
1
DEPARTMENT OF HEALTH & HUMAN SERVICES
Centers for Medicare & Medicaid Services
7500 Security Boulevard
Baltimore, Maryland 21244-1850
CENTER FOR MEDICARE
TO: All Prescription Drug Plan and Medicare Advantage-Prescription Drug Plan
Sponsors
FROM: Cynthia G. Tudor, Ph.D., Director, Medicare Drug Benefit and C&D Data Group
RE: Medicare Prescription Drug Benefit Manual – Chapter 5
DATE: September 20, 2011
CMS is pleased to release updated Chapter 5 of the Medicare Prescription Drug Benefit Manual
(Benefits and Beneficiary Protections). The revisions to Chapter 5 reflect changes previously
released in the final regulations published in the Federal Register on April 15, 2010 and 2011
and in the Calendar Year 2012 Medicare Advantage Capitation Rates and Medicare Advantage
and Part D Payment Policies and Final Call Letter released on April 4, 2011.
Specifically, CMS:
• Added the definitions of “Applicable beneficiary,” “Applicable drug,” “Coverage Gap,” and
“Non-applicable drugs” to the definition section.
• Updated the description of Standard Prescription Drug Coverage and Alternative
Prescription Drug Coverage to address coinsurance in the coverage gap.
• Clarified existing policy with respect to “Free first fill programs” by specifying that, for a
new prescription, such programs must apply to both a beneficiary switch from a brand-name
medication.
• Stipulated in the section Enhanced Alternative Gap Coverage that sponsors will no longer
indicate their level of gap coverage in the Plan Benefit Package (PBP) software, but rather,
CMS will quantify each plan’s gap coverage and assign appropriate descriptions.
• Clarified existing policy in the section Restrictions on the Offering of Enhanced Alternative
Coverage by MA Organizations to ensure that MA organizations offer at least one option for
Part D coverage for supplemental premium at the cost of basic prescription drug coverage
and announcing that two questions have been added to the PBP to help ensure this
requirement is being met.
• Added a new section Coverage Gap Coinsurance.
• Clarified and updated existing policy regarding dispensing fees to reflect the long-term care
dispensing requirements effective January 1, 2013.
• Updated the section Ensuring Meaningful Differences in Approved Bids to reflect that CMS
will only approve a bid submitted by a sponsor if its plan benefit package or cost structure is
meaningfully different from other plan offerings by the sponsor in the same service area with
respect to key characteristics.

2
• Updated the section Meaningful Differences in Basic Prescription Drug Coverage Options to
state that CMS believes that sponsors should only submit one basic offering for a stand-
alone prescription drug plan in a service area.
• Updated the section Meaningful Differences in Enhanced Alternative Coverage Options to
state that CMS will announce its meaningful differences evaluation methodology via the
annual payment notice and call letter.
• Updated the section Transition Period for Sponsors or Parent Organizations with New
Acquisitions to reflect a 2 year transition period.
• Updated the section Consolidated Renewal Plan to cover consolidation of two enhanced
alternative plans.
• Updated the section PDP Plan Benefit Package (PBP) Renewal and Crosswalk Guidance to
include a section Consolidated Plans under a Parent Organization.
• Added a new section Low Enrollment Plans.
• Added a new section Manufacturer Drug Discount Program.
• Updated the sections Costs that Count as Incurred Costs, Costs that do not Count as Incurred
Costs, Summary of TrOOP-Eligible and TrOOP-Ineligible Payers, and Pharmacy
Waiver/Reduction of Cost-Sharing and Applicability, by addressing discounts paid by
manufacturers as part of the Medicare Coverage gap Discount program, costs paid by the
Indian Health Service or an Indian tribe or organization, and costs paid by AIDS Drug
Assistance Program.
• Clarified the section on Mail-Order Pharmacy Access to state that a pharmacy that makes
some, but not all, deliveries by common carrier is not a mail order pharmacy.
• Clarified the section Level Playing Field Between Mail-Order and Retail Pharmacies by
stating that the alternative retail/mail order pharmacy rate shall not cause the standard terms
and conditions offered to similarly situated pharmacies to vary with respect to the any
willing provider pharmacy provisions.
• Revised the section Out-of-Network Pharmacy Access to add an option for sponsors to
create an out-of-network benefit structure.
• Clarified the section Public Disclosure of Pharmaceutical Prices for Equivalent Drugs to
state that CMS may modify the timing requirement for informing enrollees of any
differential between the price of a covered part D drug to an enrollee and the price of the
lowest priced generic version if the requirement becomes impracticable to administer.
• Added an Electronic Transactions Standards section to address unique BIN/PCN provisions
and Prescriber Identifiers.
• Updated Appendix 1: Adequate Access to Network Home Infusion Pharmacies by
State/Territory and Contract Type with 2011 data.
The manual revisions are available at
http://www.cms.gov/PrescriptionDrugCovContra/12_PartDManuals.asp
Any questions regarding this manual chapter may be directed to Lisa Thorpe via e-mail at

Prescription Drug Benefit Manual
Chapter 5: Benefits and Beneficiary Protections
Table of Contents
(Rev. 14, 09-30-11)
Transmittals for Chapter 5
10 - Benefits and Beneficiary Protections
10.1 - Introduction
10.2 - Definition of Terms
20 - Requirements Related to Qualified Prescription Drug Coverage
20.1 - General
20.2 - Availability of Prescription Drug Plans (PDPs)
20.3 - Standard Prescription Drug Coverage
20.3.1 - Defined Standard Coverage
20.3.2 - Actuarially Equivalent Standard Coverage
20.4 - Alternative Prescription Drug Coverage
20.4.1 - Basic Alternative Coverage
20.4.2 - Enhanced Alternative Coverage
20.4.2.1 - General
20.4.2.2 - Enhanced Alternative Gap Coverage
20.4.3 - Restrictions on the Offering of Enhanced Alternative Coverage by PDP
Sponsors
20.4.4 - Restrictions on the Offering of Enhanced Alternative Coverage by MA
Organizations
20.4.5 - Restrictions on the Offering of Enhanced Alternative Coverage by Cost
Plan Sponsors
20.5 - Coverage Gap Coinsurance
20.6 - Negotiated Prices
20.7 - Dispensing Fees
20.8 - Ensuring Meaningful Differences in Approved Bids
20.8.1 - General
20.8.2 - Meaningful Differences in Basic Prescription Drug Coverage Options
20.8.3 - Meaningful Differences in Enhanced Alternative Coverage Options
20.8.4 - Transition Period for Sponsors or Parent Organizations with New
Acquisitions
20.9 - PDP Plan Benefit Package (PBP) Renewal and Crosswalk Guidance
20.9.1 - New Plan
20.9.2 - Renewal Plan
20.9.3 - Consolidated Renewal Plan
20.9.4 - Renewal Plan with a Service Area Expansion (800 Series EGWPs only)
20.9.5 - Terminated Plan (Non-Renewal)
20.9.6 - Consolidated Plans Under a Parent Organization
20.10 - Low Enrollment Plans
20.11 - Manufacturer Drug Discount Program
30 - Incurred/ “True Out-of-Pocket” (TrOOP) Costs
30.1 - Costs that Count as Incurred Costs
30.2 - Costs that Do Not Count as Incurred Costs
30.3 - Summary of TrOOP-Eligible and TrOOP-Ineligible Payers
30.4 - Pharmacy Waiver/Reduction of Cost-Sharing and Applicability toward TrOOP
40 - Prescription Drug Plan Service Areas
50 - Access to Covered Part D Drugs
50.1 - Retail Pharmacy Access
50.2 - Mail-Order Pharmacy Access
50.3 - Limited Access Drugs and “Specialty” Pharmacies
50.4 - Home Infusion Pharmacy Access
50.5 - Long-Term Care (LTC) Pharmacy Access
50.5.1 - Convenient Access to LTC Pharmacies
50.5.2 - Performance and Service Criteria for Network Long-Term Care
Pharmacies (NLTCPs)
50.5.3 - Other LTC Contracting Terms and Conditions and Uniformity of Benefits
50.5.4 - Access to LTC Pharmacies for Enrollees Residing in Institutions for
Mental Disease (IMDs), Intermediate Care Facilities for the Mentally Retarded
(ICFs/MR), and LTC Hospitals
50.5.5 - Post-Consumption Billing
50.6 - I/T/U Pharmacy Access
50.7 - Waiver of Pharmacy Access Requirements
50.7.1 - Waiver of Retail Pharmacy Access Requirements for MA-PD Plans and
Cost Plans with Plan-Owned and Operated Pharmacies
50.7.2 - Waiver of Pharmacy Access Requirements for Private Fee-for-Service
Plans
50.8 - Pharmacy Network Contracting Requirements
50.8.1 - Any Willing Pharmacy Requirement
50.8.2 - Insurance Risk
50.9 - Differential Cost-Sharing for Preferred Pharmacies
50.10 - Level Playing Field Between Mail-Order and Retail Pharmacies
50.11 - Use of Identification Card for Accessing Negotiated Prices
50.12 - Pharmacy Access During a Federal Disaster or Other Public Health Emergency
Declaration
50.13 - Drug Shortages
50.14 - Waivers for Plans in the Territories
60 - Out-of-Network Access
60.1 - Out-of-Network Pharmacy Access
60.2 - Access to Vaccines
60.2.1 - In Network Vaccine Distribution Approaches
60.2.2 - Facilitated OON Access Approaches
60.3 - Vaccine Administration
60.3.1 - Vaccine Administration Cost-Sharing Considerations
60.3.2 - Separate Billing of the Vaccine and Vaccine Administration
60.3.3 - Claims Processing Considerations
60.3.4 - Vaccine Administration Access
70 - Public Disclosure of Pharmaceutical Prices for Equivalent Drugs
80 - Privacy, Confidentiality, and Accuracy of Enrollee Records
90 - Electronic Transaction Standards
90.1 - Unique BIN/PCN Provisions
90.1.1 - Alternate Identifiers/Crosswalking/Mapping
90.1.2 - Sponsors that Do Not Support Industry Standard Coding to Distinguish
non-Part D Covered Drugs
90.2 - Prescriber Identifiers
90.2.1 - Foreign Prescribers
90.2.2 - Beneficiary Requests for Reimbursement
90.2.3 - National Provider Identifiers (NPIs)
90.2.4 - Controlled Substances
Appendix 1 - Adequate Access to Network Home Infusion Pharmacies by State/Territory and
Contract Type
Appendix 2 - PDP Regions
Appendix 3 - MA Regions
10 - Benefits and Beneficiary Protections
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
10.1 - Introduction
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
This chapter deals with Part D sponsor requirements with regard to Part D benefits and a number
of beneficiary protections for Part D enrollees, including:
• The establishment of prescription drug plan (PDP) service areas;
• Access standards with regard to covered Part D drugs;
• Disclosure to beneficiaries of pricing information for generic versions of covered Part D
drugs; and
• Privacy, confidentiality, and accuracy of PDP sponsors’ enrollee records.
Except where specifically noted, these requirements apply to all Part D sponsors, including
PDPs, MA-PD plans, and cost plans offering Part D coverage. Other requirements related to
beneficiary protections are contained in other chapters of the Prescription Drug Benefit Manual,
which can be accessed at:
http://www.cms.hhs.gov/PrescriptionDrugCovContra/12_PartDManuals.asp#TopOfPage
10.2 - Definition of Terms
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Unless otherwise stated in this chapter, the following definitions apply:
Actual cost: The negotiated price for a covered Part D drug when the drug is purchased at a
network pharmacy, and the usual and customary price when a beneficiary purchases the drug at
an out-of network pharmacy consistent with
42 CFR 423.124(a).
Applicable beneficiary
(1) Is enrolled in a prescription drug plan or an MA-PD plan;
: Means an individual who, on the date of dispensing a covered Part D
drug--
(2) Is not enrolled in a qualified retiree prescription drug plan;
(3) Is not entitled to an income-related subsidy under section 1860D-14(a) of the Act;
(4) Has reached or exceeded the initial coverage limit under section 1860D-2(b)(3) of the Act
during the year;
(5) Has not incurred costs for covered Part D drugs in the year equal to the annual out-of-pocket
threshold specified in section 1860D-2(b)(4)(B) of the Act; and
(6) Has a claim that--
(i) Is within the coverage gap;
(ii) Straddles the initial coverage period and the coverage gap;
(iii) Straddles the coverage gap and the annual out-of-pocket threshold; or
(iv) Spans the coverage gap from the initial coverage period and exceeds the annual out-of-
pocket threshold.
Applicable drug
(1)(i) Approved under a new drug application under section 505(b) of the Federal Food, Drug,
and Cosmetic Act (FDCA); or
: Means a Part D drug that is--
(ii) In the case of a biological product, licensed under section 351 of the Public Health Service
Act (other than a product licensed under subsection (k) of such section 351); and
(2)(i) If the PDP sponsor of the prescription drug plan or the MA organization offering the MA-
PD plan uses a formulary, which is on the formulary of the prescription drug plan or MA-PD
plan that the applicable beneficiary is enrolled in;
(ii) If the PDP sponsor of the prescription drug plan or the MA organization offering the MA-PD
plan does not use a formulary, for which benefits are available under the prescription drug plan
or MA-PD plan that the applicable beneficiary is enrolled in; or
(iii) Is provided to a particular applicable beneficiary through an exception or appeal for that
particular applicable beneficiary.
Bioequivalent
: The meaning given such term in section 505(j)(8) of the Food, Drug, and
Cosmetic Act.
Catastrophic coverage: The Part D benefit phase above the annual out-of-pocket threshold
described at 42 CFR 423.104(d)(5)(iii) (and in section 20.3.1).
Contracted pharmacy network
: Licensed pharmacies, including retail, mail-order, and
institutional pharmacies, under contract with a Part D sponsor to provide covered Part D drugs at
negotiated prices to Part D enrollees.
Coverage gap
: Means the period in prescription drug coverage that occurs between the initial
coverage limit and the out-of-pocket threshold. For purposes of applying the initial coverage
limit, Part D sponsors must apply their plan specific initial coverage limit under basic
alternative, enhanced alternative or actuarially equivalent Part D benefit designs.
Employer/Union- Only Group Waiver Plan:
For the purpose of this section, Medicare-approved
prescription drug plans that qualify for waivers or modifications to their plan offerings consistent
with Pub. 100-16, Medicare Managed Care Manual, Chapter 9, Section 10 and Pub. 100-18,
Medicare Prescription Drug Benefit Manual, Chapter 12, Section 10.
Generic drug
: A drug for which an application under section 505(j) of the Federal Food, Drug,
and Cosmetic Act (21 USC 355(j)) is approved.
Government-funded health program: Any program established, maintained, or funded, in whole
or in part, by the Government of the United States, by the government of any State or political
subdivision of a State, or by any agency or instrumentality of any of the foregoing, which uses
public funds, in whole or in part, to provide to, or pay on behalf of, an individual the cost of Part
D drugs, including any of the following: (1) An approved State child health plan under title XXI
of the Act providing benefits for child health assistance that meets the requirements of section
2103 of the Act; (2) The Medicaid program under title XIX of the Act or a waiver under section
1115 of the Act; (3) The veterans' health care program under Chapter 17 of title 38 of the United
States Code; (4) The Indian Health Service program under the Indian Health Care Improvement
Act under Chapter 18 of title 25 of the United States Code; and (5) Any other government-
funded program whose principal activity is the direct provision of health care to persons.
Group health plan: For purposes of applying the definition of incurred costs in 42 CFR 423.100,
has the meaning given such term in 29 U.S.C. 1167(1), but specifically excludes a personal
health savings vehicle.
Insurance
: A health plan that provides, or pays the cost of Part D drugs, including, but not
limited to, any of the following: (1) health insurance coverage (as defined in 42 U.S.C. 300gg-
91(b)(1)); (2) a Medicare Advantage (MA) plan (as described under section 1851(a)(2) of the
Act); and (3) a PACE organization (as defined under sections 1894(a)(3) and 1934(a)(13) of the
Act). This definition specifically excludes a personal health savings vehicle.
I/T/U pharmacy
: A pharmacy operated by the Indian Health Service, an Indian tribe or tribal
organization, or an urban Indian organization, all of which are defined in section 4 of the Indian
Health Care Improvement Act, 25 U.S.C. 1603.
Long-term care (LTC) facility
: A skilled nursing facility as defined in section 1819(a) of the
Act, or a medical institution or nursing facility for which payment is made for an
institutionalized individual under section 1902(q)(1)(B) of the Act.
Long-term care pharmacy
: A pharmacy owned by or under contract with a long-term care
facility to provide prescription drugs to the facility’s residents.
Long-term care network pharmacy
: A long-term care pharmacy that is a network pharmacy.
Multiple source drug
: A drug defined in section 1927(k)(7)(A)(i) of the Social Security Act.
Network pharmacy
: A licensed pharmacy that is under contract with a Part D sponsor to provide
covered Part D drugs at negotiated prices to its Part D plan enrollees.
Non-preferred pharmacy
: A network pharmacy that offers covered Part D drugs at negotiated
prices to Part D enrollees at higher cost-sharing levels than apply at a preferred pharmacy.
Non-applicable drugs
: Covered Part D drugs that are not applicable drugs as defined in this
section. This includes generic drugs.
Or otherwise
: Through a government-funded health program.
Out-of-network (OON) pharmacy
: A licensed pharmacy that is not under contract with a Part D
sponsor to provide negotiated prices to Part D plan enrollees.
Parent organization
: An organization that holds at least the majority of the voting stock in a
legal entity that holds a Medicare Prescription Drug Plan (PDP) sponsor contract or a Medicare
Advantage (MA) Organization contract.
Part D drug: A drug described in chapter 6, section 10, of this manual.
Person
: A natural person, corporation, mutual company, unincorporated association, partnership,
joint venture, limited liability company, trust, estate, foundation, not-for-profit corporation,
unincorporated organization, government or governmental subdivision or agency.
Personal health savings vehicle
: A vehicle through which individuals can set aside their own
funds to pay for health care expenses, including covered Part D drugs, on a tax free basis
including any of the following: (1) a Health Savings Account (as defined under section 220 of
the Internal Revenue Code); (2) a Flexible Spending Account (as defined in section 106(c)(2) of
the Internal Revenue Code) offered in conjunction with a cafeteria plan under section 125 of the
Internal Revenue Code; and (3) an Archer Medical Savings Account (as defined under section
223 of the Internal Revenue Code). This definition specifically excludes a Health
Reimbursement Arrangement (as described under Internal Revenue Ruling 2002-41 and Internal
Revenue Notice 2002-45).
Plan allowance: The amount Part D plans that offer coverage, other than defined standard
coverage, may use to determine their payment and Part D enrollees’ cost-sharing for covered
Part D drugs purchased at an out-of-network pharmacy or in a physician’s office in accordance
with the requirements of
42 CFR 423.124(b).
Plan Benefit Package (PBP)
: A set of benefits for a defined MA or PDP service area. The PBP
is submitted by PDP sponsors and MA organizations to CMS for benefit analysis, marketing and
beneficiary communication purposes.
Preferred drug
: A covered Part D drug on a Part D sponsor's formulary for which beneficiary
cost-sharing is lower than for a non-preferred drug on the sponsor’s formulary.
Preferred multiple source drug
: A drug that is both a preferred drug and a multiple source drug,
meaning that one version of that drug is placed on the sponsor’s formulary with lower cost
sharing than for a non-preferred drug.
Preferred pharmacy
: A network pharmacy that offers covered Part D drugs at negotiated prices
to Part D enrollees at lower levels of cost-sharing than apply at a non-preferred pharmacy under
its pharmacy network contract with a Part D sponsor.
Retail pharmacy
: Any licensed pharmacy that is not a mail order pharmacy from which Part D
enrollees could purchase a covered Part D drug without being required to receive medical
services from a provider or institution affiliated with that pharmacy.
Rural
: A five-digit ZIP Code in which the population density is less than 1,000 individuals per
square mile.
Suburban:
A five-digit ZIP Code in which the population density is between 1,000 and 3,000
individuals per square mile.
Supplemental drugs: Drugs that would be covered Part D drugs but for the fact that they are
specifically excluded as Part D drugs under 42 CFR 423.100, and as described in section 20.1 of
chapter 6. However, because such drugs must have otherwise qualified as covered Part D drugs
(as defined in section 10.2 of chapter 6) in order to be covered as a supplemental benefit, and
because only prescription drugs are included in the definition of a Part D drug, over-the-counter
drugs cannot be supplemental drugs, as discussed in section 10.10 of chapter 6. Supplemental
drugs may be included as a supplemental benefit under enhanced alternative coverage, as
described in section 20.4.2 of this chapter.
Therapeutically equivalent
: Drugs that are rated as therapeutic equivalents under the Food and
Drug Administration’s most recent publication of “Approved Drug Products with Therapeutic
Equivalence Evaluations.”
Third party payment arrangement
: Any contractual or similar arrangement under which a person
has a legal obligation to pay for covered Part D drugs.
Urban
: A five-digit ZIP Code in which the population density is greater than 3,000 individuals
per square mile.
Usual and customary (U&C) price
: The price that an out-of-network pharmacy or a physician’s
office charges a customer who does not have any form of prescription drug coverage for a
covered Part D drug.
20 - Requirements Related to Qualified Prescription Drug Coverage
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
20.1 - General
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
A Part D sponsor must provide enrollees with qualified prescription drug coverage. Qualified
prescription drug coverage, which consists of the either of the following options, may be
provided directly by the Part D sponsor or through arrangements with other entities:
(1) Standard prescription drug coverage (as described in section 20.3), which includes both
defined standard coverage (as described in section 20.3.1) and actuarially equivalent
standard coverage (as described in section 20.3.2).
(2) Alternative prescription drug coverage (as described in section 20.4), which includes
both basic alternative coverage (as described in section 20.4.1) and enhanced
alternative coverage (as described in section 20.4.2).
For purposes of ensuring that Part D enrollees have a variety of different benefit options in a
particular service area, CMS also makes a distinction between qualified prescription drug
coverage that is basic prescription drug coverage and qualified prescription drug coverage
that provides supplemental benefits (as described in section 20.4.2). Basic prescription drug
coverage consists of any of the following:
(1) Defined standard coverage, as described in section 20.3.1;
(2) Actuarially equivalent standard coverage, as described in section 20.3.2; or
(3) Basic alternative coverage, as described in section 20.4.1
As described in section 20.4.2, plans may offer an additional type of qualified prescription drug
coverage – enhanced alternative coverage – that includes both: (1) basic prescription drug
coverage, as described above, and (2) supplemental benefits. Table 1 summarizes the difference
between qualified prescription drug coverage and basic prescription drug coverage.
Table 1
Qualified and Basic Prescription Drug Coverage
Types of Coverage that May be Included
Qualified Prescription Drug Coverage
• Defined Standard Coverage
• Actuarially Equivalent Standard
Coverage
• Basic Alternative Coverage
•
Enhanced Alternative Coverage
Basic Prescription Drug Coverage
• Defined Standard Coverage
• Actuarially Equivalent Standard
Coverage
•
Basic Alternative Coverage
20.2 - Availability of Prescription Drug Plans
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
A PDP sponsor must offer its prescription drug plans to all Part D eligible beneficiaries residing
in those plans’ service areas (refer to section 40 for more information about PDP service areas).
Unlike an MA-PD sponsor, a PDP is not eligible for a capacity limit as described in
42 CFR
422.60(b).
20.3 - Standard Prescription Drug Coverage
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Standard prescription drug coverage includes two distinct types of coverage: (1) defined standard
coverage; and (2) actuarially equivalent standard coverage. Both types of standard prescription
drug coverage consist of coverage of covered Part D drugs subject to an annual deductible; 25
percent coinsurance (or an actuarially equivalent structure) up to an initial coverage limit;
coinsurance equal to the gap coinsurance percentages (or an actuarially equivalent amount)
during the coverage gap; and catastrophic coverage after an individual incurs out-of-pocket
expenses above the annual out-of-pocket threshold. Both defined standard coverage and
actuarially equivalent standard coverage include access to negotiated prices, as described in
section 20.5.
20.3.1 - Defined Standard Coverage
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Defined standard coverage consists of coverage of covered Part D drugs subject to:
• An annual deductible
.
• Twenty-five percent coinsurance for actual costs above the annual deductible but at or
below an initial coverage limit
.
• Coinsurance that is equal to the costs of non-applicable and applicable (brand) drugs
during the coverage gap multiplied by the gap coinsurance percentages described in
section 20.5.
• Catastrophic coverage with nominal cost-sharing for the remainder of the coverage year
once an enrollee’s costs exceed the annual out-of-pocket threshold
.
The annual deductible, initial coverage limit, out-of-pocket threshold, and beneficiary cost-
sharing after the annual out-of- pocket threshold is met are adjusted annually. As provided in 42
CFR 423.104(d)(5)(iv), these amounts will be adjusted relative to the previous year’s amounts by
the annual percentage increase in average per capita aggregate expenditures for Part D drugs for
the 12-month period ending in July of the previous year. The updated benefit parameters for
2012 include an adjustment for any variations between the projected and actual amounts from the
prior period. For more information about the methodologies used to update the 2012 benefit
parameters, refer to:
http://www.cms.hhs.gov/MedicareAdvtgSpecRateStats/AD/list.asp?filtertype=none&datefilterty
pe=&datefilterinterval=&datafiltertype=1&datafiltervalue=&keyword=&intNumPerPage=10&c
mdFilterList=Show+Items
20.3.2 - Actuarially Equivalent Standard Coverage
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Part D sponsors may also offer actuarially equivalent standard coverage, under which they would
substitute certain cost-sharing requirements in defined standard coverage (including tiered
structures tied to plan formularies or preferred pharmacies in a plan’s network, as described in
section 50.9) for:
1. Costs above the annual deductible and up to the initial coverage limit, provided that those
alternative cost-sharing requirements are actuarially equivalent to the average expected
coinsurance of 25 percent for costs above the annual deductible and up to the initial
coverage limit under defined standard coverage; and/or
2. Costs for coinsurance during the coverage gap, provided that those alternative cost-
sharing requirements are actuarially equivalent to the average expected coinsurance
(that is equal to the costs of non-applicable and applicable drugs multiplied by the gap
coinsurance percentages described in section 20.5) under defined standard coverage;
and/or
3. Costs in the catastrophic portion of the benefit, provided that those alternative cost-
sharing requirements are actuarially equivalent to the average expected cost-sharing
under defined standard coverage described in the applicable annual Rate Announcement/
Call Letter found at www.cms.gov/PrescriptionDrugCovContra/01_Overview.asp.
Cost-sharing arrangements under actuarially equivalent standard coverage could include
reducing cost-sharing to $0 for generic or preferred covered Part D drugs, as long as the cost-
sharing structure is actuarially equivalent to an average expected coinsurance of 25 percent for
costs above the annual deductible and up to the initial coverage limit and/or to an average
expected cost-sharing in the catastrophic portion of the benefit equivalent to the cost-sharing
described in the applicable annual Rate Announcement/Call Letter found at
www.cms.gov/PrescriptionDrugCovContra/01_Overview.asp. Any such cost-sharing
arrangements will be reviewed, along with the rest of a plan’s benefit design, to ensure that they
do not discriminate against certain Part D eligible individuals.
20.4 - Alternative Prescription Drug Coverage
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Alternative prescription drug coverage includes two distinct types of coverage: (1) basic
alternative coverage; and (2) enhanced alternative coverage. Both basic alternative coverage and
enhanced alternative coverage include access to negotiated prices, as described in section 20.6.
In modifying the standard prescription drug coverage design to offer alternative prescription drug
coverage, Part D sponsors must use defined standard coverage (and not actuarially equivalent
standard coverage) as a fixed point of comparison. In order to receive approval to offer an
alternative prescription drug benefit design, a Part D sponsor must:
1. Include a deductible that is no greater than the deductible offered under defined standard
coverage.
2. Provide coverage above the annual out-of-pocket threshold that is at least as generous as
that provided under defined standard coverage. In other words, Part D sponsors may, at
their option, reduce cost-sharing below that required under defined standard coverage.
3. Ensure that the beneficiary premium is at least equal to the beneficiary premium under
defined standard coverage.
4. Ensure that, for individuals whose total spending exceeds the initial coverage limit under
standard prescription drug coverage, the average Part D sponsor payout is at least equal
to that under defined standard coverage.
5. Ensure that the actuarial value of the total or gross coverage is at least equal to that under
defined standard coverage.
Sponsors have flexibility to establish benefit designs within the aforementioned parameters that
include the following features, which may be particularly useful for increasing utilization of
generic drugs. All cost-sharing arrangements will be reviewed, along with the rest of a sponsor’s
benefit design, to ensure that they do not discriminate against certain Part D eligible individuals.

