Boston Soft Spinal Orthosis Corrective Order Form
Instructions
Reminder – this form is for the technicians and goes with the flow of fabrication. All items on this form need to
be completed to ensure customer service and manufacturing are able to fabricate the desired orthosis.
PLEASE DO NOT use this as your clinical note.
This form is for the fabrication of a corrective soft spinal orthosis. Use this form if your patient presents with
neuromuscular scoliosis, pelvic obliquity and the treatment goal is to improve sitting/standing posture and
head/neck control. (Refer to Decision tree at www.bostonoandp.com)
This device is designed to provide corrective forces in all three planes. Your clinical expertise and the patient’s
presentation will determine the percent correction and brace design.
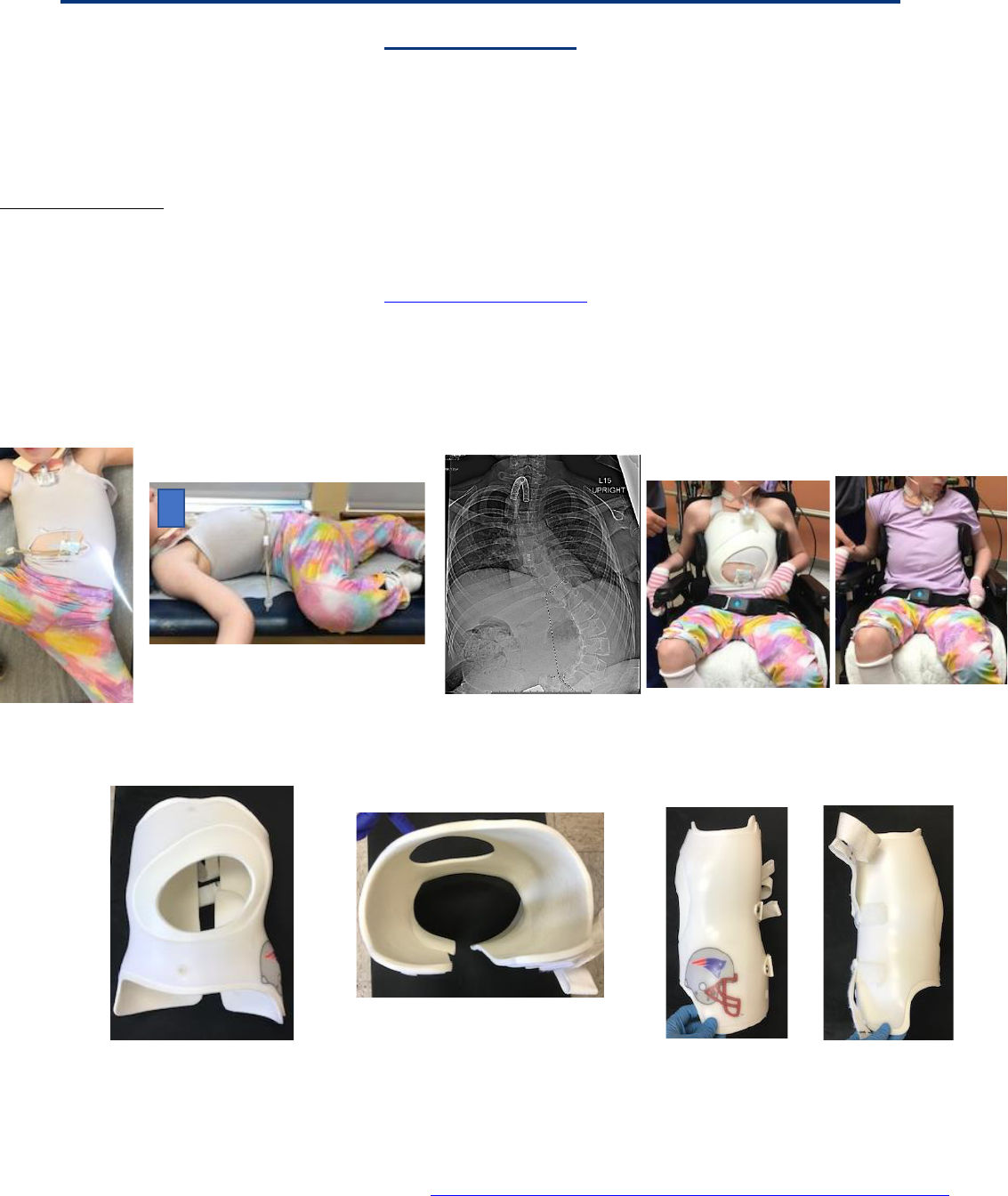
Below is an example of a CP patient, GMFCS 5, with a Boston Brace Soft Spinal Corrective orthosis to
address her needs.
