John Holahan and Michael Karpman
August 2019
AT A GLANCE
◼
Many adults are ambivalent about (neither support nor oppose) Medicare for All and other
proposals to expand health insurance coverage, though support for these proposals tends to be
greater than opposition.
◼
Young adults, nonwhite and Hispanic adults, those with low incomes, and those without private
health insurance are more likely to support than oppose Medicare for All. Those who neither
support nor oppose Medicare for All share many of these characteristics.
◼
Medicare for All supporters and opponents have different perceptions of how it will affect access
to care, with the perceptions of those who are ambivalent about the policy closer to those of
supporters.
◼
Medicare for All supporters cite universal health coverage and greater affordability as important
factors in their support. Higher taxes and concerns about wait times to see health care providers
and quality of care are more important to Medicare for All opponents.
Though support for the Affordable Care Act has grown in recent years,
1
ongoing concerns about
continuing affordability and coverage gaps, as well as political efforts to undermine the law or even
repeal it, have generated growing interest in single-payer plans, often known as Medicare for All.
Typically, a single-payer approach would establish a single government-run insurance plan in which the
entire US population would be enrolled; the costs associated with the coverage would be fully
government financed. Such approaches have been shown to significantly increase federal taxes
(Blahous 2018; Holahan et al. 2016; Liu and Eibner 2019),
2
but proponents argue that these costs would
H E A L T H R EFO R M M O N I T O R I N G S U R V E Y
What Explains Support for or
Opposition to Medicare for All?

2
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
be offset by eliminating employer and household premiums and cost sharing (Pollin et al. 2018).
Opponents raise concerns over access to and quality of care.
The Medicare for All approach was first given prominence in the 2016 presidential election cycle by
Senator Bernie Sanders; similar proposals have since been proposed or endorsed by several members of
Congress, including candidates competing for the 2020 Democratic presidential nomination.
Given concerns about Medicare for All approaches, some propose incremental reforms. These
include increasing the Affordable Care Act’s premium and out-of-pocket cost subsidies and adding a
public plan option to all or some private insurance markets. These approaches would require smaller
increases in government revenues and be less disruptive but are less likely to achieve universal
coverage.
In this brief, we assess public support for both Medicare for All proposals and some incremental
reforms. We examine support for and opposition to Medicare for All among people with different
characteristics, as well as important factors to adults who support, oppose, or are ambivalent toward
Medicare for All.
What We Did
We used data from the March 2019 round of the Health Reform Monitoring Survey (HRMS), a
nationally representative, internet-based survey of nonelderly adults.
3
Approximately half of the 9,596
respondents who participated in the survey were randomly asked questions about whether they would
support, oppose, or neither support nor oppose four approaches for expanding health insurance
coverage. The questions were presented to respondents in a randomized order. The four approaches
were
1. making health insurance coverage more affordable by increasing the amount of subsidies to
lower the premiums and out-of-pocket costs for some health insurance plans,
2. giving all Americans the option of enrolling in a government-run health insurance plan that
would be similar to Medicare (i.e., a “public option”),
3. enrolling all Americans in a single government-run health insurance plan that would be similar
to Medicare as part of a new national health insurance program (i.e., Medicare for All), and
4. enrolling all Americans in either a government-run plan that would be similar to Medicare or a
private health insurance plan as part of a new national health insurance program.
4
The 4,793 respondents who were asked these questions were then randomly assigned to questions
designed to collect additional information about their perceptions of Medicare for All. These questions
focused on
◼
perceptions about whether the respondent’s access to care would be better, about the same, or
worse under Medicare for All;

W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
3
◼
perceptions about whether the respondent’s out-of-pocket health care costs, premiums, and
federal taxes would be higher, about the same, or lower under Medicare for All; and
◼
factors that were important to the respondent in deciding whether to support Medicare for All.
We assessed support for all four approaches for expanding health insurance among all respondents
and by political party affiliation. We also examined support for Medicare for All by age, race/ethnicity,
educational attainment, family income as a percentage of the federal poverty level (FPL), census region,
and health insurance coverage at the time of the survey (i.e., private, public, and uninsured). We also
compared perceptions of how access to care and taxes would change and which factors were important
in deciding whether to support a national health insurance program among Medicare for All supporters,
opponents, and those who neither support nor oppose this approach.
Estimates of support and opposition to Medicare for All and other proposals to expand health
insurance coverage are not directly comparable to estimates from other polls, such as those conducted
by the Henry J. Kaiser Family Foundation, because of differences in the populations surveyed as well as
the response scales used in the survey questions. The HRMS included an option to select “neither
support nor oppose,” whereas other polls present a binary choice between support and opposition and
follow up to measure the intensity of that support or opposition. The inclusion of a neutral option in the
HRMS captures more ambivalence about Medicare for All and other proposals than would be suggested
by polls using a forced-choice approach, but does not fully capture weaker levels of support and
opposition.