• Brand-only deductible
: Sponsors may lower or eliminate cost sharing for generics in the
deductible period. Sponsors may not, however, increase the deductible for brands above
the defined standard benefit’s annual deductible amount in order to compensate for
decreasing the cost-sharing for generics before the deductible is met. Sponsors electing a
brand-only deductible should note that beneficiary and plan paid amounts for generic
drugs will accrue to total drug costs but not toward the brand-only deductible.
“Free first fill” program
: Sponsors may establish programs whereby enrollees are offered an
incentive in the form of a cost-sharing reduction if 1) with respect to a new prescription, the enrollee
chooses a generic version of, or a preferred brand-name therapeutic alternative to, a medication,
over a brand-name drug, and 2) with respect to a refill, the enrollee switches from a brand-name to
the generic version of, or a preferred brand-name therapeutic alternative to, a medication. The goal
of such incentive programs is to minimize drug spend and maximize compliance with plan
formularies. A
sponsor that elects this benefit design must identify these drugs in the Free First
Fill supplemental formulary flat file.
20.4.1 - Basic Alternative Coverage
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Basic alternative coverage is alternative prescription drug coverage that is actuarially equivalent
to defined standard prescription drug coverage, as described in section 20.3.1. Within the
parameters for alternative prescription drug coverage described in section 20.4, a Part D sponsor
offering a basic alternative prescription drug benefit design could combine features such as the
following to maintain an actuarial value of coverage equal to defined standard prescription drug
coverage:
• A reduction in the deductible;
• Changes in cost-sharing (e.g., benefit designs that use tiered copayments or coinsurance)
in an actuarially equivalent manner to the 25 percent cost-sharing above the deductible
and below the initial coverage limit under defined standard coverage and in an
actuarially equivalent manner to the gap coverage coinsurance (that is equal to the costs
of non-applicable and applicable drugs multiplied by the gap coinsurance percentages
described in section 20.5) during the coverage gap; and
• A modification of the initial coverage limit
20.4.2 - Enhanced Alternative Coverage
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
20.4.2.1 - General
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Enhanced alternative coverage refers to alternative prescription drug coverage whose value
exceeds that of defined standard coverage. This is only possible if a Part D sponsor offers
supplemental benefits in addition to its basic prescription drug benefit. In other words, enhanced
alternative coverage includes both: (1) basic prescription drug coverage, as described in section
20.1; and (2) supplemental benefits.
Supplemental benefits consist of:
• Reductions in cost-sharing in the coverage gap such that enrollees are liable for less than
the coinsurance in the gap for defined standard coverage, and the actuarial value of the
benefit provided is increased above the actuarial value of basic prescription drug
coverage.
• Reductions in cost-sharing that increase the actuarial value of the benefits provided above
the actuarial value of basic prescription drug coverage – for example: (1) a reduction in
the deductible; (2) a reduction in the coinsurance percentage or copayments applicable to
covered Part D drugs obtained between the annual deductible and the initial coverage
limit and/or above the annual out-of-pocket threshold; and/or (3) an increase in the initial
coverage limit; and/or
• Supplemental drugs.
20.4.2.2 - Enhanced Alternative Gap Coverage
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
As part of an enhanced alternative benefit design, Part D sponsors may include coverage of a
subset of drugs throughout the coverage gap. Sponsors may elect to provide additional coverage
for:
1. An entire drug tier;
2. A subset of a drug tier, or
3. A capped dollar amount of drugs within a tier or across the entire benefit (limited gap
coverage).
CMS will review the breadth of drugs covered through the gap, be it: (1) an entire drug tier; (2) a
subset of a drug tier, or (3) a capped dollar amount of drugs, to ensure that the coverage is
sufficient to be labeled either gap coverage or limited gap coverage. CMS reserves the right to
label coverage of a subset of all formulary drugs through the gap as something less than gap
coverage or limited gap coverage. For example, coverage of only insulin through the coverage
gap would not be sufficient to be labeled gap coverage.
In CY 2010, sponsors were required to identify their gap coverage offerings for both generic and
brand drugs in the plan benefit package (PBP) software using CMS-defined standardized
thresholds for the terms “all,” “many,” “some,” “few,” or “none.” These thresholds represented
the proportion of unique Health Plan Management System (HPMS) formulary drug entities (i.e.,
unique clinical drug component and dosage form) that are covered through the gap for drugs
described on the formulary as generic and for drugs described as brand (as specified by the drug
type label). Beginning in CY 2011, for 2012 bids, sponsors will no longer indicate their level of
gap coverage in the PBP. CMS will quantify each plan’s gap coverage based upon the
percentage of formulary drugs (brand, or generic above the standard coverage) covered through

the gap and then will assign appropriate descriptions. The gap coverage level descriptions will
reflect additional coverage above the mandated coverage gap coinsurance of non-applicable
drugs. Supplemental (excluded) drugs will not be factored into the determination of gap
coverage. For example, if a plan covers both generic Part D and supplemental drugs, only the
generic drugs as defined in this chapter, will be used in calculating the percentage of formulary
drugs covered through the gap. CMS will provide a report in HPMS describing the CMS-
assigned gap coverage levels. Gap coverage descriptions for drugs will be communicated to
beneficiaries through the SB, other marketing materials, and information dissemination
materials.
20.4.3 - Restrictions on the Offering of Enhanced Alternative Coverage by
PDP Sponsors
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
A PDP sponsor is not permitted to offer a plan that provides enhanced alternative coverage in a
particular service area unless it also offers a plan that provides only basic prescription drug
coverage, as described in section 20.1, in that same area. This requirement ensures that PDP
sponsors offer at least one option for Part D coverage for a premium at the cost of basic
prescription drug coverage. For purposes of meeting this requirement, a PDP sponsor is
considered to be a PDP parent organization.
20.4.4 - Restrictions on the Offering of Enhanced Alternative Coverage by
MA Organizations
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
An MA organization may not offer an MA coordinated care plan, as defined in 42 CFR 422.4, in
a service area unless that plan, or another MA plan offered by the same organization in the same
service area, includes required prescription drug coverage for the entire service area. MA plans,
by definition, would include private fee-for-service (PFFS) plans. For purposes of meeting this
requirement, an MA organization is considered to be an MA parent organization.
Required prescription drug coverage consists of either: (1) basic prescription drug coverage (as
described in section 20.1 of this manual), or (2) enhanced alternative coverage, provided there is
no MA monthly supplemental beneficiary premium for the drug coverage applied under the plan.
Such enhanced alternative coverage could be provided without a monthly supplemental
beneficiary premium only if a plan applied a credit of rebate dollars available under the plan’s
Part C bid against the otherwise applicable premium. Rebate dollars represent the dollars
available for supplemental (and other) benefits when an MA plan’s risk-adjusted Part C bid is
under the risk-adjusted Part C monthly benchmark amount. This requirement ensures that MA
organizations offer at least one option for Part D coverage for Part D supplemental premium at
the cost of basic prescription drug coverage. Of note, Special Needs Plans (SNPs) cannot satisfy
this requirement for non-SNPs in the same service area.
If an MA parent organization does not offer basic prescription drug coverage through a basic
plan type (defined standard, actuarial equivalent or basic alternative) in a given service area, to
the extent that an MA-PD plan chooses to provide enhanced alternative coverage with no
additional premium through the application of rebate dollars, such enhanced alternative coverage
would constitute required coverage for the purposes of meeting the requirement that an MA
organization offer a plan that includes required prescription drug coverage.
In order to help ensure that this requirement is being met, CMS has added two questions in the
PBP software for enhanced alternative plans. Sponsors must indicate that they either have
another basic (defined standard, actuarially equivalent or basic alternative) Part D plan or that
the enhanced alternative plan being submitted meets this requirement because the sponsor has
brought down the supplemental Part D premium to zero using the MA rebate dollars.
20.4.5 - Restrictions on the Offering of Enhanced Alternative Coverage by
Cost Plan Sponsors
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
A cost plan sponsor that elects to offer Part D coverage may do so only if such coverage is
provided as an optional supplemental benefit (under 42 CFR 417.440(b)(2)(ii)) and if the
coverage it offers consists of qualified prescription drug coverage. However, a cost plan sponsor
may instead elect to offer prescription drug coverage that is not qualified prescription drug
coverage, and the requirements of Part D would not apply to this coverage. However, a cost plan
sponsor may not offer both a Part D and a non-Part D drug benefit as enrollee options under the
same contract.
A cost plan sponsor that elects to offer qualified prescription drug coverage under Part D may
offer enhanced alternative coverage as an optional supplemental benefit (under 42 CFR
417.440(b)(2)(ii)), but only if the cost plan sponsor also offers basic prescription drug coverage
as an optional supplemental benefit.
If offered by a cost plan sponsor, an enrollee in the cost plan may elect to receive qualified
prescription drug coverage under the cost plan and, if so, whether to receive basic prescription
drug coverage or, if offered by the cost plan, enhanced alternative coverage. Individuals
enrolling in a Part D plan that is offered as an optional supplemental benefit by a cost plan
sponsor may do so according to the requirements for enrollment in a PDP contained in chapter 2.
As described in section 10 of
chapter 2, such an individual must be a member of the cost plan at
the time of the effective date of enrollment in the cost plan’s optional supplemental Part D
benefit. Individuals enrolled in a cost plan who do not elect Part D coverage offered by the cost
plan sponsor may elect Part D coverage offered by a PDP sponsor.
20.5 - Coverage Gap Coinsurance
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Under section 1101(b)(3) of the Health Care and Education Reconciliation Act of 2010
(HCERA), which amended section 3301 of the Patient Protections and Affordable Care Act
(PPACA), additional coverage of Part D drugs will be phased into the Part D benefit between
2011 and 2020, so that by 2020 the standard prescription drug benefit will cover 75 percent of
the cost of non-applicable drugs in the gap and 25 percent of the cost of applicable (brand)
drugs for applicable beneficiaries. Section 1860D-2(b)(2) of the Act was amended to add new
paragraphs (C)(i) and (ii) that provide gap coinsurance percentages for future years under the
standard prescription drug benefit. The gap coinsurance percentage for covered Part D drugs
that are non-applicable is equal to the following:
Year
Coinsurance Percentage
2011
93 percent
2012 through 2019
Previous year coinsurance percentage decreased by
7 percentage points
2020 and
thereafter
25 percent
For applicable (i.e., brand) drugs, the gap coinsurance percentage does not get applied until
contract year 2013. The gap coinsurance for applicable (brand) drugs is equal to the following:
Year
Coinsurance Percentage
2013 through 2014
97.5 percent
2015 through 2016
95 percent
2017
90 percent
2018
85 percent
2019
80 percent
2020 and
thereafter
75 percent
Part D sponsors offering basic Part D plans will include, as part of the bid, the coverage gap
coinsurance for all non-applicable drugs on the plan’s formulary, or an actuarially equivalent
amount using processes and methods specified under section 1860D-11(c) of the Act. The
coverage gap coinsurance applies only to applicable beneficiaries who:
1) Are enrolled in a prescription drug plan or an MA-PD plan;
2) Are not enrolled in a qualified retiree prescription drug plan;
3) Are not entitled to the Federal subsidy for low-income individuals under section 1860D-14(a)
and in Chapter 13 of this Manual;
4) Have reached or exceeded the initial coverage limit;
5) Have not incurred costs for covered Part D drugs in the year equal to the annual out-of-
pocket threshold; and
6) Have a claim that –
• Is within the coverage gap;
• Straddles the initial coverage period and the coverage gap;
• Straddles the coverage gap and the annual out-of-pocket threshold; or
• Spans the coverage gap from the initial coverage period and exceeds the annual out-of-
pocket threshold.

For alternative plans, the coverage gap begins for the purpose of applying the coverage gap
coinsurance based on the plan’s initial coverage limit (approved as part of the bid) and ends at
the point a beneficiary reaches the catastrophic threshold.
20.6 - Negotiated Prices
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Part D sponsors must provide enrollees with access to negotiated prices for covered Part D drugs
as part of their qualified prescription drug coverage. This access to negotiated prices must be
provided even when no benefits are otherwise payable on behalf of an enrollee due to the
application of a deductible or other cost-sharing. Negotiated prices will take into account
negotiated price concessions for covered Part D drugs that are passed through to enrollees at the
point of sale, such as:
• Discounts;
• Direct or indirect subsidies;
• Rebates; and
• Other direct or indirect remunerations
In addition, negotiated prices must include any applicable dispensing fees (discussed in section
20.7).
Although negotiated prices do not have to be made available for drugs that are not covered Part
D drugs, they must be made available throughout the benefit – including in any phase of the
benefit, such as the deductible, in which an enrollee is responsible for 100 percent cost-sharing –
for all covered Part D drugs. Part D sponsors must ensure that their payment systems are set up
to charge beneficiaries the lesser of a drug’s negotiated price or applicable copayment amount in
all phases of the benefit.
Example
: A beneficiary’s drug is on a $10 cost-sharing tier. However, the negotiated
price of the drug is $4. The beneficiary never pays more than $4.
In addition, uniform negotiated prices must be available to plan enrollees for a particular covered
Part D drug when purchased from the same pharmacy. In other words, the negotiated price for a
particular covered Part D drug purchased at a particular pharmacy must always be the same
regardless of what phase of the Part D benefit an enrollee is in. (To the extent that the negotiated
price fluctuates based on fluctuations in Average Wholesale Price (AWP), the actual cost to the
beneficiary may vary from purchase to purchase; however the negotiated rate, absent any
contractual changes in the reimbursement rate between the pharmacy and the Part D sponsor,
will remain constant for that drug.)
20.7 - Dispensing Fees
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
As discussed in section 20.6, negotiated prices must include any applicable dispensing fees.
Provided that Part D sponsors include only those activities allowed under CMS’ definition of
dispensing fees in the dispensing fees negotiated with network pharmacies and offer standard
contracting terms and conditions to all similarly situated pharmacies, in accordance with section
50.8.1, CMS notes that Part D sponsors have the flexibility to vary the actual dispensing fee paid
to pharmacies. For example, Part D sponsors may need to increase the dispensing fees paid to
rural or long-term care pharmacies in order to obtain their participation in networks and meet the
pharmacy access standards. Table 2 below provides a summary of the costs that may be
included in dispensing fees, as well as those that may not.
Table 2
Costs that May and May Not Be Included in Dispensing Fees
Costs That May
be Included in
Dispensing Fees
• Costs that are incurred at the point of sale and pay for costs
in excess of the ingredient cost of a covered Part D drug each
time a covered Part D drug is dispensed.
• Pharmacy costs associated with ensuring that possession of
the appropriate covered Part D drug is transferred to a Part D
enrollee. These pharmacy costs include, but are not limited
to:
o The salaries of pharmacists and other pharmacy
workers;
o Any reasonable costs associated with a pharmacist's time
in checking the computer for information about an
individual’s coverage;
o Performing quality assurance activities consistent with
42
CFR 423.153(c)(2);
o Measurement or mixing of the covered Part D drug,
including any labor costs associated with mixing a
compounded product that contains at least one Part D
drug component, as detailed in section 10.4 of
chapter 6;
o Filling the container;
o Physically providing the completed prescription to the
Part D enrollee;
o Delivery;
o Special packaging, e.g., assistive technology packaging;
and
o Overhead associated with maintaining the facility and
equipment necessary to operate the pharmacy, including
costs associated with the acquisition and maintenance of
technology.
• Reasonable pharmacy costs that are appropriate for the
typical beneficiary in that pharmacy setting, for example:
o Costs associated with postal or freight shipping (to
include air courier) to beneficiaries located in remote and
frontier areas with limited or no access to roads. While
the typical beneficiary served by a retail pharmacy in
most areas of the country would not require postage,
freight or other transport costs for delivery of drugs,
CMS believes that it is reasonable to assume that the
typical beneficiary in remote and frontier areas with
limited or no access to roads would require delivery of
drugs via postal or freight shipping (to include air
courier). Because such a circumstance constitutes a
distinct pharmacy setting, CMS believes that the costs
associated with postal or freight shipping (to include air
courier) to such remotely located beneficiaries would
constitute reasonable costs that could be reimbursed as
part of the dispensing fee negotiated between a Part D
sponsor and a contracted network pharmacy.
o Costs associated with special packaging and delivery for
residents of non-LTC facilities (e.g., assisted living
facilities and other forms of congregate residential
settings) with the same level of care need as residents of
LTC facilities. It is reasonable to assume that the typical
enrollee residing in a non-LTC facility setting who meets
the same level of care need as a beneficiary in an LTC
facility would require the provision of dispensing related
services such as unit-dose packaging and home delivery
that are provided by LTC pharmacies to the residents of
LTC facilities. For this reason, CMS believes that non-
LTC facilities in which individuals meeting an
institutionalized level of care need constitute a distinct
pharmacy setting, and one in which specialized services
such as specialized packaging and home delivery would
be appropriate for Part D sponsors to reimburse LTC
pharmacies via the dispensing fee. However, CMS notes
that it would not be appropriate for Part D sponsors to
reimburse LTC pharmacies for these specialized services
for individuals who do not meet an institutionalized level
of care need.
o With respect to LTC pharmacies, dispensing fees should
take into consideration any incremental costs associated
with any increased number of dispensing events in a
billing cycle due to the dispensing methodology used to
minimize the dispensing of unused drugs.
o Costs associated with data collection on unused Part D
drugs and restocking fees associated with return for
credit and reuse in LTC pharmacies when return for
credit and reuse is permitted under State law and is
allowed under the contract between the Part D sponsors
and the pharmacy.
Costs That May
Not be Included
in Dispensing
Fees
• Administrative costs incurred by the Part D sponsor in the
operation of the Part D benefit, including systems costs for
interfacing with pharmacies.
• Supplies, equipment, and services associated with administration
of covered Part D drugs, including those associated with home
infusion therapy of covered Part D drugs or with vaccine
administration.
1
With the exception of costs associated with
vaccine administration, these costs may also not be paid by Part
D sponsors through a separate fee or additional compensation to
home infusion pharmacies and other providers. Other than
medication therapy management programs, medical or clinical
services may not be included in administrative fees. In addition,
professional services, including those associated with home
infusion, may not be included in supplemental Part D benefits.
The costs associated with supplies, equipment, and services for
home infusion therapy of covered Part D drugs must be paid by
either the enrollee or another payer.
• Reasonable pharmacy costs that are not appropriate for the
typical beneficiary in that pharmacy setting, for example:
o Home delivery by retail pharmacies, since the typical retail
customer does not require home delivery. While it would be
appropriate for Part D sponsors to reimburse LTC, mail-
order, and home infusion pharmacies for home delivery costs
via the dispensing fee, this would not be the case for retail
pharmacies, where the term “delivery” would be limited to
the transfer of a covered Part D drug from the pharmacist to
the patient at the point of sale.
o Costs associated with delivery of drugs from manufacturers
1
The administration of a Part D-covered vaccine is included in the definition of a “Part D drug,”
effective January 1, 2008. Consequently, the Part D program covers vaccine administration costs
associated with Part D vaccines. For more information, refer to section 10.14 of chapter 6.

