Jonathan Watson, MD
REHABILITATION PROTOCOL- Nonoperative Achilles tendon rupture
The rehabilitation guidelines are presented in a criterion based progression program. General time frames are given for
reference to the average, but individual patients will progress at different rates depending on their age, associated injuries,
pre-injury health status, rehab compliance, tissue quality and injury severity. Specific time frames, restrictions, and
precautions may also be given to protect healing tissues and the surgical repair/reconstruction. It should not be a substitute
for one’s clinical decision making regarding the progression of a patient’s post-operative course based on their physical exam
findings, individual progress, and/or the presence of post-operative complications. The therapist should consult the referring
physician with any questions or concerns.
Special attention must be given to impairments that caused the initial problem. For example, if the patient is s/p partial medial
meniscectomy and they have a varus alignment, post-operative rehabilitation should include correcting muscle imbalances or
postures that create medial compartment stress.
INDIVIDUAL CONSIDERATIONS: S/p
_________________________________________________________________________________
_________________________________________
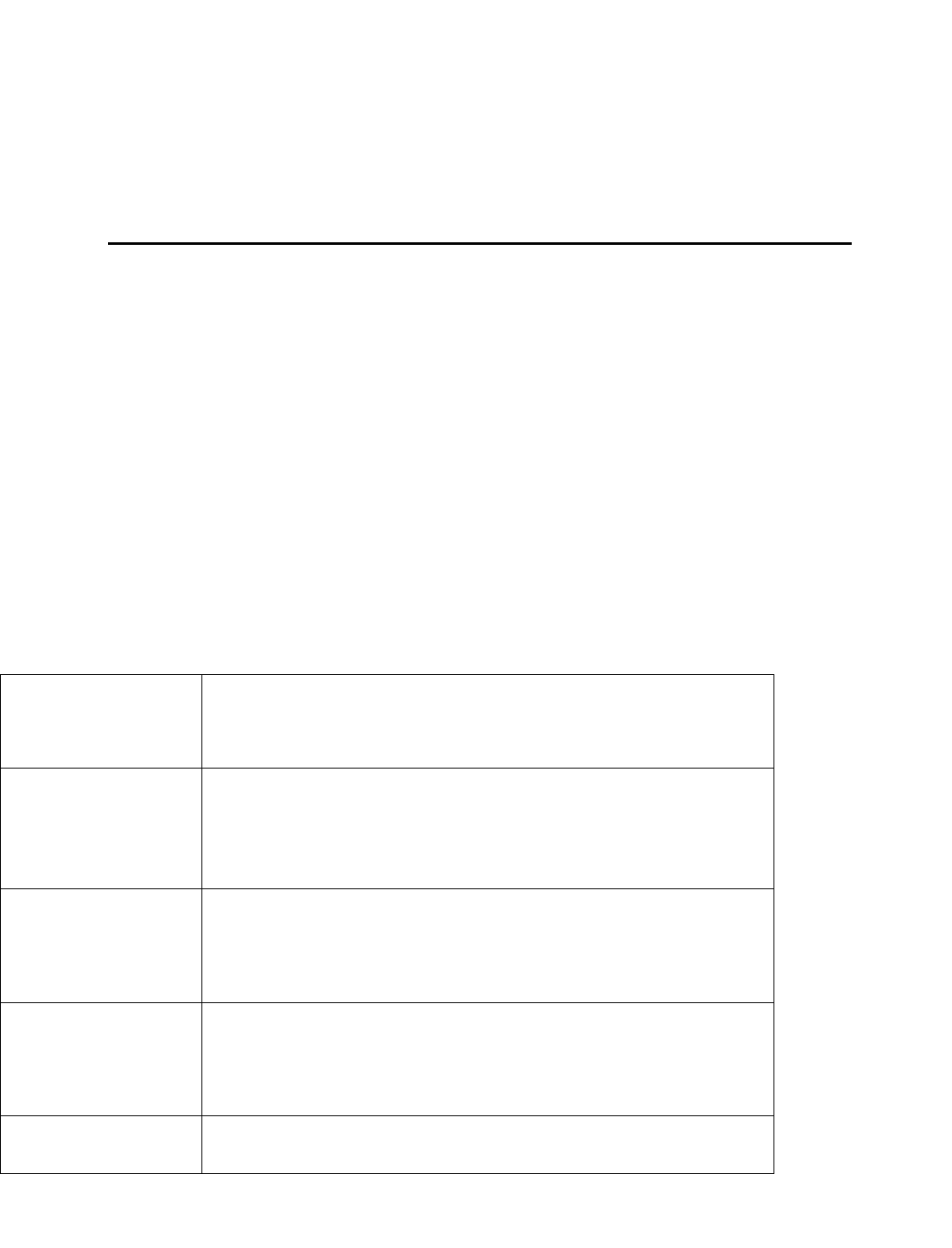
PHASE 1- ~10 days to 4 weeks
REHAB GOALS
1.