What We Found
Many adults are ambivalent about (neither support nor oppose) Medicare for All and other proposals to expand
health insurance coverage, though support for these proposals tends to be greater than opposition.
Overall, about half of adults reported that they neither supported nor opposed increasing premium
subsidies, and a plurality neither supported nor opposed a public option, Medicare for All,
5
or a national
health insurance program including both private and public health insurance (table 1), suggesting
substantial ambivalence about these policies. That ambivalence may reflect uncertainty about the
policies or what they imply, given the relatively low levels of health insurance literacy among many
Americans (Long et al. 2014). Adults were more likely to support than oppose the two incremental
approaches (i.e., increased subsidies and the public option) and a national health insurance program
with both public and private insurance, but they were more evenly divided in their support for versus
opposition to Medicare for All.
4
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
TABLE 1
Support for Proposals to Expand Health Insurance Coverage among Adults Ages 18 to 64,
Overall and by Political Party Affiliation, March 2019
All adults
Democrat or
leans Democratic
Republican or
leans Republican
Increase subsidies to lower premiums and out-of-
pocket costs
Supports
30.3%
38.6%
20.9%***
Neither supports nor opposes
51.4%^^^
51.2%^^^
48.8%^^^
Opposes
16.5%^^^
8.4%^^^
28.6%^^^***
Give all Americans the option to enroll in a
government-run health plan (public option)
Supports
32.8%
42.3%
20.4%***
Neither supports nor opposes
45.0%^^^
45.7%
40.7%^^^***
Opposes
20.5%^^^
10.0%^^^
37.6%^^^***
Enroll all Americans in a single government-run
health plan (Medicare for All)
Supports
29.8%
42.3%
13.3%***
Neither supports nor opposes
40.7%^^^
43.5%
32.6%^^^***
Opposes
27.8%
12.3%^^^
52.8%^^^***
Enroll all Americans in a government-run or
private health plan as part of a new national
health insurance program
Supports
28.2%
38.3%
16.5%***
Neither supports nor opposes
46.2%^^^
48.3%^^^
38.8%^^^***
Opposes
24.1%^^
11.6%^^^
44.0%^^^***
Sample size
4,793
2,420
1,970
Source: Health Reform Monitoring Survey, quarter 1 2019.
Notes: Estimates not shown for adults whose political party affiliation is independent, undecided, other, or not reported (less than
5 percent of the sample), though these respondents are included in the estimates for all adults. Estimates not shown for the share
of adults (less than 2 percent) who did not report whether they supported or opposed each proposal.
*/**/*** Estimate differs significantly from adults who are Democrats or lean Democratic at the 0.10/0.05/0.01 level, using two-
tailed tests.
^/^^/^^^ Estimate differs significantly from share of adults who support the proposal at the 0.10/0.05/0.01 level, using two-tailed
tests.
Table 1 also shows the support by political party for various approaches designed to expand health
coverage. More than one-third (38.6 percent) of those who report being a Democrat or leaning
Democratic (hereafter collectively referred to as Democrats) supported increasing subsidies to reduce
premiums and out-of-pocket costs, versus 20.9 percent of Republicans or those who lean Republican
(hereafter collectively referred to as Republicans). On the other hand, 28.6 percent of Republicans
opposed this proposal, compared with 8.4 percent of Democrats. About half of each group neither
supported nor opposed increasing subsidies, suggesting extensive ambivalence among both
Republicans and Democrats.
When asked about giving all Americans the option to enroll in a government-run health plan (i.e., a
public option), Democrats were far more likely to express support than Republicans (42.3 percent
versus 20.4 percent). Fewer people were ambivalent about this policy than about increasing subsidies.

W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
5
Republicans were far more likely than Democrats to oppose a public option (37.6 percent versus 10.0
percent) and were less likely than Democrats to report ambivalence toward this proposal (40.7 percent
versus 45.7 percent).
When asked about support for or opposition to enrolling all Americans in a single government-run
health plan, as would be the case under Medicare for All, 42.3 percent of Democrats expressed support
versus 13.3 percent of Republicans. On the other hand, 52.8 percent of Republicans opposed Medicare
for All versus 12.3 percent of Democrats. Democrats were more likely to neither support nor oppose
Medicare for All than were Republicans (43.5 percent versus 32.6 percent).
Republicans were less likely to oppose enrolling all Americans in a government-run or private
health plan as part of a new national health insurance program (a variant of Medicare for All) than
enrolling all Americans in a single government-run health plan (i.e., Medicare for All). Still, 44.0 percent
of Republicans opposed this approach, compared with 11.6 percent of Democrats. Democrats were
more likely to support this option than Republicans (38.3 percent versus 16.5 percent). That more
people were ambivalent about this proposal than a fully government-run plan may reflect respondents’
difficulty envisioning how this proposal would work or confusion about what the policies would be.
