
Alachua County FY20/21
Supplemental
Schedule of Fees and Charges for Services
Prepared by Office of Management & Budget
2
FY 21 Supplemental Fee Schedule Effective 05/11/2021
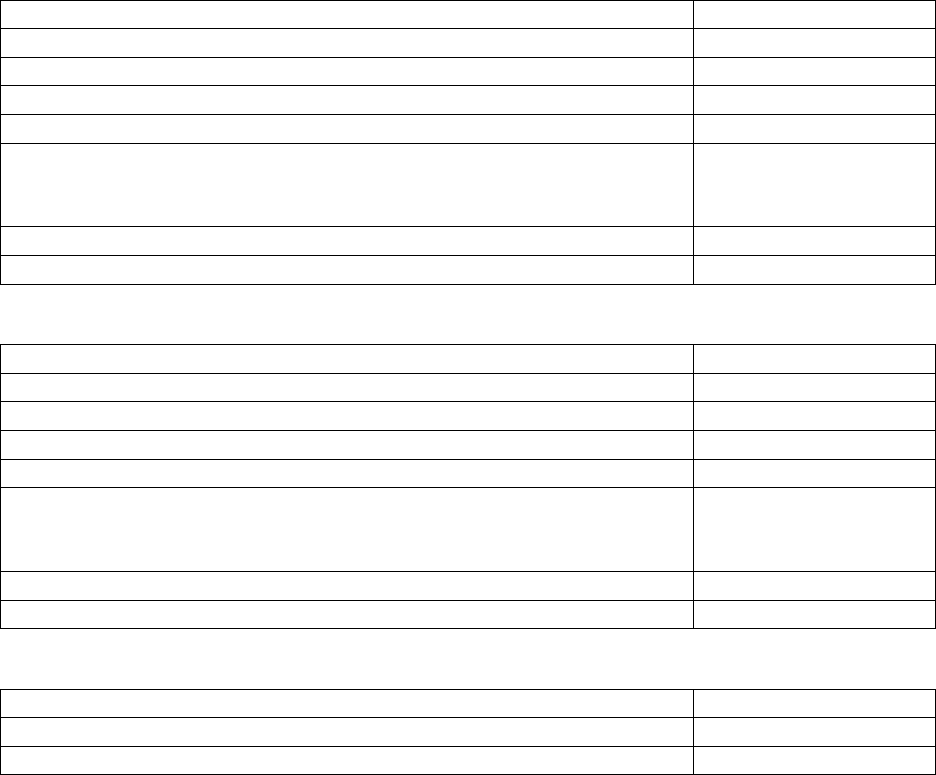
Table Of Contents
Community Support Services: Public Health Unit (PHU)
3
• Dental
3
• Immunizations
3
• Primary Care Client Fees by Procedure and Fee Group
5
• Environmental Health
7
Sheriff
9
Public Works
12
Health Department Clinic Fees
13
Health Department Dental Fees
14
Health Department Diabetes Fees
17

3
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Community Support Services: Public Health Unit (PHU)
*Some services Require an Office Visit
Administration Fee $25
Dental
Activities
Fee
Charged in accordance with current Medicaid rate
See Dental Fee Schedule
Immunizations:
Childhood Immunizations:
No charge for required immunizations of children through 12
th
grade. All children receiving
foreign travel inoculations must be charged according to the fee schedule. Medicaid does not
pay for ADULT immunizations or any immunizations for children that are not required.
Non-Childhood Immunizations
Immunizations
Fee
All non-childhood immunizations will be subject to an
administrative fee per shot
$20
All non-childhood immunizations will be subject to a
processing fee per shot
25% of cost of vaccine +
25% of administrative fee
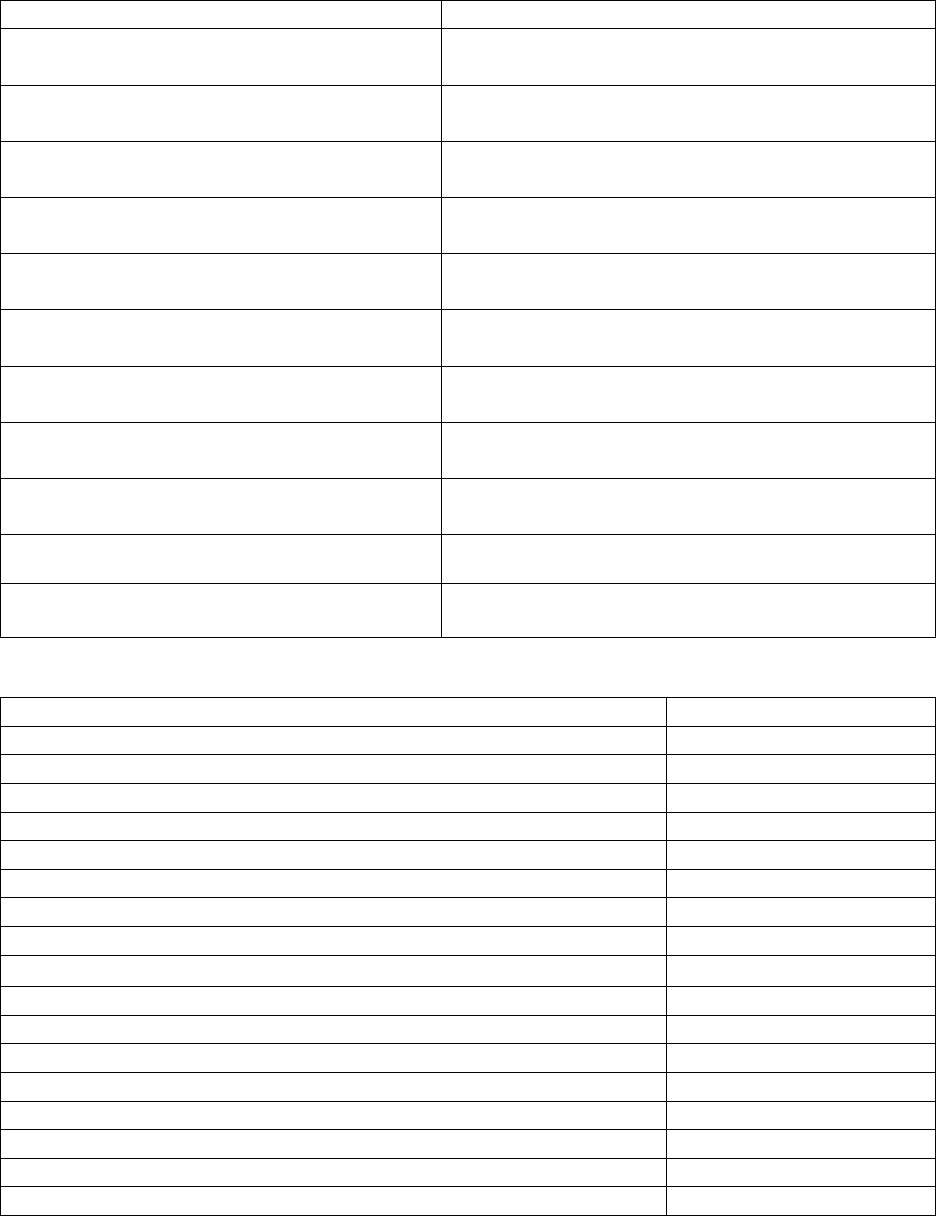
Adult Immunizations:
Immunizations
Fee
Tetanus/Diptheria
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Injectable Polio Vaccine (PIV)
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Oral Polio Vaccine (POV)
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Measles, Mumps & Rubella
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Measles only
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Mumps only
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Cholera
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Hepatitis B Immune Globulin
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Hepatitis B Immunizations
