For more information: www.cdc.gov/COVID19
Phased Allocation
of COVID-19 Vaccines
ACIP COVID-19 Vaccines Work Group
Kathleen Dooling, MD, MPH
ACIP meeting
December 20, 2020

Objective
Policy Question:
Which groups should be offered COVID-19 vaccination in Phase 1b & 1c?

Ensure safety and effectiveness of COVID-19 vaccines
Reduce transmission, morbidity, mortality of COVID-19 disease
Help minimize disruption to society and the economy, including maintaining
healthcare capacity
Ensure equity in vaccine allocation and distribution
Work Group Considerations:
Goals of the COVID-19 Vaccine Program
Work Group considerations: Balancing Goals
Prevention of
Morbidity & Mortality
Preservation of
Societal Functioning
Work Group considerations: Balancing Goals
Prevention of
Morbidity & Mortality
Preservation of
Societal Functioning
1a LTCF residents Health care personnel
●Ensure safety and effectiveness of COVID-19 vaccines●
●Ensure equity in vaccine allocation and distribution●

Work Group considerations: Balancing Goals
10 public ACIP meetings, 28 COVID-19 Work Group meetings
Evidence: Scientific, Implementation, Ethical
External Expert Advice
–
–
–
–
–
–
–
National Academies of Science Engineering Medicine
Academic Reports
International Recommendations
Public Input
Focus groups
Population surveys
Pandemic preparedness
ACIP public comment and federal register
Work Group considerations: Balancing Goals
Prevention of
Morbidity & Mortality
Preservation of
Societal Functioning
1a LTCF residents Health care personnel
1b Persons 75 years and older Frontline Essential Workers
1c
Persons 65-74 years
Persons 16-64 with high-risk
medical conditions
Other Essential Workers
●Ensure safety and effectiveness of COVID-19 vaccines●
●Ensure equity in vaccine allocation and distribution●
Work Group considerations: Balancing Goals
Prevention of
Morbidity & Mortality
Preservation of
Societal Functioning
1a LTCF residents Health care personnel
1b Persons 75 years and older Frontline Essential Workers
1c
Persons 65-74 years
Persons 16-64 with high-risk
medical conditions
Other Essential Workers
●Ensure safety and effectiveness of COVID-19 vaccines●
●Ensure equity in vaccine allocation and distribution●
Phase 1 Phase 2 Phase 3
Phase 1a “Jumpstart Phase”
• High-risk health workers
• First responders
Phase 1b
• People of all ages with
comorbid and underlying
conditions that put them
at significantly higher risk
• Older adults living in
congregate or
overcrowded settings
• K-12 teachers and school staff and child
care workers
• Critical workers in high-risk settings—
workers who are in industries essential to
the functioning of society and substantially
higher risk of exposure
• People of all ages with comorbid and
underlying conditions that put them at
moderately higher risk
• People in homeless shelters or group
homes for individuals with disabilities,
including serious mental illness,
development and intellectual disabilities,
and physical disabilities or in recovery, and
staff who work in such settings
• People in prisons, jails, detention centers,
and similar facilities, and staff who work in
such settings
• All older adults not included in Phase 1
• Young adults
• Children
• Workers in industries
and occupations
important to the
functioning of
society and at
increased risk of
exposure not
included in Phase 1
or 2
NASEM
Framework
National Academies of Sciences, Engineering, and Medicine 2020. https://www.nationalacademies.org/our-work/a-framework-for-equitable-allocation-of-vaccine-for-the-novel-coronavirus

Essential Workers* (total ~87M)
Frontline Essential Workers (~30M)
First Responders (Firefighters, Police)
Education (teachers, support staff, daycare)
Food & Agriculture
Manufacturing
Corrections workers
U.S. Postal service workers
Public transit workers
Grocery store workers
Other Essential Workers (~57M)
Transportation and logistics
Food Service
Shelter & Housing (construction)
Finance
IT & Communication
Energy
Media
Legal
Public Safety (Engineers)
Water & Wastewater
*CISA: Essential Critical Infrastructure Workers: https://www.cisa.gov/news/2020/08/18/cisa-releases-updated-guidance-essential-critical-infrastructure-workers
Frontline Essential Workers: workers who are in sectors essential to the functioning of society and are at
substantially higher risk of exposure to SARS-CoV-2
Proposed Phases of COVID-19 Vaccination
16-64 years
with high -risk
medical conditions
(>110M)
16-64 years
Without high -risk
medical conditions
(<86M)
65
-74 years (32M)
75+ years (21M)
Essential Workers
LTCF
Phase 1a
Phase 1b
Phase 1c
Phase 2
HCP
Frontline
Allocation of COVID-19 vaccine
12
Ethics
Science
Implementation
Which groups should be
recommended to receive
COVID-19 vaccines in
Phase 1b & 1c?
Science
Ethics
Science
Implementation

