Otosclerosis
Diagnosis, Evaluation, Pathology,
Surgical Techniques, and Outcomes
Chris de Souza, MS, DORL, DNB, FACS
Marcos V. Goycoolea, MD, MS, PhD
Neil M. Sperling, MD, FACS
v
Contents
List of Videos vii
Introduction ix
Contributors xi
Part I. Basic Science 1
Chapter 1. Pathology of Otosclerosis 3
Chapter 2. Genetics of Otosclerosis 9
Chapter 3. Measles and Otosclerosis 11
Chapter 4. Molecular Biology 13
Part II. Investigations 15
Chapter 5. Audiological Evaluation of the Patient with Otosclerosis 17
Chapter 6. Radiological Imaging of Otosclerosis 25
Part III. Cochlear Otosclerosis and Conservative Management of Otosclerosis 29
Chapter 7. Cochlear Otosclerosis 31
Chapter 8. Medical Treatment of Otosclerosis 37
Chapter 9. Hearing Aids and Otosclerosis 43
Part IV. Surgical Management of Otosclerosis 47
Chapter 10. Stapedectomy 49
Chapter 11. Stapedectomy Versus Stapedotomy 53
Chapter 12. Lasers in Otosclerosis 57
Chapter 13. The Stapedectomy Prosthesis 61
Chapter 14. Bilateral Otosclerosis 63
Chapter 15. Revision Stapedectomy 65
Part V. Complications of Stapedectomy 69
Chapter 16. Post-Stapedectomy Perilymph Fistula 71
Part VI. Miscellaneous 75
Chapter 17. Obliterative Otosclerosis 77
Chapter 18. The Learning Curve 81
Chapter 19. Special Conditions and Complications in Otosclerosis Surgery 83
Part VII. Atlas 91
Chapter 20. The Art of Stapes Surgery 93
Robert K. Jackler
Christine Gralapp, Chapter Illustrator

vi OtOsclerOsis: DiagnOsis, evaluatiOn, PathOlOgy, surgical techniques, anD OutcOmes
Chapter 21. Otosclerosis: Clinical Considerations 183
Richard James Wiet
Chapter 22. Obliterative Otosclerosis 195
Neil M. Sperling and Robert Vincent
Chapter 23. How to Do a Stapedotomy When the Facial Nerve Is Dehiscent 213
Thomas Linder and Christoph Schlegel-Wagner
Chapter 24. Revision Stapes Surgery: Technique of Neil M. Sperling 231
Neil M. Sperling
Chapter 25. Revision Stapedectomy: Technique of John C. Goddard 235
John C. Goddard and Audrey P. Calzada
Chapter 26. Causes of Failure of Stapedectomy 251
A. G. Pusalkar
Index 261
vii
List of Videos
1. Malleostapedectomy in Otosclerosis
Thomas Linder and Christoph Schlegel-Wagner
2. Stapedotomy in Persistent Stapedial Artery
Thomas Linder and Christoph Schlegel-Wagner
3. Full Stapedotomy Procedure
Neil M. Sperling
4. Laser-Assisted Superstructure Removal
Neil M. Sperling
5. Laser Rosette
Neil M. Sperling
6. Vein Graft Placement
Neil M. Sperling
7. Bucket-Handle Prosthesis Placement
Neil M. Sperling
8. Loop Piston Placement
Neil M. Sperling
9. Revision Stapedectomy
Neil M. Sperling
10. Revision Stapedectomy Using Double-Bend
Technique
John C. Goddard and Audrey P. Calzada
11. Persistent Stapedial Artery
John C. Goddard and Audrey P. Calzada
12. Facial Nerve Over Promontory
John C. Goddard and Audrey P. Calzada
13. Stapedectomy Surgery Using the Omniguide
CO
2
Laser System
Richard James Wiet
14. Revision Stapedectomy with Adhesions Using
the Omniguide CO
2
Laser System
Richard James Wiet
15. Stapedectomy Using the Soft Clip Prosthesis
A. G. Pusalkar
ix
Introduction
Worldwide, the number of patients suffering from
otosclerosis has declined considerably. Although
this is a cause for rejoicing, it places the modern-day
otologist in a unique predicament. It leaves him or
her with very little surgical experience in dealing
with otosclerosis. The patient who has undergone
surgery for otosclerosis many years ago and now
faces problems as a result of that surgery are among
the many challenges that the otologist of today will
need to face. The modern-day otologist will need to
overcome his or her own learning curve before being
able to perform the surgery reliably and deliver con-
sistently good results.
