a
000345 J280EVGA *0003456*
Statement date: October 15, 2016
JANE H DOE
111 AETNA STREET
HARTFORD CT 06156
Jane H Doe
W123456789
0987654-10-001 A P1 (*TO
Test INC
Contact us at aetna.com
Member ID:
Member:
Group#:
Group name:
QUESTIONS?
Track your health care costs
1-800-XXX-XXXX
Or write to the address shown above.
$0.00
Amount you owe or already paid
Amount billed $539.00
Plan payments
and discounts
- $539.00
You owe $0.00
$539.00
$0.............................................. $539.00
$249.12
Amount you saved
$1,004.23 (In-network)
Amount you have left to meet deductible
Going to a doctor or hospital in the network
saves you money.
That’s because we have arranged discounted
rates with these providers.
The online provider directory can help you nd a
doctor or other health care professional. Just go
to www.aetna.com.
Annual deductible $1,700.00
Deductible used - $695.77
Deductible remaining $1,004.23
$695.77
$0...................................................... $1,700.00
A guide to key terms
Term
This means
Your totals
Amount billed:
The amount your doctor or health care provider billed for services.
$539.00
Member rate:
The agreed upon amount the in-network doctor or health care provider accepts as their fee.
$244.88
$294.12
$0.00
The difference between the amount billed and the in-network arranged pricing.
A claim that needs more review by us or an amount we did not pay. You may or may not have to
pay this. Read ‘Your Claim Remarks’ to learn more.
The amount you pay before your health plan will pay benets.
When you pay part of the bill and we pay part of the bill. Some plans do not have coinsurance.
A xed dollar amount you pay when you visit a doctor or other health care provider.
$0.00
$0.00
$0.00
Amount you saved:
Pending or not payable:
Deductible:
Coinsurance:
Copay:
Stay healthy
When you visit your doctor, be prepared with the questions you want to ask. Write them down and bring them with you. Ask about tests, medications
Page 1 of 3
EL PASO TX 79998-1106
Aetna Life Insurance Company
P.O. BOX 981106
Explanation of Benets (EOB) - This is not a bill
This statement is called your EOB. It shows how much you may owe, the amount that was billed, and your member rate. It also shows the
amount you saved and what your plan paid. Look at this statement carefully and make sure it is correct. If you do owe anything, you will
receive a bill from your doctor or health care provider(s).
$1,004.23
and next steps you need to take over the next year.
a
000345 J280EVGA *0003456*
Statement date: October 15, 2016
JANE H DOE
111 AETNA STREET
HARTFORD CT 06156
Jane H Doe
W123456789
0987654-10-001 A P1 (*TO
Test INC
Contact us at aetna.com
Member ID:
Member:
Group#:
Group name:
QUESTIONS?
Track your health care costs
1-800-XXX-XXXX
Or write to the address shown above.
$0.00
Amount you owe or already paid
Amount billed $539.00
Plan payments
and discounts
- $539.00
You owe $0.00
$539.00
$0.............................................. $539.00
$249.12
Amount you saved
$1,004.23 (In-network)
Amount you have left to meet deductible
Going to a doctor or hospital in the network
saves you money.
That’s because we have arranged discounted
rates with these providers.
The online provider directory can help you nd a
doctor or other health care professional. Just go
to www.aetna.com.
Annual deductible $1,700.00
Deductible used - $695.77
Deductible remaining $1,004.23
$695.77
$0...................................................... $1,700.00
A guide to key terms
Term
This means
Your totals
Amount billed:
The amount your doctor or health care provider billed for services.
$539.00
Member rate:
The agreed upon amount the in-network doctor or health care provider accepts as their fee.
$244.88
$294.12
$0.00
The difference between the amount billed and the in-network arranged pricing.
A claim that needs more review by us or an amount we did not pay. You may or may not have to
pay this. Read ‘Your Claim Remarks’ to learn more.
The amount you pay before your health plan will pay benets.
When you pay part of the bill and we pay part of the bill. Some plans do not have coinsurance.
A xed dollar amount you pay when you visit a doctor or other health care provider.