or distributors to dispensing pharmacies.
20.8 - Ensuring Meaningful Differences in Approved Bids
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
20.8.1 - General
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
CMS ensures that plan offerings by Part D sponsors represent meaningful differences to
beneficiaries with respect to benefit packages and plan cost structures. Specifically,
§423.272(b)(3)(i) stipulates that CMS will only approve a bid submitted by a Part D sponsor if
its plan benefit package or plan cost structure was substantially different from those of other
plan offerings by the sponsor in the service area with respect to key characteristics such as
premiums, cost-sharing, formulary structure, or benefits offered. Section 423.265(b)(2) also
requires that Part D sponsors may submit multiple bids in the same area only if the offerings are
substantially different from each other.
While CMS supports the concept of a wide variety of prescription drug coverage choices for
Medicare beneficiaries, CMS believes it is necessary to ensure that those choices represent
meaningfully different options in order to simplify beneficiaries’ enrollment decision making
process. Ensuring that, within each service area, PDP sponsors offer only plan options that are
meaningfully different will maximize opportunities for beneficiaries to select the most
appropriate plan for their needs and reduce beneficiary confusion with respect to choices offered
by the same Part D sponsor.
To determine whether there are meaningful differences amongst plans offered by the same
sponsor, CMS will evaluate and compare plan offerings in a service area by evaluating plan-
specific benefit data (e.g., cost sharing, formulary, and benefits) for each offering. CMS will
provide additional information regarding our meaningfully different bid evaluation processes in
our annual payment notice and call letter prior to the date of plan bid submissions.
20.8.2 - Meaningful Differences in Basic Prescription Drug Coverage Options
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
To determine whether there are meaningful differences between basic prescription drug coverage
options (which includes defined standard, actuarially equivalent standard, and basic alternative
benefit designs) offered by the same PDP sponsor in a region, CMS’ analysis focuses on whether
there are significant differences in proposed beneficiary out-of-pocket costs and/or formularies.
It is important to note that, even though a sponsor may submit different formularies for different
Part D offerings, all submitted formularies must be sufficiently robust to pass CMS’ rigorous
formulary reviews and checks and be determined not to discourage enrollment by certain types
of beneficiaries. Based on CMS’ experience and given statutory actuarial equivalency
requirements, CMS does not expect that – absent substantial differences in approved formularies
– PDP sponsors can demonstrate meaningful differences between plans offering basic
prescription drug coverage. Therefore, CMS believes sponsors should submit only one basic
offering (where basic offering includes defined standard, actuarial equivalent and basic
alternative drug benefit types) for a stand-alone prescription drug plan in a service area.

20.8.3 - Meaningful Differences in Enhanced Alternative Coverage Options
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
When evaluating for differentiation among an organization’s plan offerings, CMS will scrutinize
enhanced benefit designs that add little or no additional value to its basic offering. CMS has
found that it is difficult for beneficiaries to distinguish between plan offerings of the same
sponsor when cost-sharing and premiums are similar between the enhanced and basic drug plan
offering. CMS recognizes that sponsors may have purposefully established plan benefit designs
to address different utilization patterns among sub-groups of beneficiaries and in order to
segment risk. However, CMS is concerned that some “low-additional-value” enhanced offerings
are not understood by beneficiaries in terms of expected value and may not be meaningfully
different from the basic offering.
CMS will evaluate enhanced plans to identify those enhanced plan offerings with meaningful
increases in value over basic plan offerings. CMS will announce its meaningful differences
evaluation methodology and expectations for plan sponsors via the annual payment notice and
call letter. To prepare for negotiations with CMS, Part D sponsors should consult the annual
payment notice and call letter when preparing multiple plan bids for the upcoming plan year.
CMS will request that PDP sponsors with plan benefit packages that are not substantially
different from each other either withdraw or enhance a bid in order to ensure that all offerings
are, in fact, meaningfully different. It is CMS’ experience, based on this analysis that PDP
sponsors typically must offer substantive coverage in the coverage gap as a supplemental benefit
in order to demonstrate that one enhanced alternative plan design is meaningfully different from
another.
20.8.4 - Transition Period for Sponsors or Parent Organizations with New
Acquisitions
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
PDP sponsors or parent organizations with new acquisitions on or after June 7, 2010, will be
afforded a period of 2 years to transition their plan offerings to meet the goal of ensuring that the
Part D sponsor’s offerings are substantially different from one another. PDP sponsors that have
completed a new acquisition will be expected to submit to CMS a plan that details how the 2
year transition will take place.
Example
: A PDP sponsor (or its parent organization) completing an acquisition of another PDP
sponsor in November 2010 would not be subject to requirements for offering substantially
different bids until the 2013 contract year (that is, bids would be due in June 2011 for the 2012
program year; transition would occur during 2011 and 2012; and the Part D sponsor or parent
would need to ensure that in June 2012, when it submits its bids for program year 2013, all of its
bids are for substantially different plans).
20.9 - PDP Plan Benefit Package (PBP) Renewal and Crosswalk Guidance
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
The PDP regions are defined by CMS and consist of one or more entire states (refer to Appendix
2 of this chapter for a map of the 34 PDP regions). Each of a PDP sponsor’s PBPs must be
offered in at least one entire region. A Part D sponsor’s PBP cannot be offered in only part of a
region. Note that PDP bidding rules require PDP sponsors to submit bids for PBPs that cover
only one PDP region at a time. Therefore, HPMS only allows a PDP sponsor’s PBPs to cover
one region at a time (e.g., a PDP sponsor offering a “national” PDP would, for purposes of
bidding, be said to be offering 34 plans – one in each PDP region – and would submit 34 PBPs).
A PDP sponsor may expand the service area of its offerings by submitting additional bids in the
PDP regions the sponsor expects to enter in the following contract year, provided the sponsor
submits a PDP Service Area Expansion (SAE) application and CMS approves that application
and then approves the sponsor’s submitted bids for the new region or regions.
Conversely, a PDP sponsor may reduce its service area by electing not to submit bids for those
regions from which it expects to withdraw. A PDP sponsor must notify CMS in writing of its
intent to non-renew by the first Monday in June pursuant to 42 CFR 423.507(a)(2)(i). However,
even absent written notification to CMS, a PDP sponsor’s failure to submit a timely bid to CMS
constitutes a voluntary non-renewal by the sponsor. (Note that PDP sponsors reducing their
service areas must provide notice of their action to affected beneficiaries consistent with Chapter
3, PDP Eligibility, Enrollment, and Disenrollment Guidance of this manual and CMS non-
renewal and service area reduction guidance.)
There are six renewal options for PBPs offered by current PDP sponsors: (1) new plan; (2)
renewal plan; (3) consolidated renewal plan; (4) renewal plan with a service area expansion
(applicable only to “800 series” employer/union-only group waiver plans, or EGWPs); (5)
terminated plan (non-renewal); and (6) consolidated plans under a parent organization.
20.9.1 - New Plan
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
A PDP sponsor may create a new PBP for the following contract year with no link to a PBP it
offers in the current contract year. In this situation, beneficiaries electing to enroll in the new
PBP must complete enrollment requests, and the PDP sponsor must submit enrollment
transactions to the MARx system. No beneficiary notice is required in this case.
20.9.2 - Renewal Plan
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
A PDP sponsor may retain a current PBP for the following contract year. In order for currently
enrolled beneficiaries to remain in the renewed PBP, the sponsor must retain the same PBP
identification number for the following contract year. Current enrollees are not required to make
an enrollment election to remain enrolled in the renewal PBP, and the sponsor will not submit
enrollment transactions for existing members. Current enrollees of a renewed PBP must receive
a standard Annual Notice of Change (ANOC) (described in chapter 2 of this manual) which will
include any changes to the renewing plan. Based on their review of the ANOC, beneficiaries
may elect another plan offered by either the same or another PDP sponsor or MA organization
during the Annual Coordinated Election Period.
When renewing a PBP, it is permissible to make the following benefit design changes: (1) from a
basic benefit design (meaning a defined standard, actuarially equivalent standard, or basic
alternative benefit design) to another basic benefit design; or (2) from an enhanced alternative
benefit design to a basic benefit design. As a general matter, CMS will not permit renewal of a
PBP through the HPMS Plan Crosswalk when it involves moving enrollees from a basic benefit
design to an enhanced alternative benefit design, since enrollees previously not subject to a
supplemental premium under a basic benefit design will have to pay a combined basic and
supplemental premium under an enhanced alternative benefit design that may be higher than a
basic premium.
20.9.3 -Consolidated Renewal Plan
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
PDP sponsors are permitted to combine two or more PBPs offered in the current contract year
into a single renewal plan so that all enrollees in the combined plans are offered the same
benefits under one PBP in the following contract year. When consolidating two existing PBPs
into a single renewal PBP, it is permissible for the single renewal PBP to result in a change from:
(1) a basic benefit design (meaning a defined standard, actuarially equivalent standard, or
basic alternative benefit design) to another basic benefit design;
(2) an enhanced alternative benefit design to a basic benefit design; or
(3) an enhanced alternative benefit design to another enhanced alternative benefit design.
Again, as a general matter, CMS will not permit consolidation of two existing PBPs into a single
renewal PBP through the HPMS Plan Crosswalk when it involves a change from a basic benefit
design to an enhanced alternative benefit design, since enrollees previously not subject to a
supplemental premium under a basic benefit design will have to pay a combined basic and
supplemental premium under an enhanced alternative benefit design that may be higher than a
basic premium.
PDP sponsors combining two or more PBPs into a single renewal PBP must designate which of
the consolidating plans will be retained in the following contract year after consolidation; that is,
the sponsor’s designated renewal plan ID must remain the same in order for CMS to consolidate
the beneficiary’s election by moving him or her into the designated renewal plan ID. This is
particularly important with respect to minimizing beneficiary confusion when a plan
consolidation affects a large number of enrollees. Enrollees of a plan or plans being consolidated
into a single renewal plan will not be required to take any enrollment action, and the sponsor will
not submit enrollment transactions for existing members, though it may need to submit updated
4Rx data (described in chapter 14 of this manual) for the enrollees affected by the consolidation
to CMS. The PDP sponsor will be responsible for sending a standard ANOC to any enrollees
whose current plans are being consolidated into a renewal plan. Based on their review of the
ANOC, beneficiaries whose enrollment has been consolidated into a renewal PBP may then elect
another plan offered by either the same or another PDP sponsor or MA organization during the
Annual Coordinated Election Period.
20.9.4 -Renewal Plan with a Service Area Expansion (800 Series EGWPs only)
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
A PDP sponsor offering an 800 series EGWP PBP in the current contract year may expand its
EGWP service area to include additional PDP regions for the following contract year. In order
for currently enrolled beneficiaries to remain in the renewed PBP, the sponsor must retain the
same PBP identification number for the following contract year. Current enrollees are not
required to make an enrollment election to remain enrolled in the renewal PBP, and the sponsor
will not submit enrollment transactions for existing members. New enrollees must complete an
enrollment election. Current enrollees of a renewed 800-series PBP must receive a standard
ANOC notifying them of any changes to the renewing plan.
20.9.5 - Terminated Plan (Non-Renewal)
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
A PDP sponsor may elect to terminate a current PBP for the following contract year. In this
situation, the sponsor will not submit disenrollment requests for affected enrollees. To the extent
that affected enrollees elect to enroll in a PBP offered by the current or another PBP sponsor,
they must complete an enrollment request, and the enrolling sponsor must submit enrollment
transactions so that those individuals are enrolled in the PBP they have selected. Enrollees of
terminated PBPs will be sent a termination notice and will receive a written description of
options for obtaining prescription drug coverage in their service area. For more information
about non-renewal processes and beneficiary notification requirements, refer to the annual
summer HPMS memo providing non-renewal and service area reduction guidance.
20.9.6 - Consolidated Plans Under a Parent Organization
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
For purposes of ensuring compliance with transition requirements following an acquisition or
merger under CMS’ meaningful differences policy, or to make plan transitions following a
novation, a plan sponsor may elect to combine two or more entire PBPs offered under different
contracts (the contracts may be offered by the same legal entity or represent different legal
entities). PDP sponsors cannot complete this renewal option in the HPMS Plan Crosswalk. A
PDP sponsor must complete and submit a request to CMS in accordance with its annual
renewal/non-renewal guidance.
Current enrollees of a plan or plans being consolidated across contracts in this manner will not
be required to take any enrollment action, and the sponsor will not submit enrollment
transactions for those current members, although it may need to submit updated 4Rx data to
CMS for the current enrollees affected by the consolidation. New enrollees must complete
enrollment requests, and the sponsor will submit enrollment transactions to CMS for those new
enrollees. Current enrollees of a consolidated renewal plan must receive a special notification
along with a standard ANOC.
20.10 - Low-Enrollment Plans
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
CMS will use its authority under section 1857(c)(2)(B) of the Act, as incorporated by reference
for Part D at section 1860D-12(b)(3)(B) and codified in 42 CFR §423.507(b)(1)(iii), to non-
renew plans at the benefit-package level that do not have sufficient number of enrollees after a
specified length of time to establish that they are viable plan options, because, as a general
matter, continuing low enrollment plans is not consistent with the effective and efficient
administration of the Medicare program. Consistent with that authority, CMS will be
scrutinizing low-enrollment plans during the bid review period and alerting sponsors of low-
enrollment plans that CMS expects them to withdraw or consolidate prior to submitting bids for
the next calendar year. Before CMS would take any action to non-renew a plan pursuant to 42
CFR §423.507(b)(1)(iii), CMS would take into account all relevant factors.
CMS’ scrutiny of low-enrollment plans will not apply to employer stand-alone Part D plans. At
this time, a waiver of the minimum enrollment requirements at 42 CFR 423.512(a) (minimum
enrollment requirements) for sponsors of employer group applies.
20.11 - Manufacturer Drug Discount Program
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Beginning January 1, 2011, discounts were available to applicable Medicare beneficiaries
receiving applicable drugs while in the coverage gap. Generally, the discount on each
applicable drug is 50% of the negotiated price (excluding dispensing fee). An applicable drug is
covered under Part D only if the manufacturer has signed agreement with CMS to provide the
discount on coverage gap claims for all of its applicable drugs and remains compliant with the
terms of the agreement (assuming all other coverage criteria are met). Part D sponsors provide
the discounts for applicable drugs in the coverage gap at the point-of-sale. A CMS contractor
will coordinate the collection of discount payments from manufacturers and payment to Part D
sponsors.
For additional details regarding the policies, and administration of, the Manufacturer Drug
Discount program as it evolves, Part D sponsors should consult HPMS.
30 - Incurred/ “True Out-of-Pocket” (TrOOP) Costs
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Not all enrollee out-of-pocket expenditures are considered incurred (or “true-out-of-pocket,” or
TrOOP, expenditures) for purposes of applicability toward beneficiary spending against the
annual out-of-pocket threshold described in section 20.3.1. Sections 30.1 and 30.2 provide
further detail on whether certain expenditures are TrOOP-eligible or not, and Table 3 provides a
summary of those discussions.
30.1 - Costs that Count as Incurred Costs
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Costs are considered incurred costs and can be added to an enrollee’s TrOOP balance if all of the
following conditions are met:
1. Costs are incurred against any annual deductible, any applicable cost-sharing for costs
above the deductible and up to the initial coverage limit, and any applicable cost-sharing
for costs above the initial coverage limit and up to the annual out-of-pocket threshold.
2. Costs are incurred with respect to covered Part D drugs that are either included in a PDP
or MA-PD plan’s formulary or treated as being included in a plan’s formulary as a result
of a coverage determination, redetermination, or appeal under chapter 18.
3. Costs are:
o Incurred by the enrollee;
o Incurred by another person (including charities, if they are not otherwise excluded as
TrOOP-eligible payers as provided in section 30.2) on behalf of the enrollee other
than costs reimbursed by a group health plan, insurance or otherwise (including a
government-funded health program), or another third party payment arrangement;
o Paid by Medicare on behalf of a low-income individual under the Part D subsidy
provisions described in 42 CFR 423.782;
o Discounts paid by manufacturers as part of the Medicare Coverage Gap Discount
program;
o Paid on behalf of the enrollee under a qualified State Pharmaceutical Assistance
Program (SPAP) described in 42 CFR 423.454.
o Paid by the Indian Health Service (IHS), an Indian tribe or tribal organization, or an
urban Indian organization (as defined in section 4 of the Indian Health Care
Improvement Act); and
o Paid by AIDS Drug Assistant Program (ADAP) under Part B of title XXVI of the
Public Health Service Act.
4. Costs are incurred at a network pharmacy or an out-of-network (OON) pharmacy,
consistent with the sponsor’s out-of-network access policy (refer to section 60 for more
information on out-of-network access requirements).
Following are examples of costs considered incurred costs for purposes of TrOOP calculations:
Example 1
: Any differential charged to a beneficiary between a network retail pharmacy’s
contracted rate and a network mail-order pharmacy’s contracted rate for an extended (for
example, 90-day) supply of a covered Part D drug purchased at a retail pharmacy, as
described in section 50.10.
Example 2: For a covered Part D drug obtained OON consistent with the sponsor’s OON
policy, any differential charged to the beneficiary between an OON pharmacy’s usual and
customary price for the covered Part D drug and the plan allowance for that covered Part D
drug.
Example 3: As provided in section 50.4.2 of chapter 14, costs incurred by enrollees by
using a discounted cash price, and not their Part D benefit, provided the purchase is for a
covered Part D drug; the purchase is made at a network pharmacy; the discounted cash price
is lower than the negotiated price offered by the enrollee’s Part D plan; the enrollee is in any
applicable deductible or coverage gap phase of his or her benefit; and the enrollee submits
appropriate documentation to his or her Part D plan to be credited for the purchase.
Example 4
: Covered Part D drug cost-sharing waived or reduced by a pharmacy that is not a
group health plan, insurance, government-funded health program, or party to a third party
payment arrangement with an obligation to pay for covered Part D drugs, as described in
section 30.4.
30.2 - Costs that Do Not Count as Incurred Costs
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
The following are not considered incurred costs and cannot be added to an enrollee’s TrOOP
balance:
1. Costs for non-formulary Part D drugs unless treated by the Part D sponsor as being
included in the sponsor’s formulary as a result of a coverage determination,
redetermination, or appeal as described in chapter 18.
2. Costs for non-Part D drugs, as described in section 20.1 of chapter 6.
3. Costs paid for covered Part D drugs obtained out-of-network when OON access is not
consistent with the OON access policy (refer to section 60 for more information on OON
access requirements).
4. Costs that are paid for or for which an enrollee is reimbursed by insurance or otherwise,
including a government-funded health program.
2
5. Costs that are paid for or for which an enrollee is reimbursed by a group health plan.
6. Costs that are paid for or for which an enrollee is reimbursed by another third party
payment arrangement.
7. Covered Part D drug cost-sharing waived or reduced by a pharmacy that is also a TrOOP-
ineligible payer, as described in section 30.4.
2
If an entity providing for or paying the cost of drugs receives a government grant none of which
is used to pay for drugs (for example, a low-income housing grant), such an entity is not
considered a government-funded health program. If an entity pays for Part D drugs using a mix
of private and public funds, the entity is considered a government-funded health program, and all
its drug spending is excluded from TrOOP.
Table 3
Costs that Do and Do Not Count Toward TrOOP Expenditures
Costs that Count Toward
Incurred / TrOOP
Expenditures
1. Costs that are incurred against any annual
deductible, any applicable cost-sharing for costs
above the deductible and up to the initial coverage
limit, and any applicable cost-sharing for costs
above the initial coverage limit and up to the annual
out-of-pocket threshold; AND
2. Costs that are incurred with respect to covered Part
D drugs that are either included in a prescription
drug plan or MA-PD plan’s formulary or treated as
being included in a plan’s formulary as a result of a
coverage determination, redetermination, or appeal
under chapter 18; AND
3. Costs that are:
o Incurred by the enrollee;
o Incurred by another person on behalf of the
enrollee other than costs reimbursed by a
group health plan, insurance or otherwise
(including a government-funded health
program), or another third party payment
arrangement;
o Paid by Medicare on behalf of a low-income
individual under the Part D subsidy
provisions described in
42 CFR 423.782;
o Discount paid by a manufacturer as part of
the Medicare Coverage Gap Discount
program;
o Paid on behalf of the enrollee under a
qualified State Pharmaceutical Assistance
Program (SPAP) described in
42 CFR
423.454;
o Paid by the Indian Health Service (IHS), an
Indian tribe or tribal organization, or an
urban Indian organization (as defined in
section 4 of the Indian Health Care
Improvement Act); or
o Paid by AIDS Drug Assistance Program
(ADAP) under Part B of title XXVI of the
Public Health Service Act.
4. Costs that are incurred at a network pharmacy or an
OON pharmacy, consistent with the sponsor’s OON
access policy (refer to section 60 for more
information on OON access requirements).
Costs that Do Not Count
Toward Incurred / TrOOP
Expenditures
1. Costs incurred for non-formulary Part D drugs
unless treated by a sponsor as being included in the
sponsor’s formulary as a result of a coverage
determination, redetermination, or appeal.
2. Costs incurred for non-Part D drugs.
3. Costs paid for covered Part D drugs obtained OON
when such OON access is inconsistent with the
sponsor’s OON access policy.
4. Costs paid for or reimbursed by insurance.
5. Costs paid for or reimbursed by a government-
funded health program.
6. Costs paid for or reimbursed by a group health plan.
7. Costs paid for or reimbursed by another third party
payment arrangement.
8. Covered Part D drug cost-sharing waived or
reduced by a pharmacy that is also a TrOOP-
ineligible payer, as described in section 30.4.
30.3 - Summary of TrOOP-Eligible and TrOOP-Ineligible Payers
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Part D enrollees may have coverage or receive assistance from any of a number of entities that
wrap around the benefits available under Part D. As described in sections 30.1 and 30.2 above,
this wrap-around assistance or coverage may or may not count as incurred costs. Table 4 below
provides plans with information about whether specific entities are “TrOOP-included,” meaning
that their wrap-around assistance counts as an incurred cost, or “TrOOP-excluded,” meaning that
their wrap-around assistance does not count as an incurred cost.
Table 4
Examples of TrOOP-Excluded and TrOOP-Included Entities
TrOOP-Excluded Entities TrOOP-Included Entities
• Medicaid (even when using State-
only funds)
• Medicaid 1115 demonstrations
• State Children’s Health Insurance
Program (SCHIP)
• Federally Qualified Health Centers
(FQHCs), Rural Health Clinics, and
any safety-net facilities including
public hospital systems, community
hospitals, and local health
departments that are considered
“government-funded health
programs”
• Patient assistance programs (PAPs)
operating outside the Part D benefit
• TRICARE
• Federal Employee Health Benefits
Program (FEHBP) plans
• Black Lung Funds
• State programs that do not meet the
definition of a qualified SPAP in 42
CFR 423.464.
• Health reimbursement arrangements
(HRAs)
• State Pharmaceutical Assistance
Programs (SPAPs)
• Most charities (unless established,
maintained, or otherwise controlled
by an employer or union)
• Indian Health Service (IHS), an
Indian tribe or tribal organization,
or an urban Indian organization (as
defined in section 4 of the Indian
Health Care Improvement Act)
• AIDS Drug Assistance Program
(ADAP) under Part B of title XXVI
of the Public Health Service Act
• Health savings accounts (HSAs)
• Flexible spending accounts (FSAs)
• Medical savings accounts (MSAs)
The term “incurred costs” is only defined with respect to the annual out-of-pocket threshold.
Therefore, any coverage that supplements the benefits available under basic prescription drug
coverage may be counted toward any applicable deductible even though such drug coverage is
excluded from the definition of incurred costs for purposes of TrOOP accounting.
30.4 - Pharmacy Waiver/Reduction of Cost-Sharing and Applicability Toward
TrOOP
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Pharmacies are permitted to waive or reduce Part D cost-sharing amounts, provided they do so in
an unadvertised, non-routine manner after determining that the beneficiary is financially needy
or after failing to collect the cost-sharing amount despite reasonable efforts. In addition, a
pharmacy may waive or reduce a beneficiary's Part D cost-sharing for beneficiaries eligible for
the low-income subsidy, provided the pharmacy has not advertised that the waivers or reductions
of cost-sharing are available. In other words, for low-income subsidy recipients only,
pharmacies may provide routine waivers or reductions of cost-sharing amounts and need not
ascertain financial need. However, the pharmacies will not be eligible for safe harbor protection
if they advertise in any way the availability of waivers or cost reductions.
Waivers or reductions of Part D cost-sharing by pharmacies will generally count toward TrOOP,
as will payments made by AIDS Drug Assistance Program (ADAP) under Part B of Title XXVI of
the Public Health Service Act, as well as payments made by the Indian Health Service (IHS), an
Indian tribe or tribal organizations, or an urban Indian organization (as defined in section 4 of
the Indian Health Care Improvement Act). However, in all other instances, to the extent that the
party paying for cost-sharing on behalf of a Part D enrollee is a group health plan, insurance,
government-funded health program, or party to a third party payment arrangement with an
obligation to pay for covered Part D drugs, that party’s payment will not count toward TrOOP.
Payments made for beneficiary cost-sharing by any entity – including a safety-net pharmacy –
that has an obligation to pay for covered Part D drugs on behalf of Part D enrollees, or which
voluntarily elects to use public funds, in whole or in part, for that purpose, will not count toward
that beneficiary’s TrOOP expenditures. Safety-net pharmacies typically include Federal, State,
and locally supported community health centers or clinics – many of which are deemed FQHCs
– public hospital systems, and local health departments. In some communities, they also include
mission-driven teaching hospitals, community hospitals, and ambulatory care clinics. Rural
health clinics (RHCs), small rural hospitals, critical access hospitals, clinics that receive Ryan
White HIV/AIDS grant funding, and nurse managed clinics are also key components of the
safety-net. An estimated 12,000 safety-net providers participate in the Health Resources and
Services Administration’s (HRSA) 340B Drug Pricing Program, which allows them to purchase
their prescription drugs at significantly discounted prices. Participation in the 340B Drug Pricing
Program can enable safety-net pharmacies to provide prescriptions to their patients at lower-
than-market prices.
Disproportionate Share Hospitals (DSH) may also be TrOOP-excluded entities. Receipt of
Medicaid or Medicare DSH payments by a hospital does not, in and of itself, render a DSH
facility (and any Part D network pharmacy it owns or operates) a “government-funded health
program.” CMS views Medicare and Medicaid DSH funds essentially as adjustments to the
Medicare and Medicaid reimbursements these facilities already receive for covered services.
However, any program that is operated or funded, in whole or in part, by any government
agency, and which uses public funds in whole or in part, to provide to (or pay on behalf of an
individual) the costs of Part D drugs is a government-funded health program even if it pays these
costs using a mix of private and public funds. An entity that receives DSH funds and uses non-