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
4
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Immunizations for All Ages
Immunizations
Fee
Children < 11 years old
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Children 11-19 years old
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Immune Globulin
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Japanese Encephalitis
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Influenza
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Meningococcal Vaccine
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Typhoid
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Oral Typhoid Vaccine (on request)
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Yellow Fever
(Cost of Vaccine + Administrative Fee) + 25%
of cost of vaccine and 25% of administrative fee
Foreign Travel Consultation
$40.00 per person
Immunization Booklet Replacement Fee
$20.00
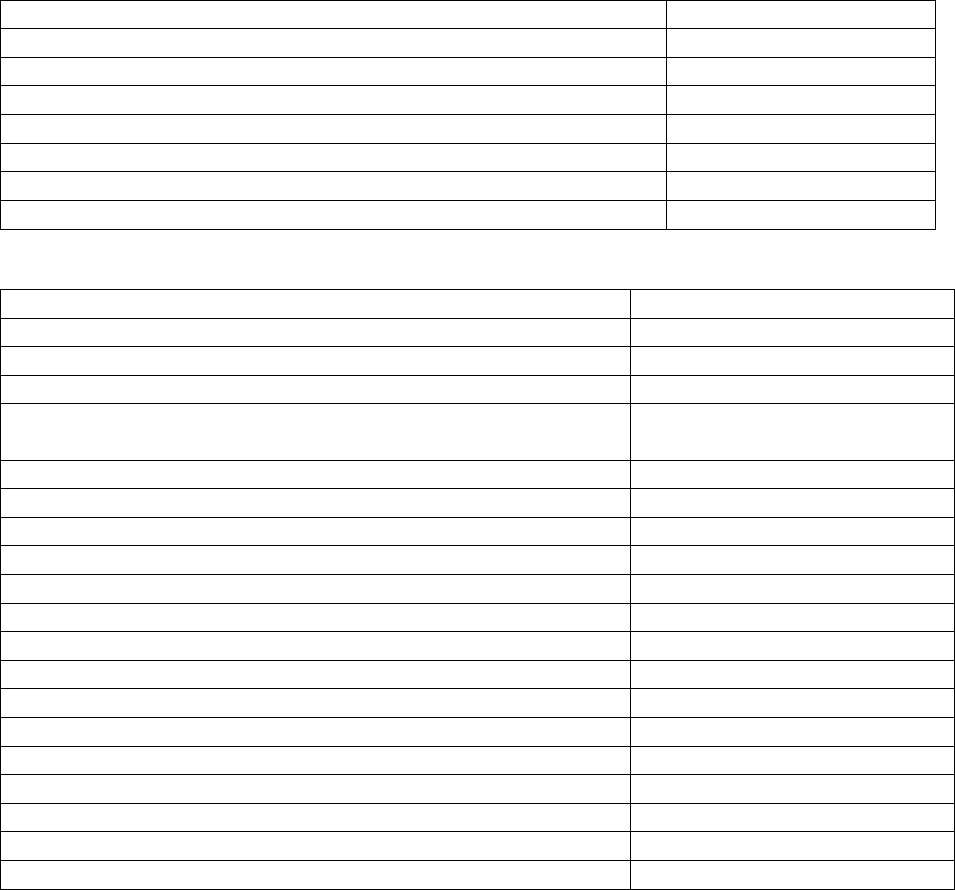
Other Services
Immunizations
Fee
Antibody Titer (Measles, Rubella)
Lab Cost + Admin Fee
Antibody Titer (Rabies)
Lab Cost + Admin Fee
Anti-HBS (Hepatitis B Antibody)
Lab Cost + Admin Fee
Body piercing Annual renewal training (4hrs + lab)
$100/participant
Childbirth/Parenting Class
$25.00
Cryo/Chemical Treatment of Genital Warts
$25.00
Diabetic Teaching
Lab Cost + Admin Fee
HBs Ag (Hepatitis Antigen)
Lab Cost + Admin Fee
Lead Testing
Lab Cost + Admin Fee
Lyme Disease/Ehrlichiosis/RMSF/Q Fever
Lab Cost + Admin Fee
Pregnancy Test HCG & Pelvis
$5.00 Supply Fee
Pregnancy Test Serum HCG Quantitative
Lab Cost + Admin Fee
RPR (Syphilis Test)
Lab Cost + Admin Fee
Signing out of state marriage license applications
$25.00
TB Skin Test
$20.00
TB Symptom Screening
$20.00
Varicella Zoster Titer
Lab Cost + Admin Fee
5
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Primary Care Client Fees by Procedure and Fee Group
Note: For laboratory and radiological services, clients will pay based on their income according
to Federal Guidelines using current provider fee schedule.
