
T aking Action for a Tobacco-Free Oregon
OREGON STATEWIDE
TOBACCO CONTROL PLAN
2005-2010

Contributors
We thank the following organizations for their participation in the series of meetings and collaborative goal
setting sessions that led to the development of this plan:
American Cancer Society
American Heart Association
American Lung Association of Oregon
Asian Family Center of IRCO
Benton County Health Department
CareOregon
Crook County Health Department
Douglas County Health Department
Group Health Cooperative
Jackson County Health and Human Services
Kaiser Permanente Northwest
Multnomah County Health Department
National Cancer Institute Cancer Information Service
Northwest Portland Area Indian Health Board
OMPRO- Oregon’s Quality Improvement Organization
Oregon Department of Education
Oregon Department of Human Services
Office of Child and Family Health Services
Office of Disease Prevention and Epidemiology, Tobacco Prevention and Education Program
Office of Medical Assistance Programs
Office of Mental Health and Addiction Services
Oregon Department of Justice Civil Enforcement Division
Oregon Human Development Corporation
Oregon Medical Association
Oregon Research Institute
PAC/WEST Communications
Portland State University
Providence Health System
Tigard-Tualatin School District
Tobacco-Free Coalition of Oregon
Umatilla County Public Health
Yamhill County Public Health

T able of Contents
Background
Taking Action 1
Tobacco’s Effects 2
Why People Use Tobacco 3
Overview of Tobacco Use in Oregon 4
Timeline 6
Goals
Oregon’s Tobacco Control Plan
Goal 1 9
Goal 2 11
Goal 3 13
Goal 4 15
Goal 5 17
Data Sources
Surveys 18
Vital Statistics 18
Other 19
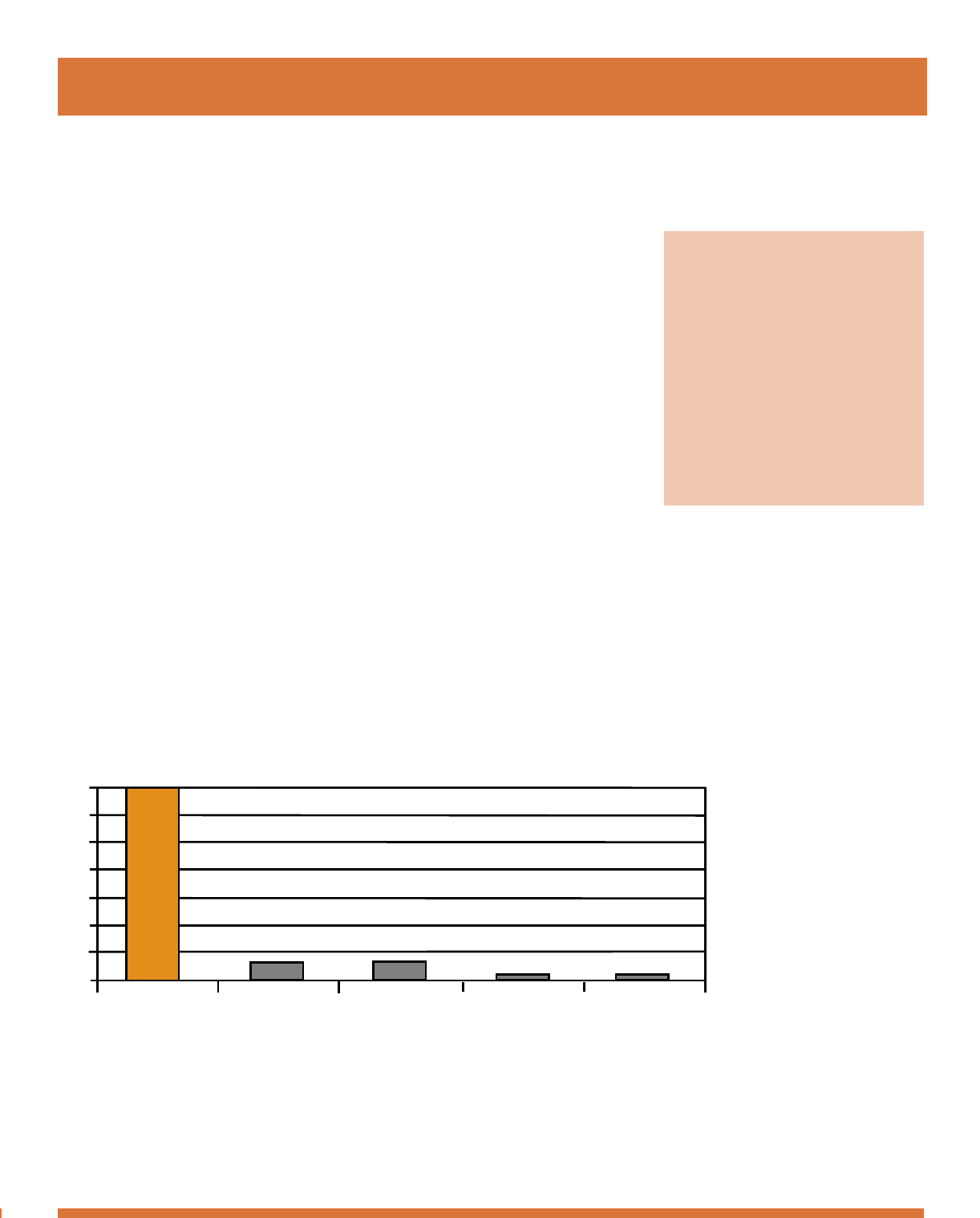
Each year in Oregon, tobacco use kills more than 6,000 people.
It claims more lives than motor vehicle crashes, suicide, AIDS, and murders
combined.
In 2003, 500,000 Oregon adults still smoked cigarettes, and 75,000
still chewed tobacco. For most smokers, addiction to tobacco began in their
youth, before they were 18. Despite gains in preventing youth from starting to
smoke, 45,000 Oregon youth still smoke and 13,000 still chew tobacco.
In addition to the cost of tobacco to Oregonians in lives, tobacco also
imposes a staggering financial burden—of particular concern at a time of seri-
ous economic difficulties in the state. Tobacco use cost Oregonians $1.8 bil-
lion in 2000. The direct cost to the healthcare system alone in Oregon was
nearly $900 million, and every pack of cigarettes sold costs our economy
$7.18—$3.45 in medical costs and $3.73 in lost productivity due to prema-
ture death and disease.
As a state, we simply cannot afford tobacco.
Taking Action
on Oregon’s
Number One
Health Problem:
Tobacco Use
7000
6000
5000
4000
3000
2000
1000
0
Tobacco Motor Vehicles Suicide AIDS Homicide
Number of Deaths-Selected Causes: Oregon, 2002
Background
T aking Action
1
T obacco’s Effects
2
Exposure to
Secondhand Smoke
Increases Risk of
Ear Infection
Asthma Attacks
Pneumonia
Bronchitis
Smoking and Spit Tobacco Cause
Stroke
Mouth Cancer
Throat Cancer
Heart Disease
Lung Cancer
and Emphysema
Pancreatic Cancer
Kidney Cancer
Cervical Cancer
Osteoporosis
Exposure to
Secondhand Smoke
Increases Risk of
Stroke
Heart Disease
Lung Cancer
Asthma Attacks
Why People Use Tobacco
The Office of the U.S. Surgeon General has been telling us since
1964 that tobacco use can cause death. Given that most everyone knows
smoking is dangerous, why do people still use tobacco?
The issue is complex. Smoking exists within a network of social
norms, political controls and tobacco industry influence. Tobacco use is a
cultural issue, with many interwoven factors ultimately affecting a person’s
decision to start or continue smoking.
Some cultures use tobacco differently than the mainstream U.S.
smoker. Sacred or traditional use of tobacco by American Indians is very
different from commercial tobacco use. Tobacco has an important role in
traditional American Indian life. For tribes throughout North America, the
use of traditional tobacco plants for spiritual, ceremonial and medicinal
purposes goes back thousands of years. This historic and enduring relation-
ship with sacred tobacco must be recognized and addressed when shaping
meaningful, culturally appropriate tobacco prevention in American Indian
communities.
In spite of all the factors that contribute to tobacco use, we do know
that when done well, tobacco control works! Comprehensive state tobacco
programs reduce tobacco use. These programs, with community and school
programs and policies, counter-marketing campaigns (such as anti-smoking
tobacco ads), and cessation programs for current smokers have proven effec-
tive time and again.
