
How to Successfully Integrate Midwives into Your Practice | Appendix 4
Appendix 4: Sample Business Plan
This sample Business Plan was developed by Heather Shannon, CNM, MS, MPH as part of her MPH
project. A small community hospital used this plan to launch a practice with two midwives and includes
plans for practice growth and the addition of more midwives. See Appendix 2 for a high-level summary
of the financial considerations as well as a sample pro forma tool to help developing a business plan for
integrating midwives.
Business Plan for
Midwifery Practice at
HOSPITAL
YEAR
By AUTHOR
Executive Summary
An opportunity exists for the development of a midwifery service at YOUR HOSPITAL and YOUR
PRACTICE to be implemented in the 20XX fiscal year. The practice model will be provider-based nurse
midwives, integrated with the existing Department of OB/GYN. As part of ongoing efforts to improve
access to care in YOUR County, HOSPITAL and YOUR DEPARTMENT jointly support this idea of a new
midwifery practice.
Midwifery care focuses on diagnosing and treating conditions related to women’s health during
their lifecycle. Midwives are primary care providers that manage medical conditions within their scope
of practice, provide educational support, and focus on prevention to increase individual health and
wellness of all gynecological and obstetrical patients. XXX Midwifery Practice will be a venue for women
in need of access to full-scope midwifery care or for women seeking an alternative to traditional
allopathic gynecological and obstetrical care.
The population that will benefit most is located on the near west side of YOUR CITY and YOUR
County and is made up of primarily of Latino, African American, and Caucasian women. By starting a
practice in this area, it offers an opportunity to care for women in zip codes with an underserved,
disparate population affected with limited access to care and adverse perinatal outcomes as well as
those women interested in midwifery care. Besides the underserved urban population, the practice will
draw on the suburban and rural population from western YOUR County. The patient mix anticipated will
be XXX% obstetrical and XXX% gynecological. The payor mix anticipated will be XXX% public insurance
(Medicaid) and XXX% private insurance.

Seed money for the XXX Midwifery Practice during the startup and first two years of operations
will need to be explored. The financial plan shows the practice will be financially dependent on seed
money for the first two years and by year three, the practice will begin to show a profit. Years four and
five will show a profit and sustainability as patient volume continues to grow. The projected start-up
costs will be $XX, which includes marketing, renovations, office furniture, equipment, and supplies, and
building rent. Year one, the anticipated practice costs will be $XX and revenues will be $XX, for a deficit
of $XX. For year two, the anticipated growth will be XXX% and practice costs will be $XX with revenues
of $XX and a deficit of $XX. In year three, the anticipated growth will be XXX% and practice costs will be
$XX with revenues of $XX. The practice will see its first profit of $XX. In year four, the anticipated
growth will be XXX% and practice costs will be $XX with revenues of $XX, yielding a profit of $XX. In year
five, the anticipated growth will be XXX% and practice costs will be $XX with revenues of $XX, yielding a
profit of $XX.
There is a need in YOUR County women’s health market for midwifery care, specifically on the
LOCAL AREA. YOUR County has the largest number of zip codes, scoring below the national average for
early prenatal care (PNC), indicating that it has a high proportion of women who do not receive PNC in
their first trimester in XXX (see Appendix A). YOUR County has eight zip codes above the national
average for low birth weight (LBW)
1
of XXX% (see Appendix A). Five of the XXX zip codes are within a
two miles of the proposed near west side location. YOUR HOSPITAL is positioned to develop a
midwifery practice, which meets the needs of the community and the hospital. The philosophy of
midwifery care will complement the culture at XXX and will serve to assist the institution in achieving its
goals of excellence in women’s services into the future.
1
LBW is defined as neonatal weight at birth of 5lb 8oz or 2,500grams from CDC
http://www.cdc.gov/pednss/what_is/pednss_health_indicators.htm
Table of Contents
Company Summary ....................................................................................................................................... 5
Scope of Services .......................................................................................................................................... 7
Management Systems................................................................................................................................... 8
Information Management and Technology .............................................................................................. 9
EMR ........................................................................................................................................................... 9
Billing ......................................................................................................................................................... 9
Financial Plan .............................................................................................................................................. 10
Five Year Plan .............................................................................................................................................. 11
Start-up ................................................................................................................................................... 11
Year One .................................................................................................................................................. 14
Year Two ................................................................................................................................................. 16
Year Three ............................................................................................................................................... 18
Year Four ................................................................................................................................................. 20
Year Five .................................................................................................................................................. 22
Market Analysis Summary .......................................................................................................................... 26
Market Segmentation ............................................................................................................................. 26
Consumers .......................................................................................................................................... 26
Competition ........................................................................................................................................ 27
Target Market Segment Strategy ........................................................................................................ 27
Service Business Analysis ........................................................................................................................ 27
Competition and Buying Patterns ....................................................................................................... 28
Marketing Strategy ..................................................................................................................................... 28
Marketing Materials ............................................................................................................................... 29
Marketing Expenses ................................................................................................................................ 29
Sales Strategy .......................................................................................................................................... 30
Keys to Success
........................................................................................................................................... 31
Appendices .................................................................................................................................................. 33
Company Summary
XXX Midwifery Practice will be a provider- and academic-based midwifery practice that offers
many advantages to XXX and its community. This practice will be folded into an existing infrastructure
through the XXX department of OB/GYN and will offer a competitive edge by working with midwives in
the XXX. Midwives will bill for services provided and will be a minimal additional liability insurance
expense.
XXX Midwifery Practice will be a premier site in that the practice will offer a unique experience
that improves access to perinatal care. The practice will improve pregnancy outcomes within the
disparate population by referring patients to public health services (i.e. Public Health Nursing, XXX, etc.).
This practice will offer a unique educational opportunity to a variety of students, and create a one of a
kind continuity service within the XXX Departments of Family Medicine and Pediatrics.
Midwives will build caseloads of patients to deliver at XXX. The vast resources of XXX will
expedite the development of a sound practice infrastructure including marketing, communications, and
contracts with outreach sites.
XXX Midwifery Practice offers both a private and public health focus in that care delivered will
be the highest quality of women’s health services available. This practice will utilize midwives prepared
at the master’s level. The midwives will also obtain a faculty appointment with XXX College of Medicine
as Voluntary Clinical Instructor, College of Nursing as Voluntary Clinical Faculty, first assistant for
cesarean sections, collaborate with public health organizations, develop a solid referral system with
health and human service providers, and collaborate with private physicians at XXX. The midwives will

be employed by XXX and be licensed in YOUR state, must also maintain membership in American College
of Nurse Midwives (ACNM) and Your State Association.
Location and Facilities
XXX Midwifery Practice will be strategically looking to draw from the LOCATION in order to
address the population in need of improved access to women’s health care and demonstrated by lowest
percentage of births receiving early prenatal natal care (PNC) and highest percentage of babies born
LBW (see Appendix A). The geographic locations of the targeted population are women who live on the
XXX- Areas in need and zip codes. This area ranges from urban to rural population and will attract
socioeconomically disadvantaged and middle-class women.
Besides drawing from this location, a steady flow of patients will come from YOUR COUNTY.
This includes NEIGHBORING TOWNS. The location of this office will be in the LOCATION OF OFFICE.
Refer to Figure 1.
The startup requirements include the rental of approximately 2500 sq feet office space to be
used by the midwifery practice. A three-year to five-year lease will be anticipated. Renovations will
need to be planned in order to create an office that optimizes patient flow and convenience.