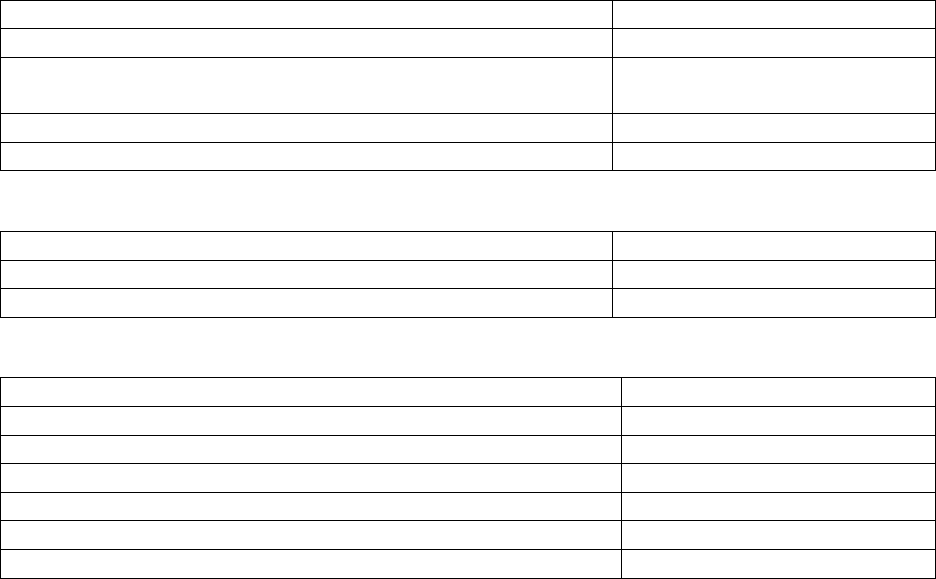
Client Net Income Levels:
Income Level
Fee
100% of federal poverty level
Zero Charge
101%-119% of federal poverty level
17% of Current Charge
120%-139% of federal poverty level
33% of Current Charge
140%-159% of federal poverty level
50% of Current Charge
160%-179% of federal poverty level
67% of Current Charge
180%-199% of federal poverty level
83% of Current Charge
Above 200% of federal poverty level
100% of Current Charge
Client Fees
Activities
Fees
Office Visit (includes any services not listed below)
Range = $65.00-$150.00
School Entrance Exam
$35.00
Sickle Cell Screen for Sports Physical
$8.00
Blood Pregnancy Test (Requires an appointment with a
Provider)
$3.00
Depo Provera
Injectable Cost + Nursing Visit
Diaphragm with Fitting
$83.00
EKG
$26.00
Cyro/Chemical Treatment of Genital Warts
$25.00
I.U.D. Insert
$250.00
I.U.D. Removal
$75.00
Counseling
$60.00
Insertion Only
$68.37
Removal Only
$60.63
Insertion & removal at the same time
$93.10
Nexplanon Device
325.00
Norplant Removal
$66.00
Physical Exam (adult or child) Primary Medical Services
$110.00-$115.00
STD Lab Screening (Asymptomatic without known contact)
$50.00
Venipuncture (Administrative Fee)
$25.00
Note: Fees (as shown above) are at $100% of current charge.
Sexually Transmitted Disease:
Note: Fees are based on sliding fee scale (as shown above) except standalone lab screening
which are fee for service.