Background
3
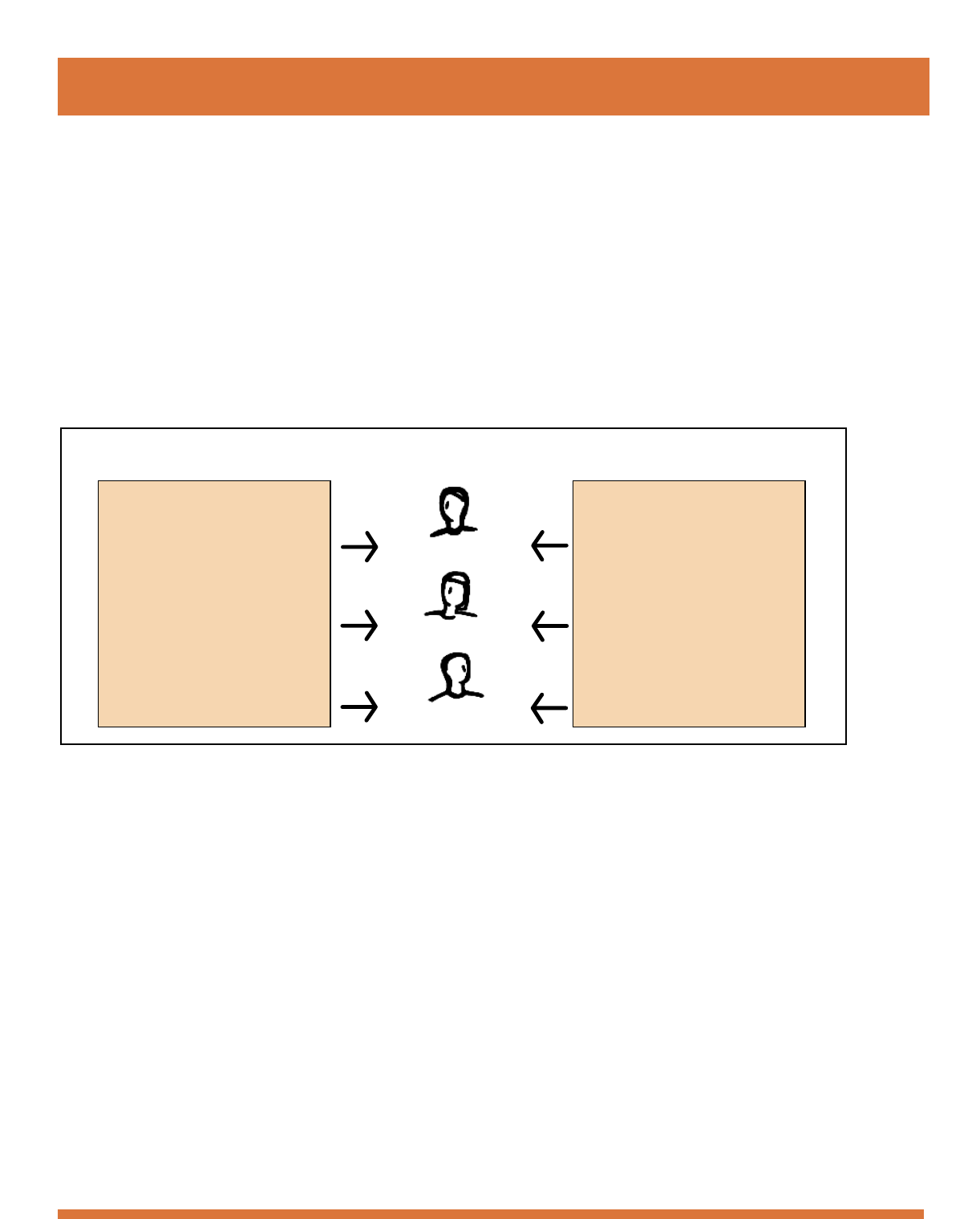
Influences on the Decision to Use Tobacco
A Young Nonsmoker
A Current Smoker
A Former Smoker
Anti -Tobacco Influences
• Health education and
information
• Price of tobacco
• Advertising policies
• Youth access to tobacco
• Smoke free environments
• Local community norms
• Behavioral treatment
• Pharmacological treatment
Pro -Tobacco Influences
• Psychosocial factors
• Adult role models
• Peer pressure
• Product availability
• Tobacco industry influence
including: advertising,
promotion and
counter education
• Addiction
A Brief Overview
of Tobacco Use
in Oregon
Smoking and chewing tobacco are prevalent among both adults and
youth in Oregon today. Twenty-one percent of adults smoke cigarettes, as do
16% of 11th graders. Chewing is less common overall, but use of this still-
deadly form of tobacco is more common among 11th grade males (11%)
than adult males (6%). Lower levels of education and income are both
linked to increased tobacco use.
These dire statistics have motivated the growing trend against tobac-
co use, and have created an increasing awareness of the dangers of second-
hand smoke. Only 17% of Oregonians in 2003 allowed smoking in their
homes, down from 29% in 1997.
The 2002 Smoke Free Workplace
Law protects a full 95% of Oregon
workers from secondhand smoke.
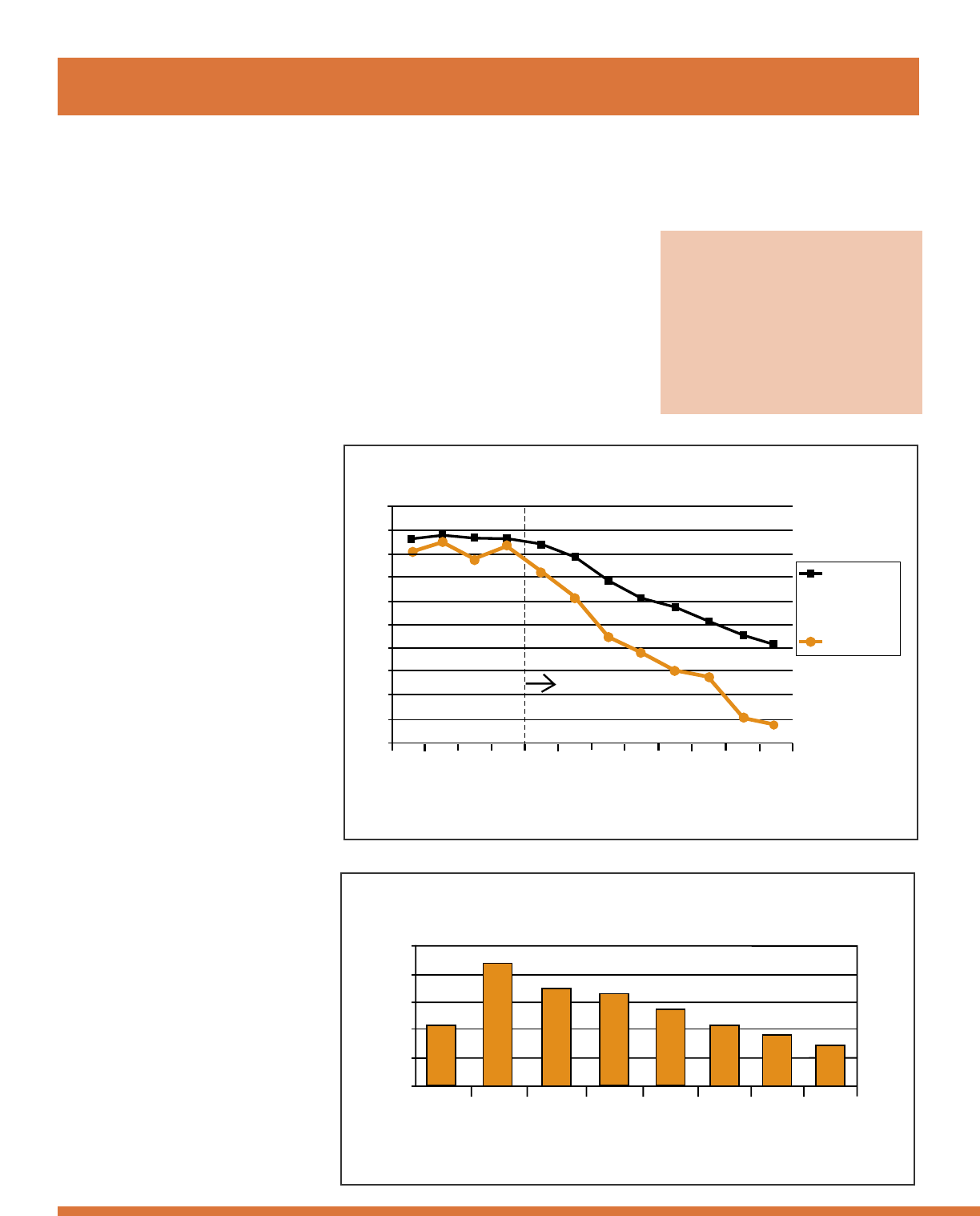
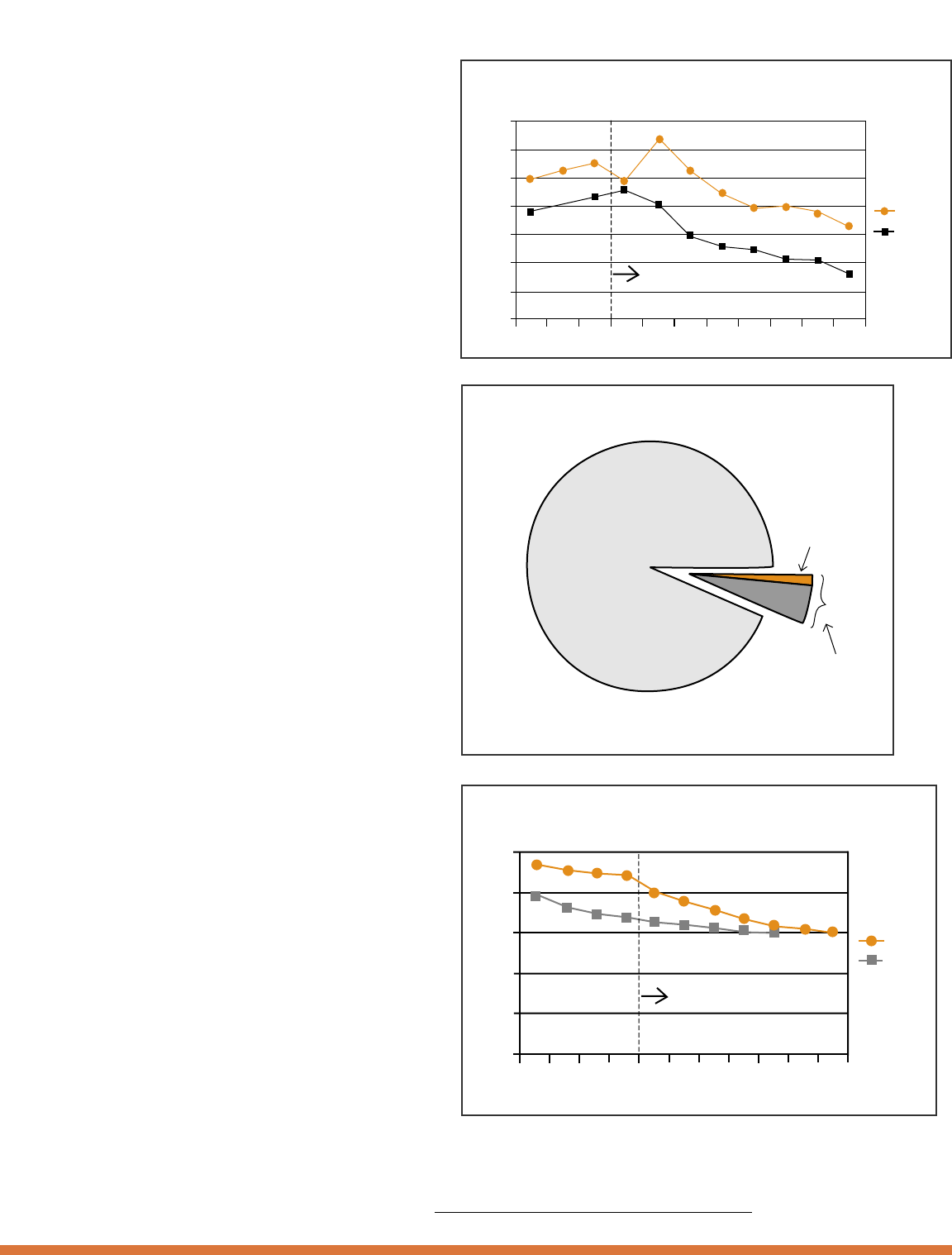
The national downward
trend in tobacco use has become
clear in per capita cigarette sales.
The dramatic drop is even more
pronounced in states like Oregon,
where comprehensive tobacco
reduction programs are in place.
While it is true that overall
cigarette consumption in Oregon is
decreasing, smoking prevalence
remains higher in some communi-
ties than in others. For example,
American Indians, the Lesbian/Gay
community and African Americans
have a high prevalence of smoking
in relation to the statewide average.
Furthermore, while the overall
prevalence among Hispanics,
Asians and Pacific Islanders is
lower than the statewide average,
some population groups within
these communities experience a
significantly higher prevalence than