Figure 1 Location of XXX Proposed Midwifery Practice in Relation to Other Providers in Location, Date
INSERT YOUR OWN CENSUS MAP WITH PLOTTED OTHER PROVIDER OFFICES
Company Ownership
This will be a provider based academic midwifery practice with XXX as the employer of the
professional staff with an onsite director, XXX.
Scope of Services
XXX Midwifery Practice will provide full-scope women’s health care to women of all ages by
offering a complete care package. The number of midwives depends upon the volume of deliveries and
patient volume in the outpatient sites. The perceived national benchmark for CNM staffing ratios is 8-10
deliveries per clinical midwife full time employees (FTE) per month. By year four, this practice should
meet this goal. An initial team of two full-time midwives, including the director, for the start-up practice
will serve XXX. This initial team will build the patient caseload and care for patients in the primary
outpatient office. Midwife staffing levels will be assessed regularly and additional midwives will be
added as the practice grows. Flexibility during the growth periods will be enhanced by the use of prn
(pro re nata - as needed) midwives. In addition, prn coverage for midwife time off will be needed.
Once the practice has demonstrated its ability to recruit patients and has a caseload of over 20
patients due to deliver each month, the first prn midwife will be recruited. A 24/7 in-house model will
provide coverage for deliveries. The aggressive growth occurs when the practice will be delivering 35-40
babies per month. Outpatient coverage at the office will be dependent upon the volume of outpatient
visits. It will be anticipated that a schedule of two midwife providers per day will be easily filled once
the volume of 20-30 births per month has been reached.
All of the patient care will be provided by a midwife. Each midwife will establish his/her own
gynecological patient base, while the obstetrical patients will be shared within the practice. This assures
continuity of care to our patients. In addition to the 24/7 midwifery coverage, there will be a 24/7
medical back up coverage available through collaborative efforts with XXX laborists. The practice
estimates that 10% of women registering for care will risk out to which a solid referral system will be in
place with XXX Department of OB/GYN and MFM faculty.
Centering Pregnancy™ is a group PNC program that will be implemented once the practice
grows. It will be offered to those interested in participating, but will be encouraged to be attended by
all pregnant teens and those with limited support systems. All clinical staff will be trained facilitators to
run the sessions. Please refer to Appendix B for further details.
XXX Midwifery Practice will have access to the XXX system’s support services (nutrition, social
work, substance abuse, etc). This will add assurance that our patients will have coordinated care within
the same medical system. With the addition of XXX electronic medical record system (EMR),
coordinated care will be more efficient (see Appendix C).
Down-stream revenue from referrals will result over time as the midwives refer complicated OB
and GYN patients to the XXX physician’s practice and to XXX. In addition, referrals to pediatric
practitioners for every baby born in the practice will help expand the pediatric caseload for pediatric
practices in the community. Referral to Family Medicine providers for pediatric and primary care will
contribute to the success of this new practice.
Management Systems
XXX Midwifery Practice will initially have two FTE midwives, two receptionists, two Registered
Nurses (RNs), and a director that is included in the two FTE midwives. The staff midwife and director
will be exempt staff and paid a predetermined salary. The receptionists and RNs will be non-exempt
staff and will be paid hourly wages. All staff will earn fringe benefits. As the practice grows, additional
midwives, RNs, medical assistants, and receptionists will be added.
The practice director, XXX, comes with the experience and knowledge of midwifery care XXX –
add qualifying skills here.
All staff and providers will be expected to continue to improve their skills and knowledge base.
All staff will be expected to complete all mandatory UMU trainings and updated trainings. Midwives will
be expected to fulfill continuing education requirements that pertain to the practice of midwifery
and/or women’s health.
Information Management and Technology
In order to comply with HIPPA and improve efficiency of billing, the practice will use a secured,
networked, EMR, also used by XXX. Using this system will allow for continuity of care with other
disciplines i.e., MFM, social work, nutritional services, medicine, etc.
EMR
XXX Midwifery Practice will utilize XXX EMR system in order to secure the success and efficiency
of the office. EMR technology will increase the systematic approach for each patient and improve
continuity of care. A benefit of the EMR will be an increase in revenues by allowing more patients to be
seen without working harder or longer as with paper charting. Collections will be improved through
optimized coding, management of referral and eligibility date, and tracking of managed care contracts.
EMR will reduce transcription costs, data analysis costs, paper shortage and access costs, staff costs, and
paper/forms costs. Risk will be reduced with the improvement of the quality of documentation,
maintaining security and integrity of patient data, safe check system with medication interactions,
allows for analysis of payor relationships, and will be compliant with the documentation and coding
laws. Tracking of patients, protocols, indicators, and recalls will improve the quality improvement of our
practice.
Billing
XXX Midwifery Practice will utilize XXX, a Management Services Organization utilized by XXX
Department of OB/GYN, as an outside billing agency. This will allow the midwifery practice to focus
primarily on patient care. XXX will use electronic claim billing and filing, which in turn will allow us to
utilize the benefits of electronic claim filing, i.e. faster payment for processing insurance claims, while at
the same time allowing us to maximize valuable clinic time and work force.
Financial Plan
XXX Midwifery Practice will need to rely on seed money for the first two years or until the
practice breaks-even. Projected losses for the first two years will be expected, but anticipate breaking
even in year three. It is anticipated that the practice will expand enrollment to XX New OB’s and XX
Established OBs per month by the end of 20XX (year four) and the maturation of these enrolled patients
to delivery would result in XX deliveries per month by mid-20XX. Developing sound referral networks
will insure the successful growth of the practice. On-going analysis of outpatient volume and deliveries
will be critical to monitor profitability of the practice. Table 1 describes the anticipated growth of
patient type by year and anticipated deliveries. Table 2 discusses the anticipated expenses, revenues,
and surplus/deficits for the first five years, including the start-up costs.
Table 1 Patient Growth by Type and Year
OB GYN
Total
Patients Total Deliveries
Year 1
Year 2
Year 3
Year 4
Year 5
Table 2 Anticipated Yearly Expenses, Revenues, and Surplus/Deficits

Years
Expenses
Revenues
Surplus/Deficit
Start up Costs
$XX
Year 1
$XX
$XX
-$XX
Year 2
$XX
$XX
-$XX
Year 3
$XX
$XX
$XX
Year 4
$XX
$XX
$XX
Year 5
$XX
$XX
$XX
An anticipated mix of insurances (XX% private, XX% public) will ensure that in three years, the
practice will break even and in five years be self-sustaining. With the advancement of XXX billing
system, efficient and quicker returns will be generated. For those patients who participate in public
insurance, the staff will offer assistance in completing any application forms in a timely manner to
assure adequate coverage during the pregnancy and post partum, and newborn care. These efforts will
be coordinated with the LHD to create a position of outreach and onsite referral programs from public
health agencies.
Payments according to procedure codes and patient growth are detailed in Appendix D. It will
be anticipated that a fast growth will occur in year two, three, and four. Year five will continue to show
growth, but at a slower pace.
Five Year Plan
Start-up
Objectives
1. Finalize seed funding through XXX.
2. Secure office space and leasing details.
3. Educate both lay and professional community members, regarding midwifery care as an
alternative to traditional women’s health care and address misconceptions of associated
with midwifery care starting early summer 20XX. This will be accomplished through
outreaches
2
and speaking engagements targeting populations that will benefit most by this
service through multiple marketing avenues.
4. Use XXX to assist in the recruiting of midwives and staff by early spring 20XX.
5. Two months prior, begin scheduling patients for the first day of operations.
6. Credential midwives (hospital and insurance) hired before the start of operations.
Costs
The estimated start-up expenses will be $XX. This sum includes the planning, marketing,
purchase of medical equipment, medical supplies, office furniture and equipment, office supplies, EMR
start up, building renovation, and rent. Marketing will be the most important expense during the six
months prior to the day of operations at $XX. Marketing efforts will be focused on educating the
community about midwifery care and the
proposed practice (Table 3). Figure 2 breaks down to the percentage of contribution of the Start-up
Costs.