COVID-19 incidence is highest in young adults
*Data sources: CDC COVID-19 data tracker. Population estimates from 2019 US Census Bureau. Data provisional, subject to change.
National Estimate of COVID-19 Incidence per 100,000 Population,
by Age Group – Data through Dec 16, 2020
1135
1944
5489
4671
4543
3993
2977
3147
5064
0 1000 2000 3000 4000 5000 6000
0-4
5-17
18-29
30-39
40-49
50-64
65-74
75-84
85+
COVID-19 Incidence per 100,000 Population
Age Group (Years)
*Data sources: CDC COVID-19 data tracker. Population estimates from 2019 US Census Bureau. Data provisional, subject to change.
COVID-19 mortality rates are highest in older adults
National Estimate of COVID-19 Deaths per 100,000 Population, by
Age Group – Data through Dec 16, 2020
0.3
0.2
2.2
6.3
15.7
50.6
143.5
366.2
1,118.3
0.0 200.0 400.0 600.0 800.0 1,000.0 1,200.0
0-4
5-17
18-29
30-39
40-49
50-64
65-74
75-84
85+
Death Rate per 100,000 Population
Age Group (Years)
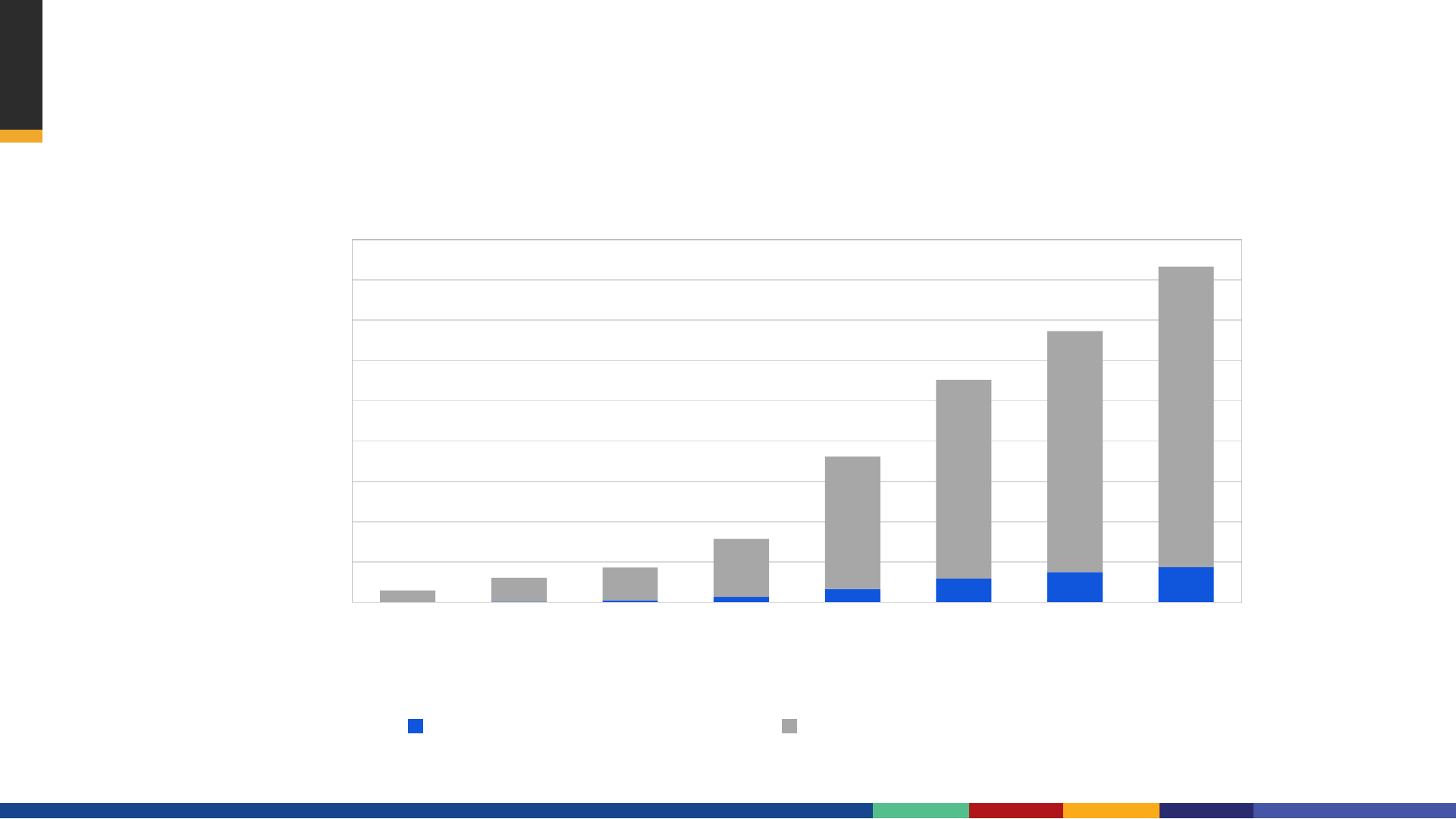
Although overall mortality increases with age, the proportion of deaths
associated with COVID-19 is similar across middle-age and older adults
16
As of December 16
th
: https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm
0
100000
200000
300000
400000
500000
600000
700000
800000
900000
15–24 25–34 35–44 45–54 55–64 65–74 75–84 85+
Number of deaths
Deaths involving COVID-19 Deaths from all causes
Age Group (years)
9%
9%
10%
11%
10%
Deaths from All Causes and Deaths Involving COVID-19, by Age Group
Data through Dec 16, 2020
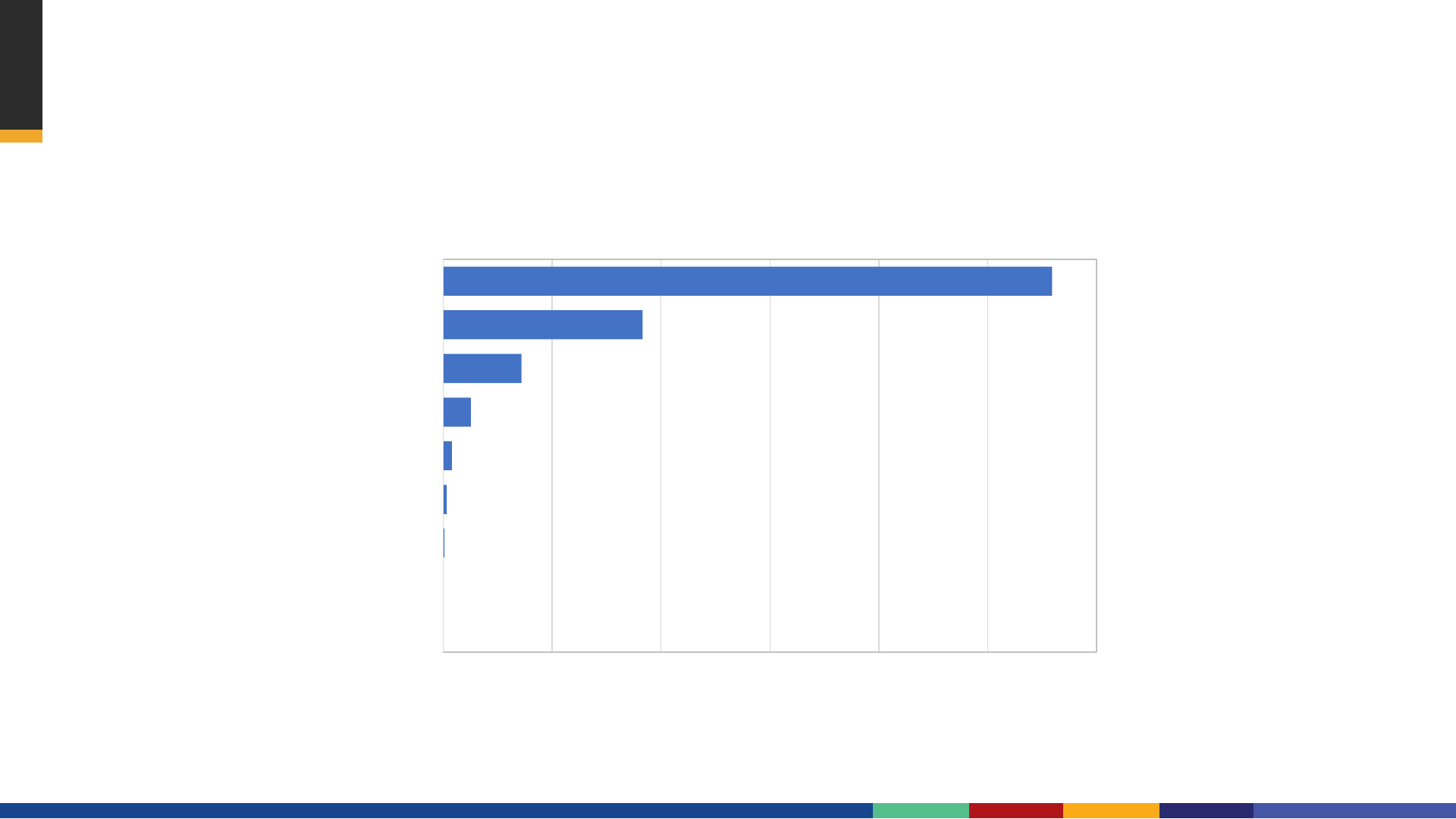
Adults 75 years and older account for 25% of COVID-19
associated hospitalizations
Data Source: COVID-19 associated hospitalizations reported to Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET) surveillance system. COVID-NET is a
population-based surveillance system that collects data on laboratory-confirmed COVID-19-associated hospitalizations among children and adults through a network of over 250 acute-care hospitals in 14 states.
12%
25%
39%
25%
0 5 10 15 20 25 30 35 40 45
15-34
35-54
55-74
75+
Percent of COVID-19 Hospitalizations
Age Group (Years)
Percent of COVID-19-Associated Hospitalizations, by Age Group
Data through Dec 5, 2020
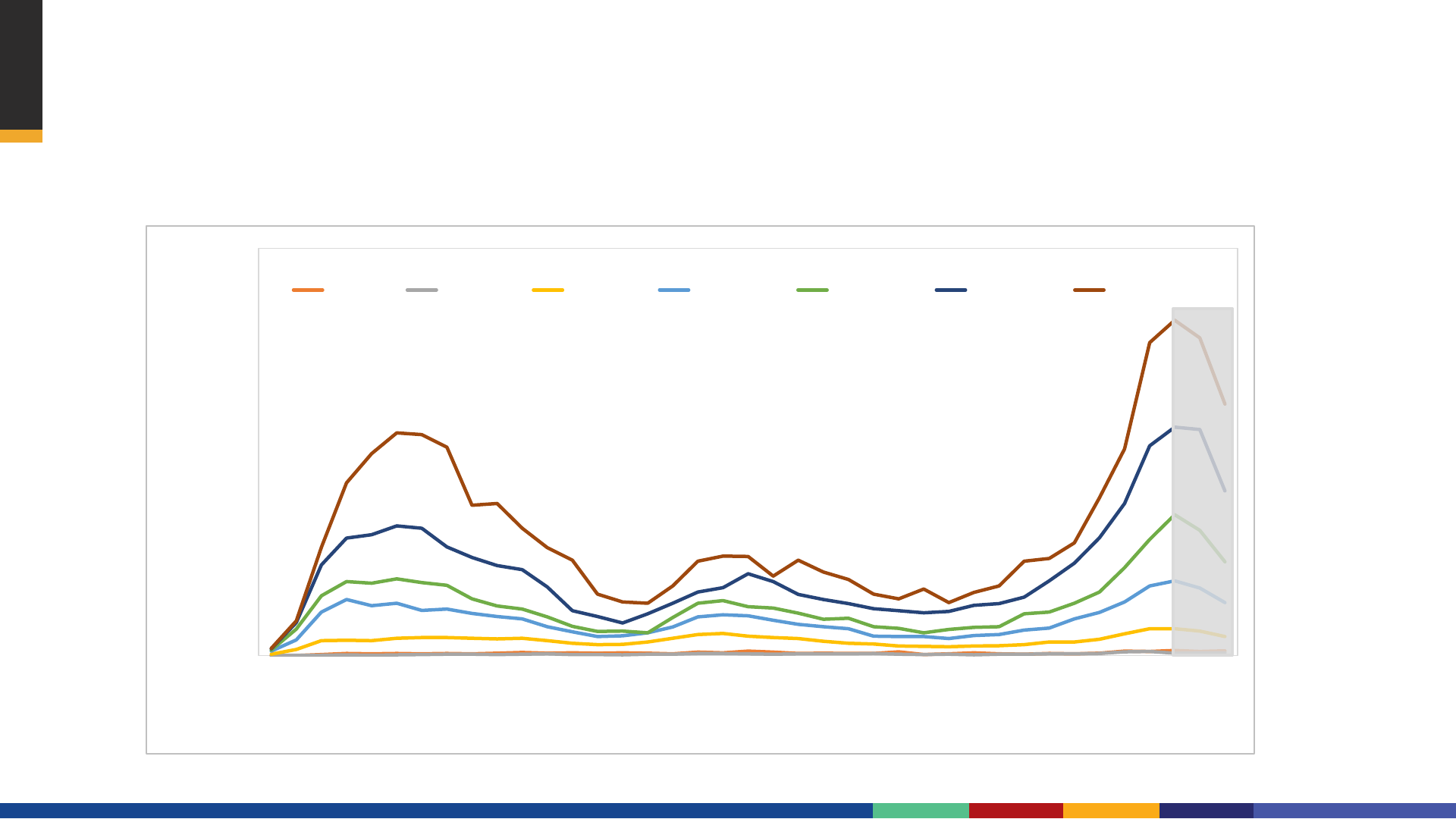
0
20
40
60
80
100
120
10 15 20 25 30 35 40 45
Hospitalization rates per 100,000
MMWR Week
0-4 yr 5-17 yr 8-49 yr 50-64 yr 65-74 yr 75-84 yr ≥85 yr