An audio review of this document is available at: Boston Soft Spinal Corrective order form instructional video
Asymmetrical
abdominal window
Enhanced lumbar support (left)
Lumbar relief (Right)
Transverse view with lumbar
pad
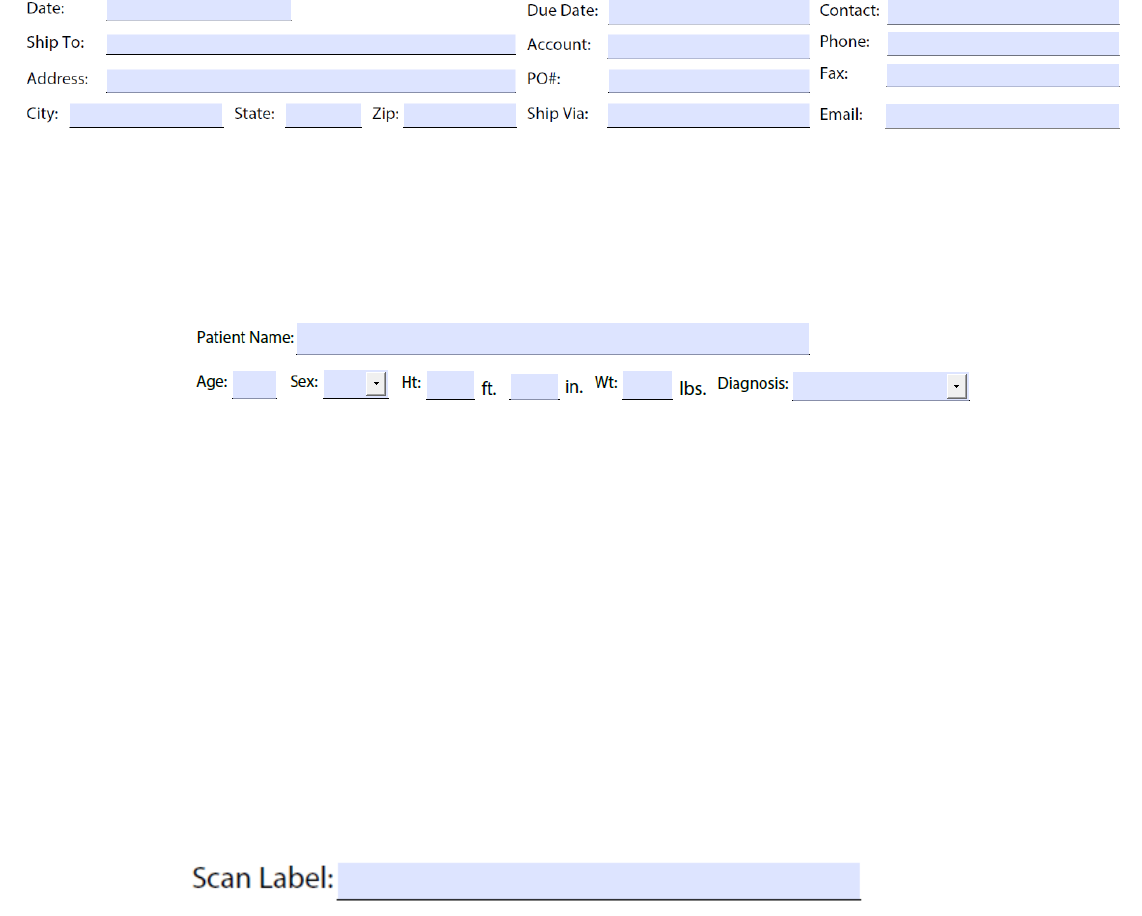
Demographics:
Customer service uses this section to initiate the fabrication process. All of the above is entered into our system.