Young adults, nonwhite and Hispanic adults, those with low incomes, and those without private health
insurance are more likely to support than oppose Medicare for All. Those who neither support nor oppose
Medicare for All share many of these characteristics.
Table 2 shows the share of respondents who support, oppose, or neither support nor oppose
Medicare for All by selected characteristics. Considerably more people reported neither supporting nor
opposing Medicare for All than took a clear position of support or opposition. Of those with an opinion,
respondents ages 18 to 34 were substantially more likely to support than oppose (33.3 percent versus
24.1 percent). The middle age group, ages 35 to 49, were slightly more likely to support than oppose
(29.3 percent versus 25.8 percent), though this difference was not statistically significant. The oldest
group, ages 50 to 64, were more likely to oppose than support (33.5 percent versus 26.5 percent).

6
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
TABLE 2
Support for Medicare for All among Adults Ages 18 to 64, Overall and by Demographic,
Socioeconomic, and Geographic Characteristics, March 2019
Share that
supports (%)
Share that neither
supports nor
opposes (%)
Share that
opposes (%)
Sample size
All adults
29.8
40.7***
27.8^^^
4,793
Ages
18–34
33.3
39.8**
24.1***^^^
1,075
35–49
29.3
43.6***
25.8^^^
1,447
50–64
26.5
39.0***
33.5**^
2,271
Race/ethnicity
Non-Hispanic white
28.0
35.6***
35.3***
3,320
Non-Hispanic black
31.2
55.6***
12.3***^^^
408
Other or more than one
race, non-Hispanic
39.5
35.0
21.9***^^^
351
Hispanic
29.9
50.4***
16.1***^^^
714
Educational attainment
Less than high school
23.7
63.5***
11.1***^^^
315
High school graduate
27.2
47.3***
23.2^^^
1,111
Some college
27.8
38.8***
31.5^^
1,370
College graduate or more
education
35.6
29.5***
33.8
1,997
Family income
At or below 138% FPL
29.1
54.2***
14.9***^^^
880
139%–399% FPL
29.7
41.3***
26.6^^^
1,800
400% FPL or higher
30.3
32.2
36.4**^
2,113
Region
Northeast
29.5
42.7***
26.7^^^
874
Midwest
31.3
38.4**
28.8^^^
1,156
South
27.9
40.5***
29.8^^^
1,634
West
31.8
41.5***
24.5**^^^
1,129
Health insurance coverage
at time of survey
Private
28.7
36.6***
33.1*
3,636
Public
32.6
50.6***
15.3***^^^
659
Uninsured
36.3
47.1**
14.1***^^^
374
Source: Health Reform Monitoring Survey, quarter 1 2019.
Note: FPL is federal poverty level. Estimates not shown for the share of adults (less than 2 percent) who did not report whether
they supported or opposed each proposal.
*/**/*** Share differs significantly from share that supports at the 0.10/0.05/0.01 level, using two-tailed tests.
^/^^/^^^ Share differs significantly from share that neither supports nor opposes at the 0.10/0.05/0.01 level, using two-tailed
tests.
Non-Hispanic whites were more likely to oppose than support Medicare for All (35.3 percent versus
28.0 percent). However, non-Hispanic blacks and Hispanics were significantly more likely to support
than oppose (31.2 percent versus 12.3 percent for non-Hispanic blacks; 29.9 percent versus 16.1
percent for Hispanics). A majority of both groups neither supported nor opposed. Support was also
greater than opposition among non-Hispanic adults of another race or more than one race.

W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
7
Those who did not complete high school were more likely to support Medicare for All than oppose.
Among those with only a high school degree or some college education, the share supporting was not
statistically different from the share opposing. Those who had a college degree or more education were
also evenly split (35.6 percent supporting versus 33.8 percent opposing). The share that neither
supported nor opposed was highest among the less educated (63.5 percent) and lowest among the most
educated (29.5 percent).
The lowest-income group, with incomes at or below 138 percent of FPL, were more likely to support
than oppose Medicare for All (29.1 percent versus 14.9 percent), though more than half of this group
(54.2 percent) neither supported nor opposed. Those with incomes between 139 percent and 399
percent of FPL were equally split between support and opposition, though, again, a large percentage
(41.3 percent) had no opinion. Of those with incomes of 400 percent of FPL or higher, more opposed
than supported (36.4 percent versus 30.3 percent).
By region, the shares of people in the Northeast, Midwest, and South who supported Medicare for
All were not statistically different from the shares that opposed. Those who live in the West were
significantly more likely to support than oppose (31.8 percent versus 24.5 percent).
Those who had private insurance were slightly more likely to oppose than support (33.1 percent
versus 28.7 percent). Those who were uninsured or had public coverage (mostly Medicaid) were more
likely to support than oppose but also more likely to have no opinion.