Table 3 Start-up Costs
Start up Costs
Non-Personnel Services
Medical equipment and supplies
$XX
Marketing
$XX
Office furniture/equipment and
supplies
$XX
Rent
$XX
Building renovation
$XX
Total
$XX
2
Outreaches are systematic attempts to provide services beyond conventional limits.
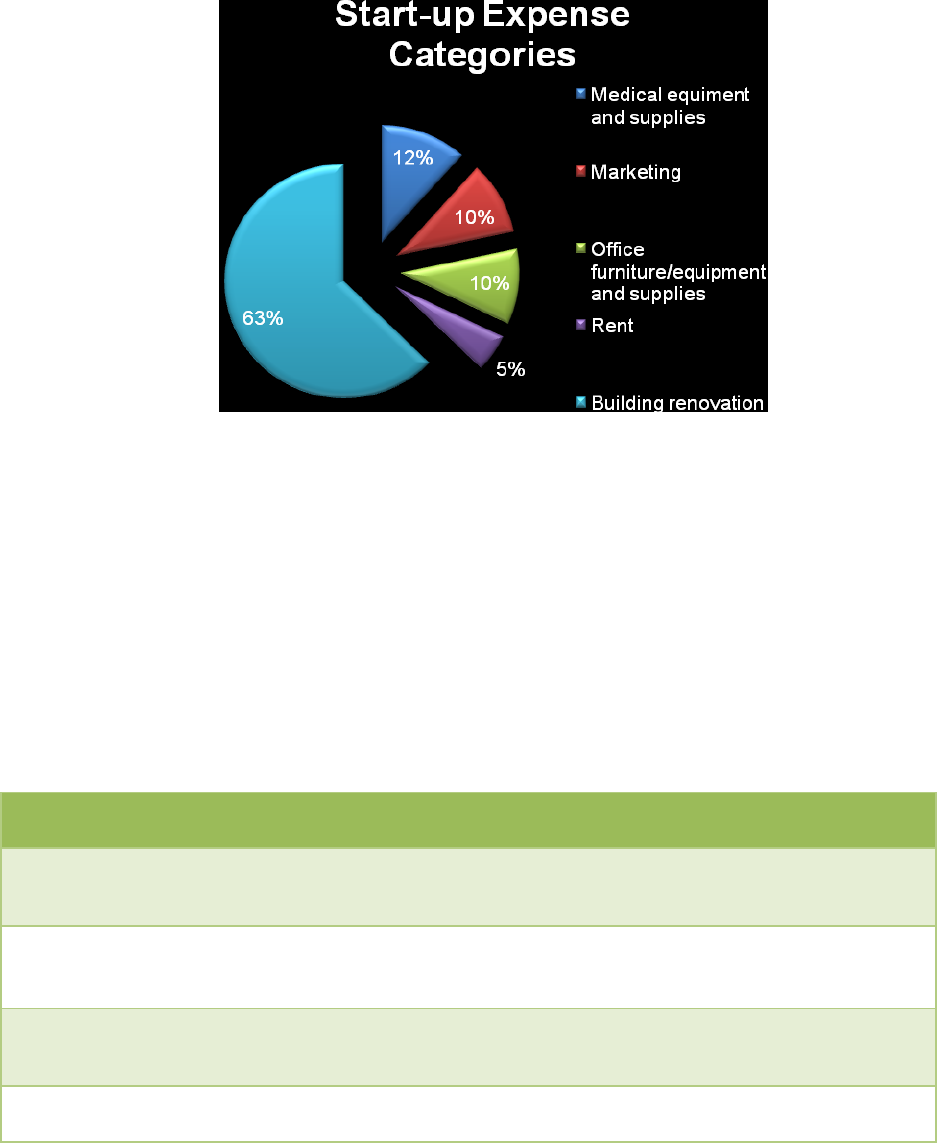
Figure 2 Categories of Start-up Costs
Table 4 Milestones
Milestone
Date
Budget
Manager
Department
Approval of Business
Plan by Hospital
1/1/2012
$0
OB/GYN/hospital
Sign lease with
Landlord
2 to 4 mos
prior to
opening
$0
OB/GYN
Design and place first
ads
Feb 2012
$0
OB/GYN and
Marketing
Begin educational
sessions
Mid-winter
2012
$1,100
OB/GYN
Sign contracts with
XXX for billing,
scheduling, and
recruiting
4 to 6 mos
prior to
opening
$0
OB/GYN
Place first ads to
recruit midwives
4 mos prior to
opening
$0
OB/GYN
Place ads for RN
3 mos prior to
opening
$600
OB/GYN
Begin scheduling
patients
2 mos prior to
opening
$0
OB/GYN
New Employee
Training
1 mo prior to
opening
$0
Human Resources
Computer and phone
line set up
1 mo prior to
opening
$0
OB/GYN, Hospital
Open house
1 day prior to
opening
$1,500
OB/GYN
Begin first
appointment
Early summer
of 2012
$0
OB/GYN
Year One
Objectives
1. Anticipate XX deliveries by end of year one and a total OB/GYN patient base of XX GYN and
XX OB patients.
2. Midwives will be appointed to the College of Medicine and College of Nursing.
3. Partner with XXX to coordinate public health referrals for those in need.
Costs
For the first year of service, the anticipated personnel costs will total $XX and non-personnel
costs will total $XX. The total costs will be $XX. Marketing efforts will continue to be a necessity and
consume a large part of the non-personnel budget at $XX. See Table 5.
Table 5 Year One Budget
Personnel Services
Annual Budget
1 Midwives annual salary
$XX
Director annual salary
$XX
Office Manager
$XX
2 RN annual salary
$XX
2 Receptionists annual salary
$XX
Sub Total
$XXX
CNM Fringe with @39%
$XX
Director Fringe RF @ 43%
$XX
Staff Fringe RF @ 43%
$XX
Personnel Total
$XXX
Non-Personnel Services
Malpractice Insurance (annually)
$XX
Overhead (telephone, pagers)
$XX
EPIC transactions per CNM per Year
$XX
EPIC transactions, Director per year
$XX
Marketing
$XX
Rent (per year)
$XX
Office supplies
$XX
Medical supplies (≤ $500/item)
$XX
Non-Personal Services Total
$XX
Total Personnel and Non-Personnel Costs
$XX
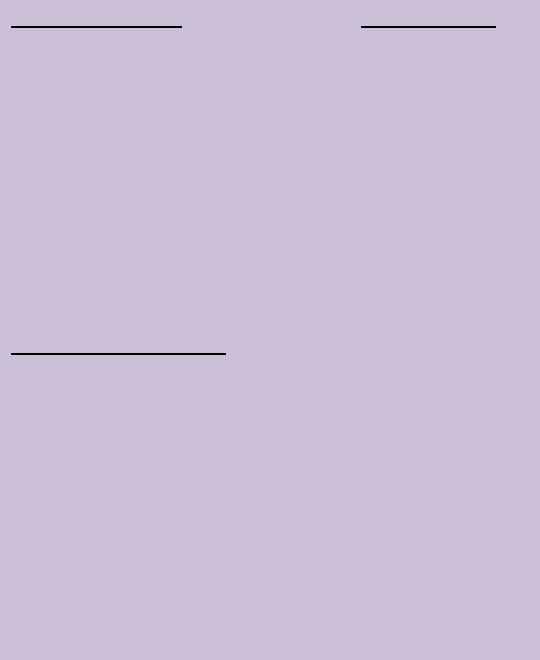
Revenues
The practice will anticipate XXX obstetrical (OB) patients and XXX gynecological patients, before
a 10% transfer or risk out rate. Of the XX patients, XX will deliver in the first year (see Appendix E). Look
to Appendix D for a breakdown of anticipated CPT codes, RVU’s, and the average reimbursement rates
for a XX% public and XX% private payor mix. The midwifery practice will estimate revenues to be $XX,
which puts the practice at a deficit of $XX. Seed money will support the difference. See Figure 3.