$0.00
$0.00
$0.00
Amount you saved:
Pending or not payable:
Deductible:
Coinsurance:
Copay:
Stay healthy
When you visit your doctor, be prepared with the questions you want to ask. Write them down and bring them with you. Ask about tests, medications
Page 1 of 3
EL PASO TX 79998-1106
Aetna Life Insurance Company
P.O. BOX 981106
Explanation of Benets (EOB) - This is not a bill
This statement is called your EOB. It shows how much you may owe, the amount that was billed, and your member rate. It also shows the
amount you saved and what your plan paid. Look at this statement carefully and make sure it is correct. If you do owe anything, you will
receive a bill from your doctor or health care provider(s).
$1,004.23
and next steps you need to take over the next year.
a
000345 J280EVGA *0003456*
Statement date: October 15, 2016
JANE H DOE
111 AETNA STREET
HARTFORD CT 06156
Jane H Doe
W123456789
0987654-10-001 A P1 (*TO
Test INC
Contact us at aetna.com
Member ID:
Member:
Group#:
Group name:
QUESTIONS?
Track your health care costs
1-800-XXX-XXXX
Or write to the address shown above.
$0.00
Amount you owe or already paid
Amount billed $539.00
Plan payments
and discounts
- $539.00
You owe $0.00
$539.00
$0.............................................. $539.00
$249.12
Amount you saved
$1,004.23 (In-network)
Amount you have left to meet deductible
Going to a doctor or hospital in the network
saves you money.
That’s because we have arranged discounted
rates with these providers.
The online provider directory can help you nd a
doctor or other health care professional. Just go
to www.aetna.com.
Annual deductible $1,700.00
Deductible used - $695.77
Deductible remaining $1,004.23
$695.77
$0...................................................... $1,700.00
A guide to key terms
Term
This means
Your totals
Amount billed:
The amount your doctor or health care provider billed for services.
$539.00
Member rate:
The agreed upon amount the in-network doctor or health care provider accepts as their fee.
$244.88
$294.12
$0.00
The difference between the amount billed and the in-network arranged pricing.
A claim that needs more review by us or an amount we did not pay. You may or may not have to
pay this. Read ‘Your Claim Remarks’ to learn more.
The amount you pay before your health plan will pay benets.
When you pay part of the bill and we pay part of the bill. Some plans do not have coinsurance.
A xed dollar amount you pay when you visit a doctor or other health care provider.
$0.00
$0.00
$0.00
Amount you saved:
Pending or not payable:
Deductible:
Coinsurance:
Copay:
Stay healthy
When you visit your doctor, be prepared with the questions you want to ask. Write them down and bring them with you. Ask about tests, medications
Page 1 of 3
EL PASO TX 79998-1106
Aetna Life Insurance Company
P.O. BOX 981106
Explanation of Benets (EOB) - This is not a bill
This statement is called your EOB. It shows how much you may owe, the amount that was billed, and your member rate. It also shows the
amount you saved and what your plan paid. Look at this statement carefully and make sure it is correct. If you do owe anything, you will
receive a bill from your doctor or health care provider(s).
$1,004.23
and next steps you need to take over the next year.
a
000345 J280EVGA *0003456*
Statement date: October 15, 2016
JANE H DOE
111 AETNA STREET
HARTFORD CT 06156
Jane H Doe
W123456789
0987654-10-001 A P1 (*TO
Test INC
Contact us at aetna.com
Member ID:
Member:
Group#:
Group name:
QUESTIONS?
Track your health care costs
1-800-XXX-XXXX
Or write to the address shown above.
$0.00
Amount you owe or already paid
Amount billed $539.00
Plan payments
and discounts
- $539.00
You owe $0.00
$539.00
$0.............................................. $539.00
$249.12
Amount you saved
$1,004.23 (In-network)
Amount you have left to meet deductible
Going to a doctor or hospital in the network
saves you money.
That’s because we have arranged discounted
rates with these providers.
The online provider directory can help you nd a
doctor or other health care professional. Just go
to www.aetna.com.
Annual deductible $1,700.00
Deductible used - $695.77
Deductible remaining $1,004.23
$695.77
$0...................................................... $1,700.00
A guide to key terms
Term
This means
Your totals
Amount billed:
The amount your doctor or health care provider billed for services.
$539.00
Member rate:
The agreed upon amount the in-network doctor or health care provider accepts as their fee.
$244.88
$294.12
$0.00
The difference between the amount billed and the in-network arranged pricing.