the non-Hispanic white popula-
tion. The Oregon Statewide
Tobacco Control Plan addresses
these disparities.
'93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04
Annual Per Capita Sales of Cigarettes
Oregon and the Nation: 1993-2004
Oregon
States without
comprehensive
tobacco control
programs*
85
100
95
90
55
50
80
75
70
65
60
Oregon's Tobacco Program
Source: state cigarette tax receipts
Annual packs per capita
*This national comparison excludes Arizona, California, Massachusetts, and Oregon because these states
have had tobacco prevention programs since at least 1997.
4
Overview of Tobacco Use in Oregon
Percentage of Adults in Selected
Subgroups Who Smoke
Percentage Who Smoke
50%
40%
30%
20%
10%
0%
Statewide
Average
American
Indian
Gay/
Lesbian/
Bisexual
Low
Socio-
economic
Status
African
American
White
Non-
Hispanic
Hispanic
Asian/
Pacific
Islander
Source: Oregon Behavioral Risk Factor Surveillance System (2003, except by race/ethnicity 2001-2002)
Youth are a group particularly at risk for
tobacco use. Eight percent of 8th graders smoke;
by 11th grade 16% smoke. There are growing
efforts to reduce and eliminate smoking among
young people. For example, the state school
board has ruled that all campuses must be tobac-
co-free by January 1, 2006.
Unfortunately, funding cuts threaten
progress. At present, Oregon’s budgets for tobac-
co control comprise only a small fraction of what
the Centers for Disease Control and Prevention
considers minimum funding for effective tobacco
prevention programs.
Interventions that reduce people’s expo-
sure to tobacco smoke, both primary and second-
ary exposure, can begin to reap immediate finan-
cial savings. Childhood pneumonia, otitis media,
certain birth defects, SIDS and heart attacks all
show immediate risk reductions and associated
cost savings with reduced exposure.
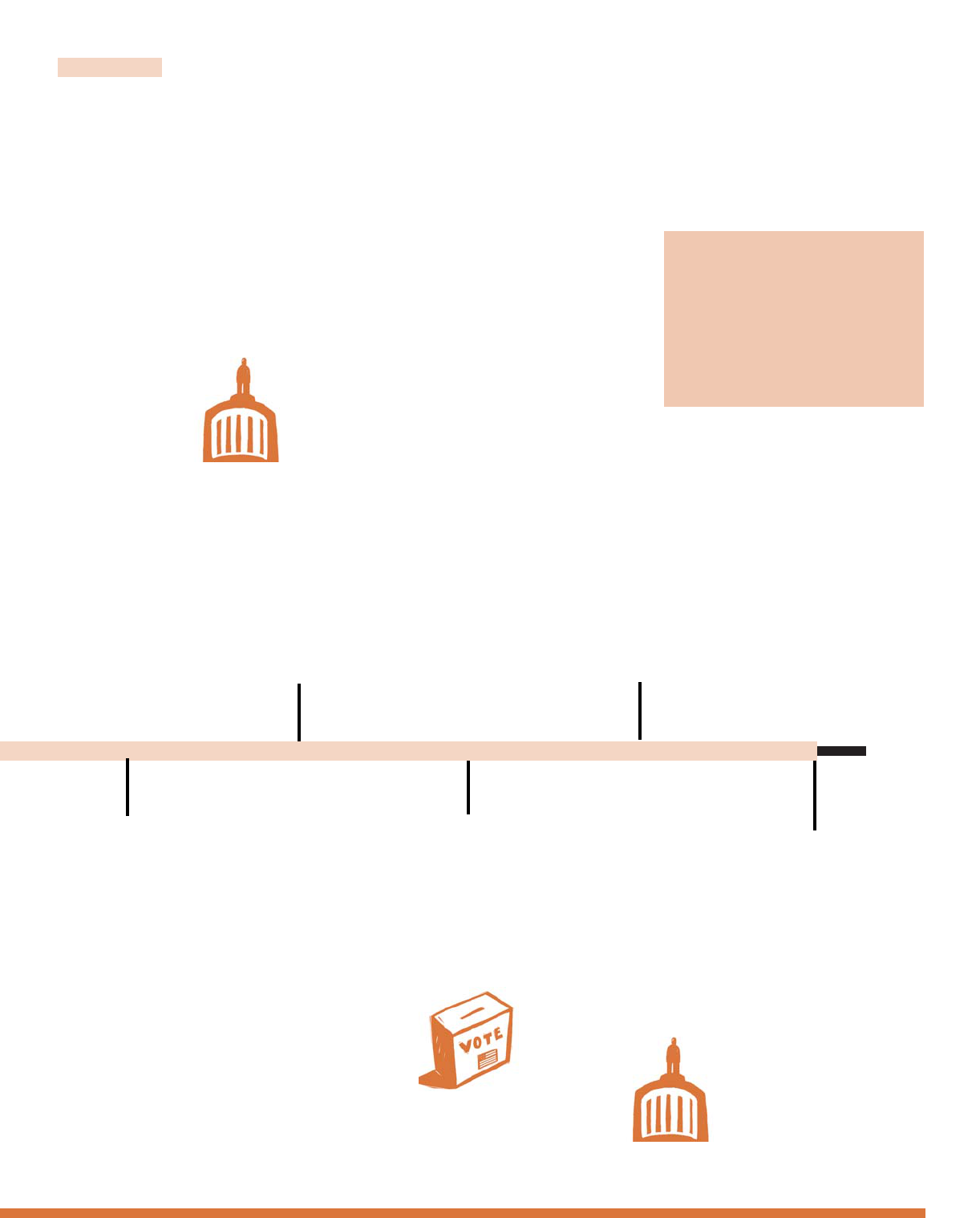
The problem of low birth weight babies
due to smoking mothers is another area where
decreased exposure gives an immediate benefit. In
Oregon, the percentage of infants born to moth-
ers who smoke has decreased 33% since 1996,
resulting in a biennial savings for Medicaid in
Oregon of $2 million.