Though slightly more people support than oppose Medicare for All (29.8 percent versus 27.8
percent; not significant), the largest percentage neither supports nor opposes. Table 2 shows that the
latter group’s demographic and socioeconomic characteristics are similar to those of Medicare for All
supporters (e.g., racial and ethnic minorities, low income, and low education levels). This suggests the
numbers could eventually tilt in favor of support.
Medicare for All supporters and opponents have different perceptions of how it will affect access to care, with
the perceptions of those who are ambivalent about the policy closer to those of supporters.
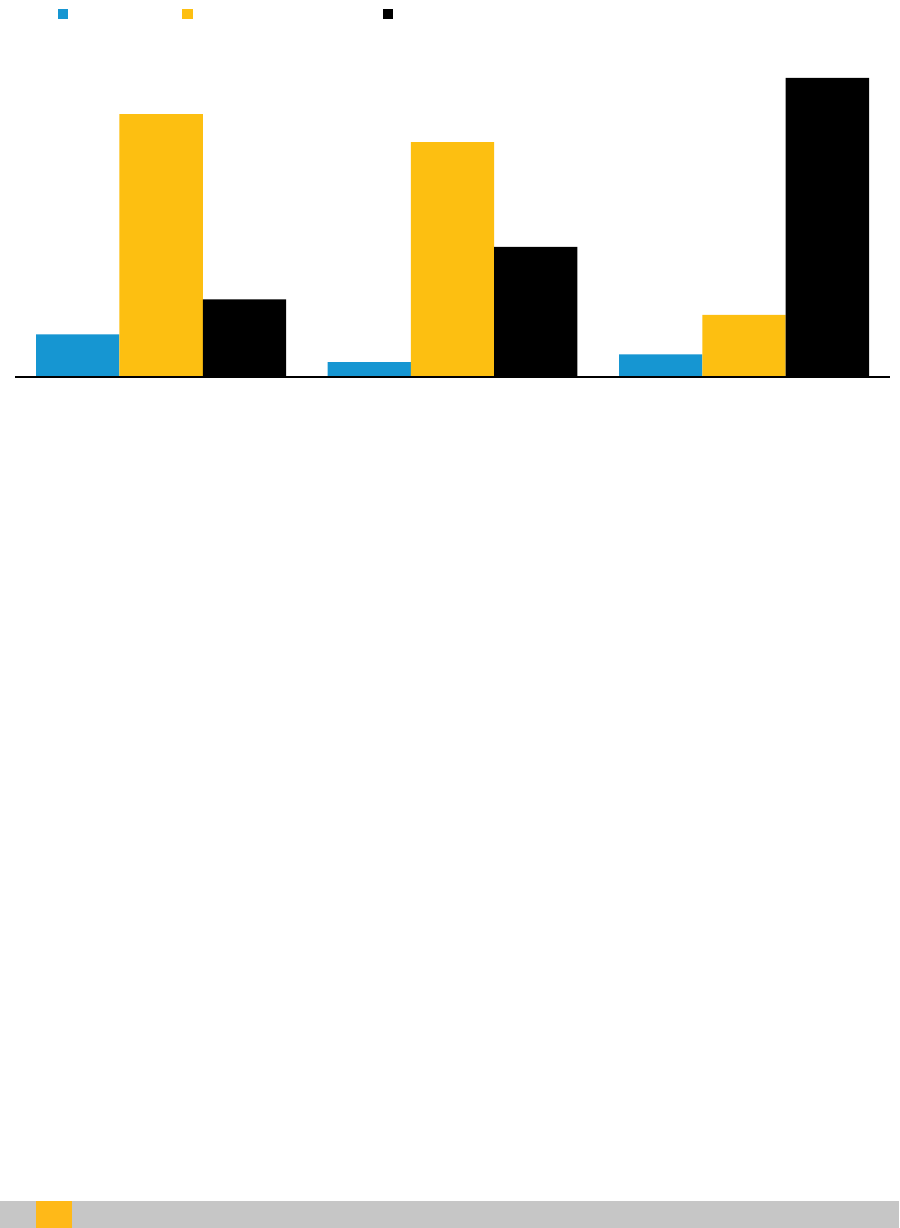
Of those who support Medicare for All, 11.0 percent thought wait times to see a doctor or other
providers would improve, 69 percent thought they would remain the same, and only about 20 percent
thought they would worsen under Medicare for All (figure 1). In contrast, 78.1 percent of Medicare for
All opponents thought wait times to see a doctor or other providers would worsen.
8
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
FIGURE 1
Perceptions of the Effects of Medicare for All on Wait Times to See Doctors and Other Providers,
among Adults Ages 18 to 64, March 2019
URBAN IN ST IT U TE
Source: Health Reform Monitoring Survey, quarter 1 2019.
