

At Horizon, we’re guiding members to achieve
their best health.
For more than 90 years, Horizon has helped New Jersey residents get the most out
of their health care coverage. As a leader in providing access to quality, affordable
health plans, we offer an extensive provider network to ensure you’re cared for
whenever, wherever. We keep things simple – every New Jersey hospital is in our
network. Plus, we provide tools and support that make navigating health care easier.
Learn more at HorizonBlue.com/shbp
Health and wellness for mind and body.
Education Resources
Get tips for healthier living with our wide range of online
health education topics.
Pregnancy Resources
PRECIOUS ADDITIONS
®
offers personalized support and
interactive resources during pregnancy and beyond –
including My Pregnancy Assistant, an online tool powered
by WebMD
®
.
Health Management Tools
Manage your health and track your progress securely and
condentially with the digital coaching and customized
tools of MyHealth Manager, powered by WebMD.
HorizonbFit
SM
Eligible SHBP members may receive a $20 reward
1
for
every month they visit a tness facility, walk 10,000+ steps
or complete certain workouts for at least 12 days a month.
Wellness Discounts
With Blue365
®
, get weekly email deals from top retailers,
including gym memberships, nutrition programs, glasses,
contacts and more.
YMCA Discount
2
Get a 15% discount on monthly memberships at
participating New Jersey YMCAs – plus, new YMCA
members can have their initiation fee waived.
HorizonBlue.com/ymca
Walgreens Discount
2
SHBP members are eligble for 30% off Walgreens-
branded health and wellness products every time they
shop in store, online or through the Walgreens app.
HorizonBlue.com/walgreens
1. Rewards are taxable.
2. Restrictions and limitations apply. For more information, please visit the associated website links
above. Walgreens discounts available as of July 1, 2024.
Learn more at HorizonBlue.com/shbpLearn more at HorizonBlue.com/shbp
Achieve your best health and
earn rewards.
The NJWELL program is a great way to make meaningful
changes to your wellness habits with program enhancements
for eligible members and their covered spouse/partner.
NJWELL can help you achieve holistic well-being including:
• Physical tness
• Emotional balance
• Preventive care
• Social connection
• Financial security
Learn more about NJWELL at HorizonBlue.com/shbp/njwell
or visit the NJ Division of Pensions and Benets website at
nj.gov/treasury/pensions.
You can earn $250 or more in
rewards* each wellness year
(November 1 to October 31).
Rewards are taxable.