Age Group
Data Source: https://gis.cdc.gov/grasp/COVIDNet/COVID19_3.html
COVID-19-Associated Hospitalization Rates per 100,000 population
Preliminary Weekly Rates as of Dec 5, 2020
COVID-19-associated hospitalization rates are highest
in older adults
Unadjusted and Adjusted
a
Rate Ratios for Number of Underlying Medical Conditions
and COVID-19-Associated Hospitalization, COVID-NET March 1- June 23, 2020
Unadjusted Rate Ratio (95%CI) Adjusted Rate Ratio
a
(95%CI)
Number of conditions
b
1 2.8 (2.7, 3.1)
2.5 (2.1, 3.0)
2 5.6 (5.2, 6.1)
4.5 (3.7, 5.5)
3+ 7.2 (6.6, 7.9)
5.0 (3.9, 6.3)
Age 45-64 years
c
-----
1.8 (1.5, 2.2)
Age 65+ years
c
-----
2.6 (2.1, 3.1)
Male sex
d
-----
1.2 (1.1, 1.4)
Non-Hispanic black
e
-----
3.9 (3.3, 4.7)
Other race/ethnicity
e
-----
3.3 (2.8, 3.9)
CI: Confidence Interval; COVID-NET: Coronavirus Disease 2019-Associated Hospitalization Surveillance Network
a
Model for number of conditions (variable) is adjusted for age, sex, and race/ethnicity
b
Reference group is no underlying medical condition; Number of conditions is a sum of underlying medical conditions excluding hypertension; the most recent
year of available BRFSS data for hypertension was 2017.
c
Reference group is 18-44 years
d
Reference group is female
e
Reference group is non-Hispanic white
Risk for COVID-19 associated hospitalization increased with
the number of underlying medical conditions
Ko, Sept 2020, doi: 10.1093/cid/ciaa1419
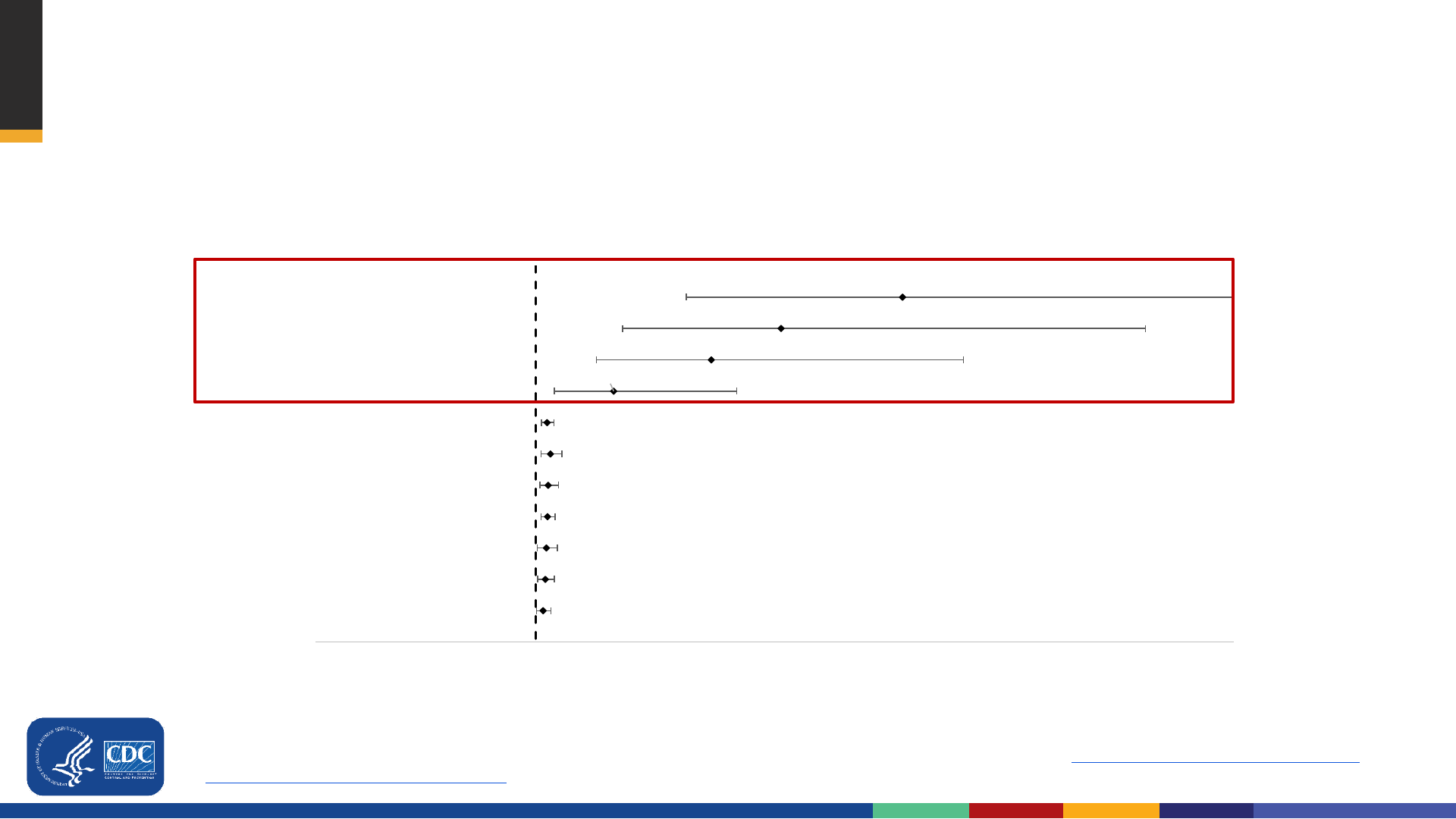
Risk of in-hospital death among patients with COVID-19 associated hospitalization,
COVID-NET March 1 - May 2, 2020
*COVID-NET Surveillance; Final model adjusted for age, sex, race/ethnicity, smoker, hypertension, obesity, diabetes, chronic lung disease, cardiovascular disease, neurologic
disease, renal disease, immunosuppression, hematologic disorders, and rheumatologic or autoimmune disease. Kim et al, 2020,
https://academic.oup.com/cid/advance-
article/doi/10.1093/cid/ciaa1012/5872581
85+ years vs 18–39 years
75–84 years vs 18–39 years
65–74 years vs 18–39 years
50–64 years vs 18–39 years
Male
Immunosuppression
Renal disease
Chronic Lung Disease
Cardiovascular Disease
Neurologic disorder
Diabetes
10.98
7.67
5.77
3.11
1.3
1.39
1.33
1.31
1.28
1.25
1.19
-5 0 5 10 15 20
Adjusted Rate Ratios and 95% Confidence Intervals
17
Risk of in-hospital death among persons hospitalized for
COVID-19 increased with age