6
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Rabies Vaccine:
Activities
Fee
Pre-Exposure Rabies
Cost of Vaccine + Admin Fee
Post-Exposure Rabies
(2 shots immunized/5 shots unimmunized)
Cost of Vaccine + Admin Fee
First session/Administration Fee
$45.00
Remaining doses/Administration Fee
$20.00
Tuberculosis
Activities
Fee
PPD
$20.00
Interferon Gamma Release Assay (TB Test)
$60.00
Vital Statistics:
Activities
Fee
Birth Certificates
$15.00
Birth Certificates: Additional Copies
$7.00
Death Certificates
$10.00
Notary Services
$5.00
Medical Records Copying
$1.00 per page
Nursing CE Provider Packet
$35.00 Processing Fee
7
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Environmental Health:
On Site Sewage Treatment and Disposal System (OSTDS):
OSTDS: Program Fees
Site Evaluation Only (no permit)
Activities
Fee
Application/Plan Review
$100.00
Application (Local PHU Surcharge)
$55.00
Site Evaluation
$115.00
Total
$270.00
New System Permit:
Activities
Fee
OSTDS Construction Application and Plan Review, New
$100.00
OSTDS Construction Site Evaluation
$115.00
OSTDS Construction Permit (New or Mod, Amendment)
$55.00
OSTDS Construction System Inspection
$75.00
OSTDS Construction System Inspection Research Fee
$5.00
Application (Local PHU Surcharge)
$55.00
Timed Inspection (Local PHU Surcharge)
$45.00
Total
$450.00
Repair Permit
Activities
Fee
OSTDS Construction Repair or Mod Site Evaluation
$115.00
OSTDS Construction System Inspection
$75.00
OSTDS Construction System Inspection Research Fee
$5.00
OSTDS Construction Application & Existing System
$55.00
OSTDS Construction Application & Existing System
$50.00
Total
$300.00
OSTDS Abandonment:
Activities
Fee
Existing Application
$50.00
Application County Surcharge
$55.00
Total
$105.00
Existing Residential Non-Bedroom Addition:
Activities
Fee
Existing Application
$35.00
Application County Surcharge
$55.00
Total
$90.00
8
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Water Program Fees:
Activities
Fee
Sample Collection Fee
$50.00
Bacteriological Analysis per Sample
$25.00
Well Survey for Site Assessment
$200.00 for ¼ mile
$800.00 for ½ mile
$1,600.00 for 1 mile
Development Review Committee Plan Review for Each
Activities
Fee
Development or Phase
$50.00
Group Care Facilities
Activities
Fee
Private school inspection Annual Operating Permit
(AOP) and Public Schools without Food Service
$100.00
Other Fees:
Activities
Fee
Late Renewal Fee for All Environmental Health Programs
$25.00
Re-Inspection for Noncompliance: Tanning Salons and
Mobile Home Parks and Swimming Pools
$40.00
9
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Sheriff
Fleet:
Activities
Fee
Vehicle Safety Violation Ticket Inspection
$4.00 each
Records
Activities
Fee
Copies – one sided
$0.15/page
Copies – double sided
$0.20/page
Concealed Weapon Permit Fingerprinting
$5.00 each
Civil
Activities
Fee
Non-Enforceable Process
$40.00
Out of State Non-Enforceable Process
$40.00
Sheriff’s Levy
$50.00
Processing Fee
$40.00
Preparations of Newspaper Ad
$40.00
Conducting Sheriff’s Sale
$40.00
Bill of Sale of Sheriff’s Deed
$40.00
Satisfaction of Judgement
$40.00
Writs of Replevin/Attachment
$90.00 each
Extra Duty (3 Hour Minimum) 30.2905 F.S.
Activities
Fee
Deputy
$53.50/hour
Sergeant
$66.25/hour
Lieutenant
$75.00/hour
Field Service Technician
$36.00/hour
Impoundment of Livestock Running At Large: 588.18 F.S.
Activities
Fee
Impound Fee
$50.00 each
Mileage Fee
IRS Standard Mileage
Feed/Care Fee
$5.00/day/animal
Disposition Fee
$5.00 each
Dart Fee
$15.00 each
10
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Alarm Permit Annual Fees
Fire Alarm Permits:
Activities
Fee
City Annual Fee
$20.00 each
City Reinstatement after Revocation
$70.50 each
County Annual Fee
$15.00 each
County Reinstatement after Revocation
$50.00 each
Burglar Alarm Permits
Activities
Fee
City Annual Fee
$23.75 each
City Reinstatement after Revocation
$74.00 each
County Annual Fee
$15.00 each
County Reinstatement after Revocation
$70.50 each
False Alarms Fines
City Fire (Gainesville Fire Rescue)
Activities
Fee
First Alarm
$0.00 each
Second Alarm
$165.50 each
Third & Fourth Alarm
$220.00 each
Fifth, Sixth, & Seventh Alarm
$441.00 each
Eighth, Ninth, and Tenth
Tenth alarm in a single year the permit will be revoked and
will be considered Non-Permitted
$882.00 each
Alarm with Non-Permitted System
$281.50 each
Unpermitted fine reduced (pending eligibility)
$232.75 each
City Burglar (Gainesville Police Department):
Activities
Fee
First Alarm
$0.00 each
Second, Third, and Fourth Alarm
$76.75 each
Fifth and Sixth Alarm
$147.75 each
Seventh and Eighth Alarm
$295.50 each
Ninth and Tenth
Tenth alarm in a single year the permit will be revoked and
will be considered Non-Permitted
$589.75 each
Alarm with Non-Permitted System
$295.50 each
Unpermitted fine reduced (pending eligibility)
$147.25 each
11
FY 21 Supplemental Fee Schedule Effective 05/11/2021
County Fire (Alachua County Fire Rescue):
Activities
Fee
First Alarm
$0.00 each
Second Alarm
$157.50 each
Third and Fourth Alarm
$210.00 each
Fifth, Sixth, and Seventh Alarm
$420.00 each
Eighth, Ninth, and Tenth Alarm
Tenth alarm in a single year the permit will be revoked and
will be considered Non-Permitted
$840.00 each
Alarm with Non-Permitted System
$268.00 each
Unpermitted fine reduced (pending eligibility)
$75.00 each
County Burglar (Alachua County Sheriff’s Office):
Activities
Fee
First Alarm
$0.00 each
Second, Third and Fourth Alarm
$73.00 each
Fifth and Sixth Alarm
$140.75 each
Seventh and Eighth Alarm
$281.50 each
Ninth and Tenth
Tenth alarm in a single year the permit will be revoked and
will be considered Non-Permitted
$562.75 each
Alarm with Non-Permitted System
$200.00 each
Unpermitted fine reduced (pending eligibility)
$75.00 each
Jail
Activities
Fee
U.S. Marshal Inmate Housing
$57.23/day
Private Transport Company Inmate Housing
$57.23/day
Note: Sheriff’s Office fees as submitted in the Sheriff’s Certified Budget.