There are still quite a few nuances that need
to be learned if the otologist is to successfully and
effectively treat patients with otosclerosis. Our
book strives to help today’s otologist achieve that
goal. The references are limited to just a few. The
atlas section on the surgical procedures is provid-
ed by internationally acknowledged experts. Their
experience and techniques have been gleaned
through years of performing this amazingly de-
manding procedure and consistently delivering
excellent results. Each beautiful picture and illustra-
tion is worth a thousand words. Their surgical vid-
eos are priceless.
We hope that the current trends continue where
otosclerosis will just be a faded memory in the his-
tory of illnesses that affect humanity. But until then,
all otologists will still need to be familiar with all the
dimensions that the treatment of otosclerosis brings.
We thank the contributors for sharing their
valuable experience, their extraordinarily beautiful
illustrations, and their videos. We appreciate their
unselfishness and their graciousness. It is their hope,
as well as ours, that all who read this book will ben-
efit from it and as a result their patients will benefit
from it too.
Chris de Souza
Marcos V. Goycoolea
Neil M. Sperling
Part I
Basic Science
3
ChaPter 1
Pathology of Otosclerosis
Chris de Souza and Marcos V. Goycoolea
INTRODUCTION
Otosclerosis is primarily a disease of localized bone
remodeling.
1
It is thought to affect only the bony
capsule of the middle and inner ear selectively.
Otosclerosis is a process occurring in two phases:
(1) active phase as characterized by bone resorption
(spongiosis), and (2) phase of remission character-
ized by bone deposition (sclerosis).
It is a disease affecting enchondral bone of the
otic capsule characterized by disordered resorption
and deposition of bone.
An otosclerotic focus consists of areas of bone
resorption, new bone formation, vascular prolifera-
tion, and a connective tissue stroma.
AGE OF ONSET
It can range from 10 to 48 years of age, however, the
mean age of onset is commonly the age of 30.
2
DeJuan
3
in his study reported the onset of clini-
cal otosclerosis to be 28% between the ages of 18 and
21 years, 40% between 21 and 30, and 22% between
31 and 40.
4
PREVALENCE
The exact incidence remains unclear and next to
impossible to determine.
However, in one report autopsy studies con-
ducted by Konigsmark and Gorlin
5
revealed an inci-
dence of 5% to 18% of the general population.
Jahn and Vernick
6
report that 10% of Caucasians
have histologic otosclerosis, but only 1% of these
develop clinical manifestations of otosclerosis.
Many authors have noted that the incidence
of patients suffering from otosclerosis has declined
steeply in recent times.
RACE
There appears to be a definite racial predisposition.
Caucasians are more predisposed than Africans.
Asians too are far less affected than Caucasians,
and the prevalence in American Indians seems to be
extremely low across the continent.
2
GENDER
Shambaugh
7
noted a female preponderance in his
study. Otosclerosis is not a genetically sex-linked
characteristic disease. Thus, a ratio of 1:1 would
have been expected.
Hueb et al
8
reported a higher incidence of bilateral
otosclerosis in women than men. This prompted them
to believe that this would more likely cause women to
seek medical advice than men. This in turn could likely
explain the gender disparity. On the other hand, endo-
crinological factors predisposing to the appearance of
otosclerotic foci is a possibility to be considered.