In the event we need to contact you, the treating orthotist, or if you have a question on the fabrication, having
this information entered allows for easy retrieval.
Patient Name, Age, Sex, Height, Weight, Diagnosis
We will keep a secondary record for you, showing the patient’s age, sex, height, and weight as well as the
diagnosis. This information may assist in justifying a new orthosis.
Make sure the patient’s name is legible.
Age and Sex are needed to complete our records in the event you need the manufacturing record.
Height is broken down into feet and inches to ensure proper record keeping. Weight is requested to be in
pounds. Diagnosis is needed to complete records.
Scan label:
Scan label is required to make sure the correct scan is modified.
Captevia: File name is auto-populated. Write Captevia as the scan label. The file will include both scans
if taking a bivalve scan.
Laser scanner: Patient’s first initial, last name; scan number; clinicians’ initials; the word spinal; date of
scan
i.e. patient John Smith is seeing clinician Jane Doe on April 1, 2020 for his first
brace.
Scan Label: jsmith#1jdspinal04012020
Bivalve scan: Follow the sequence above and add _ant and _post after the date
Anterior section: jsmith#1jdspinal04012020_ant
Posterior section: jsmith#1jdspinal04012020_post
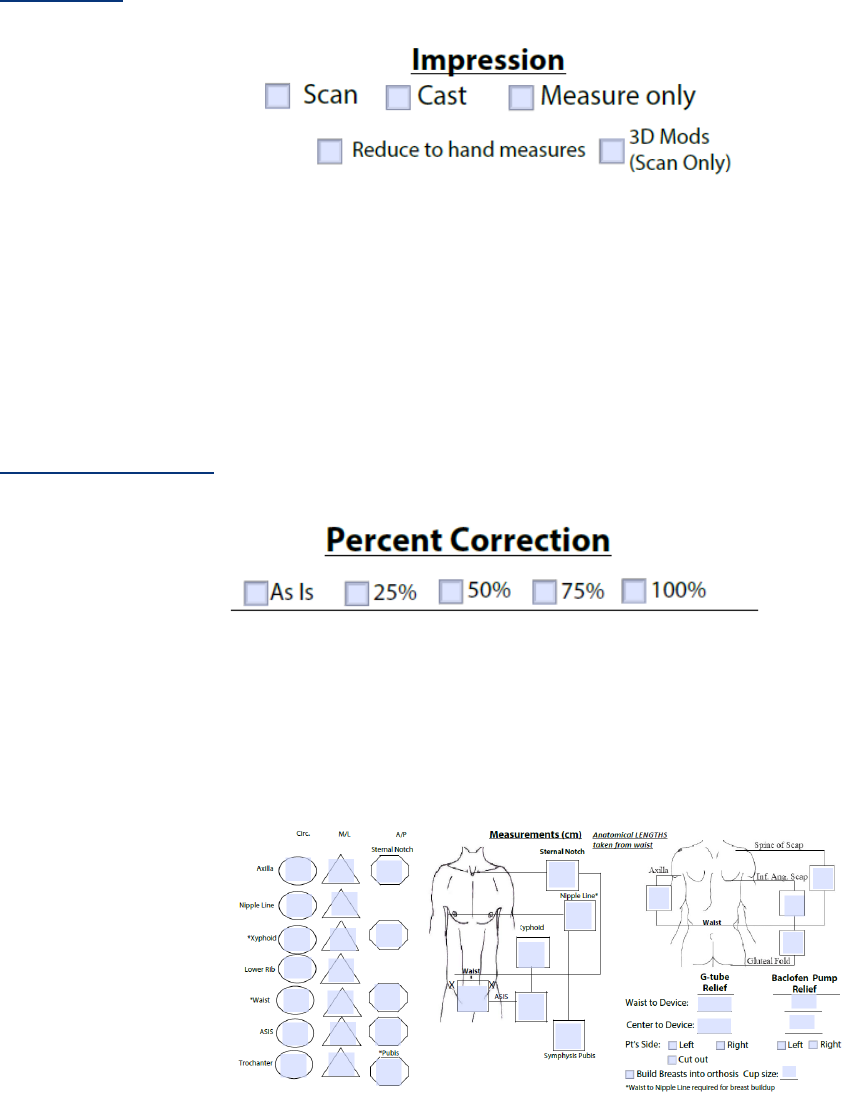
Impression:
This corrective Soft Spinal Orthosis may be fabricated from cast, measurement, or scan. Scanning is optimal.