Protection
of the tendon
2.
Decrease pain & inflammation
3.
Gait training with crutches
PRECAUTIONS
1
.
Crutches and non-weight bearing with CAM boot in 20 degrees of
plantarflexion
2. No dorsiflexion past neutral until week 4.
3. Cryocuff 3-5 times per day for 20 minutes and ice after every therapy
RANGE OF
MOTION
EXERCISES
o Toe spreads & curls
o ROM starting day 10-14
o Active dorsiflexion to neutral
o Passive plantarflexion as tolerated
o Hip ROM as tolerated
SUGGESTED
THERAPEUTIC
EXERCISES
o 4 way SLRs
o Core strengthening
o Knee extension/flexion
o At 2 weeks- submax isometric contraction of the posterior lower
leg & achilles
CARDIOVASCULAR
EXERCISE
Upper body circuit training or UBE.
PROGRESSION
CRITERIA
o Minimal pain & swelling
o Good quad set, able to perform SLR without lag
o Wound healing, no sign of infection
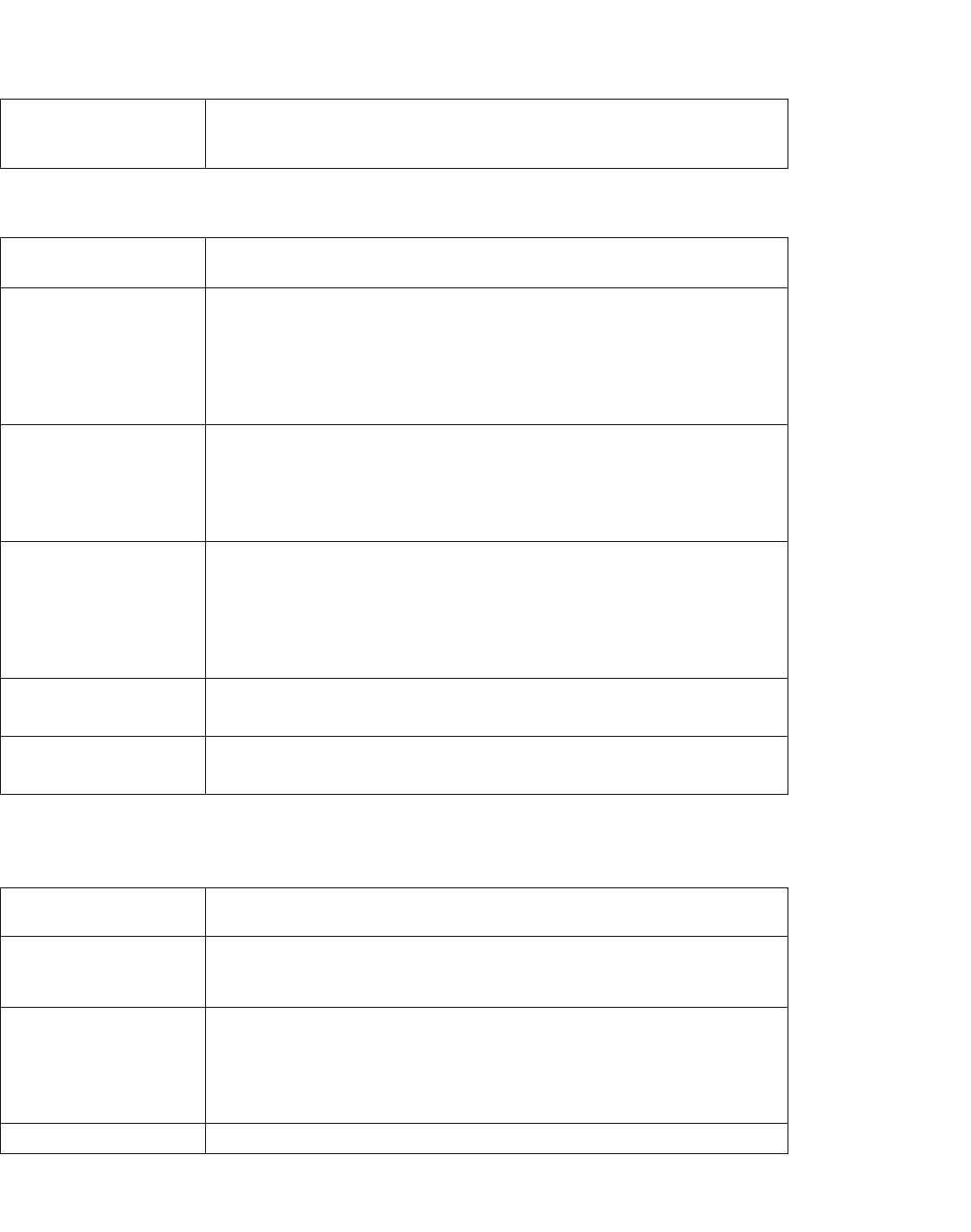
PHASE 2- 5-8 weeks
REHAB GOALS
1
.