Notes: Generally, less than 1 percent of respondents did not report their perceptions of the effects of Medicare for All.
*/**/*** Estimate differs significantly from perceptions of supporters at the 0.10/0.05/0.01 level, using two-tailed tests.
Of those who supported Medicare for All, 24.1 percent were more likely to think they would have a
better choice of providers under Medicare for All and about 62.6 percent thought provider choice
would be about the same (figure 2). For those who oppose the approach, 22.6 percent thought provider
choice would be about the same and 69.5 percent thought it would worsen.
11.0%
3.7%***
5.8%**
68.6%
61.3%*
16.1%***
20.2%
33.9%***
78.1%***
Supports Medicare for All Neither supports nor opposes
Medicare for All
Opposes Medicare for All
Better About the same Worse

W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
9
FIGURE 2
Perceptions of the Effects of Medicare for All on Choice of Doctors and Other Providers,
among Adults Ages 18 to 64, March 2019
URBAN IN ST IT U TE
Source: Health Reform Monitoring Survey, quarter 1 2019.
Notes: Generally, less than 1 percent of respondents did not report their perceptions of the effects of Medicare for All.
*/**/*** Estimate differs significantly from perceptions of supporters at the 0.10/0.05/0.01 level, using two-tailed tests.
When asked about the quality of care under Medicare for All, 23.6 percent of those who support
the strategy thought it would improve and 67.2 percent thought it would be about the same (figure 3).
Of those who oppose Medicare for All, 69.9 percent reported that they believed quality of care would
worsen.
24.1%
6.3%***
7.5%***
62.6%
66.0%
22.6%***
13.0%
26.2%***
69.5%***
Supports Medicare for All Neither supports nor opposes
Medicare for All
Opposes Medicare for All
Better About the same Worse

10
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
FIGURE 3
Perceptions of the Effects of Medicare for All on the Quality of Health Care,
among Adults Ages 18 to 64, March 2019
URBAN IN ST IT U TE
Source: Health Reform Monitoring Survey, quarter 1 2019.
Notes: Generally, less than 1 percent of respondents did not report their perceptions of the effects of Medicare for All.
*/**/*** Estimate differs significantly from perceptions of supporters at the 0.10/0.05/0.01 level, using two-tailed tests.
When asked about the ability to get needed care under Medicare for All, 31.9 percent of Medicare
for All supporters thought it would get better and 57.1 percent thought it would be the same (figure 4).
Of those who oppose the approach, 72.1 percent thought it would worsen and 19.7 percent thought it
would be about the same.
23.6%
5.8%***
5.6%***
67.2%
70.3%
23.9%***
8.6%
21.9%***
69.9%***
Supports Medicare for All Neither supports nor opposes
Medicare for All
Opposes Medicare for All
Better About the same Worse

W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
11
FIGURE 4
Perceptions of the Effects of Medicare for All on Ability to Get Needed Care,
among Adults Ages 18 to 64, March 2019
URBAN IN ST IT U TE
Source: Health Reform Monitoring Survey, quarter 1 2019.
Notes: Generally, less than 1 percent of respondents did not report their perceptions of the effects of Medicare for All.
*/**/*** Estimate differs significantly from perceptions of supporters at the 0.10/0.05/0.01 level, using two-tailed tests.
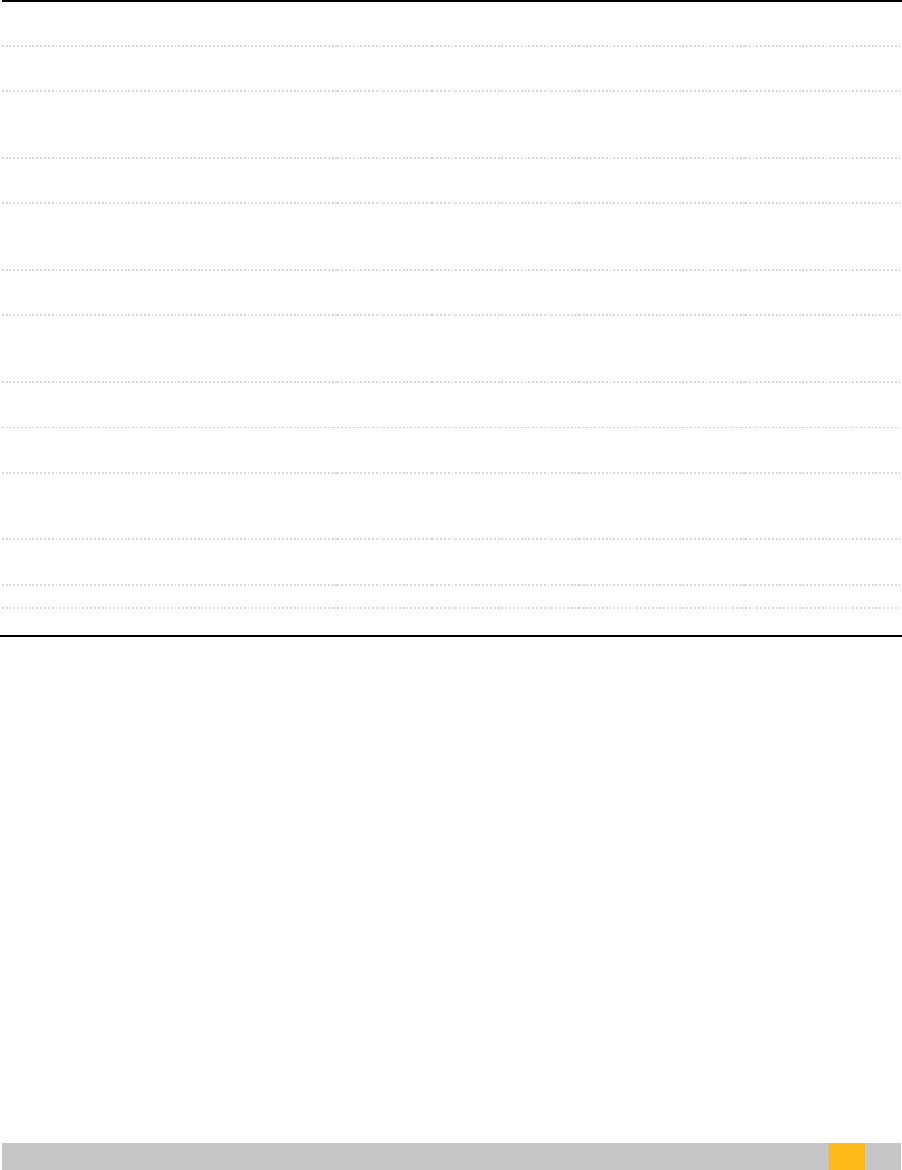
We also asked about the impact of Medicare for All on federal taxes. Of those who supported