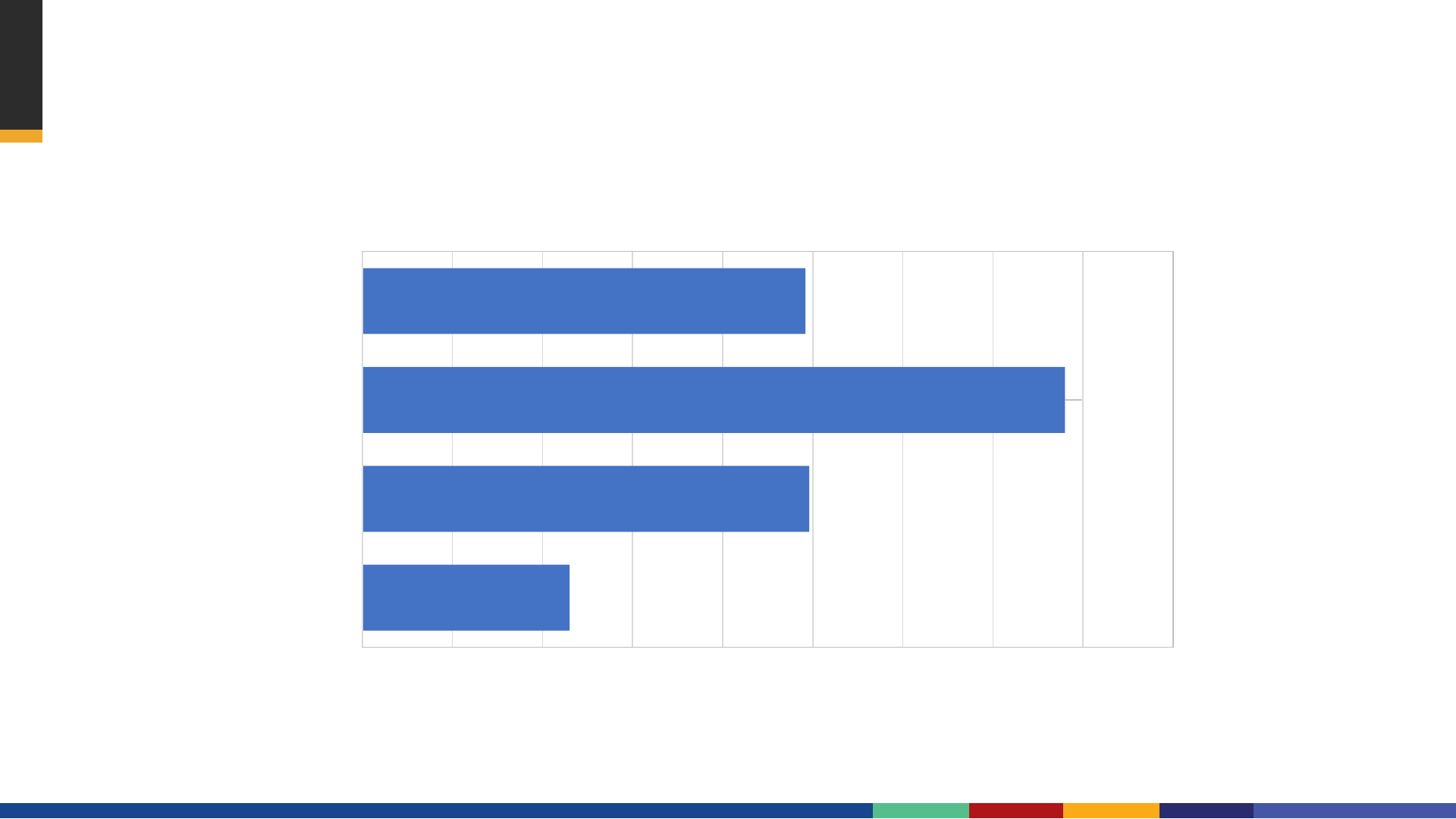
High seroprevalence
among many
frontline essential
workers groups
following first wave
of pandemic in NYC
Percent seropositive for SARS-CoV-2 IgG antibody, by occupation among
workers in public service agencies — New York City, May–July 2020
Other includes Dietary Service Staff, Environmental Service Staff and participants who selected Other and were not reassignedto an existing category
Other Health includes Student/Trainee, Respiratory Therapist, Occupational/Speech/Physical Therapist, Therapy Aide/Assistant, Pharmacist, Diagnostic Imaging Technician, Phlebotomist,
Medical Registrar, Orderly, Dietician, Dentist, Clinical Technician, Medical Assistant. Sami
et al.
Manuscript in preparation.
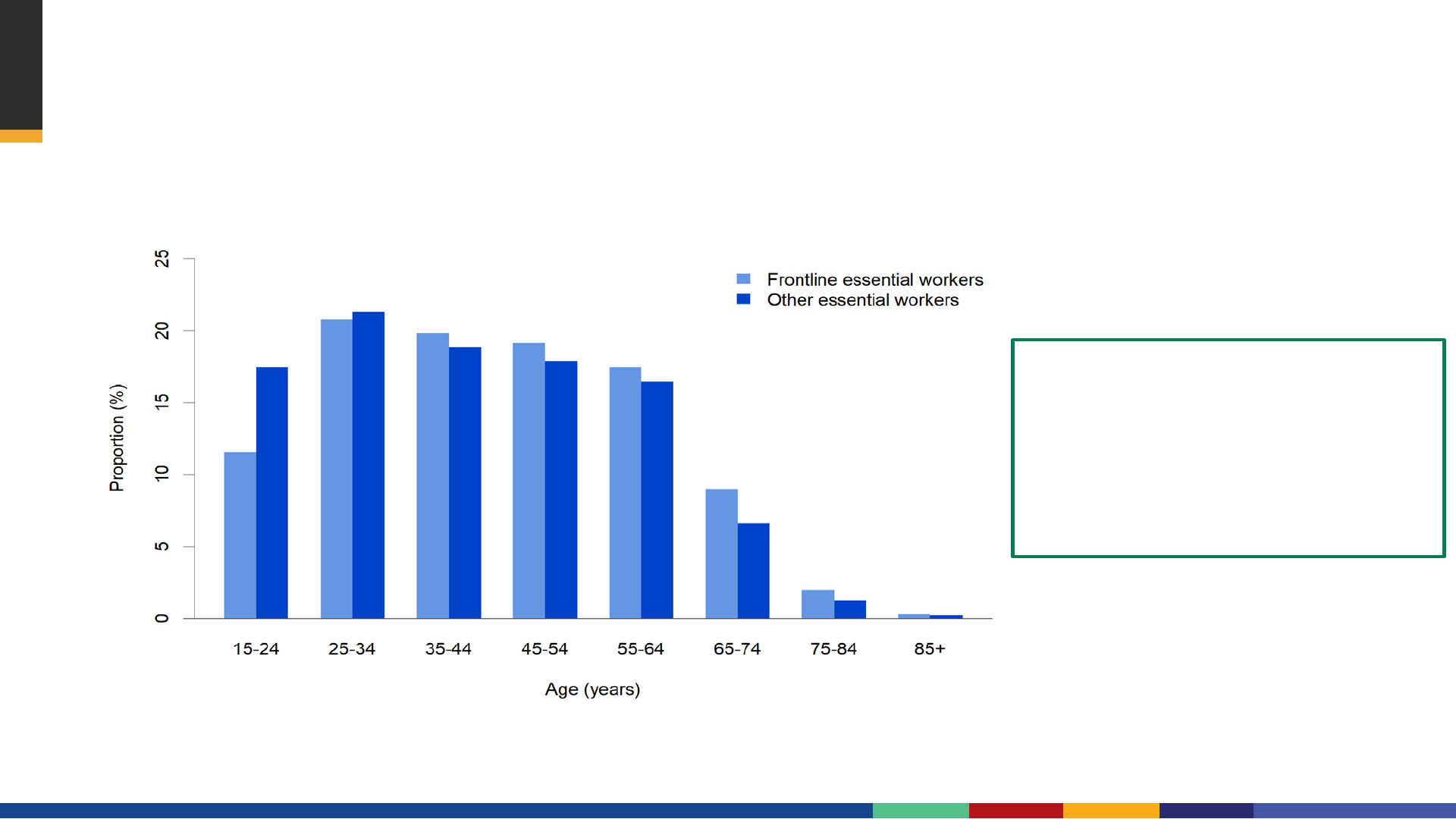
Half of essential workers are older than 40 years
1. Data Source: American Community Survey, 2019 2. Data source: 2019 Behavioral Risk Factor Surveillance System
• 8-11% are ≥65 years old
1
• >56% of adults 18-64
years have ≥1 high-risk
medical condition
2