Oregon's Tobacco Program
35%
30%
25%
20%
15%
10%
5%
0%
'94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04
Percentage of 8th and 11th Graders Who Smoke Cigarettes:
Oregon, 1994-2004
11th Grade
8th Grade
CDC minimum recommended
funding for tobacco prevention
in Oregon: $42 million
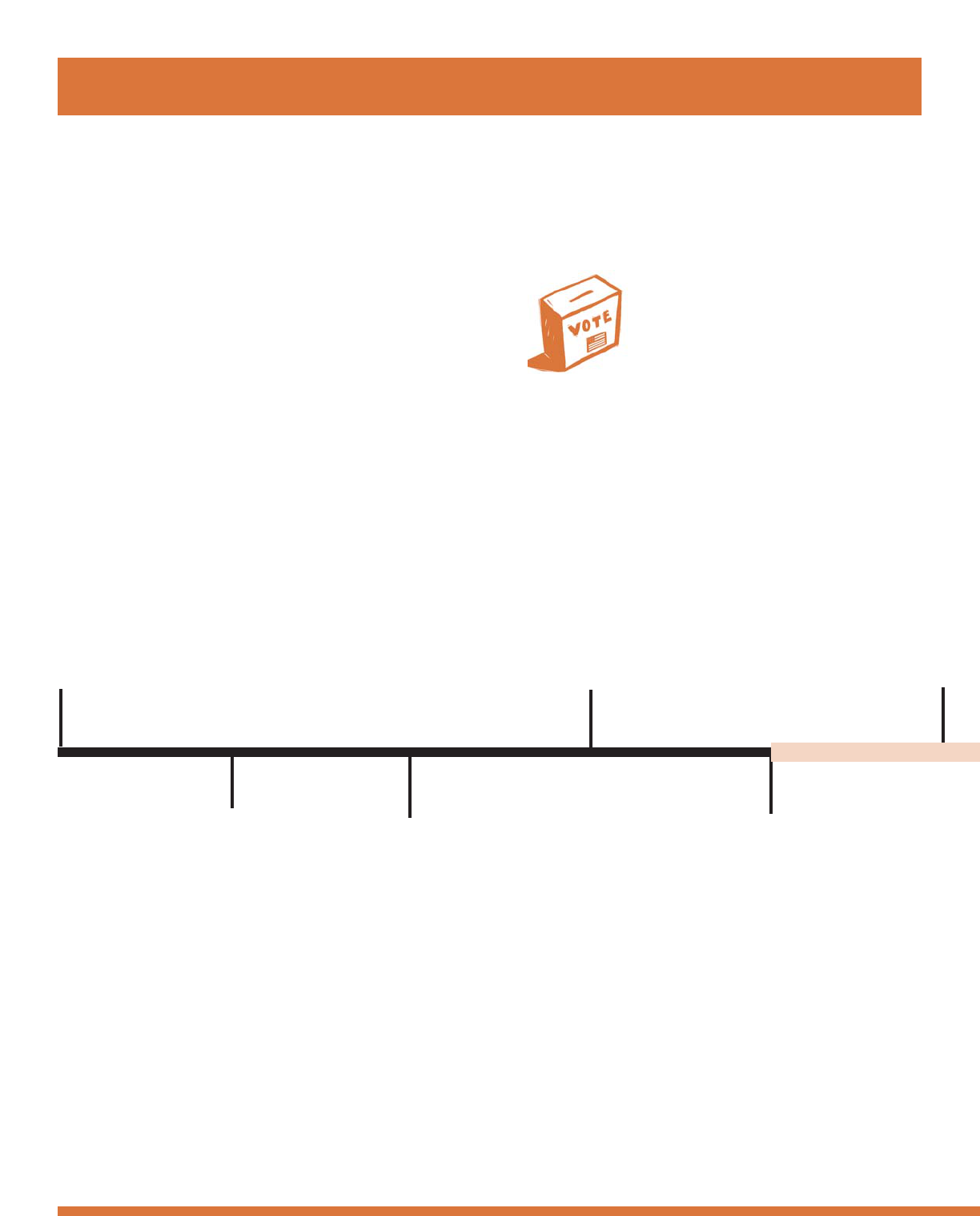
The state of Oregon receives $668 million each biennium from tobacco taxes
and payments from tobacco companies under the Master Settlement Agreement
State Tobacco Revenue and Tobacco Prevention Expenditures
2003-2005 Biennium
Total state tobacco revenue:
$668 million
Actual tobacco
prevention spending
$7 million
Oregon's Tobacco Program
20%
16%
12%
8%
4%
0%
'93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03
Oregon
U.S.
Percentage of Infants Born to Mothers Who Used Tobacco During Pregnancy
Oregon vs. U.S., 1993-2003
Background
5
For additional data about tobacco use in Oregon, please refer to Oregon Tobacco Facts. This document,
which is updated annually, is available online at www
.dhs.state.or.us/publichealth/tobacco.
Oregon Receives
CDC Funding
Oregon receives fund-
ing from the Centers
for Disease Control
and Prevention for
tobacco prevention.
1993-1994
November 1995
First State Plan for
Tobacco Control
Oregon tobacco
control advocates
launch the state’s
first Statewide
Strategic Plan for
Tobacco Control.
1994
Oregon Receives
Grant from RWJ
Foundation
Oregon receives a
grant from the
Robert Wood Johnson
Foundation
to organize statewide
tobacco control efforts.
Voters Approve Tobacco Prevention
and Education Program
Together with healthcare partners,
tobacco control advocates are success-
ful in their campaign to raise tobacco
excise taxes by 30 cents and dedicate a
portion to a tobacco use prevention
program. Ballot Measure 44 passes by
a wide margin despite millions of dol-
lars spent by tobacco companies to
defeat it.
November 1996
Master Settlement
Agreement
In a landmark agreement
in federal court, the
tobacco industry agrees
to pay out an estimated
$206 billion over 25
years to state govern-
ments. Oregon’s attorney
general joins other states
in signing the Master
Settlement Agreement.
1998
1997
A Statewide Tobacco Program is
Launched
The Oregon Department of Human
Services launches the Tobacco Prevention
and Education Program (TPEP). This
new program is grounded in one basic
premise: the only way to reduce tobacco
use is to attack the problem from multi-
ple fronts. Towards this goal, local tobac-
co control coalitions are established,
schools begin to implement comprehen-
sive prevention programs, and the
Department of Human Services estab-
lishes a statewide Quit Line for smokers.
1997 - 2004 Local
policy makers take action
T imeline
6
Making
Tobacco History
in Oregon
Oregon Indoor Clean Air Act
The Oregon State Legislature
improves Oregon’s Indoor Clean
Air Act by covering more work-
places and public places. Some
workplaces, such as bars, are
exempted.
2001
TPEP De-funded
Faced with a significant budget shortfall, the
Oregon State Legislature de-funds the Tobacco
Prevention and Education program.
2003
1997-2004
Local Policy Makers Take Action
Local policy makers on county commissions,
city councils, tribal councils, park boards,
schools boards and rodeo boards all over
Oregon change local tobacco laws. They pass
ordinances banning smoking in work and
public places, they change local regulations
about where tobacco can be placed in stores,
and they ban tobacco company sponsorship of
community events.
Background
7
2002
Measure 20
Voters approve Ballot Measure 20, which
again increases the tobacco excise tax and
dedicates a portion of the funds to the
Tobacco Prevention and Education
Program.
1999
TPEP in Full Swing
As a result of the Tobacco
Prevention and Education
Program in Oregon, ciga-
rette consumption drops,
secondhand smoke expo-
sure decreases and smok-
ing-related medical costs
are reduced.
2004
Partial Restoration of
Funding for Tobacco
Programs
The Oregon State
Legislature restores
tobacco prevention
education funding to
$5.8 million per
biennium—73% of
previous biennia, and
14% of the CDC
recommended
minimum level.
T obacco Control Plan
A Tobacco-Free
Oregon:
The Statewide
Tobacco
Prevention, Control
and Treatment
Plan
2005 - 2010
It is clear that Oregon
has made tremendous
strides in tobacco control.
