Page 1 of 7
Summary of Benefits and Coverage: What this Plan Covers & What You Pay for Covered Services Coverage Period: 01/01/2022 – 12/31/2022
Ambetter from Peach State Health Plan: Coverage for: Individual/Family | Plan Type: HMO
Ambetter Balanced Care 32
SBC-70893GA0010070-02 Underwritten by Ambetter of Peach State Inc.
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would
share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately.
This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, visit
https://ambetter.pshpgeorgia.com/2022-brochures.html, or call 1-877-687-1180 (TTY/TDD 1-877-941-9231). For general definitions of common terms, such as
allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms, see the Glossary. You can view the Glossary at
https://www.healthcare.gov/sbc-glossary or call 1-877-687-1180 (TTY/TDD 1-877-941-9231) to request a copy.
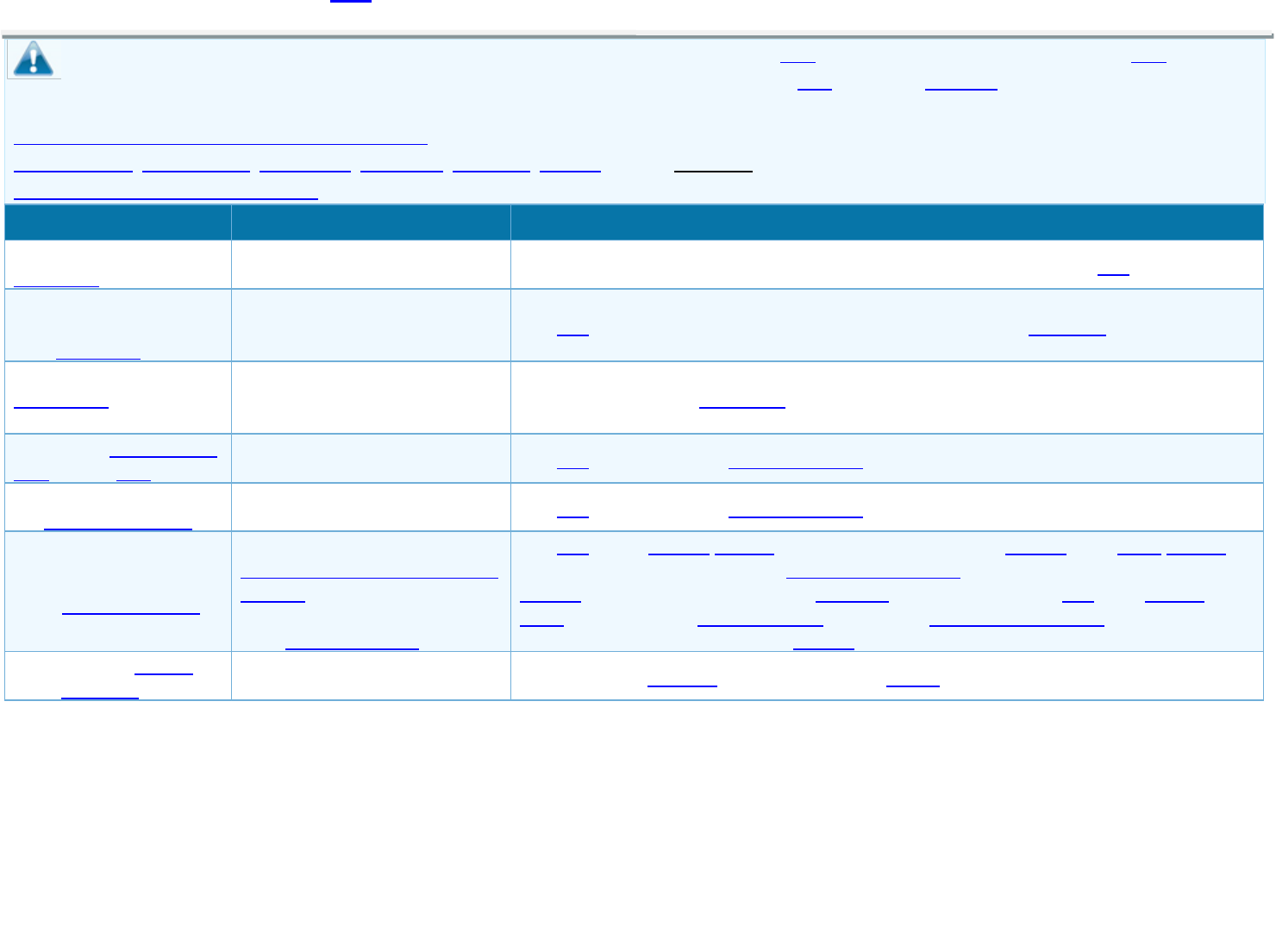
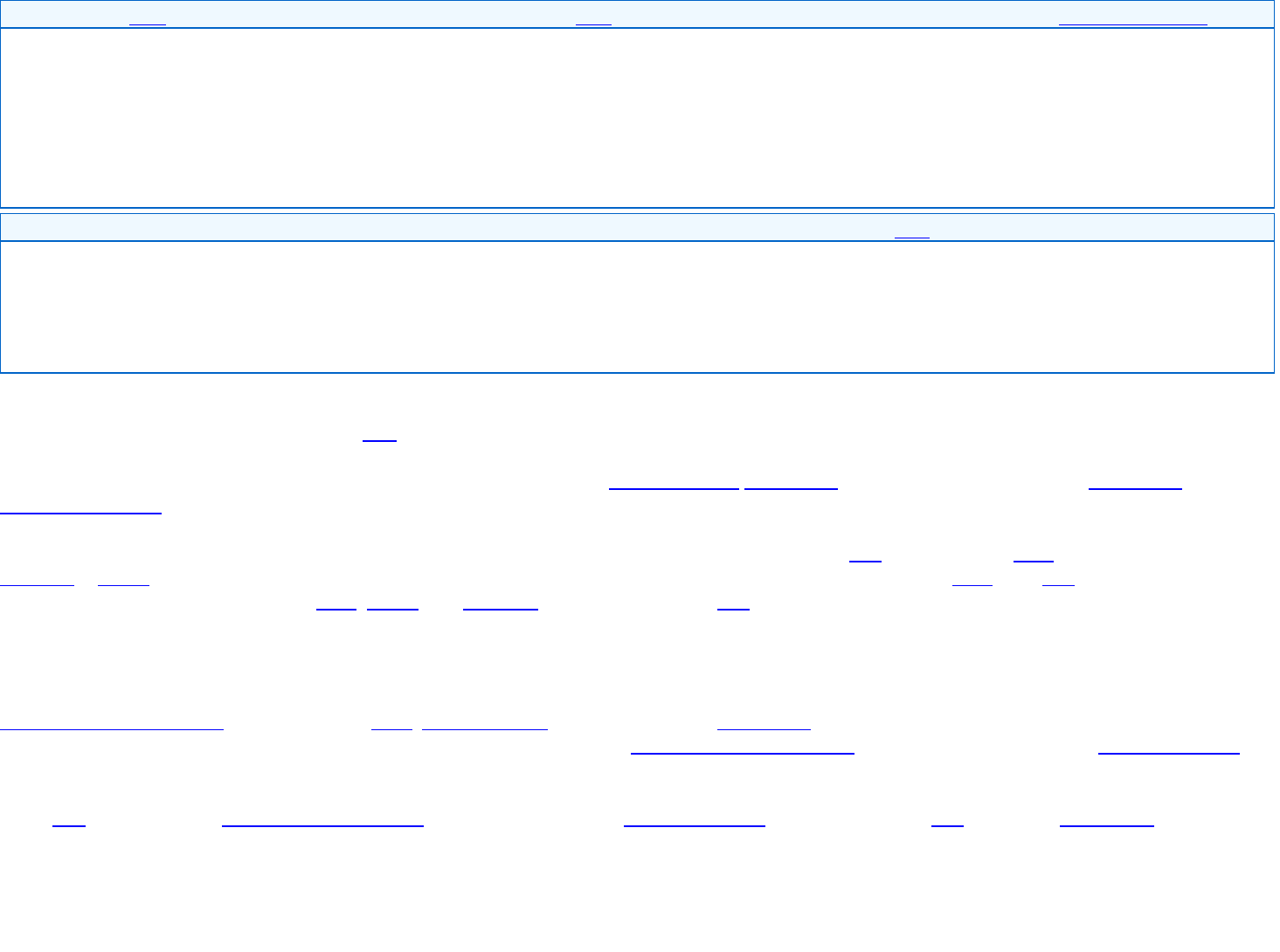
Important Questions
Answers
Why This Matters:
What is the overall
deductible?
$0
See the Common Medical Events chart below for your costs for services this plan covers.
Are there services
covered before you meet
your deductible?
Yes.
This plan covers items and services even if you haven’t yet met the deductible amount.
Are there other
deductibles for specific
services?
No.
You don’t have to meet deductibles for specific services.
What is the out-of-pocket
limit for this plan?
Not Applicable.
This plan does not have an out-of-pocket limit on your expenses.
What is not included in
the out-of-pocket limit?
Not Applicable.
This plan does not have an out-of-pocket limit on your expenses.
Will you pay less if you
use a network provider?
Yes. See
https://ambetter.pshpgeorgia.com/
findadoc or call 1-877-687-1180
(TTY/TDD 1-877-941-9231) for a
list of network providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network.
You will pay the most if you use an out-of-network provider, and you might receive a bill from a
provider for the difference between the provider’s charge and what your plan pays (balance
billing). Be aware, your network provider might use an out-of-network provider for some services
(such as lab work). Check with your provider before you get services.
Do you need a referral to
see a specialist?
No.
You can see the specialist you choose without a referral.
Page 2 of 7
* For more information about limitations and exceptions, see plan or policy document at https://api.centene.com/eoc/2022/70893GA001.pdf.