Figure 3 Year One Expenses and Revenues
Year Two
Objectives
1. Patient growth is expected at XXX%.
2. Anticipate a patient base of XXX OB patients and XXX GYN patients with XXX deliveries.
3. Consider acceptance of students of all disciplines for clinical rotation and field placement.
4. Begin Centering Pregnancy™/Parenting program
How to Successfully Integrate Midwives into Your Practice | Appendix 4
Appendix 4: Sample Business Plan
Costs
For the year two of service, the anticipated personnel costs will total $XX due to the need for
more staff. The non-personnel costs will total $XX. The total costs will be $XX. Look to Appendix D for a
breakdown of anticipated CPT codes, RVU’s, and the average reimbursement rates for a XX% public and
XXX% private payor mix. See Table 6.
Table 6 Year Two Budget
Personnel Services with 3% COLA for exempt
Annual Budget
2 Midwives annual salary
$XX
Director annual salary
$XX
Office Manager
$XX
2 RNs annual salary
$XX
1 MAs annual salary
$XX
2 Receptionists annual salary
$XX
CNM Fringe @39%
$XX
Director Fringe RF @ 43%
$XX
Staff Fringe RF @43%
$XX
Personnel Total
$XX
Non-Personnel Services
Medical supplies (≤ $500/item)
$XX
Office supplies
$XX
Rent (per year)
$XX
Malpractice Insurance (annually)
$XX
Overhead (telephone, pagers)
$XX
Marketing
$XX
EPIC transactions per CNM per Year
$XX
EPIC transactions, Director per year
$XX
Non-Personnel Services Total
$XX
Total Personnel and Non-Personnel Expenses
$XX
Revenues
The practice will anticipate a XX% growth in year two. The patient breakdown will be XXX
obstetrical (OB) patients and XXX gynecological patients, before a 10% transfer or risk out rate. Of the
XXX patients, approximately XX of OB patients will deliver in year two, increasing the revenues from year
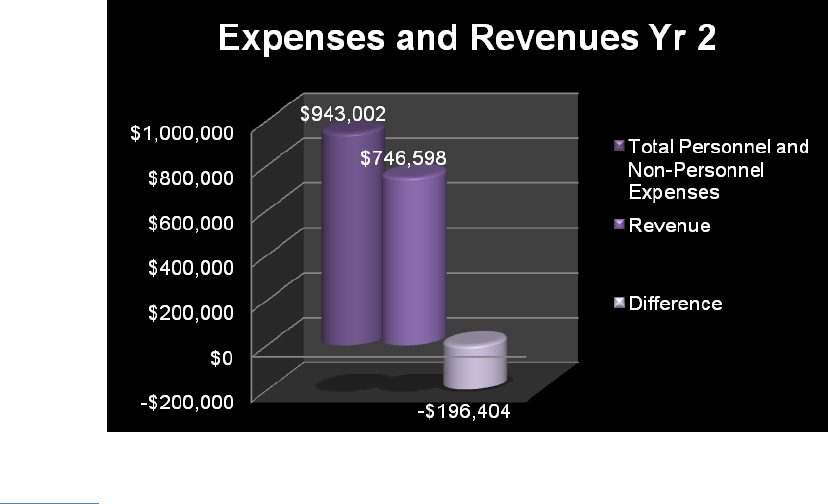
one by XX%. Look to Appendix D for a breakdown of anticipated CPT codes, RVU’s, and the average
reimbursement rates for a XX% public and XX% private payor mix. The midwifery practice will estimate
revenues to be $XX, which puts the practice at a deficit of $XX. Seed money will support the difference.
See Figure 4.
Figure 4 Year Two Expenses and Revenues
Year Three
Objectives
1. Patient growth is expected at XX%.
2. Anticipate a patient base of XXX OB patients and XXX GYN patients with XXX deliveries.
3. Increase the number of midwives to four and employ additional support staff (1-MA and 1-
RN).
4. Coordinated efforts with local universities to conduct research.
5. Contract with XXX to be a clinical site field placement for student nurse midwives.
6.
Costs
For the year three of service, the anticipated personnel costs will total $XX and non-personnel
costs will total $XX. The total costs will be $XX. See Table 7.
Table 7 Year Three Budget
Personnel Services with 3% COLA for exempt
Annual
Budget
3 Midwives annual salary
$XX
Director annual salary
$XX
Office Manager
$XX
3 RNs annual salary
$XX
2 MAs annual salary
$XX
3 Receptionists annual salary
$XX
CNM Fringe with @39%
$XX
Director Fringe RF @ 44%
$XX
Staff Fringe RF @44%
$XX
Personnel Total
$XX
Non-Personnel Services
Medical supplies (≤ $500/item)
$XX
Office supplies
$XX
Rent (per year)
$XX
Malpractice Insurance (annually)
$XX
Overhead (telephone, heat, water, gas, pagers)
$XX
Marketing
$XX
EPIC transactions per CNM per Year
$XX
EPIC transactions, Director per year
$XX
Non-Personnel Services Total
$XX
Total Personnel and Non-Personnel Expenses
$XX
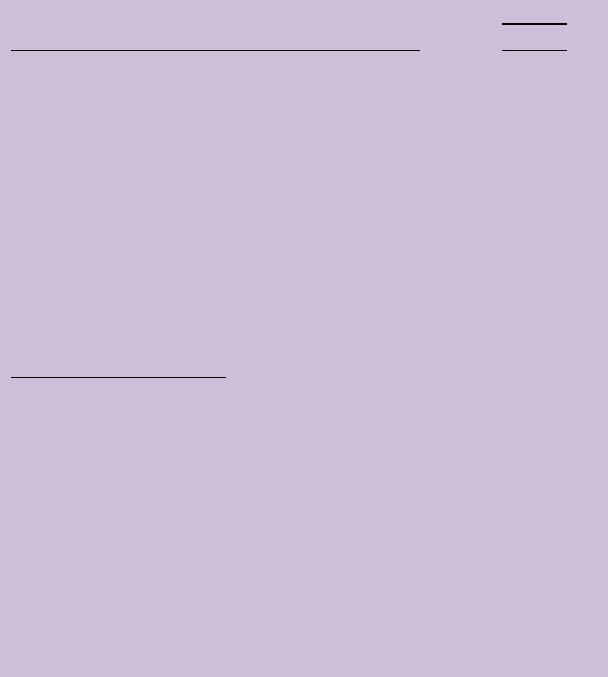
Revenues
The practice will anticipate a XX% growth in year three. The patient breakdown will be XXX
obstetrical (OB) patients and XXX gynecological patients, before a 10% transfer or risk out rate. Of the
XXX patients, approximately XXX of OB patients will deliver in year three, increasing the revenues. Look
to Appendix D for a breakdown of anticipated CPT codes, RVU’s, and the average reimbursement rates
for a XX% public and XX% private payor mix. The midwifery practice will estimate revenues to be $XX
anticipating a profit of $XX. The practice will be self-sustaining. See Figure 5.