DSH government funding streams to provide to or pay on behalf of an individual the costs of
Part D drugs will meet CMS’ definition of a government-funded health program, and any
reduction or waiver of Part D cost-sharing that it offers will not count toward a Part D enrollee’s
TrOOP balance.
Similarly, participation in the 340B Drug Pricing Program does not in and of itself render a
safety-net pharmacy a government-funded health program. However, as with DSH facilities, any
use of government funding streams to provide to or pay on behalf of an individual the costs of
Part D drugs will render a safety-net pharmacy a government-funded health program such that
any reduction or waiver of Part D cost-sharing that it offers will not count toward a Part D
enrollee’s TrOOP balance.
However, if an entity can demonstrate to a Part D sponsor that it uses only
non-public funds to
pay for the cost of Part D drugs, that sponsor may allow for cost-sharing waivers or reductions in
cost-sharing paid for by that entity’s pharmacies to count toward TrOOP. Part D sponsors
remain ultimately accountable for correctly tracking their enrollees’ TrOOP expenditures.
If, on the other hand, a pharmacy funds Part D cost-sharing waivers using a mix of private and
public funds, the pharmacy is considered a government-funded health program, and all its drug
spending is excluded from TrOOP. If a pharmacy is a government-funded health program or
other TrOOP-ineligible payer and waives or reduces any applicable Part D enrollee cost-sharing
after payment of a claim by the Part D sponsor, that claim must be flagged so that any applicable
beneficiary cost-sharing that is waived or reduced by the pharmacy is not added to a
beneficiary’s TrOOP balance. Currently, there does not exist any capability under the National
Council for Prescription Drug Programs (NCPDP) 5.1 transaction set for pharmacies to indicate
a pharmacy’s waiver or reduction of any applicable beneficiary cost-sharing so that such
subsidies are not applied to the beneficiary’s TrOOP balance. CMS recommends that Part D
sponsors set up manual processes with safety-net pharmacies in their networks in order to
accurately maintain beneficiary TrOOP balances.
40 - Prescription Drug Plan Service Areas
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Prescription drug plan regions are areas in which a contracting PDP sponsor must provide access
to covered Part D drugs. The service area for a PDP, with the exception of a fallback plan,
consists of one or more PDP regions. A PDP sponsor may offer a PDP in more than one region
– including in all PDP regions – so long as coverage is provided in all those regions in their
entirety. However, the PDP sponsor must submit separate bids for its coverage in each region of
its service area.
There are currently 34 PDP regions and 26 MA regions (refer to Appendix 2 and Appendix 3,
respectively, for maps of these PDP and MA regions). Each of the five U.S. Territories –
American Samoa, the Commonwealth of the Northern Mariana Islands, Guam, Puerto Rico, and
the Virgin Islands – constitutes an additional PDP region. While these regional boundaries are
currently in effect, CMS may revise both the PDP and MA regions in future years.

50 - Access to Covered Part D Drugs
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
Part D sponsors must establish a pharmacy network sufficient to ensure access to covered Part D
drugs for their enrollees. As detailed below, Part D sponsors must demonstrate that they
provide: (1) convenient access to retail pharmacies for all enrollees; (2) adequate access to home
infusion pharmacies for all enrollees; (3) convenient access to LTC pharmacies for enrollees
residing in LTC facilities; and (4) convenient access to I/T/U pharmacies for American
Indian/Alaska Native (AI/AN) enrollees. Except as indicated in section 50.3 for limited access
drugs, covered Part D drugs must be accessible to enrollees through network pharmacies through
all phases of the Part D benefit.
Sponsors or their pharmacy benefits manager (PBM) should maintain a contracting log
documenting their efforts to provide standard terms and conditions to prospective network
pharmacies as well as any contracting negotiations between the sponsor or PBM and prospective
network pharmacies. This contracting log will help CMS in its efforts to ensure compliance with
pharmacy access requirements, including the any willing pharmacy requirement described in
section 50.8.1.
After their initial pharmacy access submissions are approved, Part D sponsors must notify their
CMS account manager of any substantive change in their pharmacy network that may impact
their ability to maintain a Part D pharmacy network that meets CMS’ requirements. Substantive
changes to a pharmacy network include, but are not limited to:
• An inability to meet the convenient access standard for retail pharmacies, as described in
section 50.1;
• An inability to provide adequate access to home infusion drugs to enrollees within 24
hours of discharge from an acute setting, as described in section 50.4;
• An inability to provide an enrollee residing in an LTC facility convenient access to a
network LTC pharmacy that serves the LTC facility, as described in section 50.5.1; or
• Not offering Part D contracts to all I/T/U pharmacies in a Part D sponsor’s service area in
order to provide convenient access for AI/AN enrollees, as described in section 50.6.
Part D sponsors will be required to provide CMS with data on an annual basis that will allow
CMS to determine whether their retail, home infusion, and LTC pharmacy networks continue to
meet CMS’ pharmacy access standards. For more information about these reporting
requirements, refer to:
http://www.cms.hhs.gov/PrescriptionDrugCovContra/08_RxContracting_ReportingOversight.as
p#TopOfPage
A Part D sponsor must notify CMS when it changes PBMs to manage its pharmacy network mid-
year. Specifically, the sponsor must:
• Notify their CMS account manager at least 60 days prior to the effective date of the new
contract or the date the new PBM would begin providing services to beneficiaries,
whichever is earlier. In instances of a contractual change occurring within less than 60
days, then the Part D sponsor must notify their account manager within 5 days of signing
the new contract.
• Ensure the change includes an internal transition period, as any decision to change PBMs
during the last quarter of the contract year may cause disruption to beneficiary access and
services.
• Make preparations to submit appropriate documentation, upon request, to CMS Central
Office at any time after the date the contract takes effect (targeted audit). Such
documentation may include but not be limited to:
o Executed PBM contract
o Retail pharmacy contract template
o Mail order pharmacy contract template
o Home infusion pharmacy contract template
o LTC pharmacy contract template
o I/T/U pharmacy contract template
o Up-to-date Part D pharmacy network listings
o Up-to-date Part D geo-access reports
50.1 - Retail Pharmacy Access
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Part D sponsors must secure the participation in their pharmacy networks of a sufficient number
of pharmacies that dispense drugs directly to patients (other than by mail order) to ensure
convenient access to covered Part D drugs by Part D plan enrollees. CMS convenient access
rules require Part D sponsors to establish pharmacy networks in which:
• In urban areas, at least 90 percent of Medicare beneficiaries in the Part D sponsor’s
service area, on average, live within 2 miles of a retail pharmacy participating in the
sponsor’s network;
• In suburban areas, at least 90 percent of Medicare beneficiaries in the Part D sponsor’s
service areas, on average, live within 5 miles of a retail pharmacy participating in the
sponsor’s network; and
• In rural areas, at least 70 percent of Medicare beneficiaries in the Part D sponsor’s service
area, on average, live within 15 miles of a retail pharmacy participating in the sponsor’s
network.
The convenient access standards will be applied to different types of Part D sponsors as follows:
• Regional MA-PD and PDP sponsors
: Must meet or exceed the convenient access
standards across urban, suburban, and rural areas, respectively, in each State in which
they operate. To the extent that a regional MA-PD or PDP sponsor operates in a multi-
region or national service area, it will be required to meet the convenient access standards
in each State in that multi-region or national service area; the sponsor may not meet the
convenient access standards by applying those standards across the entire multi-State
geographic area it services.
• Local-MA-PD sponsors
: Must meet or exceed the convenient access standards across
urban, suburban, and rural areas, respectively, in each service area (including multi-
county service areas) in which they operate.
• Cost plans
: Must meet or exceed the convenient access standards across urban, suburban,
and rural areas, respectively, in each geographic area in which they operate.
Part D sponsors may count I/T/U pharmacies and pharmacies operated by FQHCs and RHCs
toward the standards for convenient access to retail pharmacies detailed above. However, CMS
will review Part D sponsors’ pharmacy network submissions to ensure that inclusion of I/T/U,
FQHC, and RHC pharmacies in contracted pharmacy networks does not substitute for the
inclusion in Part D plan networks of retail pharmacies.
CMS is aware that there may be some areas of the country in which meeting the rural access
standard, in particular, will be impossible or impracticable given the lack of pharmacy
infrastructure. CMS will consider modifications to the rural access standard in cases in which
Part D sponsors can demonstrate that meeting the standard is impossible or impracticable given a
lack of infrastructure.
50.2 - Mail-Order Pharmacy Access
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
The inclusion of mail-order pharmacies in Part D plan networks is optional. However, network
mail-order pharmacies will not count toward meeting the retail pharmacy access requirements
specified in section 50.1. Since network inclusion of mail-order pharmacies is optional, sponsors
may designate a subset of formulary drugs (e.g., particular tiers or “maintenance drugs” only) for
availability via network mail-order pharmacies. As described in section 50.10, to the extent that
a Part D plan offers benefits, including extended supplies of drugs (e.g., 90-day supplies),
through network mail-order pharmacies, the plan must ensure that enrollees have reasonable
access to the same benefits at network retail pharmacies. CMS recognizes that some pharmacies
may utilize common carriers in order to meet the needs of their patients, such as Part D
enrollees residing in LTC facilities or in remote areas. A pharmacy that makes some, but not
predominantly all, deliveries by common carrier is not a mail order pharmacy.
50.3 - Limited Access Drugs and “Specialty” Pharmacies
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
Part D sponsors may not limit access to certain Part D drugs to "specialty” pharmacies within
their Part D network in such a manner that contravenes the convenient access protections
described in section 50.1. In other words, limited access to a Part D drug may not be based
solely on the placement of a Part D drug in a specialty or high-cost tier because this tier
placement alone is not indicative of any special requirements associated with such drug.
Part D sponsors may only restrict access to Part D drugs to a subset of their network pharmacies
for the following reasons:
1. The FDA has restricted distribution of the drug to certain facilities or physicians; or
2. Appropriate dispensing of the Part D drug requires extraordinary special handling,
provider coordination, or patient education that cannot be met by a network pharmacy.
Additional education or counseling alone does not qualify a drug for limited distribution within
the overall pharmacy network.
Part D sponsors may specify, on a drug-by-drug basis, reasonable requirements for network
pharmacies to ensure appropriate handling and dispensing of a particular Part D drug that
requires special attention. These drug-by-drug requirements should only apply to special
handling and dispensing that may be required for a particular “specialty” drug and not to
reimbursement or other standard contracting terms and conditions. Offering pharmacies
unreasonably low reimbursement rates for certain “specialty” drugs may not be used to subvert
the convenient access standards. In other words, Part D sponsors must offer reasonable and
relevant reimbursement terms for all Part D drugs as required by 42 CFR 423.505(b)(18).
In addition, Part D sponsors may not require network pharmacies to qualify as a “specialty”
pharmacy in order to dispense any drug that requires special attention if the network pharmacy is
capable of appropriately dispensing the particular Part D drug or drugs in question. The
convenient access standards dictate that “specialty” pharmacies be used to supplement network
pharmacy access when necessary and not otherwise restrict it.
If a Part D sponsor finds it necessary to restrict access to a Part D drug for either of the two
reasons listed above, it must indicate this on the formulary information page in the Formulary
Submission module, as well as identifying these drugs in the formulary flat file. Additionally,
Part D sponsors must be prepared to provide CMS with documentation substantiating the limited
access drug criteria.
50.4 - Home Infusion Pharmacy Access
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
In order to meet the requirements for adequate access to home infusion pharmacies, Part D
sponsors must deliver home infusion drugs to enrollees within 24 hours of discharge from an
acute setting, unless the next required dose, as prescribed, is required to be administered later
than 24 hours after discharge. To ensure Part D sponsors can provide such access, as part of
their initial pharmacy access submissions, and through Part D annual reporting requirements
(Information Collection Requirements (ICF) OMB 0938-0992), each Part D sponsor must
provide a list of all contracted home infusion pharmacies licensed/legally able to serve in all
State(s) and/or territories in the service area under each CMS pending contract number. The

pharmacy list must be submitted using the CMS template, which includes NCPDP/National
Provider Identifier, pharmacy name, address, and all States and/or territories licensed in/legally
able to serve.
CMS conducts an outlier analysis using these home infusion pharmacy network submissions to
evaluate the robustness of home infusion pharmacy networks of all active Part D sponsors.
As part
of the Part D application, initial applicants to the Part D drug benefit program must demonstrate
access through submission of their home infusion pharmacy networks, which must be no less
robust than these outlier levels for their pending service area(s) as identified in Appendix 1.
CMS will evaluate access for existing sponsors through a modified outlier approach which looks
at both the number of pharmacies relative to the established outlier level combined with evidence
that the existing sponsor is meeting the 24 hour delivery standard for its enrollees.
Network robustness is assessed within contract types (e.g., PDP, Regional Prospective Payment
Organization or RPPO, and MA-PD). Outliers are those contracts that are in the lowest 25
th
percentile in terms of the number of contracted home infusion pharmacies within a given state. In
other words, 75 percent of all similarly-situated Part D sponsors have a more robust home infusion
pharmacy network than the outliers in the lowest 25
th
percentile. For organizations whose service
area comprises an entire state, Appendix 1 provides the minimum number of home infusion
pharmacies required to surpass the 2010 Reporting Requirement and 2011 Part D Application outlier
level. Organizations operating in a service area smaller than an entire state may use the provided
ratios of the number of home infusion pharmacies to the number of beneficiaries in the state and
apply it to the number of beneficiaries in the organization’s service area to calculate the minimum
required number of home infusion pharmacies for that particular service area.
CMS does not expect Part D sponsors to provide or pay for supplies, equipment, or the
professional services needed for home infusion therapy. Part D sponsors’ contracted network
pharmacies must be able to:
• Deliver home infused drugs in a form that can be easily administered in a clinically
appropriate fashion;
• Provide infusible Part D drugs for both short-term acute care and long-term chronic care
therapies;
• Ensure that the professional services and ancillary supplies necessary for the provision of
home infusion therapy are in place before dispensing home infusion drugs, consistent
with the quality assurance requirement for Part D sponsors described in 42 CFR
423.153(c); and
• Provide covered home infusion drugs within 24 hours of discharge from an acute setting,
unless the next required dose, as prescribed, is required to be administered later than 24
hours after discharge.
While Part D sponsors remain ultimately responsible for complying with all Part D requirements,
they are also permitted to delegate their responsibilities to plan contractors, such as network
pharmacies. Part D sponsors may contractually delegate the responsibility for ensuring timely
delivery of home infusion drugs to their network pharmacies provided they meet the

