UNCLASSIFIED
Army Regulation 600 – 77
Personnel-General
Administrative
Management of
Wounded, Ill,
or Injured
Soldiers
Headquarters
Department of the Army
Washington, DC
5 March 2019
SUMMARY
AR 600 – 77
Administrative Management of Wounded, Ill, or Injured Soldiers
This new Department of the Army regulation, dated 5 March 2019—
o Prescribes policy for wounded, ill, or injured Soldiers (chaps 1 through 10).
o Prescribes the following new forms: DA Form 7692 (Active Duty for Medical Care Application) and DA Form 7696
(Commander's Performance and Capability Checklist) (para 3–1e).
o Incorporates Army Directive 2011
– 22, Special Compensation for Assistance with Activities of Daily Living, dated
21 November 2011, (hereby superseded) as modified by DODI 1341.12 and DODM 1341.12 (throughout).
o Replaces Military Medical Support Office with Defense Health Agency-Great Lakes (throughout).
*This regulation supersedes Army Directive 2011–22, dated 21 November 2011.
AR 600–77 • 5 March 2019
UNCLASSIFIED
i
Headquarters
Department of the Army
Washington, DC
*Army Regulation 600
–
77
5 March 2019
Effective 5 April 2019
Personnel-General
Administrative Management of Wounded, Ill, or Injured Soldiers
History. This is a new Department of
the Army regulation.
Summary. This regulation prescribes
policy, procedures, and administrative
guidance for the management and support
of wounded, ill, or injured Soldiers.
Wounded, ill, or injured Soldiers are ad-
ministratively and medically managed by
the Soldiers' organic command, State and
Territory (for Army National Guard), re-
gional support commands (for U.S. Army
Reserves), U.S. Army Human Resources
Command (for individual ready reserve)
and Warrior Transition Units and Commu-
nity Care Units during time of injury
through return to duty, or transition to civil-
ian life through medical processing. Perti-
nent Federal statutes, regulations, and other
standards governing these programs and
services are cited throughout this regula-
tion. This regulation is supported by AR
40
– 58 which consolidates policies on the
Comprehensive Transition Plan and War-
rior Care for transitioning wounded, ill, or
injured Soldiers back into the force and/or
Veteran status. It reinforces existing De-
partment of the Army, G1 personnel policy
that remains in effect to include active duty
medical extension, medical retention pro-
cessing, medical retention processing 2, and
medical retention processing – evaluation
as well as incorporates major changes in the
Warrior Care and Transition Program. DA
Form 7692 (Active Duty for Medical Care
Application) and DA Form 7696 (Com-
mander’s Performance and Capability
Checklist) are new electronic forms pre-
scribed in this Army regulation for the man-
agement and care of wounded, ill, or injured
Soldiers by their chain of command and
medical providers and to request active
duty orders for the purpose of medical care
and/or processing.
Applicability. This regulation applies
to the Regular Army, the Army National
Guard/Army National Guard of the United
States, and the U.S. Army Reserve, unless
otherwise stated.
Proponent and exception authority.
The proponent of this regulation is the Dep-
uty Chief of Staff, G – 1. The proponent has
the authority to approve exceptions or
waivers to this regulation that are consistent
with controlling law and regulations. The
proponent may delegate this approval au-
thority, in writing, to a division chief within
the proponent agency or its direct reporting
unit or field operating agency, in the grade
of colonel or the civilian equivalent. Activ-
ities may request a waiver to this regulation
by providing justification that includes a
full analysis of the expected benefits and
must include formal review by the activity's
senior legal officer. All waiver requests will
be endorsed by the commander or senior
leader of the requesting activity and for-
warded through their higher headquarters to
the policy proponent. Refer to AR 25
– 30
for specific guidance.
Army internal control process. This
regulation contains internal control provi-
sions in accordance with AR 11 – 2 and
identifies key internal controls that must be
evaluated (see appendix B).
Supplementation. Supplementation
of this regulation and establishment of com-
mand and local forms are prohibited with-
out prior approval from the Deputy Chief of
Staff, G – 1 (DAPE – MPE), 300 Army Pen-
tagon, Washington, DC 20310
– 0300.
Suggested improvements. Users are
invited to send comments and suggested
improvements on DA Form 2028 (Recom-
mended Changes to Publications and Blank
Forms) directly to Deputy Chief of Staff,
G
– 1 (DAPE – MPE), 300 Army Pentagon,
Washington, DC 20310
– 0300.
Distribution. This regulation is availa-
ble in electronic media only and is intended
for the Regular Army, the Army National
Guard/Army National Guard of the United
States, and the U.S. Army Reserve.
Contents (Listed by paragraph and page number)
Chapter 1
General, page 1
Section I
Introduction, page 1
Purpose • 1
– 1, page 1
References • 1
– 2, page 1
Explanation of abbreviations and terms • 1
– 3, page 1
Contents—Continued
ii
AR 600–77 • 5 March 2019
Responsibilities • 1 – 4, page 1
Overview • 1
– 5, page 1
Objectives • 1
– 6, page 1
Section II
Responsibilities, page 1
Assistant Secretary of the Army (Financial Management and Comptroller) • 1
– 7, page 1
Assistant Secretary of the Army (Manpower and Reserve Affairs) • 1
– 8, page 2
Chief, National Guard Bureau • 1
– 9, page 2
Deputy Chief of Staff, G
– 1 • 1 – 10, page 2
Chief, Army Reserve • 1
– 11, page 3
The Surgeon General • 1
– 12, page 3
Assistant Chief of Staff for Installation Management • 1
– 13, page 5
The Judge Advocate General • 1
– 14, page 5
Senior commanders • 1
– 15, page 5
Warrior Transition Unit commanders • 1
– 16, page 6
Chapter 2
References to Statutes, Department of Defense Instructions and Duty Status Programs, page 6
Section I
Federal Legal Foundations and Department of Defense Guidance, page 6
Purpose • 2
– 1, page 6
Statutes • 2
– 2, page 7
Department of Defense instructions • 2
– 3, page 8
Section II
Reserve Component Duty Status Programs, page 8
Background • 2
– 4, page 8
Alternatives to active duty • 2
– 5, page 8
Medical retention processing (to include medical retention processing 2 and medical retention processing – evalua-
tion) • 2
– 6, page 8
Active duty medical extension • 2
– 7, page 9
Chapter 3
Eligibility and Application Processes for Medical Care of Wounded, Ill, and Injured Soldiers, page 9
Section I
Eligibility Criteria, page 9
Eligibility for medical care for Reserve Component Soldiers (mobilized/deployed) • 3
– 1, page 9
Continuation on active duty for medical care (medical retention processing/medical retention processing – evalua-
tion) • 3
– 2, page 10
Return to active duty for medical care (medical retention processing 2), contingency operations • 3
– 3, page 11
Return to active duty for medical care (active duty medical extension), non-contingency operations • 3
– 4, page 12
Declination of Reserve Component active duty medical care • 3
– 5, page 12
Withdrawal from Reserve Component active duty medical care • 3
– 6, page 13
Section II
Retiree recalls, retention beyond mandatory removal date, and sanctuary, page 14
Reserve Component Soldiers with 18 years but less than 20 years of active service • 3
– 7, page 14
Retiree recall retained on active duty for medical care • 3
– 8, page 15
Retention on active duty for medical care beyond mandatory removal date • 3
– 9, page 15
Section III
Resubmissions, appeals, and exceptions to policy for Reserve Component Duty Status Programs, page 15
Resubmissions • 3
– 10, page 15
Appeals • 3
– 11, page 16
Contents—Continued
AR 600–77 • 5 March 2019
iii
Exception to policy requests • 3 – 12, page 16
Section IV
Warrior Transition Unit Assignment or Attachment, page 18
Warrior Transition Unit eligibility and processing • 3
– 13, page 18
Community Care Unit • 3
– 14, page 18
Community Care Unit to Warrior Transition Unit transfer • 3
– 15, page 18
U.S. Department of Veterans Affairs medical centers • 3
– 16, page 18
Section V
Regular Army, Active Guard Reserve, and Reserve Component additional eligibility instructions, page 19
Regular Army and Active Guard Reserve • 3
– 17, page 19
Title 32 USC Army National Guard Active Guard Reserve • 3
– 18, page 23
Reserve Component • 3
– 19, page 23
Chapter 4
Application processes for medical care of wounded, ill and injured senior grade Soldiers, page 24
Senior grade or rank criteria • 4
– 1, page 24
General officer requests for entry into a Warrior Transition Unit • 4
– 2, page 24
General officer requests for extension beyond mandatory removal date • 4
– 3, page 24
General officer points of contact • 4
– 4, page 24
Chapter 5
Orders, page 24
Retention on active duty for medical treatment and evaluation (non-Active Guard Reserve) • 5
– 1, page 24
Return to active duty for medical treatment under medical retention processing 2 and the active duty medical extension
orders process • 5
– 2, page 26
Order extensions for medical retention process 2/active duty medical extension • 5
– 3, page 27
Medical temporary duty orders to the continental United States military treatment facilities • 5
– 4, page 27
Permanent change of station orders (Regular Army, Active Guard Reserve, and Soldiers on orders greater than 179
days) • 5
– 5, page 28
Retroactive modification of the effective date of orders • 5
– 6, page 28
Medical temporary duty orders • 5
– 7, page 28
Invitational travel authorizations in support of wounded Soldiers • 5
– 8, page 28
Orders distribution list for Reserve Component Soldiers • 5
– 9, page 29
Reserve Component management controls • 5
– 10, page 29
Patient movement • 5
– 11, page 30
Noncompliance • 5
– 12, page 30
Chapter 6
Personnel and Pay Actions, page 30
Section I
Personnel Functions, page 30
Line of duty determinations and access to medical and dental care • 6
– 1, page 30
Non-medical attendant and DD Form 93 • 6
– 2, page 31
Section II
Pay and Entitlements, page 32
Medical treatment and evaluation and active duty medical extension pay and entitlements • 6
– 3, page 32
Reserve Component DD Form 214 distribution • 6
– 4, page 32
Soldier pay processing within the Warrior Transition Unit or Community Care Unit • 6
– 5, page 33
Traumatic Servicemembers’ Group Life Insurance • 6
– 6, page 33
Section III
Supply and Logistics, page 33
Household goods • 6
– 7, page 33
Contents—Continued
iv
AR 600–77 • 5 March 2019
Unaccompanied personnel housing for wounded, ill, and injured Soldiers • 6 – 8, page 34
Return of personal effects from theater • 6
– 9, page 34
Chapter 7
Return to Duty, Release from Active Duty, Separation, and Retirement, page 35
Section I
Return to Duty, page 35
Assignment after completion of care • 7
– 1, page 35
Return to duty of Soldiers returned on temporary change of station or mobilization order • 7
– 2, page 35
Regular Army return to duty assignment procedures • 7
– 3, page 35
Active Guard Reserve return to duty assignment procedures • 7
– 4, page 36
Reserve Component release from active duty criteria • 7
– 5, page 36
Reserve Component released from active duty for medical condition existing prior to service • 7
– 6, page 37
Section II
Separation, page 37
Administrative separation of Regular Army and Reserve Component Soldiers found fit for duty • 7– 7, page 37
Reserve Component separation processing (non-Active Guard Reserve) • 7
– 8, page 37
Transitioning Soldiers from active duty while attached to a medical facility • 7
– 9, page 39
Process to separate an attached Warrior Transition Unit Soldier • 7– 10, page 39
Chapter 8
Benefits, page 40
Department of Veterans Affairs benefits briefing • 8
– 1, page 40
Soldier For Life - Transition Assistance Program • 8
– 2, page 40
Transitional Assistance Management Program • 8
– 3, page 40
Chapter 9
Support Sections, Agencies, and Organizations, page 40
Army retirement services • 9– 1, page
40
Legal information • 9
– 2, page 40
Soldier and Family Assistance Center • 9
– 3, page 40
U.S. Department of Veterans Affairs • 9
– 4, page 42
Chapter 10
Special Compensation for Assistance with Activities of Daily Living, page 43
Intent of the program • 10
– 1, page 43
Soldier’s application • 10
– 2, page 43
Determination of threshold eligibility • 10
– 3, page 45
Soldier is not eligible for the Special Compensation for Assistance with Activities of Daily Living compensation if re-
ceiving any of the following services • 10
– 4, page 46
Certification of DD Form 2948 • 10
– 5, page 47
Action on the application • 10
– 6, page 47
Computing compensation • 10
– 7, page 47
Regional Health Command payment authorization • 10
– 8, page 47
Notification to Soldier • 10
– 9, page 48
Special Compensation for Assistance with Activities of Daily Living packet • 10
– 10, page 48
Expiration of Special Compensation for Assistance with Activities of Daily Living eligibility • 10
– 11, page 50
Special Compensation for Assistance with Activities of Daily Living appeal process • 10
– 12, page 50
Continuation of Special Compensation for Assistance with Activities of Daily Living Compensation beyond 6
months • 10
– 13, page 50
Non-compliance to pay caregivers • 10
– 14, page 51
Appendixes
A. References, page 52
Contents—Continued
AR 600–77 • 5 March 2019
v
B. Internal Control Evaluation, page 59
Figure List
Figure 3
– 1: Declination of, or withdrawal from the Warrior Care and Transition Program, page 13
Figure 3
– 2: Exception, appeal, or resubmission request, page 17
Figure 3
– 3: Warrior Transition Unit nomination memorandum, page 21
Figure 3
– 3: Warrior Transition Unit nomination memorandum—Continued, page 21
Figure 3
– 4: Military treatment facility commander nomination memorandum, page 22
Figure 10
– 1: Sample notification memorandum to Soldiers of commander’s determination of eligibility regarding Spe-
cial Compensation for Assistance with Activities of Daily Living, page 45
Figure 10
– 1: Sample notification memorandum to Soldiers of commander’s determination of eligibility regarding Spe-
cial Compensation for Assistance with Activities of Daily Living—Continued, page 45
Figure 10
– 2: Sample memorandum from the regional health command to the defense finance and accounting service for
payment of Special Compensation for Assistance with Activities of Daily Living, page 46
Figure 10: 3. Sample language for DA Form 4856, Developmental counseling for Special Compensation for Assistance
with Activities of Daily Living, page 49
Glossary
AR 600–77 • 5 March 2019
1
Chapter 1
General
Section I
Introduction
1 – 1. Purpose
This regulation establishes policies and procedures for the administrative management of wounded, ill, or injured (WII)
Soldiers.
1 – 2. References
See appendix A.
1 – 3. Explanation of abbreviations and terms
See the glossary.
1 – 4. Responsibilities
Responsibilities are listed in chapter 1, section II.
1 – 5. Overview
This regulation governs policies and procedures necessary for the administrative management of WII Soldiers of all Army
components (Regular Army (RA) and Reserve Components (RC)). It reinforces existing personnel policy pertaining to
Soldiers in transition formerly outlined in the Warrior Transition Unit Consolidated Guidance – Administrative to include,
among other programs, active duty medical extension (ADME), medical retention processing (MRP) and medical retention
processing 2 (MRP2), and medical retention processing – evaluation (MRP
– E). It is complemented by the policies pre-
scribed in AR 40
– 58, AR 635 – 40, AR 600 – 8 – 4, and AR 40 – 400. The goal is to successfully and efficiently transition
Soldiers back to duty or to civilian life through comprehensive medical care, rehabilitation, and, if necessary, the Disability
Evaluation System (DES).
1 – 6. Objectives
a. To ensure the timely resolution of all aspects of WII Soldiers’ administrative management in the areas of personnel,
finance, and logistics, from identification of wound, illness, or injury through final disposition. Final disposition occurs
when the WII Soldier is found medically cleared and returned to duty (RTD), retires, or completes the DES process.
b. To ensure the timely resolution on the administrative aspects of medical management for the WII Soldier to include
care within either the military health system, the civilian network of care administered by the Tri-Service Medical Care
(TRICARE) health plan, or support provided by the Veterans Health Administration.
c. To ensure senior commander logistical support for WII Soldiers assigned or attached to a garrison unit, military
treatment facility (MTF), Warrior Transition Unit (WTU), Community Care Unit (CCU), or organic unit.
d. To ensure accountability and tracking during their progression through the healing process and, if necessary, the DES
process.
Section II
Responsibilities
1 – 7. Assistant Secretary of the Army (Financial Management and Comptroller)
On behalf of the ASA (FM&C), the Commander, U.S. Army Financial Management Command (USAFMCOM) will—
a. Assist, as requested, the Deputy Chief of Staff, G
– 1 (DCS, G – 1) in developing personnel policy for WII Soldiers, to
include the Warrior Care and Transition Program (WCTP).
b. Conduct oversight of finance roles and responsibilities in all aspects of WTU operations.
c. Resolve and/or assist in resolving military and travel pay issues.
d. Coordinate with Defense Finance and Accounting Service (DFAS), Army National Guard (ARNG), and U.S. Army
Reserve (USAR) pay and/or ombudsman offices for pay support and provide procedural, policy, and pay systems guidance.
2
AR 600–77 • 5 March 2019
e. Coordinate, when necessary, with DFAS, ARNG, and USAR pay and/or ombudsman offices to support WII Soldiers
and the WCTP, staff assistance visits, and the Organizational Inspection Program.
f. Ensure compliance with the DFAS Wounded Warrior Pay Management Program.
g. Coordinate and schedule military pay courses, Wounded Warrior Pay Management Program training, and travel
voucher preparation and review training for finance management specialist in WTUs and CCUs.
h. Train new ombudsman personnel on financial management matters.
i. Establish or revise financial management operations memoranda of agreement, as necessary, with the DFAS, the U.S.
Army Medical Command (MEDCOM), ARNG, and USAR.
j. Report monthly metrics on mobilization and demobilization pay (tours), medical orders, and aero medical evacuation
entitlements timeliness to the DCS, G
– 1.
1 – 8. Assistant Secretary of the Army (Manpower and Reserve Affairs)
The ASA (M&RA) will—
a. Provide policy and oversight for the administrative management (personnel, finance, and logistics) of WII Soldiers.
b. Coordinate, as necessary, personnel policy for WII Soldiers with Headquarters, Department of the Army (DA) staff
elements, other Army commands, and Army service component commands.
c. Coordinate with the DCS, G
– 1 in developing WII Soldiers’ administrative management guidance in coordination
with MEDCOM; U.S. Army Installation Management Command (IMCOM); U.S. Army Human Resources Command
(HRC); U.S. Army Physical Disability Agency (USAPDA); ARNG; U.S. Army Reserve Command (USARC);
USAFMCOM; and DFAS.
d. Oversee the Special Compensation for Assistance with Activities of Daily Living (SCAADL) Program.
1 – 9. Chief, National Guard Bureau
The CNGB will—
a. Assist the DCS, G
– 1, and MEDCOM in developing personnel policy for the WII Soldier population, to include the
WCTP.
b. Assist the local servicing finance office or WTU financial management specialist, upon request, in order to resolve
military and travel pay inquiries and assist Family members in travel voucher processing and payment, as necessary.
c. Coordinate with and assist DFAS in completing pay account reviews and maintenance.
d. Assist USAFMCOM and DFAS in responding, upon request, to inquiries or pay account audits.
e. Coordinate, when necessary, with USAFMCOM, DFAS, and USAR pay and/or ombudsman offices.
f. Provide, upon request and as available, personnel for CCU operations and task force personnel.
g. Process medical orders (initial and extensions) into the reserve pay system for the ARNG.
h. Provide primary overall pay support to WII Soldiers, including those attached or assigned to WTUs or CCUs.
i. Assist MEDCOM with analysis of personnel strength data for all WTUs and CCUs and develop a sustainable multi-
component manning strategy that supports directed Cadre-to-WII Soldier ratios.
j. Execute necessary mobilization tasks to support the ARNG portion of the developed manning strategy.
1 – 10. Deputy Chief of Staff, G – 1
The DCS, G
– 1 will—
a. Develop personnel policy for the administrative management (personnel, finance, and logistics) of WII Soldiers in
coordination with ASA (M&RA); MEDCOM; IMCOM; HRC; DCS, Warrior Care and Transition (WCT); MEDCOM
Soldier Transition Branch; USAPDA; ARNG; USAR ; USAFMCOM; and DFAS.
b. Provide policy guidance for WII Soldiers as directed by the ASA (M&RA).
c. Oversee the execution of the SCAADL Program for WII Soldiers.
d. Coordinate with the ASA (M&RA) to develop and propagate any additional administrative procedures necessary for
the SCAADL Program to include appropriate internal controls applicable to commanders and the regional health command
(RHC) in accordance with AR 11
– 2.
e. Ensure the Commanding General (CG), HRC—
(1) Develops procedures, conducts technical oversight and quality control of personnel actions, assignments, and at-
tachments, and ensures accountability and Soldier welfare.
(2) Conducts training on personnel management and strength accounting procedures, internally and externally, for key
personnel in coordination with MEDCOM and other Army commands and Army service component commands.
(3) Receives and reviews initial and extension packets for completeness.
AR 600–77 • 5 March 2019
3
(4) Maintains accountability of participants by maintaining a monthly internal tracking program and reporting metrics
to DCS, G
– 1.
(5) Assists MEDCOM with analysis of personnel strength data for all WTU or CCUs and develops a sustainable multi-
component manning strategy that supports directed Cadre-to-Soldier assigned or attached to WTU ratios.
(6) Executes necessary mobilization tasks to support the USAR and ARNG portions of the developed manning strategy.
(7) Manages pay and allowances continuation in accordance with Section 372, Title 37, United States Code (37 USC
372).
(8) Ensures the USAPDA—
(a) Assists the DCS, G
– 1 in developing personnel policy for DES processing.
(b) Trains cadre on the DES processes.
(c) Coordinates and manages all Soldiers on the temporary disability retired list (TDRL).
(d) Coordinates with Department of Defense (DOD) and other military departments to facilitate uniform interpretation
of applicable DES laws, policies, and directives among the services.
(e) Implements policies from HRC, Headquarter, Department of the Army, and DOD.
(f) Makes final decisions on behalf of the Secretary of the Army (SECARMY) concerning a Soldier’s fitness for duty
that relates to physical disability; except when a decision is reserved for a higher authority including Office of the Secretary
of Defense, Office of the Secretary of the Army, ASA (M&RA), DCS, G
– 1, or HRC.
(g) Maintains an automated database system to track and record a Soldier’s progress through the DES.
(h) Responds to requests for information about the DES from Soldiers, the Soldier’s chain of command, Headquarter,
Department of the Army, and Congressional inquiries.
(i) Conducts a weekly review and takes the appropriate action on all WTU cases received by the physical evaluation
board (PEB) or USAPDA that are older than 90 days and provides a weekly report to DCS, G
– 1.
(j) Schedules formal hearings requested by WTU Soldiers for a date within 30 calendar days of the Soldier’s request.
(k) Enters a separation/retirement date (no later than 30 calendar days from the completion of processing a Soldier’s
case) into the Transition Processing System (TRANSPROC), Veterans Tracking Application, and Integrated Disability
Evaluation System Dashboard, and provide a weekly report to the DCS, G
– 1.
(l) Manages the subordinate elements of the USAPDA.
(m) Reviews PEB proceedings to ensure that Soldiers are given uniform consideration under the applicable laws, poli-
cies, and directives.
1 – 11. Chief, Army Reserve
The CAR will—
a. Assist the DCS, G
– 1 and MEDCOM in developing personnel policy for the WII Soldier population, to include the
WCTP.
b. Assist the local servicing finance office or WTU financial management specialist, upon request, in order to resolve
military and travel pay inquiries and assist Family members in travel voucher processing and payment, as necessary.
c. Coordinate with and assist DFAS in completing pay account reviews and maintenance.
d. Assist USAFMCOM and DFAS in responding, upon request, to inquiries or pay account audits.
e. Coordinate, when necessary, with USAFMCOM, DFAS, and ARNG pay and/or ombudsman offices.
f. Provide, upon request, personnel for WTU and CCU operations on installation and USAR liaison personnel for WTU
and CCU sites.
g. Assist MEDCOM with analysis of personnel strength data for all WTUs and CCUs.
h. Develop a sustainable multi-component manning strategy that supports directed Cadre-to-WII Soldier ratios.
i. Execute necessary mobilization tasks to support the USAR portion of the developed manning strategy.
1 – 12. The Surgeon General
a. TSG will—
(1) Assist the DCS, G
– 1 in developing personnel policy for WII Soldiers to include WTU and CCU operations in
coordination with ASA (M&RA), IMCOM, HRC, USAPDA, ARNG, USAR, USAFMCOM, and DFAS.
(2) Support synchronizing efforts of ARNG, USARC, and other agencies in support of WTU and CCU operations.
(3) Maintain ownership of WTU and CCU dedicated assets, tasking authority, and funding responsibility.
(4) Establish medical decision criteria and make individual evaluations on type and location of medical treatment for
Soldiers.
(5) Ensure that the RHCs provide senior command, personnel, logistical, fiscal, legal, chaplain, and communications
coordination and support to WTUs and CCUs.
4
AR 600–77 • 5 March 2019
(6) Establish technical procedures to conduct quality assurance review of the medical evaluation board (MEB) and the
physical evaluation board liaison officer (PEBLO) functions.
(7) Conduct periodic assistance visits of WTU and CCU sites to ensure compliance with established operation stand-
ards.
(8) Develop and implement medical standards and policy to support the WII Soldier population to include provision of
clinical care, case management, monitoring outcomes, treatment tracking, ensuring appropriate and adequate clinical re-
sources and support, and providing staff orientation and education.
(9) Provide overall technical supervision and quality control over all medical aspects of the WII Soldier population,
including the WCTP.
(10) Manage and provide manpower and funding requirements to support the WII Soldier population, to include the
WCTP.
(11) Maintain ownership of WTU and CCU dedicated assets, tasking authority, and funding responsibility.
(12) Establish medical decision criteria and make individual evaluations on type and location of medical treatment for
Soldiers. Medical decision criteria will be made in a manner that conforms to and supports existing statutory and policy-
based obligations to Soldiers who require medical treatment or evaluation.
(13) Ensure that the RHCs provide senior command support, personnel, logistical, fiscal, legal, chaplain, and commu-
nications coordination and support to WTUs and CCUs.
(14) Establish technical procedures to conduct quality assurance reviews of the MEB, medical evaluation board transi-
tion office and the PEBLO functions.
(15) Ensure the provision of personnel, logistical, and finance support for the WII Soldier population, to include the
WCTP.
(16) Conduct periodic assistance visits of WTU and CCU sites to ensure compliance with established operation stand-
ards.
(17) Monitor and track all non-medical attendants (NMA) in accordance with AR 11
– 2.
(18) Serve as the orders issuing authority for orders requested under 10 USC 12301(h) (hereafter referred to as 10 USC
12301(h) orders).
(a) Contact appropriate agencies to revoke remainder of current active duty orders, if needed, when a Soldier is ap-
proved for 10 USC 12301(h) orders.
(b) Contact appropriate agencies to ensure continuation of pay and entitlements, if needed, when a Soldier is concur-
rently transitioned from an active duty order to a 10 USC 12301(h) order.