A claim that needs more review by us or an amount we did not pay. You may or may not have to
pay this. Read ‘Your Claim Remarks’ to learn more.
The amount you pay before your health plan will pay benets.
When you pay part of the bill and we pay part of the bill. Some plans do not have coinsurance.
A xed dollar amount you pay when you visit a doctor or other health care provider.
$0.00
$0.00
$0.00
Amount you saved:
Pending or not payable:
Deductible:
Coinsurance:
Copay:
Stay healthy
When you visit your doctor, be prepared with the questions you want to ask. Write them down and bring them with you. Ask about tests, medications
Page 1 of 3
EL PASO TX 79998-1106
Aetna Life Insurance Company
P.O. BOX 981106
Explanation of Benets (EOB) - This is not a bill
This statement is called your EOB. It shows how much you may owe, the amount that was billed, and your member rate. It also shows the
amount you saved and what your plan paid. Look at this statement carefully and make sure it is correct. If you do owe anything, you will
receive a bill from your doctor or health care provider(s).
$1,004.23
and next steps you need to take over the next year.
00.03.649.1 A (11/16)
Quality health plans & benefits
Healthier living
Financial well-being
Intelligent solutions
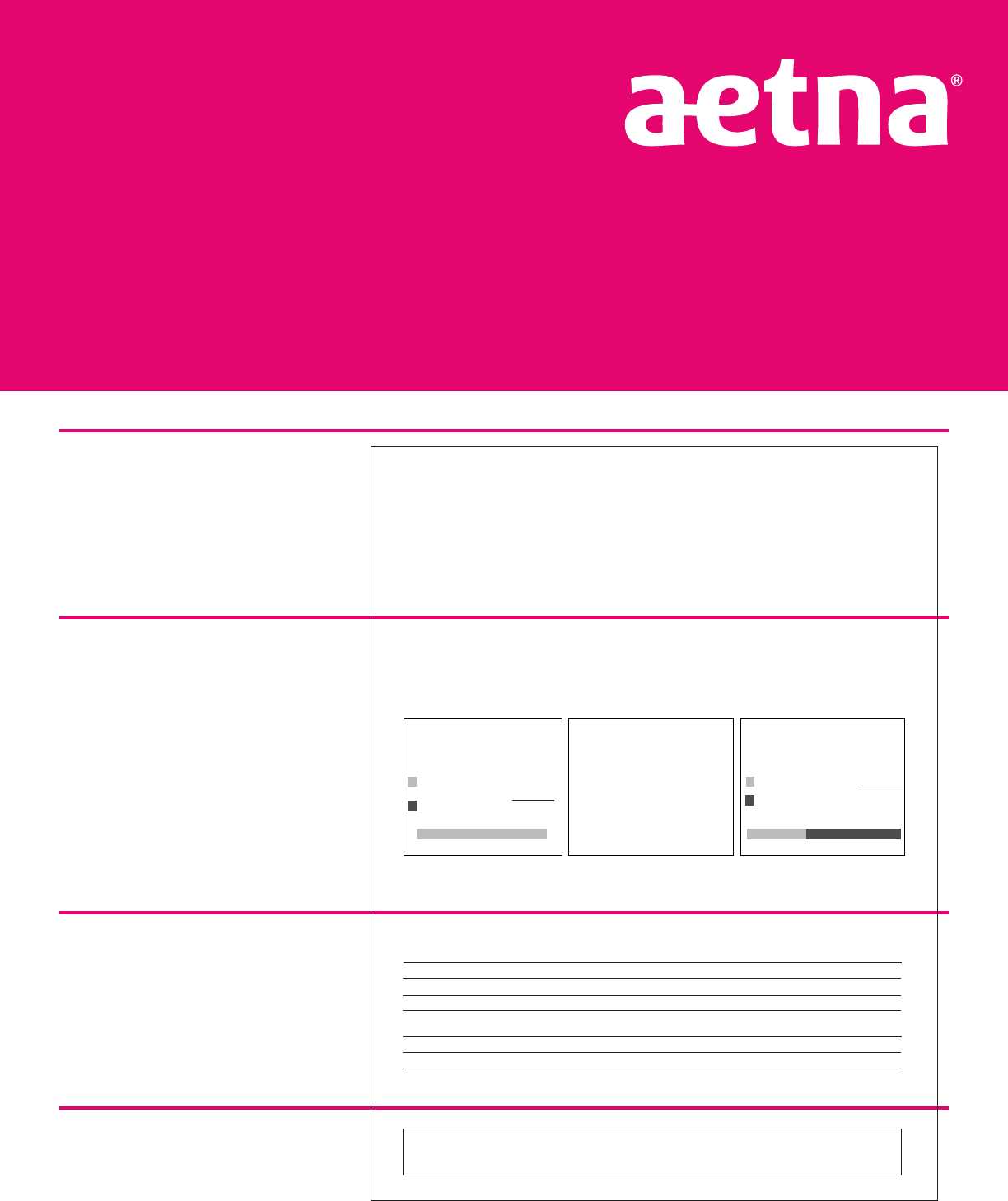
Understanding your
Explanation of Benefits (EOB)
Personal information
• Your name and address
• Member ID as shown on your ID card
• Group # identifies your plan
• Group name is your plan sponsor
• Customer-specific contact information
Track your spending, savings
and deductibles
• The first box is a summary of what you
owe and the payments already made
for the claims listed on your EOB.*
• The second box shows the amount you
save by using an in-network provider.*