Medicare for All, a slight majority, 52.3 percent, expected to pay higher taxes, and 33.1 percent thought
their taxes would be about the same (figure 5). In contrast, 85.8 percent of Medicare for All opponents
thought they would pay higher taxes.
31.9%
8.7%***
8.1%***
57.1%
67.0%**
19.7%***
10.1%
22.0%***
72.1%***
Supports Medicare for All Neither supports nor opposes
Medicare for All
Opposes Medicare for All
Better About the same Worse

12
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
FIGURE 5
Perceptions of the Effects of Medicare for All on Federal Taxes Owed,
among Adults Ages 18 to 64, March 2019
URBAN IN ST IT U TE
Source: Health Reform Monitoring Survey, quarter 1 2019.
Notes: Generally, less than 1 percent of respondents did not report their perceptions of the effects of Medicare for All.
*/**/*** Estimate differs significantly from perceptions of supporters at the 0.10/0.05/0.01 level, using two-tailed tests.
Medicare for All supporters cite universal health coverage and greater affordability as important factors in their
support. Higher taxes and concerns about wait times to see health care providers and quality of care are more
important to Medicare for All opponents.
Finally, table 3 shows responses to questions about factors that affected respondents’ support for
or opposition to Medicare for All. About 90 percent or more of Medicare for All supporters cited the
following as important factors in their decisions to support the approach: everyone would have health
insurance coverage, people would pay little to no out-of-pocket costs when they used services, people
would pay lower premiums, the health system would be simpler, and the government would have
greater ability to reduce health care costs. Another 75.6 percent reported reduced administrative
health care costs as an important factor.
52.3%
44.6%**
85.8%***
33.1%
41.7%**
9.6%***
14.3%
11.3%
2.2%***
Supports Medicare for All Neither supports nor opposes
Medicare for All
Opposes Medicare for All
Higher About the same Lower
W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
13
TABLE 3
Important Factors in Deciding Whether to Support Medicare for All among Adults Ages 18 to 64,
Overall and by Support for Medicare for All, March 2019
All
adults
Supports
Neither supports
nor opposes
Opposes
Most people would not be able to keep
their current insurance coverage
64.2%
52.9%
66.2%***
73.6%***
Everyone would have health insurance
coverage
68.6%
91.0%
69.3%***
45.0%***
People would pay little or no out-of-
pocket costs when they use health care
services
72.8%
92.6%
72.5%***
54.1%***
Most people would pay lower
premiums
75.2%
96.2%
73.4%***
56.9%***
Higher federal taxes would be needed
to finance a national health insurance
program
67.2%
58.6%
63.3%
81.2%***
The health care system would be
simpler
72.0%
89.4%
71.1%***
56.2%***
The government would have more
control over which health care benefits
are covered by insurance
63.6%
65.0%
60.6%
66.7%
The government would have a greater
ability to reduce health care costs
74.1%
91.7%
72.4%***
59.5%***
Hospitals, doctors, and other providers
might be paid less
47.4%
44.2%
47.3%
50.1%
It might be harder to get an
appointment with a provider for a
health care visit
71.0%
62.1%
70.2%**
82.8%***
Administrative spending on health care
would be reduced
64.0%
75.6%
63.1%**
54.2%***
There might be less medical innovation
66.6%
62.2%
62.7%
77.1%***
Sample size
1,153
343
407
386
Source: Health Reform Monitoring Survey, quarter 1 2019.