(c) Forward a copy of the 10 USC 12301(h) orders to the Soldier’s home address, organic unit, losing and gaining units,
RHC senior case manager, ARNG Resources Management Comptroller Financial Services Center (ARNG
– RMC – F), and,
if applicable, the Joint Forces Headquarters.
(d) Provide a monthly report to the DCS, G
– 1 on the status of 10 USC 12301(h) orders. The report will include the
following data, as a minimum:
1. List of Soldiers on 10 USC 12301(h) orders.
2. Start and end date of orders.
3. Location of attachment/assignment of the Soldier.
(19) Ensue the RHC commander—
(a) Establishes and maintains a transmittal control log for all incoming SCAADL-related documents.
(b) Appoints one regular and one alternate certifying officer who are authorized to transmit SCAADL payment data to
DFAS for payment.
(c) Submits a certified DD Form 577 (Appointment/Termination Record - Authorized Signature).
(d) No later than the 15th day of each month, submits a consolidated pay authorization roster to DFAS to effect timely
SCAADL payments for each eligible Soldier.
(e) Prepares a monthly roster of all Soldiers and their primary caregivers who are currently receiving Veterans Affairs
(VA) caregiver benefits not associated with SCAADL; ensures Soldiers are not receiving duplicative benefits.
(f) Prepares a monthly feedback report documenting all SCAADL actions completed, to include the amount of
SCAADL payments disbursed to each eligible Soldier and transmits the report by the last day of each month to WCTP,
(MCWT
– HR).
(g) Retains the records pertaining to SCAADL payments for 3 years, including—
1. The completed application.
2. The payment computation.
3. Documentation to DFAS authorizing payment.
(h) Ensures that commanders are completing Soldier’s reevaluation every 6 months to validate eligibility and assure
uninterrupted payments of SCAADL benefits.
AR 600–77 • 5 March 2019
5
(i) Ensures the RHC certification officer—
1. Becomes thoroughly familiar with Chapter 33, Volume 5 of the DOD Financial Management Regulation
(DODFMR), AR 11
– 2, and DODI 1341.12.
2. On behalf of the command, submits Soldier’s status changes to DFAS, as required, especially SCAADL eligibility
redetermination at least every 6 months or earlier should the Soldier’s medical condition or circumstances change.
(j) Ensures the DCS, WCT—
1. Serves as the lead proponent for the WCTP.
2. Executes the Army Wounded Warrior Program for MEDCOM and the Army.
3. Develops and executes an Organization Inspection Program to enforce the standardized execution of the WCTP.
4. Coordinates the movement of WTU Soldiers with MEDCOM, DCS, G
– 1, HRC, USAR, and ARNG.
5. Oversees the WCTP to ensure clinical compliance and assesses the impact policies have on recovery and reintegra-
tion for WTU Soldiers.
6. Develops and conducts training for the WTU and CCU cadre.
7. Oversees the execution of personnel and finance support within WTU and CCU operations.
8. Manages manpower and funding requirements in coordination with MEDCOM.
9. Synchronizes the efforts of ARNG, USAR, DFAS, USAFMCOM, and other agencies in support of the WII Soldier
population, to include WTU and CCU operations.
10. Receive all monthly feedback reports documenting all SCAADL actions completed, to include the amount of
SCAADL payments disbursed to each eligible Soldier and consolidate the reports into one program-wide report.
11. Provide the DCS, G
– 1 with annual SCAADL funding requirements, with input from the RHCs (Warrior Transition
offices).
1 – 13. Assistant Chief of Staff for Installation Management
ACSIM through the CG, IMCOM will—
a. Assist, as required, the MEDCOM and DCS, WCTP.
b. Provide non-clinical support service through the IMCOM Soldier and Family Assistance Center (SFAC).
c. Collaborate with MEDCOM and HRC, ARNG, or USAR, respectively, to implement procedures for the transfer of
Soldiers from IMCOM installation-to-installation, installation-to-CCU, and CCU-to-installation.
d. Support WTU and CCU commanders with installation personnel administrative processes.
e. Provide support to the WTU adjutant (S-1) to ensure the complete installation in-processing of Soldiers, including
all personnel and pay actions such as, personnel status changes to support accountability in the electronic Military Person-
nel Office (eMILPO) and updating DD Form 93 (Record of Emergency Data) and Servicemembers’ Group Life Insurance
(SGLI) forms (including SGLV 8286 (Servicemembers' Group Life Insurance Election and Certificate), SGLV 8286S
(Servicemembers' Group Life Insurance Supplemental SGLI Beneficiary Form), SGLV 8283 (Claim for Death Benefits),
SGLV 8284 (Claim for Accelerated Benefits), and SGLV 8715 (Application for the Servicemembers' Group Life Insurance
(SGLI) Disability Extension)), update the Defense Enrollment Eligibility Reporting System (DEERS), and issue Family
member identification cards, if necessary.
f. Provide Soldier for Life-Transition Assistance Program (SFL
– TAP) services at the SFAC.
g. Conduct IMCOM specific deployment cycle support, redeployment (see AR 600
– 8 – 101), and additional tasks for
WTU Soldiers and their Families.
1 – 14. The Judge Advocate General
TJAG will—
a. Provide advice and opinions to the Army Staff and, in coordination with the Army Office of the General Counsel,
Army Secretariat concerning the laws and regulations governing the Army DES.
b. In coordination with MEDCOM and through the Office of Soldiers’ Counsel, train and provide sufficient legal coun-
sel to represent Soldiers upon referral and throughout the Army DES.
c. Train Army attorneys in Army DES disability law.
1 – 15. Senior commanders
The senior commander will—
a. Serve as member of the Triad of Leadership.
b. Execute policy for the WTU entry and exit management of WII Soldiers in accordance with statutory guidance.
c. Ensure all WII Soldiers on their installation are properly managed.
6
AR 600–77 • 5 March 2019
d. Coordinate with MEDCOM and HRC to ensure quality officers and noncommissioned officers are in leadership
positions to serve as commanders, first sergeants, and platoon sergeants.
e. Ensure the WTU is staffed at the specified Cadre-to-Soldier ratios.
f. Ensure the Triad of Leadership maintains good order and discipline in the WTUs and enforces all applicable ARs.
1 – 16. Warrior Transition Unit commanders
The WTU commanders will—
a. Serve as member of the Triad of Leadership.
b. Provide command and control for WII Soldiers.
c. Evaluate and process all administrative and Uniform Code of Military Justice (UCMJ) actions for assigned or at-
tached Soldiers.
d. Establish sponsorship program for assigned or attached Soldiers and their Families.
e. In accordance with applicable Army regulations, establish policies and procedures that include initial interface or
intake procedures, Family readiness group involvement, transition procedures, process for conduct of traumatic brain in-
jury or posttraumatic stress disorder briefings, briefing on the SCAADL Program, referral to CCU procedures, conduct of
behavioral health assessment, line of duty (LOD) processing, housing procedures, and standardized new cadre or com-
mander orientation in-brief.
f. Establish conditions that facilitate Soldier’s physical, mental, and spiritual healing process.
g. Coordinate with MEDCOM to move eligible RC Soldiers from their initial order type to a 10 USC 12301(h) order.
h. Ensure for all departing Soldiers that the gaining installation WTU command element contacts the Soldier and Sol-
dier’s unit for coordination of his or her arrival.
i. Initiate requests for CCU attachment and forward to MEDCOM.
j. Ensure extension requests are completed and forwarded to MEDCOM no later than 45 days before current orders
expire in order to prevent a gap in orders.
k. Coordinate with original mobilization installation and losing installation for the transfer of records, documentation
of deployment cycle, and other administrative information, as appropriate.
l. Ensure Soldiers assigned or attached to their units who have completed DES processing and have been loaded into
the military personnel TRANSPROC report to the transition center, within 3 working days of notification by the transition
center (Soldiers assigned/attached to a CCU need not return to the supporting installation transition center for processing.
CCU will coordinate directly with supporting transition center to provide counseling statement and separation date infor-
mation within the 3-day limit).
m. Ensure the required transition counseling has occurred and DA Form 31 (Request and Authority for Leave) is pro-
vided for permissive temporary duty (TDY) and transition leave within this 3-day period.
n. Ensure that the unit finance management specialist briefs new commanders, staff, and cadre within 30 days of their
arrival to the unit on the importance of pay timeliness, pay accuracy, unit commander’s finance report (for RA), unit
commander’s pay management report (for RC), leave (DA Form 31) accountability and processing, internal controls, and
entitlements.
o. Establish and maintain a working relationship with the SFAC program and SFAC Director.
Chapter 2
References to Statutes, Department of Defense Instructions and Duty Status Programs
Section I
Federal Legal Foundations and Department of Defense Guidance
2 – 1. Purpose
This chapter includes references to the legal foundations and departmental instructions from Title 10 USC, Chapter 55 and
related DODIs, authorizing the access to care, entitlements and benefits for Soldiers in various duty statuses. These statutes
and instructions, considered collectively, ensure that Soldiers from all components have access to medical treatment and
evaluation from the point of illness or injury to final disposition determining a return to duty, retirement or separation from
the military. The guidance in this regulation is built on the purpose and intent of the various authorities listed below and
can only be superseded by guidance from this proponent.
AR 600–77 • 5 March 2019
7
2 – 2. Statutes
a. 10 USC 1074, Medical and dental care for members and certain former members. This section of Title 10 Chapter
55 states that “under joint regulations to be prescribed by the administering Secretaries, the following Soldiers are entitled
to medical and dental care in any facility of any uniformed service:” This section refers primarily to Regular Army Soldiers,
Soldiers scheduled for active duty orders, Soldiers entitled to retired or retainer pay, or Soldiers without any other health
care insurance and not covered by any other health benefits plan, listed as such:
(1) A Soldier on active duty;
(2) A member of a RC of a uniformed service who has been commissioned as an officer if—
(a) The member has requested orders to active duty for the member's initial period of active duty following the com-
missioning of the member as an officer;
(b) The request for orders has been approved;
(c) The orders are to be issued but have not been issued or the orders have been issued but the member has not entered
active duty; and
(d) The member does not have health care insurance and is not covered by any other health benefits plan;
(3) A Soldier or former Soldier who is entitled to retired or retainer pay, or equivalent pay may, upon request, be given
medical and dental care in any facility of any uniformed service, subject to the availability of space and facilities and the
capabilities of the medical and dental staff. This does not apply to a member or former member entitled to retired pay for
non-regular service under chapter 3 of Title 10 who is under 60 years of age.
b. 10 USC 1074a, Medical and dental care for members on duty other than active duty for a period of more than 30
days. Summarily, this statute authorizes each member of a uniformed service who incurs or aggravates an injury, illness,
or disease in the LOD while performing active duty for a period of 30 days or less, inactive duty training, or service on
funeral honors duty to receive medical and dental care appropriate for the treatment of the injury, illness, or disease of that
person until the resulting disability cannot be materially improved by further hospitalization or treatment. A member is not
entitled to medical and dental care appropriate for the treatment of the injury, illness, or disease if the injury, illness, or
disease, or aggravation of an injury, illness, or disease is the result of the gross negligence or misconduct of the member.
c. 10 USC 1206a, Reserve Component members unable to perform duties when ordered to active duty: disability system
processing. A member of a RC who is ordered to active duty for a period of more than 30 days and is released from active
duty within 30 days of commencing such period of active duty for failure to meet physical standards for retention due to a
preexisting condition not aggravated during the period of active duty; or failure to meet medical or dental standards for
deployment due to a preexisting condition not aggravated during the period of active duty will be considered for all pur-
poses under the authority of 10 USC 1206(a) to have been serving under an order to active duty for a period of 30 days or
less.
d. 10 USC 1218(d), Discharge or release from active duty: claims for compensation, pension, or hospitalization. A
member of an Armed Force may not be discharged or released from active duty because of physical disability until he or
she has made a claim for compensation, pension, or hospitalization, to be filed with the Department of Veterans Affairs or
has refused to make such a claim; or has signed a statement that his/her right to make such a claim has been explained to
him/her, or has refused to sign such a statement.
e. 10 USC 12301(h), Reserve components generally.
(1) RC on active duty to receive authorized medical care. When authorized by the Secretary of Defense, the Secretary
of the Army may, with the consent of the Soldier, order a member of the RC to active duty—
(a) To receive authorized medical care;
(b) To be medically evaluated for disability or other purposes; or
(c) To complete a required DOD health care study, which may include an associated medical evaluation of the member.
(2) A Soldier ordered to active duty under this subsection may, with the member's consent, be retained on active duty,
if the Secretary of the Army considers it appropriate, for medical treatment for a condition associated with the study or
evaluation, if that treatment of the member is otherwise authorized by law. A member of the ARNG of the United States
may be ordered to active duty under this subsection only with the consent of the Governor or other appropriate authority
of the State concerned.
f. 10 USC 12322, Active duty for health care. A Soldier who incurs or aggravates an injury, illness, or disease in the
line of duty may be continued on active duty, for a period of more than 30 days while the Soldier is being treated for (or
recovering from) an injury, illness, or disease when—
(1) A Soldier is performing inactive-duty training or while traveling directly to or from the place at which that member
is to perform or has performed inactive-duty training.
(2) A Soldier performs active duty for a period of 30 days or less or while traveling directly to or from the place at
which that member is to perform or has performed active duty incurred or aggravated in the line of duty.
8
AR 600–77 • 5 March 2019
2 – 3. Department of Defense instructions
a. DODI 1241.01. This Instruction establishes policy and provides guidance for determining an entitlement to medical
and dental treatment and pay and allowances for RC Service members with injury, illness, or disease incurred or aggravated
in the line of duty. Specifically, this department-wide policy instructs that an LOD determination is the mechanism for
determining an RC Servicemember entitlement to medical and dental treatment and incapacitation pay for an injury, illness,
or disease incurred or aggravated while in a qualified duty status and that is not the result of gross negligence or misconduct.
b. DODI 1332.18. This department-wide policy instructs that the DES is the mechanism for determining return to duty,
separation, or retirement of Servicemembers because of disability.
Section II
Reserve Component Duty Status Programs
2 – 4. Background
Drawing from 10 USC, the DOD has two DODIs prescribing responsibilities to the services to retain or order RC Soldiers
(with Soldier consent) to active duty for purposes of medical treatment or evaluation. The process is initiated with a duty
status determination. The Army created four distinct duty status programs with associated eligibility criteria to support RC
Soldiers who require authorized medical treatment or evaluation. The LOD determination process outlined in AR 600
– 8 – 4
serves as the basis for authorizing orders and medical treatment or evaluation. All active duty orders published specifically
for medical purposes are designated as 10 USC 12301(h) orders in accordance with the Section of Title 10 that addresses
active duty orders for medical purposes (10 USC 12301(h); 10 USC 1074a). All 10 USC 12301(h) orders are voluntary on
the part of the Soldier.
2 – 5. Alternatives to active duty
An RC Soldier may elect incapacitation pay or demobilization and pursuit of medical care through the Veterans Admin-
istration health system or outside the purview of the Army through his or her civilian medical benefit. The Office of The
Surgeon General (OTSG)/MEDCOM executes the provision of medical and dental care and provides programmatic sup-
port for eligible Soldiers who enter the WCTP through an attachment to a WTU or CCU. An OTSG/MEDCOM medical
review board executes duty status determinations for two programs (ADME and MRP2). In accordance with AR 40
– 58,
Triad of Leadership (comprised of the senior commanders and installation command sergeants major (CSMs); MTF com-
manders and MTF CSMs; and WTU commanders, CSMs and first sergeants) at Army installations provide governance for
the two remaining programs (MRP and MRP
– E). The below paragraphs describe each of the four duty status programs
that serve as the basis for voluntary retention on or an order to active duty.
2 – 6. Medical retention processing (to include medical retention processing 2 and medical retention
processing – evaluation)
The basis for the MRP programs (including MRP2 and MRP
– E) is drawn directly from DODI 1241.01 and DODI 1332.18
which state that RC Soldiers who are on active duty orders, in support of contingency operations (for example, 10 USC
12301(a), 12302, 12304(a)(b), 12301(d)), greater than 30 days will, with Soldier consent, be retained on or returned to
active duty for authorized medical treatment or evaluation.
a. Medical retention processing – evaluation. MRP
– E was created based on a recognition that Soldiers may arrive at
a mobilization force generation installation or other demobilization site without medical documentation that support MRP
orders. Short duration MRP
– E orders may be generated, affording an opportunity for a medical provider to evaluate and,
if necessary, create a medical care plan. Soldiers on MRP
– E orders will either: (1) demobilize subsequent to evaluation (if
no MRP-qualifying medical treatment or DES adjudication is required), or (2) transition to MRP orders. MRP
– E decisions
will be executed by the supporting installation Triad of Leadership based on the recommendation of the medical Soldier
readiness processing site (or other military medical provider) recommendation. The supporting WTU provides operational
and administrative support to the RC Soldier for the duration of MRP
– E orders.
b. Medical retention processing. If, during the course of a contingency mobilization or during demobilization pro-
cessing, it becomes evident that a Soldier has incurred or aggravated a duty-related medical condition, the Soldier may be
transitioned from operational mobilization orders to MRP orders. Eligibility criteria and application instructions are pre-
scribed in chapter 3. Requests for MRP orders will be produced by the Soldier’s unit of assignment with the commander’s
referral letter and forwarded to the supporting WTU. The installation Triad of Leadership of the supporting WTU location
will review the MRP packet and, subject to approval, ensure that the Soldier is directly transitioned from existing orders
to MRP orders.
AR 600–77 • 5 March 2019
9
c. Medical retention processing 2. MRP2 was created based on a recognition that RC Soldiers may demobilize from
contingency operations without receiving the appropriate guidance/support for transition to MRP orders or the medical
condition may become evident pursuant to demobilization. If, during the 180 days pursuant to demobilization, it becomes
evident that the Soldier requires authorized medical treatment or evaluation, a MRP2 application may be submitted. Eligi-
bility criteria and application instructions are prescribed in chapter 3. Requests for MRP2 orders will be produced by the
Soldier’s unit of assignment with the commander’s referral letter and forwarded to the OTSG/MEDCOM medical review
board for adjudication. If approved, MEDCOM G1 will generate MRP2 orders returning the Soldier to active duty and the
Soldier will be attached to a supporting WTU.
2 – 7. Active duty medical extension
The ADME Program was created to support RC Soldiers in a non-mobilization status. Non-mobilization duty statuses may
include, but are not limited to, active duty for operational support, active duty for training, annual training, and inactive
duty training. Non-mobilized Soldiers who incur or aggravate a medical condition documented with a LOD may be eligible
for ADME. Eligibility criteria and application instructions are prescribed in chapter 3. Requests for ADME orders will be
produced by the Soldier’s unit of assignment with the commander’s referral letter and forwarded to the OTSG/MEDCOM
medical review board for adjudication. If approved, MEDCOM G1 will generate ADME orders and the Soldier will be
attached to a supporting WTU.
Chapter 3
Eligibility and Application Processes for Medical Care of Wounded, Ill, and Injured Soldiers
Section I
Eligibility Criteria
3 – 1. Eligibility for medical care for Reserve Component Soldiers (mobilized/deployed)
a. Purpose. To establish eligibility criteria and mandated procedures for RC Soldiers seeking active duty medical care.
b. Post mobilization and/or pre-deployment.
(1) Defined as Soldiers placed on orders after mobilization date (M-date) through departure from the mobilization sta-
tion and movement to an outside the continental United States (OCONUS) or continental United States (CONUS) assign-
ment.
(2) Soldiers who have incurred or aggravated a wound, illness, or injury and are found medically non-deployable by a
military medical authority, but can receive treatment that will change their status to deployable in a reasonable timeframe
(less than 90 days), will be kept on partial mobilization orders and managed by the installation or unit to which they are
assigned or attached.
(3) If, at any time, a military medical authority determines the Soldier will not RTD within a reasonable time (less than
90 days), the Soldier will be retained on active duty to receive medical treatment or to undergo DES processing, subject to
his or her consent to remain on active duty orders.
(a) If the Soldier agrees to remain on active duty for medical treatment, he or she is attached to the installation WTU
on 10 USC 12301(h) orders.
(b) If the Soldier declines to remain on active duty for medical treatment, he or she will be released from active duty
(REFRAD) back to his or her respective RC unit.
(4) In the event of an emergent situation where the Soldier is unable to consciously make the decision to request or
decline WTU orders, the legal next of kin identified on the Soldier’s DD Form 93 has the authority to decide for the Soldier.
If there is no legal next of kin, the unit commander will treat this case as emergent and request WTU orders on behalf of
the Soldier. The commander may only utilize this authority for the initial order. All other determinations to remain on
active duty will be determined by the legal next of kin. If legal next of kin cannot be identified or found and the com-
mander’s signature is required, then a memorandum should be submitted to MEDCOM from the WTU stating, “All re-
sources have been utilized to contact the Soldier’s legal next of kin with no response; therefore, I am authorizing the
Soldier’s continued participation in the WCTP based on the Soldier’s medical need and the recommendation of the primary
physician.”
c. Deployment.
(1) Defined as Soldiers who are evacuated from a theater of operation or a CONUS mobilization assignment that incur
an LOD wound, illness, or injury or aggravate a pre-existing condition.
(2) When the medical authority determines that a Soldier evacuated from a theater or CONUS assignment will RTD
within a reasonable timeframe, the Soldier remains on his or her current mobilization order and enrolled in the WCT
10
AR 600–77 • 5 March 2019
program until medical authority determination returns the Soldier to duty. If, during that time, the medical authority deter-
mines the medical condition will not be resolved within a reasonable time (less than 90 days) the Soldier is evaluated for
placement into a WTU on a 10 USC 12301(h) order.
(3) If the medical authority determines a Soldier will not RTD within a reasonable time (less than 90 days) when he or
she is WII, the Soldier will be retained on active duty for medical treatment or to undergo DES processing, subject to his
or her consent. If the Soldier consents to remain on active duty orders, he or she will be attached to a WTU on 10 USC
12301(h) orders. If the Soldier does not consent, he or she is REFRAD back to his or her respective RC unit. See chapter
3, section II for further information on declination of/withdrawal from the WCTP.
d. Post-deployment.
(1) Defined as Soldiers arriving at the demobilization station and determined by military medical authority to have an
LOD wound, illness, or injury or aggravated pre-existing medical condition incurred during the current deployment. These
Soldiers will be evaluated for WTU placement. If the Soldier agrees, he or she is attached to the installation WTU on 10
USC 12301(h) orders. Soldiers who decline will be REFRAD to their respective RC unit.
(2) If the transition of medical care is required, the Soldiers will be counseled on access to care utilizing VA benefits,
TRICARE benefits, or the Defense Health Agency-Great Lakes (DHA
– GL).
e. In-patient. Defined as Soldiers that are hospitalized in a VA hospital, MTF, or a civilian hospital for the evaluation
and/or treatment of injuries incurred or aggravated in the LOD. The Soldier’s current command will process DA Form
7692 (Active Duty for Medical Care Application), DA Form 7696 (Commander’s Performance and Capability Checklist)
to remain on or return to active duty; if the Soldier volunteers to do so and is approved for WTU entry.
f. Rest and recuperation leave. When a Soldier is on leave and requires emergency medical care and is admitted to a
civilian facility, he or she will be processed as “absent sick” and will be picked up by the MTF responsible for that geo-
graphical location and dispositioned according to current policies and procedures. The process for an RC Soldier on rest
and recuperation leave would be no different than a RA Soldier on ordinary leave who is injured and taken to a civilian
hospital for emergency care. The Soldier will be processed through regular medical channels to ensure the responsible
MTF is aware of the location and current medical status of the Soldier. Depending on the injury or illness the Soldier may
return to theater or be assigned or attached to a WTU. Care can continue at a civilian hospital if the Soldier is unable to be
physically moved.
g. Transitional leave. If a Soldier becomes ill or injured while on transitional leave, he or she must be processed
through military medical channels. If the Soldier is treated in a civilian facility, the MTF responsible for that geographical
location will pick up the Soldier and coordinate with the nearest WTU for assignment or attachment. The previous unit of
assignment or attachment coordinates with HRC to adjust or amend the DD Form 214 (Certificate of Release or Discharge
from Active Duty).
3 – 2. Continuation on active duty for medical care (medical retention processing/medical retention
processing – evaluation)
a. Purpose. To retain Soldiers for evaluation and treatment of medical conditions requiring case management.
b. Eligibility. RC Soldiers on active duty orders for more than 30 days who incur or aggravate a wound, illness, or
injury with a definitive treatment plan requiring one of the following are eligible to request voluntarily retention on active
duty:
(1) Require definitive care; or
(2) A permanent profile that refers the Soldier into the DES. If approved, the Soldier will be retained on active duty
until he or she meets their medical retention determination point (MRDP) and is returned to duty, REFRAD, or separated
or retired as a result of the DES process.
c. Ineligibility.
(1) Soldiers ordered to active duty for more than 30 days that are REFRAD within the first 30 days for a wound, illness,
or injury that is not determined to be incurred or aggravated during the current period of active duty.
(2) Soldiers with pending actions under the UCMJ.
(3) Soldiers who are flagged or are pending adverse action are prohibited for assignment or attachment to a WTU until
the action is complete. This includes any punishment phase. Soldiers flagged solely based on Army Physical Fitness Test
failure or for enrollment in the Army Body Composition Program remain eligible for assignment or attachment to a WTU.
(4) A Soldier who is qualified for retention on active duty for the purpose of medical care and who is also pregnant
may be retained on active duty if the pregnancy will not interfere with the medical care needed for the qualifying wound,
illness, or injury.
(5) In the event of an emergent situation where the Soldier is unable to consciously make a decision to request or decline
medical orders, the legal next of kin has the authority to decide for the Soldier. If there is no legal next of kin, the unit
commander will treat this case as an emergent case and request medical orders on behalf of the Soldier.
AR 600–77 • 5 March 2019
11
Note. For application, see DA Form 7692.
3 – 3. Return to active duty for medical care (medical retention processing 2), contingency operations
a. Purpose. To voluntarily return RC Soldiers to active duty to receive evaluation and/or treatment for an unresolved
wound, illness, or injury incurred or aggravated while the Soldier was on active duty for more than 30 days.
b. Eligibility. All of the following must be met:
(1) Must be a member in good standing in the Selected Reserves, which includes ARNG and USAR troop program
unit, individual ready reserve, or an individual mobilization augmentee who was previously released from an order or call
to active duty.
(2) Must require definitive care, defined as a specific treatment or sequence of treatments of at least 30 days duration
and requiring a significant commitment of the Soldier’s time, which, in the opinion of competent medical authority may,
upon completion of treatment and care, be reasonably expected to return the Soldier to duty or be subsequently referred to
the DES.
Note. Pregnancy is not a criterion for return to active duty for medical care. A Soldier who is qualified to return and who
is also pregnant may apply if the pregnancy will not interfere with the medical care needed for the qualifying illness or
injury.
c. Process.
(1) Soldier provides documentation that he/she incurred or aggravated an illness or injury while on active duty for more
than 30 days.