Figure 5 Year Three Expenses and Revenues
Year Four
Objectives
1. Patient growth is expected at XX%.
2. Anticipate a patient base of XXX OB patients and XXX GYN patients with XXX deliveries.
3. Continue to cultivate academic and referral relationships.
Costs
For the year four of service, the anticipated personnel costs will total $XX and non-personnel
costs will total $XX. The total costs will be $XX. See Table 8.
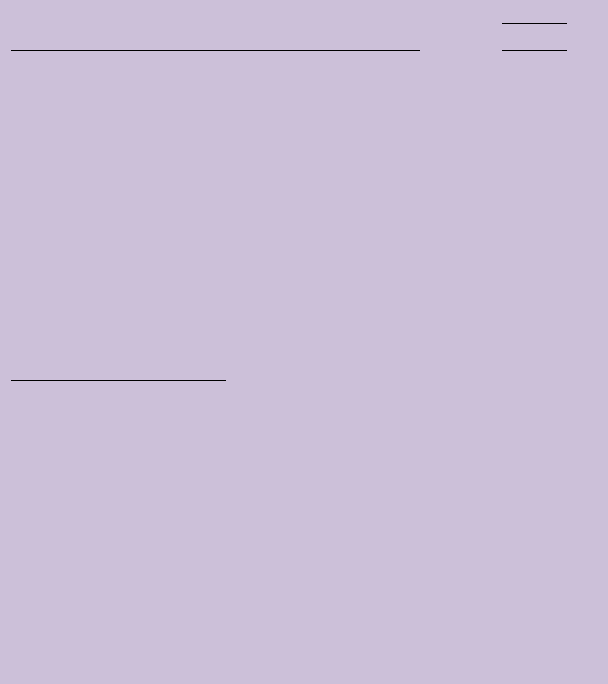
Table 8 Year Four Budget
Personnel Services with 3% COLA for exempt
Annual
Budget
4 Midwives annual salary
$XX
Director annual salary
$XX
Office Manager
$XX
4 RNs annual salary
$XX
3 MAs annual salary
$XX
3 Receptionists annual salary
$XX
CNM Fringe with @39%
$XX
Director Fringe RF @ 43%
$XX
Staff Fringe RF @43%
$XX
Personnel Total
$XX
Non-Personnel Services
Medical supplies (≤ $500/item)
$XX
Office supplies
$XX
Rent
$XX
Malpractice Insurance (annually)
$XX
Overhead (telephone, heat, water, gas, pagers)
$XX
Marketing
$XX
EPIC transactions per CNM per Year
$XX
EPIC transactions, Director per year
$XX
Non-Personnel Services Total
$XX
Total Personnel and Non-Personnel Expenses
$XX
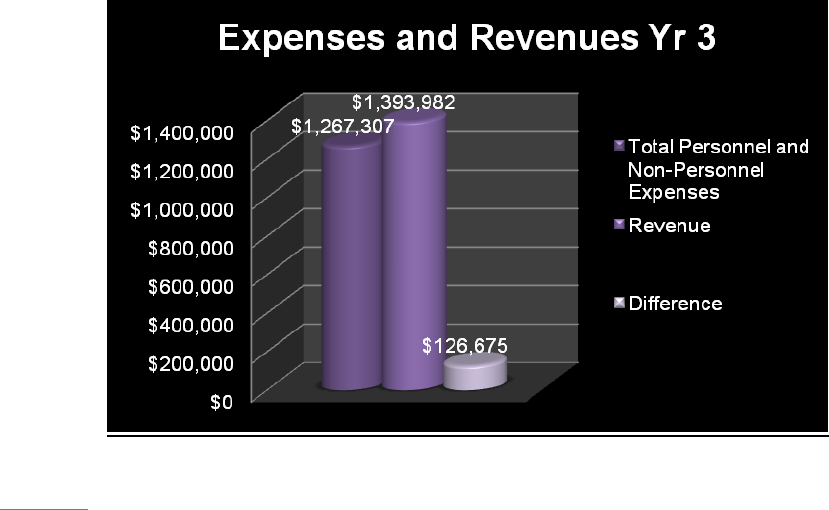
Revenues
The practice will anticipate a XX% growth in year four. The patient breakdown will be XXX
obstetrical (OB) patients and XXX gynecological patients, before a 10% transfer or risk out rate. Of the
XXX patients, approximately XXX of OB patients will deliver in year four, increasing the revenues. Look
to Appendix D for a breakdown of anticipated CPT codes, RVU’s, and the average reimbursement rates
for a XX% public and XX% private payor mix. The midwifery practice will estimate revenues to be $XX
anticipating a profit of $XX. See Figure 6.
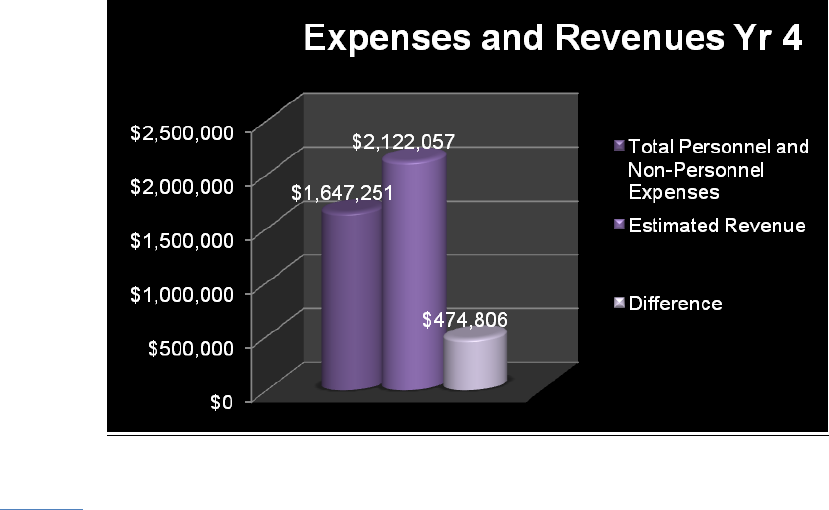
Figure 6 Year Four Expenses and Revenues
Year Five
Objectives
1. Patient growth is expected at XX%.
2. Anticipate a patient base of XXX OB patients and 877 GYN patients with XXX deliveries.
3. Increase midwives to six and employ one additional LPN and receptionist.
4. Expect to be self-sustaining.
5. Begin the development of a midwifery-training program.
Costs
For the year five of service, the anticipated personnel costs will total $XX and non-personnel
costs will total $XX. The total costs will be $XX. See Table 9.
Table 9 Year Five Budget
Personnel Services with 3% COLA for exempt
Annual
Budget
5 Midwives annual salary
$XX
Director annual salary
$XX
Office Manager
$XX
5 RNs annual salary
$XX
3 MAs annual salary
$XX
4 Receptionists annual salary
$XX
CNM Fringe with @39%
$XX
Director Fringe RF @ 45%
$XX
Staff Fringe RF @45%
$XX
Personnel Total
$XX
Non-Personnel Services
Medical supplies (≤ $500/item)
$XX
Office supplies
$XX
Rent
$XX
Malpractice Insurance (annually)
$XX
Overhead (telephone, heat, water, gas, pagers)
$XX
Marketing
$XX
EPIC transactions per CNM per Year
$XX
EPIC transactions, Director per year
$XX
Non-Personnel Services Total
$XX
Total Personnel and Non-Personnel Expenses
$XX
Revenues
The practice will anticipate a XX% growth in year five. The patient breakdown will be XXX
obstetrical (OB) patients and XXX gynecological patients, before a 10% transfer or risk out rate. Of the
XXX patients, approximately, XXX of OB patients will deliver in year five, increasing the revenues. Look
to Appendix D for a breakdown of anticipated CPT codes, RVU’s, and the average reimbursement rates
for a XX% public and XX% private payor mix. The midwifery practice will estimate revenues to be $XX
anticipating a profit of $XX. See Figure 7.