We have also experienced
significant setbacks. The
good news is we know—
from research and our own
experiences—how to reduce
tobacco use. We have been
successful in the past. With
adequate attention, funding
and energy we will continue
to reduce the terrible toll
tobacco-related death and
disease takes on our state.
The following pages of
this plan outline specific
objectives and strategies for
Oregon, which, if applied,
can reduce or eliminate
tobacco-related death and
disease.
Eliminate Exposure
to Secondhand
Smoke
Exposure to secondhand smoke is a problem almost as serious as
smoking. Those caught in this carcinogenic haze are at increased risk for
many of the same diseases afflicting smokers, such as lung cancer and heart
disease. Reducing and eliminating secondhand smoke exposure, then, must
be an integral part of tobacco control.
Objective 1
Reduce the percentage of individuals exposed to second-
hand smoke by increasing the percentage of indoor public places
and workplaces that prohibit smoking.
Strategy
a. Improve the current law by removing exemptions and strengthening
statutory enforcement, penalty language and surveillance of the State
Indoor Clean Air Act.
Objective 2
Reduce the percentage of individuals exposed to second-
hand smoke in homes and vehicles.
Strategies
a. Identify and evaluate best practices for how to reduce smoking in
homes and vehicles.
b. Pilot a research-based education/media campaign.
c. Maintain an ongoing research agenda.
d. Ensure coordination of groups around the state.
Objective 3
Increase the number of outdoor places that prohibit
smoking.
Strategy
a. Promote local policies prohibiting smoking around building entrances,
in parks, at public transit stops, and in other outdoor public places.
G oal 1
9
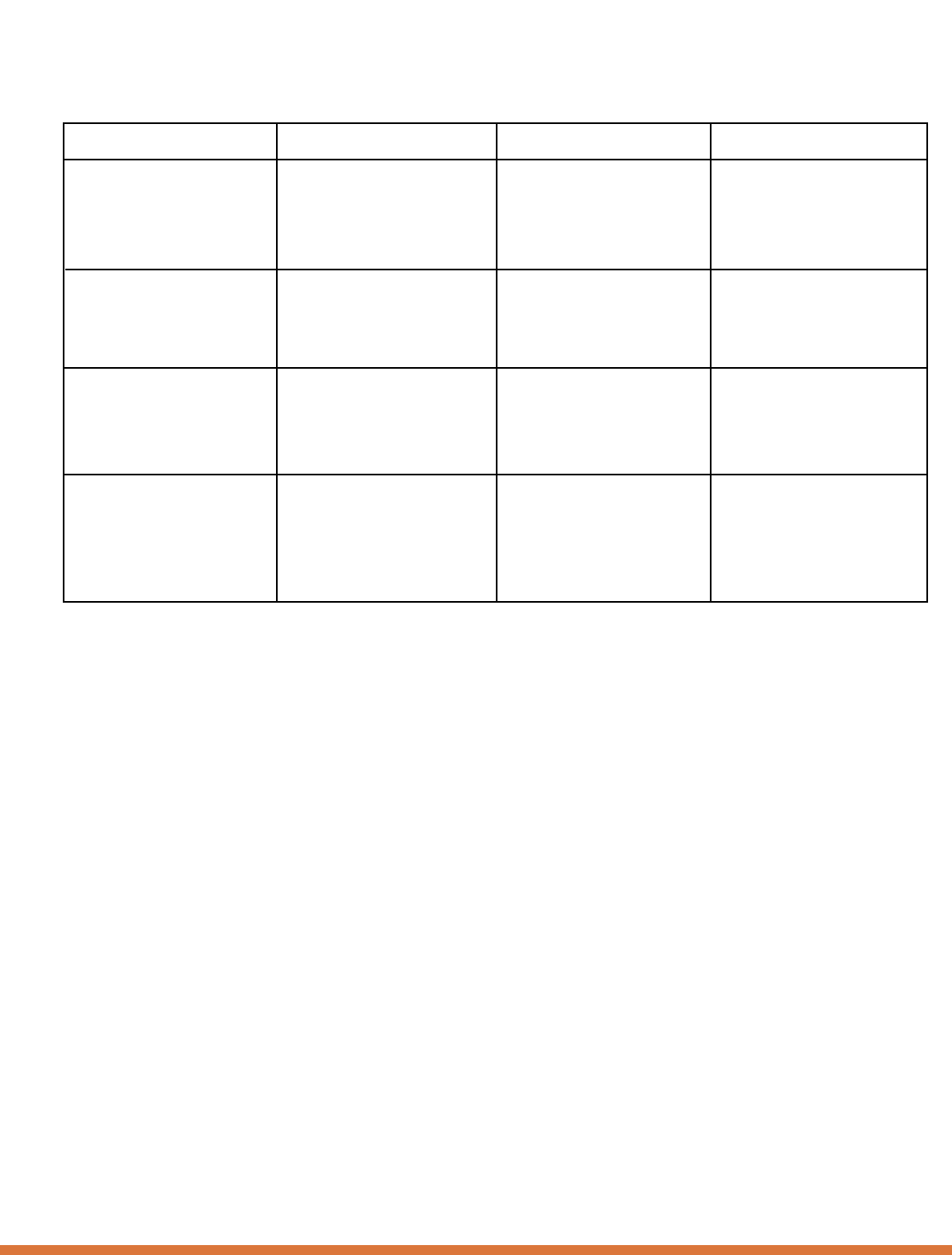
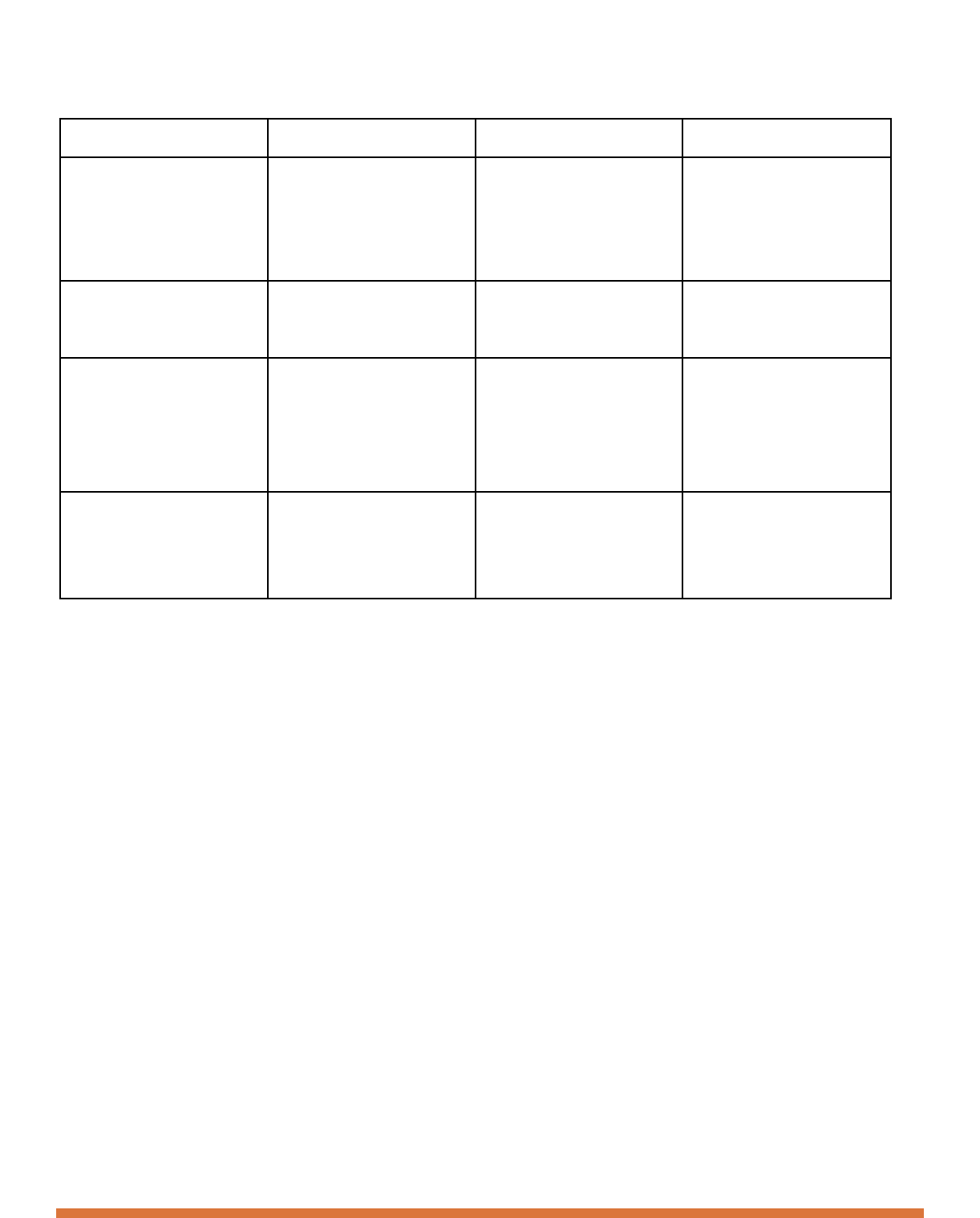
This table outlines benchmarks that will be tracked for progress towards the objectives listed
under each program goal.