12
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Public Works
Wireless Collection Fees
Activities
Fee
Collocation of a small wireless facility on an Authorized Utility Pole
$150 per pole per year
13
FY 21 Supplemental Fee Schedule Effective 05/11/2021
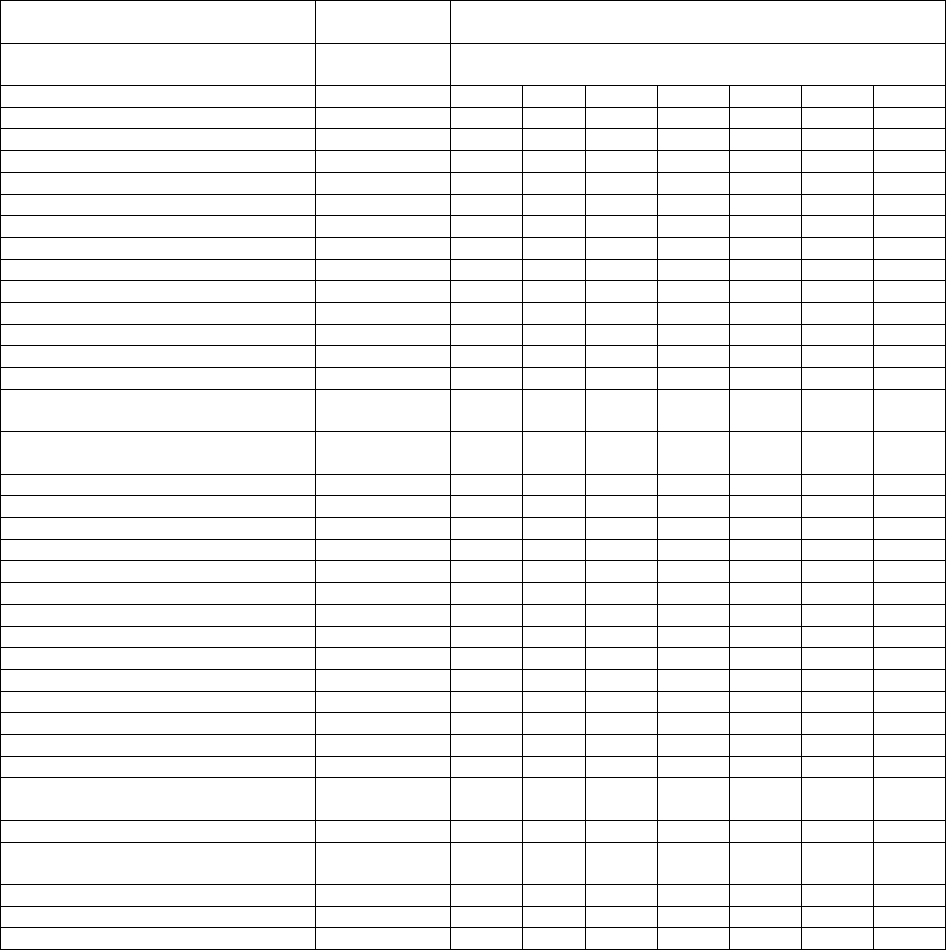
ALACHUA COUNTY HEALTH DEPARTMENT CLINIC FEES
10-1-2020 THROUGH 9-30-2021
*Some services Require an Office Visit
Procedure Name
Procedure
Code
Charge
Fee Group
(Based on Federal Poverty Guidelines)
0.00%
17%
33%
50%
67%
83%
100%
Administration Fee
25.00
25.00
25.00
25.00
25.00
25.00
25.00
Office Visit Established Patient
99212
0.00
11.05
21.45
32.50
43.55
53.95
65.00
99213
0.00
12.75
24.75
37.50
50.25
62.25
75.00
99214
0.00
15.30
29.70
45.00
60.30
74.70
90.00
99215
0.00
17.85
34.65
52.50
70.35
87.15
105.00
Office Visit New Patient
99202
0.00
11.90
23.10
35.00
46.90
58.10
70.00
99203
0.00
15.30
29.70
45.00
60.30
74.70
90.00
99204
0.00
20.40
3.60
60.00
80.40
99.60
120.00
99205
0.00
25.50
49.50
75.00
100.50
124.50
150.00
Nursing Protocol Visit
99211 (99201)
0.00
10.20
19.80
30.00
40.20
49.80
60.00
Physical Exam Established Patient
(Adult or Child)
99391-99397
0.00
18.70
36.30
55.00
73.70
91.30
110.00
Physical Exam New Patient (Adult or
Child)
99381-99387
0.00
19.55
37.95
57.50
114.33
95.45
115.00
School Entrance Exam
99212
35.00
35.00
35.00
35.00
35.00
35.00
35.00
STD Lab Screening
99402
0.00
8.50
16.50
25.00
33.50
41.50
50.00
DEPO Provera
J1055
0.00
9.01
17.49
26.50
35.51
43.99
53.00
Diaphragm With Fitting
57170
0.00
14.00
27.39
41.50
55.61
68.89
83.00
I.U.D. Insert
58300
0.00
42.50
82.50
125.00
167.50
207.50
250.00
I.U.D. Removal
58301
0.00
12.75
24.75
37.50
50.25
62.25
75.00
Norplant Removal
11976
0.00
11.22
21.78
33.00
44.22
54.78
66.00
EKG
9300
0.00
4.42
8.58
13.00
17.42
21.58
26.00
Venipuncture (Administrative Fee)
36415
25.00
25.00
25.00
25.00
25.00
25.00
25.00
Sickle Cell Screen
83020
0.00
0.51
0.99
1.50
2.01
2.49
3.00
Blood Pregnancy Test
84703
0.00
1.51
0.99
1.50
2.01
2.49
3.00
Cryo/Chemical Treatment of Warts
17110
0.00
4.25
8.25
12.50
16.75
20.75
25.00
Nexplanon:
Insertion Only with Grant Funded
Device
11981
0.00
11.62
22.56
34.19
45.81
56.75
68.37
Removal Only
11982
0.00
10.31
20.01
30.32
40.62
50.32
60.63
Insertion and Removal at the Same
Time
11983
0.00
15.83
30.72
46.55
62.38
77.27
93.10
Nexplanon Device with Insertion
J7307
0.00
66.87
129.81
196.69
263.56
326.50
393.37
Some Services Require an Office Visit
14