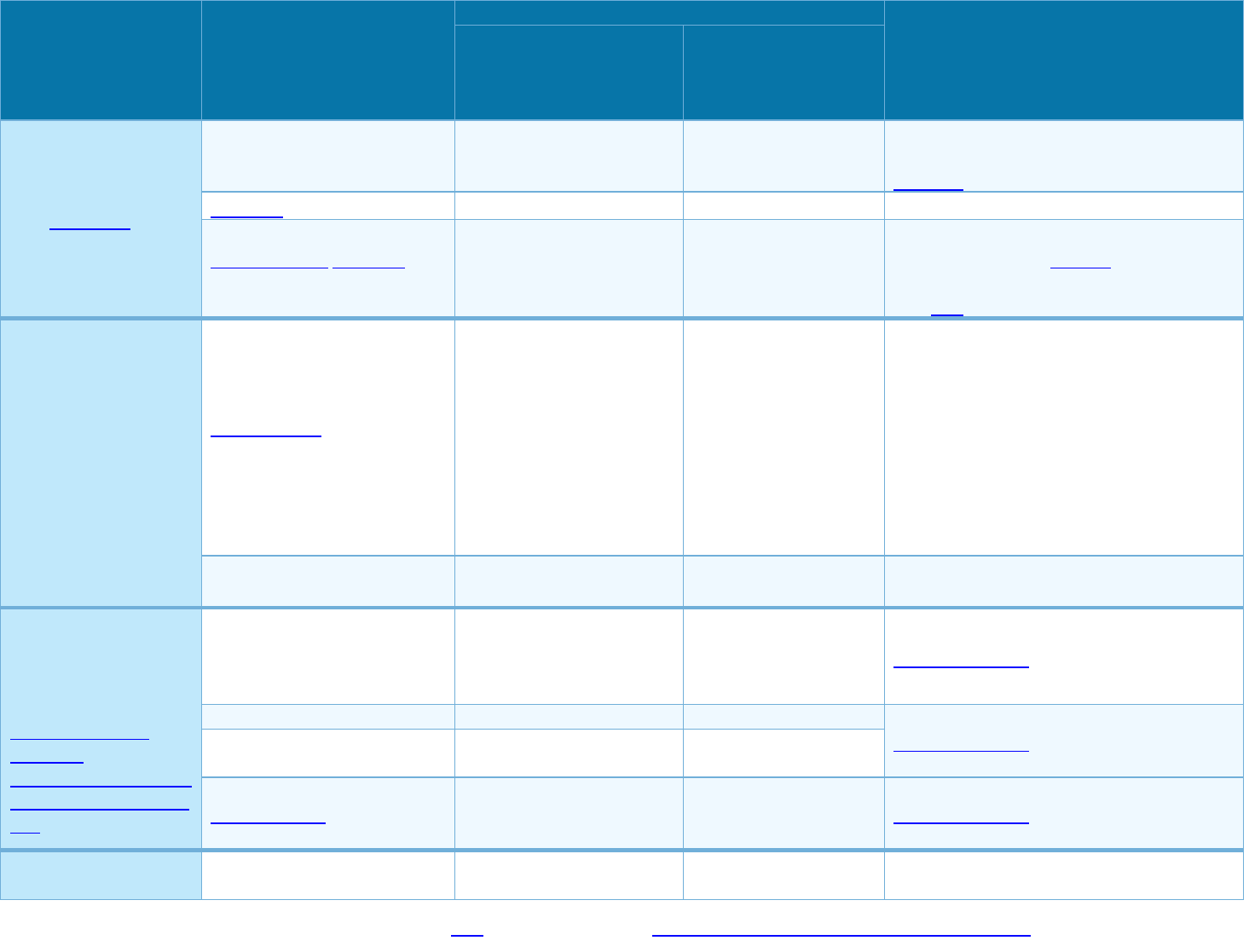
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other
Important Information
Indian Health Care
Provider (IHCP) & Non-
IHCP In-Network Provider
(You will pay the least)
Non-IHCP Out-Of-
Network Provider
(You will pay the most)
If you visit a health
care provider’s office
or clinic
Primary care visit to treat an
injury or illness
No charge
Not covered
Unlimited Virtual Care Visits received from
Ambetter Telehealth covered at No Charge,
providers covered in full.
Specialist visit
No charge
Not covered
Covered No Limit.
Preventive care/screening/
immunization
No charge
Not covered
You may have to pay for services that aren’t
preventive. Ask your provider if the services
needed are preventive. Then check what
your plan will pay for.
If you have a test
Diagnostic test (x-ray, blood
work)
No charge for laboratory &
professional services
No charge for x-ray &
diagnostic imaging
No charge for laboratory &
professional services and x-
ray & diagnostic imaging at
other places of service
Not covered
Prior authorization may be required. Covered
No Limit. Other places of service may include
Hospital, Emergency Room, or Outpatient
Facility.
Failure to obtain prior authorization for any
service that requires prior authorization will
result in a denial of benefits. See your policy
for more details.
Imaging (CT/PET scans, MRIs)
No charge
Not covered
Prior authorization may be required. Covered
No Limit.
If you need drugs to
treat your illness or
condition
More information about
prescription drug
coverage is available at
https://ambetter.pshpg
eorgia.com/2022formu
lary.
Generic drugs (Tier 1)
Preferred Generic Retail:
No charge
Generic Retail: No charge
Not covered
Prior authorization may be required.
Prescription drugs are provided up to 30 days
retail and up to 90 days through mail order.
Preferred brand drugs (Tier 2)
Retail: No charge
Not covered
Prior authorization may be required.
Prescription drugs are provided up to 30 days
retail and up to 90 days through mail order.
Non-preferred brand drugs
(Tier 3)
Retail: No charge
Not covered
Specialty drugs (Tier 4)
Retail: No charge
Not covered
Prior authorization may be required.