Summary of Work Group interpretation: Modeling
In the scenarios considered, differences between strategies is minimal
– Vaccinating older adults first averts slightly more deaths, vaccinating younger adults first
(essential workers or younger adults with high-risk conditions) averts slightly more
infections
– Ethical principles and implementation considerations also contribute to selecting the
optimal sequence in Phase 1b and 1c
Largest driver of impact in averted deaths and infections is the timing of vaccine
introduction in relation to increases in COVID-19 cases
– Emphasizes the need to continue non-pharmaceutical interventions (e.g. wearing a mask,
social distancing to prevent cases so vaccine can have maximum impact)
Vaccine’s ability to prevent transmission will further inform future modeling analysis and
interpretation
Modeling Strategies for the initial Allocation of SARS-CoV-2 Vaccines https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2020-10/COVID-Biggerstaff.pdf

Impacts of COVID-19 not represented in models:
Late Sequelae of COVID-19
Most commonly reported symptoms include:
fatigue, dyspnea, cough, arthralgia, and chest pain
More serious complications appear to be less common but have been reported:
Cardiovascular: myocardial inflammation, ventricular dysfunction
Respiratory: pulmonary function abnormalities
Renal: acute kidney injury
Dermatologic: rash, alopecia
Neurological: olfactory and gustatory dysfunction, sleep dysregulation, altered cognition,
memory impairment
Psychiatric: depression, anxiety, changes in mood
CDC, Late Sequelae of COVID-19 https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/late-sequelae.html
Implementation
Ethics
Science
Implementation