Our best coverage, for your best you.
OMNIA
SM
Health Plan
In addition to having some of our
best benets, our OMNIA Health
Plan Option gives you the exibility
to choose from one of New Jersey’s
largest networks: 70,000+ local
doctors, specialists and health
professionals and 95 hospitals in 115
convenient locations across New
Jersey and parts of Pennsylvania and
Delaware.* You also have worldwide
access to more than 2 million
providers in our BlueCard
®
PPO
program.
To save even more, choose from more
than 49,000 OMNIA Tier 1 doctors*
and some of the state’s leading
hospitals for lower copayments,
lower out-of-pocket costs and no
deductibles – all with no referrals and
no need to choose a Primary Care
Physician (PCP).
*Based on Horizon provider network data as of 10/23 and is subject to change.
PPO Plans
All of our PPO plans include:
• Care in network or out of network in
New Jersey, nationwide and abroad
• No need to select a PCP
• No referrals necessary to see a
specialist
• Lower out-of-pocket costs when
using the Horizon Managed Care
Network or the BlueCard PPO
Network nationwide and Blue Cross
Blue Shield Global
®
Core abroad
High Deductible PPO Plans
NJ DIRECT High Deductible Health
Plans (HDHPs) combine a high
deductible health plan with a health
savings account (HSA). Eligible
preventive services are covered at 100
percent if in network and do not have
a deductible. You are responsible
for eligible medical and prescription
expenses, up to the deductible.
HMO Plans
With our HMO plans, you have
access to health care professionals
and facilities in the Horizon Managed
Care Network in New Jersey and
parts of New York, Pennsylvania and
Delaware. You select a licensed PCP
from the Horizon Managed Care
Network and your PCP will refer you
to specialty care when needed. In
addition, the Away From Home Care
Program is available to eligible HMO
members who are outside the State of
New Jersey, like students living away
from home, long-term travelers and
families living apart.
Active employees:
Calculate your estimated
premium contribution at
HorizonBlue.com/shbp.
Learn more at HorizonBlue.com/shbp
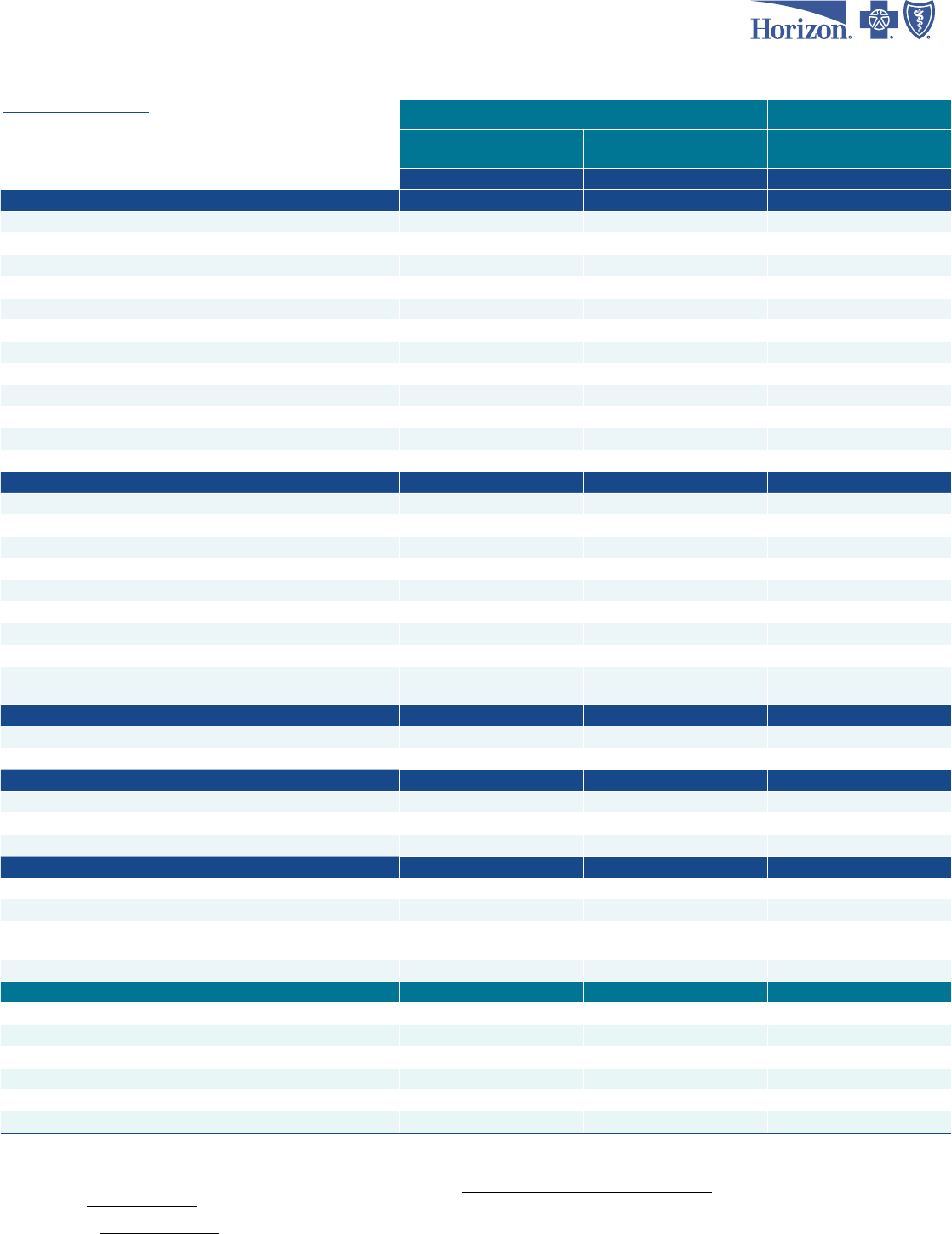
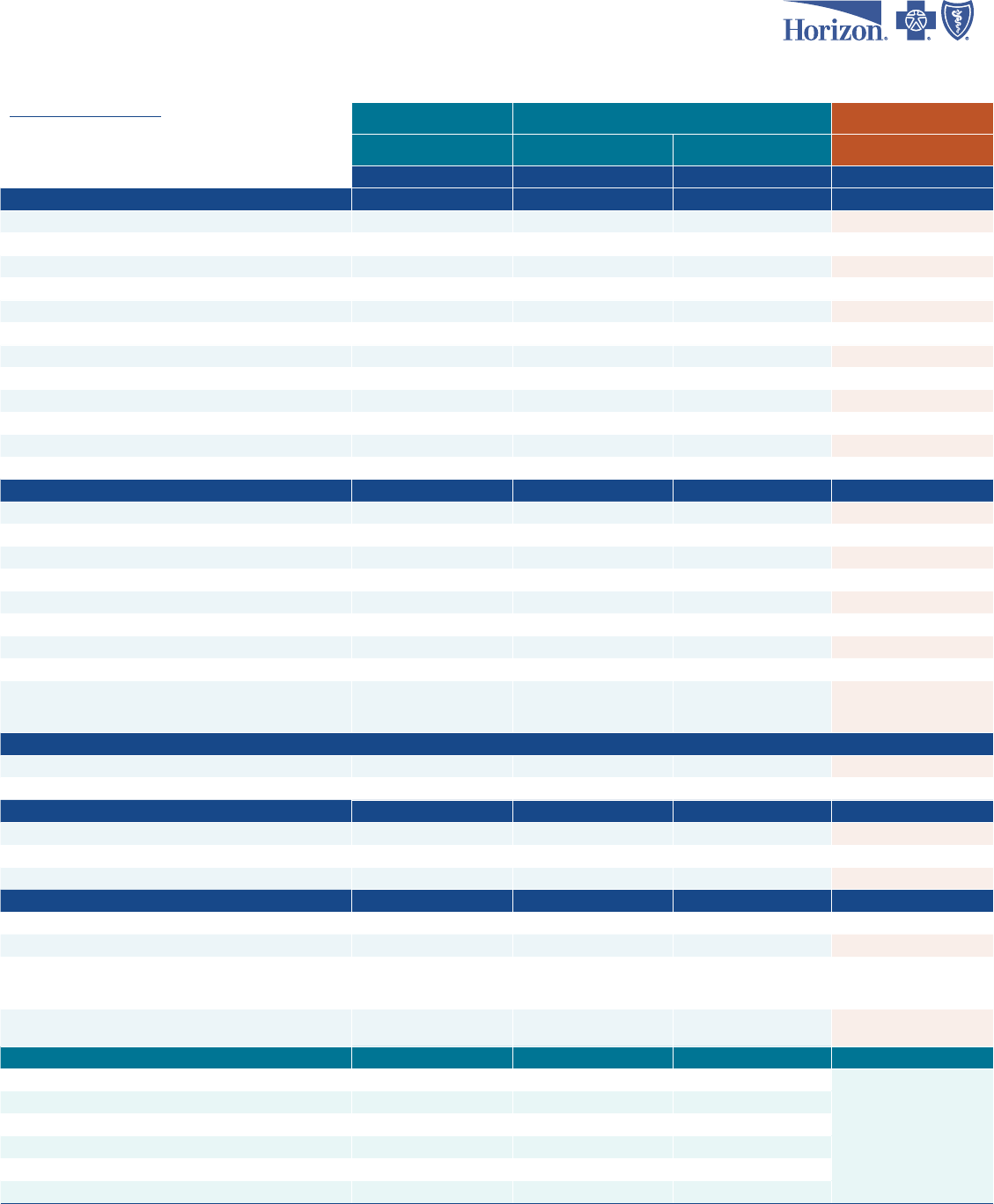
2024 NJ SHBP State and State College/University Employees
Plans for CWA and Union Negotiated Members
Plans effective 7/1/2024 (effective 6/29/2024 for biweekly employees)
HorizonBlue.com/shbp 1-800-414-SHBP (7427)
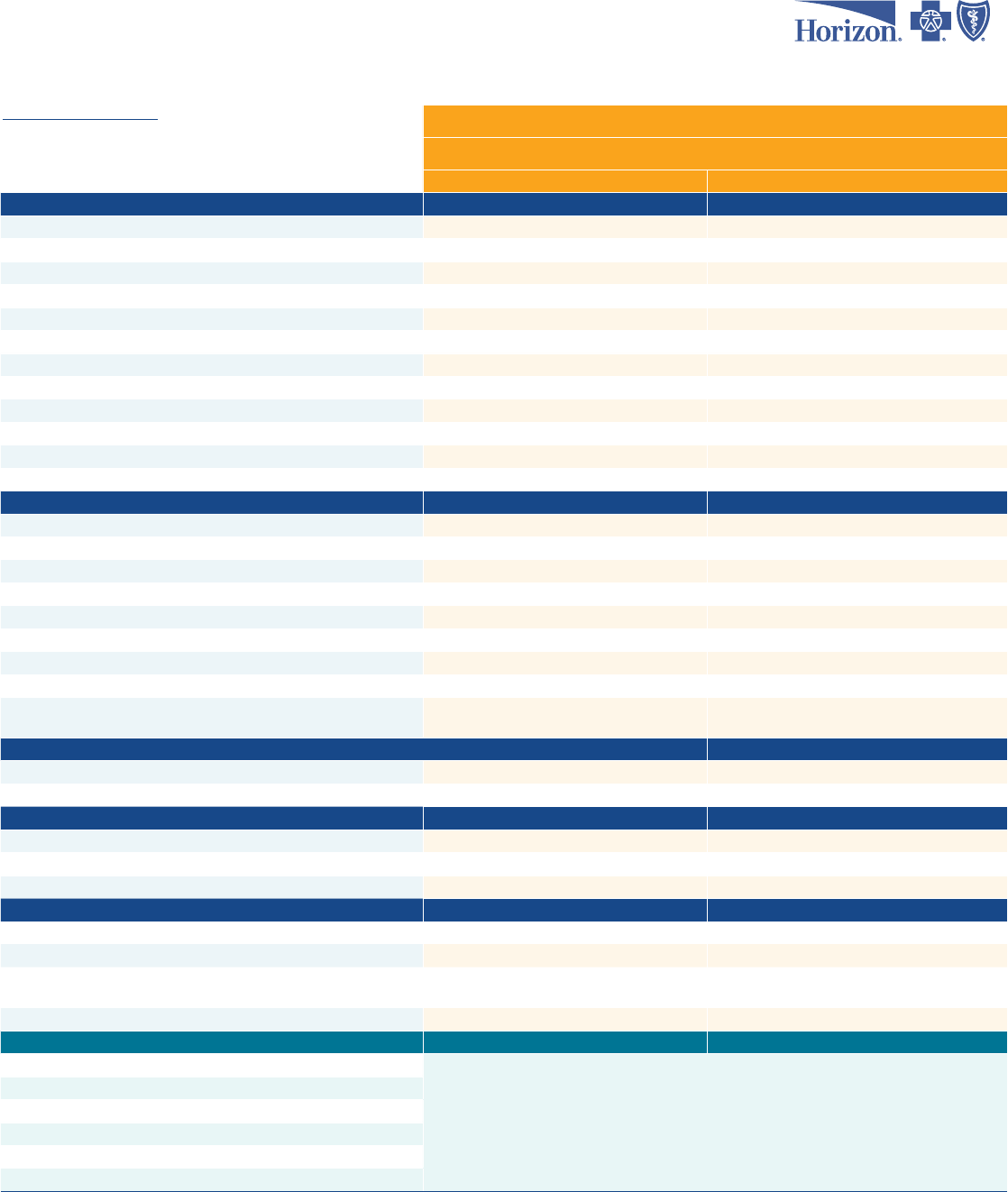
OMNIA Tiered Network Plan
OMNIA HEALTH PLAN
Tier 1 Tier 2
IN-NETWORK (IN)
Service Area Available NJ only Nationwide
Specialist Referral No referral required No referral required