Prescription drugs are provided up to 30 days
retail and up to 30 days through mail order.
If you have outpatient
surgery
Facility fee (e.g., ambulatory
surgery center)
No charge
Not covered
Prior authorization may be required. Covered
No Limit.
Page 3 of 7
* For more information about limitations and exceptions, see plan or policy document at https://api.centene.com/eoc/2022/70893GA001.pdf.
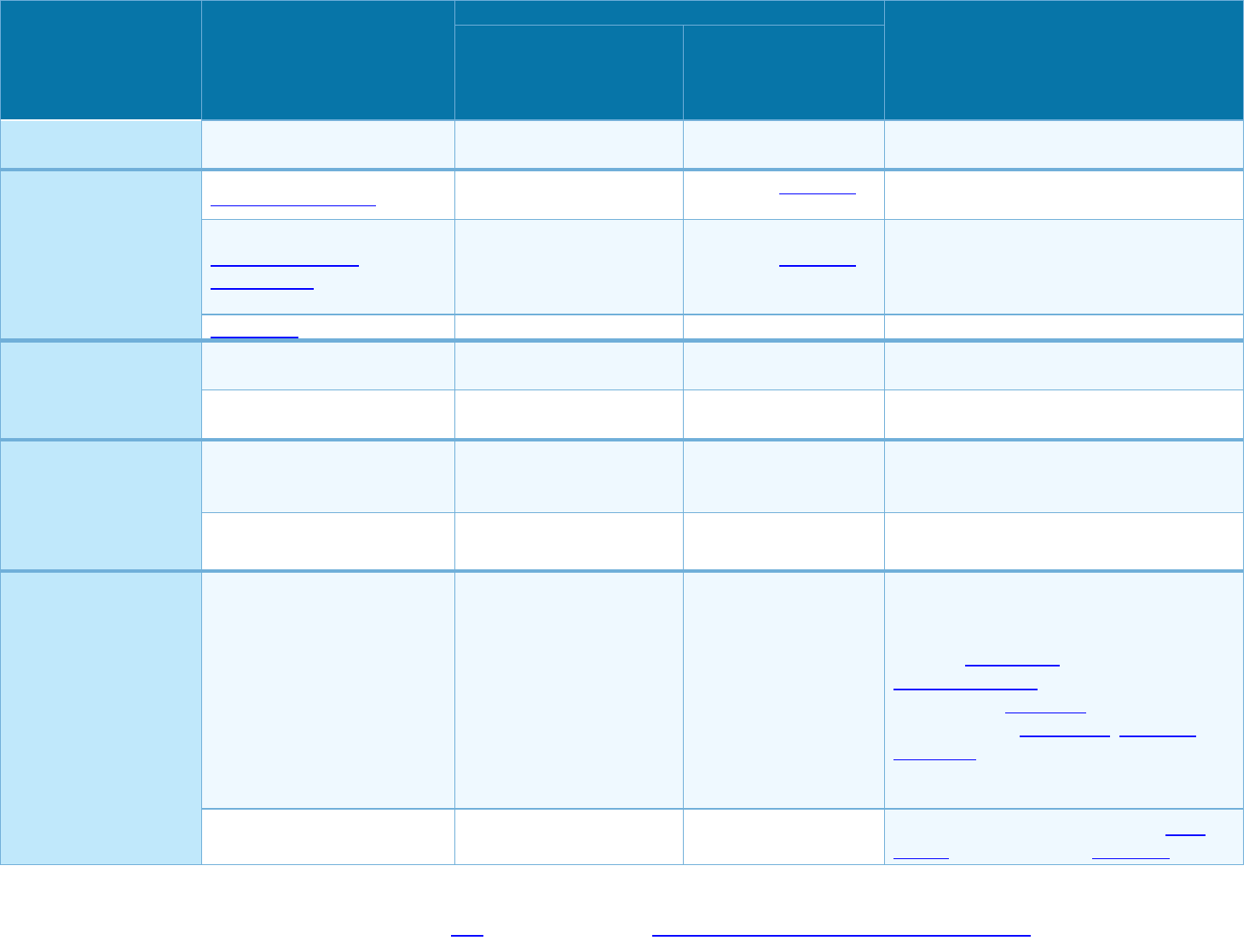
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other
Important Information
Indian Health Care
Provider (IHCP) & Non-
IHCP In-Network Provider
(You will pay the least)
Non-IHCP Out-Of-
Network Provider
(You will pay the most)
Physician/surgeon fees
No charge
Not covered
Prior authorization may be required. Covered
No Limit.
If you need immediate
medical attention
Emergency room care
No charge
No charge; deductible
does not apply
Covered No Limit.
Emergency medical
transportation
No charge
No charge; deductible
does not apply
Covered No Limit. Note: Prior authorization is
not required for emergency transport,
however, all non-emergent transport requires
prior authorization.
Urgent care
No charge
Not covered
Covered No Limit.
If you have a hospital
stay
Facility fee (e.g., hospital room)
No charge
Not covered
Prior authorization may be required. Covered
No Limit.
Physician/surgeon fees
No charge
Not covered
Prior authorization may be required. Covered
No Limit.