Goal 1
Benchmark
number of workers who are
protected from secondhand
smoke
percentage of homes where
there is smoking indoors
percentage of adults who allow
any smoking in their cars
number of local policies
that prohibit smoking in an
outdoor place
Current Status
95%
14%
28%
2
2010 Target
100%
5%
15%
15
Data Source
Local ordinances and state laws,
Oregon Department of
Employment data.
BRFSS
BRFSS
DHS Ordinance Database
10
Prevent the
Initiation of
Tobacco by Youth
Young people start to use tobacco for a variety of reasons. In spite of
their protests to the contrary, this process of youth initiation has long been a
target area for tobacco companies. The hard-fought battle to remove cartoon
advertising from cigarettes is only one example of the struggle to stop the
creation of new school-age smokers.
Only through continued efforts to prevent young people from start-
ing to smoke and chew in the first place can we decrease overall tobacco use
in Oregon.
Objective 1
Decrease young people’s desire to use tobacco.
Strategies
a. Implement culturally appropriate youth strategies using a compre-
hensive, coordinated paid and earned media campaign at the state
and local levels. Select messages based on evidence of effectiveness
with youth.
b. Develop a regionally representative, diverse youth coalition to partici-
pate in developing and implementing effective strategies and media
approaches to address the problem of tobacco use among youth.
c. Increase the percentage of school districts with comprehensive
tobacco use prevention policies and programs.
d. Support and expand the Coordinated School Health Program infra-
structure to implement and enforce a statewide comprehensive school
tobacco policy and assure effective tobacco prevention programs.
Objective 2
Decrease youth access to tobacco.
Strategy
a. Increase tobacco taxes where a portion of the revenue is dedicated in
perpetuity to support comprehensive tobacco prevention programs as
recommended by the CDC guidelines, including effective strategies
for preventing youth access to tobacco.
G oal 2
11
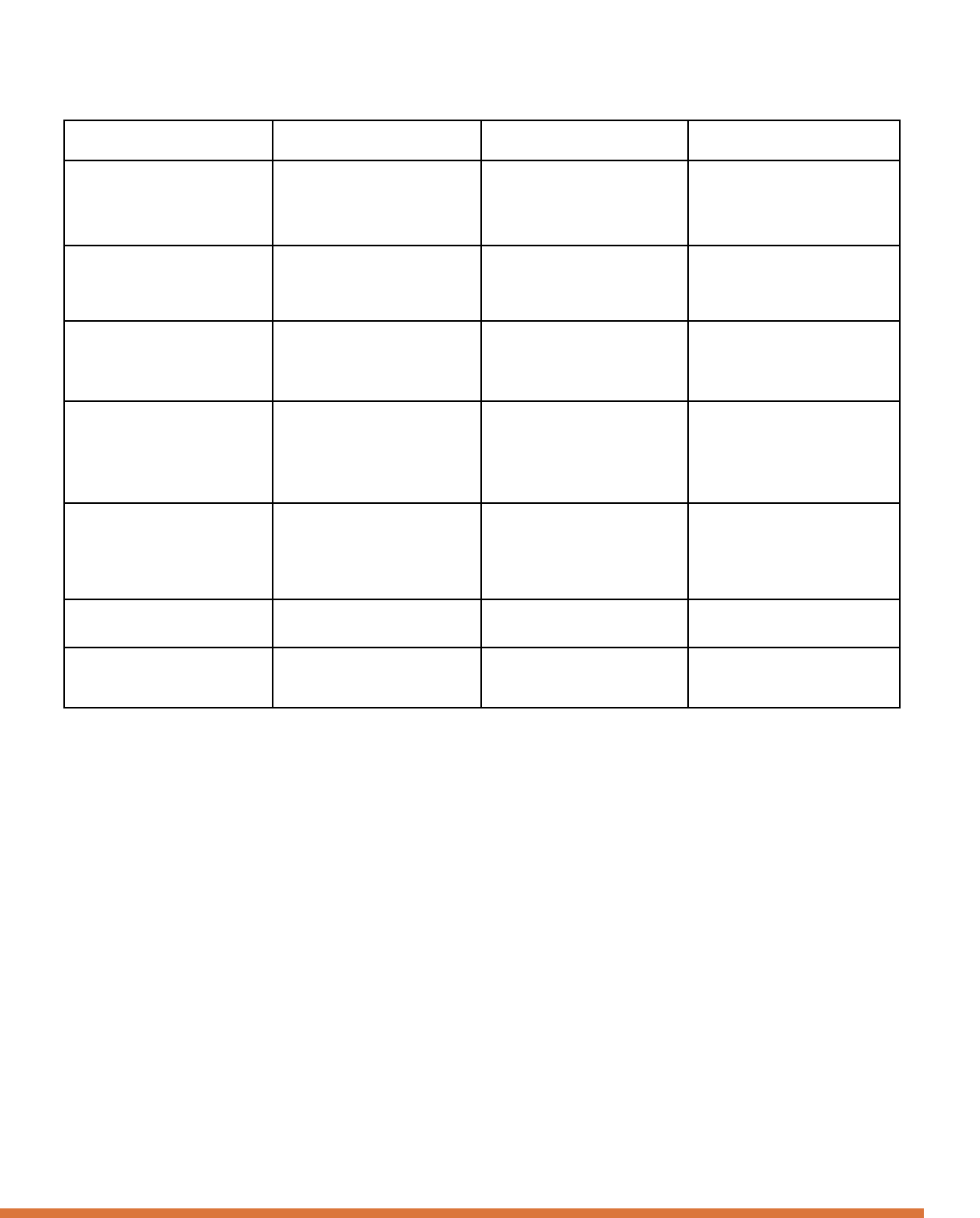
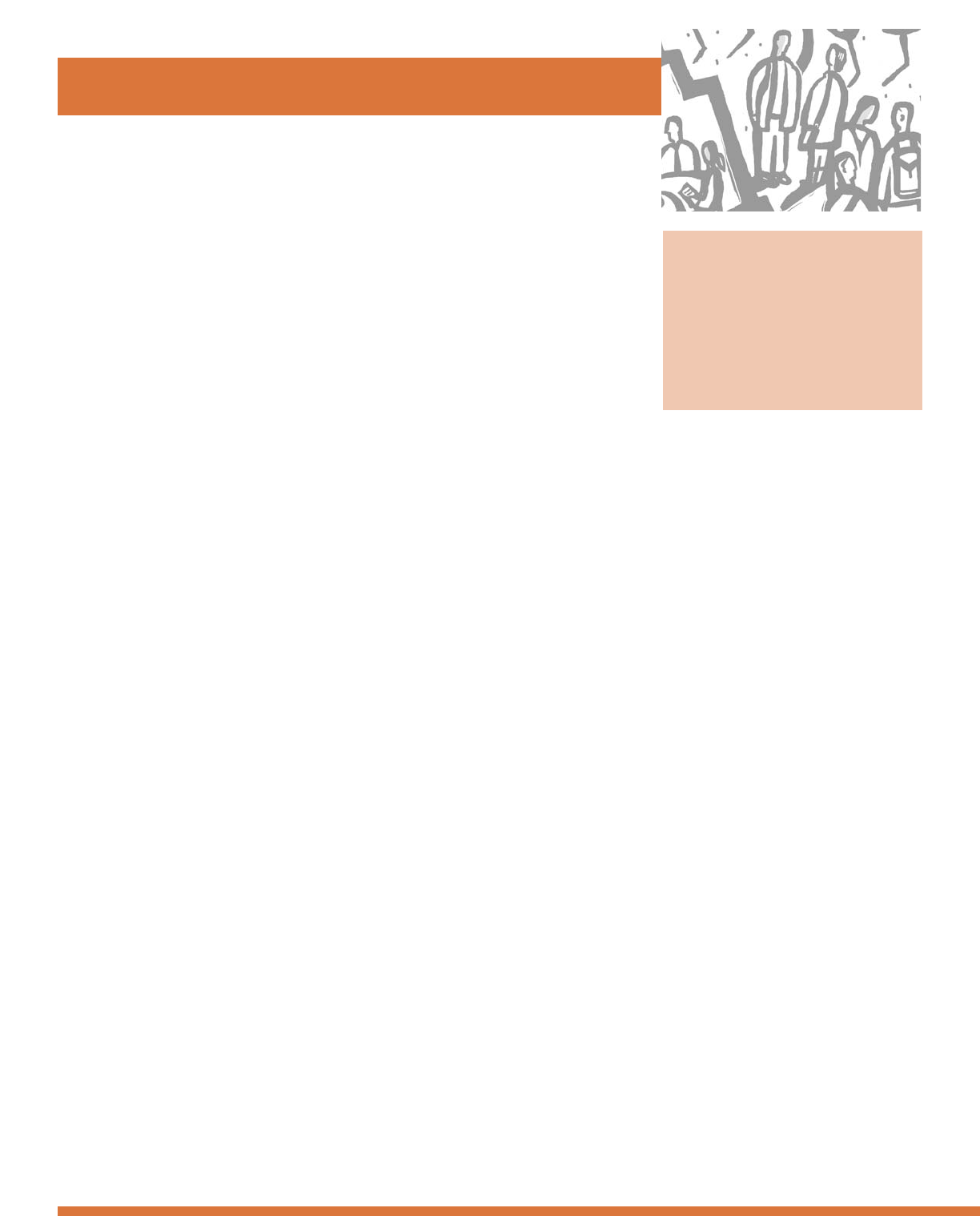
This table outlines benchmarks that will be tracked for progress towards the objectives listed
under each program goal.