requirements of 42 CFR 423.505(i) regarding relationships with pharmacies or other providers,
related entities, contractors, subcontractors, and first tier and downstream entities.
50.5 - Long-Term Care (LTC) Pharmacy Access
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
As described in section 50.5.1, Part D sponsors must demonstrate that their contracted pharmacy
network provides convenient access to LTC pharmacies for enrollees who reside in an LTC
facility. Part D sponsors must offer standard LTC pharmacy network contracts to all LTC
pharmacies operating in their service area that request such contracts. These standard
contracting terms and conditions must include the performance and service criteria for LTC
pharmacies specified in section 50.5.2 below.
50.5.1 - Convenient Access to LTC Pharmacies
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
Part D sponsors will be required to offer a contract to any pharmacy willing to participate in its
LTC pharmacy network so long as the pharmacy is capable of meeting the performance and
service criteria in section 50.5.2 (and relevant State laws governing the practice of pharmacy in
the LTC setting), as well as any other standard terms and conditions established by the Part D
sponsor for its network LTC pharmacies (NLTCPs). Once a Part D sponsor has negotiated an
agreement with an LTC pharmacy, the LTC pharmacy becomes an NLTCP and is eligible to
serve the sponsor’s enrollees who reside in LTC facilities.
CMS expects that each LTC facility will select one or possibly more than one eligible NLTCP to
provide Medicare drug benefits to its residents. A facility can continue to contract exclusively
with a single LTC pharmacy if it chooses; however, the features to promote competition
described above will likely give each facility access to a broader range of potential LTC
pharmacies than was the case before the implementation of the Part D benefit. An NLTCP that
serves a particular LTC facility must provide the same services, as delineated in its contract with
a Part D sponsor, to all of that sponsor’s enrollees who reside in that LTC facility.
Part D sponsors may not rely on OON access to meet the LTC convenient access standard. All
of a Part D sponsor’s enrollees who reside in an LTC facility must be able to routinely receive
their Part D benefits through the plan’s network of LTC pharmacies in order for a Part D sponsor
to be in compliance with CMS’ LTC convenient access standard.
In addition, Part D sponsors may not rely upon beneficiary special enrollment periods (SEPs) to
circumvent the LTC convenient access requirement. Although individuals moving into, residing
in, or moving out of an institution are entitled to an SEP, and dually eligible individuals are
entitled to an ongoing SEP for as long as they are eligible for Medicaid benefits, it is not
acceptable for Part D sponsors to rely on this beneficiary option in lieu of contracting with a
sufficient number of pharmacies to ensure that a beneficiary can remain in his or her current plan
for as long he or she resides in an LTC facility in the Part D sponsor’s service area. Ultimately,
all beneficiaries – including those who reside in LTC facilities – should have available to them
the full array of plans operating in their area.
Part D sponsors must demonstrate that they have a network of contracted LTC pharmacies that
provide convenient access to LTC pharmacies for enrollees who reside in LTC facilities. In
order to demonstrate convenient access to LTC pharmacies, Part D sponsors must include, as
part of their initial pharmacy access submissions, a list of all contracted LTC pharmacies. In
addition, Part D sponsors are required to submit an updated list of all contracted LTC pharmacies
as part of the annual Part D reporting requirements developed in accordance with 42 CFR
423.514 and OMB 0938-0992.
CMS will evaluate whether Part D sponsors provide convenient access to LTC pharmacies
through analysis of these submissions. Specifically, CMS will use these lists to verify that Part
D sponsors have contracts in place with LTC pharmacies that serve the LTC facilities where
their beneficiaries reside. Part D sponsors should have processes in place to ensure beneficiaries
residing in LTC facilities are being served by an LTC network pharmacy.
CMS expects LTC pharmacy contracting activity will be ongoing as Part D sponsors continue to
identify LTC facilities and LTC pharmacies, and as they examine their auto-enrollment
assignments and incoming enrollments. To the extent that a beneficiary is enrolled in a Part D
sponsor’s plan that does not have a contract with an LTC pharmacy that can serve the LTC
facility in which he or she resides, the appropriate action for a Part D sponsor to take is to
contract with the facility’s contracted LTC pharmacy or – if that pharmacy will not sign a
contract – with another LTC pharmacy that can serve that facility. In some cases, a retroactive
contract may be necessary.
50.5.2 - Performance and Service Criteria for Network Long-Term Care
Pharmacies (NLTCPs)
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
In order to participate in Part D sponsor LTC pharmacy networks, a pharmacy must be capable
of meeting certain minimum performance and service criteria (and relevant State laws governing
the practice of pharmacy in the LTC setting), as well as any other standard terms and conditions
established by the Part D sponsor for its network pharmacies. The following minimum
performance and service criteria for pharmacies providing LTC services are based on widely
used best practices in the market. These performance and service criteria must be incorporated
into an addendum to a Part D sponsor’s standard network contract for those pharmacies that
would like to be designated NLTCPs.
1. Comprehensive Inventory and Inventory Capacity – NLTCPs must provide a
comprehensive inventory of plan formulary drugs commonly used in the long-term care
setting. In addition, NLTCPs must provide a secured area for physical storage of drugs,
with necessary added security as required by Federal and State law for controlled
substances. This is not to be interpreted as requiring the pharmacy to have inventory or
security measures outside of the normal business setting.
2. Pharmacy Operations and Prescription Orders – NLTCPs must provide services of a
dispensing pharmacist to meet the requirements of pharmacy practice for dispensing
prescription drugs to LTC residents, including but not limited to the performance of drug
utilization review (DUR). In addition, the NLTCP pharmacist must conduct DUR to
routinely screen for allergies and drug interactions, to identify potential adverse drug
reactions, to identify inappropriate drug usage in the LTC population, and to promote
cost effective therapy in the LTC setting. The NLTCP must also be equipped with
pharmacy software and systems sufficient to meet the needs of prescription drug ordering
and distribution to an LTC facility. Further, the NLTCP must provide written copies of
the NLTCP’s pharmacy procedures manual and said manual must be available at each
LTC facility nurses’ unit. NLTCPs are also required to provide ongoing in-service
training to assure that LTC facility staff are proficient in the NLTCP’s processes for
ordering and receiving of medications. NLTCPs must be responsible for return for
destruction and/or disposal of unused medications following discontinuance, transfer,
discharge, or death as permitted by State Boards of Pharmacy. Controlled substances and
out of date substances must be disposed of within State and Federal guidelines.
3. Special Packaging – NLTCPs must have the capacity to provide specific drugs in units
of use packaging, bingo cards, cassettes, unit dose or other special packaging commonly
required by LTC facilities. NLTCPs must have access to, or arrangements with, a vendor
to furnish supplies and equipment including but not limited to labels, auxiliary labels, and
packing machines for furnishing drugs in such special packaging required by the LTC
setting.
4. IV Medications – NLTCPs must have the capacity to provide IV medications to the LTC
resident as ordered by a qualified medical professional. NLTCPs must have access to
specialized facilities for the preparation of IV prescriptions (clean room). Additionally,
NLTCPs must have access to or arrangements with a vendor to furnish special equipment
and supplies as well as IV trained pharmacists and technicians as required to safely
provide IV medications.
5. Compounding/Alternative Forms of Drug Composition – NLTCPs must be capable of
providing specialized drug delivery formulations as required for some LTC residents.
Specifically, residents unable to swallow or ingest medications through normal routes
may require tablets split or crushed or provided in suspensions or gel forms, to facilitate
effective drug delivery.
6. Pharmacist On-call Service – NLTCPs must provide on-call, 24-hour-per-day/7-day-a-
week service with a qualified pharmacist available for handling calls after hours and to
provide medication dispensing available for emergencies, holidays and after hours of
normal operations.
7. Delivery Service – NLTCPs must provide for delivery of medications to the LTC facility
up to 7 days each week (up to 3 times per day) and in-between regularly scheduled visits.
Emergency delivery service must be available 24 hours a day, 7 days a week. Specific
delivery arrangements will be determined through an agreement between the NLTCP and
the LTC facility. NLTCPs must provide safe and secure exchange systems for delivery
of medication to the LTC facility. In addition, NLTCPs must provide medication
cassettes, or other standard delivery systems, that may be exchanged on a routine basis
for automatic restocking. The NLTCP delivery of medication to carts is a part of routine
“dispensing.”
8. Emergency Boxes – NLTCPs must provide “emergency” supply of medications as
required by the facility in compliance with State requirements.
9. Emergency Log Books – NLTCPs must provide a system for logging and charging
medication used from emergency/first dose stock. Further, the pharmacy must maintain a
comprehensive record of a resident’s medication order and drug administration.
10. Miscellaneous Reports, Forms and Prescription Ordering Supplies – NLTCPs must
provide reports, forms and prescription ordering supplies necessary for the delivery of
quality pharmacy care in the LTC setting. Such reports, forms and prescription ordering
supplies may include, but will not necessarily be limited to, provider order forms,
monthly management reports to assist the LTC facility in managing orders, medication
administration records, treatment administration records, interim order forms for new
prescription orders, and boxes/folders for order storage and reconciliation in the facility.
To qualify as an LTC pharmacy for a Part D sponsor’s LTC pharmacy network, a pharmacy
must currently have the capacity – either by itself or through subcontracts with other entities – to
meet all these performance and service criteria, even if an LTC facility that pharmacy serves
does not need a particular service subsumed under those performance and service criteria.
Pharmacies subcontracting with other entities to meet the performance and service criteria must
ensure that they comply with all relevant Part D requirements, including all performance and
service criteria for the provision of LTC pharmacy services. However, it will ultimately be up to
LTC facilities and their contracted LTC pharmacy(ies) to determine which of these specific
items or services a nursing facility needs. In other words, an LTC pharmacy must be capable of
meeting all the aforementioned performance and service criteria at the time it contracts with a
Part D sponsor, but it will not be required to provide all those services to LTC facilities if those
facilities do not have a need for those certain services.
These performance and service criteria are not intended to be exclusive or exhaustive. Rather,
they are intended to be minimum requirements for becoming an NLTCP. While payment terms
for LTC pharmaceutical and dispensing services are subject to negotiations between the Part D
sponsor and its NLTCPs, CMS notes that payment to LTC pharmacies under Part D may only
cover drug ingredient costs and dispensing fees as defined in section 20.6. Specialized services
provided in the administration of drugs after they are dispensed and delivered from the LTC
pharmacy are specifically not covered by the Part D benefit.
50.5.3 - Other LTC Contracting Terms and Conditions and Uniformity of
Benefits
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Outside of the minimum performance and service criteria, Part D sponsors and pharmacies may
propose a number of contracting terms and conditions. With rare exceptions, CMS does not
generally involve itself in determining whether standard contracting terms and conditions are
“reasonable and relevant,” since these are fact-specific questions that are best left between
negotiating parties. Thus, for example, CMS generally does not opine on contracting terms and
conditions associated with compensation, billing, and business practices provided such terms and
conditions are consistent with explicit Part D statutory and regulatory requirements.

LTC pharmacies may propose other terms and conditions in their negotiations with Part D
sponsors as additional beneficiary protections. Such additional terms and conditions may be
problematic because they explicitly conflict with statutory and/or regulatory requirements for the
Part D program. Some of these proposed contracting terms and conditions not only conflict with
CMS rules, but could even be harmful to beneficiaries. Following are several examples of such
terms and conditions. While these examples are not exhaustive – and others may exist with
similar effects – ultimately, all contracting terms and conditions must comply with Part D rules
and requirements in order to protect the interests of beneficiaries and safeguard the integrity of
the Medicare prescription drug program.
Example 1
: Requirements for a longer transition period than the plan has provided for in
its transition process submission to CMS.
As described in section 30.4.4.2 of chapter 6, all plans must offer a temporary supply of
non-formulary drugs of at least 31 days with multiple refills during a 90-day transition
period in the LTC setting. Some pharmacies may wish to extend that transition period to
up to 180 days. However, given uniform benefits requirements under the statute and
CMS’ regulations, plans cannot agree to a differential transition policy for some of their
LTC enrollees. Transition policies must be applied uniformly to all similarly situated
enrollees. Moreover, extending a transition period for some plan enrollees has cost
implications for plans that may ultimately drive up costs to both beneficiaries and the
Medicare program.
Example 2
: Waivers of prior authorization or other utilization management edits for
LTC facility residents.
Plans must determine whether a particular drug is a Part D drug and, in addition, must
establish cost-effect utilization management programs. Waivers of prior authorization
management edits or other utilization management edits for some plan enrollees run
counter to these program requirements. In addition, given uniform benefits requirements
under the statute and CMS’ regulations, plans cannot apply prior authorization or other
utilization management edits differentially to a subset of their LTC enrollment.
Example 3
: Waivers of certain DUR requirements for LTC facility residents.
Plans must optimize drug regimens, which requires an up-front and thorough review of
enrollee drug files in order to ensure their safety (e.g., by preventing drug-drug
interactions). In addition – and as stated above – uniform benefits requirements under the
statute and CMS’ regulations mean that plans cannot apply DUR edits differentially to a
subset of their LTC enrollees. All plan benefits must be applied uniformly to all similarly
situated enrollees.
Part D sponsors may be out of compliance with uniform benefits requirements to the extent that
they agree to particular contracting terms and conditions that have the net result of creating a
non-uniform benefit for plan enrollees residing in LTC facilities serviced by network LTC
pharmacies whose contracts with Part D sponsors may not include these same provisions. Plan
benefits must also be applied uniformly across all enrollees (both those who reside in the

community and those residing in LTC facilities) when there is no justification for applying
different rules to enrollees residing in LTC facilities. However, there are instances in which it is
appropriate or legally required under CMS’ Part D guidance for Part D sponsors to establish
standards that differentiate between enrollees residing in LTC facilities and ambulatory patients.
For example, it is perfectly acceptable for Part D sponsors to adopt alternative standards
applicable only in the LTC setting when clinically justified, legally required, or otherwise
justified based on characteristics unique to beneficiaries residing in LTC facilities, such as
extended transition periods for enrollees residing in LTC facilities or prior authorization or other
utilization management requirements (for example, those that distinguish between Part B and
Part D covered drugs given that some drugs covered for use in the home under Part B are not
covered by Part B in LTC settings). However, Part D sponsors cannot agree to differential
benefits which would result in a non-uniform benefit among enrollees in LTC facilities, such as
an extended transition period, certain utilization management edits, or different drug utilization
review protocols that are limited to those LTC enrollees who obtain their Part D drugs from a
specific LTC pharmacy. Plan benefits must be applied uniformly to all similarly situated
enrollees, meaning that all enrollees residing in LTC facilities must be subject to the same rules.
50.5.4 - Access to LTC Pharmacies for Enrollees Residing in Institutions for
Mental Disease (IMDs), Intermediate Care Facilities for the Mentally
Retarded (ICFs/MR), and LTC Hospitals
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
To the extent that an ICF/MR or IMD designated by a State as an institution has, as an inpatient,
any institutionalized individuals – which means any full benefit dual eligible individual for
whom payment is made under Medicaid throughout a month, as provided in section
1902(q)(1)(B) of the Act – it falls within CMS’ regulatory definition of the term “LTC facility.”
There exists a statutory Federal financial participation exclusion under Medicaid affecting
residents of IMDs between the ages of 22 and 64. However, the IMD exception to the definition
of “medical assistance” under section 1902(q)(1)(B) of the Act does not apply to individuals who
are age 65 and older. Thus, all elderly full-benefit dual eligibles who are inpatients in an IMD
designated by the State as an institution for a full month are considered institutionalized
individuals for that month. Long-term care hospitals are also medical institutions and are
considered LTC facilities if they have as inpatients any institutionalized individuals.
CMS also clarifies that as medical institutions, hospitals (including long-term care hospitals) that
receive payments under section 1902(q)(1)(B) of the Act can meet the definition of an LTC
facility. As discussed in section 20.2.1 of chapter 6, to the extent that inpatients in these
hospitals exhaust their Part A inpatient days benefit, and payment is no longer available under
Part A or Part B for drugs that would otherwise meet the definition of a Part D drug, such drugs
are Part D drugs.
This means that Part D sponsors must ensure that they provide convenient access to network
LTC pharmacies for:
• All of their enrollees residing in a long-term care hospital or in an IMD or ICF/MR
designated by the State as an institution, and in which any institutionalized individuals

reside (although living in an institution that does not meet the definition of an LTC
facility does not preclude an individual from enrolling in Part D).
• All of their enrollees who are inpatients in a hospital that is a “medical institution” under
1902(q)(1)(B) of the Act – and therefore would meet the Part D definition of an LTC
facility – and whose Part A benefits have been exhausted.
Part D sponsors will not be compliant with CMS’ LTC convenient access standard if they do not
provide access to covered Part D drugs via an LTC pharmacy in their network for all of their
enrollees who reside in LTC facilities.
Many ICFs/MR, IMDs, and LTC hospitals utilize in-house pharmacies and, particularly in the
case of ICFs/MR and IMDs, such pharmacies are State run and operated. In some States,
licensing laws preclude facilities from obtaining prescription drugs and LTC services for their
residents from anyone but the facility’s in-house pharmacy. States may not be able to agree to
certain standard clauses in some LTC standard contracts because of constitutional and legal
restraints on States. Part D sponsors should be prepared to readily negotiate with States to
address these issues. To the extent that Part D sponsor contracting efforts involve
communication with State run and operated pharmacies, CMS encourages Part D sponsors to
coordinate their efforts through a single point of contact at the State level. Refer to the following
Web site for lists of State contacts for IMDs and ICFs/MR:
http://www.cms.hhs.gov/PrescriptionDrugCovContra/11_PartDContacts.asp#TopOfPage
50.5.5 - Post-Consumption Billing
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
CMS interprets the term “post-consumption” billing as billing that is performed after a drug is
dispensed and consumed by an enrollee, usually at the end of the month or the beginning of the
next month. While post-consumption billing is not typical in retail pharmacy, certain LTC
pharmacies utilize post-consumption billing procedures. A significant advantage of this type of
billing is reduction in waste because only those drugs actually consumed by an individual are
billed. Post-consumption billing arrangements are permissible under the Part D program and
should be accommodated by sponsors, assuming they are managed in a manner that is
compatible with all other Part D requirements (i.e., for a formulary drug used for a medically
accepted indication) and in a manner that provides for an accurate calculation of TrOOP
expenditures (for example, via a single claim, Point-of-Sale transaction, HIPAA compliant
format (i.e., v. NCPDP 5.1 or v .D.0)).
Network pharmacies are responsible for verifying that drugs dispensed to the beneficiary are
covered under the beneficiary’s Part D plan. Because network pharmacies utilizing post-
consumption billing will not submit the first claim to a Part D plan until after the drug has been
dispensed, the pharmacy must employ another mechanism for verifying coverage in advance of
dispensing.
50.6 - I/T/U Pharmacy Access
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
To the extent that any I/T/U pharmacies are present in their service areas, Part D sponsors must
demonstrate that their contracted pharmacy network provides convenient access to I/T/U
pharmacies. Part D sponsors must offer standard pharmacy network contracts to all I/T/U
pharmacies operating in their service area. These standard contracting terms and conditions must
conform to a model addendum developed by CMS, in collaboration with various stakeholders,
that accounts for the operational differences between I/T/U and retail pharmacies. Upon request,
sponsors must provide CMS with documentation to demonstrate that they have offered all I/T/U
pharmacies in their service area a conforming contract; such documentation may be proof of
FAX or U.S. postage or other carrier’s receipt of delivery. Refer to the following Web site for a
copy of the model I/T/U pharmacy contracting addendum:
http://www.cms.hhs.gov/PrescriptionDrugCovContra/10_RxContracting_SpecialGuidance.asp#T
opOfPage
In order to demonstrate convenient access to I/T/U pharmacies, Part D sponsors must include, as
part of their initial pharmacy access submissions, a list of all I/T/U pharmacies in their service
areas. This information must be submitted at the county level and CMS-designated contract
level and include contracting status with each of the I/T/U pharmacies listed. CMS will review
this list to ensure that sponsors are providing convenient access to I/T/U pharmacies in their
service areas.
50.7 - Waiver of Pharmacy Access Requirements
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
As detailed below, CMS will waive pharmacy access standards under two circumstances: (1) for
MA-PD plans and cost plans offering Part D coverage that operate and own their own
pharmacies, provided they demonstrate convenient access using an alternative standard; and (2)
for private fee-for-service (PFFS) plans offering Part D coverage that provide coverage for drugs
purchased from all pharmacies, regardless of whether they are network pharmacies and do not
charge additional cost-sharing to beneficiaries for obtaining their drugs at a non-network
pharmacy.
50.7.1 - Waiver of Retail Pharmacy Access Requirements for MA-PD Plans
and Cost Plans with Plan-Owned and Operated Pharmacies
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
MA-PD plans or cost plans that provide access (other than via mail order) to qualified
prescription drug coverage through retail pharmacies owned and operated by the MA
organization that offers the plan or the cost plan will not be required to meet the retail pharmacy
access standards in section 50.1. However, in order for the pharmacy access standards to be
waived, the MA-PD plan or cost plan in question must have a pharmacy network that, per CMS’
determination, provides comparable pharmacy access to its enrollees as provided under
42 CFR
422.112 or 42 CFR 417.416(e), as appropriate.
This waiver is automatically granted when the MA-PD plan or cost plan provides Part D drugs
predominantly through plan-owned and operated retail pharmacies (i.e., more than 50 percent
of prescriptions are provided through owned and operated retail pharmacies). While this waiver
of the convenient retail access standards is automatically granted to plans that meet this criteria,

MA-PD and cost plans using this waiver must initially submit information to CMS about the
number of prescriptions filled at plan-owned retail pharmacies and at contracted pharmacies, and
the percentage of prescriptions provided through plan-owned retail pharmacies during the last
complete year prior to the contract year when the waiver applies. Part D sponsors that have been
granted this waiver will be required to provide CMS with data on an annual basis on
prescriptions filled at plan-owned and operated retail pharmacies. For more information about
these reporting requirements, refer to:
http://www.cms.hhs.gov/PrescriptionDrugCovContra/08_RxContracting_ReportingOversight.as
p#TopOfPage
50.7.2 - Waiver of Pharmacy Access Requirements for Private Fee-for-Service
Plans
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Private fee-for-service (PFFS) plans offering Part D coverage will not be subject to the pharmacy
access requirements in sections 50.1, 50.4, 50.5, and 50.6, provided they:
• Provide coverage for drugs purchased from all pharmacies, regardless of whether they are
network pharmacies; and
• Do not charge additional cost-sharing to beneficiaries for obtaining their drugs at a non-
network pharmacy.
Given these two provisions, PFFS plans offering Part D coverage must provide access to
pharmacies in one of the following ways:
1. PFFS plans offering Part D coverage that meet the retail pharmacy convenient access
standards described in section 50.1, the home infusion pharmacy adequate access
standard described in section 50.4, the long-term care pharmacy convenient access
standard described in section 50.5, and the I/T/U pharmacy convenient access standard
described in section 50.6 will only have to provide access to non-network pharmacies
consistent with CMS’ out-of-network access policy as described in section 60. In other
words, they will be treated in the same way as all other Part D plans vis-à-vis the access
requirements in sections 50.1, 50.4, 50.5, and 50.6.
2. PFFS plans offering Part D coverage will not have to meet the retail pharmacy
convenient access standards described in section 50.1, the home infusion adequate access
standard described in section 50.4, the long-term care pharmacy convenient access
standard described in section 50.5, and the I/T/U pharmacy convenient access standard
described in section 50.6– either because they do not contract with any network of
pharmacies, or because they contract with a limited network that does not meet the
relevant regulatory access requirements – if they provide access to covered Part D drugs
at all pharmacies without charging beneficiaries any additional cost-sharing (relative to
the cost-sharing applicable at any network pharmacies the plan may have). Access at
non-network pharmacies would be provided by reimbursing the pharmacy its usual and
customary (U&C) price, minus any applicable beneficiary cost-sharing.