FY 21 Supplemental Fee Schedule Effective 05/11/2021
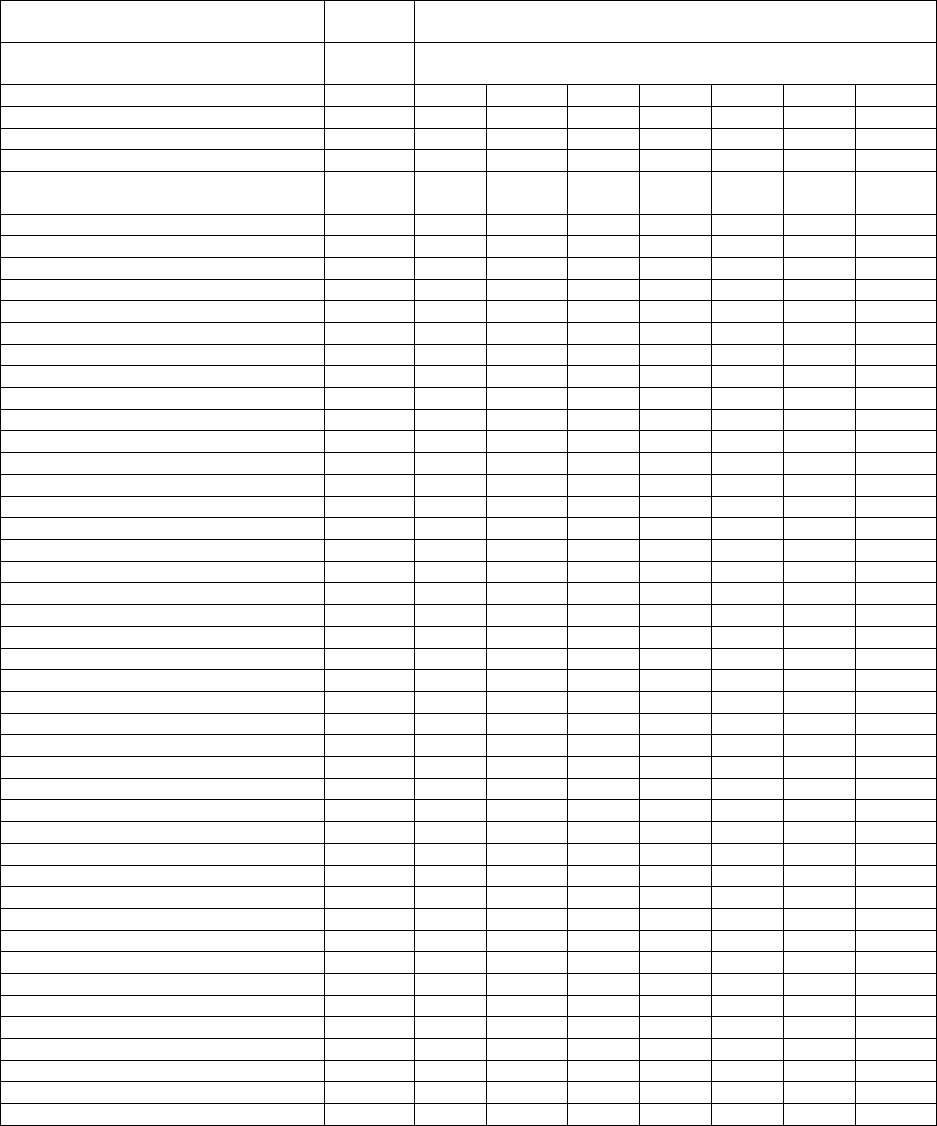
ALACHUA COUNTY HEALTH DEPARTMENT DENTAL FEES
10-01-2020 THROUGH 09-30-2021
Procedure Name
Procedu
re Code
Charge
Fee Group
(Based on Federal Poverty Guidelines)
Diagnostic Exam
0.00%
17%
33%
50%
67%
83%
100%
Per Encounter (United Health Care)
D0999
120.00
Periodic Oral Exam (Medicaid Comp)
D0120
0.00
5.31
10.30
15.61
20.91
25.90
31.21
Limited Oral Exam
D0140
0.00
2.83
5.49
8.33
11.16
13.82
16.65
Comprehensive Exam
(Medicaid Comp)
D0150
0.00
5.66
10.99
16.65
22.30
27.63
33.29
Radiographs
PA Single Film
D0220
0.00
1.42
2.75
4.17
5.58
6.91
8.33
PA – Each Additional
D0230
0.00
1.06
2.06
3.12
4.18
5.18
6.24
Intraoral Occlusal
D0240
0.00
2.83
5.49
8.33
11.16
13.82
16.65
Bitewing – Single
D0270
0.00
2.12
4.12
6.25
8.37
10.37
12.49
Bitewing – Two
D0272
0.00
3.18
6.18
9.37
12.55
15.55
18.73
Bitewing – Three
D0273
0.00
3.89
7.55
11.45
15.34
19.00
22.89
Bitewing – Four
D0274
25.00
3.89
7.55
11.45
15.34
19.00
22.89
Panoramic
D0330
0.00
10.61
20.60
31.22
41.83
51.82
62.43
Diagnostic Cast
D0470
0.00
7.78
15.11
22.89
30.67
38.00
45.78
Preventative Services
Prophylaxis – Chile
D1120
0.00
4.95
9.61
14.57
19.52
24.18
29.13
Prophylaxis – Adult
D1110
0.00
6.37
12.36
18.73
25.09
31.08
37.45
Fluoride Varnish
D1206
0.00
3.89
7.55
11.45
15.34
19.00
22.89
Oral Hygiene Instruction
D1330
0.00
2.12
4.12
6.25
8.37
10.37
12.49
Sealant – Per Tooth
D1351
0.00
4.60
8.93
13.53
18.12
22.45
27.05
Endodontics
Pulp Cap - Direct
D3110
0.00
4.60
8.93
13.53
18.12
22.45
27.05
Pulp Cap - Indirect
D3120
0.00
3.89
7.55
11.45
15.34
19.00
22.89
Therapeutic Pulpotomy
D3220
0.00
17.69
34.34
52.03
69.71
86.36
104.05
Anterior Root Canal
D3310
0.00
52.35
101.63
153.98
206.33
255.61
307.96
Apicoectomy
D3410
0.00
26.53
51.50
78.03
104.56
129.53
156.06
Scale – Cav – Per Quad
D4341
0.00
7.08
13.73
20.81
27.89
34.54
41.62
Prosthetics
Full Denture – Max
D5110
0.00
109.66
212.87
322.53
432.18
535.39
645.05
Full Denture – Mand
D5120
0.00
109.66
212.87
322.53
432.18
535.39
645.05
Upper Partial – Resin Base
D5211
0.00
58.37
113.30
171.67
230.04
284.97
343.34
Lower Partial – Resin Base
D5212
0.00
58.37
113.30
171.67
230.04
284.97
343.34
Upper Partial – Cast Metal
D5213
0.00
111.43
216.30
327.73
439.15
544.02
655.45
Lower Partial – Cast Metal
D5214
0.00
111.43
216.30
327.73
439.15
544.02
655.45
Adjust Full Denture – Max
D5410
0.00
4.95
9.61
14.57
19.52
24.18
29.13
Adjust Full Denture – Mand