Deductible
2
Individual $0 $1,500
Family $0 $3,000
Coinsurance 0% 20% after deductible
Coinsurance Out-of-Pocket Maximum
Individual Not applicable Not applicable
Family Not applicable Not applicable
Total Out-of-Pocket Maximum (Copay+Deductible+Coinsurance)
Individual $2,500 $4,500
Family $5,000 $9,000
HEALTH CARE SERVICES
Primary Care Ofce Visit $5 $20
Annual Routine Physical (In-Network Only) $0 $0
Direct Primary Care (DPC) Doctors Ofce $0 $0
First Responders Doctors Ofce (FRDOCS) $0 $0
Horizon CareOnline (Telemedicine) Cost share may apply Cost share may apply
Specialist Ofce Visit $20 $35
Annual Routine Vision (In-Network Only) $20 $35
Chiropractic
5
$20 $35
Physical/Occupational/Speech Therapy
6
$20 ofce visit/$20 outpatient facility
$35 ofce visit/
20% after deductible at an outpatient facility
DIAGNOSTIC LABORATORY
7
/RADIOLOGY/ADVANCED IMAGING
Outpatient Laboratory/Radiology/Advanced Imaging $20 20% after deductible
Freestanding Laboratory/Radiology/Advanced Imaging $0 $0
EMERGENCY/URGENT MEDICAL SERVICES
Urgent Car
e Center $35 $50
Emergency Room $100 $100
Ambulance $0 $0
OTHER SERVICES
Inpatient Facility $150 per admission
9
20% after deductible
Outpatient Facility $150 20% after deductible
Outpatient Behavioral Health $20
$35 ofce visit/
20% after deductible at an outpatient facility
Durable Medical Equipment (DME) $0 $0
OUT-OF-NETWORK (OON)
10
Deductible - Individual
No out-of-network benets
Deductible - Family
Coinsurance after Deductible
Out-of-Pocket Coinsurance Maximum - Individual
Out-of-Pocket Coinsurance Maximum - Family
Inpatient Hospital Deductible
1. High Deductible Health Plan. NJ DIRECT HDLow plan includes $300 Health Savings Account funding by employer.
2. Deductible applies to all services that require a coinsurance.
3. Includes eligible prescription cost share.
4. On select services (durable medical equipment, prosthetics, orthotics, oxygen, private duty nursing, ambulance).
5. Chiropractic: Horizon HMO: 20 visits per calendar year. OMNIA Health Plan: 25 visits per calendar year. All other plans: 30 visits per calendar year.
6. Physical, occupational and speech therapy: OMNIA Health Plan: 30 visit maximum each per calendar year. Horizon HMO: 60 visit combined maximum per calendar year. All other plans based on medical necessity.
7. Laboratory services must be rendered by an in-network participating provider, with some exceptions based on medical policy.
8. Lower copayment applies to children under 19 and physician referrals.
9. $150 per admission does not apply to inpatient childbirth, hospice or inpatient behavioral health/substance use disorder.