(2) Unit commander, or his or her representative, counsels the Soldier using DA Form 4856 (Developmental Counseling
Form) and ensures the facilitation and follow up of medical care through a DHA
– GL, VA, or a MTF utilizing clinical
assets as consultants. Incapacitation pay may be utilized in accordance with AR 135
– 381.
(3) If the Soldier’s command determines that medical treatment or the individual circumstances surrounding the Sol-
dier’s medical condition meet the criteria to return to active duty, the request for active duty is submitted through the State
Surgeon’s Office to the ARNG (ARNG
– HRP – P) for ARNG Soldiers or, for USAR Soldiers, through the Regional Support
Command Surgeon’s Office to the USAR (DAAR
– HR).
(4) The following documents are required when submitting a request for 10 USC 12301(h) orders:
(a) Unit cover letter.
(b) Completed DA Form 4187 (Personnel Action) (must be signed by the Soldier).
(c) Documentation supporting duty status at time of illness or injury, as applicable. Examples include mobilization
orders and amendments, unit sign-in roster, annual training order, and so forth.
(d) All issued DA Forms 3349 (Physical Profile) completed by the military medical authority.
(e) Statement from medical provider will include, at a minimum, diagnosis, anticipated length of care, primary care
manager (PCM) contact information, treatment plan, prognosis for recovery, and other medical documentation sufficient
to substantiate the medical condition.
(f) Statement verifying Soldier is not pending adverse administrative or UCMJ action.
(g) Statement that expiration of term of service, mandatory removal date (MRD), or retention control point will not
occur during this active duty period.
(h) DD Form 214, if applicable.
(i) DD Form 2795 (Pre-Deployment Health Assessment), if applicable.
(j) DD Form 2900 (Post Deployment Health Re-Assessment (PDHRA)), if applicable.
(5) If it is determined by ARNG or USAR that the Soldier’s medical needs cannot be met outside of a WTU, the
respective component will forward the request for 10 USC 12301(h) orders to the WCTP Surgeon’s Office for validation
and action.
(6) Once requests are validated, the DCS, WCT will coordinate with the RHC to determine the most appropriate WTU
location for the Soldier. The DCS, WCT will establish a report date, length of order, and submit the request for orders
using a DA Form 4187 and DA Form 7692 to MEDCOM.
(7) If a request is not validated, the DCS, WCT will return the request with written explanation/justification to ARNG
or USAR. Requests may also be returned to ARNG or USAR if additional information is needed to validate the request.
(8) An appeal of the DCS, WCT disapproval is forwarded through the Soldier’s chain of command to the OTSG.
(9) The following RC Soldiers are ineligible for continuum of care processing:
(a) Soldiers with conditions existing prior to service not aggravated while in a duty status.
(b) Soldiers approved for continuation on active duty or continuation on active reserve in accordance with AR 635
– 40.
(c) Soldiers discharged from the Army.
12
AR 600–77 • 5 March 2019
3 – 4. Return to active duty for medical care (active duty medical extension), non-contingency
operations
a. Purpose. To voluntarily return RC Soldiers to active duty to receive evaluation and/or treatment for an unresolved
wound, illness, or injury incurred or aggravated while the Soldier was on active duty for more than 30 days.
b. Eligibility. Must be a member in good standing in the Selected Reserves, which includes ARNG and USAR troop
program unit, individual ready reserve, or an individual mobilization augmentee who was previously released from an
order or call to active duty.
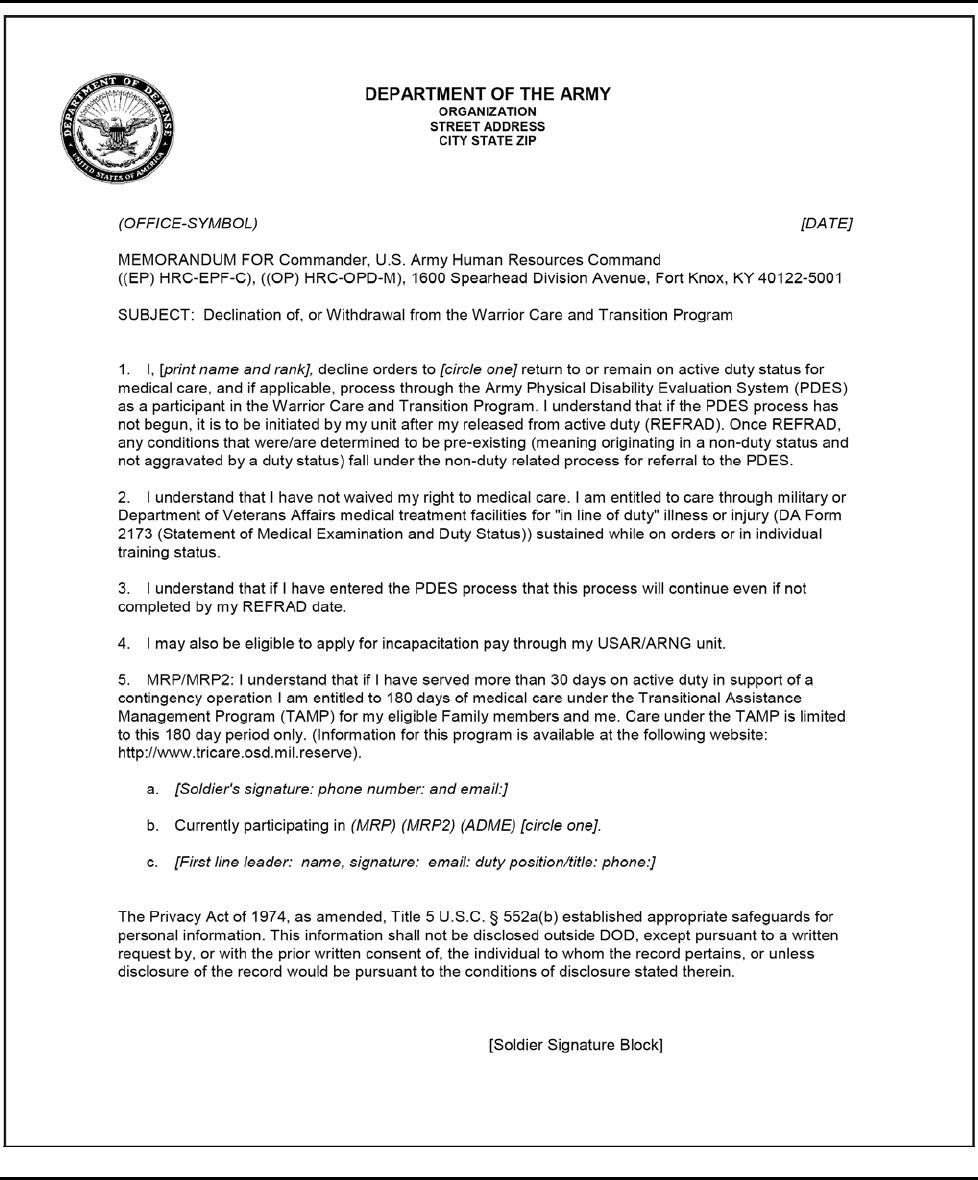
3 – 5. Declination of Reserve Component active duty medical care
Soldiers may decline Reserve Component active duty medical care up to the time of orders issuance. If the Soldier is
eligible and wishes to withdraw his or her application, the Soldier must sign a declination statement (see fig 3
– 1). If
medical care is needed after REFRAD, the Soldier’s RC unit coordinates access to medical treatment to ensure transition
in access to care. LOD will be processed in accordance with AR 600
– 8 – 4.
Note. The template memorandum should never be modified to include protected health information. A declination or with-
drawal statement is an administrative document, not a health record.
AR 600–77 • 5 March 2019
13
Figure 3 – 1. Declination of, or withdrawal from the Warrior Care and Transition Program
3 – 6. Withdrawal from Reserve Component active duty medical care
a. The decision to withdraw from RC active duty medical care will be made by the Soldier in conjunction with the
Triad of Care (PCM, Nurse Case Manager (NCM), and platoon sergeant/squad leader).
14
AR 600–77 • 5 March 2019
b. A RC Soldier may request to withdraw from active duty medical care at any time during the active duty medical
order.
c. RC Soldiers volunteer for active duty medical care. Requesting REFRAD is a Soldier’s option at any time during his
or her medical treatment and/or disability evaluation processing.
d. Release from active duty withdrawal request does not dismiss the requirement for the Soldier to maintain medical
readiness, or as applicable, does not dismiss the requirement to complete the DES process. DES processing will continue
in accordance with AR 635
– 40.
e. A Soldier must—
(1) Sign the withdrawal statement (see fig 3
– 1) after counseling by the Soldier’s chain of command. The counseling
should include information on access to medical care.
(2) Inform the PEBLO (if applicable) and unit of assignment of the intent to withdraw from active duty medical care.
f. For REFRAD requests, the Soldier must submit DA Form 4187 and the WCT Program withdrawal statement (see fig
3
– 1) through his or her chain of command to the HRC medical team. All medical and administrative REFRAD requests
should be submitted to usarmy.knox.hrc.mbx.epmd-refrad-[email protected] for enlisted Soldiers and to
usarmy.knox.hrc.mbx.opmd-[email protected] for officers. Upon REFRAD, the Soldiers return to the command and control
of their RC unit. Soldiers who require completion of any portion of the DES and elect REFRAD will have a DA Form
3349 prepared indicating the diagnosis and current status in the DES process. A copy of DA Form 3349 must be given to
the Soldier and his or her chain of command.
Section II
Retiree recalls, retention beyond mandatory removal date, and sanctuary
3 – 7. Reserve Component Soldiers with 18 years but less than 20 years of active service
a. Under the provisions of 10 USC 12686, RC Soldiers on active duty (other than for training) and are within 2 years
of eligibility for a regular retirement cannot be involuntarily REFRAD before the Soldier obtains 20 years of active service
unless the release is approved by the SECARMY or designee.
b. Prior to REFRAD from the WCTP, RC Soldiers with 18 but less than 20 years of active service may submit requests
to the HRC sanctuary team (at usarmy.knox.hrc.mbx.epmd-sanctuary-[email protected] for enlisted Soldiers and
usarmy.knox.hrc.mbx.opmd-rc-tours@mail.mil for officers) no earlier than 120 days from the end date of their 10 USC
12301(h) order.
c. RC Soldiers on active duty when referred into the DES may fall under the provisions of 10 USC 12686. However,
these Soldiers must complete a disability evaluation before any action regarding retention under sanctuary is taken. More-
over, Soldiers eligible for sanctuary are not authorized to waive referral to or completion of the DES process. If found unfit
for duty, the Soldier will be separated or retired in accordance with AR 635
– 40. If found fit for duty and has 18 but less
than 20 years of active service, the Soldier is eligible to submit a request to HRC for a sanctuary assignment. HRC will
confirm the Soldier qualifies for sanctuary, and the Soldier will, by law, be retained on active duty until he or she reaches
20 years of active service.
d. Soldiers on sanctuary orders who are wounded, ill, or injured must meet entry criteria established by MEDCOM, in
coordination with the DCS, G
– 1, for placement into a WTU. Upon receipt of acceptance into a WTU, the Soldier must
notify the HRC medical REFRAD team (usarmy.knox.hrc.mbx.epmd-refrad-[email protected] for enlisted Soldier and
usarmy.knox.hrc.mbx.opmd-[email protected] for officers) of the following in writing:
(1) Consideration to re-enter sanctuary program with the understanding he or she will be submitted for retirement at 20
years active service;
(2) Contact with a career counselor for acceptance into active duty (if Soldier is requesting to remain beyond 20 years
active service); and/or
(3) Request to return to previous status (individual ready reserve, troop program unit, or individual mobilization aug-
mentee) before submission of application.
e. Once the HRC medical REFRAD team receives the Soldier’s determination, they will forward the information back
to the HRC sanctuary team for further processing, if applicable.
f. The SECARMY or designee may direct REFRAD or separation; therefore, retention to 20 years of active service
may not occur.
Note. In accordance with AR 635
– 40, the application of the “Presumption of Fitness Rule” is reserved for determination
by the PEB or the USAPDA and only after a Soldier completes MEB processing.
AR 600–77 • 5 March 2019
15
3 – 8. Retiree recall retained on active duty for medical care
a. Will be processed in accordance with AR 601
– 10.
b. Retirees will be medically screened prior to REFRAD.
c. Retirees who incur a wound, illness, or injury or aggravate a previous condition during a period of recall are author-
ized to remain on active duty in order to receive medical care and/or DES processing.
d. Request for active duty for medical care will be submitted by the Soldier’s unit to which he or she is assigned during
the recall to MEDCOM via email to usarmy.jbsa.medcom.mbx.medcom-hr-warrior-transition-office@mail.mil.
e. If treatment plan is 30 days or less, the retiree should remain with unit assigned to during recall. If treatment plan is
greater than 30 days, the retiree should be enrolled in the WCT Program and possibly attached or reassigned to a WTU.
f. Orders may not be extended to allow the retiree to take leave.
3 – 9. Retention on active duty for medical care beyond mandatory removal date
a. Will be processed in accordance with AR 40
– 501 and 10 USC 14519.
b. Soldiers with a licensed DOD physician’s recommendation are authorized to remain on active duty beyond their
MRD to complete processing through the DES. The Soldier must consent to remain beyond his or her MRD.
c. Each request for retention beyond MRD will be adjudicated on a case-by-case basis. WTUs will submit requests
through MEDCOM human resources (MCWT
– HR) to OTSG for adjudication at least 90 days prior to the MRD.
d. MRDs must be screened during in-processing and tracked by the WTU in order to avoid late submission of retention
beyond MRD requests to OTSG.
e. Retention beyond MRD requests will be in the form of a packet with the following information and documentation:
(1) DA Form 4187 (must be complete with Soldier’s signatures and dates).
(2) DD Form 2870 (Authorization for Disclosure of Medical or Dental Information).
(3) Commissioned service date.
(4) MRD.
(5) Reason for removal (age or years of service).
(6) Copy of current orders (for example, 10 USC 12301, 12302, or other).
(7) Current orders start and end dates.
(8) Retirement point accountability.
(9) Copy of any previous retention beyond MRD approvals.
(10) Start date of MEB or PEB (if applicable).
(11) Name and address of current MTF.
(12) Name and address of current WTU (if applicable).
(13) Case manager’s name and contact information (if applicable).
(14) DCS, WCT approval memorandum.
(15) Physician’s memorandum identifying diagnosis, treatment plan, and estimated completion date of MEB and/or
PEB. Must include physician’s contact phone number and email address.
(16) Endorsement by the treatment facility’s commander (O
– 6 or above).
f. The retention beyond MRD request packet will be sent as a portable document format from the originating unit to the
MEDCOM human resources support branch via email at usarmy.jbsa.medcom.mbx.medcom-hr-warrior-transition-of-
[email protected]. Do not forward packets requesting retention beyond MRD directly to OTSG, HRC, or DCS, G
– 1.
MEDCOM human resources support branch will forward and track all MRD retention requests involving WTU Soldiers.
Section III
Resubmissions, appeals, and exceptions to policy for Reserve Component Duty Status Programs
3 – 10. Resubmissions
a. A resubmission is a request by the Soldier to have his or her original disapproval of application for active duty for
medical care reviewed based on the inclusion of additional documentation.
b. The Soldier must initiate the resubmission process and return the original packet, new information, and a letter re-
questing review directly to the DCS, WCT. The DCS, WCT will adjudicate the request for active duty for medical care in
coordination with the ARNG or USAR. If the resubmission is approved, the DCS, WCT will work directly with the Soldier,
the Soldier’s chain of command, and appropriate RHC to facilitate the request for orders through MEDCOM and coordi-
nate the WTU or CCU location, report date, and length of order.
16
AR 600–77 • 5 March 2019
c. The new information must specifically address the reason(s) for the original packet’s rejection. If the new information
does not address identified deficiencies, the two possible courses of action are either an appeal or a request for exception
to policy (ETP).
d. Resubmission is authorized one time only. Following a denial of a resubmission, any appeals or ETP requests are
authorized on time only.
3 – 11. Appeals
a. An appeal is a request by the Soldier to have his or her application packet reviewed by a higher level of authority.
The appeal should include a memorandum requesting an appeal (see fig 3
– 2) and all originally submitted documentation
for the specific request. An appeal will not include new documentation. After disapproval of application, the Soldier has 5
full duty days to appeal his or her application.
b. The administrative appeal process includes requests specific to administrative issues. Examples include report date
to WTU, utilization of privately owned vehicle (POV), and so forth.
c. The DCS, WCT is the administrative appeals authority. The appeal will originate with the Soldier and proceed
through his or her chain of command to the administrative appellate authority via email at usarmy.pentagon.medcom-
wtc.list.g1-orders-approval@mail.mil. Submission of an administrative appeal means that the Soldier asserts he or she
meets the medical criteria for WTU attachment, as determined by the appropriate medical authority. The DCS, WCT will
send an administrative appeal denial to the Soldier and the Soldier’s chain of command. The DCS, WCT has 5 full duty
days from the date he or she receives the appeal to respond to the Soldier's Component chain of command.
d. The medical appeal process includes requests specific to medical issues, that is, denial of an application due to med-
ical assessment. The medical appeal authority is OTSG, Health Policy and Services. The appeal will originate with the
Soldier and be sent through the chain of command to the medical appellate authority via email at usarmy.pentagon.med-
com-wtc.mbx.adme-mrp2processin[email protected]. If OTSG, Health Policy and Services denies an appeal, the Soldier may
not appeal the same case again. If the appeal is approved, the DCS, WCT will notify the Soldier through his or her chain
of command. The effective order date will be the date the appeal is approved.
3 – 12. Exception to policy requests
A request for an ETP is available to Soldiers to ensure that unique or special cases (those that are not covered in the written
policy) can be considered and decided on by the SECARMY. ETP requests should include a memorandum requesting
review of the application packet (see fig 3
– 2) and all originally submitted documentation for the specific request. Similar
to an appeal, an ETP will not include new documentation.
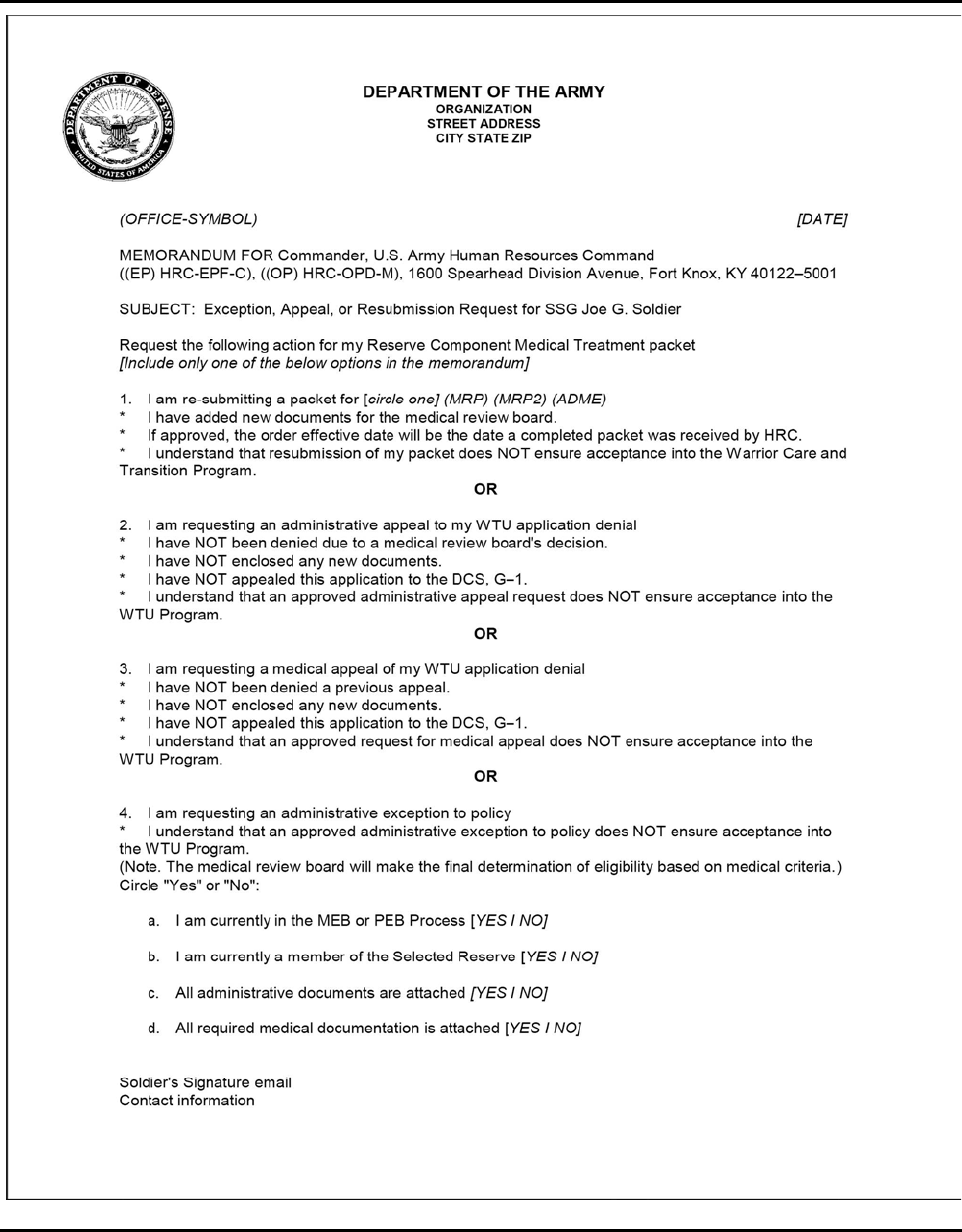
AR 600–77 • 5 March 2019
17
Figure 3 – 2. Exception, appeal, or resubmission request
18
AR 600–77 • 5 March 2019
Section IV
Warrior Transition Unit Assignment or Attachment
3 – 13. Warrior Transition Unit eligibility and processing
a. The Triad of Leadership decides on the WTU or CCU assignment/attachment location for WII Soldiers. The respec-
tive RCs (ARNG and USAR) decide on RC Soldiers’ qualifications for ADME and MRP2. RC Soldiers will be attached
and not assigned to a WTU or CCU. Regardless of the duration of orders, RC Soldiers will remain in the Reserve systems
for management and assignment to the RC unit.
b. Prior to a WTU assignment or attachment, all Soldiers must clear the losing command. The Soldier’s Triad of Lead-
ership will assist the Soldier with this task. The Soldier may be required to return to the losing command in unusual
circumstances; such as, significant missing hand receipt property. In those rare circumstances, coordination between the
senior leadership of the losing command and the gaining WTU may alleviate the requirement for the Soldier to return to
the previous assignment.
c. HRC, Personnel Management Directorate is the authority for assignment/attachment of an USAR Active Guard Re-
serve (AGR) Soldier, and ARNG, Personnel Division for ARNG AGR Soldiers. The ARNG Title 32 AGR populations are
maintained in Standard Installation and Division Personnel Reporting System within each respective State. The ARNG
Title 10 AGR population is maintained within the Full Time Management Control System.
3 – 14. Community Care Unit
a. General.
(1) The CCU is the preferred location for RC Soldiers to receive medical management and transition services. CCU
attachment allows Soldiers to live at home and perform duty at a location near home while receiving medical care from
the TRICARE network, VA, or MTF providers in or near their community. RA Soldiers may elect the basic allowance for
housing (BAH) location either at their CCU duty location or their installation WTU.
(2) RC Soldiers that meet WTU eligibility criteria with medical conditions that do not require complex medical care
management may be further attached to a CCU for completion of medical management and RTD, REFRAD, or DES
processing.
(3) RC Soldiers that meet WTU eligibility criteria with medical conditions that do not require complex medical case
management may remain attached to a WTU vice being further attached to a CCU if:
(a) The level and type of medical care required is not available in the Soldier’s community.
(b) The RC Soldier is evaluated as “High Risk” in accordance with MEDCOM’s health assessment risk criteria.
(c) The RC Soldier lives within 50 miles of a MTF with a WTU.
(4) RC senior grade Soldiers that do not receive the approval of the senior commander or first general officer (GO) in
the chain of command to remain in a WTU will transfer and further attach to a CCU within 30 days.
b. Procedures for selection.
(1) The WTU will screen all eligible RC WTU Soldiers within 30 days to determine eligibility for referral to a CCU.
The NCM coordinates with the WTU commander on the referral to the CCU. The WTU commander will consider demon-
strated reliability and accountability as a key factor in recommending Soldiers for referral. If a Soldier is not considered
ready for referral at that time, he or she may be reconsidered at a later point in his or her medical care.
(2) The NCM consults, as necessary, with the Triad of Care to determine whether the Soldier’s medical care can be
managed within the community by the CCU.
(3) The NCM coordinates with installation licensed behavioral health providers (generally, the licensed clinical social
worker) to obtain behavioral health clearance for mental health and social support status. The NCM will not refer Soldiers
who need mental health observation or treatment beyond the capacity or scope of the CCU or whose home environment is
not conducive to supporting healing and healthy outcomes.
3 – 15. Community Care Unit to Warrior Transition Unit transfer
A transfer request to the WTU is required when the Soldier is determined to need MTF/WTU level of care due to medical
complexity or non-compliance in CCU.
3 – 16. U.S. Department of Veterans Affairs medical centers
WII Soldiers should first be assigned or attached to a WTU which has a VA medical center in its catchment area. Soldiers
can then be further assigned or attached to a specific company with “duty at” the VA medical center or other facility. The
WTU maintains command responsibility during the period the place of duty is designated as the VA medical center.
AR 600–77 • 5 March 2019
19
Section V
Regular Army, Active Guard Reserve, and Reserve Component additional eligibility instructions
3 – 17. Regular Army and Active Guard Reserve
a. The Triad of Leadership will review the cases of all RA and AGR Soldiers and determine disposition for assignment
or attachment to a WTU, where the focus is to heal while receiving medical evaluation and managed treatment. This
includes all RA and AGR Soldiers who meet the following criteria:
(1) Soldier has a temporary profile or is anticipated to receive a profile for more than 6 months with duty limitations
that preclude the Soldier from training for or contributing to unit mission accomplishment (medical non-deployable is not
an automatic entrance into a WTU).
(2) The wound, illness, or injury requires clinical case management in order to ensure access to health care services to
support healing and rehabilitation.
(3) Soldiers with medical conditions that do not require case management should remain in their units and utilize the
standard health care system and access to care standards.
(4) Pregnancy is not a criterion for attachment or assignment to a WTU. A Soldier who is qualified for entry into a
WTU for a clinical condition and is also pregnant may be attached or assigned to the WTU if the pregnancy will not
interfere with the medical care needed for the qualifying illness or injury.
b. If an RA or an AGR Soldier meets the requirements, the Soldier’s commander will—
(1) Assemble a packet using DA Form 7696.
(2) Ensure that the physical capacity (P), upper extremity (U), lower extremity (L), hearing-ears (H), vision-eyes (E),
psychiatric (S) (known as the PULHES on DA Form 3349) in the Medical Protection System reflects the Soldier’s current
physical profile.