Advance weight bearing
2. Minimize pain and swelling
PRECAUTIONS
1.
Crutches and progress to full weight bearing in CAM boot with 2-3cm
lift. Discontinue crutches when walking with boot and normal gait.
2.
No dorsiflexion past 10 degrees
3.
Cryocuff 3-5 times per day for 20 minutes and ice after every therapy
session
RANGE OF
MOTION
EXERCISES
o Continue phase 1 exercises
o Active dorsiflexion to 10, passive plantarflexion as tolerated
o Active assist, active plantar flexion, inversion, eversion
SUGGESTED
THERAPEUTIC
EXERCISES
o Continue phase 1 exercises
o Static lunge with involved leg, gravity reduced squats, wall
squats/leg press (no DF past neutral)
o Core-planks
o Gentle resistance band plantarflexion
o Weight shifts if no pain
CARDIOVASCULAR
EXERCISE
Upper body circuit training (seated), core strengthening or UBE
PROGRESSION
CRITERIA
o Active dorsiflexion to 10, normal ROM otherwise
o Pain free full weight bearing
PHASE 3- 9-12 weeks
REHAB GOALS
o
Restore normal gait
o
Maintain/restore full ROM
PRECAUTIONS
o
Continue ice after PT
o
D/c CAM boot. Wear 1cm heel lift in shoe.
o
Avoid post activity swelling
RANGE OF
MOTION
EXERCISES
o
Continue exercises from phase 2.
o
Soft tissue/scar mobilizations as needed
o
Progress DF stretching to equal contralateral
SUGGESTED
o
Continue phase 2 exercises
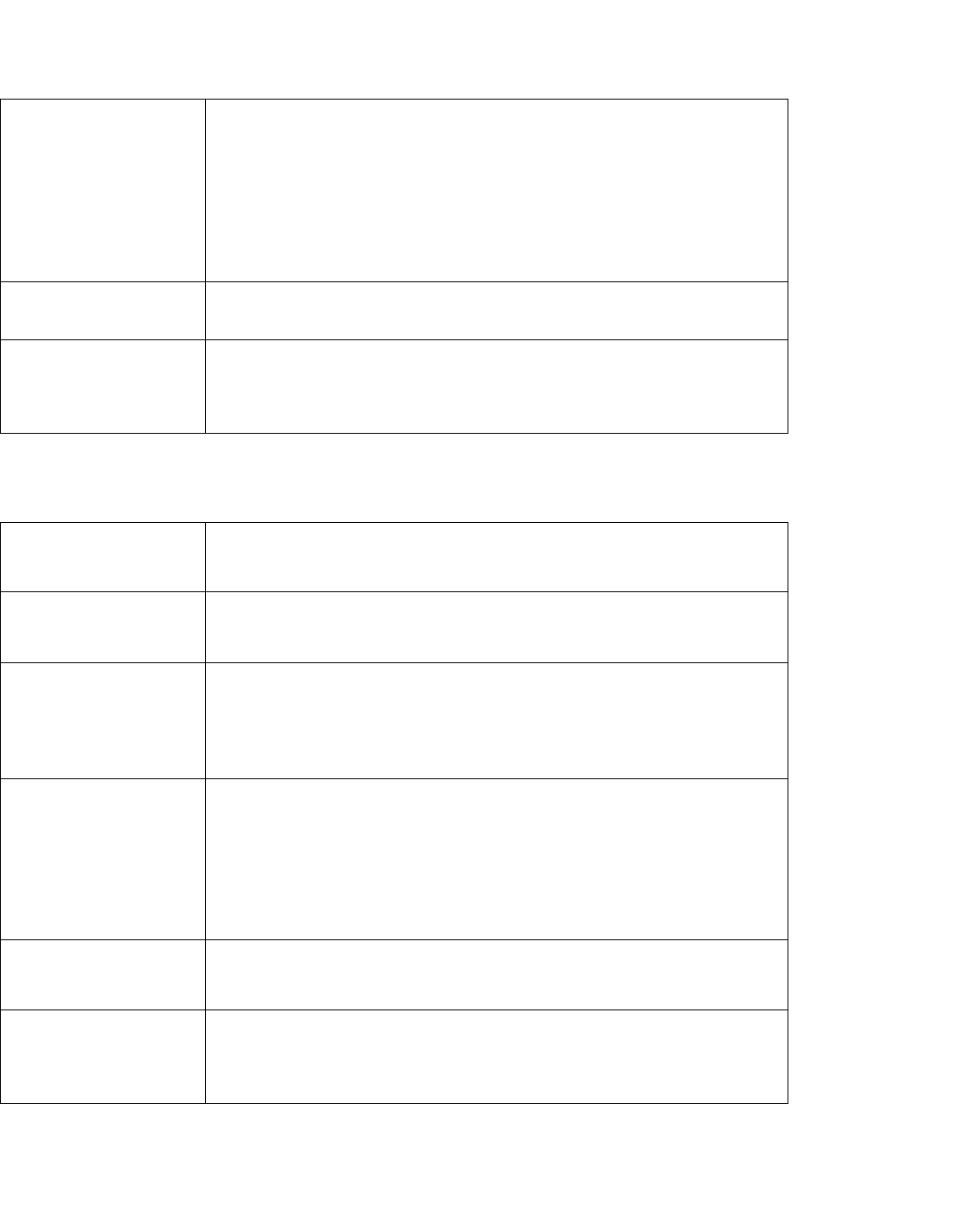
THERAPEUTIC
EXERCISES
o
LE- deadlift, straight leg deadlifts. Step ups, step downs.
o
Ankle- seated heel & toe raises. Progress to bilateral heel raises
with most weight on uninvolved leg, progress to equal weight
distribution. Low level eccentric strengthening. Week 11- can