4 OTOSCLEROSIS: DIAGNOSIS, EVALUATION, PATHOLOGY, SURGICAL TECHNIQUES, AND OUTCOMES
OTOSCLEROSIS AND PREGNANCY
There are many reports that associate the onset of
hearing loss caused by otosclerosis and the onset
of pregnancy. Shambaugh
9
found that in an analy-
sis of 475 female patients suffering from otosclerosis
that 50% suffered from hearing impairment with the
onset of pregnancy. Although he and many authors
note a correlation between the onset of hearing loss
following pregnancy, they are not clear on why or
how this occurs. As mentioned earlier, endocrino-
logic factors have been suspected for this occurrence.
TYPES OF OTOSCLEROSIS
1. Histologic otosclerosis
2. Fenestral otosclerosis
3. Cochlear otosclerosis
4. Malignant otosclerosis
5. Far advanced otosclerosis
Histologic Otosclerosis
(Figures 1–1 and 1–2)
Histologic otosclerosis is a finding on microscopic
examination of temporal bones. The location of the
otosclerotic changes is such that the patient suffers
no symptoms related to the otosclerosic changes.
Therefore, it generally does not involve the stapes
bone, the stapediovestibular joint, or the cochlear
endosteum. It is therefore asymptomatic.
Fenestral Otosclerosis
This refers to an otosclerotic lesion that involves
the stapes bone and/or the stapediovestibular joint.
This in turn causes a conductive hearing loss. This is
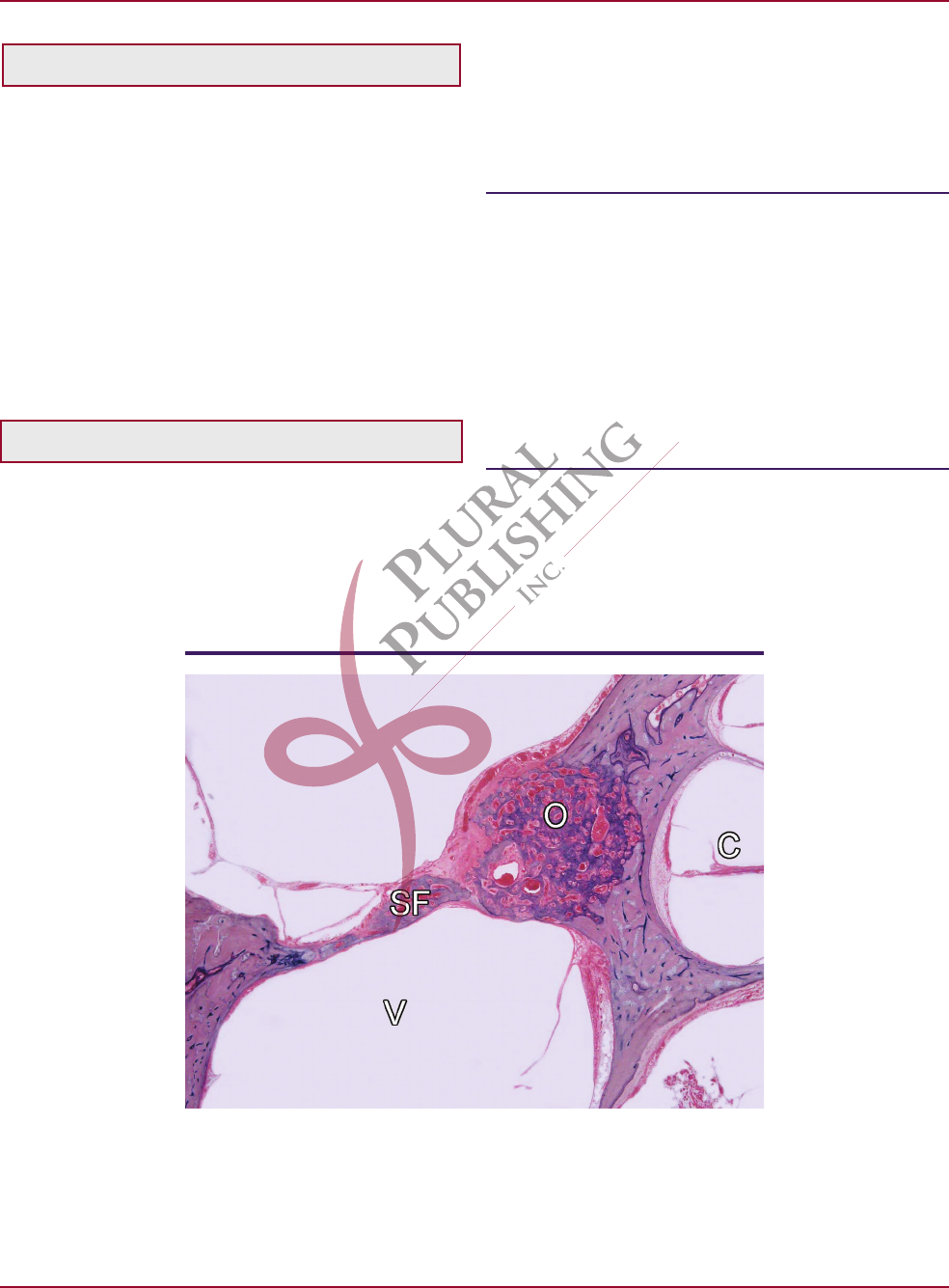
Figure 1–1. Section of human temporal bone demonstrating “his-