• The third box shows the amount you
have remaining to meet your yearly
in-network family or individual
deductible.*
Definitions of commonly
used terms
A glossary of some common terms
shown on your EOB. Following the
definitions, totals related to the
charges are displayed.
Messaging
There are helpful messages from Aetna
or your employer located in this section.
*This box may not always appear.
SAMPLE
Aetna is the brand name used for products and services provided by one or more of the Aetna group of subsidiary companies,
including Aetna Life Insurance Company and its affiliates (Aetna).
For illustrative purposes only. This is a sample EOB and does not reflect actual charges or services rendered, nor does it reflect actual
charges or services received by an actual Aetna member. Health benefits and health insurance plans contain exclusions and
limitations. Information is believed to be accurate as of the production date; however, it is subject to change. For more information
about Aetna plans, refer to www.aetna.com.
www.aetna.com
©2016 Aetna Inc.
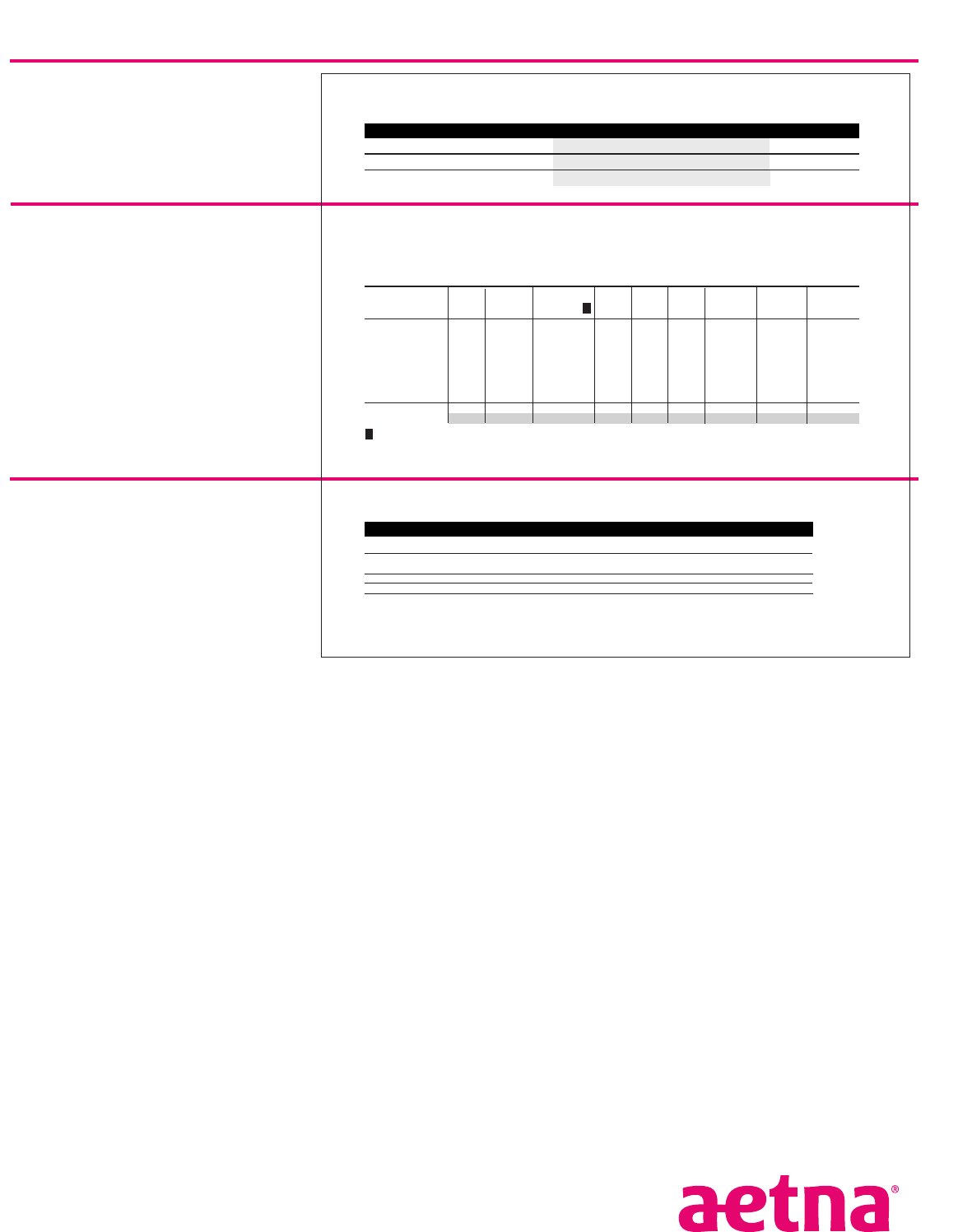
00.03.649.1 A (11/16)
Your payment summary
Includes detailed information of any
payments made for the claims on the EOB.
Your claims up close
Shows detailed information for each
claim processed on your EOB.
Columns A through I, from left to right,
break down each charge and how your
benefits were applied.
Column I reflects the amount you may
owe or have already paid.
Your benefit balances
Provides a summary of financial limits
for the benefit year listed.
You can view, print or download your EOB and other documents
anytime at www.aetna.com.
Want to stop the paper? It’s easy. Log in to your secure member website at www.aetna.com, go to “Your Profile,”
provide a valid email address and select your paper-saving preferences.