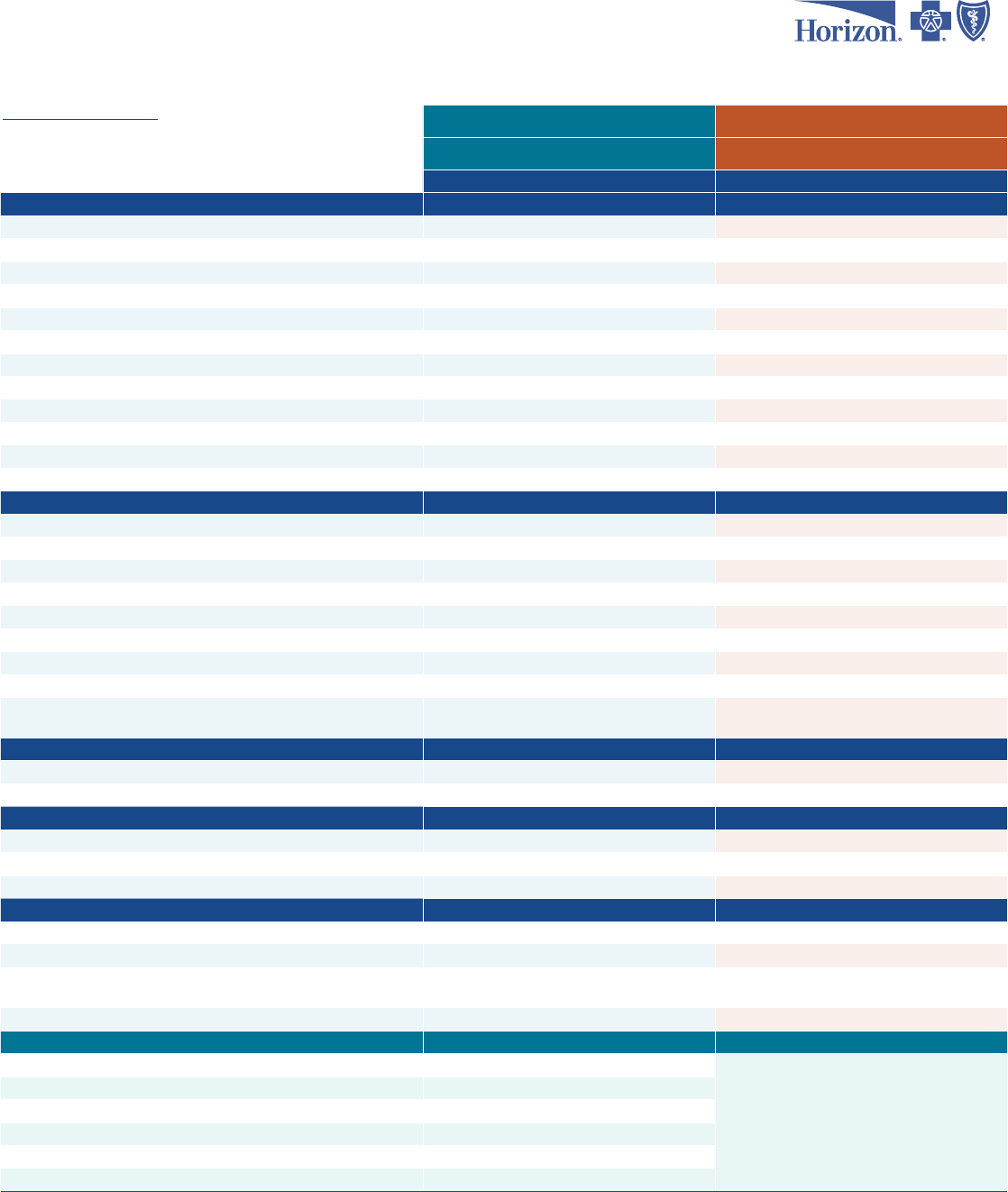
2024 NJ SHBP State and State College/University Employees
Plans for CWA and Union Negotiated Members
Plans effective 7/1/2024 (effective 6/29/2024 for biweekly employees)
HorizonBlue.com/shbp 1-800-414-SHBP (7427)
PPO Plans
High Deductible PPO Plan
CWA UNITY DIRECT
NJ DIRECT
(employees hired prior to 7/1/19)
CWA UNITY DIRECT2019
NJ DIRECT2019
(new hires on or after 7/1/19)
NJ DIRECT HDLow
1
IN-NETWORK (IN)
Service Area Available Nationwide Nationwide Nationwide
Specialist Referral No referral required No referral required No referral required
Deductible
2
Individual $0 $100
$1,600
3
Family $0 Not applicable $3,200
3
Coinsurance 10%
4
10%
after deductible
4
20% after deductible
3
Coinsurance Out-of-Pocket Maximum
Individual $800 $800 $1,000
Family $2,000 $2,000 $2,000
Total Out-of-Pocket Maximum (Copay+Deductible+Coinsurance)
Individual $7,560 $7,560 $2,600
3
Family $15,120 $15,120 $5,200
3
HEALTH CARE SERVICES
Primary Care Ofce Visit $15 $15 20% after deductible
Annual Routine Physical (In-Network Only) $0 $0 $0
Direct Primary Care (DPC) Doctors Ofce $0 $0 Not available
First Responders Doctors Ofce (FRDOCS) $0 $0 $0
Horizon CareOnline (Telemedicine) Cost share may apply Cost share may apply Cost share may apply
Specialist Ofce Visit $30 $30 20% after deductible
Annual Routine Vision (In-Network Only) $30 $30 20% after deductible
Chiropractic
5
$30 $30 20% after deductible
Physical/Occupational/Speech Therapy
6
$30 $30 20% after deductible
DIAGNOSTIC LABORATORY
7
/RADIOLOGY/ADVANCED IMAGING
Outpatient Laboratory/Radiology/Advanced Imaging $0 $0 20% after deductible
Freestanding Laboratory/Radiology/Advanced Imaging $0 $0 20% after deductible
EMERGENCY/URGENT MEDICAL SERVICES
Urgent Care Center $45 $45 20% after deductible
Emergency Room $150
8
$150
8
20% after deductible
Ambulance 10% 10% after deductible 20% after deductible
OTHER SERVICES
Inpatient Facility $0 $0 20% after deductible
Outpatient Facility $0 $0 20% after deductible
Outpatient Behavioral Health $30 $30 20% after deductible
Durable Medical Equipment (DME) 10% 10% after deductible 20% after deductible
OUT-OF-NETWORK (OON)
10
Deductible - Individual $400 $400
See in-network deductible
11
Deductible - Family $1,000 $1,000
See in-network deductible
11
Coinsurance after Deductible 30% 30% 40%
Out-of-Pocket Coinsurance Maximum - Individual $2,000 $2,000
$3,600
Out-of-Pocket Coinsurance Maximum - Family $5,000 $5,000 $7,200
Inpatient Hospital Deductible $500/stay $500/stay Not applicable
10. Out-of-network cost basis: CWA Unity DIRECT, CWA Unity DIRECT2019, NJ DIRECT and NJ DIRECT2019: 175% of CMS (Centers for Medicare & Medicaid Services) fee schedule. NJ DIRECT HD plans: 90th percentile of FAIR
Health national benchmark. All plans with an out-of-network benet also have specied dollar limits for out-of-network chiropractic ($35), physical therapy ($52) and acupuncture ($60).
11. Out-of-network deductible is combined with in-network deductible.
This is not a complete list of all covered services. Exclusions and limitations apply to some services. Visit nj.gov/treasury/pensions/member-guidebooks.shtml for more information.
You can reference HorizonBlue.com/shbp to determine your premium contribution.
Horizon Dental Choice plan available. Please visit HorizonBlue.com/shbp.
Retirees: Please visit nj.gov/treasury/pensions for information regarding available retiree plans.
This document is for informational purposes only and does not constitute a binding agreement. The information provided by this document is not intended to replace or modify the terms, conditions, limitations and exclusions
contained within health plans issued or administered by Horizon. In the event of a conict between the information contained in this document and your plan documents, your plan documents shall control.