tologic otosclerotic” focus. O = “histologic” otosclerotic focus; SF =
stapedial footplate; C = cochlea; V = vestibule. Courtesy of Univer-
sity of Minnesota temporal bone collection. Kindly contributed by
Dr. Cureoglu and Dr. Paparella.
PATHOLOGY OF OTOSCLEROSIS 5
the most common site of involvement representing
81 to 95% of cases.
10
Cochlear Otosclerosis (Figure 1–3)
Cochlear otosclerosis is a term used in cases in which
the otosclerotic lesion invades the cochlear endos-
teum and is usually reserved for the occurrence of
pure sensorineural hearing loss due to otosclerosis
without any conductive component.
“Malignant” (Obliterative) Otosclerosis
This is defined as severely active otosclerosis involving
both oval and round windows and most of the bony
labyrinth and is manifested initially by mixed hear-
ing loss, which then relentlessly progresses to severe
profound sensorineural hearing loss. Both windows
are obliterated by the otosclerotic focus. Lamellar new
bone is seen in the inner ear of such patients.
Far Advanced Otosclerosis (FAO)
Far advanced otosclerosis is defined as no measur-
able air or bone conduction or air conduction no bet-
ter than 95 dB and bone conduction at 55 dB to 60 dB
at one frequency only.
A negative Rinne’s test result with a 256 Hz
magnesium tuning fork is the best way to separate a
FAO sensorineural hearing loss from sensorineural
hearing losses of other causes.
