Flu Vaccine―Date received: ________________ Next flu vaccine due: ________________ COVID19 vaccine―Date received: _______________
Control Medicine(s) Medicine How much to take When and how oen to take it Take at
Home School
Home School
Physical Activity Use Albuterol/Levalbuterol pus, 15 minutes before activity with all activity when you feel you need it
My Asthma Action Plan
For Home and School
Name: DOB: / /
Severity Classification: Intermient Mild Persistent Moderate Persistent Severe Persistent
Asthma Triggers (list):
Peak Flow Meter Personal Best:
ALA Asthma AP Home_School V3 3 1 2023
1-800-LUNGUSA | Lung.org
Green Zone: Doing Well
Symptoms: Breathing is good – No cough or wheeze – Can work and play – Sleeps well at night
Peak Flow Meter (more than 80% of personal best)
Yellow Zone: Caution
Symptoms: Some problems breathing – Cough, wheeze, or tight chest – Problems working or playing – Wake at night
Peak Flow Meter to (between 50% and 79% of personal best)
Quick-relief Medicine(s) Albuterol/Levalbuterol pus, every 20 minutes for up to 4 hours as needed
Control Medicine(s) Continue Green Zone medicines
Add Change to
You should feel beer within 20-60 minutes of the quick-relief treatment. If you are geing worse or are in the Yellow Zone for more
than 24 hours, THEN follow the instructions in the RED ZONE and call the doctor right away!
Red Zone: Get Help Now!
Symptoms: Lots of problems breathing – Cannot work or play – Geing worse instead of beer – Medicine is not helping
Peak Flow Meter (less than 50% of personal best)
Take Quick-relief Medicine NOW! Albuterol/Levalbuterol pus, (how frequently)
Call 911 immediately if the following danger signs are present: • Trouble walking/talking due to shortness of breath
• Lips or fingernails are blue
• Still in the red zone aer 15 minutes
School Sta: Follow the Yellow and Red Zone instructions for the quick-relief medicines according to asthma symptoms.
The only control medicines to be administered in the school are those listed in the Green Zone with a check mark next to “Take at School”.
Both the Healthcare Provider and the Parent/Guardian feel that the child has demonstrated the skills to carry and self-administer their
quick-relief inhaler, including when to tell an adult if symptoms do not improve aer taking the medicine.
Healthcare Provider
Name Date Phone ( ) - Signature
Parent/Guardian
I give permission for the medicines listed in the action plan to be administered in school by the nurse or other school sta as appropriate.
I consent to communication between the prescribing health care provider or clinic, the school nurse, the school medical advisor and school-based health
clinic providers necessary for asthma management and administration of this medicine.
Name Date Phone ( ) - Signature
School Nurse
The student has demonstrated the skills to carry and self-administer their quick-relief inhaler, including when to tell an adult if symptoms do not improve
aer taking the medicine.
Name Date Phone ( ) - Signature
Please send a signed copy back to the provider listed above.
Proper inhalation
technique is important
when taking your
asthma medicine(s)
and monitoring your
breathing. Make sure to
bring all your medicines
and devices to each visit
with your primary care
provider or pharmacist
to check for correct use,
or if you have trouble
using them.
For more videos,
handouts, tutorials and
resources, visit Lung.org.
Scan the QR Code to
access How-To Videos
©2022 American Lung Association.
All rights reserved. (SEP 2022)
You can also connect
with a respiratory
therapist for one-
on-one, free support
from the American
Lung Association’s
Lung HelpLine at
1-800-LUNGUSA.
