr/index.html.
Readers who have difficulty accessing this PDF file may access the HTML file at https://www.cdc.gov/mmwr/volumes/68/rr/rr6804a1.htm?s_
cid=rr6804a1_w. Address all inquiries about the MMWR Series, including material to be considered for publication, to Executive Editor, MMWR Series,
Mailstop E-90, CDC, 1600 Clifton Rd., N.E., Atlanta, GA 30329-4027 or to mmwr[email protected].
All material in the MMWR Series is in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated.
MMWR and Morbidity and Mortality Weekly Report are service marks of the U.S. Department of Health and Human Services.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
References to non-CDC sites on the Internet are provided as a service to MMWR readers and do not constitute or imply endorsement of these organizations
or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of these sites. URL addresses
listed in MMWR were current as of the date of publication.