2024 NJ SHBP State and State College/University Employees
Plans for CWA and Union Negotiated Members
Plans effective 7/1/2024 (effective 6/29/2024 for biweekly employees)
HorizonBlue.com/shbp 1-800-414-SHBP (7427)
High Deductible PPO Plan HMO Plan
NJ DIRECT HDHigh HORIZON HMO
IN-NETWORK (IN)
Service Area Available Nationwide NJ and contiguous counties
Specialist Referral No referral required Referral required
Deductible
2
Individual $4,100
3
See DME
Family $8,200
3
See DME
Coinsurance 20%
after deductible
3
0%
Coinsurance Out-of-Pocket Maximum
Individual $1,000 Not applicable
Family $2,000 Not applicable
Total Out-of-Pocket Maximum (Copay+Deductible+Coinsurance)
Individual $5,100
3
$7,560
Family $10,200
3
$15,120
HEALTH CARE SERVICES
Primary Care Ofce Visit 20% after deductible $15
Annual Routine Physical (In-Network Only) $0 $0
Direct Primary Care (DPC) Doctors Ofce Not available Not available
First Responders Doctors Ofce (FRDOCS) $0 $0
Horizon CareOnline (Telemedicine) Cost share may apply Cost share may apply
Specialist Ofce Visit 20% after deductible $30
Annual Routine Vision (In-Network Only) 20% after deductible $30
Chiropractic
5
20% after deductible $30
Physical/Occupational/Speech Therapy
6
20% after deductible $30
DIAGNOSTIC LABORATORY
7
/RADIOLOGY/ADVANCED IMAGING
Outpatient Laboratory/Radiology/Advanced Imaging 20% after deductible $0
Freestanding Laboratory/Radiology/Advanced Imaging 20% after deductible $0
EMERGENCY/URGENT MEDICAL SERVICES
Urgent Care Center 20% after deductible $45
Emer
gency Room 20% after deductible $100
8
Ambulance 20% after deductible $0
OTHER SERVICES
Inpatient Facility 20% after deductible $0
Outpatient Facility 20% after deductible $0
Outpatient Behavioral Health 20% after deductible $30
Durable Medical Equipment (DME) 20% after deductible $100 deductible, then covered in full
OUT-OF-NETWORK (OON)
10
Deductible - Individual
See in-network deductible
11
No out-of-network benets
Deductible - Family
See in-network deductible
11
Coinsurance after Deductible 40%
Out-of-Pocket Coinsurance Maximum - Individual $6,100
Out-of-Pocket Coinsurance Maximum - Family $12,200
Inpatient Hospital Deductible Not applicable
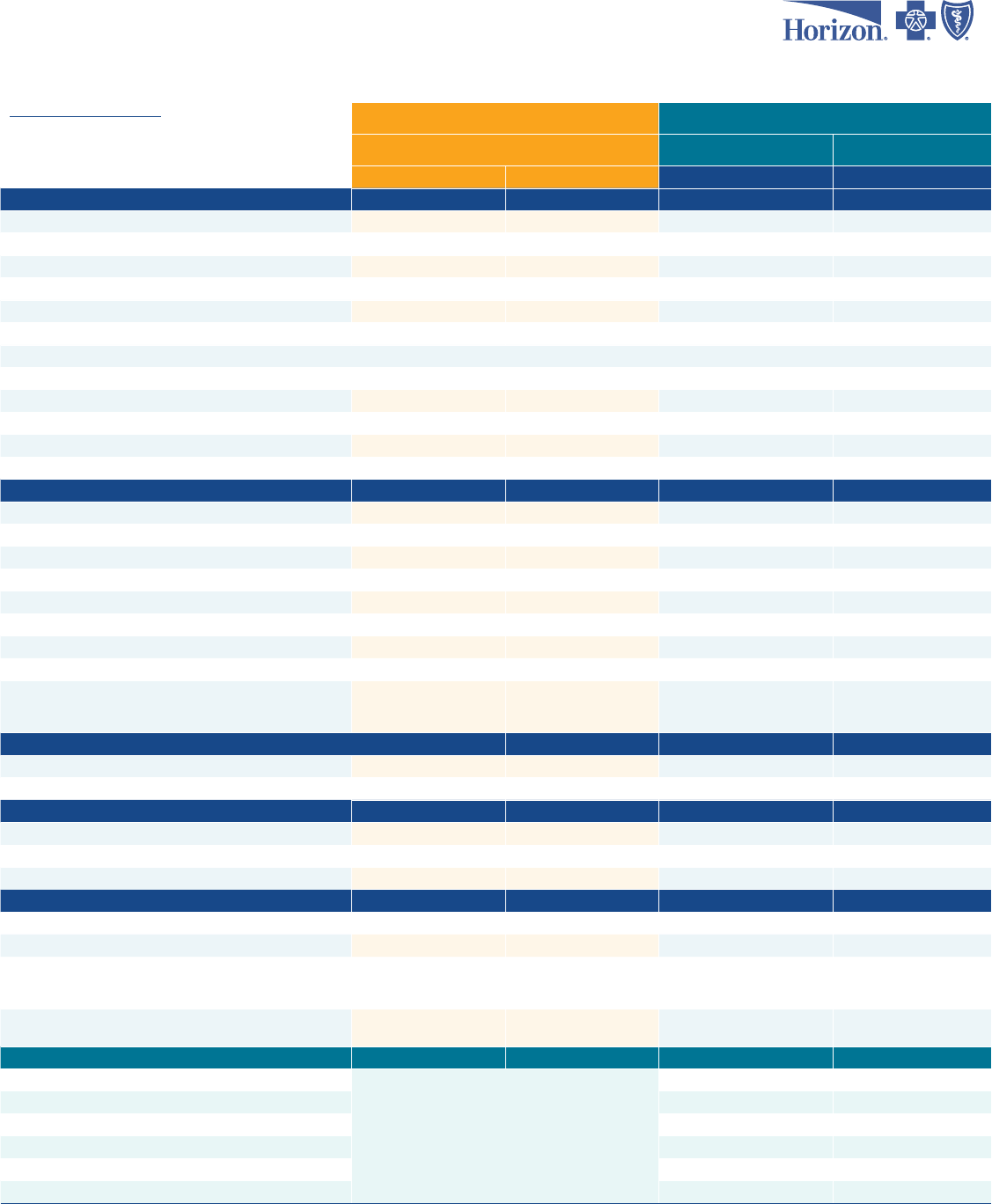
2024 NJ SHBP State and State College/University Employees
Plans for All Other State Members
Plans effective 7/1/2024 (effective 6/29/2024 for biweekly employees)
HorizonBlue.com/shbp 1-800-414-SHBP (7427)
OMNIA Tiered Network Plan
PPO Plans
OMNIA HEALTH PLAN
NJ DIRECT
(employees hired prior to 7/1/19)
NJ DIRECT2019
(new hires on or after 7/1/19)
Tier 1 Tier 2
IN-NETWORK (IN)
Service Area Available NJ only Nationwide Nationwide Nationwide
Specialist Referral No referral required No referral required No referral required No referral required
Deductible
2
Individual $0 $1,500 $0 $100
Family $0 $3,000 $0 Not applicable
Coinsurance 0%
20% after
deductible
10%
4
10%
after deductible
4
Coinsurance Out-of-Pocket Maximum
Individual Not applicable Not applicable $800 $800
Family Not applicable Not applicable $2,000 $2,000
Total Out-of-Pocket Maximum (Copay+Deductible+Coinsurance)
Individual $2,500 $4,500 $7,560 $7,560
Family $5,000 $9,000 $15,120 $15,120
HEALTH CARE SERVICES
Primary Care Ofce Visit $5 $20 $15 $15
Annual Routine Physical (In-Network Only) $0 $0 $0 $0
Direct Primary Care (DPC) Doctors Ofce $0 $0 $0 $0
First Responders Doctors Ofce (FRDOCS) $0 $0 $0 $0
Horizon CareOnline (Telemedicine)
Cost share may apply Cost share may apply Cost share may apply Cost share may apply
Specialist Ofce Visit $20 $35 $30 $30
Annual Routine Vision (In-Network Only) $20 $35 $30 $30
Chiropractic
6
$20 $35 $30 $30
Physical/Occupational/Speech Therapy
7
$20 ofce visit/
$20 outpatient facility
$35 ofce visit/
20% after deductible at
an outpatient facility
$30 $30
DIAGNOSTIC LABORATORY
8
/RADIOLOGY/ADVANCED IMAGING
Outpatient Laboratory/Radiology/Advanced Imaging $20 20% after deductible $0 $0
Freestanding Laboratory/Radiology/Advanced Imaging $0 $0 $0 $0
EMERGENCY/URGENT MEDICAL SERVICES
Urgent Care Center
$35 $50 $45 $45
Emergency Room
$100 $100 $150
9
$150
9
Ambulance
$0 $0 10% 10% after deductible