See our bivalve scanning instructions. Let us know if you want the scan or cast reduced to hand measurements.
If you want to include some corrective forces in the orthosis, let us know by checking the 3D Mods. Note this is
only available when providing a scan of the patient.
Percent Corrections:
Indicate the amount of correction, if any as a percentage. This depends on the patient’s presentation. When
taking a bivalve scan, try to
Measurements:
All measurements are required.
Linear Measurements
Linear measurements are from the waist to the anatomical landmark regardless of scan type. The axilla
measurement is to the maximum height under the arm needing an axillary extension.
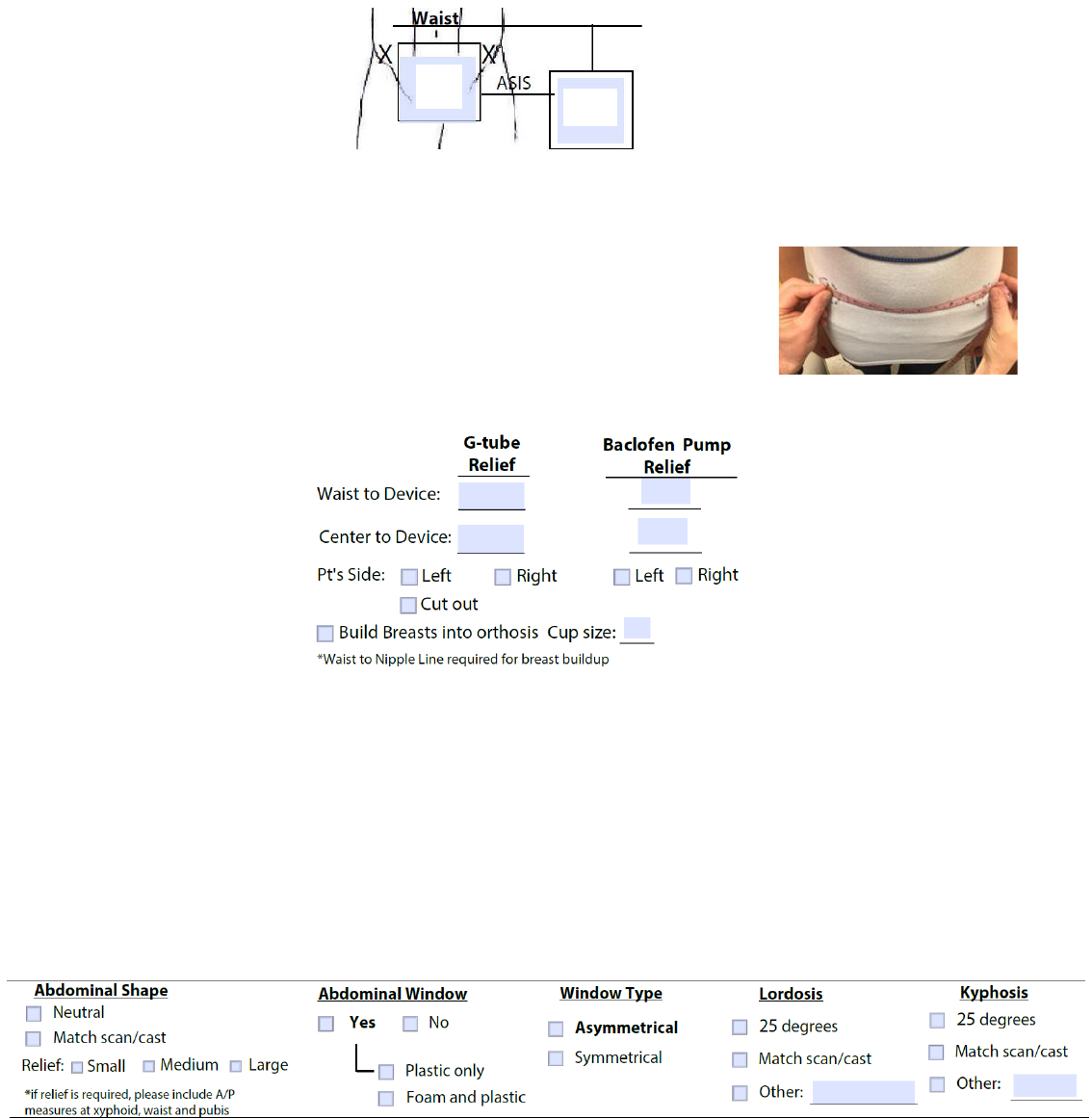
ASIS measurements
When providing ASIS to ASIS linear measurement (A), use a cloth tape
measure to follow the patient’s body contours.