If you need mental
health, behavioral
health, or substance
abuse services
Outpatient services
No charge
Not covered
Prior authorization may be required. Covered
No Limit. (PCP and other practitioner visits do
not require prior authorization).
Inpatient services
No charge
Not covered
Prior authorization may be required. Covered
No Limit.
If you are pregnant
Office visits
No charge
Not covered
Prior authorization not required for deliveries
within the standard timeframe per federal
regulation, but may be required for other
services. Cost-sharing does not apply for
preventive services, such as routine pre-natal
and post-natal screenings. Depending on the
type of services, coinsurance, deductible or
copayment may apply. Maternity care may
include tests and services described
elsewhere in the SBC (i.e. ultrasound).
Childbirth/delivery professional
services
No charge
Not covered
Prior authorization may be required. Cost-
sharing does not apply for preventive
Page 4 of 7
* For more information about limitations and exceptions, see plan or policy document at https://api.centene.com/eoc/2022/70893GA001.pdf.
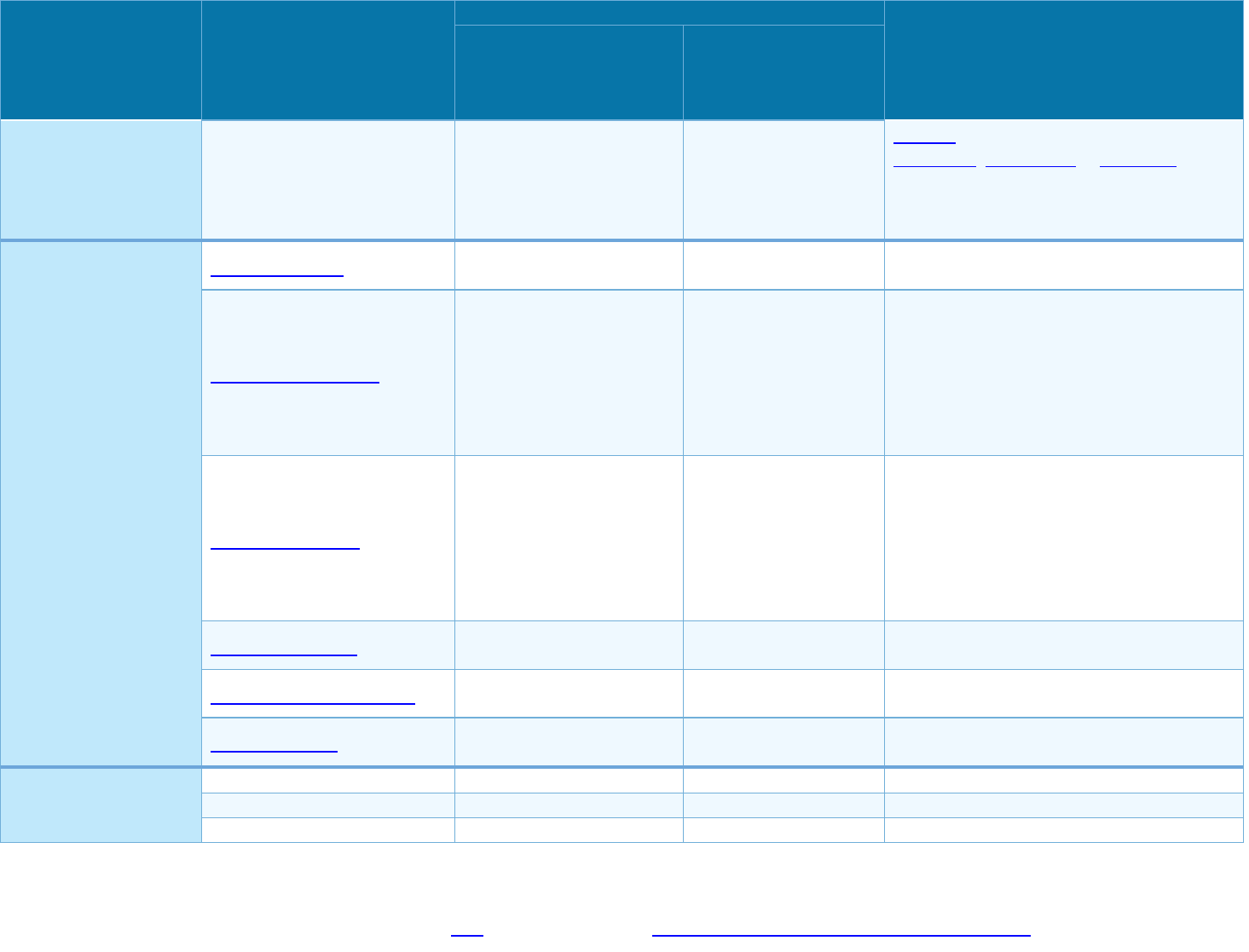
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other
Important Information
Indian Health Care
Provider (IHCP) & Non-
IHCP In-Network Provider
(You will pay the least)
Non-IHCP Out-Of-
Network Provider
(You will pay the most)
Childbirth/delivery facility
services
No charge
Not covered
services. Depending on the type of services,
copayment, coinsurance or deductible may
apply. Maternity care may include tests and
services described elsewhere in the SBC (i.e.
ultrasound).
If you need help
recovering or have
other special health
needs
Home health care
No charge
Not covered
Prior authorization may be required. Limited
to 120 visits per year.