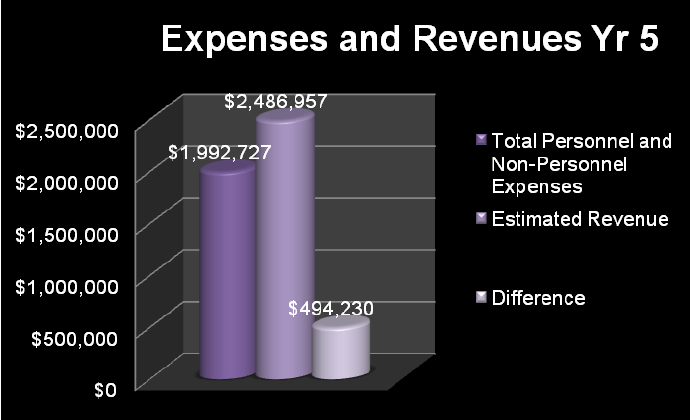
Figure 7 Year Five Expenses and Revenue
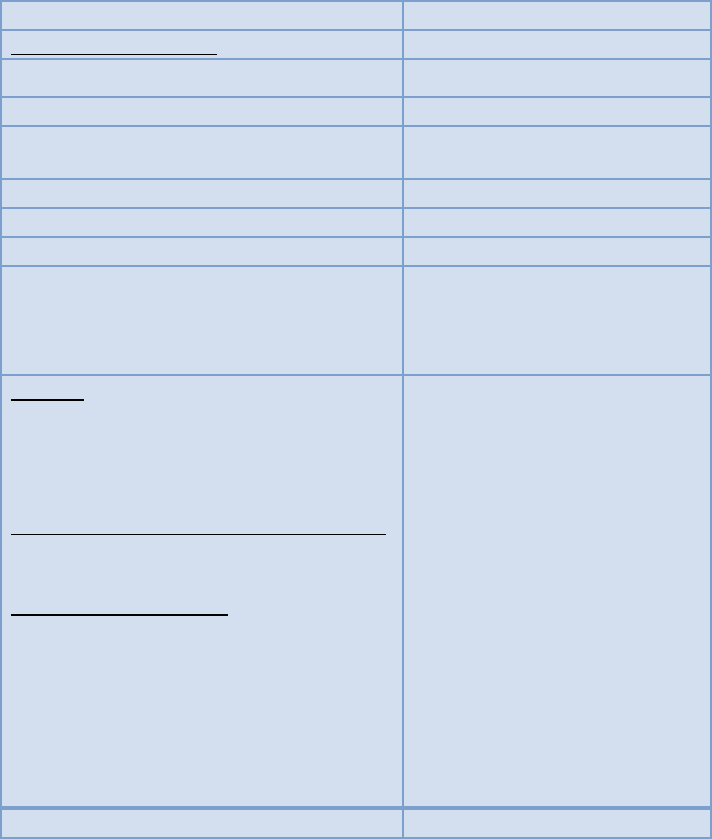
Figures 8 and 9 provide a visualization of five year anticipated patient mix of OB or GYN and the
anticipated deliveries in five years.
Figure 8 Five Year Anticipated Patient Types/Growth
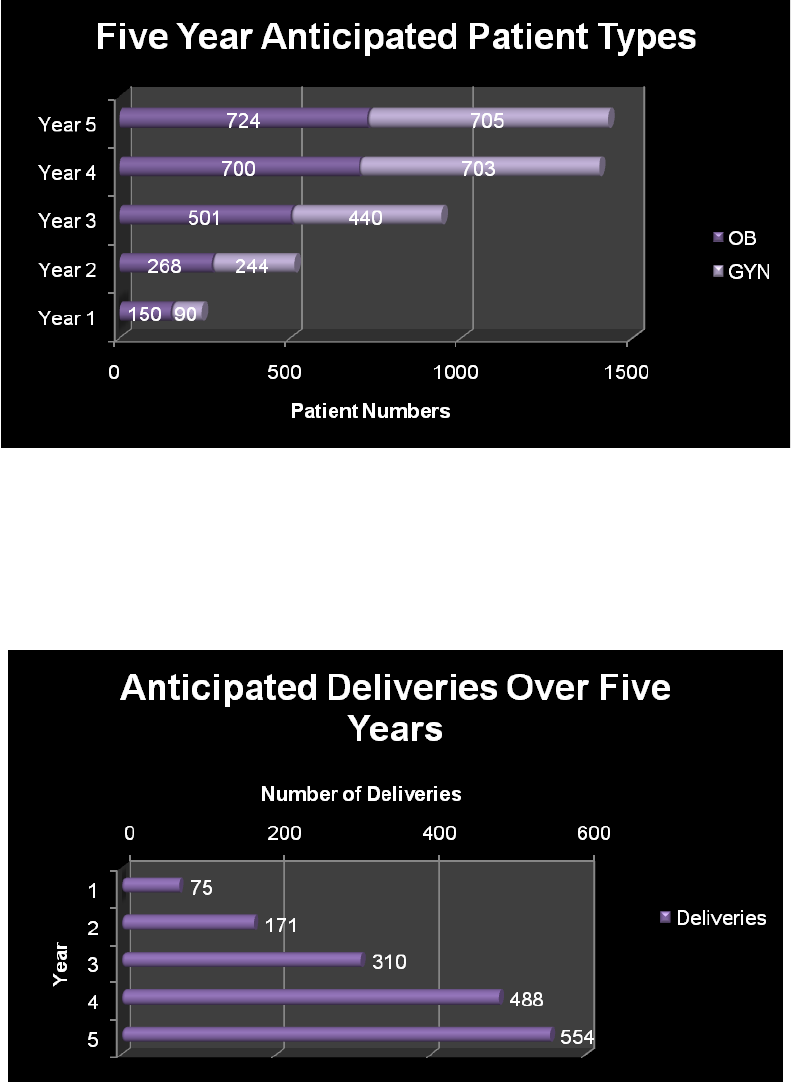
Figure 9 Five Year Anticipated Deliveries
Market Analysis Summary
According to U.S. Census Bureau (2010), XXX% of women who reside in YOUR County are of
childbearing age (15-44). The YOUR CITY area has multiple opportunities for strategic partnerships to
enhance rapid practice growth. This population of patients will positively respond to a practice with
midwifery care and a supportive caring environment. Potential community partners to enhance rapid
growth of underserved and Medicaid patients include:
YOUR PERINATAL OUTREACH
Family Planning Service
LOCAL Health Department PRENATAL PROGRAM
In addition, targeting patients with private insurance who are seeking a “high-touch” experience
associated with a tertiary care setting will be a balance to the payor mix of the practice. Contract
negotiations between XXX and private payors to add midwifery care to the existing contracts is a critical
first step.
Market Segmentation
Consumers
With nearly XX% of the population in YOUR County in 20XX comprising of women, there will be
an advantage to developing an alternative women’s health service. The advantage is to offer access to
an alternative option to traditional allopathic women’s health care. The practice will target women 15
and older who are interested in alternative women’s health care. The mean age of this community is
40; therefore, the practice will be very capable of providing routine gynecological, family planning,
perimenopausal, and postmenopausal care. One of the biggest strategies will be to educate the women
of YOUR County on the services midwives provide and disprove the myths associated with midwifery
care. The practice will strive to provide a unique experience that will cater to women by offering a
prime location that is convenient to access, a quality experience with each patient visit that includes
“high touch” concept that addresses each patients need, and modern technology to provide information
understandable by women with low levels of health literacy.