Waist to pubis measurement (B) is measured using the linear measuring device.
G-tube/Baclofen Pump/Chest Relief:
Many of the patients in this population present with a G-tube and or a Baclofen Pump. We can accommodate
both into the orthosis. To do so please provide the waist to center of the device measure as well as midline to
center of device and to what side the device is located. CAD will then make the appropriate relief in that area.
For those providing measurements only, if the patient requires accommodation for chest development,
please indicate this by checking the box and providing the chest cup size.
Sagittal Plane:
The sagittal plane alignment and support is important. This section allows you to communicate what is required
for your patient to maximize their sagittal plane control.
Abdominal Shape
A
B

We do not provide any abdominal compression. Neutral would be a convex abdomen dictated by the patient’s
measurements/shape. If a scan (recommended) or cast is provided, we will match the presentation. If the patient
requires additional relief, indicate the amount of relief in the general terms of small, medium and large. This
will provide the CAD technician some guidance.
Abdominal Window
We recommend an abdominal opening – this helps reduce any respiratory impediment and improve comfort for
the patient. If you want an abdominal opening, let us know if you want just the plastic removed or the plastic
and foam.
Window Type
Symmetrical: allows for maximum expansion of the abdomen for respiration, while still maintaining contact on
the anterior ribcage. Available with just the plastic trimmed out or both plastic and foam.
Asymmetrical: allows for expansion of the abdomen for respiration and provides some rotary control if the
patient requires additional support. Available with just the plastic trimmed out or both plastic and foam.
Lordosis
For this population, we need to provide support to the pelvis and help improve the extension response to help
these patients with postural control. The minimum amount of lordosis that we recommend is 25 degrees, but