Rehabilitation services
No charge
Not covered
Prior authorization may be required. Limited
to a combined maximum of 40 visits per year
for chiropractic care, speech therapy,
physical therapy and occupational therapy.
Note: Limits do not apply when provided for a
mental health/substance use disorder
diagnosis.
Habilitation services
No charge
Not covered
Prior authorization may be required. Limited
to a combined maximum of 40 visits per year
for chiropractic, speech therapy, physical
therapy and occupational therapy. Note:
Habilitation therapy limits do not apply when
provided for a mental health/substance use
disorder diagnosis.
Skilled nursing care
No charge
Not covered
Prior authorization may be required. Limited
to 60 days per year.
Durable medical equipment
No charge
Not covered
Prior authorization may be required. Covered
no limit.
Hospice services
No charge
Not covered
Prior authorization may be required. Covered
No Limit.
If your child needs
dental or eye care
Children’s eye exam
No charge
Not covered
Limited to 1 visit per year.
Children’s glasses
No charge
Not covered
Limited to 1 item per year.
Children’s dental check-up
Not covered
Not covered
-----None-----
Page 5 of 7
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
• Abortion (Except in cases of rape, incest, or
when the life of the mother is endangered)
• Acupuncture
• Bariatric surgery
• Cosmetic surgery
• Dental care
• Hearing aids
• Long-Term Care (Long Term Acute Care is a
covered benefit. Long Term Nursing Care/
Custodial Care is not a covered benefit.)
• Non-emergency care when traveling outside the
U.S.
• Private-duty nursing
• Routine eye care (Adult)
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
• Chiropractic care (Limited to a combined
maximum of 40 visits per year for chiropractic
care, speech therapy, physical therapy and
occupational therapy.)
• Infertility treatment (Limited to coverage for the
diagnosis of infertility only)
• Routine foot care (Coverage is limited to diabetes
care only.)
• Weight loss programs (4 Visits per year for
nutritional counseling)
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those
agencies is: Ambetter from Peach State Health Plan at 1-877-687-1180 (TTY/TDD 1-877-941-9231); Georgia Office of Insurance and Safety Fire Commissioner, Two
Martin Luther King, Jr. Drive, West Tower, Suite 716, Atlanta, Georgia 30334, Phone No. 1-404-656-2070 or 1-800-656-2298. Other coverage options may be
available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace, visit
www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a
grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide
complete information on how to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance,
contact: Georgia Office of Insurance and Safety Fire Commissioner, Two Martin Luther King, Jr. Drive, West Tower, Suite 716, Atlanta, Georgia 30334, Phone No. 1-
404-656-2070 or 1-800-656-2298.
Does this plan provide Minimum Essential Coverage? Yes.
Minimum Essential Coverage generally includes plans, health insurance available through the Marketplace or other individual market policies, Medicare, Medicaid,
CHIP, TRICARE, and certain other coverage. If you are eligible for certain types of Minimum Essential Coverage, you may not be eligible for the premium tax credit.
Does this plan meet Minimum Value Standards? Not Applicable.