progress heel rise to single leg
o
Gait training
o
Balance/proprioception- standing double leg stance, progress
to single leg
CARDIOVASCULAR
EXERCISE
Continue phase 2
Stationary bike if in athletic shoe
PROGRESSION
CRITERIA
o
Full ankle ROM
o
Able to perform single leg calf raise
o
5/5 proximal LE strength
o
Symmetrical unilateral stance
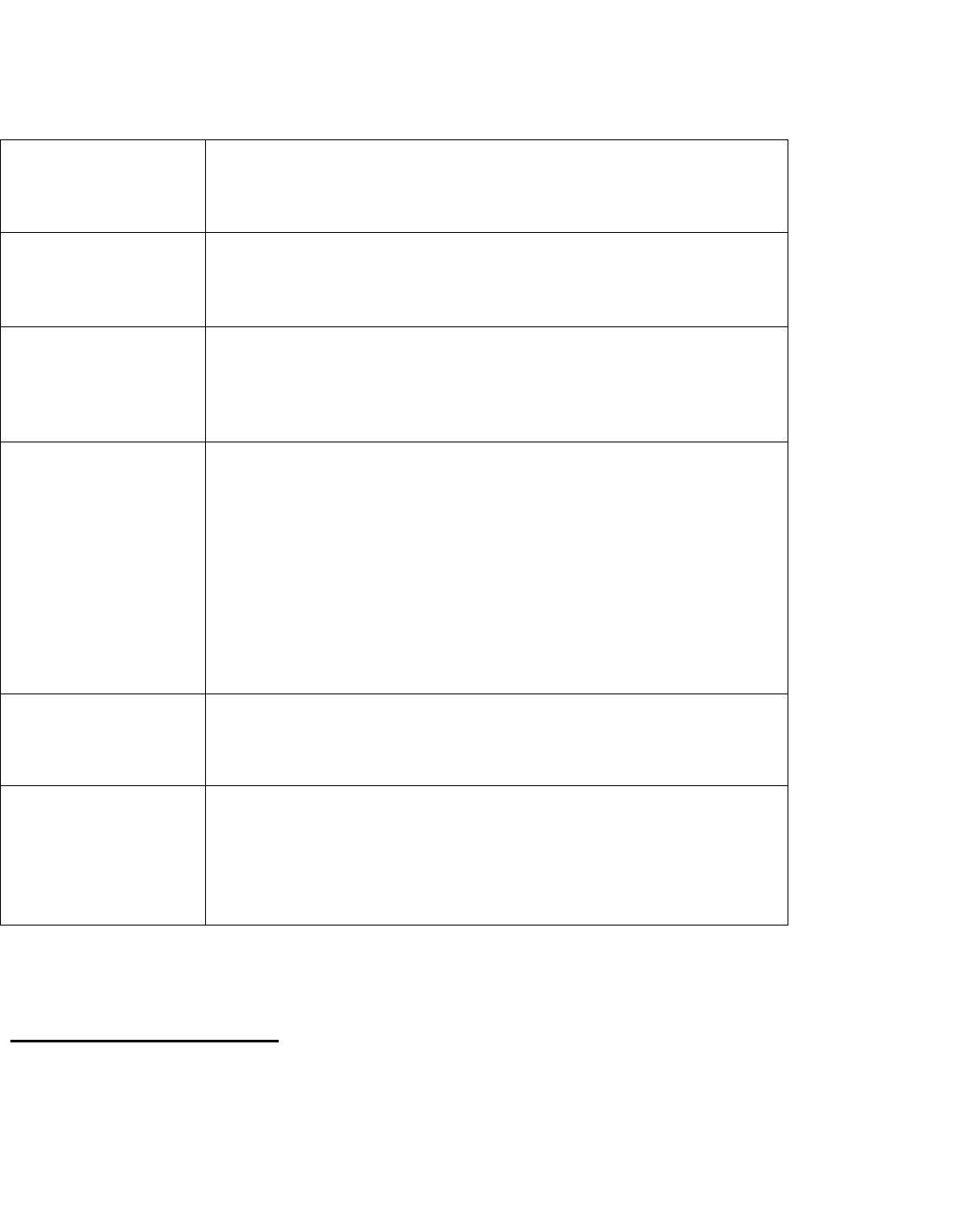
PHASE 4- 13-16 weeks
REHAB GOALS
o Restore/maintain full ROM
o Restore normal gait
o Progress strengthening
PRECAUTIONS
Post-activity soreness should resolve within 24
h
o
u
rs
Avoid post activity
s
w
el
l
in
g
Continue ice after PT
RANGE OF
MOTION
EXERCISES
Continue with flexibility exercises
Hip, IT band stretching & sport specific stretches
SUGGESTED
THERAPEUTIC
EXERCISES
o Progress phase 3 activities with resistance/weight
o LE- squats, lunges, leg press
o Core- wood chopper, diagonal chop, lift pattern
o Balance/proprioception- progress single leg activities to include
simultaneous upper body skills
o Plyometrics- week 16- gravity reduced plyometrics if able to
perform 10-15 single leg heel rises without pain
CARDIOVASCULAR
EXERCISE
Continue previous phase exercises
Aqua therapy- form walking, jogging, jumping/hopping
Elliptical
PROGRESSION
CRITERIA
o
No pain/swelling
o
Full ROM
o
Able to perform single leg heel raise
o
No issue with initiation of jogging
PHASE 5- 17-24 weeks
REHAB GOALS
o No pain/swelling
o Full ROM
o Progress in strengthening, agility & jogging
o Return to sport/activity
PRECAUTIONS
Post-activity soreness should resolve within 24
h
o
u
rs
Avoid post activity