Note: */**/*** Estimate differs significantly from adults who support Medicare for All at the 0.10/0.05/0.01 level, using two-tailed
tests.
Of those who opposed Medicare for All, 73.6 percent reported that an important factor in their
decision was that most people would not be able to keep their current insurance coverage, and 81.2
percent reported higher federal taxes to finance a national health program as an important factor.
Other important factors to opponents were that it might be harder to get an appointment with health
care providers (82.8 percent) and that there might be less medical innovation (77.1 percent). Opponents
were about half as likely as supporters (45.0 percent versus 91.0 percent) to report that everyone
having coverage was important in their decision about whether to support Medicare for All.
Nearly all factors in the survey were important to between 60 percent and 75 percent of
respondents who neither supported nor opposed Medicare for All.

14
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
What It Means
The March 2019 HRMS data showed that many Americans neither supported nor opposed a Medicare
for All or single-payer health plan. This ambivalence may partially reflect a lack of understanding of the
issues, which involve complex trade-offs that are difficult to predict. Those with an opinion were
roughly split between support and opposition. Medicare for All supporters were disproportionately
young, racial/ethnic minorities, and uninsured or publicly insured and had lower education levels and
incomes; they were also more likely to be Democrats. Opponents were disproportionately older, non-
Hispanic whites, privately insured, higher income, and Republican. Democrats were also more likely
than Republicans to support more incremental proposals, such as subsidies to low-income people and a
public option. Republican opposition to increasing subsidies, introducing a public option, or providing
universal coverage with a choice of public or private plans was weaker than their opposition to a single-
payer plan, but substantial nonetheless.
Medicare for All supporters responded that it was important that everyone have health care, that
there would be little or no out-of-pocket costs, that premiums would be lower, and that the government
would have greater ability to curb health care cost growth. They also were less likely to expect Medicare
for All to lead to less provider choice or worse quality of care. Medicare for All opponents were more
likely to be concerned about keeping their current insurance coverage, that their taxes would increase,
that it would take longer to get appointments, and that there would be less innovation in medicine.
Further, they were more likely to believe that quality of care would worsen under the approach. Those
who neither supported nor opposed Medicare for All had similar characteristics as supporters:
majorities or near-majorities of adults who were black or Hispanic, did not attend college, had low
incomes, or were uninsured or publicly insured were ambivalent toward this proposal. Their perceptions
of the effect of Medicare for All on access to care were more negative than those of supporters but were
closer to those of supporters than opponents.
This brief shows that currently there is considerable ambivalence toward Medicare for All
approaches to reforming the US health insurance system. Overall, 41 percent of respondents indicated
that they neither support nor oppose the approach. Among those presumably most in need of improved
affordability—those with low incomes and education levels, racial and ethnic minorities, and the
uninsured—support is significantly stronger than opposition, though having no opinion is still most
common. Additional premium and out-of-pocket cost subsidies and making a public option available to
consumers had levels of support similar to those of universal coverage options, though opposition to
these incremental reforms was weaker. We also found that opposition to Medicare for All was strongest
among those ages 50 to 64, non-Hispanic whites, those with higher incomes, and those with current
private coverage. In addition, opposition among Republican and Republican-leaning respondents is
considerable, making reaching political consensus challenging. However, when asked about frequently
cited concerns with Medicare for All approaches, respondents neither supporting nor opposing
Medicare for All answered more similarly to supporters than opponents, indicating some potential for
support to increase in the future and when proposals are better understood.

W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
15
About the Series
This brief is part of a series drawing on the HRMS, a survey of the nonelderly population that explores
the value of cutting-edge internet-based survey methods to monitor the Affordable Care Act before
data from federal government surveys are available. Funding for the core HRMS is provided by the
Robert Wood Johnson Foundation and the Urban Institute. For more information on the HRMS and for
other briefs in this series, visit www.urban.org/hrms.
Notes
1
“KFF Health Tracking Poll: The Public’s Views of the ACA,” Henry J. Kaiser Family Foundation, June 18, 2019,
https://www.kff.org/interactive/kff-health-tracking-poll-the-publics-views-on-the-aca/; Ashley Kirzinger, Bryan
Wu, and Mollyann Brodie, “KFF Health Tracking Poll – April 2019: Surprise Medical Bills and Public’s View of the
Supreme Court and Continuing Protections for People with Preexisting Conditions,” April 24, 2019,
https://www.kff.org/health-costs/poll-finding/kff-health-tracking-poll-april-2019/.