Safety is paramount. Vaccine safety standards will not be compromised in
efforts to accelerate COVID-19 vaccine development or distribution
Inclusive clinical trials. Study participants should reflect groups at risk for
COVID-19 to ensure safety and efficacy data are generalizable
Efficient Distribution. During a pandemic, efficient, expeditious and
equitable distribution and administration of approved vaccine is critical
Flexibility. Within national guidelines, state and local jurisdictions should have
flexibility to administer vaccine based on local epidemiology and demand
ACIP COVID-19 Vaccine Work Group: Proposed Guiding Principles
E
Q
U
I
T
Y

Efficient Distribution. During a pandemic, efficient, expeditious
and equitable distribution and administration of authorized vaccine
is critical
Flexibility. Within national guidelines, state and local jurisdictions
should have flexibility to administer vaccine based on local
epidemiology and demand
ACIP COVID-19 Vaccine Work Group: Proposed Guiding Principles
E
Q
U
I
T
Y

Feasibility
Adults ≥65 years
Challenge: long distances to central clinics and high throughput of clinics
Older adults report high intent to receive COVID-19 vaccine
Physician offices, pharmacies and public health clinics are established providers of adult vaccination
Population surveys report 73% - 82% of respondents supported priority vaccination of
persons aged ≥65 years/elderly in polls conducted in December 2020
2,3
1. 2. AP-NORC Center for Public Affairs Research. Many remain doubtful about getting COVID-19 vaccine. December
2020.
https://apnorc.org/projects/many-remain-doubtful-about-getting-covid-19-vaccine. 3. ABC/IPSOS poll. December 14,
2020.
https://www.ipsos.com/en-us/news-polls/abc-news-coronavirus-poll.

Feasibility
Essential workers
Challenge: reaching workers in rural locations, shift workers, those working multiple jobs or
working in small cohorts
Jurisdiction approaches include on site occupational clinics/pharmacies/Health Dept POD
strike teams
Population surveys report 68% - 87% of respondents supported prioritization of early
allocation of COVID-19 vaccine supply to essential workers (eg. police/fire/rescue and
teachers)
1-3
1. The Harris Poll:https://www.axios.com/who-gets-coronavirus-vaccine-first-4ff87ff8-39d7-49d6-8d25-fa2307119235.html. 2. AP-NORC Center for Public Affairs Research. Many
remain doubtful about getting COVID-19 vaccine. December 2020. https://apnorc.org/projects/many-remain-doubtful-about-getting-covid-19-vaccine. 3. ABC/IPSOS poll.
December 14, 2020. https://www.ipsos.com/en-us/news-polls/abc-news-coronavirus-poll.