SITES OF INVOLVEMENT OF THE
TEMPORAL BONE BY OTOSCLEROSIS
IN ORDER OF FREQUENCY
1. Commonly seen anterior to the oval window
2. The round window niche (Figures 1–4 and 1–5)
3. Posterior to the round window
4. Posterior wall of the internal auditory canal
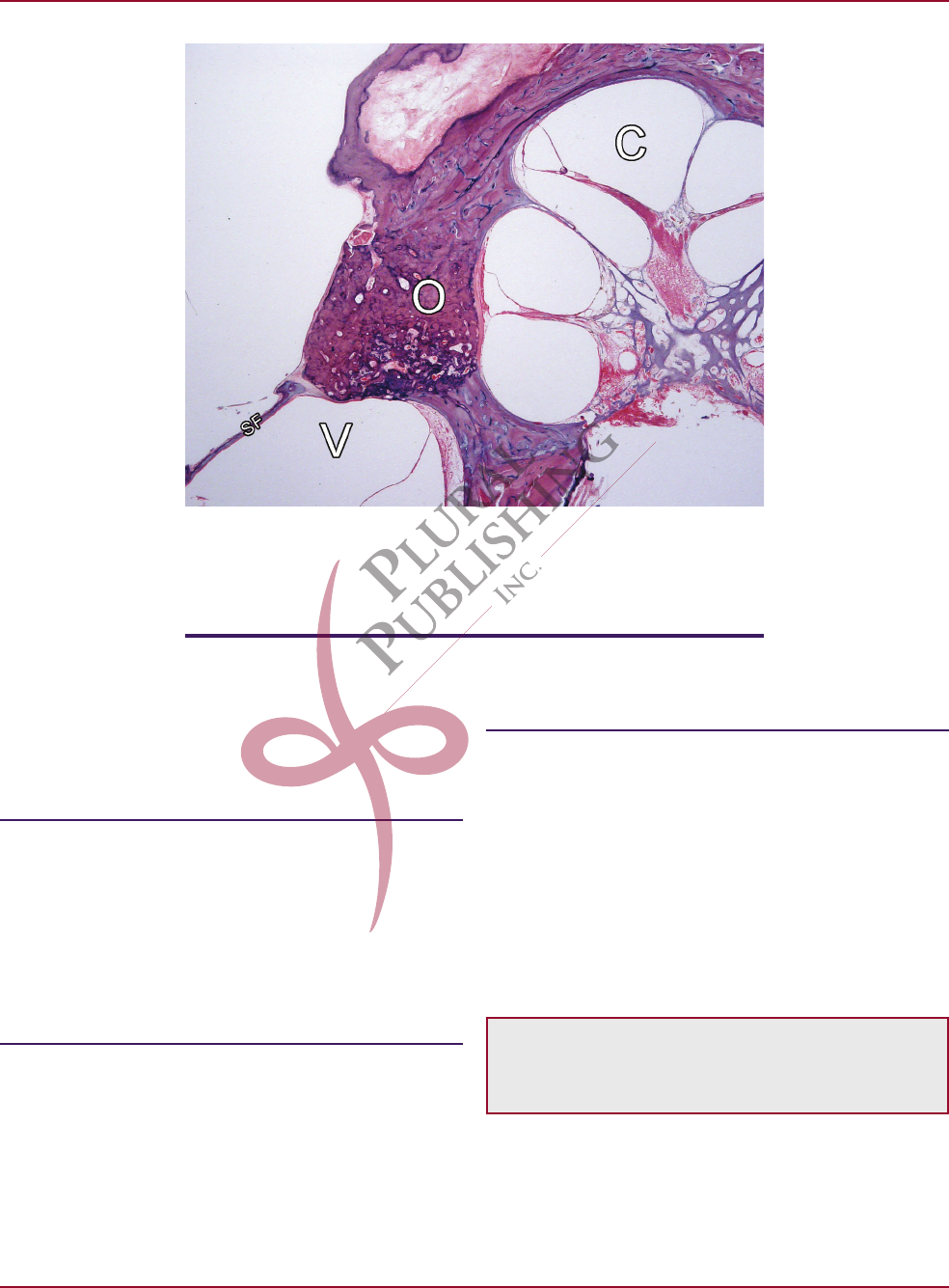
Figure 1–2. Magnified view of histologic otosclerosis. O = otoscle-
rotic focus; V = vestibule; SF = stapedial footplate. Courtesy of Uni-
versity of Minnesota temporal bone collection. Kindly contributed
by Dr. Cureoglu and Dr. Paparella.