a
Statement date: October 15, 2016
Member: Jane H Doe
Member ID: W123456789
Group#:
0987654-10-001 A P1 (*TO
Group name: Test INC
Your Payment Summary
Your plan paid You owe or already paid
Patient Provider
Amount Send Date Amount Sent to
Jane (self)
Total:
John Roe
$244.88
$244.88
John Roe 10/16/16 $0.00
$0.00
Your claims up close
Claim for Jane (self)
Claim ID: E00000000OO Amount Member Pending or Applied to
Your Amount
Plan
Your
You may
Received on 9/31/16 billed rate not payable deductible
copay
remaining
pays
coinsurance
owe
(Remarks)
X-RAY EXAM OF LOWER
SPINE on 9/31/16
72110
X-RAY EXAM NECK SPINE
4/5VWS on 9/31/16
GOOO8
John Roe
Refer to Remarks Section
Totals:
269.00
539.00
A
270.00
244.88
B
121.57
123.31
(1)
C D E
123.31
121.57
244.88
F
123.31 (100%)
121.57 (100%)
244.88
G H I
You can nd all numbered claim remarks in ‘Your Claim Remarks’ section.
Page 2 of 4
!
!
C+D+E+H=I
Your Claim Remarks
General Remarks:
Your provider may have sent diagnosis codes with your claim. You may obtain these codes and their meanings by contacting us at the
number listed at the top of the rst page. We will also provide your treatment codes and their meanings, if they do not appear on this
statement. If you have questions about your diagnosis or your treatment, please contact your provider. [H63]
(1)
Your benet balances to date
Description
Individual
Annual
Amount
Jane (self)
Medical In Network Deductible
Medical In Network Coinsurance
Medical Out of Network Deductible
$1,700.00
$6,450.00
$7,000.00
$695.77
$695.77
$0.00
limit
used
Medical Out of Network Coinsurance $12,000.00 $0.00
for 1/1/16 to 12/31/16
Amount
$1,004.23
$5754.23
$7000.00
remaining
$12,000.00
A complete list of your benet balances and plan limits can be found on your secure member website.