you can have us match the scan/cast or specify the amount of lordosis. During your evaluation, you will
determine the proper amount of lordosis needed for support.
Kyphosis
Let us know the amount that will maximize the patient’s sagittal balance.
Symmetrical window type
with plastic and foam cut
out
Asymmetrical window type
with plastic only cut out
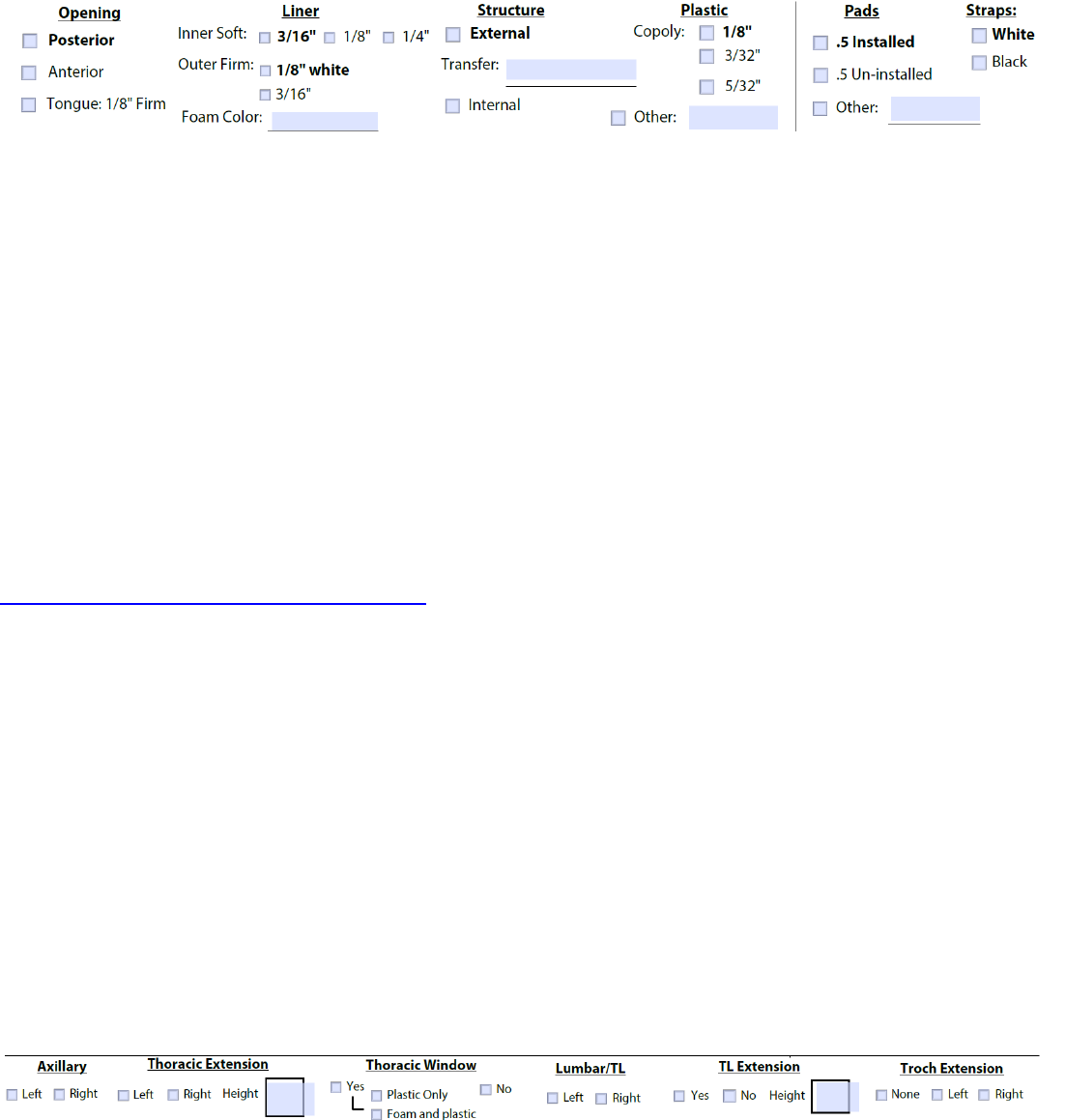
Brace Design:
Use the above section to describe the brace design.
Opening
Two options exist for the Corrective orthosis. Our clinical experience has shown the bivalve to be ineffective in
controlling the neuromuscular curve. Let us know if you want a posterior or anterior design. If anterior, indicate
if a tongue is needed.
Liner
The inner foam lining is available in different thicknesses. The outer 1/8 foam is firm and only available in
white. If you wish to have a foam with color (external foam only), it is only available in 3/16. Please state the
color requested.
Structure
The frame may be internal or external. It is one continuous structure that will follow TLSO or LSO trimline.
Indicate the type (External is recommended) and thickness of plastic. Use our transfer selection tool:
https://www.bostonoandp.com/transfers/brace/ to assist you and the parents/patients in selecting the transfer. Enter
the transfer name if requested.
Plastic
We recommend Copoly for its durability and strength. Let us know the thickness, 1/8 inch is our standard.
Pads
Let us know if you want to have the pads installed or not.
Straps
Straps are available in white or black. Strap transfers are no longer an option here as they decrease the life and
integrity of the straps.
Scoliosis Specific Trim Lines
The section above describes the specifics of your scoliosis brace design. This section is based off the patient’s
physical presentation, your clinical evaluation and the x-ray.
Our technicians can complete this section for you, or you can state the brace design.
When requesting a Thoracic or TL extension, please provide the height in CM.