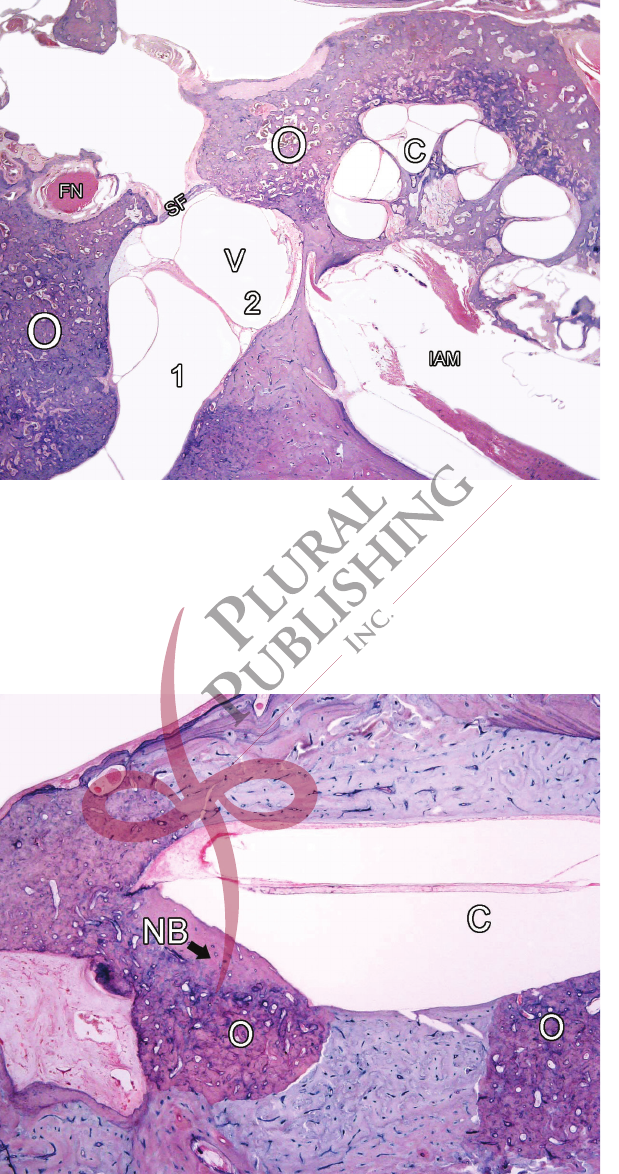
6
Figure 1–3. Histopathology section of human temporal bone
demonstrating cochlear otosclerosis. O = otosclerotic focus; C =
cochlea deformed by the otosclerosis; V = vestibule; 2 = saccule;
1 = utricle; SF = stapes footplate; FN = facial nerve. Courtesy of Uni-
versity of Minnesota temporal bone collection. Kindly contributed
by Dr. Cureoglu and Dr. Paparella.
Figure 1–4. HP section demonstrating otosclerotic focus oblit-
erating the round window. O = otosclerotic focus; C = cochlea;
NB = new bone formation. Courtesy of University of Minnesota
temporal bone collection. Kindly contributed by Dr. Cureoglu and
Dr. Paparella.
PATHOLOGY OF OTOSCLEROSIS 7
5. Around the cochlear aqueduct
6. Semicircular canals
7. Totally within the stapedial footplate
HISTOPATHOLOGY OF OTOSCLEROSIS
The otic capsule itself undergoes very little remod-
eling. The otic capsule contains small regions of
immature cartilaginous tissue called the “globuli
interossei.” This may be the loci of the earliest lesions
of otosclerosis.
Otosclerosis is characterized by the following:
1. Bone resorption
2. New bone formation
3. Vascular proliferation
4. Connective tissue stroma.
The very first stage of otosclerosis is resorption
of enchondral bone around blood vessels.
Second: This results in enlargement of perivas-
cular spaces. Vascular spaces become wider. This is
the initial stage characterized by diffuse or patchy
demineralization that coincides with preotosclerotic
lesions.
Third: This is then followed by deposition of
immature (woven) bone.
Fourth: Resorption and deposition of imma-
ture bone occurs continuously within an otosclerotic
focus with production of more mature (lamellar) bone.