(3) Forward the packet to the WTU Triad of Leadership for consideration.
c. Senior commanders will ensure that Soldiers who qualify for assignment or attachment to a WTU are referred to the
Triad of Care for evaluation.
d. The following RA and AGR Soldiers are ineligible for entry into a WTU unless unusual circumstances are present:
(1) Soldiers with uncomplicated pregnancy.
(2) Soldiers, who are in initial entry training, advanced individual training, or one station unit training. Only by excep-
tion will initial military training Soldiers be assigned or attached to a WTU.
(3) Soldiers in TDRL status.
(4) Soldiers approved for continuation on active duty (see AR 635
– 40).
e. The desire for personnel replacement should not be a consideration for assignment of a Soldier to a WTU.
f. RA Soldiers will not be in an attached status at WTUs or CCUs for longer than 180 days, unless approved as an ETP.
Soldiers attached to a WTU who are assigned to a deployed unit where travel is greater than 1 hour for continuous specialty
care will be considered for assignment no later than 30 days from date of attachment.
g. AGR Soldiers will only be attached to WTUs or CCUs.
h. When mission objectives or unusual circumstances require attachment at a WTU for more than 180 consecutive days,
the Triad of Leadership must determine if a request for attachment of greater than 180 days is appropriate.
i. ETP requests for approval of attachment greater than 180 days will be submitted by the WTU commander through
the DCS, WCT to the Director, G
– 1, Plans and Resources Directorate (DAPE – PR) at least 60 days prior to attachment
end date. Packet composition is outlined on DA Form 7692.
j. Once the MTF commander recommends that a Soldier should enter the WTU system, it is recommended that the
Soldier report to the WTU within 30 days. If the Soldier is being assigned to a WTU for treatment of greater than 180
days, a report date of no later than 90 days with early reporting authorized will be designated on the orders. Losing and
gaining units must coordinate to ensure continuity of care. The Soldier’s unit commander submits the completed entrance
request packet to the Warrior Transition Battalion (WTB) NCM. Generally, the MTF commander initiates the nomination
process and notifies the unit commander. However, the unit commander has the right to initiate the nomination process,
when appropriate. See figures 3
– 3 and 3 – 4 for sample nomination memorandums.
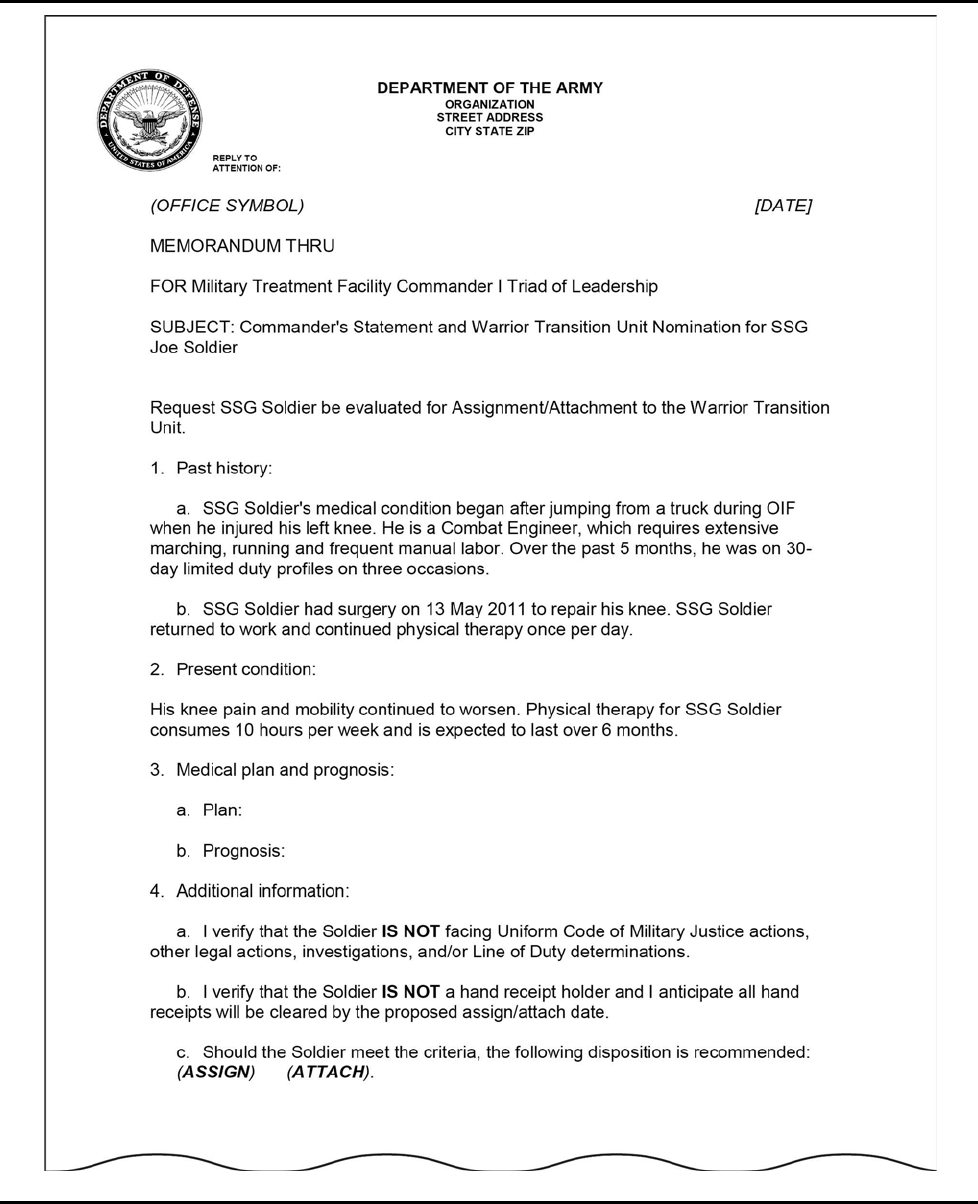
20
AR 600–77 • 5 March 2019
Figure 3 – 3. Warrior Transition Unit nomination memorandum
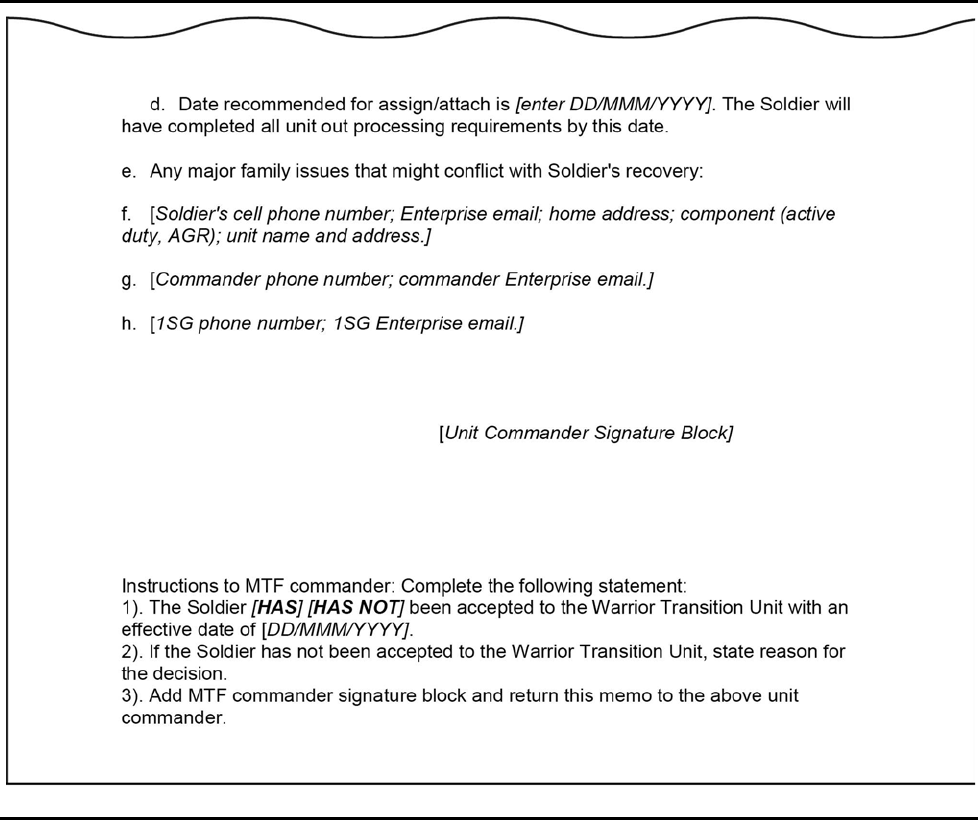
AR 600–77 • 5 March 2019
21
Figure 3 – 3. Warrior Transition Unit nomination memorandum—Continued
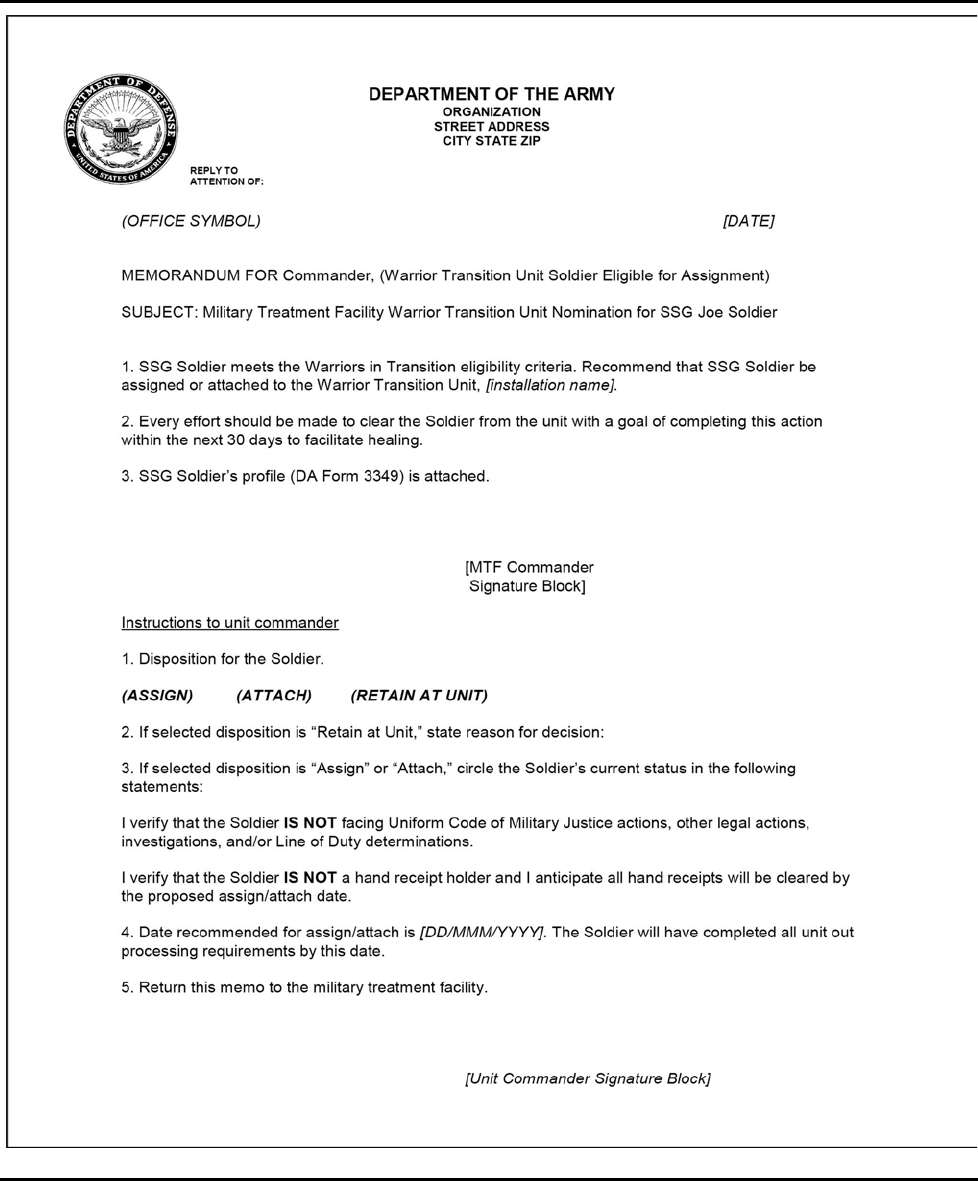
22
AR 600–77 • 5 March 2019
Figure 3 – 4. Military treatment facility commander nomination memorandum
k. Soldiers evacuated from CONUS or OCONUS who are an inpatient at a MTF, civilian, VA, or DOD medical facility
in proximity to home or Soldiers residing in a non-Army medical facility (for example, civilian, VA, and/or other Services’
MTF) must be carried as “Absent Sick” at the Army MTF or WTU with geographic responsibility.
AR 600–77 • 5 March 2019
23
(1) MTF commanders can attach RA Soldiers and coordinate per paragraph 3–2g for attachment orders for AGR Sol-
diers to a MTF or WTU. Soldiers on TDY orders should arrive at the MTF within 30 days. The MTF commander will
account for Soldiers arriving by aero medical evacuation in the headquarters company as soon as it is determined that the
evacuation process cannot be completed within 30 days. The Soldier may also move onward closer to home through the
aero medical evacuation system once seen by the specialty service evaluating the Soldier. Optionally, the Soldier is released
from attachment or assignment to the WTU as soon as the managing provider determines the level of medical management
required.
(2) The MTF commander notifies the Soldier’s unit commander of the Soldier’s status within 24 hours of arrival.
(3) The Triad of Leadership determines eligibility and assignment or attachment status for the Soldier.
(4) If a RA Soldier is assigned, orders will be published by the MTF or WTU as soon as the decision is made.
(5) For AGR Soldiers, orders must be requested via DA Form 4187. For periods greater than 180 days, the WTU will
request an assignment order (Format 452) and for periods of 180 days or less an attachment order (Format 440). However,
the report date can be no earlier than 90 days from the MTF/WTU commander’s decision date (the decision date equates
to the date the orders are published). Early report is authorized. This will allow the Soldier to clear housing, move family,
and manage other personal matters.
l. Assignment or attachment of Soldiers transferred to an MTF or WTU on installations not aero medically evacuated
will be conducted as follows:
(1) Following a Soldier’s medical evaluation, as appropriate, a nomination packet is completed and forwarded to the
gaining installation’s Triad of Leadership for disposition.
(2) If a RA Soldier is assigned, orders will be published by the MTF or WTU as soon as the decision is made.
m. Transferring a Soldier from a MTF/WTU to MTF/WTU and a WTU to CCU will be conducted as follows:
(1) The U.S. Transportation Command Regulating and Command and Control Evacuation System (TRAC2ES) will be
used to automate the transfer process. Coordination between losing and gaining WTUs through TRAC2ES facilitates pa-
tient movement and tracking.
(2) The Soldier Transfer and Regulating Tracking Center will validate the administrative and clinical information and
the DCS, WCT will approve or disapprove the request.
(3) The originating MTF/WTU will enter all patient moves into TRAC2ES based on the Soldier’s situation and the
MTF/WTU commander’s determination, thereby generating a patient movement request that is coordinated with the Sol-
dier Transfer and Regulating Tracking Center. This action will ensure positive control and accountability of Soldiers mov-
ing to medical care. This is particularly important for Soldiers moving in an inpatient status to another MTF/WTU or
medical facility at the VA or civilian community whether by ground of air evacuation mode of travel.
3 – 18. Title 32 USC Army National Guard Active Guard Reserve
a. Title 32 USC AGR Soldiers are eligible to volunteer for assignment to WTUs on 10 USC 12301(h) orders.
b. Deputy State Surgeons will validate the Soldier's illness or injury and complete a LOD determination. The State
Human Resources Personnel Management Office will coordinate with the WCTP to send the AGR Soldier to the closest
MTF via a 15-day TDY order for evaluation.
c. The WTU attachment, if warranted, will utilize entry criteria established by MEDCOM in coordination with the
DCS, G
– 1. The Soldier's unit, in conjunction with the State Human Resource Personnel Management Office, will complete
the appropriate paperwork. A packet will be assembled and forwarded to MEDCOM to process 10 USC 12301(h) orders.
The packet will include approval from the Triad of Leadership and date the Soldier will convert from Title 32 to Title 10
for assignment to a WTU.
d. Title 32 USC Soldiers approved for attachment to a WTU will have their AGR orders curtailed by the State Human
Resource Office and issued a DD Form 214 for that period of service. Attachment orders to the WTU are effective the day
after the end date on the DD Form 214.
e. Upon release from the WTU attachment, Soldiers found fit to return to active status will be reinstated into the AGR
Program in their State of assignment. If the Soldier is referred to the DES, the Soldier will remain in the WTU until the
completion of the DES process. A copy of the Soldier's Title 10 orders and DD Form 214 should be sent to the Soldier’s
respective State Human Resources Personnel Management Office.
f. The point of contact for ARNG Soldiers on Title 10 orders is the Human Capital Management Division,
(ARNG
– HCM), at 111 South George Mason Drive, Arlington, VA 22204 – 1382.
3 – 19. Reserve Component
The duty status of RC Soldiers recalled or retained in a WTU or CCU will change to active duty when the Soldier is
determined to be eligible for WTU entry. The MEDCOM will publish attachment orders to the WTU or CCU. RC Soldiers
will only be attached regardless of their location (WTU or CCU).
24
AR 600–77 • 5 March 2019
a. RC (non-AGR) Soldiers with medical conditions that occurred or were aggravated in the LOD during an active duty
status (contingency or non-contingency) or inactive duty status that meet the criteria qualify for evaluation, treatment,
and/or DES processing while in an active duty status.
b. RC Soldiers that meet WTU criteria and do not require complex medical case management will remain attached to a
WTU and not attached to a CCU if:
(1) The level and type of medical care required is not available in the Soldier’s community.
(2) The RC Soldier is evaluated as “High Risk” in accordance with MEDCOM’s health assessment risk criteria.
(3) The RC Soldier lives within 50 miles of a MTF with a WTU.
Chapter 4
Application processes for medical care of wounded, ill and injured senior grade Soldiers
4 – 1. Senior grade or rank criteria
Commissioned officers in the grade of O
– 4 and above, warrant officers in the grade of CW3 and above, and noncommis-
sioned officers in the grade of E
– 8 and above must have an endorsed approval by the senior commander or the first GO in
his or her chain of command to be retained or returned to active duty for medical care and/or DES processing.
4 – 2. General officer requests for entry into a Warrior Transition Unit
a. A GO request for retention on, or return to, active duty for medical care and/or DES processing is processed by the
GO’s unit of assignment, through the appropriate component General Officer Management Office (GOMO) for endorse-
ment, and to the DCS, WCT via email to usarmy.pentagon.medcom-wtc.list.g1-orders-[email protected] for disposition.
b. If the GO requires retention beyond MRD, this must be pre-approved and included in the request for entry onto active
duty.
4 – 3. General officer requests for extension beyond mandatory removal date
a. A GO request for retention beyond MRD is processed by the GO’s unit of assignment and forwarded through the
appropriate component GOMO for disposition.
b. WTUs will submit the request through MEDCOM human resources to OTSG for adjudication at least 90 days prior
to the MRD.
c. If OTSG approves the request for retention beyond MRD, the WTU, in coordination with the GO’s unit of assign-
ment, will forward the medical order packet, with GOMO endorsement, to MEDCOM at usarmy.jbsa.medcom.mbx.med-
com-12301h@mail.mil. MEDCOM will generate an order effective the date the completed packet is received.
4 – 4. General officer points of contact
Coordination of all GO requests for active duty for medical care must be processed through the appropriate component
GOMO:
a. Regular Army GOMO point of contact is: GOMO, Office of the Chief of Staff, Army, 200 Army Pentagon, Room
2A476, Washington, DC 20310
– 0200.
b. USAR GOMO point of contact is: USAR GOMO, Office of the Chief, Army Reserve, (DAAR
– GO), 6075 Goethals
Road, Building 1908, Fort Belvoir, VA 22060
– 5231.
c. ARNG GOMO point of contact is: NGB GOMO, Office of the Director, Army National Guard, (NGB
– GO), 111
South George Mason Drive, Arlington, VA 22204
– 1382.
Note. To ensure the timely resolution of all aspects of WII Soldiers’ administrative management in the areas of personnel,
finance, and logistics, from identification of wound, illness, or injury through final disposition. Final disposition occurs
when the WII Soldier is found medically cleared and RTD or completes the DES process.
Chapter 5
Orders
5 – 1. Retention on active duty for medical treatment and evaluation (non-Active Guard Reserve)
a. Medical retention processing orders. An RC Soldier mobilized under a 10 USC 12302 order migrates to a 10 USC
12301(h) medical order, with his or her consent, when attached to a WTU for evaluation, treatment, and/or DES processing.
AR 600–77 • 5 March 2019
25
(1) The unit commander submits a packet for entry into the WTU Program through the RHC Warrior Transition Office.
The RHC Warrior Transition Office director will determine eligibility and forward the packet to the aligned WTU's Triad
of Leadership in support of an Army MTF with the medical capability and capacity to accommodate the Soldier's treatment
needs. If approved, the gaining WTU will submit a request for orders to MEDCOM.
(2) Demobilization sites utilize established MEDCOM processes, once the clinical evaluation has been completed, to
request orders through MEDCOM.
(3) MEDCOM will publish and distribute the 10 USC 12301(h) order attaching the Soldier to a WTU under MEDCOM
derivative unit identification codes.
(4) MEDCOM will request that the issuing authority of the original partial mobilization order rescind the remaining
time on the Title 10 USC 12302 orders to eliminate the possibility of two valid concurrent orders.
(5) MEDCOM will notify the DFAS Wounded Warrior Pay Management Office of the rescinded portion of the orders
for non-AGR Soldiers.
(6) DFAS Wounded Warrior Pay Management Office will update its database and pay accounts using the newly issued
10 USC 12301(h) orders.
b. Medical retention processing – evaluation orders. These short-term 10 USC 12301(h) orders will extend a demobi-
lizing Soldier on active duty to complete medical evaluation processing when there is not enough time remaining on the
initial mobilization order.
(1) A Soldier’s mobilization order (to include amendments) and a DA Form 4187 signed by the Soldier and commander
(signature authority memorandum is required for signature other than commander) are required to process the request for
a MRP
– E Title USC 12301(h) order.
(2) MEDCOM will issue a MRP
– E Title 10 USC 12301(h) order indicating the order is for “the purpose of medical
evaluation.” These 10 USC 12301(h) orders will not exceed 60 days in length, initially.
(3) If the Soldier completes the medical evaluation and is not referred for longer- term medical care and case manage-
ment, the Soldier will be REFRAD by the WTU and MEDCOM will rescind any unused portion of the MRP
– E 10 USC
12301(h) order. A 30-day extension of the order is authorized when the WTU notifies MEDCOM that the medical evalu-
ation will not be completed within the initial 60 days.
(4) MRP
– E 10 USC 12301(h) orders for medical care for RC Soldiers will be requested by the demobilization instal-
lation after notification to the gaining WTU commander for the transition of senior commander to the WTU. The MRP
– E
10 USC 12301(h) order request will be submitted to MEDCOM via email at usarmy.jbsa.medcom.mbx.medcom-
(5) If the medical evaluation determines the Soldier does not require medical treatment or the Soldier declines care in
a WTU, the Soldier will be REFRAD from the installation where the WTU is located.
(6) Once an MRP or MRP
– E 10 USC 12301(h) order is generated by MEDCOM, the Soldier will be transferred to the
WTU closest to his or her home of record (HOR) or family support for medical management and senior commander for
the duration of the medical evaluation, while completing appointments, and until such time a disposition has been made,
resulting in REFRAD. It is the responsibility of the demobilization site to complete all aspects of the demobilization pro-
cess, except medical, prior to the Soldier moving to the WTU. It is not necessary for the Soldier to return to the demobili-
zation site for REFRAD.
(7) If, following the medical evaluation, it is determined the Soldier requires further medical treatment, a MRP appli-
cation will be submitted to the WTU. Upon approval of the completed DA Form 7692, the WTU submits the request for
orders through MEDCOM. MEDCOM will amend the original MRP
– E 10 USC 12301(h) order attaching the Soldier to
the WTU for the purpose of obtaining medical treatment.
(8) MEDCOM will provide a monthly report to the DCS, G
– 1 on the status of 10 USC 12301(h) orders. The report will
include the following data, as a minimum:
(a) List of Soldiers on 10 USC 12301(h) orders;
(b) Start and end date of orders;
(c) Location of attachment/assignment of the Soldier; and
(9) Soldiers assigned to CONUS locations should address medical conditions while at their duty location prior to arrival
at the demobilization site and the end date of their mobilization order. However, if a medical condition arises in the last
few days prior to the end date of the mobilization order, a CONUS-assigned Soldier may be considered for 10 USC
12301(h) orders for medical care.
Note: To ensure compliance with 10 USC and DOD policy, all RC Soldiers, with their consent, will be extended on active
duty 10 USC 12301(h) orders to complete the DES process. RC Soldiers who do not consent to extension will be REFRAD
to complete the DES process in their non-active duty RC status.
26
AR 600–77 • 5 March 2019
5 – 2. Return to active duty for medical treatment under medical retention processing 2 and the active
duty medical extension orders process
a. Counseling. The RC chain of command must counsel the Soldier (completing DA Form 4856 and DA Form 7692,
as applicable) before the Soldier may apply to return to active duty on 10 USC 12301(h) orders. Soldiers must volunteer
for retention or recall to active duty for medical assessment or treatment. Using a MRP2 checklist, a packet is assembled
and submitted to the OTSG via email to usarmy.pentagon.medcom-wtc.mbx.adme-mrp2processing@mail.mil.
b. Medical retention processing 2—return to active duty on a 10 USC 12301(h) initial order for medical treatment. Or-
ders that allow the voluntary return of a RC Soldier to active duty, following REFRAD from a contingency operation, for
the purpose of medical care or treatment for wounds, illnesses, or injuries incurred or aggravated in the LOD during a
period of mobilization. The Soldier must apply within 6 months of REFRAD. If additional time is required to complete
the application, the Soldier’s command will submit a justification, in writing, for the delayed submission.
c. Active duty medical extension—Return to active duty on active duty medical extension initial order.
(1) RC Soldiers and their command may apply to the ADME Program through an emergent or non-emergent request.
(a) Emergent request. The Soldier is in an inactive duty training status, not on active duty orders, and receives an injury
or sudden illness in the LOD, is hospitalized, and it is anticipated the treatment and recovery will take longer than 30 days.
Example 1: The Soldier is involved in a motor vehicle accident in route directly to inactive duty training, during drill, or
in route directly home from drill and is hospitalized. Example 2: During inactive duty training, the Soldier suffers the
sudden onset of an illness and is hospitalized.
(b) Non-emergent request. The Soldier reports an injury during inactive duty training and the unit initiates a DA Form
2173 (Statement of Medical Examination and Duty Status). Example: The Soldier received an ankle injury during inactive
duty training and receives care at a local civilian hospital. Several days later, the Soldier notifies the unit that his or her
private doctor recommends a treatment plan that requires more than 30 days to resolve the medical condition. Soldier is
unable to perform his or her military occupational specialty (MOS) and/or area of concentration in the confines of DA
Form 3349.