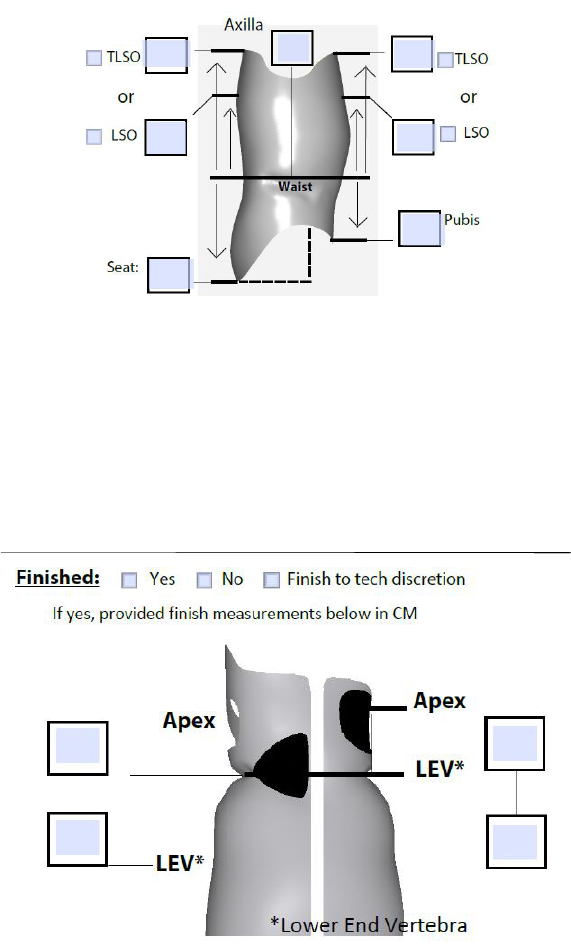
Finish
The above schematic shows the sagittal profile of the orthosis.
The TLSO/LSO check box is for you to describe the trimline of the orthosis. When controlling kyphosis, it is
recommended to have a TLSO anterior trimline, and an LSO (at the level of the kyphotic apex) posterior
trimline. All trim line measurements will be from the waist to the end point of the foam. The frame/stays will
be trimmed 2.5 cm shorter than the foam. Please provide the maximum height of the foam trimline.
The above schematic shows the coronal profile of the orthosis.
Indicate if you wish to have the orthosis finished or not. If yes, provide your finish measurements in CM. Our
finish room technicians will also finish the orthosis based on your anatomical measurements.
Each box represents the linear measurement from waist to the apical vertebra (superior box) or the bottom of the
curve (inferior box). Measurements are based on the x-ray and your clinical exam of the patient.
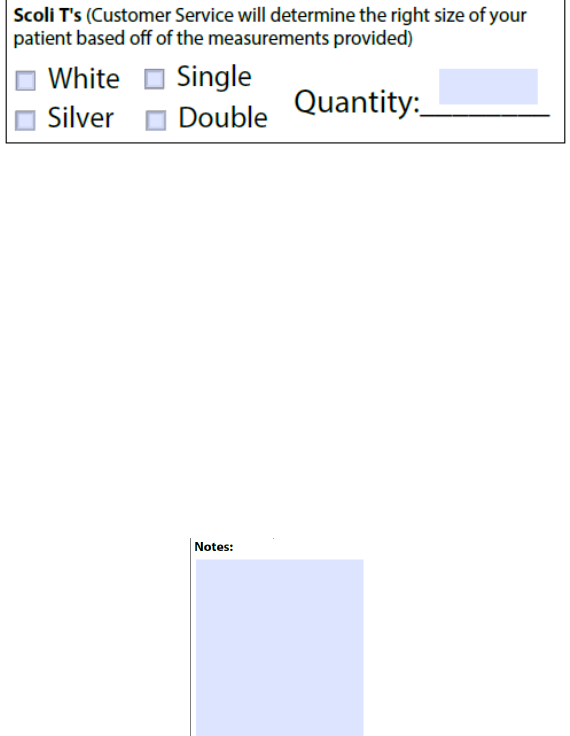
Scoli T’s
Indicate if you are providing the patient with a Boston Scoliosis T shirt. There are a few options. Standard or
silver (note that the silver is not to be worn when being MRI or HBO). Also, there are options for shirts with
two underarm flaps or a single. The T-shirts do not have a front or back, so a single axilla can be left or right.
The size is determined from the submitted measurements.
Notes
In the event a special request is made by the patient, or there is some unique anatomy or brace design needed
that is not captured in the above sections, the notes section is where you may document this information.