In effect, PFFS plans offering Part D coverage have the following options:
• Create a network that meets CMS’ regulatory access standards and limits access to out-
of-network providers consistent with CMS’ regulatory provisions regarding out-of-
network access;
• Create a network that does not meet CMS’ regulatory access standards and provides
access to all non-network pharmacies by not charging additional cost-sharing for drugs
obtained at non-network pharmacies; or
• Not create a network at all but provide access to all pharmacies at the same cost-sharing.
PFFS sponsors choosing to have either no contracted pharmacy network or a limited pharmacy
network that does not meet CMS’ pharmacy access requirements must ensure that their enrollees
are able to access their benefits at all non-network pharmacies without paying any more cost-
sharing than they would under their approved Part D benefit structure.
When accessing their drugs at non-network pharmacies in non-emergent situations, enrollees of
PFFS plans that have received waivers of the pharmacy access standards will pay only their
required cost-sharing at the point of sale. Moreover, such claims should be adjudicated
electronically whenever pharmacies support electronic billing. In other words, PFFS sponsors
with pharmacy access waivers should not routinely rely on billing practices that require an
enrollee to pay U&C price upfront and then submit a paper claim to the sponsor for
reimbursement.
CMS notes that sponsors are required to accurately track TrOOP and gross covered drug spend
amounts in order to correctly position an enrollee in the benefit. As indicated in chapter 14 of
this manual, plans are required to process claims in real-time and track TrOOP in real-time.
Consistent with those requirements, sponsors – including PFFS sponsors –receiving waivers of
the pharmacy access standards – must establish policies and procedures appropriately restricting
the use of paper claims only to situations in which online claims processing is not available at the
point of sale in order to promote accurate TrOOP accounting, to minimize administrative costs to
Part D sponsors and the Medicare program, as well as opportunities for fraudulent duplicate
claims reimbursement. Therefore, PFFS sponsors choosing to obtain a waiver rather than meet
CMS’ pharmacy access requirements must arrange for automated, online billing at non-network
pharmacies (similar to the way in which CMS’s point-of-sale contractor has allowed for online
billing by non-contracted pharmacies).
50.8 - Pharmacy Network Contracting Requirements
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
In establishing its contracted pharmacy network, a Part D sponsor must meet certain
requirements with respect to any willing pharmacy and insurance risk, as described in sections
50.8.1 and 50.8.2 below.

50.8.1 - Any Willing Pharmacy Requirement
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
“Any willing pharmacy” refers to the requirement that Part D sponsors permit the participation in
their Part D plan networks of any pharmacy – including non-retail pharmacies such as mail-order
pharmacies – that is willing to accept the sponsor’s standard contracting terms and conditions.
These standard contracting terms and conditions must be reasonable and relevant. However,
whether a Part D sponsor has permitted a pharmacy an opportunity to participate in its network,
or whether a pharmacy can meet or has met contract terms in compliance with the law and CMS’
regulations at 42 CFR 423.120(a)(8)(i) are fact-specific questions that are generally best left
between the parties.
It is unlikely that a Part D sponsor could establish a network using a uniform set of terms and
conditions throughout a service area because it will likely need to modify contracting terms and
conditions to ensure access to certain pharmacies – for example, rural and long-term care
pharmacies. Standard terms and conditions, particularly for reimbursement terms, may vary to
accommodate geographic areas or types of pharmacies, and that this is acceptable, provided that
all similarly situated pharmacies are offered the same standard terms and conditions. Thus, for
example, provided a Part D sponsor offers all mail-order pharmacies in a particular area with the
same standard terms and conditions, it may offer separate standard terms and conditions to mail-
order pharmacies than it does to retail pharmacies. With standard terms and conditions as a
“floor” of minimum requirements that all similarly situated pharmacies must abide by, Part D
sponsors may modify some of their standard terms and conditions to encourage participation by
particular pharmacies.
The any willing pharmacy requirement is waived for certain MA-PD plans or cost plans that
provide access (other than via mail order) to qualified prescription drug coverage through retail
pharmacies owned and operated by the MA organization that offers the plan or the cost plan. In
order to obtain this waiver of the any willing pharmacy requirement, an MA organization or cost
plan sponsor must generally demonstrate at the plan level that at least 98 percent of enrollee
prescriptions have been filled through pharmacies that are owned and operated by the plan
sponsor in order to be granted the waiver.
Some pharmacies, particularly independent pharmacies, work with agents or Pharmacy Services
Administration Organizations (PSAO) for purposes of negotiating and/or signing contracts with
Part D sponsors. Such agents negotiate and/or sign contracts with health plans and PBMs on
behalf of participating pharmacies to streamline the contracting process. To the extent that such
agents are authorized to act on behalf of a participating pharmacy for purposes of negotiating
and/or signing pharmacy network contracts, there is no distinction between a pharmacy and its
agent for purposes of the any willing pharmacy requirement. In other words, the any willing
pharmacy requirement at 42 CFR 423.120(b)(8)(i) extends to an agent authorized to negotiate
and/or sign contacts on behalf of a pharmacy, as long as it is in compliance with all Federal and
State laws. A Part D sponsor will be in violation of this requirement if it refuses to offer a
standard contract to an agent acting on behalf of a participating pharmacy for purposes of
negotiating and/or signing contracts. However, Part D sponsors that currently have independent
contracts with pharmacies belonging to a PSAO are only required to offer standard terms and

conditions to those pharmacies under the PSAO with no preexisting contract with the Part D
sponsor.
50.8.2 - Insurance Risk
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
A Part D sponsor may not require a network pharmacy to accept insurance risk as a condition of
participation in its pharmacy network. Insurance risk in relation to a network pharmacy refers to
risk of the type commonly assumed only by insurers licensed by a State, but not including
payment variations designed to reflect performance-based measures of activities within the
control of a pharmacy, such as formulary compliance and generic drug substitutions, or elements
potentially in the control of the pharmacy (for example, labor costs, and productivity).
More specifically, subcapitation of pharmacies is not allowed in Part D sponsor administration of
the Part D benefit. If the only contract Part D sponsors offered a pharmacy were a capitated
arrangement, this practice would equate to requiring a pharmacy to accept risk. Second, and
more importantly, subcapitated arrangements are inconsistent with the four payment mechanisms
CMS is required to use to pay plans. Part D plans must be able to report costs to CMS that
distinguish beneficiary liabilities (e.g., for TrOOP accounting and accumulation); low-income
cost-sharing subsidy payments made at the individual beneficiary level by plans to pharmacies;
costs that are considered supplemental benefits at the individual beneficiary level (supplemental
drugs and supplemental cost-sharing); and allocation of plan costs above and below the out-of-
pocket threshold at the individual beneficiary level and that subject the plan to different levels of
risk-sharing depending on which phase of the drug benefit the beneficiary is in. If the plan's
providers do not process and submit meaningful claims, this data is not available to compute
these payment streams as mandated by law. Finally, subcapitated payments to certain
pharmacies (e.g., home infusion, long-term care, and other non-retail pharmacies) could include
payment for services (e.g., clinical professional services and extensive fees for administering
drugs to patients) that are not allowed under the Part D benefit.
50.9 - Differential Cost-Sharing for Preferred Pharmacies
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
Despite the “any willing pharmacy” requirement (discussed in section 50.8.1), Part D sponsors –
with the exception of those offering defined standard coverage, since cost-sharing cannot be
altered under defined standard coverage – are permitted to reduce cost-sharing differentially for
network pharmacies. In other words, Part D sponsors may vary cost-sharing not only based on
type of covered Part D drug or formulary tier, but also on a particular pharmacy’s status within
their pharmacy network (i.e., Part D sponsors may establish distinctions between “preferred” and
“non-preferred” pharmacies within
their pharmacy networks).
While these within-network distinctions are allowed, such tiered cost-sharing arrangements must
in no way increase CMS payments to Part D sponsors. Therefore, tiered cost-sharing
arrangements based on within-network distinctions can only be included in Part D sponsors’
benefits subject to the same actuarial tests that apply to formulary-based tiered cost-sharing
structures. Thus, a reduction in cost sharing for preferred pharmacies in a Part D sponsor
network could be offered through higher cost sharing for non-preferred pharmacies (or as
alternative prescription drug coverage).
In other words, sponsors cannot designate certain network pharmacies as preferred without
designating its other network pharmacies as non-preferred. A pharmacy can only be designated
as preferred if it offers enrollees a lower level of cost-sharing than a non-preferred pharmacy.
This means that the differences in cost-sharing must be based on the designated cost-sharing
levels, and not on the actual cost to the enrollee, as illustrated in the examples below.
Example 1
: A sponsor with a benefit design based on coinsurance could offer 20%
coinsurance at preferred pharmacies and 25% coinsurance at non-preferred pharmacies.
Example 2
: A sponsor with a benefit design based on copayments could offer a $20
copayment at preferred pharmacies and a $25 copayment at non-preferred pharmacies.
CMS will permit plans to refer to non-preferred pharmacies as “other network pharmacies”
instead of “non-preferred pharmacies” in their marketing materials and other beneficiary
communications.
Differential cost-sharing in the context of preferred and non-preferred pharmacies does not raise
the cost-sharing obligation of low-income subsidy eligible enrollees above the levels specified in
42 CFR 423.782.
A Part D sponsor may not establish a differential between cost-sharing at preferred versus non-
preferred pharmacies that is so significant as to discourage enrollees in certain areas (rural areas
or inner cities, for example) from enrolling in that Part D plan – even if it otherwise meets the
retail access standards detailed in section 50.1. A pharmacy network that effectively limits
access in portions of a Part D sponsor’s service areas in this manner would be discriminatory and
disallowed as provided in
42 CFR 423.272.
50.10 - Level Playing Field Between Mail-Order and Retail Pharmacies
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Part D sponsors that include mail-order pharmacies in their networks must permit enrollees to
receive benefits, which may include an extended supply of covered Part D drugs (for example, a
90-day supply), through a network retail pharmacy rather than a network mail-order pharmacy, if
they so choose. However, a sponsor may require that enrollees choosing to receive benefits,
including an extended day supply of covered Part D drugs, at a network retail pharmacy rather
than a network mail-order pharmacy be responsible for any higher cost-sharing associated with
obtaining those benefits at a network retail pharmacy.
If a sponsor does choose to charge the beneficiary the higher cost-sharing associated with
obtaining the drug through a retail pharmacy, any increase in cost sharing must be limited to the
“differential in charge” to the sponsor in terms of any difference between higher contract rates at
a network retail pharmacy as opposed to a network mail-order pharmacy for that benefit.
Sponsors may therefore require an enrollee to pay higher cost-sharing up to an amount equal to
the mail-order cost-sharing plus any differential in contracted rates between retail and mail-
order, but plans may charge beneficiaries a lower cost sharing at retail if they so choose. This
differential in charge-based cost-sharing should be viewed as a ceiling on cost-sharing and not a
floor. In addition, Part D sponsors must ensure that the availability of benefits (including
extended day supplies) at retail rather than mail-order pharmacies does not increase costs to the
government. Enrollee cost-sharing for an extended-day supply at retail must never exceed what
the enrollee would have paid at the same retail pharmacy had the enrollee had his or her
prescription filled in multiple 1 month supply increments at retail pharmacy rates.
Sponsors electing to offer extended supplies of covered Part D drugs must make available to
retail pharmacies, on request, an “Extended Supply Addendum” to their standard contracting
terms and conditions for retail pharmacies. The addendum may allow retail pharmacies to offer
an extended supply of drugs to any enrollee at the same negotiated price, reimbursement rate
(including dispensing fee, if any), and cost-sharing as their network mail-order pharmacy or
pharmacies. CMS refers to this rate as the network mail-order pharmacy rate.
Alternatively, Part D sponsors electing to offer extended supplies of covered Part D drugs may
through their addendum allow retail pharmacies to dispense an extended supply of drugs for a
higher contracted reimbursement rate (including dispensing fee, if any) than their network mail-
order pharmacy rate. At the sponsor’s election, any differential in charge between the network
mail-order pharmacy rate and the higher contracted reimbursement rate for the extended supply
dispensed at the retail pharmacy may be reflected in higher cost-sharing paid by the beneficiary.
CMS refers to this rate as the alternative retail/mail-order pharmacy rate. Any such higher
contracted reimbursement rate shall not increase costs to the government and in no event shall
the standard terms and conditions offered to similarly situated pharmacies with respect to CMS’
any willing pharmacy provisions vary.
Below are two examples of contracting scenarios designed to illustrate the calculation of a
“difference in charge.”
Example 1
: Network Mail Order Pharmacy Rate
Suppose that a network pharmacy’s contracted retail rate is AWP-12% plus a $2
dispensing fee, and the plan’s retail cost-sharing requires 25% to be paid by the
beneficiary. Further suppose that the plan’s contracted mail-order rate is AWP-22%,
with no dispensing fee and that the plan’s mail-order cost sharing requires 20% to be paid
by the beneficiary. If the sponsor offers a 90-day supply at network mail-order
pharmacies, any retail pharmacy must be allowed to fill a 90-day prescription under the
same terms and conditions as the mail-order pharmacy provided it agrees to accept the
network mail-order pharmacy rate for that 90-day prescription – AWP – 22% (no
dispensing fee) with 20% cost sharing paid by the beneficiary.
AWP = $100
Retail Rate
Network Mail Order Rate
AWP – 12%
$88
AWP – 22%
$78
Dispensing Fee
$2
Dispensing Fee
$0
Total
$90
Total
$78
Retail beneficiary cost
sharing paid to pharmacy
(25%)
$22.50
Mail order beneficiary cost
sharing paid to pharmacy (20%)
$15.60
Plan payment to
pharmacy
$67.50
Plan payment to pharmacy
$62.40
Example 2
: Alternative Retail / Mail Order Pharmacy Rate
A Part D sponsor may establish an alternative retail/mail-order pharmacy rate for an
extended supply for retail pharmacies that cannot or will not match the network mail-
order pharmacy rate for the extended supply prescription. Suppose under this scenario,
the retail pharmacy could not match the network mail-order pharmacy rate for a 90-day
prescription (see example 1), but would accept an alternative retail/mail-order pharmacy
rate of AWP -19% (plus $2.00 dispensing fee). In this case, the sponsor could allow a
retail pharmacy to fill the 90-day prescription at the alternative retail/mail-order
pharmacy rate. The sponsor also may charge the beneficiary the difference in charge
between the network mail-order pharmacy rate for that 90-day prescription and the
alternative retail/mail-order pharmacy rate for a 90-day prescription. In this example, the
retail pharmacy would be reimbursed AWP -19% plus $2.00 and the beneficiary would
have to pay 3% of AWP plus $2.00, which would be added to the 20% cost sharing
calculated on AWP – 22%. (As stated earlier, this difference in charge-based cost-sharing
would be a ceiling, but not a floor – in other words, the cost-sharing paid at retail could
not exceed the amount described in the previous sentence, but it could be lower than such
amount.)
AWP = $100
Network Mail Order Rate
Alternative Retail / Mail
Order Pharmacy Rate
AWP – 22%
$78
AWP – 19%
$81
Dispensing Fee
$0
Dispensing Fee
$2
Total
$78
Total
$83
Beneficiary cost sharing
paid to pharmacy (20%)
$15.60
Beneficiary cost sharing based
on mail order rate (20%)
$15.60
Difference in charge
$5
Total beneficiary payment to
pharmacy
$20.60
Plan payment to pharmacy
$62.40
Plan payment to pharmacy
$62.40
NOTE
: These examples are not intended to provide guidance on specific prices or contract rates
that plans should or should not consider in contracting with pharmacies.
Part D sponsors offering benefits, including extended-day supplies of covered Part D drugs, at
network mail-order pharmacies must offer retail pharmacies a reasonable opportunity to provide
those same benefits. Part D plans must therefore contract with a sufficient number of network
retail pharmacies so as to ensure that enrollees have reasonable access to the same extended day

supply benefits at retail that are available at mail-order. CMS will review the adequacy of initial
pharmacy network submissions and may require that plans address any network access issues as
part of this review. CMS may conduct additional reviews of a Part D sponsor’s pharmacy
network and may require remedial action by Part D sponsors based upon such factors as enrollee
complaints that their access to benefits at network retail pharmacies is being unreasonably
denied. Part D sponsors will be required to provide CMS with data on an annual basis on the
number of retail pharmacies in their networks contracted to provide extended day supply
benefits. For more information about these reporting requirements, refer to:
http://www.cms.hhs.gov/PrescriptionDrugCovContra/08_RxContracting_ReportingOversight.as
p#TopOfPage
50.11 - Use of Identification Card for Accessing Negotiated Prices
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Part D sponsors must issue (and reissue, as appropriate) a card or other technology for enrollees
to use in accessing negotiated prices for covered part D drugs. CMS has developed standards
related to a standardized format for a plan identification card for this purpose. These standards
were developed after consultation with the NCPDP and are summarized in our Marketing
Guidelines, which can be accessed at:
http://www.cms.hhs.gov/PrescriptionDrugCovContra/12_PartDManuals.asp#TopOfPage
50.12 - Pharmacy Access During a Federal Disaster or Other Public Health
Emergency Declaration
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
If a Presidential major disaster or emergency declaration is issued or the Secretary declares a
public health emergency, and the underlying circumstances are reasonably expected to result in a
disruption in access to covered Part D drugs, CMS expects sponsors to lift their “refill-too-soon”
edits. Part D sponsors may exercise some operational discretion as to how these edits are lifted
during a disaster or emergency as long as access to Part D drugs is provided at the point-of-sale.
For instance, Part D sponsors could implement an edit that is readily resolvable at the point-of-
sale through the use of a pharmacist override code. CMS also expects Part D sponsors to allow
an affected enrollee to obtain the maximum extended day supply, if requested and available at
the time of refill.
CMS expects that Part D sponsors will continue to lift these edits until the termination of a
public health emergency or the end of a declared disaster or emergency. In the case of a public
health emergency, it terminates when it no longer exists or upon the expiration of the 90-day
period beginning from the initial declaration, whichever occurs first. For major disasters
declared by the President, Part D sponsors should pay particular attention to the closure of
disaster incident periods listed in the Disaster Federal Register Notice section on Federal
Emergency Management Agency’s (FEMA’s) Web site
http://www.fema.gov/news/disasters.fema, noting that in circumstances in which the incident
period has not officially closed 30 days from the initial Presidential declaration. Part D sponsors
may consider extending the implementation of the edits but are not required to do so. However,
if sponsors choose to remove the edits, they need to work closely with enrollees who indicate
that they are still displaced or otherwise impacted by the disaster or emergency.