Feasibility
Adults with high-risk medical conditions
Challenges: determining eligibility & very large group
Healthcare homes, such as physician offices or pharmacies, could be better suited to verifying
underlying medical conditions
Population surveys report 68% - 84% of respondents supported prioritization of early allocation
of COVID-19 vaccine supply to persons who are high risk because of medical problems
1-3
1. The Harris Poll:https://www.axios.com/who-gets-coronavirus-vaccine-first-4ff87ff8-39d7-49d6-8d25-fa2307119235.html. 2. AP-NORC Center for Public Affairs Research. Many
remain doubtful about getting COVID-19 vaccine. December 2020. https://apnorc.org/projects/many-remain-doubtful-about-getting-covid-19-vaccine. 3. ABC/IPSOS poll.
December 14, 2020. https://www.ipsos.com/en-us/news-polls/abc-news-coronavirus-poll.
Ethics
Ethics
Science
Implementation
Ethical Principle
Older Adults
Age 75+ years (21M) Age 65-74 Years (32M)
Maximize benefits and
minimize harms
Reduces morbidity and mortality in
persons with highest burden of COVID-
19 hospitalization and death
Reduces morbidity and mortality in
persons with high burden of COVID-
19 hospitalization and death
Promote justice
-Will require focused outreach to those who experience barriers to access
healthcare
-Persons living in multi-generational households may have greater risk of
exposure
Mitigate Health
inequities
- Racial and ethnic minority groups under-represented among adults >65
- Racial and ethnic minority persons >65 disproportionate COVID-19 related
hospitalization and death rates
Ethical Principle
Essential Workers
Frontline essential workers (~30 M) / Other essential workers (~57M)
Maximize benefits and
minimize harms
-Essential Workers are at high risk of exposure. Prevention of disease will
reduce transmission
-Preserves services essential to the COVID-19 response and overall functioning
of society. “Multiplier effect”
Promote justice
-Workers unable to work from home
-High level of interaction with public or
others in the workplace
-May be unable to control social
distancing
-Frequently interact with others in
the workplace
Mitigate Health
inequities
-Racial and ethnic minority groups disproportionately represented in many
essential industries
-~1/4 of essential workers live in low-income families
Ethical Principle
Persons 16-64 with high-risk
medical conditions
(>110 Million)
Maximize benefits and
minimize harms
Reduces morbidity and mortality in persons with moderate to high burden of
COVID-19 associated hospitalization and death
Promote justice
Will require focused outreach to those with limited or no access to healthcare
Mitigate Health
inequities
-Increased prevalence of some medical conditions in race/ethnic minority
groups & persons in rural areas
-Diagnosis of medical conditions requires access to healthcare