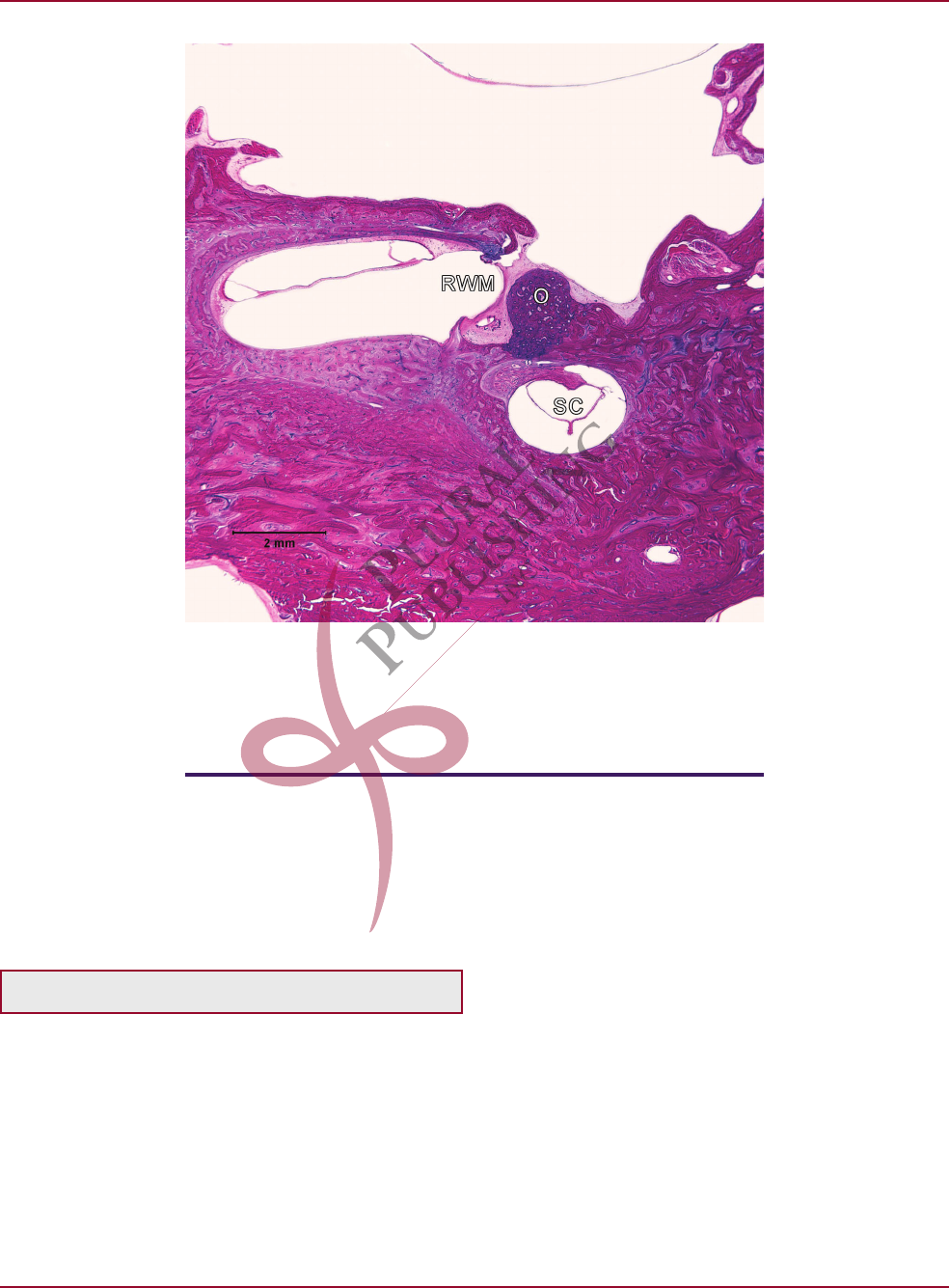
Figure 1–5. HP section demonstrating otosclerotic focus near
round window niche. O = otosclerotic focus; RWM = round win-
dow membrane; SC = Semicircular canal. Courtesy of University
of Minnesota temporal bone collection. Kindly contributed by Dr.
Cureoglu and Dr. Paparella.