In the absence of a Presidential major disaster or emergency declaration or a public health
emergency, Part D sponsors may consider lifting the edits -- for instance, in advance of an
impending disaster -- if they determine it is appropriate to do so to ensure pharmacy access.
However, at all times, and especially in disaster and/or public health emergency situations, Part
D sponsors must ensure, consistent with this chapter, that their enrollees have adequate access to
covered Part D drugs dispensed at out-of-network pharmacies when those enrollees cannot
reasonably be expected to obtain covered Part D drugs at a network pharmacy, and when such
access is not routine.
50.13 - Drug Shortages
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
This section describes the expectations of Part D sponsors when shortages impact the offering of
drug products on plan formularies. By “shortages”, CMS is referring to those drug products that
have been identified on the FDA Drug Shortage Webpage:
http://www.fda.gov/Drugs/DrugSafety/DrugShortages/default.htm
When establishing policies and procedures to address shortages, Part D sponsors should not
adopt a one-size-fits-all approach. Drug shortages may occur for differing reasons and impact
Part D sponsor application of its formulary in different ways. Therefore, when a drug shortage
occurs, Part D sponsors should begin by considering the type of drug involved, condition(s)
being treated by the drug, expected length of the drug shortage, and which enrollees are
impacted. Based on this information, Part D sponsors can work with their enrollees and
providers to find appropriate therapeutic alternatives. The Part D sponsor will need to evaluate
the availability (or unavailability) of therapeutically equivalent drug products. Different
scenarios to be addressed include:
• A single-source formulary brand drug product is temporarily unavailable—no
therapeutically equivalent products are available;
• A multiple-source formulary brand drug product is temporarily unavailable—only
therapeutically equivalent generic products are available;
• A multiple-source formulary generic drug product is temporarily unavailable (all
makers)—only therapeutically equivalent brand product is available; or
• A multiple-source formulary drug product is temporarily unavailable—no brand or
generic therapeutically equivalent product is available.
In order to minimize unnecessary changes in therapy resulting from temporary shortages of
multiple-source formulary drug products, CMS expects Part D sponsors to provide access to
therapeutically equivalent non-formulary drug products, or therapeutically equivalent formulary
drug products that otherwise require prior authorization or step therapy, for those enrollees
currently taking the drug product subject to a shortage. When applicable, Part D sponsors should
allow pharmacies to utilize a value of “8” in field 408-D8 (Dispense as Written/Product
Selection Code) of the NCPDP v5.1 Telecommunication Standard to specify that an equivalent

brand product is being dispensed due to the unavailability of any generic formulary products.
The Part D sponsor is not required to charge the same cost-sharing that applies to the unavailable
formulary product and may charge the applicable non-formulary or brand cost-sharing that
would otherwise apply to the substituted therapeutically equivalent product.
Under these circumstances, CMS does not consider access to therapeutically equivalent non-
formulary drug products, or therapeutically equivalent formulary drug products that otherwise
require prior authorization or step therapy, to be formulary exceptions and, therefore, access to
such drug products may be limited to the duration of the shortage. In the event that the shortage
becomes a market withdrawal, Part D sponsors must follow notice requirements consistent with
42 CFR 423.120(b)(5) if the Part D sponsor intends to discontinue coverage of the
therapeutically equivalent product. This policy does not preclude a beneficiary from seeking a
non-formulary or tiering exception to obtain access to a non-formulary drug product or
formulary drug product otherwise requiring prior authorization or step therapy.
50.14 - Waivers for Plans in the Territories
(Rev. 8, Issued: 12-18-09, Effective/Implementation: 01-01-10)
To ensure access to coverage in the territories, section 1860D-42(a) of the Act grants CMS the
authority to waive access requirements to secure access to qualified prescription drug coverage
for Part D eligible individuals residing in the territories. The regulations for the MMA under
42CFR 423.859(c) allow access to coverage in the territories to be waived or modified either
through an Applicant’s request or at CMS’ own determination. Under that authority, CMS has
waived the convenient access requirements for a plan’s Part D contracted retail, home infusion
and long-term care network in the Pacific territories.
60 - Out-of-Network Access
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
60.1 - Out-of-Network Pharmacy Access
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Part D sponsors must ensure that their enrollees have adequate access to covered Part D drugs
dispensed at OON pharmacies when those enrollees cannot reasonably be expected to obtain
covered Part D drugs at a network pharmacy, and when such access is not routine. The coverage
rules applicable to covered Part D drugs dispensed at OON pharmacies may generally mirror
those applicable to covered Part D drugs dispensed at network pharmacies, to the extent that the
OON pharmacy has the ability to effectuate those coverage rules. However, Part D sponsors
must develop policies and procedures governing reasonable rules for appropriately limiting OON
access (for example, quantity limits, purchase of maintenance medications via mail-order for
extended out-of-area travel, or plan notification or authorization processes). Following are
various scenarios under which CMS would expect that OON pharmacy access be guaranteed to
enrollees.
Example 1: An enrollee is traveling outside his or her Part D plan’s service area; runs
out of or loses his or her covered Part D drug(s) or becomes ill and needs a covered Part
D drug; and cannot access a network pharmacy.

Example 2
: An enrollee cannot obtain a covered Part D drug in a timely manner within
his or her service area because, for example, there is no network pharmacy within a
reasonable driving distance that provides 24-hour-a-day/7-day-per-week service.
Example 3
: An enrollee must fill a prescription for a covered Part D drug in a timely
manner, and that particular covered Part D drug (for example, an orphan drug or other
specialty pharmaceutical typically shipped directly from manufacturers or special
vendors) is not regularly stocked at accessible network retail or mail-order pharmacies.
Example 4:
An enrollee is provided covered Part D drugs dispensed by an OON
institution-based pharmacy while he or she is a patient in an emergency department,
provider-based clinic, outpatient surgery, or other outpatient setting, and as a result
cannot get his or her medications filled at a network pharmacy.
Example 5
: During any Federal disaster declaration or other public health emergency
declaration in which Part D enrollees are evacuated or otherwise displaced from their
place of residence and cannot reasonably be expected to obtain covered Part D drugs at a
network pharmacy. In addition, in circumstances in which normal distribution channels
are unavailable, Part D sponsors are expected to liberally apply their OON policies to
facilitate access to medications.
If a Part D sponsor offers coverage other than defined standard coverage, it may require enrollees
to not only be responsible for any cost-sharing, including a deductible, that would have otherwise
applied if a covered Part D drug had been purchased at a network pharmacy, but also any
differential between an OON pharmacy’s (or provider’s) U&C price and the plan allowance.
Given the cost-sharing requirements for defined standard coverage, under which the cost-sharing
between the deductible and initial coverage limit must always be 25 percent of the actual cost of
a drug at the point of sale (see section 20.3.1), Part D sponsors offering defined standard
coverage may not charge enrollees the OON differential described above. Instead, Part D
sponsors offering defined standard coverage must simply require their enrollees to pay any
deductible or cost-sharing, relative to the OON pharmacy’s (or provider’s) U&C price. The Part
D sponsor will pay the difference between the OON pharmacy’s (or provider’s) U&C price and
the enrollee’s cost-sharing.
In either case, enrollees will likely be required to pay more for a covered Part D drug purchased
OON than one purchased at a network pharmacy. However, as explained in section 30.1, any
OON differential that an enrollee is required to pay for purchases made consistent with a Part D
sponsor’s OON access policy will count toward his or her TrOOP balance. CMS will pay the
OON differential, as applicable, for appropriate OON purchases of covered Part D drugs for
individuals receiving the low-income subsidy.
Sponsors may not routinely allow more than a month’s supply of medication to be dispensed at
an OON pharmacy. In creating their out-of network benefit structure, sponsors may choose one
of the following options:
• The plan’s network cost-sharing;
• The plan’s network cost-sharing plus the differential between the OON billed charge and
their network allowable charge (applicable to all benefit structures except defined
standard prescription drug coverage);
• The plan’s network cost-sharing with a limited days supply (this limited days supply
must be greater than or equal to 10 days); or
• The plan’s network cost-sharing plus the differential between the OON billed charge
and network allowable, with a limited days supply.
Plans may override the 1 month limit on a case-by-case basis when warranted by extraordinary
circumstances.
CMS expects that enrollees obtaining covered Part D drugs at an OON pharmacy consistent with
a Part D sponsor’s OON access policy may be required to pay the OON pharmacy’s U&C price
at the point-of-sale, submit a paper claim to the sponsor, and wait for reimbursement from the
sponsor as described above.
60.2 - Access to Vaccines
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Part D vaccines may be dispensed and administered in different settings (e.g., by pharmacists in
pharmacies, by physicians in physician offices) depending on factors such as State laws
regarding the administration of vaccines and product administration complexity. While access to
Part D vaccines via a network pharmacy is likely the best method for improving enrollees’
access to Part D vaccines, Part D sponsors must ensure that enrollees have adequate access to
Part D vaccines in physician offices when those Part D vaccines are appropriately dispensed and
administered in physician offices. Such access is considered OON access because sponsor
networks are defined as pharmacy networks only.
CMS recognizes, however, that the process of upfront payment by an enrollee and subsequent
reimbursement by his or her Part D plan described for OON purchases in section 60.1 may be
less feasible in the case of enrollees who require OON access to a vaccine in a physician’s office.
As new vaccines come on the market with indications for use in the Medicare population,
network Part D vaccine access will become more critical. To address this issue, CMS offers a
range of in-network and facilitated OON approaches, described in sections 60.2.1 and 60.2.2
below, for improving access to Part D vaccines appropriately administered and dispensed by a
physician without requiring upfront beneficiary payment and subsequent reimbursement by Part
D sponsors. Part D sponsors are not limited to these approaches and are encouraged to pursue
the implementation of any cost-effective, real-time billing option at the time of vaccine
administration. Additionally, Part D sponsors may consider adopting alternative approaches,
depending upon the vaccine and its respective cost, storage requirements, and complexity of
administration. Sponsors electing to implement one or more of the options discussed below must
still meet their obligation to generally provide OON access when appropriate – including through
upfront payment by an enrollee and subsequent reimbursement by his or her Part D plan.

The administration of a Part D-covered vaccine is included in the definition of a “Part D drug,”
effective January 1, 2008. Consequently, the Part D program covers vaccine administration costs
associated with Part D vaccines. For more information, refer to section 10.14 of chapter 6.
60.2.1 - In Network Vaccine Distribution Approaches
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
While CMS is in no way limiting Part D sponsors to any specific approach to ensuring access to
Part D vaccines, CMS believes that an in-network, real time solution is the best method to
improve vaccine access. In addition to the in-network options listed below, Part D sponsors
could reduce the burden of copayment collection by establishing a benefit design with zero cost-
sharing on vaccines.
1. In Network Retail Pharmacy Access
Enrollees could obtain a prescription from the physician and bring it to their local network
retail pharmacy for filling. In some States, it might be possible for the vaccine
administration to be provided by the pharmacist. Forty-eight States currently allow
pharmacists to provide some type of vaccinations. Where it is safe to dispense these vaccines
in the pharmacy, Part D sponsors could explore utilization of their network pharmacists as a
provider of adult Medicare Part D vaccines. Pediatric vaccines should continue to be
provided by physicians, however.
2. In Network Pharmacy Distribution
A Part D sponsor’s network pharmacy could provide vaccines directly to physician offices.
Under this scenario, the physician could call or fax in a prescription, or the beneficiary could
mail a prescription for the vaccine to the pharmacy. The pharmacy would fill the
prescription for the vaccine, deliver or ship to the physician’s office, and bill the Part D
sponsor for the vaccine. This model resembles the competitive acquisition program being
implemented by Medicare Part B in that the drug is shipped to the physician but the
physician never purchases or is reimbursed for the drug.
60.2.2 - Facilitated OON Access Approaches
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
While the following options are OON arrangements between physicians and Part D sponsors,
CMS expects that these and similar options will reduce the need for up-front beneficiary
payment by facilitating other forms of payment arrangements between physicians and Part D
sponsors, increasing access beyond the current regulatory OON requirements and avoiding the
incurring of significant OON costs by beneficiaries or CMS as part of the low-income subsidy.
1. Model Vaccine Notice for Physicians (Paper Claim Enhancement)
Under this option, Part D sponsors would provide all enrollees with a vaccine-specific notice
that the enrollees could bring to their physicians. This notice would provide information

necessary for a physician to contact the enrollee’s Part D plan to receive authorization of
coverage for a particular vaccine, reimbursement rates, enrollee cost-sharing to be collected
by the physician, and billing instructions. If the Part D sponsor authorizes payment, the
physician would then bill the Part D sponsor using the physician standard claim form or ASC
X12 electronic format (which Part D sponsors must accept) and would receive payment
directly from the Part D sponsor. Alternatively, physicians could access this information
directly by calling the sponsor’s prior authorization line.
2. Web-Assisted Electronic Physician Billing
Using a commercially-developed Web-based system based on the real-time NCPDP
standard, physicians could electronically request OON reimbursement from Part D sponsors
on behalf of beneficiaries for vaccines dispensed and administered in the physician’s office.
The physician would agree to accept Part D sponsor payment as payment in full as a
condition of using the system.
60.3 - Vaccine Administration
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
60.3.1 - Vaccine Administration Cost-Sharing Considerations
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Since the vaccine administration fee is a component of a vaccine’s negotiated price, any cost-
sharing applied to a vaccine should be applied relative to the negotiated price of the vaccine and
its related component costs. If a sponsor structures its vaccine cost-sharing as coinsurance,
including 100 percent cost-sharing in any applicable deductible or coverage gap, the coinsurance
should be applied relative to the entire negotiated price (including the vaccine administration
fee). Similarly, if a sponsor structures its vaccine cost-sharing as a copayment, the copayment
should be applied relative to the entire negotiated price. In other words, a sponsor should not
charge separate copayments for the vaccine ingredient cost and its related component costs,
respectively (i.e., the vaccine administration fee and dispensing fee, if applicable), since CMS
views the vaccine and its administration as intrinsically linked. Similarly, low income subsidy
eligible individuals with copayments set by statute (see section 1860D-14(a)(1)(D) of the Social
Security Act) will pay only one copayment for a vaccine and all related charges. Thus, for
example, a low income subsidy eligible individual entitled to $1.05/$3.10 copayments in 2008
would pay only $3.10 for both the vaccine and its administration (and any applicable dispensing
fee) even if the components are billed separately.
3
3
In cases involving defined standard coverage and out-of-network vaccine administration, cost-
sharing for a vaccine is based on the usual and customary price for both the vaccine ingredient
cost and vaccine administration fee. This is because, given the cost-sharing requirements for
defined standard coverage – under which the cost-sharing between the deductible and initial
coverage limit must always be 25 percent of the actual cost of a drug at the point of sale – Part D
sponsors offering defined standard coverage may not charge enrollees any out-of-network
differential. However, sponsors offering other benefit designs (e.g., actuarially equivalent
standard coverage, basic alternative coverage, or enhanced alternative coverage), may require
enrollees being administered a vaccine out-of-network (e.g., in a physician’s office) to be
responsible for any cost-sharing that would have otherwise applied had the drug been purchased
at a network pharmacy, and also any differential between the provider’s usual and customary

60.3.2 - Separate Billing of the Vaccine and Vaccine Administration
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Although CMS prefers that all Part D vaccines be billed on one claim for both the vaccine and its
administration, CMS recognizes there are circumstances that might require vaccine
administration to be billed and reimbursed separately from the vaccine. For example, a Part D
vaccine might have very specific storage conditions that would impede most physicians’ offices
from maintaining a ready inventory for their patients. It might be more efficient for the
physician to have a pharmacy dispense and deliver the vaccine for administration. The
pharmacy will submit the vaccine ingredient cost and dispensing fee to the Part D sponsor for
reimbursement and the physician will bill the beneficiary for the administration. Part D sponsors
should establish processes necessary to separately reimburse the pharmacy for the vaccine
ingredient cost/dispensing fee and the beneficiary for physician’s administration charge.
CMS has concerns about separate billing of Part D vaccines and vaccine administration fees
because it provides an opportunity for both inappropriate and duplicate billing of administration
fees. Separate billing is more challenging for Part D sponsors to process and track, and there is
greater potential for programmatic fraud and abuse when the vaccine and its administration are
not linked at time of reimbursement. Consequently, CMS strongly encourages Part D sponsors
to link billing of a vaccine and its administration wherever possible. Where this is not possible,
and separate billing occurs, CMS expects Part D sponsors to closely scrutinize the separate
claims to ensure the beneficiary has received reimbursement for both elements and that the
sponsor has neither over- nor underpaid for both the vaccine and the vaccine administration fee.
CMS plans on monitoring Part D sponsors to ensure that when separate billing does occur, there
is a reasonable correlation of prescription drug event (PDE) records for vaccines dispensed to
PDE records for vaccine administration.
60.3.3 - Claims Processing Considerations
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Part D sponsors will implement a process that helps ensure compliance with the Health Insurance
Portability and Accountability Act of 1996 (HIPAA) vaccine billing requirements. Under the
Tax Relief and Healthcare Act of 2006 (TRHCA), a “covered Part D drug” is defined to include
the vaccine and the administration of the vaccine. For purposes of billing for vaccines, Part D
vaccine administration therefore is unique. As defined by statute, the “drug” incorporates both
the vaccine and its administration. Consequently, billing of the Part D drug vaccine must be
conducted using the NCPDP 5.1 standard for both the vaccine and its administration. When the
administration is performed by the pharmacy or facilitated by the pharmacy through an
established relationship with physician or immunizer, the administration will be included in one
standardized field in the billing transaction as part of the vaccine prescription request to the Part
D sponsor.
4
price for the vaccine and vaccine administration fee and the plan allowance for the vaccine and
vaccine administration (see section 60.1).
In other words, the pharmacy should submit the vaccine and its administration, if
4
Relative to the establishment of relationships between pharmacies and immunizers, the parties
must ensure that such arrangements do not violate the physician self-referral (‘‘Stark’’)
they are involved with the administration, as a single claim and not as two separate claims.
NCPDP has issued formal guidance regarding the standardized field to be used for vaccine
administration in the billing transaction.
When administration is billed separately from the dispensing of the vaccine, Part D sponsors or
their subcontracted PBM should review existing claims for the presence of a vaccine charge.
Should no vaccine charge be present in their claims history, the Part D sponsor should work with
the beneficiary to ensure the beneficiary did not forget to submit a paper receipt for the vaccine
and that appropriate reimbursement has been paid. For example, a sponsor could generate a
letter to an enrollee whenever it receives a claim for a vaccine but does not receive a claim for
vaccine administration within a certain time period.
A new, unique vaccine administration field has been added to the PDE elements for Part D
sponsor submission of vaccine administration. This specific vaccine administration field allows
a one-to-one claim to PDE relationship. For instance, if a sponsor receives a single claim from a
network pharmacy inclusive of the vaccine and its administration it will need to attribute the
vaccine ingredient cost, dispensing fee (if applicable), and administration to the appropriate
fields of the PDE for submission to CMS. If separate billing by a pharmacy for the dispensing of
the vaccine and by a physician for its administration occurs, the sponsor will submit one PDE
based on the pharmacy claim inclusive of the vaccine and dispensing fee and a separate PDE
based on the out-of-network claim from the beneficiary inclusive of the vaccine administration
costs attributable to physician’s administration. For this second separate PDE, the vaccine
ingredient National Drug Code (NDC) would still be identified, but the vaccine ingredient cost
and dispensing fee would be set to zero dollars. The format will be published on
www.csscoperations.com.
60.3.4 - Vaccine Administration Access
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
Part D sponsors will allow any provider so authorized by State law to administer a Part D
vaccine. Where it is safe to dispense and administer vaccines in a pharmacy, sponsors could
explore utilization of their network pharmacists as providers of adult Medicare Part D vaccines
(pediatric vaccines should continue to be provided by physicians). Out-of-network vaccines
administered in a physician’s office or by other non-network providers may be covered under the
out-of-network access rules detailed in section 60.2, where a Part D enrollee may self-pay for the
vaccine cost and its administration and submit a paper claim for reimbursement to his or her Part
D sponsor.
70 - Public Disclosure of Pharmaceutical Prices for Equivalent Drugs
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Part D sponsors must ensure that their network pharmacies inform enrollees of any differential
between the price of a covered Part D drug to an enrollee and the price of the lowest priced
generic version of that drug that is an AB-rated alternative, therapeutically equivalent and
prohibition (section 1877 of the Act), the Federal anti-kickback statute (section 1128B(b) of the
Act), or any other applicable Federal or State law or regulation.

bioequivalent, on the plan’s formulary, and available at that pharmacy. This information must be
provided:
• At the time the plan enrollee purchases the drug, if the enrollee purchases that drug at a
pharmacy; or
• At the time of delivery of that drug, in the case of drugs purchased by mail order.
CMS may modify the timing requirement (i.e., at the time of purchase or delivery) when CMS
determines the requirement to be impossible or impracticable to administer.
However, disclosure of this information will not be necessary if the particular covered Part D
drug purchased by an enrollee was the lowest-priced generic version of that drug available at a
particular pharmacy.
The requirement that information on lowest-priced generic drug equivalents be provided to
enrollees for covered Part D drugs purchased by Part D plan enrollees is not applicable when
those covered Part D drugs are purchased at:
• Any pharmacy, when the individual is enrolled in an MA private fee-for-service plan that
offers qualified prescription drug coverage and provides plan enrollees with access to
covered Part D drugs dispensed at all pharmacies, without regard to whether they are
contracted network pharmacies, and does not charge additional cost-sharing for access to
covered Part D drugs dispensed at all pharmacies;
• Out-of-network pharmacies;
• I/T/U network pharmacies;
• Network pharmacies located in any of the U.S. territories (American Samoa, the
Commonwealth of the Northern Mariana Islands, Guam, Puerto Rico, and the Virgin
Islands); and
• A long-term care pharmacy.
80 - Privacy, Confidentiality, and Accuracy of Enrollee Records
(Rev. 1, Issued: 07-03-08, Effective: 07-03-08, Implementation: 07-03-08)
To the extent that a PDP offered by a PDP sponsor maintains medical records or other health
information regarding Part D enrollees, the PDP sponsor must meet the same requirements
regarding confidentiality and accuracy of enrollee records as MA organizations offering MA
plans must currently meet under 42 CFR 422.118. These requirements do not apply to PACE
organizations and cost plans offering qualified prescription drug coverage, since these plans are
subject to similar requirements under 42 CFR 460.200(e) and 460.210, and 42 CFR 417.486,
respectively.
Specifically, PDP sponsors must:

• Abide by all Federal and State laws regarding confidentiality and disclosure of medical
records or other health and enrollment information, including the Health Insurance
Portability and Accountability Act (HIPAA) of 1996 and the privacy rule promulgated
under HIPAA;
• Ensure that medical information is released only in accordance with applicable Federal
and State law;
• Maintain the records and information in an accurate and timely manner; and
• Ensure timely access by enrollees to records and information pertaining to them.
PDP sponsors are covered entities under the HIPAA Privacy Rule because they meet the
definition of “health plan” at 45 CFR 160.103. The Department of Health and Human Services
Office for Civil Rights (OCR) is responsible for administering and enforcing the HIPAA Privacy
Rule. OCR has authority to investigate complaints, to conduct compliance reviews, and to
impose civil money penalties for HIPAA Privacy Rule violations. Thus, any violations by a PDP
sponsor for its obligations under the Privacy Rule as a covered entity are subject to such
enforcement by OCR. OCR maintains a Web site with frequently asked questions and other
compliance guidance at: http://hhs.gov/ocr/hipaa
Part D sponsors, including both PDP sponsors and MA organizations, must effectively secure all
beneficiary information, whether in paper or electronic format. This includes ensuring that data
files are not saved on public or private computers when accessing corporate e-mail through the
Internet, ensuring staff are properly trained to safeguard information, and ensuring electronic
systems are properly programmed for beneficiary mailings to avoid inadvertent disclosures of
individually identifiable health information. All sponsors should either perform an internal risk
assessment or engage an industry-recognized security expert to conduct an external risk
assessment of the organization to identify and address security vulnerabilities. Weaknesses or
gaps in Part D sponsors’ security programs should be quickly remedied. Sponsors should
annually train staff on responsibilities and consequences of failing to secure sensitive beneficiary
information. Compliance with the HIPAA Security and Privacy rules must be documented and
kept current in response to environmental or operational changes affecting the security and
privacy of the electronic protected health information. In addition to HIPAA requirements,
sponsors should notify CMS immediately upon discovery of any security breach compromising
beneficiary personally identifiable information.
90 - Electronic Transaction Standards
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
When processing Part D claims, a Part D sponsor or its intermediary must comply with the
electronic transaction standards established by 45 CFR 162.1102, which sets forth the HIPAA
administrative simplification standards for health care claims.
A Part D sponsor must also require its network pharmacies to submit claims to the Part D
sponsor or its intermediary whenever the card described in section 50.11 is presented or on file

at the pharmacy unless the enrollee expressly requests that a particular claim not be submitted
to the Part D sponsor or its intermediary.
90.1 - Unique Benefit Identification Number (BIN)/Processor Control Number
(PCN) Provisions
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
For Part D claims with a dispensing date of January 1, 2012 and later, and submitted in,
National Council for Prescription Drug Programs (NCPDP) version D.O format, a Part D
sponsor must assign and exclusively use a unique:
• Part D cardholder identification number (RxID) for each Medicare Part D enrollee to
clearly identify Medicare Part D beneficiaries (other fields such as person code may not
be used to differentiate enrollees), and
• Part D BIN or RxBIN and Part D processor control number (RxPCN) combination in its
Medicare Part D line of business, unless non-exclusive use is expressly allowed by CMS
and industry standard coding.
5
Part D sponsors that do not support industry standard coding may only process Part D- covered
drug claims under the Part D unique BIN/PCN and must reject all other claims. (See section
90.1.2 below). The intent of the unique BIN/PCN provisions is to ensure: (1) that pharmacies can
routinely identify situations in which they are billing a Part D claim; and (2) that payers
secondary to Part D can properly coordinate benefits on Part D claims. These goals cannot
reliably be met if Part D claims cannot be distinguished from other types of pharmacy claims
through unique routing and beneficiary identifiers.
Industry standard coding provides a mechanism whereby, in limited circumstances, both non-
Part D Drugs and Part D drugs not covered by the plan may be submitted to and processed
under a Part D BIN/PCN. The industry standard coding requires Part D plans to clearly
indicate on the paid response whether the drug is a non-Part D Drug covered by a Part D plan
benefit structure or a Part D drug not covered by the Part D plan but processed under the Part
D BIN/PCN.
It should be noted that in order to use Part D routing identifiers, an organization must sponsor a
Part D plan. Thus, stand-alone Medicare Advantage plans should not use Part D routing
identifiers.
With respect to which level of the sponsor’s or the sponsor’s subcontractor’s organization the
unique routing identifier (“BIN” or “BIN/PCN” combination) should be assigned, the BIN or
BIN/PCN combination should uniquely identify the Part D line of business and correspond to a
payer sheet applicable solely to Part D processing requirements. This means that the BIN or
BIN/PCN combination must be exclusively used for Part D claims processing, and must be
supported by a payer sheet, regardless of whether the routing identifiers uniquely identify the
5
E.g., NCPDP Recommendations for Effective 4Rx Usage in Medicare Part D Processing,
Version 1.Ø, July 2011, NCPDP.
processor, the sponsor’s parent organization, or a subset of the sponsor’s business. Thus, one
BIN or BIN/PCN combination could represent multiple sponsors, as long as only Part D claims
are submitted to and processed under that identifier
90.1.1 - Alternate Identifiers/Crosswalking/Mapping
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Sponsors may not utilize the unique Part D identifiers “behind the scenes” in adjudicating
claims while providing different 4Rx data (the BIN, PCN, Group, and Cardholder ID identifiers)
to CMS through the MARx system enrollment-related transaction and on PDEs. The 4Rx data
submitted to CMS following enrollment, which supports the online real-time eligibility queries
(“E1 transactions”), must be the same data that pharmacies submit on claims and that the
processor uses to adjudicate claims and prepare PDEs. This way, the plan sponsor, its claims
processor, the pharmacy, the TrOOP facilitator, and any subsequent payers that wrap around
the Part D benefit can all accurately identify and manage Part D claims.
As of January 1, 2012, CMS does not permit the use of alternate identifiers on the inbound claim
that are subsequently crosswalked or otherwise mapped to the identifiers on record with CMS
and/or then converted into PDEs. When alternate identifiers have previously been utilized prior
to the implementation of this policy change, there may be initial disruption the first time a
pharmacy claim is submitted using the old identifiers, and it will be denied. However, the
correct identifiers should be readily available through the use of an E1 query or claim reject
responses processes as defined by industry standard. Once the proper identifiers have been
submitted, subsequent claims should not reject for invalid BIN/PCN/Group or Member ID.
CMS recognizes that some plans and processors do not use all 4 data elements of 4Rx
(BIN/PCN/GROUP/Cardholder ID) or may only use a portion of the characters for matching
purposes and as such expects that sponsors consult the industry standard on how to
communicate to CMS when certain data elements or values within a data element are not used.
90.1.2 - Sponsors that do not Support Industry Standard Coding to Distinguish
non-Part D-Covered Drugs
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
If a sponsor does not support industry standard coding as described above in this section, the
sponsors must not use the Part D BIN or RxBIN and Part D processor control number (RxPCN)
for the following type claims:
• Part B Claims
The Part D routing identifiers cannot be used to process Part B claims at point of sale when
the sponsor is a Medicare Advantage Organization or an MA-PD. Processing a Part B
claim as if it were a Part D claim will cause the pharmacy to pass the Part B claim to any
secondary payer or subsequent payers that coordinate benefits with Part D. This may result
in these other payers providing benefits that they are not authorized to provide.
• Co-Administration of Part D and Secondary Payer Benefits

Unique Part D routing identifiers may only be used to process co-administered primary Part
D and secondary payer benefits, such as when a sponsor contracts with both CMS for
primary Medicare Part D benefits and with an SPAP for secondary coverage, as long as the
sponsor is reasonably certain
that no other payers are liable to coordinate benefits on Part
D claims. (In the absence of independent knowledge of any such other payers, the sponsor
may rely upon the CMS Coordination of Benefits (COB) files for this information). In this
situation, the pharmacy would correctly treat the claim as a Part D claim, and no subsequent
payer would be at risk of inappropriate coordination of benefits. However, the sponsor takes
on additional risk in segregating and reporting the components of the one transaction
properly to the two respective payers, as well as ensuring that the transaction is HIPAA
compliant.
• Discount Card Transactions
The unique Part D routing numbers cannot be used to process discount card or other
transactions that extend Part D negotiated prices to non-covered drugs (Part D or
otherwise). Such use could lead pharmacies to misidentify such claims and apply Part D
rules, terms and conditions to non-Part D claims.
90.2 - Prescriber Identifiers
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Sponsors must report on PDE records one of the following four prescriber identifiers:
• NPI,
• DEA number
• UPIN
• State license number
Beginning January 1, 2012, sponsors must ensure these identifiers are active and valid.
Sponsors may not reject a pharmacy claim solely on the basis of an invalid prescriber identifier
in order to not impede Medicare beneficiary access to needed medications unless the issue can
be resolved at point of sale. In other words, sponsors may not reject a pharmacy claim at point
of sale without prompt follow-up to ensure that the claim has been resubmitted with a corrected
and valid prescriber identifier, or new information has been otherwise received to correct the
sponsor’s information. If this is not possible, pharmacies can fill prescriptions and sponsors can
pay the associated drug claims with an unvalidated prescriber ID at the point of sale. However,
sponsors are then responsible for verifying and reporting a valid prescriber ID on the PDE
record, and, whichever type of identifier is reported on the PDE, the identifier must be valid.
Therefore, if an active and valid prescriber ID is not included on the Part D claim, either the
sponsor, or the pharmacy if in accordance with the contractual terms of the network pharmacy
agreement, must follow up retrospectively to acquire a valid ID of one of the four acceptable
types before the PDE is submitted to CMS.
Follow-up may require review of the prescription, contact with the prescriber, use of the multiple
sources of state and federal data on providers, or the purchase of prescriber ID validation
services from a commercial vendor. Among the available state and federal sources are
individual state licensing board data on licensing and sanctions, Drug Enforcement Agency
registrant files, the Social Security Administration death file, OIG and state Medicaid program
excluded provider lists, and the CMS National Plan & Provider Enumeration System (NPPES)
database. Periodically updated files are available from these databases, in some cases directly
from these agencies, or otherwise through the Department of Commerce’s National Technical
Information Service (NTIS). In addition to these resources, CMS understands that multiple
commercial firms compile databases and offer services for validation of prescriber identifiers, so
an alternative approach would be for sponsors to purchase prescriber identifier validation
services from commercial vendors who already have access to these sources of data and are
currently providing these services to pharmacy, health plan, and pharmaceutical manufacturer
clients. Thus, sponsors have the option to either build their own systems or contract with
commercial vendors for prescriber ID validation services.
Although the requirement for validation of prescriber identifiers is imposed on Part D sponsors,
CMS expects that network pharmacies may either contractually agree to provide some of these
services themselves, or will fully support any retrospective review of the prescription and other
records necessary to identify the prescriber and obtain a valid identifier. Contractual
negotiations between sponsors/their agents and network pharmacies should address the terms
and conditions as to responsibilities for these processes and any penalties for failure to perform.
However, any requirement for a pharmacy to acquire and utilize its own automated validation
capability should be a result of mutual agreement between the parties, since such a requirement
may be impractical for many smaller pharmacy organizations. Also, CMS would expect that
pharmacies will have the opportunity to correct any invalid data before payment for a claim is
reversed whether or not the applicable contract delegates any sponsor duties.
90.2.1 - Foreign Prescribers
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Certain border states permit prescriptions from foreign (e.g., non-U.S. or U.S. territory licensed)
prescribers under their applicable pharmacy laws.
The only exception to the guidance in section 90.2 of this manual is that the identifier of a
foreign prescriber cannot practically be validated. Therefore, sponsors should use the license
number assigned by the foreign jurisdiction and report it on the PDE without validation against
any official database, if the Part D claim was submitted in a state that recognizes prescriptions
from foreign-located prescribers. By license number, CMS means the one assigned by an
appropriate licensing board in the foreign jurisdiction in which the prescriber practices/resides
on the claim with the State license qualifier.
90.2.2 - Beneficiary Requests for Reimbursement
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
Beginning 2012, a valid prescriber identifier must be reported on the PDE record of non-
standard format claims, such as requests for reimbursement (“paper” claims) submitted by
Medicare beneficiaries. Sponsors may require members to furnish the prescriber’s name and
address or phone number, or the pharmacy information, to assist the sponsor in obtaining the
prescriber ID. Once the prescriber or pharmacy contact information is acquired, the sponsor
must process the request for reimbursement and the sponsor, or the pharmacy (if doing so is in
accordance with its contract terms), must follow up retrospectively to acquire a valid ID.
Follow-up may entail a review of the prescription, prescriber contact, use of state or federal
data on providers, or purchase of prescriber ID validation services from a commercial vendor.
Payment to the beneficiary cannot be made dependent upon the sponsor’s acquisition of the
prescriber ID, itself. Sponsors may withhold reimbursement to the beneficiary only if there is a
reason to suspect fraud or if there are coverage issues. In the absence of fraud, if the sponsor is
unable to retrospectively acquire a valid prescriber ID, the sponsor may not seek recovery of the
Part D payment from the beneficiary.
90.2.3 - National Provider Identifiers (NPIs)
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
CMS will begin validating the format of all prescriber identifiers on PDEs that are coded as an
NPI and will exclude from payment reconciliation PDEs with invalid NPIs. CMS will also be
assessing each sponsor’s performance regarding NPI use and validity and will be notifying plan
sponsors of their performance level. While section 90.2 of this manual has specifically
addressed prescriber identifiers, CMS reminds both Medicare Advantage organizations and Part
D sponsors that they are also required to obtain valid provider NPIs on claims. NPIs may be
deactivated for reasons such as provider death or fraud related to identity theft and other forms
of fraud. The NPPES database is updated monthly to reflect these changes. Therefore, in
addition to verifying the reported NPI is valid, sponsors must also periodically confirm the
identifiers are active. In those instances when the NPI is found to have been deactivated,
sponsors must follow up with the provider to determine the reason for the deactivation.
90.2.4 - Controlled Substances
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
In 2012, sponsors are required to confirm the validity of DEA numbers on Schedule II-V drug
claims or map NPIs on these claims to the prescriber’s DEA numbers. In addition, sponsors will
be required to confirm that the controlled substance prescribed is consistent with the
prescriber’s DEA Schedule registration. As noted in section 90.2 of this manual, sources of state
and federal data on providers are available to support sponsor efforts in this regard in addition
to prescriber identifier validation services from commercial vendors. Sponsors should
understand that this requirement supports (and does not supersede or alter) existing pharmacy
obligations relative to DEA registrants under the Controlled Substances Act and DEA rules.
Appendix 1: Adequate Access to Network Home Infusion Pharmacies by
State/Territory and Contract Type
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)
State
MA-PD PDP & RPPO
Number of HI
Pharmacies
Needed to Meet
Adequate Access
for Full-State
Service Areas
Eligible
Beneficiaries to
HI Pharmacy
(Beneficiaries: HI
Pharmacy)
Number of HI
Pharmacies
Needed to Meet
Adequate Access
Eligible
Beneficiaries
to HI
Pharmacy
(Beneficiaries:
HI Pharmacy)
AK
2
59,500:1
2
59,500:1
AL
13
67,500:1
13
67,500:1
AR
7
84,500:1
7
84,500:1
AZ
10
96,000:1
8
108,000:1
CA
60
80,000:1
49
97,500:1
CO
9
72,000:1
9
72,000:1
CT
7
91,500:1
7
91,500:1
DC
2
75.000:1
2
75,000:1
DE
2
140,000:1
2
140,000:1
FL
24
139,000:1
25
133,500:1
GA
14
88,500:1
13
95,500:1
HI
2
193,500:1
2
193,500:1
IA
8
72,500:1
6
101,000:1
ID
3
106,500:1
3
106,500:1
IL
17
111,000:1
15
126,500:1
IN
12
87,500:1
12
87,500:1
KS
8
59,500:1
8
59,500:1
KY
18
43,000:1
18
43,000:1
LA
5
163,500:1
6
131,000:1
MA
12
92,500:1
11
102,000:1
MD
9
93,000:1
9
93,000:1
ME
3
126,500:1
3
126,500:1
MI
27
63,000:1
27
63,000:1
MN
10
83,000:1
9
93,500:1
MO
11
96,500:1
11
96,500:1
MS
4
159,000:1
4
159,000:1
MT
6
32,000:1
6
32,000:1
NC
21
73,500:1
19
80,000:1
ND
2
106,500:1
2
106,500:1
NE
9
34,000:1
8
39,000:1
NH
2
204,500:1
2
204,500:1
NJ
8
183,000:1
8
183,000:1
NM
5
73,500:1
5
73,500:1
State
MA-PD PDP & RPPO
Number of HI
Pharmacies
Needed to Meet
Adequate Access
for Full-State
Service Areas
Eligible
Beneficiaries to
HI Pharmacy
(Beneficiaries: HI
Pharmacy)
Number of HI
Pharmacies
Needed to Meet
Adequate Access
Eligible
Beneficiaries
to HI
Pharmacy
(Beneficiaries:
HI Pharmacy)
NV
10
36,500:1
10
36,500:1
NY
25
120,500:1
25
120,500:1
OH
18
108,000:1
18
108,000:1
OK
7
96,000:1
7
96,000:1
OR
5
145,500:1
5
145,500:1
PA
27
85,500:1
27
85,500:1
RI
4
59,500:1
4
59,500:1
SC
9
89,500:1
7
119,500:1
SD
2
131,500:1
2
131,500:1
TN
21
52,500:1
19
57,000:1
TX
40
75,500:1
34
90,000:1
UT
3
131,500:1
3
131,500:1
VA
14
83,000:1
13
89,500:1
VT
2
104,500:1
2
104,500:1
WA
12
82,000:1
12
82,000:1
WI
7
145,500:1
7
145,500:1
WV
6
74,500:1
4
124,500:1
WY
3
38,000:1
2
76,000:1
Territory
MA-PD PDP & RPPO
Number of HI
Pharmacies
Needed to Meet
Adequate Access
for Full-Territory
Service Areas*
Eligible
Beneficiaries to
HI Pharmacy
(Beneficiaries:
HI Pharmacy)
Number of HI
Pharmacies Needed
to Meet Adequate
Access*
Eligible
Beneficiaries
to HI
Pharmacy
(Beneficiaries:
HI Pharmacy)
AS
No defined
minimum
1 3500:1
GU
No defined
minimum
2
11,500:1
MP
No defined
minimum
No defined minimum
PR
3
315,500:1
2
630,500:1
VI
2
15,000:1
2
15,000:1
NOTE: Number of pharmacies listed above is based on the Beneficiary Data Count File (release
date January 4, 2011) used for the CY2011 Reporting Requirements & CY2012 Part D
Applications. The number of pharmacies needed to meet adequate access may change annually
based on beneficiary counts.
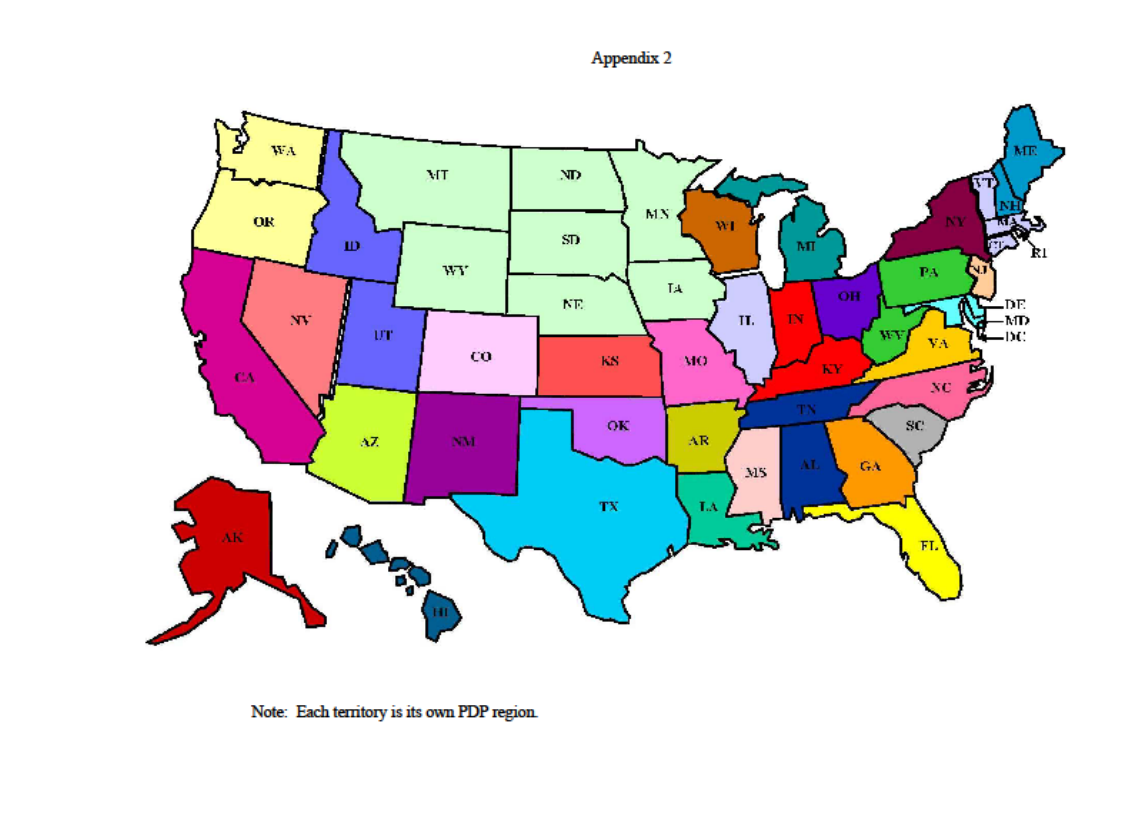
Appendix 2: PDP Regions
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)

Appendix 3: MA Regions
(Rev. 14, Issued; 09-30-11, Effective: 09-30-11, Implementation: 09-30-11)

Transmittals Issued for this Chapter
Rev #
Issue Date
Subject
Impl Date
CR#
R14PDB
09/30/2011
Chapter 5 - Benefits and Beneficiary Protections
09/30/2011
N/A
R5PDB
12/18/2009
Chapter 5 - Benefits and Beneficiary Protections
01/01/2010
N/A
R1PDB
07/03/2008
Initial release of chapter
07/03/2008
N/A