Goal 2
Benchmark
percentage of 8th graders who
smoke
percentage of 8th grade males
who use smokeless tobacco
percentage of 11th graders
who smoke cigarettes
percentage of 11th grade
males who use smokeless
tobacco
percentage of 8th graders who
say that it is very easy to get
tobacco
Oregon tax on cigarettes
SYNAR non-compliance rate
Current Status
8.1%
4%
16.5%
11%
21%
$1.18
15%
2010 Target
5%
2%
10%
6%
10%
$2.00
10%
Data Source
Oregon Healthy Teens Survey
Oregon Healthy Teens Survey
Oregon Healthy Teens Survey
Oregon Healthy Teens Survey
Oregon Healthy Teens Survey
State Law
Department of Human Services
12

Increase Access
to Cessation
Resources
for Adults and
Youth
Studies have shown that people who try to quit smoking are two to
three times more likely to succeed if they use specific medications or patches
and get professional counseling. But in 2003, of people trying to quit, only
39% tried the medications and patches that can reduce the physical crav-
ings, and only a tiny fraction (6%) received the counseling that teaches how
to quit and builds confidence. The Oregon Tobacco Quit Line, which offers
free counseling and connects tobacco users to their health systems’ assistance
programs, currently only reaches about 1% of tobacco users.
Oregon has a long way to go in helping tobacco users end their
dependence on nicotine, but the path is clear. We must make high quality
medication and counseling assistance readily available, and must increase the
number of tobacco smokers and chewers who use that assistance.
Objective 1
Increase the percentage of Oregonians who have access to
cessation benefits through their employer or health insurance.
Strategies
a. Create a widespread communication plan targeting businesses, the
uninsured, labor, the health industry, the insurance industry, and bro-
kers. The communication plan will build awareness in these target
groups, sending the message that tobacco cessation assistance works
and provides health improvements, financial benefits and productivity
gains for everyone.
b. Convene a Task Force to coordinate campaign efforts and encourage
public sector employees and major labor unions to secure cessation
benefits for their employees and families.
Objective 2
Increase the demand for and use of cessation services and
programs for adults, youth and populations with tobacco use
disparities.
Strategies
a. Raise tobacco taxes significantly, with new revenue to enhance the
comprehensive tobacco prevention program (including the expansion
of cessation services).
b. Research, promote and implement cost effective population-based
approaches to prompt large numbers of tobacco users to quit.
c. Engage a public-private partnership in finding and funding creative
ways to increase access to pharmacological interventions and cessation
counseling support.
d. Develop earned media strategies to drive calls to the Quitline, and
evaluate their effectiveness as compared to paid media strategies.
G oal 3
13
Goal 3
Benchmark
percentage of Oregonians
whose health insurance covers
cessation services
percentage of smokers who
plan to quit in the next 30 days
percentage of smokers who say
that it would be very helpful to
have assistance when
trying to quit smoking
percentage of adults who say
their health insurance
covers smoking cessation
Current Status
39%
27%
34%
19%
2010 Target
50%
32%
40%
25%
Data Source
Survey of health plans by
TOFCO
BRFSS
BRFSS
BRFSS
14
This table outlines benchmarks that will be tracked for progress towards the objectives listed
under each program goal.
Eliminate
Disparities in
Tobacco Use
Despite all of Oregon’s tobacco control successes, some population
groups are not experiencing the benefits equally. Declining tobacco use
exposes disparities among distinct populations, such as American Indians
and people of low socioeconomic status. The tobacco companies
aggressively target these and other groups in an effort to maximize profits
and expand markets.
Disparities in tobacco use prevent everyone from having equal access
to the benefits of tobacco use reduction. An effective tobacco control effort
must work to eliminate these disparities.
Objective 1
Develop and implement effective population-specific
tobacco control programs directed at specific ethnic and cultural
groups affected by tobacco use disparities.
Strategies
a. Increase the involvement of tobacco control partners and populations
affected by tobacco related disparities in the development and imple-
mentation of tobacco control programs.
b. Develop a task force to disseminate the results of the CDC - spon-
sored disparities planning project. Inform influential community
leaders from the disparate groups, advocating for tobacco control
programs and activities targeted toward specific populations.
Objective 2
Expand data collection and develop innovative data
collection strategies for populations affected by tobacco-related
disparities.
Strategy
a. Obtain funding for effective data collection on those affected by
tobacco-related disparities.
G oal 4
15
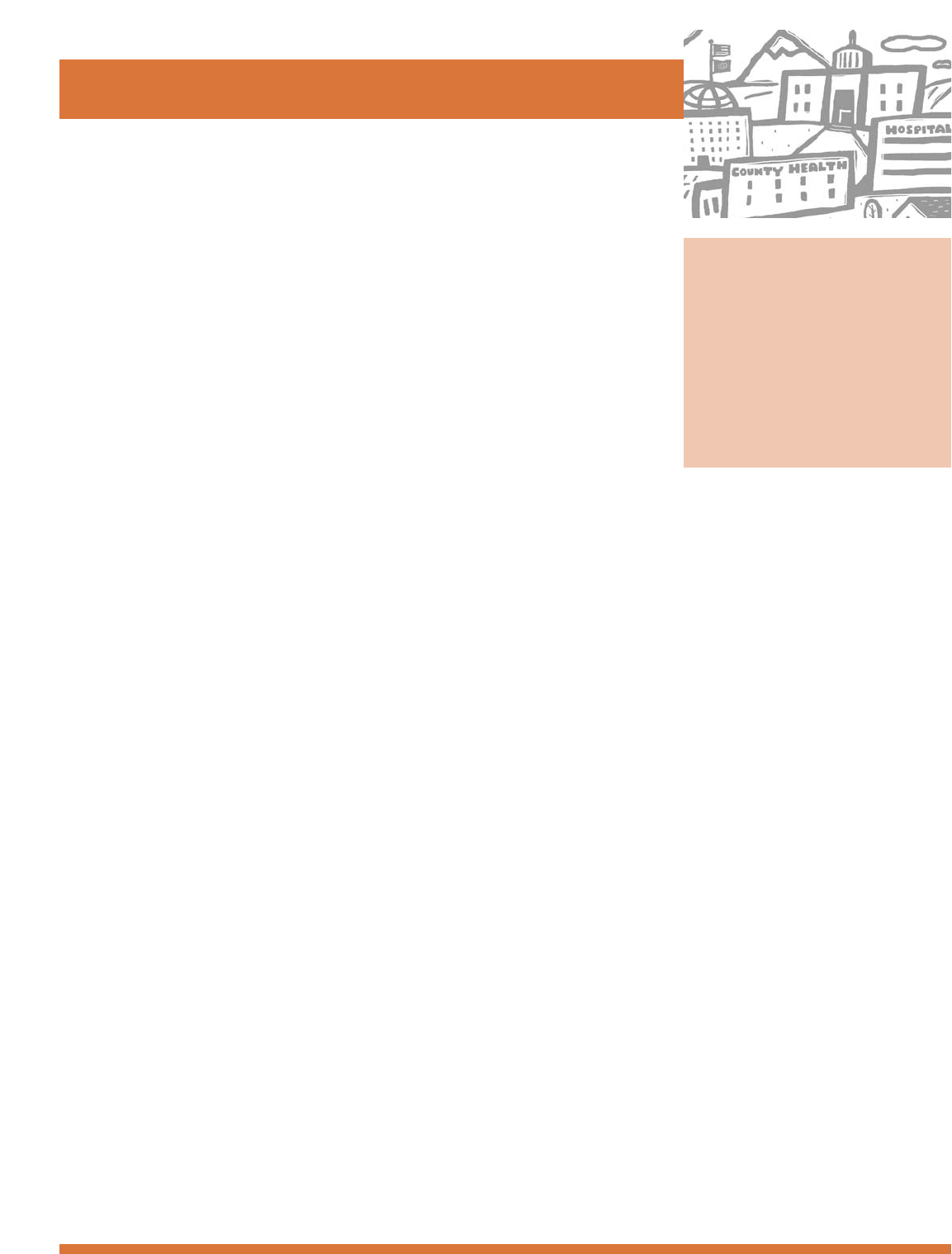
This table outlines benchmarks that will be tracked for progress towards the objectives listed
under each program goal.