OTHER SERVICES
Inpatient Facility $150 per admission
10
20% after deductible $0 $0
Outpatient Facility $150 20% after deductible $0 $0
Outpatient Behavioral Health $20
$35 ofce visit/
20% after deductible at
an outpatient facility
$30 $30
Durable Medical Equipment (DME) $0 $0 10% 10% after deductible
OUT-OF-NETWORK (OON)
11
Deductible - Individual
No out-of-network benets
$400 $400
Deductible - Family $1,000 $1,000
Coinsurance after Deductible 30% 30%
Out-of-Pocket Coinsurance Maximum - Individual $2,000 $2,000
Out-of-Pocket Coinsurance Maximum - Family $5,000 $5,000
Inpatient Hospital Deductible $500/stay $500/stay
1. High Deductible Health Plan. NJ DIRECT HDLow plan includes $300 Health Savings Account funding by employer.
2. Deductible applies to all services that require a coinsurance.
3. Includes eligible prescription cost share.
4. On select services (durable medical equipment, prosthetics, orthotics, oxygen, private duty nursing, ambulance).
5. Under age 26.
6. Chiropractic: Horizon HMO: 20 visits per calendar year. OMNIA Health Plan: 25 visits per calendar year. All other plans: 30 visits per calendar year.
7. Physical, occupational and speech therapy: OMNIA Health Plan: 30 visit maximum each per calendar year. Horizon HMO: 60 visit combined maximum per calendar year. All other plans based on medical necessity.
8. Laboratory services must be rendered by an in-network participating provider, with some exceptions based on medical policy.
9. Lower copayment applies to children under 19 and physician referrals.
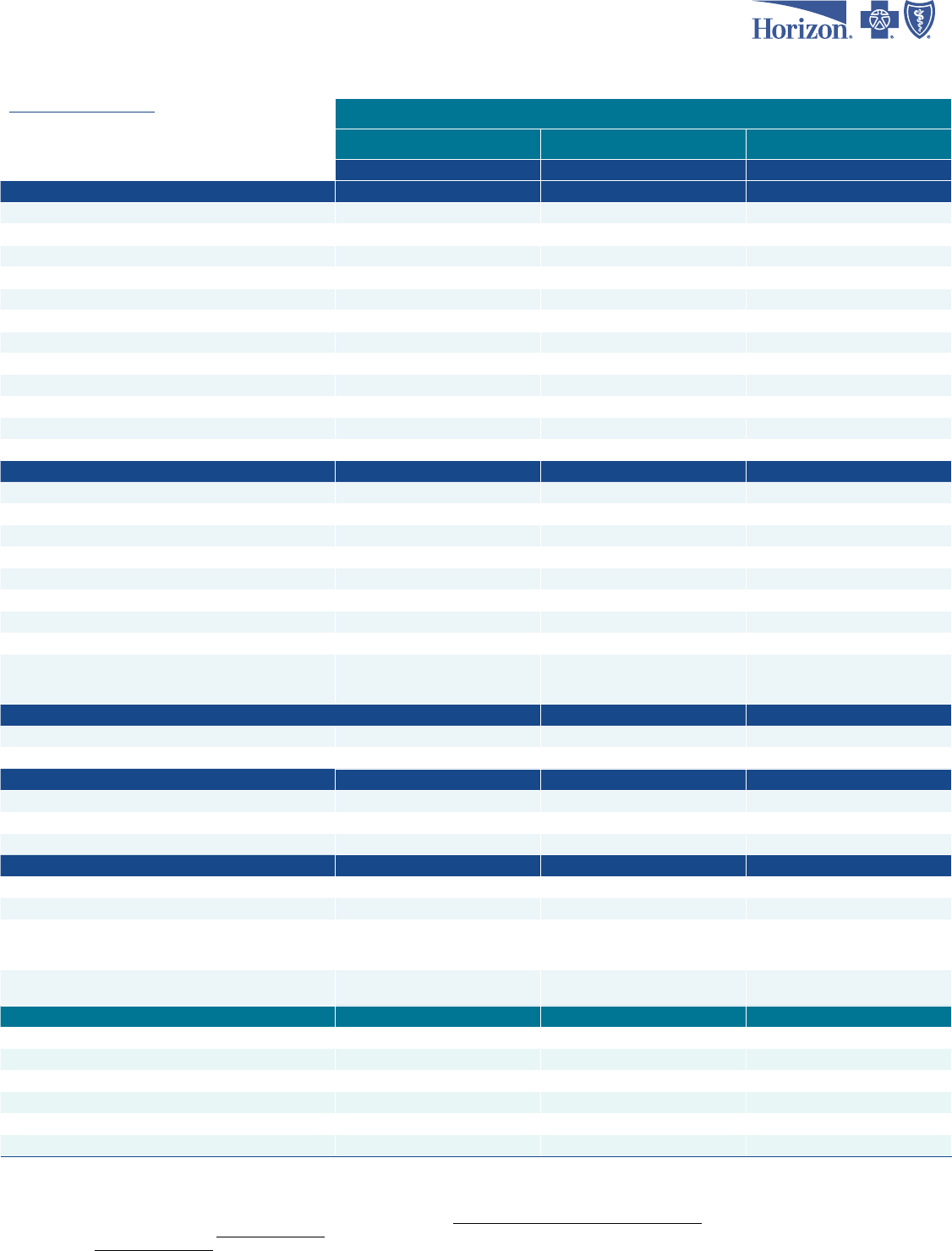
2024 NJ SHBP State and State College/University Employees
Plans for All Other State Members
Plans effective 7/1/2024 (effective 6/29/2024 for biweekly employees)
HorizonBlue.com/shbp 1-800-414-SHBP (7427)
PPO Plans
NJ DIRECT15 NJ DIRECT1525 NJ DIRECT2030
IN-NETWORK (IN)
Service Area Available Nationwide Nationwide Nationwide
Specialist Referral No referral required No referral required No referral required
Deductible
1
Individual $0 $0 $0
Family $0 $0 $0
Coinsurance 10%
4
10%
4
10%
4
Coinsurance Out-of-Pocket Maximum
Individual
$400 $400 $800
Family $1,000 $1,000 $2,000
Total Out-of-Pocket Maximum (Copay+Deductible+Coinsurance)
Individual $7,560 $7,560 $7,560
Family $15,120 $15,120 $15,120
HEALTH CARE SERVICES
Primary Care Ofce V
isit $15 $15 $20
Annual Routine Physical (In-Network Only) $0 $0 $0
Direct Primary Care (DPC) Doctors Ofce $0 $0 $0
First Responders Doctors Ofce (FRDOCS) $0 $0 $0
Horizon CareOnline (Telemedicine)
Cost share may apply Cost share may apply Cost share may apply
Specialist Ofce Visit $15 $25 $30/adult, $20/child
5
Annual Routine Vision (In-Network Only) $15 $25 $30/adult, $20/child
5
Chiropractic
5
$15 $25 $30/adult, $20/child
5
Physical/Occupational/Speech Therapy
7
$15 $25 $30/adult, $20/child
5
DIAGNOSTIC LABORATORY
8
/RADIOLOGY/ADVANCED IMAGING
Outpatient Laboratory/Radiology/Advanced Imaging $0 $0 $0
Freestanding Laboratory/Radiology/Advanced Imaging $0 $0 $0
EMERGENCY/URGENT MEDICAL SERVICES
Urgent Care Center
$15 $25 $30/adult, $20/child
5
Emergency Room
$100
9
$100
9
$125
Ambulance
10% 10% 10%
OTHER SERVICES
Inpatient Facility $0 $0 $0
Outpatient Facility $0 $0 $0
Outpatient Behavioral Health $15 $25 $30/adult, $20/child
5
Durable Medical Equipment (DME) 10% 10% 10%
OUT-OF-NETWORK (OON)
11
Deductible - Individual $100 $100 $200
Deductible - Family $250 $250 $500
Coinsurance after Deductible 30% 30% 30%
Out-of-Pocket Coinsurance Maximum - Individual $2,000 $2,000 $5,000
Out-of-Pocket Coinsurance Maximum - Family $5,000 $5,000 $12,500
Inpatient Hospital Deductible $200/stay $200/stay $500/stay
10. $150 per admission does not apply to inpatient childbirth, hospice or inpatient behavioral health/substance use disorder.
11. Out-of-network cost basis: NJ DIRECT and NJ DIRECT2019: 175% of CMS (Centers for Medicare & Medicaid Services) fee schedule. 90th percentile of FAIR Health national for all other health plans with an out-of-net-
work benet. All plans with an out-of-network benet also have specied dollar limits for out-of-network chiropractic ($35), physical therapy ($52) and acupuncture ($60).