(2) In the event of an emergent situation when it is determined by competent medical personnel that the Soldier is
unable to consciously make the decision to request or decline ADME, the legal next of kin on the Soldier’s DD Form 93
has the authority to decide for the Soldier. If the next of kin cannot be located, the unit will treat this case as an emergent
case and request ADME orders. The commander is authorized to utilize this authority for the initial order. In the event the
commander does not receive a power of attorney prior to the publication of an order, then a memorandum should be
submitted to MEDCOM from the WTU stating, “All resources have been utilized to contact the Soldier’s legal next of kin
with no response. I am authorizing the Soldier to continue participation in the ADME Program based on the Soldier’s
medical need and the recommendation of the primary physician.”
(a) The unit is only allowed to use this authority for the initial order. All other determinations to remain in the program
will have to be determined by the legal next of kin.
(b) If the unit’s authorization is required, then MEDCOM should receive a memorandum from the WTU stating, “All
resources have been exhausted in an attempt to contact the Soldier’s legal next of kin with no response; therefore, I am
authorizing the Soldier to continue participation in the ADME Program based on the Soldier’s medical need and the rec-
ommendation of the primary physician.”
(3) In the case of a Soldier of the ARNG of the United States, consent of the Governor or other appointed authority of
the State concerned is necessary before placing the Soldier on active duty in the ADME Program. It is the responsibility
of the Soldier’s unit commander to obtain this consent prior to submitting an ADME packet to OTSG/MEDCOM. The
commander’s signature, or his or her designee, on the DA Form 4187 will serve as proof that the approval has been granted.
The only exception to this policy is in an emergent situation when appropriate State authority is unavailable, and delay
will adversely affect the Soldier and his or her Family in receiving active duty entitlements.
(4) For both emergent and non-emergent cases, a Soldier’s unit is responsible for initiating the LOD investigation pro-
cess in accordance with AR 600
– 8 – 4 to protect the Soldier as well as the interest of the Army.
(5) In emergent cases, DA Form 2173 and DA Form 3349 are secondary and will not prevent the Soldier from receiving
immediate emergency medical care. These documents can be furnished by the Soldier’s unit to HRC within 10 working
days after the emergent situation is stabilized to determine whether the Soldier should continue receiving medical care
while on ADME orders.
(6) In all cases, a Soldier must be found unable to perform his or her MOS and/or area of concentration within the
confines of a DA Form 3349 to enter or continue in the ADME Program.
(7) Resolution of the medical condition must be anticipated to exceed 30 days for a Soldier to be eligible for the ADME
Program or remain in the program if entered into the program under the emergent criteria.
d. Active duty medical extension application process.
AR 600–77 • 5 March 2019
27
(1) The RC chain of command will counsel Soldiers on the Incapacitation Pay program options and provisions prior to
submitting request for orders packets for the ADME Program to the DCS, WCT.
(2) The RC chain of command will assist Soldiers in completing their ADME application packet.
(3) Soldiers will submit the DA Form 7692 to their chain of command. The Soldier’s chain of command will forward
the completed DA Form 7692 through ARNG or USAR to the DCS, WCT surgeon’s office for validation and action.
(4) The ARNG or USAR will review the application for administrative eligibility. Once the applications are adminis-
tratively approved, ARNG or USAR forwards the request for orders to the DCS, WCT surgeon’s office for validation and
action.
(5) The DCS, WCT surgeon’s office sends a response to ARNG or USAR with a brief explanation for any packets
found invalid and the process for appeal. Approved applications will be sent to the RHC within the area of the Soldier’s
HOR.
(6) The RHC senior case manager, in coordination with MEDCOM, determines the best installation MTF for attach-
ment. The installation of attachment might not be the closest one to the Soldier’s residence. If appropriate, the RHC will
coordinate with other RHCs to ensure the appropriate assignment based on medical and garrison capability and capacity
to manage the Soldier.
(7) MEDCOM will publish the 10 USC 12301(h) orders assigning the Soldier to the installation designated by the RHC.
All Soldiers will report initially to a MTF for evaluation and the development of an initial treatment plan. For ARNG
Soldiers (all grades), a copy of their orders will be provided via email to ng.ncr.ngb-arng.mbx.muarcmrp-ad-
(8) After an initial evaluation and treatment plan has been completed at the assigned MTF and WTU by a designated
medical authority, the WTU commander will coordinate with the garrison commander’s representative to determine
whether the Soldier remains at the installation or is transferred to another installation MTF or to a CCU. Decisions will be
based primarily on medical necessity. The WTU commander will determine where the Soldier will perform duty.
(9) Authorized medical and dental care will be provided until the Soldier is found fit for military duty, or the wound,
illness, injury, or disease cannot be materially improved by further hospitalization or treatment and the Soldier has been
separated or retired as the result of the DES.
(10) Physicians who identify Soldiers with medical conditions that do not meet the retention standards of AR 40
– 501
will complete a DA Form 3349. Soldiers who remain unfit to perform military duty within 1 year of diagnosis will be
referred to the DES. Delayed referral into the DES is allowed for conditions determined by a medical authority to require
more than 1 year to obtain a MRDP, however the referral may be earlier if the medical provider determines that the Soldier
will not be capable to returning to duty within 1 year. Once referred into the DES, the Soldier may remain on active duty
as part of RC active duty for medical care, with the Soldier’s consent, until final disposition of the DES.
(11) See AR 135
– 18 or AR 600 – 8 – 24 or information on processing REFRAD requests.
5 – 3. Order extensions for medical retention process 2/active duty medical extension
a. WTU commanders will submit extension requests to MEDCOM. CCU commanders will submit extension requests
through the WTU commander to MEDCOM.
b. MEDCOM will publish amended orders extending the Soldier.
c. MEDCOM will electronically distribute copies to the WTU/CCU commander and DFAS Wounded Warrior Pay
Management Office.
d. Extension requests for Soldiers assigned or attached to a WTU or CCU in excess of 1 year without a MEB referral
require a GO endorsed treatment plan to include an explanation of why there has not been a MEB referral and the expected
MRDP date.
e. For Soldiers who have completed the DES process, the separation or retirement date will normally be within the no
later than 90-day date established by USAPDA. Exceptions to exceed this date must be in accordance with AR 635
– 8.
f. MEDCOM will extend 10 USC 12301(h) orders past the original anticipated 10 USC 12301(h) orders end date to
complete approved transition, Army post deployment and/or mobilization respite absence leave, and the Yellow Ribbon
Reintegration Program.
5 – 4. Medical temporary duty orders to the continental United States military treatment facilities
a. Soldiers injured, or who sustain an illness, in theater are aero medically evacuated to the closest regional medical
center (for example, Europe, Africa, and/or Southwest Asia theaters are aero medically evacuated to the Landstuhl Re-
gional Medical Center) on the authority of their deployment TDY orders. If the regional medical center order issuing
authority determines further movement to a CONUS MTF is required, the regional medical center will amend the deploy-
ment TDY order sending the Soldier to a CONUS MTF.
28
AR 600–77 • 5 March 2019
b. If the destination in the amended TDY order changes due to treatment requirements and the Soldier is sent to another
CONUS location not matching the amendment order issued by the regional medical center, the gaining WTU is authorized
to amend the TDY order to reflect the proper final destination. Funding used for all TDY order amendments comes from
the Soldier’s original deployment TDY order. As such, requesting additional funds for the amended TDY order is unnec-
essary.
c. For individual ready reserve, drilling individual mobilization augmentee, and retiree recall Soldiers, the Automated
Orders and Resource System automatically transmits a copy of the TDY order and amendments into the Soldier’s interac-
tive Personnel Records Management System (iPERMS). DFAS must access the Soldier’s iPERMS repository to properly
settle the Soldier’s travel voucher and ensure there is no interruption in pay and entitlements.
5 – 5. Permanent change of station orders (Regular Army, Active Guard Reserve, and Soldiers on
orders greater than 179 days)
a. For RA Soldiers assigned to a WTU or CCU, the MTF/WTU commander is the order issuing authority.
b. For USAR AGR Soldiers assigned to the WTU or CCU, HRC is the order issuing authority.
c. For ARNG AGR Soldiers assigned to the WTU or CCU, ARNG is the order issuing authority.
d. ASA (M&RA) is the approval authority for more than one permanent change of station (PCS) move within the same
fiscal year.
e. MTF commanders who have WII Soldiers must request a transfer to a WTU or CCU through the Soldier Transfer
and Regulating Tracking Center prior to reassigning (intra) to and between WTUs.
f. Immediately upon transfer, MTF commanders are required to transmit all assignments to or between WTUs through
the WTU commander to the respective component authority, and OTSG, TJAG, and Chief of Chaplains, for specialty
branch officers.
g. Movement of a Soldier resulting in a second or subsequent PCS in the same fiscal year is prohibited except as au-
thorized by AR 614
– 30, AR 614 – 100, and AR 614 – 200. Approval for a second or subsequent change of station not per-
mitted by the above regulations must be sent from the MTF/WTU commander through the respective component authority
to ASA (M&RA).
5 – 6. Retroactive modification of the effective date of orders
a. In accordance with the Joint Travel Regulation (JTR), an order must not be revoked or modified retroactively to
create, deny, or change an allowance except to correct or complete an order to show the original intent (for example, it
would be improper to amend an order to “un-authorize” POV travel after travel had been completed and the order had
clearly permitted POV travel). Travel authorizations and orders cannot be retroactively modified to increase or decrease
an allowance after the travel is completed. A travel authorization or order may be retroactively corrected to show the
original intent. The original order, may be amended after travel is performed when an error is obvious or travel require-
ments change en route (JTR). A written amendment confirming a verbal order is not included in this category provided the
verbal order was issued on or before the effective date of the directed change (DODFMR, Volume 9).
b. Backdating the report date on orders is not authorized. The practice of back dating report dates on orders has resulted
in unnecessary stress and financial hardship to Soldiers and Family members. Orders may only be corrected by amend-
ments, revocations, or rescissions or as a properly approved ETP.
c. Order issuing authorities have the authority to rescind only the unexecuted portion of an order (if the order has not
been executed in its entirety) by an amendment, revocation, or rescission, as prescribed by AR 600
– 8 – 105. Commanders
are reminded that it is their responsibility to ensure full compliance with established policy and procedures.
5 – 7. Medical temporary duty orders
TDY orders should be used for Soldiers traveling to treatment facilities for temporary medical care and/or evaluation in
accordance with the JTR and TRICARE travel benefits. Soldiers should be attached, rather than assigned, to the servicing
WTU for senior commander for periods of 180 days or less. Early determination of length of treatment and/or rehabilitation
is important. If the expected outcome is greater than 180 days, Soldiers will be assigned to the WTU possessing the most
appropriate medical capabilities closest to their previously transferred unit. TDY orders cannot exceed 180 days without
the approval of the DCS, G
– 1 (DAPE – PR).
5 – 8. Invitational travel authorizations in support of wounded Soldiers
Invitational travel authorizations (ITA) are government orders that can authorize up to three designated individuals, which
may include family members of a Soldier, to travel to the medical facility providing care. Reimbursement may include
cost for hotels, meals, and incidental expenses. The lodging costs cannot exceed the approved lodging rate for the specific
AR 600–77 • 5 March 2019
29
location. The local Wounded Warrior pay management team, finance office, WTU, or CCU can provide current per diem
rates. Travelers authorized invitational travel are encouraged to contact a local military finance office or Wounded Warrior
pay management team member for any updates to the information contained in this paragraph. Soldiers may contact the
DFAS Travel Pay Customer Service Center from the DFAS website at http://www.dfas.mil/militarymembers/trav-
elpay/customerservice.html.
a. A completed travel package includes the original or a copy of the following:
(1) DD Form 1351
– 2 (Travel Voucher or Subvoucher).
(2) Orders.
(3) Amendments or endorsements (if issued).
(4) Lodging receipts, regardless of the amount.
(5) Any receipts of $75 or more.
(6) Previous travel advance(s) payments, if applicable.
(7) Rental car receipts, regardless of amount.
b. The following checklist will help ensure that DD Form 1351
– 2 is proper and complete for payment:
(1) Required signature on DD Form 1351
– 2.
(2) A daytime phone number and/or an email address.
(3) Staple attachments to DD Form 1351
– 2.
(4) Double check the DD Form 1351
– 2 to ensure all information is correct.
(5) Submit the DD Form 1351
– 2 for processing in accordance with the unit’s standard operating procedures.
c. A DD Form 1351
– 2 must be completed and submitted to ensure the traveler reconciles their official travel. This
submission will include reconciliation of any travel pay advance(s), payment for all funds due and avoidance of any debt
owed to the government for overpayment.
d. Travelers must reconcile their official travel. Travelers may submit a monthly Travel voucher (using a DD Form
1351
– 2) to pay the travel entitlements accrued from the previous month on extended stay travel. A final DD Form 1351 – 2
is required when this extended travel is completed. Travelers may elect to submit one DD Form 1351
– 2 after all official
travel is completed for a one-time payment. This DD Form 1351
– 2 would then include reimbursement for the entire period
while in an authorized travel status and would be considered the final document.
e. When a Soldier becomes an outpatient, an individual the Soldier designates may be issued NMA orders. NMA orders
are similar to ITAs with the same travel entitlements authorized. Reimbursement may include cost for hotels, meals, and
incidental expenses not to exceed the approved daily per diem rate for a specific location. Travelers should continue to file
a travel voucher once a month until the Soldier is discharged and submits a final settlement voucher after completion of
the travel.
f. When required care is not available, Soldiers will be transferred to a treatment facility that has the required care. A
medical attendant, if required and authorized by the local clinical MTF staff, is authorized to accompany the Soldier (see
AR 40
– 400 for detailed guidance).
5 – 9. Orders distribution list for Reserve Component Soldiers
The minimum distribution of a RC Soldier’s orders is:
a. Soldier’s official Army enterprise email address.
b. For USAR Soldiers, orders will be sent to their iPERMS.
c. For ARNG Soldiers, Army National Guard Resource Management Comptroller, Finance Service Center, 8899 East
56th Street, Indianapolis, IN 46249
– 0002. A courtesy copy of orders will be provided via email to sssb@ngb.army.mil.
d. DFAS Wounded Warrior Pay Management Office, when applicable.
e. WTU (gaining senior commander).
f. Regional case manager.
g. CCU commander, when applicable.
5 – 10. Reserve Component management controls
Reference policy for management of RC Soldiers on active duty for operational support and full time National Guard duty
for operational support.
a. Regardless of the duration of operational support orders, RC enlisted Soldiers will remain in the Reserve systems for
management, and RC officers will remain on the reserve active status list. RC enlisted Soldiers will move to active man-
agement and officers will move to the active duty list only if they apply and are approved for accession into the Regular
Army.
b. Soldiers on operational support orders will be released on their orders termination date unless otherwise extended.
30
AR 600–77 • 5 March 2019
c. Soldiers on active duty orders that exceeds the “3 out of 4 year” rule (1,095 days) will be counted against Regular
Army end strength. Accordingly, organizations requesting operational support orders for Soldiers that will be counted
against Regular Army end strength will include a request signed by a brigadier general (O
– 7) or senior executive service
equivalent through HRC for approval.
5 – 11. Patient movement
MTFs must notify deployed commanders of their Soldiers’ arrival to, and departure from, CONUS-based MTFs within 24
hours (see AR 40
– 400 for policy on patient movement).
a. Current patient automated tracking applications (for example, joint patient tracking application) must be maintained
in accordance with 10 USC 1074f. In accordance with DODI 6000.11, the authorized patient movement and tracking
system for DOD is the U.S. Transportation Command’s automated information system TRAC2ES. MTFs will send a
confirmation message to forward and/or rear detachments notifying them of their Soldier’s location within 24 hours of
arrival to, and departure from, CONUS-based MTFs. This requirement applies to Soldiers arriving and departing by air
evacuation or commercial means.
b. Arrival and departure notification to deployed and rear detachment commanders is not required beyond the initial
receiving treatment facility in CONUS and the Soldier’s assignment to a WTU.
c. Soldiers evacuated from CONUS or OCONUS who are inpatient at a MTF, civilian, VA, or DOD medical facility in
proximity to their homes or Soldiers residing in a non-Army medical facility (for example, civilian, VA, and/or other
Services’ MTF) must be carried as “Absent Sick” at the Army MTF or WTU with geographic responsibility.
5 – 12. Noncompliance
Soldiers who become non-compliant with the requirements of their individual treatment plan or DES process may be
REFRAD (RC Soldiers), and/or administratively separated from the Army. In such cases, the Soldier must be counseled
on the requirements of the program in which he or she is not in compliance and the consequences of non-compliance. RC
Soldiers who are REFRAD and returned to non-active duty RC status due to non-compliance with the DES process are
still required to complete the DES process or they are subject to administrative separation. Non-compliance is a subjective
command decision based on a Soldier’s unwillingness to comply with the stated or written requirements of the program or
process for which he or she was placed on active duty orders. For example, a Soldier would be considered to be non-
compliant for repeated failure to attend or cancelling medical appointments. Commanders will process medical treatment
or DES related non-compliance in accordance with the guidance found in AR 635
– 40, DA Pam 635 – 40, AR 600 – 20, AR
635
– 200, AR 600 – 8 – 24, AR 135 – 178, and AR 135 – 175.
Chapter 6
Personnel and Pay Actions
Section I
Personnel Functions
6 – 1. Line of duty determinations and access to medical and dental care
a. Line of duty determination. LOD determinations are essential for protecting the interest of both the Soldier and the
Army when service is interrupted by a wound, illness, injury, disease, or death. An LOD determination is required when-
ever a Soldier incurs a wound, illness, or injury which prevents him or her from the performance of duty.
(1) Informal line of duty investigation. See AR 600
– 8 – 4 for the processing steps for informal LOD investigations.
(2) Formal line of duty investigation. See AR 600
– 8 – 4 for the processing steps for formal LOD investigations.
(3) Reserve Component. RC Soldiers who disclose LOD illnesses and/or injuries while on active duty will have LOD
documentation completed prior to REFRAD. Soldiers will depart their active duty assignment with a hard copy of DA
Form 2173 and a commander’s memorandum.
b. Access to medical and dental care.
(1) Unit commanders will counsel their Soldiers on their rights and responsibilities for access to care.
(2) Soldiers on active duty orders are authorized medical and dental care under 10 USC 1074. This includes RC mem-
bers who are on active duty for more than 30 days and cadets of the U.S. Military Academy. Soldiers on active duty orders
and attached to WTUs or CCUs have access to care through the MTF and TRICARE system.
(3) Soldiers not on active duty orders and who incurred or aggravated a wound, illness, or injury in the LOD are eligible
for treatment of the LOD condition through the TRICARE Management Activity, Clinical Operations and Patient Care,
AR 600–77 • 5 March 2019
31
DHA – GL. See AR 40 – 400 or DHA – GL website at https://www.health.mil/greatlakes for procedures regarding obtaining
medical care and payment of claims.
(4) In accordance with AR 135
– 381, RC Soldiers maintain access to care until the LOD condition can no longer be
materially improved. If an RC Soldier’s condition is determined to not have been incurred in the LOD, medical treatment
is not authorized after the expiration of his or her active duty orders. If active duty orders have expired, funded medical
treatment entitlement ends on the date the RC Soldier is notified of the final “not in the LOD” determination; except for
those RC Soldiers who are retained in an in-patient status beyond the termination of orders.
6 – 2. Non-medical attendant and DD Form 93
a. A NMA is an individual who is designated, by a Soldier or designee, to contribute to the health and welfare of the
Soldier and has the primary responsibility of providing personal care and/or assistance with daily needs for the Soldier.
Any Soldier wounded, ill, or injured in the LOD and in need of personal care services, because of an inability to perform
one or more activities of daily living or needs supervision or protection based on symptoms or residuals of neurological or
other impairment, is eligible for a NMA.
b. A Soldier’s medical condition may prevent him or her from communicating to a health care provider his or her
preference for a NMA and the geographic location where he or she would prefer to receive medical care. Therefore, Sol-
diers may nominate one NMA and identify their preferred geographic location for medical treatment in box 14 (continua-
tion/remarks) of DD Form 93. The NMA information and geographic location for medical treatment information recorded
in box 14 should consist of the following:
(1) NMA: Name, relationship, and address of the person the Soldier nominates to be his or her NMA.
(2) Geographic location: The facility and the city and State where the Soldier prefers to receive medical care.
c. During Soldier readiness processing, Soldiers should be counseled to first consider nominating Family members who
are most likely to take a personal interest in ensuring that they receive quality care and assistance. Additionally, the Soldier
will be advised that while every effort will be made to honor his or her request, there is no assurance of the following:
(1) The person nominated will be the NMA. The factors that might preclude a nominee from performing this service
are many and varied; such as, the person nominated may not be capable of providing the proper level of care or may not
be available when needed.
(2) Medical care will be provided at the geographic location desired. Medical authorities will determine the medical
treatment facility where the best possible medical care will be provided based upon: the medical treatment plan; the avail-
ability of medical care within that geographic area; and the location of the NMA’s residence.
d. When the need arises for non-medical care and assistance during a Soldier’s treatment at a MTF, medical authorities
may authorize a NMA to assist the Soldier. The requirement for a NMA is determined by the attending physician or
surgeon and the MTF/WTU commander. Medical authorities will consult with the Soldier or designee to identify the NMA.
Additionally, medical authorities will consider the Soldier’s requests when determining the facility where care will be
provided and attempt to provide care as close to the attendant’s residence as the medical situation permits. Medical author-
ities are not restricted to providing patient care in a MTF.
(1) Non-medical attendant eligibility. The PCM must validate the NMA candidate possesses the following attributes:
(a) Is at least 18 years old.
(b) Is not involved in personal or professional activities that prevent them from assisting the Soldier with the activities
of daily living and implementing the medical and transition plan.
(c) Is physically able to provide the assistance the Soldier needs.
(d) Is able to understand the Soldier’s medication regimen.
(e) Is able to understand, communicate, and follow the Soldier’s treatment plan listing the Soldier’s specific care needs
without direct supervision.
Note. In accordance with AR 40
– 400, an active duty Soldier may serve as a NMA if his or her commander approves and
determines an official status (TDY, permissive TDY, or ordinary leave) while acting as an NMA.
(2) Non-medical attendant assignment process.
(a) The Soldier’s PCM must validate the need for a NMA and prescribe a medical order in the designated military
database (such as, the Armed Forces Health Longitudinal Technology Application (AHLTA)). If the PCM does not vali-
date the request for a NMA, the Soldier may appeal through the MTF Deputy Commander for Clinical Services. In order
to appeal the denial of a NMA request, the Soldier must complete a DA Form 4187, within 14 days of the denial determi-
nation, and include a justification for the NMA requirement.
(b) The MTF/WTU commander or the first O
– 5 commander in the Soldier’s chain of command must also validate the
need for a NMA by submitting a DA Form 4187 through the unit’s human resources office/S
– 1 to HRC or MEDCOM
human resources.
32
AR 600–77 • 5 March 2019
(3) Removal from non-medical attendant status.
(a) The requirement for a NMA must be reevaluated, at a minimum, every 6 months unless the order is terminated
sooner by the PCM.
(b) A NMA may request removal from NMA status through the MTF/WTU commander.
(c) The Soldier’s PCM may recommend the removal of the NMA status if the person is unable to perform the duties or
is impeding the Soldiers ability to heal, recover, and/or transition. The approval authority for removal of NMA status is
the MTF/WTU commander in conjunction with the PCM’s recommendation. Moreover, if any member of the Triad of
Care witnesses or receives a credible report of a NMA providing unsafe or substandard care, or impeding the Soldiers
ability to heal, recover, and/or transition, the MTF/WTU commander will report the findings to the MTF Family Advocacy
Program. If the NMA is deemed unsafe for the Soldier, then the MTF/WTU should immediately consult the servicing staff
judge advocate for guidance. Removal of a NMA from the Soldier’s immediate location must be approved through the
Triad of Leadership (under the advisement of the Family Advocacy Program and the staff judge advocate). The MTF/WTU
commander should also consult the installation for installation level policy and guidance and his or her servicing staff
judge advocate before rendering a final decision.
(d) If NMA status is removed, the NMA will lose the associated benefits and entitlements. If the removed NMA is a
spouse or parent, that individual will no longer receive NMA benefits and entitlements but may remain with the Soldier
(unless as indicated in para 6–2d(2)(c)). However, the Soldier may select another candidate as a NMA. If lodging accom-
modations do not support having the removed NMA and the new NMA in the same location, the new NMA and his or her
needs necessary to aid the Soldier will take precedence.
e. Soldiers permanently assigned (on PCS orders) to the MTF/hospital where they are being treated are not authorized
a NMA because the member is not in a travel status.
Section II
Pay and Entitlements
6 – 3. Medical treatment and evaluation and active duty medical extension pay and entitlements
a. Regular pay. A WII Soldier on active duty for medical care and/or DES processing will receive basic pay, BAH,
and other applicable entitlement(s).
b. Family separation allowance. Soldiers that are separated from their families by the military and meet regulatory
guidance may be eligible to receive family separation allowance for the period of separation.
c. Per diem (lodging, meals, and incidental expense). For travel pay, Soldiers receive per diem when they are receiving
medical treatment away from their PDS, principal, or primary home of residence.
d. Pay and allowances continuation. Soldiers medically evacuated from the theater of operations to receive medical
treatment for a wound, illness, or injury incurred in the LOD continue to receive all pay and allowances for up to 12
months, unless released sooner from a WTU. Examples include special pay (hostile fire pay and hardship duty pay –
location) and incentive pay (jump, flight, and demolition pay). However, Soldiers that are not hospitalized (outpatient) do
not continue to receive combat zone tax exclusion. Refer to the DODFMR, Volume 7A for details.
e. Designated individual or Family member. Travel, transportation allowances, and per diem are available for up to
three designated individuals, each receiving one roundtrip between the designated individual’s home and the medical fa-
cility location in any 60-day period.
6 – 4. Reserve Component DD Form 214 distribution
a. Once medical care is complete, the WTU commander will request a REFRAD order authorization from HRC at
usarmy.knox.hrc.mbx.epmd-refrad-[email protected] for enlisted and usarmy.knox.hrc.mbx.opmd-[email protected] for
officers. HRC will send the REFRAD authorization memorandum back to the WTU of origin and send copies to the
installation transition center, DFAS Wounded Warrior Pay Management Office, and the original orders issuing agency.
b. If the Soldier has completed the DES process and is to separate or retire for disability, the USAPDA will input the
Soldier’s personnel data into TRANSPROC.
c. The transition center will publish the REFRAD order and generate the DD Form 214 and forwards copies through
the local finance office. The transition center will also input any severance pay transaction before the Soldier departs the
installation or WTU.
d. Once the final discharge orders have been completed, HRC will distribute orders as listed in chapter 4 (as applicable).