Competition
There are currently XX OB/GYN practices and XX private midwife practice that are affiliated with
YOUR HOSPITAL. XX out of the XX accept GYN patients only, while the other four provide OB/GYN
services. XX of these practices employ midwives. The solo midwife is also affiliated with HOSPITAL,
located XX miles away in TOWN. XX practices are located in TOWN (XX miles); XX in the STREE/TOWN
(Xmiles) and the XX practice is located TOWN STREET (Xmiles). See Appendix F.
Target Market Segment Strategy
XXX Midwifery Practice will locate and focus its efforts on the western side of YOUR County
population. Our segmentation strategy is geographic for the reasons of: the urban, suburban, and rural
patients of this area are in need of alternative women’s health care that addresses the individual needs
and the access to care problem; the expected growth of the local population has been projected that a
few suburban towns will increase in population by XX6%.
Service Business Analysis
XX Midwifery Practice will be part of a larger medical industry. It will be associated with an
academic center, a community hospital, a high-risk obstetrical center, a hospital-based women’s health
resident clinic, a faculty generalist OB/GYN private practice, HOSPITAL private OB/GYN providers, and a
faculty family practice group. Private OB/GYN practices in YOUR County are numerous and generally
smaller (XXX providers).
According to the Census Bureau, there are nearly XXX women near the office (ZIP CODE),
suggesting an excellent patient-midwife ratio based on the number of midwives as well. With the
limited number of surrounding OB/GYN provider practices, these statistics are favorable for patient
growth.
Competition and Buying Patterns
In general, competition among midwives and OB/GYN practices in YOUR County and the
surrounding area is small. With projected growth in population of XX%, a XX% in annual pregnancies will
continue to be expected, and the limited number of women’s health providers, this practice creates a
great potential for meeting patient load goals in year three.
Marketing Strategy
The first strategy for a successful start will be based on the development of collateral materials
such as a practice brochure, which must be developed quickly. A web site will be a very important tool
for targeting all women and a link to the ACNM midwife locator engine should be established
immediately. A comprehensive marketing and communications plan will be one of the priorities during
the first few weeks that the Director is on-board. This strategy will quickly create a high profile, logo,
“look”, name recognition, and understanding of midwifery care within the community through public
speaking, networking, promotional events, and printed advertising. These marketing tools will be
followed up with a sales strategy that relies on a pleasant and accessible location, well-trained, highly
motivated employees, and a commitment to provide the best care and patient experiences possible in
every interaction. An innovative component of this program will be the linking of this midwifery
practice to public health programs, such as XXX. The advantage of this strategy is that every element of
it is within our control.
XXX Midwifery Practice will have a competitive edge based on an alternative option to women’s
health care, location, quality of care, availability to patients, 24/7 inpatient coverage, quality time spent
with each patient, focus on individual needs and providing education and support, strong social supports
and referral for those in need of additional services, pleasant staff and office environment. All of these
factors will result in high level of patient satisfaction and high self-referral rates.
In conjunction with XX Marketing Department, a momentum will be created approximately
three months prior to actual start of business to get the name and the kind of services offered
recognized. Along with this, extensive education will be provided to the community and professionals
addressing myths associated with midwives and the benefits of midwifery care.
Marketing Materials
To accomplish a visible presence, the practice will offer written materials that promote
midwifery care and the office location that is simple to read coupled with a professional and polished
look and feel. The information will include facts regarding midwifery care, roles of midwives in the
obstetrical community, biographical information, location, photos, as well as other promotional
materials. This will be available for our patients as well as potential patients.
The practice will provide multiple educational brochures from ACNM and American College of
Obstetricians and Gynecologists (ACOG). In addition, patient information handouts will be available via
Department of OB/GYN website.
Besides patient friendly written brochures and handouts (English and Spanish), there will be a
number of videos, mailings, and other materials used to promote the medical office and medical
information. This will include magazine/newspaper advertisements, movie theaters, buses, and bus
shelters, commercial announcements on the radio and television, billboards, as well as other advertising
avenues for getting the word out.
Marketing Expenses
Media Utilized / Associated Costs of the Media Budgeted Funds
Media
Budgeted Funds
Print and Social Media
Bus / Bus Shelters
$XXX (for 3 months)
Billboards
$XXX (for 2-3 months)
Print Advertising
$XXX (for 3 months)
Movie
$XXX (10 weeks, $XXX/mo.)
Radio
$XXX
Print
$XXX (flyers/brochures/posters)
Agency News Letters
XXX
WIC Tribune
March Of Dimes
$0
$0
$0
$0
Upstate
Blog , Update,
Announcements website,
Seminar Series, HOSPITAL Family Resource
Center, Physician’s Practice Magazine
Food for Outreach visits to Organizations
11 organizations @ $100per site
Website Advertisement
Business Finder
Healthcare Directories
Facebook
Twitter
$0
$XXX
$0
$0
$0
$0
Total
$XXX
Sales Strategy
The practice will offer incentives to the patients to serve as small mementos for each delivering
patient as well advertisement of the practice. This may include monogrammed bags, Onsies, pens,
coffee mugs, water bottles, stationary, etc. The marketing team will research this for comparative
pricing and quality of products once the practice is operating.
Approximately four months prior to opening, the major marketing activities will begin. These
activities will be in collaboration with the Marking Department at XXX and the lead agent will be XXX.

She will assist the Director in connecting with the most important marketing avenues. In addition, XXX
will assist with placing ads for midwifery positions and setting up interviews.
Approximately two months prior to opening the practice will begin scheduling patients to be
seen on the opening day. An arrangement will be made to have a receptionist available to operate the
telephone to schedule appointments through the Department of OB/GYN at XXX.
Once operations are commenced, emphasis in advertising will continue for the next year and
will continue to use the XXX Marketing advantage until second to third year of business, which by then
our word of mouth will take over as our main source of referrals, thus reducing the costs of advertising.
All pricing for visits and procedures will be billed according to industry standards and monitored
by the Department of OB/GYN and XXX. The practice will contract with the major private insurance
carriers (Excellus, MVP, Aetna, United Health Care, and POMCO, etc) in our area and public insurance
programs (Medicaid, Medicaid Managed Care, Medicare, etc).
Keys to Success
The keys to a successful midwifery practice will rely on patient satisfaction, the staff and office
organization, and the marketing and sales of midwifery care.
Patients
• Educate patients on the importance of preventative care and regular check-ups
• Stress the importance of follow-up care through a recall system to remind patients of their
appointments
• Focus on women’s health needs
• Alternative option in women’s health care
• Convenience of office location
Staff and Office Organization
• Unique, state of the art model that includes Centering Pregnancy™, continuity component,
teen focus, relationship with local colleges and universities to perform credible research,
and XXX
• Recognize that office staff is as crucial in the success of the business
• Progressive atmosphere
Finances
• Keep a low overhead
• Use EPIC for the latest and most accurate billing practices
• Optimize the number of patients we see in an hour while providing quality midwifery care
Marketing and Sales
• Aggressively market and create a presence in the community by catering to hospitals,
perinatal outreach programs, community organizations, schools, colleges, universities,
popular media avenues, and much more.