D5411
0.00
4.95
9.61
14.57
19.52
24.18
29.13
Adjust Partial Denture – Max
D5421
0.00
4.95
9.61
14.57
19.52
24.18
29.13
Adjust Partial Denture – Mand
D5422
0.00
4.95
9.61
14.57
19.52
24.18
29.13
Repair Full Denture – Base
D5510
0.00
15.57
30.21
45.78
61.35
75.99
91.56
Replace Teeth – Full Denture
D5520
0.00
13.80
26.78
40.58
54.38
67.36
81.16
Replace Teeth – Partial Denture
D5640
0.00
13.80
26.78
40.58
54.38
67.36
81.16
Add Tooth to Existing Partial
D5650
0.00
14.86
28.84
43.70
58.55
72.53
87.39
Reline Full Max – Chairside
D5730
0.00
22.29
43.26
65.55
87.84
108.81
131.10
Reline Full Mand – Chairside
D5731
0.00
22.29
43.26
65.55
87.84
108.81
131.10
Reline Full Max – Lab
D5750
0.00
39.97
77.59
17.57
157.54
195.16
235.13
Reline Full Man – Lab
D5751
0.00
39.97
77.59
117.57
157.54
195.16
235.13
*Any procedure not listed will be billed at 140% of Medicaid FFS Rate
15
FY 21 Supplemental Fee Schedule Effective 05/11/2021
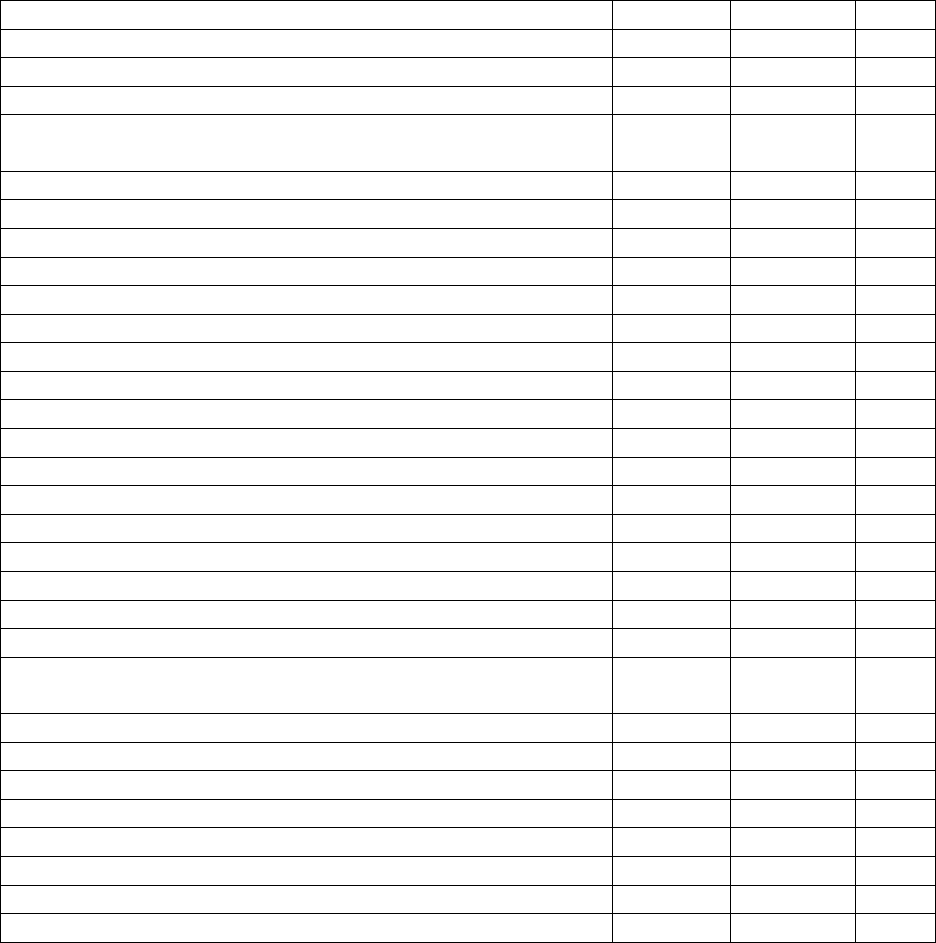
VACCINE FEE SCHEDULE
ADMINISTRATION FEE INCLUDED IF APPLICABLE
EFFECTIVE 10/01/2020
*Some services Require an Office Visit
Cholera
990725
$103.06
Z23
DTAP (Daptacel) Transplant Only
90700
$61.30
↓↓↓
*Flu (Influenza)
90658
$25.00
Flu Zone High Dose (Influenza)
90662
$43.95
Foreign Travel Consult Fee
$40 per person/ $80 family (Parents with Children)
99211
$40.00
FT Yellow Book Replacement Fee
IMFTYB
$20.00
Gardasil – 9 (HPV9)
90651
$281.55
*HEP A (Havrix)
90632
$73.01
*HEP B (Engerix)
90746
$82.06
HEP B 2 Dose (Heplisav – B)
90739
$128.38
HEP A/B (TWINRIX)
90636
$125.75
*HIB (adult)
90648
$38.80
*Meningitis (menactra – MCV4)
90734
$173.26
Meningococcal B Grp (Bexsero)
90620
$213.94
*MMR (measles, mumps, rubella)
90707
$117.30
Pneumococcal (pneumovax – PPSV23)
90732
$145.83
*Polio (IPV – IPOL)
90713
$66.80
*Prevnar 13
90670
$261.81
Rabies (IMOVAX Pre-Exposure)
90675
$432.10
Rabies (IMOVAX Post)
$432.10
Rabies (RABAVERT Pre-Exposure)
90675
$380.00
Z23
Rabies (RABAVERT POST)
90675
$380.00
Z20.3
**Post – Exposure Immune
Globulin (Per ML)
90375
$398.30
*TD (tetanus/diphtheria) Adult
90714
$68.50
*TDAP (tetanus/diphtheria/pertussis)
90715
$69.69
Typhoid (injection – Typhim)
90691
$156.68
Z23
Typhoid (Oral – Vivotif)
90690
85.80
↓↓↓
*Varicella (chickenpox)
90716
$183.98
XIARO (Japanese encephalitis-jenceph)
90738
$343.45
Yellow Fever
90717
$200.83
Shingrix (Shingles)
90750
$205.06
*Free Until 19
th
Birthday
**Add (Administration of Immune Globulin) 96372 $45.00
DH 681 (Religious Exemption Form) Replacement Fee per Copy Local Code $5.00