AR 600–77 • 5 March 2019
33
6 – 5. Soldier pay processing within the Warrior Transition Unit or Community Care Unit
a. Pay authorities and finance office. The Army must ensure accurate and timely delivery of Soldiers’ military and
travel pay to include travel pay to Family members and caregivers under ITA or NMA orders. The timely delivery of pay
is a partnership between the responsible originating activities (that is, housing office, MTF, WTU, unit commander, HRC,
IMCOM, and MEDCOM) and the responsible finance office (Army finance unit, DFAS, U.S. Property and Fiscal Office,
and USAR pay offices).
b. Standard. It is imperative that each participant in the chain of command understand the regulatory and policy stand-
ards that govern their contribution to pay timeliness and accuracy, and employ proper performance standards and corre-
sponding metrics to ensure compliance. Where feasible, all authorizing documents for military and travel pay and allow-
ances (for example, orders, personnel actions) must be delivered to the servicing finance office no later than 3 calendar
days of the effective date of the pay affecting action. Army commands, Army service component commands, and direct
reporting units must ensure their subordinate activities properly address pay timeliness and accuracy. All leadership levels
must establish appropriate metrics to manage this critical standard of support to our Soldiers and Families.
c. Counseling Soldiers, Family members, or Soldiers’ representative. To ensure Soldiers receive appropriate pay and
entitlements during assignment or attachment to an MTF, the MTF is responsible for ensuring that the Soldier or the
Soldier’s representative is properly counseled and advised regarding pay and financial obligations that may occur to in-
clude the suspension of debts.
6 – 6. Traumatic Servicemembers’ Group Life Insurance
Traumatic Servicemembers’ Group Life Insurance (TSGLI) is an automatic traumatic injury protection provision under
the SGLI. Additional information on this program can be found at http://www.insurance.va.gov. TSGLI provides for pay-
ment to Soldiers who are severely injured as the result of a traumatic event and suffer a loss that qualifies for payment
under TSGLI. TSGLI is designed to help traumatically injured Soldiers and their Families with financial burdens associated
with recovering from a severe injury. For questions about TSGLI, contact a trained TSGLI service representative at the
Army TSGLI call center via telephone at 1
or on their website at https://www.hrc.army.mil/tagd/tsgli.
Section III
Supply and Logistics
6 – 7. Household goods
a. Shipment of household goods. Point of contact for shipment of household goods (HHG) is DCS, G
– 1, Compensation
and Entitlements Branch (DAPE
– PRC), 300 Army Pentagon, Washington, DC 20310 – 0300. Further information can be
found in the JTR.
(1) RA and AGR Soldiers who remain in a TDY or attached status at an authorized health care facility (for example,
MTF, VA medical center, civilian hospital, nursing home, or other residential institution health facility) may have HHG
from their PDS shipped to them at their attached MTF or WTU. While Soldiers remain in a TDY or attached status, their
TDY or attachment orders may be amended to reflect a “TDY weight allowance authorization.” The approval authority
for such an amendment is the TDY orders issuing authority.
(2) RA WII Soldiers who are assigned or PCS to authorized health care facilities are authorized full shipment of HHG
from their previous PDS to the MTF or WTU. Shipment of HHG should be added to the Soldier’s PCS orders by the PCS
orders issuing authority.
(3) RC Soldiers attached to a WTU or CCU are authorized (if required) a TDY weight allowance for shipment of HHG
from the HOR to the MTF or WTU; the weight authorized depends on rank. The approval authority is the order issuing
authority. RC Soldiers are authorized full shipment of HHG from their HOR to the MTF or WTU for attachments greater
than 180 consecutive days. Shipment of HHG should be added to the Soldier’s orders by the Soldier’s order issuing au-
thority.
(4) In all circumstances involving shipment of HHG, medical equipment, and supportive devices issued to WII Soldiers
are considered professional gear. As such, the weight of these items does not count toward the Soldier’s total weight
allowance.
b. Special storage of household goods. RA and AGR WII Soldiers who remain in a TDY status while attached to the
hospital generally have HHG at their PDS. If the WTU and/or hospital commander, in the grade of O
– 6 or above, believes
keeping the unshipped HHG in storage is necessary, storage may be provided at government expense. The Soldier’s PDS
installation or the WTU and/or hospital will fund this storage out of existing operation and maintenance Army funds and
should seek reimbursement for these costs as an expense associated with the contingency operation. WTU and/or hospital
34
AR 600–77 • 5 March 2019
commanders will amend the Soldier’s TDY/attachment orders to reflect this authorization. After storage is authorized, and
when or if it becomes apparent that PCS entitlements to the hospital are appropriate, the Soldier’s HHG will be taken out
of storage and shipped to the new hospital PDS on the authority of the new PCS order to the hospital.
6 – 8. Unaccompanied personnel housing for wounded, ill, and injured Soldiers
a. The guidance in this regulation is provided in addition to AR 420
– 1 for the specific purpose of managing housing
for WII Soldiers. The Triad of Leadership is responsible for ensuring WII Soldiers assigned or attached to a WTU are
housed in dedicated facilities conducive to their healing and transition requirements. The Army will provide housing to
WII Soldiers that is commensurate with their service and specialized needs. This includes meeting accessibility require-
ments and co-locating NMAs.
b. Garrisons are responsible for the in- and out-processing. The Army housing office is responsible for the management
of all Government housing facilities on the installation, to include WTU unaccompanied personnel housing. Assignment
to, and termination from, quarters will be made by the Army housing office in coordination with WTU cadre. WTU cadre
will inspect the room for adequacy, ensuring it meets the conditions and requirements of the intended Soldier prior to
assignment.
c. The enterprise military housing system will be utilized (where available) to facilitate management and reporting
processes for unaccompanied personnel housing utilization and occupancy rates.
d. No distinction is made for housing unaccompanied WII Soldiers on TDY or PCS orders, and/or those who may be
geographical bachelors. Any unaccompanied WII Soldier at the WTU may be assigned space within the unaccompanied
personnel housing. WII Soldiers with Families located at another installation are authorized to be housed in unaccompanied
personnel housing without affecting their BAH entitlements.
e. The following is a list of options to meet the housing needs of unaccompanied WII Soldiers:
(1) Unaccompanied WII Soldiers without non-medical caregivers or NMAs will be housed in MEDCOM facilities or
in existing available unaccompanied personnel housing designated facilities, provided it meets their accessibility require-
ments. If unaccompanied personnel housing is unavailable or does not meet the WII Soldiers’ needs, installations may also
use U.S. Army lodging or contract with local hotels, if necessary.
(2) Unaccompanied WII Soldiers with NMAs:
(a) NMAs are authorized to live in close proximity to their Soldier (with their own bedroom space) for the duration of
their attendant orders. The Soldier and his or her NMA may be placed in two-bedroom apartment style unaccompanied
personnel housing units with shared living and kitchen areas. NMAs will not be assigned to renovated unaccompanied
personnel housing spaces where the NMA must enter the common hallway outside the module to access the WII Soldier's
room. Family members serving as NMAs are foremost considered as NMAs and may be housed in unaccompanied per-
sonnel housing.
(b) Installations may utilize Army lodging, contracted hotels, or government-leased housing in the immediate area to
provide lodging for WII Soldiers and their NMAs, if suitable unaccompanied personnel housing is unavailable.
(c) NMAs are provided compensation for their lodging, meals, and incidental expenses through a daily per diem. In
cases where the NMAs live in government-provided quarters with their Soldier, their daily lodging per diem will be zero.
(d) Garrisons may use the authority in AR 420
– 1 to temporarily divert non-privatized Army Family housing to a des-
ignated facility for WII Soldiers with NMAs. Requests will be forwarded through IMCOM to the Assistant Chief of Staff
for Installation Management for approval.
(e) The least desired option is to place unaccompanied WII Soldiers and their NMAs into privatized Residential Com-
munities Initiative Family housing. Military Families will continue to have priority for Residential Communities Initiative
housing and no Family will be displaced by an unaccompanied WII Soldier.
6 – 9. Return of personal effects from theater
For additional information on financial liability investigation of property loss procedures refer to AR 735
– 5.
a. The Joint Mortuary Affairs Program is a broad-based military program providing for the necessary care and dispo-
sition of missing and deceased personnel, including personal effects.
b. While in theater, organizational clothing and individual equipment (OCIE) will be processed as personal effects
because some OCIE items have been privately purchased.
c. The Joint Personal Effects Depot determines which OCIE is to be designated as government-owned and cleared from
the individual's hand receipt and which is to be handled as personal effects and returned to the individual or to the person(s)
eligible to receive the personal effects.
d. Considerations in regard to shipping personal effects and OCIE for Soldier’s aero medically evacuated through the
mortuary affairs collection point include the following:
(1) The ability of individuals to control the items in their possession throughout the evacuation process.
AR 600–77 • 5 March 2019
35
(2) The limit on allowable baggage that can be carried on military airlift.
e. When Soldiers are not aero medically evacuated or equipment could not accompany a Soldier that is aero medically
evacuated, commanders are responsible for inventorying equipment and shipping through the mortuary affairs collection
point.
f. Government property brought in with the patient, other than the protective gear and OCIE removed by the MTF to
treat the individual, is handled as follows:
(1) The property is inventoried using a separate DA Form 4160 (Patient’s Personal Effects and Clothing Record).
(2) The MTF will safeguard the equipment and make every effort to return the property to the individual's assigned
unit.
(3) A receipt is obtained and filed when the unit accepts the property.
g. WTUs with assigned Soldiers who have not received their personal effects from theater will contact the Casualty and
Mortuary Affairs Operations Center personal effects section via email at usarmy.knox.hrc.mbx.tagd-cmaoc-ped-
[email protected] to coordinate with the Soldiers’ previously assigned unit to identify the location and request release of the
Soldiers’ personal effects.
Chapter 7
Return to Duty, Release from Active Duty, Separation, and Retirement
Section I
Return to Duty
7 – 1. Assignment after completion of care
Every effort will be made to return the Regular Army or AGR WII Soldier to his or her previous unit of assignment once
determined fit for duty and medical treatment is complete. Release will be coordinated between MEDCOM and HRC
through normal assignment procedures.
7 – 2. Return to duty of Soldiers returned on temporary change of station or mobilization order
AGR Soldiers who are medically evacuated to CONUS for managed medical care on a previously issued mobilization
order, upon completion of managed medical care, must return to the home station on a DD Form 220 (Active Duty Report).
The unit with senior commander of the Soldier will generate this report. Generally, AGR Soldiers return to the mobilization
site upon return from theater; however, in rare cases, the Soldier may need to reside at an alternate location due to medical
necessity.
7 – 3. Regular Army return to duty assignment procedures
a. Chaplains coordinate directly with Office of Chaplains, 6608 Army Navy Drive, Washington DC, 20310
– 0300.
b. Judge Advocates coordinate directly with Office of The Judge Advocate General, Personnel, Plans and Training
Office, 2200 Army Pentagon, 2B517, Washington, DC 20310
– 0300.
c. Special Operations Commands coordinate directly with the career management field series 18 at LTG Timothy J.
Maude Human Resource Center of Excellence Complex, Building 3, 3rd Floor, Room 017, 1600 Spearhead Division
Avenue, Fort Knox, Kentucky, 40122
– 5001.
d. For CONUS WTUs, immediately upon the RA Soldier being declared RTD, the WTU commander (if WTU com-
mander is not an O
– 5 or above, the first O – 5 commander in the chain of command) will submit a DA Form 4187 directly
to HRC requesting assignment instructions (enlisted) or request for orders (officers). Requests must include verification
that all medical processing, to include any required board proceedings, is complete. For an USAR AGR Soldier, the WTU
will submit a DA Form 4187 to Commander, U.S. Army Human Resources Command (AHRC
– EPM – OMB – SAB), 1600
Spearhead Division Avenue, Fort Knox, KY 40122
– 5001 requesting follow-on assignment.
e. If the OCONUS theater G
– 1 determines the Soldier can be reassigned within the OCONUS area, the assignment
decision must be issued within 5 days of the RTD notification. Assignment report dates are outlined below. Theater G-1s
will also coordinate with the WTU servicing IMCOM military personnel division to produce PCS orders within 5 days.
OCONUS theater G-1s must establish internal metrics to track RTD processing standards.
f. If the OCONUS theater G
– 1 determines the Soldier cannot be reassigned within the OCONUS command or has a
near term or expired date eligible for return from overseas, requests for assignment instructions or request for orders follow
the procedures above. For an USAR AGR Soldier, the WTU will submit a DA Form 4187 to Commander, U.S. Army
Human Resource Command (AHRC
– EPM – OMB – SAB), 1600 Spearhead Division Avenue, Fort Knox, KY 40122 – 5001
requesting follow-on assignment. For a Soldier in the Married Army Couples Program, the RTD Soldier’s military spouse
36
AR 600–77 • 5 March 2019
should be included in the reassignment process if CONUS reassignment is identified. The RTD Soldier’s military spouse
should request a compassionate reassignment on a DA Form 3739 (Application for Compassionate Actions) upon receipt
of his or her spouse’s RTD reassignment orders.
g. RTD requests will be forwarded to HRC as follows:
(1) Enlisted requests will be sent to usarmy.knox.hrc.mbx.epmd-special-actions-branch@mail.mil. HRC will provide
assignment instructions via the Enlisted Distribution and Assignment System.
(2) Officer requests (excluding chaplains and Judge Advocates) will be sent to usarmy.knox.hrc.mbx.opmd-rc-medical-
[email protected]. RC will provide assignment instructions via the Total Officer Personnel Management Information
System.
(3) Assignment decisions must be issued within 5 working days of receipt of the RTD notification (officers will be
processed in accordance with AR 614
– 100 and enlisted in accordance with AR 614 – 200). Upon completion of all assign-
ment validations, HRC will generate an email to each Soldier’s unit of assignment, orders issuing authority, and Soldier’s
Army Enterprise email account. This notification of assignment by email is the authority to issue Soldiers individual PCS
orders. Each orders issuing authority must publish orders within 5 working days upon receipt of email notification to
include notification to HRC upon completion of task.
h. Request for assignment instructions or request for orders will include the following on a DA Form 4187:
(1) Rank and name.
(2) Social security number.
(3) Skill or primary MOS.
(4) Current WTU unit identification code (location/installation).
(5) Unit identification code of previous unit of assignment prior to WTU.
(6) Three assignment preferences.
(7) Retention memorandum (Soldier will not extend or reenlist).
(8) Statement that all medical related board proceedings have been completed and appropriate data fields updated in
the Medical Operational Data System, eMILPO, and other related data management systems, as required.
i. Enlisted Soldiers who are returned to duty and in their reenlistment eligibility window (and will reenlist) or require
reclassification must contact their retention career counselor immediately upon being declared RTD. WTUs should not
request assignment instructions for these Soldiers as outlined above unless the Soldier does not plan to extend or reenlist.
HRC will waive the remaining service requirement. HRC assignment considerations for Soldiers being RTD are as follows:
(1) Cross level to another unit on current installation or in country (if Soldier is RTD from OCONUS WTU).
(2) Army requirements.
(3) Soldier preference.
j. The report date for RTD Soldiers who are reassigned on the same installation (local move) will be within 10 days
from HRC email assignment notification to WTU and/or military personnel division. The report date for RTD Soldiers
assignment to a unit requiring a PCS will be within 90 days from HRC assignment instructions or request for orders
notification. Assignment special instructions will indicate early report is authorized.
7 – 4. Active Guard Reserve return to duty assignment procedures
AGR officers and enlisted Soldiers are RTD in accordance with AR 614
– 100 and AR 614 – 200.
7 – 5. Reserve Component release from active duty criteria
a. RC Soldiers will remain attached to the WTU or CCU until their medical condition is resolved and they are eligible
for REFRAD, complete the DES process, or they request withdrawal from the program. WTU human resources personnel
will submit a copy of the fit for duty memorandum to HRC no later than 48 hours from the date signed by the PCM.
b. When a Soldier has been medically cleared to RTD, the Soldier’s senior commander element will forward the
REFRAD checklist and a fit for duty memorandum (signed by the Soldier’s PCM) to the following email addresses: En-
listed Personnel Management Directorate at usarmy.knox.hrc.mbx.epmd-refrad-[email protected] or Officer Personnel
Management Directorate at usarmy.knox.hrc.mbx.opmd-[email protected].
c. MEDCOM, Soldier Transition Branch will forward a REFRAD authorization memorandum to the supporting WTU
and the transition center. Upon receipt of the REFRAD authorization memorandum, the WTU administrative specialist
will coordinate with the transition center and Soldier to prepare the DD Form 214.
d. The WTU administrative specialist will coordinate with the transition center to publish the final DD Form 214 and
the REFRAD order and make any corrections with supporting documents.
e. The transition center will make the appropriate changes in TRANSPROC and review with the Soldier. The transition
center will publish the final DD Form 214 and the REFRAD order (Format 523). When publishing the final DD Form 214,
AR 600–77 • 5 March 2019
37
the “mobilization service 10 USC 12302” and the “MRP/MRP2/ADME service 10 USC 12301(h)” will be listed as sepa-
rate periods in block 18 of the final DD Form 214.
f. The transition center will mail copies 1 and 4 of the DD Form 214 along with a copy of the REFRAD order to the
Soldier’s address listed on the DD Form 214 and distribute other copies of the DD Form 214, as required (to include the
organic ARNG or USAR unit).
g. Every USAR or ARNG Soldier who is demobilized must process through or be processed by a transition center. A
super server transition transaction is input on each Soldier. The transition path used is “[not Loss to Army].” This will
generate a Total Army Personnel Data Base 5010 transaction in the eMILPO system. The WTU administrative specialist
is required to complete the eMILPO 5010 transaction. The transition center will forward a copy of the final DD Form 214
to the local finance office in order to stop the individual’s pay and allowances. The local finance office will complete a
transaction in the Defense Joint Military Pay System (DJMS) to stop the Soldier’s active duty pay and allowances.
h. The Soldier may be released to his or her unit with a faxed or emailed copy of the DD Form 214 and REFRAD order.
7 – 6. Reserve Component released from active duty for medical condition existing prior to service
An RC Soldier identified within 30 days (see the Army’s Mobilization and Deployment Reference (AMDR) 25-Day Rule)
from his or her M-date as having a pre-existing medical condition that renders him or her non-deployable may be REFRAD
immediately. Administrative processing of REFRAD orders, Soldier out-processing, and return to HOR must be completed
no later than 30 days from Soldier’s M-date. Disqualifying conditions include temporary and permanent conditions that
do not meet medical retention standards. The Soldier’s command will ensure that the Soldier receives appropriate medical
care and follow-up upon return to home station. Upon reaching MRDP for the condition causing REFRAD, the Soldier
should be RTD or referred to the DES. If RTD, the Soldier is immediately subject to a subsequent order to active duty.
(see 10 USC 1206a).
Section II
Separation
7– 7. Administrative separation of Regular Army and Reserve Component Soldiers found fit for duty
A Soldier may not be administratively separated involuntarily for a medical condition which a PEB previously found the
Soldier to be fit for duty unless the condition worsens. If the condition worsens or continues to preclude the Soldier from
performing his or her duties, the Soldier may be referred back to the DES. The SECARMY or designee will have final
approval authority for any Soldier found fit for duty by the PEB but separated involuntarily as unsuitable for military
service.
7 – 8. Reserve Component separation processing (non-Active Guard Reserve)
a. Soldiers separated or retired for disability. The WTU or senior command element will only send the TRANSPROC
printout and a physical disability information report to MEDCOM to initiate the MRP, MRP2, or ADME order amendment.
b. Soldiers separated without disability benefits.
(1) When a Soldier processes through the DES and separates without physical disability benefits, the USAPDA will
input the Soldier’s personnel data into TRANSPROC.
(2) The installation transition center will notify the WTU or senior commander element when the Soldier’s information
has been located in TRANSPROC. Upon notification, the WTU or senior commander element will direct the Soldier to
begin transition proceedings. Soldiers residing on or near an installation will report with their records to the transition
center for out-processing within 24 hours of the notification. Soldiers attached to CCUs will follow WTU or CCU proce-
dures.
(3) The transition center will publish the final DD Form 214 (see AR 600
– 8 – 105 for orders format). The “mobilization
period under 10 USC 12302” and the “MRP/MRP2/ADME period under 10 USC 12301(h)” will be listed as separate
periods in block 18 of the final DD Form 214.
(4) Under provisions of 10 USC 1209, if the Soldier has 20 years of creditable Reserve service, has been issued a 20-
year notification of eligibility for non-regular retirement, and requests to transfer to the Retired Reserve, the Soldier will
be REFRAD using the appropriate order format per AR 600
– 8 – 105 and transferred directly to the Retired Reserve.
Note: Soldiers with 15 years of creditable Reserve service must request approval from HRC, the State military personnel
office, or Assistant Chief of Staff for Personnel for 15-year notification of eligibility for non-regular retirement; this is a
special request and is not an automatic action.
38
AR 600–77 • 5 March 2019
(5) Under the provisions of 10 USC 12731b, RC Soldiers of the Selected Reserve with at least 15 years of creditable
Reserve service and a disposition of separation with severance pay or separation without benefits due to non-service con-
nected disability have the option to transfer to the Retired Reserve to draw non-regular retired pay upon reaching the
required statutory age. When the Soldier elects this option and coordination has been accomplished for issuance of the 15-
year notification of eligibility for non-regular retirement, the Soldier will be REFRAD using the appropriate order format
per AR 600
– 8 – 105 and transfer directly to the Retired Reserve.
(6) The transition center will mail copies 1 and 4 of the DD Form 214, along with a copy of the REFRAD order, to the
Soldier’s address listed on the DD Form 214 and distribute other copies of the DD Form 214, as required (to include the
organic ARNG or USAR unit).
(7) The installation adjutant general is required to complete the eMILPO 5010 transaction. The transition center will
forward a copy of the final DD Form 214 to the local finance office in order to stop the Soldier’s pay and allowances. The
local finance office will complete the transaction in the DJMS to stop the Soldier’s active duty pay and allowances.
c. Soldiers separated with severance pay.
(1) When a Soldier processes through the DES and is separated with severance pay, the USAPDA will input the Sol-
dier’s personnel data into TRANSPROC.
(2) The transition center will notify the WTU or senior commander element when the Soldier’s information has been
located in TRANSPROC. Upon notification, the WTU or senior commander element will direct the Soldier to begin tran-
sition proceedings. Soldiers residing on or near installations will report with their records to the transition center for out-
processing within 24 hours of the notification. Soldiers attached to CCUs will follow WTU or CCU procedures.
(3) The transition center will publish the final DD Form 214 and the discharge order (Format 501) and the separation
program designator is directed by the USAPDA. When publishing the final DD Form 214 the “mobilization period under
10 USC 12302” and the “MRP/MRP2/ADME period under 10 USC 12301(h)” will be listed as separate periods in block
18 of the final DD Form 214.
(4) If the Soldier has 20 years of creditable service for non-regular retirement, has been issued a 20-year notification of
eligibility for non-regular retirement, and requests to be transferred to the Retired Reserve in lieu of disability severance,
the Soldier will be REFRAD using order Format 523 and transferred directly to the Retired Reserve. Soldiers with more
than 15 years of creditable service for non-regular retirement can request to be issued the 15-year notice of eligibility for
non-regular retirement and, once issued, can request to be transferred to the Retired Reserves in lieu of disability severance.
The Soldier will be REFRAD using order Format 523 and transferred directly to the Retired Reserves.
(5) The transition center will mail copies 1 and 4 of the DD Form 214, along with a copy of the REFRAD order, to the
Soldier’s address listed on the DD Form 214 and distribute all other copies of the DD Form 214, as required (to include
the organic ARNG or USAR unit).
(6) The installation adjutant general is required to complete the eMILPO 5010 transaction. The transition center will
forward a copy of the final DD Form 214 to the local finance office in order to stop the Soldier’s pay and allowances. The
local finance office will complete the transaction in the DJMS to stop the Soldier’s active duty pay and allowances.
(7) The severance pay transaction will be input before the Soldier departs the installation or the CCU.
(8) For Soldiers who accept disability severance pay under 10 USC 1209, the election is irrevocable.
d. Soldiers separated to the temporary disability retirement list or permanent disability retirement list.
(1) When a Soldier processes through the DES and is separated as TDRL or permanent disability retired list (PDRL),
the USAPDA will input the Soldier’s personnel data into TRANSPROC.
(2) The transition center will notify the WTU or senior commander element when the Soldier’s information has been
located in TRANSPROC. Upon notification, the WTU or senior commander element will direct the Soldier to begin tran-
sition proceedings. Soldiers residing on or near installations will report with their records to the transition center for out-
processing within 24 hours of the notification.
(3) The transition center will publish the final DD Form 214 and a retirement order using Format 430 (reassignment
for separation processing) and Format 610 (TDRL) or 612 (PDRL) and the separation program designator code will be
SFK or SEK (TDRL) or SFJ or SEJ (PDRL). When publishing the final DD Form 214 the “mobilization service 10 USC
12302” and the “MRP/MRP2/ADME service 10 USC 12301(h)” will be listed as separate periods in block 18 of the final
DD Form 214.
(4) The transition center will mail copies 1 and 4 of the DD Form 214, along with a copy of the retirement order, to the
Soldier’s address listed on the DD Form 214 and distribute all other copies of the DD Form 214, as required (to include
the organic ARNG or USAR unit).
(5) The installation adjutant general is required to complete the eMILPO 5010 transaction. The transition center will
forward a copy of the final DD Form 214 to the local finance office in order to stop the Soldier’s pay and allowances. The
local finance office will complete the transaction in DJMS to stop the Soldier’s active duty pay and allowances.
AR 600–77 • 5 March 2019
39
7 – 9. Transitioning Soldiers from active duty while attached to a medical facility
a. Upon separation notification from USAPDA, the transition center where the Soldier is attached or geographically
located will coordinate with the installation of assignment transition center for guidance on orders.
b. The installation of assignment transition center will—
(1) Forward a copy of the Soldier’s service records and allied papers electronically to the installation of attachment’s
transition center for the preparation of DD Form 214 and guidance of separation orders.
(2) Coordinate with the Soldier’s assigned command to appoint another Soldier to out-process the Soldier and Family
in the Soldier’s absence.
(3) Forward medical, dental, and personnel records (DD Form 93, SGLV 8286A (Family Coverage Election (SGLI)),
and Soldier Record Brief) along with the appropriate copy of the final DD Form 214 for disposition. (If those records are
located geographically with the Soldier, the attached transition center will complete this task).
c. The installation of attachment transition center will—
(1) Publish separation orders in accordance with AR 600
– 8 – 105 and provide a copy electronically to the assigned
transition center.
(2) Inform the Soldier to use his or her separation orders to make transportation and flight arrangements in order to
proceed to his or her HOR or station of choice.
(3) Inform Soldier to schedule an appointment with the local Army Wounded Warrior Program representative prior to
their final transitioning.
(4) Initiate SFL
– TAP services via DD Form 2648 (Service Member Pre-Separation/Transition Counseling and Career
Readiness Standards EForm for Service Members Separating, Retiring, Released from Active Duty (REFRAD)).
(5) Verify completion of physical exams, if appropriate.