• Network with XXX OB/GYN, MFM faculty, Family Medicine and Primary Care providers,
Family Planning Service, and XXX for referral relationship
• Location in an area with a low women’s health services
• Located close to XXX

Appendices
APPENDIX A

ZIP CODES WITH THE LOWEST PERCENTAGE OF BIRTHS RECEIVING EARLY PNC IN YOUR COUNTY
ZIP CODES WITH THE HIGHEST PERCENTAGE OF BABYS WITH LBW
IN YOUR COUNTY
3
APPENDIX B
CENTERING MODEL OVERVIEW
4
Centering is an evidence-based redesign of health care delivery that helps to promote:
• safety,
• efficiency,
• effectiveness,
• timeliness,
• culturally appropriate patient-centered care, and
• more equitable care.
Centering is a model of group healthcare, which incorporates three major components:
assessment, education, and support. Group participants meet with their care provider and other
group participants according to a regular schedule for a much longer period of time (usually 90-120
minutes) than a usual check-up visit. Centering promotes individual health empowerment and
community-building. The 13 Essential Elements of Centering secure these benefits.
At the start of a typical session, patients have a brief individual assessment by the care provider,
participate in self-care activities, complete a Self-Assessment Sheet on a particular topic, enjoy
4
https://www.centeringhealthcare.org/pages/centering-model/model-overview.php

refreshments, and have informal conversation with the other participants. When the group “circles
up” together, there is facilitated discussion about a heath topic and the exchange of corporate
wisdom on shared health experiences. Groups are lively, interactive, and patient-centered.
Agencies bill for group care in the same way as corresponding individual care visits. Centering
Pregnancy care starts around the beginning of the second trimester and goes through delivery.
Research has shown increased patient and provider satisfaction in Centering groups and improved
patient outcomes.
APPENDIX C
EMR INFO
APPENDIX D
Payments According to Procedure Code, Patient Growth, and RVU by Year
THIS IS AN EXAMPLE
Procedure Code
RVU
Avg
Pmt
Year
1
Year
2
Year
3
Year
4
Year
5
99201 - OFFICE
OUTPATIENT VISIT U/A
PG test
111
$33
36
$1,17
1
79
$2,57
5
150
$4,89
3
226
$7,339
271
$8
99202 - OFFICE
OUTPATIENT VISIT
423
$54
500
$27,0
48
1100
$59,5
05
2090
$113,
060
3135
$169,5
90
3762
$2
99203 - OFFICE
OUTPATIENT VISIT
130
7
$82
120
$9,82
4
264
$21,6
14
502
$41,0
66
752
$61,59
9
903
$7
99204 - OFFICE
OUTPATIENT VISIT
628
$113
72
$8,14
7
158
$17,9
24
301
$34,0
56
451
$51,08
3
542
$6
99205 - OFFICE
OUTPATIENT VISIT
82
$182
12
$2,18
7
26
$4,81
0
50
$9,14
0
75
$13,71
0
90
$1
99211 - OFFICE
OUTPATIENT VISIT
442
$11
4
$43
9
$95
17
$181
25
$271
30
$
99212 - OFFICE
OUTPATIENT VISIT
162
8
$31
9
$280
20
$617
38
$1,17
2
56
$1,759
68
$2
99213 - OFFICE
OUTPATIENT VISIT
801
6
$41
72
$2,92
2
158
$6,42
7
301
$12,2
12
451
$18,31
8
542
$2
99214 - OFFICE
OUTPATIENT VISIT
123
5
$55
9
$492
20
$1,08
2
38
$2,05
5
56
$3,083
68
$3
99215 - OFFICE
OUTPATIENT VISIT
236
$84
0.9
$75
2
$166
4
$315
6
$473
7
$
99221 - HOSPITAL
ADMIT, STRAIGHTF
395
$74
30
$2,22
2
76
$5,64
0
145
$10,7
16
217
$16,07
4
260
$1
99222 - HOSPITAL
ADMIT, MODERATE
863
$108
60
$6,49
0
132
$14,2
78
251
$27,1
29
376
$40,69
3
451
$4
99223 - HOSPITAL
ADMIT, HIGH COMP
242
$143
15
$2,14
4
78
$11,1
29
148
$21,1
44
222
$31,71
6
266
$3
99231 - SUBSEQUENT
HOSPITAL VISIT
167
6
$33
15
$495
15
$495
29
$941
43
$1,411
51
$1
99232 - SUBSEQUENT
HOSPITAL VISIT
121
2
$63
45
$2,84
2
54
$3,41
1
103
$6,48
0
154
$9,720
185
$1
99233 - SUBSEQUENT
HOSPITAL VISIT
303
$80
13.5
$1,07
8
70
$5,59
4
133
$10,6
29
200
$15,94
3
240
$1
99238 - HOSPITAL
DISCHARGE <30 MN
372
$50
90
$4,51
7
108
$5,42
0
205
$10,2
98
308
$15,44
8
369
$1
99239 - HOSPITAL
DISCHARGE >30 MN
98
$44
0
$0
0
$0
0
$0
0
$0
0
99384 - PREVENTIVE
VISIT, NEW, 12
41
$61
9
$549
20
$1,20
8
38
$2,29
5
56
$3,442
68
$4
99385 - PREVENTIVE
VISIT, NEW, 18
131
$80
36
$2,88
0
79
$6,33
6
150
$12,0
38
226
$18,05
8
271
$2
99386 - PREVENTIVE
VISIT, NEW, 40
78
$121
40.5
$4,90
1
89
$10,7
81
169
$20,4
84
254
$30,72
6
305
$3
99387 - PREVENTIVE
VISIT, NEW, 65
15
$146
4.5
$657
10
$1,44
6
19
$2,74
6
28
$4,120
34
$4
99394 - PREVENTIVE
VISIT, EST, 12
11
$31
0
8
$256
16
$486
24
$729
28
$
99395 - PREVENTIVE
VISIT, EST, 18
677
$73
0
66
$4,81
8
125
$9,15
4
188
$13,73
1
226
$1
99396 - PREVENTIVE
VISIT EST 40
249
$86
0
74
$6,38
6
141
$12,1
32
212
$18,19
9
254
$2
99397 - PREVENTIVE
VISIT, EST, 65
3
$114
0
2
$188
3
$357
5
$536
6
$
APPENDIX E
Number of Patient Growth Related to Percentage of Growth
Pt Visits Number of Pts % Growth
New OB
New Gyn
Total
Year 2 # Pts XXX%
Est OB
New OB
Est GYN
New GYN
Total
Year 3 # Pts XXX%
Est OB
New OB
Est GYN
New GYN
Total
Year 4 # Pts XXX%
Est OB
New OB
Est GYN
New GYN
Total
Year 5 # Pts XXX%
Est OB
New OB
Est GYN
New GYN
Total
APPENDIX F
Location of XXX Proposed Midwifery Practice in Relation to Other Providers in YOUR County, STATE,
DATE
INSERT MAP
APPENDIX G
Mission/Vision/Philosophy
XXX Midwifery Mission Statement:

The mission of the XXX Midwifery Practice is to provide safe, full scope obstetrical and
gynecological services to women of YOUR County. This care will be provided in an ethical and
humanistic manner with focuses on prevention, safety, and patient satisfaction.
Vision of XXX Midwifery Practice will:
1. Be available to our patients.
2. Be viewed as an alternative to physician care, not a substitute.
3. Function within a system that allows for independent and collaborative practice and
referrals as needed.
4. Provide a focus on the prevention of untoward outcomes through patient participation and
education.
5. Participate in state and national organizations regarding issues affecting the practice of
midwifery.
6. Participate in continuing education, to improve the quality of practice.
XXX Midwifery Philosophy:
XXX Midwifery Practice believes in a comprehensive approach to women’s health. We believe
that the woman and her family should be involved with decisions regarding greater health and well-
being during her care. This will be achieved by creating an environment where the clinical staff educate,
participate in active listening, advise, and support the woman and her family.