680 Replacement Fee Local Code $5.00
College Completion Form (Except Santa Fe) Local Code $25.00
Appointment Required

16
FY 21 Supplemental Fee Schedule Effective 05/11/2021
EFFECTIVE 10/01/2020
TITERS and HSV screening (administrative fee plus cost of test)
***ALL TITERS WILL TAKE 10-14 WORKING DAYS FOR RESULTS TO COME
BACK***
*Some services Require an Office Visit
Administrative Fee
Local Code
$25.00
Z01.84
B-12/Allergy Shot (ADM Fee Only)
J3420
$25.00
HEP A TITER
86708
$5.46
↓↓↓
HEP B Surface Antibody (State Lab)
86706
$5.68
HEP B Surface Antigen (State Lab)
87340
$5.16
HEP C TITER (State Lab)
83898
$6.99
Hepatitis Profile
86803
$23.51
*Lead Screen (Lab Corp.)
83655
$10.00
*Lyme Disease TITER (State Lab)
86618
$0.00
Measles (Rubeola)(State Lab)
86765
$5.00
MUMPS (State Lab)
86735
$5.00
PPD (purified protein derivative test)
04-86580
$20.00
Z11.1
Rabies TITER (Lab Corp)
86382
$72.50
*RPR (State Lab)
86592
$0.00
Rubella (German Measles) (State Lab)
86762
$5.00
Varicella TITER (State Lab)
87290
$5.00
*HSV Screening
86695
$10.20
A60.9
*Requires Appointment with Provider
HBIG-1CC
02-90371
$143.20
HBIG-5CC
05-90371
$666.85
TB Symptoms Screening
99211-TB
$20.00
Z11.1
IGRA QuantiFERON
86480
$60.00
Z11.1
17
FY 21 Supplemental Fee Schedule Effective 05/11/2021
Client Fees for Diabetes Self-Management Education (DSME) and Medical Nutrition
Therapy (MNT) Services for Department of Health - Alachua County
*Some services Require an Office Visit
HCPCS
Code
Short Description
Non-Facility
Rate
1.5 Times
Allowable
G0108
Diab Manage trn per indiv
$61.74
$92.61
G0109
Diab Manage trn per ind/group
$17.12
$25.68
G0270
Mnt Subs tx for change dx
$35.63
$53.45
G0271
Group mnt 2 or more mins
$18.61
$27.92
G0447
Behavior counsel obesity 15m
$29.09
$43.64
G0473
Group Behav couns 2-10
$14.09
$21.14
97802
Medical Nutrition indivin in
$41.02
$61.53
97803
Med nutrition indiv subseq
$35.63
$53.45
97804
Medical nutrition group
$18.61
$27.92
99490
Chron care mgmt srvc 20 min
$45.83
$68.75
The above services involve client education regarding the management of diabetes and
other conditions, including but not limited to, chronic kidney disease, HIV, obesity,
dyslipidemia, hypertension, congestive heart failure, food allergies/intolerance,
gastrointestinal disorders, and weight management. The fees have been selected
commensurate with other Department of Health facilities who offer the same services.