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
Language Access Services:
Spanish (Español): Para obtener asistencia en Español, llame al 1-877-687-1180 (TTY/TDD 1-877-941-9231).
Page 6 of 7
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-877-687-1180 (TTY/TDD 1-877-941-9231).
Chinese (中文): 如果需要中文的帮助,请拨打这个号码 1-877-687-1180 (TTY/TDD 1-877-941-9231).
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-877-687-1180 (TTY/TDD 1-877-941-9231).
To see examples of how this plan might cover costs for a sample medical situation, see the next section.
Page 7 of 7
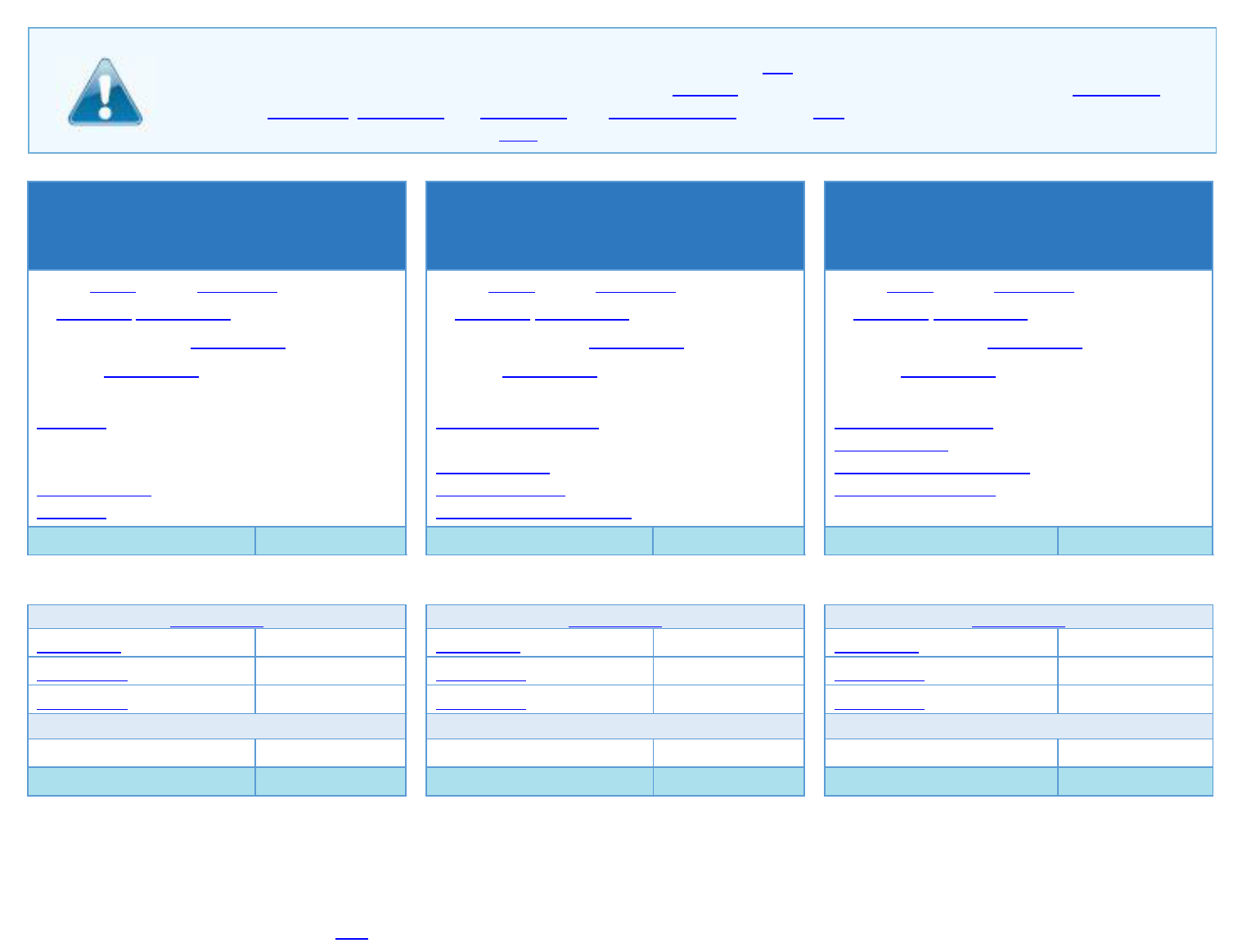
The plan would be responsible for the other costs of these EXAMPLE covered services.
Peg is Having a Baby
(9 months of in-network pre-natal care and a
hospital delivery)
Managing Joe’s Type 2 Diabetes
(a year of routine in-network care of a well-
controlled condition)
Mia’s Simple Fracture
(in-network emergency room visit and follow up
care)
◼ The plan’s overall deductible
$0
◼ The plan’s overall deductible
$0
◼ The plan’s overall deductible
$0
◼ Specialist coinsurance
0%
◼ Specialist coinsurance
0%
◼ Specialist coinsurance
0%
◼ Hospital (facility) coinsurance
0%
◼ Hospital (facility) coinsurance
0%
◼ Hospital (facility) coinsurance
0%
◼ Other coinsurance
0%
◼ Other coinsurance
0%
◼ Other coinsurance
0%
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
This EXAMPLE event includes services like:
Primary care physician office visits (including
disease education)
Diagnostic tests (blood work)
Prescription drugs
Durable medical equipment (glucose meter)
This EXAMPLE event includes services like:
Emergency room care (including medical supplies)
Diagnostic tests (x-ray)
Durable medical equipment (crutches)
Rehabilitation services (physical therapy)
Total Example Cost
$12,700
Total Example Cost
$5,600
Total Example Cost
$2,800
In this example, Peg would pay:
In this example, Joe would pay:
In this example, Mia would pay:
Cost Sharing
Cost Sharing
Cost Sharing
Deductibles
$0
Deductibles
$0
Deductibles
$0
Copayments
$0
Copayments
$0
Copayments
$0
Coinsurance
$0
Coinsurance
$0
Coinsurance
$0
What isn’t covered
What isn’t covered
What isn’t covered
Limits or exclusions
$60
Limits or exclusions
$20
Limits or exclusions
$0
The total Peg would pay is
$60
The total Joe would pay is
$20
The total Mia would pay is
$0
About these Coverage Examples:
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be
different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost-sharing
amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of
costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
AMB16-GA-C-00076
Spanish:
Si usted, o alguien a quien está ayudando, tiene preguntas acerca de Ambetter de Peach State Health Plan, tiene derecho a obtener
ayuda e información en su idioma sin costo alguno. Para hablar con un intérprete, llame al 1-877-687-1180
(TTY/TDD 1-877-941-9231).
Vietnamese:
Nếu quý vị, hay người mà quý vị đang giúp đỡ, có câu hỏi về Ambetter from Peach State Health Plan, quý vị sẽ có quyền được giúp và
có thêm thông tin bằng ngôn ngữ của mình miễn phí. Để nói chuyện với một thông dịch viên, xin gọi 1-877-687-1180
(TTY/TDD 1-877-941-9231).
Korean:
만약 귀하 또는 귀하가 돕고 있는 어떤 사람이 Ambetter from Peach State Health Plan 에 관해서 질문이 있다면 귀하는 그러한 도움과
정보를 귀하의 언어로 비용 부담없이 얻을 수 있는 권리가 있습니다. 그렇게 통역사와 얘기하기 위해서는 1-877-687-1180
(TTY/TDD 1-877-941-9231)로 전화하십시오.