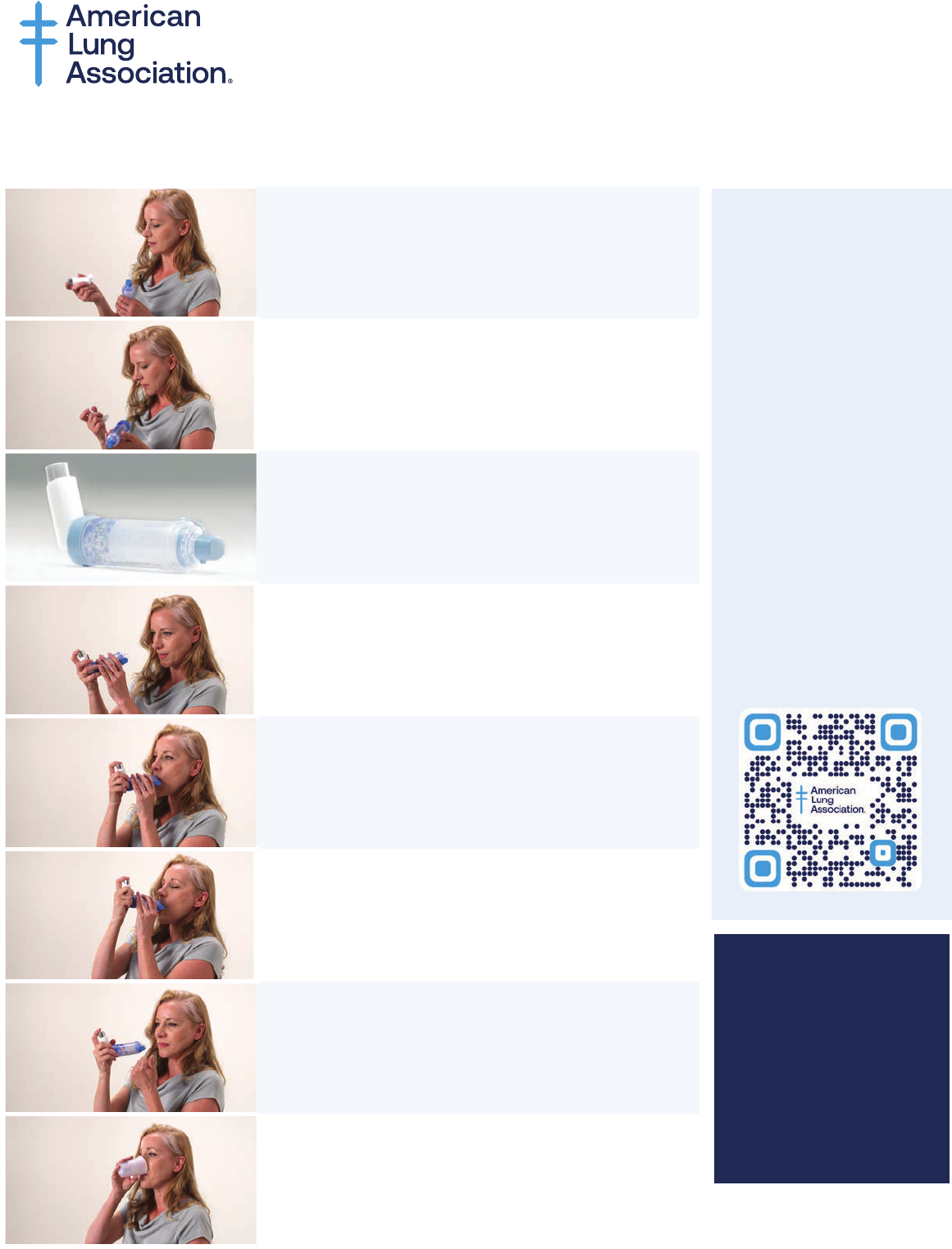
Prime a brand-new inhaler: Before using it for the first time, if you have not used
it for more than 7 days, or if it has been dropped.
1. Shake inhaler 10 seconds.
2. Take the cap o the inhaler and valved holding
chamber. Make sure the mouthpiece and valved
holding chamber are clean and there is nothing
inside the mouthpieces.
3. Put inhaler into the chamber/spacer.
4. Breathe out away from the device.
5. Put chamber mouthpiece in mouth.
6. Press inhaler once and breathe in deep and
steadily.
7. Hold your breath for 10 seconds, then breathe
out slowly.
If you need another pu of medicine, wait 1
minute and repeat steps 4-7.
8. Rinse with water and spit it out.
How to Use a Metered-Dose Inhaler with a
Valved Holding Chamber (Spacer)