a
Statement date: October 15, 2016
Member: Jane H Doe
Member ID: W123456789
Group#:
0987654-10-001 A P1 (*TO
Group name: Test INC
Your Payment Summary
Your plan paid You owe or already paid
Patient Provider Amount Send Date Amount Sent to
Jane (self)
Total:
John Roe $244.88
$244.88
John Roe 10/16/16 $0.00
$0.00
Your claims up close
Claim for Jane (self)
Claim ID: E00000000OO Amount Member Pending or Applied to
Your Amount
Plan
Your
You may
Received on 9/31/16 billed rate not payable deductible
copay
remaining
pays
coinsurance
owe
(Remarks)
X-RAY EXAM OF LOWER
SPINE on 9/31/16
72110
X-RAY EXAM NECK SPINE
4/5VWS on 9/31/16
GOOO8
John Roe
Refer to Remarks Section
Totals:
269.00
539.00
A
270.00
244.88
B
121.57
123.31
(1)
C D E
123.31
121.57
244.88
F
123.31 (100%)
121.57 (100%)
244.88
G H I
You can nd all numbered claim remarks in ‘Your Claim Remarks’ section.
Page 2 of 4
!
!
C+D+E+H=I
Your Claim Remarks
General Remarks:
Your provider may have sent diagnosis codes with your claim. You may obtain these codes and their meanings by contacting us at the
number listed at the top of the rst page. We will also provide your treatment codes and their meanings, if they do not appear on this
statement. If you have questions about your diagnosis or your treatment, please contact your provider. [H63]
(1)
Your benet balances to date
Description
Individual
Annual
Amount
Jane (self)
Medical In Network Deductible
Medical In Network Coinsurance
Medical Out of Network Deductible
$1,700.00
$6,450.00
$7,000.00
$695.77
$695.77
$0.00
limit
used
Medical Out of Network Coinsurance $12,000.00 $0.00
for 1/1/16 to 12/31/16
Amount
$1,004.23
$5754.23
$7000.00
remaining
$12,000.00
A complete list of your benet balances and plan limits can be found on your secure member website.
a
Statement date: October 15, 2016
Member: Jane H Doe
Member ID: W123456789
Group#:
0987654-10-001 A P1 (*TO
Group name: Test INC
Your Payment Summary
Your plan paid You owe or already paid
Patient Provider Amount Send Date Amount Sent to
Jane (self)
Total:
John Roe $244.88
$244.88
John Roe 10/16/16 $0.00
$0.00
Your claims up close
Claim for Jane (self)
Claim ID: E00000000OO Amount Member Pending or Applied to
Your Amount
Plan
Your
You may
Received on 9/31/16 billed rate not payable deductible
copay
remaining
pays
coinsurance
owe
(Remarks)
X-RAY EXAM OF LOWER
SPINE on 9/31/16
72110
X-RAY EXAM NECK SPINE
4/5VWS on 9/31/16
GOOO8
John Roe
Refer to Remarks Section
Totals:
269.00
539.00
A
270.00
244.88
B
121.57
123.31
(1)
C D E
123.31
121.57
244.88
F
123.31 (100%)
121.57 (100%)
244.88
G H I
You can nd all numbered claim remarks in ‘Your Claim Remarks’ section.
Page 2 of 4
!
!
C+D+E+H=I
Your Claim Remarks
General Remarks:
Your provider may have sent diagnosis codes with your claim. You may obtain these codes and their meanings by contacting us at the
number listed at the top of the rst page. We will also provide your treatment codes and their meanings, if they do not appear on this
statement. If you have questions about your diagnosis or your treatment, please contact your provider. [H63]
(1)
Your benet balances to date
Description
Individual
Annual
Amount
Jane (self)
Medical In Network Deductible
Medical In Network Coinsurance
Medical Out of Network Deductible
$1,700.00
$6,450.00
$7,000.00
$695.77
$695.77
$0.00
limit
used
Medical Out of Network Coinsurance $12,000.00 $0.00
for 1/1/16 to 12/31/16
Amount
$1,004.23
$5754.23
$7000.00
remaining
$12,000.00
A complete list of your benet balances and plan limits can be found on your secure member website.
SAMPLE