Chinese:
如果您,或是您正在協助的對象,有關於 Ambetter from Peach State Health Plan 方面的問題,您有權利免費以您的母語得到幫助和訊
息。如果要與一位翻譯員講話,請撥電話 1-877-687-1180 (TTY/TDD 1-877-941-9231)。
Gujarati:
, Ambetter from Peach State Health Plan ,
1-877-687-1180 (TTY/TDD 1-877-941-9231)
French:
Si vous-même ou une personne que vous aidez avez des questions à propos d’Ambetter from Peach State Health Plan, vous avez le
droit de bénéficier gratuitement d’aide et d’informations dans votre langue. Pour parler à un interprète, appelez le
1-877-687-1180 (TTY/TDD 1-877-941-9231).
Amharic:
እርስዎ ወይም እርሰዎ የሚርዱት ሰው ስለ Ambetter from Peach State Health Plan ግብር ጥያቄ ካለዎት ያለምንም ወጪ በቋንቋዎ ድጋፍ እንዲሁም መረጃ የማግኘት መብት
አለዎት፣ ፣ አስተርጓሚ ለማነጋገር በ 1-877-687-1180 (TTY/TDD 1-877-941-9231) ይደውሉ፤ ፤
Hindi:
, Ambetter from Peach State Health Plan
,
1-877-687-1180
(TTY/TDD 1-877-941-9231)
French
Creole:
Si oumenm, oubyen yon moun w ap ede, gen kesyon nou ta renmen poze sou Ambetter from Peach State Health Plan, ou gen tout
dwa pou w jwenn èd ak enfòmasyon nan lang manman w san sa pa koute w anyen. Pou w pale avèk yon entèprèt, sonnen nimewo
1-877-687-1180 (TTY/TDD 1-877-941-9231).
Russian:
В случае возникновения у вас или у лица, которому вы помогаете, каких-либо вопросов о программе страхования Ambetter
from Peach State Health Plan вы имеете право получить бесплатную помощь и информацию на своем родном языке. Чтобы
поговорить с переводчиком, позвоните по телефону 1-877-687-1180 (TTY/TDD 1-877-941-9231).
Arabic:
Ambetter from Peach State Health Plan
(TTY/TDD 1-877-941-9231) 1-877-687-1180
Portuguese:
Se você, ou alguém a quem você está ajudando, tem perguntas sobre o Ambetter from Peach State Health Plan, você tem o direito de
obter ajuda e informação em seu idioma e sem custos. Para falar com um intérprete, ligue para 1-877-687-1180
(TTY/TDD 1-877-941-9231).
Persian:
Ambetter from Peach State Health Plan
687-1180877 (TTY/TDD 1-877-941-9231)
German:
Falls Sie oder jemand, dem Sie helfen, Fragen zu Ambetter from Peach State Health Plan hat, haben Sie das Recht, kostenlose Hilfe
und Informationen in Ihrer Sprache zu erhalten. Um mit einem Dolmetscher zu sprechen, rufen Sie bitte die Nummer
1-877-687-1180 (TTY/TDD 1-877-941-9231) an.
Japanese:
Ambetter from Peach State Health Plan について何かご質問がございましたらご連絡ください。 ご希望の言語によるサポートや情報を無料でご提供いた
します。 通訳が必要な場合は、1-877-687-1180 (TTY/TDD 1-877-941-9231)までお電話ください。

AMB21-GA-C-00598
Statement of Non-Discrimination
Ambetter from Peach State Health Plan complies with applicable Federal civil rights laws and does not
discriminate on the basis of race, color, national origin, age, disability, or sex. Ambetter from Peach State
Health Plan does not exclude people or treat them differently because of race, color, national origin, age,
disability, or sex.
Ambetter from Peach State Health Plan:
• Provides free aids and services to people with disabilities to communicate effectively with us,
such as:
Qualified sign language interpreters
Written information in other formats (large print, audio, accessible electronic formats,
other formats)
• Provides free language services to people whose primary language is not English, such as:
Qualified interpreters
Information written in other languages
If you need these services, contact Ambetter from Peach State Health Plan at 1-877-687-1180 (TTY/TDD
1-877-941-9231).
If you believe that Ambetter from Peach State Health Plan has failed to provide these services or
discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file
a grievance with: Ambetter from Peach State Health Plan Complaints Department, 1100 Circle 75
Parkway, Suite 1100, Atlanta, GA 30339, 1-877-687-1180 (TTY/TDD 1-877-941-9231), Fax 1-866-532-
8855. You can file a grievance by mail, fax, or email. If you need help filing a grievance, Ambetter from
Peach State Health Plan is available to help you. You can also file a civil rights complaint with the U.S.
Department of Health and Human Services, Office for Civil Rights electronically through the Office for
Civil Rights Complaint Portal, available at https://ocrpor tal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone
at: U.S. Department of Health and Human Services, 200 Independence Avenue SW., Room 509F, HHH
Building, Washington, DC 20201, 1-800-368-1019, 800-537-7697 (TDD).
Complaint forms are available at http://www.hhs.gov /ocr /office/file/index.html.