2
Kenneth Thorpe, “An Analysis of Senator Sanders Single Payer Plan,” Emory University, January 27, 2016,
https://www.healthcare-now.org/296831690-Kenneth-Thorpe-s-analysis-of-Bernie-Sanders-s-single-payer-
proposal.pdf.
3
For more information about the design of the HRMS, visit http://hrms.urban.org.
4
Question wording for the March 2019 survey instrument can be found at http://hrms.urban.org/survey-
instrument/index.html.
5
These findings differ from recent estimates for all adults ages 18 and older reported by the Henry J. Kaiser Family
Foundation (KFF), which asked respondents whether they support or oppose Medicare for All without an option
for ambivalence. There are advantages and disadvantages to each approach. The forced-choice approach
prompts respondents to provide an opinion, even if their support or opposition to the policy is weak. Including a
neutral option gives respondents an opportunity to express ambivalence, but does not capture whether
respondents choosing this option lean toward support versus opposition.
The large share of HRMS respondents selecting the neutral option indicates significant ambivalence toward
Medicare for All, which is consistent with the wide fluctuation in support for Medicare for All in KFF polls when
respondents are presented with arguments in favor of and against this proposal. However, if one assumes that
those who are ambivalent about the proposals would report that they somewhat favor or somewhat oppose if
presented with a forced-choice question, KFF tabulations would be similar to those of the HRMS. We also find
that perceptions of the impact of Medicare for All on access to care and taxes among adults selecting the neutral
option are similar to those of adults who support Medicare for All, which is consistent with the KFF poll findings
that support for Medicare for All is greater than opposition when respondents are presented with a forced-
choice question. The estimates in this brief may also differ from the KFF estimates because of differences in age
(i.e., nonelderly adults versus all adults) and survey mode.

16
W H AT E X PLAIN S S U PP O R T F OR O R O PP OS I TI O N TO M E DICA R E FO R ALL ?
References
Blahous, Charles. 2018. “The Costs of a National Single-Payer Healthcare System.” Mercatus Working Paper.
Arlington, VA: George Mason University Mercatus Center.
Holahan, John, Matthew Buettgens, Lisa Clemans-Cope, Melissa M. Favreault, Linda J. Blumberg, and Siyabonga
Ndwandwe. 2016. The Sanders Single-Payer Health Care Plan: The Effect on National Health Expenditures and Federal
and Private Spending. Washington, DC: Urban Institute.
Liu, Jodi L., and Christine Eibner. 2019. National Health Spending Estimates under Medicare for All. Santa Monica, CA:
RAND Corporation.
Long, Sharon K., Genevieve M. Kenney, Stephen Zuckerman, Dana E. Goin, Douglas Wissoker, Fredric Blavin, et al.
2014. “The Health Reform Monitoring Survey: Addressing Data Gaps to Provide Timely Insights into the
Affordable Care Act.” Health Affairs 33 (1): 161–7.
Pollin, Robert, James Heintz, Peter Arno, Jeannette Wicks-Lim, and Michael Ash. 2018. Economic Analysis of
Medicare for All. Amherst, MA: University of Massachusetts Amherst Political Economy Research Institute.
About the Authors
John Holahan is an Institute fellow in the Health Policy Center at the Urban Institute.
Michael Karpman is a senior research associate in the Health Policy Center.

W H AT E X PLAIN S S U PP O R T F OR OR OP P O S I TI ON T O M E DICA R E FO R AL L ?
17
Acknowledgments
This brief was funded by the Robert Wood Johnson Foundation. The views expressed here do not
necessarily reflect the views of the Foundation.
The views expressed are those of the authors and should not be attributed to the Urban Institute,
its trustees, or its funders. Funders do not determine research findings or the insights and
recommendations of Urban experts. Further information on the Urban Institute’s funding principles is
available at urban.org/fundingprinciples.
The authors gratefully acknowledge helpful comments from Linda Blumberg, Sharon K. Long, and
Robert Reischauer.
ABOUT THE URBAN INSTITUTE
The nonprofit Urban Institute is a leading research organization dedicated to
developing evidence-based insights that improve people’s lives and strengthen
communities. For 50 years, Urban has been the trusted source for rigorous analysis
of complex social and economic issues; strategic advice to policymakers,
philanthropists, and practitioners; and new, promising ideas that expand
opportunities for all. Our work inspires effective decisions that advance fairness and
enhance the well-being of people and places.
Copyright © August 2019.
Urban Institute. Permission is granted for reproduction
of this file, with attribution to the Urban Institute.
500 L’Enfant Plaza SW
Washington, DC 20024
www.urban.org