(6) Ensure that Soldiers who may be medically retired, attend the mandatory pre-retirement and Survivor’s Benefit Plan
briefing no later than the start of the DES process. Retiring Soldiers must complete a DD Form 2656 (Data for Payment
of Retired Personnel) prior to retirement to establish their Survivor’s Benefit Plan election and retired pay account.
(7) Coordinate with the local finance office to assist the Soldier in resolving finance issues.
(8) Prepare the DD Form 214 worksheet in coordination with the assigned transition center, review the DD Form 214
worksheet with Soldier, and distribute the final DD Form 214. This includes coordination with the assigned transition
center to file a copy in the personnel and medical records.
(9) Ensure that all required actions are completed for final transitioning and records that are geographically located
with the Soldier are sent to the appropriate mailing address for disposition by the attached transition center.
d. Transition center managers must ensure the points of contact on the transition center directory are updated so that
immediate coordination can be established between transition centers upon notification of separation actions in
TRANSPROC.
7– 10. Process to separate an attached Warrior Transition Unit Soldier
a. When a Soldier is attached for medical purposes and is due to separate from active duty, the installation where the
Soldier is attached will coordinate with the installation of assignment. If the Soldier is a USAR AGR, notify the Com-
mander, U.S. Army Human Resources Command (AHRC
– OPL – PR), 1600 Spearhead Division Avenue, Fort Knox, KY,
40122
– 5001.
b. The installation of assignment transition center will publish separation orders and the two installations will coordinate
to receive the Soldier's service records and allied papers.
c. Once the attached installation receives the service records and allied papers, the Soldier will then be released from
attachment and assigned for transition purposes (usually 1 day).
d. The installation of assignment will coordinate with the Soldier's assigned unit to out-process the Soldier in his or her
absence.
e. The installation of attachment will process separation documents to include the DD Form 214.
f. The installation of attachment will coordinate with local finance to assist Soldier with final out-processing to resolve
finance issues.
g. The transition centers will need a copy of the DD Form 2648. Any retirement (TDRL or PDRL) will require a pre-
retirement briefing and DD Form 2656 to start the retired pay.
40
AR 600–77 • 5 March 2019
Chapter 8
Benefits
8 – 1. Department of Veterans Affairs benefits briefing
WII Soldiers assigned or attached to a WTU or CCU will receive a VA benefits briefing during in-processing.
8 – 2. Soldier For Life - Transition Assistance Program
a. The installation SFL
– TAP center is the designated agency to provide the pre-separation counseling to Soldiers sep-
arating from the Army and transitioning to civilian life. For installations that do not have a SFL
– TAP center, the garrison
commander will appoint a point of contact to provide pre-separation counseling in coordination with the nearest SFL
– TAP
center.
b. The SFL
– TAP pre-separation counseling for RA and RC Soldiers is standardized. The slide presentation and sup-
porting scripts can be obtained by contacting the nearest SFL
– TAP transition service manager. The SFL – TAP point of
contact is Commander, U.S. Army Human Resources Command,1600 Spearhead Division Avenue, Fort Knox, KY
40122
– 5001.
c. An booklet produced by the VA on Federal benefits for Veterans, Dependents, and Survivors is available at
https://www.va.gov/opa/publications/benefits_book.asp.
8 – 3. Transitional Assistance Management Program
The Transitional Assistance Management Program (TAMP) provides 180 days of transitional health care benefits to help
eligible Soldiers and their Families transition to civilian life.
a. For RC Soldiers, eligibility for transitional health care is based on completion of active duty for more than 30 days
in support of contingency operations pursuant to 10 USC 101(a)(13)(B). TAMP eligibility begins upon release or separa-
tion from this qualifying active duty service and remains in effect for 180 consecutive days.
(1) If—after a break in service—the Soldier returns to a subsequent active duty period (which includes health care
eligibility) that begins during the 180-day period of transition assistance, their health care eligibility will run concurrently.
(2) If the qualifying active duty period is followed by any other active duty period—without a break in service, then
the eligibility for transition assistance begins upon REFRAD.
b. Soldiers with a wound, illness, or injury incurred in the LOD while on active duty should contact their unit for
eligibility determination or authorizations for follow-up medical or dental care.
c. Changes to TRICARE programs occur when public law and/or Federal regulations are amended. MTF guidelines
and policies may be different than those outlined here. For the most current information, Soldiers should contact their
TRICARE regional contractor, TRICARE service center, or local MTF.
Chapter 9
Support Sections, Agencies, and Organizations
9– 1. Army retirement services
The Army retirement services homepage is located at https://soldierforlife.army.mil/retirement/. It is vitally important that
the Soldier and Family understand the many benefits and entitlements they are eligible for before the Soldier retires.
9 – 2. Legal information
All Soldiers referred for DES processing have access to specially trained judge advocates or DA civilian legal counsel for
issues pertaining to their DES processing. The point of contact for locating the appropriate legal counsel is the closest
servicing legal assistance office or PEBLO.
9 – 3. Soldier and Family Assistance Center
The SFAC programs are designed to support the local WTUs, WII Soldiers, and their Family members or support person-
nel. The available SFAC locations provide coordinated services on site or through coordinated appointments on site or
AR 600–77 • 5 March 2019
41
appointments at the service provider’s location. The identified services may or may not be immediately available based on
the garrison support composition.
a. Soldier and Family Assistance Center staff and personnel services.
(1) Soldier and Family Assistance Center information and referral services.
(a) Assess Soldier and Family needs; conduct specialized needs assessment to tailor services and/or complete the cen-
tralized intake process.
(b) Establish automated client case files and record client service usage in the Army Community Services Client Track-
ing System data recording system.
(c) Provide information and make service referrals within the center and to external agencies.
(d) Maintain resource listings on a variety of installation, local, state, and Federal agencies which offer support services,
assistance and information.
(e) Maintain a roster of available language translators and lodging referral resource information.
(f) Provide in person or electronic information on available services and points of contact to clients at distant, non-
resident locations.
(g) Coordinate with military personnel and the provost marshal office to establish access to installations and installation
services for NMAs arriving on an ITA.
(2) Financial counseling services.
(a) The Financial Counselor will provide financial counseling, budget information, and benefits referral for WTU Sol-
diers and their Family members. In addition, they may provide Army Emergency Relief assistance.
(b) Counsels and educates WII Soldiers and Families on personal financial self-sufficiency.
(3) Education counseling services.
(a) Education services are provided in compliance with the Army Continuing Education System.
(b) Provide access to academic and military testing.
(c) Provide mandatory GI Bill counseling and post-911 GI Bill transferability to all WII Soldiers whether they transition
within or out of the Army.
(d) Ensure all WII Soldiers are familiar with the GoArmyEd portal (https://www.goarmyed.com) procedures to apply
for educational assistance.
(e) Assist WII Soldiers and Family members in accessing State, county, or local education benefits.
(4) Military personnel service support (human resources).
(a) Provide in- and out-processing support and assistance.
(b) Provide information on common access cards, Teslin cards and assists in setting up appointments to receive cards.
When available, provides cards on site.
(c) Provide information on a wide range of personnel type issues to include updating personnel records, transition and/or
separation guidance, retirement information, and other key information topics.
(5) Outreach specialist support. Provide information, coordination and service development with a wide range of gar-
rison, local community, state and federal groups, organizations and services that support the WII Soldiers and their Family
members or NMAs. This may include development of Memoranda of Agreement, Memoranda of Understanding or other
operational agreements with partner or support services.
(6) Social services coordination and support.
(a) Provide training, information and coordination on issues that impact the well-being of the WII Soldier and their
Family members.
(b) Develop a close working relationship with the WTU and medical services so as to provide immediate referral or
connection to services, when needed.
(7) Soldier for Life-Transition Assistance Program.
(a) The contracted service provider aids the WII Servicemember in meeting their transition goals and requirements as
per the Veterans Opportunity to Work, Hire Heroes Act, their WTU Comprehensive Transition Plan goals and other related
transition requirements under SFL
– TAP.
(b) Services may be offered in varied formats and locations designed to aid the WII Soldier in their goal completion.
(8) Soldier and Family Assistance Center director. The SFAC director—
(a) Serves as the overall coordinator of direct, non-clinical services to the WTU Soldiers, their Family members, and/or
other support personnel (for example, NMAs).
(b) Coordinates SFAC services and events with the Army Community Service (ACS) director, garrison, and WTU
cadre.
(c) Coordinates with and provides overall program guidance and direction to any support personnel working in support
of or for the Soldier.
42
AR 600–77 • 5 March 2019
(d) Supervises the SFAC service providers (see paras 9–3a(1) through 9–3a(6)), operates and manages the SFAC pro-
gram and facility, and coordinates with both the WTU Command and their garrison operations supervisor and staff.
(e) Ensures all ongoing requirements and administrative actions are completed in direct support of the WII Soldiers and
their Family members or NMAs.
(9) Computer room. SFAC provides a full-service computer room with internet capability to support the specific ser-
vices and actions needed while the Soldier is in medical rehabilitation and transition.
(10) Donations management. The SFAC program, under non-appropriated fund guidance, provides support to the
WTU Soldiers and their Family members with events, activities, functions and other support or morale building actions as
a result of donations received and managed.
b. Partner service organizations, providers, agencies or non-federal organizations or entities providing services at the
SFAC or in coordination with the SFAC.
(1) Social Security liaison. SFAC coordinates with the Social Security Administration to ensure all WTU Soldiers are
aware of the services available to them and enroll for services they qualify for.
(2) Veterans Affairs. SFAC provides information and referral to the many veteran’s services offered by the VA. At
select locations the VA may be represented in the SFAC to provide these services.
(3) Traumatic Servicemembers’ Group Life Insurance and Combat-related special compensation. SFAC provides in-
formation and referral to these support services.
(4) Child, youth, and school services.
(a) Provides information on child and/or youth support programs and services and completes all registration actions.
(b) Assists with childcare services and any extended support to designated nondependent WII Soldier caregivers.
(c) Assists with coordination or arrangement of respite care services for WII Families with special needs members
through the ACS and Exceptional Family Member Program.
(5) Pastoral services (chaplain), usually located in the WTU.
(a) Provide comprehensive religious support by providing timely ministry and counseling by either direct approach or
referral to the Family Life Chaplain.
(b) Provide rites and sacraments.
(c) Provide resources such as religious literature and counseling materials.
(6) State Judge Advocate and legal assistance. Services may focus on MEB/PEB Soldiers. When available, provides
legal services and/or administrative legal assistance.
(7) Defense Financial and Accounting Service, located in or coordinated with Soldier and Family Assistance Center.
(a) Provides WII Soldiers and their Family members’ assistance with military pay and benefits information and correc-
tion in accordance with DFAS guidance.
(b) Assists with travel orders and necessary actions to complete travel document filing after all travel is completed.
(8) Non-governmental organizations, Veterans service organizations, non-federal entities and others. There are many
groups or organizations which support the military and veterans. Information about how to identify and connect with these
groups is made available.
c. Garrison services which are available to support the WII Soldiers.
(1) Army Community Service. ACS provides information on all garrison services to include locations and contact in-
formation. ACS also includes a host of services designed to assist everyone on the installation.
(2) Army Substance Abuse Program. The garrison provides a comprehensive substance abuse prevention education,
intervention, information, and referral program for WII Soldiers and their Family members. The Army Substance Abuse
Program provides guidance to assist the WTU or CCU commanders in establishing and conducting successful suicide
prevention training, hotline and resource information, and coordination of the Employee Assistance Program. The Army
Substance Abuse Program provides an information website at https://acsap.army.mil/sso/pages/public/resources/com-
manders.jsp.
(3) Survivor Outreach Services Program. The Survivor Outreach Services Program serves as the advocate for the sur-
vivor of fallen Soldiers who have paid the ultimate sacrifice.
9 – 4. U.S. Department of Veterans Affairs
a. Soldiers may be eligible for a broad range of programs and services provided by the VA. Eligibility for most VA
benefits is based upon discharge from active military service under Honorable or General, Under Honorable conditions.
Certain benefits require service during wartime. If new to the VA, the Federal Benefits for Veterans, Dependents, and
Survivors booklet may help individuals learn about the various benefits and programs.
b. The Pre-Discharge Program is a Joint VA and DOD program that affords Soldiers the opportunity to file claims for
disability compensation up to 180 days prior to separation or retirement from active duty or full time National Guard or
Reserve duty (Title 10 and 32 USC). Further information is available at http://www.benefits.va.gov/predischarge/.
AR 600–77 • 5 March 2019
43
c. Additional information is available at the nearest VA medical facility. Veterans Affairs facilities listings and tele-
phone numbers can be found at https://www.va.gov/directory/guide/home.asp. Veterans can also visit the VA health eli-
gibility website at https://www.va.gov/healthbenefits/.
Chapter 10
Special Compensation for Assistance with Activities of Daily Living
10 – 1. Intent of the program
a. The purpose of the SCAADL Program is to assist permanent catastrophically injured or ill Soldiers who require
regular aid and attendance after hospitalization as a result of injuries or illnesses sustained or aggravated in the LOD.
SCAADL is paid directly to the Soldier and is considered taxable income. This policy extends SCAADL eligibility to
those Soldiers with qualifying injuries or illnesses who meet the criteria in paragraph 10
– 3 on or after 31 August 2011.
This policy is not retroactive, and the program is voluntary for Soldiers.
b. To receive SCAADL, a DOD or VA licensed physician will determine that the Soldier has a permanent catastrophic
injury or illness to the extent that he or she would be hospitalized or institutionalized without assistance. Once determined
to have a permanent catastrophic injury or illness incurred or aggravated in the LOD that meets the criteria set forth in
DODI 1341.12 and this policy, the Soldier (RA and RC) will be authorized SCAADL; except as provided in paragraphs
10
– 4 and 10 – 11. SCAADL may be paid in addition to any other pay and allowance the Soldier is entitled or authorized.
c. Permanent catastrophically injured or ill Soldiers will be referred and processed through the DES in accordance with
AR 635
– 40 to facilitate their transition and access to eligible VA benefits.
10 – 2. Soldier’s application
a. An application will consist of—
(1) The Soldier's written request to the commander for SCAADL.
(2) The commander's verifications required by paragraphs 10
– 3, 10 – 5, and supporting documentation referenced in
paragraphs 10
– 3 and 10 – 5 (see fig 10 – 1).
b. Commanders will retain records of SCAADL payments in an appropriate system of records, including complete
applications, payment computations, and documentation provided to DFAS authorizing payments.
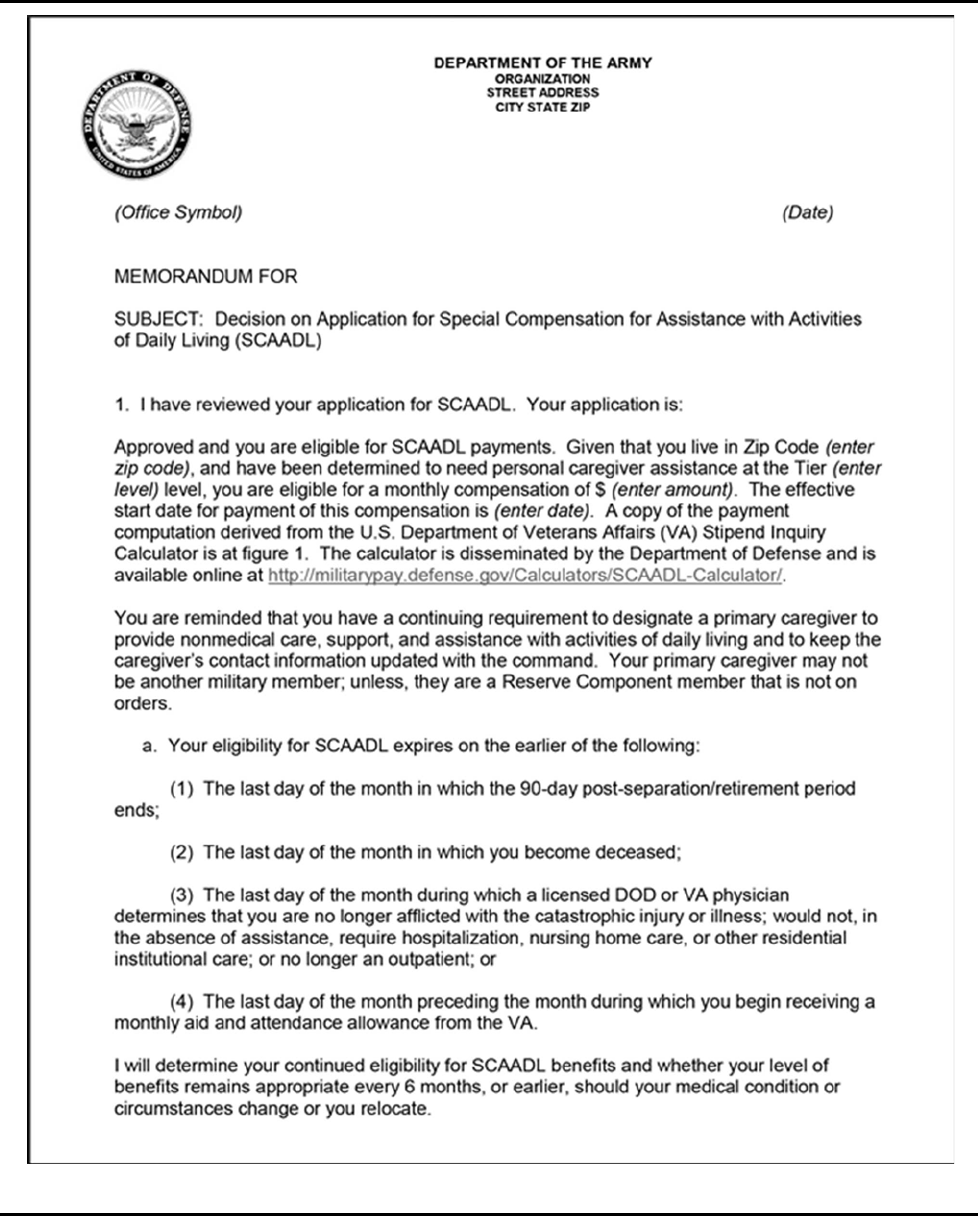
44
AR 600–77 • 5 March 2019
Figure 10 – 1. Sample notification memorandum to Soldiers of commander’s determination of eligibility regarding Special
Compensation for Assistance with Activities of Daily Living
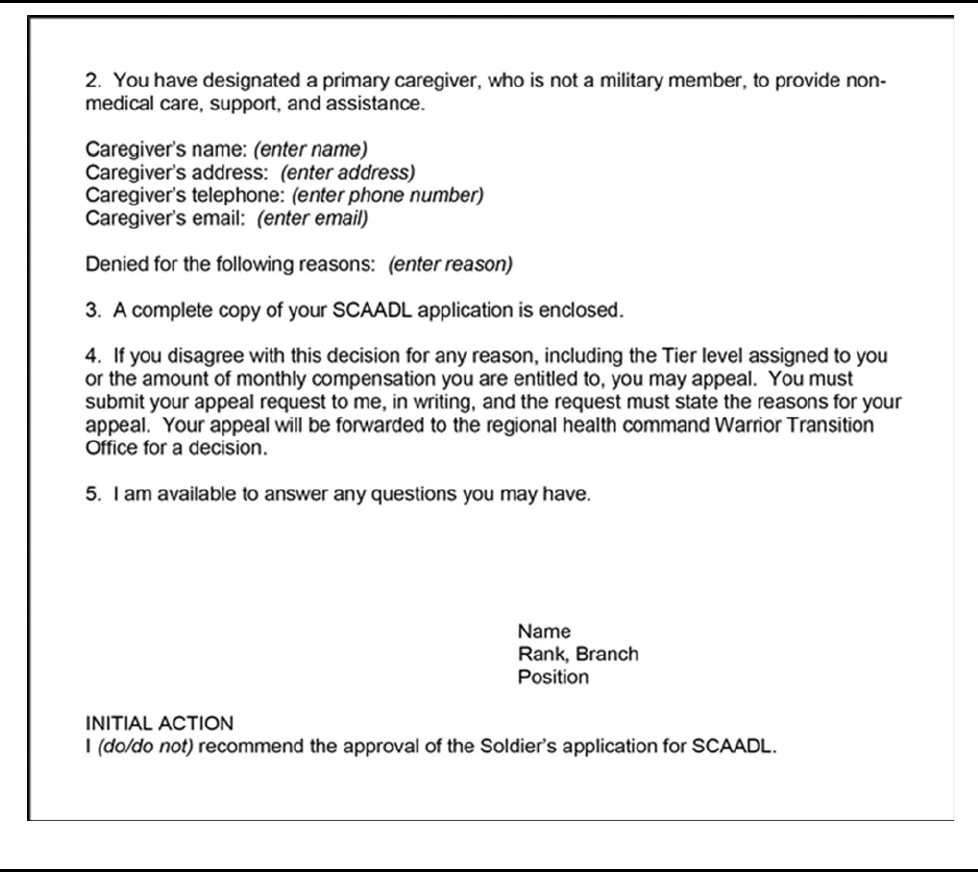
AR 600–77 • 5 March 2019
45
Figure 10 – 1. Sample notification memorandum to Soldiers of commander’s determination of eligibility regarding Special
Compensation for Assistance with Activities of Daily Living—Continued
10 – 3. Determination of threshold eligibility
Upon receipt of a written request from a Soldier (or designee) to participate in the SCAADL Program, the commander will
determine the Soldier's threshold eligibility for SCAADL by verifying that the Soldier meets all the criteria. If the Soldier
does not meet the threshold eligibility requirements, the commander will inform the Soldier, in writing, about his or her
ineligibility and the procedures for appealing the commander's determination (see para 10
– 9). The following criteria must
be met for eligibility:
a. Soldier has a permanent, catastrophic injury or illness in accordance with the definition in the glossary. Verification
will be obtained from a licensed DOD or VA physician; not a contract physician. See DD Form 2948 (Special Compensa-
tion for Assistance with Activities of Daily Living (SCAADL) Eligibility), Part I – Eligibility Criteria.
b. Soldier needs assistance from another person to perform the personal functions required in everyday living or requires
constant supervision and, in the absence of such care, would require hospitalization, nursing home care, or other residential
institutional care (see fig 10
– 2). (This certification may also be made by a licensed DOD or VA physician; not a contract
physician.);
c. The permanent catastrophic injury(ies) or illness(es) were incurred or aggravated in LOD;
d. Soldier is an outpatient and no longer determined to be an inpatient at a MTF, VA medical center, civilian hospital,
nursing home, or other residential institutional care facility. Although individuals may be temporarily placed in an inpatient
46
AR 600–77 • 5 March 2019
status during a given month for tests, examinations, or treatment, they are eligible for the full monthly SCAADL payment
provided they are in an outpatient status for the majority of the month (more than 15 days). If the Soldier is an inpatient
for 16 or more days in a given month, the amount of compensation for that month will be pro-rated based on the number
of days he or she is an inpatient, and a reevaluation will be conducted to determine continued SCAADL eligibility; and
e. Soldier has designated a primary caregiver who is at least 18 years of age to provide non-medical care, support, and
assistance with at least one of the activities of daily living as set forth in DODI 1341.12. The primary caregiver may not
be a member of the military; except RC Soldiers not on orders.
Figure 10 – 2. Sample memorandum from the regional health command to the defense finance and accounting service for
payment of Special Compensation for Assistance with Activities of Daily Living
10 – 4. Soldier is not eligible for the Special Compensation for Assistance with Activities of Daily
Living compensation if receiving any of the following services
a. Outpatient or in-home services to assist with activities of daily living or supervision to avoid harm to self or others
from another Federal agency;
b. A monthly caregiver stipend (paid directly to the Soldier's primary caregiver) from the VA pursuant to 38 USC
1720G(a)(3);
c. In-home assistance with activities of daily living (custodial care) paid with supplemental health care program funds
and provided by a TRICARE-authorized home health agency; or
AR 600–77 • 5 March 2019
47
d. If the Soldier is found fit by a PEB or RTD as unfit but continued on active duty.
Note: While receiving SCAADL, the Soldier's primary caregiver is eligible to receive the respite benefit if qualified under
TRICARE Operations Manual 6010.51M. Soldiers receiving other home health services under the TRICARE home health
benefit remain eligible for SCAADL, except as provided in paragraph 10
– 4.
10 – 5. Certification of DD Form 2948
a. After determining a Soldier meets the threshold eligibility requirements, the commander will verify that either a
DOD or VA physician has certified the DD Form 2948. The commander will help the Soldier in seeking the required
certification to include assisting the Soldier with obtaining any necessary medical examinations or chart reviews.
b. DD Form 2948 will be completed and certified by DOD or VA physician based on input from other sources as
appropriate. DD Form 2948 generally should be completed and certified by the physician acting as the Soldier's PCM. If
the assessment documented on the DD Form 2948 is conducted by a non-DOD or VA physician or the Soldier presents an
uncertified DD Form 2948, the commander will help the Soldier in seeking the required certification from a DOD or VA
physician. The commander will afford the Soldier (or designee) the opportunity to review and sign the completed DD
Form 2948. The commander will advise the Soldier about how they may appeal the determinations of their PCM, DOD,
or VA physician (see para 10
– 12).
c. A DOD or VA physician who declines to certify a DD Form 2948 must state, in writing, the reasons for the denial
to the commander. The reasons must be sufficiently detailed to permit a meaningful appeal by the Soldier. If a DOD or
VA physician will not certify the DD Form 2948, the commander will notify the Soldier, in writing, that their application
has been denied, provide the Soldier with the DD Form 2948, and the physician's written statement of the reasons for
declining certification. The commander will inform the Soldier about the procedures for appeal (see para 10
– 12).
d. If applicable, a DOD or VA physician may ask to conduct an in-home visit with the Soldier to make the assessments
needed to complete or certify the DD Form 2948. A DOD physician may request to conduct an onsite visit when verifying
a Soldier's permanent catastrophic injury or illness to determine if the Soldier would require hospitalization, nursing home
care, or other residential care in the absence of assistance. The in-home visit may be conducted by nursing personnel with
their input provided to the DOD physician for consideration as part of the physician’s assessment.
10 – 6. Action on the application
Upon the commander's verification of all information required by paragraphs 10
– 3 and 10 – 5, the Soldier's DD Form 2948
is complete and the commander will recommend its’ approval. The commander will disapprove the application if the
Soldier does not meet the required eligibility criteria.
10 – 7. Computing compensation
After recommending approval of the DD Form 2948, the commander will—
a. Compute the amount of monthly compensation the Soldier is entitled to in accordance with DODI 1341.12 using
information drawn from the Soldier's complete application and the SCAADL calculator; ensuring that the tier rating used
in the calculation is consistent with the dependence level identified on the DD Form 2948;
b. Retain the computation from the SCAADL calculator with the application materials either by printing the screen or
otherwise documenting the results; and
c. Forward a copy of the complete application and the payment computation from the SCAADL calculator to a certify-
ing officer in MEDCOM’s RHC Warrior Transition Office. For RC Soldiers not attached/assigned to a WTU or CCU, the
RC headquarters may designate additional routing channels before sending the copy of the application to the RHC Warrior
Transition Office.