Goal 4
Benchmark
African American adult smoking
prevalence
American Indian adult smoking
prevalence
Asian/Pacific Islander adult
smoking prevalence
Hispanic adult smoking
prevalence
lesbian, gay and bisexual adult
smoking prevalence
low socioeconomic status adult
smoking prevalence
percentage of African American
homes where there was
smoking indoors
percentage of American Indian
homes where there was
smoking indoors
percentage of Asian/Pacific
Islander homes where there
was smoking indoors
percentage of Hispanic homes
where there was
smoking indoors
percentage of lesbian, gay and
bisexual homes where there
was smoking indoors
percentage of low socio-
economic status homes where
there was smoking indoors
Current Status
27%
44%
14%
18%
34%
35%
17%
28%
9%
12%
29%
23%
2010 Target
15%
15%
10%
15%
15%
15%
5%
5%
5%
5%
5%
5%
Data Source
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
BRFSS
16
Develop the
Infrastructure for
Tobacco Use
Prevention
The activities that create an environment for tobacco prevention do
not happen in isolation. Legislation, medical services and counseling for the
smoker, and community education programs for the general public all
require adequate funding and organization.
Objective 1
Reevaluate and rebuild the infrastructure for tobacco use
prevention and control and the level of funding and commitment
necessary to implement the new Statewide Plan.
Strategies
a. Enhance and advance the communication, coordination and coopera-
tion among all partners to implement the Statewide Plan.
b. Develop a Communications, Coordination and Implementation Plan
that includes all stakeholders and addresses public relations, organiza-
tional activities, message development, and policy and program strate-
gies for the Statewide Plan.
c. Ensure that all partners have adequate funding to implement the
Statewide Plan.
d. Enhance and advance the systems (procedures, organizations and pro-
grams) among all partners to implement the Statewide Plan.
Benchmark
The Centers for Disease Control and Prevention (CDC) recom-
mends that Oregon spend $21 million annually on public health tobacco
prevention and education programs.
G oal 5
17
Goal 5

18
D ata Sources
A. Surveys
Behavioral Risk F
actor Surveillance System
The Behavioral Risk Factor Surveillance System
(BRFSS) is an ongoing random-digit dialed telephone
survey of adults concerning health-related behaviors.
The BRFSS was developed by the Centers for Disease
Control and Prevention (CDC) and is conducted in all
states in the U.S. Each year, between 3,000 and 7,000
adult Oregonians are interviewed. The BRFSS includes
questions on health behavior risk factors such as seat
belt use, diet, weight control, tobacco and alcohol use,
physical exercise, preventive health screenings, and use
of preventive and other healthcare services. The data are
weighted to represent all adults aged 18 years and older.
A core set of questions, which includes the question of
smoking prevalence, is asked annually and other topics
are surveyed on a rotating basis of two years. Each state
may add questions to the CDC survey, and Oregon asks
an additional sixty questions on attitudes and behaviors
regarding tobacco. Except as noted below, 2003 BRFSS
data are used in this report.
Data presented by race/ethnicity are from a special com-
bined 2000 & 2001 file which includes additional sur-
veys from an oversample among African Americans,
American Indians, and Asian/Pacific Islanders. The
oversampling ensured that there would be a minimum
of 100 surveys in each county and a minimum of 250
surveys for each racial/ethnic group. Data for each
region and each racial/ethnic group were weighted to
represent the group’s population by age and gender.
O
regon Healthy Teens Survey
Since 2000, the Youth Risk Behavior Survey and the
Oregon Public School Drug Use Survey have been com-
bined into a single annual survey, Oregon Healthy
Teens. In 2004, approximately 13,503 8th graders from
119 middle schools and 9,247 11th graders from 99
high schools were surveyed.
Y
outh Risk Behavior Survey
The YRBS was developed by the Centers for Disease
Control and Prevention and was administered in a sam-
ple of Oregon schools every other year from 1991-2000.
The sample size varied between 1,600 and 32,000 and
the final data were weighted to more accurately repre-
sent the Oregon high school population. The question-
naire assessed behavioral risks among Oregon high
school students (grades 9 through 12) in the areas of
vehicle safety, weapon carrying and violence, tobacco
use, alcohol use, other drug use, sexual activity and
pregnancy, HIV knowledge and attitudes, eating behav-
iors, nutrition, exercise, and access to healthcare includ-
ing use of school-based health centers. A sample of
middle school students (grades 6 through 8) was added
in 1997. In 2000, over 7000 students participated in
the survey.
O
regon Public School Drug Use Survey
The Oregon Office of Mental Health and Addiction
Services (OMHAS) administered this anonymous sur-
vey every other year from 1986-2000 through the
Oregon public school system. It was patterned after the
ongoing national surveys of the National Institute on
Drug Abuse and included eighth and eleventh graders
since 1986; a sixth grade sample was added in 1994.
Schools were randomly sampled using a cluster sample
design and in 2000 included over 15,000 students.
The questionnaire assessed community characteristics,
tobacco use, drug use, alcohol use, drug/alcohol use
in student’s peer and family network, refusal skills,
susceptibility to future use, and attitudes toward school
and family.
B. Vital Statistics Data
Birth Certificate Statistical File
Data from the Birth Certificate Statistical File are coded
from birth certificates collected by the State Registrar
and represent all births occurring in Oregon and all
19
births occurring out-of-state to Oregon residents. This
database includes parental demographic information,
conditions of the newborn, congenital anomalies, med-
ical factors of pregnancy, method of delivery, complica-
tions of labor and delivery, smoking, drinking, or illicit
drug use during pregnancy, antenatal and intrapartum
procedures, and payor source. The birth data analyzed
for this report consist of births to Oregon residents and
exclude missing and unknown values.
D
eath Cer
tificate Statistical File
The Death Certificate Statistical File includes all deaths
occurring in Oregon and deaths occurring out-of-state
to Oregon residents. Data are obtained from death cer-
tificates that are collected by the State Registrar. The
data are used to examine trends in mortality and causes
of death. Variables in this database include cause of
death, date and place of death, decedent demographic
information, whether the death was related to tobacco
use, and county, place, and date of injury (if applicable).
The mortality data analyzed for this report consist of
deaths of Oregon residents.
C. Other
Oregon Department of Revenue Cigarette Tax Receipts
Data on the number of cigarettes smoked by
Oregonians are estimated based on tobacco tax revenue
collected by the Oregon Department of Revenue. The
Department of Revenue’s Monthly Receipt Statements
include data on cigarette tax collections. The number of
packs of cigarettes sold is calculated by dividing the cig-
arette tax receipts by the tax rate per pack. The number
of packs per capita is calculated by dividing the total
number of cigarette packs sold by the smoking popula-
tion estimate for Oregon.
S
moking-Attributable Morbidity, Mortality and
Economic Costs (SAMMEC)
SAMMEC is a computer software program developed
by the Centers for Disease Control and Prevention to
calculate several measures of the impact of cigarette
smoking for the entire U.S. and for each state. Using
state-specific data on smoking prevalence, overall mor-
tality rates, and population data, SAMMEC generates
the number of deaths and death rates due to smoking,
years of life lost due to premature death from cigarette
smoking, and lost productivity (earnings) due to illness
and premature death from smoking-related diseases.
Tobacco Sales to Minors Inspection Repor ts (Synar)
In July 1992, Congress enacted the Alcohol, Drug
Abuse and Mental Health Administration Act, which
includes an amendment aimed at decreasing access to
tobacco products among youth under 18. Named for its
sponsor, Congressman Mike Synar, the regulation
requires states to enact and enforce laws prohibiting any
manufacturer, retailer, or distributor from selling or dis-
tributing products to individuals under 18. In addition,
the regulation requires that each state annually conduct
random, unannounced inspections of a sample of tobac-
co vendors to assess their compliance with state law.
Oregon has conducted these inspections annually since
1994. The sample size has ranges from 352 in 1995 to
860 in 2004. Oregon Liquor Control Commission lists
are used as a sampling frame after exclusion of certain
classes of licensees that customarily do not sell tobacco
products. Retired state police accompanied by a teen
"buyer" conduct the inspections. Purchase attempts are
recorded in a database which includes the following
variables: county, region, inspection data, type of busi-
ness, type of access to tobacco product, type of purchase
attempted, whether age and/or ID was requested,
results, whether illegal vending machine was present,
whether signs are posted for minimum age require-
ments, and whether single cigarettes are available.

For more information, contact:
Tobacco Prevention & Education Program
Oregon Department of Human Services
800 NE Oregon Street, Suite 730
Portland, OR 97232
(503) 731-4273
(503) 731-4082 - fax
www.healthoregon.org/tobacco
For additional copies, contact:
American Lung Association of Oregon
(503) 924-4094
1-800-LUNG-USA
www.lungoregon.org
Northwest Portland Area
Indian Health Board