s
w
el
l
in
g
Continue ice after activity
RANGE OF
MOTION
EXERCISES
Continue with flexibility exercises
SUGGESTED
THERAPEUTIC
EXERCISES
o Progress strengthening from phase 4
o LE- front squats, multiplane lunges, deadlifts, power cleans
o Ankle- continue to progress weight/resistance
o Balance/neuromuscular- continue to progress and advance
difficulty, add unstable surface, perturbations, etc
o Agility training- LE drills in controlled environment (figure 8
jogging, side shuffles, cutting) if jogging tolerated. Start with 50%
effort, progress slowly to 100%. When beginner activities tolerated
progress to form running, ladders, reactionary drills, start low
intensity.
o Plyometrics- Dry land jumping, progress to multi plane,
CARDIOVASCULAR
EXERCISE
o Continue from phase 4
o Ok to do jog/run progression at week 20 if: no gait deviation with
jogging, able to jog 2 miles without gait deviation, pain or swelling
afterward.
PROGRESSION
CRITERIA
o
No pain/swelling
o
Full ROM symmetrical
o
Single leg heel rise 90% of contralateral (reps to failure)
o
Hop test limb symmetry at least 90%
o
Completion of sport specific program, return to sport test
o
Physician clearance
RETURN TO SPORT TEST
o 10 rep max single leg squat with external weight
o Single broad jump landing on one foot
o Triple broad jump landing on one foot
o Single leg forward hop

o Single leg crossover hop
o Single leg medial and lateral hop
o Single leg medial and lateral rotating hop
o Single leg vertical hop
o Single leg triple hop
o Timed 6 meter hop
o 10 yard lower extremity functional test
10 yard pro agility run