10 – 8. Regional Health Command payment authorization
The RHC certifying officer will—
a. Notify the commander when a Soldier's SCAADL application and payment computation have been received;
b. Verify the DD Form 2948 is complete and the payment computation is accurate and work with the submitting com-
mander to resolve any discrepancies with the application or payment computation;
c. Submit DFAS required documentation to authorize SCAADL payment to the Soldier beginning on the effective start
date (the date the DOD or VA physician certified the DD Form 2948); and
d. Notify the commander when RHC authorizes DFAS to pay SCAADL to the Soldier.
Note: See figure 10
– 2 for an example of the physician certification memorandum.
48
AR 600–77 • 5 March 2019
10 – 9. Notification to Soldier
After the RHC certifying officer authorizes payment, the commander will notify the Soldier in writing that his or her
application is approved to include the amount of monthly compensation the Soldier is entitled. Upon request, the com-
mander will provide the Soldier with a complete copy of his or her application and compensation calculation. See figure
10
– 1 for an example of the notification memorandum. Commanders will make sure eligible Soldiers (or designee) are
informed of the—
a. Approval of their DD Form2948 and eligibility for SCAADL.
b. Amount of monthly compensation the Soldier is entitled, how the amount was calculated, and the effective start date
of the compensation.
c. Requirement to designate a primary caregiver of at least 18 years of age to provide non-medical care, support, and
assistance with activities of daily living and to keep the caregiver's contact information updated with the commander.
d. Duration of SCAADL eligibility, including the need for a formal reevaluation of eligibility every 6 months or earlier
should the Soldier's medical condition or circumstances change or the Soldier relocates.
e. Soldier's right to appeal the commander's decision; the appeal request must be submitted in writing and contain the
reason for the appeal.
10 – 10. Special Compensation for Assistance with Activities of Daily Living packet
As a minimum, a Soldier’s SCAADL packet will consist of the following documents:
a. DD Form 2948.
b. Notification Memorandum to Soldier of commander’s determination of eligibility (see fig 10
– 1).
c. Payment computation from the SCAADL calculator.
d. Pay authorization roster to DFAS for payment.
e. Counseling statement (see fig 10
– 3).
Note. Commanders or designees will use the language in figure 10
– 3 to execute the SCAADL counseling using a DA
Form 4856.
AR 600–77 • 5 March 2019
49
Figure 10– 3. Sample language for DA Form 4856, Developmental counseling for Special Compensation for Assistance with
Activities of Daily Living
50
AR 600–77 • 5 March 2019
10 – 11. Expiration of Special Compensation for Assistance with Activities of Daily Living eligibility
The commander will promptly notify DFAS, through the regional health command, to terminate payments when a Soldier's
eligibility expires on the earlier of the following:
a. The last day of the month in which the 90-day post-separation/retirement period ends;
b. The last day of the month during which the Soldier dies;
c. The last day of the month during which a licensed DOD or VA physician determines that the Soldier is no longer
afflicted with the catastrophic injury or illness; or
d. The last day of the month preceding the month during which the Soldier begins receiving a monthly aid and attend-
ance allowance pursuant to 38 USC 1114(r)(2).
10 – 12. Special Compensation for Assistance with Activities of Daily Living appeal process
TSG is the appellate authority and may delegate his or her appellate authority over appeals to another official at Headquar-
ters, Department of the Army. A Soldier whose application for SCAADL is denied based on failure to meet the threshold
eligibility criteria, a licensed DOD or VA physician will not certify the DD Form 2948, or for any other reason may appeal.
A Soldier who believes he or she is entitled to additional compensation based on either the DD Form 2948 criteria (for
example, the tier level) or the commander's computation may also appeal.
a. The Soldier will submit his or her appeal, in writing, to the commander within 60 days after notification of the
outcome of his or her request for SCAADL is issued. The Soldier must state the reason(s) for his or her appeal.
b. The commander will forward the Soldier's appeal, with a command recommendation, through the RHC to the
MEDCOM, DCS, WCT as the delegated authority. In all cases, the commander will assist the Soldier by forwarding a
complete copy of the Soldier's SCAADL DD Form 2948 and compensation calculation to include all available medical
reviews and opinions. TSG or his or her delegate will ensure the thorough review of all available information pertinent to
the appeal, including the determinations of eligibility, clinical evaluations, and tier scoring rendered by the Soldier's PCM
or other licensed DOD or VA physician. For appeals related to issues requiring a medical assessment or certification, TSG
or his or her delegate will request the development of a medical advisory opinion by a licensed DOD physician who did
not participate in the original evaluation.
c. Reconsideration may be granted at the lowest level practicable before transmittal to TSG or his or her delegate in an
effort to eliminate the need for the appeal. The Commander, regional health command or other appropriate official may
also elect to review applications a commander denied, regardless of an appeal. If reconsideration or further review results
in the approval of the Soldier's application, the Soldier will be notified, in writing, and his or her application returned to
the commander for computation of the payment amount.
d. The appellate authority will give the Soldier a written decision on his or her appeal and such decision will be final.
In general, such responses will be provided within 30 days of TSG's receipt of the request for appeal.
e. For an appeal relating to the amount of compensation, any portion of the SCAADL payment not in dispute will be
paid to the Soldier while the appeal is being processed. If a Soldier's appeal relating to the amount of compensation is
successful, the effective date of SCAADL payments is the date the DD Form 2948 was certified.
f. For appeals not related to the amount of compensation, TSG or his or her delegate will consult with the TJAG to
determine the effective date of SCAADL payments. The effective date will depend on the facts and circumstances of each
case.
10 – 13. Continuation of Special Compensation for Assistance with Activities of Daily Living
Compensation beyond 6 months
Commanders will continuously evaluate a Soldier's circumstances to ensure the Soldier remains eligible for SCAADL.
a. A formal reevaluation of eligibility is required every 6 months.
b. A reevaluation is also required if the Soldier relocates or his or her medical condition changes in a manner that may
warrant a change in eligibility or level of compensation. The Soldier's Triad of Care will notify the commander of any
changes in the Soldier's location, medical condition, or other eligibility criteria.
c. Except in circumstances involving relocations, a reevaluation requires a licensed DOD or VA physician to complete
and certify a new DD Form 2948. In making a reevaluation of eligibility, commanders will follow the procedures set forth
in paragraph 10
– 3.
d. A Soldier subsequently determined ineligible for SCAADL, or whose monthly compensation is reduced, may appeal
under the procedures in paragraph 10
– 12.
e. While a reevaluation is being processed, the Soldier will continue to receive SCAADL at the previously established
rate. A Soldier who has relocated will receive payments at the rate applicable to the new location, as soon as DFAS can
process the change.
AR 600–77 • 5 March 2019
51
10 – 14. Non-compliance to pay caregivers
a. The Army’s primary responsibility is the ensure the SCAADL recipient receive the required care attested to by a
competent medical authority. As a result, when applicable, Soldiers are expected to pay their caregiver(s) for services
received.
b. Commanders can refer to AR 600
– 20 to resolve issues that pertains to noncompliance of payment.
52
AR 600–77 • 5 March 2019
Appendix A
References
Section I
Required Publications
AR 600
– 20
Army Command Policy (Cited in para 5
– 12.)
AR 635
– 40
Disability Evaluation for Retention, Retirement, or Separation (Cited in para 1
– 5.)
Section II
Related Publications
A related publication is a source of additional information. The user does not have to read a related reference to understand
this publication. Unless otherwise stated, Army publications are available online from the Army Publishing Directorate
website at http://armypubs.army.mil, DOD issuances are available at http://www.dtic.mil, and the USC is available at
http://uscode.house.gov/.
AR 11
– 2
Managers’ Internal Control Program
AR 25
– 30
The Army Publishing Program
AR 25
– 400 – 2
The Army Records Information Management System (ARIMS)
AR 40
– 58
Warrior Care and Transition Program
AR 40
– 66
Medical Record Administration and Health Care Documentation
AR 40
– 400
Patient Administration
AR 40
– 501
Standards of Medical Fitness
AR 135
– 18
The Active Guard Reserve (AGR) Program
AR 135
– 155
Promotions of Commissioned Officers and Warrant Officers other than General Officers
AR 135
– 175
Separation of Officers
AR 135
– 178
Enlisted Administrative Separations
AR 135
– 381
Incapacitation of Reserve Component Soldiers
AR 420
– 1
Army Facilities Management
AR 600
– 8 – 4
Line of Duty Policy, Procedures, and Investigations
AR 600
– 8 – 7
Retirement Services Program
AR 600–77 • 5 March 2019
53
AR 600 – 8 – 10
Leaves and Passes
AR 600
– 8 – 19
Enlisted Promotions and Reductions
AR 600
– 8 – 22
Military Awards
AR 600
– 8 – 24
Officer Transfers and Discharges
AR 600
– 8 – 29
Officer Promotions
AR 600
– 8 – 101
Personnel Processing (In-, Out-, Soldier Readiness, and Deployment Cycle)
AR 600
– 8 – 105
Military Orders
AR 601
– 10
Management and Recall to Active Duty of Retired Soldiers of the Army in Support of Mobilization and Peacetime Oper-
ations
AR 601
– 280
Army Retention Program
AR 608
– 1
Army Community Service
AR 614
– 30
Overseas Service
AR 614
– 100
Officer Assignment Policies, Details, and Transfers
AR 614
– 200
Enlisted Assignments and Utilization Management
AR 623
– 3
Evaluation Reporting System
AR 635
– 8
Separation Processing and Documents
AR 635
– 200
Active Duty Enlisted Administrative Separations
AR 638
– 8
Army Casualty Program
AR 735
– 5
Property Accountability Policies
Army’s Mobilization and Deployment Reference (AMDR) 25–Day Rule
(Access by permissions only.)
DA Pam 623
– 3
Evaluation Reporting System
DA Pam 635
– 40
Procedures for Disability Evaluation For Retention, Retirement, or Separation
DOD Financial Management Regulation, Volume 7A
Military pay policy and procedures – Active Duty and Reserve pay (Available at http://comptroller.defense.gov/fmr/.)
54
AR 600–77 • 5 March 2019
DOD Financial Management Regulation, Volume 7B
Military pay policy – Retired pay (Available at http://comptroller.defense.gov/fmr/.)
DOD Travel Regulations
Joint Travel Regulation (Available at http://www.defensetravel.dod.mil/site/reference.cfm.)
DODI 1241.01
Reserve Component (RC) Line of Duty Determination for Medical and Dental Treatments and Incapacitation Pay Entitle-
ments
DODI 1300.18
Department of Defense (DOD) Personnel Casualty Matters, Policies, and Procedures
DODI 1332.18
Disability Evaluation System
DODI 1341.12
Special Compensation for Assistance with Activities of Daily Living (SCAADL) Program
DODI 4515.13
Air Transportation Eligibility
DODI 6000.11
Patient Movement (PM)
DODI 6025.20
Medical Management (MM) Programs in the Direct Care System (DCS) and Remote Areas
DODI 6025.22
Assistive Technology (AT) for Wounded, Ill, and Injured Service Members
DODM 1332.18
– V1
Disability Evaluation System (DES) Manual: General Information and Legacy Disability Evaluation System (LDES) Time
Standards
DODM 1332.18
– V2
Disability Evaluation System (DES) Manual: Integrated Disability Evaluation System (DES)
DODM 1332.18
– V3
Disability Evaluation System (DES) Manual: Quality Assurance Program (QAP)
DODM 1341.12
Special Compensation For Assistance With Activities Of Daily Living (SCAADL) Process
Federal Benefits for Veterans, Dependents, and Survivors
(Available at https://www.va.gov/opa/publications/benefits_book.asp.)
NGR 600
– 100
Commissioned Officers – Federal Recognition and Related Personnel Actions (Available at
http://www.ngbpdc.ngb.army.mil/publications.htm#ngr.)
NGR 600
– 200
Enlisted Personnel Management (Available at http://www.ngbpdc.ngb.army.mil/publications.htm#ngr.)
Personnel Policy Guidance
(Available at http://www.armyg1.army.mil/militarypersonnel/ppg.asp.)
10 USC, Chapter 55
Medical and Dental Care
10 USC 101
Definitions
10 USC 507
Extension of enlistment for members needing medical care or hospitalization
10 USC 877, et. seq.
Art. 77. Principals
AR 600–77 • 5 March 2019
55
10 USC 972
Members: effect of time lost
10 USC 1074
Medical and dental care for members and certain former members
10 USC 1074a
Medical and dental care: members on duty other than active duty for a period of more than 30 days
10 USC 1074e
Medical care: Certain Reserves who served in Southwest Asia during the Persian Gulf Conflict
10 USC 1074f
Medical tracking system for members deployed overseas
10 USC 1076
Medical and dental care for dependents: general rule
10 USC 1076d
TRICARE program: TRICARE Standard coverage for members of the Selected Reserve
10 USC 1077
Medical care for dependents: authorized care in facilities of uniformed services
10 USC 1176
Enlisted members: retention after completion of 18 or more, but less than 20, years of service
10 USC 1201
Regulars and members on active duty for more than 30 days: retirement
10 USC 1202
Regulars and members on active duty for more than 30 days: temporary disability retired list
10 USC 1203
Regulars and members on active duty for more than 30 days: separation
10 USC 1204
Members on active duty for 30 days or less or on inactive-duty training: retirement
10 USC 1205
Members on active duty for 30 days or less: temporary disability retired list
10 USC 1206
Members on active duty for 30 days or less or on inactive-duty training: separation
10 USC 1206a
Reserve component members unable to perform duties when ordered to active duty: disability system processing
10 USC 1207
Disability from intentional misconduct or willful neglect: separation
10 USC 1209
Transfer to inactive status list instead of separation
10 USC 1218
Discharge or release from active duty: Claims for compensation, pension, or hospitalization
10 USC 12301
Reserve components generally
10 USC 12302
Ready Reserve
10 USC 12322
Active duty for health care
10 USC 12686
Reserves on active duty within two years of retirement eligibility: limitation on release from active duty
56
AR 600–77 • 5 March 2019
10 USC 12731
Age and Service requirements
10 USC 14519
Deferment of retirement or separation for medical reasons
32 USC
National Guard
37 USC 204
Entitlement
37 USC 372
Continuation of pays during hospitalization and rehabilitation resulting from wounds, injury, or illness incurred while on
duty in a hostile fire area or exposed to an event of hostile fire or other hostile action
38 USC 101
Veterans’ Benefits, Part I. Definitions
38 USC 105
Line of duty and misconduct
38 USC 1114
Rates of wartime disability compensation
38 USC 1720(G)(a)(3)
Assistance and support services for caregivers
38 USC 4312
Reemployment rights of persons who serve in the uniformed services
Section III
Prescribed Forms
Unless otherwise indicated, DA forms are available on the Army Publishing Directorate website at
http://armypubs.army.mil.
DA Form 7692
Active Duty for Medical Care Application (Prescribed inthe title page.)
DA Form 7696
Commander’s Performance and Capability Checklist (Prescribed inthe title page.)
Section IV
Referenced Forms
Unless otherwise indicated, DA forms are available on the Army Publishing Directorate website at
http://armypubs.army.mil; DD forms are available on the DOD Forms Management Program website at
http://www.dtic.mil/whs/directives/forms/index.htm; and SGLI forms are available through the U.S. Department of Vet-
erans Affairs website at http://www.benefits.va.gov/insurance/resources-forms.asp#fsgli.
DA Form 11
– 2
Internal Control Evaluation Certification
DA Form 31
Request and Authority for Leave
DA Form 2028
Recommended Changes to Publications and Blank Forms
DA Form 2173
Statement of Medical Examination and Duty Status
DA Form 3349
Physical Profile (Available through
https://medpros.mods.army.mil/eprofile/default.aspx?returnurl=%2feprofile%2fadmin%2fusersmanager.aspxs.)
AR 600–77 • 5 March 2019
57
DA Form 3739
Application for Compassionate Actions (Available through normal supply channels.)
DA Form 4160
Patient’s Personal Effects and Clothing Record
DA Form 4187
Personnel Action
DA Form 4856
Developmental Counseling Form
DD Form 93
Record of Emergency Data
DD Form 214
Certificate of Release or Discharge from Active Duty (Available through normal supply channels.)
DD Form 220
Active Duty Report
DD Form 577
Appointment/Termination Record - Authorized Signature
DD Form 1351
– 2
Travel Voucher or Sub voucher
DD Form 2648
Service Member Pre-Separation/Transition Counseling and Career Readiness Standards EForm for Service Members Sep-
arating, Retiring, Released from Active Duty (REFRAD)) (Available through https://www.dodtap.mil/forms.html.)
DD Form 2656
Data for Payment of Retired Personnel
DD Form 2795
Pre-Deployment Health Assessment
DD Form 2870
Authorization for Disclosure of Medical or Dental Information
DD Form 2900
Post Deployment Health Re-Assessment Form (PDHRA)
DD Form 2948
Special Compensation for Assistance with Activities of Daily Living (SCAADL) Eligibility
SGLV 8283
Claim for Death Benefits (Available http://www.benefits.va.gov/insurance/resources-forms.asp.)
SGLV 8284
Claim for Accelerated Benefits (Available http://www.benefits.va.gov/insurance/resources-forms.asp.)
SGLV 8286
Servicemembers' Group Life Insurance Election and Certificate
(Available http://www.benefits.va.gov/insurance/resources-forms.asp.)
SGLV 8286A
Family Coverage Election (SGLI) (Available http://www.benefits.va.gov/insurance/resources-forms.asp.)
SGLV 8286S
Servicemembers' Group Life Insurance Supplemental SGLI Beneficiary Form
(Available http://www.benefits.va.gov/insurance/resources-forms.asp.)
SGLV 8715
Application for the Servicemembers' Group Life Insurance (SGLI) Disability Extension
(Available http://www.benefits.va.gov/insurance/resources-forms.asp.)
58
AR 600–77 • 5 March 2019
AR 600–77 • 5 March 2019
59
Appendix B
Internal Control Evaluation
B – 1. Function
The function covered by this evaluation is the application for, and approval of, medical care.
B
– 2. Purpose
The purpose of this evaluation is to assist HRC, commanders, supervisors, and health care personnel in evaluating the key
internal controls listed. It is intended as a guide and does not address all controls.
B
– 3. Instructions
Answers must be based on the actual testing of key internal controls (for example, document analysis, direct observation,
sampling, simulation, or other). Answers that indicate deficiencies must be explained and the corrective action identified
in supporting documentation. These internal controls must be formally evaluated at least once every 2 years. Certification
that the evaluation has been conducted must be accomplished on DA Form 11
– 2 (Internal Control Evaluation Certifica-
tion).
B
– 4. Test questions
a. Are all DA Forms 4187 indicating appropriate request for RC active duty medical care or ADME dependent upon
status of Soldier at time of LOD related medical issue?
b. Are all LOD documentation requirements completed and/or initiated for RC Soldiers entering the WTU?
c. Are all RC active duty medical care requests initiated after notification to the gaining WTU commander for the
transition of senior commander to the WTU?
d. Are all Soldiers arriving at the demobilization station and determined by military medical authority to have a LOD
related wound, illness, injury, disease, or aggravated pre-existing medical condition incurred during the current deployment
being evaluated for WTU placement?
e. Has the medical provider completed a statement verifying current diagnosis, anticipated length of care, management
plan, and prognosis for recovery?
f. Does the Soldier require an extension to his or her expiration term of service date to complete required medical care?
g. Has the senior commander ensured that all Soldiers who qualify for assignment or attachment to a WTU are referred
to the Triad of Care for evaluation?
h. Has the Triad of Leadership reviewed all RA and AGR Soldiers for eligibility criteria and determined disposition
based on, but not limited to, the following:
(1) Does the Soldier have a temporary profile for more than 6 months with duty limitations that preclude him or her
from training for, or contributing to, unit mission accomplishment?
(2) Does the Soldier have a wound, illness, or injury which requires clinical case management?
B
– 5. Supersession
Not applicable.
B
– 6. Comments
Help to make this a better tool for evaluating internal controls. Submit comments to Deputy Chief of Staff, G
– 1
(DAPE
– MPE), 300 Army Pentagon, Washington, DC 20310 – 0300.
60
AR 600–77 • 5 March 2019
Glossary
Section I
Abbreviations
ACS
Army Community Service
ACSIM
Assistant Chief of Staff for Installation Management
ADME
active duty medical extension
AGR
Active Guard Reserve
AHLTA
Armed Forces Health Longitudinal Technology Application
AR
Army Regulation
ARNG
Army National Guard
ASA (FM&C)
Assistant Secretary of the Army (Financial Management and Comptroller)
ASA (M&RA)
Assistant Secretary of the Army (Manpower and Reserve Affairs)
BAH
basic allowance for housing
CAR
Chief, Army Reserve
CCU
Community Care Unit
CG
commanding general
CNGB
Chief, National Guard Bureau
CONUS
continental United States
CSM
command sergeant major
DA
Department of the Army
DCS
Deputy Chief of Staff
DD
Department of Defense (forms)
DEERS
Defense Enrollment Eligibility Reporting System
DES
Disability Evaluation System
AR 600–77 • 5 March 2019
61
DFAS
Defense Finance and Accounting Service
DHA
– GL
Defense Health Agency-Great Lakes
DJMS
Defense Joint Military Pay System
DOD
Department of Defense
DODFMR
Department of Defense Financial Management Regulation
DODI
Department of Defense Instruction
eMILPO
electronic military personnel office
ETP
exception to policy
GO
general officer
GOMO
General Officer Management Office
HHG
household goods
HOR
home of record
HRC
Human Resources Command
IMCOM
Installation Management Command
iPERMS
interactive Personnel Records Management System
ITA
invitational travel authorization
JTR
Joint Travel Regulation
LOD
line of duty
M–date
mobilization date
MEB
medical evaluation board
MEDCOM
U.S. Army Medical Command
MOS
military occupational specialty
MRD
mandatory removal date
62
AR 600–77 • 5 March 2019
MRDP
medical retention determination point
MRP
medical retention processing
MRP2
medical retention processing 2
MRP
– E
medical retention processing - evaluation
MTF
military treatment facility
NCM
Nurse Case Manager
NGB
National Guard Bureau
NGR
National Guard regulation
NMA
non-medical attendant
OCIE
organizational clothing and individual equipment
OCONUS
outside the Continental United States
OTSG
Office of the Surgeon General
PCM
primary care manager
PCS
permanent change of station
PDRL
permanent disability retired list
PDS
permanent duty station
PEB
physical evaluation board
PEBLO
physical evaluation board liaison officer
POV
privately owned vehicle
PULHES
physical capacity, upper extremity, lower extremity, hearing-ears, vision-eyes, psychiatric
RA
Regular Army
RC
Reserve Component
REFRAD
release from active duty
AR 600–77 • 5 March 2019
63
RHC
regional health command
RTD
returned to duty
S – 1
adjutant
SCAADL
Special Compensation for Assistance with Activities of Daily Living
SECARMY
Secretary of the Army
SFAC
Soldier and Family Assistance Center
SFL
– TAP
Soldier for Life-Transition Assistance Program
SGLI
Servicemembers’ Group Life Insurance
TAMP
Transitional Assistance Management Program
TCS
temporary change of station
TDRL
temporary disability retirement list
TDY
temporary duty
TJAG
The Judge Advocate General
TRAC2ES
U.S. Transportation Command Regulating and Command and Control Evacuation System
TRANSPROC
Transition Processing System
TRICARE
tri-service medical care
TSG
The Surgeon General
TSGLI
Traumatic Servicemembers’ Group Life Insurance
UCMJ
Uniform Code of Military Justice
USAFMCOM
U. S. Army Financial Management Command
USAPDA
U.S. Army Physical Disability Agency
USAR
U.S. Army Reserve
USARC
U.S. Army Reserve Command
64
AR 600–77 • 5 March 2019
USC
United States Code
VA
Veterans Affairs
WCT
Warrior Care and Transition
WCTP
Warrior Care and Transition Program
WII
wounded, ill, injured
WTB
Warrior Transition Battalion
WTU
Warrior Transition Unit
Section II
Terms
Catastrophic injury or illness
A permanent, severely disabling injury, disorder, or illness incurred or aggravated in the line of duty that compromises the
ability to perform ADL to such a degree that a Servicemember requires personal or mechanical assistance to leave home
or bed, or requires constant supervision to avoid physical harm to self or others
Senior commander
The senior commander is normally the senior GO at the installation. The senior commander’s mission is the care of Sol-
diers, Families, and civilians, and to enable unit readiness. While the delegation of senior command authority is direct
from Headquarters, Department of the Army, the senior commander will routinely resolve installation issues with IMCOM
and, as needed, the associated Army Command, Army service component command, or direct reporting unit. The senior
commander uses the garrison as the primary organization to provide services and resources to customers in support of
accomplishing this mission. All applicable commands support the senior commander in the execution of senior commander
responsibilities; therefore, the senior commander is the supported commander by the IMCOM region director, the garrison,
and tenants.
U.S. Army Special Operations Command Soldiers
Army special operations forces Soldiers assigned, attached, or under operational control of units of the U.S. Army Special
Operations Command, its subordinate commands, or another Army special operations forces unit.
U.S. Army Special Operations Command Soldiers, 'assignment'
The Soldier’s unit has released the Soldier to the full control of the senior commander and WTU to include medical,
billeting, administrative, and financial care.
U.S. Army Special Operations Command Soldiers, 'attachment'
The Soldier remains assigned to, housed by, and under the administrative control of their unit, yet receives medical care
and services through the WTU.
Warrior Care and Transition Program
An Army-wide structure to provide support and services for WII Soldiers. WCTP enables the Army to evaluate and treat
Soldiers through a comprehensive, Soldier-centric process of medical care, rehabilitation, professional development, and
achievement of personal goals. See http://www.wtc.army.mil/modules/soldier/s1-wctpprogram.html.
Warrior Transition Unit Triad of Care
Triad of Care normally refers to the squad leader, NCM, and PCM assigned to a WII Soldier. The squad leader leads the
Soldier, the NCM coordinates his or her care, and the PCM oversees the care. The triad creates the familiar environment
of a military unit and surrounds the Soldier and his or her Family with comprehensive care and support which is all focused
on the wounded warrior’s sole mission to heal.
AR 600–77 • 5 March 2019
65
Warrior Transition Unit Triad of Leadership
The Triad of Leadership consists of senior commanders and CSMs, MTF commanders and CSMs, and WTU commanders,
CSMs, and first sergeants. This triad executes refinements to the WTU entry, management, and exit policy in order to
develop a balanced WTU structure and capability that is enduring, expandable, collapsible, and responsive to the medical
needs of every WII Soldier.
Wounded, ill, or injured
Soldiers who are WII in the LOD and require medical care and/or treatment to bring them to MRDP and/or complete
processing through the DES.
Wounded, ill, or injured Soldier’s mission
“I am a wounded, ill, or injured Soldier. My job is to heal as I transition back to duty or become a productive, responsible
citizen in society. This is not a status but a mission. I will succeed in this mission because I am a Soldier.”
UNCLASSIFIED PIN 201511–000