12. Out-of-network deductible is combined with in-network deductible.
This is not a complete list of all covered services. Exclusions and limitations apply to some services. Visit nj.gov/treasury/pensions/member-guidebooks.shtml for more information.
Horizon Dental Choice plan available. Please visit HorizonBlue.com/shbp.
Retirees: Please visit nj.gov/treasury/pensions for information regarding available retiree plans.
This document is for informational purposes only and does not constitute a binding agreement. The information provided by this document is not intended to replace or modify the terms, conditions, limitations and
exclusions contained within health plans issued or administered by Horizon. In the event of a conict between the information contained in this document and your plan documents, your plan documents shall control.
2024 NJ SHBP State and State College/University Employees
Plans for All Other State Members
Plans effective 7/1/2024 (effective 6/29/2024 for biweekly employees)
HorizonBlue.com/shbp 1-800-414-SHBP (7427)
PPO Plan High Deductible PPO Plans
HMO Plan
NJ DIRECT2035 NJ DIRECT HDLow
1
NJ DIRECT HDHigh HORIZON HMO
IN-NETWORK (IN)
Service Area Available Nationwide Nationwide Nationwide
NJ and contiguous counties
Specialist Referral No referral required No referral required No referral required Referral required
Deductible
2
Individual $200 $1,600
3
$4,100
3
See DME
Family $500 $3,200
3
$8,200
3
See DME
Coinsurance 20%
after deductible 20% after deductible
3
20% after deductible
3
0%
Coinsurance Out-of-Pocket Maximum
Individual $2,000 $1,000 $1,000 Not applicable
Family $5,000 $2,000 $2,000 Not applicable
Total Out-of-Pocket Maximum (Copay+Deductible+Coinsurance)
Individual $7,560 $2,600
3
$5,100
3
$7,560
Family $15,120 $5,200
3
$10,200
3
$15,120
HEALTH CARE SERVICES
Primary Care Ofce Visit $20 20% after deductible 20% after deductible $15
Annual Routine Physical (In-Network Only) $0 $0 $0 $0
Direct Primary Care (DPC) Doctors Ofce $0 Not available Not available Not available
First Responders Doctors Ofce (FRDOCS $0 $0 $0 $0
Horizon CareOnline (Telemedicine)
Cost share may apply Cost share may apply Cost share may apply Cost share may apply
Specialist Ofce Visit $35 20% after deductible 20% after deductible $30
Annual Routine Vision (In-Network Only) $35 20% after deductible 20% after deductible $30
Chiropractic
5
$35 20% after deductible 20% after deductible $30
Physical/Occupational/Speech Therapy
7
$35 ofce visit/
20% after deductible at
an outpatient facility
20% after deductible 20% after deductible $30
DIAGNOSTIC LABORATORY
8
/RADIOLOGY/ADVANCED IMAGING
Outpatient Laboratory/Radiology/Advanced Imaging 20% after deductible 20% after deductible 20% after deductible $0
Freestanding Laboratory/Radiology/Advanced Imaging 20% after deductible 20% after deductible 20% after deductible $0
EMERGENCY/URGENT MEDICAL SERVICES
Urgent Care Center
$35 20% after deductible 20% after deductible $45
Emergency Room
$300 20% after deductible 20% after deductible $100
9
Ambulance
20% after deductible 20% after deductible 20% after deductible $0
OTHER SERVICES
Inpatient Facility 20% after deductible 20% after deductible 20% after deductible $0
Outpatient Facility 20% after deductible
20% after deductible 20% after deductible $0
Outpatient Behavioral Health
$35 ofce visit/
20% after deductible at
an outpatient facility
20% after deductible 20% after deductible $30
Durable Medical Equipment (DME) 20% after deductible 20% after deductible 20% after deductible
$100 deductible,
then covered in full
OUT-OF-NETWORK (OON)
11
Deductible - Individual $800
See in-network deductible
12
See in-network deductible
12
No out-of-network
benets
Deductible - Family $2,000
See in-network deductible
12
See in-network deductible
12
Coinsurance after Deductible 40% 40% 40%
Out-of-Pocket Coinsurance Maximum - Individual $6,500 $3,600 $6,100
Out-of-Pocket Coinsurance Maximum - Family $13,000 $7,200 $12,200
Inpatient Hospital Deductible $600/stay Not applicable Not applicable

With Horizon health plans, we’ve got you covered.