Summary of Work Group Considerations

Summary: Work Group considerations
Scientific, implementation and ethical considerations support inclusion of groups in Phase 1b and
1c as a balance of prevention of morbidity and mortality and preservation of societal functions
This represents an interim Phase 1 sequence– allocation policy will need to be dynamic and adapt
as new information such as vaccine performance and supply and demand become clear
Gating criteria will be necessary to move expeditiously from one Phase to the next, if supply
exceeds demand
Following vaccination, measures to stop the possible spread of SARS-CoV-2, such as masks and
social distancing, will still be needed
The U.S. government is committed to making COVID-19 vaccines available to all residents, as
soon as possible
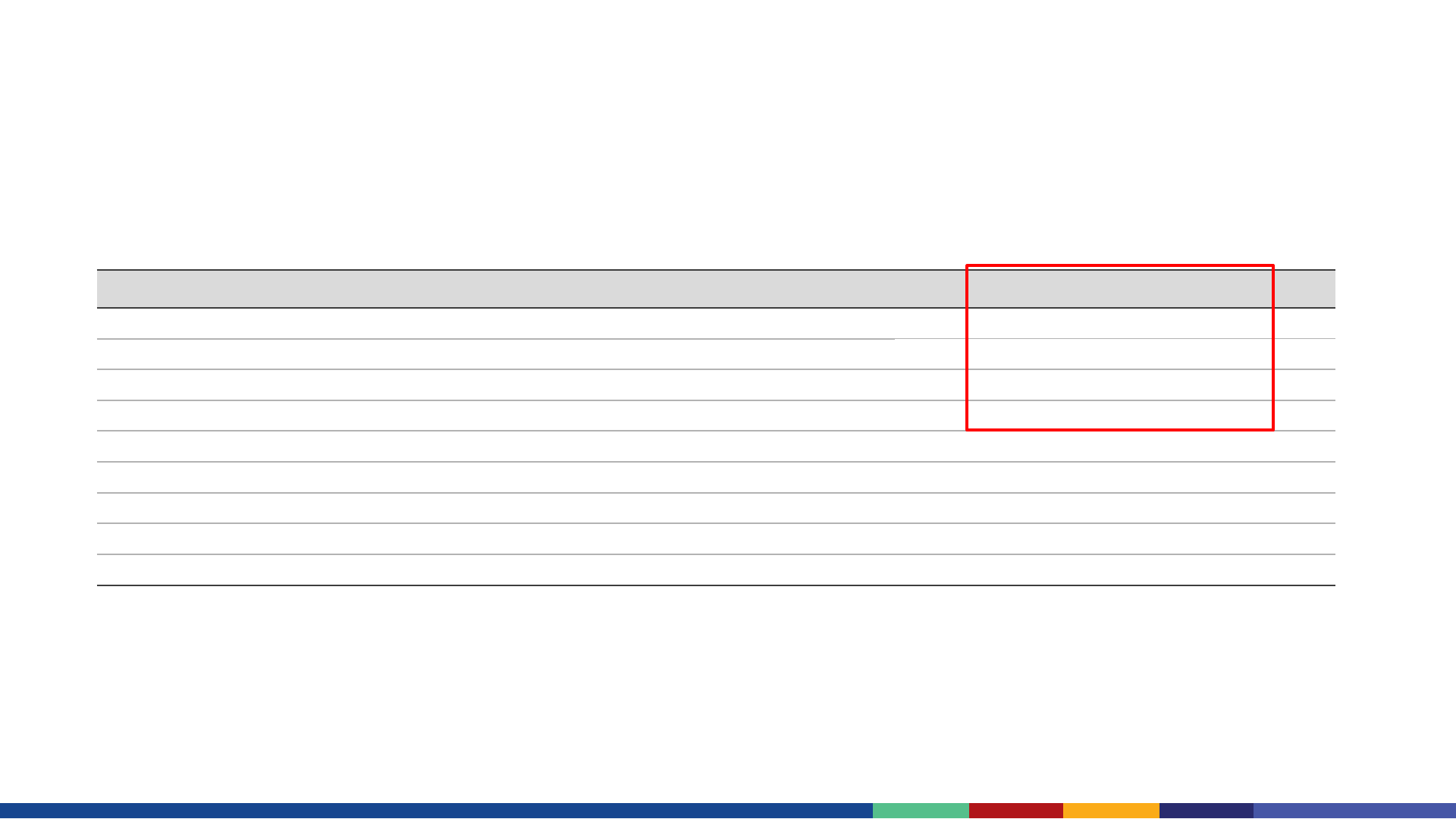
Proposed Phase 1 & 2 allocation, December 2020
*Accounts for persons recommended in prior phases or overlap within a phase
Phase
Groups recommended for vaccination
Number of
persons in each
group
(millions)
Number of unique*
persons in each
group
(millions)
Total*
(millions)
1a
Health care personnel
Long-term care facility residents
21
3
21
3
24
1b
Frontline essential workers
Persons aged 75 years and older
30
21
30
19
49
1c
Persons aged 65-74 years
Persons aged 16-64 years with high-risk conditions
Essential workers not recommended in Phase 1b
32
110
57
28
81
20
129
2
All people aged 16 years and older not in Phase 1,
who are recommended for vaccination
Proposed Phase 1 & 2 allocation, December 2020
*Accounts for persons recommended in prior phases or overlap within a phase
Phase
Groups recommended for vaccination
Number of
persons in each
group
(millions)
Number of unique*
persons in each
group
(millions)
Total*
(millions)
1a
Health care personnel
Long-term care facility residents
21
3
21
3
24
1b
Frontline essential workers
Persons aged 75 years and older
30
21
30
19
49
1c
Persons aged 65-74 years
Persons aged 16-64 years with high-risk conditions
Essential workers not recommended in Phase 1b
32
110
57
28
81
20
129
2
All people aged 16 years and older not in Phase 1,
who are recommended for vaccination
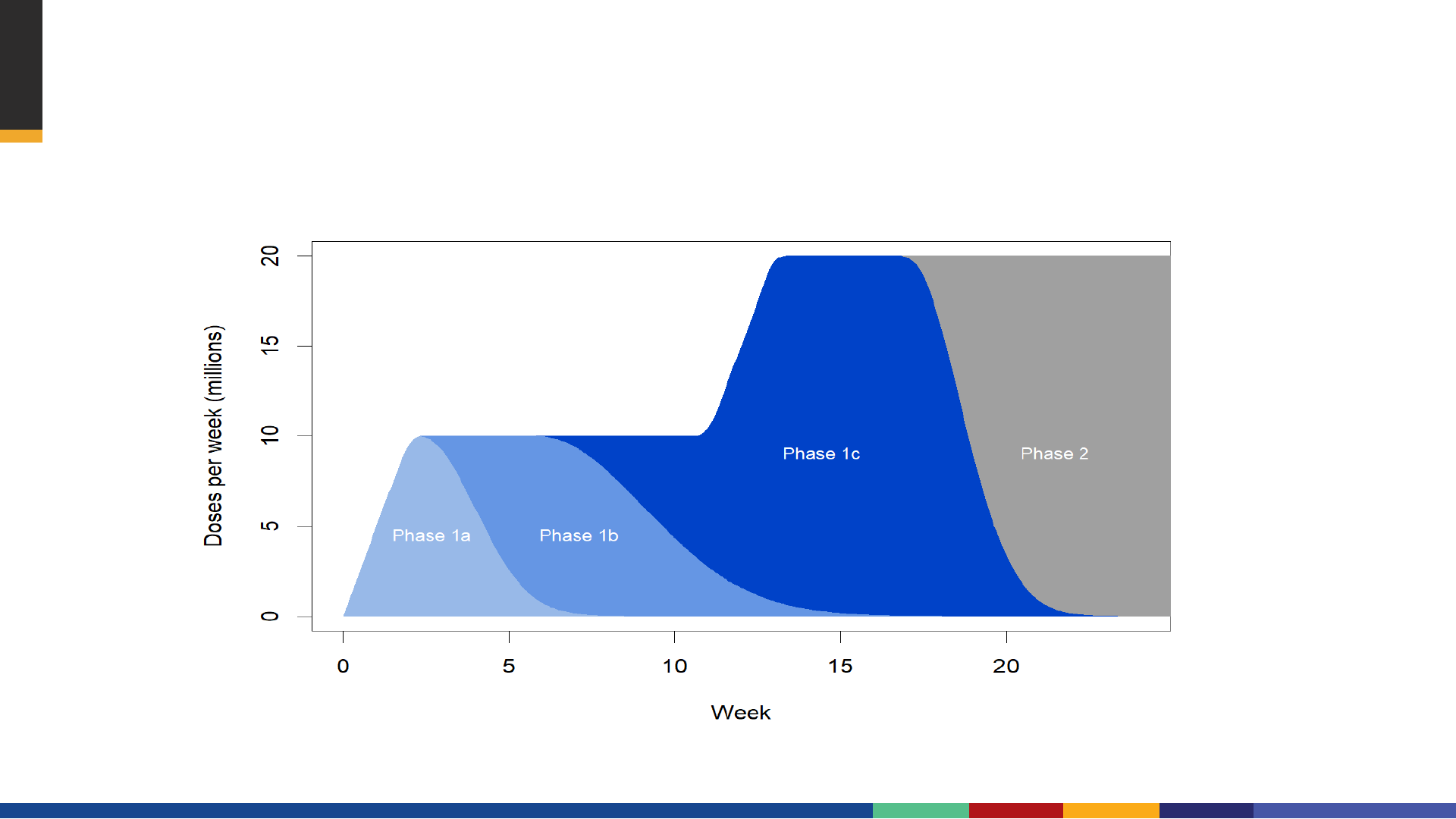
Example of Phase 1 & Phase 2 COVID-19 vaccination roll-out
Proposed Phases of COVID-19 Vaccination
16
-64 years
with high
-risk
medical conditions
(>110M)
16-
64 years
Without high -
risk
medical
conditions
(<86M)
65
-74 years (32M)
75+ years (21M)
Essential Workers
LTCF
Phase 1a
Phase 1b
Phase 1c
Phase 2
HCP
Frontline

ACIP Vote – Interim Recommendation
As an update to ACIP recommendations for vaccination in Phase 1a (health care
personnel, and long-term care facility residents), if COVID-19 vaccine supply is limited,
the following groups should be offered vaccination:
Phase 1b: persons aged ≥75 years and frontline essential workers
Phase 1c: persons aged 65–74 years, persons aged 16–64 years with high-risk medical
conditions, and other essential workers
For more information, contact CDC
1-800-CDC-INFO (232-4636)
TTY: 1-888-232-6348 www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the
official position of the Centers for Disease Control and Prevention.
Thank you