Well Care and Preventive Care
Services such as an annual physical and gynecological exam,
well baby/child medical care, immunizations and an annual
vision exam are covered when using a participating doctor.
Behavioral Health and Substance
Use Disorder
We empower our members to achieve their best physical
and mental health. Our care team will work with you,
your family, caregivers and doctors to make sure you are
getting the treatment and support you need in the most
appropriate setting. Telehealth and virtual programs are
available.
NEW- Horizon MindCare
SM
This secure online behavioral health platform offers
personalized behavioral health and resilience information,
well-being assessments, tools and resources. Plus, it can
match you to reliable in-network providers, facilities and
virtual health solutions.
In-Network Laboratories
Our members have access to in-network lab services. You
can use Quest Diagnostics
TM
(Quest) or LabCorp for blood
tests and other lab services. Our networks also include a
number of other participating labs that provide specialized
lab services.
Prescription Drug Coverage
Prescription drug coverage is available to all SHBP and
SEHBP members. To learn more, refer to the Prescription
Drug Plan information on the NJ Division of Pensions and
Benets website at nj.gov/treasury/pensions.
24/7 Nurse Line
For everyday health questions, or even a situation that
might be more serious, access trusted information by calling
the 24/7 Nurse Line at 1-888-624-3096.
Learn more at HorizonBlue.com/shbp
Making good health care more convenient.
Direct Primary Care (DPC)
Eligible members get unlimited access to personalized
care with no copays. Simply choose a DPC doctor from
Everside Health or Sanitas Medical Center for you and
your covered dependents.
If you are eligible for NJWELL, your DPC provider
will credit a well visit and follow-up ofce visit as a
completed health screening.
First Responders Program
If you are an eligible rst responder, you and your
covered family members can receive care at a First
Responders Doctors Ofce (FRDOCS) with no cost
share.
Retail Health Clinics
These clinics treat common health issues such as colds
or seasonal allergies.
• On-site board-certied nurse practitioners can
diagnose and treat conditions and prescribe
medications.
• Sites include MinuteClinics® at select CVS/
pharmacy® locations.
Telemedicine
Telemedicine is available at the touch of a button
through the Horizon Blue app for eligible members.
And depending on your doctor’s preferences, you can
also use telemedicine via video, chat or phone.
Immunizations
Getting vaccinated is more convenient with
more participating pharmacies – view our list at
HorizonBlue.com/shbpu.
• Vaccines these pharmacies administer include u,
COVID-19, shingles, hepatitis A and B, pneumococcal
and human papillomavirus (HPV).
• Medical claims are automatically submitted for you.
Urgent Care Centers
Urgent care centers provide immediate medical care
as an alternative to visiting the Emergency Room (ER).
They treat wounds, sprains and other conditions that
need immediate attention, but are not life-threatening.
• HMO members require a referral to go to a Horizon
urgent care center.
• All members are responsible for applicable
copayments/coinsurance.
• Routine ofce visits are not covered at urgent care
centers.
Learn more at HorizonBlue.com/shbp

Connect to care, benets
and support anytime.
With the Horizon Blue app, you can:
• Get help with appointment scheduling
• Get quick claim status updates
• Video chat with doctors
• View and print member ID Cards
• Locate in-network doctors
Need help registering for our Horizon Blue app or our
secure member website? Call the eService Help Desk at
1-888-777-5075 weekdays from 7 a.m. to 6 p.m., ET.
Text GetApp to
422-272 for your
free Horizon Blue
download.*
*There is no charge to download the Horizon Blue app,
but rates from your wireless provider may apply.
Here when you need us most.
Visit us online at HorizonBlue.com/shbp. Chat with us online.
Contact us toll free at 1-800-414-SHBP (7427).
CWA Unity DIRECT, NJ DIRECT and OMNIA
SM
Health Plans are administered by Horizon Blue Cross Blue Shield of New Jersey (Horizon) and Horizon HMO is administered by Horizon Healthcare of New Jersey, Inc. (HHNJ).
Horizon and HHNJ are independent licensees of the Blue Cross Blue Shield Association (BCBSA). The Blue Cross
®
and Blue Shield
®
names and symbols and BlueCard
®
, Blue365
®
and Blue Cross Blue Shield Global
®
Core
are registered marks of the Blue Cross Blue Shield Association. The Horizon
®
name and symbols and PRECIOUS ADDITIONS
®
are registered marks and Horizon MindCare
SM
, Horizon
b
Fit
SM
, OMNIA
SM
Health Plans are
service marks of Horizon. Blue365
®
offers access to savings on items and services that members may purchase directly from independent vendors. Please note that BCBSA may receive payments from Blue365 vendors.
Also, neither Horizon nor the BCBSA recommend, warrant or guarantee any specic Blue365 vendor or discounted item or service. Blue365 is not an insurance program and may be discontinued at any time. © 2024
Horizon, Three Penn Plaza East, Newark, New Jersey 07105.
All trademarks, service marks and company names are theproperty of their respective owners.
NJWELL is administered by the New Jersey Division of Pensions and Benets. All provisions of the program are established by the Division and are subject to change. *NJWELL Reward cards are issued to participants
who are eligible for NJWELL at the time the reward is earned by The Bancorp Bank, Member FDIC, pursuant to a license from Visa U.S.A. Inc. Use your Visa
®
Prepaid card anywhere Visa debit cards are accepted around
the world.
WebMD
®
provides health assessment tools and wellness education to eligible SHBP and SEHBP members. WebMD is independent from and not afliated with Horizon.
Quest Diagnostics
™
and LabCorp are independent companies that provide lab services to eligible SHBP and SEHBP members.
Everside Health and Sanitas Medical Center are independent companies that support Horizon in providing comprehensive primary care, urgent care and preventive care services to eligible SHBP and SEHBP members.
YMCA is independent company that supports Horizon in the administration of a membership discount program.
Walgreens is an independent company that supports Horizon in providing health information and preventative screenings.
Minute Clinic
®
and CVS are independent from and not afliated with Horizon.
Apple Inc. and Google LLC are independent from and not afliated with Horizon.
Horizon complies with applicable Federal civil rights laws and does not discriminate against nor does it exclude people or treat them differently on the basis of race, color, gender, national origin, age, disability, pregnancy,
gender identity, sex, sexual orientation or health status in the administration of the plan, including enrollment and benet determinations.
Spanish (Español): Para ayuda en español, llame al 1-866-660-6528 (TTY 711). Chinese (中文): 如需中文協助,請致電 1-866-660-6528 (TTY 711).
ECNA0011317 (0324)
